20 JOURNAL OF THE NATIONAL MEDICAL ASSOCIATION JANUARY, 1976 Management of Extensive Open Fractures in Children and Teen-Age Patients* RUSSELL L. ANDERSON, JR., M.D., and RAVELO ARGAMASO, M.D., Divisions of Orthopaedic Surgery and Plastic Surgery, Department of Surgery. Montefiore Hospital and Medical Center, and Morrisania Hospital, Bronx, New York E XTENSIVE skin damage in any com- minuted fracture presents an intricate problem to a surgeon; however, when the problem involves a child who develops an osteomyelitic limb, the task becomes most demanding.1 - 7 Where foot pulses are present with good skin color and venous filling of the limb manifested, despite neural deficits, all attempts should be made to salvage the limb-especially in a child. 1.6* When bone is not covered, osteomyelitis is a common sequela8 5'7'3. It is well documen- ted that in order to salvage life and limb in a chronically infected fractured extremity, antibiotics alone will not control the disease, but surgical procedures are often mandatory.6'9 Not generally emphasized, especially in pediatric orthopaedics, is the dependence of the surgeon upon the medical team'0. The team is composed of a pedia- trician, usually the team leader, a child psy- chiatrist, medical house staff, social worker and registered nurses. Few medical papers are directed towards the problem of extensive open leg fractures in children.6'9 The purpose of this paper is to show how a technique used in adults can be adapted for children who have developed osteomyelitis of compound comminuted fractures. MATERIAL During the past seven years, at the *Read at the 80th Annual Convention of the National Medical Association, Miami, Florida, August 10- 16, 1975. Montefiore-Morrisania Hospital Medical Centers, the Orthopaedic and Plastic and Reconstructive Services have combined their surgical efforts in the management of chronic osteomyelitis of comminuted non-united fractures involving massive skin tegumental defects. Of the children studied, follow-up material was found on at least three patients who displayed results of our therapeutic management. Initially, all children who had compounded leg injuries, were seen by the trauma sur- geons. The wounds were cleansed with normal saline (approximately three to six liters) until the wound appeared grossly clean. All devitalized skin, muscle, tendon and cartilage were removed, but all bone stock was preserved despite its comminution unless it was grossly contaminated. All pa- tients were started on broad spectrum anti- biotics during the operative procedure and continued after wound specimens were sent to the bacteriology laboratory for cultures of predominate organisms and chemotherapeutic sensitivity studies. The comminuted bone fragments of the child's leg were re-aligned after thorough cleansing and debridement. The limb align- ment and position were maintained utilizing threaded or non-threaded Kirschner wires or Steinman pins in plaster of paris leg casts. Following the example of treatment of open war wounds4'6, these children's wounds were not closed, using secondary methods of clo-

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

20 JOURNAL OF THE NATIONAL MEDICAL ASSOCIATION JANUARY, 1976
Management of Extensive Open Fracturesin Children and Teen-Age Patients*
RUSSELL L. ANDERSON, JR., M.D.,
and
RAVELO ARGAMASO, M.D.,Divisions of Orthopaedic Surgery
andPlastic Surgery,
Department ofSurgery.Montefiore Hospital and Medical Center,
andMorrisania Hospital,Bronx, New York
E XTENSIVE skin damage in any com-minuted fracture presents an intricate
problem to a surgeon; however, when theproblem involves a child who develops anosteomyelitic limb, the task becomes mostdemanding.1 - 7 Where foot pulses are presentwith good skin color and venous filling of thelimb manifested, despite neural deficits, allattempts should be made to salvage thelimb-especially in a child. 1.6*When bone is not covered, osteomyelitis is
a common sequela8 5'7'3. It is well documen-ted that in order to salvage life and limb in achronically infected fractured extremity,antibiotics alone will not control the disease,but surgical procedures are oftenmandatory.6'9 Not generally emphasized,especially in pediatric orthopaedics, is thedependence of the surgeon upon the medicalteam'0. The team is composed of a pedia-trician, usually the team leader, a child psy-chiatrist, medical house staff, social workerand registered nurses.Few medical papers are directed towards
the problem of extensive open leg fracturesin children.6'9 The purpose of this paper is toshow how a technique used in adults can beadapted for children who have developedosteomyelitis of compound comminutedfractures.
MATERIAL
During the past seven years, at the*Read at the 80th Annual Convention of the National Medical Association,Miami, Florida, August 10- 16, 1975.
Montefiore-Morrisania Hospital MedicalCenters, the Orthopaedic and Plastic andReconstructive Services have combined theirsurgical efforts in the management of chronicosteomyelitis of comminuted non-unitedfractures involving massive skin tegumentaldefects. Of the children studied, follow-upmaterial was found on at least three patientswho displayed results of our therapeuticmanagement.
