Mainstreaming nutrition into maternal and child health programmes: scaling up of exclusive breastfeeding Nita Bhandari*, A.K.M. Iqbal Kabir † and Mohammed Abdus Salam † *Society for Applied Studies, New Delhi, India, and † International Centre for Diarrheal Disease Research, Bangladesh, Dhaka, Bangladesh Table of Contents Summary 5 Background 6 Methods and search strategy 6 The scale-up process 7 Issues that need to be addressed while scaling up a programme for exclusive breastfeeding 7 Conclusions 13 Acknowledgements 14 References 14 Appendix 1 18 Appendix 2 22 Summary Interventions to promote exclusive breastfeeding have been estimated to have the potential to prevent 13% of all under-5 deaths in developing countries and are the single most important preventive intervention against child mortality. According to World Health Organization and United Nations Children Funds (UNICEF), only 39% infants are exclusively breastfed for less than 4 months. This review examines programme efforts to scale up exclusive breastfeeding in different countries and draws lesson for successful scale-up. Opportunities and challenges in scaling up of exclusive breastfeeding into Maternal and Child Health programmes are identified. The key processes required for exclusive breastfeeding scale-up are: (1) an evidence-based policy and science-driven technical guidelines; and (2) an implementation strategy and plan for achieving high exclusive breastfeeding rates in all strata of society, on a sustainable basis. Factors related to success include political will, strong advocacy, enabling policies, well-defined short- and long-term programme strategy, sustained financial support, clear definition of roles of multiple stakeholders and emphasis on delivery at the community level. Effective use of ante- natal, birth and post-natal contacts at homes and through community mobilization efforts is emphasized. Formative research to ensure appropriate intervention design and delivery is criti- cal particularly in areas with high HIV prevalence. Strong communication strategy and support, quality trainers and training contributed significantly to programme success. Monitoring and evaluation with feedback systems that allow for periodic programme corrections and continued innovation are central to very high coverage. Legal framework must make it possible for mothers to exclusively breastfeed for at least 4 months. Sustained programme efforts are critical to achieve high coverage and this requires strong national- and state-level leadership. Keywords: exclusive breastfeeding, scale up, breastfeeding promotion, breastfeeding programs. Correspondence: Nita Bhandari, Society for Applied Studies, 45, Kalu Sarai, New Delhi – 110017, India. E-mail: community.research@ cih.uib.no Review Article 5 © 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd. Maternal and Child Nutrition (2008), 4, pp. 5–23

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Mainstreaming nutrition into maternal and child healthprogrammes scaling up of exclusive breastfeedingNita Bhandari AKM Iqbal Kabirdagger and Mohammed Abdus Salamdagger
Society for Applied Studies New Delhi India and daggerInternational Centre for Diarrheal Disease Research Bangladesh Dhaka Bangladesh
Table of Contents
Summary 5Background 6Methods and search strategy 6The scale-up process 7Issues that need to be addressed while scaling up a programme for exclusive breastfeeding 7Conclusions 13Acknowledgements 14References 14Appendix 1 18Appendix 2 22
Summary
Interventions to promote exclusive breastfeeding have been estimated to have the potential toprevent 13 of all under-5 deaths in developing countries and are the single most importantpreventive intervention against child mortality According to World Health Organization andUnited Nations Children Funds (UNICEF) only 39 infants are exclusively breastfed for lessthan 4 months This review examines programme efforts to scale up exclusive breastfeeding indifferent countries and draws lesson for successful scale-up Opportunities and challenges inscaling up of exclusive breastfeeding into Maternal and Child Health programmes are identifiedThe key processes required for exclusive breastfeeding scale-up are (1) an evidence-basedpolicy and science-driven technical guidelines and (2) an implementation strategy and plan forachieving high exclusive breastfeeding rates in all strata of society on a sustainable basis Factorsrelated to success include political will strong advocacy enabling policies well-defined short-and long-term programme strategy sustained financial support clear definition of roles ofmultiple stakeholders and emphasis on delivery at the community level Effective use of ante-natal birth and post-natal contacts at homes and through community mobilization efforts isemphasized Formative research to ensure appropriate intervention design and delivery is criti-cal particularly in areas with high HIV prevalence Strong communication strategy and supportquality trainers and training contributed significantly to programme success Monitoring andevaluation with feedback systems that allow for periodic programme corrections and continuedinnovation are central to very high coverage Legal framework must make it possible for mothersto exclusively breastfeed for at least 4 months Sustained programme efforts are critical toachieve high coverage and this requires strong national- and state-level leadership
Keywords exclusive breastfeeding scale up breastfeeding promotion breastfeeding programs
Correspondence Nita Bhandari Society for Applied Studies 45 Kalu Sarai New Delhi ndash 110017 India E-mail communityresearch
cihuibno
Review Article
5copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Background
The Lancet series on child survival identified breast-feeding interventions to have the potential to prevent13 of all under-5 deaths in developing areas of theworld ranking it as the most important preventiveapproach for saving child lives (Jones et al 2003)Exclusive breastfeeding that is administering onlybreastmilk and no other liquids or foods (WHO 2004)for the first 6 months of life confers important benefitsto the infant and the mother ndash it protects infantsagainst many common childhood diseases includingrepeated gastrointestinal infections and pneumoniaand thereby against some of the major causes of child-hood mortality (Feachem amp Koblinsky 1984 Jasonet al 1984 Habicht et al 1986 de Zoysa et al 1991WHO Collaborative Study Team on the Role ofBreastfeeding on the Prevention of Infant Mortality2000Arifeen et al 2001)A large volume of literatureexists regarding efficacy trials that have clearly dem-onstrated the beneficial impact of exclusive breast-feeding (Green 1999)
Unfortunately exclusive breastfeeding is not prac-tised universally Global monitoring indicates thatonly 39 of infants are exclusively breastfed forless than 4 months following birth (WHOUNICEF2003) Some reasons for failure to breastfeed exclu-sively for the recommended first 6 months of lifeinclude community beliefs that result in delay in ini-tiation of breastfeeding after birth giving other fluidsandor foods to breastfeeding infants the lack ofsocial support for women in resolving breastfeedingdifficulties and lack of health system support (Green1999)
The current international optimal feeding rec-ommendations include exclusive breastfeeding for6 months these are based on a review of scientificliterature to define the optimal duration of breast-feeding (Butte et al 2002 Kramer amp Kakuma 2002WHO 2002) These are also included in UnitedNations Children Fundsrsquo (UNICEFrsquos) Facts for Life
lsquoKey MessageWhat every family and community has a
right to know about breastfeedingrsquo (UNICEF 2002)In the early 1990s the World Health Organization
(WHO) and UNICEF launched the Baby-FriendlyHospital Initiative (BFHI) for strengthening mater-
nity services to support breastfeeding practices(WHOUNICEF 1992 table 3)
Although the BFHI includes a community compo-nent its implementation in developing countries isweak and support is only available in institutionsbefore and for a short period after delivery In severalregions a large proportion of deliveries occur athome Interventions at the community level aretherefore very important for supporting exclusivebreastfeeding
Identifying effective and sustainable means forscaling up of proven interventions into child healthprogrammes remains a major problem The purposeof this review is to define a process for scaling upexclusive breastfeeding based on experiences of pro-grammes or pilot projects for promotion of exclusivebreastfeeding implemented and evaluated in differentcountries The term lsquoscale uprsquo is commonly under-stood to mean reaching a larger number of beneficia-ries with a given intervention However apart fromcoverage maintaining quality as larger numbers arereached and effectively reaching out to those difficultto reach are also important considerations (The CoreGroup 2005) The issues addressed herein pertain topolicy programme design implementation strategyresources and costs management monitoring andevaluation and the possibility of continuing innova-tion and testing of novel approaches
Methods and search strategy
We conducted a systematic literature search with notime limits defined and used data from publishedliterature programme reports and monographsdescribing effectiveness or cluster randomized trialsor implementation programmes The databasessearched included PubMed the National Library ofMedicinersquos search service and Cochrane Library(Cochrane Controlled Trials Register) using the fol-lowing keywords breastfeeding or exclusive breast-feeding or breastfeeding promotion or breastfeedingintervention or breastfeeding programme or breast-feeding education or breastfeeding effect or impact orevaluation We also reviewed reference lists of iden-tified articles and hand searched reviews bibliogra-phies of books and abstracts and proceedings of
N Bhandari and AKMI Kabir6
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
national and international conferences or meetingsAdditionally we contacted key researchers andorganizationsagencies for unpublished material ornarrowly disseminated reports
Consistent with the programmatic focus theexamples quoted in this review are demonstrationprojects that reached large populations or cluster ran-domized intervention trialsThe emphasis is on devel-oping countries and as some of these countries areburdened by HIVAIDS this review includes thiscontext as well
The scale-up process
The scale-up planning process must follow a logicalorder Several key issues that need attention are sum-marized in Table 1 It is apparent that many of thefeatures of the process are generic to neonatal andchild health programmes but there are issues in thearea of exclusive breastfeeding that requires addi-tional attention particularly in the HIV context
Issues that need to be addressedwhile scaling up a programme forexclusive breastfeeding
Policy framework
The Global Strategy on Infant and Young ChildFeeding was adopted by a World Health Assemblyresolution (5525 WHA 2002) The global strategybuilds on the BFHI (WHOUNICEF 1992) the
International Code of Marketing of Breastmilk Sub-stitutes (WHO 1981) and the Innocenti Declarationon the Protection (WHO 1989) Promotion andSupport of Breastfeeding in the overall context ofnational policies and programmes on nutrition andchild health The aim of the strategy is to improvethe feeding of infants and young children andincrease the commitment of governments societygroups and international organizations to promotethe health and nutrition of children The strategyemphasizes the need for comprehensive nationalpolicies on infant and young child feeding onan urgent basis including guidelines on ensuringoptimal feeding of infants and young children inexceptionally difficult circumstances and the need toensure that all health services protect promote andsupport infant and young child feeding (Gupta 2002WHOUNICEF 2003)
Once the decision to scale up a programme forexclusive breastfeeding is made in a region or stateor country the logical starting point is to review therelevant existing national policies and to assesswhether these address varying circumstances underwhich women deliver and live such as urban or ruralresidence working women and place of deliverySpecific features to note are the status of the imple-mentation of the BFHI in facilities where womendeliver access and support to mothers with younginfants by trained personnel during the post-natalperiod and beyond support for exclusive breastfeed-ing in community setting legislation for workingmothers that ensures leave of appropriate durationan enabling environment at the work place withingovernment and private settings and the policiesin place for discouraging promotion of breastmilksubstitutes
Existing policies are optimal in some countries(The Norwegian Government 1993 ILO 1998) butlacunae exists in others for example exclusive breast-feeding for 6 months is a policy in India but the dura-tion of maternity leave for government employees is135 days (Government of India 1997) In Norwayhowever a mother is entitled to over 6 months ofmaternity leave (The Norwegian Government 1993)Wherever weaknesses exist a decision needs to bemade on how these will be addressed during scale-up
Table 1 Steps in scaling up
Assess situation create a policy environment conducive toexclusive breastfeeding
Define roles relationships and responsibilities of all partnersestablish agreements
Review technical supportDefine programme strategyMobilize resourcesProvide training and technical assistanceDevelop and use monitoring and evaluation systemsMonitor coverage and qualityMeasure impact and costProvide for testing novel approaches and continuing innovation
Adapted from Knippenberg et al (2005) and Gonzales et al (1998)
Mainstreaming nutrition into MCH programs 7
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Prior to scale-up a policy framework for implemen-tation needs to be developed This framework shouldinclude a vision consensus on technical issues onprogramme strategy roles relationships and respon-sibilities of implementing partners measurable goalswithin defined time lines and predictable adequatefunding to achieve these (The Core Group 2005) Itshould address the capacity of all implementing part-ners and the approach to fulfilling capacity gaps at alllevels particularly at the community level The policyframework should emphasize breastfeeding promo-tion through community-based programmes Politicalcommitment and ownership by relevant governmentdepartments at national state and district levels havealso been identified to be critical for effective scale-up(The Core Group 2005)
Technical and management support andother partnerships
Creating a policy framework designing a potentiallyeffective programme and an implementation strategyrequire multiple capacities which may not always beavailable within government departments or otherconcerned agencies
Technical and managerial support may need to bemobilized more so during the planning and earlyimplementation phase If this support is not availableinvolvement of external talent ndash national or eveninternational ndash may be required Once the pro-gramme is implemented the external support couldbe phased out gradually as local capacity is built
Forging partnerships between government minis-tries donors local non-governmental organizations(NGOs) and universities was a feature of many suc-cessful programmes (Appendix 1 Van Roekel et al
2002 Bhandari et al 2005 Quinn et al 2005) In theLINKAGES projects (Appendix 1) partnershipwith Programa de Coordinacion en Salud Integral(Collaborative Program for Integrated HealthPROCOSI) and NGOs in Bolivia UNICEF NGOsand the national government in Ghana and Intersec-toral Action Group for Nutrition and Jereo SalamaIsika in Madagascar added value and quality to pro-grammes resulted in effective pooling of resources
and expertise and improved programme design andmanagement (LINKAGES 2002 Van Roekel et al
2002 Quinn et al 2005)
Programme design and strategy
This requires a systematic description of steps andprocesses that help achieve high coverage qualityequity and sustainability capacity building and pro-gramme management are particularly important fea-tures (The Core Group 2005) Experience so farsuggests that for majority of developing countriesscale-up for exclusive breastfeeding will not be pos-sible unless intervention delivery at the communitylevel receives emphasis (Appendix 1) As an increas-ing number of mothers deliver in institutions mixedmodels will be required even in developing countries
An initial step is to carefully examine the existingopportunities as vehicles for promoting exclusivebreastfeeding If use of existing opportunities is insuf-ficient to achieve high coverage with good qualitythen additional approaches would need to be evolvedin a phased manner In Bangladesh the strategy ofpeer counsellors was used as the majority of deliveriesoccur at home and a community health worker is notroutinely available in that setting (Haider et al 2000)In India on the other hand village health workersalready exist so programmes are often designedaround them (Bhandari et al 2003 2004 2005)
Hospitalinstitution-based strategies
Efforts to scale up the BFHI in countries have shownmixed results (Table 2)
In regions where hospital deliveries are the normscale-up efforts through the BFHI (WHOUNICEF1992 Table 3 Perez-Escamilla 2007) have been suc-cessful and the strategy helped increase rates ofexclusive breastfeeding (Appendix 1) However inmany countries after initial years of enthusiasm thescale-up effort seems to have plateaued perhapsreflecting changing emphasis of donors and govern-ment The initial high rates of exclusive breastfeedingmay not be sustained after mothers are dischargedfrom facilities and return to their homes (Coutinhoet al 2005) The challenge therefore is to continue at
N Bhandari and AKMI Kabir8
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
home the post-delivery support available in institu-tions through public and private providers to sustainexclusive breastfeeding or develop other mechanismsthat support recently delivered mothers to exclusivelybreastfeed once they are discharged from hospitals(de Oliveira et al 2006) Countries have addressedthis in different ways In Australia a cadre of breast-feeding counsellors exists (Australian BreastfeedingAssociation 2005) In pilot programmes in Indiaexclusive breastfeeding was promoted through healthworker home visits at immunization clinics growthmonitoring sessions and at sick-child contacts(Bhandari et al 2005) in addition to the BFHI Homevisits are particularly important in regions where cov-
erage through other channels is low or not feasibleand a cadre of community workers exists
Community-based strategies
Pilot efforts in countries or regions where home deliv-eries predominate have shown success through ver-tical as well as integrated approaches however pro-grammes integrated into ongoing activities are morelikely to be more sustainable (The Core Group 2005)In these programmes (Appendix 1) the messageswere delivered through either a single existing or newchannel or multiple delivery channels already inplace within the primary health-care systemThe deci-sion to use one or multiple channels was made basedon the ability to cover the target population In somecountries high coverage was feasible only with mul-tiple facility and community channels (Appendix 1)Multiple channels also help achieve consistency inadvice The credibility and acceptability of a givenchannel by the community was another factor in theirbeing used Routine activities of channels were modi-fied in some instances to incorporate exclusive breast-feeding counselling In India for instance it wasbelieved that immunization sessions could not beused as a counselling opportunity but better organi-zation and the presence of another available localworker during the session enabled the vaccinator tocounsel mothers (Bhandari et al 2005)Another illus-tration is the adaptation of the Integrated Manage-ment of Childhood Illness (IMCI) programme of theWHOUNICEF (2002) to the Integrated Manage-ment of Neonatal and Childhood Illness (IMNCIGovernment of India 2006) by India The IMNCIincludes three home visits for all births in the first 7days of life by an existing community worker theAnganwadi worker (ICDS 1982) to promote essentialnewborn care which includes exclusive breastfeedingIn other countries such as Bangladesh facility-basedIMCI was sought to be improved in its impact bygreater emphasis on community component of IMCIthat is C-IMCI (Gwatkin 2004)
Programme delivery
Recognizing that facility-based interventions areinsufficient countries have experimented with a
Table 2 Proportion of facilities with Baby-Friendly Hospital Initiative(WABA 2007)
Region Median (range)
West and Central Africa 013 (000ndash059)EasternSouthern Africa 023 (000ndash100)Middle East and North Africa 014 (000ndash100)South Asia 007 (001ndash100)East Asia and Pacific 0005 (000ndash087)Americas and the Caribbean 010 (000ndash100)Central and Eastern EuropeCommonwealth
of Independent States025 (004ndash093)
All Industrialized Countries 007 (000ndash097)
Table 3 The 10 steps to successful breastfeeding for hospitals andbirth centres
bull Maintain a written breastfeeding policy that is routinelycommunicated to all health-care staffbull Train all health-care staff in skills necessary to implement thispolicybull Inform all pregnant women about the benefits and managementof breastfeedingbull Help mothers initiate breastfeeding within 1 h of birthbull Show mothers how to breastfeed and how to maintain lactationeven if they are separated from their infantsbull Give infants no food or drink other than breastmilk unlessmedically indicatedbull Practise lsquorooming inrsquo ndash allow mothers and infants to remaintogether 24 hours a daybull Encourage unrestricted breastfeedingbull Give no pacifiers or artificial nipples to breastfeeding infantsbull Foster the establishment of breastfeeding support groups andrefer mothers to them on discharge from the hospital or clinic
Mainstreaming nutrition into MCH programs 9
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
variety of local workers such as peer counsellors inBangladesh (Haider et al 2000) lady health workersin Pakistan (Government of Pakistan 2003) and thelsquoAccredited Social Health Activistsrsquo (ASHA) workerin India (Government of India 2005) to promoteexclusive breastfeeding by itself or as a part of essen-tial newborn care Programmes that used peer coun-sellors as a single channel have been shown to beeffective in several efficacy (Green 1999 Lewin et al
2006) and effectiveness trials (Morrow et al 1999Haider et al 2000 Lewin et al 2006) However whilepeer or lay counsellors have been effective in theshort run long-term sustainability of this approach ona large scale is as yet not established
The possible reasons stated for the short-termsuccess of the lay health workers approach includepayment to the counsellors for performing a specificpiece of work the counsellorsrsquo own perception ofbenefits of their work and their recognition by thecommunity as being skilled These workers also feltthis opportunity to have the potential for opening upof further education and training (Haider et al 2002)An important issue would also be linking newworkers with the existing primary health system aspilot experience showed that these workers may notbe able to resolve complex breastfeeding problems(Haider et al 2002)
Recruitment of ASHA in India provides a uniqueopportunity to promote exclusive breastfeeding(Government of India 2005) Currently being re-cruited all over the country these workers will focuson essential newborn care including exclusive breast-feeding through home visitation in the first month oflife and community-based activities
While these efforts in different countries at improv-ing coverage of the target population through localworkers are of value the voluntary or semi-voluntarynature of the workers and ill-defined models of super-vision raise issues about sustainability and possiblyhigh attrition rates
Programmes that used multiple channels reportedbroader coverage (Bhandari et al 2005 Quinn et al
2005) In India formative research showed thatimmunization sessions and private providers werethe channels to which infants were most commonly(~80) exposed Following constitution of a
breastfeeding-promotion programme caregiversmost often received exclusive breastfeeding counsel-ling at immunization sessions (~40) weighing ses-sions (~25) and home visits (25ndash30) Governmentphysicians or private providers rarely (~2) coun-selled despite being trained (Bhandari et al 2005)When all the opportunities were considered together55ndash60 of caregivers had been counselled at leastonce by at least one of the channels in the last 3months indicating that multiple channels reachedmore families (Bhandari et al 2005)The frequency ofcontact with caregivers or the intensity of counsellinginfluences the cumulative benefit of the counsellingfor example six contacts with mothers resulted inhigher adoption rates for exclusive breastfeeding ascompared with three (Morrow et al 1999) In Indiathe number of channels at which caregivers werecounselled was positively associated with the rates ofexclusive breastfeeding at 3 months of age (Bhandariet al 2003) However the costs of training and theeffort will increase more than the number of channelsused and therefore this issue requires a balancedview
Another issue of interest is the value of counsellingfor the antenatal period itself Antenatal counsellinghas been used in several programmes but its effect isdifficult to delineate by itself as it was usually fol-lowed by post-natal counselling (Green 1999) In theHIV context however the importance of antenatalcounselling is obvious
Communications approach
An effective communications approach was a featureof most programmes and involvement of journalistsradio announcements and other mass media from theprogramme outset extended the reach of nutritionmessages even further (Appendix 1 Quinn et al
2005) Mass media were not used in some pro-grammes where a comparison group was present forrisk of contamination (Bhandari et al 2005) Utiliza-tion of existing or newly formed community groupsproduced the same effect (Bhandari et al 2005Quinn et al 2005) and community mobilization pro-grammes such as street plays rallies radio pro-grammes and songs helped disseminate messages
N Bhandari and AKMI Kabir10
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
and increase community involvement (Bhandari et al
2005 Quinn et al 2005)Effective counselling requires assessment of
feeding practices recognition of problems and nego-tiation with the mother in choosing improved prac-tices that are feasible (WHOUNICEF 2002) thisrequires time and patience Programmes may chooseone-on-one counselling during opportunities in whichmore time is available such as home visits and groupcounselling for opportunities with lesser availabletime (Bhandari et al 2005) One of the reasons thatpeer counsellors may have been effective was thattheir sole responsibility was counselling mothersthrough home visits (Morrow et al 1999 Haider et al
2000) The more diverse the functions of the localworker the lesser will be the emphasis on a singlecomponent such as exclusive breastfeeding
Message development
The development of messages for interpersonal com-munication and for mass media needs careful atten-tion to design and content Successful programmesincluded an element of formative research to gain anin-depth understanding of the communities wherethese programmes were implemented with regard topractices pertaining to breastfeeding the reasons forthe current practices the common breastfeedingproblems and the barriers to adoption of ideal behav-iours in that cultural setting Formative research innorth India for instance showed general unwilling-ness to offer water to infants in summer months Thisbarrier was overcome by building specific explanatorymessages using local terms within the communicationstrategy (Bhandari et al 2003)
Once the design features and broad strategy are inplace attention must then shift to the operationaliza-tion of the strategy
Training and supervision
Prior to scale-up the training needs will need to bedefined Fortunately for promotion of exclusivebreastfeeding extensive experience is available ontraining of different cadres of health workers andeven for lay counsellors Most experiences used the
adapted versions of the UNICEFWHO Breastfeed-ing Counseling Course (WHOUNICEF 1993) or theIMCI module (WHOUNICEF 2002)
Training strategy and its quality merit attentionIn successful programmes the duration of trainingextended from 3 full days to 10 part days for differentworkers The training strategies as described werelsquoconcise action orientedrsquo and included modules thataimed to equip trainers with practical skills and con-fidence to counsel effectively (Appendix 1)
Training modules for areas with high HIV preva-lence also exist (WHO 2006)
While the training modules used in studies workedwell a gap remains for referralTrained workers at thecommunity level require that referral options avail-able are easily accessible prompt and preferablyavailable free of cost to mothers with complex breast-feeding problems
Another important issue to address is handlingtraining of new staff in most developing countriesstaff turnover and absenteeism rates are high
Monitoring and evaluation
The programme strategy will need to include systemsfor monitoring and evaluation of the programmePossible markers could include the rates of exclusivebreastfeeding worker performance referral andaction As for all other national programmes therewill be a need for periodic reviews and achievabletargets by time
Costs and resources
In all pilot programmes and projects services wereprovided to mothers free of cost In many developingcountries if the government cadre of health workers isused to promote exclusive breastfeeding as a part oftheir other responsibilities (eg the IMNCI) the basicservices will remain free However a system thatrequires setting up a cadre of trained lactation coun-sellors (eg in an urban setting or as referral sources forbreastfeeding problems in rural areas) will requireadditional resources A cost-effective analysis of theBFHI was conducted in three countriesBrazilMexicoand Honduras (Horton et al 1996) Savings on health
Mainstreaming nutrition into MCH programs 11
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
care resulting from reduction in diarrhoeal and respi-ratory morbidity were estimated as a result of theeffect of BFHI on breastfeeding The study showedthat breastfeeding promotion through a BFHI-likemodel is very cost-effective (1992 US$ 2ndash19 per dis-ability adjusted life years Horton et al 1996 Perez-Escamilla 2007) Examples of cost-effectivenessanalysis of community-based programmes using lay orprofessional support in different settings could not beidentified
Testing of novel approaches andcontinuing innovation
Scaled-up programmes must have inbuilt provision totest novel approaches and the ability for continuinginnovation
Scaling up of exclusive breastfeeding in thecontext of HIV
The policy and programme design and implemen-tation issues relevant to exclusive breastfeedingscale-up discussed above are relevant to HIV-prevalent areas but there are other unique featuresthat merit consideration
Creating policies for exclusive breastfeeding pro-motion in countries with high HIV prevalence is par-ticularly challenging The revised recommendationsencourage exclusive breastfeeding for the first 6months and continued breastfeeding for 2 years andbeyond for infants whose mothers are HIV negativeor whose HIV status is unknown For women who areknown to be HIV positive the most appropriateinfant feeding option for HIV-exposed infantsdepends on individual circumstances including con-sideration of health services counselling and supportExclusive breastfeeding is the better option for suchinfants unless replacement feeding is acceptable fea-sible affordable sustainable and safe for both themother and baby This recommendation is based onthe finding that exclusive breastfeeding for up to 6months in three large cohort studies is associated witha three- to fourfold decreased risk of transmission ofHIV compared with non-exclusive breastfeeding(WHO 2006) The recommendations may need
further revision if new findings demonstrate thatexclusive breastfeeding should be the feeding ofchoice for HIV-infected women (Iliff et al 2005)
Some pilot programmes for exclusive breastfeedingpromotion in high-HIV-prevalence countries aresummarized in Appendix 2
In general exclusive breastfeeding promotionformed a part of the prevention of mother-to-childtransmission programmes LINKAGESZambiaintegrated improved counselling on infant feedingmaternal nutrition and antiretroviral therapy duringprophylaxis in both health-care and community ser-vices to enable women to make and act on informedchoice to feed their infants optimally in the context ofhigh HIV prevalence
Formative research was critical to develop locallyappropriate and feasible infant feeding recommenda-tions for individual infants and their families based onHIV status In Zambia the research included focusedgroup discussions key information interviews obser-vations of household food preparation and feedingmarket survey of replacement foods and breastmilksubstitutes and household trials of improved feedingand caring practices (LINKAGES 2005)
High quality of health workers is another criticalfactor for sensitive and accurate individual counsel-ling Programmes incorporated behaviour changecommunication methodologies in training (LINK-AGES 2005) It is important to develop skills of com-munity members as well for improved servicesreferral outreach and follow-up care and support ofHIV-positive mothers and their infants
A comprehensive communications strategy tosupport scale-up was a notable feature of the LINK-AGES programme in Zambia In 2004 an intensiveeffort was launched using brochures posters radioand television spots billboards and reference guidesfor health providers (LINKAGES 2005) Messageswere targeted to relevant stakeholders ndash pregnantand lactating mothers health providers youth andcommunity leaders and all the materials were nation-ally disseminated
Monitoring and evaluation another importantfeature of effective scale-up was a feature of pilotprogrammes (Appendix 2 Ntabaye amp Lusiola 2004Rutenberg et al 2004) in Zambia and Tanzania Moni-
N Bhandari and AKMI Kabir12
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
toring and evaluation not only provides a measure ofsuccess but identifies factors that may have contrib-uted to it and to lack of success to enable mid-coursecorrections The impact of some pilot programmes onexclusive breastfeeding is summarized in Appendix 2In most programmes exclusive breastfeeding ratesimproved In Zambia exclusive breastfeeding ratesincreased from 50 in 2002 to 64 in 2004 in Liv-ingstone from 57 in 2000 to 74 in 2004 in NdolaIn South Africa an antenatal clinic-based interven-tion led to 83 of infants born to HIV-infectedmother initiating exclusive breastfeeding InZimbabwe an intervention based on antenatal coun-selling resulted in a relatively lower exclusive breast-feeding rate of 246 at 3 months (Piwoz et al 2005)
Several barriers to success were identified Theseinclude inadequate skills of workers and non-integration of HIV counselling and tailoring into ante-natal care services (Ntabaye amp Lusiola 2004) which isthe backbone in which infant feeding counselling isbuiltWomen reported that mothers not breastfeedingtheir children were discriminated against by the com-munity and they faced the threat of domestic violenceProgramme managerrsquos understanding of barriersto effective programme implementation and impactwere emphasized as being important Governmentsupport partnerrsquos coordination increased humanresource and improving the supply system were iden-tified to be essential features to scale up programmesin the HIV context (Rutenberg et al 2004) Lowoverall exclusive breastfeeding rates prompted Piwozet al (2005) to conclude that women and their partnersshould have been reached more frequently during theantenatal and post-natal period
Conclusions
In a large number of programmes for improvingexclusive breastfeeding in developing countriesincluding in areas with high prevalence of HIV apositive impact on exclusive breastfeeding rates hasbeen achieved
Some of the factors that contributed to successfulscale-up are summarized in Table 4 Several limita-tions of the programmes reviewed merit attentionMost programmes involved special and generous
funding concentrated efforts and multiple contactsThese programmes were evaluated over relativelyshort periods of time usually 2ndash5 years and the long-term sustainability has not been really tested In theabsence of specific measures there is likely to be dilu-tion of quality as the programmes are scaled upfurther from their initial size The experience thus farleaves important questions to be addressed particu-larly on how programmes can be sustained over timeas they are scaled up at affordable costs
A key factor relevant to sustainability is to plan ona long-term basis a period of 10ndash20 years rather than5ndash10 years from the outset Experience with otherchild health programmes has shown that performancein immunization and oral rehydration therapy userates plateaued over time in many countries
Programme scale-up requires a programme man-agement capacity proportionate to the scale of opera-tions periodic assessment of barriers (Table 5) and anability to revise programme strategy to overcomethese Another key feature to sustainability ofscale-up is the extent to which capacity has been builtat the district block and community levels National-or state-level driven interventions begin with enor-mous enthusiasm which is difficult to sustain Thisfactor is particularly important as most developing
Table 4 Lessons learnt about scale-up key factors in success
bull Political will advocacy enabling policiesbull Championship by health ministries at national state and districtlevelbull Technical consensus on feeding guidelinesbull Programme strategy and measurable short- and long-term goalsbull Long-term financial commitmentbull Partners with defined roles assessment of their capacity todeliver and plans to cover gaps in capacitybull Emphasis on community-level interventions and not onlyfacility-based programmesbull Formative research as the backbone of effective scale-upprogrammes particularly in the context of HIVbull Careful selection of channels and the number required toachieve timely coverage consistency of messagesbull Communication strategy aided by formative research pre-testedvalidated messages and toolsbull Quality trainers and training centres proportionate to requiredscalebull Monitoring and evaluationbull Programme redesign when relevant through research analysisand innovation
Mainstreaming nutrition into MCH programs 13
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
countries are going through a process of decentrali-zation with increasing responsibility for planningimplementation and evaluation being delegated tolower levels of the health-care system Buildingcapacity at that level requires time resources andpatience and a longer-term perspective
Building capacity emerges to be a key factorTrainers and training centres vary in their qualitywhen training health workers and their supervisorsor programme managers As the burden of trainingincreases availability of good-quality trainersbecomes a limiting factor (WHOUNICEF 2002Government of India 2006) An effective strategymust plan for these incremental requirements includ-ing ensuring secure and sustained funding
Identifying barriers to success is a key actor Thebarriers to scaling up of health interventions havebeen elegantly described by Ranson et al (Table 5)Most of these are important for exclusive breastfeed-ing scale-up as well
Overall within the limitations discussed above anumber of programmes in countries with varying
HIV prevalence show that exclusive breastfeeding ona large scale is feasible and pilot programmes havegiven valuable guidance related to policies planningand implementation of large-scale programmes Thechallenge now is to build on these experiences whenplanning national programmes
Acknowledgements
We sincerely thank Dr MK Bhan for his constructivecriticism and sustained feedback at different stages ofdevelopment of this review
Conflicts of interest
The authors have declared no conflicts of interest
References
Arifeen S Black RE Antelman G Baqui A CaulfieldL amp Becker S (2001) Exclusive breastfeeding reducesacute respiratory infection and diarrhea deaths amonginfants in Dhaka slums Pediatrics 108 E67
Australian Breastfeeding Association (2005) Valuing Par-enthood Options for Paid Maternity Leave ndash InterimPaper 2002 Available at httpwwwbreastfeedingasnauadvocacymatleavehtml
Bhandari N Bahl R Mazumdar S Martines J BlackRE amp Bhan MK (2003) Effect of community basedpromotion of exclusive breastfeeding on diarrheal ill-nesses and growth a cluster randomized controlled trialLancet 361 1418ndash1423
Bhandari N Mazumder S Bahl R Martines J BlackRE amp Bhan MK (2004) An educational interventionto promote appropriate complementary feedingimproves child feeding practices and linear growth inrural Haryana India Journal of Nutrition 134 2342ndash2348
Bhandari N Mazumder S Bahl R Martines J BlackRE amp Bhan MK (2005) Use of multiple opportunitiesfor improving feeding practices in undertwos withinchild health programs Health Policy Plan 20 328ndash336
Bryce J Victora CG Habicht JP Vaughan JP ampBlack RE (2004) The multi-country evaluation of theintegrated management of childhood illness strategylessons for the evaluation of public health interventionsAmerican Journal of Public Health 94 406ndash415
Butte NF Lopez-Alarcon MG amp Garza C (2002) Nutri-ent Adequacy of Exclusive Breastfeeding for the TermInfant during the First Six Months of Life World HealthOrganization Geneva
Table 5 Barriers to scaling up of health interventions
Community and household levelsLack of information womenrsquos education physical financial
womenrsquos decision-making powerHealth services delivery levelShortage of qualified staff weak technical guidance programme
management and supervision inadequate supplies equipmentand infrastructure poor accessibility
Health sector policy and strategic management levelWeak and centralized system for planning and management weak
drug policies and supply system inadequate regulations lack ofintersectoral action and partnership weak incentives to useinputs efficiently and respond to user needs and preferencesreliance on donor funding
Public policies cutting across sectorsGovernment bureaucracy poor communication and transport
infrastructureEnvironmental characteristicsGovernance and overall policy frameworkCorruption weak government weak laws political instability and
insecurity low priority to social sectors weak structure for publicaccountability and opportunities for public opinions lack of freepress
Physical environmentClimatic and geographic predisposition physical environment
unfavourable to service delivery
Adapted from Ranson et al (2003)
N Bhandari and AKMI Kabir14
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Cohen J (2007) Retrovirus meeting Hope on new AIDSdrugs but breast-feeding strategy backfires Science 3151357
Coovadia HM Rollins NC Bland RM Little KCoutsoudis A Bennish ML et al (2007) Mother tochild transmission of HIV-1 infection during exclusivebreastfeeding in the first 6 months of life an interven-tion cohort study Lancet 369 1107ndash1116
Coutinho SB de Lira PI de Carvalho LM amp AshworthA (2005) Comparison of the effect of two systems forthe promotion of exclusive breastfeeding Lancet 3661094ndash1100
Feachem RG amp Koblinsky MA (1984) Interventions forthe control of diarrheal diseases among young childrenpromotion of breastfeeding Bulletin of the of the WorldHealth Organization 62 271ndash291
Gonzales A Arteaga E amp Howard-Grabman L (1998)Scaling Up the WARMI Project ndash Lessons LearnedMobilizing Bolivian Communities around ReproductiveHealth Save the Children Federation Inc Bolivia FieldOffice La Paz Available at httpwwwcoregrouporgresourcesSavebolipdf
Government of India (1997) Recommendations of the FifthCentral Pay Commission Relating to Enhancement ofQuantum of Maternity Leave and to Allow PaternityLeave in Respect of Central Government EmployeesDocument ref 13018197-Estt(L) Available at httppersminnicinesttleave2htm
Government of India (2005) National Rural HealthMission 2005ndash2012 Mission document Ministry ofHealth and Family Welfare New Delhi Government ofIndia Available at httpwwwmohfwnicinNRHM20Mission20Documentpdf
Government of India (2006) Operational Guidelines forImplementation of Integrated Management of Neonataland Childhood Illness (IMNCI) Ministry of HealthFamily Welfare New Delhi Available at httpmohfwnicindofw20websiteF20IMNCI20Operational20Plan201320june202006htm
Government of Pakistan (2003) National Programme forFamily Planning and Primary Health Care The LadyHealth Workers Programme 2003ndash2008 Ministry ofHealth Pakistan Available at httpwwwphcgovpkDownloadsPC-120augpdf
Green CP (1999) Improving Breastfeeding Behaviors Evi-dence from Two Decades of Intervention ResearchPublished for the US Agency for International Develop-ment (USAID) by the LINKAGES Project Academyfor Educational Development Washington DC
Gupta A (2002) National trends in breastfeeding andeffective strategies to improve breastfeeding ratesJournal of Neonatology 2002 4ndash14
Gwatkin DR (2004) Integrating the management of child-hood illness Lancet 364 1557ndash1558
Habicht JP DaVanzo J amp Butz WP (1986) Does breast-feeding really save lives or are apparent benefits due tobiases American Journal of Epidemiology 123279ndash290
Haider R Ashworth A Kabir I amp Huttly SR (2000)Effect of community based peer counsellors on exclusivebreastfeeding practices in Dhaka Bangladesh a ran-domized controlled trial Lancet 356 1643ndash1647
Haider R Kabir I Huttly SR amp Ashworth A (2002)Training peer counsellors to promote and support exclu-sive breastfeeding in Bangladesh Journal of HumanLactation 18 7ndash12
Horton S Sanghvi T Phillips M Fiedler J Perez-Escamilla R Lutter C et al (1996) Breastfeeding pro-motion and priority setting in health Health Policy andPlanning 11 156ndash168
ILO (1998) More than 120 Nations Provide Paid MaternityLeave Gap in Employment Treatment for Men andWomen Still Exists International Labour Office GenevaDocument ref ILO987 Available at httpwwwiloorgpublicenglishbureauinfpr19987htmr2
Iliff PJ Piwoz EG Tavengwa NV Zunguza CDMarinda ET Nathoo KJ et al (2005) Early exclusivebreastfeeding reduces the risk of postnatal HIV-1 trans-mission and increase HIV-free survival AIDS 19 699ndash708
Integrated Child Development Services Scheme (Revised)(ICDS) (1982) Ministry of Social Welfare Governmentof India New Delhi Available on URL httpwcdnicinudishahtmabouticdshtm
Jason JM Nieburg P amp Marks JS (1984) Mortality andinfectious disease associated with infant feeding prac-tices in developing countries Pediatrics 74 702ndash727
Jones G Steketee RW Black RE Bhutta ZA ampMorris SS Bellagio Child Survival Study Group (2003)How many child deaths can we prevent this yearLancet 362 65ndash71
Knippenberg R Lawn JE Darmstadt GL Begkayian GFogstad H Walelign N et al (2005) Systematic scalingup of neonatal care in countries Lancet 365 1087ndash1098
Kramer MS amp Kakuma R (2002) The optimal durationof exclusive breastfeeding a systematic reviewCochrane Database of Systematic Reviews 2002CD003517
Kramer MS Chalmers B Hodnett ED Sevkovskaya ZDzikovich I Shapiro S et al (2000) Promotion ofbreastfeeding intervention trial (PROBIT) a cluster ran-domized trial in the Republic of Belarus Design followup and data validation Advances in Experimental Medi-cine and Biology 478 327ndash345
Kramer MS Chalmers B Hodnett ED Sevkovskaya ZDzikovich I Shapiro S et al (2001) Promotion ofbreastfeeding intervention trial (PROBIT) a random-
Mainstreaming nutrition into MCH programs 15
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
ized trial in the Republic of Belarus Journal of theAmerican Medical Association 285 413ndash420
Lewin SA Dick J Pond P Zwarenstein M Aja Gvan Wyk B et al (2006) Lay health workers in primaryand community health care (Review) The CochraneLibrary 3 1ndash104
LINKAGES (2002) World LINKAGES MadagascarAcademy for Educational Development WashingtonDC
LINKAGES (2005) LINKAGES Zambia 1997ndash2005 FinalReport A Full Report on LINKAGES Infant Feedingand HIVAIDS Programs in Zambia Academy for Edu-cational Development Washington DC Available athttpwwwlinkagesprojectorgmediapublicationsFinal20draft20Zambia20final20report2012105pdf
Lutter CK Perez-Escamilla R Segall A Sanghvi TTeruya K amp Wickham C (1997) The effectiveness of ahospital based program to promote exclusive breastfeed-ing among low income women in Brazil AmericanJournal of Public Health 87 659ndash663
Morrow AL Guerrero ML Shults J Calva J Lutter CBravo J et al (1999) Efficacy of home based peer coun-selling to promote exclusive breastfeeding a randomizedcontrolled trial Lancet 353 1226ndash1231
Ntabaye MK amp Lusiola GJ (2004) Understanding barri-ers to PMTCT in Tanzania findings of a baseline surveyInternational Conference on AIDS 15 (B11396)
de Oliveira LD Giugliani ER do Espirito SLC FrancaMC Weigert EM Kohler CV et al (2006) Effect ofintervention to improve breastfeeding technique on thefrequency of exclusive breastfeeding and lactation-related problems Journal of Human Lactation 22 315ndash321
Perez-Escamilla R (2004) Effectiveness of MADLAC atImproving Breastfeeding Promotion and CounsellingIndicators in Maternity Wards in El Salvador Publishedfor the Basic Support for Institutionalizing Child Sur-vival Project (BASICS II) for the United States Agencyfor International Development Arlington VA Availableat httpwwwbasicsorgpdfFinal20MADLAC20Report20RPE20April207-2004pdf
Perez-Escamilla R (2007) Evidence based breast-feedingpromotion the Baby-Friendly Hospital InitiativeJournal of Nutrition 137 484ndash487
Piwoz EG Iliff PJ Tavengwa N Gavin L Marinda ELunney K et al (2005) An education and counselllingprogram for preventing breastfeeding associated HIVtransmission in Zimbabwe design and impact on mater-nal knowledge and behaviour Journal of Nutrition 135950ndash955
Quinn VJ Guyon AB Schubert JW Stone-Jimenez MHainsworth MD amp Martin LH (2005) Improvingbreastfeeding practices on a board scale at the commu-
nity level success stories from Africa and LatinAmerica Journal of Human Lactation 21 345ndash354
Ranson MK Hanson K Oliveira-Cruz V amp Mills A(2003) Constraints to expanding access to health inter-ventions an empirical analysis and country typologyJournal of International Development 15 15ndash40
Rea MF amp Berquo ES (1990) Impact of the Braziliannational breastfeeding programme on mothers inGreater Sao Paulo Bulletin of the of the World HealthOrganization 68 365ndash371
Rollins NC (2007) Infant feeding and HIV BritishMedical Journal 334 487ndash488
Rutenberg N Baek C Kalibala S Rosen J amp Mulenga D(2004) Evaluation of United Nations supported pilotprojects for the prevention of mother-to-child transmis-sion of HIV overview of findings International Confer-ence on AIDS 15 (WePeE6688)
The Core Group (2005) Scale and Scaling Up A COREGroup Background Paper on lsquoScaling-Uprsquo MaternalNewborn and Child Health Services CORE SpringMembership Meeting 2005 The Core Group Washing-ton DC Available at httpwwwcoregrouporgresourcesmeetingsapril05Scaling_Up_Background_Paper_7-13pdf
The Norwegian Government (1993) Women in PoliticsMinistry of Children and Equality Available at httpwwwregjeringennoendepbldRyddemappeSLA-AvdelingdoclegislationguidelinesWomen-in-Politicshtmlid=437166
Thior I Lockman S Smeaton LM Shapiro RL WesterC Heymann SJ et al (2006) Breastfeeding plus infantzidovudine prophylaxis for 6 months vs formula feedingplus infant zidovudine for 1 month to reduce mother-to-child HIV transmission in Botswana a randomized trialthe Mashi Study Journal of the American Medical Asso-ciation 296 794ndash805
UNICEF (2002) Facts for Life lsquoKey Message What EveryFamily and Community Has a Right to Know aboutBreastfeedingrsquo Available at httpwwwuniceforgffl04key_messageshtm
Van Roekel K Plowman B Griffiths M de AlvaradoVV Matute J amp Calderon M (2002) BASICS IIMidterm Evaluation of the AIN Program in Honduras2000 Basic Support for Institutionalizing Child SurvivalProject (BASICS II) for the United States Agency forInternational Development Arlington VA
WABA (2007) UNICEF Records BHFI Record UpdateAvailable at httpwwwwabaorgmydocsBFHIjan07xls 2006 Regularly updated by Miriam HLabbok Center for Infant and Young ChildFeeding and Care Department of Maternaland Child Health School of Public Health The Univer-sity of North Carolina at Chapel Hill Chapel Hill NCUSA
N Bhandari and AKMI Kabir16
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
WHA (2002) Infant and Young Child Nutrition Fifty-FifthWorld Health Assembly Agenda Item 1310 18 May2002 Available at httpwwwintgbebwhapdf_filesWHA55ewha5525pdf
WHO (1981) The International Code of Marketing ofBreastmilk Substitutes World Health OrganizationGeneva
WHO (1989) Protecting Promoting and Supporting Breast-feeding The Special Role of Maternity Services A JointWHOUNICEF Statement World Health OrganizationGeneva
WHO (2002) The Optimal Duration of Exclusive Breast-feeding Report of an Expert Consultation WHONHD0109 WHOFCHCAH0124 World HealthOrganization Geneva
WHO (2003a) Community Based Strategies for Breastfeed-ing Promotion and Support in Developing CountriesWorld Health Organization Geneva Document refISBN_92_4_159121_8 Available at httpwwwwhointchild-adolescent-healthNew_PublicationsNUTRITIONISBN_92_4_159121_8pdf
WHO (2003b) Multi-country Evaluation of IMCI Effective-ness Cost and Impact (MCE) Progress Report May2002ndashApril 2003 Document ref WHOFCHCAH035World Health Organization Geneva
WHO (2004) Promoting Proper Feeding for Infants andYoung Children World Health Organization GenevaAvailable at httpwwwwhointnutritiontopicsinfantfeedingen
WHO (2006) WHO HIV and Infant Feeding TechnicalConsultation-Consensus Statement World Health Orga-nization Geneva Available at httpwwwwhointhivmediacentreInfantfeedingconsensusstatementpfpdf
WHO Collaborative Study Team on the Role of Breast-feeding on the Prevention of Infant Mortality (2000)Effect of breastfeeding on infant and child mortality dueto infectious diseases in les developed countries apooled analysis Lancet 355 451ndash455
WHOUNICEF (1992) The global criteria for the WHOUNICEF Baby-Friendly Hospital Initiative In Baby-Friendly Hospital Initiative Part II Hospital LevelImplementation World Health Organization Geneva
WHOUNICEF (1993) Breastfeeding Counselling A Train-ing Course WHOCDR933 UNICEFNUT931 WorldHealth Organization Geneva
WHOUNICEF (2002) Protocol for Adapting the FeedingRecommendations Part III IMCI Adaptation GuideWorld Health Organization Geneva
WHOUNICEF (2003) Global Strategy for Infant andYoung Child Feeding World Health OrganizationGeneva Available at httpwwwwhointchild-adolescent-healthpublicationsNUTRITIONIYCF_GShtm
de Zoysa I Rea M amp Martines J (1991) Why promotebreastfeeding in diarrheal diseases control programmesHealth Policy and Planning 6 371ndash379
Mainstreaming nutrition into MCH programs 17
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
Cas
est
udie
so
fef
fect
iven
ess
stud
ies
or
pilo
tpr
ogra
mm
es
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Lut
ter
etal
(199
7)
Bra
zil
Low
-inc
ome
urba
nw
omen
deliv
erin
gin
hosp
ital
s
Bre
astf
eedi
ngpr
omot
ion
in
hosp
ital
sco
mpa
red
wit
h
nobr
east
feed
ing
prom
otio
n
Pro
mot
ion
ofbr
east
feed
ing
in
sele
cted
hosp
ital
s
Mea
nda
ysof
excl
usiv
e
brea
stfe
edin
g
75da
ysvs
22
days
(Plt
001
)
Rea
ampB
erqu
o
(199
0)
Wom
enw
ith
ach
ild
aged
lt2ye
ars
inSa
oP
aulo
Nat
iona
lbre
astf
eedi
ng
cam
paig
n19
81ndash1
986
BF
HI
Mas
sm
edia
cam
paig
n11
in
fant
s5ndash
6m
onth
s
excl
usiv
ely
brea
stfe
d
in19
88an
d37
in
1987
Con
foun
ding
fact
ors
over
the
6-ye
arpe
riod
not
mea
sure
d
Kra
mer
etal
(200
020
01)
PR
OB
ITtr
ial
Bel
arus
Clu
ster
rand
omiz
ed
34ho
spit
als
and
thei
rpo
lycl
inic
s
Trai
ning
inB
FH
I(W
HO
UN
ICE
F19
92)
vsr
outi
ne
prac
tice
san
dpo
licie
s
Exc
lusi
vebr
east
feed
ing
at3
(43
3vs
64
)
and
6(7
9
vs0
6
)
mon
ths
sign
ifica
ntly
high
er
Impl
emen
ted
thro
ugh
BF
HI
ina
sett
ing
whe
reho
spit
al
deliv
erie
sar
eco
mm
on
Per
ez-E
scam
illa
(200
4)
BA
SIC
SII
Mex
ico
Hon
dura
s
Bra
zil
MA
DL
AC
low
-cos
t
man
agem
ent
info
rmat
ion
syst
emto
use
an
evid
ence
-bas
edap
proa
chto
impr
ove
serv
ice
perf
orm
ance
Inte
rvie
win
gof
wom
enat
hosp
ital
disc
harg
epo
st
deliv
ery
usin
ga
ques
tion
nair
eth
atta
kes
5ndash7
min
toad
min
iste
ran
d
cont
ains
19br
east
feed
ing
prom
otio
nco
unse
lling
indi
cato
rs
Dat
aen
tere
dan
dre
sult
s
disc
usse
d3-
mon
thly
by
hosp
ital
com
mit
tee
Hos
pita
lim
plem
ents
chan
ges
in
brea
stfe
edin
g
supp
ort
base
don
anal
ysis
of
ques
tion
nair
es
Itis
aco
st-e
ffec
tive
inte
rven
tion
that
can
help
impr
ovem
ents
inth
eB
FH
I
and
isa
valu
able
tool
for
proc
ess
eval
uati
on
N Bhandari and AKMI Kabir18
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
LIN
KA
GE
S
proj
ect
inA
fric
aan
d
Lat
inA
mer
ica
(Qui
nnet
al
2005
LIN
KA
GE
S
2002
WH
O20
03a)
Bol
ivia
(1
mill
ion)
Gha
na(3
5
mill
ion)
Mad
agas
car
(6m
illio
n)
Res
ourc
e-
poor
sett
ing
Pilo
tpr
ogra
mm
e
InB
oliv
iaan
d
Gha
napr
ogra
mm
e
focu
sed
on
brea
stfe
edin
gan
d
com
plem
enta
ry
feed
ing
InM
adag
asca
r
prog
ram
me
prom
oted
brea
stfe
edin
g
wit
hin
7es
sent
ial
nutr
itio
nac
tion
san
d
subs
eque
ntly
thro
ugh
IMC
I
Bui
lton
form
ativ
ere
sear
ch
and
sust
aine
dth
roug
h
prog
ram
me
acti
viti
esth
at
focu
sed
onbr
ingi
ngab
out
the
desi
red
beha
viou
r
chan
geM
ixof
inte
rven
tion
s
reac
hed
wom
enin
divi
dual
ly
orin
grou
psin
heal
th
faci
litie
sho
mes
or
com
mun
ity
sett
ings
Con
sist
ent
mes
sage
san
d
mat
eria
lacr
oss
all
prog
ram
me
chan
nels
Bol
ivi
PR
OC
OSI
NG
Os
Gha
na
UN
ICE
F
nati
onal
nutr
itio
n
offic
eN
GO
s
Mad
agas
car
Inte
rsec
tora
l
Act
ion
Gro
upfo
r
Nut
riti
on
Jere
o
Sala
ma
Isik
a
Pro
gram
desi
gned
wit
h
part
ners
Rad
ioin
all
thre
esi
tes
Mat
eria
ls
deve
lope
d
tosu
itne
eds
oflo
cal
heal
th
wor
kers
and
com
mun
ity
mem
bers
Gre
at
emph
asis
on
deve
lopm
ent
of coun
selli
ng
and
nego
tiat
ion
skill
s
prac
tica
l
sess
ions
Sign
ifica
ntin
crea
ses
inex
clus
ive
brea
stfe
edin
gra
tes
of
0ndash6-
mon
th-o
ld
infa
nts
from
54
to65
in
Bol
ivia
68
to79
in
Gha
naan
d46
to68
in
Mad
agas
car
In
Gha
naan
d
Mad
agas
car
sign
ifica
ntre
sult
s
obse
rved
wit
hin
aye
ar
ofin
itia
tion
of
com
mun
ity
inte
rven
tion
s
App
roac
hw
asef
fect
ive
and
achi
eved
sign
ifica
nt
incr
ease
sam
ong
larg
e
popu
lati
ons
asea
rly
as
9ndash12
mo
afte
rin
itia
tion
of
com
mun
ity
acti
viti
es
Van
Roe
kele
tal
(200
2)W
HO
(200
3a)
Hon
dura
sG
row
thm
onit
orin
gan
d
prom
otio
nkn
own
as
Ate
ncioacute
nIn
tegr
ala
la
Nintilde
ez(A
IN)
or
Inte
grat
edC
hild
Car
e
Init
ially
pri
mar
ilya
grow
th
mon
itor
ing
prog
ram
me
ulti
mat
ely
thro
ugh
IMC
I
Pro
gram
me
ongr
owth
prom
otio
nndash
asse
ssm
ent
of
mon
thly
wei
ght
gain
and
focu
son
illne
ssf
eedi
ng
prac
tice
san
dge
nera
lchi
ld
care
inin
fant
sun
der
2ye
ars
Impl
emen
ted
atgo
vern
men
t
faci
litie
san
dco
mm
unit
y
Star
ted
in19
92s
tren
gthe
ned
in19
95ndash1
997
wit
hgr
eate
r
focu
son
child
feed
ing
In
1997
pro
gram
me
intr
oduc
ed
wit
hIM
CI
(WH
OU
NIC
EF
2002
)
Maj
or
part
ners
UN
ICE
F
PAH
O
Am
eric
an
and
Hon
dura
n
Red
Cro
ss
CA
RE
Rad
io
broa
dcas
ts
relig
ious
lead
ers
IMC
IM
id-t
erm
eval
uati
on
show
ed39
of
mot
hers
inin
terv
enti
on
com
mun
itie
sex
clus
ivel
y
brea
stfe
dco
mpa
red
wit
h13
in
the
cont
rol
site
s
Mainstreaming nutrition into MCH programs 19
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
cont
inue
d
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Bha
ndar
ieta
l
(200
3)
WH
O
(200
3a)
Rur
alco
mm
unit
ies
inH
arya
na
Indi
a
Clu
ster
rand
omiz
edtr
ial
8
com
mun
itie
s(t
otal
popu
lati
on~4
000
0)
Pro
mot
ion
ofex
clus
ive
brea
stfe
edin
gan
d
appr
opri
ate
com
plem
enta
ryfe
edin
g
Dev
elop
edth
roug
h
form
ativ
ere
sear
ch
ndashP
robl
emid
enti
ficat
ion
ndashP
arti
cipa
tory
desi
gnof
inte
rven
tion
impl
emen
tati
onan
d
eval
uati
on
Impl
emen
tati
onw
ithi
nan
exis
ting
prim
ary
heal
th-c
are
prog
ram
me
Opp
ortu
niti
esus
edto
deliv
erm
essa
ges
wer
e
imm
uniz
atio
ncl
inic
s
wei
ghin
gse
ssio
ns
sick
-chi
ldco
ntac
tsan
d
mon
thly
hom
evi
sits
Res
earc
hers
wit
hlo
cal
gove
rnm
ent
ICD
Ssy
stem
and
NG
O
The
atre
son
gs
Mas
sm
edia
not
used
for
risk
of
cont
amin
atio
n
Mat
eria
ls
deve
lope
d
for
heal
th
wor
kers
pos
ters
flip
book
sca
rds
Bre
astf
eedi
ng
coun
selli
ngse
ctio
n
ofth
eIM
CI
(WH
O
UN
ICE
F20
02)
Exc
lusi
ve
brea
stfe
edin
gin
the
prev
ious
24h
at3
mon
ths
of
age
79
vs4
8
The
posi
tive
effe
ct
rem
aine
dup
to
6m
onth
sof
age
(42
vs4
)
Tota
lpar
tici
pati
onof
the
dist
rict
heal
thsy
stem
from
ince
ptio
nof
the
prog
ram
me
inde
velo
ping
impl
emen
tati
onst
rate
gyt
ool
deve
lopm
ent
and
mon
itor
ing
inad
diti
onto
invo
lvem
ent
of
anN
GO
wer
eim
port
ant
feat
ures
that
cont
ribu
ted
to
the
succ
ess
ofth
e
inte
rven
tion
Mor
row
etal
(199
9)
Mex
ico
Cit
yC
lust
erra
ndom
ized
tria
l
Tota
lpop
ulat
ion
3000
0
Two
com
mun
itie
sin
the
inte
rven
tion
one
com
pari
son
130
wom
en
Hom
e-ba
sed
peer
coun
selli
ng
Pee
rco
unse
llors
mad
e3
or
6ho
me
visi
tsto
the
mot
her
Key
fam
ilym
embe
rsal
so
incl
uded
By
La
Lec
he
Lea
gue
of
Mex
ico
Exc
lusi
ve
brea
stfe
edin
g
at3
mon
ths
post
-par
tum
67
(6vi
sits
)
50
(3vi
sits
)12
(com
pari
son)
Firs
tcl
uste
rra
ndom
ized
com
mun
ity-
base
dtr
ialt
hat
used
peer
coun
sello
rsto
prom
ote
excl
usiv
e
brea
stfe
edin
g
Hai
der
etal
2000
200
2
Dha
ka
Low
mid
dle
and
low
-soc
io-
econ
omic
popu
lati
on
Clu
ster
rand
omiz
edtr
ial
20zo
nes
inin
terv
enti
on
and
20in
cont
rol
Com
mun
ity-
base
dpe
er
coun
selli
ngin
Dha
ka
15ho
me-
base
dco
unse
lling
visi
tsby
peer
coun
sello
rs
40h
(4h
yen10
days
)
WH
OU
NIC
EF
brea
stfe
edin
g
coun
selli
ngco
urse
(WH
OU
NIC
EF
1993
)
Exc
lusi
ve
brea
stfe
edin
g
at5
mon
ths
70
in
inte
rven
tion
and
6in
the
cont
rol
Com
mun
ity-
base
d
brea
stfe
edin
gpr
omot
ion
stra
tegy
was
effe
ctiv
ein
Ban
glad
esh
whe
rem
ost
deliv
erie
soc
cur
atho
me
N Bhandari and AKMI Kabir20
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Bry
ceet
al
(200
4)W
HO
(200
3b)
Bra
zil
Per
u
Tanz
ania
Uga
nda
Mul
tico
untr
yev
alua
tion
of
IMC
Ith
atin
clud
ed
effe
ctiv
enes
sco
stan
d
impa
ct(B
ryce
etal
2004
)
Bre
astf
eedi
ngpr
omot
ion
asa
part
ofIM
CI
IMC
Iis
ast
rate
gyfo
r
impr
ovin
gch
ildhe
alth
and
deve
lopm
ent
thro
ugh
the
com
bine
d
deliv
ery
ofes
sent
ial
child
heal
th
inte
rven
tion
sIM
CI
bega
nw
ith
ase
tof
case
man
agem
ent
guid
elin
es
for
the
man
agem
ent
ofsi
ckch
ildre
nat
first
-lev
elhe
alth
faci
litie
s
and
the
guid
elin
esw
ere
desi
gned
for
adap
tati
on
atco
untr
yle
vela
nd
belo
wO
ver
tim
eth
e
stra
tegy
expa
nded
to
incl
ude
ara
nge
of
guid
elin
esfo
rde
liver
ing
child
surv
ival
inte
rven
tion
at
hous
ehol
dco
mm
unit
y
and
refe
rral
leve
ls
IMC
Im
odul
e(W
HO
UN
ICE
F20
02)
Res
ults
onex
clus
ive
brea
stfe
edin
g
avai
labl
efr
om
Tanz
ania
whe
reno
sign
ifica
ntim
pact
was
seen
Des
pite
subs
tant
ial
impr
ovem
ent
inth
equ
alit
y
ofca
rede
liver
edby
IMC
Iat
heal
thfa
cilit
ies
key
fam
ily
prac
tice
ssu
chas
excl
usiv
e
brea
stfe
edin
gdi
dno
tch
ange
asco
mm
unit
yIM
CI
had
not
been
impl
emen
ted
byth
at
tim
e(W
HO
2003
b)
SA
rife
en
pers
onal
com
mun
icat
ion
Ban
glad
esh
Mat
lab
Com
mun
ity-
base
dcl
uste
r
desi
gn
Eva
luat
ion
offa
cilit
y-an
d
com
mun
ity-
base
dIM
CI
Inte
rven
tion
pack
age
incl
udes
feed
ing
asse
ssm
ent
and
coun
selli
ngon
mot
hers
ofyo
ung
child
ren
seek
ing
care
atfa
cilit
ies
for
illne
ssan
d
hom
e-ba
sed
coun
selli
ng
onim
prov
edfe
edin
gby
com
mun
ity-
base
dhe
alth
and
nutr
itio
nw
orke
rs
At
base
line
inth
e
year
2000
alit
tle
mor
eth
anha
lfth
e
0ndash5-
mon
th-o
ld
infa
nts
inth
est
udy
area
wer
ebe
ing
excl
usiv
ely
brea
stfe
dB
y20
05
this
incr
ease
dby
30
inth
eIM
CI
area
Dat
ano
t
avai
labl
efr
omth
e
com
pari
son
area
as
yet
Lac
kof
com
para
ble
data
from
the
com
pari
son
area
prev
ents
ade
finit
ive
conc
lusi
onas
tow
heth
erth
is
trul
yis
anim
pact
ofIM
CI
BA
SIC
SII
Bas
icSu
ppor
tfo
rIn
stit
utio
naliz
ing
Chi
ldSu
rviv
alP
roje
ctB
FH
IB
aby-
Frie
ndly
Hos
pita
lIni
tiat
ive
ICD
SIn
tegr
ated
Chi
ldD
evel
opm
ent
Serv
ices
IM
CI
Inte
grat
edM
anag
emen
tof
Chi
ldho
odIl
lnes
sM
AD
LA
CM
onit
oreo
deA
poyo
Dir
ecto
con
laL
acat
anci
aM
ater
naN
GO
non
-gov
ernm
enta
lorg
aniz
atio
nPA
HO
Pan
Am
eric
anH
ealt
hO
rgan
izat
ion
PR
OB
ITP
rom
otio
nof
Bre
astf
eedi
ngIn
terv
enti
onTr
ial
PR
OC
OSI
Pro
gram
ade
Coo
rdin
acio
nen
Salu
dIn
tegr
al(C
olla
bora
tive
Pro
gram
for
Inte
grat
edH
ealt
h)U
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
WH
OW
orld
Hea
lth
Org
aniz
atio
n
Mainstreaming nutrition into MCH programs 21
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x2
Cas
est
udie
sin
scal
e-up
effo
rts
inH
IVA
IDS
Stud
yde
scri
ptio
nPo
pula
tion
Inte
rven
tion
Com
mun
icat
ion
stra
tegy
Impa
cton
excl
usiv
ebr
east
feed
ing
Com
men
ts
LIN
KA
GE
S(2
005)
Zam
bia
Pro
gram
me
thro
ugh
heal
th-c
are
and
com
mun
ity
serv
ices
Rea
ched
60si
tes
in6
dist
rict
sby
2005
Inte
grat
ion
ofin
fant
feed
ing
coun
selli
ngm
ater
naln
utri
tion
and
anti
retr
ovir
aldr
ugs
prop
hyla
xis
Trai
ning
ofhe
alth
wor
kers
and
com
mun
ity
serv
ice
prov
ider
sto
coun
selw
omen
onsa
fety
opti
ons
for
thei
rsi
tuat
ion
Beh
avio
urch
ange
Com
mun
icat
ion
inte
rven
tion
sin
the
first
few
year
sM
ater
iald
evel
oped
lsquoAct
Now
rsquoM
edia
cam
paig
nsin
clud
edbr
ochu
res
post
ers
radi
oan
dte
levi
sion
Ass
esse
dth
roug
hba
selin
ean
dfo
llow
-up
hous
ehol
dan
dcl
inic
surv
eys
inse
lect
eddi
stri
cts
Exc
lusi
vebr
east
feed
ing
rate
incr
ease
dfr
om50
in
2002
to64
in
2004
inL
ivin
gsto
nean
dfr
om57
in
2000
to74
in
2004
inN
dola
Inte
grat
edde
mon
stra
tion
proj
ect
Had
seve
rals
tren
gths
inte
rms
ofth
eus
eof
form
ativ
ere
sear
chto
deve
lop
mes
sage
str
aini
ngan
dbu
ildin
gup
skill
sof
prog
ram
me
man
ager
she
alth
-car
epr
ovid
ers
and
com
mun
ity
wor
kers
adv
ocac
yfo
rna
tion
alpo
licy
stro
ngbe
havi
our
chan
geco
mm
unic
atio
nco
mpo
nent
st
reng
then
ing
com
mun
ity
capa
city
for
coun
selli
ngan
dre
ferr
als
and
mon
itor
ing
and
eval
uati
onw
ith
loca
lpar
tner
sP
iwoz
etal
(20
05)
ZV
ITA
MB
Otr
ial
Har
are
Zim
babw
eE
duca
tion
and
coun
selli
ngpr
ogra
mm
ede
liver
edan
tena
tally
1411
0m
othe
rndashba
bypa
irs
enro
lled
from
14m
ater
nity
clin
ics
wit
hin
96h
ofde
liver
yan
dfo
llow
edup
at6
wee
ks
3m
onth
san
d3-
mon
thly
inte
rval
sIn
fant
-fee
ding
patt
erns
dete
rmin
edE
xclu
sive
brea
stfe
edin
gre
com
men
ded
for
HIV
nega
tive
un
know
nor
HIV
posi
tive
who
chos
eto
brea
stfe
ed
Gro
uped
ucat
ion
indi
vidu
alco
unse
lling
vid
eos
broc
hure
sM
othe
rsw
hoen
rolle
dw
hen
prog
ram
me
was
fully
impl
emen
ted
wer
e8
4ti
mes
mor
elik
ely
toex
clus
ivel
ybr
east
feed
than
mot
hers
who
enro
lled
befo
reth
epr
ogra
mm
ebe
gan
Ove
rall
excl
usiv
ebr
east
feed
ing
rate
sti
ll3
mon
ths
was
low
at24
6
Form
ativ
ere
sear
chus
edto
desi
gna
cult
ural
lyse
nsit
ive
educ
atio
nan
dco
unse
lling
prog
ram
me
Low
over
alle
xclu
sive
brea
stfe
edin
gra
tes
prom
pted
auth
ors
toco
nclu
deth
atw
omen
and
thei
rpa
rtne
rssh
ould
have
been
reac
hed
mor
efr
eque
ntly
duri
ngan
tena
tala
ndpo
st-n
atal
peri
od
N Bhandari and AKMI Kabir22
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Thi
oret
al(
2006
)R
ollin
s(2
007)
C
ohen
(200
7)
HIV
-inf
ecte
dpr
egna
ntw
omen
atte
ndin
gan
tena
talc
linic
sin
sout
hB
otsw
ana
Inve
stig
atio
nsby
CD
Cof
adi
arrh
oea
outb
reak
inJa
nuar
y-Fe
brua
ry20
06in
the
sam
epo
pula
tion
Mat
erna
land
infa
ntan
tire
trov
iral
ther
apy
toas
cert
ain
impa
cton
HIV
tran
smis
sion
Ant
enat
alco
unse
lling
Cas
endashco
ntro
lstu
dyto
iden
tify
risk
fact
ors
for
diar
rhoe
ano
tbr
east
feed
ing
was
the
bigg
est
risk
fact
ora
djus
ted
odds
rati
o50
(95
confi
denc
ein
terv
al4
5ndash10
0)
Bot
swan
aha
sth
ebe
stpr
imar
yhe
alth
-car
est
ruct
ure
wat
ersu
pply
and
sani
tati
onsy
stem
sin
Sout
hA
fric
aFo
rmul
apr
ovid
edfr
eeby
the
gove
rnm
ent
toin
fect
edm
othe
rsL
ower
mor
talit
yin
the
brea
stfe
edin
ggr
oup
at7
mon
ths
dem
onst
rate
sri
skof
form
ula
feed
ing
and
need
for
alte
rnat
est
rate
gies
(Thi
oret
al
2006
)A
utho
rsco
nclu
deth
athe
alth
syst
ems
inw
hich
thes
epr
ogra
mm
esar
eim
plem
ente
dsh
ould
beab
leto
cope
wit
hdi
arrh
oea
and
mal
nutr
itio
nth
atre
sult
sbe
caus
eof
form
ula
feed
ing
(Rol
lins
2007
)C
oova
dia
etal
(2
007)
Kw
aZul
uNat
al
Sout
hA
fric
a27
22H
IV-i
nfec
ted
and
unin
fect
edpr
egna
ntw
omen
enro
lled
into
ano
n-ra
ndom
ized
inte
rven
tion
coho
rtst
udy
from
ante
nata
lcl
inic
sIn
fant
feed
ing
data
obta
ined
wee
kly
bloo
dsa
mpl
esfr
omin
fant
sta
ken
mon
thly
83
of13
72in
fant
sbo
rnto
HIV
-inf
ecte
dm
othe
rsin
itia
ted
excl
usiv
ebr
east
feed
ing
from
birt
hB
reas
tfed
infa
nts
who
rece
ived
solid
sw
ere
sign
ifica
ntly
mor
elik
ely
toac
quir
ein
fect
ion
com
pare
dw
ith
excl
usiv
ely
brea
stfe
d(H
R10
87
151
ndash78
P=
001
8)as
wer
ein
fant
sw
hoat
12w
eeks
rece
ived
brea
stan
dfo
rmul
am
ilk(1
82
098
ndash33
6P
=0
57)
Cum
ulat
ive
3-m
onth
mor
talit
yin
excl
usiv
ely
brea
stfe
dw
as6
1(4
74ndash
792
)vs
15
1(7
63ndash
287
3)in
infa
nts
give
nre
plac
emen
tfe
eds
(HR
206
1
0ndash4
27P
=0
05)
The
stud
ysh
ows
that
excl
usiv
ebr
east
feed
ing
can
besu
cces
sful
lysu
ppor
ted
inH
IV-i
nfec
ted
wom
enT
heau
thor
sca
llfo
rfu
rthe
rre
visi
onof
UN
ICE
FW
HO
and
USA
IDin
fant
feed
ing
guid
elin
es
CD
CC
ente
rof
Dis
ease
Con
trol
HR
haz
ards
rati
oU
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
USA
IDU
SA
genc
yfo
rIn
tern
atio
nalD
evel
opm
ent
WH
OW
orld
Hea
lth
Org
aniz
atio
nZ
VIT
AM
BO
Z
imba
bwe
Vit
amin
Afo
rM
othe
rsan
dB
abie
s
Mainstreaming nutrition into MCH programs 23
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23

Background
The Lancet series on child survival identified breast-feeding interventions to have the potential to prevent13 of all under-5 deaths in developing areas of theworld ranking it as the most important preventiveapproach for saving child lives (Jones et al 2003)Exclusive breastfeeding that is administering onlybreastmilk and no other liquids or foods (WHO 2004)for the first 6 months of life confers important benefitsto the infant and the mother ndash it protects infantsagainst many common childhood diseases includingrepeated gastrointestinal infections and pneumoniaand thereby against some of the major causes of child-hood mortality (Feachem amp Koblinsky 1984 Jasonet al 1984 Habicht et al 1986 de Zoysa et al 1991WHO Collaborative Study Team on the Role ofBreastfeeding on the Prevention of Infant Mortality2000Arifeen et al 2001)A large volume of literatureexists regarding efficacy trials that have clearly dem-onstrated the beneficial impact of exclusive breast-feeding (Green 1999)
Unfortunately exclusive breastfeeding is not prac-tised universally Global monitoring indicates thatonly 39 of infants are exclusively breastfed forless than 4 months following birth (WHOUNICEF2003) Some reasons for failure to breastfeed exclu-sively for the recommended first 6 months of lifeinclude community beliefs that result in delay in ini-tiation of breastfeeding after birth giving other fluidsandor foods to breastfeeding infants the lack ofsocial support for women in resolving breastfeedingdifficulties and lack of health system support (Green1999)
The current international optimal feeding rec-ommendations include exclusive breastfeeding for6 months these are based on a review of scientificliterature to define the optimal duration of breast-feeding (Butte et al 2002 Kramer amp Kakuma 2002WHO 2002) These are also included in UnitedNations Children Fundsrsquo (UNICEFrsquos) Facts for Life
lsquoKey MessageWhat every family and community has a
right to know about breastfeedingrsquo (UNICEF 2002)In the early 1990s the World Health Organization
(WHO) and UNICEF launched the Baby-FriendlyHospital Initiative (BFHI) for strengthening mater-
nity services to support breastfeeding practices(WHOUNICEF 1992 table 3)
Although the BFHI includes a community compo-nent its implementation in developing countries isweak and support is only available in institutionsbefore and for a short period after delivery In severalregions a large proportion of deliveries occur athome Interventions at the community level aretherefore very important for supporting exclusivebreastfeeding
Identifying effective and sustainable means forscaling up of proven interventions into child healthprogrammes remains a major problem The purposeof this review is to define a process for scaling upexclusive breastfeeding based on experiences of pro-grammes or pilot projects for promotion of exclusivebreastfeeding implemented and evaluated in differentcountries The term lsquoscale uprsquo is commonly under-stood to mean reaching a larger number of beneficia-ries with a given intervention However apart fromcoverage maintaining quality as larger numbers arereached and effectively reaching out to those difficultto reach are also important considerations (The CoreGroup 2005) The issues addressed herein pertain topolicy programme design implementation strategyresources and costs management monitoring andevaluation and the possibility of continuing innova-tion and testing of novel approaches
Methods and search strategy
We conducted a systematic literature search with notime limits defined and used data from publishedliterature programme reports and monographsdescribing effectiveness or cluster randomized trialsor implementation programmes The databasessearched included PubMed the National Library ofMedicinersquos search service and Cochrane Library(Cochrane Controlled Trials Register) using the fol-lowing keywords breastfeeding or exclusive breast-feeding or breastfeeding promotion or breastfeedingintervention or breastfeeding programme or breast-feeding education or breastfeeding effect or impact orevaluation We also reviewed reference lists of iden-tified articles and hand searched reviews bibliogra-phies of books and abstracts and proceedings of
N Bhandari and AKMI Kabir6
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
national and international conferences or meetingsAdditionally we contacted key researchers andorganizationsagencies for unpublished material ornarrowly disseminated reports
Consistent with the programmatic focus theexamples quoted in this review are demonstrationprojects that reached large populations or cluster ran-domized intervention trialsThe emphasis is on devel-oping countries and as some of these countries areburdened by HIVAIDS this review includes thiscontext as well
The scale-up process
The scale-up planning process must follow a logicalorder Several key issues that need attention are sum-marized in Table 1 It is apparent that many of thefeatures of the process are generic to neonatal andchild health programmes but there are issues in thearea of exclusive breastfeeding that requires addi-tional attention particularly in the HIV context
Issues that need to be addressedwhile scaling up a programme forexclusive breastfeeding
Policy framework
The Global Strategy on Infant and Young ChildFeeding was adopted by a World Health Assemblyresolution (5525 WHA 2002) The global strategybuilds on the BFHI (WHOUNICEF 1992) the
International Code of Marketing of Breastmilk Sub-stitutes (WHO 1981) and the Innocenti Declarationon the Protection (WHO 1989) Promotion andSupport of Breastfeeding in the overall context ofnational policies and programmes on nutrition andchild health The aim of the strategy is to improvethe feeding of infants and young children andincrease the commitment of governments societygroups and international organizations to promotethe health and nutrition of children The strategyemphasizes the need for comprehensive nationalpolicies on infant and young child feeding onan urgent basis including guidelines on ensuringoptimal feeding of infants and young children inexceptionally difficult circumstances and the need toensure that all health services protect promote andsupport infant and young child feeding (Gupta 2002WHOUNICEF 2003)
Once the decision to scale up a programme forexclusive breastfeeding is made in a region or stateor country the logical starting point is to review therelevant existing national policies and to assesswhether these address varying circumstances underwhich women deliver and live such as urban or ruralresidence working women and place of deliverySpecific features to note are the status of the imple-mentation of the BFHI in facilities where womendeliver access and support to mothers with younginfants by trained personnel during the post-natalperiod and beyond support for exclusive breastfeed-ing in community setting legislation for workingmothers that ensures leave of appropriate durationan enabling environment at the work place withingovernment and private settings and the policiesin place for discouraging promotion of breastmilksubstitutes
