Malaria & children Progress in intervention coverage Summary update 2009

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Malaria&children Progress in
intervention coverage
Summary update 2009

Copyright © 2009by the United Nations Children’s Fund
ISBN 978-92-806-4421-0
This report was prepared at UNICEF Headquarters by Emily White Johansson, Melanie Renshaw and Tessa Wardlaw. Important overall guidance and inputs were provided by Richard Steketee and Bernard Nahlen, as well as Nicholas Alipui, Nathan Bakyaita, Suprotik Basu, Francisco Blanco, Andrea Bosman, Richard Cibulskis, Misun Choi, Alan Court, Thomas Eisele, Katya Halil, Shanelle Hall, Hannah Koenker, Ryuichi Komatsu, Daniel Low-Beer, Nyein Nyein Lwin, Matthew Lynch, Richard Morgan, Khin Wit Yee Oo, Mac Otten, Peter Salama, Prudence Smith, Jan Van Erps and Neff Walker.
Financial support for this report was provided by The Global Fund to Fight AIDS, Tuberculosis and Malaria.
Communications Development Incorporated provided overall design direction, editing and layout.
Photo credit: cover, M. Hallahan/Sumitomo Chemical–Olyset® Net.
The United Nations Children’s Fund (UNICEF) welcomes requests for permission to reproduce or trans-late its publications—whether for sale or for non-commercial distribution. Applications and enquiries should be addressed to UNICEF, Division of Policy and Practice, 3 United Nations Plaza, New York, New York 10017, USA.
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of UNICEF, The Global Fund to Fight AIDS, Tuber-culosis and Malaria, or the Roll Back Malaria Partnership concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by UNICEF, The Global Fund to Fight AIDS, Tuberculosis and Malaria, or the Roll Back Malaria Partnership in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
United Nations Children’s Fund3 UN Plaza, New York, New York 10017, USA
The Global Fund to Fight AIDS, Tuberculosis and MalariaChemin de Blandonnet 8, 1214 Vernier, Geneva, Switzerland
The Roll Back Malaria Partnership Secretariat20 Avenue Appia, 1211 Geneva 27, Switzerland
1
The fight against malaria
On World Malaria Day in 2009, just over 600 days remain until 31 December 2010, UN Secretary-General Ban Ki-moon’s deadline for all endemic countries to achieve universal coverage with essential malaria control interventions.1 Data presented here highlight major signs of progress across Africa toward this goal.
The World Health Organization (WHO) has esti-mated that between 190 and 330 million malaria episodes occurred in 2006, resulting in nearly 1 million deaths. About 90 per cent of all malaria deaths occur in sub-Saharan Africa, most among children under age five (figure 1).2
Some 50 million pregnant women are exposed to malaria each year, with malaria in pregnancy
contributing to nearly 20 per cent of low birthweight babies in endemic areas.3 Malaria in pregnancy can also lead to stillbirth and maternal deaths.4
Malaria control is a major development priority. Ambitious new global goals, laid out in The Global Malaria Action Plan (Roll Back Malaria 2008), are challenging countries to implement bold plans for universal coverage (box 1).5 Malaria has also been included among major global development targets, notably the Millennium Development Goals. One of the eight goals relates specifically to malaria, AIDS and other infectious diseases, and many of the other goals, including those for child mortality and maternal health, will be diffi-cult to achieve in malaria-endemic areas without substantially reducing the malaria burden.
Box 1 Global malaria goals
The Roll Back Malaria Partnership was established in 1998 to coordinate a global approach to combating malaria. The overall goal is to halve the malaria bur-den by 2010, a vision shared by the Millennium De-velopment Goals, which call for reducing the number of malaria cases and deaths.
Since 2007, and building on the recent momentum in the fight against malaria, the UN Secretary-General, the African Union and others have called for a bolder, long-term goal of eliminating malaria as a global pub-lic health problem. To realize this vision, the Roll Back Malaria Partnership revised its goals and targets, as set out in its 2008 Global Malaria Action Plan.
Roll Back Malaria Partnership goals and targets:Achieve universal coverage for all populations at risk using locally appropriate interventions for prevention and case management by 2010 and sustain universal coverage until local field re-search suggests that coverage can gradually be targeted to high-risk areas and seasons only, without the threat of a generalized resurgence. Halve the malaria burden between 2000 and 2010 and reduce by 2015 the number of cases
by three-quarters and the number of preventable deaths to near zero.Eliminate malaria in 8-10 countries by 2015 and afterwards in all countries that are in the pre-elimination phase today. In the long term, erad-icate malaria worldwide by reducing the global incidence to zero through progressive elimina-tion in countries.
Millennium Development Goal 6: Combat HIV/AIDS, malaria and other diseases.
Target 6.C: By 2015 have halted and begun to re-verse the incidence of malaria and other major diseases.Indicator 6.6 Incidence and death rates associ-ated with malaria.Indicator 6.7 Proportion of children under age 5 sleeping under insecticide-treated nets.Indicator 6.8 Proportion of children under age 5 with fever treated with appropriate antimalarial drugs.
Source: Roll Back Malaria 2008; UN Statistics Division 2009.

2 Global funding for malaria control has risen significantly in recent years. The Roll Back Malaria Partnership estimates that interna-tional funding has grown from $250 million in 2004 to $700 million in 2007, with funding expected to have reached $1.1 billion in 2008 alone, due largely to the Global Fund to Fight AIDS, Tuberculosis and Malaria; the World Bank; the U.S. President’s Malaria Initiative and others.6 Many African countries recently achieved unprecedented success in obtaining Global Fund resources in the latest round of malaria grant applications (box 2). And in 2008, world leaders committed billions more towards malaria control.
Indeed, a new phase in the fight against malaria has begun. Data presented here show that the malaria community has accelerated efforts to deliver critical interventions, while also reduc-ing bottlenecks in their production, procure-ment and distribution. Countries have been quicker to adopt more effective strategies that would have been out of reach with less funding available, such as changing national drug poli-cies to more effective—but more expensive—
treatment courses and expanding diagnostics to better target treatment. A focus on behav-ior change communication programmes is also improving the effective use of malaria inter-ventions. Roll Back Malaria partners, includ-ing UNICEF, are supporting efforts to integrate malaria control activities into other maternal and child health services as they accelerate delivery of these essential interventions (box 3). And new actors, such as individual contribu-tors and faith-based organizations, are becom-ing increasingly involved in the fight against malaria.
We are witnessing substantial increases in cov-erage of key interventions, notably insecticide-treated nets, with 19 of 22 sub-Saharan African countries with trend data showing at least a threefold increase in insecticide-treated net use among children since around 2000—17 of them with at least a fivefold increase. Most of these nets have been distributed through maternal and child health services such as antenatal care and immunization. However, while antimalarial treatment is moderately high across Africa, many children are still using less effective medicines
Global and Africandistribution of deaths among children under age five by cause, 2004
Note: Globally, more than one-third of deaths in children under age five are attributable to undernutrition.
Source: WHO 2008a, b.
Neonatalcauses
37%
Neonatalcauses
25%
Pneumonia17%
Pneumonia21%
Diarrhea16%
Diarrhea16%
Malaria7%
Malaria16%
Measles4%
Measles4%
AIDS 5%
AIDS2% Other
13%Other13%Injuries
4%
Injuries2%
AfricaWorld
Figure 1 African children suffer the greatest malaria burden
Bon
nie
Gill
espi
e/V
oice
s fo
r a
Mal
aria
-Fre
e Fu
ture