Initially, all children who had compoundedleg injuries, were seen by the trauma sur-geons. The wounds were cleansed withnormal saline (approximately three to sixliters) until the wound appeared grosslyclean. All devitalized skin, muscle, tendonand cartilage were removed, but all bonestock was preserved despite its comminutionunless it was grossly contaminated. All pa-tients were started on broad spectrum anti-biotics during the operative procedure andcontinued after wound specimens were sentto the bacteriology laboratory for cultures ofpredominate organisms and chemotherapeuticsensitivity studies.
The comminuted bone fragments of thechild's leg were re-aligned after thoroughcleansing and debridement. The limb align-ment and position were maintained utilizingthreaded or non-threaded Kirschner wires orSteinman pins in plaster of paris leg casts.Following the example of treatment of openwar wounds4'6, these children's wounds werenot closed, using secondary methods of clo-
Vol. 68, No. 1 Open Fractures 21
sure. Usually between the fifth to seventhpost-injury day, the patient's wound was re-assessed and debrided if necessary, and thebone fragments were realigned, as necessary.Depending upon the circumstances of toiletryof the individual wounds, further debride-ment might be required at subsequent peri-ods, until the wounds were free of majordebris and necrotic tissues. The minimumamount of bone was removed, so that in mostcases, less than one-fourth of an inch of limbshortening was appreciated. With the limbwounds grossly clean, covered by sterilemoist dressings, cross-leg or abdominal tubepedicle flaps were fashioned to cover largesoft tissue and chronic osteomyelitic limbdefects.
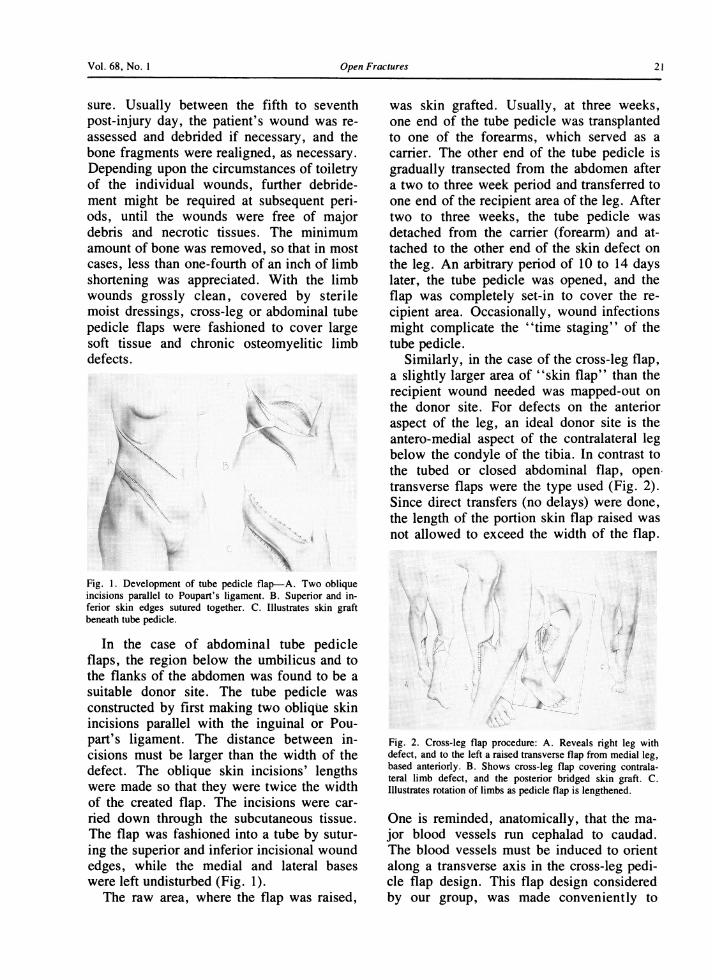
~'§,,~~~~~~~~~~~~~~~~~~~... ...... .::Fig. 1. Development of tube pedicle flap-A. Two obliqueincisions parallel to Poupart's ligament. B. Superior and in-ferior skin edges sutured together. C. Illustrates skin graftbeneath tube pedicle.
In the case of abdominal tube pedicleflaps, the region below the umbilicus and tothe flanks of the abdomen was found to be asuitable donor site. The tube pedicle wasconstructed by first making two oblique skinincisions parallel with the inguinal or Pou-part's ligament. The distance between in-cisions must be larger than the width of thedefect. The oblique skin incisions' lengthswere made so that they were twice the widthof the created flap. The incisions were car-ried down through the subcutaneous tissue.The flap was fashioned into a tube by sutur-ing the superior and inferior incisional woundedges, while the medial and lateral baseswere left undisturbed (Fig. 1).
The raw area, where the flap was raised,
was skin grafted. Usually, at three weeks,one end of the tube pedicle was transplantedto one of the forearms, which served as acarrier. The other end of the tube pedicle isgradually transected from the abdomen aftera two to three week period and transferred toone end of the recipient area of the leg. Aftertwo to three weeks, the tube pedicle wasdetached from the carrier (forearm) and at-tached to the other end of the skin defect onthe leg. An arbitrary period of 10 to 14 dayslater, the tube pedicle was opened, and theflap was completely set-in to cover the re-cipient area. Occasionally, wound infectionsmight complicate the "time staging" of thetube pedicle.
