Management of adhesive small bowel obstruction: A distinct paradigm shift in the United States Kazuhide Matsushima, MD, Andrew Sabour, BS, Caroline Park, MD, MPH, Aaron Strumwasser, MD, Kenji Inaba, MD, and Demetrios Demetriades, MD, PhD, Los Angeles, California Submitted: September 7, 2018, Revised: November 2, 2018, Accepted: November 9, 2018, Published online: November 28, 2018. From the Division of Acute Care Surgery (K.M., A.S., C.P., A.S., K.I., D.D.), University of Southern California, Los Angeles, California. This study was presented at the 77th Annual Meeting of the American Association for Surgery of Trauma and Clinical Congress of Acute Care Surgery, September 26, 2018, in San Diego, California. Address for reprints: Kazuhide Matsushima, MD, Division of Acute Care Surgery, LAC+USC Medical Center, University of Southern California, 2051 Marengo St, Inpatient Tower (C), C5L100, Los Angeles, CA 90033; email: [email protected]. DOI: 10.1097/TA.0000000000002150 AAST Continuing Medical Education Article Accreditation Statement This activity has been planned and implemented in accordance with the Es- sential Areas and Policies of the Accreditation Council for Continuing Medical Education through the joint providership of the American College of Surgeons and the American Association for the Surgery of Trauma. The American College Surgeons is accredited by the ACCME to provide continuing medical education for physicians. AMA PRA Category 1 Credits ™ The American College of Surgeons designates this journal-based CME activity for a maximum of 1 AMA PRA Category 1 Credit ™. Physicians should claim only the credit commensurate with the extent of their participation in the activity. Of the AMA PRA Category 1 Credit ™ listed above, a maximum of 1 credit meets the requirements for self-assessment. Credits can only be claimed online Objectives After reading the featured articles published in the Journal of Trauma and Acute Care Surgery, participants should be able to demonstrate increased understanding of the material specific to the article. Objectives for each article are featured at the beginning of each article and online. Test questions are at the end of the article, with a critique and specific location in the article referencing the question topic. Claiming Credit To claim credit, please visit the AAST website at http://www.aast.org/ and click on the “e-Learning/MOC” tab. You must read the article, successfully complete the post-test and evaluation. Your CME certificate will be available immediately upon receiving a passing score of 75% or higher on the post-test. Post-tests receiving a score of below 75% will require a retake of the test to receive credit. System Requirements The system requirements are as follows: Adobe® Reader 7.0 or above installed; Internet Explorer® 7 and above; Firefox® 3.0 and above, Chrome® 8.0 and above, or Safari ™ 4.0 and above. Questions If you have any questions, please contact AAST at 800-789-4006. Paper test and evaluations will not be accepted. Disclosure Information In accordance with the ACCME Accreditation Criteria, the American College of Surgeons, as the accredited provider of this journal activity, must ensure that anyone in a position to control the content of J Trauma Acute Care Surg articles selected for CME credit has disclosed all relevant financial relationships with any commercial interest. Disclosure forms are completed by the editorial staff, associate editors, reviewers, and all authors. The ACCME defines a `commercial interest' as “any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients.”“Relevant” financial relationships are those (in any amount) that may create a conflict of interest and occur within the 12’months preceding and during the time that the individual is engaged in writing the article. All reported conflicts are thoroughly managed in order to ensure any potential bias within the content is eliminated. However, if you’perceive a bias within the article, please report the circumstances on the evaluation form. Please note we have advised the authors that it is their responsibility to disclose within the article if they are describing the use of a device, product, or drug that is not FDA approved or the off-label use of an approved device, product, or drug or unapproved usage. Disclosures of Significant Relationships with Relevant Commercial Companies/Organizations by the Editorial Staff Ernest E. Moore, Editor: PI, research support and shared U.S. patents Haemonetics; PI, research support, Instrumentation Laboratory, Inc.; Co-founder, Thrombo Thera- peutics. Associate Editors David Hoyt, Ronald V. Maier and Steven Shackford have nothing to disclose. Editorial staff and Angela Sauaia have nothing to disclose. Author Disclosures The authors have nothing to disclose. Reviewer Disclosures The reviewers have nothing to disclose. Cost For AAST members and Journal of Trauma and Acute Care Surgery subscribers there is no charge to participate in this activity. For those who are not a member or subscriber, the cost for each credit is $25. AAST 2018 PODIUM P APER J Trauma Acute Care Surg Volume 86, Number 3 383 Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
AAST 2018 PODIUM PAPER
Management of adhesive small bowel obstruction: A distinctparadigm shift in the United States
Kazuhide Matsushima, MD, Andrew Sabour, BS, Caroline Park, MD, MPH, Aaron Strumwasser, MD,Kenji Inaba, MD, and Demetrios Demetriades, MD, PhD, Los Angeles, California
Submitted: September 7, 2018, Revised: November 2, 2018, Accepted: November 9, 2018, Published online: November 28, 2018.From the Division of Acute Care Surgery (K.M., A.S., C.P., A.S., K.I., D.D.), University of Southern California, Los Angeles, California.This study was presented at the 77th Annual Meeting of the American Association for Surgery of Trauma and Clinical Congress of Acute Care Surgery, September 26, 2018, in
San Diego, California.Address for reprints: Kazuhide Matsushima, MD, Division of Acute Care Surgery, LAC+USC Medical Center, University of Southern California, 2051 Marengo St, Inpatient
Tower (C), C5L100, Los Angeles, CA 90033; email: [email protected].
DOI: 10.1097/TA.0000000000002150
AAST Continuing Medical Education Article
Accreditation StatementThis activity has been planned and implemented in accordance with the Es-sential Areas and Policies of the Accreditation Council for Continuing MedicalEducation through the joint providership of the American College of Surgeonsand the American Association for the Surgery of Trauma. The AmericanCollege Surgeons is accredited by the ACCME to provide continuing medicaleducation for physicians.
AMA PRA Category 1 Credits™The American College of Surgeons designates this journal-based CME activity fora maximum of 1 AMA PRACategory 1 Credit™. Physicians should claim only the creditcommensurate with the extent of their participation in the activity.
Of the AMA PRACategory 1 Credit™ listed above, a maximum of 1 credit meetsthe requirements for self-assessment.
Credits can only be claimed online
ObjectivesAfter reading the featured articles published in the Journal of Trauma and AcuteCare Surgery, participants should be able to demonstrate increased understandingof the material specific to the article. Objectives for each article are featured atthe beginning of each article and online. Test questions are at the end of the article,with a critique and specific location in the article referencing the question topic.
Claiming CreditTo claim credit, please visit the AAST website at http://www.aast.org/ and click onthe “e-Learning/MOC” tab. You must read the article, successfully complete thepost-test and evaluation. Your CME certificate will be available immediately uponreceiving a passing score of 75% or higher on the post-test. Post-tests receiving a scoreof below 75% will require a retake of the test to receive credit.
System RequirementsThe system requirements are as follows: Adobe® Reader 7.0 or above installed; Internet Explorer® 7 and above; Firefox® 3.0 and above, Chrome® 8.0 and above, or
Safari™ 4.0 and above.
QuestionsIf you have any questions, please contact AAST at 800-789-4006. Paper test and evaluations will not be accepted.
Disclosure InformationIn accordance with the ACCME Accreditation Criteria, the American College of
Surgeons, as the accredited provider of this journal activity, must ensure that anyone
in a position to control the content of J Trauma Acute Care Surg articles selected for
CME credit has disclosed all relevant financial relationships with any commercial
interest. Disclosure forms are completed by the editorial staff, associate editors,
reviewers, and all authors. The ACCME defines a `commercial interest' as “any
entity producing, marketing, re-selling, or distributing health care goods or services
consumed by, or used on, patients.” “Relevant” financial relationships are those (in
any amount) that may create a conflict of interest and occur within the 12’months
preceding and during the time that the individual is engaged in writing the article. All
reported conflicts are thoroughly managed in order to ensure any potential bias
within the content is eliminated. However, if you’perceive a bias within the article,
please report the circumstances on the evaluation form.
Please note we have advised the authors that it is their responsibility to disclose within
the article if they are describing the use of a device, product, or drug that is not FDA
approved or the off-label use of an approved device, product, or drug or unapproved usage.
Disclosures of Significant Relationships withRelevant Commercial Companies/Organizationsby the Editorial StaffErnest E. Moore, Editor: PI, research support and shared U.S. patents Haemonetics;
PI, research support, Instrumentation Laboratory, Inc.; Co-founder, Thrombo Thera-
peutics. Associate Editors David Hoyt, Ronald V. Maier and Steven Shackford have
nothing to disclose. Editorial staff and Angela Sauaia have nothing to disclose.
Author DisclosuresThe authors have nothing to disclose.
Reviewer DisclosuresThe reviewers have nothing to disclose.
CostFor AAST members and Journal of Trauma and Acute Care Surgery subscribersthere is no charge to participate in this activity. For those who are not a memberor subscriber, the cost for each credit is $25.
J Trauma Acute Care SurgVolume 86, Number 3 383
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.

Matsushima et al.J Trauma Acute Care Surg
Volume 86, Number 3
38
BACKGROUND: R
4
ecent studies show that early operative intervention in patients who fail nonoperative management of adhesive small bowel ob-struction (ASBO) is associated with improved outcomes. The purpose of this study was to determine the trend in practice patternand outcomes of patients with ASBO in the United States.
METHODS: D
ata from the National Inpatient Sample data (2003–2013) were extracted for analysis and included patients (age ≥18 years) whowere discharged with primary diagnosis codes consistent with ASBO. We analyzed the data to examine changes in mortality andhospital length of stay in addition to any trends in rate and timing of operative interventions.RESULTS: D
uring the study period, 1,930,289 patients were identified with the diagnosis of ASBO. Over the course of the study period, therate of operative intervention declined (46.10–42.07%, p = 0.003), and the timing between admission and operative interventionwas significantly shortened (3.09–2.49 days, p < 0.001). In addition, in-hospital mortality rate decreased significantly(5.29–3.77%, p < 0.001). In the multiple logistic regression analysis, the relative risk ofmortality decreased by 5.6% per year (oddsratio, 0.944; 95% confidence interval, 0.937–0.951; p < 0.001). Hospital length of stay decreased from 10.39 to 9.06 days(p < 0.001).CONCLUSION: O
ver the last decade, fewer patients with ASBO were managed operatively, whereas those requiring an operation underwent oneearlier in their hospitalization. Although further studies are warranted, our results suggest that recent changes in practice patternmay have contributed to improved outcomes. (J Trauma Acute Care Surg. 2019;86: 383–391. Copyright © 2018 American Associ-ation for the Surgery of Trauma.)LEVEL OF EVIDENCE: T
herapeutic study, level IV. KEYWORDS: A dhesive small bowel obstruction; management; outcome; trends.A dhesive small bowel obstruction (ASBO) continues to beone of the most common emergency surgical conditions
in the United States and other developed countries. Disease bur-den and respective operative costs remain elevated in recentreports.1–3 While the majority of patients with ASBO can bemanaged nonoperatively, delays in surgical management duringcases of strangulation or complete obstruction are significantlyassociated with increased mortality and major complications.4,5
Therefore, multiple attempts have been made in previous pro-spective and retrospective studies to propose models that can re-liably predict the need for an emergent operation for ASBO.6–8
Nonetheless, the basic tenets of managing the patient withASBO have not changed for decades and include bowel rest, de-compression of the stomach, and rehydration with intravenousfluids while monitoring for signs of peritonitis, strangulation,or bowel ischemia.9 Nonetheless, in instances of complicatedclinical presentations, efforts toward further clarifying the deci-sion between operative and nonoperativemanagement are critical.
With recent advances in resolution, speed, and availability,the use of computed tomography (CT) is currently recommendedin patients with suspected ASBO.10 In addition to its diagnosticability, a combination of specific CT findings associated withstrangulation and clinical signs can be used to predict which pa-tient may require an emergent operation.7,8,11–13 Conversely, pa-tients without clinical and radiographic signs of strangulation/bowel ischemia may follow a separate path toward nonoperativemanagement; in these patients, the diagnostic and potentially ther-apeutic use of water-soluble contrast followed by serial abdominalradiographs has been proposed.14–16 The results from a recentmulticenter study suggest that the management of ASBO usingwater-soluble contrast is significantly associated with a lower rateof operative intervention and shorter hospital length of stay(HLOS) compared with conventional management.17 Thus, anincreasing number of institutions have developed and imple-mented a protocol for the management of ASBO adopting aninitial clinical evaluation with CT and subsequent water-solublecontrast challenge.18,19
To date, scarce data exist regarding the nationwide trendin the management of ASBO and patient outcomes. The purpose
Copyright © 2019 Wolters Kluwer H
of this study was to examine whether there are any recentchanges in practice patterns and patient outcomes of patientswith ASBO in the United States. We hypothesized that therewould be significant trends toward less frequent but early operativeinterventions over the last decade. In addition, we hypothesizedthat we would observe significant trends toward improved pa-tient outcomes.
PATIENTS AND METHODS
Study Design and Patient SelectionThis is a population-based, retrospective cohort study
using the National Inpatient Sample (NIS), a nationwide hospitaldischarge database organized under the federal Healthcare Costand Utilization Project. First started in 1988, the NIS continuesto release updates on an annual basis, capturing 20% of the ap-proximately 37 million annual nationwide discharges. Each up-date reports information regarding patient demographics,preexisting conditions, hospital demographics, and identified pa-tient diagnostic and procedural codes. Diagnostic and procedurecodes for each patient are provided using the InternationalClassification of Diseases, Ninth Edition, Clinical Modifica-tion (ICD-9-CM). National discharge estimates are determinedthrough sampling weights provided by the NIS database. Theweighting algorithm provides reliable estimates for nationalvolumes of a given diagnosis or procedure and updates regu-larly through every database redesign-iteration.20,21 All aspectsof this study including use of the NIS database have been ap-proved by the Institutional Review Board of the University ofSouthern California.
The NIS covers all patients, regardless of insurance status,and provides a large sample size including rare diagnoses, un-common procedures, and unique patient populations. For thisstudy, data from 2003 to 2013were compiled and retrospectivelyreviewed. Patients younger than 18 years of age were excludedusing data filters. The ICD-9-CM diagnostic codes 560.81 and560.89were used to select the subset of patients with a dischargediagnosis of ASBO. Patients within this filtered group were cat-egorized in the surgery group if they possessed an ICD-9-CM
© 2018 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.

Figure 1. Patient selection diagram.
J Trauma Acute Care SurgVolume 86, Number 3 Matsushima et al.
procedural code of either 54.11, 54.19, 54.51, 54.59, 45.61,45.62, 45.63, 45.90, or 45.91. Patients in the Surgery groupwith an ICD-9-CM procedural code of either 45.61, 45.62,45.63, 45.90, or 45.91 were further subcategorized to havinga procedure for bowel resection. Patients who fulfilled thediagnostic inclusion criteria but possessed neither of the sur-gically labeled procedural codes were categorized in the nosurgery group.
Statistical AnalysisThe counts of inpatient discharge were weighted using
sampling weights provided by the NIS database to generatea reliable estimate of nationwide discharges for patients withASBO. A Charlson comorbidity index was calculated based onICD-9-CM diagnostic codes provided by Quan et al.22 Univari-ate analysis comparing patient demographics, preexisting condi-tions, patient demographics, and hospital variables between theoperative and nonoperative group was performed. For continuousor discrete variables, a Student t test was used. For categorical var-iables, a Fisher exact test or χ2 analysis was used as appropriate.Trends in practice pattern and outcomes over time were analyzedusing a linear regression, and a p value was calculated from theslope of the line of best fit. Clinically significant patient- and hos-pital-level covariates (age, sex, Charlson comorbidity index, pri-mary payment methods, year of admission, hospital teachingstatus, hospital bed size, hospital region) were included and ad-justed for in a logistic regression model for multivariable analysis.A p value of <0.05 was considered significant. All statistical anal-yses were calculated using STATA 13.0 (StataCorp LP, CollegeStation, X).
RESULTS
Patient and Hospital CharacteristicsFrom 2003 to 2013, a total of 1,930,289 patients were
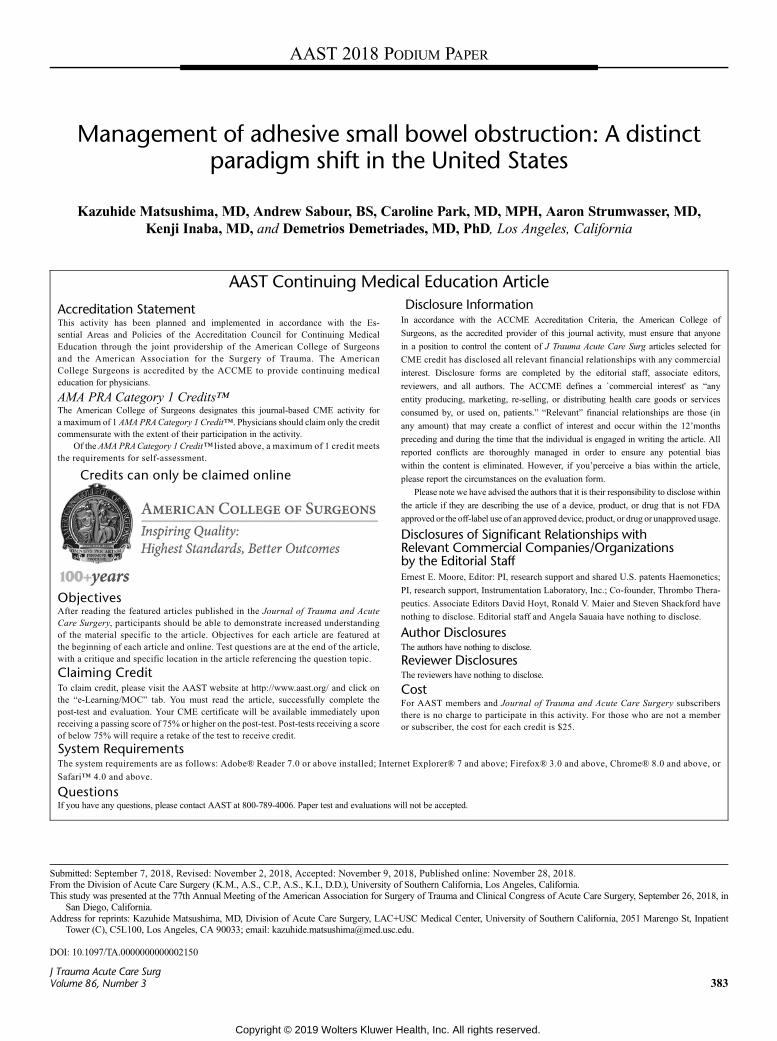
found to fit our inclusion and exclusion criteria (Fig. 1). Ofthose, 863,465 patients (44.73%) underwent surgical proceduresfor ASBO. Patient baseline demographics in the operative groupand nonoperative group were compared in Table 1. Patients whoreceived surgical management were found to be significantlyyounger (62.97 vs. 63.94 years, p < 0.001) and predominantlyfemale (61.99% vs. 57.31%, p < 0.001). Preexisting conditionssuch as congestive heart failure, obesity, and fluid and electro-lytes disorders were found more common in patients with surgi-cal management. In contrast, patients with other preexistingconditions including liver disease, metastatic cancer, and otherneurological disorders were more common in the nonoperativegroup; however, univariate analysis of total preexisting conditionsrevealed no statistical significance (2.37 vs. 2.35, p = 0.891). Hos-pital characteristics such as large bed size (62.62% vs. 61.59%,p < 0.001), nonteaching status (56.11% vs. 55.33%, p < 0.001),and urban locations (87.25% vs. 86.89%, p = 0.002) were alsofound to be significantly increased in patients receiving surgi-cal management.
Rate and Timing of Surgical Interventionsfor ASBO
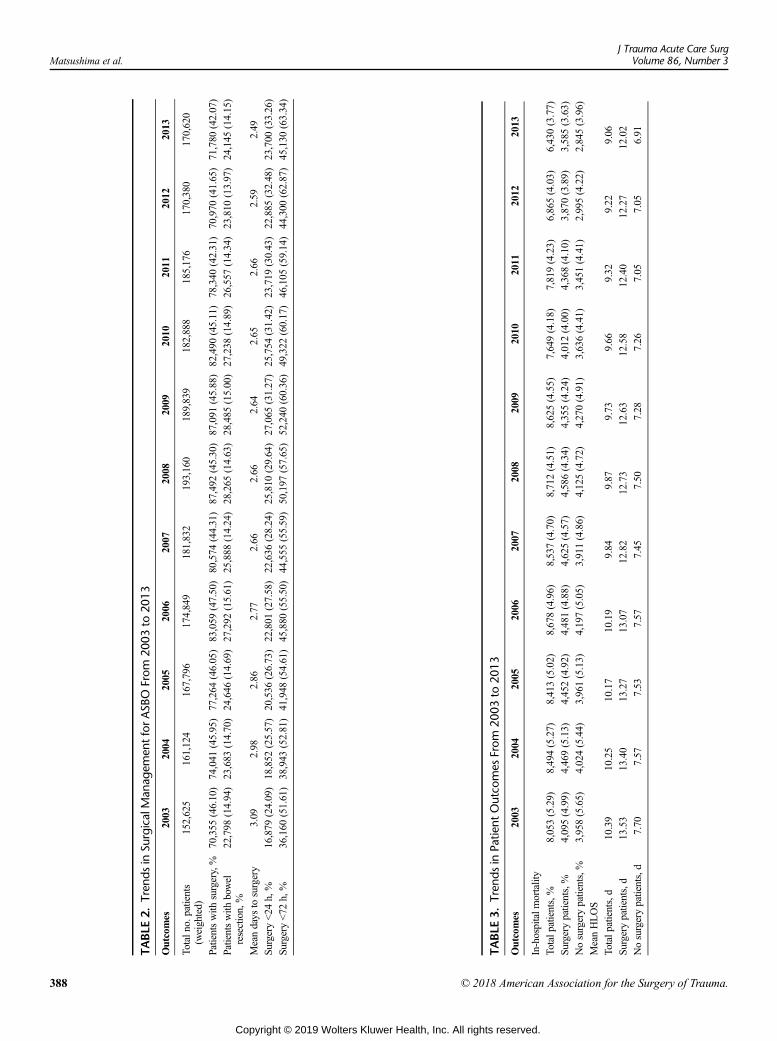
Table 2 demonstrates the rate and timing (days from hos-pital admission) of surgical interventions for ASBO in each year.
© 2018 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
The number of patients who underwent surgical interventionsdecreased from 46.10% in 2003 to 42.07% in 2013. Using logis-tic regression, each 1-year increase was significantly associatedwith a 1.1% decrease in the rate of surgical intervention (odds ra-tio [OR], 0.989; 95% confidence interval [CI], 0.986–0.992;p < 0.001). In the patients who underwent surgical interventions,the average days from admission to operation shortened from3.09 days to 2.49 days (p < 0.001). Out of all patients whounderwent surgical intervention, the rate of immediate sur-gery, defined as surgery within 24 hours of admission, in-creased from 24.09% in 2003 to 33.26% in 2013. Surgerywithin 24 and 72 hours of admission each also saw a signifi-cant steady 1-year increase (OR, 1.032 per year; 95% CI:1.027–1.038, p < 0.001 and OR, 1.026 per year; 95% CI,1.022–1.031; p < 0.001). In contrast, the rate of operative inter-vention leading to bowel resection was found to have a signifi-cant decrease in prevalence every year (OR, 0.995 per year;95% CI, 0.991–0.999; p = 0.023).
Patient OutcomesIn-hospital mortality rate and average HLOS in each year
are shown in Table 3. Overall, the rate of in-hospital mortalitydecreased from 5.29% in 2003 to 3.77% in 2013. Over the studyperiod, patients were found to have a 5.6% yearly decrease inin-hospital mortality rate (OR, 0.944 per year; 95% CI,0.937–0.951; p < 0.001). Similarly in both operative and non-operative subgroups, each increase in year brought lowersrates of in-hospital mortality (OR, 0.944 per year; 95% CI,0.935–0.954; p < 0.001 and OR, 0.948 per year; 95% CI,0.939–0.957; p < 0.001). The average HLOS decreased from10.39 to 9.06 days (p < 0.001). Patients in the operative groupwere found to have increased lengths of stay compared withthe nonoperative group (7.34 vs. 12.80 days, p < 0.001). How-ever, patients with and without surgical interventions overall
385
ealth, Inc. All rights reserved.
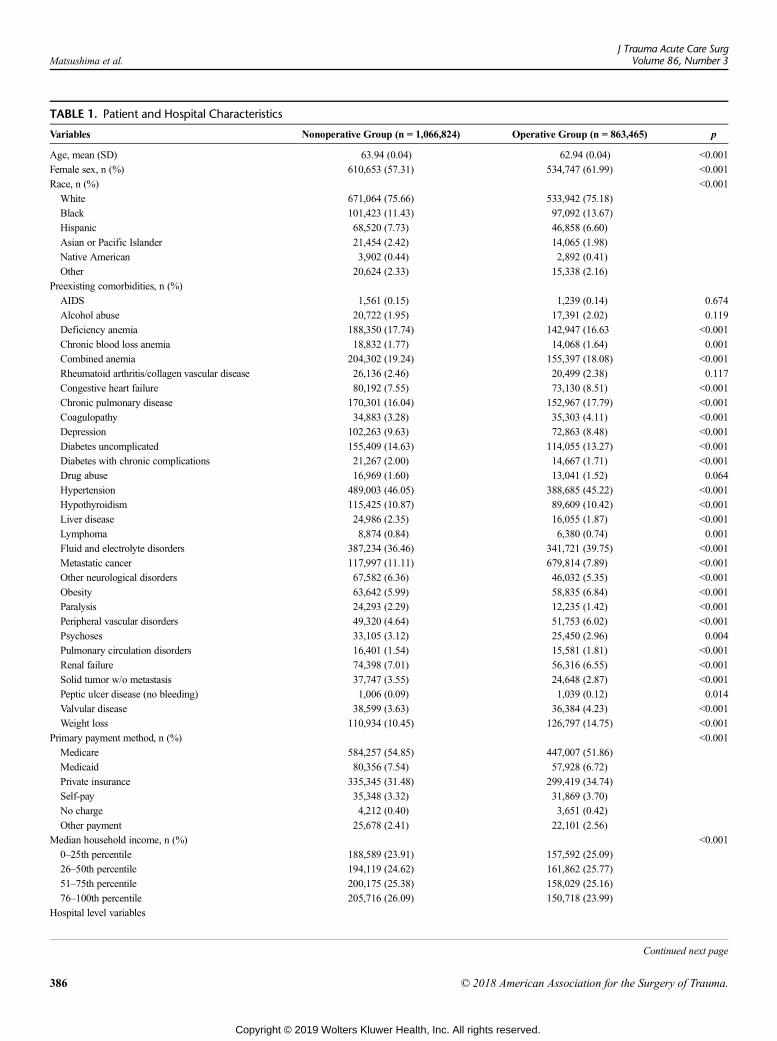
TABLE 1. Patient and Hospital Characteristics
Variables Nonoperative Group (n = 1,066,824) Operative Group (n = 863,465) p
Age, mean (SD) 63.94 (0.04) 62.94 (0.04) <0.001
Female sex, n (%) 610,653 (57.31) 534,747 (61.99) <0.001
Race, n (%) <0.001
White 671,064 (75.66) 533,942 (75.18)
Black 101,423 (11.43) 97,092 (13.67)
Hispanic 68,520 (7.73) 46,858 (6.60)
Asian or Pacific Islander 21,454 (2.42) 14,065 (1.98)
Native American 3,902 (0.44) 2,892 (0.41)
Other 20,624 (2.33) 15,338 (2.16)
Preexisting comorbidities, n (%)
AIDS 1,561 (0.15) 1,239 (0.14) 0.674
Alcohol abuse 20,722 (1.95) 17,391 (2.02) 0.119
Deficiency anemia 188,350 (17.74) 142,947 (16.63 <0.001
Chronic blood loss anemia 18,832 (1.77) 14,068 (1.64) 0.001
Combined anemia 204,302 (19.24) 155,397 (18.08) <0.001
Rheumatoid arthritis/collagen vascular disease 26,136 (2.46) 20,499 (2.38) 0.117
Congestive heart failure 80,192 (7.55) 73,130 (8.51) <0.001
Chronic pulmonary disease 170,301 (16.04) 152,967 (17.79) <0.001
Coagulopathy 34,883 (3.28) 35,303 (4.11) <0.001
Depression 102,263 (9.63) 72,863 (8.48) <0.001
Diabetes uncomplicated 155,409 (14.63) 114,055 (13.27) <0.001
Diabetes with chronic complications 21,267 (2.00) 14,667 (1.71) <0.001
Drug abuse 16,969 (1.60) 13,041 (1.52) 0.064
Hypertension 489,003 (46.05) 388,685 (45.22) <0.001
Hypothyroidism 115,425 (10.87) 89,609 (10.42) <0.001
Liver disease 24,986 (2.35) 16,055 (1.87) <0.001
Lymphoma 8,874 (0.84) 6,380 (0.74) 0.001
Fluid and electrolyte disorders 387,234 (36.46) 341,721 (39.75) <0.001
Metastatic cancer 117,997 (11.11) 679,814 (7.89) <0.001
Other neurological disorders 67,582 (6.36) 46,032 (5.35) <0.001
Obesity 63,642 (5.99) 58,835 (6.84) <0.001
Paralysis 24,293 (2.29) 12,235 (1.42) <0.001
Peripheral vascular disorders 49,320 (4.64) 51,753 (6.02) <0.001
Psychoses 33,105 (3.12) 25,450 (2.96) 0.004
Pulmonary circulation disorders 16,401 (1.54) 15,581 (1.81) <0.001
Renal failure 74,398 (7.01) 56,316 (6.55) <0.001
Solid tumor w/o metastasis 37,747 (3.55) 24,648 (2.87) <0.001
Peptic ulcer disease (no bleeding) 1,006 (0.09) 1,039 (0.12) 0.014
Valvular disease 38,599 (3.63) 36,384 (4.23) <0.001
Weight loss 110,934 (10.45) 126,797 (14.75) <0.001
Primary payment method, n (%) <0.001
Medicare 584,257 (54.85) 447,007 (51.86)
Medicaid 80,356 (7.54) 57,928 (6.72)
Private insurance 335,345 (31.48) 299,419 (34.74)
Self-pay 35,348 (3.32) 31,869 (3.70)
No charge 4,212 (0.40) 3,651 (0.42)
Other payment 25,678 (2.41) 22,101 (2.56)
Median household income, n (%) <0.001
0–25th percentile 188,589 (23.91) 157,592 (25.09)
26–50th percentile 194,119 (24.62) 161,862 (25.77)
51–75th percentile 200,175 (25.38) 158,029 (25.16)
76–100th percentile 205,716 (26.09) 150,718 (23.99)
Hospital level variables
Continued next page
Matsushima et al.J Trauma Acute Care Surg
Volume 86, Number 3
386 © 2018 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
TABLE 1. (Continued)
Variables Nonoperative Group (n = 1,066,824) Operative Group (n = 863,465) p
Bed size of hospital, n (%) <0.001
Small 139,078 (13.09) 104,969 (12.22)
Medium 269,052 (25.32) 216,255 (25.17)
Large 654,521 (61.59) 538,078 (62.62)
Hospital location setting, n (%) 0.002
Rural 113,315 (13.11) 91,375 (12.75)
Urban 751,086 (86.89) 625,178 (87.25)
Region of hospital, n (%) <0.001
Northeast 240,972 (22.59) 164,286 (19.03)
Midwest 242,117 (22.70) 205,175 (23.76)
South 363,742 (34.10) 322,085 (37.30)
West 219,993 (20.62) 171,920 (19.91)
Teaching status of hospital, n (%) <0.001
Nonteaching 478,265 (55.33) 402,037 (56.11)
Teaching 386,136 (44.67) 314,516 (43.89)
AIDS, acquired immune deficiency syndrome.
J Trauma Acute Care SurgVolume 86, Number 3 Matsushima et al.
stayed fewer days in the hospital during the course of thestudy period.
DISCUSSION
In this study using a large national database, we reportedseveral important findings to suggest significant trends in themanagement of ASBO and patient outcomes. While patientsless frequently undergo operative interventions for ASBO, thetiming of operation has shifted earlier in their hospital stay. Ap-proximately one third of operative interventions were performedwithin 24 hours after the admission, increased from one quarterin previous years. The in-hospital mortality in ASBO patientswith and without operative intervention significantly decreasedover the study period. Similarly, the length of hospital stay trendeddown regardless of operative intervention. To our knowledge, thisis one of the largest studies in the modern era to report the con-temporary management of ASBO and patient outcomes.
One of the most significant findings we observed in thisstudy was the trend toward earlier operation for ASBO. A long-standing dilemma surgeons have faced for centuries is on themanagement of ASBO, particularly (1) whether to operateand (2) when to operate. In the past, a mandatory surgical inter-vention was considered as the mainstay of treatment for ASBO.This practice pattern is well-represented in the motto, “Neverlet the sun rise or set on a small bowel obstruction.” However,it has been recently reported that up to 70% of patients withSBO were managed nonoperatively at 13 hospitals acrossNorth America, all of which participated in the American Col-lege of Surgeons National Surgical Quality Improvement Pro-gram.23 On the other hand, a failure to identify the patientwith strangulated ASBO and subsequent bowel ischemia is as-sociated with the significant delay in surgical interventions. Inthese cases, the mortality rate was reported to be as high as 40%in previous literature.24
The ultimate goal in the management of ASBO is to iden-tify patients who require an operation and then operate early in
© 2018 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
their hospital stay. Any delay in surgical intervention, even morethan 24 hours after admission, is significantly associated withhigher mortality and complication rate.4 Multiple studies fromthe 20th century have challenged to create the best model to pre-dict the need for surgical interventions using clinical and labora-tory variables without success.25 In many cases, the experiencedsurgeon's gestalt may not be sufficiently accurate or reliable. Inthe last decade, an increased number of studies have focusedon the utility of CT features in addition to clinical symptomsand signs to achieve the aforementioned goals in the manage-ment of ASBO.6–9,11,26 Zielinski et al.6,7 created a predictionmodel including clinical and CT signs in a retrospective study,then conducted a prospective study to validate their model. Theyfound that 86% of patients with all three variables including clin-ical symptoms and CT features (obstipation, lack of small bowelfeces sign, and mesenteric edema) required surgical exploration,with 29% of these explorations demonstrating strangulation.Another recent (2011–2013) prospective observational studyfrom three US trauma centers also identified one clinical symp-tom (no flatus) and two CT findings (free fluid, high-grade ob-struction) were identified as significant predictors for earlyoperation in ASBO patients who underwent a trial of nonopera-tive management.11 With the presence of these three variablesbeing positive, 56% of patients required an early operation. Ofnote, the median days from admission to operation among threeparticipating centers was 1.5 days. Furthermore, the medianlength of stay in patients successfully managed nonoperativelywas 2 days.
There are an increasing number of institutions where theuse of water-soluble contrast in a trial of nonoperative manage-ment of ASBO is standard practice. In a recent multi-institutionalstudy of water-soluble contrast for ASBO, 11 (79%) of 14 partic-ipating institutions had previously implemented the water-solublecontrast challenge for the management of ASBO. There was alsoa significantly lower rate of operative exploration in the water-soluble contrast group (20.8% vs. 49.0%, p < 0.0001) and a sig-nificant trend toward lower operative rate, the latter of which
387
ealth, Inc. All rights reserved.
TABLE
2.Tren
dsin
SurgicalMan
agem
entforASB
OFrom
2003
to20
13
Outcomes
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Totaln
o.patients
(weighted)
152,625
161,124
167,796
174,849
181,832
193,160
189,839
182,888
185,176
170,380
170,620
Patientswith
surgery,%
70,355
(46.10)
74,041
(45.95)
77,264
(46.05)
83,059
(47.50)
80,574
(44.31)
87,492
(45.30)
87,091
(45.88)
82,490
(45.11)
78,340
(42.31)
70,970
(41.65)
71,780
(42.07)
Patientswith
bowel
resection,%
22,798
(14.94)
23,683
(14.70)
24,646
(14.69)
27,292
(15.61)
25,888
(14.24)
28,265
(14.63)
28,485
(15.00)
27,238
(14.89)
26,557
(14.34)
23,810
(13.97)
24,145
(14.15)
Meandays
tosurgery
3.09
2.98
2.86
2.77
2.66
2.66
2.64
2.65
2.66
2.59
2.49
Surgery<24
h,%
16,879
(24.09)
18,852
(25.57)
20,536
(26.73)
22,801
(27.58)
22,636
(28.24)
25,810
(29.64)
27,065
(31.27)
25,754
(31.42)
23,719
(30.43)
22,885
(32.48)
23,700
(33.26)
Surgery<72
h,%
36,160
(51.61)
38,943
(52.81)
41,948
(54.61)
45,880
(55.50)
44,555
(55.59)
50,197
(57.65)
52,240
(60.36)
49,322
(60.17)
46,105
(59.14)
44,300
(62.87)
45,130
(63.34)
TABLE
3.Tren
dsin
Patie
ntOutco
mes
From
2003
to20
13
Outcomes
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
In-hospitalm
ortality
Totalp
atients,%
8,053(5.29)
8,494(5.27)
8,413(5.02)
8,678(4.96)
8,537(4.70)
8,712(4.51)
8,625(4.55)
7,649(4.18)
7,819(4.23)
6,865(4.03)
6,430(3.77)
Surgerypatients,%
4,095(4.99)
4,469(5.13)
4,452(4.92)
4,481(4.88)
4,625(4.57)
4,586(4.34)
4,355(4.24)
4,012(4.00)
4,368(4.10)
3,870(3.89)
3,585(3.63)
Nosurgerypatients,%
3,958(5.65)
4,024(5.44)
3,961(5.13)
4,197(5.05)
3,911(4.86)
4,125(4.72)
4,270(4.91)
3,636(4.41)
3,451(4.41)
2,995(4.22)
2,845(3.96)
MeanHLOS
Totalp
atients,d
10.39
10.25
10.17
10.19
9.84
9.87
9.73
9.66
9.32
9.22
9.06
Surgerypatients,d
13.53
13.40
13.27
13.07
12.82
12.73
12.63
12.58
12.40
12.27
12.02
Nosurgerypatients,d
7.70
7.57
7.53
7.57
7.45
7.50
7.28
7.26
7.05
7.05
6.91
Matsushima et al.J Trauma Acute Care Surg
Volume 86, Number 3
388 © 2018 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Matsushima et al.
may be contributed by an increase in the administration ofwater-soluble contrast.17 This algorithm includes administra-tion of water-soluble contrast via nasogastric tube, and thenserial abdominal radiographs are taken every 4 to 6 hours.The indication for surgical intervention is usually defined asa failure to pass contrast to the ascending colon within 8 to24 hours.15 The benefits of this protocol are twofold: serialradiographs follow the passage of contrast and can help diag-nose whether the patient has a complete obstruction in an ob-jective fashion. The second potential benefit is therapeuticfrom the contrast's high osmolarity that facilitates decreasein edema of the small intestine and help relieve intraluminalpressure. While this protocol helps guide the surgeon, the mostimportant decision is to determine, within 24 to 48 hours,whether to a patient with ABSO requires an operation.
To date, little has been described about recent changes inthe practice patterns and patient outcomes for ASBO inpopulation-based studies. Our study clearly demonstratesan improved survival of patients with ASBO in the UnitedStates over the last decade. In the United Kingdom, Peacocket al27 reported the data from the National Emergency Laparot-omy Audit, a nationwide surgical quality improvement programdatabase in England and Wales. Between December 2013 andNovember 2015, 31.3% of emergency laparotomies with eitheradhesiolysis or bowel resection for SBO were performed lessthan 24 hours after admission. The overall 30-day mortalitywas 7.2% in their cohort. Behman et al.28 conducted a retrospec-tive population-based study using a Canadian administrative da-tabase to evaluate the trends in the management of ASBO from2005 to 2014. While their study also showed a significant in-crease in the proportion of patients who underwent surgerywithin 1 day, the proportion of patients who underwent surgeryoverall increased significantly.
There are several limitations to our study. First, the NISdatabase is an administrative database, thus not structured forthe use in research. Although the database includes a large num-ber of patients discharged from the US hospitals, limited clinicaldata are available to be adjusted in the multivariable analysis.There are several important factors associated with patient out-comes in ASBO, including previous history of abdominal sur-geries, previous admissions for ASBO, severity grades, andprimary admitting service (surgery vs. others).29,30 For that rea-son, this study focused on describing the trends in practice pat-tern and patient outcomes.31 Furthermore, we determined toinclude ASBO patients between 2003 and 2013, as we believethat water-soluble contrast have been more commonly used forASBO in the United States since the early 2000s, although thisperiod can be arbitrary.14,15,32 Second, we were unable to eval-uate the impact of laparoscopic procedures. The utility of lapa-roscopic procedure for ASBO remains controversial.33,34 Webelieve that the NIS database is not suitable to perform theanalysis to compare patient outcomes between different treat-ment options because of limitations of the database. Third, sig-nificant trends observed in our study may not apply to eachsurgeon- and hospital-level across the country. Significant dis-parities in the practice pattern and outcome may still exist inASBO.35 Finally, we would like to emphasize that the resultsof this study should not interpreted as if the change in practicepatterns have improved the outcome of patients with ASBO.
© 2018 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
There are several factors, including recent advances in initialresuscitation, medical optimization of patients with comorbidi-ties, and postoperative care in the intensive care unit, all of whichmay have contributed to these improved patient outcomes.
CONCLUSIONS
The results of this study suggest that there has been a sig-nificant paradigm shift in the management of ASBO from 2003to 2013. We observed an overall decrease in the number of pa-tients who underwent an operative intervention but a shift tointervention earlier during hospitalization. At the same time,in-hospital mortality and HLOS have significantly improved.Further studies are warranted whether recent changes in practicepattern are associated with improved patient outcomes.
DISCLOSURE
The authors declare no conflicts of interest.
AUTHORSHIP
Corresponding author: Matsushima; study concept, design: Matsushima,Sabour, Park, Strumwasser, Inaba, Demetriades; data collection and anal-ysis: Matsushima, Sabour, Park; writing: Matsushima, Sabour; critical revi-sion: Park, Strumwasser, Inaba, Demetriades.
REFERENCES1. Scott JW, Olufajo OA, Brat GA, Rose JA, Zogg CK, Haider AH, Salim A,
Havens JM. Use of national burden to define operative emergency generalsurgery. JAMA Surg. 2016;151(6):e160480.
2. Menzies D, Ellis H. Intestinal obstruction from adhesions—how big is theproblem? Ann R Coll Surg Engl. 1990;72:60–63.
3. Ray NF, Denton WG, Thamer M, Henderson SC, Perry S. Abdominaladhesiolysis: inpatient care and expenditures in the United States in 1994.J Am Coll Surg. 1998;186:1–9.
4. Teixeira PG, Karamanos E, Talving P, Inaba K, Lam L, Demetriades D. Earlyoperation is associated with a survival benefit for patients with adhesivebowel obstruction. Ann Surg. 2013;258:459–465.
5. Keenan JE, Turley RS, McCoy CC, Migaly J, Shapiro ML, Scarborough JE.Trials of nonoperative management exceeding 3 days are associated withincreased morbidity in patients undergoing surgery for uncomplicatedadhesive small bowel obstruction. J Trauma Acute Care Surg. 2014;76:1367–1372.
6. Zielinski MD, Eiken PW, Bannon MP, Heller SF, Lohse CM, Huebner M,Sarr MG. Small bowel obstruction—who needs an operation? Amultivariateprediction model. World J Surg. 2010;34:910–919.
7. Zielinski MD, Eiken PW, Heller SF, Lohse CM, Huebner M, Sarr MG,Bannon MP. Prospective, observational validation of a multivariate small-bowel obstruction model to predict the need for operative intervention.J Am Coll Surg. 2011;212:1068–1076.
8. Jancelewicz T, Vu LT, Shawo AE, Yeh B, Gasper WJ, Harris HW. Predictingstrangulated small bowel obstruction: an old problem revisited. J GastrointestSurg. 2009;13:93–99.
9. Diaz JJ Jr., Bokhari F, Mowery NT, Acosta JA, Block EF, Bromberg WJ,Collier BR, Cullinane DC, Dwyer KM, Griffen MM, et al. Guidelines formanagement of small bowel obstruction. J Trauma. 2008;64:1651–1664.
10. Ten Broek RPG, Krielen P, Di Saverio S, Coccolini F, Biffl WL, Ansaloni L,Velmahos GC, Sartelli M, Fraga GP, Kelly MD, et al. Bologna guidelines fordiagnosis and management of adhesive small bowel obstruction (ASBO):2017 update of the evidence-based guidelines from the world society ofemergency surgery ASBOworking group.World J Emerg Surg. 2018;13:24.
11. Kulvatunyou N, Pandit V, Moutamn S, Inaba K, Chouliaras K, DeMoya M,Naraghi L, Kalb B, Arif H, Sravanthi R, et al. A multi-institution prospectiveobservational study of small bowel obstruction: clinical and computerized to-mography predictors of which patients may require early surgery. J TraumaAcute Care Surg. 2015;79:393–398.
389
ealth, Inc. All rights reserved.
Matsushima et al.J Trauma Acute Care Surg
Volume 86, Number 3
12. Millet I, Boutot D, Faget C, Pages-Bouic E, Molinari N, Zins M, Taourel P.Assessment of strangulation in adhesive small bowel obstruction on the basisof combined CT findings: implications for clinical care. Radiology. 2017;285:798–808.
13. Scrima A, Lubner MG, King S, Pankratz J, Kennedy G, Pickhardt PJ. ValueofMDCTand clinical and laboratory data for predicting the need for surgicalintervention in suspected small-bowel obstruction. AJR Am J Roentgenol.2017;208:785–793.
14. Biondo S, Parés D, Mora L, Martí Ragué J, Kreisler E, Jaurrieta E. Random-ized clinical study of Gastrografin administration in patients with adhesivesmall bowel obstruction. Br J Surg. 2003;90:542–546.
15. Branco BC, Barmparas G, Schnüriger B, Inaba K, Chan LS, Demetriades D.Systematic review andmeta-analysis of the diagnostic and therapeutic role ofwater-soluble contrast agent in adhesive small bowel obstruction. Br J Surg.2010;97:470–478.
16. Mori H, Kaneoka Y,MaedaA, TakayamaY, Takahashi T, Onoe S, Fukami Y.Determination of therapeutic strategy for adhesive small bowel obstructionusing water-soluble contrast agents: an audit of 776 cases in a single center.Surgery. 2017;162:139–146.
17. Zielinski MD, Haddad NN, Cullinane DC, Inaba K, Yeh DD, Wydo S,Turay D, Pakula A, Duane TM, Watras J, et al. Multi-institutional, prospec-tive, observational study comparing the Gastrografin challenge versus stan-dard treatment in adhesive small bowel obstruction. J Trauma Acute CareSurg. 2017;83:47–54.
18. Loftus T, Moore F, VanZant E, Bala T, Brakenridge S, Croft C, Lottenberg L,Richards W, Mozingo D, Atteberry L, et al. A protocol for the managementof adhesive small bowel obstruction. J Trauma Acute Care Surg. 2015;78:13–19.
19. Azagury D, Liu RC, Morgan A, Spain DA. Small bowel obstruction: a prac-tical step-by-step evidence-based approach to evaluation, decision making,and management. J Trauma Acute Care Surg. 2015;79:661–668.
20. Houchens R, Ross D, Elixhauser A, Jiang J. Nationwide Inpatient Sample(NIS) Redesign Final Report. 2014; HCUP Methods Series Report No.2014-04. April 4, 2014. U.S. Agency for Healthcare Research and Quality.Available at: http://www.hcup-us.ahrq.gov/reports/methods/methods.jsp.Accessed August 15, 2018.
21. HCUPNIS TrendWeights. Healthcare Cost and Utilization Project (HCUP).2015. Agency for Healthcare Research and Quality, Rockville, MD. Avail-able at: www.hcup-us.ahrq.gov/db/nation/nis/trendwghts.jsp. Accessed onAugust 15, 2018.
22. Quan H, Sundararajan V, Halfon P, Fong A, Burnand B, Luthi JC,Saunders LD, Beck CA, Feasby TE, Ghali WA. Coding algorithms for defin-ing comorbidities in ICD-9-CM and ICD-10 administrative data.Med Care.2005;43:1130–1139.
23. WandlingMW, Ko CY, Bankey PE, Cribari C, Cryer HG, Diaz JJ, Duane TM,Hameed SM, Hutter MM, Metzler MH 3rd, et al. Expanding the scope ofquality measurement in surgery to include nonoperative care: results fromthe American College of Surgeons National Surgical Quality ImprovementProgram emergency general surgery pilot. J Trauma Acute Care Surg. 2017;83:837–845.
24. Silen W, hein MF, Goldman L. Strangulation obstruction of the small intes-tine. Arch Surg. 1962;85:121–129.
25. Sarr MG, Bulkley GB, Zuidema GD. Preoperative recognition of intestinalstrangulation obstruction. Prospective evaluation of diagnostic capability.Am J Surg. 1983;145:176–182.
26. Schwenter F, Poletti PA, Platon A, Perneger T, Morel P, Gervaz P.Clinicoradiological score for predicting the risk of strangulated small bowelobstruction. Br J Surg. 2010;97:1119–1125.
27. Peacock O, Bassett MG, Kuryba A, Walker K, Davies E, Anderson I,Vohra RS: National Emergency Laparotomy Audit (NELA) Project Team.Thirty-day mortality in patients undergoing laparotomy for small bowel ob-struction. Br J Surg. 2018;105:1006–1013.
28. Behman R, Nathens AB, Look Hong N, Pechlivanoglou P, Karanicolas PJ.Evolving management strategies in patients with adhesive small bowelobstruction: a population-based analysis. J Gastrointest Surg. 2018;22:2133–2141.
29. Hernandez MC, Haddad NN, Cullinane DC, Yeh DD, Wydo S, Inaba K,Duane TM, Pakula A, Skinner R, Rodriguez CJ, et al. The American Asso-ciation for the Surgery of Trauma Severity Grade is valid and generalizable
390
Copyright © 2019 Wolters Kluwer H
in adhesive small bowel obstruction. J Trauma Acute Care Surg. 2018;84:372–378.
30. Aquina CT, Becerra AZ, Probst CP, Xu Z, Hensley BJ, Iannuzzi JC, Noyes K,Monson JR, Fleming FJ. Patients with adhesive small bowel obstruction shouldbe primarily managed by a surgical team. Ann Surg. 2016;264:437–447.
31. Stulberg JJ, Haut ER. Practical guide to surgical data sets: healthcare cost andutilization project National Inpatient Sample (NIS). JAMA Surg. 2018;153:586–587.
32. Choi HK, Chu KW, LawWL. Therapeutic value of gastrografin in adhesivesmall bowel obstruction after unsuccessful conservative treatment: a pro-spective randomized trial. Ann Surg. 2002;236:1–6.
33. Behman R, Nathens AB, Byrne JP, Mason S, Look Hong N, Karanicolas PJ.Laparoscopic surgery for adhesive small bowel obstruction is associatedwitha higher risk of bowel injury: a population-based analysis of 8584 Patients.Ann Surg. 2017;266:489–498.
34. Patel R, Borad NP, Merchant AM. Comparison of outcomes following lapa-roscopic and open treatment of emergent small bowel obstruction: an 11-yearanalysis of ACS NSQIP. Surg Endosc. 2018;32:4900–4911.
35. Thornblade LW, Truitt AR, Davidson GH, Flum DR, Lavallee DC. Surgeonattitudes and practice patterns in managing small bowel obstruction: a qual-itative analysis. J Surg Res. 2017;219:347–353.
DISCUSSIONMartin D. Zielinski, M.D. (Rochester, Minnesota): Good
morning. Drs. Rotondo and Reilly, Publication and Program Com-mittee, thank you for the opportunity to discuss this outstandingpaper. Dr. Matsushima, thank you for highlighting the care ofsmall bowel obstruction patients.
My interest in this field was actually due to a delayed diag-nosis of a strangulation obstruction as a chief resident, and that re-ally drove me into doing some research in this area, because Iknew there must be a better way to manage small bowel obstruc-tion patients which the authors have successfully highlighted.
They present a secondary analysis of the National InpatientSample and have studied non-operative versus operative manage-ment of adhesive small bowel obstruction in the setting of increas-ing national trends to use small bowel obstruction protocols, whichheavily rely on CT imaging and Gastrografin challenge protocols.
They hypothesize that there would be trends towards lessfrequent operations, but that the operations would be earlier inthe patients' critical course.
To answer their questions, the NIS was utilized from 2003to 2013, and identified nearly two million patients. Of these pa-tients, almost half of them underwent operative exploration.
They were able to show multiple improvements over thatdecade in terms of mortality, lesser rates of bowel resection, andlesser durations of stay.
The authors also highlighted, however, that there was noability to proscribe a cause and effect relationship with these im-provements in clinical outcomes to the protocols, but their re-sults certainly are intriguing. This was really a quite well-donepaper, so I only have a few questions:
Why did you choose the years 2003 – 2013? TheGastrografinchallenge has been around since the early 1990's, and the pushto move small bowel obstruction protocols really was comingin in the late 2000's. I would also bet that there would be a con-tinued and probably even stronger national trends to further sup-port your hypothesis after 2013.
Secondly, why didn't you stratify for hospital characteris-tics, particularly the ones with differences such as bed size andteaching status?
© 2018 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Matsushima et al.
This study highlights the inability to really use some ofthese national databases designed for purposes other than qual-ity and research. For instance, we have no idea which hospitalsare using small bowel obstruction protocols, and how manymore protocols were implemented in these institutions acrossthe country throughout the study period.
Really, to me, there are two major takeaways from this pa-per. First, the clinical protocols for emergency general surgerydiseases will likely become more commonplace, and hopefullyimprove patient outcomes in the next years and decades;
And secondly, that we need a reliable national data sourcethat captures both operatively and non-operatively managed pa-tients, that also contains data points specific to disease processesto allow us to control for disease severity, physiologic status, andhospital parameters, instead of relying on billing databases todrive our research. With this more specific information, we asa community of emergency surgeons can determine the causeand effect this and other similar protocols will have to furtherimprove patient care. Thank you.
David Harrington, M.D. (Providence, Rhode Island):Thank you. The rate of surgery of 40 percent was a shocker tome, and I was wondering if you could give us some informationas to whether those were immediate operations – people came inwith, you know, compromised bowel and went to surgery – andhowmany of thosewere, kind of, failure of management, meaning,detected later. That would be an important distinction for me.
Kimberly A. Davis, M.D., M.B.A. (New Haven,Connecticut): Thank you very much for your excellent presen-tation and an interesting study. A number of papers have previ-ously demonstrated that the type of surgery performed is morelikely to be linked to lengths of stay and outcomes, so can yougive us some insight as to howmany of these patients underwent
© 2018 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
their surgeries laparoscopically versus via more traditional opentechniques? Thank you.
KazuhideMatsushima,M.D. (Los Angeles, California):Dr. Zielinski, thank you so much for your kind and invaluablecomments. We certainly acknowledge your contribution to thisarea. Please let me start to address your questions first.
In terms of a study period, I agree, the Gastrografin chal-lenge has been around since 1990's, but we felt that the surgeonsin the U.S. became familiar with the Gastrografin study in early2000, that's whywe chose the 2003. I know it's an arbitrary num-ber, so that's one of the limitations.
The second question regarding the hospital level charac-teristics, we did control in our logistical regression model; how-ever, like I briefly mentioned, I can imagine there is a significantvariations in terms of management of small bowel obstructionbetween institutions, so that's something we have to address infuture studies.
The rate of operative intervention – 46 percent in 2003 –it's higher than described; however, I think the rate of successfulnon-operative management – 70-80 percent – in previous litera-ture, is based on the data at institutions with a high-volume ofpatients with small bowel obstruction; however, if you includeentire hospital across the country, the rate of operating interven-tion can be increased, such as 45-50 percent.
The question regarding laparoscopic surgery, which is an-other hot topic in adhesive small bowel obstruction, we did in-crease ICD-9 code for laparoscopic procedures, such as lysisof adhesions. I don't have an exact number, but in the previousstudy, the use of laparoscopic surgery has been increasing signif-icantly in the last ten years, so I would think the number wouldbe much higher in the last ten years.
Thank you so much.
391
ealth, Inc. All rights reserved.

AAST 2018 PODIUM PAPER
Management of duodenal trauma: A retrospective reviewfrom the Panamerican Trauma Society
Paula Ferrada, MD, Luke Wolfe, MS, Juan Duchesne, MD, Gustavo P. Fraga, MD,Elizabeth Benjamin, MD, Augustin Alvarez, MD, Andre Campbell, MD, Christopher Wybourn, MD,
Alberto Garcia, MD, Carlos Morales, MD, Julieta Correa, MD, Bruno M. Pereira, MD, Marcelo Ribeiro, MD,Martha Quiodettis, MD, Gregory Peck, DO, Juan C. Salamea, MD, Victor F. Kruger, MD,
Rao R. Ivatury, MD, and Thomas Scalea, MD, Richmond, Virginia
Fro
Add
Pre
DO
39
INTRODUCTION: T
mtheVirginiaCommonwealthUnUniversity (J.D.), NewOrleans,Campinas, Brazil; Keck SchoolCalifornia, Los Angeles, CalifSan Francisco, California; ClinLili, Cali, Colombia; UniversidaFundación (C.M.J.C.), MedelliSanto Amaro (M.R.), São Paulde Panamá, Panamá; RobertVicente Corral Moscoso–UnivShock Trauma Centre (T.S.), Uress for reprints: Paula Ferrada,MDSurgery, POBox 980454, Richsented as an oral presentation atTrauma annual meeting in San
I: 10.1097/TA.00000000000021
2
he operative management of duodenal trauma remains controversial. Our hypothesis is that a simplified operative approach couldlead to better outcomes.
METHODS: W
e conducted an international multicenter study, involving 13 centers. We performed a retrospective review from January 2007 toDecember of 2016. Data on demographics, mechanism of trauma, blood loss, operative time, and associated injured organs werecollected. Outcomes included postoperative intra-abdominal sepsis, leak, need for unplanned surgery, length of stay, renal failure,and mortality. We used the Research Electronic Data Capture tool to store the data. Poisson regression using a backward selectionmethod was used to identify independent predictors of mortality.RESULTS: W
e collected data of 372 patients with duodenal injuries. Although the duodenal trauma was complex (median Injury SeverityScore [ISS], 18 [interquartile range, 2–3]; Abbreviated Injury Scale, 3.5 [3–4]; American Association for the Surgery of Traumagrade, 3 [2–3]), primary repair alone was the most common type of operative management (80%, n = 299). Overall mortality was24%.On univariate analysis, mortality was associatedwithmale gender, lower admission systolic blood pressure, need for transfusionbefore operative repair, higher intraoperative blood loss, longer operative time, renal failure requiring renal replacement therapy,higher ISS, and associated pancreatic injury. Poisson regression showed higher ISS, associated pancreatic injury, postoperative renalfailure requiring renal replacement therapy, the need for preoperative transfusion, and male gender remained significant predictorsof mortality. Duodenal suture line leak was statistically significantly lower, and patients had primary repair over every AmericanAssociation for the Surgery of Trauma grade of injury.CONCLUSIONS: T
he need for transfusion prior to the operating room, associated pancreatic injuries, and postoperative renal failure are predictors ofmortality for patients with duodenal injuries. Primary repair alone is a common and safe operative repair even for complex injurieswhen feasible. (J Trauma Acute Care Surg. 2019;86: 392–396. Copyright © 2018 American Association for the Surgery of Trauma.)LEVEL OF EVIDENCE: T
herapeutic study, level IV. KEYWORDS: B lunt and penetrating duodenal trauma; duodenal trauma; surgical management of duodena trauma.D uodenal injuries requiring surgical repair are rare. Higher-grade injuries are even more unusual. Hence, the best sur-
gical treatment for complex duodenal injuries is controversial.1,2
Over the years, there have been many techniques described inthe treatment of these injuries, especially when involving otherorgans.2–10 Primary repair is technically possible most of thetime.More advanced procedures exist, largely to protect the sutureline form dehiscence as leak from the duodenal repair, and can
iversity (P.F., L.W., R.I.), Richmond,Virginia; TulaneLouisiana; University of Campinas (G.P.F., B.M.P.),of Medicine (E.B., A.A.), University of Southernornia; University of San Francisco (A.C., C.W.),ical Research Center (A.G.), Fundación Valle deld deAntioquia-Hospital Universitario SanVicenten, Colombia; Hospital Geral Grajaú–Universidadeo, Brazil; Hospital Santo Tomas (M.Q.), CuidadaWood Johnson Medical School (G.P.); Hospitalersidad del Azuay (J.C.S.), Cuenca, Ecuador; andniversity of Maryland, College Park, Maryland.,VCUSurgeryTrauma,CriticalCare andEmergency
mond, VA 23298; email: [email protected] 77th American Association for the Surgery ofDiego, California, September 2018.
57
Copyright © 2019 Wolters Kluwer H
result in life-threatening complications such as septic shock and,in some cases, an increased mortality.2–10
Some of the techniques used to protect the suture line of theduodenum include duodenal diverticulization, pyloric exclusionwith or without gastrojejunostomy, and primary repair with aretrograde duodenostomy tube and distal feeding tube.7,11–13
For more complex injuries with devascularization of the duode-num, other options such as resection with enteric anastomosisand the Whipple procedure have been described.7,16–21
We hypothesized that a primary repair alone can be usedfor duodenal injuries without increased complications such asintra-abdominal sepsis or increased mortality even in cases ofhigh-grade duodenal injuries.
METHODS
A retrospective multicenter trial was conducted including11 Panamerican Trauma Society centers. An international chatcreated by the society, including surgeons from internationalcenters, was used as a recruitment tool.
Each center obtained its own approval of its institutionalreview board (IRB). Virginia Commonwealth Center was the site
J Trauma Acute Care SurgVolume 86, Number 3
ealth, Inc. All rights reserved.
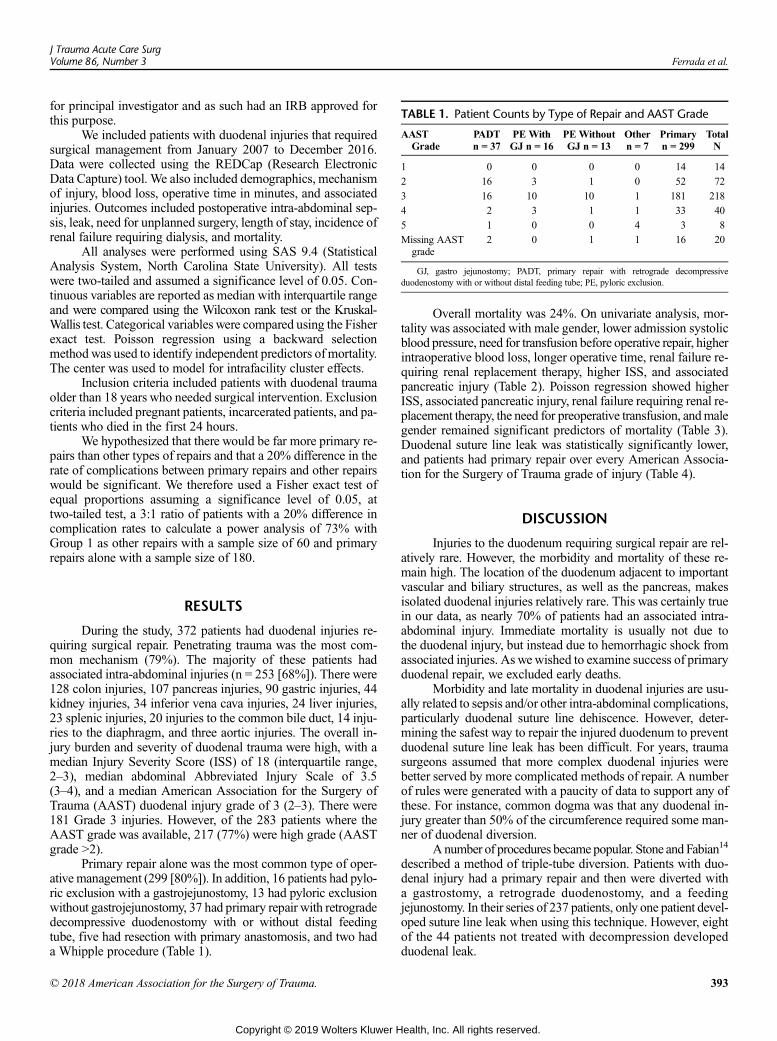
TABLE 1. Patient Counts by Type of Repair and AAST Grade
AASTGrade
PADTn = 37
PE WithGJ n = 16
PEWithoutGJ n = 13
Othern = 7
Primaryn = 299
TotalN
1 0 0 0 0 14 14
2 16 3 1 0 52 72
3 16 10 10 1 181 218
4 2 3 1 1 33 40
5 1 0 0 4 3 8
Missing AASTgrade
2 0 1 1 16 20
GJ, gastro jejunostomy; PADT, primary repair with retrograde decompressiveduodenostomy with or without distal feeding tube; PE, pyloric exclusion.
J Trauma Acute Care SurgVolume 86, Number 3 Ferrada et al.
for principal investigator and as such had an IRB approved forthis purpose.
We included patients with duodenal injuries that requiredsurgical management from January 2007 to December 2016.Data were collected using the REDCap (Research ElectronicData Capture) tool. We also included demographics, mechanismof injury, blood loss, operative time in minutes, and associatedinjuries. Outcomes included postoperative intra-abdominal sep-sis, leak, need for unplanned surgery, length of stay, incidence ofrenal failure requiring dialysis, and mortality.
All analyses were performed using SAS 9.4 (StatisticalAnalysis System, North Carolina State University). All testswere two-tailed and assumed a significance level of 0.05. Con-tinuous variables are reported as median with interquartile rangeand were compared using the Wilcoxon rank test or the Kruskal-Wallis test. Categorical variables were compared using the Fisherexact test. Poisson regression using a backward selectionmethod was used to identify independent predictors of mortality.The center was used to model for intrafacility cluster effects.
Inclusion criteria included patients with duodenal traumaolder than 18 years who needed surgical intervention. Exclusioncriteria included pregnant patients, incarcerated patients, and pa-tients who died in the first 24 hours.
We hypothesized that there would be far more primary re-pairs than other types of repairs and that a 20% difference in therate of complications between primary repairs and other repairswould be significant. We therefore used a Fisher exact test ofequal proportions assuming a significance level of 0.05, attwo-tailed test, a 3:1 ratio of patients with a 20% difference incomplication rates to calculate a power analysis of 73% withGroup 1 as other repairs with a sample size of 60 and primaryrepairs alone with a sample size of 180.
RESULTS
During the study, 372 patients had duodenal injuries re-quiring surgical repair. Penetrating trauma was the most com-mon mechanism (79%). The majority of these patients hadassociated intra-abdominal injuries (n = 253 [68%]). There were128 colon injuries, 107 pancreas injuries, 90 gastric injuries, 44kidney injuries, 34 inferior vena cava injuries, 24 liver injuries,23 splenic injuries, 20 injuries to the common bile duct, 14 inju-ries to the diaphragm, and three aortic injuries. The overall in-jury burden and severity of duodenal trauma were high, with amedian Injury Severity Score (ISS) of 18 (interquartile range,2–3), median abdominal Abbreviated Injury Scale of 3.5(3–4), and a median American Association for the Surgery ofTrauma (AAST) duodenal injury grade of 3 (2–3). There were181 Grade 3 injuries. However, of the 283 patients where theAAST grade was available, 217 (77%) were high grade (AASTgrade >2).
Primary repair alone was the most common type of oper-ative management (299 [80%]). In addition, 16 patients had pylo-ric exclusion with a gastrojejunostomy, 13 had pyloric exclusionwithout gastrojejunostomy, 37 had primary repair with retrogradedecompressive duodenostomy with or without distal feedingtube, five had resection with primary anastomosis, and two hada Whipple procedure (Table 1).
© 2018 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
Overall mortality was 24%. On univariate analysis, mor-tality was associated with male gender, lower admission systolicblood pressure, need for transfusion before operative repair, higherintraoperative blood loss, longer operative time, renal failure re-quiring renal replacement therapy, higher ISS, and associatedpancreatic injury (Table 2). Poisson regression showed higherISS, associated pancreatic injury, renal failure requiring renal re-placement therapy, the need for preoperative transfusion, andmalegender remained significant predictors of mortality (Table 3).Duodenal suture line leak was statistically significantly lower,and patients had primary repair over every American Associa-tion for the Surgery of Trauma grade of injury (Table 4).
DISCUSSION
Injuries to the duodenum requiring surgical repair are rel-atively rare. However, the morbidity and mortality of these re-main high. The location of the duodenum adjacent to importantvascular and biliary structures, as well as the pancreas, makesisolated duodenal injuries relatively rare. This was certainly truein our data, as nearly 70% of patients had an associated intra-abdominal injury. Immediate mortality is usually not due tothe duodenal injury, but instead due to hemorrhagic shock fromassociated injuries. As wewished to examine success of primaryduodenal repair, we excluded early deaths.
Morbidity and late mortality in duodenal injuries are usu-ally related to sepsis and/or other intra-abdominal complications,particularly duodenal suture line dehiscence. However, deter-mining the safest way to repair the injured duodenum to preventduodenal suture line leak has been difficult. For years, traumasurgeons assumed that more complex duodenal injuries werebetter served by more complicated methods of repair. A numberof rules were generated with a paucity of data to support any ofthese. For instance, common dogma was that any duodenal in-jury greater than 50% of the circumference required some man-ner of duodenal diversion.
A number of procedures became popular. Stone and Fabian14
described a method of triple-tube diversion. Patients with duo-denal injury had a primary repair and then were diverted witha gastrostomy, a retrograde duodenostomy, and a feedingjejunostomy. In their series of 237 patients, only one patient devel-oped suture line leak when using this technique. However, eightof the 44 patients not treated with decompression developedduodenal leak.
393
ealth, Inc. All rights reserved.
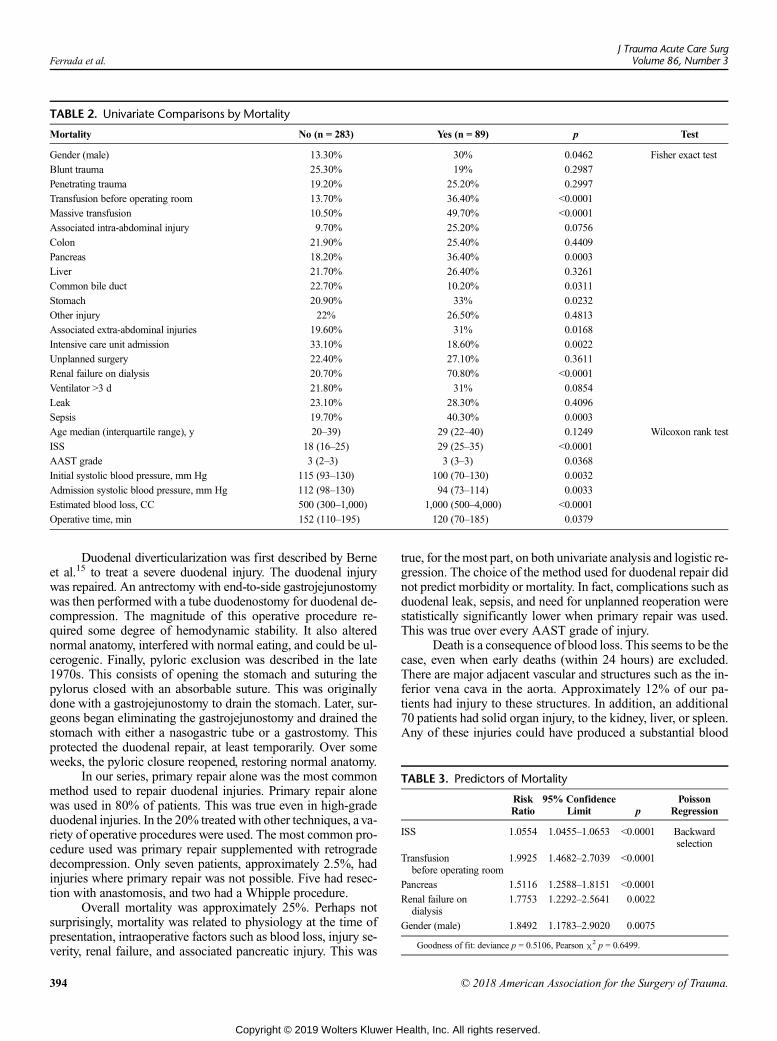
TABLE 2. Univariate Comparisons by Mortality
Mortality No (n = 283) Yes (n = 89) p Test
Gender (male) 13.30% 30% 0.0462 Fisher exact test
Blunt trauma 25.30% 19% 0.2987
Penetrating trauma 19.20% 25.20% 0.2997
Transfusion before operating room 13.70% 36.40% <0.0001
Massive transfusion 10.50% 49.70% <0.0001
Associated intra-abdominal injury 9.70% 25.20% 0.0756
Colon 21.90% 25.40% 0.4409
Pancreas 18.20% 36.40% 0.0003
Liver 21.70% 26.40% 0.3261
Common bile duct 22.70% 10.20% 0.0311
Stomach 20.90% 33% 0.0232
Other injury 22% 26.50% 0.4813
Associated extra-abdominal injuries 19.60% 31% 0.0168
Intensive care unit admission 33.10% 18.60% 0.0022
Unplanned surgery 22.40% 27.10% 0.3611
Renal failure on dialysis 20.70% 70.80% <0.0001
Ventilator >3 d 21.80% 31% 0.0854
Leak 23.10% 28.30% 0.4096
Sepsis 19.70% 40.30% 0.0003
Age median (interquartile range), y 20–39) 29 (22–40) 0.1249 Wilcoxon rank test
ISS 18 (16–25) 29 (25–35) <0.0001
AAST grade 3 (2–3) 3 (3–3) 0.0368
Initial systolic blood pressure, mm Hg 115 (93–130) 100 (70–130) 0.0032
Admission systolic blood pressure, mm Hg 112 (98–130) 94 (73–114) 0.0033
Estimated blood loss, CC 500 (300–1,000) 1,000 (500–4,000) <0.0001
Operative time, min 152 (110–195) 120 (70–185) 0.0379
TABLE 3. Predictors of Mortality
RiskRatio
95% ConfidenceLimit p
PoissonRegression
ISS 1.0554 1.0455–1.0653 <0.0001 Backwardselection
Transfusionbefore operating room
1.9925 1.4682–2.7039 <0.0001
Pancreas 1.5116 1.2588–1.8151 <0.0001
Renal failure ondialysis
1.7753 1.2292–2.5641 0.0022
Gender (male) 1.8492 1.1783–2.9020 0.0075
Goodness of fit: deviance p = 0.5106, Pearson χ2 p = 0.6499.
Ferrada et al.J Trauma Acute Care Surg
Volume 86, Number 3
Duodenal diverticularization was first described by Berneet al.15 to treat a severe duodenal injury. The duodenal injurywas repaired. An antrectomy with end-to-side gastrojejunostomywas then performed with a tube duodenostomy for duodenal de-compression. The magnitude of this operative procedure re-quired some degree of hemodynamic stability. It also alterednormal anatomy, interfered with normal eating, and could be ul-cerogenic. Finally, pyloric exclusion was described in the late1970s. This consists of opening the stomach and suturing thepylorus closed with an absorbable suture. This was originallydone with a gastrojejunostomy to drain the stomach. Later, sur-geons began eliminating the gastrojejunostomy and drained thestomach with either a nasogastric tube or a gastrostomy. Thisprotected the duodenal repair, at least temporarily. Over someweeks, the pyloric closure reopened, restoring normal anatomy.
In our series, primary repair alone was the most commonmethod used to repair duodenal injuries. Primary repair alonewas used in 80% of patients. This was true even in high-gradeduodenal injuries. In the 20% treated with other techniques, a va-riety of operative procedures were used. The most common pro-cedure used was primary repair supplemented with retrogradedecompression. Only seven patients, approximately 2.5%, hadinjuries where primary repair was not possible. Five had resec-tion with anastomosis, and two had a Whipple procedure.
Overall mortality was approximately 25%. Perhaps notsurprisingly, mortality was related to physiology at the time ofpresentation, intraoperative factors such as blood loss, injury se-verity, renal failure, and associated pancreatic injury. This was
394
Copyright © 2019 Wolters Kluwer H
true, for the most part, on both univariate analysis and logistic re-gression. The choice of the method used for duodenal repair didnot predict morbidity or mortality. In fact, complications such asduodenal leak, sepsis, and need for unplanned reoperation werestatistically significantly lower when primary repair was used.This was true over every AAST grade of injury.
Death is a consequence of blood loss. This seems to be thecase, even when early deaths (within 24 hours) are excluded.There are major adjacent vascular and structures such as the in-ferior vena cava in the aorta. Approximately 12% of our pa-tients had injury to these structures. In addition, an additional70 patients had solid organ injury, to the kidney, liver, or spleen.Any of these injuries could have produced a substantial blood
© 2018 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.
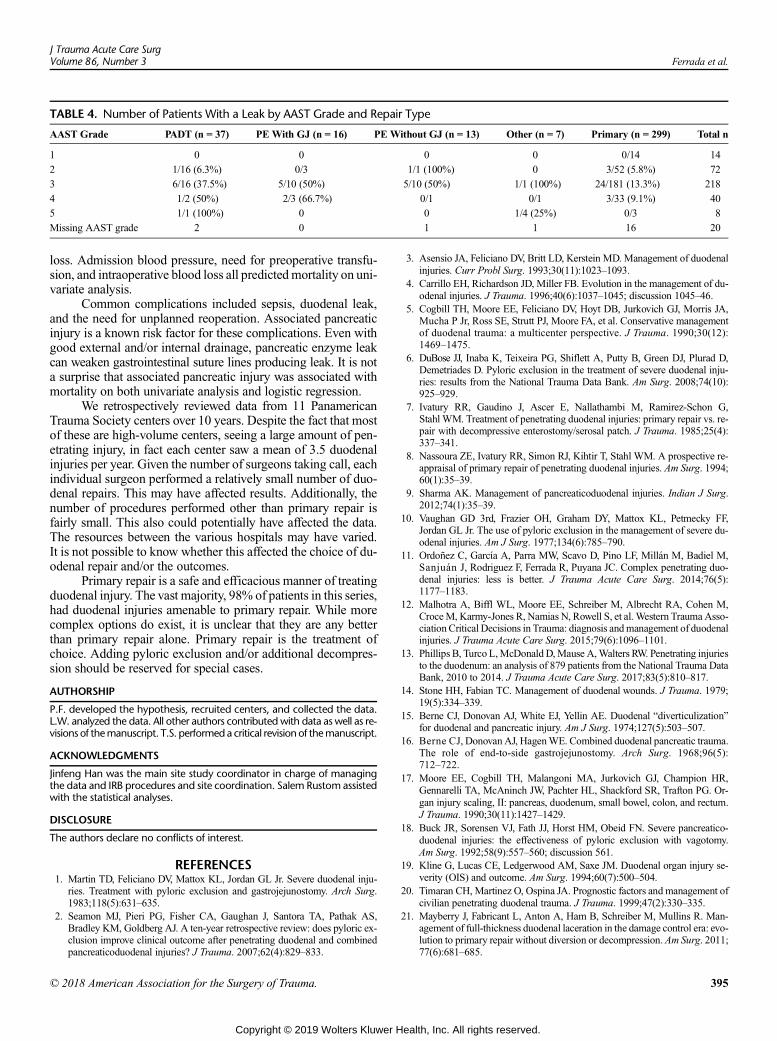
TABLE 4. Number of Patients With a Leak by AAST Grade and Repair Type
AAST Grade PADT (n = 37) PEWith GJ (n = 16) PE Without GJ (n = 13) Other (n = 7) Primary (n = 299) Total n
1 0 0 0 0 0/14 14
2 1/16 (6.3%) 0/3 1/1 (100%) 0 3/52 (5.8%) 72
3 6/16 (37.5%) 5/10 (50%) 5/10 (50%) 1/1 (100%) 24/181 (13.3%) 218
4 1/2 (50%) 2/3 (66.7%) 0/1 0/1 3/33 (9.1%) 40
5 1/1 (100%) 0 0 1/4 (25%) 0/3 8
Missing AAST grade 2 0 1 1 16 20
J Trauma Acute Care SurgVolume 86, Number 3 Ferrada et al.
loss. Admission blood pressure, need for preoperative transfu-sion, and intraoperative blood loss all predicted mortality on uni-variate analysis.
Common complications included sepsis, duodenal leak,and the need for unplanned reoperation. Associated pancreaticinjury is a known risk factor for these complications. Even withgood external and/or internal drainage, pancreatic enzyme leakcan weaken gastrointestinal suture lines producing leak. It is nota surprise that associated pancreatic injury was associated withmortality on both univariate analysis and logistic regression.
We retrospectively reviewed data from 11 PanamericanTrauma Society centers over 10 years. Despite the fact that mostof these are high-volume centers, seeing a large amount of pen-etrating injury, in fact each center saw a mean of 3.5 duodenalinjuries per year. Given the number of surgeons taking call, eachindividual surgeon performed a relatively small number of duo-denal repairs. This may have affected results. Additionally, thenumber of procedures performed other than primary repair isfairly small. This also could potentially have affected the data.The resources between the various hospitals may have varied.It is not possible to know whether this affected the choice of du-odenal repair and/or the outcomes.
Primary repair is a safe and efficacious manner of treatingduodenal injury. The vast majority, 98% of patients in this series,had duodenal injuries amenable to primary repair. While morecomplex options do exist, it is unclear that they are any betterthan primary repair alone. Primary repair is the treatment ofchoice. Adding pyloric exclusion and/or additional decompres-sion should be reserved for special cases.
AUTHORSHIP
P.F. developed the hypothesis, recruited centers, and collected the data.L.W. analyzed the data. All other authors contributed with data as well as re-visions of themanuscript. T.S. performeda critical revisionof themanuscript.
ACKNOWLEDGMENTS
Jinfeng Han was the main site study coordinator in charge of managingthe data and IRB procedures and site coordination. Salem Rustom assistedwith the statistical analyses.
DISCLOSURE
The authors declare no conflicts of interest.
REFERENCES1. Martin TD, Feliciano DV, Mattox KL, Jordan GL Jr. Severe duodenal inju-
ries. Treatment with pyloric exclusion and gastrojejunostomy. Arch Surg.1983;118(5):631–635.
2. Seamon MJ, Pieri PG, Fisher CA, Gaughan J, Santora TA, Pathak AS,Bradley KM, Goldberg AJ. A ten-year retrospective review: does pyloric ex-clusion improve clinical outcome after penetrating duodenal and combinedpancreaticoduodenal injuries? J Trauma. 2007;62(4):829–833.
© 2018 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
3. Asensio JA, Feliciano DV, Britt LD, Kerstein MD. Management of duodenalinjuries. Curr Probl Surg. 1993;30(11):1023–1093.
4. Carrillo EH, Richardson JD, Miller FB. Evolution in the management of du-odenal injuries. J Trauma. 1996;40(6):1037–1045; discussion 1045–46.
5. Cogbill TH, Moore EE, Feliciano DV, Hoyt DB, Jurkovich GJ, Morris JA,Mucha P Jr, Ross SE, Strutt PJ, Moore FA, et al. Conservative managementof duodenal trauma: a multicenter perspective. J Trauma. 1990;30(12):1469–1475.
6. DuBose JJ, Inaba K, Teixeira PG, Shiflett A, Putty B, Green DJ, Plurad D,Demetriades D. Pyloric exclusion in the treatment of severe duodenal inju-ries: results from the National Trauma Data Bank. Am Surg. 2008;74(10):925–929.
7. Ivatury RR, Gaudino J, Ascer E, Nallathambi M, Ramirez-Schon G,Stahl WM. Treatment of penetrating duodenal injuries: primary repair vs. re-pair with decompressive enterostomy/serosal patch. J Trauma. 1985;25(4):337–341.
8. Nassoura ZE, Ivatury RR, Simon RJ, Kihtir T, Stahl WM. A prospective re-appraisal of primary repair of penetrating duodenal injuries. Am Surg. 1994;60(1):35–39.
9. Sharma AK. Management of pancreaticoduodenal injuries. Indian J Surg.2012;74(1):35–39.
10. Vaughan GD 3rd, Frazier OH, Graham DY, Mattox KL, Petmecky FF,Jordan GL Jr. The use of pyloric exclusion in the management of severe du-odenal injuries. Am J Surg. 1977;134(6):785–790.
11. Ordoñez C, García A, Parra MW, Scavo D, Pino LF, Millán M, Badiel M,Sanjuán J, Rodriguez F, Ferrada R, Puyana JC. Complex penetrating duo-denal injuries: less is better. J Trauma Acute Care Surg. 2014;76(5):1177–1183.
12. Malhotra A, Biffl WL, Moore EE, Schreiber M, Albrecht RA, Cohen M,CroceM, Karmy-Jones R, Namias N, Rowell S, et al. Western Trauma Asso-ciationCritical Decisions in Trauma: diagnosis andmanagement of duodenalinjuries. J Trauma Acute Care Surg. 2015;79(6):1096–1101.
13. Phillips B, Turco L,McDonald D,Mause A,Walters RW. Penetrating injuriesto the duodenum: an analysis of 879 patients from the National Trauma DataBank, 2010 to 2014. J Trauma Acute Care Surg. 2017;83(5):810–817.
14. Stone HH, Fabian TC. Management of duodenal wounds. J Trauma. 1979;19(5):334–339.
15. Berne CJ, Donovan AJ, White EJ, Yellin AE. Duodenal “diverticulization”for duodenal and pancreatic injury. Am J Surg. 1974;127(5):503–507.
16. Berne CJ, DonovanAJ, HagenWE. Combined duodenal pancreatic trauma.The role of end-to-side gastrojejunostomy. Arch Surg. 1968;96(5):712–722.
17. Moore EE, Cogbill TH, Malangoni MA, Jurkovich GJ, Champion HR,Gennarelli TA, McAninch JW, Pachter HL, Shackford SR, Trafton PG. Or-gan injury scaling, II: pancreas, duodenum, small bowel, colon, and rectum.J Trauma. 1990;30(11):1427–1429.
18. Buck JR, Sorensen VJ, Fath JJ, Horst HM, Obeid FN. Severe pancreatico-duodenal injuries: the effectiveness of pyloric exclusion with vagotomy.Am Surg. 1992;58(9):557–560; discussion 561.
19. Kline G, Lucas CE, Ledgerwood AM, Saxe JM. Duodenal organ injury se-verity (OIS) and outcome. Am Surg. 1994;60(7):500–504.
20. Timaran CH, Martinez O, Ospina JA. Prognostic factors and management ofcivilian penetrating duodenal trauma. J Trauma. 1999;47(2):330–335.
21. Mayberry J, Fabricant L, Anton A, Ham B, Schreiber M, Mullins R. Man-agement of full-thickness duodenal laceration in the damage control era: evo-lution to primary repair without diversion or decompression. Am Surg. 2011;77(6):681–685.
395
ealth, Inc. All rights reserved.

Ferrada et al.J Trauma Acute Care Surg
Volume 86, Number 3
DISCUSSIONGregory J. “Jerry” Jurkovich, M.D. (Sacramento,
California): Good afternoon, members and guests, President-ElectCroce, Dr. Winchell. Thank you for the honor of discussing thisimportant paper.
The presentation was based, as you heard, on a multi-centerreview from North, Central and South American trauma hospi-tals. It represents an effort from the Panamerican Trauma Society,and this collaboration is representative of this landmark meetingof the AAST and the World Trauma Congress, so well done.
Dr. Ferrada and her colleagues have emphasized the greatvariability that exists in the management of duodenal injuries.
Over the decade of this retrospective review, the 13 traumacenters who compiled the data managed a large number – 372patients – with duodenal injuries. It is not a common entity,but also not so rare that every surgeon will eventually have toface this management dilemma.
I have a few observations about this cohort of duodenaltrauma patients that are worth noting, and along with that willbe my questions.
Number one, 80 percent of this population suffered pene-trating trauma. Are the factors that influence the outcome anydifferent between penetrating and blunt trauma mechanisms?
Secondly, associated injuries are highly common, and Ipresume that hemorrhage control and control of contaminationremain the highest priorities of initial trauma care.
To that end, mortality was high, at 24 percent, and whilemany of these deaths are likely due to acute blood loss, the au-thors did not provide us with data on the timeline nor the causeof mortality, sowhat was the time of death and the cause of deathin these 24 percent of patients?
And fourth, four of the study centers were from NorthAmerica, but the remainder were from Central or South Amer-ica. Are there any differences in management style and outcomenoted based on the geography of the trauma centers?
And finally, I would like to emphasize the operative tech-niques utilized. Primary repair alone was performed in 80 per-cent of the patients, as we heard.
Are any of the adjuncts to simple primary repair or resec-tion in primary anastomosis really necessary or beneficial in themanagement of duodenal trauma?
I believe that's the crux of the dilemma of judgment thatfaces the trauma surgeon in the middle of the night in trying todecide how to manage these patients.
Perhaps for the very rare circumstance of significant lossof duodenal tissue, a resection and primary anastomosis will berequired – that was five patients in this series –, or if tension ex-ists, a roux-en-Y limb of intestine will need to be sutured to theproximal duodenum to establish continuity – none in this series– or even rarer, a pancreatic-duodenectomy and Whipple recon-struction will be needed for a complete destruction of the duode-num and pancreatic head – and there were two in this series.
But the role of pyloric exclusion, duodenostomy tube, pro-grade or retrograde duodenal lumen decompression, buttressingof the duodenal repairs, et cetera, their role remains unanswered.And I wonder what the authors could suggest as a way to help re-solve some of these uncommon intra-operative questions aboutmanagement.
396
Copyright © 2019 Wolters Kluwer H
Finally, my sincere congratulations on this accomplishment,as this is the first multi-center trial study from the PanAmericanTrauma Society.
Sheldon H. Tepperman (Bronx, New York):Dr. Ferrada,I, too, offer my congratulations. Awesome.
So, Dr. Ron Gross is sitting here in the audience on hiscomputer, and he is about to update the definitive textbook on thisquestion, which would be the Advanced Trauma Operative Man-agement course. And so there is a chapter on duodenal injury.
And as we are teaching this course, it's confusing for ouryoung surgeons. So is it time to turn to Dr. Gross and offerthe advice of, let's down-regulate all of these tubes and thingsand just tell people to do a primary repair?
Omar Bekdache, M.D., F.R.C.S., F.A.C.S. (Montreal,Canada): My question is, how was the assessment of the asso-ciated pancreatic injury done intra-operatively, and how did thisimpact your management protocol intra-operatively for the pri-mary type of repair? Thank you.
MarcA. deMoya, (Milwaukee,Wisconsin):Thank you,Dr. Ferrada, always great presentations, and my question actuallyhas to do with the leaks.
You had a significant number of patients in this cohort,and so it would be nice to kind of drill down into the type ofleak, and whether or not, if you separated those that had a leakversus those who didn't have a leak, rather than look at themortality.
Was there any difference at all among the groups, in termsof the technique of closure, and then also the management, be-cause not all leaks are the same, right? So, if you could just shedsome light on that, perhaps.
Ari K. Leppaniemi, M.D., Ph.D. (Helsinki, Finland):Nice work, Paula. Congratulations. As Marc was saying, thekey to duodenal injuries is really the leak. And I saw you showedsome data on that, but I would be interested if you could elaboratea little bit more how you managed the leaks, and how much theleaks actually contributed to the outcomes in terms of not justmortality, but complications, length of stay, and so on.
Paula Ferrada, M.D.(Glen Allen, Virginia): Thank youeverybody for the wonderful comments and support.
We excluded the deaths within the first 24 hours, be-cause we wanted to hone in on the deaths secondary to intra-abdominal sepsis.
Regarding how many patients had a leak, those thatunderwent primary repair leaked less however no repair showeda decreased mortality.
To answer the question about if there was a difference be-tween North America and Latin America, the large majority ofthe patients underwent primary repair, and surgeons in LatinAmerica almost exclusively used primary repair.
I agree with the statement that perhaps it's time to at thevery least attempt primary repair, if there is adequate bloodsupply, and no other injuries that can prevent this repair. It ismore likely the patients would heal one anastomosis than severalother enterotomies that can cause further morbidity for ourpatients.
Thank you so much for the opportunity to present this pa-per. It is an honor for the Panamerican Trauma Society to presentour fist multicenter trial in this forum.
© 2018 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.

AAST 2018 PODIUM PAPER
Development of a geospatial approach for the quantitativeanalysis of trauma center access
Robert J.Winchell, MD, Paige Xu,MPH, Lauren E.Mount, MD, andReedHuegerich,MCRP, New York, New York
AAST Continuing Medical Education Article
Accreditation StatementThis activity has been planned and implemented in accordance with the Es-sential Areas and Policies of the Accreditation Council for Continuing MedicalEducation through the joint providership of the American College of Surgeonsand the American Association for the Surgery of Trauma. The AmericanCollege Surgeons is accredited by the ACCME to provide continuing medicaleducation for physicians.
AMA PRA Category 1 Credits™The American College of Surgeons designates this journal-based CME activity fora maximum of 1 AMA PRACategory 1 Credit™. Physicians should claim only the creditcommensurate with the extent of their participation in the activity.
Of the AMA PRACategory 1 Credit™ listed above, a maximum of 1 credit meetsthe requirements for self-assessment.
Credits can only be claimed online
ObjectivesAfter reading the featured articles published in the Journal of Trauma and AcuteCare Surgery, participants should be able to demonstrate increased understandingof the material specific to the article. Objectives for each article are featured atthe beginning of each article and online. Test questions are at the end of the article,with a critique and specific location in the article referencing the question topic.
Claiming CreditTo claim credit, please visit the AAST website at http://www.aast.org/ and click onthe “e-Learning/MOC” tab. You must read the article, successfully complete thepost-test and evaluation. Your CME certificate will be available immediately uponreceiving a passing score of 75% or higher on the post-test. Post-tests receiving a scoreof below 75% will require a retake of the test to receive credit.
System RequirementsThe system requirements are as follows: Adobe® Reader 7.0 or above installed; Internet Explorer® 7 and above; Firefox® 3.0 and above, Chrome® 8.0 and above, or
Safari™ 4.0 and above.
QuestionsIf you have any questions, please contact AAST at 800-789-4006. Paper test and evaluations will not be accepted.
Disclosure InformationIn accordance with the ACCME Accreditation Criteria, the American College of
Surgeons, as the accredited provider of this journal activity, must ensure that anyone
in a position to control the content of J Trauma Acute Care Surg articles selected for
CME credit has disclosed all relevant financial relationships with any commercial
interest. Disclosure forms are completed by the editorial staff, associate editors,
reviewers, and all authors. The ACCME defines a `commercial interest' as “any
entity producing, marketing, re-selling, or distributing health care goods or services
consumed by, or used on, patients.” “Relevant” financial relationships are those (in
any amount) that may create a conflict of interest and occur within the 12’months
preceding and during the time that the individual is engaged in writing the article. All
reported conflicts are thoroughly managed in order to ensure any potential bias
within the content is eliminated. However, if you’perceive a bias within the article,
please report the circumstances on the evaluation form.
Please note we have advised the authors that it is their responsibility to disclose within
the article if they are describing the use of a device, product, or drug that is not FDA
approved or the off-label use of an approved device, product, or drug or unapproved usage.
Disclosures of Significant Relationships withRelevant Commercial Companies/Organizationsby the Editorial StaffErnest E. Moore, Editor: PI, research support and shared U.S. patents Haemonetics;
PI, research support, Instrumentation Laboratory, Inc.; Co-founder, Thrombo Thera-
peutics. Associate Editors David Hoyt, Ronald V. Maier and Steven Shackford have
nothing to disclose. Editorial staff and Angela Sauaia have nothing to disclose.
Author DisclosuresRobert J.Winchell, MD – Stryker Corporation/CRICO Insurance Company, received moneyas consultant/expert witness.
Reviewer DisclosuresThe reviewers have nothing to disclose.
CostFor AAST members and Journal of Trauma and Acute Care Surgery subscribersthere is no charge to participate in this activity. For those who are not a memberor subscriber, the cost for each credit is $25.
J Trauma Acute Care SurgVolume 86, Number 3 397
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.

Fro
Ad
Pre
DO
Winchell et al.J Trauma Acute Care Surg
Volume 86, Number 3
39
INTRODUCTION: D
m the Weill Cornell Medicine,University Mailman School ofCornell University, Ithaca, Newdress for reprints: Robert J. WinMedical Center, 525 E 68th Stemail: [email protected] at the 77th Annual MeetiTrauma, September 26, 2018, i
I: 10.1097/TA.00000000000021
8
ecisions around trauma center (TC) designation have become contentious in many areas. There is no consensus regarding theideal number and location of TC and no accepted metrics to assess the effect of changes in system structure. We aimed to developmetrics of TC access, using publicly available data and analytic tools. We hypothesize that geospatial analysis can provide a repro-ducible approach to quantitatively asses potential changes in trauma system structure.
METHODS: A
region in New York State was chosen for evaluation. Geospatial data and analytic tools in ArcGIS Online were used. Transporttime polygons were created around TC, and the population covered was estimated by summing the census tracts within thesepolygons. Transport time from each census tract to the nearest TC was calculated. The baseline model includes the singledesignated TC. Model 1 includes one additional TC, andModel 2 includes two additional TC, chosen to maximize coverage.The population covered, population-weighted distribution of transport times, and population covered by a specific TC werecalculated for each model.RESULTS: T
he baseline model covered 1.12� 106 people. The median transport time was 19.2 minutes. In Model 1, the population coveredincreased by 14.4%, while the population catchment, and thus the estimated trauma volume, of the existing TC decreased by 12%.Median transport time to the nearest TC increased to 20.4 minutes. Model 2 increased coverage by 18% above baseline, while thecatchment, and thus the estimated trauma volume, of the existing TC decreased by 22%. Median transport time to the nearest TCdecreased to 19.6 minutes.CONCLUSIONS: G
eospatial analysis can provide objective measures of population access to trauma care. The analysis can be performed usingdifferent numbers and locations of TC, allowing direct comparison of changes in coverage and impact on existing centers. Thistype of data is essential for guiding difficult decisions regarding trauma system design. (J Trauma Acute Care Surg. 2019;86:397–405. Copyright © 2018 American Association for the Surgery of Trauma.)LEVEL OF EVIDENCE: C
are management, level IV. KEYWORDS: G eospatial analysis; Trauma systems; Trauma center; Needs assessment; Health policy.C are at a designated trauma center has been shown to improveoutcomes after injury,1–3 and systems of care that ensure
rapid access to trauma centers have been shown to be a criticalpredictor of survival and recovery.4–6 From the inception oftrauma system development, it has been recognized that the leadagency for the system should have the authority to designatetrauma centers based on the capabilities of the facility and theneeds of the population served.7–10 Despite this recognition,processes and standards for trauma center designation in theUnited States remain highly variable.11 There are no federalstandards; thus, statutory authority to designate trauma centersexists at the level of state or county agencies, if it exists at all.Moreover, there are no accepted benchmarks to establish theoptimum number of trauma centers or their location in a givencommunity.
This lack of objective guidance was rarely an issue beforethe early 21st century, a period when economic pressures onhospitals made trauma care an almost untenable mission. Thedecision to designate a new trauma center was not controversialin this era in which trauma center closings far outnumbered newtrauma center designations, with more than 300 trauma centersclosing their doors between 1990 and 2005.12 Conversely, bythe mid 2000s, the economic climate had shifted, and the numberof new hospitals claiming trauma center status began to dwarf thenumber of trauma centers closing. According to self-designationdata collected annually by the American Hospital Association,13
in the year 2000, 258 (6.1%) of hospitals reported having a Level
New York, New York (R.J.W., L.E.M.); ColumbiaPublic Health, New York, New York (P.X.); andYork (R.H.).chell, MD, New York-Presbyterian Weill Cornell, Payson 7-714, Box 116, New York, NY 10065;du.ng of the American Association for the Surgery ofn San Diego, California.
56
Copyright © 2019 Wolters Kluwer H
I trauma center. In 2010, the number had risen to 387 (9.4%); andin 2013, there were 416 hospitals claiming Level I trauma centerstatus. Data from the American College of Surgeons Committeeon Trauma (ACS COT) Verification, Review, and Consultation(VRC) program shows a similarly dramatic rise between 2005and 2015; the number of verified Level I and Level II traumacenters increased from 166 to 290.14 These new trauma centersoften arise in more affluent urban and suburban areas rather thanin underserved or economically depressed areas, and maycompete with existing centers for patient volume as well asrevenue. Despite an increase in the overall number of traumacenters, this trend may actually result in decreased access totrauma center resources for vulnerable populations.15
The shift from a predominance of trauma center closingsto trauma center proliferation, coupled with a strong politicalshift away from government regulation of free markets that in-cludes heath care, has made the process of trauma center des-ignation a highly contentious one, and one with significantfinancial implications. Lacking clear standards, processes, andpolitical support, state and county agencies are often challengedto exert their authority to control trauma center designation inthe face of opposition from large health care organizations. Asa result, the decision to open a new trauma center or close anexisting one is most commonly left to individual health carefacilities, driven by market factors and the hospital's perceptionof its mission.15
In response to this trend, the ACS COT released a positionstatement in 2015 outlining a set of principles that should guidedecisions around trauma system development, and advocatingfor the establishment of a transparent and objective needs-basedprocess to guide trauma center placement and designation.16
The statement put forward a list of parameters that could be usedto assess the need for trauma centers in a region, includingEmergency Medical Services (EMS) transport times and thepercentage of population within 60 minutes’ transport time ofa Level I or Level II trauma center as metrics of trauma system
© 2018 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Winchell et al.
access. The statement also outlined fundamental principles thatshould guide system development, including the preservationof a sufficient patient volume at existing centers. Although theACS COT statement provides general guidance, to date, thereis no accepted set of metrics to provide objective assessmentof trauma center access or the impact of new centers on existingfacilities as part of a needs-based assessment.
The purpose of this study was to describe a systematic andeasily reproducible method to calculate metrics of trauma centeraccess using publicly available data and analytic routines. Ourgoal is to utilize geospatial analysis to quantitatively assess theeffects of potential changes in trauma system structure, such asthe number and location of trauma centers in the region, to helpguide policy decisions related to trauma system planning anddevelopment.
MATERIALS AND METHODS
Data SourcesBasic cartographic information, including ground trans-
portation network data, was obtained through ArcGIS Online(ESRI; Redlands, CA). Population density information at thelevel of county census tract was derived fromUSCensus Bureaudata for 2014, presented as a publicly available map layer (USCensus Tract Areas, updated May 22, 2017) within ArcGISOnline. For the purposes of population coverage and transportationtime estimates, the population of each census tract was placed at thegeographic centroid of the individual census tract. Hospital data,including location, reported trauma center designation level, andother characteristics, were obtained in spreadsheet format fromthe Homeland Infrastructure Foundation-Level Data website17
and cross-checked with data from the ASC COT Verification,Review, and Consultation.18
AnalysisWe evaluated a single region in NewYork state. This region
was chosen based on availability of necessary geospatial data inthe public domain, and because of its relative geographic isola-tion, being functionally served by a single designated trauma cen-ter. Our intent was to analyze the effects of adding new traumacenters to an existing system as a hypothetical case, not to modelthe current situation in the chosen region. Therefore, for simplicity,we did not include existing trauma centers located at the periph-ery of the chosen region, nor did we include population-densecensus tracts located at the periphery of the region. We evalu-ated three different models for the index region: the current base-line, served by the single existing designated adult trauma center,Model 1 including one additional designated adult center chosento optimize population coverage, and Model 2 including two ad-ditional designated adult centers, also chosen to optimize popula-tion coverage. This method for picking new candidate centers wasused to facilitate demonstration of the modeling approach in aneutral fashion, without reference to hospital capabilities or po-tential interest in becoming a trauma center. For each model, sev-eral metrics were calculated: total population coverage within60 minutes’ estimated transport time, subdivided into 10-minutebands, the distribution of estimated transport times to the nearesttrauma center within 60 minutes, and the estimated populationcatchment for each trauma center. To more accurately model the
© 2018 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
region as geographically isolated, several densely populated urbancensus tracts in adjacent cities located at the outer limits of the60-minute drive time range were excluded from the analysis.
To calculate population coverage, the ArcGIS network an-alyst tools, availablewithin ArcGISOnline, were used to create aset of transport-time polygons capturing the geographic areawithin 60 minutes’ estimated transport time of the trauma cen-ters in the model, divided in 10-minute segments. Populationcoveragewas estimated by joining these transport-time polygonswith the population density layer, summing the population forall included census tract centroids. We used the ArcGIS networkanalyst tools to estimate the shortest transport time from eachcensus tract centroid to its nearest allocated trauma center, limit-ing the analysis to census tracts with transport times less than60 minutes. Estimated transport times from each centroid wereweighted by population, and the distribution was analyzed foreach model. Population weighting was used to improve estima-tion over purely geographic methods.19 Trauma center catch-ment population for each model was estimated by summingthe population for all census tract centroids that had the shortesttransport time to the index trauma center. For the model, we as-sume patient volume at the index trauma center to be propor-tional to this catchment population.
Geospatial and Statistical AnalysisAll geospatial analyseswere performed using ArcGISOn-
line, versions 5.1 [June 2017] through 6.2 [June 2018] (ESRI),and ArcGIS Desktop version 10.5 (ESRI). All descriptive statis-tical and graphic analyses were performed using R version 3.5.0(R Core Team)20 with the ggplot2 package.21
RESULTS
The baseline model includes a total population of1.12� 106 within 60 minutes of the trauma center. The popula-tion catchment of the single trauma center was the full coveredpopulation of 1.12 � 106. Addition of a second trauma centerin Model 1 increased the population covered within 60 minutesof either trauma center by 14% to 1.28 � 106 while decreasingthe population catchment of the existing trauma center, and thusthe estimated trauma volume at that center, by 12% from base-line, to 9.86 � 105. The addition of a third trauma center inModel 2 further increased the population covered within60 minutes of any trauma center to 1.32� 106, an 18% increaseabove the baseline model, while the population catchment of theexisting trauma center, and thus estimated trauma volume at thatcenter, decreased by 22% from baseline to 8.72 � 105. A geo-graphic representation of these models is presented in Figure 1,and summary data on the relative changes in population andtrauma center volume are presented in Table 1. A more detailedexamination of population coverage within 10-minute transporttime bands for each model is presented in Figure 2. These datashow that in addition to increasing total population coverage,the sequential addition of trauma centers inModels 1 and 2moststrongly increases population coverage in the 10- to 40-minutetransport time bands while decreasing population coverage intime bands over 40 minutes.
The distribution of population-weighted transport timesbetween each population centroid and its nearest trauma center
399
ealth, Inc. All rights reserved.
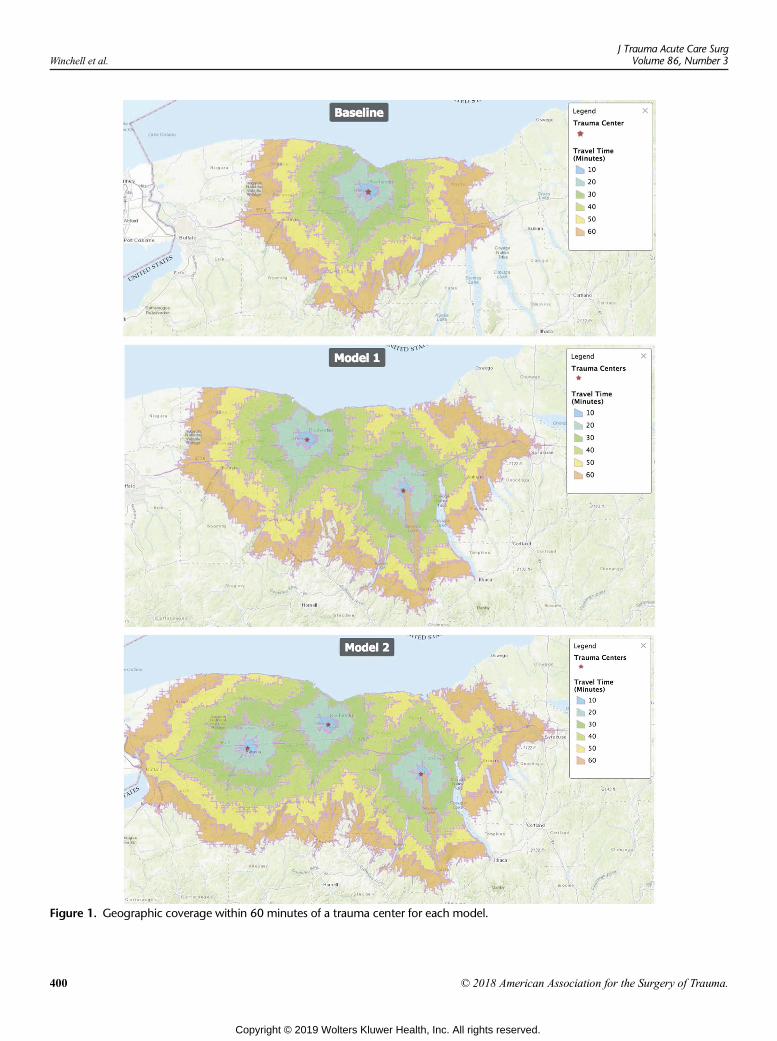
Figure 1. Geographic coverage within 60 minutes of a trauma center for each model.
Winchell et al.J Trauma Acute Care Surg
Volume 86, Number 3
400 © 2018 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.

TABLE 1. Population Coverage and Estimated Changes inTrauma Center Volume
PopulationCoverage
Change inPopulationCoverage
Change inExisting
Trauma CenterVolume
Change inSecond TraumaCenter Volume
Baseline 1.12 � 106
Model 1 1.28 � 106 + 14% −12%Model 2 1.32 � 106 + 18% −22% −32%
TABLE 2. Central Tendency of Population-Weighted TransportTimes (in Minutes)
Mean SD Median IQR
Baseline 25.7 14.5 20.6 14.5-15.7
Model 1 25.5 13.6 21.3 14.7-34.5
Model 2 23.7 12.6 20.6 14.5-30.1
SD, Standard deviation; IQR, interquartile range.
J Trauma Acute Care SurgVolume 86, Number 3 Winchell et al.
was also evaluated. The central tendency of the weighted aver-age travel times, shown in Table 2, changed very little betweenmodels, whether evaluated as the mean or the median; however,the variance of the weighted transport times decreased as the ad-ditional trauma centers were added to the model. The weightedtransport time histograms are shown in Figure 3. The histogramshave been smoothed using a local regression (LOESS) approachto simplify display. These data also demonstrate the increase intransport times between 20 and 40 minutes and concomitant de-crease in times over 40 minutes seen in Model 1 and Model 2.
DISCUSSION
The determination of need and optimal location for atrauma center is often framed as a multidimensional optimiza-tion problem. For example, the proposed center should be placedin such a way as to maximize the number of patients who canreach the trauma center within an hour to minimize transporttimes for patients overall and to maintain individual center vol-umes above a minimum level felt to be needed to maintain com-petency while allowing for system surge capacity in case ofmass casualties. Geographic Information Systems (GIS) andgeospatial techniques are ideally suited for this type of approach,allowing the simultaneous analysis of many important variables
Figure 2. Population coverage with 60 minutes of a trauma center fo
© 2018 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
including population density, injury severity, and the existingtransportation grid. The depth of such potential modeling is lim-ited only by the availability of data and the complexities of theoptimization routines, offering the attractive potential to de-scribe the perfect system. Examples of this geospatial optimiza-tion approach include the work of Jansen et al. who developedtheir own optimization algorithm to evaluate trauma systems inScotland and Colorado22–24 and Horst et al. who used the sameArcGIS network analyst tools used in our study to evaluatetrauma center placement in Pennsylvania.25–27 These ap-proaches yield elegant solutions, but they can fall short in prac-tical application.
In actual practice, trauma centers and trauma systems havedeveloped organically, not as the result of a comprehensive plan.In most cases, trauma centers have arisen in places where need,interest, and resources overlapped by happenstance, not by in-tent. Furthermore, trauma centers are expensive to establish, ex-pensive to operate, and require extensive support for hospitalresources and specialty personnel, making it nearly impossible,both financially and functionally, to simply create a new traumacenter where it might be needed. It is equally difficult to simplyremove an existing trauma center or to move it 10 miles downthe road to a geospatially optimized location. This challenge ismagnified by the use of population density data or injury sever-ity data for optimization, as both of these change with time. As a
r each model.
401
ealth, Inc. All rights reserved.
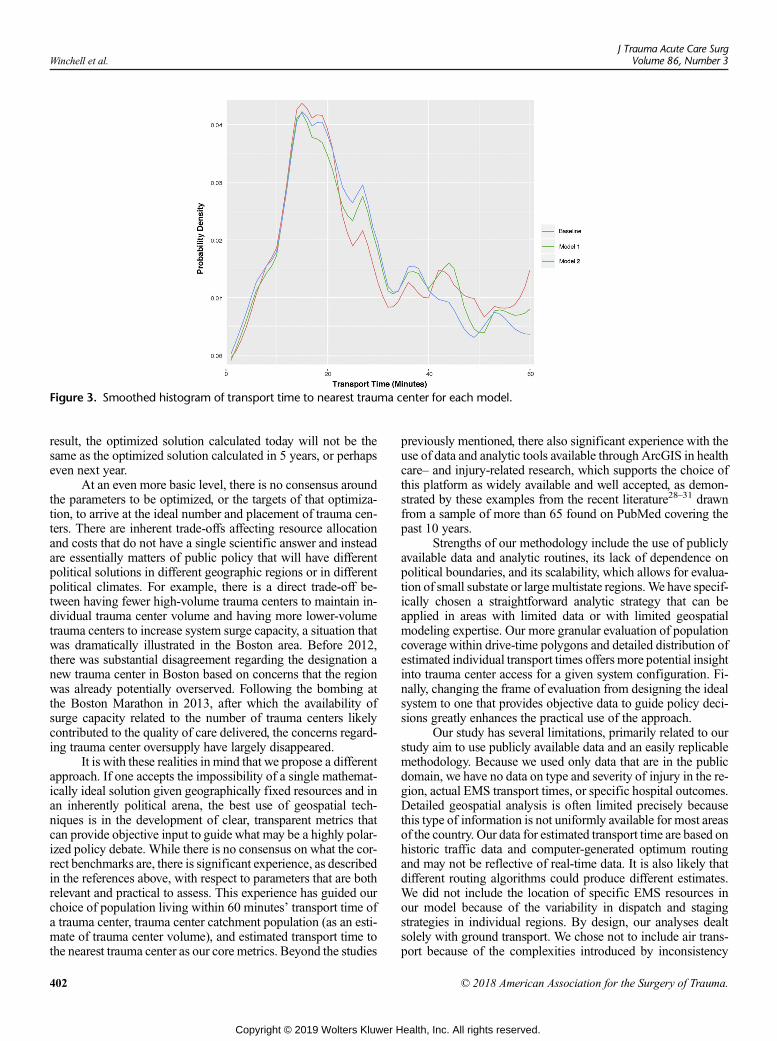
Figure 3. Smoothed histogram of transport time to nearest trauma center for each model.
Winchell et al.J Trauma Acute Care Surg
Volume 86, Number 3
result, the optimized solution calculated today will not be thesame as the optimized solution calculated in 5 years, or perhapseven next year.
At an even more basic level, there is no consensus aroundthe parameters to be optimized, or the targets of that optimiza-tion, to arrive at the ideal number and placement of trauma cen-ters. There are inherent trade-offs affecting resource allocationand costs that do not have a single scientific answer and insteadare essentially matters of public policy that will have differentpolitical solutions in different geographic regions or in differentpolitical climates. For example, there is a direct trade-off be-tween having fewer high-volume trauma centers to maintain in-dividual trauma center volume and having more lower-volumetrauma centers to increase system surge capacity, a situation thatwas dramatically illustrated in the Boston area. Before 2012,there was substantial disagreement regarding the designation anew trauma center in Boston based on concerns that the regionwas already potentially overserved. Following the bombing atthe Boston Marathon in 2013, after which the availability ofsurge capacity related to the number of trauma centers likelycontributed to the quality of care delivered, the concerns regard-ing trauma center oversupply have largely disappeared.
It is with these realities in mind that we propose a differentapproach. If one accepts the impossibility of a single mathemat-ically ideal solution given geographically fixed resources and inan inherently political arena, the best use of geospatial tech-niques is in the development of clear, transparent metrics thatcan provide objective input to guide what may be a highly polar-ized policy debate. While there is no consensus on what the cor-rect benchmarks are, there is significant experience, as describedin the references above, with respect to parameters that are bothrelevant and practical to assess. This experience has guided ourchoice of population living within 60 minutes’ transport time ofa trauma center, trauma center catchment population (as an esti-mate of trauma center volume), and estimated transport time tothe nearest trauma center as our core metrics. Beyond the studies
402
Copyright © 2019 Wolters Kluwer H
previously mentioned, there also significant experience with theuse of data and analytic tools available through ArcGIS in healthcare– and injury-related research, which supports the choice ofthis platform as widely available and well accepted, as demon-strated by these examples from the recent literature28–31 drawnfrom a sample of more than 65 found on PubMed covering thepast 10 years.
Strengths of our methodology include the use of publiclyavailable data and analytic routines, its lack of dependence onpolitical boundaries, and its scalability, which allows for evalua-tion of small substate or largemultistate regions.We have specif-ically chosen a straightforward analytic strategy that can beapplied in areas with limited data or with limited geospatialmodeling expertise. Our more granular evaluation of populationcoverage within drive-time polygons and detailed distribution ofestimated individual transport times offers more potential insightinto trauma center access for a given system configuration. Fi-nally, changing the frame of evaluation from designing the idealsystem to one that provides objective data to guide policy deci-sions greatly enhances the practical use of the approach.
Our study has several limitations, primarily related to ourstudy aim to use publicly available data and an easily replicablemethodology. Because we used only data that are in the publicdomain, we have no data on type and severity of injury in the re-gion, actual EMS transport times, or specific hospital outcomes.Detailed geospatial analysis is often limited precisely becausethis type of information is not uniformly available for most areasof the country. Our data for estimated transport time are based onhistoric traffic data and computer-generated optimum routingand may not be reflective of real-time data. It is also likely thatdifferent routing algorithms could produce different estimates.We did not include the location of specific EMS resources inour model because of the variability in dispatch and stagingstrategies in individual regions. By design, our analyses dealtsolely with ground transport. We chose not to include air trans-port because of the complexities introduced by inconsistency
© 2018 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Winchell et al.
in criteria for its use in primary scene transport, shifting cover-age by air medical providers and differences in availability dueto local weather. For most trauma centers, ground transportationremains the most common mode. Furthermore, contested deci-sions regarding trauma center designation are more commonlybased on local factors and local ground transport patterns. Fordemonstration purposes, we assumed that patients would betransported to the nearest trauma center, based on estimatedtransport time. This approach does not take into account otherfactors that can affect the choice of EMS destination. In addition,our approach assesses population access only and does not di-rectly address the capabilities or level of designation of a partic-ular facility. The determination of optimal level and capacity ofcenters in a given model is a different facet of needs assessmentthat would occur in parallel with the analysis we describe. Finally,for simplicity, we assumed our test area to be geographically iso-lated without interaction with other trauma centers whose temporalcatchment areas might overlap. In actual practice, both temporalbarriers and state, county, or regional boundaries are blurred byconvenience and historic patterns of transportation.
We believe that this exploratory analysis demonstrates awidely available, meaningful, objective, and easily reproduciblemethod to assess the current status of trauma center access andto estimate the effect of potential changes in trauma systemconfiguration. Future work will be directed at evaluating theapproach in a wide variety of geographies and system config-urations, and validating the test metrics by comparison withexisting data in specific regional trauma systems.
CONCLUSIONS
Geospatial analysis can provide objective measures ofpopulation access to trauma care, including the estimated popu-lation within 60 minutes of a trauma center, the population cov-ered by a specific trauma center (as an estimate for trauma centervolume), and the distribution of transport times to a trauma cen-ter. The analysis can be easily performed using publicly avail-able data and software to model trauma system configurationsthat contain different numbers and locations of trauma centers,thus allowing direct comparison of potential changes in cover-age and impact on existing centers. This type of data is vital toguide difficult decisions regarding trauma center designationto optimize access to care and allocation of resources.
AUTHORSHIP
R.J.W. contributed to literature search, study design, data analysis, data in-terpretation, writing of the manuscript, and critical revision of the manu-script. P.X. contributed to literature search, study design, data analysis,data interpretation, and writing of themanuscript. L.M. contributed to lit-erature search, data analysis, and critical review of the manuscript. R.H.contributed to data analysis and critical reviewof themanuscript, and pro-vided software support.
DISCLOSURE
The authors declare no conflicts of interest.This study received no funding support.
REFERENCES1. MacKenzie EJ, Rivara FP, Jurkovich GJ, Nathens AB, Frey KP, Egleston BL,
Salkever DS, Scharfstein DO. A national evaluation of the effect of trauma-center care on mortality. N Engl J Med. 2006;354(4):366–378.
© 2018 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
2. MacKenzie EJ, Weir S, Rivara FP, Jurkovich GJ, Nathens AB, Wang W,Scharfstein DO, Salkever DS. The value of trauma center care. J Trauma.2010;69(1):1–10.
3. Morshed S, Knops S, Jurkovich GJ, Wang J, MacKenzie E, Rivara FP.The impact of trauma-center care on mortality and function followingpelvic ring and acetabular injuries. J Bone Joint Surg Am. 2015;97(4):265–272.
4. Nathens AB, Jurkovich GJ, Rivara FP, Maier RV. Effectiveness of statetrauma systems in reducing injury-related mortality: a national evaluation.J Trauma. 2000;48(1):25–30; discussion 30–1.
5. Nathens AB, Brunet FP, Maier RV. Development of trauma systems and ef-fect on outcomes after injury. Lancet. 2004;363(9423):1794–1801.
6. Eastman AB,Mackenzie EJ, Nathens AB. Sustaining a coordinated, regionalapproach to trauma and emergency care is critical to patient health careneeds. Health Aff (Millwood). 2013;32(12):2091–2098.
7. Boyd DR, DuneaMM, Flashner BA. The Illinois plan for a statewide systemof trauma centers. J Trauma. 1973;13(1):24–31.
8. Bazzoli GJ, Madura KJ, Cooper GF, MacKenzie EJ, Maier RV. Progress inthe development of trauma systems in the United States. Results of a nationalsurvey. JAMA. 1995;273(5):395–401.
9. Bazzoli GJ, Harmata R, Chan C. Community-based trauma systems in theUnited States: an examination of structural development. Soc Sci Med.1998;46(9):1137–1149.
10. West JG, Williams MJ, Trunkey DD, Wolferth CC Jr. Trauma systems. Cur-rent status—future challenges. JAMA. 1988;259(24):3597–3600.
11. Eastman AB. Wherever the dart lands: toward the ideal trauma system. J AmColl Surg. 2010;211(2):153–168.
12. Shen YC, Hsia RY, Kuzma K. Understanding the risk factors of trauma cen-ter closures: do financial pressure and community characteristics matter?Med Care. 2009;47(9):968–978.
13. Friedman E. The Roller-Coaster Supply of Burn and Trauma Care:American Hospital Association. 2015. Available at: http://www.hhnmag.com/Daily/2015/April/trauma-burn-centers-vary-article-friedman. AccessedAugust 22, 2015.
14. RJW MD, ed. Growth of verified trauma centers. Chicago, IL: AmericanCollege of Surgeons Committee on Trauma Verification, Review and Con-sultation Program; 2015.
15. Hsia RY, ShenYC. Changes in geographical access to trauma centers for vul-nerable populations in the United States. Health Affairs (Project Hope).2011;30(10):1912–1920.
16. The Trauma Systems Evaluation and Planning Committee, American Col-lege of Surgeons Committee on Trauma. Statement on trauma center desig-nation based upon system need. Bull Am Coll Surg. 2015;100(1):51–52.
17. Homeland Infrastructure Foundation-Level Data (HIFLD)—Hospitalsdataset [Internet]. US Department of Homeland Security; 2017. Avail-able at: https://hifld-geoplatform.opendata.arcgis.com/datasets/hospitals. Accessed May 10, 2017.
18. Verification, Review, and Consultation Program for Hospitals [Internet].American College of Surgeons Committee on Trauma. Available at: https://www.facs.org/quality-programs/trauma/vrc. Accessed May 10, 2017.
19. Berke EM, Shi X. Computing travel time when the exact address is un-known: a comparison of point and polygon ZIP code approximationmethods. Int J Health Geogr. 2009;8:23.
20. R Core Team. R: A Language and Environment for Statistical Computing.Vienna, Austria: R Foundation for Statistical Computing; 2018.
21. Wickham H. ggplot2: Elegant Graphics for Data Analysis. New York, NY:Springer-Verlag; 2016.
22. Jansen JO, Campbell MK. The GEOS study: designing a geospatiallyoptimised trauma system for Scotland. Surgeon. 2014;12(2):61–63.
23. Jansen JO, Morrison JJ, Wang H, Lawrenson R, Egan G, He S,Campbell MK. Optimizing trauma system design: the GEOS (GeospatialEvaluation of Systems of Trauma Care) approach. J Trauma Acute CareSurg. 2014;76(4):1035–1040.
24. Jansen JO, Moore EE, Wang H, Morrison JJ, Hutchison JD, Campbell MK,Sauaia A. Maximizing geographical efficiency: an analysis of the configura-tion of Colorado's trauma system. J Trauma Acute Care Surg. 2018;84(5):762–770.
25. Horst MA, Gross BW, Cook AD, Osler TM, Bradburn EH, Rogers FB. Anovel approach to optimal placement of new trauma centers within an
403
ealth, Inc. All rights reserved.

Winchell et al.J Trauma Acute Care Surg
Volume 86, Number 3
existing trauma system using geospatial mapping. J Trauma Acute CareSurg. 2017;83(4):705–710.
26. Horst MA, Jammula S, Gross BW, Bradburn EH, Cook AD, Altenburg J,Morgan M, Von Nieda D, Rogers FB. Development of a trauma systemand optimal placement of trauma centers using geospatial mapping.J Trauma Acute Care Surg. 2018;84(3):441–448.
27. Horst MA, Jammula S, Gross BW, Cook AD, Bradburn EH, Altenburg J,Von Nieda D, Morgan M, Rogers FB. Undertriage in trauma: does an orga-nized trauma network capture themajor trauma victim?A statewide analysis.J Trauma Acute Care Surg. 2018;84(3):497–504.
28. Wen M, Fan JX, Kowaleski-Jones L, Wan N. Rural-urban disparities in obe-sity prevalence among working age adults in the united states: exploring themechanisms. Am J Health Promot. 2018;32(2):400–408.
29. Nuhu KM, McDaniel JT, Alorbi GA, Ruiz JI. Effect of healthcare spendingon the relationship between the Human Development Index and maternaland neonatal mortality. Int Health. 2018;10(1):33–39.
30. Brown SC, Wang K, Dong C, Yi L, Marinovic Gutierrez C, Di Tullio MR,Farrell MB, Burgess P, Gornik HL, Hamburg NM, et al. Accreditation statusand geographic location of outpatient echocardiographic testing facilitiesamong medicare beneficiaries: the VALUE-ECHO Study. J UltrasoundMed. 2018;37(2):397–402.
31. Ahmed AK, Duhaime AC, Smith TR. Geographic proximity to specializedpediatric neurosurgical care in the contiguous United States. J NeurosurgPediatr. 2018;21(4):434–438.
DISCUSSIONFrederick B. Rogers, M.D. (Lancaster, Pennsylvania):
I would like to congratulate Dr. Winchell and his co-authorson a well-performed study, and also acknowledge Dr. Winchell'sleadership through the American College of Surgeons in devel-oping objective measures, such as the needs-based assessmentof trauma systems to guide trauma center placement within atrauma system.
In the past 15 to 20 years, there has been an enormousgrowth in the number of trauma centers throughout the UnitedStates. While superficially this may seem like a good thing, un-fortunately, this growth is not guided by intelligent design, butrather by financial considerations and large healthcare systemconglomerate imperatives.
The net result is a clustering of trauma centers in more af-fluent urban and suburban regions, with each trauma centerencroaching on each other's catchment areas, and as a result, di-luting the experience of each individual trauma center. Con-versely, many rural and less affluent areas are bereft of traumacenter coverage for the major trauma victim.
There are now a number of studies which are beginning toaddress this disparity in care and look to other ways to managethe growth of new trauma centers within a defined trauma sys-tem. The geo-spacial approach for analysis of trauma center ac-cess presented here today is one such approach.
The beauty of this approach is that it uses readily availableoff-the-shelf software, which is frequently used by many com-mercial enterprises, and also publicly available, easily obtainabledata that could be incorporated within any area that the data isavailable, without resorting to capturing sophisticated traumademographics.
I would also add this is probably also the inherent weak-ness of such a preliminary analysis in that we really don't knowthe particulars of the trauma system they studied: the volume oftrauma; the severity and the size and capabilities of the individ-ual trauma hospitals within the trauma system.
I have two questions for the authors.
404
Copyright © 2019 Wolters Kluwer H
You state that Strong Memorial Hospital in Rochester isthe center of your study area. You then remove census tracts fromurban areas on the outer areas of the 60-minute drive to Rochester,which in this case would be both Buffalo and Syracuse.
Both these cities have existing Level 1 trauma centers,whose catchment area would presumably cover parts of the pop-ulation included in your model.
Have you conducted sensitivity analysis to determine theimpact of the service areas of those two trauma centers and theirresults? Including these trauma centers and their service areaswould most likely change where the next trauma center wouldbe located in their model.
And second, this is more of a philosophical question,while these models of theoretical trauma center placement arehelpful to define the ideal location of the next trauma centerwithin a trauma system, how do you translate that into the realworld of practical application of these methods into the morassof politics and monetary demands that are currently surroundingthe placement of trauma centers?
Thank you very much for the opportunity to comment onthis paper.
Charles E. Lucas, M.D. (Detroit, Michigan): Robertthat was an excellent presentation. The principles that yououtlined need to be followed by the Committee on Traumathroughout the country.
I have one question. Most of us trauma surgeons makemost of our living by taking care of non-trauma patients.When you look at your model, have you considered how thetrauma people from all specialties are going to make a livingrelated to diseases that are not related to trauma at these newtrauma centers?
JamesW. Davis, M.D. (Fresno, California):Dr. Winchell,excellent presentation. I am concerned that with your expertisein system development and system evaluation that your analysisis flawed, because you've used logic, and it seems to be notice-ably lacking in where trauma centers get put.
I'd also like to understand better what it would do for areaslike mine in Central California, which is relatively underserved,and how this model could be used to identify centers that shouldparticipate, and if this could be used to perhaps provide some in-fluence from the College to help people see the light. Thank you.
Michael B. Aboutanos, M.D. (Richmond, Virginia):Bob, thank you so much for this wonderful presentation. I alsowant to thank you for representing our state for our trauma sys-tem plan. We actually just finalized our plan.
The issue I have with the model – I think that it is ex-tremely useful, but mainly in comparison to an existing model.It sounds like it's almost a fictitious aspect.
So, one question I have, your model is really based on thepopulation increase as you have centers. That seemed to have in-creased as far as how many more population can be covered.
What if you keep that population constant, that does notincrease, and see how the model works with additional centersbeing created within this same area, not being allowed to in-crease, and seewhat that does with regard to the actual plan? Be-cause I think that's really the reality of it.
We're not adding something; we're leveling up existing fa-cilities that are present. So how does the model apply to that?Again, I think it would be very useful, taking the reality, you
© 2018 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Winchell et al.
know, how the model works and how it should have worked.Thank you.
Robert J. Winchell, M.D. (New York, New York):Thank you very much, and thanks, Fred, for your comments. I'llsee if I can get these all figured out.
So, as to the reason that we picked that area, when I starteddoing this twoyears ago, wewere approaching the GIS data a lit-tle differently. We actually were working from the ground up at avery basic level, and so we tried to pick an area that was simple,but that had all of the data that we needed. As time went on andour knowledge of the software improved, in fact, you don't haveto dig to find the data, it's all out there. So we modified the pro-cess a little bit but did not change the selected geographic area.
The idea was not to pick a real-world trauma center or areal-world situation; it was to pick a test area and see how themetrics changed. And so if you put the two cities – if you putErie and Syracuse back in at the corners of that, what you find,in fact, is that 60 minutes transport time picks up downtownSyracuse, and that's also not the real world. We could haveput those population centers in the model, but it just muddlesit up, and makes it that much harder to demonstrate what thedifferences are in a five-center model rather than a two-centermodel or a three-center model.
We were really just trying to pick an area to demonstratethe metrics that could be generated and how the metrics couldbe used to differentiate between different configurations, ratherthan actually trying to figure out what's going on in Rochester.I think that is the first question.
The second question was about validation, and how doweknow this works. And further, still in part of Dr. Rogers' presen-tation, is the idea that this methodology is going to try and tellyou where to put the trauma centers. I would say that, in fact,the idea behind this set of metrics is “you tell mewhere youwantto put the trauma center, I can tell you what that's going to do toyour existing center”. It won't say whether it's the best or theworst configuration, just what the impact will likely be, to helpguide the decisions around whether it is, in fact, an intelligentchoice within a given system. As Dr. Davis noted, decisionsaround trauma center placement are not logical, they're political.There is no ideal solution.
Our concept in putting this together is to generate the datathat will at least help guide some rationality in what is intrinsi-cally a political decision.
We are working on trying to validate how well the transpor-tation calculations model real transportation times. I think that canbe validated. We're going to look at some before and after areaswhere centers have already been added and we have the data tosee if the predictions are accurate. But for the most part, the useof this tool would be to hopefully figure out what might happenif you put in trauma center Awithout actually having to do it.
© 2018 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
Let's see, then, so, Dr. Lucas, I'm not sure if I understoodyour question with respect to how we're going to be able to tellus in the trauma centers what to do in addition to trauma.
The idea of population coverage could certainly be ex-tended to other time-sensitive illnesses. In that context, the con-cept of population coverage still works.
When you try to start adding more detail, and the data cer-tainly exists to stratify the population by age groups, or groups atrisk for certain types of injury, these are dynamic factors that tellme what's happening today, but will almost certainly changewith time while the distribution of trauma centers is likely tobe fixed.
Dr. Davis, I completely concur that there is an absence oflogic. The whole idea behind this approach is to try and at leastprovide some reproduceable objective data so that I'll get thesame answer that you will, and at least we don't have to fightabout how we crunched the numbers. Whether that actuallywill introduce a change in the debate, I think remains to be seenas well.
And, finally, Dr. Aboutanos, if my memory now serves,we weren't really seeking to compare our outcome to a realworld – the proposed models certainly do not reflect any real-world thing that was happening around the Rochester area –but more to try and demonstrate what changes in populationcoverage would be predicted with the addition of new centers.
The way the model works is it goes out 60 minutes basedon network transport time, and that will encompass more peopleas those coverage areas geometrically get bigger. The pop-ulation data that underlies all three models is the same. It'sjust you're increasing population coverage, and I think that'sstill valid.
Themodel could be easily adapted to a specific catchmentdistrict, and I could cut it off at the borders of five counties andsay I'm only going to look within here, and in which case youwon't add much in terms of coverage.
But having played with the model, I can tell you that if Iput another trauma center right next door to Strong, thosetravel-time polygons don't get bigger and I won't increase thepopulation coverage, either. It just simply will decrease the num-ber of people that go to each hospital.
Going back to Dr. Davis's last piece, if I put a hospital inthe middle of the Central Valley, the model very eloquently dem-onstrates that that's a brand new group of people who are cov-ered within 60 minutes of a trauma center who weren't coveredbefore. There is no impact on the existing centers in the region,because those polygons don't overlap, so that's not usually con-tentious, but again, the tools will certainly outline the need andhow well those holes get plugged.
Once again, my thanks for the opportunity to presentour approach.
405
ealth, Inc. All rights reserved.

