The Journal of Applied Research • Vol. 5, No. 2, 2005 305 Malignant Ascites Associated with Carcinoma of the Prostate Muhammad Wasif Saif, MD University of Alabama at Birmingham (UAB), Comprehensive Cancer Center, Birmingham, Alabama patients with history of prostate cancer develop malignant effusions, prostate specific antigen (PSA) immunohis- tostaining of the fluid can serve as a valuable adjunctive study for the diag- nosis. This clinical situation becomes particularly important in patients with ascites with a carcinoma of unknown primary. Palliation can be achieved in patients with ascites secondary to prostate cancer using hormone manipu- lation. Lack of knowledge about this complication of prostate cancer may delay the diagnosis and treatment of this hormonally responsive malignancy. INTRODUCTION Carcinoma of the prostate is predomi- nantly a tumor of older men. Some patients have prolonged survival even after the cancer has metastasized to dis- tant sites, such as to bone. 1 Since the median age at diagnosis is 72 years, many patients, especially those with localized tumor, may die of other ill- nesses without ever having suffered sig- nificant morbidity from their cancer. 2 Survival of the patient with prostate carcinoma is related to the extent of the tumor. Patients with locally advanced cancer are not usually curable, and a substantial fraction will eventually die as a result of their tumor, although median survival may be as long as 5 years. 1,2 If prostate cancer has spread to distant organs, current therapy is not curative. Median survival is usually 1 to 3 years, and the majority of such KEY WORDS: prostate cancer, ascites, malignant effusion, hormonal treatment, PSA, cancer of unknown primary ABSTRACT: Background: Prostate cancer is the most common malignancy in men in the United States. Both at diagnosis and throughout the disease progression, it can metastasize to multiple organs, most commonly bone and lymph nodes. Effusions (either pleural or abdominal) are relatively uncommon. Patients and Methods: We reviewed the medical literature including the case reports and post-mortem studies relating ascites to prostate cancer, identified through a MEDLINE search (human; all languages; 1969-2004). Results: We found 12 published cases. Forty two percent of patients presented initially with ascites, in 50% ascites developed later with progressive disease, and 8% had ascites being the only site of recurrence. The response rate to endocrine therapy, including orchiecto- my, was 25%. Ascites in these patients conferred a poorer prognosis. Conclusion: The development of ascites secondary to prostate cancer, either as an initial manifestation or recurrent dis- ease, is not well known and may be unfamiliar to many physicians. If

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
The Journal of Applied Research • Vol. 5, No. 2, 2005 305
Malignant Ascites Associated withCarcinoma of the ProstateMuhammad Wasif Saif, MD
University of Alabama at Birmingham (UAB), Comprehensive Cancer Center, Birmingham,Alabama
patients with history of prostate cancerdevelop malignant effusions, prostatespecific antigen (PSA) immunohis-tostaining of the fluid can serve as avaluable adjunctive study for the diag-nosis. This clinical situation becomesparticularly important in patients withascites with a carcinoma of unknownprimary. Palliation can be achieved inpatients with ascites secondary toprostate cancer using hormone manipu-lation. Lack of knowledge about thiscomplication of prostate cancer maydelay the diagnosis and treatment ofthis hormonally responsive malignancy.
INTRODUCTIONCarcinoma of the prostate is predomi-nantly a tumor of older men. Somepatients have prolonged survival evenafter the cancer has metastasized to dis-tant sites, such as to bone.1 Since themedian age at diagnosis is 72 years,many patients, especially those withlocalized tumor, may die of other ill-nesses without ever having suffered sig-nificant morbidity from their cancer.2
Survival of the patient with prostatecarcinoma is related to the extent of thetumor. Patients with locally advancedcancer are not usually curable, and asubstantial fraction will eventually dieas a result of their tumor, althoughmedian survival may be as long as 5years.1,2 If prostate cancer has spread todistant organs, current therapy is notcurative. Median survival is usually 1 to3 years, and the majority of such
KEY WO R D S : prostate cancer, a s c i t e s,malignant effusion, hormonal t r e a t m e n t , P S A , cancer of unknown p r i m a r y
ABSTRACT:Background: Prostate cancer is the mostcommon malignancy in men in theUnited States. Both at diagnosis andthroughout the disease progression, itcan metastasize to multiple organs, mostcommonly bone and lymph nodes.Effusions (either pleural or abdominal)are relatively uncommon.
