Malignant Sarcoma of the Pelvic Bones Treatment Outcomes and Prognostic Factors Vary by Histopathology Muhammad Umar Jawad, MD 1 ; Abdul Ahad Haleem, MD 2 ; and Sean P. Scully, MD, PhD 3 BACKGROUND: Treatment of malignant sarcomas of the pelvis poses a challenge for local disease control and onco- logic outcome. Many reports have described the dismal outcomes. Most studies are retrospective series coming out of single centers, thus biased toward patient selection and are of limited statistical power. METHODS: The authors used the Surveillance, Epidemiology, and End Results database to analyze 1185 pelvic sarcoma cases from 1987 to 2006. Kaplan-Meier and Cox regression were used to analyze the significance of prognostic factors.The analysis was repeated for different histopathological subtypes to determine specific prognostic factors in each case. RESULTS: Incidence of pelvic sarcoma in 2006 was 89 per 100,000 persons; it has significantly increased since 1973 (P < .05). The overall 5-year survival for all the patients with pelvic sarcoma was 47%, with osteosarcoma having the worst 5- year survival at 19% and patients with chordoma having the best 5-year survival at 60%. Independent prognostic fac- tors included age, stage, grade, size of primary lesion, histopathology, and treatment-related factors. Comparing the patients only with high-grade lesions, patients with Ewing sarcoma have the best prognosis. CONCLUSIONS: This is an analysis of patients with pelvic sarcomas derived from a population-based registry. Survival and prognostics vary with histopathological diagnoses. Although surgical resection was associated with superior outcomes for osteosar- coma and chondrosarcoma, there was no significant difference in outcomes of patients with Ewing sarcoma treated with surgery and/or radiotherapy. Cancer 2011;117:1529–41. V C 2010 American Cancer Society . KEYWORDS: malignant sarcoma, pelvic sarcoma, prognostic factors, treatment outcomes. Malignant tumors involving the pelvis pose a challenge in achieving local disease control and improving patient sur- vival. 1 Previous reports have described the significant morbidity and complications associated with surgical resection, and provide conflicting data regarding treatment outcomes and prognosis. 2-16 The reasons behind such conflicting evidence are severalfold. Most of the reports emanate from a single center and thus carry a bias toward the selection of patient popu- lation and treatment modalities used. 1,13,17,18 Second, the small number of patients analyzed has limited the statistical power for each of the studies. Lastly, there is inconsistency in the analysis of the data, with some reports providing an anal- ysis of outcomes and prognostic factors with respect to a particular histopathological subtype of tumor, 19-29 whereas others have grouped different histopathological subtypes affecting pelvic bones as a single cohort. 1,13,17,18 The clinician is thus left wondering whether a uniform treatment strategy should be applied to all the patients regardless of the histopathology, as previously suggested, or each disease should be treated as a separate entity. 1 An example of such a controversy is illus- trated in the treatment recommendations for pelvic Ewing sarcoma, in which some authors have suggested considering radiotherapy as an alternative to surgery in pelvic Ewing sarcoma, 30-34 whereas others have stressed the importance of wide excision of the primary disease for this and other sarcomas. 25,35-43 In the current study, we have made an attempt to resolve these controversies by analyzing the outcomes of all patients with sarcomas of the pelvis from 1987 to 2006 using the Surveillance, Epidemiology, and End Results (SEER) database. The data were analyzed as a single cohort and also separately with respect to different histopathological subtypes. The selection was limited to the years 1987 to 2006, because imaging such as computed tomography and magnetic resonance imaging were routinely used, permitting determination of tumor size and extent. DOI: 10.1002/cncr.25684, Received: May 26, 2010; Revised: August 19, 2010; Accepted: September 7, 2010, Published online November 8, 2010 in Wiley Online Library (wileyonlinelibrary.com) Corresponding author: Muhammad Umar Jawad, MD, Department of Orthopedics, Edwards Building, 300 Pasteur Drive, R116, Stanford, CA 94301; Fax: (305) 325-4784; [email protected] 1 Department of Orthopedics, Stanford University Hospital and Clinics, Stanford, California; 2 Department of Orthopedic Surgery, Hays Medical Center, Hays, Kansas; 3 Department of Orthopedics, University of Miami Miller School of Medicine, Miami, Florida Cancer April 1, 2011 1529 Original Article

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Malignant Sarcoma of the Pelvic BonesTreatment Outcomes and Prognostic Factors Vary by Histopathology
Muhammad Umar Jawad, MD1; Abdul Ahad Haleem, MD2; and Sean P. Scully, MD, PhD3
BACKGROUND: Treatment of malignant sarcomas of the pelvis poses a challenge for local disease control and onco-
logic outcome. Many reports have described the dismal outcomes. Most studies are retrospective series coming out
of single centers, thus biased toward patient selection and are of limited statistical power. METHODS: The authors
used the Surveillance, Epidemiology, and End Results database to analyze 1185 pelvic sarcoma cases from 1987 to
2006. Kaplan-Meier and Cox regression were used to analyze the significance of prognostic factors. The analysis was
repeated for different histopathological subtypes to determine specific prognostic factors in each case. RESULTS:
Incidence of pelvic sarcoma in 2006 was 89 per 100,000 persons; it has significantly increased since 1973 (P < .05).
The overall 5-year survival for all the patients with pelvic sarcoma was 47%, with osteosarcoma having the worst 5-
year survival at 19% and patients with chordoma having the best 5-year survival at 60%. Independent prognostic fac-
tors included age, stage, grade, size of primary lesion, histopathology, and treatment-related factors. Comparing the
patients only with high-grade lesions, patients with Ewing sarcoma have the best prognosis. CONCLUSIONS: This is
an analysis of patients with pelvic sarcomas derived from a population-based registry. Survival and prognostics vary
with histopathological diagnoses. Although surgical resection was associated with superior outcomes for osteosar-
coma and chondrosarcoma, there was no significant difference in outcomes of patients with Ewing sarcoma treated
with surgery and/or radiotherapy. Cancer 2011;117:1529–41. VC 2010 American Cancer Society.
KEYWORDS: malignant sarcoma, pelvic sarcoma, prognostic factors, treatment outcomes.
Malignant tumors involving the pelvis pose a challenge in achieving local disease control and improving patient sur-vival.1 Previous reports have described the significant morbidity and complications associated with surgical resection, andprovide conflicting data regarding treatment outcomes and prognosis.2-16 The reasons behind such conflicting evidenceare severalfold. Most of the reports emanate from a single center and thus carry a bias toward the selection of patient popu-lation and treatment modalities used.1,13,17,18 Second, the small number of patients analyzed has limited the statisticalpower for each of the studies. Lastly, there is inconsistency in the analysis of the data, with some reports providing an anal-ysis of outcomes and prognostic factors with respect to a particular histopathological subtype of tumor,19-29 whereas othershave grouped different histopathological subtypes affecting pelvic bones as a single cohort.1,13,17,18 The clinician is thusleft wondering whether a uniform treatment strategy should be applied to all the patients regardless of the histopathology,as previously suggested, or each disease should be treated as a separate entity.1 An example of such a controversy is illus-trated in the treatment recommendations for pelvic Ewing sarcoma, in which some authors have suggested consideringradiotherapy as an alternative to surgery in pelvic Ewing sarcoma,30-34 whereas others have stressed the importance ofwide excision of the primary disease for this and other sarcomas.25,35-43
In the current study, we have made an attempt to resolve these controversies by analyzing the outcomes of all patientswith sarcomas of the pelvis from 1987 to 2006 using the Surveillance, Epidemiology, and End Results (SEER) database.The data were analyzed as a single cohort and also separately with respect to different histopathological subtypes. Theselection was limited to the years 1987 to 2006, because imaging such as computed tomography and magnetic resonanceimaging were routinely used, permitting determination of tumor size and extent.
