Maladie de Crohn de l’enfant Frank Rümmele Université Paris Descartes, Sorbonne Paris Cité INSERM U989 Hôpital Necker Enfants Malades, PARIS [email protected]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Maladie de Crohn de l’enfant
Frank RümmeleUniversité Paris Descartes, Sorbonne Paris Cité
INSERM U989Hôpital Necker Enfants Malades, PARIS

F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité
La maladie de Crohn

F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité
Cause(s) ?
La maladie de Crohn

Pathogenesis of IBD
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité
endogenous factors
genetics
exogenous factors
environnement
microbial flora
immune responses
intestinal mucosa
intestinal
inflammationhomeostasis
down-regulationno down-regulation
IBD
Pathophysiology of IBD
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité

Mucosal Immune SystemSystème immunitaire de l’intestin
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité

5p13
10q21
ATG16L
PTPN2
NKX2-3
IRGM
3p21
7p12 ICOSLG
6q27 21q21
6q21 17q21
CDKAL1 17q21
IL12B 13q14
1q32 12q12
1q24 c11orf30
1q23 10p11
1q13 9p24
8q24
IL23RTNFSF15IBD5
NOD2
2007 2008200620052000
Prior to GWAS WTCCC GWAS
Early GWAS GWAS meta-analysis
Summary of Confirmed CD Loci
~20% genetic risk
~ 10% overall risk
Pediatric Specific Genes ?
Kugathasan et al. Nature Genetics 2008 2 loci (DcR3?)Imielinski et al. Nature Genetics 2009 5 loci (IL27?)
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité
Genetic factors and IBD
2012
150 Susceptibiltyloci for IBD
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité

Evolution naturelle de la MC
Cure?
Health
Death
Subclinical inflammation
Symptomatic inflammation
Complications
Disability
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité

– Contrôle/disparition des symptômes
– Maintenir la rémission
– Croissance de rattrapage
– Prévention de complications
– Eviter une chirurgie de résection
– Qualité de vie
Importance de la
croissance
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris CitéF. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité
Stratégies thérapeutiques

Disease progression
Years
Late intervention
Disease modifying drug or strategy
Stratégies thérapeutiques
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité

Early intervention
Disease modifying drug or strategy
Disease progression
Years
Stratégies thérapeutiques
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité

Stratégies thérapeutiques
Comment reconnaître les patients avec une maladie à risque ?
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité

Consensus Guidelines of ECCO/ESPGHAN on the medical management of pediatric Crohn’s
disease

Stratégies thérapeutiques
Comment reconnaître les patients avec une maladie à risque ?
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité
Facteurs potentiels de mauvais pronostique• Ulcérations creusantes• Maladie étendue (iléopancolique)• Poussée sévère et difficile à traiter• Retard de taille <-2,5DS• Ostéoporose• Maladie périnéale sévère• Complications d’emblée (B2/B3)

Quel choix thérapeutique pour ce jeune homme avec un nouveau diagnostic de
maladie de Crohn?
Frank Rümmele, Université Sorbonne Paris

Frank Rümmele, Université Sorbonne Paris
Présentation iléo-cecale L1
Multiples ulcerations superficielles
et une ulcération creusante
CRP très élévée (69mg/dl) B1
Pas d’abcès, pas de fistule
Retard de croissance importante G1
11 ans (age osseux 9.5 ans)
Quel choix thérapeutique pour ce jeune homme avec un nouveau diagnostic de
maladie de Crohn?

Frank Rümmele, Université Sorbonne Paris
A- 5-ASA, maladie moderée
B- AZATHIOPRINE car patient jeune
C- Anti-TNF car très efficace
D- Je ne sais pas, il me faut des guidelines
Quel choix thérapeutique pour ce jeune homme avec un nouveau diagnostic de
maladie de Crohn?

