Management of cervical spine injury* Colin F. Mackenzie MBChB, FRCA, FCCM Professor and Vice-Chairman Department of Anesthesiology Director Trauma Anesthesiology, R Adams Cowley Shock Trauma Center, University of Maryland School of Medicine, Baltimore, Maryland 21201, USA Fred H. Geisler MD PhD Director Comprehensive Spinal Care Center, Chicago Institute of Neurosurgery and Neuroresearch Medical Group, S.C., Chicago, Illinois 60614, USA Field assessment, neck immobilization, oxygenation and maintenance of the airway occur in suspected cervical-spine-injured patients before transport to a regional spinal cord injury centre. After cervical spine radiography, bony alignment of the spinal column is re-established and mean blood pressure is maintained at 80–90 mmHg with fluids and, if necessary, inotropic support. Predetermined guidelines are used for intubation and ventilation and for invasive monitoring of patients in spinal shock. Fluid challenge is used to assess reserve cardiac function and the need for fluid infusion, restriction or inotropic support. Evoked potential monitoring provides a non-invasive, objective and sensitive method to assess neuroconduction through a spinal cord injury and may be used to replace a wake-up test intraoperatively. There are no randomized prospective studies showing that surgical decompression and/or internal stabiliza- tion improves outcome compared with non-surgical treatment of acute cervical spine injury. Respiratory failure is managed by long-term ventilator support, diaphragm pacing or use of glossopharyngeal breathing. Chest physiotherapy is helpful in reducing the occurrence of atelectasis and pneumonia. Hyperreflexic syndromes during surgery are avoided with adequate anaesthesia during stimulation. An area with a population near one million should designate a regional spinal cord injury centre. Such centres decrease the proportion of patients with complete neurological injury. Key words: cervical spine; trauma; resuscitation; anaesthesia; surgery; critical care. The diagnosis and acute management of cervical spinal cord injury (SCI) can be divided into six separate phases: (1) initial assessment and immobilization; (2) resuscitation and medical management; (3) radiological diagnostics; (4) anaesthesia management; (5) surgical therapy; and (6) post-operative critical care management. 1521–6896/99/040643+16 $12.00/00 * c 1999 Harcourt Publishers Ltd. Baillie`re’s Clinical Anaesthesiology Vol. 13, No. 4, pp. 643–658, 1999 11 *Parts of this chapter have previously been published in: Albin M (ed). Management of Acute Cervical Spinal Cord Injury , pp. 1083–1136, New York: McGraw-Hill, 1997. The material is reproduced here with the permission of The McGraw-Hill Companies.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Management of cervical spine injury*
Colin F. Mackenzie MBChB, FRCA, FCCM
Professor and Vice-ChairmanDepartment of Anesthesiology
DirectorTrauma Anesthesiology, R Adams Cowley Shock Trauma Center, University of Maryland School of Medicine,Baltimore, Maryland 21201, USA
Fred H. Geisler MD PhD
DirectorComprehensive Spinal Care Center, Chicago Institute of Neurosurgery and Neuroresearch Medical Group,S.C., Chicago, Illinois 60614, USA
Field assessment, neck immobilization, oxygenation and maintenance of the airway occur insuspected cervical-spine-injured patients before transport to a regional spinal cord injurycentre. After cervical spine radiography, bony alignment of the spinal column is re-establishedand mean blood pressure is maintained at 80±90 mmHg with ¯uids and, if necessary, inotropicsupport. Predetermined guidelines are used for intubation and ventilation and for invasivemonitoring of patients in spinal shock. Fluid challenge is used to assess reserve cardiac functionand the need for ¯uid infusion, restriction or inotropic support. Evoked potential monitoringprovides a non-invasive, objective and sensitive method to assess neuroconduction through aspinal cord injury and may be used to replace a wake-up test intraoperatively. There are norandomized prospective studies showing that surgical decompression and/or internal stabiliza-tion improves outcome compared with non-surgical treatment of acute cervical spine injury.Respiratory failure is managed by long-term ventilator support, diaphragm pacing or use ofglossopharyngeal breathing. Chest physiotherapy is helpful in reducing the occurrence ofatelectasis and pneumonia. Hyperre¯exic syndromes during surgery are avoided withadequate anaesthesia during stimulation. An area with a population near one million shoulddesignate a regional spinal cord injury centre. Such centres decrease the proportion ofpatients with complete neurological injury.
Key words: cervical spine; trauma; resuscitation; anaesthesia; surgery; critical care.
The diagnosis and acute management of cervical spinal cord injury (SCI) can be dividedinto six separate phases: (1) initial assessment and immobilization; (2) resuscitationand medical management; (3) radiological diagnostics; (4) anaesthesia management;(5) surgical therapy; and (6) post-operative critical care management.
1521±6896/99/040643+16 $12.00/00 *c 1999 Harcourt Publishers Ltd.
BaillieÁ re's Clinical AnaesthesiologyVol. 13, No. 4, pp. 643±658, 1999
11
*Parts of this chapter have previously been published in: Albin M (ed). Management of Acute CervicalSpinal Cord Injury, pp. 1083±1136, New York: McGraw-Hill, 1997. The material is reproduced here with thepermission of The McGraw-Hill Companies.

INITIAL ASSESSMENT AND IMMOBILIZATION
The ®rst care phase begins in the ®eld. A patient with a possible SCI is identi®edutilizing an initial ®eld screening and a neurological examination for motor andsensory de®cits in all extremities. A protocol for splinting and immobilizing the spineis followed; the patient is placed on a backboard with the head and neck immobilizedin a neutral position with a hard cervical collar and tape. A spine board can beslipped behind the victim in a car seat prior to extraction. The major goal is toreduce the risk of neurological deterioration from repeated mechanical insults to thespinal cord; ¯exion of the neck o�ers the greatest potential for additional damage. Ahard cervical collar is routinely used on seriously head-injured patients because asmany as 4% of these victims will have an unsuspected cervical spine fracture.Distribution of neurological status and frequency of cervical injury are shown inFigure 1.
Maintenance of an airway and adequate ventilation during assessment and transportmust supersede total neck immobilization. Jaw thrust and slight head extension canimprove oxygenation while occipital±C1 movement should not provoke damage tolower cervical areas (C3±C7).1
If the patient requires intubation, in-line manual stabilization facilitates placement ofthe endotracheal tube without compromising the spinal cord. Patients with acute SCIsshould proceed directly to an SCI centre, not just the nearest hospital.