DOI: 10.1002/cncr.25684, Received: May 26, 2010; Revised: August 19, 2010; Accepted: September 7, 2010, Published online November 8, 2010 in Wiley Online
Library (wileyonlinelibrary.com)
Corresponding author: Muhammad Umar Jawad, MD, Department of Orthopedics, Edwards Building, 300 Pasteur Drive, R116, Stanford, CA 94301; Fax: (305)
325-4784; [email protected]
1Department of Orthopedics, Stanford University Hospital and Clinics, Stanford, California; 2Department of Orthopedic Surgery, Hays Medical Center, Hays, Kansas;3Department of Orthopedics, University of Miami Miller School of Medicine, Miami, Florida
Cancer April 1, 2011 1529
Original Article

MATERIALS AND METHODSThe population analyzed was extracted from population-based cancer registries that participate in the NationalCancer Institute (NCI)’s SEER program.44 A total of1185 patients with a diagnosis of sarcoma and a primarydisease location of pelvic bones were identified over theinterval from 1987 to 2006. Sarcoma cases were identifiedby the designated histologic International Classificationof Diseases for Oncology, Third Edition codes. Informa-tion regarding patient demographics, stage at diagnosis,size, number of primaries, cause of death, year of diagno-sis, surgical and radiation treatment, and survival timeuntil death or loss to follow-up was identified. Patientswith missing data were excluded from each respective uni-variate and multivariate analysis.
Patient age was arbitrarily converted to a categoricalvariable (0-16, 17-40, 41-60, �60 years) for the purposeof analysis. Staging categories of local, regional, and dis-tant disease were used according to the SEER staging sys-tem. Tumor size was converted into a categorical variable(<5, 5-10, >10) according to the American JointCommittee on Cancer recommendations and previousreports.1,17,20
SEER* Stat software (version 6.4.4, NCI) was usedto analyze incidence rates, which were age adjusted andnormalized using the 2000 US standard population. Sta-tistical analysis was performed using the SPSS statisticalpackage version 16.0 (SPSS Inc., Chicago, Ill). The effectsof demographic, clinical, pathological, and treatment var-iables were tested using the log-rank test for categoricalvalues. A multivariate analysis was carried out for determi-nation of independent prognostic factors using the Coxproportional hazards model.
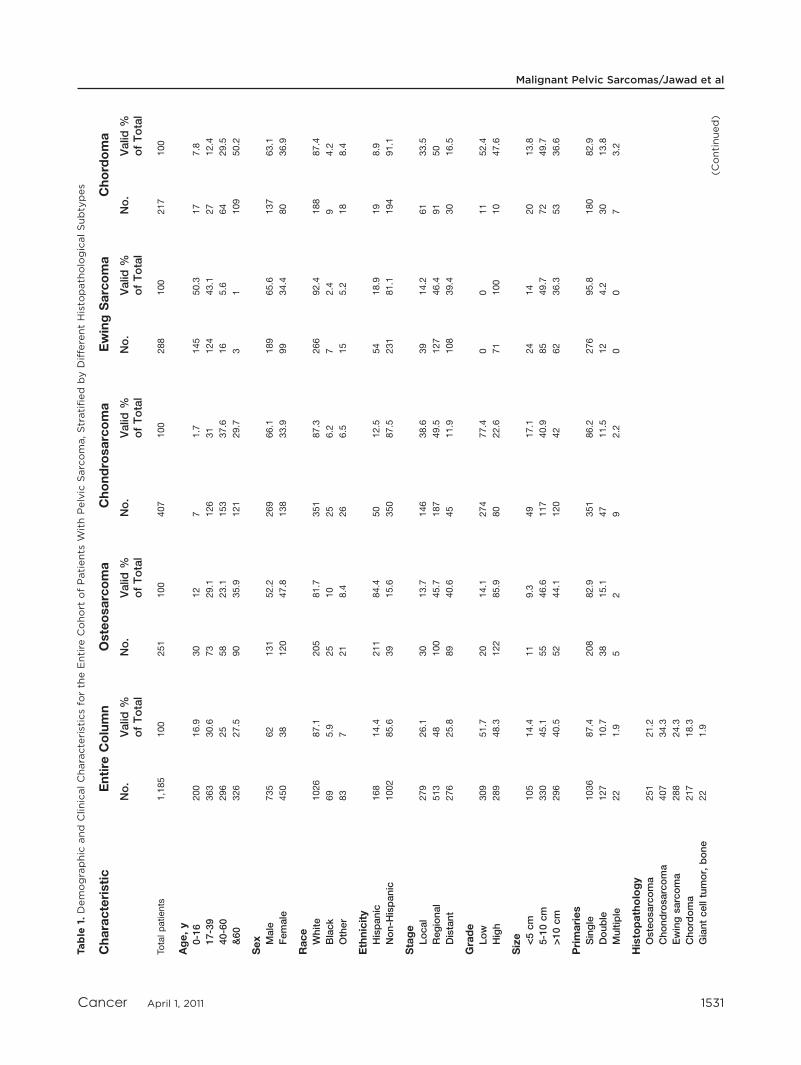
RESULTSThe demographic characteristics of the 1185 patients withsarcomas involving the pelvic bones identified in theSEER database are displayed in Table 1. The specific his-topathological diagnosis was chondrosarcoma (31.3%),osteosarcoma (19%), and Ewing sarcoma (22.1%). Grade(664 patients) and size (775 patients) data were availableonly for a proportion of the cohort. Location was specifiedas pelvic bones for most of the patients (97.9%), and mostof the patients (86.7%) presented with a single lesion.Incidence of pelvic sarcoma in 2006 was 89 per 100,000persons and has shown a significant increase since 1973,with an annual percentage change of 5.39 (P< .05).
Patients with osteosarcoma of the pelvis constituted19.3% of the cohort and had a mode age of >60 years(35.9%). The pediatric age group contributed the fewestnumbers to patients with pelvic osteosarcoma (12%). Todetermine whether there is a statistically significant associ-ation between pelvic location for osteosarcoma and age, across table analysis was performed. Chi-square testrevealed a statistically significant association between pel-vic location and age >60 years (P < .001). Only 16 ofthese cases were diagnosed as Paget osteosarcoma. Allother patients had primary osteosarcoma.
A total of 407 patients had the diagnosis of chondro-sarcoma, with only 7 (1.7%) patients in the pediatric agegroup. Only 11.9% of patients presented with a distantstage of disease, and most of the patients with availablegrade information presented with low-grade lesions(77.4%). Most of these patients underwent surgical resec-tion (74.6%), only 16.9% of patients underwent radio-therapy, and the latter did not significantly impactsurvival (P¼ .667).