Patients and Methods: We reviewed themedical literature including the casereports and post-mortem studies relatingascites to prostate cancer, identifiedthrough a MEDLINE search (human; alllanguages; 1969-2004).
Results: We found 12 published cases.Forty two percent of patients presentedinitially with ascites, in 50% ascitesdeveloped later with progressive disease,and 8% had ascites being the only siteof recurrence. The response rate toendocrine therapy, including orchiecto-my, was 25%. Ascites in these patientsconferred a poorer prognosis.
Conclusion: The development of ascitessecondary to prostate cancer, either asan initial manifestation or recurrent dis-ease, is not well known and may beunfamiliar to many physicians. If
Saif-Ascites-vol5no2 6/1/05 8:58 PM Page 305

Vol. 5, No. 2, 2005 • The Journal of Applied Research306
patients will die of prostate cancer.3Even in this group of patients, however,indolent clinical courses lasting for manyyears may be observed. Other factorsaffecting the prognosis of patients withprostate cancer that are useful in mak-ing therapeutic decisions include histo-logical grade of the tumor, patient’s age,other medical illnesses, and the serumlevel of PSA.4 Poorly differentiatedtumors are more likely to have metasta-sized at the time of diagnosis and areassociated with a poorer prognosis.5
The evaluation of metastatic carci-noma of an unknown primary site isoften a challenging problem encoun-tered by oncologists. Despite extensiveclinical evaluation, the origin of the pri-mary tumor may remain undetected.This clinical situation can be moreexhausting if a patient presents with anatypical feature of the underlying tumor.Prostate cancer usually presents asobstructive uropathy with a predilectionto spread to the axial skeleton. This situ-ation can be compounded if ascites aremanifested as an initial presentation orthe only site of recurrent disease. Thisassociation of prostate cancer andascites may be unknown to many physi-cians, and thereby, diagnosis of a hor-mone-responsive tumor may be delayed.
PATIENTS AND METHODSWe reviewed the medical literatureincluding the case reports and post-mortem studies relating ascites toprostate cancer, identified through aMEDLINE search (human; all lan-guages; 1969-2004). A manual retrievalof bibliographies of the identified litera-ture was performed to collect informa-tion pertaining to age, race, clinicalfeatures, sites of metastases, treatment,outcome to treatment, and survival.
RESULTSWe found 12 published cases with wherethe patients’ mean age was 70 years
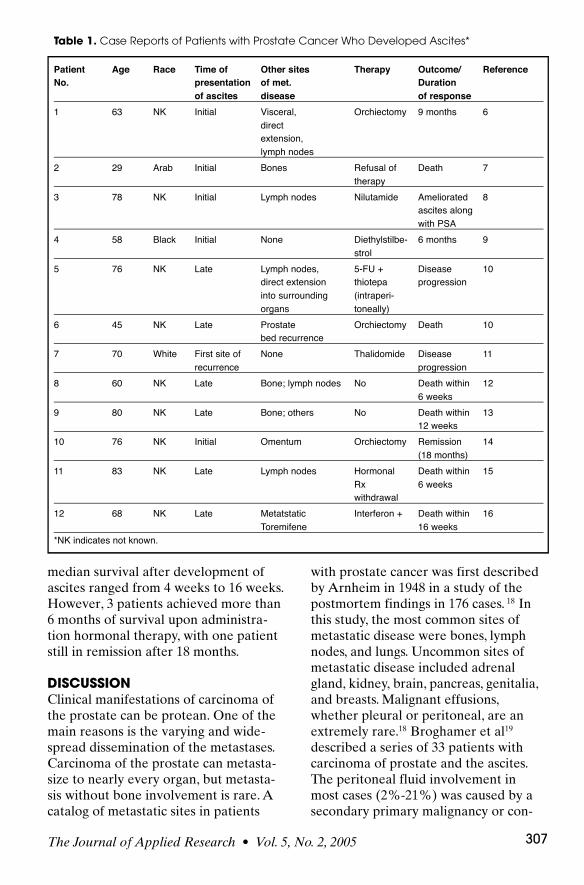
(range: 29–83).6-16 Five patients werediagnosed with ascites at the time of ini-tial diagnosis (42%), while six patientsdeveloped ascites later with wide-spreadmetastatic cancer (50%). Only onepatient had ascites manifesting as thesole manifestation of recurrent prostatecancer (8%) (Table 1).
