Malnutrition. and Mortality Lincoln C. Chen, M.D. Ford Foundation, New Delhi Recent scholarly exchanges in India on the magnitude and nature of the malnutrition problem have made several enquiries and references with regard to my research papers, "Anthropometric assessment of energy-protein malnutrition and subsequent risk of mortality among preschool aged children" and "The use of anthropometry for nutritional surveillance in mortality control programmes. The paper and the letter to the edi- tor, respectively, were both pub- lished in the American Journal of Clinical Nutrition (Chen, L.C., AK.MA Chowdhury, and S.L Huf- fman. Anthropometric assessment of energy-protein malnutrition and subsequent risk of mortality among preschool aged children.Am. J. Clin. Nutr. 33: 1836-1845, 1980; Chen L.c, AK.MA Chowdhury, and S.L Huffman. The use of anthropometry for nutritional surveillance in mortal- ity control programmes. Am. J. Clin. Nutr. 34:2596-2599, 1981). These notes are intended to summa rise the published evidence and to clarify which conclusions are (and are not) supported by the reported findings. The paper cited is an epidemio- logic investigation of the relation- ship between various anthropometric indicators of energy-protein malnu- trition and the subsequent risk of murtality among children in a rural area of Bangladesh Cross-sectional anthropometric measurements of 2,091 children aged 13 to 23 months were under- taken in an earlier study on nutrition and fertility. These children were all residing in an area which has been under independent longitudinal demographic surveillance (registra- tion of birth, death, and migration) for 15 years. (Chen L.C., M. Rahman, and AM. Sardar. Epidemiology and causes of death among children in a rural area of Bangladesh. Intern. J. Epidem. 9:25-33, 1980).' By linking the cross-sectional anthropometric data with the mor- tality experience of the same study children over the following 24 months, the relationship of anthro- pometry and the subsequent risk of mortality was examined 24 Months Comparison Children were grouped according to standard anthropometric classifi- cations (weight-for-age, weight-for- height. height-for-age, arm circumference-for-age, and arm circumference-far-height) and their mortality experiences over the sub- sequent 24 months were compared. The major findings were that: all classifications were able to prog- nosticate subsequent mortality risk; weight-far-age and arm circum- ference-far-age possessed the highest discriminatory power: and the discriminatory capacity was enhanced with maternal nutritional status and socioeconomic indica- tors were also included. The results showed that severely malnourished children according to all indices, experienced markedly higher mortality risk whereas nor- mally nourished and mildly and moderately malnourished children all experienced lower but similar risks (Table 1). It is this last finding, graphically depicted in Figure 1, that has gener- ated widespread interest. The remainder of this note elaborates on this key finding and discusses the validity of various. interpretations It is important to recognise at the outset that the study's objective was epidemiologic; to determine the usefulness of anthropometric classi- fications for screening of high mor- tality risk children to facilitate preventive nutritional interve·ntions. The study design did not address the definition of malnutrition, and the analysis used the epidemiologic concept of "risk". Risk connotes associative relationships, and is only one component of proving direct causal links (Lilienfeld, A.M. Foun- dations of Epidemiology. New York: Oxford University Press, 1976). Thus, while the study showed a strong association between severe malnutrition and mortality, it does not prove necessarily that the former caused the latter. In fact. the analysis showed that othervariables, such as maternal nutritional status and the socioeconomic condition of the family, were also powerful predic- tors of mortality. The study used anthropometry exclusively as an indicator of nutri-

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Malnutrition. and Mortality
Lincoln C. Chen, M.D.Ford Foundation, New Delhi
Recent scholarly exchanges inIndia on the magnitude and nature ofthe malnutrition problem have madeseveral enquiries and referenceswith regard to my research papers,"Anthropometric assessment ofenergy-protein malnutrition and
subsequent risk of mortality amongpreschool aged children" and "Theuse of anthropometry for nutritionalsurveillance in mortality controlprogrammes.
The paper and the letter to the edi
tor, respectively, were both published in the American Journal ofClinical Nutrition (Chen, L.C.,AK.MA Chowdhury, and S.L Huffman. Anthropometric assessmentof energy-protein malnutrition andsubsequent risk of mortality amongpreschool aged children.Am. J. Clin.Nutr. 33: 1836-1845, 1980; ChenL.c, AK.MA Chowdhury, and S.LHuffman. The use of anthropometryfor nutritional surveillance in mortality control programmes. Am. J. Clin.Nutr. 34:2596-2599, 1981). Thesenotes are intended to summa rise the
published evidence and to clarifywhich conclusions are (and are not)supported by the reported findings.
The paper cited is an epidemiologic investigation of the relationship between various anthropometricindicators of energy-protein malnutrition and the subsequent risk ofmurtality among children in a ruralarea of Bangladesh
Cross-sectional anthropometricmeasurements of 2,091 childrenaged 13 to 23 months were undertaken in an earlier study on nutritionand fertility. These children were allresiding in an area which has beenunder independent longitudinaldemographic surveillance (registration of birth, death, and migration)for 15 years. (Chen L.C., M. Rahman,and AM. Sardar. Epidemiology andcauses of death among children in arural area of Bangladesh. Intern. J.Epidem. 9:25-33, 1980).'