Le patient est jeune, la maladie ne semble pas si
sévère ?
Approche step-up ?
PENTASA 100mg/kg en 3 prises?
Frank Rümmele, Université Sorbonne Paris
Stratégies thérapeutiques

STATEMENT 175-ASA and derivates are only recommended to be used in selected patients with a very mild
disease (EL2) 88% agreement
• Inflammation colique à minima• Sulfasalazine superior chez les patients adultes• Posologie 50-80 mg/kg/jour(max 4g/jour).• Pas de “mucosal healing”
Frank Rümmele, Université Sorbonne Paris
Stratégies thérapeutiques
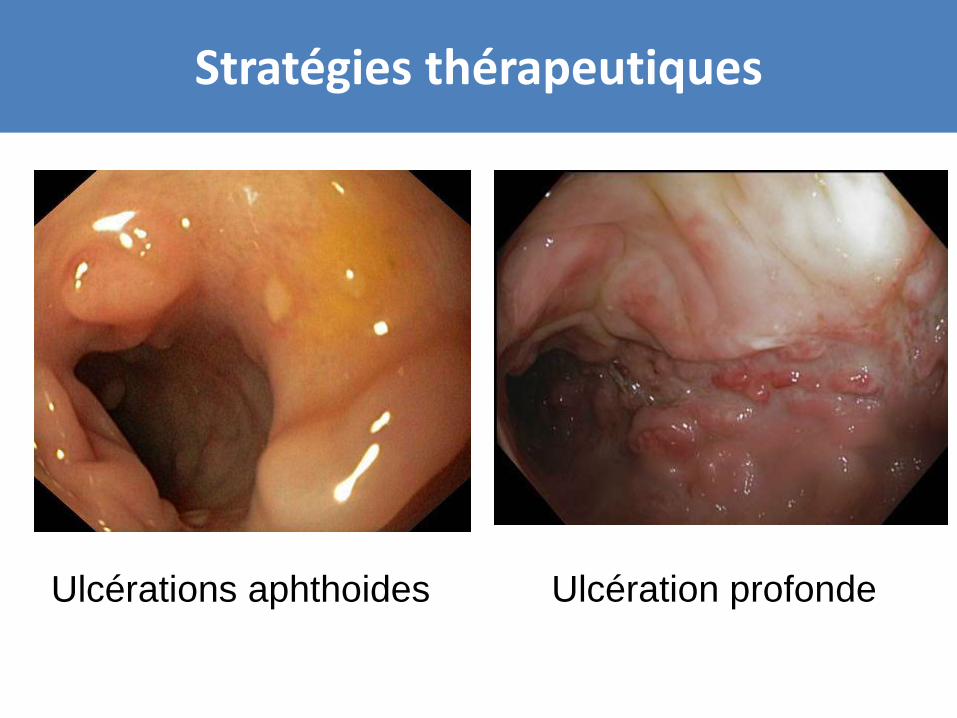
Ulcérations aphthoides Ulcération profonde
Stratégies thérapeutiques

Le patient est jeune, la maladie ne semble pas si
sévère ?
Approche step-up ?
PENTASA 100mg/kg en 3 prises?
Frank Rümmele, Université Sorbonne Paris
Stratégies thérapeutiques
NO

Il est jeune, il a une ulcérations creusante et un
retard de croissance important
C’est une indication pour l’AZATHIOPRINE
Frank Rümmele, Université Sorbonne Paris
Stratégies thérapeutiques
STATEMENT 8Thiopurines (azathioprine or 6-mercaptopurine) are
recommended as one option for maintenance of steroid free remission in children at risk for adverse
outcome [EL2 (pediatrics), EL1 (adults) 96% agreement
Frank Rümmele, Université Sorbonne Paris
Stratégies thérapeutiques

Markowitz J et al., Gastroenterology 2000;119:895-902
6MP
placebo
Frank Rümmele, Université Sorbonne Paris
Stratégies thérapeutiques

• Mode d’action retardé (effect au bout de 14 semaines)
• AZA: 2.0-2.5 mg/kg, (6-MP1.0-1.5 mg/kg)
• La determination de l’activité TPMT (genotypage ou phenotypage) permet d’identifier les patients à risque d’aplasie
• Reduction de la dose chez les patients hétérozygote ou activité TPMT intermédiaire
• Thiopurines contraindiqués chez les patients homozygotes ou activitéTPMT très basse
• Bilan biologique: NFS, transaminase, etc. 6TGN/6MMP utiles
Frank Rümmele, Université Sorbonne Paris
Stratégies thérapeutiques