Figure 1. Distribution of neurological status and frequency of cervical injury level among 696 cervical spineinjury patients: , complete; h, incomplete; , intact. Data redrawn from Meyer PR (ed.) (1989, Surgery ofSpine Trauma. New York: Churchill-Livingstone).
644 C. F. Mackenzie and F. H. Geisler
RESUSCITATION AND MEDICAL MANAGEMENT
The second care phase involves the medical support necessary to reverse thephysiological changes that occur as a consequence of a cervical SCI. A severe cervicalSCI physiologically interrupts the out¯ow of the entire sympathetic nervous system asit passes through the cervical spinal cord before it exits in the thoracic region. Thisinterruption causes loss of vascular tone and of the body's ability to maintain normalblood pressure. Patients in neurogenic or `spinal' shock typically present withhypotension and bradycardia, a state di�ering from that of hypovolaemic hypotensionassociated with blood loss from other injuries because of the absence of tachycardia.The hypotension associated with the neurogenic shock of SCI usually can be reversedwith ¯uids and small doses of dopamine (3±5 mcg/kg per minute), which can beadjusted to maintain a mean blood pressure of 80±90 mmHg in a previously normal,young healthy individual. By bony realignment and relief of pressure on the spinal cordwithin hours of injury, tissue perfusion is enhanced at the site of spinal cord damageand this may improve neurological outcome.
Initial medical management
Although treatment priorities for the multitrauma patient mandate management oflife-threatening injuries as the ®rst priority, the displaced spinal column can often bereduced rapidly with cervical traction and stabilized while any required multisystemdiagnostic studies take place. The initial management goals are to preserve theneurological function present on arrival and to reverse the presenting neurologicalde®cits. These initial goals also include maintaining arterial blood gases and vital signsin the normal range. All SCI patients, despite the severity of the initial injuries, arepresumed to have incomplete SCIs with a potential for recovery until serialneurological examinations conducted at 472 hours document irrecoverable motorand/or sensory loss.
Medical management includes a lateral cervical spine radiograph with at least oneview showing structures inferior to C7.2 After the diagnosis of a cervical fracture orSCI, bony alignment of the spinal column is re-established with Gardner±Wellscervical traction or Halo vest immobilization. Two large-bore i.v. catheters, a Foleycatheter and a nasogastric tube are inserted. A pulmonary artery catheter is alsoinserted in an SCI patient with acute neurological de®cit who requires surgery andanaesthesia. A baseline laboratory work-up is conducted including a complete bloodcount, electrolytes, amylase, lactate, coagulation pro®le, blood type and cross-match,urinalysis, arterial blood gas and electrocardiogram. In addition to diagnosing the SCI,the diagnostic work-up of a patient with multitrauma should exclude other life-threatening injuries.
During the ®rst 72 hours following an SCI, the patient's mean arterial bloodpressure is maintained between 80 and 90 mmHg with optimization of circulatingvolume by ¯uid challenge (see below). Cardiac output is maintained in a normal tohigh-normal (1.5 times the normal output) range.3 Inotropic support with dopamineor dobutamine may be necessary after ¯uid infusion to attain these physiological goals.The hyperdynamic cardiac output enhances spinal cord perfusion during theneurogenic shock state, which begins at the time of injury. The augmented cardio-vascular parameters are carefully monitored and maintained throughout induction ofanaesthesia or during surgery, in those patients requiring early spinal decompression
Management of cervical spine injury 645

or emergency surgery. The patient receives methylprednislone in a 30 mg/kg bolusfollowed by 5.4 mg/kg per hour for 23 hours.4
RADIOLOGICAL DIAGNOSTICS
The third care phase involves detailed, diagnostic radiological procedures to de®ne thebony damage and to verify decompression of the spinal cord and nerve roots. Afteroptimal closed reduction of the cervical fracture±dislocation has been obtained, asdetermined from an X-ray ®lm, a C1±C2 iohexol myelogram is obtained (Figure 2(A))and then a computerized tomography (CT) myelogram. Magnetic resonance imaging(MRI) or cervical tomograms can image the injury and may be used instead of the CTmyelogram. The CT myelogram provides superb bony detail of the fracture site andthe anatomic relation of fractured or dislocated fragments to the spinal cord, whereasthe MRI view provides better images of anterior discs, posterior ligamentum ¯ava orspinal cord contusion5 (Figure 2(B)).
The bony injuries may be classi®ed into ¯exion, ¯exion compression, compression,extension, and the rare distraction injury. All require di�erent positioning and weight
Figure 2. (A) Myleogram showing extravasation of contrast through torn annulus and posterior ligamentand a cord transection at C5. (B) Nuclear magnetic resonance image of C5±C6 hyper¯exion injury showingligamentum ¯avum, posterior longitudinal ligament and posterior annulus ®brosis. There is cord narrowing,oedema and contusion. Courtesy Stuart Mirvis, MD.
(A)(B)
646 C. F. Mackenzie and F. H. Geisler

traction. The neurological de®cit may be less if reduction is achieved rapidly. Fewpatients will not realign, and, in these, operative reduction is required to achieve canalrestoration.
ANAESTHESIA MANAGEMENT
Pre-operative considerations
During spinal shock, which lasts from 3 days to 6 weeks following the onset ofquadriplegia6, anaesthesia may be especially hazardous because of impaired cardiac andrespiratory function. An electrocardiogram should be taken because myocardialischaemia may be present in the elderly quadriplegic or even in the younger popula-tion who may have su�ered hypoxaemia from, for example, near drowning following adiving accident. In persistently bradycardic patients, a pacemaker may be useful inincreasing cardiac output and improving cardiac reserve by chronotropy, without useof infused inotropic agents (Figure 3).
Pulmonary artery and radial artery catherization is advisable to make an assessmentof reserve cardiac function pre-operatively and to optimize circulating volume for allquadriplegic patients undergoing general anaesthesia during the spinal shock period.During elevation of cardiac ®lling pressures by rapid ¯uid infusion through the rightatrial line in these mechanically ventilated patients, pulmonary artery and capillarywedge pressures and ventilator end inspiratory pressure (lung±thorax compliance)
Figure 3. The pulse ( ), systolic blood pressure (-- - - - - -) and diastolic blood pressure (ÐÐÐ) of aquadriplegic patient with a C5±C6 spinal cord injury are shown from the time of admission (day 1) andincluding day 7 when spinal cord fusion occurred. Persistent bradycardia in the low 40s/min responded tointravenous atropine on days 4 and 5. A transvenous pacemaker was inserted on day 6 before surgery. Theincreased heart rate to 70 beats/min with pacing caused an increase in blood pressure and resulted in markedincrease in urinary ¯ow (2110 ml in 6 hours on day 7) suggesting improved perfusion of the kidneys. Thepacing rate was changed and cardiac output measured intraoperatively before an optimal rate of 80 beats/minwas established on day 8. Reproduced from Mackenzie & Geisler (1997, Albin MS (ed.) Textbook of Neuro-anesthesia. New York: McGraw-Hill) with permission.