AAST 2018 PODIUM PAPER
Interhospital variability in time to discharge to rehabilitationamong insured trauma patients
LisaM. Knowlton,MD,MPH, Alex H.S. Harris, MS, PhD, Lakshika Tennakoon,MD,Mary T. Hawn,MD,MPH,David A. Spain, MD, and Kristan L. Staudenmayer, MD, MS, Stanford, California
Fro
Ad
Thi
DO
40
BACKGROUND: H
m the Department of SurgeryUniversity School of Medicinesearch and Education (A.H.S.Hdress for reprints: Lisa Marie KnCare and Acute Care SurgeryStanford, CA 94305; email: drls article will be presented as a poof the American Association foin San Diego, CA.
I: 10.1097/TA.00000000000021
6
ospital costs are partly a function of length of stay (LOS), which can be impacted by the local availability of postacute care (PAC)resources (inpatient rehabilitation and skilled nursing facilities), particularly for injured patients. We hypothesized that LOS fortrauma patients destined for PAC would be variable based on insurance type and hospitals from which they are discharged.
METHODS: W
e used the 2014 to 2015 National Inpatient Sample from the Healthcare Cost and Utilization Project. We included all adult ad-missions with a primary diagnosis of trauma (International Classification of Diseases, 9th Revision, Clinical Modification codes),who were insured and discharged to PAC. We then ranked hospitals based upon mean LOS and divided them into quartiles to de-termine differences. The primary outcome was inpatient LOS; secondary outcome was cost.RESULTS: T
here are 958,005 trauma patients that met the inclusion criteria. Mean LOS varied based upon insurance type (Medicaid vs. Private vs.Medicare: 12.7 days vs. 8.8 days and 5.7 days; p < 0.001). Shortest LOS hospitals had a marginal variation in LOS (Medicaid vs.Private vs. Medicare: 5.5 days vs. 4.8 days vs. 4.2 days; p < 0.001). Longest LOS hospitals hadmean LOS that varied substantially(16.4 days vs. 11.0 days vs. 6.7 days; p < 0.001). Multivariate regression controlling for patient and hospital characteristics re-vealed that Medicaid patients spent Medicaid patients spent an additional 0.4 days in shortest LOS hospitals and an additional2.6 days in longest LOS hospitals (p < 0.001). The average daily cost of inpatient care was US $3,500 (SD, US $132). Even withconservative estimates, Medicaid patients at hospitals without easy access to rehabilitation incur significant additional inpatientcosts over $10,000 in some hospitals.CONCLUSION: P
rolonged LOS is likely a function of access to postacute facilities, which is largely out of the hands of trauma centers. Efficienciesin care are magnified by access to postacute beds, suggesting that increased availability of rehabilitation facilities, particularly forMedicaid patients, might help to reduce LOS. (J Trauma Acute Care Surg. 2019;86: 406–414. Copyright © 2018 American Associ-ation for the Surgery of Trauma.)LEVEL OF EVIDENCE: E
pidemiologic, level III; care management, level IV. KEYWORDS: R ehabilitation; postacute services; insurance status; trauma systems; healthcare utilization.H ospital costs are partly a function of length of stay (LOS),which has been previously associated with patient and hos-
pital process-related factors.1 However, LOSmay also be impactedby the local availability of postacute care (PAC) resources such asinpatient rehabilitation facilities or skilled nursing facilities. Fur-thermore, even when facilities are available, access to those re-sources may depend on the type of insurance a patient possesses.The Institute of Medicine (IOM) has documented substantialvariation in spending for PAC spending, as well as variabilityin the number of rehabilitation and skilled nursing facilities byState. In fact, the IOM found that PAC spending accounted for73% of the geographic variation in Medicare spending per ben-eficiary.2 This suggests that variability in access exists. If so, thismay directly impact a hospital's ability to discharge patients,
(L.M.K., L.T., M.T.H., D.A.S., K.L.S.), Stanford; and Stanford-Surgery Policy Improvement Re-.) Center (S-SPIRE), Stanford, California.owlton, MD, Section of Trauma, Surgical CriticalStanford University 300 Pasteur Drive, [email protected] oral presentation at the 77th AnnualMeetingr the Surgery of Trauma; September 26–29, 2018
63
Copyright © 2019 Wolters Kluwer H
resulting in unnecessarily longer lengths of stay, higher inpatienthospitalization costs, and impacting hospital benchmarking.3
Access to rehabilitation is particularly important for traumapatients, who frequently require discharge to rehabilitation andskilled nursing facilities postinjury to regain function and restoretheir quality of life. A recent study in Washington State found a40% lower odds of mortality 1 year after injury for injuredpatients discharged to rehabilitation compared to similar patientswhowere not provided rehabilitation.4 PAC is also becomingincreasingly important given that elderly patients are the fastest-growing trauma population, many of whom require rehabilitationpostinjury due to falls.5,6
Even after controlling for sociodemographics and injuryseverity, uninsured hospitalized young adult trauma patientsare less likely to receive rehabilitative care after serious injuryand spendmuch longer recovering in hospital compared to thosewith insurance.7,8 However, differences in time spent awaitingrehabilitation for trauma patients with different types and qualityof insurance are less well documented.We hypothesized that for alltrauma patients destined for PAC, LOS would vary based on insur-ance type.We further postulated that this would vary based on hos-pital, as different hospitals likely have different access to PAC beds.If true, this would suggest that a focus on improving access to PACdestinations might help to improve patient outcomes as well ascosts associated with excessive inpatient acute care hospital days.
J Trauma Acute Care SurgVolume 86, Number 3
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Knowlton et al.
METHODS
We queried the National Inpatient Sample (NIS) from theHealthcare Cost and Utilization Project (HCUP), a nationallyrepresentative all-payer database for inpatient hospitalizationsthat provides data for approximately 35 million weighted dis-charges from US hospitals annually.
We used the 2014 database and the first 9 months of 2015(January–September) that were consistent with InternationalClassification of Diseases, 9th Revision, Clinical Modification(ICD-9CM) coding, as the last 3 months of the 2015 databasecontained ICD-10CM coding. We included all admissions witha primary diagnosis of trauma based upon ICD-9CM codes(ICD-9-CM 800.0 to 959.0, excluding 905 to 924), who were18 years and older, insured, and whose discharge dispositionwas PAC. We defined PAC using the HCUP standard, which in-cluded discharge to inpatient rehabilitation facilities, skilled nurs-ing facilities, or long-term care hospitals. We excluded patientswith missing cost data.
Patient demographic and healthcare utilization characteris-tics were compared across three primary insurance groups;Medicare, Medicaid and Private (including commercial andemployer-based plans). Injury Severity Score (ISS) was calculatedfor each patient using the ICDPIC version 3.0 within Stata/SEversion 14.2 (StataCorp, College Station, TX).9 Major proce-dures were defined by the NIS as any procedure with an ICD-9-CM procedure indicator that is performed in the operatingroom, whether for diagnostic or therapeutic reasons.
To test the hypothesis that LOS prior to discharge to PACvaries by insurance type, we conducted a mixed-effects negativebinominal regression with LOS as the outcome, insurance type(Medicare, Medicaid, Private) as the primary independent vari-able, and a random effect to account for clustering of patientsin hospital. Patient-level control variables included in the modelwere age, sex, race/ethnicity, ISS calculated for using the ICDPICversion 3.0, income quartile for zip code of residence, and whetherthe admission included a major surgery/procedure. Hospital-levelcontrol variable included in the model were bed size (small, me-dium, large), region, ownership (government, private nonprofit,private investor-owned), and hospital teaching location (rural,urban nonteaching, urban teaching). The secondary outcome ofcost was determined by converting charges to cost using conver-sion ratios provided by HCUP.
Subanalysis was then performed based on patient age, dueto differences in insurance type in patients younger than andolder than 65 years. Patients 65 years and older, for example,would be far more likely to qualify for and be insured by Medi-care. We therefore analyzed patients aged 18 years to 64 yearsanalyzed separately from patients 65 years and older.
To examine whether the effects of insurance status varieddepending on hospital average LOS, we also repeated the analy-ses in patients treated in hospitals in the longest and, separately,the shortest quartiles of average LOS. Centers were rank orderedbased on shortest to longest LOS to rehabilitation, and subsequentlydivided into quartiles bymean LOS. Hospital region, ownership,teaching status, and bed size were compared between groups.
The NIS is a nationally representative, all-payer databasethat provides data for approximately 35 million weighted dis-charges from US hospitals annually. Survey weights were used
© 2018 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
to provide national estimates. As recommended, weights were notused in conducting regression analyses in this trauma-focused sub-sample of discharges.10 All analyses were conducted using StataSE v14.2 andR. The studywas exempted for review by the StanfordIRB as data were provided by HCUP in a deidentified format.Use of the NIS follows regulations within the data use agreementas defined by the Agency of Healthcare Research and Quality.
RESULTS
A total of 464,119 patients had a primary diagnosis oftrauma. When weighted, this represented approximately 2.4 millionpatients nationwide. The percent of patients discharged to PACvaried with insurance type. Of all adult trauma patients, 34.5%Medicare patients (n = 160,128), 5.5% Private patients(n = 25,357), and only 1.9% (n = 8,915) Medicaid and 0.4%(n = 2,016) self-pay patients were discharged to PAC. We thenrestricted our study sample to our defined conditions of being in-sured and discharged to PAC. Thus, 190,352 patients (weighted:958,005) or 41% met inclusion criteria. Approximately 82%(n = 156,793) were insured byMedicare, 5% (n = 8,756) byMed-icaid, and 13% (n = 24,803) by Private insurance. The additional2,016 self-pay patients who were discharged to PAC (1.0% of allpatients discharged to PAC) were excluded from analysis.
Patient demographic and utilization characteristics differedsignificantly across insurance types (Table 1). Medicaid patientswere younger (50.5 years vs. 61.8 years and 80.4 years for Privateand Medicare, respectively: p < 0.001) and more often male(55.7% vs. 45.2% and 29.6% for Private and Medicare, respec-tively; p < 0.001). Injury severity score was greatest amongMedicaid patients discharged to rehabilitation (ISS greater than15 in 27.6% vs. 24.8% and 9.0% for Private and Medicare, re-spectively: p < 0.001). Operative intervention for trauma wasalso highest among Medicaid patients (72.0% vs. 70.8% and65.0% for Private vs. Medicare, respectively, p < 0.001).
The distribution of LOS across the overall sample is presentedin Table 2. Overall, mean LOS for trauma patients discharged torehabilitation was 6.4 days (SD, 0.1). Medicaid trauma patientsdischarged to rehabilitation had the longest LOS (12.7 days vs.8.8 days and 5.7 days for Private and Medicare, respectively:p < 0.001). Mean costs were also highest for Medicaid patients(US $40,528 vs. US $30,087 and US $15,558 for Private andMedicare, respectively; p < 0.001). The differences in costs be-tween Medicaid and Private insurance were explained by theLOS, as the average daily costs for Medicaid and Private pa-tients awaiting rehabilitation were the same (US $3,201 andUS $3,407 per day, respectively; p = 0.23). In contrast, the lowermean costs for Medicare patients destined for rehab were due toboth lower costs per day as well as shorter lengths of stay (Medi-care, US $2,739 per day; p < 0.001).
Subanalysis was then performed analyzing separately pa-tient groups ages 18 years to 64 years, and 65 years and older.Among 196,616 trauma patients ages 18 years to 64 years,16% (n = 31,246 patients) were discharged to rehabilitation.For this younger cohort discharged to rehabilitation, 30%(n = 9,464) were insured byMedicare, 25% (n = 7,787) byMed-icaid and 45% (n = 13,995) by Private insurance.When compar-ing clinical characteristics, younger patients being discharged toPAC had higher injury severity (ISS > 15: 25% vs. 9% in
407
ealth, Inc. All rights reserved.
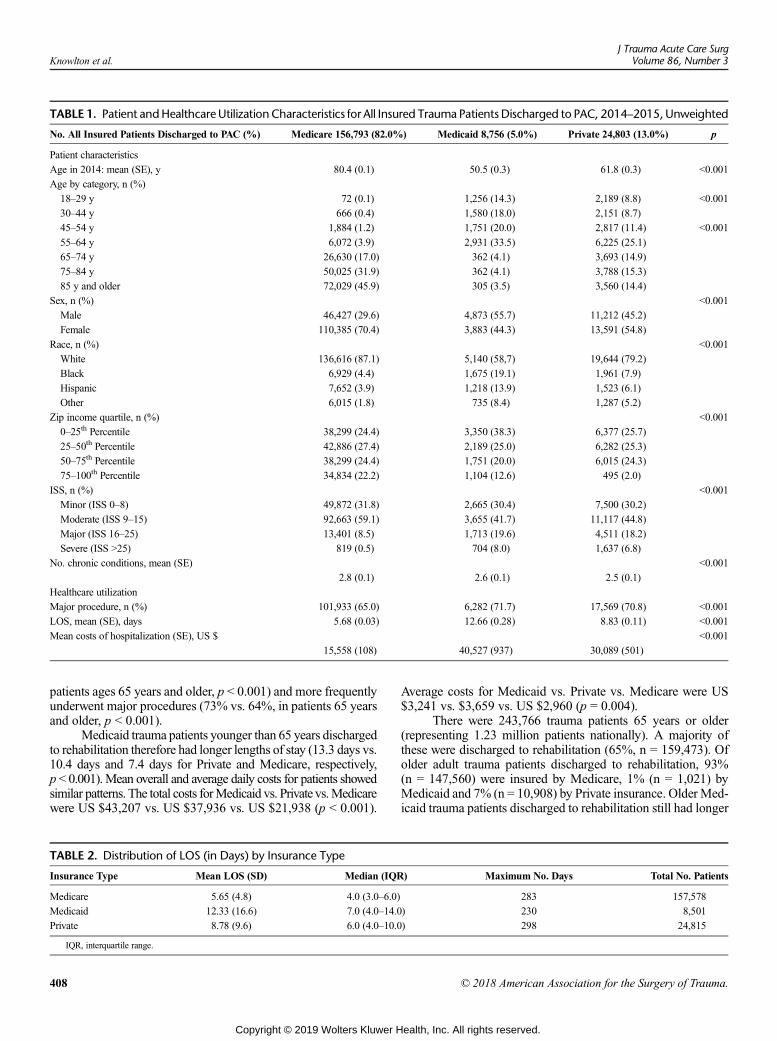
TABLE 1. Patient andHealthcareUtilizationCharacteristics for All Insured Trauma PatientsDischarged to PAC, 2014–2015, Unweighted
No. All Insured Patients Discharged to PAC (%) Medicare 156,793 (82.0%) Medicaid 8,756 (5.0%) Private 24,803 (13.0%) p
Patient characteristics
Age in 2014: mean (SE), y 80.4 (0.1) 50.5 (0.3) 61.8 (0.3) <0.001
Age by category, n (%)
18–29 y 72 (0.1) 1,256 (14.3) 2,189 (8.8) <0.001
30–44 y 666 (0.4) 1,580 (18.0) 2,151 (8.7)
45–54 y 1,884 (1.2) 1,751 (20.0) 2,817 (11.4) <0.001
55–64 y 6,072 (3.9) 2,931 (33.5) 6,225 (25.1)
65–74 y 26,630 (17.0) 362 (4.1) 3,693 (14.9)
75–84 y 50,025 (31.9) 362 (4.1) 3,788 (15.3)
85 y and older 72,029 (45.9) 305 (3.5) 3,560 (14.4)
Sex, n (%) <0.001
Male 46,427 (29.6) 4,873 (55.7) 11,212 (45.2)
Female 110,385 (70.4) 3,883 (44.3) 13,591 (54.8)
Race, n (%) <0.001
White 136,616 (87.1) 5,140 (58,7) 19,644 (79.2)
Black 6,929 (4.4) 1,675 (19.1) 1,961 (7.9)
Hispanic 7,652 (3.9) 1,218 (13.9) 1,523 (6.1)
Other 6,015 (1.8) 735 (8.4) 1,287 (5.2)
Zip income quartile, n (%) <0.001
0–25th Percentile 38,299 (24.4) 3,350 (38.3) 6,377 (25.7)
25–50th Percentile 42,886 (27.4) 2,189 (25.0) 6,282 (25.3)
50–75th Percentile 38,299 (24.4) 1,751 (20.0) 6,015 (24.3)
75–100th Percentile 34,834 (22.2) 1,104 (12.6) 495 (2.0)
ISS, n (%) <0.001
Minor (ISS 0–8) 49,872 (31.8) 2,665 (30.4) 7,500 (30.2)
Moderate (ISS 9–15) 92,663 (59.1) 3,655 (41.7) 11,117 (44.8)
Major (ISS 16–25) 13,401 (8.5) 1,713 (19.6) 4,511 (18.2)
Severe (ISS >25) 819 (0.5) 704 (8.0) 1,637 (6.8)
No. chronic conditions, mean (SE) <0.001
2.8 (0.1) 2.6 (0.1) 2.5 (0.1)
Healthcare utilization
Major procedure, n (%) 101,933 (65.0) 6,282 (71.7) 17,569 (70.8) <0.001
LOS, mean (SE), days 5.68 (0.03) 12.66 (0.28) 8.83 (0.11) <0.001
Mean costs of hospitalization (SE), US $ <0.001
15,558 (108) 40,527 (937) 30,089 (501)
Knowlton et al.J Trauma Acute Care Surg
Volume 86, Number 3
patients ages 65 years and older, p < 0.001) and more frequentlyunderwent major procedures (73% vs. 64%, in patients 65 yearsand older, p < 0.001).
Medicaid trauma patients younger than 65 years dischargedto rehabilitation therefore had longer lengths of stay (13.3 days vs.10.4 days and 7.4 days for Private and Medicare, respectively,p < 0.001).Mean overall and average daily costs for patients showedsimilar patterns. The total costs forMedicaid vs. Private vs.Medicarewere US $43,207 vs. US $37,936 vs. US $21,938 (p < 0.001).
TABLE 2. Distribution of LOS (in Days) by Insurance Type
Insurance Type Mean LOS (SD) Median (IQR
Medicare 5.65 (4.8) 4.0 (3.0–6.0)
Medicaid 12.33 (16.6) 7.0 (4.0–14.0
Private 8.78 (9.6) 6.0 (4.0–10.0
IQR, interquartile range.
408
Copyright © 2019 Wolters Kluwer H
Average costs for Medicaid vs. Private vs. Medicare were US$3,241 vs. $3,659 vs. US $2,960 (p = 0.004).
There were 243,766 trauma patients 65 years or older(representing 1.23 million patients nationally). A majority ofthese were discharged to rehabilitation (65%, n = 159,473). Ofolder adult trauma patients discharged to rehabilitation, 93%(n = 147,560) were insured by Medicare, 1% (n = 1,021) byMedicaid and 7% (n = 10,908) by Private insurance. Older Med-icaid trauma patients discharged to rehabilitation still had longer
) Maximum No. Days Total No. Patients
283 157,578
) 230 8,501
) 298 24,815
© 2018 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Knowlton et al.
lengths of stay (7.5 days vs. 6.9 days and. 5.6 days for Privateand Medicare, respectively; p < 0.001), but the total costs forcosts for Medicaid vs. Private vs. Medicare were smaller in mag-nitude than the younger rehabilitation cohort at US $20,139 ver-sus US $20,059 versus US $15,150, (p < 0.001).
Hospital-level analysis was then performed to analyze dif-ferences in time to discharge to rehabilitation. Among the 4,700hospitals in the NIS sample, 4,456 met the two inclusion criteriaof (1) treating adult trauma patients of one of three insurancetypes, and (2) having evidence that they discharged patients torehabilitation (to ensure hospitals in areas without ready accessto rehabilitation were not included in the analysis). Hospitalswere rank ordered based upon mean LOS for their trauma pa-tients and divided into quartiles based upon the mean LOS.Mean LOS differed between shortest LOS hospitals and longestLOS hospitals (4.3 days vs. 8.0 days, p < 0.001). When compar-ing LOS by insurance type within each hospital group, therewere significant differences (Fig. 1). The shortest LOS hospitalshad a marginal variation in LOS based on insurance types (Med-icaid vs. Private vs. Medicare: 5.5 days vs. 4.8 days vs. 4.2 days,p < 0.001). In contrast, the longest LOS hospitals varied by asmuch as 1 week (Medicaid vs. Private vs. Medicare: 16.4 days vs.11.0 days vs. 6.7 days, p < 0.001). Mean costs of care were alsolower across insurance types in the shortest LOS hospitals(Medicaid vs. Private vs. Medicare: US $19,055 vs. US$16,617 vs. US $13,762, p < 0.001), as compared to the longestLOS hospitals (daily costs of Medicaid patients vs. Private vs.Medicare: US $51,582 vs. US $37,923 vs. US $17,525, p < 0.001).
Patients within the hospitals with shortest LOS differedsignificantly from those with the longest LOS. Patients in theshortest LOShospitalswere overall older (79.3 years vs. 74.0 years,p< 0.001), more often female (72.1%vs. 63.2%, p< 0.001), and ofa higher income (zip income quartile 50–100%: 50.1% vs. 42.8%,p < 0.001). Hospitals with the shortest LOS also had fewerMed-icaid patients (3.1% vs. 6.3%), and more Medicare patients(88.2% vs. 77.2%, p < 0.001).
Access to rehabilitation differed across the United States.Hospital-level analysis revealed that the shortest LOS hospitalswere more commonly found in the Midwest (41.6% of the top
Figure 1. Differences in LOS by insurance type among hospital quar
© 2018 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
25%). This included hospitals in the West North Central statesincluding Missouri, the Dakotas, and Nebraska (n = 267, 24.2%),and East North Central states such as Ohio, Illinois, Wisconsin,and Michigan (n = 192, 17.4%). Hospitals in the longest LOSquartile were more often in the Southern part of the UnitedStates (47.1% of the bottom 25%). This included the South At-lantic states such as the Carolinas, Georgia and Florida (n = 236,21.1%), the West South Central states such as Oklahoma andArkansas (n = 221, 19.7%) and the East South central states in-cluding Kentucky, Tennessee and Alabama (n = 71, 6.3%)(Fig. 2). A full list of States by hospital division are availablethrough HCUP.
Finally, to satisfy the statistical assumptions of our linearregression model, we performed a multivariate mixed-effectsnegative binomial regression controlling for hospital, patientcharacteristics and injury factors (Table 3). Compared to patientswithMedicare, patientswithMedicaid had an additional 1.6 dayslonger LOS (p < 0.001). In contrast, patients with private insur-ance had 0.5 more days compared to Medicare (p < 0.001). Thedifference between insurance type became more pronouncedwhen evaluating hospitals by LOS quartile. In hospitals withthe longest LOS, patients with Medicaid or private insurancehad an additional 2.6 days or 0.8 days longer LOS, respectively(p < 0.001). In hospitals in the shortest LOS quartile, patientswith Medicaid or private insurance had an additional 0.4 daysand additional 0.2 days longer LOS, respectively (p < 0.001).
DISCUSSION
Our study revealed that over 40% of trauma patients aredischarged to rehabilitation postinjury, reflecting the urgentand increasing need for access to postacute services, regardlessof insurance status.11–13 This is an underestimate of true need,as this does not include those patients who require PAC, but donot have access due to lack of insurance. As expected, patientswithMedicare and private plansweremore often discharged to re-habilitation, but this could not fully be explained by patient char-acteristics. Medicaid patients in fact had a higher injury severityscore andmore often underwent operative intervention, indicating
tiles.
409
ealth, Inc. All rights reserved.
Figure 2. Regional distribution of hospitals discharging patients to rehabilitation, based on hospital quartiles.
Knowlton et al.J Trauma Acute Care Surg
Volume 86, Number 3
a greater burden of injury that would suggest need for rehabilita-tion. This also meant that they had the longest LOS, with patientsyounger than 65 years spending nearly an additional week in hos-pital awaiting discharge to PAC. Although trauma care often fo-cuses on the acute period, rehabilitation has been shown to havea significant impact on outcomes.14–16 The findings of this work
TABLE 3. Negative Binomial Mixed-effects Regression to PredictLOS, Based on Insurance Type
Variables Exp (coefficient) Additional Days p
Intercept 4.71 — <0.001
Payer status
Medicare Reference
Medicaid 1.33 1.55 <0.001
Private insurance 1.10 0.47 <0.001
Race
White Reference
Black 1.08 0.37 <0.001
Hispanic 1.03 0.14 <0.001
Zip income quartile
0–25th percentile Reference
25–50th percentile 0.99 −0.04 <0.001
50–75th percentile 0.98 −0.09 <0.001
75–100th percentile 0.97 −0.14 <0.001
ISS
0–8 (Minor) Reference
9–15 (Moderate) 1.07 0.33 <0.001
16–25 (Major) 1.54 2.54 <0.001
>25 (Severe) 2.22 5.75 <0.001
Had major OR procedure 1.27 1.37 <0.001
Hospital region
Northeast Reference
Midwest 0.92 −0.38 <0.001
South 0.99 −0.01 <0.001
West 0.89 −0.52 <0.001
Hospital teaching location
Rural Reference
Urban nonteaching 1.06 0.28 <0.001
Urban teaching 1.17 0.80 <0.001
Hospital control
Government Reference
Private, nonprofit 0.90 −0.47 <0.001
Private, for-profit 0.92 −0.38 <0.001
410
Copyright © 2019 Wolters Kluwer H
suggest a lack of alignment between patient need and resourcesavailable based on insurance status.
Furthermore, LOS for those patients with insurance whowere ultimately discharged to rehabilitation varied substantiallyby insurance type. Overall, mean LOS for trauma patientsdischarged to PAC was 6.4 days (SD, 0.1 days), with LOS by in-surance type varying by as much as 1 week. Medicaid traumapatients discharged to rehabilitation stayed approximately 13 days,compared to only 6 days for Medicare patients. This effect isseen across age groups, but particularly among patients underthe age of 65. Within this younger group, the LOS stay differ-ence is preserved, but youngMedicare patients spend an averageof 1 day longer in hospital than their elderly Medicare coun-terparts. This is likely due to the fact that Medicare patientsyounger than 65 years are a special cohort of patients with com-plex needs who qualify for coverage either through disability,end-stage renal disease or other select criteria.17 These patientsyounger than 65 years meeting such criteria comprise 16%of the current US Medicare population.17 They likely repre-sent 30% of our younger than 65 years cohort given that welimited our study sample to injured patients with a dischargedestination of PAC, thereby potentially selecting for a group ofpatients with poorer baseline functional status.
Variability in LOS based upon type of insurance is likely adirect result of policy differences between Medicare and state-by-state Medicaid programs. For example, Medicare will payfor inpatient rehabilitation for up to 100 days in a benefit periodafter a hospitalization lasting three or more days.18 In contrast,Medicaid plans vary widely in their coverage for rehabilitation.Furthermore, variability exists in state-by-state Medicaid policieson approval for rehabilitation, exacerbating these differences.19
Therefore, Medicaid patients who require rehabilitation mayspend longer in hospital while awaiting administrative approvalfor rehabilitation or end up doing most of their rehab duringtheir acute hospitalization. Sensitivity of access to rehabilitationand public policy has been documented in the past. Immediatelyfollowing implementation of the Inpatient Rehabilitation Facil-ity (IPF) Prospective Payment System (PPS) Final Rule ofMay 2004, access to rehabilitation steadily declined.20,21
As there is much focus on reducing healthcare costs andimproving outcomes, it is important to recognize that limitationsin access to PAC – particularly for Medicaid patients –contribute significantly to inpatient costs. The mean daily inpa-tient cost of Medicaid patients US $3,201 and they are admitted6.5 days longer than the mean LOS of patients being dischargedto PAC. This represents US $20,807 in excess inpatient costs per
© 2018 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Knowlton et al.
Medicaid patient, and approximately US $915 billion dollarswhen extrapolated to our weighted national Medicaid sample.It is worthwhile considering how redirecting these funds towardimproved availability of PAC sites could result in both signifi-cant improvement in patient outcomes and improved inpatientresource utilization.
In addition to patient and policy differences, geographiclocation of a hospital may determine the number of beds locallyavailable for rehabilitation. We discovered regional discrepan-cies in time to rehabilitation, as well as differences based uponrural vs. urban setting, and teaching status. Interestingly, hospi-tals with presumed good access to rehabilitation beds (as deter-mined by shortest LOS for patients destined to rehabilitation)were most often located in the Midwest, and there was little dif-ference between payer types in LOS. Although this againmay bea result of state Medicaid policy, the noticeable difference be-tween LOS in each quartile suggests that some hospitals and re-gions have better access to PAC than others.
Our findings are consistent with the national distributionof PACs by region, as described in a study by the Office of theAssistant Secretary for Planning and Evaluation.22 The highestvolumes of PAC facilities were concentrated in the Midwestand Pacific regions, as well as in Texas. Furthermore, a KaiserFamily Foundation report on the national distribution of PACsimilarly mapped the highest number of skilled nursing facilityto the Midwestern states of Illinois and Ohio.23 Previous studieshave also highlighted issues surrounding supply and demand ofpostacute services in large urban settings where patients likelyspend additional days in hospital waiting for rehab beds to be-come available, as the ratio of hospitals to PAC facilities ishigh.24 Ultimately, further study is required to understand the re-gional and state-level factors by specific insurance beneficiaryin order ensure that trauma patients in all areas of the country re-ceive the best possible care.
There are several limitations to this study. This is a retro-spective study, with inherent limitations determining causationbased upon our findings. The NIS is a nationally representativeadministrative databases which provides valuable demographic,cost and healthcare utilization data. However, it does not includegranular clinical data, nor trauma-specific information such astrauma center status or mechanism of injury. All trauma-related information (injuries and injury severity) was derivedfrom ICD-9-CM codes, converted using the ICDPIC tool. Fur-thermore, the NIS does not differentiate between discharge to in-patient rehabilitation or skilled nursing facility, therefore wewere not able to determine which proportion of patients weredischarged to either type of PAC. As well, the NIS uniquelycaptures data associated with inpatient hospitalizations. Conse-quently, wewere not able to extrapolate on outpatient outcomes oftrauma patients discharged to rehabilitation, the burden of long-term disability, nor the out-of-hospital mortality rate (i.e., forpatients who never survived to be admitted to hospital, or thosewho later died after discharge to rehabilitation). Finally, we didnot have detailed geographic data regarding hospital location,therefore we were not able to confirm at the state or county levelwhether hospitals with the shortest mean lengths of stay weresituated in areas with greater density of postacute services. Wehope that the findings from this study will lead to follow-upanalyses with more robust clinical data from trauma registries
© 2018 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
and possibly linking to additional data regarding distributionof postacute services throughout the country.
To build truly inclusive trauma systems within the UnitedStates, ensuring appropriate access to postacute facilities is anintegral part of strengthening trauma care, as well as supportingthe best possible functional and long-term outcomes for in-jured patients.
CONCLUSION
Differences in time to discharge to rehabilitation and costsof hospitalization are based only on patient demographics andinsurance status. Our findings highlight that efficiencies in dis-charge are magnified at the facility level within certain traumahospitals regardless of patient factors. This suggests that thesecenters likely had improved access to PAC which helped to re-duce LOS. For trauma systems to be able to better integrate withPAC, a more comprehensive approach to resource planning isneeded. Future studies should evaluate how to better inform policyaimed at incorporating access to rehabilitation for all insur-ance types to streamline inpatient healthcare utilization and re-duce healthcare costs.
AUTHORSHIP
L.K. participated in study design, data analysis and article preparation. A.H.S.H. participated in data analysis and interpretation, article revisions.L.T. participated in data collection andmanagement. M.T.H. participatedin data interpretation and article revisions. D.S. participated in data analy-sis and article revisions. K.S. participated in study design, data analysis,and article preparation.
DISCLOSURE
There are no conflicts of interest to report for any of the authors.K.L.S. is currently receiving a grant (1K08AG04442801A1) from the Na-tional Institute of Health.
REFERENCES1. Epstein AM, Bogen J, Dreyer P, Thorpe KE. Trends in length of stay and
rates of readmission in Massachusetts: implications for monitoring qualityof care. Inquiry. 1991;28(1):19–28.
2. Institute of Medicine. Variation in health care spending: target decision mak-ing, not geography. 2013; https://www.nap.edu/catalog/18393/variation-in-health-care-spending-target-decision-making-not-geography. Accessed July16, 2018.
3. Daras LC, Ingber MJ, Deutsch A, Hefele JG, Perloff J. Geographic regionand profit status drive variation in hospital readmission outcomes among in-patient rehabilitation facilities in the United States. Arch Phys Med Rehabil.2018;99(6):1060–1066.
4. Nehra D, Nixon ZA, Lengenfelder C, Bulger EM, Cuschieri J, Maier RV,Arbabi S. Acute rehabilitation after trauma: does it really matter? J Am CollSurg. 2016;223(6):755–763.
5. Ayoung-Chee PR, Rivara FP,Weiser T,Maier RV, Arbabi S. Beyond the hospitaldoors: improving long-term outcomes for elderly trauma patients. J TraumaAcute Care Surg. 2015;78(4):837–843.
6. Inaba K, Goecke M, Sharkey P, Brenneman F. Long-term outcomes after in-jury in the elderly. J Trauma. 2003;54(3):486–491.
7. Englum BR, Villegas C, Bolorunduro O, Haut ER, Cornwell EE 3rd,Efron DT, Haider AH. Racial, ethnic, and insurance status disparities inuse of posthospitalization care after trauma. J Am Coll Surg. 2011;213(6):699–708.
8. Chan L, Doctor J, Temkin N,MacLehose RF, Esselman P, Bell K, Dikmen S.Discharge disposition from acute care after traumatic brain injury: the effectof insurance type. Arch Phys Med Rehabil. 2001;82(9):1151–1154.
9. Clark OT, Hahn DR. ICDPIC: State Module to provide methods for translat-ing International Classification of Diseases (Ninth Revision) diagnosis codes
411
ealth, Inc. All rights reserved.
Knowlton et al.J Trauma Acute Care Surg
Volume 86, Number 3
into standard injury categories and/or scores. 2010; http://econpapers.repec.org/software/bocbocode/s457028.htm. Accessed July 20, 2018.
10. Winship C. SamplingWeights and Regression Analysis. 1994; http://scholar.harvard.edu/files/cwinship/files/sampling_weights.pdf. Accessed August 22, 2018.
11. Zogg CK, Payro Chew F, Scott JW, Wolf LL, Tsai TC, Najjar P, Olufajo OA,Schneider EB, Haut ER, Haider AH, et al. Implications of the patient protec-tion and affordable care act on insurance coverage and rehabilitation useamong young adult trauma patients. JAMA Surg. 2016;151(12):e163609.
12. Akande M, Minneci PC, Deans KJ, Xiang H, Cooper JN. Association ofMedicaid expansion under the affordable care act with outcomes and accessto rehabilitation in young adult trauma patients. JAMA Surg. 2018;e181630.
13. Olufajo OA, Cooper Z, Yorkgitis BK, Najjar PA, Metcalfe D, Havens JM,Askari R, Brat GA, Haider AH, Salim A. The truth about trauma readmis-sions. Am J Surg. 2016;211(4):649–655.
14. Haider AH,Weygandt PL, Bentley JM,MonnMF, Rehman KA, Zarzaur BL, Crandall ML, Cornwell EE, Cooper LA. Disparities in trauma care and out-comes in the United States: a systematic review and meta-analysis. J TraumaAcute Care Surg. 2013;74(5):1195–1205.
15. Lancaster CW, DiMaggio C,Marshall G,Wall S, Ayoung-Chee P. Functionaloutcomes after inpatient rehabilitation for trauma-improved but unable to re-turn home. J Surg Res. 2018;222:187–194 e183.
16. Luthi F, Stiefel F, Gobelet C, Rivier G, Deriaz O. Rehabilitation outcomes fororthopaedic trauma individuals as measured by the INTERMED. DisabilRehabil. 2011;33(25–26):2544–2552.
17. Henry J. Kaiser Family Foundation. Medicare's role for people under age 65with disabilities. 2016; https://www.kff.org/medicare/issue-brief/medicares-role-for-people-under-age-65-with-disabilities/. Accessed November 5, 2018.
18. Zorowitz RD, Chen E, Tong KB, Laouri M. Costs and rehabilitation use ofstroke survivors: a retrospective study of Medicare beneficiaries. Top StrokeRehabil. 2009;16(5):309–320.
19. Meagher AD, Beadles CA, Doorey J, Charles AG. Racial and ethnic dispar-ities in discharge to rehabilitation following traumatic brain injury. J Neurosurg.2015;122(3):595–601.
20. Medicare Program. Hospital inpatient prospective payment systems for acutecare hospitals and the long-term care hospital prospective payment systemand policy changes and fiscal year 2017 rates; final rule. Fed Regist. 2016;81(162):56761–57345.
21. Smith TR, Rambachan A, Cote D, Cybulski G, Laws ER. Market-basedhealth care in specialty surgery: finding patient-Centered shared value. Neu-rosurgery. 2015;77(4):509–516.
22. U.S. Department of Health and Human Services, Office of the Assistant Sec-retary for Planning and Evaluation. Examining post acute care relationshipsin an integrated hospital system, geographic distribution of providers. 2009;https://aspe.hhs.gov/report/examining-post-acute-care-relationships-integrated-hospital-system/31-geographic-distribution-providers. AccessedOctober 30, 2018.
23. Henry J. Kaiser Family Foundation. Total Number of CertifiedNursing Facilities.2016; https://www.kff.org/other/state-indicator/number-of-nursing-facilities/?activeTab=map¤tTimeframe=0&selectedDistributions=number-of-nursing-facilities&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D. Accessed August 1, 2018.
24. Allen L, McIntyre A, Janzen S, Richardson M, Meyer M, Ure D, Teasell R.Community stroke rehabilitation: how do rural residents fare compared withtheir urban counterparts? Can J Neurol Sci. 2016;43(1):98–104.
DISCUSSIONJay J. Doucet, M.D., M.Sc. (San Diego, California):
Thank you very much for the chance to discuss this paper, tothe members of the Association and to President Rotondo.
Congratulations to Dr. Knowlton and the Stanford SPIREgroup collaborators for a nice paper. It was sent to me in a timelyfashion, and it was a great presentation.
It's an admirable attempt to try to examinewhat I think is agreatly neglected area in trauma care – the econometrics of inad-equate insurance delaying access to post-injury rehabilitation.
412
Copyright © 2019 Wolters Kluwer H
As the authors pointed out, the IOM found that post-acutecare accounted for 73 percent of the geographic variation inMedicare spending. The ACA and Medicaid expansion in manystates have provided insurance that may cover acute phase of care,but generally don't do as good a job at the post-acute care phase.
The authors used the Nationwide Inpatient Sample to de-termine length of stay for all trauma patients destined for reha-bilitation based on insurance type.
They also showed us that there is considerable variationdepending on hospital type, and probably on the post-acute caremarket. And they've really clearly shown that Medicaid patientsare clearly the lowest on the pecking order when it comes to re-hab placement, after Medicare and private payer patients. Med-icaid patients have longer length of stay and increased costsbefore post-acute care placement.
I have a few questions. Firstly, since 2012, and NIS unfor-tunately lumps acute rehab facilities, SNFs and LTACs – long-term care facilities – all in the same group, and so I think mostof the patients you identify are either elderly patients who are go-ing to SNFs, and also younger patients who need acute rehab,and are lumped together in the same group, and I think those pa-tients are obviously very different.
The Medicaid patients obviously had more surgery at ahigher ISS, and so, do you have any kind of ICD code differ-ences between these groups? Is there a big difference in thegroups we're seeing here?
I suspect one group is mostly elderly folks who fell downwith a hip fracture or head injuries, where the other group mayhave much more severe trauma.
The other question I have is about your risk adjustment.Medicaid had an odds ratio of about 1.55 for extra days of lengthof stay, which was the second strongest effect. But the verystrongest effect, of course, was on ISS.
And for those over 16, the ISS ranges from 2.54 to 5.75.How confident are you that you've totally disentangled the typeof injury from ISS and other confounders for Medicaid status inyour analysis?
And thirdly, you excluded self-pay patients from analysis,and I suspect that's because there's very fewof those patients thatactually get to go to post-acute care placement but it does show asignificant limitation in the approach.
We're kind of looking at the patients who do get rehab. ButI think a very big issue is patients who never get access to rehab.And another way to look at this, maybe using NIS, is to first lookat ICD-9 codes and try to get odds ratios for those patients actu-ally getting to post-acute care placement. There I would suggestyou may want to include self-payer rehab patients, only becausetheir relative rarity may be illuminating.
And finally, about your paper's conclusion, you suggestedthat hospitals or trauma systems need to plan for rehab resourcesfor all payer groups.
I've spent some time on rounds and on the phone trying totalk to payers or to rehab facilities, and I suspect that it's reallythe reluctance of payers to cover rehab that's actually the prob-lem here, and not a problem with trauma systems planning.
And therefore, I think this is really not a trauma systemsissue, but a health policy and political issue. And if that's true,do you have any idea of how much we should be asking for,and how we're going to get that to happen?
© 2018 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Knowlton et al.
I'd like to thank the Association for the opportunity to dis-cuss this important paper.
Carl J. Hauser, M.D. (Boston, Massachusetts): Thankyou very much. Very nice paper. I have two questions. One ofour problems is with older people who are sort of nearing theend of their ability to care for themselves, who fall down andhave minor injuries, and then need a room at the inn for a coupleof days before they can actually get coverage to go to rehab or tofacilities – there's this so-called three-day rule.
And I'm wondering, how many of your patients in theMedicare group have low ISS – fractured radius, something likethat – and are actually being kept in the hospital because of thatMedicare three-day rule?
Secondly, I'm wondering, how many of your patients inthe Medicaid group, who are younger, are staying in the hospitalfor longer because they have head injuries and are considered tobe very difficult rehab candidates or need specialized rehab, andthat's part of the problem? Very nice data.
Lawrence Sue, M.D. (Fresno, California):Very nice pa-per. A lot of our Medicaid patients come into the hospital asno-pays first, with no insurance, and undergo a process by whichthey become qualified eligible, they get enrolled into it – and theprocess takes time. Could this be contributing to your increasedlength of stay for these patients?
Krista L. Kaups, M.D., M.Sc. (Fresno, California):This is really terrifying, because my colleague asked the samequestion I was going to ask.
But I was going to suggest that for analysis, you mightwant to take your highest performing quartiles, and comparethem to the lowest for some of those diagnoses, and see the dif-ference there, in terms of costs. We frequently have the issuewith patients where rehab beds are available, they just don't havefunding – yet – until they get their presumptive Medi-Cal, thusprolonging length of hospital stay.
R. Lawrence Reed, M.D. (Indianapolis, Indiana):Thank you. Acute care hospitals like trauma centers are beinggamed here, because Medicaid pays something like 10 centson the dollar and is always the lowest among payers unlessyou include self-pay. The problem acute care hospitals have isthat they cannot restrict admission. However, a rehab facilitycan restrict admission to their institution if they perceive the pa-tient’s coverage to be inadequate. They can therefore selectivelypick better paying patients to enter the rehab facility, while theunderfunded patients must be retained by the acute care hospital.The unfair aspect in the system is that an acute-care facility like atertiary trauma center cannot selectively accept or rejecttransfers; our doors are open for any emergency that comesour way whether the patient has financial resources or not.However, that financial risk is not distributed equally through-out the system.
Have you considered evaluating the adequacy of pay-ments for acute care hospitals relative to their costs versus theadequacy of payments for the costs at post-acute care facilities?In other words, are acute care hospitals unfairly bearing theburden of inadequate patient coverage compared to post-acutecare facilities?
LisaM.Knowlton,M.D.,M.P.H. (Stanford, California):Thank you all, in particular Dr. Doucet, for your insightfulcomments and questions.
© 2018 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
To address Dr. Doucet's commentary, I agree that muchlike in the NTDB, we were not able to differentiate between re-hab and SNF discharge destination. This is a limitation of theNIS database.
We attempted to address this issue by doing a subset anal-ysis based upon age, with the assumption being that youngerpatients would be discharged to rehabilitation and older patientswould be going to SNF.
Although we did not use injury ICD-9 codes specifically –that would be a great study– we did identify, as you mentioned,that younger patients had higher Injury Severity Scores (25%ISS greater than 15 vs. 9% in patients over 65) and a higher per-cent of them underwent operations (73% vs 64%).
To address the second question about our risk adjustment,with our mixed effects negative binomial regression, we wereactually looking at additional days spent in hospital rather thantraditional odds ratio, and the objective of the regression wasto control for confounders. That said, it would be interesting tolook at the interaction term of insurance type and injury severityand add it to our model.
In terms of the self-pay group, I agree that this is a particu-larly important population when discussing the need for post-acute care. We specifically decided to exclude uninsured patientsbecause their limitation in access has already been demon-strated. I do recall that within the NIS database, the percentof self-pay patients discharged to post-acute care is less than0.5% and out of all patients going to post-acute care, self-payaccounted for 1%.
I also suspect some portion of the Medicaid populationand the self-paid population that we're seeing in this data is ex-actly as you described, patients who are becoming temporarilyinsured while in-hospital and then go on to lose their insuranceonce they've been discharged to rehabilitation.
Finally, in terms of our conclusion, I think in order forthis very complex problem to truly be solved, we really needto approach it from multiple angles, as there are multiplestakeholders.
It certainly is a policy problem. The significance of ourwork is that we can show that by reducing LOS, there are tre-mendous resource and cost savings on the inpatient side whichcan be shifted toward rehabilitation resources. As providers,we should be invested and engaging payors and policymakers,because we have the opportunity to free up resources in the hos-pital and improving long-term outcomes of our patients by re-distributing funds to the post-acute care setting. We alreadyknow that post-injury disability is a huge burden in our societyand this may be a first-step toward finding solutions.
Dr. Hauser, in terms of the elderly injury severity patterns,approximately 70% of the patients had an ISS less than 15. Thislikely represents a group of elderly falls patients who were notvery severely injured, but then subsequently debilitated fromtheir baseline status and required post-acute care. It would bevery interesting to look specifically at the TBI group, whichwe are doing in our other work.
Dr. Sue, you raise an important point about patients be-coming insured at the time of hospitalization and the delays indischarge that this may impose. We are in the midst of study thisissue in our other work, as these patients who acquire Medicaidin-hospital cannot be differentiated from otherMedicaid patients
413
ealth, Inc. All rights reserved.

Knowlton et al.J Trauma Acute Care Surg
Volume 86, Number 3
in an administrative database like NIS. We know that even ifpatients do acquire this insurance temporarily, there are stilllimitations on access to care and the number of rehabilitationand SNF facilities that will accept post-discharge. Furthermore,their insurance does not always get sustained after discharge.
As Dr. Reed mentioned, rehab centers are presently ableto select for patients based on better reimbursements, so thisfunnels back to the cost conundrum that was raised earlier.
414
Copyright © 2019 Wolters Kluwer H
An interesting study would certainly be to compare under-payments for post-acute care facilities with underpaymentsfor hospitals.
My hope for a first step is that we can make a convincingargument for shifting some of the inpatient costs associated withtime spent waiting for an accepting facility toward much neededresources in the post-acute care setting.
Thank you very much.
© 2018 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.
ORIGINAL ARTICLE
Traumatic brain injury may worsen clinical outcomes afterprolonged partial resuscitative endovascular balloon occlusion
of the aorta in severe hemorrhagic shock model
Aaron M. Williams, MD, Umar F. Bhatti, MD, Isabel S. Dennahy, MD, Nathan J. Graham, BS,Vahagn C. Nikolian, MD, Kiril Chtraklin, DVM, Panpan Chang, MD, Jing Zhou, MD, Ben E. Biesterveld, MD,
Jonathan Eliason, MD, and Hasan B. Alam, MD, Arbor, Michigan
Sub
FroThi
Ad
DO
J TrVol
BACKGROUND: T
mitted: August 4, 2018Published online: Novm the Department of Ss study was presented athe Surgery of Traumadress for reprints: HasMichigan Hospital, UnMedical Center Dr, An
I: 10.1097/TA.000000
auma Acute Care Suume 86, Number 3
he use of partial resuscitative endovascular balloon occlusion of the aorta (pREBOA) in combined hemorrhagic shock (HS) and traumaticbrain injury (TBI) has not beenwell studied.We hypothesized that the use of pREBOA in the setting of TBI would be associatedwith worseclinical outcomes.
METHODS: F
emale Yorkshire swine were randomized to the following groups: HS-TBI, HS-TBI-pREBOA, and HS-pREBOA (n = 5/cohort). Animalsin the HS-TBI group were left in shock for a total of 2 hours, whereas animals assigned to pREBOA groups were treated with supraceliacpREBOA deployment (60minutes) 1 hour into the shock period. All animals were then resuscitated, and physiologic parameters were mon-itored for 6 hours. Further fluid resuscitation and vasopressors were administered as needed. At the end of the observation period, brainhemispheric swelling (%) and lesion size (mm3) were assessed.RESULTS: M
ortality was highest in the HS-TBI-pREBOAgroup (40% [2/5] vs. 0% [0/5] in the other groups, p = 0.1). Severity of shockwas greatest inthe HS-TBI-pREBOAgroup, as defined by peak lactate levels and pH nadir (p < 0.05). Fluid resuscitation and norepinephrine requirementswere significantly higher in the HS-TBI-pREBOA group (p < 0.05). No significant differences were noted in brain hemispheric swellingand lesion size between the groups.CONCLUSION: P
rolonged application of pREBOA in the setting of TBI does not contribute to early worsening of brain lesion size and edema. However, theaddition of TBI to HS-pREBOAmay worsen the severity of shock. Providers should be aware of the potential physiologic sequelae inducedby TBI. (J Trauma Acute Care Surg. 2019;86: 415–423. Copyright © 2018 Wolters Kluwer Health, Inc. All rights reserved.)KEYWORDS: T
raumatic brain injury; hemorrhagic shock; partial aortic occlusion; noncompressible torso hemorrhage; swine.H emorrhagic shock (HS) and traumatic brain injury (TBI)remain leading causes of immediate and early death in
trauma patients.1,2 Hemorrhagic shock accounts for the majorityof trauma deaths during the first hour of care, while TBI is re-sponsible for a large segment thereafter.3 In traumatic settings,TBI is often accompanied by other insults, including vascularinjury and hemorrhage. When HS and TBI are found in combi-nation, the likelihood of early death is approximately 80%.4 Al-though TBI contributes to significant morbidity and mortality,the priority in these patients is hemorrhage control to preventearly deaths due to exsanguination.5,6
Within recent years, resuscitative endovascular balloonocclusion of the aorta (REBOA) has gained attention as a techniquefor the management of noncompressible torso hemorrhage(NCTH).7–9 Use of REBOA has been shown to confer earlysurvival advantages in HS; however, concerns have been raisedregarding the risk of end-organ ischemiawith complete REBOA(cREBOA).10,11 As a result, alternative endovascular strategies,
, Revised: October 28, 2018, Accepted: November 9, 2018,ember 28, 2018.urgery, University of Michigan, Ann Arbor, Michigan.t the 77th Annual Meeting of the American Association for, September 26–29, 2018, in San Diego, California.an B. Alam, MD, Department of Surgery, University ofiversity of Michigan, 2920 Taubman Center/5331, 1500 En Arbor, MI 48109-5331; email: [email protected].
0000002149
rg
Copyright © 2019 Wolters Kluwer H
like partial REBOA (pREBOA), have been devised to overcomethis limitation.12,13 Although early in its adoption, pREBOAmay afford better distal perfusion, more physiologic proximalaortic mean arterial pressures (MAPs), and less reperfusion injuryfollowing balloon deflation.12,13 However, despite promising earlydata, further studies are required to fully define the consequences ofpREBOA deployment in the setting of severe hemorrhage.
Although REBOA has been widely believed to be usefulin NCTH, its utility in the setting of concurrent TBI has not beenwell studied. Some have reported exacerbation of TBI followingREBOA deployment, raising concerns about guidelines for useand patient selection.14,15 Moreover, preclinical studies of bothcREBOA and pREBOA have been limited to mild traumamodelsof HS and TBI with several clinical limitations.16 In this study, wesought to investigate the effects of pREBOA deployment in aswine model of severe HS and TBI with limited resuscitationstrategies.We hypothesized that the use of pREBOA in the settingof TBI would be associated with worse clinical outcomes.
MATERIALS AND METHODS
The study protocol was approved by the University ofMichigan Institutional Animal Care and Use Committee. Experi-ments were conducted in compliance with all guidelines and reg-ulations regarding animal welfare and research. Figure 1 providesa schematic representation of the model used in this experiment.
415
ealth, Inc. All rights reserved.
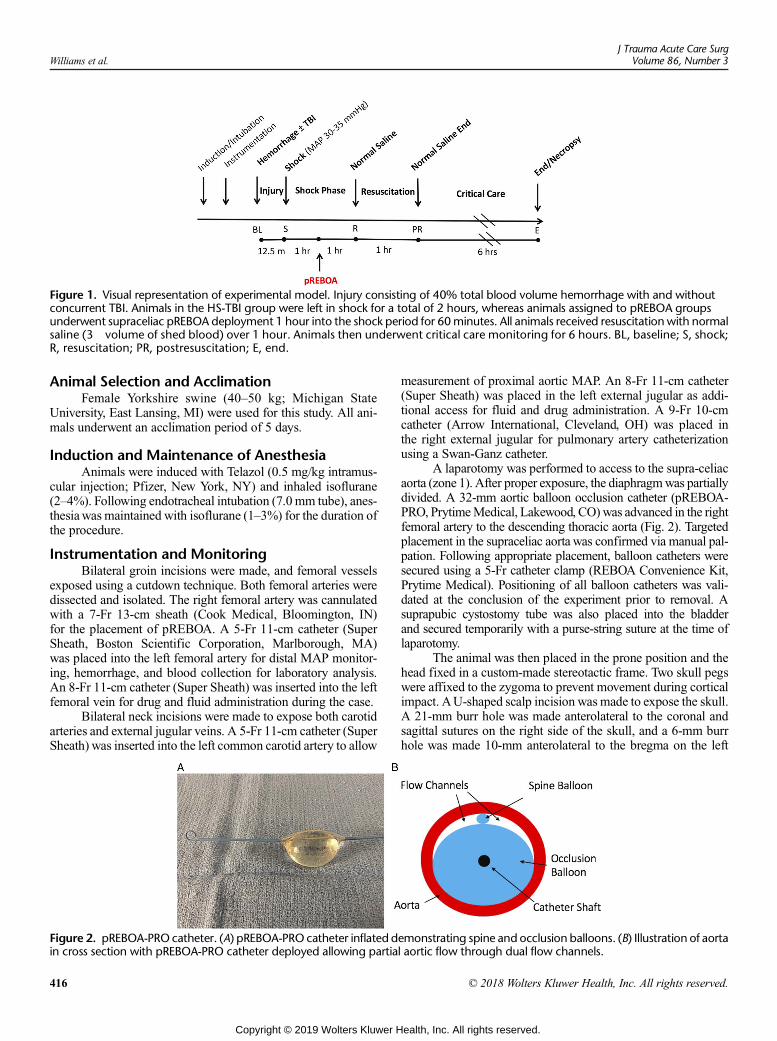
Figure 1. Visual representation of experimental model. Injury consisting of 40% total blood volume hemorrhage with and withoutconcurrent TBI. Animals in the HS-TBI group were left in shock for a total of 2 hours, whereas animals assigned to pREBOA groupsunderwent supraceliac pREBOA deployment 1 hour into the shock period for 60minutes. All animals received resuscitationwith normalsaline (3� volume of shed blood) over 1 hour. Animals then underwent critical care monitoring for 6 hours. BL, baseline; S, shock;R, resuscitation; PR, postresuscitation; E, end.
Williams et al.J Trauma Acute Care Surg
Volume 86, Number 3
Animal Selection and AcclimationFemale Yorkshire swine (40–50 kg; Michigan State
University, East Lansing, MI) were used for this study. All ani-mals underwent an acclimation period of 5 days.
Induction and Maintenance of AnesthesiaAnimals were induced with Telazol (0.5 mg/kg intramus-
cular injection; Pfizer, New York, NY) and inhaled isoflurane(2–4%). Following endotracheal intubation (7.0 mm tube), anes-thesiawas maintained with isoflurane (1–3%) for the duration ofthe procedure.
Instrumentation and MonitoringBilateral groin incisions were made, and femoral vessels
exposed using a cutdown technique. Both femoral arteries weredissected and isolated. The right femoral artery was cannulatedwith a 7-Fr 13-cm sheath (Cook Medical, Bloomington, IN)for the placement of pREBOA. A 5-Fr 11-cm catheter (SuperSheath, Boston Scientific Corporation, Marlborough, MA)was placed into the left femoral artery for distal MAP monitor-ing, hemorrhage, and blood collection for laboratory analysis.An 8-Fr 11-cm catheter (Super Sheath) was inserted into the leftfemoral vein for drug and fluid administration during the case.
Bilateral neck incisions were made to expose both carotidarteries and external jugular veins. A 5-Fr 11-cm catheter (SuperSheath) was inserted into the left common carotid artery to allow
Figure 2. pREBOA-PRO catheter. (A) pREBOA-PRO catheter inflated din cross section with pREBOA-PRO catheter deployed allowing partia
416
Copyright © 2019 Wolters Kluwer H
measurement of proximal aortic MAP. An 8-Fr 11-cm catheter(Super Sheath) was placed in the left external jugular as addi-tional access for fluid and drug administration. A 9-Fr 10-cmcatheter (Arrow International, Cleveland, OH) was placed inthe right external jugular for pulmonary artery catheterizationusing a Swan-Ganz catheter.
A laparotomy was performed to access to the supra-celiacaorta (zone 1). After proper exposure, the diaphragmwas partiallydivided. A 32-mm aortic balloon occlusion catheter (pREBOA-PRO, PrytimeMedical, Lakewood, CO) was advanced in the rightfemoral artery to the descending thoracic aorta (Fig. 2). Targetedplacement in the supraceliac aorta was confirmed via manual pal-pation. Following appropriate placement, balloon catheters weresecured using a 5-Fr catheter clamp (REBOA Convenience Kit,Prytime Medical). Positioning of all balloon catheters was vali-dated at the conclusion of the experiment prior to removal. Asuprapubic cystostomy tube was also placed into the bladderand secured temporarily with a purse-string suture at the time oflaparotomy.
The animal was then placed in the prone position and thehead fixed in a custom-made stereotactic frame. Two skull pegswere affixed to the zygoma to prevent movement during corticalimpact. AU-shaped scalp incision was made to expose the skull.A 21-mm burr hole was made anterolateral to the coronal andsagittal sutures on the right side of the skull, and a 6-mm burrhole was made 10-mm anterolateral to the bregma on the left
emonstrating spine and occlusion balloons. (B) Illustration of aortal aortic flow through dual flow channels.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Williams et al.
side. The 21-mm burr hole was used for brain injury, and the6-mm burr hole was used for intracranial pressure (ICP) and ox-ygenation monitoring.
Following instrumentation, animals were block random-ized to three groups: (1) HS-TBI, (2) HS-TBI-pREBOA, and(3) HS-pREBOA (n = 5/cohort).
TBI and HemorrhageAnimals were then subjected to their respective randomized
injury patterns, including HS, or HS-TBI. Forty percent esti-mated total blood volume (estimated total blood volume(mL) = weight (g) � 0.06 + 0.77) was hemorrhaged over12.5 minutes using a Masterflex pump (Cole-Palmer, VernonHills, IL). Blood was collected in standard blood collection bagscontaining anticoagulants (CPDA, AS-5; Terumo, Ann Arbor,MI). If randomized to undergo TBI, a computer-controlled cor-tical impact (CCI) device (University of Michigan InnovationCentre, Ann Arbor, MI) was used to create an impact concur-rently (cylindrical impactor, 20 mm; velocity, 4 m/s; dwell time,100 millisecond; cortical penetration depth, 12 mm). This insulthas been shown to reliably produce a severe TBI.17,18
During the hemorrhage period, if MAP decreased below30 mm Hg, hemorrhage was held, isoflurane was turned off,and a 50 to 100 mL bolus of 0.9% normal saline (NS) was ad-ministered. Hemorrhage was restarted when MAP returnedabove 30mmHg. The bone fragment from the 21-mmBurr holewas replaced, and bone wax was used to seal the hole. Thisprevented cerebrospinal fluid leakage and ensured accurateICP monitoring. The scalp incision was temporarily closed fol-lowing TBI using silk suture.
HS, Treatment, and ResuscitationOnce hemorrhage was complete, animals were subjected
to shock (MAP goal of 30–35 mm Hg). Following 60 minutesof shock, HS-TBI animals were kept in shock for an additional60 minutes, while HS-TBI-pREBOA and HS-pREBOA animalsunderwent 60 minutes of supraceliac (zone 1) partial aortic bal-loon occlusion. For animals randomized to pREBOA deploy-ment, a distal MAP of 20 to 25 mm Hg was targeted, achievinga 60–70% systolic-to-diastolic pressure gradient. Aortic balloonswere inflated with NS and manually adjusted as needed to meetthis target. A standard balloon titration device (Encore AdvantageKit, Boston Scientific Corporation, Natick, MA) was used for bal-loon volume titration. In the HS-TBI group, pREBOA catheterswere maintained in the supraceliac aorta during the 60-minuteshock period, but balloons were not inflated.
At the end of the 60-minute pREBOA deployment period,aortic occlusion balloons were deflated manually at a rate of0.5 mL/min using the balloon titration device until completelydeflated. pREBOA catheters were then withdrawn followingballoon deflation. Concurrently, all animals were resuscitatedwith NS (3� hemorrhage volume) over a 1-hour period.
Critical Care MonitoringAnimals were observed for 6 hours following resuscita-
tion with continuous monitoring of physiological and laboratoryparameters. Maintenance intravenous fluids were administeredat a rate of 50 mL/hr of NS. Additional fluids and vasopressortherapy were administered according to objective thresholds.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
Animals received a 500 mL NS fluid bolus if the central venouspressure (CVP) was less than 6 mm Hg and were reassessed.Fluid boluses were repeated as needed to a maximum volumeof 100 mL/kg. A norepinephrine (24 μg/mL) infusion was initi-ated and titrated to maintain a MAP of 55 to 60 mmHg. Electro-lyte abnormalities, including hypoglycemia and hyperkalemia,were corrected throughout the critical care monitoring phase.A Bair Hugger (Arizant Healthcare, Inc., Eden Prairie, MN)was used to maintain physiologic temperature.
Intraoperative Hemodynamic andLaboratory Monitoring
Physiologic parameters were measured continuously aspreviously described.19–21 Parameters measured included heartrate; proximal and distal systolic, diastolic, andMAP;CVP; cardiacoutput (CO); core body temperature; pulse oxygenation; and ICP.
Arterial blood gases (Nova Biochemical, Waltham, MA)and whole blood samples were obtained at baseline, postshock,postresuscitation, and at the end of the observation phase. Addi-tional arterial blood gases were performed as needed throughoutthe experiment. Whole blood samples were withdrawn intovacuum-sealed tubes, centrifuged for separation into serumand plasma, and flash frozen for future analysis. All laboratorysamples were included in the calculation of hemorrhage volume.
Tissue CollectionAnimals were euthanized with Euthasol (Virbac, Fort
Worth, TX) at the end of the 6-hour observation period. Brainswere harvested and sliced into 5-mm coronal sections using asectioning block (University of Michigan Medical InnovationCenter, Ann Arbor, MI). Sections were then stained with 2%2,3,5-triphenyltetrazolium chloride (SigmaChemical Co., St.Louis, MO) to detect viable tissue. Brain lesion size (mm3)and hemispheric volumes were calculated using ImageJ analysissoftware (National Institutes of Health, Bethesda, MD). Hemi-spheric swelling ipsilateral to the brain lesion was calculatedusing the following equation: ipsilateral hemispheric swell-ing = (volume of ipsilateral hemisphere/volume of contralateralhemisphere − 1) � 100%.22,23
Statistical AnalysesPrimary endpoints involved clinical outcomes (laboratory
parameters and rescuscitation requirements) following pREBOAdeployment. Pilot experiments, which were not included in thisstudy, were used to conduct an a priori power analysis by a bio-statistician. Using pilot data comparing the primary endpointsfor the HS-TBI-pREBOA and HS-pREBOA groups, effect size(d) was determined. Sample sizes were then planned with 90%power and 95% confidence for each variable followingpREBOA deployment: lactate levels (d = 5; n = 2), pH levels(d = 2.6; n = 4), total fluid resuscitation (d = 3; n = 3), and va-sopressor requirements (d = 10; n = 2). The HS-TBI group isused for reference.
All statistical analyses were performed using GraphPadPrism v6.00 (GraphPad Software, San Diego, CA). Survivalrates were compared using Kaplan-Meier method with log-rank testing. One-way analysis of variance with Tukey posthoc testing was used for all discrete time points. The Brown-Forsythe test was used to check for differences in variance
417
ealth, Inc. All rights reserved.
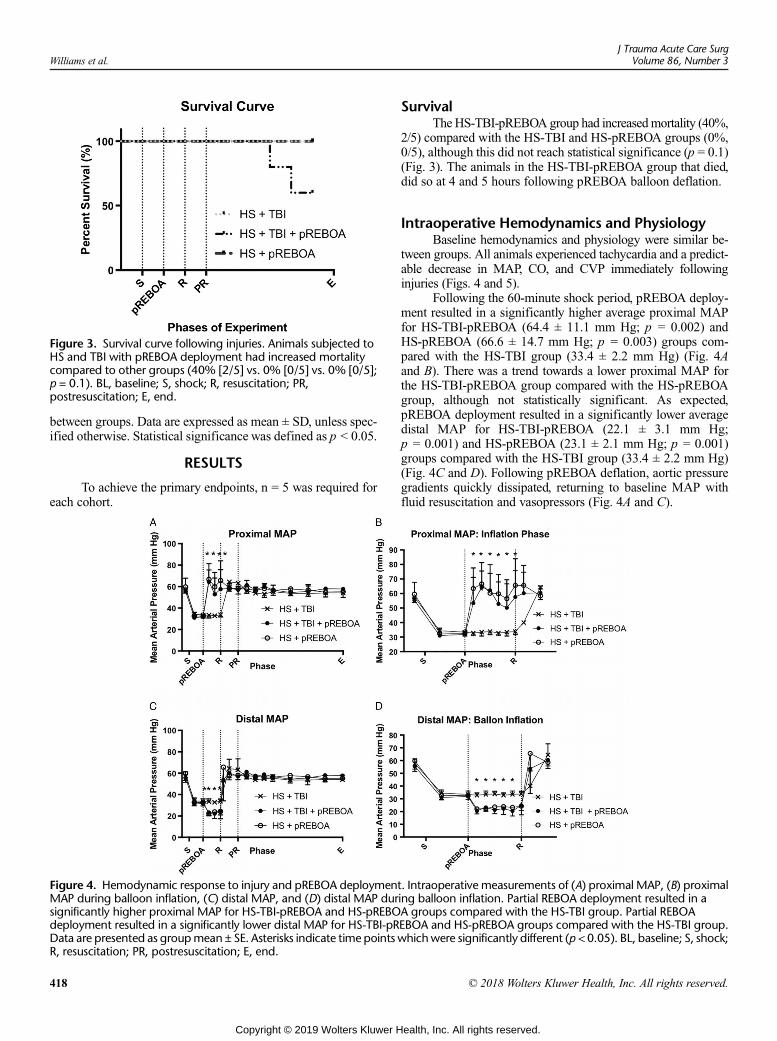
Figure 3. Survival curve following injuries. Animals subjected toHS and TBI with pREBOA deployment had increased mortalitycompared to other groups (40% [2/5] vs. 0% [0/5] vs. 0% [0/5];p = 0.1). BL, baseline; S, shock; R, resuscitation; PR,postresuscitation; E, end.
Williams et al.J Trauma Acute Care Surg
Volume 86, Number 3
between groups. Data are expressed as mean ± SD, unless spec-ified otherwise. Statistical significance was defined as p < 0.05.
RESULTS
To achieve the primary endpoints, n = 5 was required foreach cohort.
Figure 4. Hemodynamic response to injury and pREBOA deploymentMAP during balloon inflation, (C) distal MAP, and (D) distal MAP dursignificantly higher proximal MAP for HS-TBI-pREBOA and HS-pREBOdeployment resulted in a significantly lower distal MAP for HS-TBI-pRData are presented as groupmean ± SE. Asterisks indicate time points wR, resuscitation; PR, postresuscitation; E, end.
418
Copyright © 2019 Wolters Kluwer H
SurvivalTheHS-TBI-pREBOA group had increasedmortality (40%,
2/5) compared with the HS-TBI and HS-pREBOA groups (0%,0/5), although this did not reach statistical significance (p = 0.1)(Fig. 3). The animals in the HS-TBI-pREBOA group that died,did so at 4 and 5 hours following pREBOA balloon deflation.
Intraoperative Hemodynamics and PhysiologyBaseline hemodynamics and physiology were similar be-
tween groups. All animals experienced tachycardia and a predict-able decrease in MAP, CO, and CVP immediately followinginjuries (Figs. 4 and 5).
Following the 60-minute shock period, pREBOA deploy-ment resulted in a significantly higher average proximal MAPfor HS-TBI-pREBOA (64.4 ± 11.1 mm Hg; p = 0.002) andHS-pREBOA (66.6 ± 14.7 mm Hg; p = 0.003) groups com-pared with the HS-TBI group (33.4 ± 2.2 mm Hg) (Fig. 4Aand B). There was a trend towards a lower proximal MAP forthe HS-TBI-pREBOA group compared with the HS-pREBOAgroup, although not statistically significant. As expected,pREBOA deployment resulted in a significantly lower averagedistal MAP for HS-TBI-pREBOA (22.1 ± 3.1 mm Hg;p = 0.001) and HS-pREBOA (23.1 ± 2.1 mm Hg; p = 0.001)groups compared with the HS-TBI group (33.4 ± 2.2 mm Hg)(Fig. 4C and D). Following pREBOA deflation, aortic pressuregradients quickly dissipated, returning to baseline MAP withfluid resuscitation and vasopressors (Fig. 4A and C).
. Intraoperative measurements of (A) proximal MAP, (B) proximaling balloon inflation. Partial REBOA deployment resulted in aA groups compared with the HS-TBI group. Partial REBOAEBOA and HS-pREBOA groups compared with the HS-TBI group.hichwere significantly different (p < 0.05). BL, baseline; S, shock;
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
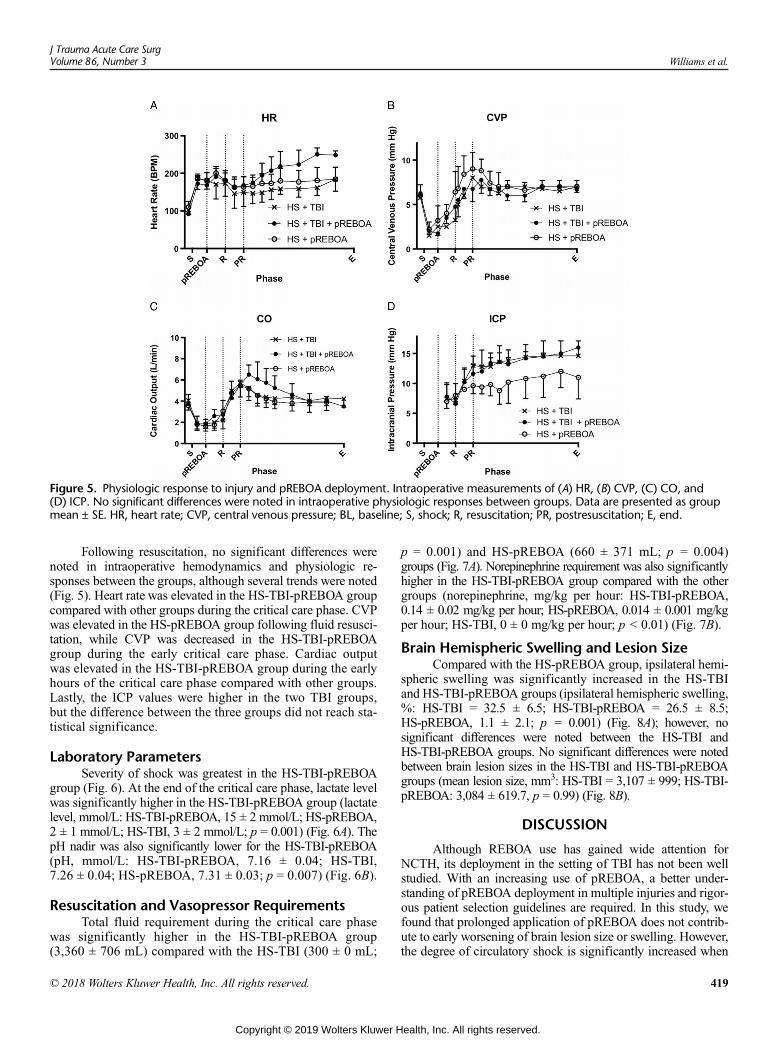
Figure 5. Physiologic response to injury and pREBOA deployment. Intraoperative measurements of (A) HR, (B) CVP, (C) CO, and(D) ICP. No significant differences were noted in intraoperative physiologic responses between groups. Data are presented as groupmean ± SE. HR, heart rate; CVP, central venous pressure; BL, baseline; S, shock; R, resuscitation; PR, postresuscitation; E, end.
J Trauma Acute Care SurgVolume 86, Number 3 Williams et al.
Following resuscitation, no significant differences werenoted in intraoperative hemodynamics and physiologic re-sponses between the groups, although several trends were noted(Fig. 5). Heart rate was elevated in the HS-TBI-pREBOA groupcompared with other groups during the critical care phase. CVPwas elevated in the HS-pREBOA group following fluid resusci-tation, while CVP was decreased in the HS-TBI-pREBOAgroup during the early critical care phase. Cardiac outputwas elevated in the HS-TBI-pREBOA group during the earlyhours of the critical care phase compared with other groups.Lastly, the ICP values were higher in the two TBI groups,but the difference between the three groups did not reach sta-tistical significance.
Laboratory ParametersSeverity of shock was greatest in the HS-TBI-pREBOA
group (Fig. 6). At the end of the critical care phase, lactate levelwas significantly higher in the HS-TBI-pREBOA group (lactatelevel, mmol/L: HS-TBI-pREBOA, 15 ± 2 mmol/L; HS-pREBOA,2 ± 1 mmol/L; HS-TBI, 3 ± 2 mmol/L; p = 0.001) (Fig. 6A). ThepH nadir was also significantly lower for the HS-TBI-pREBOA(pH, mmol/L: HS-TBI-pREBOA, 7.16 ± 0.04; HS-TBI,7.26 ± 0.04; HS-pREBOA, 7.31 ± 0.03; p = 0.007) (Fig. 6B).
Resuscitation and Vasopressor RequirementsTotal fluid requirement during the critical care phase
was significantly higher in the HS-TBI-pREBOA group(3,360 ± 706 mL) compared with the HS-TBI (300 ± 0 mL;
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
p = 0.001) and HS-pREBOA (660 ± 371 mL; p = 0.004)groups (Fig. 7A). Norepinephrine requirement was also significantlyhigher in the HS-TBI-pREBOA group compared with the othergroups (norepinephrine, mg/kg per hour: HS-TBI-pREBOA,0.14 ± 0.02 mg/kg per hour; HS-pREBOA, 0.014 ± 0.001 mg/kgper hour; HS-TBI, 0 ± 0 mg/kg per hour; p < 0.01) (Fig. 7B).
Brain Hemispheric Swelling and Lesion SizeCompared with the HS-pREBOA group, ipsilateral hemi-
spheric swelling was significantly increased in the HS-TBIand HS-TBI-pREBOA groups (ipsilateral hemispheric swelling,%: HS-TBI = 32.5 ± 6.5; HS-TBI-pREBOA = 26.5 ± 8.5;HS-pREBOA, 1.1 ± 2.1; p = 0.001) (Fig. 8A); however, nosignificant differences were noted between the HS-TBI andHS-TBI-pREBOA groups. No significant differences were notedbetween brain lesion sizes in the HS-TBI and HS-TBI-pREBOAgroups (mean lesion size, mm3: HS-TBI = 3,107 ± 999; HS-TBI-pREBOA: 3,084 ± 619.7, p = 0.99) (Fig. 8B).
DISCUSSION
Although REBOA use has gained wide attention forNCTH, its deployment in the setting of TBI has not been wellstudied. With an increasing use of pREBOA, a better under-standing of pREBOA deployment in multiple injuries and rigor-ous patient selection guidelines are required. In this study, wefound that prolonged application of pREBOA does not contrib-ute to early worsening of brain lesion size or swelling. However,the degree of circulatory shock is significantly increased when
419
ealth, Inc. All rights reserved.
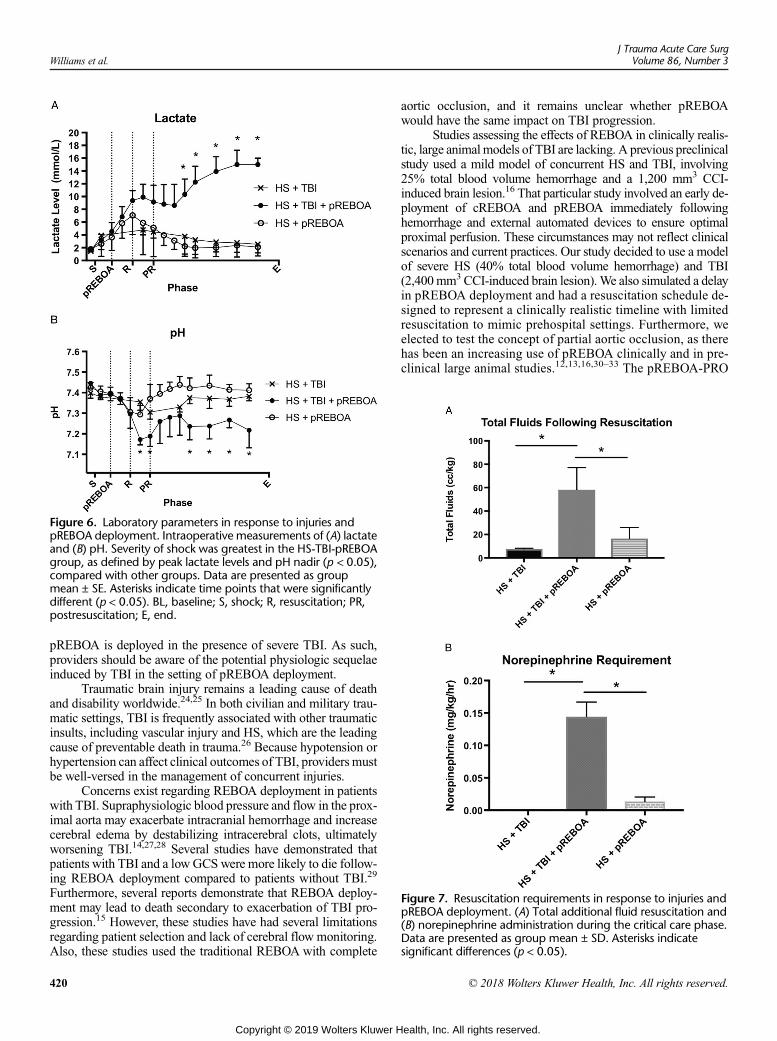
Figure 6. Laboratory parameters in response to injuries andpREBOA deployment. Intraoperative measurements of (A) lactateand (B) pH. Severity of shock was greatest in the HS-TBI-pREBOAgroup, as defined by peak lactate levels and pH nadir (p < 0.05),compared with other groups. Data are presented as groupmean ± SE. Asterisks indicate time points that were significantlydifferent (p < 0.05). BL, baseline; S, shock; R, resuscitation; PR,postresuscitation; E, end.
Figure 7. Resuscitation requirements in response to injuries andpREBOA deployment. (A) Total additional fluid resuscitation and(B) norepinephrine administration during the critical care phase.Data are presented as group mean ± SD. Asterisks indicatesignificant differences (p < 0.05).
Williams et al.J Trauma Acute Care Surg
Volume 86, Number 3
pREBOA is deployed in the presence of severe TBI. As such,providers should be aware of the potential physiologic sequelaeinduced by TBI in the setting of pREBOA deployment.
Traumatic brain injury remains a leading cause of deathand disability worldwide.24,25 In both civilian and military trau-matic settings, TBI is frequently associated with other traumaticinsults, including vascular injury and HS, which are the leadingcause of preventable death in trauma.26 Because hypotension orhypertension can affect clinical outcomes of TBI, providers mustbe well-versed in the management of concurrent injuries.
Concerns exist regarding REBOA deployment in patientswith TBI. Supraphysiologic blood pressure and flow in the prox-imal aorta may exacerbate intracranial hemorrhage and increasecerebral edema by destabilizing intracerebral clots, ultimatelyworsening TBI.14,27,28 Several studies have demonstrated thatpatients with TBI and a low GCS were more likely to die follow-ing REBOA deployment compared to patients without TBI.29
Furthermore, several reports demonstrate that REBOA deploy-ment may lead to death secondary to exacerbation of TBI pro-gression.15 However, these studies have had several limitationsregarding patient selection and lack of cerebral flow monitoring.Also, these studies used the traditional REBOA with complete
420
Copyright © 2019 Wolters Kluwer H
aortic occlusion, and it remains unclear whether pREBOAwould have the same impact on TBI progression.
Studies assessing the effects of REBOA in clinically realis-tic, large animal models of TBI are lacking. A previous preclinicalstudy used a mild model of concurrent HS and TBI, involving25% total blood volume hemorrhage and a 1,200 mm3 CCI-induced brain lesion.16 That particular study involved an early de-ployment of cREBOA and pREBOA immediately followinghemorrhage and external automated devices to ensure optimalproximal perfusion. These circumstances may not reflect clinicalscenarios and current practices. Our study decided to use a modelof severe HS (40% total blood volume hemorrhage) and TBI(2,400mm3 CCI-induced brain lesion).We also simulated a delayin pREBOA deployment and had a resuscitation schedule de-signed to represent a clinically realistic timeline with limitedresuscitation to mimic prehospital settings. Furthermore, weelected to test the concept of partial aortic occlusion, as therehas been an increasing use of pREBOA clinically and in pre-clinical large animal studies.12,13,16,30–33 The pREBOA-PRO
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
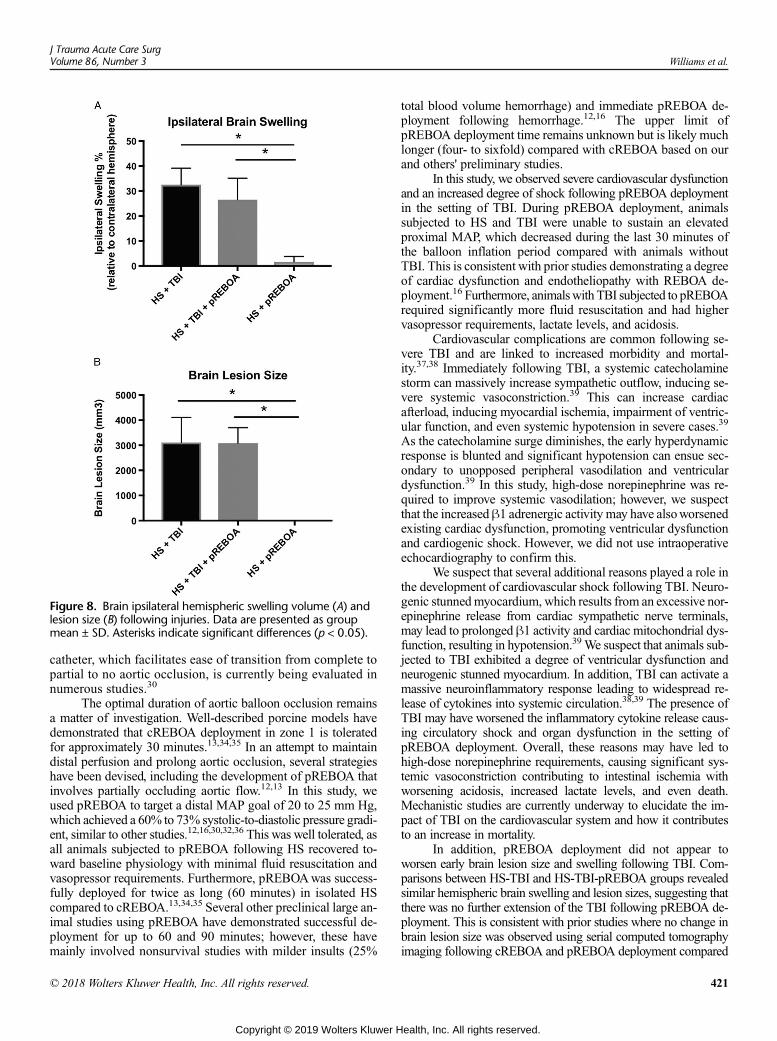
Figure 8. Brain ipsilateral hemispheric swelling volume (A) andlesion size (B) following injuries. Data are presented as groupmean ± SD. Asterisks indicate significant differences (p < 0.05).
J Trauma Acute Care SurgVolume 86, Number 3 Williams et al.
catheter, which facilitates ease of transition from complete topartial to no aortic occlusion, is currently being evaluated innumerous studies.30
The optimal duration of aortic balloon occlusion remainsa matter of investigation. Well-described porcine models havedemonstrated that cREBOA deployment in zone 1 is toleratedfor approximately 30 minutes.13,34,35 In an attempt to maintaindistal perfusion and prolong aortic occlusion, several strategieshave been devised, including the development of pREBOA thatinvolves partially occluding aortic flow.12,13 In this study, weused pREBOA to target a distal MAP goal of 20 to 25 mm Hg,which achieved a 60% to 73% systolic-to-diastolic pressure gradi-ent, similar to other studies.12,16,30,32,36 This was well tolerated, asall animals subjected to pREBOA following HS recovered to-ward baseline physiology with minimal fluid resuscitation andvasopressor requirements. Furthermore, pREBOAwas success-fully deployed for twice as long (60 minutes) in isolated HScompared to cREBOA.13,34,35 Several other preclinical large an-imal studies using pREBOA have demonstrated successful de-ployment for up to 60 and 90 minutes; however, these havemainly involved nonsurvival studies with milder insults (25%
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
total blood volume hemorrhage) and immediate pREBOA de-ployment following hemorrhage.12,16 The upper limit ofpREBOA deployment time remains unknown but is likely muchlonger (four- to sixfold) compared with cREBOA based on ourand others' preliminary studies.
In this study, we observed severe cardiovascular dysfunctionand an increased degree of shock following pREBOA deploymentin the setting of TBI. During pREBOA deployment, animalssubjected to HS and TBI were unable to sustain an elevatedproximal MAP, which decreased during the last 30 minutes ofthe balloon inflation period compared with animals withoutTBI. This is consistent with prior studies demonstrating a degreeof cardiac dysfunction and endotheliopathy with REBOA de-ployment.16 Furthermore, animalswith TBI subjected to pREBOArequired significantly more fluid resuscitation and had highervasopressor requirements, lactate levels, and acidosis.
Cardiovascular complications are common following se-vere TBI and are linked to increased morbidity and mortal-ity.37,38 Immediately following TBI, a systemic catecholaminestorm can massively increase sympathetic outflow, inducing se-vere systemic vasoconstriction.39 This can increase cardiacafterload, inducing myocardial ischemia, impairment of ventric-ular function, and even systemic hypotension in severe cases.39
As the catecholamine surge diminishes, the early hyperdynamicresponse is blunted and significant hypotension can ensue sec-ondary to unopposed peripheral vasodilation and ventriculardysfunction.39 In this study, high-dose norepinephrine was re-quired to improve systemic vasodilation; however, we suspectthat the increasedβ1 adrenergic activity may have alsoworsenedexisting cardiac dysfunction, promoting ventricular dysfunctionand cardiogenic shock. However, we did not use intraoperativeechocardiography to confirm this.
We suspect that several additional reasons played a role inthe development of cardiovascular shock following TBI. Neuro-genic stunnedmyocardium, which results from an excessive nor-epinephrine release from cardiac sympathetic nerve terminals,may lead to prolonged β1 activity and cardiac mitochondrial dys-function, resulting in hypotension.39We suspect that animals sub-jected to TBI exhibited a degree of ventricular dysfunction andneurogenic stunned myocardium. In addition, TBI can activate amassive neuroinflammatory response leading to widespread re-lease of cytokines into systemic circulation.38,39 The presence ofTBI may have worsened the inflammatory cytokine release caus-ing circulatory shock and organ dysfunction in the setting ofpREBOA deployment. Overall, these reasons may have led tohigh-dose norepinephrine requirements, causing significant sys-temic vasoconstriction contributing to intestinal ischemia withworsening acidosis, increased lactate levels, and even death.Mechanistic studies are currently underway to elucidate the im-pact of TBI on the cardiovascular system and how it contributesto an increase in mortality.
In addition, pREBOA deployment did not appear toworsen early brain lesion size and swelling following TBI. Com-parisons between HS-TBI and HS-TBI-pREBOA groups revealedsimilar hemispheric brain swelling and lesion sizes, suggesting thatthere was no further extension of the TBI following pREBOA de-ployment. This is consistent with prior studies where no change inbrain lesion size was observed using serial computed tomographyimaging following cREBOA and pREBOA deployment compared
421
ealth, Inc. All rights reserved.

Williams et al.J Trauma Acute Care Surg
Volume 86, Number 3
with controls.16 Furthermore, no significant increase in ICP wasobserved with pREBOA deployment in the setting of TBI com-pared to the HS-TBI group.
Several reasons may explain why pREBOA deploymentdid not worsen brain lesion size and swelling. First, supraphysiologicproximal MAP during pREBOA deployment may not be as ex-treme as that observed with cREBOA; furthermore, the proxi-mal MAP may be higher in milder HS models due todecreased hemorrhage volumes. In this study, however, we fo-cused on the effects of pREBOA deployment in a severe HSmodel. Second, the increase in proximal MAP followingpREBOA deployment may help maintain an appropriate cere-bral perfusion pressure despite an increase in ICP; this may haveminimized any exacerbation of TBI. Third, only a subset of pa-tients demonstrate TBI progression during the first 24 hours fol-lowing injury; therefore, detection of TBI progression isdifficult early following injury as was the case in this experi-ment.40,41 Despite the absence of early worsening in brain lesionsize and swelling following pREBOA deployment seen in thisstudy, survival studies are required to further assess the effectsof pREBOA deployment on neurologic outcomes and mortalityfollowing TBI and HS.
Although the presence of TBI is not a contraindication forpREBOA in HS, it is crucial for providers to be aware of the po-tential physiologic sequelae induced by TBI. The presence of TBImay significantly affect patient physiology, hemodynamics, andclinical outcomes following pREBOA deployment. For example,patients may require more fluid resuscitation, vasopressors, andpharmacologic therapies. Ultimately, this may translate into moreutilization of resources, which is especially relevant for far-forwardand other austere settings.
There are several limitations to this study. First, samplesize in this study was limited by ethical considerations and costs,and therefore, the results may be prone to a type II error. Further-more, there were unbalanced groups at the completion of thestudy given the increased mortality observed in the HS-TBI-pREBOA group; this finding may also affect the statistical anal-yses. Second, although swine are commonly used for humantranslation, they serve as an imperfect surrogate for human sub-jects. Studies of pREBOA application in patients with TBI areneeded to confirm the results of this study. Third, we used acontrolled-hemorrhage model for proof-of-concept testing ofpREBOA in the setting of TBI and to minimize variability; how-ever, uncontrolled hemorrhage models (from vascular injuries inthe abdomen and pelvis) are more clinically realistic and optimalfor testing pREBOA deployment. Fourth, objective thresholdswere used to guide fluid resuscitation and vasopressor requirementseven though resuscitation is often guided by fluid responsiveness inthe clinical setting. Fluid responsiveness as a benchmark for re-suscitation is highly subjective and operator dependent. There-fore, we used predefined thresholds to minimize investigatorbias. Fifth, animals were not transfused blood during the study.We realize that this may not reflect clinical practice in urban cen-ters; however, we sought to attain aworst case scenariowith lim-ited resuscitation and vasopressors, reflecting military or austeresettings with delayed evacuation where blood products may notbe available. Lastly, this study involved a short-term nonsurvivalmodel. In the future, the effects of pREBOA deployment onlong-term TBI progression and neurologic outcomes should be
422
Copyright © 2019 Wolters Kluwer H
tested. Our team is planning follow-up studies to address manyof these issues.
CONCLUSION
In conclusion, this study demonstrates that prolonged ap-plication of pREBOA in the setting of TBI does not contribute toearly worsening of brain lesion size and swelling. However, theaddition of TBI to HS-pREBOA may worsen the severity ofshock and create a situation that is difficult to reversewith resus-citation. Although the presence of TBI is not a contraindicationfor pREBOA in HS, it is crucial for providers to be aware of thepotential physiologic sequelae induced by TBI. Overall, thefindings of this study support continued evaluation of pREBOAdeployment in preclinical models of polytraumatic injuries, in-cluding HS, TBI, and multiorgan injuries.
AUTHORSHIP
A.M.W., J.E., and H.B.A. contributed in the conception and design. A.M.W.,U.F.B., I.S.D., N.J.G., V.C.N., K.C., P.C., J.Z., and B.E.B. contributed in thedata acquisition. A.M.W., U.F.B., I.S.D., N.J.G., V.C.N., K.C., P.C., J.Z.,B.E.B., J.E., and H.B.A. contributed in the data interpretation. A.M.W.,U.F.B., I.S.D., N.J.G., V.C.N., K.C., P.C., J.Z., B.E.B., J.E., and H.B.A. contrib-uted in the article preparation. All authors contributed in the critical revisionof the article.
ACKNOWLEDGMENTS
We thank Dr. Patrick Georgoff, Dr. Yongqing Li, Rachael O'Connell, andJessica Lee for their assistance with animal experiments. Wewould also liketo acknowledge Prytime Medical (Lakewood, CO) who provided thepREBOA catheters for testing.
DISCLOSURE
A.M.W. andH.B.A. received grant funding. For all other authors, no conflictsare declared. This work was funded by the US Army Materiel and ResearchCommand (contract W81XWH-09-1-0520), National Institutes of Healthgrant 2 R01 GM084127, and the Frederick A. Coller Surgical Society Re-search Grant.
REFERENCES1. Sauaia A, Moore FA, Moore EE, Moser KS, Brennan R, Read RA, Pons PT.
Epidemiology of trauma deaths: a reassessment. J Trauma. 1995;38(2):185–193.
2. Acosta JA, Yang JC, Winchell RJ, Simons RK, Fortlage DA,Hollingsworth-Fridlund P, Hoyt DB. Lethal injuries and time to death in alevel I trauma center. J Am Coll Surg. 1998;186(5):528–533.
3. Kauvar DS, Wade CE. The epidemiology and modern management of trau-matic hemorrhage: US and international perspectives. Crit Care.2005;9 Suppl 5:S1–S9.
4. Meislin H, Criss EA, Judkins D, Berger R, Conroy C, Parks B, Spaite DW,Valenzuela TD. Fatal trauma: the modal distribution of time to death is afunction of patient demographics and regional resources. J Trauma. 1997;43(3):433–440.
5. MartinM,Oh J, Currier H, Tai N, Beekley A, EckertM,Holcomb J. An anal-ysis of in-hospital deaths at a modern combat support hospital. J Trauma.2009;66(4 Suppl):S51–S60; discussion S-1.
6. Eastridge BJ, Jenkins D, Flaherty S, Schiller H, Holcomb JB. Trauma systemdevelopment in a theater of war: Experiences from Operation Iraqi Freedomand Operation Enduring Freedom. J Trauma. 2006;61(6):1366–1372;discussion 1372–73.
7. Napolitano LM. Resuscitative endovascular balloon occlusion of the aorta:indications, outcomes, and training. Crit Care Clin. 2017;33(1):55–70.
8. DuBose JJ, Scalea TM, Brenner M, Skiada D, Inaba K, Cannon J, Moore L,Holcomb J, Turay D, Arbabi CN, et al. The AAST prospective Aortic Occlu-sion for Resuscitation in Trauma and Acute Care Surgery (AORTA) registry:data on contemporary utilization and outcomes of aortic occlusion and
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
J Trauma Acute Care SurgVolume 86, Number 3 Williams et al.
resuscitative balloon occlusion of the aorta (REBOA). J Trauma Acute CareSurg. 2016;81(3):409–419.
9. Biffl WL, Fox CJ, Moore EE. The role of REBOA in the control of exsan-guinating torso hemorrhage. J Trauma Acute Care Surg. 2015;78(5):1054–1058.
10. Gupta BK, Khaneja SC, Flores L, Eastlick L, Longmore W, Shaftan GW.The role of intra-aortic balloon occlusion in penetrating abdominal trauma.J Trauma. 1989;29(6):861–865.
11. Inoue J, Shiraishi A, Yoshiyuki A, Haruta K, Matsui H, Otomo Y. Resusci-tative endovascular balloon occlusion of the aorta might be dangerous in pa-tients with severe torso trauma: a propensity score analysis. J Trauma AcuteCare Surg. 2016;80(4):559–566. discussion 66–67.
12. Russo RM,Williams TK, Grayson JK, Lamb CM, Cannon JW, Clement NF,Galante JM, Neff LP. Extending the golden hour: partial resuscitativeendovascular balloon occlusion of the aorta in a highly lethal swine liver in-jury model. J Trauma Acute Care Surg. 2016;80(3):372–378; discussion378–80.
13. Russo RM, Neff LP, Lamb CM, Cannon JW, Galante JM, Clement NF,Grayson JK, Williams TK. Partial resuscitative endovascular balloon occlu-sion of the aorta in swine model of hemorrhagic shock. J Am Coll Surg.2016;223(2):359–368.
14. Sellmann T, Miersch D, Kienbaum P, Flohe S, Schneppendahl J, Lefering R.The impact of arterial hypertension on polytrauma and traumatic brain injury.Dtsch Arztebl Int. 2012;109(49):849–856.
15. Uchino H, Tamura N, Echigoya R, Ikegami T, Fukuoka T. “REBOA”— is itreally safe? A case with massive intracranial hemorrhage possibly due toendovascular balloon occlusion of the aorta (REBOA). Am J Case Rep.2016;17:810–813.
16. Johnson MA, Williams TK, Ferencz SE, Davidson AJ, Russo RM,O'BrienWTSr., Galante JM,Grayson JK, Neff LP. The effect of resuscitativeendovascular balloon occlusion of the aorta, partial aortic occlusion and ag-gressive blood transfusion on traumatic brain injury in a swine multiple inju-ries model. J Trauma Acute Care Surg. 2017;83(1):61–70.
17. Jin G, DeMoya MA, Duggan M, Knightly T, Mejaddam AY, Hwabejire J,Lu J, Smith WM, Kasotakis G, Velmahos GC, et al. Traumatic brain injuryand hemorrhagic shock: evaluation of different resuscitation strategies in alarge animal model of combined insults. Shock. 2012;38(1):49–56.
18. Imam AM, Jin G, Duggan M, Sillesen M, Hwabejire JO, Jepsen CH,DePeralta D, Liu B, Lu J, deMoya MA, et al. Synergistic effects of fresh fro-zen plasma and valproic acid treatment in a combined model of traumaticbrain injury and hemorrhagic shock. Surgery. 2013;154(2):388–396.
19. Halaweish I, Bambakidis T, Chang Z, Wei H, Liu B, Li Y, Bonthrone T,Srinivasan A, Bonham T, Chtraklin K, et al. Addition of low-dose valproicacid to saline resuscitation provides neuroprotection and improves long-term out-comes in a large animal model of combined traumatic brain injury and hemor-rhagic shock. J Trauma Acute Care Surg. 2015;79(6):911–919. discussion 919.
20. Williams AM, Dennahy IS, Bhatti UF, Halaweish I, Xiong Y, Chang P,Nikolian VC, Chtraklin K, Brown J, Zhang Y, et al. Mesenchymal stemcell-derived exosomes provide neuroprotection and improve long-term neu-rologic outcomes in a swine model of traumatic brain injury and hemor-rhagic shock. J Neurotrauma. 2018; Jul 30. doi: 10.1089/neu.2018.5711.
21. Nikolian VC, Georgoff PE, Pai MP, Dehaney IS, Chtraklin K, Eidy H,Ghandour M, Han Y, Srinivasan A, Li Y, et al. Valproic acid decreases brainlesion size and improves neurologic recovery in swine subjected to traumaticbrain injury, hemorrhagic shock, and polytrauma. J Trauma Acute CareSurg. 2017. 83(6):1066–1073.
22. Rhee P, Talon E, Eifert S, Anderson D, Stanton K, Koustova E, Ling G,Burris D, Kaufmann C, Mongan P, et al. Induced hypothermia during emer-gency department thoracotomy: an animal model. J Trauma. 2000;48(3):439–447; discussion 447–50.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
23. Jin G, Duggan M, Imam A, Demoya MA, Sillesen M, Hwabejire J,Jepsen CH, Liu B, Mejaddam AY, Lu J, et al. Pharmacologic resuscitationfor hemorrhagic shock combined with traumatic brain injury. J TraumaAcute Care Surg. 2012;73(6):1461–1470.
24. Chauhan NB. Chronic neurodegenerative consequences of traumatic braininjury. Restor Neurol Neurosci. 2014;32(2):337–365.
25. Menon DK, Schwab K, Wright DW, Maas AI. Position statement: definitionof traumatic brain injury. Arch Phys Med Rehabil. 2010;91(11):1637–1640.
26. Alam HB. Trauma care: Finding a better way. PLoS Med. 2017;14(7):e1002350.
27. Freeman WD, Aguilar MI. Intracranial hemorrhage: diagnosis and manage-ment. Neurol Clin. 2012;30(1):211–240. ix.
28. Mori T, Katayama Y, Kawamata T. Acute hemispheric swelling associatedwith thin subdural hematomas: pathophysiology of repetitive head injury insports. Acta Neruochir Suppl. 2006;96:40–43.
29. Norii T, Crandall C, Terasaka Y. Survival of severe blunt trauma patientstreated with resuscitative endovascular balloon occlusion of the aorta com-pared with propensity score-adjusted untreated patients. J Trauma AcuteCare Surg. 2015;78(4):721–728.
30. Madurska MJ, Jansen JO, Reva VA, Mirghani M, Morrison JJ. The compat-ibility of computed tomography scanning and partial REBOA: a large animalpilot study. J Trauma Acute Care Surg. 2017;83(3):557–561.
31. Matsumura Y, Matsumoto J, Kondo H, Idoguchi K, Ishida T, Kon Y,Tomita K, Ishida K, Hirose T, Umakoshi K, et al. Fewer REBOA complica-tions with smaller devices and partial occlusion: evidence from a multicentreregistry in Japan. Emerg Med J. 2017;34(12):793–799.
32. DuBose JJ. How I do it: partial resuscitative endovascular balloon occlusionof the aorta (P-REBOA). J Trauma Acute Care Surg. 2017;83(1):197–199.
33. Johnson MA, Neff LP, Williams TK, DuBose JJ. Partial resuscitative bal-loon occlusion of the aorta (P-REBOA): clinical technique and rationale.J Trauma Acute Care Surg. 2016;81(5 Suppl 2 Proceedings of the 2015Mil-itary Health System Research Symposium):S133–s7.
34. Causey MW, Miller S, Hoffer Z, Hempel J, Stallings JD, Jin G, Alam H,Martin M. Beneficial effects of histone deacetylase inhibition with severehemorrhage and ischemia-reperfusion injury. J Surg Res. 2013;184(1):533–540.
35. Sokol KK, Black GE, Shawhan R, Marko ST, Eckert MJ, Tran NT,Starnes BW, Martin MJ. Efficacy of a novel fluoroscopy-free endovascularballoon device with pressure release capabilities in the setting of uncon-trolled junctional hemorrhage. J Trauma Acute Care Surg. 2016;80(6):907–914.
36. Williams TK, Neff LP, Johnson MA, Ferencz SA, Davidson AJ, Russo RM,Rasmussen TE. Extending resuscitative endovascular balloon occlusion ofthe aorta: endovascular variable aortic control in a lethal model of hemor-rhagic shock. J Trauma Acute Care Surg. 2016;81(2):294–301.
37. Krishnamoorthy V, Mackensen GB, Gibbons EF, Vavilala MS. Cardiac dys-function after neurologic injury: what do we know and where are we going?Chest. 2016;149(5):1325–1331.
38. Lim HB, Smith M. Systemic complications after head injury: a clinical re-view. Anaesthesia. 2007;62(5):474–482.
39. Nguyen H, Zaroff JG. Neurogenic stunned myocardium. Curr NeurolNeurosci Rep. 2009;9(6):486–491.
40. Juratli TA, Zang B, Litz RJ, Sitoci KH, Aschenbrenner U, Gottschlich B,Daubner D, Schackert G, Sobottka SB. Early hemorrhagic progression oftraumatic brain contusions: frequency, correlation with coagulation disor-ders, and patient outcome: a prospective study. J Neurotrauma. 2014;31(17):1521–1527.
41. Kurland D, Hong C, Aarabi B, Gerzanich V, Simard JM. Hemorrhagic pro-gression of a contusion after traumatic brain injury: a review. J Neurotrauma.2012;29(1):19–31.
423
ealth, Inc. All rights reserved.

ORIGINAL ARTICLE
Initial evaluation of the efficacy and safety of in-hospitalexpandable hemostatic minisponge use in penetrating trauma
Zachary Warriner, MD, Lydia Lam, MD, Kazuhide Matsushima, MD, Elizabeth Benjamin, MD, PhD,Aaron Strumwasser, MD, Demetrios Demetriades, MD, PhD, and Kenji Inaba, MD, Los Angeles, California
Sub
Fro
Ad
DO
42
BACKGROUND: H
mitted: July 28, 2018, RevisedPublished online: October 23, 2m the Division of Trauma and SD.D., K.I.), LAC+USC MedicAngeles, California.dress for reprints: Kenji Inaba, MLAC + USC Medical Center, USt, Inpatient Tower, C5L100, Lusc.edu.
I: 10.1097/TA.00000000000020
4
emorrhage remains the leading cause of preventable death after trauma. The XSTATexpandable minisponge hemostatic devicewas developed for the control of severe, life-threatening bleeding from junctional wounds not amenable to tourniquet application.This is an initial report of the clinical use of this novel method of hemorrhage control for civilian penetrating injury.
METHODS: A
review of trauma admissions at a high-volume Level I trauma center was performed from July 2016 to November 2017. Allpatients sustaining penetrating trauma with active hemorrhage were evaluated for XSTAT use. Ten device deployments occurredduring this time. Each deployment was reviewed in detail, capturing patient and injury data, efficacy of hemorrhage control, andevaluation of any potential device or treatment related complications.RESULTS: S
ix thousand three hundred sixty-three trauma admissions were reviewed with 22.1% sustaining a penetrating mechanism of in-jury. XSTATwas deployed in 10 (0.7%) penetrating trauma admissions with a mean age of 38.3 (range, 16–59) years, systolicblood pressure (SBP) of 126.7 (range, 74–194)mmHg, GlasgowComa Scale (GCS) score of 14.5 (range, 13–15), and New InjurySeverity Score (NISS) of 9.5 (range, 1–27). Eight patients had an identifiable arterial injury; the remainder had vein or soft tissuebleeding. Overall, half were junctional injuries. XSTATwas able to stop bleeding in nine of ten patients on the first deployment,with the remaining patient requiring one repeat injection. Dwell times ranged from 1 hour to 40 hours (median, 15 hours). There wereno technical device failures or embolic complications. Retained sponges were identified in two patients on initial postremoval x-raysfollowing wound exploration for definitive hemorrhage control and sponge removal. No patient died during the study period.CONCLUSION: X
STAT use appears safe. It is rapid, reliable, and provides a high degree of hemorrhage control on first deployment. Sponge re-moval should always be followed by radiographic clearance. For patients with hemorrhage from cavitary wounds not amenableto tourniquet placement, this device was effective. Further study is warranted as XSTATuse becomes morewidespread. (J TraumaAcute Care Surg. 2019;86: 424–430. Copyright © 2018 Wolters Kluwer Health, Inc. All rights reserved.)LEVEL OF EVIDENCE: T
herapeutic study, level V. KEYWORDS: T opical hemostatic; balloon tamponade; junctional hemorrhage; minisponge dressing; XSTAT.A 20-year-old female presented to our Level I trauma centeras a top tier trauma activation in hemorrhagic shock. She
had sustained multiple gunshot wounds with large-volumeblood loss reported at the scene and arrived with a blood pres-sure of 88/77 mmHg and heart rate of 148 bpm. Physical exam-ination revealed two injuries to her right lower quadrant as wellas an injury to her right groin. The junctional wound had a largeunderlying hematoma and active bleeding. This was controlledwith direct pressure, a plain radiograph of the abdomen was ob-tained, and the patient was transported immediately to the oper-ating room for definitive hemorrhage control. In order for thelaparotomy to be safely performed, temporary groin hemorrhagecontrolwas necessary. The location of the injurywas not amenableto tourniquet placement, and attempts at Foley catheter balloon
: October 6, 2018, Accepted: October 11, 2018,018.urgical Critical Care (Z.W., L.L., K.M., E.B., A.S.,al Center, University of Southern California, Los
D, Division of Trauma and Surgical Critical Care,niversity of Southern California, 2051 Marengoos Angeles, CA 90033; email: kinaba@surgery.
91
Copyright © 2019 Wolters Kluwer H
tamponade were unsuccessful due to balloon extrusion. OneXSTAT 30 device was then deployed into the wound, resultingin immediate hemorrhage control allowing for completion ofthe abdominal exploration (Fig. 1). The laparotomy demonstratedno source of hemorrhage and the blood loss was attributed to thejunctionalwound. Attentionwas then returned to this area. At thispoint, after the infusion of 5 units of packed red blood cells and 1unit of plasma, the patient's hemodynamics were normalizing. Aplain radiograph was obtained to rule out an associated fractureand the groin was explored. The wound was extended, theXSTAT sponges removed, and a complete transection of theright profunda femoris artery just beyond the common femoralbifurcation (Fig. 2) was found. This was ligated. Repeat intraop-erative radiograph was obtained to ensure complete removal ofthe sponges (Fig. 3). Hemodynamics continued to improve, andthe patient was transferred to the intensive care unit and ulti-mately discharged home.
This case highlights the challenge of effective junctionalor other noncompressible hemorrhage control where a tourni-quet cannot be used and other means are unsuccessful. The im-portance of immediate hemorrhage control cannot be overstated,as hemorrhage remains the leading cause of preventable death,accounting for 30% to 40% of trauma related mortality.1 Withany visible external bleeding, achieving immediate hemorrhagecontrol is the priority.2,3
J Trauma Acute Care SurgVolume 86, Number 3
ealth, Inc. All rights reserved.
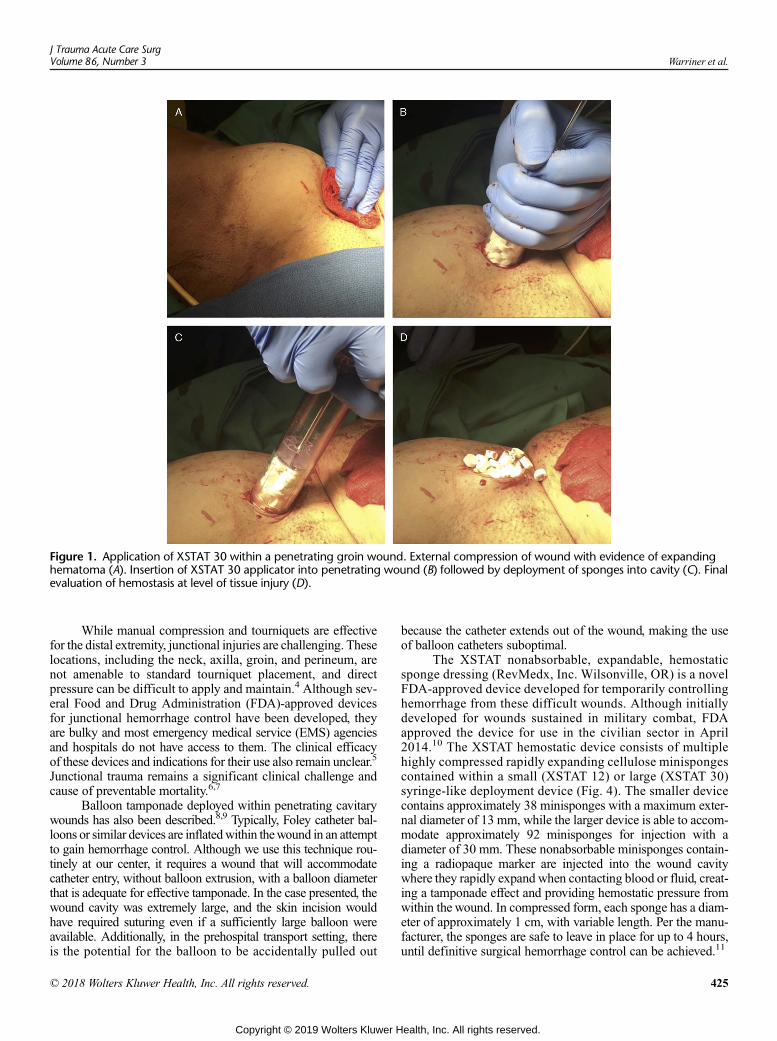
Figure 1. Application of XSTAT 30 within a penetrating groin wound. External compression of wound with evidence of expandinghematoma (A). Insertion of XSTAT 30 applicator into penetrating wound (B) followed by deployment of sponges into cavity (C). Finalevaluation of hemostasis at level of tissue injury (D).
J Trauma Acute Care SurgVolume 86, Number 3 Warriner et al.
While manual compression and tourniquets are effectivefor the distal extremity, junctional injuries are challenging. Theselocations, including the neck, axilla, groin, and perineum, arenot amenable to standard tourniquet placement, and directpressure can be difficult to apply and maintain.4 Although sev-eral Food and Drug Administration (FDA)-approved devicesfor junctional hemorrhage control have been developed, theyare bulky and most emergency medical service (EMS) agenciesand hospitals do not have access to them. The clinical efficacyof these devices and indications for their use also remain unclear.5
Junctional trauma remains a significant clinical challenge andcause of preventable mortality.6,7
Balloon tamponade deployed within penetrating cavitarywounds has also been described.8,9 Typically, Foley catheter bal-loons or similar devices are inflatedwithin thewound in an attemptto gain hemorrhage control. Although we use this technique rou-tinely at our center, it requires a wound that will accommodatecatheter entry, without balloon extrusion, with a balloon diameterthat is adequate for effective tamponade. In the case presented, thewound cavity was extremely large, and the skin incision wouldhave required suturing even if a sufficiently large balloon wereavailable. Additionally, in the prehospital transport setting, thereis the potential for the balloon to be accidentally pulled out
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
because the catheter extends out of the wound, making the useof balloon catheters suboptimal.
The XSTAT nonabsorbable, expandable, hemostaticsponge dressing (RevMedx, Inc. Wilsonville, OR) is a novelFDA-approved device developed for temporarily controllinghemorrhage from these difficult wounds. Although initiallydeveloped for wounds sustained in military combat, FDAapproved the device for use in the civilian sector in April2014.10 The XSTAT hemostatic device consists of multiplehighly compressed rapidly expanding cellulose minispongescontained within a small (XSTAT 12) or large (XSTAT 30)syringe-like deployment device (Fig. 4). The smaller devicecontains approximately 38 minisponges with a maximum exter-nal diameter of 13 mm, while the larger device is able to accom-modate approximately 92 minisponges for injection with adiameter of 30 mm. These nonabsorbable minisponges contain-ing a radiopaque marker are injected into the wound cavitywhere they rapidly expand when contacting blood or fluid, creat-ing a tamponade effect and providing hemostatic pressure fromwithin the wound. In compressed form, each sponge has a diam-eter of approximately 1 cm, with variable length. Per the manu-facturer, the sponges are safe to leave in place for up to 4 hours,until definitive surgical hemorrhage control can be achieved.11
425
ealth, Inc. All rights reserved.
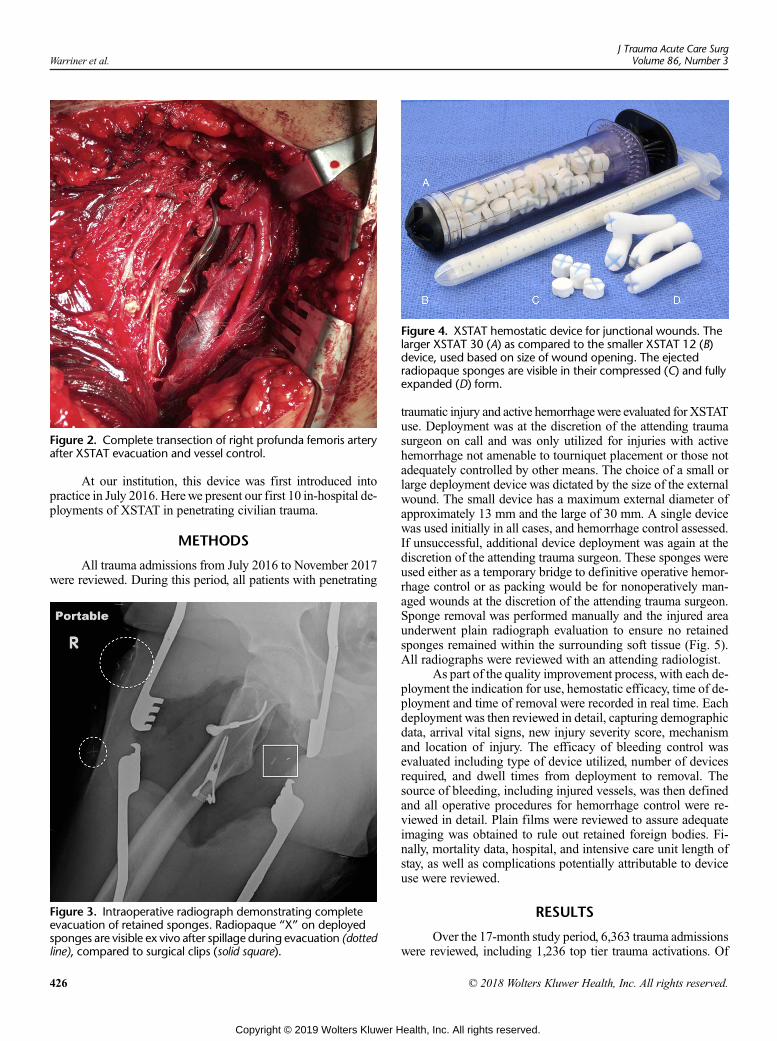
Figure 4. XSTAT hemostatic device for junctional wounds. Thelarger XSTAT 30 (A) as compared to the smaller XSTAT 12 (B)device, used based on size of wound opening. The ejectedradiopaque sponges are visible in their compressed (C) and fullyexpanded (D) form.
Figure 2. Complete transection of right profunda femoris arteryafter XSTAT evacuation and vessel control.
Warriner et al.J Trauma Acute Care Surg
Volume 86, Number 3
At our institution, this device was first introduced intopractice in July 2016. Herewe present our first 10 in-hospital de-ployments of XSTAT in penetrating civilian trauma.
METHODS
All trauma admissions from July 2016 to November 2017were reviewed. During this period, all patients with penetrating
Figure 3. Intraoperative radiograph demonstrating completeevacuation of retained sponges. Radiopaque “X” on deployedsponges are visible ex vivo after spillage during evacuation (dottedline), compared to surgical clips (solid square).
426
Copyright © 2019 Wolters Kluwer H
traumatic injury and active hemorrhagewere evaluated for XSTATuse. Deployment was at the discretion of the attending traumasurgeon on call and was only utilized for injuries with activehemorrhage not amenable to tourniquet placement or those notadequately controlled by other means. The choice of a small orlarge deployment device was dictated by the size of the externalwound. The small device has a maximum external diameter ofapproximately 13 mm and the large of 30 mm. A single devicewas used initially in all cases, and hemorrhage control assessed.If unsuccessful, additional device deployment was again at thediscretion of the attending trauma surgeon. These sponges wereused either as a temporary bridge to definitive operative hemor-rhage control or as packing would be for nonoperatively man-aged wounds at the discretion of the attending trauma surgeon.Sponge removal was performed manually and the injured areaunderwent plain radiograph evaluation to ensure no retainedsponges remained within the surrounding soft tissue (Fig. 5).All radiographs were reviewed with an attending radiologist.
As part of the quality improvement process, with each de-ployment the indication for use, hemostatic efficacy, time of de-ployment and time of removal were recorded in real time. Eachdeployment was then reviewed in detail, capturing demographicdata, arrival vital signs, new injury severity score, mechanismand location of injury. The efficacy of bleeding control wasevaluated including type of device utilized, number of devicesrequired, and dwell times from deployment to removal. Thesource of bleeding, including injured vessels, was then definedand all operative procedures for hemorrhage control were re-viewed in detail. Plain films were reviewed to assure adequateimaging was obtained to rule out retained foreign bodies. Fi-nally, mortality data, hospital, and intensive care unit length ofstay, as well as complications potentially attributable to deviceuse were reviewed.
RESULTS
Over the 17-month study period, 6,363 trauma admissionswere reviewed, including 1,236 top tier trauma activations. Of
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
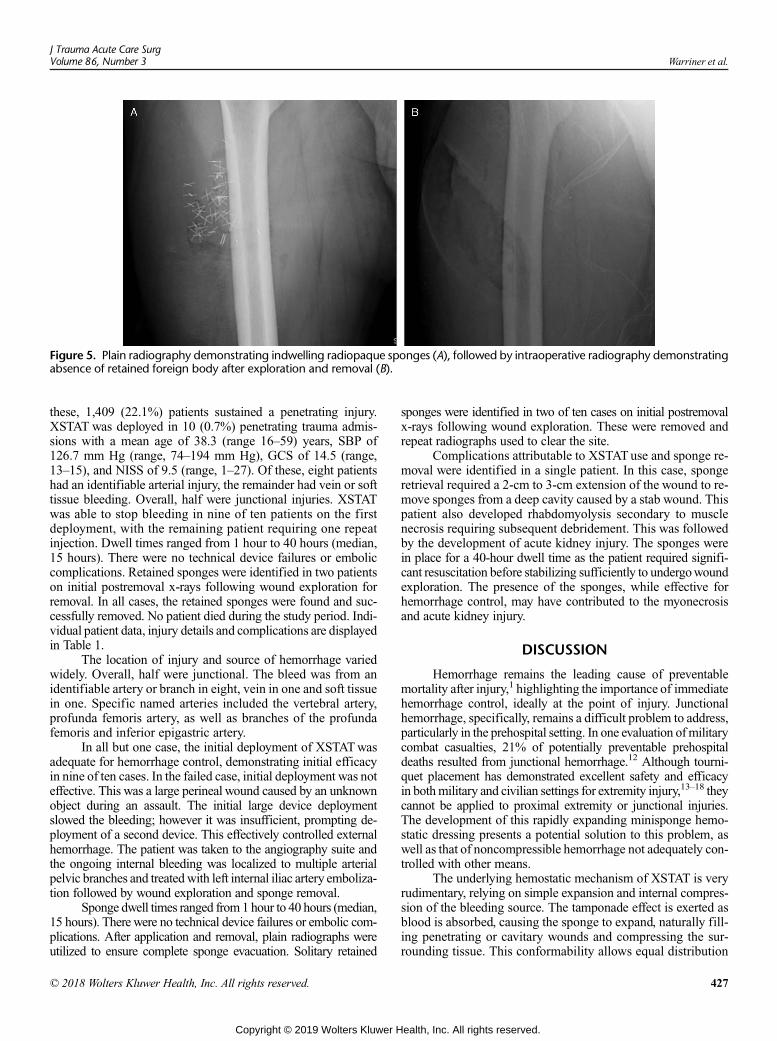
Figure 5. Plain radiography demonstrating indwelling radiopaque sponges (A), followed by intraoperative radiography demonstratingabsence of retained foreign body after exploration and removal (B).
J Trauma Acute Care SurgVolume 86, Number 3 Warriner et al.
these, 1,409 (22.1%) patients sustained a penetrating injury.XSTAT was deployed in 10 (0.7%) penetrating trauma admis-sions with a mean age of 38.3 (range 16–59) years, SBP of126.7 mm Hg (range, 74–194 mm Hg), GCS of 14.5 (range,13–15), and NISS of 9.5 (range, 1–27). Of these, eight patientshad an identifiable arterial injury, the remainder had vein or softtissue bleeding. Overall, half were junctional injuries. XSTATwas able to stop bleeding in nine of ten patients on the firstdeployment, with the remaining patient requiring one repeatinjection. Dwell times ranged from 1 hour to 40 hours (median,15 hours). There were no technical device failures or emboliccomplications. Retained sponges were identified in two patientson initial postremoval x-rays following wound exploration forremoval. In all cases, the retained sponges were found and suc-cessfully removed. No patient died during the study period. Indi-vidual patient data, injury details and complications are displayedin Table 1.
The location of injury and source of hemorrhage variedwidely. Overall, half were junctional. The bleed was from anidentifiable artery or branch in eight, vein in one and soft tissuein one. Specific named arteries included the vertebral artery,profunda femoris artery, as well as branches of the profundafemoris and inferior epigastric artery.
In all but one case, the initial deployment of XSTATwasadequate for hemorrhage control, demonstrating initial efficacyin nine of ten cases. In the failed case, initial deployment was noteffective. This was a large perineal wound caused by an unknownobject during an assault. The initial large device deploymentslowed the bleeding; however it was insufficient, prompting de-ployment of a second device. This effectively controlled externalhemorrhage. The patient was taken to the angiography suite andthe ongoing internal bleeding was localized to multiple arterialpelvic branches and treatedwith left internal iliac artery emboliza-tion followed by wound exploration and sponge removal.
Sponge dwell times ranged from 1 hour to 40 hours (median,15 hours). There were no technical device failures or embolic com-plications. After application and removal, plain radiographs wereutilized to ensure complete sponge evacuation. Solitary retained
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
sponges were identified in two of ten cases on initial postremovalx-rays following wound exploration. These were removed andrepeat radiographs used to clear the site.
Complications attributable to XSTATuse and sponge re-moval were identified in a single patient. In this case, spongeretrieval required a 2-cm to 3-cm extension of the wound to re-move sponges from a deep cavity caused by a stab wound. Thispatient also developed rhabdomyolysis secondary to musclenecrosis requiring subsequent debridement. This was followedby the development of acute kidney injury. The sponges werein place for a 40-hour dwell time as the patient required signifi-cant resuscitation before stabilizing sufficiently to undergowoundexploration. The presence of the sponges, while effective forhemorrhage control, may have contributed to the myonecrosisand acute kidney injury.
DISCUSSION
Hemorrhage remains the leading cause of preventablemortality after injury,1 highlighting the importance of immediatehemorrhage control, ideally at the point of injury. Junctionalhemorrhage, specifically, remains a difficult problem to address,particularly in the prehospital setting. In one evaluation ofmilitarycombat casualties, 21% of potentially preventable prehospitaldeaths resulted from junctional hemorrhage.12 Although tourni-quet placement has demonstrated excellent safety and efficacyin bothmilitary and civilian settings for extremity injury,13–18 theycannot be applied to proximal extremity or junctional injuries.The development of this rapidly expanding minisponge hemo-static dressing presents a potential solution to this problem, aswell as that of noncompressible hemorrhage not adequately con-trolled with other means.
The underlying hemostatic mechanism of XSTAT is veryrudimentary, relying on simple expansion and internal compres-sion of the bleeding source. The tamponade effect is exerted asblood is absorbed, causing the sponge to expand, naturally fill-ing penetrating or cavitary wounds and compressing the sur-rounding tissue. This conformability allows equal distribution
427
ealth, Inc. All rights reserved.
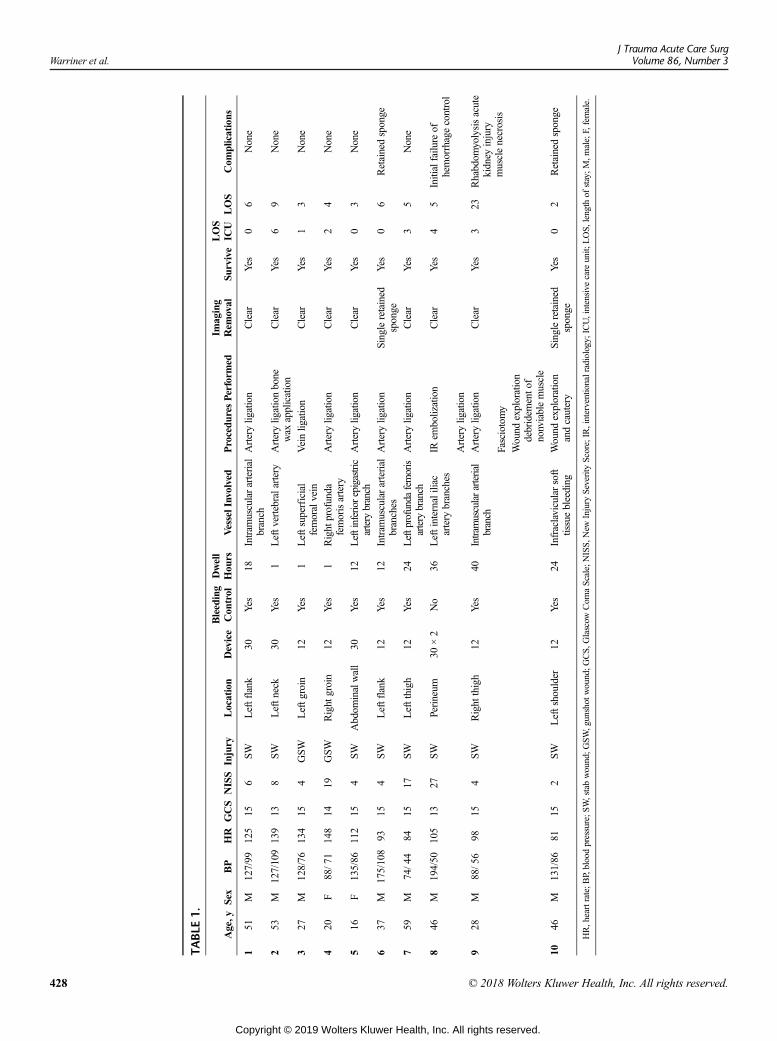
TABLE
1.
Age,y
Sex
BP
HR
GCS
NISS
Injury
Location
Device
Bleeding
Con
trol
Dwell
Hou
rsVesselInvolved
Procedu
resPerform
edIm
aging
Rem
oval
Survive
LOS
ICU
LOS
Com
plications
151
M127/99
125
156
SWLeftflank
30Yes
18Intram
usculararterial
branch
Arteryligation
Clear
Yes
06
None
253
M127/109
139
138
SWLeftn
eck
30Yes
1Leftv
ertebralartery
Arteryligationbone
wax
application
Clear
Yes
69
None
327
M128/76
134
154
GSW
Leftg
roin
12Yes
1Leftsuperficial
femoralvein
Veinlig
ation
Clear
Yes
13
None
420
F88/7
1148
1419
GSW
Right
groin
12Yes
1Right
profunda
femorisartery
Arteryligation
Clear
Yes
24
None
516
F135/86
112
154
SWAbdom
inalwall
30Yes
12Leftinferiorepigastric
artery
branch
Arteryligation
Clear
Yes
03
None
637
M175/108
9315
4SW
Leftflank
12Yes
12Intram
usculararterial
branches
Arterylig
ation
Singleretained
sponge
Yes
06
Retainedsponge
759
M74/4
484
1517
SWLeftthigh
12Yes
24Leftprofundafemoris
artery
branch
Arteryligation
Clear
Yes
35
None
846
M194/50
105
1327
SWPerineum
30×2
No
36Leftinternaliliac
artery
branches
IRem
bolization
Clear
Yes
45
Initialfailu
reof
hemorrhagecontrol
Arteryligation
928
M88/5
698
154
SWRight
thigh
12Yes
40Intramusculararterial
branch
Arterylig
ation
Clear
Yes
323
Rhabdom
yolysisacute
kidney
injury
musclenecrosis
Fasciotomy
Wound
exploration
debridem
ento
fnonviablemuscle
1046
M131/86
8115
2SW
Leftshoulder
12Yes
24Infraclavicularsoft
tissuebleeding
Wound
exploration
andcautery
Singleretained
sponge
Yes
02
Retainedsponge
HR,heartrate;B
P,bloodpressure;S
W,stabwound;G
SW,gunshot
wound;G
CS,
Glascow
Com
aScale;N
ISS,N
ewInjury
Severity
Score;IR,interventionalradiology;ICU,intensive
care
unit;
LOS,
length
ofstay;M
,male;F,female.
Warriner et al.J Trauma Acute Care Surg
Volume 86, Number 3
428 © 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Warriner et al.
of pressure uniformly throughout the defect, ensuring applica-tion of pressure at the point of injury, without the need for anydiagnostics or knowledge of the underlying vascular injury.This proof of concept has been verified in a penetrating woundmodel study by Kragh, demonstrating improved maintenanceof pressure at both the side and bottom of thewound asmeasuredby manometry when compared to standard gauze dressing.19
XSTATexpanded evenly with a balanced distribution of pressure,as opposed to the asymmetrical pressure distribution of packedgauze. Additionally, time to application strongly favored XSTATwith an eight-fold reduction, as well as an absence of mechanicalwound shear which was seen with gauze packing.
In the preclinical evaluation of XSTAT, swine femoral ar-tery injuries (6.0 mm arteriotomy) were controlled in 100% ofcases, with a decrease in wound packing time from 4.6 minutesto 1.1 minutes as compared to standard gauze packing.10 An ad-ditional analysis of swine subclavian artery and vein transectiondemonstrated hemorrhage control in 87.5% of injuries, with asolitary failure related to the loss of an applicator tip within thewound, preventing sponges from accessing the point of bleed-ing.10 Applicator tips are now secured to the device with glueto remedy this problem.
In the current data set, the first reported clinical applicationof XSTAT in penetrating civilian trauma, the initial deploymentefficacy was 90%. Temporary hemorrhage control was achieved,even in the setting of significant arterial bleeding. The solitaryfailure ultimately required embolization of the left internal iliacartery for definitive control of bleeding from multiple pelvicbranches caused by a deep perineal laceration. Tamponade wasdifficult to achieve due to the size of the cavity and the largewound opening, which allowed spillage of injected sponges,rather than expansion within a contained cavity. These large cav-itary wounds are potentially ideal for XSTAT use, but highlightthe need for a penetrating skin wound smaller than the underlyingcavity, accommodating sponge insertion but preventing unwantedextrusion. In these cases, skin suturing may be required. Forpatients where the initial deployment is ineffective, a secondinjection remains an option, which in this case was effective.
XSTAT placement was found to be straightforward. Thesyringe type deployment device is intuitive and no diagnosticsare necessary before use. Determination of the exact natureand location of the injured blood vessel is not necessary. In auser evaluation of XSTAT device and applicator use, controlledapplicationwas performed in under 90 seconds in all first attemptsby civilian EMS or military medics, with a mean application timeof 50.1 seconds.10 The device itself is portable, lightweight, andmay be stored at room temperature. The self-sustaining natureof tamponade with XSTAT use would allow rescuers to focus onother tasks during extrication or transport to definitive care. Thesequalities make it ideal for prehospital application.
Although application is straightforward and rapid, the re-moval of hemostatic material is more difficult and time intensivewhen compared to simple gauze packing. In the previouslydiscussed woundmodel study by Kragh, the mean time of spongeremoval required a 22-fold increase when compared to a contin-uous standard gauze roll.19 Animal data supports a fivefold in-crease in time required for removal.10 In addition, within thiscase series, extension of the skin incision to enlarge the woundwas required in one case for complete sponge evacuation.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
Retained sponges were identified in 2 of 10 cases afterattempted removal. This highlights the importance of obtainingimaging at the time of sponge retrieval to ensure the absence ofretained foreign bodies. In practice, even when adequate woundexploration appears to have been completed, sponges may beoverlooked and could result in potentially serious complicationsif left undetected. While attempts at localizing all sponges basedon number per applicator would be ideal, in practice, sponges areoften lost due towound extrusion, incomplete syringe evacuation,or many other variables. Additionally, the manufacturer stateseach applicator contains an approximate rather than exact numberof sponges, further invalidating this practice. For these reasons,postevacuation radiography is mandatory.
The development of rhabdomyolysis potentially related toprolonged dwell time highlights the importance of this device asa temporary method of hemorrhage control, bridging the patientto definitive care. It is important to note that this complicationdeveloped in the setting of a 40-hour sponge dwell time, as thepatient was unable to tolerate an operative procedure before this.While the recommended safe dwell time is 4 hours, as demon-strated in this case series, longer dwell times may be required,and should be dictated by the patient's clinical condition. Unfor-tunately, the maximum safe dwell time has yet to be established.However, because complications due to local tissue ischemia arepossible, as soon as the patient is able to tolerate it, sponge re-moval and definitive hemorrhage control should be obtained.
CONCLUSION
Junctional and noncompressible hemorrhage control re-mains a challenge, particularly in the prehospital setting. XSTATis a rapid, reliable and hands free device for achieving control ofhemorrhage within wounds not amenable to tourniquet place-ment or other simple methods. While there is a high rate ofbleeding control with initial deployment, repeat injection maybe required. The sponges should be used as a temporary bridgeto definitive hemorrhage control. Removal should be followedby radiographic confirmation. Further evaluation of this prod-uct is warranted as its use expands.
AUTHORSHIP
Z.W. and K.I. provided the conceptual study design. Z.W. and K.I. partic-ipated in the literature search. L.L., K.M., E.B., A.S., D.D., and K.I. per-formed surgical procedures. Z.W., K.M., A.S., and K.I. participated in thedata collection. Z.W., L.L., E.B., and K.I. performed the data analysis. Z.W.,L.L., K.M., E.B., A.S., D.D., and K.I. performed the data interpretation.All authors participated in writing and critically reviewing the final article.
DISCLOSURE
The authors have no conflicts of interest or disclosures of funding to declare.
REFERENCES1. Teixeira PG, Inaba K, Hadjizacharia P, Brown C, Salim A, Rhee P,
Browder T, Noguchi TT, Demetriades D. Preventable or potentially prevent-able mortality at a mature trauma center. J Trauma. 2007;63(6):1338–1346;discussion 1346-7.
2. Kauvar DS, Lefering R, Wade CE. Impact of hemorrhage on trauma out-come: an overview of epidemiology, clinical presentations, and therapeuticconsiderations. J Trauma. 2006;60(Suppl 6):S3–S11.
3. Eastridge BJ, Mabry RL, Seguin P, Cantrell J, Tops T, Uribe P, Mallett O,Zubko T, Oetjen-Gerdes L, Rasmussen TE, et al. Death on the battlefield(2001-2011): implications for the future of combat casualty care. J TraumaAcute Care Surg. 2012;73(6 Suppl 5):S431–S437.
429
ealth, Inc. All rights reserved.