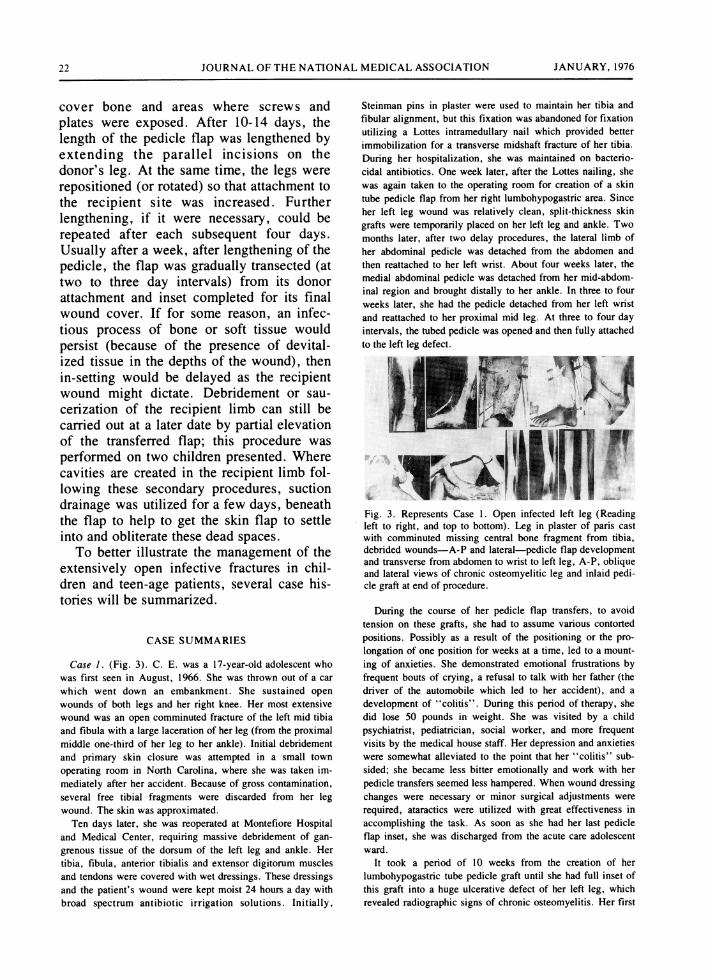
Similarly, in the case of the cross-leg flap,a slightly larger area of "skin flap" than therecipient wound needed was mapped-out onthe donor site. For defects on the anterioraspect of the leg, an ideal donor site is theantero-medial aspect of the contralateral legbelow the condyle of the tibia. In contrast tothe tubed or closed abdominal flap, open,transverse flaps were the type used (Fig. 2).Since direct transfers (no delays) were done,the length of the portion skin flap raised wasnot allowed to exceed the width of the flap.
Fig. 2. Cross-leg flap procedure: A. Reveals right leg withdefect, and to the left a raised transverse flap from medial leg,based anteriorly. B. Shows cross-leg flap covering contrala-teral limb defect, and the posterior bridged skin graft. C.Illustrates rotation of limbs as pedicle flap is lengthened.
One is reminded, anatomically, that the ma-jor blood vessels run cephalad to caudad.The blood vessels must be induced to orientalong a transverse axis in the cross-leg pedi-cle flap design. This flap design consideredby our group, was made conveniently to
22 JOURNAL OF THE NATIONAL MEDICAL ASSOCIATION JANUARY, 1976
cover bone and areas where screws andplates were exposed. After 10-14 days, thelength of the pedicle flap was lengthened byextending the parallel incisions on thedonor's leg. At the same time, the legs wererepositioned (or rotated) so that attachment tothe recipient site was increased. Furtherlengthening, if it were necessary, could berepeated after each subsequent four days.Usually after a week, after lengthening of thepedicle, the flap was gradually transected (attwo to three day intervals) from its donorattachment and inset completed for its finalwound cover. If for some reason, an infec-tious process of bone or soft tissue wouldpersist (because of the presence of devital-ized tissue in the depths of the wound), thenin-setting would be delayed as the recipientwound might dictate. Debridement or sau-cerization of the recipient limb can still becarried out at a later date by partial elevationof the transferred flap; this procedure wasperformed on two children presented. Wherecavities are created in the recipient limb fol-lowing these secondary procedures, suctiondrainage was utilized for a few days, beneaththe flap to help to get the skin flap to settleinto and obliterate these dead spaces.To better illustrate the management of the
extensively open infective fractures in chil-dren and teen-age patients, several case his-tories will be summarized.