3and many countries have shown little or no progress in expanding coverage since 2000. But important steps have been taken to improve cov-erage with effective treatment. Based on recent
efforts to scale up programs, some areas are now showing major reductions in the number of malaria cases and deaths, with more declines expected in coming years.7
Global funding for malaria control has risen significantly in recent years. Indeed, a new phase in the fight against malaria has begun
Box 3 UNICEF’s role in malaria control and monitoring progress
UNICEF works closely with Roll Back Malaria part-ners to support malaria-endemic countries to achieve universal coverage with key malaria control interven-tions. In 2007, UNICEF spent $1.4 billion on child survival programming, including funding for malaria control. It actively supports countries in leveraging other resources to support their malaria programmes through the Global Fund to Fight AIDS, Tuberculosis and Malaria, UNITAID and others.
UNICEF supports integrated programming, including net distribution through maternal and child health ser-vices, such as antenatal care, child health days and integrated campaigns alongside measles immuniza-tion, deworming and vitamin A supplementation.
UNICEF is also the largest global procurer and distrib-utor of insecticide-treated nets worldwide and pro-vides extensive technical and operational support in countries for procurement and supply chain manage-ment, behavior change communication programmes and operational research (such as intermittent pre-ventive treatment for infants).
UNICEF provides technical and financial support to countries to collect data through the Multiple Indi-cator Cluster Surveys, implemented in about 100 countries since 1995. Alongside the Demographic and Health Surveys, the surveys are a major source of data for monitoring the Millennium Development Goals.
Box 2 Success in leveraging resources for scaling up malaria prevention and treatment
The global financial crisis has raised concerns about international funding for global health, includ-ing malaria. In September 2008, the UN Secretary- General’s office concluded that funding is already below what is needed to reach the Millennium Devel-opment Goals in 2015. This situation makes it even more important for countries to develop strong pro-grammes, to spend their resources effectively and demonstrate tangible results.
The Roll Back Malaria partners can support govern-ments in these efforts, including through partner har-monisation efforts such as the Roll Back Malaria Harmonisation Working Group, currently co-chaired by UNICEF and the UN Special Envoy’s Office. This group provided critical support to countries
submitting malaria proposals to the Global Fund to Fight AIDS, Tuberculosis and Malaria. African coun-tries had experienced low malaria proposal success rates, with only 23 per cent of proposals successful in 2005 and 32 per cent in 2006. Countries were sup-ported with technical assistance, training workshops and country peer review of proposals. In 2007, $1 bil-lion was mobilized to support scale-up in endemic countries. In 2008, $2.4 billion was leveraged, rep-resenting 78 per cent success rate in malaria grant proposals among countries receiving support. Most countries submitted proposals that supported univer-sal coverage of malaria interventions by 2010.
Source: Roll Back Malaria Harmonisation Working Group 2009;
Garrett 2008.

4 Insecticide-treated mosquito nets are one of the most effective ways to prevent malaria transmis-sion. Studies show that high coverage and regu-lar use can reduce all-cause mortality rates in children under age five by nearly 20 per cent in malaria-endemic areas.8 Since 2004 the num-ber of insecticide-treated nets produced world-wide has more than tripled—from 30 million to 100 million in 2008 (figure 2)—leading to a
Prevention
rapid rise in the number of nets procured and distributed. The number of nets procured by UNICEF—the largest global net procurer—is 20 times greater today than in 2000 (figure 3). Programs supported by the Global Fund to Fight AIDS, Tuberculosis and Malaria distrib-uted 70 million nets by the end of 2008. Most nets are distributed through integrated mater-nal and child health services, such as in Mada-gascar (box 4). Many countries are now working to develop monthly distribution plans to help ensure distribution by the 31 December 2010 deadline to achieve universal coverage.
Manufacturers’ estimates indicate that more than 150 million nets were delivered to African coun-tries during 2004–2008 and are available for use out of the more than 340 million nets needed to achieve universal coverage in areas with malaria transmission (defined here as one net for every two people).9 Based on these estimates, endemic African countries overall have received enough nets during 2004–2008 to cover more than 40 per cent of their at-risk populations (map 1), and financing is available to purchase an esti-mated 240 million additional nets in 2009–2010. Nigeria, for example, has funding to support the distribution of 60 million nets to work towards universal coverage. The next round of surveys is expected to show higher coverage in many coun-tries based on these estimates.10
The wealth of new malaria data from house-hold surveys shows that sub-Saharan Africa has quickly scaled up insecticide-treated net use among children—rising from 2 per cent in 2000 to 20 per cent in 2006. Indeed, 19 of 22 African countries with trend data at least tripled coverage during this time, with 17 of them experiencing at least a fivefold increase (figure 4). Although overall net use still falls short of global targets—and children in rural areas or in the poorest households are even less likely to use insecticide-treated nets (figures 5 and 6)—the next round of surveys is expected to show higher coverage.
Figure 2 Global production of mosquito nets has more than tripled since 2004
Global production oflong-lasting insecticidal nets, 2004–2008(millions)
Note: Data for 2007 and 2008 are estimated production capacity.
Source: UNICEF Supply Division data 2009, based on estimates from insecticide-treated net manufacturers.
0
20
40
60
80
100
120
20082007200620052004
100
95
63
43
30
Figure 3 UNICEF insecticide-treated net procurement is 20 times greater today than in 2000
12
4 4
7
17
Number of insecticide-treated nets procured by UNICEF, 2000–2008 (millions)
Note: UNICEF is the largest global net procurer. Data are for insecticide-treated nets treated by the user and long-lasting insecticidal nets. Since 2004, data refer mostly to long- lasting insecticidal nets.
Source: UNICEF Supply Division data 2009.0
5
10
15
20
25
30
20082006200420022000
25
18
20

5
Since 2004 the number of insecticide-treated nets produced worldwide has more than tripled—from 30 million to 100 million in 2008—leading to a rapid rise in the number of nets procured and distributed
Map 1 African countries overall have received enough nets from manufacturers to cover more than 40 per cent of their at-risk population
Available long-lasting insecticidal nets as a percentage of nets needed to reach universal coverage,sub-Saharan Africa, 2004–2008
Less than 20 per cent
20–59 per cent
60–79 per cent
80 per cent or more
Non-malaria-endemic
Note: Data are as of 1 April 2009. Universal coverage is defined here as one net for every two people at risk for malaria transmission. Available long-lasting insecticidal nets include cumulative deliveries between 2004 and 2008, less worn-out nets. The Net Mapping Project is a project of the Alliance for Malaria Prevention, a workstream of the Roll Back Malaria Harmonisation Working Group.
Source: Milliner 2009.
The designations employed in this publication and the presentation of the material do not imply on the part of the United Nations Children’s Fund or the Roll Back Malaria Partnership the expression of any opinion whatsoever concerning the legal status of any country or territory, or of its authorities or the delimitations of its frontiers.
In October 2007 Madagascar’s Ministry of Health and its partners implemented a national mother-child health campaign focusing on 2.8 million children under age five. The campaign combined distribution of long-lasting insecticidal nets with measles vacci-nation, vitamin A supplementation and treatment for intestinal worms. Distribution took place in 59 of the country’s 111 districts, primarily in the western and southern areas, which had not previously benefited from mass distribution of nets.
A follow-up campaign evaluation in 2008 indicated that six months after the campaign more than half of
households owned at least one long-lasting insecti-cidal net. A Demographic and Health Survey is now under way to provide further data on national cover-age of key malaria control interventions. Madagascar is also a leading country for the roll-out of commu-nity based treatment with artemisinin-based com-bination therapies and widespread use of malaria diagnostics. It also supports indoor residual spraying in highland areas as part of its overall malaria control programming.
Source: Madagascar Ministry of Health 2007.
Box 4 Madagascar rapidly scaled up insecticide-treated nets through integrated campaigns

6
Insecticide-treated nets are one of the most effective ways to prevent malaria transmission. Much progress has been made across sub-Saharan Africa in quickly scaling up insecticide-treated net coverage in recent years
Indoor residual spraying is also an effective pre-vention method where epidemiologically and logistically appropriate. National programme records may provide the most useful data for monitoring coverage since this intervention is often targeted to subnational areas. In col-laboration with national malaria control pro-grammes, the U.S. President’s Malaria Initiative has supported implementation and scale-up of indoor residual spraying programmes in 14 of the initiative’s 15 countries. In 2008 alone, more than 6 million houses were sprayed and more than 24 million people were protected by indoor residual spraying as a result of these efforts.11
Figure 4 Rapid progress in scaling up insecticide-treated net use among children across all African countries with trend data
Around 2000
Percentage of children underage five sleeping under an insecticide-treated net the night before the survey, sub-Saharan Africa, 2000–2006
Around 2006
Note: Some sub-Saharan African countries have a significant share of their population living in non-malarious areas. National-level estimates may obscure higher coverage in endemic subnational areas targeted by programmes.
Source: UNICEF global malaria databases 2009, based on 22 countries with trend data for around 2000 and 2006, covering 53 per cent of children under age five.
Trends in insecticide-treated net use
0
20
40
60
80
15
49
23
42
1
41
7
39
2
38
2
33
2
26
2
26
3
25
4
22
7
20
2
16
2
15
4
56
1
13
2
10
0
10
1
8
1
7
1
6
13
01
Rwanda
(200
0, 20
07–20
08)
Gambia
, The
(200
0, 20
05–20
06)
São To
mé & Pr
incipe
(200
0, 20
06)
Zambia
(199
9, 20
08)
Guinea
–Bissau
(200
0, 20
06)
Togo
(200
0, 20
06)
Ethio
pia (2
005,
2007
)
Sierra
Leon
e (20
00, 2
008)
Tanz
ania
(1999
, 200
7–20
08)
Mala
wi (200
0, 20
06)
Ghana
(200
3, 20
06)
Benin
(2001
–2002
, 200
6)
Seneg
al (20
00, 2
006)
Centra
l Afri
can R
epub
lic (2
000,
2006
)
Camer
oon (
2000
, 200
6)
Burkin
a Fas
o (20
03, 2
006)
Ugand
a (20
00–20
01, 2
006)
Burun
di (20
00, 2
005)
Niger (
2000
, 200
6)
Congo
, Dem
. Rep
. (200
1, 20
07)
Côte d
’Ivoir
e (20
00, 2
006)
Swazila
nd (2
000,
2006
–2007
)
Figure 5 Use of insecticide-treated nets is lowest among African children in rural areas and the poorest households
0 10 20 30
Poorest
Second
Middle
Fourth
Richest
Rural
Urban
Female
Male 20
20
18
25
18
26
20
18
17
Percentage of children under age five sleeping under insecticide-treated nets, sub-Saharan Africa, by gender, residence and wealth index quintiles
Source: UNICEF global malaria databases 2009, based on 24 (gender), 26 (residence) and 25 (wealth) surveys for 2006–2008, covering around 58 per cent of children under age five.