Stratégies thérapeutiques
Frank Rümmele, Université Sorbonne Paris
STATEMENTS 9
Thiopurines alone are not recommended as induction therapy (EL3)
100% agreement
Frank Rümmele, Université Sorbonne Paris
Stratégies thérapeutiques
Traitement d’induction – lequel choisir ?
Frank Rümmele, Université Sorbonne Paris
• Corticoides
• Nutrition enterale exclusive
• Anti-TNF
Stratégies thérapeutiques

STATEMENTS 1 and 2
Exclusive Enteral Nutrition (EEN) is recommended as first line therapy to induce remission in children
with active luminal CD [EL1]
96% agreement
Partial Enteral Nutrition should not be used for induction of remission [EL2]
100% agreement
Frank Rümmele, Université Sorbonne Paris
Stratégies thérapeutiques

NEE et Mucosal Healing
2 mois de Nutrition entérale+ AZA
Heuschkel, Beattie, Ruemmele JPGN 2007
Frank Rümmele, Université Sorbonne Paris

1. Borrelli O, et al. Clin. Gastroenterol. Hepatol.; 2006:4(6):744-753.
EEN
CS
His
tolo
gic
al S
core
Borrelli O, et al. Clin. Gastroenterol. Hepatol. 2006
Frank Rümmele, Université Sorbonne Paris
NEE et Mucosal Healing

NPO – NE en exclusifpo (préféré) ou par SNGPolymerique > elementaire6 – 8 semainesMaladie endo-luminale B1 (grêle et/ou colon)
Frank Rümmele, Université Sorbonne Paris
NEE pour la maladie de Crohn
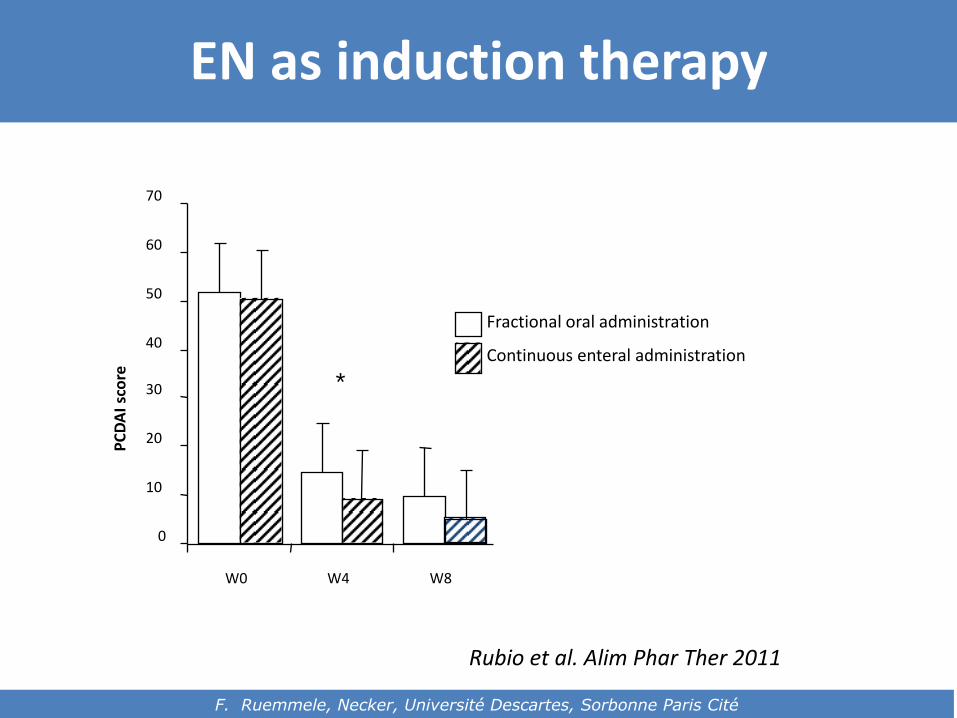
Oral versus tube EN
Fractional oral administration
Continuous enteral administration
0
10
20
30
40
50
60
70
W0 W4 W8
PC
DA
I sc
ore *
Rubio et al. Alim Phar Ther 2011
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité
EN as induction therapy
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité
STATEMENTS 3,4
Oral corticosteroids are recommended for inducing remission in children with moderate to severe active
luminal CD if EEN is not an option [EL2 (Pediatrics), EL1 (Adults)]
96% agreementIn children with mild to moderate ileo-cecal CD,
budesonide may be used as alternative to systemic steroids for induction of remission [EL2 (Pediatrics) EL2
(Adults)] 96% agreement
Frank Rümmele, Université Sorbonne Paris
Stratégies thérapeutiques
STATEMENT 5Steroids should not be used as a maintenance
therapy (EL4) 100% agreement
Frank Rümmele, Université Sorbonne Paris
Stratégies thérapeutiques