After review of these cases withprostate carcinoma, it is apparent thatmetastatic effusions responded toendocrine therapy. Heffner et al17
reported a case of a 64-year-old manwith metastatic prostate cancer whoresponded to diethylstilbestrol dipropri-onate therapy evidenced by resolvingpleural effusion, partial clearing of theparenchymal infiltrates, and improvedoxygenation. Disdier et al8 reported a78-year-old man whose ascites respond-ed to nilutamide (150 mg/24 hours x 2months) along with a decrease in serumPSA level from 150 ng/mL to 40 ng/mL.Catton et al6 reported a response toorchiectomy with control of ascites for 9months in which no other immediatetherapy was instituted. Orchiectomy hasalso been tried in patients with prostatecancer who developed ascites and result-ed in mixed responses.6,10,14
Intraperitoneal chemotherapy (5-FU,thiotepa) was not successful in anotherpatient.10 These data support thatendocrine or hormonal therapy shouldbe tried in patients with ascites resultingfrom prostate cancer. In patients withandrogen independent prostate cancer, asecondary hormonal therapy,chemotherapy or experimental agentsshould be tried. The role of the newanti-angiogenesis therapy, either as atherapy or a potential cause resulting influid retention, is not known at present.However, one patient was on thalido-mide at the time when he developedascites.11
Malignant effusion development incases of prostatic adenocarcinoma seemsto correlate with a poorer outcome. The
Saif-Ascites-vol5no2 6/1/05 8:58 PM Page 306
The Journal of Applied Research • Vol. 5, No. 2, 2005 307
median survival after development ofascites ranged from 4 weeks to 16 weeks.However, 3 patients achieved more than6 months of survival upon administra-tion hormonal therapy, with one patientstill in remission after 18 months.
DISCUSSIONClinical manifestations of carcinoma ofthe prostate can be protean. One of themain reasons is the varying and wide-spread dissemination of the metastases.Carcinoma of the prostate can metasta-size to nearly every organ, but metasta-sis without bone involvement is rare. Acatalog of metastatic sites in patients
with prostate cancer was first describedby Arnheim in 1948 in a study of thepostmortem findings in 176 cases. 18 Inthis study, the most common sites ofmetastatic disease were bones, lymphnodes, and lungs. Uncommon sites ofmetastatic disease included adrenalgland, kidney, brain, pancreas, genitalia,and breasts. Malignant effusions,whether pleural or peritoneal, are anextremely rare.18 Broghamer et al19
described a series of 33 patients withcarcinoma of prostate and the ascites.The peritoneal fluid involvement inmost cases (2%-21%) was caused by asecondary primary malignancy or con-
Table 1. Case Reports of Patients with Prostate Cancer Who Developed Ascites*
Patient Age Race Time of Other sites Therapy Outcome/ ReferenceNo. presentation of met. Duration
of ascites disease of response1 63 NK Initial Visceral, Orchiectomy 9 months 6
direct extension, lymph nodes
2 29 Arab Initial Bones Refusal of Death 7therapy
3 78 NK Initial Lymph nodes Nilutamide Ameliorated 8ascites along with PSA
4 58 Black Initial None Diethylstilbe- 6 months 9strol
5 76 NK Late Lymph nodes, 5-FU + Disease 10direct extension thiotepa progressioninto surrounding (intraperi-organs toneally)
6 45 NK Late Prostate Orchiectomy Death 10bed recurrence
7 70 White First site of None Thalidomide Disease 11recurrence progression
8 60 NK Late Bone; lymph nodes No Death within 126 weeks
9 80 NK Late Bone; others No Death within 1312 weeks
10 76 NK Initial Omentum Orchiectomy Remission 14(18 months)
11 83 NK Late Lymph nodes Hormonal Death within 15Rx 6 weekswithdrawal
12 68 NK Late Metatstatic Interferon + Death within 16Toremifene 16 weeks
*NK indicates not known.