Management of cervical spine injury 647
should be continuously monitored (see Fluid challenge below). The central venouspressure that provides optimum cardiac function can be determined intraoperativelywhen the patient has a pulmonary artery catheter in position and this can be used as abaseline for volume loading should oliguria or other evidence of impaired tissueperfusion occur post-operatively, after removal of the pulmonary artery catheter.Unless sepsis or hypoxaemia occurs, it is unusual to require pulmonary arterycatheterization outside the peri-operative period.
Pre-medicant drugs are avoided in spontaneously breathing quadriplegics until thepatient reaches the operating room, where i.v. midazolam may be given and its e�ectsobserved. Atropine should be given as a pre-medicant especially if the patient has apulse rate less than 70 beats/min, because the myocardial depressant e�ects ofanaesthetic agentsmay be reversed by atropine. Doses reportedly as high as 0.04 mg/kgi.v. may be required to elevate the pulse rate7, although we have found 0.02 mg/kg tobe satisfactory.8 The operative procedure and patient positioning should be discussedand plannedwith the surgeon pre-operatively and baseline values of pulse, intravascularpressures and electrocardiogram obtained before induction of anaesthesia.
Indications for tracheal intubation and mechanical ventilation
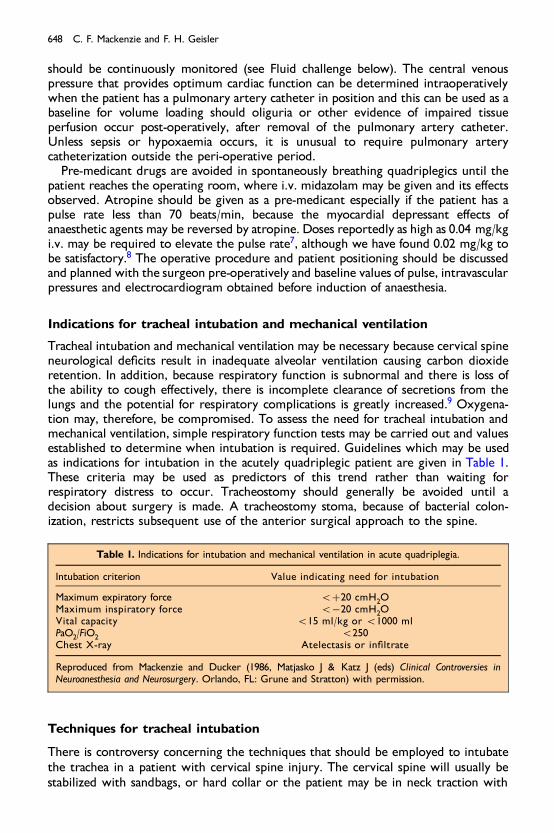
Tracheal intubation and mechanical ventilation may be necessary because cervical spineneurological de®cits result in inadequate alveolar ventilation causing carbon dioxideretention. In addition, because respiratory function is subnormal and there is loss ofthe ability to cough e�ectively, there is incomplete clearance of secretions from thelungs and the potential for respiratory complications is greatly increased.9 Oxygena-tion may, therefore, be compromised. To assess the need for tracheal intubation andmechanical ventilation, simple respiratory function tests may be carried out and valuesestablished to determine when intubation is required. Guidelines which may be usedas indications for intubation in the acutely quadriplegic patient are given in Table 1.These criteria may be used as predictors of this trend rather than waiting forrespiratory distress to occur. Tracheostomy should generally be avoided until adecision about surgery is made. A tracheostomy stoma, because of bacterial colon-ization, restricts subsequent use of the anterior surgical approach to the spine.
Techniques for tracheal intubation
There is controversy concerning the techniques that should be employed to intubatethe trachea in a patient with cervical spine injury. The cervical spine will usually bestabilized with sandbags, or hard collar or the patient may be in neck traction with
Table 1. Indications for intubation and mechanical ventilation in acute quadriplegia.
Intubation criterion Value indicating need for intubation
Maximum expiratory force 5�20 cmH2OMaximum inspiratory force 5ÿ20 cmH2OVital capacity 515 ml/kg or 51000 mlPaO2/FiO2 5250Chest X-ray Atelectasis or in®ltrate
Reproduced from Mackenzie and Ducker (1986, Matjasko J & Katz J (eds) Clinical Controversies inNeuroanesthesia and Neurosurgery. Orlando, FL: Grune and Stratton) with permission.
648 C. F. Mackenzie and F. H. Geisler

tongs or a Halo ring. The techniques used to intubate the trachea in patients withcervical spine injury depend on the general condition of the patient, the neurologicalde®cit and on how recently the spine injury occurred. There is no single acceptabletechnique for tracheal intubation for all cervical-spine-injured patients.
In the non-emergency `elective intubation', it appears that nasal intubation undertopical anaesthesia with a ®bre-optic bronchoscopy performed with the patient awakeis the technique of choice. Neurological function may then be assessed before and afterthe tracheal tube is secured in place and the patient appropriately positioned forinduction of general anaesthesia or other elective intervention.
The SCI patient who is in acute respiratory distress or shock, or who has su�eredother injuries, should not undergo heavy sedation and prolonged e�orts to provideadequate topical anaesthesia for awake intubation. In our experience, when attemptsare made to perform awake intubation in the shocked, recently admitted, cervical-spine-injured patient who may also be under the in¯uence of alcohol and have a fullstomach, neck movement is increased and incomplete anaesthesia results in a highfrequency of vomiting and aspiration. Topical anaesthesia has been abandoned for theinitial intubation in such patients. Rather, following pre-oxygenation and application ofcricoid pressure10, intubation is performed using succinylcholine after administration ofa sleep dose of barbiturate. If di�culty is encountered in intubation because ofweighted traction, a second person, preferably a neurosurgeon, assists by reducing thetraction weight until the trachea can be intubated. In our hands, this technique hasbeen used successfully for many years without producing any alterations in neuro-logical function. In the patient without traction, the front half of the hard collar isremoved to allow application of cricoid pressure and a second person holds the head inthe neutral position and applies in-line neck stabilization. These techniques are notrecommended for novice laryngoscopists.