Existing policies are optimal in some countries(The Norwegian Government 1993 ILO 1998) butlacunae exists in others for example exclusive breast-feeding for 6 months is a policy in India but the dura-tion of maternity leave for government employees is135 days (Government of India 1997) In Norwayhowever a mother is entitled to over 6 months ofmaternity leave (The Norwegian Government 1993)Wherever weaknesses exist a decision needs to bemade on how these will be addressed during scale-up
Table 1 Steps in scaling up
Assess situation create a policy environment conducive toexclusive breastfeeding
Define roles relationships and responsibilities of all partnersestablish agreements
Review technical supportDefine programme strategyMobilize resourcesProvide training and technical assistanceDevelop and use monitoring and evaluation systemsMonitor coverage and qualityMeasure impact and costProvide for testing novel approaches and continuing innovation
Adapted from Knippenberg et al (2005) and Gonzales et al (1998)
Mainstreaming nutrition into MCH programs 7
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Prior to scale-up a policy framework for implemen-tation needs to be developed This framework shouldinclude a vision consensus on technical issues onprogramme strategy roles relationships and respon-sibilities of implementing partners measurable goalswithin defined time lines and predictable adequatefunding to achieve these (The Core Group 2005) Itshould address the capacity of all implementing part-ners and the approach to fulfilling capacity gaps at alllevels particularly at the community level The policyframework should emphasize breastfeeding promo-tion through community-based programmes Politicalcommitment and ownership by relevant governmentdepartments at national state and district levels havealso been identified to be critical for effective scale-up(The Core Group 2005)
Technical and management support andother partnerships
Creating a policy framework designing a potentiallyeffective programme and an implementation strategyrequire multiple capacities which may not always beavailable within government departments or otherconcerned agencies
Technical and managerial support may need to bemobilized more so during the planning and earlyimplementation phase If this support is not availableinvolvement of external talent ndash national or eveninternational ndash may be required Once the pro-gramme is implemented the external support couldbe phased out gradually as local capacity is built
Forging partnerships between government minis-tries donors local non-governmental organizations(NGOs) and universities was a feature of many suc-cessful programmes (Appendix 1 Van Roekel et al
2002 Bhandari et al 2005 Quinn et al 2005) In theLINKAGES projects (Appendix 1) partnershipwith Programa de Coordinacion en Salud Integral(Collaborative Program for Integrated HealthPROCOSI) and NGOs in Bolivia UNICEF NGOsand the national government in Ghana and Intersec-toral Action Group for Nutrition and Jereo SalamaIsika in Madagascar added value and quality to pro-grammes resulted in effective pooling of resources
and expertise and improved programme design andmanagement (LINKAGES 2002 Van Roekel et al
2002 Quinn et al 2005)
Programme design and strategy
This requires a systematic description of steps andprocesses that help achieve high coverage qualityequity and sustainability capacity building and pro-gramme management are particularly important fea-tures (The Core Group 2005) Experience so farsuggests that for majority of developing countriesscale-up for exclusive breastfeeding will not be pos-sible unless intervention delivery at the communitylevel receives emphasis (Appendix 1) As an increas-ing number of mothers deliver in institutions mixedmodels will be required even in developing countries
An initial step is to carefully examine the existingopportunities as vehicles for promoting exclusivebreastfeeding If use of existing opportunities is insuf-ficient to achieve high coverage with good qualitythen additional approaches would need to be evolvedin a phased manner In Bangladesh the strategy ofpeer counsellors was used as the majority of deliveriesoccur at home and a community health worker is notroutinely available in that setting (Haider et al 2000)In India on the other hand village health workersalready exist so programmes are often designedaround them (Bhandari et al 2003 2004 2005)
Hospitalinstitution-based strategies
Efforts to scale up the BFHI in countries have shownmixed results (Table 2)
In regions where hospital deliveries are the normscale-up efforts through the BFHI (WHOUNICEF1992 Table 3 Perez-Escamilla 2007) have been suc-cessful and the strategy helped increase rates ofexclusive breastfeeding (Appendix 1) However inmany countries after initial years of enthusiasm thescale-up effort seems to have plateaued perhapsreflecting changing emphasis of donors and govern-ment The initial high rates of exclusive breastfeedingmay not be sustained after mothers are dischargedfrom facilities and return to their homes (Coutinhoet al 2005) The challenge therefore is to continue at
N Bhandari and AKMI Kabir8
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
home the post-delivery support available in institu-tions through public and private providers to sustainexclusive breastfeeding or develop other mechanismsthat support recently delivered mothers to exclusivelybreastfeed once they are discharged from hospitals(de Oliveira et al 2006) Countries have addressedthis in different ways In Australia a cadre of breast-feeding counsellors exists (Australian BreastfeedingAssociation 2005) In pilot programmes in Indiaexclusive breastfeeding was promoted through healthworker home visits at immunization clinics growthmonitoring sessions and at sick-child contacts(Bhandari et al 2005) in addition to the BFHI Homevisits are particularly important in regions where cov-
erage through other channels is low or not feasibleand a cadre of community workers exists
Community-based strategies
Pilot efforts in countries or regions where home deliv-eries predominate have shown success through ver-tical as well as integrated approaches however pro-grammes integrated into ongoing activities are morelikely to be more sustainable (The Core Group 2005)In these programmes (Appendix 1) the messageswere delivered through either a single existing or newchannel or multiple delivery channels already inplace within the primary health-care systemThe deci-sion to use one or multiple channels was made basedon the ability to cover the target population In somecountries high coverage was feasible only with mul-tiple facility and community channels (Appendix 1)Multiple channels also help achieve consistency inadvice The credibility and acceptability of a givenchannel by the community was another factor in theirbeing used Routine activities of channels were modi-fied in some instances to incorporate exclusive breast-feeding counselling In India for instance it wasbelieved that immunization sessions could not beused as a counselling opportunity but better organi-zation and the presence of another available localworker during the session enabled the vaccinator tocounsel mothers (Bhandari et al 2005)Another illus-tration is the adaptation of the Integrated Manage-ment of Childhood Illness (IMCI) programme of theWHOUNICEF (2002) to the Integrated Manage-ment of Neonatal and Childhood Illness (IMNCIGovernment of India 2006) by India The IMNCIincludes three home visits for all births in the first 7days of life by an existing community worker theAnganwadi worker (ICDS 1982) to promote essentialnewborn care which includes exclusive breastfeedingIn other countries such as Bangladesh facility-basedIMCI was sought to be improved in its impact bygreater emphasis on community component of IMCIthat is C-IMCI (Gwatkin 2004)
Programme delivery
Recognizing that facility-based interventions areinsufficient countries have experimented with a
Table 2 Proportion of facilities with Baby-Friendly Hospital Initiative(WABA 2007)
Region Median (range)
West and Central Africa 013 (000ndash059)EasternSouthern Africa 023 (000ndash100)Middle East and North Africa 014 (000ndash100)South Asia 007 (001ndash100)East Asia and Pacific 0005 (000ndash087)Americas and the Caribbean 010 (000ndash100)Central and Eastern EuropeCommonwealth
of Independent States025 (004ndash093)
All Industrialized Countries 007 (000ndash097)
Table 3 The 10 steps to successful breastfeeding for hospitals andbirth centres
bull Maintain a written breastfeeding policy that is routinelycommunicated to all health-care staffbull Train all health-care staff in skills necessary to implement thispolicybull Inform all pregnant women about the benefits and managementof breastfeedingbull Help mothers initiate breastfeeding within 1 h of birthbull Show mothers how to breastfeed and how to maintain lactationeven if they are separated from their infantsbull Give infants no food or drink other than breastmilk unlessmedically indicatedbull Practise lsquorooming inrsquo ndash allow mothers and infants to remaintogether 24 hours a daybull Encourage unrestricted breastfeedingbull Give no pacifiers or artificial nipples to breastfeeding infantsbull Foster the establishment of breastfeeding support groups andrefer mothers to them on discharge from the hospital or clinic
Mainstreaming nutrition into MCH programs 9
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
variety of local workers such as peer counsellors inBangladesh (Haider et al 2000) lady health workersin Pakistan (Government of Pakistan 2003) and thelsquoAccredited Social Health Activistsrsquo (ASHA) workerin India (Government of India 2005) to promoteexclusive breastfeeding by itself or as a part of essen-tial newborn care Programmes that used peer coun-sellors as a single channel have been shown to beeffective in several efficacy (Green 1999 Lewin et al
2006) and effectiveness trials (Morrow et al 1999Haider et al 2000 Lewin et al 2006) However whilepeer or lay counsellors have been effective in theshort run long-term sustainability of this approach ona large scale is as yet not established
The possible reasons stated for the short-termsuccess of the lay health workers approach includepayment to the counsellors for performing a specificpiece of work the counsellorsrsquo own perception ofbenefits of their work and their recognition by thecommunity as being skilled These workers also feltthis opportunity to have the potential for opening upof further education and training (Haider et al 2002)An important issue would also be linking newworkers with the existing primary health system aspilot experience showed that these workers may notbe able to resolve complex breastfeeding problems(Haider et al 2002)
Recruitment of ASHA in India provides a uniqueopportunity to promote exclusive breastfeeding(Government of India 2005) Currently being re-cruited all over the country these workers will focuson essential newborn care including exclusive breast-feeding through home visitation in the first month oflife and community-based activities
While these efforts in different countries at improv-ing coverage of the target population through localworkers are of value the voluntary or semi-voluntarynature of the workers and ill-defined models of super-vision raise issues about sustainability and possiblyhigh attrition rates
Programmes that used multiple channels reportedbroader coverage (Bhandari et al 2005 Quinn et al
2005) In India formative research showed thatimmunization sessions and private providers werethe channels to which infants were most commonly(~80) exposed Following constitution of a
breastfeeding-promotion programme caregiversmost often received exclusive breastfeeding counsel-ling at immunization sessions (~40) weighing ses-sions (~25) and home visits (25ndash30) Governmentphysicians or private providers rarely (~2) coun-selled despite being trained (Bhandari et al 2005)When all the opportunities were considered together55ndash60 of caregivers had been counselled at leastonce by at least one of the channels in the last 3months indicating that multiple channels reachedmore families (Bhandari et al 2005)The frequency ofcontact with caregivers or the intensity of counsellinginfluences the cumulative benefit of the counsellingfor example six contacts with mothers resulted inhigher adoption rates for exclusive breastfeeding ascompared with three (Morrow et al 1999) In Indiathe number of channels at which caregivers werecounselled was positively associated with the rates ofexclusive breastfeeding at 3 months of age (Bhandariet al 2003) However the costs of training and theeffort will increase more than the number of channelsused and therefore this issue requires a balancedview
Another issue of interest is the value of counsellingfor the antenatal period itself Antenatal counsellinghas been used in several programmes but its effect isdifficult to delineate by itself as it was usually fol-lowed by post-natal counselling (Green 1999) In theHIV context however the importance of antenatalcounselling is obvious
Communications approach
An effective communications approach was a featureof most programmes and involvement of journalistsradio announcements and other mass media from theprogramme outset extended the reach of nutritionmessages even further (Appendix 1 Quinn et al
2005) Mass media were not used in some pro-grammes where a comparison group was present forrisk of contamination (Bhandari et al 2005) Utiliza-tion of existing or newly formed community groupsproduced the same effect (Bhandari et al 2005Quinn et al 2005) and community mobilization pro-grammes such as street plays rallies radio pro-grammes and songs helped disseminate messages
N Bhandari and AKMI Kabir10
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
and increase community involvement (Bhandari et al
2005 Quinn et al 2005)Effective counselling requires assessment of
feeding practices recognition of problems and nego-tiation with the mother in choosing improved prac-tices that are feasible (WHOUNICEF 2002) thisrequires time and patience Programmes may chooseone-on-one counselling during opportunities in whichmore time is available such as home visits and groupcounselling for opportunities with lesser availabletime (Bhandari et al 2005) One of the reasons thatpeer counsellors may have been effective was thattheir sole responsibility was counselling mothersthrough home visits (Morrow et al 1999 Haider et al
2000) The more diverse the functions of the localworker the lesser will be the emphasis on a singlecomponent such as exclusive breastfeeding
Message development
The development of messages for interpersonal com-munication and for mass media needs careful atten-tion to design and content Successful programmesincluded an element of formative research to gain anin-depth understanding of the communities wherethese programmes were implemented with regard topractices pertaining to breastfeeding the reasons forthe current practices the common breastfeedingproblems and the barriers to adoption of ideal behav-iours in that cultural setting Formative research innorth India for instance showed general unwilling-ness to offer water to infants in summer months Thisbarrier was overcome by building specific explanatorymessages using local terms within the communicationstrategy (Bhandari et al 2003)
Once the design features and broad strategy are inplace attention must then shift to the operationaliza-tion of the strategy
Training and supervision
Prior to scale-up the training needs will need to bedefined Fortunately for promotion of exclusivebreastfeeding extensive experience is available ontraining of different cadres of health workers andeven for lay counsellors Most experiences used the
adapted versions of the UNICEFWHO Breastfeed-ing Counseling Course (WHOUNICEF 1993) or theIMCI module (WHOUNICEF 2002)
Training strategy and its quality merit attentionIn successful programmes the duration of trainingextended from 3 full days to 10 part days for differentworkers The training strategies as described werelsquoconcise action orientedrsquo and included modules thataimed to equip trainers with practical skills and con-fidence to counsel effectively (Appendix 1)
Training modules for areas with high HIV preva-lence also exist (WHO 2006)
While the training modules used in studies workedwell a gap remains for referralTrained workers at thecommunity level require that referral options avail-able are easily accessible prompt and preferablyavailable free of cost to mothers with complex breast-feeding problems
Another important issue to address is handlingtraining of new staff in most developing countriesstaff turnover and absenteeism rates are high
Monitoring and evaluation
The programme strategy will need to include systemsfor monitoring and evaluation of the programmePossible markers could include the rates of exclusivebreastfeeding worker performance referral andaction As for all other national programmes therewill be a need for periodic reviews and achievabletargets by time
Costs and resources
In all pilot programmes and projects services wereprovided to mothers free of cost In many developingcountries if the government cadre of health workers isused to promote exclusive breastfeeding as a part oftheir other responsibilities (eg the IMNCI) the basicservices will remain free However a system thatrequires setting up a cadre of trained lactation coun-sellors (eg in an urban setting or as referral sources forbreastfeeding problems in rural areas) will requireadditional resources A cost-effective analysis of theBFHI was conducted in three countriesBrazilMexicoand Honduras (Horton et al 1996) Savings on health
Mainstreaming nutrition into MCH programs 11
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
care resulting from reduction in diarrhoeal and respi-ratory morbidity were estimated as a result of theeffect of BFHI on breastfeeding The study showedthat breastfeeding promotion through a BFHI-likemodel is very cost-effective (1992 US$ 2ndash19 per dis-ability adjusted life years Horton et al 1996 Perez-Escamilla 2007) Examples of cost-effectivenessanalysis of community-based programmes using lay orprofessional support in different settings could not beidentified
Testing of novel approaches andcontinuing innovation
Scaled-up programmes must have inbuilt provision totest novel approaches and the ability for continuinginnovation
Scaling up of exclusive breastfeeding in thecontext of HIV
The policy and programme design and implemen-tation issues relevant to exclusive breastfeedingscale-up discussed above are relevant to HIV-prevalent areas but there are other unique featuresthat merit consideration
Creating policies for exclusive breastfeeding pro-motion in countries with high HIV prevalence is par-ticularly challenging The revised recommendationsencourage exclusive breastfeeding for the first 6months and continued breastfeeding for 2 years andbeyond for infants whose mothers are HIV negativeor whose HIV status is unknown For women who areknown to be HIV positive the most appropriateinfant feeding option for HIV-exposed infantsdepends on individual circumstances including con-sideration of health services counselling and supportExclusive breastfeeding is the better option for suchinfants unless replacement feeding is acceptable fea-sible affordable sustainable and safe for both themother and baby This recommendation is based onthe finding that exclusive breastfeeding for up to 6months in three large cohort studies is associated witha three- to fourfold decreased risk of transmission ofHIV compared with non-exclusive breastfeeding(WHO 2006) The recommendations may need
further revision if new findings demonstrate thatexclusive breastfeeding should be the feeding ofchoice for HIV-infected women (Iliff et al 2005)
Some pilot programmes for exclusive breastfeedingpromotion in high-HIV-prevalence countries aresummarized in Appendix 2
In general exclusive breastfeeding promotionformed a part of the prevention of mother-to-childtransmission programmes LINKAGESZambiaintegrated improved counselling on infant feedingmaternal nutrition and antiretroviral therapy duringprophylaxis in both health-care and community ser-vices to enable women to make and act on informedchoice to feed their infants optimally in the context ofhigh HIV prevalence
Formative research was critical to develop locallyappropriate and feasible infant feeding recommenda-tions for individual infants and their families based onHIV status In Zambia the research included focusedgroup discussions key information interviews obser-vations of household food preparation and feedingmarket survey of replacement foods and breastmilksubstitutes and household trials of improved feedingand caring practices (LINKAGES 2005)
High quality of health workers is another criticalfactor for sensitive and accurate individual counsel-ling Programmes incorporated behaviour changecommunication methodologies in training (LINK-AGES 2005) It is important to develop skills of com-munity members as well for improved servicesreferral outreach and follow-up care and support ofHIV-positive mothers and their infants
A comprehensive communications strategy tosupport scale-up was a notable feature of the LINK-AGES programme in Zambia In 2004 an intensiveeffort was launched using brochures posters radioand television spots billboards and reference guidesfor health providers (LINKAGES 2005) Messageswere targeted to relevant stakeholders ndash pregnantand lactating mothers health providers youth andcommunity leaders and all the materials were nation-ally disseminated
Monitoring and evaluation another importantfeature of effective scale-up was a feature of pilotprogrammes (Appendix 2 Ntabaye amp Lusiola 2004Rutenberg et al 2004) in Zambia and Tanzania Moni-
N Bhandari and AKMI Kabir12
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
toring and evaluation not only provides a measure ofsuccess but identifies factors that may have contrib-uted to it and to lack of success to enable mid-coursecorrections The impact of some pilot programmes onexclusive breastfeeding is summarized in Appendix 2In most programmes exclusive breastfeeding ratesimproved In Zambia exclusive breastfeeding ratesincreased from 50 in 2002 to 64 in 2004 in Liv-ingstone from 57 in 2000 to 74 in 2004 in NdolaIn South Africa an antenatal clinic-based interven-tion led to 83 of infants born to HIV-infectedmother initiating exclusive breastfeeding InZimbabwe an intervention based on antenatal coun-selling resulted in a relatively lower exclusive breast-feeding rate of 246 at 3 months (Piwoz et al 2005)
Several barriers to success were identified Theseinclude inadequate skills of workers and non-integration of HIV counselling and tailoring into ante-natal care services (Ntabaye amp Lusiola 2004) which isthe backbone in which infant feeding counselling isbuiltWomen reported that mothers not breastfeedingtheir children were discriminated against by the com-munity and they faced the threat of domestic violenceProgramme managerrsquos understanding of barriersto effective programme implementation and impactwere emphasized as being important Governmentsupport partnerrsquos coordination increased humanresource and improving the supply system were iden-tified to be essential features to scale up programmesin the HIV context (Rutenberg et al 2004) Lowoverall exclusive breastfeeding rates prompted Piwozet al (2005) to conclude that women and their partnersshould have been reached more frequently during theantenatal and post-natal period
Conclusions
In a large number of programmes for improvingexclusive breastfeeding in developing countriesincluding in areas with high prevalence of HIV apositive impact on exclusive breastfeeding rates hasbeen achieved
Some of the factors that contributed to successfulscale-up are summarized in Table 4 Several limita-tions of the programmes reviewed merit attentionMost programmes involved special and generous
funding concentrated efforts and multiple contactsThese programmes were evaluated over relativelyshort periods of time usually 2ndash5 years and the long-term sustainability has not been really tested In theabsence of specific measures there is likely to be dilu-tion of quality as the programmes are scaled upfurther from their initial size The experience thus farleaves important questions to be addressed particu-larly on how programmes can be sustained over timeas they are scaled up at affordable costs
A key factor relevant to sustainability is to plan ona long-term basis a period of 10ndash20 years rather than5ndash10 years from the outset Experience with otherchild health programmes has shown that performancein immunization and oral rehydration therapy userates plateaued over time in many countries
Programme scale-up requires a programme man-agement capacity proportionate to the scale of opera-tions periodic assessment of barriers (Table 5) and anability to revise programme strategy to overcomethese Another key feature to sustainability ofscale-up is the extent to which capacity has been builtat the district block and community levels National-or state-level driven interventions begin with enor-mous enthusiasm which is difficult to sustain Thisfactor is particularly important as most developing
Table 4 Lessons learnt about scale-up key factors in success
bull Political will advocacy enabling policiesbull Championship by health ministries at national state and districtlevelbull Technical consensus on feeding guidelinesbull Programme strategy and measurable short- and long-term goalsbull Long-term financial commitmentbull Partners with defined roles assessment of their capacity todeliver and plans to cover gaps in capacitybull Emphasis on community-level interventions and not onlyfacility-based programmesbull Formative research as the backbone of effective scale-upprogrammes particularly in the context of HIVbull Careful selection of channels and the number required toachieve timely coverage consistency of messagesbull Communication strategy aided by formative research pre-testedvalidated messages and toolsbull Quality trainers and training centres proportionate to requiredscalebull Monitoring and evaluationbull Programme redesign when relevant through research analysisand innovation
Mainstreaming nutrition into MCH programs 13
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
countries are going through a process of decentrali-zation with increasing responsibility for planningimplementation and evaluation being delegated tolower levels of the health-care system Buildingcapacity at that level requires time resources andpatience and a longer-term perspective
Building capacity emerges to be a key factorTrainers and training centres vary in their qualitywhen training health workers and their supervisorsor programme managers As the burden of trainingincreases availability of good-quality trainersbecomes a limiting factor (WHOUNICEF 2002Government of India 2006) An effective strategymust plan for these incremental requirements includ-ing ensuring secure and sustained funding
Identifying barriers to success is a key actor Thebarriers to scaling up of health interventions havebeen elegantly described by Ranson et al (Table 5)Most of these are important for exclusive breastfeed-ing scale-up as well
Overall within the limitations discussed above anumber of programmes in countries with varying
HIV prevalence show that exclusive breastfeeding ona large scale is feasible and pilot programmes havegiven valuable guidance related to policies planningand implementation of large-scale programmes Thechallenge now is to build on these experiences whenplanning national programmes
Acknowledgements
We sincerely thank Dr MK Bhan for his constructivecriticism and sustained feedback at different stages ofdevelopment of this review
Conflicts of interest
The authors have declared no conflicts of interest
References
Arifeen S Black RE Antelman G Baqui A CaulfieldL amp Becker S (2001) Exclusive breastfeeding reducesacute respiratory infection and diarrhea deaths amonginfants in Dhaka slums Pediatrics 108 E67
Australian Breastfeeding Association (2005) Valuing Par-enthood Options for Paid Maternity Leave ndash InterimPaper 2002 Available at httpwwwbreastfeedingasnauadvocacymatleavehtml
Bhandari N Bahl R Mazumdar S Martines J BlackRE amp Bhan MK (2003) Effect of community basedpromotion of exclusive breastfeeding on diarrheal ill-nesses and growth a cluster randomized controlled trialLancet 361 1418ndash1423
Bhandari N Mazumder S Bahl R Martines J BlackRE amp Bhan MK (2004) An educational interventionto promote appropriate complementary feedingimproves child feeding practices and linear growth inrural Haryana India Journal of Nutrition 134 2342ndash2348
Bhandari N Mazumder S Bahl R Martines J BlackRE amp Bhan MK (2005) Use of multiple opportunitiesfor improving feeding practices in undertwos withinchild health programs Health Policy Plan 20 328ndash336
Bryce J Victora CG Habicht JP Vaughan JP ampBlack RE (2004) The multi-country evaluation of theintegrated management of childhood illness strategylessons for the evaluation of public health interventionsAmerican Journal of Public Health 94 406ndash415
Butte NF Lopez-Alarcon MG amp Garza C (2002) Nutri-ent Adequacy of Exclusive Breastfeeding for the TermInfant during the First Six Months of Life World HealthOrganization Geneva
Table 5 Barriers to scaling up of health interventions
Community and household levelsLack of information womenrsquos education physical financial
womenrsquos decision-making powerHealth services delivery levelShortage of qualified staff weak technical guidance programme
management and supervision inadequate supplies equipmentand infrastructure poor accessibility
Health sector policy and strategic management levelWeak and centralized system for planning and management weak
drug policies and supply system inadequate regulations lack ofintersectoral action and partnership weak incentives to useinputs efficiently and respond to user needs and preferencesreliance on donor funding
Public policies cutting across sectorsGovernment bureaucracy poor communication and transport
infrastructureEnvironmental characteristicsGovernance and overall policy frameworkCorruption weak government weak laws political instability and
insecurity low priority to social sectors weak structure for publicaccountability and opportunities for public opinions lack of freepress
Physical environmentClimatic and geographic predisposition physical environment
unfavourable to service delivery
Adapted from Ranson et al (2003)
N Bhandari and AKMI Kabir14
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Cohen J (2007) Retrovirus meeting Hope on new AIDSdrugs but breast-feeding strategy backfires Science 3151357
Coovadia HM Rollins NC Bland RM Little KCoutsoudis A Bennish ML et al (2007) Mother tochild transmission of HIV-1 infection during exclusivebreastfeeding in the first 6 months of life an interven-tion cohort study Lancet 369 1107ndash1116
Coutinho SB de Lira PI de Carvalho LM amp AshworthA (2005) Comparison of the effect of two systems forthe promotion of exclusive breastfeeding Lancet 3661094ndash1100
Feachem RG amp Koblinsky MA (1984) Interventions forthe control of diarrheal diseases among young childrenpromotion of breastfeeding Bulletin of the of the WorldHealth Organization 62 271ndash291
Gonzales A Arteaga E amp Howard-Grabman L (1998)Scaling Up the WARMI Project ndash Lessons LearnedMobilizing Bolivian Communities around ReproductiveHealth Save the Children Federation Inc Bolivia FieldOffice La Paz Available at httpwwwcoregrouporgresourcesSavebolipdf
Government of India (1997) Recommendations of the FifthCentral Pay Commission Relating to Enhancement ofQuantum of Maternity Leave and to Allow PaternityLeave in Respect of Central Government EmployeesDocument ref 13018197-Estt(L) Available at httppersminnicinesttleave2htm
Government of India (2005) National Rural HealthMission 2005ndash2012 Mission document Ministry ofHealth and Family Welfare New Delhi Government ofIndia Available at httpwwwmohfwnicinNRHM20Mission20Documentpdf
Government of India (2006) Operational Guidelines forImplementation of Integrated Management of Neonataland Childhood Illness (IMNCI) Ministry of HealthFamily Welfare New Delhi Available at httpmohfwnicindofw20websiteF20IMNCI20Operational20Plan201320june202006htm
Government of Pakistan (2003) National Programme forFamily Planning and Primary Health Care The LadyHealth Workers Programme 2003ndash2008 Ministry ofHealth Pakistan Available at httpwwwphcgovpkDownloadsPC-120augpdf
Green CP (1999) Improving Breastfeeding Behaviors Evi-dence from Two Decades of Intervention ResearchPublished for the US Agency for International Develop-ment (USAID) by the LINKAGES Project Academyfor Educational Development Washington DC
Gupta A (2002) National trends in breastfeeding andeffective strategies to improve breastfeeding ratesJournal of Neonatology 2002 4ndash14
Gwatkin DR (2004) Integrating the management of child-hood illness Lancet 364 1557ndash1558
Habicht JP DaVanzo J amp Butz WP (1986) Does breast-feeding really save lives or are apparent benefits due tobiases American Journal of Epidemiology 123279ndash290
Haider R Ashworth A Kabir I amp Huttly SR (2000)Effect of community based peer counsellors on exclusivebreastfeeding practices in Dhaka Bangladesh a ran-domized controlled trial Lancet 356 1643ndash1647
Haider R Kabir I Huttly SR amp Ashworth A (2002)Training peer counsellors to promote and support exclu-sive breastfeeding in Bangladesh Journal of HumanLactation 18 7ndash12
Horton S Sanghvi T Phillips M Fiedler J Perez-Escamilla R Lutter C et al (1996) Breastfeeding pro-motion and priority setting in health Health Policy andPlanning 11 156ndash168
ILO (1998) More than 120 Nations Provide Paid MaternityLeave Gap in Employment Treatment for Men andWomen Still Exists International Labour Office GenevaDocument ref ILO987 Available at httpwwwiloorgpublicenglishbureauinfpr19987htmr2
Iliff PJ Piwoz EG Tavengwa NV Zunguza CDMarinda ET Nathoo KJ et al (2005) Early exclusivebreastfeeding reduces the risk of postnatal HIV-1 trans-mission and increase HIV-free survival AIDS 19 699ndash708
Integrated Child Development Services Scheme (Revised)(ICDS) (1982) Ministry of Social Welfare Governmentof India New Delhi Available on URL httpwcdnicinudishahtmabouticdshtm
Jason JM Nieburg P amp Marks JS (1984) Mortality andinfectious disease associated with infant feeding prac-tices in developing countries Pediatrics 74 702ndash727
Jones G Steketee RW Black RE Bhutta ZA ampMorris SS Bellagio Child Survival Study Group (2003)How many child deaths can we prevent this yearLancet 362 65ndash71
Knippenberg R Lawn JE Darmstadt GL Begkayian GFogstad H Walelign N et al (2005) Systematic scalingup of neonatal care in countries Lancet 365 1087ndash1098
Kramer MS amp Kakuma R (2002) The optimal durationof exclusive breastfeeding a systematic reviewCochrane Database of Systematic Reviews 2002CD003517
Kramer MS Chalmers B Hodnett ED Sevkovskaya ZDzikovich I Shapiro S et al (2000) Promotion ofbreastfeeding intervention trial (PROBIT) a cluster ran-domized trial in the Republic of Belarus Design followup and data validation Advances in Experimental Medi-cine and Biology 478 327ndash345
Kramer MS Chalmers B Hodnett ED Sevkovskaya ZDzikovich I Shapiro S et al (2001) Promotion ofbreastfeeding intervention trial (PROBIT) a random-
Mainstreaming nutrition into MCH programs 15
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
ized trial in the Republic of Belarus Journal of theAmerican Medical Association 285 413ndash420
Lewin SA Dick J Pond P Zwarenstein M Aja Gvan Wyk B et al (2006) Lay health workers in primaryand community health care (Review) The CochraneLibrary 3 1ndash104
LINKAGES (2002) World LINKAGES MadagascarAcademy for Educational Development WashingtonDC
LINKAGES (2005) LINKAGES Zambia 1997ndash2005 FinalReport A Full Report on LINKAGES Infant Feedingand HIVAIDS Programs in Zambia Academy for Edu-cational Development Washington DC Available athttpwwwlinkagesprojectorgmediapublicationsFinal20draft20Zambia20final20report2012105pdf
Lutter CK Perez-Escamilla R Segall A Sanghvi TTeruya K amp Wickham C (1997) The effectiveness of ahospital based program to promote exclusive breastfeed-ing among low income women in Brazil AmericanJournal of Public Health 87 659ndash663
Morrow AL Guerrero ML Shults J Calva J Lutter CBravo J et al (1999) Efficacy of home based peer coun-selling to promote exclusive breastfeeding a randomizedcontrolled trial Lancet 353 1226ndash1231
Ntabaye MK amp Lusiola GJ (2004) Understanding barri-ers to PMTCT in Tanzania findings of a baseline surveyInternational Conference on AIDS 15 (B11396)
de Oliveira LD Giugliani ER do Espirito SLC FrancaMC Weigert EM Kohler CV et al (2006) Effect ofintervention to improve breastfeeding technique on thefrequency of exclusive breastfeeding and lactation-related problems Journal of Human Lactation 22 315ndash321
Perez-Escamilla R (2004) Effectiveness of MADLAC atImproving Breastfeeding Promotion and CounsellingIndicators in Maternity Wards in El Salvador Publishedfor the Basic Support for Institutionalizing Child Sur-vival Project (BASICS II) for the United States Agencyfor International Development Arlington VA Availableat httpwwwbasicsorgpdfFinal20MADLAC20Report20RPE20April207-2004pdf
Perez-Escamilla R (2007) Evidence based breast-feedingpromotion the Baby-Friendly Hospital InitiativeJournal of Nutrition 137 484ndash487
Piwoz EG Iliff PJ Tavengwa N Gavin L Marinda ELunney K et al (2005) An education and counselllingprogram for preventing breastfeeding associated HIVtransmission in Zimbabwe design and impact on mater-nal knowledge and behaviour Journal of Nutrition 135950ndash955
Quinn VJ Guyon AB Schubert JW Stone-Jimenez MHainsworth MD amp Martin LH (2005) Improvingbreastfeeding practices on a board scale at the commu-
nity level success stories from Africa and LatinAmerica Journal of Human Lactation 21 345ndash354
Ranson MK Hanson K Oliveira-Cruz V amp Mills A(2003) Constraints to expanding access to health inter-ventions an empirical analysis and country typologyJournal of International Development 15 15ndash40
Rea MF amp Berquo ES (1990) Impact of the Braziliannational breastfeeding programme on mothers inGreater Sao Paulo Bulletin of the of the World HealthOrganization 68 365ndash371
Rollins NC (2007) Infant feeding and HIV BritishMedical Journal 334 487ndash488
Rutenberg N Baek C Kalibala S Rosen J amp Mulenga D(2004) Evaluation of United Nations supported pilotprojects for the prevention of mother-to-child transmis-sion of HIV overview of findings International Confer-ence on AIDS 15 (WePeE6688)
The Core Group (2005) Scale and Scaling Up A COREGroup Background Paper on lsquoScaling-Uprsquo MaternalNewborn and Child Health Services CORE SpringMembership Meeting 2005 The Core Group Washing-ton DC Available at httpwwwcoregrouporgresourcesmeetingsapril05Scaling_Up_Background_Paper_7-13pdf
The Norwegian Government (1993) Women in PoliticsMinistry of Children and Equality Available at httpwwwregjeringennoendepbldRyddemappeSLA-AvdelingdoclegislationguidelinesWomen-in-Politicshtmlid=437166
Thior I Lockman S Smeaton LM Shapiro RL WesterC Heymann SJ et al (2006) Breastfeeding plus infantzidovudine prophylaxis for 6 months vs formula feedingplus infant zidovudine for 1 month to reduce mother-to-child HIV transmission in Botswana a randomized trialthe Mashi Study Journal of the American Medical Asso-ciation 296 794ndash805
UNICEF (2002) Facts for Life lsquoKey Message What EveryFamily and Community Has a Right to Know aboutBreastfeedingrsquo Available at httpwwwuniceforgffl04key_messageshtm
Van Roekel K Plowman B Griffiths M de AlvaradoVV Matute J amp Calderon M (2002) BASICS IIMidterm Evaluation of the AIN Program in Honduras2000 Basic Support for Institutionalizing Child SurvivalProject (BASICS II) for the United States Agency forInternational Development Arlington VA
WABA (2007) UNICEF Records BHFI Record UpdateAvailable at httpwwwwabaorgmydocsBFHIjan07xls 2006 Regularly updated by Miriam HLabbok Center for Infant and Young ChildFeeding and Care Department of Maternaland Child Health School of Public Health The Univer-sity of North Carolina at Chapel Hill Chapel Hill NCUSA
N Bhandari and AKMI Kabir16
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
WHA (2002) Infant and Young Child Nutrition Fifty-FifthWorld Health Assembly Agenda Item 1310 18 May2002 Available at httpwwwintgbebwhapdf_filesWHA55ewha5525pdf
WHO (1981) The International Code of Marketing ofBreastmilk Substitutes World Health OrganizationGeneva
WHO (1989) Protecting Promoting and Supporting Breast-feeding The Special Role of Maternity Services A JointWHOUNICEF Statement World Health OrganizationGeneva
WHO (2002) The Optimal Duration of Exclusive Breast-feeding Report of an Expert Consultation WHONHD0109 WHOFCHCAH0124 World HealthOrganization Geneva
WHO (2003a) Community Based Strategies for Breastfeed-ing Promotion and Support in Developing CountriesWorld Health Organization Geneva Document refISBN_92_4_159121_8 Available at httpwwwwhointchild-adolescent-healthNew_PublicationsNUTRITIONISBN_92_4_159121_8pdf
WHO (2003b) Multi-country Evaluation of IMCI Effective-ness Cost and Impact (MCE) Progress Report May2002ndashApril 2003 Document ref WHOFCHCAH035World Health Organization Geneva
WHO (2004) Promoting Proper Feeding for Infants andYoung Children World Health Organization GenevaAvailable at httpwwwwhointnutritiontopicsinfantfeedingen
WHO (2006) WHO HIV and Infant Feeding TechnicalConsultation-Consensus Statement World Health Orga-nization Geneva Available at httpwwwwhointhivmediacentreInfantfeedingconsensusstatementpfpdf
WHO Collaborative Study Team on the Role of Breast-feeding on the Prevention of Infant Mortality (2000)Effect of breastfeeding on infant and child mortality dueto infectious diseases in les developed countries apooled analysis Lancet 355 451ndash455
WHOUNICEF (1992) The global criteria for the WHOUNICEF Baby-Friendly Hospital Initiative In Baby-Friendly Hospital Initiative Part II Hospital LevelImplementation World Health Organization Geneva
WHOUNICEF (1993) Breastfeeding Counselling A Train-ing Course WHOCDR933 UNICEFNUT931 WorldHealth Organization Geneva
WHOUNICEF (2002) Protocol for Adapting the FeedingRecommendations Part III IMCI Adaptation GuideWorld Health Organization Geneva
WHOUNICEF (2003) Global Strategy for Infant andYoung Child Feeding World Health OrganizationGeneva Available at httpwwwwhointchild-adolescent-healthpublicationsNUTRITIONIYCF_GShtm
de Zoysa I Rea M amp Martines J (1991) Why promotebreastfeeding in diarrheal diseases control programmesHealth Policy and Planning 6 371ndash379
Mainstreaming nutrition into MCH programs 17
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
Cas
est
udie
so
fef
fect
iven
ess
stud
ies
or
pilo
tpr
ogra
mm
es
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Lut
ter
etal
(199
7)
Bra
zil
Low
-inc
ome
urba
nw
omen
deliv
erin
gin
hosp
ital
s
Bre
astf
eedi
ngpr
omot
ion
in
hosp
ital
sco
mpa
red
wit
h
nobr
east
feed
ing
prom
otio
n
Pro
mot
ion
ofbr
east
feed
ing
in
sele
cted
hosp
ital
s
Mea
nda
ysof
excl
usiv
e
brea
stfe
edin
g
75da
ysvs
22
days
(Plt
001
)
Rea
ampB
erqu
o
(199
0)
Wom
enw
ith
ach
ild
aged
lt2ye
ars
inSa
oP
aulo
Nat
iona
lbre
astf
eedi
ng
cam
paig
n19
81ndash1
986
BF
HI
Mas
sm
edia
cam
paig
n11
in
fant
s5ndash
6m
onth
s
excl
usiv
ely
brea
stfe
d
in19
88an
d37
in
1987
Con
foun
ding
fact
ors
over
the
6-ye
arpe
riod
not
mea
sure
d
Kra
mer
etal
(200
020
01)
PR
OB
ITtr
ial
Bel
arus
Clu
ster
rand
omiz
ed
34ho
spit
als
and
thei
rpo
lycl
inic
s
Trai
ning
inB
FH
I(W
HO
UN
ICE
F19
92)
vsr
outi
ne
prac
tice
san
dpo
licie
s
Exc
lusi
vebr
east
feed
ing
at3
(43
3vs
64
)
and
6(7
9
vs0
6
)
mon
ths
sign
ifica
ntly
high
er
Impl
emen
ted
thro
ugh
BF
HI
ina
sett
ing
whe
reho
spit
al
deliv
erie
sar
eco
mm
on
Per
ez-E
scam
illa
(200
4)
BA
SIC
SII
Mex
ico
Hon
dura
s
Bra
zil
MA
DL
AC
low
-cos
t
man
agem
ent
info
rmat
ion
syst
emto
use
an
evid
ence
-bas
edap
proa
chto
impr
ove
serv
ice
perf
orm
ance
Inte
rvie
win
gof
wom
enat
hosp
ital
disc
harg
epo
st
deliv
ery
usin
ga
ques
tion
nair
eth
atta
kes
5ndash7
min
toad
min
iste
ran
d
cont
ains
19br
east
feed
ing
prom
otio
nco
unse
lling
indi
cato
rs
Dat
aen
tere
dan
dre
sult
s
disc
usse
d3-
mon
thly
by
hosp
ital
com
mit
tee
Hos
pita
lim
plem
ents
chan
ges
in
brea
stfe
edin
g
supp
ort
base
don
anal
ysis
of
ques
tion
nair
es
Itis
aco
st-e
ffec
tive
inte
rven
tion
that
can
help
impr
ovem
ents
inth
eB
FH
I
and
isa
valu
able
tool
for
proc
ess
eval
uati
on
N Bhandari and AKMI Kabir18
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
LIN
KA
GE
S
proj
ect
inA
fric
aan
d
Lat
inA
mer
ica
(Qui
nnet
al
2005
LIN
KA
GE
S
2002
WH
O20
03a)
Bol
ivia
(1
mill
ion)
Gha
na(3
5
mill
ion)
Mad
agas
car
(6m
illio
n)
Res
ourc
e-
poor
sett
ing
Pilo
tpr
ogra
mm
e
InB
oliv
iaan
d
Gha
napr
ogra
mm
e
focu
sed
on
brea
stfe
edin
gan
d
com
plem
enta
ry
feed
ing
InM
adag
asca
r
prog
ram
me
prom
oted
brea
stfe
edin
g
wit
hin
7es
sent
ial
nutr
itio
nac
tion
san
d
subs
eque
ntly
thro
ugh
IMC
I
Bui
lton
form
ativ
ere
sear
ch
and
sust
aine
dth
roug
h
prog
ram
me
acti
viti
esth
at
focu
sed
onbr
ingi
ngab
out
the
desi
red
beha
viou
r
chan
geM
ixof
inte
rven
tion
s
reac
hed
wom
enin
divi
dual
ly
orin
grou
psin
heal
th
faci
litie
sho
mes
or
com
mun
ity
sett
ings
Con
sist
ent
mes
sage
san
d
mat
eria
lacr
oss
all
prog
ram
me
chan
nels
Bol
ivi
PR
OC
OSI
NG
Os
Gha
na
UN
ICE
F
nati
onal
nutr
itio
n
offic
eN
GO
s
Mad
agas
car
Inte
rsec
tora
l
Act
ion
Gro
upfo
r
Nut
riti
on
Jere
o
Sala
ma
Isik
a
Pro
gram
desi
gned
wit
h
part
ners
Rad
ioin
all
thre
esi
tes
Mat
eria
ls
deve
lope
d
tosu
itne
eds
oflo
cal
heal
th
wor
kers
and
com
mun
ity
mem
bers
Gre
at
emph
asis
on
deve
lopm
ent
of coun
selli
ng
and
nego
tiat
ion
skill
s
prac
tica
l
sess
ions
Sign
ifica
ntin
crea
ses
inex
clus
ive
brea
stfe
edin
gra
tes
of
0ndash6-
mon
th-o
ld
infa
nts
from
54
to65
in
Bol
ivia
68
to79
in
Gha
naan
d46
to68
in
Mad
agas
car
In
Gha
naan
d
Mad
agas
car
sign
ifica
ntre
sult
s
obse
rved
wit
hin
aye
ar
ofin
itia
tion
of
com
mun
ity
inte
rven
tion
s
App
roac
hw
asef
fect
ive
and
achi
eved
sign
ifica
nt
incr
ease
sam
ong
larg
e
popu
lati
ons
asea
rly
as
9ndash12
mo
afte
rin
itia
tion
of
com
mun
ity
acti
viti
es
Van
Roe
kele
tal
(200
2)W
HO
(200
3a)
Hon
dura
sG
row
thm
onit
orin
gan
d
prom
otio
nkn
own
as
Ate
ncioacute
nIn
tegr
ala
la
Nintilde
ez(A
IN)
or
Inte
grat
edC
hild
Car
e
Init
ially
pri
mar
ilya
grow
th
mon
itor
ing
prog
ram
me
ulti
mat
ely
thro
ugh
IMC
I
Pro
gram
me
ongr
owth
prom
otio
nndash
asse
ssm
ent
of
mon
thly
wei
ght
gain
and
focu
son
illne
ssf
eedi
ng
prac
tice
san
dge
nera
lchi
ld
care
inin
fant
sun
der
2ye
ars
Impl
emen
ted
atgo
vern
men
t
faci
litie
san
dco
mm
unit
y
Star
ted
in19
92s
tren
gthe
ned
in19
95ndash1
997
wit
hgr
eate
r
focu
son
child
feed
ing
In
1997
pro
gram
me
intr
oduc
ed
wit
hIM
CI
(WH
OU
NIC
EF
2002
)
Maj
or
part
ners
UN
ICE
F
PAH
O
Am
eric
an
and
Hon
dura
n
Red
Cro
ss
CA
RE
Rad
io
broa
dcas
ts
relig
ious
lead
ers
IMC
IM
id-t
erm
eval
uati
on
show
ed39
of
mot
hers
inin
terv
enti
on
com
mun
itie
sex
clus
ivel
y
brea
stfe
dco
mpa
red
wit
h13
in
the
cont
rol
site
s
Mainstreaming nutrition into MCH programs 19
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
cont
inue
d
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Bha
ndar
ieta
l
(200
3)
WH
O
(200
3a)
Rur
alco
mm
unit
ies
inH
arya
na
Indi
a
Clu
ster
rand
omiz
edtr
ial
8
com
mun
itie
s(t
otal
popu
lati
on~4
000
0)
Pro
mot
ion
ofex
clus
ive
brea
stfe
edin
gan
d
appr
opri
ate
com
plem
enta
ryfe
edin
g
Dev
elop
edth
roug
h
form
ativ
ere
sear
ch
ndashP
robl
emid
enti
ficat
ion
ndashP
arti
cipa
tory
desi
gnof
inte
rven
tion
impl
emen
tati
onan
d
eval
uati
on
Impl
emen
tati
onw
ithi
nan
exis
ting
prim
ary
heal
th-c
are
prog
ram
me
Opp
ortu
niti
esus
edto
deliv
erm
essa
ges
wer
e
imm
uniz
atio
ncl
inic
s
wei
ghin
gse
ssio
ns
sick
-chi
ldco
ntac
tsan
d
mon
thly
hom
evi
sits
Res
earc
hers
wit
hlo
cal
gove
rnm
ent
ICD
Ssy
stem
and
NG
O
The
atre
son
gs
Mas
sm
edia
not
used
for
risk
of
cont
amin
atio
n
Mat
eria
ls
deve
lope
d
for
heal
th
wor
kers
pos
ters
flip
book
sca
rds
Bre
astf
eedi
ng
coun
selli
ngse
ctio
n
ofth
eIM
CI
(WH
O
UN
ICE
F20
02)
Exc
lusi
ve
brea
stfe
edin
gin
the
prev
ious
24h
at3
mon
ths
of
age
79
vs4
8
The
posi
tive
effe
ct
rem
aine
dup
to
6m
onth
sof
age
(42
vs4
)
Tota
lpar
tici
pati
onof
the
dist
rict
heal
thsy
stem
from
ince
ptio
nof
the
prog
ram
me
inde
velo
ping
impl
emen
tati
onst
rate
gyt
ool
deve
lopm
ent
and
mon
itor
ing
inad
diti
onto
invo
lvem
ent
of
anN
GO
wer
eim
port
ant
feat
ures
that
cont
ribu
ted
to
the
succ
ess
ofth
e
inte
rven
tion
Mor
row
etal
(199
9)
Mex
ico
Cit
yC
lust
erra
ndom
ized
tria
l
Tota
lpop
ulat
ion
3000
0
Two
com
mun
itie
sin
the
inte
rven
tion
one
com
pari
son
130
wom
en
Hom
e-ba
sed
peer
coun
selli
ng
Pee
rco
unse
llors
mad
e3
or
6ho
me
visi
tsto
the
mot
her
Key
fam
ilym
embe
rsal
so
incl
uded
By
La
Lec
he
Lea
gue
of
Mex
ico
Exc
lusi
ve
brea
stfe
edin
g
at3
mon
ths
post
-par
tum
67
(6vi
sits
)
50
(3vi
sits
)12
(com
pari
son)
Firs
tcl
uste
rra
ndom
ized
com
mun
ity-
base
dtr
ialt
hat
used
peer
coun
sello
rsto
prom
ote
excl
usiv
e
brea
stfe
edin
g
Hai
der
etal
2000
200
2
Dha
ka
Low
mid
dle
and
low
-soc
io-
econ
omic
popu
lati
on
Clu
ster
rand
omiz
edtr
ial
20zo
nes
inin
terv
enti
on
and
20in
cont
rol
Com
mun
ity-
base
dpe
er
coun
selli
ngin
Dha
ka
15ho
me-
base
dco
unse
lling
visi
tsby
peer
coun
sello
rs
40h
(4h
yen10
days
)
WH
OU
NIC
EF
brea
stfe
edin
g
coun
selli
ngco
urse
(WH
OU
NIC
EF
1993
)
Exc
lusi
ve
brea
stfe
edin
g
at5
mon
ths
70
in
inte
rven
tion
and
6in
the
cont
rol
Com
mun
ity-
base
d
brea
stfe
edin
gpr
omot
ion
stra
tegy
was
effe
ctiv
ein
Ban
glad
esh
whe
rem
ost
deliv
erie
soc
cur
atho
me
N Bhandari and AKMI Kabir20
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Bry
ceet
al
(200
4)W
HO
(200
3b)
Bra
zil
Per
u
Tanz
ania
Uga
nda
Mul
tico
untr
yev
alua
tion
of
IMC
Ith
atin
clud
ed
effe
ctiv
enes
sco
stan
d
impa
ct(B
ryce
etal
2004
)
Bre
astf
eedi
ngpr
omot
ion
asa
part
ofIM
CI
IMC
Iis
ast
rate
gyfo
r
impr
ovin
gch
ildhe
alth
and
deve
lopm
ent
thro
ugh
the
com
bine
d
deliv
ery
ofes
sent
ial
child
heal
th
inte
rven
tion
sIM
CI
bega
nw
ith
ase
tof
case
man
agem
ent
guid
elin
es
for
the
man
agem
ent
ofsi
ckch
ildre
nat
first
-lev
elhe
alth
faci
litie
s
and
the
guid
elin
esw
ere
desi
gned
for
adap
tati
on
atco
untr
yle
vela
nd
belo
wO
ver
tim
eth
e
stra
tegy
expa
nded
to
incl
ude
ara
nge
of
guid
elin
esfo
rde
liver
ing
child
surv
ival
inte
rven
tion
at
hous
ehol
dco
mm
unit
y
and
refe
rral
leve
ls
IMC
Im
odul
e(W
HO
UN
ICE
F20
02)
Res
ults
onex
clus
ive
brea
stfe
edin
g
avai
labl
efr
om
Tanz
ania
whe
reno
sign
ifica
ntim
pact
was
seen
Des
pite
subs
tant
ial
impr
ovem
ent
inth
equ
alit
y
ofca
rede
liver
edby
IMC
Iat
heal
thfa
cilit
ies
key
fam
ily
prac
tice
ssu
chas
excl
usiv
e
brea
stfe
edin
gdi
dno
tch
ange
asco
mm
unit
yIM
CI
had
not
been
impl
emen
ted
byth
at
tim
e(W
HO
2003
b)
SA
rife
en
pers
onal
com
mun
icat
ion
Ban
glad
esh
Mat
lab
Com
mun
ity-
base
dcl
uste
r
desi
gn
Eva
luat
ion
offa
cilit
y-an
d
com
mun
ity-
base
dIM
CI
Inte
rven
tion
pack
age
incl
udes
feed
ing
asse
ssm
ent
and
coun
selli
ngon
mot
hers
ofyo
ung
child
ren
seek
ing
care
atfa
cilit
ies
for
illne
ssan
d
hom
e-ba
sed
coun
selli
ng
onim
prov
edfe
edin
gby
com
mun
ity-
base
dhe
alth
and
nutr
itio
nw
orke
rs
At
base
line
inth
e
year
2000
alit
tle
mor
eth
anha
lfth
e
0ndash5-
mon
th-o
ld
infa
nts
inth
est
udy
area
wer
ebe
ing
excl
usiv
ely
brea
stfe
dB
y20
05
this
incr
ease
dby
30
inth
eIM
CI
area
Dat
ano
t
avai
labl
efr
omth
e
com
pari
son
area
as
yet
Lac
kof
com
para
ble
data
from
the
com
pari
son
area
prev
ents
ade
finit
ive
conc
lusi
onas
tow
heth
erth
is
trul
yis
anim
pact
ofIM
CI
BA
SIC
SII
Bas
icSu
ppor
tfo
rIn
stit
utio
naliz
ing
Chi
ldSu
rviv
alP
roje
ctB
FH
IB
aby-
Frie
ndly
Hos
pita
lIni
tiat
ive
ICD
SIn
tegr
ated
Chi
ldD
evel
opm
ent
Serv
ices
IM
CI
Inte
grat
edM
anag
emen
tof
Chi
ldho
odIl
lnes
sM
AD
LA
CM
onit
oreo
deA
poyo
Dir
ecto
con
laL
acat
anci
aM
ater
naN
GO
non
-gov
ernm
enta
lorg
aniz
atio
nPA
HO
Pan
Am
eric
anH
ealt
hO
rgan
izat
ion
PR
OB
ITP
rom
otio
nof
Bre
astf
eedi
ngIn
terv
enti
onTr
ial
PR
OC
OSI
Pro
gram
ade
Coo
rdin
acio
nen
Salu
dIn
tegr
al(C
olla
bora
tive
Pro
gram
for
Inte
grat
edH
ealt
h)U
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
WH
OW
orld
Hea
lth
Org
aniz
atio
n
Mainstreaming nutrition into MCH programs 21
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x2
Cas
est
udie
sin
scal
e-up
effo
rts
inH
IVA
IDS
Stud
yde
scri
ptio
nPo
pula
tion
Inte
rven
tion
Com
mun
icat
ion
stra
tegy
Impa
cton
excl
usiv
ebr
east
feed
ing
Com
men
ts
LIN
KA
GE
S(2
005)
Zam
bia
Pro
gram
me
thro
ugh
heal
th-c
are
and
com
mun
ity
serv
ices
Rea
ched
60si
tes
in6
dist
rict
sby
2005
Inte
grat
ion
ofin
fant
feed
ing
coun
selli
ngm
ater
naln
utri
tion
and
anti
retr
ovir
aldr
ugs
prop
hyla
xis
Trai
ning
ofhe
alth
wor
kers
and
com
mun
ity
serv
ice
prov
ider
sto
coun
selw
omen
onsa
fety
opti
ons
for
thei
rsi
tuat
ion
Beh
avio
urch
ange
Com
mun
icat
ion
inte
rven
tion
sin
the
first
few
year
sM
ater
iald
evel
oped
lsquoAct
Now
rsquoM
edia
cam
paig
nsin
clud
edbr
ochu
res
post
ers
radi
oan
dte
levi
sion
Ass
esse
dth
roug
hba
selin
ean
dfo
llow
-up
hous
ehol
dan
dcl
inic
surv
eys
inse
lect
eddi
stri
cts
Exc
lusi
vebr
east
feed
ing
rate
incr
ease
dfr
om50
in
2002
to64
in
2004
inL
ivin
gsto
nean
dfr
om57
in
2000
to74
in
2004
inN
dola
Inte
grat
edde
mon
stra
tion
proj
ect
Had
seve
rals
tren
gths
inte
rms
ofth
eus
eof
form
ativ
ere
sear
chto
deve
lop
mes
sage
str
aini
ngan
dbu
ildin
gup
skill
sof
prog
ram
me
man
ager
she
alth
-car
epr
ovid
ers
and
com
mun
ity
wor
kers
adv
ocac
yfo
rna
tion
alpo
licy
stro
ngbe
havi
our
chan
geco
mm
unic
atio
nco
mpo
nent
st
reng
then
ing
com
mun
ity
capa
city
for
coun
selli
ngan
dre
ferr
als
and
mon
itor
ing
and
eval
uati
onw
ith
loca
lpar
tner
sP
iwoz
etal
(20
05)
ZV
ITA
MB
Otr
ial
Har
are
Zim
babw
eE
duca
tion
and
coun
selli
ngpr
ogra
mm
ede
liver
edan
tena
tally
1411
0m
othe
rndashba
bypa
irs
enro
lled
from
14m
ater
nity
clin
ics
wit
hin
96h
ofde
liver
yan
dfo
llow
edup
at6
wee
ks
3m
onth
san
d3-
mon
thly
inte
rval
sIn
fant
-fee
ding
patt
erns
dete
rmin
edE
xclu
sive
brea
stfe
edin
gre
com
men
ded
for
HIV
nega
tive
un
know
nor
HIV
posi
tive
who
chos
eto
brea
stfe
ed
Gro
uped
ucat
ion
indi
vidu
alco
unse
lling
vid
eos
broc
hure
sM
othe
rsw
hoen
rolle
dw
hen
prog
ram
me
was
fully
impl
emen
ted
wer
e8
4ti
mes
mor
elik
ely
toex
clus
ivel
ybr
east
feed
than
mot
hers
who
enro
lled
befo
reth
epr
ogra
mm
ebe
gan
Ove
rall
excl
usiv
ebr
east
feed
ing
rate
sti
ll3
mon
ths
was
low
at24
6
Form
ativ
ere
sear
chus
edto
desi
gna
cult
ural
lyse
nsit
ive
educ
atio
nan
dco
unse
lling
prog
ram
me
Low
over
alle
xclu
sive
brea
stfe
edin
gra
tes
prom
pted
auth
ors
toco
nclu
deth
atw
omen
and
thei
rpa
rtne
rssh
ould
have
been
reac
hed
mor
efr
eque
ntly
duri
ngan
tena
tala
ndpo
st-n
atal
peri
od
N Bhandari and AKMI Kabir22
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Thi
oret
al(
2006
)R
ollin
s(2
007)
C
ohen
(200
7)
HIV
-inf
ecte
dpr
egna
ntw
omen
atte
ndin
gan
tena
talc
linic
sin
sout
hB
otsw
ana
Inve
stig
atio
nsby
CD
Cof
adi
arrh
oea
outb
reak
inJa
nuar
y-Fe
brua
ry20
06in
the
sam
epo
pula
tion
Mat
erna
land
infa
ntan
tire
trov
iral
ther
apy
toas
cert
ain
impa
cton
HIV
tran
smis
sion
Ant
enat
alco
unse
lling
Cas
endashco
ntro
lstu
dyto
iden
tify
risk
fact
ors
for
diar
rhoe
ano
tbr
east
feed
ing
was
the
bigg
est
risk
fact
ora
djus
ted
odds
rati
o50
(95
confi
denc
ein
terv
al4
5ndash10
0)
Bot
swan
aha
sth
ebe
stpr
imar
yhe
alth
-car
est
ruct
ure
wat
ersu
pply
and
sani
tati
onsy
stem
sin
Sout
hA
fric
aFo
rmul
apr
ovid
edfr
eeby
the
gove
rnm
ent
toin
fect
edm
othe
rsL
ower
mor
talit
yin
the
brea
stfe
edin
ggr
oup
at7
mon
ths
dem
onst
rate
sri
skof
form
ula
feed
ing
and
need
for
alte
rnat
est
rate
gies
(Thi
oret
al
2006
)A
utho
rsco
nclu
deth
athe
alth
syst
ems
inw
hich
thes
epr
ogra
mm
esar
eim
plem
ente
dsh
ould
beab
leto
cope
wit
hdi
arrh
oea
and
mal
nutr
itio
nth
atre
sult
sbe
caus
eof
form
ula
feed
ing
(Rol
lins
2007
)C
oova
dia
etal
(2
007)
Kw
aZul
uNat
al
Sout
hA
fric
a27
22H
IV-i
nfec
ted
and
unin
fect
edpr
egna
ntw
omen
enro
lled
into
ano
n-ra
ndom
ized
inte
rven
tion
coho
rtst
udy
from
ante
nata
lcl
inic
sIn
fant
feed
ing
data
obta
ined
wee
kly
bloo
dsa
mpl
esfr
omin
fant
sta
ken
mon
thly
83
of13
72in
fant
sbo
rnto
HIV
-inf
ecte
dm
othe
rsin
itia
ted
excl
usiv
ebr
east
feed
ing
from
birt
hB
reas
tfed
infa
nts
who
rece
ived
solid
sw
ere
sign
ifica
ntly
mor
elik
ely
toac
quir
ein
fect
ion
com
pare
dw
ith
excl
usiv
ely
brea
stfe
d(H
R10
87
151
ndash78
P=
001
8)as
wer
ein
fant
sw
hoat
12w
eeks
rece
ived
brea
stan
dfo
rmul
am
ilk(1
82
098
ndash33
6P
=0
57)
Cum
ulat
ive
3-m
onth
mor
talit
yin
excl
usiv
ely
brea
stfe
dw
as6
1(4
74ndash
792
)vs
15
1(7
63ndash
287
3)in
infa
nts
give
nre
plac
emen
tfe
eds
(HR
206
1
0ndash4
27P
=0
05)
The
stud
ysh
ows
that
excl
usiv
ebr
east
feed
ing
can
besu
cces
sful
lysu
ppor
ted
inH
IV-i
nfec
ted
wom
enT
heau
thor
sca
llfo
rfu
rthe
rre
visi
onof
UN
ICE
FW
HO
and
USA
IDin
fant
feed
ing
guid
elin
es
CD
CC
ente
rof
Dis
ease
Con
trol
HR
haz
ards
rati
oU
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
USA
IDU
SA
genc
yfo
rIn
tern
atio
nalD
evel
opm
ent
WH
OW
orld
Hea
lth
Org
aniz
atio
nZ
VIT
AM
BO
Z
imba
bwe
Vit
amin
Afo
rM
othe
rsan
dB
abie
s
Mainstreaming nutrition into MCH programs 23
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23

national and international conferences or meetingsAdditionally we contacted key researchers andorganizationsagencies for unpublished material ornarrowly disseminated reports
Consistent with the programmatic focus theexamples quoted in this review are demonstrationprojects that reached large populations or cluster ran-domized intervention trialsThe emphasis is on devel-oping countries and as some of these countries areburdened by HIVAIDS this review includes thiscontext as well
The scale-up process
The scale-up planning process must follow a logicalorder Several key issues that need attention are sum-marized in Table 1 It is apparent that many of thefeatures of the process are generic to neonatal andchild health programmes but there are issues in thearea of exclusive breastfeeding that requires addi-tional attention particularly in the HIV context
Issues that need to be addressedwhile scaling up a programme forexclusive breastfeeding
Policy framework
The Global Strategy on Infant and Young ChildFeeding was adopted by a World Health Assemblyresolution (5525 WHA 2002) The global strategybuilds on the BFHI (WHOUNICEF 1992) the
International Code of Marketing of Breastmilk Sub-stitutes (WHO 1981) and the Innocenti Declarationon the Protection (WHO 1989) Promotion andSupport of Breastfeeding in the overall context ofnational policies and programmes on nutrition andchild health The aim of the strategy is to improvethe feeding of infants and young children andincrease the commitment of governments societygroups and international organizations to promotethe health and nutrition of children The strategyemphasizes the need for comprehensive nationalpolicies on infant and young child feeding onan urgent basis including guidelines on ensuringoptimal feeding of infants and young children inexceptionally difficult circumstances and the need toensure that all health services protect promote andsupport infant and young child feeding (Gupta 2002WHOUNICEF 2003)
Once the decision to scale up a programme forexclusive breastfeeding is made in a region or stateor country the logical starting point is to review therelevant existing national policies and to assesswhether these address varying circumstances underwhich women deliver and live such as urban or ruralresidence working women and place of deliverySpecific features to note are the status of the imple-mentation of the BFHI in facilities where womendeliver access and support to mothers with younginfants by trained personnel during the post-natalperiod and beyond support for exclusive breastfeed-ing in community setting legislation for workingmothers that ensures leave of appropriate durationan enabling environment at the work place withingovernment and private settings and the policiesin place for discouraging promotion of breastmilksubstitutes
Existing policies are optimal in some countries(The Norwegian Government 1993 ILO 1998) butlacunae exists in others for example exclusive breast-feeding for 6 months is a policy in India but the dura-tion of maternity leave for government employees is135 days (Government of India 1997) In Norwayhowever a mother is entitled to over 6 months ofmaternity leave (The Norwegian Government 1993)Wherever weaknesses exist a decision needs to bemade on how these will be addressed during scale-up
Table 1 Steps in scaling up
Assess situation create a policy environment conducive toexclusive breastfeeding
Define roles relationships and responsibilities of all partnersestablish agreements
Review technical supportDefine programme strategyMobilize resourcesProvide training and technical assistanceDevelop and use monitoring and evaluation systemsMonitor coverage and qualityMeasure impact and costProvide for testing novel approaches and continuing innovation
Adapted from Knippenberg et al (2005) and Gonzales et al (1998)
Mainstreaming nutrition into MCH programs 7
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Prior to scale-up a policy framework for implemen-tation needs to be developed This framework shouldinclude a vision consensus on technical issues onprogramme strategy roles relationships and respon-sibilities of implementing partners measurable goalswithin defined time lines and predictable adequatefunding to achieve these (The Core Group 2005) Itshould address the capacity of all implementing part-ners and the approach to fulfilling capacity gaps at alllevels particularly at the community level The policyframework should emphasize breastfeeding promo-tion through community-based programmes Politicalcommitment and ownership by relevant governmentdepartments at national state and district levels havealso been identified to be critical for effective scale-up(The Core Group 2005)
Technical and management support andother partnerships
Creating a policy framework designing a potentiallyeffective programme and an implementation strategyrequire multiple capacities which may not always beavailable within government departments or otherconcerned agencies
Technical and managerial support may need to bemobilized more so during the planning and earlyimplementation phase If this support is not availableinvolvement of external talent ndash national or eveninternational ndash may be required Once the pro-gramme is implemented the external support couldbe phased out gradually as local capacity is built
Forging partnerships between government minis-tries donors local non-governmental organizations(NGOs) and universities was a feature of many suc-cessful programmes (Appendix 1 Van Roekel et al
2002 Bhandari et al 2005 Quinn et al 2005) In theLINKAGES projects (Appendix 1) partnershipwith Programa de Coordinacion en Salud Integral(Collaborative Program for Integrated HealthPROCOSI) and NGOs in Bolivia UNICEF NGOsand the national government in Ghana and Intersec-toral Action Group for Nutrition and Jereo SalamaIsika in Madagascar added value and quality to pro-grammes resulted in effective pooling of resources
and expertise and improved programme design andmanagement (LINKAGES 2002 Van Roekel et al
2002 Quinn et al 2005)
Programme design and strategy
This requires a systematic description of steps andprocesses that help achieve high coverage qualityequity and sustainability capacity building and pro-gramme management are particularly important fea-tures (The Core Group 2005) Experience so farsuggests that for majority of developing countriesscale-up for exclusive breastfeeding will not be pos-sible unless intervention delivery at the communitylevel receives emphasis (Appendix 1) As an increas-ing number of mothers deliver in institutions mixedmodels will be required even in developing countries
An initial step is to carefully examine the existingopportunities as vehicles for promoting exclusivebreastfeeding If use of existing opportunities is insuf-ficient to achieve high coverage with good qualitythen additional approaches would need to be evolvedin a phased manner In Bangladesh the strategy ofpeer counsellors was used as the majority of deliveriesoccur at home and a community health worker is notroutinely available in that setting (Haider et al 2000)In India on the other hand village health workersalready exist so programmes are often designedaround them (Bhandari et al 2003 2004 2005)
Hospitalinstitution-based strategies
Efforts to scale up the BFHI in countries have shownmixed results (Table 2)
In regions where hospital deliveries are the normscale-up efforts through the BFHI (WHOUNICEF1992 Table 3 Perez-Escamilla 2007) have been suc-cessful and the strategy helped increase rates ofexclusive breastfeeding (Appendix 1) However inmany countries after initial years of enthusiasm thescale-up effort seems to have plateaued perhapsreflecting changing emphasis of donors and govern-ment The initial high rates of exclusive breastfeedingmay not be sustained after mothers are dischargedfrom facilities and return to their homes (Coutinhoet al 2005) The challenge therefore is to continue at
N Bhandari and AKMI Kabir8
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
home the post-delivery support available in institu-tions through public and private providers to sustainexclusive breastfeeding or develop other mechanismsthat support recently delivered mothers to exclusivelybreastfeed once they are discharged from hospitals(de Oliveira et al 2006) Countries have addressedthis in different ways In Australia a cadre of breast-feeding counsellors exists (Australian BreastfeedingAssociation 2005) In pilot programmes in Indiaexclusive breastfeeding was promoted through healthworker home visits at immunization clinics growthmonitoring sessions and at sick-child contacts(Bhandari et al 2005) in addition to the BFHI Homevisits are particularly important in regions where cov-
erage through other channels is low or not feasibleand a cadre of community workers exists
Community-based strategies
Pilot efforts in countries or regions where home deliv-eries predominate have shown success through ver-tical as well as integrated approaches however pro-grammes integrated into ongoing activities are morelikely to be more sustainable (The Core Group 2005)In these programmes (Appendix 1) the messageswere delivered through either a single existing or newchannel or multiple delivery channels already inplace within the primary health-care systemThe deci-sion to use one or multiple channels was made basedon the ability to cover the target population In somecountries high coverage was feasible only with mul-tiple facility and community channels (Appendix 1)Multiple channels also help achieve consistency inadvice The credibility and acceptability of a givenchannel by the community was another factor in theirbeing used Routine activities of channels were modi-fied in some instances to incorporate exclusive breast-feeding counselling In India for instance it wasbelieved that immunization sessions could not beused as a counselling opportunity but better organi-zation and the presence of another available localworker during the session enabled the vaccinator tocounsel mothers (Bhandari et al 2005)Another illus-tration is the adaptation of the Integrated Manage-ment of Childhood Illness (IMCI) programme of theWHOUNICEF (2002) to the Integrated Manage-ment of Neonatal and Childhood Illness (IMNCIGovernment of India 2006) by India The IMNCIincludes three home visits for all births in the first 7days of life by an existing community worker theAnganwadi worker (ICDS 1982) to promote essentialnewborn care which includes exclusive breastfeedingIn other countries such as Bangladesh facility-basedIMCI was sought to be improved in its impact bygreater emphasis on community component of IMCIthat is C-IMCI (Gwatkin 2004)
Programme delivery
Recognizing that facility-based interventions areinsufficient countries have experimented with a
Table 2 Proportion of facilities with Baby-Friendly Hospital Initiative(WABA 2007)
Region Median (range)
West and Central Africa 013 (000ndash059)EasternSouthern Africa 023 (000ndash100)Middle East and North Africa 014 (000ndash100)South Asia 007 (001ndash100)East Asia and Pacific 0005 (000ndash087)Americas and the Caribbean 010 (000ndash100)Central and Eastern EuropeCommonwealth
of Independent States025 (004ndash093)
All Industrialized Countries 007 (000ndash097)
Table 3 The 10 steps to successful breastfeeding for hospitals andbirth centres
bull Maintain a written breastfeeding policy that is routinelycommunicated to all health-care staffbull Train all health-care staff in skills necessary to implement thispolicybull Inform all pregnant women about the benefits and managementof breastfeedingbull Help mothers initiate breastfeeding within 1 h of birthbull Show mothers how to breastfeed and how to maintain lactationeven if they are separated from their infantsbull Give infants no food or drink other than breastmilk unlessmedically indicatedbull Practise lsquorooming inrsquo ndash allow mothers and infants to remaintogether 24 hours a daybull Encourage unrestricted breastfeedingbull Give no pacifiers or artificial nipples to breastfeeding infantsbull Foster the establishment of breastfeeding support groups andrefer mothers to them on discharge from the hospital or clinic
Mainstreaming nutrition into MCH programs 9
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
variety of local workers such as peer counsellors inBangladesh (Haider et al 2000) lady health workersin Pakistan (Government of Pakistan 2003) and thelsquoAccredited Social Health Activistsrsquo (ASHA) workerin India (Government of India 2005) to promoteexclusive breastfeeding by itself or as a part of essen-tial newborn care Programmes that used peer coun-sellors as a single channel have been shown to beeffective in several efficacy (Green 1999 Lewin et al
2006) and effectiveness trials (Morrow et al 1999Haider et al 2000 Lewin et al 2006) However whilepeer or lay counsellors have been effective in theshort run long-term sustainability of this approach ona large scale is as yet not established
The possible reasons stated for the short-termsuccess of the lay health workers approach includepayment to the counsellors for performing a specificpiece of work the counsellorsrsquo own perception ofbenefits of their work and their recognition by thecommunity as being skilled These workers also feltthis opportunity to have the potential for opening upof further education and training (Haider et al 2002)An important issue would also be linking newworkers with the existing primary health system aspilot experience showed that these workers may notbe able to resolve complex breastfeeding problems(Haider et al 2002)
Recruitment of ASHA in India provides a uniqueopportunity to promote exclusive breastfeeding(Government of India 2005) Currently being re-cruited all over the country these workers will focuson essential newborn care including exclusive breast-feeding through home visitation in the first month oflife and community-based activities
While these efforts in different countries at improv-ing coverage of the target population through localworkers are of value the voluntary or semi-voluntarynature of the workers and ill-defined models of super-vision raise issues about sustainability and possiblyhigh attrition rates
Programmes that used multiple channels reportedbroader coverage (Bhandari et al 2005 Quinn et al
2005) In India formative research showed thatimmunization sessions and private providers werethe channels to which infants were most commonly(~80) exposed Following constitution of a
breastfeeding-promotion programme caregiversmost often received exclusive breastfeeding counsel-ling at immunization sessions (~40) weighing ses-sions (~25) and home visits (25ndash30) Governmentphysicians or private providers rarely (~2) coun-selled despite being trained (Bhandari et al 2005)When all the opportunities were considered together55ndash60 of caregivers had been counselled at leastonce by at least one of the channels in the last 3months indicating that multiple channels reachedmore families (Bhandari et al 2005)The frequency ofcontact with caregivers or the intensity of counsellinginfluences the cumulative benefit of the counsellingfor example six contacts with mothers resulted inhigher adoption rates for exclusive breastfeeding ascompared with three (Morrow et al 1999) In Indiathe number of channels at which caregivers werecounselled was positively associated with the rates ofexclusive breastfeeding at 3 months of age (Bhandariet al 2003) However the costs of training and theeffort will increase more than the number of channelsused and therefore this issue requires a balancedview
Another issue of interest is the value of counsellingfor the antenatal period itself Antenatal counsellinghas been used in several programmes but its effect isdifficult to delineate by itself as it was usually fol-lowed by post-natal counselling (Green 1999) In theHIV context however the importance of antenatalcounselling is obvious
Communications approach
An effective communications approach was a featureof most programmes and involvement of journalistsradio announcements and other mass media from theprogramme outset extended the reach of nutritionmessages even further (Appendix 1 Quinn et al
2005) Mass media were not used in some pro-grammes where a comparison group was present forrisk of contamination (Bhandari et al 2005) Utiliza-tion of existing or newly formed community groupsproduced the same effect (Bhandari et al 2005Quinn et al 2005) and community mobilization pro-grammes such as street plays rallies radio pro-grammes and songs helped disseminate messages
N Bhandari and AKMI Kabir10
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
and increase community involvement (Bhandari et al
2005 Quinn et al 2005)Effective counselling requires assessment of
feeding practices recognition of problems and nego-tiation with the mother in choosing improved prac-tices that are feasible (WHOUNICEF 2002) thisrequires time and patience Programmes may chooseone-on-one counselling during opportunities in whichmore time is available such as home visits and groupcounselling for opportunities with lesser availabletime (Bhandari et al 2005) One of the reasons thatpeer counsellors may have been effective was thattheir sole responsibility was counselling mothersthrough home visits (Morrow et al 1999 Haider et al
2000) The more diverse the functions of the localworker the lesser will be the emphasis on a singlecomponent such as exclusive breastfeeding
Message development
The development of messages for interpersonal com-munication and for mass media needs careful atten-tion to design and content Successful programmesincluded an element of formative research to gain anin-depth understanding of the communities wherethese programmes were implemented with regard topractices pertaining to breastfeeding the reasons forthe current practices the common breastfeedingproblems and the barriers to adoption of ideal behav-iours in that cultural setting Formative research innorth India for instance showed general unwilling-ness to offer water to infants in summer months Thisbarrier was overcome by building specific explanatorymessages using local terms within the communicationstrategy (Bhandari et al 2003)
Once the design features and broad strategy are inplace attention must then shift to the operationaliza-tion of the strategy
Training and supervision
Prior to scale-up the training needs will need to bedefined Fortunately for promotion of exclusivebreastfeeding extensive experience is available ontraining of different cadres of health workers andeven for lay counsellors Most experiences used the
adapted versions of the UNICEFWHO Breastfeed-ing Counseling Course (WHOUNICEF 1993) or theIMCI module (WHOUNICEF 2002)
Training strategy and its quality merit attentionIn successful programmes the duration of trainingextended from 3 full days to 10 part days for differentworkers The training strategies as described werelsquoconcise action orientedrsquo and included modules thataimed to equip trainers with practical skills and con-fidence to counsel effectively (Appendix 1)
Training modules for areas with high HIV preva-lence also exist (WHO 2006)
While the training modules used in studies workedwell a gap remains for referralTrained workers at thecommunity level require that referral options avail-able are easily accessible prompt and preferablyavailable free of cost to mothers with complex breast-feeding problems
Another important issue to address is handlingtraining of new staff in most developing countriesstaff turnover and absenteeism rates are high
Monitoring and evaluation
The programme strategy will need to include systemsfor monitoring and evaluation of the programmePossible markers could include the rates of exclusivebreastfeeding worker performance referral andaction As for all other national programmes therewill be a need for periodic reviews and achievabletargets by time
Costs and resources
In all pilot programmes and projects services wereprovided to mothers free of cost In many developingcountries if the government cadre of health workers isused to promote exclusive breastfeeding as a part oftheir other responsibilities (eg the IMNCI) the basicservices will remain free However a system thatrequires setting up a cadre of trained lactation coun-sellors (eg in an urban setting or as referral sources forbreastfeeding problems in rural areas) will requireadditional resources A cost-effective analysis of theBFHI was conducted in three countriesBrazilMexicoand Honduras (Horton et al 1996) Savings on health
