1 Malignant Lymphomas Donald Innes, M.D. with special thanks to John Cousar, M.D. Hodgkin Lymphoma and Non-Hodgkin Lymphomas I. Overview of the Lymphoid System: 1. The lymphoid system consists of circulating T and B lymphocytes and the lymphoid organs, including lymph nodes, thymus, spleen, tonsils, and adenoids. Less well-organized lymphoid tissue is also present in the gastrointestinal tract and lung (referred to as Mucosal Associated Lymphoid Tissue, or MALT), marrow and skin. 2. Lymphopoiesis: Lymphocytes are derived from marrow stem cells. T- lymphocytes undergo differentiation and maturation in the thymus and then migrate to peripheral lymphoid tissue (nodes, spleen, etc.), and function as T- helper (CD4+) or T-suppressor (CD8+) cells. B-lymphocytes develop in the marrow, and likewise migrate to specific B-cell compartments of peripheral lymphoid tissue. The effector cell, and most differentiated cell of the B-cell system, is the plasma cell, which produces immunoglobulin. The maturation and differentiation of T and B cells are associated with changes in the DNA of the cells (which can be detected by molecular genetic techniques) and sequential gain and loss of surface and cytoplasmic antigens (which can be detected by monoclonal antibodies using flow cytometry or immunohistochemistry). 3. Lymph Nodes: The major function of lymph nodes is to detect and inactivate foreign antigens arriving via lymphatics. Lymph nodes are principally located to receive lymph from those organs in major contact with the environment (i.e. skin, respiratory tract, gastrointestinal tract). Lymph nodes are encapsulated, and are organized into B and T cell subcompartments. In the cortex of the

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
Malignant Lymphomas Donald Innes, M.D.
with special thanks to John Cousar, M.D.
Hodgkin Lymphoma and Non-Hodgkin Lymphomas
I. Overview of the Lymphoid System:
1. The lymphoid system consists of circulating T and B lymphocytes and the
lymphoid organs, including lymph nodes, thymus, spleen, tonsils, and
adenoids. Less well-organized lymphoid tissue is also present in the
gastrointestinal tract and lung (referred to as Mucosal Associated Lymphoid
Tissue, or MALT), marrow and skin.
2. Lymphopoiesis: Lymphocytes are derived from marrow stem cells. T-
lymphocytes undergo differentiation and maturation in the thymus and then
migrate to peripheral lymphoid tissue (nodes, spleen, etc.), and function as T-
helper (CD4+) or T-suppressor (CD8+) cells. B-lymphocytes develop in the
marrow, and likewise migrate to specific B-cell compartments of peripheral
lymphoid tissue. The effector cell, and most differentiated cell of the B-cell
system, is the plasma cell, which produces immunoglobulin. The maturation
and differentiation of T and B cells are associated with changes in the DNA of
the cells (which can be detected by molecular genetic techniques) and sequential
gain and loss of surface and cytoplasmic antigens (which can be detected by
monoclonal antibodies using flow cytometry or immunohistochemistry).
