2/29/2016 1 Management of Acute Heart Failure and Cardiogenic Shock www.fshp.org Brittany D. Bissell, Pharm.D. PGY-2 Critical Care Pharmacy Resident Jackson Memorial Hospital | Miami, Florida DISCLOSURE STATEMENT I have no actual or potential conflicts of interest in relation to this presentation. 2 TECHNICIAN OBJECTIVES • Explain management principles for left ventricular failure • Describe treatment options for end-stage heart failure • List pharmacologic therapies for cardiogenic shock 3 PHARMACIST OBJECTIVES • Assess the hemodynamic dysregulation implicated in the pathophysiology of heart failure • Develop recommendations for preload optimization • Investigate evidence for current options for the management of cardiogenic shock 4

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

2/29/2016
1
Management of Acute Heart Failure and Cardiogenic Shock
www.fshp.org
Brittany D. Bissell, Pharm.D.PGY-2 Critical Care Pharmacy Resident
Jackson Memorial Hospital | Miami, Florida
DISCLOSURE STATEMENT
I have no actual or potential conflicts of interest in relation to this presentation.
2
TECHNICIAN OBJECTIVES
• Explain management principles for left ventricular failure
• Describe treatment options for end-stage heart failure
• List pharmacologic therapies for cardiogenic shock
3
PHARMACIST OBJECTIVES
• Assess the hemodynamic dysregulation implicated in the pathophysiology of heart failure
• Develop recommendations for preload optimization
• Investigate evidence for current options for the management of cardiogenic shock
4
2/29/2016
2
PATHOPHYSIOLOGY OF
ACUTE HEART FAILURE
6
Afterload mismatch
Insulting Event
PATHOPHYSIOLOGY
Fluid Overload
Neurohormonal Activation
Diastolic Dysfunction
Afterload Mismatch
Cotter, et al. Am Heart J. 2008;155(1):9-18.
• Cardiac changes– Decreased stroke volume (SV)
– Increased end-diastolic pressure
• Vascular changes– Increased systemic vascular resistance
– Increased venous pressure
– Decreased arterial pressure
– Decreased compliance
HEMODYNAMIC DYSREGULATION
7
CARDIAC PHYSIOLOGY
Sinoatrial node automaticity
Vagal innervation
Sympathetic activity and catecholamines8
Inotropy: Contractile force
Afterload: Resistance against ejection
Preload: Pre-contraction stretch of cardiac myocyte
Heart Rate Stroke Volume

2/29/2016
3
IMPROVING STROKE VOLUME
9
Decreased Afterload↓ Systemic vascular resistance↓Aortic pressure
Increased Preload
↑Aortic Pressure↓ Heart Rate ↑Atrial Contractility ↑ Central Venous Pressure↑ Ventricular Compliance
Increased Inotropy
↑ Catecholamines↓ Vagal Inhibition↑ Sympathetic Activation↑Afterload↑ Heart Rate
EDV = End Diastolic Volume | ESV = End Systolic Volume
CARDIAC FUNCTION PARAMETERS
• Central venous pressure (CVP)
– Representative of right ventricular end diastolic pressure / preload
– Normal: 2 - 6 mmHg
• Cardiac index (CI)
– Correction of cardiac output for body surface area
– Normal: 2.5 - 4.0 L/min/m2
• Systemic vascular resistance index (SVRI)
– Resistance of blood flow by systemic vasculature corrected for surface area
– Normal: 800 - 1200 dynes - sec/cm-5
10
ACUTE MANAGEMENT
11
Preload optimization
Afterload optimization
Inotropic support
Congestion
Poor Systemic Perfusion
• Jugular vein distension• Hepatomegaly• Peripheral edema• Pulmonary edema
• Cold extremities• Alteration in mental status• Decreased urine output• Elevated lactate
Patient Evaluation
Mebazza, et al. Intensive Care Med. 2016 Feb;42(2):147-63.
ACUTE MANAGEMENT
12
ACUTE HEART FAILURE
CONGESTION CONGESTION & LOW OUTPUT
MILDMODERATE-
SEVERE
SBP >90 SBP <90
DobutamineVasopressors
MilrinoneDobutamine
IV furosemide Furosemide infusion
plus nitroglycerin
Howlett. Can J Cardiol. 2011;27(3):284-95.
MILD-MODERATE
SEVERE
Consider PA line

2/29/2016
4
PRELOAD
OPTIMIZATION
14
OPTIMIZATION OF PRELOAD
DIURETICS DOPAMINEHYPERTONIC
SALINEULTRAFILTRATION
LOOP DIURETIC RESISTANCE
15
Ter Maaten, et al. Nat Rev Cardiol. 2015;12(3):184-92.
Alternative therapies
DIURETIC RESISTANCE MANAGEMENT
16
DOSE: No differences in responsewith continuous infusion
Dose-dependent mortality with furosemide over 300 mg
Diuretic Response0.5 L net fluid outputOr 0.4 kg weight loss
HYPERTONIC
SALINEDOPAMINE ULTRAFILTRATION
Ter Maaten, et al. Nat Rev Cardiol. 2015;12(3):184-92.
LOOP DIURETIC
INTRAVENOUS LOOP
ALTERNATIVE LOOP
COMBINATION
THERAPY

2/29/2016
5
CHOICE OF DIURETIC
STANDARD THERAPY = FUROSEMIDE
TORSEMIDE
• Liver clearance and increased bioavailability
• Correction of collagen cross-linking and left ventricular stiffness
• Decreased sympathetic nerve response and remodeling
• Significant improvement in NYHA class compared to furosemide
• Decreased mortality compared to furosemide
Ter Maaten, et al. Nat Rev Cardiol. 2015;12(3):184-92.Di Somma, et al. Rev Esp Cardiol. 2015;68(8):706-13.