Mainstreaming nutrition into MCH programs 11
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
care resulting from reduction in diarrhoeal and respi-ratory morbidity were estimated as a result of theeffect of BFHI on breastfeeding The study showedthat breastfeeding promotion through a BFHI-likemodel is very cost-effective (1992 US$ 2ndash19 per dis-ability adjusted life years Horton et al 1996 Perez-Escamilla 2007) Examples of cost-effectivenessanalysis of community-based programmes using lay orprofessional support in different settings could not beidentified
Testing of novel approaches andcontinuing innovation
Scaled-up programmes must have inbuilt provision totest novel approaches and the ability for continuinginnovation
Scaling up of exclusive breastfeeding in thecontext of HIV
The policy and programme design and implemen-tation issues relevant to exclusive breastfeedingscale-up discussed above are relevant to HIV-prevalent areas but there are other unique featuresthat merit consideration
Creating policies for exclusive breastfeeding pro-motion in countries with high HIV prevalence is par-ticularly challenging The revised recommendationsencourage exclusive breastfeeding for the first 6months and continued breastfeeding for 2 years andbeyond for infants whose mothers are HIV negativeor whose HIV status is unknown For women who areknown to be HIV positive the most appropriateinfant feeding option for HIV-exposed infantsdepends on individual circumstances including con-sideration of health services counselling and supportExclusive breastfeeding is the better option for suchinfants unless replacement feeding is acceptable fea-sible affordable sustainable and safe for both themother and baby This recommendation is based onthe finding that exclusive breastfeeding for up to 6months in three large cohort studies is associated witha three- to fourfold decreased risk of transmission ofHIV compared with non-exclusive breastfeeding(WHO 2006) The recommendations may need
further revision if new findings demonstrate thatexclusive breastfeeding should be the feeding ofchoice for HIV-infected women (Iliff et al 2005)
Some pilot programmes for exclusive breastfeedingpromotion in high-HIV-prevalence countries aresummarized in Appendix 2
In general exclusive breastfeeding promotionformed a part of the prevention of mother-to-childtransmission programmes LINKAGESZambiaintegrated improved counselling on infant feedingmaternal nutrition and antiretroviral therapy duringprophylaxis in both health-care and community ser-vices to enable women to make and act on informedchoice to feed their infants optimally in the context ofhigh HIV prevalence
Formative research was critical to develop locallyappropriate and feasible infant feeding recommenda-tions for individual infants and their families based onHIV status In Zambia the research included focusedgroup discussions key information interviews obser-vations of household food preparation and feedingmarket survey of replacement foods and breastmilksubstitutes and household trials of improved feedingand caring practices (LINKAGES 2005)
High quality of health workers is another criticalfactor for sensitive and accurate individual counsel-ling Programmes incorporated behaviour changecommunication methodologies in training (LINK-AGES 2005) It is important to develop skills of com-munity members as well for improved servicesreferral outreach and follow-up care and support ofHIV-positive mothers and their infants
A comprehensive communications strategy tosupport scale-up was a notable feature of the LINK-AGES programme in Zambia In 2004 an intensiveeffort was launched using brochures posters radioand television spots billboards and reference guidesfor health providers (LINKAGES 2005) Messageswere targeted to relevant stakeholders ndash pregnantand lactating mothers health providers youth andcommunity leaders and all the materials were nation-ally disseminated
Monitoring and evaluation another importantfeature of effective scale-up was a feature of pilotprogrammes (Appendix 2 Ntabaye amp Lusiola 2004Rutenberg et al 2004) in Zambia and Tanzania Moni-
N Bhandari and AKMI Kabir12
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
toring and evaluation not only provides a measure ofsuccess but identifies factors that may have contrib-uted to it and to lack of success to enable mid-coursecorrections The impact of some pilot programmes onexclusive breastfeeding is summarized in Appendix 2In most programmes exclusive breastfeeding ratesimproved In Zambia exclusive breastfeeding ratesincreased from 50 in 2002 to 64 in 2004 in Liv-ingstone from 57 in 2000 to 74 in 2004 in NdolaIn South Africa an antenatal clinic-based interven-tion led to 83 of infants born to HIV-infectedmother initiating exclusive breastfeeding InZimbabwe an intervention based on antenatal coun-selling resulted in a relatively lower exclusive breast-feeding rate of 246 at 3 months (Piwoz et al 2005)
Several barriers to success were identified Theseinclude inadequate skills of workers and non-integration of HIV counselling and tailoring into ante-natal care services (Ntabaye amp Lusiola 2004) which isthe backbone in which infant feeding counselling isbuiltWomen reported that mothers not breastfeedingtheir children were discriminated against by the com-munity and they faced the threat of domestic violenceProgramme managerrsquos understanding of barriersto effective programme implementation and impactwere emphasized as being important Governmentsupport partnerrsquos coordination increased humanresource and improving the supply system were iden-tified to be essential features to scale up programmesin the HIV context (Rutenberg et al 2004) Lowoverall exclusive breastfeeding rates prompted Piwozet al (2005) to conclude that women and their partnersshould have been reached more frequently during theantenatal and post-natal period
Conclusions
In a large number of programmes for improvingexclusive breastfeeding in developing countriesincluding in areas with high prevalence of HIV apositive impact on exclusive breastfeeding rates hasbeen achieved
Some of the factors that contributed to successfulscale-up are summarized in Table 4 Several limita-tions of the programmes reviewed merit attentionMost programmes involved special and generous
funding concentrated efforts and multiple contactsThese programmes were evaluated over relativelyshort periods of time usually 2ndash5 years and the long-term sustainability has not been really tested In theabsence of specific measures there is likely to be dilu-tion of quality as the programmes are scaled upfurther from their initial size The experience thus farleaves important questions to be addressed particu-larly on how programmes can be sustained over timeas they are scaled up at affordable costs
A key factor relevant to sustainability is to plan ona long-term basis a period of 10ndash20 years rather than5ndash10 years from the outset Experience with otherchild health programmes has shown that performancein immunization and oral rehydration therapy userates plateaued over time in many countries
Programme scale-up requires a programme man-agement capacity proportionate to the scale of opera-tions periodic assessment of barriers (Table 5) and anability to revise programme strategy to overcomethese Another key feature to sustainability ofscale-up is the extent to which capacity has been builtat the district block and community levels National-or state-level driven interventions begin with enor-mous enthusiasm which is difficult to sustain Thisfactor is particularly important as most developing
Table 4 Lessons learnt about scale-up key factors in success
bull Political will advocacy enabling policiesbull Championship by health ministries at national state and districtlevelbull Technical consensus on feeding guidelinesbull Programme strategy and measurable short- and long-term goalsbull Long-term financial commitmentbull Partners with defined roles assessment of their capacity todeliver and plans to cover gaps in capacitybull Emphasis on community-level interventions and not onlyfacility-based programmesbull Formative research as the backbone of effective scale-upprogrammes particularly in the context of HIVbull Careful selection of channels and the number required toachieve timely coverage consistency of messagesbull Communication strategy aided by formative research pre-testedvalidated messages and toolsbull Quality trainers and training centres proportionate to requiredscalebull Monitoring and evaluationbull Programme redesign when relevant through research analysisand innovation
Mainstreaming nutrition into MCH programs 13
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
countries are going through a process of decentrali-zation with increasing responsibility for planningimplementation and evaluation being delegated tolower levels of the health-care system Buildingcapacity at that level requires time resources andpatience and a longer-term perspective
Building capacity emerges to be a key factorTrainers and training centres vary in their qualitywhen training health workers and their supervisorsor programme managers As the burden of trainingincreases availability of good-quality trainersbecomes a limiting factor (WHOUNICEF 2002Government of India 2006) An effective strategymust plan for these incremental requirements includ-ing ensuring secure and sustained funding
Identifying barriers to success is a key actor Thebarriers to scaling up of health interventions havebeen elegantly described by Ranson et al (Table 5)Most of these are important for exclusive breastfeed-ing scale-up as well
Overall within the limitations discussed above anumber of programmes in countries with varying
HIV prevalence show that exclusive breastfeeding ona large scale is feasible and pilot programmes havegiven valuable guidance related to policies planningand implementation of large-scale programmes Thechallenge now is to build on these experiences whenplanning national programmes
Acknowledgements
We sincerely thank Dr MK Bhan for his constructivecriticism and sustained feedback at different stages ofdevelopment of this review
Conflicts of interest
The authors have declared no conflicts of interest
References
Arifeen S Black RE Antelman G Baqui A CaulfieldL amp Becker S (2001) Exclusive breastfeeding reducesacute respiratory infection and diarrhea deaths amonginfants in Dhaka slums Pediatrics 108 E67
Australian Breastfeeding Association (2005) Valuing Par-enthood Options for Paid Maternity Leave ndash InterimPaper 2002 Available at httpwwwbreastfeedingasnauadvocacymatleavehtml
Bhandari N Bahl R Mazumdar S Martines J BlackRE amp Bhan MK (2003) Effect of community basedpromotion of exclusive breastfeeding on diarrheal ill-nesses and growth a cluster randomized controlled trialLancet 361 1418ndash1423
Bhandari N Mazumder S Bahl R Martines J BlackRE amp Bhan MK (2004) An educational interventionto promote appropriate complementary feedingimproves child feeding practices and linear growth inrural Haryana India Journal of Nutrition 134 2342ndash2348
Bhandari N Mazumder S Bahl R Martines J BlackRE amp Bhan MK (2005) Use of multiple opportunitiesfor improving feeding practices in undertwos withinchild health programs Health Policy Plan 20 328ndash336
Bryce J Victora CG Habicht JP Vaughan JP ampBlack RE (2004) The multi-country evaluation of theintegrated management of childhood illness strategylessons for the evaluation of public health interventionsAmerican Journal of Public Health 94 406ndash415
Butte NF Lopez-Alarcon MG amp Garza C (2002) Nutri-ent Adequacy of Exclusive Breastfeeding for the TermInfant during the First Six Months of Life World HealthOrganization Geneva
Table 5 Barriers to scaling up of health interventions
Community and household levelsLack of information womenrsquos education physical financial
womenrsquos decision-making powerHealth services delivery levelShortage of qualified staff weak technical guidance programme
management and supervision inadequate supplies equipmentand infrastructure poor accessibility
Health sector policy and strategic management levelWeak and centralized system for planning and management weak
drug policies and supply system inadequate regulations lack ofintersectoral action and partnership weak incentives to useinputs efficiently and respond to user needs and preferencesreliance on donor funding
Public policies cutting across sectorsGovernment bureaucracy poor communication and transport
infrastructureEnvironmental characteristicsGovernance and overall policy frameworkCorruption weak government weak laws political instability and
insecurity low priority to social sectors weak structure for publicaccountability and opportunities for public opinions lack of freepress
Physical environmentClimatic and geographic predisposition physical environment
unfavourable to service delivery
Adapted from Ranson et al (2003)
N Bhandari and AKMI Kabir14
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Cohen J (2007) Retrovirus meeting Hope on new AIDSdrugs but breast-feeding strategy backfires Science 3151357
Coovadia HM Rollins NC Bland RM Little KCoutsoudis A Bennish ML et al (2007) Mother tochild transmission of HIV-1 infection during exclusivebreastfeeding in the first 6 months of life an interven-tion cohort study Lancet 369 1107ndash1116
Coutinho SB de Lira PI de Carvalho LM amp AshworthA (2005) Comparison of the effect of two systems forthe promotion of exclusive breastfeeding Lancet 3661094ndash1100
Feachem RG amp Koblinsky MA (1984) Interventions forthe control of diarrheal diseases among young childrenpromotion of breastfeeding Bulletin of the of the WorldHealth Organization 62 271ndash291
Gonzales A Arteaga E amp Howard-Grabman L (1998)Scaling Up the WARMI Project ndash Lessons LearnedMobilizing Bolivian Communities around ReproductiveHealth Save the Children Federation Inc Bolivia FieldOffice La Paz Available at httpwwwcoregrouporgresourcesSavebolipdf
Government of India (1997) Recommendations of the FifthCentral Pay Commission Relating to Enhancement ofQuantum of Maternity Leave and to Allow PaternityLeave in Respect of Central Government EmployeesDocument ref 13018197-Estt(L) Available at httppersminnicinesttleave2htm
Government of India (2005) National Rural HealthMission 2005ndash2012 Mission document Ministry ofHealth and Family Welfare New Delhi Government ofIndia Available at httpwwwmohfwnicinNRHM20Mission20Documentpdf
Government of India (2006) Operational Guidelines forImplementation of Integrated Management of Neonataland Childhood Illness (IMNCI) Ministry of HealthFamily Welfare New Delhi Available at httpmohfwnicindofw20websiteF20IMNCI20Operational20Plan201320june202006htm
Government of Pakistan (2003) National Programme forFamily Planning and Primary Health Care The LadyHealth Workers Programme 2003ndash2008 Ministry ofHealth Pakistan Available at httpwwwphcgovpkDownloadsPC-120augpdf
Green CP (1999) Improving Breastfeeding Behaviors Evi-dence from Two Decades of Intervention ResearchPublished for the US Agency for International Develop-ment (USAID) by the LINKAGES Project Academyfor Educational Development Washington DC
Gupta A (2002) National trends in breastfeeding andeffective strategies to improve breastfeeding ratesJournal of Neonatology 2002 4ndash14
Gwatkin DR (2004) Integrating the management of child-hood illness Lancet 364 1557ndash1558
Habicht JP DaVanzo J amp Butz WP (1986) Does breast-feeding really save lives or are apparent benefits due tobiases American Journal of Epidemiology 123279ndash290
Haider R Ashworth A Kabir I amp Huttly SR (2000)Effect of community based peer counsellors on exclusivebreastfeeding practices in Dhaka Bangladesh a ran-domized controlled trial Lancet 356 1643ndash1647
Haider R Kabir I Huttly SR amp Ashworth A (2002)Training peer counsellors to promote and support exclu-sive breastfeeding in Bangladesh Journal of HumanLactation 18 7ndash12
Horton S Sanghvi T Phillips M Fiedler J Perez-Escamilla R Lutter C et al (1996) Breastfeeding pro-motion and priority setting in health Health Policy andPlanning 11 156ndash168
ILO (1998) More than 120 Nations Provide Paid MaternityLeave Gap in Employment Treatment for Men andWomen Still Exists International Labour Office GenevaDocument ref ILO987 Available at httpwwwiloorgpublicenglishbureauinfpr19987htmr2
Iliff PJ Piwoz EG Tavengwa NV Zunguza CDMarinda ET Nathoo KJ et al (2005) Early exclusivebreastfeeding reduces the risk of postnatal HIV-1 trans-mission and increase HIV-free survival AIDS 19 699ndash708
Integrated Child Development Services Scheme (Revised)(ICDS) (1982) Ministry of Social Welfare Governmentof India New Delhi Available on URL httpwcdnicinudishahtmabouticdshtm
Jason JM Nieburg P amp Marks JS (1984) Mortality andinfectious disease associated with infant feeding prac-tices in developing countries Pediatrics 74 702ndash727
Jones G Steketee RW Black RE Bhutta ZA ampMorris SS Bellagio Child Survival Study Group (2003)How many child deaths can we prevent this yearLancet 362 65ndash71
Knippenberg R Lawn JE Darmstadt GL Begkayian GFogstad H Walelign N et al (2005) Systematic scalingup of neonatal care in countries Lancet 365 1087ndash1098
Kramer MS amp Kakuma R (2002) The optimal durationof exclusive breastfeeding a systematic reviewCochrane Database of Systematic Reviews 2002CD003517
Kramer MS Chalmers B Hodnett ED Sevkovskaya ZDzikovich I Shapiro S et al (2000) Promotion ofbreastfeeding intervention trial (PROBIT) a cluster ran-domized trial in the Republic of Belarus Design followup and data validation Advances in Experimental Medi-cine and Biology 478 327ndash345
Kramer MS Chalmers B Hodnett ED Sevkovskaya ZDzikovich I Shapiro S et al (2001) Promotion ofbreastfeeding intervention trial (PROBIT) a random-
Mainstreaming nutrition into MCH programs 15
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
ized trial in the Republic of Belarus Journal of theAmerican Medical Association 285 413ndash420
Lewin SA Dick J Pond P Zwarenstein M Aja Gvan Wyk B et al (2006) Lay health workers in primaryand community health care (Review) The CochraneLibrary 3 1ndash104
LINKAGES (2002) World LINKAGES MadagascarAcademy for Educational Development WashingtonDC
LINKAGES (2005) LINKAGES Zambia 1997ndash2005 FinalReport A Full Report on LINKAGES Infant Feedingand HIVAIDS Programs in Zambia Academy for Edu-cational Development Washington DC Available athttpwwwlinkagesprojectorgmediapublicationsFinal20draft20Zambia20final20report2012105pdf
Lutter CK Perez-Escamilla R Segall A Sanghvi TTeruya K amp Wickham C (1997) The effectiveness of ahospital based program to promote exclusive breastfeed-ing among low income women in Brazil AmericanJournal of Public Health 87 659ndash663
Morrow AL Guerrero ML Shults J Calva J Lutter CBravo J et al (1999) Efficacy of home based peer coun-selling to promote exclusive breastfeeding a randomizedcontrolled trial Lancet 353 1226ndash1231
Ntabaye MK amp Lusiola GJ (2004) Understanding barri-ers to PMTCT in Tanzania findings of a baseline surveyInternational Conference on AIDS 15 (B11396)
de Oliveira LD Giugliani ER do Espirito SLC FrancaMC Weigert EM Kohler CV et al (2006) Effect ofintervention to improve breastfeeding technique on thefrequency of exclusive breastfeeding and lactation-related problems Journal of Human Lactation 22 315ndash321
Perez-Escamilla R (2004) Effectiveness of MADLAC atImproving Breastfeeding Promotion and CounsellingIndicators in Maternity Wards in El Salvador Publishedfor the Basic Support for Institutionalizing Child Sur-vival Project (BASICS II) for the United States Agencyfor International Development Arlington VA Availableat httpwwwbasicsorgpdfFinal20MADLAC20Report20RPE20April207-2004pdf
Perez-Escamilla R (2007) Evidence based breast-feedingpromotion the Baby-Friendly Hospital InitiativeJournal of Nutrition 137 484ndash487
Piwoz EG Iliff PJ Tavengwa N Gavin L Marinda ELunney K et al (2005) An education and counselllingprogram for preventing breastfeeding associated HIVtransmission in Zimbabwe design and impact on mater-nal knowledge and behaviour Journal of Nutrition 135950ndash955
Quinn VJ Guyon AB Schubert JW Stone-Jimenez MHainsworth MD amp Martin LH (2005) Improvingbreastfeeding practices on a board scale at the commu-
nity level success stories from Africa and LatinAmerica Journal of Human Lactation 21 345ndash354
Ranson MK Hanson K Oliveira-Cruz V amp Mills A(2003) Constraints to expanding access to health inter-ventions an empirical analysis and country typologyJournal of International Development 15 15ndash40
Rea MF amp Berquo ES (1990) Impact of the Braziliannational breastfeeding programme on mothers inGreater Sao Paulo Bulletin of the of the World HealthOrganization 68 365ndash371
Rollins NC (2007) Infant feeding and HIV BritishMedical Journal 334 487ndash488
Rutenberg N Baek C Kalibala S Rosen J amp Mulenga D(2004) Evaluation of United Nations supported pilotprojects for the prevention of mother-to-child transmis-sion of HIV overview of findings International Confer-ence on AIDS 15 (WePeE6688)
The Core Group (2005) Scale and Scaling Up A COREGroup Background Paper on lsquoScaling-Uprsquo MaternalNewborn and Child Health Services CORE SpringMembership Meeting 2005 The Core Group Washing-ton DC Available at httpwwwcoregrouporgresourcesmeetingsapril05Scaling_Up_Background_Paper_7-13pdf
The Norwegian Government (1993) Women in PoliticsMinistry of Children and Equality Available at httpwwwregjeringennoendepbldRyddemappeSLA-AvdelingdoclegislationguidelinesWomen-in-Politicshtmlid=437166
Thior I Lockman S Smeaton LM Shapiro RL WesterC Heymann SJ et al (2006) Breastfeeding plus infantzidovudine prophylaxis for 6 months vs formula feedingplus infant zidovudine for 1 month to reduce mother-to-child HIV transmission in Botswana a randomized trialthe Mashi Study Journal of the American Medical Asso-ciation 296 794ndash805
UNICEF (2002) Facts for Life lsquoKey Message What EveryFamily and Community Has a Right to Know aboutBreastfeedingrsquo Available at httpwwwuniceforgffl04key_messageshtm
Van Roekel K Plowman B Griffiths M de AlvaradoVV Matute J amp Calderon M (2002) BASICS IIMidterm Evaluation of the AIN Program in Honduras2000 Basic Support for Institutionalizing Child SurvivalProject (BASICS II) for the United States Agency forInternational Development Arlington VA
WABA (2007) UNICEF Records BHFI Record UpdateAvailable at httpwwwwabaorgmydocsBFHIjan07xls 2006 Regularly updated by Miriam HLabbok Center for Infant and Young ChildFeeding and Care Department of Maternaland Child Health School of Public Health The Univer-sity of North Carolina at Chapel Hill Chapel Hill NCUSA
N Bhandari and AKMI Kabir16
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
WHA (2002) Infant and Young Child Nutrition Fifty-FifthWorld Health Assembly Agenda Item 1310 18 May2002 Available at httpwwwintgbebwhapdf_filesWHA55ewha5525pdf
WHO (1981) The International Code of Marketing ofBreastmilk Substitutes World Health OrganizationGeneva
WHO (1989) Protecting Promoting and Supporting Breast-feeding The Special Role of Maternity Services A JointWHOUNICEF Statement World Health OrganizationGeneva
WHO (2002) The Optimal Duration of Exclusive Breast-feeding Report of an Expert Consultation WHONHD0109 WHOFCHCAH0124 World HealthOrganization Geneva
WHO (2003a) Community Based Strategies for Breastfeed-ing Promotion and Support in Developing CountriesWorld Health Organization Geneva Document refISBN_92_4_159121_8 Available at httpwwwwhointchild-adolescent-healthNew_PublicationsNUTRITIONISBN_92_4_159121_8pdf
WHO (2003b) Multi-country Evaluation of IMCI Effective-ness Cost and Impact (MCE) Progress Report May2002ndashApril 2003 Document ref WHOFCHCAH035World Health Organization Geneva
WHO (2004) Promoting Proper Feeding for Infants andYoung Children World Health Organization GenevaAvailable at httpwwwwhointnutritiontopicsinfantfeedingen
WHO (2006) WHO HIV and Infant Feeding TechnicalConsultation-Consensus Statement World Health Orga-nization Geneva Available at httpwwwwhointhivmediacentreInfantfeedingconsensusstatementpfpdf
WHO Collaborative Study Team on the Role of Breast-feeding on the Prevention of Infant Mortality (2000)Effect of breastfeeding on infant and child mortality dueto infectious diseases in les developed countries apooled analysis Lancet 355 451ndash455
WHOUNICEF (1992) The global criteria for the WHOUNICEF Baby-Friendly Hospital Initiative In Baby-Friendly Hospital Initiative Part II Hospital LevelImplementation World Health Organization Geneva
WHOUNICEF (1993) Breastfeeding Counselling A Train-ing Course WHOCDR933 UNICEFNUT931 WorldHealth Organization Geneva
WHOUNICEF (2002) Protocol for Adapting the FeedingRecommendations Part III IMCI Adaptation GuideWorld Health Organization Geneva
WHOUNICEF (2003) Global Strategy for Infant andYoung Child Feeding World Health OrganizationGeneva Available at httpwwwwhointchild-adolescent-healthpublicationsNUTRITIONIYCF_GShtm
de Zoysa I Rea M amp Martines J (1991) Why promotebreastfeeding in diarrheal diseases control programmesHealth Policy and Planning 6 371ndash379
Mainstreaming nutrition into MCH programs 17
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
Cas
est
udie
so
fef
fect
iven
ess
stud
ies
or
pilo
tpr
ogra
mm
es
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Lut
ter
etal
(199
7)
Bra
zil
Low
-inc
ome
urba
nw
omen
deliv
erin
gin
hosp
ital
s
Bre
astf
eedi
ngpr
omot
ion
in
hosp
ital
sco
mpa
red
wit
h
nobr
east
feed
ing
prom
otio
n
Pro
mot
ion
ofbr
east
feed
ing
in
sele
cted
hosp
ital
s
Mea
nda
ysof
excl
usiv
e
brea
stfe
edin
g
75da
ysvs
22
days
(Plt
001
)
Rea
ampB
erqu
o
(199
0)
Wom
enw
ith
ach
ild
aged
lt2ye
ars
inSa
oP
aulo
Nat
iona
lbre
astf
eedi
ng
cam
paig
n19
81ndash1
986
BF
HI
Mas
sm
edia
cam
paig
n11
in
fant
s5ndash
6m
onth
s
excl
usiv
ely
brea
stfe
d
in19
88an
d37
in
1987
Con
foun
ding
fact
ors
over
the
6-ye
arpe
riod
not
mea
sure
d
Kra
mer
etal
(200
020
01)
PR
OB
ITtr
ial
Bel
arus
Clu
ster
rand
omiz
ed
34ho
spit
als
and
thei
rpo
lycl
inic
s
Trai
ning
inB
FH
I(W
HO
UN
ICE
F19
92)
vsr
outi
ne
prac
tice
san
dpo
licie
s
Exc
lusi
vebr
east
feed
ing
at3
(43
3vs
64
)
and
6(7
9
vs0
6
)
mon
ths
sign
ifica
ntly
high
er
Impl
emen
ted
thro
ugh
BF
HI
ina
sett
ing
whe
reho
spit
al
deliv
erie
sar
eco
mm
on
Per
ez-E
scam
illa
(200
4)
BA
SIC
SII
Mex
ico
Hon
dura
s
Bra
zil
MA
DL
AC
low
-cos
t
man
agem
ent
info
rmat
ion
syst
emto
use
an
evid
ence
-bas
edap
proa
chto
impr
ove
serv
ice
perf
orm
ance
Inte
rvie
win
gof
wom
enat
hosp
ital
disc
harg
epo
st
deliv
ery
usin
ga
ques
tion
nair
eth
atta
kes
5ndash7
min
toad
min
iste
ran
d
cont
ains
19br
east
feed
ing
prom
otio
nco
unse
lling
indi
cato
rs
Dat
aen
tere
dan
dre
sult
s
disc
usse
d3-
mon
thly
by
hosp
ital
com
mit
tee
Hos
pita
lim
plem
ents
chan
ges
in
brea
stfe
edin
g
supp
ort
base
don
anal
ysis
of
ques
tion
nair
es
Itis
aco
st-e
ffec
tive
inte
rven
tion
that
can
help
impr
ovem
ents
inth
eB
FH
I
and
isa
valu
able
tool
for
proc
ess
eval
uati
on
N Bhandari and AKMI Kabir18
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
LIN
KA
GE
S
proj
ect
inA
fric
aan
d
Lat
inA
mer
ica
(Qui
nnet
al
2005
LIN
KA
GE
S
2002
WH
O20
03a)
Bol
ivia
(1
mill
ion)
Gha
na(3
5
mill
ion)
Mad
agas
car
(6m
illio
n)
Res
ourc
e-
poor
sett
ing
Pilo
tpr
ogra
mm
e
InB
oliv
iaan
d
Gha
napr
ogra
mm
e
focu
sed
on
brea
stfe
edin
gan
d
com
plem
enta
ry
feed
ing
InM
adag
asca
r
prog
ram
me
prom
oted
brea
stfe
edin
g
wit
hin
7es
sent
ial
nutr
itio
nac
tion
san
d
subs
eque
ntly
thro
ugh
IMC
I
Bui
lton
form
ativ
ere
sear
ch
and
sust
aine
dth
roug
h
prog
ram
me
acti
viti
esth
at
focu
sed
onbr
ingi
ngab
out
the
desi
red
beha
viou
r
chan
geM
ixof
inte
rven
tion
s
reac
hed
wom
enin
divi
dual
ly
orin
grou
psin
heal
th
faci
litie
sho
mes
or
com
mun
ity
sett
ings
Con
sist
ent
mes
sage
san
d
mat
eria
lacr
oss
all
prog
ram
me
chan
nels
Bol
ivi
PR
OC
OSI
NG
Os
Gha
na
UN
ICE
F
nati
onal
nutr
itio
n
offic
eN
GO
s
Mad
agas
car
Inte
rsec
tora
l
Act
ion
Gro
upfo
r
Nut
riti
on
Jere
o
Sala
ma
Isik
a
Pro
gram
desi
gned
wit
h
part
ners
Rad
ioin
all
thre
esi
tes
Mat
eria
ls
deve
lope
d
tosu
itne
eds
oflo
cal
heal
th
wor
kers
and
com
mun
ity
mem
bers
Gre
at
emph
asis
on
deve
lopm
ent
of coun
selli
ng
and
nego
tiat
ion
skill
s
prac
tica
l
sess
ions
Sign
ifica
ntin
crea
ses
inex
clus
ive
brea
stfe
edin
gra
tes
of
0ndash6-
mon
th-o
ld
infa
nts
from
54
to65
in
Bol
ivia
68
to79
in
Gha
naan
d46
to68
in
Mad
agas
car
In
Gha
naan
d
Mad
agas
car
sign
ifica
ntre
sult
s
obse
rved
wit
hin
aye
ar
ofin
itia
tion
of
com
mun
ity
inte
rven
tion
s
App
roac
hw
asef
fect
ive
and
achi
eved
sign
ifica
nt
incr
ease
sam
ong
larg
e
popu
lati
ons
asea
rly
as
9ndash12
mo
afte
rin
itia
tion
of
com
mun
ity
acti
viti
es
Van
Roe
kele
tal
(200
2)W
HO
(200
3a)
Hon
dura
sG
row
thm
onit
orin
gan
d
prom
otio
nkn
own
as
Ate
ncioacute
nIn
tegr
ala
la
Nintilde
ez(A
IN)
or
Inte
grat
edC
hild
Car
e
Init
ially
pri
mar
ilya
grow
th
mon
itor
ing
prog
ram
me
ulti
mat
ely
thro
ugh
IMC
I
Pro
gram
me
ongr
owth
prom
otio
nndash
asse
ssm
ent
of
mon
thly
wei
ght
gain
and
focu
son
illne
ssf
eedi
ng
prac
tice
san
dge
nera
lchi
ld
care
inin
fant
sun
der
2ye
ars
Impl
emen
ted
atgo
vern
men
t
faci
litie
san
dco
mm
unit
y
Star
ted
in19
92s
tren
gthe
ned
in19
95ndash1
997
wit
hgr
eate
r
focu
son
child
feed
ing
In
1997
pro
gram
me
intr
oduc
ed
wit
hIM
CI
(WH
OU
NIC
EF
2002
)
Maj
or
part
ners
UN
ICE
F
PAH
O
Am
eric
an
and
Hon
dura
n
Red
Cro
ss
CA
RE
Rad
io
broa
dcas
ts
relig
ious
lead
ers
IMC
IM
id-t
erm
eval
uati
on
show
ed39
of
mot
hers
inin
terv
enti
on
com
mun
itie
sex
clus
ivel
y
brea
stfe
dco
mpa
red
wit
h13
in
the
cont
rol
site
s
Mainstreaming nutrition into MCH programs 19
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
cont
inue
d
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Bha
ndar
ieta
l
(200
3)
WH
O
(200
3a)
Rur
alco
mm
unit
ies
inH
arya
na
Indi
a
Clu
ster
rand
omiz
edtr
ial
8
com
mun
itie
s(t
otal
popu
lati
on~4
000
0)
Pro
mot
ion
ofex
clus
ive
brea
stfe
edin
gan
d
appr
opri
ate
com
plem
enta
ryfe
edin
g
Dev
elop
edth
roug
h
form
ativ
ere
sear
ch
ndashP
robl
emid
enti
ficat
ion
ndashP
arti
cipa
tory
desi
gnof
inte
rven
tion
impl
emen
tati
onan
d
eval
uati
on
Impl
emen
tati
onw
ithi
nan
exis
ting
prim
ary
heal
th-c
are
prog
ram
me
Opp
ortu
niti
esus
edto
deliv
erm
essa
ges
wer
e
imm
uniz
atio
ncl
inic
s
wei
ghin
gse
ssio
ns
sick
-chi
ldco
ntac
tsan
d
mon
thly
hom
evi
sits
Res
earc
hers
wit
hlo
cal
gove
rnm
ent
ICD
Ssy
stem
and
NG
O
The
atre
son
gs
Mas
sm
edia
not
used
for
risk
of
cont
amin
atio
n
Mat
eria
ls
deve
lope
d
for
heal
th
wor
kers
pos
ters
flip
book
sca
rds
Bre
astf
eedi
ng
coun
selli
ngse
ctio
n
ofth
eIM
CI
(WH
O
UN
ICE
F20
02)
Exc
lusi
ve
brea
stfe
edin
gin
the
prev
ious
24h
at3
mon
ths
of
age
79
vs4
8
The
posi
tive
effe
ct
rem
aine
dup
to
6m
onth
sof
age
(42
vs4
)
Tota
lpar
tici
pati
onof
the
dist
rict
heal
thsy
stem
from
ince
ptio
nof
the
prog
ram
me
inde
velo
ping
impl
emen
tati
onst
rate
gyt
ool
deve
lopm
ent
and
mon
itor
ing
inad
diti
onto
invo
lvem
ent
of
anN
GO
wer
eim
port
ant
feat
ures
that
cont
ribu
ted
to
the
succ
ess
ofth
e
inte
rven
tion
Mor
row
etal
(199
9)
Mex
ico
Cit
yC
lust
erra
ndom
ized
tria
l
Tota
lpop
ulat
ion
3000
0
Two
com
mun
itie
sin
the
inte
rven
tion
one
com
pari
son
130
wom
en
Hom
e-ba
sed
peer
coun
selli
ng
Pee
rco
unse
llors
mad
e3
or
6ho
me
visi
tsto
the
mot
her
Key
fam
ilym
embe
rsal
so
incl
uded
By
La
Lec
he
Lea
gue
of
Mex
ico
Exc
lusi
ve
brea
stfe
edin
g
at3
mon
ths
post
-par
tum
67
(6vi
sits
)
50
(3vi
sits
)12
(com
pari
son)
Firs
tcl
uste
rra
ndom
ized
com
mun
ity-
base
dtr
ialt
hat
used
peer
coun
sello
rsto
prom
ote
excl
usiv
e
brea
stfe
edin
g
Hai
der
etal
2000
200
2
Dha
ka
Low
mid
dle
and
low
-soc
io-
econ
omic
popu
lati
on
Clu
ster
rand
omiz
edtr
ial
20zo
nes
inin
terv
enti
on
and
20in
cont
rol
Com
mun
ity-
base
dpe
er
coun
selli
ngin
Dha
ka
15ho
me-
base
dco
unse
lling
visi
tsby
peer
coun
sello
rs
40h
(4h
yen10
days
)
WH
OU
NIC
EF
brea
stfe
edin
g
coun
selli
ngco
urse
(WH
OU
NIC
EF
1993
)
Exc
lusi
ve
brea
stfe
edin
g
at5
mon
ths
70
in
inte
rven
tion
and
6in
the
cont
rol
Com
mun
ity-
base
d
brea
stfe
edin
gpr
omot
ion
stra
tegy
was
effe
ctiv
ein
Ban
glad
esh
whe
rem
ost
deliv
erie
soc
cur
atho
me
N Bhandari and AKMI Kabir20
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Bry
ceet
al
(200
4)W
HO
(200
3b)
Bra
zil
Per
u
Tanz
ania
Uga
nda
Mul
tico
untr
yev
alua
tion
of
IMC
Ith
atin
clud
ed
effe
ctiv
enes
sco
stan
d
impa
ct(B
ryce
etal
2004
)
Bre
astf
eedi
ngpr
omot
ion
asa
part
ofIM
CI
IMC
Iis
ast
rate
gyfo
r
impr
ovin
gch
ildhe
alth
and
deve
lopm
ent
thro
ugh
the
com
bine
d
deliv
ery
ofes
sent
ial
child
heal
th
inte
rven
tion
sIM
CI
bega
nw
ith
ase
tof
case
man
agem
ent
guid
elin
es
for
the
man
agem
ent
ofsi
ckch
ildre
nat
first
-lev
elhe
alth
faci
litie
s
and
the
guid
elin
esw
ere
desi
gned
for
adap
tati
on
atco
untr
yle
vela
nd
belo
wO
ver
tim
eth
e
stra
tegy
expa
nded
to
incl
ude
ara
nge
of
guid
elin
esfo
rde
liver
ing
child
surv
ival
inte
rven
tion
at
hous
ehol
dco
mm
unit
y
and
refe
rral
leve
ls
IMC
Im
odul
e(W
HO
UN
ICE
F20
02)
Res
ults
onex
clus
ive
brea
stfe
edin
g
avai
labl
efr
om
Tanz
ania
whe
reno
sign
ifica
ntim
pact
was
seen
Des
pite
subs
tant
ial
impr
ovem
ent
inth
equ
alit
y
ofca
rede
liver
edby
IMC
Iat
heal
thfa
cilit
ies
key
fam
ily
prac
tice
ssu
chas
excl
usiv
e
brea
stfe
edin
gdi
dno
tch
ange
asco
mm
unit
yIM
CI
had
not
been
impl
emen
ted
byth
at
tim
e(W
HO
2003
b)
SA
rife
en
pers
onal
com
mun
icat
ion
Ban
glad
esh
Mat
lab
Com
mun
ity-
base
dcl
uste
r
desi
gn
Eva
luat
ion
offa
cilit
y-an
d
com
mun
ity-
base
dIM
CI
Inte
rven
tion
pack
age
incl
udes
feed
ing
asse
ssm
ent
and
coun
selli
ngon
mot
hers
ofyo
ung
child
ren
seek
ing
care
atfa
cilit
ies
for
illne
ssan
d
hom
e-ba
sed
coun
selli
ng
onim
prov
edfe
edin
gby
com
mun
ity-
base
dhe
alth
and
nutr
itio
nw
orke
rs
At
base
line
inth
e
year
2000
alit
tle
mor
eth
anha
lfth
e
0ndash5-
mon
th-o
ld
infa
nts
inth
est
udy
area
wer
ebe
ing
excl
usiv
ely
brea
stfe
dB
y20
05
this
incr
ease
dby
30
inth
eIM
CI
area
Dat
ano
t
avai
labl
efr
omth
e
com
pari
son
area
as
yet
Lac
kof
com
para
ble
data
from
the
com
pari
son
area
prev
ents
ade
finit
ive
conc
lusi
onas
tow
heth
erth
is
trul
yis
anim
pact
ofIM
CI
BA
SIC
SII
Bas
icSu
ppor
tfo
rIn
stit
utio
naliz
ing
Chi
ldSu
rviv
alP
roje
ctB
FH
IB
aby-
Frie
ndly
Hos
pita
lIni
tiat
ive
ICD
SIn
tegr
ated
Chi
ldD
evel
opm
ent
Serv
ices
IM
CI
Inte
grat
edM
anag
emen
tof
Chi
ldho
odIl
lnes
sM
AD
LA
CM
onit
oreo
deA
poyo
Dir
ecto
con
laL
acat
anci
aM
ater
naN
GO
non
-gov
ernm
enta
lorg
aniz
atio
nPA
HO
Pan
Am
eric
anH
ealt
hO
rgan
izat
ion
PR
OB
ITP
rom
otio
nof
Bre
astf
eedi
ngIn
terv
enti
onTr
ial
PR
OC
OSI
Pro
gram
ade
Coo
rdin
acio
nen
Salu
dIn
tegr
al(C
olla
bora
tive
Pro
gram
for
Inte
grat
edH
ealt
h)U
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
WH
OW
orld
Hea
lth
Org
aniz
atio
n
Mainstreaming nutrition into MCH programs 21
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x2
Cas
est
udie
sin
scal
e-up
effo
rts
inH
IVA
IDS
Stud
yde
scri
ptio
nPo
pula
tion
Inte
rven
tion
Com
mun
icat
ion
stra
tegy
Impa
cton
excl
usiv
ebr
east
feed
ing
Com
men
ts
LIN
KA
GE
S(2
005)
Zam
bia
Pro
gram
me
thro
ugh
heal
th-c
are
and
com
mun
ity
serv
ices
Rea
ched
60si
tes
in6
dist
rict
sby
2005
Inte
grat
ion
ofin
fant
feed
ing
coun
selli
ngm
ater
naln
utri
tion
and
anti
retr
ovir
aldr
ugs
prop
hyla
xis
Trai
ning
ofhe
alth
wor
kers
and
com
mun
ity
serv
ice
prov
ider
sto
coun
selw
omen
onsa
fety
opti
ons
for
thei
rsi
tuat
ion
Beh
avio
urch
ange
Com
mun
icat
ion
inte
rven
tion
sin
the
first
few
year
sM
ater
iald
evel
oped
lsquoAct
Now
rsquoM
edia
cam
paig
nsin
clud
edbr
ochu
res
post
ers
radi
oan
dte
levi
sion
Ass
esse
dth
roug
hba
selin
ean
dfo
llow
-up
hous
ehol
dan
dcl
inic
surv
eys
inse
lect
eddi
stri
cts
Exc
lusi
vebr
east
feed
ing
rate
incr
ease
dfr
om50
in
2002
to64
in
2004
inL
ivin
gsto
nean
dfr
om57
in
2000
to74
in
2004
inN
dola
Inte
grat
edde
mon
stra
tion
proj
ect
Had
seve
rals
tren
gths
inte
rms
ofth
eus
eof
form
ativ
ere
sear
chto
deve
lop
mes
sage
str
aini
ngan
dbu
ildin
gup
skill
sof
prog
ram
me
man
ager
she
alth
-car
epr
ovid
ers
and
com
mun
ity
wor
kers
adv
ocac
yfo
rna
tion
alpo
licy
stro
ngbe
havi
our
chan
geco
mm
unic
atio
nco
mpo
nent
st
reng
then
ing
com
mun
ity
capa
city
for
coun
selli
ngan
dre
ferr
als
and
mon
itor
ing
and
eval
uati
onw
ith
loca
lpar
tner
sP
iwoz
etal
(20
05)
ZV
ITA
MB
Otr
ial
Har
are
Zim
babw
eE
duca
tion
and
coun
selli
ngpr
ogra
mm
ede
liver
edan
tena
tally
1411
0m
othe
rndashba
bypa
irs
enro
lled
from
14m
ater
nity
clin
ics
wit
hin
96h
ofde
liver
yan
dfo
llow
edup
at6
wee
ks
3m
onth
san
d3-
mon
thly
inte
rval
sIn
fant
-fee
ding
patt
erns
dete
rmin
edE
xclu
sive
brea
stfe
edin
gre
com
men
ded
for
HIV
nega
tive
un
know
nor
HIV
posi
tive
who
chos
eto
brea
stfe
ed
Gro
uped
ucat
ion
indi
vidu
alco
unse
lling
vid
eos
broc
hure
sM
othe
rsw
hoen
rolle
dw
hen
prog
ram
me
was
fully
impl
emen
ted
wer
e8
4ti
mes
mor
elik
ely
toex
clus
ivel
ybr
east
feed
than
mot
hers
who
enro
lled
befo
reth
epr
ogra
mm
ebe
gan
Ove
rall
excl
usiv
ebr
east
feed
ing
rate
sti
ll3
mon
ths
was
low
at24
6
Form
ativ
ere
sear
chus
edto
desi
gna
cult
ural
lyse
nsit
ive
educ
atio
nan
dco
unse
lling
prog
ram
me
Low
over
alle
xclu
sive
brea
stfe
edin
gra
tes
prom
pted
auth
ors
toco
nclu
deth
atw
omen
and
thei
rpa
rtne
rssh
ould
have
been
reac
hed
mor
efr
eque
ntly
duri
ngan
tena
tala
ndpo
st-n
atal
peri
od
N Bhandari and AKMI Kabir22
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Thi
oret
al(
2006
)R
ollin
s(2
007)
C
ohen
(200
7)
HIV
-inf
ecte
dpr
egna
ntw
omen
atte
ndin
gan
tena
talc
linic
sin
sout
hB
otsw
ana
Inve
stig
atio
nsby
CD
Cof
adi
arrh
oea
outb
reak
inJa
nuar
y-Fe
brua
ry20
06in
the
sam
epo
pula
tion
Mat
erna
land
infa
ntan
tire
trov
iral
ther
apy
toas
cert
ain
impa
cton
HIV
tran
smis
sion
Ant
enat
alco
unse
lling
Cas
endashco
ntro
lstu
dyto
iden
tify
risk
fact
ors
for
diar
rhoe
ano
tbr
east
feed
ing
was
the
bigg
est
risk
fact
ora
djus
ted
odds
rati
o50
(95
confi
denc
ein
terv
al4
5ndash10
0)
Bot
swan
aha
sth
ebe
stpr
imar
yhe
alth
-car
est
ruct
ure
wat
ersu
pply
and
sani
tati
onsy
stem
sin
Sout
hA
fric
aFo
rmul
apr
ovid
edfr
eeby
the
gove
rnm
ent
toin
fect
edm
othe
rsL
ower
mor
talit
yin
the
brea
stfe
edin
ggr
oup
at7
mon
ths
dem
onst
rate
sri
skof
form
ula
feed
ing
and
need
for
alte
rnat
est
rate
gies
(Thi
oret
al
2006
)A
utho
rsco
nclu
deth
athe
alth
syst
ems
inw
hich
thes
epr
ogra
mm
esar
eim
plem
ente
dsh
ould
beab
leto
cope
wit
hdi
arrh
oea
and
mal
nutr
itio
nth
atre
sult
sbe
caus
eof
form
ula
feed
ing
(Rol
lins
2007
)C
oova
dia
etal
(2
007)
Kw
aZul
uNat
al
Sout
hA
fric
a27
22H
IV-i
nfec
ted
and
unin
fect
edpr
egna
ntw
omen
enro
lled
into
ano
n-ra
ndom
ized
inte
rven
tion
coho
rtst
udy
from
ante
nata
lcl
inic
sIn
fant
feed
ing
data
obta
ined
wee
kly
bloo
dsa
mpl
esfr
omin
fant
sta
ken
mon
thly
83
of13
72in
fant
sbo
rnto
HIV
-inf
ecte
dm
othe
rsin
itia
ted
excl
usiv
ebr
east
feed
ing
from
birt
hB
reas
tfed
infa
nts
who
rece
ived
solid
sw
ere
sign
ifica
ntly
mor
elik
ely
toac
quir
ein
fect
ion
com
pare
dw
ith
excl
usiv
ely
brea
stfe
d(H
R10
87
151
ndash78
P=
001
8)as
wer
ein
fant
sw
hoat
12w
eeks
rece
ived
brea
stan
dfo
rmul
am
ilk(1
82
098
ndash33
6P
=0
57)
Cum
ulat
ive
3-m
onth
mor
talit
yin
excl
usiv
ely
brea
stfe
dw
as6
1(4
74ndash
792
)vs
15
1(7
63ndash
287
3)in
infa
nts
give
nre
plac
emen
tfe
eds
(HR
206
1
0ndash4
27P
=0
05)
The
stud
ysh
ows
that
excl
usiv
ebr
east
feed
ing
can
besu
cces
sful
lysu
ppor
ted
inH
IV-i
nfec
ted
wom
enT
heau
thor
sca
llfo
rfu
rthe
rre
visi
onof
UN
ICE
FW
HO
and
USA
IDin
fant
feed
ing
guid
elin
es
CD
CC
ente
rof
Dis
ease
Con
trol
HR
haz
ards
rati
oU
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
USA
IDU
SA
genc
yfo
rIn
tern
atio
nalD
evel
opm
ent
WH
OW
orld
Hea
lth
Org
aniz
atio
nZ
VIT
AM
BO
Z
imba
bwe
Vit
amin
Afo
rM
othe
rsan
dB
abie
s
Mainstreaming nutrition into MCH programs 23
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23

Prior to scale-up a policy framework for implemen-tation needs to be developed This framework shouldinclude a vision consensus on technical issues onprogramme strategy roles relationships and respon-sibilities of implementing partners measurable goalswithin defined time lines and predictable adequatefunding to achieve these (The Core Group 2005) Itshould address the capacity of all implementing part-ners and the approach to fulfilling capacity gaps at alllevels particularly at the community level The policyframework should emphasize breastfeeding promo-tion through community-based programmes Politicalcommitment and ownership by relevant governmentdepartments at national state and district levels havealso been identified to be critical for effective scale-up(The Core Group 2005)
Technical and management support andother partnerships
Creating a policy framework designing a potentiallyeffective programme and an implementation strategyrequire multiple capacities which may not always beavailable within government departments or otherconcerned agencies
Technical and managerial support may need to bemobilized more so during the planning and earlyimplementation phase If this support is not availableinvolvement of external talent ndash national or eveninternational ndash may be required Once the pro-gramme is implemented the external support couldbe phased out gradually as local capacity is built
Forging partnerships between government minis-tries donors local non-governmental organizations(NGOs) and universities was a feature of many suc-cessful programmes (Appendix 1 Van Roekel et al
2002 Bhandari et al 2005 Quinn et al 2005) In theLINKAGES projects (Appendix 1) partnershipwith Programa de Coordinacion en Salud Integral(Collaborative Program for Integrated HealthPROCOSI) and NGOs in Bolivia UNICEF NGOsand the national government in Ghana and Intersec-toral Action Group for Nutrition and Jereo SalamaIsika in Madagascar added value and quality to pro-grammes resulted in effective pooling of resources
and expertise and improved programme design andmanagement (LINKAGES 2002 Van Roekel et al
2002 Quinn et al 2005)
Programme design and strategy
This requires a systematic description of steps andprocesses that help achieve high coverage qualityequity and sustainability capacity building and pro-gramme management are particularly important fea-tures (The Core Group 2005) Experience so farsuggests that for majority of developing countriesscale-up for exclusive breastfeeding will not be pos-sible unless intervention delivery at the communitylevel receives emphasis (Appendix 1) As an increas-ing number of mothers deliver in institutions mixedmodels will be required even in developing countries
An initial step is to carefully examine the existingopportunities as vehicles for promoting exclusivebreastfeeding If use of existing opportunities is insuf-ficient to achieve high coverage with good qualitythen additional approaches would need to be evolvedin a phased manner In Bangladesh the strategy ofpeer counsellors was used as the majority of deliveriesoccur at home and a community health worker is notroutinely available in that setting (Haider et al 2000)In India on the other hand village health workersalready exist so programmes are often designedaround them (Bhandari et al 2003 2004 2005)
Hospitalinstitution-based strategies
Efforts to scale up the BFHI in countries have shownmixed results (Table 2)
In regions where hospital deliveries are the normscale-up efforts through the BFHI (WHOUNICEF1992 Table 3 Perez-Escamilla 2007) have been suc-cessful and the strategy helped increase rates ofexclusive breastfeeding (Appendix 1) However inmany countries after initial years of enthusiasm thescale-up effort seems to have plateaued perhapsreflecting changing emphasis of donors and govern-ment The initial high rates of exclusive breastfeedingmay not be sustained after mothers are dischargedfrom facilities and return to their homes (Coutinhoet al 2005) The challenge therefore is to continue at
N Bhandari and AKMI Kabir8
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
home the post-delivery support available in institu-tions through public and private providers to sustainexclusive breastfeeding or develop other mechanismsthat support recently delivered mothers to exclusivelybreastfeed once they are discharged from hospitals(de Oliveira et al 2006) Countries have addressedthis in different ways In Australia a cadre of breast-feeding counsellors exists (Australian BreastfeedingAssociation 2005) In pilot programmes in Indiaexclusive breastfeeding was promoted through healthworker home visits at immunization clinics growthmonitoring sessions and at sick-child contacts(Bhandari et al 2005) in addition to the BFHI Homevisits are particularly important in regions where cov-
erage through other channels is low or not feasibleand a cadre of community workers exists
Community-based strategies
Pilot efforts in countries or regions where home deliv-eries predominate have shown success through ver-tical as well as integrated approaches however pro-grammes integrated into ongoing activities are morelikely to be more sustainable (The Core Group 2005)In these programmes (Appendix 1) the messageswere delivered through either a single existing or newchannel or multiple delivery channels already inplace within the primary health-care systemThe deci-sion to use one or multiple channels was made basedon the ability to cover the target population In somecountries high coverage was feasible only with mul-tiple facility and community channels (Appendix 1)Multiple channels also help achieve consistency inadvice The credibility and acceptability of a givenchannel by the community was another factor in theirbeing used Routine activities of channels were modi-fied in some instances to incorporate exclusive breast-feeding counselling In India for instance it wasbelieved that immunization sessions could not beused as a counselling opportunity but better organi-zation and the presence of another available localworker during the session enabled the vaccinator tocounsel mothers (Bhandari et al 2005)Another illus-tration is the adaptation of the Integrated Manage-ment of Childhood Illness (IMCI) programme of theWHOUNICEF (2002) to the Integrated Manage-ment of Neonatal and Childhood Illness (IMNCIGovernment of India 2006) by India The IMNCIincludes three home visits for all births in the first 7days of life by an existing community worker theAnganwadi worker (ICDS 1982) to promote essentialnewborn care which includes exclusive breastfeedingIn other countries such as Bangladesh facility-basedIMCI was sought to be improved in its impact bygreater emphasis on community component of IMCIthat is C-IMCI (Gwatkin 2004)
Programme delivery
Recognizing that facility-based interventions areinsufficient countries have experimented with a
Table 2 Proportion of facilities with Baby-Friendly Hospital Initiative(WABA 2007)
Region Median (range)
West and Central Africa 013 (000ndash059)EasternSouthern Africa 023 (000ndash100)Middle East and North Africa 014 (000ndash100)South Asia 007 (001ndash100)East Asia and Pacific 0005 (000ndash087)Americas and the Caribbean 010 (000ndash100)Central and Eastern EuropeCommonwealth
of Independent States025 (004ndash093)
All Industrialized Countries 007 (000ndash097)
Table 3 The 10 steps to successful breastfeeding for hospitals andbirth centres
bull Maintain a written breastfeeding policy that is routinelycommunicated to all health-care staffbull Train all health-care staff in skills necessary to implement thispolicybull Inform all pregnant women about the benefits and managementof breastfeedingbull Help mothers initiate breastfeeding within 1 h of birthbull Show mothers how to breastfeed and how to maintain lactationeven if they are separated from their infantsbull Give infants no food or drink other than breastmilk unlessmedically indicatedbull Practise lsquorooming inrsquo ndash allow mothers and infants to remaintogether 24 hours a daybull Encourage unrestricted breastfeedingbull Give no pacifiers or artificial nipples to breastfeeding infantsbull Foster the establishment of breastfeeding support groups andrefer mothers to them on discharge from the hospital or clinic
Mainstreaming nutrition into MCH programs 9
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
variety of local workers such as peer counsellors inBangladesh (Haider et al 2000) lady health workersin Pakistan (Government of Pakistan 2003) and thelsquoAccredited Social Health Activistsrsquo (ASHA) workerin India (Government of India 2005) to promoteexclusive breastfeeding by itself or as a part of essen-tial newborn care Programmes that used peer coun-sellors as a single channel have been shown to beeffective in several efficacy (Green 1999 Lewin et al
2006) and effectiveness trials (Morrow et al 1999Haider et al 2000 Lewin et al 2006) However whilepeer or lay counsellors have been effective in theshort run long-term sustainability of this approach ona large scale is as yet not established
The possible reasons stated for the short-termsuccess of the lay health workers approach includepayment to the counsellors for performing a specificpiece of work the counsellorsrsquo own perception ofbenefits of their work and their recognition by thecommunity as being skilled These workers also feltthis opportunity to have the potential for opening upof further education and training (Haider et al 2002)An important issue would also be linking newworkers with the existing primary health system aspilot experience showed that these workers may notbe able to resolve complex breastfeeding problems(Haider et al 2002)
Recruitment of ASHA in India provides a uniqueopportunity to promote exclusive breastfeeding(Government of India 2005) Currently being re-cruited all over the country these workers will focuson essential newborn care including exclusive breast-feeding through home visitation in the first month oflife and community-based activities
While these efforts in different countries at improv-ing coverage of the target population through localworkers are of value the voluntary or semi-voluntarynature of the workers and ill-defined models of super-vision raise issues about sustainability and possiblyhigh attrition rates
Programmes that used multiple channels reportedbroader coverage (Bhandari et al 2005 Quinn et al
2005) In India formative research showed thatimmunization sessions and private providers werethe channels to which infants were most commonly(~80) exposed Following constitution of a
breastfeeding-promotion programme caregiversmost often received exclusive breastfeeding counsel-ling at immunization sessions (~40) weighing ses-sions (~25) and home visits (25ndash30) Governmentphysicians or private providers rarely (~2) coun-selled despite being trained (Bhandari et al 2005)When all the opportunities were considered together55ndash60 of caregivers had been counselled at leastonce by at least one of the channels in the last 3months indicating that multiple channels reachedmore families (Bhandari et al 2005)The frequency ofcontact with caregivers or the intensity of counsellinginfluences the cumulative benefit of the counsellingfor example six contacts with mothers resulted inhigher adoption rates for exclusive breastfeeding ascompared with three (Morrow et al 1999) In Indiathe number of channels at which caregivers werecounselled was positively associated with the rates ofexclusive breastfeeding at 3 months of age (Bhandariet al 2003) However the costs of training and theeffort will increase more than the number of channelsused and therefore this issue requires a balancedview
Another issue of interest is the value of counsellingfor the antenatal period itself Antenatal counsellinghas been used in several programmes but its effect isdifficult to delineate by itself as it was usually fol-lowed by post-natal counselling (Green 1999) In theHIV context however the importance of antenatalcounselling is obvious
Communications approach
An effective communications approach was a featureof most programmes and involvement of journalistsradio announcements and other mass media from theprogramme outset extended the reach of nutritionmessages even further (Appendix 1 Quinn et al
2005) Mass media were not used in some pro-grammes where a comparison group was present forrisk of contamination (Bhandari et al 2005) Utiliza-tion of existing or newly formed community groupsproduced the same effect (Bhandari et al 2005Quinn et al 2005) and community mobilization pro-grammes such as street plays rallies radio pro-grammes and songs helped disseminate messages
N Bhandari and AKMI Kabir10
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
and increase community involvement (Bhandari et al
2005 Quinn et al 2005)Effective counselling requires assessment of
feeding practices recognition of problems and nego-tiation with the mother in choosing improved prac-tices that are feasible (WHOUNICEF 2002) thisrequires time and patience Programmes may chooseone-on-one counselling during opportunities in whichmore time is available such as home visits and groupcounselling for opportunities with lesser availabletime (Bhandari et al 2005) One of the reasons thatpeer counsellors may have been effective was thattheir sole responsibility was counselling mothersthrough home visits (Morrow et al 1999 Haider et al
2000) The more diverse the functions of the localworker the lesser will be the emphasis on a singlecomponent such as exclusive breastfeeding
Message development
The development of messages for interpersonal com-munication and for mass media needs careful atten-tion to design and content Successful programmesincluded an element of formative research to gain anin-depth understanding of the communities wherethese programmes were implemented with regard topractices pertaining to breastfeeding the reasons forthe current practices the common breastfeedingproblems and the barriers to adoption of ideal behav-iours in that cultural setting Formative research innorth India for instance showed general unwilling-ness to offer water to infants in summer months Thisbarrier was overcome by building specific explanatorymessages using local terms within the communicationstrategy (Bhandari et al 2003)
Once the design features and broad strategy are inplace attention must then shift to the operationaliza-tion of the strategy
Training and supervision
Prior to scale-up the training needs will need to bedefined Fortunately for promotion of exclusivebreastfeeding extensive experience is available ontraining of different cadres of health workers andeven for lay counsellors Most experiences used the
adapted versions of the UNICEFWHO Breastfeed-ing Counseling Course (WHOUNICEF 1993) or theIMCI module (WHOUNICEF 2002)
Training strategy and its quality merit attentionIn successful programmes the duration of trainingextended from 3 full days to 10 part days for differentworkers The training strategies as described werelsquoconcise action orientedrsquo and included modules thataimed to equip trainers with practical skills and con-fidence to counsel effectively (Appendix 1)
Training modules for areas with high HIV preva-lence also exist (WHO 2006)
While the training modules used in studies workedwell a gap remains for referralTrained workers at thecommunity level require that referral options avail-able are easily accessible prompt and preferablyavailable free of cost to mothers with complex breast-feeding problems
Another important issue to address is handlingtraining of new staff in most developing countriesstaff turnover and absenteeism rates are high
Monitoring and evaluation
The programme strategy will need to include systemsfor monitoring and evaluation of the programmePossible markers could include the rates of exclusivebreastfeeding worker performance referral andaction As for all other national programmes therewill be a need for periodic reviews and achievabletargets by time
Costs and resources
In all pilot programmes and projects services wereprovided to mothers free of cost In many developingcountries if the government cadre of health workers isused to promote exclusive breastfeeding as a part oftheir other responsibilities (eg the IMNCI) the basicservices will remain free However a system thatrequires setting up a cadre of trained lactation coun-sellors (eg in an urban setting or as referral sources forbreastfeeding problems in rural areas) will requireadditional resources A cost-effective analysis of theBFHI was conducted in three countriesBrazilMexicoand Honduras (Horton et al 1996) Savings on health
Mainstreaming nutrition into MCH programs 11
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
care resulting from reduction in diarrhoeal and respi-ratory morbidity were estimated as a result of theeffect of BFHI on breastfeeding The study showedthat breastfeeding promotion through a BFHI-likemodel is very cost-effective (1992 US$ 2ndash19 per dis-ability adjusted life years Horton et al 1996 Perez-Escamilla 2007) Examples of cost-effectivenessanalysis of community-based programmes using lay orprofessional support in different settings could not beidentified
Testing of novel approaches andcontinuing innovation
Scaled-up programmes must have inbuilt provision totest novel approaches and the ability for continuinginnovation
Scaling up of exclusive breastfeeding in thecontext of HIV
The policy and programme design and implemen-tation issues relevant to exclusive breastfeedingscale-up discussed above are relevant to HIV-prevalent areas but there are other unique featuresthat merit consideration
Creating policies for exclusive breastfeeding pro-motion in countries with high HIV prevalence is par-ticularly challenging The revised recommendationsencourage exclusive breastfeeding for the first 6months and continued breastfeeding for 2 years andbeyond for infants whose mothers are HIV negativeor whose HIV status is unknown For women who areknown to be HIV positive the most appropriateinfant feeding option for HIV-exposed infantsdepends on individual circumstances including con-sideration of health services counselling and supportExclusive breastfeeding is the better option for suchinfants unless replacement feeding is acceptable fea-sible affordable sustainable and safe for both themother and baby This recommendation is based onthe finding that exclusive breastfeeding for up to 6months in three large cohort studies is associated witha three- to fourfold decreased risk of transmission ofHIV compared with non-exclusive breastfeeding(WHO 2006) The recommendations may need
further revision if new findings demonstrate thatexclusive breastfeeding should be the feeding ofchoice for HIV-infected women (Iliff et al 2005)
Some pilot programmes for exclusive breastfeedingpromotion in high-HIV-prevalence countries aresummarized in Appendix 2
In general exclusive breastfeeding promotionformed a part of the prevention of mother-to-childtransmission programmes LINKAGESZambiaintegrated improved counselling on infant feedingmaternal nutrition and antiretroviral therapy duringprophylaxis in both health-care and community ser-vices to enable women to make and act on informedchoice to feed their infants optimally in the context ofhigh HIV prevalence
Formative research was critical to develop locallyappropriate and feasible infant feeding recommenda-tions for individual infants and their families based onHIV status In Zambia the research included focusedgroup discussions key information interviews obser-vations of household food preparation and feedingmarket survey of replacement foods and breastmilksubstitutes and household trials of improved feedingand caring practices (LINKAGES 2005)
High quality of health workers is another criticalfactor for sensitive and accurate individual counsel-ling Programmes incorporated behaviour changecommunication methodologies in training (LINK-AGES 2005) It is important to develop skills of com-munity members as well for improved servicesreferral outreach and follow-up care and support ofHIV-positive mothers and their infants
A comprehensive communications strategy tosupport scale-up was a notable feature of the LINK-AGES programme in Zambia In 2004 an intensiveeffort was launched using brochures posters radioand television spots billboards and reference guidesfor health providers (LINKAGES 2005) Messageswere targeted to relevant stakeholders ndash pregnantand lactating mothers health providers youth andcommunity leaders and all the materials were nation-ally disseminated
Monitoring and evaluation another importantfeature of effective scale-up was a feature of pilotprogrammes (Appendix 2 Ntabaye amp Lusiola 2004Rutenberg et al 2004) in Zambia and Tanzania Moni-
N Bhandari and AKMI Kabir12
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
toring and evaluation not only provides a measure ofsuccess but identifies factors that may have contrib-uted to it and to lack of success to enable mid-coursecorrections The impact of some pilot programmes onexclusive breastfeeding is summarized in Appendix 2In most programmes exclusive breastfeeding ratesimproved In Zambia exclusive breastfeeding ratesincreased from 50 in 2002 to 64 in 2004 in Liv-ingstone from 57 in 2000 to 74 in 2004 in NdolaIn South Africa an antenatal clinic-based interven-tion led to 83 of infants born to HIV-infectedmother initiating exclusive breastfeeding InZimbabwe an intervention based on antenatal coun-selling resulted in a relatively lower exclusive breast-feeding rate of 246 at 3 months (Piwoz et al 2005)
Several barriers to success were identified Theseinclude inadequate skills of workers and non-integration of HIV counselling and tailoring into ante-natal care services (Ntabaye amp Lusiola 2004) which isthe backbone in which infant feeding counselling isbuiltWomen reported that mothers not breastfeedingtheir children were discriminated against by the com-munity and they faced the threat of domestic violenceProgramme managerrsquos understanding of barriersto effective programme implementation and impactwere emphasized as being important Governmentsupport partnerrsquos coordination increased humanresource and improving the supply system were iden-tified to be essential features to scale up programmesin the HIV context (Rutenberg et al 2004) Lowoverall exclusive breastfeeding rates prompted Piwozet al (2005) to conclude that women and their partnersshould have been reached more frequently during theantenatal and post-natal period
Conclusions
In a large number of programmes for improvingexclusive breastfeeding in developing countriesincluding in areas with high prevalence of HIV apositive impact on exclusive breastfeeding rates hasbeen achieved
Some of the factors that contributed to successfulscale-up are summarized in Table 4 Several limita-tions of the programmes reviewed merit attentionMost programmes involved special and generous
funding concentrated efforts and multiple contactsThese programmes were evaluated over relativelyshort periods of time usually 2ndash5 years and the long-term sustainability has not been really tested In theabsence of specific measures there is likely to be dilu-tion of quality as the programmes are scaled upfurther from their initial size The experience thus farleaves important questions to be addressed particu-larly on how programmes can be sustained over timeas they are scaled up at affordable costs
A key factor relevant to sustainability is to plan ona long-term basis a period of 10ndash20 years rather than5ndash10 years from the outset Experience with otherchild health programmes has shown that performancein immunization and oral rehydration therapy userates plateaued over time in many countries
Programme scale-up requires a programme man-agement capacity proportionate to the scale of opera-tions periodic assessment of barriers (Table 5) and anability to revise programme strategy to overcomethese Another key feature to sustainability ofscale-up is the extent to which capacity has been builtat the district block and community levels National-or state-level driven interventions begin with enor-mous enthusiasm which is difficult to sustain Thisfactor is particularly important as most developing
Table 4 Lessons learnt about scale-up key factors in success
bull Political will advocacy enabling policiesbull Championship by health ministries at national state and districtlevelbull Technical consensus on feeding guidelinesbull Programme strategy and measurable short- and long-term goalsbull Long-term financial commitmentbull Partners with defined roles assessment of their capacity todeliver and plans to cover gaps in capacitybull Emphasis on community-level interventions and not onlyfacility-based programmesbull Formative research as the backbone of effective scale-upprogrammes particularly in the context of HIVbull Careful selection of channels and the number required toachieve timely coverage consistency of messagesbull Communication strategy aided by formative research pre-testedvalidated messages and toolsbull Quality trainers and training centres proportionate to requiredscalebull Monitoring and evaluationbull Programme redesign when relevant through research analysisand innovation
Mainstreaming nutrition into MCH programs 13
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
countries are going through a process of decentrali-zation with increasing responsibility for planningimplementation and evaluation being delegated tolower levels of the health-care system Buildingcapacity at that level requires time resources andpatience and a longer-term perspective
Building capacity emerges to be a key factorTrainers and training centres vary in their qualitywhen training health workers and their supervisorsor programme managers As the burden of trainingincreases availability of good-quality trainersbecomes a limiting factor (WHOUNICEF 2002Government of India 2006) An effective strategymust plan for these incremental requirements includ-ing ensuring secure and sustained funding
Identifying barriers to success is a key actor Thebarriers to scaling up of health interventions havebeen elegantly described by Ranson et al (Table 5)Most of these are important for exclusive breastfeed-ing scale-up as well
Overall within the limitations discussed above anumber of programmes in countries with varying
HIV prevalence show that exclusive breastfeeding ona large scale is feasible and pilot programmes havegiven valuable guidance related to policies planningand implementation of large-scale programmes Thechallenge now is to build on these experiences whenplanning national programmes
Acknowledgements
We sincerely thank Dr MK Bhan for his constructivecriticism and sustained feedback at different stages ofdevelopment of this review
Conflicts of interest
The authors have declared no conflicts of interest
References
Arifeen S Black RE Antelman G Baqui A CaulfieldL amp Becker S (2001) Exclusive breastfeeding reducesacute respiratory infection and diarrhea deaths amonginfants in Dhaka slums Pediatrics 108 E67
Australian Breastfeeding Association (2005) Valuing Par-enthood Options for Paid Maternity Leave ndash InterimPaper 2002 Available at httpwwwbreastfeedingasnauadvocacymatleavehtml
Bhandari N Bahl R Mazumdar S Martines J BlackRE amp Bhan MK (2003) Effect of community basedpromotion of exclusive breastfeeding on diarrheal ill-nesses and growth a cluster randomized controlled trialLancet 361 1418ndash1423
Bhandari N Mazumder S Bahl R Martines J BlackRE amp Bhan MK (2004) An educational interventionto promote appropriate complementary feedingimproves child feeding practices and linear growth inrural Haryana India Journal of Nutrition 134 2342ndash2348
Bhandari N Mazumder S Bahl R Martines J BlackRE amp Bhan MK (2005) Use of multiple opportunitiesfor improving feeding practices in undertwos withinchild health programs Health Policy Plan 20 328ndash336
Bryce J Victora CG Habicht JP Vaughan JP ampBlack RE (2004) The multi-country evaluation of theintegrated management of childhood illness strategylessons for the evaluation of public health interventionsAmerican Journal of Public Health 94 406ndash415
Butte NF Lopez-Alarcon MG amp Garza C (2002) Nutri-ent Adequacy of Exclusive Breastfeeding for the TermInfant during the First Six Months of Life World HealthOrganization Geneva
Table 5 Barriers to scaling up of health interventions
Community and household levelsLack of information womenrsquos education physical financial
womenrsquos decision-making powerHealth services delivery levelShortage of qualified staff weak technical guidance programme
management and supervision inadequate supplies equipmentand infrastructure poor accessibility
Health sector policy and strategic management levelWeak and centralized system for planning and management weak
drug policies and supply system inadequate regulations lack ofintersectoral action and partnership weak incentives to useinputs efficiently and respond to user needs and preferencesreliance on donor funding
Public policies cutting across sectorsGovernment bureaucracy poor communication and transport
infrastructureEnvironmental characteristicsGovernance and overall policy frameworkCorruption weak government weak laws political instability and
insecurity low priority to social sectors weak structure for publicaccountability and opportunities for public opinions lack of freepress
Physical environmentClimatic and geographic predisposition physical environment
unfavourable to service delivery
Adapted from Ranson et al (2003)
N Bhandari and AKMI Kabir14
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Cohen J (2007) Retrovirus meeting Hope on new AIDSdrugs but breast-feeding strategy backfires Science 3151357
Coovadia HM Rollins NC Bland RM Little KCoutsoudis A Bennish ML et al (2007) Mother tochild transmission of HIV-1 infection during exclusivebreastfeeding in the first 6 months of life an interven-tion cohort study Lancet 369 1107ndash1116
Coutinho SB de Lira PI de Carvalho LM amp AshworthA (2005) Comparison of the effect of two systems forthe promotion of exclusive breastfeeding Lancet 3661094ndash1100
Feachem RG amp Koblinsky MA (1984) Interventions forthe control of diarrheal diseases among young childrenpromotion of breastfeeding Bulletin of the of the WorldHealth Organization 62 271ndash291
Gonzales A Arteaga E amp Howard-Grabman L (1998)Scaling Up the WARMI Project ndash Lessons LearnedMobilizing Bolivian Communities around ReproductiveHealth Save the Children Federation Inc Bolivia FieldOffice La Paz Available at httpwwwcoregrouporgresourcesSavebolipdf
Government of India (1997) Recommendations of the FifthCentral Pay Commission Relating to Enhancement ofQuantum of Maternity Leave and to Allow PaternityLeave in Respect of Central Government EmployeesDocument ref 13018197-Estt(L) Available at httppersminnicinesttleave2htm
Government of India (2005) National Rural HealthMission 2005ndash2012 Mission document Ministry ofHealth and Family Welfare New Delhi Government ofIndia Available at httpwwwmohfwnicinNRHM20Mission20Documentpdf
Government of India (2006) Operational Guidelines forImplementation of Integrated Management of Neonataland Childhood Illness (IMNCI) Ministry of HealthFamily Welfare New Delhi Available at httpmohfwnicindofw20websiteF20IMNCI20Operational20Plan201320june202006htm
Government of Pakistan (2003) National Programme forFamily Planning and Primary Health Care The LadyHealth Workers Programme 2003ndash2008 Ministry ofHealth Pakistan Available at httpwwwphcgovpkDownloadsPC-120augpdf
Green CP (1999) Improving Breastfeeding Behaviors Evi-dence from Two Decades of Intervention ResearchPublished for the US Agency for International Develop-ment (USAID) by the LINKAGES Project Academyfor Educational Development Washington DC
Gupta A (2002) National trends in breastfeeding andeffective strategies to improve breastfeeding ratesJournal of Neonatology 2002 4ndash14
Gwatkin DR (2004) Integrating the management of child-hood illness Lancet 364 1557ndash1558
Habicht JP DaVanzo J amp Butz WP (1986) Does breast-feeding really save lives or are apparent benefits due tobiases American Journal of Epidemiology 123279ndash290
Haider R Ashworth A Kabir I amp Huttly SR (2000)Effect of community based peer counsellors on exclusivebreastfeeding practices in Dhaka Bangladesh a ran-domized controlled trial Lancet 356 1643ndash1647
Haider R Kabir I Huttly SR amp Ashworth A (2002)Training peer counsellors to promote and support exclu-sive breastfeeding in Bangladesh Journal of HumanLactation 18 7ndash12
Horton S Sanghvi T Phillips M Fiedler J Perez-Escamilla R Lutter C et al (1996) Breastfeeding pro-motion and priority setting in health Health Policy andPlanning 11 156ndash168
ILO (1998) More than 120 Nations Provide Paid MaternityLeave Gap in Employment Treatment for Men andWomen Still Exists International Labour Office GenevaDocument ref ILO987 Available at httpwwwiloorgpublicenglishbureauinfpr19987htmr2
Iliff PJ Piwoz EG Tavengwa NV Zunguza CDMarinda ET Nathoo KJ et al (2005) Early exclusivebreastfeeding reduces the risk of postnatal HIV-1 trans-mission and increase HIV-free survival AIDS 19 699ndash708
Integrated Child Development Services Scheme (Revised)(ICDS) (1982) Ministry of Social Welfare Governmentof India New Delhi Available on URL httpwcdnicinudishahtmabouticdshtm
Jason JM Nieburg P amp Marks JS (1984) Mortality andinfectious disease associated with infant feeding prac-tices in developing countries Pediatrics 74 702ndash727
Jones G Steketee RW Black RE Bhutta ZA ampMorris SS Bellagio Child Survival Study Group (2003)How many child deaths can we prevent this yearLancet 362 65ndash71
Knippenberg R Lawn JE Darmstadt GL Begkayian GFogstad H Walelign N et al (2005) Systematic scalingup of neonatal care in countries Lancet 365 1087ndash1098
Kramer MS amp Kakuma R (2002) The optimal durationof exclusive breastfeeding a systematic reviewCochrane Database of Systematic Reviews 2002CD003517
Kramer MS Chalmers B Hodnett ED Sevkovskaya ZDzikovich I Shapiro S et al (2000) Promotion ofbreastfeeding intervention trial (PROBIT) a cluster ran-domized trial in the Republic of Belarus Design followup and data validation Advances in Experimental Medi-cine and Biology 478 327ndash345
Kramer MS Chalmers B Hodnett ED Sevkovskaya ZDzikovich I Shapiro S et al (2001) Promotion ofbreastfeeding intervention trial (PROBIT) a random-
Mainstreaming nutrition into MCH programs 15
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
ized trial in the Republic of Belarus Journal of theAmerican Medical Association 285 413ndash420
Lewin SA Dick J Pond P Zwarenstein M Aja Gvan Wyk B et al (2006) Lay health workers in primaryand community health care (Review) The CochraneLibrary 3 1ndash104
LINKAGES (2002) World LINKAGES MadagascarAcademy for Educational Development WashingtonDC
LINKAGES (2005) LINKAGES Zambia 1997ndash2005 FinalReport A Full Report on LINKAGES Infant Feedingand HIVAIDS Programs in Zambia Academy for Edu-cational Development Washington DC Available athttpwwwlinkagesprojectorgmediapublicationsFinal20draft20Zambia20final20report2012105pdf
Lutter CK Perez-Escamilla R Segall A Sanghvi TTeruya K amp Wickham C (1997) The effectiveness of ahospital based program to promote exclusive breastfeed-ing among low income women in Brazil AmericanJournal of Public Health 87 659ndash663
Morrow AL Guerrero ML Shults J Calva J Lutter CBravo J et al (1999) Efficacy of home based peer coun-selling to promote exclusive breastfeeding a randomizedcontrolled trial Lancet 353 1226ndash1231
Ntabaye MK amp Lusiola GJ (2004) Understanding barri-ers to PMTCT in Tanzania findings of a baseline surveyInternational Conference on AIDS 15 (B11396)
de Oliveira LD Giugliani ER do Espirito SLC FrancaMC Weigert EM Kohler CV et al (2006) Effect ofintervention to improve breastfeeding technique on thefrequency of exclusive breastfeeding and lactation-related problems Journal of Human Lactation 22 315ndash321
Perez-Escamilla R (2004) Effectiveness of MADLAC atImproving Breastfeeding Promotion and CounsellingIndicators in Maternity Wards in El Salvador Publishedfor the Basic Support for Institutionalizing Child Sur-vival Project (BASICS II) for the United States Agencyfor International Development Arlington VA Availableat httpwwwbasicsorgpdfFinal20MADLAC20Report20RPE20April207-2004pdf
Perez-Escamilla R (2007) Evidence based breast-feedingpromotion the Baby-Friendly Hospital InitiativeJournal of Nutrition 137 484ndash487
Piwoz EG Iliff PJ Tavengwa N Gavin L Marinda ELunney K et al (2005) An education and counselllingprogram for preventing breastfeeding associated HIVtransmission in Zimbabwe design and impact on mater-nal knowledge and behaviour Journal of Nutrition 135950ndash955
Quinn VJ Guyon AB Schubert JW Stone-Jimenez MHainsworth MD amp Martin LH (2005) Improvingbreastfeeding practices on a board scale at the commu-
nity level success stories from Africa and LatinAmerica Journal of Human Lactation 21 345ndash354
Ranson MK Hanson K Oliveira-Cruz V amp Mills A(2003) Constraints to expanding access to health inter-ventions an empirical analysis and country typologyJournal of International Development 15 15ndash40
Rea MF amp Berquo ES (1990) Impact of the Braziliannational breastfeeding programme on mothers inGreater Sao Paulo Bulletin of the of the World HealthOrganization 68 365ndash371
Rollins NC (2007) Infant feeding and HIV BritishMedical Journal 334 487ndash488
Rutenberg N Baek C Kalibala S Rosen J amp Mulenga D(2004) Evaluation of United Nations supported pilotprojects for the prevention of mother-to-child transmis-sion of HIV overview of findings International Confer-ence on AIDS 15 (WePeE6688)