By linking the cross-sectionalanthropometric data with the mortality experience of the same studychildren over the following 24months, the relationship of anthropometry and the subsequent risk ofmortality was examined
24 Months Comparison
Children were grouped accordingto standard anthropometric classifications (weight-for-age, weight-forheight. height-for-age, armcircumference-for-age, and armcircumference-far-height) and theirmortality experiences over the subsequent 24 months were compared.
The major findings were that: allclassifications were able to prognosticate subsequent mortality risk;weight-far-age and arm circumference-far-age possessed thehighest discriminatory power: and
the discriminatory capacity wasenhanced with maternal nutritionalstatus and socioeconomic indicators were also included.
The results showed that severelymalnourished children according toall indices, experienced markedlyhigher mortality risk whereas normally nourished and mildly andmoderately malnourished childrenall experienced lower but similarrisks (Table 1).
It is this last finding, graphicallydepicted in Figure 1, that has generated widespread interest. Theremainder of this note elaborates onthis key finding and discusses thevalidity of various. interpretations
It is important to recognise at theoutset that the study's objective wasepidemiologic; to determine theusefulness of anthropometric classifications for screening of high mortality risk children to facilitatepreventive nutritional interve·ntions.The study design did not address thedefinition of malnutrition, and the
analysis used the epidemiologicconcept of "risk". Risk connotesassociative relationships, and is onlyone component of proving directcausal links (Lilienfeld, A.M. Foundations of Epidemiology. New York:Oxford University Press, 1976).Thus, while the study showed astrong association between severemalnutrition and mortality, it doesnot prove necessarily that the formercaused the latter. In fact. the analysisshowed that othervariables, such asmaternal nutritional status and thesocioeconomic condition of thefamily, were also powerful predictors of mortality.
The study used anthropometryexclusively as an indicator of nutri-

Mortality rate (per 1000) 0 to 11 and 12 to 23 months after nutritional assessmentclassified by percentage wt/a'ge, wt/ht and ht/age of the Harvard standard.
Table I
NUTRITIONAL STATUS
NO. OF CHILDRENFOllOW-UPMORTALITYRATE
Degree
%0-11 mo12-23 mo0-23 moStandard
Wt/age
Normal/mild75 ,54623.812.836.6
Moderate60-74104626.815.342.1
Severe
6042746.865.6112.4
WtI HtNormal
9039935.117.552.6Mild
80-8997926.626.653.2Moderate
70-7956628.321.249.5Severe
707566.780.0146.7
Ht/ageNormal
9518216.516.533.0Mild
90-9465622.916.839.6Moderate
85-8971328.09.837.9Severe
8546851.362.0113.2
All
201930.225.355.5tiona I status. The current debate in
India focusses primarily on nutrientintake. not anthropometry. to definemalnutrition (Chen. L.C.. E. Huq. andS.L. Huffman. A prospective study ofthe risk of the diarrhoeal diseasesaccording to nutritional status ofchildren. Am. J. Epidem. 114:284292. 1981). The concept of malnutrition is elusive and controversial. Itmay be reflected in many indicators,including dietary. biochemical. clinical. and functional performanceparameters. Each parameter contains inherent strengths and weaknesses. There is unfortunately littleempirical data b.etween populationsor amongst individuals on thedegree of congruence betweenthese various measures.
The use of mortality also hasstrengths and weaknesses. The definition of mortality is unambiguous.and quantitative measurement ispossible. Because it reflects the ultimate consequence of ill-health,mortality is affected by multiple,simultaneous, and inter-active processes (Chen. L.C., M. Rahman, a'ndA.M. Sardar. Epidemiology andcauses of death among children in arural area of Bangladesh. Intern. J.Epidem. 9:25-33. 1980). As such,measurement of mortality can detectindirect and difficult-to-predicteffects. Attempts to dissect the unidirectional impact of any single factor on mortality. however, may bedifficult and subject to high "background noise" of other importantfactors.
There are at least three possiblehypotheses to explain the centralfinding (Figure 1) that the severelymalnourished experienced significantly higher mortality risk while thenormally no.urished and mildly andmoderately malnourished all experienced the same but lower risk:
The reported findings are incorrect. There is indeed a difference ofmortality risk between the normallynourished and the mildly and moderately malnourished. but the differences are small and thus were not
detected because of methodologicalconstraints.
The reported findings are correct,but the explanation lies in the asso-.ciative. not necessarily causal. linksbetween nutritional status and mor-
tality and on the complex interactionbetween nutrition and infection.
The reported findings are correct.Mortality risk is indeed similarbetween the normally nourished andthe mildly and moderately malnourished. This is due to "homeostasis"
or "adaptation," which imply physiologic normality.
Let us deal with each in turn. The
first hypothesis seems unlikely. Itshould be noted that the demographic registration system in this studypopulation is one of the most accurate and reliable in the world. (Chen,L.C., M. Rahman, and A.M. Sardar.
Epidemiology and causes of deathamong children in a rural area ofBangladesh. Intern J. Epidem. 9:2533, 1980).
All children aged 13-23 monthsresiding in 86 ,villages weresampled, and the age of the studychildren was known with precisionbecause all births were registered.However, as described in the paper'smethods section, about 450 children were excluded from the final
analysis because of infant mortality(deaths from birth to the study agel.unavailability for anthropometrymeasl)r'emnt. or mis-linkagebetween anthropometry and mortality records. (C.hen, L.C., A.K.MAChowdhury. and S.L. Huffman.Anthropometric assessment of
2
energy-protein malnutrition andsubsequent risk of mortality amongpreschool aged children.Am. J. ClinNutr. 33: 1845, 1980).