7
UN
ICE
F/H
Q07
-05
88
/Gia
com
o P
irozz
i
M. H
alla
han/
Sum
itom
o C
hem
ical
–Oly
set®
Net
Figure 6 Household ownership of any type of net is relatively high, but increases are needed in ownership of insecticide-treated nets
Households with at least one insecticide-treated net
Percentage of households owning at least one insecticide-treated net and at least one net of any type,2004–2008
Households with at least one mosquito net of any type
Note: Some sub-Saharan African countries have a significant share of their population living in non-malarious areas. National-level estimates may obscure higher coverage in endemic subnational areas targeted by programmes.
a. Data on household availability of insecticide-treated nets are not available.
Source: UNICEF global malaria databases 2009. The estimate for sub-Saharan Africa is based on the 28 countries with data for 2006–2008 and covers 56 per cent of children under age five.
Household ownershipof mosquito nets
0 20 40 60 80 100
Sub-Saharan Africa average (2006–2008)b
Swaziland (2006–2007)
Burundi (2005)
Zimbabwe (2005–2006)
Somalia (2006)
Namibia (2006–2007)
Djibouti (2006)
Guinea (2005)
Côte d’Ivoire (2006)
Congo, Dem. Rep. (2007)
Ghana (2006)
Liberiaa (2007)
Cameroon (2006)
Angola (2006–2007)
Uganda (2006)
Central African Republic (2006)
Sudan (2006)
Madagascara (2003–2004)
Sierra Leone (2008)
Togo (2006)
São Tomé & Principe (2006)
Malawi (2006)
Burkina Faso (2006)
Ethiopia (2007)
Tanzania (2007–2008)
Benin (2006)
Mauritania (2007)
Senegal (2006)
Rwanda (2007–2008)
Gambia, The (2005–2006)
Chada (2004)
Mali (2006)
Niger (2006)
Zambia (2008)
Congo (2005)
Guinea-Bissau (2006) 79
76
72
69
69
64
59
59
57
57
56
56
56
52
51
49
46
39
37
36
34
33
32
30
30
28
27
27
26
22
25
20
40
13
44
6

8
Treatment
Prompt and effective treatment of malaria within 24 hours of the onset of symptoms is important to prevent life-threatening complications. In recent years, the sub-Saharan Africa region has experi-enced a major transition, with nearly all countries rapidly shifting national drug policies to include
artemisinin-based combination therapies and sub-stantially increasing financing and procurement for these medicines since around 2005 (figure 7).
The use of these newer medicines, rather than traditional monotherapies, is critical for improv-ing treatment efficacy and delaying the develop-ment of drug resistance. While most studies still conclude that the efficacy of artemisinin-based combination therapies remains high, new evi-dence suggests increased tolerance along the Cambodian and Thailand border.12
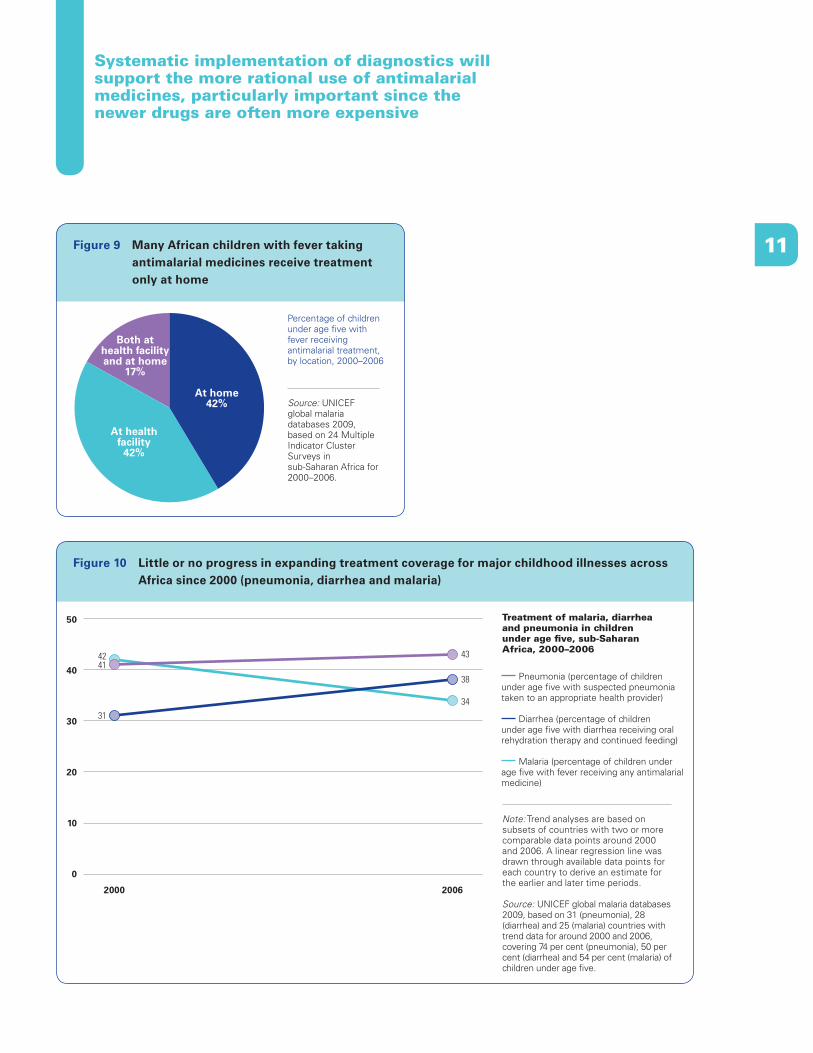
While antimalarial treatment in children with fever is moderately high across Africa, many febrile children are still being treated at home and with less effective medicines (figures 8 and 9). Many African countries also have made little or no progress in expanding treatment coverage since 2000, which mirrors trends across Africa in the treatment of other major childhood illnesses, such as diarrheal diseases and pneumonia (figure 10). This underscores the urgent need to strengthen integrated community- based case management of major childhood illnesses (box 5).
Number of doses ofartemisinin-based combination therapiesprocured worldwide,2001–2008 (millions)
Source: World Health Organization Global Malaria Programme database 2009.
0
30
60
90
120
150
20082007200620052004200320022001
0.5 0.6 2.1 5.0
31.3
82.7
97.0
130.0
Figure 7 Recent and rapid scale-up in the global procurement of artemisinin-based combination therapies
Box 5 Scaling up home management of malaria in Zambia
Zambia is actively working to expand treatment cov-erage by strengthening its community-based case management of malaria. This is an essential mea-sure since most malaria cases occur in rural or poor areas, often without good access to health facilities. Fourteen districts have already implemented training of community health workers and health facility staff in the home management of malaria, and expansion to another 14 districts is planned for mid-2009. Such training includes instruction on national malaria diag-nostic and treatment guidelines, appropriate use of antimalarial medicines, stronger referral procedures and reinforced links between health facilities and community health workers, as well as improved ma-laria surveillance at the community level.
Because functional microscopy is limited in most rural areas, the training teaches community health workers to diagnose malaria using rapid diagnostic tests. These rapid tests are becoming more widely available as international funding increasingly sup-ports their purchase and use. A recent study in Zam-bia found that community health workers could use these rapid diagnostic tests safely and effectively when provided with clear instructions and appro-priate training. Use of the tests has better targeted prompt and effective treatment to children with malaria and is extending the front-line fight against malaria deeper into affected populations.
Source: Harvey and others 2008.