The Core Group (2005) Scale and Scaling Up A COREGroup Background Paper on lsquoScaling-Uprsquo MaternalNewborn and Child Health Services CORE SpringMembership Meeting 2005 The Core Group Washing-ton DC Available at httpwwwcoregrouporgresourcesmeetingsapril05Scaling_Up_Background_Paper_7-13pdf
The Norwegian Government (1993) Women in PoliticsMinistry of Children and Equality Available at httpwwwregjeringennoendepbldRyddemappeSLA-AvdelingdoclegislationguidelinesWomen-in-Politicshtmlid=437166
Thior I Lockman S Smeaton LM Shapiro RL WesterC Heymann SJ et al (2006) Breastfeeding plus infantzidovudine prophylaxis for 6 months vs formula feedingplus infant zidovudine for 1 month to reduce mother-to-child HIV transmission in Botswana a randomized trialthe Mashi Study Journal of the American Medical Asso-ciation 296 794ndash805
UNICEF (2002) Facts for Life lsquoKey Message What EveryFamily and Community Has a Right to Know aboutBreastfeedingrsquo Available at httpwwwuniceforgffl04key_messageshtm
Van Roekel K Plowman B Griffiths M de AlvaradoVV Matute J amp Calderon M (2002) BASICS IIMidterm Evaluation of the AIN Program in Honduras2000 Basic Support for Institutionalizing Child SurvivalProject (BASICS II) for the United States Agency forInternational Development Arlington VA
WABA (2007) UNICEF Records BHFI Record UpdateAvailable at httpwwwwabaorgmydocsBFHIjan07xls 2006 Regularly updated by Miriam HLabbok Center for Infant and Young ChildFeeding and Care Department of Maternaland Child Health School of Public Health The Univer-sity of North Carolina at Chapel Hill Chapel Hill NCUSA
N Bhandari and AKMI Kabir16
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
WHA (2002) Infant and Young Child Nutrition Fifty-FifthWorld Health Assembly Agenda Item 1310 18 May2002 Available at httpwwwintgbebwhapdf_filesWHA55ewha5525pdf
WHO (1981) The International Code of Marketing ofBreastmilk Substitutes World Health OrganizationGeneva
WHO (1989) Protecting Promoting and Supporting Breast-feeding The Special Role of Maternity Services A JointWHOUNICEF Statement World Health OrganizationGeneva
WHO (2002) The Optimal Duration of Exclusive Breast-feeding Report of an Expert Consultation WHONHD0109 WHOFCHCAH0124 World HealthOrganization Geneva
WHO (2003a) Community Based Strategies for Breastfeed-ing Promotion and Support in Developing CountriesWorld Health Organization Geneva Document refISBN_92_4_159121_8 Available at httpwwwwhointchild-adolescent-healthNew_PublicationsNUTRITIONISBN_92_4_159121_8pdf
WHO (2003b) Multi-country Evaluation of IMCI Effective-ness Cost and Impact (MCE) Progress Report May2002ndashApril 2003 Document ref WHOFCHCAH035World Health Organization Geneva
WHO (2004) Promoting Proper Feeding for Infants andYoung Children World Health Organization GenevaAvailable at httpwwwwhointnutritiontopicsinfantfeedingen
WHO (2006) WHO HIV and Infant Feeding TechnicalConsultation-Consensus Statement World Health Orga-nization Geneva Available at httpwwwwhointhivmediacentreInfantfeedingconsensusstatementpfpdf
WHO Collaborative Study Team on the Role of Breast-feeding on the Prevention of Infant Mortality (2000)Effect of breastfeeding on infant and child mortality dueto infectious diseases in les developed countries apooled analysis Lancet 355 451ndash455
WHOUNICEF (1992) The global criteria for the WHOUNICEF Baby-Friendly Hospital Initiative In Baby-Friendly Hospital Initiative Part II Hospital LevelImplementation World Health Organization Geneva
WHOUNICEF (1993) Breastfeeding Counselling A Train-ing Course WHOCDR933 UNICEFNUT931 WorldHealth Organization Geneva
WHOUNICEF (2002) Protocol for Adapting the FeedingRecommendations Part III IMCI Adaptation GuideWorld Health Organization Geneva
WHOUNICEF (2003) Global Strategy for Infant andYoung Child Feeding World Health OrganizationGeneva Available at httpwwwwhointchild-adolescent-healthpublicationsNUTRITIONIYCF_GShtm
de Zoysa I Rea M amp Martines J (1991) Why promotebreastfeeding in diarrheal diseases control programmesHealth Policy and Planning 6 371ndash379
Mainstreaming nutrition into MCH programs 17
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
Cas
est
udie
so
fef
fect
iven
ess
stud
ies
or
pilo
tpr
ogra
mm
es
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Lut
ter
etal
(199
7)
Bra
zil
Low
-inc
ome
urba
nw
omen
deliv
erin
gin
hosp
ital
s
Bre
astf
eedi
ngpr
omot
ion
in
hosp
ital
sco
mpa
red
wit
h
nobr
east
feed
ing
prom
otio
n
Pro
mot
ion
ofbr
east
feed
ing
in
sele
cted
hosp
ital
s
Mea
nda
ysof
excl
usiv
e
brea
stfe
edin
g
75da
ysvs
22
days
(Plt
001
)
Rea
ampB
erqu
o
(199
0)
Wom
enw
ith
ach
ild
aged
lt2ye
ars
inSa
oP
aulo
Nat
iona
lbre
astf
eedi
ng
cam
paig
n19
81ndash1
986
BF
HI
Mas
sm
edia
cam
paig
n11
in
fant
s5ndash
6m
onth
s
excl
usiv
ely
brea
stfe
d
in19
88an
d37
in
1987
Con
foun
ding
fact
ors
over
the
6-ye
arpe
riod
not
mea
sure
d
Kra
mer
etal
(200
020
01)
PR
OB
ITtr
ial
Bel
arus
Clu
ster
rand
omiz
ed
34ho
spit
als
and
thei
rpo
lycl
inic
s
Trai
ning
inB
FH
I(W
HO
UN
ICE
F19
92)
vsr
outi
ne
prac
tice
san
dpo
licie
s
Exc
lusi
vebr
east
feed
ing
at3
(43
3vs
64
)
and
6(7
9
vs0
6
)
mon
ths
sign
ifica
ntly
high
er
Impl
emen
ted
thro
ugh
BF
HI
ina
sett
ing
whe
reho
spit
al
deliv
erie
sar
eco
mm
on
Per
ez-E
scam
illa
(200
4)
BA
SIC
SII
Mex
ico
Hon
dura
s
Bra
zil
MA
DL
AC
low
-cos
t
man
agem
ent
info
rmat
ion
syst
emto
use
an
evid
ence
-bas
edap
proa
chto
impr
ove
serv
ice
perf
orm
ance
Inte
rvie
win
gof
wom
enat
hosp
ital
disc
harg
epo
st
deliv
ery
usin
ga
ques
tion
nair
eth
atta
kes
5ndash7
min
toad
min
iste
ran
d
cont
ains
19br
east
feed
ing
prom
otio
nco
unse
lling
indi
cato
rs
Dat
aen
tere
dan
dre
sult
s
disc
usse
d3-
mon
thly
by
hosp
ital
com
mit
tee
Hos
pita
lim
plem
ents
chan
ges
in
brea
stfe
edin
g
supp
ort
base
don
anal
ysis
of
ques
tion
nair
es
Itis
aco
st-e
ffec
tive
inte
rven
tion
that
can
help
impr
ovem
ents
inth
eB
FH
I
and
isa
valu
able
tool
for
proc
ess
eval
uati
on
N Bhandari and AKMI Kabir18
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
LIN
KA
GE
S
proj
ect
inA
fric
aan
d
Lat
inA
mer
ica
(Qui
nnet
al
2005
LIN
KA
GE
S
2002
WH
O20
03a)
Bol
ivia
(1
mill
ion)
Gha
na(3
5
mill
ion)
Mad
agas
car
(6m
illio
n)
Res
ourc
e-
poor
sett
ing
Pilo
tpr
ogra
mm
e
InB
oliv
iaan
d
Gha
napr
ogra
mm
e
focu
sed
on
brea
stfe
edin
gan
d
com
plem
enta
ry
feed
ing
InM
adag
asca
r
prog
ram
me
prom
oted
brea
stfe
edin
g
wit
hin
7es
sent
ial
nutr
itio
nac
tion
san
d
subs
eque
ntly
thro
ugh
IMC
I
Bui
lton
form
ativ
ere
sear
ch
and
sust
aine
dth
roug
h
prog
ram
me
acti
viti
esth
at
focu
sed
onbr
ingi
ngab
out
the
desi
red
beha
viou
r
chan
geM
ixof
inte
rven
tion
s
reac
hed
wom
enin
divi
dual
ly
orin
grou
psin
heal
th
faci
litie
sho
mes
or
com
mun
ity
sett
ings
Con
sist
ent
mes
sage
san
d
mat
eria
lacr
oss
all
prog
ram
me
chan
nels
Bol
ivi
PR
OC
OSI
NG
Os
Gha
na
UN
ICE
F
nati
onal
nutr
itio
n
offic
eN
GO
s
Mad
agas
car
Inte
rsec
tora
l
Act
ion
Gro
upfo
r
Nut
riti
on
Jere
o
Sala
ma
Isik
a
Pro
gram
desi
gned
wit
h
part
ners
Rad
ioin
all
thre
esi
tes
Mat
eria
ls
deve
lope
d
tosu
itne
eds
oflo
cal
heal
th
wor
kers
and
com
mun
ity
mem
bers
Gre
at
emph
asis
on
deve
lopm
ent
of coun
selli
ng
and
nego
tiat
ion
skill
s
prac
tica
l
sess
ions
Sign
ifica
ntin
crea
ses
inex
clus
ive
brea
stfe
edin
gra
tes
of
0ndash6-
mon
th-o
ld
infa
nts
from
54
to65
in
Bol
ivia
68
to79
in
Gha
naan
d46
to68
in
Mad
agas
car
In
Gha
naan
d
Mad
agas
car
sign
ifica
ntre
sult
s
obse
rved
wit
hin
aye
ar
ofin
itia
tion
of
com
mun
ity
inte
rven
tion
s
App
roac
hw
asef
fect
ive
and
achi
eved
sign
ifica
nt
incr
ease
sam
ong
larg
e
popu
lati
ons
asea
rly
as
9ndash12
mo
afte
rin
itia
tion
of
com
mun
ity
acti
viti
es
Van
Roe
kele
tal
(200
2)W
HO
(200
3a)
Hon
dura
sG
row
thm
onit
orin
gan
d
prom
otio
nkn
own
as
Ate
ncioacute
nIn
tegr
ala
la
Nintilde
ez(A
IN)
or
Inte
grat
edC
hild
Car
e
Init
ially
pri
mar
ilya
grow
th
mon
itor
ing
prog
ram
me
ulti
mat
ely
thro
ugh
IMC
I
Pro
gram
me
ongr
owth
prom
otio
nndash
asse
ssm
ent
of
mon
thly
wei
ght
gain
and
focu
son
illne
ssf
eedi
ng
prac
tice
san
dge
nera
lchi
ld
care
inin
fant
sun
der
2ye
ars
Impl
emen
ted
atgo
vern
men
t
faci
litie
san
dco
mm
unit
y
Star
ted
in19
92s
tren
gthe
ned
in19
95ndash1
997
wit
hgr
eate
r
focu
son
child
feed
ing
In
1997
pro
gram
me
intr
oduc
ed
wit
hIM
CI
(WH
OU
NIC
EF
2002
)
Maj
or
part
ners
UN
ICE
F
PAH
O
Am
eric
an
and
Hon
dura
n
Red
Cro
ss
CA
RE
Rad
io
broa
dcas
ts
relig
ious
lead
ers
IMC
IM
id-t
erm
eval
uati
on
show
ed39
of
mot
hers
inin
terv
enti
on
com
mun
itie
sex
clus
ivel
y
brea
stfe
dco
mpa
red
wit
h13
in
the
cont
rol
site
s
Mainstreaming nutrition into MCH programs 19
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
cont
inue
d
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Bha
ndar
ieta
l
(200
3)
WH
O
(200
3a)
Rur
alco
mm
unit
ies
inH
arya
na
Indi
a
Clu
ster
rand
omiz
edtr
ial
8
com
mun
itie
s(t
otal
popu
lati
on~4
000
0)
Pro
mot
ion
ofex
clus
ive
brea
stfe
edin
gan
d
appr
opri
ate
com
plem
enta
ryfe
edin
g
Dev
elop
edth
roug
h
form
ativ
ere
sear
ch
ndashP
robl
emid
enti
ficat
ion
ndashP
arti
cipa
tory
desi
gnof
inte
rven
tion
impl
emen
tati
onan
d
eval
uati
on
Impl
emen
tati
onw
ithi
nan
exis
ting
prim
ary
heal
th-c
are
prog
ram
me
Opp
ortu
niti
esus
edto
deliv
erm
essa
ges
wer
e
imm
uniz
atio
ncl
inic
s
wei
ghin
gse
ssio
ns
sick
-chi
ldco
ntac
tsan
d
mon
thly
hom
evi
sits
Res
earc
hers
wit
hlo
cal
gove
rnm
ent
ICD
Ssy
stem
and
NG
O
The
atre
son
gs
Mas
sm
edia
not
used
for
risk
of
cont
amin
atio
n
Mat
eria
ls
deve
lope
d
for
heal
th
wor
kers
pos
ters
flip
book
sca
rds
Bre
astf
eedi
ng
coun
selli
ngse
ctio
n
ofth
eIM
CI
(WH
O
UN
ICE
F20
02)
Exc
lusi
ve
brea
stfe
edin
gin
the
prev
ious
24h
at3
mon
ths
of
age
79
vs4
8
The
posi
tive
effe
ct
rem
aine
dup
to
6m
onth
sof
age
(42
vs4
)
Tota
lpar
tici
pati
onof
the
dist
rict
heal
thsy
stem
from
ince
ptio
nof
the
prog
ram
me
inde
velo
ping
impl
emen
tati
onst
rate
gyt
ool
deve
lopm
ent
and
mon
itor
ing
inad
diti
onto
invo
lvem
ent
of
anN
GO
wer
eim
port
ant
feat
ures
that
cont
ribu
ted
to
the
succ
ess
ofth
e
inte
rven
tion
Mor
row
etal
(199
9)
Mex
ico
Cit
yC
lust
erra
ndom
ized
tria
l
Tota
lpop
ulat
ion
3000
0
Two
com
mun
itie
sin
the
inte
rven
tion
one
com
pari
son
130
wom
en
Hom
e-ba
sed
peer
coun
selli
ng
Pee
rco
unse
llors
mad
e3
or
6ho
me
visi
tsto
the
mot
her
Key
fam
ilym
embe
rsal
so
incl
uded
By
La
Lec
he
Lea
gue
of
Mex
ico
Exc
lusi
ve
brea
stfe
edin
g
at3
mon
ths
post
-par
tum
67
(6vi
sits
)
50
(3vi
sits
)12
(com
pari
son)
Firs
tcl
uste
rra
ndom
ized
com
mun
ity-
base
dtr
ialt
hat
used
peer
coun
sello
rsto
prom
ote
excl
usiv
e
brea
stfe
edin
g
Hai
der
etal
2000
200
2
Dha
ka
Low
mid
dle
and
low
-soc
io-
econ
omic
popu
lati
on
Clu
ster
rand
omiz
edtr
ial
20zo
nes
inin
terv
enti
on
and
20in
cont
rol
Com
mun
ity-
base
dpe
er
coun
selli
ngin
Dha
ka
15ho
me-
base
dco
unse
lling
visi
tsby
peer
coun
sello
rs
40h
(4h
yen10
days
)
WH
OU
NIC
EF
brea
stfe
edin
g
coun
selli
ngco
urse
(WH
OU
NIC
EF
1993
)
Exc
lusi
ve
brea
stfe
edin
g
at5
mon
ths
70
in
inte
rven
tion
and
6in
the
cont
rol
Com
mun
ity-
base
d
brea
stfe
edin
gpr
omot
ion
stra
tegy
was
effe
ctiv
ein
Ban
glad
esh
whe
rem
ost
deliv
erie
soc
cur
atho
me
N Bhandari and AKMI Kabir20
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Bry
ceet
al
(200
4)W
HO
(200
3b)
Bra
zil
Per
u
Tanz
ania
Uga
nda
Mul
tico
untr
yev
alua
tion
of
IMC
Ith
atin
clud
ed
effe
ctiv
enes
sco
stan
d
impa
ct(B
ryce
etal
2004
)
Bre
astf
eedi
ngpr
omot
ion
asa
part
ofIM
CI
IMC
Iis
ast
rate
gyfo
r
impr
ovin
gch
ildhe
alth
and
deve
lopm
ent
thro
ugh
the
com
bine
d
deliv
ery
ofes
sent
ial
child
heal
th
inte
rven
tion
sIM
CI
bega
nw
ith
ase
tof
case
man
agem
ent
guid
elin
es
for
the
man
agem
ent
ofsi
ckch
ildre
nat
first
-lev
elhe
alth
faci
litie
s
and
the
guid
elin
esw
ere
desi
gned
for
adap
tati
on
atco
untr
yle
vela
nd
belo
wO
ver
tim
eth
e
stra
tegy
expa
nded
to
incl
ude
ara
nge
of
guid
elin
esfo
rde
liver
ing
child
surv
ival
inte
rven
tion
at
hous
ehol
dco
mm
unit
y
and
refe
rral
leve
ls
IMC
Im
odul
e(W
HO
UN
ICE
F20
02)
Res
ults
onex
clus
ive
brea
stfe
edin
g
avai
labl
efr
om
Tanz
ania
whe
reno
sign
ifica
ntim
pact
was
seen
Des
pite
subs
tant
ial
impr
ovem
ent
inth
equ
alit
y
ofca
rede
liver
edby
IMC
Iat
heal
thfa
cilit
ies
key
fam
ily
prac
tice
ssu
chas
excl
usiv
e
brea
stfe
edin
gdi
dno
tch
ange
asco
mm
unit
yIM
CI
had
not
been
impl
emen
ted
byth
at
tim
e(W
HO
2003
b)
SA
rife
en
pers
onal
com
mun
icat
ion
Ban
glad
esh
Mat
lab
Com
mun
ity-
base
dcl
uste
r
desi
gn
Eva
luat
ion
offa
cilit
y-an
d
com
mun
ity-
base
dIM
CI
Inte
rven
tion
pack
age
incl
udes
feed
ing
asse
ssm
ent
and
coun
selli
ngon
mot
hers
ofyo
ung
child
ren
seek
ing
care
atfa
cilit
ies
for
illne
ssan
d
hom
e-ba
sed
coun
selli
ng
onim
prov
edfe
edin
gby
com
mun
ity-
base
dhe
alth
and
nutr
itio
nw
orke
rs
At
base
line
inth
e
year
2000
alit
tle
mor
eth
anha
lfth
e
0ndash5-
mon
th-o
ld
infa
nts
inth
est
udy
area
wer
ebe
ing
excl
usiv
ely
brea
stfe
dB
y20
05
this
incr
ease
dby
30
inth
eIM
CI
area
Dat
ano
t
avai
labl
efr
omth
e
com
pari
son
area
as
yet
Lac
kof
com
para
ble
data
from
the
com
pari
son
area
prev
ents
ade
finit
ive
conc
lusi
onas
tow
heth
erth
is
trul
yis
anim
pact
ofIM
CI
BA
SIC
SII
Bas
icSu
ppor
tfo
rIn
stit
utio
naliz
ing
Chi
ldSu
rviv
alP
roje
ctB
FH
IB
aby-
Frie
ndly
Hos
pita
lIni
tiat
ive
ICD
SIn
tegr
ated
Chi
ldD
evel
opm
ent
Serv
ices
IM
CI
Inte
grat
edM
anag
emen
tof
Chi
ldho
odIl
lnes
sM
AD
LA
CM
onit
oreo
deA
poyo
Dir
ecto
con
laL
acat
anci
aM
ater
naN
GO
non
-gov
ernm
enta
lorg
aniz
atio
nPA
HO
Pan
Am
eric
anH
ealt
hO
rgan
izat
ion
PR
OB
ITP
rom
otio
nof
Bre
astf
eedi
ngIn
terv
enti
onTr
ial
PR
OC
OSI
Pro
gram
ade
Coo
rdin
acio
nen
Salu
dIn
tegr
al(C
olla
bora
tive
Pro
gram
for
Inte
grat
edH
ealt
h)U
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
WH
OW
orld
Hea
lth
Org
aniz
atio
n
Mainstreaming nutrition into MCH programs 21
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x2
Cas
est
udie
sin
scal
e-up
effo
rts
inH
IVA
IDS
Stud
yde
scri
ptio
nPo
pula
tion
Inte
rven
tion
Com
mun
icat
ion
stra
tegy
Impa
cton
excl
usiv
ebr
east
feed
ing
Com
men
ts
LIN
KA
GE
S(2
005)
Zam
bia
Pro
gram
me
thro
ugh
heal
th-c
are
and
com
mun
ity
serv
ices
Rea
ched
60si
tes
in6
dist
rict
sby
2005
Inte
grat
ion
ofin
fant
feed
ing
coun
selli
ngm
ater
naln
utri
tion
and
anti
retr
ovir
aldr
ugs
prop
hyla
xis
Trai
ning
ofhe
alth
wor
kers
and
com
mun
ity
serv
ice
prov
ider
sto
coun
selw
omen
onsa
fety
opti
ons
for
thei
rsi
tuat
ion
Beh
avio
urch
ange
Com
mun
icat
ion
inte
rven
tion
sin
the
first
few
year
sM
ater
iald
evel
oped
lsquoAct
Now
rsquoM
edia
cam
paig
nsin
clud
edbr
ochu
res
post
ers
radi
oan
dte
levi
sion
Ass
esse
dth
roug
hba
selin
ean
dfo
llow
-up
hous
ehol
dan
dcl
inic
surv
eys
inse
lect
eddi
stri
cts
Exc
lusi
vebr
east
feed
ing
rate
incr
ease
dfr
om50
in
2002
to64
in
2004
inL
ivin
gsto
nean
dfr
om57
in
2000
to74
in
2004
inN
dola
Inte
grat
edde
mon
stra
tion
proj
ect
Had
seve
rals
tren
gths
inte
rms
ofth
eus
eof
form
ativ
ere
sear
chto
deve
lop
mes
sage
str
aini
ngan
dbu
ildin
gup
skill
sof
prog
ram
me
man
ager
she
alth
-car
epr
ovid
ers
and
com
mun
ity
wor
kers
adv
ocac
yfo
rna
tion
alpo
licy
stro
ngbe
havi
our
chan
geco
mm
unic
atio
nco
mpo
nent
st
reng
then
ing
com
mun
ity
capa
city
for
coun
selli
ngan
dre
ferr
als
and
mon
itor
ing
and
eval
uati
onw
ith
loca
lpar
tner
sP
iwoz
etal
(20
05)
ZV
ITA
MB
Otr
ial
Har
are
Zim
babw
eE
duca
tion
and
coun
selli
ngpr
ogra
mm
ede
liver
edan
tena
tally
1411
0m
othe
rndashba
bypa
irs
enro
lled
from
14m
ater
nity
clin
ics
wit
hin
96h
ofde
liver
yan
dfo
llow
edup
at6
wee
ks
3m
onth
san
d3-
mon
thly
inte
rval
sIn
fant
-fee
ding
patt
erns
dete
rmin
edE
xclu
sive
brea
stfe
edin
gre
com
men
ded
for
HIV
nega
tive
un
know
nor
HIV
posi
tive
who
chos
eto
brea
stfe
ed
Gro
uped
ucat
ion
indi
vidu
alco
unse
lling
vid
eos
broc
hure
sM
othe
rsw
hoen
rolle
dw
hen
prog
ram
me
was
fully
impl
emen
ted
wer
e8
4ti
mes
mor
elik
ely
toex
clus
ivel
ybr
east
feed
than
mot
hers
who
enro
lled
befo
reth
epr
ogra
mm
ebe
gan
Ove
rall
excl
usiv
ebr
east
feed
ing
rate
sti
ll3
mon
ths
was
low
at24
6
Form
ativ
ere
sear
chus
edto
desi
gna
cult
ural
lyse
nsit
ive
educ
atio
nan
dco
unse
lling
prog
ram
me
Low
over
alle
xclu
sive
brea
stfe
edin
gra
tes
prom
pted
auth
ors
toco
nclu
deth
atw
omen
and
thei
rpa
rtne
rssh
ould
have
been
reac
hed
mor
efr
eque
ntly
duri
ngan
tena
tala
ndpo
st-n
atal
peri
od
N Bhandari and AKMI Kabir22
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Thi
oret
al(
2006
)R
ollin
s(2
007)
C
ohen
(200
7)
HIV
-inf
ecte
dpr
egna
ntw
omen
atte
ndin
gan
tena
talc
linic
sin
sout
hB
otsw
ana
Inve
stig
atio
nsby
CD
Cof
adi
arrh
oea
outb
reak
inJa
nuar
y-Fe
brua
ry20
06in
the
sam
epo
pula
tion
Mat
erna
land
infa
ntan
tire
trov
iral
ther
apy
toas
cert
ain
impa
cton
HIV
tran
smis
sion
Ant
enat
alco
unse
lling
Cas
endashco
ntro
lstu
dyto
iden
tify
risk
fact
ors
for
diar
rhoe
ano
tbr
east
feed
ing
was
the
bigg
est
risk
fact
ora
djus
ted
odds
rati
o50
(95
confi
denc
ein
terv
al4
5ndash10
0)
Bot
swan
aha
sth
ebe
stpr
imar
yhe
alth
-car
est
ruct
ure
wat
ersu
pply
and
sani
tati
onsy
stem
sin
Sout
hA
fric
aFo
rmul
apr
ovid
edfr
eeby
the
gove
rnm
ent
toin
fect
edm
othe
rsL
ower
mor
talit
yin
the
brea
stfe
edin
ggr
oup
at7
mon
ths
dem
onst
rate
sri
skof
form
ula
feed
ing
and
need
for
alte
rnat
est
rate
gies
(Thi
oret
al
2006
)A
utho
rsco
nclu
deth
athe
alth
syst
ems
inw
hich
thes
epr
ogra
mm
esar
eim
plem
ente
dsh
ould
beab
leto
cope
wit
hdi
arrh
oea
and
mal
nutr
itio
nth
atre
sult
sbe
caus
eof
form
ula
feed
ing
(Rol
lins
2007
)C
oova
dia
etal
(2
007)
Kw
aZul
uNat
al
Sout
hA
fric
a27
22H
IV-i
nfec
ted
and
unin
fect
edpr
egna
ntw
omen
enro
lled
into
ano
n-ra
ndom
ized
inte
rven
tion
coho
rtst
udy
from
ante
nata
lcl
inic
sIn
fant
feed
ing
data
obta
ined
wee
kly
bloo
dsa
mpl
esfr
omin
fant
sta
ken
mon
thly
83
of13
72in
fant
sbo
rnto
HIV
-inf
ecte
dm
othe
rsin
itia
ted
excl
usiv
ebr
east
feed
ing
from
birt
hB
reas
tfed
infa
nts
who
rece
ived
solid
sw
ere
sign
ifica
ntly
mor
elik
ely
toac
quir
ein
fect
ion
com
pare
dw
ith
excl
usiv
ely
brea
stfe
d(H
R10
87
151
ndash78
P=
001
8)as
wer
ein
fant
sw
hoat
12w
eeks
rece
ived
brea
stan
dfo
rmul
am
ilk(1
82
098
ndash33
6P
=0
57)
Cum
ulat
ive
3-m
onth
mor
talit
yin
excl
usiv
ely
brea
stfe
dw
as6
1(4
74ndash
792
)vs
15
1(7
63ndash
287
3)in
infa
nts
give
nre
plac
emen
tfe
eds
(HR
206
1
0ndash4
27P
=0
05)
The
stud
ysh
ows
that
excl
usiv
ebr
east
feed
ing
can
besu
cces
sful
lysu
ppor
ted
inH
IV-i
nfec
ted
wom
enT
heau
thor
sca
llfo
rfu
rthe
rre
visi
onof
UN
ICE
FW
HO
and
USA
IDin
fant
feed
ing
guid
elin
es
CD
CC
ente
rof
Dis
ease
Con
trol
HR
haz
ards
rati
oU
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
USA
IDU
SA
genc
yfo
rIn
tern
atio
nalD
evel
opm
ent
WH
OW
orld
Hea
lth
Org
aniz
atio
nZ
VIT
AM
BO
Z
imba
bwe
Vit
amin
Afo
rM
othe
rsan
dB
abie
s
Mainstreaming nutrition into MCH programs 23
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23

home the post-delivery support available in institu-tions through public and private providers to sustainexclusive breastfeeding or develop other mechanismsthat support recently delivered mothers to exclusivelybreastfeed once they are discharged from hospitals(de Oliveira et al 2006) Countries have addressedthis in different ways In Australia a cadre of breast-feeding counsellors exists (Australian BreastfeedingAssociation 2005) In pilot programmes in Indiaexclusive breastfeeding was promoted through healthworker home visits at immunization clinics growthmonitoring sessions and at sick-child contacts(Bhandari et al 2005) in addition to the BFHI Homevisits are particularly important in regions where cov-
erage through other channels is low or not feasibleand a cadre of community workers exists
Community-based strategies
Pilot efforts in countries or regions where home deliv-eries predominate have shown success through ver-tical as well as integrated approaches however pro-grammes integrated into ongoing activities are morelikely to be more sustainable (The Core Group 2005)In these programmes (Appendix 1) the messageswere delivered through either a single existing or newchannel or multiple delivery channels already inplace within the primary health-care systemThe deci-sion to use one or multiple channels was made basedon the ability to cover the target population In somecountries high coverage was feasible only with mul-tiple facility and community channels (Appendix 1)Multiple channels also help achieve consistency inadvice The credibility and acceptability of a givenchannel by the community was another factor in theirbeing used Routine activities of channels were modi-fied in some instances to incorporate exclusive breast-feeding counselling In India for instance it wasbelieved that immunization sessions could not beused as a counselling opportunity but better organi-zation and the presence of another available localworker during the session enabled the vaccinator tocounsel mothers (Bhandari et al 2005)Another illus-tration is the adaptation of the Integrated Manage-ment of Childhood Illness (IMCI) programme of theWHOUNICEF (2002) to the Integrated Manage-ment of Neonatal and Childhood Illness (IMNCIGovernment of India 2006) by India The IMNCIincludes three home visits for all births in the first 7days of life by an existing community worker theAnganwadi worker (ICDS 1982) to promote essentialnewborn care which includes exclusive breastfeedingIn other countries such as Bangladesh facility-basedIMCI was sought to be improved in its impact bygreater emphasis on community component of IMCIthat is C-IMCI (Gwatkin 2004)
Programme delivery
Recognizing that facility-based interventions areinsufficient countries have experimented with a
Table 2 Proportion of facilities with Baby-Friendly Hospital Initiative(WABA 2007)
Region Median (range)
West and Central Africa 013 (000ndash059)EasternSouthern Africa 023 (000ndash100)Middle East and North Africa 014 (000ndash100)South Asia 007 (001ndash100)East Asia and Pacific 0005 (000ndash087)Americas and the Caribbean 010 (000ndash100)Central and Eastern EuropeCommonwealth
of Independent States025 (004ndash093)
All Industrialized Countries 007 (000ndash097)
Table 3 The 10 steps to successful breastfeeding for hospitals andbirth centres
bull Maintain a written breastfeeding policy that is routinelycommunicated to all health-care staffbull Train all health-care staff in skills necessary to implement thispolicybull Inform all pregnant women about the benefits and managementof breastfeedingbull Help mothers initiate breastfeeding within 1 h of birthbull Show mothers how to breastfeed and how to maintain lactationeven if they are separated from their infantsbull Give infants no food or drink other than breastmilk unlessmedically indicatedbull Practise lsquorooming inrsquo ndash allow mothers and infants to remaintogether 24 hours a daybull Encourage unrestricted breastfeedingbull Give no pacifiers or artificial nipples to breastfeeding infantsbull Foster the establishment of breastfeeding support groups andrefer mothers to them on discharge from the hospital or clinic
Mainstreaming nutrition into MCH programs 9
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
variety of local workers such as peer counsellors inBangladesh (Haider et al 2000) lady health workersin Pakistan (Government of Pakistan 2003) and thelsquoAccredited Social Health Activistsrsquo (ASHA) workerin India (Government of India 2005) to promoteexclusive breastfeeding by itself or as a part of essen-tial newborn care Programmes that used peer coun-sellors as a single channel have been shown to beeffective in several efficacy (Green 1999 Lewin et al
2006) and effectiveness trials (Morrow et al 1999Haider et al 2000 Lewin et al 2006) However whilepeer or lay counsellors have been effective in theshort run long-term sustainability of this approach ona large scale is as yet not established
The possible reasons stated for the short-termsuccess of the lay health workers approach includepayment to the counsellors for performing a specificpiece of work the counsellorsrsquo own perception ofbenefits of their work and their recognition by thecommunity as being skilled These workers also feltthis opportunity to have the potential for opening upof further education and training (Haider et al 2002)An important issue would also be linking newworkers with the existing primary health system aspilot experience showed that these workers may notbe able to resolve complex breastfeeding problems(Haider et al 2002)
Recruitment of ASHA in India provides a uniqueopportunity to promote exclusive breastfeeding(Government of India 2005) Currently being re-cruited all over the country these workers will focuson essential newborn care including exclusive breast-feeding through home visitation in the first month oflife and community-based activities
While these efforts in different countries at improv-ing coverage of the target population through localworkers are of value the voluntary or semi-voluntarynature of the workers and ill-defined models of super-vision raise issues about sustainability and possiblyhigh attrition rates
Programmes that used multiple channels reportedbroader coverage (Bhandari et al 2005 Quinn et al
2005) In India formative research showed thatimmunization sessions and private providers werethe channels to which infants were most commonly(~80) exposed Following constitution of a
breastfeeding-promotion programme caregiversmost often received exclusive breastfeeding counsel-ling at immunization sessions (~40) weighing ses-sions (~25) and home visits (25ndash30) Governmentphysicians or private providers rarely (~2) coun-selled despite being trained (Bhandari et al 2005)When all the opportunities were considered together55ndash60 of caregivers had been counselled at leastonce by at least one of the channels in the last 3months indicating that multiple channels reachedmore families (Bhandari et al 2005)The frequency ofcontact with caregivers or the intensity of counsellinginfluences the cumulative benefit of the counsellingfor example six contacts with mothers resulted inhigher adoption rates for exclusive breastfeeding ascompared with three (Morrow et al 1999) In Indiathe number of channels at which caregivers werecounselled was positively associated with the rates ofexclusive breastfeeding at 3 months of age (Bhandariet al 2003) However the costs of training and theeffort will increase more than the number of channelsused and therefore this issue requires a balancedview
Another issue of interest is the value of counsellingfor the antenatal period itself Antenatal counsellinghas been used in several programmes but its effect isdifficult to delineate by itself as it was usually fol-lowed by post-natal counselling (Green 1999) In theHIV context however the importance of antenatalcounselling is obvious
Communications approach
An effective communications approach was a featureof most programmes and involvement of journalistsradio announcements and other mass media from theprogramme outset extended the reach of nutritionmessages even further (Appendix 1 Quinn et al
2005) Mass media were not used in some pro-grammes where a comparison group was present forrisk of contamination (Bhandari et al 2005) Utiliza-tion of existing or newly formed community groupsproduced the same effect (Bhandari et al 2005Quinn et al 2005) and community mobilization pro-grammes such as street plays rallies radio pro-grammes and songs helped disseminate messages
N Bhandari and AKMI Kabir10
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
and increase community involvement (Bhandari et al
2005 Quinn et al 2005)Effective counselling requires assessment of
feeding practices recognition of problems and nego-tiation with the mother in choosing improved prac-tices that are feasible (WHOUNICEF 2002) thisrequires time and patience Programmes may chooseone-on-one counselling during opportunities in whichmore time is available such as home visits and groupcounselling for opportunities with lesser availabletime (Bhandari et al 2005) One of the reasons thatpeer counsellors may have been effective was thattheir sole responsibility was counselling mothersthrough home visits (Morrow et al 1999 Haider et al
2000) The more diverse the functions of the localworker the lesser will be the emphasis on a singlecomponent such as exclusive breastfeeding
Message development
The development of messages for interpersonal com-munication and for mass media needs careful atten-tion to design and content Successful programmesincluded an element of formative research to gain anin-depth understanding of the communities wherethese programmes were implemented with regard topractices pertaining to breastfeeding the reasons forthe current practices the common breastfeedingproblems and the barriers to adoption of ideal behav-iours in that cultural setting Formative research innorth India for instance showed general unwilling-ness to offer water to infants in summer months Thisbarrier was overcome by building specific explanatorymessages using local terms within the communicationstrategy (Bhandari et al 2003)
Once the design features and broad strategy are inplace attention must then shift to the operationaliza-tion of the strategy
Training and supervision
Prior to scale-up the training needs will need to bedefined Fortunately for promotion of exclusivebreastfeeding extensive experience is available ontraining of different cadres of health workers andeven for lay counsellors Most experiences used the
adapted versions of the UNICEFWHO Breastfeed-ing Counseling Course (WHOUNICEF 1993) or theIMCI module (WHOUNICEF 2002)
Training strategy and its quality merit attentionIn successful programmes the duration of trainingextended from 3 full days to 10 part days for differentworkers The training strategies as described werelsquoconcise action orientedrsquo and included modules thataimed to equip trainers with practical skills and con-fidence to counsel effectively (Appendix 1)
Training modules for areas with high HIV preva-lence also exist (WHO 2006)
While the training modules used in studies workedwell a gap remains for referralTrained workers at thecommunity level require that referral options avail-able are easily accessible prompt and preferablyavailable free of cost to mothers with complex breast-feeding problems
Another important issue to address is handlingtraining of new staff in most developing countriesstaff turnover and absenteeism rates are high
Monitoring and evaluation
The programme strategy will need to include systemsfor monitoring and evaluation of the programmePossible markers could include the rates of exclusivebreastfeeding worker performance referral andaction As for all other national programmes therewill be a need for periodic reviews and achievabletargets by time
Costs and resources
In all pilot programmes and projects services wereprovided to mothers free of cost In many developingcountries if the government cadre of health workers isused to promote exclusive breastfeeding as a part oftheir other responsibilities (eg the IMNCI) the basicservices will remain free However a system thatrequires setting up a cadre of trained lactation coun-sellors (eg in an urban setting or as referral sources forbreastfeeding problems in rural areas) will requireadditional resources A cost-effective analysis of theBFHI was conducted in three countriesBrazilMexicoand Honduras (Horton et al 1996) Savings on health
Mainstreaming nutrition into MCH programs 11
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
care resulting from reduction in diarrhoeal and respi-ratory morbidity were estimated as a result of theeffect of BFHI on breastfeeding The study showedthat breastfeeding promotion through a BFHI-likemodel is very cost-effective (1992 US$ 2ndash19 per dis-ability adjusted life years Horton et al 1996 Perez-Escamilla 2007) Examples of cost-effectivenessanalysis of community-based programmes using lay orprofessional support in different settings could not beidentified
Testing of novel approaches andcontinuing innovation
Scaled-up programmes must have inbuilt provision totest novel approaches and the ability for continuinginnovation
Scaling up of exclusive breastfeeding in thecontext of HIV
The policy and programme design and implemen-tation issues relevant to exclusive breastfeedingscale-up discussed above are relevant to HIV-prevalent areas but there are other unique featuresthat merit consideration
Creating policies for exclusive breastfeeding pro-motion in countries with high HIV prevalence is par-ticularly challenging The revised recommendationsencourage exclusive breastfeeding for the first 6months and continued breastfeeding for 2 years andbeyond for infants whose mothers are HIV negativeor whose HIV status is unknown For women who areknown to be HIV positive the most appropriateinfant feeding option for HIV-exposed infantsdepends on individual circumstances including con-sideration of health services counselling and supportExclusive breastfeeding is the better option for suchinfants unless replacement feeding is acceptable fea-sible affordable sustainable and safe for both themother and baby This recommendation is based onthe finding that exclusive breastfeeding for up to 6months in three large cohort studies is associated witha three- to fourfold decreased risk of transmission ofHIV compared with non-exclusive breastfeeding(WHO 2006) The recommendations may need
further revision if new findings demonstrate thatexclusive breastfeeding should be the feeding ofchoice for HIV-infected women (Iliff et al 2005)
Some pilot programmes for exclusive breastfeedingpromotion in high-HIV-prevalence countries aresummarized in Appendix 2
In general exclusive breastfeeding promotionformed a part of the prevention of mother-to-childtransmission programmes LINKAGESZambiaintegrated improved counselling on infant feedingmaternal nutrition and antiretroviral therapy duringprophylaxis in both health-care and community ser-vices to enable women to make and act on informedchoice to feed their infants optimally in the context ofhigh HIV prevalence
Formative research was critical to develop locallyappropriate and feasible infant feeding recommenda-tions for individual infants and their families based onHIV status In Zambia the research included focusedgroup discussions key information interviews obser-vations of household food preparation and feedingmarket survey of replacement foods and breastmilksubstitutes and household trials of improved feedingand caring practices (LINKAGES 2005)
High quality of health workers is another criticalfactor for sensitive and accurate individual counsel-ling Programmes incorporated behaviour changecommunication methodologies in training (LINK-AGES 2005) It is important to develop skills of com-munity members as well for improved servicesreferral outreach and follow-up care and support ofHIV-positive mothers and their infants
A comprehensive communications strategy tosupport scale-up was a notable feature of the LINK-AGES programme in Zambia In 2004 an intensiveeffort was launched using brochures posters radioand television spots billboards and reference guidesfor health providers (LINKAGES 2005) Messageswere targeted to relevant stakeholders ndash pregnantand lactating mothers health providers youth andcommunity leaders and all the materials were nation-ally disseminated
Monitoring and evaluation another importantfeature of effective scale-up was a feature of pilotprogrammes (Appendix 2 Ntabaye amp Lusiola 2004Rutenberg et al 2004) in Zambia and Tanzania Moni-
N Bhandari and AKMI Kabir12
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
toring and evaluation not only provides a measure ofsuccess but identifies factors that may have contrib-uted to it and to lack of success to enable mid-coursecorrections The impact of some pilot programmes onexclusive breastfeeding is summarized in Appendix 2In most programmes exclusive breastfeeding ratesimproved In Zambia exclusive breastfeeding ratesincreased from 50 in 2002 to 64 in 2004 in Liv-ingstone from 57 in 2000 to 74 in 2004 in NdolaIn South Africa an antenatal clinic-based interven-tion led to 83 of infants born to HIV-infectedmother initiating exclusive breastfeeding InZimbabwe an intervention based on antenatal coun-selling resulted in a relatively lower exclusive breast-feeding rate of 246 at 3 months (Piwoz et al 2005)
Several barriers to success were identified Theseinclude inadequate skills of workers and non-integration of HIV counselling and tailoring into ante-natal care services (Ntabaye amp Lusiola 2004) which isthe backbone in which infant feeding counselling isbuiltWomen reported that mothers not breastfeedingtheir children were discriminated against by the com-munity and they faced the threat of domestic violenceProgramme managerrsquos understanding of barriersto effective programme implementation and impactwere emphasized as being important Governmentsupport partnerrsquos coordination increased humanresource and improving the supply system were iden-tified to be essential features to scale up programmesin the HIV context (Rutenberg et al 2004) Lowoverall exclusive breastfeeding rates prompted Piwozet al (2005) to conclude that women and their partnersshould have been reached more frequently during theantenatal and post-natal period
Conclusions
In a large number of programmes for improvingexclusive breastfeeding in developing countriesincluding in areas with high prevalence of HIV apositive impact on exclusive breastfeeding rates hasbeen achieved
Some of the factors that contributed to successfulscale-up are summarized in Table 4 Several limita-tions of the programmes reviewed merit attentionMost programmes involved special and generous
funding concentrated efforts and multiple contactsThese programmes were evaluated over relativelyshort periods of time usually 2ndash5 years and the long-term sustainability has not been really tested In theabsence of specific measures there is likely to be dilu-tion of quality as the programmes are scaled upfurther from their initial size The experience thus farleaves important questions to be addressed particu-larly on how programmes can be sustained over timeas they are scaled up at affordable costs
A key factor relevant to sustainability is to plan ona long-term basis a period of 10ndash20 years rather than5ndash10 years from the outset Experience with otherchild health programmes has shown that performancein immunization and oral rehydration therapy userates plateaued over time in many countries
Programme scale-up requires a programme man-agement capacity proportionate to the scale of opera-tions periodic assessment of barriers (Table 5) and anability to revise programme strategy to overcomethese Another key feature to sustainability ofscale-up is the extent to which capacity has been builtat the district block and community levels National-or state-level driven interventions begin with enor-mous enthusiasm which is difficult to sustain Thisfactor is particularly important as most developing
Table 4 Lessons learnt about scale-up key factors in success
bull Political will advocacy enabling policiesbull Championship by health ministries at national state and districtlevelbull Technical consensus on feeding guidelinesbull Programme strategy and measurable short- and long-term goalsbull Long-term financial commitmentbull Partners with defined roles assessment of their capacity todeliver and plans to cover gaps in capacitybull Emphasis on community-level interventions and not onlyfacility-based programmesbull Formative research as the backbone of effective scale-upprogrammes particularly in the context of HIVbull Careful selection of channels and the number required toachieve timely coverage consistency of messagesbull Communication strategy aided by formative research pre-testedvalidated messages and toolsbull Quality trainers and training centres proportionate to requiredscalebull Monitoring and evaluationbull Programme redesign when relevant through research analysisand innovation
Mainstreaming nutrition into MCH programs 13
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
countries are going through a process of decentrali-zation with increasing responsibility for planningimplementation and evaluation being delegated tolower levels of the health-care system Buildingcapacity at that level requires time resources andpatience and a longer-term perspective
Building capacity emerges to be a key factorTrainers and training centres vary in their qualitywhen training health workers and their supervisorsor programme managers As the burden of trainingincreases availability of good-quality trainersbecomes a limiting factor (WHOUNICEF 2002Government of India 2006) An effective strategymust plan for these incremental requirements includ-ing ensuring secure and sustained funding
Identifying barriers to success is a key actor Thebarriers to scaling up of health interventions havebeen elegantly described by Ranson et al (Table 5)Most of these are important for exclusive breastfeed-ing scale-up as well
Overall within the limitations discussed above anumber of programmes in countries with varying
HIV prevalence show that exclusive breastfeeding ona large scale is feasible and pilot programmes havegiven valuable guidance related to policies planningand implementation of large-scale programmes Thechallenge now is to build on these experiences whenplanning national programmes
Acknowledgements
We sincerely thank Dr MK Bhan for his constructivecriticism and sustained feedback at different stages ofdevelopment of this review
Conflicts of interest
The authors have declared no conflicts of interest
References
Arifeen S Black RE Antelman G Baqui A CaulfieldL amp Becker S (2001) Exclusive breastfeeding reducesacute respiratory infection and diarrhea deaths amonginfants in Dhaka slums Pediatrics 108 E67
Australian Breastfeeding Association (2005) Valuing Par-enthood Options for Paid Maternity Leave ndash InterimPaper 2002 Available at httpwwwbreastfeedingasnauadvocacymatleavehtml
Bhandari N Bahl R Mazumdar S Martines J BlackRE amp Bhan MK (2003) Effect of community basedpromotion of exclusive breastfeeding on diarrheal ill-nesses and growth a cluster randomized controlled trialLancet 361 1418ndash1423
Bhandari N Mazumder S Bahl R Martines J BlackRE amp Bhan MK (2004) An educational interventionto promote appropriate complementary feedingimproves child feeding practices and linear growth inrural Haryana India Journal of Nutrition 134 2342ndash2348
Bhandari N Mazumder S Bahl R Martines J BlackRE amp Bhan MK (2005) Use of multiple opportunitiesfor improving feeding practices in undertwos withinchild health programs Health Policy Plan 20 328ndash336
Bryce J Victora CG Habicht JP Vaughan JP ampBlack RE (2004) The multi-country evaluation of theintegrated management of childhood illness strategylessons for the evaluation of public health interventionsAmerican Journal of Public Health 94 406ndash415
Butte NF Lopez-Alarcon MG amp Garza C (2002) Nutri-ent Adequacy of Exclusive Breastfeeding for the TermInfant during the First Six Months of Life World HealthOrganization Geneva
Table 5 Barriers to scaling up of health interventions
Community and household levelsLack of information womenrsquos education physical financial
womenrsquos decision-making powerHealth services delivery levelShortage of qualified staff weak technical guidance programme
management and supervision inadequate supplies equipmentand infrastructure poor accessibility
Health sector policy and strategic management levelWeak and centralized system for planning and management weak
drug policies and supply system inadequate regulations lack ofintersectoral action and partnership weak incentives to useinputs efficiently and respond to user needs and preferencesreliance on donor funding
Public policies cutting across sectorsGovernment bureaucracy poor communication and transport
infrastructureEnvironmental characteristicsGovernance and overall policy frameworkCorruption weak government weak laws political instability and
insecurity low priority to social sectors weak structure for publicaccountability and opportunities for public opinions lack of freepress
Physical environmentClimatic and geographic predisposition physical environment
unfavourable to service delivery
Adapted from Ranson et al (2003)
N Bhandari and AKMI Kabir14
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Cohen J (2007) Retrovirus meeting Hope on new AIDSdrugs but breast-feeding strategy backfires Science 3151357
Coovadia HM Rollins NC Bland RM Little KCoutsoudis A Bennish ML et al (2007) Mother tochild transmission of HIV-1 infection during exclusivebreastfeeding in the first 6 months of life an interven-tion cohort study Lancet 369 1107ndash1116
Coutinho SB de Lira PI de Carvalho LM amp AshworthA (2005) Comparison of the effect of two systems forthe promotion of exclusive breastfeeding Lancet 3661094ndash1100
Feachem RG amp Koblinsky MA (1984) Interventions forthe control of diarrheal diseases among young childrenpromotion of breastfeeding Bulletin of the of the WorldHealth Organization 62 271ndash291
Gonzales A Arteaga E amp Howard-Grabman L (1998)Scaling Up the WARMI Project ndash Lessons LearnedMobilizing Bolivian Communities around ReproductiveHealth Save the Children Federation Inc Bolivia FieldOffice La Paz Available at httpwwwcoregrouporgresourcesSavebolipdf
Government of India (1997) Recommendations of the FifthCentral Pay Commission Relating to Enhancement ofQuantum of Maternity Leave and to Allow PaternityLeave in Respect of Central Government EmployeesDocument ref 13018197-Estt(L) Available at httppersminnicinesttleave2htm
Government of India (2005) National Rural HealthMission 2005ndash2012 Mission document Ministry ofHealth and Family Welfare New Delhi Government ofIndia Available at httpwwwmohfwnicinNRHM20Mission20Documentpdf
Government of India (2006) Operational Guidelines forImplementation of Integrated Management of Neonataland Childhood Illness (IMNCI) Ministry of HealthFamily Welfare New Delhi Available at httpmohfwnicindofw20websiteF20IMNCI20Operational20Plan201320june202006htm
Government of Pakistan (2003) National Programme forFamily Planning and Primary Health Care The LadyHealth Workers Programme 2003ndash2008 Ministry ofHealth Pakistan Available at httpwwwphcgovpkDownloadsPC-120augpdf
Green CP (1999) Improving Breastfeeding Behaviors Evi-dence from Two Decades of Intervention ResearchPublished for the US Agency for International Develop-ment (USAID) by the LINKAGES Project Academyfor Educational Development Washington DC
Gupta A (2002) National trends in breastfeeding andeffective strategies to improve breastfeeding ratesJournal of Neonatology 2002 4ndash14
Gwatkin DR (2004) Integrating the management of child-hood illness Lancet 364 1557ndash1558
Habicht JP DaVanzo J amp Butz WP (1986) Does breast-feeding really save lives or are apparent benefits due tobiases American Journal of Epidemiology 123279ndash290
Haider R Ashworth A Kabir I amp Huttly SR (2000)Effect of community based peer counsellors on exclusivebreastfeeding practices in Dhaka Bangladesh a ran-domized controlled trial Lancet 356 1643ndash1647
Haider R Kabir I Huttly SR amp Ashworth A (2002)Training peer counsellors to promote and support exclu-sive breastfeeding in Bangladesh Journal of HumanLactation 18 7ndash12
Horton S Sanghvi T Phillips M Fiedler J Perez-Escamilla R Lutter C et al (1996) Breastfeeding pro-motion and priority setting in health Health Policy andPlanning 11 156ndash168
ILO (1998) More than 120 Nations Provide Paid MaternityLeave Gap in Employment Treatment for Men andWomen Still Exists International Labour Office GenevaDocument ref ILO987 Available at httpwwwiloorgpublicenglishbureauinfpr19987htmr2
Iliff PJ Piwoz EG Tavengwa NV Zunguza CDMarinda ET Nathoo KJ et al (2005) Early exclusivebreastfeeding reduces the risk of postnatal HIV-1 trans-mission and increase HIV-free survival AIDS 19 699ndash708
Integrated Child Development Services Scheme (Revised)(ICDS) (1982) Ministry of Social Welfare Governmentof India New Delhi Available on URL httpwcdnicinudishahtmabouticdshtm
Jason JM Nieburg P amp Marks JS (1984) Mortality andinfectious disease associated with infant feeding prac-tices in developing countries Pediatrics 74 702ndash727
Jones G Steketee RW Black RE Bhutta ZA ampMorris SS Bellagio Child Survival Study Group (2003)How many child deaths can we prevent this yearLancet 362 65ndash71
Knippenberg R Lawn JE Darmstadt GL Begkayian GFogstad H Walelign N et al (2005) Systematic scalingup of neonatal care in countries Lancet 365 1087ndash1098
Kramer MS amp Kakuma R (2002) The optimal durationof exclusive breastfeeding a systematic reviewCochrane Database of Systematic Reviews 2002CD003517
Kramer MS Chalmers B Hodnett ED Sevkovskaya ZDzikovich I Shapiro S et al (2000) Promotion ofbreastfeeding intervention trial (PROBIT) a cluster ran-domized trial in the Republic of Belarus Design followup and data validation Advances in Experimental Medi-cine and Biology 478 327ndash345
Kramer MS Chalmers B Hodnett ED Sevkovskaya ZDzikovich I Shapiro S et al (2001) Promotion ofbreastfeeding intervention trial (PROBIT) a random-
Mainstreaming nutrition into MCH programs 15
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
ized trial in the Republic of Belarus Journal of theAmerican Medical Association 285 413ndash420
Lewin SA Dick J Pond P Zwarenstein M Aja Gvan Wyk B et al (2006) Lay health workers in primaryand community health care (Review) The CochraneLibrary 3 1ndash104
LINKAGES (2002) World LINKAGES MadagascarAcademy for Educational Development WashingtonDC
LINKAGES (2005) LINKAGES Zambia 1997ndash2005 FinalReport A Full Report on LINKAGES Infant Feedingand HIVAIDS Programs in Zambia Academy for Edu-cational Development Washington DC Available athttpwwwlinkagesprojectorgmediapublicationsFinal20draft20Zambia20final20report2012105pdf
Lutter CK Perez-Escamilla R Segall A Sanghvi TTeruya K amp Wickham C (1997) The effectiveness of ahospital based program to promote exclusive breastfeed-ing among low income women in Brazil AmericanJournal of Public Health 87 659ndash663
Morrow AL Guerrero ML Shults J Calva J Lutter CBravo J et al (1999) Efficacy of home based peer coun-selling to promote exclusive breastfeeding a randomizedcontrolled trial Lancet 353 1226ndash1231
Ntabaye MK amp Lusiola GJ (2004) Understanding barri-ers to PMTCT in Tanzania findings of a baseline surveyInternational Conference on AIDS 15 (B11396)
de Oliveira LD Giugliani ER do Espirito SLC FrancaMC Weigert EM Kohler CV et al (2006) Effect ofintervention to improve breastfeeding technique on thefrequency of exclusive breastfeeding and lactation-related problems Journal of Human Lactation 22 315ndash321
Perez-Escamilla R (2004) Effectiveness of MADLAC atImproving Breastfeeding Promotion and CounsellingIndicators in Maternity Wards in El Salvador Publishedfor the Basic Support for Institutionalizing Child Sur-vival Project (BASICS II) for the United States Agencyfor International Development Arlington VA Availableat httpwwwbasicsorgpdfFinal20MADLAC20Report20RPE20April207-2004pdf
Perez-Escamilla R (2007) Evidence based breast-feedingpromotion the Baby-Friendly Hospital InitiativeJournal of Nutrition 137 484ndash487
Piwoz EG Iliff PJ Tavengwa N Gavin L Marinda ELunney K et al (2005) An education and counselllingprogram for preventing breastfeeding associated HIVtransmission in Zimbabwe design and impact on mater-nal knowledge and behaviour Journal of Nutrition 135950ndash955
Quinn VJ Guyon AB Schubert JW Stone-Jimenez MHainsworth MD amp Martin LH (2005) Improvingbreastfeeding practices on a board scale at the commu-
nity level success stories from Africa and LatinAmerica Journal of Human Lactation 21 345ndash354
Ranson MK Hanson K Oliveira-Cruz V amp Mills A(2003) Constraints to expanding access to health inter-ventions an empirical analysis and country typologyJournal of International Development 15 15ndash40
Rea MF amp Berquo ES (1990) Impact of the Braziliannational breastfeeding programme on mothers inGreater Sao Paulo Bulletin of the of the World HealthOrganization 68 365ndash371
Rollins NC (2007) Infant feeding and HIV BritishMedical Journal 334 487ndash488
Rutenberg N Baek C Kalibala S Rosen J amp Mulenga D(2004) Evaluation of United Nations supported pilotprojects for the prevention of mother-to-child transmis-sion of HIV overview of findings International Confer-ence on AIDS 15 (WePeE6688)
The Core Group (2005) Scale and Scaling Up A COREGroup Background Paper on lsquoScaling-Uprsquo MaternalNewborn and Child Health Services CORE SpringMembership Meeting 2005 The Core Group Washing-ton DC Available at httpwwwcoregrouporgresourcesmeetingsapril05Scaling_Up_Background_Paper_7-13pdf
The Norwegian Government (1993) Women in PoliticsMinistry of Children and Equality Available at httpwwwregjeringennoendepbldRyddemappeSLA-AvdelingdoclegislationguidelinesWomen-in-Politicshtmlid=437166
Thior I Lockman S Smeaton LM Shapiro RL WesterC Heymann SJ et al (2006) Breastfeeding plus infantzidovudine prophylaxis for 6 months vs formula feedingplus infant zidovudine for 1 month to reduce mother-to-child HIV transmission in Botswana a randomized trialthe Mashi Study Journal of the American Medical Asso-ciation 296 794ndash805
UNICEF (2002) Facts for Life lsquoKey Message What EveryFamily and Community Has a Right to Know aboutBreastfeedingrsquo Available at httpwwwuniceforgffl04key_messageshtm
Van Roekel K Plowman B Griffiths M de AlvaradoVV Matute J amp Calderon M (2002) BASICS IIMidterm Evaluation of the AIN Program in Honduras2000 Basic Support for Institutionalizing Child SurvivalProject (BASICS II) for the United States Agency forInternational Development Arlington VA
WABA (2007) UNICEF Records BHFI Record UpdateAvailable at httpwwwwabaorgmydocsBFHIjan07xls 2006 Regularly updated by Miriam HLabbok Center for Infant and Young ChildFeeding and Care Department of Maternaland Child Health School of Public Health The Univer-sity of North Carolina at Chapel Hill Chapel Hill NCUSA
N Bhandari and AKMI Kabir16
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
WHA (2002) Infant and Young Child Nutrition Fifty-FifthWorld Health Assembly Agenda Item 1310 18 May2002 Available at httpwwwintgbebwhapdf_filesWHA55ewha5525pdf
WHO (1981) The International Code of Marketing ofBreastmilk Substitutes World Health OrganizationGeneva
WHO (1989) Protecting Promoting and Supporting Breast-feeding The Special Role of Maternity Services A JointWHOUNICEF Statement World Health OrganizationGeneva
WHO (2002) The Optimal Duration of Exclusive Breast-feeding Report of an Expert Consultation WHONHD0109 WHOFCHCAH0124 World HealthOrganization Geneva
WHO (2003a) Community Based Strategies for Breastfeed-ing Promotion and Support in Developing CountriesWorld Health Organization Geneva Document refISBN_92_4_159121_8 Available at httpwwwwhointchild-adolescent-healthNew_PublicationsNUTRITIONISBN_92_4_159121_8pdf
WHO (2003b) Multi-country Evaluation of IMCI Effective-ness Cost and Impact (MCE) Progress Report May2002ndashApril 2003 Document ref WHOFCHCAH035World Health Organization Geneva
WHO (2004) Promoting Proper Feeding for Infants andYoung Children World Health Organization GenevaAvailable at httpwwwwhointnutritiontopicsinfantfeedingen
WHO (2006) WHO HIV and Infant Feeding TechnicalConsultation-Consensus Statement World Health Orga-nization Geneva Available at httpwwwwhointhivmediacentreInfantfeedingconsensusstatementpfpdf
WHO Collaborative Study Team on the Role of Breast-feeding on the Prevention of Infant Mortality (2000)Effect of breastfeeding on infant and child mortality dueto infectious diseases in les developed countries apooled analysis Lancet 355 451ndash455
WHOUNICEF (1992) The global criteria for the WHOUNICEF Baby-Friendly Hospital Initiative In Baby-Friendly Hospital Initiative Part II Hospital LevelImplementation World Health Organization Geneva
WHOUNICEF (1993) Breastfeeding Counselling A Train-ing Course WHOCDR933 UNICEFNUT931 WorldHealth Organization Geneva
WHOUNICEF (2002) Protocol for Adapting the FeedingRecommendations Part III IMCI Adaptation GuideWorld Health Organization Geneva
WHOUNICEF (2003) Global Strategy for Infant andYoung Child Feeding World Health OrganizationGeneva Available at httpwwwwhointchild-adolescent-healthpublicationsNUTRITIONIYCF_GShtm
de Zoysa I Rea M amp Martines J (1991) Why promotebreastfeeding in diarrheal diseases control programmesHealth Policy and Planning 6 371ndash379
Mainstreaming nutrition into MCH programs 17
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
Cas
est
udie
so
fef
fect
iven
ess
stud
ies
or
pilo
tpr
ogra
mm
es
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Lut
ter
etal
(199
7)
Bra
zil
Low
-inc
ome
urba
nw
omen
deliv
erin
gin
hosp
ital
s
Bre
astf
eedi
ngpr
omot
ion
in
hosp
ital
sco
mpa
red
wit
h
nobr
east
feed
ing
prom
otio
n
Pro
mot
ion
ofbr
east
feed
ing
in
sele
cted
hosp
ital
s
Mea
nda
ysof
excl
usiv
e
brea
stfe
edin
g
75da
ysvs
22
days
(Plt
001
)
Rea
ampB
erqu
o
(199
0)
Wom
enw
ith
ach
ild
aged
lt2ye
ars
inSa
oP
aulo
Nat
iona
lbre
astf
eedi
ng
cam
paig
n19
81ndash1
986
BF
HI
Mas
sm
edia
cam
paig
n11
in
fant
s5ndash
6m
onth
s
excl
usiv
ely
brea
stfe
d
in19
88an
d37
in
1987
Con
foun
ding
fact
ors
over
the
6-ye
arpe
riod
not
mea
sure
d
Kra
mer
etal
(200
020
01)
PR
OB
ITtr
ial
Bel
arus
Clu
ster
rand
omiz
ed
34ho
spit
als
and
thei
rpo
lycl
inic
s
Trai
ning
inB
FH
I(W
HO
UN
ICE
F19
92)
vsr
outi
ne
prac
tice
san
dpo
licie
s
Exc
lusi
vebr
east
feed
ing
at3
(43
3vs
64
)
and
6(7
9
vs0
6
)
mon
ths
sign
ifica
ntly
high
er
Impl
emen
ted
thro
ugh
BF
HI
ina
sett
ing
whe
reho
spit
al
deliv
erie
sar
eco
mm
on
Per
ez-E
scam
illa
(200
4)
BA
SIC
SII
Mex
ico
Hon
dura
s
Bra
zil
MA
DL
AC
low
-cos
t
man
agem
ent
info
rmat
ion
syst
emto
use
an
evid
ence
-bas
edap
proa
chto
impr
ove
serv
ice
perf
orm
ance
Inte
rvie
win
gof
wom
enat
hosp
ital
disc
harg
epo
st
deliv
ery
usin
ga
ques
tion
nair
eth
atta
kes
5ndash7
min
toad
min
iste
ran
d
cont
ains
19br
east
feed
ing
prom
otio
nco
unse
lling
indi
cato
rs
Dat
aen
tere
dan
dre
sult
s
disc
usse
d3-
mon
thly
by
hosp
ital
com
mit
tee
Hos
pita
lim
plem
ents
chan
ges
in
brea
stfe
edin
g
supp
ort
base
don
anal
ysis
of
ques
tion
nair
es
Itis
aco
st-e
ffec
tive
inte
rven
tion
that
can
help
impr
ovem
ents
inth
eB
FH
I
and
isa
valu
able
tool
for
proc
ess
eval
uati
on
N Bhandari and AKMI Kabir18
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
LIN
KA
GE
S
proj
ect
inA
fric
aan
d
Lat
inA
mer
ica
(Qui
nnet
al
2005
LIN
KA
GE
S
2002
WH
O20
03a)
Bol
ivia
(1
mill
ion)
Gha
na(3
5
mill
ion)
Mad
agas
car
(6m
illio
n)
Res
ourc
e-
poor
sett
ing
Pilo
tpr
ogra
mm
e
InB
oliv
iaan
d
Gha
napr
ogra
mm
e
focu
sed
on
brea
stfe
edin
gan
d
com
plem
enta
ry
feed
ing
InM
adag
asca
r
prog
ram
me
prom
oted
brea
stfe
edin
g
wit
hin
7es
sent
ial
nutr
itio
nac
tion
san
d
subs
eque
ntly
thro
ugh
IMC
I
Bui
lton
form
ativ
ere
sear
ch
and
sust
aine
dth
roug
h
prog
ram
me
acti
viti
esth
at
focu
sed
onbr
ingi
ngab
out
the
desi
red
beha
viou
r
chan
geM
ixof
inte
rven
tion
s
reac
hed
wom
enin
divi
dual
ly
orin
grou
psin
heal
th
faci
litie
sho
mes
or
com
mun
ity
sett
ings
Con
sist
ent
mes
sage
san
d
mat
eria
lacr
oss
all
prog
ram
me
chan
nels
Bol
ivi
PR
OC
OSI
NG
Os
Gha
na
UN
ICE
F
nati
onal
nutr
itio
n
offic
eN
GO
s
Mad
agas
car
Inte
rsec
tora
l
Act
ion
Gro
upfo
r
Nut
riti
on
Jere
o
Sala
ma
Isik
a
Pro
gram
desi
gned
wit
h
part
ners
Rad
ioin
all
thre
esi
tes
Mat
eria
ls
deve
lope
d
tosu
itne
eds
oflo
cal
heal
th
wor
kers
and
com
mun
ity
mem
bers
Gre
at
emph
asis
on
deve
lopm
ent
of coun
selli
ng
and
nego
tiat
ion
skill
s
prac
tica
l
sess
ions
Sign
ifica
ntin
crea
ses
inex
clus
ive
brea
stfe
edin
gra
tes
of
0ndash6-
mon
th-o
ld
infa
nts
from
54
to65
in
Bol
ivia
68
to79
in
Gha
naan
d46
to68
in
Mad
agas
car
In
Gha
naan
d
Mad
agas
car
sign
ifica
ntre
sult
s
obse
rved
wit
hin
aye
ar
ofin
itia
tion
of
com
mun
ity
inte
rven
tion
s
App
roac
hw
asef
fect
ive
and
achi
eved
sign
ifica
nt
incr
ease
sam
ong
larg
e
popu
lati
ons
asea
rly
as
9ndash12
mo
afte
rin
itia
tion
of
com
mun
ity
acti
viti
es
Van
Roe
kele
tal
(200
2)W
HO
(200
3a)
Hon
dura
sG
row
thm
onit
orin
gan
d
prom
otio
nkn
own
as
Ate
ncioacute
nIn
tegr
ala
la
Nintilde
ez(A
IN)
or
Inte
grat
edC
hild
Car
e
Init
ially
pri
mar
ilya
grow
th
mon
itor
ing
prog
ram
me
ulti
mat
ely
thro
ugh
IMC
I
Pro
gram
me
ongr
owth
prom
otio
nndash
asse
ssm
ent
of
mon
thly
wei
ght
gain
and
focu
son
illne
ssf
eedi
ng
prac
tice
san
dge
nera
lchi
ld
care
inin
fant
sun
der
2ye
ars
Impl
emen
ted
atgo
vern
men
t
faci
litie
san
dco
mm
unit
y
Star
ted
in19
92s
tren
gthe
ned
in19
95ndash1
997
wit
hgr
eate
r
focu
son
child
feed
ing
In
1997
pro
gram
me
intr
oduc
ed
wit
hIM
CI
(WH
OU
NIC
EF
2002
)
Maj
or
part
ners
UN
ICE
F
PAH
O
Am
eric
an
and
Hon
dura
n
Red
Cro
ss
CA
RE
Rad
io
broa
dcas
ts
relig
ious
lead
ers
IMC
IM
id-t
erm
eval
uati
on
show
ed39
of
mot
hers
inin
terv
enti
on
com
mun
itie
sex
clus
ivel
y
brea
stfe
dco
mpa
red
wit
h13
in
the
cont
rol
site
s
Mainstreaming nutrition into MCH programs 19
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
cont
inue
d
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Bha
ndar
ieta
l
(200
3)
WH
O
(200
3a)
Rur
alco
mm
unit
ies
inH
arya
na
Indi
a
Clu
ster
rand
omiz
edtr
ial
8
com
mun
itie
s(t
otal
popu
lati
on~4
000
0)
Pro
mot
ion
ofex
clus
ive
brea
stfe
edin
gan
d
appr
opri
ate
com
plem
enta
ryfe
edin
g
Dev
elop
edth
roug
h
form
ativ
ere
sear
ch
ndashP
robl
emid
enti
ficat
ion
ndashP
arti
cipa
tory
desi
gnof
inte
rven
tion
impl
emen
tati
onan
d
eval
uati
on
Impl
emen
tati
onw
ithi
nan
exis
ting
prim
ary
heal
th-c
are
prog
ram
me
Opp
ortu
niti
esus
edto
deliv
erm
essa
ges
wer
e
imm
uniz
atio
ncl
inic
s
wei
ghin
gse
ssio
ns
sick
-chi
ldco
ntac
tsan
d
mon
thly
hom
evi
sits
Res
earc
hers
wit
hlo
cal
gove
rnm
ent
ICD
Ssy
stem
and
NG
O
The
atre
son
gs
Mas
sm
edia
not
used
for
risk
of
cont
amin
atio
n
Mat
eria
ls
deve
lope
d
for
heal
th
wor
kers
pos
ters
flip
book
sca
rds
Bre
astf
eedi
ng
coun
selli
ngse
ctio
n
ofth
eIM
CI
(WH
O
UN
ICE
F20
02)
Exc
lusi
ve
brea
stfe
edin
gin
the
prev
ious
24h
at3
mon
ths
of
age
79
vs4
8
The
posi
tive
effe
ct
rem
aine
dup
to
6m
onth
sof
age
(42
vs4
)
Tota
lpar
tici
pati
onof
the
dist
rict
heal
thsy
stem
from
ince
ptio
nof
the
prog
ram
me
inde
velo
ping
impl
emen
tati
onst
rate
gyt
ool
deve
lopm
ent
and
mon
itor
ing
inad
diti
onto
invo
lvem
ent
of
anN
GO
wer
eim
port
ant
feat
ures
that
cont
ribu
ted
to
the
succ
ess
ofth
e
inte
rven
tion
Mor
row
etal
(199
9)
Mex
ico
Cit
yC
lust
erra
ndom
ized
tria
l
Tota
lpop
ulat
ion
3000
0
Two
com
mun
itie
sin
the
inte
rven
tion
one
com
pari
son
130
wom
en
Hom
e-ba
sed
peer
coun
selli
ng
Pee
rco
unse
llors
mad
e3
or
6ho
me
visi
tsto
the
mot
her
Key
fam
ilym
embe
rsal
so
incl
uded
By
La
Lec
he
Lea
gue
of
Mex
ico
Exc
lusi
ve
brea
stfe
edin
g
at3
mon
ths
post
-par
tum
67
(6vi
sits
)
50
(3vi
sits
)12
(com
pari
son)
Firs
tcl
uste
rra
ndom
ized
com
mun
ity-
base
dtr
ialt
hat
used
peer
coun
sello
rsto
prom
ote
excl
usiv
e
brea
stfe
edin
g
Hai
der
etal
2000
200
2
Dha
ka
Low
mid
dle
and
low
-soc
io-
econ
omic
popu
lati
on
Clu
ster
rand
omiz
edtr
ial
20zo
nes
inin
terv
enti
on
and
20in
cont
rol
Com
mun
ity-
base
dpe
er
coun
selli
ngin
Dha
ka
15ho
me-
base
dco
unse
lling
visi
tsby
peer
coun
sello
rs
40h
(4h
yen10
days
)
WH
OU
NIC
EF
brea
stfe
edin
g
coun
selli
ngco
urse
(WH
OU
NIC
EF
1993
)
Exc
lusi
ve
brea
stfe
edin
g
at5
mon
ths
70
in
inte
rven
tion
and
6in
the
cont
rol
Com
mun
ity-
base
d
brea
stfe
edin
gpr
omot
ion
stra
tegy
was
effe
ctiv
ein
Ban
glad
esh
whe
rem
ost
deliv
erie
soc
cur
atho
me
N Bhandari and AKMI Kabir20
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Bry
ceet
al
(200
4)W
HO
(200
3b)
Bra
zil
Per
u
Tanz
ania
Uga
nda
Mul
tico
untr
yev
alua
tion
of
IMC
Ith
atin
clud
ed
effe
ctiv
enes
sco
stan
d
impa
ct(B
ryce
etal
2004
)
Bre
astf
eedi
ngpr
omot
ion
asa
part
ofIM
CI
IMC
Iis
ast
rate
gyfo
r
impr
ovin
gch
ildhe
alth
and
deve
lopm
ent
thro
ugh
the
com
bine
d
deliv
ery
ofes
sent
ial
child
heal
th
inte
rven
tion
sIM
CI
bega
nw
ith
ase
tof
case
man
agem
ent
guid
elin
es
for
the
man
agem
ent
ofsi
ckch
ildre
nat
first
-lev
elhe
alth
faci
litie
s
and
the
guid
elin
esw
ere
desi
gned
for
adap
tati
on
atco
untr
yle
vela
nd
belo
wO
ver
tim
eth
e
stra
tegy
expa
nded
to
incl
ude
ara
nge
of
guid
elin
esfo
rde
liver
ing
child
surv
ival
inte
rven
tion
at
hous
ehol
dco
mm
unit
y
and
refe
rral
leve
ls
IMC
Im
odul
e(W
HO
UN
ICE
F20
02)
Res
ults
onex
clus
ive
brea
stfe
edin
g
avai
labl
efr
om
Tanz
ania
whe
reno
sign
ifica
ntim
pact
was
seen
Des
pite
subs
tant
ial
impr
ovem
ent
inth
equ
alit
y
ofca
rede
liver
edby
IMC
Iat
heal
thfa
cilit
ies
key
fam
ily
prac
tice
ssu
chas
excl
usiv
e
brea
stfe
edin
gdi
dno
tch
ange
asco
mm
unit
yIM
CI
had
not
been
impl
emen
ted
byth
at
tim
e(W
HO
2003
b)
SA
rife
en
pers
onal
com
mun
icat
ion
Ban
glad
esh
Mat
lab
Com
mun
ity-
base
dcl
uste
r
desi
gn
Eva
luat
ion
offa
cilit
y-an
d
com
mun
ity-
base
dIM
CI
Inte
rven
tion
pack
age
incl
udes
feed
ing
asse
ssm
ent
and
coun
selli
ngon
mot
hers
ofyo
ung
child
ren
seek
ing
care
atfa
cilit
ies
for
illne
ssan
d
hom
e-ba
sed
coun
selli
ng
onim
prov
edfe
edin
gby
com
mun
ity-
base
dhe
alth
and
nutr
itio
nw
orke
rs
At
base
line
inth
e
year
2000
alit
tle
mor
eth
anha
lfth
e
0ndash5-
mon
th-o
ld
infa
nts
inth
est
udy
area
wer
ebe
ing
excl
usiv
ely
brea
stfe
dB
y20
05
this
incr
ease
dby
30
inth
eIM
CI
area
Dat
ano
t
avai
labl
efr
omth
e
com
pari
son
area
as
yet
Lac
kof
com
para
ble
data
from
the
com
pari
son
area
prev
ents
ade
finit
ive
conc
lusi
onas
tow
heth
erth
is
trul
yis
anim
pact
ofIM
CI
BA
SIC
SII
Bas
icSu
ppor
tfo
rIn
stit
utio
naliz
ing
Chi
ldSu
rviv
alP
roje
ctB
FH
IB
aby-
Frie
ndly
Hos
pita
lIni
tiat
ive
ICD
SIn
tegr
ated
Chi
ldD
evel
opm
ent
Serv
ices
IM
CI
Inte
grat
edM
anag
emen
tof
Chi
ldho
odIl
lnes
sM
AD
LA
CM
onit
oreo
deA
poyo
Dir
ecto
con
laL
acat
anci
aM
ater
naN
GO
non
-gov
ernm
enta
lorg
aniz
atio
nPA
HO
Pan
Am
eric
anH
ealt
hO
rgan
izat
ion
PR
OB
ITP
rom
otio
nof
Bre
astf
eedi
ngIn
terv
enti
onTr
ial
PR
OC
OSI
Pro
gram
ade
Coo
rdin
acio
nen
Salu
dIn
tegr
al(C
olla
bora
tive
Pro
gram
for
Inte
grat
edH
ealt
h)U
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
WH
OW
orld
Hea
lth
Org
aniz
atio
n
Mainstreaming nutrition into MCH programs 21
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x2
Cas
est
udie
sin
scal
e-up
effo
rts
inH
IVA
IDS
Stud
yde
scri
ptio
nPo
pula
tion
Inte
rven
tion
Com
mun
icat
ion
stra
tegy
Impa
cton
excl
usiv
ebr
east
feed
ing
Com
men
ts
LIN
KA
GE
S(2
005)
Zam
bia
Pro
gram
me
thro
ugh
heal
th-c
are
and
com
mun
ity
serv
ices
Rea
ched
60si
tes
in6
dist
rict
sby
2005
Inte
grat
ion
ofin
fant
feed
ing
coun
selli
ngm
ater
naln
utri
tion
and
anti
retr
ovir
aldr
ugs
prop
hyla
xis
Trai
ning
ofhe
alth
wor
kers
and
com
mun
ity
serv
ice
prov
ider
sto
coun
selw
omen
onsa
fety
opti
ons
for
thei
rsi
tuat
ion
Beh
avio
urch
ange
Com
mun
icat
ion
inte
rven
tion
sin
the
first
few
year
sM
ater
iald
evel
oped
lsquoAct
Now
rsquoM
edia
cam
paig
nsin
clud
edbr
ochu
res
post
ers
radi
oan
dte
levi
sion
Ass
esse
dth
roug
hba
selin
ean
dfo
llow
-up
hous
ehol
dan
dcl
inic
surv
eys
inse
lect
eddi
stri
cts
Exc
lusi
vebr
east
feed
ing
rate
incr
ease
dfr
om50
in
2002
to64
in
2004
inL
ivin
gsto
nean
dfr
om57
in
2000
to74
in
2004
inN
dola
Inte
grat
edde
mon
stra
tion
proj
ect
Had
seve
rals
tren
gths
inte
rms
ofth
eus
eof
form
ativ
ere
sear
chto
deve
lop
mes
sage
str
aini
ngan
dbu
ildin
gup
skill
sof
prog
ram
me
man
ager
she
alth
-car
epr
ovid
ers
and
com
mun
ity
wor
kers
adv
ocac
yfo
rna
tion
alpo
licy
stro
ngbe
havi
our
chan
geco
mm
unic
atio
nco
mpo
nent
st
reng
then
ing
com
mun
ity
capa
city
for
coun
selli
ngan
dre
ferr
als
and
mon
itor
ing
and
eval
uati
onw
ith
loca
lpar
tner
sP
iwoz
etal
(20
05)
ZV
ITA
MB
Otr
ial
Har
are
Zim
babw
eE
duca
tion
and
coun
selli
ngpr
ogra
mm
ede
liver
edan
tena
tally
1411
0m
othe
rndashba
bypa
irs
enro
lled
from
14m
ater
nity
clin
ics
wit
hin
96h
ofde
liver
yan
dfo
llow
edup
at6
wee
ks
3m
onth
san
d3-
mon
thly
inte
rval
sIn
fant
-fee
ding
patt
erns
dete
rmin
edE
xclu
sive
brea
stfe
edin
gre
com
men
ded
for
HIV
nega
tive
un
know
nor
HIV
posi
tive
who
chos
eto
brea
stfe
ed
Gro
uped
ucat
ion
indi
vidu
alco
unse
lling
vid
eos
broc
hure
sM
othe
rsw
hoen
rolle
dw
hen
prog
ram
me
was
fully
impl
emen
ted
wer
e8
4ti
mes
mor
elik
ely
toex
clus
ivel
ybr
east
feed
than
mot
hers
who
enro
lled
befo
reth
epr
ogra
mm
ebe
gan
Ove
rall
excl
usiv
ebr
east
feed
ing
rate
sti
ll3
mon
ths
was
low
at24
6
Form
ativ
ere
sear
chus
edto
desi
gna
cult
ural
lyse
nsit
ive
educ
atio
nan
dco
unse
lling
prog
ram
me
Low
over
alle
xclu
sive
brea
stfe
edin
gra
tes
prom
pted
auth
ors
toco
nclu
deth
atw
omen
and
thei
rpa
rtne
rssh
ould
have
been
reac
hed
mor
efr
eque
ntly
duri
ngan
tena
tala
ndpo
st-n
atal
peri
od
N Bhandari and AKMI Kabir22
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Thi
oret
al(
2006
)R
ollin
s(2
007)
C
ohen
(200
7)
HIV
-inf
ecte
dpr
egna
ntw
omen
atte
ndin
gan
tena
talc
linic
sin
sout
hB
otsw
ana
Inve
stig
atio
nsby
CD
Cof
adi
arrh
oea
outb
reak
inJa
nuar
y-Fe
brua
ry20
06in
the
sam
epo
pula
tion
Mat
erna
land
infa
ntan
tire
trov
iral
ther
apy
toas
cert
ain
impa
cton
HIV
tran
smis
sion
Ant
enat
alco
unse
lling
Cas
endashco
ntro
lstu
dyto
iden
tify
risk
fact
ors
for
diar
rhoe
ano
tbr
east
feed
ing
was
the
bigg
est
risk
fact
ora
djus
ted
odds
rati
o50
(95
confi
denc
ein
terv
al4
5ndash10
0)
Bot
swan
aha
sth
ebe
stpr
imar
yhe
alth
-car
est
ruct
ure
wat
ersu
pply
and
sani
tati
onsy
stem
sin
Sout
hA
fric
aFo
rmul
apr
ovid
edfr
eeby
the
gove
rnm
ent
toin
fect
edm
othe
rsL
ower
mor
talit
yin
the
brea
stfe
edin
ggr
oup
at7
mon
ths
dem
onst
rate
sri
skof
form
ula
feed
ing
and
need
for
alte
rnat
est
rate
gies
(Thi
oret
al
2006
)A
utho
rsco
nclu
deth
athe
alth
syst
ems
inw
hich
thes
epr
ogra
mm
esar
eim
plem
ente
dsh
ould
beab
leto
cope
wit
hdi
arrh
oea
and
mal
nutr
itio
nth
atre
sult
sbe
caus
eof
form
ula
feed
ing
(Rol
lins
2007
)C
oova
dia
etal
(2
007)
Kw
aZul
uNat
al
Sout
hA
fric
a27
22H
IV-i
nfec
ted
and
unin
fect
edpr
egna
ntw
omen
enro
lled
into
ano
n-ra
ndom
ized
inte
rven
tion
coho
rtst
udy
from
ante
nata
lcl
inic
sIn
fant
feed
ing
data
obta
ined
wee
kly
bloo
dsa
mpl
esfr
omin
fant
sta
ken
mon
thly
83
of13
72in
fant
sbo
rnto
HIV
-inf
ecte
dm
othe
rsin
itia
ted
excl
usiv
ebr
east
feed
ing
from
birt
hB
reas
tfed
infa
nts
who
rece
ived
solid
sw
ere
sign
ifica
ntly
mor
elik
ely
toac
quir
ein
fect
ion
com
pare
dw
ith
excl
usiv
ely
brea
stfe
d(H
R10
87
151
ndash78
P=
001
8)as
wer
ein
fant
sw
hoat
12w
eeks
rece
ived
brea
stan
dfo
rmul
am
ilk(1
82
098
ndash33
6P
=0
57)
Cum
ulat
ive
3-m
onth
mor
talit
yin
excl
usiv
ely
brea
stfe
dw
as6
1(4
74ndash
792
)vs
15
1(7
63ndash
287
3)in
infa
nts
give
nre
plac
emen
tfe
eds
(HR
206
1
0ndash4
27P
=0
05)
The
stud
ysh
ows
that
excl
usiv
ebr
east
feed
ing
can
besu
cces
sful
lysu
ppor
ted
inH
IV-i
nfec
ted
wom
enT
heau
thor
sca
llfo
rfu
rthe
rre
visi
onof
UN
ICE
FW
HO
and
USA
IDin
fant
feed
ing
guid
elin
es
CD
CC
ente
rof
Dis
ease
Con
trol
HR
haz
ards
rati
oU
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
USA
IDU
SA
genc
yfo
rIn
tern
atio
nalD
evel
opm
ent
WH
OW
orld
Hea
lth
Org
aniz
atio
nZ
VIT
AM
BO
Z
imba
bwe
Vit
amin
Afo
rM
othe
rsan
dB
abie
s
Mainstreaming nutrition into MCH programs 23
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23

variety of local workers such as peer counsellors inBangladesh (Haider et al 2000) lady health workersin Pakistan (Government of Pakistan 2003) and thelsquoAccredited Social Health Activistsrsquo (ASHA) workerin India (Government of India 2005) to promoteexclusive breastfeeding by itself or as a part of essen-tial newborn care Programmes that used peer coun-sellors as a single channel have been shown to beeffective in several efficacy (Green 1999 Lewin et al
2006) and effectiveness trials (Morrow et al 1999Haider et al 2000 Lewin et al 2006) However whilepeer or lay counsellors have been effective in theshort run long-term sustainability of this approach ona large scale is as yet not established
The possible reasons stated for the short-termsuccess of the lay health workers approach includepayment to the counsellors for performing a specificpiece of work the counsellorsrsquo own perception ofbenefits of their work and their recognition by thecommunity as being skilled These workers also feltthis opportunity to have the potential for opening upof further education and training (Haider et al 2002)An important issue would also be linking newworkers with the existing primary health system aspilot experience showed that these workers may notbe able to resolve complex breastfeeding problems(Haider et al 2002)
Recruitment of ASHA in India provides a uniqueopportunity to promote exclusive breastfeeding(Government of India 2005) Currently being re-cruited all over the country these workers will focuson essential newborn care including exclusive breast-feeding through home visitation in the first month oflife and community-based activities
While these efforts in different countries at improv-ing coverage of the target population through localworkers are of value the voluntary or semi-voluntarynature of the workers and ill-defined models of super-vision raise issues about sustainability and possiblyhigh attrition rates
Programmes that used multiple channels reportedbroader coverage (Bhandari et al 2005 Quinn et al
2005) In India formative research showed thatimmunization sessions and private providers werethe channels to which infants were most commonly(~80) exposed Following constitution of a
breastfeeding-promotion programme caregiversmost often received exclusive breastfeeding counsel-ling at immunization sessions (~40) weighing ses-sions (~25) and home visits (25ndash30) Governmentphysicians or private providers rarely (~2) coun-selled despite being trained (Bhandari et al 2005)When all the opportunities were considered together55ndash60 of caregivers had been counselled at leastonce by at least one of the channels in the last 3months indicating that multiple channels reachedmore families (Bhandari et al 2005)The frequency ofcontact with caregivers or the intensity of counsellinginfluences the cumulative benefit of the counsellingfor example six contacts with mothers resulted inhigher adoption rates for exclusive breastfeeding ascompared with three (Morrow et al 1999) In Indiathe number of channels at which caregivers werecounselled was positively associated with the rates ofexclusive breastfeeding at 3 months of age (Bhandariet al 2003) However the costs of training and theeffort will increase more than the number of channelsused and therefore this issue requires a balancedview
Another issue of interest is the value of counsellingfor the antenatal period itself Antenatal counsellinghas been used in several programmes but its effect isdifficult to delineate by itself as it was usually fol-lowed by post-natal counselling (Green 1999) In theHIV context however the importance of antenatalcounselling is obvious
Communications approach
An effective communications approach was a featureof most programmes and involvement of journalistsradio announcements and other mass media from theprogramme outset extended the reach of nutritionmessages even further (Appendix 1 Quinn et al
2005) Mass media were not used in some pro-grammes where a comparison group was present forrisk of contamination (Bhandari et al 2005) Utiliza-tion of existing or newly formed community groupsproduced the same effect (Bhandari et al 2005Quinn et al 2005) and community mobilization pro-grammes such as street plays rallies radio pro-grammes and songs helped disseminate messages
N Bhandari and AKMI Kabir10
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
and increase community involvement (Bhandari et al
2005 Quinn et al 2005)Effective counselling requires assessment of
feeding practices recognition of problems and nego-tiation with the mother in choosing improved prac-tices that are feasible (WHOUNICEF 2002) thisrequires time and patience Programmes may chooseone-on-one counselling during opportunities in whichmore time is available such as home visits and groupcounselling for opportunities with lesser availabletime (Bhandari et al 2005) One of the reasons thatpeer counsellors may have been effective was thattheir sole responsibility was counselling mothersthrough home visits (Morrow et al 1999 Haider et al
2000) The more diverse the functions of the localworker the lesser will be the emphasis on a singlecomponent such as exclusive breastfeeding
Message development
The development of messages for interpersonal com-munication and for mass media needs careful atten-tion to design and content Successful programmesincluded an element of formative research to gain anin-depth understanding of the communities wherethese programmes were implemented with regard topractices pertaining to breastfeeding the reasons forthe current practices the common breastfeedingproblems and the barriers to adoption of ideal behav-iours in that cultural setting Formative research innorth India for instance showed general unwilling-ness to offer water to infants in summer months Thisbarrier was overcome by building specific explanatorymessages using local terms within the communicationstrategy (Bhandari et al 2003)
Once the design features and broad strategy are inplace attention must then shift to the operationaliza-tion of the strategy
Training and supervision
Prior to scale-up the training needs will need to bedefined Fortunately for promotion of exclusivebreastfeeding extensive experience is available ontraining of different cadres of health workers andeven for lay counsellors Most experiences used the
adapted versions of the UNICEFWHO Breastfeed-ing Counseling Course (WHOUNICEF 1993) or theIMCI module (WHOUNICEF 2002)