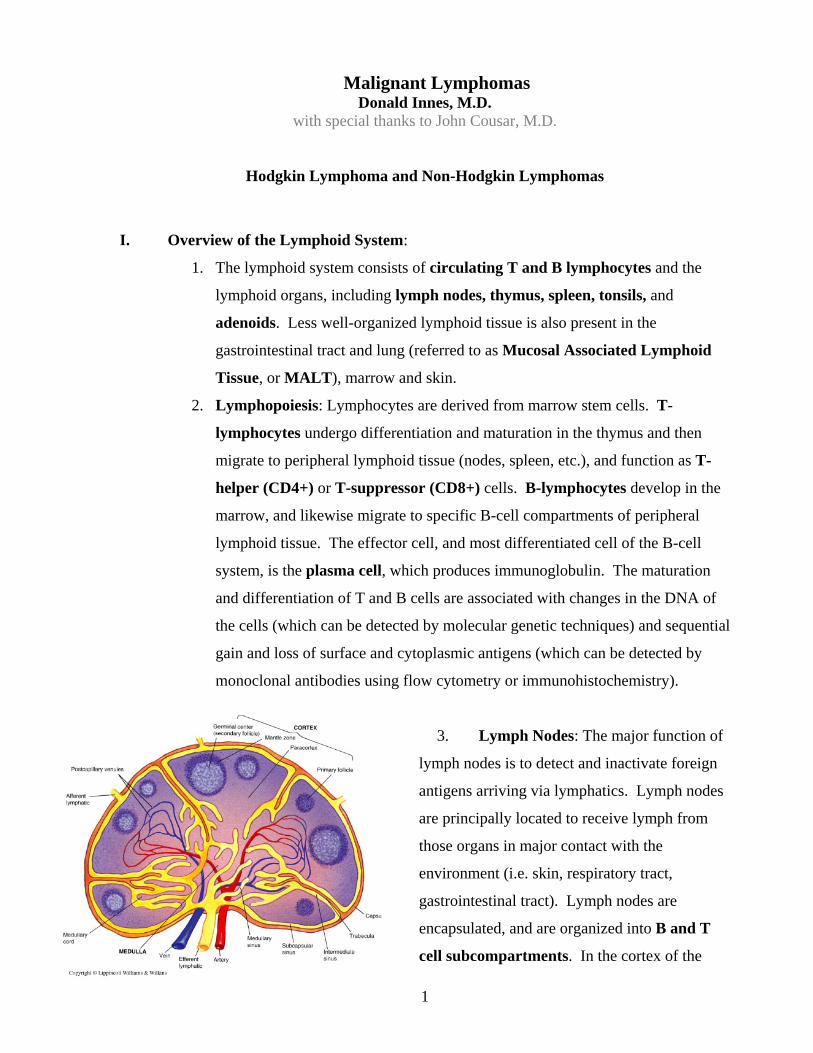
3. Lymph Nodes: The major function of
lymph nodes is to detect and inactivate foreign
antigens arriving via lymphatics. Lymph nodes
are principally located to receive lymph from
those organs in major contact with the
environment (i.e. skin, respiratory tract,
gastrointestinal tract). Lymph nodes are
encapsulated, and are organized into B and T
cell subcompartments. In the cortex of the

2
node are spherical aggregates of lymphoid cells called primary follicles, which are B-
cell domains. With antigenic stimulation, primary follicles develop germinal or
follicular centers composed of follicular center cells. Surrounding the follicular
center is a cuff or mantle of small B-cells which have not been challenged by
antigen. The paracortex of the node is a T-cell dependent area.
4. Spleen: The spleen consists of a filtering component, the red pulp, and a lymphoid
component, the white pulp. The white pulp is organized into B-cell domains similar
to the follicles of nodes and T-dependent areas, the periarteriolar lymphoid sheath.
5. Mucosa-Associated Lymphoid Tissue: Extranodal specialized lymphoid tissue
present in the GI tract, lung, and other sites is termed Mucosa-Associated Lymphoid
Tissue, or MALT, and is composed of lymphocytes that provide mucosal immunity.
II. Malignant Lymphomas:
1. Lymphomas are malignancies which arise from lymphocytes residing in lymphoid
tissue outside of the marrow (i.e. lymph nodes, spleen, etc.). Lymphomas are broadly
separated into Hodgkin lymphoma (identified in part by its neoplastic cell – the
Reed-Sternberg cell), and all other types of lymphomas referred to as non-Hodgkin
lymphomas. There are no recognized benign neoplasms of the hematopoietic-
lymphoid system.
2. Important Features of Malignant Lymphomas:
Lymphomas are clonal. There is abundant immunologic and karyotypic
evidence indicating these neoplasms contain clonal expansions of a single
functional subpopulation.
The cause of most lymphomas is generally unknown.