The final study cohort. therefore.may contain hidden biases; thisexclusion may have implications forthe interpret~tion of the data. Thereare no reasons to suspect. however,that had all children been included,the pattern of mortality risk wouldhave differed from the observed.
The second hypothesis is moreplausible. Although the analysisdemonstrated an associative rela
tionship between anthropometryand mortality, many other factors(which are also associated with poorgrowth) could be importantdeterminants of mortality as well.
The study, in fact. showed thatmaternal nutritional status and the
economic condition of the family aretwo such variables. These collinear
determinants could generate high"background noise", which couldobscure whatever modest differen
ces actually exist. In this regard, therole of parental child care and parental response to illness may beimportant. Children who 'areseverely malnourished may constitute a subgroup for whom maternalcompetence or family social factorsmay playa critical role. (Chen, L.CWhere have the women gone:
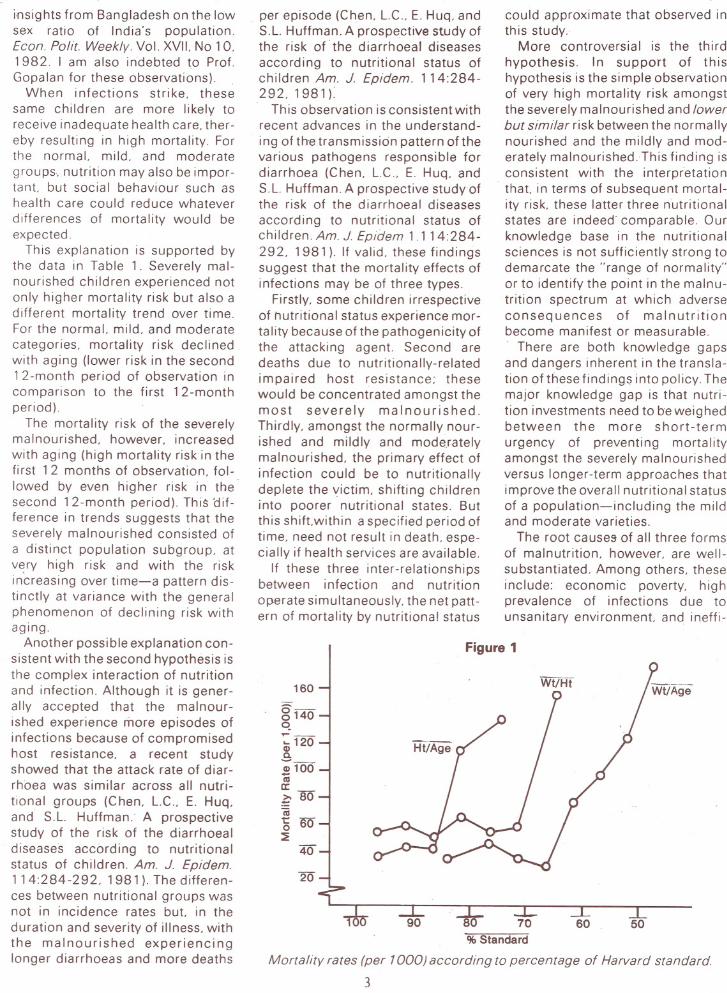
Figure 1
Mortalitv rates (per 1000) according to percentage of Harvard standard
3
insights from Bangladesh on the lowsex ratio of India's populationEcon. Polit Weeklv. Vol. XVII. No 10.1982 I am also indebted to Prof.Gopalan for these observations)
When infections strike. these
same children are more likely toreceive inadequate health care. thereby resulting in high mortality. Forthe normal. mild. and moderategroups. nutrition may also be important. but social behaviour such ashealth care could reduce whateverdifferences of mortality would beexpected.
This explanation is supported bythe data in Table 1. Severely malnourished children experienced notonly hIgher mortality risk but also adifferent mortality trend over time.For the normal. mild. and moderatecategories. mortality risk declinedwith aging (lower risk in the second12-month period of observation incomparison to the first 12-monthperiod)
The mortality risk of the severelymalnourished. however. increasedwith aging (high mortality riskin thefirst 12 months of observation. followed by even higher risk in thesecond 12-month period). This 'difference in trends suggests that theseverely malnourished consisted ofa distinct population subgroup. atvery high risk and with the riskincreasing over time-a pattern distinctly at variance with the generalphenomenon of declining risk withaging.
Another possible explanation consistent with the second hypothesis isthe complex interaction of nutritionand infection. Although it is generally accepted that the malnourIshed experience more episodes ofinfections because of compromisedhost resistance, a recent studyshowed that the attack rate of diarrhoea was similar across all nutri
tional groups (Chen, L.C., E. Huq,and S.L. Huffman. A prospectivestudy of the risk of the diarrhoealdiseases according to nutritionalstatus of children. Am. J. Epidem.114:284-292, 1981). The differences between nutritional groups wasnot in incidence rates but. in theduration and severity of illness, withthe malnourished experiencinglonger diarrhoeas and more deaths
per episode (Chen, L.C, E. Huq, andS.L. Huffman. A prospective study ofthe risk of' the diarrhoeal diseases
according to nutritional status ofchildren Am. J. Epidem. 114:284292. 1981):
This observation is consistent withrecent advances in the understand
ing of the transmission pattern of thevarious pathogens responsible fordiarrhoea (Chen, L.C. E. Huq, andS.L. Huffma n. A prospective study ofthe risk of the diarrhoeal diseases
according to nutritional status ofchildren. Am. J. Epidem 1.114:284292, 1981). If valid, these findingssuggest that the mortality effects ofinfections may be of three types.