Warriner et al.J Trauma Acute Care Surg
Volume 86, Number 3
4. Kragh JF Jr, Murphy C, DubickMA, Baer DG, Johnson J, Blackbourne LH.New tourniquet device concepts for battlefield hemorrhage control.US ArmyMed Dep J. 2011;38–48.
5. van Oostendorp SE, Tan EC, Geeraedts LM Jr. Prehospital control oflife-threatening truncal and junctional haemorrhage is the ultimate chal-lenge in optimizing trauma care; a review of treatment options and their ap-plicability in the civilian trauma setting. Scand J Trauma Resusc EmergMed.2016;24:110.
6. Holcomb JB,McMullin NR, Pearse L, Caruso J,Wade CE, Oetjen-Gerdes L,Champion HR, Lawnick M, Farr W, Rodriguez S, et al. Causes of death inU.S. special operations forces in the global war on terrorism: 2001-2004.Ann Surg. 2007;245:986–991.
7. Kelly JF, Ritenour AE,McLaughlin DF, BaggKA, ApodacaAN,Mallak CT,Pearse L, Lawnick MM, Champion HR, Wade CE, et al. Injury severityand causes of death from operation iraqi freedom and operation enduringfreedom: 2003-2004 versus 2006. J Trauma. 2008;64(Suppl 2):S21–S27;discussion S26-7.
8. Ball CG, Wyrzykowski AD, Nicholas JM, Rozycki GS, Feliciano DV. Adecade's experiencewith balloon catheter tamponade for the emergency con-trol of hemorrhage. J Trauma. 2011;70(2):330–333.
9. FelicianoDV, Burch JM,MattoxKL,Bitondo CG, Fields G. Balloon cathetertamponade in cardiovascular wounds. Am J Surg. 1990;160:583–587.
10. U.S. Food andDrug Administration (FDA) (2014). De novo classification re-quest for XStat. http://www.accessdata.fda.gov/cdrh_docs/reviews/k130218.pdf. Accessed May 17, 2018.
11. XSTAT® RevMedx™. XSTAT® product website. https://www.revmedx.com/xstat. Accessed July 22, 2018.
430
Copyright © 2019 Wolters Kluwer H
12. Eastridge BJ, Hardin M, Cantrell J, Oetjen-Gerdes L, Zubko T, Mallak C,Wade CE, Simmons J, Mace J, Mabry R, et al. Died of wounds on the battle-field: causation and implications for improving combat casualty care.J Trauma. 2011;71(Suppl 1):S4–S8.
13. Inaba K, Siboni S, Resnick S, Zhu J, Wong MD, Haltmeier T, Benjamin E,Demetriades D. Tourniquet use for civilian extremity trauma. J Trauma AcuteCare Surg. 2015;79(2):232–237.
14. Kragh JF Jr, Littrel ML, Jones JA, Walters TJ, Baer DG, Wade CE,Holcomb JB. Battle casualty survival with emergency tourniquet use to stoplimb bleeding. J Emerg Med. 2011;41(6):590–597.
15. Kragh JF Jr, Walters TJ, Baer DG, Fox CJ, Wade CE, Salinas J, Holcomb JB.Survival with emergency tourniquet use to stop bleeding in major limbtrauma. Ann Surg. 2009;249(1):1–43.
16. Lairet JR, Bebarta VS, Burns CJ, Lairet KF, Rasmussen TE, Renz EM,King BT, Fernandez W, Gerhardt R, Butler F, et al. Prehospital interventionsperformed in a combat zone: a prospective multicenter study of 1,003 com-bat wounded. J Trauma Acute Care Surg. 2012;73(2 Suppl 1):S38–S42.
17. Kragh JF Jr, Walters TJ, Baer DG, Fox CJ, Wade CE, Salinas J, Holcomb JB.Practical use of emergency tourniquets to stop bleeding in major limbtrauma. J Trauma. 2008;64(Suppl 2):S38–S49; discussion S49-50.
18. Teixeira PGR, Brown CVR, Emigh B, Long M, Foreman M, Eastridge B,Gale S, Truitt MS, Dissanaike S, Duane T, et al. Civilian prehospital tourni-quet use is associated with improved survival in patients with peripheral vas-cular injury. J Am Coll Surg. 2018;226(5):769–776.e1.
19. Kragh JF Jr, Aden JK, Steinbaugh J, Bullard M, Dubick MA. Gauze vsXSTAT® in wound packing for hemorrhage control. Am J Emerg Med.2015;33:974–976.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

ORIGINAL ARTICLE
Caspase-(8/3) activation and organ inflammation in a rat modelof resuscitated hemorrhagic shock: A role for uric acid
Kim Gilbert, PhD, Guy Rousseau, PhD, Caroline Bouchard, Sophie Dunberry-Poissant, MD,Frédérique Baril, BSc, Anne Marie Cardinal, BSc, François Khazoom, MD, Melissa Aubin Vega,
Emmanuelle Brochiero, PhD, and Emmanuel Charbonney, MD, PhD, Québec,Canada; on behalf of the Canadian Critical Care Translational Biology Group (CCCTBG)
Sub
Fro
Me
Ad
Sup
DO
J TrVol
BACKGROUND: M
mitted: February 13, 22018, Published onlinm the Centre de Rech(K.G.,G.R.,C.B.,E.C.)Département de MédF.K.,M.A.V., E.B.); ande Montréal (CRCHUeting presentation: Partthe Canadian Criticaldress for reprints: EmmMontréal 5400 Boul.emmanuel.charbonneyplemental digital contethe printed text, and linarticle on the journal’s
I: 10.1097/TA.000000
auma Acute Care Suume 86, Number 3
ultiple organ failure can develop after hemorrhagic shock (HS). Uric acid (UA) is released from dying cells and can be proinflammatory.We hypothesized that UA could be an alternative mediator of organ apoptosis and inflammation after HS.
METHODS: V
entilatedmaleWistar rats were used for the HSmodel. Two durations of shock (5minutes vs. 60minutes) were compared, and shamswereinstrumented only; animals were resuscitated and observed for 24 hours/72 hours. Caspases-(8/3), myeloperoxidase (MPO), TNF-α weremeasured in lungs and kidneys. Plasma UA and cytokine (IL-1β, IL-18, TNF-α) were measured. A second set of animals were randomizedto vehicle versus Rasburicase intraperitoneal intervention (to degrade UA) during resuscitation. Another group received exogenous UA in-traperitoneally without HS. Measures mentioned above, in addition to organs UA, were performed at 24 hours. In vitro, caspases-(8/3) ac-tivity was tested in epithelial cells exposed to UA.RESULTS: H
emorrhagic shock increased organ (kidney and lung) TNF-α, MPO, and caspases activity in various patterns while caspase-8 remainedelevated over time. Hemorrhagic shock led to increased plasma UA at 2 hours, which remained high until 72 hours; TNF-α and IL-18 wereelevated at 24 hours. The exogenous UA administration in sham animals reproduced the activation of caspase-8 and MPO in organs, andTNF-α in the lung. The increased plasma and organ UA levels, plasma and lung TNF-α, as well as organ caspase-(8/3) andMPO, observedat 24 hours after HS, were prevented by the administration of Rasburicase during resuscitation. In vitro, soluble UA induced caspases-(3/8)activity in epithelial cells.CONCLUSION: U
ric acid is persistently high after HS and leads to the activation of caspases-8 and organ inflammation; these can be prevented by anintervention to degrade UA. Therefore, UA is an important biomarker and mediator that could be considered a therapeutic target dur-ing HS resuscitation in human. (J Trauma Acute Care Surg. 2019;86: 431–439. Copyright © 2018 Wolters Kluwer Health, Inc. Allrights reserved.)KEYWORDS: H
emorrhagic shock; uric acid; apoptosis; inflammation; organ failure.F ollowing severe injury, hemorrhagic shock (HS) is responsi-ble for early death or late morbidity in resuscitated survi-
vors.1 Organ failure, most frequently involving the lungs andkidneys, represents a major cause of morbidity, driving the needfor new therapeutic approaches.2 Numerous mediators are im-plicated in systemic inflammation and organ failure after resus-citated HS, but the understanding of secondary tissue damage isstill incomplete.3
In the quest for mediators released by dying cells, uric acid(UA) was identified as one potential candidate.4 Uric acid is the
018, Revised: October 27, 2018, Accepted: November 14,e: December 3, 2018.erche de l'Hôpital du Sacré-Cœur de Montréal (HSCM); Département de Pharmacologie et Physiologie (G.R.),ecine (S.D.-P.,E.C.), Université de Montréal (F.B.,A.M.C.,d Centre de Recherche du Centre Hospitalier de l'UniversitéM) (M.A.V.,E.B.), Montréal, QC, Canada.of the data have been presented at 4th Annual Meeting ofCare Forum, October 25-28, 2015 in Toronto, Canada.anuel Charbonney, MD, PhD, Hôpital du Sacré-Coeur deGouin Ouest Montréal, Québec, Canada H4J 1C5; email:@umontreal.ca.nt is available for this article. Direct URL citations appear inks to the digital files are provided in the HTML text of thisWeb site (www.jtrauma.com).
0000002152
rg
Copyright © 2019 Wolters Kluwer H
metabolic product of xanthine oxidase, secondary to DNA break-down and purine degradation, or can be released from necroticcells.5,6 Previous works on HS implicated xanthine oxidase in ox-idative products generation, responsible for ischemia-reperfusioninjury, with UA only measured as metabolite.7 The circulation ofUA followingHS is known, but without investigation of its role inorgan injury pathogenesis.8–10
Uric acid is a potent activator of the immune system as acrystal,11 but also in its soluble form,12 released from necroticcells.5,13 It triggers inflammation through a Toll-like receptor(TLR)/inflammasome (NLRP3) caspase-1–dependent activa-tion, which can alter the lung alveolar barrier14,15 or provokeacute renal failure.16
After ischemia-reperfusion, unlike the accepted usual con-cept, apoptosis is able to induce inflammation leading to second-ary tissue injury.17,18 Uric acid itself can induce cellular apoptosisthrough caspases19 The caspases, enzymes responsible for theprocess of induced-cell death are described to have a role inthe induction of local inflammation.18,20 Particularly caspase-8, which represents the classical inducer of the death receptorextrinsic pathway leading to caspase-3 activation, can have adual role as an inducer of quiescent cell death and a promoterof inflammation.21 Classically, the extrinsic pathway of apopto-sis is triggered by extracellular cell death ligands includingTNF-α.22 However, new insights on caspase-8 roles have shown
431
ealth, Inc. All rights reserved.

Gilbert et al.J Trauma Acute Care Surg
Volume 86, Number 3
its capacity to regulate the inflammasome (NLRP3), an intracel-lular complex sensor responding to various stimuli includingUA and promoting the release of cytokines (IL-1β, IL-18) in re-sponse to danger.23 The activation of the inflammasome in re-sponse to TLR stimulation by crystals is reported in the lung,but potential soluble ligands are incompletely characterized.24
We hypothesized that UA, a mediator that could circulatedepending on ischemia duration, would be an important inducerof caspase activation and organ inflammation. Our first aim wasto characterize caspase-8/3 activation and organ inflammation(lungs and kidneys) over time, as well as circulatory UA, in asurvival rat model of HS. Our second aimwas to test its systemicrole using an intervention (uricase) to metabolize it.
MATERIALS AND METHODS
Animal Procedures and SamplingsExperimental Design
MaleWistar rats (Rattus norvegicus) weighing 400 g to 450 g(12–15 weeks) were obtained from Charles River (Canada). Theywere handled in compliance with local animal care committee reg-ulation and guidelines of the Canadian Council on Animal Care.The animal research ethical board of our institution approved theprotocol (REB-CHAE01/02/04). Animals were housed individu-ally, under constant conditions (temperature, 21–22°C; humidity,40–50%), including a 12-hour dark-light cycle. Chow pellets andtap water were available ad libitum. Three days acclimatizationwas applied before allocation to experimental groups.
To answer the study aims, 73 animals were assigned totwo different protocols.
For each experiment, two animals were randomly assignedto two different conditions, in parallel. Protocol 1: three experi-mental groups were performed, including two magnitude ofshock (as described precisely in the next paragraph): (1) shock(n = 17), (2) sustained shock (n = 17), (3) sham (n = 16). Eachgroup was exposed to three different reperfusion time (five tosix animals per groups): 2 hours, 24 hours, or 72 hours.
Protocol 2: the four experimental groups were: (1) sham(n = 5), (2) sham + UA administration (n = 6), (3) sustainedshock (n = 6), (4) sustained shock + Rasburicase (n = 6).Rasburicase is a recombinant urate oxidase enzyme (uricase)that specifically metabolizes UA into allantoin, for its elimina-tion. All rats were euthanized at 24 hours. In the group 2 only,UA (250 mg/kg dissolved in 0.5 mL of saline 0.9%) was admin-istered intraperitoneally (IP), as described elsewhere,25 after in-tubation and 4 hours after. Rasburicase (1.5 mg/kg dissolved in0.5 mL of saline 0.9%; Sanofi-Aventis Canada Inc.) was givenIP at the beginning of the reperfusion period and controls re-ceived saline 0.9% only. For experiments, two rats were ran-domly allocated in parallel to the experimental groups. Thedeath rate was 10% (n = 5) in protocol 1, of asystole at 2 hours(n = 3) and overnight (n = 2). No animal died during protocol 2.
Surgical Procedure and Hemorrhagic ShockIn all animals, including shams: (1) anesthesia was in-
duced by IP ketamine/xylazine injection (50 and 10 mg/kg, re-spectively) and maintained with isoflurane (1–2%); (2) animalswere intubated and ventilated in volume controlled (6 mL/kg);
432
Copyright © 2019 Wolters Kluwer H
(3) after local lidocaine administration (5 mg/kg subcutaneous),catheters were placed and fixed in the femoral vein (withdrawal,sampling, and fluid administration) and the femoral artery (mon-itoring) sterilely. The saturation, temperature (rectal probe), elec-trocardiogram were monitored, and animals kept on a warmingblanket to prevent hypothermia.
Blood was drawn until a mean arterial pressure (MAP) of30 mmHg. One group (shock) was immediately resuscitated af-ter 5 minutes (in protocol 1), another (sustained shock) was re-suscitated after 60 minutes. Resuscitation was performed usingshed blood (with citrate and kept at 37°C) mixed with RingerLactate (1:1), administered by 1 to 2 mL to reach and maintainMAP above 60 mm Hg; 85% to 100% of shed blood was re-turned, with up to 3 mL of NaCl after sustained shock. Animalswere kept under anesthesia for 2 hours, then catheters were re-moved, and the vessels were ligated. One group was immedi-ately euthanized in the first protocol. Others were wakened,allowed to drink and eat, and observed for 24 hours or 72 hours.A subcutaneous analgesic injection (2 mg/kg buprenorphine)had been administered before extubation and another the nextday. Lower limb saturation was measured. Animals were eutha-nized through decapitation, following an IP ketamine/xylazineinjection (50 and 10 mg/kg, respectively). An overview of theexperimental timeline is presented in Supplemental Figure 1,Supplemental Digital Content 1, http://links.lww.com/TA/B252.
Blood and Tissue SamplingBlood samples were collected (kept on ice), at baseline
(time 0: 0.5 mL), after the reperfusion period (time 1 at 2 hours,before catheter removal; 0.5 mL) and at euthanasia (time 2 at24 hours or time 3 at 72 hours of reperfusion period; 2 mL). Theywere centrifuged at 3,000g (15 minutes at 4°C), aliquoted andstored at −80°C. At the time of euthanasia, organs (kidney andlung) were retrieved, frozen in liquid nitrogen, and stored at −80°C.
Biochemical Analysis and AssaysCreatinine Concentration
Creatinine concentration value were assessed in the shamand sustained shock groups at baseline, at the end of the reperfu-sion and at 24 hours, using a VetScan i-Stat (Abaxis Inc., UnionCIty, CA).
Caspase-3 and -8 ActivitiesCaspase-3 and -8 activitieswere measured in triplicate, ac-
cording to a previously described protocol.26 Tissues were ho-mogenized by sonication in lysis buffer and incubated for30 minutes on ice. After 3 freeze/thaw cycles, tissue homogenateswere centrifuged at 4°C for 10 minutes. Enzymatic reactions wereundertaken in a buffer with 25 mg of protein (confirmed by theBradford method) and 40 μM of fluorescent substrates (Ac-DEVD-AMC and Ac-IETD-AMC for caspase-3 and caspase-8,respectively). Reactions were assessed after a 3-hour incubation(37°C) in the dark and stopped with the addition of 0.4 M NaOHand 0.4Mglycine buffer. Fluorescencewas quantified by spectro-fluorometry (Photon Technology International, Lawrenceville,NJ) at excitation wavelength 365 nm and emission wavelength465 or 430 nm for caspase-3 and -8 activity, respectively.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
TABLE 1. Hemodynamic Parameters
Baseline Shock Reperfusion
Sham (n = 17)
MAP, mm Hg 69 (3) 71 (3) 64 (1)
HR, beats/min 261 (6) 250 (8) 226 (18)
Shock (n = 15)
MAP, mm Hg 65 (3) 31 (1) 62 (2)
HR, beats/min 246 (7) 239 (9) 251 (8)
Sustained shock (n = 14)
MAP, mm Hg 68 (3) 35 (1) 62 (2)
HR, beats/min 253 (5) 228 (11) 273 (12)
The data represented are from the first protocol.All values are reported as mean (SEM).HR, heart rate.
J Trauma Acute Care SurgVolume 86, Number 3 Gilbert et al.
Myeloperoxidase Assay: Neutrophil AccumulationNeutrophil accumulation in the tissue was estimated by
myeloperoxidase (MPO) activity assay, performed in triplicate.Tissues were weighed, added to hexadecytrimethylamonium bro-mide buffer (0.5% hexadecytrimethylamonium bromide +50 mMpotassium phosphate, pH 6.0) and pulverized by sonication. Ly-sates were subjected to 3 freeze/thaw cycles and centrifuged at10,000g for 15 minutes. For activity, 0.1 mL of supernatant wasadded to 2.9 mL of 50 mM sodium phosphate (pH 6.0) with0.167mg/mL of o-dianisidine hydrochloride and 0.0005% hydro-gen peroxide. Absorbance of the orange product wasmeasured byspectrophotometer every 10 seconds at 460 nm for 2 minutes.Difference was generated between the maximum and minimumdivided by 2 (UI/mg of tissue per minute).
UAConcentrationUric acid was measured in the plasma sampled at 2 hours,
24 hours, and 72 hours in triplicate. Uric acid in organswasmea-sured at 24 hours. Briefly, tissues were weighed and homoge-nized by sonication in lysis buffer (MAPK buffer: 50 mM tripsHCL, 20 mM Glycérophosphate, 20 mM NaF, 5 mM EDTA,10 mM EGTA, 1 mM Na3VO4, benzamidine, PMSF, DTT,microcystin, triton X-100 10%), incubated 30minutes on ice un-der continuous agitation, then centrifuged at 13,000g for15 minutes. Uric acid concentration was assessed according tothe protocol provided by the manufacturer (STA-375 400 assays,Cell Biolabs Inc.)
Xanthine Oxidase ActivityXanthine oxidase was measure in the plasma sampled in
duplicate at the different timepoints. Xanthine oxidase plasma con-centration was assessed according to the protocol provided by themanufacturer (Xanthine oxidase Fluorometric Assay Kit, CaymanChemicals).
Plasma Cytokine Concentrations (IL-1β,IL-18, TNF-α)
Cytokines were measured in plasma (100 μL) at the time ofeuthanasia. Plasma IL-1β and IL-18 (interleukins) were assessed induplicate according to the protocol provided by the manufacturer(Rat IL-1beta/IL-1F2 DuoSet Elisa; R&D systems and Rat IL-18Elisa Kit; Biorbyt Company). Plasma and tissue TNF-α concentra-tion were assessed in duplicate according to the protocol providedby themanufacturer (Rat TNF-alpha DuoSet Elisa; R&D systems).
In Vitro ExperimentsCell Culture
Human embryonic kidney (HEK) cells were obtainedfrom ATCC (293 CRL-3216) and cultured in Dulbecco's Modi-fied Eagle's Medium supplemented with 10% FBS. They weremaintained at 37°C with 5% CO2.
Primary alveolar type II (ATII) cells were isolated frommale Sprague-Dawley rats (6–7 weeks), according to a proce-dure approved by a committee at the Centre de Recherche duCentre Hospitalier de l'Université de Montréal. In brief, lungswere washed to remove the blood cells and macrophages beforetreatment with elastase (Worthington, Lakewood, NJ), mincedand alveolar cells were purified from the resulting suspension
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
using a differentiated adherence technique. Primary alveolarcells were cultured in MEM (Gibco, Life technologies Inc,Burlington, ON, Canada), supplemented with 10% FBS (Gibco),0.08 mg/mL gentamicin, septra (3 μg/mL trimethoprime +17 μg/mLsulfamethoxazole), 0.2% NaHCO3 (Sigma-Aldrich, Oakville,ON, Canada), 10 mM HEPES (Hyclone, Fisher Scientific Ltd.),and 2 mM L-glutamine (Gibco), at 37°C with 5% CO2. The MEM-FBS-Septra was replaced after 3 days by the same MEM-FBSwithout septra; experiments were performed on day 4.
UATreatmentsUric acid sodium salt (UA sodium salt, U2875-25G;
SIGMA)was dissolved inDMEMmedium and filteredwith a ster-ile 0.22-μm filter to obtain a concentration of 0.2 M. Subconfluentcells were treated with a 5 � 10−4 M concentration overnight(18 hours) at room air oxygen concentration and the reaction wasstopped by plunging the flasks into ice. Control microscopy wasperformed at the beginning and the end of treatment period to as-sure the absence of crystals. After three washes with PBS, cellswere recovered using a scraper. After centrifugation for removingPBS, caspases were measured, as described previously.26
Statistical AnalysisResults are reported as means (±SEM). Statistical analyses
were performed with SPSS 19. Data were compared by analysis ofvariance, followed by post hoc multiple comparisons (Dunnett),when significant. If variances were heterogeneous, Brown-Forsythecorrection was followed by Games-Howell comparisons whenapplicable. p Value less than 0.05 was considered significant.
RESULTS
Physiological Parameters and ResuscitationThe animals exposed toHSwere closelymonitored, including
the reached lower MAP, during HS. In every group, saturation re-mained 97% or greater and the mean rectal temperature was 35°C.
Mean arterial pressure and heart rate during the threephases of the study are reported in Table 1; the MAP graphicpattern over time is reported in the Supplemental Figure 2, Sup-plemental Digital Content 2, http://links.lww.com/TA/B253. Toreach the target MAP, sustained shock group had more mean vol-ume of blood drawn than shock (14.4 ± 1.0mL vs. 10.3 ± 0.7mL,
433
ealth, Inc. All rights reserved.
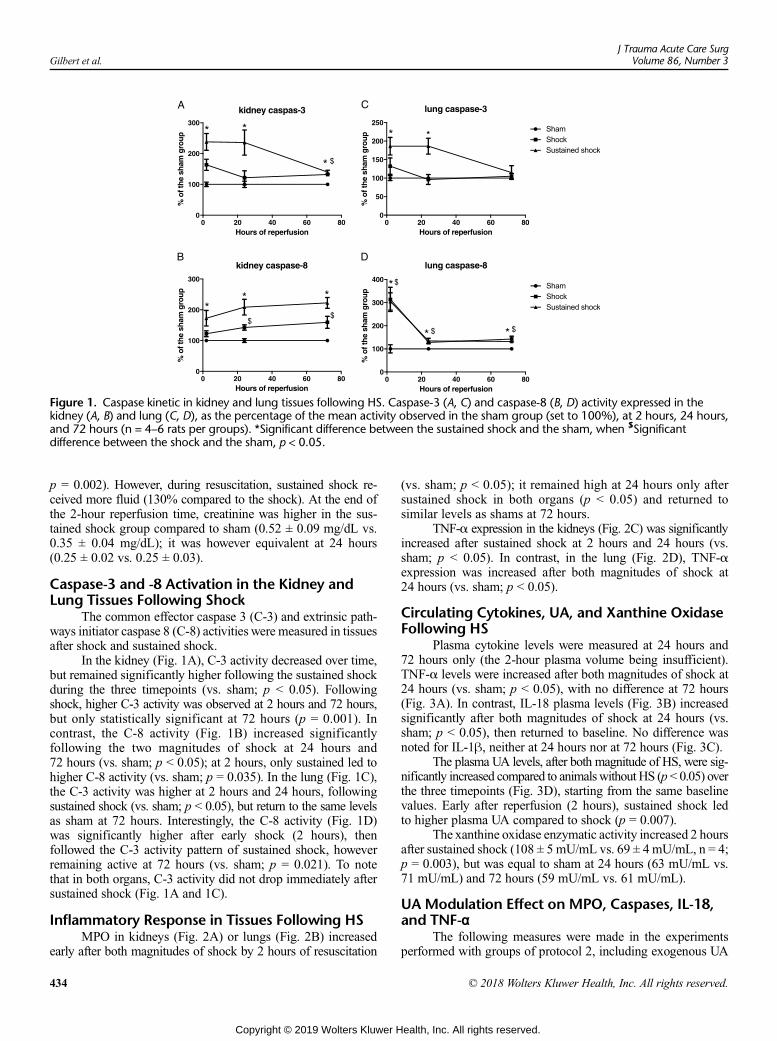
Figure 1. Caspase kinetic in kidney and lung tissues following HS. Caspase-3 (A, C) and caspase-8 (B, D) activity expressed in thekidney (A, B) and lung (C, D), as the percentage of the mean activity observed in the sham group (set to 100%), at 2 hours, 24 hours,and 72 hours (n = 4–6 rats per groups). *Significant difference between the sustained shock and the sham, when $Significantdifference between the shock and the sham, p < 0.05.
Gilbert et al.J Trauma Acute Care Surg
Volume 86, Number 3
p = 0.002). However, during resuscitation, sustained shock re-ceived more fluid (130% compared to the shock). At the end ofthe 2-hour reperfusion time, creatinine was higher in the sus-tained shock group compared to sham (0.52 ± 0.09 mg/dL vs.0.35 ± 0.04 mg/dL); it was however equivalent at 24 hours(0.25 ± 0.02 vs. 0.25 ± 0.03).
Caspase-3 and -8 Activation in the Kidney andLung Tissues Following Shock
The common effector caspase 3 (C-3) and extrinsic path-ways initiator caspase 8 (C-8) activities were measured in tissuesafter shock and sustained shock.
In the kidney (Fig. 1A), C-3 activity decreased over time,but remained significantly higher following the sustained shockduring the three timepoints (vs. sham; p < 0.05). Followingshock, higher C-3 activity was observed at 2 hours and 72 hours,but only statistically significant at 72 hours (p = 0.001). Incontrast, the C-8 activity (Fig. 1B) increased significantlyfollowing the two magnitudes of shock at 24 hours and72 hours (vs. sham; p < 0.05); at 2 hours, only sustained led tohigher C-8 activity (vs. sham; p = 0.035). In the lung (Fig. 1C),the C-3 activity was higher at 2 hours and 24 hours, followingsustained shock (vs. sham; p < 0.05), but return to the same levelsas sham at 72 hours. Interestingly, the C-8 activity (Fig. 1D)was significantly higher after early shock (2 hours), thenfollowed the C-3 activity pattern of sustained shock, howeverremaining active at 72 hours (vs. sham; p = 0.021). To notethat in both organs, C-3 activity did not drop immediately aftersustained shock (Fig. 1A and 1C).
Inflammatory Response in Tissues Following HSMPO in kidneys (Fig. 2A) or lungs (Fig. 2B) increased
early after both magnitudes of shock by 2 hours of resuscitation
434
Copyright © 2019 Wolters Kluwer H
(vs. sham; p < 0.05); it remained high at 24 hours only aftersustained shock in both organs (p < 0.05) and returned tosimilar levels as shams at 72 hours.
TNF-α expression in the kidneys (Fig. 2C) was significantlyincreased after sustained shock at 2 hours and 24 hours (vs.sham; p < 0.05). In contrast, in the lung (Fig. 2D), TNF-αexpression was increased after both magnitudes of shock at24 hours (vs. sham; p < 0.05).
Circulating Cytokines, UA, and Xanthine OxidaseFollowing HS
Plasma cytokine levels were measured at 24 hours and72 hours only (the 2-hour plasma volume being insufficient).TNF-α levels were increased after both magnitudes of shock at24 hours (vs. sham; p < 0.05), with no difference at 72 hours(Fig. 3A). In contrast, IL-18 plasma levels (Fig. 3B) increasedsignificantly after both magnitudes of shock at 24 hours (vs.sham; p < 0.05), then returned to baseline. No difference wasnoted for IL-1β, neither at 24 hours nor at 72 hours (Fig. 3C).
The plasma UA levels, after both magnitude of HS, were sig-nificantly increased compared to animalswithout HS (p< 0.05) overthe three timepoints (Fig. 3D), starting from the same baselinevalues. Early after reperfusion (2 hours), sustained shock ledto higher plasma UA compared to shock (p = 0.007).
The xanthine oxidase enzymatic activity increased 2 hoursafter sustained shock (108 ± 5 mU/mL vs. 69 ± 4 mU/mL, n = 4;p = 0.003), but was equal to sham at 24 hours (63 mU/mL vs.71 mU/mL) and 72 hours (59 mU/mL vs. 61 mU/mL).
UA Modulation Effect on MPO, Caspases, IL-18,and TNF-α
The following measures were made in the experimentsperformed with groups of protocol 2, including exogenous UA
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
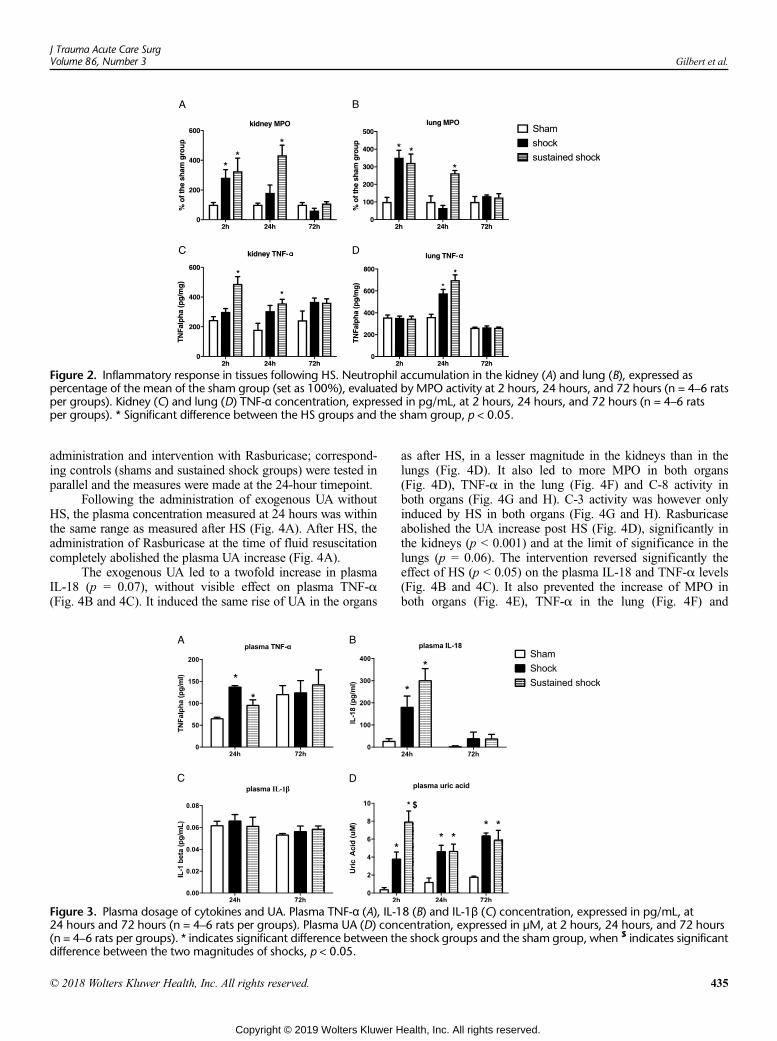
Figure 2. Inflammatory response in tissues following HS. Neutrophil accumulation in the kidney (A) and lung (B), expressed aspercentage of the mean of the sham group (set as 100%), evaluated by MPO activity at 2 hours, 24 hours, and 72 hours (n = 4–6 ratsper groups). Kidney (C) and lung (D) TNF-α concentration, expressed in pg/mL, at 2 hours, 24 hours, and 72 hours (n = 4–6 ratsper groups). * Significant difference between the HS groups and the sham group, p < 0.05.
J Trauma Acute Care SurgVolume 86, Number 3 Gilbert et al.
administration and intervention with Rasburicase; correspond-ing controls (shams and sustained shock groups) were tested inparallel and the measures were made at the 24-hour timepoint.
Following the administration of exogenous UA withoutHS, the plasma concentration measured at 24 hours was withinthe same range as measured after HS (Fig. 4A). After HS, theadministration of Rasburicase at the time of fluid resuscitationcompletely abolished the plasma UA increase (Fig. 4A).
The exogenous UA led to a twofold increase in plasmaIL-18 (p = 0.07), without visible effect on plasma TNF-α(Fig. 4B and 4C). It induced the same rise of UA in the organs
Figure 3. Plasma dosage of cytokines and UA. Plasma TNF-α (A), IL-124 hours and 72 hours (n = 4–6 rats per groups). Plasma UA (D) con(n = 4–6 rats per groups). * indicates significant difference between thdifference between the two magnitudes of shocks, p < 0.05.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
as after HS, in a lesser magnitude in the kidneys than in thelungs (Fig. 4D). It also led to more MPO in both organs(Fig. 4D), TNF-α in the lung (Fig. 4F) and C-8 activity inboth organs (Fig. 4G and H). C-3 activity was however onlyinduced by HS in both organs (Fig. 4G and H). Rasburicaseabolished the UA increase post HS (Fig. 4D), significantly inthe kidneys (p < 0.001) and at the limit of significance in thelungs (p = 0.06). The intervention reversed significantly theeffect of HS (p < 0.05) on the plasma IL-18 and TNF-α levels(Fig. 4B and 4C). It also prevented the increase of MPO inboth organs (Fig. 4E), TNF-α in the lung (Fig. 4F) and
8 (B) and IL-1β (C) concentration, expressed in pg/mL, atcentration, expressed in μM, at 2 hours, 24 hours, and 72 hourse shock groups and the sham group, when $ indicates significant
435
ealth, Inc. All rights reserved.
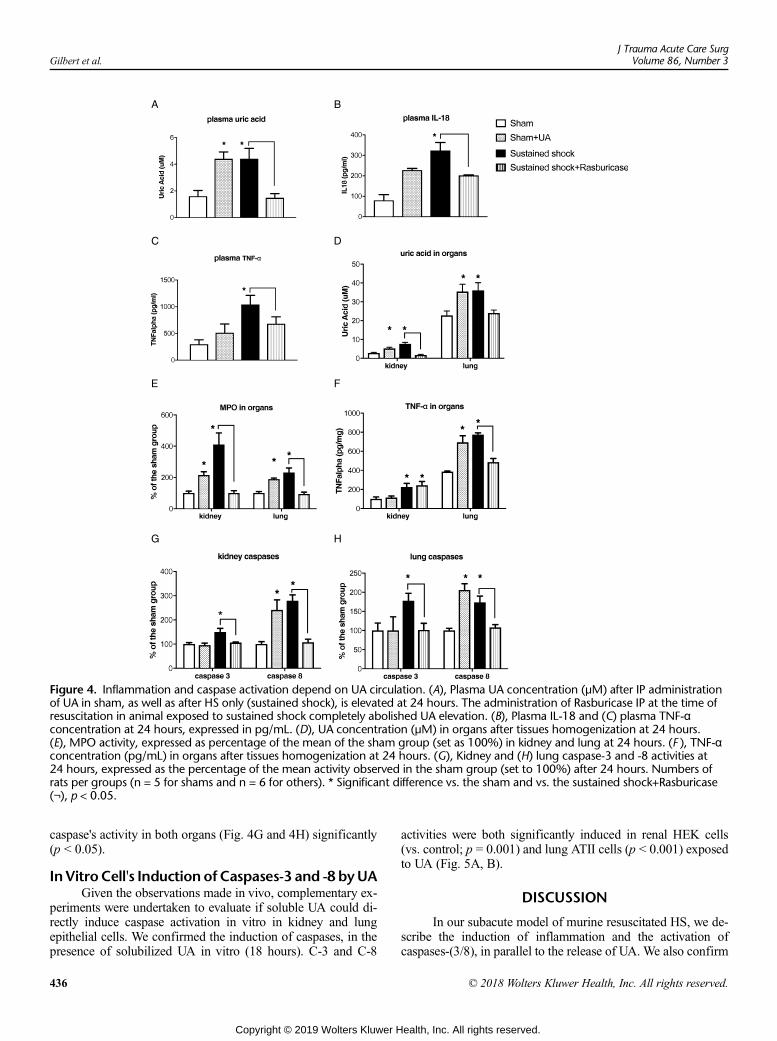
Figure 4. Inflammation and caspase activation depend on UA circulation. (A), Plasma UA concentration (μM) after IP administrationof UA in sham, as well as after HS only (sustained shock), is elevated at 24 hours. The administration of Rasburicase IP at the time ofresuscitation in animal exposed to sustained shock completely abolished UA elevation. (B), Plasma IL-18 and (C) plasma TNF-αconcentration at 24 hours, expressed in pg/mL. (D), UA concentration (μM) in organs after tissues homogenization at 24 hours.(E), MPO activity, expressed as percentage of the mean of the sham group (set as 100%) in kidney and lung at 24 hours. (F ), TNF-αconcentration (pg/mL) in organs after tissues homogenization at 24 hours. (G), Kidney and (H) lung caspase-3 and -8 activities at24 hours, expressed as the percentage of the mean activity observed in the sham group (set to 100%) after 24 hours. Numbers ofrats per groups (n = 5 for shams and n = 6 for others). * Significant difference vs. the sham and vs. the sustained shock+Rasburicase(¬), p < 0.05.
Gilbert et al.J Trauma Acute Care Surg
Volume 86, Number 3
caspase's activity in both organs (Fig. 4G and 4H) significantly(p < 0.05).
In Vitro Cell's Induction of Caspases-3 and -8 byUAGiven the observations made in vivo, complementary ex-
periments were undertaken to evaluate if soluble UA could di-rectly induce caspase activation in vitro in kidney and lungepithelial cells. We confirmed the induction of caspases, in thepresence of solubilized UA in vitro (18 hours). C-3 and C-8
436
Copyright © 2019 Wolters Kluwer H
activities were both significantly induced in renal HEK cells(vs. control; p = 0.001) and lung ATII cells (p < 0.001) exposedto UA (Fig. 5A, B).
DISCUSSION
In our subacute model of murine resuscitated HS, we de-scribe the induction of inflammation and the activation ofcaspases-(3/8), in parallel to the release of UA. We also confirm
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
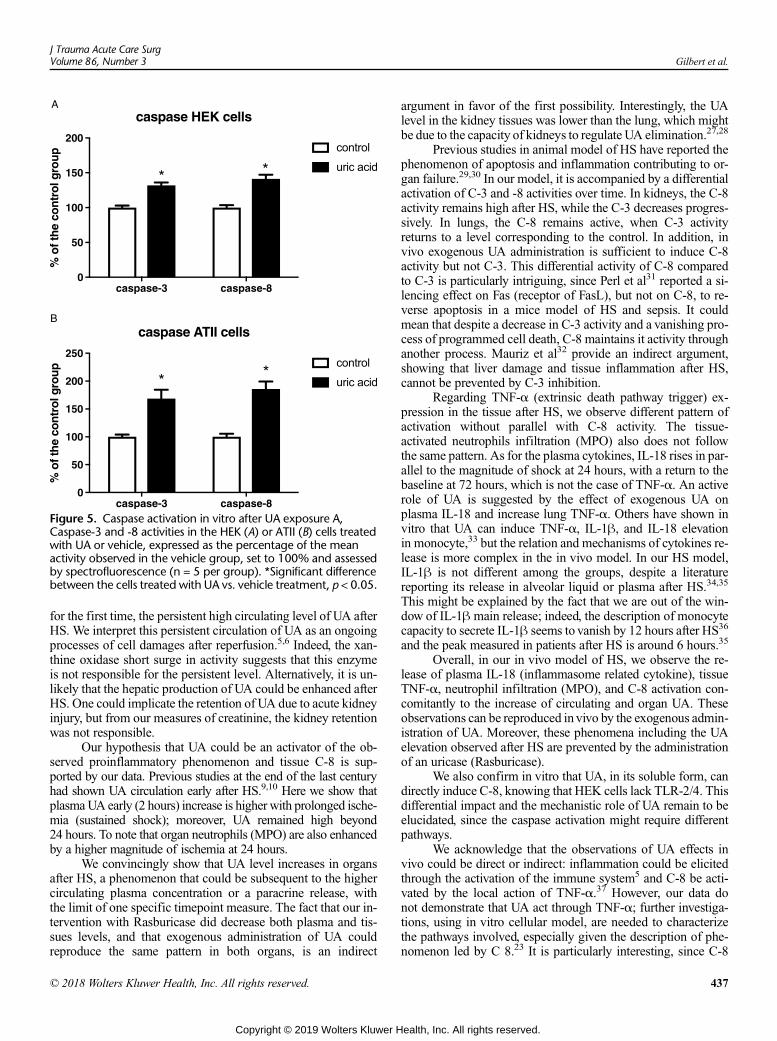
Figure 5. Caspase activation in vitro after UA exposure A,Caspase-3 and -8 activities in the HEK (A) or ATII (B) cells treatedwith UA or vehicle, expressed as the percentage of the meanactivity observed in the vehicle group, set to 100% and assessedby spectrofluorescence (n = 5 per group). *Significant differencebetween the cells treated with UA vs. vehicle treatment, p < 0.05.
J Trauma Acute Care SurgVolume 86, Number 3 Gilbert et al.
for the first time, the persistent high circulating level of UA afterHS. We interpret this persistent circulation of UA as an ongoingprocesses of cell damages after reperfusion.5,6 Indeed, the xan-thine oxidase short surge in activity suggests that this enzymeis not responsible for the persistent level. Alternatively, it is un-likely that the hepatic production of UA could be enhanced afterHS. One could implicate the retention of UA due to acute kidneyinjury, but from our measures of creatinine, the kidney retentionwas not responsible.
Our hypothesis that UA could be an activator of the ob-served proinflammatory phenomenon and tissue C-8 is sup-ported by our data. Previous studies at the end of the last centuryhad shown UA circulation early after HS.9,10 Here we show thatplasmaUA early (2 hours) increase is higher with prolonged ische-mia (sustained shock); moreover, UA remained high beyond24 hours. To note that organ neutrophils (MPO) are also enhancedby a higher magnitude of ischemia at 24 hours.
We convincingly show that UA level increases in organsafter HS, a phenomenon that could be subsequent to the highercirculating plasma concentration or a paracrine release, withthe limit of one specific timepoint measure. The fact that our in-tervention with Rasburicase did decrease both plasma and tis-sues levels, and that exogenous administration of UA couldreproduce the same pattern in both organs, is an indirect
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
argument in favor of the first possibility. Interestingly, the UAlevel in the kidney tissues was lower than the lung, which mightbe due to the capacity of kidneys to regulate UA elimination.27,28
Previous studies in animal model of HS have reported thephenomenon of apoptosis and inflammation contributing to or-gan failure.29,30 In our model, it is accompanied by a differentialactivation of C-3 and -8 activities over time. In kidneys, the C-8activity remains high after HS, while the C-3 decreases progres-sively. In lungs, the C-8 remains active, when C-3 activityreturns to a level corresponding to the control. In addition, invivo exogenous UA administration is sufficient to induce C-8activity but not C-3. This differential activity of C-8 comparedto C-3 is particularly intriguing, since Perl et al31 reported a si-lencing effect on Fas (receptor of FasL), but not on C-8, to re-verse apoptosis in a mice model of HS and sepsis. It couldmean that despite a decrease in C-3 activity and a vanishing pro-cess of programmed cell death, C-8 maintains it activity throughanother process. Mauriz et al32 provide an indirect argument,showing that liver damage and tissue inflammation after HS,cannot be prevented by C-3 inhibition.
Regarding TNF-α (extrinsic death pathway trigger) ex-pression in the tissue after HS, we observe different pattern ofactivation without parallel with C-8 activity. The tissue-activated neutrophils infiltration (MPO) also does not followthe same pattern. As for the plasma cytokines, IL-18 rises in par-allel to the magnitude of shock at 24 hours, with a return to thebaseline at 72 hours, which is not the case of TNF-α. An activerole of UA is suggested by the effect of exogenous UA onplasma IL-18 and increase lung TNF-α. Others have shown invitro that UA can induce TNF-α, IL-1β, and IL-18 elevationin monocyte,33 but the relation and mechanisms of cytokines re-lease is more complex in the in vivo model. In our HS model,IL-1β is not different among the groups, despite a literaturereporting its release in alveolar liquid or plasma after HS.34,35
This might be explained by the fact that we are out of the win-dow of IL-1β main release; indeed, the description of monocytecapacity to secrete IL-1β seems to vanish by 12 hours after HS36
and the peak measured in patients after HS is around 6 hours.35
Overall, in our in vivo model of HS, we observe the re-lease of plasma IL-18 (inflammasome related cytokine), tissueTNF-α, neutrophil infiltration (MPO), and C-8 activation con-comitantly to the increase of circulating and organ UA. Theseobservations can be reproduced in vivo by the exogenous admin-istration of UA. Moreover, these phenomena including the UAelevation observed after HS are prevented by the administrationof an uricase (Rasburicase).
We also confirm in vitro that UA, in its soluble form, candirectly induce C-8, knowing that HEK cells lack TLR-2/4. Thisdifferential impact and the mechanistic role of UA remain to beelucidated, since the caspase activation might require differentpathways.
We acknowledge that the observations of UA effects invivo could be direct or indirect: inflammation could be elicitedthrough the activation of the immune system5 and C-8 be acti-vated by the local action of TNF-α.37 However, our data donot demonstrate that UA act through TNF-α; further investiga-tions, using in vitro cellular model, are needed to characterizethe pathways involved, especially given the description of phe-nomenon led by C 8.23 It is particularly interesting, since C-8
437
ealth, Inc. All rights reserved.

Gilbert et al.J Trauma Acute Care Surg
Volume 86, Number 3
induces pyroptosis (inflammation by cell death), inflammatoryresponse through the inflammasome,23 or NF-kB activation.38
This potential central switch position of C-839 points toward apossible effect of other mediators, like UA, besides other knowntriggers (TNF-α or FasL).
Another point of discussion is the benefit of UA accumula-tion, due to the loss of gene programing for uricase in human.40
On one aspect, UA has been shown to have anti-oxidant and scav-enger effects on radicals in plasma, but it requires the presence ofascorbic acid.41,42 Alternatively, UA can form oxidative radicals,particularly in a lipid environment, likewithin cells.43 Even amildhyperuricemia can induce the elevation of reactive oxygen speciesleading to apoptosis.19 Despite its earlier advocated anti-oxidanteffect after HS,44 UA is certainly a contributor of secondary dam-age to organs. Foremost, its incrimination in chronic cardiovascu-lar disease,45 as well as recent data pointing toward its role inacute lung and kidney injuries support the argument.14,16
We acknowledge the following limitations of our work.Our survival model is descriptive of a few selected phenomenaof cellular injury through caspase activation and induction of or-gan inflammation; we did not measure specific cellular apopto-sis endpoints in the tissue. However, the role of UA in theprocess of secondary inflammatory processes and tissues injuryis suggested by our specific modulations of UA in vivo and invitro. Further in vitro studies are warranted to understand betterthe relationship between the UA, TNF-α, and the induction ofcaspase 8.46 Our findings point toward a mechanistic relation-ship, which remains to be elucidated.
CONCLUSION
We describe the activation of the extrinsic caspase path-way in the lung and kidney after HS. We also depict the inflam-matory response after HS. We confirm for the first time that UAis persistently high after HS and can activate C-8, as well as or-gan inflammation. Therefore, UA is an important biomarker andmediator in HS. It could be considered a therapeutic target dur-ing HS resuscitation in human.
AUTHORSHIP
K.G., G.R., and E.C. contributed to the design, the acquisition of data, theanalysis and interpretation of the results. They drafted the article and re-vised the final version. C.B., S.D.B., F.B., A.M.C., and F.K. contributed tothe acquisition of data, the analysis and interpretation of the results. Theyactively participated to the drafting of the article, the critical revision of itand the approval of the final version. M.A.V. and E.B. contributed to the ac-quisition of data (particularly the cellular in vitro experiments), the analysisand interpretation of the results. They actively participated to the critical re-vision of the article and the approval of the final version. The Canadian Crit-ical Care Translational Biology Group (CCCTBG): the group providedguidance and advices on the design, concept and results interpretation.All authors have provided their final approval to the final article.
ACKNOWLEDGMENTS
We are grateful to John Marshall, Alison Fox-Robichaud and JenniferTsang, members of the CCCTBG, for their critical review of the article.We also thank Marie-Claude Battista for her critical appraisal of the article.
DISCLOSURE
E. Charbonney received financial support for his programof research fromSanofi Genzyme Canada. The other authors have no conflict of interest toreport. The research was funded locally by the Centre de RechercheHôpital du Sacré-Cœur de Montréal.
438
Copyright © 2019 Wolters Kluwer H
REFERENCES1. Liu H, Xiao X, Sun C, Sun D, Li Y, Yang M. Systemic inflammation and
multiple organ injury in traumatic hemorrhagic shock. Front Biosci (Land-mark Ed). 2015;20:927–933.
2. Regel G, Grotz M,Weltner T, Sturm JA, Tscherne H. Pattern of organ failurefollowing severe trauma. World J Surg. 1996;20(4):422–429.
3. Chen CJ, Kono H, Golenbock D, Reed G, Akira S, Rock KL. Identificationof a key pathway required for the sterile inflammatory response triggered bydying cells. Nat Med. 2007;13(7):851–856.
4. Shi Y, Evans JE, Rock KL. Molecular identification of a danger signal thatalerts the immune system to dying cells. Nature. 2003;425(6957):516–521.
5. Kono H, Chen CJ, Ontiveros F, Rock KL. Uric acid promotes an acute in-flammatory response to sterile cell death in mice. J Clin Invest. 2010;120(6):1939–1949.
6. Poulsen JP, Oyasaeter S, Saugstad OD. Hypoxanthine, xanthine, and uricacid in newborn pigs during hypoxemia followed by resuscitation with roomair or 100% oxygen. Crit Care Med. 1993;21(7):1058–1065.
7. Matsumura F, Yamaguchi Y, Goto M, Ichiguchi O, Akizuki E, Matsuda T,Okabe K, Liang J, Ohshiro H, Iwamoto T, et al. Xanthine oxidase inhibitionattenuates Kupffer cell production of neutrophil chemoattractant followingischemia-reperfusion in rat liver. Hepatology. 1998;28(6):1578–1587.
8. Flynn WJ Jr, Hoover EL. Allopurinol plus standard resuscitation preserveshepatic blood flow and function following hemorrhagic shock. J Trauma.1994;37(6):956–961.
9. Crowell JW, Jones CE, Smith EE. Effect of allopurinol on hemorrhagicshock. Am J Phys. 1969;216(4):744–748.
10. Adachi H. The preventive effect of allopurinol on experimental shock(author's transl). Masui. 1977;26(8):864–871.
11. Martinon F, Petrilli V, Mayor A, Tardivel A, Tschopp J. Gout-associated uricacid crystals activate the NALP3 inflammasome. Nature. 2006;440(7081):237–241.
12. Braga TT, Forni MF, Correa-Costa M, Ramos RN, Barbuto JA, Branco P,Castoldi A, Hiyane MI, Davanso MR, Latz E, et al. Soluble uric acid acti-vates the NLRP3 Inflammasome. Sci Rep. 2017;7:39884.
13. Xiao J, Zhang XL, Fu C, Han R, Chen W, Lu Y, Ye Z. Soluble uric acid in-creases NALP3 inflammasome and interleukin-1β expression in human pri-mary renal proximal tubule epithelial cells through the toll-like receptor4-mediated pathway. Int J Mol Med. 2015;35(5):1347–1354.
14. Kuipers MT, Aslami H, Vlaar AP, Juffermans NP, Tuip-de Boer AM,Hegeman MA, Jongsma G, Roelofs JJ, van der Poll T, Schultz MJ, et al.Pre-treatment with allopurinol or uricase attenuates barrier dysfunction butnot inflammation during murine ventilator-induced lung injury. PLoS One.2012;7(11):e50559.
15. Gasse P, Riteau N, Charron S, Girre S, Fick L, Petrilli V, Tschopp J,Lagente V, Quesniaux VF, Ryffel B, et al. Uric acid is a danger signal activat-ing NALP3 inflammasome in lung injury inflammation and fibrosis. Am JRespir Crit Care Med. 2009;179(10):903–913.
16. Roncal CA, Mu W, Croker B, Reungjui S, Ouyang X, Tabah-Fisch I,Johnson RJ, Ejaz AA. Effect of elevated serum uric acid on cisplatin-induced acute renal failure. AJP: Renal Physiology. 2007;292(1):F116–F122.
17. BeeriR, SymonZ, BrezisM, Ben-Sasson SA, Baehr PH, Rosen S, Zager RA.Rapid DNA fragmentation from hypoxia along the thick ascending limb ofrat kidneys. Kidney Int. 1995;47(6):1806–1810.
18. Daemen MA, van 't Veer C, Denecker G, Heemskerk VH, Wolfs TG,Clauss M, Vandenabeele P, Buurman WA. Inhibition of apoptosis inducedby ischemia-reperfusion prevents inflammation. J Clin Invest. 1999;104(5):541–549.
19. Verzola D, Ratto E, Villaggio B, Parodi EL, Pontremoli R, Garibotto G,Viazzi F. Uric acid promotes apoptosis in human proximal tubule cells by ox-idative stress and the activation of NADPH oxidase NOX 4. PLoS One.2014;9(12):e115210.
20. Leist M, Jaattela M. Four deaths and a funeral: from caspases to alternativemechanisms. Nat Rev Mol Cell Biol. 2001;2(8):589–598.
21. Gurung P, Kanneganti TD. Novel roles for caspase-8 in IL-1β andinflammasome regulation. Am J Pathol. 2015;185(1):17–25.
22. Ashkenazi A, Dixit VM. Death receptors: signaling and modulation. Sci-ence. 1998;281(5381):1305–1308.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Gilbert et al.
23. Gurung P, Anand PK, Malireddi RK, Vande Walle L, Van Opdenbosch N,Dillon CP, Weinlich R, Green DR, Lamkanfi M, Kanneganti TD. FADDand caspase-8 mediate priming and activation of the canonical and nonca-nonical Nlrp3 inflammasomes. J Immunol. 2014;192(4):1835–1846.
24. Dostert C, Petrilli V, Van Bruggen R, Steele C, Mossman BT, Tschopp J. In-nate immune activation through Nalp3 inflammasome sensing of asbestosand silica. Science. 2008;320(5876):674–677.
25. Romero F, Perez M, Chavez M, Parra G, Durante P. Effect of uric acid ongentamicin-induced nephrotoxicity in rats—role of matrix metalloprotein-ases 2 and 9. Basic Clin Pharmacol Toxicol. 2009;105(6):416–424.
26. Boucher M, Wann BP, Kaloustian S, Cardinal R, Godbout R, Rousseau G.Reduction of apoptosis in the amygdala by an A2A adenosine receptor ago-nist following myocardial infarction. Apoptosis. 2006;11(7):1067–1074.
27. Anzai N, Ichida K, Jutabha P, Kimura T, Babu E, Jin CJ, Srivastava S,Kitamura K, Hisatome I, Endou H, et al. Plasma urate level is directly regu-lated by a voltage-driven urate efflux transporter URATv1 (SLC2A9) inhumans. J Biol Chem. 2008;283(40):26834–26838.
28. Enomoto A, Kimura H, Chairoungdua A, Shigeta Y, Jutabha P, Cha SH,Hosoyamada M, Takeda M, Sekine T, Igarashi T, et al. Molecular identifica-tion of a renal urate anion exchanger that regulates blood urate levels.Nature.2002;417(6887):447–452.
29. Arikan AA, Yu B, Mastrangelo MA, Tweardy DJ. Interleukin-6 treatment re-verses apoptosis and blunts susceptibility to intraperitoneal bacterial chal-lenge following hemorrhagic shock. Crit Care Med. 2006;34(3):771–777.
30. Barlos D, Deitch EA, Watkins AC, Caputo FJ, Lu Q, Abungu B, Colorado I,XuD-Z, FeinmanR. Trauma-hemorrhagic shock-induced pulmonary epithe-lial and endothelial cell injury utilizes different programmed cell death sig-naling pathways. Am J Phys Lung Cell Mol Phys. 2009;296(3):L404–L417.
31. Perl M, Chung C-S, Lomas-Neira J, Rachel TM, Biffl WL, Cioffi WG,Ayala A. Silencing of Fas, but not caspase-8, in lung epithelial cells amelio-rates pulmonary apoptosis, inflammation, and neutrophil influx after hemor-rhagic shock and sepsis. Am J Pathol. 2005;167(6):1545–1559.
32. Mauriz JL, González P, Jorquera F, Olcoz JL, González-Gallego J. Caspaseinhibition does not protect against liver damage in hemorrhagic shock.Shock. 2003;19(1):33–37.
33. Kinoshita T, Imamura R, KushiyamaH, Suda T. NLRP3mediates NF-κB ac-tivation and cytokine induction in microbially induced and sterile inflamma-tion. PLoS One. 2015;10(3):e0119179.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
34. XiangM, Shi X, Li Y, Xu J, Yin L, Xiao G, Scott MJ, Billiar TR,Wilson MA,Fan J. Hemorrhagic shock activation of NLRP3 inflammasome in lung endo-thelial cells. J Immunol. 2011;187(9):4809–4817.
35. Roumen RM, Hendriks T, van der Ven-Jongekrijg J, Nieuwenhuijzen GA,Sauerwein RW, Van der Meer JW, Goris RJ. Cytokine patterns in patients af-ter major vascular surgery, hemorrhagic shock, and severe blunt trauma. Re-lation with subsequent adult respiratory distress syndrome and multipleorgan failure. Ann Surg. 1993;218(6):769–776.
36. Abraham E, Richmond NJ, Chang YH. Effects of hemorrhage oninterleukin-1 production. Circ Shock. 1988;25(1):33–40.
37. Wang L, Du F,Wang X. TNF-alpha induces two distinct caspase-8 activationpathways. Cell. 2008;133(4):693–703.
38. Su H, Bidere N, Zheng L, Cubre A, Sakai K, Dale J, Salmena L, Hakem R,Straus S, LenardoM. Requirement for caspase-8 in NF-kappaB activation byantigen receptor. Science. 2005;307(5714):1465–1468.
39. Vince JE, Silke J. The intersection of cell death and inflammasome activa-tion. Cell Mol Life Sci. 2016;73(11–12):2349–2367.
40. Sautin YY, Johnson RJ. Uric acid: the oxidant-antioxidant paradox. Nucleo-sides Nucleotides Nucleic Acids. 2008;27(6–7):608–619.
41. Frei B, Stocker R, Ames BN. Antioxidant defenses and lipid peroxidation inhuman blood plasma. Proc Natl Acad Sci U S A. 1988;85(24):9748–9752.
42. Ames BN, Cathcart R, Schwiers E, Hochstein P. Uric acid provides anantioxidant defense in humans against oxidant- and radical-causedaging and cancer: a hypothesis. Proc Natl Acad Sci U S A. 1981;78(11):6858–6862.
43. Santos CX, Anjos EI, Augusto O. Uric acid oxidation by peroxynitrite: mul-tiple reactions, free radical formation, and amplification of lipid oxidation.Arch Biochem Biophys. 1999;372(2):285–294.
44. Tsukada K, Hasegawa T, Tsutsumi S, Katoh H, Kuwano H, Miyazaki T,Yamamoto Y. Effect of uric acid on liver injury during hemorrhagic shock.Surgery. 2000;127(4):439–446.
45. Feig DI, Kang DH, Johnson RJ. Uric acid and cardiovascular risk. N Engl JMed. 2009;359(17):1811–1821.
46. Bordoni V, De Cal M, Rassu M, Cazzavillan S, Segala C, Bonello M,Ranishta R, Andrikos E, Yavuz A, Salvatori G, et al. Protective effect of urateoxidase on uric acid induced-monocyte apoptosis. Curr Drug DiscovTechnol. 2005;2(1):29–36.
439
ealth, Inc. All rights reserved.
ORIGINAL ARTICLE
Clinical relevance of single nucleotide polymorphisms in theCXCL1 and CXCL12 genes in patients with major trauma
Xiao Wang, MD, An-Qiang Zhang, MD, Wei Gu, MD, Da-Lin Wen, MPH, Hong-Xiang Lu, MD,Jian-Hua Yang, MD, Xu Wang, MD, Jin Deng, MD, Hong-Qi Zhang, MD, Ding-Yuan Du, MD,
Lian-Yang Zhang, MD, Ling Zeng, MD, and Jian-Xin Jiang, MD, Chongqing, China
Sub
Fro
Ad
Sup
DO
44
BACKGROUND: G
mitted: February 11, 2018, RevPublished online: November 28m the State Key Laboratory of TrW.G., D.-L.W., H.-X.L., J.-H.Ysearch, Daping Hospital, ThirdMedical University (X.W.), Wmatic Orthopedics (J.D.), The AGuiyang, Guizhou Province; anD.-Y.D.), Chongqing, China.dress for reprints: Ling Zeng, MCombined Injury, Institute of SMedical University, [email protected] digital content is avaithe printed text, and links to thearticle in the journal's Web site
I: 10.1097/TA.00000000000021
0
enetic backgrounds have been recognized as significant determinants of susceptibility to sepsis. CXC chemokines play a signif-icant role in innate immunity against infectious diseases. Genetic polymorphisms of CXC chemokine genes have been widely stud-ied in inflammatory and infectious diseases but not in sepsis. Thus, we aimed to investigate the clinical relevance of CXCchemokine gene polymorphisms and susceptibility to sepsis in a traumatically injured population.
METHODS: T
hirteen tag single nucleotide polymorphismswere selected fromCXC chemokine genes using amultimarker tagging algorithm inthe Tagger software. Three independent cohorts of injured patients (n = 1700) were prospectively recruited. Selected single nucle-otide polymorphisms were genotyped using an improved multiplex ligation detection reaction method. Cytokine production in li-popolysaccharide-stimulated whole blood was measured using an enzyme-linked immunosorbent assay.RESULTS: A
mong the 13 tag single nucleotide polymorphisms, four single nucleotide polymorphisms (rs1429638, rs266087, rs2297630, andrs2839693) were significantly associated with the susceptibility to sepsis, and three (rs3117604, rs1429638, and rs4074) were sig-nificantly associated with an increased multiple organ dysfunction score in the derivation cohort. However, only the clinical rele-vance of rs1429638 and rs266087 was confirmed in the validation cohorts. In addition, rs2297630 was significantly associatedwith interleukin 6 production.CONCLUSION: T
he rs1429638 polymorphism in the CXCL1 gene and the rs2297630 polymorphism in the CXCL12 gene were associatedwith altered susceptibility to sepsis and might be used as important genetic markers to assess the risks of sepsis in trauma patients.(J Trauma Acute Care Surg. 2019;86: 440–447. Copyright © 2018 Wolters Kluwer Health, Inc. All rights reserved.)LEVEL OF EVIDENCE: P
rognostic and epidemiologic study, level II. KEYWORDS: T rauma; sepsis; CXC chemokines; polymorphisms; SNP.I n 2013, approximately 973 million people sustained injuriesthat required medical attention, and 4.8 million people died
from trauma worldwide.1 In addition, trauma accounted formore than 10% of the global burden of disease. Thus, trauma re-mains a severe public health problem worldwide.2,3 Despite sig-nificant advances in the emergency care system in recent years,patients who survive an initial trauma still suffer from a series ofcomplications after admission. Sepsis and multiple organ dys-function syndrome (MODS) are common serious complicationsin major trauma patients.4,5 Therefore, it is important to preventsepsis and MODS when treating trauma.
ised: June 1, 2018, Accepted: October 25, 2018,, 2018.auma, Burns and Combined Injury (X.W., A.-Q.Z.,., L.-Y.Z., L.Z., J.-X.J.), Institute of Surgery Re-Military Medical University, Chongqing; Wenzhouenzhou, Zhejiang Province; Department of Trau-ffiliated Hospital of Guizhou Medical University,d Chongqing EmergencyMedical Center (H.Q.-Z.,
D, State Key Laboratory of Trauma, Burns andurgery Research, Daping Hospital, Third Militaryg 400042, China; email: [email protected] or
lable for this article. Direct URL citations appear indigital files are provided in the HTML text of this(www.jtrauma.com).
41
Copyright © 2019 Wolters Kluwer H
Chemokines are a subfamily of small cytokines or signal-ing proteins. According to the arrangement of their conservedcysteine residues, chemokines have been classified into fourmain subfamilies: CXC, XC, CC, and CX3C.6 Chemokinesare critical mediators of the homeostatic processes and inflam-matory response by regulating inflammatory cell recruitmentand activation. In particular, CXC chemokines play an impor-tant role in defending against bacterial infection and sepsis.CXCL1 reduces bacterial burden in sepsis via modulating theactivities and functions of neutrophils and T lymphocytes.7 In-creased CXCL2 expression is associated with increased sepsisseverity. Attenuating CXCL2 activity by antibody blocking orgene silencing reduces the inflammatory response and de-creases mortality.8,9 CXCL10 mediates the function of immunecells and serves as an early diagnostic marker for sepsis.10,11
CXCL12 activates anti-inflammatory signaling pathways andpredicts mortality in septic patients.12,13
Increasing evidence suggests that single nucleotide poly-morphisms (SNPs) are important determinants of interindivid-ual differences in the degree of inflammation and clinicaloutcome in septic patients.14–16 In addition, a growing body ofevidence has indicated that genetic variants within CXC chemo-kine genes may influence the susceptibility to inflammatory andinfectious diseases.17–19 Therefore, we hypothesized that SNPsin CXC chemokine genes influence susceptibility to sepsis andMODS. In this study, we surveyed a set of tag SNPs (tSNPs)within the CXCL1, CXCL2, CXCL10, and CXCL12 genes to
J Trauma Acute Care SurgVolume 86, Number 3
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Wang et al.
investigate the relevance between these SNPs and the suscepti-bility to sepsis and MODS in a traumatically injured population.
PATIENTS AND METHODS
Study Population and Clinical EvaluationOur study was approved by the Ethical and Protocol Re-
view Committee of the Third Military Medical University andother participating institutions. Informed consent was obtainedfrom the patients or their next of kin.
First, 734 consecutive patients admitted to the Departmentof Trauma Surgery in the Daping Hospital and the ChongqingEmergency Medical Center between January 1, 2005, andJanuary 1, 2014, were prospectively enrolled in the study. Thesepatients constituted the derivation cohort, which was used to ex-plore the relevance of candidate SNPs. Then, an additional 966patients were prospectively enrolled in the study as validationcohort. Among them, 683 patients were enrolled from DapingHospital and the Chongqing Emergency Medical Center be-tween January 2, 2014, and January 1, 2016. The remaining283 patients were enrolled from the Department of TraumaticOrthopedics in the Affiliated Hospital of Guizhou Medical Uni-versity between January 1, 2007, and January 1, 2016. Patientswere enrolled if they met all of the inclusion criteria: (1) age be-tween 18 and 65 years, (2) Injury Severity Score (ISS) greaterthan 16, and (3) surviving for longer than 48 hours. Patientswere not eligible if they had penetrating injuries, severe brain in-jury (Abbreviated Injury Scale of head ≥3), preexisting organdysfunction, or immune diseases. Preexisting respiratory failurewas deemed present when mechanical ventilation was necessaryfor at least 72 hours, when PaO2/FiO2 less than 37.3 kPa positiveend-expiratory pressure was over 8 cm H2O and when there wasradio graphically confirmed acute respiratory distress syndromeor a respiratory rate less than or equal to 5/min or greater than orequal to 49/min. Preexisting hepatic failure was defined asbilirubinemia over 51 μmol/L for at least 48 hours. Preexisting re-nal insufficiencywas defined as serum creatinine over 177 μmol/Lor at least 48 hours. Preexisting heart failure was defined as car-diac index of less than 3.0�min−1�m−2, obligatory applicationof inotropic therapy, heart rate of less than or equal to 54/min,present ventricular tachicardy and/or fibrillation, and mean ar-terial pressure of less than or equal to 49 mm Hg or pH lessthan or equal to 7.24. Preexisting hematologic insufficiencywas defined as a platelet count of less than 20,000 or a whiteblood cell count of less than 1 � 10−9/L. Preexisting immunediseases include diabetes mellitus type 1, Graves disease, in-flammatory bowel disease, multiple sclerosis, psoriasis, rheu-matoid arthritis, celiac disease, systemic lupus erythematosus,and so on. The ISS of patients was calculated according to theAbbreviated Injury Scale (2005 revision) by two independent in-vestigators. All included patients received standard treatment ac-cording to international guidelines for management of sepsisand sepsis shock.20
Demographic characteristics, laboratory, and clinical datawere collected by expert physicians who did not know the pa-tients' genotypes. Sepsis diagnosis was based on the guidelinesof the American College of Chest Physicians/Society of CriticalCare Medicine Consensus Conference.21 Infection was definedas a clinically obvious source or positive bacterial cultures.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
Pneumonia was diagnosed when a predominant organism wasisolated from appropriately obtained sputum cultures in the set-ting of purulent sputum production and/or a new or changingpulmonary infiltrate on chest x-ray film. Bloodstream infectionswere diagnosed based on isolation of a predominant organismfrom blood cultures obtained under sterile conditions. Criteriafor urinary tract infections included greater than10 white bloodcells/high-power field on microscopic examination or isolationof greater than 105 organisms/mL urine or greater than 104 or-ganisms with symptoms. Criteria for catheter-related infectionsincluded isolation of greater than 15 colony forming units fromcatheter tips cultured only in the setting of suspected infection.Wound infection was identified by drainage of purulent materialfrom the wound. Multiple organ dysfunction (MOD) score wascalculated as the sum of the simultaneously obtained individualorgan scores on each hospital day.22 Neurological scoring wasnot performed because every patient was sedated. Multiple or-gan dysfunction score is defined as a Marshall score of 4 orgreater for at least consecutive 2 days on the basis of the compar-ative studies reported by Sauaia et al.23 Multiple organ dysfunc-tion scores and the presence of sepsis were determined byindividuals who did not know the patients' genotypes.
SNP SelectionThe full sequences of the human CXCL1, CXCL2,
CXCL10, and CXCL12 genes, including all exons and introns3 kb upstream of the transcription start site and 3 kb downstreamof the stop codon, were retrieved from GenBank at the NationalCenter for Biotechnology Information (NCBI)Web site. Geneticvariation data for CXCL1, CXCL2, CXCL10, andCXCL12 geneswere obtained fromChineseHanBeijing population of theHapMapproject. From this database, a total of 91 SNPs (7 in CXCL1, 7in CXCL2, 19 in CXCL10, and 58 in CXCL12) were identified.Among them, 43 SNPs (7 in CXCL1, 3 in CXCL2, 3 in CXCL10,and 30 in CXCL12) with minor allele frequency (MAF) greaterthan or equal to 0.05 were selected for tSNP analysis. Tag SNPsfor these genes were identified using a multimarker tagging al-gorithm in the Tagger software.24 Single nucleotide polymor-phisms with potential biological functions were also selected,even if they could not constitute a bin with other SNPs.
GenotypingDuring the first 24 hours after admission, 5 mL of venous
blood was collected in tripotassium ethylenediaminetetraaceticacid sterile tubes. For DNA isolation, 2.5 mL blood was used,and the remaining blood was used for lipopolysaccharide(LPS) stimulation. Genomic DNAwas isolated from peripheralwhole blood using QuickGene DNA whole blood kit L withQuickGene-610 L equipment (Fujifilm, Tokyo, Japan). Theconcentration and purity of the isolated DNA samples werequantitated using the Thermo Scientific Nanodrop ND-1000Spectrophotometer (Isogen Life Science, De Meern, Nether-lands). DNA samples were diluted to 40 μg/mL and stored at−80°C until use. Single nucleotide polymorphism genotypingwas performed by an improved multiplex ligation detection re-action technique according to a previous report.25 Approxi-mately 10% of the samples were genotyped in duplicate toassess the stability of improved multiplex ligation detection
441
ealth, Inc. All rights reserved.
Wang et al.J Trauma Acute Care Surg
Volume 86, Number 3
reaction method. Genotyping was performed by researcherswho did not know the patients' clinical data.
Ex Vivo Inflammatory Cytokines ProductionWe detected interferon γ, interleukin (IL) 1-β, IL-4, IL-6,
IL-8, IL-10, tumor necrosis factor α, lipopolysaccharide bindingprotein (LBP), and high mobility group box 1 (HMGB1) in LPS-stimulated whole blood according to our previous report.26 Inbrief, whole blood collected from trauma patients was mixed1:1 with Roswell Park Memorial Institute 1640 culture mediumand incubated with 100 ng/mL of LPS (Escherichia coli O26:B6; Difco Laboratories, Detroit, MI) in a sample mixer at 37°Cfor 4 hours. Then, the supernatants were collected after centrifu-gation and stored at −80°C until use. The concentrations of theseinflammatory cytokines were detected using an enzyme-linkedimmunosorbent assay.
Statistical AnalysisSample size was calculated using online Power and Sam-
ple Size Program software (http://biostat.mc.vanderbilt.edu/twiki/bin/view/Main/PowerSampleSize). The desired power ofour study was set at 80% with a significance level of 0.05 in atwo-sided test. We chose the log-additive inheritance model,which is the most suitable for polygenic diseases. Categoricaldata are presented as counts and percentages. Continuous dataare presented as the mean ± SD or median and interquartileranges. The χ2 or Fisher exact test was used to compare categor-ical variables, and the Mann-Whitney U test or Student t test wasused for continuous variables. The Hardy-Weinberg equilibriumof each SNP was tested using χ2 tests. Hazard ratio (HR) with
TABLE 1. Overall Clinical Characteristics of Trauma Patients
Clinical characteristics
Derivation cohort
(n = 734)
Age, mean ± SD, y 41.3 ± 12.1
Males/females, n 591/143
ISS, mean ± SD 22.3 ± 9.4
Organ dysfunction, n (%)
One, n 258 (35.1)
Two, n 95 (12.9)
Three or above, n 21 (2.9)
Sepsis, n (%) 300 (40.9)
Source of infection, %
Respiratory tract infection 46.3
Primary bloodstream infection 19.7
Urinary tract infection 15.0
Catheter-associated infection 9.7
Wound infection 7.3
Others* 2.0
Pathogens (positive blood cultures), %
Gram-negative 21.7
Gram-positive 11.3
Fungi 3.3
Mixed Gram-negative and Gram-positive 9.7
Negative blood cultures 54.0
*Other sites of infection included soft-tissue infection, bone infection and ear infection.
442
Copyright © 2019 Wolters Kluwer H
95% confidence intervals (CIs) were calculated usingmultivariateCox models. We tested recessive, codominant, and allele-dosemodels that were adjusted for confounding variables of ISS,age, injury sites, and sex ratio. Intrafacility correlation wastested byχ2 test and one-way analysis of variance. False discov-ery rate correction was applied to adjust for multiple compari-sons.27 p Values of less than 0.05 were considered statisticallysignificant. All data analyses were performed using SPSS soft-ware version 19.0 (SPSS Inc., Chicago).
RESULTS
Characteristics of the Study PopulationThere were three independent cohorts consisting of 734,
683, and 283 Chinese Han trauma patients. By means of thePower and Sample Size program, our sample was consideredadequate to study both polymorphisms. Demographics andother characteristics of the included patients are summarizedin Table 1 and Supplemental Figure (Figure, Supplemental Dig-ital Content 1, http://links.lww.com/TA/B238). The majority ofincluded patients were young male. The mean ± SD ISS valueswere 22.3 ± 9.4, 18.3 ± 9.1, and 20.8 ± 8.8, respectively, and thesepsis morbidity rates were 40.9%, 27.8%, and 35.0%. The maintypes of infection were respiratory tract infection, bloodstreaminfection, and urinary tract infection. The most common patho-gens in our study were Klebsiella pneumonia, Acinetobacterbaumannii, Pseudomonas aeruginosa, Staphylococcus aureus,Escherichia coli, and Enterococcus faecium. Organ dysfunctionoccurred in 50.9%, 46.7%, and 51.0% of the three cohorts. Pa-tients with sepsis had higher incidences of MODS.
Validation cohort 1 Validation cohort 2
p(n = 683) (n = 283)
42.1 ± 12.8 37.8 ± 12.4 0.59
547/136 229/54 0.83
18.3 ± 9.1 20.8 ± 8.8 0.37
214 (31.3) 87 (30.6) 0.219
75 (11.0) 47 (16.5) 0.057
30 (4.4) 11 (3.9) 0.299
190 (27.8) 99 (35.0) <0.01
50.3 39.4 0.286
18.3 24.2 0.566
15.2 14.1 0.974
5.8 8.1 0.581
8.4 9.1 0.873
2.0 5.1 0.357
24.3 16.7 0.457
11.4 13.9 0.753
2.9 5.6 0.458
8.6 8.3 0.885
52.8 55.5 0.941
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
J Trauma Acute Care SurgVolume 86, Number 3 Wang et al.
Selection of SNPsA total of 43 SNPs with a MAF of greater than or equal to
0.05 were identified within the CXCL1, CXCL2, CXCL10, andCXCL12 genes from the HapMap database for the Chinese HanBeijing population. Three SNPs in CXCL1, 1 in CXCL2, 2 inCXCL10, and 7 in CXCL12were selected as tSNPs by the Taggersoftware. Overall, 13 SNPs were selected in this study (Table 2).
Clinical Relevance of the Selected SNPs in theDerivation Cohort
First, we selected 734 patients to investigate the clinicalrelevance of the 13 selected tSNPs (Table 3). The MAFs of alltSNPs in the derivation cohort were similar to those in the ChineseHan Beijing population reported in the HapMap database. Thegenotype distributions of the selected tSNPswere consistent withHardy-Weinberg equilibrium. There were no significant differ-ences in age, sex ratio, or ISS among trauma patients with differ-ent genotypes of each tSNPs. Among the 13 SNPs, four SNPs(rs1429638, rs266087, rs2297630, and rs2839693) were signifi-cantly associated with susceptibility to sepsis in trauma patients.Three SNPs (rs3117604, rs1429638, and rs4074) were signifi-cantly associated with increased MOD scores in trauma patients.After adjusting for possible confounders by multiple logistic re-gression analyses, we identified an association of rs1429638,rs2297630, and rs2839693 that remained significant in the al-lele-dose effect for the sepsis morbidity rate (HR, 1.436; 95%confidence interval [CI], 1.249–3.732; p = 0.035; HR, 1.306;95% CI, 1.390–2.976; p = 0.025; and HR, 1.418; 95% CI,1.092–3.172; p = 0.039).
Clinical Relevance of SNPs in theValidation Cohort
To confirm the clinical relevance of rs266087, rs2839693,rs2297630, rs1429638, rs3117604, and rs4074, we further in-vestigated these SNPs in two validation cohorts (Table 4). Thegenotype distributions of these six SNPs were also consistentwith Hardy-Weinberg equilibrium, except for rs4074 in valida-tion cohort 1. The MAFs of these SNPs in the validation cohortwere similar to those in the derivation cohort. However, only twoSNPs (rs2297630 and rs1429638) were significantly associatedwith the risk for developing sepsis in the two validation cohorts.
TABLE 2. SNPs Identified Within the CXC Chemokine Family Genes
Gene rs Number Location
CXCL1 rs3117604 Chr 4: 74734668
rs4074 Chr 4: 74736144
rs1429638 Chr 4: 74737930
CXCL2 rs3806792 Chr 4: 74965274
CXCL10 rs4256246 Chr 4: 76945522
rs4508917 Chr 4: 76946097
CXCL12 rs1065297 Chr 10: 44865976
rs1029153 Chr 10: 44867146
rs1801157 Chr 10: 44868257
rs266087 Chr 10: 44871062
rs2297630 Chr 10: 44871548
rs2839693 Chr 10: 44874567
rs1413519 Chr 10: 44882561
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
One SNP (rs1429638) was significantly associated with an in-creased MOD score in validation cohort 1, and no significantassociation was observed in validation cohort 2. Data frommultiple logistic regression analyses also revealed the associa-tion of both SNPs with the sepsis morbidity rate. Sincers1429638 and rs2297630 were associated with the sepsis mor-bidity rate in all cohorts, we assessed the combined effects of thetwo SNPs in the study. Patients with both variants exhibited aslightly higher sepsis morbidity rate than did the patients witha single variant (Table 5). However, no statistically significantdifference was noted.
Association of rs1429638 and rs2297630Polymorphisms With InflammatoryResponsiveness in Trauma Patients
Since inflammatory cytokines drive the pathophysiologicprocess in sepsis, we further evaluated whether the variant influ-ences the expression of interferon γ, IL1-β, IL-4, IL-6, IL-8,IL-10, tumor necrosis factor α, LBP, and HMGB1. The A alleleof rs2297630 was significantly associated with increased IL-6production (Fig. 1). Data from linear regression analysis indicatedthat the association between rs2297630 and IL-6 production wassignificant (p = 0.005). After multiple testing correctionsusing the Bonferroni method, the association remained signifi-cant (p < 0.006). There was no significant difference in the pro-duction of other inflammatory cytokines between the differentgenotypes of the two SNPs.
DISCUSSION
Trauma is the leading cause of death in young adults underage 49 and the third leading cause of death worldwide.28 Sepsisafter trauma is associated with longer antibiotic use periods, lon-ger hospital stays, higher overall costs, increased incidence ofMODS, and increased in-hospital mortality. The improved mo-lecular diagnostic techniques provide disease-gene associationstudies to investigate the role of genetic variations in sepsisand MODS. To the best of our knowledge, the present study isthe first to investigate the potential clinical relevance of geneticvariations in CXC chemokine genes in relation to the suscepti-bility to sepsis and MODS in patients with major trauma.
in Chinese Han Population
Variation MAF, % Region
C/T 48.5 5′FLANKING
A/G 44.4 Intron
A/C 27.4 3′FLANKING
C/T 33.6 5′FLANKING
A/G 31.4 5′FLANKING
A/G 47.8 5′FLANKING
C/T 6.6 3′UTR
C/T 22.4 3′UTR
A/G 25.2 3′UTR
A/G 49.3 Intron
A/G 16.4 Intron
A/G 6.4 Intron
C/G 24.4 5′FLANKING
443
ealth, Inc. All rights reserved.
TABLE 3. Clinical Relevance of the Selected SNPs Among Trauma Patients in Derivation Cohort
Gene SNPs Genotypes N ISS Sepsis, n (%) p MOD Score p HWE Test
CXCL1 rs3117604 C/C 169 22.3 ± 9.0 66 (39.1) 5.1 ± 2.5 0.86
C/T 368 22.2 ± 9.3 151 (41.0) 0.561* 5.0 ± 2.6 0.290†
T/T 195 22.5 ± 10.1 83 (42.6) 0.600** 4.5 ± 2.3 0.014‡
CXCL1 rs4074 A/A 150 21.6 ± 8.3 56 (37.3) 4.9 ± 2.4 0.55
A/G 371 22.9 ± 9.8 158 (42.6) 0.301* 5.0 ± 2.6 0.834†
G/G 210 21.8 ± 9.6 86 (41.0) 0.976** 4.6 ± 2.4 0.040‡
CXCL1 rs1429638 A/A 49 21.8 ± 8.8 22 (44.9) 4.7 ± 2.4 0.19
A/C 307 22.8 ± 9.4 140 (45.6) 0.570* 5.2 ± 2.6 0.579†
C/C 375 21.9 ± 9.6 138 (36.8) 0.017** 4.7 ± 2.4 0.040‡
CXCL2 rs3806792 C/C 67 22.1 ± 7.1 31 (46.3) 5.1 ± 3.0 0.67
C/T 297 22.2 ± 9.4 122 (41.1) 0.422* 4.9 ± 2.3 0.740†
T/T 356 22.5 ± 9.9 147 (41.3) 0.840** 4.8 ± 2.4 0.539‡
CXCL10 rs4256246 A/A 95 21.3 ± 9.1 34 (35.8) 4.8 ± 2.8 0.70
A/G 344 22.4 ± 9.8 144 (41.9) 0.270* 4.9 ± 2.5 0.790†
G/G 293 22.5 ± 9.2 122 (41.6) 0.769** 4.9 ± 2.4 0.885‡
CXCL10 rs4508917 A/A 176 21.6 ± 9.2 69 (39.2) 4.7 ± 2.6 0.71
A/G 371 22.5 ± 9.8 158 (42.6) 0.582* 5.0 ± 2.6 0.191†
G/G 185 22.7 ± 9.0 73 (41.5) 0.626** 4.8 ± 2.3 0.872‡
CXCL12 rs1065297 C/C 3 35 ± 16.7 1 (33.3) 5.3 ± 3.5 0.74
C/T 96 23.5 ± 8.7 37 (38.5) 1.000* 4.9 ± 2.2 0.885†
T/T 627 22.1 ± 9.5 262 (41.8) 0.523** 4.9 ± 2.5 0.580‡
CXCL12 rs1029153 C/C 29 21.2 ± 7.6 12 (41.4) 5.0 ± 2.5 0.56
C/T 246 22.3 ± 9.2 104 (42.3) 0.970* 4.7 ± 2.3 0.296†
T/T 456 22.4 ± 9.7 184 (40.4) 0.626** 4.9 ± 2.6 0.837‡
CXCL12 rs1801157 A/A 60 21.8 ± 10.5 26 (43.3) 4.8 ± 2.4 0.19
A/G 274 21.8 ± 9.7 109 (39.8) 0.699* 4.8 ± 2.6 0.853†
G/G 398 22.7 ± 9.1 165 (41.5) 0.776** 4.9 ± 2.5 0.594‡
CXCL12 rs266087 G/G 174 21.8 ± 8.4 70 (40.2) 4.7 ± 2.3 0.73
G/A 361 22.5 ± 9.5 163 (45.2) 0.817* 5.0 ± 2.6 0.705†
A/A 197 22.4 ± 10.3 67 (34.0) 0.020** 4.8 ± 2.5 0.426‡
CXCL12 rs2297630 A/A 11 18.8 ± 5.3 5 (45.5) 4.8 ± 2.3 0.58
A/G 171 21.9 ± 8.8 84 (49.1) 1.000* 4.8 ± 2.4 0.879†
G/G 550 22.5 ± 9.7 211 (38.4) 0.012** 4.9 ± 2.5 0.574‡
CXCL12 rs2839693 A/A 12 19.6 ± 6.1 5 (41.7) 4.5 ± 2.3 0.85
A/G 168 22.0 ± 8.2 82 (48.8) 1.000* 5.1 ± 2.7 0.648†
G/G 552 22.5 ± 9.9 213 (38.6) 0.021** 4.8 ± 2.4 0.175‡
CXCL12 rs1413519 C/C 30 22.6 ± 9.2 8 (26.7) 5.1 ± 2.8 0.94
C/G 4238 22.8 ± 8.4 109 (45.8) 0.103* 5.0 ± 2.5 0.303†
G/G 464 22.0 ± 10.0 183 (39.4) 0.264** 4.8 ± 2.5 0.668‡
*Recessive effect for sepsis morbidity.**Dominant effect for sepsis morbidity.†Recessive effect for MOD score.‡Dominant effect for MOD score.HWE, Hardy-Weinberg equilibrium.
Wang et al.J Trauma Acute Care Surg
Volume 86, Number 3
In the study, 13 tSNPswere selected fromCXC chemokinegenes. The use of tag SNPs is an efficient and powerful methodfor investigating the clinical relevance of SNPs in the full genesequence.29 In the derivation cohort, we identified 6 SNPs thatwere significantly associated with the development of sepsis orMOD score. Because the accuracy of the results was influencedsignificantly by the sample size, we further verified the resultsin two additional cohorts. Finally, we found that rs1429638 inthe CXCL1 gene and rs2297630 in the CXCL12 gene were sig-nificantly associated with sepsis in two validation cohorts and
444
Copyright © 2019 Wolters Kluwer H
that rs1429638 was significantly associated with the MOD scorein validation cohort 1. Taken together, the association betweenthe two SNPs (rs1429638 and rs2297630) and sepsis was con-firmed by three independent trauma cohorts, and the associationbetween rs1429638 andMOD score was confirmed by two inde-pendent trauma cohorts. It is possible that rs1429638 was notsignificantly associated with theMOD score in validation cohort2 because of the small sample size or population heterogeneity.
CXCL1 is a small cytokine that belongs to the CXC chemo-kine family and is mainly secreted by macrophages/monocytes,
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
TABLE 4. Clinical Relevance of the Selected SNPs Among Trauma Patients in Validation Cohort
Gene SNPs Genotypes N ISS Sepsis, n (%) p MOD Score p HWE Test
Validation cohort 1
CXCL1 rs3117604 C/C 150 17.9 ± 8.8 43 (28.7) 4.7 ± 2.6 0.22
C/T 357 18.8 ± 9.2 97 (27.2) 0.793* 4.4 ± 2.4 0.482†
T/T 176 17.8 ± 9.0 50 (28.4) 0.839† 4.5 ± 2.4 0.215‡
CXCL1 rs4074 A/A 137 17.9 ± 8.8 44 (32.1) 4.7 ± 2.8 0.03
A/G 369 18.8 ± 9.2 94 (25.5) 0.209* 4.4 ± 2.4 0.211†
G/G 177 17.8 ± 9.0 52 (29.4) 0.590† 4.4 ± 2.3 0.654‡
CXCL1 rs1429638 A/A 48 18.0 ± 9.1 17 (35.4) 4.8 ± 2.7 0.79
A/C 261 18.7 ± 9.5 81 (31.0) 0.223* 4.7 ± 2.3 0.418†
C/C 374 18.1 ± 8.8 92 (24.6) 0.039† 4.3 ± 2.6 0.035‡
CXCL12 rs266087 G/G 166 18.7 ± 9.7 54 (32.5) 4.8 ± 2.6 0.68
G/A 336 18.1 ± 9.0 89 (26.5) 0.119* 4.3 ± 2.4 0.254†
A/A 181 18.4 ± 8.7 47 (26.0) 0.517** 4.5 ± 2.5 0.547‡
CXCL12 rs2297630 A/A 16 18.9 ± 8.3 7 (43.8) 4.5 ± 1.9 0.35
A/G 157 17.5 ± 9.4 53 (33.8) 0.247* 4.3 ± 2.4 0.824†
G/G 510 18.6 ± 9.0 130 (25.5) 0.020** 4.6 ± 2.5 0.793‡
CXCL12 rs2839693 A/A 12 17.3 ± 6.6 2 (16.7) 5.8 ± 3.0 0.97
A/G 157 17.7 ± 8.8 49 (31.2) 0.581* 4.6 ± 2.6 0.815†
G/G 508 18.6 ± 9.2 138 (27.2) 0.450** 4.5 ± 2.4 0.329‡
Validation cohort 2
CXCL1 rs3117604 C/C 58 20.3 ± 8.3 17 (29.3) 4.7 ± 2.5 0.10
C/T 155 21.4 ± 9.1 55 (35.5) 0.310* 4.5 ± 2.4 0.626†
T/T 70 19.7 ± 8.5 27 (38.6) 0.468** 4.3 ± 2.6 0.352‡
CXCL1 rs4074 A/A 59 20.5 ± 8.3 20 (33.9) 5.1 ± 2.6 0.78
A/G 143 21.4 ± 8.6 47 (32.9) 0.844* 4.1 ± 2.4 0.418†
G/G 81 19.9 ± 9.4 32 (39.5) 0.312** 4.7 ± 2.6 0.763‡
CXCL1 rs1429638 A/A 26 22.0 ± 9.4 11 (42.3) 4.8 ± 2.8 0.76
A/C 116 20.5 ± 8.2 47 (40.5) 0.411* 4.3 ± 2.4 0.714†
C/C 141 20.7 ± 9.1 41 (29.1) 0.038** 4.5 ± 2.5 0.636‡
CXCL12 rs266087 G/G 57 20.7 ± 8.1 19 (33.3) 4.6 ± 2.6 0.67
G/A 144 21.2 ± 8.3 55 (38.2) 0.770* 4.7 ± 2.4 0.824†
A/A 82 20.0 ± 9.9 25 (30.5) 0.311** 4.4 ± 2.3 0.635‡
CXCL12 rs2297630 A/A 2 29.5 ± 6.4 1 (50.0) 2.0 ± 1.4 0.24
A/G 64 20.7 ± 7.8 29 (45.3) 1.000* 4.6 ± 2.7 0.952‡
G/G 217 20.7 ± 9.1 69 (31.8) 0.042** 4.5 ± 2.4 0.833‡
CXCL12 rs2839693 A/A 3 17.3 ± 2.3 0 (0.0) 3.7 ± 1.5 0.29
A/G 69 20.7 ± 8.4 24 (34.8) 0.496* 4.6 ± 2.7 0.895†
G/G 205 21.0 ± 9.1 74 (36.1) 0.673** 4.5 ± 2.3 0.863‡
*Recessive effect for sepsis morbidity.**Dominant effect for sepsis morbidity.†Recessive effect for MOD score.‡Dominant effect for MOD score.HWE, Hardy-Weinberg equilibrium.
TABLE 5. The Combined Effects of rs1429638 and rs2297630 inAll Included Patients
Variants (n) N ISS Sepsis, n (%) MOD Score
0 685 20.4 ± 9.4 212 (30.9) 4.6 ± 2.5
1 796 20.5 ± 9.5 289 (36.3) 4.6 ± 2.5
2 216 20.5 ± 8.7 88 (40.7) 4.8 ± 2.6
* **
*p = 0.232.**p = 0.925.
J Trauma Acute Care SurgVolume 86, Number 3 Wang et al.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
fibroblasts, and endothelial cells. Biondo et al.30 demonstratedthat CXCL1 induces the recruitment of neutrophils to infectionsites. Cai et al.31 demonstrated that CXCL1 regulates the hostdefense to bacterial infection via CXCL2, CXCL5, NF-κB,and MAPKs. Jin et al.7 demonstrated that CXCL1 contributesto host defense in polymicrobial sepsis by modulating the activ-ities and functions of neutrophils and T lymphocyte. Rs1429638is located in the 3′ flanking region of CXCL1. This region maycontain enhancers or other sites to which proteins may bind. Wefurther examined the polymorphism map to assess the reportedexpression quantitative trait loci for nearby genes and found that
445
ealth, Inc. All rights reserved.
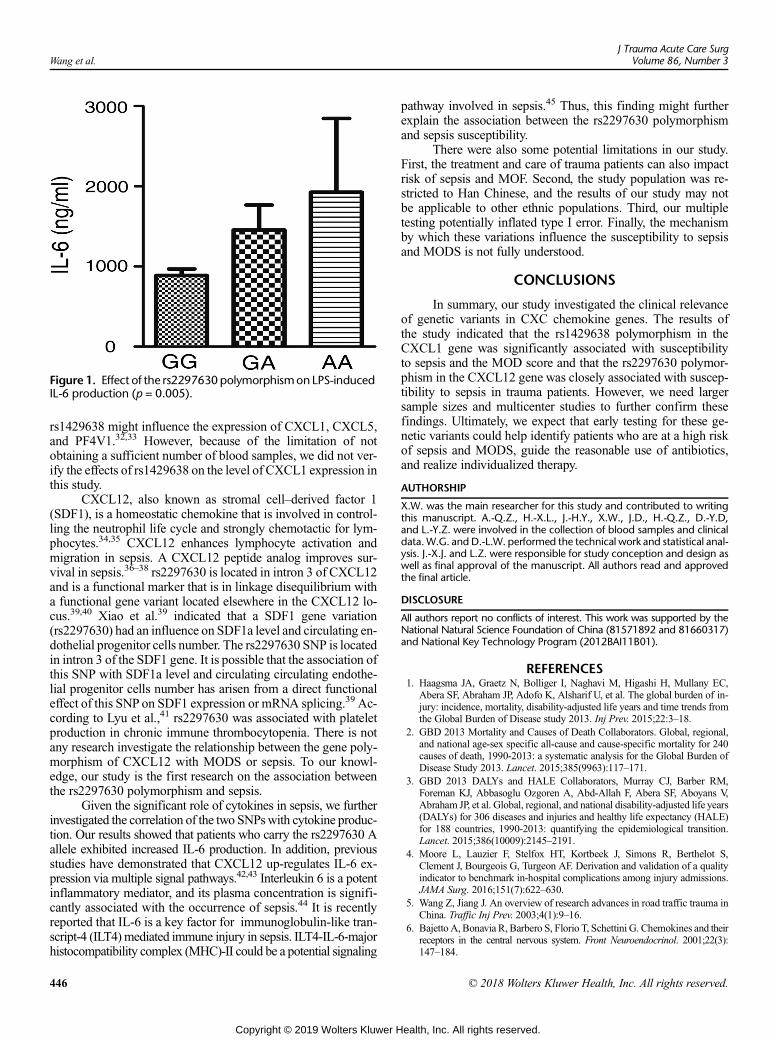
Figure 1. Effect of the rs2297630polymorphismonLPS-inducedIL-6 production (p = 0.005).
Wang et al.J Trauma Acute Care Surg
Volume 86, Number 3
rs1429638 might influence the expression of CXCL1, CXCL5,and PF4V1.32,33 However, because of the limitation of notobtaining a sufficient number of blood samples, we did not ver-ify the effects of rs1429638 on the level of CXCL1 expression inthis study.
CXCL12, also known as stromal cell–derived factor 1(SDF1), is a homeostatic chemokine that is involved in control-ling the neutrophil life cycle and strongly chemotactic for lym-phocytes.34,35 CXCL12 enhances lymphocyte activation andmigration in sepsis. A CXCL12 peptide analog improves sur-vival in sepsis.36–38 rs2297630 is located in intron 3 of CXCL12and is a functional marker that is in linkage disequilibrium witha functional gene variant located elsewhere in the CXCL12 lo-cus.39,40 Xiao et al.39 indicated that a SDF1 gene variation(rs2297630) had an influence on SDF1a level and circulating en-dothelial progenitor cells number. The rs2297630 SNP is locatedin intron 3 of the SDF1 gene. It is possible that the association ofthis SNP with SDF1a level and circulating circulating endothe-lial progenitor cells number has arisen from a direct functionaleffect of this SNP on SDF1 expression or mRNA splicing.39 Ac-cording to Lyu et al.,41 rs2297630 was associated with plateletproduction in chronic immune thrombocytopenia. There is notany research investigate the relationship between the gene poly-morphism of CXCL12 with MODS or sepsis. To our knowl-edge, our study is the first research on the association betweenthe rs2297630 polymorphism and sepsis.
Given the significant role of cytokines in sepsis, we furtherinvestigated the correlation of the two SNPswith cytokine produc-tion. Our results showed that patients who carry the rs2297630 Aallele exhibited increased IL-6 production. In addition, previousstudies have demonstrated that CXCL12 up-regulates IL-6 ex-pression via multiple signal pathways.42,43 Interleukin 6 is a potentinflammatory mediator, and its plasma concentration is signifi-cantly associated with the occurrence of sepsis.44 It is recentlyreported that IL-6 is a key factor for immunoglobulin-like tran-script-4 (ILT4) mediated immune injury in sepsis. ILT4-IL-6-majorhistocompatibility complex (MHC)-II could be a potential signaling
446
Copyright © 2019 Wolters Kluwer H
pathway involved in sepsis.45 Thus, this finding might furtherexplain the association between the rs2297630 polymorphismand sepsis susceptibility.
There were also some potential limitations in our study.First, the treatment and care of trauma patients can also impactrisk of sepsis and MOF. Second, the study population was re-stricted to Han Chinese, and the results of our study may notbe applicable to other ethnic populations. Third, our multipletesting potentially inflated type I error. Finally, the mechanismby which these variations influence the susceptibility to sepsisand MODS is not fully understood.
CONCLUSIONS
In summary, our study investigated the clinical relevanceof genetic variants in CXC chemokine genes. The results ofthe study indicated that the rs1429638 polymorphism in theCXCL1 gene was significantly associated with susceptibilityto sepsis and the MOD score and that the rs2297630 polymor-phism in the CXCL12 gene was closely associated with suscep-tibility to sepsis in trauma patients. However, we need largersample sizes and multicenter studies to further confirm thesefindings. Ultimately, we expect that early testing for these ge-netic variants could help identify patients who are at a high riskof sepsis and MODS, guide the reasonable use of antibiotics,and realize individualized therapy.
AUTHORSHIP
X.W. was the main researcher for this study and contributed to writingthis manuscript. A.-Q.Z., H.-X.L., J.-H.Y., X.W., J.D., H.-Q.Z., D.-Y.D,and L.-Y.Z. were involved in the collection of blood samples and clinicaldata.W.G. and D.-L.W. performed the technical work and statistical anal-ysis. J.-X.J. and L.Z. were responsible for study conception and design aswell as final approval of the manuscript. All authors read and approvedthe final article.
DISCLOSURE
All authors report no conflicts of interest. This work was supported by theNational Natural Science Foundation of China (81571892 and 81660317)and National Key Technology Program (2012BAI11B01).
REFERENCES1. Haagsma JA, Graetz N, Bolliger I, Naghavi M, Higashi H, Mullany EC,
Abera SF, Abraham JP, Adofo K, Alsharif U, et al. The global burden of in-jury: incidence, mortality, disability-adjusted life years and time trends fromthe Global Burden of Disease study 2013. Inj Prev. 2015;22:3–18.
2. GBD 2013 Mortality and Causes of Death Collaborators. Global, regional,and national age-sex specific all-cause and cause-specific mortality for 240causes of death, 1990-2013: a systematic analysis for the Global Burden ofDisease Study 2013. Lancet. 2015;385(9963):117–171.
3. GBD 2013 DALYs and HALE Collaborators, Murray CJ, Barber RM,Foreman KJ, Abbasoglu Ozgoren A, Abd-Allah F, Abera SF, Aboyans V,Abraham JP, et al. Global, regional, and national disability-adjusted life years(DALYs) for 306 diseases and injuries and healthy life expectancy (HALE)for 188 countries, 1990-2013: quantifying the epidemiological transition.Lancet. 2015;386(10009):2145–2191.
4. Moore L, Lauzier F, Stelfox HT, Kortbeek J, Simons R, Berthelot S,Clement J, Bourgeois G, Turgeon AF. Derivation and validation of a qualityindicator to benchmark in-hospital complications among injury admissions.JAMA Surg. 2016;151(7):622–630.
5. Wang Z, Jiang J. An overview of research advances in road traffic trauma inChina. Traffic Inj Prev. 2003;4(1):9–16.
6. Bajetto A, Bonavia R, Barbero S, Florio T, Schettini G. Chemokines and theirreceptors in the central nervous system. Front Neuroendocrinol. 2001;22(3):147–184.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
J Trauma Acute Care SurgVolume 86, Number 3 Wang et al.
7. Jin L, Batra S, Douda DN, Palaniyar N, Jeyaseelan S. CXCL1 contributes tohost defense in polymicrobial sepsis via modulating T cell and neutrophilfunctions. J Immunol. 2014;193(7):3549–3558.
8. Walley KR, Lukacs NW, Standiford TJ, Strieter RM, Kunkel SL. Elevatedlevels of macrophage inflammatory protein 2 in severe murine peritonitisincrease neutrophil recruitment and mortality. Infect Immun. 1997;65(9):3847–3851.
9. Ebong S, Call D, Nemzek J, Bolgos G, Newcomb D, Remick D. Immuno-pathologic alterations in murine models of sepsis of increasing severity.Infect Immun. 1999;67(12):6603–6610.
10. CuencaAG,Wynn JL, Kelly-Scumpia KM, Scumpia PO, Vila L,DelanoMJ,Mathews CE, Wallet SM, Reeves WH, Behrns KE, et al. Critical role forCXC ligand 10/CXC receptor 3 signaling in the murine neonatal responseto sepsis. Infect Immun. 2011;79(7):2746–2754.
11. Chan T, Gu F. Early diagnosis of sepsis using serum biomarkers. Expert RevMol Diagn. 2011;11(5):487–496.
12. Hu X, Dai S, Wu WJ, Tan W, Zhu X, Mu J, Guo Y, Bolli R, Rokosh G.Stromal cell derived factor-1 alpha confers protection against myocardialischemia/reperfusion injury: role of the cardiac stromal cell derived factor-1alpha CXCR4 axis. Circulation. 2007;116(6):654–663.
13. Franchini S, Marciano T, Sorlini C, Campochiaro C, Tresoldi M,Sabbadini MG, Dagna L. Serum CXCL12 levels on hospital admission pre-dict mortality in patients with severe sepsis/septic shock. Am J Emerg Med.2015;33(12):1802–1804.
14. Namath A, Patterson AJ. Genetic polymorphisms in sepsis. Crit Care Clin.2009;25(4):835–856, x.
15. Zeng L, Du J, Gu W, Zhang AQ, Wang HY, Wen DL, Qiu L, Yang XT,Sun JH, Zhang M, et al. Rs1800625 in the receptor for advanced glycationend products gene predisposes to sepsis and multiple organ dysfunction syn-drome in patients with major trauma. Crit Care. 2015;19:6.
16. Zeng L, Zhang AQ, Gu W, Zhou J, Zhang LY, Du DY, Zhang M, Wang HY,Yan J, Yang C, et al. Identification of haplotype tag single nucleotide poly-morphisms within the receptor for advanced glycation end products geneand their clinical relevance in patients with major trauma. Crit Care. 2012;16(4):R131.
17. Kotrych D, Dziedziejko V, Safranow K, DrozdzikM, Pawlik A. CXCL9 andCXCL10 gene polymorphisms in patients with rheumatoid arthritis.Rheumatol Int. 2015;35(8):1319–1323.
18. Selvaraj P, Alagarasu K, Singh B. Stromal cell-derived factor-1 (SDF-1/CXCL12) gene polymorphisms in pulmonary tuberculosis patients of southIndia. Int J Immunogenet. 2012;39(1):26–31.
19. Wang B, Suo P, Chen B,Wei Z, Yang L, Zhou S,Wang J, Cao Y,Ma X. Hap-lotype analysis of chemokine CXCL12 polymorphisms and susceptibility topremature ovarian failure in Chinese women. Hum Reprod. 2011;26(4):950–954.
20. Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM,Sevransky JE, Sprung CL, Douglas IS, Jaeschke R, et al. Surviving SepsisCampaign: international guidelines for management of severe sepsis andseptic shock, 2012. Intensive Care Med. 2013;39(2):165–228.
21. Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, Cohen J,Opal SM, Vincent JL, Ramsay G, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med. 2003;31(4):1250–1256.
22. Marshall JC, Cook DJ, Christou NV, Bernard GR, Sprung CL, Sibbald WJ.Multiple organ dysfunction score: a reliable descriptor of a complex clinicaloutcome. Crit Care Med. 1995;23(10):1638–1652.
23. Sauaia A, Moore EE, Johnson JL, Ciesla DJ, Biffl WL, Banerjee A. Valida-tion of postinjury multiple organ failure scores. Shock. 2009;31(5):438–447.
24. de Bakker PI, Yelensky R, Pe'er I, Gabriel SB, Daly MJ, Altshuler D. Effi-ciency and power in genetic association studies. Nat Genet. 2005;37(11):1217–1223.
25. Dai Q, Luo H, Li XP, Huang J, Zhou TJ, Yang ZH. XRCC1 and ERCC1polymorphisms are related to susceptibility and survival of colorectal cancerin the Chinese population.Mutagenesis. 2015;30(3):441–449.
26. Gu W, Shan YA, Zhou J, Jiang DP, Zhang L, Du DY, Wang ZG, Jiang JX.Functional significance of gene polymorphisms in the promoter of myeloiddifferentiation-2. Ann Surg. 2007;246(1):151–158.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
27. Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practicaland powerful approach to multiple testing. J R Stat Soc B Methodol. 1995;57:289–300.
28. World Health Organization. Global health estimates 2014 summary ta-bles — deaths by cause, age and sex, by WHO region. In: 2000–2012.2015: Available at: http://www.who.int/healthinfo/global_burden_disease/GHE_DthWHOReg6_2000_2012.xls. Accessed July 6, 2015.
29. Barrett JC, Fry B, Maller J, Daly MJ. Haploview: analysis and visualizationof LD and haplotype maps. Bioinformatics. 2005;21(2):263–265.
30. Biondo C, Mancuso G, Midiri A, Signorino G, Domina M, Lanza Cariccio V,Mohammadi N, VenzaM, Venza I, Teti G, et al. The interleukin-1β/CXCL1/2/neutrophil axis mediates host protection against group B streptococcal infec-tion. Infect Immun. 2014;82(11):4508–4517.
31. Cai S, Batra S, Lira SA, Kolls JK, Jeyaseelan S. CXCL1 regulates pulmo-nary host defense to Klebsiella Infection via CXCL2, CXCL5, NF-kappaB,and MAPKs. J Immunol. 2010;185(10):6214–6225.
32. Fehrmann RS, Jansen RC, Veldink JH, Westra HJ, Arends D, Bonder MJ,Fu J, Deelen P, Groen HJ, Smolonska A, et al. Trans-eQTLs reveal that inde-pendent genetic variants associated with a complex phenotype converge onintermediate genes, with a major role for the HLA. PLoS Genet. 2011;7(8):e1002197.
33. Westra HJ, Peters MJ, Esko T, Yaghootkar H, Schurmann C, Kettunen J,ChristiansenMW, Fairfax BP, SchrammK, Powell JE, et al. Systematic iden-tification of trans eQTLs as putative drivers of known disease associations.Nat Genet. 2013;45(10):1238–1243.
34. Yamada M, Kubo H, Kobayashi S, Ishizawa K, He M, Suzuki T, Fujino N,Kunishima H, Hatta M, Nishimaki K, et al. The increase in surface CXCR4expression on lung extravascular neutrophils and its effects on neutrophilsduring endotoxin-induced lung injury. Cell Mol Immunol. 2011;8(4):305–314.
35. Bleul CC, Fuhlbrigge RC, Casasnovas JM, Aiuti A, Springer TA. A highlyefficacious lymphocyte chemoattractant, stromal cell-derived factor 1 (SDF-1).J Exp Med. 1996;184(3):1101–1109.
36. Ding Z, Jia SH, Marshall JC, Downey GP, Waddell TK. Up-regulation offunctional CXCR4 expression on human lymphocytes in sepsis. Crit CareMed. 2006;34(12):3011–3017.
37. Fan H, Wong D, Ashton SH, Borg KT, Halushka PV, Cook JA. Beneficialeffect of a CXCR4 agonist in murine models of systemic inflammation.Inflammation. 2012;35(1):130–137.
38. Guan S, Guo C, Zingarelli B, Wang L, Halushka PV, Cook JA, Fan H. Com-bined treatment with a CXCL12 analogue and antibiotics improves survivaland neutrophil recruitment and function in murine sepsis. Immunology. 2014.
39. Xiao Q, Ye S, Oberhollenzer F, Mayr A, Jahangiri M, Willeit J, Kiechl S,Xu Q. SDF1 gene variation is associated with circulating SDF1alpha leveland endothelial progenitor cell number: the Bruneck Study. PLoS One.2008;3(12):e4061.
40. Ku FC, Tsai CR, Der Wang J, Wang CH, Chang TK, Hwang WL. Stromal-derived factor-1 gene variations in pediatric patients with primary immunethrombocytopenia. Eur J Haematol. 2013;90(1):25–30.
41. Lyu M, Li Y, Hao Y, Sun T, Liu W, Lyu C, Fu R, Li H, Xue F, Liu X, et al.Stromal cell-derived factor-1 rs2297630 polymorphism associated withplatelet production and treatment response in Chinese patients with chronicimmune thrombocytopenia. Platelets. 2016;27(4):338–343.
42. Zhang H, Wu H, Guan J, Wang L, Ren X, Shi X, Liang Z, Liu T. ParacrineSDF-1α signaling mediates the effects of PSCs on GEM chemoresistancethrough an IL-6 autocrine loop in pancreatic cancer cells. Oncotarget.2015;6(5):3085–3097.
43. Lin L, Han MM, Wang F, Xu LL, Yu HX, Yang PY. CXCR7 stimulatesMAPK signaling to regulate hepatocellular carcinoma progression. CellDeath Dis. 2014;5:e1488.
44. Tranca S, Oever JT, Ciuce C, Netea M, Slavcovici A, Petrisor C, Hagau N.sTREM-1, sIL-2Rα, and IL-6, but not sCD163, might predict sepsis inpolytrauma patients: a prospective cohort study. Eur J Trauma Emerg Surg.2017;43(3):363–3670.
45. Zhang W, He J. Interleukin-6 is a key factor for immunoglobulin-like tran-script-4-mediated immune injury in sepsis. J Intensive Care. 2018;10(6):22.
447
ealth, Inc. All rights reserved.