There are major clinicopathologic differences between childhood and adult
lymphomas. The great majority of non-Hodgkin lymphoma occurring in
children are of high histologic grade, and are clinically aggressive. Low-
grade lymphomas are rare in children. Non-Hodgkin lymphomas of adults
may be either low or high-grade.
Prognosis is closely correlated with histologic grade of the neoplasm. For
example, follicular lymphoma grade 1-2, (composed predominantly of
dormant, non-dividing B-cells, called centrocytes) is a low-grade neoplasm,

3
while diffuse large B-cell lymphoma (composed predominantly of larger,
more rapidly dividing B-cell) is a higher-grade process.
III. Classification of Non-Hodgkin Lymphomas (NHLs):
1. NHLs are heterogeneous (much more so than Hodgkin Lymphoma), and can
develop as a result of malignant transformation at any stage of B and T cell
differentiation. Therefore, NHLs are broadly grouped into B or T cell types. In
this country, B cell NHLs are much more common than T cell types. The
classification system most widely used for NHLs is the 2008 World Health
Organization Classification (W.H.O.)]. It is not necessary that you memorize
this system in its entirety, but it is important that you understand several
principles of classification of NHLs:
NHLs are classified on the basis of the morphologic, immunologic,
cytogenetic, and molecular genetic similarity of the predominant
neoplastic cell to the various stages of B and T cell differentiation.
For example, the lymphoma that is comprised predominantly of
centrocytes (small cleaved cells) of the follicular (germinal) center is
called a follicular lymphoma. It is a B-cell neoplasm that
morphologically and immunologically resembles the cell of origin
(i.e. centrocyte).
When classification is based on the cell of origin, distinct
clinicopathologic entities emerge which better predict prognosis and
facilitate therapy.
In general, NHLs in which the predominant cell is small and
dormant-appearing tend to be more indolent than those in which
the predominant cell is a transformed lymphocyte, and are more
aggressive.
Site of the primary disease (i.e. node vs. spleen vs. gastrointestinal
tract vs skin, etc.) is important.
Currently, the most widely used classification system is the 2008
W.H.O. system. A listing of the W.H.O. lymphomas is shown in
Table 1 on the next page.
4
2008 World Health Organization Classification of B cell, T cell, Hodgkin Lymphoma, Histiocytic/Dendritic Cell Neoplasms, and Post-Transplant Lymphoproliferative Disorders (Swerdlow SH et al editors)
PrecursorLymphoidNeoplasms
B lymphoblastic leukemia / lymphoma NOS B lymphoblastic leukemia / lymphoma with recurrent genetic abnormalities T lymphoblastic leukemia / lymphoma
MatureB‐CellNeoplasms
Chronic lymphocytic leukemia / small lymphocytic lymphoma B-cell prolymphocytic leukemia Splenic marginal zone lymphoma Hairy cell leukemia Lymphoplasmacytic lymphoma / Waldenstrom macroglobulinemia Heavy chain disease Plasma cell myeloma Solitary plasmacytoma of bone Extraosseous plasmacytoma Extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue (MALT) type Nodal marginal zone lymphoma Follicular lymphoma Primary cutaneous follicular lymphoma Mantle cell lymphoma Diffuse large B-cell lymphoma, NOS (T-cell / histiocyte-rich type; primary CNS type ; primary leg skin type & EBV+ elderly type) Diffuse large B-cell lymphoma with chronic inflammation Lymphomatoid granulomatosis Primary mediastinal large B-cell lymphoma Intravascular large B-cell lymphoma ALK+ large B-cell lymphoma Plasmablastic lymphoma Large B-cell lymphoma associated with HHV8+ Castleman disease Primary effusion lymphoma Burkitt lymphoma B cell lymphoma, unclassifiable, Burkitt-like B cell lymphoma, unclassifiable, Hodgkin lymphoma-like
MatureT‐Cell&NK‐CellNeoplasms
T-cell prolymphocytic leukemia T-cell large granular lymphocytic leukemia Chronic lymphoproliferative disorder of NK-cells.