Training strategy and its quality merit attentionIn successful programmes the duration of trainingextended from 3 full days to 10 part days for differentworkers The training strategies as described werelsquoconcise action orientedrsquo and included modules thataimed to equip trainers with practical skills and con-fidence to counsel effectively (Appendix 1)
Training modules for areas with high HIV preva-lence also exist (WHO 2006)
While the training modules used in studies workedwell a gap remains for referralTrained workers at thecommunity level require that referral options avail-able are easily accessible prompt and preferablyavailable free of cost to mothers with complex breast-feeding problems
Another important issue to address is handlingtraining of new staff in most developing countriesstaff turnover and absenteeism rates are high
Monitoring and evaluation
The programme strategy will need to include systemsfor monitoring and evaluation of the programmePossible markers could include the rates of exclusivebreastfeeding worker performance referral andaction As for all other national programmes therewill be a need for periodic reviews and achievabletargets by time
Costs and resources
In all pilot programmes and projects services wereprovided to mothers free of cost In many developingcountries if the government cadre of health workers isused to promote exclusive breastfeeding as a part oftheir other responsibilities (eg the IMNCI) the basicservices will remain free However a system thatrequires setting up a cadre of trained lactation coun-sellors (eg in an urban setting or as referral sources forbreastfeeding problems in rural areas) will requireadditional resources A cost-effective analysis of theBFHI was conducted in three countriesBrazilMexicoand Honduras (Horton et al 1996) Savings on health
Mainstreaming nutrition into MCH programs 11
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
care resulting from reduction in diarrhoeal and respi-ratory morbidity were estimated as a result of theeffect of BFHI on breastfeeding The study showedthat breastfeeding promotion through a BFHI-likemodel is very cost-effective (1992 US$ 2ndash19 per dis-ability adjusted life years Horton et al 1996 Perez-Escamilla 2007) Examples of cost-effectivenessanalysis of community-based programmes using lay orprofessional support in different settings could not beidentified
Testing of novel approaches andcontinuing innovation
Scaled-up programmes must have inbuilt provision totest novel approaches and the ability for continuinginnovation
Scaling up of exclusive breastfeeding in thecontext of HIV
The policy and programme design and implemen-tation issues relevant to exclusive breastfeedingscale-up discussed above are relevant to HIV-prevalent areas but there are other unique featuresthat merit consideration
Creating policies for exclusive breastfeeding pro-motion in countries with high HIV prevalence is par-ticularly challenging The revised recommendationsencourage exclusive breastfeeding for the first 6months and continued breastfeeding for 2 years andbeyond for infants whose mothers are HIV negativeor whose HIV status is unknown For women who areknown to be HIV positive the most appropriateinfant feeding option for HIV-exposed infantsdepends on individual circumstances including con-sideration of health services counselling and supportExclusive breastfeeding is the better option for suchinfants unless replacement feeding is acceptable fea-sible affordable sustainable and safe for both themother and baby This recommendation is based onthe finding that exclusive breastfeeding for up to 6months in three large cohort studies is associated witha three- to fourfold decreased risk of transmission ofHIV compared with non-exclusive breastfeeding(WHO 2006) The recommendations may need
further revision if new findings demonstrate thatexclusive breastfeeding should be the feeding ofchoice for HIV-infected women (Iliff et al 2005)
Some pilot programmes for exclusive breastfeedingpromotion in high-HIV-prevalence countries aresummarized in Appendix 2
In general exclusive breastfeeding promotionformed a part of the prevention of mother-to-childtransmission programmes LINKAGESZambiaintegrated improved counselling on infant feedingmaternal nutrition and antiretroviral therapy duringprophylaxis in both health-care and community ser-vices to enable women to make and act on informedchoice to feed their infants optimally in the context ofhigh HIV prevalence
Formative research was critical to develop locallyappropriate and feasible infant feeding recommenda-tions for individual infants and their families based onHIV status In Zambia the research included focusedgroup discussions key information interviews obser-vations of household food preparation and feedingmarket survey of replacement foods and breastmilksubstitutes and household trials of improved feedingand caring practices (LINKAGES 2005)
High quality of health workers is another criticalfactor for sensitive and accurate individual counsel-ling Programmes incorporated behaviour changecommunication methodologies in training (LINK-AGES 2005) It is important to develop skills of com-munity members as well for improved servicesreferral outreach and follow-up care and support ofHIV-positive mothers and their infants
A comprehensive communications strategy tosupport scale-up was a notable feature of the LINK-AGES programme in Zambia In 2004 an intensiveeffort was launched using brochures posters radioand television spots billboards and reference guidesfor health providers (LINKAGES 2005) Messageswere targeted to relevant stakeholders ndash pregnantand lactating mothers health providers youth andcommunity leaders and all the materials were nation-ally disseminated
Monitoring and evaluation another importantfeature of effective scale-up was a feature of pilotprogrammes (Appendix 2 Ntabaye amp Lusiola 2004Rutenberg et al 2004) in Zambia and Tanzania Moni-
N Bhandari and AKMI Kabir12
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
toring and evaluation not only provides a measure ofsuccess but identifies factors that may have contrib-uted to it and to lack of success to enable mid-coursecorrections The impact of some pilot programmes onexclusive breastfeeding is summarized in Appendix 2In most programmes exclusive breastfeeding ratesimproved In Zambia exclusive breastfeeding ratesincreased from 50 in 2002 to 64 in 2004 in Liv-ingstone from 57 in 2000 to 74 in 2004 in NdolaIn South Africa an antenatal clinic-based interven-tion led to 83 of infants born to HIV-infectedmother initiating exclusive breastfeeding InZimbabwe an intervention based on antenatal coun-selling resulted in a relatively lower exclusive breast-feeding rate of 246 at 3 months (Piwoz et al 2005)
Several barriers to success were identified Theseinclude inadequate skills of workers and non-integration of HIV counselling and tailoring into ante-natal care services (Ntabaye amp Lusiola 2004) which isthe backbone in which infant feeding counselling isbuiltWomen reported that mothers not breastfeedingtheir children were discriminated against by the com-munity and they faced the threat of domestic violenceProgramme managerrsquos understanding of barriersto effective programme implementation and impactwere emphasized as being important Governmentsupport partnerrsquos coordination increased humanresource and improving the supply system were iden-tified to be essential features to scale up programmesin the HIV context (Rutenberg et al 2004) Lowoverall exclusive breastfeeding rates prompted Piwozet al (2005) to conclude that women and their partnersshould have been reached more frequently during theantenatal and post-natal period
Conclusions
In a large number of programmes for improvingexclusive breastfeeding in developing countriesincluding in areas with high prevalence of HIV apositive impact on exclusive breastfeeding rates hasbeen achieved
Some of the factors that contributed to successfulscale-up are summarized in Table 4 Several limita-tions of the programmes reviewed merit attentionMost programmes involved special and generous
funding concentrated efforts and multiple contactsThese programmes were evaluated over relativelyshort periods of time usually 2ndash5 years and the long-term sustainability has not been really tested In theabsence of specific measures there is likely to be dilu-tion of quality as the programmes are scaled upfurther from their initial size The experience thus farleaves important questions to be addressed particu-larly on how programmes can be sustained over timeas they are scaled up at affordable costs
A key factor relevant to sustainability is to plan ona long-term basis a period of 10ndash20 years rather than5ndash10 years from the outset Experience with otherchild health programmes has shown that performancein immunization and oral rehydration therapy userates plateaued over time in many countries
Programme scale-up requires a programme man-agement capacity proportionate to the scale of opera-tions periodic assessment of barriers (Table 5) and anability to revise programme strategy to overcomethese Another key feature to sustainability ofscale-up is the extent to which capacity has been builtat the district block and community levels National-or state-level driven interventions begin with enor-mous enthusiasm which is difficult to sustain Thisfactor is particularly important as most developing
Table 4 Lessons learnt about scale-up key factors in success
bull Political will advocacy enabling policiesbull Championship by health ministries at national state and districtlevelbull Technical consensus on feeding guidelinesbull Programme strategy and measurable short- and long-term goalsbull Long-term financial commitmentbull Partners with defined roles assessment of their capacity todeliver and plans to cover gaps in capacitybull Emphasis on community-level interventions and not onlyfacility-based programmesbull Formative research as the backbone of effective scale-upprogrammes particularly in the context of HIVbull Careful selection of channels and the number required toachieve timely coverage consistency of messagesbull Communication strategy aided by formative research pre-testedvalidated messages and toolsbull Quality trainers and training centres proportionate to requiredscalebull Monitoring and evaluationbull Programme redesign when relevant through research analysisand innovation
Mainstreaming nutrition into MCH programs 13
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
countries are going through a process of decentrali-zation with increasing responsibility for planningimplementation and evaluation being delegated tolower levels of the health-care system Buildingcapacity at that level requires time resources andpatience and a longer-term perspective
Building capacity emerges to be a key factorTrainers and training centres vary in their qualitywhen training health workers and their supervisorsor programme managers As the burden of trainingincreases availability of good-quality trainersbecomes a limiting factor (WHOUNICEF 2002Government of India 2006) An effective strategymust plan for these incremental requirements includ-ing ensuring secure and sustained funding
Identifying barriers to success is a key actor Thebarriers to scaling up of health interventions havebeen elegantly described by Ranson et al (Table 5)Most of these are important for exclusive breastfeed-ing scale-up as well
Overall within the limitations discussed above anumber of programmes in countries with varying
HIV prevalence show that exclusive breastfeeding ona large scale is feasible and pilot programmes havegiven valuable guidance related to policies planningand implementation of large-scale programmes Thechallenge now is to build on these experiences whenplanning national programmes
Acknowledgements
We sincerely thank Dr MK Bhan for his constructivecriticism and sustained feedback at different stages ofdevelopment of this review
Conflicts of interest
The authors have declared no conflicts of interest
References
Arifeen S Black RE Antelman G Baqui A CaulfieldL amp Becker S (2001) Exclusive breastfeeding reducesacute respiratory infection and diarrhea deaths amonginfants in Dhaka slums Pediatrics 108 E67
Australian Breastfeeding Association (2005) Valuing Par-enthood Options for Paid Maternity Leave ndash InterimPaper 2002 Available at httpwwwbreastfeedingasnauadvocacymatleavehtml
Bhandari N Bahl R Mazumdar S Martines J BlackRE amp Bhan MK (2003) Effect of community basedpromotion of exclusive breastfeeding on diarrheal ill-nesses and growth a cluster randomized controlled trialLancet 361 1418ndash1423
Bhandari N Mazumder S Bahl R Martines J BlackRE amp Bhan MK (2004) An educational interventionto promote appropriate complementary feedingimproves child feeding practices and linear growth inrural Haryana India Journal of Nutrition 134 2342ndash2348
Bhandari N Mazumder S Bahl R Martines J BlackRE amp Bhan MK (2005) Use of multiple opportunitiesfor improving feeding practices in undertwos withinchild health programs Health Policy Plan 20 328ndash336
Bryce J Victora CG Habicht JP Vaughan JP ampBlack RE (2004) The multi-country evaluation of theintegrated management of childhood illness strategylessons for the evaluation of public health interventionsAmerican Journal of Public Health 94 406ndash415
Butte NF Lopez-Alarcon MG amp Garza C (2002) Nutri-ent Adequacy of Exclusive Breastfeeding for the TermInfant during the First Six Months of Life World HealthOrganization Geneva
Table 5 Barriers to scaling up of health interventions
Community and household levelsLack of information womenrsquos education physical financial
womenrsquos decision-making powerHealth services delivery levelShortage of qualified staff weak technical guidance programme
management and supervision inadequate supplies equipmentand infrastructure poor accessibility
Health sector policy and strategic management levelWeak and centralized system for planning and management weak
drug policies and supply system inadequate regulations lack ofintersectoral action and partnership weak incentives to useinputs efficiently and respond to user needs and preferencesreliance on donor funding
Public policies cutting across sectorsGovernment bureaucracy poor communication and transport
infrastructureEnvironmental characteristicsGovernance and overall policy frameworkCorruption weak government weak laws political instability and
insecurity low priority to social sectors weak structure for publicaccountability and opportunities for public opinions lack of freepress
Physical environmentClimatic and geographic predisposition physical environment
unfavourable to service delivery
Adapted from Ranson et al (2003)
N Bhandari and AKMI Kabir14
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Cohen J (2007) Retrovirus meeting Hope on new AIDSdrugs but breast-feeding strategy backfires Science 3151357
Coovadia HM Rollins NC Bland RM Little KCoutsoudis A Bennish ML et al (2007) Mother tochild transmission of HIV-1 infection during exclusivebreastfeeding in the first 6 months of life an interven-tion cohort study Lancet 369 1107ndash1116
Coutinho SB de Lira PI de Carvalho LM amp AshworthA (2005) Comparison of the effect of two systems forthe promotion of exclusive breastfeeding Lancet 3661094ndash1100
Feachem RG amp Koblinsky MA (1984) Interventions forthe control of diarrheal diseases among young childrenpromotion of breastfeeding Bulletin of the of the WorldHealth Organization 62 271ndash291
Gonzales A Arteaga E amp Howard-Grabman L (1998)Scaling Up the WARMI Project ndash Lessons LearnedMobilizing Bolivian Communities around ReproductiveHealth Save the Children Federation Inc Bolivia FieldOffice La Paz Available at httpwwwcoregrouporgresourcesSavebolipdf
Government of India (1997) Recommendations of the FifthCentral Pay Commission Relating to Enhancement ofQuantum of Maternity Leave and to Allow PaternityLeave in Respect of Central Government EmployeesDocument ref 13018197-Estt(L) Available at httppersminnicinesttleave2htm
Government of India (2005) National Rural HealthMission 2005ndash2012 Mission document Ministry ofHealth and Family Welfare New Delhi Government ofIndia Available at httpwwwmohfwnicinNRHM20Mission20Documentpdf
Government of India (2006) Operational Guidelines forImplementation of Integrated Management of Neonataland Childhood Illness (IMNCI) Ministry of HealthFamily Welfare New Delhi Available at httpmohfwnicindofw20websiteF20IMNCI20Operational20Plan201320june202006htm
Government of Pakistan (2003) National Programme forFamily Planning and Primary Health Care The LadyHealth Workers Programme 2003ndash2008 Ministry ofHealth Pakistan Available at httpwwwphcgovpkDownloadsPC-120augpdf
Green CP (1999) Improving Breastfeeding Behaviors Evi-dence from Two Decades of Intervention ResearchPublished for the US Agency for International Develop-ment (USAID) by the LINKAGES Project Academyfor Educational Development Washington DC
Gupta A (2002) National trends in breastfeeding andeffective strategies to improve breastfeeding ratesJournal of Neonatology 2002 4ndash14
Gwatkin DR (2004) Integrating the management of child-hood illness Lancet 364 1557ndash1558
Habicht JP DaVanzo J amp Butz WP (1986) Does breast-feeding really save lives or are apparent benefits due tobiases American Journal of Epidemiology 123279ndash290
Haider R Ashworth A Kabir I amp Huttly SR (2000)Effect of community based peer counsellors on exclusivebreastfeeding practices in Dhaka Bangladesh a ran-domized controlled trial Lancet 356 1643ndash1647
Haider R Kabir I Huttly SR amp Ashworth A (2002)Training peer counsellors to promote and support exclu-sive breastfeeding in Bangladesh Journal of HumanLactation 18 7ndash12
Horton S Sanghvi T Phillips M Fiedler J Perez-Escamilla R Lutter C et al (1996) Breastfeeding pro-motion and priority setting in health Health Policy andPlanning 11 156ndash168
ILO (1998) More than 120 Nations Provide Paid MaternityLeave Gap in Employment Treatment for Men andWomen Still Exists International Labour Office GenevaDocument ref ILO987 Available at httpwwwiloorgpublicenglishbureauinfpr19987htmr2
Iliff PJ Piwoz EG Tavengwa NV Zunguza CDMarinda ET Nathoo KJ et al (2005) Early exclusivebreastfeeding reduces the risk of postnatal HIV-1 trans-mission and increase HIV-free survival AIDS 19 699ndash708
Integrated Child Development Services Scheme (Revised)(ICDS) (1982) Ministry of Social Welfare Governmentof India New Delhi Available on URL httpwcdnicinudishahtmabouticdshtm
Jason JM Nieburg P amp Marks JS (1984) Mortality andinfectious disease associated with infant feeding prac-tices in developing countries Pediatrics 74 702ndash727
Jones G Steketee RW Black RE Bhutta ZA ampMorris SS Bellagio Child Survival Study Group (2003)How many child deaths can we prevent this yearLancet 362 65ndash71
Knippenberg R Lawn JE Darmstadt GL Begkayian GFogstad H Walelign N et al (2005) Systematic scalingup of neonatal care in countries Lancet 365 1087ndash1098
Kramer MS amp Kakuma R (2002) The optimal durationof exclusive breastfeeding a systematic reviewCochrane Database of Systematic Reviews 2002CD003517
Kramer MS Chalmers B Hodnett ED Sevkovskaya ZDzikovich I Shapiro S et al (2000) Promotion ofbreastfeeding intervention trial (PROBIT) a cluster ran-domized trial in the Republic of Belarus Design followup and data validation Advances in Experimental Medi-cine and Biology 478 327ndash345
Kramer MS Chalmers B Hodnett ED Sevkovskaya ZDzikovich I Shapiro S et al (2001) Promotion ofbreastfeeding intervention trial (PROBIT) a random-
Mainstreaming nutrition into MCH programs 15
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
ized trial in the Republic of Belarus Journal of theAmerican Medical Association 285 413ndash420
Lewin SA Dick J Pond P Zwarenstein M Aja Gvan Wyk B et al (2006) Lay health workers in primaryand community health care (Review) The CochraneLibrary 3 1ndash104
LINKAGES (2002) World LINKAGES MadagascarAcademy for Educational Development WashingtonDC
LINKAGES (2005) LINKAGES Zambia 1997ndash2005 FinalReport A Full Report on LINKAGES Infant Feedingand HIVAIDS Programs in Zambia Academy for Edu-cational Development Washington DC Available athttpwwwlinkagesprojectorgmediapublicationsFinal20draft20Zambia20final20report2012105pdf
Lutter CK Perez-Escamilla R Segall A Sanghvi TTeruya K amp Wickham C (1997) The effectiveness of ahospital based program to promote exclusive breastfeed-ing among low income women in Brazil AmericanJournal of Public Health 87 659ndash663
Morrow AL Guerrero ML Shults J Calva J Lutter CBravo J et al (1999) Efficacy of home based peer coun-selling to promote exclusive breastfeeding a randomizedcontrolled trial Lancet 353 1226ndash1231
Ntabaye MK amp Lusiola GJ (2004) Understanding barri-ers to PMTCT in Tanzania findings of a baseline surveyInternational Conference on AIDS 15 (B11396)
de Oliveira LD Giugliani ER do Espirito SLC FrancaMC Weigert EM Kohler CV et al (2006) Effect ofintervention to improve breastfeeding technique on thefrequency of exclusive breastfeeding and lactation-related problems Journal of Human Lactation 22 315ndash321
Perez-Escamilla R (2004) Effectiveness of MADLAC atImproving Breastfeeding Promotion and CounsellingIndicators in Maternity Wards in El Salvador Publishedfor the Basic Support for Institutionalizing Child Sur-vival Project (BASICS II) for the United States Agencyfor International Development Arlington VA Availableat httpwwwbasicsorgpdfFinal20MADLAC20Report20RPE20April207-2004pdf
Perez-Escamilla R (2007) Evidence based breast-feedingpromotion the Baby-Friendly Hospital InitiativeJournal of Nutrition 137 484ndash487
Piwoz EG Iliff PJ Tavengwa N Gavin L Marinda ELunney K et al (2005) An education and counselllingprogram for preventing breastfeeding associated HIVtransmission in Zimbabwe design and impact on mater-nal knowledge and behaviour Journal of Nutrition 135950ndash955
Quinn VJ Guyon AB Schubert JW Stone-Jimenez MHainsworth MD amp Martin LH (2005) Improvingbreastfeeding practices on a board scale at the commu-
nity level success stories from Africa and LatinAmerica Journal of Human Lactation 21 345ndash354
Ranson MK Hanson K Oliveira-Cruz V amp Mills A(2003) Constraints to expanding access to health inter-ventions an empirical analysis and country typologyJournal of International Development 15 15ndash40
Rea MF amp Berquo ES (1990) Impact of the Braziliannational breastfeeding programme on mothers inGreater Sao Paulo Bulletin of the of the World HealthOrganization 68 365ndash371
Rollins NC (2007) Infant feeding and HIV BritishMedical Journal 334 487ndash488
Rutenberg N Baek C Kalibala S Rosen J amp Mulenga D(2004) Evaluation of United Nations supported pilotprojects for the prevention of mother-to-child transmis-sion of HIV overview of findings International Confer-ence on AIDS 15 (WePeE6688)
The Core Group (2005) Scale and Scaling Up A COREGroup Background Paper on lsquoScaling-Uprsquo MaternalNewborn and Child Health Services CORE SpringMembership Meeting 2005 The Core Group Washing-ton DC Available at httpwwwcoregrouporgresourcesmeetingsapril05Scaling_Up_Background_Paper_7-13pdf
The Norwegian Government (1993) Women in PoliticsMinistry of Children and Equality Available at httpwwwregjeringennoendepbldRyddemappeSLA-AvdelingdoclegislationguidelinesWomen-in-Politicshtmlid=437166
Thior I Lockman S Smeaton LM Shapiro RL WesterC Heymann SJ et al (2006) Breastfeeding plus infantzidovudine prophylaxis for 6 months vs formula feedingplus infant zidovudine for 1 month to reduce mother-to-child HIV transmission in Botswana a randomized trialthe Mashi Study Journal of the American Medical Asso-ciation 296 794ndash805
UNICEF (2002) Facts for Life lsquoKey Message What EveryFamily and Community Has a Right to Know aboutBreastfeedingrsquo Available at httpwwwuniceforgffl04key_messageshtm
Van Roekel K Plowman B Griffiths M de AlvaradoVV Matute J amp Calderon M (2002) BASICS IIMidterm Evaluation of the AIN Program in Honduras2000 Basic Support for Institutionalizing Child SurvivalProject (BASICS II) for the United States Agency forInternational Development Arlington VA
WABA (2007) UNICEF Records BHFI Record UpdateAvailable at httpwwwwabaorgmydocsBFHIjan07xls 2006 Regularly updated by Miriam HLabbok Center for Infant and Young ChildFeeding and Care Department of Maternaland Child Health School of Public Health The Univer-sity of North Carolina at Chapel Hill Chapel Hill NCUSA
N Bhandari and AKMI Kabir16
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
WHA (2002) Infant and Young Child Nutrition Fifty-FifthWorld Health Assembly Agenda Item 1310 18 May2002 Available at httpwwwintgbebwhapdf_filesWHA55ewha5525pdf
WHO (1981) The International Code of Marketing ofBreastmilk Substitutes World Health OrganizationGeneva
WHO (1989) Protecting Promoting and Supporting Breast-feeding The Special Role of Maternity Services A JointWHOUNICEF Statement World Health OrganizationGeneva
WHO (2002) The Optimal Duration of Exclusive Breast-feeding Report of an Expert Consultation WHONHD0109 WHOFCHCAH0124 World HealthOrganization Geneva
WHO (2003a) Community Based Strategies for Breastfeed-ing Promotion and Support in Developing CountriesWorld Health Organization Geneva Document refISBN_92_4_159121_8 Available at httpwwwwhointchild-adolescent-healthNew_PublicationsNUTRITIONISBN_92_4_159121_8pdf
WHO (2003b) Multi-country Evaluation of IMCI Effective-ness Cost and Impact (MCE) Progress Report May2002ndashApril 2003 Document ref WHOFCHCAH035World Health Organization Geneva
WHO (2004) Promoting Proper Feeding for Infants andYoung Children World Health Organization GenevaAvailable at httpwwwwhointnutritiontopicsinfantfeedingen
WHO (2006) WHO HIV and Infant Feeding TechnicalConsultation-Consensus Statement World Health Orga-nization Geneva Available at httpwwwwhointhivmediacentreInfantfeedingconsensusstatementpfpdf
WHO Collaborative Study Team on the Role of Breast-feeding on the Prevention of Infant Mortality (2000)Effect of breastfeeding on infant and child mortality dueto infectious diseases in les developed countries apooled analysis Lancet 355 451ndash455
WHOUNICEF (1992) The global criteria for the WHOUNICEF Baby-Friendly Hospital Initiative In Baby-Friendly Hospital Initiative Part II Hospital LevelImplementation World Health Organization Geneva
WHOUNICEF (1993) Breastfeeding Counselling A Train-ing Course WHOCDR933 UNICEFNUT931 WorldHealth Organization Geneva
WHOUNICEF (2002) Protocol for Adapting the FeedingRecommendations Part III IMCI Adaptation GuideWorld Health Organization Geneva
WHOUNICEF (2003) Global Strategy for Infant andYoung Child Feeding World Health OrganizationGeneva Available at httpwwwwhointchild-adolescent-healthpublicationsNUTRITIONIYCF_GShtm
de Zoysa I Rea M amp Martines J (1991) Why promotebreastfeeding in diarrheal diseases control programmesHealth Policy and Planning 6 371ndash379
Mainstreaming nutrition into MCH programs 17
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
Cas
est
udie
so
fef
fect
iven
ess
stud
ies
or
pilo
tpr
ogra
mm
es
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Lut
ter
etal
(199
7)
Bra
zil
Low
-inc
ome
urba
nw
omen
deliv
erin
gin
hosp
ital
s
Bre
astf
eedi
ngpr
omot
ion
in
hosp
ital
sco
mpa
red
wit
h
nobr
east
feed
ing
prom
otio
n
Pro
mot
ion
ofbr
east
feed
ing
in
sele
cted
hosp
ital
s
Mea
nda
ysof
excl
usiv
e
brea
stfe
edin
g
75da
ysvs
22
days
(Plt
001
)
Rea
ampB
erqu
o
(199
0)
Wom
enw
ith
ach
ild
aged
lt2ye
ars
inSa
oP
aulo
Nat
iona
lbre
astf
eedi
ng
cam
paig
n19
81ndash1
986
BF
HI
Mas
sm
edia
cam
paig
n11
in
fant
s5ndash
6m
onth
s
excl
usiv
ely
brea
stfe
d
in19
88an
d37
in
1987
Con
foun
ding
fact
ors
over
the
6-ye
arpe
riod
not
mea
sure
d
Kra
mer
etal
(200
020
01)
PR
OB
ITtr
ial
Bel
arus
Clu
ster
rand
omiz
ed
34ho
spit
als
and
thei
rpo
lycl
inic
s
Trai
ning
inB
FH
I(W
HO
UN
ICE
F19
92)
vsr
outi
ne
prac
tice
san
dpo
licie
s
Exc
lusi
vebr
east
feed
ing
at3
(43
3vs
64
)
and
6(7
9
vs0
6
)
mon
ths
sign
ifica
ntly
high
er
Impl
emen
ted
thro
ugh
BF
HI
ina
sett
ing
whe
reho
spit
al
deliv
erie
sar
eco
mm
on
Per
ez-E
scam
illa
(200
4)
BA
SIC
SII
Mex
ico
Hon
dura
s
Bra
zil
MA
DL
AC
low
-cos
t
man
agem
ent
info
rmat
ion
syst
emto
use
an
evid
ence
-bas
edap
proa
chto
impr
ove
serv
ice
perf
orm
ance
Inte
rvie
win
gof
wom
enat
hosp
ital
disc
harg
epo
st
deliv
ery
usin
ga
ques
tion
nair
eth
atta
kes
5ndash7
min
toad
min
iste
ran
d
cont
ains
19br
east
feed
ing
prom
otio
nco
unse
lling
indi
cato
rs
Dat
aen
tere
dan
dre
sult
s
disc
usse
d3-
mon
thly
by
hosp
ital
com
mit
tee
Hos
pita
lim
plem
ents
chan
ges
in
brea
stfe
edin
g
supp
ort
base
don
anal
ysis
of
ques
tion
nair
es
Itis
aco
st-e
ffec
tive
inte
rven
tion
that
can
help
impr
ovem
ents
inth
eB
FH
I
and
isa
valu
able
tool
for
proc
ess
eval
uati
on
N Bhandari and AKMI Kabir18
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
LIN
KA
GE
S
proj
ect
inA
fric
aan
d
Lat
inA
mer
ica
(Qui
nnet
al
2005
LIN
KA
GE
S
2002
WH
O20
03a)
Bol
ivia
(1
mill
ion)
Gha
na(3
5
mill
ion)
Mad
agas
car
(6m
illio
n)
Res
ourc
e-
poor
sett
ing
Pilo
tpr
ogra
mm
e
InB
oliv
iaan
d
Gha
napr
ogra
mm
e
focu
sed
on
brea
stfe
edin
gan
d
com
plem
enta
ry
feed
ing
InM
adag
asca
r
prog
ram
me
prom
oted
brea
stfe
edin
g
wit
hin
7es
sent
ial
nutr
itio
nac
tion
san
d
subs
eque
ntly
thro
ugh
IMC
I
Bui
lton
form
ativ
ere
sear
ch
and
sust
aine
dth
roug
h
prog
ram
me
acti
viti
esth
at
focu
sed
onbr
ingi
ngab
out
the
desi
red
beha
viou
r
chan
geM
ixof
inte
rven
tion
s
reac
hed
wom
enin
divi
dual
ly
orin
grou
psin
heal
th
faci
litie
sho
mes
or
com
mun
ity
sett
ings
Con
sist
ent
mes
sage
san
d
mat
eria
lacr
oss
all
prog
ram
me
chan
nels
Bol
ivi
PR
OC
OSI
NG
Os
Gha
na
UN
ICE
F
nati
onal
nutr
itio
n
offic
eN
GO
s
Mad
agas
car
Inte
rsec
tora
l
Act
ion
Gro
upfo
r
Nut
riti
on
Jere
o
Sala
ma
Isik
a
Pro
gram
desi
gned
wit
h
part
ners
Rad
ioin
all
thre
esi
tes
Mat
eria
ls
deve
lope
d
tosu
itne
eds
oflo
cal
heal
th
wor
kers
and
com
mun
ity
mem
bers
Gre
at
emph
asis
on
deve
lopm
ent
of coun
selli
ng
and
nego
tiat
ion
skill
s
prac
tica
l
sess
ions
Sign
ifica
ntin
crea
ses
inex
clus
ive
brea
stfe
edin
gra
tes
of
0ndash6-
mon
th-o
ld
infa
nts
from
54
to65
in
Bol
ivia
68
to79
in
Gha
naan
d46
to68
in
Mad
agas
car
In
Gha
naan
d
Mad
agas
car
sign
ifica
ntre
sult
s
obse
rved
wit
hin
aye
ar
ofin
itia
tion
of
com
mun
ity
inte
rven
tion
s
App
roac
hw
asef
fect
ive
and
achi
eved
sign
ifica
nt
incr
ease
sam
ong
larg
e
popu
lati
ons
asea
rly
as
9ndash12
mo
afte
rin
itia
tion
of
com
mun
ity
acti
viti
es
Van
Roe
kele
tal
(200
2)W
HO
(200
3a)
Hon
dura
sG
row
thm
onit
orin
gan
d
prom
otio
nkn
own
as
Ate
ncioacute
nIn
tegr
ala
la
Nintilde
ez(A
IN)
or
Inte
grat
edC
hild
Car
e
Init
ially
pri
mar
ilya
grow
th
mon
itor
ing
prog
ram
me
ulti
mat
ely
thro
ugh
IMC
I
Pro
gram
me
ongr
owth
prom
otio
nndash
asse
ssm
ent
of
mon
thly
wei
ght
gain
and
focu
son
illne
ssf
eedi
ng
prac
tice
san
dge
nera
lchi
ld
care
inin
fant
sun
der
2ye
ars
Impl
emen
ted
atgo
vern
men
t
faci
litie
san
dco
mm
unit
y
Star
ted
in19
92s
tren
gthe
ned
in19
95ndash1
997
wit
hgr
eate
r
focu
son
child
feed
ing
In
1997
pro
gram
me
intr
oduc
ed
wit
hIM
CI
(WH
OU
NIC
EF
2002
)
Maj
or
part
ners
UN
ICE
F
PAH
O
Am
eric
an
and
Hon
dura
n
Red
Cro
ss
CA
RE
Rad
io
broa
dcas
ts
relig
ious
lead
ers
IMC
IM
id-t
erm
eval
uati
on
show
ed39
of
mot
hers
inin
terv
enti
on
com
mun
itie
sex
clus
ivel
y
brea
stfe
dco
mpa
red
wit
h13
in
the
cont
rol
site
s
Mainstreaming nutrition into MCH programs 19
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
cont
inue
d
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Bha
ndar
ieta
l
(200
3)
WH
O
(200
3a)
Rur
alco
mm
unit
ies
inH
arya
na
Indi
a
Clu
ster
rand
omiz
edtr
ial
8
com
mun
itie
s(t
otal
popu
lati
on~4
000
0)
Pro
mot
ion
ofex
clus
ive
brea
stfe
edin
gan
d
appr
opri
ate
com
plem
enta
ryfe
edin
g
Dev
elop
edth
roug
h
form
ativ
ere
sear
ch
ndashP
robl
emid
enti
ficat
ion
ndashP
arti
cipa
tory
desi
gnof
inte
rven
tion
impl
emen
tati
onan
d
eval
uati
on
Impl
emen
tati
onw
ithi
nan
exis
ting
prim
ary
heal
th-c
are
prog
ram
me
Opp
ortu
niti
esus
edto
deliv
erm
essa
ges
wer
e
imm
uniz
atio
ncl
inic
s
wei
ghin
gse
ssio
ns
sick
-chi
ldco
ntac
tsan
d
mon
thly
hom
evi
sits
Res
earc
hers
wit
hlo
cal
gove
rnm
ent
ICD
Ssy
stem
and
NG
O
The
atre
son
gs
Mas
sm
edia
not
used
for
risk
of
cont
amin
atio
n
Mat
eria
ls
deve
lope
d
for
heal
th
wor
kers
pos
ters
flip
book
sca
rds
Bre
astf
eedi
ng
coun
selli
ngse
ctio
n
ofth
eIM
CI
(WH
O
UN
ICE
F20
02)
Exc
lusi
ve
brea
stfe
edin
gin
the
prev
ious
24h
at3
mon
ths
of
age
79
vs4
8
The
posi
tive
effe
ct
rem
aine
dup
to
6m
onth
sof
age
(42
vs4
)
Tota
lpar
tici
pati
onof
the
dist
rict
heal
thsy
stem
from
ince
ptio
nof
the
prog
ram
me
inde
velo
ping
impl
emen
tati
onst
rate
gyt
ool
deve
lopm
ent
and
mon
itor
ing
inad
diti
onto
invo
lvem
ent
of
anN
GO
wer
eim
port
ant
feat
ures
that
cont
ribu
ted
to
the
succ
ess
ofth
e
inte
rven
tion
Mor
row
etal
(199
9)
Mex
ico
Cit
yC
lust
erra
ndom
ized
tria
l
Tota
lpop
ulat
ion
3000
0
Two
com
mun
itie
sin
the
inte
rven
tion
one
com
pari
son
130
wom
en
Hom
e-ba
sed
peer
coun
selli
ng
Pee
rco
unse
llors
mad
e3
or
6ho
me
visi
tsto
the
mot
her
Key
fam
ilym
embe
rsal
so
incl
uded
By
La
Lec
he
Lea
gue
of
Mex
ico
Exc
lusi
ve
brea
stfe
edin
g
at3
mon
ths
post
-par
tum
67
(6vi
sits
)
50
(3vi
sits
)12
(com
pari
son)
Firs
tcl
uste
rra
ndom
ized
com
mun
ity-
base
dtr
ialt
hat
used
peer
coun
sello
rsto
prom
ote
excl
usiv
e
brea
stfe
edin
g
Hai
der
etal
2000
200
2
Dha
ka
Low
mid
dle
and
low
-soc
io-
econ
omic
popu
lati
on
Clu
ster
rand
omiz
edtr
ial
20zo
nes
inin
terv
enti
on
and
20in
cont
rol
Com
mun
ity-
base
dpe
er
coun
selli
ngin
Dha
ka
15ho
me-
base
dco
unse
lling
visi
tsby
peer
coun
sello
rs
40h
(4h
yen10
days
)
WH
OU
NIC
EF
brea
stfe
edin
g
coun
selli
ngco
urse
(WH
OU
NIC
EF
1993
)
Exc
lusi
ve
brea
stfe
edin
g
at5
mon
ths
70
in
inte
rven
tion
and
6in
the
cont
rol
Com
mun
ity-
base
d
brea
stfe
edin
gpr
omot
ion
stra
tegy
was
effe
ctiv
ein
Ban
glad
esh
whe
rem
ost
deliv
erie
soc
cur
atho
me
N Bhandari and AKMI Kabir20
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Bry
ceet
al
(200
4)W
HO
(200
3b)
Bra
zil
Per
u
Tanz
ania
Uga
nda
Mul
tico
untr
yev
alua
tion
of
IMC
Ith
atin
clud
ed
effe
ctiv
enes
sco
stan
d
impa
ct(B
ryce
etal
2004
)
Bre
astf
eedi
ngpr
omot
ion
asa
part
ofIM
CI
IMC
Iis
ast
rate
gyfo
r
impr
ovin
gch
ildhe
alth
and
deve
lopm
ent
thro
ugh
the
com
bine
d
deliv
ery
ofes
sent
ial
child
heal
th
inte
rven
tion
sIM
CI
bega
nw
ith
ase
tof
case
man
agem
ent
guid
elin
es
for
the
man
agem
ent
ofsi
ckch
ildre
nat
first
-lev
elhe
alth
faci
litie
s
and
the
guid
elin
esw
ere
desi
gned
for
adap
tati
on
atco
untr
yle
vela
nd
belo
wO
ver
tim
eth
e
stra
tegy
expa
nded
to
incl
ude
ara
nge
of
guid
elin
esfo
rde
liver
ing
child
surv
ival
inte
rven
tion
at
hous
ehol
dco
mm
unit
y
and
refe
rral
leve
ls
IMC
Im
odul
e(W
HO
UN
ICE
F20
02)
Res
ults
onex
clus
ive
brea
stfe
edin
g
avai
labl
efr
om
Tanz
ania
whe
reno
sign
ifica
ntim
pact
was
seen
Des
pite
subs
tant
ial
impr
ovem
ent
inth
equ
alit
y
ofca
rede
liver
edby
IMC
Iat
heal
thfa
cilit
ies
key
fam
ily
prac
tice
ssu
chas
excl
usiv
e
brea
stfe
edin
gdi
dno
tch
ange
asco
mm
unit
yIM
CI
had
not
been
impl
emen
ted
byth
at
tim
e(W
HO
2003
b)
SA
rife
en
pers
onal
com
mun
icat
ion
Ban
glad
esh
Mat
lab
Com
mun
ity-
base
dcl
uste
r
desi
gn
Eva
luat
ion
offa
cilit
y-an
d
com
mun
ity-
base
dIM
CI
Inte
rven
tion
pack
age
incl
udes
feed
ing
asse
ssm
ent
and
coun
selli
ngon
mot
hers
ofyo
ung
child
ren
seek
ing
care
atfa
cilit
ies
for
illne
ssan
d
hom
e-ba
sed
coun
selli
ng
onim
prov
edfe
edin
gby
com
mun
ity-
base
dhe
alth
and
nutr
itio
nw
orke
rs
At
base
line
inth
e
year
2000
alit
tle
mor
eth
anha
lfth
e
0ndash5-
mon
th-o
ld
infa
nts
inth
est
udy
area
wer
ebe
ing
excl
usiv
ely
brea
stfe
dB
y20
05
this
incr
ease
dby
30
inth
eIM
CI
area
Dat
ano
t
avai
labl
efr
omth
e
com
pari
son
area
as
yet
Lac
kof
com
para
ble
data
from
the
com
pari
son
area
prev
ents
ade
finit
ive
conc
lusi
onas
tow
heth
erth
is
trul
yis
anim
pact
ofIM
CI
BA
SIC
SII
Bas
icSu
ppor
tfo
rIn
stit
utio
naliz
ing
Chi
ldSu
rviv
alP
roje
ctB
FH
IB
aby-
Frie
ndly
Hos
pita
lIni
tiat
ive
ICD
SIn
tegr
ated
Chi
ldD
evel
opm
ent
Serv
ices
IM
CI
Inte
grat
edM
anag
emen
tof
Chi
ldho
odIl
lnes
sM
AD
LA
CM
onit
oreo
deA
poyo
Dir
ecto
con
laL
acat
anci
aM
ater
naN
GO
non
-gov
ernm
enta
lorg
aniz
atio
nPA
HO
Pan
Am
eric
anH
ealt
hO
rgan
izat
ion
PR
OB
ITP
rom
otio
nof
Bre
astf
eedi
ngIn
terv
enti
onTr
ial
PR
OC
OSI
Pro
gram
ade
Coo
rdin
acio
nen
Salu
dIn
tegr
al(C
olla
bora
tive
Pro
gram
for
Inte
grat
edH
ealt
h)U
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
WH
OW
orld
Hea
lth
Org
aniz
atio
n
Mainstreaming nutrition into MCH programs 21
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x2
Cas
est
udie
sin
scal
e-up
effo
rts
inH
IVA
IDS
Stud
yde
scri
ptio
nPo
pula
tion
Inte
rven
tion
Com
mun
icat
ion
stra
tegy
Impa
cton
excl
usiv
ebr
east
feed
ing
Com
men
ts
LIN
KA
GE
S(2
005)
Zam
bia
Pro
gram
me
thro
ugh
heal
th-c
are
and
com
mun
ity
serv
ices
Rea
ched
60si
tes
in6
dist
rict
sby
2005
Inte
grat
ion
ofin
fant
feed
ing
coun
selli
ngm
ater
naln
utri
tion
and
anti
retr
ovir
aldr
ugs
prop
hyla
xis
Trai
ning
ofhe
alth
wor
kers
and
com
mun
ity
serv
ice
prov
ider
sto
coun
selw
omen
onsa
fety
opti
ons
for
thei
rsi
tuat
ion
Beh
avio
urch
ange
Com
mun
icat
ion
inte
rven
tion
sin
the
first
few
year
sM
ater
iald
evel
oped
lsquoAct
Now
rsquoM
edia
cam
paig
nsin
clud
edbr
ochu
res
post
ers
radi
oan
dte
levi
sion
Ass
esse
dth
roug
hba
selin
ean
dfo
llow
-up
hous
ehol
dan
dcl
inic
surv
eys
inse
lect
eddi
stri
cts
Exc
lusi
vebr
east
feed
ing
rate
incr
ease
dfr
om50
in
2002
to64
in
2004
inL
ivin
gsto
nean
dfr
om57
in
2000
to74
in
2004
inN
dola
Inte
grat
edde
mon
stra
tion
proj
ect
Had
seve
rals
tren
gths
inte
rms
ofth
eus
eof
form
ativ
ere
sear
chto
deve
lop
mes
sage
str
aini
ngan
dbu
ildin
gup
skill
sof
prog
ram
me
man
ager
she
alth
-car
epr
ovid
ers
and
com
mun
ity
wor
kers
adv
ocac
yfo
rna
tion
alpo
licy
stro
ngbe
havi
our
chan
geco
mm
unic
atio
nco
mpo
nent
st
reng
then
ing
com
mun
ity
capa
city
for
coun
selli
ngan
dre
ferr
als
and
mon
itor
ing
and
eval
uati
onw
ith
loca
lpar
tner
sP
iwoz
etal
(20
05)
ZV
ITA
MB
Otr
ial
Har
are
Zim
babw
eE
duca
tion
and
coun
selli
ngpr
ogra
mm
ede
liver
edan
tena
tally
1411
0m
othe
rndashba
bypa
irs
enro
lled
from
14m
ater
nity
clin
ics
wit
hin
96h
ofde
liver
yan
dfo
llow
edup
at6
wee
ks
3m
onth
san
d3-
mon
thly
inte
rval
sIn
fant
-fee
ding
patt
erns
dete
rmin
edE
xclu
sive
brea
stfe
edin
gre
com
men
ded
for
HIV
nega
tive
un
know
nor
HIV
posi
tive
who
chos
eto
brea
stfe
ed
Gro
uped
ucat
ion
indi
vidu
alco
unse
lling
vid
eos
broc
hure
sM
othe
rsw
hoen
rolle
dw
hen
prog
ram
me
was
fully
impl
emen
ted
wer
e8
4ti
mes
mor
elik
ely
toex
clus
ivel
ybr
east
feed
than
mot
hers
who
enro
lled
befo
reth
epr
ogra
mm
ebe
gan
Ove
rall
excl
usiv
ebr
east
feed
ing
rate
sti
ll3
mon
ths
was
low
at24
6
Form
ativ
ere
sear
chus
edto
desi
gna
cult
ural
lyse
nsit
ive
educ
atio
nan
dco
unse
lling
prog
ram
me
Low
over
alle
xclu
sive
brea
stfe
edin
gra
tes
prom
pted
auth
ors
toco
nclu
deth
atw
omen
and
thei
rpa
rtne
rssh
ould
have
been
reac
hed
mor
efr
eque
ntly
duri
ngan
tena
tala
ndpo
st-n
atal
peri
od
N Bhandari and AKMI Kabir22
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Thi
oret
al(
2006
)R
ollin
s(2
007)
C
ohen
(200
7)
HIV
-inf
ecte
dpr
egna
ntw
omen
atte
ndin
gan
tena
talc
linic
sin
sout
hB
otsw
ana
Inve
stig
atio
nsby
CD
Cof
adi
arrh
oea
outb
reak
inJa
nuar
y-Fe
brua
ry20
06in
the
sam
epo
pula
tion
Mat
erna
land
infa
ntan
tire
trov
iral
ther
apy
toas
cert
ain
impa
cton
HIV
tran
smis
sion
Ant
enat
alco
unse
lling
Cas
endashco
ntro
lstu
dyto
iden
tify
risk
fact
ors
for
diar
rhoe
ano
tbr
east
feed
ing
was
the
bigg
est
risk
fact
ora
djus
ted
odds
rati
o50
(95
confi
denc
ein
terv
al4
5ndash10
0)
Bot
swan
aha
sth
ebe
stpr
imar
yhe
alth
-car
est
ruct
ure
wat
ersu
pply
and
sani
tati
onsy
stem
sin
Sout
hA
fric
aFo
rmul
apr
ovid
edfr
eeby
the
gove
rnm
ent
toin
fect
edm
othe
rsL
ower
mor
talit
yin
the
brea
stfe
edin
ggr
oup
at7
mon
ths
dem
onst
rate
sri
skof
form
ula
feed
ing
and
need
for
alte
rnat
est
rate
gies
(Thi
oret
al
2006
)A
utho
rsco
nclu
deth
athe
alth
syst
ems
inw
hich
thes
epr
ogra
mm
esar
eim
plem
ente
dsh
ould
beab
leto
cope
wit
hdi
arrh
oea
and
mal
nutr
itio
nth
atre
sult
sbe
caus
eof
form
ula
feed
ing
(Rol
lins
2007
)C
oova
dia
etal
(2
007)
Kw
aZul
uNat
al
Sout
hA
fric
a27
22H
IV-i
nfec
ted
and
unin
fect
edpr
egna
ntw
omen
enro
lled
into
ano
n-ra
ndom
ized
inte
rven
tion
coho
rtst
udy
from
ante
nata
lcl
inic
sIn
fant
feed
ing
data
obta
ined
wee
kly
bloo
dsa
mpl
esfr
omin
fant
sta
ken
mon
thly
83
of13
72in
fant
sbo
rnto
HIV
-inf
ecte
dm
othe
rsin
itia
ted
excl
usiv
ebr
east
feed
ing
from
birt
hB
reas
tfed
infa
nts
who
rece
ived
solid
sw
ere
sign
ifica
ntly
mor
elik
ely
toac
quir
ein
fect
ion
com
pare
dw
ith
excl
usiv
ely
brea
stfe
d(H
R10
87
151
ndash78
P=
001
8)as
wer
ein
fant
sw
hoat
12w
eeks
rece
ived
brea
stan
dfo
rmul
am
ilk(1
82
098
ndash33
6P
=0
57)
Cum
ulat
ive
3-m
onth
mor
talit
yin
excl
usiv
ely
brea
stfe
dw
as6
1(4
74ndash
792
)vs
15
1(7
63ndash
287
3)in
infa
nts
give
nre
plac
emen
tfe
eds
(HR
206
1
0ndash4
27P
=0
05)
The
stud
ysh
ows
that
excl
usiv
ebr
east
feed
ing
can
besu
cces
sful
lysu
ppor
ted
inH
IV-i
nfec
ted
wom
enT
heau
thor
sca
llfo
rfu
rthe
rre
visi
onof
UN
ICE
FW
HO
and
USA
IDin
fant
feed
ing
guid
elin
es
CD
CC
ente
rof
Dis
ease
Con
trol
HR
haz
ards
rati
oU
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
USA
IDU
SA
genc
yfo
rIn
tern
atio
nalD
evel
opm
ent
WH
OW
orld
Hea
lth
Org
aniz
atio
nZ
VIT
AM
BO
Z
imba
bwe
Vit
amin
Afo
rM
othe
rsan
dB
abie
s
Mainstreaming nutrition into MCH programs 23
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23

and increase community involvement (Bhandari et al
2005 Quinn et al 2005)Effective counselling requires assessment of
feeding practices recognition of problems and nego-tiation with the mother in choosing improved prac-tices that are feasible (WHOUNICEF 2002) thisrequires time and patience Programmes may chooseone-on-one counselling during opportunities in whichmore time is available such as home visits and groupcounselling for opportunities with lesser availabletime (Bhandari et al 2005) One of the reasons thatpeer counsellors may have been effective was thattheir sole responsibility was counselling mothersthrough home visits (Morrow et al 1999 Haider et al
2000) The more diverse the functions of the localworker the lesser will be the emphasis on a singlecomponent such as exclusive breastfeeding
Message development
The development of messages for interpersonal com-munication and for mass media needs careful atten-tion to design and content Successful programmesincluded an element of formative research to gain anin-depth understanding of the communities wherethese programmes were implemented with regard topractices pertaining to breastfeeding the reasons forthe current practices the common breastfeedingproblems and the barriers to adoption of ideal behav-iours in that cultural setting Formative research innorth India for instance showed general unwilling-ness to offer water to infants in summer months Thisbarrier was overcome by building specific explanatorymessages using local terms within the communicationstrategy (Bhandari et al 2003)
Once the design features and broad strategy are inplace attention must then shift to the operationaliza-tion of the strategy
Training and supervision
Prior to scale-up the training needs will need to bedefined Fortunately for promotion of exclusivebreastfeeding extensive experience is available ontraining of different cadres of health workers andeven for lay counsellors Most experiences used the
adapted versions of the UNICEFWHO Breastfeed-ing Counseling Course (WHOUNICEF 1993) or theIMCI module (WHOUNICEF 2002)
Training strategy and its quality merit attentionIn successful programmes the duration of trainingextended from 3 full days to 10 part days for differentworkers The training strategies as described werelsquoconcise action orientedrsquo and included modules thataimed to equip trainers with practical skills and con-fidence to counsel effectively (Appendix 1)
Training modules for areas with high HIV preva-lence also exist (WHO 2006)
While the training modules used in studies workedwell a gap remains for referralTrained workers at thecommunity level require that referral options avail-able are easily accessible prompt and preferablyavailable free of cost to mothers with complex breast-feeding problems
Another important issue to address is handlingtraining of new staff in most developing countriesstaff turnover and absenteeism rates are high
Monitoring and evaluation
The programme strategy will need to include systemsfor monitoring and evaluation of the programmePossible markers could include the rates of exclusivebreastfeeding worker performance referral andaction As for all other national programmes therewill be a need for periodic reviews and achievabletargets by time
Costs and resources
In all pilot programmes and projects services wereprovided to mothers free of cost In many developingcountries if the government cadre of health workers isused to promote exclusive breastfeeding as a part oftheir other responsibilities (eg the IMNCI) the basicservices will remain free However a system thatrequires setting up a cadre of trained lactation coun-sellors (eg in an urban setting or as referral sources forbreastfeeding problems in rural areas) will requireadditional resources A cost-effective analysis of theBFHI was conducted in three countriesBrazilMexicoand Honduras (Horton et al 1996) Savings on health
Mainstreaming nutrition into MCH programs 11
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
care resulting from reduction in diarrhoeal and respi-ratory morbidity were estimated as a result of theeffect of BFHI on breastfeeding The study showedthat breastfeeding promotion through a BFHI-likemodel is very cost-effective (1992 US$ 2ndash19 per dis-ability adjusted life years Horton et al 1996 Perez-Escamilla 2007) Examples of cost-effectivenessanalysis of community-based programmes using lay orprofessional support in different settings could not beidentified
Testing of novel approaches andcontinuing innovation
Scaled-up programmes must have inbuilt provision totest novel approaches and the ability for continuinginnovation
Scaling up of exclusive breastfeeding in thecontext of HIV
The policy and programme design and implemen-tation issues relevant to exclusive breastfeedingscale-up discussed above are relevant to HIV-prevalent areas but there are other unique featuresthat merit consideration
Creating policies for exclusive breastfeeding pro-motion in countries with high HIV prevalence is par-ticularly challenging The revised recommendationsencourage exclusive breastfeeding for the first 6months and continued breastfeeding for 2 years andbeyond for infants whose mothers are HIV negativeor whose HIV status is unknown For women who areknown to be HIV positive the most appropriateinfant feeding option for HIV-exposed infantsdepends on individual circumstances including con-sideration of health services counselling and supportExclusive breastfeeding is the better option for suchinfants unless replacement feeding is acceptable fea-sible affordable sustainable and safe for both themother and baby This recommendation is based onthe finding that exclusive breastfeeding for up to 6months in three large cohort studies is associated witha three- to fourfold decreased risk of transmission ofHIV compared with non-exclusive breastfeeding(WHO 2006) The recommendations may need
further revision if new findings demonstrate thatexclusive breastfeeding should be the feeding ofchoice for HIV-infected women (Iliff et al 2005)
Some pilot programmes for exclusive breastfeedingpromotion in high-HIV-prevalence countries aresummarized in Appendix 2
In general exclusive breastfeeding promotionformed a part of the prevention of mother-to-childtransmission programmes LINKAGESZambiaintegrated improved counselling on infant feedingmaternal nutrition and antiretroviral therapy duringprophylaxis in both health-care and community ser-vices to enable women to make and act on informedchoice to feed their infants optimally in the context ofhigh HIV prevalence
Formative research was critical to develop locallyappropriate and feasible infant feeding recommenda-tions for individual infants and their families based onHIV status In Zambia the research included focusedgroup discussions key information interviews obser-vations of household food preparation and feedingmarket survey of replacement foods and breastmilksubstitutes and household trials of improved feedingand caring practices (LINKAGES 2005)
High quality of health workers is another criticalfactor for sensitive and accurate individual counsel-ling Programmes incorporated behaviour changecommunication methodologies in training (LINK-AGES 2005) It is important to develop skills of com-munity members as well for improved servicesreferral outreach and follow-up care and support ofHIV-positive mothers and their infants
A comprehensive communications strategy tosupport scale-up was a notable feature of the LINK-AGES programme in Zambia In 2004 an intensiveeffort was launched using brochures posters radioand television spots billboards and reference guidesfor health providers (LINKAGES 2005) Messageswere targeted to relevant stakeholders ndash pregnantand lactating mothers health providers youth andcommunity leaders and all the materials were nation-ally disseminated
Monitoring and evaluation another importantfeature of effective scale-up was a feature of pilotprogrammes (Appendix 2 Ntabaye amp Lusiola 2004Rutenberg et al 2004) in Zambia and Tanzania Moni-
N Bhandari and AKMI Kabir12
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
toring and evaluation not only provides a measure ofsuccess but identifies factors that may have contrib-uted to it and to lack of success to enable mid-coursecorrections The impact of some pilot programmes onexclusive breastfeeding is summarized in Appendix 2In most programmes exclusive breastfeeding ratesimproved In Zambia exclusive breastfeeding ratesincreased from 50 in 2002 to 64 in 2004 in Liv-ingstone from 57 in 2000 to 74 in 2004 in NdolaIn South Africa an antenatal clinic-based interven-tion led to 83 of infants born to HIV-infectedmother initiating exclusive breastfeeding InZimbabwe an intervention based on antenatal coun-selling resulted in a relatively lower exclusive breast-feeding rate of 246 at 3 months (Piwoz et al 2005)
Several barriers to success were identified Theseinclude inadequate skills of workers and non-integration of HIV counselling and tailoring into ante-natal care services (Ntabaye amp Lusiola 2004) which isthe backbone in which infant feeding counselling isbuiltWomen reported that mothers not breastfeedingtheir children were discriminated against by the com-munity and they faced the threat of domestic violenceProgramme managerrsquos understanding of barriersto effective programme implementation and impactwere emphasized as being important Governmentsupport partnerrsquos coordination increased humanresource and improving the supply system were iden-tified to be essential features to scale up programmesin the HIV context (Rutenberg et al 2004) Lowoverall exclusive breastfeeding rates prompted Piwozet al (2005) to conclude that women and their partnersshould have been reached more frequently during theantenatal and post-natal period
Conclusions
In a large number of programmes for improvingexclusive breastfeeding in developing countriesincluding in areas with high prevalence of HIV apositive impact on exclusive breastfeeding rates hasbeen achieved
Some of the factors that contributed to successfulscale-up are summarized in Table 4 Several limita-tions of the programmes reviewed merit attentionMost programmes involved special and generous
funding concentrated efforts and multiple contactsThese programmes were evaluated over relativelyshort periods of time usually 2ndash5 years and the long-term sustainability has not been really tested In theabsence of specific measures there is likely to be dilu-tion of quality as the programmes are scaled upfurther from their initial size The experience thus farleaves important questions to be addressed particu-larly on how programmes can be sustained over timeas they are scaled up at affordable costs
A key factor relevant to sustainability is to plan ona long-term basis a period of 10ndash20 years rather than5ndash10 years from the outset Experience with otherchild health programmes has shown that performancein immunization and oral rehydration therapy userates plateaued over time in many countries
Programme scale-up requires a programme man-agement capacity proportionate to the scale of opera-tions periodic assessment of barriers (Table 5) and anability to revise programme strategy to overcomethese Another key feature to sustainability ofscale-up is the extent to which capacity has been builtat the district block and community levels National-or state-level driven interventions begin with enor-mous enthusiasm which is difficult to sustain Thisfactor is particularly important as most developing
Table 4 Lessons learnt about scale-up key factors in success
bull Political will advocacy enabling policiesbull Championship by health ministries at national state and districtlevelbull Technical consensus on feeding guidelinesbull Programme strategy and measurable short- and long-term goalsbull Long-term financial commitmentbull Partners with defined roles assessment of their capacity todeliver and plans to cover gaps in capacitybull Emphasis on community-level interventions and not onlyfacility-based programmesbull Formative research as the backbone of effective scale-upprogrammes particularly in the context of HIVbull Careful selection of channels and the number required toachieve timely coverage consistency of messagesbull Communication strategy aided by formative research pre-testedvalidated messages and toolsbull Quality trainers and training centres proportionate to requiredscalebull Monitoring and evaluationbull Programme redesign when relevant through research analysisand innovation
Mainstreaming nutrition into MCH programs 13
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
countries are going through a process of decentrali-zation with increasing responsibility for planningimplementation and evaluation being delegated tolower levels of the health-care system Buildingcapacity at that level requires time resources andpatience and a longer-term perspective
Building capacity emerges to be a key factorTrainers and training centres vary in their qualitywhen training health workers and their supervisorsor programme managers As the burden of trainingincreases availability of good-quality trainersbecomes a limiting factor (WHOUNICEF 2002Government of India 2006) An effective strategymust plan for these incremental requirements includ-ing ensuring secure and sustained funding
Identifying barriers to success is a key actor Thebarriers to scaling up of health interventions havebeen elegantly described by Ranson et al (Table 5)Most of these are important for exclusive breastfeed-ing scale-up as well
Overall within the limitations discussed above anumber of programmes in countries with varying
HIV prevalence show that exclusive breastfeeding ona large scale is feasible and pilot programmes havegiven valuable guidance related to policies planningand implementation of large-scale programmes Thechallenge now is to build on these experiences whenplanning national programmes
Acknowledgements
We sincerely thank Dr MK Bhan for his constructivecriticism and sustained feedback at different stages ofdevelopment of this review
Conflicts of interest
The authors have declared no conflicts of interest
References
Arifeen S Black RE Antelman G Baqui A CaulfieldL amp Becker S (2001) Exclusive breastfeeding reducesacute respiratory infection and diarrhea deaths amonginfants in Dhaka slums Pediatrics 108 E67
Australian Breastfeeding Association (2005) Valuing Par-enthood Options for Paid Maternity Leave ndash InterimPaper 2002 Available at httpwwwbreastfeedingasnauadvocacymatleavehtml
Bhandari N Bahl R Mazumdar S Martines J BlackRE amp Bhan MK (2003) Effect of community basedpromotion of exclusive breastfeeding on diarrheal ill-nesses and growth a cluster randomized controlled trialLancet 361 1418ndash1423
Bhandari N Mazumder S Bahl R Martines J BlackRE amp Bhan MK (2004) An educational interventionto promote appropriate complementary feedingimproves child feeding practices and linear growth inrural Haryana India Journal of Nutrition 134 2342ndash2348
Bhandari N Mazumder S Bahl R Martines J BlackRE amp Bhan MK (2005) Use of multiple opportunitiesfor improving feeding practices in undertwos withinchild health programs Health Policy Plan 20 328ndash336
Bryce J Victora CG Habicht JP Vaughan JP ampBlack RE (2004) The multi-country evaluation of theintegrated management of childhood illness strategylessons for the evaluation of public health interventionsAmerican Journal of Public Health 94 406ndash415
Butte NF Lopez-Alarcon MG amp Garza C (2002) Nutri-ent Adequacy of Exclusive Breastfeeding for the TermInfant during the First Six Months of Life World HealthOrganization Geneva
Table 5 Barriers to scaling up of health interventions
Community and household levelsLack of information womenrsquos education physical financial
womenrsquos decision-making powerHealth services delivery levelShortage of qualified staff weak technical guidance programme
management and supervision inadequate supplies equipmentand infrastructure poor accessibility
Health sector policy and strategic management levelWeak and centralized system for planning and management weak
drug policies and supply system inadequate regulations lack ofintersectoral action and partnership weak incentives to useinputs efficiently and respond to user needs and preferencesreliance on donor funding
Public policies cutting across sectorsGovernment bureaucracy poor communication and transport
infrastructureEnvironmental characteristicsGovernance and overall policy frameworkCorruption weak government weak laws political instability and
insecurity low priority to social sectors weak structure for publicaccountability and opportunities for public opinions lack of freepress
Physical environmentClimatic and geographic predisposition physical environment
unfavourable to service delivery
Adapted from Ranson et al (2003)
N Bhandari and AKMI Kabir14
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Cohen J (2007) Retrovirus meeting Hope on new AIDSdrugs but breast-feeding strategy backfires Science 3151357
Coovadia HM Rollins NC Bland RM Little KCoutsoudis A Bennish ML et al (2007) Mother tochild transmission of HIV-1 infection during exclusivebreastfeeding in the first 6 months of life an interven-tion cohort study Lancet 369 1107ndash1116
Coutinho SB de Lira PI de Carvalho LM amp AshworthA (2005) Comparison of the effect of two systems forthe promotion of exclusive breastfeeding Lancet 3661094ndash1100
Feachem RG amp Koblinsky MA (1984) Interventions forthe control of diarrheal diseases among young childrenpromotion of breastfeeding Bulletin of the of the WorldHealth Organization 62 271ndash291
Gonzales A Arteaga E amp Howard-Grabman L (1998)Scaling Up the WARMI Project ndash Lessons LearnedMobilizing Bolivian Communities around ReproductiveHealth Save the Children Federation Inc Bolivia FieldOffice La Paz Available at httpwwwcoregrouporgresourcesSavebolipdf
Government of India (1997) Recommendations of the FifthCentral Pay Commission Relating to Enhancement ofQuantum of Maternity Leave and to Allow PaternityLeave in Respect of Central Government EmployeesDocument ref 13018197-Estt(L) Available at httppersminnicinesttleave2htm
Government of India (2005) National Rural HealthMission 2005ndash2012 Mission document Ministry ofHealth and Family Welfare New Delhi Government ofIndia Available at httpwwwmohfwnicinNRHM20Mission20Documentpdf
Government of India (2006) Operational Guidelines forImplementation of Integrated Management of Neonataland Childhood Illness (IMNCI) Ministry of HealthFamily Welfare New Delhi Available at httpmohfwnicindofw20websiteF20IMNCI20Operational20Plan201320june202006htm
Government of Pakistan (2003) National Programme forFamily Planning and Primary Health Care The LadyHealth Workers Programme 2003ndash2008 Ministry ofHealth Pakistan Available at httpwwwphcgovpkDownloadsPC-120augpdf
Green CP (1999) Improving Breastfeeding Behaviors Evi-dence from Two Decades of Intervention ResearchPublished for the US Agency for International Develop-ment (USAID) by the LINKAGES Project Academyfor Educational Development Washington DC
Gupta A (2002) National trends in breastfeeding andeffective strategies to improve breastfeeding ratesJournal of Neonatology 2002 4ndash14
Gwatkin DR (2004) Integrating the management of child-hood illness Lancet 364 1557ndash1558
Habicht JP DaVanzo J amp Butz WP (1986) Does breast-feeding really save lives or are apparent benefits due tobiases American Journal of Epidemiology 123279ndash290
Haider R Ashworth A Kabir I amp Huttly SR (2000)Effect of community based peer counsellors on exclusivebreastfeeding practices in Dhaka Bangladesh a ran-domized controlled trial Lancet 356 1643ndash1647
Haider R Kabir I Huttly SR amp Ashworth A (2002)Training peer counsellors to promote and support exclu-sive breastfeeding in Bangladesh Journal of HumanLactation 18 7ndash12
Horton S Sanghvi T Phillips M Fiedler J Perez-Escamilla R Lutter C et al (1996) Breastfeeding pro-motion and priority setting in health Health Policy andPlanning 11 156ndash168
ILO (1998) More than 120 Nations Provide Paid MaternityLeave Gap in Employment Treatment for Men andWomen Still Exists International Labour Office GenevaDocument ref ILO987 Available at httpwwwiloorgpublicenglishbureauinfpr19987htmr2
Iliff PJ Piwoz EG Tavengwa NV Zunguza CDMarinda ET Nathoo KJ et al (2005) Early exclusivebreastfeeding reduces the risk of postnatal HIV-1 trans-mission and increase HIV-free survival AIDS 19 699ndash708
Integrated Child Development Services Scheme (Revised)(ICDS) (1982) Ministry of Social Welfare Governmentof India New Delhi Available on URL httpwcdnicinudishahtmabouticdshtm
Jason JM Nieburg P amp Marks JS (1984) Mortality andinfectious disease associated with infant feeding prac-tices in developing countries Pediatrics 74 702ndash727
Jones G Steketee RW Black RE Bhutta ZA ampMorris SS Bellagio Child Survival Study Group (2003)How many child deaths can we prevent this yearLancet 362 65ndash71
Knippenberg R Lawn JE Darmstadt GL Begkayian GFogstad H Walelign N et al (2005) Systematic scalingup of neonatal care in countries Lancet 365 1087ndash1098
Kramer MS amp Kakuma R (2002) The optimal durationof exclusive breastfeeding a systematic reviewCochrane Database of Systematic Reviews 2002CD003517
Kramer MS Chalmers B Hodnett ED Sevkovskaya ZDzikovich I Shapiro S et al (2000) Promotion ofbreastfeeding intervention trial (PROBIT) a cluster ran-domized trial in the Republic of Belarus Design followup and data validation Advances in Experimental Medi-cine and Biology 478 327ndash345
Kramer MS Chalmers B Hodnett ED Sevkovskaya ZDzikovich I Shapiro S et al (2001) Promotion ofbreastfeeding intervention trial (PROBIT) a random-
Mainstreaming nutrition into MCH programs 15
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
ized trial in the Republic of Belarus Journal of theAmerican Medical Association 285 413ndash420
Lewin SA Dick J Pond P Zwarenstein M Aja Gvan Wyk B et al (2006) Lay health workers in primaryand community health care (Review) The CochraneLibrary 3 1ndash104
LINKAGES (2002) World LINKAGES MadagascarAcademy for Educational Development WashingtonDC
LINKAGES (2005) LINKAGES Zambia 1997ndash2005 FinalReport A Full Report on LINKAGES Infant Feedingand HIVAIDS Programs in Zambia Academy for Edu-cational Development Washington DC Available athttpwwwlinkagesprojectorgmediapublicationsFinal20draft20Zambia20final20report2012105pdf
Lutter CK Perez-Escamilla R Segall A Sanghvi TTeruya K amp Wickham C (1997) The effectiveness of ahospital based program to promote exclusive breastfeed-ing among low income women in Brazil AmericanJournal of Public Health 87 659ndash663
Morrow AL Guerrero ML Shults J Calva J Lutter CBravo J et al (1999) Efficacy of home based peer coun-selling to promote exclusive breastfeeding a randomizedcontrolled trial Lancet 353 1226ndash1231
Ntabaye MK amp Lusiola GJ (2004) Understanding barri-ers to PMTCT in Tanzania findings of a baseline surveyInternational Conference on AIDS 15 (B11396)
de Oliveira LD Giugliani ER do Espirito SLC FrancaMC Weigert EM Kohler CV et al (2006) Effect ofintervention to improve breastfeeding technique on thefrequency of exclusive breastfeeding and lactation-related problems Journal of Human Lactation 22 315ndash321
Perez-Escamilla R (2004) Effectiveness of MADLAC atImproving Breastfeeding Promotion and CounsellingIndicators in Maternity Wards in El Salvador Publishedfor the Basic Support for Institutionalizing Child Sur-vival Project (BASICS II) for the United States Agencyfor International Development Arlington VA Availableat httpwwwbasicsorgpdfFinal20MADLAC20Report20RPE20April207-2004pdf
Perez-Escamilla R (2007) Evidence based breast-feedingpromotion the Baby-Friendly Hospital InitiativeJournal of Nutrition 137 484ndash487
Piwoz EG Iliff PJ Tavengwa N Gavin L Marinda ELunney K et al (2005) An education and counselllingprogram for preventing breastfeeding associated HIVtransmission in Zimbabwe design and impact on mater-nal knowledge and behaviour Journal of Nutrition 135950ndash955
Quinn VJ Guyon AB Schubert JW Stone-Jimenez MHainsworth MD amp Martin LH (2005) Improvingbreastfeeding practices on a board scale at the commu-
nity level success stories from Africa and LatinAmerica Journal of Human Lactation 21 345ndash354
Ranson MK Hanson K Oliveira-Cruz V amp Mills A(2003) Constraints to expanding access to health inter-ventions an empirical analysis and country typologyJournal of International Development 15 15ndash40
Rea MF amp Berquo ES (1990) Impact of the Braziliannational breastfeeding programme on mothers inGreater Sao Paulo Bulletin of the of the World HealthOrganization 68 365ndash371
Rollins NC (2007) Infant feeding and HIV BritishMedical Journal 334 487ndash488
Rutenberg N Baek C Kalibala S Rosen J amp Mulenga D(2004) Evaluation of United Nations supported pilotprojects for the prevention of mother-to-child transmis-sion of HIV overview of findings International Confer-ence on AIDS 15 (WePeE6688)
The Core Group (2005) Scale and Scaling Up A COREGroup Background Paper on lsquoScaling-Uprsquo MaternalNewborn and Child Health Services CORE SpringMembership Meeting 2005 The Core Group Washing-ton DC Available at httpwwwcoregrouporgresourcesmeetingsapril05Scaling_Up_Background_Paper_7-13pdf
The Norwegian Government (1993) Women in PoliticsMinistry of Children and Equality Available at httpwwwregjeringennoendepbldRyddemappeSLA-AvdelingdoclegislationguidelinesWomen-in-Politicshtmlid=437166
Thior I Lockman S Smeaton LM Shapiro RL WesterC Heymann SJ et al (2006) Breastfeeding plus infantzidovudine prophylaxis for 6 months vs formula feedingplus infant zidovudine for 1 month to reduce mother-to-child HIV transmission in Botswana a randomized trialthe Mashi Study Journal of the American Medical Asso-ciation 296 794ndash805
UNICEF (2002) Facts for Life lsquoKey Message What EveryFamily and Community Has a Right to Know aboutBreastfeedingrsquo Available at httpwwwuniceforgffl04key_messageshtm
Van Roekel K Plowman B Griffiths M de AlvaradoVV Matute J amp Calderon M (2002) BASICS IIMidterm Evaluation of the AIN Program in Honduras2000 Basic Support for Institutionalizing Child SurvivalProject (BASICS II) for the United States Agency forInternational Development Arlington VA
WABA (2007) UNICEF Records BHFI Record UpdateAvailable at httpwwwwabaorgmydocsBFHIjan07xls 2006 Regularly updated by Miriam HLabbok Center for Infant and Young ChildFeeding and Care Department of Maternaland Child Health School of Public Health The Univer-sity of North Carolina at Chapel Hill Chapel Hill NCUSA
N Bhandari and AKMI Kabir16
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
WHA (2002) Infant and Young Child Nutrition Fifty-FifthWorld Health Assembly Agenda Item 1310 18 May2002 Available at httpwwwintgbebwhapdf_filesWHA55ewha5525pdf
WHO (1981) The International Code of Marketing ofBreastmilk Substitutes World Health OrganizationGeneva
WHO (1989) Protecting Promoting and Supporting Breast-feeding The Special Role of Maternity Services A JointWHOUNICEF Statement World Health OrganizationGeneva
WHO (2002) The Optimal Duration of Exclusive Breast-feeding Report of an Expert Consultation WHONHD0109 WHOFCHCAH0124 World HealthOrganization Geneva
WHO (2003a) Community Based Strategies for Breastfeed-ing Promotion and Support in Developing CountriesWorld Health Organization Geneva Document refISBN_92_4_159121_8 Available at httpwwwwhointchild-adolescent-healthNew_PublicationsNUTRITIONISBN_92_4_159121_8pdf
WHO (2003b) Multi-country Evaluation of IMCI Effective-ness Cost and Impact (MCE) Progress Report May2002ndashApril 2003 Document ref WHOFCHCAH035World Health Organization Geneva
WHO (2004) Promoting Proper Feeding for Infants andYoung Children World Health Organization GenevaAvailable at httpwwwwhointnutritiontopicsinfantfeedingen
WHO (2006) WHO HIV and Infant Feeding TechnicalConsultation-Consensus Statement World Health Orga-nization Geneva Available at httpwwwwhointhivmediacentreInfantfeedingconsensusstatementpfpdf
WHO Collaborative Study Team on the Role of Breast-feeding on the Prevention of Infant Mortality (2000)Effect of breastfeeding on infant and child mortality dueto infectious diseases in les developed countries apooled analysis Lancet 355 451ndash455
WHOUNICEF (1992) The global criteria for the WHOUNICEF Baby-Friendly Hospital Initiative In Baby-Friendly Hospital Initiative Part II Hospital LevelImplementation World Health Organization Geneva
WHOUNICEF (1993) Breastfeeding Counselling A Train-ing Course WHOCDR933 UNICEFNUT931 WorldHealth Organization Geneva
WHOUNICEF (2002) Protocol for Adapting the FeedingRecommendations Part III IMCI Adaptation GuideWorld Health Organization Geneva
WHOUNICEF (2003) Global Strategy for Infant andYoung Child Feeding World Health OrganizationGeneva Available at httpwwwwhointchild-adolescent-healthpublicationsNUTRITIONIYCF_GShtm
de Zoysa I Rea M amp Martines J (1991) Why promotebreastfeeding in diarrheal diseases control programmesHealth Policy and Planning 6 371ndash379
Mainstreaming nutrition into MCH programs 17
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
Cas
est
udie
so
fef
fect
iven
ess
stud
ies
or
pilo
tpr
ogra
mm
es
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Lut
ter
etal
(199
7)
Bra
zil
Low
-inc
ome
urba
nw
omen
deliv
erin
gin
hosp
ital
s
Bre
astf
eedi
ngpr
omot
ion
in
hosp
ital
sco
mpa
red
wit
h
nobr
east
feed
ing
prom
otio
n
Pro
mot
ion
ofbr
east
feed
ing
in
sele
cted
hosp
ital
s
Mea
nda
ysof
excl
usiv
e
brea
stfe
edin
g
75da
ysvs
22
days
(Plt
001
)
Rea
ampB
erqu
o
(199
0)
Wom
enw
ith
ach
ild
aged
lt2ye
ars
inSa
oP
aulo
Nat
iona
lbre
astf
eedi
ng
cam
paig
n19
81ndash1
986
BF
HI
Mas
sm
edia
cam
paig
n11
in
fant
s5ndash
6m
onth
s
excl
usiv
ely
brea
stfe
d
in19
88an
d37
in
1987
Con
foun
ding
fact
ors
over
the
6-ye
arpe
riod
not
mea
sure
d
Kra
mer
etal
(200
020
01)
PR
OB
ITtr
ial
Bel
arus
Clu
ster
rand
omiz
ed
34ho
spit
als
and
thei
rpo
lycl
inic
s
Trai
ning
inB
FH
I(W
HO
UN
ICE
F19
92)
vsr
outi
ne
prac
tice
san
dpo
licie
s
Exc
lusi
vebr
east
feed
ing
at3
(43
3vs
64
)
and
6(7
9
vs0
6
)
mon
ths
sign
ifica
ntly
high
er
Impl
emen
ted
thro
ugh
BF
HI
ina
sett
ing
whe
reho
spit
al
deliv
erie
sar
eco
mm
on
Per
ez-E
scam
illa
(200
4)
BA
SIC
SII
Mex
ico
Hon
dura
s
Bra
zil
MA
DL
AC
low
-cos
t
man
agem
ent
info
rmat
ion
syst
emto
use
an
evid
ence
-bas
edap
proa
chto
impr
ove
serv
ice
perf
orm
ance
Inte
rvie
win
gof
wom
enat
hosp
ital
disc
harg
epo
st
deliv
ery
usin
ga
ques
tion
nair
eth
atta
kes
5ndash7
min
toad
min
iste
ran
d
cont
ains
19br
east
feed
ing
prom
otio
nco
unse
lling
indi
cato
rs
Dat
aen
tere
dan
dre
sult
s
disc
usse
d3-
mon
thly
by
hosp
ital
com
mit
tee
Hos
pita
lim
plem
ents
chan
ges
in
brea
stfe
edin
g
supp
ort
base
don
anal
ysis
of
ques
tion
nair
es
Itis
aco
st-e
ffec
tive
inte
rven
tion
that
can
help
impr
ovem
ents
inth
eB
FH
I
and
isa
valu
able
tool
for
proc
ess
eval
uati
on
N Bhandari and AKMI Kabir18
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
LIN
KA
GE
S
proj
ect
inA
fric
aan
d
Lat
inA
mer
ica
(Qui
nnet
al
2005
LIN
KA
GE
S
2002
WH
O20
03a)
Bol
ivia
(1
mill
ion)
Gha
na(3
5
mill
ion)
Mad
agas
car
(6m
illio
n)
Res
ourc
e-
poor
sett
ing
Pilo
tpr
ogra
mm
e
InB
oliv
iaan
d
Gha
napr
ogra
mm
e
focu
sed
on
brea
stfe
edin
gan
d
com
plem
enta
ry
feed
ing
InM
adag
asca
r
prog
ram
me
prom
oted
brea
stfe
edin
g
wit
hin
7es
sent
ial
nutr
itio
nac
tion
san
d
subs
eque
ntly
thro
ugh
IMC
I
Bui
lton
form
ativ
ere
sear
ch
and
sust
aine
dth
roug
h
prog
ram
me
acti
viti
esth
at
focu
sed
onbr
ingi
ngab
out
the
desi
red
beha
viou
r
chan
geM
ixof
inte
rven
tion
s
reac
hed
wom
enin
divi
dual
ly
orin
grou
psin
heal
th
faci
litie
sho
mes
or
com
mun
ity
sett
ings
Con
sist
ent
mes
sage
san
d
mat
eria
lacr
oss
all
prog
ram
me
chan
nels
Bol
ivi
PR
OC
OSI
NG
Os
Gha
na
UN
ICE
F
nati
onal
nutr
itio
n
offic
eN
GO
s
Mad
agas
car
Inte
rsec
tora
l
Act
ion
Gro
upfo
r
Nut
riti
on
Jere
o
Sala
ma
Isik
a
Pro
gram
desi
gned
wit
h
part
ners
Rad
ioin
all
thre
esi
tes
Mat
eria
ls
deve
lope
d
tosu
itne
eds
oflo
cal
heal
th
wor
kers
and
com
mun
ity
mem
bers
Gre
at
emph
asis
on
deve
lopm
ent
of coun
selli
ng
and
nego
tiat
ion
skill
s
prac
tica
l
sess
ions
Sign
ifica
ntin
crea
ses
inex
clus
ive
brea
stfe
edin
gra
tes
of
0ndash6-
mon
th-o
ld
infa
nts
from
54
to65
in
Bol
ivia
68
to79
in
Gha
naan
d46
to68
in
Mad
agas
car
In
Gha
naan
d
Mad
agas
car
sign
ifica
ntre
sult
s
obse
rved
wit
hin
aye
ar
ofin
itia
tion
of
com
mun
ity
inte
rven
tion
s
App
roac
hw
asef
fect
ive
and
achi
eved
sign
ifica
nt
incr
ease
sam
ong
larg
e
popu
lati
ons
asea
rly
as
9ndash12
mo
afte
rin
itia
tion
of
com
mun
ity
acti
viti
es
Van
Roe
kele
tal
(200
2)W
HO
(200
3a)
Hon
dura
sG
row
thm
onit
orin
gan
d
prom
otio
nkn
own
as
Ate
ncioacute
nIn
tegr
ala
la
Nintilde
ez(A
IN)
or
Inte
grat
edC
hild
Car
e
Init
ially
pri
mar
ilya
grow
th
mon
itor
ing
prog
ram
me
ulti
mat
ely
thro
ugh
IMC
I
Pro
gram
me
ongr
owth
prom
otio
nndash
asse
ssm
ent
of
mon
thly
wei
ght
gain
and
focu
son
illne
ssf
eedi
ng
prac
tice
san
dge
nera
lchi
ld
care
inin
fant
sun
der
2ye
ars
Impl
emen
ted
atgo
vern
men
t
faci
litie
san
dco
mm
unit
y
Star
ted
in19
92s
tren
gthe
ned
in19
95ndash1
997
wit
hgr
eate
r
focu
son
child
feed
ing
In
1997
pro
gram
me
intr
oduc
ed
wit
hIM
CI
(WH
OU
NIC
EF
2002
)
Maj
or
part
ners
UN
ICE
F
PAH
O
Am
eric
an
and
Hon
dura
n
Red
Cro
ss
CA
RE
Rad
io
broa
dcas
ts
relig
ious
lead
ers
IMC
IM
id-t
erm
eval
uati
on
show
ed39
of
mot
hers
inin
terv
enti
on
com
mun
itie
sex
clus
ivel
y
brea
stfe
dco
mpa
red
wit
h13
in
the
cont
rol
site
s
Mainstreaming nutrition into MCH programs 19
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
cont
inue
d
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Bha
ndar
ieta
l
(200
3)
WH
O
(200
3a)
Rur
alco
mm
unit
ies
inH
arya
na
Indi
a
Clu
ster
rand
omiz
edtr
ial
8
com
mun
itie
s(t
otal
popu
lati
on~4
000
0)
Pro
mot
ion
ofex
clus
ive
brea
stfe
edin
gan
d
appr
opri
ate
com
plem
enta
ryfe
edin
g
Dev
elop
edth
roug
h
form
ativ
ere
sear
ch
ndashP
robl
emid
enti
ficat
ion
ndashP
arti
cipa
tory
desi
gnof
inte
rven
tion
impl
emen
tati
onan
d
eval
uati
on
Impl
emen
tati
onw
ithi
nan
exis
ting
prim
ary
heal
th-c
are
prog
ram
me
Opp
ortu
niti
esus
edto
deliv
erm
essa
ges
wer
e
imm
uniz
atio
ncl
inic
s
wei
ghin
gse
ssio
ns
sick
-chi
ldco
ntac
tsan
d
mon
thly
hom
evi
sits
Res
earc
hers
wit
hlo
cal
gove
rnm
ent
ICD
Ssy
stem
and
NG
O
The
atre
son
gs
Mas
sm
edia
not
used
for
risk
of
cont
amin
atio
n
Mat
eria
ls
deve
lope
d
for
heal
th
wor
kers
pos
ters
flip
book
sca
rds
Bre
astf
eedi
ng
coun
selli
ngse
ctio
n
ofth
eIM
CI
(WH
O
UN
ICE
F20
02)
Exc
lusi
ve
brea
stfe
edin
gin
the
prev
ious
24h
at3
mon
ths
of
age
79
vs4
8
The
posi
tive
effe
ct
rem
aine
dup
to
6m
onth
sof
age
(42
vs4
)
Tota
lpar
tici
pati
onof
the
dist
rict
heal
thsy
stem
from
ince
ptio
nof
the
prog
ram
me
inde
velo
ping
impl
emen
tati
onst
rate
gyt
ool
deve
lopm
ent
and
mon
itor
ing
inad
diti
onto
invo
lvem
ent
of
anN
GO
wer
eim
port
ant
feat
ures
that
cont
ribu
ted
to
the
succ
ess
ofth
e
inte
rven
tion
Mor
row
etal
(199
9)
Mex
ico
Cit
yC
lust
erra
ndom
ized
tria
l
Tota
lpop
ulat
ion
3000
0
Two
com
mun
itie
sin
the
inte
rven
tion
one
com
pari
son
130
wom
en
Hom
e-ba
sed
peer
coun
selli
ng
Pee
rco
unse
llors
mad
e3
or
6ho
me
visi
tsto
the
mot
her
Key
fam
ilym
embe
rsal
so
incl
uded
By
La
Lec
he
Lea
gue
of
Mex
ico
Exc
lusi
ve
brea
stfe
edin
g
at3
mon
ths
post
-par
tum
67
(6vi
sits
)
50
(3vi
sits
)12
(com
pari
son)
Firs
tcl
uste
rra
ndom
ized
com
mun
ity-
base
dtr
ialt
hat
used
peer
coun
sello
rsto
prom
ote
excl
usiv
e
brea
stfe
edin
g
Hai
der
etal
2000
200
2
Dha
ka
Low
mid
dle
and
low
-soc
io-
econ
omic
popu
lati
on
Clu
ster
rand
omiz
edtr
ial
20zo
nes
inin
terv
enti
on
and
20in
cont
rol
Com
mun
ity-
base
dpe
er
coun
selli
ngin
Dha
ka
15ho
me-
base
dco
unse
lling
visi
tsby
peer
coun
sello
rs
40h
(4h
yen10
days
)
WH
OU
NIC
EF
brea
stfe
edin
g
coun
selli
ngco
urse
(WH
OU
NIC
EF
1993
)
Exc
lusi
ve
brea
stfe
edin
g
at5
mon
ths
70
in
inte
rven
tion
and
6in
the
cont
rol
Com
mun
ity-
base
d
brea
stfe
edin
gpr
omot
ion
stra
tegy
was
effe
ctiv
ein
Ban
glad
esh
whe
rem
ost
deliv
erie
soc
cur
atho
me
N Bhandari and AKMI Kabir20
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Bry
ceet
al
(200
4)W
HO
(200
3b)
Bra
zil