CASE SUMMARIES
Case 1. (Fig. 3). C. E. was a 17-year-old adolescent whowas first seen in August, 1966. She was thrown out of a carwhich went down an embankment. She sustained openwounds of both legs and her right knee. Her most extensivewound was an open comminuted fracture of the left mid tibiaand fibula with a large laceration of her leg (from the proximalmiddle one-third of her leg to her ankle). Initial debridementand primary skin closure was attempted in a small townoperating room in North Carolina, where she was taken im-mediately after her accident. Because of gross contamination,several free tibial fragments were discarded from her legwound. The skin was approximated.Ten days later, she was reoperated at Montefiore Hospital
and Medical Center, requiring massive debridement of gan-grenous tissue of the dorsum of the left leg and ankle. Hertibia, fibula, anterior tibialis and extensor digitorum musclesand tendons were covered with wet dressings. These dressingsand the patient's wound were kept moist 24 hours a day withbroad spectrum antibiotic irrigation solutions. Initially,
Steinman pins in plaster were used to maintain her tibia andfibular alignment, but this fixation was abandoned for fixationutilizing a Lottes intramedullary nail which provided betterimmobilization for a transverse midshaft fracture of her tibia.During her hospitalization, she was maintained on bacterio-cidal antibiotics. One week later, after the Lottes nailing, shewas again taken to the operating room for creation of a skintube pedicle flap from her right lumbohypogastric area. Sinceher left leg wound was relatively clean, split-thickness skingrafts were temporarily placed on her left leg and ankle. Twomonths later, after two delay procedures, the lateral limb ofher abdominal pedicle was detached from the abdomen andthen reattached to her left wrist. About four weeks later, themedial abdominal pedicle was detached from her mid-abdom-inal region and brought distally to her ankle. In three to fourweeks later, she had the pedicle detached from her left wristand reattached to her proximal mid leg. At three to four dayintervals, the tubed pedicle was opened and then fully attachedto the left leg defect.
Fig. 3. Represents Case 1. Open infected left leg (Readingleft to right, and top to bottom). Leg in plaster of paris castwith comminuted missing central bone fragment from tibia,debrided wounds-A-P and lateral-pedicle flap developmentand transverse from abdomen to wrist to left leg, A-P, obliqueand lateral views of chronic osteomyelitic leg and inlaid pedi-cle graft at end of procedure.
During the course of her pedicle flap transfers, to avoidtension on these grafts, she had to assume various contortedpositions. Possibly as a result of the positioning or the pro-longation of one position for weeks at a time, led to a mount-ing of anxieties. She demonstrated emotional frustrations byfrequent bouts of crying, a refusal to talk with her father (thedriver of the automobile which led to her accident), and adevelopment of "colitis". During this period of therapy, shedid lose 50 pounds in weight. She was visited by a childpsychiatrist, pediatrician, social worker, and more frequentvisits by the medical house staff. Her depression and anxietieswere somewhat alleviated to the point that her "colitis" sub-sided; she became less bitter emotionally and work with herpedicle transfers seemed less hampered. When wound dressingchanges were necessary or minor surgical adjustments wererequired, ataractics were utilized with great effectiveness inaccomplishing the task. As soon as she had her last pedicleflap inset, she was discharged from the acute care adolescentward.
It took a period of 10 weeks from the creation of herlumbohypogastric tube pedicle graft until she had full inset ofthis graft into a huge ulcerative defect of her left leg, whichrevealed radiographic signs of chronic osteomyelitis. Her first

Vol. 68, No. I Open Fractures 23
18 months postoperatively were complicated by several epi-sodes of severe left leg pain, chills and fever, and develop-ment of sinuses over the dorsal and lateral surfaces of her legdespite continued large doses of bacteriocidal and bacterio-static antibiotics. Her bacterial flora included Staphylococcusaureus, Proteus mirabilis and Pseudomonas arugenosa. Thelatter bacterial organisms have proved to be the most resistantand persistent organisms to therapeutic management. One yearfrom the time of her auto accident, the Lottes nail was re-moved from her left tibia; tibial union was radiographicallypresent as well as a synostosis between her tibia and fibula;and she had an arthrodesis of her ankle joint. Six months afterthe Lottes nail was removed, she developed sinuses of her leg.Sinograms demonstrated radiopaque dye pooling at the mid-shaft of her tibia. The medial aspect of her tubed pedicle graftwas raised as a single flap, and a sequestrectomy and saucer-ization was performed. Since that major procedure, she hashad two defatting procedures of her leg and foot pediclegrafts. She has otherwise led a rather benign clinical course.She has been followed by the present authors for seven yearswith occasional skin ulceration complaints but without signs ofacute bone involvement.Case 2. (Fig. 4). W. E. was a 13-year-old male when
admitted to Morrisania Hospital with a severe injury of hisright leg. He had stuck his right foot into a washing machinewhile it was spinning in an attempt to stop the machine. Hesustained a comminuted open fracture of his right tibial shaft
i'
....
