
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
-Trishna Kattelroll no. 20
INTRODUCTION

MALARIA
• Name is derived from Italian Mal’ aria or bad air• Malaria is a mosquito-borne infectious
disease of caused by parasitic protozoan of the genus Plasmodium.
• the disease is transmitted by a bite from an infected female Anopheles mosquito
• In humans, the parasites multiply in liver and infect the RBCs.

• Malaria is the fifth cause of death of infectious diseases worldwide.
• It is a disease that can be cured within 48 hours, yet it can cause fatal complications if the diagnosis and treatment are delayed.
• Malaria Kills more people than AIDS
• Malaria kills in one year what AIDS kills in 15 years. For every death due to HIV/AIDS there are about 50 deaths due to malaria.
Malaria – Early History
• The symptoms of malaria were described in ancient Chinese medical writings. In 2700 BC, several characteristic symptoms of what would later be named malaria were described in the Nei Ching.

Hippocrates and Malaria
Hippocrates, who is regarded as the "Father of Medicine", was the first to describe the manifestations of the disease, and relate them to the time of year and to where the patients lived. He is the first known malariologist.
History – Events on Malaria
• 1880 - Charles Louis Alphose Lavern discovered malarial parasite in wet mount
• 1883 - Methylene blue stain - Marchafava• 1891 - Polychrome stain- Romanowsky• 1898 - Roland Ross - Life cycle of
parasite transmission, wins Nobel Prize in 1902
• 1948 - Site of Exoerythrocytic development in Liver by Shortt and Garnham

EPIDEMIOLOGY
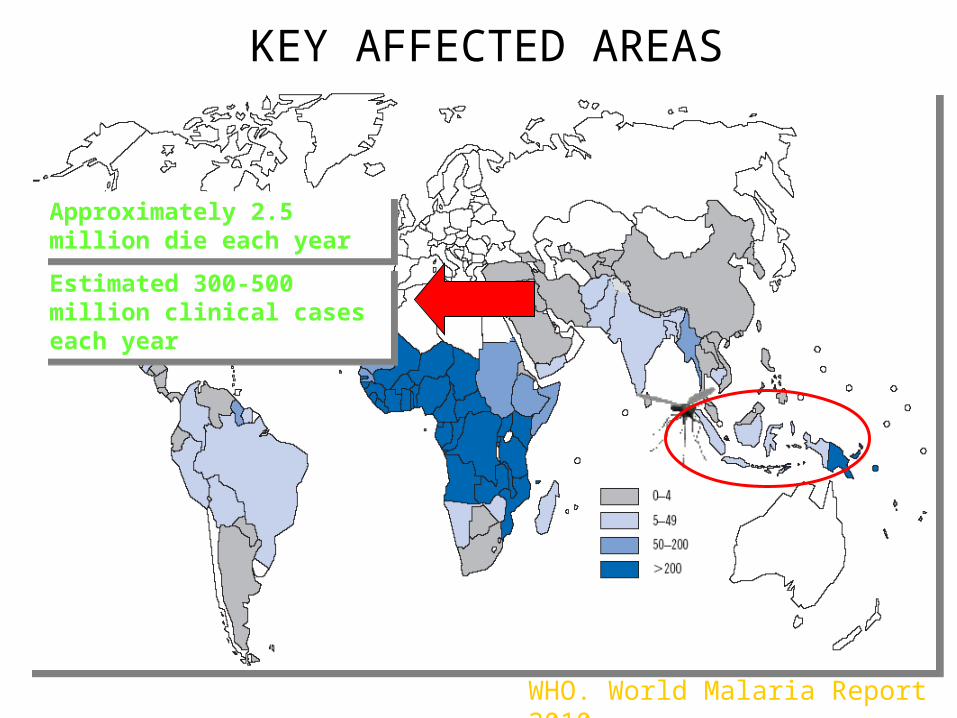
KEY AFFECTED AREAS
WHO. World Malaria Report 2010
Estimated 300-500 million clinical cases each year
Estimated 300-500 million clinical cases each year
Approximately 2.5 million die each year
Approximately 2.5 million die each year
CAUSATIVE AGENTS OF MALARIA
PRESENTED BY: SOFIYA MAKAJOOROLL NO:27

• Malaria is an infectious disease caused by plasmodium species.
• Plasmodium is a protozoa discovered by Alphonse Laveran.
• Transmission of this parasite to human is by blood sucking bite of female anopheles mosquito of various species.
ANOPHELES MOSQUITO

Four species of plasmodium which typically infect humans are;
1. Plasmodium falciparum2. Plasmodium vivax3. Plasmodium malariae4. Plasmodium ovale
• The genus plasmodium includes about 200 named species of intra-erythrocytic parasites.
• These species infect a wide range of mammals, birds, reptiles, and amphibians.

SPECIES TYPES OF MALARIA
Plasmodium falciparum Malignant tertian malariaPlasmodium vivax Benign tertian malariaPlasmodium malariae Benign quartan malaria Plasmodium ovale Benign tertian malaria
• Out of the four species PLASMODIUM VIVAX and PLASMODIUM FALCIPARUM are the most common.
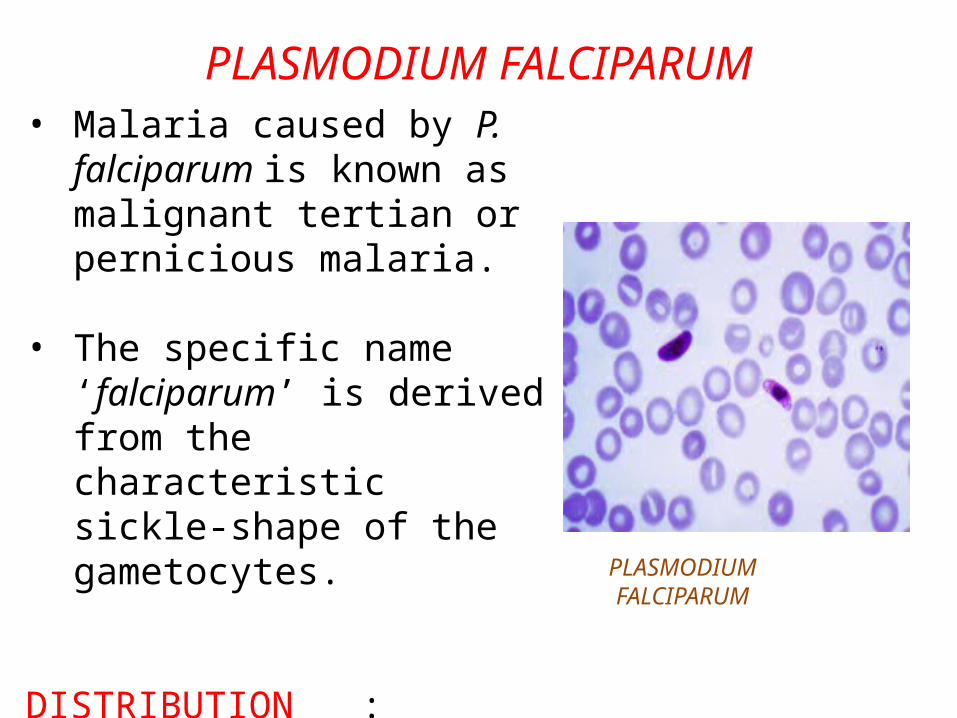
PLASMODIUM FALCIPARUM• Malaria caused by P. falciparum
is known as malignant tertian or pernicious malaria.
• The specific name ‘falciparum’ is derived from the characteristic sickle-shape of the gametocytes.
DISTRIBUTION : Found mainly in tropical, sub- tropical, Africa, South America and Asia.
PLASMODIUM FALCIPARUM
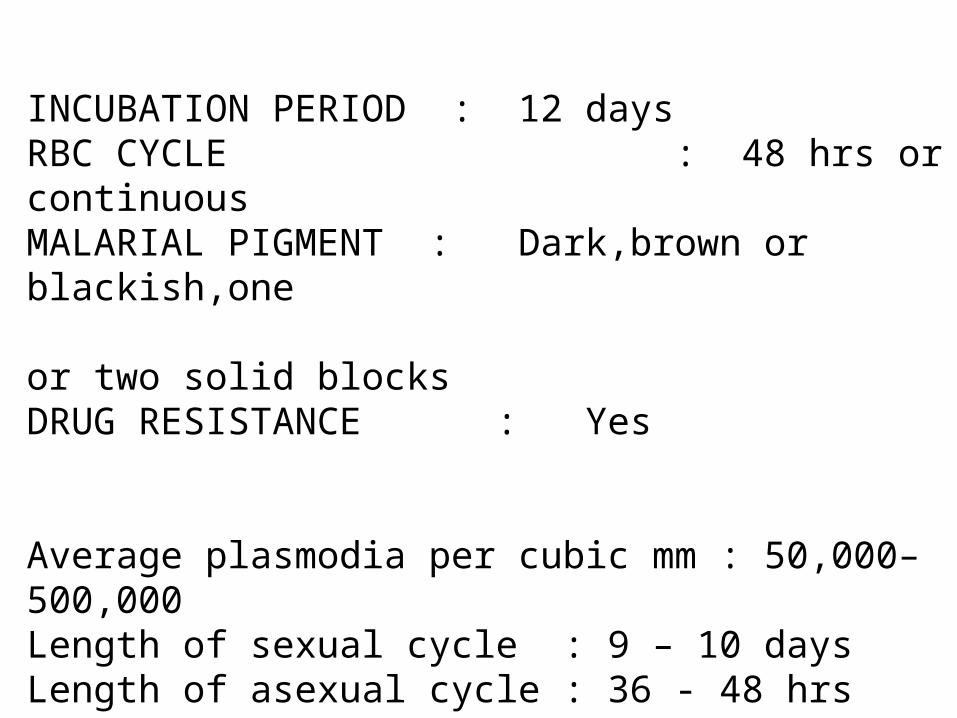
INCUBATION PERIOD : 12 days RBC CYCLE : 48 hrs or continuousMALARIAL PIGMENT : Dark,brown or blackish,one or two solid blocksDRUG RESISTANCE : Yes
Average plasmodia per cubic mm : 50,000–500,000Length of sexual cycle : 9 – 10 daysLength of asexual cycle : 36 - 48 hrs
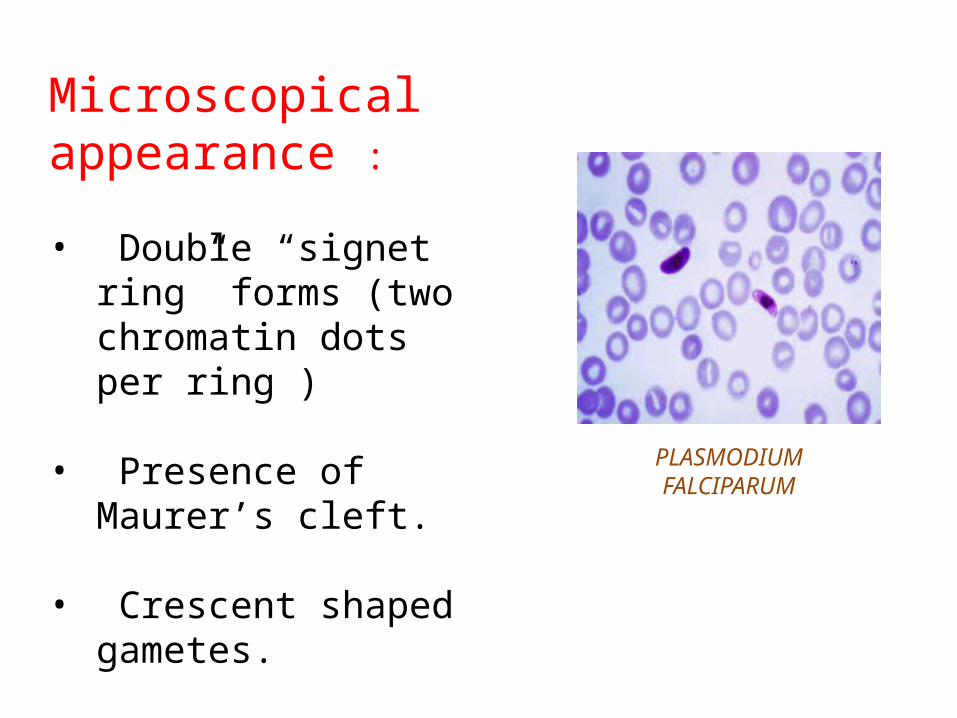
Microscopical appearance :
• Double “signet ring” forms (two chromatin dots per ring )
• Presence of Maurer’s cleft.
• Crescent shaped gametes.
PLASMODIUM FALCIPARUM