Stratégies thérapeutiques
Frank Rümmele, Université Sorbonne Paris
R. Heusckel JPGN 2000

Frank Rümmele, Université Sorbonne Paris
Stratégies thérapeutiques
• 1mg/kg/j (max 40mg/j) recommandé Eventuellement 1,5 mg/kg/j (max 60mg) Eventuellement IV
• ENTOCORT (Budesonide) (9mg) comme alternative pour les formes ileo-caecales (L1)
• Baisse progressive sur 10 semaines
Il est jeune, il a une ulcération creusante et un
retard de croissance important
C’est une indication pour l’AZATHIOPRINE
Traitement d’induction par NEE
Frank Rümmele, Université Sorbonne Paris
Stratégies thérapeutiques
Quid au MTX, quid aux anti-TNF

STATEMENTS 10+11
Methotrexate is recommended as one option for maintenance of steroid free remission in children at
risk for adverse outcome (EL4 (Pediatrics) EL1 (adults)) 96% agreement
Methotrexate can be used as a primary maintenance therapy or as an alternative to thiopurines (EL 4 (Pediatrics), EL1 (Adults))
92% agreement
Stratégies thérapeutiques
STATEMENTS 12 +13Anti-TNF therapy is recommended for inducing and maintaining remission in children with chronically
active luminal CD despite prior optimised immunomodulator therapy (EL2) 100% agreement
Anti-TNF therapy is recommended for inducing remission in children with active steroid-refractory
disease (EL2) 100% agreement
Stratégies thérapeutiques

REACH – IFX study
Réponse clinique Remission clinique
Hyams Gastroenterology 2007
Frank Rümmele, Université Sorbonne Paris
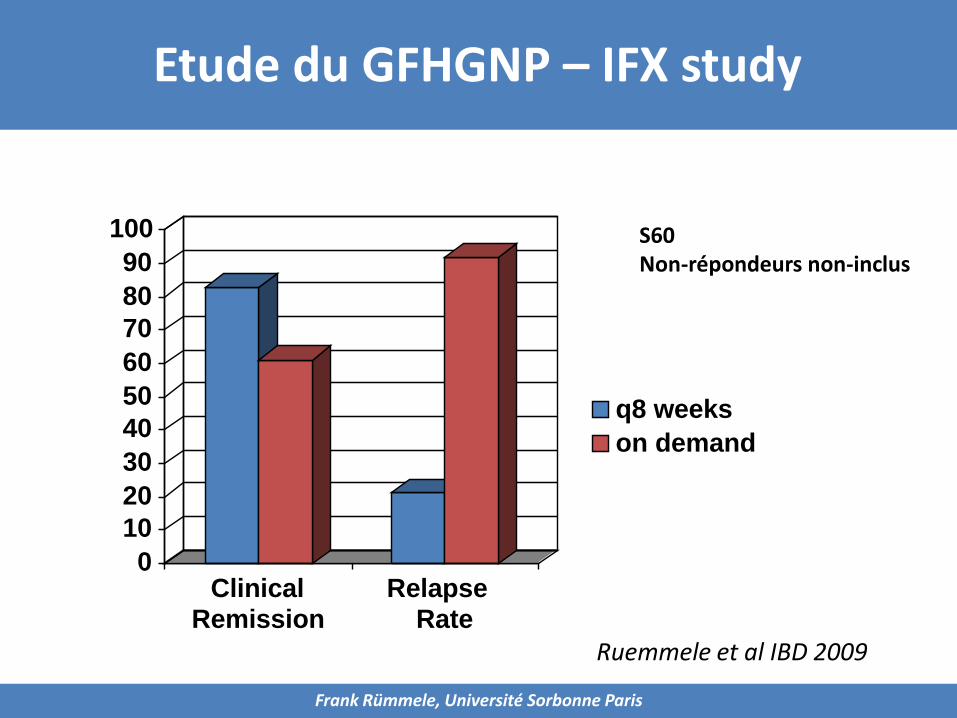
S60Non-répondeurs non-inclus
0
10
20
30
40
50
60
70
80
90
100
ClinicalRemission
Relapse Rate
q8 weeks
on demand
Ruemmele et al IBD 2009
Etude du GFHGNP – IFX study
Frank Rümmele, Université Sorbonne Paris