COMBINATION THERAPY
18
Ter Maaten, et al. Nat Rev Cardiol. 2015;12(3):184-92.
DOPAMINE
•5 mcg/kg/min with furosemide 5 mg/hour•As effective as furosemide 20 mg/hour with decrease in worsened renal function
DAD-HF
•2 mcg/kg/minute•No effect on urine volume or cystatin C
ROSE
•5 mcg/kg/minute•No difference in urine output or mortality
DAD-HF II
19
Ter Maaten, et al. Nat Rev Cardiol. 2015;12(3):184-92.
HYPERTONIC SALINE
• Mobilization of extravascular fluid into the intravascular space
• Increases cardiac output, renal blood flow, and quick excretion
• SMAC-HF Trial
– 150 mL of hypertonic saline twice daily
– Increased diuresis
– Decreased creatinine
– Reduction in hospitalization and readmission
– Decreased mortality
20
Ter Maaten, et al. Nat Rev Cardiol. 2015;12(3):184-92.

2/29/2016
6
ULTRAFILTRATION
RAPID-CHF
• 8 hour ultrafiltration versus pharmacologic treatment
• Increased fluid removal
• No difference in 24-hour weight loss
UNLOAD
• Ultrafiltration versus intravenous diuretics
• Increased fluid removal
• No difference in dyspnea
• Decrease in rehospitalization and hospital visits
CARRESS-HF
• Fixed-rate ultrafiltration versus stepwise diuretics
• Increased serum creatinine
• Increased adverse events
21
Semipermeable membrane yields iso-osmotic ultrafiltrate
Added benefit of removal of myocardial depressant cytokines
Ter Maaten, et al. Nat Rev Cardiol. 2015;12(3):184-92.
AFTERLOAD
OPTIMIZATION
23
OPTIMIZATION OF AFTERLOAD
NITRATES NESIRITIDE CLEVIDIPINE
24
NITRATE THERAPY
Nitroglycerin
•5- 200 mcg/min
•Primarily venodilation with coronary vasodilation
•Decreased rates of endotracheal intubation and ICU admission
•Tachyphylaxis problematic
Nitroprusside
•0.25 - 3 mcg/kg/min
•Primarily arterial with some venous vasodilation
•Retrospective study evidence
•Concern in renal dysfunction
Mebazza, et al. Intensive Care Med. 2016 Feb;42(2):147-63.

2/29/2016
7
NESIRITIDE
– Arterial and venous vasodilation with natriuretic effects
– Significant improvement in cardiac output and dyspnea
– Increased short-term mortality and symptomatic hypotension
CLEVIDIPINE
– Selective arterial vasodilation
– 2 - 32 mg/hour
– Rapid reduction in blood pressure without worsening of heart failure
– Higher rates of target blood pressure and dyspnea improvement compared to standard of care
25
NITRATE ALTERNATIVES
Mebazza, et al. Intensive Care Med. 2016 Feb;42(2):147-63.Di Somma, et al. Rev Esp Cardiol. 2015;68(8):706-13.
INOTROPIC SUPPORT
27
CARDIOGENIC SHOCK
• Less than 5% of acute heart failure cases
• 80% of cases secondary to acute coronary syndromes with or without mechanical complications
• 40% short-term mortality rates
28
ACUTE MANAGEMENT
CARDIOGENIC
SHOCK
CATH LAB OR
SURGERY
RESPIRATORY
DISTRESSHYPOPERFUSION
NONINVASIVE
VENTILATION
INVASIVE
MONITORING
INOTROPES ±VASOPRESSORS
MECHANICAL
SUPPORT
RENAL
REPLACEMENT
INVASIVE
VENTILATION
IDENTIFY CAUSE
Mebazza, et al. Intensive Care Med. 2016 Feb;42(2):147-63.
2/29/2016
8
29
POSITIVE PRESSURE VENTILATION
• Decreased …
– Transthoracic pulmonary pressure decreases LV afterload
– Venous return decreases preload
– Breathing efforts decreases metabolic demand
– Hypoxia decreases pulmonary vasoconstriction
• Studies show increased cardiac output, decreased pulmonary pressures, improved oxygenation, increased ventilator weaning, and increased survival
BIPAP CPAP INVASIVE
Positive end-expiratory pressure (PEEP) = Aveolar pressure above atmospheric pressure after expiration
Wiesen, et al. Heart. 2013;99(24):1812-7.
30
INOTROPIC SUPPORT
DOPAMINE DOBUTAMINE MILRINONE
31
DOSE-DEPENDENCY OF DOPAMINE
Low doses (<5 mcg/kg/minute) vasodilate, including coronary and renal arteries
• Increased renal perfusion not seen in cohort studies
Intermediate doses (5 - 10 mcg/kg/minute) produce inotropic and chronotropic effects
High doses (>10 mcg/kg/minute) induce vasoconstriction and increases in afterload
Tariq, et al. Int J Mol Sci. 2015;16(12):29060-8.
32
DOPAMINE
Tariq, et al. Int J Mol Sci. 2015;16(12):29060-8.