Why P. falciparum is most highly pathogenic ??
• This species infects all RBCs, resulting in prominent anemia.
• Its changes the RBC surface which causes endothelial adherence with decreased microcirculation and
cerebral malaria.
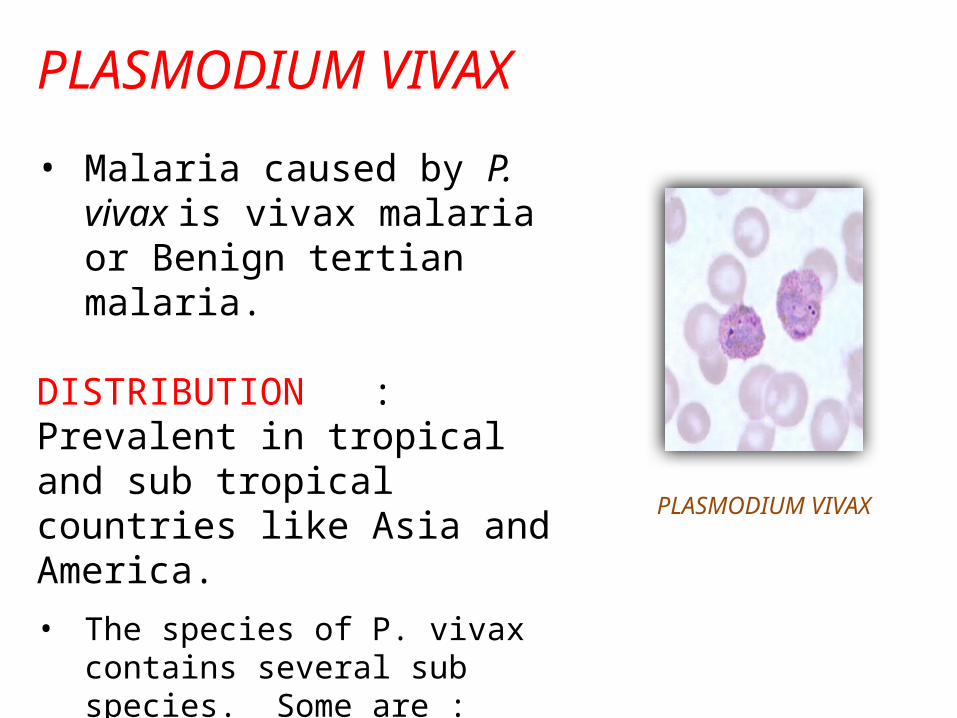
PLASMODIUM VIVAX
• Malaria caused by P. vivax is vivax malaria or Benign tertian malaria.
DISTRIBUTION : Prevalent in tropical and sub tropical countries like Asia and America.• The species of P. vivax contains
several sub species. Some are :• Plasmodium vivax multinucleatum• Plasmodium vivax hybernans
PLASMODIUM VIVAX
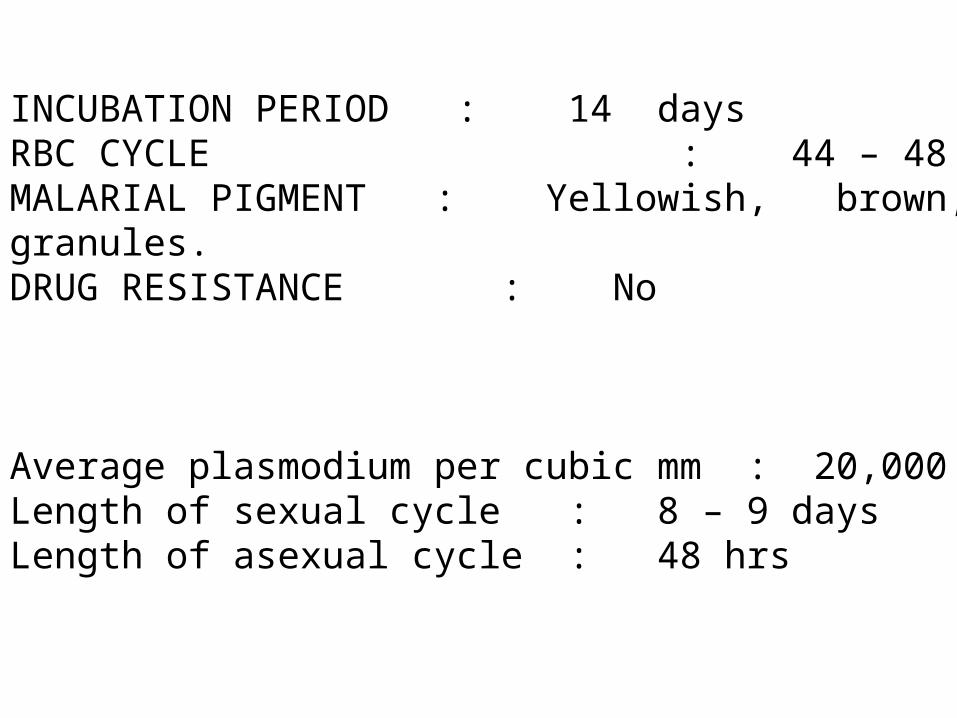
INCUBATION PERIOD : 14 daysRBC CYCLE : 44 – 48 hrsMALARIAL PIGMENT : Yellowish, brown, fine granules.DRUG RESISTANCE : No
Average plasmodium per cubic mm : 20,000Length of sexual cycle : 8 – 9 days Length of asexual cycle : 48 hrs
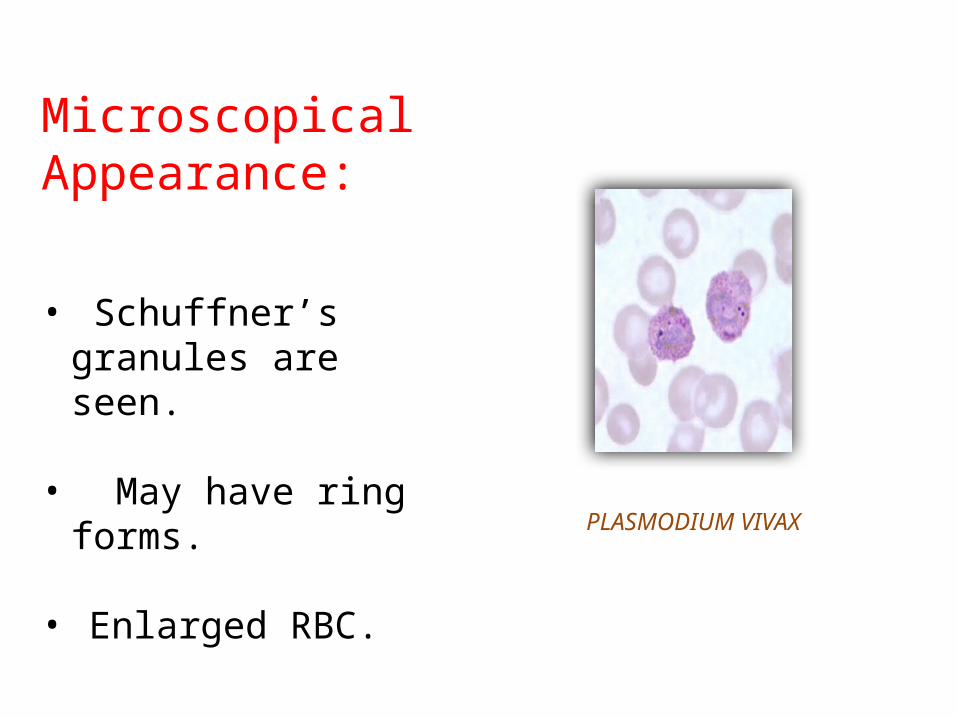
Microscopical Appearance:
• Schuffner’s granules are seen.
• May have ring forms. • Enlarged RBC. PLASMODIUM VIVAX
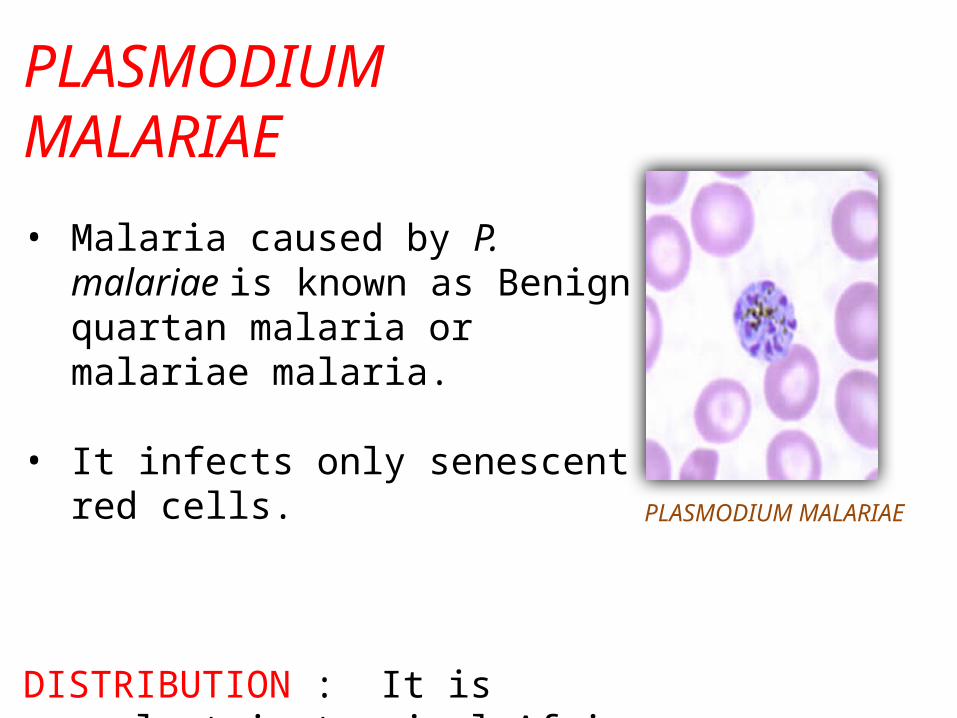
PLASMODIUM MALARIAE
• Malaria caused by P. malariae is known as Benign quartan malaria or malariae malaria.
• It infects only senescent red cells.
DISTRIBUTION : It is prevalent in tropical Africa and accounts for upto 25% of Plasmodium infection.
PLASMODIUM MALARIAE
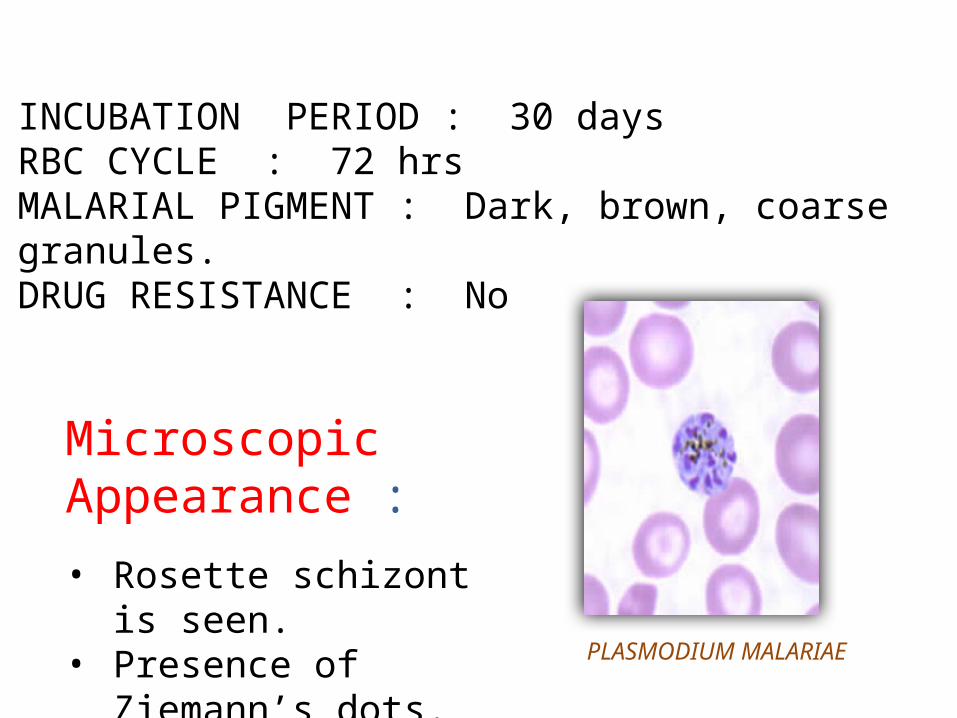
Microscopic Appearance :
• Rosette schizont is seen.• Presence of Ziemann’s
dots.
INCUBATION PERIOD : 30 daysRBC CYCLE : 72 hrsMALARIAL PIGMENT : Dark, brown, coarse granules.DRUG RESISTANCE : No
PLASMODIUM MALARIAE
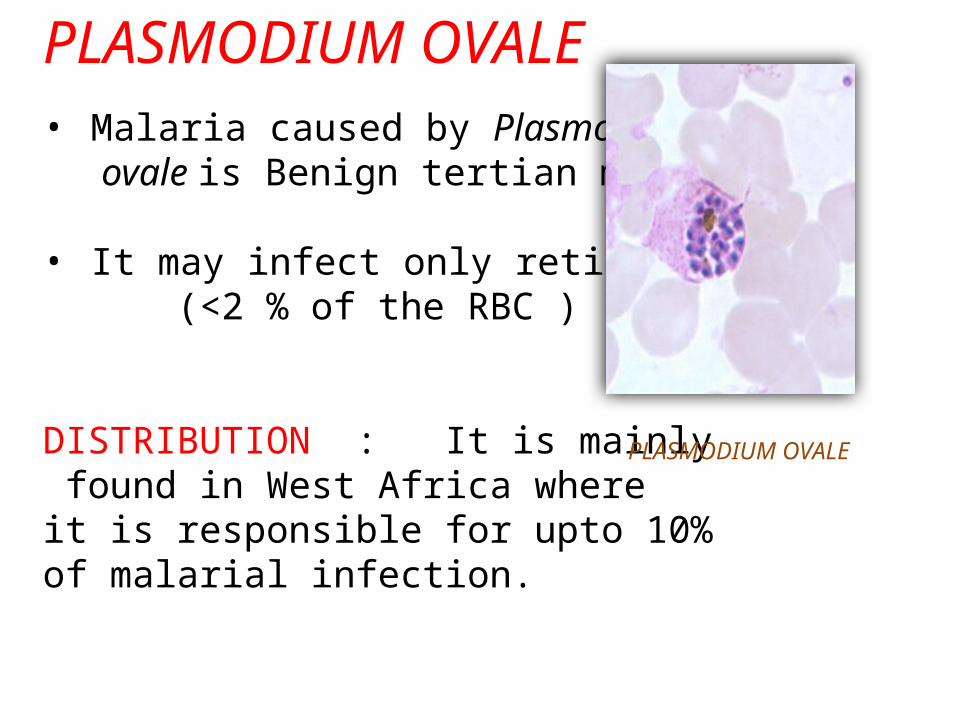
PLASMODIUM OVALE• Malaria caused by Plasmodium ovale is Benign tertian malaria.
• It may infect only reticulocytes. (<2 % of the RBC )
DISTRIBUTION : It is mainly found in West Africa where it is responsible for upto 10% of malarial infection.
PLASMODIUM OVALE

