Male circumcision for prevention of homosexual acquisition of HIV in men (Review) Wiysonge CS, Kongnyuy EJ, Shey M, Muula AS, Navti OB, Akl EA, Lo YR This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library 2011, Issue 6 http://www.thecochranelibrary.com Male circumcision for prevention of homosexual acquisition of HIV in men (Review) Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Male circumcision for prevention of homosexual acquisition of
HIV in men (Review)
Wiysonge CS, Kongnyuy EJ, Shey M, Muula AS, Navti OB, Akl EA, Lo YR
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2011, Issue 6
http://www.thecochranelibrary.com
Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2SUMMARY OF FINDINGS FOR THE MAIN COMPARISON . . . . . . . . . . . . . . . . . . .
5BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
8RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Figure 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Figure 2. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
11DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
12AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
12ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
13REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
16CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
40DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Analysis 1.1. Comparison 1 Male circumcision versus no male circumcision, Outcome 1 HIV infection (all MSM). . 40
Analysis 1.2. Comparison 1 Male circumcision versus no male circumcision, Outcome 2 HIV infection (by sexual
position). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
Analysis 1.3. Comparison 1 Male circumcision versus no male circumcision, Outcome 3 Sexually transmitted infection. 44
44HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
45CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
45DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
45SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
45DIFFERENCES BETWEEN PROTOCOL AND REVIEW . . . . . . . . . . . . . . . . . . . . .
45INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iMale circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

[Intervention Review]
Male circumcision for prevention of homosexual acquisition ofHIV in men
Charles Shey Wiysonge1 , Eugene J Kongnyuy2, Muki Shey3, Adamson S Muula4, Osric B Navti5, Elie A Akl6, Ying-Ru Lo7
1School of Child and Adolescent Health, University of Cape Town, Cape Town, South Africa. 2Child and Reproductive Health Group,
Liverpool School of Tropical Medicine, Liverpool, UK. 3Institute of Infectious Disease and Molecular Medicine (IIDMM), University
of Cape Town, Cape Town, South Africa. 4Department of Public Health; College of Medicine, University of Malawi, Blantyre,
Malawi. 5Directorate of Women’s, Perinatal and Sexual Health Services, University Hospitals of Leicester NHS Trust, Leicester, UK.6Department of Medicine, State University of New York at Buffalo, Buffalo, NY, USA. 7Department of HIV/AIDS, World Health
Organization, Geneva, Switzerland
Contact address: Charles Shey Wiysonge, School of Child and Adolescent Health, University of Cape Town, Institute of Infec-
tious Disease and Molecular Medicine, Anzio Road, Observatory, Cape Town, 7925, South Africa. [email protected].
Editorial group: Cochrane HIV/AIDS Group.
Publication status and date: New, published in Issue 6, 2011.
Review content assessed as up-to-date: 9 May 2011.
Citation: Wiysonge CS, Kongnyuy EJ, Shey M, Muula AS, Navti OB, Akl EA, Lo YR. Male circumcision for prevention of
homosexual acquisition of HIV in men. Cochrane Database of Systematic Reviews 2011, Issue 6. Art. No.: CD007496. DOI:
10.1002/14651858.CD007496.pub2.
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A B S T R A C T
Background
Previous systematic reviews found inconsistent effects of male circumcision on HIV acquisition in men who have sex with men (MSM).
However, a number of new studies have become available in the three years since the last systematic review.
Objectives
To assess the effects of male circumcision for preventing HIV acquisition by men through sex with men.
Search strategy
In June 2010 we electronically searched the Cochrane Central Register of Controlled Trials, PubMed, EMBASE, AIDS Education
Global Information System, ClinicalTrials.gov, and WHO International Clinical Trials Registry Platform; hand-searched reference lists
of relevant articles; and contacted relevant organisations and experts. We updated the search in March 2011.
Selection criteria
We looked for randomised controlled trials (RCTs) and observational studies that assessed the effects of male circumcision on HIV
acquisition in MSM.
Data collection and analysis
Two authors independently assessed study eligibility and methodological quality, and extracted data. We expressed study results as odds
ratios (OR) with 95% confidence intervals (CI), and conducted random-effects meta-analysis.
1Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Main results
We found no completed RCT and included 21 observational studies with 71,693 participants. The only eligible RCT is currently
ongoing among MSM in China. The pooled effect estimate for HIV acquisition was not statistically significant (20 studies; 65,784
participants; OR 0.86, 95% CI 0.70 to 1.06) and showed significant heterogeneity (I²=53%). In a subgroup analysis, the results were
statistically significant in studies of men reporting an insertive role (7 studies, 3465 participants; OR 0.27, 95% CI 0.17 to 0.44; I²=
0%) but not in studies of men reporting a receptive role (3 studies, 1792 participants; OR 1.20, 95% CI 0.63 to 2.29; I² = 0%). There
was no significant association between male circumcision and syphilis (8 studies; 34,999 participants: OR 0.96, 95% CI 0.82 to 1.13;
I² = 0%), herpes simplex virus 1 (2 studies, 2740 participants; OR 0.90, 95% CI 0.53 to 1.52; I²=0%), or herpes simplex virus 2 (5
studies;10,285 participants; OR 0.86, 95% CI 0.62 to 1.21; I²=0%). The overall GRADE quality of evidence was low. None of the
included studies assessed adverse effects associated with male circumcision.
Authors’ conclusions
Current evidence suggests that male circumcision may be protective among MSM who practice primarily insertive anal sex, but the
role of male circumcision overall in the prevention of HIV and other sexually transmitted infections among MSM remains to be
determined. Therefore, there is not enough evidence to recommend male circumcision for HIV prevention among MSM at present.
Further research should be of high quality and further explore interaction with the predominant sexual role.
P L A I N L A N G U A G E S U M M A R Y
Male circumcision for prevention of homosexual acquisition of HIV in men
At present there is no completed randomised controlled trial that has assessed the effects of male circumcision on acquisition of HIV
and other sexually transmitted infections among men who have sex with men (MSM). Results from observational studies suggest that
circumcision may be protective among MSM who practice primarily insertive anal sex, but the role of male circumcision overall in the
prevention of HIV and other sexually transmitted infections among MSM remains to be determined.
2Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

S U M M A R Y O F F I N D I N G S F O R T H E M A I N C O M P A R I S O N [Explanation]
Male circumcision for prevention of HIV and other STIs among men who have sex with men and transgender people
Patient or population: Men who have sex with men and transgender persons
Settings: High-income countries (16 studies), low and middle-income countries (5)
Intervention: Male circumcision
Comparison: No male circumcision
Outcomes Illustrative comparative risks* (95% CI) Relative effect
(95% CI)
No of Participants
(studies)
Quality of the evidence
(GRADE)
Assumed risk Corresponding risk
No male circumcision Male circumcision
HIV infection (all studies to-
gether, regardless of sexual
role)
Lab test or self report
268 per 1000 239 per 1000
(204 to 280)
OR 0.86
(0.7 to 1.06)164915
(20 studies)
⊕⊕©©
low
HIV infection (mainly recep-
tive anal sex)
294 per 1000 333 per 1000
(208 to 488)
OR 1.20
(0.63 to 2.29)2876
(3 studies)
⊕©©©
very low3
HIV infection (mainly in-
sertive anal sex)
126 per 1000 37 per 1000
(24 to 60)
OR 0.27
(0.17 to 0.44)42098
(7 studies)
⊕⊕©©
low
Syphilis 13 per 1000 12 per 1000
(11 to 15)
OR 0.96
(0.82 to 1.13)
31174
(6 studies)
⊕⊕©©
low
Herpes simplex virus - 1 415 per 1000 390 per 1000
(273 to 519)
OR 0.90
(0.53 to 1.52)
2740
(2 studies)
⊕©©©
very low3
Herpes simplex virus - 2 178 per 1000 157 per 1000
(118 to 208)
OR 0.86
(0.62 to 1.21)
10285
(4 studies)
⊕©©©
very low3
3M
ale
circ
um
cisio
nfo
rp
reven
tion
of
ho
mo
sexu
alacq
uisitio
no
fH
IVin
men
(Revie
w)
Co
pyrig
ht
©2011
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

*The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the
assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
CI: Confidence interval; OR: Odds ratio;
GRADE Working Group grades of evidence
High quality: Further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low quality: We are very uncertain about the estimate.
1 Two studies (Reissen 2007 and Tabot 2002) reported the adjusted OR for the association between MC and HIV; with no corresponding
count data. The 2 studies had a total of 869 participants with complete data on MC and HIV status. The total number of participants is
therefore 65,784; and not 64,915.2 The Sanchez 2007 study (with 906 participants who self-identified as mainly receptive) reported the adjusted OR for the association
between MC and HIV; with no corresponding count data.The total number of participants is therefore 1,782; and not 876.3 Very small proportion of the 21 studies reported separate data for this outcome (possibility of publication bias); rated down by 1.4 The Sanchez 2007 study (with 1931 participants who self-identified as mainly insertive) reported the adjusted OR for the association
between MC and HIV; with no corresponding count data.The total number of participants is therefore 4,029; and not 2,098.
4M
ale
circ
um
cisio
nfo
rp
reven
tion
of
ho
mo
sexu
alacq
uisitio
no
fH
IVin
men
(Revie
w)
Co
pyrig
ht
©2011
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

B A C K G R O U N D
Male circumcision is the surgical removal of the foreskin of the
penis. Starting in the mid-1980s (Fink 1986), two decades of ob-
servational data indicated that circumcised heterosexual men have
lower incidence and prevalence of HIV infection than uncircum-
cised men (Fink 1986; Moses 1990; O’Farrell 2000; Weiss 2000;
Auvert 2001; Drain 2004; Baeten 2005). However, it was unclear
whether this observation is the result of a biological effect of male
circumcision, or due to cultural, social, or behavioural factors that
occur in association with or as a consequence of male circumci-
sion. Subsequently, three randomised controlled trials were set up
to examine the impact of adult male circumcision on HIV acqui-
sition in heterosexual men in South Africa (Auvert 2005), Kenya
(Bailey 2007), and Uganda (Gray 2007). A meta-analysis of all
three trials shows that medical adult male circumcision reduces the
acquisition of HIV by heterosexual men by 54% (95% confidence
intervals (CI): 38% to 66%) over 24 months (Siegfried 2009).
There are many concerns about the applicability of these results to
men who have sex with men (MSM) and male-to-female transexu-
als as well as their generalisability to other contexts. First, the HIV
epidemic in Africa occurs largely among heterosexuals, whereas
MSM remain the most affected risk group in other parts of the
World (Hall 2008; UNAIDS 2008; Le Vu 2010). Second, the
African data would be most relevant to MSM who only take the
insertive role during anal sex, because being the receptive partner
during anal sex would involve an HIV transmission route that
is likely to be unaffected by circumcision (Koblin 2006; Sullivan
2007). Third, the concentration of HIV in rectal secretions may be
greater than in vaginal secretions, which may increase HIV trans-
mission risk per act of unprotected insertive anal sex compared
with unprotected vaginal sex (Koblin 2006; Sullivan 2007).
Two systematic reviews published in 2008 (Fankem 2008; Millet
2008) pooled published and unpublished observational studies
and found insufficient evidence that male circumcision prevents
the acquisition of HIV or other sexually transmitted infections
(STIs) in MSM. However, more studies on the effect of male
circumcision on HIV transmission through anal sex have been
published since then (Templeton 2009; Thornton 2009; Gust
2010; Jameson 2010; McDaid 2010; Jozkowski 2010; Lane 2011;
Sanchez 2011).
O B J E C T I V E S
To assess the effects of male circumcision for preventing acquisition
of HIV by men through sex with men.
M E T H O D S
Criteria for considering studies for this review
Types of studies
We preferentially looked for randomised controlled trials. Since
we did not find completed randomised controlled trials (RCTs)
or controlled clinical trials, we included observational studies i.e.
cohort, case-control, and cross-sectional studies.
Types of participants
Men who have sex with men.
Types of interventions
Intervention: Surgical removal of the foreskin of the penis as de-
termined by direct observation, objective medical records, self re-
port, or partner-report.
Comparison: No circumcision
Types of outcome measures
Primary outcome: HIV infection (incidence or prevalence), as
defined by the authors.
Secondary outcomes: Other sexually transmitted infections
(STIs) and adverse effects associated with circumcision, as defined
by the authors.
Search methods for identification of studies
See: Cochrane HIV/AIDS Review Group search strategy.
We attempted to identify all relevant studies regardless of language
or publication status. In June 2010 we electronically searched
PubMed (Table 1), EMBASE (Table 2), the Cochrane Central
Register of Controlled Trials (CENTRAL: Table 3), Clinical-
Trials.gov, and the WHO International Clinical Trials Registry
Platform (http://www.who.int/ictrp/search/en/) using terms spe-
cific to male circumcision, HIV, and MSM. We also conducted
an electronic search for conference abstracts in the GATEWAY
and the AIDS Education Global Information System (AEGIS:
www.aegis.com) databases, and the web sites of relevant scien-
tific conferences (i.e. International AIDS Conference, Interna-
tional AIDS Society Conference on HIV Pathogenesis and Treat-
ment, British HIV/AIDS Association, Conference on Retroviruses
and Opportunistic Infections, European AIDS Conference, HIV
Pathogenesis & Treatment, National HIV Prevention Conference,
and Australasian Society for HIV Medicine Conference). We re-
peated these electronic searches in March 2011.
5Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
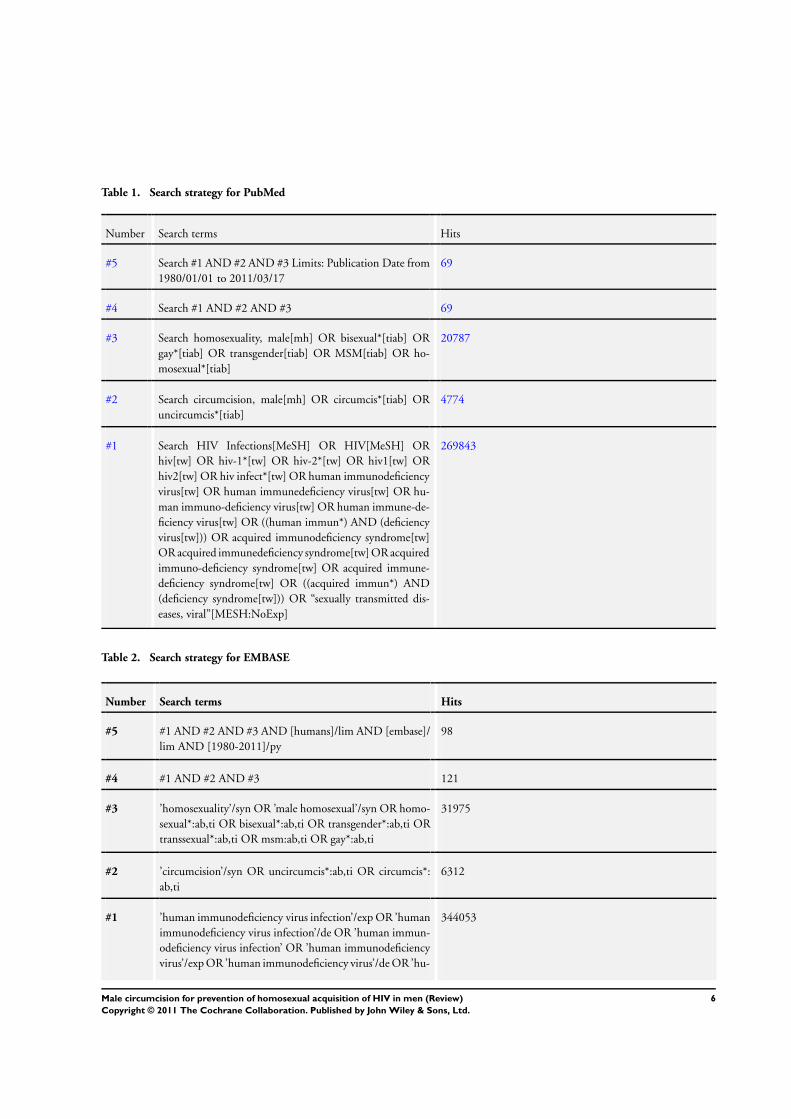
Table 1. Search strategy for PubMed
Number Search terms Hits
#5 Search #1 AND #2 AND #3 Limits: Publication Date from
1980/01/01 to 2011/03/17
69
#4 Search #1 AND #2 AND #3 69
#3 Search homosexuality, male[mh] OR bisexual*[tiab] OR
gay*[tiab] OR transgender[tiab] OR MSM[tiab] OR ho-
mosexual*[tiab]
20787
#2 Search circumcision, male[mh] OR circumcis*[tiab] OR
uncircumcis*[tiab]
4774
#1 Search HIV Infections[MeSH] OR HIV[MeSH] OR
hiv[tw] OR hiv-1*[tw] OR hiv-2*[tw] OR hiv1[tw] OR
hiv2[tw] OR hiv infect*[tw] OR human immunodeficiency
virus[tw] OR human immunedeficiency virus[tw] OR hu-
man immuno-deficiency virus[tw] OR human immune-de-
ficiency virus[tw] OR ((human immun*) AND (deficiency
virus[tw])) OR acquired immunodeficiency syndrome[tw]
OR acquired immunedeficiency syndrome[tw] OR acquired
immuno-deficiency syndrome[tw] OR acquired immune-
deficiency syndrome[tw] OR ((acquired immun*) AND
(deficiency syndrome[tw])) OR “sexually transmitted dis-
eases, viral”[MESH:NoExp]
269843
Table 2. Search strategy for EMBASE
Number Search terms Hits
#5 #1 AND #2 AND #3 AND [humans]/lim AND [embase]/
lim AND [1980-2011]/py
98
#4 #1 AND #2 AND #3 121
#3 ’homosexuality’/syn OR ’male homosexual’/syn OR homo-
sexual*:ab,ti OR bisexual*:ab,ti OR transgender*:ab,ti OR
transsexual*:ab,ti OR msm:ab,ti OR gay*:ab,ti
31975
#2 ’circumcision’/syn OR uncircumcis*:ab,ti OR circumcis*:
ab,ti
6312
#1 ’human immunodeficiency virus infection’/exp OR ’human
immunodeficiency virus infection’/de OR ’human immun-
odeficiency virus infection’ OR ’human immunodeficiency
virus’/exp OR ’human immunodeficiency virus’/de OR ’hu-
344053
6Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 2. Search strategy for EMBASE (Continued)
man immunodeficiency virus’ OR hiv:ti OR hiv:ab OR ’hiv-
1’:ti OR ’hiv-1’:ab OR ’hiv-2’:ti OR ’hiv-2’:ab OR ’human
immunodeficiency virus’:ti OR ’human immunodeficiency
virus’:ab OR ’human immuno-deficiency virus’:ti OR ’hu-
man immuno-deficiency virus’:ab OR ’human immuned-
eficiency virus’:ti OR ’human immunedeficiency virus’:ab
OR ’human immune-deficiency virus’:ti OR ’human im-
mune-deficiency virus’:ab OR ’acquired immune-deficiency
syndrome’:ti OR ’acquired immune-deficiency syndrome’:
ab OR ’acquired immunedeficiency syndrome’:ti OR ’ac-
quired immunedeficiency syndrome’:ab OR ’acquired im-
munodeficiency syndrome’:ti OR ’acquired immunodefi-
ciency syndrome’:ab OR ’acquired immuno-deficiency syn-
drome’:ti OR ’acquired immuno-deficiency syndrome’:ab
Table 3. Search strategy for CENTRAL
Number Search terms Hits
#1 MeSH descriptor HIV Infections explode all trees 6413
#2 MeSH descriptor HIV explode all trees 2045
#3 hiv OR hiv-1* OR hiv-2* OR hiv1 OR hiv2 OR HIV
INFECT* OR HUMAN IMMUNODEFICIENCY
VIRUS OR HUMAN IMMUNEDEFICIENCY VIRUS
OR HUMAN IMMUNE-DEFICIENCY VIRUS
OR HUMAN IMMUNO-DEFICIENCY VIRUS
OR HUMAN IMMUN* DEFICIENCY VIRUS OR
ACQUIRED IMMUNODEFICIENCY SYNDROME
OR ACQUIRED IMMUNEDEFICIENCY
SYNDROME OR ACQUIRED IMMUNO-
DEFICIENCY SYNDROME OR ACQUIRED
IMMUNE-DEFICIENCY SYNDROME OR
ACQUIRED IMMUN* DEFICIENCY SYNDROME
9888
#4 MeSH descriptor Lymphoma, AIDS-Related, this term
only
21
#5 MeSH descriptor Sexually Transmitted Diseases, Viral,
this term only
19
#6 (#1 OR #2 OR #3 OR #4 OR #5) 9976
#7 MeSH descriptor Circumcision, Male, this term only 179
#8 circumcis*:ti,ab,kw OR uncircumcis*:ti,ab,kw 251
7Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 3. Search strategy for CENTRAL (Continued)
#9 (#7 OR #8) 251
#10 MeSH descriptor Homosexuality, Male, this term only 139
#11 MeSH descriptor Bisexuality, this term only 33
#12 homosexual*:ti,ab,kw OR bisexual*:ti,ab,kw OR
gay*:ti,ab,kw OR transgender*:ti,ab,kw OR msm:ti,ab,kw
469
#13 (#10 OR #11 OR #12) 469
#14 (#6 AND #9 AND #13) 3
#15 (#6 AND #9 AND #13), from 1980 to 2011 3
We complemented the electronic search by hand searching the
reference lists of identified articles and relevant previous reviews
(Fankem 2008; Millet 2008; Templeton 2010). We identified pre-
vious reviews of male circumcision for prevention of HIV acqui-
sition in MSM by searching PubMed, EMBASE, the Cochrane
Database of Systematic Reviews, and the York Database of Ab-
stracts of Reviews of Effectiveness (DARE). In addition, we con-
sulted the WHO Department of HIV/AIDS in Geneva and mem-
bers of the WHO MSM guideline development working group,
and presented the findings of an earlier version of this review to
experts attending the WHO meeting on “Development of Guid-
ance for the Prevention and Treatment of HIV and other Sexu-
ally Transmitted Infections among Men having Sex with Men and
Transgender People” in September 2010 in Beijing, China.
The Cochrane HIV/AIDS Group assisted with the electronic
search.
Data collection and analysis
Each of four review authors (CSW, EJK, MS, OBN) indepen-
dently screened the titles, abstracts and descriptor terms of cita-
tions identified by the searches for potential eligibility. We then
obtained full articles for citations judged as potentially eligible by
at least one author. The authors screened in duplicate and inde-
pendently the full texts for eligibility based on types of partic-
ipants, exposures, and outcome measures. The authors resolved
disagreements by discussion and consensus.
For each included study, two authors (CSW, MS) conducted dupli-
cate and independent extraction of data on study methods (study
design and time period), participant characteristics (sample size,
location, population demographics, and risk characteristics), in-
terventions (method for assessing circumcision status, and preva-
lence of circumcision), outcomes (HIV or STI incidence or preva-
lence, measures of effect and their 95% CI, adverse effects, and
methods used to diagnose HIV infection), and other notes. The
two authors (CSW, MS) then assessed the possibility of bias in
included studies by evaluating the adequacy of the methods used
to ascertain circumcision status and outcomes, the handling of
confounding, and the completeness of outcome data. The authors
resolved disagreements by discussion and consensus.
We calculated the natural logarithm of the odds ratio and its stan-
dard error for each study. We then expressed each study result as
an odds ratio (OR) with its 95% CI using inverse variance. We
examined statistical heterogeneity between studies using the chi-
square test of homogeneity and the Higgins I2 statistic (Higgins
2003). Due to the variation in study designs (i.e. cohort, case-con-
trol, and cross-sectional), we decided to combine the study results
using the random-effects method; irrespective of whether there
was significant statistical heterogeneity or not. We conducted a
subgroup analysis to explore the cause of significant statistical het-
erogeneity in study results, with subgroups defined by predomi-
nant role during sexual intercourse.
R E S U L T S
Description of studies
See: Characteristics of included studies; Characteristics of excluded
studies; Characteristics of ongoing studies.
The search yielded 320 records, 56 of which were judged to be
potentially eligible by at least one reviewer. Following independent
duplicate screening of the full-text of each of the potentially eligible
8Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

records, we included 21 primary studies which were reported in
30 separate publications. Among the other 26 potentially eligible
records is an ongoing RCT being conducted among MSM in 8
cities in China by the National Center for AIDS/STD Control and
Prevention, China CDC (MSM Trial 2010). We provide a more
detailed describtion of this study in the table of Characteristics of
ongoing studies.
The 21 included studies with a total of 71,693 participants are
all observational: 6 cohort (Buchbinder 2005; Bartholow 2006;
Buchbinder 2007; Templeton 2009; Gust 2010; Jameson 2010),
1 case-control (Calzavara 2007), and 14 cross-sectional (Kreiss
1993; Reid 2001; Kumta 2002; Tabet 2002; Lai 2004; Millett
2007 (Black); Millet 2007 (Latino); Mor 2007; Reisen 2007;
Sanchez 2007; Xu 2007; Begley 2008; McDaid 2010; Lane 2011)
studies. One study (Mor 2007) reported STI data separately for
HIV-positive (Mor 2007 (HIV-pos)) and HIV-negative partici-
pants (Mor 2007 (HIV-neg)), and the latter are treated as sepa-
rate studies in the STI meta-analyses. Another study (Templeton
2009) reported STI data separately for the baseline and prospec-
tive components of the study (Templeton 2009 (CS); Templeton
2009 (P)) respectively; and these are also treated as separate studies
in the analyses. A detailed description of each included study is
provided in the table of Characteristics of included studies.
Each of the remainining 25 records (Beyrer 2010; Botros 2009;
Coplan 1996; Dandona 2008; Fankem 2008; Farr 2010; Grulich
2001; Jewkes 2006; Jin 2010; Jozkowski 2010; Kloos 2007;
Lafferty 1997; Lau 2010; MacDonald 2008; McKinney 2008;
Millet 2008; Perisse 2009; Sanchez 2011; Smith 2010; Sullivan
2007; Templeton 2010; Thornton 2009; Vermund 2008; Wei
2010) was excluded either because the (primary) study does not
report analysable data or because it is a review article, view point
or editorial with no relevant primary data. We provide detailed
reasons for excluding each of these publications in the table of
Characteristics of excluded studies.
Risk of bias in included studies
All the included studies, as indicated earlier, were observational in
nature. In six studies, circumcision status was assessed by genital
examination while in the remaining 15 it was assessed by self-
report. We judged the ascertainment of outcomes in 18 studies
to be adequate because the HIV or STI status was determined
by appropriate laboratory diagnostic tests; and we presume that
the laboratory technicians did not know the circumcision status
of the participants. Ascertainment of outcomes in the remaining
three studies was judged to be inadequate because HIV status
was assessed by self-report. Attrition and exclusions from analyses
were minimal and we, therefore, judged that incomplete outcome
data were adequately addressed by all studies. However, given the
observational nature of the studies there might be other factors
that confound the relationship between male circumcision and
HIV. We therefore agreed that none of the studies was free of other
sources of bias.