1679 patients receiving dopamine 2– 20 mcg/kg/minute or norepinephrine 0.02-0.19 mcg/kg/minute for shock
2/29/2016
9
33
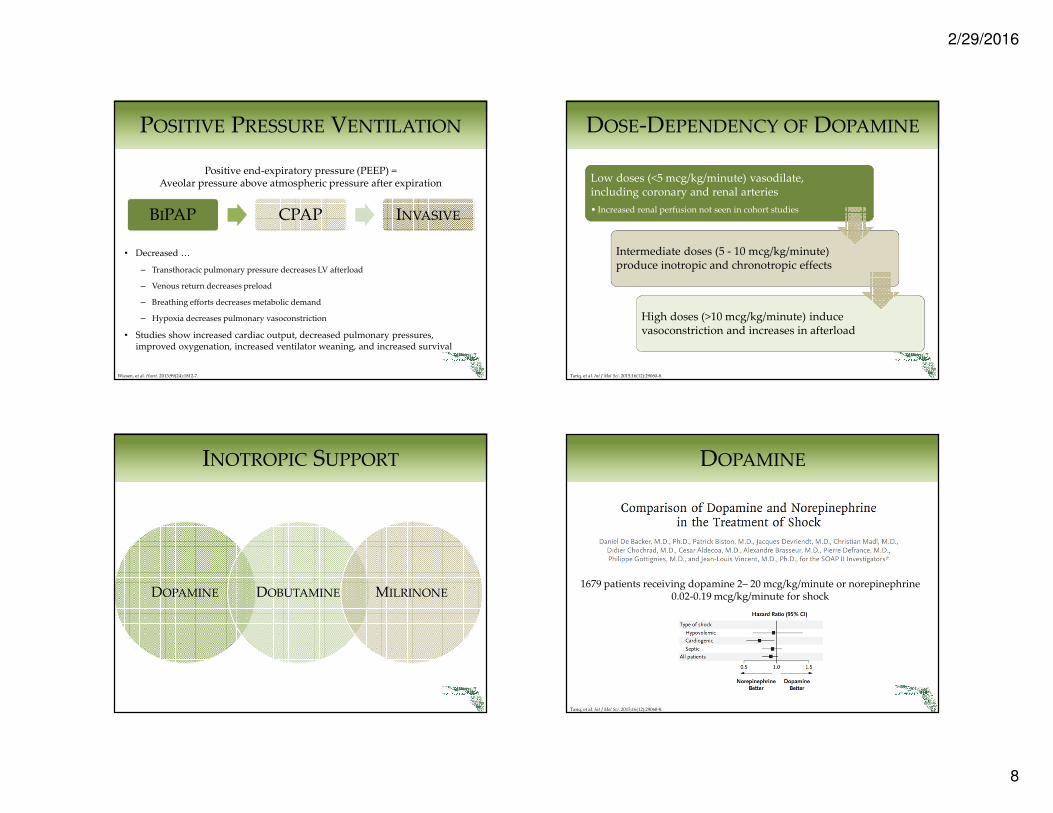
DOBUTAMINE
• Dose range: 5-20 mcg/kg/minute
• β effects improve myocardial contractility and output
• Increased left ventricular end diastolic pressure
• May induce hypotension
• Risk of eosinophilic myocarditis and arrhythmias
• Increased myocardial oxygen demand
Tariq, et al. Int J Mol Sci. 2015;16(12):29060-8.
34
MILRINONE
Inhibits phosphodiesterase-3, preventing cAMP degradation
Positive inotrope activity independent of β stimulation
Reduction of pulmonary artery pressure
Significantly higher rates of hypotension compared to placebo
Dose range: 0.25 - 0.75 mcg/kg/min
Tariq, et al. Int J Mol Sci. 2015;16(12):29060-8.
35
MILRINONE
Felker, et al. . J Am Coll Cardiol. 2003;41(6):997-1003
949 patients receiving milrinone or placebo for
48-72 hours
36
MILRINONE
Abraham, et al. J Am Coll Cardiol. 2005;46(1):57-64.

2/29/2016
10
MECHANICAL
CIRCULATORY SUPPORT
38
MECHANICAL CIRCULATORY SUPPORT
INTRA-AORTIC
BALLOON PUMP
(IABP)
VENTRICULAR
ASSIST DEVICE
(VAD)
EXTRACORPOREAL
MEMBRANE
OXYGENATION
(ECMO)
Inflation facilitates coronary perfusion with increased diastolic pressure
Deflation augments left ventricular (LV) ejection through negative pressure
MECHANICAL CIRCULATORY SUPPORT
Long-term support of cardiac output
Blood removed from left ventricle and returned to ascending aorta
Pulmonary artery return for right ventricular support
Extracorporeal controller and power supply
Blood removed from femoral vein or inferior vena cava
Blood returned to right heart or femoral artery
Separate modes for goal outcomes
Subramaniam, et al. Best Pract Res Clin Anaesthesiol. 2015;29(2):203-27.Pratt, et al. Crit Care Med. 2014; 42:158–168Russell, et al. Circulation. 2009;120(23):2352-7.