Induction of anaesthesia may be unnecessary or contraindicated for the unconsciousrecently injured patient with spinal cord trauma or those in severe shock with anunrecordable blood pressure. In these circumstances, after pre-oxygenation andapplication of cricoid pressure, succinylcholine alone is used to facilitate rapid trachealintubation with a cu�ed tube by the oral route. Nasal intubation is not used inemergencies because, unless there is extensive pre-intubation use of e�ective mucosalvasoconstrictors such as cocaine, bleeding is precipitated by passage of a nasal tube.This further complicates visualization of the larynx. An orotracheal tube can bechanged to a nasal tube under controlled, ideal circumstances of optimumoxygenation at some future time after the patient is stabilized. Prolonged nasalintubation is not often used for the SCI patient in our institution because of therelatively high incidence of purulent sinusitis associated with nasotracheal andnasogastric tubes.11
Induction and maintenance of anaesthesia: techniques and precautions
Several reports in the literature have addressed cardiovascular collapse following i.v.succinylcholine in patients and animals with spinal cord and neural injury.12±14 Stoneet al13 reported that a C6 spine-injured quadriplegic developed cardiac arrest whensuccinylcholine was injected i.v. 46 days after SCI. The patient's serum potassium wasincreased from 4.6 to 11.6 meq/l within 2 min of succinylcholine administration. Thesame authors found that, in laboratory animals with transected spinal cords, hyper-kalaemia after succinylcholine infusion was signi®cant after 14 days and highlysigni®cant 28 days following spinal cord transection.
Management of cervical spine injury 649

The pharmacological receptor area of the end plate at the neuromuscular junction ishypertrophied and spreads into the muscle as extra junctional receptors followingdenervation. Sensitivity to depolarizing muscle relaxants such as succinylcholine isdeveloped over a period of several weeks15 and may be increased to 104±105 timesabove normal. In addition, there is a decreased re-entry permeability to potassium indenervated muscle.16 These factors appear to account for the dramatic hyperkalaemiafound clinically. The spread and hypertrophy of cholinergic receptors is ®rst detectableat about 3±4 days after injury and reaches its peak 7±14 days later.12 The duration ofthe hypersensitivity to succinylcholine is not well documented. Smith17 reportedcardiac arrest following D-tubocurarine pre-treatment and succinylcholine given to aquadriplegic patient 6 months after injury. It is generally recommended that succinyl-choline be avoided and not be given until at least 8 months after injury. Nowadays,alternative such as rocuronium give rapid onset muscular relaxation and may be usedto replace succinylcholine in all SCI patients requiring rapid sequence induction ofanaesthesia with tracheal intubation.
Induction agents commonly used include thiopental (2.5±4.0 mg/kg), propofol(2.0±2.5 mg/kg), etomidate (0.3 mg/kg) and ketamine (1±2 mg/kg). Maintenanceagents such as nitrous oxide, halothane, en¯urane, iso¯urane and des¯urane allappear to be satisfactory in controlling blood pressure during surgery or autonomichyperre¯exia. Inhalation agents have the advantage over i.v. agents in that, shouldhypotension occur, they are rapidly excreted through the lungs after reduction of theinspired concentration. Rapid excretion is proportional to blood±gas solubility(des¯urane4 iso¯urane4 en¯urane4 halothane).
Intraoperative monitoring
Cervical SCI patients in spinal shock require specialized monitoring for anaesthesia(Table 2); an arterial line and pulmonary artery catheter are inserted pre-operatively.These enable beat-to-beat determination of intravascular pressures, frequent arterialand mixed venous blood gas sampling and cardiac output determination. In stable,chronically injured patients, arterial and pulmonary artery catheterization is notnormally necessary for elective surgery. Electrocardiogram, end-tidal carbon dioxideand pulse oximetry, urine output by indwelling catheter, and temperature aremonitored during anaesthesia.
Table 2. Intraoperative monitoring and equipment for management of acute spinal cord injury patient inspinal shock.
Electrocardiograph Urinary catheterInvasive arterial blood pressure Airway pressurePulmonary artery catheterization Blood warner±external warmer humidi®erCardiac output computer±temperature Arterial and venous blood gasesEnd-tidal CO2 Somatosensory evoked potentialsPulse oximeter
Reproduced from Mackenzie and Geisler (1997, Albin MS (ed.) Textbook of Neuroanesthesia. New York:McGraw-Hill) with permission.
650 C. F. Mackenzie and F. H. Geisler
Fluid challenge
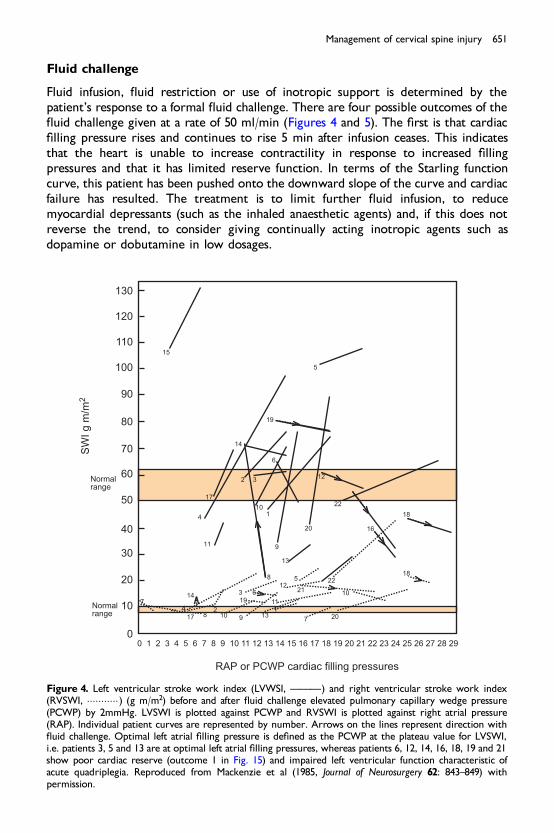
Fluid infusion, ¯uid restriction or use of inotropic support is determined by thepatient's response to a formal ¯uid challenge. There are four possible outcomes of the¯uid challenge given at a rate of 50 ml/min (Figures 4 and 5). The ®rst is that cardiac®lling pressure rises and continues to rise 5 min after infusion ceases. This indicatesthat the heart is unable to increase contractility in response to increased ®llingpressures and that it has limited reserve function. In terms of the Starling functioncurve, this patient has been pushed onto the downward slope of the curve and cardiacfailure has resulted. The treatment is to limit further ¯uid infusion, to reducemyocardial depressants (such as the inhaled anaesthetic agents) and, if this does notreverse the trend, to consider giving continually acting inotropic agents such asdopamine or dobutamine in low dosages.