Firstly, some children irrespectiveof hutritional status experience mortality because of the pathogenicity ofthe attacking agent. Second aredeaths due to nutritionally-relatedimpaired host resistance; thesewould be concentrated amongst themost severely malnourished.Thirdly, amongst the normally nourished and mildly and moderatelymalnourished, the primary effect ofinfection could be to nutritionallydeplete the victim, shifting childreninto poorer nutritional states. Butthis shift.within a specified period oftime. need not result in death, especially if health services are available.
If these three inter-relationshipsbetween infection and nutrition
operate simultaneously. the net pattern of mortality by nutritional status
could approximate that observed inthis study.
More controversial is the third
hypothesis. In support of thishypothesis is the simple observationof very high mortality risk amongstthe severely malnourished and lowerbut similar risk between the normallynourished and the mildly and moderately malnourished This finding isconsistent with the interpretationthat. in terms of subsequent mortality risk. these latter three nutritionalstates are indeed- comparable. Ourknowledge base in the nutritionalsciences is not sufficiently strong todemarcate the "range of normality"or to identify the point in the malnutrition spectrum at which adverseconsequences of malnutritionbecome manifest or measurable.
There are both knowledge gapsand dangers inherent in the translation of these findings into policy Themajor knowledge gap is that nutrition investments need to be weighedbetween the more short-term
urgency of preventi ng marta Iityamongst the severely malnourishedversus longer-term approaches thatimprove the overall nutritional statusof a population-including the mildand moderate varieties.
The root causes of all three formsof malnutrition, however, are well
substantiated. Among others, theseinclude: economic poverty. highprevalence of infections due tounsanitary environment. and ineffi-

cient uses of household resources.
Any long or short-range attack onmalnutrition must deal with all three
One danger of the third hypothesisis not with.regard to its validity. butto its possible misinterpretation fornutrition policy. Derived conclusions may go too far beyond cautious hypothesis formulation. If theterms "homeostatis" or "adaptation"are used to imply successful andharmless adjustment to stress. orthat mild and moderate malnutrition
are not a problem. the overwhelmingweight of scientific evidence. in thispaper and in the published literature. is inconsistent with this policyconclusion. for several reasons:
First. the pattern of risk (Figure 1)overshadows the key finding that themortality level reported even for thenormally nourished Bangaladeshichildren is 30-50 deaths per 1.000per year (Figure 1). This level isapproximately tenfold that of moreprivileged children in rich and poorcountries (Chen. L.C .. M. Rahman.and A.M Sardar. Epidemiology andcauses of death among children in arural area of Bangladesh. Intern J£pidem. 9:25-33. 1980) Thus irrespective of the demarcation between"normal" and "abnormal." the level
of mortality among even "normal"children in rural Bangladesh is staggering and largely preventable
Second. privileged children inBangladesh. as elsewhere. attaingrowth standards remarkably similarto their counterparts in rich populations (Institute of Nutrition and FoodSciences. Nutrition Survey of RuralBangladesh. Dacca. University ofDacca. 1978). In other words. stunting and retardation are not the consequences of varying geneticpotential. but reflect primarily biologic insult-due predominantly toinsufficient nutrient intake andrepeated infections.
In biologic terms. the human organism. appears to recognise theabnormality of stunting and retardation During the convalescent phaseafter acute nutrition insult. for exam~pie. the phenomenon of "catch-up"growth is well documented (Rohde.J.E. Preparing for the next round:convalescent care after acute infection. Am. J Clin. Nutr. 31: 2258.1978)
Catch-up growth involves physiologic adjustments of increasingappetite and enhancing efficiency inthe deposition of body mass. Liketissue repair after injury. the bodyappears to recognise growth slowdowns as abnormal and attempts toadjust b'y more-rapia-than-normalgrowth recovery. After a child attainsnorma I weight for height. "catch-up"growth ceases.
Third. the study examined only thesurvivors Those who died prior tothe study period are excluded. InBangladesh. the infant mortality rateis about 140 per 1.000 live births(Chen. L.e. M. Rahman. and A.M.Sardar Epidemiology and causes ofdeath among children in a rural areaof Bangladesh. Intern J Epidem. 9:25-33. 1980).
Low Birth Weight Mortality
For a study beginning with 13-23months old children. at least 14 percent of the same birth cohort have
already died. One effect of this biasis illustrated by low birth weight. Lowbirth weight babies possess significantly higher mortality risk than theirheavier counterparts (Habicht. J.P ..A. Lechtig. C. Yarborough. and R.E.Klein. Maternal nutrition. birthweight. and infant mortality in Size atBirtf). CIBA Foundation Symposium27. Elsevier. London. 1974).