Patients with Ewing sarcoma of the pelvis repre-sented 22.1% of the cohort with a modal age group of 0to 16 years (50.3%). Most of the patients were male(66.1%), and only 14.2% of the patients presented withlocal stage of disease. Surgery was performed in 35.1% ofthe patients, and radiotherapy was administered in 62.5%of the patients. A total of 56 (20.7%) patients underwentsurgical resection as well as radiotherapy. A Kaplan-Meiercurve predicting the effects of treatment on survival isshown in Figure 1B. It shows that patients undergoingsurgical resection, radiation therapy, or a combination ofboth fared similarly and significantly better than those notreceiving either therapy.
Chordoma was the histopathological diagnosis in217 (16.7%) patients. The most common age group was>60 years (50.2%); most of the patients were male(63.1%), and 50% of all the patients presented with re-gional disease. Surgical resection was performed in 68.6%of the patients.
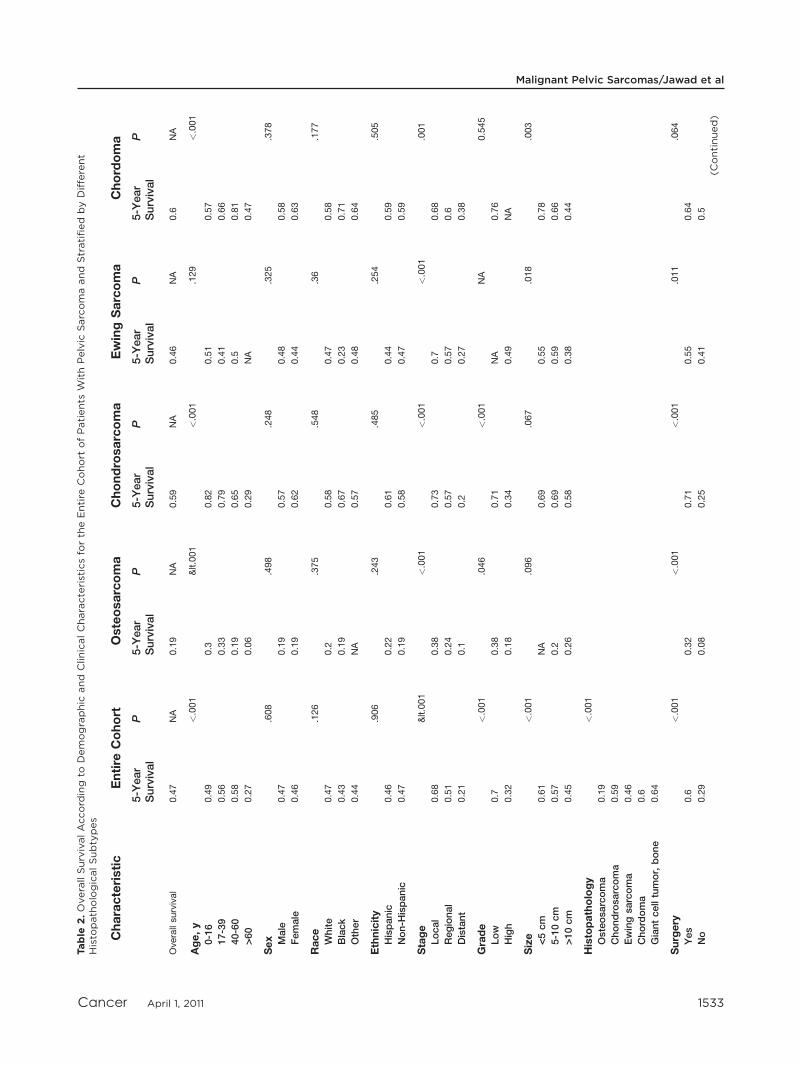
The 5-year survival of all the patients with pelvic sar-coma was 45%, for patients with osteosarcoma it was19%, for chondrosarcoma it was 59%, for Ewing sarcomait was 46%, and for chordoma the 5-year survival was60%. When only high-grade tumors are considered, the5-year survival for pelvic osteosarcoma and chondrosar-coma was 18% and 34%, respectively.
Univariate and multivariate analysis of parametersthat influence survival are demonstrated in Table 2 andTable 3, respectively. Univariate analysis demonstrated a
Original Article
1530 Cancer April 1, 2011
Table
1.Demographic
and
ClinicalCharacteristicsfo
rth
eEntire
Cohort
ofPatients
WithPelvic
Sarcoma,Stratified
byDifferentHisto
path
ologicalSubtypes
Characteristic
Entire
Column
Osteosarcoma
Chondrosarcoma
EwingSarcoma
Chordoma
No.
Valid
%ofTotal
No.
Valid
%ofTotal
No.
Valid
%ofTotal
No.
Valid
%ofTotal
No.
Valid
%ofTotal
Totalpatients
1,185
100
251
100
407
100
288
100
217
100
Age,y
0-16
200
16.9
30
12
71.7
145
50.3
17
7.8
17-39
363
30.6
73
29.1
126
31
124
43.1
27
12.4
40-60
296
25
58
23.1
153
37.6
16
5.6
64
29.5
&60
326
27.5
90
35.9
121
29.7
31
109
50.2
Sex Male
735
62
131
52.2
269
66.1
189
65.6
137
63.1
Female
450
38
120
47.8
138
33.9
99
34.4
80
36.9
Race
White
1026
87.1
205
81.7
351
87.3
266
92.4
188
87.4
Black
69
5.9
25
10
25
6.2
72.4
94.2
Other
83
721
8.4
26
6.5
15
5.2
18
8.4
Ethnicity
Hispanic
168
14.4
211
84.4
50
12.5
54
18.9
19
8.9
Non-H
ispanic
1002
85.6
39
15.6
350
87.5
231
81.1
194
91.1
Stage
Local
279
26.1
30
13.7
146
38.6
39
14.2
61
33.5
Regional
513
48
100
45.7
187
49.5
127
46.4
91
50
Distant
276
25.8
89
40.6
45
11.9
108
39.4
30
16.5
Grade
Low
309
51.7
20
14.1
274
77.4
00
11
52.4
High
289
48.3
122
85.9
80
22.6
71
100
10
47.6
Size <5cm
105
14.4
11
9.3
49
17.1
24
14
20
13.8
5-10cm
330
45.1
55
46.6
117
40.9
85
49.7
72
49.7
>10cm
296
40.5
52
44.1
120
42
62
36.3
53
36.6
Primaries
Single
1036
87.4
208
82.9
351
86.2
276
95.8
180
82.9
Double
127
10.7
38
15.1
47
11.5
12
4.2
30
13.8
Multiple
22
1.9
52
92.2
00
73.2
Histopathology
Osteosarcoma
251
21.2
Chondrosarcoma
407
34.3
Ewingsarcoma
288
24.3
Chordoma
217
18.3
Giantcelltumor,bone
22
1.9
(Continued)
Malignant Pelvic Sarcomas/Jawad et al
Cancer April 1, 2011 1531

survival advantage for patients with pelvic sarcomas withage <60 years (P < .001), local stage of disease with nosystemic disease involvement (P < .001), low grade (P <
.001), smaller size (P < .001), single primary lesion (P <
.001), histology other than osteosarcoma (P< .001), per-formance of surgical resection (P < .001), and nonuse ofradiation therapy (P¼ .006). Association between nonuseT
able
1.(C
ontinued)
Characteristic
Entire
Column
Osteosarcoma
Chondrosarcoma
EwingSarcoma
Chordoma
No.