Figure 4. Left ventricular stroke work index (LVWSI, ÐÐÐ) and right ventricular stroke work index(RVSWI, �����������) (g m/m2) before and after ¯uid challenge elevated pulmonary capillary wedge pressure(PCWP) by 2mmHg. LVSWI is plotted against PCWP and RVSWI is plotted against right atrial pressure(RAP). Individual patient curves are represented by number. Arrows on the lines represent direction with¯uid challenge. Optimal left atrial ®lling pressure is de®ned as the PCWP at the plateau value for LVSWI,i.e. patients 3, 5 and 13 are at optimal left atrial ®lling pressures, whereas patients 6, 12, 14, 16, 18, 19 and 21show poor cardiac reserve (outcome 1 in Fig. 15) and impaired left ventricular function characteristic ofacute quadriplegia. Reproduced from Mackenzie et al (1985, Journal of Neurosurgery 62: 843±849) withpermission.
Management of cervical spine injury 651

The second possible outcome is that wedge pressure rises 3±4 mmHg abovebaseline but falls within 5 min to a level of 2 mmHg above the starting point. Thisresponse is interpreted as indicating that myocardial contractility is adequate for theprevailing vascular tone and increase in cardiac preload. The patient is, therefore,approaching the highest point on the Starling function curve, and any further increasein ®lling pressures will precipitate the situation found in the ®rst outcome. Thetreatment is to increase ¯uids and to maintain cardiac ®lling pressures within thisrange for optimum cardiac function and tissue O2 supply.
The third possible outcome is that cardiac ®lling pressures do not change or theyrise immediately but then fall to the same baseline within 5 min of ceasing ¯uidinfusion. This response indicates that the patient has considerable reserve cardiacfunction and that a greater circulating volume may be tolerated. Therefore, if thispatient is hypotensive or oliguric or has a low mixed venous oxygen partial pressureindicating inadequate tissue oxygen delivery, cardiac output should be increased by¯uid infusion until the response seen in the second outcome is achieved. Inotropicagents, vasoconstrictors and diuretics are not indicated and should be avoided. Rather,the inadequate tissue perfusion, hypotension and oliguria should be reversed byincreasing cardiac output with the infusion.
The fourth outcome from ¯uid challenge is uncommonly seen and results in aninitial lack of change in cardiac ®lling pressures but an increase in systemic arterialpressure and a fall in pulse rate. After infusion of 500 ml or more, cardiac ®llingpressures fall 2±3 mmHg below baseline and on measuring cardiac output this isfound to be increased. The Starling function shifts to the left either as a result ofsystemic vasodilation due to rapid infusion of ¯uids or by slowing of heart rate withresulting improvement in myocardial perfusion and contractility. Further therapeutic
Figure 5. Outcome possibilities in response to ¯uid challenge. Reproduced from Mackenzie et al (1985,Journal of Neurosurgery 62: 843±849) with permission.
652 C. F. Mackenzie and F. H. Geisler
intervention is usually not required because the increased cardiac output improves O2delivery and tissue perfusion.18
Evoked potential monitoring
Somatosensory and cortical evoked potentials provide a non-invasive, objective,sensitive and reproducible method to assess conduction through an SCI. Alteration inwave pattern, amplitude and latency can be used to assess neurological function. Thepossibility of motor injury without sensory evoked response alteration means that insome centres wake-up tests are used to evaluate motor neurological function.However, in cervical spine surgery the head is pinned or immobilized on a head restso that any movement of the patient during such a test could cause cervical vertebralmovement and cord injury. In addition, if the patient is prone there is a potentiallydisastrous risk of extubation. Apart from those risks, including that of emotionaldistress for the patient (although they may be amnesic of such tests), the only bene®t isa single con®rmation that motor function is intact. The wake-up test does not excludethe possibility that subsequent damage from surgical or anaesthetic manoeuvres occursafter anaesthesia is re-induced. As an alternative to the wake-up test, the patient maybe intubated awake and positioned for surgery before repeat evaluation to con®rmlack of change in neurological function. Anaesthesia is then induced. Again this onlyprovides a single point of view to con®rm that tracheal intubation and patientpositioning did not alter motor function.19
SURGICAL THERAPY OF CERVICAL FRACTURES
The ®fth phase includes a potential urgent surgical decompression of mechanicallycompressed neurological elements. Radiological studies will identify elements thatwere not decompressed by the anatomic bony alignment procedure of phase 3. Themajority of these cases are bilateral locked facets that cannot be reduced with traction.Additional cases of anterior disc dislocation in the spinal canal or bone fragments maybe found. Although most surgeons agree that the deteriorating neurological statuswith a mass lesion causing compression requires urgent removal if possible, not allsurgeons agree with the timing of surgery in a patient with a stable neurologicalde®cit.
Timing of surgical intervention
Both the use and the timing of surgical intervention in cervical SCI remain contro-versial because no conclusive scienti®c evidence has been presented for either aspect.Surgical decompression and/or internal stabilization occurs in one-half to three-quarters of all patients in acute hospitalization in North America.20,21 These incidencestudies were both prospective and retrospective.21 In the United Kingdom andAustralia, the non-surgical treatment of acute SCI utilizing postural reduction andprolonged bed rest is the standard, with surgery reserved only for the most extremecases.22,23
A series of non-randomized studies have reported that urgent fracture reduction didnot improve outcome.24,25 However, no randomized, prospective study relative tosurgical timing has been conducted.
Management of cervical spine injury 653
Mechanical stabilization and post-operative complications
Rarely will patients show immediate post-operative improvement. Consequently, pre-operative and post-operative examinations must be performed. If the patient is worsepost-operatively or if the patient deteriorates after operation, diagnostic studies mustbe carried out to pinpoint the aetiology.
Recurrent compression may occur as a result of bony malalignment, haematoma,swelling or delayed abscess formation. Ischaemia can occur with compression oroedema or from reduced circulating blood volume and poor perfusion pressure.Breakdown of the wound can lead to leakage of cerebrospinal ¯uid and, in turn,contribute to wound infection and even meningitis. Certain wounds will requirerevision. Recurrent compression is the greatest fear. Post-operative haematomas,although rare, may cause deterioration over a few hours. Rapid identi®cation of thehaematoma and operative removal are necessary.