Aggressive NK-cell leukemia Systemic EBV+ T-cell lymphoproliferative disorder of childhood Hydroa vacciniforme-like lymphoma Adult T-cell lymphoma/leukemia Extranodal T-cell/NK-cell lymphoma, nasal type Enteropathy-associated T-cell lymphoma Hepato-splenic T-cell lymphoma Subcutaneous panniculitis-like T-cell lymphoma Mycosis fungoides Sézary syndrome Primary cutaneous CD30+ T-cell lymphoproliferative disorder Primary cutaneous gamma-delta T-cell lymphoma Peripheral T-cell lymphoma, NOS Angioimmunoblastic T-cell lymphoma Anaplastic large cell lymphoma, ALK+ type Anaplastic large cell lymphoma, ALK- type
Hodgkinlymphoma(Hodgkindisease)
Nodular lymphocyte-predominant Hodgkin lymphomas
Classic Hodgkin lymphomas Nodular sclerosis Hodgkin lymphoma Lymphocyte-rich classic Hodgkin lymphoma Mixed cellularity Hodgkin lymphoma Lymphocyte depletion Hodgkin lymphoma
Post‐TransplantLymphoproliferativeDisorders(PTLD)
Plasmacytic hyperplasia Infectious mononucleosis like PTLD Polymorphic PTLD Monomorphic PTLD (B & T/NK cell types) Classic HD type PTLD
HistiocyticandDendriticCellNeoplasms
Histiocytic sarcoma Langerhans cell histiocytosis Langerhans cell sarcoma Interdigitating dendritic cell sarcoma Follicular dendritic cell sarcoma Fibroblastic reticular cell tumor Indeterminate dendritic cell sarcoma Disseminated juvenile xanthogranuloma

5

6
IV. Diagnosis of Lymphomas:
1. Clinical Information: Age, symptoms, distribution of disease,
organomegaly, and lab data are often useful in determining the type of
neoplasm and the extent of disease.
2. Morphologic Evaluation: Most lymphomas are very distinctive on
histologic sections, and are actually recognizable at a glance (by the
experienced eye).
3. Immunophenotypic Analysis: The cell lineage of most lymphomas can be
determined by immunologic techniques using monoclonal antibodies and
flow cytometry (requires viable cell suspensions) or immunoperoxidase
techniques (can be performed on frozen or fixed paraffin embedded tissue).
Clonality can also be detected in B-cell neoplasms by immunoglobulin light
chain restriction (presence of single light chain type on the surface or in the
cytoplasm of neoplastic cells).
4. Karyotypic and Molecular Techniques: Certain lymphomas have
characteristic chromosomal abnormalities (i.e. follicular lymphomas often
demonstrate a 14;18 translocation). Clonality and lineage can be determined
using molecular techniques for immunoglobulin or T-cell receptor
rearrangements.
V. B-cell Non-Hodgkin Lymphomas (B-NHL):
1. Introduction: B-NHLs are the most common group of lymphomas in
Western countries (85-90% of all non-Hodgkin lymphomas), and the
frequency of these malignancies has dramatically increased over the last 20
years.
2. Important Features of B-NHLs:
All B-NHLs demonstrate clonal rearrangement of the
immunoglobulin gene, detectable by Southern blot or PCR.
Most B-NHLs express monotypic immunoglobulin which is easily
detectable on the cell surface (with flow cytometry), or in the cell
cytoplasm (immunohistochemistry), or occasionally as a monoclonal
protein in the serum.
7
The B-lineage of many B-NHLs can be accurately and simply
determined by histopathologic features such as follicular nodulation,
plasmacytic differentiation, and other morphologic features.