Saif-Ascites-vol5no2 6/1/05 8:58 PM Page 307
Vol. 5, No. 2, 2005 • The Journal of Applied Research308
comitant reactive conditions, such aspancreatic cancer, bronchogenic cancerand gastric carcinoma.19 In contrast, gas-trointestinal malignancies are the mostfrequent etiology of malignant ascites inmen.20 Megalli et al9 noted that ascites inpatients with prostate cancer were alsocaused by second primary malignancies,and gastrointestinal malignancies werethe most common among them.
Rapoport et al10 reviewed the autop-sy of 523 cases of prostate cancer andfound 13 cases with peritoneal depositswith no disease elsewhere, demonstrat-ing the fact that effusions can occur inpatients with prostate cancer withoutthe involvement of the more commonsites of metastatic disease.
There are several aspects of thesepublished cases of ascites in patientswith prostate cancer, which warrantcomment: First, malignant effusions,whether peritoneal or pleural, are asso-ciated extremely rarely with carcinomaof prostate and so much less so withoutosseous or lymph node involvement.Second, 42% patients developed ascitesas their first presenting sign, but onlytwo of these patients had ascites with noother sites of metastatic disease (includ-ing bones and lymph nodes). Only onepatient developed ascites as the onlysign of recurrent disease. Third, theexudative nature of the effusion andpositive papanicolou stain for malignantcells supports a pathogenetc mechanismof mesothelial invasion. This in contrastto the transudative nature of ascitic fluidreported in few of these cases suggestinglymphatic obstruction as the mechanismin the development of malignant effu-sion associated with carcinoma ofprostate. Two patients had chylousascites.7,15 One patient had hemorrhagicascites.16 Fourth, the mean age of thesepatients was 70 years. The relationshipto race cannot be assessed due to theunavailability of such information in thereported cases. Fifth, malignant effusions
secondary to carcinoma of the prostatehave been reported to resolve withendocrine therapy, even if ascites consti-tutes the initial manifestation of prostatecancer and in patients with or withoutprevious hormonal ablation. This fact isfurther strengthened by the presence ofmalignant prostate cells in the malignanteffusion, as evidenced by special stainingby Broghamer et al.19 He suggested thatthe benefit from hormonal therapy maybe derived in such conditions and henceshould be used.19 Sixth, we also foundthat these malignant effusions inpatients with prostate cancer are associ-ated with a poorer prognosis. Finally, adifficult problem for the physician andthe patient can be the evaluation ofmetastatic carcinoma of unknown pri-mary site.21 Despite extensive clinicalevaluation, the original tumor mayremain undetected, especially if the solepresenting feature is a malignant effu-sion. In this situation, it may be prudentto stain the fluid for both PSA andprostate acid phosphatase (PAP).