INCUBATION PERIOD : 14 days RBC CYCLE : 48 hrs MALARIAL PIGMENT : Dark, yellowish, brown, coarse granules. DRUG RESISTANCE : No
Microscopic Appearance :
• Enlarged oval red cells.
• Schuffner’s granules are seen.
PLASMODIUM OVALE
Life Cycle of Malarial Parasite
Presented by,Rajitha Kodithuwakku ArachchiRoll No 22
• Four species of genus plasmodium infect human with malaria1. Pasmodium vivax2. Plasmodium falciparum3. Plasmodium malariae4. Plasmodium ovale
• P.vivax and P.falciparum are more common.• Requires 2 hosts to complete it’s life cycle.• Human acts as the intermediate host.• Female anopheles mosquito acts as the vector and the definitive
host.
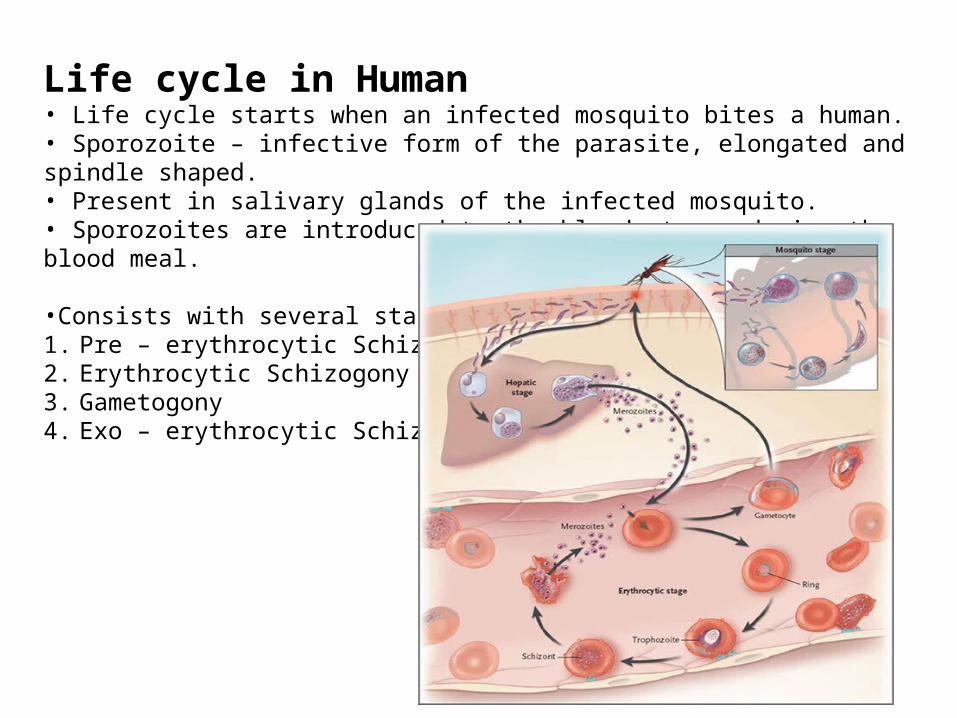
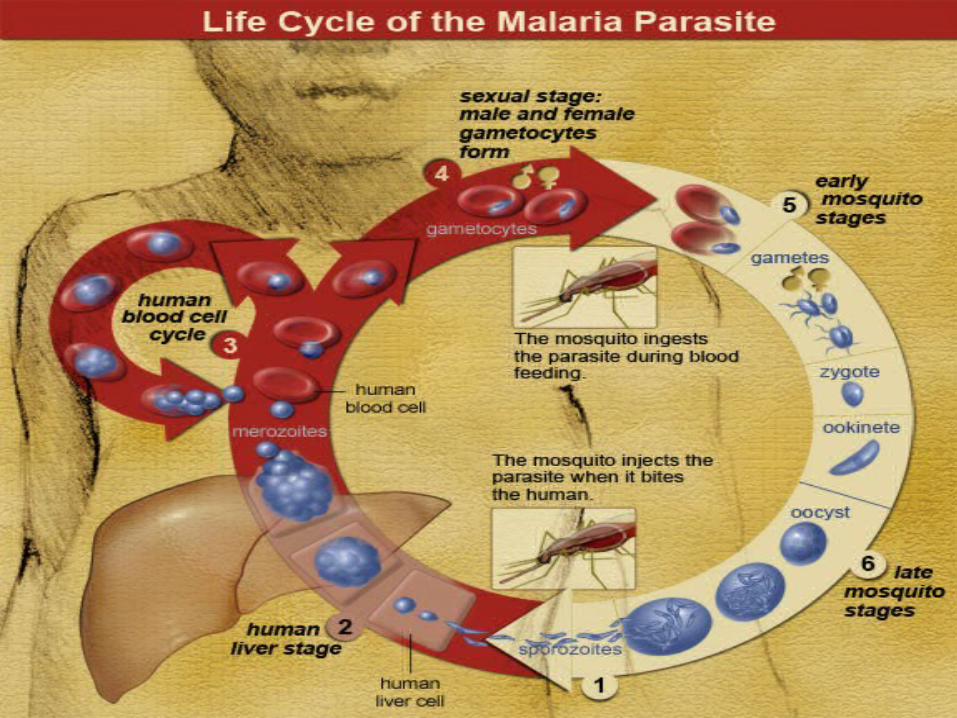
Life cycle in Human• Life cycle starts when an infected mosquito bites a human.• Sporozoite – infective form of the parasite, elongated and spindle shaped.• Present in salivary glands of the infected mosquito.• Sporozoites are introduced to the blood stream during the blood meal.
•Consists with several stages1. Pre – erythrocytic Schizogony2. Erythrocytic Schizogony3. Gametogony4. Exo – erythrocytic Schizogony