9
The use of artemisinin-based combination therapies, rather than traditional monotherapies, is critical for improving treatment efficacy and delaying the development of drug resistance
Figure 8 Despite moderately high treatment coverage, many children are still using less effective medicines
Children under age five with fever receiving artemisinin-based combination therapy
Percentage of children under age five with fever receiving artemisinin-based combination therapy, chloroquine or any antimalarial medicine, sub-Saharan Africa, 2004–2008
Children under age five with fever receiving chloroquine
Children under age five with fever receiving any antimalarial medicine
Note: Some sub-Saharan African countries have a significant share of their population living in non-malarious areas. National-level estimates may obscure higher coverage in endemic subnational areas targeted by programmes.
a. Data for chloroquine, artemisinin-based combination therapies or both not available. Data by drug types are insufficient to calculate a sub-Saharan African average.
Source: UNICEF global malaria databases 2009. The estimate for Sub-Saharan Africa is based on the 28 countries with data for 2006–2008 and covers 59 per cent of children under age five.
Malaria treatment by drug type
0 20 40 60 80 100
63
61
61
59
58
57
57
54
54
53
48
48
48
46
44
43
36
34
33
32
30
30
30
29
25
25
22
21
15
10
10
10
8
6
5
34
1
Sub-Saharan Africa averagea (2006–2008)
Swazilanda (2006–2007)
Zimbabwea (2005–2006)
Rwandaa (2007–2008)
Somalia (2006)
Djibouti (2006)
Namibiaa (2006–2007)
Ethiopiaa (2007)
Mozambiquea (2003–2004)
Mauritania (2007)
Senegala (2006)
São Tomé & Principe (2006)
Malawi (2006)
Angola (2006–2007)
Burundi (2005)
Congo, Dem. Rep. (2007)
Sierra Leonea (2008)
Malia (2006)
Nigera (2006)
Madagascara (2003–2004)
Côte d’Ivoire (2006)
Zambiaa (2008)
Guineaa (2005)
Guinea-Bissaua (2006)
Togo (2006)
Burkina Fasoa (2006)
Congoa (2005)
Chada (2004)
Benin (2006)
Sudan (2006)
Central African Republic (2006)
Tanzania (2007–2008)
Cameroon (2006)
Liberiaa (2007)
Ghana (2006)
Uganda (2006)
Gambia (2006)

10 But in this rapidly changing malaria environ-ment, trends in treatment coverage will become increasingly difficult to interpret, particularly in areas with substantial declines in the number of malaria cases due to scaled up prevention measures and in areas with more widely avail-able diagnostics (box 6). Other data sources may provide useful information to interpret trends in case management, such as health facility data.
Some countries are greatly expanding the use of diagnostics to better target treatment only to febrile patients with a positive diagnosis. Sys-tematic implementation will support the more
rational use of anti-malarial medicines. There is also increasing emphasis on integrated com-munity case management of major childhood diseases, particularly malaria, diarrhea and pneumonia, and on strengthening private sector support for treatment, such as the through the Affordable Medicines Facility for Malaria, which is hosted by the Global Fund to Fight AIDS, Tuberculosis and Malaria.
These actions, coupled with investments in strengthening health facilities and distribution mechanisms within countries, suggest that many more children suffering from malaria will receive prompt and effective treatment in coming years.
Box 6 Interpretation of malaria treatment data
Interpreting malaria treatment data from population-based household surveys can be complicated, par-ticularly where scaling up prevention measures has substantially lowered the number of malaria cases and where diagnostics are becoming more widely available.
In areas of high malaria transmission and where qual-ity diagnostics are not available, the World Health Organization (WHO) currently recommends that all febrile children under age five be treated presump-tively for malaria. Household surveys collect treat-ment data for children experiencing fever at some point in the two weeks before the survey. Some countries are moving away from presumptive ma-laria treatment by scaling up the use of diagnostics through microscopy in health facilities and rapid diag-nostic tests at peripheral levels of the health system. In these areas, measuring treatment among all febrile
children will become less useful for monitoring the success of programmes that are better targeted to-wards treating only confirmed cases. In addition, comparisons of historical survey data reflecting pre-sumptive treatment with newer data based on lab-oratory-confirmed malaria would inevitably show a downward trend in treatment coverage among all fe-brile children. This issue becomes more critical as countries scale up preventive measures, resulting in even fewer febrile cases due to malaria.
The Roll Back Malaria Monitoring and Evaluation Ref-erence Group is currently reviewing this treatment indicator in light of the major scale-up of malaria con-trol activities across Africa and has recommended collecting data on diagnostics use in the next round of surveys to help interpret trends.
Source: Roll Back Malaria Monitoring and Evaluation Reference Group.
UN
ICE
F/H
Q07
-012
7/G
iaco
mo
Piro
zzi
BA
SF
AG
Pub
lic H
ealth
/ME
NTO
R/V
OIC
ES
/Ben
oist
Car
pent
ier
11
Systematic implementation of diagnostics will support the more rational use of antimalarial medicines, particularly important since the newer drugs are often more expensive
Figure 10 Little or no progress in expanding treatment coverage for major childhood illnesses across Africa since 2000 (pneumonia, diarrhea and malaria)
Treatment of malaria, diarrhea and pneumonia in children under age five, sub-Saharan Africa, 2000–2006
Note: Trend analyses are based on subsets of countries with two or more comparable data points around 2000 and 2006. A linear regression line was drawn through available data points for each country to derive an estimate for the earlier and later time periods.
Source: UNICEF global malaria databases 2009, based on 31 (pneumonia), 28 (diarrhea) and 25 (malaria) countries with trend data for around 2000 and 2006, covering 74 per cent (pneumonia), 50 per cent (diarrhea) and 54 per cent (malaria) of children under age five.
43
38
34
31
4241
20062000
Pneumonia (percentage of children under age five with suspected pneumonia taken to an appropriate health provider)
Diarrhea (percentage of children under age five with diarrhea receiving oral rehydration therapy and continued feeding)
Malaria (percentage of children under age five with fever receiving any antimalarial medicine)
0
10
20
30
40
50
Figure 9 Many African children with fever taking antimalarial medicines receive treatment only at home
Percentage of children under age five with fever receiving antimalarial treatment, by location, 2000–2006
Source: UNICEF global malaria databases 2009, based on 24 Multiple Indicator Cluster Surveys in sub-Saharan Africa for 2000–2006.
Both athealth facilityand at home
17%
At home42%
At healthfacility
42%

12 Together with regular use of insecticide-treated nets, intermittent preventive treatment dur-ing pregnancy is critical for preventing malaria among pregnant women in stable malarious areas. The treatment consists of at least two doses of an effective antimalarial drug during the sec-ond and third trimesters of pregnancy. This intervention is highly effective in reducing the proportion of women with anemia and placen-tal malaria infection at delivery. Sulfadoxine- pyrimethamine is a safe and appropriate drug for intermittent preventive treatment for pregnant women.13
Most countries have only recently adopted inter-mittent preventive treatment as a recommended regimen for pregnant women. The next round of
surveys is expected to show higher coverage. Some countries have already achieved relatively high levels, including Zambia (60 per cent in 2008) and Senegal (49 per cent in 2006; fig-ure 11). The higher coverage is due largely to early adoption and implementation of intermit-tent preventive treatment as a key part of national reproductive health and malaria control activi-ties. Indeed, many countries with more recent data show higher values, and better coverage is expected in the next round of surveys.
Use of insecticide-treated nets by pregnant women is also low across Africa, although many countries with more recent survey data show higher coverage, and further gains are expected in coming years (figure 12).
Figure 12 Insecticide-treated net use among pregnant women is too low in most African countries
0 20 40 60 80 100
Guinea (2005)
Swaziland (2006–2007)
Cameroon (2006)
Zimbabwe (2005–2006)
Congo (2005)
Niger (2006)
Congo, Dem. Rep. (2007)
Namibia (2006–2007)
Uganda (2006)
Malawi (2006)
Senegal (2006)
Benin (2006)
Angola (2006–2007)
Tanzania (2007–2008)
Sierra Leone (2008)
Mali (2006)
Ethiopia (2007)
Zambia (2008)
Rwanda (2007–2008)Percentage of pregnant women sleeping under an insecticide-treated net, sub-Saharan Africa, 2004–2008
Source: UNICEF global malaria databases 2009.
1
1
1
3
4
7
7
9
10
15
17
20
22
28
27
29
35
60
43
Malaria during pregnancy
Figure 11 Despite major progress in some countries, intermittent preventive treatment coverage remains too low
0 20 40 60 80 100
Niger (2006)
Swazilanda (2006–2007)
Somaliaa (2006)
Burkina Faso (2006)
Angola (2006–2007)
Guinea (2005)
Benina (2006)
Mali (2006)
Congo, Dem. Rep. (2007)
Cameroon (2004)
Zimbabwe (2005–2006)
Guinea-Bissaua (2006)
Côte d’Ivoirea (2006)
Central African Rep. (2006)
Namibia (2006–2007)
Sierra Leone (2008)
Uganda (2006)
Togoa (2006)
Ghana (2006)
Tanzania (2007–2008)
Gambiaa (2006)
Malawia (2006)
Senegal (2006)
Zambia (2008)
0
1
1
1
3
3
3
4
5
6
6
7
8
9
10
12
16
18
30
27
33
45
49
60 Percentage of women ages 15–49 who received intermittent preventive treatment during pregnancybefore last live birth, sub-Saharan Africa, 2004–2008
a. Treatment during antenatal care visit not specified.
Source: UNICEF global malaria databases 2009.