Valid
%ofTotal
No.
Valid
%ofTotal
No.
Valid
%ofTotal
No.
Valid
%ofTotal
No.
Valid
%ofTotal
Surgery
Yes
717
58.1
118
48
300
74.6
98
35.1
144
68.6
No
554
41.9
128
52
102
25.4
181
64.9
66
31.4
Radiation
Yes
392
34.1
65
26.2
67
16.9
173
62.5
80
38.6
No
757
65.9
183
73.8
330
83.1
104
37.5
127
61.4
Yearofdiagnosis
1987-1996
372
31.4
90
35.9
128
31.4
84
29.2
65
30
1997-2006
813
68.6
161
64.1
279
68.6
204
70.8
152
70
Figure 1. Survival for patients with pelvic Ewing sarcoma isshown with respect to (A) stage and (B) treatment modality.
Original Article
1532 Cancer April 1, 2011
Table
2.OverallSurvivalAccord
ing
toDemographic
and
ClinicalCharacteristicsfo
rth
eEntire
Cohort
ofPatients
WithPelvic
Sarcomaand
Stratified
byDifferent
Histo
path
ologicalSubtypes
Characteristic
Entire
Cohort
Osteosarcoma
Chondrosarcoma
EwingSarcoma
Chordoma
5-Y
ear
Survival
P5-Y
ear
Survival
P5-Y
ear
Survival
P5-Y
ear
Survival
P5-Y
ear
Survival
P
Overallsurvival
0.47
NA
0.19
NA
0.59
NA
0.46
NA
0.6
NA
Age,y
<.001
<.001
<.001
.129
<.001
0-16
0.49
0.3
0.82
0.51
0.57
17-39
0.56
0.33
0.79
0.41
0.66
40-60
0.58
0.19
0.65
0.5
0.81
>60
0.27
0.06
0.29
NA
0.47
Sex
.608
.498
.248
.325
.378
Male
0.47
0.19
0.57
0.48
0.58
Female
0.46
0.19
0.62
0.44
0.63
Race
.126
.375
.548
.36
.177
White
0.47
0.2
0.58
0.47
0.58
Black
0.43
0.19
0.67
0.23
0.71
Other
0.44
NA
0.57
0.48
0.64
Ethnicity
.906
.243
.485
.254
.505
Hispanic
0.46
0.22
0.61
0.44
0.59
Non-H
ispanic
0.47
0.19
0.58
0.47
0.59
Stage
<.001
<.001
<.001
<.001
.001
Local
0.68
0.38
0.73
0.7
0.68
Regional
0.51
0.24
0.57
0.57
0.6
Distant
0.21
0.1
0.2
0.27
0.38
Grade
<.001
.046
<.001
NA
0.545
Low
0.7
0.38
0.71
NA
0.76
High
0.32
0.18
0.34
0.49
NA
Size
<.001
.096
.067
.018
.003
<5cm
0.61
NA
0.69
0.55
0.78
5-10cm
0.57
0.2
0.69
0.59
0.66
>10cm
0.45
0.26
0.58
0.38
0.44
Histopathology
<.001
Osteosarcoma
0.19
Chondrosarcoma
0.59
Ewingsarcoma
0.46
Chordoma
0.6
Giantcelltumor,bone
0.64
Surgery
<.001
<.001
<.001
.011
.064
Yes
0.6
0.32
0.71
0.55
0.64
No
0.29
0.08
0.25
0.41
0.5
(Continued)
Malignant Pelvic Sarcomas/Jawad et al
Cancer April 1, 2011 1533

Table
2.(C
ontinued)
Characteristic
Entire
Cohort
Osteosarcoma
Chondrosarcoma
EwingSarcoma
Chordoma
5-Y
ear
Survival
P5-Y
ear
Survival
P5-Y
ear
Survival
P5-Y
ear
Survival
P5-Y
ear
Survival
P
Radiation
.006
<.001
<.001
.014
.781
Yes
0.42
0.04
0.35
0.52
0.59
No
0.49
0.25
0.64
0.37
0.6
Yearofdiagnosis
.351
.507
.745
.174
.413
1987-1996
0.45
0.16
0.61
0.39
0.61
1997-2006
0.48
0.21
0.57
0.5
0.59
NAindicatesnotapplicable.
Forentire
cohort,age:P<.001is
trueonly
for>60years
vstherest;0-16vs17-40years,P¼.153;0-16vs41-60years,P¼.168;17-40vs41-60years,P¼.935;race:P¼.126only
forwhitesvsothers;
whitesvsblacks,P¼.148;blacksvsothers,P¼.982;stage:P<.001is
trueforcomparisonbetw
eenallcategories;size:P<.001is
trueonly
for<5cm
vs>10cm;<5cm
vs5-10cm,P¼.104;5-10cm
vs>10cm,P¼.002;primaries:P¼.007is
trueonly
forsingle
vsdouble;single
vsmultiple,P¼.353;double
vsmultiple,P¼.777;histopathology:P<.001is
trueforosteosarcomavstherest;chondrosar-
comavsgiantcelltumorofthebone,P¼.461;chondrosarcomavsEwing,P¼.008;chondrosarcomavschordoma,P¼.205;Ewingvsgiantcelltumorofthebone,P¼.154;chordomavsgiantcelltumor
ofthebone,P¼.395;Ewingvschordoma,P¼.067.
Forosteosarcoma,age:P<.001is
trueonly
for>60years
vstherest;0-16vs17-40years,P¼.725;0-16vs41-60years,P¼.160;17-40vs41-60years,P¼.026;race:P¼.375only
forwhitesvsothers;
whitesvsblacks,P¼.590;blacksvsothers,P¼.692;stage:P<.001is
trueforcomparisonbetw
eenallcategoriesexceptlocalvsregional,P¼.851;size:P<.096is
trueonly
for<5cm
vs5-10cm;<5
cm
vs>10cm,P¼.212;5-10cm
vs>10cm,P¼.605;primaries:P<.097is
trueonly
forsingle
vsdouble;single
vsmultiple,P¼.511;double
vsmultiple,P¼.953.
Forchondrosarcoma,age:P<.001is
trueonly
for>
60years
vstherest,except>60vs0-16years,P¼.010;0-16vs17-40years,P¼.654;0-16vs41-60years,P¼.266;17-40vs41-60years,P¼.008;
race:P
¼.548only
forblacksvsothers;whitesvsblacks,P¼.627;others
vswhites,P
¼.844;stage:P
<.001is
trueforcomparisonbetw
eenallcategories;size:P
¼.067is
trueforall,
except<5cm
vs
5-10cm,P¼.554;primaries,P¼.013is
trueonly
forsingle
vsdouble;single
vsmultiple,P¼.545;double
vsmultiple,P¼.765.