Pre – erythrocytic Schizogony• Sporozoites leave the blood stream and enter in to liver parenchymal cells.• Elongated and spindle shaped sporozoites become round in shape.• Undergo multiple nuclear division and develop in to merozoites.• 20,000 – 50,000 merozoites.• After compleion of the cycle liver cells rupture and release merozoites in to the blood stream
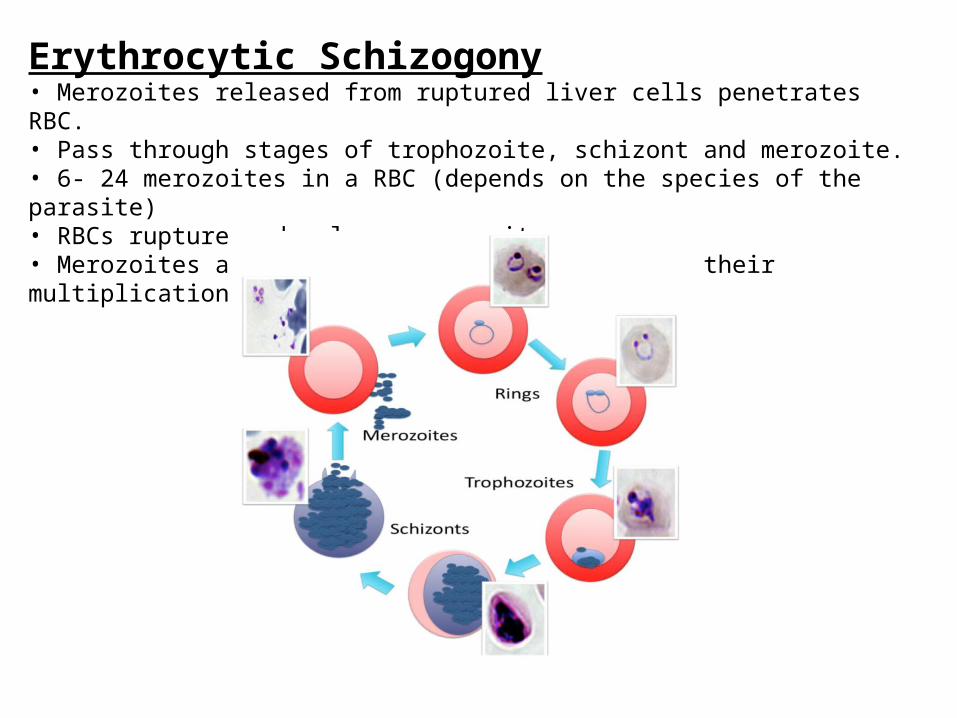
Erythrocytic Schizogony• Merozoites released from ruptured liver cells penetrates RBC.• Pass through stages of trophozoite, schizont and merozoite.• 6- 24 merozoites in a RBC (depends on the species of the parasite)• RBCs rupture and release merozoites.• Merozoites attacks healthy RBCs and continue their multiplication.

Gametogony• Some merozoites develop in to male and female gametocytes.• Known as microgametocytes and macrogametocytes respectively.• Develop in the RBCs of the capillaries of the internal organs such as spleen and bone marrow.• Microgametocytes – Smaller in size, large nucleus, light blue stained cytoplasm • Macrogametocytes – Larger in size, small and compact nucleus, deep blue stained cytoplasm
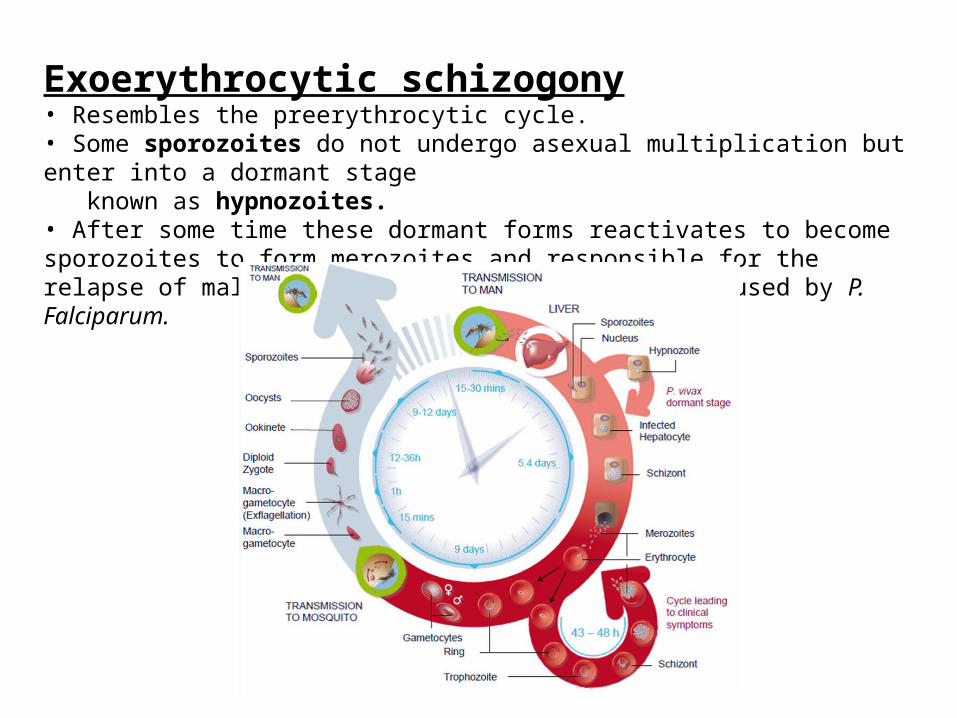
Exoerythrocytic schizogony• Resembles the preerythrocytic cycle.• Some sporozoites do not undergo asexual multiplication but enter into a dormant stage known as hypnozoites.• After some time these dormant forms reactivates to become sporozoites to form merozoites and responsible for the relapse of malaria. Cannot be seen in malaria caused by P. Falciparum.

Life cycle in mosquito• Male and female gametocytes enter in to the female anopheles mosquito during a blood meal from an infected human.• In the mid gut of the mosquito each microgametocytes develops into 4 to 8 micro gametes by the process of exflagellation.• one macrogametocyte forms only one macrogamete and does not show any exflagellation.• Macrogamete and microgamete fuse together to form a zygote which develops in to ookinete.• Ookinete develops into oocyst. Oosyct matures and develops into thousanda of sporozoites.


MALARIAL PATHOGENESIS
By: Prithul Koirala
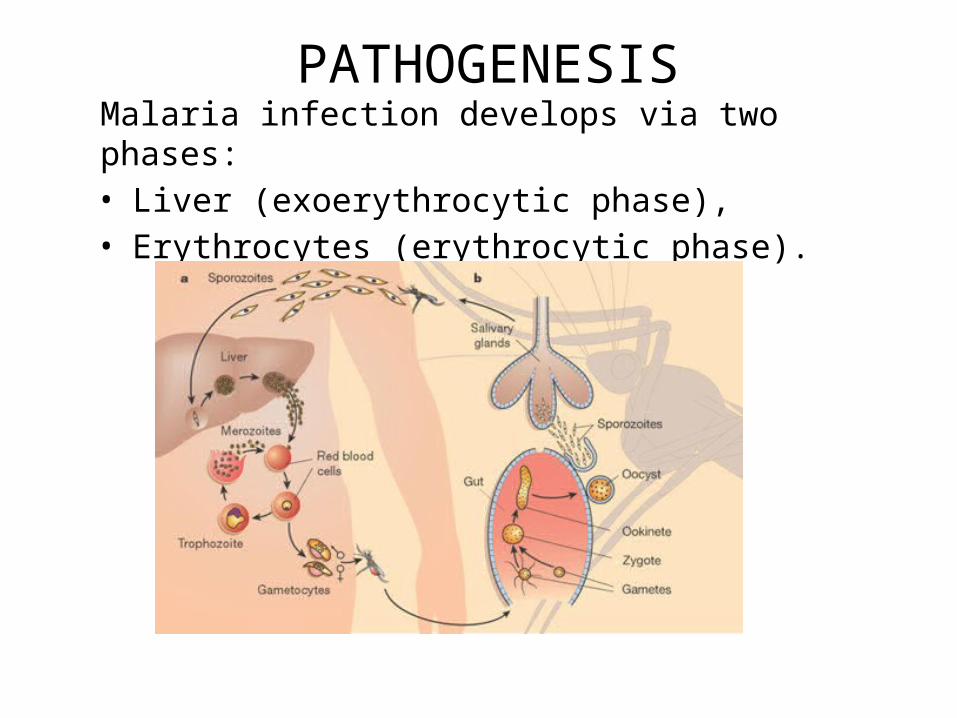
PATHOGENESISMalaria infection develops via two phases: • Liver (exoerythrocytic phase),• Erythrocytes (erythrocytic phase).
HEPATIC PHASE
• Sporozoites from mosquito's saliva enter the bloodstream
• Migrate to the liver where they infect hepatocytes, multiplying asexually for a period of 8–30 days.
• After a dormant period organisms differentiate to yield merozoites
• Rupture host cells, escape into the blood and infect red blood cells
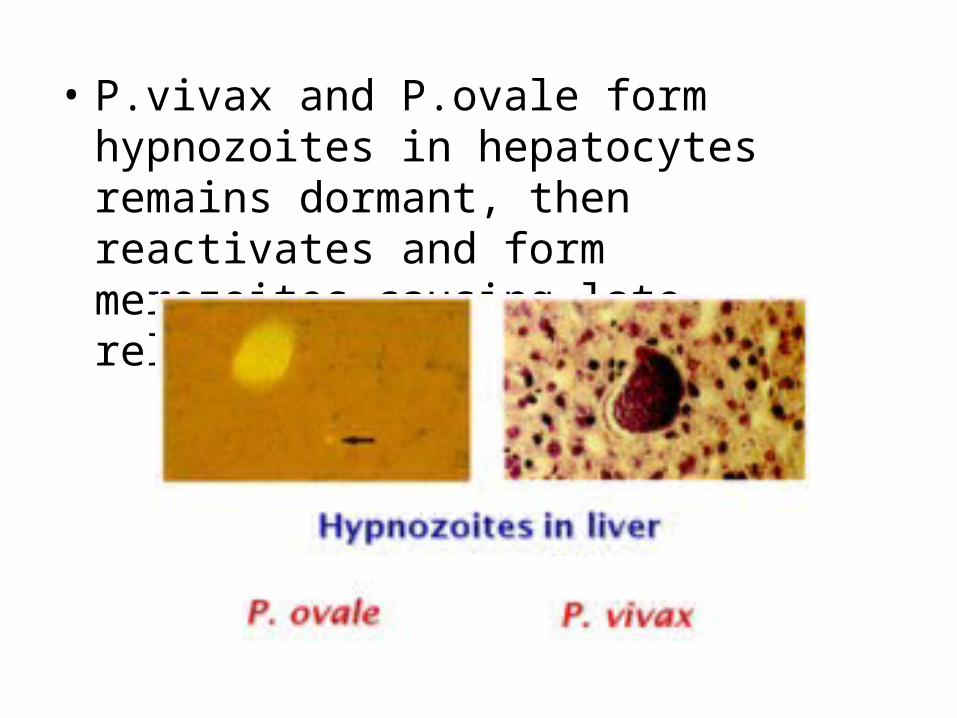
• P.vivax and P.ovale form hypnozoites in hepatocytes remains dormant, then reactivates and form merozoites causing late relapse in P.vivax malaria.