IABP INDICATIONS FOR USE
40
Acute Coronary Syndromes•Cardiogenic shock in STEMI
•High-risk PCI or CABG
•STEMI and NSTEMI complications
•Refractory angina
Ventricular Arrhythmias
Refractory Heart Failure
Ihdayhid, et al. Curr Opin Cardiol. 2014, 29:285–292
2/29/2016
11
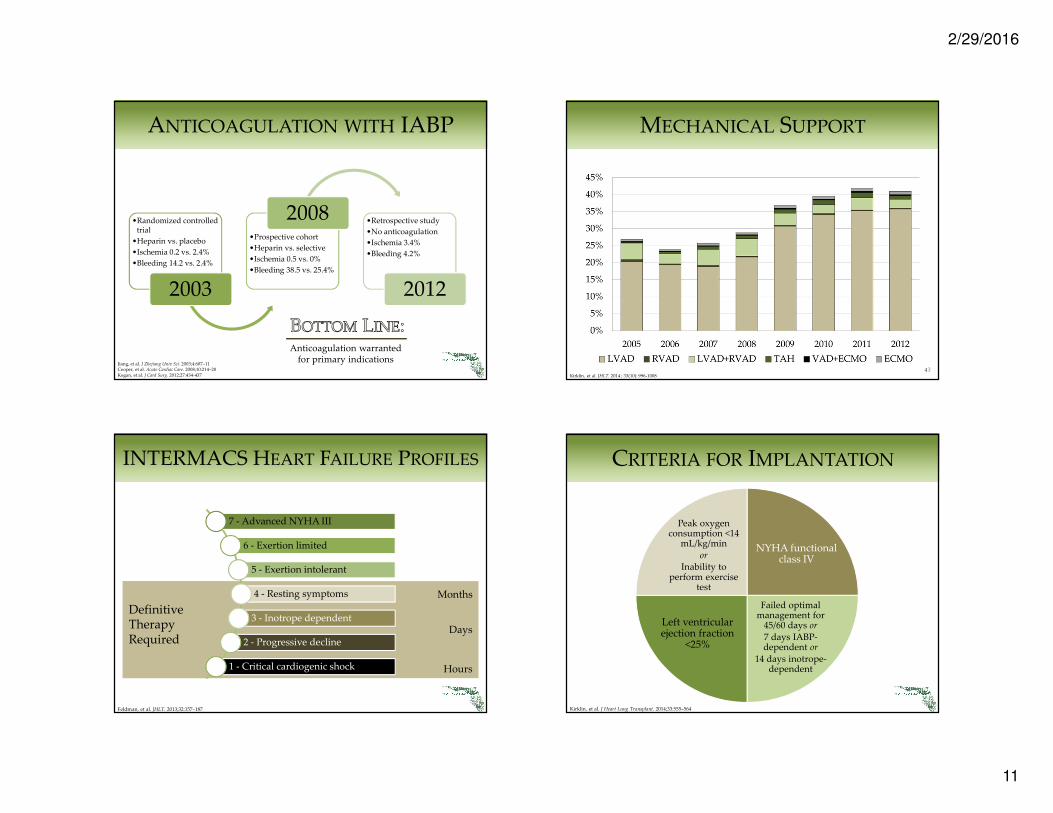
ANTICOAGULATION WITH IABP
41
•Randomized controlled trial
•Heparin vs. placebo
•Ischemia 0.2 vs. 2.4%
•Bleeding 14.2 vs. 2.4%
2003
•Prospective cohort
•Heparin vs. selective
•Ischemia 0.5 vs. 0%
•Bleeding 38.5 vs. 25.4%
2008 •Retrospective study
•No anticoagulation
•Ischemia 3.4%
•Bleeding 4.2%
2012
Anticoagulation warranted for primary indications
Jiang, et al. J Zhejiang Univ Sci. 2003;4:607–11Cooper, et al. Acute Cardiac Care. 2008;10:214–20Kogan, et al. J Card Surg. 2012;27:434-437
42
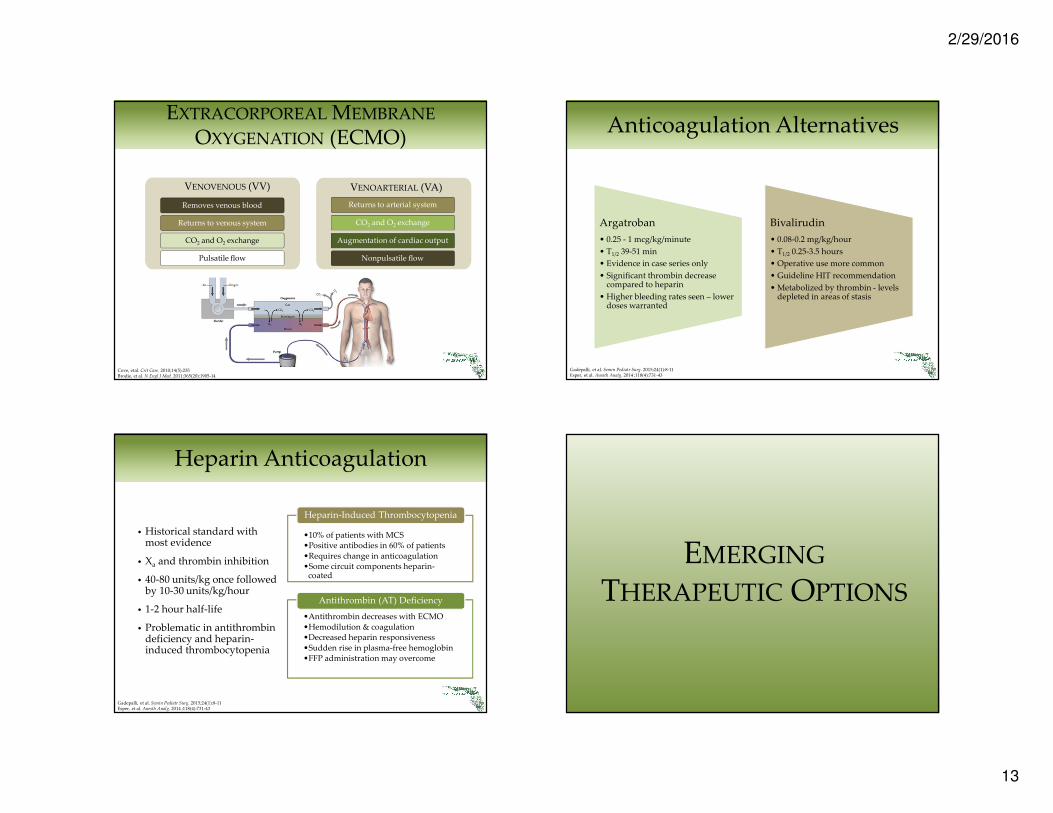
7 - Advanced NYHA III
6 - Exertion limited
5 - Exertion intolerant
4 - Resting symptoms
3 - Inotrope dependent
2 - Progressive decline
1 - Critical cardiogenic shock
Definitive Therapy Required
Months
Hours
Days
Feldman, et al. JHLT. 2013;32:157–187
INTERMACS HEART FAILURE PROFILES
43
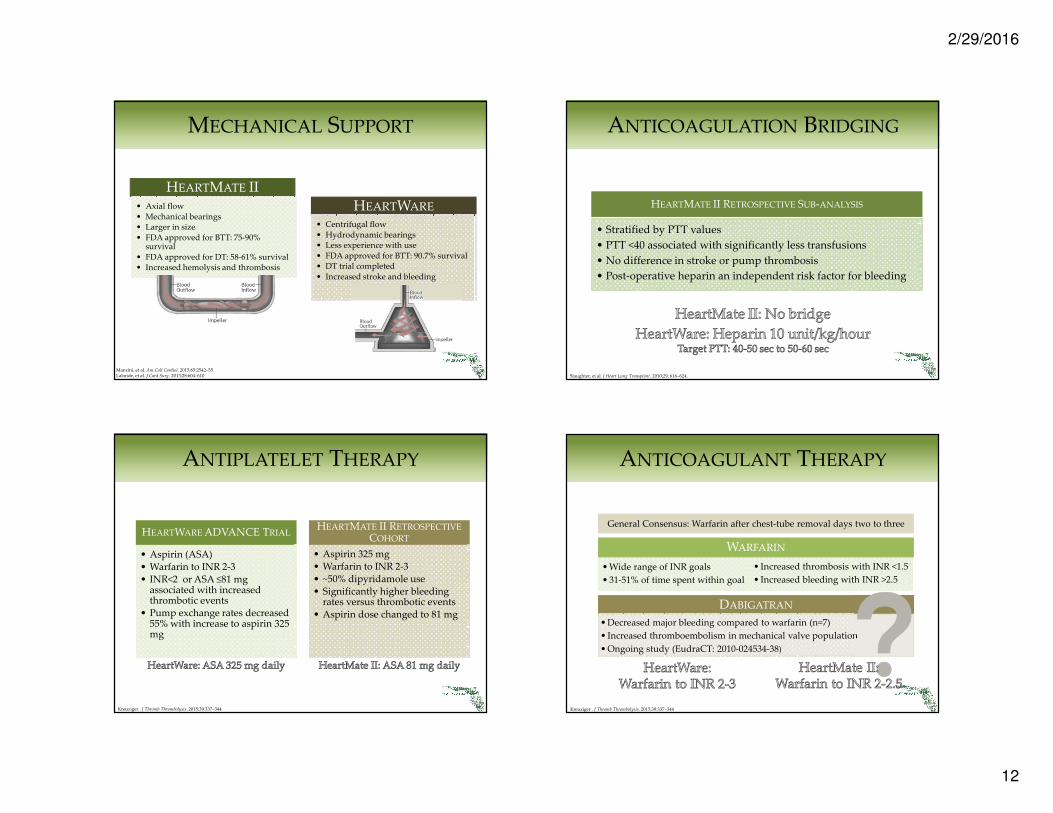
MECHANICAL SUPPORT
Kirklin, et al. JHLT. 2014 ; 33(10): 996-1008
44
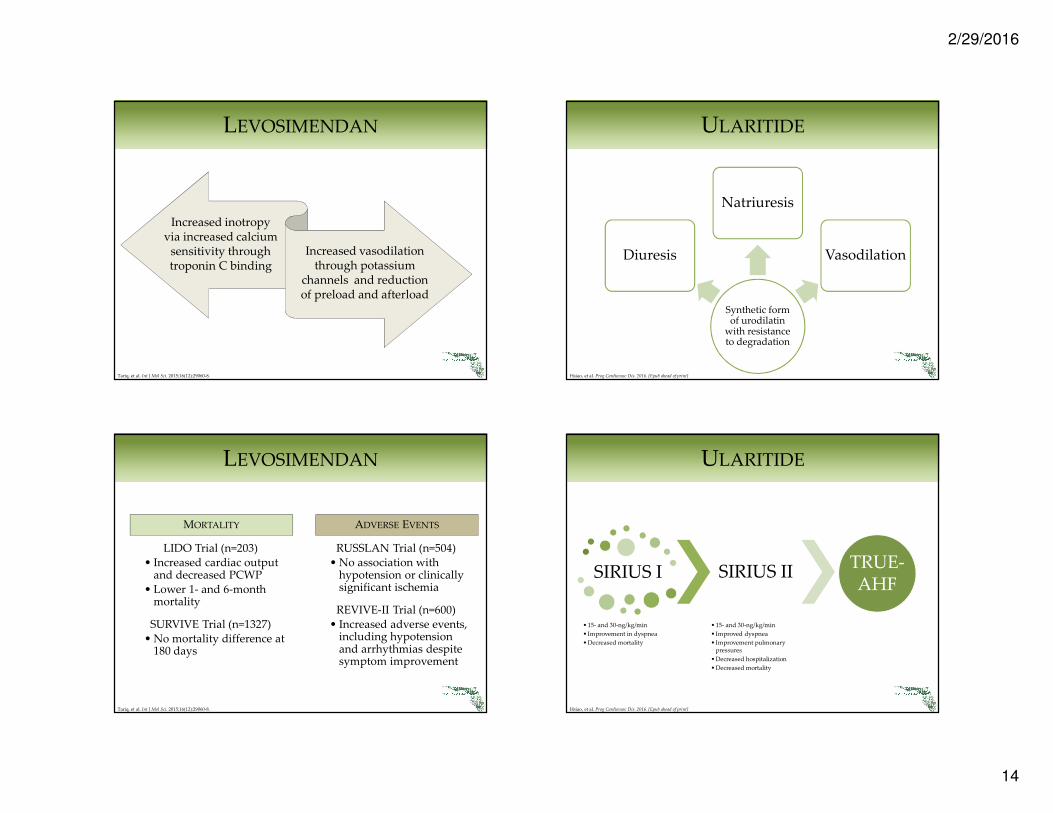
CRITERIA FOR IMPLANTATION
Peak oxygen consumption <14
mL/kg/minor
Inability to perform exercise
test
NYHA functional class IV
Left ventricular ejection fraction
<25%
Failed optimal management for
45/60 days or
7 days IABP-dependent or
14 days inotrope-dependent
Kirklin, et al. J Heart Lung Transplant. 2014;33:555–564
2/29/2016
12
45
MECHANICAL SUPPORT
Destination
Therapy (DT)
HEARTMATE II• Axial flow• Mechanical bearings• Larger in size• FDA approved for BTT: 75-90%