Fig. 4. Case 2. (Reading from left to right, top to bottom)Initial open comminuted fracture, clean open wound weekslater, transverse pedicle flap, flap covering compound wound,flap inset, and lateral and A-P radiographs of healing osteo-myelitic limb.
and fractures of the proximal and distal thirds of his fibula.The tibial shaft pierced through a four and one-half inchoblique anterior laceration. He had good function, sensationand bounding pulses of his right foot. He was taken to theoperating room several hours after admission to the hospital,
where, after thorough wound debridement, pins in plastertechnique was utilized. There was some tension at the midportion of the lacerated skin, and this area of skin was notclosed.On the fourth post-operative day, the central wound was
found non-viable. On the 10th day, the orthopaedic and plasticsurgical teams took the patient to the operating room, andunder Ketamine anesthesia, performed further debridement,cultured the wound, and firmer fixation of the fractured tibiawas provided. Following the second debridement procedure,the skin defect measured 2-Y4 x 31/2" exposing the fracturedtibia and the metallic fixation. A cross-leg pedicle flap wasdesigned from the left calf. The tibial wound cultures revealedKlebsiella, Aspergillus and E. coli. All cultured bacterialorganisms were sensitive to Nafcillin and Ampicillin, andboth antibiotics were given intravenously. One week later, thepatient was again operated upon for further right leg debride-ment, and at this time, a transverse calf pedicle flap (mediallybased) was elevated from the left gastrocnemius musculature.An initial attachment was made to the right leg coveringone-half of the wound, particularly including the fracturedtibial site. After two and one-half weeks, the pedicle waslengthened by 1½12". At the same time, the legs were reposi-tioned to increase the area of contact between the donor siteand left recipient site. A week later, the distal portion of thepedicle flap was gradually transected until the flap was com-pletely detached. Final inset was accomplished at that time.There was no further complication to the cross-leg pediclegrafting. But during the patient's hospitalization, he wastroubled, fearful and anxious after every procedure, althoughhe seemed to tolerate the positioning and fixation of his limbsin plaster casts. It was felt that the medical team greatly aidedthe patient through the two month period of surgery-espe-cially, during the period when the patient "felt he was goingcrazy". He was placed on Thorazine at intervals, which alsoseemed to be effective-especially at times of dressingchanges.Case 3. (Figs. 5 & 6) F. T., a 101/2 year old boy, was admitted
to Morrisania Hospital after being pushed in front of aninterstate passenger train. Upon hospital admission, he re-vealed a partially degloving wound at the distal right calf andankle with dirt and cinders noted ground up and sprayed upinto the intramedullary cavities of the distal tibia and fibula.His posterior tibial neurovascular bundle had been "avulsedout", as was his left posterior tibial tendon and flexor digi-torum longus tendon to the foot. Several hours after his ad-mission to the hospital and after he was normotensive, he wastaken to the operating room, where he had an initial debride-ment and fixation of his comminuted tibial and fibular frac-tures. Within four weeks, he was taken to the operating roomon four specific occasions for debridement of his left leg andankle wounds. On each occasion, more dirt-mainly railroadbed cinders-were washed from his open leg wound; from hisfirst operative day, he was placed on massive doses of peni-cillin, but the wounds of his leg and ankle cultured and "grewout" organisms of Enterobacter, Pseudomonas aeroginosa,Proteus mirabilis and Klebsiella. His antibiotic therapy fre-quently was changed based upon wound cultures and sensitiv-ity studies. He received the following antibiotics: Oxacillin,Ampicillin, Nafacillin, Gentamycin and Carbenicillin.
On the sixth hospital week, he was again taken to the
24 JOURNAL OF THE NATIONAL MEDICAL ASSOCIATION JANUARY, 1976
operating room, and with the plastic and orthopaedic surgeryteams, a transverse cross-leg pedicle flap 31/2 x 10½/2" basedanteromedially, was raised from the patient's left leg andtransferred to the right distal tibial ankle defect and the legswere held in place by Steinman pins and plaster of paris casts.The underlying donor defect was grafted with a split-thicknessskin graft. After 21/2 weeks, the large pedicle graft waslengthened by one inch, and the lengthening was repeatedtwice (on the fourth and seventh day following the firstlengthening). The legs were repositioned during each pro-cedural lengthening.