ERYTHROCYTIC PHASE• Binds to RBCS• Hydrolyze Hb by enzymes• Trophozoites formed(single chromatin)• Formation of schizonts• Lysis of RBCs

• Gametocytes are formed by parasites in RBCs which infect mosquito when it bites infected person
• Parasite is protected from body's immune system because it resides within the liver and blood cells invisible to immune surveillance.

CEREBRAL MALARIA• P.Falciparum infect RBCs leading to parasitic burden and
anemia• RBCs clump together(rosette)and stick to endothelial
cells of blood vessel(sequestration)

• Sequestered red blood cells can breach the blood–brain barrier
• Proteins like PfEMP1 forms knob
• Stimulates production of cytokines TNF,IL-1
• Induce fever,suppreses RBCs production, stimulate Nitric oxide production(tissue damage)


IMPACT OF SICKLE CELL TRAIT
Sickle cell trait causes cell to distort into curved shapeThe molecule is ineffective in releasing oxygen. Reduces the frequency with which malaria parasites complete their life cycle in the cell.
CLINICAL FEATURESOF MALARIA
By: Aishath Maeesha Roll no. 26

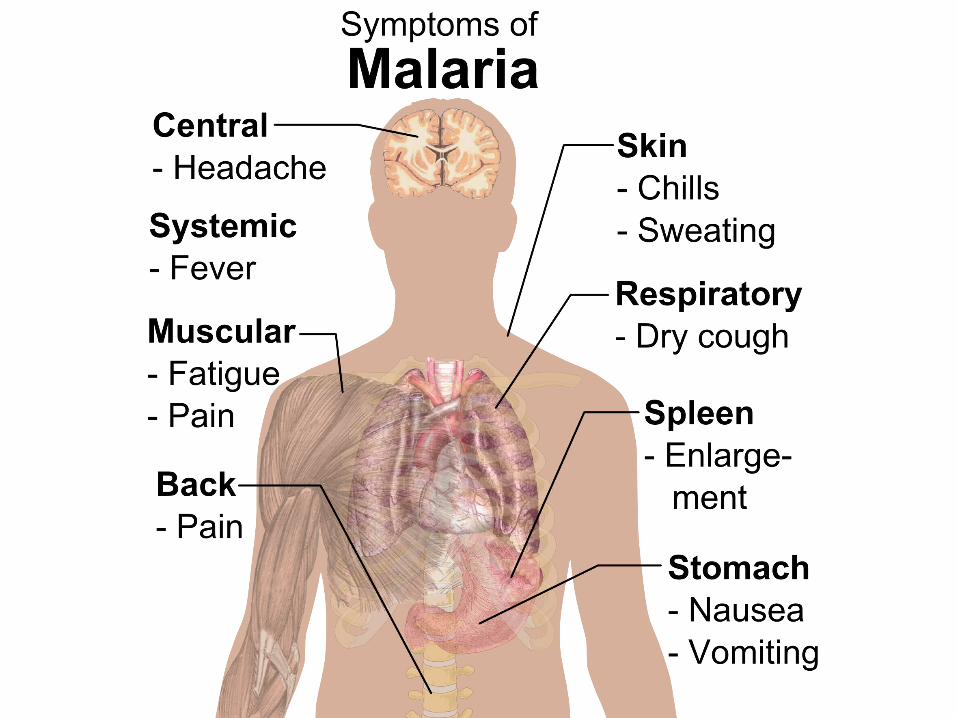
• The signs and symptoms of malaria typically begin 8–25 days following infection.
• Symptoms may occur later in those who have taken antimalarial medications as prevention.
• Initial manifestations of the disease—common to all malaria species—are similar to flu-like symptoms and can resemble other conditions such as septicemia, gastroenteritis and viral diseases
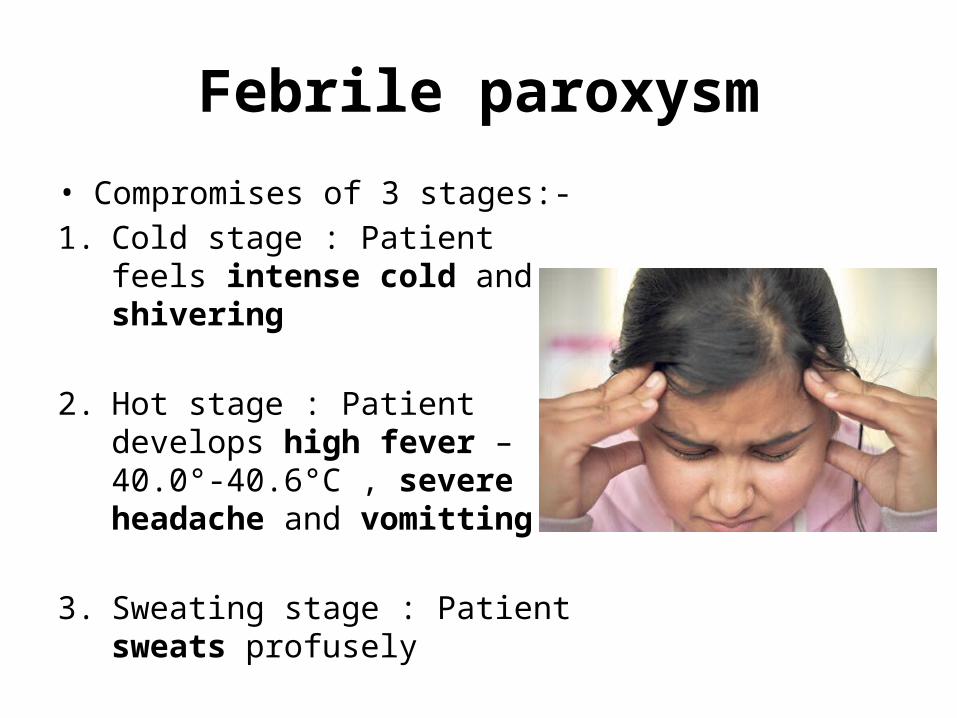
Febrile paroxysm
• Compromises of 3 stages:-1. Cold stage : Patient feels
intense cold and shivering
2. Hot stage : Patient develops high fever – 40.0°-40.6°C , severe headache and vomitting
3. Sweating stage : Patient sweats profusely
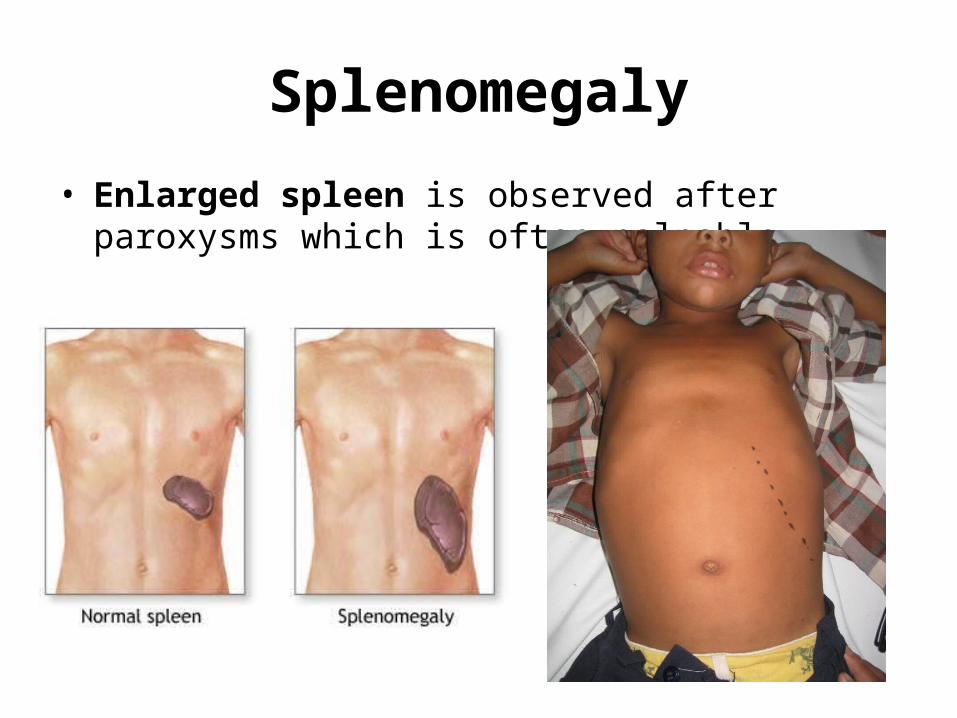
Splenomegaly
• Enlarged spleen is observed after paroxysms which is often palpable
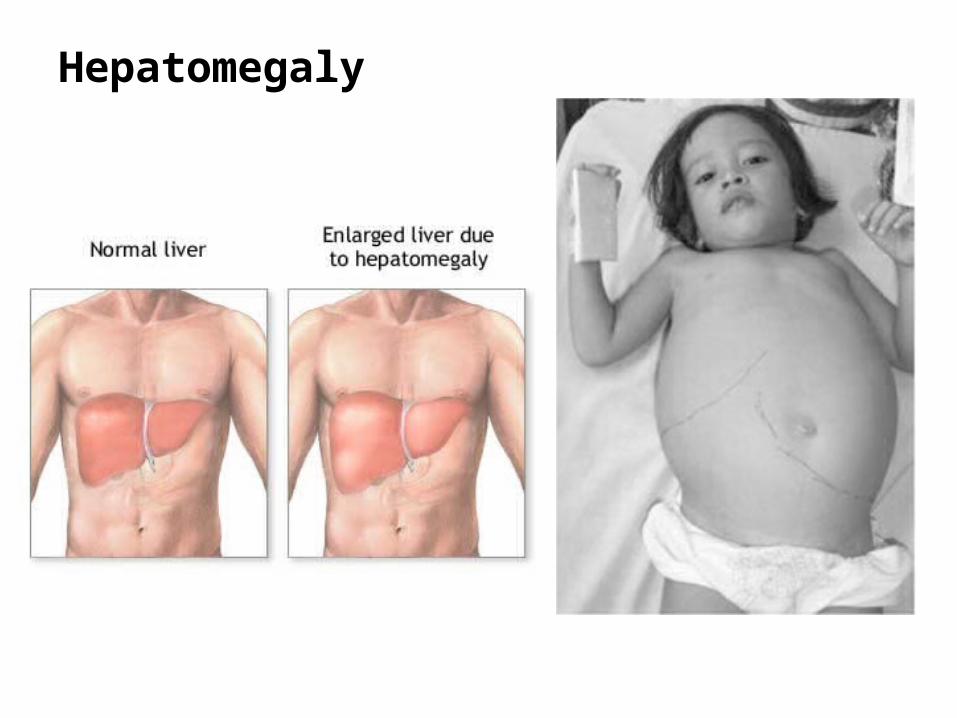
Hepatomegaly
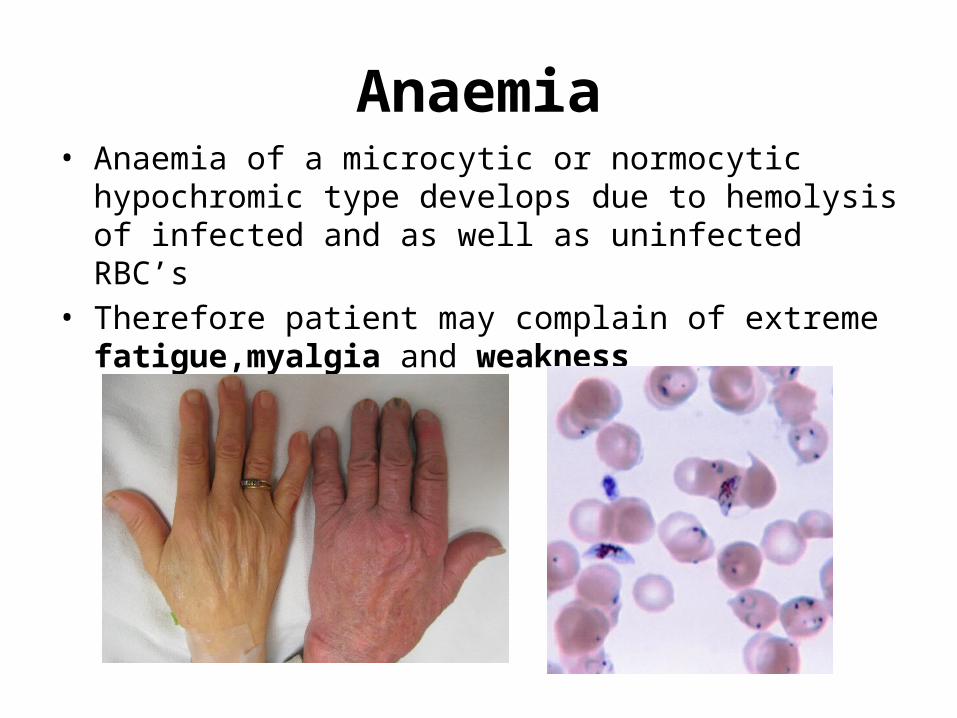
Anaemia• Anaemia of a microcytic or normocytic
hypochromic type develops due to hemolysis of infected and as well as uninfected RBC’s
• Therefore patient may complain of extreme fatigue,myalgia and weakness