Pe
rce
nta
ge
of
Pati
en
ts
in R
em
issio
n
Low-Dose High-Dose
0
20
40
60
80
100
28%
39%
N=95 N=93
P=0.075
Pe
rce
nta
ge
of
Pati
en
ts
in R
em
issio
n
Low-Dose High-Dose
0
20
40
60
80
100
23%
33%
N=95 N=93
P=0.100
Remission clinique = PCDAI ≤ 10
Etude IMAgINE ADA
S26 S52Hyams J Gastroenterology 2012
Frank Rümmele, Université Sorbonne Paris

Il est jeune, il a une ulcération creusante et un
retard de croissance important
Apparition rapidement d’une fistule périnéale
Frank Rümmele, Université Sorbonne Paris
Stratégies thérapeutiques

STATEMENTS 14+15Anti-TNF therapy is recommended as primary induction
and maintenance therapy for children with perianal fistulising disease in combination with appropriate
surgical intervention [EL2] 84% agreement
Regularly scheduled and not episodic treatment should be used to maintain remission in patients responding
to induction therapy with anti-TNF agents [EL2] 100% agreement
Stratégies thérapeutiques

Frank Rümmele, Université Sorbonne Paris
Stratégies thérapeutiques
• Les anti-TNF sont le traitement de premièreintention des fistules perinéales (après ttt par ATBet drainage/seton de la fistule/abcès)
• Les anti-TNF sont le traitement de premièreintention des patients avec un ou plusieurs facteursde mauvais prognostic

Frank Rümmele, Université Sorbonne Paris
Stratégies thérapeutiques
• Indiqué pour le ttt les manifestations extraintestinales(arthrite sévère, pyoderma gangrenosum)
• L’efficacité doit être évaluée après la 2eme ou 3eme dose
• Pour l’instant nous manquons d’études permettant de mieuxdéfinir le rapport bénéfice/risque pour une mono- oucombothérapie
• Rôle de MTX ? Combo permettant d’éviter une combothiopurine/anti-TNF et le risque d’un lymphome T hépato-splénique

A practical guide: the consensus work of ECCO/ESPGHAN
Frank Rümmele, Université Sorbonne Paris
EEN for 6-8
W
Anti-TNF-therapy
No response after 2 or 3 adm