Per
u
Tanz
ania
Uga
nda
Mul
tico
untr
yev
alua
tion
of
IMC
Ith
atin
clud
ed
effe
ctiv
enes
sco
stan
d
impa
ct(B
ryce
etal
2004
)
Bre
astf
eedi
ngpr
omot
ion
asa
part
ofIM
CI
IMC
Iis
ast
rate
gyfo
r
impr
ovin
gch
ildhe
alth
and
deve
lopm
ent
thro
ugh
the
com
bine
d
deliv
ery
ofes
sent
ial
child
heal
th
inte
rven
tion
sIM
CI
bega
nw
ith
ase
tof
case
man
agem
ent
guid
elin
es
for
the
man
agem
ent
ofsi
ckch
ildre
nat
first
-lev
elhe
alth
faci
litie
s
and
the
guid
elin
esw
ere
desi
gned
for
adap
tati
on
atco
untr
yle
vela
nd
belo
wO
ver
tim
eth
e
stra
tegy
expa
nded
to
incl
ude
ara
nge
of
guid
elin
esfo
rde
liver
ing
child
surv
ival
inte
rven
tion
at
hous
ehol
dco
mm
unit
y
and
refe
rral
leve
ls
IMC
Im
odul
e(W
HO
UN
ICE
F20
02)
Res
ults
onex
clus
ive
brea
stfe
edin
g
avai
labl
efr
om
Tanz
ania
whe
reno
sign
ifica
ntim
pact
was
seen
Des
pite
subs
tant
ial
impr
ovem
ent
inth
equ
alit
y
ofca
rede
liver
edby
IMC
Iat
heal
thfa
cilit
ies
key
fam
ily
prac
tice
ssu
chas
excl
usiv
e
brea
stfe
edin
gdi
dno
tch
ange
asco
mm
unit
yIM
CI
had
not
been
impl
emen
ted
byth
at
tim
e(W
HO
2003
b)
SA
rife
en
pers
onal
com
mun
icat
ion
Ban
glad
esh
Mat
lab
Com
mun
ity-
base
dcl
uste
r
desi
gn
Eva
luat
ion
offa
cilit
y-an
d
com
mun
ity-
base
dIM
CI
Inte
rven
tion
pack
age
incl
udes
feed
ing
asse
ssm
ent
and
coun
selli
ngon
mot
hers
ofyo
ung
child
ren
seek
ing
care
atfa
cilit
ies
for
illne
ssan
d
hom
e-ba
sed
coun
selli
ng
onim
prov
edfe
edin
gby
com
mun
ity-
base
dhe
alth
and
nutr
itio
nw
orke
rs
At
base
line
inth
e
year
2000
alit
tle
mor
eth
anha
lfth
e
0ndash5-
mon
th-o
ld
infa
nts
inth
est
udy
area
wer
ebe
ing
excl
usiv
ely
brea
stfe
dB
y20
05
this
incr
ease
dby
30
inth
eIM
CI
area
Dat
ano
t
avai
labl
efr
omth
e
com
pari
son
area
as
yet
Lac
kof
com
para
ble
data
from
the
com
pari
son
area
prev
ents
ade
finit
ive
conc
lusi
onas
tow
heth
erth
is
trul
yis
anim
pact
ofIM
CI
BA
SIC
SII
Bas
icSu
ppor
tfo
rIn
stit
utio
naliz
ing
Chi
ldSu
rviv
alP
roje
ctB
FH
IB
aby-
Frie
ndly
Hos
pita
lIni
tiat
ive
ICD
SIn
tegr
ated
Chi
ldD
evel
opm
ent
Serv
ices
IM
CI
Inte
grat
edM
anag
emen
tof
Chi
ldho
odIl
lnes
sM
AD
LA
CM
onit
oreo
deA
poyo
Dir
ecto
con
laL
acat
anci
aM
ater
naN
GO
non
-gov
ernm
enta
lorg
aniz
atio
nPA
HO
Pan
Am
eric
anH
ealt
hO
rgan
izat
ion
PR
OB
ITP
rom
otio
nof
Bre
astf
eedi
ngIn
terv
enti
onTr
ial
PR
OC
OSI
Pro
gram
ade
Coo
rdin
acio
nen
Salu
dIn
tegr
al(C
olla
bora
tive
Pro
gram
for
Inte
grat
edH
ealt
h)U
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
WH
OW
orld
Hea
lth
Org
aniz
atio
n
Mainstreaming nutrition into MCH programs 21
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x2
Cas
est
udie
sin
scal
e-up
effo
rts
inH
IVA
IDS
Stud
yde
scri
ptio
nPo
pula
tion
Inte
rven
tion
Com
mun
icat
ion
stra
tegy
Impa
cton
excl
usiv
ebr
east
feed
ing
Com
men
ts
LIN
KA
GE
S(2
005)
Zam
bia
Pro
gram
me
thro
ugh
heal
th-c
are
and
com
mun
ity
serv
ices
Rea
ched
60si
tes
in6
dist
rict
sby
2005
Inte
grat
ion
ofin
fant
feed
ing
coun
selli
ngm
ater
naln
utri
tion
and
anti
retr
ovir
aldr
ugs
prop
hyla
xis
Trai
ning
ofhe
alth
wor
kers
and
com
mun
ity
serv
ice
prov
ider
sto
coun
selw
omen
onsa
fety
opti
ons
for
thei
rsi
tuat
ion
Beh
avio
urch
ange
Com
mun
icat
ion
inte
rven
tion
sin
the
first
few
year
sM
ater
iald
evel
oped
lsquoAct
Now
rsquoM
edia
cam
paig
nsin
clud
edbr
ochu
res
post
ers
radi
oan
dte
levi
sion
Ass
esse
dth
roug
hba
selin
ean
dfo
llow
-up
hous
ehol
dan
dcl
inic
surv
eys
inse
lect
eddi
stri
cts
Exc
lusi
vebr
east
feed
ing
rate
incr
ease
dfr
om50
in
2002
to64
in
2004
inL
ivin
gsto
nean
dfr
om57
in
2000
to74
in
2004
inN
dola
Inte
grat
edde
mon
stra
tion
proj
ect
Had
seve
rals
tren
gths
inte
rms
ofth
eus
eof
form
ativ
ere
sear
chto
deve
lop
mes
sage
str
aini
ngan
dbu
ildin
gup
skill
sof
prog
ram
me
man
ager
she
alth
-car
epr
ovid
ers
and
com
mun
ity
wor
kers
adv
ocac
yfo
rna
tion
alpo
licy
stro
ngbe
havi
our
chan
geco
mm
unic
atio
nco
mpo
nent
st
reng
then
ing
com
mun
ity
capa
city
for
coun
selli
ngan
dre
ferr
als
and
mon
itor
ing
and
eval
uati
onw
ith
loca
lpar
tner
sP
iwoz
etal
(20
05)
ZV
ITA
MB
Otr
ial
Har
are
Zim
babw
eE
duca
tion
and
coun
selli
ngpr
ogra
mm
ede
liver
edan
tena
tally
1411
0m
othe
rndashba
bypa
irs
enro
lled
from
14m
ater
nity
clin
ics
wit
hin
96h
ofde
liver
yan
dfo
llow
edup
at6
wee
ks
3m
onth
san
d3-
mon
thly
inte
rval
sIn
fant
-fee
ding
patt
erns
dete
rmin
edE
xclu
sive
brea
stfe
edin
gre
com
men
ded
for
HIV
nega
tive
un
know
nor
HIV
posi
tive
who
chos
eto
brea
stfe
ed
Gro
uped
ucat
ion
indi
vidu
alco
unse
lling
vid
eos
broc
hure
sM
othe
rsw
hoen
rolle
dw
hen
prog
ram
me
was
fully
impl
emen
ted
wer
e8
4ti
mes
mor
elik
ely
toex
clus
ivel
ybr
east
feed
than
mot
hers
who
enro
lled
befo
reth
epr
ogra
mm
ebe
gan
Ove
rall
excl
usiv
ebr
east
feed
ing
rate
sti
ll3
mon
ths
was
low
at24
6
Form
ativ
ere
sear
chus
edto
desi
gna
cult
ural
lyse
nsit
ive
educ
atio
nan
dco
unse
lling
prog
ram
me
Low
over
alle
xclu
sive
brea
stfe
edin
gra
tes
prom
pted
auth
ors
toco
nclu
deth
atw
omen
and
thei
rpa
rtne
rssh
ould
have
been
reac
hed
mor
efr
eque
ntly
duri
ngan
tena
tala
ndpo
st-n
atal
peri
od
N Bhandari and AKMI Kabir22
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Thi
oret
al(
2006
)R
ollin
s(2
007)
C
ohen
(200
7)
HIV
-inf
ecte
dpr
egna
ntw
omen
atte
ndin
gan
tena
talc
linic
sin
sout
hB
otsw
ana
Inve
stig
atio
nsby
CD
Cof
adi
arrh
oea
outb
reak
inJa
nuar
y-Fe
brua
ry20
06in
the
sam
epo
pula
tion
Mat
erna
land
infa
ntan
tire
trov
iral
ther
apy
toas
cert
ain
impa
cton
HIV
tran
smis
sion
Ant
enat
alco
unse
lling
Cas
endashco
ntro
lstu
dyto
iden
tify
risk
fact
ors
for
diar
rhoe
ano
tbr
east
feed
ing
was
the
bigg
est
risk
fact
ora
djus
ted
odds
rati
o50
(95
confi
denc
ein
terv
al4
5ndash10
0)
Bot
swan
aha
sth
ebe
stpr
imar
yhe
alth
-car
est
ruct
ure
wat
ersu
pply
and
sani
tati
onsy
stem
sin
Sout
hA
fric
aFo
rmul
apr
ovid
edfr
eeby
the
gove
rnm
ent
toin
fect
edm
othe
rsL
ower
mor
talit
yin
the
brea
stfe
edin
ggr
oup
at7
mon
ths
dem
onst
rate
sri
skof
form
ula
feed
ing
and
need
for
alte
rnat
est
rate
gies
(Thi
oret
al
2006
)A
utho
rsco
nclu
deth
athe
alth
syst
ems
inw
hich
thes
epr
ogra
mm
esar
eim
plem
ente
dsh
ould
beab
leto
cope
wit
hdi
arrh
oea
and
mal
nutr
itio
nth
atre
sult
sbe
caus
eof
form
ula
feed
ing
(Rol
lins
2007
)C
oova
dia
etal
(2
007)
Kw
aZul
uNat
al
Sout
hA
fric
a27
22H
IV-i
nfec
ted
and
unin
fect
edpr
egna
ntw
omen
enro
lled
into
ano
n-ra
ndom
ized
inte
rven
tion
coho
rtst
udy
from
ante
nata
lcl
inic
sIn
fant
feed
ing
data
obta
ined
wee
kly
bloo
dsa
mpl
esfr
omin
fant
sta
ken
mon
thly
83
of13
72in
fant
sbo
rnto
HIV
-inf
ecte
dm
othe
rsin
itia
ted
excl
usiv
ebr
east
feed
ing
from
birt
hB
reas
tfed
infa
nts
who
rece
ived
solid
sw
ere
sign
ifica
ntly
mor
elik
ely
toac
quir
ein
fect
ion
com
pare
dw
ith
excl
usiv
ely
brea
stfe
d(H
R10
87
151
ndash78
P=
001
8)as
wer
ein
fant
sw
hoat
12w
eeks
rece
ived
brea
stan
dfo
rmul
am
ilk(1
82
098
ndash33
6P
=0
57)
Cum
ulat
ive
3-m
onth
mor
talit
yin
excl
usiv
ely
brea
stfe
dw
as6
1(4
74ndash
792
)vs
15
1(7
63ndash
287
3)in
infa
nts
give
nre
plac
emen
tfe
eds
(HR
206
1
0ndash4
27P
=0
05)
The
stud
ysh
ows
that
excl
usiv
ebr
east
feed
ing
can
besu
cces
sful
lysu
ppor
ted
inH
IV-i
nfec
ted
wom
enT
heau
thor
sca
llfo
rfu
rthe
rre
visi
onof
UN
ICE
FW
HO
and
USA
IDin
fant
feed
ing
guid
elin
es
CD
CC
ente
rof
Dis
ease
Con
trol
HR
haz
ards
rati
oU
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
USA
IDU
SA
genc
yfo
rIn
tern
atio
nalD
evel
opm
ent
WH
OW
orld
Hea
lth
Org
aniz
atio
nZ
VIT
AM
BO
Z
imba
bwe
Vit
amin
Afo
rM
othe
rsan
dB
abie
s
Mainstreaming nutrition into MCH programs 23
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23

care resulting from reduction in diarrhoeal and respi-ratory morbidity were estimated as a result of theeffect of BFHI on breastfeeding The study showedthat breastfeeding promotion through a BFHI-likemodel is very cost-effective (1992 US$ 2ndash19 per dis-ability adjusted life years Horton et al 1996 Perez-Escamilla 2007) Examples of cost-effectivenessanalysis of community-based programmes using lay orprofessional support in different settings could not beidentified
Testing of novel approaches andcontinuing innovation
Scaled-up programmes must have inbuilt provision totest novel approaches and the ability for continuinginnovation
Scaling up of exclusive breastfeeding in thecontext of HIV
The policy and programme design and implemen-tation issues relevant to exclusive breastfeedingscale-up discussed above are relevant to HIV-prevalent areas but there are other unique featuresthat merit consideration
Creating policies for exclusive breastfeeding pro-motion in countries with high HIV prevalence is par-ticularly challenging The revised recommendationsencourage exclusive breastfeeding for the first 6months and continued breastfeeding for 2 years andbeyond for infants whose mothers are HIV negativeor whose HIV status is unknown For women who areknown to be HIV positive the most appropriateinfant feeding option for HIV-exposed infantsdepends on individual circumstances including con-sideration of health services counselling and supportExclusive breastfeeding is the better option for suchinfants unless replacement feeding is acceptable fea-sible affordable sustainable and safe for both themother and baby This recommendation is based onthe finding that exclusive breastfeeding for up to 6months in three large cohort studies is associated witha three- to fourfold decreased risk of transmission ofHIV compared with non-exclusive breastfeeding(WHO 2006) The recommendations may need
further revision if new findings demonstrate thatexclusive breastfeeding should be the feeding ofchoice for HIV-infected women (Iliff et al 2005)
Some pilot programmes for exclusive breastfeedingpromotion in high-HIV-prevalence countries aresummarized in Appendix 2
In general exclusive breastfeeding promotionformed a part of the prevention of mother-to-childtransmission programmes LINKAGESZambiaintegrated improved counselling on infant feedingmaternal nutrition and antiretroviral therapy duringprophylaxis in both health-care and community ser-vices to enable women to make and act on informedchoice to feed their infants optimally in the context ofhigh HIV prevalence
Formative research was critical to develop locallyappropriate and feasible infant feeding recommenda-tions for individual infants and their families based onHIV status In Zambia the research included focusedgroup discussions key information interviews obser-vations of household food preparation and feedingmarket survey of replacement foods and breastmilksubstitutes and household trials of improved feedingand caring practices (LINKAGES 2005)
High quality of health workers is another criticalfactor for sensitive and accurate individual counsel-ling Programmes incorporated behaviour changecommunication methodologies in training (LINK-AGES 2005) It is important to develop skills of com-munity members as well for improved servicesreferral outreach and follow-up care and support ofHIV-positive mothers and their infants
A comprehensive communications strategy tosupport scale-up was a notable feature of the LINK-AGES programme in Zambia In 2004 an intensiveeffort was launched using brochures posters radioand television spots billboards and reference guidesfor health providers (LINKAGES 2005) Messageswere targeted to relevant stakeholders ndash pregnantand lactating mothers health providers youth andcommunity leaders and all the materials were nation-ally disseminated
Monitoring and evaluation another importantfeature of effective scale-up was a feature of pilotprogrammes (Appendix 2 Ntabaye amp Lusiola 2004Rutenberg et al 2004) in Zambia and Tanzania Moni-
N Bhandari and AKMI Kabir12
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
toring and evaluation not only provides a measure ofsuccess but identifies factors that may have contrib-uted to it and to lack of success to enable mid-coursecorrections The impact of some pilot programmes onexclusive breastfeeding is summarized in Appendix 2In most programmes exclusive breastfeeding ratesimproved In Zambia exclusive breastfeeding ratesincreased from 50 in 2002 to 64 in 2004 in Liv-ingstone from 57 in 2000 to 74 in 2004 in NdolaIn South Africa an antenatal clinic-based interven-tion led to 83 of infants born to HIV-infectedmother initiating exclusive breastfeeding InZimbabwe an intervention based on antenatal coun-selling resulted in a relatively lower exclusive breast-feeding rate of 246 at 3 months (Piwoz et al 2005)
Several barriers to success were identified Theseinclude inadequate skills of workers and non-integration of HIV counselling and tailoring into ante-natal care services (Ntabaye amp Lusiola 2004) which isthe backbone in which infant feeding counselling isbuiltWomen reported that mothers not breastfeedingtheir children were discriminated against by the com-munity and they faced the threat of domestic violenceProgramme managerrsquos understanding of barriersto effective programme implementation and impactwere emphasized as being important Governmentsupport partnerrsquos coordination increased humanresource and improving the supply system were iden-tified to be essential features to scale up programmesin the HIV context (Rutenberg et al 2004) Lowoverall exclusive breastfeeding rates prompted Piwozet al (2005) to conclude that women and their partnersshould have been reached more frequently during theantenatal and post-natal period
Conclusions
In a large number of programmes for improvingexclusive breastfeeding in developing countriesincluding in areas with high prevalence of HIV apositive impact on exclusive breastfeeding rates hasbeen achieved
Some of the factors that contributed to successfulscale-up are summarized in Table 4 Several limita-tions of the programmes reviewed merit attentionMost programmes involved special and generous
funding concentrated efforts and multiple contactsThese programmes were evaluated over relativelyshort periods of time usually 2ndash5 years and the long-term sustainability has not been really tested In theabsence of specific measures there is likely to be dilu-tion of quality as the programmes are scaled upfurther from their initial size The experience thus farleaves important questions to be addressed particu-larly on how programmes can be sustained over timeas they are scaled up at affordable costs
A key factor relevant to sustainability is to plan ona long-term basis a period of 10ndash20 years rather than5ndash10 years from the outset Experience with otherchild health programmes has shown that performancein immunization and oral rehydration therapy userates plateaued over time in many countries
Programme scale-up requires a programme man-agement capacity proportionate to the scale of opera-tions periodic assessment of barriers (Table 5) and anability to revise programme strategy to overcomethese Another key feature to sustainability ofscale-up is the extent to which capacity has been builtat the district block and community levels National-or state-level driven interventions begin with enor-mous enthusiasm which is difficult to sustain Thisfactor is particularly important as most developing
Table 4 Lessons learnt about scale-up key factors in success
bull Political will advocacy enabling policiesbull Championship by health ministries at national state and districtlevelbull Technical consensus on feeding guidelinesbull Programme strategy and measurable short- and long-term goalsbull Long-term financial commitmentbull Partners with defined roles assessment of their capacity todeliver and plans to cover gaps in capacitybull Emphasis on community-level interventions and not onlyfacility-based programmesbull Formative research as the backbone of effective scale-upprogrammes particularly in the context of HIVbull Careful selection of channels and the number required toachieve timely coverage consistency of messagesbull Communication strategy aided by formative research pre-testedvalidated messages and toolsbull Quality trainers and training centres proportionate to requiredscalebull Monitoring and evaluationbull Programme redesign when relevant through research analysisand innovation
Mainstreaming nutrition into MCH programs 13
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
countries are going through a process of decentrali-zation with increasing responsibility for planningimplementation and evaluation being delegated tolower levels of the health-care system Buildingcapacity at that level requires time resources andpatience and a longer-term perspective
Building capacity emerges to be a key factorTrainers and training centres vary in their qualitywhen training health workers and their supervisorsor programme managers As the burden of trainingincreases availability of good-quality trainersbecomes a limiting factor (WHOUNICEF 2002Government of India 2006) An effective strategymust plan for these incremental requirements includ-ing ensuring secure and sustained funding
Identifying barriers to success is a key actor Thebarriers to scaling up of health interventions havebeen elegantly described by Ranson et al (Table 5)Most of these are important for exclusive breastfeed-ing scale-up as well
Overall within the limitations discussed above anumber of programmes in countries with varying
HIV prevalence show that exclusive breastfeeding ona large scale is feasible and pilot programmes havegiven valuable guidance related to policies planningand implementation of large-scale programmes Thechallenge now is to build on these experiences whenplanning national programmes
Acknowledgements
We sincerely thank Dr MK Bhan for his constructivecriticism and sustained feedback at different stages ofdevelopment of this review
Conflicts of interest
The authors have declared no conflicts of interest
References
Arifeen S Black RE Antelman G Baqui A CaulfieldL amp Becker S (2001) Exclusive breastfeeding reducesacute respiratory infection and diarrhea deaths amonginfants in Dhaka slums Pediatrics 108 E67
Australian Breastfeeding Association (2005) Valuing Par-enthood Options for Paid Maternity Leave ndash InterimPaper 2002 Available at httpwwwbreastfeedingasnauadvocacymatleavehtml
Bhandari N Bahl R Mazumdar S Martines J BlackRE amp Bhan MK (2003) Effect of community basedpromotion of exclusive breastfeeding on diarrheal ill-nesses and growth a cluster randomized controlled trialLancet 361 1418ndash1423
Bhandari N Mazumder S Bahl R Martines J BlackRE amp Bhan MK (2004) An educational interventionto promote appropriate complementary feedingimproves child feeding practices and linear growth inrural Haryana India Journal of Nutrition 134 2342ndash2348
Bhandari N Mazumder S Bahl R Martines J BlackRE amp Bhan MK (2005) Use of multiple opportunitiesfor improving feeding practices in undertwos withinchild health programs Health Policy Plan 20 328ndash336
Bryce J Victora CG Habicht JP Vaughan JP ampBlack RE (2004) The multi-country evaluation of theintegrated management of childhood illness strategylessons for the evaluation of public health interventionsAmerican Journal of Public Health 94 406ndash415
Butte NF Lopez-Alarcon MG amp Garza C (2002) Nutri-ent Adequacy of Exclusive Breastfeeding for the TermInfant during the First Six Months of Life World HealthOrganization Geneva
Table 5 Barriers to scaling up of health interventions
Community and household levelsLack of information womenrsquos education physical financial
womenrsquos decision-making powerHealth services delivery levelShortage of qualified staff weak technical guidance programme
management and supervision inadequate supplies equipmentand infrastructure poor accessibility
Health sector policy and strategic management levelWeak and centralized system for planning and management weak
drug policies and supply system inadequate regulations lack ofintersectoral action and partnership weak incentives to useinputs efficiently and respond to user needs and preferencesreliance on donor funding
Public policies cutting across sectorsGovernment bureaucracy poor communication and transport
infrastructureEnvironmental characteristicsGovernance and overall policy frameworkCorruption weak government weak laws political instability and
insecurity low priority to social sectors weak structure for publicaccountability and opportunities for public opinions lack of freepress
Physical environmentClimatic and geographic predisposition physical environment
unfavourable to service delivery
Adapted from Ranson et al (2003)
N Bhandari and AKMI Kabir14
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Cohen J (2007) Retrovirus meeting Hope on new AIDSdrugs but breast-feeding strategy backfires Science 3151357
Coovadia HM Rollins NC Bland RM Little KCoutsoudis A Bennish ML et al (2007) Mother tochild transmission of HIV-1 infection during exclusivebreastfeeding in the first 6 months of life an interven-tion cohort study Lancet 369 1107ndash1116
Coutinho SB de Lira PI de Carvalho LM amp AshworthA (2005) Comparison of the effect of two systems forthe promotion of exclusive breastfeeding Lancet 3661094ndash1100
Feachem RG amp Koblinsky MA (1984) Interventions forthe control of diarrheal diseases among young childrenpromotion of breastfeeding Bulletin of the of the WorldHealth Organization 62 271ndash291
Gonzales A Arteaga E amp Howard-Grabman L (1998)Scaling Up the WARMI Project ndash Lessons LearnedMobilizing Bolivian Communities around ReproductiveHealth Save the Children Federation Inc Bolivia FieldOffice La Paz Available at httpwwwcoregrouporgresourcesSavebolipdf
Government of India (1997) Recommendations of the FifthCentral Pay Commission Relating to Enhancement ofQuantum of Maternity Leave and to Allow PaternityLeave in Respect of Central Government EmployeesDocument ref 13018197-Estt(L) Available at httppersminnicinesttleave2htm
Government of India (2005) National Rural HealthMission 2005ndash2012 Mission document Ministry ofHealth and Family Welfare New Delhi Government ofIndia Available at httpwwwmohfwnicinNRHM20Mission20Documentpdf
Government of India (2006) Operational Guidelines forImplementation of Integrated Management of Neonataland Childhood Illness (IMNCI) Ministry of HealthFamily Welfare New Delhi Available at httpmohfwnicindofw20websiteF20IMNCI20Operational20Plan201320june202006htm
Government of Pakistan (2003) National Programme forFamily Planning and Primary Health Care The LadyHealth Workers Programme 2003ndash2008 Ministry ofHealth Pakistan Available at httpwwwphcgovpkDownloadsPC-120augpdf
Green CP (1999) Improving Breastfeeding Behaviors Evi-dence from Two Decades of Intervention ResearchPublished for the US Agency for International Develop-ment (USAID) by the LINKAGES Project Academyfor Educational Development Washington DC
Gupta A (2002) National trends in breastfeeding andeffective strategies to improve breastfeeding ratesJournal of Neonatology 2002 4ndash14
Gwatkin DR (2004) Integrating the management of child-hood illness Lancet 364 1557ndash1558
Habicht JP DaVanzo J amp Butz WP (1986) Does breast-feeding really save lives or are apparent benefits due tobiases American Journal of Epidemiology 123279ndash290
Haider R Ashworth A Kabir I amp Huttly SR (2000)Effect of community based peer counsellors on exclusivebreastfeeding practices in Dhaka Bangladesh a ran-domized controlled trial Lancet 356 1643ndash1647
Haider R Kabir I Huttly SR amp Ashworth A (2002)Training peer counsellors to promote and support exclu-sive breastfeeding in Bangladesh Journal of HumanLactation 18 7ndash12
Horton S Sanghvi T Phillips M Fiedler J Perez-Escamilla R Lutter C et al (1996) Breastfeeding pro-motion and priority setting in health Health Policy andPlanning 11 156ndash168
ILO (1998) More than 120 Nations Provide Paid MaternityLeave Gap in Employment Treatment for Men andWomen Still Exists International Labour Office GenevaDocument ref ILO987 Available at httpwwwiloorgpublicenglishbureauinfpr19987htmr2
Iliff PJ Piwoz EG Tavengwa NV Zunguza CDMarinda ET Nathoo KJ et al (2005) Early exclusivebreastfeeding reduces the risk of postnatal HIV-1 trans-mission and increase HIV-free survival AIDS 19 699ndash708
Integrated Child Development Services Scheme (Revised)(ICDS) (1982) Ministry of Social Welfare Governmentof India New Delhi Available on URL httpwcdnicinudishahtmabouticdshtm
Jason JM Nieburg P amp Marks JS (1984) Mortality andinfectious disease associated with infant feeding prac-tices in developing countries Pediatrics 74 702ndash727
Jones G Steketee RW Black RE Bhutta ZA ampMorris SS Bellagio Child Survival Study Group (2003)How many child deaths can we prevent this yearLancet 362 65ndash71
Knippenberg R Lawn JE Darmstadt GL Begkayian GFogstad H Walelign N et al (2005) Systematic scalingup of neonatal care in countries Lancet 365 1087ndash1098
Kramer MS amp Kakuma R (2002) The optimal durationof exclusive breastfeeding a systematic reviewCochrane Database of Systematic Reviews 2002CD003517
Kramer MS Chalmers B Hodnett ED Sevkovskaya ZDzikovich I Shapiro S et al (2000) Promotion ofbreastfeeding intervention trial (PROBIT) a cluster ran-domized trial in the Republic of Belarus Design followup and data validation Advances in Experimental Medi-cine and Biology 478 327ndash345
Kramer MS Chalmers B Hodnett ED Sevkovskaya ZDzikovich I Shapiro S et al (2001) Promotion ofbreastfeeding intervention trial (PROBIT) a random-
Mainstreaming nutrition into MCH programs 15
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
ized trial in the Republic of Belarus Journal of theAmerican Medical Association 285 413ndash420
Lewin SA Dick J Pond P Zwarenstein M Aja Gvan Wyk B et al (2006) Lay health workers in primaryand community health care (Review) The CochraneLibrary 3 1ndash104
LINKAGES (2002) World LINKAGES MadagascarAcademy for Educational Development WashingtonDC
LINKAGES (2005) LINKAGES Zambia 1997ndash2005 FinalReport A Full Report on LINKAGES Infant Feedingand HIVAIDS Programs in Zambia Academy for Edu-cational Development Washington DC Available athttpwwwlinkagesprojectorgmediapublicationsFinal20draft20Zambia20final20report2012105pdf
Lutter CK Perez-Escamilla R Segall A Sanghvi TTeruya K amp Wickham C (1997) The effectiveness of ahospital based program to promote exclusive breastfeed-ing among low income women in Brazil AmericanJournal of Public Health 87 659ndash663
Morrow AL Guerrero ML Shults J Calva J Lutter CBravo J et al (1999) Efficacy of home based peer coun-selling to promote exclusive breastfeeding a randomizedcontrolled trial Lancet 353 1226ndash1231
Ntabaye MK amp Lusiola GJ (2004) Understanding barri-ers to PMTCT in Tanzania findings of a baseline surveyInternational Conference on AIDS 15 (B11396)
de Oliveira LD Giugliani ER do Espirito SLC FrancaMC Weigert EM Kohler CV et al (2006) Effect ofintervention to improve breastfeeding technique on thefrequency of exclusive breastfeeding and lactation-related problems Journal of Human Lactation 22 315ndash321
Perez-Escamilla R (2004) Effectiveness of MADLAC atImproving Breastfeeding Promotion and CounsellingIndicators in Maternity Wards in El Salvador Publishedfor the Basic Support for Institutionalizing Child Sur-vival Project (BASICS II) for the United States Agencyfor International Development Arlington VA Availableat httpwwwbasicsorgpdfFinal20MADLAC20Report20RPE20April207-2004pdf
Perez-Escamilla R (2007) Evidence based breast-feedingpromotion the Baby-Friendly Hospital InitiativeJournal of Nutrition 137 484ndash487
Piwoz EG Iliff PJ Tavengwa N Gavin L Marinda ELunney K et al (2005) An education and counselllingprogram for preventing breastfeeding associated HIVtransmission in Zimbabwe design and impact on mater-nal knowledge and behaviour Journal of Nutrition 135950ndash955
Quinn VJ Guyon AB Schubert JW Stone-Jimenez MHainsworth MD amp Martin LH (2005) Improvingbreastfeeding practices on a board scale at the commu-
nity level success stories from Africa and LatinAmerica Journal of Human Lactation 21 345ndash354
Ranson MK Hanson K Oliveira-Cruz V amp Mills A(2003) Constraints to expanding access to health inter-ventions an empirical analysis and country typologyJournal of International Development 15 15ndash40
Rea MF amp Berquo ES (1990) Impact of the Braziliannational breastfeeding programme on mothers inGreater Sao Paulo Bulletin of the of the World HealthOrganization 68 365ndash371
Rollins NC (2007) Infant feeding and HIV BritishMedical Journal 334 487ndash488
Rutenberg N Baek C Kalibala S Rosen J amp Mulenga D(2004) Evaluation of United Nations supported pilotprojects for the prevention of mother-to-child transmis-sion of HIV overview of findings International Confer-ence on AIDS 15 (WePeE6688)
The Core Group (2005) Scale and Scaling Up A COREGroup Background Paper on lsquoScaling-Uprsquo MaternalNewborn and Child Health Services CORE SpringMembership Meeting 2005 The Core Group Washing-ton DC Available at httpwwwcoregrouporgresourcesmeetingsapril05Scaling_Up_Background_Paper_7-13pdf
The Norwegian Government (1993) Women in PoliticsMinistry of Children and Equality Available at httpwwwregjeringennoendepbldRyddemappeSLA-AvdelingdoclegislationguidelinesWomen-in-Politicshtmlid=437166
Thior I Lockman S Smeaton LM Shapiro RL WesterC Heymann SJ et al (2006) Breastfeeding plus infantzidovudine prophylaxis for 6 months vs formula feedingplus infant zidovudine for 1 month to reduce mother-to-child HIV transmission in Botswana a randomized trialthe Mashi Study Journal of the American Medical Asso-ciation 296 794ndash805
UNICEF (2002) Facts for Life lsquoKey Message What EveryFamily and Community Has a Right to Know aboutBreastfeedingrsquo Available at httpwwwuniceforgffl04key_messageshtm
Van Roekel K Plowman B Griffiths M de AlvaradoVV Matute J amp Calderon M (2002) BASICS IIMidterm Evaluation of the AIN Program in Honduras2000 Basic Support for Institutionalizing Child SurvivalProject (BASICS II) for the United States Agency forInternational Development Arlington VA
WABA (2007) UNICEF Records BHFI Record UpdateAvailable at httpwwwwabaorgmydocsBFHIjan07xls 2006 Regularly updated by Miriam HLabbok Center for Infant and Young ChildFeeding and Care Department of Maternaland Child Health School of Public Health The Univer-sity of North Carolina at Chapel Hill Chapel Hill NCUSA
N Bhandari and AKMI Kabir16
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
WHA (2002) Infant and Young Child Nutrition Fifty-FifthWorld Health Assembly Agenda Item 1310 18 May2002 Available at httpwwwintgbebwhapdf_filesWHA55ewha5525pdf
WHO (1981) The International Code of Marketing ofBreastmilk Substitutes World Health OrganizationGeneva
WHO (1989) Protecting Promoting and Supporting Breast-feeding The Special Role of Maternity Services A JointWHOUNICEF Statement World Health OrganizationGeneva
WHO (2002) The Optimal Duration of Exclusive Breast-feeding Report of an Expert Consultation WHONHD0109 WHOFCHCAH0124 World HealthOrganization Geneva
WHO (2003a) Community Based Strategies for Breastfeed-ing Promotion and Support in Developing CountriesWorld Health Organization Geneva Document refISBN_92_4_159121_8 Available at httpwwwwhointchild-adolescent-healthNew_PublicationsNUTRITIONISBN_92_4_159121_8pdf
WHO (2003b) Multi-country Evaluation of IMCI Effective-ness Cost and Impact (MCE) Progress Report May2002ndashApril 2003 Document ref WHOFCHCAH035World Health Organization Geneva
WHO (2004) Promoting Proper Feeding for Infants andYoung Children World Health Organization GenevaAvailable at httpwwwwhointnutritiontopicsinfantfeedingen
WHO (2006) WHO HIV and Infant Feeding TechnicalConsultation-Consensus Statement World Health Orga-nization Geneva Available at httpwwwwhointhivmediacentreInfantfeedingconsensusstatementpfpdf
WHO Collaborative Study Team on the Role of Breast-feeding on the Prevention of Infant Mortality (2000)Effect of breastfeeding on infant and child mortality dueto infectious diseases in les developed countries apooled analysis Lancet 355 451ndash455
WHOUNICEF (1992) The global criteria for the WHOUNICEF Baby-Friendly Hospital Initiative In Baby-Friendly Hospital Initiative Part II Hospital LevelImplementation World Health Organization Geneva
WHOUNICEF (1993) Breastfeeding Counselling A Train-ing Course WHOCDR933 UNICEFNUT931 WorldHealth Organization Geneva
WHOUNICEF (2002) Protocol for Adapting the FeedingRecommendations Part III IMCI Adaptation GuideWorld Health Organization Geneva
WHOUNICEF (2003) Global Strategy for Infant andYoung Child Feeding World Health OrganizationGeneva Available at httpwwwwhointchild-adolescent-healthpublicationsNUTRITIONIYCF_GShtm
de Zoysa I Rea M amp Martines J (1991) Why promotebreastfeeding in diarrheal diseases control programmesHealth Policy and Planning 6 371ndash379
Mainstreaming nutrition into MCH programs 17
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
Cas
est
udie
so
fef
fect
iven
ess
stud
ies
or
pilo
tpr
ogra
mm
es
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Lut
ter
etal
(199
7)
Bra
zil
Low
-inc
ome
urba
nw
omen
deliv
erin
gin
hosp
ital
s
Bre
astf
eedi
ngpr
omot
ion
in
hosp
ital
sco
mpa
red
wit
h
nobr
east
feed
ing
prom
otio
n
Pro
mot
ion
ofbr
east
feed
ing
in
sele
cted
hosp
ital
s
Mea
nda
ysof
excl
usiv
e
brea
stfe
edin
g
75da
ysvs
22
days
(Plt
001
)
Rea
ampB
erqu
o
(199
0)
Wom
enw
ith
ach
ild
aged
lt2ye
ars
inSa
oP
aulo
Nat
iona
lbre
astf
eedi
ng
cam
paig
n19
81ndash1
986
BF
HI
Mas
sm
edia
cam
paig
n11
in
fant
s5ndash
6m
onth
s
excl
usiv
ely
brea
stfe
d
in19
88an
d37
in
1987
Con
foun
ding
fact
ors
over
the
6-ye
arpe
riod
not
mea
sure
d
Kra
mer
etal
(200
020
01)
PR
OB
ITtr
ial
Bel
arus
Clu
ster
rand
omiz
ed
34ho
spit
als
and
thei
rpo
lycl
inic
s
Trai
ning
inB
FH
I(W
HO
UN
ICE
F19
92)
vsr
outi
ne
prac
tice
san
dpo
licie
s
Exc
lusi
vebr
east
feed
ing
at3
(43
3vs
64
)
and
6(7
9
vs0
6
)
mon
ths
sign
ifica
ntly
high
er
Impl
emen
ted
thro
ugh
BF
HI
ina
sett
ing
whe
reho
spit
al
deliv
erie
sar
eco
mm
on
Per
ez-E
scam
illa
(200
4)
BA
SIC
SII
Mex
ico
Hon
dura
s
Bra
zil
MA
DL
AC
low
-cos
t
man
agem
ent
info
rmat
ion
syst
emto
use
an
evid
ence
-bas
edap
proa
chto
impr
ove
serv
ice
perf
orm
ance
Inte
rvie
win
gof
wom
enat
hosp
ital
disc
harg
epo
st
deliv
ery
usin
ga
ques
tion
nair
eth
atta
kes
5ndash7
min
toad
min
iste
ran
d
cont
ains
19br
east
feed
ing
prom
otio
nco
unse
lling
indi
cato
rs
Dat
aen
tere
dan
dre
sult
s
disc
usse
d3-
mon
thly
by
hosp
ital
com
mit
tee
Hos
pita
lim
plem
ents
chan
ges
in
brea
stfe
edin
g
supp
ort
base
don
anal
ysis
of
ques
tion
nair
es
Itis
aco
st-e
ffec
tive
inte
rven
tion
that
can
help
impr
ovem
ents
inth
eB
FH
I
and
isa
valu
able
tool
for
proc
ess
eval
uati
on
N Bhandari and AKMI Kabir18
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
LIN
KA
GE
S
proj
ect
inA
fric
aan
d
Lat
inA
mer
ica
(Qui
nnet
al
2005
LIN
KA
GE
S
2002
WH
O20
03a)
Bol
ivia
(1
mill
ion)
Gha
na(3
5
mill
ion)
Mad
agas
car
(6m
illio
n)
Res
ourc
e-
poor
sett
ing
Pilo
tpr
ogra
mm
e
InB
oliv
iaan
d
Gha
napr
ogra
mm
e
focu
sed
on
brea
stfe
edin
gan
d
com
plem
enta
ry
feed
ing
InM
adag
asca
r
prog
ram
me
prom
oted
brea
stfe
edin
g
wit
hin
7es
sent
ial
nutr
itio
nac
tion
san
d
subs
eque
ntly
thro
ugh
IMC
I
Bui
lton
form
ativ
ere
sear
ch
and
sust
aine
dth
roug
h
prog
ram
me
acti
viti
esth
at
focu
sed
onbr
ingi
ngab
out
the
desi
red
beha
viou
r
chan
geM
ixof
inte
rven
tion
s
reac
hed
wom
enin
divi
dual
ly
orin
grou
psin
heal
th
faci
litie
sho
mes
or
com
mun
ity
sett
ings
Con
sist
ent
mes
sage
san
d
mat
eria
lacr
oss
all
prog
ram
me
chan
nels
Bol
ivi
PR
OC
OSI
NG
Os
Gha
na
UN
ICE
F
nati
onal
nutr
itio
n
offic
eN
GO
s
Mad
agas
car
Inte
rsec
tora
l
Act
ion
Gro
upfo
r
Nut
riti
on
Jere
o
Sala
ma
Isik
a
Pro
gram
desi
gned
wit
h
part
ners
Rad
ioin
all
thre
esi
tes
Mat
eria
ls
deve
lope
d
tosu
itne
eds
oflo
cal
heal
th
wor
kers
and
com
mun
ity
mem
bers
Gre
at
emph
asis
on
deve
lopm
ent
of coun
selli
ng
and
nego
tiat
ion
skill
s
prac
tica
l
sess
ions
Sign
ifica
ntin
crea
ses
inex
clus
ive
brea
stfe
edin
gra
tes
of
0ndash6-
mon
th-o
ld
infa
nts
from
54
to65
in
Bol
ivia
68
to79
in
Gha
naan
d46
to68
in
Mad
agas
car
In
Gha
naan
d
Mad
agas
car
sign
ifica
ntre
sult
s
obse
rved
wit
hin
aye
ar
ofin
itia
tion
of
com
mun
ity
inte
rven
tion
s
App
roac
hw
asef
fect
ive
and
achi
eved
sign
ifica
nt
incr
ease
sam
ong
larg
e
popu
lati
ons
asea
rly
as
9ndash12
mo
afte
rin
itia
tion
of
com
mun
ity
acti
viti
es
Van
Roe
kele
tal
(200
2)W
HO
(200
3a)
Hon
dura
sG
row
thm
onit
orin
gan
d
prom
otio
nkn
own
as
Ate
ncioacute
nIn
tegr
ala
la
Nintilde
ez(A
IN)
or
Inte
grat
edC
hild
Car
e
Init
ially
pri
mar
ilya
grow
th
mon
itor
ing
prog
ram
me
ulti
mat
ely
thro
ugh
IMC
I
Pro
gram
me
ongr
owth
prom
otio
nndash
asse
ssm
ent
of
mon
thly
wei
ght
gain
and
focu
son
illne
ssf
eedi
ng
prac
tice
san
dge
nera
lchi
ld
care
inin
fant
sun
der
2ye
ars
Impl
emen
ted
atgo
vern
men
t
faci
litie
san
dco
mm
unit
y
Star
ted
in19
92s
tren
gthe
ned
in19
95ndash1
997
wit
hgr
eate
r
focu
son
child
feed
ing
In
1997
pro
gram
me
intr
oduc
ed
wit
hIM
CI
(WH
OU
NIC
EF
2002
)
Maj
or
part
ners
UN
ICE
F
PAH
O
Am
eric
an
and
Hon
dura
n
Red
Cro
ss
CA
RE
Rad
io
broa
dcas
ts
relig
ious
lead
ers
IMC
IM
id-t
erm
eval
uati
on
show
ed39
of
mot
hers
inin
terv
enti
on
com
mun
itie
sex
clus
ivel
y
brea
stfe
dco
mpa
red
wit
h13
in
the
cont
rol
site
s
Mainstreaming nutrition into MCH programs 19
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
cont
inue
d
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Bha
ndar
ieta
l
(200
3)
WH
O
(200
3a)
Rur
alco
mm
unit
ies
inH
arya
na
Indi
a
Clu
ster
rand
omiz
edtr
ial
8
com
mun
itie
s(t
otal
popu
lati
on~4
000
0)
Pro
mot
ion
ofex
clus
ive
brea
stfe
edin
gan
d
appr
opri
ate
com
plem
enta
ryfe
edin
g
Dev
elop
edth
roug
h
form
ativ
ere
sear
ch
ndashP
robl
emid
enti
ficat
ion
ndashP
arti
cipa
tory
desi
gnof
inte
rven
tion
impl
emen
tati
onan
d
eval
uati
on
Impl
emen
tati
onw
ithi
nan
exis
ting
prim
ary
heal
th-c
are
prog
ram
me
Opp
ortu
niti
esus
edto
deliv
erm
essa
ges
wer
e
imm
uniz
atio
ncl
inic
s
wei
ghin
gse
ssio
ns
sick
-chi
ldco
ntac
tsan
d
mon
thly
hom
evi
sits
Res
earc
hers
wit
hlo
cal
gove
rnm
ent
ICD
Ssy
stem
and
NG
O
The
atre
son
gs
Mas
sm
edia
not
used
for
risk
of
cont
amin
atio
n
Mat
eria
ls
deve
lope
d
for
heal
th
wor
kers
pos
ters
flip
book
sca
rds
Bre
astf
eedi
ng
coun
selli
ngse
ctio
n
ofth
eIM
CI
(WH
O
UN
ICE
F20
02)
Exc
lusi
ve
brea
stfe
edin
gin
the
prev
ious
24h
at3
mon
ths
of
age
79
vs4
8
The
posi
tive
effe
ct
rem
aine
dup
to
6m
onth
sof
age
(42
vs4
)
Tota
lpar
tici
pati
onof
the
dist
rict
heal
thsy
stem
from
ince
ptio
nof
the
prog
ram
me
inde
velo
ping
impl
emen
tati
onst
rate
gyt
ool
deve
lopm
ent
and
mon
itor
ing
inad
diti
onto
invo
lvem
ent
of
anN
GO
wer
eim
port
ant
feat
ures
that
cont
ribu
ted
to
the
succ
ess
ofth
e
inte
rven
tion
Mor
row
etal
(199
9)
Mex
ico
Cit
yC
lust
erra
ndom
ized
tria
l
Tota
lpop
ulat
ion
3000
0
Two
com
mun
itie
sin
the
inte
rven
tion
one
com
pari
son
130
wom
en
Hom
e-ba
sed
peer
coun
selli
ng
Pee
rco
unse
llors
mad
e3
or
6ho
me
visi
tsto
the
mot
her
Key
fam
ilym
embe
rsal
so
incl
uded
By
La
Lec
he
Lea
gue
of
Mex
ico
Exc
lusi
ve
brea
stfe
edin
g
at3
mon
ths
post
-par
tum
67
(6vi
sits
)
50
(3vi
sits
)12
(com
pari
son)
Firs
tcl
uste
rra
ndom
ized
com
mun
ity-
base
dtr
ialt
hat
used
peer
coun
sello
rsto
prom
ote
excl
usiv
e
brea
stfe
edin
g
Hai
der
etal
2000
200
2
Dha
ka
Low
mid
dle
and
low
-soc
io-
econ
omic
popu
lati
on
Clu
ster
rand
omiz
edtr
ial
20zo
nes
inin
terv
enti
on
and
20in
cont
rol
Com
mun
ity-
base
dpe
er
coun
selli
ngin
Dha
ka
15ho
me-
base
dco
unse
lling
visi
tsby
peer
coun
sello
rs
40h
(4h
yen10
days
)
WH
OU
NIC
EF
brea
stfe
edin
g
coun
selli
ngco
urse
(WH
OU
NIC
EF
1993
)
Exc
lusi
ve
brea
stfe
edin
g
at5
mon
ths
70
in
inte
rven
tion
and
6in
the
cont
rol
Com
mun
ity-
base
d
brea
stfe
edin
gpr
omot
ion
stra
tegy
was
effe
ctiv
ein
Ban
glad
esh
whe
rem
ost
deliv
erie
soc
cur
atho
me
N Bhandari and AKMI Kabir20
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Bry
ceet
al
(200
4)W
HO
(200
3b)
Bra
zil
Per
u
Tanz
ania
Uga
nda
Mul
tico
untr
yev
alua
tion
of
IMC
Ith
atin
clud
ed
effe
ctiv
enes
sco
stan
d
impa
ct(B
ryce
etal
2004
)
Bre
astf
eedi
ngpr
omot
ion
asa
part
ofIM
CI
IMC
Iis
ast
rate
gyfo
r
impr
ovin
gch
ildhe
alth
and
deve
lopm
ent
thro
ugh
the
com
bine
d
deliv
ery
ofes
sent
ial
child
heal
th
inte
rven
tion
sIM
CI
bega
nw
ith
ase
tof
case
man
agem
ent
guid
elin
es
for
the
man
agem
ent
ofsi
ckch
ildre
nat
first
-lev
elhe
alth
faci
litie
s
and
the
guid
elin
esw
ere
desi
gned
for
adap
tati
on
atco
untr
yle
vela
nd
belo
wO
ver
tim
eth
e
stra
tegy
expa
nded
to
incl
ude
ara
nge
of
guid
elin
esfo
rde
liver
ing
child
surv
ival
inte
rven
tion
at
hous
ehol
dco
mm
unit
y
and
refe
rral
leve
ls
IMC
Im
odul
e(W
HO
UN
ICE
F20
02)
Res
ults
onex
clus
ive
brea
stfe
edin
g
avai
labl
efr
om
Tanz
ania
whe
reno
sign
ifica
ntim
pact
was
seen
Des
pite
subs
tant
ial
impr
ovem
ent
inth
equ
alit
y
ofca
rede
liver
edby
IMC
Iat
heal
thfa
cilit
ies
key
fam
ily
prac
tice
ssu
chas
excl
usiv
e
brea
stfe
edin
gdi
dno
tch
ange
asco
mm
unit
yIM
CI
had
not
been
impl
emen
ted
byth
at
tim
e(W
HO
2003
b)
SA
rife
en
pers
onal
com
mun
icat
ion
Ban
glad
esh
Mat
lab
Com
mun
ity-
base
dcl
uste
r
desi
gn
Eva
luat
ion
offa
cilit
y-an
d
com
mun
ity-
base
dIM
CI
Inte
rven
tion
pack
age
incl
udes
feed
ing
asse
ssm
ent
and
coun
selli
ngon
mot
hers
ofyo
ung
child
ren
seek
ing
care
atfa
cilit
ies
for
illne
ssan
d
hom
e-ba
sed
coun
selli
ng
onim
prov
edfe
edin
gby
com
mun
ity-
base
dhe
alth
and
nutr
itio
nw
orke
rs
At
base
line
inth
e
year
2000
alit
tle
mor
eth
anha
lfth
e
0ndash5-
mon
th-o
ld
infa
nts
inth
est
udy
area
wer
ebe
ing
excl
usiv
ely
brea
stfe
dB
y20
05
this
incr
ease
dby
30
inth
eIM
CI
area
Dat
ano
t
avai
labl
efr
omth
e
com
pari
son
area
as
yet
Lac
kof
com
para
ble
data
from
the
com
pari
son
area
prev
ents
ade
finit
ive
conc
lusi
onas
tow
heth
erth
is
trul
yis
anim
pact
ofIM
CI
BA
SIC
SII
Bas
icSu
ppor
tfo
rIn
stit
utio
naliz
ing
Chi
ldSu
rviv
alP
roje
ctB
FH
IB
aby-
Frie
ndly
Hos
pita
lIni
tiat
ive
ICD
SIn
tegr
ated
Chi
ldD
evel
opm
ent
Serv
ices
IM
CI
Inte
grat
edM
anag
emen
tof
Chi
ldho
odIl
lnes
sM
AD
LA
CM
onit
oreo
deA
poyo
Dir
ecto
con
laL
acat
anci
aM
ater
naN
GO
non
-gov
ernm
enta
lorg
aniz
atio
nPA
HO
Pan
Am
eric
anH
ealt
hO
rgan
izat
ion
PR
OB
ITP
rom
otio
nof
Bre
astf
eedi
ngIn
terv
enti
onTr
ial
PR
OC
OSI
Pro
gram
ade
Coo
rdin
acio
nen
Salu
dIn
tegr
al(C
olla
bora
tive
Pro
gram
for
Inte
grat
edH
ealt
h)U
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
WH
OW
orld
Hea
lth
Org
aniz
atio
n
Mainstreaming nutrition into MCH programs 21
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x2
Cas
est
udie
sin
scal
e-up
effo
rts
inH
IVA
IDS
Stud
yde
scri
ptio
nPo
pula
tion
Inte
rven
tion
Com
mun
icat
ion
stra
tegy
Impa
cton
excl
usiv
ebr
east
feed
ing
Com
men
ts
LIN
KA
GE
S(2
005)
Zam
bia
Pro
gram
me
thro
ugh
heal
th-c
are
and
com
mun
ity
serv
ices
Rea
ched
60si
tes
in6
dist
rict
sby
2005
Inte
grat
ion
ofin
fant
feed
ing
coun
selli
ngm
ater
naln
utri
tion
and
anti
retr
ovir
aldr
ugs
prop
hyla
xis
Trai
ning
ofhe
alth
wor
kers
and
com
mun
ity
serv
ice
prov
ider
sto
coun
selw
omen
onsa
fety
opti
ons
for
thei
rsi
tuat
ion
Beh
avio
urch
ange
Com
mun
icat
ion
inte
rven
tion
sin
the
first
few
year
sM
ater
iald
evel
oped
lsquoAct
Now
rsquoM
edia
cam
paig
nsin
clud
edbr
ochu
res
post
ers
radi
oan
dte
levi
sion
Ass
esse
dth
roug
hba
selin
ean
dfo
llow
-up
hous
ehol
dan
dcl
inic
surv
eys
inse
lect
eddi
stri
cts
Exc
lusi
vebr
east
feed
ing
rate
incr
ease
dfr
om50
in
2002
to64
in
2004
inL
ivin
gsto
nean
dfr
om57
in
2000
to74
in
2004
inN
dola
Inte
grat
edde
mon
stra
tion
proj
ect
Had
seve
rals
tren
gths
inte
rms
ofth
eus
eof
form
ativ
ere
sear
chto
deve
lop
mes
sage
str
aini
ngan
dbu
ildin
gup
skill
sof
prog
ram
me
man
ager
she
alth
-car
epr
ovid
ers
and
com
mun
ity
wor
kers
adv
ocac
yfo
rna
tion
alpo
licy
stro
ngbe
havi
our
chan
geco
mm
unic
atio
nco
mpo
nent
st
reng
then
ing
com
mun
ity
capa
city
for
coun
selli
ngan
dre
ferr
als
and
mon
itor
ing
and
eval
uati
onw
ith
loca
lpar
tner
sP
iwoz
etal
(20
05)
ZV
ITA
MB
Otr
ial
Har
are
Zim
babw
eE
duca
tion
and
coun
selli
ngpr
ogra
mm
ede
liver
edan
tena
tally
1411
0m
othe
rndashba
bypa
irs
enro
lled
from
14m
ater
nity
clin
ics
wit
hin
96h
ofde
liver
yan
dfo
llow
edup
at6
wee
ks
3m
onth
san
d3-
mon
thly
inte
rval
sIn
fant
-fee
ding
patt
erns
dete
rmin
edE
xclu
sive
brea
stfe
edin
gre
com
men
ded
for
HIV
nega
tive
un
know
nor
HIV
posi
tive
who
chos
eto
brea
stfe
ed
Gro
uped
ucat
ion
indi
vidu
alco
unse
lling
vid
eos
broc
hure
sM
othe
rsw
hoen
rolle
dw
hen
prog
ram
me
was
fully
impl
emen
ted
wer
e8
4ti
mes
mor
elik
ely
toex
clus
ivel
ybr
east
feed
than
mot
hers
who
enro
lled
befo
reth
epr
ogra
mm
ebe
gan
Ove
rall
excl
usiv
ebr
east
feed
ing
rate
sti
ll3
mon
ths
was
low
at24
6
Form
ativ
ere
sear
chus
edto
desi
gna
cult
ural
lyse
nsit
ive
educ
atio
nan
dco
unse
lling
prog
ram
me
Low
over
alle
xclu
sive
brea
stfe
edin
gra
tes
prom
pted
auth
ors
toco
nclu
deth
atw
omen
and
thei
rpa
rtne
rssh
ould
have
been
reac
hed
mor
efr
eque
ntly
duri
ngan
tena
tala
ndpo
st-n
atal
peri
od
N Bhandari and AKMI Kabir22
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Thi
oret
al(
2006
)R
ollin
s(2
007)
C
ohen
(200
7)
HIV
-inf
ecte
dpr
egna
ntw
omen
atte
ndin
gan
tena
talc
linic
sin
sout
hB
otsw
ana
Inve
stig
atio
nsby
CD
Cof
adi
arrh
oea
outb
reak
inJa
nuar
y-Fe
brua
ry20
06in
the
sam
epo
pula
tion
Mat
erna
land
infa
ntan
tire
trov
iral
ther
apy
toas
cert
ain
impa
cton
HIV
tran
smis
sion
Ant
enat
alco
unse
lling
Cas
endashco
ntro
lstu
dyto
iden
tify
risk
fact
ors
for
diar
rhoe
ano
tbr
east
feed
ing
was
the
bigg
est
risk
fact
ora
djus
ted
odds
rati
o50
(95
confi
denc
ein
terv
al4
5ndash10
0)
Bot
swan
aha
sth
ebe
stpr
imar
yhe
alth
-car
est
ruct
ure
wat
ersu
pply
and
sani
tati
onsy
stem
sin
Sout
hA
fric
aFo
rmul
apr
ovid
edfr
eeby
the
gove
rnm
ent
toin
fect
edm
othe
rsL
ower
mor
talit
yin
the
brea
stfe
edin
ggr
oup
at7
mon
ths
dem
onst
rate
sri
skof
form
ula
feed
ing
and
need
for
alte
rnat
est
rate
gies
(Thi
oret
al
2006
)A
utho
rsco
nclu
deth
athe
alth
syst
ems
inw
hich
thes
epr
ogra
mm
esar
eim
plem
ente
dsh
ould
beab
leto
cope
wit
hdi
arrh
oea
and
mal
nutr
itio
nth
atre
sult
sbe
caus
eof
form
ula
feed
ing
(Rol
lins
2007
)C
oova
dia
etal
(2
007)
Kw
aZul
uNat
al
Sout
hA
fric
a27
22H
IV-i
nfec
ted
and
unin
fect
edpr
egna
ntw
omen
enro
lled
into
ano
n-ra
ndom
ized
inte
rven
tion
coho
rtst
udy
from
ante
nata
lcl
inic
sIn
fant
feed
ing
data
obta
ined
wee
kly
bloo
dsa
mpl
esfr
omin
fant
sta
ken
mon
thly
83
of13
72in
fant
sbo
rnto
HIV
-inf
ecte
dm
othe
rsin
itia
ted
excl
usiv
ebr
east
feed
ing
from
birt
hB
reas
tfed
infa
nts
who
rece
ived
solid
sw
ere
sign
ifica
ntly
mor
elik
ely
toac
quir
ein
fect
ion
com
pare
dw
ith
excl
usiv
ely
brea
stfe
d(H
R10
87
151
ndash78
P=
001
8)as
wer
ein
fant
sw
hoat
12w
eeks
rece
ived
brea
stan
dfo
rmul
am
ilk(1
82
098
ndash33
6P
=0
57)
Cum
ulat
ive
3-m
onth
mor
talit
yin
excl
usiv
ely
brea
stfe
dw
as6
1(4
74ndash
792
)vs
15
1(7
63ndash
287
3)in
infa
nts
give
nre
plac
emen
tfe
eds
(HR
206
1
0ndash4
27P
=0
05)
The
stud
ysh
ows
that
excl
usiv
ebr
east
feed
ing
can
besu
cces
sful
lysu
ppor
ted
inH
IV-i
nfec
ted
wom
enT
heau
thor
sca
llfo
rfu
rthe
rre
visi
onof
UN
ICE
FW
HO
and
USA
IDin
fant
feed
ing
guid
elin
es
CD
CC
ente
rof
Dis
ease
Con
trol
HR
haz
ards
rati
oU
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
USA
IDU
SA
genc
yfo
rIn
tern
atio
nalD
evel
opm
ent
WH
OW
orld
Hea
lth
Org
aniz
atio
nZ
VIT
AM
BO
Z
imba
bwe
Vit
amin
Afo
rM
othe
rsan
dB
abie
s
Mainstreaming nutrition into MCH programs 23
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23

toring and evaluation not only provides a measure ofsuccess but identifies factors that may have contrib-uted to it and to lack of success to enable mid-coursecorrections The impact of some pilot programmes onexclusive breastfeeding is summarized in Appendix 2In most programmes exclusive breastfeeding ratesimproved In Zambia exclusive breastfeeding ratesincreased from 50 in 2002 to 64 in 2004 in Liv-ingstone from 57 in 2000 to 74 in 2004 in NdolaIn South Africa an antenatal clinic-based interven-tion led to 83 of infants born to HIV-infectedmother initiating exclusive breastfeeding InZimbabwe an intervention based on antenatal coun-selling resulted in a relatively lower exclusive breast-feeding rate of 246 at 3 months (Piwoz et al 2005)
Several barriers to success were identified Theseinclude inadequate skills of workers and non-integration of HIV counselling and tailoring into ante-natal care services (Ntabaye amp Lusiola 2004) which isthe backbone in which infant feeding counselling isbuiltWomen reported that mothers not breastfeedingtheir children were discriminated against by the com-munity and they faced the threat of domestic violenceProgramme managerrsquos understanding of barriersto effective programme implementation and impactwere emphasized as being important Governmentsupport partnerrsquos coordination increased humanresource and improving the supply system were iden-tified to be essential features to scale up programmesin the HIV context (Rutenberg et al 2004) Lowoverall exclusive breastfeeding rates prompted Piwozet al (2005) to conclude that women and their partnersshould have been reached more frequently during theantenatal and post-natal period
Conclusions
In a large number of programmes for improvingexclusive breastfeeding in developing countriesincluding in areas with high prevalence of HIV apositive impact on exclusive breastfeeding rates hasbeen achieved
Some of the factors that contributed to successfulscale-up are summarized in Table 4 Several limita-tions of the programmes reviewed merit attentionMost programmes involved special and generous
funding concentrated efforts and multiple contactsThese programmes were evaluated over relativelyshort periods of time usually 2ndash5 years and the long-term sustainability has not been really tested In theabsence of specific measures there is likely to be dilu-tion of quality as the programmes are scaled upfurther from their initial size The experience thus farleaves important questions to be addressed particu-larly on how programmes can be sustained over timeas they are scaled up at affordable costs
A key factor relevant to sustainability is to plan ona long-term basis a period of 10ndash20 years rather than5ndash10 years from the outset Experience with otherchild health programmes has shown that performancein immunization and oral rehydration therapy userates plateaued over time in many countries
Programme scale-up requires a programme man-agement capacity proportionate to the scale of opera-tions periodic assessment of barriers (Table 5) and anability to revise programme strategy to overcomethese Another key feature to sustainability ofscale-up is the extent to which capacity has been builtat the district block and community levels National-or state-level driven interventions begin with enor-mous enthusiasm which is difficult to sustain Thisfactor is particularly important as most developing
Table 4 Lessons learnt about scale-up key factors in success
bull Political will advocacy enabling policiesbull Championship by health ministries at national state and districtlevelbull Technical consensus on feeding guidelinesbull Programme strategy and measurable short- and long-term goalsbull Long-term financial commitmentbull Partners with defined roles assessment of their capacity todeliver and plans to cover gaps in capacitybull Emphasis on community-level interventions and not onlyfacility-based programmesbull Formative research as the backbone of effective scale-upprogrammes particularly in the context of HIVbull Careful selection of channels and the number required toachieve timely coverage consistency of messagesbull Communication strategy aided by formative research pre-testedvalidated messages and toolsbull Quality trainers and training centres proportionate to requiredscalebull Monitoring and evaluationbull Programme redesign when relevant through research analysisand innovation
Mainstreaming nutrition into MCH programs 13
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
countries are going through a process of decentrali-zation with increasing responsibility for planningimplementation and evaluation being delegated tolower levels of the health-care system Buildingcapacity at that level requires time resources andpatience and a longer-term perspective
Building capacity emerges to be a key factorTrainers and training centres vary in their qualitywhen training health workers and their supervisorsor programme managers As the burden of trainingincreases availability of good-quality trainersbecomes a limiting factor (WHOUNICEF 2002Government of India 2006) An effective strategymust plan for these incremental requirements includ-ing ensuring secure and sustained funding
Identifying barriers to success is a key actor Thebarriers to scaling up of health interventions havebeen elegantly described by Ranson et al (Table 5)Most of these are important for exclusive breastfeed-ing scale-up as well
Overall within the limitations discussed above anumber of programmes in countries with varying
HIV prevalence show that exclusive breastfeeding ona large scale is feasible and pilot programmes havegiven valuable guidance related to policies planningand implementation of large-scale programmes Thechallenge now is to build on these experiences whenplanning national programmes
Acknowledgements
We sincerely thank Dr MK Bhan for his constructivecriticism and sustained feedback at different stages ofdevelopment of this review
Conflicts of interest
The authors have declared no conflicts of interest
References
Arifeen S Black RE Antelman G Baqui A CaulfieldL amp Becker S (2001) Exclusive breastfeeding reducesacute respiratory infection and diarrhea deaths amonginfants in Dhaka slums Pediatrics 108 E67
Australian Breastfeeding Association (2005) Valuing Par-enthood Options for Paid Maternity Leave ndash InterimPaper 2002 Available at httpwwwbreastfeedingasnauadvocacymatleavehtml
Bhandari N Bahl R Mazumdar S Martines J BlackRE amp Bhan MK (2003) Effect of community basedpromotion of exclusive breastfeeding on diarrheal ill-nesses and growth a cluster randomized controlled trialLancet 361 1418ndash1423
Bhandari N Mazumder S Bahl R Martines J BlackRE amp Bhan MK (2004) An educational interventionto promote appropriate complementary feedingimproves child feeding practices and linear growth inrural Haryana India Journal of Nutrition 134 2342ndash2348
Bhandari N Mazumder S Bahl R Martines J BlackRE amp Bhan MK (2005) Use of multiple opportunitiesfor improving feeding practices in undertwos withinchild health programs Health Policy Plan 20 328ndash336
Bryce J Victora CG Habicht JP Vaughan JP ampBlack RE (2004) The multi-country evaluation of theintegrated management of childhood illness strategylessons for the evaluation of public health interventionsAmerican Journal of Public Health 94 406ndash415
Butte NF Lopez-Alarcon MG amp Garza C (2002) Nutri-ent Adequacy of Exclusive Breastfeeding for the TermInfant during the First Six Months of Life World HealthOrganization Geneva
Table 5 Barriers to scaling up of health interventions
Community and household levelsLack of information womenrsquos education physical financial
womenrsquos decision-making powerHealth services delivery levelShortage of qualified staff weak technical guidance programme
management and supervision inadequate supplies equipmentand infrastructure poor accessibility
Health sector policy and strategic management levelWeak and centralized system for planning and management weak
drug policies and supply system inadequate regulations lack ofintersectoral action and partnership weak incentives to useinputs efficiently and respond to user needs and preferencesreliance on donor funding
Public policies cutting across sectorsGovernment bureaucracy poor communication and transport
infrastructureEnvironmental characteristicsGovernance and overall policy frameworkCorruption weak government weak laws political instability and
insecurity low priority to social sectors weak structure for publicaccountability and opportunities for public opinions lack of freepress
Physical environmentClimatic and geographic predisposition physical environment
unfavourable to service delivery
Adapted from Ranson et al (2003)
N Bhandari and AKMI Kabir14
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Cohen J (2007) Retrovirus meeting Hope on new AIDSdrugs but breast-feeding strategy backfires Science 3151357
Coovadia HM Rollins NC Bland RM Little KCoutsoudis A Bennish ML et al (2007) Mother tochild transmission of HIV-1 infection during exclusivebreastfeeding in the first 6 months of life an interven-tion cohort study Lancet 369 1107ndash1116
Coutinho SB de Lira PI de Carvalho LM amp AshworthA (2005) Comparison of the effect of two systems forthe promotion of exclusive breastfeeding Lancet 3661094ndash1100
Feachem RG amp Koblinsky MA (1984) Interventions forthe control of diarrheal diseases among young childrenpromotion of breastfeeding Bulletin of the of the WorldHealth Organization 62 271ndash291
Gonzales A Arteaga E amp Howard-Grabman L (1998)Scaling Up the WARMI Project ndash Lessons LearnedMobilizing Bolivian Communities around ReproductiveHealth Save the Children Federation Inc Bolivia FieldOffice La Paz Available at httpwwwcoregrouporgresourcesSavebolipdf
Government of India (1997) Recommendations of the FifthCentral Pay Commission Relating to Enhancement ofQuantum of Maternity Leave and to Allow PaternityLeave in Respect of Central Government EmployeesDocument ref 13018197-Estt(L) Available at httppersminnicinesttleave2htm
Government of India (2005) National Rural HealthMission 2005ndash2012 Mission document Ministry ofHealth and Family Welfare New Delhi Government ofIndia Available at httpwwwmohfwnicinNRHM20Mission20Documentpdf
Government of India (2006) Operational Guidelines forImplementation of Integrated Management of Neonataland Childhood Illness (IMNCI) Ministry of HealthFamily Welfare New Delhi Available at httpmohfwnicindofw20websiteF20IMNCI20Operational20Plan201320june202006htm
Government of Pakistan (2003) National Programme forFamily Planning and Primary Health Care The LadyHealth Workers Programme 2003ndash2008 Ministry ofHealth Pakistan Available at httpwwwphcgovpkDownloadsPC-120augpdf
Green CP (1999) Improving Breastfeeding Behaviors Evi-dence from Two Decades of Intervention ResearchPublished for the US Agency for International Develop-ment (USAID) by the LINKAGES Project Academyfor Educational Development Washington DC
Gupta A (2002) National trends in breastfeeding andeffective strategies to improve breastfeeding ratesJournal of Neonatology 2002 4ndash14
Gwatkin DR (2004) Integrating the management of child-hood illness Lancet 364 1557ndash1558
Habicht JP DaVanzo J amp Butz WP (1986) Does breast-feeding really save lives or are apparent benefits due tobiases American Journal of Epidemiology 123279ndash290
Haider R Ashworth A Kabir I amp Huttly SR (2000)Effect of community based peer counsellors on exclusivebreastfeeding practices in Dhaka Bangladesh a ran-domized controlled trial Lancet 356 1643ndash1647
Haider R Kabir I Huttly SR amp Ashworth A (2002)Training peer counsellors to promote and support exclu-sive breastfeeding in Bangladesh Journal of HumanLactation 18 7ndash12
Horton S Sanghvi T Phillips M Fiedler J Perez-Escamilla R Lutter C et al (1996) Breastfeeding pro-motion and priority setting in health Health Policy andPlanning 11 156ndash168
ILO (1998) More than 120 Nations Provide Paid MaternityLeave Gap in Employment Treatment for Men andWomen Still Exists International Labour Office GenevaDocument ref ILO987 Available at httpwwwiloorgpublicenglishbureauinfpr19987htmr2
Iliff PJ Piwoz EG Tavengwa NV Zunguza CDMarinda ET Nathoo KJ et al (2005) Early exclusivebreastfeeding reduces the risk of postnatal HIV-1 trans-mission and increase HIV-free survival AIDS 19 699ndash708
Integrated Child Development Services Scheme (Revised)(ICDS) (1982) Ministry of Social Welfare Governmentof India New Delhi Available on URL httpwcdnicinudishahtmabouticdshtm
Jason JM Nieburg P amp Marks JS (1984) Mortality andinfectious disease associated with infant feeding prac-tices in developing countries Pediatrics 74 702ndash727
Jones G Steketee RW Black RE Bhutta ZA ampMorris SS Bellagio Child Survival Study Group (2003)How many child deaths can we prevent this yearLancet 362 65ndash71
Knippenberg R Lawn JE Darmstadt GL Begkayian GFogstad H Walelign N et al (2005) Systematic scalingup of neonatal care in countries Lancet 365 1087ndash1098
Kramer MS amp Kakuma R (2002) The optimal durationof exclusive breastfeeding a systematic reviewCochrane Database of Systematic Reviews 2002CD003517
Kramer MS Chalmers B Hodnett ED Sevkovskaya ZDzikovich I Shapiro S et al (2000) Promotion ofbreastfeeding intervention trial (PROBIT) a cluster ran-domized trial in the Republic of Belarus Design followup and data validation Advances in Experimental Medi-cine and Biology 478 327ndash345
Kramer MS Chalmers B Hodnett ED Sevkovskaya ZDzikovich I Shapiro S et al (2001) Promotion ofbreastfeeding intervention trial (PROBIT) a random-
Mainstreaming nutrition into MCH programs 15
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
ized trial in the Republic of Belarus Journal of theAmerican Medical Association 285 413ndash420
Lewin SA Dick J Pond P Zwarenstein M Aja Gvan Wyk B et al (2006) Lay health workers in primaryand community health care (Review) The CochraneLibrary 3 1ndash104
LINKAGES (2002) World LINKAGES MadagascarAcademy for Educational Development WashingtonDC
LINKAGES (2005) LINKAGES Zambia 1997ndash2005 FinalReport A Full Report on LINKAGES Infant Feedingand HIVAIDS Programs in Zambia Academy for Edu-cational Development Washington DC Available athttpwwwlinkagesprojectorgmediapublicationsFinal20draft20Zambia20final20report2012105pdf
Lutter CK Perez-Escamilla R Segall A Sanghvi TTeruya K amp Wickham C (1997) The effectiveness of ahospital based program to promote exclusive breastfeed-ing among low income women in Brazil AmericanJournal of Public Health 87 659ndash663
Morrow AL Guerrero ML Shults J Calva J Lutter CBravo J et al (1999) Efficacy of home based peer coun-selling to promote exclusive breastfeeding a randomizedcontrolled trial Lancet 353 1226ndash1231
Ntabaye MK amp Lusiola GJ (2004) Understanding barri-ers to PMTCT in Tanzania findings of a baseline surveyInternational Conference on AIDS 15 (B11396)
de Oliveira LD Giugliani ER do Espirito SLC FrancaMC Weigert EM Kohler CV et al (2006) Effect ofintervention to improve breastfeeding technique on thefrequency of exclusive breastfeeding and lactation-related problems Journal of Human Lactation 22 315ndash321
Perez-Escamilla R (2004) Effectiveness of MADLAC atImproving Breastfeeding Promotion and CounsellingIndicators in Maternity Wards in El Salvador Publishedfor the Basic Support for Institutionalizing Child Sur-vival Project (BASICS II) for the United States Agencyfor International Development Arlington VA Availableat httpwwwbasicsorgpdfFinal20MADLAC20Report20RPE20April207-2004pdf
Perez-Escamilla R (2007) Evidence based breast-feedingpromotion the Baby-Friendly Hospital InitiativeJournal of Nutrition 137 484ndash487
Piwoz EG Iliff PJ Tavengwa N Gavin L Marinda ELunney K et al (2005) An education and counselllingprogram for preventing breastfeeding associated HIVtransmission in Zimbabwe design and impact on mater-nal knowledge and behaviour Journal of Nutrition 135950ndash955
Quinn VJ Guyon AB Schubert JW Stone-Jimenez MHainsworth MD amp Martin LH (2005) Improvingbreastfeeding practices on a board scale at the commu-
nity level success stories from Africa and LatinAmerica Journal of Human Lactation 21 345ndash354
Ranson MK Hanson K Oliveira-Cruz V amp Mills A(2003) Constraints to expanding access to health inter-ventions an empirical analysis and country typologyJournal of International Development 15 15ndash40
Rea MF amp Berquo ES (1990) Impact of the Braziliannational breastfeeding programme on mothers inGreater Sao Paulo Bulletin of the of the World HealthOrganization 68 365ndash371
Rollins NC (2007) Infant feeding and HIV BritishMedical Journal 334 487ndash488
Rutenberg N Baek C Kalibala S Rosen J amp Mulenga D(2004) Evaluation of United Nations supported pilotprojects for the prevention of mother-to-child transmis-sion of HIV overview of findings International Confer-ence on AIDS 15 (WePeE6688)
The Core Group (2005) Scale and Scaling Up A COREGroup Background Paper on lsquoScaling-Uprsquo MaternalNewborn and Child Health Services CORE SpringMembership Meeting 2005 The Core Group Washing-ton DC Available at httpwwwcoregrouporgresourcesmeetingsapril05Scaling_Up_Background_Paper_7-13pdf
The Norwegian Government (1993) Women in PoliticsMinistry of Children and Equality Available at httpwwwregjeringennoendepbldRyddemappeSLA-AvdelingdoclegislationguidelinesWomen-in-Politicshtmlid=437166
Thior I Lockman S Smeaton LM Shapiro RL WesterC Heymann SJ et al (2006) Breastfeeding plus infantzidovudine prophylaxis for 6 months vs formula feedingplus infant zidovudine for 1 month to reduce mother-to-child HIV transmission in Botswana a randomized trialthe Mashi Study Journal of the American Medical Asso-ciation 296 794ndash805
UNICEF (2002) Facts for Life lsquoKey Message What EveryFamily and Community Has a Right to Know aboutBreastfeedingrsquo Available at httpwwwuniceforgffl04key_messageshtm
Van Roekel K Plowman B Griffiths M de AlvaradoVV Matute J amp Calderon M (2002) BASICS IIMidterm Evaluation of the AIN Program in Honduras2000 Basic Support for Institutionalizing Child SurvivalProject (BASICS II) for the United States Agency forInternational Development Arlington VA
WABA (2007) UNICEF Records BHFI Record UpdateAvailable at httpwwwwabaorgmydocsBFHIjan07xls 2006 Regularly updated by Miriam HLabbok Center for Infant and Young ChildFeeding and Care Department of Maternaland Child Health School of Public Health The Univer-sity of North Carolina at Chapel Hill Chapel Hill NCUSA
N Bhandari and AKMI Kabir16
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
WHA (2002) Infant and Young Child Nutrition Fifty-FifthWorld Health Assembly Agenda Item 1310 18 May2002 Available at httpwwwintgbebwhapdf_filesWHA55ewha5525pdf
WHO (1981) The International Code of Marketing ofBreastmilk Substitutes World Health OrganizationGeneva
WHO (1989) Protecting Promoting and Supporting Breast-feeding The Special Role of Maternity Services A JointWHOUNICEF Statement World Health OrganizationGeneva
WHO (2002) The Optimal Duration of Exclusive Breast-feeding Report of an Expert Consultation WHONHD0109 WHOFCHCAH0124 World HealthOrganization Geneva
WHO (2003a) Community Based Strategies for Breastfeed-ing Promotion and Support in Developing CountriesWorld Health Organization Geneva Document refISBN_92_4_159121_8 Available at httpwwwwhointchild-adolescent-healthNew_PublicationsNUTRITIONISBN_92_4_159121_8pdf
WHO (2003b) Multi-country Evaluation of IMCI Effective-ness Cost and Impact (MCE) Progress Report May2002ndashApril 2003 Document ref WHOFCHCAH035World Health Organization Geneva
WHO (2004) Promoting Proper Feeding for Infants andYoung Children World Health Organization GenevaAvailable at httpwwwwhointnutritiontopicsinfantfeedingen
WHO (2006) WHO HIV and Infant Feeding TechnicalConsultation-Consensus Statement World Health Orga-nization Geneva Available at httpwwwwhointhivmediacentreInfantfeedingconsensusstatementpfpdf
WHO Collaborative Study Team on the Role of Breast-feeding on the Prevention of Infant Mortality (2000)Effect of breastfeeding on infant and child mortality dueto infectious diseases in les developed countries apooled analysis Lancet 355 451ndash455
WHOUNICEF (1992) The global criteria for the WHOUNICEF Baby-Friendly Hospital Initiative In Baby-Friendly Hospital Initiative Part II Hospital LevelImplementation World Health Organization Geneva
WHOUNICEF (1993) Breastfeeding Counselling A Train-ing Course WHOCDR933 UNICEFNUT931 WorldHealth Organization Geneva
WHOUNICEF (2002) Protocol for Adapting the FeedingRecommendations Part III IMCI Adaptation GuideWorld Health Organization Geneva
WHOUNICEF (2003) Global Strategy for Infant andYoung Child Feeding World Health OrganizationGeneva Available at httpwwwwhointchild-adolescent-healthpublicationsNUTRITIONIYCF_GShtm
de Zoysa I Rea M amp Martines J (1991) Why promotebreastfeeding in diarrheal diseases control programmesHealth Policy and Planning 6 371ndash379
Mainstreaming nutrition into MCH programs 17
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
Cas
est
udie
so
fef
fect
iven
ess
stud
ies
or
pilo
tpr
ogra
mm
es
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Lut
ter
etal
(199
7)
Bra
zil
Low
-inc
ome
urba
nw
omen
deliv
erin
gin
hosp
ital
s
Bre
astf
eedi
ngpr
omot
ion
in
hosp
ital
sco
mpa
red
wit
h
nobr
east
feed
ing
prom
otio
n
Pro
mot
ion
ofbr
east
feed
ing
in
sele
cted
hosp
ital
s
Mea
nda
ysof
excl
usiv
e
brea
stfe
edin
g
75da
ysvs
22
days
(Plt
001
)
Rea
ampB
erqu
o
(199
0)
Wom
enw
ith
ach
ild
aged
lt2ye
ars
inSa
oP
aulo
Nat
iona
lbre
astf
eedi
ng
cam
paig
n19
81ndash1
986
BF
HI
Mas
sm
edia
cam
paig
n11
in
fant
s5ndash
6m
onth
s
excl
usiv
ely
brea
stfe
d
in19
88an
d37
in
1987
Con
foun
ding
fact
ors
over
the
6-ye
arpe
riod
not
mea
sure
d
Kra
mer
etal
(200
020
01)
PR
OB
ITtr
ial
Bel
arus
Clu
ster
rand
omiz
ed
34ho
spit
als
and
thei
rpo
lycl
inic
s
Trai
ning
inB
FH
I(W
HO
UN
ICE
F19
92)
vsr
outi
ne
prac
tice
san
dpo
licie
s
Exc
lusi
vebr
east
feed
ing
at3
(43
3vs
64
)
and
6(7
9
vs0
6
)
mon
ths
sign
ifica
ntly
high
er
Impl
emen
ted
thro
ugh
BF
HI
ina
sett
ing
whe
reho
spit
al
deliv
erie
sar
eco
mm
on
Per
ez-E
scam
illa
(200
4)
BA
SIC
SII
Mex
ico
Hon
dura
s
Bra
zil
MA
DL
AC
low
-cos
t
man
agem
ent
info
rmat
ion
syst
emto
use
an
evid
ence
-bas
edap
proa
chto
impr
ove
serv
ice
perf
orm
ance
Inte
rvie
win
gof
wom
enat
hosp
ital
disc
harg
epo
st
deliv
ery
usin
ga
ques
tion
nair
eth
atta
kes
5ndash7
min
toad
min
iste
ran
d
cont
ains
19br
east
feed
ing
prom
otio
nco
unse
lling
indi
cato
rs
Dat
aen
tere
dan
dre
sult
s
disc
usse
d3-
mon
thly
by
hosp
ital
com
mit
tee
Hos
pita
lim
plem
ents
chan
ges
in
brea
stfe
edin
g
supp
ort
base
don
anal
ysis
of
ques
tion
nair
es
Itis
aco
st-e
ffec
tive
inte
rven
tion
that
can
help
impr
ovem
ents
inth
eB
FH
I
and
isa
valu
able
tool
for
proc
ess
eval
uati
on
N Bhandari and AKMI Kabir18
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
LIN
KA
GE
S
proj
ect
inA
fric
aan
d
Lat
inA
mer
ica
(Qui
nnet
al
2005
LIN
KA
GE
S
2002
WH
O20
03a)
Bol
ivia
(1
mill
ion)
Gha
na(3
5
mill
ion)
Mad
agas
car
(6m
illio
n)
Res
ourc
e-
poor
sett
ing
Pilo
tpr
ogra
mm
e
InB
oliv
iaan
d
Gha
napr
ogra
mm
e
focu
sed
on
brea
stfe
edin
gan
d
com
plem
enta
ry
feed
ing
InM
adag
asca
r
prog
ram
me
prom
oted
brea
stfe
edin
g
wit
hin
7es
sent
ial
nutr
itio
nac
tion
san
d
subs
eque
ntly
thro
ugh
IMC
I
Bui
lton
form
ativ
ere
sear
ch
and
sust
aine
dth
roug
h
prog
ram
me
acti
viti
esth
at
focu
sed
onbr
ingi
ngab
out
the
desi
red
beha
viou
r
chan
geM
ixof
inte
rven
tion
s
reac
hed
wom
enin
divi
dual
ly
orin
grou
psin
heal
th
faci
litie
sho
mes
or
com
mun
ity
sett
ings
Con
sist
ent
mes
sage
san
d
mat
eria
lacr
oss
all
prog
ram
me
chan
nels
Bol
ivi
PR
OC
OSI
NG
Os
Gha
na
UN
ICE
F
nati
onal
nutr
itio
n
offic
eN
GO
s
Mad
agas
car
Inte
rsec
tora
l
Act
ion
Gro
upfo
r
Nut
riti
on
Jere
o
Sala
ma
Isik
a
Pro
gram
desi
gned
wit
h
part
ners
Rad
ioin
all
thre
esi
tes
Mat
eria
ls
deve
lope
d
tosu
itne
eds
oflo
cal
heal
th
wor
kers
and
com
mun
ity
mem
bers
Gre
at
emph
asis
on
deve
lopm
ent
of coun
selli
ng
and
nego
tiat
ion
skill
s
prac
tica
l
sess
ions
Sign
ifica
ntin
crea
ses
inex
clus
ive
brea
stfe
edin
gra
tes
of
0ndash6-
mon
th-o
ld
infa
nts
from
54
to65
in
Bol
ivia
68
to79
in
Gha
naan
d46
to68
in
Mad
agas
car
In
Gha
naan
d
Mad
agas
car
sign
ifica
ntre
sult
s
obse
rved
wit
hin
aye
ar
ofin
itia
tion
of
com
mun
ity
inte
rven
tion
s
App
roac
hw
asef
fect
ive
and
achi
eved
sign
ifica
nt
incr
ease
sam
ong
larg
e
popu
lati
ons
asea
rly
as
9ndash12
mo
afte
rin
itia
tion
of
com
mun
ity
acti
viti
es
Van
Roe
kele
tal
(200
2)W
HO
(200
3a)
Hon
dura
sG
row
thm
onit
orin
gan
d
prom
otio
nkn
own
as
Ate
ncioacute
nIn
tegr
ala
la
Nintilde
ez(A
IN)
or
Inte
grat
edC
hild
Car
e
Init
ially
pri
mar
ilya
grow
th
mon
itor
ing
prog
ram
me
ulti
mat
ely
thro
ugh
IMC
I
Pro
gram
me
ongr
owth
prom
otio
nndash
asse
ssm
ent
of
mon
thly
wei
ght
gain
and
focu
son
illne
ssf
eedi
ng
prac
tice
san
dge
nera
lchi
ld
care
inin
fant
sun
der
2ye
ars
Impl
emen
ted
atgo
vern
men
t
faci
litie
san
dco
mm
unit
y
Star
ted
in19
92s
tren
gthe
ned
in19
95ndash1
997
wit
hgr
eate
r
focu
son
child
feed
ing
In
1997
pro
gram
me
intr
oduc
ed
wit
hIM
CI
(WH
OU
NIC
EF
2002
)
Maj
or
part
ners
UN
ICE
F
PAH
O
Am
eric
an
and
Hon
dura
n
Red
Cro
ss
CA
RE
Rad
io
broa
dcas
ts
relig
ious
lead
ers
IMC
IM
id-t
erm
eval
uati
on
show
ed39
of
mot
hers
inin
terv
enti
on
com
mun
itie
sex
clus
ivel
y
brea
stfe
dco
mpa
red
wit
h13
in
the
cont
rol
site
s
Mainstreaming nutrition into MCH programs 19
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
cont
inue
d
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Bha
ndar
ieta
l
(200
3)
WH
O
(200
3a)
Rur
alco
mm
unit
ies
inH
arya
na
Indi
a
Clu
ster
rand
omiz
edtr
ial
8
com
mun
itie
s(t
otal
popu
lati
on~4
000
0)
Pro
mot
ion
ofex
clus
ive
brea
stfe
edin
gan
d
appr
opri
ate
com
plem
enta
ryfe
edin
g
Dev
elop
edth
roug
h
form
ativ
ere
sear
ch
ndashP
robl
emid
enti
ficat
ion
ndashP
arti
cipa
tory
desi
gnof
inte
rven
tion
impl
emen
tati
onan
d
eval
uati
on
Impl
emen
tati
onw
ithi
nan
exis
ting
prim
ary
heal
th-c
are
prog
ram
me
Opp
ortu
niti
esus
edto
deliv
erm
essa
ges
wer
e
imm
uniz
atio
ncl
inic
s
wei
ghin
gse
ssio
ns
sick
-chi
ldco
ntac
tsan
d
mon
thly
hom
evi
sits
Res
earc
hers
wit
hlo
cal
gove
rnm
ent
ICD
Ssy
stem
and
NG
O
The
atre
son
gs
Mas
sm
edia
not
used
for
risk
of
cont
amin
atio
n
Mat
eria
ls
deve
lope
d
for
heal
th
wor
kers
pos
ters
flip
book
sca
rds
Bre
astf
eedi
ng
coun
selli
ngse
ctio
n
ofth
eIM
CI
(WH
O
UN
ICE
F20
02)
Exc
lusi
ve
brea
stfe
edin
gin
the
prev
ious
24h
at3
mon
ths
of
age
79
vs4
8
The
posi
tive
effe
ct
rem
aine
dup
to
6m
onth
sof
age
(42
vs4
)
Tota
lpar
tici
pati
onof
the
dist
rict
heal
thsy
stem
from
ince
ptio
nof
the
prog
ram
me
inde
velo
ping
impl
emen
tati
onst
rate
gyt
ool
deve
lopm
ent
and
mon
itor
ing
inad
diti
onto
invo
lvem
ent
of
anN
GO
wer
eim
port
ant
feat
ures
that
cont
ribu
ted
to
the
succ
ess
ofth
e
inte
rven
tion
Mor
row
etal
(199
9)
Mex
ico
Cit
yC
lust
erra
ndom
ized
tria
l
Tota
lpop
ulat
ion
3000
0
Two
com
mun
itie
sin
the
inte
rven
tion
one
com
pari
son
130
wom
en
Hom
e-ba
sed
peer
coun
selli
ng
Pee
rco
unse
llors
mad
e3
or
6ho
me
visi
tsto
the
mot
her
Key
fam
ilym
embe
rsal
so
incl
uded
By
La
Lec
he
Lea
gue
of
Mex
ico
Exc
lusi
ve
brea
stfe
edin
g
at3
mon
ths
post
-par
tum
67
(6vi
sits
)
50
(3vi
sits
)12
(com
pari
son)
Firs
tcl
uste
rra
ndom
ized
com
mun
ity-
base
dtr
ialt
hat
used
peer
coun
sello
rsto
prom
ote
excl
usiv
e
brea
stfe
edin
g
Hai
der
etal
2000
200
2
Dha
ka
Low
mid
dle
and
low
-soc
io-
econ
omic
popu
lati
on
Clu
ster
rand
omiz
edtr
ial
20zo
nes
inin
terv
enti
on
and
20in
cont
rol
Com
mun
ity-
base
dpe
er
coun
selli
ngin
Dha
ka
15ho
me-
base
dco
unse
lling
visi
tsby
peer
coun
sello
rs
40h
(4h
yen10
days
)
WH
OU
NIC
EF
brea
stfe
edin
g
coun
selli
ngco
urse
(WH
OU
NIC
EF
1993
)
Exc
lusi
ve
brea
stfe
edin
g
at5
mon
ths
70
in
inte
rven
tion
and
6in
the
cont
rol
Com
mun
ity-
base
d
brea
stfe
edin
gpr
omot
ion
stra
tegy
was
effe
ctiv
ein
Ban
glad
esh
whe
rem
ost
deliv
erie
soc
cur
atho
me
N Bhandari and AKMI Kabir20
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Bry
ceet
al
(200
4)W
HO
(200
3b)
Bra
zil
Per
u
Tanz
ania
Uga
nda
Mul
tico
untr
yev
alua
tion
of
IMC
Ith
atin
clud
ed
effe
ctiv
enes
sco
stan
d
impa
ct(B
ryce
etal
2004
)
Bre
astf
eedi
ngpr
omot
ion
asa
part
ofIM
CI
IMC
Iis
ast
rate
gyfo
r
impr
ovin
gch
ildhe
alth
and
deve
lopm
ent
thro
ugh
the
com
bine
d
deliv
ery
ofes
sent
ial
child
heal
th
inte
rven
tion
sIM
CI
bega
nw
ith
ase
tof
case
man
agem
ent
guid
elin
es
for
the
man
agem
ent
ofsi
ckch
ildre
nat
first
-lev
elhe
alth
faci
litie
s
and
the
guid
elin
esw
ere
desi
gned
for
adap
tati
on
atco
untr
yle
vela
nd
belo
wO
ver
tim
eth
e
stra
tegy
expa
nded
to
incl
ude
ara
nge
of
guid
elin
esfo
rde
liver
ing
child
surv
ival
inte
rven
tion
at
hous
ehol
dco
mm
unit
y
and
refe
rral
leve
ls
IMC
Im
odul
e(W
HO
UN
ICE
F20
02)
Res
ults
onex
clus
ive
brea
stfe
edin
g
avai
labl
efr
om
Tanz
ania
whe
reno
sign
ifica
ntim
pact
was
seen
Des
pite
subs
tant
ial
impr
ovem
ent
inth
equ
alit
y
ofca
rede
liver
edby
IMC
Iat
heal
thfa
cilit
ies
key
fam
ily
prac
tice
ssu
chas
excl
usiv
e
brea
stfe
edin
gdi
dno
tch
ange
asco
mm
unit
yIM
CI
had
not
been
impl
emen
ted
byth
at
tim
e(W
HO
2003
b)
SA
rife
en
pers
onal
com
mun
icat
ion
Ban
glad
esh
Mat
lab
Com
mun
ity-
base
dcl
uste
r
desi
gn
Eva
luat
ion
offa
cilit
y-an
d
com
mun
ity-
base
dIM
CI
Inte
rven
tion
pack
age
incl
udes
feed
ing
asse
ssm
ent
and
coun
selli
ngon
mot
hers
ofyo
ung
child
ren
seek
ing
care
atfa
cilit
ies
for
illne
ssan
d
hom
e-ba
sed
coun
selli
ng
onim
prov
edfe
edin
gby
com
mun
ity-
base
dhe
alth
and
nutr
itio
nw
orke
rs
At
base
line
inth
e
year
2000
alit
tle
mor
eth
anha
lfth
e
0ndash5-
mon
th-o
ld
infa
nts
inth
est
udy
area
wer
ebe
ing
excl
usiv
ely
brea
stfe
dB
y20
05
this
incr
ease
dby
30
inth
eIM
CI
area
Dat
ano
t
avai
labl
efr
omth
e
com
pari
son
area
as
yet
Lac
kof
com
para
ble
data
from
the
com
pari
son
area
prev
ents
ade
finit
ive
conc
lusi
onas
tow
heth
erth
is
trul
yis
anim
pact
ofIM
CI
BA
SIC
SII
Bas
icSu
ppor
tfo
rIn
stit
utio
naliz
ing
Chi
ldSu
rviv
alP
roje
ctB
FH
IB
aby-
Frie
ndly
Hos
pita
lIni
tiat
ive
ICD
SIn
tegr
ated
Chi
ldD
evel
opm
ent
Serv
ices
IM
CI
Inte
grat
edM
anag
emen
tof
Chi
ldho
odIl
lnes
sM
AD
LA
CM
onit
oreo
deA
poyo
Dir
ecto
con
laL
acat
anci
aM
ater
naN
GO
non
-gov
ernm
enta
lorg
aniz
atio
nPA
HO
Pan
Am
eric
anH
ealt
hO
rgan
izat
ion
PR
OB
ITP
rom
otio
nof
Bre
astf
eedi
ngIn
terv
enti
onTr
ial
PR
OC
OSI
Pro