survival• FDA approved for DT: 58-61% survival• Increased hemolysis and thrombosis
HEARTWARE
• Centrifugal flow• Hydrodynamic bearings• Less experience with use• FDA approved for BTT: 90.7% survival• DT trial completed• Increased stroke and bleeding
Mancini, et al. Am Coll Cardiol. 2015;65:2542–55Lalonde, et al. J Card Surg. 2013;28:604–610
46
ANTIPLATELET THERAPY
HEARTWARE ADVANCE TRIAL
• Aspirin (ASA)• Warfarin to INR 2-3• INR<2 or ASA ≤81 mg
associated with increased thrombotic events
• Pump exchange rates decreased 55% with increase to aspirin 325 mg
HEARTMATE II RETROSPECTIVE
COHORT
• Aspirin 325 mg• Warfarin to INR 2-3• ~50% dipyridamole use• Significantly higher bleeding
rates versus thrombotic events• Aspirin dose changed to 81 mg
Kreuziger . J Thromb Thrombolysis. 2015;39:337–344
47
ANTICOAGULATION BRIDGING
Slaughter, et al. J Heart Lung Transplant. 2010;29, 616–624.
HEARTMATE II RETROSPECTIVE SUB-ANALYSIS
• Stratified by PTT values
• PTT <40 associated with significantly less transfusions
• No difference in stroke or pump thrombosis
• Post-operative heparin an independent risk factor for bleeding
48
ANTICOAGULANT THERAPY
WARFARIN
DABIGATRAN
• Decreased major bleeding compared to warfarin (n=7)
• Increased thromboembolism in mechanical valve population
• Ongoing study (EudraCT: 2010-024534-38)
General Consensus: Warfarin after chest-tube removal days two to three
• Increased thrombosis with INR <1.5
• Increased bleeding with INR >2.5
• Wide range of INR goals
• 31-51% of time spent within goal
Kreuziger . J Thromb Thrombolysis. 2015;39:337–344
2/29/2016
13
49
EXTRACORPOREAL MEMBRANE
OXYGENATION (ECMO)
Returns to arterial system
CO2 and O2 exchange
Augmentation of cardiac output