ORIGINAL ARTICLE
An unambiguous definition of pediatric hypotension is still lacking:Gaps between two percentile-based definitions and Pediatric
Advanced Life Support/Advanced Trauma Life Support guidelines
Giselle Sarganas, MD, PhD, MScIH, Angelika Schaffrath Rosario, MSc,Steffen Berger, MD, and Hannelore K. Neuhauser, MD, PhD, MPH, Berlin, Germany
Sub
Fro
Ad
Sup
DO
44
BACKGROUND: D
mitted: April 23, 2018, Revised:Published online: November 27m the Department of EpidemiolBerlin, Germany (G.S., A.S.R.cular Research), Partner Site BUniversitätsspital Bern, Departmdress for reprints: Giselle SargDepartment of Epidemiology12101 Berlin, Germany; email:plemental digital content is avaithe printed text, and links to thearticle on the journal’s Web sit
I: 10.1097/TA.00000000000021
8
ata are lacking to provide cutoffs for hypotension in children based on outcome studies and Pediatric Advanced Life Support(PALS), and Advanced Trauma Life Support (ATLS) definitions are based on normal populations. The goal of this study wasto compare different normal population based cutoffs including fifth percentile of systolic blood pressure (P5-SBP) in childrenand adolescents from the GermanHealth Examination Survey for Children and Adolescents (KiGGS), US population data (FourthReport), and cutoffs from PALS and ATLS guidelines.
METHODS: F
ifth percentile of systolic blood pressure according to age, sex, and height was modeled based on standardized restingoscillometric BP measurements (12,199 children aged 3–17 years) from KiGGS 2003–2006. In addition, we applied the age-adjusted pediatric shock index in the KiGGS study.RESULTS: T
he KiGGS P5-SBP was on average 7 mm Hg higher than Fourth Report P5-SBP (5–10 mm Hg depending on age-sex group).For children aged 3 to 9 years, KIGGS P5-SBP at median height follows the formula 82 mm Hg + age; for age 10 to 17 years,the increase was not linear and is presented in a simplified table. Pediatric Advanced Life Support/ATLS thresholds were betweenKiGGS and Fourth Report until age of 11 years. The adult threshold of 90 mmHg was reached by KiGGS P5-SBPmedian heightat 8 years, PALS/ATLS at age of 10 years, and Fourth Report P5-SBP at 12 years. The pediatric shock index, which is supposed toidentify severely injured children, was exceeded by 2.3% nonacutely ill KiGGS participants.CONCLUSION: O
ur study shows that percentile cutoffs vary by reference population. The 90 mmHg cutoff for adolescents targets only those in theless than 1% of the low SBP range and represents an undertriage compared with P5 at younger ages according to both KiGGS andFourth Report. Finally, current pediatric shock index cutoffs when applied to a healthy cohort lead to a relevant percentage of falsepositives. (J Trauma Acute Care Surg. 2019;86: 448–453. Copyright © 2018 Wolters Kluwer Health, Inc. All rights reserved.)LEVEL OF EVIDENCE: E
pidemiologic/prognostic, level III. KEYWORDS: B lood pressure; hypotension; percentiles; epidemiology; children.L ow blood pressure (BP) (hypotension) is an important vital pa-rameter when evaluating and treating critically ill or injured
children in the emergency department or intensive care unit.1–3
The Pediatric Advanced Life Support (PALS)4 through theAmerican Heart Association Guidelines for CardiopulmonaryResuscitation and Emergency Cardiovascular Care defines hy-potension in children based on a systolic blood pressure (SBP)below the fifth percentile (P5) for agewithout specifying the ref-erence population as follows:
<70 mm Hg + (2 � age in years) in children 1 to 10 years<90 mm Hg in children ≥10 years of age
The Advanced Trauma Life Support (ATLS) guideline5
recommends an identical formula to the PALS formula;
September 15, 2018, Accepted: October 29, 2018,, 2018.ogy and HealthMonitoring, Robert Koch Institute,, H.K.N.), DZHK (German Center for Cardiovas-erlin, Berlin, Germany (G.S., H.K.N.) Inselspital,ent of Pediatric Surgery Bern, Switzerland (S.B.).
anas, MD, PhD, MScIH, Robert Koch Institute,and Health Monitoring, General-Pape-Str. 62-66,[email protected] for this article. Direct URL citations appear indigital files are provided in the HTML text of thise (www.jtrauma.com).
39
Copyright © 2019 Wolters Kluwer H
however, it is not explicitly mentioned that, starting at age10 years, 90 mm Hg is the threshold for hypotension.
Even though these or similar cutoffs are published in mostof the relevant pediatric emergency and critical care manuals andtextbooks, it remains often unclear on which samples and statisti-cal methods the percentiles are based.6–9 Furthermore, no justify-ing evidence is presented for using thresholds irrespective of sexand height, in contrast to thresholds for elevated pediatric BP.
It is also important to consider that children have a re-markable ability to maintain their BP even with significant vol-ume loss; therefore, BP alone is not an accurate reflection ofcirculatory status.10 Hypotension must be interpreted withinthe context of the entire clinical picture4; therefore, there areother tools that help clinicians to better identify and evaluate crit-ically ill children, that is, shock in trauma patients, such as theshock index (heart rate/SBP).11 Cutoffs for shock index for iden-tification of most severe injured patients suggested in a previousstudy were greater than 1.22 (age 4–6 years), greater than 1.0(age 7–12 years), and greater than 0.9 (age 13–16 years).12
The aim of this study is to present the BP P1 and P5 byage, height, and sex from children and adolescents aged 3 to17 years from a nationally representative sample of 12,199nonoverweight children and adolescents who participated inthe German Health Interview and Examination Survey on Chil-dren and Adolescents (KiGGS) 2003–2006. Furthermore, we
J Trauma Acute Care SurgVolume 86, Number 3
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Sarganas et al.
compared these references with the corresponding percentilesfrom the United States based on data from the Fourth Report onthe diagnosis, evaluation, and treatment of high BP in childrenand adolescents,13,14 with the PALS4/ATLS5 cutoffs. In addition,we explore the prevalence of children exceeding current cutoffsfor pediatric shock index in a noninjured normal population.
PATIENTS AND METHODS
Study PopulationThe KiGGS 2003–2006 study is a population-based cross-
sectional study used to collect representative information on thehealth of children and adolescents aged 0 to 17 years living inGermany. The two-stage sampling procedure involved the selec-tion of 167 study locations from strata formed according to fed-eral state, community type, and population size.15 In a secondstep, an equal number of children per birth year from each loca-tion as identified through local population registries and invitedto participate in the study. The response rate was 66.6%, and17,640 children and adolescents aged 0 to 17 years participatedin the study (8,654 girls and 8,986 boys). The study was approvedby the ethical committee of Charité—University Medicine, Ber-lin, and by the Federal Commissioner for Data Protection andFreedom of Information. Informed written consent and assentwere obtained from all parents and from adolescents aged14 years or older. The KiGGS study includes 17% of childrenwith a two-sided migration background; migrants from Turkeyand the former Soviet Union were the two largest groups.15 Acomputer-assisted personal interview by a study physician cov-ered current and past medical conditions andmedication within the7 days preceding the interview. The girls' median age at menarchewas 12.8 years, and the boys' voices started breaking/reached fulladult pitch at a median of 13.5/15.1 years.16
MeasurementsIn children aged 3 to 17 years, two readings of SBP,
diastolic blood pressure (DBP), and mean arterial BP andheart rate were obtained by using an automated oscillometricdevice (Datascope Accutorr Plus) at 2-minute intervals aftera nonstrenuous part of the examination and an additional5-minute rest.17 The measurements were taken using the rightarm, in the sitting position with the elbow at the level of theright atrium, using one of four cuff sizes (6 � 12, 9 � 18,12 � 23, or 17 � 38.6 cm), which had to cover at least twothirds of the upper arm length (from the axilla to theantecubital fossa). The mean of the two measurements wasused for analysis. Body height was measured by trained staffaccording to a standardized protocol to the nearest 0.1 cmby using portable devices (Harpenden Stadiometer; HoltainLtd., Crymych, United Kingdom). Body weight was mea-sured with the child wearing only underwear to the nearest0.1 kg with a calibrated scale (Seca, Birmingham, UnitedKingdom).15 Body mass index (BMI) was calculated as theratio of weight (in kg) by height2 (in m2) and rounded to threedigits. A BMI at greater than 90th percentile for sex and agewas categorized as overweight according to the German refer-ence system.18
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
Inclusion and Exclusion Criteria for the Sample onWhich the Percentiles Are Based
Of 14 836 KiGGS participants aged 3 to 17 years, we ex-cluded 149 children with missing or invalid BP or height data, par-ticipants with chronic conditions possibly influencing growth(n = 302)19 or BP (n = 30 [i.e., chronic renal diseases, aortic coarc-tation, hyperthyroidism, congenital adrenal hyperplasia, porphyria])and children taking antihypertensive agents (n = 25 [AnatomicalTherapeutic Chemical Classification System codes C01-03 andC07-09 or any medication given with the indication hypertension]).Seventeen children had more than one exclusion criterion, leaving7038 girls and 7311 boys for analysis. A decision was taken to ex-clude overweight children (n = 2150) from the reference populationfrom which BP percentiles by sex, age, and height were derived.Similarly to other countries,13 this was done to avoid that rising pro-portions of overweight children raise the threshold for normal BP.However, for comparison, the sample including overweight chil-dren was also used for percentile derivation, however in a sim-plified form, that is, only by sex and age (not height).
STATISTICAL ANALYSIS
Blood pressure percentiles as a function of age only weremodeled using the L (skewness parameter), M (median), and S(coefficient of variation)method20with the programLMSChartMakerPro 2.2 (Medical Research Council, London, United Kingdom).
The reference curves from nonoverweight children by ageand height simultaneously were fitted by using an extension ofthe LMS method for two covariates, namely, the generalized ad-ditive models for location scale and shape with the Box-Cox-Cole-Green distribution family21–23 fitted with gamlss 1.9-4 inthe free statistical software R 2.8.0 (www.cran.r-project.org).Both models require neither the assumption of a normal distribu-tion nor of a constant variance of BP values with age and/orheight; however, if the data follow a distribution, then the modelcan be simplified and uses the normal distribution. Moreover, ifnecessary, it incorporates the use of cubic spline functions. Ifthese are not necessary to describe the data, the model can be sim-plified using parametric terms and a formula can be given for cal-culating percentiles. Another important aspect is that not only themean is modeled (as for example in linear regression) but also theentire distribution, including the more extreme percentiles, whichare most interesting from a clinical perspective.24,25
RESULTS
Baseline characteristics of the KiGGS nonoverweight ref-erence population consisting of 12,199 children and adolescents(6210 boys and 5989 girls) aged 3 to 17 years are shown in Table 1.
Smoothed SBP and DBP for P1, P5, P50, and P95 fromboys and girls by age and height (given in cm) are shown in Sup-plemental Tables 1 and 2 (Tables, Supplemental Digital Con-tents 1 and 2, http://links.lww.com/TA/B235 and http://links.lww.com/TA/B236). Blood pressure increased in children andadolescents aged 3 to 17 years both with age and height. Nosex difference was observed in DBP P1 and P5. For SBP P1and P5 this was also the case until the age of 13 years; however,older boys had higher SBP P1 and P5 compared with girls (atmedian height P5-SBP was up to 6 mm Hg higher in boys at
449
ealth, Inc. All rights reserved.
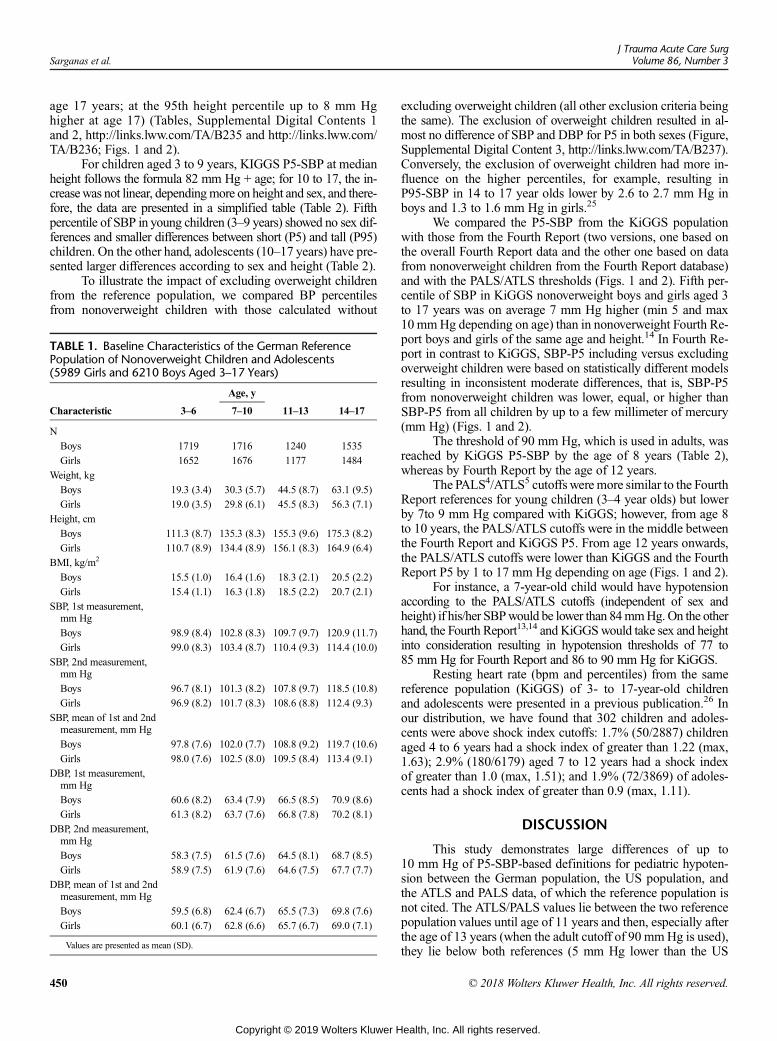
Sarganas et al.J Trauma Acute Care Surg
Volume 86, Number 3
age 17 years; at the 95th height percentile up to 8 mm Hghigher at age 17) (Tables, Supplemental Digital Contents 1and 2, http://links.lww.com/TA/B235 and http://links.lww.com/TA/B236; Figs. 1 and 2).
For children aged 3 to 9 years, KIGGS P5-SBP at medianheight follows the formula 82 mm Hg + age; for 10 to 17, the in-creasewas not linear, dependingmore on height and sex, and there-fore, the data are presented in a simplified table (Table 2). Fifthpercentile of SBP in young children (3–9 years) showed no sex dif-ferences and smaller differences between short (P5) and tall (P95)children. On the other hand, adolescents (10–17 years) have pre-sented larger differences according to sex and height (Table 2).
To illustrate the impact of excluding overweight childrenfrom the reference population, we compared BP percentilesfrom nonoverweight children with those calculated without
TABLE 1. Baseline Characteristics of the German ReferencePopulation of Nonoverweight Children and Adolescents(5989 Girls and 6210 Boys Aged 3–17 Years)
Age, y
Characteristic 3–6 7–10 11–13 14–17
N
Boys 1719 1716 1240 1535
Girls 1652 1676 1177 1484
Weight, kg
Boys 19.3 (3.4) 30.3 (5.7) 44.5 (8.7) 63.1 (9.5)
Girls 19.0 (3.5) 29.8 (6.1) 45.5 (8.3) 56.3 (7.1)
Height, cm
Boys 111.3 (8.7) 135.3 (8.3) 155.3 (9.6) 175.3 (8.2)
Girls 110.7 (8.9) 134.4 (8.9) 156.1 (8.3) 164.9 (6.4)
BMI, kg/m2
Boys 15.5 (1.0) 16.4 (1.6) 18.3 (2.1) 20.5 (2.2)
Girls 15.4 (1.1) 16.3 (1.8) 18.5 (2.2) 20.7 (2.1)
SBP, 1st measurement,mm Hg
Boys 98.9 (8.4) 102.8 (8.3) 109.7 (9.7) 120.9 (11.7)
Girls 99.0 (8.3) 103.4 (8.7) 110.4 (9.3) 114.4 (10.0)
SBP, 2nd measurement,mm Hg
Boys 96.7 (8.1) 101.3 (8.2) 107.8 (9.7) 118.5 (10.8)
Girls 96.9 (8.2) 101.7 (8.3) 108.6 (8.8) 112.4 (9.3)
SBP, mean of 1st and 2ndmeasurement, mm Hg
Boys 97.8 (7.6) 102.0 (7.7) 108.8 (9.2) 119.7 (10.6)
Girls 98.0 (7.6) 102.5 (8.0) 109.5 (8.4) 113.4 (9.1)
DBP, 1st measurement,mm Hg
Boys 60.6 (8.2) 63.4 (7.9) 66.5 (8.5) 70.9 (8.6)
Girls 61.3 (8.2) 63.7 (7.6) 66.8 (7.8) 70.2 (8.1)
DBP, 2nd measurement,mm Hg
Boys 58.3 (7.5) 61.5 (7.6) 64.5 (8.1) 68.7 (8.5)
Girls 58.9 (7.5) 61.9 (7.6) 64.6 (7.5) 67.7 (7.7)
DBP, mean of 1st and 2ndmeasurement, mm Hg
Boys 59.5 (6.8) 62.4 (6.7) 65.5 (7.3) 69.8 (7.6)
Girls 60.1 (6.7) 62.8 (6.6) 65.7 (6.7) 69.0 (7.1)
Values are presented as mean (SD).
450
Copyright © 2019 Wolters Kluwer H
excluding overweight children (all other exclusion criteria beingthe same). The exclusion of overweight children resulted in al-most no difference of SBP and DBP for P5 in both sexes (Figure,Supplemental Digital Content 3, http://links.lww.com/TA/B237).Conversely, the exclusion of overweight children had more in-fluence on the higher percentiles, for example, resulting inP95-SBP in 14 to 17 year olds lower by 2.6 to 2.7 mm Hg inboys and 1.3 to 1.6 mm Hg in girls.25
We compared the P5-SBP from the KiGGS populationwith those from the Fourth Report (two versions, one based onthe overall Fourth Report data and the other one based on datafrom nonoverweight children from the Fourth Report database)and with the PALS/ATLS thresholds (Figs. 1 and 2). Fifth per-centile of SBP in KiGGS nonoverweight boys and girls aged 3to 17 years was on average 7 mm Hg higher (min 5 and max10 mmHg depending on age) than in nonoverweight Fourth Re-port boys and girls of the same age and height.14 In Fourth Re-port in contrast to KiGGS, SBP-P5 including versus excludingoverweight children were based on statistically different modelsresulting in inconsistent moderate differences, that is, SBP-P5from nonoverweight children was lower, equal, or higher thanSBP-P5 from all children by up to a few millimeter of mercury(mm Hg) (Figs. 1 and 2).
The threshold of 90 mm Hg, which is used in adults, wasreached by KiGGS P5-SBP by the age of 8 years (Table 2),whereas by Fourth Report by the age of 12 years.
The PALS4/ATLS5 cutoffs were more similar to the FourthReport references for young children (3–4 year olds) but lowerby 7to 9 mm Hg compared with KiGGS; however, from age 8to 10 years, the PALS/ATLS cutoffs were in the middle betweenthe Fourth Report and KiGGS P5. From age 12 years onwards,the PALS/ATLS cutoffs were lower than KiGGS and the FourthReport P5 by 1 to 17 mm Hg depending on age (Figs. 1 and 2).
For instance, a 7-year-old child would have hypotensionaccording to the PALS/ATLS cutoffs (independent of sex andheight) if his/her SBPwould be lower than 84mmHg.On the otherhand, the Fourth Report13,14 and KiGGSwould take sex and heightinto consideration resulting in hypotension thresholds of 77 to85 mm Hg for Fourth Report and 86 to 90 mm Hg for KiGGS.
Resting heart rate (bpm and percentiles) from the samereference population (KiGGS) of 3- to 17-year-old childrenand adolescents were presented in a previous publication.26 Inour distribution, we have found that 302 children and adoles-cents were above shock index cutoffs: 1.7% (50/2887) childrenaged 4 to 6 years had a shock index of greater than 1.22 (max,1.63); 2.9% (180/6179) aged 7 to 12 years had a shock indexof greater than 1.0 (max, 1.51); and 1.9% (72/3869) of adoles-cents had a shock index of greater than 0.9 (max, 1.11).
DISCUSSION
This study demonstrates large differences of up to10 mm Hg of P5-SBP-based definitions for pediatric hypoten-sion between the German population, the US population, andthe ATLS and PALS data, of which the reference population isnot cited. The ATLS/PALS values lie between the two referencepopulation values until age of 11 years and then, especially afterthe age of 13 years (when the adult cutoff of 90 mmHg is used),they lie below both references (5 mm Hg lower than the US
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
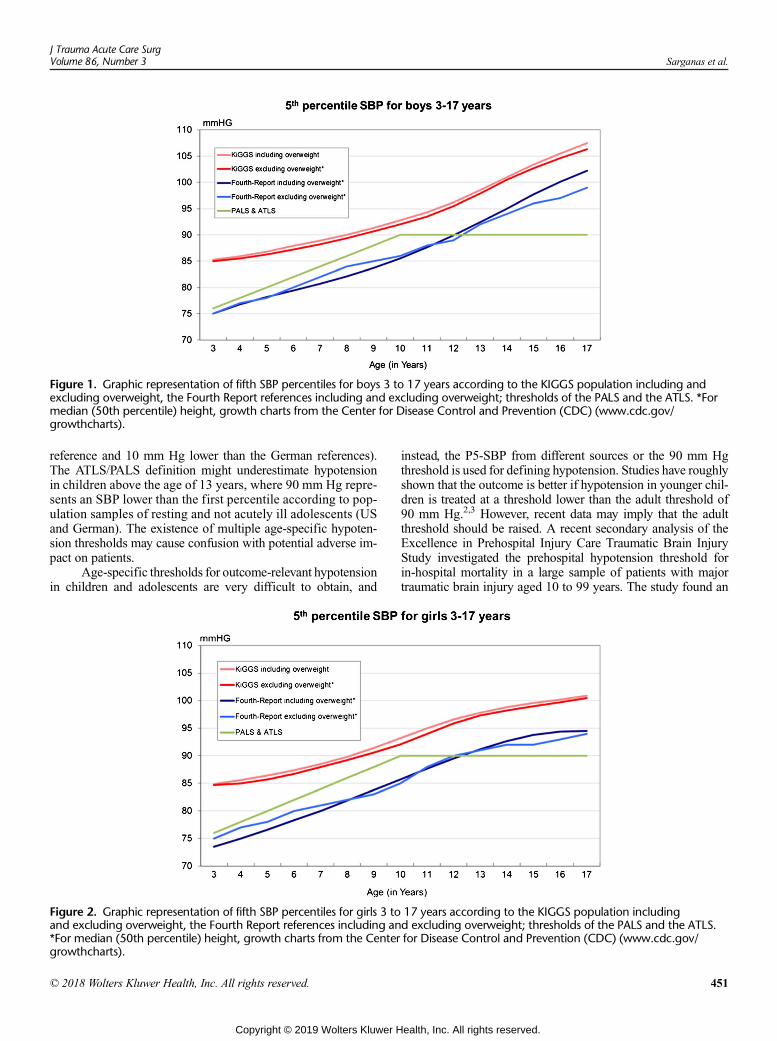
Figure 1. Graphic representation of fifth SBP percentiles for boys 3 to 17 years according to the KIGGS population including andexcluding overweight, the Fourth Report references including and excluding overweight; thresholds of the PALS and the ATLS. *Formedian (50th percentile) height, growth charts from the Center for Disease Control and Prevention (CDC) (www.cdc.gov/growthcharts).
J Trauma Acute Care SurgVolume 86, Number 3 Sarganas et al.
reference and 10 mm Hg lower than the German references).The ATLS/PALS definition might underestimate hypotensionin children above the age of 13 years, where 90 mm Hg repre-sents an SBP lower than the first percentile according to pop-ulation samples of resting and not acutely ill adolescents (USand German). The existence of multiple age-specific hypoten-sion thresholds may cause confusion with potential adverse im-pact on patients.
Age-specific thresholds for outcome-relevant hypotensionin children and adolescents are very difficult to obtain, and
Figure 2. Graphic representation of fifth SBP percentiles for girls 3 toand excluding overweight, the Fourth Report references including an*For median (50th percentile) height, growth charts from the Centergrowthcharts).
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
instead, the P5-SBP from different sources or the 90 mm Hgthreshold is used for defining hypotension. Studies have roughlyshown that the outcome is better if hypotension in younger chil-dren is treated at a threshold lower than the adult threshold of90 mm Hg.2,3 However, recent data may imply that the adultthreshold should be raised. A recent secondary analysis of theExcellence in Prehospital Injury Care Traumatic Brain InjuryStudy investigated the prehospital hypotension threshold forin-hospital mortality in a large sample of patients with majortraumatic brain injury aged 10 to 99 years. The study found an
17 years according to the KIGGS population includingd excluding overweight; thresholds of the PALS and the ATLS.for Disease Control and Prevention (CDC) (www.cdc.gov/
451
ealth, Inc. All rights reserved.

TABLE 2. Simplified P5 BP for Boys and Girls (KiGGS Survey2003–2006)
Age, y
P5-SBP, mm Hg
Boys and Girls (Height P50)
3 85
4 86
5 87
6 88
7 89
8 90
9 91
Boys (Height P5-P95) Girls (Height P5-P95)
10 91–95 90–95
11 92–97 92–97
12 93–99 94–99
13 96–102 96–100
14 98–104 97–100
15 100–106 98–101
16 102–108 99–101
17 104–110 100–102
BP percentiles apply exactly for the midpoint of each age group (i.e., 3 years and6 months old) and can be applied to all children of that age.
Sarganas et al.J Trauma Acute Care Surg
Volume 86, Number 3
association between lowest prehospital SBP and adjusted proba-bility of death across the SBP range of 40 to 119 mm Hg, witheach 10-point increase in SBP associated with a decrease of19% in the adjusted odds of death.27 The association was mono-tonic, that is, no threshold was suggested by the data. The au-thors concluded that clinically the threshold for meaningfulhypotension might be higher than current guidelines suggest;which would coincidewith the percentile-based US and Germandata in adolescents. This is largely a study in adults, and thereare several major limitations to the analysis (the treatment ofhypotension was not accounted for, only SBP documented bythe emergency physicians could be used, no BP measurementstandardization). Other studies have shown that, in childrenwith se-vere traumatic brain injury, early hypotension is common and asso-ciatedwith poorer outcomes including in-hospital mortality.2,3,28–31
A pediatric registry of prehospital BP in trauma patients that canbe linked to mortality data would be of great benefit for deter-mining outcome-based thresholds for pediatric hypotension.Such a registry should be simple enough to remain feasiblebut should still include data on BP treatment and on height.
The clinical cause of hypotension may justify different BPtargets. A study in children with severe CNS infections and sep-sis demonstrated that therapies targeted to preservation of a min-imum cerebral perfusion pressure (CPP) rather than to intracranialpressure reduced mortality from 38% in the intracranial pressurecontrol group to 18% in the CPP preservation group, where themean BP in the CPP targeted group was the 90th percentile forage supporting targeting a mean BP greater than 50th percentilefor age.32 Another study showed a significant association be-tween poor outcomes after severe pediatric traumatic brain injuryand an age-appropriate SBP below the 75th percentile (odds ratio,4.2; 95% confidence interval, 2.1–8.3).3 A pediatric neurotraumastudy suggested that it might be beneficial to maintain SBP of
452
Copyright © 2019 Wolters Kluwer H
greater than or equal to 50th percentile.33 On the other hand, inchildren post cardiac arrest, the BP target recommended by thePaediatric Task Force of the International Liaison Committee onResuscitation is the P5.34 For pediatric sepsis resuscitation, thereare no agreed BP targets.35 While some data suggest benefitsfrom higher BP targets at least in patient subgroups, the evidencebase is still not satisfactory and higher targets can be associatedwith additional risks such as side effects of vasoactive agents.35
A recent study has demonstrated that a pediatric age-adjusted shock index was superior to age-adjusted hypotensionin identifying injured children likely to require emergency oper-ation, endotracheal intubation, or early blood transfusion.36 Inthe KiGGS sample of nonacutely ill and noninjured nationalhealth survey participants, 302 children corresponding to 1.7%to 2.9% of children in the respective age group exceeded the cut-offs for the pediatric shock index, which have been suggested foridentification of most severely injured children and are false-positive cases, suggesting further research on optimal cutoffs.
Major strengths of the KiGGS BP percentiles are the largeand nationally representative sample, coverage of awide age range,standardized measurements of BP and height, use of a BP devicevalidated in children, averaging of two BP measurements at restper participant, and themodeling by age and height simultaneouslywith flexible statistical techniques that do not impose normality orconstant variance assumptions on the data. A limitation of KiGGSis possible selection bias (ill children may be underrepresented);however, this is the case with all health survey data.
Possible reasons for the difference between KiGGS andFourth Report percentiles, which have well-described referencepopulations, include statistical differences, differential BP mea-surement by auscultatory and oscillometric techniques, and ac-tual BP distribution differences in the samples. The PALS andATLS population on the other hand is not referenced and cantherefore not be commented on.4,5 In any case, our results con-firm that guidelines should not only mention a specific BP per-centile but also specify the reference population.
A further strength of our analysis is that we investigatedthe need to have an age-, sex-, and height-stratified definitionof hypotension. Our analysis shows that, in contrast to the 90thand 95th percentiles used for definition of prehypertension and hy-pertension,25 the lower BP percentiles are not sensitive to includingor excluding overweight children in the reference population. Sexdifferences become evident at pubertal age and differences betweenshort (P5 for height) and tall (P95 for height) children exceed5 mm Hg from age 13 years in boys. Therefore, even a simpli-fied table as the one we present should differentiate by sex andheight in adolescents. We conclude that clinical outcome studiesinvestigating hypotension should adjust for height.
In summary, at present, the P5-SBP from general pediatricpopulation samples is used as hypotension threshold in guidelinesfor treatment of critically ill or injured children with a transition toa fixed (adult) cutoff in adolescents. Our analyses show that P5-SBP varies considerably depending on the reference populationand statistical method used. However, in adolescents, the90 mm Hg fixed adult cutoff identifies considerably less adoles-cents as hypotensive than a P5-SBP definition would, leading toan age-gap in the triage. Clinically meaningful BP targets in acuteclinical situations need more and better outcome studies that takeinto consideration sex and height differences in adolescents.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
J Trauma Acute Care SurgVolume 86, Number 3 Sarganas et al.
AUTHORSHIP
G.S. carried out the literature review and interpretation of results, draftedthe initial article, and coordinated the revision of the article. A.S.R. per-formed the statistical analysis, contributed with the interpretation of re-sults, and revised the article. S.B. contributed in the interpretation ofresults and revised the article. H.K.N. conceptualized and supervised thestudy and contributed in the interpretation of results and in the writingof the article. All authors critically reviewed and approved the final article.
ACKNOWLEDGMENTS
We thank the study participants and all our colleagues who contributed tothe KiGGS study.
DISCLOSURE
For all authors, no conflicts of interest were declared. The study has beenfinanced by the German Federal Ministry of Health and by the RobertKoch Institute.
REFERENCES1. Zubrow AB, Hulman S, Kushner H, Falkner B. Determinants of blood
pressure in infants admitted to neonatal intensive care units: a prospective mul-ticenter study. Philadelphia Neonatal Blood Pressure StudyGroup. J Perinatol.1995;15:470–479.
2. Coates BM, Vavilala MS, Mack CD, Muangman S, Suz P, Sharar SR,Bulger E, Lam AM. Influence of definition and location of hypotension onoutcome following severe pediatric traumatic brain injury. Crit Care Med.2005;33:2645–2650.
3. Vavilala MS, Bowen A, Lam AM, Uffman JC, Powell J, Winn HR,Rivara FP. Blood pressure and outcome after severe pediatric traumatic braininjury. J Trauma. 2003;55:1039–1044.
4. Kleinman ME, Chameides L, Schexnayder SM, Samson RA, Hazinski MF,Atkins DL, Berg MD, de Caen AR, Fink EL, Freid EB, et al. Part 14: pedi-atric advanced life support: 2010 American Heart Association Guidelinesfor Cardiopulmonary Resuscitation and Emergency Cardiovascular Care.Circulation. 2010;122:S876–S908.
5. American College of Surgeons. Committee on Trauma. Advanced TraumaLife Support ATLS Student Course Manual. Chicago, IL: American Collegeof Surgeons; 2012.
6. FuhrmanBP, Zimmerman JJ. Pediatric Critical Care. 2nd ed. St. Louis, MO:Mosby; 1998.
7. Rogers MC, Nichols DG. Textbook of Pediatric Intensive Care. 3rd ed.Baltimore: Williams & Wilkins; 1996.
8. Baren JM, Rothrock SG. Pediatric Emergency Medicine. Philadelphia, PA:Saunders Elsevier; 2008.
9. Hazinski MF. Manual of Pediatric Critical Care. London: Mosby; 1999.10. Leeper CM, McKenna C, Gaines BA. Too little too late: hypotension and
blood transfusion in the trauma bay are independent predictors of death in in-jured children. J Trauma Acute Care Surg. 2018.
11. Cannon CM, Braxton CC, Kling-Smith M, Mahnken JD, Carlton E,Moncure M. Utility of the shock index in predicting mortality in traumati-cally injured patients. J Trauma. 2009;67:1426–1430.
12. Acker SN, Ross JT, Partrick DA, Tong S, Bensard DD. Pediatric specificshock index accurately identifies severely injured children. J Pediatr Surg.2015;50:331–334.
13. National High Blood Pressure Education Program Working Group on HighBlood Pressure in Children and Adolescents. The fourth report on the diag-nosis, evaluation, and treatment of high blood pressure in children and ado-lescents. Pediatrics. 2004;114:555–576.
14. Rosner B, CookN, Portman R, Daniels S, Falkner B. Determination of bloodpressure percentiles in normal-weight children: some methodological issues.Am J Epidemiol. 2008;167:653–666.
15. Kurth BM, Kamtsiuris P, Holling H, Schlaud M, Dolle R, Ellert U, Kahl H,Knopf H, Lange M, Mensink GB, et al. The challenge of comprehensivelymapping children's health in a nation-wide health survey: design of the Ger-man KiGGS-Study. BMC Public Health. 2008;8:196.
16. Kahl H, Schaffrath Rosario A, SchlaudM. Sexual maturation of children andadolescents in Germany. results of the German Health Interview and Examina-tion Survey for Children and Adolescents (KiGGS). BundesgesundheitsblattGesundheitsforschung Gesundheitsschutz. 2007;50:677–685.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
17. Neuhauser H, Thamm M. Blood pressure measurement in the GermanHealth Interview and Examination Survey for Children and Adolescents(KiGGS). Methodology and initial results. BundesgesundheitsblattGesundheitsforschung Gesundheitsschutz. 2007;50:728–735.
18. Kromeyer-Hauschild K, Wabitsch M, Kunze D, Geller F, Geiß HC, Hesse V,von Hippel A, Jaeger U, Johnsen D, Korte W, et al. Percentiles of body massindex in children and adolescents evaluated from different regional Germanstudies [in German]. Monatsschr Kinderheilkd. 2001;149:807–818.
19. Schaffrath Rosario A, Schienkiewitz A, Neuhauser H. German height refer-ences for children aged 0 to under 18 years compared to WHO and CDCgrowth charts. Ann Hum Biol. 2011;38:121–130.
20. Cole TJ, Green PJ. Smoothing reference centile curves: the LMSmethod andpenalized likelihood. Stat Med. 1992;11:1305–1319.
21. Cole TJ, Stanojevic S, Stocks J, Coates AL, Hankinson JL, Wade AM. Age-and size-related reference ranges: a case study of spirometry through child-hood and adulthood. Stat Med. 2009;28:880–898.
22. Ribgy R, Stasinopoulos D. Generalized additive models for location, scaleand shape. Appl Statist. 2005;54:507–554.
23. Stanojevic S,WadeA, Stocks J, Hankinson J, Coates AL, PanH, RosenthalM,Corey M, Lebecque P, Cole TJ. Reference ranges for spirometry across allages: a new approach. Am J Respir Crit Care Med. 2008;177:253–260.
24. Neuhauser HK, Schienkiewitz A, Schaffrath Rosario A, Dortschy R,Kurth BM. Reference percentiles for anthropometric measures and bloodpressure based on the German Health Interview and Examination Surveyfor Children and Adolescents 2003–2006 (KiGGS). Berlin: Robert Koch-Institut; 2016. Available at: http://www.rki.de/EN/Content/Health_Monitoring/Health_Reporting/Contributions/beitraege_node.html. AccessedSeptember 10, 2018.
25. Neuhauser HK, ThammM, Ellert U, Hense HW, Rosario AS. Blood pressurepercentiles by age and height from nonoverweight children and adolescentsin Germany. Pediatrics. 2011;127:e978–e988.
26. Sarganas G, Schaffrath Rosario A, Neuhauser HK. Resting heart rate percen-tiles and associated factors in children and adolescents. J Pediatr. 2017;187:174–181.e3.
27. Spaite DW, Hu C, Bobrow BJ, Chikani V, Sherrill D, Barnhart B, Gaither JB,Denninghoff KR, Viscusi C,Mullins T, et al. Mortality and prehospital bloodpressure in patients with major traumatic brain injury: implications for thehypotension threshold. JAMA Surg. 2017;152:360–368.
28. Chiaretti A, De Benedictis R, Della Corte F, Piastra M, Viola L, Polidori G,Di Rocco C. The impact of initial management on the outcome of childrenwith severe head injury. Childs Nerv Syst. 2002;18:54–60.
29. Kannan N,Wang J,Mink RB,WainwrightMS, Groner JI, Bell MJ, Giza CC,Zatzick DF, Ellenbogen RG, Boyle LN, et al. Timely hemodynamic resusci-tation and outcomes in severe pediatric traumatic brain injury: preliminaryfindings. Pediatr Emerg Care. 2016.
30. Kokoska ER, Smith GS, Pittman T, Weber TR. Early hypotension worsensneurological outcome in pediatric patients with moderately severe headtrauma. J Pediatr Surg. 1998;33:333–338.
31. Pigula FA, Wald SL, Shackford SR, Vane DW. The effect of hypotensionand hypoxia on children with severe head injuries. J Pediatr Surg. 1993;28:310–314; discussion 315–6.
32. Kumar R, Singhi S, Singhi P, Jayashree M, Bansal A, Bhatti A. Randomizedcontrolled trial comparing cerebral perfusion pressure-targeted therapy versusintracranial pressure-targeted therapy for raised intracranial pressure due toacute CNS infections in children. Crit Care Med. 2014;42:1775–1787.
33. Kannan N, Ramaiah R, VavilalaMS. Pediatric neurotrauma. Int J Crit Illn InjSci. 2014;4:131–137.
34. de Caen AR, Maconochie IK, Aickin R, Atkins DL, Biarent D,Guerguerian AM, Kleinman ME, Kloeck DA, Meaney PA, Nadkarni VM,et al. Part 6: Pediatric basic life support and pediatric advanced life support:2015 International Consensus on Cardiopulmonary Resuscitation and Emer-gency Cardiovascular Care Science With Treatment Recommendations(Reprint). Pediatrics. 2015;136(Suppl 2):S88–S119.
35. MarlaisM, Lyttle MD, Inwald D. Ten concerns about blood pressuremeasure-ment and targets in paediatric sepsis. Intensive Care Med. 2017;43:433–435.
36. Acker SN, Bredbeck B, Partrick DA, Kulungowski AM, Barnett CC,Bensard DD. Shock index, pediatric age-adjusted (SIPA) is more accuratethan age-adjusted hypotension for trauma team activation. Surgery. 2017;161:803–807.
453
ealth, Inc. All rights reserved.

ORIGINAL ARTICLE
Near hangings: Epidemiology, injuries, and investigations
Morgan Schellenberg, MD, MPH, Kenji Inaba, MD, Zachary Warriner, MD, Daniel Alfson, MD,Jordan Roman, Valery Van Velsen, Lydia Lam, MD, and Demetrios Demetriades, MD, PhD,
Los Angeles, California
Sub
Fro
Ad
DO
45
BACKGROUND: N
mitted: June 11, 2018, Revised: Alished online: November 16, 201m the Division of Trauma and SV.V.V., L.L., D.D.), LAC+USCLos Angeles, California.dress for reprints: Kenji Inaba,Critical Care, LAC+USC Me2051 Marengo St, Inpatient [email protected].
I: 10.1097/TA.00000000000021
4
ear hangings are an infrequent cause of trauma, and the optimalworkup for these patients is unclear. The study objectives were todefine the epidemiology, injury patterns, and use of investigations, including computed tomographic angiography (CTA) neck,after near hangings.
METHODS: A
ll patients presenting to LAC+USC Medical Center (2008–2015) after near hanging (International Classification of Diseases,Ninth Revision, code of E913.8, E953.0, E963, or E983.0) were screened for inclusion. Transferred patients were excluded. Patientdemographics, clinical data, injury data, investigations performed, and outcomes were collected.RESULTS: O
ver the study period, 71 patients were identified. Median age was 32 years (interquartile range [IQR], 24-44), and 85% (n=64)were male.Median GlasgowComa Scalewas 12 [IQR 5-15], andmedian Injury Severity Scorewas 1 [IQR 1-2].Mortality ratewas14% (n = 10). The most common finding on physical examination was a ligature mark (n = 38, 54%). Cervical injuries after nearhangings occurred infrequently (five injuries in four patients [6%]: 3 [4%] arterial injuries and 2 [3%] laryngotracheal injuries).Only one patient (1%) required surgical and/or endovascular intervention. Two (3%) arrived in cardiac arrest, underwent resusci-tative thoracotomy, and were pronounced dead. All others (n = 69, 97%) underwent CTA of the neck. No patient in this series man-ifested signs or symptoms of cervical injury during hospitalization after a normal CTA neck on presentation.CONCLUSION: N
ear hangings infrequently result in cervical injury, and intervention is rarely needed. When injuries are sustained, they occur tocritical structures such as the larynx, trachea, and cervical vasculature. Therefore, effective injury screening is important. We rec-ommend CTA of the neck as the optimal initial imaging investigation after near hangings. (J Trauma Acute Care Surg. 2019;86:454–457. Copyright © 2018 Wolters Kluwer Health, Inc. All rights reserved.)LEVEL OF EVIDENCE: E
pidemiologic, level IV; therapeutic/care management, level IV. KEYWORDS: N ear hangings; ligature mark; computed tomographic angiography; blunt cerebrovascular injury; laryngotracheal injury.H angings are an infrequent cause of trauma. There are twomajor subsets of hanging patients: judicial hangings, which
involve a drop in height followed by suspension, and suicidalhangings, which involve self suspension. Suicidal hangings arerelevant in the current era to North American trauma care pro-viders, as these are the patients who present to emergency de-partments (EDs) if they survive the attempted hanging. Termednear hangings, these patients are at risk for blunt injury to neckstructures because of direct compression or cervical flexion/extension. These patients can also have systemic sequelae as aresult of cardiac, respiratory, and neurological injuries. The optimalworkup for patients after near hangings is unclear.
The utility investigation for blunt cervical trauma is com-puted tomographic angiography (CTA) of the neck. However,the use of contemporary CTA in patients who present after nearhangings is not well described by the current literature. The ob-jectives of this study were to define the epidemiology, physicalexamination findings, and injury patterns after near hangings
ugust 17, 2018, Accepted: November 5, 2018, Pub-8.urgical Critical Care (M.S., K.I., Z.W., D.A., J.R.,Medical Center, University of Southern California,
MD, FRCSC, Division of Trauma and Surgicaldical Center, University of Southern California,ower, C5L100, Los Angeles, CA 90033; email:
34
Copyright © 2019 Wolters Kluwer H
and to examine the use of CTA after this mechanism of injury.In addition, the utility of other investigations (laryngoscopy/bronchoscopy, esophagogastroduodenoscopy [EGD], gastrografinswallow, duplex ultrasound of the neck, and catheter-based an-giogram of the neck) in diagnosing or excluding injuries afternear hangings was investigated. The aim was to define nearhangings in terms of the epidemiology, type and frequency ofinjuries, and diagnostic investigations utilized among patientswho sustain this mechanism of injury.
METHODS
In this retrospective observational study, all patients whopresented to LAC+USC Medical Center between January 1,2008, and September 30, 2015, after near hanging (defined asInternational Classification of Diseases, Ninth Revision, codeof E913.8, E953.0, E963, or E983.0) were screened for inclu-sion. Patients were excluded if they were transferred to or froman outside hospital. Institutional review board approval wassought and obtained from the University of Southern California.
Data were obtained from the LAC+USC Medical Centertrauma registry and patient charts. Patient demographics (age,sex, race, ethnicity), clinical data (physical examination of theneck, vital signs, and Glasgow Coma Scale [GCS] score on ad-mission), injury data (Injury Severity Score [ISS], AbbreviatedInjury Score by body region, injuries sustained), investiga-tions performed (CTA neck, laryngoscopy/bronchoscopy, EGD,gastrografin swallow, duplex ultrasound, and catheter-based
J Trauma Acute Care SurgVolume 86, Number 3
ealth, Inc. All rights reserved.
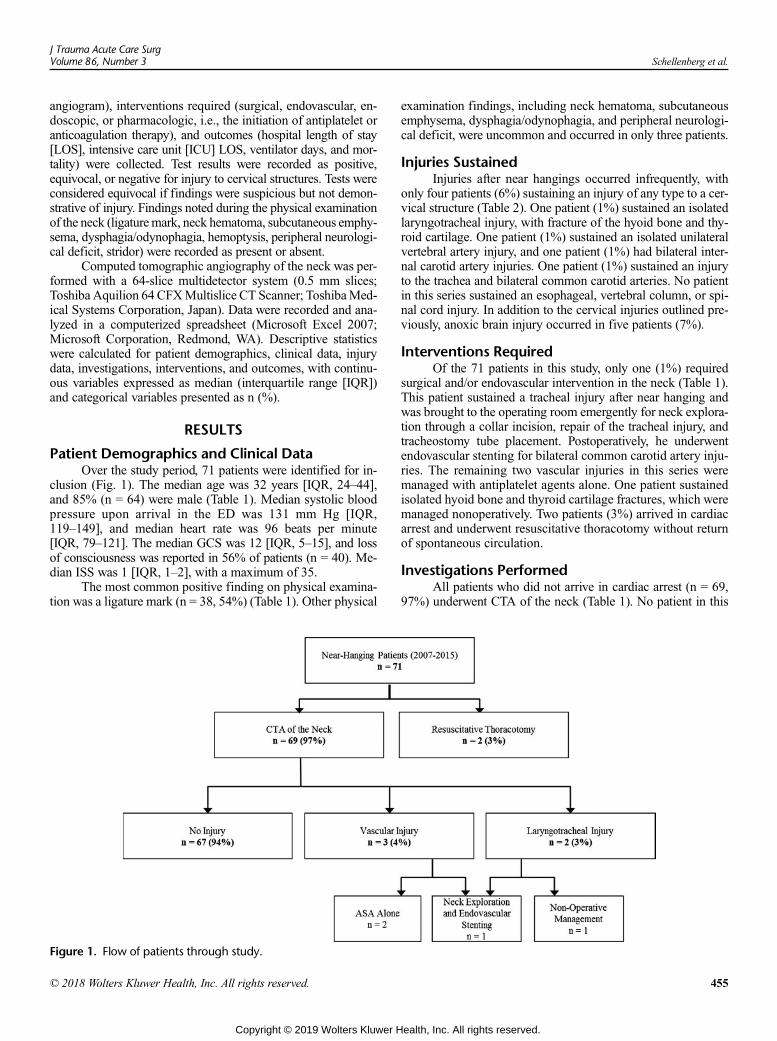
J Trauma Acute Care SurgVolume 86, Number 3 Schellenberg et al.
angiogram), interventions required (surgical, endovascular, en-doscopic, or pharmacologic, i.e., the initiation of antiplatelet oranticoagulation therapy), and outcomes (hospital length of stay[LOS], intensive care unit [ICU] LOS, ventilator days, and mor-tality) were collected. Test results were recorded as positive,equivocal, or negative for injury to cervical structures. Tests wereconsidered equivocal if findings were suspicious but not demon-strative of injury. Findings noted during the physical examinationof the neck (ligaturemark, neck hematoma, subcutaneous emphy-sema, dysphagia/odynophagia, hemoptysis, peripheral neurologi-cal deficit, stridor) were recorded as present or absent.
Computed tomographic angiography of the neck was per-formed with a 64-slice multidetector system (0.5 mm slices;Toshiba Aquilion 64 CFXMultislice CT Scanner; ToshibaMed-ical Systems Corporation, Japan). Data were recorded and ana-lyzed in a computerized spreadsheet (Microsoft Excel 2007;Microsoft Corporation, Redmond, WA). Descriptive statisticswere calculated for patient demographics, clinical data, injurydata, investigations, interventions, and outcomes, with continu-ous variables expressed as median (interquartile range [IQR])and categorical variables presented as n (%).
RESULTS
Patient Demographics and Clinical DataOver the study period, 71 patients were identified for in-
clusion (Fig. 1). The median age was 32 years [IQR, 24–44],and 85% (n = 64) were male (Table 1). Median systolic bloodpressure upon arrival in the ED was 131 mm Hg [IQR,119–149], and median heart rate was 96 beats per minute[IQR, 79–121]. The median GCS was 12 [IQR, 5–15], and lossof consciousness was reported in 56% of patients (n = 40). Me-dian ISS was 1 [IQR, 1–2], with a maximum of 35.
The most common positive finding on physical examina-tion was a ligature mark (n = 38, 54%) (Table 1). Other physical
Figure 1. Flow of patients through study.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
examination findings, including neck hematoma, subcutaneousemphysema, dysphagia/odynophagia, and peripheral neurologi-cal deficit, were uncommon and occurred in only three patients.
Injuries SustainedInjuries after near hangings occurred infrequently, with
only four patients (6%) sustaining an injury of any type to a cer-vical structure (Table 2). One patient (1%) sustained an isolatedlaryngotracheal injury, with fracture of the hyoid bone and thy-roid cartilage. One patient (1%) sustained an isolated unilateralvertebral artery injury, and one patient (1%) had bilateral inter-nal carotid artery injuries. One patient (1%) sustained an injuryto the trachea and bilateral common carotid arteries. No patientin this series sustained an esophageal, vertebral column, or spi-nal cord injury. In addition to the cervical injuries outlined pre-viously, anoxic brain injury occurred in five patients (7%).
Interventions RequiredOf the 71 patients in this study, only one (1%) required
surgical and/or endovascular intervention in the neck (Table 1).This patient sustained a tracheal injury after near hanging andwas brought to the operating room emergently for neck explora-tion through a collar incision, repair of the tracheal injury, andtracheostomy tube placement. Postoperatively, he underwentendovascular stenting for bilateral common carotid artery inju-ries. The remaining two vascular injuries in this series weremanaged with antiplatelet agents alone. One patient sustainedisolated hyoid bone and thyroid cartilage fractures, which weremanaged nonoperatively. Two patients (3%) arrived in cardiacarrest and underwent resuscitative thoracotomy without returnof spontaneous circulation.
Investigations PerformedAll patients who did not arrive in cardiac arrest (n = 69,
97%) underwent CTA of the neck (Table 1). No patient in this
455
ealth, Inc. All rights reserved.
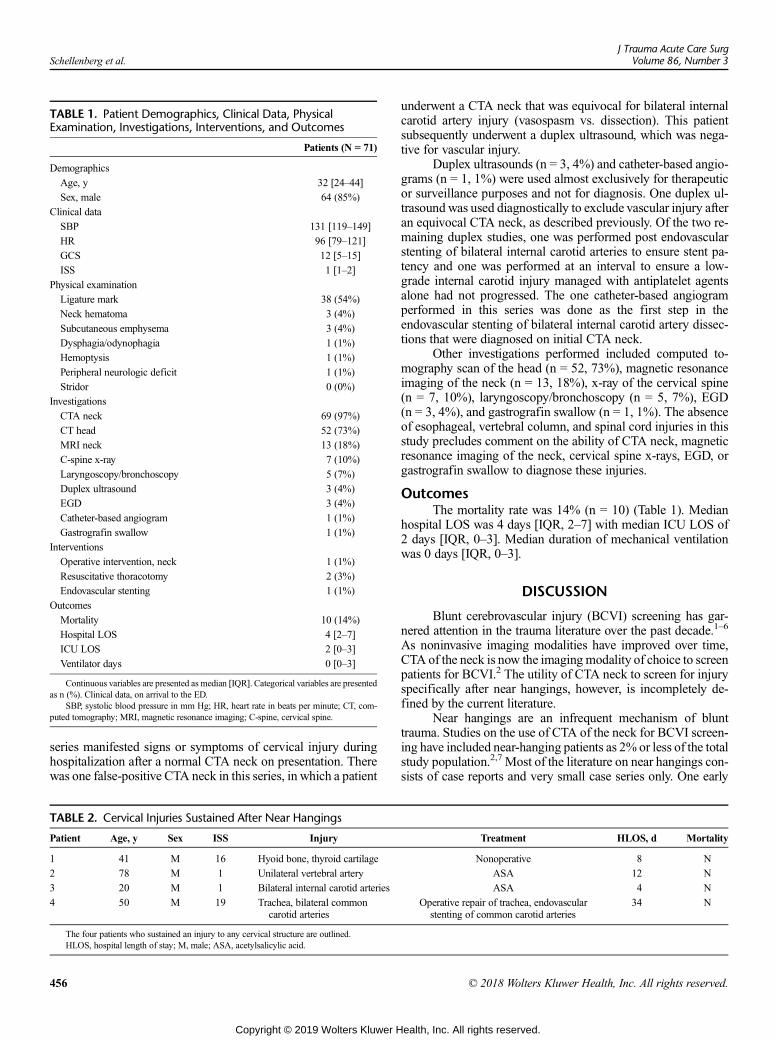
TABLE 1. Patient Demographics, Clinical Data, PhysicalExamination, Investigations, Interventions, and Outcomes
Patients (N = 71)
Demographics
Age, y 32 [24–44]
Sex, male 64 (85%)
Clinical data
SBP 131 [119–149]
HR 96 [79–121]
GCS 12 [5–15]
ISS 1 [1–2]
Physical examination
Ligature mark 38 (54%)
Neck hematoma 3 (4%)
Subcutaneous emphysema 3 (4%)
Dysphagia/odynophagia 1 (1%)
Hemoptysis 1 (1%)
Peripheral neurologic deficit 1 (1%)
Stridor 0 (0%)
Investigations
CTA neck 69 (97%)
CT head 52 (73%)
MRI neck 13 (18%)
C-spine x-ray 7 (10%)
Laryngoscopy/bronchoscopy 5 (7%)
Duplex ultrasound 3 (4%)
EGD 3 (4%)
Catheter-based angiogram 1 (1%)
Gastrografin swallow 1 (1%)
Interventions
Operative intervention, neck 1 (1%)
Resuscitative thoracotomy 2 (3%)
Endovascular stenting 1 (1%)
Outcomes
Mortality 10 (14%)
Hospital LOS 4 [2–7]
ICU LOS 2 [0–3]
Ventilator days 0 [0–3]
Continuous variables are presented as median [IQR]. Categorical variables are presentedas n (%). Clinical data, on arrival to the ED.
SBP, systolic blood pressure in mm Hg; HR, heart rate in beats per minute; CT, com-puted tomography; MRI, magnetic resonance imaging; C-spine, cervical spine.
Schellenberg et al.J Trauma Acute Care Surg
Volume 86, Number 3
series manifested signs or symptoms of cervical injury duringhospitalization after a normal CTA neck on presentation. Therewas one false-positive CTA neck in this series, in which a patient
TABLE 2. Cervical Injuries Sustained After Near Hangings
Patient Age, y Sex ISS Injury
1 41 M 16 Hyoid bone, thyroid cartilage
2 78 M 1 Unilateral vertebral artery
3 20 M 1 Bilateral internal carotid arteries
4 50 M 19 Trachea, bilateral commoncarotid arteries
The four patients who sustained an injury to any cervical structure are outlined.HLOS, hospital length of stay; M, male; ASA, acetylsalicylic acid.
456
Copyright © 2019 Wolters Kluwer H
underwent a CTA neck that was equivocal for bilateral internalcarotid artery injury (vasospasm vs. dissection). This patientsubsequently underwent a duplex ultrasound, which was nega-tive for vascular injury.
Duplex ultrasounds (n = 3, 4%) and catheter-based angio-grams (n = 1, 1%) were used almost exclusively for therapeuticor surveillance purposes and not for diagnosis. One duplex ul-trasound was used diagnostically to exclude vascular injury afteran equivocal CTA neck, as described previously. Of the two re-maining duplex studies, one was performed post endovascularstenting of bilateral internal carotid arteries to ensure stent pa-tency and one was performed at an interval to ensure a low-grade internal carotid injury managed with antiplatelet agentsalone had not progressed. The one catheter-based angiogramperformed in this series was done as the first step in theendovascular stenting of bilateral internal carotid artery dissec-tions that were diagnosed on initial CTA neck.
Other investigations performed included computed to-mography scan of the head (n = 52, 73%), magnetic resonanceimaging of the neck (n = 13, 18%), x-ray of the cervical spine(n = 7, 10%), laryngoscopy/bronchoscopy (n = 5, 7%), EGD(n = 3, 4%), and gastrografin swallow (n = 1, 1%). The absenceof esophageal, vertebral column, and spinal cord injuries in thisstudy precludes comment on the ability of CTA neck, magneticresonance imaging of the neck, cervical spine x-rays, EGD, orgastrografin swallow to diagnose these injuries.
OutcomesThe mortality rate was 14% (n = 10) (Table 1). Median
hospital LOS was 4 days [IQR, 2–7] with median ICU LOS of2 days [IQR, 0–3]. Median duration of mechanical ventilationwas 0 days [IQR, 0–3].
DISCUSSION
Blunt cerebrovascular injury (BCVI) screening has gar-nered attention in the trauma literature over the past decade.1–6
As noninvasive imaging modalities have improved over time,CTA of the neck is now the imaging modality of choice to screenpatients for BCVI.2 The utility of CTA neck to screen for injuryspecifically after near hangings, however, is incompletely de-fined by the current literature.
Near hangings are an infrequent mechanism of blunttrauma. Studies on the use of CTA of the neck for BCVI screen-ing have included near-hanging patients as 2% or less of the totalstudy population.2,7 Most of the literature on near hangings con-sists of case reports and very small case series only. One early
Treatment HLOS, d Mortality
Nonoperative 8 N
ASA 12 N
ASA 4 N
Operative repair of trachea, endovascularstenting of common carotid arteries
34 N
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Schellenberg et al.
study on near hangings did not examine the necessary diagnosticworkup nor the accuracy of commonly used investigations.8
More recently, a thorough study on near hangings advocated thatdiagnostic tests should be minimized among patients presentingwith a GCS of 15 and no concerning physical examination find-ings but did not systematically examine the diagnostic yield ofCTA of the neck after this mechanism of injury.9
The current study examined a cohort of 71 patients whopresented to our high-volume, American College of Surgeonslevel I trauma center over an 8-year study period after near hangings.Injuries occurred uncommonly in this population, with cervicalinjuries or anoxic brain injury present in only 14% of the studypopulation. Despite the low potential for injury, injuries that didoccur were clinically significant and consisted of internal carotidartery, vertebral artery, and laryngotracheal injuries. This is inagreement with previous studies that reported predominantly an-oxic brain injuries, laryngeal fractures, and carotid artery injuries.8,10
The need for surgical intervention after near hanging was ex-ceedingly rare and required in only one patient in this series.
In this series, CTA of the neckwas used in all patients whopresented after near hangings who did not undergo ED thoracot-omy. After a normal CTA neck on presentation, no patient in thisstudy went on to develop signs or symptoms of cervical injury orhad a cervical injury diagnosed by another imaging modalityduring hospital admission. One CTAwas falsely positive for vas-cular injury and required a duplex ultrasound to exclude internalcarotid injury. Taken together, these findings suggest that CTAneck may be an optimal screening investigation for injury to cer-vical structures after near hangings.
There are limitations to this study. First, there is a lack of agold standard against which to compare CTA results. Because ofthis, asymptomatic neck injuries may be missed by CTA. Thisprecludes comment on the diagnostic accuracy of CTA neck af-ter near hangings. Furthermore, this is a single-center retrospec-tive study. Because the rate of injury after near hangings is lowand diagnostic tests other than CTA neck are used infrequently,in the future, a large prospective multicenter study should bepursued to better understand this mechanism of injury.
In conclusion, near hangings are an infrequent cause ofblunt trauma that rarely cause cervical injury or require interven-tion. However, when injuries are sustained, they tend to occur tocritical structures such as the carotid and vertebral arteries, larynx,
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
and trachea. Therefore, effective injury screening in these patientsremains important. Although there is likely a subpopulation ofnear-hanging patients who do not require imaging investigations,these patients are undefined at the present time. We recommendCTA of the neck as the initial imaging investigation of choicein patients who present to the ED after near hangings.
AUTHORSHIP
M.S., K.I., and D.A. provided the study concept. M.S., Z.W., D.A., J.R., andV.V.V. performed the data collection. M.S., K.I., and Z.W. performed thedata analysis. M.S., K.I., L.L., and D.D. performed the data interpretation.All authors participated in writing and critically reviewing the final article.
DISCLOSURE
The authors declare no conflicts of interest.
REFERENCES1. Bruns BR, Tesoriero R, Kufera J, Sliker C, Laser A, Scalea TM, Stein DM.
Blunt cerebrovascular injury screening guidelines: what are we willing tomiss? J Trauma. 2014;76(3):691–695.
2. Wang AC, Charters MA, Thawani JP, Than KD, Sullivan SE, Graziano GP.Evaluating the use and utility of noninvasive angiography in diagnosing trau-matic blunt cerebrovascular injury. J Trauma. 2012;72(6):1599–1608.
3. BrombergWJ, Collier BC, Diebel LN, Dwyer KM, Holevar MR, Jacobs DG,Kurek SJ, Schreiber MA, Shapiro ML, Vogel TR. Blunt cerebrovascular in-jury practice management guidelines: the Eastern Association for the Sur-gery of Trauma. J Trauma. 2010;68(2):471–477.
4. Eastman AL, Chason DP, Perez CL, McAnulty AL, Minei JP. Computed to-mographic angiography for the diagnosis of blunt cervical vascular injury: isit ready for primetime? J Trauma. 2006;60(5):925–959.
5. Schneidereit NP, Simons R, Nicolaou S, GraebD, Brown DR,Kirkpatrick A,Redekop G, McKevitt EC, Neyestani A. Utility of screening for blunt vascu-lar neck injuries with computed tomographic angiography. J Trauma. 2006;60(1):209–215.
6. Cothren CC,Moore EE, RayCE, Ciesla DJ, Johnson JL,Moore JB, Burch JM.Screening for blunt cerebrovascular injuries is cost-effective. Am J Surg. 2005;190:849–854.
7. Emmett KP, Fabian TC,DiCocco JM, Zarzaur BL, CroceMA. Improving thescreening criteria for blunt cerebrovascular injury: the appropriate role forcomputed tomography angiography. J Trauma. 2011;70(5):1058–1063.
8. Salim A, Martin M, Sangthong B, Brown C, Rhee P, Demetriades D. Near-hanging injuries: a 10-year experience. Injury. 2006;37:435–439.
9. Subramanian M, Hranjec T, Liu L, Hodgman EI, Minshall CT, Minei JP. Acase for less workup in near hanging. J Trauma Acute Care Surg. 2016;81(5):925–930.
10. Nichols SD, McCarthy MC, Ekeh AP, Woods RJ, Walusimbi MS, Saxe JM.Outcome of cervical near-hanging injuries. J Trauma. 2009;66(1):174–178.
457
ealth, Inc. All rights reserved.
ORIGINAL ARTICLE
The impact of hypothermia on outcomes in massivelytransfused patients
Erica Louise Walsh Lester, MD, MSc, Erin E. Fox, PhD, John B. Holcomb, MD, Karen J. Brasel, MD, MPH,Eileen M. Bulger, MD, Mitchell J. Cohen, MD, Bryan A. Cotton, MD, MPH, Timothy C. Fabian, MD,
Jeffery D. Kerby, MD, PhD, Terrence O'Keefe, MB, ChB, MSPH, Sandro B. Rizoli, MD, PhD,Thomas M. Scalea, MD, Martin A. Schreiber, MD, Kenji Inaba, MD, and On behalf of the
PROPPR study group, Los Angeles, California
AAST Continuing Medical Education Article
Accreditation StatementThis activity has been planned and implemented in accordance with the Es-sential Areas and Policies of the Accreditation Council for Continuing MedicalEducation through the joint providership of the American College of Surgeonsand the American Association for the Surgery of Trauma. The AmericanCollege Surgeons is accredited by the ACCME to provide continuing medicaleducation for physicians.
AMA PRA Category 1 Credits™The American College of Surgeons designates this journal-based CME activity fora maximum of 1 AMA PRACategory 1 Credit™. Physicians should claim only the creditcommensurate with the extent of their participation in the activity.
Of the AMA PRACategory 1 Credit™ listed above, a maximum of 1 credit meetsthe requirements for self-assessment.
Credits can only be claimed online
ObjectivesAfter reading the featured articles published in the Journal of Trauma and AcuteCare Surgery, participants should be able to demonstrate increased understandingof the material specific to the article. Objectives for each article are featured atthe beginning of each article and online. Test questions are at the end of the article,with a critique and specific location in the article referencing the question topic.
Claiming CreditTo claim credit, please visit the AAST website at http://www.aast.org/ and click onthe “e-Learning/MOC” tab. You must read the article, successfully complete thepost-test and evaluation. Your CME certificate will be available immediately uponreceiving a passing score of 75% or higher on the post-test. Post-tests receiving a scoreof below 75% will require a retake of the test to receive credit.
System RequirementsThe system requirements are as follows: Adobe® Reader 7.0 or above installed; Internet Explorer® 7 and above; Firefox® 3.0 and above, Chrome® 8.0 and above, or
Safari™ 4.0 and above.
QuestionsIf you have any questions, please contact AAST at 800-789-4006. Paper test and evaluations will not be accepted.
Disclosure InformationIn accordance with the ACCME Accreditation Criteria, the American College of
Surgeons, as the accredited provider of this journal activity, must ensure that anyone
in a position to control the content of J Trauma Acute Care Surg articles selected for
CME credit has disclosed all relevant financial relationships with any commercial
interest. Disclosure forms are completed by the editorial staff, associate editors,
reviewers, and all authors. The ACCME defines a `commercial interest' as “any
entity producing, marketing, re-selling, or distributing health care goods or services
consumed by, or used on, patients.” “Relevant” financial relationships are those (in
any amount) that may create a conflict of interest and occur within the 12’months
preceding and during the time that the individual is engaged in writing the article. All
reported conflicts are thoroughly managed in order to ensure any potential bias
within the content is eliminated. However, if you’perceive a bias within the article,
please report the circumstances on the evaluation form.
Please note we have advised the authors that it is their responsibility to disclose within
the article if they are describing the use of a device, product, or drug that is not FDA
approved or the off-label use of an approved device, product, or drug or unapproved usage.
Disclosures of Significant Relationships withRelevant Commercial Companies/Organizationsby the Editorial StaffErnest E. Moore, Editor: PI, research support and shared U.S. patents Haemonetics;
PI, research support, Instrumentation Laboratory, Inc.; Co-founder, Thrombo Thera-
peutics. Associate Editors David Hoyt, Ronald V. Maier and Steven Shackford have
nothing to disclose. Editorial staff and Angela Sauaia have nothing to disclose.
Author DisclosuresJohn B. Holcomb, MD – Decisio Health/Prytime Medical/Terumo BCT, received money asconsultant/employment; Martin A. Schreiber, MD – Arsenal Medical/Velico Medical/Haemonetics, received grants as principal investigator.
Reviewer DisclosuresThe reviewers have nothing to disclose.
CostFor AAST members and Journal of Trauma and Acute Care Surgery subscribersthere is no charge to participate in this activity. For those who are not a memberor subscriber, the cost for each credit is $25.
458J Trauma Acute Care Surg
Volume 86, Number 3
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.

Sub
Fro
Ad
DO
J Trauma Acute Care SurgVolume 86, Number 3 Lester et al.
©
BACKGROUND: H
mitted: August 2, 2018, Accept15, 2018.m the Division of General Surgof Alberta, Edmonton, Alberta,(E.E.F., J.H.), Division of AcuSchool, University of Texas HeTrauma (K.B.), Critical CareOregon Health and Science Uand Critical Care (E.M.B.), Desity of Washington, Seattle, Wasity of Colorado, Denver, ColoA.C.), Division of Acute CareUniversity of Texas Health Sciand Surgical Critical Care (T.Ccine, University of Tennessee Hsion of Trauma (J.D.K.), BurnsSchool of Medicine, UniversityTrauma (T.O.), Critical Care andversity of Arizona, Tucson, AriMichael's Hospital, Toronto, OCenter (T.S.), University of Ma(M.A.S.), Critical Care and AcHealth and Science UniversityCritical Care (K.I.), LAC+UCalifornia, Los Angeles, Califodress for reprints: Kenji Inaba,+USC Medical Center, UniveIPT, C5L100, Los Angeles, CA
I: 10.1097/TA.00000000000021
2018 Wolters Kluwer Heal
ypothermia is associated with poor outcomes after injury. The relationship between hypothermia during contemporary large vol-ume resuscitation and blood product consumption is unknown.We evaluated this association, and the predictive value of hypother-mia on mortality.
METHODS: P
atients predicted to receive massive transfusion at 12 level 1 trauma centers were randomized in the Pragmatic Randomized Op-timal Platelet and Plasma Ratios (PROPPR) trial and were grouped into those who were hypothermic (<36°C) or normothermic(36–38.5°C) within the first 6 hours of emergency department arrival. The impact of hypothermia or normothermia on the volumeof blood product required during the first 24 hours was determined via negative binomial regression, adjusting for treatment arm,injury severity score, mechanism, demographics, pre–emergency department fluid volume, blood administered before becominghypothermic, pulse and systolic blood pressure on arrival, and the time exposed to hypothermic or normothermic temperatures.RESULTS: O
f 680 patients, 590 had a temperaturemeasured during the first 6 hours in hospital, and 399 experienced hypothermia. Themean numberof red blood cell (RBC) units given to all patients in the first 24 hours of admission was 8.8 (95% confidence interval [CI], 7.9–9.6). Inmultivariable analysis, every 1°C decrease in temperature below 36.0°C was associated with a 10% increase (incidence rate ratio, 0.90;95% CI, 0.89–0.92; p < 0.00) in consumption of RBCs during the first 24 hours of admission. There was no association betweenRBC administration and a temperature above 36°C. Hypothermia on arrival was an independent predictor of mortality, with an adjustedodds ratio of 2.7 (95% CI, 1.7–4.5; p < 0.00) for 24-hour mortality and 1.8 (95% CI, 1.3–2.4; p < 0.00) for 30-day mortality.CONCLUSION: H
ypothermia is associated with increase in blood product consumption and mortality. These findings support the maintenance of nor-mothermia in trauma patients and suggest that further investigation on the impact of cooling or rewarming during massive transfusionis warranted. (J Trauma Acute Care Surg. 2019;86: 458–463. Copyright © 2018 Wolters Kluwer Health, Inc. All rights reserved.)LEVEL OF EVIDENCE: P
rognostic, level III. KEYWORDS: H ypothermia; normothermia; massive transfusion; resuscitation; hemorrhage.T he mechanism underlying the coagulopathy associated withtrauma is an area of ongoing investigation. It is described
by varying and combined degrees of dysfibrinogenemia,hyperfibrinolysis, endothelial dysfunction, and impaired plateletactivity, dependent upon the magnitude of injury and severity ofshock.1–3 The impact of hypothermia on this process is a clini-cally relevant consideration, as the presence of decreased bodytemperature has been shown to impair clotting factor activityand platelet function.1,4
Trauma-induced hypothermia has an incidence of approxi-mately 43% to 65% and is associated with progression of coagulop-athy and poor outcomes in trauma patients.5–16 Jurkovich et al.9
ed: October 2, 2018, Published online: November
ery (E.L.W.L.), Department of Surgery, UniversityCanada; Center for Translational Injury Researchte Care Surgery, Department of Surgery, Medicalalth Science Center, Houston, Texas; Division ofand Acute Care Surgery, School of Medicine,niversity, Portland, Oregon; Division of Traumapartment of Surgery, School of Medicine, Univer-shington; Department of Surgery (M.C.), Univer-rado; Center for Translational Injury Research (B.Surgery, Department of Surgery, Medical School,ence Center, Houston, Texas; Division of Trauma.T.C.F.), Department of Surgery, College of Medi-ealth Science Center, Memphis, Tennessee; Divi-and Surgical Critical Care, Department of Surgery,of Alabama, Birmingham, Alabama; Division ofEmergency Surgery, Department of Surgery, Uni-
zona; Trauma and Acute Care Service (S.B.R.), St.ntario, Canada; R Adams Crowley Shock Traumaryland, Baltimore, Maryland; Division of Traumaute Care Surgery, Department of Surgery, Oregon, Portland, Oregon; and Division of Trauma andSC Medical Center, University of Southernrnia.MD, Division of Trauma and Critical Care, LACrsity of Southern California, 2051 Marengo St,90033; email: [email protected].
44
th, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
demonstrated that mortality increases as temperature decreasesacross groups with similar injury severity scores (ISSs) and fluidrequirements. In this seminal work, 32°C was identified as thecritical temperature, below which mortality was 100%.9 Subse-quently Gentilello et al.17 determined that rapid rewarming de-creases mortality and reduces fluid requirements. Hypothermiaafter cavitary exploration for traumatic injury has also been foundto be an independent predictor of mortality, with a stepwise de-crease in morality with increasing postoperative temperature.6
While it has been suggested that hypothermia contributesto operative blood loss, its impact on blood product requirementin trauma patients undergoing contemporary large volume resus-citation has, to the best of our knowledge, not been deter-mined.14,18,19 The objective of this study was to ascertain theindependent impact of hypothermia on blood product require-ments during initial resuscitation. Furthermore, we sought to ex-amine the association of hypothermia with mortality in criticallyinjured trauma patients undergoing contemporary large volumebalanced resuscitation.
METHODS
This secondary analysis was conducted using the data setthat was collected during the Pragmatic Randomized OptimalPlatelet and Plasma Ratios (PROPPR) trial.20 This was an Ex-ception From Informed Consent (EFIC) trial and was approvedby all institutional review boards at each of the 12 study sitesas well as the Human Research Protection Office of the USArmy. The study design and results have been described in detailpreviously.21 Briefly, severely injured patients, 15 years or older,expected to require a massive transfusion and admitted to a levelI trauma center were randomized to a 1:1:1 or 1:1:2 ratio ofplasma to platelets to red blood cells (RBCs). Clinical parame-ters including vital signs, diagnostic tests, and resuscitation mea-sures, as well as the time of each intervention or measurementwere captured in detail.
459
ealth, Inc. All rights reserved.
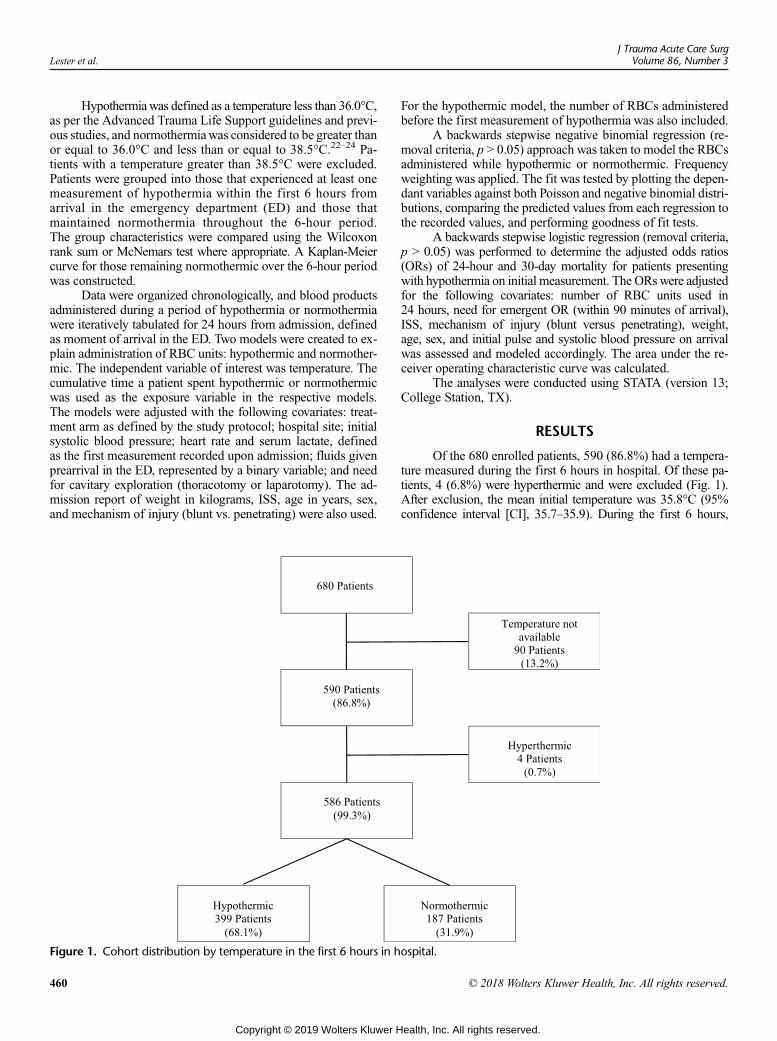
Lester et al.J Trauma Acute Care Surg
Volume 86, Number 3
Hypothermiawas defined as a temperature less than 36.0°C,as per the Advanced Trauma Life Support guidelines and previ-ous studies, and normothermiawas considered to be greater thanor equal to 36.0°C and less than or equal to 38.5°C.22–24 Pa-tients with a temperature greater than 38.5°C were excluded.Patients were grouped into those that experienced at least onemeasurement of hypothermia within the first 6 hours fromarrival in the emergency department (ED) and those thatmaintained normothermia throughout the 6-hour period.The group characteristics were compared using the Wilcoxonrank sum or McNemars test where appropriate. A Kaplan-Meiercurve for those remaining normothermic over the 6-hour periodwas constructed.
Data were organized chronologically, and blood productsadministered during a period of hypothermia or normothermiawere iteratively tabulated for 24 hours from admission, definedas moment of arrival in the ED. Two models were created to ex-plain administration of RBC units: hypothermic and normother-mic. The independent variable of interest was temperature. Thecumulative time a patient spent hypothermic or normothermicwas used as the exposure variable in the respective models.The models were adjusted with the following covariates: treat-ment arm as defined by the study protocol; hospital site; initialsystolic blood pressure; heart rate and serum lactate, definedas the first measurement recorded upon admission; fluids givenprearrival in the ED, represented by a binary variable; and needfor cavitary exploration (thoracotomy or laparotomy). The ad-mission report of weight in kilograms, ISS, age in years, sex,and mechanism of injury (blunt vs. penetrating) were also used.
Figure 1. Cohort distribution by temperature in the first 6 hours in h
460
Copyright © 2019 Wolters Kluwer H
For the hypothermic model, the number of RBCs administeredbefore the first measurement of hypothermia was also included.
A backwards stepwise negative binomial regression (re-moval criteria, p > 0.05) approach was taken to model the RBCsadministered while hypothermic or normothermic. Frequencyweighting was applied. The fit was tested by plotting the depen-dant variables against both Poisson and negative binomial distri-butions, comparing the predicted values from each regression tothe recorded values, and performing goodness of fit tests.
A backwards stepwise logistic regression (removal criteria,p > 0.05) was performed to determine the adjusted odds ratios(ORs) of 24-hour and 30-day mortality for patients presentingwith hypothermia on initial measurement. The ORswere adjustedfor the following covariates: number of RBC units used in24 hours, need for emergent OR (within 90 minutes of arrival),ISS, mechanism of injury (blunt versus penetrating), weight,age, sex, and initial pulse and systolic blood pressure on arrivalwas assessed and modeled accordingly. The area under the re-ceiver operating characteristic curve was calculated.
The analyses were conducted using STATA (version 13;College Station, TX).
RESULTS
Of the 680 enrolled patients, 590 (86.8%) had a tempera-ture measured during the first 6 hours in hospital. Of these pa-tients, 4 (6.8%) were hyperthermic and were excluded (Fig. 1).After exclusion, the mean initial temperature was 35.8°C (95%confidence interval [CI], 35.7–35.9). During the first 6 hours,
ospital.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
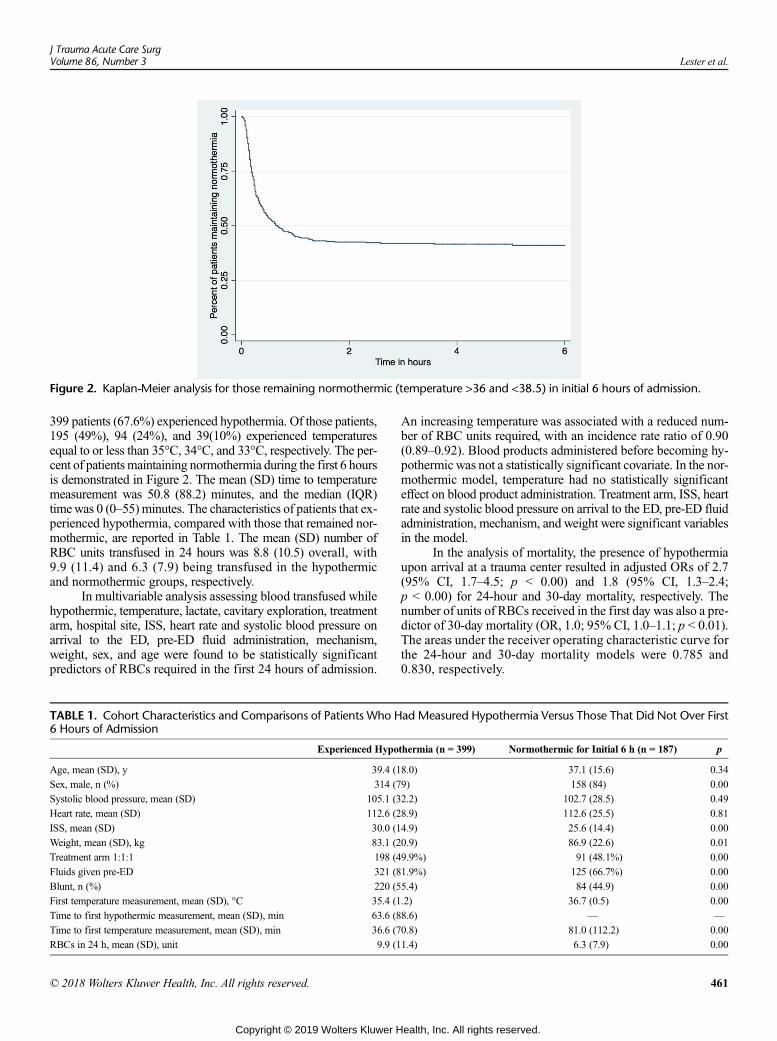
Figure 2. Kaplan-Meier analysis for those remaining normothermic (temperature >36 and <38.5) in initial 6 hours of admission.
J Trauma Acute Care SurgVolume 86, Number 3 Lester et al.
399 patients (67.6%) experienced hypothermia. Of those patients,195 (49%), 94 (24%), and 39(10%) experienced temperaturesequal to or less than 35°C, 34°C, and 33°C, respectively. The per-cent of patientsmaintaining normothermia during the first 6 hoursis demonstrated in Figure 2. The mean (SD) time to temperaturemeasurement was 50.8 (88.2) minutes, and the median (IQR)timewas 0 (0–55) minutes. The characteristics of patients that ex-perienced hypothermia, compared with those that remained nor-mothermic, are reported in Table 1. The mean (SD) number ofRBC units transfused in 24 hours was 8.8 (10.5) overall, with9.9 (11.4) and 6.3 (7.9) being transfused in the hypothermicand normothermic groups, respectively.
In multivariable analysis assessing blood transfused whilehypothermic, temperature, lactate, cavitary exploration, treatmentarm, hospital site, ISS, heart rate and systolic blood pressure onarrival to the ED, pre-ED fluid administration, mechanism,weight, sex, and age were found to be statistically significantpredictors of RBCs required in the first 24 hours of admission.
TABLE 1. Cohort Characteristics and Comparisons of Patients Who H6 Hours of Admission
Experienced Hypo
Age, mean (SD), y 39.4 (1
Sex, male, n (%) 314 (7
Systolic blood pressure, mean (SD) 105.1 (3
Heart rate, mean (SD) 112.6 (2
ISS, mean (SD) 30.0 (1
Weight, mean (SD), kg 83.1 (2
Treatment arm 1:1:1 198 (4
Fluids given pre-ED 321 (8
Blunt, n (%) 220 (5
First temperature measurement, mean (SD), °C 35.4 (1
Time to first hypothermic measurement, mean (SD), min 63.6 (8
Time to first temperature measurement, mean (SD), min 36.6 (7
RBCs in 24 h, mean (SD), unit 9.9 (1
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
An increasing temperature was associated with a reduced num-ber of RBC units required, with an incidence rate ratio of 0.90(0.89–0.92). Blood products administered before becoming hy-pothermic was not a statistically significant covariate. In the nor-mothermic model, temperature had no statistically significanteffect on blood product administration. Treatment arm, ISS, heartrate and systolic blood pressure on arrival to the ED, pre-ED fluidadministration, mechanism, and weight were significant variablesin the model.
In the analysis of mortality, the presence of hypothermiaupon arrival at a trauma center resulted in adjusted ORs of 2.7(95% CI, 1.7–4.5; p < 0.00) and 1.8 (95% CI, 1.3–2.4;p < 0.00) for 24-hour and 30-day mortality, respectively. Thenumber of units of RBCs received in the first day was also a pre-dictor of 30-day mortality (OR, 1.0; 95% CI, 1.0–1.1; p < 0.01).The areas under the receiver operating characteristic curve forthe 24-hour and 30-day mortality models were 0.785 and0.830, respectively.
ad Measured Hypothermia Versus Those That Did Not Over First
thermia (n = 399) Normothermic for Initial 6 h (n = 187) p
8.0) 37.1 (15.6) 0.34
9) 158 (84) 0.00
2.2) 102.7 (28.5) 0.49
8.9) 112.6 (25.5) 0.81
4.9) 25.6 (14.4) 0.00
0.9) 86.9 (22.6) 0.01
9.9%) 91 (48.1%) 0.00
1.9%) 125 (66.7%) 0.00
5.4) 84 (44.9) 0.00
.2) 36.7 (0.5) 0.00
8.6) — —
0.8) 81.0 (112.2) 0.00
1.4) 6.3 (7.9) 0.00
461
ealth, Inc. All rights reserved.

Lester et al.J Trauma Acute Care Surg
Volume 86, Number 3
DISCUSSION
In this large cohort of critically ill, massively transfusedpatients admitted to a level 1 trauma center, we described the in-dependent association between hypothermic temperatures andboth mortality and blood product requirement. Confirming pre-vious work, despite the aggressive contemporary resuscitationefforts, hypothermia at ED presentation remained an indepen-dent predictor of mortality, with adjusted ORs of 2.7 (95% CI,1.7–4.5; p < 0.00) and 1.8 (95% CI, 1.3–2.4; p < 0.00) for24-hour and 30-day mortality, respectively. Furthermore, analy-sis of this comprehensive transfusion data set demonstrated thatan increase in temperature by 1°C, when hypothermic, is associ-ated with a 10% reduction in the RBC transfusion requirement.This relationship is independent of other factors thought to in-fluence transfusion requirements. When normothermia ismaintained during the first 6 hours in hospital, temperature in-crease is not a predictor of blood cell transfusion requirement.The implication is that, using the mean number of RBCs trans-fused in this study, a patient with a temperature of 34°C will re-quire one more unit of RBCswhen compared with a patient witha temperature of 36°C, after adjustment for injury severity andother factors influencing transfusion requirements. This repre-sents a significant increase in resource use, cost, and patient risk,supporting the avoidance of hypothermia in trauma patients.
The size of our study cohort was suitable for determiningthe impact of hypothermia on both blood product use and mor-tality. The study exclusion criteria, which included the exclusionof patients requiring CPR for greater than 5 minutes and thoseundergoing an emergency thoracotomy, increase the homogene-ity of the cohort. The rate of hypothermia and other patient de-mographics in our study was similar to that published in theliterature.1,15 The ISS was higher in the hypothermic group,which concurs with the findings of Beilman et al.15 The hypo-thermic group weighed less than the normothermic group. Thismay suggest a protective effect of body mass, with regards tobody temperature. Similarly, there were more females in the hy-pothermic group, which may be reflective of body compositionand a subsequent protective effect. Importantly, the hypothermicpatients were more likely to receive fluids before arrival in theED. Whether this represents a more severe injury and tenuoushemodynamic state or a causal mechanism for hypothermia it-self cannot be determined from this study. Adjusting for theuse of prearrival fluids in the explanatory models parses itspotential effect on transfusion requirements from that of tem-perature itself.
There was a statistically significant difference between thedistribution of treatment arms between the two temperaturegroups. However, the difference may not be clinically relevant,as it was less than 2%. The presence of more 1:1:1 patients,who by definition received more blood product then the 1:1:2patients, in the hypothermic arm may reflect the use of bloodproducts or may simply be stochastic. The reported incidencerate ratios were adjusted for patient treatment arm.
While the granular and frequent data collection of the ran-domized controlled trial protocol creates an advantageous cohortin which to study the impact of hypothermia, several limitationsof this work merit consideration. First, the anatomical locationand method of temperature measurement were not standardized
462
Copyright © 2019 Wolters Kluwer H
or documented. Given the variability in the devices used and theheterogeneity of temperatures taken at different locations, alongwith the pooling of data from 12 sites, the temperature measure-ments may have introduced endogeneity into the models. More-over, warming protocols differ between sites and may haveintroduced bias as well.
The design of the trial was such that the massive transfu-sion protocol ceased once the most responsible physiciandeemed hemostasis had been achieved. However, further bloodproducts could be administered based on institutional guide-lines, local laboratory results, and clinical judgment.25 There-fore, our use of RBC units as a surrogate for overall productuse, based on the study ratios, may introduce error because ofadditional blood product use after protocol termination.
Of the 680 patients enrolled in the PROPPR study,90 patients, or 13.2%, did not have temperature measured within6 hours of ED arrival. The mean (SD) time to temperature mea-surement was 50.8 (88.2) minutes; however, the median (IQR)time was 0 (0–55) minutes. This demonstrates that, while mostpatients had a temperature measured, there was variability inthe time to temperature measurement. As well, hypothermic pa-tients had their temperature measured earlier: this may representan increased propensity to check temperature in sicker, more se-verely injured patients. Given the evidence that hypothermia isassociated with increased blood product use and mortality, thisstudy illustrates possible areas for improvement in baseline vitalsign assessment.
Caution should be applied to extracting causation from as-sociation within the context of this study. While initial tempera-ture measurements occurred before few, or any, blood productswere administered, many of the subsequent temperatures occur-ring during the initial 6 hours occurred after transfusions had oc-curred and thus may be influenced by the product temperatureitself. Unfortunately, too few patients had temperatures recordedby EMS or before initiation of massive transfusion to power amodel isolating the influence of body temperature during thetime between injury and ED arrival or commencement of mas-sive transfusion. Collecting this information is difficult, as thedecision to commence a transfusion protocol is made based onparameters other than temperature, making temperature mea-surement lower priority than other metrics. Therefore, whiletemperature and transfusion requirements are associated in awell-adjusted model, supporting the paradigm that normothermiais superior, further work is needed to elicit the effect of activelywarming hypothermic trauma patients. Furthermore, given thesuccess of controlled hypothermia in organ preservation and car-diac arrest models, the interface between trauma-induced, uncon-trolled hypothermia and induced hypothermia merits furtherinvestigation.26 Studying the role of hypothermia in trauma onthe full complex state of injury, rather than isolated componentssuch as energy stores, acidosis, and coagulopathy, will aid inelucidating the optimal approach to resuscitation of the severelyinjured patient.26,27
CONCLUSION
Hypothermia is associated with an increase in blood prod-uct consumption and is an independent predictor of mortality.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Lester et al.
Measuring the impact of restoring normothermia in severely in-jured patients warrants further investigation.
AUTHORSHIP
E.L.W.L. collaborated on the study design, performed the statistical anddata analysis, and drafted and extensively revised the final article. E.E.F col-laborated on the study design, reviewed the data analysis, aided with thenavigation of the retrospective data, and contributed to the editing of thearticle. J.B.H., K.J.B., E.M.B.,M.J.C., B.A.C., T.C.F., J.D.K., T.O., S.R., T.M.S.,and M.A.S. extensively revised the final article. K.I. provided content ex-pertise, oversaw and collaborated on the study design, and assisted exten-sively with the article revision. All authors have approved the final article.
DISCLOSURE
The authors declare no conflicts of interest.
REFERENCES1. Soreide K. Clinical and translational aspects of hypothermia in major trauma
patients: from pathophysiology to prevention, prognosis and potential preser-vation. Injury. 2014;45(4):647–654.
2. Lier H, Krep H, Schroeder S, Stuber F. Preconditions of hemostasis intrauma: a review. The influence of acidosis, hypocalcemia, anemia, andhypothermia on functional hemostasis in trauma. J Trauma. 2008;65(4):951–960.
3. Watts DD, Trask A, Soeken K, Perdue P, Dols S, Kaufmann C. Hypothermiccoagulopathy in trauma: effect of varying levels of hypothermia on enzymespeed, platelet function, and fibrinolytic activity. J Trauma. 1998;44(5):846–854.
4. Ferrara A, MacArthur JD, Wright HK, Modlin IM, McMillen MA. Hypo-thermia and acidosis worsen coagulopathy in the patient requiring massivetransfusion. Am J Surg. 1990;160(5):515–518.
5. Trentzsch H, Huber-Wagner S, Hildebrand F, Kanz KG, Faist E, Piltz S,Lefering R, TraumaRegistry DGU. Hypothermia for prediction of death inseverely injured blunt trauma patients. Shock. 2012;37(2):131–139.
6. Inaba K, Teixeira PG, Rhee P, Brown C, Salim A, DuBose J, Chan LS,Demetriades D. Mortality impact of hypothermia after cavitary explorationsin trauma.World J Surg. 2009;33(4):864–869.
7. Engels PT, Rezende-Neto JB, Al Mahroos M, Scarpelini S, Rizoli SB,Tien HC. The natural history of trauma-related coagulopathy: implicationsfor treatment. J Trauma. 2011;71(5 Suppl 1):S448–S455.
8. Kashuk JL, Moore EE, Millikan JS, Moore JB. Major abdominal vasculartrauma—a unified approach. J Trauma. 1982;22(8):672–679.
9. Jurkovich GJ, Greiser WB, LutermanA, Curreri PW. Hypothermia in traumavictims: an ominous predictor of survival. J Trauma. 1987;27(9):1019–1024.
10. Beale E, Zhu J, Chan L, Shulman I, HarwoodR,DemetriadesD. Blood trans-fusion in critically injured patients: a prospective study. Injury. 2006;37(5):455–465.
11. Martin RS, Kilgo PD, Miller PR, Hoth JJ, Meredith JW, Chang MC. Injury-associated hypothermia: an analysis of the 2004National TraumaData Bank.Shock. 2005;24(2):114–118.
12. Gregory JS, Flancbaum L, Townsend MC, Cloutier CT, Jonasson O. Inci-dence and timing of hypothermia in trauma patients undergoing operations.J Trauma. 1991;31(6):795–800.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
13. Kongsayreepong S, Chaibundit C, Chadpaibool J, Komoltri C,Suraseranivongse S, Suwannanonda P, Raksamanee EO, Noocharoen P,Silapadech A, Parakkamodom S, et al. Predictor of core hypothermia andthe surgical intensive care unit. Anesth Analg. 2003;96(3):826–833; tableof contents.
14. Garrison JR, Richardson JD, Hilakos AS, Spain DA,WilsonMA,Miller FB,Fulton RL. Predicting the need to pack early for severe intra-abdominal hem-orrhage. J Trauma. 1996;40(6):923–927; discussion 927-9.
15. Beilman GJ, Blondet JJ, Nelson TR, Nathens AB, Moore FA, Rhee P,Puyana JC, Moore EE, Cohn SM. Early hypothermia in severely injuredtrauma patients is a significant risk factor for multiple organ dysfunction syn-drome but not mortality. Ann Surg. 2009;249(5):845–850.
16. Bennett BL, Holcomb JB. Battlefield trauma-induced hypothermia: transitioningthe preferred method of casualty rewarming. Wilderness Environ Med.2017;28(2S):S82–S89.
17. Gentilello LM, Jurkovich GJ, Stark MS, Hassantash SA, O'Keefe GE. Is hy-pothermia in the victim of major trauma protective or harmful? A random-ized, prospective study. Ann Surg. 1997;226(4):439–449.
18. Bernabei AF, Levison MA, Bender JS. The effects of hypothermia andinjury severity on blood loss during trauma laparotomy. J Trauma.1992;33(6):835–839.
19. Arthurs Z, Cuadrado D, Beekley A, Grathwohl K, Perkins J, Rush R,Sebesta J. The impact of hypothermia on trauma care at the 31st combat sup-port hospital. Am J Surg. 2006;191(5):610–614.
20. Holcomb JB, Tilley BC, Baraniuk S, Fox EE, Wade CE, Podbielski JM,del Junco DJ, Brasel KJ, Bulger EM, Callcut RA, et al. Transfusion ofplasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortalityin patients with severe trauma: the PROPPR randomized clinical trial. JAMA.2015;313(5):471–482.
21. Baraniuk S, Tilley BC, del Junco DJ, Fox EE, van Belle G, Wade CE,Podbielski JM, Beeler AM, Hess JR, Bulger EM, et al. Pragmatic Random-ized Optimal Platelet and Plasma Ratios (PROPPR) trial: design, rationaleand implementation. Injury. 2014;45(9):1287–1295.
22. Wade CE, Salinas J, Eastridge BJ, McManus JG, Holcomb JB. Admissionhypo- or hyperthermia and survival after trauma in civilian and military en-vironments. Int J Emerg Med. 2011;4(1):35.
23. Klauke N, Graff I, Fleischer A, Boehm O, Guttenthaler V, Baumgarten G,Meybohm P,WittmannM. Effects of prehospital hypothermia on transfusionrequirements and outcomes: a retrospective observatory trial. BMJ Open.2016;6(3):e009913.
24. ATLSSubcommittee, American College of Surgeonsâ Committee on Trauma;International ATLS working group. Advanced trauma life support (ATLS(R)):the ninth edition. J Trauma Acute Care Surg. 2013;74(5):1363–1366.
25. UTHeatlh. Pragmatic, Randomized Optimal Platelet and Plasma Ratios(PROPPR) Protocol. UTHeatlh; Houston, TX: 2012.
26. Alam HB, Pusateri AE, Kindzelski A, Egan D, Hoots K, Andrews MT,Rhee P, Tisherman S, Mann K, Vostal J, et al. Hypothermia and hemostasisin severe trauma: a new crossroads workshop report. J Trauma Acute CareSurg. 2012;73(4):809–817.
27. Tisherman SA, Alam HB, Rhee PM, Scalea TM, Drabek T, Forsythe RM,Kochanek McCm PM. Development of the Emergency Preservation andResuscitation for Cardiac Arrest from Trauma (EPR-CAT) Clinical Trial.J Trauma Acute Care Surg. 2017;83(5):803–809.
463
ealth, Inc. All rights reserved.

ORIGINAL ARTICLE
Recurring emergency general surgery: Characterizinga vulnerable population
Nicole Lunardi, MSPH, Ambar Mehta, MD, MPH, Hiba Ezzeddine, MD, Joseph K. Canner, MHS,Mohammad Hamidi, MD, Faisal Jehan, MD, Bellal A. Joseph, MD, Avery B. Nathens, MD, MPH, PhD,David T. Efron, MD, Jose Diaz, Jr, MD, and Joseph V. Sakran, MD, MPH, MPA, Baltimore, Maryland
AAST Continuing Medical Education Article
Accreditation StatementThis activity has been planned and implemented in accordance with the Es-sential Areas and Policies of the Accreditation Council for Continuing MedicalEducation through the joint providership of the American College of Surgeonsand the American Association for the Surgery of Trauma. The AmericanCollege Surgeons is accredited by the ACCME to provide continuing medicaleducation for physicians.
AMA PRA Category 1 Credits™The American College of Surgeons designates this journal-based CME activity fora maximum of 1 AMA PRA Category 1 Credit™. Physicians should claim only thecredit commensurate with the extent of their participation in the activity.
Of the AMA PRA Category 1 Credit™ listed above, a maximum of 1 creditmeets the requirements for self-assessment.
Credits can only be claimed online
ObjectivesAfter reading the featured articles published in the Journal of Trauma and AcuteCare Surgery, participants should be able to demonstrate increased understandingof the material specific to the article. Objectives for each article are featured at thebeginning of each article and online. Test questions are at the end of the article,with a critique and specific location in the article referencing the question topic.
Claiming CreditTo claim credit, please visit the AAST website at http://www.aast.org/ and click onthe “e-Learning/MOC” tab. You must read the article, successfully complete thepost-test and evaluation. Your CME certificate will be available immediately uponreceiving a passing score of 75% or higher on the post-test. Post-tests receiving ascore of below 75% will require a retake of the test to receive credit.
System RequirementsThe system requirements are as follows: Adobe® Reader 7.0 or above installed; Internet Explorer® 7 and above; Firefox® 3.0 and above, Chrome® 8.0 and above, or
Safari™ 4.0 and above.
QuestionsIf you have any questions, please contact AAST at 800-789-4006. Paper test and evaluations will not be accepted.
Disclosure InformationIn accordance with the ACCME Accreditation Criteria, the American College of
Surgeons, as the accredited provider of this journal activity, must ensure that anyone
in a position to control the content of J Trauma Acute Care Surg articles selected for
CME credit has disclosed all relevant financial relationships with any commercial
interest. Disclosure forms are completed by the editorial staff, associate editors,
reviewers, and all authors. The ACCME defines a `commercial interest' as “any
entity producing, marketing, re-selling, or distributing health care goods or services
consumed by, or used on, patients.” “Relevant” financial relationships are those (in
any amount) that may create a conflict of interest and occur within the 12’months
preceding and during the time that the individual is engaged in writing the article. All
reported conflicts are thoroughly managed in order to ensure any potential bias
within the content is eliminated. However, if you’perceive a bias within the article,
please report the circumstances on the evaluation form.
Please note we have advised the authors that it is their responsibility to disclose within
the article if they are describing the use of a device, product, or drug that is not FDA
approved or the off-label use of an approved device, product, or drug or unapproved usage.
Disclosures of Significant Relationships withRelevant Commercial Companies/Organizationsby the Editorial StaffErnest E. Moore, Editor: PI, research support and shared U.S. patents Haemonetics;
PI, research support, Instrumentation Laboratory, Inc.; Co-founder, Thrombo Thera-
peutics. Associate Editors David Hoyt, Ronald V. Maier and Steven Shackford have
nothing to disclose. Editorial staff and Angela Sauaia have nothing to disclose.
Author DisclosuresJose Diaz, Jr, MD – Acute Innovations, received money as a consultant.
Reviewer DisclosuresThe reviewers have nothing to disclose.
CostFor AAST members and Journal of Trauma and Acute Care Surgery subscribersthere is no charge to participate in this activity. For those who are not a memberor subscriber, the cost for each credit is $25.
464J Trauma Acute Care Surg
Volume 86, Number 3
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.

Sub
Fro
Thi
Ad
Sup
DO
J Trauma Acute Care SurgVolume 86, Number 3 Lunardi et al.
©
BACKGROUND: L
mitted: September 7, 2018, Rev2018, Published online: Novemm the School of Medicine (N.L.Department of Surgery (A.MMedical Center, New York, ND.T.E.,J.V.S.), Johns HopkinsSurgery (M.H., F.J., B.A.J.),Tucson, Arizona; DepartmenToronto, Ontario, Canada; andShock Trauma, School of Medis study was presented at the 77thof Acute Care Surgery, Septemdress for reprints: Joseph V. SaSurgery, Department of SurgerSuite 61078, Baltimore, MD 21plemental digital content is avaithe printed text, and links to thearticle on the journal’s Web sit
I: 10.1097/TA.00000000000021
2018 American Associatio
imited data exist for long-term outcomes after emergency general surgeries (EGSs) in the United States. This study aimed to char-acterize the incidence of inpatient readmissions and additional operations within 6 months of an EGS procedure.
METHODS: I
n this retrospective observational study, we identified adults (≥18 years old) undergoing one of seven common EGS procedures(appendectomies, cholecystectomies, small bowel resections, large bowel resections, control of gastrointestinal [GI] ulcers andbleeding, peritoneal adhesiolysis, and exploratory laparotomies) who were discharged alive in the 2010–2015 National Readmis-sions Database. Outcomes included the rates of all-cause inpatient readmissions and of undergoing a second EGS procedure, bothwithin 6 months. Multivariable logistic regression models identified risk factors of reoperation, adjusting for patient, clinical, andhospital factors.RESULTS: O
f 706,678 patients undergoing an EGS procedure 131,291 (18.6%) had an inpatient readmission within 6 months. Among thosereadmitted, 15,178 (11.6%) underwent a second EGS procedure, occurring at a median of 45 days (interquartile range, 15–95).After adjustment, notable predictors of reoperation included male sex (adjusted odds ratio [aOR], 1.06 [95% confidence interval,1.01–1.10]); private, nonprofit hospitals (aOR, 1.09 [1.02–1.17]); private, investor-owned hospitals (aOR, 1.09 [1.00–1.85]); dis-charge to short-term hospital (aOR, 1.35 [1.04–1.74]); discharge with home health care (aOR, 1.19 [1.13–1.25]); and index pro-cedure of control of GI ulcer and bleeding (aOR, 9.38 [8.75–10.05]), laparotomy (aOR, 7.62 [6.92–8.40]), or large bowel resection(aOR, 6.94 [6.44–7.47]).CONCLUSION: O
ne fifth of patients undergoing an EGS procedure had an inpatient readmission within 6 months, where one in nine of thoseunderwent a second EGS procedure. As half of all second EGS procedures occurred within 6 weeks of the index procedure, iden-tifying patients with the highest health care needs (index procedure type and discharge needs) may identify patients at risk for sub-sequent reoperation in nonemergency settings. (J Trauma Acute Care Surg. 2019;86: 464–470. Copyright © 2018 AmericanAssociation for the Surgery of Trauma)LEVEL OF EVIDENCE: E
pidemiological, level III. KEYWORDS: E mergency general surgery; readmissions; outcomes; recurring operation.T rauma and acute care surgeons care for a growing number ofacutely ill high-risk patients who require emergency general
surgery (EGS) procedures. Currently, 7.1% of all inpatienthospital admissions, or more than 3 million patients annually,undergo an EGS evaluation, of which 30% undergo a surgicalprocedure.1 EGS procedures have been independently associ-ated with increased odds of morbidity and mortality in numer-ous studies. Specifically, half of all EGS patients experiencea postoperative complication, with 33% having a majorcomplication.2–4 Postoperative complications have been corre-lated with 30-day readmission rates, along with patient comor-bidities and hospital disposition.5,6 Thirty-day postoperativemortality rate is as high as 13%, which is significantly higherthan patients undergoing the same procedures electively.2
In 2013, the American Association for the Surgery ofTrauma Committee of Severity Assessment and Patient Outcomesdefined the scope of EGS as “Any patient (inpatient or emergencydepartment) requiring an emergency surgical evaluation (operative
ised: October 25, 2018, Accepted: November 11,ber 28, 2018.), Johns Hopkins University, Baltimore, Maryland;.), NewYork-Presbyterian Columbia Universityew York; Department of Surgery (H.E., J.K.C.,Hospital, Baltimore, Maryland; Department ofUniversity of Arizona College of Medicine,t of Surgery (A.B.N.), University of Toronto,Department of Surgery (J.D.J.), R Adams Cowleycine, University of Maryland, Maryland.Annual Meeting of AASTand Clinical Congressber 26–29, 2018, in San Diego, California.kran, MD, MPH, MPA, Division of Acute Carey, Johns Hopkins Hospital, Sheikh Zayed Tower,287; email: [email protected] for this article. Direct URL citations appear indigital files are provided in the HTML text of thise (www.jtrauma.com).
51
n for the Surgery of Trauma
Copyright © 2019 Wolters Kluwer H
or non-operative) for diseases within the realm of general surgeryas defined by the American Board of Surgery.” The diseases andprocedures of EGS span 621 International Classification ofDiseases, Ninth Revision, Schedule Modification (ICD-9) codesand 149 Current Procedural Terminology codes, respectively.7
Despite the recent advances in defining the scope and out-comes of EGS, there is a paucity of data regarding long-termEGS outcomes. In 2013, Shafi et al.8 published a comprehensiveassessment, on behalf of the American Association for theSurgery of Trauma, to define EGS, providing the first listof ICD-9 diagnosis codes. Other studies followed lookingat outcomes, readmissions, and their risk factors in EGSfrom national databases within 30 days of operation.2,6,9
To our knowledge, few have carefully characterized long-termEGS outcomes. As such, this study sought to characterize read-mission rates and subsequent EGS operations within 6 monthsof an index EGS procedure.
METHODS
Study PopulationThe Healthcare Cost and Utilization Project maintains the
Nationwide Readmissions Database (NRD). Annually, the NRDcaptures approximately 17 million unweighted, all payer hos-pital discharges from up to 27 states in the United States.10 Weused the 2010–2015NRD to identify patients at least 18 years ofage who underwent an EGS procedure, were discharged alive,and had 6 months of discharge data available. Given that thisis a retrospective observational study, no power analysis wasperformed to determine sample size a priori.
Despite the breadth of the EGS field, seven proceduresaccount for 80% of EGS volume, complications, death, andcost.7 As such, we used ICD-9 Clinical Modification codes toidentify patients who underwent one of the seven procedures:appendectomy (47.0X), cholecystectomy (51.263X), small bowel
465
ealth, Inc. All rights reserved.
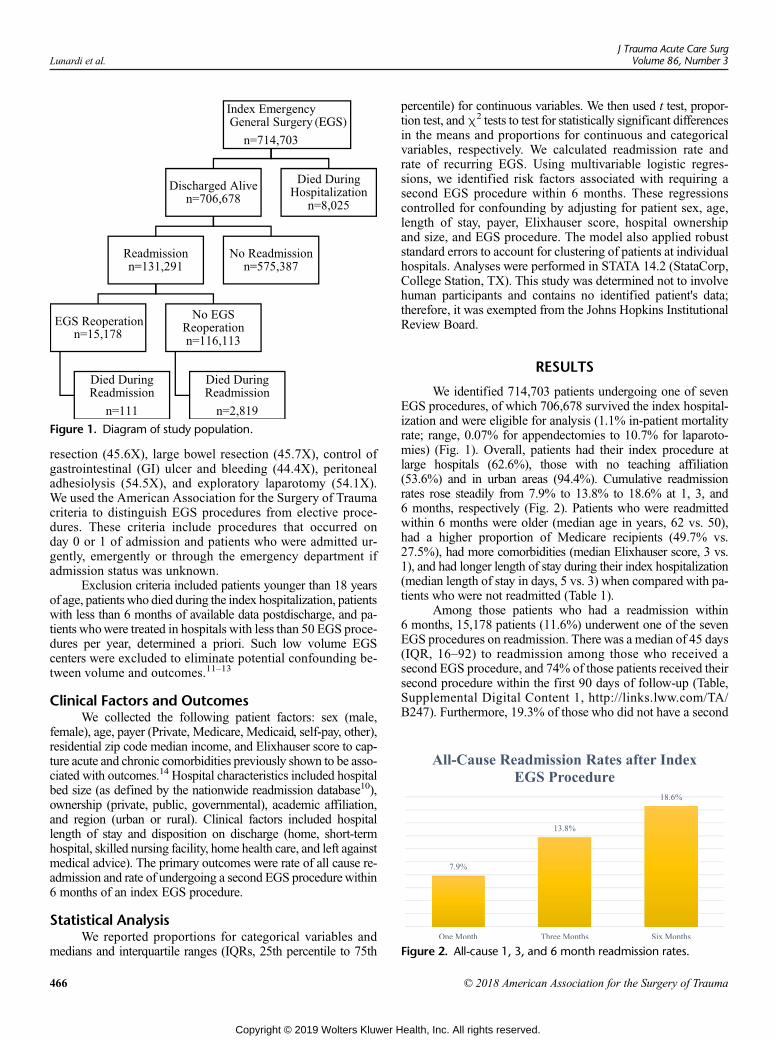
Figure 2. All-cause 1, 3, and 6 month readmission rates.
Figure 1. Diagram of study population.
Lunardi et al.J Trauma Acute Care Surg
Volume 86, Number 3
resection (45.6X), large bowel resection (45.7X), control ofgastrointestinal (GI) ulcer and bleeding (44.4X), peritonealadhesiolysis (54.5X), and exploratory laparotomy (54.1X).We used the American Association for the Surgery of Traumacriteria to distinguish EGS procedures from elective proce-dures. These criteria include procedures that occurred onday 0 or 1 of admission and patients who were admitted ur-gently, emergently or through the emergency department ifadmission status was unknown.
Exclusion criteria included patients younger than 18 yearsof age, patientswho died during the index hospitalization, patientswith less than 6 months of available data postdischarge, and pa-tients whowere treated in hospitals with less than 50 EGS proce-dures per year, determined a priori. Such low volume EGScenters were excluded to eliminate potential confounding be-tween volume and outcomes.11–13
Clinical Factors and OutcomesWe collected the following patient factors: sex (male,
female), age, payer (Private, Medicare, Medicaid, self-pay, other),residential zip code median income, and Elixhauser score to cap-ture acute and chronic comorbidities previously shown to be asso-ciated with outcomes.14 Hospital characteristics included hospitalbed size (as defined by the nationwide readmission database10),ownership (private, public, governmental), academic affiliation,and region (urban or rural). Clinical factors included hospitallength of stay and disposition on discharge (home, short-termhospital, skilled nursing facility, home health care, and left againstmedical advice). The primary outcomes were rate of all cause re-admission and rate of undergoing a second EGS procedurewithin6 months of an index EGS procedure.
Statistical AnalysisWe reported proportions for categorical variables and
medians and interquartile ranges (IQRs, 25th percentile to 75th
466
Copyright © 2019 Wolters Kluwer H
percentile) for continuous variables. We then used t test, propor-tion test, andχ2 tests to test for statistically significant differencesin the means and proportions for continuous and categoricalvariables, respectively. We calculated readmission rate andrate of recurring EGS. Using multivariable logistic regres-sions, we identified risk factors associated with requiring asecond EGS procedure within 6 months. These regressionscontrolled for confounding by adjusting for patient sex, age,length of stay, payer, Elixhauser score, hospital ownershipand size, and EGS procedure. The model also applied robuststandard errors to account for clustering of patients at individualhospitals. Analyses were performed in STATA 14.2 (StataCorp,College Station, TX). This study was determined not to involvehuman participants and contains no identified patient's data;therefore, it was exempted from the Johns Hopkins InstitutionalReview Board.
RESULTS
We identified 714,703 patients undergoing one of sevenEGS procedures, of which 706,678 survived the index hospital-ization and were eligible for analysis (1.1% in-patient mortalityrate; range, 0.07% for appendectomies to 10.7% for laparoto-mies) (Fig. 1). Overall, patients had their index procedure atlarge hospitals (62.6%), those with no teaching affiliation(53.6%) and in urban areas (94.4%). Cumulative readmissionrates rose steadily from 7.9% to 13.8% to 18.6% at 1, 3, and6 months, respectively (Fig. 2). Patients who were readmittedwithin 6 months were older (median age in years, 62 vs. 50),had a higher proportion of Medicare recipients (49.7% vs.27.5%), had more comorbidities (median Elixhauser score, 3 vs.1), and had longer length of stay during their index hospitalization(median length of stay in days, 5 vs. 3) when compared with pa-tients who were not readmitted (Table 1).
Among those patients who had a readmission within6 months, 15,178 patients (11.6%) underwent one of the sevenEGS procedures on readmission. There was a median of 45 days(IQR, 16–92) to readmission among those who received asecond EGS procedure, and 74% of those patients received theirsecond procedure within the first 90 days of follow-up (Table,Supplemental Digital Content 1, http://links.lww.com/TA/B247). Furthermore, 19.3% of those who did not have a second
© 2018 American Association for the Surgery of Trauma
ealth, Inc. All rights reserved.
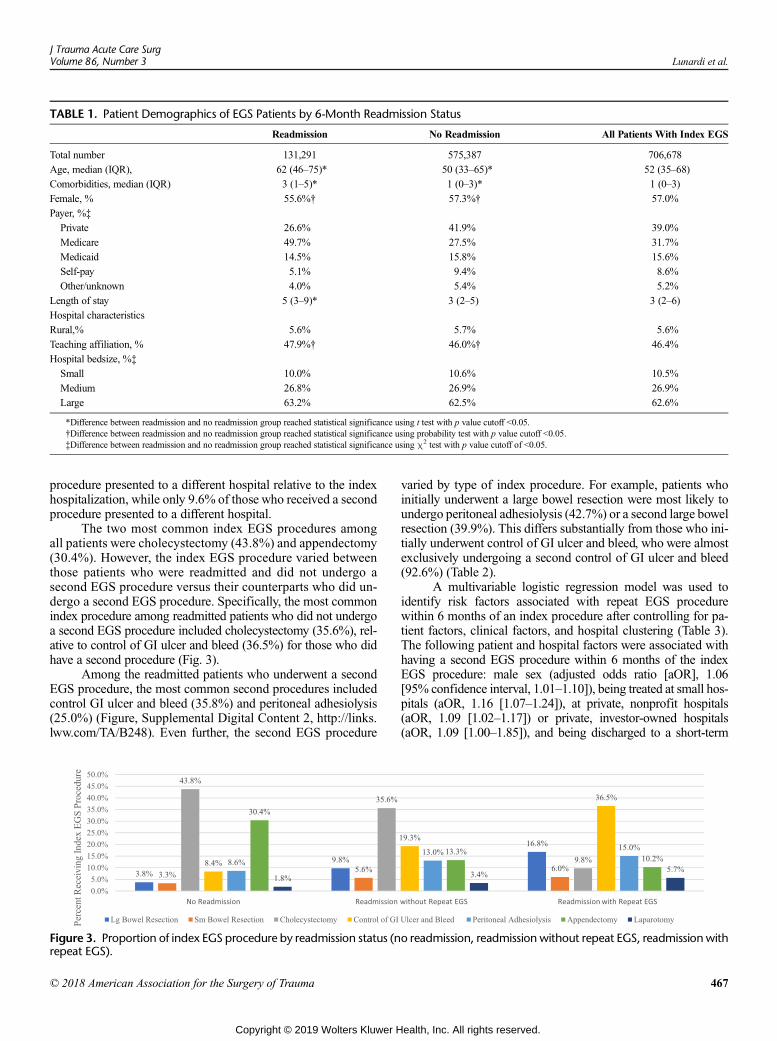
TABLE 1. Patient Demographics of EGS Patients by 6-Month Readmission Status
Readmission No Readmission All Patients With Index EGS
Total number 131,291 575,387 706,678
Age, median (IQR), 62 (46–75)* 50 (33–65)* 52 (35–68)
Comorbidities, median (IQR) 3 (1–5)* 1 (0–3)* 1 (0–3)
Female, % 55.6%† 57.3%† 57.0%
Payer, %‡
Private 26.6% 41.9% 39.0%
Medicare 49.7% 27.5% 31.7%
Medicaid 14.5% 15.8% 15.6%
Self-pay 5.1% 9.4% 8.6%
Other/unknown 4.0% 5.4% 5.2%
Length of stay 5 (3–9)* 3 (2–5) 3 (2–6)
Hospital characteristics
Rural,% 5.6% 5.7% 5.6%
Teaching affiliation, % 47.9%† 46.0%† 46.4%
Hospital bedsize, %‡
Small 10.0% 10.6% 10.5%
Medium 26.8% 26.9% 26.9%
Large 63.2% 62.5% 62.6%
*Difference between readmission and no readmission group reached statistical significance using t test with p value cutoff <0.05.†Difference between readmission and no readmission group reached statistical significance using probability test with p value cutoff <0.05.‡Difference between readmission and no readmission group reached statistical significance using χ2 test with p value cutoff of <0.05.
J Trauma Acute Care SurgVolume 86, Number 3 Lunardi et al.
procedure presented to a different hospital relative to the indexhospitalization, while only 9.6% of those who received a secondprocedure presented to a different hospital.
The two most common index EGS procedures amongall patients were cholecystectomy (43.8%) and appendectomy(30.4%). However, the index EGS procedure varied betweenthose patients who were readmitted and did not undergo asecond EGS procedure versus their counterparts who did un-dergo a second EGS procedure. Specifically, the most commonindex procedure among readmitted patients who did not undergoa second EGS procedure included cholecystectomy (35.6%), rel-ative to control of GI ulcer and bleed (36.5%) for those who didhave a second procedure (Fig. 3).
Among the readmitted patients who underwent a secondEGS procedure, the most common second procedures includedcontrol GI ulcer and bleed (35.8%) and peritoneal adhesiolysis(25.0%) (Figure, Supplemental Digital Content 2, http://links.lww.com/TA/B248). Even further, the second EGS procedure
Figure 3. Proportion of index EGS procedure by readmission status (nrepeat EGS).
© 2018 American Association for the Surgery of Trauma
Copyright © 2019 Wolters Kluwer H
varied by type of index procedure. For example, patients whoinitially underwent a large bowel resection were most likely toundergo peritoneal adhesiolysis (42.7%) or a second large bowelresection (39.9%). This differs substantially from those who ini-tially underwent control of GI ulcer and bleed, who were almostexclusively undergoing a second control of GI ulcer and bleed(92.6%) (Table 2).
A multivariable logistic regression model was used toidentify risk factors associated with repeat EGS procedurewithin 6 months of an index procedure after controlling for pa-tient factors, clinical factors, and hospital clustering (Table 3).The following patient and hospital factors were associated withhaving a second EGS procedure within 6 months of the indexEGS procedure: male sex (adjusted odds ratio [aOR], 1.06[95% confidence interval, 1.01–1.10]), being treated at small hos-pitals (aOR, 1.16 [1.07–1.24]), at private, nonprofit hospitals(aOR, 1.09 [1.02–1.17]) or private, investor-owned hospitals(aOR, 1.09 [1.00–1.85]), and being discharged to a short-term
o readmission, readmission without repeat EGS, readmissionwith
467
ealth, Inc. All rights reserved.

TABLE 2. Type of EGS Procedure on Readmission Stratified by Index EGS Procedure Type
Index EGS Procedure n, %
LargeBowel
Resection
SmallBowel
Resection Cholecystectomy
Control of GIUlcer andBleed
PeritonealAdhesiolysis Appendectomy Laparotomy
EGS Procedure onReadmission(n, %)
Large bowel resection 1,016 (39.9) 49 (5.4) 112 (7.6) 43 (0.8) 129 (5.7) 285 (18.4) 93 (10.8)
Small bowel resection 195 (7.7) 462 (50.4) 91 (6.1) 37 (0.7) 217 (9.5) 76 (4.9) 48 (5.6)
Cholecystectomy 82 (3.2) 58 (6.3) 475 (32.1) 162 (2.9) 164 (7.2) 324 (20.9) 37 (4.3)
Control of GI ulcer and bleed 33 (1.3) 20 (2.2) 149 (10.1) 5,130 (92.6) 69 (3.0) 32 (2.1) 7 (0.8)
Peritoneal adhesiolysis 1,087 (42.7) 231 (25.2) 297 (20.1) 112 (2.0) 1,549 (67.9) 371 (23.9) 147 (17.1)
Appendectomy 24 (0.9) 20 (2.2) 230 (15.5) 14 (0.3) 37 (1.6) 261 (16.8) 18 (2.1)
Laparotomy 107 (4.2) 76 (8.3) 127 (8.6) 44 (0.8) 118 (5.2) 204 (13.1) 509 (59.3)
Total (n) 2,544 (100) 916 (100) 1,481 (100) 5,542 (100) 2,283 (100) 1,553 (100) 859 (100)
Lunardi et al.J Trauma Acute Care Surg
Volume 86, Number 3
hospital (aOR, 1.35 [1.04–1.74]) or with home health care (aOR,1.19 [1.13–1.25]) (Table 3).
Patients undergoing certain index EGS procedureswere associated with higher odds of undergoing a secondEGS procedure. All index procedures, when compared withindex cholecystectomy, had increased odds of repeat EGSwithin 6 months. The following procedures are listed inorder of greatest to smallest increased odds of repeat EGS:control of GI ulcer and bleeding (aOR, 9.38 [8.75–10.05]),laparotomy (aOR, 7.62 [6.92–8.40]), large bowel resection(aOR, 6.94 [6.44–7.47]), peritoneal adhesiolysis (aOR, 4.90[4.56–5.26]), small bowel resection (aOR, 4.67 [4.25–5.13]),and appendectomy (aOR, 2.07 (1.93–2.22]).
Self-pay patients (aOR, 0.80 [0.72–0.89]), Medicare pa-tients (aOR, 0.90 [0.84–0.96]), Medicaid patients (aOR, 0.83[0.77–0.89]), and those discharged to skilled nursing facilities(aOR, 0.71 [0.66–0.76]) had decreased odds of repeat EGS.Slight decrease in odds of repeat EGS was also found amongolder patients (aOR, 1.00 [0.99–1.00]), patients with more co-morbidities (aOR, 0.93 [0.92–0.94]), patients with longerlengths of stay (aOR, 0.98 [0.98–0.99]), and patients in the low-est income quartile relative to the highest (aOR, 0.93 [0.88–1.00]) (Table 3).
DISCUSSION
While EGS procedures continue to rise in the UnitedStates, there exists limited literature on the long-term outcomesof these procedures, especially with respect to patients under-going a second EGS procedure postdischarge. In this study,we found that the cumulative readmission rates among patientsreceiving one of seven common EGS procedures rose from7.9% to 13.8% to 18.6% at 1, 3, and 6 months, respectively. Fur-thermore, at least half of all second EGS procedures occurwithin 6 weeks of discharge from the index EGS procedure, ourdata suggest that certain patients undergoing higher-risk EGSprocedures are more likely to require a second EGS procedure.These findings can appropriately inform clinical practices forsurgeons taking care of patients undergoing various EGS pro-cedures, warranting further discussion.
Patients undergoing emergent procedures represent a sickerand more acutely ill population relative to those undergoing elec-tive procedures. Even further, the life-saving measures of an
468
Copyright © 2019 Wolters Kluwer H
emergent intervention eliminate the opportunity for preoperativeoptimization of comorbidities. It follows that these patients havehigh postoperative morbidity and mortality rates. Many amongthose discharged alive will subsequently experience a surgicalcomplication requiring a readmission. The findings of this studyare consistent with previously published 30-day readmission rates(6–15%) among EGS patients.6,9,15,16 The current analysis pro-vides further granularity in that it shows cumulative readmissionrates continue to rise beyond the initial 30 days.
Even further, this study suggests that not all EGS readmis-sions are the same. Of the total 131,291 readmissions, there wasa subset of patients (n = 15,178, 11.6%) who underwent one ofseven EGS procedures at the time of readmission. Control of GIulcer and bleeding and laparotomy were associated with ninefoldand eightfold increase in odds respectively (the two highest odds)of undergoing a second EGS procedure. Of the seven readmissionEGS procedures, more than half of patients underwent control ofGI ulcer and bleed and peritoneal adhesiolysis. This may point toa clinically relevant framework with which to identify patients atrisk of requiring future EGS procedures. Of the patients who ini-tially underwent a control of GI ulcer and bleed and had a subse-quent operation, 93% underwent a reoperation of a control of GIulcer and bleed. This trend warrants the question of whether thereare preventable behaviors, such as non-steroidal anti-inflamma-tory drug overuse, or unidentified, reversible acid hypersecretorystates, which may provide opportunities to reduce the likelihoodof requiring a future reoperation. This trend is different, for exam-ple, among patients receiving an index large bowel resection.Among these patients receiving a second operation, 43% un-derwent a peritoneal adhesiolysis and 40% underwent a secondlarge bowel resection. In this clinical scenario, a subset of patientsmay require further intervention given the natural disease courseof the index procedure itself, namely, adhesiolysis for obstructivesymptoms following a large abdominal procedure. Careful atten-tion in the outpatient setting for common complications ofmorbidprocedures and also for opportunities to change health behaviorsmay present the opportunity to plan elective safer procedures ormay potentially prevent the need for reoperation all together.
A smaller proportion of those who underwent a secondEGS procedure (9.6%) presented to a different hospital on read-mission compared with those who were readmitted without asecond EGS procedure (19.3%). This suggests that patients withthe highest acute care need are more likely to receive care at the
© 2018 American Association for the Surgery of Trauma
ealth, Inc. All rights reserved.
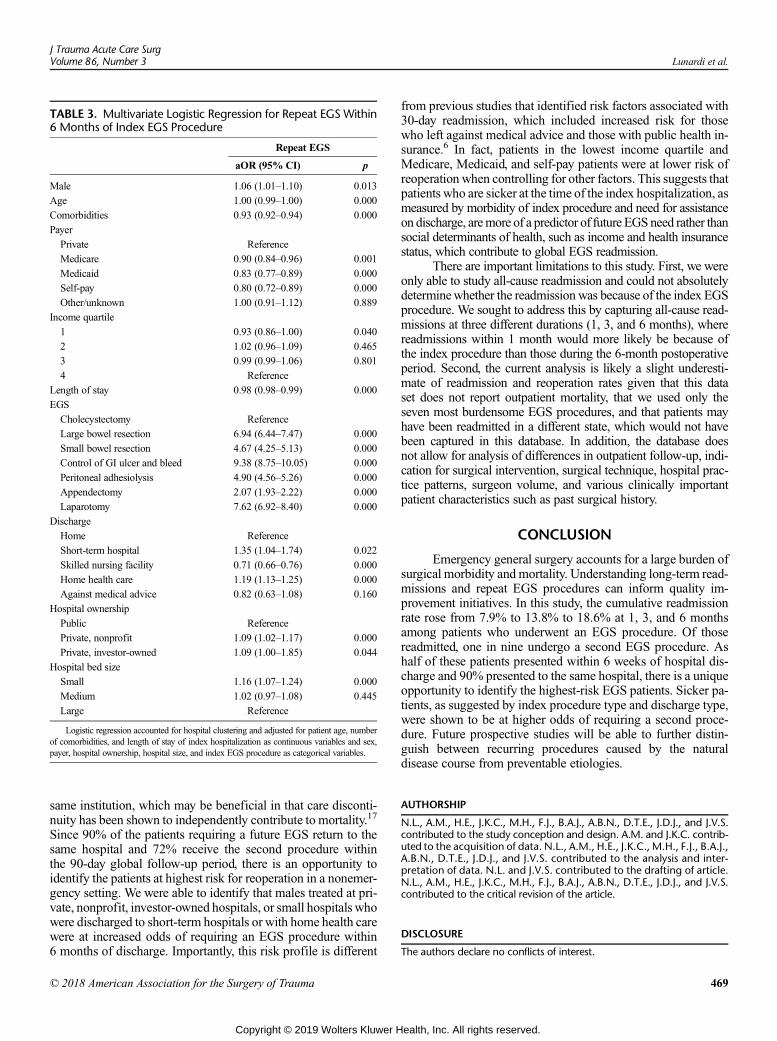
TABLE 3. Multivariate Logistic Regression for Repeat EGS Within6 Months of Index EGS Procedure
Repeat EGS
aOR (95% CI) p
Male 1.06 (1.01–1.10) 0.013
Age 1.00 (0.99–1.00) 0.000
Comorbidities 0.93 (0.92–0.94) 0.000
Payer
Private Reference
Medicare 0.90 (0.84–0.96) 0.001
Medicaid 0.83 (0.77–0.89) 0.000
Self-pay 0.80 (0.72–0.89) 0.000
Other/unknown 1.00 (0.91–1.12) 0.889
Income quartile
1 0.93 (0.86–1.00) 0.040
2 1.02 (0.96–1.09) 0.465
3 0.99 (0.99–1.06) 0.801
4 Reference
Length of stay 0.98 (0.98–0.99) 0.000
EGS
Cholecystectomy Reference
Large bowel resection 6.94 (6.44–7.47) 0.000
Small bowel resection 4.67 (4.25–5.13) 0.000
Control of GI ulcer and bleed 9.38 (8.75–10.05) 0.000
Peritoneal adhesiolysis 4.90 (4.56–5.26) 0.000
Appendectomy 2.07 (1.93–2.22) 0.000
Laparotomy 7.62 (6.92–8.40) 0.000
Discharge
Home Reference
Short-term hospital 1.35 (1.04–1.74) 0.022
Skilled nursing facility 0.71 (0.66–0.76) 0.000
Home health care 1.19 (1.13–1.25) 0.000
Against medical advice 0.82 (0.63–1.08) 0.160
Hospital ownership
Public Reference
Private, nonprofit 1.09 (1.02–1.17) 0.000
Private, investor-owned 1.09 (1.00–1.85) 0.044
Hospital bed size
Small 1.16 (1.07–1.24) 0.000
Medium 1.02 (0.97–1.08) 0.445
Large Reference
Logistic regression accounted for hospital clustering and adjusted for patient age, numberof comorbidities, and length of stay of index hospitalization as continuous variables and sex,payer, hospital ownership, hospital size, and index EGS procedure as categorical variables.
J Trauma Acute Care SurgVolume 86, Number 3 Lunardi et al.
same institution, which may be beneficial in that care disconti-nuity has been shown to independently contribute to mortality.17
Since 90% of the patients requiring a future EGS return to thesame hospital and 72% receive the second procedure withinthe 90-day global follow-up period, there is an opportunity toidentify the patients at highest risk for reoperation in a nonemer-gency setting. We were able to identify that males treated at pri-vate, nonprofit, investor-owned hospitals, or small hospitals whowere discharged to short-term hospitals or with home health carewere at increased odds of requiring an EGS procedure within6 months of discharge. Importantly, this risk profile is different
© 2018 American Association for the Surgery of Trauma
Copyright © 2019 Wolters Kluwer H
from previous studies that identified risk factors associated with30-day readmission, which included increased risk for thosewho left against medical advice and those with public health in-surance.6 In fact, patients in the lowest income quartile andMedicare, Medicaid, and self-pay patients were at lower risk ofreoperation when controlling for other factors. This suggests thatpatients who are sicker at the time of the index hospitalization, asmeasured by morbidity of index procedure and need for assistanceon discharge, aremore of a predictor of future EGSneed rather thansocial determinants of health, such as income and health insurancestatus, which contribute to global EGS readmission.
There are important limitations to this study. First, we wereonly able to study all-cause readmission and could not absolutelydeterminewhether the readmission was because of the index EGSprocedure. We sought to address this by capturing all-cause read-missions at three different durations (1, 3, and 6 months), wherereadmissions within 1 month would more likely be because ofthe index procedure than those during the 6-month postoperativeperiod. Second, the current analysis is likely a slight underesti-mate of readmission and reoperation rates given that this dataset does not report outpatient mortality, that we used only theseven most burdensome EGS procedures, and that patients mayhave been readmitted in a different state, which would not havebeen captured in this database. In addition, the database doesnot allow for analysis of differences in outpatient follow-up, indi-cation for surgical intervention, surgical technique, hospital prac-tice patterns, surgeon volume, and various clinically importantpatient characteristics such as past surgical history.
CONCLUSION
Emergency general surgery accounts for a large burden ofsurgical morbidity and mortality. Understanding long-term read-missions and repeat EGS procedures can inform quality im-provement initiatives. In this study, the cumulative readmissionrate rose from 7.9% to 13.8% to 18.6% at 1, 3, and 6 monthsamong patients who underwent an EGS procedure. Of thosereadmitted, one in nine undergo a second EGS procedure. Ashalf of these patients presented within 6 weeks of hospital dis-charge and 90% presented to the same hospital, there is a uniqueopportunity to identify the highest-risk EGS patients. Sicker pa-tients, as suggested by index procedure type and discharge type,were shown to be at higher odds of requiring a second proce-dure. Future prospective studies will be able to further distin-guish between recurring procedures caused by the naturaldisease course from preventable etiologies.
AUTHORSHIP
N.L., A.M., H.E., J.K.C., M.H., F.J., B.A.J., A.B.N., D.T.E., J.D.J., and J.V.S.contributed to the study conception and design. A.M. and J.K.C. contrib-uted to the acquisition of data. N.L., A.M., H.E., J.K.C., M.H., F.J., B.A.J.,A.B.N., D.T.E., J.D.J., and J.V.S. contributed to the analysis and inter-pretation of data. N.L. and J.V.S. contributed to the drafting of article.N.L., A.M., H.E., J.K.C., M.H., F.J., B.A.J., A.B.N., D.T.E., J.D.J., and J.V.S.contributed to the critical revision of the article.
DISCLOSURE
The authors declare no conflicts of interest.
469
ealth, Inc. All rights reserved.