ForEwingsarcoma,age:P
¼.129is
trueonly
for0-16vs17-40years;0-16vs>60years,P
¼.137;0-16vs41-60years,P¼.965;17-40vs41-60years,P¼.507;17-40vs>60years,P¼.362;41-60vs
>60years,P¼
0.411;race:P¼.360only
forothers
vsblacks;whitevsothers,P¼.611;blackvswhite,P¼.400;stage:P<.001is
trueforcomparisonbetw
eenallcategoriesexceptlocalvsregional,P¼
.343;size,P¼.018is
trueonly
for5-10cm
vs>10cm;<5cm
vs5-10cm,P¼.680;<5cm
vs>10cm,P¼.055;primaries:P¼.429is
trueonly
forsingle
vsdouble.There
were
nopatients
withmultiple
lesions.
Forchordoma,age:P
<.001is
trueonly
for>60vs41-60years;0-16vs17-40years,P
¼.512;0-16vs41-60years,P
¼.345;0-16vs>60years,P
¼.057;17-40vs41-60years;P
¼.034;17-40vs>60
years,P¼.044;race:P¼.177only
forothers
vsblacks;whitesvsothers,P¼.219;blacksvswhites,P¼.990;stage:P¼.001is
trueforlocalvsdistantonly;localvsregional,P¼.083;regionalvsdistant,
P¼.039;size:P¼.003is
trueonly
for<5cm
vs>10cm;<5cm
vs5-10cm,P¼.175;5-10cm
vs>10cm,P¼.006;primaries:P¼.459is
trueonly
forsingle
vsmultiple;single
vsdouble,P¼.631;dou-
ble
vsmultiple,P¼.748.
Original Article
1534 Cancer April 1, 2011

Table
3.Multivariate
Analysis
forth
eEntire
Cohort
ofPatients
WithPelvic
Sarcomaand
Stratified
byDifferentHisto
path
ologicalSubtypes
Characteristic
Entire
Cohort
Osteosarcoma
Chondrosarcoma
EwingSarcoma
Chordoma
No.
Haza
rdRatio
PNo.
Haza
rdRatio
PNo.
Haza
rdRatio
PNo.
Haza
rdRatio
PNo.
Haza
rdRatio
P
Overall
376
NA
NA
125
NA
NA
324
NA
NA
257
NA
NA
136
NA
NA
Age,y
0-16
37
0.205
<.001
15
0.283
.003
60.164
.077
60.654
.473
17-39
129
0.254
<.001
42
0.308
<.001
104
0.255
<.001
15
0.497
.127
40-60
134
0.366
<.001
41
0.474
.022
124
0.425
<.001
40
0.211
<.001
>60
80
Referencegroup
29
Referencegroup
90
Referencegroup
75
Referencegroup
Stage
Local
118
0.31
<.001
17
0.413
.022
128
0.258
<.001
38
0.346
.001
46
0.177
<.001
Regional
195
0.562
.016
61
0.441
.001
166
0.513
.007
115
0.449
<.001
74
0.251
.002
Distant
67
Referencegroup
49
Referencegroup
30
Referencegroup
105
Referencegroup
16
Referencegroup
Grade
<.001
.924
<.001
Low
216
0.328
19
0.964
250
0.376
Grade
164
Referencegroup
108
Referencegroup
74
Referencegroup
Size <5cm
57
0.939
.828
20
0.36
.029
5-10cm
158
0.684
.036
66
0.579
.056
>10cm
165
Referencegroup
50
Referencegroup
Primaries
Single
337
0.386
.029
283
0.793
.722
Double
33
0.377
.047
33
0.671
.509
Multiple
10
Referencegroup
8Referencegroup
Histopathology
Osteosarcoma
77
3.298
.029
Chondrosarcoma
243
1.501
.441
Ewingsarcoma
42
1.075
.902
Chordoma
13
Referencegroup
Giantcelltumor,bone
52.906
.229
Surgery
Yes
291
0.512
.004
76
0.635
.095
263
0.352
<.001
90
0.626
.023
No
89
Referencegroup
51
Referencegroup
61
Referencegroup
168
Referencegroup
Radiation
Yes
86
1.366
.139
31
1.73
.032
47
1.112
.667
163
0.6
.005
No
294
Referencegroup
96
Referencegroup
277
Referencegroup
95
Referencegroup
NAindicatesnotapplicable.
of radiotherapy and improved survival may representselection bias in patients’ selection for radiotherapy for ei-ther close surgical margins or unresectable disease.
For osteosarcoma, survival advantage was found tobe associated with younger age (P< .001), localized stage(P < .001), low grade (P < .046), surgical resection (P <
.001), and nonuse of radiotherapy (P < .001). For chon-drosarcoma, the significant prognostic factors on univari-ate analysis included age<60 years (P< .001), local stage(P< .001), low grade (P< .001), absence of multiple pri-maries (P¼ .013), surgery (P< .001), and radiation (P<
.001). We suspect that association of radiotherapy andpoor survival is probably attributable to selection bias inselecting patients for radiotherapy.
Prognostic factors for Ewing sarcoma include localstage (P < .001), tumor size <10 cm (P < .018), surgery(P ¼ .011), and radiotherapy (P ¼ .014) for local controlof disease. On univariate analysis, significant prognosticfactors for chordoma patients included age <60 years (P< .001), local stage (P ¼ .001), tumor size <10 cm (P ¼.003), and primary location pelvis not otherwise specified(P¼ .005).
On multivariate analysis for all patients with pelvicsarcoma, factors affecting survival independently includedage, stage, grade, size of primary tumor, histopathology, andsurgery. Because grade and size information was availablefor only a fraction of patients, 376 patients were included inthe analysis. To determine the effects of this censoring, we
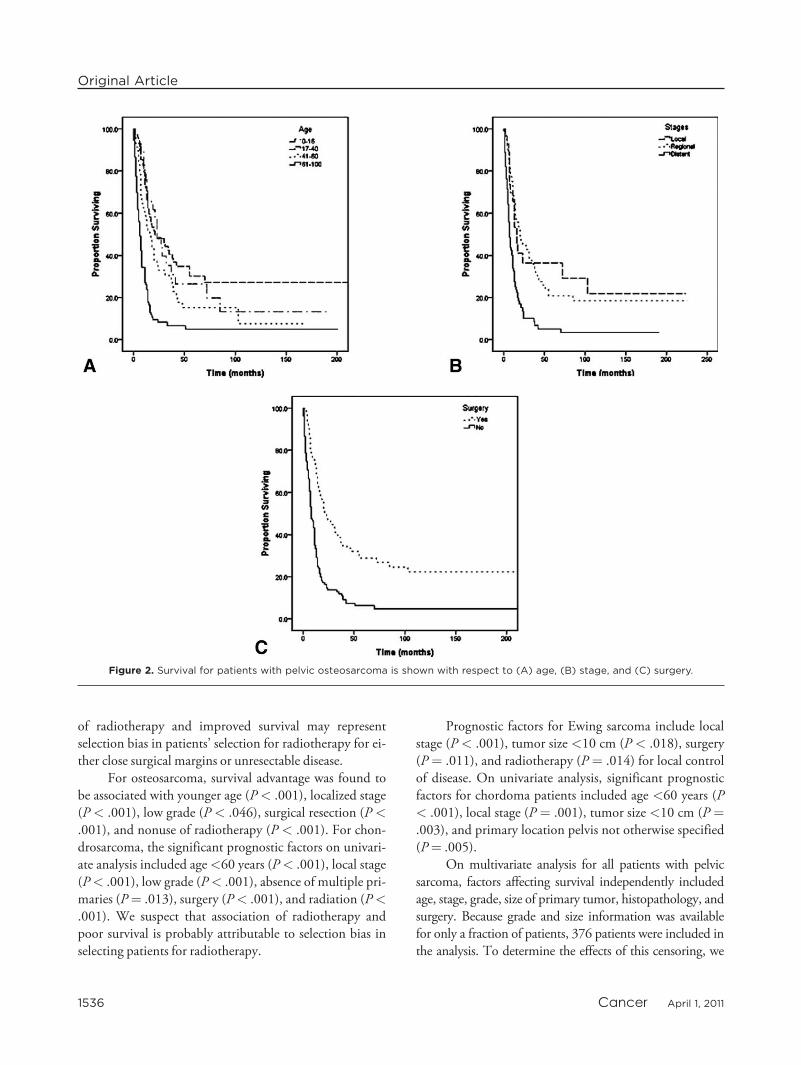
Figure 2. Survival for patients with pelvic osteosarcoma is shown with respect to (A) age, (B) stage, and (C) surgery.