3. Common B-NHL:
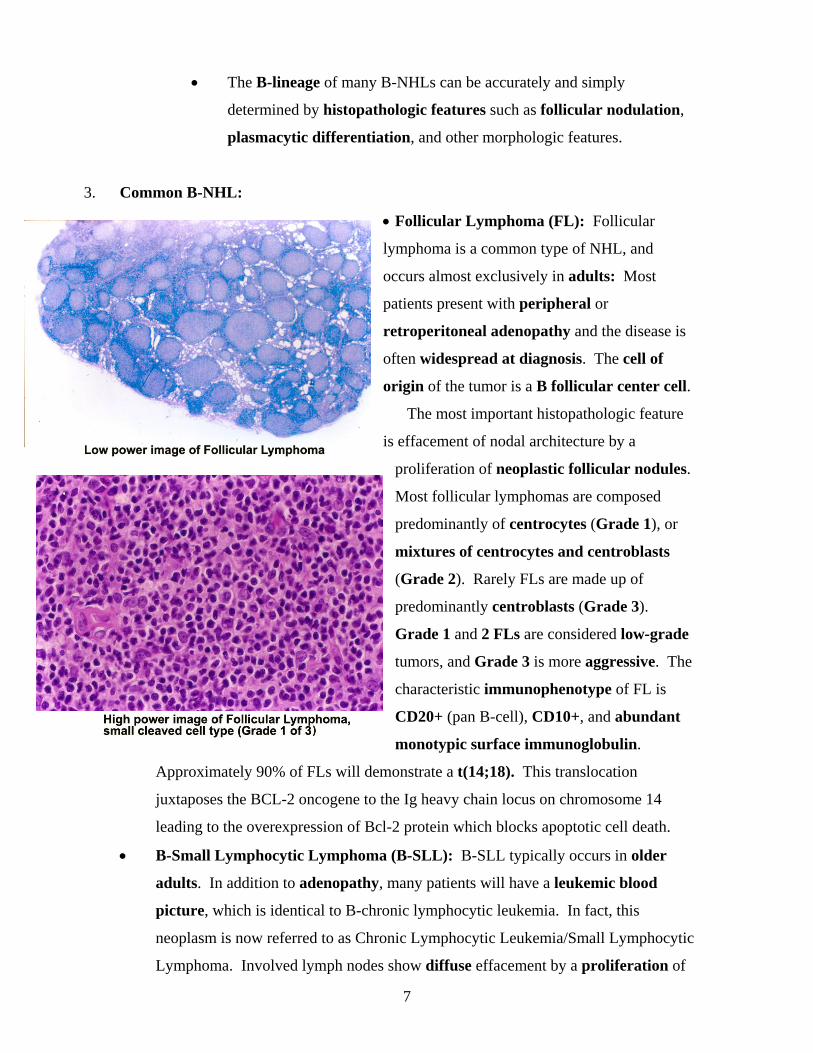
Follicular Lymphoma (FL): Follicular
lymphoma is a common type of NHL, and
occurs almost exclusively in adults: Most
patients present with peripheral or
retroperitoneal adenopathy and the disease is
often widespread at diagnosis. The cell of
origin of the tumor is a B follicular center cell.
The most important histopathologic feature
is effacement of nodal architecture by a
proliferation of neoplastic follicular nodules.
Most follicular lymphomas are composed
predominantly of centrocytes (Grade 1), or
mixtures of centrocytes and centroblasts
(Grade 2). Rarely FLs are made up of
predominantly centroblasts (Grade 3).
Grade 1 and 2 FLs are considered low-grade
tumors, and Grade 3 is more aggressive. The
characteristic immunophenotype of FL is
CD20+ (pan B-cell), CD10+, and abundant
monotypic surface immunoglobulin.
Approximately 90% of FLs will demonstrate a t(14;18). This translocation
juxtaposes the BCL-2 oncogene to the Ig heavy chain locus on chromosome 14
leading to the overexpression of Bcl-2 protein which blocks apoptotic cell death.