Lunardi et al.J Trauma Acute Care Surg
Volume 86, Number 3
REFERENCES1. Gale SC, Shafi S, Dombrovskiy VY, Arumugam D, Crystal JS. The public
health burden of emergency general surgery in the United States: a 10-yearanalysis of theNationwide Inpatient Sample—2001 to 2010. J Trauma AcuteCare Surg. 2014;77(2):202–208.
2. Havens JM, Peetz AB, DoWS. The excess morbidity and mortality of emer-gency general surgery. J Trauma Acute Care Surg. 2015;78(2):306–311.
3. Mullen MG, Michaels AD, Mehaffey JH, Guidry CA, Turrentine FE,Hedrick TL, Friel CM. Risk associated with complications and mortality af-ter urgent surgery vs elective and emergency surgery: implications for defin-ing “quality” and reporting outcomes for urgent surgery. JAMA Surg. 2017;152(8):768–774.
4. Mehta A, Efron DT, Stevens K, Manukyan MC, Joseph B, Sakran JV.Hospital variation in mortality after emergent bowel resections: the role offailure-to-rescue. J Trauma Acute Care Surg. 2018;84(5):702–710.
5. Kassin MT, Owen RM, Perez SD, Leeds I, Cox JC, Schnier K, Sweeney JF.Risk factors for 30-day hospital readmission among general surgery patients.J Am Coll Surg. 2012;215(3):322–330.
6. Havens JM, Olufajo OA, Cooper ZR, Haider AH, ShahAA, Salim A. Defin-ing rates and risk factors for readmissions following emergency general sur-gery. JAMA Surg. 2016;151(4):330–336.
7. Scott JW, Olufajo OA, Brat GA, Rose JA, Zogg CK, Haider AH, Havens JM.Use of national burden to define operative emergency general surgery. JAMASurg. 2016;151(6):e160480.
8. Shafi S, AboutanosMB, Agarwal S Jr., BrownCV, CrandallM, Feliciano DV,Ross S. Emergency general surgery: definition and estimated burden of dis-ease. J Trauma Acute Care Surg. 2013;74(4):1092–1097.
470
Copyright © 2019 Wolters Kluwer H
9. McIntyre LK, Arbabi S, Robinson EF, Maier RV. Analysis of risk factors forpatient readmission 30 days following discharge from general surgery. JAMASurg. 2016;151(9):855–861.
10. Healthcare Cost and Utilization Project (HCUP) NRD Notes. Availableat: https://www.hcup-us.ahrq.gov/db/vars/hosp_bedsize/nrdnote.jsp. AccessedFebruary 15, 2018.
11. Mehta A, Efron DT, Canner JK, Dultz L, Xu T, Jones C, Sakran JV. Effect ofsurgeon and hospital volume on emergency general surgery outcomes. J AmColl Surg. 2017;225(5):666–675.e2.
12. Mehta A, Dultz LA, Joseph B, Canner JK, Stevens K, Jones C, Haut ER,Efron DT, Sakran JV. Emergency general surgery in geriatrics patients: astatewide analysis of surgery and hospital volume with outcomes. J TraumaAcute Care Surg. 2018;84(6):864–874.
13. Mehta A, Efron DT, Canner JK, Manukyan MC, Dultz L, Burns C,Stevens K, Sakran JV. Surgeon variation in operating times and charges foremergency general surgery. J Surg Res. 2018;227:101–111.
14. Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures foruse with administrative data.Med Care. 1998;36(1):8–27.
15. Muthuvel G, Tevis SE, Liepert AE, Agarwal SK, Kennedy GD. A compositeindex for predicting readmission following emergency general surgery.J Trauma Acute Care Surg. 2014;76(6):1467–1472.
16. Glance LG, Kellermann AL, Osler TM, Li Y, Mukamel DB, Lustik SJ,Eaton MP, Dick AW. Hospital readmission after noncardiac surgery: the roleof major complications. JAMA Surg. 2014;149(5):439–445.
17. Havens JM, Olufajo OA, Tsai TC, Jiang W, Nitzschke SL, Cooper Z,Salim A. Hospital factors associated with care discontinuity following emer-gency general surgery. JAMA Surg. 2017;152(3):242–249.
© 2018 American Association for the Surgery of Trauma
ealth, Inc. All rights reserved.

ORIGINAL ARTICLE
A comparison of cholecystitis grading scales
Tarik D. Madni, MD, MBA, Paul A. Nakonezny, PhD, Jonathan B. Imran, MD, Luis Taveras, MD,Holly B. Cunningham, MD, Ryan Vela, MD, Audra T. Clark, MD, Christian T. Minshall, MD, PhD,
Alexander L. Eastman, MD, MPH, Stephen Luk, MD, Herb A. Phelan, MD, MSCS,and Michael W. Cripps, MD, MSCS, Dallas, Texas
Sub
Fro
Thi
Ad
DO
J TrVol
BACKGROUND: P
mitted: July 15, 2018, RevisedPublished online: November 5,m the Department of Surgery (Tof General and Acute Care SurDivision of Biostatistics, DepaTexas Southwestern, Dallas, Tes original work will be presentegeons Clinical Congress, Octohas not been published elsewhedress for reprints: Michael W. CSurgery, University of Texas SBlvd., Dallas, TX 75390-9158;
I: 10.1097/TA.00000000000021
auma Acute Care Surgume 86, Number 3
reviously, our group developed the Parkland grading scale for cholecystitis (PGS) to stratify gallbladder (GB) disease severity thatcan be determined immediately when performing laparoscopic cholecystectomy (LC). In prior studies, PGS demonstrated excel-lent interrater reliability and was internally validated as an accurate measure of LC outcomes. Here, we compare PGS against amore complex cholecystitis severity score developed by the national trauma society, American Association for the Surgery ofTrauma (AAST), which requires clinical, operative, imaging, and pathologic inputs, as a predictor of LC outcomes.
METHODS: E
leven acute care surgeons prospectively graded 179 GBs using PGS and filled out a postoperative questionnaire regarding thedifficulty of the surgery. Three independent raters retrospectively graded these GBs using PGS from images stored in the electronicmedical record. Three additional surgeons then assigned separate AAST scores to each GB. The intraclass correlation coefficientstatistic assessed rater reliability for both PGS and AAST. The PGS score and the median AAST score became predictors in sep-arate linear, logistic, and negative binomial regression models to estimate perioperative outcomes.RESULTS: T
he average intraclass correlation coefficient of PGS and AASTwas 0.8647 and 0.8341, respectively. Parkland grading scale forcholecystitis was found to be a superior predictor of increasing operative difficulty (R2, 0.566 vs. 0.202), case length (R2, 0.217 vs.0.037), open conversion rates (area under the curve, 0.904 vs. 0.757), and complication rates (area under the curve, 0.7039 vs.0.6474) defined as retained stone, small-bowel obstruction, wound infection, or postoperative biliary leak. Parkland grading scalefor cholecystitis performed similar to AAST in predicting partial cholecystectomy, readmission, bile leak rates, and length of stay.CONCLUSION: B
oth PGS and AASTare accurate predictors of LC outcomes. Parkland grading scale for cholecystitis was found to be a superiorpredictor of subjective operative difficulty, case length, open conversion rates, and complication rates. Parkland grading scale forcholecystitis has the advantage of being a simpler, operative-based scale which can be scored at a single point in time. (J TraumaAcute Care Surg. 2018;86: 471–478. Copyright © 2018 Wolters Kluwer Health, Inc. All rights reserved.)LEVEL OF EVIDENCE: S
ingle institution, retrospective review, level IV. KEYWORDS: G allbladder; cholecystitis; score; grade; outcomes.B ased on the Agency for Healthcare Research and Quality'sNationwide Inpatient Sample, between 2001 and 2010, emer-
gency general surgery (EGS) accounted for over 27 million hos-pital admissions and over 7% of all hospitalizations.1 Unlike itselective equivalents, EGS diseases are often associated with in-creased rates ofmedical errors, complications, and deaths.2–4Givenboth the substantial and continuously increasing socioeconomicburden of such disease, the costs of EGS in the United States is ex-pected to rise fromUS $28 billion in 2010 to over US $41 billionby 2060.5 In an era of increasing costs, declining reimbursements,and financial penalties associated with quality comparisons, phy-sicians and health care systems associated with EGS services arecontinuously searching for ways to risk-adjust patients for quality
: September 7, 2018, Accepted: October 8, 2018,2018..D.M., J.B.I., L.T., H.B.C., R.V., A.T.C.), Divisiongery (C.T.M., A.L.E., S.L., H.A.P., M.W.C.), andrtment of Clinical Sciences (P.A.N), University ofxas.d as an oral at the 2018 American College of Sur-ber 21–25, 2018 in Boston, Massachusetts andre.ripps, MD, Division of General and Acute Careouthwestern Medical Center, 5323 Harry Hinesemail: [email protected].
25
Copyright © 2019 Wolters Kluwer H
assessment to compare outcomes fairly to their less severe, potentiallyelective counterparts.3,6 Of the 31 classified EGS diseases, the ninemost common disorders account for over 80% of EGS diseaseburden, with gallbladder (GB) disease accounting for 12% alone.5
Gallbladder disease affects more than 20 million Americansannually, and roughly 20% of patients who become symptom-atic will develop acute cholecystitis if left untreated.7 As such,the laparoscopic cholecystectomy (LC) is one of the most com-mon operations performed by the general surgeon.8 However, notall cholecystitis is created equal. Anatomical and inflammatorychanges during LCs can lead to more difficult, time-consumingoperations that are more prone to adverse postoperative events.As such, it is imperative that an accurate measure for outcomecomparisons is developed for LCs, and other EGS operations, toavoid penalizing a surgeon or a hospital for complications that mayin fact be associated with disease severity and not clinical care.9
In response to these growing needs, the American Associ-ation for the Surgery of Trauma (AAST) developed a gradingsystem for 16 common EGS diseases as a method to qualify dis-ease severity and risk-adjust patients to allow for accurate out-come comparison between surgeons and institutions.10,11 Whileits acute cholecystitis scale (AAST-C) was recently validated, thescale's complexity, exclusion criteria, and lack of granularity be-tween grades suggests it needs to be further refined.12 As such,we believe our previously created Parkland grading scale for
471
ealth, Inc. All rights reserved.
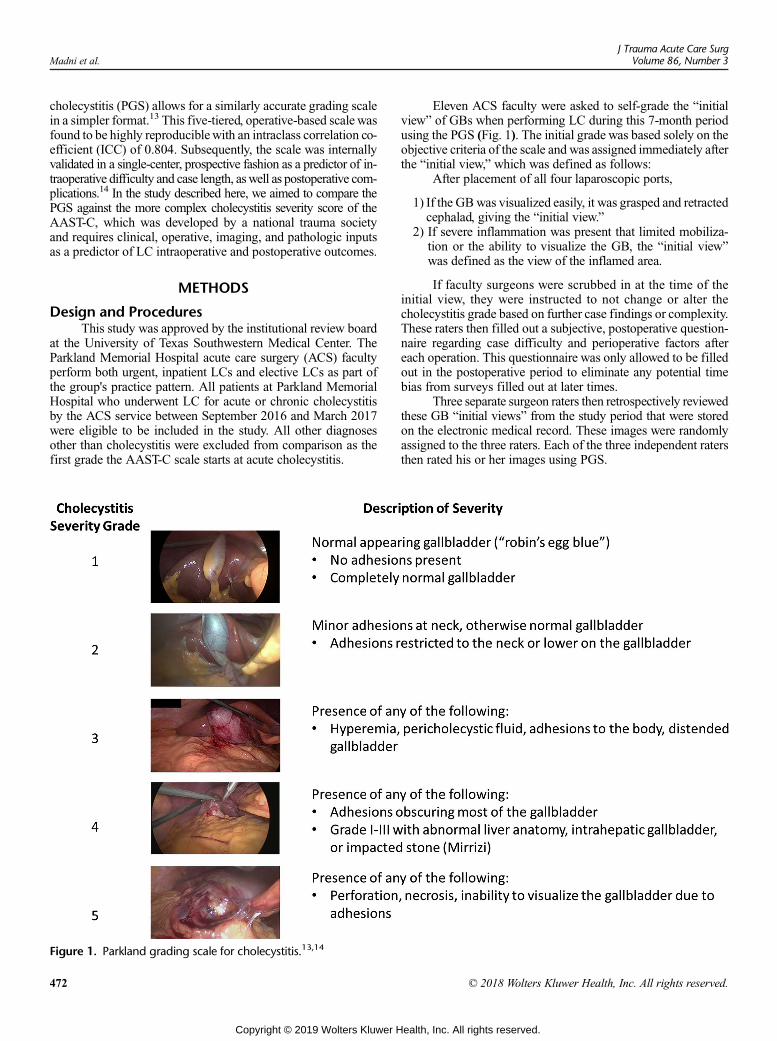
Madni et al.J Trauma Acute Care Surg
Volume 86, Number 3
cholecystitis (PGS) allows for a similarly accurate grading scalein a simpler format.13 This five-tiered, operative-based scale wasfound to be highly reproduciblewith an intraclass correlation co-efficient (ICC) of 0.804. Subsequently, the scale was internallyvalidated in a single-center, prospective fashion as a predictor of in-traoperative difficulty and case length, aswell as postoperative com-plications.14 In the study described here, we aimed to compare thePGS against the more complex cholecystitis severity score of theAAST-C, which was developed by a national trauma societyand requires clinical, operative, imaging, and pathologic inputsas a predictor of LC intraoperative and postoperative outcomes.
METHODS
Design and ProceduresThis study was approved by the institutional review board
at the University of Texas Southwestern Medical Center. TheParkland Memorial Hospital acute care surgery (ACS) facultyperform both urgent, inpatient LCs and elective LCs as part ofthe group's practice pattern. All patients at Parkland MemorialHospital who underwent LC for acute or chronic cholecystitisby the ACS service between September 2016 and March 2017were eligible to be included in the study. All other diagnosesother than cholecystitis were excluded from comparison as thefirst grade the AAST-C scale starts at acute cholecystitis.
Figure 1. Parkland grading scale for cholecystitis.13,14
472
Copyright © 2019 Wolters Kluwer H
Eleven ACS faculty were asked to self-grade the “initialview” of GBs when performing LC during this 7-month periodusing the PGS (Fig. 1). The initial grade was based solely on theobjective criteria of the scale and was assigned immediately afterthe “initial view,” which was defined as follows:
After placement of all four laparoscopic ports,
1) If the GBwas visualized easily, it was grasped and retractedcephalad, giving the “initial view.”
2) If severe inflammation was present that limited mobiliza-tion or the ability to visualize the GB, the “initial view”was defined as the view of the inflamed area.
If faculty surgeons were scrubbed in at the time of theinitial view, they were instructed to not change or alter thecholecystitis grade based on further case findings or complexity.These raters then filled out a subjective, postoperative question-naire regarding case difficulty and perioperative factors aftereach operation. This questionnaire was only allowed to be filledout in the postoperative period to eliminate any potential timebias from surveys filled out at later times.
Three separate surgeon raters then retrospectively reviewedthese GB “initial views” from the study period that were storedon the electronic medical record. These images were randomlyassigned to the three raters. Each of the three independent ratersthen rated his or her images using PGS.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
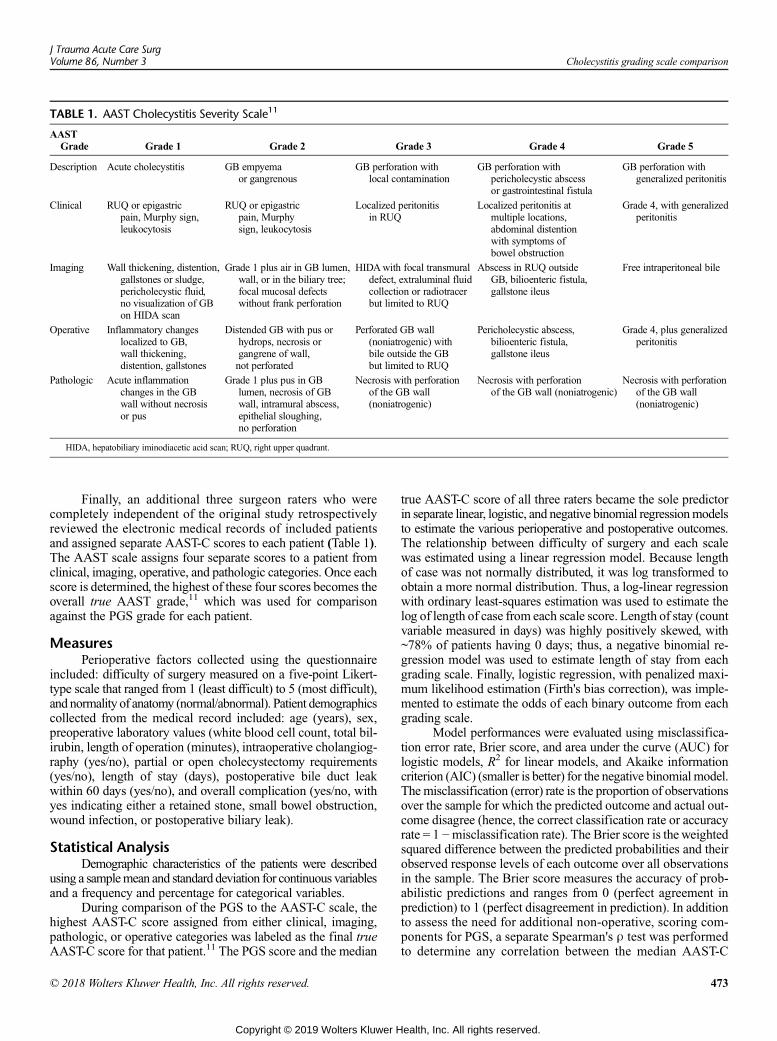
TABLE 1. AAST Cholecystitis Severity Scale11
AASTGrade Grade 1 Grade 2 Grade 3 Grade 4 Grade 5
Description Acute cholecystitis GB empyemaor gangrenous
GB perforation withlocal contamination
GB perforation withpericholecystic abscessor gastrointestinal fistula
GB perforation withgeneralized peritonitis
Clinical RUQ or epigastricpain, Murphy sign,leukocytosis
RUQ or epigastricpain, Murphysign, leukocytosis
Localized peritonitisin RUQ
Localized peritonitis atmultiple locations,abdominal distentionwith symptoms ofbowel obstruction
Grade 4, with generalizedperitonitis
Imaging Wall thickening, distention,gallstones or sludge,pericholecystic fluid,no visualization of GBon HIDA scan
Grade 1 plus air in GB lumen,wall, or in the biliary tree;focal mucosal defectswithout frank perforation
HIDAwith focal transmuraldefect, extraluminal fluidcollection or radiotracerbut limited to RUQ
Abscess in RUQ outsideGB, bilioenteric fistula,gallstone ileus
Free intraperitoneal bile
Operative Inflammatory changeslocalized to GB,wall thickening,distention, gallstones
Distended GB with pus orhydrops, necrosis organgrene of wall,not perforated
Perforated GB wall(noniatrogenic) withbile outside the GBbut limited to RUQ
Pericholecystic abscess,bilioenteric fistula,gallstone ileus
Grade 4, plus generalizedperitonitis
Pathologic Acute inflammationchanges in the GBwall without necrosisor pus
Grade 1 plus pus in GBlumen, necrosis of GBwall, intramural abscess,epithelial sloughing,no perforation
Necrosis with perforationof the GB wall(noniatrogenic)
Necrosis with perforationof the GB wall (noniatrogenic)
Necrosis with perforationof the GB wall(noniatrogenic)
HIDA, hepatobiliary iminodiacetic acid scan; RUQ, right upper quadrant.
J Trauma Acute Care SurgVolume 86, Number 3 Cholecystitis grading scale comparison
Finally, an additional three surgeon raters who werecompletely independent of the original study retrospectivelyreviewed the electronic medical records of included patientsand assigned separate AAST-C scores to each patient (Table 1).The AAST scale assigns four separate scores to a patient fromclinical, imaging, operative, and pathologic categories. Once eachscore is determined, the highest of these four scores becomes theoverall true AAST grade,11 which was used for comparisonagainst the PGS grade for each patient.
MeasuresPerioperative factors collected using the questionnaire
included: difficulty of surgery measured on a five-point Likert-type scale that ranged from 1 (least difficult) to 5 (most difficult),and normality of anatomy (normal/abnormal). Patient demographicscollected from the medical record included: age (years), sex,preoperative laboratory values (white blood cell count, total bil-irubin, length of operation (minutes), intraoperative cholangiog-raphy (yes/no), partial or open cholecystectomy requirements(yes/no), length of stay (days), postoperative bile duct leakwithin 60 days (yes/no), and overall complication (yes/no, withyes indicating either a retained stone, small bowel obstruction,wound infection, or postoperative biliary leak).
Statistical AnalysisDemographic characteristics of the patients were described
using a samplemean and standard deviation for continuous variablesand a frequency and percentage for categorical variables.
During comparison of the PGS to the AAST-C scale, thehighest AAST-C score assigned from either clinical, imaging,pathologic, or operative categories was labeled as the final trueAAST-C score for that patient.11 The PGS score and the median
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
true AAST-C score of all three raters became the sole predictorin separate linear, logistic, and negative binomial regressionmodelsto estimate the various perioperative and postoperative outcomes.The relationship between difficulty of surgery and each scalewas estimated using a linear regression model. Because lengthof case was not normally distributed, it was log transformed toobtain a more normal distribution. Thus, a log-linear regressionwith ordinary least-squares estimation was used to estimate thelog of length of case from each scale score. Length of stay (countvariable measured in days) was highly positively skewed, with~78% of patients having 0 days; thus, a negative binomial re-gression model was used to estimate length of stay from eachgrading scale. Finally, logistic regression, with penalized maxi-mum likelihood estimation (Firth's bias correction), was imple-mented to estimate the odds of each binary outcome from eachgrading scale.
Model performances were evaluated using misclassifica-tion error rate, Brier score, and area under the curve (AUC) forlogistic models, R2 for linear models, and Akaike informationcriterion (AIC) (smaller is better) for the negative binomial model.The misclassification (error) rate is the proportion of observationsover the sample for which the predicted outcome and actual out-come disagree (hence, the correct classification rate or accuracyrate = 1 −misclassification rate). The Brier score is the weightedsquared difference between the predicted probabilities and theirobserved response levels of each outcome over all observationsin the sample. The Brier score measures the accuracy of prob-abilistic predictions and ranges from 0 (perfect agreement inprediction) to 1 (perfect disagreement in prediction). In additionto assess the need for additional non-operative, scoring com-ponents for PGS, a separate Spearman's ρ test was performedto determine any correlation between the median AAST-C
473
ealth, Inc. All rights reserved.

TABLE 2. Patient and Surgical Characteristics
n (%)
Sex
Female 132 (26.3)
Male 47 (73.7)
Diagnosis
Acute cholecystitis 165 (92.2)
Chronic cholecystitis 14 (7.8)
Partial cholecystectomy 14 (7.8)
Open conversion 8 (4.5)
Abnormal anatomy 26 (14.5)
Difficulty of surgery
1 18 (10.1)
2 59 (33.0)
3 37 (20.7)
4 37 (20.7)
5 34 (19.0)
Parkland cholecystitis grade
1 22 (12.3)
2 38 (21.2)
3 63 (35.2)
4 22 (12.3)
5 34 (19.0)
Median true AAST grade*
1 132 (73.7)
2 39 (21.8)
3 5 (2.8)
4 3 (1.7)
5 0 (0.0)
Performance of IOC 3 (1.7)
60-d ER return visit 31 (17.3)
60-d readmission to ACS services 16 (8.9)
Postoperative biliary leak 5 (2.8)
Complication 7 (3.9)
Mean ± SD
Age, y 41.7 ± 13.8
Preoperative WBC 10.9 ± 3.7
Preoperative total bilirubin 0.6 ± 0.6
Length of stay, d 0.6 ± 1.5
Length of operation, min 85.0 ± 32.4
*True AAST grade is the highest grade from either clinical, imaging, operative, or path-ologic AAST scores assigned to a patient.
ER, emergency room, IOC, intraoperative cholangiogram;WBC,white blood cell count.
Madni et al.J Trauma Acute Care Surg
Volume 86, Number 3
imaging only grade (see Table 1 for imaging componentscore) and PGS.
We assessed the reliability (or consistency) of all fiveAAST-C components (clinical, imaging, operative, pathologic,highest score) from the three independent raters using the ICCstatistic. In addition, we assessed the reliability of the PGS scoreof the faculty who performed the operation to the PGS score ofthe three independent raters using the ICC statistic.
The α level for all tests was set at 0.05 (two-tailed), andto address multiple testing, p values were adjusted using thefalse discovery rate procedure. Statistical analyses were per-formed using SAS software, version 9.4 (SAS Institute, Inc,Cary NC).
474
Copyright © 2019 Wolters Kluwer H
RESULTS
A total of 179 LCs were used to evaluate the PGS alongwith the true AAST-C score. Demographic, perioperative, andpostoperative outcomes, as well as the frequency distributionfor the PGS and median true AAST-C are shown in Table 2.
Score Reliability (ICC)The ICC between the PGS score assigned by the three sep-
arate raters and the faculty surgeons who performed the opera-tion demonstrated excellent reliability (ICC, 0.8647; 95%confidence interval, 0.8065–0.9054; p = 0.0001). The averageICC for each of the AAST-C scoring components was as fol-lows: clinical (0.3472), imaging (0.9243), operative (0.9182),pathologic (0.7023), and true (i.e., highest, 0.8341).
Comparison of Predictive PerformanceParkland grading scale for cholecystitis was found to be
superior to the AAST-C in predicting increasing operative diffi-culty (R2 of 0.566 vs. 0.202), case length (R2 0.217 vs. 0.037),but similar in predicting length of stay (AIC of 314.01 vs.318.86; Table 3). Logistic model performance comparisons areshown in Table 4, where the PGSwas found to be a superior pre-dictor of open conversion (AUC, 0.903 vs. 0.756), partial chole-cystectomy (AUC, 0.878 vs. 0.833), and overall complicationrates (AUC, 0.703 vs. 0.647). Both the PGS and AAST-C weresimilar in discriminating postoperative bile leak (AUC, 0.777 vs.0.758). However, neither the PGS nor AAST-C seemed to dis-criminate abnormal anatomy (AUC, 0.565 vs. 0.578), 60-dayemergency room return visit (AUC, 0.509 vs. 0.491), or 60-dayACS readmission (AUC, 0.505 vs. 0.552). In a separate post hocanalysis, PGS was further compared against the median, stand-alone AAST-C operative grade. The pattern of predictive perfor-mance, not reported, for the median AAST-C operative gradeversus PGS was found similar to that of the median true AASTscore versus PGS (i.e., similar towhat is reported in Tables 3 and 4).
Finally, when comparing PGS to the median AAST-C imag-ing grade, the Spearman's ρ, the rank-order correlation coefficient,showed a significant, positive relationship (0.19904, p < 0.0076).
DISCUSSION
Starting with the National Surgical Quality ImprovementProgram (NSQIP) and at VA systems in the 1990s, health careoutcome measurements and comparisons have come under thenational spotlight in both the private and public sectors.15 Now,both the American College of Surgeons' NSQIP and the Centersfor Medicare and Medicaid Services have begun to publicly re-port clinical outcome measures as a way to improve overall carequality through transparency.15,16 While such endeavors haveassisted hospitals and providers in achieving safer and better pa-tient care,15 the downsides of publicly, available outcomes com-parison cannot be ignored. Specifically, centers or providerswho treat higher-risk patients with worse disease severity couldbe potentially penalized if their outcomes are not adjusted ac-cordingly. Demographics of an institution (i.e., public vs. pri-vate, geographic location, etc.) could substantially sway certainpatient populations toward one hospital versus another (i.e., safetynet hospitals). In a regulatory era where the Affordable Care Acthas created programs such as the Hospital Readmission Reduction
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
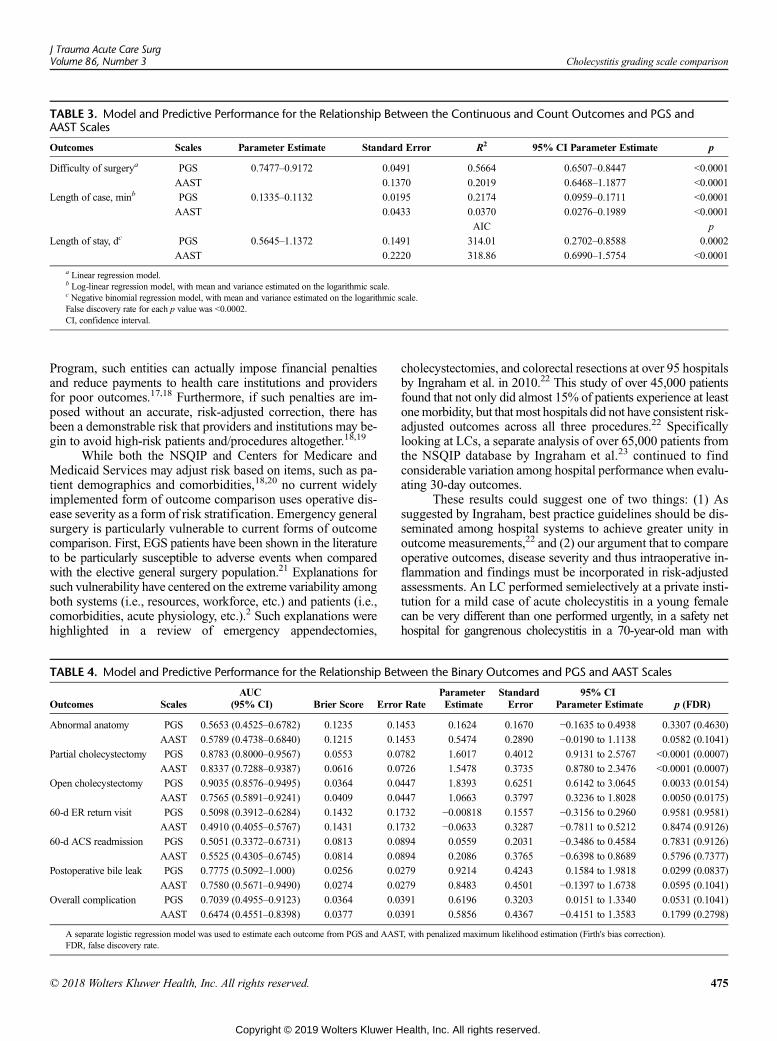
TABLE 3. Model and Predictive Performance for the Relationship Between the Continuous and Count Outcomes and PGS andAAST Scales
Outcomes Scales Parameter Estimate Standard Error R2 95% CI Parameter Estimate p
Difficulty of surgerya PGS 0.7477–0.9172 0.0491 0.5664 0.6507–0.8447 <0.0001
AAST 0.1370 0.2019 0.6468–1.1877 <0.0001
Length of case, minb PGS 0.1335–0.1132 0.0195 0.2174 0.0959–0.1711 <0.0001
AAST 0.0433 0.0370 0.0276–0.1989 <0.0001
AIC p
Length of stay, dc PGS 0.5645–1.1372 0.1491 314.01 0.2702–0.8588 0.0002
AAST 0.2220 318.86 0.6990–1.5754 <0.0001
a Linear regression model.b Log-linear regression model, with mean and variance estimated on the logarithmic scale.c Negative binomial regression model, with mean and variance estimated on the logarithmic scale.False discovery rate for each p value was <0.0002.CI, confidence interval.
J Trauma Acute Care SurgVolume 86, Number 3 Cholecystitis grading scale comparison
Program, such entities can actually impose financial penaltiesand reduce payments to health care institutions and providersfor poor outcomes.17,18 Furthermore, if such penalties are im-posed without an accurate, risk-adjusted correction, there hasbeen a demonstrable risk that providers and institutions may be-gin to avoid high-risk patients and/procedures altogether.18,19
While both the NSQIP and Centers for Medicare andMedicaid Services may adjust risk based on items, such as pa-tient demographics and comorbidities,18,20 no current widelyimplemented form of outcome comparison uses operative dis-ease severity as a form of risk stratification. Emergency generalsurgery is particularly vulnerable to current forms of outcomecomparison. First, EGS patients have been shown in the literatureto be particularly susceptible to adverse events when comparedwith the elective general surgery population.21 Explanations forsuch vulnerability have centered on the extreme variability amongboth systems (i.e., resources, workforce, etc.) and patients (i.e.,comorbidities, acute physiology, etc.).2 Such explanations werehighlighted in a review of emergency appendectomies,
TABLE 4. Model and Predictive Performance for the Relationship Bet
Outcomes ScalesAUC
(95% CI) Brier Score Erro
Abnormal anatomy PGS 0.5653 (0.4525–0.6782) 0.1235 0.1
AAST 0.5789 (0.4738–0.6840) 0.1215 0.1
Partial cholecystectomy PGS 0.8783 (0.8000–0.9567) 0.0553 0.0
AAST 0.8337 (0.7288–0.9387) 0.0616 0.0
Open cholecystectomy PGS 0.9035 (0.8576–0.9495) 0.0364 0.0
AAST 0.7565 (0.5891–0.9241) 0.0409 0.0
60-d ER return visit PGS 0.5098 (0.3912–0.6284) 0.1432 0.1
AAST 0.4910 (0.4055–0.5767) 0.1431 0.1
60-d ACS readmission PGS 0.5051 (0.3372–0.6731) 0.0813 0.0
AAST 0.5525 (0.4305–0.6745) 0.0814 0.0
Postoperative bile leak PGS 0.7775 (0.5092–1.000) 0.0256 0.0
AAST 0.7580 (0.5671–0.9490) 0.0274 0.0
Overall complication PGS 0.7039 (0.4955–0.9123) 0.0364 0.0
AAST 0.6474 (0.4551–0.8398) 0.0377 0.0
A separate logistic regression model was used to estimate each outcome from PGS and AASFDR, false discovery rate.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
cholecystectomies, and colorectal resections at over 95 hospitalsby Ingraham et al. in 2010.22 This study of over 45,000 patientsfound that not only did almost 15% of patients experience at leastonemorbidity, but that most hospitals did not have consistent risk-adjusted outcomes across all three procedures.22 Specificallylooking at LCs, a separate analysis of over 65,000 patients fromthe NSQIP database by Ingraham et al.23 continued to findconsiderable variation among hospital performance when evalu-ating 30-day outcomes.
These results could suggest one of two things: (1) Assuggested by Ingraham, best practice guidelines should be dis-seminated among hospital systems to achieve greater unity inoutcome measurements,22 and (2) our argument that to compareoperative outcomes, disease severity and thus intraoperative in-flammation and findings must be incorporated in risk-adjustedassessments. An LC performed semielectively at a private insti-tution for a mild case of acute cholecystitis in a young femalecan be very different than one performed urgently, in a safety nethospital for gangrenous cholecystitis in a 70-year-old man with
ween the Binary Outcomes and PGS and AAST Scales
r RateParameterEstimate
StandardError
95% CIParameter Estimate p (FDR)
453 0.1624 0.1670 −0.1635 to 0.4938 0.3307 (0.4630)
453 0.5474 0.2890 −0.0190 to 1.1138 0.0582 (0.1041)
782 1.6017 0.4012 0.9131 to 2.5767 <0.0001 (0.0007)
726 1.5478 0.3735 0.8780 to 2.3476 <0.0001 (0.0007)
447 1.8393 0.6251 0.6142 to 3.0645 0.0033 (0.0154)
447 1.0663 0.3797 0.3236 to 1.8028 0.0050 (0.0175)
732 −0.00818 0.1557 −0.3156 to 0.2960 0.9581 (0.9581)
732 −0.0633 0.3287 −0.7811 to 0.5212 0.8474 (0.9126)
894 0.0559 0.2031 −0.3486 to 0.4584 0.7831 (0.9126)
894 0.2086 0.3765 −0.6398 to 0.8689 0.5796 (0.7377)
279 0.9214 0.4243 0.1584 to 1.9818 0.0299 (0.0837)
279 0.8483 0.4501 −0.1397 to 1.6738 0.0595 (0.1041)
391 0.6196 0.3203 0.0151 to 1.3340 0.0531 (0.1041)
391 0.5856 0.4367 −0.4151 to 1.3583 0.1799 (0.2798)
T, with penalized maximum likelihood estimation (Firth's bias correction).
475
ealth, Inc. All rights reserved.

Madni et al.J Trauma Acute Care Surg
Volume 86, Number 3
10 comorbidities. Complications, length of stay, and mortalityshould all be judged differently in these two examples. However,what if we are comparing two LCs with almost identical demo-graphics and comorbidities? The two operations can still be vastlydifferent, pending the amount of inflation or anatomic variability.One operation could take less than 20minutes, and one could takemultiple hours via a fairly unclear and risky dissection. Given thatthe latter operation has a higher risk for future complications, itis imperative that both patient factors as well as disease severitybe factored into the risk-adjustment of comparable outcomes.
In addition to outcome comparison, we believe that anintraoperative-based grading scale could also be used to assistin management decisions. If certain patient-specific factors(i.e., abnormal anatomy, inflation, etc.) can be realized earlyon, then it is feasible to assume that an LC may be managedor approached differently. For instance, recognition of key intra-operative factors may allow for a more senior resident or facultyto take over the dissection in an academic setting. Or, perhaps acertain degree of intraoperative inflammationmay lower a surgeon'sthreshold for an open conversion if the data suggest that this surgeryis a likely outcome in the future. Currently, the most widespreadscoring system used for management of GB disease, specificallyacute cholecystitis, has been a three-tiered grading system, theTokyo guidelines.24 From its inception, however, the Tokyo guide-lines have been criticized for not leading to improved outcomesregardless if its management recommendations were followedor not.25 A more recent study by Joseph et al. found similar re-sults in addition to finding no difference in outcomes (i.e., com-plications, conversion to open, hospital length of stay, mortality)between grades.26
In our previous work, we have reviewed several additionalscoring systems that have been developed for LC outcome pre-diction; however, most are complex, based on preoperative data,and have been in limited use since their inception.13 In responseto the need for more uniform risk stratification, the AAST createda grading scale for the 16 most common EGS conditions.10,11 Thisscale has been found reliable and validated as a method of outcomeprediction in several EGS diseases to date, including small-bowelobstruction27 skin and soft tissue infections,28 pancreatitis,29 ap-pendicitis,30 and diverticulitis,31 as well as cholecystitis.12 Spe-cifically looking at cholecystitis, in addition to its AAST scalevalidation, Hernandez et al. compared the AAST-C scale againstthe gold standard Tokyo guidelines. In a single-center study of443 patients, the AAST-C scale was found to outperform the To-kyo guidelines for key clinical outcomes: mortality, complica-tions, and cholecystostomy tube placement.32 However, thereare several limitations that this scale has failed to address. First,the scale is complex, and it requires one through five grades infour components (clinical, operative, imaging, and pathology)as shown in Table 1. The true AAST grade is the highest of thefour separate grades. Thus, the scale requires extensive data col-lection, and the user must wait days toweeks for pathological re-sults prior to determining a grade.
Second, the AAST scale starts (grade 1) at the diagnosis ofacute cholecystitis, and as such, excludes the comparison of poten-tial other EGS GB disease (biliary colic, biliary pancreatitis, etc.).Furthermore, in a validation article by Vera et al.12, the majorityof the patient population had lowAAST grade for disease: grade1 (69.5%), grade 2 (23.8%), grade 3 (5.7%), grade 4 (0.0%), and
476
Copyright © 2019 Wolters Kluwer H
grade 5 (1.0%). As such, and acknowledged by the authors, theAAST scale does not offer true granularity for less severe dis-ease, with 90% of the disease appearing in grades 1 and 2.12
We found similar results in our current study, as 96% of our pa-tients received either an AAST-C grade 1 or 2 score (Table 2)with an ICC of 0.8341 among three raters.
In contrast to the AAST-C, PGS has a number ofstrengths. First, it is an operative-based scale where the gradecan be determined upon the initial view of the GB during LC.No further data collection is required. This allows the grade tobe notated in the operative report, and thus easily used for futureoutcome comparisons. Furthermore, our results demonstratethat when PGS was compared against the median, stand-aloneAAST-C operative grade (i.e., ignoring the clinical, imaging, andpathologic components) the pattern of predictive performance forthe median AAST-C operative grade versus PGS is similar to thatof the median trueAAST score versus PGS (i.e., similar to whatis reported in Tables 3 and 4). Summarized, our operative-onlygrading scale (PGS) was found to be a similar predictor oflength of stay and bile leak rate in addition to superior predictorof operative difficulty, case length, open and partial cholecystec-tomy rates, and overall complication rates compared with boththe trueAAST-C score as well as the stand-alone operative grad-ing component of the AAST-C scale. Second, the PGS encom-passes a wider spectrum of disease and is not specific to justcholecystitis. Any GB observed during LC, regardless of its pa-thology, can be included. During our study period, 316 GBs re-ceived a PGS grade; however, only 179 (57%) could becompared against the AAST-C grade as the other LCs were per-formed for reasons other than acute cholecystitis (i.e., symptom-atic cholelithiasis, choledocholithiasis, biliary pancreatitis, etc.),which is the first grade of the AAST-C scale. Finally, even withinour acute cholecystitis cohort, the PGS offered better granularity,demonstrating an almost normal distribution among grades(Table 2). In summary, PGS is a simpler, superior scale whencompared with either the true AAST-C grade or the AAST-C'sstand-alone operative grade component.
In addition, while the AAST-C scale demonstrated excellentrater reliability with a κ of 1.00 among two raters in its validationarticle12 and within this study (ICC, 0.8341), our study founddiscrepancies in the ICC among the individual scoring compo-nents and question their need. With regards to PGS, we havedemonstrated excellent reliability among 11 raters in our originalwork (ICC, 0.804),13 and between three independent, retrospectivesurgeon raters of “still” images and the surgeon who performedthe operation and assigned the “live” grade (ICC, 0.8647). Onthe other hand, the clinical component of the AAST-C score,demonstrated an ICC of 0.3472 in this study, suggesting perhapsthis as an unnecessary point of data collection. In addition, whilethe AAST-C imaging grade demonstrated excellent rater reli-ability with an ICC of 0.9243, we find this grading componentlargely unnecessary to further define disease severity. It is in ouropinion that true anatomical disease severity for cholecystitis isbest defined and classified in the operating room and is superiorto any imaging findings. To further support such a hypothesis,we performed a separate Spearman's ρ test to determine any cor-relation between the median AAST-C imaging grade and PGS.The results showed a significant relationship between PGS andthe median AAST-C imaging grade, but the magnitude of the
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Cholecystitis grading scale comparison
association was quite modest. The statistical significance waslikely secondary to the relatively large N of 179. Since PGSwas found to be either a similar, or superior, predictor of out-comes to the true AAST-C grade in an operative-only–basedscale, we believe there is little need for an extra imaging com-ponent to such a scale. Finally, while the ICC of the AAST-Cpathology component was found to be excellent (ICC = 0.7023),the limited added value of waiting for days to weeks for a pa-thology report for a final true AAST-C score may limit thewidespread utility of such a scale. As such, we believe the PGSis a superior predictor of LC outcomes, in a highly reliable,simple-to-use scale.
We acknowledge a few limitations within our study. First,while three raters assigned AAST-C grades to GBs to find a truegrade, only one PGS score was assigned per LC. However, sucha limitation is minimal as our previous work demonstrated ex-cellent interrater reliability among raters.13 Second, it is possiblea rater who assigns a higher PGS score during the “initial view”may assign a higher difficulty score postoperatively as a self-fulfilling bias. In the study design itself, we attempted to mini-mize this potential bias by making the grading scale based onobjective anatomical and inflammatory changes to be assignedduring the initial viewof the GB fossa before the dissection begins.Operative difficultywas graded separately during the postoperativeperiod with no referral or prior stated relationship to the chole-cystitis operative grade. A difficulty correlation, however, wasnot the only outcome assessed in this study. Even if one wereto assume too much subjectivity in the difficulty ratings, objec-tive superiority was demonstrated by the PGS in several otheroutcomes. Third, one may argue hybrid scores inclusive of mul-tiple data points (i.e., preoperative, perioperative, and postoper-ative data) may provide the most information to the level ofdisease severity being assessed (i.e., more data may providemore valid and reliable results); however, our results suggestthe opposite. Parkland grading scale for cholecystitis was foundto perform either similarly or superiorly to the hybrid AAST-Cscale in several perioperative outcomes. In addition, hybridscores of multiple findings require cumbersome data collec-tion at different time points, and thus limit the utility of thescale for widespread use. Additional components require fur-ther time for both data mining as well as interpretation, whichmay disincentivize the practitioner to incorporate such a toolinto his or her practice. A final limitation is our focus on postop-erative complications defined as either a retained stone, smallbowel obstruction, wound infection, or postoperative biliaryleak. Other validation studies for the AAST-C scale include out-comes, such as acute renal failure, urinary tract infection, pneu-monia, deep venous thrombosis, and so on.12 Given the rarity ofthese complications after LC, we did not think our study wouldhave sufficient power to detect such differences. On post hoc re-view, however, no patients showed any such complications.
CONCLUSION
In conclusion, while the PGS and AAST-C both demon-strate excellent reliability among raters, the PGS was found tobe a superior predictor of operative difficulty, case length, openand partial cholecystectomy rates, and overall complication rates.The PGS does so in a simpler, easy-to-understand scale with data
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
collection only occurring during the operative portion of thepatient's stay (i.e., a single time point). Future work will focuson multicenter trial assessment for external validation as wellas comparison against both the AAST-C scale as well as theTokyo guidelines.
AUTHORSHIP
T.D.M., P.A.N., J.B.I., A.T.C., H.A.P., M.W.C., C.T.M. participated in thestudy conception and design. T.D.M., J.B.I., A.T.C., L.T., H.B.C., R.V., M.W.C., H.A.P., S.L., A.L.E., C.T.M. participated in the acquisition of data.T.D.M., P.A.N., H.A.P., M.W.C., C.T.M. participated in the analysis and in-terpretation of data. T.D.M., P.A.N., A.T.C., J.B.I., H.B.C., R.V., L.T., H.A.P.,M.W.C., S.L., A.L.E., C.T.M. participated in the drafting of the article. T.D.M.,P.A.N., A.T.C., J.B.I., H.A.P., M.W.C., A.L.E., C.T.M. participated in thecritical revision.
ACKNOWLEDGMENTS
The authors acknowledge the following: Inna Donovan, NP, for data col-lection; Karen Garofalo, PA, for data collection; Cynthia Chernyakhovsky,PA, for data collection; David Primm as the medical editor.
DISCLOSURE
The authors declare no funding or conflicts of interest.
REFERENCES1. Gale SC, Shafi S, Dombrovskiy VY, Arumugam D, Crystal JS. The public
health burden of emergency general surgery in the United States: a 10-yearanalysis of the nationwide inpatient sample—2001 to 2010. J Trauma AcuteCare Surg. 2014;77(2):202–208.
2. Columbus AB, Morris MA, Lilley EJ, Harlow AF, Haider AH, Salim A,Havens JM. Critical differences between elective and emergency surgery:identifying domains for quality improvement in emergency general surgery.Surgery. 2018;163(4):832–838.
3. Shafi S, AboutanosMB, Agarwal S Jr., Brown CV, CrandallM, FelicianoDV,Guillamondegui O, Haider A, Inaba K, Osler TM, et al. Emergency generalsurgery: definition and estimated burden of disease. J Trauma Acute CareSurg. 2013;74(4):1092–1097.
4. Havens JM, Peetz AB, Do WS, Cooper Z, Kelly E, Askari R, Reznor G,Salim A. The excess morbidity and mortality of emergency general surgery.J Trauma Acute Care Surg. 2015;78(2):306–311.
5. Ogola GO, Gale SC, Haider A, Shafi S. The financial burden of emergencygeneral surgery: national estimates 2010 to 2060. J Trauma Acute Care Surg.2015;79(3):444–448.
6. Neary WD, Prytherch D, Foy C, Heather BP, Earnshaw JJ. Comparison ofdifferent methods of risk stratification in urgent and emergency surgery.Br J Surg. 2007;94(10):1300–1305.
7. Strasberg SM.Clinical practice. Acute calculous cholecystitis.NEngl JMed.2008;358(26):2804–2811.
8. Agency forHealthcareResearch andQuality—Healthcare Cost andUtilizationProject (H-CUP). Most frequent operating room procedures performed in U.S.hospitals, 2003-2012 2014. [updated 12/2014; Accessed: 10/23/2017].
9. Havens JM, Columbus AB, Seshadri AJ, Brown CVR, Tominaga GT,Mowery NT, Crandall M. Risk stratification tools in emergency general sur-gery. Trauma Surg Acute Care Open. 2018;3(1):e000160.
10. Shafi S, Aboutanos M, Brown CV, Ciesla D, Cohen MJ, Crandall ML,Inaba K, Miller PR, Mowery NT. Measuring anatomic severity of diseasein emergency general surgery. J Trauma Acute Care Surg. 2014;76(3):884–887.
11. TominagaGT, Staudenmayer KL, Shafi S, Schuster KM, Savage SA, Ross S,Muskat P, Mowery NT, Miller P, Inaba K, et al. The American Associationfor the Surgery of Trauma grading scale for 16 emergency general surgeryconditions: disease-specific criteria characterizing anatomic severity grading.J Trauma Acute Care Surg. 2016;81(3):593–602.
12. Vera K, Pei KY, Schuster KM, Davis KA. Validation of a new American As-sociation for the Surgery of Trauma (AAST) anatomic severity grading sys-tem for acute cholecystitis. J Trauma Acute Care Surg. 2018;84(4):650–654.
477
ealth, Inc. All rights reserved.
Madni et al.J Trauma Acute Care Surg
Volume 86, Number 3
13. Madni TD, Leshikar DE, Minshall CT, Nakonezny PA, Cornelius CC,Imran JB, Clark AT,Williams BH, EastmanAL,Minei JP, et al. The Parklandgrading scale for cholecystitis. Am J Surg. 2017.
14. Madni TD, Nakonezny PA, Barrios E, Imran JB, Clark AT, Taveras L,Cunningham HB, Christie A, Eastman AL, Minshall CT, et al. Prospectivevalidation of the Parkland grading scale for cholecystitis. Am J Surg. 2018;S0002-9610:30848–30841.
15. Ko CY, Hall BL, Hart AJ, Cohen ME, Hoyt DB. The American College ofSurgeons National Surgical Quality Improvement Program: achieving betterand safer surgery. Jt Comm J Qual Patient Saf. 2015;41(5):199–204.
16. Centers for Medicare &Medicaid Services. Outcomes Measures [Accessed:06/04/2018]. Available from: https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/HospitalQualityInits/OutcomeMeasures.html.
17. Gupta A, Fonarow GC. The hospital readmissions reduction program-learning from failure of a healthcare policy. Eur J Heart Fail. 2018;20:1169–1174.
18. Maggard-Gibbons M. The use of report cards and outcomemeasurements toimprove the safety of surgical care: the American College of Surgeons Na-tional Surgical Quality Improvement Program. BMJ Qual Saf. 2014;23(7):589–599.
19. Omoigui NA, Miller DP, Brown KJ, Annan K, Cosgrove D 3rd, Lytle B,Loop F, Topol EJ. Outmigration for coronary bypass surgery in an era of pub-lic dissemination of clinical outcomes. Circulation. 1996;93(1):27–33.
20. Centers for Medicare & Medicaid Services. Fact Sheet: Risk Adjustment2015 [Accessed: 06/08/2018]. Available from: https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeedbackProgram/Downloads/Risk-Adjustment-Fact-Sheet.pdf.
21. Ingraham AM, Cohen ME, Raval MV, Ko CY, Nathens AB. Comparison ofhospital performance in emergency versus elective general surgery opera-tions at 198 hospitals. J Am Coll Surg. 2011;212(1):20–8.e1.
22. Ingraham AM, Cohen ME, Bilimoria KY, Raval MV, Ko CY, Nathens AB,Hall BL. Comparison of 30-day outcomes after emergency general surgeryprocedures: potential for targeted improvement. Surgery. 2010;148(2):217–238.
23. Ingraham AM, Cohen ME, Ko CY, Hall BL. A current profile and assess-ment of North American cholecystectomy: results from the American
478
Copyright © 2019 Wolters Kluwer H
College of Surgeon's National Surgical Quality Improvement Program.J Am Coll Surg. 2010;211(2):176–186.
24. Hirota M, Takada T, Kawarada Y, Nimura Y, Miura F, Hirata K, Mayumi T,Yoshida M, Strasberg S, Pitt H, et al. Diagnostic criteria and severity assess-ment of acute cholecystitis: Tokyo guidelines. J Hepato-Biliary-PancreatSurg. 2007;14(1):78–82.
25. Lee SW, Yang SS, Chang CS, Yeh HJ. Impact of the Tokyo guidelines on themanagement of patients with acute calculous cholecystitis. J GastroenterolHepatol. 2009;24(12):1857–1861.
26. Joseph B, Jehan F, Dacey M, Kulvatunyou N, KhanM, ZeeshanM, Gries L,O'Keeffe T, Riall TS. Evaluating the relevance of the 2013 Tokyo guidelinesfor the diagnosis and management of cholecystitis. J Am Coll Surg. 2018;227:38–43.e1.
27. Baghdadi YMK, Morris DS, Choudhry AJ, Thiels CA, Khasawneh MA,Polites SF, Goussous N, Jenkins DH, Zielinski MD. Validation of the ana-tomic severity score developed by the American Association for the Surgeryof Trauma in small bowel obstruction. J Surg Res. 2016;204(2):428–434.
28. Ray-Zack MD, Hernandez MC, Younis M, Hoch WB, Soukup DS,Haddad NN, Zielinski MD. Validation of the American Association for theSurgery of Trauma emergency general surgery grade for skin and soft tissueinfection. J Trauma Acute Care Surg. 2018;84(6):939–945.
29. Younis M, Hernandez M, Ray-Zack M, Haddad NN, Choudhry A, Reddy P,Zielinski MD. Validation of AAST EGS grade for acute pancreatitis.J Gastrointest Surg. 2018;22(3):430–437.
30. Hernandez MC, Aho JM, Habermann EB, Choudhry AJ, Morris DS,Zielinski MD. Increased anatomic severity predicts outcomes: validation ofthe American Association for the Surgery of Trauma's Emergency GeneralSurgery Score in appendicitis. J Trauma Acute Care Surg. 2017;82(1):73–79.
31. Shafi S, Priest EL,CrandallML,Klekar CS,NazimA,AboutanosM,Agarwal S,Bhattacharya B, Byrge N, Dhillon TS, et al. Multicenter validation of AmericanAssociation for the Surgery of Trauma grading system for acute colonic divertic-ulitis and its use for emergency general surgery quality improvement pro-gram. J Trauma Acute Care Surg. 2016;80(3):405–410; discussion 410-1.
32. HernandezM,Murphy B, Aho JM, Haddad NN, SaleemH, ZebM,Morris DS,Jenkins DH, Zielinski M. Validation of the AAST EGS acute cholecystitisgrade and comparison with the Tokyo guidelines. Surgery. 2018;163:739–746.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
ORIGINAL ARTICLE
Symptomatic human immunodeficiency virus–infected patientshave poorer outcomes following emergency general surgery:
A study of the nationwide inpatient sample
Britt J. Sandler, MD, MHS, Kimberly A. Davis, MD, MBA,and Kevin M. Schuster, MD, MPH, New Haven, Connecticut
Sub
Fro
Ad
Pre
DO
J TrVol
BACKGROUND: T
mitted: May 7, 2016, Revised:Published online: December 10m the Section of General Surgerof Surgery (B.J.S., K.A.D., KConnecticutdress for reprints: KevinM. SchuNew Haven, CT 06520; email:sented as a poster at the EasterMeeting, San Antonio, TX, Jan
I: 10.1097/TA.00000000000021
auma Acute Care Surgume 86, Number 3
he impact of human immunodeficiency virus (HIV) infection on outcomes following common emergency general surgery pro-cedures has not been evaluated since the widespread introduction of highly active antiretroviral therapy.
METHODS: A
retrospective cohort study was conducted using the Nationwide Inpatient Sample. Records of patients who underwent laparo-scopic or open appendectomy, cholecystectomy, or colon resection after emergency admission from 2004 to 2011 were obtained.Outcomes analyzed included in-hospital mortality, length of stay, total charges, and selected postoperative complications. Patientswere divided among three groups, HIV-negative controls, asymptomatic HIV-positive patients, and symptomatic HIV/acquired im-mune deficiency syndrome (AIDS) patients. Data were analyzed using χ2 and multivariable regression with propensity scorematching among the three groups, with p value less than 0.05 significant.RESULTS: T
here were 974,588 patients identified, of which 1,489 were HIV-positive and 1,633 were HIV/AIDS-positive. The HIV/AIDSpatients were more likely to die during their hospital stay than HIV-negative patients (4.4% vs. 1.6%, adjusted odds ratio, 3.53;95% confidence interval [CI], 2.67–4.07; p < 0.001). The HIV/AIDS patients had longer hospital stays (7 days vs. 3 days; adjusteddifference, 3.66 days; 95% CI, 3.53–4.00; p < 0.001) and higher median total charges than HIV-negative patients (US $47,714 vs.US $28,405; adjusted difference, US $15,264; 95% CI, US $13,905–US $16,623; p < 0.001). The HIV/AIDS patients also hadsignificantly increased odds of certain postoperative complications, including sepsis, septic shock, pneumonia, urinary tract infec-tion, acute renal failure and need for transfusion (p < 0.05 for each). Differences persisted irrespective of case complexity and overthe study period. Asymptomatic HIV-positive patients had outcomes similar to HIV-negative patients.CONCLUSION: T
he HIV/AIDS patients have a greater risk of death, infectious, and noninfectious complications after emergency surgery regard-less of operative complexity and despite advanced highly active antiretroviral therapy. Patients who have not developed advanceddisease, however, have similar outcomes to HIV-negative patients. (J Trauma Acute Care Surg. 2019;86: 479–488. Copyright ©2018 Wolters Kluwer Health, Inc. All rights reserved.)LEVEL OF EVIDENCE: P
rognostic and epidemiologic study, level III. KEYWORDS: H IV; emergency general surgery; surgical outcomes; nationwide inpatient sample.N ational statistics indicate that there are 1.2 million peopleinfected with human immunodeficiency virus (HIV) in
the United States. The prevalence of HIV infection has increasedby 20% over the past decade, due to new infections (approxi-mately 45,000 per year), and a decrease in mortality from the ac-quired immune deficiency syndrome (AIDS).1
Surgical outcomes in HIV-infected patients have improvedsubstantially over the course of the 30-year epidemic. Some of theearliest reports of surgical outcomes in this population describedpatients with advanced disease receiving surgery for AIDS-related pathologies, such as Candida cholecystitis and perforatedcytomegalovirus colitis. Unsurprisingly, mortality was high
August 7, 2018, Accepted: November 21, 2018,, 2018.y, Trauma, and Surgical Critical Care, Department.M.S.), Yale School of Medicine, New Haven,
ster, MD, 330 Cedar St., BB 310, POBox [email protected] Association for the Surgery of Trauma Annualuary 2016.
61
Copyright © 2019 Wolters Kluwer H
(22–70%) in these early cohorts, due to severely compromisedimmune function, the presence of opportunistic infections, andprotein-calorie malnutrition.2–4
The introduction of highly active antiretroviral therapy(HAART) in the mid-1990s has changed HIV from a rapidlyprogressive and fatal disease to a chronic disease. However, con-cerns still remain about the impact of HIV infection on patients'ability to tolerate and recover from surgery. Human immunodefi-ciency virus–related immunosuppression diminishes the ability todefend against postoperative infections, such as pneumonia, urinarytract infection (UTI), and bacterial sepsis.2–4 CD4 counts below200 cells/mm3 and viral load of 30,000 copies/mL or greaterhave been associated with increases in infectious complicationsand mortality.5–7
Human immunodeficiency virus infection is also associatedwith delayedwound healing and increasedwound-related complica-tions. CD4-positive T lymphocytes and macrophages, the cell typesinfected by HIV, both play an important role in wound healing,and the targeted depletion of CD4 cells is associated with de-creased wound strength.8,9 Prior studies have demonstrated sig-nificant delays in wound healing among HIV-infected patientsand higher rates of wound dehiscence and anastomotic leak.2,9–11
479
ealth, Inc. All rights reserved.

Sandler et al.J Trauma Acute Care Surg
Volume 86, Number 3
Studies of surgical outcomes in the HAART era have fre-quently found inferior outcomes among HIV-infected patients,including increased risk of postoperative infection, higher ratesof complications, and increased mortality, although the absoluterates of adverse outcomes remain low.5,12–18 However, thesestatements mask a great deal of heterogeneity depending onthe specific clinical picture of HIV infection, including CD4count, viral load, antiretroviral (ARV) treatment regimen and ad-herence, age, comorbidities, and associated risk factors, and thetype and complexity of surgery performed.
Separately, efforts within the field of acute care surgery todescribe the patient cohort undergoing emergency general sur-gery (EGS) and the burden of disease from these pathologiesand procedures are ongoing.19,20 Emergency general surgery pa-tients appear to have poorer outcomes than patients undergoingelective procedures, for reasons that remain unclear but may re-flect the pathophysiology behind the need for an emergent sur-gery as well as issues surrounding the delivery of care.21–23
Further characterization of this patient population is a necessarystep in measuring quality, developing evidence-based guide-lines, and improving the delivery of EGS care.20,24
Our objective was to examine the effect of HIV on out-comes following emergency general surgery. To our knowledge,this is the first study in the HAARTera to specifically investigatepostoperative outcomes following emergency general surgery.We hypothesized that, given the unique effects of HIV infectionon healing and the immune response, HIV-infected patients un-dergoing these procedures would have higher rates of infectiousand wound-related complications and as a result would have lon-ger hospitalizations, increased hospital charges, and higher ratesof death following emergency general surgery. Identifying thespecific impact of HIV infection on patients receiving emer-gency surgery would generate valuable information to informsurgical decision making and informed consent regarding therisks and benefits of surgery.
METHODS
Patient IdentificationWe conducted a retrospective cohort study using the Na-
tionwide Inpatient Sample (NIS), the largest all-payer inpatientadministrative database available in the United States. The NIS,a part of the Healthcare Cost and Utilization Project (HCUP), ismaintained by the Agency for Healthcare Research and Quality.The NIS contains discharge records from more than 7 millionhospitalizations annually and is collected as a stratified samplefrom approximately 20% of hospitals nationwide.25 The NIS'slarge sample size enables analyses of patient populations with
TABLE 1. ICD-9-CM Codes Used to Identify Patients Undergoing Co
Procedure Type
Laparoscopic appendectomy
Open appendectomy
Laparoscopic cholecystectomy
Open cholecystectomy
Laparoscopic colon resection
Open colon resection 45
480
Copyright © 2019 Wolters Kluwer H
relatively rare conditions. The Yale Human Investigation Com-mittee deemed this study exempt from review as the NIS con-tains de-identified records.
Discharge records of patients at least 18 years of age whounderwent common emergency general surgery (EGS) proceduresafter emergent or urgent admission between 2004 and 2011 wereabstracted into a database for analysis. The operative proceduresincluded were based on prior studies examining common diag-noses and procedures among EGS patients.19,20,26 Procedureswere organized into six categories: laparoscopic appendectomy,open appendectomy, laparoscopic cholecystectomy, opencholecystectomy, laparoscopic colon resection, and open colonresection. Patient records were selected using the InternationalClassification of Diseases, Ninth Revision, Clinical Modifica-tion (ICD-9-CM) codes for these procedures (Table 1).27 Re-cords were excluded if important values for risk stratificationor outcome purposes were missing including, age, gender,or any primary outcome.
From this cohort, three groups were identified: (1) a controlgroup of patients without HIV, and (2) patients with HIV infectionwho also carried a diagnosis of AIDS, having manifestations oftheir HIV disease and (3) patients with asymptomatic HIV infec-tion. Patients with HIV infection were selected using ICD-9-CMdiagnosis codes 042 (human immunodeficiency virus disease)and V08 (asymptomatic human immunodeficiency virus infec-tion status). To receive a 042 code, a patient must be describedas having a condition or disease resulting from their HIV-positive status or have a diagnosis of AIDS.16
Analytic MethodsDemographic variables and the rates of comorbid condi-
tions were compared between EGS patients with HIV/AIDS,asymptomatic HIV infection and controls using Pearson'sχ2 test.The demographic variables examined included age, gender, race,hospital type (urban teaching, urban nonteaching, and rural), pri-mary payer, and median income in the patient's zip code, a proxyvariable for socioeconomic status. These have all been shown topotentially impact outcomes either after injury or in other medicalconditions.28,29
Comorbid conditions were chosen from the list of individualdiagnoses that comprise the Charlson-Deyo comorbidity index andincluded diabetes, chronic pulmonary disease, malignancy andmetastatic cancer, congestive heart failure, chronic kidney disease,liver disease, peripheral vascular disease, a history of myocardialinfarction, rheumatoid arthritis, cerebrovascular disease, paralysis,dementia, and peptic ulcer disease.30 Rates of three potentially rel-evant risk factors (obesity, smoking, and a history of drug abuse)were also compared between HIV/AIDS patients, as well as,
mmon Emergency General Surgery Procedures
ICD-9-CM Code(s) Included in Analysis
47.01
47.09
51.23
51.22
17.31, 17.32, 17.33, 17.34, 17.35, 17.36, 17.39, 45.81, 48.42, 48.51
.71, 45.72, 45.73, 45.74, 45.75, 45.76, 45.79, 45.82, 45.83, 48.50, 48.52, 48.69
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
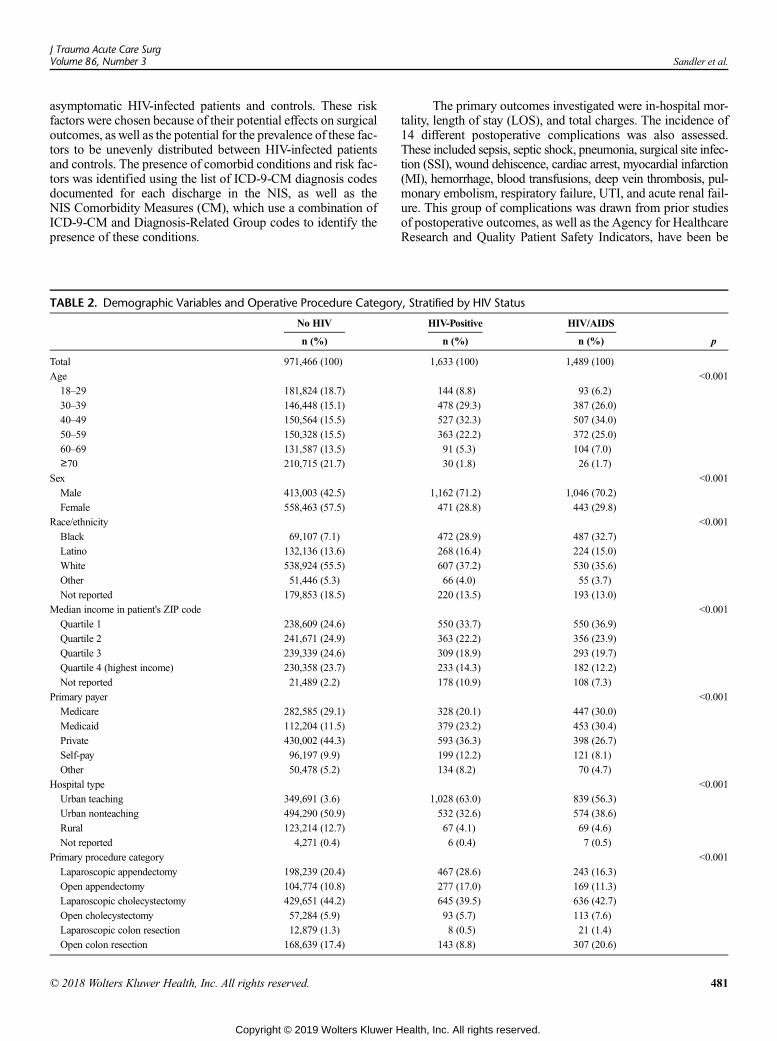
J Trauma Acute Care SurgVolume 86, Number 3 Sandler et al.
asymptomatic HIV-infected patients and controls. These riskfactors were chosen because of their potential effects on surgicaloutcomes, as well as the potential for the prevalence of these fac-tors to be unevenly distributed between HIV-infected patientsand controls. The presence of comorbid conditions and risk fac-tors was identified using the list of ICD-9-CM diagnosis codesdocumented for each discharge in the NIS, as well as theNIS Comorbidity Measures (CM), which use a combination ofICD-9-CM and Diagnosis-Related Group codes to identify thepresence of these conditions.
TABLE 2. Demographic Variables and Operative Procedure Category
No HIV
n (%)
Total 971,466 (100)
Age
18–29 181,824 (18.7)
30–39 146,448 (15.1)
40–49 150,564 (15.5)
50–59 150,328 (15.5)
60–69 131,587 (13.5)
≥70 210,715 (21.7)
Sex
Male 413,003 (42.5)
Female 558,463 (57.5)
Race/ethnicity
Black 69,107 (7.1)
Latino 132,136 (13.6)
White 538,924 (55.5)
Other 51,446 (5.3)
Not reported 179,853 (18.5)
Median income in patient's ZIP code
Quartile 1 238,609 (24.6)
Quartile 2 241,671 (24.9)
Quartile 3 239,339 (24.6)
Quartile 4 (highest income) 230,358 (23.7)
Not reported 21,489 (2.2)
Primary payer
Medicare 282,585 (29.1)
Medicaid 112,204 (11.5)
Private 430,002 (44.3)
Self-pay 96,197 (9.9)
Other 50,478 (5.2)
Hospital type
Urban teaching 349,691 (3.6)
Urban nonteaching 494,290 (50.9)
Rural 123,214 (12.7)
Not reported 4,271 (0.4)
Primary procedure category
Laparoscopic appendectomy 198,239 (20.4)
Open appendectomy 104,774 (10.8)
Laparoscopic cholecystectomy 429,651 (44.2)
Open cholecystectomy 57,284 (5.9)
Laparoscopic colon resection 12,879 (1.3)
Open colon resection 168,639 (17.4)
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
The primary outcomes investigated were in-hospital mor-tality, length of stay (LOS), and total charges. The incidence of14 different postoperative complications was also assessed.These included sepsis, septic shock, pneumonia, surgical site infec-tion (SSI), wound dehiscence, cardiac arrest, myocardial infarction(MI), hemorrhage, blood transfusions, deep vein thrombosis, pul-monary embolism, respiratory failure, UTI, and acute renal fail-ure. This group of complications was drawn from prior studiesof postoperative outcomes, as well as the Agency for HealthcareResearch and Quality Patient Safety Indicators, have been be
, Stratified by HIV Status
HIV-Positive HIV/AIDS
n (%) n (%) p
1,633 (100) 1,489 (100)
<0.001
144 (8.8) 93 (6.2)
478 (29.3) 387 (26.0)
527 (32.3) 507 (34.0)
363 (22.2) 372 (25.0)
91 (5.3) 104 (7.0)
30 (1.8) 26 (1.7)
<0.001
1,162 (71.2) 1,046 (70.2)
471 (28.8) 443 (29.8)
<0.001
472 (28.9) 487 (32.7)
268 (16.4) 224 (15.0)
607 (37.2) 530 (35.6)
66 (4.0) 55 (3.7)
220 (13.5) 193 (13.0)
<0.001
550 (33.7) 550 (36.9)
363 (22.2) 356 (23.9)
309 (18.9) 293 (19.7)
233 (14.3) 182 (12.2)
178 (10.9) 108 (7.3)
<0.001
328 (20.1) 447 (30.0)
379 (23.2) 453 (30.4)
593 (36.3) 398 (26.7)
199 (12.2) 121 (8.1)
134 (8.2) 70 (4.7)
<0.001
1,028 (63.0) 839 (56.3)
532 (32.6) 574 (38.6)
67 (4.1) 69 (4.6)
6 (0.4) 7 (0.5)
<0.001
467 (28.6) 243 (16.3)
277 (17.0) 169 (11.3)
645 (39.5) 636 (42.7)
93 (5.7) 113 (7.6)
8 (0.5) 21 (1.4)
143 (8.8) 307 (20.6)
481
ealth, Inc. All rights reserved.
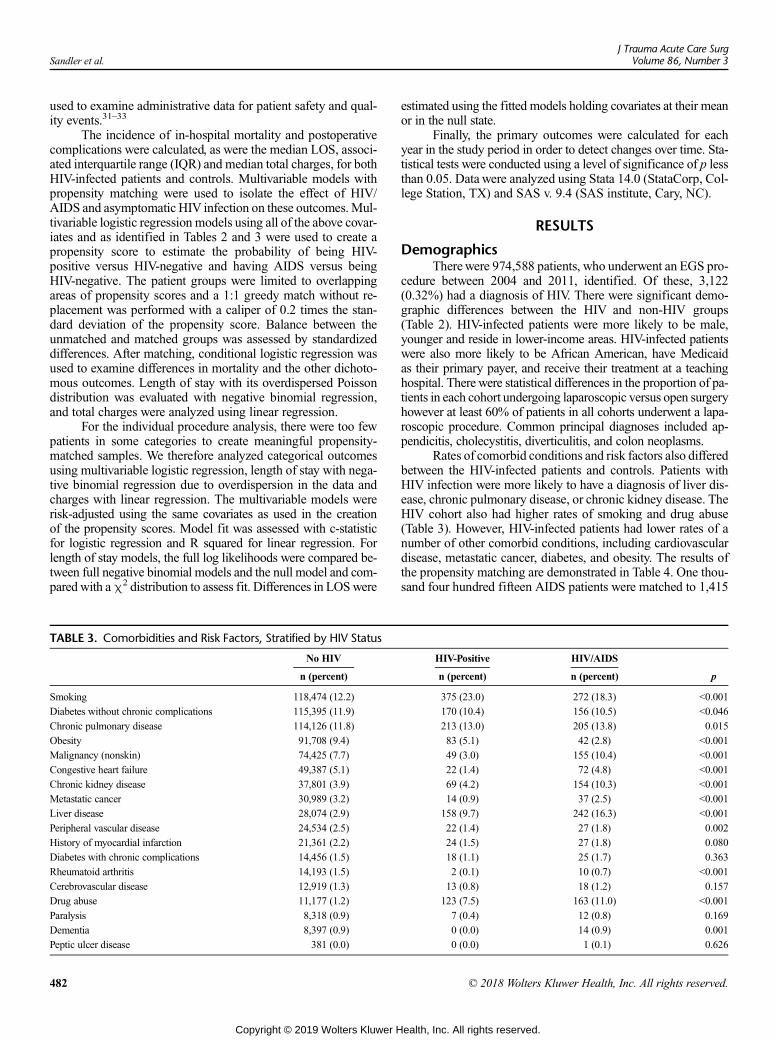
Sandler et al.J Trauma Acute Care Surg
Volume 86, Number 3
used to examine administrative data for patient safety and qual-ity events.31–33
The incidence of in-hospital mortality and postoperativecomplications were calculated, as were the median LOS, associ-ated interquartile range (IQR) and median total charges, for bothHIV-infected patients and controls. Multivariable models withpropensity matching were used to isolate the effect of HIV/AIDS and asymptomatic HIV infection on these outcomes.Mul-tivariable logistic regression models using all of the above covar-iates and as identified in Tables 2 and 3 were used to create apropensity score to estimate the probability of being HIV-positive versus HIV-negative and having AIDS versus beingHIV-negative. The patient groups were limited to overlappingareas of propensity scores and a 1:1 greedy match without re-placement was performed with a caliper of 0.2 times the stan-dard deviation of the propensity score. Balance between theunmatched and matched groups was assessed by standardizeddifferences. After matching, conditional logistic regression wasused to examine differences in mortality and the other dichoto-mous outcomes. Length of stay with its overdispersed Poissondistribution was evaluated with negative binomial regression,and total charges were analyzed using linear regression.
For the individual procedure analysis, there were too fewpatients in some categories to create meaningful propensity-matched samples. We therefore analyzed categorical outcomesusing multivariable logistic regression, length of stay with nega-tive binomial regression due to overdispersion in the data andcharges with linear regression. The multivariable models wererisk-adjusted using the same covariates as used in the creationof the propensity scores. Model fit was assessed with c-statisticfor logistic regression and R squared for linear regression. Forlength of stay models, the full log likelihoods were compared be-tween full negative binomial models and the null model and com-pared with aχ2 distribution to assess fit. Differences in LOSwere
TABLE 3. Comorbidities and Risk Factors, Stratified by HIV Status
No HIV
n (percent)
Smoking 118,474 (12.2)
Diabetes without chronic complications 115,395 (11.9)
Chronic pulmonary disease 114,126 (11.8)
Obesity 91,708 (9.4)
Malignancy (nonskin) 74,425 (7.7)
Congestive heart failure 49,387 (5.1)
Chronic kidney disease 37,801 (3.9)
Metastatic cancer 30,989 (3.2)
Liver disease 28,074 (2.9)
Peripheral vascular disease 24,534 (2.5)
History of myocardial infarction 21,361 (2.2)
Diabetes with chronic complications 14,456 (1.5)
Rheumatoid arthritis 14,193 (1.5)
Cerebrovascular disease 12,919 (1.3)
Drug abuse 11,177 (1.2)
Paralysis 8,318 (0.9)
Dementia 8,397 (0.9)
Peptic ulcer disease 381 (0.0)
482
Copyright © 2019 Wolters Kluwer H
estimated using the fitted models holding covariates at their meanor in the null state.
Finally, the primary outcomes were calculated for eachyear in the study period in order to detect changes over time. Sta-tistical tests were conducted using a level of significance of p lessthan 0.05. Data were analyzed using Stata 14.0 (StataCorp, Col-lege Station, TX) and SAS v. 9.4 (SAS institute, Cary, NC).
RESULTS
DemographicsTherewere 974,588 patients, who underwent an EGS pro-
cedure between 2004 and 2011, identified. Of these, 3,122(0.32%) had a diagnosis of HIV. There were significant demo-graphic differences between the HIV and non-HIV groups(Table 2). HIV-infected patients were more likely to be male,younger and reside in lower-income areas. HIV-infected patientswere also more likely to be African American, have Medicaidas their primary payer, and receive their treatment at a teachinghospital. There were statistical differences in the proportion of pa-tients in each cohort undergoing laparoscopic versus open surgeryhowever at least 60% of patients in all cohorts underwent a lapa-roscopic procedure. Common principal diagnoses included ap-pendicitis, cholecystitis, diverticulitis, and colon neoplasms.
Rates of comorbid conditions and risk factors also differedbetween the HIV-infected patients and controls. Patients withHIV infection were more likely to have a diagnosis of liver dis-ease, chronic pulmonary disease, or chronic kidney disease. TheHIV cohort also had higher rates of smoking and drug abuse(Table 3). However, HIV-infected patients had lower rates of anumber of other comorbid conditions, including cardiovasculardisease, metastatic cancer, diabetes, and obesity. The results ofthe propensity matching are demonstrated in Table 4. One thou-sand four hundred fifteen AIDS patients were matched to 1,415
HIV-Positive HIV/AIDS
n (percent) n (percent) p
375 (23.0) 272 (18.3) <0.001
170 (10.4) 156 (10.5) <0.046
213 (13.0) 205 (13.8) 0.015
83 (5.1) 42 (2.8) <0.001
49 (3.0) 155 (10.4) <0.001
22 (1.4) 72 (4.8) <0.001
69 (4.2) 154 (10.3) <0.001
14 (0.9) 37 (2.5) <0.001
158 (9.7) 242 (16.3) <0.001
22 (1.4) 27 (1.8) 0.002
24 (1.5) 27 (1.8) 0.080
18 (1.1) 25 (1.7) 0.363
2 (0.1) 10 (0.7) <0.001
13 (0.8) 18 (1.2) 0.157
123 (7.5) 163 (11.0) <0.001
7 (0.4) 12 (0.8) 0.169
0 (0.0) 14 (0.9) 0.001
0 (0.0) 1 (0.1) 0.626
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
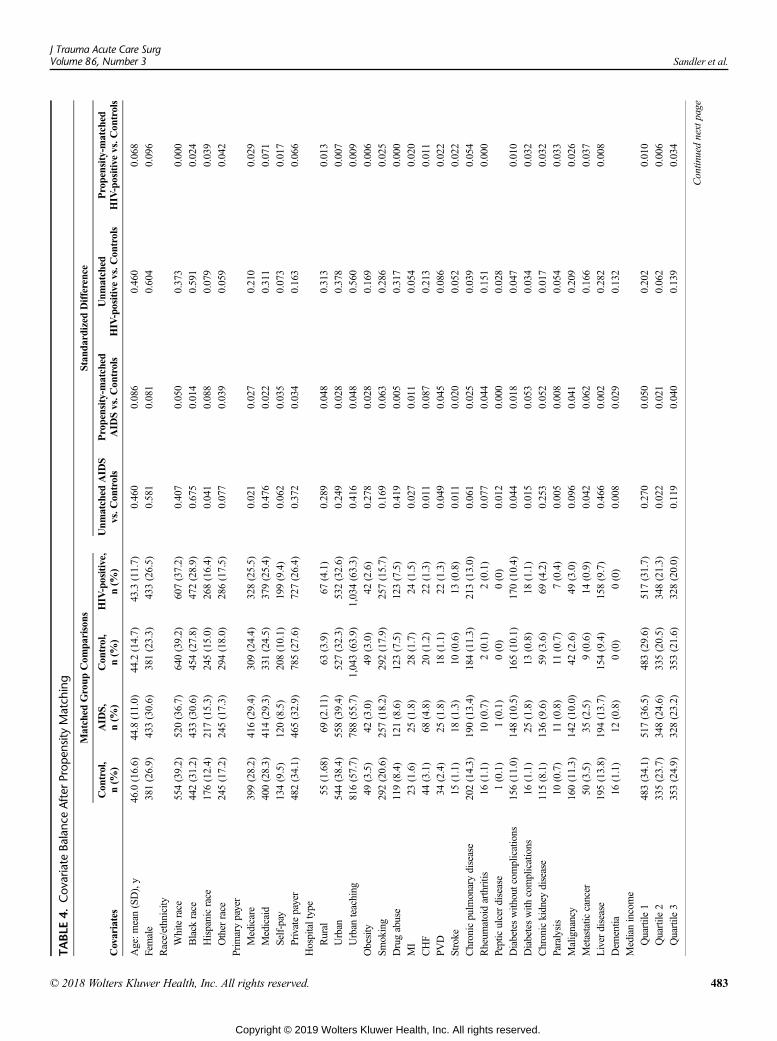
TABLE
4.Cov
ariate
Balanc
eAfterProp
ensityMatch
ing
Matched
Group
Com
parisons
Stan
dardized
Difference
Covariates
Con
trol,
n(%
)AID
S,n(%
)Con
trol,
n(%
)HIV-positive,
n(%
)Unm
atched
AID
Svs.C
ontrols
Propensity-matched
AID
Svs.C
ontrols
Unm
atched
HIV-positivevs.C
ontrols
Propensity-matched
HIV-positivevs.C
ontrols
Age:m
ean(SD),y
46.0(16.6)
44.8(11.0)
44.2(14.7)
43.3(11.7)
0.460
0.086
0.460
0.068
Female
381(26.9)
433(30.6)
381(23.3)
433(26.5)
0.581
0.081
0.604
0.096
Race/ethnicity
Whiterace
554(39.2)
520(36.7)
640(39.2)
607(37.2)
0.407
0.050
0.373
0.000
Black
race
442(31.2)
433(30.6)
454(27.8)
472(28.9)
0.675
0.014
0.591
0.024
Hispanicrace
176(12.4)
217(15.3)
245(15.0)
268(16.4)
0.041
0.088
0.079
0.039
Other
race
245(17.2)
245(17.3)
294(18.0)
286(17.5)
0.077
0.039
0.059
0.042
Prim
arypayer
Medicare
399(28.2)
416(29.4)
309(24.4)
328(25.5)
0.021
0.027
0.210
0.029
Medicaid
400(28.3)
414(29.3)
331(24.5)
379(25.4)
0.476
0.022
0.311
0.071
Self-pay
134(9.5)
120(8.5)
208(10.1)
199(9.4)
0.062
0.035
0.073
0.017
Privatepayer
482(34.1)
465(32.9)
785(27.6)
727(26.4)
0.372
0.034
0.163
0.066
Hospitaltype
Rural
55(1.68)
69(2.11)
63(3.9)
67(4.1)
0.289
0.048
0.313
0.013
Urban
544(38.4)
558(39.4)
527(32.3)
532(32.6)
0.249
0.028
0.378
0.007
Urban
teaching
816(57.7)
788(55.7)
1,043(63.9)
1,034(63.3)
0.416
0.048
0.560
0.009
Obesity
49(3.5)
42(3.0)
49(3.0)
42(2.6)
0.278
0.028
0.169
0.006
Smoking
292(20.6)
257(18.2)
292(17.9)
257(15.7)
0.169
0.063
0.286
0.025
Drugabuse
119(8.4)
121(8.6)
123(7.5)
123(7.5)
0.419
0.005
0.317
0.000
MI
23(1.6)
25(1.8)
28(1.7)
24(1.5)
0.027
0.011
0.054
0.020
CHF
44(3.1)
68(4.8)
20(1.2)
22(1.3)
0.011
0.087
0.213
0.011
PVD
34(2.4)
25(1.8)
18(1.1)
22(1.3)
0.049
0.045
0.086
0.022
Stroke
15(1.1)
18(1.3)
10(0.6)
13(0.8)
0.011
0.020
0.052
0.022
Chronicpulm
onarydisease
202(14.3)
190(13.4)
184(11.3)
213(13.0)
0.061
0.025
0.039
0.054
Rheum
atoidarthritis
16(1.1)
10(0.7)
2(0.1)
2(0.1)
0.077
0.044
0.151
0.000
Pepticulcerdisease
1(0.1)
1(0.1)
0(0)
0(0)
0.012
0.000
0.028
Diabeteswithoutcom
plications
156(11.0)
148(10.5)
165(10.1)
170(10.4)
0.044
0.018
0.047
0.010
Diabeteswith
complications
16(1.1)
25(1.8)
13(0.8)
18(1.1)
0.015
0.053
0.034
0.032
Chronickidney
disease
115(8.1)
136(9.6)
59(3.6)
69(4.2)
0.253
0.052
0.017
0.032
Paralysis
10(0.7)
11(0.8)
11(0.7)
7(0.4)
0.005
0.008
0.054
0.033
Malignancy
160(11.3)
142(10.0)
42(2.6)
49(3.0)
0.096
0.041
0.209
0.026
Metastatic
cancer
50(3.5)
35(2.5)
9(0.6)
14(0.9)
0.042
0.062
0.166
0.037
Liver
disease
195(13.8)
194(13.7)
154(9.4)
158(9.7)
0.466
0.002
0.282
0.008
Dem
entia
16(1.1)
12(0.8)
0(0)
0(0)
0.008
0.029
0.132
Medianincome
Quartile
1483(34.1)
517(36.5)
483(29.6)
517(31.7)
0.270
0.050
0.202
0.010
Quartile
2335(23.7)
348(24.6)
335(20.5)
348(21.3)
0.022
0.021
0.062
0.006
Quartile
3353(24.9)
328(23.2)
353(21.6)
328(20.0)
0.119
0.040
0.139
0.034
Continuednextpage
J Trauma Acute Care SurgVolume 86, Number 3 Sandler et al.
© 2018 Wolters Kluwer Health, Inc. All rights reserved. 4
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
83
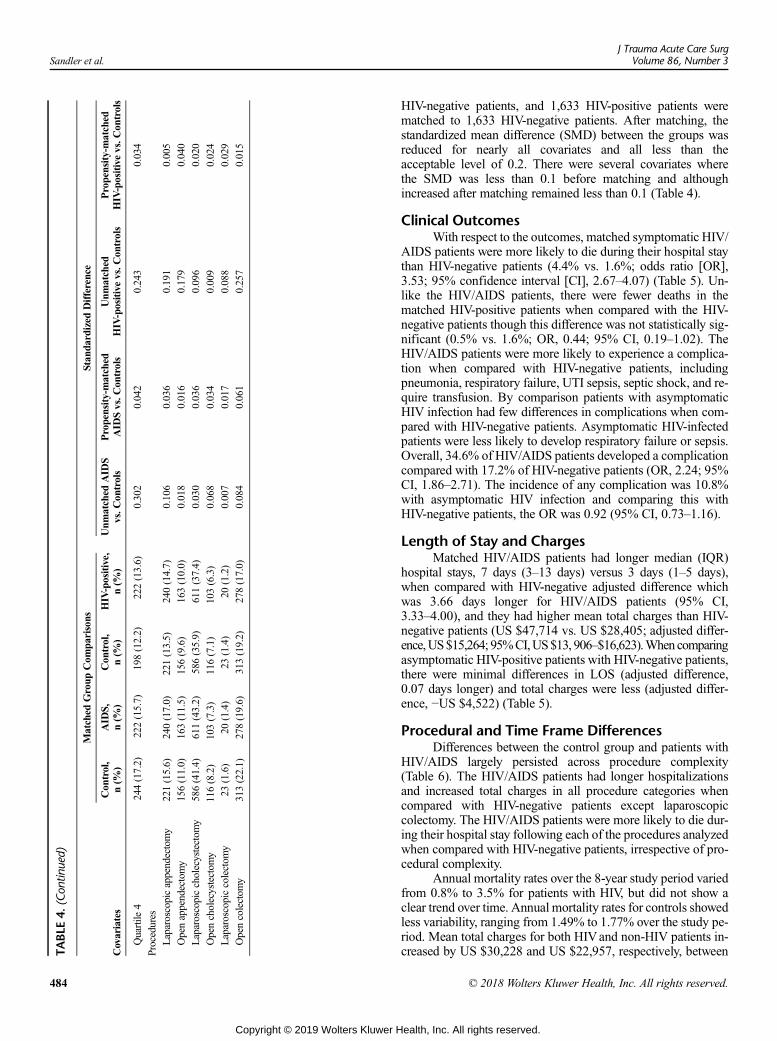
TABLE
4.(Con
tinued)
Matched
Group
Com
parisons
Stan
dardized
Difference
Covariates
Con
trol,
n(%
)AID
S,n(%
)Con
trol,
n(%
)HIV-positive,
n(%
)Unm
atched
AID
Svs.C
ontrols
Propensity-matched
AID
Svs.C
ontrols
Unm
atched
HIV-positivevs.C
ontrols
Propensity-matched
HIV-positivevs.C
ontrols
Quartile
4244(17.2)
222(15.7)
198(12.2)
222(13.6)
0.302
0.042
0.243
0.034
Procedures
Laparoscopicappendectomy
221(15.6)
240(17.0)
221(13.5)
240(14.7)
0.106
0.036
0.191
0.005
Openappendectomy
156(11.0)
163(11.5)
156(9.6)
163(10.0)
0.018
0.016
0.179
0.040
Laparoscopiccholecystectom
y586(41.4)
611(43.2)
586(35.9)
611(37.4)
0.030
0.036
0.096
0.020
Opencholecystectom
y116(8.2)
103(7.3)
116(7.1)
103(6.3)
0.068
0.034
0.009
0.024
Laparoscopiccolectom
y23
(1.6)
20(1.4)
23(1.4)
20(1.2)
0.007
0.017
0.088
0.029
Opencolectom
y313(22.1)
278(19.6)
313(19.2)
278(17.0)
0.084
0.061
0.257
0.015
Sandler et al.J Trauma Acute Care Surg
Volume 86, Number 3
484
Copyright © 2019 Wolters Kluwer H
HIV-negative patients, and 1,633 HIV-positive patients werematched to 1,633 HIV-negative patients. After matching, thestandardized mean difference (SMD) between the groups wasreduced for nearly all covariates and all less than theacceptable level of 0.2. There were several covariates wherethe SMD was less than 0.1 before matching and althoughincreased after matching remained less than 0.1 (Table 4).
Clinical OutcomesWith respect to the outcomes, matched symptomatic HIV/
AIDS patients were more likely to die during their hospital staythan HIV-negative patients (4.4% vs. 1.6%; odds ratio [OR],3.53; 95% confidence interval [CI], 2.67–4.07) (Table 5). Un-like the HIV/AIDS patients, there were fewer deaths in thematched HIV-positive patients when compared with the HIV-negative patients though this difference was not statistically sig-nificant (0.5% vs. 1.6%; OR, 0.44; 95% CI, 0.19–1.02). TheHIV/AIDS patients were more likely to experience a complica-tion when compared with HIV-negative patients, includingpneumonia, respiratory failure, UTI sepsis, septic shock, and re-quire transfusion. By comparison patients with asymptomaticHIV infection had few differences in complications when com-pared with HIV-negative patients. Asymptomatic HIV-infectedpatients were less likely to develop respiratory failure or sepsis.Overall, 34.6% of HIV/AIDS patients developed a complicationcompared with 17.2% of HIV-negative patients (OR, 2.24; 95%CI, 1.86–2.71). The incidence of any complication was 10.8%with asymptomatic HIV infection and comparing this withHIV-negative patients, the OR was 0.92 (95% CI, 0.73–1.16).
Length of Stay and ChargesMatched HIV/AIDS patients had longer median (IQR)
hospital stays, 7 days (3–13 days) versus 3 days (1–5 days),when compared with HIV-negative adjusted difference whichwas 3.66 days longer for HIV/AIDS patients (95% CI,3.33–4.00), and they had higher mean total charges than HIV-negative patients (US $47,714 vs. US $28,405; adjusted differ-ence,US$15,264; 95%CI,US$13, 906–$16,623).Whencomparingasymptomatic HIV-positive patients with HIV-negative patients,there were minimal differences in LOS (adjusted difference,0.07 days longer) and total charges were less (adjusted differ-ence, −US $4,522) (Table 5).
Procedural and Time Frame DifferencesDifferences between the control group and patients with
HIV/AIDS largely persisted across procedure complexity(Table 6). The HIV/AIDS patients had longer hospitalizationsand increased total charges in all procedure categories whencompared with HIV-negative patients except laparoscopiccolectomy. The HIV/AIDS patients were more likely to die dur-ing their hospital stay following each of the procedures analyzedwhen compared with HIV-negative patients, irrespective of pro-cedural complexity.
Annual mortality rates over the 8-year study period variedfrom 0.8% to 3.5% for patients with HIV, but did not show aclear trend over time. Annual mortality rates for controls showedless variability, ranging from 1.49% to 1.77% over the study pe-riod. Mean total charges for both HIVand non-HIV patients in-creased by US $30,228 and US $22,957, respectively, between
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
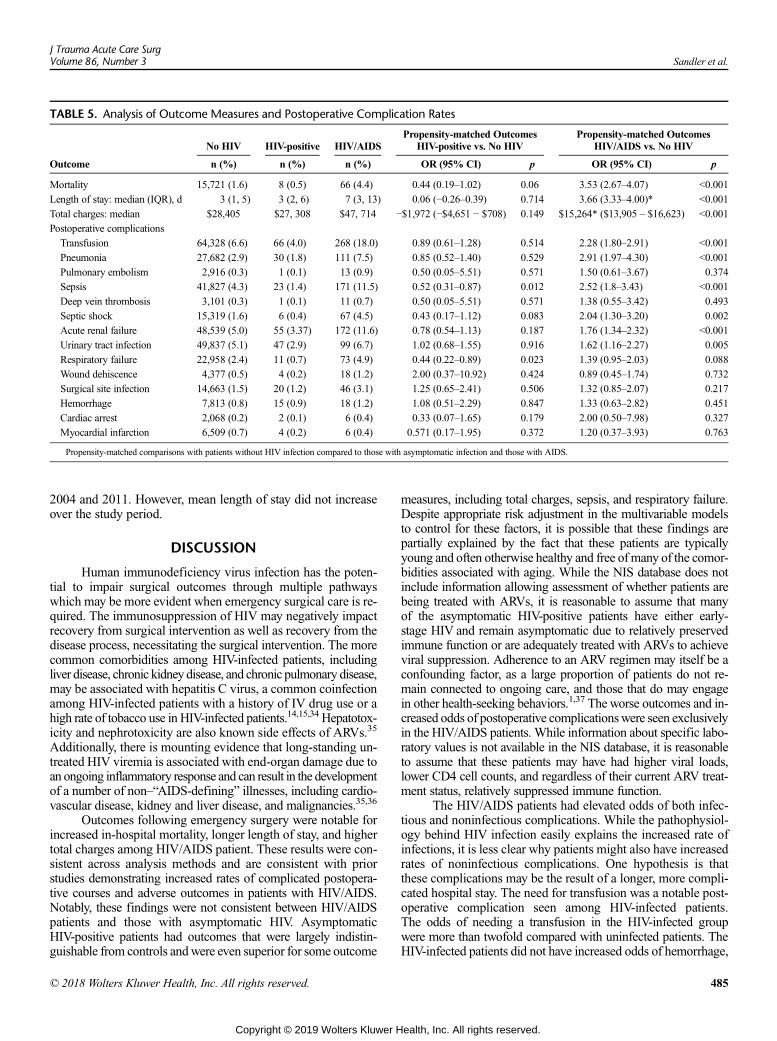
TABLE 5. Analysis of Outcome Measures and Postoperative Complication Rates
No HIV HIV-positive HIV/AIDSPropensity-matched Outcomes
HIV-positive vs. No HIVPropensity-matched Outcomes
HIV/AIDS vs. No HIV
Outcome n (%) n (%) n (%) OR (95% CI) p OR (95% CI) p
Mortality 15,721 (1.6) 8 (0.5) 66 (4.4) 0.44 (0.19–1.02) 0.06 3.53 (2.67–4.07) <0.001
Length of stay: median (IQR), d 3 (1, 5) 3 (2, 6) 7 (3, 13) 0.06 (−0.26–0.39) 0.714 3.66 (3.33–4.00)* <0.001
Total charges: median $28,405 $27, 308 $47, 714 −$1,972 (−$4,651 − $708) 0.149 $15,264* ($13,905 – $16,623) <0.001
Postoperative complications
Transfusion 64,328 (6.6) 66 (4.0) 268 (18.0) 0.89 (0.61–1.28) 0.514 2.28 (1.80–2.91) <0.001
Pneumonia 27,682 (2.9) 30 (1.8) 111 (7.5) 0.85 (0.52–1.40) 0.529 2.91 (1.97–4.30) <0.001
Pulmonary embolism 2,916 (0.3) 1 (0.1) 13 (0.9) 0.50 (0.05–5.51) 0.571 1.50 (0.61–3.67) 0.374
Sepsis 41,827 (4.3) 23 (1.4) 171 (11.5) 0.52 (0.31–0.87) 0.012 2.52 (1.8–3.43) <0.001
Deep vein thrombosis 3,101 (0.3) 1 (0.1) 11 (0.7) 0.50 (0.05–5.51) 0.571 1.38 (0.55–3.42) 0.493
Septic shock 15,319 (1.6) 6 (0.4) 67 (4.5) 0.43 (0.17–1.12) 0.083 2.04 (1.30–3.20) 0.002
Acute renal failure 48,539 (5.0) 55 (3.37) 172 (11.6) 0.78 (0.54–1.13) 0.187 1.76 (1.34–2.32) <0.001
Urinary tract infection 49,837 (5.1) 47 (2.9) 99 (6.7) 1.02 (0.68–1.55) 0.916 1.62 (1.16–2.27) 0.005
Respiratory failure 22,958 (2.4) 11 (0.7) 73 (4.9) 0.44 (0.22–0.89) 0.023 1.39 (0.95–2.03) 0.088
Wound dehiscence 4,377 (0.5) 4 (0.2) 18 (1.2) 2.00 (0.37–10.92) 0.424 0.89 (0.45–1.74) 0.732
Surgical site infection 14,663 (1.5) 20 (1.2) 46 (3.1) 1.25 (0.65–2.41) 0.506 1.32 (0.85–2.07) 0.217
Hemorrhage 7,813 (0.8) 15 (0.9) 18 (1.2) 1.08 (0.51–2.29) 0.847 1.33 (0.63–2.82) 0.451
Cardiac arrest 2,068 (0.2) 2 (0.1) 6 (0.4) 0.33 (0.07–1.65) 0.179 2.00 (0.50–7.98) 0.327
Myocardial infarction 6,509 (0.7) 4 (0.2) 6 (0.4) 0.571 (0.17–1.95) 0.372 1.20 (0.37–3.93) 0.763
Propensity-matched comparisons with patients without HIV infection compared to those with asymptomatic infection and those with AIDS.
J Trauma Acute Care SurgVolume 86, Number 3 Sandler et al.
2004 and 2011. However, mean length of stay did not increaseover the study period.
DISCUSSION
Human immunodeficiency virus infection has the poten-tial to impair surgical outcomes through multiple pathwayswhich may be more evident when emergency surgical care is re-quired. The immunosuppression of HIV may negatively impactrecovery from surgical intervention as well as recovery from thedisease process, necessitating the surgical intervention. The morecommon comorbidities among HIV-infected patients, includingliver disease, chronic kidney disease, and chronic pulmonary disease,may be associated with hepatitis C virus, a common coinfectionamong HIV-infected patients with a history of IV drug use or ahigh rate of tobacco use in HIV-infected patients.14,15,34 Hepatotox-icity and nephrotoxicity are also known side effects of ARVs.35
Additionally, there is mounting evidence that long-standing un-treated HIV viremia is associated with end-organ damage due toan ongoing inflammatory response and can result in the developmentof a number of non–“AIDS-defining” illnesses, including cardio-vascular disease, kidney and liver disease, and malignancies.35,36
Outcomes following emergency surgery were notable forincreased in-hospital mortality, longer length of stay, and highertotal charges among HIV/AIDS patient. These results were con-sistent across analysis methods and are consistent with priorstudies demonstrating increased rates of complicated postopera-tive courses and adverse outcomes in patients with HIV/AIDS.Notably, these findings were not consistent between HIV/AIDSpatients and those with asymptomatic HIV. AsymptomaticHIV-positive patients had outcomes that were largely indistin-guishable from controls andwere even superior for some outcome
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
measures, including total charges, sepsis, and respiratory failure.Despite appropriate risk adjustment in the multivariable modelsto control for these factors, it is possible that these findings arepartially explained by the fact that these patients are typicallyyoung and often otherwise healthy and free ofmany of the comor-bidities associated with aging. While the NIS database does notinclude information allowing assessment of whether patients arebeing treated with ARVs, it is reasonable to assume that manyof the asymptomatic HIV-positive patients have either early-stage HIV and remain asymptomatic due to relatively preservedimmune function or are adequately treated with ARVs to achieveviral suppression. Adherence to an ARV regimen may itself be aconfounding factor, as a large proportion of patients do not re-main connected to ongoing care, and those that do may engagein other health-seeking behaviors.1,37 The worse outcomes and in-creased odds of postoperative complicationswere seen exclusivelyin the HIV/AIDS patients. While information about specific labo-ratory values is not available in the NIS database, it is reasonableto assume that these patients may have had higher viral loads,lower CD4 cell counts, and regardless of their current ARV treat-ment status, relatively suppressed immune function.
The HIV/AIDS patients had elevated odds of both infec-tious and noninfectious complications. While the pathophysiol-ogy behind HIV infection easily explains the increased rate ofinfections, it is less clear why patients might also have increasedrates of noninfectious complications. One hypothesis is thatthese complications may be the result of a longer, more compli-cated hospital stay. The need for transfusion was a notable post-operative complication seen among HIV-infected patients.The odds of needing a transfusion in the HIV-infected groupwere more than twofold compared with uninfected patients. TheHIV-infected patients did not have increased odds of hemorrhage,
485
ealth, Inc. All rights reserved.
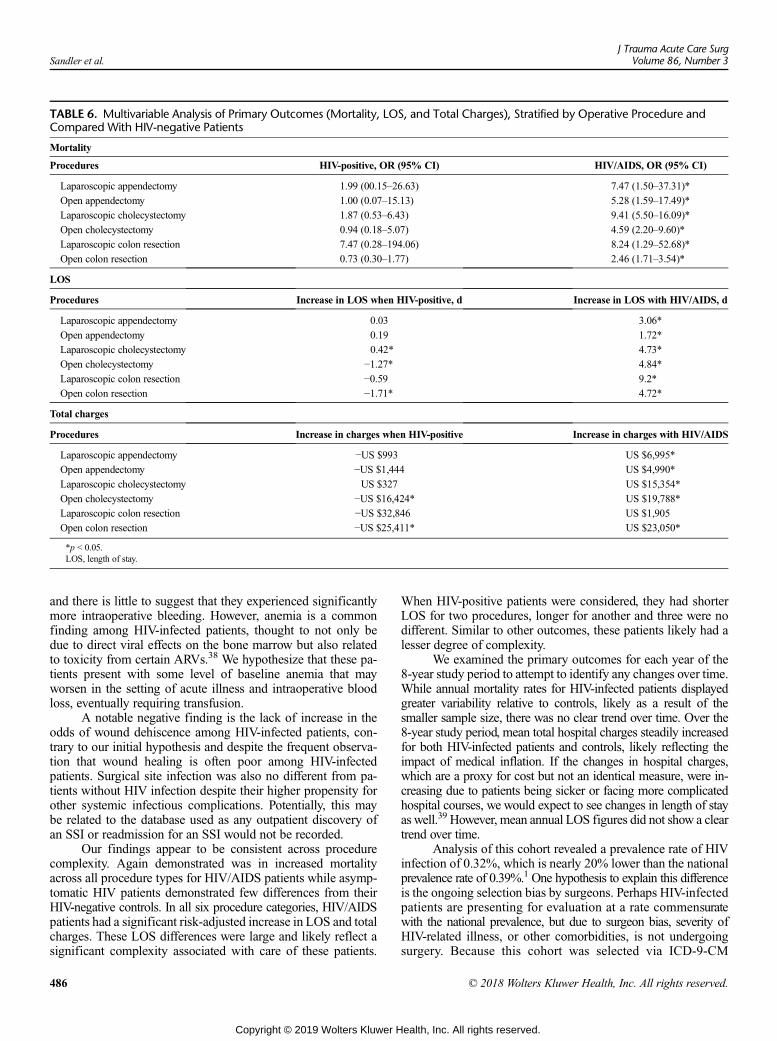
TABLE 6. Multivariable Analysis of Primary Outcomes (Mortality, LOS, and Total Charges), Stratified by Operative Procedure andCompared With HIV-negative Patients
Mortality
Procedures HIV-positive, OR (95% CI) HIV/AIDS, OR (95% CI)
Laparoscopic appendectomy 1.99 (00.15–26.63) 7.47 (1.50–37.31)*
Open appendectomy 1.00 (0.07–15.13) 5.28 (1.59–17.49)*
Laparoscopic cholecystectomy 1.87 (0.53–6.43) 9.41 (5.50–16.09)*
Open cholecystectomy 0.94 (0.18–5.07) 4.59 (2.20–9.60)*
Laparoscopic colon resection 7.47 (0.28–194.06) 8.24 (1.29–52.68)*
Open colon resection 0.73 (0.30–1.77) 2.46 (1.71–3.54)*
LOS
Procedures Increase in LOS when HIV-positive, d Increase in LOS with HIV/AIDS, d
Laparoscopic appendectomy 0.03 3.06*
Open appendectomy 0.19 1.72*
Laparoscopic cholecystectomy 0.42* 4.73*
Open cholecystectomy −1.27* 4.84*
Laparoscopic colon resection −0.59 9.2*
Open colon resection −1.71* 4.72*
Total charges
Procedures Increase in charges when HIV-positive Increase in charges with HIV/AIDS
Laparoscopic appendectomy −US $993 US $6,995*
Open appendectomy −US $1,444 US $4,990*
Laparoscopic cholecystectomy US $327 US $15,354*
Open cholecystectomy −US $16,424* US $19,788*
Laparoscopic colon resection −US $32,846 US $1,905
Open colon resection −US $25,411* US $23,050*
*p < 0.05.LOS, length of stay.
Sandler et al.J Trauma Acute Care Surg
Volume 86, Number 3
and there is little to suggest that they experienced significantlymore intraoperative bleeding. However, anemia is a commonfinding among HIV-infected patients, thought to not only bedue to direct viral effects on the bone marrow but also relatedto toxicity from certain ARVs.38 We hypothesize that these pa-tients present with some level of baseline anemia that mayworsen in the setting of acute illness and intraoperative bloodloss, eventually requiring transfusion.
A notable negative finding is the lack of increase in theodds of wound dehiscence among HIV-infected patients, con-trary to our initial hypothesis and despite the frequent observa-tion that wound healing is often poor among HIV-infectedpatients. Surgical site infection was also no different from pa-tients without HIV infection despite their higher propensity forother systemic infectious complications. Potentially, this maybe related to the database used as any outpatient discovery ofan SSI or readmission for an SSI would not be recorded.
Our findings appear to be consistent across procedurecomplexity. Again demonstrated was in increased mortalityacross all procedure types for HIV/AIDS patients while asymp-tomatic HIV patients demonstrated few differences from theirHIV-negative controls. In all six procedure categories, HIV/AIDSpatients had a significant risk-adjusted increase in LOS and totalcharges. These LOS differences were large and likely reflect asignificant complexity associated with care of these patients.
486
Copyright © 2019 Wolters Kluwer H
When HIV-positive patients were considered, they had shorterLOS for two procedures, longer for another and three were nodifferent. Similar to other outcomes, these patients likely had alesser degree of complexity.
We examined the primary outcomes for each year of the8-year study period to attempt to identify any changes over time.While annual mortality rates for HIV-infected patients displayedgreater variability relative to controls, likely as a result of thesmaller sample size, there was no clear trend over time. Over the8-year study period, mean total hospital charges steadily increasedfor both HIV-infected patients and controls, likely reflecting theimpact of medical inflation. If the changes in hospital charges,which are a proxy for cost but not an identical measure, were in-creasing due to patients being sicker or facing more complicatedhospital courses, we would expect to see changes in length of stayas well.39 However, mean annual LOS figures did not show a cleartrend over time.
Analysis of this cohort revealed a prevalence rate of HIVinfection of 0.32%, which is nearly 20% lower than the nationalprevalence rate of 0.39%.1 One hypothesis to explain this differenceis the ongoing selection bias by surgeons. Perhaps HIV-infectedpatients are presenting for evaluation at a rate commensuratewith the national prevalence, but due to surgeon bias, severity ofHIV-related illness, or other comorbidities, is not undergoingsurgery. Because this cohort was selected via ICD-9-CM
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Sandler et al.
procedure codes, rather than diagnosis codes for EGS condi-tions (e.g., appendicitis, cholecystitis, perforation), theremay be bias introduced by this selection mechanism, whichonly includes patients who have been deemed appropriate sur-gical candidates and therefore well enough to undergo sur-gery. Another hypothesis is that many HIV-infected patientsare young and otherwise healthy, and are less likely to presentwith some of the pathologies that necessitate emergency sur-gery, such as acute cholecystitis, perforated diverticulitis, orobstructing colonic neoplasms.
The demographic findings in this cohort are consistent withthe overall picture of the HIV epidemic in the United States,which is increasingly concentrated in African-Americans andother racial and ethnic minorities and men who have sex withmen.1,40 New infections primarily occur among younger individ-uals, which reflects the age distribution seen in this analysis. Thedifferences seen in comorbid conditions may be explained bythese factors as well, as the non–HIV-infected controls had higherrates of comorbid conditions associated with aging, including car-diovascular disease, diabetes, and cancer.
To our knowledge, this is the first HAART era study tospecifically examine the association of HIV infection with out-comes following emergency general surgery. We postulate thatthis issue will become increasingly relevant to acute care sur-geons. While our risk-adjusted multivariable models suggestthat HIV/AIDS is associated with inferior outcomes, the abso-lute rates of adverse outcomes remain relatively low. This is pre-sumably due to the fact that many HIV-infected patients areyoung and otherwise healthy and remain unaffected by manyof the significant comorbidities related to age, such as cardiovas-cular illness. However, decreases in AIDS-related mortalitymeans that there are increasing numbers of HIV-infected patientssurviving long enough to experience the illnesses of older age,and causes of death among HIV patients are increasingly attrib-utable to cancer, cardiovascular disease, and other common ill-nesses.36 As these patients age, more will present for care fornon–HIV-related illnesses, including emergency general surgicalcare. Patients with asymptomatic HIV infection had outcomessimilar to their uninfected counterparts. Provided HIV-positivepatients can avoid the development of AIDS and AIDS-relatedillnesses potentially, their outcomes will remain equivalent touninfected cohorts as they age.
This analysis is constrained by the inherent limitations ofworking with administrative databases. While the NIS and otheradministrative databases offer a number of beneficial features,including the ability to rapidly collect data on large cohorts, theyalso are limited by the motivation for recording the data, hospitalbilling. Additionally, code modifiers that indicate that a diagno-sis was present on admission are not consistently reported by thestate-based entities that submit data to the NIS and are thereforenot included in the national database.25 However, studies com-paring administrative claims data to chart review data have val-idated the use of ICD-9-CM codes to identify complications to areasonable level of accuracy.41 Finally, as previously mentioned,the samplingmethodologymay have introduced bias into the co-hort by only examining patients who were well enough to bedeemed operative candidates.
These results indicate that HIV/AIDS patients have agreater risk of death, infectious, and noninfectious complications
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
after common emergency general surgery procedures regardlessof operative complexity. Equally important was the finding thatHIV-positive patients without a diagnosis of AIDS have equiva-lent outcomes to uninfected patients. Accordingly, patients withHIV/AIDS have longer and costlier hospital stays. Despitethe availability of advanced therapy for HIV/AIDS, it continuesto negatively impact emergency surgery outcomes while anHIV-positive status does not. Surgeons should be aware of theserisks and HIV/AIDS patients and HIV-positive patients shouldbe counseled accordingly.
AUTHORSHIP
B.S. participated in the literature search. K.S., K.D., B.S. participated in thestudy design. B.S. participated in the data collection. K.S. and B.S. partici-pated in the data analysis. K.S., K.D., and B.S. participated in the data inter-pretation. K.S. and B.S. participated in the writing of the article. K.S., K.D.,and B.S. participated in the critical revision.
ACKNOWLEDGMENTS
Wewish to acknowledgeDaniel Bohl and James Tooley for their assistancewith data analysis.
DISCLOSURE
No conflicts of interest are declared.Work supported by the Yale School ofMedicine Office of Student Research.
REFERENCES1. Frieden TR, Foti KE,Mermin J. Applying public health principles to the HIV
epidemic—how are we doing? N Engl J Med. 2015;373(23):2281–2287.2. Burack JH, Mandel MS, Bizer LS. Emergency abdominal operations in
the patient with acquired immunodeficiency syndrome. Arch Surg. 1989;124(3):285–286.
3. LaRaja RD, Rothenberg RE, Odom JW, Mueller SC. The incidence of intra-abdominal surgery in acquired immunodeficiency syndrome: a statistical re-view of 904 patients. Surgery. 1989;105(2 Pt 1):175–179.
4. Robinson G,Wilson SE,Williams RA. Surgery in patients with acquired im-munodeficiency syndrome. Arch Surg. 1987;122(2):170–175.
5. Horberg MA, Hurley LB, Klein DB, Follansbee SE, Quesenberry C,Flamm JA, Green GM, Luu T. Surgical outcomes in human immunodefi-ciency virus-infected patients in the era of highly active antiretroviral therapy.Arch Surg. 2006;141(12):1238–1245.
6. Albaran RG, Webber J, Steffes CP. CD4 cell counts as a prognostic factor ofmajor abdominal surgery in patients infected with the human immunodefi-ciency virus. Arch Surg. 1998;133(6):626–631.
7. Tran HS, Moncure M, Tarnoff M, Goodman M, Puc MM, Kroon D,Eydelman J, Ross SE. Predictors of operative outcome in patients with hu-man immunodeficiency virus infection and acquired immunodeficiency syn-drome. Am J Surg. 2000;180(3):228–233.
8. Baum CL, Arpey CJ. Normal cutaneous wound healing: clinical correlationwith cellular and molecular events. Dermatol Surg. 2005;31(6):674–686;discussion 686.
9. Morandi E, Merlini D, Salvaggio A, Foschi D, Trabucchi E. Prospectivestudy of healing time after hemorrhoidectomy: influence of HIV infection,acquired immunodeficiency syndrome, and analwound infection.Dis ColonRectum. 1999;42(9):1140–1144.
10. Burke EC, Orloff SL, Freise CE,Macho JR, SchecterWP.Wound healing af-ter anorectal surgery in human immunodeficiency virus-infected patients.Arch Surg. 1991;126(10):1267–1270; discussion 1270–1.
11. Consten EC, Slors FJ, Noten HJ, Oosting H, Danner SA, van Lanschot JJ.Anorectal surgery in human immunodeficiency virus-infected patients. Clin-ical outcome in relation to immune status. Dis Colon Rectum. 1995;38(11):1169–1175.
12. King JT Jr., Perkal MF, Rosenthal RA, Gordon AJ, Crystal S,Rodriguez-Barradas MC, Butt AA, Gibert CL, Rimland D, Simberkoff MS,et al. Thirty-day postoperative mortality among individuals with HIV infec-tion receiving antiretroviral therapy and procedure-matched, uninfected com-parators. JAMA Surg. 2015;150(4):343–351.
487
ealth, Inc. All rights reserved.
Sandler et al.J Trauma Acute Care Surg
Volume 86, Number 3
13. Locke JE, Durand C, Reed RD, MacLennan PA, Mehta S, Massie A,Nellore A, DuBay D, Segev DL. Long-term outcomes after liver transplanta-tion among human immunodeficiency virus-infected recipients. Transplan-tation. 2016;100(1):141–146.
14. Eisenbach C, Merle U, Stremmel W, Encke J. Liver transplantation in HIV-positive patients. Clin Transplant. 2009;23(Suppl 21):68–74.
15. Landin L, Rodriguez-Perez JC, Garcia-Bello MA, Cavadas PC, Thione A,Nthumba P, Blanes M, Ibanez J. Kidney transplants in HIV-positive recipi-ents under HAART. A comprehensive review and meta-analysis of 12 series.Nephrol Dial Transplant. 2010;25(9):3106–3115.
16. Polanco A, Itagaki S, Chiang Y, Chikwe J. Changing prevalence, profile, andoutcomes of patients with HIV undergoing cardiac surgery in the UnitedStates. Am Heart J. 2014;167(3):363–368.
17. Hooker CM, Meguid RA, Hulbert A, Taylor JT, Shin J, Wrangle J,Rodgers K, Lee B, Laskshmanan S, Brown T, et al. Human immunodefi-ciency virus infection as a prognostic factor in surgical patients with non-small cell lung cancer. Ann Thorac Surg. 2012;93(2):405–412.
18. Ferrero S, Bentivoglio G. Post-operative complications after caesarean sec-tion in HIV-infected women. Arch Gynecol Obstet. 2003;268(4):268–273.
19. Gale SC, Shafi S, Dombrovskiy VY, Arumugam D, Crystal JS. The publichealth burden of emergency general surgery in the United States: a 10-yearanalysis of the Nationwide inpatient sample—2001 to 2010. J Trauma AcuteCare Surg. 2014;77(2):202–208.
20. Shafi S, Aboutanos MB, Agarwal S Jr., Brown CV, Crandall M,Feliciano DV, Guillamondegui O, Haider A, Inaba K, Osler TM, et al. Emer-gency general surgery: definition and estimated burden of disease. J TraumaAcute Care Surg. 2013;74(4):1092–1097.
21. Ingraham AM, Cohen ME, Raval MV, Ko CY, Nathens AB. Comparison ofhospital performance in emergency versus elective general surgery opera-tions at 198 hospitals. J Am Coll Surg. 2011;212(1):20–28 e1.
22. Obirieze AC, Kisat M, Hicks CW, Oyetunji TA, Schneider EB, Gaskin DJ,Haut ER, Efron DT, Cornwell EE 3rd, Haider AH. State-by-state variationin emergency versus elective colon resections: room for improvement.J Trauma Acute Care Surg. 2013;74(5):1286–1291.
23. Becher RD, Hoth JJ, Miller PR, Mowery NT, Chang MC, Meredith JW. Acritical assessment of outcomes in emergency versus nonemergency generalsurgery using the American College of Surgeons National Surgical QualityImprovement Program database. Am Surg. 2011;77(7):951–959.
24. Becher RD, Meredith JW, Chang MC, Hoth JJ, Beard HR, Miller PR. Crea-tion and implementation of an emergency general surgery registry modeledafter the National Trauma Data Bank. J Am Coll Surg. 2012;214(2):156–163.
25. Agency for Healthcare Research and Quality (AHRQ), Healthcare Cost andUtilization Project (HCUP). Introduction to the HCUP Nationwide InpatientSample (NIS). Rockville, MD; 2011: [December 18, 2015]. Available from:http://www.hcup-us.ahrq.gov/.
26. Ingraham AM, Cohen ME, Bilimoria KY, Raval MV, Ko CY, Nathens AB,Hall BL. Comparison of 30-day outcomes after emergency general surgeryprocedures: potential for targeted improvement. Surgery. 2010;148(2):217–238.
488
Copyright © 2019 Wolters Kluwer H
27. United States. Public Health Service., United States. Health Care FinancingAdministration., National Center for Health Statistics (U.S.). ICD-9-CM in-ternational classification of diseases, ninth revision, clinical modification,sixth edition. Washington, D.C.: U.S. Dept. of Health and Human Services,Public Health Service, Health Care Financing Administration; 1996.
28. Wojcik G, Latanich R, Mosbruger T, Astemborski J, Kirk GD, Mehta SH,Goedert JJ, Kim AY, Seaberg EC, Busch M, Thomas DL, Duggal P,Thio CL. Variants in HAVCR1 gene region contribute to hepatitis C persis-tence in African Americans. J Infect Dis. 2014;209:355–359.
29. McQuistion K, Zens T, Jung HS, Beems M, Leverson G, Liepert A,Scarborough J, Agarwal S. Insurance status and race affect treatment and out-come of traumatic brain injury. J Surg Res. 2016;205:261–271.
30. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index foruse with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613–619.
31. Romano PS, Mull HJ, Rivard PE, Zhao S, Henderson WG, Loveland S,Tsilimingras D, Christiansen CL, Rosen AK. Validity of selected AHRQ Pa-tient Safety Indicators based on VA National Surgical Quality ImprovementProgram data. Health Serv Res. 2009;44(1):182–204.
32. West J, Khan Y, Murray DM, Stevenson KB. Assessing specific secondaryICD-9-CM codes as potential predictors of surgical site infections. Am J In-fect Control. 2010;38(9):701–705.
33. Dimick JB, Pronovost PJ, Cowan JA Jr., Lipsett PA, Stanley JC,Upchurch GR Jr. Variation in postoperative complication rates after high-risk surgery in the United States. Surgery. 2003;134(4):534–540; discussion540–1.
34. Edelman EJ, Tetrault JM, Fiellin DA. Substance use in older HIV-infectedpatients. Curr Opin HIVAIDS. 2014;9(4):317–324.
35. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelinesfor the use of antiretroviral agents in HIV-1-infected adults and adolescents.Department of Health andHuman Services [cited 2015 December 17]. Availablefrom: http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf.
36. Lewden C,May T, Rosenthal E, Burty C, Bonnet F, Costagliola D, Jougla E,Semaille C, Morlat P, Salmon D, et al. Changes in causes of death amongadults infected by HIV between 2000 and 2005: the “Mortalite 2000 and2005” surveys (ANRS EN19 and Mortavic). J Acquir Immune Defic Syndr.2008;48(5):590–598.
37. Dasgupta S, Oster AM, Li J, Hall HI. Disparities in consistent retention inHIV care—11 states and theDistrict of Columbia, 2011-2013.MMWRMorbMortal Wkly Rep. 2016;65(4):77–82.
38. Belperio PS, Rhew DC. Prevalence and outcomes of anemia in individualswith human immunodeficiency virus: a systematic review of the literature.Am J Med. 2004;116(Suppl 7A):27S–43S.
39. Finkler SA. The distinction between cost and charges.Ann InternMed. 1982;96(1):102–109.
40. Hall HI, Song R, Rhodes P, Prejean J, An Q, Lee LM, Karon J,Brookmeyer R, Kaplan EH, McKenna MT, et al. Estimation of HIV inci-dence in the United States. JAMA. 2008;300(5):520–529.
41. Lawthers AG,McCarthy EP, Davis RB, Peterson LE, Palmer RH, Iezzoni LI.Identification of in-hospital complications from claims data. Is it valid?MedCare. 2000;38(8):785–795.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
SPECIAL REPORT
The American Trauma Society’s 50th anniversary:Saving lives. Improving care. Empowering survivors.
Christopher P. Michetti, MD, Falls Church, Virginia
S aving lives. Improving care. Empowering survivors.1 This isthe mission of the American Trauma Society (ATS) and the
driving force behind its members and leadership for the last fivedecades.
In 2018, the ATS celebrated its 50th anniversary. Since itsinception in 1968, the ATS has been on a journey of service to thetrauma community and advancing trauma care through profes-sional and public education, injury prevention, and a special focuson the unique needs of trauma patients and survivors. AmericanTrauma Society membership is diverse, including physiciansand nurses, trauma program managers, trauma registrars, injuryprevention professionals, trauma survivors, and others from all50 states and several countries. In addition, the ATS has longrecognized the need to support the people it really works for:trauma patients and their families. Through its Trauma Survi-vors Network program, patients receive much needed ongoingcare long after their physical wounds have healed. Some survi-vors in turn become peer visitors and provide support to othertrauma patients. In this report, we highlight milestones of theATS from the past 50 years that embody the evolution of the So-ciety and its ongoing work to fulfill its mission.
A CALL TO ACTION
TheATSwas born out of the need for an organized nationaleffort to address the “wicked menace to life and good health”2
that was traumatic injury in the 1960s. At that time, like today, in-juries were common. Unlike today, emergency medical andtrauma systems were in their infancy, and trauma was largelyviewed as the result of unfortunate accidents. These “accidents”were addressed on a case-by-case basis by the medical professionwith little organizational or government support to delve into theroot causes of injury or to approach the problem more broadlywith a public health strategy.3 Such an approach was used to suc-cessfully tackle polio in the prior decade, an effort at the forefrontof popular consciousness that benefited from massive public sup-port through donations to The March of Dimes Foundation.4
Trauma, in contrast, received little recognition or support.In 1964, at the meeting of the Committee on Shock, Dr.
John W. Howard, a surgeon at Hahnemann Medical College in
Submitted: November 13, 2018, Accepted: November 14, 2018, Published online:December 10, 2018.
From the Inova Fairfax Hospital, Falls Church, Virginia.Address for reprints: Christopher P. Michetti, MD, Inova Trauma Center, Inova Fairfax
Medical Campus, 3300 Gallows Rd, Falls Church, VA 22042; email: [email protected].
DOI: 10.1097/TA.0000000000002153
J Trauma Acute Care SurgVolume 86, Number 3
Copyright © 2019 Wolters Kluwer H
Philadelphia and later the first Secretary-Treasurer of the ATS,proposed the formation of an “American Trauma Society” asan independent volunteer health organization to help counterthe trauma epidemic. In 1966, the landmark white paper “Acci-dental Death and Disability: the Neglected Disease of ModernSociety”was prepared by the Committees on Trauma and Shockof the National Academy of Sciences, National Research Coun-cil.3 This publication spurred a national call to action to combatthe public apathy toward the devastating toll that traumawas tak-ing on America. One of the five major steps suggested by thewhite paper was the establishment of a National Trauma Associ-ation to drive public demand for injury prevention.
FOUNDING AND EARLY YEARS
The American Association for the Surgery of Trauma(AAST) took on the task of bringing these ideas to fruition, andthe ATS was incorporated on June 27, 1968. With the support ofthe AAST, the American College of Surgeons, the AmericanAcademy of Orthopedic Surgeons, individual ATS FoundingMembers, and other organizations, the ATS steadily built mo-mentum. Luminaries of the American surgery community helpedguide the nascent organization, including Dr. Preston A. Wade(the first President of the ATS), Dr. William T. Fitts, Dr. BasilA. Pruitt, Dr. James “Red”Duke, and Dr. Howard, among others.
In 1974, the ATS introduced its distinctive logo (Fig. 1),which became emblematic of the organization for decades tocome. The design was the product of a contest that attracted al-most 700 entries, with the $1000 award going to the image ofdamaged beauty symbolic of the injured patient: the broken-stemmed tulip.
In 1972, Dr. Howard provided the ATS's first central officein his department at Crozier-Chester Medical Center outside ofPhiladelphia. Over the ensuing years, the National Office mi-grated to Toledo, Chicago, and Baltimore; Landover, MD, UpperMarlboro, MD, and finally Falls Church, VA, its current location.
From early on, the ATS sought to actively engage its mem-bers, initially through published newsletters sent by mail, and laterthrough e-mail. Traumagram had begun publication in 1974, andTraumaviewwasmailed bimonthly while Congress was in sessionto update the membership on pertinent trauma-related legislativeactivities. This focus on advocacy has remained a pillar of theorganization. Today, members receive The Pulse newsletter bye-mail, providing a monthly update on State and Federal legisla-tion and other health policy information relevant to the ATSMission. ATS Inform, another monthly newsletter, highlights in-formation of interest to the trauma community including events,
489
ealth, Inc. All rights reserved.