The risk is highest immediatelyafter birth and. with aging. tends tomove towards the population mean.Surviving low birth weight babiesoften follow growth tracks thatparallel. but remain lower at eachage than. their heavier counterparts(Yarborough. C.. J.P. Habicht. A.Lechtig. and R.E. Klein. Length andweight in rural Latino children.Phys.Anthropol. 42: 390. 1975).
Thus. mildly and moderately malnourished children at 13-23 months
would consist of disproportionatelymore surviving low birth weightbabies than normally nourishedchildren. Even if the subsequentmortality risk of the malnourishedapproached that of normally nourished children. the high mortality tollof low birth weight babies in theearly years should be an integralconsideration in interpreting thestudy
4
Fourth. mortality is only one of themany well-documented adverseconsequences of malnutrition. Thepattern of function'al impairmentdue to malnutrition will vary according to the parameter examined.Some of the more important effects.in contrast to mortality. may be themost difficult to measure and quantify. Of possible relevance here aresubtle. less-discernible. anddifficult-to-measure changes ofexploratory activity. initiative. creativity. learning.and social interaction(Calloway. D.H. Functional consequences of malnutrition. Paper prepared for the Workshop onInteraction of Parasitic Diseases and
Malnutrition. Bellagio. Italy. September 27 -October 1. 1980).
Fifth. even if mildly and moderately malnourished children experience the same mortality risk asnormally nourished children. thephenomenon does not assess thehuman cost of the adjustment process High mortality at younger agesis one such cost. Other possiblecosts include hunger and dietaryinsufficiency. repeated onslaught ofinfections. other morbidities. compromised exploration and learning.
Take as a parallel example. notmalnutrition. but contaminated
drinking water. Repeated exposureto pathogens from contaminatedwater leads to gastrointestinal infections. With each episode. somechildren die while others experiencetransitory illness. Among the survivors. each infectious insult alsostimulates an immune response.
Thus. at some future time. one mayobserve surviving children with noapparent problems (and even possessing immunity against manyinfections). It would be fallacious toconclude that since children
exposed to contaminated waterappear healthy (even healthier thanothers). contaminated drinkingwater is not a problem.
These notes have summarised thesalient features of the relationshipbetween malnutrition and mortality.Particular attention was devoted to
three alternative hypothesesexplaining the reported findings. Ifthe hypotheses are extended too farto derive the conclusions that mildand moderate malnutrition does not

C. Gopalan
The Nutrition Policy ofBrinkmanship
constitute a problem, the interpretation is fallacious.
Too much attention may be paid tothe future risk of those who arealready mildly, moderately orseverely malnourished. The centralquestion ought to be to the past aswell. All forms of malnourishmentare due to antecedent root causes,such as lack of income and infec
tions. These deserve the highestpriority in any nutrition policy.
A study that focuses on only survivors. on mortality measurements.and on subsequent or future riskdoes not deal with the central issueof the human cost absorbed in thepast which has resulted in less-thanoptimal growth. Clearly. there is aneed to address all forms of malnutrition, mild to severe. and to workdirectly on the root causes of theproblem.
The role of the nutritional sciences
should be to provide insights thatgenerate more political commitment, higher priority. and operationally effective interventionson-the-ground that wi II confrontsquarely one ofthe major challengesof contemporary humankind.
While intellectual dialogue on themagnitude of malnutrition is nodoubt stimulating. we should notmiss the main point with which we allconcur. namely that poverty andmalnutrition are massive, and itsprevention and control demand thehighest priority through effective
action on-the-ground.
FOUNDATIONNEWS
A meeting of the task force onstudies on health/nutrition consequences of developmental programmes in Punjab and Uttar Pradeshwas held in New Delhi on July 23.under the chairmanship of Dr. Srikantia.
A meeting of the task force onstudies on disabilities in schoolchildren related to malnutrition washeld in New Delhi on September 11.under the chairmanship of Dr. V.N.Rao. Director (Research). KEMHospital. Pune.
Brinkmanship is defined as the artof advancing to the very brink ofwar or catastrophe but stoppingjust short of it. It would seem thatbrinkmanship is now being activelypromoted and propagated as part ofthe nutrition policy of developingcountries.
The art of brinkmanship in nutrition consists essentially in advocating that children who suffer frommalnutrition of the so-called 'mild'and 'moderate' grades-a classification devoid of proven physiologicalvalidity-may be left severely aloneto fend for themselves. and "nutri
tion intervention" need be attemptedonly when they reach the "severe"
stage of impending death. In otherwords, saving children from thecatastrophe of death. rather thanensuring their normal health andnutrition is the essence of the policyof brinkmanship.