B-Small Lymphocytic Lymphoma (B-SLL): B-SLL typically occurs in older
adults. In addition to adenopathy, many patients will have a leukemic blood
picture, which is identical to B-chronic lymphocytic leukemia. In fact, this
neoplasm is now referred to as Chronic Lymphocytic Leukemia/Small Lymphocytic
Lymphoma. Involved lymph nodes show diffuse effacement by a proliferation of

8
small lymphocytes with round nuclei and dense chromatin. This neoplasm is
considered to be low-grade. Phenotypically, the neoplastic cells of B-SLL express
weak CD20, CD5, CD23, and weak surface immunoglobulin.
Low-grade B-cell Lymphoma of Mucosa-Associated Lymphoid Tissue (MALT
Lymphoma): MALT lymphomas are usually low-grade lymphomas of adults
that arise in extranodal lymphoid tissue, especially the GI tract and lung. The
lymphoid tissue in which MALT lymphomas arise may be a normal constituent of
the site of origin (for example, Peyer’s patches of the small intestine), or may be
acquired as part of an autoimmune disorder (for example, Hashimoto thyroiditis) or
infection (for example, H. pylori-associated chronic gastritis).
Mantle Cell Lymphoma (MCL): Mantle cell lymphoma
occurs in adults and is a clinically aggressive neoplasm,
although the histologic appearance is low grade. Involved
nodes usually show a diffuse effacement by a very
homogenous population of small lymphoid cells with
virtually no large cells. Phenotypically, the neoplastic cell is
CD 20+ and SIg+. Like B-SLL, the tumor cells co-express
CD5 but unlike B-SLL usually do not express CD 23. A
characteristic t(11;14)(q13;q32) translocation is seen and
involves the immunoglobulin heavy chain genes and the
CYCLIN D1 (a.k.a. BCL-1) gene, which leads to the
overexpression of CYCLIN D1. The CYCLIN D1 protein
can be detected by immunohistochemistry.
Diffuse Large B-cell Lymphoma (DLBCL): DLBCL is
the most common type of NHL that occurs in adults, and
rarely in children. Morphologically, it is a diffuse
proliferation of large
neoplastic B-lymphoid cells. Within this group of
lymphomas, there have been a variety of subtypes
recognized. Most cases are CD20+, and express surface
immunoglobulin. This neoplasm behaves in an
aggressive fashion.

9
Burkitt Lymphoma (BL): BL is a highly aggressive lymphoma that
occurs in children as well as adults, and often presents in extra-nodal
sites, such as the jaws, distal ileum and ovaries. It is endemic in young
children in Africa, and sporadic in children of all ages in the U.S.A.
Morphologically, it demonstrates a diffuse proliferation of small
noncleaved cells with a very high mitotic rate, and a background of
“starry sky” macrophages. Epstein-Barr virus is thought to play an
important role in the pathogenesis of BL, especially the endemic form.
Phenotypically, the neoplastic cells are CD20+, CD10+, and surface
immunoglobulin positive. All cases have a translocation of the MYC gene
on chromosome 8 to the Ig heavy chain on chromosome 14, or, less
commonly, to the light chain loci on chromosome 2 or 22.
VI. T-cell Lymphomas:
1. Introduction: Only 10-15% of lymphomas in Western countries are T-cell origin.
Despite their relative rarity, T-cell lymphomas are important because they are
difficult to diagnose, tend to be more aggressive than most B-cell lymphomas, can
occur in young patients, and may be associated with paraneoplastic syndromes
such as hypercalcemia, hypergammaglobulinemia, and erythrophagocytosis.
2. Classification of T-cell Neoplasms: T-cell neoplasms are broadly classified
according to the anatomic compartment from which they arise, and their level of
maturity. Immature or precursor T-cell neoplasms arise in the marrow (T-
lymphoblastic leukemia), or in the thymus (T-lymphoblastic lymphoma). T-cell
lymphomas arising in other sites as a group are called peripheral (peripheral to the
thymus) T-cell lymphomas, and they arise in lymph nodes or extranodal sites
(skin, lung, nasopharynx, intestine, liver, spleen). In addition, some T-cell
lymphomas are classified according to histologic features (anaplastic large cell
lymphoma, angioimmunoblastic T-cell lymphoma).