We provide a summary of the methodological quality for the in-
cluded studies in Figure 1 and Figure 2.
Figure 1. Risk of bias graph: review authors’ judgements about each risk of bias item presented as
percentages across all included studies.
9Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 2. Risk of bias summary: review authors’ judgements about each risk of bias item for each included
study.
10Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Effects of interventions
See: Summary of findings for the main comparison Male
circumcision for prevention of HIV and other STIs among men
who have sex with men and transgender people
HIV infection
The main analysis found no significant association between male
circumcision status and HIV infection in men who have sex with
men (Analysis 1.1: 20 studies with 65,784 participants; OR 0.86,
95% CI 0.70 to 1.06). However, there was significant statistical
heterogeneity in study results (P = 0.003, I² = 53%).
The inconsistency in study results seemed to be explained by sexual
roles during anal sex (Analysis 1.2). There was a statistically sig-
nificant decrease in HIV infection in studies of circumcised men
who reported a predominantly or exclusively insertive role during
anal sex: 7 studies with 3465 participants (Calzavara 2007; Reisen
2007; Sanchez 2007; Templeton 2009; Jameson 2010; McDaid
2010; Lane 2011) (OR 0.27, 95% CI 0.17 to 0.44; I² = 0%). In
contrast, there was no statistically significant association between
male circumcision status and HIV infection in studies of men who
reported mainly a receptive role during anal sex (3 studies with
1792 participants; OR 1.20, 95% CI 0.63 to 2.29; I² = 0%), and
in studies in which the differentiation between men who reported
insertive versus receptive role was not clear or was not done (17
studies, 64,538 participants; OR 1.00, 95% CI 0.92 to 1.09; (P
= 0.90); I² = 0%).
Other sexually transmitted infections
There was no significant association (Analysis 1.3) between male
circumcision and acquisition of syphilis (8 studies; 34,999 partic-
ipants: OR 0.96, 95% CI 0.82 to 1.13; Chi² = 2.54, df = 7 (P
= 0.92); I² = 0%), herpes simplex virus 1 (2 studies, 2740 par-
ticipants; OR 0.90, 95% CI 0.53 to 1.52; Chi² = 0.11, df = 1
(P = 0.74); I² = 0%), or herpes simplex virus 2 (5 studies;10,285
participants; OR 0.86, 95% CI 0.62 to 1.21; Chi² = 0.48, df = 4
(P = 0.98); I² = 0%).
Adverse effects associated with circumcision
None of the included studies reported this outcome.
D I S C U S S I O N
Summary of main results
Current evidence suggests that male circumcision may be protec-
tive among MSM who practice primarily insertive anal sex, but
the role of male circumcision overall in the prevention of HIV and
other sexually transmitted infections among MSM remains to be
determined. Adverse effects of male circumcision have not been
studied among MSM but potentially include risk compensation,
surgical complications, pain, and stigma (if circumcision is offered
only to MSM).
Overall completeness and applicability ofevidence
The strength of this systematic review lies in the large number of
study participants and our adherence to the standardised guide-
lines on the conduct and reporting of systematic reviews (Higgins
2011; Moher 2009). However, there are limitations to our finding
that male circumcision conferred significant benefit among men
who primarily or exclusively practised insertive anal sex including
the low quality of data in the studies and the observational rather
than experimental nature of the studies. In addition, most MSM
who become infected are likely infected through receptive rather
than insertive anal sex so the impact of circumcision in this pop-
ulation may not be substantial. Furthermore, circumcision status
and predominant role during sexual intercourse were self-reported
by study participants. To the effect that these were mis-reported,
the findings from the individual studies could be biased. However,
Templeton and colleagues have found self-report to be a valid mea-
sure of circumcision status in a group of predominantly Anglo gay-
community-attached men in Sydney, Australia (Templeton 2008).
RCTs are the “gold standard” for testing the effects of an interven-
tion, but there are several concerns with conducting RCTs to assess
the effects of male circumcision on HIV acquisition in MSM. First,
the only subgroup of MSM who would plausibly gain benefit are
the “insertive” MSM (as shown in our subgroup analysis). Second,
most MSM are “versatile” and there are some studies suggesting
that a minority of MSM predominantly practice the insertive role
(Calzavara 2007; Reisen 2007; Sanchez 2007; Templeton 2009;
Jameson 2010; McDaid 2010; Lane 2011). Thus, huge numbers
of participants with low baseline circumcision prevalence and high
incidence of HIV would be needed for an adequately powered
RCT to answer this question definitely. Despite these difficulties,
we have found a registered ongoing RCT being conducted among
MSM in 8 cities in China.
There are also significant concerns with the feasibility of imple-
menting adult male circumcision among men who have sex with
men. First, significant resources are needed for introduction of
the surgical services in settings where male circumcision is not a
standard intervention. Second, there are concerns about discrim-
11Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

ination and stigma within an already stigmatised population such
as men who have sex with men.
Protective benefits of male circumcision could be weakened by
risk compensation i.e. increases in unsafe sexual behaviour such as
non-use of condoms and multiple concurrent sex partners, sparked
by decreases in perceived risk (Cassell 2006). In addition, having
sex shortly after circumcision (during the wound healing process)
could increase the risk of HIV infection. These risks are not limited
to men who have sex with men, but are potential adverse effects
associated with male circumcision.
Quality of the evidence
In making healthcare decisions, policymakers, patients and clini-
cians should be influenced not only by the best estimates of the ex-
pected advantages and disadvantages of alternative strategies, but
also by their confidence in these estimates i.e. the quality of the
evidence. We used the GRADE system (Guyatt 2011) to assess
quality of evidence. GRADE provides a structured and transpar-
ent system for making judgements about the quality of evidence.
Overall, the quality of the available evidence on the effect of male
circumcision on HIV or STI acquisition in men who have sex
with men is low; as shown in Summary of findings for the main
comparison. The implication of the low quality of the evidence
is that further research (especially randomised controlled trials)
on this topic is very likely to have an important impact on our
confidence in the estimate of effect and is likely to change the
pooled odd ratios found in this review.
The subgroup effect meets some but not all of the methodological
criteria for believability (Sun 2010). It is plausible, consistent, and
is the only one that we hypothesised and explored. However, the
effect is suggested by a comparison between rather than within
studies, and we do not have a formal interaction test for the sub-
group effect.
Potential biases in the review process
We minimised bias in the process of conducting and reporting the
current review by adhering to standardised international guidelines
(Higgins 2011; Moher 2009).
Agreements and disagreements with otherstudies or reviews
The most comprehensive previous systematic review was published
by Millett and colleagues in 2008 (Millet 2008). These authors
pooled the published and unpublished observational studies avail-
able by February 2008 and found insufficient evidence that male
circumcision prevents acquisition of HIV or other sexually trans-
mitted infections in men who have sex with men. Our findings
are consistent with theirs. However, our systematic review has the
added advantage of subgroup analysis by sexual positioning dur-
ing anal sex and inclusion of more recent data.
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
Subgroup analysis suggests that male circumcision may be more
effective among MSM with mainly an insertive role in anal sex,
but the overall role of male circumcision in the prevention of HIV
and other sexually transmitted infections among MSM remains
to be determined. Therefore, there is not enough evidence to rec-
ommend male circumcision for HIV prevention among men who
have sex with men at present. However, in settings where adult
male circumcision is being scaled up, men who have sex with men
should not be excluded from the circumcision programmes. In
other settings, individual men who have sex with men who request
circumcision should not be denied this intervention.
Implications for research
Further research (especially RCTs) is needed to examine the ef-
fect of adult male circumcision for prevention of HIV and STI
acquisition among men who have sex with men. Such studies will
better inform if they include data on the predominant role (in-
sertive or receptive) during sexual intercourse. Further disaggre-
gation regarding the various groups of MSM (e.g. bisexual, exclu-
sively MSM) may be valuable. However, there are several concerns
with conducting RCTs to assess the effects of male circumcision on
HIV acquisition in MSM. First, the only subgroup of MSM who
would plausibly gain benefit are the “insertive” MSM. Second,
most MSM are “versatile” and there are some studies suggesting
that a minority of MSM predominantly practice the insertive role.
Thus, huge numbers of participants with low baseline circumci-
sion prevalence and high incidence of HIV would be needed for
an adequately powered RCT to answer this question definitely.
A C K N O W L E D G E M E N T S
We gratefully acknowledge the support obtained from the HIV/
AIDS Department at WHO Headquarters and the contribution
of the Cochrane HIV/AIDS Group editorial base in the comple-
tion of this review. In addition, we are grateful to four enthusi-
astic anonymous referees who reviewed an earlier version of the
manuscript and provided very useful comments and suggestions.
12Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

R E F E R E N C E S
References to studies included in this review
Bartholow 2006 {published data only}
Bartholow BN, Vamshidar G, Ackers M, et a.
Demographicand behavioral contextual risk groups
amongmen who have sex with men participating in a
phase 3HIV vaccine efficacy trial: implications for HIV
preventionand behavioral/biomedical intervention trials.. J
AcquirImmune Defic Syndr 2006;43:594–602.
Begley 2008 {published data only}
Begley E, Jafa K, Voetsch A, Heffelfinger J, SullivanPS.
Willingness of men who have sex with men in theUS to
be circumcised as adults to reduce risk of HIVinfection
[abstract 983]. Poster abstract presented at:14th Conference onRetroviruses and OpportunisticInfections; February 3-7, 2007;
Boston, MA. http://www.retroconference.org/2007/Abstracts/28594.htm.∗ Begley EB, Jafa K, Voetsch AC, Heffelfinger JD, Borkowf
CB, et al.Willingness of Men Who Have Sex with Men
(MSM) in the United States to Be Circumcised as Adults to
Reduce the Risk of HIV Infection. PLoS One 2008;3(7):
e2731. doi:10.1371/journal.pone.0002731.
Buchbinder 2005 {published data only}
Buchbinder SP, Vittinghoff E, Heagerty PJ, et al.Sexual risk,
nitrile inhalant use, and lack of circumcision associated with
HIV seroconversion in men who have sex with men in the
United States. J Acquir Immune Defic Syndr 2005;39:82-89.
Buchbinder 2007 {published data only}∗ Buchbinder S. STEP Trial: exploring hypotheses
for differential HIV acquisition rates. HIV VaccinesTrialNetwork Conference; November 12, 2007; Seattle,WA.
http://www.hvtn.org/fgm/1107slides/Buchbinder.pdf.Buchbinder SP, Mehrotra DV, Duerr A, Fitzgerald DW,
Mogg R, et al.Efficacy assessment of a cell-mediated
immunity HIV-1 vaccine (the Step Study): a double-
blind, randomised, placebo-controlled, test-of-concept trial.
Lancet 2008;372:1881–93.
Calzavara 2007 {published data only}
Calzavara LM, Remis R, Myers T, Polaris StudyTeam.
Circumcision and HIV/STI among men who have sex
with men (MSM) in the Polaris HIV seroconversion study
[abstract 0100]. Abstract presented at: the16th AnnualCanadian Association for HIV Research;April 24-27, 2007;
Toronto, Ontario, Canada.
Gust 2010 {published data only}
Gust DA, Wiegand RE, Kretsinger K, et al.Circumcision
status and HIV infection among MSM: reanalysis of a Phase
III HIV vaccine clinical trial. AIDS 2010, 24:1135-1143
2010;24:1135–43.
Jameson 2010 {published data only}
Jameson DR, Celum CL, Manhart L, Menza TW, Golden
MR. The association between lack of circumcision and
HIV, HSV-2, and other sexually transmitted infections
among men who have sex with men. Sex Transm Dis 2010;
37:147–52.
Kreiss 1993 {published data only}
Kreiss JK, Hopkins SG. The association between
circumcision status and human immunodeficiency virus
infection among homosexual men. J Infect Dis 1993;168:
1404-08.
Kumta 2002 {published data only}
Kumta S, Setia M, Jerjani HR, Mathur MS, RaoKavi A,
Lindan CP. Men who have sex with men (MSM) and male-
to-female transgender (TG) in Mumbai: a critical emerging
risk group for HIV and sexually transmitted infections
(STI) in India [abstract TuOrC1149]. 14th International
AIDS Conference; 7-12 July 2002; Barcelona, Spain.
Lai 2004 {published data only}
Lai SF, Hong CP, Lan YC, et al.Molecular epidemiology of
HIV-1 in men who have sex with men from gay saunas in
Taiwanfrom 2000 to 2003 [abstract WePeC6097]. 15th
International AIDS Conference; 11-16 July 2004; Bangkok,
Thailand..
Lane 2011 {published data only}
Lane T, Raymond HF, Dladla S, et al.High HIV prevalence
among men who have sex with men in Soweto, South
Africa: results from the Soweto Mens Study. AIDS Behav
2009;Aug 7 [Epub ahead of print].∗ Lane T, Raymond HF, Dladla S, et al.High HIV
prevalence among men who have sex with men in Soweto,
South Africa: results from the Soweto Mens Study. AIDS
Behav 2011;15:626-34.
Lane T, Raymond HF, Dladla S, et al.Lower risk of hiv
infection among circumcised MSM: results from the Soweto
Men’s Study [Abstract No. MOPDC105]. 5th International
AIDS Society Conference on HIV Pathogenesis and
Treatment; 19-22 July 2009; Cape Town, South Africa.
McDaid 2010 {published data only}
McDaid LM, Weiss HA, Hart GJ. Circumcision among
men who have sex with men in Scotland: limited potential
for HIV prevention. Sex Transm Infect 2010;86:404–06.