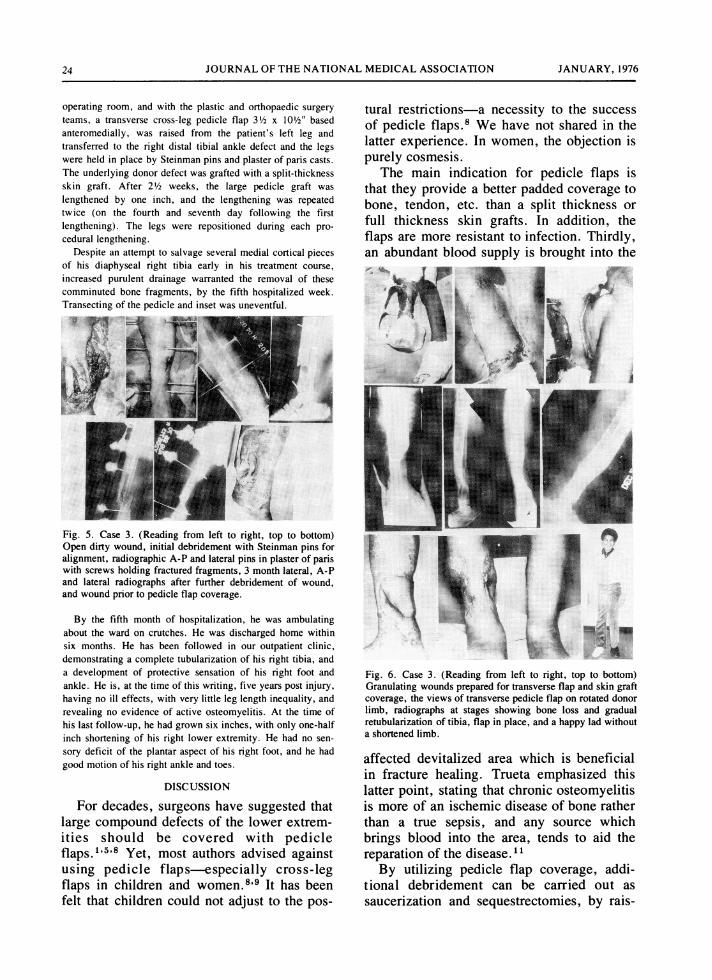
Despite an attempt to salvage several medial cortical piecesof his diaphyseal right tibia early in his treatment course,increased purulent drainage warranted the removal of thesecomminuted bone fragments, by the fifth hospitalized week.Transecting of the pedicle and inset was uneventful.
7i~~c.
Fig. 5. Case 3. (Reading from left to right, top to bottom)Open dirty wound, initial debridement with Steinman pins foralignment, radiographic A-P and lateral pins in plaster of pariswith screws holding fractured fragments, 3 month lateral, A-Pand lateral radiographs after further debridement of wound,and wound prior to pedicle flap coverage.
By the fifth month of hospitalization, he was ambulatingabout the ward on crutches. He was discharged home withinsix months. He has been followed in our outpatient clinic,demonstrating a complete tubularization of his right tibia, anda development of protective sensation of his right foot andankle. He is, at the time of this writing, five years post injury,having no ill effects, with very little leg length inequality, andrevealing no evidence of active osteomyelitis. At the time ofhis last follow-up, he had grown six inches, with only one-halfinch shortening of his right lower extremity. He had no sen-sory deficit of the plantar aspect of his right foot, and he hadgood motion of his right ankle and toes.
DISCUSSION
For decades, surgeons have suggested thatlarge compound defects of the lower extrem-ities should be covered with pedicleflaps."15'8 Yet, most authors advised againstusing pedicle flaps-especially cross-legflaps in children and women.8'9 It has beenfelt that children could not adjust to the pos-
tural restrictions-a necessity to the successof pedicle flaps.8 We have not shared in thelatter experience. In women, the objection ispurely cosmesis.
The main indication for pedicle flaps isthat they provide a better padded coverage tobone, tendon, etc. than a split thickness orfull thickness skin grafts. In addition, theflaps are more resistant to infection. Thirdly,an abundant blood supply is brought into the
.....x.....
......~~~~~~~~~~~~~~~~~~~~~~~.......
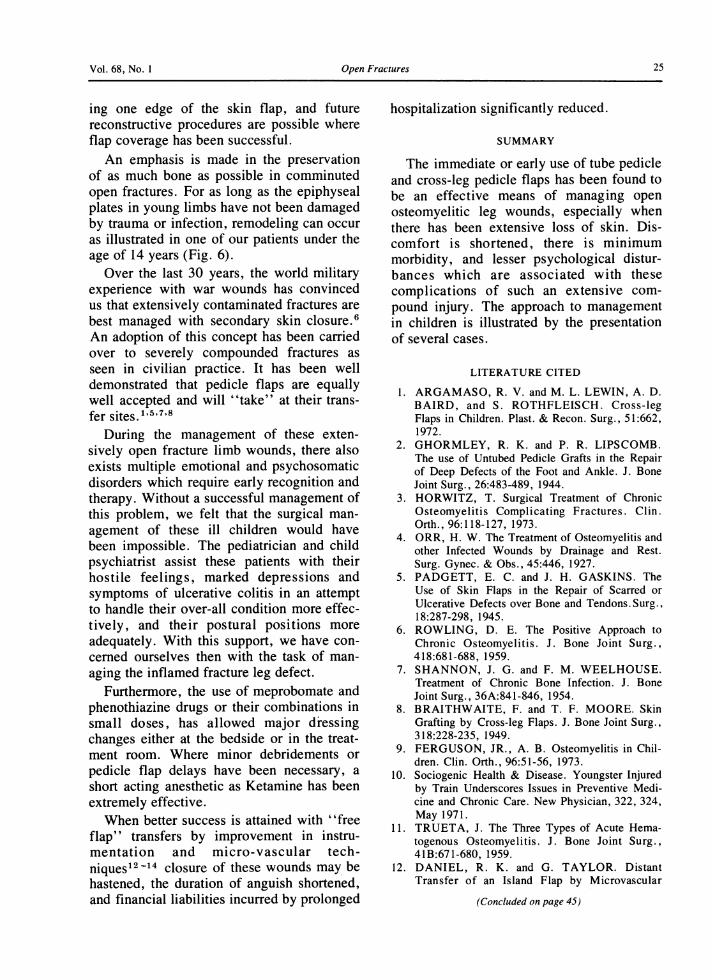
Fig. 6. Case 3. (Reading from left to right, top to bottom)Granulating wounds prepared for transverse flap and skin graftcoverage, the views of transverse pedicle flap on rotated donorlimb, radiographs at stages showing bone loss and gradualretubularization of tibia, flap in place, and a happy lad withouta shortened limb.