Original Article
1536 Cancer April 1, 2011

repeated the multivariate analysis without size and stageconsiderations (data not shown). There was no markedchange with respect to independent prognostic factors.
For osteosarcoma, independent prognostic factors asshown in Figure 2 include age (A), stage (B), and surgery(C). Independent predictors of survival for patients withpelvic chondrosarcoma are age, stage, surgery, and grade.
Corresponding Kaplan-Meier curves are shown in Figure3A-D, respectively. Factors governing survival independ-ently among patients with Ewing sarcoma included stage,surgery, and radiotherapy (Fig 1). Survival in patientswith chordoma was dictated by age, stage, and size of theprimary tumor. Primary tumor size <5 cm was an inde-pendent predictor of improved survival among patients
Figure 3. Survival for patients with pelvic chondrosarcoma is shown with respect to (A) age, (B) stage, (C) surgery, and (D)grade.
Malignant Pelvic Sarcomas/Jawad et al
Cancer April 1, 2011 1537

with pelvic chordoma, probably because of ease ofresection.
DISCUSSIONThe current study analyzes a population-based cohort ofpatients with a diagnosis of malignant pelvic bone sar-coma. The SEER database compiles its data from 17 regis-tries across the United States, and completeness is 98%.44
There is a general consensus in the literature regarding thepoor outcomes among patients with a malignant sarcomainvolving the pelvic bones or adjacent soft tissues.1,13,17,18
A study by Mankin et al1 represents a retrospective analy-sis of 206 patients and reports mean 5-year survival at51%. An earlier study by Kawai et al showed a 5-year sur-vival of 55%17 in a cohort of 102 patients. Wirbel et al18
presented a retrospective analysis of 93 patients from1978 to 1998 and reported a mean survival of 21.5months for 46 patients dying of disease. The current anal-ysis shows an overall 5-year survival of 45% in a cohort ofpatients from 1987 to 2006, which is lower but still com-parable to survival reported in earlier studies. Mankin etal1 and Wirbel et al18 both recognized surgical marginand stage of the disease as independent predictors of sur-vival. In addition to surgical margin and stage, Kawai et alsuggested the size of primary tumor and type of surgery asindependent prognostic factors.17 In contrast, Shin et al13
reported grade as the only independent prognostic factorin their cohort of 46 patients. In the current analysis, wewere unable to evaluate the prognostic significance of sur-gical margin, because this information is not included inthe SEER data set. The independent predictors of survivalin the current analysis included age, stage, grade, size ofthe tumor, histopathology, and use of surgical treatmentfor pelvic sarcomas as a group. Age >50 years was also asignificant factor predicting poor survival on univariateanalysis in the data reported.1 Multivariate analysis wasnot carried out, probably because of a relatively smallercohort, and the authors attributed the difference in sur-vival with respect to age to other factors, such as older ageand lower survival among patients with malignant fibroushistiocytoma and metastatic carcinoma. However, thecurrent study clearly demonstrates age as an independentpredictor of survival among patients with pelvic sarcomas(P< .001) (Table 3).
There has been contradictory evidence about theprognostic significance of grade versus stage for pelvic sar-comas.1,13,17,18 Wirbel et al18 reported a prognostic sig-nificance for grade only if surgical stage of the tumor is
excluded from the analysis. The current analysis clearlydemonstrates with substantial statistical significance thatboth grade and stage are independent predictors of sur-vival for pelvic sarcomas. Mankin et al1 identified varia-tion in survival according to different histopathologicaldiagnoses, but failed to suggest histopathology as an inde-pendent predictor of survival. In our analysis, a histopath-ological diagnosis of osteosarcoma was an independentpredictor of poor survival. This observation is consistentwith the study byMankin et al.1
Patients with the diagnosis of osteosarcoma (251patients) of the pelvis had the lowest 5-year survival(19%) in the cohort. Some of the larger published seriesreport the 5-year survival ranging from 4% to32%.22,27,45-48 A recent investigation by Fuchs et al20
reported a 5-year survival of 38% in a cohort of 43patients. Only 18% of patients in the abovementionedstudy presented with a distant stage of disease. The differ-ence in survival can be partially explained by a higher pro-portion of patients (40.6%) included in the currentanalysis with distant stage of disease. Mankin et al1
reported a 5-year survival rate as high as 58% in a cohortof 45 patients. The independent predictors of survival inpatients with pelvic osteosarcoma in the current analysisincluded age, stage, and absence of radiotherapy. Stageand surgery have been widely recognized as predictors ofsurvival in the literature for patients with pelvic osteosar-coma.20,22,27,45-48 Although there is a statistical trendtoward improved survival with surgical resection in multi-variate analysis, we failed to identify surgical resection asan independent predictor of survival. Other prognosticfactors suggested in the literature include surgical margins,response to chemotherapy, and involvement of sac-rum.20,22,27,45-48 Because this information is not availablein the SEER database, we are unable to make a commenton the importance of these prognostic factors. An impor-tant observation with osteosarcoma of the pelvis was theabsence of characteristic bimodal distribution at extremeages. Only 12% of all the patients with pelvic osteosar-coma were in the pediatric age group, and the mode of agedistribution was >60 years (35.9%, Table 1). Moreover,in this group of patients grade was not a prognostic factor.This likely reflects the overwhelming predominance ofhigh-grade lesions in this cohort (86%).