Millet 2007 (Latino) {published data only}
Millett GA, Ding H, Lauby J, et al.Circumcision status and
HIV infection among black and Latino men who have sex
with men in 3 US cities. J Acquir Immune Defic Syndr 2007;
46:643–50.
Millett 2007 (Black) {published data only}
Millett GA, Ding H, Lauby J, et al.Circumcision status and
HIV infection among black and Latino men who have sex
with men in 3 US cities. J Acquir Immune Defic Syndr 2007;
46:643–50.
Mor 2007 {published data only}
Mor Z, Kent CK, Kohn RP, Klausner JD. Declining rates in
male circumcision amidst increasing evidence of its public
health benefit. PLoS One 2007;2(9):e861. doi:10.1371/
journal.pone.0000861.
13Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Mor 2007 (HIV-neg) {published data only}
Mor Z, Kent CK, Kohn RP, Klausner JD. Declining rates
in male circumcision amidst increasing evidence of its
public health benefit. PLoS One 2007;2(9):doi:10.1371/
journal.pone.0000861.
Mor 2007 (HIV-pos) {published data only}
Mor Z, Kent CK, Kohn RP, Klausner JD. Declining rates in
male circumcision amidst increasing evidence of its public
health benefit.. PLoS One 2007;2(9):e861. doi:10.1371/
journal.pone.0000861..
Reid 2001 {published data only}
Reid D, Weatherburn P, Hickson F, Stephens M. Know
the score: findings from a national gay men’s sex survey
2001: September 2002. http://www.sigmaresearch.org.uk/
downloads/report02d.pdf (accessed 22 September 2010).
Reisen 2007 {published data only}
Reisen CA, Zea MC, Poppen PJ, Bianchi FT. Male
circumcision and HIV status among Latino immigrant
MSM in New York City. J LGBT Health Res 2007;3:29–36.
Sanchez 2007 {published data only}∗ Sanchez J. Cutting the edge of the HIV epidemic among
MSM. Presented at: The Center for HIV Identification,
Prevention, and Treatment Services (CHIPTS) The Future
Direction of Male Circumcision in HIV Prevention
working conference; April 9, 2007; Los Angeles, CA.
http://chipts.ucla.edu/TEMPMAT/MaleCirc2007/
Sanchez%20LA.pdf (accessed 22 September 2010).
Sanchez J, Lama JR, Peinado J, et al.High HIV and
ulcerative sexually transmitted infection incidence estimates
among men who have sex with men in Peru: awaiting for
an effective preventive intervention. J Acquir Immune Defic
Syndr 2009;51(Suppl 1):S47–S51.
Tabet 2002 {published data only}
Tabet S, Sanchez J, Lama J, et al.HIV, syphilis and
heterosexual bridging among Peruvian men who have sex
with men. AIDS 2002;16:1271–77.
Templeton 2009 {published data only}
Mao L, Templeton DJ, Imrie J, Prestage GP, et al.Does
circumcision make a difference to the sexual experience of
gay men? Findings from the Health in Men (HIM) cohort.
J Sex Med 2008;5:2557–61.∗ Templeton DJ, Jin F, Mao L, et al.Circumcision and risk
of HIV infection in Australian homosexual men. AIDS2009;23:2347–51.
Templeton DJ, Jin F, Prestage G, et al.Circumcision status
and risk of HIV seroconversion in the HIM cohort of
homosexually active men in Sydney [abstract WEAC103].
4th International AIDS Society Conference on HIV
Pathogenesis, Treatment and Prevention; 22-25 July 2007;
Sydney, Australia.
Templeton 2009 (CS) {published data only}∗ Templeton DJ, Jin F, Prestage GP, et al.Circumcision and
risk of sexually transmissible infections in a community-
based cohort of HIV-negative homosexual men in Sydney,
Australia. J Infect Dis 2009;200:1813–19.
Templeton DJ, Jin F, Prestage GP, et al.Circumcision and
risk of sexually transmitted infections in the HIM cohort
of homosexual men in Sydney, Australia[abstract 6]. The
International Society for Sexually Transmitted Disease
Research; 29 July ? 1 August 2007; Seattle, WA.
Templeton 2009 (P) {published data only}∗ Templeton DJ, Jin F, Prestage GP, et al.Circumcision and
risk of sexually transmissible infections in a community-
based cohort of HIV-negative homosexual men in Sydney,
Australia. J Infect Dis 2009;200:1813–19.
Templeton DJ, Jin F, Prestage GP, et al.Circumcision and
risk of sexually transmitted infections in the HIM cohort
of homosexual men in Sydney, Australia [abstract 6]. The
International Society for Sexually Transmitted Disease
Research; 29 July -1 August 2007; Seattle, WA.
Xu 2007 {published data only}
Xu F, Markowitz LE, Sternberg MR, Aral SO. Prevalence
of circumcision and herpes simplex virus type 2 infection
in men in the United States: the National Health and
Nutrition Examination Survey (NHANES), 1999-2004.
Sex Transm Dis 2007;34:479–84.
References to studies excluded from this review
Beyrer 2010 {published data only}
Beyrer C. Global prevention of HIV infection for neglected
populations: men who have sex with men. Clin Infect Dis2010;50 Suppl 3:S108–13.
Botros 2009 {published data only}
Botros BA, Aliyev QM, Saad MD, Michael AA, Sanchez JL,
et al.HIV infection and associated risk factors among long-
distance truck drivers travelling through Azerbaijan. Int JSTD AIDS 2009;20:477–82.
Coplan 1996 {published data only}
Coplan PM, Gortmaker S, Hernandez-Avila M, et
al.Human immunodeficiency virus infection in Mexico
City: rectal bleeding and anal warts as risk factors among
men reporting sex with men. Am J Epidemiol 1996;144:
817–27.
Dandona 2008 {published data only}
Dandona L, Dandona R, Kumar GA, Reddy GB, Ameer
MA, et al.Risk factors associated with HIV in a population-
based study in Andhra Pradesh state of India. Int J Epidemiol
2008;37:1274–86.
Fankem 2008 {published data only}
Fankem SL, Wiysonge CS, Hankins CA. Male circumcision
and the risk of HIV infection in men who have sex with
men. Int J Epidemiol 2008;37:353–55.
Farr 2010 {published data only}
Farr AC, Wilson DP. An HIV epidemic is ready to emerge
in the Philippines. J Int AIDS Soc 2010;13:16.
Grulich 2001 {published data only}
Grulich AE, Hendry O, Clark E, Kippax S, Kaldor JM.
Circumcision and male-to-male sexual transmission of HIV.
AIDS 2001;15:1188–89.
14Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Jewkes 2006 {published data only}
Jewkes R, Dunkle K, Nduna M, Levin J, Jama N, et
al.Factors associated with HIV sero-positivity in young,
rural South African men. Int J Epidemiol 2006;35:1455–60.
Jin 2010 {published data only}
Jin F, Jansson J, Law M, Prestage GP, Zablotska I, et al.Per-
contact probability of HIV transmission in homosexual men
in Sydney in the era of HAART. AIDS 2010;24:907–13.
Jozkowski 2010 {published data only}
Jozkowski K, Rosenberger JG, Schick V, Herbenick D,
Novak DS, Reece M. Relations between circumcision status,
sexually transmitted infection history, and HIV serostatus
among a national sample of men who have sex with men
in the United States. AIDS Patient Care STDS 2010;24:
465–70.
Kloos 2007 {published data only}
Kloos H, Mariam DH. Some neglected and emerging
factors in HIV transmission in Ethiopia. Ethiop Med J2007;45:103–07.
Lafferty 1997 {published data only}
Lafferty WE, Hughes JP, Handsfield HH. Sexually
transmitted diseases in men who have sex with men:
acquisition of gonorrhea and nongonococcal urethritis by
fellatio and implications for STD/HIV prevention. Sex
Transm Dis 1997;24:272–78.
Lau 2010 {published data only}
Lau JT, Yan H, Lin C, Zhang J, Choi KC, et al.How
Willing are Men Who Have Sex with Men in China to
be Circumcised for the Sake of Protecting His Female Sex
Partner?. J Sex Med 2010;Nov 22. doi: 10.1111/j.1743-
6109.2010.02050.
MacDonald 2008 {published data only}
Macdonald A, Humphreys J, Jaffe HW. Prevention of
HIV transmission in the UK: what is the role of male
circumcision?. Sex Transm Infect 2008;84:158–60.
McKinney 2008 {published data only}
McKinney CM, Klingler EJ, Paneth-Pollak R, Schillinger
JA, Gwynn RC, Frieden TR. Prevalence of adult male
circumcision in the general population and a population at
increased risk for HIV/AIDS in New York City. Sex TransmDis 2008;35:814–47.
Millet 2008 {published data only}
Millett GA, Flores SA, Marks G, Reed JB, Herbst
JH. Circumcision status and risk of HIV and sexually
transmitted infections among men who have sex with men:
a meta-analysis. JAMA 2008;300:1674–84.
Perisse 2009 {published data only}
Périssé AR, Schechter M, Blattner W. Association between
male circumcision and prevalent HIV infections in Rio
de Janeiro, Brazil. J Acquir Immune Defic Syndr 2009;50:
435–37.
Sanchez 2011 {published data only}
Sánchez J, Sal Y Rosas VG, Hughes JP, Baeten JM, Fuchs J,
et al.Male circumcision and risk of HIV acquisition among
MSM. AIDS 2011;25:519–23.
Smith 2010 {published data only}
Smith DK, Taylor A, Kilmarx PH, Sullivan P, Warner L, et
al.Male circumcision in the United States for the prevention
of HIV infection and other adverse health outcomes: report
from a CDC consultation. Public Health Rep 2010;125
Suppl 1:72–82.
Sullivan 2007 {published data only}
Sullivan PS, Kilmarx PH, Peterman TA, Taylor AW,
Nakashima AK, et al.Male circumcision for prevention
of HIV transmission: what the new data mean for HIV
prevention in the United States. PLoS Med 2007;4:e223.
Templeton 2010 {published data only}
Templeton DJ, Millett GA, Grulich AE. Male circumcision
to reduce the risk of HIV and sexually transmitted infections
among men who have sex with men. Curr Opin Infect Dis
2010;23:45-52.
Thornton 2009 {published data only (unpublished sought but not
used)}
Lattimore S, Thornton A, Delpech V, Elford J. Changing
patterns of sexual risk behavior among London gay men:
1998-2008. Sex Transm Dis 2011;38:221–29.∗ Thornton A, Lattimore S, Delpech V, Elford J.
Circumcision among men who have sex with men in
London (Abstract No P4.62). 18th Biennial Meeting of
the International Society for STD Research. 28 June - 1
July 2009; London, UK. International Society for STD
Research/British Association for Sexual Health and HIV.
Vermund 2008 {published data only}
Vermund SH, Qian HZ. Circumcision and HIV prevention
among men who have sex with men: no final word. JAMA
2008;300:1698–700.
Wei 2010 {published data only}
Wei C, Raymond HF, McFarland W, Buchbinder S, Fuchs
JD. What Is the Potential Impact of Adult Circumcision on
the HIV Epidemic Among Men Who Have Sex With Men
in San Francisco?. Sex Transm Dis 2010;Nov 16 [Epub
ahead of print].
References to ongoing studies
MSM Trial 2010 {published data only}
National Center for AIDS/STD Control and Prevention,
China CDC. A community-based, randomized controlled
trial to evaluate the efficacy of comprehensive HIV/STIs
intervention among men who have sex with men in 8 cities
in China. http://clinicaltrials.gov/show/NCT01068015
(accessed 09 May 2011).
Additional references
Auvert 2001
Auvert B, Buvé A, Lagarde E, Kahindo M, Chege J,
Rutenberg N, et al.Male circumcision and HIV infection in
four cities in sub-Saharan Africa. AIDS 2001;15:S31–S40.
Auvert 2005
Auvert B, Taljaard D, Lagarde E, Sonbngwi-Tambekou J,
Sitta R, Puren A. Randomized, controlled intervention trial
15Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

of male circumcision for reduction of HIV infection risks:
The ANRS 1265 Trial. PLoS Med 2005;2(11):e298.
Baeten 2005
Baeten JM, Richardson BA, Lavreys L, Rakwar JP,
Mandaliya K, Bwayo JJ, Kreiss JK. Female-to-male
infectivity of HIV-1 among circumcised and uncircumcised
Kenyan men. JID 2005;191:546–553.
Bailey 2007
Bailey RC, Moses S, Parker CB, Agot K, Maclean I, Krieger
JN, et al.Male circumcision for HIV prevention in young
men in Kisumu, Kenya: a randomised controlled trial.
Lancet 2007;369:643–656.
Cassell 2006
Cassell MM, Halperin DT, Shelton JD, Stanton D. Risk
compensation: the Achilles’ heel of innovations in HIV
prevention?. BMJ 2006;332:605-07.
Drain 2004
Drain PK, Smith JS, Hughes JP, Halperin DT, Holmes KK.
Correlates of national HIV seroprevalence. An ecologic
analysis of 122 developing countries. J Acquir Immune Defic
Syndr 2004;35:407–420.
Fink 1986
Fink AJ. A possible explanation for heterosexual male
infection with AIDS. N Engl J Med 1986;315(18):1167.
Gray 2007
Gray RH, Kigozi G, Serwadda D, Makumbi F, Watya S,
Nalugoda F, et al.Male circumcision for HIV prevention in
men in Rakai, Uganda: a randomised trial. Lancet 2007;
369:657–666.
Guyatt 2011
Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, et
al.GRADE guidelines: Introduction-GRADE evidence
profiles and summary of findings tables.. J Clin Epidemiol
2011;64:383–94.