POST-OPERATIVE CRITICAL CARE MANAGEMENT
Long-term ventilatory management
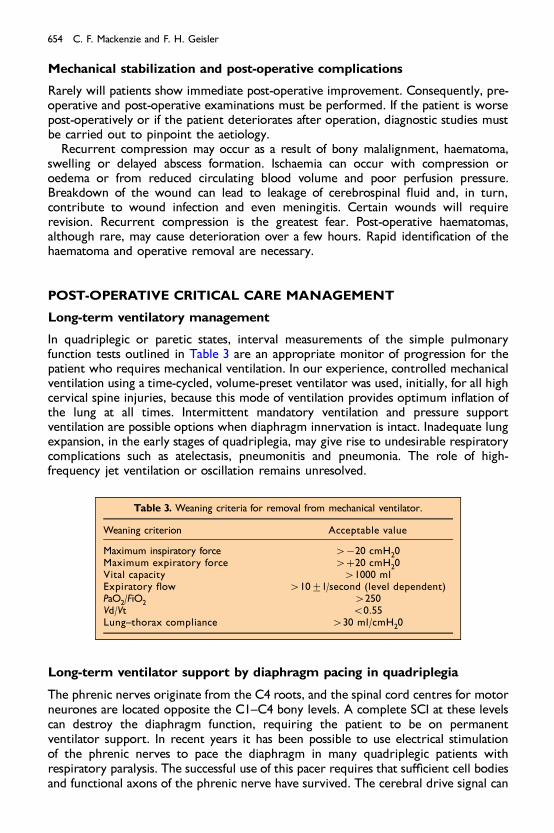
In quadriplegic or paretic states, interval measurements of the simple pulmonaryfunction tests outlined in Table 3 are an appropriate monitor of progression for thepatient who requires mechanical ventilation. In our experience, controlled mechanicalventilation using a time-cycled, volume-preset ventilator was used, initially, for all highcervical spine injuries, because this mode of ventilation provides optimum in¯ation ofthe lung at all times. Intermittent mandatory ventilation and pressure supportventilation are possible options when diaphragm innervation is intact. Inadequate lungexpansion, in the early stages of quadriplegia, may give rise to undesirable respiratorycomplications such as atelectasis, pneumonitis and pneumonia. The role of high-frequency jet ventilation or oscillation remains unresolved.
Long-term ventilator support by diaphragm pacing in quadriplegia
The phrenic nerves originate from the C4 roots, and the spinal cord centres for motorneurones are located opposite the C1±C4 bony levels. A complete SCI at these levelscan destroy the diaphragm function, requiring the patient to be on permanentventilator support. In recent years it has been possible to use electrical stimulationof the phrenic nerves to pace the diaphragm in many quadriplegic patients withrespiratory paralysis. The successful use of this pacer requires that su�cient cell bodiesand functional axons of the phrenic nerve have survived. The cerebral drive signal can
Table 3. Weaning criteria for removal from mechanical ventilator.
Weaning criterion Acceptable value
Maximum inspiratory force 4ÿ20 cmH20Maximum expiratory force 4�20 cmH20Vital capacity 41000 mlExpiratory ¯ow 410+l/second (level dependent)PaO2/FiO2 4250Vd/Vt 50.55Lung±thorax compliance 430 ml/cmH20
654 C. F. Mackenzie and F. H. Geisler

be totally disrupted as it is replaced by the pacing signal. Non-ventilator breathingprovides a tremendous increase in independence and psychological advantage for thepatient. Tibballs26 has reviewed the history of phrenic pacing.
Chest physiotherapy
Both spontaneously breathing and mechanically ventilated patients can bene®t fromprophylactic chest physiotherapy to prevent atelectasis and the development ofpneumonia.9,27 Because the quadriplegic patient has decreased vital capacity, total lungcapacity, expiratory reserve volume and forced expiratory volume in 1 second,pulmonary complications are common.9,28±33 In addition, paralysis of the trunk andextremity muscles makes patients unable to turn themselves and to cough, anddiaphragm function is limited by abdominal muscle and intercostal muscle paralysis.
Glossopharyngeal breathing
Dail34 published the ®rst report of the bene®cial e�ect of glossopharyngeal breathingin a paralysed polio patient. The technique was termed glossopharyngeal breathing orfrog breathing35 because it uses the muscles of the mouth, pharynx and larynx as arespiratory pump to in¯ate the lungs in a similar manner to the respiratory move-ments of the frog and other amphibia. The use of glossopharyngeal breathing isreported in many patients with paralysis following poliomyelitis and in acute quad-riplegia.36±40 The bene®ts include an increase in vital capacity from 11% to 50% ofpredicted normal by use of an average of 20 glossopharyngeal strokes of 80 ml each41
and an increase in duration of breathing without mechanical assistance from 1 min toover 3 hours, on the average. Maximal glossopharyngeal breathing resulted inincreased lung volume and better cough and mucus clearance than unaided breath-ing.35 Lung±thorax compliance and peak expiratory ¯ow were increased by glosso-pharyngeal breathing.37 Glossopharyngeal breathing helps speech by allowing longerphrases to be formed in one large breath.
Glossopharyngeal breathing is a breathing substitute that requires none of theordinary muscles of respiration and no mechanical equipment. It increases vitalcapacity, lung±thorax compliance and expiratory ¯ow and improves cough.35,40
Hyperre¯exic syndromes
Muscle spasms
Following spinal shock, which is an are¯exic state, recovery begins with return of thebulbocavernosus, cremasteric and Babinski re¯exes. As spasticity develops, uncon-trolled hyperre¯exic spasms ofmuscles occur. Thismass re¯ex is probably caused by thehyperactive spinal re¯exes controlling muscle tone. In the quadriplegic patient it isthought that thesemass re¯exes causemuscle contraction bymultiple-level spinal re¯exarcs in response to stimuli below the level of the SCI. Cervical cord transectionfunctionally separates the nuclei in the brain stem and hypothalamus from thethoracolumbar spinal sympathetic out¯ow. This causes spinal re¯ex activity from severalsegments below the level of the lesion with no inhibition by the higher centres.42
Autonomic hyperre¯exia
This is characterized by acute generalized sympathetic activity in response to anendogenous or exogenous stimulus below the level of spinal cord transection.