Invasion of the mesothelial lining bymalignant cells is regarded as a trigger-ing factor in the pathogenesis of a bodycavity effusion such as ascites. It is sug-gested that neoplastic cells in an effu-sion may be exfoliated from the cancerof the origin, if the cytological examina-tion of these fluids reveals the presenceof cancer cells. It is also suggested thatthe effusion may develop secondary tolymphatic obstruction, or that it may bethe result of prostatic lymphatic carcino-matosis. Other benign and malignant eti-ologies should be excluded in thesepatients, as suggested by the literaturereview of cancers of non-prostatic ori-gin, especially in cancer of the gastroin-testinal tract, which can be the reasonfor the development of ascites inpatients with carcinoma of the prostate.9
Two cases of chylous ascites as a pre-senting sign of prostate adenocarcinomahave also been reported.7,15 In these
Saif-Ascites-vol5no2 6/1/05 8:58 PM Page 308
The Journal of Applied Research • Vol. 5, No. 2, 2005 309
patients, with enlarged retroperitoneallymph nodes and wide dissemination ofthe carcinoma, development of chylousascites were thought to be secondary todiffuse metastases to periaortic lymphnodes and regional lymphatics drainingthe prostate carcinoma.7,15 We reported asimilar case earlier in which thalidomidewas initially thought to be the cause ofthe patient’s ascites and leg edema.11
This presumption was based on the pre-liminary data from a Phase II trialinvolving thalidomide that revealed thedevelopment of peripheral edema inapproximately 50% of cases, but noascites or other effusions were seen.However, immunostaining of the ascitic
fluid confirmed the diagnosis of prostatecancer. 11
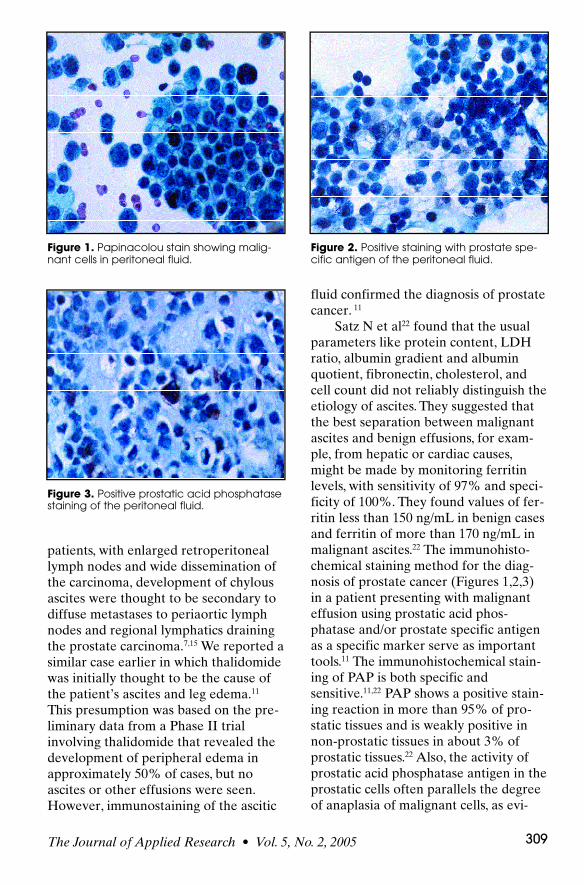
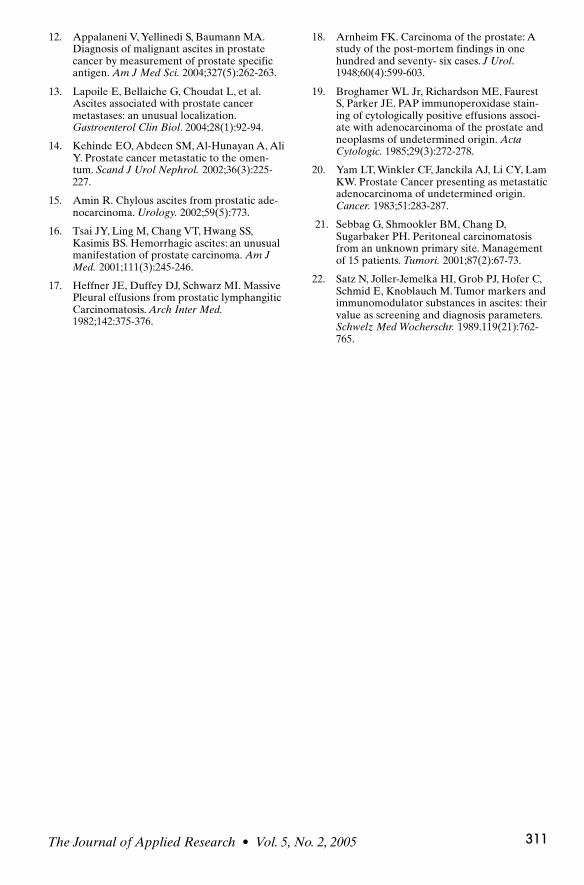
Satz N et al22 found that the usualparameters like protein content, LDHratio, albumin gradient and albuminquotient, fibronectin, cholesterol, andcell count did not reliably distinguish theetiology of ascites. They suggested thatthe best separation between malignantascites and benign effusions, for exam-ple, from hepatic or cardiac causes,might be made by monitoring ferritinlevels, with sensitivity of 97% and speci-ficity of 100%. They found values of fer-ritin less than 150 ng/mL in benign casesand ferritin of more than 170 ng/mL inmalignant ascites.22 The immunohisto-chemical staining method for the diag-nosis of prostate cancer (Figures 1,2,3)in a patient presenting with malignanteffusion using prostatic acid phos-phatase and/or prostate specific antigenas a specific marker serve as importanttools.11 The immunohistochemical stain-ing of PAP is both specific andsensitive.11,22 PAP shows a positive stain-ing reaction in more than 95% of pro-static tissues and is weakly positive innon-prostatic tissues in about 3% ofprostatic tissues.22 Also, the activity ofprostatic acid phosphatase antigen in theprostatic cells often parallels the degreeof anaplasia of malignant cells, as evi-
Figure 1. Papinacolou stain showing malig-nant cells in peritoneal fluid.