gram
ade
Coo
rdin
acio
nen
Salu
dIn
tegr
al(C
olla
bora
tive
Pro
gram
for
Inte
grat
edH
ealt
h)U
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
WH
OW
orld
Hea
lth
Org
aniz
atio
n
Mainstreaming nutrition into MCH programs 21
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x2
Cas
est
udie
sin
scal
e-up
effo
rts
inH
IVA
IDS
Stud
yde
scri
ptio
nPo
pula
tion
Inte
rven
tion
Com
mun
icat
ion
stra
tegy
Impa
cton
excl
usiv
ebr
east
feed
ing
Com
men
ts
LIN
KA
GE
S(2
005)
Zam
bia
Pro
gram
me
thro
ugh
heal
th-c
are
and
com
mun
ity
serv
ices
Rea
ched
60si
tes
in6
dist
rict
sby
2005
Inte
grat
ion
ofin
fant
feed
ing
coun
selli
ngm
ater
naln
utri
tion
and
anti
retr
ovir
aldr
ugs
prop
hyla
xis
Trai
ning
ofhe
alth
wor
kers
and
com
mun
ity
serv
ice
prov
ider
sto
coun
selw
omen
onsa
fety
opti
ons
for
thei
rsi
tuat
ion
Beh
avio
urch
ange
Com
mun
icat
ion
inte
rven
tion
sin
the
first
few
year
sM
ater
iald
evel
oped
lsquoAct
Now
rsquoM
edia
cam
paig
nsin
clud
edbr
ochu
res
post
ers
radi
oan
dte
levi
sion
Ass
esse
dth
roug
hba
selin
ean
dfo
llow
-up
hous
ehol
dan
dcl
inic
surv
eys
inse
lect
eddi
stri
cts
Exc
lusi
vebr
east
feed
ing
rate
incr
ease
dfr
om50
in
2002
to64
in
2004
inL
ivin
gsto
nean
dfr
om57
in
2000
to74
in
2004
inN
dola
Inte
grat
edde
mon
stra
tion
proj
ect
Had
seve
rals
tren
gths
inte
rms
ofth
eus
eof
form
ativ
ere
sear
chto
deve
lop
mes
sage
str
aini
ngan
dbu
ildin
gup
skill
sof
prog
ram
me
man
ager
she
alth
-car
epr
ovid
ers
and
com
mun
ity
wor
kers
adv
ocac
yfo
rna
tion
alpo
licy
stro
ngbe
havi
our
chan
geco
mm
unic
atio
nco
mpo
nent
st
reng
then
ing
com
mun
ity
capa
city
for
coun
selli
ngan
dre
ferr
als
and
mon
itor
ing
and
eval
uati
onw
ith
loca
lpar
tner
sP
iwoz
etal
(20
05)
ZV
ITA
MB
Otr
ial
Har
are
Zim
babw
eE
duca
tion
and
coun
selli
ngpr
ogra
mm
ede
liver
edan
tena
tally
1411
0m
othe
rndashba
bypa
irs
enro
lled
from
14m
ater
nity
clin
ics
wit
hin
96h
ofde
liver
yan
dfo
llow
edup
at6
wee
ks
3m
onth
san
d3-
mon
thly
inte
rval
sIn
fant
-fee
ding
patt
erns
dete
rmin
edE
xclu
sive
brea
stfe
edin
gre
com
men
ded
for
HIV
nega
tive
un
know
nor
HIV
posi
tive
who
chos
eto
brea
stfe
ed
Gro
uped
ucat
ion
indi
vidu
alco
unse
lling
vid
eos
broc
hure
sM
othe
rsw
hoen
rolle
dw
hen
prog
ram
me
was
fully
impl
emen
ted
wer
e8
4ti
mes
mor
elik
ely
toex
clus
ivel
ybr
east
feed
than
mot
hers
who
enro
lled
befo
reth
epr
ogra
mm
ebe
gan
Ove
rall
excl
usiv
ebr
east
feed
ing
rate
sti
ll3
mon
ths
was
low
at24
6
Form
ativ
ere
sear
chus
edto
desi
gna
cult
ural
lyse
nsit
ive
educ
atio
nan
dco
unse
lling
prog
ram
me
Low
over
alle
xclu
sive
brea
stfe
edin
gra
tes
prom
pted
auth
ors
toco
nclu
deth
atw
omen
and
thei
rpa
rtne
rssh
ould
have
been
reac
hed
mor
efr
eque
ntly
duri
ngan
tena
tala
ndpo
st-n
atal
peri
od
N Bhandari and AKMI Kabir22
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Thi
oret
al(
2006
)R
ollin
s(2
007)
C
ohen
(200
7)
HIV
-inf
ecte
dpr
egna
ntw
omen
atte
ndin
gan
tena
talc
linic
sin
sout
hB
otsw
ana
Inve
stig
atio
nsby
CD
Cof
adi
arrh
oea
outb
reak
inJa
nuar
y-Fe
brua
ry20
06in
the
sam
epo
pula
tion
Mat
erna
land
infa
ntan
tire
trov
iral
ther
apy
toas
cert
ain
impa
cton
HIV
tran
smis
sion
Ant
enat
alco
unse
lling
Cas
endashco
ntro
lstu
dyto
iden
tify
risk
fact
ors
for
diar
rhoe
ano
tbr
east
feed
ing
was
the
bigg
est
risk
fact
ora
djus
ted
odds
rati
o50
(95
confi
denc
ein
terv
al4
5ndash10
0)
Bot
swan
aha
sth
ebe
stpr
imar
yhe
alth
-car
est
ruct
ure
wat
ersu
pply
and
sani
tati
onsy
stem
sin
Sout
hA
fric
aFo
rmul
apr
ovid
edfr
eeby
the
gove
rnm
ent
toin
fect
edm
othe
rsL
ower
mor
talit
yin
the
brea
stfe
edin
ggr
oup
at7
mon
ths
dem
onst
rate
sri
skof
form
ula
feed
ing
and
need
for
alte
rnat
est
rate
gies
(Thi
oret
al
2006
)A
utho
rsco
nclu
deth
athe
alth
syst
ems
inw
hich
thes
epr
ogra
mm
esar
eim
plem
ente
dsh
ould
beab
leto
cope
wit
hdi
arrh
oea
and
mal
nutr
itio
nth
atre
sult
sbe
caus
eof
form
ula
feed
ing
(Rol
lins
2007
)C
oova
dia
etal
(2
007)
Kw
aZul
uNat
al
Sout
hA
fric
a27
22H
IV-i
nfec
ted
and
unin
fect
edpr
egna
ntw
omen
enro
lled
into
ano
n-ra
ndom
ized
inte
rven
tion
coho
rtst
udy
from
ante
nata
lcl
inic
sIn
fant
feed
ing
data
obta
ined
wee
kly
bloo
dsa
mpl
esfr
omin
fant
sta
ken
mon
thly
83
of13
72in
fant
sbo
rnto
HIV
-inf
ecte
dm
othe
rsin
itia
ted
excl
usiv
ebr
east
feed
ing
from
birt
hB
reas
tfed
infa
nts
who
rece
ived
solid
sw
ere
sign
ifica
ntly
mor
elik
ely
toac
quir
ein
fect
ion
com
pare
dw
ith
excl
usiv
ely
brea
stfe
d(H
R10
87
151
ndash78
P=
001
8)as
wer
ein
fant
sw
hoat
12w
eeks
rece
ived
brea
stan
dfo
rmul
am
ilk(1
82
098
ndash33
6P
=0
57)
Cum
ulat
ive
3-m
onth
mor
talit
yin
excl
usiv
ely
brea
stfe
dw
as6
1(4
74ndash
792
)vs
15
1(7
63ndash
287
3)in
infa
nts
give
nre
plac
emen
tfe
eds
(HR
206
1
0ndash4
27P
=0
05)
The
stud
ysh
ows
that
excl
usiv
ebr
east
feed
ing
can
besu
cces
sful
lysu
ppor
ted
inH
IV-i
nfec
ted
wom
enT
heau
thor
sca
llfo
rfu
rthe
rre
visi
onof
UN
ICE
FW
HO
and
USA
IDin
fant
feed
ing
guid
elin
es
CD
CC
ente
rof
Dis
ease
Con
trol
HR
haz
ards
rati
oU
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
USA
IDU
SA
genc
yfo
rIn
tern
atio
nalD
evel
opm
ent
WH
OW
orld
Hea
lth
Org
aniz
atio
nZ
VIT
AM
BO
Z
imba
bwe
Vit
amin
Afo
rM
othe
rsan
dB
abie
s
Mainstreaming nutrition into MCH programs 23
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
countries are going through a process of decentrali-zation with increasing responsibility for planningimplementation and evaluation being delegated tolower levels of the health-care system Buildingcapacity at that level requires time resources andpatience and a longer-term perspective
Building capacity emerges to be a key factorTrainers and training centres vary in their qualitywhen training health workers and their supervisorsor programme managers As the burden of trainingincreases availability of good-quality trainersbecomes a limiting factor (WHOUNICEF 2002Government of India 2006) An effective strategymust plan for these incremental requirements includ-ing ensuring secure and sustained funding
Identifying barriers to success is a key actor Thebarriers to scaling up of health interventions havebeen elegantly described by Ranson et al (Table 5)Most of these are important for exclusive breastfeed-ing scale-up as well
Overall within the limitations discussed above anumber of programmes in countries with varying
HIV prevalence show that exclusive breastfeeding ona large scale is feasible and pilot programmes havegiven valuable guidance related to policies planningand implementation of large-scale programmes Thechallenge now is to build on these experiences whenplanning national programmes
Acknowledgements
We sincerely thank Dr MK Bhan for his constructivecriticism and sustained feedback at different stages ofdevelopment of this review
Conflicts of interest
The authors have declared no conflicts of interest
References
Arifeen S Black RE Antelman G Baqui A CaulfieldL amp Becker S (2001) Exclusive breastfeeding reducesacute respiratory infection and diarrhea deaths amonginfants in Dhaka slums Pediatrics 108 E67
Australian Breastfeeding Association (2005) Valuing Par-enthood Options for Paid Maternity Leave ndash InterimPaper 2002 Available at httpwwwbreastfeedingasnauadvocacymatleavehtml
Bhandari N Bahl R Mazumdar S Martines J BlackRE amp Bhan MK (2003) Effect of community basedpromotion of exclusive breastfeeding on diarrheal ill-nesses and growth a cluster randomized controlled trialLancet 361 1418ndash1423
Bhandari N Mazumder S Bahl R Martines J BlackRE amp Bhan MK (2004) An educational interventionto promote appropriate complementary feedingimproves child feeding practices and linear growth inrural Haryana India Journal of Nutrition 134 2342ndash2348
Bhandari N Mazumder S Bahl R Martines J BlackRE amp Bhan MK (2005) Use of multiple opportunitiesfor improving feeding practices in undertwos withinchild health programs Health Policy Plan 20 328ndash336
Bryce J Victora CG Habicht JP Vaughan JP ampBlack RE (2004) The multi-country evaluation of theintegrated management of childhood illness strategylessons for the evaluation of public health interventionsAmerican Journal of Public Health 94 406ndash415
Butte NF Lopez-Alarcon MG amp Garza C (2002) Nutri-ent Adequacy of Exclusive Breastfeeding for the TermInfant during the First Six Months of Life World HealthOrganization Geneva
Table 5 Barriers to scaling up of health interventions
Community and household levelsLack of information womenrsquos education physical financial
womenrsquos decision-making powerHealth services delivery levelShortage of qualified staff weak technical guidance programme
management and supervision inadequate supplies equipmentand infrastructure poor accessibility
Health sector policy and strategic management levelWeak and centralized system for planning and management weak
drug policies and supply system inadequate regulations lack ofintersectoral action and partnership weak incentives to useinputs efficiently and respond to user needs and preferencesreliance on donor funding
Public policies cutting across sectorsGovernment bureaucracy poor communication and transport
infrastructureEnvironmental characteristicsGovernance and overall policy frameworkCorruption weak government weak laws political instability and
insecurity low priority to social sectors weak structure for publicaccountability and opportunities for public opinions lack of freepress
Physical environmentClimatic and geographic predisposition physical environment
unfavourable to service delivery
Adapted from Ranson et al (2003)
N Bhandari and AKMI Kabir14
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Cohen J (2007) Retrovirus meeting Hope on new AIDSdrugs but breast-feeding strategy backfires Science 3151357
Coovadia HM Rollins NC Bland RM Little KCoutsoudis A Bennish ML et al (2007) Mother tochild transmission of HIV-1 infection during exclusivebreastfeeding in the first 6 months of life an interven-tion cohort study Lancet 369 1107ndash1116
Coutinho SB de Lira PI de Carvalho LM amp AshworthA (2005) Comparison of the effect of two systems forthe promotion of exclusive breastfeeding Lancet 3661094ndash1100
Feachem RG amp Koblinsky MA (1984) Interventions forthe control of diarrheal diseases among young childrenpromotion of breastfeeding Bulletin of the of the WorldHealth Organization 62 271ndash291
Gonzales A Arteaga E amp Howard-Grabman L (1998)Scaling Up the WARMI Project ndash Lessons LearnedMobilizing Bolivian Communities around ReproductiveHealth Save the Children Federation Inc Bolivia FieldOffice La Paz Available at httpwwwcoregrouporgresourcesSavebolipdf
Government of India (1997) Recommendations of the FifthCentral Pay Commission Relating to Enhancement ofQuantum of Maternity Leave and to Allow PaternityLeave in Respect of Central Government EmployeesDocument ref 13018197-Estt(L) Available at httppersminnicinesttleave2htm
Government of India (2005) National Rural HealthMission 2005ndash2012 Mission document Ministry ofHealth and Family Welfare New Delhi Government ofIndia Available at httpwwwmohfwnicinNRHM20Mission20Documentpdf
Government of India (2006) Operational Guidelines forImplementation of Integrated Management of Neonataland Childhood Illness (IMNCI) Ministry of HealthFamily Welfare New Delhi Available at httpmohfwnicindofw20websiteF20IMNCI20Operational20Plan201320june202006htm
Government of Pakistan (2003) National Programme forFamily Planning and Primary Health Care The LadyHealth Workers Programme 2003ndash2008 Ministry ofHealth Pakistan Available at httpwwwphcgovpkDownloadsPC-120augpdf
Green CP (1999) Improving Breastfeeding Behaviors Evi-dence from Two Decades of Intervention ResearchPublished for the US Agency for International Develop-ment (USAID) by the LINKAGES Project Academyfor Educational Development Washington DC
Gupta A (2002) National trends in breastfeeding andeffective strategies to improve breastfeeding ratesJournal of Neonatology 2002 4ndash14
Gwatkin DR (2004) Integrating the management of child-hood illness Lancet 364 1557ndash1558
Habicht JP DaVanzo J amp Butz WP (1986) Does breast-feeding really save lives or are apparent benefits due tobiases American Journal of Epidemiology 123279ndash290
Haider R Ashworth A Kabir I amp Huttly SR (2000)Effect of community based peer counsellors on exclusivebreastfeeding practices in Dhaka Bangladesh a ran-domized controlled trial Lancet 356 1643ndash1647
Haider R Kabir I Huttly SR amp Ashworth A (2002)Training peer counsellors to promote and support exclu-sive breastfeeding in Bangladesh Journal of HumanLactation 18 7ndash12
Horton S Sanghvi T Phillips M Fiedler J Perez-Escamilla R Lutter C et al (1996) Breastfeeding pro-motion and priority setting in health Health Policy andPlanning 11 156ndash168
ILO (1998) More than 120 Nations Provide Paid MaternityLeave Gap in Employment Treatment for Men andWomen Still Exists International Labour Office GenevaDocument ref ILO987 Available at httpwwwiloorgpublicenglishbureauinfpr19987htmr2
Iliff PJ Piwoz EG Tavengwa NV Zunguza CDMarinda ET Nathoo KJ et al (2005) Early exclusivebreastfeeding reduces the risk of postnatal HIV-1 trans-mission and increase HIV-free survival AIDS 19 699ndash708
Integrated Child Development Services Scheme (Revised)(ICDS) (1982) Ministry of Social Welfare Governmentof India New Delhi Available on URL httpwcdnicinudishahtmabouticdshtm
Jason JM Nieburg P amp Marks JS (1984) Mortality andinfectious disease associated with infant feeding prac-tices in developing countries Pediatrics 74 702ndash727
Jones G Steketee RW Black RE Bhutta ZA ampMorris SS Bellagio Child Survival Study Group (2003)How many child deaths can we prevent this yearLancet 362 65ndash71
Knippenberg R Lawn JE Darmstadt GL Begkayian GFogstad H Walelign N et al (2005) Systematic scalingup of neonatal care in countries Lancet 365 1087ndash1098
Kramer MS amp Kakuma R (2002) The optimal durationof exclusive breastfeeding a systematic reviewCochrane Database of Systematic Reviews 2002CD003517
Kramer MS Chalmers B Hodnett ED Sevkovskaya ZDzikovich I Shapiro S et al (2000) Promotion ofbreastfeeding intervention trial (PROBIT) a cluster ran-domized trial in the Republic of Belarus Design followup and data validation Advances in Experimental Medi-cine and Biology 478 327ndash345
Kramer MS Chalmers B Hodnett ED Sevkovskaya ZDzikovich I Shapiro S et al (2001) Promotion ofbreastfeeding intervention trial (PROBIT) a random-
Mainstreaming nutrition into MCH programs 15
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
ized trial in the Republic of Belarus Journal of theAmerican Medical Association 285 413ndash420
Lewin SA Dick J Pond P Zwarenstein M Aja Gvan Wyk B et al (2006) Lay health workers in primaryand community health care (Review) The CochraneLibrary 3 1ndash104
LINKAGES (2002) World LINKAGES MadagascarAcademy for Educational Development WashingtonDC
LINKAGES (2005) LINKAGES Zambia 1997ndash2005 FinalReport A Full Report on LINKAGES Infant Feedingand HIVAIDS Programs in Zambia Academy for Edu-cational Development Washington DC Available athttpwwwlinkagesprojectorgmediapublicationsFinal20draft20Zambia20final20report2012105pdf
Lutter CK Perez-Escamilla R Segall A Sanghvi TTeruya K amp Wickham C (1997) The effectiveness of ahospital based program to promote exclusive breastfeed-ing among low income women in Brazil AmericanJournal of Public Health 87 659ndash663
Morrow AL Guerrero ML Shults J Calva J Lutter CBravo J et al (1999) Efficacy of home based peer coun-selling to promote exclusive breastfeeding a randomizedcontrolled trial Lancet 353 1226ndash1231
Ntabaye MK amp Lusiola GJ (2004) Understanding barri-ers to PMTCT in Tanzania findings of a baseline surveyInternational Conference on AIDS 15 (B11396)
de Oliveira LD Giugliani ER do Espirito SLC FrancaMC Weigert EM Kohler CV et al (2006) Effect ofintervention to improve breastfeeding technique on thefrequency of exclusive breastfeeding and lactation-related problems Journal of Human Lactation 22 315ndash321
Perez-Escamilla R (2004) Effectiveness of MADLAC atImproving Breastfeeding Promotion and CounsellingIndicators in Maternity Wards in El Salvador Publishedfor the Basic Support for Institutionalizing Child Sur-vival Project (BASICS II) for the United States Agencyfor International Development Arlington VA Availableat httpwwwbasicsorgpdfFinal20MADLAC20Report20RPE20April207-2004pdf
Perez-Escamilla R (2007) Evidence based breast-feedingpromotion the Baby-Friendly Hospital InitiativeJournal of Nutrition 137 484ndash487
Piwoz EG Iliff PJ Tavengwa N Gavin L Marinda ELunney K et al (2005) An education and counselllingprogram for preventing breastfeeding associated HIVtransmission in Zimbabwe design and impact on mater-nal knowledge and behaviour Journal of Nutrition 135950ndash955
Quinn VJ Guyon AB Schubert JW Stone-Jimenez MHainsworth MD amp Martin LH (2005) Improvingbreastfeeding practices on a board scale at the commu-
nity level success stories from Africa and LatinAmerica Journal of Human Lactation 21 345ndash354
Ranson MK Hanson K Oliveira-Cruz V amp Mills A(2003) Constraints to expanding access to health inter-ventions an empirical analysis and country typologyJournal of International Development 15 15ndash40
Rea MF amp Berquo ES (1990) Impact of the Braziliannational breastfeeding programme on mothers inGreater Sao Paulo Bulletin of the of the World HealthOrganization 68 365ndash371
Rollins NC (2007) Infant feeding and HIV BritishMedical Journal 334 487ndash488
Rutenberg N Baek C Kalibala S Rosen J amp Mulenga D(2004) Evaluation of United Nations supported pilotprojects for the prevention of mother-to-child transmis-sion of HIV overview of findings International Confer-ence on AIDS 15 (WePeE6688)
The Core Group (2005) Scale and Scaling Up A COREGroup Background Paper on lsquoScaling-Uprsquo MaternalNewborn and Child Health Services CORE SpringMembership Meeting 2005 The Core Group Washing-ton DC Available at httpwwwcoregrouporgresourcesmeetingsapril05Scaling_Up_Background_Paper_7-13pdf
The Norwegian Government (1993) Women in PoliticsMinistry of Children and Equality Available at httpwwwregjeringennoendepbldRyddemappeSLA-AvdelingdoclegislationguidelinesWomen-in-Politicshtmlid=437166
Thior I Lockman S Smeaton LM Shapiro RL WesterC Heymann SJ et al (2006) Breastfeeding plus infantzidovudine prophylaxis for 6 months vs formula feedingplus infant zidovudine for 1 month to reduce mother-to-child HIV transmission in Botswana a randomized trialthe Mashi Study Journal of the American Medical Asso-ciation 296 794ndash805
UNICEF (2002) Facts for Life lsquoKey Message What EveryFamily and Community Has a Right to Know aboutBreastfeedingrsquo Available at httpwwwuniceforgffl04key_messageshtm
Van Roekel K Plowman B Griffiths M de AlvaradoVV Matute J amp Calderon M (2002) BASICS IIMidterm Evaluation of the AIN Program in Honduras2000 Basic Support for Institutionalizing Child SurvivalProject (BASICS II) for the United States Agency forInternational Development Arlington VA
WABA (2007) UNICEF Records BHFI Record UpdateAvailable at httpwwwwabaorgmydocsBFHIjan07xls 2006 Regularly updated by Miriam HLabbok Center for Infant and Young ChildFeeding and Care Department of Maternaland Child Health School of Public Health The Univer-sity of North Carolina at Chapel Hill Chapel Hill NCUSA
N Bhandari and AKMI Kabir16
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
WHA (2002) Infant and Young Child Nutrition Fifty-FifthWorld Health Assembly Agenda Item 1310 18 May2002 Available at httpwwwintgbebwhapdf_filesWHA55ewha5525pdf
WHO (1981) The International Code of Marketing ofBreastmilk Substitutes World Health OrganizationGeneva
WHO (1989) Protecting Promoting and Supporting Breast-feeding The Special Role of Maternity Services A JointWHOUNICEF Statement World Health OrganizationGeneva
WHO (2002) The Optimal Duration of Exclusive Breast-feeding Report of an Expert Consultation WHONHD0109 WHOFCHCAH0124 World HealthOrganization Geneva
WHO (2003a) Community Based Strategies for Breastfeed-ing Promotion and Support in Developing CountriesWorld Health Organization Geneva Document refISBN_92_4_159121_8 Available at httpwwwwhointchild-adolescent-healthNew_PublicationsNUTRITIONISBN_92_4_159121_8pdf
WHO (2003b) Multi-country Evaluation of IMCI Effective-ness Cost and Impact (MCE) Progress Report May2002ndashApril 2003 Document ref WHOFCHCAH035World Health Organization Geneva
WHO (2004) Promoting Proper Feeding for Infants andYoung Children World Health Organization GenevaAvailable at httpwwwwhointnutritiontopicsinfantfeedingen
WHO (2006) WHO HIV and Infant Feeding TechnicalConsultation-Consensus Statement World Health Orga-nization Geneva Available at httpwwwwhointhivmediacentreInfantfeedingconsensusstatementpfpdf
WHO Collaborative Study Team on the Role of Breast-feeding on the Prevention of Infant Mortality (2000)Effect of breastfeeding on infant and child mortality dueto infectious diseases in les developed countries apooled analysis Lancet 355 451ndash455
WHOUNICEF (1992) The global criteria for the WHOUNICEF Baby-Friendly Hospital Initiative In Baby-Friendly Hospital Initiative Part II Hospital LevelImplementation World Health Organization Geneva
WHOUNICEF (1993) Breastfeeding Counselling A Train-ing Course WHOCDR933 UNICEFNUT931 WorldHealth Organization Geneva
WHOUNICEF (2002) Protocol for Adapting the FeedingRecommendations Part III IMCI Adaptation GuideWorld Health Organization Geneva
WHOUNICEF (2003) Global Strategy for Infant andYoung Child Feeding World Health OrganizationGeneva Available at httpwwwwhointchild-adolescent-healthpublicationsNUTRITIONIYCF_GShtm
de Zoysa I Rea M amp Martines J (1991) Why promotebreastfeeding in diarrheal diseases control programmesHealth Policy and Planning 6 371ndash379
Mainstreaming nutrition into MCH programs 17
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
Cas
est
udie
so
fef
fect
iven
ess
stud
ies
or
pilo
tpr
ogra
mm
es
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Lut
ter
etal
(199
7)
Bra
zil
Low
-inc
ome
urba
nw
omen
deliv
erin
gin
hosp
ital
s
Bre
astf
eedi
ngpr
omot
ion
in
hosp
ital
sco
mpa
red
wit
h
nobr
east
feed
ing
prom
otio
n
Pro
mot
ion
ofbr
east
feed
ing
in
sele
cted
hosp
ital
s
Mea
nda
ysof
excl
usiv
e
brea
stfe
edin
g
75da
ysvs
22
days
(Plt
001
)
Rea
ampB
erqu
o
(199
0)
Wom
enw
ith
ach
ild
aged
lt2ye
ars
inSa
oP
aulo
Nat
iona
lbre
astf
eedi
ng
cam
paig
n19
81ndash1
986
BF
HI
Mas
sm
edia
cam
paig
n11
in
fant
s5ndash
6m
onth
s
excl
usiv
ely
brea
stfe
d
in19
88an
d37
in
1987
Con
foun
ding
fact
ors
over
the
6-ye
arpe
riod
not
mea
sure
d
Kra
mer
etal
(200
020
01)
PR
OB
ITtr
ial
Bel
arus
Clu
ster
rand
omiz
ed
34ho
spit
als
and
thei
rpo
lycl
inic
s
Trai
ning
inB
FH
I(W
HO
UN
ICE
F19
92)
vsr
outi
ne
prac
tice
san
dpo
licie
s
Exc
lusi
vebr
east
feed
ing
at3
(43
3vs
64
)
and
6(7
9
vs0
6
)
mon
ths
sign
ifica
ntly
high
er
Impl
emen
ted
thro
ugh
BF
HI
ina
sett
ing
whe
reho
spit
al
deliv
erie
sar
eco
mm
on
Per
ez-E
scam
illa
(200
4)
BA
SIC
SII
Mex
ico
Hon
dura
s
Bra
zil
MA
DL
AC
low
-cos
t
man
agem
ent
info
rmat
ion
syst
emto
use
an
evid
ence
-bas
edap
proa
chto
impr
ove
serv
ice
perf
orm
ance
Inte
rvie
win
gof
wom
enat
hosp
ital
disc
harg
epo
st
deliv
ery
usin
ga
ques
tion
nair
eth
atta
kes
5ndash7
min
toad
min
iste
ran
d
cont
ains
19br
east
feed
ing
prom
otio
nco
unse
lling
indi
cato
rs
Dat
aen
tere
dan
dre
sult
s
disc
usse
d3-
mon
thly
by
hosp
ital
com
mit
tee
Hos
pita
lim
plem
ents
chan
ges
in
brea
stfe
edin
g
supp
ort
base
don
anal
ysis
of
ques
tion
nair
es
Itis
aco
st-e
ffec
tive
inte
rven
tion
that
can
help
impr
ovem
ents
inth
eB
FH
I
and
isa
valu
able
tool
for
proc
ess
eval
uati
on
N Bhandari and AKMI Kabir18
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
LIN
KA
GE
S
proj
ect
inA
fric
aan
d
Lat
inA
mer
ica
(Qui
nnet
al
2005
LIN
KA
GE
S
2002
WH
O20
03a)
Bol
ivia
(1
mill
ion)
Gha
na(3
5
mill
ion)
Mad
agas
car
(6m
illio
n)
Res
ourc
e-
poor
sett
ing
Pilo
tpr
ogra
mm
e
InB
oliv
iaan
d
Gha
napr
ogra
mm
e
focu
sed
on
brea
stfe
edin
gan
d
com
plem
enta
ry
feed
ing
InM
adag
asca
r
prog
ram
me
prom
oted
brea
stfe
edin
g
wit
hin
7es
sent
ial
nutr
itio
nac
tion
san
d
subs
eque
ntly
thro
ugh
IMC
I
Bui
lton
form
ativ
ere
sear
ch
and
sust
aine
dth
roug
h
prog
ram
me
acti
viti
esth
at
focu
sed
onbr
ingi
ngab
out
the
desi
red
beha
viou
r
chan
geM
ixof
inte
rven
tion
s
reac
hed
wom
enin
divi
dual
ly
orin
grou
psin
heal
th
faci
litie
sho
mes
or
com
mun
ity
sett
ings
Con
sist
ent
mes
sage
san
d
mat
eria
lacr
oss
all
prog
ram
me
chan
nels
Bol
ivi
PR
OC
OSI
NG
Os
Gha
na
UN
ICE
F
nati
onal
nutr
itio
n
offic
eN
GO
s
Mad
agas
car
Inte
rsec
tora
l
Act
ion
Gro
upfo
r
Nut
riti
on
Jere
o
Sala
ma
Isik
a
Pro
gram
desi
gned
wit
h
part
ners
Rad
ioin
all
thre
esi
tes
Mat
eria
ls
deve
lope
d
tosu
itne
eds
oflo
cal
heal
th
wor
kers
and
com
mun
ity
mem
bers
Gre
at
emph
asis
on
deve
lopm
ent
of coun
selli
ng
and
nego
tiat
ion
skill
s
prac
tica
l
sess
ions
Sign
ifica
ntin
crea
ses
inex
clus
ive
brea
stfe
edin
gra
tes
of
0ndash6-
mon
th-o
ld
infa
nts
from
54
to65
in
Bol
ivia
68
to79
in
Gha
naan
d46
to68
in
Mad
agas
car
In
Gha
naan
d
Mad
agas
car
sign
ifica
ntre
sult
s
obse
rved
wit
hin
aye
ar
ofin
itia
tion
of
com
mun
ity
inte
rven
tion
s
App
roac
hw
asef
fect
ive
and
achi
eved
sign
ifica
nt
incr
ease
sam
ong
larg
e
popu
lati
ons
asea
rly
as
9ndash12
mo
afte
rin
itia
tion
of
com
mun
ity
acti
viti
es
Van
Roe
kele
tal
(200
2)W
HO
(200
3a)
Hon
dura
sG
row
thm
onit
orin
gan
d
prom
otio
nkn
own
as
Ate
ncioacute
nIn
tegr
ala
la
Nintilde
ez(A
IN)
or
Inte
grat
edC
hild
Car
e
Init
ially
pri
mar
ilya
grow
th
mon
itor
ing
prog
ram
me
ulti
mat
ely
thro
ugh
IMC
I
Pro
gram
me
ongr
owth
prom
otio
nndash
asse
ssm
ent
of
mon
thly
wei
ght
gain
and
focu
son
illne
ssf
eedi
ng
prac
tice
san
dge
nera
lchi
ld
care
inin
fant
sun
der
2ye
ars
Impl
emen
ted
atgo
vern
men
t
faci
litie
san
dco
mm
unit
y
Star
ted
in19
92s
tren
gthe
ned
in19
95ndash1
997
wit
hgr
eate
r
focu
son
child
feed
ing
In
1997
pro
gram
me
intr
oduc
ed
wit
hIM
CI
(WH
OU
NIC
EF
2002
)
Maj
or
part
ners
UN
ICE
F
PAH
O
Am
eric
an
and
Hon
dura
n
Red
Cro
ss
CA
RE
Rad
io
broa
dcas
ts
relig
ious
lead
ers
IMC
IM
id-t
erm
eval
uati
on
show
ed39
of
mot
hers
inin
terv
enti
on
com
mun
itie
sex
clus
ivel
y
brea
stfe
dco
mpa
red
wit
h13
in
the
cont
rol
site
s
Mainstreaming nutrition into MCH programs 19
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
cont
inue
d
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Bha
ndar
ieta
l
(200
3)
WH
O
(200
3a)
Rur
alco
mm
unit
ies
inH
arya
na
Indi
a
Clu
ster
rand
omiz
edtr
ial
8
com
mun
itie
s(t
otal
popu
lati
on~4
000
0)
Pro
mot
ion
ofex
clus
ive
brea
stfe
edin
gan
d
appr
opri
ate
com
plem
enta
ryfe
edin
g
Dev
elop
edth
roug
h
form
ativ
ere
sear
ch
ndashP
robl
emid
enti
ficat
ion
ndashP
arti
cipa
tory
desi
gnof
inte
rven
tion
impl
emen
tati
onan
d
eval
uati
on
Impl
emen
tati
onw
ithi
nan
exis
ting
prim
ary
heal
th-c
are
prog
ram
me
Opp
ortu
niti
esus
edto
deliv
erm
essa
ges
wer
e
imm
uniz
atio
ncl
inic
s
wei
ghin
gse
ssio
ns
sick
-chi
ldco
ntac
tsan
d
mon
thly
hom
evi
sits
Res
earc
hers
wit
hlo
cal
gove
rnm
ent
ICD
Ssy
stem
and
NG
O
The
atre
son
gs
Mas
sm
edia
not
used
for
risk
of
cont
amin
atio
n
Mat
eria
ls
deve
lope
d
for
heal
th
wor
kers
pos
ters
flip
book
sca
rds
Bre
astf
eedi
ng
coun
selli
ngse
ctio
n
ofth
eIM
CI
(WH
O
UN
ICE
F20
02)
Exc
lusi
ve
brea
stfe
edin
gin
the
prev
ious
24h
at3
mon
ths
of
age
79
vs4
8
The
posi
tive
effe
ct
rem
aine
dup
to
6m
onth
sof
age
(42
vs4
)
Tota
lpar
tici
pati
onof
the
dist
rict
heal
thsy
stem
from
ince
ptio
nof
the
prog
ram
me
inde
velo
ping
impl
emen
tati
onst
rate
gyt
ool
deve
lopm
ent
and
mon
itor
ing
inad
diti
onto
invo
lvem
ent
of
anN
GO
wer
eim
port
ant
feat
ures
that
cont
ribu
ted
to
the
succ
ess
ofth
e
inte
rven
tion
Mor
row
etal
(199
9)
Mex
ico
Cit
yC
lust
erra
ndom
ized
tria
l
Tota
lpop
ulat
ion
3000
0
Two
com
mun
itie
sin
the
inte
rven
tion
one
com
pari
son
130
wom
en
Hom
e-ba
sed
peer
coun
selli
ng
Pee
rco
unse
llors
mad
e3
or
6ho
me
visi
tsto
the
mot
her
Key
fam
ilym
embe
rsal
so
incl
uded
By
La
Lec
he
Lea
gue
of
Mex
ico
Exc
lusi
ve
brea
stfe
edin
g
at3
mon
ths
post
-par
tum
67
(6vi
sits
)
50
(3vi
sits
)12
(com
pari
son)
Firs
tcl
uste
rra
ndom
ized
com
mun
ity-
base
dtr
ialt
hat
used
peer
coun
sello
rsto
prom
ote
excl
usiv
e
brea
stfe
edin
g
Hai
der
etal
2000
200
2
Dha
ka
Low
mid
dle
and
low
-soc
io-
econ
omic
popu
lati
on
Clu
ster
rand
omiz
edtr
ial
20zo
nes
inin
terv
enti
on
and
20in
cont
rol
Com
mun
ity-
base
dpe
er
coun
selli
ngin
Dha
ka
15ho
me-
base
dco
unse
lling
visi
tsby
peer
coun
sello
rs
40h
(4h
yen10
days
)
WH
OU
NIC
EF
brea
stfe
edin
g
coun
selli
ngco
urse
(WH
OU
NIC
EF
1993
)
Exc
lusi
ve
brea
stfe
edin
g
at5
mon
ths
70
in
inte
rven
tion
and
6in
the
cont
rol
Com
mun
ity-
base
d
brea
stfe
edin
gpr
omot
ion
stra
tegy
was
effe
ctiv
ein
Ban
glad
esh
whe
rem
ost
deliv
erie
soc
cur
atho
me
N Bhandari and AKMI Kabir20
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Bry
ceet
al
(200
4)W
HO
(200
3b)
Bra
zil
Per
u
Tanz
ania
Uga
nda
Mul
tico
untr
yev
alua
tion
of
IMC
Ith
atin
clud
ed
effe
ctiv
enes
sco
stan
d
impa
ct(B
ryce
etal
2004
)
Bre
astf
eedi
ngpr
omot
ion
asa
part
ofIM
CI
IMC
Iis
ast
rate
gyfo
r
impr
ovin
gch
ildhe
alth
and
deve
lopm
ent
thro
ugh
the
com
bine
d
deliv
ery
ofes
sent
ial
child
heal
th
inte
rven
tion
sIM
CI
bega
nw
ith
ase
tof
case
man
agem
ent
guid
elin
es
for
the
man
agem
ent
ofsi
ckch
ildre
nat
first
-lev
elhe
alth
faci
litie
s
and
the
guid
elin
esw
ere
desi
gned
for
adap
tati
on
atco
untr
yle
vela
nd
belo
wO
ver
tim
eth
e
stra
tegy
expa
nded
to
incl
ude
ara
nge
of
guid
elin
esfo
rde
liver
ing
child
surv
ival
inte
rven
tion
at
hous
ehol
dco
mm
unit
y
and
refe
rral
leve
ls
IMC
Im
odul
e(W
HO
UN
ICE
F20
02)
Res
ults
onex
clus
ive
brea
stfe
edin
g
avai
labl
efr
om
Tanz
ania
whe
reno
sign
ifica
ntim
pact
was
seen
Des
pite
subs
tant
ial
impr
ovem
ent
inth
equ
alit
y
ofca
rede
liver
edby
IMC
Iat
heal
thfa
cilit
ies
key
fam
ily
prac
tice
ssu
chas
excl
usiv
e
brea
stfe
edin
gdi
dno
tch
ange
asco
mm
unit
yIM
CI
had
not
been
impl
emen
ted
byth
at
tim
e(W
HO
2003
b)
SA
rife
en
pers
onal
com
mun
icat
ion
Ban
glad
esh
Mat
lab
Com
mun
ity-
base
dcl
uste
r
desi
gn
Eva
luat
ion
offa
cilit
y-an
d
com
mun
ity-
base
dIM
CI
Inte
rven
tion
pack
age
incl
udes
feed
ing
asse
ssm
ent
and
coun
selli
ngon
mot
hers
ofyo
ung
child
ren
seek
ing
care
atfa
cilit
ies
for
illne
ssan
d
hom
e-ba
sed
coun
selli
ng
onim
prov
edfe
edin
gby
com
mun
ity-
base
dhe
alth
and
nutr
itio
nw
orke
rs
At
base
line
inth
e
year
2000
alit
tle
mor
eth
anha
lfth
e
0ndash5-
mon
th-o
ld
infa
nts
inth
est
udy
area
wer
ebe
ing
excl
usiv
ely
brea
stfe
dB
y20
05
this
incr
ease
dby
30
inth
eIM
CI
area
Dat
ano
t
avai
labl
efr
omth
e
com
pari
son
area
as
yet
Lac
kof
com
para
ble
data
from
the
com
pari
son
area
prev
ents
ade
finit
ive
conc
lusi
onas
tow
heth
erth
is
trul
yis
anim
pact
ofIM
CI
BA
SIC
SII
Bas
icSu
ppor
tfo
rIn
stit
utio
naliz
ing
Chi
ldSu
rviv
alP
roje
ctB
FH
IB
aby-
Frie
ndly
Hos
pita
lIni
tiat
ive
ICD
SIn
tegr
ated
Chi
ldD
evel
opm
ent
Serv
ices
IM
CI
Inte
grat
edM
anag
emen
tof
Chi
ldho
odIl
lnes
sM
AD
LA
CM
onit
oreo
deA
poyo
Dir
ecto
con
laL
acat
anci
aM
ater
naN
GO
non
-gov
ernm
enta
lorg
aniz
atio
nPA
HO
Pan
Am
eric
anH
ealt
hO
rgan
izat
ion
PR
OB
ITP
rom
otio
nof
Bre
astf
eedi
ngIn
terv
enti
onTr
ial
PR
OC
OSI
Pro
gram
ade
Coo
rdin
acio
nen
Salu
dIn
tegr
al(C
olla
bora
tive
Pro
gram
for
Inte
grat
edH
ealt
h)U
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
WH
OW
orld
Hea
lth
Org
aniz
atio
n
Mainstreaming nutrition into MCH programs 21
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x2
Cas
est
udie
sin
scal
e-up
effo
rts
inH
IVA
IDS
Stud
yde
scri
ptio
nPo
pula
tion
Inte
rven
tion
Com
mun
icat
ion
stra
tegy
Impa
cton
excl
usiv
ebr
east
feed
ing
Com
men
ts
LIN
KA
GE
S(2
005)
Zam
bia
Pro
gram
me
thro
ugh
heal
th-c
are
and
com
mun
ity
serv
ices
Rea
ched
60si
tes
in6
dist
rict
sby
2005
Inte
grat
ion
ofin
fant
feed
ing
coun
selli
ngm
ater
naln
utri
tion
and
anti
retr
ovir
aldr
ugs
prop
hyla
xis
Trai
ning
ofhe
alth
wor
kers
and
com
mun
ity
serv
ice
prov
ider
sto
coun
selw
omen
onsa
fety
opti
ons
for
thei
rsi
tuat
ion
Beh
avio
urch
ange
Com
mun
icat
ion
inte
rven
tion
sin
the
first
few
year
sM
ater
iald
evel
oped
lsquoAct
Now
rsquoM
edia
cam
paig
nsin
clud
edbr
ochu
res
post
ers
radi
oan
dte
levi
sion
Ass
esse
dth
roug
hba
selin
ean
dfo
llow
-up
hous
ehol
dan
dcl
inic
surv
eys
inse
lect
eddi
stri
cts
Exc
lusi
vebr
east
feed
ing
rate
incr
ease
dfr
om50
in
2002
to64
in
2004
inL
ivin
gsto
nean
dfr
om57
in
2000
to74
in
2004
inN
dola
Inte
grat
edde
mon
stra
tion
proj
ect
Had
seve
rals
tren
gths
inte
rms
ofth
eus
eof
form
ativ
ere
sear
chto
deve
lop
mes
sage
str
aini
ngan
dbu
ildin
gup
skill
sof
prog
ram
me
man
ager
she
alth
-car
epr
ovid
ers
and
com
mun
ity
wor
kers
adv
ocac
yfo
rna
tion
alpo
licy
stro
ngbe
havi
our
chan
geco
mm
unic
atio
nco
mpo
nent
st
reng
then
ing
com
mun
ity
capa
city
for
coun
selli
ngan
dre
ferr
als
and
mon
itor
ing
and
eval
uati
onw
ith
loca
lpar
tner
sP
iwoz
etal
(20
05)
ZV
ITA
MB
Otr
ial
Har
are
Zim
babw
eE
duca
tion
and
coun
selli
ngpr
ogra
mm
ede
liver
edan
tena
tally
1411
0m
othe
rndashba
bypa
irs
enro
lled
from
14m
ater
nity
clin
ics
wit
hin
96h
ofde
liver
yan
dfo
llow
edup
at6
wee
ks
3m
onth
san
d3-
mon
thly
inte
rval
sIn
fant
-fee
ding
patt
erns
dete
rmin
edE
xclu
sive
brea
stfe
edin
gre
com
men
ded
for
HIV
nega
tive
un
know
nor
HIV
posi
tive
who
chos
eto
brea
stfe
ed
Gro
uped
ucat
ion
indi
vidu
alco
unse
lling
vid
eos
broc
hure
sM
othe
rsw
hoen
rolle
dw
hen
prog
ram
me
was
fully
impl
emen
ted
wer
e8
4ti
mes
mor
elik
ely
toex
clus
ivel
ybr
east
feed
than
mot
hers
who
enro
lled
befo
reth
epr
ogra
mm
ebe
gan
Ove
rall
excl
usiv
ebr
east
feed
ing
rate
sti
ll3
mon
ths
was
low
at24
6
Form
ativ
ere
sear
chus
edto
desi
gna
cult
ural
lyse
nsit
ive
educ
atio
nan
dco
unse
lling
prog
ram
me
Low
over
alle
xclu
sive
brea
stfe
edin
gra
tes
prom
pted
auth
ors
toco
nclu
deth
atw
omen
and
thei
rpa
rtne
rssh
ould
have
been
reac
hed
mor
efr
eque
ntly
duri
ngan
tena
tala
ndpo
st-n
atal
peri
od
N Bhandari and AKMI Kabir22
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Thi
oret
al(
2006
)R
ollin
s(2
007)
C
ohen
(200
7)
HIV
-inf
ecte
dpr
egna
ntw
omen
atte
ndin
gan
tena
talc
linic
sin
sout
hB
otsw
ana
Inve
stig
atio
nsby
CD
Cof
adi
arrh
oea
outb
reak
inJa
nuar
y-Fe
brua
ry20
06in
the
sam
epo
pula
tion
Mat
erna
land
infa
ntan
tire
trov
iral
ther
apy
toas
cert
ain
impa
cton
HIV
tran
smis
sion
Ant
enat
alco
unse
lling
Cas
endashco
ntro
lstu
dyto
iden
tify
risk
fact
ors
for
diar
rhoe
ano
tbr
east
feed
ing
was
the
bigg
est
risk
fact
ora
djus
ted
odds
rati
o50
(95
confi
denc
ein
terv
al4
5ndash10
0)
Bot
swan
aha
sth
ebe
stpr
imar
yhe
alth
-car
est
ruct
ure
wat
ersu
pply
and
sani
tati
onsy
stem
sin
Sout
hA
fric
aFo
rmul
apr
ovid
edfr
eeby
the
gove
rnm
ent
toin
fect
edm
othe
rsL
ower
mor
talit
yin
the
brea
stfe
edin
ggr
oup
at7
mon
ths
dem
onst
rate
sri
skof
form
ula
feed
ing
and
need
for
alte
rnat
est
rate
gies
(Thi
oret
al
2006
)A
utho
rsco
nclu
deth
athe
alth
syst
ems
inw
hich
thes
epr
ogra
mm
esar
eim
plem
ente
dsh
ould
beab
leto
cope
wit
hdi
arrh
oea
and
mal
nutr
itio
nth
atre
sult
sbe
caus
eof
form
ula
feed
ing
(Rol
lins
2007
)C
oova
dia
etal
(2
007)
Kw
aZul
uNat
al
Sout
hA
fric
a27
22H
IV-i
nfec
ted
and
unin
fect
edpr
egna
ntw
omen
enro
lled
into
ano
n-ra
ndom
ized
inte
rven
tion
coho
rtst
udy
from
ante
nata
lcl
inic
sIn
fant
feed
ing
data
obta
ined
wee
kly
bloo
dsa
mpl
esfr
omin
fant
sta
ken
mon
thly
83
of13
72in
fant
sbo
rnto
HIV
-inf
ecte
dm
othe
rsin
itia
ted
excl
usiv
ebr
east
feed
ing
from
birt
hB
reas
tfed
infa
nts
who
rece
ived
solid
sw
ere
sign
ifica
ntly
mor
elik
ely
toac
quir
ein
fect
ion
com
pare
dw
ith
excl
usiv
ely
brea
stfe
d(H
R10
87
151
ndash78
P=
001
8)as
wer
ein
fant
sw
hoat
12w
eeks
rece
ived
brea
stan
dfo
rmul
am
ilk(1
82
098
ndash33
6P
=0
57)
Cum
ulat
ive
3-m
onth
mor
talit
yin
excl
usiv
ely
brea
stfe
dw
as6
1(4
74ndash
792
)vs
15
1(7
63ndash
287
3)in
infa
nts
give
nre
plac
emen
tfe
eds
(HR
206
1
0ndash4
27P
=0
05)
The
stud
ysh
ows
that
excl
usiv
ebr
east
feed
ing
can
besu
cces
sful
lysu
ppor
ted
inH
IV-i
nfec
ted
wom
enT
heau
thor
sca
llfo
rfu
rthe
rre
visi
onof
UN
ICE
FW
HO
and
USA
IDin
fant
feed
ing
guid
elin
es
CD
CC
ente
rof
Dis
ease
Con
trol
HR
haz
ards
rati
oU
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
USA
IDU
SA
genc
yfo
rIn
tern
atio
nalD
evel
opm
ent
WH
OW
orld
Hea
lth
Org
aniz
atio
nZ
VIT
AM
BO
Z
imba
bwe
Vit
amin
Afo
rM
othe
rsan
dB
abie
s
Mainstreaming nutrition into MCH programs 23
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Cohen J (2007) Retrovirus meeting Hope on new AIDSdrugs but breast-feeding strategy backfires Science 3151357
Coovadia HM Rollins NC Bland RM Little KCoutsoudis A Bennish ML et al (2007) Mother tochild transmission of HIV-1 infection during exclusivebreastfeeding in the first 6 months of life an interven-tion cohort study Lancet 369 1107ndash1116
Coutinho SB de Lira PI de Carvalho LM amp AshworthA (2005) Comparison of the effect of two systems forthe promotion of exclusive breastfeeding Lancet 3661094ndash1100
Feachem RG amp Koblinsky MA (1984) Interventions forthe control of diarrheal diseases among young childrenpromotion of breastfeeding Bulletin of the of the WorldHealth Organization 62 271ndash291
Gonzales A Arteaga E amp Howard-Grabman L (1998)Scaling Up the WARMI Project ndash Lessons LearnedMobilizing Bolivian Communities around ReproductiveHealth Save the Children Federation Inc Bolivia FieldOffice La Paz Available at httpwwwcoregrouporgresourcesSavebolipdf
Government of India (1997) Recommendations of the FifthCentral Pay Commission Relating to Enhancement ofQuantum of Maternity Leave and to Allow PaternityLeave in Respect of Central Government EmployeesDocument ref 13018197-Estt(L) Available at httppersminnicinesttleave2htm
Government of India (2005) National Rural HealthMission 2005ndash2012 Mission document Ministry ofHealth and Family Welfare New Delhi Government ofIndia Available at httpwwwmohfwnicinNRHM20Mission20Documentpdf
Government of India (2006) Operational Guidelines forImplementation of Integrated Management of Neonataland Childhood Illness (IMNCI) Ministry of HealthFamily Welfare New Delhi Available at httpmohfwnicindofw20websiteF20IMNCI20Operational20Plan201320june202006htm
Government of Pakistan (2003) National Programme forFamily Planning and Primary Health Care The LadyHealth Workers Programme 2003ndash2008 Ministry ofHealth Pakistan Available at httpwwwphcgovpkDownloadsPC-120augpdf
Green CP (1999) Improving Breastfeeding Behaviors Evi-dence from Two Decades of Intervention ResearchPublished for the US Agency for International Develop-ment (USAID) by the LINKAGES Project Academyfor Educational Development Washington DC
Gupta A (2002) National trends in breastfeeding andeffective strategies to improve breastfeeding ratesJournal of Neonatology 2002 4ndash14
Gwatkin DR (2004) Integrating the management of child-hood illness Lancet 364 1557ndash1558
Habicht JP DaVanzo J amp Butz WP (1986) Does breast-feeding really save lives or are apparent benefits due tobiases American Journal of Epidemiology 123279ndash290
Haider R Ashworth A Kabir I amp Huttly SR (2000)Effect of community based peer counsellors on exclusivebreastfeeding practices in Dhaka Bangladesh a ran-domized controlled trial Lancet 356 1643ndash1647
Haider R Kabir I Huttly SR amp Ashworth A (2002)Training peer counsellors to promote and support exclu-sive breastfeeding in Bangladesh Journal of HumanLactation 18 7ndash12
Horton S Sanghvi T Phillips M Fiedler J Perez-Escamilla R Lutter C et al (1996) Breastfeeding pro-motion and priority setting in health Health Policy andPlanning 11 156ndash168
ILO (1998) More than 120 Nations Provide Paid MaternityLeave Gap in Employment Treatment for Men andWomen Still Exists International Labour Office GenevaDocument ref ILO987 Available at httpwwwiloorgpublicenglishbureauinfpr19987htmr2
Iliff PJ Piwoz EG Tavengwa NV Zunguza CDMarinda ET Nathoo KJ et al (2005) Early exclusivebreastfeeding reduces the risk of postnatal HIV-1 trans-mission and increase HIV-free survival AIDS 19 699ndash708
Integrated Child Development Services Scheme (Revised)(ICDS) (1982) Ministry of Social Welfare Governmentof India New Delhi Available on URL httpwcdnicinudishahtmabouticdshtm
Jason JM Nieburg P amp Marks JS (1984) Mortality andinfectious disease associated with infant feeding prac-tices in developing countries Pediatrics 74 702ndash727
Jones G Steketee RW Black RE Bhutta ZA ampMorris SS Bellagio Child Survival Study Group (2003)How many child deaths can we prevent this yearLancet 362 65ndash71
Knippenberg R Lawn JE Darmstadt GL Begkayian GFogstad H Walelign N et al (2005) Systematic scalingup of neonatal care in countries Lancet 365 1087ndash1098
Kramer MS amp Kakuma R (2002) The optimal durationof exclusive breastfeeding a systematic reviewCochrane Database of Systematic Reviews 2002CD003517
Kramer MS Chalmers B Hodnett ED Sevkovskaya ZDzikovich I Shapiro S et al (2000) Promotion ofbreastfeeding intervention trial (PROBIT) a cluster ran-domized trial in the Republic of Belarus Design followup and data validation Advances in Experimental Medi-cine and Biology 478 327ndash345
Kramer MS Chalmers B Hodnett ED Sevkovskaya ZDzikovich I Shapiro S et al (2001) Promotion ofbreastfeeding intervention trial (PROBIT) a random-
Mainstreaming nutrition into MCH programs 15
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
ized trial in the Republic of Belarus Journal of theAmerican Medical Association 285 413ndash420
Lewin SA Dick J Pond P Zwarenstein M Aja Gvan Wyk B et al (2006) Lay health workers in primaryand community health care (Review) The CochraneLibrary 3 1ndash104
LINKAGES (2002) World LINKAGES MadagascarAcademy for Educational Development WashingtonDC
LINKAGES (2005) LINKAGES Zambia 1997ndash2005 FinalReport A Full Report on LINKAGES Infant Feedingand HIVAIDS Programs in Zambia Academy for Edu-cational Development Washington DC Available athttpwwwlinkagesprojectorgmediapublicationsFinal20draft20Zambia20final20report2012105pdf
Lutter CK Perez-Escamilla R Segall A Sanghvi TTeruya K amp Wickham C (1997) The effectiveness of ahospital based program to promote exclusive breastfeed-ing among low income women in Brazil AmericanJournal of Public Health 87 659ndash663
Morrow AL Guerrero ML Shults J Calva J Lutter CBravo J et al (1999) Efficacy of home based peer coun-selling to promote exclusive breastfeeding a randomizedcontrolled trial Lancet 353 1226ndash1231
Ntabaye MK amp Lusiola GJ (2004) Understanding barri-ers to PMTCT in Tanzania findings of a baseline surveyInternational Conference on AIDS 15 (B11396)
de Oliveira LD Giugliani ER do Espirito SLC FrancaMC Weigert EM Kohler CV et al (2006) Effect ofintervention to improve breastfeeding technique on thefrequency of exclusive breastfeeding and lactation-related problems Journal of Human Lactation 22 315ndash321
Perez-Escamilla R (2004) Effectiveness of MADLAC atImproving Breastfeeding Promotion and CounsellingIndicators in Maternity Wards in El Salvador Publishedfor the Basic Support for Institutionalizing Child Sur-vival Project (BASICS II) for the United States Agencyfor International Development Arlington VA Availableat httpwwwbasicsorgpdfFinal20MADLAC20Report20RPE20April207-2004pdf
Perez-Escamilla R (2007) Evidence based breast-feedingpromotion the Baby-Friendly Hospital InitiativeJournal of Nutrition 137 484ndash487
Piwoz EG Iliff PJ Tavengwa N Gavin L Marinda ELunney K et al (2005) An education and counselllingprogram for preventing breastfeeding associated HIVtransmission in Zimbabwe design and impact on mater-nal knowledge and behaviour Journal of Nutrition 135950ndash955
Quinn VJ Guyon AB Schubert JW Stone-Jimenez MHainsworth MD amp Martin LH (2005) Improvingbreastfeeding practices on a board scale at the commu-
nity level success stories from Africa and LatinAmerica Journal of Human Lactation 21 345ndash354
Ranson MK Hanson K Oliveira-Cruz V amp Mills A(2003) Constraints to expanding access to health inter-ventions an empirical analysis and country typologyJournal of International Development 15 15ndash40
Rea MF amp Berquo ES (1990) Impact of the Braziliannational breastfeeding programme on mothers inGreater Sao Paulo Bulletin of the of the World HealthOrganization 68 365ndash371
Rollins NC (2007) Infant feeding and HIV BritishMedical Journal 334 487ndash488
Rutenberg N Baek C Kalibala S Rosen J amp Mulenga D(2004) Evaluation of United Nations supported pilotprojects for the prevention of mother-to-child transmis-sion of HIV overview of findings International Confer-ence on AIDS 15 (WePeE6688)
The Core Group (2005) Scale and Scaling Up A COREGroup Background Paper on lsquoScaling-Uprsquo MaternalNewborn and Child Health Services CORE SpringMembership Meeting 2005 The Core Group Washing-ton DC Available at httpwwwcoregrouporgresourcesmeetingsapril05Scaling_Up_Background_Paper_7-13pdf
The Norwegian Government (1993) Women in PoliticsMinistry of Children and Equality Available at httpwwwregjeringennoendepbldRyddemappeSLA-AvdelingdoclegislationguidelinesWomen-in-Politicshtmlid=437166
Thior I Lockman S Smeaton LM Shapiro RL WesterC Heymann SJ et al (2006) Breastfeeding plus infantzidovudine prophylaxis for 6 months vs formula feedingplus infant zidovudine for 1 month to reduce mother-to-child HIV transmission in Botswana a randomized trialthe Mashi Study Journal of the American Medical Asso-ciation 296 794ndash805
UNICEF (2002) Facts for Life lsquoKey Message What EveryFamily and Community Has a Right to Know aboutBreastfeedingrsquo Available at httpwwwuniceforgffl04key_messageshtm
Van Roekel K Plowman B Griffiths M de AlvaradoVV Matute J amp Calderon M (2002) BASICS IIMidterm Evaluation of the AIN Program in Honduras2000 Basic Support for Institutionalizing Child SurvivalProject (BASICS II) for the United States Agency forInternational Development Arlington VA
WABA (2007) UNICEF Records BHFI Record UpdateAvailable at httpwwwwabaorgmydocsBFHIjan07xls 2006 Regularly updated by Miriam HLabbok Center for Infant and Young ChildFeeding and Care Department of Maternaland Child Health School of Public Health The Univer-sity of North Carolina at Chapel Hill Chapel Hill NCUSA
N Bhandari and AKMI Kabir16
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
WHA (2002) Infant and Young Child Nutrition Fifty-FifthWorld Health Assembly Agenda Item 1310 18 May2002 Available at httpwwwintgbebwhapdf_filesWHA55ewha5525pdf
WHO (1981) The International Code of Marketing ofBreastmilk Substitutes World Health OrganizationGeneva
WHO (1989) Protecting Promoting and Supporting Breast-feeding The Special Role of Maternity Services A JointWHOUNICEF Statement World Health OrganizationGeneva
WHO (2002) The Optimal Duration of Exclusive Breast-feeding Report of an Expert Consultation WHONHD0109 WHOFCHCAH0124 World HealthOrganization Geneva
WHO (2003a) Community Based Strategies for Breastfeed-ing Promotion and Support in Developing CountriesWorld Health Organization Geneva Document refISBN_92_4_159121_8 Available at httpwwwwhointchild-adolescent-healthNew_PublicationsNUTRITIONISBN_92_4_159121_8pdf
WHO (2003b) Multi-country Evaluation of IMCI Effective-ness Cost and Impact (MCE) Progress Report May2002ndashApril 2003 Document ref WHOFCHCAH035World Health Organization Geneva
WHO (2004) Promoting Proper Feeding for Infants andYoung Children World Health Organization GenevaAvailable at httpwwwwhointnutritiontopicsinfantfeedingen
WHO (2006) WHO HIV and Infant Feeding TechnicalConsultation-Consensus Statement World Health Orga-nization Geneva Available at httpwwwwhointhivmediacentreInfantfeedingconsensusstatementpfpdf
WHO Collaborative Study Team on the Role of Breast-feeding on the Prevention of Infant Mortality (2000)Effect of breastfeeding on infant and child mortality dueto infectious diseases in les developed countries apooled analysis Lancet 355 451ndash455
WHOUNICEF (1992) The global criteria for the WHOUNICEF Baby-Friendly Hospital Initiative In Baby-Friendly Hospital Initiative Part II Hospital LevelImplementation World Health Organization Geneva
WHOUNICEF (1993) Breastfeeding Counselling A Train-ing Course WHOCDR933 UNICEFNUT931 WorldHealth Organization Geneva
WHOUNICEF (2002) Protocol for Adapting the FeedingRecommendations Part III IMCI Adaptation GuideWorld Health Organization Geneva
WHOUNICEF (2003) Global Strategy for Infant andYoung Child Feeding World Health OrganizationGeneva Available at httpwwwwhointchild-adolescent-healthpublicationsNUTRITIONIYCF_GShtm
de Zoysa I Rea M amp Martines J (1991) Why promotebreastfeeding in diarrheal diseases control programmesHealth Policy and Planning 6 371ndash379
Mainstreaming nutrition into MCH programs 17
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
Cas
est
udie
so
fef
fect
iven
ess
stud
ies
or
pilo
tpr
ogra
mm
es
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Lut
ter
etal
(199
7)
Bra
zil
Low
-inc
ome
urba
nw
omen
deliv
erin
gin
hosp
ital
s
Bre
astf
eedi
ngpr
omot
ion
in
hosp
ital
sco
mpa
red
wit
h
nobr
east
feed
ing
prom
otio
n
Pro
mot
ion
ofbr
east
feed
ing
in
sele
cted
hosp
ital
s
Mea
nda
ysof
excl
usiv
e
brea
stfe
edin
g
75da
ysvs
22
days
(Plt
001
)
Rea
ampB
erqu
o
(199
0)
Wom
enw
ith
ach
ild
aged
lt2ye
ars
inSa
oP
aulo
Nat
iona
lbre
astf
eedi
ng
cam
paig
n19
81ndash1
986
BF
HI
Mas
sm
edia
cam
paig
n11
in
fant
s5ndash
6m
onth
s
excl
usiv
ely
brea
stfe
d
in19
88an
d37
in
1987
Con
foun
ding
fact
ors
over
the
6-ye
arpe
riod
not
mea
sure
d
Kra
mer
etal
(200
020
01)
PR
OB
ITtr
ial
Bel
arus
Clu
ster
rand
omiz
ed
34ho
spit
als
and
thei
rpo
lycl
inic
s
Trai
ning
inB
FH
I(W
HO
UN
ICE
F19
92)
vsr
outi
ne
prac
tice
san
dpo
licie
s
Exc
lusi
vebr
east
feed
ing
at3
(43
3vs
64
)
and
6(7
9
vs0
6
)
mon
ths
sign
ifica
ntly
high
er
Impl
emen
ted
thro
ugh
BF
HI
ina
sett
ing
whe
reho
spit
al
deliv
erie
sar
eco
mm
on
Per
ez-E
scam
illa
(200
4)
BA
SIC
SII
Mex
ico
Hon
dura
s
Bra
zil
MA
DL
AC
low
-cos
t
man
agem
ent
info
rmat
ion
syst
emto
use
an
evid
ence
-bas
edap
proa
chto
impr
ove
serv
ice
perf
orm
ance
Inte
rvie
win
gof
wom
enat
hosp
ital
disc
harg
epo
st
deliv
ery
usin
ga
ques
tion
nair
eth
atta
kes
5ndash7
min
toad
min
iste
ran
d
cont
ains
19br
east
feed
ing
prom
otio
nco
unse
lling
indi
cato
rs
Dat
aen
tere
dan
dre
sult
s
disc
usse
d3-
mon
thly
by
hosp
ital
com
mit
tee
Hos
pita
lim
plem
ents
chan
ges
in
brea
stfe
edin
g
supp
ort
base
don
anal
ysis
of
ques
tion
nair
es
Itis
aco
st-e
ffec
tive
inte
rven
tion
that
can
help
impr
ovem
ents
inth
eB
FH
I
and
isa
valu
able
tool
for
proc
ess
eval
uati
on
N Bhandari and AKMI Kabir18
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
LIN
KA
GE
S
proj
ect
inA
fric
aan
d
Lat
inA
mer
ica
(Qui
nnet
al
2005
LIN
KA
GE
S
2002
WH
O20
03a)
Bol
ivia
(1
mill
ion)
Gha
na(3
5
mill
ion)
Mad
agas
car
(6m
illio
n)
Res
ourc
e-
poor
sett
ing
Pilo
tpr
ogra
mm
e
InB
oliv
iaan
d
Gha
napr
ogra
mm
e
focu
sed
on
brea
stfe
edin
gan
d
com
plem
enta
ry
feed
ing
InM
adag
asca
r
prog
ram
me
prom
oted
brea
stfe
edin
g
wit
hin
7es
sent
ial
nutr
itio
nac
tion
san
d
subs
eque
ntly
thro
ugh
IMC
I
Bui
lton
form
ativ
ere
sear
ch
and
sust
aine
dth
roug
h
prog
ram
me
acti
viti
esth
at
focu
sed
onbr
ingi
ngab
out
the
desi
red
beha
viou
r
chan
geM
ixof
inte
rven
tion
s
reac
hed
wom
enin
divi
dual
ly
orin
grou
psin
heal
th
faci
litie
sho
mes
or
com
mun
ity
sett
ings
Con
sist
ent
mes
sage
san
d
mat
eria
lacr
oss
all
prog
ram
me
chan
nels
Bol
ivi
PR
OC
OSI
NG
Os
Gha
na
UN
ICE
F
nati
onal
nutr
itio
n
offic
eN
GO
s
Mad
agas
car
Inte
rsec
tora
l
Act
ion
Gro
upfo
r
Nut
riti
on
Jere
o
Sala
ma
Isik
a
Pro
gram
desi
gned
wit
h
part
ners
Rad
ioin
all
thre
esi
tes
Mat
eria
ls
deve
lope
d
tosu
itne
eds
oflo
cal
heal
th
wor
kers
and
com
mun
ity
mem
bers
Gre
at
emph
asis
on
deve
lopm
ent
of coun
selli
ng
and
nego
tiat
ion
skill
s
prac
tica
l
sess
ions
Sign
ifica
ntin
crea
ses
inex
clus
ive
brea
stfe
edin
gra
tes
of
0ndash6-
mon
th-o
ld
infa
nts
from
54
to65
in
Bol
ivia
68
to79
in
Gha
naan
d46
to68
in
Mad
agas
car
In
Gha
naan
d
Mad
agas
car
sign
ifica
ntre
sult
s
obse
rved
wit
hin
aye
ar
ofin
itia
tion
of
com
mun
ity
inte
rven
tion
s
App
roac
hw
asef
fect
ive
and
achi
eved
sign
ifica
nt
incr
ease
sam
ong
larg
e
popu
lati
ons
asea
rly
as
9ndash12
mo
afte
rin
itia
tion
of
com
mun
ity
acti
viti
es
Van
Roe
kele
tal
(200
2)W
HO
(200
3a)
Hon
dura
sG
row
thm
onit
orin
gan
d
prom
otio
nkn
own
as
Ate
ncioacute
nIn
tegr
ala
la
Nintilde
ez(A
IN)
or
Inte
grat
edC
hild
Car
e
Init
ially
pri
mar
ilya
grow
th
mon
itor
ing
prog
ram
me
ulti
mat
ely
thro
ugh
IMC
I
Pro
gram
me
ongr
owth
prom
otio
nndash
asse
ssm
ent
of
mon
thly
wei
ght
gain
and
focu
son
illne
ssf
eedi
ng
prac
tice
san
dge
nera
lchi
ld
care
inin
fant
sun
der
2ye
ars
Impl
emen
ted
atgo
vern
men
t
faci
litie
san
dco
mm
unit
y
Star
ted
in19
92s
tren
gthe
ned
in19
95ndash1
997
wit
hgr
eate
r
focu
son
child
feed
ing
In
1997
pro
gram
me
intr
oduc
ed
wit
hIM
CI
(WH
OU
NIC
EF
2002
)
Maj
or
part
ners
UN
ICE
F
PAH
O
Am
eric
an
and
Hon
dura
n
Red
Cro
ss
CA
RE
Rad
io
broa
dcas
ts
relig
ious
lead
ers
IMC
IM
id-t
erm
eval
uati
on
show
ed39
of
mot
hers
inin
terv
enti
on
com
mun
itie
sex
clus
ivel
y
brea
stfe
dco
mpa
red
wit
h13
in
the
cont
rol
site
s
Mainstreaming nutrition into MCH programs 19
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
cont
inue
d
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Bha
ndar
ieta
l
(200
3)
WH
O
(200
3a)
Rur
alco
mm
unit
ies
inH
arya
na
Indi
a
Clu
ster
rand
omiz
edtr
ial
8
com
mun
itie
s(t
otal
popu
lati
on~4
000
0)
Pro
mot
ion
ofex
clus
ive
brea
stfe
edin
gan
d
appr
opri
ate
com
plem
enta
ryfe
edin
g
Dev
elop
edth
roug
h
form
ativ
ere
sear
ch
ndashP
robl
emid
enti
ficat
ion
ndashP
arti
cipa
tory
desi
gnof
inte
rven
tion
impl
emen
tati
onan
d
eval
uati
on
Impl
emen
tati
onw
ithi
nan
exis
ting
prim
ary
heal
th-c
are
prog
ram
me
Opp
ortu
niti
esus
edto
deliv
erm
essa
ges
wer
e
imm
uniz
atio
ncl
inic
s
wei
ghin
gse
ssio
ns
sick
-chi
ldco
ntac
tsan
d
mon
thly
hom
evi
sits
Res
earc
hers
wit
hlo
cal
gove
rnm
ent
ICD
Ssy
stem
and
NG
O
The
atre
son
gs
Mas
sm
edia
not
used
for
risk
of
cont
amin
atio
n
Mat
eria
ls
deve
lope
d
for
heal
th
wor
kers
pos
ters
flip
book
sca
rds
Bre
astf
eedi
ng
coun
selli
ngse
ctio
n
ofth
eIM
CI
(WH
O
UN
ICE
F20
02)
Exc
lusi
ve
brea
stfe
edin
gin
the
prev
ious
24h
at3
mon
ths
of
age
79
vs4
8
The
posi
tive
effe
ct
rem
aine
dup
to
6m
onth
sof
age
(42
vs4
)
Tota
lpar
tici
pati
onof
the
dist
rict
heal
thsy
stem
from
ince
ptio
nof
the
prog
ram
me
inde
velo
ping
impl
emen
tati
onst
rate
gyt
ool
deve
lopm
ent
and
mon
itor
ing
inad
diti
onto
invo
lvem
ent
of
anN
GO
wer
eim
port
ant
feat
ures
that
cont
ribu
ted
to
the
succ
ess
ofth
e
inte
rven
tion
Mor
row
etal
(199
9)
Mex
ico
Cit
yC
lust
erra
ndom
ized
tria
l
Tota
lpop
ulat
ion
3000
0
Two
com
mun
itie
sin
the
inte
rven
tion
one
com
pari
son
130
wom
en
Hom
e-ba
sed
peer
coun
selli
ng
Pee
rco
unse
llors
mad
e3
or
6ho
me
visi
tsto
the
mot
her
Key
fam
ilym
embe
rsal
so
incl
uded
By
La
Lec
he
Lea
gue
of
Mex
ico
Exc
lusi
ve
brea
stfe
edin
g
at3
mon
ths
post
-par
tum
67
(6vi
sits
)
50
(3vi
sits
)12
(com
pari
son)
Firs
tcl
uste
rra
ndom
ized
com
mun
ity-
base
dtr
ialt
hat
used
peer
coun
sello
rsto
prom
ote
excl
usiv
e
brea
stfe
edin
g
Hai
der
etal
2000
200
2
Dha
ka
Low
mid
dle
and
low
-soc
io-
econ
omic
popu
lati
on
Clu
ster
rand
omiz
edtr
ial
20zo
nes
inin
terv
enti
on
and
20in
cont
rol
Com
mun
ity-
base
dpe
er
coun
selli
ngin
Dha
ka
15ho
me-
base
dco
unse
lling
visi
tsby
peer
coun
sello
rs
40h
(4h
yen10
days
)
WH
OU
NIC
EF
brea
stfe
edin
g
coun
selli
ngco
urse
(WH
OU
NIC
EF
1993
)
Exc
lusi
ve
brea
stfe
edin
g
at5
mon
ths
70
in
inte
rven
tion
and
6in
the
cont
rol
Com
mun
ity-
base
d
brea
stfe
edin
gpr
omot
ion
stra
tegy
was
effe
ctiv
ein
Ban
glad
esh
whe
rem
ost
deliv
erie
soc
cur
atho
me
N Bhandari and AKMI Kabir20
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Bry
ceet
al
(200
4)W
HO
(200
3b)
Bra
zil
Per
u
Tanz
ania
Uga
nda
Mul
tico
untr
yev
alua
tion
of
IMC
Ith
atin
clud
ed
effe
ctiv
enes
sco
stan
d
impa
ct(B
ryce
etal
2004
)
Bre
astf
eedi
ngpr
omot
ion
asa
part
ofIM
CI
IMC
Iis
ast
rate
gyfo
r
impr
ovin
gch
ildhe
alth
and
deve
lopm
ent
thro
ugh
the
com
bine
d
deliv
ery
ofes
sent
ial
child
heal
th
inte
rven
tion
sIM
CI
bega
nw
ith
ase
tof
case
man
agem
ent
guid
elin
es
for
the
man
agem
ent
ofsi
ckch
ildre
nat
first
-lev
elhe
alth
faci
litie
s
and
the
guid
elin
esw
ere
desi
gned
for
adap
tati
on
atco
untr
yle
vela
nd
belo
wO
ver
tim
eth
e
stra
tegy
expa
nded
to
incl
ude
ara
nge
of
guid
elin
esfo
rde
liver
ing
child
surv
ival
inte
rven
tion
at
hous
ehol
dco
mm
unit
y
and
refe
rral
leve
ls
IMC
Im
odul
e(W
HO
UN
ICE
F20
02)
Res
ults
onex
clus
ive
brea
stfe
edin
g
avai
labl
efr
om
Tanz
ania
whe
reno
sign
ifica
ntim
pact
was
seen
Des
pite
subs
tant
ial
impr
ovem
ent
inth
equ
alit
y
ofca
rede
liver
edby
IMC
Iat
heal
thfa
cilit
ies
key
fam
ily
prac
tice
ssu
chas
excl
usiv
e
brea
stfe
edin
gdi
dno
tch
ange
asco
mm
unit
yIM
CI
had
not
been
impl
emen
ted
byth
at
tim
e(W
HO
2003
b)
SA
rife
en
pers
onal
com
mun
icat
ion
Ban
glad
esh
Mat
lab
Com
mun
ity-
base
dcl
uste
r
desi
gn
Eva
luat
ion
offa
cilit
y-an
d
com
mun
ity-
base
dIM
CI
Inte
rven
tion
pack
age
incl
udes
feed
ing
asse
ssm
ent
and
coun
selli
ngon
mot
hers
ofyo
ung
child
ren
seek
ing
care
atfa
cilit
ies
for
illne
ssan
d
hom
e-ba
sed
coun
selli
ng
onim
prov
edfe
edin
gby
com
mun
ity-
base
dhe
alth
and
nutr
itio
nw
orke
rs
At
base
line
inth
e
year
2000
alit
tle
mor
eth
anha
lfth
e
0ndash5-
mon
th-o
ld
infa
nts
inth
est
udy
area
wer
ebe
ing
excl
usiv
ely
brea
stfe
dB
y20
05
this
incr
ease
dby
30
inth
eIM
CI
area
Dat
ano
t
avai
labl
efr
omth
e
com
pari
son
area
as
yet
Lac
kof
com
para
ble
data
from
the
com
pari
son
area
prev
ents
ade
finit
ive
conc
lusi
onas
tow
heth
erth
is
trul
yis
anim
pact
ofIM
CI
BA
SIC
SII
Bas
icSu
ppor
tfo
rIn
stit
utio
naliz
ing
Chi
ldSu
rviv
alP
roje
ctB
FH
IB
aby-
Frie
ndly
Hos
pita
lIni
tiat
ive
ICD
SIn
tegr
ated
Chi
ldD
evel
opm
ent
Serv
ices
IM
CI
Inte
grat
edM
anag
emen
tof
Chi
ldho
odIl
lnes
sM
AD
LA
CM
onit
oreo
deA
poyo
Dir
ecto
con
laL
acat
anci
aM
ater
naN
GO
non
-gov
ernm
enta
lorg
aniz
atio
nPA
HO
Pan
Am
eric
anH
ealt
hO
rgan
izat
ion
PR
OB
ITP
rom
otio
nof
Bre
astf
eedi
ngIn
terv
enti
onTr
ial
PR
OC
OSI
Pro
gram
ade
Coo
rdin
acio
nen
Salu
dIn
tegr
al(C
olla
bora
tive
Pro
gram
for
Inte
grat
edH
ealt
h)U
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
WH
OW
orld
Hea
lth
Org
aniz
atio
n
Mainstreaming nutrition into MCH programs 21
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x2
Cas
est
udie
sin
scal
e-up
effo
rts
inH
IVA
IDS
Stud
yde
scri
ptio
nPo
pula
tion
Inte
rven
tion
Com
mun
icat
ion
stra
tegy
Impa
cton
excl
usiv
ebr
east
feed
ing
Com
men
ts
LIN
KA
GE
S(2
005)
Zam
bia
Pro
gram
me
thro
ugh
heal
th-c
are
and
com
mun
ity
serv
ices
Rea
ched
60si
tes
in6
dist
rict
sby
2005
Inte
grat
ion
ofin
fant
feed
ing
coun
selli
ngm
ater
naln
utri
tion
and
anti
retr
ovir
aldr
ugs
prop
hyla
xis
Trai
ning
ofhe
alth
wor
kers
and
com
mun
ity
serv
ice
prov
ider
sto
coun
selw
omen
onsa
fety
opti
ons
for
thei
rsi
tuat
ion
Beh
avio
urch
ange
Com
mun
icat
ion
inte
rven
tion
sin
the
first
few
year
sM
ater
iald
evel
oped
lsquoAct
Now
rsquoM
edia
cam
paig
nsin
clud
edbr
ochu
res
post
ers
radi
oan
dte
levi
sion
Ass
esse
dth
roug
hba
selin
ean
dfo
llow
-up
hous
ehol
dan
dcl
inic
surv
eys
inse
lect
eddi
stri
cts
Exc
lusi
vebr
east
feed
ing
rate
incr
ease
dfr
om50
in
2002
to64
in
2004
inL
ivin
gsto
nean
dfr
om57
in
2000
to74
in
2004
inN
dola
Inte
grat
edde
mon
stra
tion
proj
ect
Had
seve
rals
tren
gths
inte
rms
ofth
eus
eof
form
ativ
ere
sear
chto
deve
lop
mes
sage
str
aini
ngan
dbu
ildin
gup
skill
sof
prog
ram
me
man
ager
she
alth
-car
epr
ovid
ers
and
com
mun
ity
wor
kers
adv
ocac
yfo
rna
tion
alpo
licy
stro
ngbe
havi
our
chan
geco
mm
unic
atio
nco
mpo
nent
st
reng
then
ing
com
mun
ity
capa
city
for
coun
selli
ngan
dre
ferr
als
and
mon
itor
ing
and
eval
uati
onw
ith
loca
lpar
tner
sP
iwoz
etal
(20
05)
ZV
ITA
MB
Otr
ial
Har
are
Zim
babw
eE
duca
tion
and
coun
selli
ngpr
ogra
mm
ede
liver
edan
tena
tally
1411
0m
othe
rndashba
bypa
irs
enro
lled
from
14m
ater
nity
clin
ics
wit
hin
96h
ofde
liver
yan
dfo
llow
edup
at6
wee
ks
3m
onth
san
d3-
mon
thly
inte
rval
sIn
fant
-fee
ding
patt
erns
dete
rmin
edE
xclu
sive
brea
stfe
edin
gre
com
men
ded
for
HIV
nega
tive
un
know
nor
HIV
posi
tive
who
chos
eto
brea
stfe
ed
Gro
uped
ucat
ion
indi
vidu
alco
unse
lling
vid
eos
broc
hure
sM
othe
rsw
hoen
rolle
dw
hen
prog
ram
me
was
fully
impl
emen
ted
wer
e8
4ti
mes
mor
elik
ely
toex
clus
ivel
ybr
east
feed
than
mot
hers
who
enro
lled
befo
reth
epr
ogra
mm
ebe
gan
Ove
rall
excl
usiv
ebr
east
feed
ing
rate
sti
ll3
mon
ths
was
low
at24
6
Form
ativ
ere
sear
chus
edto
desi
gna
cult
ural
lyse
nsit
ive
educ
atio
nan
dco
unse
lling
prog
ram
me
Low
over
alle
xclu
sive
brea
stfe
edin
gra
tes
prom
pted
auth
ors
toco
nclu
deth
atw
omen
and
thei
rpa
rtne
rssh
ould
have
been
reac
hed
mor
efr
eque
ntly
duri
ngan
tena
tala
ndpo
st-n
atal
peri
od
N Bhandari and AKMI Kabir22
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Thi
oret
al(
2006
)R
ollin
s(2
007)
C
ohen
(200
7)
HIV
-inf
ecte
dpr
egna
ntw
omen
atte
ndin
gan
tena
talc
linic
sin
sout
hB
otsw
ana
Inve
stig
atio
nsby
CD
Cof
adi
arrh
oea
outb
reak
inJa
nuar
y-Fe
brua
ry20
06in
the
sam
epo
pula
tion
Mat
erna
land
infa
ntan
tire
trov
iral
ther
apy
toas
cert
ain
impa
cton
HIV
tran
smis
sion
Ant
enat
alco
unse
lling
Cas
endashco
ntro
lstu
dyto
iden
tify
risk
fact
ors
for
diar
rhoe
ano
tbr
east
feed
ing
was
the
bigg
est
risk
fact
ora
djus
ted
odds
rati
o50
(95
confi
denc
ein
terv
al4
5ndash10
0)
Bot
swan
aha
sth
ebe
stpr
imar
yhe
alth
-car
est
ruct
ure
wat
ersu
pply
and
sani
tati
onsy
stem
sin
Sout
hA
fric
aFo
rmul
apr
ovid
edfr
eeby
the
gove
rnm
ent
toin
fect
edm
othe
rsL
ower
mor
talit
yin
the
brea
stfe
edin
ggr
oup
at7
mon
ths
dem
onst
rate
sri
skof
form
ula
feed
ing
and
need
for
alte
rnat
est
rate
gies
(Thi
oret
al
2006
)A
utho
rsco
nclu
deth
athe
alth
syst
ems
inw
hich
thes
epr
ogra
mm
esar
eim
plem
ente
dsh
ould
beab
leto
cope
wit
hdi
arrh
oea
and
mal
nutr
itio
nth
atre
sult
sbe
caus
eof
form
ula
feed
ing
(Rol
lins
2007
)C
oova
dia
etal
(2
007)
Kw
aZul
uNat
al
Sout
hA
fric
a27
22H
IV-i
nfec
ted
and
unin
fect
edpr
egna
ntw
omen
enro
lled
into
ano
n-ra
ndom
ized
inte
rven
tion
coho
rtst
udy
from
ante
nata
lcl
inic
sIn
fant
feed
ing
data
obta
ined
wee
kly
bloo
dsa
mpl
esfr
omin
fant
sta
ken
mon
thly
83
of13
72in
fant
sbo
rnto
HIV
-inf
ecte
dm
othe
rsin
itia
ted
excl
usiv
ebr
east
feed
ing
from
birt
hB
reas
tfed
infa
nts
who
rece
ived
solid
sw
ere
sign
ifica
ntly
mor
elik
ely
toac
quir
ein
fect
ion
com
pare
dw
ith
excl
usiv
ely
brea
stfe
d(H
R10
87
151
ndash78
P=
001
8)as
wer
ein
fant
sw
hoat
12w
eeks
rece
ived
brea
stan
dfo
rmul
am
ilk(1
82
098
ndash33
6P
=0
57)
Cum
ulat
ive
3-m
onth
mor
talit
yin
excl
usiv
ely
brea
stfe
dw
as6
1(4
74ndash
792
)vs
15
1(7
63ndash
287
3)in
infa
nts
give
nre
plac
emen
tfe
eds
(HR
206
1
0ndash4
27P
=0
05)
The
stud
ysh
ows
that
excl
usiv
ebr
east
feed
ing
can
besu
cces
sful
lysu
ppor
ted
inH
IV-i
nfec
ted
wom
enT
heau
thor
sca
llfo
rfu
rthe
rre
visi
onof
UN
ICE
FW
HO
and
USA
IDin
fant
feed
ing
guid
elin
es
CD
CC
ente
rof
Dis
ease
Con
trol
HR
haz
ards
rati
oU
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
USA
IDU
SA
genc
yfo
rIn
tern
atio
nalD
evel
opm
ent
WH
OW
orld
Hea
lth
Org
aniz
atio
nZ
VIT
AM
BO
Z
imba
bwe
Vit
amin
Afo
rM
othe
rsan
dB
abie
s
Mainstreaming nutrition into MCH programs 23
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
ized trial in the Republic of Belarus Journal of theAmerican Medical Association 285 413ndash420
Lewin SA Dick J Pond P Zwarenstein M Aja Gvan Wyk B et al (2006) Lay health workers in primaryand community health care (Review) The CochraneLibrary 3 1ndash104
LINKAGES (2002) World LINKAGES MadagascarAcademy for Educational Development WashingtonDC
LINKAGES (2005) LINKAGES Zambia 1997ndash2005 FinalReport A Full Report on LINKAGES Infant Feedingand HIVAIDS Programs in Zambia Academy for Edu-cational Development Washington DC Available athttpwwwlinkagesprojectorgmediapublicationsFinal20draft20Zambia20final20report2012105pdf
Lutter CK Perez-Escamilla R Segall A Sanghvi TTeruya K amp Wickham C (1997) The effectiveness of ahospital based program to promote exclusive breastfeed-ing among low income women in Brazil AmericanJournal of Public Health 87 659ndash663
Morrow AL Guerrero ML Shults J Calva J Lutter CBravo J et al (1999) Efficacy of home based peer coun-selling to promote exclusive breastfeeding a randomizedcontrolled trial Lancet 353 1226ndash1231
Ntabaye MK amp Lusiola GJ (2004) Understanding barri-ers to PMTCT in Tanzania findings of a baseline surveyInternational Conference on AIDS 15 (B11396)
de Oliveira LD Giugliani ER do Espirito SLC FrancaMC Weigert EM Kohler CV et al (2006) Effect ofintervention to improve breastfeeding technique on thefrequency of exclusive breastfeeding and lactation-related problems Journal of Human Lactation 22 315ndash321
Perez-Escamilla R (2004) Effectiveness of MADLAC atImproving Breastfeeding Promotion and CounsellingIndicators in Maternity Wards in El Salvador Publishedfor the Basic Support for Institutionalizing Child Sur-vival Project (BASICS II) for the United States Agencyfor International Development Arlington VA Availableat httpwwwbasicsorgpdfFinal20MADLAC20Report20RPE20April207-2004pdf
Perez-Escamilla R (2007) Evidence based breast-feedingpromotion the Baby-Friendly Hospital InitiativeJournal of Nutrition 137 484ndash487
Piwoz EG Iliff PJ Tavengwa N Gavin L Marinda ELunney K et al (2005) An education and counselllingprogram for preventing breastfeeding associated HIVtransmission in Zimbabwe design and impact on mater-nal knowledge and behaviour Journal of Nutrition 135950ndash955
Quinn VJ Guyon AB Schubert JW Stone-Jimenez MHainsworth MD amp Martin LH (2005) Improvingbreastfeeding practices on a board scale at the commu-
nity level success stories from Africa and LatinAmerica Journal of Human Lactation 21 345ndash354
Ranson MK Hanson K Oliveira-Cruz V amp Mills A(2003) Constraints to expanding access to health inter-ventions an empirical analysis and country typologyJournal of International Development 15 15ndash40
Rea MF amp Berquo ES (1990) Impact of the Braziliannational breastfeeding programme on mothers inGreater Sao Paulo Bulletin of the of the World HealthOrganization 68 365ndash371
Rollins NC (2007) Infant feeding and HIV BritishMedical Journal 334 487ndash488
Rutenberg N Baek C Kalibala S Rosen J amp Mulenga D(2004) Evaluation of United Nations supported pilotprojects for the prevention of mother-to-child transmis-sion of HIV overview of findings International Confer-ence on AIDS 15 (WePeE6688)
The Core Group (2005) Scale and Scaling Up A COREGroup Background Paper on lsquoScaling-Uprsquo MaternalNewborn and Child Health Services CORE SpringMembership Meeting 2005 The Core Group Washing-ton DC Available at httpwwwcoregrouporgresourcesmeetingsapril05Scaling_Up_Background_Paper_7-13pdf
The Norwegian Government (1993) Women in PoliticsMinistry of Children and Equality Available at httpwwwregjeringennoendepbldRyddemappeSLA-AvdelingdoclegislationguidelinesWomen-in-Politicshtmlid=437166
Thior I Lockman S Smeaton LM Shapiro RL WesterC Heymann SJ et al (2006) Breastfeeding plus infantzidovudine prophylaxis for 6 months vs formula feedingplus infant zidovudine for 1 month to reduce mother-to-child HIV transmission in Botswana a randomized trialthe Mashi Study Journal of the American Medical Asso-ciation 296 794ndash805
UNICEF (2002) Facts for Life lsquoKey Message What EveryFamily and Community Has a Right to Know aboutBreastfeedingrsquo Available at httpwwwuniceforgffl04key_messageshtm
Van Roekel K Plowman B Griffiths M de AlvaradoVV Matute J amp Calderon M (2002) BASICS IIMidterm Evaluation of the AIN Program in Honduras2000 Basic Support for Institutionalizing Child SurvivalProject (BASICS II) for the United States Agency forInternational Development Arlington VA
WABA (2007) UNICEF Records BHFI Record UpdateAvailable at httpwwwwabaorgmydocsBFHIjan07xls 2006 Regularly updated by Miriam HLabbok Center for Infant and Young ChildFeeding and Care Department of Maternaland Child Health School of Public Health The Univer-sity of North Carolina at Chapel Hill Chapel Hill NCUSA
N Bhandari and AKMI Kabir16
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
WHA (2002) Infant and Young Child Nutrition Fifty-FifthWorld Health Assembly Agenda Item 1310 18 May2002 Available at httpwwwintgbebwhapdf_filesWHA55ewha5525pdf
WHO (1981) The International Code of Marketing ofBreastmilk Substitutes World Health OrganizationGeneva
WHO (1989) Protecting Promoting and Supporting Breast-feeding The Special Role of Maternity Services A JointWHOUNICEF Statement World Health OrganizationGeneva
WHO (2002) The Optimal Duration of Exclusive Breast-feeding Report of an Expert Consultation WHONHD0109 WHOFCHCAH0124 World HealthOrganization Geneva
WHO (2003a) Community Based Strategies for Breastfeed-ing Promotion and Support in Developing CountriesWorld Health Organization Geneva Document refISBN_92_4_159121_8 Available at httpwwwwhointchild-adolescent-healthNew_PublicationsNUTRITIONISBN_92_4_159121_8pdf
WHO (2003b) Multi-country Evaluation of IMCI Effective-ness Cost and Impact (MCE) Progress Report May2002ndashApril 2003 Document ref WHOFCHCAH035World Health Organization Geneva
WHO (2004) Promoting Proper Feeding for Infants andYoung Children World Health Organization GenevaAvailable at httpwwwwhointnutritiontopicsinfantfeedingen
WHO (2006) WHO HIV and Infant Feeding TechnicalConsultation-Consensus Statement World Health Orga-nization Geneva Available at httpwwwwhointhivmediacentreInfantfeedingconsensusstatementpfpdf
WHO Collaborative Study Team on the Role of Breast-feeding on the Prevention of Infant Mortality (2000)Effect of breastfeeding on infant and child mortality dueto infectious diseases in les developed countries apooled analysis Lancet 355 451ndash455
WHOUNICEF (1992) The global criteria for the WHOUNICEF Baby-Friendly Hospital Initiative In Baby-Friendly Hospital Initiative Part II Hospital LevelImplementation World Health Organization Geneva
WHOUNICEF (1993) Breastfeeding Counselling A Train-ing Course WHOCDR933 UNICEFNUT931 WorldHealth Organization Geneva
WHOUNICEF (2002) Protocol for Adapting the FeedingRecommendations Part III IMCI Adaptation GuideWorld Health Organization Geneva
WHOUNICEF (2003) Global Strategy for Infant andYoung Child Feeding World Health OrganizationGeneva Available at httpwwwwhointchild-adolescent-healthpublicationsNUTRITIONIYCF_GShtm
de Zoysa I Rea M amp Martines J (1991) Why promotebreastfeeding in diarrheal diseases control programmesHealth Policy and Planning 6 371ndash379
Mainstreaming nutrition into MCH programs 17
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
Cas
est
udie
so
fef
fect
iven
ess
stud
ies
or
pilo
tpr
ogra
mm
es
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Lut
ter
etal
(199
7)
Bra
zil
Low
-inc
ome
urba
nw
omen
deliv
erin
gin
hosp
ital
s
Bre
astf
eedi
ngpr
omot
ion
in
hosp
ital
sco
mpa
red
wit
h
nobr
east
feed
ing
prom
otio
n
Pro
mot
ion
ofbr
east
feed
ing
in
sele
cted
hosp
ital
s
Mea
nda
ysof
excl
usiv
e
brea
stfe
edin
g
75da
ysvs
22
days
(Plt
001
)
Rea
ampB
erqu
o
(199
0)
Wom
enw
ith
ach
ild
aged
lt2ye
ars
inSa
oP
aulo
Nat
iona
lbre
astf
eedi
ng
cam
paig
n19
81ndash1
986
BF
HI
Mas
sm
edia
cam
paig
n11
in
fant
s5ndash
6m
onth
s
excl
usiv
ely
brea
stfe
d
in19
88an
d37
in
1987
Con
foun
ding
fact
ors
over
the
6-ye
arpe
riod
not
mea
sure
d
Kra
mer
etal
(200
020
01)
PR
OB
ITtr
ial
Bel
arus
Clu
ster
rand
omiz
ed
34ho
spit
als
and
thei
rpo
lycl
inic
s
Trai
ning
inB
FH
I(W
HO
UN
ICE
F19
92)
vsr
outi
ne
prac
tice
san
dpo
licie
s
Exc
lusi
vebr
east
feed
ing
at3
(43
3vs
64
)
and
6(7
9
vs0
6
)
mon
ths
sign
ifica
ntly
high
er
Impl
emen
ted
thro
ugh
BF
HI
ina
sett
ing
whe
reho
spit
al
deliv
erie
sar
eco
mm
on
Per
ez-E
scam
illa
(200
4)
BA
SIC
SII
Mex
ico
Hon
dura
s
Bra
zil
MA
DL
AC
low
-cos
t
man
agem
ent
info
rmat
ion
syst
emto
use
an
evid
ence
-bas
edap
proa
chto
impr
ove
serv
ice
perf
orm
ance
Inte
rvie
win
gof
wom
enat
hosp
ital
disc
harg
epo
st
deliv
ery
usin
ga
ques
tion
nair
eth
atta
kes
5ndash7
min
toad
min
iste
ran
d
cont
ains
19br
east
feed
ing
prom
otio
nco
unse
lling
indi
cato
rs
Dat
aen
tere
dan
dre
sult
s
disc
usse
d3-
mon
thly
by
hosp
ital
com
mit
tee
Hos
pita
lim
plem
ents
chan
ges
in
brea
stfe
edin
g
supp
ort
base
don
anal
ysis
of
ques
tion
nair
es
Itis
aco
st-e
ffec
tive
inte
rven
tion
that
can
help
impr
ovem
ents
inth
eB
FH
I
and
isa
valu
able
tool
for
proc
ess
eval
uati
on
N Bhandari and AKMI Kabir18
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
LIN
KA
GE
S
proj
ect
inA
fric
aan
d
Lat
inA
mer
ica
(Qui
nnet
al
2005
LIN
KA
GE
S
2002
WH
O20
03a)
Bol
ivia
(1
mill
ion)
Gha
na(3
5
mill
ion)
Mad
agas
car
(6m
illio
n)
Res
ourc
e-
poor
sett
ing
Pilo
tpr
ogra
mm
e
InB
oliv
iaan
d
Gha
napr
ogra
mm
e
focu
sed
on
brea
stfe
edin
gan
d
com
plem
enta
ry
feed
ing
InM
adag
asca
r
prog
ram
me
prom
oted
brea
stfe
edin
g
wit
hin
7es
sent
ial
nutr
itio
nac
tion
san
d
subs
eque
ntly
thro
ugh
IMC
I
Bui
lton
form
ativ
ere
sear
ch
and
sust
aine
dth
roug
h
prog
ram
me
acti
viti
esth
at
focu
sed
onbr
ingi
ngab
out
the
desi
red
beha
viou
r
chan
geM
ixof
inte
rven
tion
s
reac
hed
wom
enin
divi
dual
ly
orin
grou
psin
heal
th
faci
litie
sho
mes
or
com
mun
ity
sett
ings
Con
sist
ent
mes
sage
san
d
mat
eria
lacr
oss
all
prog
ram
me
chan
nels
Bol
ivi
PR
OC
OSI
NG
Os
Gha
na
UN
ICE
F
nati
onal
nutr
itio
n
offic
eN
GO
s
Mad
agas
car
Inte
rsec
tora
l
Act
ion
Gro
upfo
r
Nut
riti
on
Jere
o
Sala
ma
Isik
a
Pro
gram
desi
gned
wit
h
part
ners
Rad
ioin
all
thre
esi
tes
Mat
eria
ls
deve
lope
d
tosu
itne
eds
oflo
cal
heal
th
wor
kers
and
com
mun
ity
mem
bers
Gre
at
emph
asis
on
deve
lopm
ent
of coun
selli
ng
and
nego
tiat
ion
skill
s
prac
tica
l
sess
ions
Sign
ifica
ntin
crea
ses
inex
clus
ive
brea
stfe
edin
gra
tes
of
0ndash6-
mon
th-o
ld
infa
nts
from
54
to65
in
Bol
ivia
68
to79
in
Gha
naan
d46
to68
in
Mad
agas
car
In
Gha
naan
d
Mad
agas
car
sign
ifica
ntre
sult
s
obse
rved
wit
hin
aye
ar
ofin
itia
tion
of
com
mun
ity
inte
rven
tion
s
App
roac
hw
asef
fect
ive
and
achi
eved
sign
ifica
nt
incr
ease
sam
ong
larg
e
popu
lati
ons
asea
rly
as
9ndash12
mo
afte
rin
itia
tion
of
com
mun
ity
acti
viti
es
Van
Roe
kele
tal
(200
2)W
HO
(200
3a)
Hon
dura
sG
row
thm
onit
orin
gan
d
prom
otio
nkn
own
as
Ate
ncioacute
nIn
tegr
ala
la
Nintilde
ez(A
IN)
or
Inte
grat
edC
hild
Car
e
Init
ially
pri
mar
ilya
grow
th
mon
itor
ing
prog
ram
me
ulti
mat
ely
thro
ugh
IMC
I
Pro
gram
me
ongr
owth
prom
otio
nndash
asse
ssm
ent
of
mon
thly
wei
ght
gain
and
focu
son
illne
ssf
eedi
ng
prac
tice
san
dge
nera
lchi
ld
care
inin
fant
sun
der
2ye
ars
Impl
emen
ted
atgo
vern
men
t
faci
litie
san
dco
mm
unit
y
Star
ted
in19
92s
tren
gthe
ned
in19
95ndash1
997
wit
hgr
eate
r
focu
son
child
feed
ing
In
1997
pro
gram
me
intr
oduc
ed
wit
hIM
CI
(WH
OU
NIC
EF
2002
)
Maj
or
part
ners
UN
ICE
F
PAH
O
Am
eric
an
and
Hon
dura
n
Red
Cro
ss
CA
RE
Rad
io
broa
dcas
ts
relig
ious
lead
ers
IMC
IM
id-t
erm
eval
uati
on
show
ed39
of
mot
hers
inin
terv
enti
on
com
mun
itie
sex
clus
ivel
y
brea
stfe
dco
mpa
red
wit
h13
in
the
cont
rol
site
s
Mainstreaming nutrition into MCH programs 19
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
cont
inue
d
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Bha
ndar
ieta
l
(200
3)
WH
O
(200
3a)
Rur
alco
mm
unit
ies
inH
arya
na
Indi
a
Clu
ster
rand
omiz
edtr
ial
8
com
mun
itie
s(t
otal
popu
lati
on~4
000
0)
Pro
mot
ion
ofex
clus
ive
brea
stfe
edin
gan
d
appr
opri
ate
com
plem
enta
ryfe
edin
g
Dev
elop
edth
roug
h
form
ativ
ere
sear
ch
ndashP
robl
emid
enti
ficat
ion
ndashP
arti
cipa
tory
desi
gnof
inte
rven
tion
impl
emen
tati
onan
d
eval
uati
on
Impl
emen
tati
onw
ithi
nan
exis
ting
prim
ary
heal
th-c
are
prog
ram
me
Opp
ortu
niti
esus
edto
deliv
erm
essa
ges
wer
e
imm
uniz
atio
ncl
inic
s
wei
ghin
gse
ssio
ns
sick
-chi
ldco
ntac
tsan
d
mon
thly
hom
evi
sits
Res
earc
hers
wit
hlo
cal
gove
rnm
ent
ICD
Ssy
stem
and
NG
O
The
atre
son
gs
Mas
sm
edia
not
used
for
risk
of
cont
amin
atio
n
Mat
eria
ls
deve
lope
d
for
heal
th
wor
kers
pos
ters
flip
book
sca
rds
Bre
astf
eedi
ng
coun
selli
ngse
ctio
n
ofth
eIM
CI
(WH
O
UN
ICE
F20
02)
Exc
lusi
ve
brea
stfe
edin
gin
the
prev
ious
24h
at3
mon
ths
of
age
79
vs4
8
The
posi
tive
effe
ct
rem
aine
dup
to
6m
onth
sof
age
(42
vs4
)
Tota
lpar
tici
pati
onof
the
dist
rict
heal
thsy
stem
from
ince
ptio
nof
the
prog
ram
me
inde
velo
ping
impl
emen
tati
onst
rate
gyt
ool
deve
lopm
ent
and
mon
itor
ing
inad
diti
onto
invo
lvem
ent
of
anN
GO
wer
eim
port
ant
feat
ures
that
cont
ribu
ted
to
the
succ
ess
ofth
e
inte
rven
tion
Mor
row
etal
(199
9)
Mex
ico
Cit
yC
lust
erra
ndom
ized
tria
l
Tota
lpop
ulat
ion
3000
0
Two
com
mun
itie
sin
the
inte
rven
tion
one
com
pari
son
130
wom
en
Hom
e-ba
sed
peer
coun
selli
ng
Pee
rco
unse
llors
mad
e3
or
6ho
me
visi
tsto
the
mot
her
Key
fam
ilym
embe
rsal
so
incl
uded
By
La
Lec
he
Lea
gue
of
Mex
ico
Exc
lusi
ve
brea
stfe
edin
g
at3
mon
ths
post
-par
tum
67
(6vi
sits
)
50
(3vi
sits
)12
(com
pari
son)
Firs
tcl
uste
rra
ndom
ized
com
mun
ity-
base
dtr
ialt
hat
used
peer
coun
sello
rsto
prom
ote
excl
usiv
e
brea
stfe
edin
g
Hai
der
etal
2000
200
2
Dha
ka
Low
mid
dle
and
low
-soc
io-
econ
omic
popu
lati
on
Clu
ster
rand
omiz
edtr
ial
20zo
nes
inin
terv
enti
on
and
20in
cont
rol
Com
mun
ity-
base
dpe
er
coun
selli
ngin
Dha
ka
15ho
me-
base
dco
unse
lling
visi
tsby
peer
coun
sello
rs
40h
(4h
yen10
days
)
WH
OU
NIC
EF
brea
stfe
edin
g
coun
selli
ngco
urse
(WH
OU
NIC
EF
1993
)
Exc
lusi
ve
brea
stfe
edin
g
at5
mon
ths
70
in
inte
rven
tion
and
6in
the
cont
rol
Com
mun
ity-
base
d
brea
stfe
edin
gpr
omot
ion
stra
tegy
was
effe
ctiv
ein
Ban
glad
esh
whe
rem
ost
deliv
erie
soc
cur
atho
me
N Bhandari and AKMI Kabir20
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Bry
ceet
al
(200
4)W
HO
(200
3b)
Bra
zil
Per
u
Tanz
ania
Uga
nda
Mul
tico
untr
yev
alua
tion
of
IMC
Ith
atin
clud
ed
effe