10
3. Specific T-cell Neoplasms:
T-lymphoblastic
Lymphoma (T-LL): TLLs often
present as a rapidly growing anterior
mediastinal mass in young patients,
most often male, who may have
respiratory or cardiovascular
compromise and pleural or pericardial
effusions. These lymphomas
disseminate rapidly to the marrow, peripheral blood, and regional lymph
nodes, and, therefore, at that stage, closely resemble T-lymphoblastic
leukemias. The tumor cells have a blastic appearance which a high nuclear
to cytoplasmic ratio, finely dispersed chromatin, and inconspicuous nucleoli.
Thymic tissue is effaced by a diffuse growth of these monomorphic tumor
cells that have a high mitotic rate, and invade the capsule. The tumor cells
mark immunophenotypically as immature T-cells.
Mycosis Fungoides (MF): Mycosis fungoides is a tumor of small, skin-
based T-cells, predominantly of the CD4+ subset that occurs in adults. MF
produces a band-like superficial dermal infiltrate adjacent to, and invading
the epidermis (epidermotropism) with formation of small collections of
lymphocytes in the epidermis (Pautrier’s microabscess). The lymphocytes
are small and have a characteristic folded, cerebriform nucleus.
Peripheral T-cell Lymphoma (PTCL): PTCL is usually a nodal disease of
adults, and encompasses a variety of morphological variants. Most patients
have advanced stage disease with constitutional symptoms and paraneoplastic
features such as eosinophilia, and hemophagocytosis may be seen. Most cases
demonstrate a T-phenotype with loss or aberrant expression of pan T-cell
antigens.
VII. Hodgkin Lymphoma (HL):

11
1. Introduction: In 1832, Thomas Hodgkin was the first to report that
lymphadenopathy could occur as a primary disorder, rather than secondary
to infection or carcinoma. Three decades later, primary diseases of the
lymph node well called Hodgkin Disease, in honor of Dr. Hodgkin’s
important observation. Between 1898 and 1902, Dorothy Reed and Carl
Sternberg described the histologic features of HL, including the diagnostic
dysplastic Reed-Sternberg (RS) cell that bears their names.
2. General Features of Hodgkin Lymphoma: HL represents 30% of all
lymphomas. HL is separated from NHL for several reasons. 1) The
cellular composition of HL is unique in that the neoplastic cell (Reed-
Sternberg cell) accounts for only a minority of the tumor mass, most
of which is reactive inflammatory cells. Thus the general principles for
the histopathologic diagnosis of HL differ from NHL. 2) The clinical
features and response to therapy of HL differ from those of NHLs. HL
mostly affects young adults (15-35 years) but also occurs in older adults
(>50 years). The spread of HL is nonrandom, with dissemination via
lymphatics to contiguous lymph node groups including the spleen.
Prognosis in large part is related to stage of disease. Limited stage
disease (stage I or II) has a better prognosis than advanced stage disease
(stage III or IV). In addition, asymptomatic patients (A) fare better than
those with B symptoms – fever, night sweats or weight loss >10% of
body weight. The therapy for HL is usually determined by the stage of
disease, as well as histopathologic subtype, and includes radiotherapy, and
specific combination chemotherapy. Long-term survival is usually quite
good.