A practical guide: the consensus work of ECCO/ESPGHAN
Frank Rümmele, Université Sorbonne Paris
no therapy
PEN
5 ASA
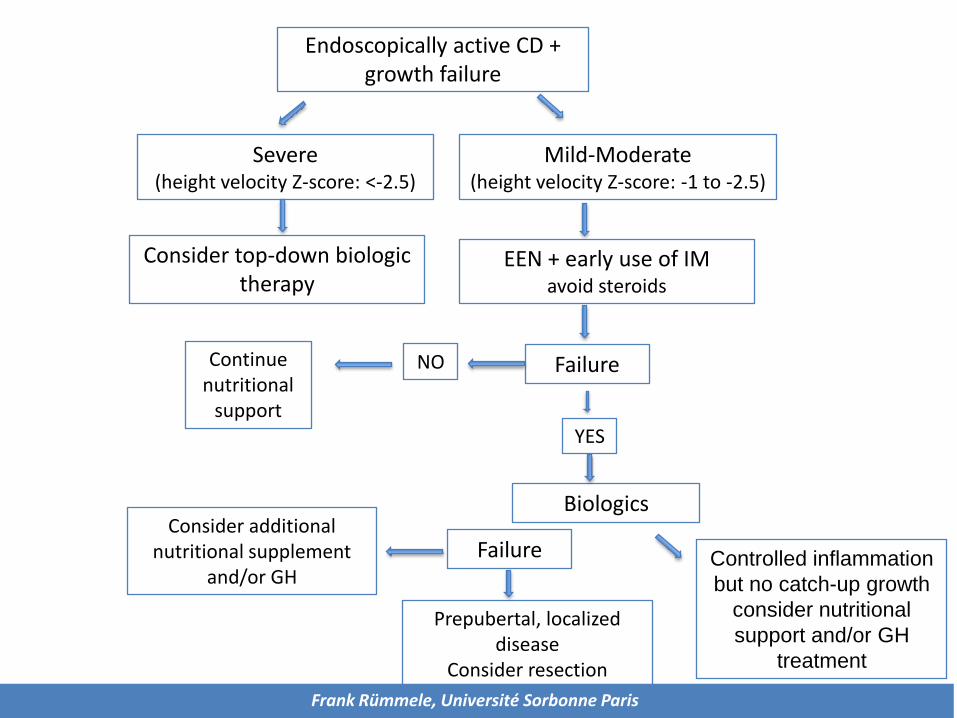
Endoscopically active CD + growth failure
Severe (height velocity Z-score: <-2.5)
Mild-Moderate(height velocity Z-score: -1 to -2.5)
Consider top-down biologic therapy
EEN + early use of IMavoid steroids
FailureNO
YES
Continue nutritional
support
Biologics
FailureConsider additional
nutritional supplement and/or GH
Prepubertal, localized disease
Consider resection surgeryFrank Rümmele, Université Sorbonne Paris
Controlled inflammation
but no catch-up growth
consider nutritional
support and/or GH
treatment

Hyams J, et al. DDW. 2009; Abstract W1181 (Data on file, Centocor).
Résumé
oPremier guidelines pour la maladie de Crohn de
l’enfant (guidelines=aide pour les décisions
thérapeutique, mais pas une référence opposable)
oDéfinition de l’objectif du ttt: « Deep Remission »
(Mucosal healing)
o Introduction de facteurs de risque de mauvais
pronostique
oUtilisation très fréquente (>80%) d’IM
o « Safety » à surveiller à longtemr
o Consider safety profile and longterm evolutionFrank Rümmele, Université Sorbonne Paris

Hyams J, et al. DDW. 2009; Abstract W1181 (Data on file, Centocor).
Frank M. Ruemmele, FranceGabor Veres, BudapestKaija Leena Kolho, Finnland Anne Griffiths, Canada Arie Levine, Israel Johanna Escher, The Netherlands Jorge Amil Dias, PortugalArrigo Barabino, Italy Christian Bragger, SwitzerlandJiri Bronsky, Czech RepublicStephan Buderus, GermanyJavier de Carpi, Spain Lissy de Ridder, The NetherlandsUlrika L. Fagerberg, SwedenJean-Pierre Hugot, FranceJaroslaw Kierkus, Poland
Sanja Kolacek, Croatia
Sibylle Koletzko, Germany
Paulo Lionetti, Italy
Erasmo Miele, Italy
Victor Navas Lopez, Spain
Anders Paerregaard, Danemark
Richard Russell, Scotland
Daniela Serban, Roumania
Ron Shaoul, Israel
Patrick Van Rheenen, Netherlands
Geneviève Veereman, Belgium
Batia Weiss, Israel
David Wilson, UK
Axel Dignass, Germany
Abraham Eliakim, Israel
Harland Winter, USA
Dan Turner, Israel
https://www.ecco-ibd.eu/publications/ecco-guidelines-science/published-ecco-guidelines.html