13
Impact on children’s lives
2001–2007 through the scaling up of insecticide-treated nets (figure 13).14 This estimate does not reflect the impact of changes in the other malaria control interventions, such as antimalarial treat-ment. Based on this model’s predictions, the Global Fund evaluation suggests that most of these deaths were averted since 2006, reflecting the recent and significant gains made in malaria control across a number of African countries.
There are significant challenges to monitoring changes in the malaria burden over time. Fur-ther investments are needed in the quality of vital registration and in health information systems in high-burden African countries with poor access to health care and inadequate disease surveillance systems. In some areas, data from these sources do suggest that major declines in the malaria bur-den are becoming increasingly evident.
While improving these data systems in high- burden countries is the long-term objective, modeling efforts provide crude estimates of the potential number of deaths averted due to scal-ing up malaria control interventions over time and may be used alongside data from other sources to provide an overall indication of mor-tality impact of programs. This model, known as the Lives Saved Tool (or LiST model), links cover-age of key child survival interventions (including those for malaria) with their known impact on mortality in children under age five (box 7).
A recent evaluation for The Global Fund to Fight AIDS, Tuberculosis and Malaria using this model indicates that an estimated 125,000 malaria deaths were averted in 10 African countries in
Figure 13 An estimated 125,000 malaria deaths averted in 10 African countries by scaling up insecticide-treated nets, most since 2006
Estimated number of deaths due to malaria averted in children under age five by insecticide-treated-net scale-up in 10 African countries included in the GFATM evaluation, 2001–2007, by year
Note: Countries include Benin, Burkina Faso, Burundi, Democratic Republic of the Congo, Ethiopia, Ghana, Malawi, Rwanda,Tanzania and Zambia.
Source: GFATM forthcoming.
2006(32,000 deaths
averted)
2001–2004(31,000 deaths
averted)2007
(41,000 deathsaverted)
2005(21,000deaths
averted)
A consortium of academic and international organiza-tions, led by Institute of International Programs at the Johns Hopkins Bloomberg School, has developed a user-friendly tool (Lives Saved Tool, LiST) to esti-mate the impact of scaling up maternal, newborn and child health interventions. The model derives its esti-mates of trends in cause-specific under-five mortality based on the methods outlined in Jones and others (2003), which were incorporated into the Spectrum Demographic Software (1,2). This model estimates the potential number of deaths averted in children under age five by cause through changes in key child survival intervention coverage (including those
for malaria) with empirical evidence of the effect of these interventions on preventing deaths in children under age five. Estimates of the impact of insecti-cide-treated nets on all-cause under-five mortality in Africa are based on the work of Lengeler (2004). The model’s predictions also takes into account current demographic projections and country-specific cause of death profiles for children under age five. More in-formation on the model is available at: www.jhsph.edu/dept/IH/IIP/list/index.html.
Source: Johns Hopkins University 2009; Jones and others 2003;
Lengeler 2004.
Box 7 Lives Saved Tool (LiST)
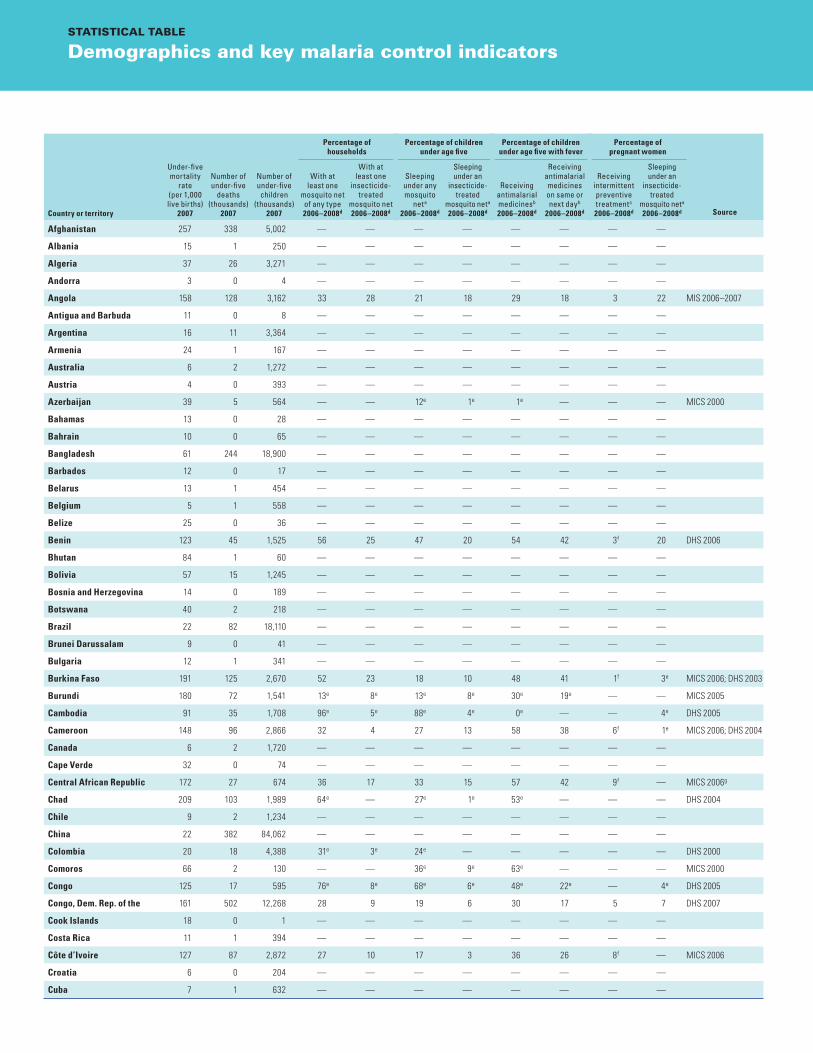
Country or territory
Under-five mortality
rate (per 1,000 live births)
2007
Number of under-five
deaths (thousands)
2007
Number of under-five children
(thousands) 2007
Percentage of households
Percentage of children under age five
Percentage of children under age five with fever
Percentage of pregnant women
Source
With at least one
mosquito net of any type 2006–2008d
With at least one
insecticide-treated
mosquito net 2006–2008d
Sleeping under any mosquito
neta 2006–2008d
Sleeping under an
insecticide-treated
mosquito neta 2006–2008d
Receiving antimalarial medicinesb 2006–2008d
Receiving antimalarial medicines on same or next dayb
2006–2008d
Receiving intermittent preventive treatmentc 2006–2008d
Sleeping under an
insecticide-treated
mosquito neta 2006–2008d
Afghanistan 257 338 5,002 — — — — — — — —
Albania 15 1 250 — — — — — — — —
Algeria 37 26 3,271 — — — — — — — —
Andorra 3 0 4 — — — — — — — —
Angola 158 128 3,162 33 28 21 18 29 18 3 22 MIS 2006–2007
Antigua and Barbuda 11 0 8 — — — — — — — —
Argentina 16 11 3,364 — — — — — — — —
Armenia 24 1 167 — — — — — — — —
Australia 6 2 1,272 — — — — — — — —
Austria 4 0 393 — — — — — — — —
Azerbaijan 39 5 564 — — 12e 1e 1e — — — MICS 2000
Bahamas 13 0 28 — — — — — — — —
Bahrain 10 0 65 — — — — — — — —
Bangladesh 61 244 18,900 — — — — — — — —
Barbados 12 0 17 — — — — — — — —
Belarus 13 1 454 — — — — — — — —
Belgium 5 1 558 — — — — — — — —
Belize 25 0 36 — — — — — — — —
Benin 123 45 1,525 56 25 47 20 54 42 3f 20 DHS 2006
Bhutan 84 1 60 — — — — — — — —
Bolivia 57 15 1,245 — — — — — — — —
Bosnia and Herzegovina 14 0 189 — — — — — — — —
Botswana 40 2 218 — — — — — — — —
Brazil 22 82 18,110 — — — — — — — —
Brunei Darussalam 9 0 41 — — — — — — — —
Bulgaria 12 1 341 — — — — — — — —
Burkina Faso 191 125 2,670 52 23 18 10 48 41 1f 3e MICS 2006; DHS 2003
Burundi 180 72 1,541 13e 8e 13e 8e 30e 19e — — MICS 2005
Cambodia 91 35 1,708 96e 5e 88e 4e 0e — — 4e DHS 2005
Cameroon 148 96 2,866 32 4 27 13 58 38 6f 1e MICS 2006; DHS 2004
Canada 6 2 1,720 — — — — — — — —
Cape Verde 32 0 74 — — — — — — — —
Central African Republic 172 27 674 36 17 33 15 57 42 9f — MICS 2006g
Chad 209 103 1,989 64e — 27e 1e 53e — — — DHS 2004
Chile 9 2 1,234 — — — — — — — —
China 22 382 84,062 — — — — — — — —
Colombia 20 18 4,388 31e 3e 24e — — — — — DHS 2000
Comoros 66 2 130 — — 36e 9e 63e — — — MICS 2000
Congo 125 17 595 76e 8e 68e 6e 48e 22e — 4e DHS 2005
Congo, Dem. Rep. of the 161 502 12,268 28 9 19 6 30 17 5 7 DHS 2007
Cook Islands 18 0 1 — — — — — — — —
Costa Rica 11 1 394 — — — — — — — —
Côte d’Ivoire 127 87 2,872 27 10 17 3 36 26 8f — MICS 2006
Croatia 6 0 204 — — — — — — — —
Cuba 7 1 632 — — — — — — — —
STATISTICAL TABLE
Demographics and key malaria control indicators
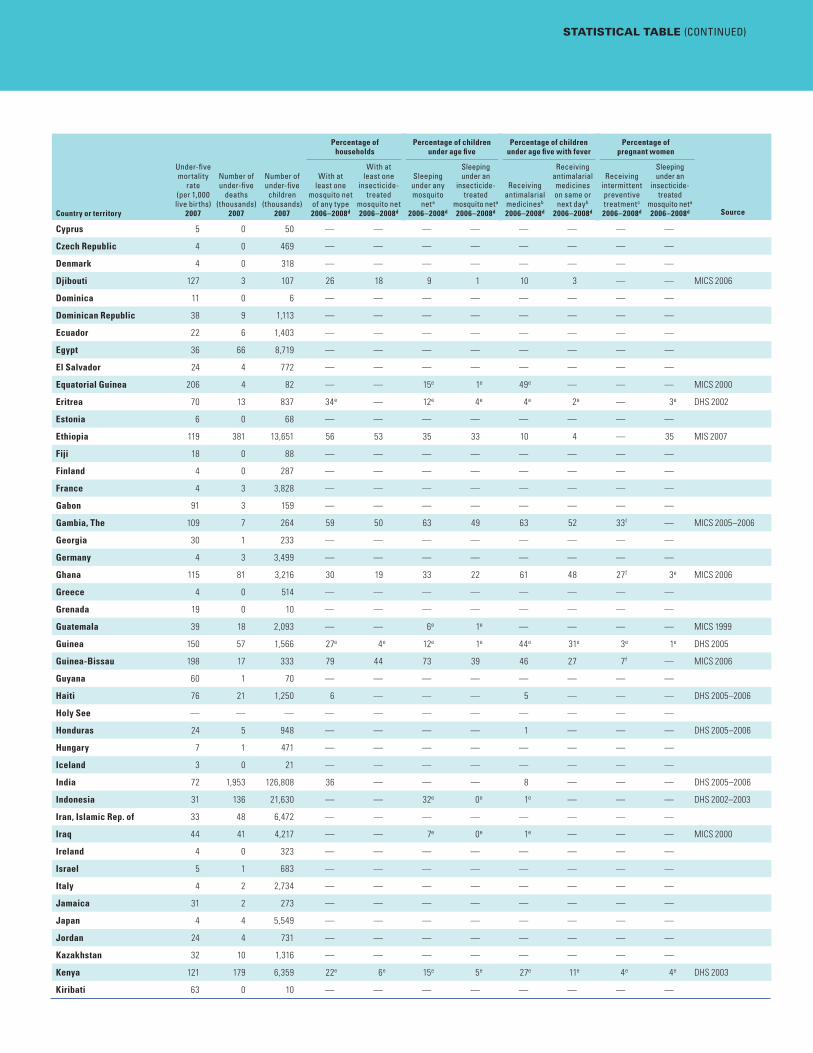
STATISTICAL TABLE (CONTINUED)
Country or territory
Under-five mortality
rate (per 1,000 live births)
2007
Number of under-five
deaths (thousands)
2007
Number of under-five children
(thousands) 2007
Percentage of households
Percentage of children under age five
Percentage of children under age five with fever
Percentage of pregnant women
Source
With at least one
mosquito net of any type 2006–2008d
With at least one
insecticide-treated
mosquito net 2006–2008d
Sleeping under any mosquito
neta 2006–2008d
Sleeping under an
insecticide-treated
mosquito neta 2006–2008d
Receiving antimalarial medicinesb 2006–2008d
Receiving antimalarial medicines on same or next dayb
2006–2008d
Receiving intermittent preventive treatmentc 2006–2008d
Sleeping under an
insecticide-treated
mosquito neta 2006–2008d
Cyprus 5 0 50 — — — — — — — —
Czech Republic 4 0 469 — — — — — — — —
Denmark 4 0 318 — — — — — — — —
Djibouti 127 3 107 26 18 9 1 10 3 — — MICS 2006
Dominica 11 0 6 — — — — — — — —
Dominican Republic 38 9 1,113 — — — — — — — —
Ecuador 22 6 1,403 — — — — — — — —
Egypt 36 66 8,719 — — — — — — — —
El Salvador 24 4 772 — — — — — — — —
Equatorial Guinea 206 4 82 — — 15e 1e 49e — — — MICS 2000
Eritrea 70 13 837 34e — 12e 4e 4e 2e — 3e DHS 2002
Estonia 6 0 68 — — — — — — — —
Ethiopia 119 381 13,651 56 53 35 33 10 4 — 35 MIS 2007
Fiji 18 0 88 — — — — — — — —
Finland 4 0 287 — — — — — — — —
France 4 3 3,828 — — — — — — — —
Gabon 91 3 159 — — — — — — — —
Gambia, The 109 7 264 59 50 63 49 63 52 33f — MICS 2005–2006
Georgia 30 1 233 — — — — — — — —
Germany 4 3 3,499 — — — — — — — —
Ghana 115 81 3,216 30 19 33 22 61 48 27f 3e MICS 2006
Greece 4 0 514 — — — — — — — —
Grenada 19 0 10 — — — — — — — —
Guatemala 39 18 2,093 — — 6e 1e — — — — MICS 1999
Guinea 150 57 1,566 27e 4e 12e 1e 44e 31e 3e 1e DHS 2005
Guinea-Bissau 198 17 333 79 44 73 39 46 27 7f — MICS 2006
Guyana 60 1 70 — — — — — — — —
Haiti 76 21 1,250 6 — — — 5 — — — DHS 2005–2006
Holy See — — — — — — — — — — —
Honduras 24 5 948 — — — — 1 — — — DHS 2005–2006
Hungary 7 1 471 — — — — — — — —
Iceland 3 0 21 — — — — — — — —
India 72 1,953 126,808 36 — — — 8 — — — DHS 2005–2006
Indonesia 31 136 21,630 — — 32e 0e 1e — — — DHS 2002–2003
Iran, Islamic Rep. of 33 48 6,472 — — — — — — — —
Iraq 44 41 4,217 — — 7e 0e 1e — — — MICS 2000
Ireland 4 0 323 — — — — — — — —
Israel 5 1 683 — — — — — — — —
Italy 4 2 2,734 — — — — — — — —
Jamaica 31 2 273 — — — — — — — —
Japan 4 4 5,549 — — — — — — — —
Jordan 24 4 731 — — — — — — — —
Kazakhstan 32 10 1,316 — — — — — — — —
Kenya 121 179 6,359 22e 6e 15e 5e 27e 11e 4e 4e DHS 2003
Kiribati 63 0 10 — — — — — — — —