Figure 2. Positive staining with prostate spe-cific antigen of the peritoneal fluid.
Figure 3. Positive prostatic acid phosphatasestaining of the peritoneal fluid.
Saif-Ascites-vol5no2 6/1/05 8:58 PM Page 309

Vol. 5, No. 2, 2005 • The Journal of Applied Research310
denced by scarce enzyme antigen in cellsof poorly differentiated carcinoma. PSAis a nonenzymatic protein which showsno cross antigenicity with the PAP. PSAmay be found in anaplastic tumor cellswhere there is scanty PAP activity.22
Therefore, the use of PSA in conjunc-tion with PAP enhances the diagnosticsensitivity in metastatic carcinoma of theprostate. Hence, it may be prudent tostain the tumor or cell in a malignanteffusion associated with a tumor toestablish its origin.11,12,22
The general management of ascitesincluding the three D’s—that is D1 fordiet, D2 for diuretic, and D3 fordrainage, should be applied in individualcases. Our review supports the view thatendocrine therapy should be tried inpatients with ascites resulting from theprostate cancer. In patients with andro-gen independent prostate cancer, a sec-ondary hormonal therapy, chemotherapyor experimental agents should be tried.The role of intraperitoneal chemothera-py remains investigative. Similarly, theeffect and role of newer chemotherapiessuch as docetaxel, which can potentiallycause fluid retention, needs to beexplored in this rare presentation ofprostate cancer.
CONCLUSIONWe conclude that malignant effusionslike ascites are a potential complicationof carcinoma of the prostate. Althoughthese effusions may constitute the initialmanifestation of prostatic adenocarcino-ma, such effusions may be the only signsof recurrence of prostate cancer.Prostate cancer is a common disease inelderly men and presents typically withobstructive uropathy or disease in theaxial skeleton. However, an unusualpresentation like malignant effusionsmay be encountered, therefore, oncolo-gists, urologists, and primary care physi-cians should be aware of thiscomplication of the prostate cancer. We
suggest that PSA measurement may bea valuable adjunctive study for the diag-nosis of malignant effusions in prostatecancer. This situation is of particular sig-nificance in cases of metastatic carcino-ma of unknown primary site, whereascites may be the only manifestation.Immunohistochemical staining shouldbe performed in sorting out the tumororigin. Worthwhile palliation can beachieved in patients with massive effu-sions secondary to metastatic prostatecancer using hormone manipulation.
REFERENCES1. American Cancer Society. Cancer Facts and
Figures 2004. Atlanta, Ga: American CancerSociety; 2004.
2. Garnick MB. Prostate cancer: screening, dia-gnosis, and management. Ann Intern Med.1993;118(10):804-818.
3. Helgesen F, Holmberg L, Johansson JE, et al.Trends in prostate cancer survival in Sweden,1960 through 1988: evidence of increasingdiagnosis of nonlethal tumors. J Natl CancerInst. 1996;88(17):1216-1221.