Removes venous blood
Returns to venous system
CO2 and O2 exchange
Nonpulsatile flowPulsatile flow
VENOVENOUS (VV) VENOARTERIAL (VA)
Cove, etal. Crit Care. 2010;14(5):235Brodie, et al. N Engl J Med. 2011;365(20):1905-14
50
Heparin Anticoagulation
• Historical standard with most evidence
• Xa and thrombin inhibition
• 40-80 units/kg once followed by 10-30 units/kg/hour
• 1-2 hour half-life
• Problematic in antithrombin deficiency and heparin-induced thrombocytopenia
•Antithrombin decreases with ECMO •Hemodilution & coagulation•Decreased heparin responsiveness•Sudden rise in plasma-free hemoglobin•FFP administration may overcome
Antithrombin (AT) Deficiency
•10% of patients with MCS•Positive antibodies in 60% of patients•Requires change in anticoagulation•Some circuit components heparin-
coated
Heparin-Induced Thrombocytopenia
Gadepalli, et al. Semin Pediatr Surg. 2015;24(1):8-11Esper, et al. Anesth Analg. 2014 ;118(4):731-43
51
Anticoagulation Alternatives
Argatroban
• 0.25 - 1 mcg/kg/minute
• T1/2 39-51 min
• Evidence in case series only
• Significant thrombin decrease compared to heparin
• Higher bleeding rates seen – lower doses warranted
Bivalirudin
• 0.08-0.2 mg/kg/hour
• T1/2 0.25-3.5 hours
• Operative use more common
• Guideline HIT recommendation
• Metabolized by thrombin - levels depleted in areas of stasis
Gadepalli, et al. Semin Pediatr Surg. 2015;24(1):8-11Esper, et al. Anesth Analg. 2014 ;118(4):731-43
EMERGING
THERAPEUTIC OPTIONS
2/29/2016
14
53
LEVOSIMENDAN
Increased inotropy via increased calcium
sensitivity through troponin C binding
Increased vasodilation through potassium
channels and reduction of preload and afterload
Tariq, et al. Int J Mol Sci. 2015;16(12):29060-8.