STATISTICAL TABLE (CONTINUED)
Demographics and key malaria control indicators
Country or territory
Under-five mortality
rate (per 1,000 live births)
2007
Number of under-five
deaths (thousands)
2007
Number of under-five children
(thousands) 2007
Percentage of households
Percentage of children under age five
Percentage of children under age five with fever
Percentage of pregnant women
Source
With at least one
mosquito net of any type 2006–2008d
With at least one
insecticide-treated
mosquito net 2006–2008d
Sleeping under any mosquito
neta 2006–2008d
Sleeping under an
insecticide-treated
mosquito neta 2006–2008d
Receiving antimalarial medicinesb 2006–2008d
Receiving antimalarial medicines on same or next dayb
2006–2008d
Receiving intermittent preventive treatmentc 2006–2008d
Sleeping under an
insecticide-treated
mosquito neta 2006–2008d
Korea, Dem. People’s Rep. of 55 17 1,562 — — — — — — — —
Korea, Rep. of 5 2 2,319 — — — — — — — —
Kuwait 11 1 242 — — — — — — — —
Kyrgyzstan 38 4 514 — — — — — — — —
Lao People’s Dem. Rep. 70 11 720 — — 82e 18e 9e — — — MICS 2000
Latvia 9 0 103 — — — — — — — —
Lebanon 29 2 362 — — — — — — — —
Lesotho 84 5 271 — — — — — — — —
Liberia 133 25 725 30 — — — 59 — — — DHS 2007
Libyan Arab Jamahiriya 18 3 688 — — — — — — — —
Liechtenstein 3 0 2 — — — — — — — —
Lithuania 8 0 150 — — — — — — — —
Luxembourg 3 0 27 — — — — — — — —
Macedonia, TFYR 17 0 115 — — — — — — — —
Madagascar 112 81 3,190 39e — 30e 0e 34e — — — DHS 2003–2004
Malawi 111 64 2,461 51 38 31 25 25 21 45f 15e MICS 2006; DHS 2004
Malaysia 11 6 2,756 — — — — — — — —
Maldives 30 0 31 — — — — — — — —
Mali 196 117 2,321 69 50 41 27 32 15 4 29 DHS 2006
Malta 5 0 20 — — — — — — — —
Marshall Islands 54 0 6 — — — — — — — —
Mauritania 119 12 462 57 12 31e 2e 21 10 — — MICS 2007
Mauritius 15 0 94 — — — — — — — —
Mexico 35 73 10,342 — — — — — — — —
Micronesia, Fed. Sts. of 40 0 14 — — — — — — — —
Moldova 18 1 211 — — — — — — — —
Monaco 4 0 2 — — — — — — — —
Mongolia 43 2 232 — — — — — — — —
Montenegro 10 0 38 — — — — — — — —
Morocco 34 22 3,005 — — — — — — — —
Mozambique 168 144 3,700 — — 10e — 15e 8e — — DHS 2003–2004h
Myanmar 103 92 4,132 — — — — — — — —
Namibia 68 4 248 25 20 12 11 10 — 10 9 DHS 2006–2007
Nauru 30 0 1 — — — — — — — —
Nepal 55 44 3,651 — — — — 0 — — — DHS 2006
Netherlands 5 1 969 — — — — — — — —
New Zealand 6 0 285 — — — — — — — —
Nicaragua 35 5 673 42e — — — 2e — — — DHS 2001
Niger 176 123 2,797 69 43 15 7 33 25 0 7 DHS 2006
Nigeria 189 1,126 24,823 12e 2e 6e 1e 34e 25e 1e 1e DHS 2003
Niue — — 0 — — — — — — — —
Norway 4 0 284 — — — — — — — —
Occupied Palestinian Terr. 27 4 685 — — — — — — — —
Oman 12 1 271 — — — — — — — —
Pakistan 90 400 19,333 6 0 2 — 3 3 — — DHS 2006–2007

