Magnification chromoendoscopy for the diagnosis of gastric intestinal metaplasia and dysplasia Mdrio Dinis-Ribeiro, MD, Altamiro da Costa-Pereira, MD, PhD, Carlos Lopes, MD, PhD, Ldcio Lara-Santos, MD, Mateus Guilherme, MD, Luis Moreira-Dias, MD, Helena Lomba-Viana, MD, Armando Ribeiro, MD, Costa Santos, MD, Jos6 Soares, MD, Nuno Mesquita, MD, Rui Silva, MD, Rafael Lomba-Viana, MD, PhD Porto, Portugal Background: The aim of this study was to define the reproducibility and accuracy of magnification chromoendoscopy for the diagnosis of lesions associated with gastric cancer (intestinal metapla- sia and dysplasia). Methods: A total of 136 patients with previously diagnosed lesions and 5 gastrectomy specimens were studied. Endoscopic examination was performed with a magnification endoscope after meth- ylene blue (1%) spraying. According to differences in color and mucosal pattern, groups and sub- groups of endoscopic images were defined, and biopsies taken (n = 462). Five endoscopists were asked to classify individually 2 endoscopic images per subgroup on 2 separate occasions. Results: Three groups of endoscopic images were defined: nonmetaplastic, nondysplastic mucosa (I); metaplastic mucosa (11); and dysplastic mucosa (111). Ten subgroups were defined according to pit pattern: round small (IA), round and tubular small (IB), coarse round (IC), and course round pits with a straight pit (ID); blue irregular marks (IIA), blue round and tubular pits (liB), blue villi (IIC), and blue small pits (liD); and loss of clear pattern, with depression (IliA) or with slight elevation (lllB).The kappa statistic for intraobserver agreement on the classification of endo- scopic images in groups was 0.86; for interobserver agreement, it was 0.74. For classification into subgroups, kappa values ranged from 0.48 to 0.78. For 85% of the areas classified endoscopical- ly as Group I (n = 146), no mucosal lesions or gastritis was described at histologic examination; for83% of those in Group II (n = 198), intestinal metaplasia was found. Subgroups IIA and liB were more often associated with complete intestinal metaplasia (62%), and IIC and liD with incomplete metaplasia (67%); in Group III (n = 118), dysplasia was diagnosed histopathologically in 33%. For the diagnosis of dysplasia, specificity was 81% (95% CI [77%, 85%]) and negative predictive value 99% (95% CI [99%, 100%]). Conclusions: Gastric endoscopic patterns with chromoendoscopy and magnification seem repro- ducible and valid for the diagnosis of lesions associated with gastric cancer. This procedure may improve the follow-up of individuals at high-risk of gastric cancer, at least for the exclusion of severe lesions. (Gastrointest Endosc 2003;57:498-504.) Gastric cancer is the second most lethal diges- tive neoplasm in the world and the first in Portugal.I, 2 The prognosis for patients with this cancer clearly depends on stage at diagnosis. 3 At least for the intestinal subtype of gastric adenocar- cinoma, 4-6 a cascade of histopathologic lesions has been defined: chronic gastritis, atrophic chronic Received April 1, 2002. For revision September 4, 2002. Accepted December 4, 2002. Current affiliations: Instituto Portugu~s de Oncologia "Francisco Gentil," Centro do Porto, Faculdade de Medicina do Porto, Hospital de S. Jo~o and Hospital Geral de Santo Ant6nio, Porto, Portugal. Supported by grants from the Portuguese Health Ministry and from the Portuguese Society of Gastrointestinal Endoscopy. Reprint requests: Mdrio Dinis-Ribeiro, MD, Instituto Portugu~s de Oncologia "Francisco Gentil," Rua Dr. Ant6nio. Bernardino de Almeida, 4200-072 Porto, Portugal. Copyright 2003 by the American Saciety for Gastrointestinal Endoscopy 0016-5107/2003/$30.00 + 0 doi:10.1067 / mge.2003.145 gastritis, intestinal metaplasia, and dysplasia.4,7, s The identification of these lesions and follow-up of patients in whom they are found could lead to diag- nosis of gastric cancer at an early stage, thus improving patient survival. The