54
LEVOSIMENDAN
MORTALITY
LIDO Trial (n=203)• Increased cardiac output
and decreased PCWP• Lower 1- and 6-month
mortality
SURVIVE Trial (n=1327)• No mortality difference at
180 days
ADVERSE EVENTS
RUSSLAN Trial (n=504)• No association with
hypotension or clinically significant ischemia
REVIVE-II Trial (n=600)• Increased adverse events,
including hypotension and arrhythmias despite symptom improvement
Tariq, et al. Int J Mol Sci. 2015;16(12):29060-8.
ULARITIDE
55
Synthetic form of urodilatin
with resistance to degradation
Diuresis
Natriuresis
Vasodilation
Hsiao, et al. Prog Cardiovasc Dis. 2016. [Epub ahead of print]
ULARITIDE
56
SIRIUS I
• 15- and 30-ng/kg/min
• Improvement in dyspnea
• Decreased mortality
SIRIUS II
• 15- and 30-ng/kg/min
• Improved dyspnea
• Improvement pulmonary pressures
• Decreased hospitalization
• Decreased mortality
TRUE-AHF
Hsiao, et al. Prog Cardiovasc Dis. 2016. [Epub ahead of print]

2/29/2016
15
TRUE-AHF
57
Co-Primary Outcome:
• Improved global assessment at 6, 24, and 48 hours without meeting criteria for worsening, including:
• Death within 48 hours
• Worsening of disease warranting intervention
• Worsening global assessment
Co-Primary Outcome:
• Freedom from cardiovascular mortality
Secondary Outcomes:
• N-terminal pro-BNP changes
• All-cause mortality and rehospitalization
• Cardiovascular rehospitaliation
Anker, et al. Eur Heart J. 2015;36(12):715-2
SERELAXIN
58
Human recombinant form
of relaxin
Upregulator of endothelin B receptors and nitric oxide production
Inhibition of angiotensin II
and endothelin potentiates
systemic and renal vasodilation
Anti-inflammatory
and anti-fibrotic properties
Hsiao, et al. Prog Cardiovasc Dis. 2016. [Epub ahead of print]
RELAX-AHF
59
Significantly reduced hospital stay, time to dyspnea improvement, and worsening of heart failure
Significant improvement in symptomatic visual analog scale
30 mcg/kg/day serelaxin versus placebo
Teerlink, et al, Lancet. 2013;381(9860):29-39.
RELAX-AHF
60
Felker, et al. J Am Coll Cardiol. 2014 ;64(15):1591-8.

2/29/2016
16
Medication correlation with decompensation
Half-life longer than initial
critical period
Paradoxical activation of sympathetic
nervous system
61
BETA-BLOCKER CONSIDERATIONS
Jondeau , et al. JACC Heart Fail. 2015;3(8):654-6
62
BETA-BLOCKER THERAPY
IN-HOSPITAL MORTALITY
Prins, et al. JACC Heart Fail. 2015;3(8):647-53.
63
BETA-BLOCKER THERAPY
SHORT-TERM MORTALITY OR REHOSPITALIZATION
Prins, et al. JACC Heart Fail. 2015;3(8):647-53.
ASSESSMENT QUESTION
Increasing preload and/or inotropy are strategies for optimization of cardiac
output.
64
2/29/2016
17
A primary principle in the management of left heart failure is
reduction of venous congestion.
65
ASSESSMENT QUESTION
The patient receives a HeartMate II ventricular assist device. The patient
should be bridged with heparin.
66
ASSESSMENT QUESTION
Management of Acute Heart Failure and Cardiogenic Shock
www.fshp.org
Brittany D. Bissell, Pharm.D.PGY-2 Critical Care Pharmacy Resident
Jackson Memorial Hospital | Miami, Florida
• Abraham WT, Adams KF, Fonarow GC, et al. In-hospital mortality in patients with acute decompensated heart failure requiringintravenous vasoactive medications: an analysis from the Acute Decompensated Heart Failure National Registry (ADHERE). J Am CollCardiol. 2005;46(1):57-64.
• Anker SD, Ponikowski P, Mitrovic V, Peacock WF, Filippatos G. Ularitide for the treatment of acute decompensated heart failure: frompreclinical to clinical studies. Eur Heart J. 2015;36(12):715-2
• Brodie D, Bacchetta M. Extracorporeal membrane oxygenation for ARDS in adults. N Engl J Med. 2011;365(20):1905-14.• Cooper HA, Thompson E, Panza JA. The role of heparin anticoagulation during intra-aortic balloon counterpulsation in the coronary
care unit. Acute Cardiac Care 2008;10:214–20.• Cotter G, Felker GM, Adams KF, Milo-Cotter O, O'Connor CM. The pathophysiology of acute heart failure--is it all about fluid
accumulation? Am Heart J. 2008;155(1):9-18.• Cove ME, MacLaren G. Clinical review: mechanical circulatory support for cardiogenic shock complicating acute myocardial infarction.