Complications of P.Falciparum Malaria
• Pernicious Malaria: Arises due to heavy parasitization Manifestations are grouped as:
Cerebral malaria : Hyperpyrexia, confusion, palsy, abnormal posturing coma and paralysis
Algid Malaria: severe abdominal pain, vomitting, diarhhea, low blood pressure, hypodermia and cold clammy skin
Septicaemic Malaria: continuous fever, shock, liver or kidney failure

• Black water fever:
A complication of malaria in which RBC’s burst in the bloodstream releasing hemoglobin directly into the blood vessels and into the urine, frequently leading to kidney failure.
Occurs in persons who have been previously infected.
Clinical manifestations include:
Bilious vommiting Intense Jaundice Anuria Passage of dark red or blackish urine

LABORATORY DIAGNOSIS OF
MALARIA
SRUTHI KRISHNANROLL NO. 24
SEM- II
Presented by

Lab Diagnostic Techniques
• Light Microscopy• Fluorescent Microscopy• Quantitative buffy coat test• Serological tests• Molecular methods• Rapid diagnostic tests

Light Microscopy Most reliable, economic and preferred diagnostic procedure in malaria. Specimen : Peripheral Blood Two types of peripheral blood smears are prepared:
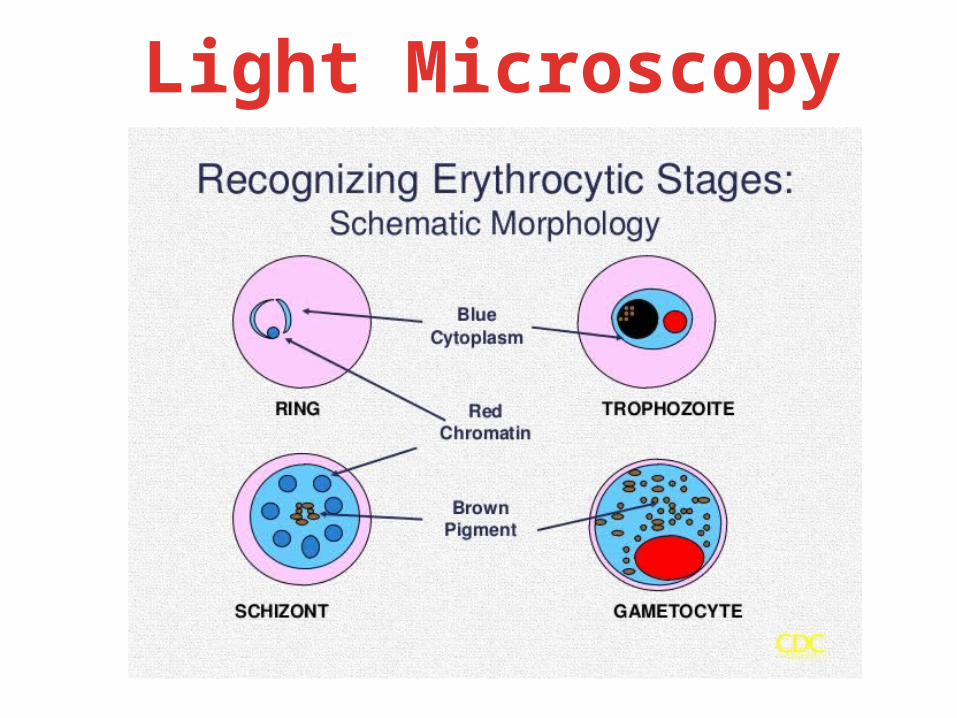
Light Microscopy
Light Microscopy All asexual erythrocytic stages (ring forms, trophozoites, schizonts) as well as gametocytes detected in P. vivax, P. malariae, P. ovale.
Only ring forms and gametocytes detected in P. falciparum.