affected devitalized area which is beneficialin fracture healing. Trueta emphasized thislatter point, stating that chronic osteomyelitisis more of an ischemic disease of bone ratherthan a true sepsis, and any source whichbrings blood into the area, tends to aid thereparation of the disease."By utilizing pedicle flap coverage, addi-
tional debridement can be carried out assaucerization and sequestrectomies, by rais-
Vol. 68, No. 1 Open Fractures 25
ing one edge of the skin flap, and futurereconstructive procedures are possible whereflap coverage has been successful.An emphasis is made in the preservation
of as much bone as possible in comminutedopen fractures. For as long as the epiphysealplates in young limbs have not been damagedby trauma or infection, remodeling can occuras illustrated in one of our patients under theage of 14 years (Fig. 6).
Over the last 30 years, the world militaryexperience with war wounds has convincedus that extensively contaminated fractures arebest managed with secondary skin closure.6An adoption of this concept has been carriedover to severely compounded fractures asseen in civilian practice. It has been welldemonstrated that pedicle flaps are equallywell accepted and will "take" at their trans-fer sites.1'5'7'8
During the management of these exten-sively open fracture limb wounds, there alsoexists multiple emotional and psychosomaticdisorders which require early recognition andtherapy. Without a successful management ofthis problem, we felt that the surgical man-agement of these ill children would havebeen impossible. The pediatrician and childpsychiatrist assist these patients with theirhostile feelings, marked depressions andsymptoms of ulcerative colitis in an attemptto handle their over-all condition more effec-tively, and their postural positions moreadequately. With this support, we have con-cerned ourselves then with the task of man-aging the inflamed fracture leg defect.
Furthermore, the use of meprobomate andphenothiazine drugs or their combinations insmall doses, has allowed major dressingchanges either at the bedside or in the treat-ment room. Where minor debridements orpedicle flap delays have been necessary, ashort acting anesthetic as Ketamine has beenextremely effective.When better success is attained with "free
flap" transfers by improvement in instru-mentation and micro-vascular tech-niques12 -14 closure of these wounds may behastened, the duration of anguish shortened,and financial liabilities incurred by prolonged
hospitalization significantly reduced.
SUMMARY
The immediate or early use of tube pedicleand cross-leg pedicle flaps has been found tobe an effective means of managing openosteomyelitic leg wounds, especially whenthere has been extensive loss of skin. Dis-comfort is shortened, there is minimummorbidity, and lesser psychological distur-bances which are associated with thesecomplications of such an extensive com-pound injury. The approach to managementin children is illustrated by the presentationof several cases.
LITERATURE CITED
1. ARGAMASO, R. V. and M. L. LEWIN, A. D.BAIRD, and S. ROTHFLEISCH. Cross-legFlaps in Children. Plast. & Recon. Surg., 51:662,1972.
2. GHORMLEY, R. K. and P. R. LIPSCOMB.The use of Untubed Pedicle Grafts in the Repairof Deep Defects of the Foot and Ankle. J. BoneJoint Surg., 26:483-489, 1944.
3. HORWITZ, T. Surgical Treatment of ChronicOsteomyelitis Complicating Fractures. Clin.Orth., 96:118-127, 1973.
4. ORR, H. W. The Treatment of Osteomyelitis andother Infected Wounds by Drainage and Rest.Surg. Gynec. & Obs., 45:446, 1927.
5. PADGETT, E. C. and J. H. GASKINS. TheUse of Skin Flaps in the Repair of Scarred orUlcerative Defects over Bone and Tendons. Surg.,18:287-298, 1945.