Strange Justification
The justification proffered for thispolicy is that children who are not soseverely malnourished as to be onthe verge of death, may somehow"muddle through" and manage tosurvive-in which case they could bedescribed as "adapted", meaningthat they have come to terms with.and have learnt to reconcile themselves to, their bad lot. Unfortu
nately, many of those who are usingthe word "adaptation", in the debatedo so rather loo~ely. A person withhigh blood pressure can "adapt"himself to his condition throughhypertrophy of his heart; such"adaptation" helps him to buy sometime before the inevitable disasterstrikes, but he IS by no means normal.The fact that between death and nor
malcy, there exists a broad twilightzone of morbidity, functional impairment of various kinds, apathy. lack ofsense of well-being, poor physicalstamina, low productivity, etc., is lar-
5
gely lost sight of.The policy of brinkmanship
withholding nutrition intervention tochildren till they reach the verge ofdeath, the so-called "severe" stageof malnutrition, is calculated to
undermine and erode the quality ofour human resources. Intervention
in the last stages of malnutritioncannot help to build a strong andhealthy nation, but will only serve toincrease the pool of survivors of substandard physical stamina andproductivity-the scars of childhoodmalnutrition: it will be akin to boltingthe stable door after the horse hasescaped, for many children whohave reached the 'severe' stage ofmalnutrition cannot be restored to
full normalcy
Policy of Bankruptcy
To say this is not to advocate
"triage": for it is not implied here that'severe' cases of malnutrition should
be left alone to d.ie. What is emphasised here is that a nutrition policywhich consists in apportioning thepredominant part of the NutritionBudget only to saving severely malnourished children from the jaws ofdeath, and in according little importance and support to improving thelot of other malnourished children in
the community and in preventingthem from sliding into the 'severe'stage. will be a policy of bankruptcyand brinkmanship.
What is objectionable is theattempt to justify exclusive emphasison 'severely' malnourished childrennot on the basis of lack of adequateresources for a broader coverage,but on the basis thatchildren in poorcommunities. other than those"severely malnourished" and on theverge of death, are all normal and'adapted' in spite of their very significant growth-retardation In otherwords, we are being persuaded toaccept mild and moderate malnutri-

tion in our children as our normalnational feature.
When it is pointed out to thosewho advocate this policy of brinkmanship that malnourished children
who may escape death eventuallygrow into stunted adults of low bodysize and poor productivity. it isargued that low body size is welcome because the energy requirement of such subjects will be low;the resultant low productivity andlow earning capacity should notmatter because in any case we are alabour-intensive, cheap-laboureconomy! "Improve the economyfirst. and then talk aboUt improvingnutrition of children and body-sizeof adults. Our labourers have the
body-size suited to our economy," isthe answer. Without questioning thebonafides of scientists who advo
cate this policy and with all duerespect to them, it must be clear that
this policy will only serve to perpetuate the current nutrition scenario~ \
and .the 'underlying povertysyndrome-the vicious cycle of poverty, undernutrition, low productivity. poor fncome and poverty. Thisvicious cycle must be broken at several points and not in an ordainedsequence.
A sensible National Nutrition Pol
icy should aim at preventing malnourished children of poorcommunities from reaching thesevere terminal stage, and not wait·passively for them to arrive there in
oorder to start rescue and repair operations, which, besides being expensive, will in any case not restore themto full normalcy.
It is from this point of view that wewelcome Dr. Linc.oln Chen's foregoing excellent paper; his earlier communications in the AmericanJournal of Clinical Nutrition had led
to unwarranted interpretationswhich were clearly not intended byhim.
Dr. Chen's communication clearlyunderscores the need for a nutrition
policy which seeks to· attack thebasic factors that underlie all forms
of malnutrition. including the "mild"and "moderate" degress. His paperrepresents a cogent well-reasonedand forceful plea against the policyof brinkmanship ionnutrition.
REVIEWS ANDCOMMENTS
On Brinkmanshipin Nutrition
I am thankful to Dr. C. Gopalan forsharing with me the draft of hispaper on "The Nutrition Policy of
Brinkmanship". I agree heartily withwhat he has written. and especiallyendorse his objection to attempts tojustify a nutrition policy of exclusiveemphasis on 'severely' malnourishedchildren, on the assumption that allother malnourished children in thecommunity (the so-called mild/moderately malnourished) are normaland ·adapted'. Indeed, I would gofurther and say that in India, a countrywith enough food. no baby shouldbe expected to adapt to deprivationoffood.lnsteadofdevising a nutritionpolicy based on such expectationand consisting mainly of dealingwith severe' malnutrition after it hasset in, the country should embark ona war-footing upon a policy ofpreventing such 'severe' malnutritionin children.
In every village of the countrytoday, all the time, "horses are bolting out of open stable doors"infants and children, victims of the
. inexorable interaction of chronicstarvation and diseases die. often tobe replaced by the next. with themother progressively worn out andnutritionally depleted. I w0L!ld callthis a progressive spiral of descentinto the state of misery (not just avicious circle). Our .experience inCMC Ludhiana. working with thehealth functionaries in a communitydevelopment block. has shown usthat all this misery can be avoided .. 0
In every village. though the overallcommunity nutrition profile mayshow little change over severalmonths. in individual households itis all the time rapidly changing.New high-risk subjects will haveemerged in families which did nothave them before-new pregnancies, new births, and babies who
were in good nutritio,n on exclusivebreast-feeding just a few weeks aqo.now steadily descending into malnutrition. Under the circumstances,
6
what is needed for an effective preventive programme (as against arepair operation) is a strategy of continuous monitoring of thecommunity for rapidly updating the data onchanging nutrition profile in individual house holds and for timely identification of the high-risk su bjects.This cannot be achieved throughelaborate resurveys, following on aninitial base-line survey, each ofwhich resurvey may take at leastthree months for a team of multi
purpose workers, working fourhours a day, to complete in a subcentre area. Such resurveys wouldprove as much tiresome and frustrating to the communities as to thehealth-personnel. for, in the meanwhile "several horses would havebolted out of the stables".