Crit Care. 2010;14(5):235.• Di Somma S, Magrini L. Drug Therapy for Acute Heart Failure. Rev Esp Cardiol. 2015;68(8):706-13.• Esper SA, Levy JH, Waters JH, Welsby IJ. Extracorporeal membrane oxygenation in the adult: a review of anticoagulation monitoring
and transfusion. Anesth Analg. 2014;118(4):731-43• Feldman D, Pamboukian SV, Teuteberg JJ, et al. The 2013 International Society for Heart and Lung Transplantation Guidelines for
mechanical circulatory support: executive summary. J Heart Lung Transplant. 2013;32(2):157-87.• Felker GM, Benza RL, Chandler AB, et al. Heart failure etiology and response to milrinone in decompensated heart failure: results from
the OPTIME-CHF study. J Am Coll Cardiol. 2003;41(6):997-1003.• Felker GM, Teerlink JR, Butler J, et al. Effect of serelaxin on mode of death in acute heart failure: results from the RELAX-AHF study. J
Am Coll Cardiol. 2014 ;64(15):1591-8.• Gadepalli SK, Hirschl RB. Extracorporeal life support: updates and controversies. Semin Pediatr Surg. 2015;24(1):8-11.• Howlett JG. Acute heart failure: lessons learned so far. Can J Cardiol. 2011;27(3):284-95.• Hsiao R, Greenberg B. Contemporary Treatment of Acute Heart Failure. Prog Cardiovasc Dis. 2016 Jan 4. [Epub ahead of print]• Ihdayhid AR, Chopra S, Rankin J. Intra-aortic balloon pump: indications, efficacy, guidelines and future directions.Curr Opin Cardiol.
2014, 29:285–292• Jiang CY, Zhao LL, Wang JA, Mohammod B. Anticoagulation therapy in intra-aortic balloon counterpulsation: does IABP really need
anti-coagulation? J Zhejiang Univ Sci 2003;4:607–11.• Jondeau G, Milleron O. Beta-Blockers in Acute Heart Failure: Do They Cause Harm? JACC Heart Fail. 2015;3(8):654-6
68
REFERENCES

2/29/2016
18
• Kirklin JK, Naftel DC, Pagani FD, et al. Sixth INTERMACS annual report: a 10,000-patient database. J Heart Lung Transplant.2014;33:555–564
• Kogan A, Preisman S, Sternik, et al. Heparin-free management of intra-aortic balloon pump after cardiac surgery. J Card Surg2012;27:434-437.
• Kreuziger LM. Management of anticoagulation and antiplatelet therapy in patients with left ventricular assist devices. J ThrombThrombolysis. 2015;39:337–344.
• Lalonde SD, Alba AC, Rigobon A, et al. Clinical Differences Between Continuous Flow Ventricular Assist Devices: A ComparisonBetween HeartMate II and HeartWare HVAD. 2013; J Card Surg, 28: 604–610
• Liu C, Liu K. Effects of glucocorticoids in potentiating diuresis in heart failure patients with diuretic resistance. J Card Fail.2014;20(9):625-9.
• Mancini D, Colombo PC. Left Ventricular Assist Devices: A Rapidly Evolving Alternative to Transplant. J Am Coll Cardiol.2015;65(23):2542-55
• Mebazaa A, Tolppanen H, Mueller C, et al. Acute heart failure and cardiogenic shock: a multidisciplinary practical guidance. IntensiveCare Med. 2016 Feb;42(2):147-63.
• Pratt AK, Shah NS, Boyce SW. Left ventricular assist device management in the ICU. Crit Care Med. 2014; 42:158–168• Prins KW, Neill JM, Tyler JO, Eckman PM, Duval S. Effects of Beta-Blocker Withdrawal in Acute Decompensated Heart Failure: A
Systematic Review and Meta-Analysis. JACC Heart Fail. 2015;3(8):647-53.• Russell SD, Rogers JG, Milano CA, et al. Renal and hepatic function improve in advanced heart failure patients during continuous-flow
support with the HeartMate II left ventricular assist device. Circulation. 2009;120(23):2352-7.• Slaughter MS, Naka Y, John R, et al. Post-operative heparin may not be required for transitioning patients with a HeartMate II left
ventricular assist system to long-term warfarin therapy. J Heart Lung Transplant. 2010;29, 616–624.• Subramaniam K. Mechanical circulatory support. Best Pract Res Clin Anaesthesiol. 2015;29(2):203-27.• Teerlink JR, Cotter G, Davison BA, et al. Serelaxin, recombinant human relaxin-2, for treatment of acute heart failure (RELAX-AHF): a
randomised, placebo-controlled trial. Lancet. 2013;381(9860):29-39.• Tariq S, Aronow WS. Use of Inotropic Agents in Treatment of Systolic Heart Failure. Int J Mol Sci. 2015;16(12):29060-8.• ter Maaten JM, Valente MA, Damman K, Hillege HL, Navis G, Voors AA. Diuretic response in acute heart failure-pathophysiology,
evaluation, and therapy. Nat Rev Cardiol. 2015;12(3):184-92.• Wiesen J, Ornstein M, Tonelli AR, Menon V, Ashton RW. State of the evidence: mechanical ventilation with PEEP in patients with
cardiogenic shock. Heart. 2013;99(24):1812-7.
69
REFERENCES
Related Documents