Chondrosarcoma is the most common histopatho-logic diagnosis (407 patients) in the current analysis,which is consistent with previous studies.1,13,17,18 The 5-year survival for patients with pelvic chondrosarcoma inthe current study was 59%. This is comparable to the
Original Article
1538 Cancer April 1, 2011

survival reported in some of the previous studies,1,29
whereas others have reported a 5-year survival rangingfrom 72% to 92%.19,21,23 This difference in survival canbe explained on the basis of clinical characteristics of thepatients analyzed. Pring et al21 (64 patients) and Donatiet al23 (124 patients) did not include any patients withdistant stage of disease in their respective analysis. Only 2of 69 patients had metastasis in the series reported byBergh et al.19 On the contrary, 11.9% of all the chondro-sarcoma patients in the current analysis presented with adistant stage of disease. In the current investigation, inde-pendent prognostic factors on multivariate analysisincluded age, stage, grade, and surgical resection. Gradeand operability of the tumor have also been previouslydescribed as independent predictors of survival.19,21,23
Bergh et al19 have also suggested age as a prognostic factorfor outcome. Although stage has not been implicated as aprognostic factor in previous studies, we have clearlyshown that stage is an independent factor affecting sur-vival in patients with pelvic chondrosarcoma (P < .001,Table 3).
Pelvis has been implicated as the single most com-mon site for Ewing sarcoma.35,49 A total of 288 (22.1%)patients with Ewing sarcoma were included in the currentanalysis, with a 5-year survival rate of 46%. The earlierreports on pelvic Ewing sarcoma reported survival ratesonly as high as 20% to 30%.32,34We believe that improve-ment in survival among patients over the past 2 decadescan be attributed to improvements in multimodal therapyfor Ewing sarcoma and radiological imaging. Other recentinvestigations, including those originating in Europe, havereported similar 5-year overall survival.33,35,36,43 The inde-pendent predictors of survival in the current analysisincluded stage and local treatment, that is, surgery orradiotherapy. This observation has been validated by pre-vious investigations.32-36,43 As mentioned in the introduc-tion section, 1 of the controversies in literature is about theefficacy of radiotherapy30-34 as compared with sur-gery25,35-43 for local disease control. In the current investi-gation, both surgery and radiotherapy were independentlyassociated with improved survival on multivariate analysis,without a clear advantage of 1 over the other.
Limitations of the current study include lack of anyinformation on specific chemotherapy or any other medi-cal therapy in the SEER database. Thus we are unable tocomment directly on survival benefit conferred by the useof chemotherapy or efficacy of a particular regimen in aparticular subset of patients. The database consists ofpatient information from tertiary treatment centers within
the United States, and hence it may be reasonable toassume that appropriate chemotherapy was administered,but the data are lacking. Also, chemotherapeutic regimensand protocols in regard to various patient factors such asage are usually standardized across such facilities, facilitat-ing an unbiased analysis. Similarly, no informationregarding medical history, radiological studies, or serolog-ical workup is provided in the database, limiting our anal-ysis regarding prognostic significance of fever, duration ofsymptoms, tumor volume, anemia, hypoalbuminemia, orhigh lactate dehydrogenase. The absence of images makesit impossible to verify the stage at diagnosis. Havingacknowledged these limitations, the current article bringsnovel observations to the literature.
The current article clearly demonstrates that the his-tologic diagnosis in patients with pelvic sarcomas has aprofound influence on long-term disease outcome. Thecomparison of different diagnoses on the basis of ana-tomic location as has been done in the past in the litera-ture is not warranted. The current analysis clearly outlinesthe important prognostic factors for patients with pelvicsarcoma within each of the histologic diagnoses. We haveoutlined the specific prognostic factors and oncologicaloutcomes for different histological subtypes of pelvic sar-coma. A novel observation is the age bias in patients withpelvic osteosarcoma. This has not been previouslyreported. It is only with the use of a large data set such asused in this analysis that these conclusions can be reached.
CONFLICT OF INTEREST DISCLOSURESThe authors made no disclosures.
REFERENCES
1. Mankin HJ, Hornicek FJ, Temple HT, Gebhardt MC. Ma-lignant tumors of the pelvis: an outcome study. Clin OrthopRelat Res. 2004:212-217.
2. Apffelstaedt JP, Zhang PJ, Driscoll DL, Karakousis CP.Various types of hemipelvectomy for soft tissue sarcomas:complications, survival and prognostic factors. Surg Oncol.1995;4:217-222.
3. Campanacci M, Capanna R. Pelvic resections: the RizzoliInstitute experience. Orthop Clin North Am. 1991;22:65-86.
4. Damron TA, Sim FH. Surgical treatment for metastatic dis-ease of the pelvis and the proximal end of the femur. InstrCourse Lect. 2000;49:461-470.
5. Eilber FR, Grant TT, Sakai D, Morton DL. Internal hemi-pelvectomy–excision of the hemipelvis with limb preserva-tion. An alternative to hemipelvectomy. Cancer. 1979;43:806-809.
6. Enneking WF, Dunham WK. Resection and reconstructionfor primary neoplasms involving the innominate bone.J Bone Joint Surg Am. 1978;60:731-746.
Malignant Pelvic Sarcomas/Jawad et al
Cancer April 1, 2011 1539

7. Harrington KD. The use of hemipelvic allografts or auto-claved grafts for reconstruction after wide resections of ma-lignant tumors of the pelvis. J Bone Joint Surg Am.1992;74:331-341.
8. O’Connor MI. Malignant pelvic tumors: limb-sparingresection and reconstruction. Semin Surg Oncol. 1997;13:49-54.
9. O’Connor MI, Sim FH. Salvage of the limb in the treat-ment of malignant pelvic tumors. J Bone Joint Surg Am.1989;71:481-494.
10. Masterson EL, Davis AM, Wunder JS, Bell RS. Hindquarteramputation for pelvic tumors. The importance of patientselection. Clin Orthop Relat Res. 1998;(350):187-194.
11. Patterson FR, Peabody TD. Operative management of me-tastases to the pelvis and acetabulum. Orthop Clin NorthAm. 2000;31:623-631.
12. Prewitt TW, Alexander HR, Sindelar WF. Hemipelvectomyfor soft tissue sarcoma: clinical results in fifty-three patients.Surg Oncol. 1995;4:261-269.
13. Shin KH, Rougraff BT, Simon MA. Oncologic outcomes ofprimary bone sarcomas of the pelvis. Clin Orthop Relat Res.1994;(304):207-217.
14. Ozaki T, Hillmann A, Bettin D, Wuisman P, WinkelmannW. High complication rates with pelvic allografts. Experi-ence of 22 sarcoma resections. Acta Orthop Scand.1996;67:333-338.
15. Ozaki T, Hillmann A, Winkelmann W. Treatment outcomeof pelvic sarcomas in young children: orthopaedic and onco-logic analysis. J Pediatr Orthop. 1998;18:350-355.
16. Ozaki T, Rodl R, Gosheger G, et al. Sacral infiltration inpelvic sarcomas: joint infiltration analysis II. Clin OrthopRelat Res. 2003;(407):152-158.
17. Kawai A, Healey JH, Boland PJ, Lin PP, Huvos AG,Meyers Pa. Prognostic factors for patients with sarcomas ofthe pelvic bones. Cancer. 1998;82:851-859.
18. Wirbel RJ, Schulte M, Mutschler WE. Surgical treatment ofpelvic sarcomas: oncologic and functional outcome. ClinOrthop Relat Res. 2001;(390):190-205.
19. Bergh P, Gunterberg B, Meis-Kindblom JM, KindblomLG. Prognostic factors and outcome of pelvic, sacral, andspinal chondrosarcomas: a center-based study of 69 cases.Cancer. 2001;91:1201-1212.