STATISTICAL TABLE (CONTINUED)
Country or territory
Under-five mortality
rate (per 1,000 live births)
2007
Number of under-five
deaths (thousands)
2007
Number of under-five children
(thousands) 2007
Percentage of households
Percentage of children under age five
Percentage of children under age five with fever
Percentage of pregnant women
Source
With at least one
mosquito net of any type 2006–2008d
With at least one
insecticide-treated
mosquito net 2006–2008d
Sleeping under any mosquito
neta 2006–2008d
Sleeping under an
insecticide-treated
mosquito neta 2006–2008d
Receiving antimalarial medicinesb 2006–2008d
Receiving antimalarial medicines on same or next dayb
2006–2008d
Receiving intermittent preventive treatmentc 2006–2008d
Sleeping under an
insecticide-treated
mosquito neta 2006–2008d
Palau 10 0 2 — — — — — — — —
Panama 23 2 344 — — — — — — — —
Papua New Guinea 65 12 894 — — — — — — — —
Paraguay 29 4 734 — — — — — — — —
Peru 20 12 2,817 — — — — — — — —
Philippines 28 64 11,095 — — — — — — — —
Poland 7 3 1,767 — — — — — — — —
Portugal 4 0 558 — — — — — — — —
Qatar 15 0 65 — — — — — — — —
Romania 15 3 1,051 — — — — — — — —
Russian Federation 15 23 7,302 — — — — — — — —
Rwanda 181 79 1,685 59 56 60 56 6 0 — 60 DHS 2007–2008
Saint Kitts and Nevis 18 0 5 — — — — — — — —
Saint Lucia 18 0 15 — — — — — — — —
Saint Vincent & Grenadines 19 0 12 — — — — — — — —
Samoa 27 0 24 — — — — — — — —
San Marino 4 0 2 — — — — — — — —
São Tomé and Principe 99 0 23 49 36 53 42 25 17 — — MICS 2006
Saudi Arabia 25 15 2,921 — — — — — — — —
Senegal 114 50 1,942 57 36 28 16 22 11 49 17 MIS 2006
Serbia 8 1 610 — — — — — — — —
Seychelles 13 0 15 — — — — — — — —
Sierra Leone 262 70 1,019 40 37 28 26 30 15 12 28 DHS 2008g
Singapore 3 0 200 — — — — — — — —
Slovakia 8 0 260 — — — — — — — —
Slovenia 4 0 89 — — — — — — — —
Solomon Islands 70 1 71 — — — — — — — —
Somalia 142 54 1,539 22 12 18 11 8 3 1f — MICS 2006
South Africa 59 64 5,235 — — — — — — — —
Spain 4 2 2,321 — — — — — — — —
Sri Lanka 21 6 1,464 62 5 62 3 0 — — 2 DHS 2006–2007h
Sudan 109 134 5,528 37 18 — 28 54 3 — — ONS 2006
Suriname 29 0 44 — — 77e 3e — — — — MICS 2000
Swaziland 91 3 147 6 4 1 1 1 — 1i 1 DHS 2006–2007
Sweden 3 0 505 — — — — — — — —
Switzerland 5 0 358 — — — — — — — —
Syrian Arab Republic 17 9 2,544 — — — — — — — —
Tajikistan 67 12 857 5e 2e 2e 1e 2e 1e — — MICS 2005
Tanzania, United Rep. of 116 186 7,050 56 39 36 26 57 34 30 27 MIS 2007–2008
Thailand 7 7 4,518 — — — — — — — —
Timor-Leste 97 5 199 — — 48e 8e 47e — — — MICS 2002
Togo 100 25 1,061 46 40 41 38 48 38 18f — MICS 2006
Tonga 23 0 12 — — — — — — — —
Trinidad and Tobago 35 1 94 — — — — — — — —
Tunisia 21 4 830 — — — — — — — —

STATISTICAL TABLE (CONTINUED)
Demographics and key malaria control indicators
Country or territory
Under-five mortality
rate (per 1,000 live births)
2007
Number of under-five
deaths (thousands)
2007
Number of under-five children
(thousands) 2007
Percentage of households
Percentage of children under age five
Percentage of children under age five with fever
Percentage of pregnant women
Source
With at least one
mosquito net of any type 2006–2008d
With at least one
insecticide-treated
mosquito net 2006–2008d
Sleeping under any mosquito
neta 2006–2008d
Sleeping under an
insecticide-treated
mosquito neta 2006–2008d
Receiving antimalarial medicinesb 2006–2008d
Receiving antimalarial medicines on same or next dayb
2006–2008d
Receiving intermittent preventive treatmentc 2006–2008d
Sleeping under an
insecticide-treated
mosquito neta 2006–2008d
Turkey 23 32 6,646 — — — — — — — —
Turkmenistan 50 5 494 — — — — — — — —
Tuvalu 37 0 1 — — — — — — — —
Uganda 130 188 6,028 34 16 22 10 61 29 16 10 DHS 2006
Ukraine 24 10 2,025 — — — — — — — —
United Arab Emirates 8 1 327 — — — — — — — —
United Kingdom 6 4 3,503 — — — — — — — —
United States 8 34 20,957 — — — — — — — —
Uruguay 14 1 252 — — — — — — — —
Uzbekistan 41 26 2,879 — — — — — — — —
Vanuatu 34 0 31 — — — — — — — —
Venezuela, B.R. 19 11 2,896 — — — — — — — —
Viet Nam 15 25 8,109 97 19 95 5 3 2 — 15e MICS 2006; ONS 2005
Yemen 73 63 3,740 — — — — — — — —
Zambia 170 80 2,030 72 62 48 41 43 29 60 43 MIS 2008
Zimbabwe 90 34 1,706 20 9 7 3 5 3 6 3 DHS 2005–2006
Regional groupings
Sub-Saharan Africa 148 4,480 127,624 44 30 28 20 34 21 — —
Eastern & Southern Africa 123 1,761 61,296 48 39 31 26 30 16 — 32
Western & Central Africa 169 2,719 66,328 40 21 25 13 39 26 — —
Middle East & North Africa 46 445 44,789 — — — — — — — —
South Asia 78 2,985 175,250 32 — — — 7 — — —
East Asia & the Pacific 27 799 144,441 — — — — — — — —
Latin America & Caribbean 26 302 55,622 — — — — — — — —
CEE/CIS 25 138 26,458 — — — — — — — —
Industrialized countries 6 66 54,922 — — — — — — — —
Developing countries 74 9,109 562,128 — — — — — — — —
Least developed countries 130 3,775 124,237 46 32 30 21 32 18 — —
World 68 9,216 629,106 — — — — — — — —
— not available.
Note: Data are from the UNICEF malaria databases, which include survey data from Demographic and Health Surveys (DHS), Malaria Indicator Surveys (MIS), Multiple Indicator Cluster Surveys (MICS) and
other national surveys (ONS). The complete databases (including time series, disparities and detailed source information) are available at www.childinfo.org. Demographic information is based on United
Nations Population Division estimates (children under age five) and Interagency Group for Child Mortality Estimation (under-five deaths).
Data are for the night before the survey.a. Data are for the two weeks before the survey.b. Data are for women ages 15–49 with a live birth in the previous two years who received two or more doses of sulfadoxine-pyrimethamine/Fansidar during pregnancy through an antenatal care visit.c. Data are for the most recent year available during the period specified.d. Data are for years or periods other than those specified.e. Data do not specify that intermittent preventive treatment was received through an antenatal care visit.f. Preliminary report.g. National report.h. Data are for two or more doses of chloroquine received during pregnancy.i.