Hall 2008
Hall HI, Song R, Rhodes P, Prejean J, An Q, et al.Estimation
of HIV incidence in the United States. JAMA 2008;300:
520–29.
Higgins 2003
Higgins JP, Thompson SG, Deeks JJ, Altman DG.
Measuring inconsistency in meta-analyses. BMJ 2003;327:
557–560.
Higgins 2011
Higgins JPT, Green S (editors). Cochrane Handbook forSystematic Reviews of Interventions Version 5.1.0 [updated
March 2011]. The Cochrane Collaboration, 2011.
Available from www.cochrane–handbook.org.
Koblin 2006
Koblin BA, Husnik MJ, Colfax G, Huang Y, Madison M,
Mayer K, et al.Risk factors for HIV infection among men
who have sex with men. AIDS 2006;20:731–39.
Le Vu 2010
Le Vu S, Le Strat Y, Barin F, Pillonel J, Cazein F, et
al.Population-based HIV-1 incidence in France, 2003-08: a
modelling analysis. Lancet Infect Dis 2010;10:682–87.
Moher 2009
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA
Group. Preferred reporting items for systematic reviews and
meta-analyses: the PRISMA statement. PLoS Med 2009 Jul
21;6(7):e1000097.
Moses 1990
Moses S, Bradley JE, Nagelkerre NJD, Ronald AR, Ndinya-
Achola JA, Plummer FA. Geographical patterns of male
circumcision practices in Africa: association with HIV
seroprevalence. Int J Epidemiol 1990;19:693–697.
O’Farrell 2000
O’Farrell N, Egger M. Circumcision in men and the
prevention of HIV infection: a ’meta-analysis’ revisited. IntJ STD & AIDS 2000;11:137–142.
Siegfried 2009
Siegfried N, Muller M, Deeks JJ, Volmink J. Male
circumcision for prevention of heterosexual acquisition
of HIV in men. Cochrane Database of Systematic Reviews
2009, Issue 2. Art. No.: CD003362. DOI: 10.1002/
14651858.CD003362.pub2.
Sun 2010
Sun X, Briel M, Walter SD, Guyatt GH. Is a subgroup effect
believable? Updating criteria to evaluate the credibility of
subgroup analyses. BMJ 2010;340:c117.
Templeton 2008
Templeton DJ, Mao L, Prestage GP, Jin F, Kaldor JM,
Grulich AE. Self-report is a valid measure of circumcision
status in homosexual men. Sex Transm Infect 2008;84:
187–88.
UNAIDS 2008
UNAIDS. Report on the global AIDS epidemic-2008.
Geneva: Joint United Nations Programme on HIV/AIDS,
2008.
Weiss 2000
Weiss HA, Quigley MA, Hayes RJ. Male circumcision and
risk of HIV infection in sub-Saharan Africa: a systematic
review and meta-analysis. AIDS 2000;14:2361–2370.∗ Indicates the major publication for the study
16Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Bartholow 2006
Methods Prospective study.
Duration of enrolment: June 1998 to November 1999.
Participants 5,095 HIV-seronegative MSM, 18 to 60 years of age. enrolled in a 36-month phase 3
HIV vaccine efficacy trial (VAX004 trial) across 61 sites primarily in North America and
Europe.
Whites 86%, Hispanic 6%, Black 4%, Asian 2%, Other 2%. High school 37%, college
graduate 42%, graduate degree 22%.
Interventions Male circumcision status assessed by self-report. 4381(86%) men were circumcised.
Outcomes HIV status established by ELISA test and confirmed using immunoblot kits.
Notes The VAX004 trial was a randomised, double-blind, placebo-controlled efficacy trial of a
bivalent rgp120 HIV-1 subtype B vaccine and was conducted at 61 sites in the United
States (n = 57), Canada (n = 3), and The Netherlands (n = 1).
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Unclear risk Male circumcision status assessed by self-
report
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk HIV status was determined by appropriate
diagnostic tests, and we presume the lab-
oratory technicians did not know the cir-
cumcision status of the participants.
Incomplete outcome data (attrition bias)
All outcomes
Low risk The authors report findings on 5090
(99.9%) participants.
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
17Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Begley 2008
Methods Cross-sectional study.
Duration of enrolment: June to October 2006.
Participants 780 HIV-positive who were interviewed at 7 Gay Pride events in 2006 in 7 US cities
(170 at minority Gay Pride events in Chicago, IL, Charlotte, NC, and St. Louis, MO,
and 609 at Gay Pride events in Birmingham, AL, Anchorage, AK, Raleigh-Durham,
NC, and Springdale, UT)
Of the 780, 43 were Hispanic, 198 non-Hispanic Black, 436 non-Hispanic White, and
103 others.
Interventions Male circumcision status assessed by self-report. 667 (86%) men were circumcised.
Outcomes HIV status assessed by self-report
Notes 914 men met definition of MSM. Authors excluded 100 respondents because they were
HIV-positive; an additional 31 respondents were excluded due to missing demographic or
risk characteristics. The authors report findings on 780 (75%) eligible survey respondents
who met their definition of MSM, who were not HIV-positive by self-report, and who
provided complete survey data. 83% circumcised.
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Unclear risk Male circumcision status assessed by self-
report
Blinding of outcome assessment (detection
bias)
All outcomes
Unclear risk HIV status assessed by self-report
Incomplete outcome data (attrition bias)
All outcomes
Low risk The authors report findings on all 780
(75%) eligible survey respondents who met
their definition of MSM, who self-iden-
tified as HIV-negative by self-report, and
who provided complete survey data.
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
18Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
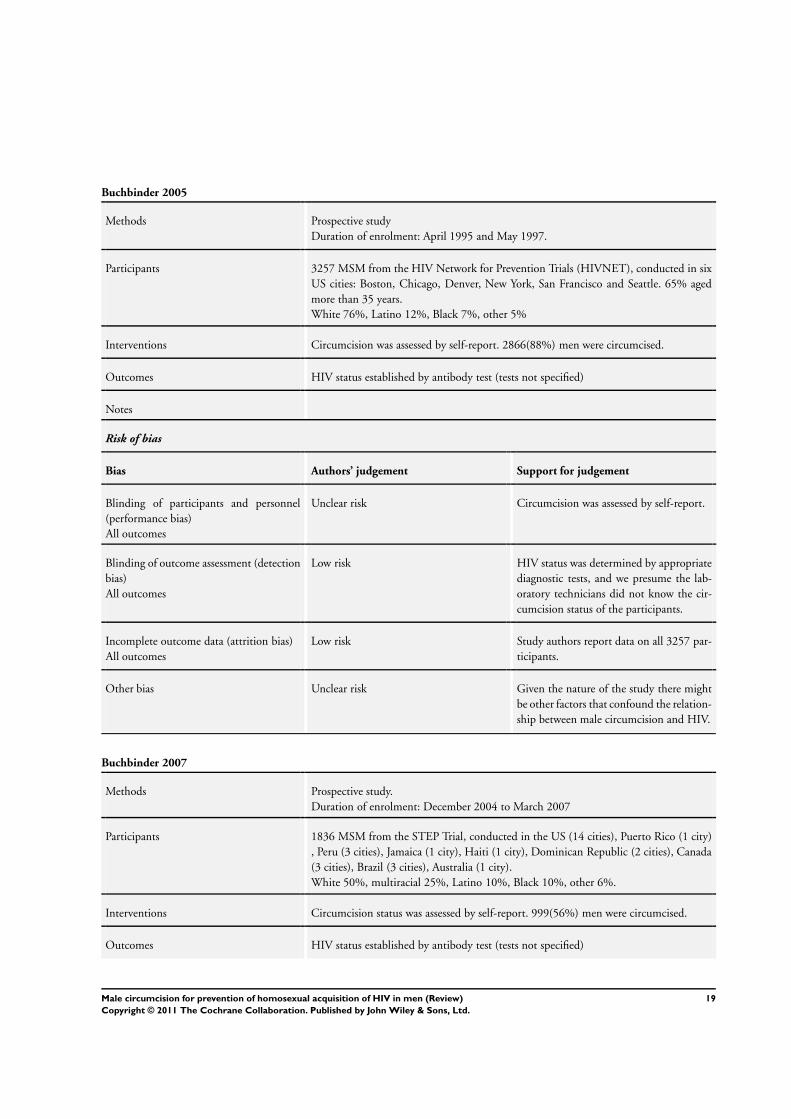
Buchbinder 2005
Methods Prospective study
Duration of enrolment: April 1995 and May 1997.
Participants 3257 MSM from the HIV Network for Prevention Trials (HIVNET), conducted in six
US cities: Boston, Chicago, Denver, New York, San Francisco and Seattle. 65% aged
more than 35 years.
White 76%, Latino 12%, Black 7%, other 5%
Interventions Circumcision was assessed by self-report. 2866(88%) men were circumcised.
Outcomes HIV status established by antibody test (tests not specified)
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Unclear risk Circumcision was assessed by self-report.
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk HIV status was determined by appropriate
diagnostic tests, and we presume the lab-
oratory technicians did not know the cir-
cumcision status of the participants.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Study authors report data on all 3257 par-
ticipants.
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
Buchbinder 2007
Methods Prospective study.
Duration of enrolment: December 2004 to March 2007
Participants 1836 MSM from the STEP Trial, conducted in the US (14 cities), Puerto Rico (1 city)
, Peru (3 cities), Jamaica (1 city), Haiti (1 city), Dominican Republic (2 cities), Canada
(3 cities), Brazil (3 cities), Australia (1 city).
White 50%, multiracial 25%, Latino 10%, Black 10%, other 6%.
Interventions Circumcision status was assessed by self-report. 999(56%) men were circumcised.
Outcomes HIV status established by antibody test (tests not specified)
19Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Buchbinder 2007 (Continued)
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Unclear risk Circumcision status was assessed by self-
report.
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk HIV status was determined by appropriate
diagnostic tests, and we presume the lab-
oratory technicians did not know the cir-
cumcision status of the participants.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Study authors report data on 1787 (97%)
participants.
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
Calzavara 2007
Methods Case-control study
Duration of enrolment: 2001 to 2005.
Participants 165 MSM enrolled in the Polaris cohort in Ontario, Canada. Participants in this study
are recruited through Ontario’s HIV diagnostic testing database, physicians, community
organizations and media.
White 85%, Latino 4%, Native American 2%, other 9%
Interventions Circumcision status was assessed by self-report. 11(73%) men were circumcised.
Outcomes HIV status established by diagnostic test (tests not specified).
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Unclear risk Circumcision was assessed by self-report.
20Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Calzavara 2007 (Continued)
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk HIV status was determined by appropriate
diagnostic tests, and we presume the lab-
oratory technicians did not know the cir-
cumcision status of the participants.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Study authors report data on all 165 par-
ticipants.
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
Gust 2010
Methods Prospective study
Duration of enrolment: June 1998 to October 1999.
Participants 4,889 MSM (median age 36.8 years) who participated in the VAXGen VAX004 HIV
vaccine clinical trial, which was conducted in 61 sites primarily in North America and
Europe.
Whites 86%, Hispanic 6%, Black 4%, Asian 2%, Other 2%. High school 37%, college
graduate 42%, graduate degree 22%.
Interventions Male circumcision status assessed by self-report. 4209(86%) men were circumcised.
Outcomes HIV status established by ELISA test and confirmed using immunoblot kits.
Notes The VaxGen VAX004 was a randomized, double-blind, placebo-controlled efficacy trial
of an HIV vaccine (bivalent rgp120 HIV-1 subtype B). It was carried out at 61 sites (US:
n=57, Canada: n=3; The Netherlands: n=1).
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Unclear risk Circumcision was assessed by self-report.
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk HIV status was determined by appropriate
diagnostic tests, and we presume the lab-
oratory technicians did not know the cir-
cumcision status of the participants.
Incomplete outcome data (attrition bias)
All outcomes
Low risk A total of 5417 participants enrolled in the
study. Removed from the analysis were 309
women, 13 men who were indicated by
21Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Gust 2010 (Continued)
nucleic acid testing to be HIV-infected at
baseline, 1 participant who reported a sex
change, and 5 whose circumcision status
changed during the study. The final num-
ber of participants for this analysis, which
excluded 200 participants who only at-
tended the baseline visit, was 4889. Of
participants in the analysis, 80.2% (3921/
4889) were recorded as completing the
study.
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
Jameson 2010
Methods Prospective study.
Duration of enrolment: October 2001 to May 2006.
Participants 3,828 MSM attending the Public Health-Seattle and King County STD clinic, who
reported anal intercourse in the previous 12 months. 75.7% older than 25 years.
Whites 74.5%, Hispanic 7.9%, Black 6.5%, Asian and Pacific Islander 5.4%, Other
4.8%.
Interventions Clinicians determined circumcision status by examination. 3241(85%) men were cir-
cumcised.
Outcomes HIV status established by ELISA test and confirmed using independently-validated,
quantitative,
real-time polymerase chain reaction assay.
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Circumcision was assessed by clinical ex-
amination.
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk HIV status was determined by appropriate
diagnostic tests, and we presume the lab-
oratory technicians did not know the cir-
cumcision status of the participants.
22Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Jameson 2010 (Continued)
Incomplete outcome data (attrition bias)
All outcomes
Low risk Of 4,749 men who visited the clinic during
the study, circumcision status was not as-
sessed or was inconsistently noted for 729
men (15%), and anal sexual repertoire was
incomplete for an additional 192 men (4%)
; the authors excluded these men from fur-
ther analysis. Participants whose circumci-
sion status was not noted were similar to
those whose status was noted .
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
Kreiss 1993
Methods Cross-sectional study.
Duration of enrolment: April 1989 and March 1991.