2. Plasmodium vivaxPresence of Schuffner’s dotsEnlarged RBCs.
1. Plasmodium ovalePresence of Schuffner’s dotsSchizonts do not have more than 12 nuclei.
Light Microscopy
Light Microscopy
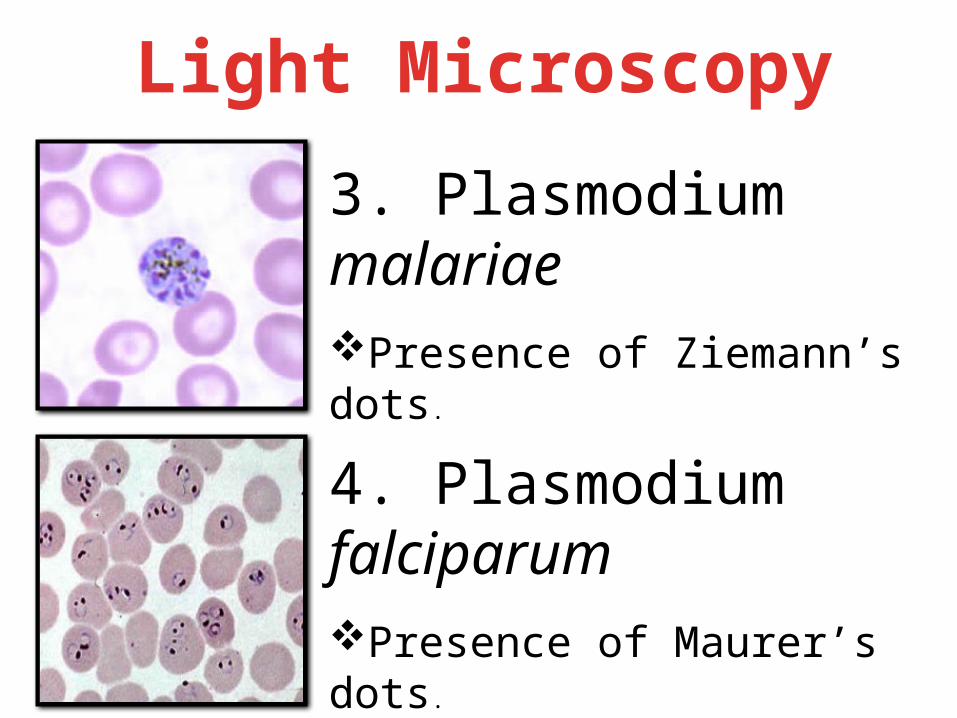
3. Plasmodium malariaePresence of Ziemann’s dots.
4. Plasmodium falciparumPresence of Maurer’s dots.
Multiple rings in individual RBCs with accole forms.
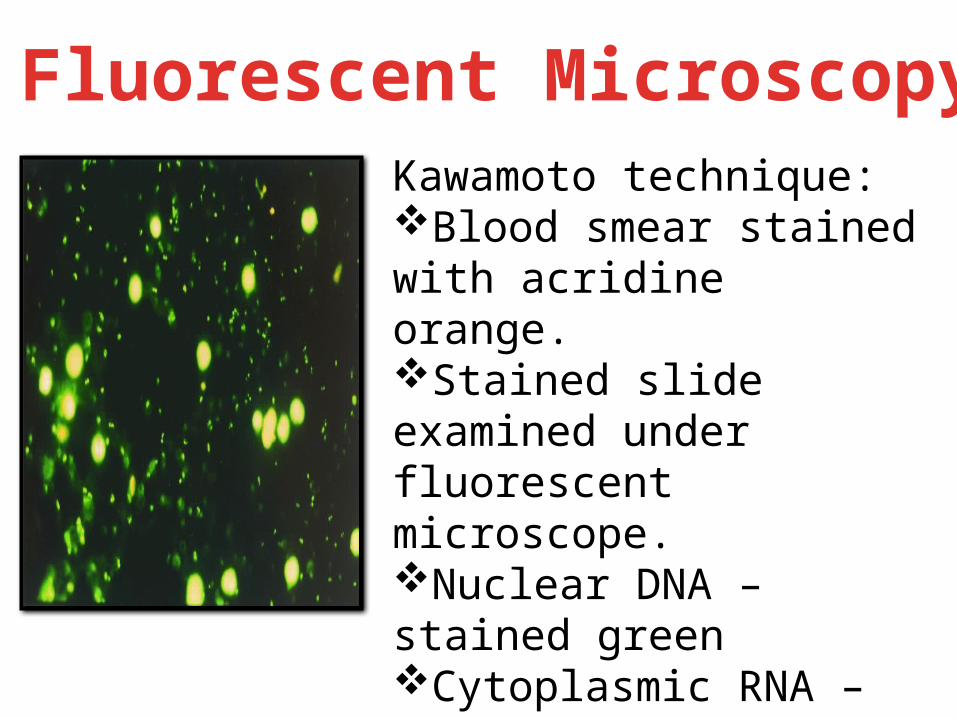
Fluorescent MicroscopyKawamoto technique:Blood smear stained with acridine orange.Stained slide examined under fluorescent microscope.Nuclear DNA – stained greenCytoplasmic RNA – stained red
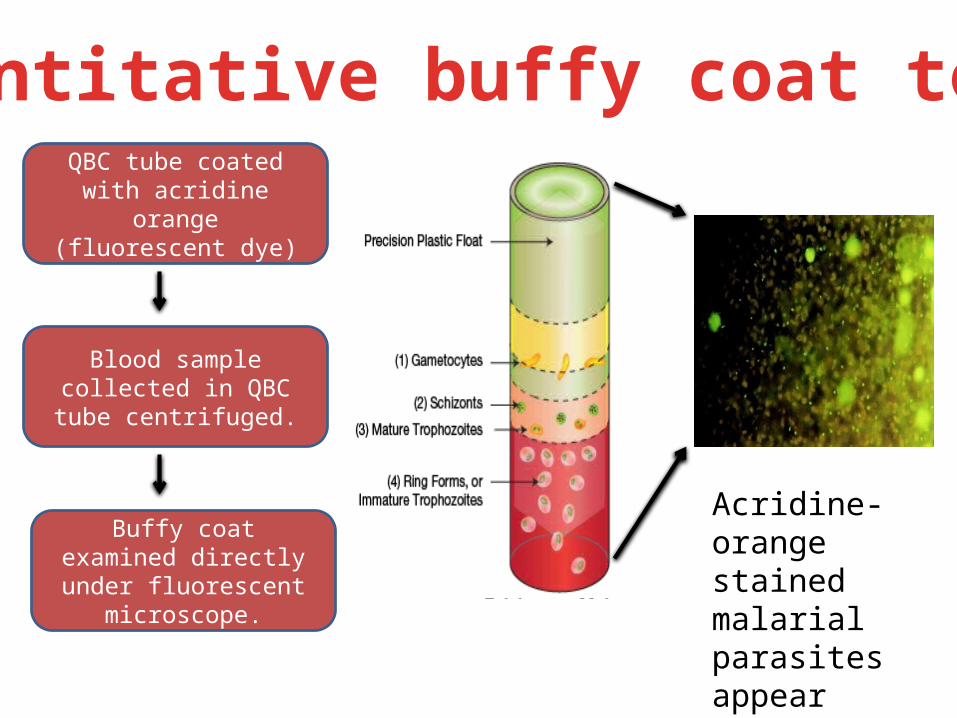
Quantitative buffy coat testQBC tube coated with
acridine orange (fluorescent dye)
Blood sample collected in QBC tube centrifuged.
Buffy coat examined directly under fluorescent
microscope.
Acridine-orange stained malarial parasites appear brilliant green.
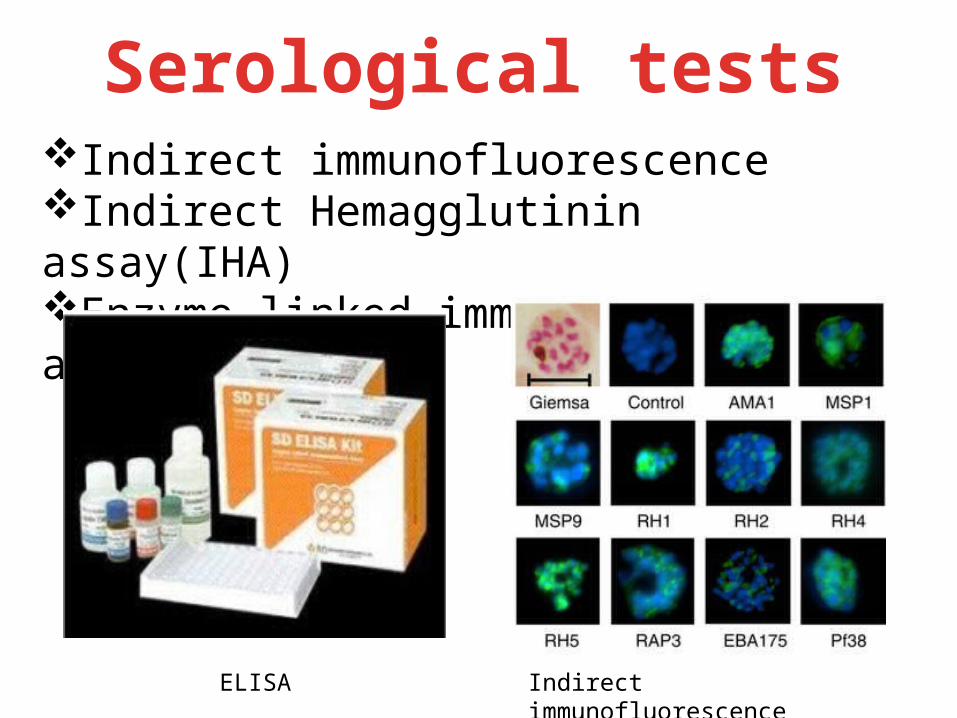
Serological testsIndirect immunofluorescenceIndirect Hemagglutinin assay(IHA)Enzyme linked immmunosorbent assay (ELISA)
ELISA Indirect immunofluorescence

Molecular MethodsPolymerase Chain ReactionMore sensitive than microscopy.Amplification of 18S rRNA genes.ExpensiveRequires specialized laboratory set-up.
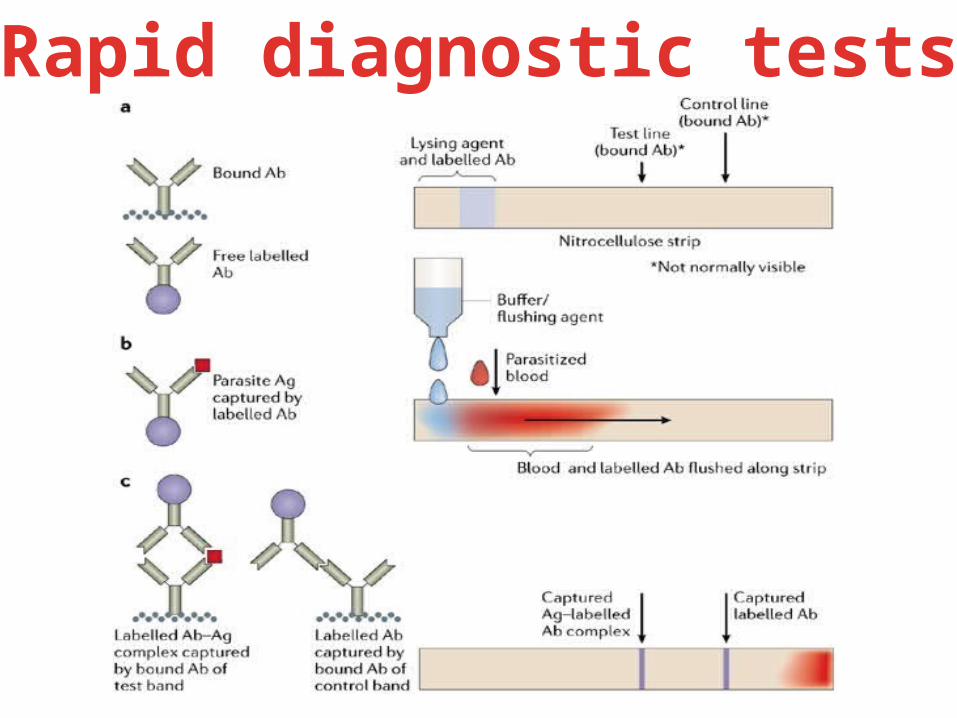
Rapid diagnostic tests
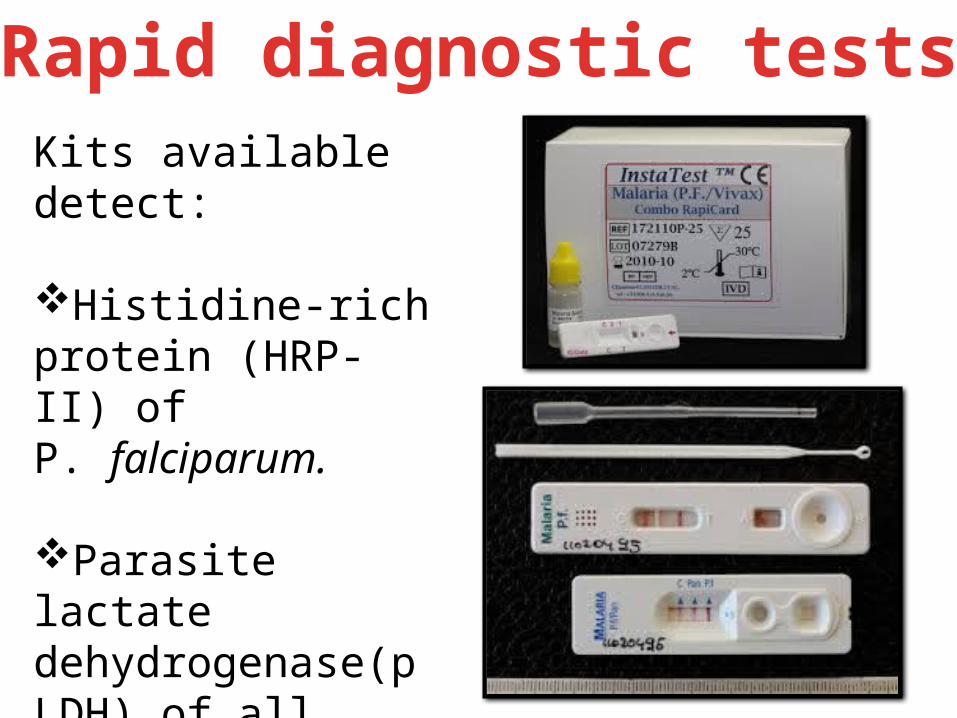
Rapid diagnostic testsKits available detect:
Histidine-rich protein (HRP-II) of P. falciparum.
Parasite lactate dehydrogenase(pLDH) of all four Plasmodium species can also be detected.


Chloroquine Rapidly acting erythrocytic schizontocide Controls most clinical attacks within 1-2 days Acts mainly on trophozoite blood stage; kills gametocytes of P. vivax, P.
ovale, and P. malariae (but not P. falciparum); no action on liver stages
Dose: 600 mg stat, followed by 300 mg after 6 hours and 300 mg for the next 2 days.
Adverse effect: Nausea, dysphoria, pruritus in dark-skinned patients, postural hypotension Hypotensive shock (parenteral), cardiac arrhythmias, neuropsychiatric
reactions,Retinopathy (cumulative dose, >g), skeletal and cardiac myopathy

Quinine• Obtained from cinchona bark• Acts mainly on trophozoite blood stage• Kills gametocytes of P. vivax, P. ovale, and P. malariae (but not P. falciparum)• No action on pre-erythrocytic stages
Adverse Effect• Cinchonism: A large single dose or higher therapeutic dose taken is k/a
CINCHONISM. It includes: - Ringing of ear -Nausea & vomiting -headache & mental confusion -Vertigo -difficulty in hearing -visual defect

Primaquine
• It is highly active against gametocytes and hypnozoites.
• Active against the pre-erythrocytic stage • Poor erythrocytic schizontocide
Adverse effects Abdominal pain GI upset Leucopenia Hemolysis in G6PD deficient patients.