diagnosis of these lesions, which often appear in flat mucosa,9, TM is currently based on histopathologic examination of endoscopic biopsy specimens. However, endoscopy for this purpose has high interobserver variabili- tyll, 12 and a poor correlation with histopathologic findings.13-20 The use of new methods, such as mag- nification endoscopy, could increase diagnostic yield for these lesions. The aims of the present study were to define the endoscopic findings (patterns) for intestinal metaplasia and dysplasia with magnification chromoendoscopy, to measure intraobserver and interobserver variability for the recognition of these endoscopic patterns in gastric mucosa, and to determine the diagnostic accuracy of these patterns. 498 GASTROINTESTINAL ENDOSCOPY VOLUME 57. NO. 4. 2003

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Magnification chromoendoscopy for the diagnosis of gastric intestinal metaplasia and dysplasia Mdrio Dinis-Ribeiro, MD, Altamiro da Costa-Pereira, MD, PhD, Carlos Lopes, MD, PhD, Ldcio Lara-Santos, MD, Mateus Guilherme, MD, Luis Moreira-Dias, MD, Helena Lomba-Viana, MD, Armando Ribeiro, MD, Costa Santos, MD, Jos6 Soares, MD, Nuno Mesquita, MD, Rui Silva, MD, Rafael Lomba-Viana, MD, PhD Porto, Portugal
Background: The aim of this study was to define the reproducibility and accuracy of magnification chromoendoscopy for the diagnosis of lesions associated with gastric cancer (intestinal metapla- sia and dysplasia). Methods: A total of 136 patients with previously diagnosed lesions and 5 gastrectomy specimens were studied. Endoscopic examination was performed with a magnification endoscope after meth- ylene blue (1%) spraying. According to differences in color and mucosal pattern, groups and sub- groups of endoscopic images were defined, and biopsies taken (n = 462). Five endoscopists were asked to classify individually 2 endoscopic images per subgroup on 2 separate occasions. Results: Three groups of endoscopic images were defined: nonmetaplastic, nondysplastic mucosa (I); metaplastic mucosa (11); and dysplastic mucosa (111). Ten subgroups were defined according to pit pattern: round small (IA), round and tubular small (IB), coarse round (IC), and course round pits with a straight pit (ID); blue irregular marks (IIA), blue round and tubular pits (liB), blue villi (IIC), and blue small pits (liD); and loss of clear pattern, with depression (IliA) or with slight elevation (lllB).The kappa statistic for intraobserver agreement on the classification of endo- scopic images in groups was 0.86; for interobserver agreement, it was 0.74. For classification into subgroups, kappa values ranged from 0.48 to 0.78. For 85% of the areas classified endoscopical- ly as Group I (n = 146), no mucosal lesions or gastritis was described at histologic examination; for83% of those in Group II (n = 198), intestinal metaplasia was found. Subgroups IIA and liB were more often associated with complete intestinal metaplasia (62%), and IIC and liD with incomplete metaplasia (67%); in Group III (n = 118), dysplasia was diagnosed histopathologically in 33%. For the diagnosis of dysplasia, specificity was 81% (95% CI [77%, 85%]) and negative predictive value 99% (95% CI [99%, 100%]). Conclusions: Gastric endoscopic patterns with chromoendoscopy and magnification seem repro- ducible and valid for the diagnosis of lesions associated with gastric cancer. This procedure may improve the follow-up of individuals at high-risk of gastric cancer, at least for the exclusion of severe lesions. (Gastrointest Endosc 2003;57:498-504.)
Gastric cancer is the second most lethal diges- tive neoplasm in the world and the first in Portugal.I, 2 The prognosis for patients with this cancer clearly depends on stage at diagnosis. 3 At least for the intestinal subtype of gastric adenocar- cinoma, 4-6 a cascade of histopathologic lesions has been defined: chronic gastritis, atrophic chronic
Received April 1, 2002. For revision September 4, 2002. Accepted December 4, 2002.