Participants Men, 17 to 64 years old, reporting a history of homosexual behaviour and attending
any of two AIDS clinic or AIDS Prevention Project (in Seattle, Washington, USA) were
included. 503 men enrolled into the study, (316 HIV-seropositive and 186 seronegative)
. Final analysis included 499 men (97%). 4% Hispanic, 4% non-Hispanic Black, 90%
white, 1% others.
Interventions Circumcision status assessed by self-report. 442(85%) men were circumcised.
Outcomes HIV status established by ELISA test and confirmed by Western Blot or immunofluo-
rescent assays.
Sexually transmitted infections assessed by self-report.
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Unclear risk Circumcision status was assessed by self-
report.
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk HIV status was determined by appropriate
diagnostic tests, and we presume the lab-
oratory technicians did not know the cir-
cumcision status of the participants.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Final analysis included 499 men (97%).
23Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Kreiss 1993 (Continued)
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
Kumta 2002
Methods Cross-sectional study.
Duration of enrolment: March 2001 to July 2002
Participants 122 MSM in Mumbia, India. Ethnicity not reported.
Interventions Male circumcision status assessed by genital examination. 27(22%) men were circum-
cised.
Outcomes HIV status assessed by laboratory test.
Notes This is one of the few studies conducted in a low or middle-income country. 22%
circumcised
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Circumcision status was assessed by clinical
examination.
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk HIV status was determined by appropriate
diagnostic tests, and we presume the lab-
oratory technicians did not know the cir-
cumcision status of the participants.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Information obtained from all study par-
ticipants.
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
Lai 2004
Methods Cross-sectional study.
Study conducted in 2003.
Participants 556 MSM in Taipei, Taiwan. Ethnicity not reported.
Interventions Circumcision status assessed by self-report. 154(28%) men were circumcised.
24Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Lai 2004 (Continued)
Outcomes HIV status assessed by laboratory test.
Notes 28% circumcised.
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Unclear risk Circumcision status was assessed by self-
report.
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk HIV status was determined by appropriate
diagnostic tests, and we presume the lab-
oratory technicians did not know the cir-
cumcision status of the participants.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Information obtained from all study par-
ticipants.
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
Lane 2011
Methods Cross-sectional study.
Duration of enrolment: 30 weeks in 2008.
Participants 378 MSM from Soweto, South Africa, were recruited via respondent-driven sampling.
Black 100%, 19% post-secondary education.
Interventions Circumcision status assessed by self-report. 124(34%) men were circumcised.
Outcomes HIV status was determined though rapid antibody testing.
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Unclear risk Circumcision status was assessed by self-
report.
25Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
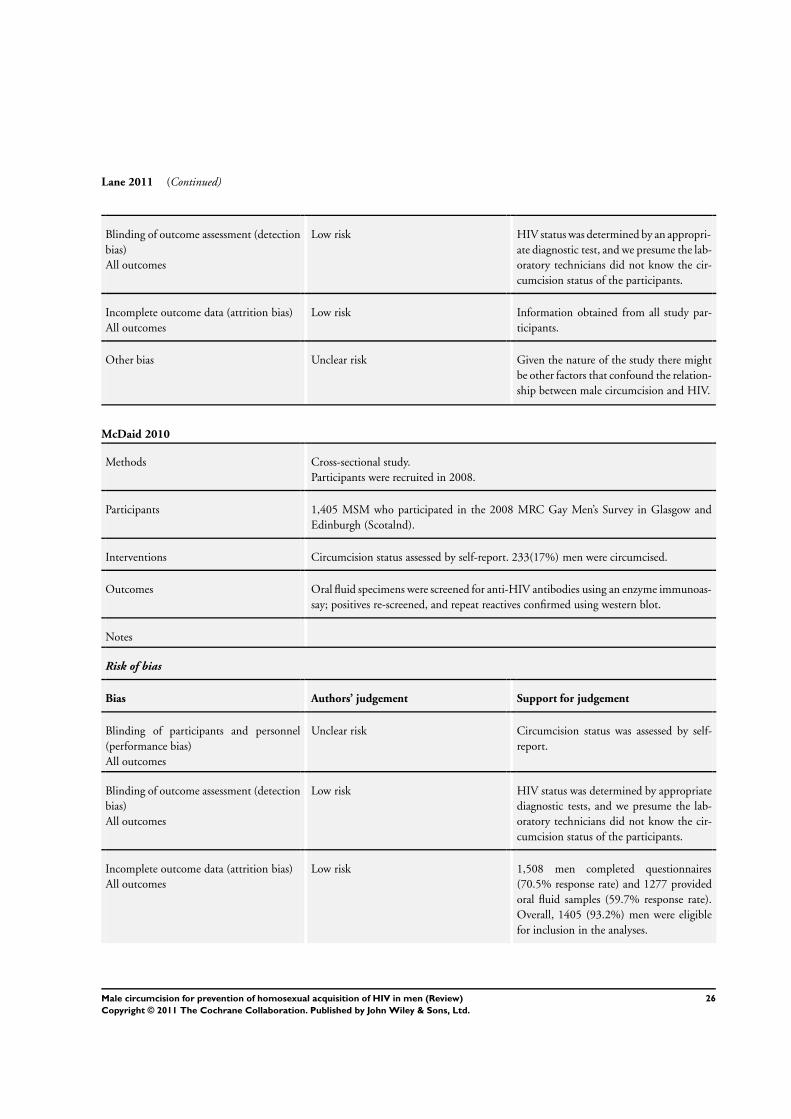
Lane 2011 (Continued)
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk HIV status was determined by an appropri-
ate diagnostic test, and we presume the lab-
oratory technicians did not know the cir-
cumcision status of the participants.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Information obtained from all study par-
ticipants.
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
McDaid 2010
Methods Cross-sectional study.
Participants were recruited in 2008.
Participants 1,405 MSM who participated in the 2008 MRC Gay Men’s Survey in Glasgow and
Edinburgh (Scotalnd).
Interventions Circumcision status assessed by self-report. 233(17%) men were circumcised.
Outcomes Oral fluid specimens were screened for anti-HIV antibodies using an enzyme immunoas-
say; positives re-screened, and repeat reactives confirmed using western blot.
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Unclear risk Circumcision status was assessed by self-
report.
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk HIV status was determined by appropriate
diagnostic tests, and we presume the lab-
oratory technicians did not know the cir-
cumcision status of the participants.
Incomplete outcome data (attrition bias)
All outcomes
Low risk 1,508 men completed questionnaires
(70.5% response rate) and 1277 provided
oral fluid samples (59.7% response rate).
Overall, 1405 (93.2%) men were eligible
for inclusion in the analyses.
26Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

McDaid 2010 (Continued)
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
Millet 2007 (Latino)
Methods Cross-sectional study.
Duration of enrolment: May 2005 to April 2006.
Participants 1,091 Latino MSM were recruited from 3 US cities (New York City, Philadelphia, and
Los Angeles) using respondent-driven sampling.
100% Latino, median age 33.1 years.
Interventions Circumcision status assessed by self-report. 317(33%) men were circumcised.
Outcomes Participants were tested for HIV antibodies using a rapid oral fluid HIV antibody test.
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Unclear risk Circumcision status was assessed by self-
report.
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk HIV status was determined by an appropri-
ate diagnostic test, and we presume the lab-
oratory technicians did not know the cir-
cumcision status of the participants.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Data available on 957 (87.7%) participants
and missing data not related to intervention
or outcome.
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
27Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Millett 2007 (Black)
Methods Cross-sectional study.
Duration of enrolment: May 2005 and April 2006.
Participants 1,154 Black MSM were recruited from 3 US cities (New York City, Philadelphia, and
Los Angeles) using respondent-driven sampling.
100% Black, median age 42.5 years.
Interventions Circumcision status assessed by self-report. 794(74%) men were circumcised.
Outcomes Participants were tested for HIV antibodies using a rapid oral fluid HIV antibody test.
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Unclear risk Circumcision status was assessed by self-
report.
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk HIV status was determined by an appropri-
ate diagnostic test, and we presume the lab-
oratory technicians did not know the cir-
cumcision status of the participants.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Data available on 1,079 (93.5%) partici-
pants and missing data not related to inter-
vention or outcome.
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
Mor 2007
Methods Cross-sectional study.
Duration of enrolment: January 1996 to December 2005.
Participants 20,832 MSM attending the San Francisco municipal STD clinic, California, USA. 7%
non-Hispanic Blak, 10% Asian/Pacific Islander, 16% Hispanic, 66% White.
Interventions Male circumcision status assessed by genital examination. 15,207(73%) men were cir-
cumcised.
Outcomes HIV status assessed by laboratory test. STI status assessed by laboratory test.
Notes 73% circumcised.
28Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Mor 2007 (Continued)
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Circumcision status was assessed by clinical
examination
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk HIV status was determined by appropriate
diagnostic tests, and we presume the lab-
oratory technicians did not know the cir-
cumcision status of the participants.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Information obtained from all participants.
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
Mor 2007 (HIV-neg)
Methods Cross-sectional study.
Duration of enrolment: January 1996 to December 2005.
Participants 20,832 MSM attending the San Francisco municipal STD clinic, California, USA. 7%
non-Hispanic Blak, 10% Asian/Pacific Islander, 16% Hispanic, 66% White.
Interventions Male circumcision status assessed by genital examination. 15,207(73%) men were cir-
cumcised.
Outcomes HIV status assessed by laboratory test. STI status assessed by laboratory test.
Notes 73% circumcised.
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Circumcision was assessed by clinical ex-
amination.
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk HIV status was determined by appropriate
diagnostic tests, and we presume the lab-
oratory technicians did not know the cir-
cumcision status of the participants.
29Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
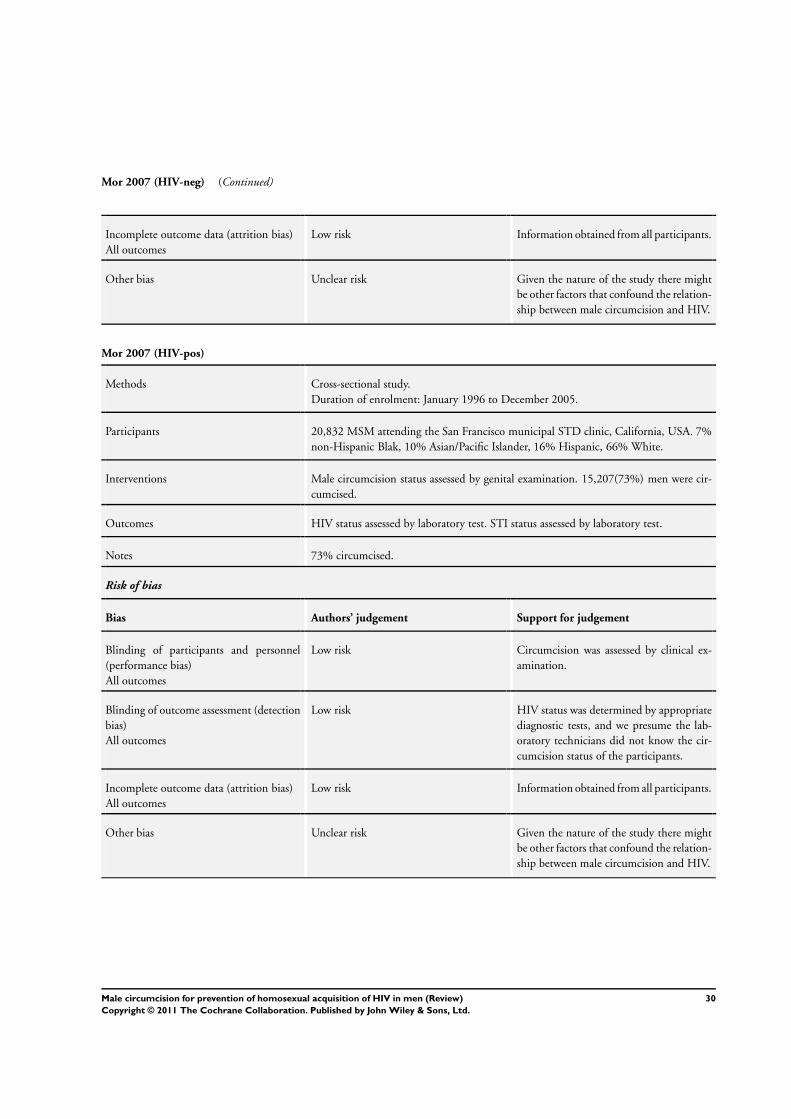
Mor 2007 (HIV-neg) (Continued)
Incomplete outcome data (attrition bias)
All outcomes
Low risk Information obtained from all participants.
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
Mor 2007 (HIV-pos)
Methods Cross-sectional study.
Duration of enrolment: January 1996 to December 2005.
Participants 20,832 MSM attending the San Francisco municipal STD clinic, California, USA. 7%
non-Hispanic Blak, 10% Asian/Pacific Islander, 16% Hispanic, 66% White.
Interventions Male circumcision status assessed by genital examination. 15,207(73%) men were cir-
cumcised.
Outcomes HIV status assessed by laboratory test. STI status assessed by laboratory test.
Notes 73% circumcised.
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Circumcision was assessed by clinical ex-
amination.
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk HIV status was determined by appropriate
diagnostic tests, and we presume the lab-
oratory technicians did not know the cir-
cumcision status of the participants.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Information obtained from all participants.
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
30Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Reid 2001
Methods Cross-sectional study.
Duration of enrolment: May 2001 to September 2001.
Participants 13,851 MSM who participated in Vital Statistics 2001 (i.e. the 5th annual national Gay
Men’s Sex Survey in England and Wales). 1% Blak, 2% mixed race, 3% Asian, 93%
White.