ctiv
enes
sco
stan
d
impa
ct(B
ryce
etal
2004
)
Bre
astf
eedi
ngpr
omot
ion
asa
part
ofIM
CI
IMC
Iis
ast
rate
gyfo
r
impr
ovin
gch
ildhe
alth
and
deve
lopm
ent
thro
ugh
the
com
bine
d
deliv
ery
ofes
sent
ial
child
heal
th
inte
rven
tion
sIM
CI
bega
nw
ith
ase
tof
case
man
agem
ent
guid
elin
es
for
the
man
agem
ent
ofsi
ckch
ildre
nat
first
-lev
elhe
alth
faci
litie
s
and
the
guid
elin
esw
ere
desi
gned
for
adap
tati
on
atco
untr
yle
vela
nd
belo
wO
ver
tim
eth
e
stra
tegy
expa
nded
to
incl
ude
ara
nge
of
guid
elin
esfo
rde
liver
ing
child
surv
ival
inte
rven
tion
at
hous
ehol
dco
mm
unit
y
and
refe
rral
leve
ls
IMC
Im
odul
e(W
HO
UN
ICE
F20
02)
Res
ults
onex
clus
ive
brea
stfe
edin
g
avai
labl
efr
om
Tanz
ania
whe
reno
sign
ifica
ntim
pact
was
seen
Des
pite
subs
tant
ial
impr
ovem
ent
inth
equ
alit
y
ofca
rede
liver
edby
IMC
Iat
heal
thfa
cilit
ies
key
fam
ily
prac
tice
ssu
chas
excl
usiv
e
brea
stfe
edin
gdi
dno
tch
ange
asco
mm
unit
yIM
CI
had
not
been
impl
emen
ted
byth
at
tim
e(W
HO
2003
b)
SA
rife
en
pers
onal
com
mun
icat
ion
Ban
glad
esh
Mat
lab
Com
mun
ity-
base
dcl
uste
r
desi
gn
Eva
luat
ion
offa
cilit
y-an
d
com
mun
ity-
base
dIM
CI
Inte
rven
tion
pack
age
incl
udes
feed
ing
asse
ssm
ent
and
coun
selli
ngon
mot
hers
ofyo
ung
child
ren
seek
ing
care
atfa
cilit
ies
for
illne
ssan
d
hom
e-ba
sed
coun
selli
ng
onim
prov
edfe
edin
gby
com
mun
ity-
base
dhe
alth
and
nutr
itio
nw
orke
rs
At
base
line
inth
e
year
2000
alit
tle
mor
eth
anha
lfth
e
0ndash5-
mon
th-o
ld
infa
nts
inth
est
udy
area
wer
ebe
ing
excl
usiv
ely
brea
stfe
dB
y20
05
this
incr
ease
dby
30
inth
eIM
CI
area
Dat
ano
t
avai
labl
efr
omth
e
com
pari
son
area
as
yet
Lac
kof
com
para
ble
data
from
the
com
pari
son
area
prev
ents
ade
finit
ive
conc
lusi
onas
tow
heth
erth
is
trul
yis
anim
pact
ofIM
CI
BA
SIC
SII
Bas
icSu
ppor
tfo
rIn
stit
utio
naliz
ing
Chi
ldSu
rviv
alP
roje
ctB
FH
IB
aby-
Frie
ndly
Hos
pita
lIni
tiat
ive
ICD
SIn
tegr
ated
Chi
ldD
evel
opm
ent
Serv
ices
IM
CI
Inte
grat
edM
anag
emen
tof
Chi
ldho
odIl
lnes
sM
AD
LA
CM
onit
oreo
deA
poyo
Dir
ecto
con
laL
acat
anci
aM
ater
naN
GO
non
-gov
ernm
enta
lorg
aniz
atio
nPA
HO
Pan
Am
eric
anH
ealt
hO
rgan
izat
ion
PR
OB
ITP
rom
otio
nof
Bre
astf
eedi
ngIn
terv
enti
onTr
ial
PR
OC
OSI
Pro
gram
ade
Coo
rdin
acio
nen
Salu
dIn
tegr
al(C
olla
bora
tive
Pro
gram
for
Inte
grat
edH
ealt
h)U
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
WH
OW
orld
Hea
lth
Org
aniz
atio
n
Mainstreaming nutrition into MCH programs 21
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x2
Cas
est
udie
sin
scal
e-up
effo
rts
inH
IVA
IDS
Stud
yde
scri
ptio
nPo
pula
tion
Inte
rven
tion
Com
mun
icat
ion
stra
tegy
Impa
cton
excl
usiv
ebr
east
feed
ing
Com
men
ts
LIN
KA
GE
S(2
005)
Zam
bia
Pro
gram
me
thro
ugh
heal
th-c
are
and
com
mun
ity
serv
ices
Rea
ched
60si
tes
in6
dist
rict
sby
2005
Inte
grat
ion
ofin
fant
feed
ing
coun
selli
ngm
ater
naln
utri
tion
and
anti
retr
ovir
aldr
ugs
prop
hyla
xis
Trai
ning
ofhe
alth
wor
kers
and
com
mun
ity
serv
ice
prov
ider
sto
coun
selw
omen
onsa
fety
opti
ons
for
thei
rsi
tuat
ion
Beh
avio
urch
ange
Com
mun
icat
ion
inte
rven
tion
sin
the
first
few
year
sM
ater
iald
evel
oped
lsquoAct
Now
rsquoM
edia
cam
paig
nsin
clud
edbr
ochu
res
post
ers
radi
oan
dte
levi
sion
Ass
esse
dth
roug
hba
selin
ean
dfo
llow
-up
hous
ehol
dan
dcl
inic
surv
eys
inse
lect
eddi
stri
cts
Exc
lusi
vebr
east
feed
ing
rate
incr
ease
dfr
om50
in
2002
to64
in
2004
inL
ivin
gsto
nean
dfr
om57
in
2000
to74
in
2004
inN
dola
Inte
grat
edde
mon
stra
tion
proj
ect
Had
seve
rals
tren
gths
inte
rms
ofth
eus
eof
form
ativ
ere
sear
chto
deve
lop
mes
sage
str
aini
ngan
dbu
ildin
gup
skill
sof
prog
ram
me
man
ager
she
alth
-car
epr
ovid
ers
and
com
mun
ity
wor
kers
adv
ocac
yfo
rna
tion
alpo
licy
stro
ngbe
havi
our
chan
geco
mm
unic
atio
nco
mpo
nent
st
reng
then
ing
com
mun
ity
capa
city
for
coun
selli
ngan
dre
ferr
als
and
mon
itor
ing
and
eval
uati
onw
ith
loca
lpar
tner
sP
iwoz
etal
(20
05)
ZV
ITA
MB
Otr
ial
Har
are
Zim
babw
eE
duca
tion
and
coun
selli
ngpr
ogra
mm
ede
liver
edan
tena
tally
1411
0m
othe
rndashba
bypa
irs
enro
lled
from
14m
ater
nity
clin
ics
wit
hin
96h
ofde
liver
yan
dfo
llow
edup
at6
wee
ks
3m
onth
san
d3-
mon
thly
inte
rval
sIn
fant
-fee
ding
patt
erns
dete
rmin
edE
xclu
sive
brea
stfe
edin
gre
com
men
ded
for
HIV
nega
tive
un
know
nor
HIV
posi
tive
who
chos
eto
brea
stfe
ed
Gro
uped
ucat
ion
indi
vidu
alco
unse
lling
vid
eos
broc
hure
sM
othe
rsw
hoen
rolle
dw
hen
prog
ram
me
was
fully
impl
emen
ted
wer
e8
4ti
mes
mor
elik
ely
toex
clus
ivel
ybr
east
feed
than
mot
hers
who
enro
lled
befo
reth
epr
ogra
mm
ebe
gan
Ove
rall
excl
usiv
ebr
east
feed
ing
rate
sti
ll3
mon
ths
was
low
at24
6
Form
ativ
ere
sear
chus
edto
desi
gna
cult
ural
lyse
nsit
ive
educ
atio
nan
dco
unse
lling
prog
ram
me
Low
over
alle
xclu
sive
brea
stfe
edin
gra
tes
prom
pted
auth
ors
toco
nclu
deth
atw
omen
and
thei
rpa
rtne
rssh
ould
have
been
reac
hed
mor
efr
eque
ntly
duri
ngan
tena
tala
ndpo
st-n
atal
peri
od
N Bhandari and AKMI Kabir22
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Thi
oret
al(
2006
)R
ollin
s(2
007)
C
ohen
(200
7)
HIV
-inf
ecte
dpr
egna
ntw
omen
atte
ndin
gan
tena
talc
linic
sin
sout
hB
otsw
ana
Inve
stig
atio
nsby
CD
Cof
adi
arrh
oea
outb
reak
inJa
nuar
y-Fe
brua
ry20
06in
the
sam
epo
pula
tion
Mat
erna
land
infa
ntan
tire
trov
iral
ther
apy
toas
cert
ain
impa
cton
HIV
tran
smis
sion
Ant
enat
alco
unse
lling
Cas
endashco
ntro
lstu
dyto
iden
tify
risk
fact
ors
for
diar
rhoe
ano
tbr
east
feed
ing
was
the
bigg
est
risk
fact
ora
djus
ted
odds
rati
o50
(95
confi
denc
ein
terv
al4
5ndash10
0)
Bot
swan
aha
sth
ebe
stpr
imar
yhe
alth
-car
est
ruct
ure
wat
ersu
pply
and
sani
tati
onsy
stem
sin
Sout
hA
fric
aFo
rmul
apr
ovid
edfr
eeby
the
gove
rnm
ent
toin
fect
edm
othe
rsL
ower
mor
talit
yin
the
brea
stfe
edin
ggr
oup
at7
mon
ths
dem
onst
rate
sri
skof
form
ula
feed
ing
and
need
for
alte
rnat
est
rate
gies
(Thi
oret
al
2006
)A
utho
rsco
nclu
deth
athe
alth
syst
ems
inw
hich
thes
epr
ogra
mm
esar
eim
plem
ente
dsh
ould
beab
leto
cope
wit
hdi
arrh
oea
and
mal
nutr
itio
nth
atre
sult
sbe
caus
eof
form
ula
feed
ing
(Rol
lins
2007
)C
oova
dia
etal
(2
007)
Kw
aZul
uNat
al
Sout
hA
fric
a27
22H
IV-i
nfec
ted
and
unin
fect
edpr
egna
ntw
omen
enro
lled
into
ano
n-ra
ndom
ized
inte
rven
tion
coho
rtst
udy
from
ante
nata
lcl
inic
sIn
fant
feed
ing
data
obta
ined
wee
kly
bloo
dsa
mpl
esfr
omin
fant
sta
ken
mon
thly
83
of13
72in
fant
sbo
rnto
HIV
-inf
ecte
dm
othe
rsin
itia
ted
excl
usiv
ebr
east
feed
ing
from
birt
hB
reas
tfed
infa
nts
who
rece
ived
solid
sw
ere
sign
ifica
ntly
mor
elik
ely
toac
quir
ein
fect
ion
com
pare
dw
ith
excl
usiv
ely
brea
stfe
d(H
R10
87
151
ndash78
P=
001
8)as
wer
ein
fant
sw
hoat
12w
eeks
rece
ived
brea
stan
dfo
rmul
am
ilk(1
82
098
ndash33
6P
=0
57)
Cum
ulat
ive
3-m
onth
mor
talit
yin
excl
usiv
ely
brea
stfe
dw
as6
1(4
74ndash
792
)vs
15
1(7
63ndash
287
3)in
infa
nts
give
nre
plac
emen
tfe
eds
(HR
206
1
0ndash4
27P
=0
05)
The
stud
ysh
ows
that
excl
usiv
ebr
east
feed
ing
can
besu
cces
sful
lysu
ppor
ted
inH
IV-i
nfec
ted
wom
enT
heau
thor
sca
llfo
rfu
rthe
rre
visi
onof
UN
ICE
FW
HO
and
USA
IDin
fant
feed
ing
guid
elin
es
CD
CC
ente
rof
Dis
ease
Con
trol
HR
haz
ards
rati
oU
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
USA
IDU
SA
genc
yfo
rIn
tern
atio
nalD
evel
opm
ent
WH
OW
orld
Hea
lth
Org
aniz
atio
nZ
VIT
AM
BO
Z
imba
bwe
Vit
amin
Afo
rM
othe
rsan
dB
abie
s
Mainstreaming nutrition into MCH programs 23
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
WHA (2002) Infant and Young Child Nutrition Fifty-FifthWorld Health Assembly Agenda Item 1310 18 May2002 Available at httpwwwintgbebwhapdf_filesWHA55ewha5525pdf
WHO (1981) The International Code of Marketing ofBreastmilk Substitutes World Health OrganizationGeneva
WHO (1989) Protecting Promoting and Supporting Breast-feeding The Special Role of Maternity Services A JointWHOUNICEF Statement World Health OrganizationGeneva
WHO (2002) The Optimal Duration of Exclusive Breast-feeding Report of an Expert Consultation WHONHD0109 WHOFCHCAH0124 World HealthOrganization Geneva
WHO (2003a) Community Based Strategies for Breastfeed-ing Promotion and Support in Developing CountriesWorld Health Organization Geneva Document refISBN_92_4_159121_8 Available at httpwwwwhointchild-adolescent-healthNew_PublicationsNUTRITIONISBN_92_4_159121_8pdf
WHO (2003b) Multi-country Evaluation of IMCI Effective-ness Cost and Impact (MCE) Progress Report May2002ndashApril 2003 Document ref WHOFCHCAH035World Health Organization Geneva
WHO (2004) Promoting Proper Feeding for Infants andYoung Children World Health Organization GenevaAvailable at httpwwwwhointnutritiontopicsinfantfeedingen
WHO (2006) WHO HIV and Infant Feeding TechnicalConsultation-Consensus Statement World Health Orga-nization Geneva Available at httpwwwwhointhivmediacentreInfantfeedingconsensusstatementpfpdf
WHO Collaborative Study Team on the Role of Breast-feeding on the Prevention of Infant Mortality (2000)Effect of breastfeeding on infant and child mortality dueto infectious diseases in les developed countries apooled analysis Lancet 355 451ndash455
WHOUNICEF (1992) The global criteria for the WHOUNICEF Baby-Friendly Hospital Initiative In Baby-Friendly Hospital Initiative Part II Hospital LevelImplementation World Health Organization Geneva
WHOUNICEF (1993) Breastfeeding Counselling A Train-ing Course WHOCDR933 UNICEFNUT931 WorldHealth Organization Geneva
WHOUNICEF (2002) Protocol for Adapting the FeedingRecommendations Part III IMCI Adaptation GuideWorld Health Organization Geneva
WHOUNICEF (2003) Global Strategy for Infant andYoung Child Feeding World Health OrganizationGeneva Available at httpwwwwhointchild-adolescent-healthpublicationsNUTRITIONIYCF_GShtm
de Zoysa I Rea M amp Martines J (1991) Why promotebreastfeeding in diarrheal diseases control programmesHealth Policy and Planning 6 371ndash379
Mainstreaming nutrition into MCH programs 17
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
Cas
est
udie
so
fef
fect
iven
ess
stud
ies
or
pilo
tpr
ogra
mm
es
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Lut
ter
etal
(199
7)
Bra
zil
Low
-inc
ome
urba
nw
omen
deliv
erin
gin
hosp
ital
s
Bre
astf
eedi
ngpr
omot
ion
in
hosp
ital
sco
mpa
red
wit
h
nobr
east
feed
ing
prom
otio
n
Pro
mot
ion
ofbr
east
feed
ing
in
sele
cted
hosp
ital
s
Mea
nda
ysof
excl
usiv
e
brea
stfe
edin
g
75da
ysvs
22
days
(Plt
001
)
Rea
ampB
erqu
o
(199
0)
Wom
enw
ith
ach
ild
aged
lt2ye
ars
inSa
oP
aulo
Nat
iona
lbre
astf
eedi
ng
cam
paig
n19
81ndash1
986
BF
HI
Mas
sm
edia
cam
paig
n11
in
fant
s5ndash
6m
onth
s
excl
usiv
ely
brea
stfe
d
in19
88an
d37
in
1987
Con
foun
ding
fact
ors
over
the
6-ye
arpe
riod
not
mea
sure
d
Kra
mer
etal
(200
020
01)
PR
OB
ITtr
ial
Bel
arus
Clu
ster
rand
omiz
ed
34ho
spit
als
and
thei
rpo
lycl
inic
s
Trai
ning
inB
FH
I(W
HO
UN
ICE
F19
92)
vsr
outi
ne
prac
tice
san
dpo
licie
s
Exc
lusi
vebr
east
feed
ing
at3
(43
3vs
64
)
and
6(7
9
vs0
6
)
mon
ths
sign
ifica
ntly
high
er
Impl
emen
ted
thro
ugh
BF
HI
ina
sett
ing
whe
reho
spit
al
deliv
erie
sar
eco
mm
on
Per
ez-E
scam
illa
(200
4)
BA
SIC
SII
Mex
ico
Hon
dura
s
Bra
zil
MA
DL
AC
low
-cos
t
man
agem
ent
info
rmat
ion
syst
emto
use
an
evid
ence
-bas
edap
proa
chto
impr
ove
serv
ice
perf
orm
ance
Inte
rvie
win
gof
wom
enat
hosp
ital
disc
harg
epo
st
deliv
ery
usin
ga
ques
tion
nair
eth
atta
kes
5ndash7
min
toad
min
iste
ran
d
cont
ains
19br
east
feed
ing
prom
otio
nco
unse
lling
indi
cato
rs
Dat
aen
tere
dan
dre
sult
s
disc
usse
d3-
mon
thly
by
hosp
ital
com
mit
tee
Hos
pita
lim
plem
ents
chan
ges
in
brea
stfe
edin
g
supp
ort
base
don
anal
ysis
of
ques
tion
nair
es
Itis
aco
st-e
ffec
tive
inte
rven
tion
that
can
help
impr
ovem
ents
inth
eB
FH
I
and
isa
valu
able
tool
for
proc
ess
eval
uati
on
N Bhandari and AKMI Kabir18
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
LIN
KA
GE
S
proj
ect
inA
fric
aan
d
Lat
inA
mer
ica
(Qui
nnet
al
2005
LIN
KA
GE
S
2002
WH
O20
03a)
Bol
ivia
(1
mill
ion)
Gha
na(3
5
mill
ion)
Mad
agas
car
(6m
illio
n)
Res
ourc
e-
poor
sett
ing
Pilo
tpr
ogra
mm
e
InB
oliv
iaan
d
Gha
napr
ogra
mm
e
focu
sed
on
brea
stfe
edin
gan
d
com
plem
enta
ry
feed
ing
InM
adag
asca
r
prog
ram
me
prom
oted
brea
stfe
edin
g
wit
hin
7es
sent
ial
nutr
itio
nac
tion
san
d
subs
eque
ntly
thro
ugh
IMC
I
Bui
lton
form
ativ
ere
sear
ch
and
sust
aine
dth
roug
h
prog
ram
me
acti
viti
esth
at
focu
sed
onbr
ingi
ngab
out
the
desi
red
beha
viou
r
chan
geM
ixof
inte
rven
tion
s
reac
hed
wom
enin
divi
dual
ly
orin
grou
psin
heal
th
faci
litie
sho
mes
or
com
mun
ity
sett
ings
Con
sist
ent
mes
sage
san
d
mat
eria
lacr
oss
all
prog
ram
me
chan
nels
Bol
ivi
PR
OC
OSI
NG
Os
Gha
na
UN
ICE
F
nati
onal
nutr
itio
n
offic
eN
GO
s
Mad
agas
car
Inte
rsec
tora
l
Act
ion
Gro
upfo
r
Nut
riti
on
Jere
o
Sala
ma
Isik
a
Pro
gram
desi
gned
wit
h
part
ners
Rad
ioin
all
thre
esi
tes
Mat
eria
ls
deve
lope
d
tosu
itne
eds
oflo
cal
heal
th
wor
kers
and
com
mun
ity
mem
bers
Gre
at
emph
asis
on
deve
lopm
ent
of coun
selli
ng
and
nego
tiat
ion
skill
s
prac
tica
l
sess
ions
Sign
ifica
ntin
crea
ses
inex
clus
ive
brea
stfe
edin
gra
tes
of
0ndash6-
mon
th-o
ld
infa
nts
from
54
to65
in
Bol
ivia
68
to79
in
Gha
naan
d46
to68
in
Mad
agas
car
In
Gha
naan
d
Mad
agas
car
sign
ifica
ntre
sult
s
obse
rved
wit
hin
aye
ar
ofin
itia
tion
of
com
mun
ity
inte
rven
tion
s
App
roac
hw
asef
fect
ive
and
achi
eved
sign
ifica
nt
incr
ease
sam
ong
larg
e
popu
lati
ons
asea
rly
as
9ndash12
mo
afte
rin
itia
tion
of
com
mun
ity
acti
viti
es
Van
Roe
kele
tal
(200
2)W
HO
(200
3a)
Hon
dura
sG
row
thm
onit
orin
gan
d
prom
otio
nkn
own
as
Ate
ncioacute
nIn
tegr
ala
la
Nintilde
ez(A
IN)
or
Inte
grat
edC
hild
Car
e
Init
ially
pri
mar
ilya
grow
th
mon
itor
ing
prog
ram
me
ulti
mat
ely
thro
ugh
IMC
I
Pro
gram
me
ongr
owth
prom
otio
nndash
asse
ssm
ent
of
mon
thly
wei
ght
gain
and
focu
son
illne
ssf
eedi
ng
prac
tice
san
dge
nera
lchi
ld
care
inin
fant
sun
der
2ye
ars
Impl
emen
ted
atgo
vern
men
t
faci
litie
san
dco
mm
unit
y
Star
ted
in19
92s
tren
gthe
ned
in19
95ndash1
997
wit
hgr
eate
r
focu
son
child
feed
ing
In
1997
pro
gram
me
intr
oduc
ed
wit
hIM
CI
(WH
OU
NIC
EF
2002
)
Maj
or
part
ners
UN
ICE
F
PAH
O
Am
eric
an
and
Hon
dura
n
Red
Cro
ss
CA
RE
Rad
io
broa
dcas
ts
relig
ious
lead
ers
IMC
IM
id-t
erm
eval
uati
on
show
ed39
of
mot
hers
inin
terv
enti
on
com
mun
itie
sex
clus
ivel
y
brea
stfe
dco
mpa
red
wit
h13
in
the
cont
rol
site
s
Mainstreaming nutrition into MCH programs 19
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
cont
inue
d
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Bha
ndar
ieta
l
(200
3)
WH
O
(200
3a)
Rur
alco
mm
unit
ies
inH
arya
na
Indi
a
Clu
ster
rand
omiz
edtr
ial
8
com
mun
itie
s(t
otal
popu
lati
on~4
000
0)
Pro
mot
ion
ofex
clus
ive
brea
stfe
edin
gan
d
appr
opri
ate
com
plem
enta
ryfe
edin
g
Dev
elop
edth
roug
h
form
ativ
ere
sear
ch
ndashP
robl
emid
enti
ficat
ion
ndashP
arti
cipa
tory
desi
gnof
inte
rven
tion
impl
emen
tati
onan
d
eval
uati
on
Impl
emen
tati
onw
ithi
nan
exis
ting
prim
ary
heal
th-c
are
prog
ram
me
Opp
ortu
niti
esus
edto
deliv
erm
essa
ges
wer
e
imm
uniz
atio
ncl
inic
s
wei
ghin
gse
ssio
ns
sick
-chi
ldco
ntac
tsan
d
mon
thly
hom
evi
sits
Res
earc
hers
wit
hlo
cal
gove
rnm
ent
ICD
Ssy
stem
and
NG
O
The
atre
son
gs
Mas
sm
edia
not
used
for
risk
of
cont
amin
atio
n
Mat
eria
ls
deve
lope
d
for
heal
th
wor
kers
pos
ters
flip
book
sca
rds
Bre
astf
eedi
ng
coun
selli
ngse
ctio
n
ofth
eIM
CI
(WH
O
UN
ICE
F20
02)
Exc
lusi
ve
brea
stfe
edin
gin
the
prev
ious
24h
at3
mon
ths
of
age
79
vs4
8
The
posi
tive
effe
ct
rem
aine
dup
to
6m
onth
sof
age
(42
vs4
)
Tota
lpar
tici
pati
onof
the
dist
rict
heal
thsy
stem
from
ince
ptio
nof
the
prog
ram
me
inde
velo
ping
impl
emen
tati
onst
rate
gyt
ool
deve
lopm
ent
and
mon
itor
ing
inad
diti
onto
invo
lvem
ent
of
anN
GO
wer
eim
port
ant
feat
ures
that
cont
ribu
ted
to
the
succ
ess
ofth
e
inte
rven
tion
Mor
row
etal
(199
9)
Mex
ico
Cit
yC
lust
erra
ndom
ized
tria
l
Tota
lpop
ulat
ion
3000
0
Two
com
mun
itie
sin
the
inte
rven
tion
one
com
pari
son
130
wom
en
Hom
e-ba
sed
peer
coun
selli
ng
Pee
rco
unse
llors
mad
e3
or
6ho
me
visi
tsto
the
mot
her
Key
fam
ilym
embe
rsal
so
incl
uded
By
La
Lec
he
Lea
gue
of
Mex
ico
Exc
lusi
ve
brea
stfe
edin
g
at3
mon
ths
post
-par
tum
67
(6vi
sits
)
50
(3vi
sits
)12
(com
pari
son)
Firs
tcl
uste
rra
ndom
ized
com
mun
ity-
base
dtr
ialt
hat
used
peer
coun
sello
rsto
prom
ote
excl
usiv
e
brea
stfe
edin
g
Hai
der
etal
2000
200
2
Dha
ka
Low
mid
dle
and
low
-soc
io-
econ
omic
popu
lati
on
Clu
ster
rand
omiz
edtr
ial
20zo
nes
inin
terv
enti
on
and
20in
cont
rol
Com
mun
ity-
base
dpe
er
coun
selli
ngin
Dha
ka
15ho
me-
base
dco
unse
lling
visi
tsby
peer
coun
sello
rs
40h
(4h
yen10
days
)
WH
OU
NIC
EF
brea
stfe
edin
g
coun
selli
ngco
urse
(WH
OU
NIC
EF
1993
)
Exc
lusi
ve
brea
stfe
edin
g
at5
mon
ths
70
in
inte
rven
tion
and
6in
the
cont
rol
Com
mun
ity-
base
d
brea
stfe
edin
gpr
omot
ion
stra
tegy
was
effe
ctiv
ein
Ban
glad
esh
whe
rem
ost
deliv
erie
soc
cur
atho
me
N Bhandari and AKMI Kabir20
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Bry
ceet
al
(200
4)W
HO
(200
3b)
Bra
zil
Per
u
Tanz
ania
Uga
nda
Mul
tico
untr
yev
alua
tion
of
IMC
Ith
atin
clud
ed
effe
ctiv
enes
sco
stan
d
impa
ct(B
ryce
etal
2004
)
Bre
astf
eedi
ngpr
omot
ion
asa
part
ofIM
CI
IMC
Iis
ast
rate
gyfo
r
impr
ovin
gch
ildhe
alth
and
deve
lopm
ent
thro
ugh
the
com
bine
d
deliv
ery
ofes
sent
ial
child
heal
th
inte
rven
tion
sIM
CI
bega
nw
ith
ase
tof
case
man
agem
ent
guid
elin
es
for
the
man
agem
ent
ofsi
ckch
ildre
nat
first
-lev
elhe
alth
faci
litie
s
and
the
guid
elin
esw
ere
desi
gned
for
adap
tati
on
atco
untr
yle
vela
nd
belo
wO
ver
tim
eth
e
stra
tegy
expa
nded
to
incl
ude
ara
nge
of
guid
elin
esfo
rde
liver
ing
child
surv
ival
inte
rven
tion
at
hous
ehol
dco
mm
unit
y
and
refe
rral
leve
ls
IMC
Im
odul
e(W
HO
UN
ICE
F20
02)
Res
ults
onex
clus
ive
brea
stfe
edin
g
avai
labl
efr
om
Tanz
ania
whe
reno
sign
ifica
ntim
pact
was
seen
Des
pite
subs
tant
ial
impr
ovem
ent
inth
equ
alit
y
ofca
rede
liver
edby
IMC
Iat
heal
thfa
cilit
ies
key
fam
ily
prac
tice
ssu
chas
excl
usiv
e
brea
stfe
edin
gdi
dno
tch
ange
asco
mm
unit
yIM
CI
had
not
been
impl
emen
ted
byth
at
tim
e(W
HO
2003
b)
SA
rife
en
pers
onal
com
mun
icat
ion
Ban
glad
esh
Mat
lab
Com
mun
ity-
base
dcl
uste
r
desi
gn
Eva
luat
ion
offa
cilit
y-an
d
com
mun
ity-
base
dIM
CI
Inte
rven
tion
pack
age
incl
udes
feed
ing
asse
ssm
ent
and
coun
selli
ngon
mot
hers
ofyo
ung
child
ren
seek
ing
care
atfa
cilit
ies
for
illne
ssan
d
hom
e-ba
sed
coun
selli
ng
onim
prov
edfe
edin
gby
com
mun
ity-
base
dhe
alth
and
nutr
itio
nw
orke
rs
At
base
line
inth
e
year
2000
alit
tle
mor
eth
anha
lfth
e
0ndash5-
mon
th-o
ld
infa
nts
inth
est
udy
area
wer
ebe
ing
excl
usiv
ely
brea
stfe
dB
y20
05
this
incr
ease
dby
30
inth
eIM
CI
area
Dat
ano
t
avai
labl
efr
omth
e
com
pari
son
area
as
yet
Lac
kof
com
para
ble
data
from
the
com
pari
son
area
prev
ents
ade
finit
ive
conc
lusi
onas
tow
heth
erth
is
trul
yis
anim
pact
ofIM
CI
BA
SIC
SII
Bas
icSu
ppor
tfo
rIn
stit
utio
naliz
ing
Chi
ldSu
rviv
alP
roje
ctB
FH
IB
aby-
Frie
ndly
Hos
pita
lIni
tiat
ive
ICD
SIn
tegr
ated
Chi
ldD
evel
opm
ent
Serv
ices
IM
CI
Inte
grat
edM
anag
emen
tof
Chi
ldho
odIl
lnes
sM
AD
LA
CM
onit
oreo
deA
poyo
Dir
ecto
con
laL
acat
anci
aM
ater
naN
GO
non
-gov
ernm
enta
lorg
aniz
atio
nPA
HO
Pan
Am
eric
anH
ealt
hO
rgan
izat
ion
PR
OB
ITP
rom
otio
nof
Bre
astf
eedi
ngIn
terv
enti
onTr
ial
PR
OC
OSI
Pro
gram
ade
Coo
rdin
acio
nen
Salu
dIn
tegr
al(C
olla
bora
tive
Pro
gram
for
Inte
grat
edH
ealt
h)U
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
WH
OW
orld
Hea
lth
Org
aniz
atio
n
Mainstreaming nutrition into MCH programs 21
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x2
Cas
est
udie
sin
scal
e-up
effo
rts
inH
IVA
IDS
Stud
yde
scri
ptio
nPo
pula
tion
Inte
rven
tion
Com
mun
icat
ion
stra
tegy
Impa
cton
excl
usiv
ebr
east
feed
ing
Com
men
ts
LIN
KA
GE
S(2
005)
Zam
bia
Pro
gram
me
thro
ugh
heal
th-c
are
and
com
mun
ity
serv
ices
Rea
ched
60si
tes
in6
dist
rict
sby
2005
Inte
grat
ion
ofin
fant
feed
ing
coun
selli
ngm
ater
naln
utri
tion
and
anti
retr
ovir
aldr
ugs
prop
hyla
xis
Trai
ning
ofhe
alth
wor
kers
and
com
mun
ity
serv
ice
prov
ider
sto
coun
selw
omen
onsa
fety
opti
ons
for
thei
rsi
tuat
ion
Beh
avio
urch
ange
Com
mun
icat
ion
inte
rven
tion
sin
the
first
few
year
sM
ater
iald
evel
oped
lsquoAct
Now
rsquoM
edia
cam
paig
nsin
clud
edbr
ochu
res
post
ers
radi
oan
dte
levi
sion
Ass
esse
dth
roug
hba
selin
ean
dfo
llow
-up
hous
ehol
dan
dcl
inic
surv
eys
inse
lect
eddi
stri
cts
Exc
lusi
vebr
east
feed
ing
rate
incr
ease
dfr
om50
in
2002
to64
in
2004
inL
ivin
gsto
nean
dfr
om57
in
2000
to74
in
2004
inN
dola
Inte
grat
edde
mon
stra
tion
proj
ect
Had
seve
rals
tren
gths
inte
rms
ofth
eus
eof
form
ativ
ere
sear
chto
deve
lop
mes
sage
str
aini
ngan
dbu
ildin
gup
skill
sof
prog
ram
me
man
ager
she
alth
-car
epr
ovid
ers
and
com
mun
ity
wor
kers
adv
ocac
yfo
rna
tion
alpo
licy
stro
ngbe
havi
our
chan
geco
mm
unic
atio
nco
mpo
nent
st
reng
then
ing
com
mun
ity
capa
city
for
coun
selli
ngan
dre
ferr
als
and
mon
itor
ing
and
eval
uati
onw
ith
loca
lpar
tner
sP
iwoz
etal
(20
05)
ZV
ITA
MB
Otr
ial
Har
are
Zim
babw
eE
duca
tion
and
coun
selli
ngpr
ogra
mm
ede
liver
edan
tena
tally
1411
0m
othe
rndashba
bypa
irs
enro
lled
from
14m
ater
nity
clin
ics
wit
hin
96h
ofde
liver
yan
dfo
llow
edup
at6
wee
ks
3m
onth
san
d3-
mon
thly
inte
rval
sIn
fant
-fee
ding
patt
erns
dete
rmin
edE
xclu
sive
brea
stfe
edin
gre
com
men
ded
for
HIV
nega
tive
un
know
nor
HIV
posi
tive
who
chos
eto
brea
stfe
ed
Gro
uped
ucat
ion
indi
vidu
alco
unse
lling
vid
eos
broc
hure
sM
othe
rsw
hoen
rolle
dw
hen
prog
ram
me
was
fully
impl
emen
ted
wer
e8
4ti
mes
mor
elik
ely
toex
clus
ivel
ybr
east
feed
than
mot
hers
who
enro
lled
befo
reth
epr
ogra
mm
ebe
gan
Ove
rall
excl
usiv
ebr
east
feed
ing
rate
sti
ll3
mon
ths
was
low
at24
6
Form
ativ
ere
sear
chus
edto
desi
gna
cult
ural
lyse
nsit
ive
educ
atio
nan
dco
unse
lling
prog
ram
me
Low
over
alle
xclu
sive
brea
stfe
edin
gra
tes
prom
pted
auth
ors
toco
nclu
deth
atw
omen
and
thei
rpa
rtne
rssh
ould
have
been
reac
hed
mor
efr
eque
ntly
duri
ngan
tena
tala
ndpo
st-n
atal
peri
od
N Bhandari and AKMI Kabir22
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Thi
oret
al(
2006
)R
ollin
s(2
007)
C
ohen
(200
7)
HIV
-inf
ecte
dpr
egna
ntw
omen
atte
ndin
gan
tena
talc
linic
sin
sout
hB
otsw
ana
Inve
stig
atio
nsby
CD
Cof
adi
arrh
oea
outb
reak
inJa
nuar
y-Fe
brua
ry20
06in
the
sam
epo
pula
tion
Mat
erna
land
infa
ntan
tire
trov
iral
ther
apy
toas
cert
ain
impa
cton
HIV
tran
smis
sion
Ant
enat
alco
unse
lling
Cas
endashco
ntro
lstu
dyto
iden
tify
risk
fact
ors
for
diar
rhoe
ano
tbr
east
feed
ing
was
the
bigg
est
risk
fact
ora
djus
ted
odds
rati
o50
(95
confi
denc
ein
terv
al4
5ndash10
0)
Bot
swan
aha
sth
ebe
stpr
imar
yhe
alth
-car
est
ruct
ure
wat
ersu
pply
and
sani
tati
onsy
stem
sin
Sout
hA
fric
aFo
rmul
apr
ovid
edfr
eeby
the
gove
rnm
ent
toin
fect
edm
othe
rsL
ower
mor
talit
yin
the
brea
stfe
edin
ggr
oup
at7
mon
ths
dem
onst
rate
sri
skof
form
ula
feed
ing
and
need
for
alte
rnat
est
rate
gies
(Thi
oret
al
2006
)A
utho
rsco
nclu
deth
athe
alth
syst
ems
inw
hich
thes
epr
ogra
mm
esar
eim
plem
ente
dsh
ould
beab
leto
cope
wit
hdi
arrh
oea
and
mal
nutr
itio
nth
atre
sult
sbe
caus
eof
form
ula
feed
ing
(Rol
lins
2007
)C
oova
dia
etal
(2
007)
Kw
aZul
uNat
al
Sout
hA
fric
a27
22H
IV-i
nfec
ted
and
unin
fect
edpr
egna
ntw
omen
enro
lled
into
ano
n-ra
ndom
ized
inte
rven
tion
coho
rtst
udy
from
ante
nata
lcl
inic
sIn
fant
feed
ing
data
obta
ined
wee
kly
bloo
dsa
mpl
esfr
omin
fant
sta
ken
mon
thly
83
of13
72in
fant
sbo
rnto
HIV
-inf
ecte
dm
othe
rsin
itia
ted
excl
usiv
ebr
east
feed
ing
from
birt
hB
reas
tfed
infa
nts
who
rece
ived
solid
sw
ere
sign
ifica
ntly
mor
elik
ely
toac
quir
ein
fect
ion
com
pare
dw
ith
excl
usiv
ely
brea
stfe
d(H
R10
87
151
ndash78
P=
001
8)as
wer
ein
fant
sw
hoat
12w
eeks
rece
ived
brea
stan
dfo
rmul
am
ilk(1
82
098
ndash33
6P
=0
57)
Cum
ulat
ive
3-m
onth
mor
talit
yin
excl
usiv
ely
brea
stfe
dw
as6
1(4
74ndash
792
)vs
15
1(7
63ndash
287
3)in
infa
nts
give
nre
plac
emen
tfe
eds
(HR
206
1
0ndash4
27P
=0
05)
The
stud
ysh
ows
that
excl
usiv
ebr
east
feed
ing
can
besu
cces
sful
lysu
ppor
ted
inH
IV-i
nfec
ted
wom
enT
heau
thor
sca
llfo
rfu
rthe
rre
visi
onof
UN
ICE
FW
HO
and
USA
IDin
fant
feed
ing
guid
elin
es
CD
CC
ente
rof
Dis
ease
Con
trol
HR
haz
ards
rati
oU
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
USA
IDU
SA
genc
yfo
rIn
tern
atio
nalD
evel
opm
ent
WH
OW
orld
Hea
lth
Org
aniz
atio
nZ
VIT
AM
BO
Z
imba
bwe
Vit
amin
Afo
rM
othe
rsan
dB
abie
s
Mainstreaming nutrition into MCH programs 23
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
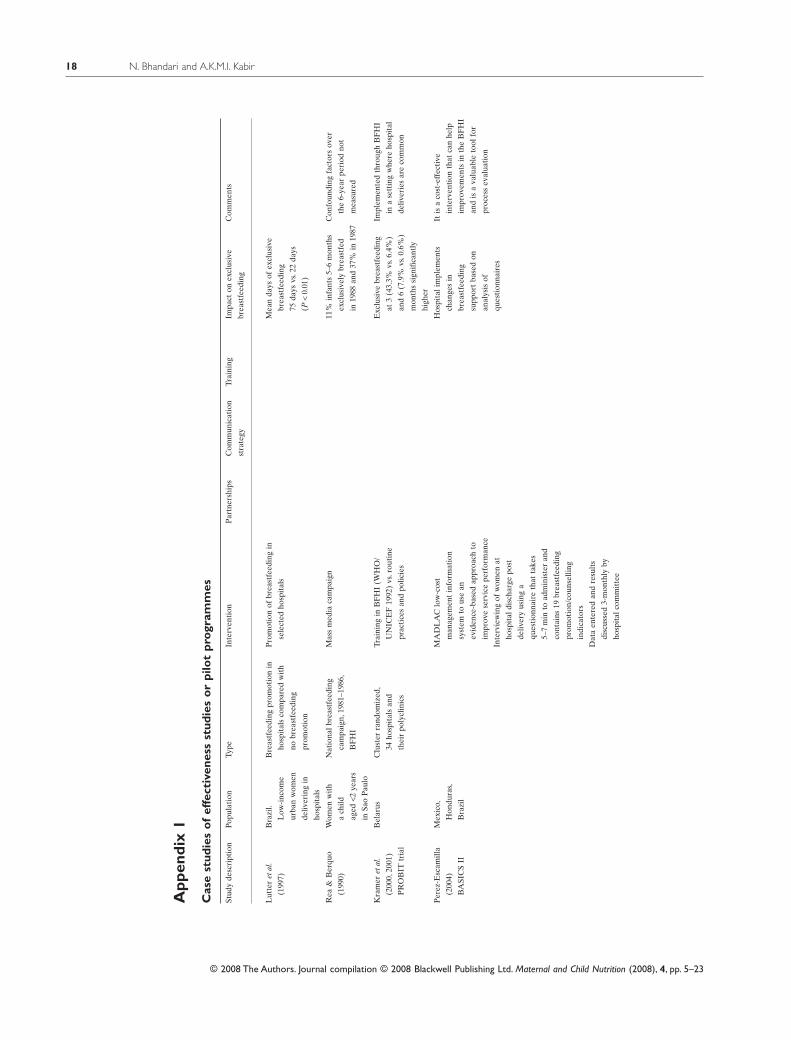
App
endi
x1
Cas
est
udie
so
fef
fect
iven
ess
stud
ies
or
pilo
tpr
ogra
mm
es
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Lut
ter
etal
(199
7)
Bra
zil
Low
-inc
ome
urba
nw
omen
deliv
erin
gin
hosp
ital
s
Bre
astf
eedi
ngpr
omot
ion
in
hosp
ital
sco
mpa
red
wit
h
nobr
east
feed
ing
prom
otio
n
Pro
mot
ion
ofbr
east
feed
ing
in
sele
cted
hosp
ital
s
Mea
nda
ysof
excl
usiv
e
brea
stfe
edin
g
75da
ysvs
22
days
(Plt
001
)
Rea
ampB
erqu
o
(199
0)
Wom
enw
ith
ach
ild
aged
lt2ye
ars
inSa
oP
aulo
Nat
iona
lbre
astf
eedi
ng
cam
paig
n19
81ndash1
986
BF
HI
Mas
sm
edia
cam
paig
n11
in
fant
s5ndash
6m
onth
s
excl
usiv
ely
brea
stfe
d
in19
88an
d37
in
1987
Con
foun
ding
fact
ors
over
the
6-ye
arpe
riod
not
mea
sure
d
Kra
mer
etal
(200
020
01)
PR
OB
ITtr
ial
Bel
arus
Clu
ster
rand
omiz
ed
34ho
spit
als
and
thei
rpo
lycl
inic
s
Trai
ning
inB
FH
I(W
HO
UN
ICE
F19
92)
vsr
outi
ne
prac
tice
san
dpo
licie
s
Exc
lusi
vebr
east
feed
ing
at3
(43
3vs
64
)
and
6(7
9
vs0
6
)
mon
ths
sign
ifica
ntly
high
er
Impl
emen
ted
thro
ugh
BF
HI
ina
sett
ing
whe
reho
spit
al
deliv
erie
sar
eco
mm
on
Per
ez-E
scam
illa
(200
4)
BA
SIC
SII
Mex
ico
Hon
dura
s
Bra
zil
MA
DL
AC
low
-cos
t
man
agem
ent
info
rmat
ion
syst
emto
use
an
evid
ence
-bas
edap
proa
chto
impr
ove
serv
ice
perf
orm
ance
Inte
rvie
win
gof
wom
enat
hosp
ital
disc
harg
epo
st
deliv
ery
usin
ga
ques
tion
nair
eth
atta
kes
5ndash7
min
toad
min
iste
ran
d
cont
ains
19br
east
feed
ing
prom
otio
nco
unse
lling
indi
cato
rs
Dat
aen
tere
dan
dre
sult
s
disc
usse
d3-
mon
thly
by
hosp
ital
com
mit
tee
Hos
pita
lim
plem
ents
chan
ges
in
brea
stfe
edin
g
supp
ort
base
don
anal
ysis
of
ques
tion
nair
es
Itis
aco
st-e
ffec
tive
inte
rven
tion
that
can
help
impr
ovem
ents
inth
eB
FH
I
and
isa
valu
able
tool
for
proc
ess
eval
uati
on
N Bhandari and AKMI Kabir18
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
LIN
KA
GE
S
proj
ect
inA
fric
aan
d
Lat
inA
mer
ica
(Qui
nnet
al
2005
LIN
KA
GE
S
2002
WH
O20
03a)
Bol
ivia
(1
mill
ion)
Gha
na(3
5
mill
ion)
Mad
agas
car
(6m
illio
n)
Res
ourc
e-
poor
sett
ing
Pilo
tpr
ogra
mm
e
InB
oliv
iaan
d
Gha
napr
ogra
mm
e
focu
sed
on
brea
stfe
edin
gan
d
com
plem
enta
ry
feed
ing
InM
adag
asca
r
prog
ram
me
prom
oted
brea
stfe
edin
g
wit
hin
7es
sent
ial
nutr
itio
nac
tion
san
d
subs
eque
ntly
thro
ugh
IMC
I
Bui
lton
form
ativ
ere
sear
ch
and
sust
aine
dth
roug
h
prog
ram
me
acti
viti
esth
at
focu
sed
onbr
ingi
ngab
out
the
desi
red
beha
viou
r
chan
geM
ixof
inte
rven
tion
s
reac
hed
wom
enin
divi
dual
ly
orin
grou
psin
heal
th
faci
litie
sho
mes
or
com
mun
ity
sett
ings
Con
sist
ent
mes
sage
san
d
mat
eria
lacr
oss
all
prog
ram
me
chan
nels
Bol
ivi
PR
OC
OSI
NG
Os
Gha
na
UN
ICE
F
nati
onal
nutr
itio
n
offic
eN
GO
s
Mad
agas
car
Inte
rsec
tora
l
Act
ion
Gro
upfo
r
Nut
riti
on
Jere
o
Sala
ma
Isik
a
Pro
gram
desi
gned
wit
h
part
ners
Rad
ioin
all
thre
esi
tes
Mat
eria
ls
deve
lope
d
tosu
itne
eds
oflo
cal
heal
th
wor
kers
and
com
mun
ity
mem
bers
Gre
at
emph
asis
on
deve
lopm
ent
of coun
selli
ng
and
nego
tiat
ion
skill
s
prac
tica
l
sess
ions
Sign
ifica
ntin
crea
ses
inex
clus
ive
brea
stfe
edin
gra
tes
of
0ndash6-
mon
th-o
ld
infa
nts
from
54
to65
in
Bol
ivia
68
to79
in
Gha
naan
d46
to68
in
Mad
agas
car
In
Gha
naan
d
Mad
agas
car
sign
ifica
ntre
sult
s
obse
rved
wit
hin
aye
ar
ofin
itia
tion
of
com
mun
ity
inte
rven
tion
s
App
roac
hw
asef
fect
ive
and
achi
eved
sign
ifica
nt
incr
ease
sam
ong
larg
e
popu
lati
ons
asea
rly
as
9ndash12
mo
afte
rin
itia
tion
of
com
mun
ity
acti
viti
es
Van
Roe
kele
tal
(200
2)W
HO
(200
3a)
Hon
dura
sG
row
thm
onit
orin
gan
d
prom
otio
nkn
own
as
Ate
ncioacute
nIn
tegr
ala
la
Nintilde
ez(A
IN)
or
Inte
grat
edC
hild
Car
e
Init
ially
pri
mar
ilya
grow
th
mon
itor
ing
prog
ram
me
ulti
mat
ely
thro
ugh
IMC
I
Pro
gram
me
ongr
owth
prom
otio
nndash
asse
ssm
ent
of
mon
thly
wei
ght
gain
and
focu
son
illne
ssf
eedi
ng
prac
tice
san
dge
nera
lchi
ld
care
inin
fant
sun
der
2ye
ars
Impl
emen
ted
atgo
vern
men
t
faci
litie
san
dco
mm
unit
y
Star
ted
in19
92s
tren
gthe
ned
in19
95ndash1
997
wit
hgr
eate
r
focu
son
child
feed
ing
In
1997
pro
gram
me
intr
oduc
ed
wit
hIM
CI
(WH
OU
NIC
EF
2002
)
Maj
or
part
ners
UN
ICE
F
PAH
O
Am
eric
an
and
Hon
dura
n
Red
Cro
ss
CA
RE
Rad
io
broa
dcas
ts
relig
ious
lead
ers
IMC
IM
id-t
erm
eval
uati
on
show
ed39
of
mot
hers
inin
terv
enti
on
com
mun
itie
sex
clus
ivel
y
brea
stfe
dco
mpa
red
wit
h13
in
the
cont
rol
site
s
Mainstreaming nutrition into MCH programs 19
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
cont
inue
d
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Bha
ndar
ieta
l
(200
3)
WH
O
(200
3a)
Rur
alco
mm
unit
ies
inH
arya
na
Indi
a
Clu
ster
rand
omiz
edtr
ial
8
com
mun
itie
s(t
otal
popu
lati
on~4
000
0)
Pro
mot
ion
ofex
clus
ive
brea
stfe
edin
gan
d
appr
opri
ate
com
plem
enta
ryfe
edin
g
Dev
elop
edth
roug
h
form
ativ
ere
sear
ch
ndashP
robl
emid
enti
ficat
ion
ndashP
arti
cipa
tory
desi
gnof
inte
rven
tion
impl
emen
tati
onan
d
eval
uati
on
Impl
emen
tati
onw
ithi
nan
exis
ting
prim
ary
heal
th-c
are
prog
ram
me
Opp
ortu
niti
esus
edto
deliv
erm
essa
ges
wer
e
imm
uniz
atio
ncl
inic
s
wei
ghin
gse
ssio
ns
sick
-chi
ldco
ntac
tsan
d
mon
thly
hom
evi
sits
Res
earc
hers
wit
hlo
cal
gove
rnm
ent
ICD
Ssy
stem
and
NG
O
The
atre
son
gs
Mas
sm
edia
not
used
for
risk
of
cont
amin
atio
n
Mat
eria
ls
deve
lope
d
for
heal
th
wor
kers
pos
ters
flip
book
sca
rds
Bre
astf
eedi
ng
coun
selli
ngse
ctio
n
ofth
eIM
CI
(WH
O
UN
ICE
F20
02)
Exc
lusi
ve
brea
stfe
edin
gin
the
prev
ious
24h
at3
mon
ths
of
age
79
vs4
8
The
posi
tive
effe
ct
rem
aine
dup
to
6m
onth
sof
age
(42
vs4
)
Tota
lpar
tici
pati
onof
the
dist
rict
heal
thsy
stem
from
ince
ptio
nof
the
prog
ram
me
inde
velo
ping
impl
emen
tati
onst
rate
gyt
ool
deve
lopm
ent
and
mon
itor
ing
inad
diti
onto
invo
lvem
ent
of
anN
GO
wer
eim
port
ant
feat
ures
that
cont
ribu
ted
to
the
succ
ess
ofth
e
inte
rven
tion
Mor
row
etal
(199
9)
Mex
ico
Cit
yC
lust
erra
ndom
ized
tria
l
Tota
lpop
ulat
ion
3000
0
Two
com
mun
itie
sin
the
inte
rven
tion
one
com
pari
son
130
wom
en
Hom
e-ba
sed
peer
coun
selli
ng
Pee
rco
unse
llors
mad
e3
or
6ho
me
visi
tsto
the
mot
her
Key
fam
ilym
embe
rsal
so
incl
uded
By
La
Lec
he
Lea
gue
of
Mex
ico
Exc
lusi
ve
brea
stfe
edin
g
at3
mon
ths
post
-par
tum
67
(6vi
sits
)
50
(3vi
sits
)12
(com
pari
son)
Firs
tcl
uste
rra
ndom
ized
com
mun
ity-
base
dtr
ialt
hat
used
peer
coun
sello
rsto
prom
ote
excl
usiv
e
brea
stfe
edin
g
Hai
der
etal
2000
200
2
Dha
ka
Low
mid
dle
and
low
-soc
io-
econ
omic
popu
lati
on
Clu
ster
rand
omiz
edtr
ial
20zo
nes
inin
terv
enti
on
and
20in
cont
rol
Com
mun
ity-
base
dpe
er
coun
selli
ngin
Dha
ka
15ho
me-
base
dco
unse
lling
visi
tsby
peer
coun
sello
rs
40h
(4h
yen10
days
)
WH
OU
NIC
EF
brea
stfe
edin
g
coun
selli
ngco
urse
(WH
OU
NIC
EF
1993
)
Exc
lusi
ve
brea
stfe
edin
g
at5
mon
ths
70
in
inte
rven
tion
and
6in
the
cont
rol
Com
mun
ity-
base
d
brea
stfe
edin
gpr
omot
ion
stra
tegy
was
effe
ctiv
ein
Ban
glad
esh
whe
rem
ost
deliv
erie
soc
cur
atho
me
N Bhandari and AKMI Kabir20
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Bry
ceet
al
(200
4)W
HO
(200
3b)
Bra
zil
Per
u
Tanz
ania
Uga
nda
Mul
tico
untr
yev
alua
tion
of
IMC
Ith
atin
clud
ed
effe
ctiv
enes
sco
stan
d
impa
ct(B
ryce
etal
2004
)
Bre
astf
eedi
ngpr
omot
ion
asa
part
ofIM
CI
IMC
Iis
ast
rate
gyfo
r
impr
ovin
gch
ildhe
alth
and
deve
lopm
ent
thro
ugh
the
com
bine
d
deliv
ery
ofes
sent
ial
child
heal
th
inte
rven
tion
sIM
CI
bega
nw
ith
ase
tof
case
man
agem
ent
guid
elin
es
for
the
man
agem
ent
ofsi
ckch
ildre
nat
first
-lev
elhe
alth
faci
litie
s
and
the
guid
elin
esw
ere
desi
gned
for
adap
tati
on
atco
untr
yle
vela
nd
belo
wO
ver
tim
eth
e
stra
tegy
expa
nded
to
incl
ude
ara
nge
of
guid
elin
esfo
rde
liver
ing
child
surv
ival
inte
rven
tion
at
hous
ehol
dco
mm
unit
y
and
refe
rral
leve
ls
IMC
Im
odul
e(W
HO
UN
ICE
F20
02)
Res
ults
onex
clus
ive
brea
stfe
edin
g
avai
labl
efr
om
Tanz
ania
whe
reno
sign
ifica
ntim
pact
was
seen
Des
pite
subs
tant
ial
impr
ovem
ent
inth
equ
alit
y
ofca
rede
liver
edby
IMC
Iat
heal
thfa
cilit
ies
key
fam
ily
prac
tice
ssu
chas
excl
usiv
e
brea
stfe
edin
gdi
dno
tch
ange
asco
mm
unit
yIM
CI
had
not
been
impl
emen
ted
byth
at
tim
e(W
HO
2003
b)
SA
rife
en
pers
onal
com
mun
icat
ion
Ban
glad
esh
Mat
lab
Com
mun
ity-
base
dcl
uste
r
desi
gn
Eva
luat
ion
offa
cilit
y-an
d
com
mun
ity-
base
dIM
CI
Inte
rven
tion
pack
age
incl
udes
feed
ing
asse
ssm
ent
and
coun
selli
ngon
mot
hers
ofyo
ung
child
ren
seek
ing
care
atfa
cilit
ies
for
illne
ssan
d
hom
e-ba
sed
coun
selli
ng
onim
prov
edfe
edin
gby
com
mun
ity-
base
dhe
alth
and
nutr
itio
nw
orke
rs
At
base
line
inth
e
year
2000
alit
tle
mor
eth
anha
lfth
e
0ndash5-
mon
th-o
ld
infa
nts
inth
est
udy
area
wer
ebe
ing
excl
usiv
ely
brea
stfe
dB
y20
05
this
incr
ease
dby
30
inth
eIM
CI
area
Dat
ano
t
avai
labl
efr
omth
e
com
pari
son
area
as
yet
Lac
kof
com
para
ble
data
from
the
com
pari
son
area
prev
ents
ade
finit
ive
conc
lusi
onas
tow
heth
erth
is
trul
yis
anim
pact
ofIM
CI
BA
SIC
SII
Bas
icSu
ppor
tfo
rIn
stit
utio
naliz
ing
Chi
ldSu
rviv
alP
roje
ctB
FH
IB
aby-
Frie
ndly
Hos
pita
lIni
tiat
ive
ICD
SIn
tegr
ated
Chi
ldD
evel
opm
ent
Serv
ices
IM
CI
Inte
grat
edM
anag
emen
tof
Chi
ldho
odIl
lnes
sM
AD
LA
CM
onit
oreo
deA
poyo
Dir
ecto
con
laL
acat
anci
aM
ater
naN
GO
non
-gov
ernm
enta
lorg
aniz
atio
nPA
HO
Pan
Am
eric
anH
ealt
hO
rgan
izat
ion
PR
OB
ITP
rom
otio
nof
Bre
astf
eedi
ngIn
terv
enti
onTr
ial
PR
OC
OSI
Pro
gram
ade
Coo
rdin
acio
nen
Salu
dIn
tegr
al(C
olla
bora
tive
Pro
gram
for
Inte
grat
edH
ealt
h)U
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
WH
OW
orld
Hea
lth
Org
aniz
atio
n
Mainstreaming nutrition into MCH programs 21
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x2
Cas
est
udie
sin
scal
e-up
effo
rts
inH
IVA
IDS
Stud
yde
scri
ptio
nPo
pula
tion
Inte
rven
tion
Com
mun
icat
ion
stra
tegy
Impa
cton
excl
usiv
ebr
east
feed
ing
Com
men
ts
LIN
KA
GE
S(2
005)
Zam
bia
Pro
gram
me
thro
ugh
heal
th-c
are
and
com
mun
ity
serv
ices
Rea
ched
60si
tes
in6
dist
rict
sby
2005
Inte
grat
ion
ofin
fant
feed
ing
coun
selli
ngm
ater
naln
utri
tion
and
anti
retr
ovir
aldr
ugs
prop
hyla
xis
Trai
ning
ofhe
alth
wor
kers
and
com
mun
ity
serv
ice
prov
ider
sto
coun
selw
omen
onsa
fety
opti
ons
for
thei
rsi
tuat
ion
Beh
avio
urch
ange
Com
mun
icat
ion
inte
rven
tion
sin
the
first
few
year
sM
ater
iald
evel
oped
lsquoAct
Now
rsquoM
edia
cam
paig
nsin
clud
edbr
ochu
res
post
ers
radi
oan
dte
levi
sion
Ass
esse
dth
roug
hba
selin
ean
dfo
llow
-up
hous
ehol
dan
dcl
inic
surv
eys
inse
lect
eddi
stri
cts
Exc
lusi
vebr
east
feed
ing
rate
incr
ease
dfr
om50
in
2002
to64
in
2004
inL
ivin
gsto
nean
dfr
om57
in
2000
to74
in
2004
inN
dola
Inte
grat
edde
mon
stra
tion
proj
ect
Had
seve
rals
tren
gths
inte
rms
ofth
eus
eof
form
ativ
ere
sear
chto
deve
lop
mes
sage
str
aini
ngan
dbu
ildin
gup
skill
sof
prog
ram
me
man
ager
she
alth
-car
epr
ovid
ers
and
com
mun
ity
wor
kers
adv
ocac
yfo
rna
tion
alpo
licy
stro
ngbe
havi
our
chan
geco
mm
unic
atio
nco
mpo
nent
st
reng
then
ing
com
mun
ity
capa
city
for
coun
selli
ngan
dre
ferr
als
and
mon
itor
ing
and
eval
uati
onw
ith
loca
lpar
tner
sP
iwoz
etal
(20
05)
ZV
ITA
MB
Otr
ial
Har
are
Zim
babw
eE
duca
tion
and
coun
selli
ngpr
ogra
mm
ede
liver
edan
tena
tally
1411
0m
othe
rndashba
bypa
irs
enro
lled
from
14m
ater
nity
clin
ics
wit
hin
96h
ofde
liver
yan
dfo
llow
edup
at6
wee
ks
3m
onth
san
d3-
mon
thly
inte
rval
sIn
fant
-fee
ding
patt
erns
dete
rmin
edE
xclu
sive
brea
stfe
edin
gre
com
men
ded
for
HIV
nega
tive
un
know
nor
HIV
posi
tive
who
chos
eto
brea
stfe
ed
Gro
uped
ucat
ion
indi
vidu
alco
unse
lling
vid
eos
broc
hure
sM
othe
rsw
hoen
rolle
dw
hen
prog
ram
me
was
fully
impl
emen
ted
wer
e8
4ti
mes
mor
elik
ely
toex
clus
ivel
ybr
east
feed
than
mot
hers
who
enro
lled
befo
reth
epr
ogra
mm
ebe
gan
Ove
rall
excl
usiv
ebr
east
feed
ing
rate
sti
ll3
mon
ths
was
low
at24
6
Form
ativ
ere
sear
chus
edto
desi
gna
cult
ural
lyse
nsit
ive
educ
atio
nan
dco
unse
lling
prog
ram
me
Low
over
alle
xclu
sive
brea
stfe
edin
gra
tes
prom
pted
auth
ors
toco
nclu
deth
atw
omen
and
thei
rpa
rtne
rssh
ould
have
been
reac
hed
mor
efr
eque
ntly
duri
ngan
tena
tala
ndpo
st-n
atal
peri
od
N Bhandari and AKMI Kabir22
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Thi
oret
al(
2006
)R
ollin
s(2
007)
C
ohen
(200
7)
HIV
-inf
ecte
dpr
egna
ntw
omen
atte
ndin
gan
tena
talc
linic
sin
sout
hB
otsw
ana
Inve
stig
atio
nsby
CD
Cof
adi
arrh
oea
outb
reak
inJa
nuar
y-Fe
brua
ry20
06in
the
sam
epo
pula
tion
Mat
erna
land
infa
ntan
tire
trov
iral
ther
apy
toas
cert
ain
impa
cton
HIV
tran
smis
sion
Ant
enat
alco
unse
lling
Cas
endashco
ntro
lstu
dyto
iden
tify
risk
fact
ors
for
diar
rhoe
ano
tbr
east
feed
ing
was
the
bigg
est
risk
fact
ora
djus
ted
odds
rati
o50
(95
confi
denc
ein
terv
al4
5ndash10
0)
Bot
swan
aha
sth
ebe
stpr
imar
yhe
alth
-car
est
ruct
ure
wat
ersu
pply
and
sani
tati
onsy
stem
sin
Sout
hA
fric
aFo
rmul
apr
ovid
edfr
eeby
the
gove
rnm
ent
toin
fect
edm
othe
rsL
ower
mor
talit
yin
the
brea
stfe
edin
ggr
oup
at7
mon
ths
dem
onst
rate
sri
skof
form
ula
feed
ing
and
need
for
alte
rnat
est
rate
gies
(Thi
oret
al
2006
)A
utho
rsco
nclu
deth
athe
alth
syst
ems
inw
hich
thes
epr
ogra
mm
esar
eim
plem
ente
dsh
ould
beab
leto
cope
wit
hdi
arrh
oea
and
mal
nutr
itio
nth
atre
sult
sbe
caus
eof
form
ula
feed
ing
(Rol
lins
2007
)C
oova
dia
etal
(2
007)
Kw
aZul
uNat
al
Sout
hA
fric
a27
22H
IV-i
nfec
ted
and
unin
fect
edpr
egna
ntw
omen
enro
lled
into
ano
n-ra
ndom
ized
inte
rven
tion
coho
rtst
udy
from
ante
nata
lcl
inic
sIn
fant
feed
ing
data
obta
ined
wee
kly
bloo
dsa
mpl
esfr
omin
fant
sta
ken
mon
thly
83
of13
72in
fant
sbo
rnto
HIV
-inf
ecte
dm
othe
rsin
itia
ted
excl
usiv
ebr
east
feed
ing
from
birt
hB
reas
tfed
infa
nts
who
rece
ived
solid
sw
ere
sign
ifica
ntly
mor
elik
ely
toac
quir
ein
fect
ion
com
pare
dw
ith
excl
usiv
ely
brea
stfe
d(H
R10
87
151
ndash78
P=
001
8)as
wer
ein
fant
sw
hoat
12w
eeks
rece
ived
brea
stan
dfo
rmul
am
ilk(1
82
098
ndash33
6P
=0
57)
Cum
ulat
ive
3-m
onth
mor
talit
yin
excl
usiv
ely
brea
stfe
dw
as6
1(4
74ndash
792
)vs
15
1(7
63ndash
287
3)in
infa
nts
give
nre
plac
emen
tfe
eds
(HR
206
1
0ndash4
27P
=0
05)
The
stud
ysh
ows
that
excl
usiv
ebr
east
feed
ing
can
besu
cces
sful
lysu
ppor
ted
inH
IV-i
nfec
ted
wom
enT
heau
thor
sca
llfo
rfu
rthe
rre
visi
onof
UN
ICE
FW
HO
and
USA
IDin
fant
feed
ing
guid
elin
es
CD
CC
ente
rof
Dis
ease
Con
trol
HR
haz
ards
rati
oU
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
USA
IDU
SA
genc
yfo
rIn
tern
atio
nalD
evel
opm
ent
WH
OW
orld
Hea
lth
Org
aniz
atio
nZ
VIT
AM
BO
Z
imba
bwe
Vit
amin
Afo
rM
othe
rsan
dB
abie
s
Mainstreaming nutrition into MCH programs 23
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
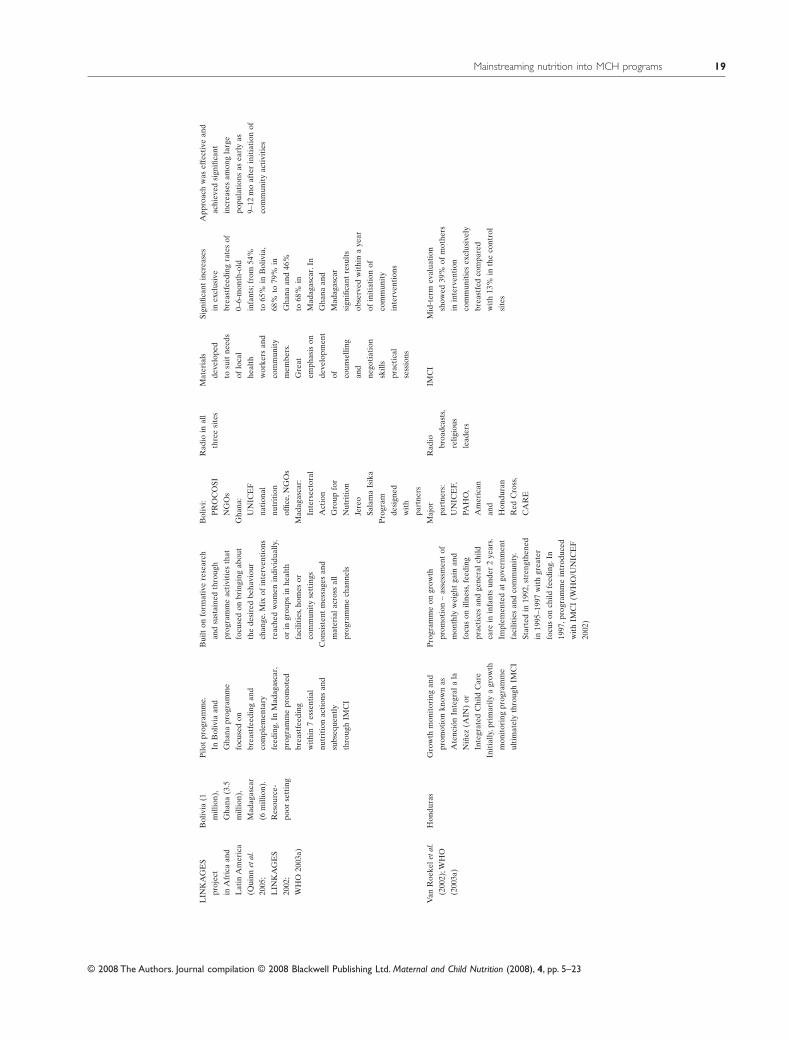
LIN
KA
GE
S
proj
ect
inA
fric
aan
d
Lat
inA
mer
ica
(Qui
nnet
al
2005
LIN
KA
GE
S
2002
WH
O20
03a)
Bol
ivia
(1
mill
ion)
Gha
na(3
5
mill
ion)
Mad
agas
car
(6m
illio
n)
Res
ourc
e-
poor
sett
ing
Pilo
tpr
ogra
mm
e
InB
oliv
iaan
d
Gha
napr
ogra
mm
e
focu
sed
on
brea
stfe
edin
gan
d
com
plem
enta
ry
feed
ing
InM
adag
asca
r
prog
ram
me
prom
oted
brea
stfe
edin
g
wit
hin
7es
sent
ial
nutr
itio
nac
tion
san
d
subs
eque
ntly
thro
ugh
IMC
I
Bui
lton
form
ativ
ere
sear
ch
and
sust
aine
dth
roug
h
prog
ram
me
acti
viti
esth
at
focu
sed
onbr
ingi
ngab
out
the
desi
red
beha
viou
r
chan
geM
ixof
inte
rven
tion
s
reac
hed
wom
enin
divi
dual
ly
orin
grou
psin
heal
th
faci
litie
sho
mes
or
com
mun
ity
sett
ings
Con
sist
ent
mes
sage
san
d
mat
eria
lacr
oss
all
prog
ram
me
chan
nels
Bol
ivi
PR
OC
OSI
NG
Os
Gha
na
UN
ICE
F
nati
onal
nutr
itio
n
offic
eN
GO
s
Mad
agas
car
Inte
rsec
tora
l
Act
ion
Gro
upfo
r
Nut
riti
on
Jere
o
Sala
ma
Isik
a
Pro
gram
desi
gned
wit
h
part
ners
Rad
ioin
all
thre
esi
tes
Mat
eria
ls
deve
lope
d
tosu
itne
eds
oflo
cal
heal
th
wor
kers
and
com
mun
ity
mem
bers
Gre
at
emph
asis
on
deve
lopm
ent
of coun
selli
ng
and
nego
tiat
ion
skill
s
prac
tica
l
sess
ions
Sign
ifica
ntin
crea
ses
inex
clus
ive
brea
stfe
edin
gra
tes
of
0ndash6-
mon
th-o
ld
infa
nts
from
54
to65
in
Bol
ivia
68
to79
in
Gha
naan
d46
to68
in
Mad
agas
car
In
Gha
naan
d
Mad
agas
car
sign
ifica
ntre
sult
s
obse
rved
wit
hin
aye
ar
ofin
itia
tion
of
com
mun
ity
inte
rven
tion
s
App
roac
hw
asef
fect
ive
and
achi
eved
sign
ifica
nt
incr
ease
sam
ong
larg
e
popu
lati
ons
asea
rly
as
9ndash12
mo
afte
rin
itia
tion
of
com
mun
ity
acti
viti
es
Van
Roe
kele
tal
(200
2)W
HO
(200
3a)
Hon
dura
sG
row
thm
onit
orin
gan
d
prom
otio
nkn
own
as
Ate
ncioacute
nIn
tegr
ala
la
Nintilde
ez(A
IN)
or
Inte
grat
edC
hild
Car
e
Init
ially
pri
mar
ilya
grow
th
mon
itor
ing
prog
ram
me
ulti
mat
ely
thro
ugh
IMC
I
Pro
gram
me
ongr
owth
prom
otio
nndash
asse
ssm
ent
of
mon
thly
wei
ght
gain
and
focu
son
illne
ssf
eedi
ng
prac
tice
san
dge
nera
lchi
ld
care
inin
fant
sun
der
2ye
ars
Impl
emen
ted
atgo
vern
men
t
faci
litie
san
dco
mm
unit
y
Star
ted
in19
92s
tren
gthe
ned
in19
95ndash1
997
wit
hgr
eate
r
focu
son
child
feed
ing
In
1997
pro
gram
me
intr
oduc
ed
wit
hIM
CI
(WH
OU
NIC
EF
2002
)
Maj
or
part
ners
UN
ICE
F
PAH
O
Am
eric
an
and
Hon
dura
n
Red
Cro
ss
CA
RE
Rad
io
broa
dcas
ts
relig
ious
lead
ers
IMC
IM
id-t
erm
eval
uati
on
show
ed39
of
mot
hers
inin
terv
enti
on
com
mun
itie
sex
clus
ivel
y
brea
stfe
dco
mpa
red
wit
h13
in
the
cont
rol
site
s
Mainstreaming nutrition into MCH programs 19
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x1
cont
inue
d
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Bha
ndar
ieta
l
(200
3)
WH
O
(200
3a)
Rur
alco
mm
unit
ies
inH
arya
na
Indi
a
Clu
ster
rand
omiz
edtr
ial
8
com
mun
itie
s(t
otal
popu
lati
on~4
000
0)
Pro
mot
ion
ofex
clus
ive
brea
stfe
edin
gan
d
appr
opri
ate
com
plem
enta
ryfe
edin
g
Dev
elop
edth
roug
h
form
ativ
ere
sear
ch
ndashP
robl
emid
enti
ficat
ion
ndashP
arti
cipa
tory
desi
gnof
inte
rven
tion
impl
emen
tati
onan
d
eval
uati
on
Impl
emen
tati
onw
ithi
nan
exis
ting
prim
ary
heal
th-c
are
prog
ram
me
Opp
ortu
niti
esus
edto
deliv
erm
essa
ges
wer
e
imm
uniz
atio
ncl
inic
s
wei
ghin
gse
ssio
ns
sick
-chi
ldco
ntac
tsan
d
mon
thly
hom
evi
sits
Res
earc
hers
wit
hlo
cal
gove
rnm
ent
ICD
Ssy
stem
and
NG
O
The
atre
son
gs
Mas
sm
edia
not
used
for
risk
of
cont
amin
atio
n
Mat
eria
ls
deve
lope
d
for
heal
th
wor
kers
pos
ters
flip
book
sca
rds
Bre
astf
eedi
ng
coun
selli
ngse
ctio
n
ofth
eIM
CI
(WH
O
UN
ICE
F20
02)
Exc
lusi
ve
brea
stfe
edin
gin
the
prev
ious
24h
at3
mon
ths
of
age
79
vs4
8
The
posi
tive
effe
ct
rem
aine
dup
to
6m
onth
sof
age
(42
vs4
)
Tota
lpar
tici
pati
onof
the
dist
rict
heal
thsy
stem
from
ince
ptio
nof
the
prog
ram
me
inde
velo
ping
impl
emen
tati
onst
rate
gyt
ool
deve
lopm
ent
and
mon
itor
ing
inad
diti
onto
invo
lvem
ent
of
anN
GO
wer
eim
port
ant
feat
ures
that
cont
ribu
ted
to
the
succ
ess
ofth
e
inte
rven
tion
Mor
row
etal
(199
9)
Mex
ico
Cit
yC
lust
erra
ndom
ized
tria
l
Tota
lpop
ulat
ion
3000
0
Two
com
mun
itie
sin
the
inte
rven
tion
one
com
pari
son
130
wom
en
Hom
e-ba
sed
peer
coun
selli
ng
Pee
rco
unse
llors
mad
e3
or
6ho
me
visi
tsto
the
mot
her
Key
fam
ilym
embe
rsal
so
incl
uded
By
La
Lec
he
Lea
gue
of
Mex
ico
Exc
lusi
ve
brea
stfe
edin
g
at3
mon
ths
post
-par
tum
67
(6vi
sits
)
50
(3vi
sits
)12
(com
pari
son)
Firs
tcl
uste
rra
ndom
ized
com
mun
ity-
base
dtr
ialt
hat
used
peer
coun
sello
rsto
prom
ote
excl
usiv
e
brea
stfe
edin
g
Hai
der
etal
2000
200
2
Dha
ka
Low
mid
dle
and
low
-soc
io-
econ
omic
popu
lati
on
Clu
ster
rand
omiz
edtr
ial
20zo
nes
inin
terv
enti
on
and
20in
cont
rol
Com
mun
ity-
base
dpe
er
coun
selli
ngin
Dha
ka
15ho
me-
base
dco
unse
lling
visi
tsby
peer
coun
sello
rs
40h
(4h
yen10
days
)
WH
OU
NIC
EF
brea
stfe
edin
g
coun
selli
ngco
urse
(WH
OU
NIC
EF
1993
)
Exc
lusi
ve
brea
stfe
edin
g
at5
mon
ths
70
in
inte
rven
tion
and
6in
the
cont
rol
Com
mun
ity-
base
d
brea
stfe
edin
gpr
omot
ion
stra
tegy
was
effe
ctiv
ein
Ban
glad
esh
whe
rem
ost
deliv
erie
soc
cur
atho
me
N Bhandari and AKMI Kabir20
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Bry
ceet
al
(200
4)W
HO
(200
3b)
Bra
zil
Per
u
Tanz
ania
Uga
nda
Mul
tico
untr
yev
alua
tion
of
IMC
Ith
atin
clud
ed
effe
ctiv
enes
sco
stan
d
impa
ct(B
ryce
etal
2004
)
Bre
astf
eedi
ngpr
omot
ion
asa
part
ofIM
CI
IMC
Iis
ast
rate
gyfo
r
impr
ovin
gch
ildhe
alth
and
deve
lopm
ent
thro
ugh
the
com
bine
d
deliv
ery
ofes
sent
ial
child
heal
th
inte
rven
tion
sIM
CI
bega
nw
ith
ase
tof
case
man
agem
ent
guid
elin
es
for
the
man
agem
ent
ofsi
ckch
ildre
nat
first
-lev
elhe
alth
faci
litie
s
and
the
guid
elin
esw
ere
desi
gned
for
adap
tati
on
atco
untr
yle
vela
nd
belo
wO
ver
tim
eth
e
stra
tegy
expa
nded
to
incl
ude
ara
nge
of
guid
elin
esfo
rde
liver
ing
child
surv
ival
inte
rven
tion
at
hous
ehol
dco
mm
unit
y
and
refe
rral
leve
ls
IMC
Im
odul
e(W
HO
UN
ICE
F20
02)
Res
ults
onex
clus
ive
brea
stfe
edin
g
avai
labl
efr
om
Tanz
ania
whe
reno
sign
ifica
ntim
pact
was
seen
Des
pite
subs
tant
ial
impr
ovem
ent
inth
equ
alit
y
ofca
rede
liver
edby
IMC
Iat
heal
thfa
cilit
ies
key
fam
ily
prac
tice
ssu
chas
excl
usiv
e
brea
stfe
edin
gdi
dno
tch
ange
asco
mm
unit
yIM
CI
had
not
been
impl
emen
ted
byth
at
tim
e(W
HO
2003
b)
SA
rife
en
pers
onal
com
mun
icat
ion
Ban
glad
esh
Mat
lab
Com
mun
ity-
base
dcl
uste
r
desi
gn
Eva
luat
ion
offa
cilit
y-an
d
com
mun
ity-
base
dIM
CI
Inte
rven
tion
pack
age
incl
udes
feed
ing
asse
ssm
ent
and
coun
selli
ngon
mot
hers
ofyo
ung
child
ren
seek
ing
care
atfa
cilit
ies
for
illne
ssan
d
hom
e-ba
sed
coun
selli
ng
onim
prov
edfe
edin
gby
com
mun
ity-
base
dhe
alth
and
nutr
itio
nw
orke
rs
At
base
line
inth
e
year
2000
alit
tle
mor
eth
anha
lfth
e
0ndash5-
mon
th-o
ld
infa
nts
inth
est
udy
area
wer
ebe
ing
excl
usiv
ely
brea
stfe
dB
y20
05
this
incr
ease
dby
30
inth
eIM
CI
area
Dat
ano
t
avai
labl
efr
omth
e
com
pari
son
area
as
yet
Lac
kof
com
para
ble
data
from
the
com
pari
son
area
prev
ents
ade
finit
ive
conc
lusi
onas
tow
heth
erth
is
trul
yis
anim
pact
ofIM
CI
BA
SIC
SII
Bas
icSu
ppor
tfo
rIn
stit
utio
naliz
ing
Chi
ldSu
rviv
alP
roje
ctB
FH
IB
aby-
Frie
ndly
Hos
pita
lIni
tiat
ive
ICD
SIn
tegr
ated
Chi
ldD
evel
opm
ent
Serv
ices
IM
CI
Inte
grat
edM
anag
emen
tof
Chi
ldho
odIl
lnes
sM
AD
LA
CM
onit
oreo
deA
poyo
Dir
ecto
con
laL
acat
anci
aM
ater
naN
GO
non
-gov
ernm
enta
lorg
aniz
atio
nPA
HO
Pan
Am
eric
anH
ealt
hO
rgan
izat
ion
PR
OB
ITP
rom
otio
nof
Bre
astf
eedi
ngIn
terv
enti
onTr
ial
PR
OC
OSI
Pro
gram
ade
Coo
rdin
acio
nen
Salu
dIn
tegr
al(C
olla
bora
tive
Pro
gram
for
Inte
grat
edH
ealt
h)U
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
WH
OW
orld
Hea
lth
Org
aniz
atio
n
Mainstreaming nutrition into MCH programs 21
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x2
Cas
est
udie
sin
scal
e-up
effo
rts
inH
IVA
IDS
Stud
yde
scri
ptio
nPo
pula
tion
Inte
rven
tion
Com
mun
icat
ion
stra
tegy
Impa
cton
excl
usiv
ebr
east
feed
ing
Com
men
ts
LIN
KA
GE
S(2
005)
Zam
bia
Pro
gram
me
thro
ugh
heal
th-c
are
and
com
mun
ity
serv
ices
Rea
ched
60si
tes
in6
dist
rict
sby
2005
Inte
grat
ion
ofin
fant
feed
ing
coun
selli
ngm
ater
naln
utri
tion
and
anti
retr
ovir
aldr
ugs
prop
hyla
xis
Trai
ning
ofhe
alth
wor
kers
and
com
mun
ity
serv
ice
prov
ider
sto
coun
selw
omen
onsa
fety
opti
ons
for
thei
rsi
tuat
ion
Beh
avio
urch
ange
Com
mun
icat
ion
inte
rven
tion
sin
the
first
few
year
sM
ater
iald
evel
oped
lsquoAct
Now
rsquoM
edia
cam
paig
nsin
clud
edbr
ochu
res
post
ers
radi
oan
dte
levi
sion
Ass
esse
dth
roug
hba
selin
ean
dfo
llow
-up
hous
ehol
dan
dcl
inic
surv
eys
inse
lect
eddi
stri
cts
Exc
lusi
vebr
east
feed
ing
rate
incr
ease
dfr
om50
in
2002
to64
in
2004
inL
ivin
gsto
nean
dfr
om57
in
2000
to74
in
2004
inN
dola
Inte
grat
edde
mon
stra
tion
proj
ect
Had
seve
rals
tren
gths
inte
rms
ofth
eus
eof
form
ativ
ere
sear
chto
deve
lop
mes
sage
str
aini
ngan
dbu
ildin
gup
skill
sof
prog
ram
me
man
ager
she
alth
-car
epr
ovid
ers
and
com
mun
ity
wor
kers
adv
ocac
yfo
rna
tion
alpo
licy
stro
ngbe
havi
our
chan
geco
mm
unic
atio
nco
mpo
nent
st
reng
then
ing
com
mun
ity
capa
city
for
coun
selli
ngan
dre
ferr
als
and
mon
itor
ing
and
eval
uati
onw
ith
loca
lpar
tner
sP
iwoz
etal
(20
05)
ZV
ITA
MB
Otr
ial
Har
are
Zim
babw
eE
duca
tion
and
coun
selli
ngpr
ogra
mm
ede
liver
edan
tena
tally
1411
0m
othe
rndashba
bypa
irs
enro
lled
from
14m
ater
nity
clin
ics
wit
hin
96h
ofde
liver
yan
dfo
llow
edup
at6
wee
ks
3m
onth
san
d3-
mon
thly
inte
rval
sIn
fant
-fee
ding
patt
erns
dete
rmin
edE
xclu
sive
brea
stfe
edin
gre
com
men
ded
for
HIV
nega
tive
un
know
nor
HIV
posi
tive
who
chos
eto
brea
stfe
ed
Gro
uped
ucat
ion
indi
vidu
alco
unse
lling
vid
eos
broc
hure
sM
othe
rsw
hoen
rolle
dw
hen
prog
ram
me
was
fully
impl
emen
ted
wer
e8
4ti
mes
mor
elik
ely
toex
clus
ivel
ybr
east
feed
than
mot
hers
who
enro
lled
befo
reth
epr
ogra
mm
ebe
gan
Ove
rall
excl
usiv
ebr
east
feed
ing
rate
sti
ll3
mon
ths
was
low
at24
6
Form
ativ
ere
sear
chus
edto
desi
gna
cult
ural
lyse
nsit
ive
educ
atio
nan
dco
unse
lling
prog
ram
me
Low
over
alle
xclu
sive
brea
stfe
edin
gra
tes
prom
pted
auth
ors
toco
nclu
deth
atw
omen
and
thei
rpa
rtne
rssh
ould
have
been
reac
hed
mor
efr
eque
ntly
duri
ngan
tena
tala
ndpo
st-n
atal
peri
od
N Bhandari and AKMI Kabir22
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Thi
oret
al(
2006
)R
ollin
s(2
007)
C
ohen
(200
7)
HIV
-inf
ecte
dpr
egna
ntw
omen
atte
ndin
gan
tena
talc
linic
sin
sout
hB
otsw
ana
Inve
stig
atio
nsby
CD
Cof
adi
arrh
oea
outb
reak
inJa
nuar
y-Fe
brua
ry20
06in
the
sam
epo
pula
tion
Mat
erna
land
infa
ntan
tire
trov
iral
ther
apy
toas
cert
ain
impa
cton
HIV
tran
smis
sion
Ant
enat
alco
unse
lling
Cas
endashco
ntro
lstu
dyto
iden
tify
risk
fact
ors
for
diar
rhoe
ano
tbr
east
feed
ing
was
the
bigg
est
risk
fact
ora
djus
ted
odds
rati
o50
(95
confi
denc
ein
terv
al4
5ndash10
0)
Bot
swan
aha
sth
ebe
stpr
imar
yhe
alth
-car
est
ruct
ure
wat
ersu
pply
and
sani
tati
onsy
stem
sin
Sout
hA
fric
aFo
rmul
apr
ovid
edfr
eeby
the
gove
rnm
ent
toin
fect
edm
othe
rsL
ower
mor
talit
yin
the
brea
stfe
edin
ggr
oup
at7
mon
ths
dem
onst
rate
sri
skof
form
ula
feed
ing
and
need
for
alte
rnat
est
rate
gies
(Thi
oret
al
2006
)A
utho
rsco
nclu
deth
athe
alth
syst
ems
inw
hich
thes
epr
ogra
mm
esar
eim
plem
ente
dsh
ould
beab
leto
cope
wit
hdi
arrh
oea
and
mal
nutr
itio
nth
atre
sult
sbe
caus
eof
form
ula
feed
ing
(Rol
lins
2007
)C
oova
dia
etal
(2
007)
Kw
aZul
uNat
al
Sout
hA
fric
a27
22H
IV-i
nfec
ted
and
unin
fect
edpr
egna
ntw
omen
enro
lled
into
ano
n-ra
ndom
ized
inte
rven
tion
coho
rtst
udy
from
ante
nata
lcl
inic
sIn
fant
feed
ing
data
obta
ined
wee
kly
bloo
dsa
mpl
esfr
omin
fant
sta
ken
mon
thly
83
of13
72in
fant
sbo
rnto
HIV
-inf
ecte
dm
othe
rsin
itia
ted
excl
usiv
ebr
east
feed
ing
from
birt
hB
reas
tfed
infa
nts
who
rece
ived
solid
sw
ere
sign
ifica
ntly
mor
elik
ely
toac
quir
ein
fect
ion
com
pare
dw
ith
excl
usiv
ely
brea
stfe
d(H
R10
87
151
ndash78
P=
001
8)as
wer
ein
fant
sw
hoat
12w
eeks
rece
ived
brea
stan
dfo
rmul
am
ilk(1
82
098
ndash33
6P
=0
57)
Cum
ulat
ive
3-m
onth
mor
talit
yin
excl
usiv
ely
brea
stfe
dw
as6
1(4
74ndash
792
)vs
15
1(7
63ndash
287
3)in
infa
nts
give
nre
plac
emen
tfe
eds
(HR
206
1
0ndash4
27P
=0
05)
The
stud
ysh
ows
that
excl
usiv
ebr
east
feed
ing
can
besu
cces
sful
lysu
ppor
ted
inH
IV-i
nfec
ted
wom
enT
heau
thor
sca
llfo
rfu
rthe
rre
visi
onof
UN
ICE
FW
HO
and
USA
IDin
fant
feed
ing
guid
elin
es
CD
CC
ente
rof
Dis
ease
Con
trol
HR
haz
ards
rati
oU
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
USA
IDU
SA
genc
yfo
rIn
tern
atio
nalD
evel
opm
ent
WH
OW
orld
Hea
lth
Org
aniz
atio
nZ
VIT
AM
BO
Z
imba
bwe
Vit
amin
Afo
rM
othe
rsan
dB
abie
s
Mainstreaming nutrition into MCH programs 23
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
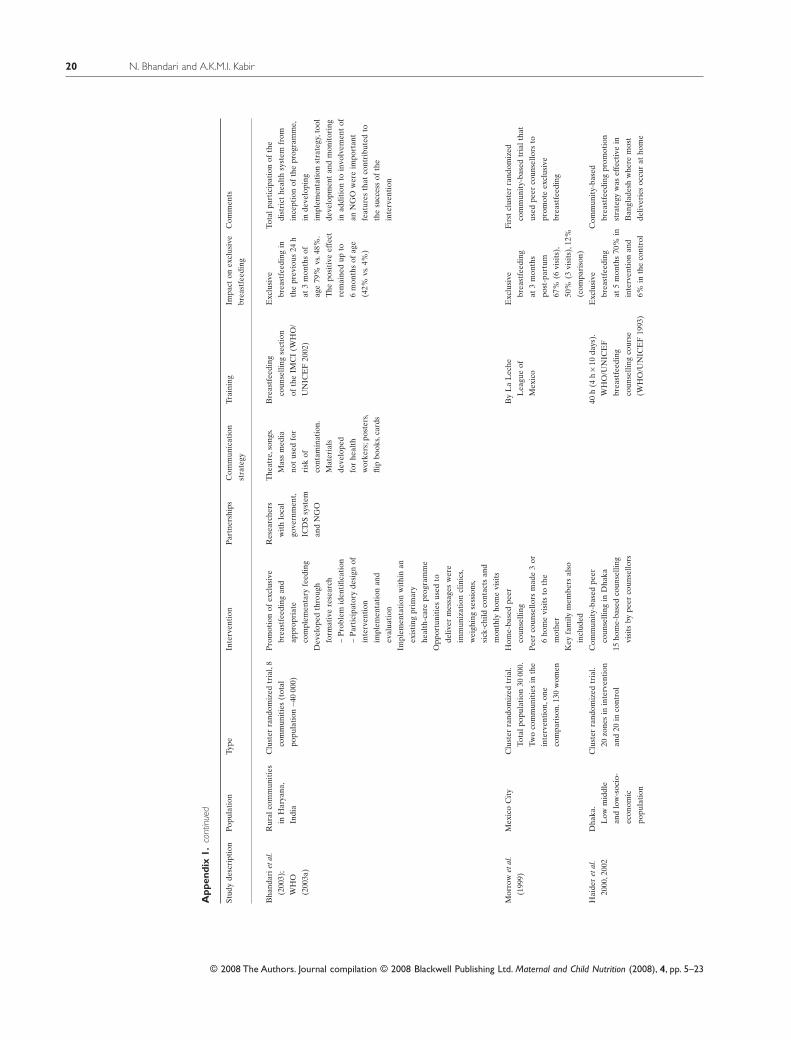
App
endi
x1
cont
inue
d
Stud
yde
scri
ptio
nPo
pula
tion
Type
Inte
rven
tion
Par
tner
ship
sC
omm
unic
atio
n
stra
tegy
Trai
ning
Impa
cton
excl
usiv
e
brea
stfe
edin
g
Com
men
ts
Bha
ndar
ieta
l
(200
3)
WH
O
(200
3a)
Rur
alco
mm
unit
ies
inH
arya
na
Indi
a
Clu
ster
rand
omiz
edtr
ial
8
com
mun
itie
s(t
otal
popu
lati
on~4
000
0)
Pro
mot
ion
ofex
clus
ive
brea
stfe
edin
gan
d
appr
opri
ate
com
plem
enta
ryfe
edin
g
Dev
elop
edth
roug
h
form
ativ
ere
sear
ch
ndashP
robl
emid
enti
ficat
ion
ndashP
arti
cipa
tory
desi
gnof
inte
rven
tion
impl
emen
tati
onan
d
eval
uati
on
Impl
emen
tati
onw
ithi
nan
exis
ting
prim
ary
heal
th-c
are
prog
ram
me
Opp
ortu
niti
esus
edto
deliv
erm
essa
ges
wer
e
imm
uniz
atio
ncl
inic
s
wei
ghin
gse
ssio
ns
sick
-chi
ldco
ntac
tsan
d
mon
thly
hom
evi
sits
Res
earc
hers
wit
hlo
cal
gove
rnm
ent
ICD
Ssy
stem
and
NG
O
The
atre
son
gs
Mas
sm
edia
not
used
for
risk
of
cont
amin
atio
n
Mat
eria
ls
deve
lope
d
for
heal
th
wor
kers
pos
ters
flip
book
sca
rds
Bre
astf
eedi
ng
coun
selli
ngse
ctio
n
ofth
eIM
CI
(WH
O
UN
ICE
F20
02)
Exc
lusi
ve
brea
stfe
edin
gin
the
prev
ious
24h
at3
mon
ths
of
age
79
vs4
8
The
posi
tive
effe
ct
rem
aine
dup
to
6m
onth
sof
age
(42
vs4
)
Tota
lpar
tici
pati
onof
the
dist
rict
heal
thsy
stem
from
ince
ptio
nof
the
prog
ram
me
inde
velo
ping
impl
emen
tati
onst
rate
gyt
ool
deve
lopm
ent
and
mon
itor
ing
inad
diti
onto
invo
lvem
ent
of
anN
GO
wer
eim
port
ant
feat
ures
that
cont
ribu
ted
to
the
succ
ess
ofth
e
inte
rven
tion
Mor
row
etal
(199
9)
Mex
ico
Cit
yC
lust
erra
ndom
ized
tria
l
Tota
lpop
ulat
ion
3000
0
Two
com
mun
itie
sin
the
inte
rven
tion
one
com
pari
son
130
wom
en
Hom
e-ba
sed
peer
coun
selli
ng
Pee
rco
unse
llors
mad
e3
or
6ho
me
visi
tsto
the
mot
her
Key
fam
ilym
embe
rsal
so
incl
uded
By
La
Lec
he
Lea
gue
of
Mex
ico
Exc
lusi
ve
brea
stfe
edin
g
at3
mon
ths
post
-par
tum
67
(6vi
sits
)
50
(3vi
sits
)12
(com
pari
son)
Firs
tcl
uste
rra
ndom
ized
com
mun
ity-
base
dtr
ialt
hat
used
peer
coun
sello
rsto
prom
ote
excl
usiv
e
brea
stfe
edin
g
Hai
der
etal
2000
200
2
Dha
ka
Low
mid
dle
and
low
-soc
io-
econ
omic
popu
lati
on
Clu
ster
rand
omiz
edtr
ial
20zo
nes
inin
terv
enti
on
and
20in
cont
rol
Com
mun
ity-
base
dpe
er
coun
selli
ngin
Dha
ka
15ho
me-
base
dco
unse
lling
visi
tsby
peer
coun
sello
rs
40h
(4h
yen10
days
)
WH
OU
NIC
EF
brea
stfe
edin
g
coun
selli
ngco
urse
(WH
OU
NIC
EF
1993
)
Exc
lusi
ve
brea
stfe
edin
g
at5
mon
ths
70
in
inte
rven
tion
and
6in
the
cont
rol
Com
mun
ity-
base
d
brea
stfe
edin
gpr
omot
ion
stra
tegy
was
effe
ctiv
ein
Ban
glad
esh
whe
rem
ost
deliv
erie
soc
cur
atho
me
N Bhandari and AKMI Kabir20
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Bry
ceet
al
(200
4)W
HO
(200
3b)
Bra
zil
Per
u
Tanz
ania
Uga
nda
Mul
tico
untr
yev
alua
tion
of
IMC
Ith
atin
clud
ed
effe
ctiv
enes
sco
stan
d
impa
ct(B
ryce
etal
2004
)
Bre
astf
eedi
ngpr
omot
ion
asa
part
ofIM
CI
IMC
Iis
ast
rate
gyfo
r
impr
ovin
gch
ildhe
alth
and
deve
lopm
ent
thro
ugh
the
com
bine
d
deliv
ery
ofes
sent
ial
child
heal
th
inte
rven
tion
sIM
CI
bega
nw
ith
ase
tof
case
man
agem
ent
guid
elin
es
for
the
man
agem
ent
ofsi
ckch
ildre
nat
first
-lev
elhe
alth
faci
litie
s
and
the
guid
elin
esw
ere
desi
gned
for
adap
tati
on
atco
untr
yle
vela
nd
belo
wO
ver
tim
eth
e
stra
tegy
expa
nded
to
incl
ude
ara
nge
of
guid
elin
esfo
rde
liver
ing
child
surv
ival
inte
rven
tion
at
hous
ehol
dco
mm
unit
y
and
refe
rral
leve
ls
IMC
Im
odul
e(W
HO
UN
ICE
F20
02)
Res
ults
onex
clus
ive
brea
stfe
edin
g
avai
labl
efr
om
Tanz
ania
whe
reno
sign
ifica
ntim
pact
was
seen
Des
pite
subs
tant
ial
impr
ovem
ent
inth
equ
alit
y
ofca
rede
liver
edby
IMC
Iat
heal
thfa
cilit
ies
key
fam
ily
prac
tice
ssu
chas
excl
usiv
e
brea
stfe
edin
gdi
dno
tch
ange
asco
mm
unit
yIM
CI
had
not
been
impl
emen
ted
byth
at
tim
e(W
HO
2003
b)
SA
rife
en
pers
onal
com
mun
icat
ion
Ban
glad
esh
Mat
lab
Com
mun
ity-
base
dcl
uste
r
desi
gn
Eva
luat
ion
offa
cilit
y-an
d
com
mun
ity-
base
dIM
CI
Inte
rven
tion
pack
age
incl
udes
feed
ing
asse
ssm
ent
and
coun
selli
ngon
mot
hers
ofyo
ung
child
ren
seek
ing
care
atfa
cilit
ies
for
illne
ssan
d
hom
e-ba
sed
coun
selli
ng
onim
prov
edfe
edin
gby
com
mun
ity-
base
dhe
alth
and
nutr
itio
nw
orke
rs
At
base
line
inth
e
year
2000
alit
tle
mor
eth
anha
lfth
e
0ndash5-
mon
th-o
ld
infa
nts
inth
est
udy
area
wer
ebe
ing
excl
usiv
ely
brea
stfe
dB
y20
05
this
incr
ease
dby
30
inth
eIM
CI
area
Dat
ano
t
avai
labl
efr
omth
e
com
pari
son
area
as
yet
Lac
kof
com
para
ble
data
from
the
com
pari
son
area
prev
ents
ade
finit
ive
conc
lusi
onas
tow
heth
erth
is
trul
yis
anim
pact
ofIM
CI
BA
SIC
SII
Bas
icSu
ppor
tfo
rIn
stit
utio
naliz
ing
Chi
ldSu
rviv
alP
roje
ctB
FH
IB
aby-
Frie
ndly
Hos
pita
lIni
tiat
ive
ICD
SIn
tegr
ated
Chi
ldD
evel
opm
ent
Serv
ices
IM
CI
Inte
grat
edM
anag
emen
tof
Chi
ldho
odIl
lnes
sM
AD
LA
CM
onit
oreo
deA
poyo
Dir
ecto
con
laL
acat
anci
aM
ater
naN
GO
non
-gov
ernm
enta
lorg
aniz
atio
nPA
HO
Pan
Am
eric
anH
ealt
hO
rgan
izat
ion
PR
OB
ITP
rom
otio
nof
Bre
astf
eedi
ngIn
terv
enti
onTr
ial
PR
OC
OSI
Pro
gram
ade
Coo
rdin
acio
nen
Salu
dIn
tegr
al(C
olla
bora
tive
Pro
gram
for
Inte
grat
edH
ealt
h)U
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
WH
OW
orld
Hea
lth
Org
aniz
atio
n
Mainstreaming nutrition into MCH programs 21
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x2
Cas
est
udie
sin
scal
e-up
effo
rts
inH
IVA
IDS
Stud
yde
scri
ptio
nPo
pula
tion
Inte
rven
tion
Com
mun
icat
ion
stra
tegy
Impa
cton
excl
usiv
ebr
east
feed
ing
Com
men
ts
LIN
KA
GE
S(2
005)
Zam
bia
Pro
gram
me
thro
ugh
heal
th-c
are
and
com
mun
ity
serv
ices
Rea
ched
60si
tes
in6
dist
rict
sby
2005
Inte
grat
ion
ofin
fant
feed
ing
coun
selli
ngm
ater
naln
utri
tion
and
anti
retr
ovir
aldr
ugs
prop
hyla
xis
Trai
ning
ofhe
alth
wor
kers
and
com
mun
ity
serv
ice
prov
ider
sto
coun
selw
omen
onsa
fety
opti
ons
for
thei
rsi
tuat
ion
Beh
avio
urch
ange
Com
mun
icat
ion
inte
rven
tion
sin
the
first
few
year
sM
ater
iald
evel
oped
lsquoAct
Now
rsquoM
edia
cam
paig
nsin
clud
edbr
ochu
res
post
ers
radi
oan
dte
levi
sion
Ass
esse
dth
roug
hba
selin
ean
dfo
llow
-up
hous
ehol
dan
dcl
inic
surv
eys
inse
lect
eddi
stri
cts
Exc
lusi
vebr
east
feed
ing
rate
incr
ease
dfr
om50
in
2002
to64
in
2004
inL
ivin
gsto
nean
dfr
om57
in
2000
to74
in
2004
inN
dola
Inte
grat
edde
mon
stra
tion
proj
ect
Had
seve
rals
tren
gths
inte
rms
ofth
eus
eof
form
ativ
ere
sear
chto
deve
lop
mes
sage
str
aini
ngan
dbu
ildin
gup
skill
sof
prog
ram
me
man
ager
she
alth
-car
epr
ovid
ers
and
com
mun
ity
wor
kers
adv
ocac
yfo
rna
tion
alpo
licy
stro
ngbe
havi
our
chan
geco
mm
unic
atio
nco
mpo
nent
st
reng
then
ing
com
mun
ity
capa
city
for
coun
selli
ngan
dre
ferr
als
and
mon
itor
ing
and
eval
uati
onw
ith
loca
lpar
tner
sP
iwoz
etal
(20
05)
ZV
ITA
MB
Otr
ial
Har
are
Zim
babw
eE
duca
tion
and
coun
selli
ngpr
ogra
mm
ede
liver
edan
tena
tally
1411
0m
othe
rndashba
bypa
irs
enro
lled
from
14m
ater
nity
clin
ics
wit
hin
96h
ofde
liver
yan
dfo
llow
edup
at6
wee
ks
3m
onth
san
d3-
mon
thly
inte
rval
sIn
fant
-fee
ding
patt
erns
dete
rmin
edE
xclu
sive
brea
stfe
edin
gre
com
men
ded
for
HIV
nega
tive
un
know
nor
HIV
posi
tive
who
chos
eto
brea
stfe
ed
Gro
uped
ucat
ion
indi
vidu
alco
unse
lling
vid
eos
broc
hure
sM
othe
rsw
hoen
rolle
dw
hen
prog
ram
me
was
fully
impl
emen
ted
wer
e8
4ti
mes
mor
elik
ely
toex
clus
ivel
ybr
east
feed
than
mot
hers
who
enro
lled
befo
reth
epr
ogra
mm
ebe
gan
Ove
rall
excl
usiv
ebr
east
feed
ing
rate
sti
ll3
mon
ths
was
low
at24
6
Form
ativ
ere
sear
chus
edto
desi
gna
cult
ural
lyse
nsit
ive
educ
atio
nan
dco
unse
lling
prog
ram
me
Low
over
alle
xclu
sive
brea
stfe
edin
gra
tes
prom
pted
auth
ors
toco
nclu
deth
atw
omen
and
thei
rpa
rtne
rssh
ould
have
been
reac
hed
mor
efr
eque
ntly
duri
ngan
tena
tala
ndpo
st-n
atal
peri
od
N Bhandari and AKMI Kabir22
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Thi
oret
al(
2006
)R
ollin
s(2
007)
C
ohen
(200
7)
HIV
-inf
ecte
dpr
egna
ntw
omen
atte
ndin
gan
tena
talc
linic
sin
sout
hB
otsw
ana
Inve
stig
atio
nsby
CD
Cof
adi
arrh
oea
outb
reak
inJa
nuar
y-Fe
brua
ry20
06in
the
sam
epo
pula
tion
Mat
erna
land
infa
ntan
tire
trov
iral
ther
apy
toas
cert
ain
impa
cton
HIV
tran
smis
sion
Ant
enat
alco
unse
lling
Cas
endashco
ntro
lstu
dyto
iden
tify
risk
fact
ors
for
diar
rhoe
ano
tbr
east
feed
ing
was
the
bigg
est
risk
fact
ora
djus
ted
odds
rati
o50
(95
confi
denc
ein
terv
al4
5ndash10
0)
Bot
swan
aha
sth
ebe
stpr
imar
yhe
alth
-car
est
ruct
ure
wat
ersu
pply
and
sani
tati
onsy
stem
sin
Sout
hA
fric
aFo
rmul
apr
ovid
edfr
eeby
the
gove
rnm
ent
toin
fect
edm
othe
rsL
ower
mor
talit
yin
the
brea
stfe
edin
ggr
oup
at7
mon
ths
dem
onst
rate
sri
skof
form
ula
feed
ing
and
need
for
alte
rnat
est
rate
gies
(Thi
oret
al
2006
)A
utho
rsco
nclu
deth
athe
alth
syst
ems
inw
hich
thes
epr
ogra
mm
esar
eim
plem
ente
dsh
ould
beab
leto
cope
wit
hdi
arrh
oea
and
mal
nutr
itio
nth
atre
sult
sbe
caus
eof
form
ula
feed
ing
(Rol
lins
2007
)C
oova
dia
etal
(2
007)
Kw
aZul
uNat
al
Sout
hA
fric
a27
22H
IV-i
nfec
ted
and
unin
fect
edpr
egna
ntw
omen
enro
lled
into
ano
n-ra
ndom
ized
inte
rven
tion
coho
rtst
udy
from
ante
nata
lcl
inic
sIn
fant
feed
ing
data
obta
ined
wee
kly
bloo
dsa
mpl
esfr
omin
fant
sta
ken
mon
thly
83
of13
72in
fant
sbo
rnto
HIV
-inf
ecte
dm
othe
rsin
itia
ted
excl
usiv
ebr
east
feed
ing
from
birt
hB
reas
tfed
infa
nts
who
rece
ived
solid
sw
ere
sign
ifica
ntly
mor
elik
ely
toac
quir
ein
fect
ion
com
pare
dw
ith
excl
usiv
ely
brea
stfe
d(H
R10
87
151
ndash78
P=
001
8)as
wer
ein
fant
sw
hoat
12w
eeks
rece
ived
brea
stan
dfo
rmul
am
ilk(1
82
098
ndash33
6P
=0
57)
Cum
ulat
ive
3-m
onth
mor
talit
yin
excl
usiv
ely
brea
stfe
dw
as6
1(4
74ndash
792
)vs
15
1(7
63ndash
287
3)in
infa
nts
give
nre
plac
emen
tfe
eds
(HR
206
1
0ndash4
27P
=0
05)
The
stud
ysh
ows
that
excl
usiv
ebr
east
feed
ing
can
besu
cces
sful
lysu
ppor
ted
inH
IV-i
nfec
ted
wom
enT
heau
thor
sca
llfo
rfu
rthe
rre
visi
onof
UN
ICE
FW
HO
and
USA
IDin
fant
feed
ing
guid
elin
es
CD
CC
ente
rof
Dis
ease
Con
trol
HR
haz
ards
rati
oU
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
USA
IDU
SA
genc
yfo
rIn
tern
atio
nalD
evel
opm
ent
WH
OW
orld
Hea
lth
Org
aniz
atio
nZ
VIT
AM
BO
Z
imba
bwe
Vit
amin
Afo
rM
othe
rsan
dB
abie
s
Mainstreaming nutrition into MCH programs 23
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
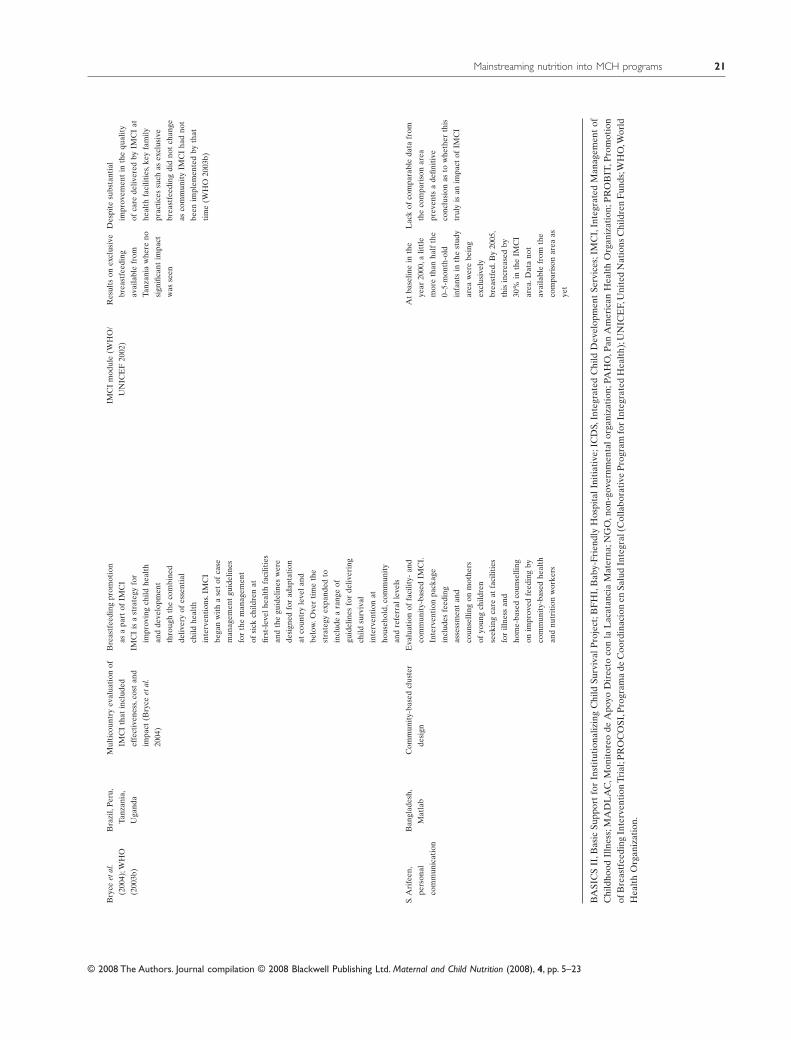
Bry
ceet
al
(200
4)W
HO
(200
3b)
Bra
zil
Per
u
Tanz
ania
Uga
nda
Mul
tico
untr
yev
alua
tion
of
IMC
Ith
atin
clud
ed
effe
ctiv
enes
sco
stan
d
impa
ct(B
ryce
etal
2004
)
Bre
astf
eedi
ngpr
omot
ion
asa
part
ofIM
CI
IMC
Iis
ast
rate
gyfo
r
impr
ovin
gch
ildhe
alth
and
deve
lopm
ent
thro
ugh
the
com
bine
d
deliv
ery
ofes
sent
ial
child
heal
th
inte
rven
tion
sIM
CI
bega
nw
ith
ase
tof
case
man
agem
ent
guid
elin
es
for
the
man
agem
ent
ofsi
ckch
ildre
nat
first
-lev
elhe
alth
faci
litie
s
and
the
guid
elin
esw
ere
desi
gned
for
adap
tati
on
atco
untr
yle
vela
nd
belo
wO
ver
tim
eth
e
stra
tegy
expa
nded
to
incl
ude
ara
nge
of
guid
elin
esfo
rde
liver
ing
child
surv
ival
inte
rven
tion
at
hous
ehol
dco
mm
unit
y
and
refe
rral
leve
ls
IMC
Im
odul
e(W
HO
UN
ICE
F20
02)
Res
ults
onex
clus
ive
brea
stfe
edin
g
avai
labl
efr
om
Tanz
ania
whe
reno
sign
ifica
ntim
pact
was
seen
Des
pite
subs
tant
ial
impr
ovem
ent
inth
equ
alit
y
ofca
rede
liver
edby
IMC
Iat
heal
thfa
cilit
ies
key
fam
ily
prac
tice
ssu
chas
excl
usiv
e
brea
stfe
edin
gdi
dno
tch
ange
asco
mm
unit
yIM
CI
had
not
been
impl
emen
ted
byth
at
tim
e(W
HO
2003
b)
SA
rife
en
pers
onal
com
mun
icat
ion
Ban
glad
esh
Mat
lab
Com
mun
ity-
base
dcl
uste
r
desi
gn
Eva
luat
ion
offa
cilit
y-an
d
com
mun
ity-
base
dIM
CI
Inte
rven
tion
pack
age
incl
udes
feed
ing
asse
ssm
ent
and
coun
selli
ngon
mot
hers
ofyo
ung
child
ren
seek
ing
care
atfa
cilit
ies
for
illne
ssan
d
hom
e-ba
sed
coun
selli
ng
onim
prov
edfe
edin
gby
com
mun
ity-
base
dhe
alth
and
nutr
itio
nw
orke
rs
At
base
line
inth
e
year
2000
alit
tle
mor
eth
anha
lfth
e
0ndash5-
mon
th-o
ld
infa
nts
inth
est
udy
area
wer
ebe
ing
excl
usiv
ely
brea
stfe
dB
y20
05
this
incr
ease
dby
30
inth
eIM
CI
area
Dat
ano
t
avai
labl
efr
omth
e
com
pari
son
area
as
yet
Lac
kof
com
para
ble
data
from
the
com
pari
son
area
prev
ents
ade
finit
ive
conc
lusi
onas
tow
heth
erth
is
trul
yis
anim
pact
ofIM
CI
BA
SIC
SII
Bas
icSu
ppor
tfo
rIn
stit
utio
naliz
ing
Chi
ldSu
rviv
alP
roje
ctB
FH
IB
aby-
Frie
ndly
Hos
pita
lIni
tiat
ive
ICD
SIn
tegr
ated
Chi
ldD
evel
opm
ent
Serv
ices
IM
CI
Inte
grat
edM
anag
emen
tof
Chi
ldho
odIl
lnes
sM
AD
LA
CM
onit
oreo
deA
poyo
Dir
ecto
con
laL
acat
anci
aM
ater
naN
GO
non
-gov
ernm
enta
lorg
aniz
atio
nPA
HO
Pan
Am
eric
anH
ealt
hO
rgan
izat
ion
PR
OB
ITP
rom
otio
nof
Bre
astf
eedi
ngIn
terv
enti
onTr
ial
PR
OC
OSI
Pro
gram
ade
Coo
rdin
acio
nen
Salu
dIn
tegr
al(C
olla
bora
tive
Pro
gram
for
Inte
grat
edH
ealt
h)U
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
WH
OW
orld
Hea
lth
Org
aniz
atio
n
Mainstreaming nutrition into MCH programs 21
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
App
endi
x2
Cas
est
udie
sin
scal
e-up
effo
rts
inH
IVA
IDS
Stud
yde
scri
ptio
nPo
pula
tion
Inte
rven
tion
Com
mun
icat
ion
stra
tegy
Impa
cton
excl
usiv
ebr
east
feed
ing
Com
men
ts
LIN
KA
GE
S(2
005)
Zam
bia
Pro
gram
me
thro
ugh
heal
th-c
are
and
com
mun
ity
serv
ices
Rea
ched
60si
tes
in6
dist
rict
sby
2005
Inte
grat
ion
ofin
fant
feed
ing
coun
selli
ngm
ater
naln
utri
tion
and
anti
retr
ovir
aldr
ugs
prop
hyla
xis
Trai
ning
ofhe
alth
wor
kers
and
com
mun
ity
serv
ice
prov
ider
sto
coun
selw
omen
onsa
fety
opti
ons
for
thei
rsi
tuat
ion
Beh
avio
urch
ange
Com
mun
icat
ion
inte
rven
tion
sin
the
first
few
year
sM
ater
iald
evel
oped
lsquoAct
Now
rsquoM
edia
cam
paig
nsin
clud
edbr
ochu
res
post
ers
radi
oan
dte
levi
sion
Ass
esse
dth
roug
hba
selin
ean
dfo
llow
-up
hous
ehol
dan
dcl
inic
surv
eys
inse
lect
eddi
stri
cts
Exc
lusi
vebr
east
feed
ing
rate
incr
ease
dfr
om50
in
2002
to64
in
2004
inL
ivin
gsto
nean
dfr
om57
in
2000
to74
in
2004
inN
dola
Inte
grat
edde
mon
stra
tion
proj
ect
Had
seve
rals
tren
gths
inte
rms
ofth
eus
eof
form
ativ
ere
sear
chto
deve
lop
mes
sage
str
aini
ngan
dbu
ildin
gup
skill
sof
prog
ram
me
man
ager
she
alth
-car
epr
ovid
ers
and
com
mun
ity
wor
kers
adv
ocac
yfo
rna
tion
alpo
licy
stro
ngbe
havi
our
chan
geco
mm
unic
atio
nco
mpo
nent
st
reng
then
ing
com
mun
ity
capa
city
for
coun
selli
ngan
dre
ferr
als
and
mon
itor
ing
and
eval
uati
onw
ith
loca
lpar
tner
sP
iwoz
etal
(20
05)
ZV
ITA
MB
Otr
ial
Har
are
Zim
babw
eE
duca
tion
and
coun
selli
ngpr
ogra
mm
ede
liver
edan
tena
tally
1411
0m
othe
rndashba
bypa
irs
enro
lled
from
14m
ater
nity
clin
ics
wit
hin
96h
ofde
liver
yan
dfo
llow
edup
at6
wee
ks
3m
onth
san
d3-
mon
thly
inte
rval
sIn
fant
-fee
ding
patt
erns
dete
rmin
edE
xclu
sive
brea
stfe
edin
gre
com
men
ded
for
HIV
nega
tive
un
know
nor
HIV
posi
tive
who
chos
eto
brea
stfe
ed
Gro
uped
ucat
ion
indi
vidu
alco
unse
lling
vid
eos
broc
hure
sM
othe
rsw
hoen
rolle
dw
hen
prog
ram
me
was
fully
impl
emen
ted
wer
e8
4ti
mes
mor
elik
ely
toex
clus
ivel
ybr
east
feed
than
mot
hers
who
enro
lled
befo
reth
epr
ogra
mm
ebe
gan
Ove
rall
excl
usiv
ebr
east
feed
ing
rate
sti
ll3
mon
ths
was
low
at24
6
Form
ativ
ere
sear
chus
edto
desi
gna
cult
ural
lyse
nsit
ive
educ
atio
nan
dco
unse
lling
prog
ram
me
Low
over
alle
xclu
sive
brea
stfe
edin
gra
tes
prom
pted
auth
ors
toco
nclu
deth
atw
omen
and
thei
rpa
rtne
rssh
ould
have
been
reac
hed
mor
efr
eque
ntly
duri
ngan
tena
tala
ndpo
st-n
atal
peri
od
N Bhandari and AKMI Kabir22
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Thi
oret
al(
2006
)R
ollin
s(2
007)
C
ohen
(200
7)
HIV
-inf
ecte
dpr
egna
ntw
omen
atte
ndin
gan
tena
talc
linic
sin
sout
hB
otsw
ana
Inve
stig
atio
nsby
CD
Cof
adi
arrh
oea
outb
reak
inJa
nuar
y-Fe
brua
ry20
06in
the
sam
epo
pula
tion
Mat
erna
land
infa
ntan
tire
trov
iral
ther
apy
toas
cert
ain
impa
cton
HIV
tran
smis
sion
Ant
enat
alco
unse
lling
Cas
endashco
ntro
lstu
dyto
iden
tify
risk
fact
ors
for
diar
rhoe
ano
tbr
east
feed
ing
was
the
bigg
est
risk
fact
ora
djus
ted
odds
rati
o50
(95
confi
denc
ein
terv
al4
5ndash10
0)
Bot
swan
aha
sth
ebe
stpr
imar
yhe
alth
-car
est
ruct
ure
wat
ersu
pply
and
sani
tati
onsy
stem
sin
Sout
hA
fric
aFo
rmul
apr
ovid
edfr
eeby
the
gove
rnm
ent
toin
fect
edm
othe
rsL
ower
mor
talit
yin
the
brea
stfe
edin
ggr
oup
at7
mon
ths
dem
onst
rate
sri
skof
form
ula
feed
ing
and
need
for
alte
rnat
est
rate
gies
(Thi
oret
al
2006
)A
utho
rsco
nclu
deth
athe
alth
syst
ems
inw
hich
thes
epr
ogra
mm
esar
eim
plem
ente
dsh
ould
beab
leto
cope
wit
hdi
arrh
oea
and
mal
nutr
itio
nth
atre
sult
sbe
caus
eof
form
ula
feed
ing
(Rol
lins
2007
)C
oova
dia
etal
(2
007)
Kw
aZul
uNat
al
Sout
hA
fric
a27
22H
IV-i
nfec
ted
and
unin
fect
edpr
egna
ntw
omen
enro
lled
into
ano
n-ra
ndom
ized
inte
rven
tion
coho
rtst
udy
from
ante
nata
lcl
inic
sIn
fant
feed
ing
data
obta
ined
wee
kly
bloo
dsa
mpl
esfr
omin
fant
sta
ken
mon
thly
83
of13
72in
fant
sbo
rnto
HIV
-inf
ecte
dm
othe
rsin
itia
ted
excl
usiv
ebr
east
feed
ing
from
birt
hB
reas
tfed
infa
nts
who
rece
ived
solid
sw
ere
sign
ifica
ntly
mor
elik
ely
toac
quir
ein
fect
ion
com
pare
dw
ith
excl
usiv
ely
brea
stfe
d(H
R10
87
151
ndash78
P=
001
8)as
wer
ein
fant
sw
hoat
12w
eeks
rece
ived
brea
stan
dfo
rmul
am
ilk(1
82
098
ndash33
6P
=0
57)
Cum
ulat
ive
3-m
onth
mor
talit
yin
excl
usiv
ely
brea
stfe
dw
as6
1(4
74ndash
792
)vs
15
1(7
63ndash
287
3)in
infa
nts
give
nre
plac
emen
tfe
eds
(HR
206
1
0ndash4
27P
=0
05)
The
stud
ysh
ows
that
excl
usiv
ebr
east
feed
ing
can
besu
cces
sful
lysu
ppor
ted
inH
IV-i
nfec
ted
wom
enT
heau
thor
sca
llfo
rfu
rthe
rre
visi
onof
UN
ICE
FW
HO
and
USA
IDin
fant
feed
ing
guid
elin
es
CD
CC
ente
rof
Dis
ease
Con
trol
HR
haz
ards
rati
oU
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
USA
IDU
SA
genc
yfo
rIn
tern
atio
nalD
evel
opm
ent
WH
OW
orld
Hea
lth
Org
aniz
atio
nZ
VIT
AM
BO
Z
imba
bwe
Vit
amin
Afo
rM
othe
rsan
dB
abie
s
Mainstreaming nutrition into MCH programs 23
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
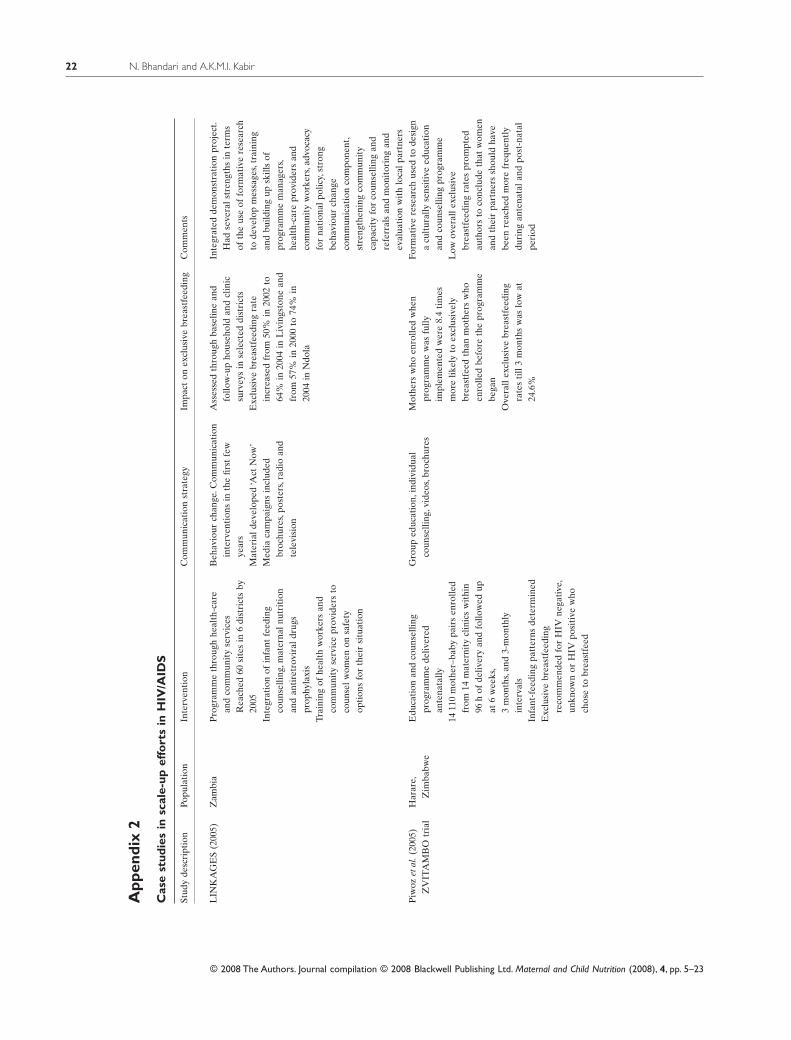
App
endi
x2
Cas
est
udie
sin
scal
e-up
effo
rts
inH
IVA
IDS
Stud
yde
scri
ptio
nPo
pula
tion
Inte
rven
tion
Com
mun
icat
ion
stra
tegy
Impa
cton
excl
usiv
ebr
east
feed
ing
Com
men
ts
LIN
KA
GE
S(2
005)
Zam
bia
Pro
gram
me
thro
ugh
heal
th-c
are
and
com
mun
ity
serv
ices
Rea
ched
60si
tes
in6
dist
rict
sby
2005
Inte
grat
ion
ofin
fant
feed
ing
coun
selli
ngm
ater
naln
utri
tion
and
anti
retr
ovir
aldr
ugs
prop
hyla
xis
Trai
ning
ofhe
alth
wor
kers
and
com
mun
ity
serv
ice
prov
ider
sto
coun
selw
omen
onsa
fety
opti
ons
for
thei
rsi
tuat
ion
Beh
avio
urch
ange
Com
mun
icat
ion
inte
rven
tion
sin
the
first
few
year
sM
ater
iald
evel
oped
lsquoAct
Now
rsquoM
edia
cam
paig
nsin
clud
edbr
ochu
res
post
ers
radi
oan
dte
levi
sion
Ass
esse
dth
roug
hba
selin
ean
dfo
llow
-up
hous
ehol
dan
dcl
inic
surv
eys
inse
lect
eddi
stri
cts
Exc
lusi
vebr
east
feed
ing
rate
incr
ease
dfr
om50
in
2002
to64
in
2004
inL
ivin
gsto
nean
dfr
om57
in
2000
to74
in
2004
inN
dola
Inte
grat
edde
mon
stra
tion
proj
ect
Had
seve
rals
tren
gths
inte
rms
ofth
eus
eof
form
ativ
ere
sear
chto
deve
lop
mes
sage
str
aini
ngan
dbu
ildin
gup
skill
sof
prog
ram
me
man
ager
she
alth
-car
epr
ovid
ers
and
com
mun
ity
wor
kers
adv
ocac
yfo
rna
tion
alpo
licy
stro
ngbe
havi
our
chan
geco
mm
unic
atio
nco
mpo
nent
st
reng
then
ing
com
mun
ity
capa
city
for
coun
selli
ngan
dre
ferr
als
and
mon
itor
ing
and
eval
uati
onw
ith
loca
lpar
tner
sP
iwoz
etal
(20
05)
ZV
ITA
MB
Otr
ial
Har
are
Zim
babw
eE
duca
tion
and
coun
selli
ngpr
ogra
mm
ede
liver
edan
tena
tally
1411
0m
othe
rndashba
bypa
irs
enro
lled
from
14m
ater
nity
clin
ics
wit
hin
96h
ofde
liver
yan
dfo
llow
edup
at6
wee
ks
3m
onth
san
d3-
mon
thly
inte
rval
sIn
fant
-fee
ding
patt
erns
dete
rmin
edE
xclu
sive
brea
stfe
edin
gre
com
men
ded
for
HIV
nega
tive
un
know
nor
HIV
posi
tive
who
chos
eto
brea
stfe
ed
Gro
uped
ucat
ion
indi
vidu
alco
unse
lling
vid
eos
broc
hure
sM
othe
rsw
hoen
rolle
dw
hen
prog
ram
me
was
fully
impl
emen
ted
wer
e8
4ti
mes
mor
elik
ely
toex
clus
ivel
ybr
east
feed
than
mot
hers
who
enro
lled
befo
reth
epr
ogra
mm
ebe
gan
Ove
rall
excl
usiv
ebr
east
feed
ing
rate
sti
ll3
mon
ths
was
low
at24
6
Form
ativ
ere
sear
chus
edto
desi
gna
cult
ural
lyse
nsit
ive
educ
atio
nan
dco
unse
lling
prog
ram
me
Low
over
alle
xclu
sive
brea
stfe
edin
gra
tes
prom
pted
auth
ors
toco
nclu
deth
atw
omen
and
thei
rpa
rtne
rssh
ould
have
been
reac
hed
mor
efr
eque
ntly
duri
ngan
tena
tala
ndpo
st-n
atal
peri
od
N Bhandari and AKMI Kabir22
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Thi
oret
al(
2006
)R
ollin
s(2
007)
C
ohen
(200
7)
HIV
-inf
ecte
dpr
egna
ntw
omen
atte
ndin
gan
tena
talc
linic
sin
sout
hB
otsw
ana
Inve
stig
atio
nsby
CD
Cof
adi
arrh
oea
outb
reak
inJa
nuar
y-Fe
brua
ry20
06in
the
sam
epo
pula
tion
Mat
erna
land
infa
ntan
tire
trov
iral
ther
apy
toas
cert
ain
impa
cton
HIV
tran
smis
sion
Ant
enat
alco
unse
lling
Cas
endashco
ntro
lstu
dyto
iden
tify
risk
fact
ors
for
diar
rhoe
ano
tbr
east
feed
ing
was
the
bigg
est
risk
fact
ora
djus
ted
odds
rati
o50
(95
confi
denc
ein
terv
al4
5ndash10
0)
Bot
swan
aha
sth
ebe
stpr
imar
yhe
alth
-car
est
ruct
ure
wat
ersu
pply
and
sani
tati
onsy
stem
sin
Sout
hA
fric
aFo
rmul
apr
ovid
edfr
eeby
the
gove
rnm
ent
toin
fect
edm
othe
rsL
ower
mor
talit
yin
the
brea
stfe
edin
ggr
oup
at7
mon
ths
dem
onst
rate
sri
skof
form
ula
feed
ing
and
need
for
alte
rnat
est
rate
gies
(Thi
oret
al
2006
)A
utho
rsco
nclu
deth
athe
alth
syst
ems
inw
hich
thes
epr
ogra
mm
esar
eim
plem
ente
dsh
ould
beab
leto
cope
wit
hdi
arrh
oea
and
mal
nutr
itio
nth
atre
sult
sbe
caus
eof
form
ula
feed
ing
(Rol
lins
2007
)C
oova
dia
etal
(2
007)
Kw
aZul
uNat
al
Sout
hA
fric
a27
22H
IV-i
nfec
ted
and
unin
fect
edpr
egna
ntw
omen
enro
lled
into
ano
n-ra
ndom
ized
inte
rven
tion
coho
rtst
udy
from
ante
nata
lcl
inic
sIn
fant
feed
ing
data
obta
ined
wee
kly
bloo
dsa
mpl
esfr
omin
fant
sta
ken
mon
thly
83
of13
72in
fant
sbo
rnto
HIV
-inf
ecte
dm
othe
rsin
itia
ted
excl
usiv
ebr
east
feed
ing
from
birt
hB
reas
tfed
infa
nts
who
rece
ived
solid
sw
ere
sign
ifica
ntly
mor
elik
ely
toac
quir
ein
fect
ion
com
pare
dw
ith
excl
usiv
ely
brea
stfe
d(H
R10
87
151
ndash78
P=
001
8)as
wer
ein
fant
sw
hoat
12w
eeks
rece
ived
brea
stan
dfo
rmul
am
ilk(1
82
098
ndash33
6P
=0
57)
Cum
ulat
ive
3-m
onth
mor
talit
yin
excl
usiv
ely
brea
stfe
dw
as6
1(4
74ndash
792
)vs
15
1(7
63ndash
287
3)in
infa
nts
give
nre
plac
emen
tfe
eds
(HR
206
1
0ndash4
27P
=0
05)
The
stud
ysh
ows
that
excl
usiv
ebr
east
feed
ing
can
besu
cces
sful
lysu
ppor
ted
inH
IV-i
nfec
ted
wom
enT
heau
thor
sca
llfo
rfu
rthe
rre
visi
onof
UN
ICE
FW
HO
and
USA
IDin
fant
feed
ing
guid
elin
es
CD
CC
ente
rof
Dis
ease
Con
trol
HR
haz
ards
rati
oU
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
USA
IDU
SA
genc
yfo
rIn
tern
atio
nalD
evel
opm
ent
WH
OW
orld
Hea
lth
Org
aniz
atio
nZ
VIT
AM
BO
Z
imba
bwe
Vit
amin
Afo
rM
othe
rsan
dB
abie
s
Mainstreaming nutrition into MCH programs 23
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
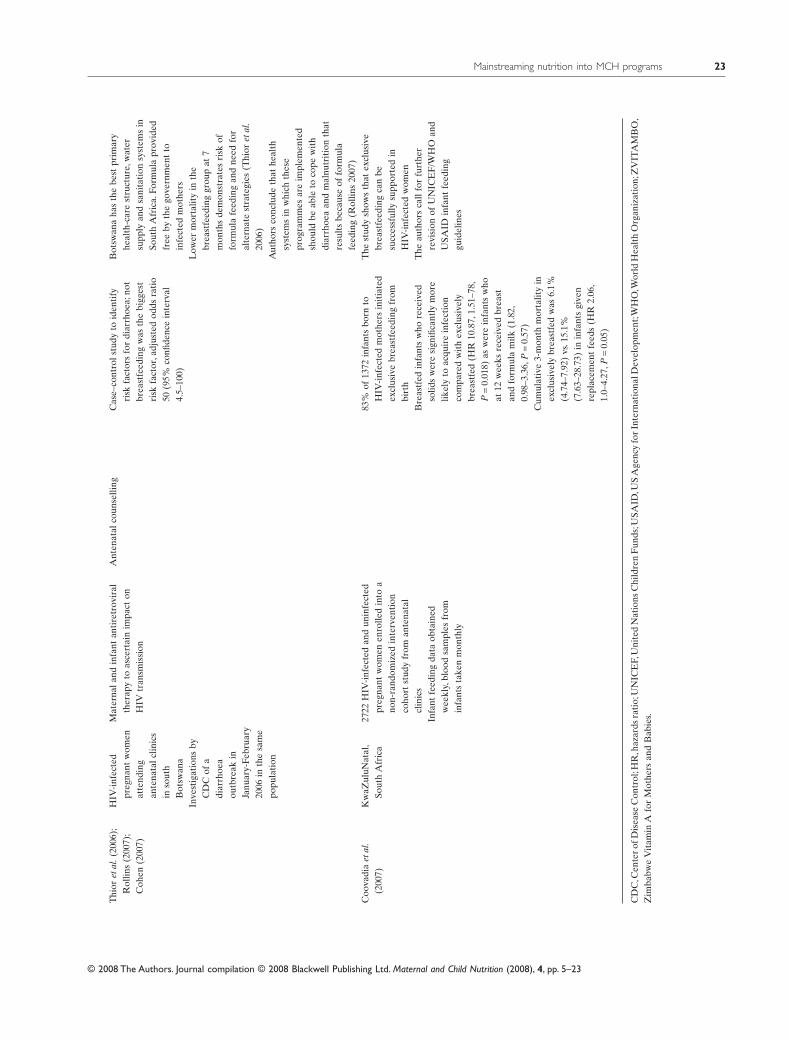
Thi
oret
al(
2006
)R
ollin
s(2
007)
C
ohen
(200
7)
HIV
-inf
ecte
dpr
egna
ntw
omen
atte
ndin
gan
tena
talc
linic
sin
sout
hB
otsw
ana
Inve
stig
atio
nsby
CD
Cof
adi
arrh
oea
outb
reak
inJa
nuar
y-Fe
brua
ry20
06in
the
sam
epo
pula
tion
Mat
erna
land
infa
ntan
tire
trov
iral
ther
apy
toas
cert
ain
impa
cton
HIV
tran
smis
sion
Ant
enat
alco
unse
lling
Cas
endashco
ntro
lstu
dyto
iden
tify
risk
fact
ors
for
diar
rhoe
ano
tbr
east
feed
ing
was
the
bigg
est
risk
fact
ora
djus
ted
odds
rati
o50
(95
confi
denc
ein
terv
al4
5ndash10
0)
Bot
swan
aha
sth
ebe
stpr
imar
yhe
alth
-car
est
ruct
ure
wat
ersu
pply
and
sani
tati
onsy
stem
sin
Sout
hA
fric
aFo
rmul
apr
ovid
edfr
eeby
the
gove
rnm
ent
toin
fect
edm
othe
rsL
ower
mor
talit
yin
the
brea
stfe
edin
ggr
oup
at7
mon
ths
dem
onst
rate
sri
skof
form
ula
feed
ing
and
need
for
alte
rnat
est
rate
gies
(Thi
oret
al
2006
)A
utho
rsco
nclu
deth
athe
alth
syst
ems
inw
hich
thes
epr
ogra
mm
esar
eim
plem
ente
dsh
ould
beab
leto
cope
wit
hdi
arrh
oea
and
mal
nutr
itio
nth
atre
sult
sbe
caus
eof
form
ula
feed
ing
(Rol
lins
2007
)C
oova
dia
etal
(2
007)
Kw
aZul
uNat
al
Sout
hA
fric
a27
22H
IV-i
nfec
ted
and
unin
fect
edpr
egna
ntw
omen
enro
lled
into
ano
n-ra
ndom
ized
inte
rven
tion
coho
rtst
udy
from
ante
nata
lcl
inic
sIn
fant
feed
ing
data
obta
ined
wee
kly
bloo
dsa
mpl
esfr
omin
fant
sta
ken
mon
thly
83
of13
72in
fant
sbo
rnto
HIV
-inf
ecte
dm
othe
rsin
itia
ted
excl
usiv
ebr
east
feed
ing
from
birt
hB
reas
tfed
infa
nts
who
rece
ived
solid
sw
ere
sign
ifica
ntly
mor
elik
ely
toac
quir
ein
fect
ion
com
pare
dw
ith
excl
usiv
ely
brea
stfe
d(H
R10
87
151
ndash78
P=
001
8)as
wer
ein
fant
sw
hoat
12w
eeks
rece
ived
brea
stan
dfo
rmul
am
ilk(1
82
098
ndash33
6P
=0
57)
Cum
ulat
ive
3-m
onth
mor
talit
yin
excl
usiv
ely
brea
stfe
dw
as6
1(4
74ndash
792
)vs
15
1(7
63ndash
287
3)in
infa
nts
give
nre
plac
emen
tfe
eds
(HR
206
1
0ndash4
27P
=0
05)
The
stud
ysh
ows
that
excl
usiv
ebr
east
feed
ing
can
besu
cces
sful
lysu
ppor
ted
inH
IV-i
nfec
ted
wom
enT
heau
thor
sca
llfo
rfu
rthe
rre
visi
onof
UN
ICE
FW
HO
and
USA
IDin
fant
feed
ing
guid
elin
es
CD
CC
ente
rof
Dis
ease
Con
trol
HR
haz
ards
rati
oU
NIC
EF
Uni
ted
Nat
ions
Chi
ldre
nF
unds
USA
IDU
SA
genc
yfo
rIn
tern
atio
nalD
evel
opm
ent
WH
OW
orld
Hea
lth
Org
aniz
atio
nZ
VIT
AM
BO
Z
imba
bwe
Vit
amin
Afo
rM
othe
rsan
dB
abie
s
Mainstreaming nutrition into MCH programs 23
copy 2008 The Authors Journal compilation copy 2008 Blackwell Publishing Ltd Maternal and Child Nutrition (2008) 4 pp 5ndash23
Related Documents