19NotesChambers 2009.1.WHO 2008b. 2. Crawley and others 2007.3. Desai and others 2007.4. Roll Back Malaria Partnership 2008. 5. Roll Back Malaria Partnership 2008. 6. WHO 2008b.7. Lengeler 2004. 8. Different definitions of universal coverage 9. have been used by different countries and their development partners. For planning purposes, many countries currently use the definition of one net for every two people at risk of malaria, which is used by the Net Map-ping Project assessment.Estimates are derived from the Roll Back 10. Malaria Harmonisation Working Group database.U.S. President’s Malaria Initiative 2009. 11. WHO 2007.12. Marchesini and Crawley 2004; Ter Kuile, van 13. Eik, and Filler 2007; Crawley and others 2007; WHO 2005.GFATM forthcoming.14.
Technical noteFigures presented in this booklet have been adapted and updated from the publication: UNICEF and RBM, 2007, Malaria and Chil-dren: Progress in Intervention Coverage, New York: UNICEF.
UNICEF headquarters maintains a series of public- access databases on key malaria preven-tion and treatment indicators. Data are derived from national-level households surveys, including the UNICEF-supported Multiple Indicator Clus-ter Surveys (MICS), USAID-supported Demo-graphic and Health Surveys (DHS) and Malaria Indicator Surveys (MIS). Most of the indica-tors presented in this booklet draw on the UNI-CEF malaria databases. The complete databases (including time series, disparities and detailed source information), along with information on
data interpretation, are available at www.child-info.org.
ReferencesChambers, Raymond. 2009. “United Nations
Secretary- General’s Special Envoy for Malaria Progress Report.” Office of the UN Secretary-General Special Envoy for Malaria, New York. www.malariaenvoy.com/tabid/61/Default.aspx?udt_373_param_detail=57.
Crawley, J. J., J. Hill, J. Yartley, M. Robalo, A. Seru-filira, A. Ba-Nguz, E. Roman, A. Palmer, K. Asamoa, and R. Steketee. 2007. “From Evi-dence to Action? Challenges to Policy Change and Programme Delivery for Malaria in Preg-nancy.” The Lancet Infectious Diseases 7(2): 145–55.
Desai, M., F.O. ter Kuile, F. Nosten, R. McGready, K. Asamoa, B. Brabin, and R. D. Newman. 2007. “Epidemiology and Burden of Malaria in Pregnancy.” The Lancet Infectious Diseases 7(2): 93–104.
Garrett, Laurie. 2008. “Development and Global Health Aid Cuts Would Be Cruelest of All.” Council on Foreign Relations, Novem-ber 2008. www.cfr.org/publication/17811/development_and_global_health_aid_cuts_would_be_cruelest_of_all.html.(Accessed March 2009).
GFATM (Global Fund to Fight AIDS, Tuber-culosis and Malaria). Forthcoming. Global Fund Five-Year Evaluation: Study Area 3 (Health Impact). May 2009. Geneva: Global Fund to Fight AIDS, Tuberculosis and Malaria.
Harvey, S.A., L. Jennings, M. Chinyama, F. Masan-inga, K. Mulholland, and D. R Bell. 2008. “Improving Community Health Worker Use of Malaria Rapid Diagnostic Tests in Zam-bia: Package Instructions, Job Aid and Job Aid-Plus-Training.” Malaria Journal 7 doi: 10.1186/1475–2875-7-160. http://rbm.who.int/partnership/wg/wg_itn/docs/Cochrane_reviewITNs2004.pdf.
Notes, technical note and references

20 Jones G., R. Steketee, R.E. Black, Z.A. Bhutta, S.S. Morris, and The Bellagio Child Survival Group. 2003. “How Many Child Deaths Can We Prevent This Year?” Lancet 362 (9377): 65–71.
Lengeler, C. 2004. “Insecticide-treated Bed Nets and Curtains for Preventing Malaria.” Cochrane Database of Systematic Reviews issue 2, article CD000363, doi: 10.1002/14651858.CD000363.pub2. http://rbm.who.int/partnership/wg/wg_itn/docs/Cochrane_reviewITNs2004.pdf.
Marchesini, P., and J. Crawley. 2004. “Reducing the Burden of Malaria in Pregnancy.” Roll Back Malaria, Geneva. www.who.int/malaria/rbm/Attachment/20040713/MeraJan2003.pdf.
Madagascar Ministry of Health. 2007. “Evaluation of the ownership and usage of LLINs in Mad-agascar six months after the October 2007 measles and malaria integrated campaign.” Final report.
Milliner, John. 2009. “Net Mapping Project.” President’s Malaria Initiative. United States Agency for International Development, Wash-ington, DC. www.malariaenvoy.org.
Roll Back Malaria Harmonisation Working Group. 2009. Personal communication regarding sup-port for malaria grant proposals. 1 April 2009. New York.
Roll Back Malaria Monitoring and Evaluation Ref-erence Group. 2009. Personal communica-tion regarding interpreting malaria treatment data. 1 April 2009. New York.
Roll Back Malaria Partnership. 2008. The Global Malaria Action Plan for a Malaria-free World. Geneva: Roll Back Malaria Partnership.
Ter Kuile, F.O., A.M. van Eik, and S.J. Filler. 2007. “Effect of Sulfadoxine-Pyrimethamine Resis-tance on the Efficacy of Intermittent Pre-ventive Therapy for Malaria Control during Pregnancy.” Journal of the American Medical Association 297: 2603–16.
U.S. President’s Malaria Initiative. 2009. Annual Report 2009. Washington, DC: U.S. Agency for International Development.
WHO (World Health Organization). 2005. “Malaria Control Today: Current WHO Rec-ommendations.” Working Document. World Health Organization, Geneva.
———. 2007. “Containment of Malaria Multi drug Resistance on the Cambodia- Thailand Border.” Report on an informal consultation. Phnom Penh, 29–30 Janu-ary, 2007. http://malaria.who.int/docs/drugresistance/ReportThaiCam.pdf.
———.2008a.The Global Burden of Disease: 2004 Update. Geneva: World Health Organization.
———. 2008b. World Malaria Report 2008. Geneva: World Health Organization.


On World Malaria Day in 2009, just over 600 days remain until the 31 December 2010 deadline set by UN Secretary-General Ban Ki-moon for all endemic countries to achieve universal coverage with key malaria control interventions. Data presented here highlight major signs of progress across sub-Saharan Africa toward this goal.
Malaria has become a major development priority. New and ambitious goals are challenging countries to implement bold plans to scale up their programs—critical for achieving the Millennium Development Goals in affected countries. There have also been major increases in funding for malaria control in recent years, and in 2008 world leaders again committed billions more towards malaria control.
Indeed, a new phase in the fight against malaria has begun. Net manufacturers’ estimates indicate that malaria-endemic countries in Africa have now received enough nets to cover more than 40 per cent of their at-risk populations. Across sub-Saharan Africa, more children are using insecticide-treated nets, with 19 of the 22 countries with trend data showing at least a threefold increase since around 2000 and 17 showing at least a fivefold increase. Most of these nets are distributed through integrated maternal and child health services, such as antenatal care and immunization.
Despite major increases in procurement of artemisinin-based combination therapy since around 2005, many African children are still using less effective medicines and there has been little or no progress in expanding coverage in most countries since 2000. But important work is now under way to improve coverage with effective treatment.
Based on these efforts, some areas are now showing major reductions in the number of malaria cases and deaths, with more declines expected in the coming years.
2009
ISBN: 978-92-806-4421-0
Related Documents