Interventions Male circumcision status assessed by self-report. 3089(22%) men were circumcised.
Outcomes HIV status assessed by self-report.
Notes 22% circumcised.
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Unclear risk Circumcision status was assessed by self-
report.
Blinding of outcome assessment (detection
bias)
All outcomes
Unclear risk HIV status assessed by self-report.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Information obtained from all participants.
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
Reisen 2007
Methods Cross-sectional study.
Duration of enrolment: Not stated.
Participants 482 immigrant Latino MSM living in the New York Metropolitan Area.
Interventions Male circumcision status assessed by self-report. About 120 (25%) men were circumcised.
Outcomes HIV status assessed by self-report.
Notes Brazilians = 146, Colombians = 169, Dominicans = 167.
Risk of bias
Bias Authors’ judgement Support for judgement
31Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Reisen 2007 (Continued)
Blinding of participants and personnel
(performance bias)
All outcomes
Unclear risk Circumcision status was assessed by self-
report.
Blinding of outcome assessment (detection
bias)
All outcomes
Unclear risk HIV status was determined by self-report.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Information obtained from all participants.
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
Sanchez 2007
Methods Cross-sectional study.
Duration of enrolment: February 2006 and June 2006.
Participants 2,884 MSM recruited from Peru (3 cities) and Ecuador (1 city). Ethnicity not reported..
Interventions Male circumcision status assessed by genital examination. 123(4%) men were circum-
cised.
Outcomes HIV status assessed by means of enzyme immunoassay and confirmed by Western blot.
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Circumcision status was assessed by self-
report.
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk HIV status was determined by appropriate
diagnostic tests, and we presume the lab-
oratory technicians did not know the cir-
cumcision status of the participants.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Information obtained from all participants.
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
32Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Tabet 2002
Methods Cross-sectional study.
Study conducted in 1996.
Participants 442 MSM (over 17 years of age) recruited in Lima, Peru. Ethnicity not reported.
Interventions Male circumcision status assessed by genital examination. 36(8%) men were circumcised
men.
Outcomes Antibodies to HIV were detected by ELISA and repeatedly reactive sera were confirmed
using Western blot.
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Circumcision status was assessed by clinical
examination.
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk HIV status was determined by appropriate
diagnostic tests, and we presume the lab-
oratory technicians did not know the cir-
cumcision status of the participants.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Complete information available for 440
(99.5%) participants.
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
Templeton 2009
Methods Prospective study.
Duration of enrolment: 2001 through 2004
Participants 1,426 HIV-negative MSM recruited from community-based sources into the Health in
Men (HIM) study in Sydney, Australia. Median age at enrolment was 35 years (range
18-75 years), 68% Australian-born and 74% of Anglo ethnicity.
Interventions Circumcision status was reported at baseline and self-reported circumcision status was
validated by clinical examination in a subgroup of 240 consecutively presenting partici-
pants. 938(66%) men were circumcised.
Outcomes Participants were tested annually for HIV with western blot confirmation.
33Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Templeton 2009 (Continued)
Notes Study participants followed up until mid-2007.
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Circumcision status was assessed by clinical
examination.
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk HIV status was determined by appropriate
diagnostic tests, and we presume the lab-
oratory technicians did not know the cir-
cumcision status of the participants.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Complete information available on all par-
ticipants.
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
Templeton 2009 (CS)
Methods Cross-sectional study
Duration of enrolment: 2001 through 2004
In the Templeton 2009 study, the association between circumcision status and STIs were
assessed at baseline (prevalent STIs) and prospectively (incident STIs). Templeton 2009
(CS) refers to the prevalence study.
Participants 1,426 HIV-negative MSM recruited from community-based sources into the Health in
Men (HIM) study in Sydney, Australia. Median age at enrolment was 35 years (range
18-75 years), 68% Australian-born and 74% of Anglo ethnicity.
Interventions Circumcision status was reported at baseline and self-reported circumcision status was
validated by clinical examination in a subgroup of 240 consecutively presenting partici-
pants. 938(66%) men were circumcised.
Outcomes Syphilis: Participants were screened annually by enzyme immunoassay, and positive
assay results confirmed with the Treponema pallidum particle agglutination assay and
fluorescent treponemal antibody absorption test. The rapid plasma reagin test was used
to assist clinical staging and to detect reinfection.
HSV: Baseline serum samples and sequential specimens were tested for antibody to HSV
using ELISA. Equivocal results were resolved by Western blot analysis.
Notes Paticipants were followed up until mid-2007.
34Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Templeton 2009 (CS) (Continued)
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Circumcision status was assessed by clinical
examination.
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk HIV status was determined by appropriate
diagnostic tests, and we presume the lab-
oratory technicians did not know the cir-
cumcision status of the participants.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Complete information available on all par-
ticipants.
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
Templeton 2009 (P)
Methods Prospective study.
Duration of enrolment: 2001 through 2004
In the Templeton 2009 study, the association between circumcision status and STIs were
assessed at baseline (prevalent STIs) and prospectively (incident STIs). Templeton 2009
(P) refers to the incidence study.
Participants 1,426 HIV-negative MSM recruited from community-based sources into the Health in
Men (HIM) study in Sydney, Australia. Median age at enrolment was 35 years (range
18-75 years), 68% Australian-born and 74% of Anglo ethnicity.
Interventions Circumcision status was reported at baseline and self-reported circumcision status was
validated by clinical examination in a subgroup of 240 consecutively presenting partici-
pants. 938(66%) men were circumcised.
Outcomes Participants were tested annually for HIV with western blot confirmation.
Notes Paticipants were followed up until mid-2007.
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Circumcision status was assessed by clinical
examination.
35Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Templeton 2009 (P) (Continued)
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk HIV status was determined by appropriate
diagnostic tests, and we presume the lab-
oratory technicians did not know the cir-
cumcision status of the participants.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Complete information available on all par-
ticipants.
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
Xu 2007
Methods Cross-sectional study
Duration of enrolment: 1999 to 2004.
Participants 6174 MSM participating in the National Health and Nutrition Examination Surveys
(NHANES) in the US from 1999 to 2004.
This analysis was limited to 3850 boys/men 14 to 49 years of age who reported having
had sex and were tested for HSV-2 antibodies
Interventions Circumcision status was assessed by self-report. The overall prevalence of circumcision
was 79% (95% CI 77 to 80).
Outcomes Participants were tested for HSV-2 by antibody tests.
Notes The NHANES is a series of cross-sectional surveys using a complex, stratified, multi-
stage probability sampling design. Briefly, during each year of the survey, a nationally
representative sample of the US civilian, noninstitutionalized population was selected,
interviewed, and examined by medical professionals.
During NHANES 1999-2004, health examinations were conducted in specially
equipped mobile examination Centers.
Risk of bias
Bias Authors’ judgement Support for judgement
Blinding of participants and personnel
(performance bias)
All outcomes
Unclear risk Circumcision status was assessed by self-
report.
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk HIV status was determined by appropriate
diagnostic tests, and we presume the lab-
oratory technicians did not know the cir-
cumcision status of the participants.
36Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Xu 2007 (Continued)
Incomplete outcome data (attrition bias)
All outcomes
Low risk Of 6313 interviewed (“Are you circumcised
or uncircumcised?”), 53 refused to answer
the question and 86 responded with “Don’t
know,” leaving a sample of 6174 persons
(90% of those examined at mobile exami-
nation Centers) for further analyses.
Other bias Unclear risk Given the nature of the study there might
be other factors that confound the relation-
ship between male circumcision and HIV.
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Beyrer 2010 This is a review and not a primary study.
Botros 2009 The study did not report either the number of persons with HIV (or syphilis or herpes simplex virus) in the
circumcised and uncircumcised groups or the odds ratio and its 95% confidence intervals for the association
between male circumcision and HIV (or syphilis or herpes simplex virus).
Coplan 1996 The study did not report either the number of persons with HIV (or syphilis or herpes simplex virus) in the
circumcised and uncircumcised groups or the odds ratio and its 95% confidence intervals for the association
between male circumcision and HIV (or syphilis or herpes simplex virus).
Dandona 2008 The study did not report either the number of persons with HIV (or syphilis or herpes simplex virus) in the
circumcised and uncircumcised groups or the odds ratio and its 95% confidence intervals for the association
between male circumcision and HIV (or syphilis or herpes simplex virus).
Fankem 2008 This is a review and not a primary study.
Farr 2010 The study did not report either the number of persons with HIV (or syphilis or herpes simplex virus) in the
circumcised and uncircumcised groups or the odds ratio and its 95% confidence intervals for the association
between male circumcision and HIV (or syphilis or herpes simplex virus).
Grulich 2001 At baseline all the participants were HIV infected.
Jewkes 2006 The study did not report either the number of persons with HIV (or syphilis or herpes simplex virus) in the
circumcised and uncircumcised groups or the odds ratio and its 95% confidence intervals for the association
between male circumcision and HIV (or syphilis or herpes simplex virus).
Jin 2010 The study did not report either the number of persons with HIV (or syphilis or herpes simplex virus) in the
circumcised and uncircumcised groups or the odds ratio and its 95% confidence intervals for the association
between male circumcision and HIV (or syphilis or herpes simplex virus).
37Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Jozkowski 2010 We need additional information before deciding whether to include this potentially eligible study or not. When
we decide on the final eligibility of this study, we will update this review and move this reference to the appropriate
section.
Kloos 2007 This is a review and not a primary study.
Lafferty 1997 The study did not report either the number of persons with HIV (or syphilis or herpes simplex virus) in the
circumcised and uncircumcised groups or the odds ratio and its 95% confidence intervals for the association
between male circumcision and HIV (or syphilis or herpes simplex virus).
Lau 2010 The study did not report either the number of persons with HIV (or syphilis or herpes simplex virus) in the
circumcised and uncircumcised groups or the odds ratio and its 95% confidence intervals for the association
between male circumcision and HIV (or syphilis or herpes simplex virus).
MacDonald 2008 This is a review and not a primary study.
McKinney 2008 The study did not report either the number of persons with HIV (or syphilis or herpes simplex virus) in the
circumcised and uncircumcised groups or the odds ratio and its 95% confidence intervals for the association
between male circumcision and HIV (or syphilis or herpes simplex virus).
Millet 2008 This is a review and not a primary study.
Perisse 2009 The study did not report either the number of persons with HIV (or syphilis or herpes simplex virus) in the
circumcised and uncircumcised groups or the odds ratio and its 95% confidence intervals for the association
between male circumcision and HIV (or syphilis or herpes simplex virus).
Sanchez 2011 We need additional information before deciding whether to include this potentially eligible study or not. When
we decide on the final eligibility of this study, we will update this review and move this reference to the appropriate
section.
Smith 2010 This is a review and not a primary study.
Sullivan 2007 This is a review and not a primary study.
Templeton 2010 This is a review and not a primary study.
Thornton 2009 We need additional information before deciding whether to include this potentially eligible study or not. When
we decide on the final eligibility of this study, we will update this review and move this reference to the appropriate
section.
Vermund 2008 This is an editorial and not a primary study.
Wei 2010 The study did not report either the number of persons with HIV (or syphilis or herpes simplex virus) in the
circumcised and uncircumcised groups or the odds ratio and its 95% confidence intervals for the association
between male circumcision and HIV (or syphilis or herpes simplex virus).
38Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Characteristics of ongoing studies [ordered by study ID]
MSM Trial 2010
Trial name or title Public title: (Men Who Have Sex With Men) MSM Community Intervention Trial
Scientific title: A community-based, randomized controlled trial to evaluate the efficacy of comprehensive
HIV/STIs intervention among men who have sex with men in 8 cities in China.
Main ID: NCT01068015
Methods Allocation: Randomized
Endpoint Classification: Efficacy Study
Intervention Model: Parallel Assignment
Masking: Open Label
Primary Purpose: Prevention
Phases: Phase III
Register: ClinicalTrials.gov
First Received: February 11, 2010
Last Updated: April 7, 2010
Last Verified: April 2010
Participants Target sample size: 3214
Inclusion Criteria: 18 years or above; Male have oral sex or anal sex within 6 months with a man; Accept
questionnaire survey and blood test; Can participate in three surveys in one year; HIV Negative; No mental
disease and can understand informed consent
Interventions Behavior intervention and male circumcision
Outcomes HIV incidence, Syphilis, HSV-2 incidence
Frequency of condom uses, number of sexual partners
The proportion of people who have intention to be circumcised
The proportion of people who have been circumcised
Starting date Start Date: June 2009
Completion Date: December 2010
Primary Completion Date: November 2010
Recruitment status: Active, not recruiting
Contact information Jie Xu, MD, MS, MPH: National Center for AIDS/STD Control and Prevention, China CDC
Zunyou Wu, MD, PhD: National Center for AIDS/STD Control and Prevention, China CDC
Notes URL: http://ClinicalTrials.gov/show/NCT01068015
39Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D A T A A N D A N A L Y S E S
Comparison 1. Male circumcision versus no male circumcision
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 HIV infection (all MSM) 20 Odds Ratio (Random, 95% CI) 0.86 [0.70, 1.06]
2 HIV infection (by sexual
position)
20 Odds Ratio (Random, 95% CI) Subtotals only
2.1 Receptive anal 3 Odds Ratio (Random, 95% CI) 1.20 [0.63, 2.29]
2.2 No differentiation 17 Odds Ratio (Random, 95% CI) 1.00 [0.92, 1.09]
2.3 Insertive anal 7 Odds Ratio (Random, 95% CI) 0.27 [0.17, 0.44]
3 Sexually transmitted infection 9 Odds Ratio (Random, 95% CI) Subtotals only
3.1 Syphilis 8 Odds Ratio (Random, 95% CI) 0.96 [0.82, 1.13]
3.2 Herpes simplex virus - 1 2 Odds Ratio (Random, 95% CI) 0.90 [0.53, 1.52]
3.3 Herpes simplex virus - 2 5 Odds Ratio (Random, 95% CI) 0.86 [0.62, 1.21]
Analysis 1.1. Comparison 1 Male circumcision versus no male circumcision, Outcome 1 HIV infection (all
MSM).