At present the MultipurposeWorkers attached to each Subsi
diary Health Centre (population5,000) in Punjab. visit every homeonce in 6-8 weeks. Their emphasis ison maternal and child health and
family planning but the continuinghigh infant and toddler mortality andthe prevalence of so much malnutrition, esp'ecially in the second andthird year. shows that the goals ofthese 0 workers are not beingachieved. In the Community Development Block allocated in 19BO toour medical college. without disturbing the basic working pattern ot theexisting work force. we have simplymore effectively deployed that forceso that they have adopted the "needbased" approach developed by us.
The workers, realising that attitudes and long-standing practicescannot be changed during a homevisit lasting 3-5 minutes every 6-8weeks have recognised that allhomes do not need 5 minutes, andthat in the homes of more than halfof the family folders they take outdaily, they need spend only 2 minutes monitoring any change whichhas taken place.
In these homes there will be no
potentially "at risk" individual andthis allows them 15-20 minutes in
homes where there are pregnantwomen and/or under-five children.
especially when these high risk subjects do not attend the local clinicsfor mothers and children. This"intensive care" approach allows the

Dr. P.V. Indiresan, Director,Indian Institute of Technology, Madras
Integrated Rural Development:The Narayanapuram Experience
workers time to teach mothers, no
matter how poor or over-worked,how to make the best use of whatever is available in that home.
Having spent half an hour daily inthe centre recording in appropriatesection of the Master Register, allchanges found on that day's homevisiting, the workers andsupervisor-who may be a medicalofficer or Lady Health Visitor. discuss all priority persons seen thatday and make a plan for each. Thusfor a clinic attender of 18 months.
eating adequately, there may be noneed to see her till the routine visit
However, a female of 10 monthsfrom a poor home, eating inadequately in spite of earlier advice andwhose mother's pregnancy wasnoted that day, is of very high risk.Even though she is on the "Road toHealth"-she must go on a high risklist so that the home receives visits
every 4 or even 2 weeks until thechild is out of danger as a result ofthe mother's acceptance of the oftrepeated nutrition health education.
Through such a programme, wehave shown that women of poorcommunities can have splendidbabies through encouraging exclusive breast feeding for 6 to 7months; and that through timelyadvice on the use of inexpensivelocally available supplements(based just on roti. vegetables andtea) which can be eaten by theseven-month old, even first degreemalnutrition can be prevented inthem, We can ensure that a very highpercentage of children avail offacilities for immunisation, and the practice of timely oral hydration ofchildren with diarrhoea is promotedand propagated.
We are convinced from our experience in CMC-Ludhiana that thisstrategy of preventing infants andyoung children from sliding intosevere malnutrition (rather than astrategy of belated repair andrescue-brinkmanship) is perfectlyfeasible, with the existing infrastructure, facilities and resources, andthat this is not a "pipe-dream".
Dr. Betty CowanChristian Medical CollegeLudhiana
Some years ago. the Indian Institute of Technology. Madras,obtained from the' Tamil NaduGovernment a 94 acre tract of land
near the southern boundary of thecity to establish a Rural Development Project This land, part of a seasonal swamp, which gets inundatedby knee-deep water for about fourmonths in a year. was uncultivatedand uncultivable. with not even
water hyacinth surviving on it.On this inhospitable land. the
Institute has established during thepast two years, an integrated development complex, employing about300 people with monthly wagesranging from Rs 300 to Rs 1200.The main resource available on site
was plenty of subsoil, brackishwater. with salt content as high as30,000 parts per million. It wasdecided that the best way to utilisethis asset was to cultivate the fishthat thrive in brackish water.
From the earth that came out of
digging this fish pond, bricks weremade, and to help make bricks, a biogas plant was established, naturallyalong with a dairy farm. To facilitateboth dairy farming and brick making,a rice r1iill was started, the branbeing used for the cattle and thehusk for making bricks. In addition abakery was established to use thebiogas.
As this project involved considerable construction work-worth overRs 20 lakh during the past oneyear-a carpentry and a weldingsection, were formed, which haveproved to be profitable industrialactivities in their own right.
It so happened that the ScienceCentre of the liT-Madras had alreadydeveloped kits for teaching electronics in schools, and had secured substantial orders from various stategovernments. The fabrication ofthese kits also was taken up by theCentre
During fabrication, a need was feltfor screen printing and for plasticbags. It was found far more convenient to have these things done inhouse hence a screen printing unitand a small plastic moulding plantwere also started.
As an adjunct to screen printing. aprinting press was also establishedFinally, to utilise the considerableamount of waste paper that is available from the liT and elsewhere, a
Paper Recycling Plant of one ton'capacity per day was erected.
Thanks to the considerableamount of sludge from the biogasplant. the uncultivable land in whicheven water hyacinth would notgrowis now gradually being reclaimed.Today, there are hundreds of cOCQnut plants and thousands of kubabui'trees. Further expansion will be inthe direction of providing varioussocial, municipal and commercialamenities, as well as housing. A dis-_pensary is already in 9peration and abank is about to start Together,these constitute the NarayanapuramIntegrated Development ProJect.