12
3. Diagnostic Criteria: HL typically
effaces nodal architecture, forming a mass
of characteristic reactive inflammatory
cells with an admixed smaller population
of large dysplastic RS cells. The RS cell
is a large binucleate cell with dispersed
chromatin, inclusion-like macronucleoli,
and abundant eosinophilic cytoplasm. For
diagnostic purposes, recognition of the
characteristic inflammatory component is
just as important as identifying the RS cell. Although the histologic features of HL
are often diagnostic, “RS-like” cells may be seen in reactive conditions such as
infectious mononucleosis and other lymphomas. Immunologic studies are useful in
confirming the diagnosis, as classical RS cells have a characteristic
immunophenotype: LeuM1 (CD15)+, Ki-1 (CD30)+ and leukocyte common antigen
[(LCA) CD45–]. It is now known that the RS cells of almost all types of classical
HL are of B-lineage. However, in contrast to normal B-cells, the RS cells of classical
HL show a global shut down of the B-cell transcription program. Thus, markers of
B-lineage, such as CD 20 or surface Ig, are usually not expressed by classical RS
cells.
4. Classification: The W.H.O. Classification recognizes two major
categories of HL: Classical HL and nodular lymphocyte predominant HL.
These two categories differ with respect to morphologic appearance,
clinical behavior and immunophenotype. There are four types of classical
HL that are distinguished by the pattern of nodal infiltration, the mixture
of reactive cells, and the number and appearance of RS cells. The four
types of HL include nodular sclerosis, lymphocyte -rich, mixed cellularity,
and lymphocyte depleted.

13
Nodular Sclerosis (NS): NSHL is the most
common type of HL. It occurs most often in
young adults, and is the only type of HL that
affects females more than males. Patients usually
present with cervical adenopathy and/or a
mediastinal mass. Histologic features include
capsular fibrosis, and dense bands of connective
tissue that efface nodal architecture and give a
nodular appearance. The nodules often contain
numerous inflammatory cells and scattered RS
cells. Most RS cells have a lacunar appearance
where the cytoplasm retracts against the nucleus,
giving the appearance of a hole or lacuna.

14
Mixed Cellularity (MC): MCHL is the second most common type. The most
common presentation is a symptomatic (fever, weight loss, night sweats) middle-aged
to elderly male. The prognosis is intermediate. Typically, nodal architecture is
completely effaced with numerous inflammatory cells (lymphocytes, histocytes,
eosinophils, and plasma cells) and a readily identifiable RS-cells including
“diagnostic” binucleate forms.
Lymphocyte Depletion (LD): LDHL is uncommon, representing <5% of HL. Most
patients have fever and peripheral blood cytopenias. Generally, there is little
peripheral and more abdominal adenopathy. As the name implies, lymphocytes are
fewer in number, and RS cells may predominate over the reactive component. RS
cells vary from diagnostic to bizarre, multinucleated cells that may have sarcomatous
appearance.
Lymphocyte – rich (LR): LPHL is rare and mimics LPHL but has an
immunophenotype of classical HL.
NOTE: NSHL, MCHL, LRHL, and LDHL subtypes of HL are grouped together as
classical Hodgkin Lymphoma, as RS cells have the characteristic immunophenotype
(CD 45-, CD 15+, CD 30+) described above.
Lymphocyte Predominance (LP): LPHL represents 5-10% of all HL cases.
Patients typically are asymptomatic young males with cervical or axillary
adenopathy. The prognosis is excellent. Histologically, the predominant cell is a
small lymphocyte. RS cells are few in number, and have a folded, vesiculated
nucleus with less prominent nucleoli than seen in other types of HL. These RS cells
are sometimes called “popcorn cells” based on this morphology.
NOTE: LPHL has a characteristic immunophenotype (CD 45+, CD 15-, CD 30-,
CD20+) that is different from “classical HL”, and molecular genetic studies have
shown a B-cell origin for LPHL. In contrast to classical HL, the neoplastic cells of
LPHL express B-lineage markers, such as CD 20.
Related Documents


![Indolent T- and NK-cell lymphoproliferative disorders of ... · extranodal site of occurrence of non-Hodgkin lymphomas [1]. Most GI lymphomas are of B-cell lineage, and T-cell lymphomas](https://static.cupdf.com/doc/110x72/5f93d293a1c10d3ed34c6b11/indolent-t-and-nk-cell-lymphoproliferative-disorders-of-extranodal-site-of.jpg)