Figure 1. AmericanTraumaSociety logo, thebroken-stemmed tulip.
Figure 2. National TraumaAwarenessMonth30thanniversary logo.
MichettiJ Trauma Acute Care Surg
Volume 86, Number 3
research, professional development opportunities, and links toarticles in the press.
In the 1970s and 1980s, while trauma continued to affectmillions of Americans each year, there remained a deficit in pub-lic acknowledgment of injury as a preventable disease andawareness of the role of trauma centers and trauma systems.The ATS advocated for the Emergency Medical Services Sys-tems Act of 1973,5 the first federal program to build EMS andtrauma systems throughout the country.6 This Act authorizedthe Department of Health, Education and Welfare to developmore than 300 EMS systems in the United States, effectively ini-tiating the coordinated approach to delivery of trauma and emer-gency care.
TRAUMA AWARENESS AND INJURY PREVENTION
In 1985, the National Research Council provided anothercall to action through its publication “Injury in America: ACon-tinuing Public Health Problem.”7 This document called for theestablishment of a program within the Centers for Disease Con-trol and Prevention (CDC) to address injury, and was also nota-ble for its branding of trauma as a public health issue. In 1990,Congress subsequently passed the Injury Control Act8 authoriz-ing the creation of the National Center for Injury Prevention andControl at the CDC. The ATS worked with the Center's first di-rector, Dr. Mark Rosenberg, to press Congress for appropria-tions for injury prevention. The issue of firearm violence was apriority for the Center. At the time, ATS President Dr. JonathanRhodes and Executive Director Harry Teter joined others inhelping to obtain the votes necessary to move the Federal
490
Copyright © 2019 Wolters Kluwer H
Assault Weapons Ban through Congress. For their efforts on be-half of the ATS, each received a personal letter of thanks fromPresident Bill Clinton.
The ATS alsoworked with the US Congress and the Exec-utive Branch in 1987 to help designate May as National TraumaAwareness Month, which was established by Presidential Proc-lamation 5806 by Ronald Reagan on April 29, 1988. Over theensuing years the ATS has worked with an expanding numberof organizations and partners to identify and publicize a differenttheme each May and to develop materials about injury preven-tion and trauma awareness. National Trauma Awareness Monthcampaigns have focused on topics including drunk and dis-tracted driving, school violence and bullying, concussions andsports injuries, falls in the elderly, and Stop the Bleed. In 2018,the 30th anniversary of National Trauma Awareness Month, theATS chose the overarching theme of “Injury is No Accident”[Fig. 2] to highlight its public health perspective on injury and toemphasize the preventable nature of traumatic injury. The injuryprevention community is carrying this message forward: throughits Injury Prevention Coordinators' course, the ATS supports andprepares injury prevention professionals to serve their local andnational communities and shine a light on the effort to prevent in-jury. In this decade, the ATS became a founding member of theTrauma Prevention Coalition, and in 2018 hosted the Coalition'sfourth annual injury prevention symposium in Washington, DC.
Recognizing that teaching injury prevention is also criticalin the pediatric population, TraumaRoo was developed to helpeducate children from ages 3 to 7 years about injury preventionin a friendly, nonthreatening way. “Troo” the TraumaRoo is akangaroo costume that has been used in visitations to hospitals,schools, fairs, and other locations to support activities and safetyeducation for kids. It has been estimated that TraumaRoo hashelped teachmore than onemillion children about the importance
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
Figure 3. American Trauma Society’s 50th anniversary logo.
J Trauma Acute Care SurgVolume 86, Number 3 Michetti
of safety and trauma prevention (personal communication,Harry Teter, Jr., 2018).
TRAUMA SURVIVORS NETWORK
An integral part of the mission of the ATS is “empoweringsurvivors.” Recognizing that recovery and healing extend far be-yond the hospital and rehabilitation center and that many pa-tients harbor ongoing challenges for months or years after theirinjury, the ATS developed the Trauma Survivors Network(TSN).9 The TSN brings together trauma survivors and familiesto support one another, share experiences and information aboutrecovery, and help enhance survivor skills to manage the dailychallenges that come with injury recovery. By means of peersupport from other survivors, peer visitation programs, and otherresources, patients and families receive much needed psycholog-ical and emotional support in the hospital and beyond. In addi-tion, TSN members lend their unique perspective to fuel injuryprevention efforts locally and nationally.
The TSN has its roots in a local support group for traumasurvivors called “Rebuild,” formed in 1995 at Inova Fairfax Hos-pital in Virginia. In 2003, the ATS began exploring the develop-ment of a peer support network for trauma survivors andcollaborated with Inova Fairfax Hospital to develop materialsfor a national program, supported by a grant from the TempletonFoundation. By 2008, the TSN was officially up and running.
As more hospitals began adopting the TSN, the JohnsHopkins School of Public Health, with a grant from the Depart-ment of Defense, funded six Level 1 trauma centers from 2013to 2015 with full-time TSN coordinators to develop the TSNprogram and study program outcomes. Building on the training,development, and experience from the Johns Hopkins School ofPublic Health study, the ATS continued to expand the program.Today, close to 100 hospitals and rehabilitation centers in theUnited States and Canada use the TSN program to supporttrauma survivors.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
IMPROVING CARE
The ATS is not an academic society, but it works to ensurethe optimal care of trauma patients through professional educa-tion and support of the people who are essential to making atrauma center run, such as program managers, registrars, and in-jury prevention specialists. The ATS Trauma ProgramManagers'course provides leaders with the tools to build and manage acomprehensive trauma program. Its core curriculum was initiallydeveloped by past ATS President Maurine Goehring, DianeRogers Balderson, and Jan Price. Trauma registry professionals,another group that forms the infrastructure of a trauma center,have also found a home at the ATS for decades. A focus ontrauma registry education was started in the late 1980s by pastATS President Dr. Carl Valenziano and Dr. Richard Cales. In1994, the ATS launched its trauma registry education programand course, and in 2000 established the first national certifica-tion for trauma registry professionals, the Certified Specialistin Trauma Registries (CSTR).
Dr. Valenziano also initiated the ATS Bystander Care ofthe Injured Program in 1996. This program, prompted by theUS Department of Transportation National Highway TrafficSafety Administration and predating the Stop the Bleed courseby many years, taught participants basic skills that could be ap-plied in the field, such as at the scene of an automobile crash.Like Stop the Bleed, the program aimed to empower citizenswith basic medical skills and tools to build resilience.
The 2nd Trauma program was developed in 2002 to 2003to help trauma surgeons and other trauma teammembers improvecommunication with the families of their patients. This programteaches compassionate, effective communication for the most dif-ficult situations, such as the death of a patient. Participants learnhow to give devastating news during the critical first meetingwith families and loved ones and afterward during the intensivecare unit stay and beyond. Even before the practice of patient-centered and family-centered care was at the forefront of themedical consciousness, 2nd Trauma was teaching crucial com-munication skills with these concepts in mind.
Another valuable asset provided by the ATS is its inventoryof trauma centers throughout the United States, which is main-tained as part of the Trauma Information Exchange Program.The Trauma Information Exchange Program database containsinformation about trauma centers and injury and facilitates shar-ing of such data among trauma centers, providers, researchers,payers, and policy makers. The inventory map allows the generalpublic to locate trauma centers and learn about the differences be-tween trauma center levels.
50TH ANNIVERSARY AND A LOOK FORWARD
In its golden anniversary year (Fig. 3), the ATS looks backwith pride on its first half-century and its contributions to traumacare in the United States. Yet, injury is still a leading cause ofdeath and disability, and many challenges remain: firearm vio-lence, mass shootings, an aging population with increasing lon-gevity, underfunding of trauma research relative to its massiveburden on society, under-recognition of trauma's lingering psycho-social aftereffects, and a heavy skew toward treating instead ofpreventing injury. The ATS looks forward to continue its work
491
ealth, Inc. All rights reserved.

MichettiJ Trauma Acute Care Surg
Volume 86, Number 3
with ATS members and partners as it strives to meet thesechallenges and fulfill its mission to save lives, improve care,and empower survivors.
ACKNOWLEDGMENTS
For their insight, perspective, and historical accounts, I thank Basil Pruitt,MD, Anna Newcomb, PhD, Samir Fakhry, MD, Marc Levison, MD, andHarry Teter, Esq.
DISCLOSURE
The author declares no conflict of interest. No funding was received forthis work.
REFERENCES1. American Trauma Society. Mission statement, American Trauma Society
Website. Available at: www.amtrauma.org. Accessed June 27, 2018.2. Walker R. American Trauma Society, 23rd annual Stone Lecture. American
Trauma Society Archives. May 1, 1998.
492
Copyright © 2019 Wolters Kluwer H
3. Committee on Trauma, and Committee on Shock, Division of Medical Sci-ences, National Academy of Sciences/National Research Council (US). Acci-dental Death and Disability: the Neglected Disease of Modern Society.Washington, DC: National Academy of Sciences; 1966.
4. Oshinsky DM. Polio: An American Story. 1st Ed. NewYork, NY: Oxford Uni-versity Press; 2005.
5. Emergency Medical Services Systems Act of 1973, Public Law 93–154.Available at: https://www.congress.gov/bill/93rd-congress/senate-bill/2410.Accessed July 4, 2018.
6. Harvey JC. The Emergency Medical Service Systems Act of 1973. JAMA.1974;230(8):1139–1140.
7. Committee on Trauma Research. Injury in America: A Continuing PublicHealth Problem. Washington, DC: National Academy Press; 1985.
8. Injury Control Act of 1990, Public Law 101-558. Available at: https://www.congress.gov/bill/101st-congress/house-bill/5113. Accessed July 18, 2018.
9. BradfordAN, Castillo RC, Carlini AR,Wegener ST, Teter H Jr, Mackenzie EJ.The Trauma Survivors Network: survive connect. rebuild. J Trauma. 2011;70:1557–1560.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

SYSTEMATIC REVIEW
Massive transfusion protocols in nontrauma patients:A systematic review and meta-analysis
Nora Sommer, Beat Schnüriger, MD, Daniel Candinas, MD, and Tobias Haltmeier, MD, Bern, Switzerland
Sub
Fro
Ad
DO
J TrVol
BACKGROUND: M
mitted: June 11, 2018, Revised: July 16, 2lished online: October 29, 2018.m the Division of Acute Care Surgery,Medicine (N.S., B.S., D.C., T.H.), InselsSwitzerland.dress for reprints: Tobias Haltmeier, MD, FDepartment of Visceral Surgery and MedicBern, Switzerland; email: tobias.haltmeie
I: 10.1097/TA.0000000000002101
auma Acute Care Surgume 86, Number 3
assive bleeding is a major cause of death both in trauma and nontrauma patients. In trauma patients, the implementa-tion of massive transfusion protocols (MTP) led to improved outcomes. However, the majority of patients with massivebleeding are nontrauma patients.
OBJECTIVES: T
o assess if the implementation of MTP in nontrauma patients with massive bleeding leads to improved survival. DATA SOURCES: N ational Library of Medicine's Medline database (PubMed). STUDY ELIGIBILITY CRITERIA: O riginal research articles in English language investigating MTP in nontrauma patients. PARTICIPANTS: N ontrauma patients with massive bleeding 18 years or older. INTERVENTION: T ransfusion according to MTP versus off-protocol. STUDYAPPRAISAL ANDSYNTHESIS METHODS:St
ystematic literature review using PubMed. Outcomes assessed were mortality and transfused blood products. Studieshat compared mortality of MTP and non-MTP groups were included in meta-analysis using Mantel-Haenszel randomeffect models.RESULTS: A
total of 252 abstracts were screened. Of these, 12 studies published 2007 to 2017were found to be relevant to the topic,including 2,475 patients. All studies were retrospective and comprised different patient populations. Most frequent indi-cations for massive transfusion were perioperative, obstetrical and gastrointestinal bleeding, as well as vascular emergen-cies. Four of the five studies that compared the number of transfused blood products in MTP and non-MTP groupsrevealed no significant difference. Meta-analysis revealed no significant effect of MTP on the 24-hour mortality (oddsratio 0.42; 95% confidence interval 0.01–16.62; p = 0.65) and a trend toward lower 1-month mortality (odds ratio 0.56;95% confidence interval 0.30–1.07; p = 0.08).LIMITATIONS: H
eterogeneous patient populations and MTP in the studies included. CONCLUSION: T here is limited evidence that the implementation of MTP may be associated with decreased mortality in nontrauma pa-tients. However, patient characteristics, as well as the indication and definition of MTPwere highly heterogeneous in theavailable studies. Further prospective investigation into this topic is warranted. (J Trauma Acute Care Surg. 2019;86:493–504. Copyright © 2018 Wolters Kluwer Health, Inc. All rights reserved.)
LEVEL OF EVIDENCE: S
ystematic review and meta-analysis, level III. KEYWORDS: H emorrhage; nontrauma emergency; blood component transfusion; transfusion protocol; meta-analysis.I n patients receiving massive transfusion a high mortality ratehas been described, both in the trauma and nontrauma
setting.1–3 Rose et al.2 report an in-hospital mortality rate of34% in a mixed patient population receiving massive transfu-sion. Halmin et al.,1 in a nationwide cohort study assessing theepidemiology of massive transfusion in Sweden and Denmark,report a 30-day mortality of 24.8%.1 Turan et al.3 investigatedthe mortality after massive transfusion in patients undergoingnoncardiac surgery using the American College of SurgeonsNational Surgical Quality Improvement Program database. Inthis study, a postoperative 30-day mortality of 17% was foundin patients undergoing massive transfusion. Common causesfor massive hemorrhage in nontrauma patients are gastrointesti-nal bleeding, ruptured abdominal aortic aneurisms, as well as
018, Accepted: October 8, 2018, Pub-
Department of Visceral Surgery andpital, Bern University Hospital, Bern,
ACS, Division of Acute Care Surgery,ine, Inselspital, Bern University Hospital,[email protected].
Copyright © 2019 Wolters Kluwer H
surgical or obstetrical bleeding.4–7 In the abovementioned co-hort study conducted in Sweden and Denmark, massive transfu-sion was reported with an incidence of 2.5 (Sweden) and 4.5(Denmark) per 10,000 person years.1 Turan et al.3 report mas-sive transfusion in 7,485 of 917,651 patients in National Surgi-cal Quality Improvement Program 2006 to 2009, correspondingto 0.8%. Most recent studies investigating the pathophysiologyand treatment of hemorrhage focused on trauma patients.4,6–11
However, major surgery for nontraumatic disease has been re-ported to be the most common cause of massive bleeding,followed by trauma and obstetric bleeding. Although the overallincidence of massive bleeding is relatively small, it remains animportant source of mortality in nontrauma patients.1,3
The goal of massive transfusion protocols (MTP) is to rap-idly provide blood products to hemodynamically unstable bleed-ing patients and to treat coagulopathy. This includes theavailability of blood products in predefined ratios and the rapidtransport and transfusion of these products.12 Massive transfu-sion protocols have been successfully implemented in traumapatients and have been shown to improve outcomes in this pa-tient population,12 including lower mortality,13 a lower risk ofmultiorgan failure, higher rate of fascial closure,14 and decreaseduse of blood products.15 The current guidelines of the American
493
ealth, Inc. All rights reserved.
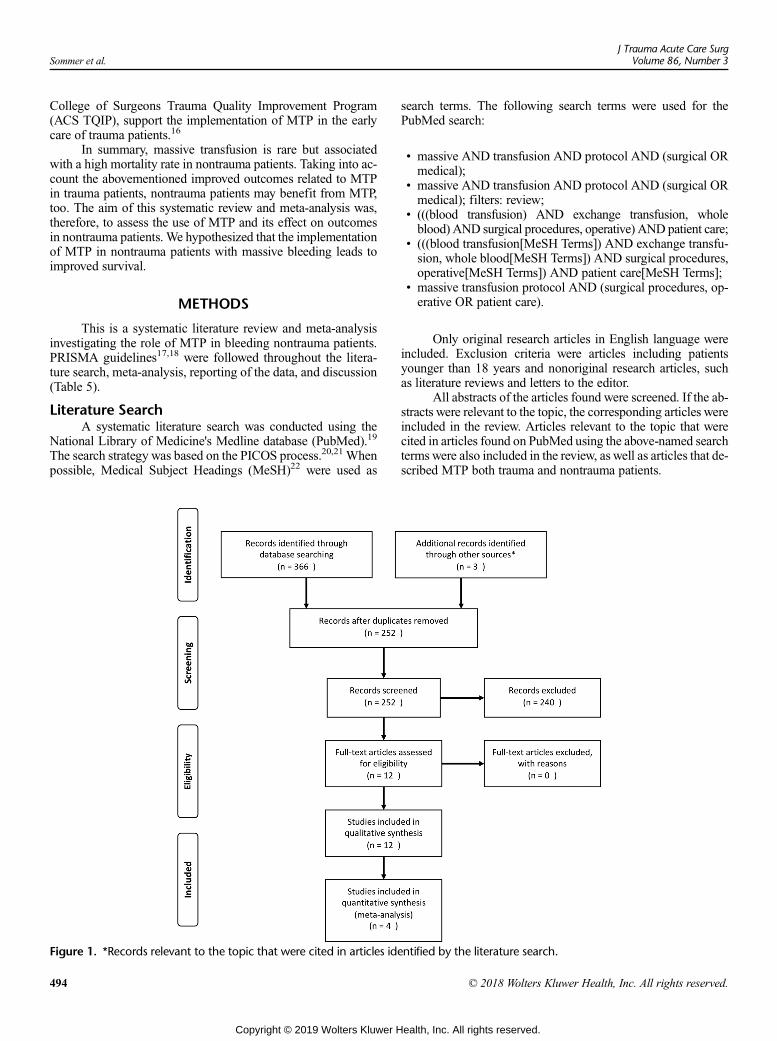
Sommer et al.J Trauma Acute Care Surg
Volume 86, Number 3
College of Surgeons Trauma Quality Improvement Program(ACS TQIP), support the implementation of MTP in the earlycare of trauma patients.16
In summary, massive transfusion is rare but associatedwith a high mortality rate in nontrauma patients. Taking into ac-count the abovementioned improved outcomes related to MTPin trauma patients, nontrauma patients may benefit from MTP,too. The aim of this systematic review and meta-analysis was,therefore, to assess the use of MTP and its effect on outcomesin nontrauma patients. We hypothesized that the implementationof MTP in nontrauma patients with massive bleeding leads toimproved survival.
METHODS
This is a systematic literature review and meta-analysisinvestigating the role of MTP in bleeding nontrauma patients.PRISMA guidelines17,18 were followed throughout the litera-ture search, meta-analysis, reporting of the data, and discussion(Table 5).
Literature SearchA systematic literature search was conducted using the
National Library of Medicine's Medline database (PubMed).19
The search strategy was based on the PICOS process.20,21 Whenpossible, Medical Subject Headings (MeSH)22 were used as
Figure 1. *Records relevant to the topic that were cited in articles ide
494
Copyright © 2019 Wolters Kluwer H
search terms. The following search terms were used for thePubMed search:
• massive AND transfusion AND protocol AND (surgical ORmedical);
• massive AND transfusion AND protocol AND (surgical ORmedical); filters: review;
• (((blood transfusion) AND exchange transfusion, wholeblood) AND surgical procedures, operative) AND patient care;
• (((blood transfusion[MeSH Terms]) AND exchange transfu-sion, whole blood[MeSH Terms]) AND surgical procedures,operative[MeSH Terms]) AND patient care[MeSH Terms];
• massive transfusion protocol AND (surgical procedures, op-erative OR patient care).
Only original research articles in English language wereincluded. Exclusion criteria were articles including patientsyounger than 18 years and nonoriginal research articles, suchas literature reviews and letters to the editor.
All abstracts of the articles found were screened. If the ab-stracts were relevant to the topic, the corresponding articles wereincluded in the review. Articles relevant to the topic that werecited in articles found on PubMed using the above-named searchterms were also included in the review, as well as articles that de-scribed MTP both trauma and nontrauma patients.
ntified by the literature search.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
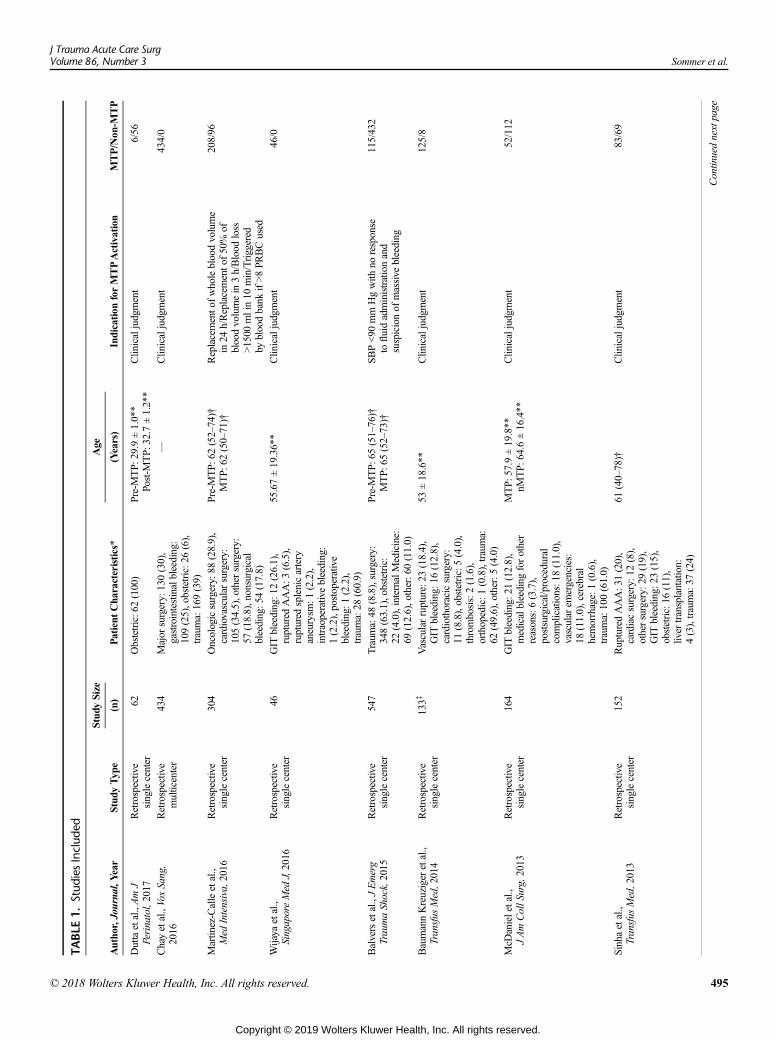
TABLE
1.Stud
iesInclud
ed
Stud
ySize
Age
Autho
r,Journal,Y
ear
Stud
yTyp
e(n)
Patient
Cha
racteristics*
(Years)
Indication
forMTPActivation
MTP/Non
-MTP
Duttaetal.,AmJ
Perinatol,2017
Retrospective
singlecenter
62Obstetric:6
2(100)
Pre-MTP:
29.9±1.0**
Post-M
TP:
32.7±1.2**
Clin
icaljudgment
6/56
Chayetal.,VoxSang,
2016
Retrospective
multicenter
434
Major
surgery:
130(30),
gastrointestinalbleeding:
109(25),obstetric:2
6(6),
trauma:169(39)
—Clin
icaljudgment
434/0
Martin
ez-Calleetal.,
Med
Intensiva,2016
Retrospective
singlecenter
304
Oncologicsurgery:
88(28.9),
cardiovascular
surgery:
105(34.5),other
surgery:
57(18.8),nonsurgical
bleeding:5
4(17.8)
Pre-MTP:
62(52–74)†
MTP:
62(50–71)†
Replacemento
fwholebloodvolume
in24
h/Replacemento
f50%
ofbloodvolumein
3h/Blood
loss
>1500
mlin10
min/Triggered
bybloodbank
if>8PR
BCused
208/96
Wijaya
etal.,
SingaporeMed
J,2016
Retrospective
singlecenter
46GIT
bleeding:1
2(26.1),
ruptured
AAA:3
(6.5),
ruptured
splenicartery
aneurysm
:1(2.2),
intraoperativebleeding:
1(2.2),postoperative
bleeding:1
(2.2),
trauma:28
(60.9)
55.67±19.36**
Clinicaljudgment
46/0
Balversetal.,JEmerg
TraumaShock,2015
Retrospective
singlecenter
547
Traum
a:48
(8.8),surgery:
348(63.1),obstetric:
22(4.0),internalMedicine:
69(12.6),other:6
0(11.0)
Pre-MTP:
65(51–76)†
MTP:
65(52–73)†
SBP<90
mm
Hgwith
noresponse
tofluidadministrationand
suspicionof
massive
bleeding
115/432
BaumannKreuziger
etal.,
Transfus
Med,2014
Retrospective
singlecenter
133‡
Vascularrupture:23
(18.4),
GIT
bleeding:1
6(12.8),
cardiothoracicsurgery:
11(8.8),obstetric:5(4.0),
thrombosis:2(1.6),
orthopedic:1
(0.8),trauma:
62(49.6),other:5
(4.0)
53±18.6**
Clinicaljudgment
125/8
McD
anieletal.,
JAmCollS
urg,2013
Retrospective
singlecenter
164
GIT
bleeding:2
1(12.8),
medicalbleeding
forother
reasons:6(3.7),
postsurgical/procedural
complications:1
8(11.0),
vascular
emergencies:
18(11.0),cerebral
hemorrhage:1(0.6),
trauma:100(61.0)
MTP:
57.9±19.8**
nMTP:
64.6±16.4**
Clin
icaljudgment
52/112
Sinhaetal.,
Transfus
Med,2013
Retrospective
singlecenter
152
RupturedAAA:3
1(20),
cardiacsurgery:
12(8),
othersurgery:
29(19),
GIT
bleeding:2
3(15),
obstetric:16
(11),
liver
transplantation:
4(3),trauma:37
(24)
61(40–78)†
Clin
icaljudgment
83/69
Continuednextpage
J Trauma Acute Care SurgVolume 86, Number 3 Sommer et al.
© 2018 Wolters Kluwer Health, Inc. All rights reserved. 495
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
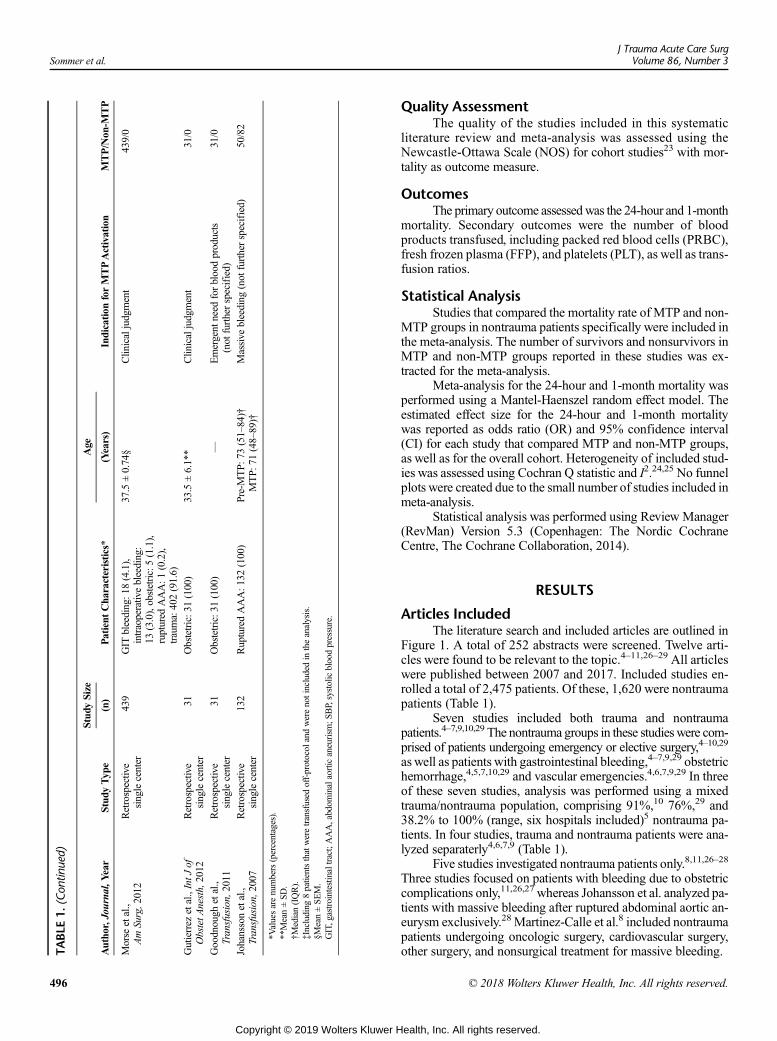
TABLE
1.(Con
tinued)
Stud
ySize
Age
Autho
r,Journal,Y
ear
Stud
yTyp
e(n)
Patient
Cha
racteristics*
(Years)
Indication
forMTPActivation
MTP/Non
-MTP
Morse
etal.,
AmSurg,2012
Retrospective
singlecenter
439
GIT
bleeding:1
8(4.1),
intraoperativebleeding:
13(3.0),obstetric:5(1.1),
ruptured
AAA:1
(0.2),
trauma:402(91.6)
37.5±0.74§
Clin
icaljudgment
439/0
Gutierrez
etal.,IntJ
ofObstetA
nesth,2012
Retrospective
singlecenter
31Obstetric:3
1(100)
33.5±6.1**
Clinicaljudgment
31/0
Goodnough
etal.,
Transfusion,2011
Retrospective
singlecenter
31Obstetric:3
1(100)
—Emergent
need
forbloodproducts
(not
furtherspecified)
31/0
Johanssonetal.,
Transfusion,2007
Retrospective
singlecenter
132
RupturedAAA:1
32(100)
Pre-MTP:
73(51–84)†
MTP:
71(48–89)†
Massive
bleeding
(not
furtherspecified)
50/82
*Valuesarenumbers(percentages).
**Mean±SD
.†M
edian(IQR).
‡Including
8patientsthatweretransfused
off-protocol
andwerenotincludedin
theanalysis.
§Mean±SEM.
GIT,gastrointestinaltract;AAA,abdom
inalaorticaneurism
;SBP,systolicbloodpressure.
Sommer et al.J Trauma Acute Care Surg
Volume 86, Number 3
496
Copyright © 2019 Wolters Kluwer H
Quality AssessmentThe quality of the studies included in this systematic
literature review and meta-analysis was assessed using theNewcastle-Ottawa Scale (NOS) for cohort studies23 with mor-tality as outcome measure.
OutcomesThe primary outcome assessedwas the 24-hour and 1-month
mortality. Secondary outcomes were the number of bloodproducts transfused, including packed red blood cells (PRBC),fresh frozen plasma (FFP), and platelets (PLT), as well as trans-fusion ratios.
Statistical AnalysisStudies that compared the mortality rate of MTP and non-
MTP groups in nontrauma patients specifically were included inthe meta-analysis. The number of survivors and nonsurvivors inMTP and non-MTP groups reported in these studies was ex-tracted for the meta-analysis.
Meta-analysis for the 24-hour and 1-month mortality wasperformed using a Mantel-Haenszel random effect model. Theestimated effect size for the 24-hour and 1-month mortalitywas reported as odds ratio (OR) and 95% confidence interval(CI) for each study that compared MTP and non-MTP groups,as well as for the overall cohort. Heterogeneity of included stud-ies was assessed using Cochran Q statistic and I2.24,25 No funnelplots were created due to the small number of studies included inmeta-analysis.
Statistical analysis was performed using Review Manager(RevMan) Version 5.3 (Copenhagen: The Nordic CochraneCentre, The Cochrane Collaboration, 2014).
RESULTS
Articles IncludedThe literature search and included articles are outlined in
Figure 1. A total of 252 abstracts were screened. Twelve arti-cles were found to be relevant to the topic.4–11,26–29 All articleswere published between 2007 and 2017. Included studies en-rolled a total of 2,475 patients. Of these, 1,620 were nontraumapatients (Table 1).
Seven studies included both trauma and nontraumapatients.4–7,9,10,29 The nontrauma groups in these studieswere com-prised of patients undergoing emergency or elective surgery,4–10,29
as well as patients with gastrointestinal bleeding,4–7,9,29 obstetrichemorrhage,4,5,7,10,29 and vascular emergencies.4,6,7,9,29 In threeof these seven studies, analysis was performed using a mixedtrauma/nontrauma population, comprising 91%,10 76%,29 and38.2% to 100% (range, six hospitals included)5 nontrauma pa-tients. In four studies, trauma and nontrauma patients were ana-lyzed separaterly4,6,7,9 (Table 1).
Five studies investigated nontrauma patients only.8,11,26–28
Three studies focused on patients with bleeding due to obstetriccomplications only,11,26,27 whereas Johansson et al. analyzed pa-tients with massive bleeding after ruptured abdominal aortic an-eurysm exclusively.28 Martinez-Calle et al.8 included nontraumapatients undergoing oncologic surgery, cardiovascular surgery,other surgery, and nonsurgical treatment for massive bleeding.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
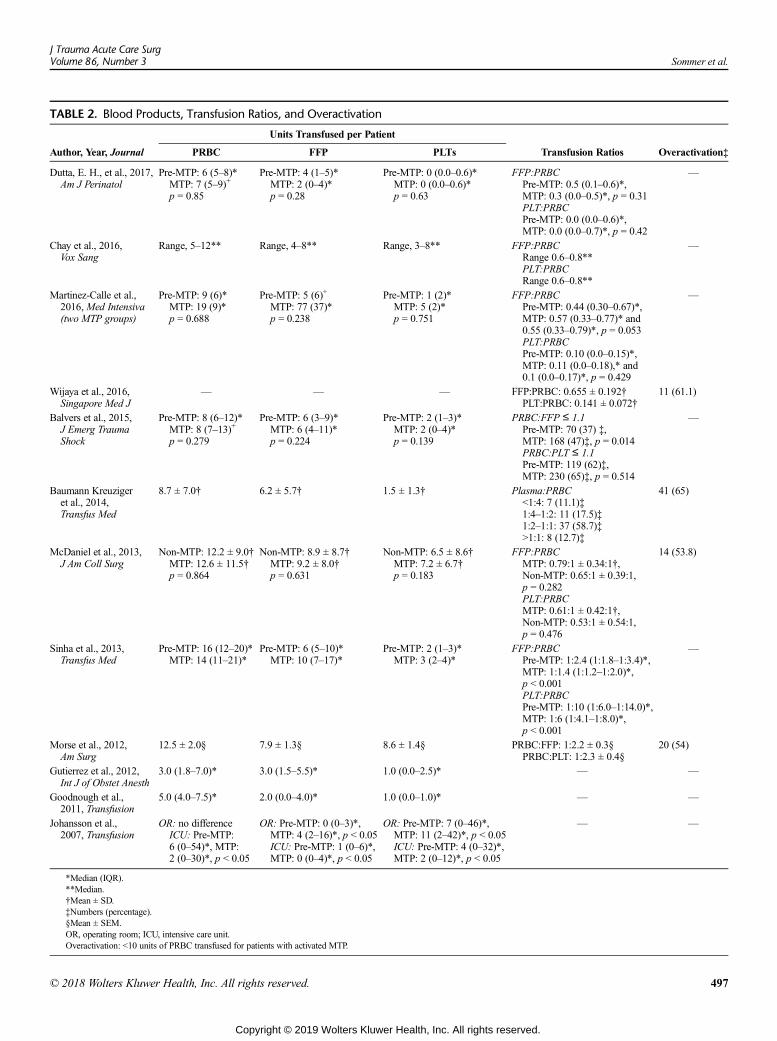
TABLE 2. Blood Products, Transfusion Ratios, and Overactivation
Units Transfused per Patient
Author, Year, Journal PRBC FFP PLTs Transfusion Ratios Overactivation‡
Dutta, E. H., et al., 2017,Am J Perinatol
Pre-MTP: 6 (5–8)*MTP: 7 (5–9)+
p = 0.85
Pre-MTP: 4 (1–5)*MTP: 2 (0–4)*p = 0.28
Pre-MTP: 0 (0.0–0.6)*MTP: 0 (0.0–0.6)*p = 0.63
FFP:PRBCPre-MTP: 0.5 (0.1–0.6)*,MTP: 0.3 (0.0–0.5)*, p = 0.31PLT:PRBCPre-MTP: 0.0 (0.0–0.6)*,MTP: 0.0 (0.0–0.7)*, p = 0.42
—
Chay et al., 2016,Vox Sang
Range, 5–12** Range, 4–8** Range, 3–8** FFP:PRBCRange 0.6–0.8**PLT:PRBCRange 0.6–0.8**
—
Martinez-Calle et al.,2016,Med Intensiva(two MTP groups)
Pre-MTP: 9 (6)*MTP: 19 (9)*p = 0.688
Pre-MTP: 5 (6)+
MTP: 77 (37)*p = 0.238
Pre-MTP: 1 (2)*MTP: 5 (2)*p = 0.751
FFP:PRBCPre-MTP: 0.44 (0.30–0.67)*,MTP: 0.57 (0.33–0.77)* and0.55 (0.33–0.79)*, p = 0.053PLT:PRBCPre-MTP: 0.10 (0.0–0.15)*,MTP: 0.11 (0.0–0.18),* and0.1 (0.0–0.17)*, p = 0.429
—
Wijaya et al., 2016,Singapore Med J
— — — FFP:PRBC: 0.655 ± 0.192†PLT:PRBC: 0.141 ± 0.072†
11 (61.1)
Balvers et al., 2015,J Emerg TraumaShock
Pre-MTP: 8 (6–12)*MTP: 8 (7–13)+
p = 0.279
Pre-MTP: 6 (3–9)*MTP: 6 (4–11)*p = 0.224
Pre-MTP: 2 (1–3)*MTP: 2 (0–4)*p = 0.139
PRBC:FFP ≤ 1.1Pre-MTP: 70 (37) ‡,MTP: 168 (47)‡, p = 0.014PRBC:PLT ≤ 1.1Pre-MTP: 119 (62)‡,MTP: 230 (65)‡, p = 0.514
—
Baumann Kreuzigeret al., 2014,Transfus Med
8.7 ± 7.0† 6.2 ± 5.7† 1.5 ± 1.3† Plasma:PRBC<1:4: 7 (11.1)‡1:4–1:2: 11 (17.5)‡1:2–1:1: 37 (58.7)‡>1:1: 8 (12.7)‡
41 (65)
McDaniel et al., 2013,J Am Coll Surg
Non-MTP: 12.2 ± 9.0†MTP: 12.6 ± 11.5†p = 0.864
Non-MTP: 8.9 ± 8.7†MTP: 9.2 ± 8.0†p = 0.631
Non-MTP: 6.5 ± 8.6†MTP: 7.2 ± 6.7†p = 0.183
FFP:PRBCMTP: 0.79:1 ± 0.34:1†,Non-MTP: 0.65:1 ± 0.39:1,p = 0.282PLT:PRBCMTP: 0.61:1 ± 0.42:1†,Non-MTP: 0.53:1 ± 0.54:1,p = 0.476
14 (53.8)
Sinha et al., 2013,Transfus Med
Pre-MTP: 16 (12–20)*MTP: 14 (11–21)*
Pre-MTP: 6 (5–10)*MTP: 10 (7–17)*
Pre-MTP: 2 (1–3)*MTP: 3 (2–4)*
FFP:PRBCPre-MTP: 1:2.4 (1:1.8–1:3.4)*,MTP: 1:1.4 (1:1.2–1:2.0)*,p < 0.001PLT:PRBCPre-MTP: 1:10 (1:6.0–1:14.0)*,MTP: 1:6 (1:4.1–1:8.0)*,p < 0.001
—
Morse et al., 2012,Am Surg
12.5 ± 2.0§ 7.9 ± 1.3§ 8.6 ± 1.4§ PRBC:FFP: 1:2.2 ± 0.3§PRBC:PLT: 1:2.3 ± 0.4§
20 (54)
Gutierrez et al., 2012,Int J of Obstet Anesth
3.0 (1.8–7.0)* 3.0 (1.5–5.5)* 1.0 (0.0–2.5)* — —
Goodnough et al.,2011, Transfusion
5.0 (4.0–7.5)* 2.0 (0.0–4.0)* 1.0 (0.0–1.0)* — —
Johansson et al.,2007, Transfusion
OR: no differenceICU: Pre-MTP:6 (0–54)*, MTP:2 (0–30)*, p < 0.05
OR: Pre-MTP: 0 (0–3)*,MTP: 4 (2–16)*, p < 0.05ICU: Pre-MTP: 1 (0–6)*,MTP: 0 (0–4)*, p < 0.05
OR: Pre-MTP: 7 (0–46)*,MTP: 11 (2–42)*, p < 0.05ICU: Pre-MTP: 4 (0–32)*,MTP: 2 (0–12)*, p < 0.05
— —
*Median (IQR).**Median.†Mean ± SD.‡Numbers (percentage).§Mean ± SEM.OR, operating room; ICU, intensive care unit.Overactivation: <10 units of PRBC transfused for patients with activated MTP.
J Trauma Acute Care SurgVolume 86, Number 3 Sommer et al.
© 2018 Wolters Kluwer Health, Inc. All rights reserved. 497
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
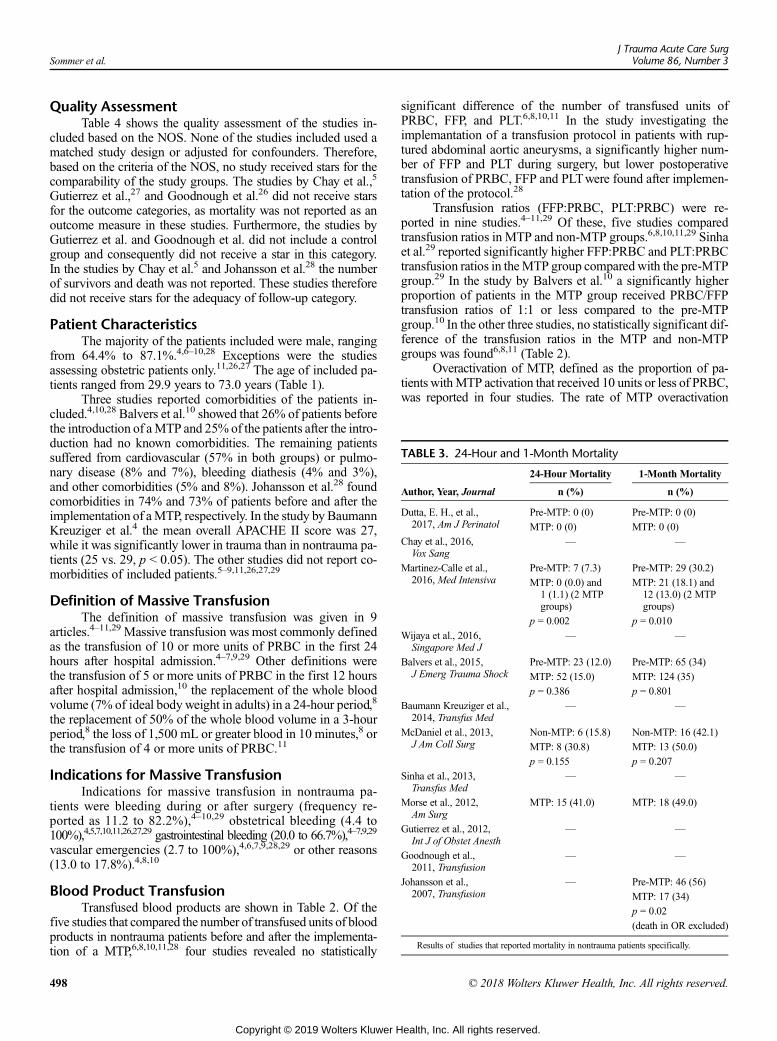
TABLE 3. 24-Hour and 1-Month Mortality
24-Hour Mortality 1-Month Mortality
Author, Year, Journal n (%) n (%)
Dutta, E. H., et al.,2017, Am J Perinatol
Pre-MTP: 0 (0) Pre-MTP: 0 (0)
MTP: 0 (0) MTP: 0 (0)
Chay et al., 2016,Vox Sang
— —
Martinez-Calle et al.,2016, Med Intensiva
Pre-MTP: 7 (7.3) Pre-MTP: 29 (30.2)
MTP: 0 (0.0) and1 (1.1) (2 MTPgroups)
MTP: 21 (18.1) and12 (13.0) (2 MTPgroups)
p = 0.002 p = 0.010
Wijaya et al., 2016,Singapore Med J
— —
Balvers et al., 2015,J Emerg Trauma Shock
Pre-MTP: 23 (12.0) Pre-MTP: 65 (34)
MTP: 52 (15.0) MTP: 124 (35)
p = 0.386 p = 0.801
Baumann Kreuziger et al.,2014, Transfus Med
— —
McDaniel et al., 2013,J Am Coll Surg
Non-MTP: 6 (15.8) Non-MTP: 16 (42.1)
MTP: 8 (30.8) MTP: 13 (50.0)
p = 0.155 p = 0.207
Sinha et al., 2013,Transfus Med
— —
Morse et al., 2012,Am Surg
MTP: 15 (41.0) MTP: 18 (49.0)
Gutierrez et al., 2012,Int J of Obstet Anesth
— —
Goodnough et al.,2011, Transfusion
— —
Johansson et al.,2007, Transfusion
— Pre-MTP: 46 (56)
MTP: 17 (34)
p = 0.02
(death in OR excluded)
Results of studies that reported mortality in nontrauma patients specifically.
Sommer et al.J Trauma Acute Care Surg
Volume 86, Number 3
Quality AssessmentTable 4 shows the quality assessment of the studies in-
cluded based on the NOS. None of the studies included used amatched study design or adjusted for confounders. Therefore,based on the criteria of the NOS, no study received stars for thecomparability of the study groups. The studies by Chay et al.,5
Gutierrez et al.,27 and Goodnough et al.26 did not receive starsfor the outcome categories, as mortality was not reported as anoutcome measure in these studies. Furthermore, the studies byGutierrez et al. and Goodnough et al. did not include a controlgroup and consequently did not receive a star in this category.In the studies by Chay et al.5 and Johansson et al.28 the numberof survivors and death was not reported. These studies thereforedid not receive stars for the adequacy of follow-up category.
Patient CharacteristicsThe majority of the patients included were male, ranging
from 64.4% to 87.1%.4,6–10,28 Exceptions were the studiesassessing obstetric patients only.11,26,27 The age of included pa-tients ranged from 29.9 years to 73.0 years (Table 1).
Three studies reported comorbidities of the patients in-cluded.4,10,28 Balvers et al.10 showed that 26% of patients beforethe introduction of aMTP and 25% of the patients after the intro-duction had no known comorbidities. The remaining patientssuffered from cardiovascular (57% in both groups) or pulmo-nary disease (8% and 7%), bleeding diathesis (4% and 3%),and other comorbidities (5% and 8%). Johansson et al.28 foundcomorbidities in 74% and 73% of patients before and after theimplementation of aMTP, respectively. In the study by BaumannKreuziger et al.4 the mean overall APACHE II score was 27,while it was significantly lower in trauma than in nontrauma pa-tients (25 vs. 29, p < 0.05). The other studies did not report co-morbidities of included patients.5–9,11,26,27,29
Definition of Massive TransfusionThe definition of massive transfusion was given in 9
articles.4–11,29 Massive transfusion was most commonly definedas the transfusion of 10 or more units of PRBC in the first 24hours after hospital admission.4–7,9,29 Other definitions werethe transfusion of 5 or more units of PRBC in the first 12 hoursafter hospital admission,10 the replacement of the whole bloodvolume (7% of ideal body weight in adults) in a 24-hour period,8
the replacement of 50% of the whole blood volume in a 3-hourperiod,8 the loss of 1,500 mL or greater blood in 10 minutes,8 orthe transfusion of 4 or more units of PRBC.11
Indications for Massive TransfusionIndications for massive transfusion in nontrauma pa-
tients were bleeding during or after surgery (frequency re-ported as 11.2 to 82.2%),4–10,29 obstetrical bleeding (4.4 to100%),4,5,7,10,11,26,27,29 gastrointestinal bleeding (20.0 to 66.7%),4–7,9,29
vascular emergencies (2.7 to 100%),4,6,7,9,28,29 or other reasons(13.0 to 17.8%).4,8,10
Blood Product TransfusionTransfused blood products are shown in Table 2. Of the
five studies that compared the number of transfused units of bloodproducts in nontrauma patients before and after the implementa-tion of a MTP,6,8,10,11,28 four studies revealed no statistically
498
Copyright © 2019 Wolters Kluwer H
significant difference of the number of transfused units ofPRBC, FFP, and PLT.6,8,10,11 In the study investigating theimplemantation of a transfusion protocol in patients with rup-tured abdominal aortic aneurysms, a significantly higher num-ber of FFP and PLT during surgery, but lower postoperativetransfusion of PRBC, FFP and PLTwere found after implemen-tation of the protocol.28
Transfusion ratios (FFP:PRBC, PLT:PRBC) were re-ported in nine studies.4–11,29 Of these, five studies comparedtransfusion ratios in MTP and non-MTP groups.6,8,10,11,29 Sinhaet al.29 reported significantly higher FFP:PRBC and PLT:PRBCtransfusion ratios in theMTP group compared with the pre-MTPgroup.29 In the study by Balvers et al.10 a significantly higherproportion of patients in the MTP group received PRBC/FFPtransfusion ratios of 1:1 or less compared to the pre-MTPgroup.10 In the other three studies, no statistically significant dif-ference of the transfusion ratios in the MTP and non-MTPgroups was found6,8,11 (Table 2).
Overactivation of MTP, defined as the proportion of pa-tients withMTP activation that received 10 units or less of PRBC,was reported in four studies. The rate of MTP overactivation
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
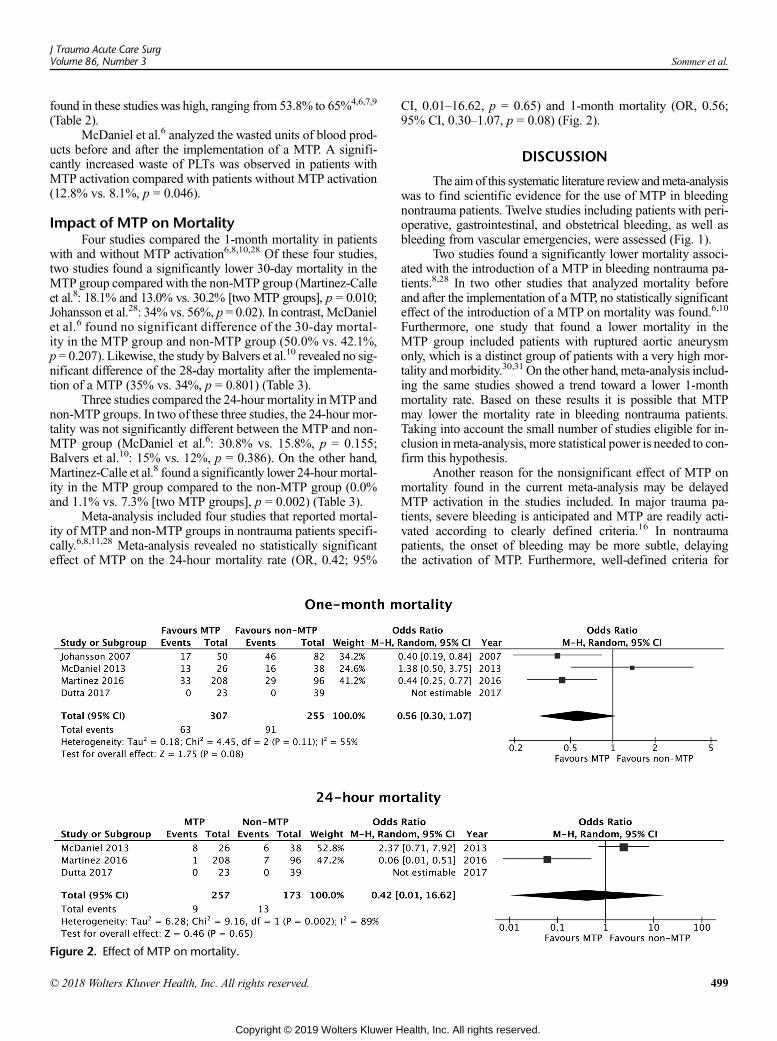
J Trauma Acute Care SurgVolume 86, Number 3 Sommer et al.
found in these studies was high, ranging from 53.8% to 65%4,6,7,9
(Table 2).McDaniel et al.6 analyzed the wasted units of blood prod-
ucts before and after the implementation of a MTP. A signifi-cantly increased waste of PLTs was observed in patients withMTP activation compared with patients without MTP activation(12.8% vs. 8.1%, p = 0.046).
Impact of MTP on MortalityFour studies compared the 1-month mortality in patients
with and without MTP activation6,8,10,28 Of these four studies,two studies found a significantly lower 30-day mortality in theMTP group compared with the non-MTP group (Martinez-Calleet al.8: 18.1% and 13.0% vs. 30.2% [two MTP groups], p = 0.010;Johansson et al.28: 34% vs. 56%, p = 0.02). In contrast, McDanielet al.6 found no significant difference of the 30-day mortal-ity in the MTP group and non-MTP group (50.0% vs. 42.1%,p = 0.207). Likewise, the study by Balvers et al.10 revealed no sig-nificant difference of the 28-day mortality after the implementa-tion of a MTP (35% vs. 34%, p = 0.801) (Table 3).
Three studies compared the 24-hour mortality inMTP andnon-MTP groups. In two of these three studies, the 24-hour mor-tality was not significantly different between the MTP and non-MTP group (McDaniel et al.6: 30.8% vs. 15.8%, p = 0.155;Balvers et al.10: 15% vs. 12%, p = 0.386). On the other hand,Martinez-Calle et al.8 found a significantly lower 24-hour mortal-ity in the MTP group compared to the non-MTP group (0.0%and 1.1% vs. 7.3% [two MTP groups], p = 0.002) (Table 3).
Meta-analysis included four studies that reported mortal-ity of MTP and non-MTP groups in nontrauma patients specifi-cally.6,8,11,28 Meta-analysis revealed no statistically significanteffect of MTP on the 24-hour mortality rate (OR, 0.42; 95%
Figure 2. Effect of MTP on mortality.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
CI, 0.01–16.62, p = 0.65) and 1-month mortality (OR, 0.56;95% CI, 0.30–1.07, p = 0.08) (Fig. 2).
DISCUSSION
The aim of this systematic literature reviewandmeta-analysiswas to find scientific evidence for the use of MTP in bleedingnontrauma patients. Twelve studies including patients with peri-operative, gastrointestinal, and obstetrical bleeding, as well asbleeding from vascular emergencies, were assessed (Fig. 1).
Two studies found a significantly lower mortality associ-ated with the introduction of a MTP in bleeding nontrauma pa-tients.8,28 In two other studies that analyzed mortality beforeand after the implementation of a MTP, no statistically significanteffect of the introduction of a MTP on mortality was found.6,10
Furthermore, one study that found a lower mortality in theMTP group included patients with ruptured aortic aneurysmonly, which is a distinct group of patients with a very high mor-tality andmorbidity.30,31 On the other hand, meta-analysis includ-ing the same studies showed a trend toward a lower 1-monthmortality rate. Based on these results it is possible that MTPmay lower the mortality rate in bleeding nontrauma patients.Taking into account the small number of studies eligible for in-clusion inmeta-analysis, more statistical power is needed to con-firm this hypothesis.
Another reason for the nonsignificant effect of MTP onmortality found in the current meta-analysis may be delayedMTP activation in the studies included. In major trauma pa-tients, severe bleeding is anticipated and MTP are readily acti-vated according to clearly defined criteria.16 In nontraumapatients, the onset of bleeding may be more subtle, delayingthe activation of MTP. Furthermore, well-defined criteria for
499
ealth, Inc. All rights reserved.
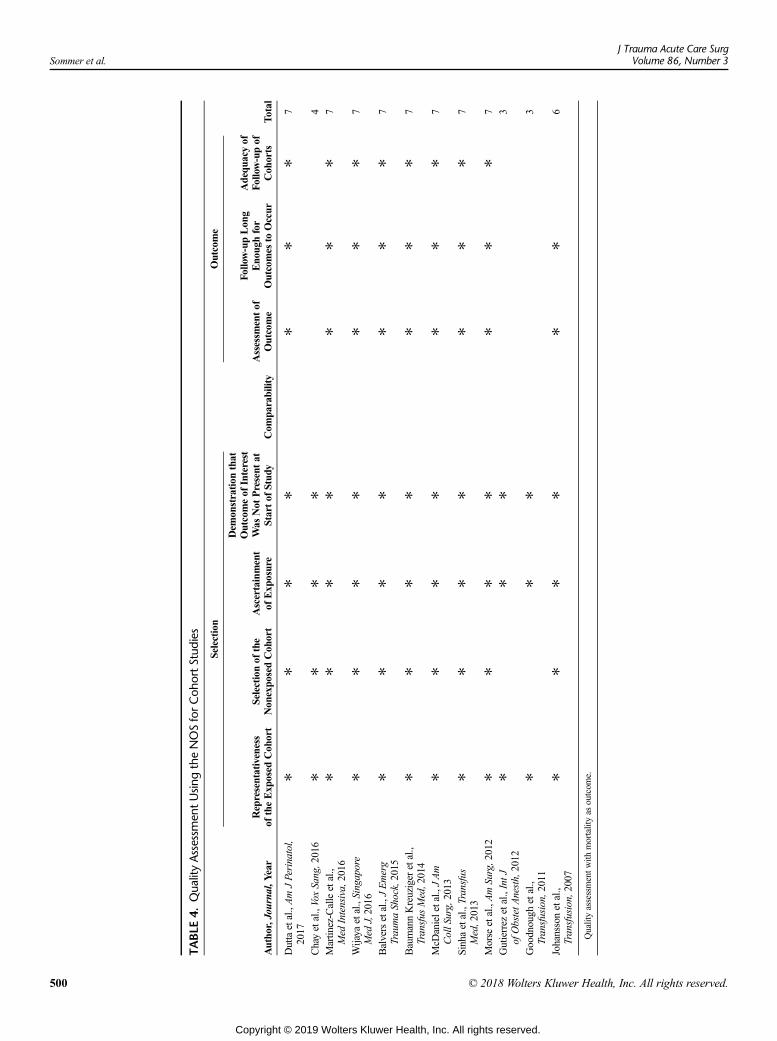
TABLE
4.Qua
lityAssessm
entUsin
gtheNOSforCoh
ortStud
ies
Selection
Outcome
Autho
r,Journal,Y
ear
Representativeness
oftheExp
osed
Coh
ort
Selectionof
the
Non
expo
sedCoh
ort
Ascertainment
ofExp
osure
Dem
onstration
that
Outcomeof
Interest
Was
Not
Present
atStartof
Stud
yCom
parability
Assessm
entof
Outcome
Follow-upLon
gEno
ughfor
Outcomes
toOccur
Adequ
acyof
Follow-upof
Coh
orts
Total
Duttaetal.,AmJPerinatol,
2017
✻✻
✻✻
✻✻
✻7
Chayetal.,VoxSang,2016
✻✻
✻✻
4
Martin
ez-Calleetal.,
Med
Intensiva,2016
✻✻
✻✻
✻✻
✻7
Wijaya
etal.,Singapore
Med
J,2016
✻✻
✻✻
✻✻
✻7
Balversetal.,JEmerg
TraumaShock,2015
✻✻
✻✻
✻✻
✻7
BaumannKreuziger
etal.,
Transfus
Med,2014
✻✻
✻✻
✻✻
✻7
McD
anieletal.,JAm
CollS
urg,2013
✻✻
✻✻
✻✻
✻7
Sinhaetal.,Transfus
Med,2013
✻✻
✻✻
✻✻
✻7
Morse
etal.,AmSurg,2012
✻✻
✻✻
✻✻
✻7
Gutierrez
etal.,IntJ
ofObstetA
nesth,2012
✻✻
✻3
Goodnough
etal.,
Transfusion,2011
✻✻
✻3
Johanssonetal.,
Transfusion,2007
✻✻
✻✻
✻✻
6
Qualityassessmentw
ithmortalityas
outcom
e.
Sommer et al.J Trauma Acute Care Surg
Volume 86, Number 3
500 © 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
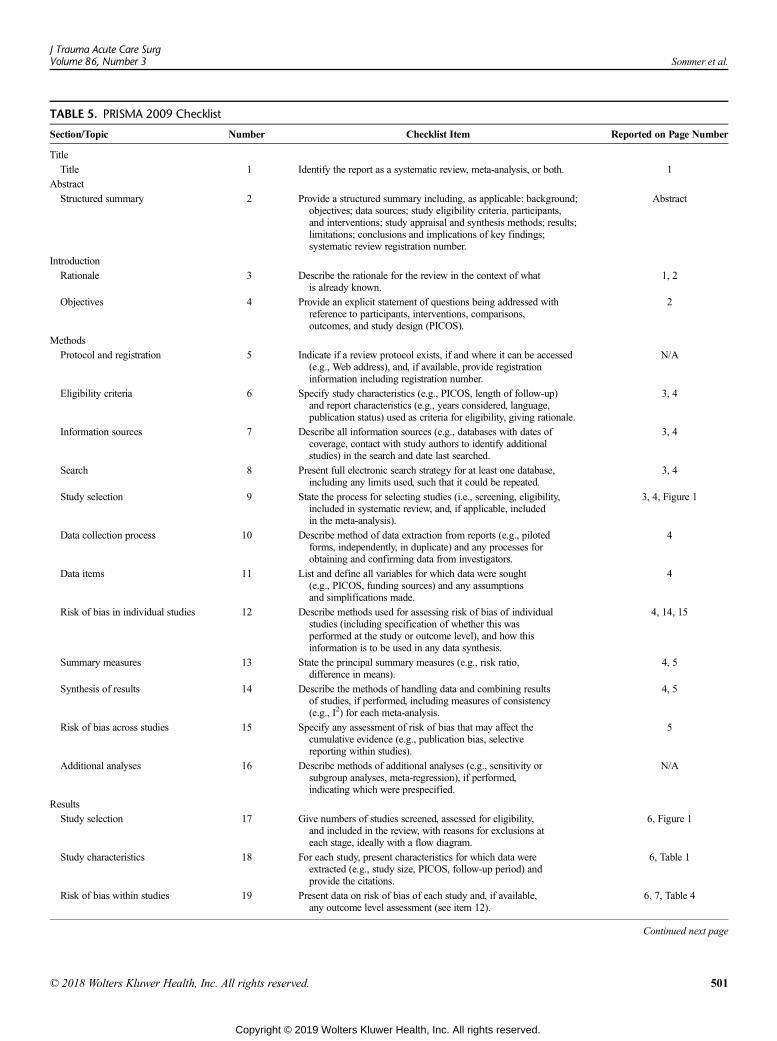
TABLE 5. PRISMA 2009 Checklist
Section/Topic Number Checklist Item Reported on Page Number
Title
Title 1 Identify the report as a systematic review, meta-analysis, or both. 1
Abstract
Structured summary 2 Provide a structured summary including, as applicable: background;objectives; data sources; study eligibility criteria, participants,and interventions; study appraisal and synthesis methods; results;limitations; conclusions and implications of key findings;systematic review registration number.
Abstract
Introduction
Rationale 3 Describe the rationale for the review in the context of whatis already known.
1, 2
Objectives 4 Provide an explicit statement of questions being addressed withreference to participants, interventions, comparisons,outcomes, and study design (PICOS).
2
Methods
Protocol and registration 5 Indicate if a review protocol exists, if and where it can be accessed(e.g., Web address), and, if available, provide registrationinformation including registration number.
N/A
Eligibility criteria 6 Specify study characteristics (e.g., PICOS, length of follow-up)and report characteristics (e.g., years considered, language,publication status) used as criteria for eligibility, giving rationale.
3, 4
Information sources 7 Describe all information sources (e.g., databases with dates ofcoverage, contact with study authors to identify additionalstudies) in the search and date last searched.
3, 4
Search 8 Present full electronic search strategy for at least one database,including any limits used, such that it could be repeated.
3, 4
Study selection 9 State the process for selecting studies (i.e., screening, eligibility,included in systematic review, and, if applicable, includedin the meta-analysis).
3, 4, Figure 1
Data collection process 10 Describe method of data extraction from reports (e.g., pilotedforms, independently, in duplicate) and any processes forobtaining and confirming data from investigators.
4
Data items 11 List and define all variables for which data were sought(e.g., PICOS, funding sources) and any assumptionsand simplifications made.
4
Risk of bias in individual studies 12 Describe methods used for assessing risk of bias of individualstudies (including specification of whether this wasperformed at the study or outcome level), and how thisinformation is to be used in any data synthesis.
4, 14, 15
Summary measures 13 State the principal summary measures (e.g., risk ratio,difference in means).
4, 5
Synthesis of results 14 Describe the methods of handling data and combining resultsof studies, if performed, including measures of consistency(e.g., I2) for each meta-analysis.
4, 5
Risk of bias across studies 15 Specify any assessment of risk of bias that may affect thecumulative evidence (e.g., publication bias, selectivereporting within studies).
5
Additional analyses 16 Describe methods of additional analyses (e.g., sensitivity orsubgroup analyses, meta-regression), if performed,indicating which were prespecified.
N/A
Results
Study selection 17 Give numbers of studies screened, assessed for eligibility,and included in the review, with reasons for exclusions ateach stage, ideally with a flow diagram.
6, Figure 1
Study characteristics 18 For each study, present characteristics for which data wereextracted (e.g., study size, PICOS, follow-up period) andprovide the citations.
6, Table 1
Risk of bias within studies 19 Present data on risk of bias of each study and, if available,any outcome level assessment (see item 12).
6, 7, Table 4
Continued next page
J Trauma Acute Care SurgVolume 86, Number 3 Sommer et al.
© 2018 Wolters Kluwer Health, Inc. All rights reserved. 501
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.

TABLE 5. (Continued)
Section/Topic Number Checklist Item Reported on Page Number
Results of individual studies 20 For all outcomes considered (benefits or harms), present,for each study: (a) simple summary data for eachintervention group (b) effect estimates and confidenceintervals, ideally with a forest plot.
10, 11, Table 3, Figure 2
Synthesis of results 21 Present results of each meta-analysis performed, includingconfidence intervals and measures of consistency.
10, 11, Figure 2
Risk of bias across studies 22 Present results of any assessment of risk of bias acrossstudies (see Item 15).
4, 5, 14, 15, Figure 2
Additional analysis 23 Give results of additional analyses, if performed (e.g., sensitivityor subgroup analyses, meta-regression [see Item 16]).
N/A
Discussion
Summary of evidence 24 Summarize the main findings including the strength of evidencefor each main outcome; consider their relevance to key groups(e.g., healthcare providers, users, and policy makers).
12, 13, 14
Limitations 25 Discuss limitations at study and outcome level (e.g., riskof bias), and at review-level (e.g., incomplete retrievalof identified research, reporting bias).
14, 15
Conclusion 26 Provide a general interpretation of the results in the contextof other evidence, and implications for future research.
16
Funding
Funding 27 Describe sources of funding for the systematic review andother support (e.g., supply of data); role of funders forthe systematic review.
N/A
Sommer et al.J Trauma Acute Care Surg
Volume 86, Number 3
massive transfusion in nontrauma patients are lacking. Martinezet al. report proactive triggering of MTP in only 20% in non-trauma patients. In the other 80%, MTP was automatically acti-vated by the blood bank after the transfusion of more than 8units of PRBC.8 In the study by McDaniel et al. MTP activationaccelerated the delivery of FFP and PLTs. However, MTP acti-vation was not associated with improved survival in this study.6
Although one of the goals of MTP is to achieve higherplasma and PLTs to PRBC transfusion ratios, FFP:PRBC and/or PLT:PRBC transfusion ratios did not meet the currently recom-mended ratios of 1:1:1 or 1:1:232 in four studies8,9,11,29 (Table 2).This finding is surprising, as with the introduction of a MTP,predefined ratios of blood products should be available fortransfusion.12,15,33–35 A possible explanation for the lower thanrecommended transfusion ratios in these studies may be a de-layed MTP activation with unbalanced PRBC transfusion priorto the activation of the protocol.8
A high rate of MTP overactivation was found in four stud-ies.4,6,7,9 The identification of nontrauma patients that requireMTP activation may be challenging as specific criteria arestill lacking. In trauma patients, on the contrary, there are well-established criteria for massive transfusion and MTP activation,such as the ACS TQIP Best Practice Guidelines,16 the Assess-ment of Blood Consumption score,36–38 the Trauma AssociatedSevere Hemorrhage score,39 the algorithm developed for combatcasualty patients by McLaughlin and collegues,40 the RevisedAssessment of Bleeding and Transfusion score,41 and the Mas-sive Transfusion Score.42 The absence of defined criteria formassive transfusion in nontrauma patients most likely explainsthe high overactivation rate in this patient population.
The study of McDaniel et al.6 was the only one that ana-lyzed the waste of blood products. An increased waste of PLTs
502
Copyright © 2019 Wolters Kluwer H
was found after the introduction of a MTP. The waste of bloodproducts associated with MTP could potentially be prevented,as unused blood products may be provided to other patients ifthey are returned promptly to the blood bank.6 Furthermore,timely termination of the MTP once the endpoints of transfusionare achieved may reduce the waste of blood products. The ACSTQIP lists several criteria for the termination of MTP, includingdowngrading to goal-directed transfusion if bleeding has beencontrolled by surgery or angioembolization, further resuscitationis futile, and—in patients with no active bleeding—laboratoryfindings indicate adequate blood coagulation.16 Although theACS TQIP criteria for the termination of MTP were elaboratedfor trauma patients, they may also be useful in nontrauma pa-tients. Further studies will need to evaluate the criteria forMTP termination in nontrauma patients specifically.
Nontrauma patients included in the current reviewhad many comorbidities, especially from cardiovascular or-igin4,10,28,29 (Table 1). Trauma patients are typically youngerand have less comorbidities than the nontrauma patients in-cluded in the current review. Furthermore, trauma patients maybleed frommultiple injuries, whereas bleeding is often localizedin nontrauma patients, for example, in patients with gastrointes-tinal bleeding or bleeding during cardiovascular surgery. Bothtrauma and nontrauma patients may suffer from profuse bleedingdue to coagulopathy. However, due to the abovementioned cardio-vascular comorbidities, drug-induced coagulopathy is more likelyin nontrauma than in trauma patients.43 When extrapolating indi-cations and goals of MTP from trauma to nontrauma patients, thedifferent characteristics of these two patient populations need tobe considered.
This systematic literature review and meta-analysis hasseveral limitations. First, all studies were retrospective. Second,
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Sommer et al.
three studies analyzed mixed cohorts of nontrauma and traumapatients,5,10,29 while others focused on a specific group ofpatients.11,26–28 Third, the total number of patients that were in-cluded inmeta-analysis was relatively small, limiting the validityof the results. Fourth, the quality of the studies included variedand was poor in some studies (Table 4). Fifth, MTPs, includingthe indication for MTP activation and predefined transfusionratios, differed between the studies included. To take into ac-count the heterogeneity of the studies included, only studiesreporting outcomes ofMTP and non-MTP groups in nontraumapatients specifically were included in the quantitative analysis.Furthermore, a random-effects model was chosen for meta-analysis.
CONCLUSION
Based on the current literature review and meta-analysis,there is limited evidence that the implementation of MTP maybe associated with decreased mortality in nontrauma patients.Both, overactivation and an increased waste of blood productshave been reported with the introduction of MTP. However, pa-tient characteristics, as well as the indication and definition ofMTPwere highly heterogeneous in the available studies. Furtherprospective investigation into this topic is warranted.
AUTHORSHIP
N.S. and T.H. participated in the literature search. T.H. and B.S. partici-pated in the study design. N.S. and T.H. participated in the data collection.T.H. and B.S. participated in the data analysis. T.H., N.S., B.S., and D.C.participated in the data interpretation. N.S., T.H., and B.S. participatedin the writing. T.H., B.S., and D.C. participated in the critical revision.
DISCLOSURE
The authors declare no funding or conflicts of interest.
REFERENCES1. Halmin M, Chiesa F, Vasan SK, Wikman A, Norda R, Rostgaard K,
Vesterager PedersenOB, Erikstrup C, NielsenKR, Titlestad K, et al. Epidemi-ology of massive transfusion: a binational study from Sweden and Denmark.Crit Care Med. 2016;44(3):468–477.
2. Rose AH, Kotze A, Doolan D, Norfolk DR, Bellamy MC. Massivetransfusion—evaluation of current clinical practice and outcome in twolarge teaching hospital trusts in Northern England. Vox Sang. 2009;97(3):247–253.
3. TuranA,YangD, Bonilla A, Shiba A, Sessler DI, Saager L, Kurz A.Morbidityand mortality after massive transfusion in patients undergoing non-cardiacsurgery. Can J Anaesth. 2013;60(8):761–770.
4. Baumann Kreuziger LM, Morton CT, Subramanian AT, Anderson CP,Dries DJ. Not only in trauma patients: hospital-wide implementation of amassive transfusion protocol. Transfus Med. 2014;24(3):162–168.
5. Chay J, Koh M, Tan HH, Ng J, Ng HJ, Chia N, Kuperan P, Tan J, Lew E,Tan LK, et al. A national common massive transfusion protocol (MTP) is afeasible and advantageous option for centralized blood services and hospi-tals. Vox Sang. 2016;110(1):36–50.
6. McDaniel LM, Neal MD, Sperry JL, Alarcon LH, Forsythe RM, Triulzi D,Peitzman AB, Raval JS. Use of a massive transfusion protocol in nontraumapatients: activate away. J Am Coll Surg. 2013;216(6):1103–1109.
7. Morse BC, Dente CJ, Hodgman EI, Shaz BH, Winkler A, Nicholas JM,Wyrzykowski AD, Rozycki GS, Feliciano DV. Outcomes after massive trans-fusion in nontrauma patients in the era of damage control resuscitation. AmSurg. 2012;78(6):679–684.
8. Martinez-Calle N, Hidalgo F, Alfonso A, Munoz M, Hernandez M,Lecumberri R, Paramo JA. Implementation of a management protocol formassive bleeding reduces mortality in non-trauma patients: results from asingle centre audit. Med Intensiva. 2016;40(9):550–559.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
9. Wijaya R, Cheng HM, Chong CK. The use of massive transfusion protocolfor trauma and non-trauma patients in a civilian setting: what can be donebetter? Singapore Med J. 2016;57(5):238–241.
10. Balvers K, Coppens M, van Dieren S, van Rooyen-Schreurs IH,Klinkspoor HJ, Zeerleder SS, Baumann HM, Goslings JC, Juffermans NP.Effects of a hospital-wide introduction of a massive transfusion protocol onblood product ratio and blood product waste. J Emerg Trauma Shock.2015;8(4):199–204.
11. Dutta EH, Poole AT, Behnia F, Dunn HE, Clark SM, Pacheco LD, Saade GR,Hankins GD. Hemostatic resuscitation in peripartum hysterectomy pre- andpostmassive transfusion protocol initiation. Am J Perinatol. 2017;34(9):861–866.
12. Nunez TC, Young PP, Holcomb JB, Cotton BA. Creation, implementation,and maturation of a massive transfusion protocol for the exsanguinatingtrauma patient. J Trauma. 2010;68(6):1498–1505.
13. RiskinDJ, Tsai TC, Riskin L,Hernandez-Boussard T, Purtill M,Maggio PM,Spain DA, Brundage SI. Massive transfusion protocols: the role of aggres-sive resuscitation versus product ratio in mortality reduction. J AmColl Surg.2009;209(2):198–205.
14. Cotton BA, Au BK, Nunez TC, Gunter OL, Robertson AM, Young PP.Predefined massive transfusion protocols are associated with a reduction inorgan failure and postinjury complications. J Trauma. 2009;66(1):41–48;discussion 48–9.
15. O'Keeffe T, Refaai M, Tchorz K, Forestner JE, Sarode R. A massive transfu-sion protocol to decrease blood component use and costs. Arch Surg. 2008;143(7):686–690; discussion 690–1.
16. ACS TQIP Best Practice Guidelines. Accessed 08-20-2018. Available from:https://www.facs.org/quality-programs/trauma/tqip/best-practice.
17. Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C,Ioannidis JP, Straus S, Thorlund K, Jansen JP, et al. The PRISMA extensionstatement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann InternMed. 2015;162(11):777–784.
18. Preferred Reporting Items for Systematic Reviews and Meta-Analyses(PRISMA). Accessed 08-20-2018. Available from: http://prisma-statement.org/Default.aspx.
19. PubMed—US National Library of Medicine. Accessed 08-20-2018. Avail-able from: https://www.ncbi.nlm.nih.gov/mesh.
20. Cochrane Handbook for Systematic Reviews of Interventions. Accessed 08-20-2018. Available from: http://training.cochrane.org/handbook.
21. Methley AM, Campbell S, Chew-Graham C, McNally R, Cheraghi-Sohi S.PICO, PICOS and SPIDER: a comparison study of specificity and sensitivityin three search tools for qualitative systematic reviews. BMC Health ServRes. 2014;14:579.
22. Medical Subject Headings (MeSH). Accessed 08-20-2018. Available from:https://www.ncbi.nlm.nih.gov/mesh.
23. Newcastle-Ottawa Scale (NOS). Accessed 08-20-2018. Available from:http://www.ohri.ca/Programs/clinical_epidemiology/oxford.asp.
24. Sedgwick P. Meta-analyses: what is heterogeneity? BMJ. 2015;350:h1435.25. Hak T, Rhee HV, Suurmond R. How to interpret results of meta-analysis
(version 1.3). Accessed 08-20-2018. Available from: https://repub.eur.nl/pub/80102.
26. Goodnough LT, Daniels K, Wong AE, Viele M, Fontaine MF, Butwick AJ.Howwe treat: transfusion medicine support of obstetric services. Transfusion.2011;51(12):2540–2548.
27. Gutierrez MC, Goodnough LT, Druzin M, Butwick AJ. Postpartum hemor-rhage treatedwith a massive transfusion protocol at a tertiary obstetric center:a retrospective study. Int J Obstet Anesth. 2012;21(3):230–235.
28. Johansson PI, Stensballe J, Rosenberg I, Hilslov TL, Jorgensen L,Secher NH. Proactive administration of platelets and plasma for patients witha ruptured abdominal aortic aneurysm: evaluating a change in transfusionpractice. Transfusion. 2007;47(4):593–598.
29. Sinha R, Roxby D, Bersten A. Experience with a massive transfusion proto-col in the management of massive haemorrhage. Transfus Med. 2013;23(2):108–113.
30. Bown MJ, Sutton AJ, Bell PR, Sayers RD. A meta-analysis of 50 years ofruptured abdominal aortic aneurysm repair. Br J Surg. 2002;89(6):714–730.
503
ealth, Inc. All rights reserved.

Sommer et al.J Trauma Acute Care Surg
Volume 86, Number 3
31. Rayt HS, Sutton AJ, London NJ, Sayers RD, Bown MJ. A systematic reviewand meta-analysis of endovascular repair (EVAR) for ruptured abdominalaortic aneurysm. Eur J Vasc Endovasc Surg. 2008;36(5):536–544.
32. Holcomb JB, Tilley BC, Baraniuk S, Fox EE, Wade CE, Podbielski JM,del Junco DJ, Brasel KJ, Bulger EM, Callcut RA, et al. Transfusion ofplasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortalityin patients with severe trauma: the PROPPR randomized clinical trial. JAMA.2015;313(5):471–482.
33. Cotton BA, Gunter OL, Isbell J, Au BK, Robertson AM, Morris JA Jr.,St Jacques P, Young PP. Damage control hematology: the impact of a traumaexsanguination protocol on survival and blood product utilization. J Trauma.2008;64(5):1177–1182; discussion 1182–3.
34. Gonzalez EA, Moore FA, Holcomb JB, Miller CC, Kozar RA, Todd SR,Cocanour CS, Balldin BC, McKinley BA. Fresh frozen plasma should begiven earlier to patients requiring massive transfusion. J Trauma. 2007;62(1):112–119.
35. Repine TB, Perkins JG, Kauvar DS, Blackborne L. The use of fresh wholeblood in massive transfusion. J Trauma. 2006;60(Suppl 6):S59–S69.
36. Nunez TC, Voskresensky IV, Dossett LA, Shinall R, DuttonWD, Cotton BA.Early prediction of massive transfusion in trauma: simple as ABC (assess-ment of blood consumption)? J Trauma. 2009;66(2):346–352.
37. Cotton BA, Dossett LA, Haut ER, Shafi S, Nunez TC, Au BK, ZaydfudimV,Johnston M, Arbogast P, Young PP. Multicenter validation of a simplified
504
Copyright © 2019 Wolters Kluwer H
score to predict massive transfusion in trauma. J Trauma. 2010;69(Suppl 1):S33–S39.
38. Cantle PM, Cotton BA. Prediction of massive transfusion in trauma. CritCare Clin. 2017;33(1):71–84.
39. Yücel N, Lefering R, Maegele M, Vorweg M, Tjardes T, Ruchholtz S,Neugebauer EA,Wappler F, Bouillon B, Rixen D. TraumaAssociated SevereHemorrhage (TASH)-score: probability of mass transfusion as surrogate forlife threatening hemorrhage after multiple trauma. J Trauma. 2006;60(6):1228–1236; discussion 1236–7.
40. McLaughlin DF, Niles SE, Salinas J, Perkins JG, Cox ED, Wade CE,Holcomb JB. A predictive model for massive transfusion in combat casualtypatients. J Trauma. 2008;64(Suppl 2):S57–S63; discussion S63.
41. Joseph B, Khan M, Truitt M, Jehan F, Kulvatunyou N, Azim A, Jain A,Zeeshan M, Tang A, O'Keeffe T. Massive transfusion: the Revised Assess-ment of Bleeding and Transfusion (RABT) score. World J Surg. 2018;42:3560–3567.
42. Callcut RA, Cotton BA, Muskat P, Fox EE, Wade CE, Holcomb JB,Schreiber MA, Rahbar MH, Cohen MJ, Knudson MM, et al. Defining whento initiate massive transfusion: a validation study of individual massive trans-fusion triggers in PROMMTT patients. J Trauma Acute Care Surg. 2013;74(1):59–65, 7–8; discussion 66–7.
43. Kreuziger LMB, Salzman J, SubramanianAT,MortonCT, Dries DJ.Massivetransfusion in non-trauma patients. Blood. 2011;118(21):3376.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
SYSTEMATIC REVIEW
Management of penetrating intraperitoneal colon injuries:A meta-analysis and practice management guideline from
the Eastern Association for the Surgery of Trauma
Daniel C. Cullinane, MD, Randeep S. Jawa, MD, John J. Como, MD, MPH, Ashlee E. Moore, MD,David S. Morris, MD, Jerry Cheriyan, MD, Oscar D. Guillamondegui, MD, Stephanie R. Goldberg, MD,
Laura Petrey,MD,Gregory P. Schaefer, DO, Kosar A. Khwaja,MD, Susan E. Rowell, MD, Ronald R. Barbosa,MD,Gary A. Bass, MD, MSc, George Kasotakis, MD, MPH, and Bryce R.H. Robinson, MD, MS, Marshfield, Wisconsin
Sub
Fro
Ad
Thi
DO
J TrVol
BACKGROUND: T
mitted: June 20, 2018, RevisedPublished online: November 21m theDepartment of Surgery,Mavision of Trauma, Stony BrookYork (R.S.J.); Department of SOhio (J.J.C.); Department of Su(A.M.); Department of SurgeryM.); Department of Surgery, KDepartment of Surgery, VanTennessee (O.D.G.); DepartmenRichmond, Virginia (S.R.G.); DCenter, Dallas, Texas (L.P.); Depical Center, Morgantown, WestGeneral Hospital, Montreal, QOregon Health & Science Univegery, Legacy Emmanuel MedicaSurgery, St. Vincent's Hospital,Boston Medical Center, Boston,University of Washington, Seattdress for reprints: Daniel C. CAvenue, Marshfield, WI 54449s manuscript was not presented
I: 10.1097/TA.00000000000021
auma Acute Care Surgume 86, Number 3
he management of penetrating colon injuries in civilians has evolved over the last four decades. The objectives of thismeta-analysis are to evaluate the current treatment regimens available for penetrating colon injuries and assess the role ofanastomosis in damage control surgery to develop a practice management guideline for surgeons.
METHODS: U
sing the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) methodology, a subcommittee ofthe Practice Management Guidelines section of EAST conducted a systematic review using MEDLINE and EMBASE articlesfrom 1980 through 2017. We developed three relevant problem, intervention, comparison, and outcome (PICO) questionsregarding penetrating colon injuries. Outcomes of interest included mortality and infectious abdominal complications.RESULTS: T
hirty-seven studies were identified for analysis, of which 16 met criteria for quantitative meta-analysis and included 705 patientsconsidered low-risk in six prospective randomized studies. Seven hundred thirty-eight patients in 10 studies undergoing damagecontrol laparotomy and repair or resection and anastomosis (R&A) were included in a separate meta-analysis. Meta-analysis ofhigh-risk patients undergoing repair or R&Awas not feasible due to inadequate data.CONCLUSIONS: I
n adult civilian patients sustaining penetrating colon injury without signs of shock, significant hemorrhage, severe contamination,or delay to surgical intervention we recommend that colon repair or R&A be performed rather than routine colostomy. In adulthigh-risk civilian trauma patients sustaining penetrating colon injury, we conditionally recommend that colon repair or R&A beperformed rather than routine colostomy. In adult civilian trauma patients sustaining penetrating colon injury who had damagecontrol laparotomy, we conditionally recommend that routine colostomy not be performed; instead, definitive repair or delayedR&A or anastomosis at initial operation should be performed rather than routine colostomy. (J Trauma Acute Care Surg.2019;86: 505–515. Copyright © 2018 Wolters Kluwer Health, Inc. All rights reserved.)LEVEL OF EVIDENCE: S
ystematic review/meta-analysis, level III. KEYWORDS: C olon injury; colon trauma; colon repair; penetrating abdominal trauma; damage control surgery.M anagement of penetrating colon wounds has evolved overthe past four decades as primary repair has become
: July 11, 2018, Accepted: November 11, 2018,, 2018.rshfield Clinic,Marshfield,Wisconsin (D.C.C.); Di-University School of Medicine, Stony Brook, Newurgery, MetroHealth Medical Center, Cleveland,rgery, Holmes Medical Center, Melbourne, Florida, Intermountain Health Care, Murray, Utah (D.S.ern Medical Center, Bakersfield, California (J.C.);derbilt University Medical Center, Nashville,t of Surgery, Virginia Commonwealth University,epartment of Surgery, Baylor University Medicalartment of Surgery, West Virginia University Med-Virginia (G.S.); Department of Surgery, Montrealuebec, Canada (K.A.K.); Department of Surgery,rsity, Portland, Oregon (S.E.R.); Department of Sur-l Center, Portland, Oregon (R.R.B.); Department ofDublin, Ireland (G.A.B.); Department of Surgery,Massachusetts (G.K.); and Department of Surgery,le, Washington (B.R.H.R.).ullinane, MD, Marshfield Clinic, 1000 N Oak; email: [email protected] any meeting or conference.
46
Copyright © 2019 Wolters Kluwer H
commonplace. Traditionally, most colon injuries in the civilianpopulation were managed by colostomy.1,2 Since the publicationof several prospective randomized studies (PRS) on thesubject3–7 and Eastern Association for the Surgery of Trauma(EAST) 1998 Guidelines for the Management of PenetratingColon Injury,8 there has been increasing experience with coloninjury repair at time of intervention. Repair avoids colostomyand its associated psychosocial stigmata, reduces morbidityfrom the colostomy itself (25%),9 and obviates the costs10 andhigh complication rates associated with colostomy closure.11–15
In 1998, EAST published a practice management guide-line (PMG) for the management of penetrating colon injuries.8
At the time, most trauma surgeons were likely to perform repaireven with significant contamination.16,17 Since this publication,larger observational studies have been reported, more patients arehaving resection and anastomosis (R&A), and newer techniquesare being used including delayed anastomosis (DA) after damagecontrol laparotomy (DCL) and increased implementation ofresuscitation strategies limiting crystalloid use. Therefore, wehave performed a systematic review and meta-analysis to developupdated evidence-based recommendations for the managementof penetrating colon injuries in the adult civilian population.
505
ealth, Inc. All rights reserved.
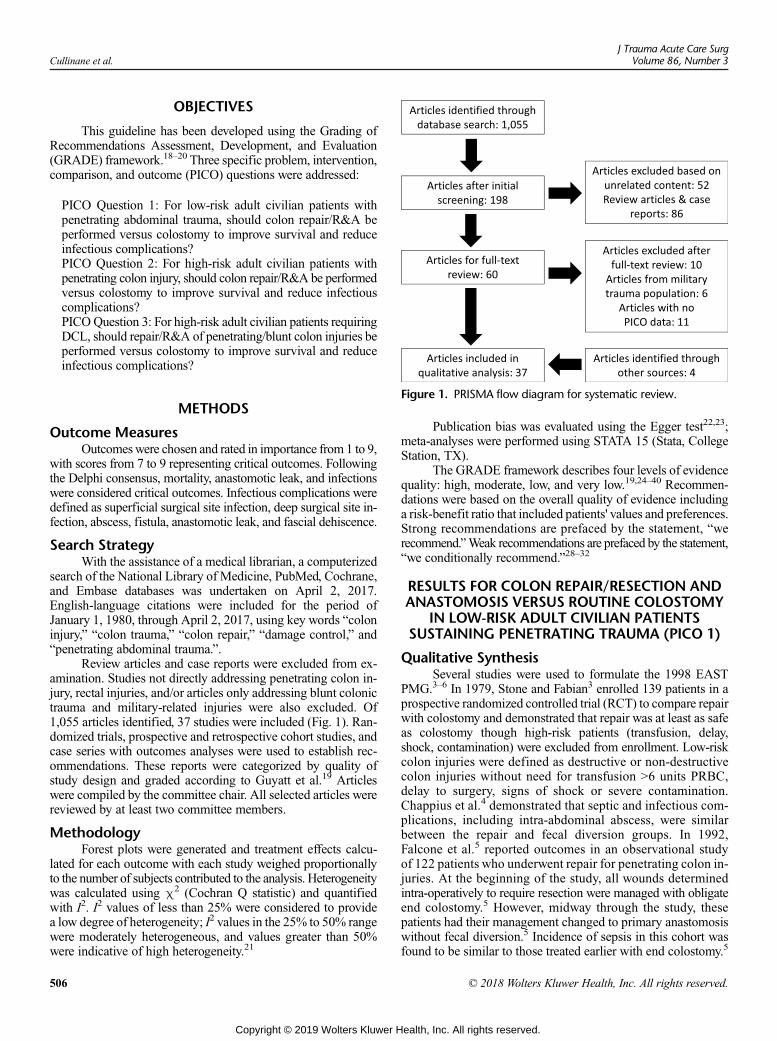
Cullinane et al.J Trauma Acute Care Surg
Volume 86, Number 3
OBJECTIVES
This guideline has been developed using the Grading ofRecommendations Assessment, Development, and Evaluation(GRADE) framework.18–20 Three specific problem, intervention,comparison, and outcome (PICO) questions were addressed:
PICO Question 1: For low-risk adult civilian patients withpenetrating abdominal trauma, should colon repair/R&A beperformed versus colostomy to improve survival and reduceinfectious complications?PICO Question 2: For high-risk adult civilian patients withpenetrating colon injury, should colon repair/R&A be performedversus colostomy to improve survival and reduce infectiouscomplications?PICOQuestion 3: For high-risk adult civilian patients requiringDCL, should repair/R&A of penetrating/blunt colon injuries beperformed versus colostomy to improve survival and reduceinfectious complications?
Figure 1. PRISMA flow diagram for systematic review.
METHODSOutcome MeasuresOutcomeswere chosen and rated in importance from 1 to 9,
with scores from 7 to 9 representing critical outcomes. Followingthe Delphi consensus, mortality, anastomotic leak, and infectionswere considered critical outcomes. Infectious complications weredefined as superficial surgical site infection, deep surgical site in-fection, abscess, fistula, anastomotic leak, and fascial dehiscence.
Search StrategyWith the assistance of a medical librarian, a computerized
search of the National Library of Medicine, PubMed, Cochrane,and Embase databases was undertaken on April 2, 2017.English-language citations were included for the period ofJanuary 1, 1980, through April 2, 2017, using key words “coloninjury,” “colon trauma,” “colon repair,” “damage control,” and“penetrating abdominal trauma.”.
Review articles and case reports were excluded from ex-amination. Studies not directly addressing penetrating colon in-jury, rectal injuries, and/or articles only addressing blunt colonictrauma and military-related injuries were also excluded. Of1,055 articles identified, 37 studies were included (Fig. 1). Ran-domized trials, prospective and retrospective cohort studies, andcase series with outcomes analyses were used to establish rec-ommendations. These reports were categorized by quality ofstudy design and graded according to Guyatt et al.19 Articleswere compiled by the committee chair. All selected articles werereviewed by at least two committee members.
MethodologyForest plots were generated and treatment effects calcu-
lated for each outcome with each study weighed proportionallyto the number of subjects contributed to the analysis. Heterogeneitywas calculated using χ2 (Cochran Q statistic) and quantifiedwith I2. I2 values of less than 25% were considered to providea low degree of heterogeneity; I2 values in the 25% to 50% rangewere moderately heterogeneous, and values greater than 50%were indicative of high heterogeneity.21
506
Copyright © 2019 Wolters Kluwer H
Publication bias was evaluated using the Egger test22,23;meta-analyses were performed using STATA 15 (Stata, CollegeStation, TX).
The GRADE framework describes four levels of evidencequality: high, moderate, low, and very low.19,24–40 Recommen-dations were based on the overall quality of evidence includinga risk-benefit ratio that included patients' values and preferences.Strong recommendations are prefaced by the statement, “werecommend.”Weak recommendations are prefaced by the statement,“we conditionally recommend.”28–32
RESULTS FOR COLON REPAIR/RESECTION ANDANASTOMOSIS VERSUS ROUTINE COLOSTOMY
IN LOW-RISK ADULT CIVILIAN PATIENTSSUSTAINING PENETRATING TRAUMA (PICO 1)
Qualitative SynthesisSeveral studies were used to formulate the 1998 EAST
PMG.3–6 In 1979, Stone and Fabian3 enrolled 139 patients in aprospective randomized controlled trial (RCT) to compare repairwith colostomy and demonstrated that repair was at least as safeas colostomy though high-risk patients (transfusion, delay,shock, contamination) were excluded from enrollment. Low-riskcolon injuries were defined as destructive or non-destructivecolon injuries without need for transfusion >6 units PRBC,delay to surgery, signs of shock or severe contamination.Chappius et al.4 demonstrated that septic and infectious com-plications, including intra-abdominal abscess, were similarbetween the repair and fecal diversion groups. In 1992,Falcone et al.5 reported outcomes in an observational studyof 122 patients who underwent repair for penetrating colon in-juries. At the beginning of the study, all wounds determinedintra-operatively to require resection were managed with obligateend colostomy.5 However, midway through the study, thesepatients had their management changed to primary anastomosiswithout fecal diversion.5 Incidence of sepsis in this cohort wasfound to be similar to those treated earlier with end colostomy.5
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Cullinane et al.
In contrast, Sasaki et al.6 noted a higher rate of infectious com-plications in the colostomy group versus primary repair/R&A ina prospective RCT of 71 patients though the authors noted thatsome complications were attributable to colostomy reversal.
Since the 1998 EAST PMG, two additional RCTs havebeen published. In a follow-up study, Gonzalez et al.7,41 reportedthat patients treated with colostomy had higher rates of compli-cations (abdominal abscess, wound dehiscence, enterocutaneousfistula, gangrenous stoma, peristomal abscess, or parastomalsmall bowel volvulus) than patients treated with primary repair.41
Kamwendo et al.42 published a trial with 238 patients randomizedto repair or diversion and analyzed the effect of a delay of surgery(<12 and >12 hours) on outcomes. Patients managed with colos-tomy had higher rates of complications (sepsis, pulmonary com-plications, wound dehiscence, enterocutaneous fistula, and woundcomplications) regardless of surgical delay.42 The consensus fromthese trials was that primary repair of penetrating colon injuriesseemed to be at least as safe as fecal diversion,3 if not safer.4–7
A 2003 Cochrane meta-analysis43 comparing primary re-pair with colostomy, in low-risk patients, demonstrated no differ-ence in mortality between patients undergoing primary repairversus those receiving colostomy (odds ratio (OR) for mortality,1.22; 95% confidence interval (CI), 0.4–3.74) and demonstrateda lower rate of complications in the groupmanaged with primaryrepair (OR, 0.54; 95% CI, 0.39–0.76). Specifically, the primaryrepair group had a lower OR of infectious complications (OR,0.44; 95% CI, 0.17–1.1), abdominal infection (OR, 0.67; 95%CI, 0.35–1.3), and wound complications (OR, 0.73; 95% CI,0.38–1.39) although wide confidence intervals precluded statis-tical significance.43 The authors concluded that all penetratingcolon injuries could be safelymanaged by primary repair, includingR&A, and rated the evidence at Level 1B (from randomizedtrials).43 Observations from retrospective studies support theconclusion that nearly all colon injuries in low-risk patientscan be successfully repaired.44–48
Colon Resection/Anastomosis for Destructive InjuriesIn 1998, available data regarding patients with destructive
colon injuries (>50% of the circumference of the colon) werescarce, and the PRS available included only a small number ofpatients managed with R&A.3–7 Around the time of the 1998EAST PMG, two additional studies demonstrated concerningcomplication rates in patients with destructive colon injuries.48,49
As a result, the 1998 Guideline recommended R&A for man-agement of destructive injuries only if the patient did not haveconcurrent shock (systolic blood pressure (SBP) <90 mm Hg),underlying comorbid disease, significant associated injuries,penetrating abdominal trauma injury (PATI) score > 25, injuryseverity score (ISS) > 25, Flint grade > 11,50 or peritonitis.8
Destructive colon injuries alone do not necessarily qualifyas high-risk colonic injuries.
In an effort to address the conflicting evidence, anAmericanAssociation for the Surgery of Trauma (AAST) prospective multi-center trial was performed in 2001.51 This study included297 patientswhowere treatedwith colon resection; 66% of patientsunderwent R&A and 34% were managed with colostomy.51 De-spite including high-risk patients as defined by the 1998 Guideline,a lower mortality rate was discovered for primary anastomosis (0%
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
versus 4%, p = 0.012), and no significant difference in complica-tion rates (intra-abdominal abscess, colon leak, fascial dehiscence)were noted.51 Although the groups were well-matched, there werehigher rates of shock, colon injury severity, and PATI scores inthe colostomy group.51 The authors concluded that the surgicalprocedure for colon injuries did not affect mortality regardless ofassociated risk factors, despite some differences in the populationsexamined.51
Quantitative Synthesis (Meta-Analysis)A total of 705 subjects with colon injury from six PRS
were included in our analysis for PICO 1. Separating recommen-dations for repair versus R&Awere not possible given limitationsand variability of the current prospective studies. Analysis ofpooled data demonstrated similar mortality between patientshaving repair/R&A versus colostomy (OR, 1.218; 95% CI,0.40–3.74; p = 0.73). Regarding infections, patients havingrepair/R&A tended to have improved outcomes versus thosewho had colostomy (OR, 0.42; 95% CI, 0.17–1.03; p = 0.059).Heterogeneity was low for analysis of mortality (I2 = 0.0%,p = 0.61), and high with regard to surgical infections (I2 = 80.8%,p < 0.001). The data regarding mortality and infectious compli-cations are summarized in Figure 2.
Grading the EvidenceNo serious publication bias was detected for either analyzed
outcome although some inconsistency was found in smaller stud-ies. There are several prospective randomized trials that addressedthis question. The overall quality of evidence is high (Table 1).
RECOMMENDATION
Based on the evidence, 15 of 16 authors voted in favor of astrong recommendation for colon repair or R&A in low-riskpatients. Therefore, in adult civilian patients with penetratingcolon injury without signs of shock, significant hemorrhage,severe contamination, or delay to surgical intervention, we recom-mend that colon repair or R&Abe performed rather than colostomy.
RESULTS FOR COLON REPAIR/RESECTION ANDANASTOMOSIS VERSUS ROUTINE COLOSTOMY
IN HIGH-RISK ADULT CIVILIAN PATIENTSSUSTAINING PENETRATING TRAUMA (PICO 2)
Qualitative SynthesisHigh-level recommendations cannot be provided for high-
risk civilian penetrating colon injuries due to confounding vari-ables, limited population, and few prospectively designed trials.Many studies had variable inclusion of different penetratingmechanisms, namely stab wounds, gunshot wounds, and blunttraumatic injuries, that may influence risk for infectious com-plications.52–55 Furthermore, differences in intra- and post-operative management of colonic injuries can alter patientrisk for complications.6,15,54,56–58 However, even with theseinconsistencies, some general conclusions can be made specif-ically that R&A has similar complication rates to colostomyin high-risk patients, and certain patient-specific factors can
507
ealth, Inc. All rights reserved.
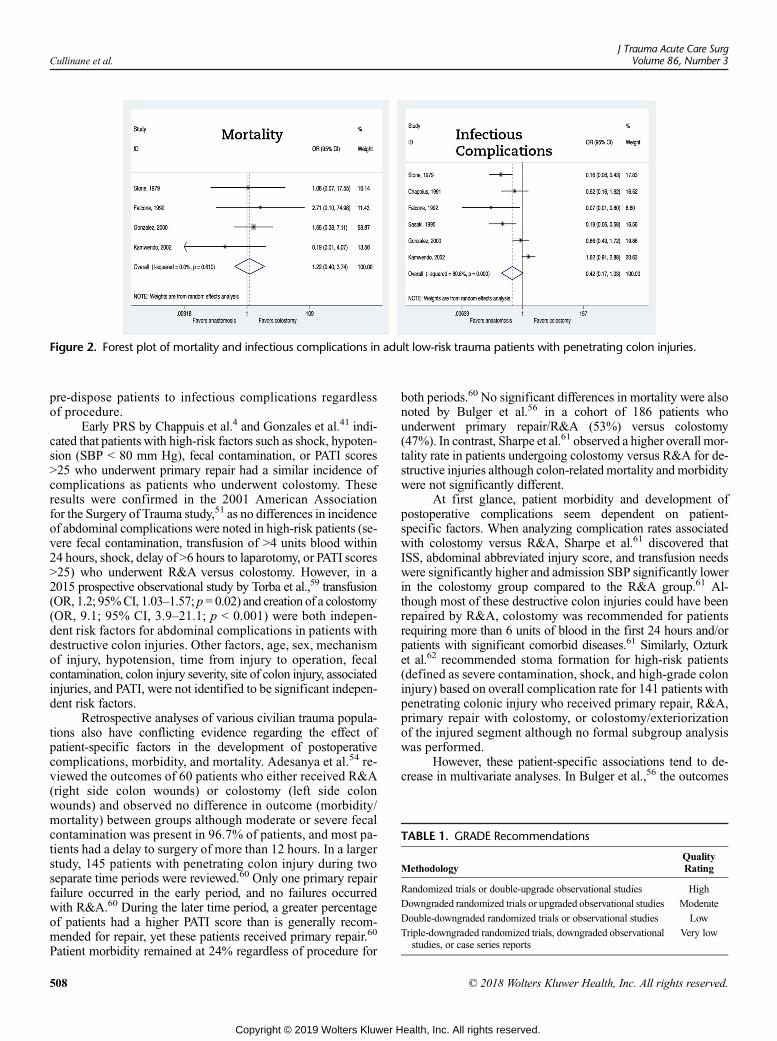
Figure 2. Forest plot of mortality and infectious complications in adult low-risk trauma patients with penetrating colon injuries.
TABLE 1. GRADE Recommendations
MethodologyQualityRating
Randomized trials or double-upgrade observational studies High
Downgraded randomized trials or upgraded observational studies Moderate
Double-downgraded randomized trials or observational studies Low
Triple-downgraded randomized trials, downgraded observationalstudies, or case series reports
Very low
Cullinane et al.J Trauma Acute Care Surg
Volume 86, Number 3
pre-dispose patients to infectious complications regardlessof procedure.
Early PRS by Chappuis et al.4 and Gonzales et al.41 indi-cated that patients with high-risk factors such as shock, hypoten-sion (SBP < 80 mm Hg), fecal contamination, or PATI scores>25 who underwent primary repair had a similar incidence ofcomplications as patients who underwent colostomy. Theseresults were confirmed in the 2001 American Associationfor the Surgery of Trauma study,51 as no differences in incidenceof abdominal complications were noted in high-risk patients (se-vere fecal contamination, transfusion of >4 units blood within24 hours, shock, delay of >6 hours to laparotomy, or PATI scores>25) who underwent R&A versus colostomy. However, in a2015 prospective observational study by Torba et al.,59 transfusion(OR, 1.2; 95%CI, 1.03–1.57; p= 0.02) and creation of a colostomy(OR, 9.1; 95% CI, 3.9–21.1; p < 0.001) were both indepen-dent risk factors for abdominal complications in patients withdestructive colon injuries. Other factors, age, sex, mechanismof injury, hypotension, time from injury to operation, fecalcontamination, colon injury severity, site of colon injury, associatedinjuries, and PATI, were not identified to be significant indepen-dent risk factors.
Retrospective analyses of various civilian trauma popula-tions also have conflicting evidence regarding the effect ofpatient-specific factors in the development of postoperativecomplications, morbidity, and mortality. Adesanya et al.54 re-viewed the outcomes of 60 patients who either received R&A(right side colon wounds) or colostomy (left side colonwounds) and observed no difference in outcome (morbidity/mortality) between groups although moderate or severe fecalcontamination was present in 96.7% of patients, and most pa-tients had a delay to surgery of more than 12 hours. In a largerstudy, 145 patients with penetrating colon injury during twoseparate time periods were reviewed.60 Only one primary repairfailure occurred in the early period, and no failures occurredwith R&A.60 During the later time period, a greater percentageof patients had a higher PATI score than is generally recom-mended for repair, yet these patients received primary repair.60
Patient morbidity remained at 24% regardless of procedure for
508
Copyright © 2019 Wolters Kluwer H
both periods.60 No significant differences in mortality were alsonoted by Bulger et al.56 in a cohort of 186 patients whounderwent primary repair/R&A (53%) versus colostomy(47%). In contrast, Sharpe et al.61 observed a higher overall mor-tality rate in patients undergoing colostomy versus R&A for de-structive injuries although colon-related mortality and morbiditywere not significantly different.
At first glance, patient morbidity and development ofpostoperative complications seem dependent on patient-specific factors. When analyzing complication rates associatedwith colostomy versus R&A, Sharpe et al.61 discovered thatISS, abdominal abbreviated injury score, and transfusion needswere significantly higher and admission SBP significantly lowerin the colostomy group compared to the R&A group.61 Al-though most of these destructive colon injuries could have beenrepaired by R&A, colostomy was recommended for patientsrequiring more than 6 units of blood in the first 24 hours and/orpatients with significant comorbid diseases.61 Similarly, Ozturket al.62 recommended stoma formation for high-risk patients(defined as severe contamination, shock, and high-grade coloninjury) based on overall complication rate for 141 patients withpenetrating colonic injury who received primary repair, R&A,primary repair with colostomy, or colostomy/exteriorizationof the injured segment although no formal subgroup analysiswas performed.
However, these patient-specific associations tend to de-crease in multivariate analyses. In Bulger et al.,56 the outcomes
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Cullinane et al.
of 186 patients with penetrating colon injuries were comparedbetween two groups: 53% received primary repair/R&A and47% received colostomy.While the total complication rate of pa-tients requiring colostomy was significantly higher (57% vs42%), when adjusting for ISS and hypotension, colostomy wasnot associated with a significant increase in total complicationrate.56 Furthermore, the incidence of abdominal abscess, woundinfection, wound dehiscence, and anastomotic leak were not sig-nificantly different. Subgroup analysis indicated that develop-ment of infectious complications was related to ISS and shock,not the operation performed. Dente et al.63 reported that PATIscores greater than 30, ISS greater than 16, transfusion of morethan 2 units of blood, and a revised trauma score greater than 7.8were all significantly associated with infections based on univar-iate analysis of outcomes for 311 patients with penetrating coloninjuries. With multivariate logistic regression, all factors with theexception of revised trauma score had a significant associationwith infectious complications, and no high-risk groups wereidentified for whom a colostomy had fewer septic complica-tions.63 The authors concluded that the presence of a colostomywas associated with a greater burden of septic abdominal com-plications than primary repair.63 Similarly, Girgin et al.55 wereunable to identify a high-risk group where colostomy preventedseptic complications. Univariate analysis indicated that gunshotwounds, delay to operation of more than 6 hours, shock, opera-tion duration of more than 6 hours, PATI score greater than 25,ISS greater than 20, colonic ISS greater than 3, major fecal con-tamination, more than two extra-abdominal injuries, transfusiongreater than 4 units of blood, and colostomy were significantlyassociated with increased morbidity.55 Only colostomy andtransfusion remained independent factors for colon-related mor-bidity in subsequent multivariate regression.55
Contrary to Dente et al. and Girgin et al., Durham et al.64
noted that presence of a colostomy was not associated with infec-tion. No significant differences in wound or intra-abdominal com-plication rates were found among high-risk patients (PATI score>30 or colonic injury score (CIS) >4) undergoing primary repairversus colostomy although the abdominal trauma index and CISwere significantly higher in the colostomy group.64 Furtherevaluation of risk factors for intra-abdominal and woundcomplications using stepwise regression revealed that onlyabdominal trauma index, CIS, and gross contamination wereindependent predictors of complications.64 Therefore, repairor R&A of penetrating colon injuries should be consideredin the context of patient-specific factors and colostomy maybe warranted in some patients.
Quantitative Synthesis (Meta-Analysis)Meta-analysis was not appropriate owing to heterogeneity
and variability in data reporting. A summary table of availableevidence for PICO 2 was created (Table 2).
Grading the EvidenceNo serious publication bias was detected although some
inconsistency was found in smaller studies.58,65 Although thereare prospective trials (high quality) addressing this question,most of the data are retrospective (low quality). The overall qual-ity of evidence is low (Table 1).
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
RECOMMENDATION
Based on the evidence, 15 of 16 authors voted in favor ofthe following recommendation: In adult, high-risk (delay>12 hours, shock, associated injury, transfusion >6 units ofblood, contamination, or left side colon injuries) trauma patientswith penetrating colon injury, we conditionally recommend thatcolon repair or R&A be performed rather than mandatory colos-tomy. Colostomy may have a limited role in select patients.
RESULTS FOR COLON REPAIR/RESECTION ANDANASTOMOSIS VERSUS ROUTINE COLOSTOMY
IN THOSE REQUIRING DCL (PICO 3)
Qualitative SynthesisA question not addressed by the 1998 Guideline was the
management of colon injuries in the setting of DCL. There areno prospective trials that specifically address this question, andavailable studies have conflicting recommendations. By defini-tion, patients requiring DCL have high-risk physiology with ex-pected higher rates of sepsis and anastomotic leak, which skewthe data. Furthermore, surgeons are concerned about performingan anastomosis in DCL due to bowel edema and the negativepressure produced from temporary abdominal closure.
Initial studies suggested that R&A is safe to perform in thecontext of a DCL. Johnson et al.66 reported the earliest colonR&A in the setting of DCL in 2001. Since then, managementof colon injuries shifted from colostomy in all surviving DCLpatients to primary repair or R&A at their institution.66 Compar-ing results from the two studies, there was no statistically signif-icant difference in abdominal septic complications. Milleret al.67 compared DA in DCL to R&A at initial operation. De-spite more severe initial shock in the DCL group, there wereno anastomotic leaks in the DA group, and abscess rate andcolon-related mortality were similar in both groups.67
Chavarria-Aguilar et al.65 reviewed destructive colon injuriesin DCL over an 11-year period. The incidence of intra-abdominal abscesses were not significantly different betweenprimary colonic repairs and diverting stomas in 104 patients re-quiring resection (29 requiring DCL).65 Similarly, Ordoñezet al.68 reported that R&A can be safely performed with DCLin patients with colon injury. Two patients in the DA groupleaked versus one in the single laparotomy (SL) group(p = 0.6), and there was one colon-related death (DCL) in thisstudy.68 Combined, these studies suggest that DA during DCLis safe.
However, other studies indicate that DAwith DCL is notthe safest option for patients with colon trauma. Ott et al.69 pub-lished a cohort study of 174 trauma colon resections using bothdamage control and immediate abdominal closure. The authorsreported an “unacceptable” leak rate with DA after DCL(27%) compared to SL (6%; p < 0.01).69 Unsurprisingly, theDCL group had a significantly greater length of stay (LOS),mortality, intensive care unit days, transfusion requirements,and physiologic derangement compared to the immediate repairgroup, as these patients were intrinsically sicker than patients re-ceiving immediate abdominal closure.69 Although the conse-quences of leak led to more complications and longer LOS,the mortality rates were not statistically different between
509
ealth, Inc. All rights reserved.
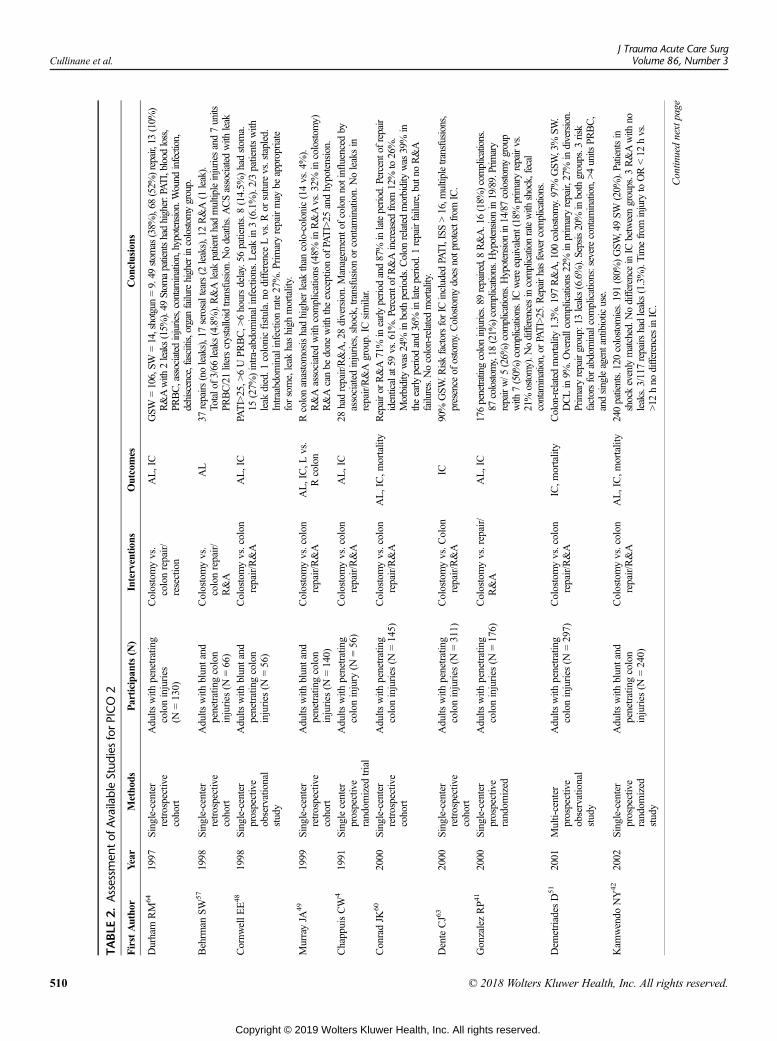
TABLE
2.Assessmen
tof
AvailableStud
iesforPICO
2
FirstAutho
rYear
Metho
dsParticipa
nts(N
)Intervention
sOutcomes
Con
clusions
Durham
RM
641997
Single-center
retrospective
cohort
Adults
with
penetrating
coloninjuries
(N=130)
Colostomyvs.
colonrepair/
resection
AL,IC
GSW
=106,SW
=14,shotgun
=9.49
stom
as(38%
),68
(52%
)repair,13
(10%
)R&Awith
2leaks(15%
).49
Stom
apatientshadhigher:PATI,bloodloss,
PRBC,associatedinjuries,contam
ination,hypotension.Wound
infection,
dehiscence,fasciitis,organfailurehigherincolostom
ygroup.
Behrm
anSW
571998
Single-center
retrospective
cohort
Adults
with
bluntand
penetratingcolon
injuries
(N=66)
Colostomyvs.
colonrepair/
R&A
AL
37repairs
(noleaks),17serosaltears(2
leaks),12R&A(1
leak).
Totalof3/66
leaks(4.8%).R&Aleak
patienthadmultipleinjuriesand7units
PRBC/21literscrystalloidtransfusion.N
odeaths.A
CSassociated
with
leak
Cornw
ellE
E48
1998
Single-center
prospective
observational
study
Adults
with
bluntand
penetratingcolon
injuries
(N=56)
Colostomyvs.colon
repair/R&A
AL,IC
PATI>25,>
6UPR
BC,>
6hoursdelay.56
patients.8(14.5%
)hadstom
a.15
(27%
)intra-abdom
inalinfections.L
eakin3(6.1%).2/3patientswith
leak
died.1
colonicfistula.no
difference
Lvs.R
orsuturevs.stapled.
Intraabdominalinfectionrate27%.P
rimaryrepairmay
beappropriate
forsome,leak
hashigh
mortality.
MurrayJA
491999
Single-center
retrospective
cohort
Adults
with
bluntand
penetratingcolon
injuries
(N=140)
Colostomyvs.colon
repair/R&A
AL,IC,L
vs.
Rcolon
Rcolonanastomosishadhigherleak
than
colo-colonic(14vs.4%).
R&Aassociated
with
complications
(48%
inR&Avs.32%
incolostom
y)R&Acanbe
done
with
theexceptionof
PATI>25
andhypotension.
ChappuisCW
41991
Singlecenter
prospective
random
ized
trial
Adults
with
penetrating
coloninjury
(N=56)
Colostomyvs.colon
repair/R&A
AL,IC
28hadrepair/R&A,28diversion.Managem
entofcolonnotinfluencedby
associated
injuries,shock,transfusion
orcontam
ination.Noleaksin
repair/R&Agroup.IC
similar.
ConradJK
602000
Single-center
retrospective
cohort
Adults
with
penetrating
coloninjuries
(N=145)
Colostomyvs.colon
repair/R&A
AL,IC,m
ortality
Repairor
R&A71%
inearly
periodand87%
inlateperiod.Percentofrepair
identicalat59
vs.61%
.Percentof
R&Aincreasedfrom
12%
to26%.
Morbiditywas
24%
inbothperiods.C
olon
relatedmorbiditywas
39%
intheearly
periodand36%
inlateperiod.1repairfailure,butno
R&A
failures.Nocolon-relatedmortality.
DenteCJ63
2000
Single-center
retrospective
cohort
Adults
with
penetrating
coloninjuries
(N=311)
Colostomyvs.C
olon
repair/R&A
IC90%
GSW
.RiskfactorsforIC
included
PATI,ISS>16,m
ultipletransfusions,
presence
ofostomy.Colostomydoes
notprotectfrom
IC.
GonzalezRP4
12000
Single-center
prospective
random
ized
Adults
with
penetrating
coloninjuries
(N=176)
Colostomyvs.repair/
R&A
AL,IC
176penetratingcoloninjuries.89
repaired,8R&A.16(18%
)com
plications.
87colostom
y,18
(21%
)com
plications.H
ypotension
in19/89.Primary
repairw/5
(26%
)complications.H
ypotension
in14/87colostom
ygroup
with
7(50%
)complications.ICwereequivalent(18%
primaryrepairvs.
21%
ostomy).N
odifferencesincomplicationratewith
shock,fecal
contam
ination,orPATI>25.R
epairhasfewercomplications.
Dem
etriades
D51
2001
Multi-center
prospective
observational
study
Adults
with
penetrating
coloninjuries
(N=297)
Colostomyvs.colon
repair/R&A
IC,m
ortality
Colon-related
mortality1.3%
.197
R&A,100
colostom
y.97%
GSW
,3%
SW.
DCLin9%
.Overallcomplications
22%
inprimaryrepair,27%
indiversion.
Primaryrepairgroup:13
leaks(6.6%).Sepsis20%
inbothgroups.3
risk
factorsforabdominalcomplications:severecontam
ination,>4
units
PRBC,
andsingleagentantibiotic
use.
Kam
wendo
NY42
2002
Single-center
prospective
random
ized
study
Adults
with
bluntand
penetratingcolon
injuries
(N=240)
Colostomyvs.colon
repair/R&A
AL,IC,m
ortality
240patients.120colostom
ies.191(80%
)GSW
,49SW
(20%
).Patientsin
shockevenlymatched.N
odifference
inIC
betweengroups.3
R&Awith
noleaks.3/117repairs
hadleaks(1.3%).Timefrom
injury
toOR<12
hvs.
>12hno
differencesinIC.
Contin
uednextpage
Cullinane et al.J Trauma Acute Care Surg
Volume 86, Number 3
510 © 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
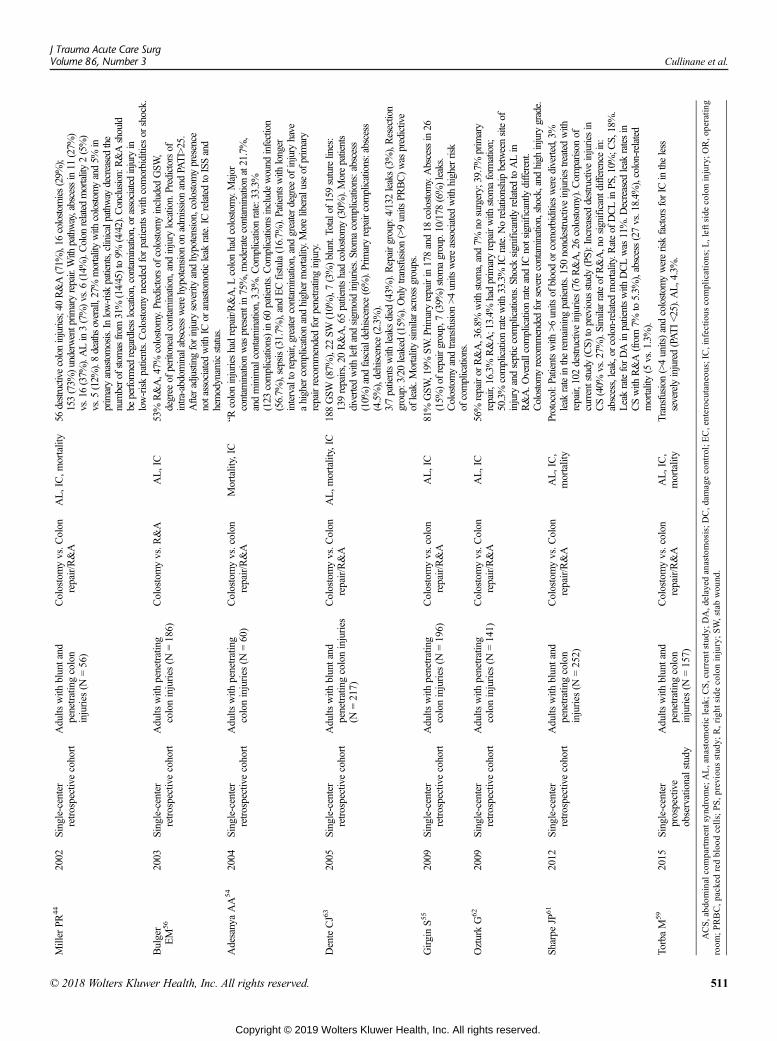
Miller
PR44
2002
Single-center
retrospectivecohort
Adults
with
bluntand
penetratingcolon
injuries
(N=56)
Colostomyvs.C
olon
repair/R&A
AL,IC,m
ortality
56destructivecoloninjuries;40
R&A(71%
),16
colostom
ies(29%
);153(73%
)underwentprim
aryrepair.With
pathway,abscessin11
(27%
)vs.16(37%
).ALin3(7%)vs.6
(14%
).Colon
relatedmortality2(5%)
vs.5
(12%
).8deaths
overall,27%
mortalitywith
colostom
yand5%
inprimaryanastomosis.Inlow-risk
patients,clinicalpathway
decreasedthe
numberofstom
asfrom
31%
(14/45)to9%
(4/42).C
onclusion:R&Ashould
beperform
edregardlesslocation,contam
ination,orassociated
injury
inlow-riskpatients.Colostomyneeded
forpatientswith
comorbiditiesor
shock.
Bulger
EM
562003
Single-center
retrospectivecohort
Adults
with
penetrating
coloninjuries
(N=186)
Colostomyvs.R
&A
AL,IC
53%
R&A,47%
colostom
y.Predictorsof
colostom
yincluded
GSW
,degree
ofperitonealcontamination,andinjury
location.Predictorsof
intra-abdom
inalabscesswerehypotensionon
admission
andPATI>25.
Afteradjustingforinjury
severityandhypotension,colostom
ypresence
notassociatedwith
ICor
anastomoticleak
rate.ICrelatedtoISSand
hemodynam
icstatus.
AdesanyaAA54
2004
Single-center
retrospectivecohort
Adults
with
penetrating
coloninjuries
(N=60)
Colostomyvs.colon
repair/R&A
Mortality,IC
“Rcoloninjurieshadrepair/R&A,L
colonhadcolostom
y.Major
contam
inationwas
presentin75%,m
oderatecontam
inationat21.7%,
andminimalcontam
ination,3.3%
.Com
plicationrate:33.3%
(123
complications)in60
patients.Com
plications
includewound
infection
(56.7%
),sepsis(31.7%
),andECfistula(16.7%
).Patientswith
longer
intervaltorepair,greatercontam
ination,andgreaterdegree
ofinjury
have
ahighercomplicationandhighermortality.Moreliberaluseof
primary
repairrecommendedforpenetratinginjury.
DenteCJ63
2005
Single-center
retrospectivecohort
Adults
with
bluntand
penetratingcoloninjuries
(N=217)
Colostomyvs.C
olon
repair/R&A
AL,m
ortality,IC
188GSW
(87%
),22
SW(10%
),7(3%)blunt.Totalof159suturelines:
139repairs,20R&A,65patientshadcolostom
y(30%
).Morepatients
divertedwith
leftandsigm
oidinjuries.Stom
acomplications:abscess
(10%
)andfascialdehiscence(6%).Primaryrepaircomplications:abscess
(4.5%),dehiscence
(2.3%).
3/7patientswith
leaksdied
(43%
).Repairgroup:4/132leaks(3%),Resection
group:3/20
leaked
(15%
).Onlytransfusion
(>9units
PRBC)was
predictive
ofleak.M
ortalitysimilaracrossgroups.
GirginS5
52009
Single-center
retrospectivecohort
Adults
with
penetrating
coloninjuries
(N=196)
Colostomyvs.colon
repair/R&A
AL,IC
81%
GSW
,19%
SW.Prim
aryrepairin178and18
colostom
y.Abscessin26
(15%
)of
repairgroup,7(39%
)stom
agroup.10/178
(6%)leaks.
Colostomyandtransfusion
>4units
wereassociated
with
higherrisk
ofcomplications.
OzturkG62
2009
Single-center
retrospectivecohort
Adults
with
penetrating
coloninjuries
(N=141)
Colostomyvs.C
olon
repair/R&A
AL,IC
56%
repairor
R&A,36.8%
with
stom
a,and7%
nosurgery;39.7%
primary
repair,16.3%
R&A;13.4%
hadprimaryrepairwith
stom
aform
ation;
50.3%
complicationratewith
33.3%
ICrate.N
orelationshipbetweensiteof
injury
andsepticcomplications.Shock
significantly
relatedtoALin
R&A.O
verallcomplicationrateandIC
notsignificantlydifferent.
Colostomyrecommendedforseverecontam
ination,shock,andhigh
injury
grade.
Sharpe
JP61
2012
Single-center
retrospectivecohort
Adults
with
bluntand
penetratingcolon
injuries
(N=252)
Colostomyvs.C
olon
repair/R&A
AL,IC,
mortality
Protocol:P
atientswith
>6units
ofbloodor
comorbiditieswerediverted,3%
leak
rateintheremaining
patients.150nondestructiveinjuriestreated
with
repair,102destructiveinjuries(76R&A,26colostom
y).C
omparison
ofcurrentstudy
(CS)
toprevious
study(PS):Increased
destructiveinjuriesin
CS(40%
vs.27%
).Similarrateof
R&A,nosignificantdifference
in:
abscess,leak,orcolon-relatedmortality.Rateof
DCLinPS
,10%
;CS,18%.
LeakrateforDAinpatientswith
DCLwas
11%.D
ecreased
leak
ratesin
CSwith
R&A(from7%
to5.3%
),abscess(27vs.18.4%
),colon-related
mortality(5
vs.1.3%).
TorbaM
592015
Single-center
prospective
observationalstudy
Adults
with
bluntand
penetratingcolon
injuries
(N=157)
Colostomyvs.colon
repair/R&A
AL,IC,
mortality
Transfusion(>4units)andcolostom
ywereriskfactorsforIC
intheless
severelyinjured(PATI<25).A
L,4.3%.
ACS,abd
ominalcompartmentsyn
drom
e;AL,anastom
oticleak;C
S,current
stud
y;DA,d
elayed
anastomosis;D
C,d
amagecontrol;EC,enterocutaneous;IC,infectiou
scomplications;L
,leftsidecoloninjury;O
R,o
perating
room
;PRBC,packed
redbloo
dcells;PS,p
reviou
sstud
y;R,righ
tside
coloninjury;SW,stabwou
nd.
J Trauma Acute Care SurgVolume 86, Number 3 Cullinane et al.
© 2018 Wolters Kluwer Health, Inc. All rights reserved. 511
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
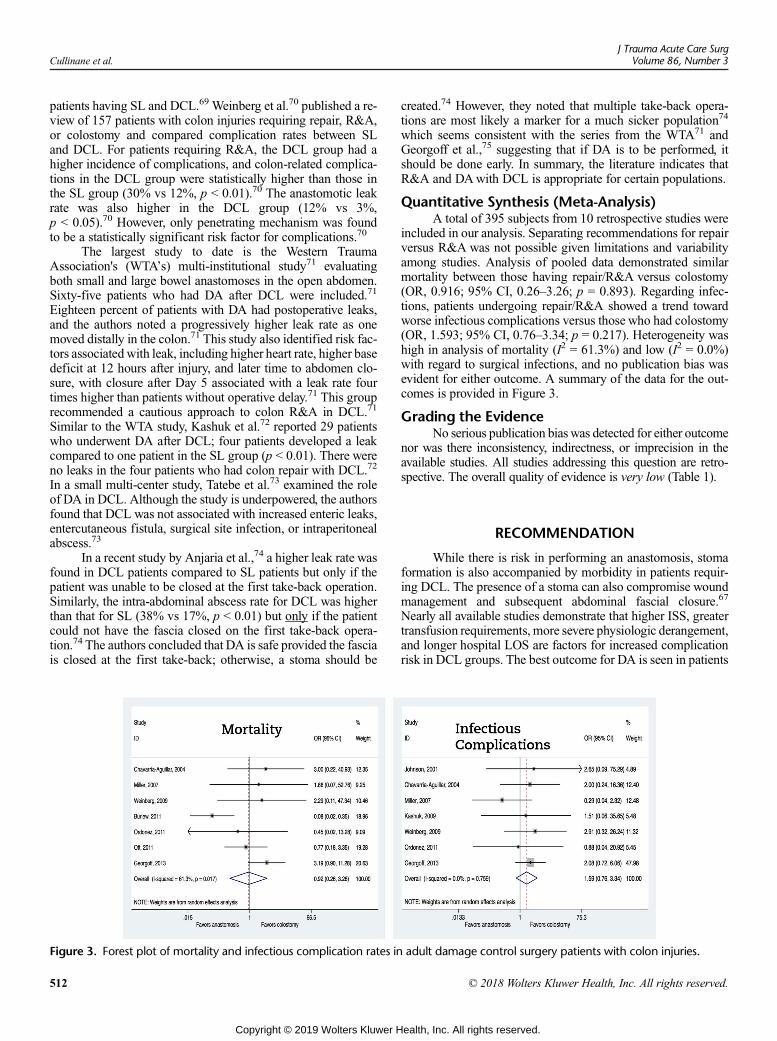
Cullinane et al.J Trauma Acute Care Surg
Volume 86, Number 3
patients having SL and DCL.69 Weinberg et al.70 published a re-view of 157 patients with colon injuries requiring repair, R&A,or colostomy and compared complication rates between SLand DCL. For patients requiring R&A, the DCL group had ahigher incidence of complications, and colon-related complica-tions in the DCL group were statistically higher than those inthe SL group (30% vs 12%, p < 0.01).70 The anastomotic leakrate was also higher in the DCL group (12% vs 3%,p < 0.05).70 However, only penetrating mechanism was foundto be a statistically significant risk factor for complications.70
The largest study to date is the Western TraumaAssociation's (WTA’s) multi-institutional study71 evaluatingboth small and large bowel anastomoses in the open abdomen.Sixty-five patients who had DA after DCL were included.71
Eighteen percent of patients with DA had postoperative leaks,and the authors noted a progressively higher leak rate as onemoved distally in the colon.71 This study also identified risk fac-tors associated with leak, including higher heart rate, higher basedeficit at 12 hours after injury, and later time to abdomen clo-sure, with closure after Day 5 associated with a leak rate fourtimes higher than patients without operative delay.71 This grouprecommended a cautious approach to colon R&A in DCL.71
Similar to the WTA study, Kashuk et al.72 reported 29 patientswho underwent DA after DCL; four patients developed a leakcompared to one patient in the SL group (p < 0.01). There wereno leaks in the four patients who had colon repair with DCL.72
In a small multi-center study, Tatebe et al.73 examined the roleof DA in DCL. Although the study is underpowered, the authorsfound that DCL was not associated with increased enteric leaks,entercutaneous fistula, surgical site infection, or intraperitonealabscess.73
In a recent study by Anjaria et al.,74 a higher leak rate wasfound in DCL patients compared to SL patients but only if thepatient was unable to be closed at the first take-back operation.Similarly, the intra-abdominal abscess rate for DCL was higherthan that for SL (38% vs 17%, p < 0.01) but only if the patientcould not have the fascia closed on the first take-back opera-tion.74 The authors concluded that DA is safe provided the fasciais closed at the first take-back; otherwise, a stoma should be
Figure 3. Forest plot of mortality and infectious complication rates in
512
Copyright © 2019 Wolters Kluwer H
created.74 However, they noted that multiple take-back opera-tions are most likely a marker for a much sicker population74
which seems consistent with the series from the WTA71 andGeorgoff et al.,75 suggesting that if DA is to be performed, itshould be done early. In summary, the literature indicates thatR&A and DAwith DCL is appropriate for certain populations.
Quantitative Synthesis (Meta-Analysis)A total of 395 subjects from 10 retrospective studies were
included in our analysis. Separating recommendations for repairversus R&A was not possible given limitations and variabilityamong studies. Analysis of pooled data demonstrated similarmortality between those having repair/R&A versus colostomy(OR, 0.916; 95% CI, 0.26–3.26; p = 0.893). Regarding infec-tions, patients undergoing repair/R&A showed a trend towardworse infectious complications versus those who had colostomy(OR, 1.593; 95% CI, 0.76–3.34; p = 0.217). Heterogeneity washigh in analysis of mortality (I2 = 61.3%) and low (I2 = 0.0%)with regard to surgical infections, and no publication bias wasevident for either outcome. A summary of the data for the out-comes is provided in Figure 3.
Grading the EvidenceNo serious publication bias was detected for either outcome
nor was there inconsistency, indirectness, or imprecision in theavailable studies. All studies addressing this question are retro-spective. The overall quality of evidence is very low (Table 1).
RECOMMENDATION
While there is risk in performing an anastomosis, stomaformation is also accompanied by morbidity in patients requir-ing DCL. The presence of a stoma can also compromise woundmanagement and subsequent abdominal fascial closure.67
Nearly all available studies demonstrate that higher ISS, greatertransfusion requirements, more severe physiologic derangement,and longer hospital LOS are factors for increased complicationrisk in DCL groups. The best outcome for DA is seen in patients
adult damage control surgery patients with colon injuries.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Cullinane et al.
who resuscitate and achieve abdominal closure earlier althoughthe quality of evidence in this area is very low.65,68,70 Based onthe literature, 10 authors voted in favor of a strong recommenda-tion and six voted in favor of a conditional recommendation.Therefore, in adult trauma patients with penetrating colon injurywho had DCL, we conditionally recommend that mandatory co-lostomy not be performed; instead, definitive repair, delayedR&A, or anastomosis (if resection already took place in the set-ting of DCL) may be performed rather than colostomy. Clinicaljudgment in these situations is paramount.
APPLYING THIS GUIDELINE TOCLINICAL PRACTICE
This PMGpresents qualitative and quantitative data to for-mulate recommendations based on available studies on the treat-ment of penetrating colon injury. We recognize that everysituation is different and that patient, personnel, institutional,and situational factors may warrant or require deviation fromour recommendations. We encourage institutions to use thisPMG to formulate their own protocols for surgically managingpenetrating colon injuries.
CONCLUSION
Three evidence-based recommendations have been pro-vided for adult civilian patients with penetrating colonic trauma.In patients without signs of shock, hemorrhage, severe con-tamination, or delay to surgical intervention, we recommendthat colon repair or R&A be performed rather than colostomy.For high-risk patients, including those receiving DCL, we condi-tionally recommend that colon repair or R&A be performedrather than mandatory colostomy except in patients withthe most severe injuries.
AUTHORSHIP
DCC and RSJ designed the study and performed PICO development,literature review, data extraction, data interpretation, manuscript devel-opment, andmanuscript editing. JJC and BRHR performed PICO develop-ment, literature review, data extraction, data interpretation, manuscriptdevelopment, and manuscript editing. AM performed literature review,data extraction, manuscript development, and manuscript editing.DSM, and GAB performed literature review, data extraction, data inter-pretation, manuscript development, and manuscript editing. JC per-formed data extraction, data interpretation, manuscript development,and manuscript editing. ODG designed the study and performed PICOdevelopment, literature review, data extraction, data interpretation, andmanuscript editing. SRG and KAK performed literature review, data ex-traction, and manuscript editing. LP and RRB performed PICO develop-ment, literature review, data extraction, data interpretation, manuscriptediting. GS and SER performed literature review, data extraction, data inter-pretation, manuscript editing. GK performed PICO development, data ex-traction,data interpretation, manuscript development, manuscript editing.
ACKNOWLEDGMENTS
The authors thank Emily Andreae, PhD, for assistance with manuscriptediting and Brian J. Finnegan, MLIS, for assistance with the documentsearch.
DISCLOSURE
The authors declare no conflicts of interest.No external sources of funding were used in the preparation of thismanuscript.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
REFERENCES1. Mulherin JL Jr., Sawyers JL. Evaluation of three methods for managing pen-
etrating colon injuries. J Trauma. 1975;15(7):580–587.2. Adkins RB Jr., Zirkle PK, Waterhouse G. Penetrating colon trauma.
J Trauma. 1984;24(6):491–499.3. Stone HH, Fabian TC.Management of perforating colon trauma: randomiza-
tion between primary closure and exteriorization. Ann Surg. 1979;190(4):430–436.
4. Chappuis CW, Frey DJ, Dietzen CD, Panetta TP, Buechter KJ, Cohn I Jr.Management of penetrating colon injuries. A prospective randomized trial.Ann Surg. 1991;213(5):492–498.
5. Falcone RE, Wanamaker SR, Santanello SA, Carey LC. Colorectal trauma:primary repair or anastomosis with intracolonic bypass vs. ostomy. Dis ColonRectum. 1992;35(10):957–963.
6. Sasaki LS, Allaben RD, Golwala R, Mittal VK. Primary repair of colon inju-ries: a prospective randomized study. J Trauma. 1995;39(5):891–901.
7. Gonzalez RP, Merlotti GJ, Holevar MR. Colostomy in penetrating colon in-jury: Is it necessary? J Trauma. 1996;41(2):271–275.
8. Cayten CG, Fabian TC, Garcia VF, Ivatury RR, Morris JA. Penetrating coloninjuries, management of. J Trauma. 1998;44(6):941–956.
9. Park JJ, Del PinoA, Orsay CP, Nelson RL, Pearl RK, Cintron JR, Abcarian H.Stoma complications: the Cook County hospital experience. Dis ColonRectum. 1999;42(12):1575–1580.
10. Pachter HL, Hoballah JJ, Corcoran TA, Hofstetter SR. The morbidity and fi-nancial impact of colostomy closure in trauma patients. J Trauma. 1990;30(12):1510–1513.
11. Crass RA, Salbi F, Trunkey DD. Colostomy closure after colon injury: a low-morbidity procedure. J Trauma. 1987;27(11):1237–1239.
12. Sola JE, Bender JS, Buchman TG. Morbidity and timing of colostomy clo-sure in trauma patients. Injury. 1993;24(7):438–440.
13. Thal ER, Yeary EC. Morbidity of colostomy closure following colonictrauma. J Trauma. 1980;20(4):287–291.
14. Williams RA, Csepanyi E, Hiatt J, Wilson SE. Analysis of the morbidity,mortality, and cost of colostomy closure in traumatic compared with non-traumatic colorectal diseases. Dis Colon Rectum. 1987;30(3):164–167.
15. Berne JD, Velmahos GC, Chan LS, Asensio JA, Demetriades D. The highmorbidity of colostomy closure after trauma: Further support for the primaryrepair of colon injuries. Surgery. 1998;123(2):157–164.
16. Eshraghi N, Mullins RJ, Mayberry JC, Brand DM, Crass RA, Trunkey DD.Surveyed opinion of American trauma surgeons in management of colon in-juries. J Trauma. 1998;44(1):93–97.
17. Pezim ME, Vestrup JA. Canadian attitudes toward use of primary repair inmanagement of colon trauma. A survey of 317members of the CanadianAs-sociation of General Surgeons. Dis Colon Rectum. 1996;39(1):40–44.
18. Kerwin AJ, Haut ER, Burns JB, Como JJ, Haider A, Stassen N, Dahm P.Eastern Association for the Surgery of Trauma PracticeManagement Guide-lines Ad Hoc Committee. The Eastern Association of the Surgery of Traumaapproach to practice management guideline development using Grading ofRecommendations, Assessment, Development, and Evaluation (GRADE)methodology. J Trauma Acute Care Surg. 2012;73(5 Suppl 4):S283–S287.
19. Guyatt G, Gutterman D, Baumann MH, Addrizzo-Harris D, Hylek EM,Phillips B, Raskob G, Lewis SZ, SchünemannH. Grading strength of recom-mendations and quality of evidence in clinical guidelines: report from anAmerican College of Chest Physicians task force. Chest. 2006;129(1):174–181.
20. RhodesM. Practice management guidelines for trauma care: presidential ad-dress, Seventh Scientific Assembly of the Eastern Association for the Sur-gery of Trauma. J Trauma. 1994;37(4):635–644.
21. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis.Stat Med. 2002;21(11):1539–1558.
22. Egger M, Smith G, Altman D. Systematic Reviews in Health Care: Meta-Analysis in Context. London: BMJ Books; 2011.
23. Sterne JA, Egger M, Smith GD. Systematic reviews in health care: Investi-gating and dealing with publication and other biases in meta-analysis.BMJ. 2001;323(7304):101–105.
24. Guyatt GH, Oxman AD, Kunz R, Falck-Ytter Y, Vist GE, Liberati A,Schünemann HJ. GRADE Working Group. Going from evidence to recom-mendations. BMJ. 2008;336(7652):1049–1051.
513
ealth, Inc. All rights reserved.
Cullinane et al.J Trauma Acute Care Surg
Volume 86, Number 3
25. Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, Norris S,Falck-Ytter Y, Glasziou P, DeBeer H, et al. GRADE guidelines: 1.Introduction—GRADE evidence profiles and summary of findings tables.J Clin Epidemiol. 2011;64(4):383–394.
26. Guyatt GH, Oxman AD, Kunz R, Atkins D, Brozek J, Vist G, Alderson P,Glasziou P, Falck-Ytter Y, Schünemann HJ. GRADE guidelines: 2. Framingthe question and deciding on important outcomes. J Clin Epidemiol. 2011;64(4):395–400.
27. Balshem H, Helfand M, Schünemann HJ, Oxman AD, Kunz R, Brozek J,Vist GE, Falck-Ytter Y, Meerpohl J, et al. GRADE guidelines: 3. Ratingthe quality of evidence. J Clin Epidemiol. 2011;64(4):401–406.
28. Guyatt GH, Oxman AD, Vist G, Kunz R, Brozek J, Alonso-Coello P,Montori V, Akl EA, Djulbegovic B, Falck-Ytter Y, et al. GRADE guidelines:4. Rating the quality of evidence - study limitations (risk of bias). J ClinEpidemiol. 2011;64(4):407–415.
29. Guyatt GH, Oxman AD, Montori V, Vist G, Kunz R, Brozek J,Alonso-Coello P, Djulbegovic B, Atkins D, Falck-Ytter Y, et al. GRADEguidelines: 5. Rating the quality of evidence—publication bias. J ClinEpidemiol. 2011;64(12):1277–1282.
30. Guyatt GH, Oxman AD, Kunz R, Brozek J, Alonso-Coello P, Rind D,Devereaux PJ, Montori VM, Freyschuss B, Vist G, et al. GRADE guidelines6. Rating the quality of evidence—imprecision. J Clin Epidemiol. 2011;64(12):1283–1293.
31. Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M,Alonso-Coello P, Glasziou P, Jaeschke R, Akl EA, et al. GRADE guidelines:7. Rating the quality of evidence—inconsistency. J Clin Epidemiol. 2011;64(12):1294–1302.
32. Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M,Alonso-Coello P, Falck-Ytter Y, Jaeschke R, Vist G, et al. GRADE guide-lines: 8. Rating the quality of evidence–indirectness. J Clin Epidemiol.2011;64(12):1303–1310.
33. Guyatt GH, Oxman AD, Sultan S, Glasziou P, Akl EA, Alonso-Coello P,Atkins D, Kunz R, Brozek J, Montori V, et al. GRADE guidelines: 9. Ratingup the quality of evidence. J Clin Epidemiol. 2011;64(12):1311–1316.
34. Guyatt GH, OxmanAD, SchünemannHJ. GRADE guidelines—an introduc-tion to the 10th-13th articles in the series. J Clin Epidemiol. 2013;66(2):121–123.
35. Brunetti M, Shemilt I, Pregno S, Vale L, Oxman AD, Lord J, Sisk J, Ruiz F,Hill S, Guyatt GH, et al. GRADE guidelines: 10. Considering resource useand rating the quality of economic evidence. J Clin Epidemiol. 2013;66(2):140–150.
36. Guyatt G, Oxman AD, Sultan S, Brozek J, Glasziou P, Alonso-Coello P,Atkins D, Kunz R, Montori V, Jaeschke R, et al. GRADE guidelines: 11.Making an overall rating of confidence in effect estimates for a single out-come and for all outcomes. J Clin Epidemiol. 2013;66(2):151–157.
37. Guyatt GH, Oxman AD, Santesso N, Helfand M, Vist G, Kunz R, Brozek J,Norris S, Meerpohl J, Djulbegovic B, et al. GRADE guidelines: 12. Prepar-ing summary of findings tables-binary outcomes. J Clin Epidemiol. 2013;66(2):158–172.
38. Guyatt GH, Thorlund K, Oxman AD, Walter SD, Patrick D, Furukawa TA,Johnston BC, Karanicolas P, Akl EA, Vist G, et al. GRADE guidelines:13. Preparing summary of findings tables and evidence profiles-continuousoutcomes. J Clin Epidemiol. 2013;66(2):173–183.
39. Andrews J, Guyatt G, Oxman AD, Alderson P, Dahm P, Falck-Ytter Y,Nasser M, Meerpohl J, Post PN, Kunz R, et al. GRADE guidelines: 14. Go-ing from evidence to recommendations: the significance and presentation ofrecommendations. J Clin Epidemiol. 2013;66(7):719–725.
40. Andrews JC, Schünemann HJ, Oxman AD, Pottie K, Meerpohl JJ,Coello PA, Rind D, Montori VM, Brito JP, Norris S, et al. GRADE guide-lines: 15. Going from evidence to recommendation-determinants of arecommendation's direction and strength. J Clin Epidemiol. 2013;66(7):726–735.
41. Gonzalez RP, Falimirski ME, Holevar MR. Further evaluation of colostomyin penetrating colon injury. Am Surg. 2000;66(4):342–347.
42. Kamwendo NY, Modiba MC, Matlala NS, Becker PJ. Randomized clinicaltrial to determine if delay from time of penetrating colonic injury precludesprimary repair. Br J Surg. 2002;89(8):993–998.
43. Nelson RL, Singer M. Primary repair for penetrating colon injuries (review).Cochrane Library. 2009;4: doi: 10.1002/14651858.CD002247.
514
Copyright © 2019 Wolters Kluwer H
44. Miller PR, Fabian TC, Croce MA, Magnotti LJ, Elizabeth Pritchard F,Minard G, Stewart RM. Improving outcomes following penetrating colonwounds: application of a clinical pathway. Ann Surg. 2002;235(6):775–781.
45. Fealk M, Osipov R, Foster K, Caruso D, Kassir A. The conundrum of trau-matic colon injury. Am J Surg. 2004;188(6):663–670.
46. Mihmanli M, Erzurumlu K, Güney M. Primary repairing in penetrating co-lon injuries. Hepatogastroenterology. 1996;43(10):819–822.
47. Kuzma J, Jaworski J. Primary repair of colonic injuries at the Kundiawa andMadangGeneral Hospitals, Papua NewGuinea.PNGMed J. 2008;51(1–2):43–46.
48. Cornwell EE 3rd, Velmahos GC, Berne TV, Murray JA, Chahwan S,Asensio J, Demetriades D. The fate of colonic suture lines in high-risktrauma patients: a prospective analysis. J Am Coll Surg. 1998;187(1):58–63.
49. Murray JA, Demetriades D, Colson M, Song Z, Velmahos GC, Cornwell EE3rd, Asensio JA, Belzberg H, Berne TV. Colonic resection in trauma: Colos-tomy versus anastomosis. J Trauma. 1999;46(2):250–254.
50. Flint LM, Vitale GC, Richardson JD, Polk HC Jr. The injured colon: re-lationships of management to complications. Ann Surg. 1981;193(5):619–623.
51. Demetriades D, Murray JA, Chan L, Ordoñez C, Bowley D, Nagy KK,Cornwell EE 3rd, Velmahos GC,Muñoz N, Hatzitheofilou C, et al. Penetrat-ing colon injuries requiring resection: diversion or primary anastomosis? AnAAST prospective multicenter study. J Trauma. 2001;50(5):765–775.
52. Steel M, Danne P, Jones I. Colon trauma: Royal Melbourne Hospital experi-ence. ANZ J Surg. 2002;72(5):357–359.
53. Sambasivan CN, Underwood SJ, Kuehn RB, Cho SD, Kiraly LN,Hamilton GJ, Flaherty SF, DorlacWC, Schreiber MA.Management and out-comes of traumatic colon injury in civilian and military patients. Am Surg.2011;77(12):1685–1691.
54. Adesanya AA, Ekanem EE. A ten-year study of penetrating injuries of thecolon. Dis Colon Rectum. 2004;47(12):2169–2177.
55. Girgin S, Gedik E, Uysal E, Taçyildiz IH. Independent risk factors of mor-bidity in penetrating colon injuries. Ulus Travma Acil Cerrahi Derg. 2009;15(3):232–238.
56. Bulger EM, McMahon K, Jurkovich GJ. The morbidity of penetrating coloninjury. Injury. 2003;34(1):41–46.
57. Behrman SW, Bertken KA, Stefanacci HA, Parks SN. Breakdown of intesti-nal repair after laparotomy for trauma: incidence, risk factors, and strategiesfor prevention. J Trauma. 1998;45(2):227–233.
58. Schnüriger B, Inaba K,Wu T, Eberle BM, Belzberg H, Demetriades D. Crys-talloids after primary colon resection and anastomosis at initial trauma lapa-rotomy: excessive volumes are associated with anastomotic leakage.J Trauma. 2011;70(3):603–610.
59. Torba M, Gjata A, Buci S, Bushi G, Zenelaj A, Kajo I, Koceku S, Kagjini K,Subashi K. The influence of the risk factor on the abdominal complicationsin colon injury management. G Chir. 2015;36(2):57–62.
60. Conrad JK, Ferry KM, Foreman ML, Gogel BM, Fisher TL, Livingston SA.Changing management trends in penetrating colon trauma.Dis Colon Rectum.2000;43(4):466–471.
61. Sharpe JP, Magnotti LJ, Weinberg JA, Parks NA, Maish GO, Shahan CP,Fabian TC, CroceMA. Adherence to a simplified management algorithm re-duces morbidity and mortality after penetrating colon injuries: a 15-year ex-perience. J Am Coll Surg. 2012;214(4):591–598.
62. Oztürk G, Aydinli B, Selcuk Atamanalp S, Celebi F, Ilhan Yildirgan M,Donmez R. Penetrating colon injury: experience of a single centre. Acta ChirBelg. 2009;109(2):185–190.
63. Dente CJ, Tyburski J,WilsonRF, Collinge J, Steffes C, Carlin A. Ostomy as arisk factor for posttraumatic infection in penetrating colonic injuries: univar-iate and multivariate analyses. J Trauma. 2000;49(4):628–637.
64. Durham RM, Pruitt C, Moran J, Longo WE. Civilian colon trauma: factorsthat predict success by primary repair. Dis Colon Rectum. 1997;40(6):685–692.
65. Chavarria-AguilarM, CockerhamWT, Barker DE, Ciraulo DL, Richart CM,Maxwell RA.Management of destructive bowel injury in the open abdomen.J Trauma. 2004;56(3):560–564.
66. Johnson JW, Gracias VH, Schwab CW, Reilly PM, Kauder DR, ShapiroMB,Dabrowski GP, Rotondo MF. Evolution in damage control for exsanguinat-ing penetrating abdominal injury. J Trauma. 2001;51(2):261–271.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Cullinane et al.
67. Miller PR, ChangMC, Hoth JJ, Holmes JH 4th,Meredith JW. Colonic resec-tion in the setting of damage control laparotomy: is delayed anastomosissafe? Am Surg. 2007;73(6):606–610.
68. Ordoñez CA, Pino LF, BadielM, Sánchez AI, Loaiza J, Ballestas L, Puyana JC.Safety of performing a delayed anastomosis during damage control laparotomyin patients with destructive colon injuries. J Trauma. 2011;71(6):1512–1518.
69. Ott MM, Norris PR, Diaz JJ, Collier BR, Jenkins JM, Gunter OL, Morris JAJr. Colon anastomosis after damage control laparotomy: recommendationsfrom 174 trauma colectomies. J Trauma. 2011;70(3):595–602.
70. Weinberg JA, Griffin RL, Vandromme MJ, Melton SM, George RL,Reiff DA, Kerby JD, Rue LW 3rd. Management of colon wounds in the set-ting of damage control laparotomy: a cautionary tale. J Trauma. 2009;67(5):929–935.
71. Burlew CC, Moore EE, Cuschieri J, Jurkovich GJ, Codner P, Crowell K,Nirula R, Haan J, Rowell SE, Kato CM, et al. Sew it up! AWestern Trauma
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
Association multi-institutional study of enteric injury management in thepostinjury open abdomen. J Trauma. 2011;70(2):273–277.
72. Kashuk JL, Cothren CC, Moore EE, Johnson JL, Biffl WL, Barnett CC. Pri-mary repair of civilian colon injuries is safe in the damage control scenario.Surgery. 2009;146(4):663–670.
73. Tatebe LC, Jennings A, Tatebe K, Handy A, Prajapati P, Smith M, Do T,Ogola GO, Gandhi RR, Duane TM, et al. Traumatic colon injury in damagecontrol laparotomy—Amulticenter trial: is it safe to do a delayed anastomo-sis? J Trauma Acute Care Surg. 2017;82(4):742–749.
74. Anjaria DJ, Ullmann TM, Lavery RL, Livingston DH. Management of co-lonic injuries in the setting of damage-control laparotomy: one shot to getit right. J Trauma Acute Care Surg. 2014;76(3):594–600.
75. Georgoff P, Perales P, Laguna B, Holena D, Reilly P, Sims C. Colonic injuriesand the damage control abdomen: does management strategy matter? J SurgRes. 2013;181(2):293–299.
515
ealth, Inc. All rights reserved.