Clinical CaseBoy 12 years old with several episodes ofabdominal pain and diarrheaWhat are the arguments that orientate youtowards the diagnosis of Crohn’s disease ?A) Chronicity of abdominal painB) Typical age for the onset of Crohn’s diseaseC) Combination of diarrhea and abdominal painD) If there is a family history of IBD it will be more
like to be Crohn’s diseaseE) I need more details (type of abdominal pain,
detailled history of how long and when, andsome inflammatory parameters

Clinical CaseBoy 12 years old with several episodes ofabdominal pain and diarrheaWhat are the arguments that orientate youtowards the diagnosis of Crohn’s disease ?A) Chronicity of abdominal painB) Typical age for the onset of Crohn’s diseaseC) Combination of diarrhea and abdominal painD) If there is a family history of IBD it will be more
like to be Crohn’s diseaseE) I need more details (type of abdominal pain,
detailled history of how long and when, andsome inflammatory parameters

IBD starts before the age of 18 years in
A) 10% of patients
B) 25% of patients
C) 50% of patients
D) 75% of patients
E) All answers are wrong

IBD starts before the age of 18 years in
A) 10% of patients
B) 25% of patients
C) 50% of patients
D) 75% of patients
E) All answers are wrong

The diagnosis of IBD in childrenrequires
A) Analysis of growth chart
B) Inflammatory parameters (CRP, ESR)
C) Radiological investigation (best by MRI)
D) Endoscopic evaluation with histology
E) All answers are correct

The diagnosis of IBD in childrenrequires
A) Analysis of growth chart
B) Inflammatory parameters (CRP, ESR)
C) Radiological investigation (best by MRI)
D) Endoscopic evaluation with histology
E) All answers are correct

How do you classify pediatric IBD ?
A) I can use the Montreal classification
B) I prefere the Paris classification
C) I consider Disease location (L1-L4)
D) I consider Disease behaviour (B1-B3)
E) All answers are correct
How do you classify pediatric IBD ?
A) I can use the Montreal classification
B) I prefere the Paris classification
C) I consider Disease location (L1-L4)
D) I consider Disease behaviour (B1-B3)
E) All answers are correct

Questions 1
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité
What is the youngest age of onset of IBD ?
A) 1st year of lifeB) Not before 5 yearsC) Not before 10 yearsD) Most often in pre-/or adolescents, but
younger age is also possible
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité

Questions 1
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité
What is the youngest age of onset of IBD ?
A) 1st year of lifeB) Not before 5 yearsC) Not before 10 yearsD) Most often in pre-/or adolescents, but
younger age is also possible
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité

Questions 2
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité
Why are pediatric gastroenterologists « obsessional » about growth charts of their patients
A) Since they are pediatricians and that’s normalB) Since they have a lot of time for their patientsC) Since all their patients are smallD) Since therapeutic option depend on growth pattern
and monitoring is important
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité

Questions 2
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité
Why are pediatric gastroenterologists « obsessional » about growth charts of their patients
A) Since they are pediatricians and that’s normalB) Since they have a lot of time for their patientsC) Since all their patients are smallD) Since therapeutic option depend on growth pattern
and monitoring is important
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité

Questions 3
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité
Do pediatric gastroenterologists use more oftenImmunosuppressors for their patients
A) YesB) NoC) They are crazy, since they believe this makes theirs
patients grow faster
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité

Questions 3
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité
Do pediatric gastroenterologists use more oftenImmunosuppressors for their patients
A) YesB) NoC) They are crazy, since they believe this makes theirs
patients grow faster
F. Ruemmele, Necker, Université Descartes, Sorbonne Paris Cité
Related Documents