6. ROWLING, D. E. The Positive Approach toChronic Osteomyelitis. J. Bone Joint Surg.,418:681-688, 1959.
7. SHANNON, J. G. and F. M. WEELHOUSE.Treatment of Chronic Bone Infection. J. BoneJoint Surg., 36A:841-846, 1954.
8. BRAITHWAITE, F. and T. F. MOORE. SkinGrafting by Cross-leg Flaps. J. Bone Joint Surg.,318:228-235, 1949.
9. FERGUSON, JR., A. B. Osteomyelitis in Chil-dren. Clin. Orth., 96:51-56, 1973.
10. Sociogenic Health & Disease. Youngster Injuredby Train Underscores Issues in Preventive Medi-cine and Chronic Care. New Physician, 322, 324,May 1971.
11. TRUETA, J. The Three Types of Acute Hema-togenous Osteomyelitis. J. Bone Joint Surg.,41B:671-680, 1959.
12. DANIEL, R. K. and G. TAYLOR. DistantTransfer of an Island Flap by Microvascular
(Concluded on page 45)
Vol. 68, No. 1 Bronchial Stump Closure 45
and seven, when the inflammatory responseto silk was most intense, collagen productionin the silk closures was minimal. At thissame time (postoperative days 5-7), thestaple closures demonstrated only a moderateinflammatory response and the production ofcollagen was rapidly accelerating. Althoughby the tenth day the difference in collagenproduction between the two closures was lessmarked, the silk closed stumps never devel-oped the foci of solid collagen noted in thestaple closures. Nylon collagen levels werealways intermediate between those of silkand staple closures.
The strength of bronchial stump closuresas determined by leakage pressures also cor-related closely with histological evaluation.Between postoperative days three and seven,the strength of staple closed stumps was ap-preciably greater than that of silk closures.This developed while the exudative reactionin the staple closures was much less than thatin the silk closures and collagen production
in staple closures demonstrably greater thanthat present in the silk closures. However,after seven days postoperatively the strengthof the silk closed bronchial stumps rapidlyincreased as the inflammatory response de-creased and collagen production increased.Nevertheless, the strength of the silk closuresnever approached that of the stronger stapleclosures. Again, nylon closures were alwaysintermediate in strength between the weakersilk and the stronger staple closures.
In conclusion, we feel any exudative reac-tion in a bronchial stump is undesirable be-cause it delays the onset and extent of col-lagen production. Inflammation thus contrib-utes to a weaker closure and enhances thedevelopment of a bronchopleural fistula.With the staple bronchial stump closure, theonset and severity of the exudative reaction isdelayed and wound healing accelerated. Thestrength of staple closed stumps appears su-perior to that of silk and nylon closed stumpsat all postoperative days studied.
(Anderson and Argamasofrom page 25)
Anastomosis-A Clinical Technique. Plastic andReconstr. Surg., 52:111-117, 1973.
13. O'BRIEN, B. M. and A. M. MacLEOD, J. W.HAYHURST, and W. A. MORRISON. Suc-cessful Transfer of a Large Island Flap from theGroin to the Foot by Microvascular Anastomosis.Plast. Reconstr. Surg., 52:271, 1973.
14. HARRIS, K. and K. OHMARI. Direct Transferof Larger Free Groin Skin Flaps for the Lower
Extremity Using Microvascular Anastomosis.Chir. Plastic, 3:1-14, 1975.
SEE ALSO
KELLY, P. J. and C. J. WILKOWSKE, and J.A. WASHINGTON. Comparison of Gram-nega-tive Bacillary and Staphylococcal Osteomyelitis ofthe Femur and Tibia. Clin. Orth., 96:70-75,1973.
NUTRITION, DIET, AND CANCER
Cancer is the second leading cause of death in the United States. It is estimated that 80-90% of all human cancer may berelated to several environmental factors and, therefore, potentially preventable. Nutrition and diet have been suggested to beamong these environmental factors, and nutritional effects in tumor development in experimental animals have been demon-strated. Caloric restriction, type and amount of dietary fat, deficiencies of certain vitamins and minerals, and dietary content ofprotein and amino acids all influence induction or growth of tumors in animals. Certain amino acid deficiencies are reported tohave tumor-suppressing action. Some vitamin deficiencies enhance tumor development; other deficiencies suppress it. Epidemio-logic studies in human populations have implicated high levels of fat or a lack of fiber in the diet in the causation of breast andcolon cancer. Differences in the diet may bring about differences in the intestinal microflora which have been associated withvariations in the incidence of cancer of the large bowel. More studies are needed to elucidate the mechanism(s) by whichnutrition and diet can influence carcinogenesis and to document associations between dietary practices and cancer. While thescientific evidence in experimental animals is suggestive of a relationship between nutrition and cancer, confirmation of thesefindings in humans is fragmentary. Therefore, other than maintenance of desirable body weight, it is premature to make specificdietary recommendations at present to minimize the risk of cancer.
Dairy Council Digest, Sept.-Oct., 1975
Related Documents