Commercial Venture
There are several novel conceptsin this scheme. Firstly, it is not a welfare project but a commercial venture. Most rural development
. projects run mainly with subsidiesfrom Government and other agencies. However, this project has.beenfinanced by commercial loans takenfrom the United Commercial Bank atthe usual rates of interest. Most ruraldevelopment schemes were notreplicable because they did notinspire adequate confidence regarding their economic viability. The bestway to demonstrate such a viabilityis to .have a bankable project
A bankable project has also theadvantage that. as and when theloan is repaid, there will be funds to

start another similar project. andwhen the loan is repaid with interest.one can actually generate funds tostart more than one such project.Subsidies. on the other hand. tend todry up sooner or later. Thus. only abankable project is self-regenerativeand has the ability to growexponentially
Secondly. most rural projects aimat marginal improvement in the conditions of life and the economic status of the concerned individuals. As
already stated. the salary levels thathave been established. range fromRs 300/ - to Rs 1200/- per month.These are muCh higher than what isnormally obtained in village development schemes.
A Quantum Jump
Thus. the attempt is to ensure aquantum jump rather than a marginal improvement. In fact. this quantum jump is much more substantialthan what may appear from the kindof salaries that are being paid. It isplanned that the people working onthis project will get subsidised modern housing. protected water supply.proper sewage systems. fuel andother amenities such as schools.health centres. commercial andtransportation systems.
The effective income and qualityof life will. therefore. be far higherthan what the salaries indicate.
The reason why we consider itfeasible to establish an improvementin the quality of life as listed above isbecause the main basis of development is not agriculture but industryAgriculture has the limitation thatthe consumption of agricultural products is comparatively inelastic. Onthe other hand. there is an insatiabledemand for industrial goods andhence. the rr.argin of developmentthrough industrial development isimmensely higher.
Most major schemes of rural technology are based on maximisingemployment and mlnlmlslngprod uctivity.
In Narayanapuram. on the contrary. the aim has been to maxi miseproductivity and to minimise directemployment in every field of activityThe overall employment is madehigh. however. by increasing the
number of such activities. To ensure
high productivity we have to use thebest possible technology in contrastwith the accepted norms of appropriate technology which usuallyimplies minimum of technology
Such a minimum technology isgenerally advocated because of theworkers' illiteracy and the cost ofsophisticated equipment. Webelieve these arguments to beincorrect.
Firstly. there is a distinctionbetween a sophisticated equipmentand equipment which requiressophistication to handle. QUite alarge variety of modern sophisticated production equipment requirevery simple skills indeed In fact. theentire growth of the industry In theWest has been based on the employment of more and more unskilledlabour. as for instance. in the manufacture of automobiles. Thus.
sophistication in machines actuallydemands less. not more. skill fromlabour and is better adapted tounskilled people than are simpletools
No·doubt. it is true that sophisticated equipment is expensive and. ina poor cQuntry like ours. funds arelimited. Strictiy speaking. howeverthe real limitation is not funds forinvestment. but profitable ideas forinvestment. One of the main reasonswhy rural development works arestarved of funds is because of thefear that. in most cases. the loanswill never be repaid. Where theinvestment is profitable. there willbe-in fact. this is our experienceno dearth of funds.
It might have been noticed that the300 workers who have been
employed under the scheme are allwage-employees. This again is indirect contrast to the traditional wisdom of rural development. whichemphasises self-employment. Toprovide an additional cow. or pig. orloom to help an individual supplement his income. is no answer; selfemployment requires a standard offoresight and entrepreneurshipwhich even highly educated peoplerarely enjoy. It is far too much toexpect an illiterate villager to 5UCceed where even the best educatedfear to tread.
Secondly. self-employment can
never be properly integrated. whereas wage employment can be. Thereason why we are able to generate alarge amount of employment isbecause a variety of things havebeen integrated and such an integration is not possible where all theworkers are self-employed with eachone ploughing his own lonelyfurrow.
We were fortunate to get a reasonably large tract of unoccupied land.Thereby. we have avoided the pitfallsof adopting a village. Adopting a village implies that we have to come toterms with the internal social. political and economic structure within
the village. By establishing the project outside any village. we haveavoided many such problems. Infact. we draw our workers from as
many as five villages in the vicinity.This further diffuses the problem ofinternal rivalries common in villagecommunities.
Ideas for Investment
We have also more or lessexcluded the local leadership fromthe functioning or organisation ofthe project. In fact. apart from thesenior faculty of the liT-Madras whoare working in this project. most ofthe functional leadership is with thehired supervisory staff who had to bedrawn from outside the neighbourhood.
By insisting on such professionalmanagement. we have. at least sofar. avoided the local caste. groupand political pressures We do notadvocate enlargment of a schemeto obtain growth. but suggest replication instead. Incidentally. replica-
. tion is also the only way a ruralproject remains rural.
Although these projects havedrawn on the expertise of the IndianInstitute of Technology. Madras. thisis not strictly necessary In fact. whatliT-Madras has provided is not somuch technical expertise asmanagerial ideas. There is no reasonwhy the concepts enumerated herecannot be implemented by others.As mentioned already the cost ofinvestment. although substantial. isunlikely to be a. problem. but a minimum of 100-200 acres is needed totryout such a scheme.
Edited by Dr (Mrsl S Malhan. PhD for Nutrition Foundation of India. B 37 Gulmohar Park. New Deihl. DeSigned and produced by Media Workshlp and printed at Veerendra Printers
Related Documents
![Malnutrition [Autosaved]](https://static.cupdf.com/doc/110x72/577cd2051a28ab9e7895192c/malnutrition-autosaved.jpg)