4. Thompson IM, Pauler DK, Goodman PJ, etal. Prevalence of prostate cancer among menwith a prostate-specific antigen level < or=4.0 ng per milliliter. N Engl J Med.2004;350(22):2239-2246.
5. Gittes RF. Carcinoma of the prostate. N EnglJ Med. 1991;324(4):236-245.
6 . Catton PA , Hartwick RW, Srigley JR, et al.Prostate Cancer presenting with malignanta s c i t e s : Signet-ring cell variant of prostatea d e n o c a r c i n o m a . U r o l o g y. 1 9 9 2 ; 3 9 ( 5 ) : 4 9 5 - 4 9 7 .
7. Beigel Y, Zelikovski A, Shimoni S, Ekstein J,Melloul M, Mor C, Fuchs J. Chylous ascites asa presenting sign of prostate adenocarcino-ma. Lymphology. 1990; 23(4):183-186.
8. Disdier P, Harle JR, Swiader L, Coulange C,Mongin M, Weiller PJ. Prostate carcinomarevealed by ascites with cachexia. PresseMedicale.1990;19(5):220.
9. Megalli MR, Gursel EO, Veenema RJ. Ascitesas an unusual presentation of carcinoma ofthe prostate. J Urol. 1973:110(2):232-234.
10. Rapoport AH, Omenn GS. Dermatomyositisand Malignant Effusions: Rare manifestationof cancer. J Urol. 1968;100(2):183-187.
11. Saif MW, Figg WD, Hewitt S, Dahut W.Malignant ascites as only manifestation ofmetastatic prostate cancer. Prostate CancerDis. 1999;2:290-293.
Saif-Ascites-vol5no2 6/1/05 8:58 PM Page 310
The Journal of Applied Research • Vol. 5, No. 2, 2005 311
12. Appalaneni V, Yellinedi S, Baumann MA.Diagnosis of malignant ascites in prostatecancer by measurement of prostate specificantigen. Am J Med Sci. 2004;327(5):262-263.
13. Lapoile E, Bellaiche G, Choudat L, et al.Ascites associated with prostate cancermetastases: an unusual localization.Gastroenterol Clin Biol. 2004;28(1):92-94.
14. Kehinde EO, Abdeen SM, Al-Hunayan A, AliY. Prostate cancer metastatic to the omen-tum. Scand J Urol Nephrol. 2002;36(3):225-227.
15. Amin R. Chylous ascites from prostatic ade-nocarcinoma. Urology. 2002;59(5):773.
16. Tsai JY, Ling M, Chang VT, Hwang SS,Kasimis BS. Hemorrhagic ascites: an unusualmanifestation of prostate carcinoma. Am JMed. 2001;111(3):245-246.
17. Heffner JE, Duffey DJ, Schwarz MI. MassivePleural effusions from prostatic lymphangiticCarcinomatosis. Arch Inter Med.1982;142:375-376.
18. Arnheim FK. Carcinoma of the prostate: Astudy of the post-mortem findings in onehundred and seventy- six cases. J Urol.1948;60(4):599-603.
19. Broghamer WL Jr, Richardson ME, FaurestS, Parker JE. PAP immunoperoxidase stain-ing of cytologically positive effusions associ-ate with adenocarcinoma of the prostate andneoplasms of undetermined origin. ActaCytologic. 1985;29(3):272-278.
20. Yam LT, Winkler CF, Janckila AJ, Li CY, LamKW. Prostate Cancer presenting as metastaticadenocarcinoma of undetermined origin.Cancer. 1983;51:283-287.
21. Sebbag G, Shmookler BM, Chang D,Sugarbaker PH. Peritoneal carcinomatosisfrom an unknown primary site. Managementof 15 patients. Tumori. 2001;87(2):67-73.
22. Satz N, Joller-Jemelka HI, Grob PJ, Hofer C,Schmid E, Knoblauch M. Tumor markers andimmunomodulator substances in ascites: theirvalue as screening and diagnosis parameters.Schwelz Med Wocherschr. 1989.119(21):762-765.
Saif-Ascites-vol5no2 6/1/05 8:58 PM Page 311
Related Documents