Review: Male circumcision for prevention of homosexual acquisition of HIV in men
Comparison: 1 Male circumcision versus no male circumcision
Outcome: 1 HIV infection (all MSM)
Study or subgroup log [Odds Ratio] Odds Ratio Weight Odds Ratio
(SE) IV,Random,95% CI IV,Random,95% CI
Kreiss 1993 -0.69314718 (0.70729304) 2.0 % 0.50 [ 0.13, 2.00 ]
Reid 2001 0.20701417 (0.17306925) 11.5 % 1.23 [ 0.88, 1.73 ]
Tabet 2002 -1.42711636 (1.43541363) 0.5 % 0.24 [ 0.01, 4.00 ]
Kumta 2002 -0.07257069 (0.26062532) 8.2 % 0.93 [ 0.56, 1.55 ]
Lai 2004 -0.7985077 (0.98850576) 1.1 % 0.45 [ 0.06, 3.12 ]
Buchbinder 2005 -0.69314718 (0.61990951) 2.5 % 0.50 [ 0.15, 1.69 ]
Bartholow 2006 0.0861777 (0.32713645) 6.4 % 1.09 [ 0.57, 2.07 ]
Millett 2007 (Black) 0.20701417 (0.35364652) 5.8 % 1.23 [ 0.62, 2.46 ]
Reisen 2007 -0.63487827 (0.64434456) 2.3 % 0.53 [ 0.15, 1.87 ]
0.01 0.1 1 10 100
Favours circumcision Favours no circumcision
(Continued . . . )
40Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup log [Odds Ratio] Odds Ratio Weight Odds Ratio
(SE) IV,Random,95% CI IV,Random,95% CI
Sanchez 2007 -0.03045921 (0.59697513) 2.6 % 0.97 [ 0.30, 3.13 ]
Buchbinder 2007 0.39877612 (0.47942407) 3.7 % 1.49 [ 0.58, 3.81 ]
Millet 2007 (Latino) 0.09531018 (0.41914712) 4.6 % 1.10 [ 0.48, 2.50 ]
Mor 2007 -0.03045921 (0.05375537) 16.0 % 0.97 [ 0.87, 1.08 ]
Calzavara 2007 -1.51412773 (2.49699055) 0.2 % 0.22 [ 0.00, 29.37 ]
Begley 2008 -0.51082562 (0.49173116) 3.6 % 0.60 [ 0.23, 1.57 ]
Templeton 2009 -0.24846136 (0.63217557) 2.4 % 0.78 [ 0.23, 2.69 ]
McDaid 2010 -0.24846136 (0.81527731) 1.5 % 0.78 [ 0.16, 3.86 ]
Jameson 2010 0.10436002 (0.10145452) 14.4 % 1.11 [ 0.91, 1.35 ]
Gust 2010 0.0295588 (0.5576741) 2.9 % 1.03 [ 0.35, 3.07 ]
Lane 2011 -1.51412773 (0.27499821) 7.8 % 0.22 [ 0.13, 0.38 ]
Total (95% CI) 100.0 % 0.86 [ 0.70, 1.06 ]
Heterogeneity: Tau2 = 0.07; Chi2 = 40.20, df = 19 (P = 0.003); I2 =53%
Test for overall effect: Z = 1.38 (P = 0.17)
0.01 0.1 1 10 100
Favours circumcision Favours no circumcision
41Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.2. Comparison 1 Male circumcision versus no male circumcision, Outcome 2 HIV infection (by
sexual position).
Review: Male circumcision for prevention of homosexual acquisition of HIV in men
Comparison: 1 Male circumcision versus no male circumcision
Outcome: 2 HIV infection (by sexual position)
Study or subgroup log [Odds Ratio] Odds Ratio Weight Odds Ratio
(SE) IV,Random,95% CI IV,Random,95% CI
1 Receptive anal
Sanchez 2007 0.19062036 (0.8867629) 13.7 % 1.21 [ 0.21, 6.88 ]
Reisen 2007 -0.09431068 (0.54751694) 36.0 % 0.91 [ 0.31, 2.66 ]
Jameson 2010 0.3852624 (0.46313453) 50.3 % 1.47 [ 0.59, 3.64 ]
Subtotal (95% CI) 100.0 % 1.20 [ 0.63, 2.29 ]
Heterogeneity: Tau2 = 0.0; Chi2 = 0.45, df = 2 (P = 0.80); I2 =0.0%
Test for overall effect: Z = 0.57 (P = 0.57)
2 No differentiation
Kreiss 1993 -0.69314718 (0.70729304) 0.4 % 0.50 [ 0.13, 2.00 ]
Reid 2001 0.20701417 (0.17306925) 6.2 % 1.23 [ 0.88, 1.73 ]
Kumta 2002 -0.07257069 (0.26062532) 2.7 % 0.93 [ 0.56, 1.55 ]
Tabet 2002 -1.42711636 (1.43541363) 0.1 % 0.24 [ 0.01, 4.00 ]
Lai 2004 -0.7985077 (0.98850576) 0.2 % 0.45 [ 0.06, 3.12 ]
Buchbinder 2005 -0.69314718 (0.61990951) 0.5 % 0.50 [ 0.15, 1.69 ]
Bartholow 2006 0.0861777 (0.32713645) 1.7 % 1.09 [ 0.57, 2.07 ]
Millet 2007 (Latino) 0.09531018 (0.41914712) 1.1 % 1.10 [ 0.48, 2.50 ]
Buchbinder 2007 0.39877612 (0.47942407) 0.8 % 1.49 [ 0.58, 3.81 ]
Sanchez 2007 -0.03045921 (0.59697513) 0.5 % 0.97 [ 0.30, 3.13 ]
Mor 2007 -0.03045921 (0.05375537) 64.2 % 0.97 [ 0.87, 1.08 ]
Millett 2007 (Black) 0.20701417 (0.35364652) 1.5 % 1.23 [ 0.62, 2.46 ]
Begley 2008 -0.51082562 (0.49173116) 0.8 % 0.60 [ 0.23, 1.57 ]
Templeton 2009 -0.24846136 (0.63217557) 0.5 % 0.78 [ 0.23, 2.69 ]
Jameson 2010 0.10436002 (0.10145452) 18.0 % 1.11 [ 0.91, 1.35 ]
McDaid 2010 -0.24846136 (0.81527731) 0.3 % 0.78 [ 0.16, 3.86 ]
Gust 2010 0.0295588 (0.5576741) 0.6 % 1.03 [ 0.35, 3.07 ]
Subtotal (95% CI) 100.0 % 1.00 [ 0.92, 1.09 ]
0.01 0.1 1 10 100
Favours circumcision Favours no circumcision
(Continued . . . )
42Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup log [Odds Ratio] Odds Ratio Weight Odds Ratio
(SE) IV,Random,95% CI IV,Random,95% CI
Heterogeneity: Tau2 = 0.0; Chi2 = 9.22, df = 16 (P = 0.90); I2 =0.0%
Test for overall effect: Z = 0.10 (P = 0.92)
3 Insertive anal
Reisen 2007 -1.42711636 (1.60415933) 2.3 % 0.24 [ 0.01, 5.57 ]
Sanchez 2007 -1.23787436 (1.20237363) 4.0 % 0.29 [ 0.03, 3.06 ]
Calzavara 2007 -1.51412773 (2.49699055) 0.9 % 0.22 [ 0.00, 29.37 ]
Templeton 2009 -2.20727491 (1.6752114) 2.1 % 0.11 [ 0.00, 2.93 ]
Jameson 2010 0.13102826 (0.66446934) 13.2 % 1.14 [ 0.31, 4.19 ]
McDaid 2010 -0.5798185 (3.06152523) 0.6 % 0.56 [ 0.00, 226.03 ]
Lane 2011 -1.51412773 (0.27499821) 76.9 % 0.22 [ 0.13, 0.38 ]
Subtotal (95% CI) 100.0 % 0.27 [ 0.17, 0.44 ]
Heterogeneity: Tau2 = 0.0; Chi2 = 5.61, df = 6 (P = 0.47); I2 =0.0%
Test for overall effect: Z = 5.36 (P < 0.00001)
0.01 0.1 1 10 100
Favours circumcision Favours no circumcision
43Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.3. Comparison 1 Male circumcision versus no male circumcision, Outcome 3 Sexually
transmitted infection.
Review: Male circumcision for prevention of homosexual acquisition of HIV in men
Comparison: 1 Male circumcision versus no male circumcision
Outcome: 3 Sexually transmitted infection
Study or subgroup log [Odds Ratio] Odds Ratio Weight Odds Ratio
(SE) IV,Random,95% CI IV,Random,95% CI
1 Syphilis
Kreiss 1993 -0.69314718 (0.86976943) 0.9 % 0.50 [ 0.09, 2.75 ]
Tabet 2002 -0.24846136 (1.29233421) 0.4 % 0.78 [ 0.06, 9.82 ]
Mor 2007 (HIV-pos) 0 (0.14235919) 33.2 % 1.00 [ 0.76, 1.32 ]
Sanchez 2007 -0.27443685 (0.79112113) 1.1 % 0.76 [ 0.16, 3.58 ]
Mor 2007 (HIV-neg) -0.02020271 (0.10448695) 61.7 % 0.98 [ 0.80, 1.20 ]
Templeton 2009 (P) -1.02165125 (0.90846233) 0.8 % 0.36 [ 0.06, 2.14 ]
Templeton 2009 (CS) -0.34249031 (0.72166594) 1.3 % 0.71 [ 0.17, 2.92 ]
Jameson 2010 -0.69314718 (1.02801175) 0.6 % 0.50 [ 0.07, 3.75 ]
Subtotal (95% CI) 100.0 % 0.96 [ 0.82, 1.13 ]
Heterogeneity: Tau2 = 0.0; Chi2 = 2.54, df = 7 (P = 0.92); I2 =0.0%
Test for overall effect: Z = 0.48 (P = 0.63)
2 Herpes simplex virus - 1
Templeton 2009 (CS) -0.13926207 (0.28330479) 90.2 % 0.87 [ 0.50, 1.52 ]
Templeton 2009 (P) 0.16551444 (0.85780738) 9.8 % 1.18 [ 0.22, 6.34 ]
Subtotal (95% CI) 100.0 % 0.90 [ 0.53, 1.52 ]
Heterogeneity: Tau2 = 0.0; Chi2 = 0.11, df = 1 (P = 0.74); I2 =0.0%
Test for overall effect: Z = 0.41 (P = 0.68)
3 Herpes simplex virus - 2
Sanchez 2007 -0.34249031 (0.44943306) 14.5 % 0.71 [ 0.29, 1.71 ]
Xu 2007 -0.09431068 (0.31817404) 28.9 % 0.91 [ 0.49, 1.70 ]
Templeton 2009 (P) -0.41551544 (0.91100383) 3.5 % 0.66 [ 0.11, 3.94 ]
Templeton 2009 (CS) -0.02020271 (0.3207187) 28.5 % 0.98 [ 0.52, 1.84 ]
Jameson 2010 -0.19845094 (0.34477318) 24.6 % 0.82 [ 0.42, 1.61 ]
Subtotal (95% CI) 100.0 % 0.86 [ 0.62, 1.21 ]
Heterogeneity: Tau2 = 0.0; Chi2 = 0.48, df = 4 (P = 0.98); I2 =0.0%
Test for overall effect: Z = 0.85 (P = 0.39)
0.01 0.1 1 10 100
Favours circumcision Favours no circumcision
44Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

H I S T O R Y
Protocol first published: Issue 4, 2008
Review first published: Issue 6, 2011
C O N T R I B U T I O N S O F A U T H O R S
CSW, EJK, ASM and OBN wrote the protocol for the review and CSW, EJK, MS, ASM, OBN, EA and YL contributed important
intellectual content to the review. All authors read and approved the final version.
D E C L A R A T I O N S O F I N T E R E S T
None known.
S O U R C E S O F S U P P O R T
Internal sources
• University of Cape Town (CSW, MSS), South Africa.
• Liverpool School of Tropical Medicine, Liverpool (EJK), UK.
• Leicester Royal Infirmary (OBN), UK.
• University of Malawi, College of Medicine, Blantyre (ASM), Malawi.
External sources
• Department of HIV/AIDS, World Health Organization, Switzerland.
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
MS, EAA and YRL were not authors in the published protocol, but they are included as authors in the review because they have made
substantive contributions in the selection of studies, data extraction and analyses, and/or interpretation of findings.
In addition, in the published protocol, we indicated that we would add transgendered persons as participants in this review. Our aim of
lumping MSM and transgenders was to be able to identify all studies where transmission routes for HIV would likely be similar to that
for MSM (i.e. through anal sex). However, our comprehensive search did not identify any study on transgenders. More importantly,
all four peer-referees expressed concerns about this lumping and we decided to exclude this group of participants from this review.
I N D E X T E R M S
45Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Medical Subject Headings (MeSH)
∗Circumcision, Male; ∗Homosexuality, Male; HIV Infections [∗prevention & control; transmission]; Herpes Simplex [prevention &
control; transmission]; Herpesvirus 1, Human; Herpesvirus 2, Human; Syphilis [prevention & control; transmission]
MeSH check words
Humans; Male
46Male circumcision for prevention of homosexual acquisition of HIV in men (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Related Documents