SYSTEMATIC REVIEW
Comparing short-, long-, and oblique-axis approaches toultrasound-guided internal jugular venous catheterization:
A meta-analysis of randomized controlled trials
Jen-Yin Chen, MD, PhD, Li-Kai Wang, MD, Yao-Tsung Lin, MD, Kuo-Mao Lan, MD, El-Wui Loh, PhD,Chih-Heng Chen, MD, and Ka-Wai Tam, MD, PhD, New Taipei City Taiwan
Sub
Fro
Ad
Sup
DO
51
BACKGROUND: I
mitted: September 7, 2018, Rev2018, Published online: Novemm the Department of AnesthesiMedical Center; Department ofNan University of Pharmacy andApplied Biotechnology (Y-T.L., KTaiwan; Center for Evidence-BaMedical Research (E-W.L., K-WNewTaipei City; School ofMedieral Surgery, Department of Surgcine, Taipei Medical University,Surgery (K-W.T.), Taipei Medicaand Cochrane Taiwan (K-W.T.),dress for reprints: Ka-Wai Tam,Taipei Medical University-ShuDistrict, New Taipei City, 2356plemental digital content is avaithe printed text, and links to thearticle on the journal’s Web sit
I: 10.1097/TA.00000000000021
6
nternal jugular venous catheterization is performed for numerous therapeutic interventions. Although ultrasound-guided internaljugular venous catheterization is the gold standard for this procedure, complications can still occur. Various scanning axes, namely,the short axis (SA), long axis (LA), and oblique axis (OA), have been developed to ameliorate these complications. This studycompared the efficacy and safety of SA, LA, and OA approaches.
METHODS: P
ubMed, Embase, and Cochrane Library databases were searched for studies published before September 2018. Only randomizedcontrolled trials were included. We conducted meta-analyses using a random-effects model. Treatment efficacy was measured bytotal success rate, first-pass success rate, number of needle passes, and incidence of complications, namely, arterial puncture, he-matoma, and catheter-related bloodstream infection.RESULTS: S
ix randomized controlled trials with 621 patients were included. No significant differences were observed in total success rate andfirst-pass success rate, as well as in the arterial puncture, hematoma, or catheter-related bloodstream infection complications be-tween SA and LA approaches. Moreover, no significant difference was found between SA and OA approaches in terms of totalsuccess rate, first-pass success rate, number of needle passes, and complications of arterial puncture and hematoma. However,the number of needle passes was significantly fewer in SA approach than in LA approach (weighted mean difference, −0.18;95% confidence interval, −0.35 to −0.01).CONCLUSION: N
one of the scanning axes exhibited unique features that could enhance their suitability for application. Hence, scanning axesshould be selected by considering various factors that include patient characteristics, clinician expertise, and ease of procedures.(J Trauma Acute Care Surg. 2019;86: 516–523. Copyright © 2018 Wolters Kluwer Health, Inc. All rights reserved.)LEVEL OF EVIDENCE: S
ystematic review and meta-analysis, level I. KEYWORDS: C atheterization; central venous; internal jugular vein; scanning axis; ultrasonography; meta-analysis.I nternal jugular venous catheterization (IJVC) is per-formed in operating rooms and critical care settings for
numerous therapeutic interventions. Providing secure vas-cular access for the administration of vasoactive drugs orinitiating rapid fluid resuscitation, long-term total par-enteral nutrition, accessing alternative kidney therapies, and
ised: December 19, 2018, Accepted: October 29,ber 30, 2018.ology (J-Y.C., L-K.W., Y-T.L., K-M.L.), Chi MeiSenior Citizen ServiceManagement (J-Y.C.), ChiaScience, Tainan; Department of Food Science and-M.L.), National Chung Hsing University, Taichung,sed Health Care (E-W.L., K-W.T.), Department of.T.), Taipei Medical University-Shuang Ho Hospital,cine (C-H.C.), College ofMedicine, Division of Gen-ery (K-W.T.), School of Medicine, College of Medi-Taipei; Division of General Surgery, Department ofl University-Shuang Ho Hospital, New Taipei City;Taipei Medical University, Taipei, Taiwan.MD, PhD, Center for Evidence-based Health Care,ang Ho Hospital, 291 Zhongzheng Rd, Zhonghe1, Taiwan; email: [email protected] for this article. Direct URL citations appear indigital files are provided in the HTML text of thise (www.jtrauma.com).
58
Copyright © 2019 Wolters Kluwer H
cardiopulmonary resuscitation when accessing peripheral veinsis difficult.1 Despite the prevalent usage of IJVC, the rate ofcomplications, such as arterial puncture, pneumothorax, air em-bolism, catheter embolism, and cardiac arrhythmia range from5% to 19%.2
The IJVC technique is based on anatomical landmarks;however, current evidence-based recommendations revealthat real-time ultrasound guidance of the needle tip duringvascular puncture is the gold standard for this procedure.3–5
This reduces the incidence of complications, as well as thetime and number of attempts until successful catheterization,and increases the success rate compared with the landmarktechnique.6,7
Studies have described various imaging approaches.Ultrasound-guided IJVC is performed through three main scan-ning axes: short axis (SA), long axis (LA), and oblique axis(OA).8–10 The SA view allows simultaneous visualization ofthe artery and vein but can make needle tip control difficult.11,12
The LAview can optimize needle visualization but usually onlydisplays the vein in the ultrasound image, meaning accidental ar-terial puncture can occur.11 The OA view uses the strengths ofboth previous approaches by using a probe alignment that ismidway between SA and LA. Thus, the OA can optimize visu-alization of the needle and jugular vein with all surroundingstructures.8
J Trauma Acute Care SurgVolume 86, Number 3
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Chen et al.
Currently, the outcome of any one ultrasound-guidedIJVC approach has not been systematically proven superior.Therefore, we performed a meta-analysis of available randomizedcontrolled trials (RCTs) to compare the efficacy and safety of theSA, LA, and OA approaches for ultrasound-guided IJVC.
MATERIALS AND METHODS
Inclusion CriteriaPeer review RCTs comparing the SA, LA, and OA ap-
proaches in patients who underwent ultrasound-guided IJVCwere included. The trials were required to clearly report the in-clusion and exclusion criteria for patients, the technique ofultrasound-guided IJVC, the scanning axis approaches, and thedefinitions and methods of evaluation for success rates, numberof needle passes, and complications. We excluded studies thatmet one or more of the following criteria: (1) inclusion of pedi-atric patients (<18 years old); (2) patients without indications ofIJVC; or (3) duplicate reporting of patient cohorts.
Search Strategy and Study SelectionRelevant trials published before September 2018 were
identified from the databases of PubMed, Embase, and theCochrane Library. The following medical subject headingswere used: vascular access OR venous catheterization ORvenous cannulation, central vein OR central venous OR inter-nal jugular vein OR internal jugular venous, ultrasound ORultrasound-guided OR ultrasonography OR echography, andshort axis OR long axis OR OA OR scanning axis. The“related articles” option in PubMed was used to broadenthe search, and all abstracts, studies, and citations thusretrieved were reviewed. Finally, unpublished studies were col-lected from the ClinicalTrials.gov registry (http://clinicaltrials.gov/). No language restrictions were applied. The systematicreview described herein has been accepted by PROSPERO(CRD42018090457).
Data ExtractionBaseline and outcome datawere independently retrieved by
two reviewers (C.H.C. and K.W.T.). Furthermore, data regardingstudy designs, study population characteristics, inclusion andexclusion criteria, total success rate, first needle pass successrate, number of needle passes, procedure time, and complica-tions were extracted. Decisions recorded individually by the re-viewers were compared and disagreements were resolved by athird reviewer (J.Y.C.).
Appraisal of Methodological QualityTwo reviewers (C.H.C. and K.W.T.) independently
assessed the methodological quality of each study using theCochrane risk of bias tool (RoB 2.0).13 Studies were awardedan overall risk of bias grade of high, some, or low risk of bias.This grade was calculated by assessing five domains: biasarising from the randomization process, bias owing to devia-tions from intended interventions, bias owing to missing out-come data, bias in measurement of the outcome, and bias inselection of the reported results.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
OutcomesThe primary outcomes were the total success rate and
first needle pass success rate. The secondary outcomes werenumber of needle passes, procedure time, and complicationsof hematoma, arterial puncture, and catheter-related blood-stream infection (CRBSI).
Statistical AnalysesData were entered and analyzed using Review Man-
ager 5.3 (The Cochrane Collaboration, Oxford, England).A meta-analysis was performed following the PreferredReporting Items for Systematic Review and Meta-Analysesguidelines.14 Standard deviations were estimated using theprovided confidence interval (CI) limits or standard errors.Dichotomous outcomes were analyzed using risk ratios(RR) as the summary statistics. The effect sizes of the con-tinuous outcomes were reported as the weighted mean differ-ence (WMD). The precision of the effect sizes was reportedat a CI of 95%. A pooled estimate of the RRs andWMDs wascomputed using the DerSimonian and Laird random effectsmodel.15 A statistically significant result was indicated by ap value less than 0.05 or 95% CI not including one in RR andzero in WMD.
Statistical heterogeneity and the inconsistency of thetreatment effects across studies were evaluated using CochraneQ tests and I2 statistics, respectively. Statistical significancewas set at p less than 0.10 for the Cochrane Q tests. Statisticalheterogeneity across studies was assessed using the I2 test,which quantifies the proportion of the total outcome variabilityacross studies. Moreover, subgroup analyses were performedby pooling available estimates for similar subsets of patientsacross trials.
RESULTS
Trial CharacteristicsFigure 1 illustrates the flowchart of the studies'
screening and selection. The initial screen yielded 684 cita-tions, of which 565 were ineligible based on the criteriaused for screening titles and abstracts. Thus, the full texts of119 studies were retrieved. However, 74 studies featured an in-appropriate topic, 21 discussed inappropriate intervention, and18 were not RCTs. Thus, six trials were eligible for inclusionin this meta-analysis.1,16–20
These six trials were published between 2011 and2016 and included a total of 621 patients. Three trials in-vestigated the SA and LA approaches,17,19,20 two com-pared the SA and OA approaches,1,18 and one evaluated allthree approaches.16 In most of the included trials, the patientswere older than 18 years to minimize variables during compar-ison. Five trials recruited patients undergoing surgery1,16–19
and two trials included critical or hemodialysis patients.19,20
The SA and LA approaches were similar in technique in allsix trials. However, the OA approaches were slightly different:the conventional OA approach,16 the “syringe-free” OA ap-proach,18 and the medial-oblique approach were used.1
Baseline patient characteristics in the six trials are shownin Table 1.
517
ealth, Inc. All rights reserved.
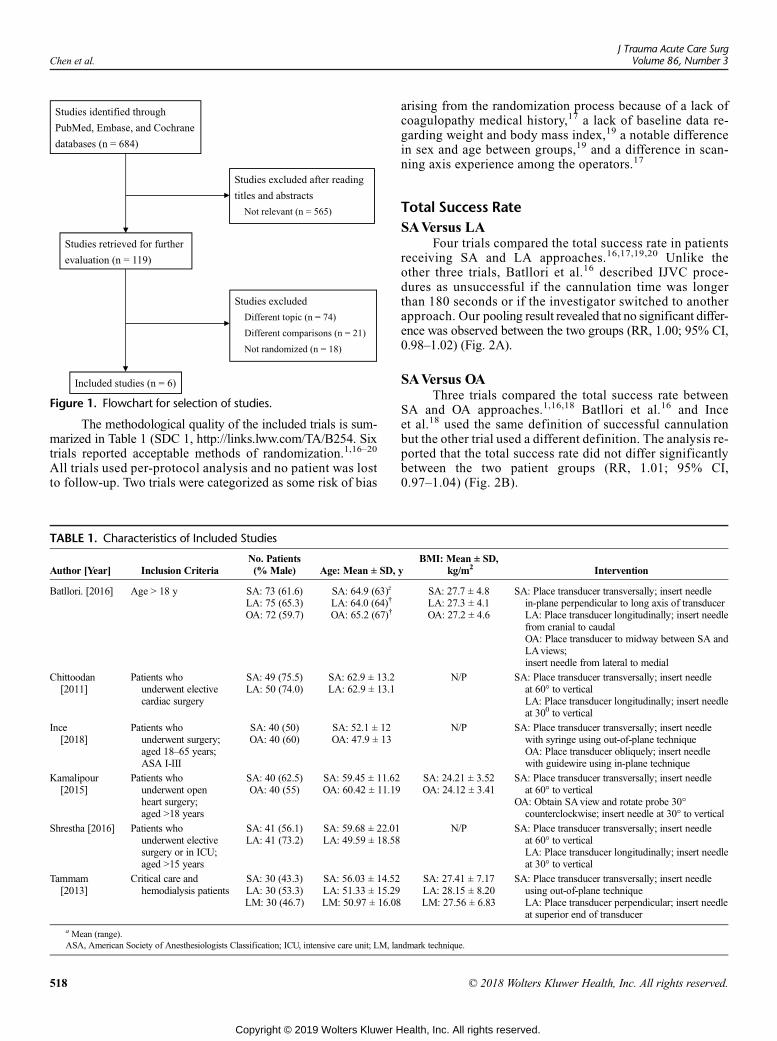
Figure 1. Flowchart for selection of studies.
Chen et al.J Trauma Acute Care Surg
Volume 86, Number 3
The methodological quality of the included trials is sum-marized in Table 1 (SDC 1, http://links.lww.com/TA/B254. Sixtrials reported acceptable methods of randomization.1,16–20
All trials used per-protocol analysis and no patient was lostto follow-up. Two trials were categorized as some risk of bias
TABLE 1. Characteristics of Included Studies
Author [Year] Inclusion CriteriaNo. Patients(% Male) Age: Mean ± SD,
Batllori. [2016] Age > 18 y SA: 73 (61.6)LA: 75 (65.3)OA: 72 (59.7)
SA: 64.9 (63)z
LA: 64.0 (64)†
OA: 65.2 (67)†
Chittoodan[2011]
Patients whounderwent electivecardiac surgery
SA: 49 (75.5)LA: 50 (74.0)
SA: 62.9 ± 13.2LA: 62.9 ± 13.1
Ince[2018]
Patients whounderwent surgery;aged 18–65 years;ASA I-III
SA: 40 (50)OA: 40 (60)
SA: 52.1 ± 12OA: 47.9 ± 13
Kamalipour[2015]
Patients whounderwent openheart surgery;aged >18 years
SA: 40 (62.5)OA: 40 (55)
SA: 59.45 ± 11.62OA: 60.42 ± 11.19
Shrestha [2016] Patients whounderwent electivesurgery or in ICU;aged >15 years
SA: 41 (56.1)LA: 41 (73.2)
SA: 59.68 ± 22.01LA: 49.59 ± 18.58
Tammam[2013]
Critical care andhemodialysis patients
SA: 30 (43.3)LA: 30 (53.3)LM: 30 (46.7)
SA: 56.03 ± 14.52LA: 51.33 ± 15.29LM: 50.97 ± 16.08
a Mean (range).ASA, American Society of Anesthesiologists Classification; ICU, intensive care unit; LM, la
518
Copyright © 2019 Wolters Kluwer H
arising from the randomization process because of a lack ofcoagulopathy medical history,17 a lack of baseline data re-garding weight and body mass index,19 a notable differencein sex and age between groups,19 and a difference in scan-ning axis experience among the operators.17
Total Success RateSAVersus LA
Four trials compared the total success rate in patientsreceiving SA and LA approaches.16,17,19,20 Unlike theother three trials, Batllori et al.16 described IJVC proce-dures as unsuccessful if the cannulation time was longerthan 180 seconds or if the investigator switched to anotherapproach. Our pooling result revealed that no significant differ-ence was observed between the two groups (RR, 1.00; 95% CI,0.98–1.02) (Fig. 2A).
SAVersus OAThree trials compared the total success rate between
SA and OA approaches.1,16,18 Batllori et al.16 and Inceet al.18 used the same definition of successful cannulationbut the other trial used a different definition. The analysis re-ported that the total success rate did not differ significantlybetween the two patient groups (RR, 1.01; 95% CI,0.97–1.04) (Fig. 2B).
yBMI: Mean ± SD,
kg/m2 Intervention
SA: 27.7 ± 4.8LA: 27.3 ± 4.1OA: 27.2 ± 4.6
SA: Place transducer transversally; insert needlein-plane perpendicular to long axis of transducerLA: Place transducer longitudinally; insert needlefrom cranial to caudalOA: Place transducer to midway between SA andLAviews;insert needle from lateral to medial
N/P SA: Place transducer transversally; insert needleat 60° to verticalLA: Place transducer longitudinally; insert needleat 300 to vertical
N/P SA: Place transducer transversally; insert needlewith syringe using out-of-plane techniqueOA: Place transducer obliquely; insert needlewith guidewire using in-plane technique
SA: 24.21 ± 3.52OA: 24.12 ± 3.41
SA: Place transducer transversally; insert needleat 60° to vertical
OA: Obtain SAview and rotate probe 30°counterclockwise; insert needle at 30° to vertical
N/P SA: Place transducer transversally; insert needleat 60° to verticalLA: Place transducer longitudinally; insert needleat 30° to vertical
SA: 27.41 ± 7.17LA: 28.15 ± 8.20LM: 27.56 ± 6.83
SA: Place transducer transversally; insert needleusing out-of-plane techniqueLA: Place transducer perpendicular; insert needleat superior end of transducer
ndmark technique.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
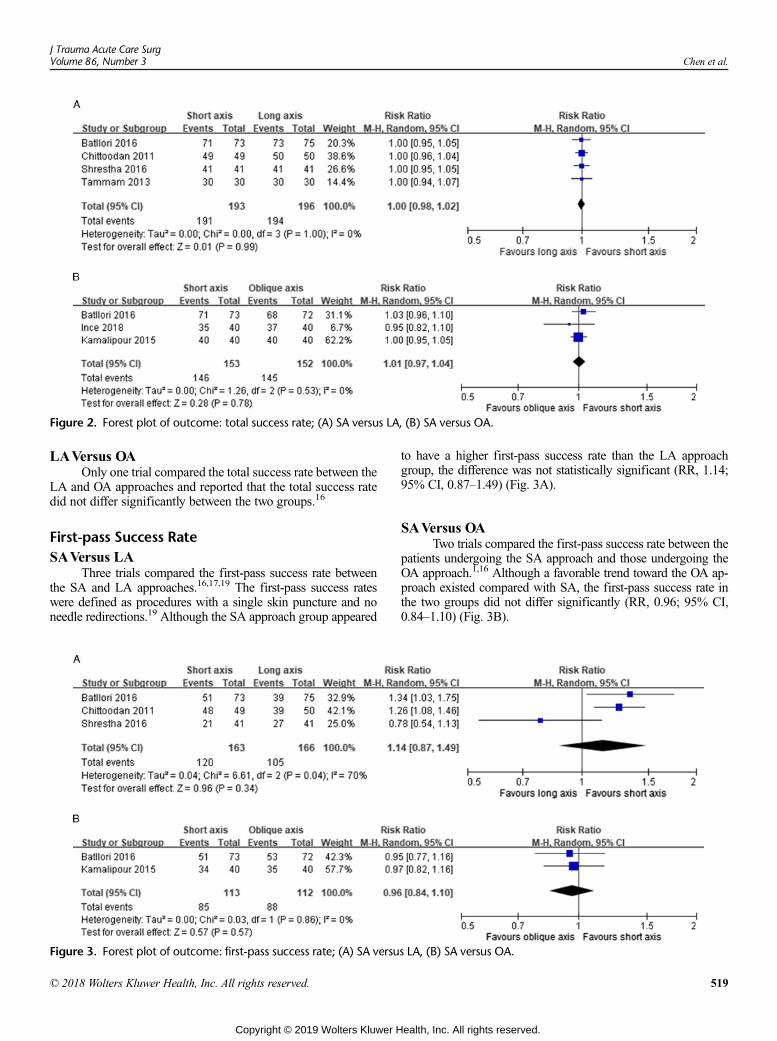
Figure 2. Forest plot of outcome: total success rate; (A) SA versus LA, (B) SA versus OA.
J Trauma Acute Care SurgVolume 86, Number 3 Chen et al.
LAVersus OAOnly one trial compared the total success rate between the
LA and OA approaches and reported that the total success ratedid not differ significantly between the two groups.16
First-pass Success RateSAVersus LA
Three trials compared the first-pass success rate betweenthe SA and LA approaches.16,17,19 The first-pass success rateswere defined as procedures with a single skin puncture and noneedle redirections.19 Although the SA approach group appeared
Figure 3. Forest plot of outcome: first-pass success rate; (A) SA versu
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
to have a higher first-pass success rate than the LA approachgroup, the difference was not statistically significant (RR, 1.14;95% CI, 0.87–1.49) (Fig. 3A).
SAVersus OATwo trials compared the first-pass success rate between the
patients undergoing the SA approach and those undergoing theOA approach.1,16 Although a favorable trend toward the OA ap-proach existed compared with SA, the first-pass success rate inthe two groups did not differ significantly (RR, 0.96; 95% CI,0.84–1.10) (Fig. 3B).
s LA, (B) SA versus OA.
519
ealth, Inc. All rights reserved.
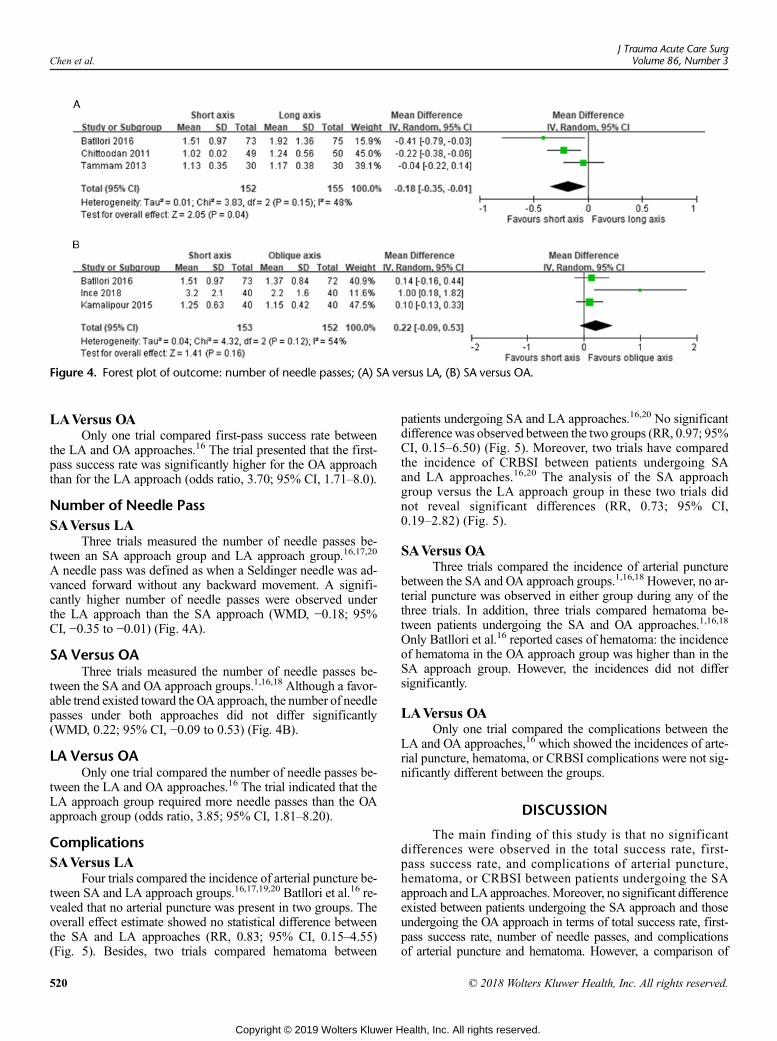
Figure 4. Forest plot of outcome: number of needle passes; (A) SA versus LA, (B) SA versus OA.
Chen et al.J Trauma Acute Care Surg
Volume 86, Number 3
LAVersus OAOnly one trial compared first-pass success rate between
the LA and OA approaches.16 The trial presented that the first-pass success rate was significantly higher for the OA approachthan for the LA approach (odds ratio, 3.70; 95% CI, 1.71–8.0).
Number of Needle PassSAVersus LA
Three trials measured the number of needle passes be-tween an SA approach group and LA approach group.16,17,20
A needle pass was defined as when a Seldinger needle was ad-vanced forward without any backward movement. A signifi-cantly higher number of needle passes were observed underthe LA approach than the SA approach (WMD, −0.18; 95%CI, −0.35 to −0.01) (Fig. 4A).
SA Versus OAThree trials measured the number of needle passes be-
tween the SA and OA approach groups.1,16,18 Although a favor-able trend existed toward the OA approach, the number of needlepasses under both approaches did not differ significantly(WMD, 0.22; 95% CI, −0.09 to 0.53) (Fig. 4B).
LA Versus OAOnly one trial compared the number of needle passes be-
tween the LA and OA approaches.16 The trial indicated that theLA approach group required more needle passes than the OAapproach group (odds ratio, 3.85; 95% CI, 1.81–8.20).
ComplicationsSAVersus LA
Four trials compared the incidence of arterial puncture be-tween SA and LA approach groups.16,17,19,20 Batllori et al.16 re-vealed that no arterial puncture was present in two groups. Theoverall effect estimate showed no statistical difference betweenthe SA and LA approaches (RR, 0.83; 95% CI, 0.15–4.55)(Fig. 5). Besides, two trials compared hematoma between
520
Copyright © 2019 Wolters Kluwer H
patients undergoing SA and LA approaches.16,20 No significantdifferencewas observed between the two groups (RR, 0.97; 95%CI, 0.15–6.50) (Fig. 5). Moreover, two trials have comparedthe incidence of CRBSI between patients undergoing SAand LA approaches.16,20 The analysis of the SA approachgroup versus the LA approach group in these two trials didnot reveal significant differences (RR, 0.73; 95% CI,0.19–2.82) (Fig. 5).
SAVersus OAThree trials compared the incidence of arterial puncture
between the SA and OA approach groups.1,16,18 However, no ar-terial puncture was observed in either group during any of thethree trials. In addition, three trials compared hematoma be-tween patients undergoing the SA and OA approaches.1,16,18
Only Batllori et al.16 reported cases of hematoma: the incidenceof hematoma in the OA approach group was higher than in theSA approach group. However, the incidences did not differsignificantly.
LAVersus OAOnly one trial compared the complications between the
LA and OA approaches,16 which showed the incidences of arte-rial puncture, hematoma, or CRBSI complications were not sig-nificantly different between the groups.
DISCUSSION
The main finding of this study is that no significantdifferences were observed in the total success rate, first-pass success rate, and complications of arterial puncture,hematoma, or CRBSI between patients undergoing the SAapproach and LA approaches.Moreover, no significant differenceexisted between patients undergoing the SA approach and thoseundergoing the OA approach in terms of total success rate, first-pass success rate, number of needle passes, and complicationsof arterial puncture and hematoma. However, a comparison of
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
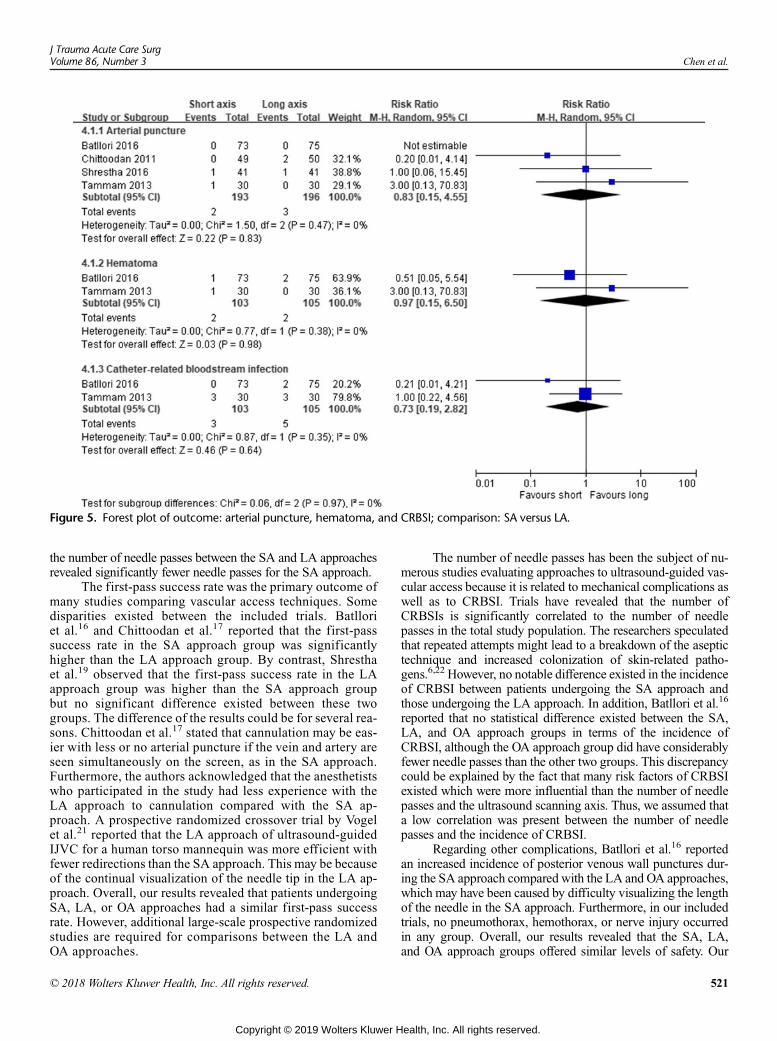
Figure 5. Forest plot of outcome: arterial puncture, hematoma, and CRBSI; comparison: SA versus LA.
J Trauma Acute Care SurgVolume 86, Number 3 Chen et al.
the number of needle passes between the SA and LA approachesrevealed significantly fewer needle passes for the SA approach.
The first-pass success rate was the primary outcome ofmany studies comparing vascular access techniques. Somedisparities existed between the included trials. Batlloriet al.16 and Chittoodan et al.17 reported that the first-passsuccess rate in the SA approach group was significantlyhigher than the LA approach group. By contrast, Shresthaet al.19 observed that the first-pass success rate in the LAapproach group was higher than the SA approach groupbut no significant difference existed between these twogroups. The difference of the results could be for several rea-sons. Chittoodan et al.17 stated that cannulation may be eas-ier with less or no arterial puncture if the vein and artery areseen simultaneously on the screen, as in the SA approach.Furthermore, the authors acknowledged that the anesthetistswho participated in the study had less experience with theLA approach to cannulation compared with the SA ap-proach. A prospective randomized crossover trial by Vogelet al.21 reported that the LA approach of ultrasound-guidedIJVC for a human torso mannequin was more efficient withfewer redirections than the SA approach. This may be becauseof the continual visualization of the needle tip in the LA ap-proach. Overall, our results revealed that patients undergoingSA, LA, or OA approaches had a similar first-pass successrate. However, additional large-scale prospective randomizedstudies are required for comparisons between the LA andOA approaches.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
The number of needle passes has been the subject of nu-merous studies evaluating approaches to ultrasound-guided vas-cular access because it is related to mechanical complications aswell as to CRBSI. Trials have revealed that the number ofCRBSIs is significantly correlated to the number of needlepasses in the total study population. The researchers speculatedthat repeated attempts might lead to a breakdown of the aseptictechnique and increased colonization of skin-related patho-gens.6,22 However, no notable difference existed in the incidenceof CRBSI between patients undergoing the SA approach andthose undergoing the LA approach. In addition, Batllori et al.16
reported that no statistical difference existed between the SA,LA, and OA approach groups in terms of the incidence ofCRBSI, although the OA approach group did have considerablyfewer needle passes than the other two groups. This discrepancycould be explained by the fact that many risk factors of CRBSIexisted which were more influential than the number of needlepasses and the ultrasound scanning axis. Thus, we assumed thata low correlation was present between the number of needlepasses and the incidence of CRBSI.
Regarding other complications, Batllori et al.16 reportedan increased incidence of posterior venous wall punctures dur-ing the SA approach compared with the LA and OA approaches,which may have been caused by difficulty visualizing the lengthof the needle in the SA approach. Furthermore, in our includedtrials, no pneumothorax, hemothorax, or nerve injury occurredin any group. Overall, our results revealed that the SA, LA,and OA approach groups offered similar levels of safety. Our
521
ealth, Inc. All rights reserved.

Chen et al.J Trauma Acute Care Surg
Volume 86, Number 3
findings necessitate the execution of additional, larger studies tovalidate this observation.
Procedural difficulty and time required for insertion repre-sent other factors for consideration during scanning axis selec-tion. Blaivas et al.23 reported that novice ultrasound usersobtained vascular access faster using an SA approach than anLA approach on an inanimate model. Operators tended to ratethe SA approach as easier but the difference in mean difficultyscore was not statistically significant. By contrast, Shresthaet al.19 revealed comparable mean times required for insertionof guidewire between the SA and LA approaches, with no tech-nical difficulties encountered in either group. However, Batlloriet al.16 revealed that mean cannulation time was significantlygreater in the LA approach than in the SA and OA approaches.Moreover, the authors noted that operators encountered difficul-ties during the procedures, namely, advancing the guidewire inthe SA approach, identifying the needle in the LA approach,and piercing the vein wall in the OA approach. In conclusion,all three approaches have strengths and weaknesses; therefore,operators should choose an approach depending on their experi-ence and preference.
New ultrasound-guided IJVC techniques based on the SA,LA, and OA approaches have been proposed.1,18,24 In one of ourincluded trials, Ince et al.18 reported that an innovative “syringe-free” OA approach had a lower performance time, number ofneedle passes, and skin punctures in comparison with the SA ap-proach. In a syringe-free technique, the guidewire is placed intothe puncture needle and insertion is performed without blood as-piration.25 In another trial, Kamalipour et al.1 revealed that a new“medial-oblique” approach and the SA approach had the sameduration for different catheterization steps, total success rate,and primary mechanical complications. As opposed to the OAapproach where the needle's direction is from lateral to medial,in the “medial-oblique” approach the needle's direction is frommedial-cephalad to lateral-cauded. Thus, the IJVand carotid ar-tery can be seen beside each other, and the needle's shaft and tipdirection are observable in their entirety.9 Moreover, a crossoverrandomized controlled manikin trial by Takeshita et al.24 indi-cated that that a combined SA-LA approach considerably im-proved the success rate of IJV puncture performed by novicephysicians on a manikin model, without increasing proceduralduration in comparison with the SA approach. For the combinedSA-LA approach, the transducer was initially positioned in theSAview. After inserting the needle into the vein, the transducerchanged to the LAview and maintained visualization of the nee-dle tip. Although these new techniques appear efficient and safe,additional large-scale prospective randomized studies are re-quired to provide a definite recommendation.
The trials included in our meta-analysis exhibited consid-erable heterogeneity because of various clinical factors. First, thepatients in the included trials were under various conditions.Most of the trials included patients in a stable condition, butTammam et al.20 included patients in critical care or hemodialy-sis and did not exclude patient undergoing coagulopathy. Sec-ond, certain approaches regarding the same group differedamong the included trials. For example, the OA approach inthe included trials comprised the conventional OA,16 medialOA,1 and OAwith a syringe-free technique.18 Third, differencesin ultrasound instruments existed between the trials. Finally, as
522
Copyright © 2019 Wolters Kluwer H
described previously, the total success rate of outcome evalua-tion differed in some trials.16,18 Such differences explain the ob-served heterogeneity among the trials.
This study has several limitations. First, the patients in ourincluded trials were all adults. Thus, on the basis of our meta-analysis, we cannot deduce the outcomes of scanning axes inchildren. Second, experienced operators performed theultrasound-guided IJVC in the trials. Therefore, the data ob-tained may only be extrapolated to operators experienced inultrasound-guided IJVC. Finally, because of the nature of the re-search, blinding the operators to the scanning axis approach dur-ing the trials was impossible, which may have resulted in biasowing to deviations from the intended interventions.
In conclusion, three types of approach were comparable intotal success rate, first-pass success rate, and complications ofarterial puncture, hematoma, and CRBSI. Although the SA ap-proach could slightly improve the number of needle passes, nopotential benefit was observed in complication rates. None ofthe approaches indicated unique features that may enhance theirsuitability for application; hence, a scanning axis can be selectedafter considering the ease of procedure, patient characteristics,and clinician expertise.
AUTHORSHIP
C.-H.C. and K.-W.T. devised and designed the study. J.-Y.C., C.-H.C. andK.-W.T. extracted the data. J.-Y.C., L.-K.W., Y.-T.L., K.-M.L., C.-H.C., andK.-W.T. analyzed and interpreted the data. E.-W.L., C.-H.C., and K.-W.T.wrote the first draft. All authors contributed to subsequent versions andapproved the final article. C.-H.C. and K.-W.T. are the guarantors.
ACKNOWLEDGMENT
We acknowledge Wallace Academic Editing for editing this article.K.-W.T. and C.-H.C. contributed equally to this work.
DISCLOSURE
The authors have no conflicts of interest or financial ties to disclose.Funding: This workwas supported by a research grant fromChi Mei Med-ical Center and Taipei Medical University (grant: 106CM-TMU-14). Thesponsoring organization was not involved in the study design, data anal-ysis, or interpretation.
REFERENCES1. Kamalipour H, Shahbazi S, Derakhshan MM, Moinvaziri MT, Allahyari E.
Comparison of US-guided catheterization of the right internal jugular veinusing medial-oblique and short axis techniques. Int Cardiovasc Res J.2015;9(4):210–215.
2. MFS Filho LP, de Souza K, Palitot I, Magalhaes I, Vasconceloset H. Com-parison between ultrasound-guided and anatomic landmark puncture of theright internal jugular vein. J Cardiovasc Dis Diagn. 2013;1:128.
3. Troianos CA, Hartman GS, Glas KE, Skubas NJ, Eberhardt RT, Walker JD,Reeves ST. Councils on Intraoperative Echocardiography and Vascular Ul-trasound of the American Society of Echocardiography; Society of Cardio-vascular Anesthesiologists. Special articles: guidelines for performingultrasound guided vascular cannulation: recommendations of the AmericanSociety of Echocardiography and the Society of Cardiovascular Anesthesiol-ogists. Anesth Analg. 2012;114(1):46–72.
4. Lamperti M, Bodenham AR, Pittiruti M, Blaivas M, Augoustides JG,Elbarbary M, Pirotte T, Karakitsos D, Ledonne J, Doniger S, et al. Interna-tional evidence-based recommendations on ultrasound-guided vascular ac-cess. Intensive Care Med. 2012;38(7):1105–1117.
5. Feller-Kopman D. Ultrasound-guided internal jugular access: a proposedstandardized approach and implications for training and practice. Chest.2007;132(1):302–309.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Chen et al.
6. Karakitsos D, Labropoulos N, De Groot E, Patrianakos AP, Kouraklis G,Poularas J, Samonis G, Tsoutsos DA, Konstadoulakis MM, Karabinis A.Real-time ultrasound-guided catheterisation of the internal jugular vein: aprospective comparison with the landmark technique in critical care patients.Crit Care. 2006;10(6):R162.
7. Milling TJ Jr., Rose J, Briggs WM, Birkhahn R, Gaeta TJ, Bove JJ,Melniker LA. Randomized, controlled clinical trial of point-of-care limitedultrasonography assistance of central venous cannulation: the third Sonogra-phy outcomes assessment program (SOAP-3) trial. Crit Care Med. 2005;33(8):1764–1769.
8. Phelan M, Hagerty D. The oblique view: an alternative approach forultrasound-guided central line placement. J Emerg Med. 2009;37(4):403–408.
9. Dilisio R,Mittnacht AJ. The ‘medial-oblique’ approach to ultrasound-guidedcentral venous cannulation–maximize the view, minimize the risk.J Cardiothorac Vasc Anesth. 2012;26(6):982–984.
10. Ho AM, Ricci CJ, Ng CS, Critchley LA, Ho AK, Karmakar MK,Cheung CW, Ng SK. The medial-transverse approach for internal jugularvein cannulation: an example of lateral thinking. J Emerg Med. 2012;42(2):174–177.
11. French JL, Raine-Fenning NJ, Hardman JG, Bedforth NM. Pitfalls of ultra-sound guided vascular access: the use of three/four-dimensional ultrasound.Anaesthesia. 2008;63(8):806–813.
12. BlaivasM, Adhikari S. An unseen danger: frequency of posterior vessel wallpenetration by needles during attempts to place internal jugular vein centralcatheters using ultrasound guidance.Crit CareMed. 2009;37(8):2345–2349.
13. Chandler J, McKenzie J, Boutron I, Welch V (editors). Cochrane Methods.Cochrane Database Syst Rev. 2016, Issue 10 (Suppl 1).
14. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP,Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement forreporting systematic reviews and meta-analyses of studies that evaluatehealth care interventions: explanation and elaboration. J Clin Epidemiol.2009;62(10):e1–e34.
15. DerSimonian R, Laird N. Meta-analysis in clinical trials.Control Clin Trials.1986;7(3):177–188.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
16. Batllori M, Urra M, Uriarte E, Romero C, Pueyo J, López-Olaondo L,Cambra K, Ibáñez B. Randomized comparison of three transducer orienta-tion approaches for ultrasound guided internal jugular venous cannulation.Br J Anaesth. 2016;116(3):370–376.
17. Chittoodan S, Breen D, O'Donnell BD, Iohom G. Long versus short axis ul-trasound guided approach for internal jugular vein cannulation: a prospectiverandomised controlled trial. Med Ultrason. 2011;13(1):21–25.
18. Ince I, Arı MA, Sulak MM, Aksoy M. Comparison of transverse short-axisclassic and oblique long-axis “syringe-free” approaches for internal jugularvenous catheterization under ultrasound guidance. Rev Bras Anestesiol.2018;68(3):260–265.
19. Shrestha GS, Gurung A, Koirala S. Comparison between long- and short-axis techniques for ultrasound-guided cannulation of internal jugular vein.Ann Card Anaesth. 2016;19(2):288–292.
20. Tammam TF, El-Shafey EM, Tammam HF. Ultrasound-guided internal jug-ular vein access: comparison between short axis and long axis techniques.Saudi J Kidney Dis Transpl. 2013;24(4):707–713.
21. Vogel JA, Haukoos JS, Erickson CL, Liao MM, Theoret J, Sanz GE,Kendall J. Is long-axis view superior to short-axis view in ultrasound-guided central venous catheterization? Crit Care Med. 2015;43(4):832–839.
22. Center for Disease Control and Prevention DC. National Nosocomial Infec-tions Surveillance (NNIS) system report, data summary from January 1992–June 2001, issued August 2001. Am J Infect Control. 2001;29(6):404–421.
23. BlaivasM, BrannamL, Fernandez E. Short-axis versus long-axis approachesfor teaching ultrasound-guided vascular access on a new inanimate model.Acad Emerg Med. 2003;10(12):1307–1311.
24. Takeshita J, Nishiyama K, Beppu S, Sasahashi N, Shime N. Combined short-and long-axis ultrasound-guided central venous catheterization is superior toconventional techniques: a cross-over randomized controlled manikin trial.PLoS One. 2017;12(12): e0189258.
25. Matias F, Semedo E, Carreira C, Pereira P. Ultrasound-guided central venouscatheterization “syringe-free” approach. Rev Bras Anestesiol. 2017;67(3):314–317.
523
ealth, Inc. All rights reserved.
SYSTEMATIC REVIEW
The current status of clinical trials in emergency gastrointestinalsurgery: A systematic analysis of contemporary clinical trials
Amelia Milton, MPH, Thomas M. Drake, MBChB, and Matthew J. Lee, MBChB, Sheffield, UK
Sub
Fro
Ad
Sup
DO
52
BACKGROUND: E
mitted: September 4, 2018, Rev2018, Published online: Novemm the Medical School (A.M., MKingdom; Department of ClinRoyal Infirmary of Edinburgh,Sciences (T.M.D.), University oand Department of General SuFoundation Trust, Sheffield, Udress for reprints: Mr MatthewGeneral Hospital, Sheffield S5plemental digital content is avaithe printed text, and links to thearticle on the journal’s Web sit
I: 10.1097/TA.00000000000021
4
mergency gastrointestinal surgery (EGS) conditions represent a significant healthcare burden globally requiring emer-gency operations that are associated with mortality rates as high as 80%. EGS is currently focused on quality improvementand internal audits, which occurs at a national or local level. An appreciation ofwhat EGS trials are being conducted is important toreduce research wastage and develop coordinated research strategies in surgery. The primary aim of this study was to identify andquantify recent and active trials in EGS. The secondary aim was to identify conditions of interest and which aspects of care werebeing modified.
METHODS: A
systematic search of WHO, UK, US, Australian, and Canadian trials databases was undertaken using broad terms to identifystudies addressing emergency abdominal surgery and specific high-risk diagnoses. Studies registered between 2013 and 2018 wereeligible for inclusion. Data on study topic, design, and funding body were collected. Interventionswere classified into “perioperative”,“procedural”, “postoperative”, “non-surgical”, and “other” categories.RESULTS: S
earches identified 5603 registered trials. After removal of duplicates, 4492 studies remained and 42 were eligible for inclusion.Almost 50% of trials were located in Europe and 17% (n = 7) in the United States. The most common condition addressed wasacute appendicitis (n = 11), with the most common intervention being procedure based (n = 23). Hospital-based funding wasthe most common funder (n = 30).CONCLUSION: T
here is large disparity in the number of surgical trials in emergency surgery, which are primarily focused on high-volume conditions.More research is needed into high-mortality conditions. (J Trauma Acute Care Surg. 2019;86: 524–531. Copyright © 2018Wolters Kluwer Health, Inc. All rights reserved.)LEVEL OF EVIDENCE: S
ystematic review, level III. KEYWORDS: E mergency surgery; randomized trials; research methodology.E mergency general surgery (EGS) conditions represent a sig-nificant healthcare burden globally.1 Many of these condi-
tions require emergency operations, with associated mortalityrates ranging from 1.1% at 24 hours to 8.6% at 30 days. Evenin high-income countries such as the UK where high-risk emer-gency surgical procedures account for 12.5% of total operations,death rates are as high as 80%.1,2 In addition, routine proceduresin emergency surgery such as small bowel resection are associ-ated with high morbidity rates, which has further implicationsfor patient recovery and healthcare costs.1–3
EGS activity is currently focused on quality improvementand audits at a local or national level. These include the NationalEmergency Laparotomy Audit in the UK and the National Sur-gical Quality Improvement Partnership in the United States.2,4
Quality improvement relies on a high-quality evidence base to
ised: September 21, 2018, Accepted: October 23,ber 5, 2018..J.L.), University of Sheffield, Sheffield, Unitedical Surgery (T.M.D.), University of Edinburgh,Edinburgh, United Kingdom; Institute for Cancerf Glasgow, Bearsden, Glasgow, United Kingdom;rgery (M.J.L.), Sheffield Teaching Hospitals NHSnited Kingdom.Lee, Department of General Surgery, Northern7AU, UK; email: [email protected] for this article. Direct URL citations appear indigital files are provided in the HTML text of thise (www.jtrauma.com).
23
Copyright © 2019 Wolters Kluwer H
guide efforts that are primarily designed to improve patient out-comes. It is recognized that EGS lacks a high-quality evidencebase,5 which may account for why many aspects of surgicalpractice are based upon dogma.6
To generate high-quality evidence to improve patient out-comes, it is necessary to conduct randomized clinical trials. Theconduct of a clinical trial can take many years as funding andgovernance approvals must be secured, along with delivery of thestudy and analysis of findings. This means that there can be asignificant period between the registration of a trial and the pub-lication of findings. Knowing which trials are in progress is im-portant to reduce research wastage and develop coordinatedresearch strategies in surgery. It is considered standard practicefor clinical trials to be registered on a database. This helps to pre-vent duplication and may also protect against publication bias.
The primary aim of this study was to identify and quantifyrecent and active trials in EGS. The secondary aim was to cate-gorize research according to geographic base, funding body,condition of interest, and intervention being trialed to grasp abetter idea of what evidence-based research in emergency sur-gery is currently being undertaken.
METHODS
This study was conducted with reference to the Cochranehandbook and is reported in line with the applicable fields of thePreferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.7,8
J Trauma Acute Care SurgVolume 86, Number 3
ealth, Inc. All rights reserved.
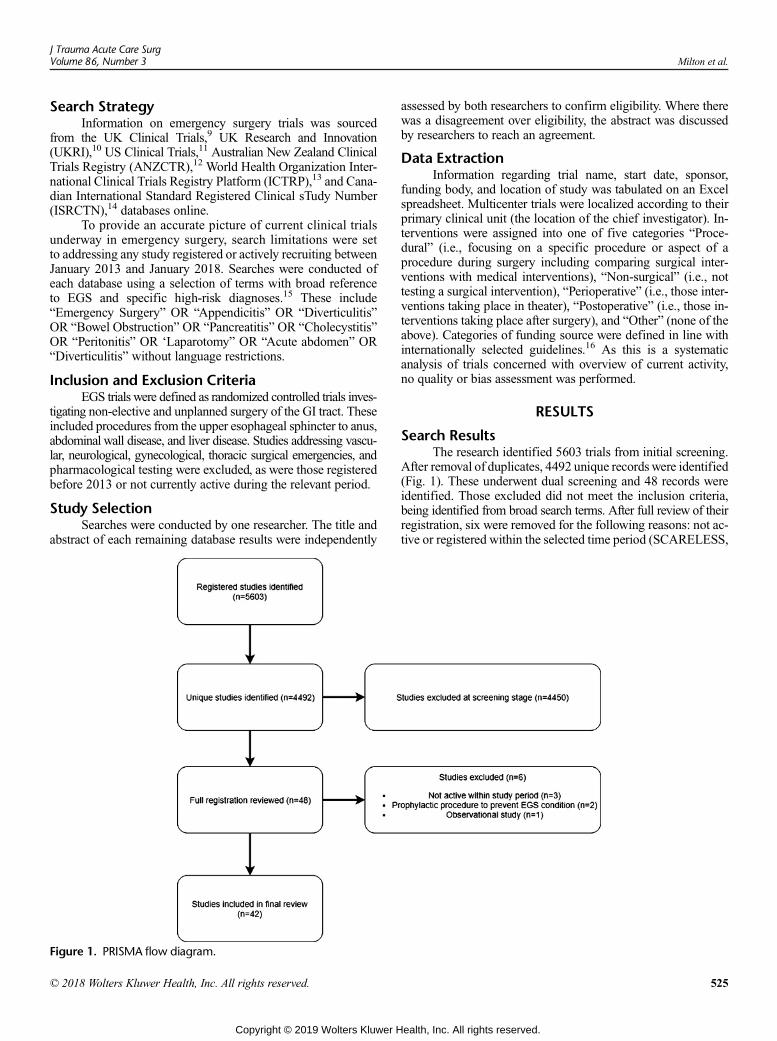
J Trauma Acute Care SurgVolume 86, Number 3 Milton et al.
Search StrategyInformation on emergency surgery trials was sourced
from the UK Clinical Trials,9 UK Research and Innovation(UKRI),10 US Clinical Trials,11 Australian New Zealand ClinicalTrials Registry (ANZCTR),12 World Health Organization Inter-national Clinical Trials Registry Platform (ICTRP),13 and Cana-dian International Standard Registered Clinical sTudy Number(ISRCTN),14 databases online.
To provide an accurate picture of current clinical trialsunderway in emergency surgery, search limitations were setto addressing any study registered or actively recruiting betweenJanuary 2013 and January 2018. Searches were conducted ofeach database using a selection of terms with broad referenceto EGS and specific high-risk diagnoses.15 These include“Emergency Surgery” OR “Appendicitis” OR “Diverticulitis”OR “Bowel Obstruction” OR “Pancreatitis” OR “Cholecystitis”OR “Peritonitis” OR ‘Laparotomy” OR “Acute abdomen” OR“Diverticulitis” without language restrictions.
Inclusion and Exclusion CriteriaEGS trials were defined as randomized controlled trials inves-
tigating non-elective and unplanned surgery of the GI tract. Theseincluded procedures from the upper esophageal sphincter to anus,abdominal wall disease, and liver disease. Studies addressing vascu-lar, neurological, gynecological, thoracic surgical emergencies, andpharmacological testing were excluded, as were those registeredbefore 2013 or not currently active during the relevant period.
Study SelectionSearches were conducted by one researcher. The title and
abstract of each remaining database results were independently
Figure 1. PRISMA flow diagram.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
assessed by both researchers to confirm eligibility. Where therewas a disagreement over eligibility, the abstract was discussedby researchers to reach an agreement.
Data ExtractionInformation regarding trial name, start date, sponsor,
funding body, and location of study was tabulated on an Excelspreadsheet. Multicenter trials were localized according to theirprimary clinical unit (the location of the chief investigator). In-terventions were assigned into one of five categories “Proce-dural” (i.e., focusing on a specific procedure or aspect of aprocedure during surgery including comparing surgical inter-ventions with medical interventions), “Non-surgical” (i.e., nottesting a surgical intervention), “Perioperative” (i.e., those inter-ventions taking place in theater), “Postoperative” (i.e., those in-terventions taking place after surgery), and “Other” (none of theabove). Categories of funding source were defined in line withinternationally selected guidelines.16 As this is a systematicanalysis of trials concerned with overview of current activity,no quality or bias assessment was performed.
RESULTS
Search ResultsThe research identified 5603 trials from initial screening.
After removal of duplicates, 4492 unique records were identified(Fig. 1). These underwent dual screening and 48 records wereidentified. Those excluded did not meet the inclusion criteria,being identified from broad search terms. After full review of theirregistration, six were removed for the following reasons: not ac-tive or registered within the selected time period (SCARELESS,
525
ealth, Inc. All rights reserved.

Milton et al.J Trauma Acute Care Surg
Volume 86, Number 3
CReST, and LEONARDO; n = 3); observational study (STELLA;n = 1); preventative or diagnostic procedure (prophylaxis of post-ERCP pancreatitis using temporary pancreatic stent vs. rectal non-steroidal anti-inflammatory drug and the use of different-sizedUS-guided needles in the diagnosis of acute appendicitis; n = 2).
In total, 42 trials were identified. Fourteen were identifiedfrom ICTRP, 11 from the US clinical trials database, 10 fromUKclinical trials, three from the ANZCTR and ISRCTN, respec-tively, and one from UKRI (see Table, Supplemental DigitalContent 1, http://links.lww.com/TA/B231). These addressed emer-gency surgery (n = 9), cholecystitis (n = 6), pancreatitis (n = 3), lap-arotomy (n = 5), appendicitis (n = 11), bowel obstruction (n = 2),acute abdomen (n = 1), and diverticulitis (n = 5). A summary listof trials identified is presented in Table 1.
Timing and Type of InterventionOver 50% (n = 23) studies were found to be investigating
a procedure within the operating theater, for example, using dif-ferent techniques or different equipment. Nine studies investi-gated non-surgical management, such as using antibiotics totreat appendicitis followed by a delayed appendicectomy or theuse of gastrografin for bowel obstruction. Six studies were focusedon addressing perioperative factors, for example, the use of IVfluids during operating to improve outcomes or the insertionof rectus sheath blocks at the end of surgery to improve postop-erative pain intensity. Three of the studies were focused on post-operative outcomes mainly looking at physiotherapy and qualityimprovement in postoperative care. Two studies were classifiedas “other” focusing on the use of telemedicine in the remote man-agement of damage control surgery and the use of a smartphonein assessing surgical site infections. Graphical representationof intervention categories is highlighted in Figure 2.
Funding SourceHospital-based funding was the most common funding
category accounting for 30 trials. The category named affiliatedmedical research bodies was the second most common fundingcategory with eight trials. These included the NIHR (NationalInstitute of Health Research), the UK MRC (Medical ResearchCouncil), Canadian ForcesMedical Services, Hungarian PancreaticStudy Group, and Southwest Oncology Group. Private sponsors(n = 3) are individually named sponsors. Commercially basedsponsors included Bupa, a private health insurance company.
Emergency SurgeryNine studies addressed emergency surgery in general.
Three of these trials focused on EGS procedures, such as laparo-scopic versus open surgery (LaCeS), using nanotechnologies asa fixing method for prosthetic materials in emergency laparo-scopic procedures, and the role of endoluminal stenting in theacute management of obstructing colorectal cancer. Two trialswere categorized as perioperative management, investigating fluidoptimization in emergency laparotomy (FLO-ELA) and compar-ing direct and guidewire-assisted techniques to artery cannulationin patients posted for emergency surgery and the association be-tween oxygen saturations and postoperative cognitive dysfunc-tion in the elderly undergoing EGS. The single postoperative trialinvestigated the outcomes of enhanced rehabilitation in patientsafter EGS. One trial was categorized as “other” investigating
526
Copyright © 2019 Wolters Kluwer H
whether the use of a smartphone tool aided the earlier identifica-tion and management of surgical site infections in EGS patients.Four of the studies were carried out in the UK, one in China, France,India, Italy, and Tasmania, respectively. Five studies received hospitalfunding; three were funded by affiliated medical research bodies.The remaining study was privately funded.
LaparotomyFive studies investigating laparotomy were identified.
Two studies were categorized as procedural, investigating theoutcomes of damage control surgery and comparing endoscopi-cally assisted colostomy with colopexy to laparotomy (EACC).Two other trials were categorized as “perioperative”; one wasbased in the UK looking at interventions for quality improve-ment for patients undergoing emergency laparotomy (EPOCH)and the other was based in Dubai investigating the post-surgicaluse of rectal sheath blocks for pain management. One trial ad-dressing laparotomy was categorized as “other”, investigatingthe use of telemedicine to mentor surgeons in damage controlsurgery for critically injured trauma patients from afar. This trialtook place in Canada and was funded by the Canadian ArmedForces. One trial (EPOCH) was funded by the NIHR, two trialsreceived hospital-based funding, and one trial was privatelyfunded in Dubai.
AppendicitisEleven trials addressing acute appendicitis were identified.
Six trials were categorized as “non-surgical” and investigated theoutcomes of antibiotics for the treatment of appendicitis whencompared with surgery. Notably, four of these trials (CONTRACT,APPY, COMMA, and CHINA) were focused exclusively on pe-diatric populations. Four trials investigated procedural tech-niques for appendicectomy. This included the use of polymerclips versus endoloops (PECAS), clips versus staples, the useof single versus multiple ports, and an interval appendicectomypost-antibiotic therapy for acute appendicitis (CHINA). Four(36%) of the trials originated from the United States, three inthe UK, one in Taiwan, and the remaining three in Europe (seeFigure, Supplemental Digital Content 2, http://links.lww.com/TA/B232). The majority (n = 8) of trials identified from thesearch term appendicitis received hospital-based funding.
CholecystitisSix EGS trials addressed cholecystitis, five (83%) of which
focused on EGS procedures, including intra-operative ERCP ver-sus laparoscopic bile duct exploration for bile duct clearance inpatients undergoing emergency cholecystitis, immediate versusdelayed laparoscopic cholecystectomy in two trials, laparoscopicversus conservative treatment in acute cholecystitis, and intra-gallbladder or systemic Indocyanine green injection to facilitatecholecystectomy in patients with acute cholecystitis. One studyinvestigated the use of extended antibiotic therapy postopera-tively in reducing infections. Five (83%) of the studies were hospitalfunded, and one was privately funded. All six of the trials werecarried out in different countries including Australia, Argentina,Finland, Japan, Taiwan, and Saudi Arabia.
Bowel ObstructionTwo studies addressing bowel obstruction were identified.
The first study investigated the non-surgical use of water-soluble
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
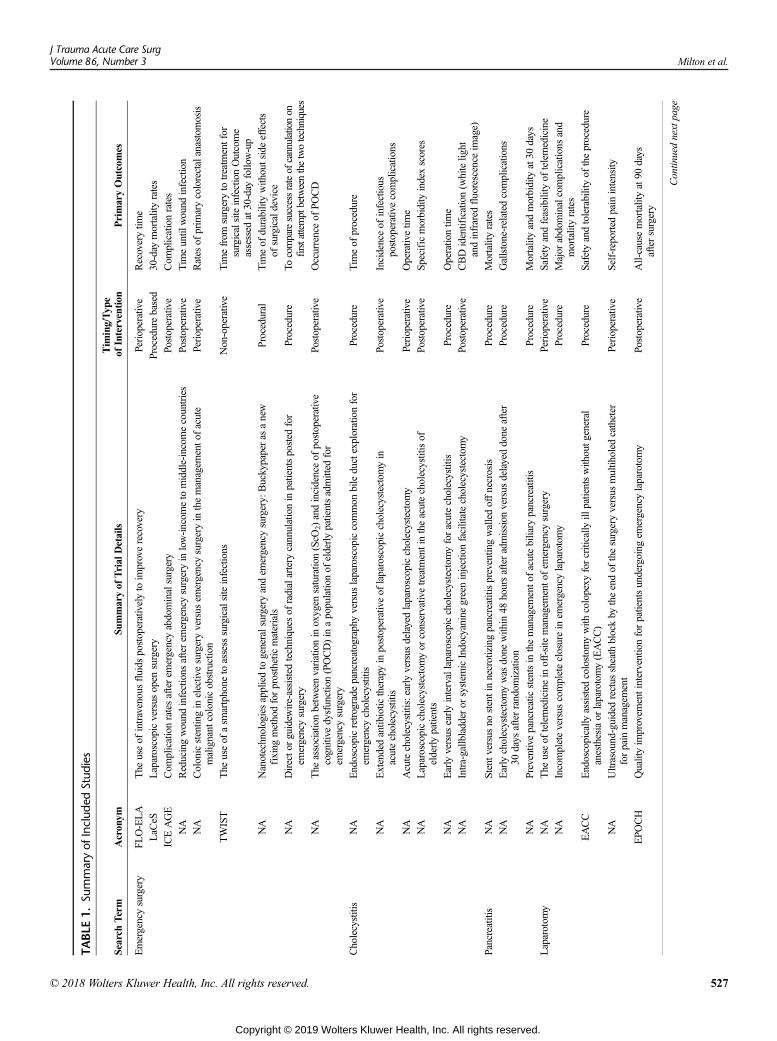
TABLE
1.Su
mmaryof
Includ
edStud
ies
Search
Term
Acronym
Summaryof
Trial
Details
Tim
ing/Typ
eof
Intervention
PrimaryOutcomes
Emergencysurgery
FLO-ELA
The
useof
intravenousfluids
postoperativelyto
improverecovery
Perioperative
Recoverytim
e
LaC
eSLaparoscopicversus
open
surgery
Procedurebased
30-day
mortalityrates
ICEAGE
Com
plicationratesafterem
ergencyabdominalsurgery
Postoperative
Com
plicationrates
NA
Reducingwound
infections
afterem
ergencysurgeryin
low-incom
eto
middle-incomecountries
Postoperative
Tim
euntil
wound
infection
NA
Colonicstentingin
electivesurgeryversus
emergencysurgeryin
themanagem
ento
facute
malignant
colonicobstruction
Perioperative
Rates
ofprim
arycolorectalanastomosis
TWIST
The
useof
asm
artphone
toassess
surgicalsiteinfections
Non-operative
Tim
efrom
surgeryto
treatm
entfor
surgicalsiteinfectionOutcome
assessed
at30-day
follow-up
NA
Nanotechnologiesappliedtogeneralsurgery
andem
ergencysurgery:
Buckypaperas
anew
fixing
methodforprostheticmaterials
Procedural
Tim
eof
durabilitywithoutsideeffects
ofsurgicaldevice
NA
Directo
rguidew
ire-assisted
techniques
ofradialartery
cannulationin
patientsposted
for
emergencysurgery
Procedure
Tocomparesuccessrateof
cannulationon
firstattemptbetweenthetwotechniques
NA
The
associationbetweenvariationin
oxygen
saturatio
n(ScO
2)andincidenceof
postoperative
cognitive
dysfunction(POCD)in
apopulatio
nof
elderlypatientsadmitted
for
emergencysurgery
Postoperative
Occurrenceof
POCD
Cholecystitis
NA
Endoscopicretrograde
pancreatographyversus
laparoscopiccommon
bileductexplorationfor
emergencycholecystitis
Procedure
Tim
eof
procedure
NA
Extendedantib
iotic
therapyin
postoperativeof
laparoscopiccholecystectom
yin
acutecholecystitis
Postoperative
Incidenceof
infectious
postoperativecomplications
NA
Acutecholecystitis:earlyversus
delayedlaparoscopiccholecystectom
yPerioperative
Operativetim
e
NA
Laparoscopiccholecystectom
yor
conservativetreatm
entintheacutecholecystitisof
elderlypatients
Postoperative
Specificmorbidity
indexscores
NA
Earlyversus
earlyintervallaparoscopiccholecystectom
yforacutecholecystitis
Procedure
Operatio
ntim
e
NA
Intra-gallbladderor
system
icIndocyaninegreeninjectionfacilitatecholecystectom
yPostoperative
CBDidentification(w
hitelig
htandinfrared
fluorescence
image)
Pancreatitis
NA
Stentv
ersusno
stentinnecrotizingpancreatitispreventin
gwalledoffnecrosis
Procedure
Mortalityrates
NA
Earlycholecystectom
ywas
done
with
in48
hoursafteradmission
versus
delayeddone
after
30days
afterrandom
ization
Procedure
Gallstone-related
complications
NA
Preventivepancreaticstentsin
themanagem
ento
facutebiliary
pancreatitis
Procedure
Mortalityandmorbidity
at30
days
Laparotom
yNA
The
useof
telemedicinein
off-sitemanagem
ento
fem
ergencysurgery
Perioperative
Safety
andfeasibility
oftelemedicine
NA
Incompleteversus
completeclosurein
emergencylaparotomy
Procedure
Major
abdominalcomplications
and
mortalityrates
EACC
Endoscopically
assisted
colostom
ywith
colopexy
forcritically
illpatientswithoutg
eneral
anesthesiaor
laparotomy(EACC)
Procedure
Safety
andtolerabilityof
theprocedure
NA
Ultrasound-guidedrectus
sheath
blockby
theendof
thesurgeryversus
multiholed
catheter
forpain
managem
ent
Perioperative
Self-reportedpain
intensity
EPO
CH
Qualityim
provem
entinterventionforpatientsundergoing
emergencylaparotomy
Postoperative
All-causemortalityat90
days
aftersurgery
Continuednextpage
J Trauma Acute Care SurgVolume 86, Number 3 Milton et al.
© 2018 Wolters Kluwer Health, Inc. All rights reserved. 52
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
7
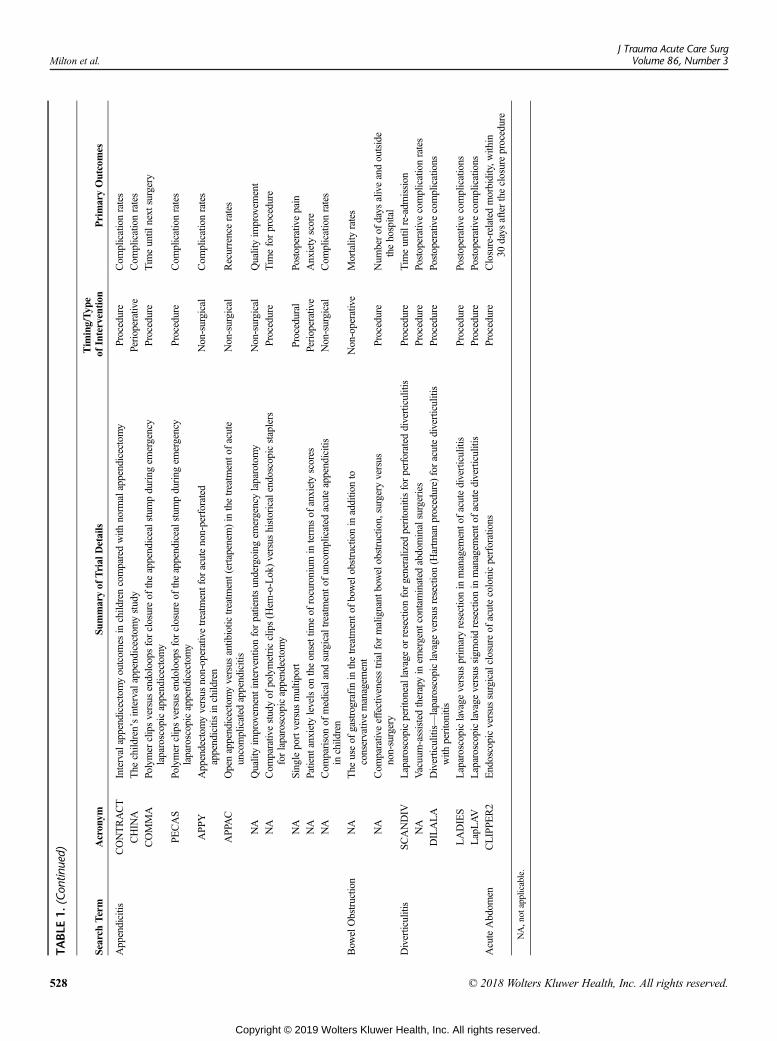
TABLE
1.(Con
tinued)
Search
Term
Acronym
Summaryof
Trial
Details
Tim
ing/Typ
eof
Intervention
PrimaryOutcomes
Appendicitis
CONTRACT
Intervalappendicectomyoutcom
esin
childrencomparedwith
norm
alappendicectomy
Procedure
Com
plicationrates
CHINA
The
child
ren’sintervalappendicectomystudy
Perioperative
Com
plicationrates
COMMA
Polymer
clipsversus
endoloopsforclosureof
theappendicealstumpduring
emergency
laparoscopicappendicectomy
Procedure
Tim
euntil
next
surgery
PECAS
Polymer
clipsversus
endoloopsforclosureof
theappendicealstumpduring
emergency
laparoscopicappendicectomy
Procedure
Com
plicationrates
APP
YAppendectom
yversus
non-operativetreatm
entfor
acutenon-perforated
appendicitisin
child
ren
Non-surgical
Com
plicationrates
APPAC
Openappendicectomyversus
antibiotic
treatm
ent(ertapenem)in
thetreatm
ento
facute
uncomplicated
appendicitis
Non-surgical
Recurrencerates
NA
Qualityim
provem
entinterventionforpatientsundergoing
emergencylaparotomy
Non-surgical
Qualityim
provem
ent
NA
Com
parativestudyof
polymetricclips(H
em-o-Lok)versus
historicalendoscopicstaplers
forlaparoscopicappendectomy
Procedure
Tim
eforprocedure
NA
Singleportversus
multiport
Procedural
Postoperativepain
NA
Patient
anxietylevelson
theonsettim
eof
rocuronium
interm
sof
anxietyscores
Perioperative
Anxiety
score
NA
Com
parisonof
medicalandsurgicaltreatm
ento
funcomplicated
acuteappendicitis
inchild
ren
Non-surgical
Com
plicationrates
Bow
elObstruction
NA
The
useof
gastrografin
inthetreatm
ento
fbowelobstructionin
additionto
conservativemanagem
ent
Non-operative
Mortalityrates
NA
Com
parativeeffectivenesstrialfor
malignant
bowelobstruction,surgeryversus
non-surgery
Procedure
Num
berof
days
aliveandoutside
thehospital
Diverticulitis
SCANDIV
Laparoscopicperitoneallavage
orresectionforgeneralized
peritonitis
forperforated
diverticulitis
Procedure
Tim
euntil
re-adm
ission
NA
Vacuum-assistedtherapyin
emergent
contam
inated
abdominalsurgeries
Procedure
Postoperativecomplicationrates
DILALA
Diverticulitis—
laparoscopiclavage
versus
resection(H
artm
anprocedure)
foracutediverticulitis
with
peritonitis
Procedure
Postoperativecomplications
LADIES
Laparoscopiclavage
versus
prim
aryresectionin
managem
ento
facutediverticulitis
Procedure
Postoperativecomplications
LapLAV
Laparoscopiclavage
versus
sigm
oidresectionin
managem
ento
facutediverticulitis
Procedure
Postoperativecomplications
AcuteAbdom
enCLIPPE
R2
Endoscopicversus
surgicalclosureof
acutecolonicperforations
Procedure
Closure-related
morbidity,w
ithin
30days
aftertheclosureprocedure
NA,not
applicable.
Milton et al.J Trauma Acute Care Surg
Volume 86, Number 3
528 © 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
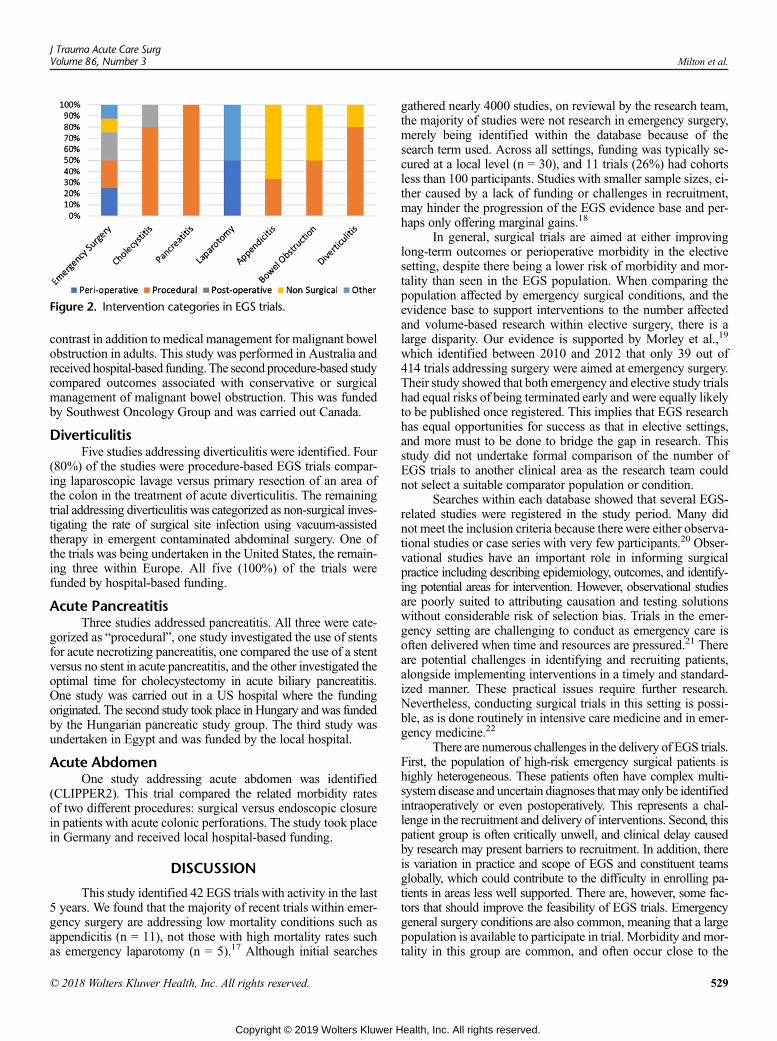
Figure 2. Intervention categories in EGS trials.
J Trauma Acute Care SurgVolume 86, Number 3 Milton et al.
contrast in addition to medical management for malignant bowelobstruction in adults. This study was performed in Australia andreceived hospital-based funding. The second procedure-based studycompared outcomes associated with conservative or surgicalmanagement of malignant bowel obstruction. This was fundedby Southwest Oncology Group and was carried out Canada.
DiverticulitisFive studies addressing diverticulitis were identified. Four
(80%) of the studies were procedure-based EGS trials compar-ing laparoscopic lavage versus primary resection of an area ofthe colon in the treatment of acute diverticulitis. The remainingtrial addressing diverticulitis was categorized as non-surgical inves-tigating the rate of surgical site infection using vacuum-assistedtherapy in emergent contaminated abdominal surgery. One ofthe trials was being undertaken in the United States, the remain-ing three within Europe. All five (100%) of the trials werefunded by hospital-based funding.
Acute PancreatitisThree studies addressed pancreatitis. All three were cate-
gorized as “procedural”, one study investigated the use of stentsfor acute necrotizing pancreatitis, one compared the use of a stentversus no stent in acute pancreatitis, and the other investigated theoptimal time for cholecystectomy in acute biliary pancreatitis.One study was carried out in a US hospital where the fundingoriginated. The second study took place in Hungary and was fundedby the Hungarian pancreatic study group. The third study wasundertaken in Egypt and was funded by the local hospital.
Acute AbdomenOne study addressing acute abdomen was identified
(CLIPPER2). This trial compared the related morbidity ratesof two different procedures: surgical versus endoscopic closurein patients with acute colonic perforations. The study took placein Germany and received local hospital-based funding.
DISCUSSION
This study identified 42 EGS trials with activity in the last5 years. We found that the majority of recent trials within emer-gency surgery are addressing low mortality conditions such asappendicitis (n = 11), not those with high mortality rates suchas emergency laparotomy (n = 5).17 Although initial searches
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
gathered nearly 4000 studies, on reviewal by the research team,the majority of studies were not research in emergency surgery,merely being identified within the database because of thesearch term used. Across all settings, funding was typically se-cured at a local level (n = 30), and 11 trials (26%) had cohortsless than 100 participants. Studies with smaller sample sizes, ei-ther caused by a lack of funding or challenges in recruitment,may hinder the progression of the EGS evidence base and per-haps only offering marginal gains.18
In general, surgical trials are aimed at either improvinglong-term outcomes or perioperative morbidity in the electivesetting, despite there being a lower risk of morbidity and mor-tality than seen in the EGS population. When comparing thepopulation affected by emergency surgical conditions, and theevidence base to support interventions to the number affectedand volume-based research within elective surgery, there is alarge disparity. Our evidence is supported by Morley et al.,19
which identified between 2010 and 2012 that only 39 out of414 trials addressing surgery were aimed at emergency surgery.Their study showed that both emergency and elective study trialshad equal risks of being terminated early and were equally likelyto be published once registered. This implies that EGS researchhas equal opportunities for success as that in elective settings,and more must to be done to bridge the gap in research. Thisstudy did not undertake formal comparison of the number ofEGS trials to another clinical area as the research team couldnot select a suitable comparator population or condition.
Searches within each database showed that several EGS-related studies were registered in the study period. Many didnot meet the inclusion criteria because there were either observa-tional studies or case series with very few participants.20 Obser-vational studies have an important role in informing surgicalpractice including describing epidemiology, outcomes, and identify-ing potential areas for intervention. However, observational studiesare poorly suited to attributing causation and testing solutionswithout considerable risk of selection bias. Trials in the emer-gency setting are challenging to conduct as emergency care isoften delivered when time and resources are pressured.21 Thereare potential challenges in identifying and recruiting patients,alongside implementing interventions in a timely and standard-ized manner. These practical issues require further research.Nevertheless, conducting surgical trials in this setting is possi-ble, as is done routinely in intensive care medicine and in emer-gency medicine.22
There are numerous challenges in the delivery of EGS trials.First, the population of high-risk emergency surgical patients ishighly heterogeneous. These patients often have complex multi-system disease and uncertain diagnoses that may only be identifiedintraoperatively or even postoperatively. This represents a chal-lenge in the recruitment and delivery of interventions. Second, thispatient group is often critically unwell, and clinical delay causedby research may present barriers to recruitment. In addition, thereis variation in practice and scope of EGS and constituent teamsglobally, which could contribute to the difficulty in enrolling pa-tients in areas less well supported. There are, however, some fac-tors that should improve the feasibility of EGS trials. Emergencygeneral surgery conditions are also common, meaning that a largepopulation is available to participate in trial. Morbidity and mor-tality in this group are common, and often occur close to the
529
ealth, Inc. All rights reserved.

Milton et al.J Trauma Acute Care Surg
Volume 86, Number 3
index event of surgery,23 potentially meaning shorter-term follow-ups are necessary to assess outcomes.
Our study identified very few EGS trials outside of high-income settings with clinically significant sample sizes. Popula-tions in low-income and middle-income settings have a higherrequirement for emergency surgical services and poorer out-comes than high-income populations.24 However, in our study,the studies we identified within low-income to middle-incomecountries had very few participants. Four out of the nine studiesidentified with fewer than 100 participants were carried out inlow-income to middle-income countries (EACC, single-incisionlaparoscopic surgery in acute abdomen, acute biliary pancreatitis—optimal time for cholecystectomy, and the onset time ofrocuronium in emergency and elective surgery). These settingspresent unique challenges and may be where the greatest gainsin outcome may be. Identifying interventions that are effectivein improving outcomes from emergency surgery across the worldwould enable a far larger population to benefit. There are multiplereasons why surgical trials may not have been identified in thesesettings. First, these countries may not have requirements to reg-ister clinical trials prospectively and hence would not have beenidentified by our searches. This is unlikely as we searched mul-tiple international databases and the requirement for prospectiveregistration is common. Secondly, resource and ethical limitationsmay play a role. Clinicians in these settings are more stretched,dedicatingmost of their time to service provision and leaving verylimited time for participant recruitment or data collection. More-over, they may lack the necessary resources to undertake re-search. International initiatives are aiming to change this, withcapacity-building networks being formed in surgery, such asthe GlobalSurg collaborative,25 who have just launched a facto-rial randomized trial investigating skin preparation.
This study is not without limitations. Although it is ex-pected that all trials are registered after the legislation imple-mented by the International Committee of Medical JournalEditors in 2005,26 it is possible that some may not be identifiedthrough the searches. We did not search for resulting publica-tions and were unable to account for unpublished research, norresearch that remains within the hospital or country where itwas carried out, meaning it is available globally. This could beresolved by streamlining the regulation process, making all stud-ies from the various databases available on one global databasewith unlimited international access. This would also make itsimpler for authors to both recruit and register trials globally.However, a recent study suggests that 46% of EGS trials arepublished.19 We recognize that the findings of our study mayage if significant changes are made to encourage future emer-gency surgery research; however, it will provide a useful bench-mark progress in this field. The strengths of this study includeadherence to methodological principles, dual review of candi-date studies, and interrogation of multiple databases using mul-tiple search terms, meaning the majority of candidate studiesshould have been identified. This allows a robust estimate of in-ternational trial activity in EGS.
For elective surgery, time for preoperative optimizationand careful planning provide a controlled environment to un-dertake research aimed at improving surgical and perioperativeoutcomes. This is not a luxury afforded to research in the emer-gency setting. Nevertheless, this study highlights that there is a
530
Copyright © 2019 Wolters Kluwer H
large disparity in the number of randomized trials in elective ver-sus emergency surgery that are currently being performed. It isimperative that this gap is addressed to improve both the quan-tity and quality of the literature in this field, which is key forimproving EGS outcomes. Future studies should focus onhigh-risk groups (i.e., emergency laparotomy), in addition tohigh-volume groups (i.e., appendicitis) for maximal benefit.Researcher teams should include the wider surgical team, anes-thetists, intensivists, emergency physicians, and methodologists.Teams should work to optimize trial designs to answer importantresearch questions robustly, while adequately addressing thecomplex challenges to research in the emergency setting.27
One way to improve outcomes in emergency surgeries isby making funding more accessible. It was notable in this reviewthat many of the studies were supported by local hospital funds,rather than national-level funders such as the NIHR in the UKor the National Institute for Health in the use. These strategicfunding bodies could consider commissioned calls for EGS pro-jects and incentivization of units to deliver emergency surgeryresearch. This may help to increase the number of trials thatare addressing high-morbidity conditions such as laparotomyand bowel obstruction.
There is large disparity in the number of surgical trials inemergency surgery, which are primarily focused on high-volumeconditions.More research is needed into high-mortality conditions.Future efforts should focus on improving both the quantity andquality of research in these patients and ensuring findings aregeneralizable for patients across the world.
AUTHORSHIP
All authors were involved in the conception, design, analysis, articledrafting, and critical revision of this work. All authors meet the ICMJEcriteria for authorship.
ACKNOWLEDGMENTS
None.
DISCLOSURE
Declarations: Ethics: This study did not use patient data and therefore noethical approval was required.Consent for publication: This study did not use patient data and thereforedid not require any consent from patients for publication.Availability of data andmaterial: Data are available on request to investiga-tors and is presented in Table 1.Competing interests: No competing interests.Funding: This study is unfunded.Authors’ contributions: All authors contributed equally to all aspects of thework. M.J.L. is the study guarantor.
REFERENCES1. GlobalSurg Collaborative. Mortality of emergency abdominal surgery in
high-, middle- and low-income countries. Br J Surg. 2016;103(8):632–632.2. NELA Project Team. The third Patient Report of the National Emergency
Laparotomy Audit (NELA). 2017.3. Scott J, Olubode O, Gabriel B. Use of national burden to define operative
emergency general surgery. JAMA Surg. 2016;151(6):e160480.4. American College of Surgeons. ACS National Surgical Quality Improve-
ment Program. ACS. 2017.5. EMSurg Collaborators. Methodological overview of systematic reviews to
establish the evidence base for emergency general surgery. Br J Surg.2017;104(5):513–524.
6. Jenkins T. It’s time to challenge surgical dogma with evidence-based data.Am J Obstet Gynecol. 2003;189(2):423–427.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Milton et al.
7. Moher D, Liberati A, Tetzlaff J, Liberati A, Tetzlaff J, Altman D. PreferredReporting Items for Systematic Reviews and Meta-Analyses: The PRISMAStatement. PLoS Med. 2009;6(7).
8. The Cochrane Collaboration. Part 2: general methods for Cochrane reviews.In: Higgins J, Green S, editors. Cochrane Handbook for Systematic Reviewsof Interventions. Version 5.1. 2011.
9. UKCTG. UK Clinical trials Gateway [Internet]. Date last accessed: 01/08/2018. Available from: https://www.ukctg.nihr.ac.uk/.
10. UKRI Gateway. UK Research and Innovation.11. NIH. Clinical Trials.gov [Internet]. Date last accessed: 01/08/2018. Available
from: https://clinicaltrials.gov/.12. ANZCTR. Australian New Zealand Clinical Trials Registry.13. WHO. WHO International Clinical Trials Registry Platform.14. ISRCTN. Canadian International Standard Registered Clinical sTudy Num-
ber Registry [Internet]. Date last accessed: 01/08/2018. Available from:http://www.isrctn.com/.
15. Symons N, Moorthy K, Almoudaris AM, Bottle A, Aylin P, Vincent CA,Faiz OD. Mortality in high-risk emergency general surgical admissions. BrJ Surg. 2013;100(10):1318–1325.
16. Ravinetto R, Nys K, Boelaert M, Diro E, Meintjes G, Adoke Y, Tagbor H,Casteels M. Sponsorship in non-commercial clinical trials: definitions, chal-lenges and the role of Good Clinical Practice guidelines. BioMed Cent IntHeal Hum Rights. 2015;15(34).
17. Boney O, Bell M, Conquest A, Cumbers M, Drake S, GalsworthyM, Gath J,Grocott MPW, Harris E, Howell S, et al. Identifying research priorities in an-aesthesia and perioperative care: final report of the joint National Institute ofAcademic Anaesthesia/James Lind Alliance Research Priority Setting Part-nership. BMJ Open. 2015;5(12).
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
18. Sakpal T. Sample size estimation in clinical trial. Perspect Clin Res. 2010;1(2):67–69.
19. MorleyRL, EdmondsonMJ,RowlandsC,Blazeby JM,HinchliffeRJ. Registrationand publication of emergency and elective randomised controlled trials insurgery: a cohort study from trial registries. BMJ Open. 2018;8(7):e021700.
20. Horton R. Surgical research or comic opera: questions, but few answers.Lancet. 1996;13(347):984–985.
21. Good A, Driscoll P. Clinical research in emergency medicine: putting it to-gether. BMJ Open. 19(3):242–246.
22. Patterson T, Perkins A, Perkins GD, Clayton T, Evans R, Nguyen H,Wilson K,Whitbread M, Hughes J, Fothergill RT, et al. Rationale and designof: A Randomized tRial of Expedited transfer to a cardiac arrest center fornon-ST elevation out-of-hospital cardiac arrest: the ARREST randomizedcontrolled trial. Am Heart J. 2018;6(204):92–101.
23. Tengberg LT, Cihoric M, Foss NB, Bay-NielsenM, Gögenur I, Henriksen R,Jensen TK, Tolstrup MB, Nielsen LB. Complications after emergency lapa-rotomy beyond the immediate postoperative period—a retrospective, obser-vational cohort study of 1139 patients. Anaesthesia. 2017;72(3):309–316.
24. Meara JG, Leather AJ, Hagander L, Alkire BC, Alonso N, Ameh EA,Bickler SW, Conteh L, Dare AJ, Davies J, et al. Global Surgery 2030: evi-dence and solutions for achieving health, welfare, and economic develop-ment. Lancet Comm. 2015;386(9993):569–624.
25. GlobalSurg Collaborative. Surgical site infection after gastrointestinal sur-gery in high-income, middle-income, and low-income countries: a prospec-tive, international, multicentre cohort study. Lancet Infect Dis. 2018;18(5):516–525.
26. What is the ICMJE definition of a clinical Trial. ICMJE. 2018.27. The G4 Alliance. Global Surgery & Anaesthesia Statistics The Importance
of Data Collection.
531
ealth, Inc. All rights reserved.