Management of cervical spine injury 655
Symptoms of autonomic hyperre¯exia include severe headache, sweating, nasalobstruction, desire to vomit and blurring of vision; the person may complain of feeling¯ushed. The signs of autonomic hyperre¯exia are hypertension, bradycardia,dysrhythmias, sweating and goose¯esh. Sweating rarely extends below T10 and ismost marked at the level of the lesion.6 Below the level of transection, sweating ismore likely to be part of the general sympathetic response.43 There is cutaneousvasodilatation above and vasoconstriction below the SCI.44 Normally, hypertensionthat follows peripheral vasoconstriction results in stimulation of the carotid and aorticarch baroreceptors, resulting in vasodilation, bradycardia and a fall in blood pressure.In the quadriplegic patient, because there is loss of inhibition of the spinal re¯ex by thehigher centres, vasodilatation does not occur and the hypertension is not relieved.Additional signs that may occur include changes in skin and rectal temperature,convulsions or loss of consciousness, cessation of respiration, visual ®eld defects andsigns of cerebrovascular accident.6,45±47 In the SCI patient with a lesion above T7,hypertension, resulting from autonomic hyperre¯exia during surgery performedbelow the level of the spinal cord lesion without anaesthesia, occurs in 65±85% ofpatients.48 Hypertension is seen despite compensatory upper extremity vasodilatationand is accompanied by baroreceptor-mediated bradycardia. In high levels of SCI, ifsympathetic innervation of the heart is included in the autonomic e�erent activity,tachycardia can result.
Autonomic hyperre¯exia should be anticipated before it occurs and preparationsshould be made to treat hypertension. If autonomic hyperre¯exia occurs duringsurgery, the precipitating cause should be stopped immediately while therapy isinitiated. Patients at risk for developing autonomic hyperre¯exia are protected fromintraoperative hypertension by either general or spinal anaesthesia. Topicalanaesthesia, sedation or no anaesthesia did not prevent hypertension.48
Regional spinal cord injury centres
Patients with acute SCIs should not be taken to the nearest hospital. Within any state,there should be a designated hospital or hospitals where neurosurgeons and criticalcare physicians are immediately available to treat these injured persons. While it israre, immediate realignment of fracture dislocation has led to functional recovery.A designated centre is essential for these few patients.
There are 35 patients/million per year who will su�er these injuries; any area thathas a population near one million people should, therefore, designate a centre whereexpertise in the resuscitation and treatment of these victims is immediately available.The medical and economic consequences of permanent quadriplegia or paraplegia areso devastating that anything less than an all-out medical e�ort for these victims can nolonger be justi®ed. Evidence con®rms the bene®ts of early admission to an SCI centreincluding reduced hospital length of stay, decreased patient care costs, reductions inassociated complications and less mortality.49±52 As a result of changes in therapy andadmission to regional SCI centres, there has been a signi®cant decrease in theproportion of patients with complete neurological injuries.49,53,54
Acknowledgements
The authors wish to acknowledge the contributions of Alice Eissele, Paul Delaney, Rene e Kahn,Doris Scheihing and Sue Tavitas for their extensive typing, editing and management of thereferences.
656 C. F. Mackenzie and F. H. Geisler
REFERENCES
1. Cowley RA, Hudson F, Scanlan E et al. An economical and proven helicopter program for transportingthe emergency critically ill and injured patient in Maryland. Journal of Trauma 1973; 13: 1029±1038.
2. Dunham M & Cowley RA. Shock Trauma/Critical Care Handbook. Rockville, MD: Aspen PublishingCompany, 1986.
3. Guha A, Tator CH & Rochon J. Spinal cord blood ¯ow and systemic blood pressure after experimentalspinal cord injury in rats. Stroke 1989; 20: 372±377.
* 4. Bracken MB, Shepard MJ, Collins WF et al. A randomized, controlled trial of methylprednisolone ornaloxone in the treatment of acute spinal cord injury. Results of the second National Acute Spinal CordInjury Study. New England Journal of Medicine 1990; 322: 1405±1411.
5. Stover SL & Fine PR. Spinal Cord Injury: The Facts and Figures. Birmingham, AL: National Spinal CordInjury Statistical Center, The University of Alabama at Birmingham, 1986.
* 6. Guttman L. Patterns of re¯ex disturbances. In Guttman L (ed.) Spinal Cord Injuries: ComprehensiveManagement and Research, pp 243±245. London: Blackwell, 1976.
7. Greene NM & Bachaud RG. Vagal components of the chronotropic response to baroreceptorstimulation in man. American Heart Journal 1971; 82: 22±27.
8. Mackenzie CF & Shin B. Cardiac e�ects of atropine in bradycardic quadriplegics during spinal shock.Critical Care Medicine 1981; 9: 150.
* 9. McMichan JC, Michel L & Westbrook PR. Pulmonary dysfunction following traumatic quadriplegia.Journal of the American Medical Association 1980; 243: 528±531.
10. Sellick BA. Cricoid pressure to control regurgitation of stomach contents during induction ofanaesthesia. Lancet 1961; 2: 404±406.
11. Caplan ES & Hoyt NJ. Nosocomial sinusitis. Journal of the American Medical Association 1982; 247:639±641.
12. John DA, Tobey RE, Homer LD et al. Onset of succinylcholine induced hyperkalemia followingdenervation. Anesthesiology 1976; 45: 294±299.
13. Stone WA, Beach TP & Hamelberg W. Succinylcholine ± danger in the spinal cord injured patient.Anesthesiology 1970; 32: 168±169.
*14. Tobey RE, Jacobsen PM, Kahle CT et al. The serum potassium response to muscle relaxants in neuralinjury. Anesthesiology 1972; 37: 332±337.
15. Axelsson J & Thesle� S. A study of supersensitivity in denervated mammalian skeletal muscle. Journal ofPhysiology 1957; 149: 178±193.
16. Harris EJ & Nicholls JG. The e�ect of denervation on the rate of entry of potassium into the frog muscle.Journal of Physiology 1956; 131: 473±476.
17. Smith RB. Hyperkalemia following succinylcholine administration in neurological disorders: a review.Canadian Anaesthesiology Society Journal 1971; 18: 199±201.
*18. Mackenzie CF, Shin B, Kashnaprasad D et al. Assessment of cardiac and respiratory function duringsurgery on patients with acute quadriplegia. Journal of Neurosurgery 1985; 62: 843±849.
19. Schriebman DL & Mackenzie CF. The trauma victim with an acute spinal cord injury. In Shin B &Matjasko J (eds) Problems in Anesthesia, pp 459±476. Hagerstown, MD: Lippincott, 1994.
20. Ahn JH, Ragnarsson KT, GordonWA et al. Current trends in stabilizing high thoracic and thoracolumbarspinal fractures. Archives of Physical Medicine and Rehabilitation 1984; 65: 366±369.
*21. Tator CH, Duncan EG, Edmonds VE et al. Comparison of surgical and conservative management in 208patients with acute spinal cord injury. Canadian Journal of Neurological Science 1987; 14: 60±69.