20. Fuchs B, Hoekzema N, Larson DR, Inwards CY, Sim FH.Osteosarcoma of the pelvis: outcome analysis of surgicaltreatment. Clin Orthop Relat Res. 2009;467:510-518.
21. Pring ME, Weber KL, Unni KK, Sim FH. Chondrosarcomaof the pelvis. A review of sixty-four cases. J Bone Joint SurgAm. 2001;83-A:1630-1642.
22. Saab R, Rao BN, Rodriguez-Galindo C, Billups CA, For-tenberry TN, Daw NC. Osteosarcoma of the pelvis in chil-dren and young adults: the St. Jude Children’s ResearchHospital experience. Cancer. 2005;103:1468-1474.
23. Donati D, El Ghoneimy A, Bertoni F, Di Bella C, MercuriM. Surgical treatment and outcome of conventionalpelvic chondrosarcoma. J Bone Joint Surg Br. 2005;87:1527-1530.
24. Donati D, Wafa H, Di Bella C, Colangeli M, Colangeli S,Bertoni F. Management of pelvic giant cell tumours in-volving the acetabular bone. Acta Orthop Belg. 2008;74:773-778.
25. Donati D, Yin J, Di Bella C, et al. Local and distant con-trol in non-metastatic pelvic Ewing’s sarcoma patients.J Surg Oncol. 2007;96:19-25.
26. Gradinger R, Rechl H, Hipp E. Pelvic osteosarcoma. Resec-tion, reconstruction, local control, and survival statistics.Clin Orthop Relat Res. 1991;(270):149-158.
27. Kawai A, Huvos AG, Meyers PA, Healey JH. Osteosarcomaof the pelvis. Oncologic results of 40 patients. Clin OrthopRelat Res. 1998;(348):196-207.
28. Matsuo T, Sugita T, Sato K, et al. Clinical outcomes of 54pelvic osteosarcomas registered by Japanese musculoskeletaloncology group. Oncology. 2005;68:375-381.
29. Ozaki T, Hillmann A, Lindner N, Blasius S, WinkelmannW. Chondrosarcoma of the pelvis. Clin Orthop Relat Res.1997;(166):226-239.
30. Indelicato DJ, Keole SR, Shahlaee AH, et al. Impact of localmanagement on long-term outcomes in Ewing tumors ofthe pelvis and sacral bones: the University of Florida experi-ence. Int J Radiat Oncol Biol Phys. 2008;72:41-48.
31. Indelicato DJ, Keole SR, Shahlaee AH, Shi W, Morris CG,Marcus RB Jr. Definitive radiotherapy for Ewing tumors ofextremities and pelvis: long-term disease control, limb func-tion, and treatment toxicity. Int J Radiat Oncol Biol Phys.2008;72:871-877.
32. Scully SP, Temple HT, O’Keefe RJ, Scarborough MT,Mankin HJ, Gebhardt MC. Role of surgical resectionin pelvic Ewing’s sarcoma. J Clin Oncol. 1995;13:2336-2341.
33. Yock TI, Krailo M, Fryer CJ, et al. Local control in pelvicEwing sarcoma: analysis from INT-0091–a report from theChildren’s Oncology Group. J Clin Oncol. 2006;24:3838-3843.
34. Bhagat S, Sharma H, Pillai DS, Jane MJ. Pelvic Ewing’s sar-coma: a review from Scottish Bone Tumour Registry.J Orthop Surg (Hong Kong). 2008;16:333-338.
35. Sucato DJ, Rougraff B, McGrath BE, et al. Ewing’s sarcomaof the pelvis. Long-term survival and functional outcome.Clin Orthop Relat Res. 2000;(373):193-201.
36. Hoffmann C, Ahrens S, Dunst J, et al. Pelvic Ewing sar-coma: a retrospective analysis of 241 cases. Cancer. 1999;85:869-877.
37. Bacci G, Ferrari S, Bertoni F, et al. Prognostic factors innonmetastatic Ewing’s sarcoma of bone treated with adju-vant chemotherapy: analysis of 359 patients at the IstitutoOrtopedico Rizzoli. J Clin Oncol. 2000;18:4-11.
38. Bacci G, Ferrari S, Longhi A, et al. Role of surgery in localtreatment of Ewing’s sarcoma of the extremities in patientsundergoing adjuvant and neoadjuvant chemotherapy. OncolRep. 2004;11:111-120.
39. Bacci G, Ferrari S, Longhi A, et al. Therapy and survival afterrecurrence of Ewing’s tumors: the Rizzoli experience in 195patients treated with adjuvant and neoadjuvant chemotherapyfrom 1979 to 1997. Ann Oncol. 2003;14:1654-1659.
40. Bacci G, Ferrari S, Longhi A, et al. Local and systemic con-trol in Ewing’s sarcoma of the femur treated with chemo-therapy, and locally by radiotherapy and/or surgery. J BoneJoint Surg Br. 2003;85:107-114.
41. Bacci G, Forni C, Longhi A, et al. Long-term outcome forpatients with non-metastatic Ewing’s sarcoma treated withadjuvant and neoadjuvant chemotherapies. 402 patientstreated at Rizzoli between 1972 and 1992. Eur J Cancer.2004;40:73-83.
42. Bacci G, Mercuri M, Longhi A, et al. Neoadjuvant chemo-therapy for Ewing’s tumour of bone: recent experience atthe Rizzoli Orthopaedic Institute. Eur J Cancer. 2002;38:2243-2251.
Original Article
1540 Cancer April 1, 2011

43. Rodl RW, Hoffmann C, Gosheger G, Leidinger B, JurgensH, Winkelmann W. Ewing’s sarcoma of the pelvis: com-bined surgery and radiotherapy treatment. J Surg Oncol.2003;83:154-160.
44. NCI. Surveillance Epidemiology and End Results 2008.Available at: http://seer.cancer.gov/ Accessed August 26,2010.
45. Donati D, Giacomini S, Gozzi E, et al. Osteosarcoma ofthe pelvis. Eur J Surg Oncol. 2004;30:332-340.
46. Fahey M, Spanier SS, Vander Griend RA. Osteosarcoma ofthe pelvis. A clinical and histopathological study of twenty-five patients. J Bone Joint Surg Am. 1992;74:321-330.
47. Grimer RJ, Carter SR, Tillman RM, Spooner D, ManghamDC, Kabukcuoglu Y. Osteosarcoma of the pelvis. J BoneJoint Surg Br. 1999;81:796-802.
48. Ozaki T, Flege S, Kevric M, et al. Osteosarcoma of thepelvis: experience of the Cooperative Osteosarcoma StudyGroup. J Clin Oncol. 2003;21:334-341.
49. Jawad MU, Cheung MC, Min ES, Schneiderbauer MM,Koniaris LG, Scully SP. Ewing sarcoma demonstrates racialdisparities in incidence-related and sex-related differences inoutcome: an analysis of 1631 cases from the SEER database,1973-2005. Cancer. 2009;115:3526-3536.
Cancer April 1, 2011 1541
Malignant Pelvic Sarcomas/Jawad et al
Related Documents