Artemisinins
• The most important of these analogs are artesunate, artemether, and arteether.
• act very rapidly against all erythrocytic-stage human malaria parasites
• increasing role in the treatment of malaria, including multidrug-resistant P falciparum malaria
• Artesunate • Artemether • Quinidine
Treatment During Pregnancy
1. IV quinine2. Chloroquine3. SP4. Artesunate combinations5. Quinine and clindamycin6. Amodiaquine
What Is Drug Resistance?
• The ability of a parasite strain to survive and/or multiply
despite administration & absorption of a drug given in
doses equal to or higher than those usually
recommended but within the limit of tolerance of the
subject .
• Drug resistance is complicated by cross-resistance, which can occur among drugs that belong to the same chemical family or which have similar modes of action.
• Drug resistance results in a delay in or failure to clear asexual parasites from the blood, which allows production of the gametocytes that are responsible for transmission of the resistant genotype.
MALARIAL DRUG RESISTANCE

Malaria Endemic Areas and Drug Resistance
Chloroquine resistanceSP resistanceMulti-drug resistance

Prevention of Malaria
Dristi LamichhaneRoll No. 19
• Be Aware: risk factor, incubation period, symptom • Avoid being Bitten by mosquitoes
• Chemoprophylaxis • Immediately seek Diagnosis & treatment: if fever
occur 1 week – 3 months after arrival in endemic areas
Key tools of prevention

What determines the spread of malaria?
Female Anopheles mosquito
Malaria spread depends on:• Rainfall pattern
• Types of mosquitoes in the area• How close are people to the breeding sites?
Some areas constantly have a high rate of malaria.Other areas have “malaria seasons” or occasional epidemics of malaria.

How often does malaria occur in your area?
• Is it common and frequent throughout the year?– Young children and pregnant women are at
highest risk in these areas– With frequent exposure, adults develop some
immunity to malaria• Or is it seasonal, occurring in bursts during
rainy season or times of flooding

Where do mosquitoes breed?
Tire tracks Irrigation water
Rice paddiesRice paddies
Any place there is water!
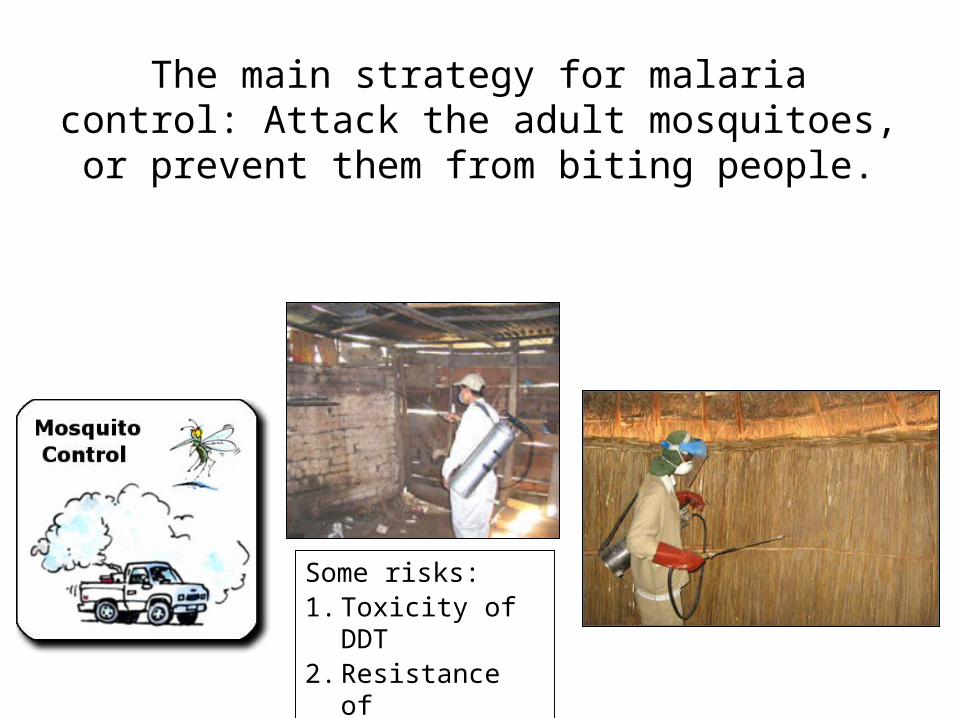
The main strategy for malaria control: Attack the adult mosquitoes, or
prevent them from biting people.
Some risks:1. Toxicity of DDT2. Resistance of
mosquitoes

What are ways to prevent mosquito bites?
• Use mosquito repellants.• Wear long pants and long sleeves.• Wear light-colored clothes.• Use window screens• Use bed nets.
Other Ways to Prevent MalariaWho is at the highest risk of malaria?– Travelers to an area high in malaria• Travelers often take prophylactic (preventive) medicines
to prevent malaria.
– Pregnant women (especially those with HIV)• Pregnant women are given intermittent preventive
treatment. They are given at least 2 doses of a malaria drug during their pregnancy.
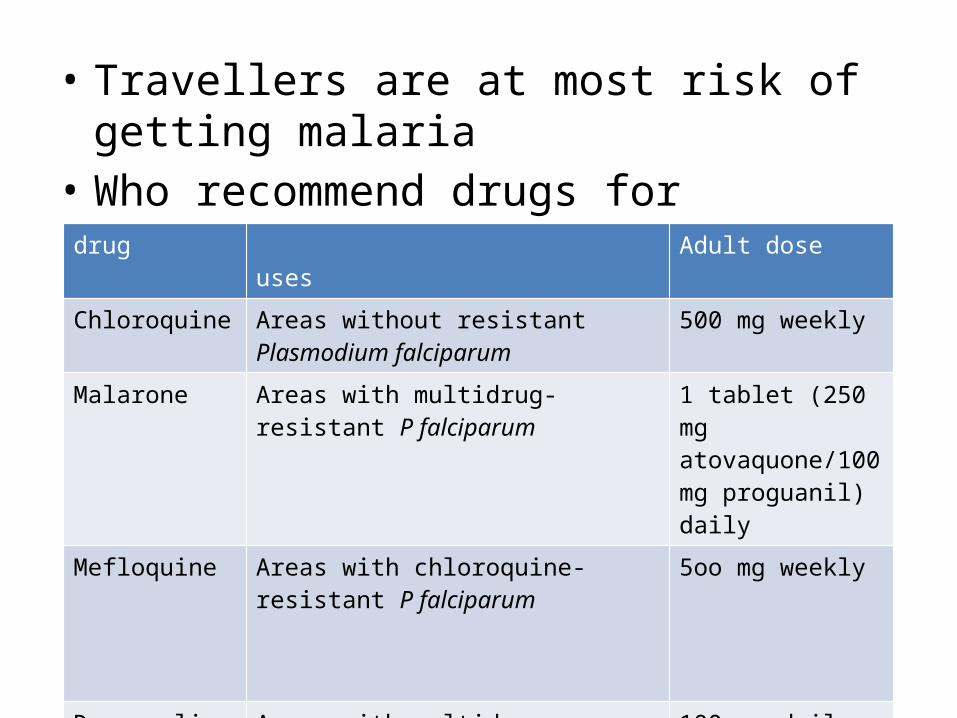
• Travellers are at most risk of getting malaria• Who recommend drugs for travellers
drug uses Adult dose
Chloroquine Areas without resistant Plasmodium falciparum
500 mg weekly
Malarone Areas with multidrug-resistant P falciparum
1 tablet (250 mg atovaquone/100 mg proguanil) daily
Mefloquine Areas with chloroquine-resistant P falciparum
5oo mg weekly
Doxycycline Areas with multidrug-resistant P falciparum
100 mg daily
1. Find out about malaria in your community
• Visit families to ask them about their experiences with malaria.
• Ask about bed nets.• Check for standing water.

2.Teach about malaria
• Teach about malaria and malaria prevention.• Use health stories for malaria teaching.• You will enjoy the malaria comic book.• Do skits; make posters; tell stories; be
creative!
Where can you teach about malaria?
1. During home visits2. In community
meetings3. At the health center
and local school
3. Do community cleanup
• Encourage the community for cleaning programs so that they work together with you on this.
• Get rid of any sources of standing water (old tires, cans, jars, pools of water).
• Cover any water containers.

4. Encourage the use of long-lasting nets and insecticides
RECENT ADVANCES
PRASUN KHANALROLL NO. - 21
• An effective vaccine is not yet available for malaria although several are under development
• The highly polymorphic nature of many P. falciparum proteins results in significant challenges to vaccine design
• Malaria vaccines in development include:– Pre-erythrocytic or liver-stage vaccinesThat aims to protect against the early stage of malaria infection– Blood-stage vaccinesThat aims to reduce the severity of disease– Transmission blocking vaccinesThat are intended to prevent mosquitoes that fed on an infected person from spreading malaria to new hosts
• Vaccine candidates that target antigens on gametes, zygotes, or ookinetes in the mosquito aims to block the transmission of malaria.
• These transmission-blocking vaccines induce antibodies in the human blood; when a mosquito takes a blood meal from a protected individual, these antibodies prevent the parasite from completing its development in the mosquito.

Vaccines
• SPf66• RTS,S or Mosquirix• PfSPZ
SPf66
• This vaccine was tested extensively in endemic areas in the 90s, but clinical trials showed it to be ineffective.

RTS,S
• RTS,S or Mosquirix is an experimental recombinant protein-based vaccine for malaria expected to be licensed in 2015.
• It targets the pre-erythrocytic stage of the parasite’s life cycle.
• Infection is prevented by inducing high antibody titers that block the parasite from infecting the liver.

PfSPZ
• It is a pre-erythrocytic attenuated vaccine that uses whole sporozoites to induce an immune response
• Sanaria, a US biotech company, is involved in it.

Different Approach To Immunization• Genomics is now central to malaria research.
With the sequencing of P. falciparum, one of its vectors Anopheles gambiae, and the human genome, the genetics of all three organisms in the malaria lifecycle can be studied.
• The ability to produce genetically modified mosquitoes that do not transmit malaria, potentially allowing biological control of malaria transmission.

World Malaria Day, April 25
• The theme for 2014 and 2015 is:
“Invest in the future. Defeat malaria”

Thank YouThank You

Related Documents






![MALARIA [Descriptive Epidemiology of Malaria] Dr …wp.cune.org/.../11/MALARIA-descriptive-epidemiology-of-malaria.pdfMALARIA [Descriptive Epidemiology of Malaria] Dr Adeniyi Mofoluwake](https://static.cupdf.com/doc/110x72/5ac17de07f8b9ad73f8cf6b2/malaria-descriptive-epidemiology-of-malaria-dr-wpcuneorg11malaria-descriptive-epidemiology-of-.jpg)