22. Bedbrook G. Recovery of spinal cord function. Paraplegia 1980; 18: 315±323.23. Guttman L. Disturbances of the bladder and urinary tract. In Guttman L (ed.) Spinal Cord Injuries:
Comprehensive Management and Research, pp 352±367. London: Blackwell, 1976.24. Dall DM. Injuries of the cervical spine. II. Does anatomical reduction of the bony injuries improve the
prognosis for spinal cord recovery? South African Medical Journal 1972; 46: 1083±1090.25. Harris P, Karmi M, McClemont E et al. The prognosis of patients sustaining severe cervical spine injury
(C2±C7 inclusive). Paraplegia 1980; 18: 324±330.26. Tibballs J. Diaphragmatic packing: an alternative to long-term mechanical ventilation. Anesthesiology
Intensive Care 1991; 19: 597±601.27. Mackenzie CF. Clinical usage and chest physiotherapy indications for acute lung pathology. In Mackenzie
CF (ed.) Chest Physiotherapy in the Intensive Care Unit, 2nd edn, pp 53±92. Baltimore, MD: Williams andWilkins, 1989.
*28. Fugl-Meyer AR. E�ects of respiratory muscle paralysis in tetraplegic and paraplegic patients. ScandinavianJournal of Rehabilitative Medicine 1971; 3: 141±150.
Management of cervical spine injury 657
29. Bake B, Fugl-Meyer AR & Grimby G. Breathing patterns and regional ventilation distribution intetraplegic patients and in normal subjects. Clinical Science 1972; 42: 117±128.
30. Bergofsky EH. Mechanisms for respiratory insu�ciency after cervical cord injury. Annals of InternalMedicine 1964; 61: 435±447.
31. Haas A, Lowman EW & Bergofsky EH. Impairment of respiration after spinal cord injury. Archives ofPhysical Medicine and Rehabilitation 1965; 46: 399±405.
32. Odry A, Molho M & Rozin R. Alterations in pulmonary function in spinal cord injured patients.Paraplegia 1975; 13: 101±108.
33. Stone DJ & Keltz H. The e�ect of respiratory muscle dysfunction on pulmonary function. AmericanReview of Respiratory Disorders 1963; 88: 621±629.
34. Dail CW. Glossopharyngeal breathing by paralyzed patients: preliminary report. California Medicine1951; 75: 217.
35. Dail CW, A�eldt JE & Collier CR. Clinical aspects of glossopharyngeal breathing. Journal of the AmericanMedical Association 1955; 158: 445±449.
36. Aidran GM, Kelleher WH & Kemp FH. Cineradiographic studies of glossopharyngeal breathing. Journalof Radiology 1959; 32: 322±328.
37. Feigelson CI, Dickinson DG & Tolner NS. Glossopharyngeal breathing as an aid to the coughingmechanism in the patient with chronic poliomyelitis in a respirator. New England Journal of Medicine1956; 254: 611±613.
38. Kelleher WH & Parida RK. Glossopharyngeal breathing, its value in respiratory muscle paralysis ofpoliomyelitis. British Medical Journal 1957; 2: 740±743.
39. Metcalf VA. Vital capacity and glossopharyngeal breathing in traumatic quadriplegia. Physical Therapy1966; 46: 835±838.
40. Montero JC, Feldman DJ & Montero D. E�ects of glossopharyngeal breathing on respiratory functionafter cervical cord transection. Archives of Physical Medicine and Rehabilitation 1967; 48: 650±653.
41. A�eldt JE, Dail CW & Cother CR. Glossopharyngeal breathing: ventilation studies. Journal of AppliedPhysiology 1955; 18: 111±113.
42. Desmond J. Paraplegia: problems confronting the anaesthesiologist. Canadian Anaesthesiology SocietyJournal 1970; 17: 435±451.
43. List CF & Pimenta AD. Sweat secretion in man: spinal re¯ex sweating. Archives of Neurological Psychology1944; 51: 501±507.
44. Rocco AG & Vandam LD. Problems in anesthesia for paraplegics. Anesthesiology 1959; 20: 348±354.45. Head M & Riddoch G. The autonomic bladder, excessive sweating and some other re¯ex conditions in
gross injuries of the spinal cord. Brain 1917; 40: 188±263.46. Guttman L & Whitteridge D. E�ects of bladder distension on autonomic mechanisms after spinal cord
injuries. Brain 1947; 70: 361±404.47. Kurnick NB. Autonomic hyperre¯exia and its control in patients with spinal cord lesions. Annals of
Internal Medicine 1956; 44: 678±686.*48. Lambert DH, Deane RS & Mazuzan JE. Anesthesia and the control of blood pressure in patients with
spinal cord injury. Anesthesia and Analgesia 1982; 61: 344±348.49. Buchanan LE, Ditunno JF Jr, Osterholm JL et al. Spinal cord injury: a ten-year report. Pennsylvania
Medicine 1990; 93: 36±39.50. Donovan WH & Carter RE. Incidence of medical complications in spinal cord injury: patients in
specialized compared with non specialized centers. Paraplegia 1984; 22: 282±290.51. Oakes DD, Wilmot CB, Hall KM et al. Bene®ts of early admission to a comprehensive trauma center for
patients with spinal cord injury. Archives of Physical Medicine and Rehabilitation 1990; 71: 637±643.52. Tator CH. Acute management of spinal cord injury. British Journal of Surgery 1990; 77: 485±486.*53. Duncan EG, Tator CH, Edmonds VE & Polk HC. Treatment in a specialized unit improves three
measures of outcome after acute spinal cord injury: statistical analysis of 552 cases. Surgical Forum 1987;38: 501±503.
54. Meyers PR & Greesan GT. Management of acute spinal cord injured patients by the mid-west regionalspinal cord injury system. Topics in Acute Care and Trauma Rehabilitation 1987; 1: 1±31.
55. Hayes RL, Galinet BJ, Kulkame P et al. E�ects of naloxone on systemic and cerebral responses toexperimental concussive brain injury in cats. Journal of Neurosurgery 1983; 58: 720±728.
56. Mackenzie CF & Ducker TB. Cervical spinal cord injury. In Matjasko J & Katz J (eds) Clinical Controversiesin Neuroanesthesia and Neurosurgery, pp 77±134. Orlando, FL: Grune and Stratton, 1986.
*57. Mackenzie CF & Geisler FH. Management of acute cervical spinal cord injury. In Albin MS (ed.) Textbookof Neuroanesthesia, chap. 33, pp 1083±1136. New York: McGraw-Hill, 1997.
658 C. F. Mackenzie and F. H. Geisler
Related Documents