SYSTEMATIC REVIEW
The effectiveness of junctional tourniquets: A systematic reviewand meta-analysis
Shane Smith, MD, John White, Kerollos Nashat Wanis, MD, Andrew Beckett, MD,Vivian C. McAlister, MB, and Richard Hilsden, MD, London, Ontario Canada
Sub
Fro
Ad
DO
53
BACKGROUND: J
mitted: July 4, 2018, Revised: SPublished online: November 30,m the Royal Canadian MedicalDepartment of Surgery (S.S., J.WLondon, ON; Department of SuCanada; and Department of Epiof Public Health, Boston, Massadress for reprints: Shane Smith,Hospital, Room C8-144, 339 W5A5; email: [email protected]
I: 10.1097/TA.00000000000021
2
unctional tourniquets have been incorporated into tactical combat casualty care for junctional vascular trauma. They apply exter-nal compression to stop blood flow in the groin and axilla.
OBJECTIVES: T
he primary outcomewas effectiveness in achieving arterial occlusion. Secondary outcomes included time to application and painscores.DATA SOURCES: M
edline and EMBASE databases were searched. STUDYAPPRAISAL ANDSYNTHESIS METHODS:Ad
random-effects meta-analysis was conducted to estimate the average effectiveness and time to effective application for eachevice.
RESULTS: E
ight studies reported the effectiveness of junctional tourniquets in healthy volunteers. The average effectiveness was 52% (95%confidence interval [CI], 15–87%) for the abdominal application of the abdominal aortic and junctional tourniquet (AAJT), 83%(95% CI, 73–89%; 26%) for the junctional Emergency Treatment Tool, 87% (95% CI, 79–92%; 15%) for the SAM junctionaltourniquet (SJT), and 95% (95% CI, 90–98%) for the Combat Ready Clamp. The groin application of the AAJTwas studiedin two articles with 100% in both studies. The average time to application was 101 seconds for the SAM junctional tourniquet(95% CI, 50–152 seconds) and the Combat Ready Clamp (95% CI, 63–139 seconds), while it was 130 seconds (95% CI, 85–-176 seconds) for the Junctional Emergency Treatment Tool. The abdominal application of AAJT had an average time to applica-tion of 92 and 171 seconds in two studies.LIMITATIONS: A
ll studies were conducted in healthy volunteers. CONCLUSION ANDIMPLICATIONS:Jd
unctional tourniquets may meet a medical need in combat, and in the civilian environment, to control hemorrhage from theseifficult injuries. All four Food and Drug Administration–approved devices demonstrate the ability to achieve vascular occlusionin healthy volunteers; however, effectiveness in patient transport has not been evaluated, and outcomes of their use in the fieldneed to be captured and reported. (J Trauma Acute Care Surg. 2019;86: 532–539. Copyright © 2018 Wolters Kluwer Health,Inc. All rights reserved.)LEVEL OF EVIDENCE: S
ystematic review, level III. KEYWORDS: J unctional injuries; tourniquet; hemorrhage; vascular trauma.J unctional tourniquets are external compression devices thatocclude blood flow from the iliac or axillary arteries to prevent
hemorrhage. They were designed to meet a military need; how-ever, with domestic terrorist activity, such as the Boston mara-thon bombing and mass civilian shootings,1,2 there may be arole for them to treat civilians with the difficult problem of junc-tional bleeding. There may be a future role for integrating these
eptember 9, 2018, Accepted: October 8, 2018,2018.Service (S.S., J.W., A.B., V.C.M., R.H.), Ottawa;., V.C.M., R.H.), University of Western Ontario,rgery (A.B.), McGill University, Montreal, QC,demiology (K.N.W.), Harvard T.H. Chan Schoolchusetts.MD, University of Western Ontario, Universityindermere Road. London, Ontario, Canada N6An.ca.
59
Copyright © 2019 Wolters Kluwer H
devices into the civilian prehospital management of junctionalbleeding.
In modern conflicts, soldiers have become more likely tobe injured by improvised explosive devices than by bullets orconventional weapons.3 These weapons cause multiple amputa-tions, severe perineal injury, and pelvic disruption.4,5 New casu-alty care strategies have been developed in order for soldiers andmedical responders to be able to better treat our combat casual-ties. The Tactical Combat Casualty Care (TCCC) approach,which includes rapid tourniquet application, has resulted inmore casualties surviving injuries that would have once been le-thal.6 However, a conventional tourniquet will not control bleed-ing if an improvised explosive device disrupts a soldier's pelvisor injures their common femoral artery or iliac artery. The neces-sity of treating these difficult injuries has prompted the develop-ment of new techniques, such as resuscitative endovascularballoon occlusion of the aorta (REBOA)7,8 and junctional tour-niquets. The latter devices are designed to occlude the iliac ar-tery or aorta to prevent exsanguination from injuries thatwould otherwise not be compressible without constant care
J Trauma Acute Care SurgVolume 86, Number 3
ealth, Inc. All rights reserved.
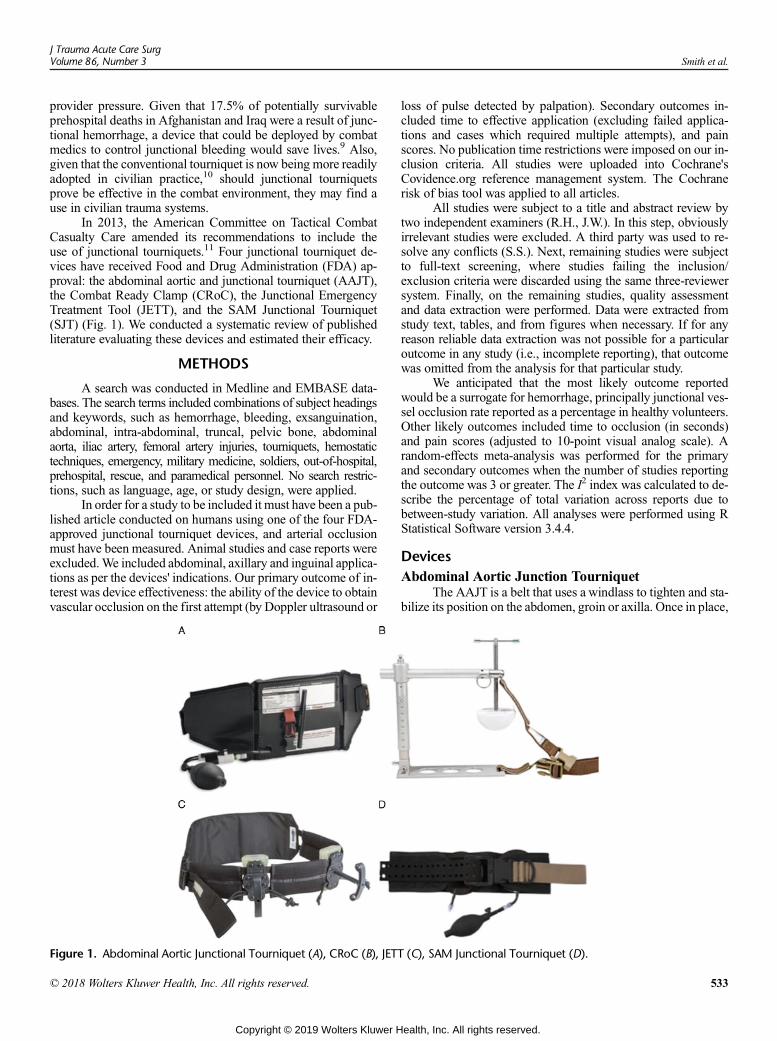
J Trauma Acute Care SurgVolume 86, Number 3 Smith et al.
provider pressure. Given that 17.5% of potentially survivableprehospital deaths in Afghanistan and Iraq were a result of junc-tional hemorrhage, a device that could be deployed by combatmedics to control junctional bleeding would save lives.9 Also,given that the conventional tourniquet is now being more readilyadopted in civilian practice,10 should junctional tourniquetsprove be effective in the combat environment, they may find ause in civilian trauma systems.
In 2013, the American Committee on Tactical CombatCasualty Care amended its recommendations to include theuse of junctional tourniquets.11 Four junctional tourniquet de-vices have received Food and Drug Administration (FDA) ap-proval: the abdominal aortic and junctional tourniquet (AAJT),the Combat Ready Clamp (CRoC), the Junctional EmergencyTreatment Tool (JETT), and the SAM Junctional Tourniquet(SJT) (Fig. 1). We conducted a systematic review of publishedliterature evaluating these devices and estimated their efficacy.
METHODS
A search was conducted in Medline and EMBASE data-bases. The search terms included combinations of subject headingsand keywords, such as hemorrhage, bleeding, exsanguination,abdominal, intra-abdominal, truncal, pelvic bone, abdominalaorta, iliac artery, femoral artery injuries, tourniquets, hemostatictechniques, emergency, military medicine, soldiers, out-of-hospital,prehospital, rescue, and paramedical personnel. No search restric-tions, such as language, age, or study design, were applied.
In order for a study to be included it must have been a pub-lished article conducted on humans using one of the four FDA-approved junctional tourniquet devices, and arterial occlusionmust have been measured. Animal studies and case reports wereexcluded.We included abdominal, axillary and inguinal applica-tions as per the devices' indications. Our primary outcome of in-terest was device effectiveness: the ability of the device to obtainvascular occlusion on the first attempt (by Doppler ultrasound or
Figure 1. Abdominal Aortic Junctional Tourniquet (A), CRoC (B), JETT
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
loss of pulse detected by palpation). Secondary outcomes in-cluded time to effective application (excluding failed applica-tions and cases which required multiple attempts), and painscores. No publication time restrictions were imposed on our in-clusion criteria. All studies were uploaded into Cochrane'sCovidence.org reference management system. The Cochranerisk of bias tool was applied to all articles.
All studies were subject to a title and abstract review bytwo independent examiners (R.H., J.W.). In this step, obviouslyirrelevant studies were excluded. A third party was used to re-solve any conflicts (S.S.). Next, remaining studies were subjectto full-text screening, where studies failing the inclusion/exclusion criteria were discarded using the same three-reviewersystem. Finally, on the remaining studies, quality assessmentand data extraction were performed. Data were extracted fromstudy text, tables, and from figures when necessary. If for anyreason reliable data extraction was not possible for a particularoutcome in any study (i.e., incomplete reporting), that outcomewas omitted from the analysis for that particular study.
We anticipated that the most likely outcome reportedwould be a surrogate for hemorrhage, principally junctional ves-sel occlusion rate reported as a percentage in healthy volunteers.Other likely outcomes included time to occlusion (in seconds)and pain scores (adjusted to 10-point visual analog scale). Arandom-effects meta-analysis was performed for the primaryand secondary outcomes when the number of studies reportingthe outcome was 3 or greater. The I2 index was calculated to de-scribe the percentage of total variation across reports due tobetween-study variation. All analyses were performed using RStatistical Software version 3.4.4.
DevicesAbdominal Aortic Junction Tourniquet
The AAJT is a belt that uses a windlass to tighten and sta-bilize its position on the abdomen, groin or axilla. Once in place,
(C), SAM Junctional Tourniquet (D).
533
ealth, Inc. All rights reserved.
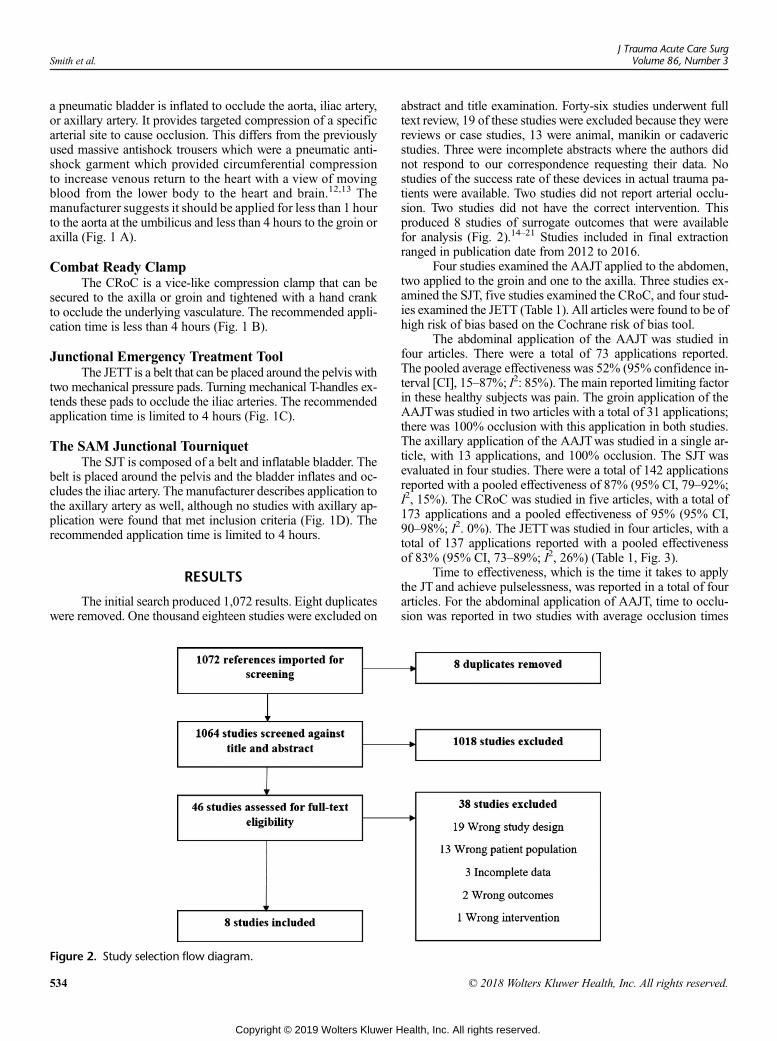
Smith et al.J Trauma Acute Care Surg
Volume 86, Number 3
a pneumatic bladder is inflated to occlude the aorta, iliac artery,or axillary artery. It provides targeted compression of a specificarterial site to cause occlusion. This differs from the previouslyused massive antishock trousers which were a pneumatic anti-shock garment which provided circumferential compressionto increase venous return to the heart with a view of movingblood from the lower body to the heart and brain.12,13 Themanufacturer suggests it should be applied for less than 1 hourto the aorta at the umbilicus and less than 4 hours to the groin oraxilla (Fig. 1 A).
Combat Ready ClampThe CRoC is a vice-like compression clamp that can be
secured to the axilla or groin and tightened with a hand crankto occlude the underlying vasculature. The recommended appli-cation time is less than 4 hours (Fig. 1 B).
Junctional Emergency Treatment ToolThe JETT is a belt that can be placed around the pelvis with
two mechanical pressure pads. Turning mechanical T-handles ex-tends these pads to occlude the iliac arteries. The recommendedapplication time is limited to 4 hours (Fig. 1C).
The SAM Junctional TourniquetThe SJT is composed of a belt and inflatable bladder. The
belt is placed around the pelvis and the bladder inflates and oc-cludes the iliac artery. The manufacturer describes application tothe axillary artery as well, although no studies with axillary ap-plication were found that met inclusion criteria (Fig. 1D). Therecommended application time is limited to 4 hours.
RESULTS
The initial search produced 1,072 results. Eight duplicateswere removed. One thousand eighteen studies were excluded on
Figure 2. Study selection flow diagram.
534
Copyright © 2019 Wolters Kluwer H
abstract and title examination. Forty-six studies underwent fulltext review, 19 of these studies were excluded because they werereviews or case studies, 13 were animal, manikin or cadavericstudies. Three were incomplete abstracts where the authors didnot respond to our correspondence requesting their data. Nostudies of the success rate of these devices in actual trauma pa-tients were available. Two studies did not report arterial occlu-sion. Two studies did not have the correct intervention. Thisproduced 8 studies of surrogate outcomes that were availablefor analysis (Fig. 2).14–21 Studies included in final extractionranged in publication date from 2012 to 2016.
Four studies examined the AAJT applied to the abdomen,two applied to the groin and one to the axilla. Three studies ex-amined the SJT, five studies examined the CRoC, and four stud-ies examined the JETT (Table 1). All articles were found to be ofhigh risk of bias based on the Cochrane risk of bias tool.
The abdominal application of the AAJT was studied infour articles. There were a total of 73 applications reported.The pooled average effectiveness was 52% (95% confidence in-terval [CI], 15–87%; I2: 85%). The main reported limiting factorin these healthy subjects was pain. The groin application of theAAJTwas studied in two articles with a total of 31 applications;there was 100% occlusion with this application in both studies.The axillary application of the AAJTwas studied in a single ar-ticle, with 13 applications, and 100% occlusion. The SJT wasevaluated in four studies. There were a total of 142 applicationsreported with a pooled effectiveness of 87% (95% CI, 79–92%;I2, 15%). The CRoC was studied in five articles, with a total of173 applications and a pooled effectiveness of 95% (95% CI,90–98%; I2. 0%). The JETTwas studied in four articles, with atotal of 137 applications reported with a pooled effectivenessof 83% (95% CI, 73–89%; I2, 26%) (Table 1, Fig. 3).
Time to effectiveness, which is the time it takes to applythe JT and achieve pulselessness, was reported in a total of fourarticles. For the abdominal application of AAJT, time to occlu-sion was reported in two studies with average occlusion times
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
TABLE 1. Results Summary
Study Intervention Occlusion Time to Application (s) Pain Score No. Subjects
Lyon et al., 2012 AAJT-abdomen 7/9 (78%) — 7/10* 9
Lyon et al., 2015 AAJT-groin 13/13 (100%) — 4/10* 13
AAJT-axillary 13/13 (100%) — 4/10* 13
Taylor et al., 2013 AAJT-abdomen 15/16 (94%) — 6/10 16
Kragh and Parsons et al., 2014 AAJT-abdomen 2/18 (11%) 92 — 9
SJT 18/18 (100%) 78 — 9
CRoC 17/18 (94%) 80 — 9
JETT 16/18 (89%) 212 — 9
Kragh and Kotwal et al., 2015 AAJT-abdomen 8/30 (27%) 171 76/100 10
SJT 28/30 (93%) 174 43/100 10
CRoC 29/30 (97%) 123 30/100 10
JETT 25/30 (83%) 203 45/100 10
Chen et al., 2016 AAJT-groin 18/18 (100%) 98 — 5
SJT 46/56 (82%) 65 — 14
CRoC 55/56 (98%) 128 — 14
JETT 42/56 (75%) 77 — 14
Meusnier et al., 2016 SJT 33/38 (86.8%) 34 1.76/5 38
CRoC 33/36 (92%) 41 1.64/5 36
Theodoridis et al., 2016 CRoC 33/33 (100%) 72 — 33
JETT 30/33 (91%) 55 — 33
*Reported as a median remainder of pain scores reported as mean.
J Trauma Acute Care SurgVolume 86, Number 3 Smith et al.
of 92 and 171 seconds. No time to effectiveness was reported forthe axillary use of the AJTT. For the groin use of the AAJT, thesingle study reporting this outcome reported a mean time to ap-plication of 98 seconds. For the SJT, the time to effectivenesswas reported in three studies with a pooled time to applicationof 101 seconds (95% CI, 50 to 152 seconds; I2, 90%). Time to ef-fectiveness for the CRoCwas reported in four studieswith a pooledtime of 101 seconds (95% CI, 63–139 seconds; I2, 97%). Time toeffectiveness for the JETTwas reported in three studies. The pooledtimewas 130 seconds (95%CI, 85–176 seconds; I2, 98%) (Fig. 4).
Pain scores with the application of the junctional tourni-quets were reported in five articles. For the abdominal applica-tion of the AAJT, pain scores were reported in two articles
Figure 3. Forest plots for junctional tourniquet device effectiveness (
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
with a mean pain score of 7.6/10 and a median score of 7/10 re-spectively. The groin application of the AAJT reported in a singlestudy had a median pain score of 4/10. The axillary application ofthe AAJTwas reported in a single study with a pain score of 4/10.For the SJT two articles reported mean pain scores of 4.3/10 and3.52/10. For the CRoC two studies reported mean pain scores of3/10 and 3.28/10, respectively. Finally, the JETTwas reported ina single article with a mean pain score of 5/10.
DISCUSSION
The prevalence of junctional injury in modern combat ne-cessitates creative solutions to save patients' lives.9 Junctional
seconds).
535
ealth, Inc. All rights reserved.
Figure 4. Forest plots for time to successful application of junctional tourniquet devices (effective/total applications).
Smith et al.J Trauma Acute Care Surg
Volume 86, Number 3
tourniquets have been developed as a technique to prevent junc-tional exsanguination while freeing-up the care provider frommaintaining direct pressure. This technique may also facilitatetransportation of injured patients when having continuous man-ual pressure may be difficult or impossible. External compres-sion devices for vascular control are not a new idea; in factexternal compression tools have been used as far back as theCrimean War.22 Despite the assertion that a device to occludethe external iliac artery was “in general use” in the British Armyin 1851 to treat aneurysms, these devices disappeared into ob-scurity presumably due to lack of effectiveness (Fig. 5).22 How-ever, the application of an external compression device is new tothe modern combat environment and is now been incorporatedinto Tactical Combat Casualty Care. We estimated the effective-ness of the four available junctional tourniquet devices andfound that the SJT, CRoC, and JETT had high effectiveness inhealthy volunteers and a mean time to application of approxi-mately 2 minutes. The CRoC device requires some assembly,and the various studies reported the time to application from var-ious states of assembly. The strategy to externally occlude theabdominal aorta was the least effective strategy in our review,with a pooled effectiveness of only 52% in healthy volunteers.The authors reported that the main limiting factor preventing oc-clusion was the subject's report of pain. In a tactical environment,a hypotensive and nonresponsive patient may be expected to
536
Copyright © 2019 Wolters Kluwer H
tolerate this device, possibly increasing its effectiveness in prac-tice; however, it has not been studied in this population. It is alsoa consideration that the SJT has an FDA-approved indication forpelvic immobilization; however, the effectiveness of any of thedevices as a pelvic binder was not tested in these studies.
Unfortunately, sparse data are currently available on theuse of junctional tourniquets in injured patients, and all of the re-viewed studies examined healthy volunteers. Animal studieshave tried to characterize the tourniquets' safety profiles. Rallet al.23 used a porcine hemorrhaging model to test the AAJT.They showed an increase in mean arterial pressure without anyevidence of pulmonary dysfunction or bowel injury. Kheirabadiand colleagues24 analyzed physiological effects of 2-hour ab-dominal application of the AAJT in the porcine model. Theyfound that AAJT application resulted in increases in both bloodpressure and hemorrhagic control. However, minor injury toperineural sheets of femoral and saphenous nerves, 5% to 10%myocyte degeneration of lumbar and peroneus muscles, andendothelial swelling in iliac vessels were observed. Interstitialbleeding of the ovaries was observed and may have resultedfrom external compression. Release of the AAJT after 2 hoursresulted in sudden increases in serum potassium and lactate, aswell as a drop in total pH. Importantly, sudden respiratory arrestoccurred in all of the spontaneously breathing animals when theAAJTwas removed, necessitating CPR and resulting in a fatality
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
Figure 5. Staff surgeon George Russell Dartnell's device toocclude the external iliac artery for treatment of aneurysms was“in general use” in the British Army in 1851.21
J Trauma Acute Care SurgVolume 86, Number 3 Smith et al.
rate of 50%. It is important to note that 2 hours of occlusion atthe umbilicus is outside of the FDA-approved parameters forthe device.
Although these devices may achieve arterial occlusion inhuman volunteers in the research setting, the present body of re-search has limitations. Casualties with junctional injuries mayhave significantly disrupted anatomy.4,5 Will junctional tourni-quets be as effective in traumatic junctional anatomy? The stud-ies reviewed only examined static subjects. Will junctionaltourniquets be able to obtain and maintain hemorrhagic controlof an evacuated casualty? One conference abstract by Gasparyet al.25 found that the SJTwas 43% effective on litter-carried pa-tients, whereas the CRoC and JETTwere 37% and 16% success-ful, respectively. For junctional tourniquets to be a useful combattool, they must remain effective during transport of the casualty.
Algorithms have been proposed for the chain of evacua-tion and systematic approach to removal of REBOA balloons.7
Similar algorithms should be implemented for removal of junc-tional tourniquet devices; in fact, there is a case report of junc-tional tourniquet application providing successful hemorrhagiccontrol, only to have the patient die upon removal.26 As withall types of tourniquets, time of application and ischemic burdenneed to be considered. The FDA limits SJT, JETT, CRoC, andgroin and axillary application of the AAJT to 4 hours and the ab-dominal application of the AAJT to 1 hour. Tourniquet applica-tion time should be recorded for each casualty and the deviceremoved as soon as clinically safe to do so. We would suggestthat the moment a junctional tourniquet is applied, the patientshould be urgently evacuated to an operating room, and thatthe junctional tourniquet should be removed only when a sur-geon is able to obtain proximal control.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
Junctional tourniquets have been incorporated intoTCCC; as such, there are published case reports of their use intactical environments. Croushourn et al.27 describe a successfulcivilian application of an AAJT to a gunshot wound of the ax-illa.27 The device was applied in the emergency departmentand hemorrhagic control was maintained until it was removedin the operating room. Although this was a successful use ofthe device, when the patient regained consciousness with resus-citation the device came loose and needed to be adjusted.Croushorn has also highlighted successful civilian applicationof the AAJT to the groin.28 In an emergency department, multi-ple attempts at applying direct pressure and tourniquets were un-successful at controlling hemorrhage from this wound. AnAAJTwas placed over the left groin achieving hemorrhagic con-trol. During resuscitation and transport to a level I trauma centerthe AAJT remained inflated and in place; the patient survivedvascular surgery and has had no complications related to theAAJT in posthospitalization follow-up. An AAJTwas success-fully deployed to the abdomen of a soldier in Afghanistan withbilateral traumatic amputations of his lower extremities.29 Thepatient was transferred via helicopter with the AAJT in place,and he ultimately survived with a through-knee and an above-knee amputation. No bowel injury or renal failure was noted48 hours postsurgery. Tovmassian et al.26 describe an instancewhere an Afghan adult male was injured in an explosionresulting in traumatic left lower extremity amputation throughthe groin. Application of the CRoC resulted in immediate hem-orrhage control. The patient was evacuated to a nearby Afghanhospital. Klotz et al.30 describe the use of the SJT in treating acasualty who received a gunshot wound to the left proximalthigh. After placement and inflation of the pneumatic bladder,peripheral pulses were promptly eliminated. The casualty wasthen evacuated by air to a nearby hospital and survived. No casereports for the JETTwere found.
More invasive intra-arterial occlusion techniques, such asREBOA, have been used in combat settings even in the forwardenvironment.31,32 These techniques have been applied by sur-geons and emergency physicians, whereas junctional tourniquetsmay be used by medics and first responders. The REBOA regis-tries and literature may provide valuable data with respect to thesafety of prolonged vascular occlusion but will not reflect the po-tential for harm to viscera and tissue that is compressed by junc-tional tourniquets or challenges of transporting a patient with ajunctional tourniquet in place.33 A registry of junctional tourni-quet use will be required to determine best practices for theiruse in the care of junctional vessel injury. This is especially im-portant because the majority of the data available regardingjunctional tourniquet application is preclinical. Massive anti-shock trousers were widely implemented based on preclinicaldata,12 only to eventually be shown to have no impact onmortal-ity.13 The studies reviewed show the ability of junction tourni-quets to occlude blood flow in a research setting, but cautionis required in extrapolating from these preclinical static experi-ments into the clinical prehospital environment. Hopefully, junc-tional tourniquets will prove to be a valuable tool to treat adifficult combat injury; however, they are presently being imple-mented with a paucity of data. The effectiveness of junctionaltourniquets in a transport and evacuation environment, and oninjured anatomy needs to be studies. Data from the current use
537
ealth, Inc. All rights reserved.
Smith et al.J Trauma Acute Care Surg
Volume 86, Number 3
of junctional tourniquets should be captured and studied to con-firm their safety profile and effectiveness.
CONCLUSION
There is a need to control junction hemorrhage on the bat-tlefield and in civilian trauma. Junctional tourniquets are a sim-ple tool that are being used in the combat environment and havealready been incorporated into TCCC. These devices have beenshown to be able to occlude blood flow in healthy volunteers.None of the published studies have measured effectiveness ofthese devices in trauma patients or during transport. Our reviewdemonstrated similar rates of successful occlusion between thedifferent devices, with the exception of lower rates for abdomi-nal application of the AAJT. Since these devices are already inuse, it behooves those using these devices to continue to studytheir use and report on their experiences.
AUTHORSHIP
S.S., J.W., and R.H. conducted the search, reviewed the articles, andwrotethe article. K.W. performed the data analysis. All authors participated indata interpretation and critical revisions.
DISCLOSURE
S.S., J.W., A.B., V.M., and R.H. are members of the Canadian ArmedForces. The views expressed in this article are those of the authors anddo not constitute the views or policies of the Canadian Armed Forces.S.S., J.W., A.B., and R.H. are members of the Canadian Armed Forces. Theviews expressed in this article are those of the authors and do not consti-tute the views or policies of the Canadian Armed Forces.S.S., J.W., A.B., V.M., and R.H. are all employed by the Canadian ArmedForces. There are no other sources of funding to declare.
REFERENCES1. Smith ER, Shapiro G, Sarani B. The profile of wounding in civilian pub-
lic mass shooting fatalities. J Trauma Acute Care Surg. 2016;81(1):86–92.
2. Gates JD, Arabian S, Biddinger P, Blansfield J, Burke P, Chung S, Fischer J,Friedman F, Gervasini A, Goralnick E, et al. The initial response to theBoston marathon bombing: lessons learned to prepare for the next disaster.Ann Surg. 2014;260(6):960–966.
3. Beckett A, Pelletier P, Mamczak C, Benfield R, Elster E. Multidisciplinarytrauma team care in Kandahar, Afghanistan: current injury patterns and carepractices. Injury. 2012;43(12):2072–2077.
4. Smith S, Devine M, Taddeo J, McAlister VC. Injury profile suffered by tar-gets of antipersonnel improvised explosive devices: prospective cohort study.BMJ Open. 2017;7(7):e014697.
5. Cannon JW, Hofmann LJ, Glasgow SC, Potter BK, Rodriguez CJ, Cancio LC,Rasmussen TE, Fries CA, Davis MR, Jezior JR, et al. Dismounted complexblast injuries: a comprehensive review of the modern combat experience.J Am Coll Surg. 2016;223(4):652–64.e8.
6. Savage E, Forestier C, Withers N, Tien H, Pannell D. Tactical combat casu-alty care in the Canadian forces: lessons learned from the Afghan war. Can JSurg. 2011;54(6):S118–S123.
7. Smith SA, Hilsden R, Beckett A, McAlister VC. The future of resuscita-tive endovascular balloon occlusion in combat operations. J R Army MedCorps. 2017.
8. Fisher AD, Teeter WA, Cordova CB, Brenner ML, Szczepanski MP,Miles EA, Galante JM, DuBose JJ, Rasmussen TE. The role I resuscitationteam and resuscitative endovascular balloon occlusion of the aorta. J SpecOper Med. 17(2):65–73.
9. Eastridge BJ, Mabry RL, Seguin P, Cantrell J, Tops T, Uribe P, Mallett O,Zubko T, Oetjen-Gerdes L, Rasmussen TE, et al. Death on the battlefield
538
Copyright © 2019 Wolters Kluwer H
(2001–2011): implications for the future of combat casualty care. J TraumaAcute Care Surg. 2012;73(6 Suppl 5):S431–S437.
10. Stop the bleed Department of Homeland Security. 2016 Available from:https://www.dhs.gov/stopthebleed. Accessed 27 January 2017.
11. Kotwal RS, Butler FK, Gross KR, Kheirabadi BS, Baer DG, Dubick MA,Rasmussen TE, Weber MA, Bailey JA. Management of Junctional Hemor-rhage in tactical combat casualty care: TCCC guidelines? Proposed change13-03. J Spec Oper Med. 2013;13(4):85–93.
12. Kaback KR, Sanders AB, Meislin HW. MAST suit update. JAMA. 1984;252(18):2598–2603.
13. Dickinson K, Roberts I. Medical anti-shock trousers (pneumatic anti-shockgarments) for circulatory support in patients with trauma. Cochrane Data-base Syst Rev. 2000(2):Cd001856.
14. LyonM, Shiver SA, Greenfield EM, Reynolds BZ, Lerner EB, Wedmore IS,Schwartz RB. Use of a novel abdominal aortic tourniquet to reduce or elim-inate flow in the common femoral artery in human subjects. J Trauma AcuteCare Surg. 2012;73(2 Suppl 1):S103–S105.
15. Lyon M, Johnson D, Gordon R. Use of a novel abdominal aortic andjunctional tourniquet to reduce or eliminate flow in the brachial and pop-liteal arteries in human subjects. Prehosp Emerg Care. 2015;19(3):405–408.
16. Taylor DM, Coleman M, Parker PJ. The evaluation of an abdominal aortictourniquet for the control of pelvic and lower limb hemorrhage. Mil Med.2013;178(11):1196–1201.
17. Kragh JF Jr, Parsons DL, Kotwal RS, Kheirabadi BS, Aden JK 3rd,Gerhardt RT, Dubick MA. Testing of junctional tourniquets by militarymedics to control simulated groin hemorrhage. J Spec Oper Med. 2014;14(3):58–63.
18. Kragh JF, Kotwal RS, Cap AP, Aden JK, Walters TJ, Kheirabadi BS,Gerhardt RT, DeLorenzo RA, Pidcoke HF, Cancio LC. Performance of junc-tional tourniquets in normal human volunteers. Prehosp Emerg Care. 2015;19(3):391–398.
19. Chen J, Benov A, Nadler R, Landau G, Sorkin A, Aden JK 3rd, Kragh JF Jr,Glassberg E. Testing of junctional tourniquets by medics of the Israeli De-fense Force in control of simulated groin hemorrhage. J Spec Oper Med.2016;16(1):36–42.
20. Meusnier JG, Dewar C, Mavrovi E, Caremil F, Wey PF, Martinez JY. Evalu-ation of two junctional tourniquets used on the battlefield: CombatReady Clamp® versus SAM® junctional tourniquet. J Spec Oper Med.2016;16(3):41–46.
21. Theodoridis CA, Kafka KE, Perez AM, Curlee JB, Yperman PC,Oppermann N, Holmstroem E, Niegsch DD, Mannino A, Ramundo N.Evaluation and testing of junctional tourniquets by special operationforces personnel: a comparison of the Combat Ready Clamp and theJunctional Emergency Treatment Tool. J Spec Oper Med. 2016;16(1):44–50.
22. Dartnell GR. Femoral aneurism. Compression-cure in 24 hours. MedicalTimes & Gazette. 1851;148–149.
23. Rall JM, Ross JD, Clemens MS, Cox JM, Buckley TA, Morrison JJ. Hemo-dynamic effects of the abdominal aortic and Junctional tourniquet in a hem-orrhagic swine model. J Surg Res. 2017;212:159–166.
24. Kheirabadi BS, Terrazas IB, Miranda N, Voelker AN, GrimmR, Kragh JF Jr,Dubick MA. Physiological consequences of Abdominal Aortic And Junc-tional Tourniquet (AAJT) application to control hemorrhage in a swinemodel. Shock. 2016;46(3 Suppl 1):160–166.
25. Gaspary M, Walchak AC, Conley S, Zarow G. The Comparitive Effective-ness of Three Junctional Tourniquet Devices in Human Volunteers. ACEPResearch Forum: Annals of Emergency Medicine; 2016.
26. Tovmassian RV, Kragh JF Jr, Dubick MA, Baer DG, Blackbourne LH.Combat ready clamp medic technique. J Spec Oper Med. 2012;12(4):72–78.
27. Croushorn J, Thomas G, McCord SR. Abdominal aortic tourniquet controlsjunctional hemorrhage from a gunshot wound of the axilla. J SpecOperMed.2013;13(3):1–4.
28. Croushorn J. Abdominal aortic and junctional tourniquet controls hemor-rhage from a gunshot wound of the left groin. J Spec Oper Med. 2014;14(2):6–8.
29. Anonymous. Abdominal aortic tourniquet? Use in Afghanistan. J Spec OperMed. 2013;13(2):1–2.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Smith et al.
30. Klotz JK, Leo M, Andersen BL, Nkodo AA, Garcia G, Wichern AM,Chambers MJ, Gonzalez ON, Pahle MU, Wagner JA, et al. First case reportof SAM(r) Junctional tourniquet use in Afghanistan to control inguinal hem-orrhage on the battlefield. J Spec Oper Med. 2014;14(2):1–5.
31. Manley JD,Mitchell BJ, DuBose JJ, Rasmussen TE. Amodern case series ofresuscitative endovascular balloon occlusion of the aorta (REBOA) in an out-of-hospital, combat casualty care setting. J Spec Oper Med. 2017;17(1):1–8.
32. Northern DM,Manley JD, Lyon R, Farber D, Mitchell BJ, Filak KJ, Lundy J,DuBose JJ, Rasmussen TE, Holcomb JB. Recent advances in austere combat
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
surgery: use of aortic balloon occlusion as well as blood challenges by spe-cial operations medical forces in recent combat operations. J Trauma AcuteCare Surg. 2018;85(1S Suppl 2):S98–S103.
33. DuBose JJ, Scalea TM, Brenner M, Skiada D, Inaba K, Cannon J, Moore L,Holcombe J, Turay D, Arbabi CN, et al. The AAST prospective Aortic Oc-clusion for Resuscitation in Trauma and Acute Care Surgery (AORTA) reg-istry: data on contemporary utilization and outcomes of aortic occlusion andresuscitative balloon occlusion of the aorta (REBOA). J Trauma Acute CareSurg. 2016;81(3):409–419.
539
ealth, Inc. All rights reserved.

REVIEWARTICLE
A review of racial/ethnic disparities in pediatrictrauma care, treatment, and outcomes
Melanie B. LaPlant, MPH and Donavon J. Hess, MD, PhD
Sub
Fro
Ad
Sup
DO
54
ABSTRACT: H
mitted: July 12, 2018, Revised:Published online: December 7,m the Division of Pediatric Surgversity of Minnesota, Minneapdress for reprints: Donavon J. Hof Minnesota, 2450 [email protected], hessx006@plemental digital content is avaithe printed text, and links to thearticle on the journal’s Web sit
I: 10.1097/TA.00000000000021
0
ealth disparities are an increasingly researched topic in the United States. Evidence of disparities found across the spectrum ofhealth care includes pediatric patients. The purpose of this review is to comprehensively summarize disparities among pediatrictrauma patients, evaluating both emergency department and hospital treatment and outcomes. Multiple studies describe disparitiesin a variety of areas of trauma care including emergency department, radiology, surgery, abuse evaluation, and discharge rehabil-itation. More concerning, multiple studies report disparities in length of stay, disability, recidivism, and mortality. This review alsohighlights several gaps in disparity research including specialty care, inclusion of all racial/ethnic groups, and geographic differ-ences. Few of the reviewed studies described disparity interventions; however, research regarding abuse evaluations showed thatcare guidelines diminished disparity. Trauma care, a routinized patient service, is subject to existing care guidelines and qualityimprovement programs, and may be the ideal health care setting for disparity intervention. (J Trauma Acute Care Surg.2019;86: 540–550. Copyright © 2018 Wolters Kluwer Health, Inc. All rights reserved.)
LEVEL OF EVIDENCE: S
tudy type review, level V. KEYWORDS: T rauma; pediatric; disparity; ethnic groups; continental population groups.A considerable amount of research in the past decades has es-tablished a multitude of racial and ethnic health disparities.
The Institute of Medicine, now the National Academy of Medicine,published a landmark report in 2003,Unequal Treatment, that detailedthe current state of disparity and recommended further researchon health care access and utilization by patient race and ethnic-ity.1 Later, a systematic reviewwas published establishing healthand health care disparities among children in the United States.2
Pediatric trauma is a leading cause of emergency depart-ment (ED) presentation in the United States, and a leading causeof death.3,4 A recent review summarizes pediatric injury epidemi-ology as showing disparities in incidence, morbidity, and mor-tality.5 We sought to review disparity literature to examineevidence of disparity, not only in outcomes from pediatric injury,but also in the antecedent medical treatment that may impactthose outcomes. The objective was to review the literature forevidence of disparities in pediatric trauma evaluation and treat-ment and to summarize the existing evidence of disparities intrauma care. We included all racial/ethnic groups in our review,but restricted the literature to the United States.
METHODS
We searched PubMed for a combination of the followingkey words “child,” “pediatric,” “trauma,” “wound and injuries,”
October 16, 2018, Accepted: November 25, 2018,2018.ery, Department of Surgery (M.B.L., D.J.H.), Uni-olis, Minnesota.ess, MD, PhD, Department of Surgery, Universitye Ave S. MB 505, Minneapolis, MN; email:umn.edu.
lable for this article. Direct URL citations appear indigital files are provided in the HTML text of thise (www.jtrauma.com).
60
Copyright © 2019 Wolters Kluwer H
“emergencymedical services,” “mortality,” “disparity,” “continentalpopulation groups,” “ethnic groups,” “African American,” “His-panic Americans,” “Asian Americans,” and “American NativeContinental Group.” Articles were included if their study popu-lation was in the United States. We found 508 articles, 329 afterremoving duplicates. We assessed 103 full text articles. Articleswere excluded if they studied chronic conditions, infectiousdiseases, mental illness, or other acute noninjury conditions(25 articles). Additionally, articles were excluded if they onlydescribed injury incidence or prevalence without mention ortreatment or outcomes (nine articles). Articles were also ex-cluded if the data was pulled from death records (11 articles)or prehospital emergency services (eight articles). Fifty articleswere included in the review. The results were grouped by ED,hospital treatment, and outcomes. Within each group, categorieswere not identified a priori. Instead, categories formed based onthe literature search results (Appendix, Supplemental DigitalContent 1, http://links.lww.com/JAAOS/A305).
Emergency DepartmentA study in 2007 found that white patients were more likely
to be admitted than black or Hispanic patients, especially amongpatients with low illness severity.6 A few studies have examineddisparity in ED wait times using the National Hospital Ambula-tory Medical Care Survey. In 2005, a study found that Hispanicpatients waited 18% longer than white patients, but found no dif-ference for black patients as compared with white patients.7 In2009, a study found that wait times were 14.2% longer for blackpatients and 26.1% longer for Hispanic patients, compared withwhite patients.8 Zook et al.9 found that black, Hispanic, andAmerican Indian patients were more likely to receive a lower-acuity triage score in the ED compared towhite patients. Hispanicpatients, but not black, Asian, or other patients, were found to bemore likely to have a prolonged ED length of stay (8 hours ormore) compared with whites (adjusted odds ratio [AOR], 1.76;95% confidence interval [CI], 1.10–2.81).10 Black, American
J Trauma Acute Care SurgVolume 86, Number 3
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 LaPlant and Hess
Indian/Alaskan Native, and Hispanic patients were all morelikely to have a return ED visit within 1 year of dischargecompared to white patients.11 From admission to recidivism,there appears to be evidence for racial/ethnic disparities inaspects of the ED experience (Table 1).
Hospital TreatmentAnalgesia Use
There have been several studies examining analgesia usefor patients with orthopedic fractures. Three studies looked atanalgesia use in the ED, and found no significant difference byrace (Table 2).12–14 A 2013 study looked at whether patientswere given an analgesia prescription at discharge, and found thatblack, biracial, and Hispanic patients, compared with white pa-tients, were significantly less likely to receive a prescription foran opioid-containing analgesic.15 An earlier 2010 study exam-ined the use of nonpharmacological anxiolysis, pharmacologi-cal anxiolysis, or procedural sedation with the treatment for askin laceration, and found that race was not significant.16
RadiologyRadiology, especially among pediatric patients, represents
a clinical trade-off. An imaging study may be advantageous indiagnostics; however, it also may be disadvantageous in exposureto radiation. Therefore, conclusions about the cause and conse-quences of disparities found in the use of radiology are less clear.Among patients with blunt torso trauma, black patients were 20%less likely to receive an abdominal computed tomography (CT)
TABLE 1. Summary of Evidence for ED Treatment Disparities
Treatment Study Population Race/Ethnicities
Admission rate 16 EDs that randomly enrolledtwo patients per day
Hispanic and black comparedwith white
Wait time National Hospital AmbulatoryMedical Care Survey, patients15 years and younger presentingto the ED from 1997 to 2000
Hispanic white andnon-Hispanic black comparwith non-Hispanic white
Wait time National Hospital AmbulatoryMedical Care Survey, patients16 years and younger presentingto the ED from 2005 to 2006
Hispanic, non-Hispanic black,and other race comparedwith non-Hispanic white
Triage score Two urban pediatric EDs, allpatients discharged homeor admitted
African American, Hispanic,and American Indiancompared with white
Prolonged EDlength of stay
National Hospital AmbulatoryMedical Care Survey, patients18 years and younger admittedfrom 2001 to 2006
Hispanic, black, Asian, andother race comparedwith white
Recurrent EDvisit
PECARN EDs, patients 17 yearsand younger with 12-monthfollow-up visit
Hispanic, non-Hispanic black,Asian/Pacific Islander, AmIndian/Alaskan Native, andother race compared withnon-Hispanic white
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
scan, compared with white patients (AOR, 0.8; 95% CI,0.7–0.9). However, there was no difference observed for His-panic patients compared to white patients.17 More researchhas been done with radiology and head trauma. A 2010 studyfound that white patients were 50% more likely than nonwhitepatients to receive a CT for head trauma (AOR, 1.5; 95% CI,1.02–2.1).18 A 2012 study of patients with minor head trauma,a Glascow Coma Scale score of 14 or 15, presented resultsstratified by the risk of clinically important traumatic brain injury(TBI). They found that there was no difference in the rate of cra-nial CT scan at the highest risk, but there was a significant differ-ence among the intermediate and low risk groups. IntermediateTBI risk nonwhite patients were 16% less likely to receive a CTscan (AOR, 0.84; 95%CI, 0.76–0.94), and lowTBI risk nonwhitepatients were 26% less likely to receive a CT scan (AOR, 0.73;95% CI, 0.66–0.81).19 Payne and Puumala20 examined total radi-ology charges for patients with a head injury. Because their pro-viders used a decision algorithm for imaging use, there was nosignificant difference in total radiology charges by race.20
SurgeryFew studies have looked at disparities in surgical trauma
care. In a national sample ofmotor vehicle crash injures of patients16 years and younger, researchers found a difference in need foremergency surgery by race/ethnicity. African American patientswere 23% less likely (AOR, 0.77; 95% CI, 0.69–0.87), Hispanicpatients were 22% less likely (AOR, 0.88; 95% CI, 0.78–0.99),and Native American patients were 81% less likely (AOR, 0.19;
Disparity ResultsEvidence
of Disparity YearReference
No.
Adjusted odds of admission:black/Hispanic, 0.54 (0.33–0.88)
Yes 2007 6
edAdjusted change in wait time:
Hispanic white, 18%(6%–30%) non-Hispanicblack, 6% (−3% to 16%)
Yes 2005 7
Adjusted change in wait time:non-Hispanic black, 14.2%(3.3%–26.4%) Hispanic, 26.1%(15.1%–38.3%) Other race,−3.4% (−18.0% to 13.9%)
Yes 2009 8
Adjusted odds of lower acuity score:African American, 1.89 (1.69–2.12)Hispanic, 1.77 (1.55–2.02)American Indian, 2.57 (1.80–3.66)
Yes 2016 9
Adjusted odds of ED length ofstay longer than 8 hours:Hispanic, 1.76 (1.10–2.81)Black, 1.33 (0.86–2.07)Asian, 0.36 (0.09–1.35)Other race, 1.37 (0.40–4.66)
Yes 2011 10
ericanAdjusted rate of recurrent ED
visit within 1 year: Hispanic,1.47 (1.33–1.62) non-Hispanicblack, 1.62 (1.49–1.76_Asian/Pacific Islander, 1.06(0.95–1.18) American Indian/AlaskanNative, 1.40 (1.25–1.56)Other race, 1.16 (1.06–1.28)
Yes 2014 11
541
ealth, Inc. All rights reserved.
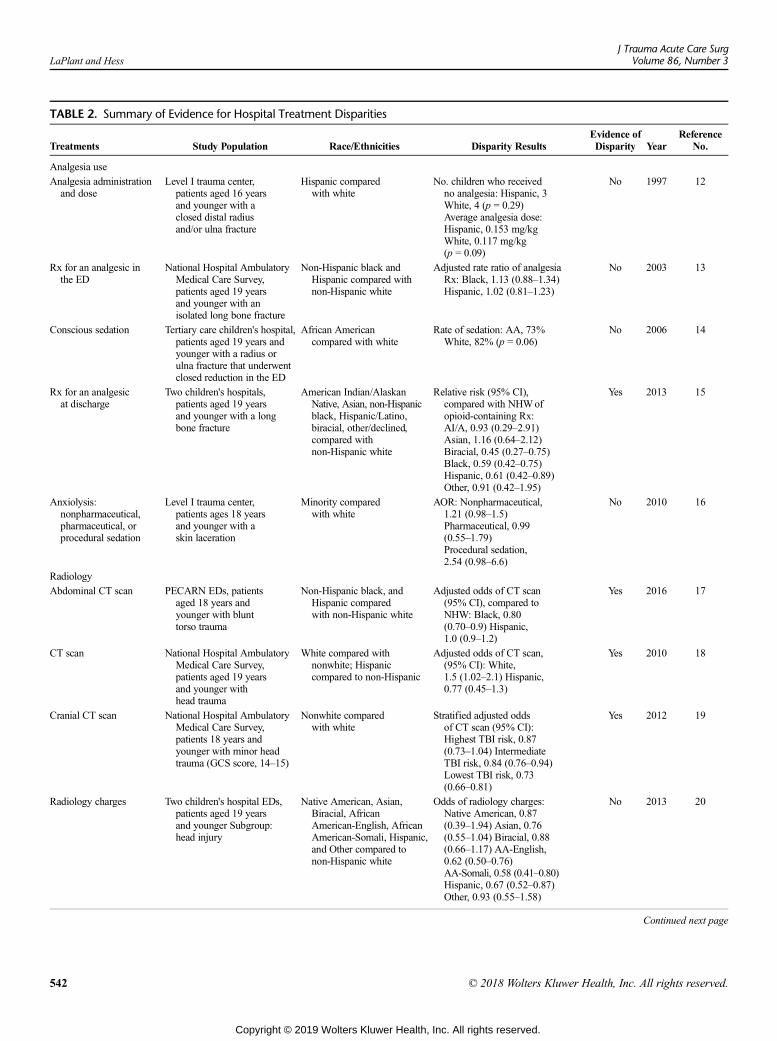
TABLE 2. Summary of Evidence for Hospital Treatment Disparities
Treatments Study Population Race/Ethnicities Disparity ResultsEvidence ofDisparity Year
ReferenceNo.
Analgesia use
Analgesia administrationand dose
Level I trauma center,patients aged 16 yearsand younger with aclosed distal radiusand/or ulna fracture
Hispanic comparedwith white
No. children who receivedno analgesia: Hispanic, 3White, 4 (p = 0.29)Average analgesia dose:Hispanic, 0.153 mg/kgWhite, 0.117 mg/kg(p = 0.09)
No 1997 12
Rx for an analgesic inthe ED
National Hospital AmbulatoryMedical Care Survey,patients aged 19 yearsand younger with anisolated long bone fracture
Non-Hispanic black andHispanic compared withnon-Hispanic white
Adjusted rate ratio of analgesiaRx: Black, 1.13 (0.88–1.34)Hispanic, 1.02 (0.81–1.23)
No 2003 13
Conscious sedation Tertiary care children's hospital,patients aged 19 years andyounger with a radius orulna fracture that underwentclosed reduction in the ED
African Americancompared with white
Rate of sedation: AA, 73%White, 82% (p = 0.06)
No 2006 14
Rx for an analgesicat discharge
Two children's hospitals,patients aged 19 yearsand younger with a longbone fracture
American Indian/AlaskanNative, Asian, non-Hispanicblack, Hispanic/Latino,biracial, other/declined,compared withnon-Hispanic white
Relative risk (95% CI),compared with NHWofopioid-containing Rx:AI/A, 0.93 (0.29–2.91)Asian, 1.16 (0.64–2.12)Biracial, 0.45 (0.27–0.75)Black, 0.59 (0.42–0.75)Hispanic, 0.61 (0.42–0.89)Other, 0.91 (0.42–1.95)
Yes 2013 15
Anxiolysis:nonpharmaceutical,pharmaceutical, orprocedural sedation
Level I trauma center,patients ages 18 yearsand younger with askin laceration
Minority comparedwith white
AOR: Nonpharmaceutical,1.21 (0.98–1.5)Pharmaceutical, 0.99(0.55–1.79)Procedural sedation,2.54 (0.98–6.6)
No 2010 16
Radiology
Abdominal CT scan PECARN EDs, patientsaged 18 years andyounger with blunttorso trauma
Non-Hispanic black, andHispanic comparedwith non-Hispanic white
Adjusted odds of CT scan(95% CI), compared toNHW: Black, 0.80(0.70–0.9) Hispanic,1.0 (0.9–1.2)
Yes 2016 17
CT scan National Hospital AmbulatoryMedical Care Survey,patients aged 19 yearsand younger withhead trauma
White compared withnonwhite; Hispaniccompared to non-Hispanic
Adjusted odds of CT scan,(95% CI): White,1.5 (1.02–2.1) Hispanic,0.77 (0.45–1.3)
Yes 2010 18
Cranial CT scan National Hospital AmbulatoryMedical Care Survey,patients 18 years andyounger with minor headtrauma (GCS score, 14–15)
Nonwhite comparedwith white
Stratified adjusted oddsof CT scan (95% CI):Highest TBI risk, 0.87(0.73–1.04) IntermediateTBI risk, 0.84 (0.76–0.94)Lowest TBI risk, 0.73(0.66–0.81)
Yes 2012 19
Radiology charges Two children's hospital EDs,patients aged 19 yearsand younger Subgroup:head injury
Native American, Asian,Biracial, AfricanAmerican-English, AfricanAmerican-Somali, Hispanic,and Other compared tonon-Hispanic white
Odds of radiology charges:Native American, 0.87(0.39–1.94) Asian, 0.76(0.55–1.04) Biracial, 0.88(0.66–1.17) AA-English,0.62 (0.50–0.76)AA-Somali, 0.58 (0.41–0.80)Hispanic, 0.67 (0.52–0.87)Other, 0.93 (0.55–1.58)
No 2013 20
Continued next page
LaPlant and HessJ Trauma Acute Care Surg
Volume 86, Number 3
542 © 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
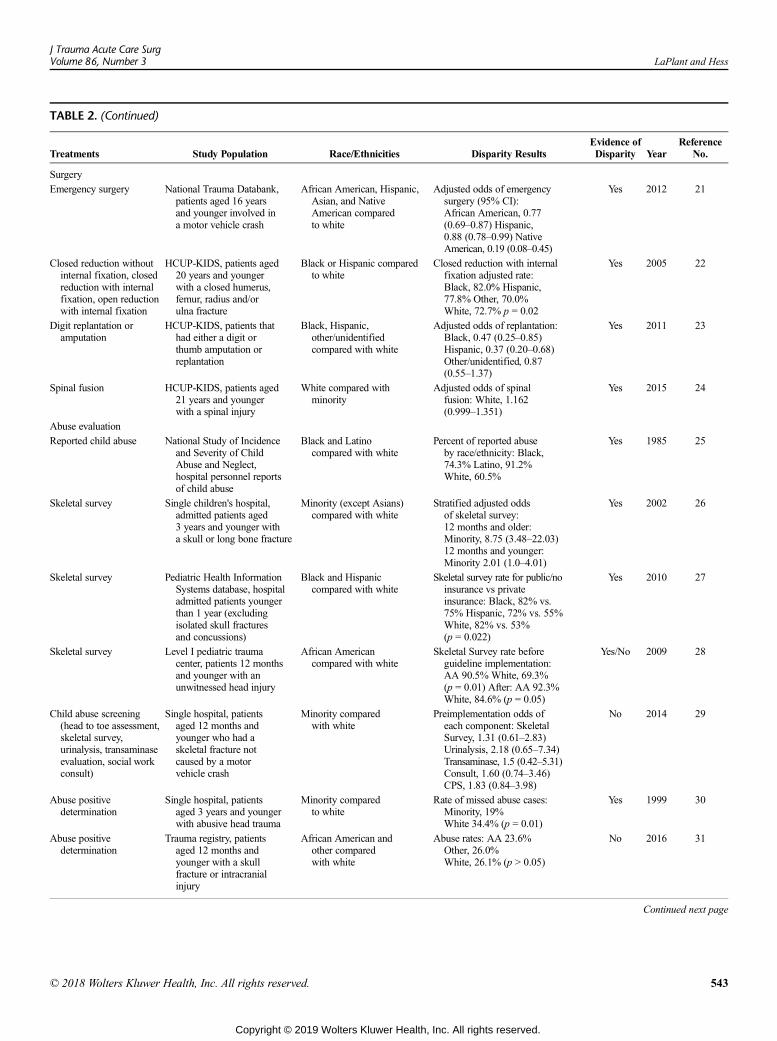
TABLE 2. (Continued)
Treatments Study Population Race/Ethnicities Disparity ResultsEvidence ofDisparity Year
ReferenceNo.
Surgery
Emergency surgery National Trauma Databank,patients aged 16 yearsand younger involved ina motor vehicle crash
African American, Hispanic,Asian, and NativeAmerican comparedto white
Adjusted odds of emergencysurgery (95% CI):African American, 0.77(0.69–0.87) Hispanic,0.88 (0.78–0.99) NativeAmerican, 0.19 (0.08–0.45)
Yes 2012 21
Closed reduction withoutinternal fixation, closedreduction with internalfixation, open reductionwith internal fixation
HCUP-KIDS, patients aged20 years and youngerwith a closed humerus,femur, radius and/orulna fracture
Black or Hispanic comparedto white
Closed reduction with internalfixation adjusted rate:Black, 82.0% Hispanic,77.8% Other, 70.0%White, 72.7% p = 0.02
Yes 2005 22
Digit replantation oramputation
HCUP-KIDS, patients thathad either a digit orthumb amputation orreplantation
Black, Hispanic,other/unidentifiedcompared with white
Adjusted odds of replantation:Black, 0.47 (0.25–0.85)Hispanic, 0.37 (0.20–0.68)Other/unidentified, 0.87(0.55–1.37)
Yes 2011 23
Spinal fusion HCUP-KIDS, patients aged21 years and youngerwith a spinal injury
White compared withminority
Adjusted odds of spinalfusion: White, 1.162(0.999–1.351)
Yes 2015 24
Abuse evaluation
Reported child abuse National Study of Incidenceand Severity of ChildAbuse and Neglect,hospital personnel reportsof child abuse
Black and Latinocompared with white
Percent of reported abuseby race/ethnicity: Black,74.3% Latino, 91.2%White, 60.5%
Yes 1985 25
Skeletal survey Single children's hospital,admitted patients aged3 years and younger witha skull or long bone fracture
Minority (except Asians)compared with white
Stratified adjusted oddsof skeletal survey:12 months and older:Minority, 8.75 (3.48–22.03)12 months and younger:Minority 2.01 (1.0–4.01)
Yes 2002 26
Skeletal survey Pediatric Health InformationSystems database, hospitaladmitted patients youngerthan 1 year (excludingisolated skull fracturesand concussions)
Black and Hispaniccompared with white
Skeletal survey rate for public/noinsurance vs privateinsurance: Black, 82% vs.75% Hispanic, 72% vs. 55%White, 82% vs. 53%(p = 0.022)
Yes 2010 27
Skeletal survey Level I pediatric traumacenter, patients 12 monthsand younger with anunwitnessed head injury
African Americancompared with white
Skeletal Survey rate beforeguideline implementation:AA 90.5% White, 69.3%(p = 0.01) After: AA 92.3%White, 84.6% (p = 0.05)
Yes/No 2009 28
Child abuse screening(head to toe assessment,skeletal survey,urinalysis, transaminaseevaluation, social workconsult)
Single hospital, patientsaged 12 months andyounger who had askeletal fracture notcaused by a motorvehicle crash
Minority comparedwith white
Preimplementation odds ofeach component: SkeletalSurvey, 1.31 (0.61–2.83)Urinalysis, 2.18 (0.65–7.34)Transaminase, 1.5 (0.42–5.31)Consult, 1.60 (0.74–3.46)CPS, 1.83 (0.84–3.98)
No 2014 29
Abuse positivedetermination
Single hospital, patientsaged 3 years and youngerwith abusive head trauma
Minority comparedto white
Rate of missed abuse cases:Minority, 19%White 34.4% (p = 0.01)
Yes 1999 30
Abuse positivedetermination
Trauma registry, patientsaged 12 months andyounger with a skullfracture or intracranialinjury
African American andother comparedwith white
Abuse rates: AA 23.6%Other, 26.0%White, 26.1% (p > 0.05)
No 2016 31
Continued next page
J Trauma Acute Care SurgVolume 86, Number 3 LaPlant and Hess
© 2018 Wolters Kluwer Health, Inc. All rights reserved. 543
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
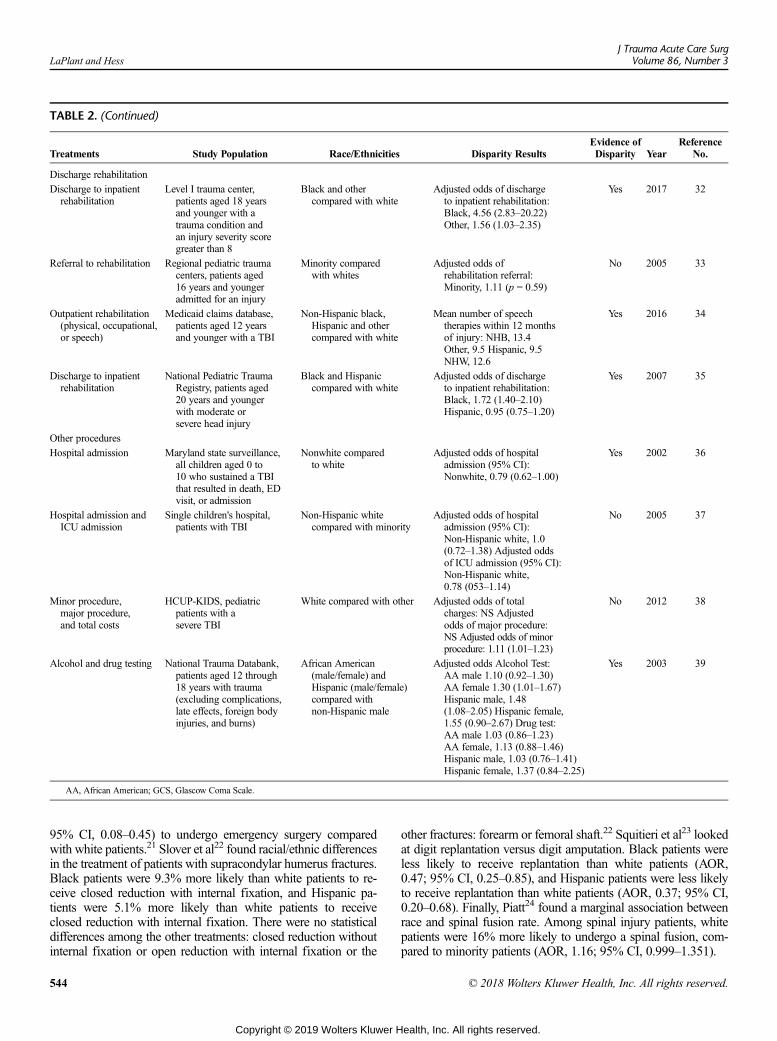
TABLE 2. (Continued)
Treatments Study Population Race/Ethnicities Disparity ResultsEvidence ofDisparity Year
ReferenceNo.
Discharge rehabilitation
Discharge to inpatientrehabilitation
Level I trauma center,patients aged 18 yearsand younger with atrauma condition andan injury severity scoregreater than 8
Black and othercompared with white
Adjusted odds of dischargeto inpatient rehabilitation:Black, 4.56 (2.83–20.22)Other, 1.56 (1.03–2.35)
Yes 2017 32
Referral to rehabilitation Regional pediatric traumacenters, patients aged16 years and youngeradmitted for an injury
Minority comparedwith whites
Adjusted odds ofrehabilitation referral:Minority, 1.11 (p = 0.59)
No 2005 33
Outpatient rehabilitation(physical, occupational,or speech)
Medicaid claims database,patients aged 12 yearsand younger with a TBI
Non-Hispanic black,Hispanic and othercompared with white
Mean number of speechtherapies within 12 monthsof injury: NHB, 13.4Other, 9.5 Hispanic, 9.5NHW, 12.6
Yes 2016 34
Discharge to inpatientrehabilitation
National Pediatric TraumaRegistry, patients aged20 years and youngerwith moderate orsevere head injury
Black and Hispaniccompared with white
Adjusted odds of dischargeto inpatient rehabilitation:Black, 1.72 (1.40–2.10)Hispanic, 0.95 (0.75–1.20)
Yes 2007 35
Other procedures
Hospital admission Maryland state surveillance,all children aged 0 to10 who sustained a TBIthat resulted in death, EDvisit, or admission
Nonwhite comparedto white
Adjusted odds of hospitaladmission (95% CI):Nonwhite, 0.79 (0.62–1.00)
Yes 2002 36
Hospital admission andICU admission
Single children's hospital,patients with TBI
Non-Hispanic whitecompared with minority
Adjusted odds of hospitaladmission (95% CI):Non-Hispanic white, 1.0(0.72–1.38) Adjusted oddsof ICU admission (95% CI):Non-Hispanic white,0.78 (053–1.14)
No 2005 37
Minor procedure,major procedure,and total costs
HCUP-KIDS, pediatricpatients with asevere TBI
White compared with other Adjusted odds of totalcharges: NS Adjustedodds of major procedure:NS Adjusted odds of minorprocedure: 1.11 (1.01–1.23)
No 2012 38
Alcohol and drug testing National Trauma Databank,patients aged 12 through18 years with trauma(excluding complications,late effects, foreign bodyinjuries, and burns)
African American(male/female) andHispanic (male/female)compared withnon-Hispanic male
Adjusted odds Alcohol Test:AA male 1.10 (0.92–1.30)AA female 1.30 (1.01–1.67)Hispanic male, 1.48(1.08–2.05) Hispanic female,1.55 (0.90–2.67) Drug test:AA male 1.03 (0.86–1.23)AA female, 1.13 (0.88–1.46)Hispanic male, 1.03 (0.76–1.41)Hispanic female, 1.37 (0.84–2.25)
Yes 2003 39
AA, African American; GCS, Glascow Coma Scale.
LaPlant and HessJ Trauma Acute Care Surg
Volume 86, Number 3
95% CI, 0.08–0.45) to undergo emergency surgery comparedwith white patients.21 Slover et al22 found racial/ethnic differencesin the treatment of patients with supracondylar humerus fractures.Black patients were 9.3% more likely than white patients to re-ceive closed reduction with internal fixation, and Hispanic pa-tients were 5.1% more likely than white patients to receiveclosed reduction with internal fixation. There were no statisticaldifferences among the other treatments: closed reduction withoutinternal fixation or open reduction with internal fixation or the
544
Copyright © 2019 Wolters Kluwer H
other fractures: forearm or femoral shaft.22 Squitieri et al23 lookedat digit replantation versus digit amputation. Black patients wereless likely to receive replantation than white patients (AOR,0.47; 95% CI, 0.25–0.85), and Hispanic patients were less likelyto receive replantation than white patients (AOR, 0.37; 95% CI,0.20–0.68). Finally, Piatt24 found a marginal association betweenrace and spinal fusion rate. Among spinal injury patients, whitepatients were 16% more likely to undergo a spinal fusion, com-pared to minority patients (AOR, 1.16; 95% CI, 0.999–1.351).
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 LaPlant and Hess
Abuse EvaluationProvider evaluation of suspected nonaccidental trauma
abuse has been primarily conducted with very young children.These children are unable to report abuse themselves; therefore,providers may attempt to deduce abuse by examining injuries. Acommon method used is a skeletal survey. An early study ofchild abuse reporting found that hospitals were more likely to re-port minority families.25 A study in 2002 found that, amongchildren 12 months to 3 years, minority children, who sustaineda skull or long bone fracture, were significantly more likely toundergo a skeletal survey than white children (AOR, 8.75; 95%CI, 3.48–22.03); this association was also significant amongchildren 12 months and younger (AOR, 2.01; 95% CI, 1.0–4.01).Minority children 12 months to 3 years were also more likelyto be reported to Child Protective Services, compared with whitechildren (AOR, 4.32; 1.63–11.43).26 A 2010 study found an in-teraction between insurance and race in the utilization of skeletalsurveys. Among infants younger than 1 year with TBI, therewasa significantly greater difference in performance of skeletalsurvey between privately insured patients and patients publiclyinsured or uninsured (82% vs. 53%) for white patients com-pared with black patients (85% vs. 75%) and Hispanic patients(72% vs. 55%; p = 0.022). The same study found that white pa-tients evaluated with a skeletal survey were more likely to be di-agnosed as abused (61%) compared with black patients (51%)and Hispanic patients (51%; p = 0.009).27 Many facilities haveimplemented guidelines for child abuse screening. At one facil-ity, prior to implementing guidelines for a skeletal survey forchildren 12 months and younger who sustained an unwitnessedhead injury, African American children were significantly morelikely than white children to undergo a skeletal survey (90.5%vs. 69.3%, p = 0.01). However, after guideline implementation,there was no difference by race.28 Another facility implementedabuse-screening guidelines and found no difference by race inthe use of the screening components before or after guidelineimplementation.29 After using screening methods, providers at-tempt to positively determine cases of abuse. A retrospective re-viewofmedical records determined the time to correct diagnosisfor abused children. They found that white patients were signif-icantly more likely to have a missed abuse diagnosis (37.4% vs.19%, p = 0.01).30 Recently, a 2016 study examined all of thecases of positively determined abuse and found that there wasno difference in the rate of abuse by race.31
Discharge RehabilitationDifferences in discharge to inpatient rehabilitation have
been observed, though the reasons for these differences havenot been discovered. Nguyen et al.32 broadly examined the rateof discharge to inpatient rehabilitation for any nonmild traumacondition. Black children were significantly more likely to bedischarged to inpatient rehabilitation compared with white chil-dren (AOR, 7.56; 95% CI, 2.80–20.22). They grouped all otherrace/ethnicities together and found that this group was 56%more likely compared with white patients to be discharged to in-patient rehabilitation (AOR, 1.56; 95% CI 1.03–2.35).32 A re-gional study of all injury emergency inpatient patients youngerthan 16 years found no difference by race in referral to rehabili-tation.33 Discharge to outpatient rehabilitation, physical, occu-pational, or speech was analyzed for TBI patients in a different
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
study. The only significant difference found by race/ethnicitywas that Hispanics were slightly less likely to receive speech re-habilitation.34 Finally, Haider et al.35 specifically examined dis-charge to inpatient rehabilitation for TBI and found that blackpatients were 72%more likely to be discharged to inpatient reha-bilitation compared with white patients (AOR, 1.72; 95% CI,1.40–2.10).35
Other ProceduresA few studies with trauma patients and disparity did not fit
into the categories presented above. The TBI surveillance inMaryland showed that nonwhite patients were less likely to beadmitted than white patients (AOR, 0.79; 95% CI, 0.62–1.0).36
However, an independent children's hospital found no differencein hospital admission or ICU admission by race for TBI pa-tients.37 A national database study that examined total charges,major procedure rate, and minor procedure rate for TBI patientsfound no difference by race/ethnicity, except that white patientswere slightly more likely to undergo a minor procedure.38 Astudy in California evaluated drug and alcohol testing for trauma(excluding complications, late effects, foreign body injuries, andburns) patients aged 12 to 18 years. The comparison group wasnon-Hispanic white males. There was no difference by race/ethnicity and gender for drug testing. Although, for alcohol test-ing, African American females were 30% more likely (AOR,1.30; 95% CI, 1.01–1.67), and Hispanic males were 48% morelikely (AOR, 1.48; 95% CI, 1.08–2.05).39
OutcomesLength of Stay and Disability
A National Trauma Databank study evaluating length ofstay following an injury sustained at home, among patients5 years and younger, found a slightly longer length of stay forblack patients and a shorter length of stay for Asian or Pacific Is-lander patients compared with white patients.40 A regional studyof all pediatric injury emergency inpatients found no differencein length of stay by race.33 Another National Trauma Databankstudy found no difference in length of stay by race/ethnicity formotor vehicle crash injury patients. The same study found ahigher odds of complication for Asian patients compared withwhite patients (AOR, 3.6; 95% CI, 2.5–5.1).21
All other studies that have evaluated disability disparitieshave been with TBI patients. A 2013 study found that Hispanicpatients, compared with non-Hispanic white patients, had lowerscored on both the Pediatric Quality of Life Inventory and theAdaptive Behavior Assessment System-Second Edition at 3,12, 24, and 36 months of follow-up.41 A 2015 study found nodifference by race/ethnicity in functional independence measureat discharge.42 Finally, an earlier 2007 study found a 29% higherodds of speech deficit (AOR, 1.29; 95% CI, 1.02–1.57), a 40%higher odds of a locomotion deficit (AOR, 1.40; 95% CI,1.15–1.70), and a 32% higher odds of a feeding deficit (AOR,1.32; 95% CI, 1.06–1.63) (Table 3).35
RecidivismA single institution study that evaluated all trauma patients
found no race/ethnicity difference in a trauma-related return visitwithin 30 days after discharge.43 A statewide study in New Yorkamong patients discharged with an upper- or lower-extremity
545
ealth, Inc. All rights reserved.
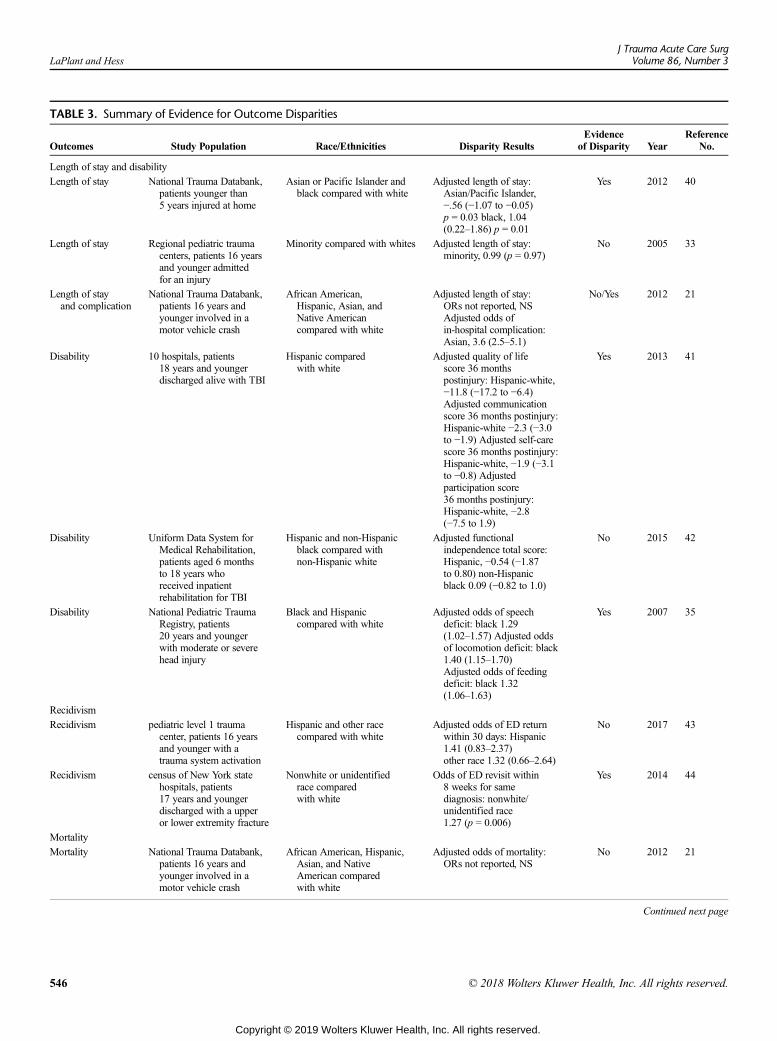
TABLE 3. Summary of Evidence for Outcome Disparities
Outcomes Study Population Race/Ethnicities Disparity ResultsEvidence
of Disparity YearReference
No.
Length of stay and disability
Length of stay National Trauma Databank,patients younger than5 years injured at home
Asian or Pacific Islander andblack compared with white
Adjusted length of stay:Asian/Pacific Islander,−.56 (−1.07 to −0.05)p = 0.03 black, 1.04(0.22–1.86) p = 0.01
Yes 2012 40
Length of stay Regional pediatric traumacenters, patients 16 yearsand younger admittedfor an injury
Minority compared with whites Adjusted length of stay:minority, 0.99 (p = 0.97)
No 2005 33
Length of stayand complication
National Trauma Databank,patients 16 years andyounger involved in amotor vehicle crash
African American,Hispanic, Asian, andNative Americancompared with white
Adjusted length of stay:ORs not reported, NSAdjusted odds ofin-hospital complication:Asian, 3.6 (2.5–5.1)
No/Yes 2012 21
Disability 10 hospitals, patients18 years and youngerdischarged alive with TBI
Hispanic comparedwith white
Adjusted quality of lifescore 36 monthspostinjury: Hispanic-white,−11.8 (−17.2 to −6.4)Adjusted communicationscore 36 months postinjury:Hispanic-white −2.3 (−3.0to −1.9) Adjusted self-carescore 36 months postinjury:Hispanic-white, −1.9 (−3.1to −0.8) Adjustedparticipation score36 months postinjury:Hispanic-white, −2.8(−7.5 to 1.9)
Yes 2013 41
Disability Uniform Data System forMedical Rehabilitation,patients aged 6 monthsto 18 years whoreceived inpatientrehabilitation for TBI
Hispanic and non-Hispanicblack compared withnon-Hispanic white
Adjusted functionalindependence total score:Hispanic, −0.54 (−1.87to 0.80) non-Hispanicblack 0.09 (−0.82 to 1.0)
No 2015 42
Disability National Pediatric TraumaRegistry, patients20 years and youngerwith moderate or severehead injury
Black and Hispaniccompared with white
Adjusted odds of speechdeficit: black 1.29(1.02–1.57) Adjusted oddsof locomotion deficit: black1.40 (1.15–1.70)Adjusted odds of feedingdeficit: black 1.32(1.06–1.63)
Yes 2007 35
Recidivism
Recidivism pediatric level 1 traumacenter, patients 16 yearsand younger with atrauma system activation
Hispanic and other racecompared with white
Adjusted odds of ED returnwithin 30 days: Hispanic1.41 (0.83–2.37)other race 1.32 (0.66–2.64)
No 2017 43
Recidivism census of New York statehospitals, patients17 years and youngerdischarged with a upperor lower extremity fracture
Nonwhite or unidentifiedrace comparedwith white
Odds of ED revisit within8 weeks for samediagnosis: nonwhite/unidentified race1.27 (p = 0.006)
Yes 2014 44
Mortality
Mortality National Trauma Databank,patients 16 years andyounger involved in amotor vehicle crash
African American, Hispanic,Asian, and NativeAmerican comparedwith white
Adjusted odds of mortality:ORs not reported, NS
No 2012 21
Continued next page
LaPlant and HessJ Trauma Acute Care Surg
Volume 86, Number 3
546 © 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
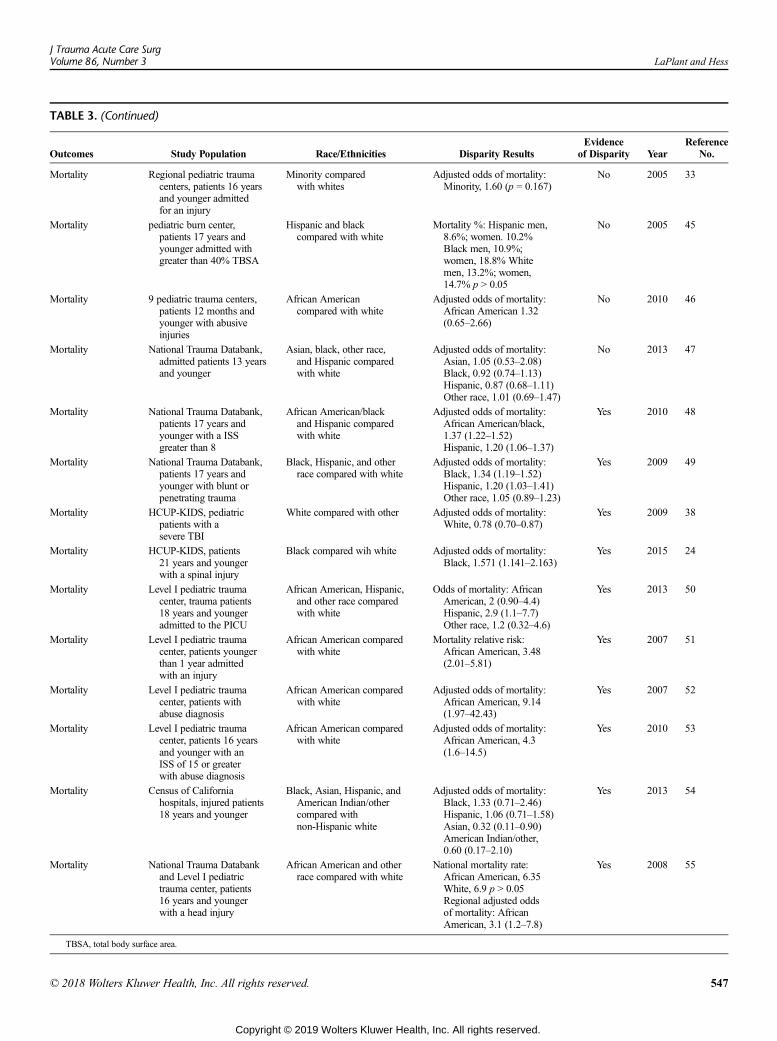
TABLE 3. (Continued)
Outcomes Study Population Race/Ethnicities Disparity ResultsEvidence
of Disparity YearReference
No.
Mortality Regional pediatric traumacenters, patients 16 yearsand younger admittedfor an injury
Minority comparedwith whites
Adjusted odds of mortality:Minority, 1.60 (p = 0.167)
No 2005 33
Mortality pediatric burn center,patients 17 years andyounger admitted withgreater than 40% TBSA
Hispanic and blackcompared with white
Mortality %: Hispanic men,8.6%; women. 10.2%Black men, 10.9%;women, 18.8% Whitemen, 13.2%; women,14.7% p > 0.05
No 2005 45
Mortality 9 pediatric trauma centers,patients 12 months andyounger with abusiveinjuries
African Americancompared with white
Adjusted odds of mortality:African American 1.32(0.65–2.66)
No 2010 46
Mortality National Trauma Databank,admitted patients 13 yearsand younger
Asian, black, other race,and Hispanic comparedwith white
Adjusted odds of mortality:Asian, 1.05 (0.53–2.08)Black, 0.92 (0.74–1.13)Hispanic, 0.87 (0.68–1.11)Other race, 1.01 (0.69–1.47)
No 2013 47
Mortality National Trauma Databank,patients 17 years andyounger with a ISSgreater than 8
African American/blackand Hispanic comparedwith white
Adjusted odds of mortality:African American/black,1.37 (1.22–1.52)Hispanic, 1.20 (1.06–1.37)
Yes 2010 48
Mortality National Trauma Databank,patients 17 years andyounger with blunt orpenetrating trauma
Black, Hispanic, and otherrace compared with white
Adjusted odds of mortality:Black, 1.34 (1.19–1.52)Hispanic, 1.20 (1.03–1.41)Other race, 1.05 (0.89–1.23)
Yes 2009 49
Mortality HCUP-KIDS, pediatricpatients with asevere TBI
White compared with other Adjusted odds of mortality:White, 0.78 (0.70–0.87)
Yes 2009 38
Mortality HCUP-KIDS, patients21 years and youngerwith a spinal injury
Black compared wih white Adjusted odds of mortality:Black, 1.571 (1.141–2.163)
Yes 2015 24
Mortality Level I pediatric traumacenter, trauma patients18 years and youngeradmitted to the PICU
African American, Hispanic,and other race comparedwith white
Odds of mortality: AfricanAmerican, 2 (0.90–4.4)Hispanic, 2.9 (1.1–7.7)Other race, 1.2 (0.32–4.6)
Yes 2013 50
Mortality Level I pediatric traumacenter, patients youngerthan 1 year admittedwith an injury
African American comparedwith white
Mortality relative risk:African American, 3.48(2.01–5.81)
Yes 2007 51
Mortality Level I pediatric traumacenter, patients withabuse diagnosis
African American comparedwith white
Adjusted odds of mortality:African American, 9.14(1.97–42.43)
Yes 2007 52
Mortality Level I pediatric traumacenter, patients 16 yearsand younger with anISS of 15 or greaterwith abuse diagnosis
African American comparedwith white
Adjusted odds of mortality:African American, 4.3(1.6–14.5)
Yes 2010 53
Mortality Census of Californiahospitals, injured patients18 years and younger
Black, Asian, Hispanic, andAmerican Indian/othercompared withnon-Hispanic white
Adjusted odds of mortality:Black, 1.33 (0.71–2.46)Hispanic, 1.06 (0.71–1.58)Asian, 0.32 (0.11–0.90)American Indian/other,0.60 (0.17–2.10)
Yes 2013 54
Mortality National Trauma Databankand Level I pediatrictrauma center, patients16 years and youngerwith a head injury
African American and otherrace compared with white
National mortality rate:African American, 6.35White, 6.9 p > 0.05Regional adjusted oddsof mortality: AfricanAmerican, 3.1 (1.2–7.8)
Yes 2008 55
TBSA, total body surface area.
J Trauma Acute Care SurgVolume 86, Number 3 LaPlant and Hess
© 2018 Wolters Kluwer Health, Inc. All rights reserved. 547
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.

LaPlant and HessJ Trauma Acute Care Surg
Volume 86, Number 3
fractures found that nonwhite or unidentified race patients had ahigher odds of return visit for the same diagnosis within 8 weeks(odds ratio [OR], 1.27; p < 0.001).44
MortalitySeveral studies, examining TBI, burns, nonaccidental
trauma, or blunt trauma, have found no race/ethnicity mortalitydisparities.21,33,45–47 However, several other studies have foundsignificant mortality disparities. In a National Trauma Databankstudy, among patients with blunt or penetrating trauma, the mor-tality odds was 37% higher for African American patients(AOR, 1.37; 95% CI, 1.22–1.52), and 20% higher for Hispanicpatients (AOR, 1.20; 95% CI, 1.06–1.37) compared with whitepatients.48 A similar National Trauma Databank study amongpatients 17 and younger who sustained blunt or penetratingtrauma found that black patients had 82% higher mortality odds(AOR, 1.82; 95% CI, 1.61–2.06) and Hispanic patients had 46%higher mortality odds (AOR, 1.46; 95%CI, 1.21–1.75) comparedwith white patients.49 A Kids' Inpatient Database study showedthat white TBI patients had a 22% lower mortality odds comparedto minority TBI patients (AOR, 0.78; 95% CI, 0.70–0.87).38 Spe-cifically among spinal injury patients, black patients had a 57%higher mortality odds compared with all other patients (AOR,1.57; 95% CI, 1.14–2.16).24 Disparities have also been shown re-gionally. AWisconsin study found that among all trauma patients,18 years and younger, admitted to the pediatric intensive care unit,Hispanic patients had a higher odds of mortality (OR, 2.09; 95%CI, 1.1–1.7).50 A Cincinnati Children's Hospital study showedthat infants, aged 28 to 364 days, had an injury mortality ratiofor African American patients, compared with white patients, of3.48 (95% CI, 2.01–5.81).51 Another Cincinnati Children'sHospital study found an abuse mortality ratio, adjusted for in-jury severity and other patient characteristics, for pediatric pa-tients to be 9.14 for African American patients compared withwhite patients (95% CI, 1.97–42.43).52 Despite similar findingson initial head CT scans, African American patients had anabuse mortality OR of 4.3 compared with white patients in an-other study (95% CI, 1.6–11.5).53 Additionally, a Californiastudy did find that Asian trauma patients had a decreased like-lihood of mortality compared with white patients (AOR, 0.32;95% CI, 0.11–0.90).54 Finally, one study combined a nationalsample, National Trauma Databank, with a regional sample,Cincinnati Children's Hospital. They demonstrated that nation-ally, there was no difference in head injury mortality odds byrace, but regionally, African American patients had significantlyincreased head injury mortality odds compared with white pa-tients (AOR, 3.1; 95% CI, 1.2 7.8).55
DISCUSSION
This review of the existing evidence for disparities in theevaluation and treatment of pediatric trauma patients, whichwas very broadly defined, shows that the overall state of this lineof inquiry is incomplete and early in its development. While thecare of the trauma patient is wide ranging and involves manyspecialty areas, the literature evaluating disparities in such careis sparse, focusing on the characteristics of the experience in theED, radiographic evaluation, evaluation for nonaccidental trauma,discharge to inpatient rehabilitation, and some orthopedic
548
Copyright © 2019 Wolters Kluwer H
procedures. Other areas of research into evaluation and treat-ment have been limited to single publications. Vast areas oftrauma treatment and evaluation remain unexamined in thepublished literature. Work in this area is hampered by theavailability of multi-institutional data sets and the extent ofinformation therein. Such data sets are important becausethere tends to be a relatively low number of patients with aparticular injury on a per-institution basis. Ongoing effortsare required to develop the means to meaningfully measuredisparities in pediatric trauma, both through better data setsand through different analytic approaches.
The results of this review show that researchers have ex-amined disparities throughout the course of care for injured pe-diatric patients, from the ED, to the hospital, and for outcomes.The studies presented in this review are observational studies,and do not allow for causational or conclusive interpretation.As is often found with the social determinants of health, thefindings of some studies contradict the findings of others. As re-searchers and health practitioners, we should aim to continue toevaluate disparities in asmany populations as possible to attemptto understand this phenomenon.
While the literature covers a range of trauma care dispar-ities, there are several gaps. We were not able to find many stud-ies regarding surgical care and other specialties. Most studiesonly evaluated black/African American patients or Hispanic pa-tients comparing them to non-Hispanic white patients. Few stud-ies were able to include Native American, Asian, Biracial, orMultiracial patients. Most studies focused on adjusting for so-cioeconomic status variables, such as insurance status or medianhousehold income. This is important, because socioeconomicstatus affects patients' resources in terms of both finances andeducation. Finances impact injury not only in terms of insurancebut also in terms of use of safety devices and neighborhoodsafety. Education influences injury in terms of not only literacybut also health literacy and injury prevention. However, few ad-justed for other sociodemographic variables, such as rurality,language, nationality, or sex. We were only able to find onestudy that evaluated sex disparity in trauma care.56 Further, theremay be geographic differences within the United States that maybe obscured by national data samples. Finally, the majority of re-search on trauma disparities is with mortality. More research isnecessary to understand the treatment and other factors that affectmortality and that evaluate other outcomes, such as disability.
Lacking from the existing evidence of disparities intrauma evaluation and care are studies that attempt to delve intothe origins of disparities. Disparities may be attributable to indi-vidual or systemic bias, or other causality, or combination thereof.Etiologic investigations of disparities are difficult andmay requireexpertise in mixed methods research, which is not always avail-able or accepted in surgical circles.
Finally, there is little evidence available regarding effec-tive methods to eliminate disparities. Early evidence that guide-lines can diminish disparities is encouraging, particularly astrauma evaluation and care tends to be amenable to protocols,and practitioners are accustomed to the use of protocol directedtrauma care. However, there are aspects of care that cannot andshould not be governed by protocol. Thus, some efforts to elim-inate disparities will necessarily rest on identifying the underly-ing etiology and addressing it directly. The extensive use of
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 LaPlant and Hess
protocols in trauma care does present an interesting opportunityfor future research, namely, to investigate whether there is dis-parity evident in the adherence to or compliance with protocolsin trauma centers.
Some may believe that trauma care is an area of healthcare that is often subject to protocols, and therefore not subjectto differential or unequal treatment. However, an increasingbody of health disparity research is showing unequal treatmentin all areas of health care. Because trauma care is often subjectto protocol, it may represent an area of health care that may bemore amenable to intervention. Previous research with CT scansfor head injury and abuse evaluation found that after imple-menting guidelines, racial disparities diminished.20,28 Further-more, the American College of Surgeons has a long history oftrauma care quality improvement. Therefore, it may be effectiveto use existing quality improvement infrastructure to addressdisparities. We are investigating the possibilities of using dispar-ities as a trauma quality indicator.
AUTHORSHIP
M.LP. and D.H. were both responsible for literature search, literature re-view, drafting the article, and revisions.The authors do not have any conflicts of interest to disclose.No funding was received for this review.
DISCLOSURE
The authors do not have any conflicts of interest to disclose.No funding was received for this review.
REFERENCES1. Smedley B, Stith A, Nelson A. Unequal Treatment Confronting Racial and
Ethnic Disparities in Health Care. Washington, DC; 2003.2. Flores G. Technical report—racial and ethnic disparities in the health and
health care of children. Pediatrics. 2010;125(4):e979–e1020.3. Avraham JB, Bhandari M, Frangos SG, Levine DA, Tunik MG,
DiMaggio CJ. Epidemiology of paediatric trauma presenting to US emer-gency departments: 2006-2012. Inj Prev. 2017; injuryprev-2017-042435.
4. Centers for Disease Control and Prevention. Leading Causes of Death inMales, 2014. 2014;2014.
5. Brown RL. Epidemiology of injury and the impact of health disparities.CurrOpin Pediatr. 2010;22(3):321–325.
6. Chamberlain JM, Joseph JG, Patel KM, Pollack MM. Differences inseverity-adjusted pediatric hospitalization rates are associated with race/ethnicity. Pediatrics. 2007;119(6):e1319–e1324.
7. James CA, Bourgeois FT, Shannon MW. Association of race/ethnicity withemergency department wait times. Pediatrics. 2005;115(3):e310–e315.
8. Park CY, LeeMA, EpsteinAJ. Variation in emergency department wait timesfor children by race/ethnicity and payment source: children’s care and cover-age. Health Serv Res. 2009;44(6):2022–2039.
9. Zook HG, Kharbanda AB, Flood A, Harmon B, Puumala SE, Payne NR. Ra-cial differences in pediatric emergency department triage scores. J EmergMed. 2016;50(5):720–727.
10. Bekmezian A, Chung PJ, CabanaMD,Maselli JH, Hilton JF, Hersh AL. Fac-tors associated with prolonged emergency department length of stay for ad-mitted children. Pediatr Emerg Care. 2011;27(2):110–115.
11. Alpern ER, Clark AE, Alessandrini EA, Gorelick MH, Kittick M,Stanley RM, Dean JM, Teach SJ, Chamberlain JM. Recurrent and high-frequency use of the emergency department by pediatric patients. AcadEmerg Med. 2014;21(4):365–373.
12. Karpman RR, Del Mar N, Bay C. Analgesia for emergency centers' ortho-paedic patients: does an ethnic bias exist? Clin Orthop Relat Res. 1997;334:270–275.
13. Yen K, Kim M, Stremski ES, Gorelick MH. Effect of ethnicity and race onthe use of pain medications in children with long bone fractures in the emer-gency department. Ann Emerg Med. 2003;42(1):41–47.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
14. VanderBeek BL, Mehlman CT, Foad SL, Wall EJ, Crawford AH. The use ofconscious sedation for pain control during forearm fracture reduction in chil-dren: does race matter? J Pediatr Orthop. 2006;26(1):53–57.
15. Ortega HW,Vander VeldenH, Lin CW, Reid S. Race, ethnicity, and analgesiaprovision at discharge among children with long-bone fractures requiringemergency care. Pediatr Emerg Care. 2013;29(4):492–497.
16. Brodzinski H, Iyer S, Grupp-Phelan J. Assessment of disparities in the use ofanxiolysis and sedation among children undergoing laceration repair. AcadPediatr. 2010;10(3):194–199.
17. Natale JE, Joseph JG, Rogers AJ, TunikM,Monroe D, Kerrey B, Bonsu BK,Cook LJ, Page K, Adelgais K, et al. Relationship of physician-identified pa-tient race and ethnicity to use of computed tomography in Pediatric blunttorso trauma. Acad Emerg Med. 2016;23(5):584–590.
18. Mannix R, Bourgeois FT, Schutzman SA, Bernstein A, Lee LK. Neuroimag-ing for pediatric head trauma: do patient and hospital characteristics influ-ence who gets imaged? Acad Emerg Med. 2010;17(7):694–700.
19. Natale JE, Joseph JG, Rogers AJ, Mahajan P, Cooper A, Wisner DH,MiskinML, Hoyle JD Jr, Atabaki SM, Dayan PS, et al. Cranial computed to-mography use among children with minor blunt head trauma: associationwith race/ethnicity. Arch Pediatr Adolesc Med. 2012;166(8):732–737.
20. Payne NR, Puumala SE. Racial disparities in ordering laboratory and radiol-ogy tests for pediatric patients in the emergency department. Pediatr EmergCare. 2013;29(5):598–606.
21. Lee SL, Yaghoubian A, Stark R, Munoz V, Kaji AH. Are there racial dispar-ities in the use of restraints and outcomes in children after motor vehiclecrashes? J Pediatr Surg. 2012;47(6):1192–1195.
22. Slover J, Gibson J, Tosteson T, Smith B, Koval K. Racial and economic dis-parity and the treatment of pediatric fractures. J Pediatr Orthop. 2005;25(6):717–721.
23. Squitieri L, Reichert H, Kim HM, Steggerda J, Chung KC. Patterns of surgi-cal care and health disparities of treating pediatric finger amputation injuriesin the United States. J Am Coll Surg. 2011;213(4):475–485.
24. Piatt JH Jr. Pediatric spinal injury in the US: epidemiology and disparities.J Neurosurg Pediatr. 2015;16(4):463–471.
25. Hampton RL, Newberger EH. Child abuse incidence and reporting by hospi-tals: significance of severity, class, and race. AmJ Public Health. 1985;75(1):56–60.
26. Lane WG, Rubin DM, Monteith R, Christian CW. Racial differences in theevaluation of pediatric fractures for physical abuse. JAMA. 2002;288(13):1603–1609.
27. Wood JN, Hall M, Schilling S, Keren R, Mitra N, Rubin DM. Disparities inthe evaluation and diagnosis of abuse among infants with traumatic brain in-jury. Pediatrics. 2010;126(3):408–414.
28. Rangel EL, Cook BS, Bennett BL, Shebesta K, Ying J, Falcone RA. Elimi-nating disparity in evaluation for abuse in infants with head injury: use of ascreening guideline. J Pediatr Surg. 2009;44(6):1229–1235.
29. HigginbothamN, LawsonKA, Gettig K, Roth J, Hopper E,HigginbothamE,George TM, Maxson T, Edwards G, Garcia NM. Utility of a child abusescreening guideline in an urban pediatric emergency department. J TraumaAcute Care Surg. 2014;76(3):871–877.
30. Jenny C, Hymel KP, Ritzen A, Reinert SE, Hay TC. Analysis of missed casesof abusive head trauma. JAMA. 1999;281(7):621–626.
31. Kim PT, McCagg J, Dundon A, Ziesler Z, Moody S, Falcone RA Jr. Consis-tent screening of admitted infants with head injuries reveals high rate ofnonaccidental trauma. J Pediatr Surg. 2017;52(11):1827–1830.
32. Nguyen HT, Newton C, Pirrotta EA, Aguilar C, Wang NE. Variations in uti-lization of inpatient rehabilitation services among pediatric trauma patients.J Pediatr. 2017;182:342–348.e1.
33. Hayes JR, Groner JI. Minority status and the risk of serious childhood injuryand death. J Natl Med Assoc. 2005;97(3):362–369.
34. Jimenez N, Symons RG, Wang J, Ebel BH, Vavilala MS, Buchwald D,Temkin N, Jaffe KM, Rivara FP. Outpatient rehabilitation for Medicaid-insured children hospitalized with traumatic brain injury. Pediatrics. 2016;137(6):e20153500–e20153500.
35. Haider AH, Efron DT, Haut ER, Dirusso SM, Sullivan T, Cornwell EE 3rd.Black children experience worse clinical and functional outcomes aftertraumatic brain injury: an analysis of the National Pediatric Trauma Registry.J Trauma. 2007;62(5):1259–1262.
549
ealth, Inc. All rights reserved.
LaPlant and HessJ Trauma Acute Care Surg
Volume 86, Number 3
36. McCarthy ML, Serpi T, Kufera JA, Demeter LA, Paidas C. Factors influenc-ing admission among children with a traumatic brain injury. Acad EmergMed. 2002;9(7):684–693.
37. Howard I, Joseph JG, Natale JE. Pediatric traumatic brain injury: do racial/ethnic disparities exist in brain injury severity, mortality, or medical disposi-tion? Ethn Dis. 2005;15(4 Suppl 5):S5-51–S5-56.
38. Piatt JH Jr, Neff DA. Hospital care of childhood traumatic brain injury in theUnited States, 1997-2009: a neurosurgical perspective. J Neurosurg Pediatr.2012;10(4):257–267.
39. Marcin JP, Pretzlaff RK,Whittaker HL, Kon AA. Evaluation of race and eth-nicity on alcohol and drug testing of adolescents admitted with trauma. AcadEmerg Med. 2003;10(11):1253–1259.
40. Oyetunji TA, Stevenson AA, Oyetunji AO, Onguti SK, Ames SA,Haider AH, Nwomeh BC. Profiling the ethnic characteristics of domestic in-juries in children younger than age 5 years. Am Surg. 2012;78(4):426–431.
41. Jimenez N, Ebel BE, Wang J, Koepsell TD, Jaffe KM, Dorsch A, Durbin D,Vavilala MS, Temkin N, Rivara FP. Disparities in disability after traumaticbrain injury among Hispanic children and adolescents. Pediatrics. 2013;131(6):e1850–e1856.
42. Jimenez N, Osorio M, Ramos JL, Apkon S, Ebel BE, Rivara FP. Functionalindependence after inpatient rehabilitation for traumatic brain injury amongminority children and adolescents. Arch Phys Med Rehabil. 2015;96(7):1255–1261.
43. Ruttan T, Lawson KA, Piper K, Wilkinson M. Visits following trauma sys-tem discharge. 2017;0(0):1–6.
44. Dy CJ, Lyman S, Do HT, Fabricant PD, Marx RG, Green DW. Socioeco-nomic factors are associated with frequency of repeat emergency departmentvisits for pediatric closed fractures. J Pediatr Orthop. 2014;34(5):548–551.
45. Barrow RE, Przkora R, Hawkins HK, Barrow LN, Jeschke MG,Herndon DN. Mortality related to gender, age, sepsis, and ethnicity in se-verely burned children. Shock. 2005;23(6):485–487.
550
Copyright © 2019 Wolters Kluwer H
46. Rangel EL, Burd RS, Falcone RA Jr. Socioeconomic disparities in infantmortality after nonaccidental trauma: a multicenter study. J Trauma. 2010;69(1):20–25.
47. Short SS, Liou DZ, Singer MB, Bloom MB, Margulies DR, Bukur M,Salim A, Ley EJ. Insurance type, not race, predicts mortality after pediatrictrauma. J Surg Res. 2013;184(1):383–387.
48. Hakmeh W, Barker J, Szpunar SM, Fox JM, Irvin CB. Effect of race andinsurance on outcome of pediatric trauma. Acad Emerg Med. 2010;17(8):809–812.
49. Rosen H, Saleh F, Lipsitz SR, Meara JG, Rogers SO Jr. Lack of insurancenegatively affects trauma mortality in US children. J Pediatr Surg. 2009;44(10):1952–1957.
50. Cassidy LD, Lambropoulos D, Enters J, Gourlay D, Farahzad M, Lal DR.Health disparities analysis of critically ill pediatric trauma patients in Mil-waukee, Wisconsin. J Am Coll Surg. 2013;217(2):233–239.
51. Falcone RA Jr, Brown RL, Garcia VF. The epidemiology of infant injuriesand alarming health disparities. J Pediatr Surg. 2007;42(1):172–176.
52. Falcone RA Jr, BrownRL, Garcia VF. Disparities in child abuse mortality arenot explained by injury severity. J Pediatr Surg. 2007;42(6):1031–1036.
53. Martin CA, Care M, Rangel EL, Brown RL, Garcia VF, Falcone RA Jr.Severity of head computed tomography scan findings fail to explain racialdifferences inmortality following child abuse.AmJ Surg. 2010;199(2):210–215.
54. Ramirez M, Chang DC, Bickler SW. Pediatric injury outcomes in racial/ethnic minorities in California: diversity may reduce disparity. JAMA Surg.2013;148(1):76–80.
55. Falcone RA Jr, Martin C, Brown RL, Garcia VF. Despite overall low pediat-ric head injury mortality, disparities exist between races. J Pediatr Surg.2008;43(10):1858–1864.
56. Haider AH, Efron DT, Haut ER, Chang DC, Paidas CN, Cornwell EE 3rd.Mortality in adolescent girls vs boys following traumatic shock: an analysisof the national pediatric trauma registry. Arch Surg. 2007;142(9):875–880.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

PROCEDURES AND TECHNIQUES
Periosteal flap repair for traumatic lung hernia.An old technique revisited
Hani Saiedi, MD, Nasir Bustangi, MD, Gabrielle Drevet, MD, and Francois Tronc, MD, PhD, France
L ung hernia can be defined as a protrusion of pulmonary tis-sue and pleural membranes through a defect in the chest
wall.1 These are rare and most commonly secondary to bluntor penetrating trauma. There are approximately 300 cases re-ported in the literature.2 Repair techniques vary, ranging fromprimary closure to implantation of prosthetic or autologous ma-terial. The periosteal flap technique was first described in 1933.We have an experience of four cases, three after blunt traumaand one after previous chest surgery, which were repaired usingsuch technique.
CASESA 60-year-old gentleman who suffered a direct chest trauma
while rowing was diagnosed with right hemopneumothorax sec-ondary to ninth rib fracture and a chest tubewas inserted. Duringhis follow-up appointment, physical examination revealed amass with paradoxical protrusion during expiration. Computedtomographic (CT) scan showed a segment of the right lung pa-renchyma protruding beyond the confines of the musculoskele-tal thorax into the subcutaneous space and a widened intercostalspace at the previous injury site. The second case is an 11-year-old boy whowas managed conservatively after falling off his bi-cycle and sustaining a handlebar injury to his chest. On thefollow-up visit, he complained of a painful, bulging, crepitantmass within the chest wall, on the left. The pain he felt was ex-acerbated by coughing and efforts. Clinical examination andchest CT scan confirmed the presence of left anterior pulmonaryhernia at the level of the fifth intercostal space (Fig. 1A). Thenext case is an 8-year-old boy who suffered a chest trauma dueto a fall on a round metal object and developed a chest wallhematoma. He was treated conservatively. One year later, hepresented a lump in the right side of the chest, and clinical andradiographic examination confirmed the presence of hernia atthe level of the sixth intercostal space. Our fourth patient is a44-year-old gentleman who had a minimally invasive mitralvalve repair. One year later, he presented with a painful bulgein the right side of the chest. Clinical examination revealed areducible lump at the site of previous minithoracotomy at the
From the Department of Thoracic Surgery, Louis Pradel Hospital, Lyon, France (H.S.,G.D., F.T.); and Department of Pediatric Surgery, King Abdul-Aziz UniversityHospital, Jeddah, KSA (N.B.).
Address for reprints: Hani Saiedi, MD,Department of Thoracic Surgery, Louis Pradel Hos-pital, 28 AvenueDoyen Jean Lépine, Bron 69500, France; email: [email protected].
DOI: 10.1097/TA.0000000000002154
J Trauma Acute Care SurgVolume 86, Number 3
Copyright © 2019 Wolters Kluwer H
level of the fourth intercostal space, which was confirmed byValsalva maneuver during CT scan examination.(Fig. 1B).
TECHNIQUE
At surgery, the patients were placed in a position allowingthe surgeon to access the hernia. A skin incision was made overthe affected intercostal space. Muscles were found unharmed inall patients, so muscle-sparing dissection was performed andhernial sac was identified as a mushroom in the intercostalspace. The sac was assessed to make sure that the lung wasnot incarcerated. It was freed and excised with preservation ofpleural edges. Using electrocautery, the periosteum coveringthe upper and lower ribs of the affected space was incised. Thelower half of periosteum covering the upper rib and the upperhalf of the periosteum over the lower rib were then elevated toform periosteal flaps using bone elevator in caudal and cephaladdirections, respectively. The flap was easy to create for the twochildren, since periosteal tissues were thick at this age. In adults,such tissues were much thinner. The flap was first delineatedwith electrocautery and afterward gently separated from the lat-eral part of the rib with a bone elevator. A chest tubewas insertedin preparation for repair of the hernia to drain potential air leak-age due to the liberation of pleural adhesions related to thetrauma and to stabilize the chest wall repair. With the use of a2–0 Vicryl suture, the pleura was closed in continuous fashion,followed by approximating the superior and inferior flaps using2–0 Vicryl repair in continuous manner. Thus, the gap betweenthe ribs was bridged by a complete layer of periosteum. To en-force the repair, three interrupted absorbable sutures were placedto approximate the upper and lower ribs (Fig. 2). Then, closureof the wound was done in layers.
Postoperative course for all four patients went smoothly,with hospital stays ranging from 3 to 5 days. Therewere no com-plications and no recurrence during follow-up.
DISCUSSION
The basic classification of lung hernias was suggested byMorel-Lavellee according to both anatomic location and etiol-ogy as congenital or acquired. He further differentiated the ac-quired hernias as spontaneous or pathologic, but the mostcommon causative factors of acquired lung hernias are blunt orpenetrating trauma and surgery.2 Recently, lung hernia aftervideo-assisted thoracic surgery and minithoracotomies has beenreported. In such cases, the cause is mainly inadequate closure ofthe wound undertaken by surgeons due to its limited size. Blunt
551
ealth, Inc. All rights reserved.
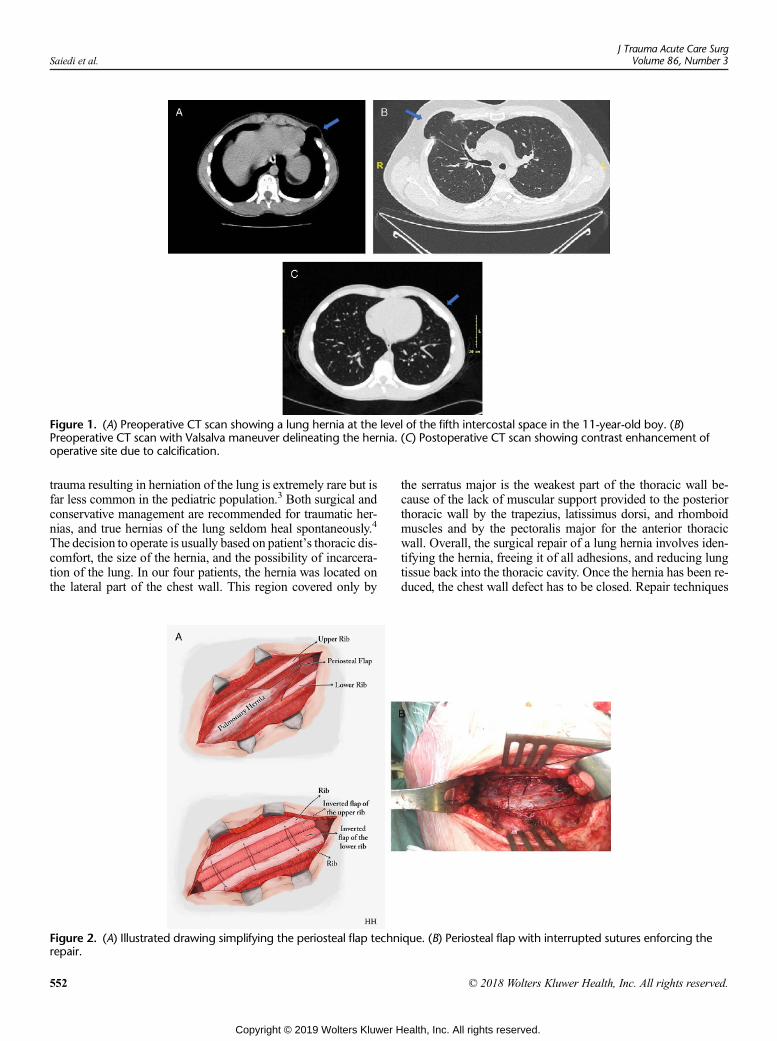
Figure 1. (A) Preoperative CT scan showing a lung hernia at the level of the fifth intercostal space in the 11-year-old boy. (B)Preoperative CT scan with Valsalva maneuver delineating the hernia. (C) Postoperative CT scan showing contrast enhancement ofoperative site due to calcification.
Saiedi et al.J Trauma Acute Care Surg
Volume 86, Number 3
trauma resulting in herniation of the lung is extremely rare but isfar less common in the pediatric population.3 Both surgical andconservative management are recommended for traumatic her-nias, and true hernias of the lung seldom heal spontaneously.4
The decision to operate is usually based on patient’s thoracic dis-comfort, the size of the hernia, and the possibility of incarcera-tion of the lung. In our four patients, the hernia was located onthe lateral part of the chest wall. This region covered only by
Figure 2. (A) Illustrated drawing simplifying the periosteal flap technrepair.
552
Copyright © 2019 Wolters Kluwer H
the serratus major is the weakest part of the thoracic wall be-cause of the lack of muscular support provided to the posteriorthoracic wall by the trapezius, latissimus dorsi, and rhomboidmuscles and by the pectoralis major for the anterior thoracicwall. Overall, the surgical repair of a lung hernia involves iden-tifying the hernia, freeing it of all adhesions, and reducing lungtissue back into the thoracic cavity. Once the hernia has been re-duced, the chest wall defect has to be closed. Repair techniques
ique. (B) Periosteal flap with interrupted sutures enforcing the
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 3 Saiedi et al.
vary, and smaller defects can be repaired with absorbable suturesto close the intercostal space.5 Some surgeons prefer to use pros-thetic mesh or muscle flaps especially for large defects throughthoracotomy or with video-assisted thoracic surgery.2,5
Periosteal flap repair was first described by Goodman in1933.6 Maurer and Blades reported five other cases after blunttrauma for one patient and secondary to emergent thoracotomyfor penetrating wound of the chest for the other four patients.7
These four soldiers suffered war injuries during World War II.In the late 1960s, Thomas Smith described the periosteal flap re-pair using nylon sutures with the enforcement by stainless steelwires to overcome the tendency of the ribs to spring apart andthereby to reduce tension on the periosteal flap suture line.8
We report here four other cases, and for the first time, oftwo children of 8 and 11 years of age, respectively. In our expe-rience, although performed in insufficient numbers to draw de-finitive conclusions, periosteal flap repair using absorbablesutures with approximation of ribs is safe and easy to performwith an excellent outcome and no recurrence observed in eitherof the four cases. We have no experience of the periosteal flaprepair in an acute setting. However, it will be probably harderto perform with crushed tissues and parietal hematoma. More-over, the presence of a rib fracture will contraindicate the proce-dure by the disruption of periosteal tissue, which is not the caseafter bone consolidation with thicker periosteal tissues due to fi-brosis as demonstrated in the first patient reported here.
The use of native tissue has the advantage of cost savingsand a theoretical benefit of reducing the risk of infection. More-over, foreign bodymaterial in children could have a negative im-pact on harmonious thoracic and spine growth and arepotentially subjected to surgical removal at some point of theirlife. The most important feature in the repair of pulmonary her-nias is the covering of the defect with sturdy tissue as perios-teum, which will produce bone, especially in pediatric patients,
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
as demonstrated in the 11-year-old boy (Fig. 1B). There is nosufficient experience in the surgical treatment of hernias of thechest wall to establish any one acceptable surgical technique.However, in the seven cases published to date as well as in ourfour new cases, periosteal flap suture seems to be a satisfactoryrepair of average-sized defects even in the pediatric population.
ACKNOWLEDGMENT
The authors thank Karine Debbasch for reviewing the English manuscriptand Hotaf Hamid for the realization of the drawing.
AUTHORSHIP
HS contributed tomanuscript writing, revision, and paper design. NB con-tributed to data collection. GD contributed to literature review. FT, the se-nior author, supervised this work and critically revised this paper.
DISCLOSURE
The authors declare no conflicts of interest.
REFERENCES1. Khalil MW, Masala N, Walter DA, Cardillo G. Surgical repair of post trau-
matic lung hernia using a video-assisted open technique. Interact CardiovascThorac Surg. 2008;7:506–507.
2. Johnson C, Weksler B. Lung hernia after video-assisted thoracoscopic lobec-tomy. Innovations. 2010;5:300–302.
3. Fine J, Walters BS, Agnoni AA, Coppola CP, Scorpio RJ, Kennedy AP. Pul-monary hernia in a two-year-old child. In: Case Reports in Surgery, Volume2014. London, UK: Hindawi Publishing Corporation, Article ID 792376.
4. Bikhchandani J, BaltersMW, Sugimoto JT. Conservative management of trau-matic lung hernia. Ann Thorac Surg. 2012;93(3):992–994.
5. Seder CW, Allen MS, Nichols FC, Wigle DA, Shen KR, Deschamps C,Cassivi SD. Primary and prosthetic repair of acquired chest wall hernias: a20-year experience. Ann Thorac Surg. 2014;98(2):484–489.
6. Goodman HI. Hernia of the lung. J Thorac Surg. 1933;2:368–379.7. Maurer E, Blades B. Hernia of the Lung. J Thorac Surg. 1946;15(2):77–98.8. Smith AT, Jamplis RW. Lung hernia: a technic for repair. Ann Surg. 1972;
176(6):711–712.
553
ealth, Inc. All rights reserved.

LETTERS TO THE EDITOR
In replyTrauma pneumonectomy
for major thoracicbleeding:When should we
consider it?
W e would like to thank Dr. Tonglet andcolleagues for their valuable com-
ments and questions regarding the indicationsfor pneumonectomy in severe chest trauma.Because of the limited information provided,we are unable to make any specific recom-mendations on their morality case. However,it would be important to note that the type oflung resection should be carefully chosenbased on intraoperative findings without anydelay.While pneumonectomy is not necessaryin many patients even with hilar injuries, afailure to control ongoing hemorrhage withless invasive lung resections can lead to per-sistent hemorrhagic shock and refractory co-agulopathy, which often cannot be recoveredwith pneumonectomy as a rescue procedure.
As we reported in our study, 70% of alldeaths following trauma pneumonectomy oc-curred within 24 hours after hospital admis-sion.1 Therefore, once the surgeons decided toperform pneumonectomy, postoperative man-agement should really be focused on optimizingthe patient's cardiopulmonary status in the inten-sive care unit. Although acute right-sided heartfailure and acute respiratory distress syndromeare known complications following pneumonec-tomy and associated with high mortality, recentdata suggest that the use of inhaled nitric oxideand extracorporeal membrane oxygenation canbe considered to improve the outcome of pneu-monectomy patients with hemodynamic insta-bility or severe respiratory failure.2,3 Certainly,further prospective studies are warranted toprovide a clear answer to the question by Dr.Tonglet and colleagues. In the meantime, wehope that the results of our study may be usedto guide the surgeons in making an importantdecision in the operating room, whether or notto perform pneumonectomy.
Kazuhide Matsushima, MDDemetrios Demetriades, MD, PhD
Division of Acute Care Surgery (K.M., D.D.)University of Southern California
Los Angeles, California
The authors declare no conflicts of interest.
554
Copyright
REFERENCES1. Matsushima K, Aiolfi A, Park C, Rosen D,
Strumwasser A, Benjamin E, Inaba K,Demetriades D. Surgical outcomes after traumapneumonectomy: revisited. J Trauma Acute CareSurg. 2017;82:927–932.
2. Lubitz AL, Sjoholm LO, Goldberg A, Pathak A,SantoraT, Sharp TE 3rd,WallnerM, Berretta RM,Poole LA, Wu J, Wolfson MR. Acute right heartfailure after hemorrhagic shock and traumapneumonectomy-a management approach: ablinded randomized controlled animal trial usinginhaled nitric oxide. J Trauma Acute Care Surg.2017;82:243–251.
3. Ahmad SB, Menaker J, Kufera J, O'Connor J,Scalea TM, Stein DM. Extracorporeal membraneoxygenation after traumatic injury. J TraumaAcute Care Surg. 2017;82:554–555.
Re: Use of anevidence-based
algorithm for patients withtraumatic hemothorax
reduces need foradditional interventions
S imilar to abdominal damage control sur-gery, damage control in the chest is a nec-
essary tool for every trauma surgeon, but itsuse must come with appropriate discretion.As cited in the Matsushima et al. article, bothtrauma pneumonectomy and hilar twist comewith significant consequence to the patient withregard to morbidity andmortality and should beavoided unless absolutely necessary. In initialhemorrhage control, a hilar twist should provideno advantage over simple clamping, either man-ually or with a shodded vascular clamp. On thepresumption that this is occurring in a resuscita-tive thoracotomy outside the operating room,this will allow for temporary hemorrhage con-trol until the patient can be taken to the operat-ing room and allow for continued resuscitation.
In contrast to damage control in the ab-domen, which focuses on hemorrhage andcontamination control, damage control in thechest requires maintenance ventilation and ox-ygenation in addition to hemorrhage control.The typical trauma patient will be able to sup-port adequate ventilation and oxygenationwith a single lung for the duration of a damagecontrol operation so long as there is not a sig-nificant portion of shunted blood through thenonventilated and injured lung, which would beprevented by a vascular clamp across the hilum.While thiswill not allow for temporary chest clo-sure and egress from the operating room, it willafford the surgeon time to carefully evaluate thesurgical options. In the setting of instability, we
© 2019 Wolters Kluwer Health, Inc. All rights res
strongly favor nonanatomic wedge resection ofinjured areas of the lung with an awareness ofthe course of the major vascular and bronchialstructures over total pneumonectomy.
The difficulty with initial pneumonec-tomy as damage control is the resultant pul-monary hypertension in the unaffected lungand the subsequent development of failure ofthe right side of the heart, which is the likelyreason for the failure to achieve a return ofspontaneous circulation in the mentioned case.In the event that pneumonectomy is absolutelynecessary, we emphasize the importance ofpreserving the function of the right side of theheart through several means. First, a focus oncrystalloid-free resuscitation and avoidanceof hypervolemia is critical, even in the initialphase of resuscitation. Second, intraoperativeplacement of a pulmonary arterial catheter willallow for continuous monitoring of pressuresof the right side of the heart postoperativelywithout the risk of perforating pulmonary arte-rial staple line. Finally, a tight closure of thepericardium should be avoided to prevent aneffective constrictive pericarditis, and insteadeither loose or no closure should be performed.
In summary, it is these authors' opinionthat both trauma pneumonectomy and hilar twistshould be avoided at all costs, with a preferencetoward simple manual control of the hilum orvascular clamping followed by nonanatomicwedge resection and temporary closure of thechest. For very proximal injuries to the hilumthat mandate pneumonectomy, a crystalloid-free, right-side-of-the-heart protective resuscita-tion strategy should be implemented.
Stephen Gondek, MD, MPHOscar Guillamondegui, MD, MPH
Bradley Dennis, MDTrauma and Acute Care Surgery
(S.G., O.G., B.D.)Vanderbilt University Medical Center
Nashville, Tennessee
Authors Responseto Commentary onour Manuscript
Dear Dr. Moore,
W e read with interest the letter to the ed-itor by Venketaraman et al. referring to
our study, “A cohort study of blunt cerebrovas-cular injury screening in children: Are they justlittle adults?” and appreciate their thoughtful
J Trauma Acute Care SurgVolume 86, Number 3
erved.

LETTERS TO THE EDITOR
In replyTrauma pneumonectomy
for major thoracicbleeding:When should we
consider it?
W e would like to thank Dr. Tonglet andcolleagues for their valuable com-
ments and questions regarding the indicationsfor pneumonectomy in severe chest trauma.Because of the limited information provided,we are unable to make any specific recom-mendations on their morality case. However,it would be important to note that the type oflung resection should be carefully chosenbased on intraoperative findings without anydelay.While pneumonectomy is not necessaryin many patients even with hilar injuries, afailure to control ongoing hemorrhage withless invasive lung resections can lead to per-sistent hemorrhagic shock and refractory co-agulopathy, which often cannot be recoveredwith pneumonectomy as a rescue procedure.
As we reported in our study, 70% of alldeaths following trauma pneumonectomy oc-curred within 24 hours after hospital admis-sion.1 Therefore, once the surgeons decided toperform pneumonectomy, postoperative man-agement should really be focused on optimizingthe patient's cardiopulmonary status in the inten-sive care unit. Although acute right-sided heartfailure and acute respiratory distress syndromeare known complications following pneumonec-tomy and associated with high mortality, recentdata suggest that the use of inhaled nitric oxideand extracorporeal membrane oxygenation canbe considered to improve the outcome of pneu-monectomy patients with hemodynamic insta-bility or severe respiratory failure.2,3 Certainly,further prospective studies are warranted toprovide a clear answer to the question by Dr.Tonglet and colleagues. In the meantime, wehope that the results of our study may be usedto guide the surgeons in making an importantdecision in the operating room, whether or notto perform pneumonectomy.
Kazuhide Matsushima, MDDemetrios Demetriades, MD, PhD
Division of Acute Care Surgery (K.M., D.D.)University of Southern California
Los Angeles, California
The authors declare no conflicts of interest.
554
Copyright
REFERENCES1. Matsushima K, Aiolfi A, Park C, Rosen D,
Strumwasser A, Benjamin E, Inaba K,Demetriades D. Surgical outcomes after traumapneumonectomy: revisited. J Trauma Acute CareSurg. 2017;82:927–932.
2. Lubitz AL, Sjoholm LO, Goldberg A, Pathak A,SantoraT, Sharp TE 3rd,WallnerM, Berretta RM,Poole LA, Wu J, Wolfson MR. Acute right heartfailure after hemorrhagic shock and traumapneumonectomy-a management approach: ablinded randomized controlled animal trial usinginhaled nitric oxide. J Trauma Acute Care Surg.2017;82:243–251.
3. Ahmad SB, Menaker J, Kufera J, O'Connor J,Scalea TM, Stein DM. Extracorporeal membraneoxygenation after traumatic injury. J TraumaAcute Care Surg. 2017;82:554–555.
Re: Use of anevidence-based
algorithm for patients withtraumatic hemothorax
reduces need foradditional interventions
S imilar to abdominal damage control sur-gery, damage control in the chest is a nec-
essary tool for every trauma surgeon, but itsuse must come with appropriate discretion.As cited in the Matsushima et al. article, bothtrauma pneumonectomy and hilar twist comewith significant consequence to the patient withregard to morbidity andmortality and should beavoided unless absolutely necessary. In initialhemorrhage control, a hilar twist should provideno advantage over simple clamping, either man-ually or with a shodded vascular clamp. On thepresumption that this is occurring in a resuscita-tive thoracotomy outside the operating room,this will allow for temporary hemorrhage con-trol until the patient can be taken to the operat-ing room and allow for continued resuscitation.
In contrast to damage control in the ab-domen, which focuses on hemorrhage andcontamination control, damage control in thechest requires maintenance ventilation and ox-ygenation in addition to hemorrhage control.The typical trauma patient will be able to sup-port adequate ventilation and oxygenationwith a single lung for the duration of a damagecontrol operation so long as there is not a sig-nificant portion of shunted blood through thenonventilated and injured lung, which would beprevented by a vascular clamp across the hilum.While thiswill not allow for temporary chest clo-sure and egress from the operating room, it willafford the surgeon time to carefully evaluate thesurgical options. In the setting of instability, we
© 2019 Wolters Kluwer Health, Inc. All rights res
strongly favor nonanatomic wedge resection ofinjured areas of the lung with an awareness ofthe course of the major vascular and bronchialstructures over total pneumonectomy.
The difficulty with initial pneumonec-tomy as damage control is the resultant pul-monary hypertension in the unaffected lungand the subsequent development of failure ofthe right side of the heart, which is the likelyreason for the failure to achieve a return ofspontaneous circulation in the mentioned case.In the event that pneumonectomy is absolutelynecessary, we emphasize the importance ofpreserving the function of the right side of theheart through several means. First, a focus oncrystalloid-free resuscitation and avoidanceof hypervolemia is critical, even in the initialphase of resuscitation. Second, intraoperativeplacement of a pulmonary arterial catheter willallow for continuous monitoring of pressuresof the right side of the heart postoperativelywithout the risk of perforating pulmonary arte-rial staple line. Finally, a tight closure of thepericardium should be avoided to prevent aneffective constrictive pericarditis, and insteadeither loose or no closure should be performed.
In summary, it is these authors' opinionthat both trauma pneumonectomy and hilar twistshould be avoided at all costs, with a preferencetoward simple manual control of the hilum orvascular clamping followed by nonanatomicwedge resection and temporary closure of thechest. For very proximal injuries to the hilumthat mandate pneumonectomy, a crystalloid-free, right-side-of-the-heart protective resuscita-tion strategy should be implemented.
Stephen Gondek, MD, MPHOscar Guillamondegui, MD, MPH
Bradley Dennis, MDTrauma and Acute Care Surgery
(S.G., O.G., B.D.)Vanderbilt University Medical Center
Nashville, Tennessee
Authors Responseto Commentary onour Manuscript
Dear Dr. Moore,
W e read with interest the letter to the ed-itor by Venketaraman et al. referring to
our study, “A cohort study of blunt cerebrovas-cular injury screening in children: Are they justlittle adults?” and appreciate their thoughtful
J Trauma Acute Care SurgVolume 86, Number 3
erved.

J Trauma Acute Care SurgVolume 86, Number 3 Letters to the Editor
analysis.1 We do, however, respectfully dis-agree on several points that we believe war-rant discussion and consideration.
The primary finding of our study is thatthe rate of blunt cerebrovascular injury (BCVI)in pediatric patients is higher than previouslyexpected and that the currently clinical screen-ing tools available to us are insufficiently sensi-tive. As a result, there are likely a number ofmissed BCVIs in the pediatric population, al-though we do agree with Venketaraman et al.that these injuries are likely clinically minor.To maximize injury identification and mini-mize missed injuries, we therefore recommendapplication of more liberal clinically screeningcriteria. The authors of the letter advocate foruse of theMcGovern score to minimize missedinjuries and, in effect, are actualizing our rec-ommendation by adding mechanism of injuryto the previously described Utah score to pro-vide a more liberal indication for imaging.2
While their commentary is correct inpointing out that our cohort represents a combi-nation of adolescents and children, it reflects theinjury patterns and patient demographics of alarger trauma center and thus provides pragmaticdata for the practicing trauma surgeon. Wefurthermore agree that ionizing radiation ex-posure is always a concern in the pediatric pa-tient; however, this must be balanced againstthe potential clinical significance of a missedBCVI and risk of permanent neurologic se-quelae. Balancing future oncologic risk with
© 2018 Wolters Kluwer Health, Inc. All rights re
Copyrigh
immediate injury risk is one of the more chal-lenging problems in trauma care. We wouldbe cautious to limit the evaluation of a poten-tially acutely injured trauma patient due tofears of low-incidence future events and thussubjecting them to immediate risk to mitigatefuture risk. We recognize that this is likely asmuch a philosophical argument as it is a clinicalargument. Without a validated clinical screeningtool with acceptable sensitivity and specific-ity, one is forced to make a subjective choice,balancing a future small risk of malignancywith a more immediate, and 10-fold higher,risk of BCVI and attended risk of stroke.
The McGovern score, while conceptu-ally interesting and worthy of further investi-gation, is currently not clinically validated;and 19% of patients were misclassified intheir small cohort. Their analysis is basedon a retrospective cohort of patients who actu-ally received imaging and thus, their study andours suffer from the same fundamental lim-itation, namely, there is likely a larger-than-appreciated incidence of clinically silent andthus undiagnosed BCVIs in children who arenot radiographically screened and followedin the long term. This likely raises the missedinjury rate of the McGovern score, further sup-ports more liberal imaging to reduce themissedinjury rate, and limits immediate clinical ap-plication of their score for further validation.
Despite these concerns, we sincerelyapplaud their work, and we are all clearly in
served.
t © 2019 Wolters Kluwer Health, Inc. All rights re
agreement that better clinical screening toolsare needed for children and a large, multicenter,prospective trial is warranted. Wewould like tothank Venketaraman et al. for their thoughtfulcommentary on our work, and we look forwardto their future investigations on the subject.
SincerelyMackenzie Cook, MDJoseph Cuschieri, MD
Mackenzie Rainier Cook, MDJoseph Cuschieri, MD
Oregon Health and Science UniversityPortland, Oregon
Author contributions: MC wrote and crit-ically revised the letter. JC critically revisedthe letter.
REFERENCES1. Cook MR, Witt CE, Bonow RH, Bulger EM,
Linnau KF, Arbabi S, Robinson BRH, Cuschieri J.A cohort study of blunt cerebrovascular injuryscreening in children: are they just little adults? JTrauma Acute Care Surg. 2018;84(1):50–57.
2. Ravindra VM, Bollo RJ, Sivakumar W, Akbari H,Naftel RP, Limbrick DD Jr., Jea A, Gannon S,ShannonC, Birkas Y, et al. Predicting blunt cere-brovascular injury in pediatric trauma: validationof the “Utah score”. J Neurotrauma. 2017;34(2):391–399.
555
served.
2019 JOHN M. TEMPLETON, JR.PEDIATRIC TRAUMA SYMPOSIUM
March 1Y2, 2019Omni William Penn Hotel Pittsburgh, PAWestin Snowmass ResortTempletontrauma.org
49TH ANNUAL MEETING OF THEWESTERN TRAUMA ASSOCIATION
March 3Y8, 2019Westin Snowmass ResortSnowmass, COhttps://westerntrauma.org/
TRAUMA CENTER ASSOCIATIONOF AMERICA’S 22ND
ANNUAL CONFERENCE
April 28 - May 3, 2019Luxor Hotel 18, 2019Luxor Hotel &Casino in Las Vegas, NVhttps://www.traumacenters.org
ENDOVASCULAR RESUSCITATIONAND TRAUMA
MANAGEMENT (EVTM) SYMPOSIUM
November 17Y18, 2019Pan-American EVTM Denver,Colorado (#panamevtm2019)http://www.jevtm.com/evtm-symposium/
Please send your meeting and course information to [email protected] to be included in the Meetings/Courses sectionof the journal. Please contact [email protected] if you would like to highlight your event in The Journal of Traumaand Acute Care Surgery with a paid advertising placement.
MEETINGS/COURSES
J Trauma Acute Care SurgVolume 86, Number 3556
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.

Featured Articles for CME Credit March 2019
Recurring Emergency General Surgery: Characterizing aVulnerable PopulationNicole Lunardi, MSPH, Ambar Mehta, MD, MPH, Hiba Ezzeddine, MD, Joseph K Canner, MHS, Mohammad Hamidi,MD, Faisal Jehan, MD, Bellal A Joseph, MD, Avery B Nathens, MD, MPH, PhD, Jose Diaz Jr, MD, CNS, David T Efron,MD, Joseph V. Sakran, MD, MPA, MPH, FACS(J Trauma Acute Care Surg. 2019;86(3):465Y471)
The Impact of Hypothermia on Outcomes in MassivelyTransfused PatientsErica Louise Walsh Lester, MD, MSc, Erin E. Fox, PhD, John Holcomb, MD, Karen Brasel, MD, MPH, Eileen M. Bulger, MD,Mitchell Cohen, MD, Bryan A. Cotton, MD, MPH, Timothy C. T.C. Fabian, MD, Jeffery D. Kerby, MD, PhD, TerrenceO’Keefe, MB, ChB, MSPH, Sandro B. Rizoli, MD, PhD, Thomas Scalea, MD, Martin A. Schreiber, MD, Kenji Inaba, MD,FRCSC, FACS(J Trauma Acute Care Surg. 2019;86(3):459Y464)
Management of Adhesive Small Bowel Obstruction: A Distinct ParadigmShift in the United StatesKazuhide Matsushima, M.D. Andrew Sabour, BS Caroline Park, MD, MPH, Aaron Strumwasser, MD, Kenji Inaba, MD,Demetrios Demetriades, MD, PhD(J Trauma Acute Care Surg. 2019;86(3):383Y391)
Development of a Geospatial Approach for the Quantitative Analysis ofTrauma Center AccessRobert J. Winchell, MD, Paige Xu, MPH, Lauren E. Mount, MD, Reed Huegerich, MCRP, AICP(J Trauma Acute Care Surg. 2019;86(2):398Y406)
CME ARTICLE 1
Recurring Emergency General Surgery: Characterizing aVulnerable Population
Nicole Lunardi, MSPH Ambar Mehta, MD, MPH Hiba Ezzeddine,MD Joseph K Canner, MHS Mohammad Hamidi, MD Faisal Jehan,MD Bellal A Joseph, MD Avery B Nathens, MD, MPH, PhD JoseDiaz Jr, MD, CNS David T Efron, MD Joseph V. Sakran, MD, MPA,MPH, FACS(J Trauma Acute Care Surg. 2019;86(3):465Y471)
Impact Statement:There is a subset (11.6%) of readmitted emergency generalsurgery (EGS) patients who undergo a second EGS procedure.The majority of these patients present to the same hospital andwithin the 90-day global follow up period. As such, our studysuggests that there may be a unique opportunity to preventfuture emergency surgical interventions by identifying thehighest risk patients at the time of discharge from the indexhospitalization.
Article Objective:This study aimed to characterize the incidence of inpatientreadmissions and additional operations within 6-months of anEGS procedure.
QUESTION 1:Which of the following statements is true regarding Emergency GeneralSurgery (EGS) procedure outcomes based on previous literature?
A. EGS is independently associated with morbidity, but notmortality
B. EGS is independently associated with mortality, but notmorbidity
C. EGS is independently associated with both morbidity andmortality
D. EGS is not associated with morbidity or mortality relativeto elective procedures
QUESTION 2:
What is the trend in all cause inpatient readmission rates amongEGS patients within 6 months of discharge?
A. Readmission rates continue to rise between 1, 3 and 6monthsB. Readmission rates rise until 3 months, then flattenC. Readmission rates peak at 1 month and downtrend thereafterD. Readmission rates rise exponentially between 1, 3 and 6months
QUESTION 3:
Which of the following statements best characterizes the patientswho underwent a second EGS procedure in this study?
CONTINUING MEDICAL EDUCATION PROGRAM
J Trauma Acute Care SurgVolume 86, Number 3 e7
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.

A. Most patients received the second EGS procedure at adifferent hospital relative to the index procedure
B. The majority presented within the 90 day follow up periodC. The most common index procedure was a cholecystectomyD. The second procedure did not vary by index procedure type
QUESTION 4:A 58-year-old male with a past medical history of hypertension,osteoarthritis and obesity presented to the emergency departmentwith an upper GI bleed secondary to an ulcer. He required anemergency surgical procedure. His pos-operative course wasunremarkable and he was discharged home on post-operativeday 4.Which of the following risk factors specific to this patientincrease his odds the most for a second EGS procedure withinthe next 6 months?
A. Male sexB. Number of comorbiditiesC. Type of index procedureD. Discharge to home
CME ARTICLE 2
The Impact of Hypothermia on Outcomes in Massively Trans-fused Patients
Erica LouiseWalsh Lester, MD,MSc, Erin E. Fox, PhD John Holcomb,MD, Karen Brasel, MD, MPH, Eileen M. Bulger, MD, Mitchell Cohen,MD, Bryan A. Cotton, MD,MPH, Timothy C. T.C. Fabian, MD, JefferyD. Kerby, MD, PhD, Terrence O’Keefe, MB, ChB, MSPH, Sandro B.Rizoli, MD, PhD, Thomas Scalea, MD,Martin A. Schreiber, MD, KenjiInaba, MD, FRCSC, FACS
(J Trauma Acute Care Surg. 2019;86(3):459Y464)
Impact Statement:This cohort study is a secondary analysis of the PROPPR trial, whichwas a randomized control trial that compared the outcomes of 1:1:1versus 1:1:2 resuscitation in patients expected to require massivetransfusion and admitted to a Level I trauma center. This study illustratesthe association between temperature and blood product requirement inthe massively transfused trauma patient. The results indicate that everyone-degree decrease in temperature below 36.0 degrees is associatedwith a 10% increase in consumption of red blood cells during the first24 hours of admission.
Article Objective:The primary objective of this study was to ascertain the independentimpact of hypothermia on blood product requirements during initialresuscitation, and to examine the association of hypothermia withmortality in critically injured trauma patients undergoing contemporarylarge volume balanced resuscitation.
QUESTION 1:What proportion of patients requiring massive transfusion are hypo-thermic within the first 6 hours of hospital arrival?
A. 1/4B. 1/3C. 2/3D. 3/4
QUESTION 2:In this study, what percentage of patients have a temperaturerecorded within the first 6 hours?
A. 93%B. 72%C. 66%D. 87%
QUESTION 3:In patients that requiremassive transfusion protocol, arriving in the traumabay hypothermic has an adjusted odds ratio of 24-hour mortality of:
A. 1.0B. 1.7C. 2.7D. 4.5
QUESTION 4:A patient arrives in the trauma bay with a temperature of 35.5-C.Within one hour, his temperature is 34.5-C. Independent of othervariables, what percentage change in blood product requirement willthis be associated with?
A. j10%B. +10%C. j30%D. +30%
CME ARTICLE 3
Management of Adhesive Small Bowel Obstruction: ADistinctParadigm Shift in the United States
KazuhideMatsushima, M.D. Andrew Sabour, BS, Caroline Park, MD,MPH,Aaron Strumwasser,MD,Kenji Inaba,MD,DemetriosDemetriades,MD, PhD
(J Trauma Acute Care Surg. 2019;86(3):383Y391)
Impact Statement:In the United States, we have observed significant trends in the man-agement of adhesive small bowel obstruction; less frequent but earliersurgical interventions. Also, the in-hospital mortality has significantlydecreased over the last decade.
Article Objective:The purpose of this study was to evaluate the recent trends in managingpatients with adhesive small bowel obstruction and their outcomes.
QUESTION 1:What is the percentage of patients who underwent surgical interventionfor adhesive small bowel obstruction in 2013?
A. 20Y30%B. 30Y40%C. 40Y50%D. 50Y60%
QUESTION 2:In the patientswho underwent surgical interventions for adhesivesmall bowel obstruction, what is the percentage of patients whounderwent surgery within 24 hours of admission in 2013?
J Trauma Acute Care SurgVolume 86, Number 3Continuing Medical Education Program
e8 * 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
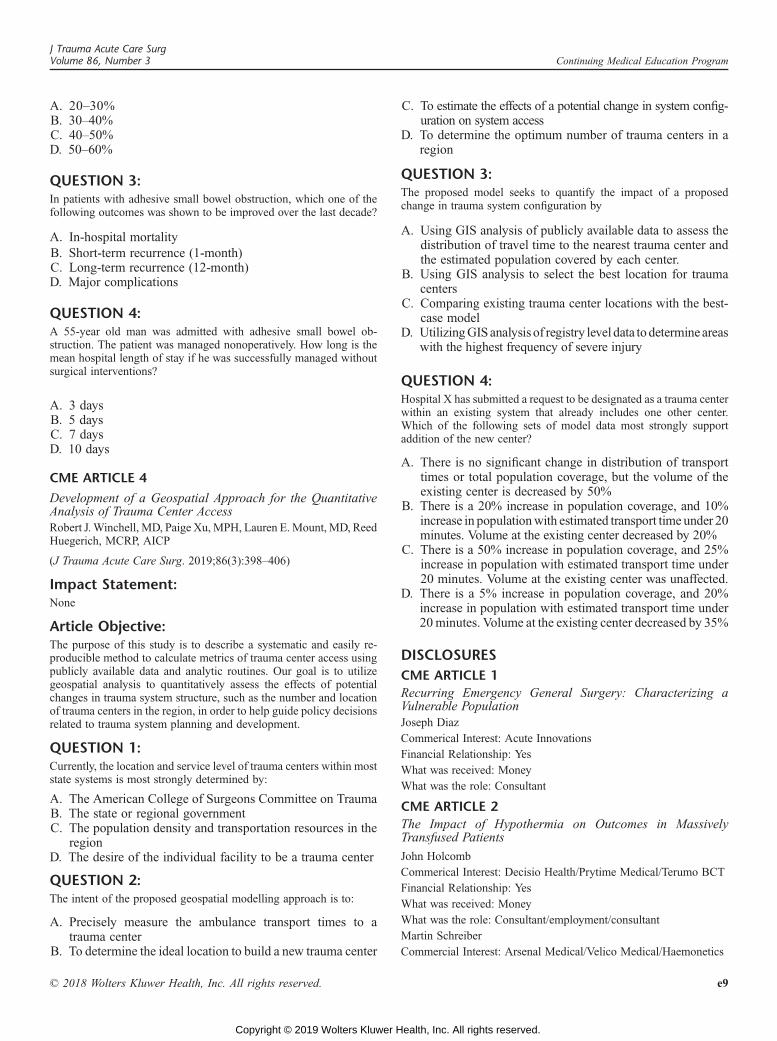
A. 20Y30%B. 30Y40%C. 40Y50%D. 50Y60%
QUESTION 3:In patients with adhesive small bowel obstruction, which one of thefollowing outcomes was shown to be improved over the last decade?
A. In-hospital mortalityB. Short-term recurrence (1-month)C. Long-term recurrence (12-month)D. Major complications
QUESTION 4:A 55-year old man was admitted with adhesive small bowel ob-struction. The patient was managed nonoperatively. How long is themean hospital length of stay if he was successfully managed withoutsurgical interventions?
A. 3 daysB. 5 daysC. 7 daysD. 10 days
CME ARTICLE 4
Development of a Geospatial Approach for the QuantitativeAnalysis of Trauma Center AccessRobert J.Winchell, MD, Paige Xu,MPH, Lauren E.Mount, MD, ReedHuegerich, MCRP, AICP
(J Trauma Acute Care Surg. 2019;86(3):398Y406)
Impact Statement:None
Article Objective:The purpose of this study is to describe a systematic and easily re-producible method to calculate metrics of trauma center access usingpublicly available data and analytic routines. Our goal is to utilizegeospatial analysis to quantitatively assess the effects of potentialchanges in trauma system structure, such as the number and locationof trauma centers in the region, in order to help guide policy decisionsrelated to trauma system planning and development.
QUESTION 1:Currently, the location and service level of trauma centers within moststate systems is most strongly determined by:
A. The American College of Surgeons Committee on TraumaB. The state or regional governmentC. The population density and transportation resources in the
regionD. The desire of the individual facility to be a trauma center
QUESTION 2:The intent of the proposed geospatial modelling approach is to:
A. Precisely measure the ambulance transport times to atrauma center
B. To determine the ideal location to build a new trauma center
C. To estimate the effects of a potential change in system config-uration on system access
D. To determine the optimum number of trauma centers in aregion
QUESTION 3:The proposed model seeks to quantify the impact of a proposedchange in trauma system configuration by
A. Using GIS analysis of publicly available data to assess thedistribution of travel time to the nearest trauma center andthe estimated population covered by each center.
B. Using GIS analysis to select the best location for traumacenters
C. Comparing existing trauma center locations with the best-case model
D. UtilizingGIS analysis of registry level data todetermine areaswith the highest frequency of severe injury
QUESTION 4:Hospital X has submitted a request to be designated as a trauma centerwithin an existing system that already includes one other center.Which of the following sets of model data most strongly supportaddition of the new center?
A. There is no significant change in distribution of transporttimes or total population coverage, but the volume of theexisting center is decreased by 50%
B. There is a 20% increase in population coverage, and 10%increase in populationwith estimated transport time under 20minutes. Volume at the existing center decreased by 20%
C. There is a 50% increase in population coverage, and 25%increase in population with estimated transport time under20 minutes. Volume at the existing center was unaffected.
D. There is a 5% increase in population coverage, and 20%increase in population with estimated transport time under20minutes. Volume at the existing center decreased by 35%
DISCLOSURES
CME ARTICLE 1
Recurring Emergency General Surgery: Characterizing aVulnerable PopulationJoseph DiazCommerical Interest: Acute InnovationsFinancial Relationship: YesWhat was received: MoneyWhat was the role: Consultant
CME ARTICLE 2
The Impact of Hypothermia on Outcomes in MassivelyTransfused Patients
John HolcombCommerical Interest: Decisio Health/Prytime Medical/Terumo BCTFinancial Relationship: YesWhat was received: MoneyWhat was the role: Consultant/employment/consultantMartin SchreiberCommercial Interest: Arsenal Medical/Velico Medical/Haemonetics
J Trauma Acute Care SurgVolume 86, Number 3 Continuing Medical Education Program
* 2018 Wolters Kluwer Health, Inc. All rights reserved. e9
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.

Financial Relationship: YesWhat was received: GrantsWhat was the role: PI
CME ARTICLE 3
Management of adhesive small bowel obstruction: a distinctparadigm shift in the United StatesNONE
CME ARTICLE 4
Development of a Geospatial Approach for the QuantitativeAnalysis of Trauma Center Access
Robert WinchellCommercial Interest: Stryker Corporation/CRICO Insurance companyFinancial Relationship: YesWhat was received: MoneyWhat was the role: Consultant/Expert Witness
J Trauma Acute Care SurgVolume 86, Number 3Continuing Medical Education Program
e10 * 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
Related Documents