Current affiliations: Instituto Portugu~s de Oncologia "Francisco Gentil," Centro do Porto, Faculdade de Medicina do Porto, Hospital de S. Jo~o and Hospital Geral de Santo Ant6nio, Porto, Portugal.
Supported by grants from the Portuguese Health Ministry and from the Portuguese Society of Gastrointestinal Endoscopy.
Reprint requests: Mdrio Dinis-Ribeiro, MD, Instituto Portugu~s de Oncologia "Francisco Gentil," Rua Dr. Ant6nio. Bernardino de Almeida, 4200-072 Porto, Portugal.
Copyright �9 2003 by the American Saciety for Gastrointestinal Endoscopy 0016-5107/2003/$30.00 + 0
doi:10.1067 / mge.2003.145
gastritis, intestinal metaplasia, and dysplasia.4,7, s The identification of these lesions and follow-up of patients in whom they are found could lead to diag- nosis of gastric cancer at an early stage, thus improving patient survival. The diagnosis of these lesions, which often appear in flat mucosa,9, TM is currently based on histopathologic examination of endoscopic biopsy specimens. However, endoscopy for this purpose has high interobserver variabili- tyll, 12 and a poor correlation with histopathologic findings.13-20 The use of new methods, such as mag- nification endoscopy, could increase diagnostic yield for these lesions. The aims of the present study were to define the endoscopic findings (patterns) for intestinal metaplasia and dysplasia with magnification chromoendoscopy, to measure intraobserver and interobserver variability for the recognition of these endoscopic patterns in gastric mucosa, and to determine the diagnostic accuracy of these patterns.
498 GASTROINTESTINAL ENDOSCOPY VOLUME 57. NO. 4. 2003

Magnification chromoendoscopy for intestinal metaplasia and gastric dysplasia M Dinis-Ribeiro, A da Costa-Pereira, C Lopes, et al.
0oo^
? i,
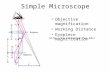
Figure 1. Magnification chromoendoscopic Group I images (nonmetaplastic, nondysplastic mucosa; no color change, regular mucosal pattern) subgrouped by pit pattern: A, round small pits (IA); B, round and tubular-small pits (IB); C, coarse round pits (IC); D, course round-pits with straight pit (ID).
PATIENTS AND METHODS Participants
The study included 141 patients seen between June and December 2001, who were being followed at our insti- tution (minimum 12 months follow-up; median follow-up, 3 years) because endoscopic biopsies had formerly revealed gastric mucosal changes such as dysplasia, meta- plasia, and chronic gastritis. Gastric cancer had recently developed in 5 of the pat ients (ulcerated early-stage, Lauren's intestinal type), which was located in the proxi- mal body (1), angularis (2), or antrum (2), with dimensions ranging from 30 to 34 mm. After surgery, the patients per- mit ted the gastrectomy specimens to be studied for mucosa] dysplasia and metaplasia. Informed consent was obtained from all participating patients. This study proto- col was approved by the ethical committee of our institute.
Endoscopic procedures The endoscopic examinations were performed by 2
endoscopists (M.D-R., R.L-V.) with a magnification endo- scope (Q240Z, Olympus Optical Co., Ltd., Tokyo, Japan) and videotaped for detailed analysis. All examinations were performed with the patients under conscious sedation. Before the procedure, all patients ingested simethicone (20 mL). A mucolytic agent (10% N-acetylcistein, 20 to 30 mL) was sprayed on the mucosal surface. For the purpose of staining areas with intestinal metaplasia, a 1% solution of methylene blue was sprayed over the gastric mucosa (medi- an volume 30 mL) with a spray catheter (PW-5L-1, Olympus). After 2 minutes, water was used to wash excess methylene blue from the gastric mucosa, which was then observed systematically. Mucosal patterns were observed by using the maximum magnification possible (_--105• and defined according to differences in color and homogeneity. In gastrectomy specimens, the malignancy was identified by endoscopy and the surrounding mucosa described.
The median time for performance of these endoscopic examinations was 16 minutes (range 12-24 minutes). Although patient satisfaction was not evaluated specifi- cally, the procedure was generally well-tolerated. However, it was aborted in 5 cases: 4 because of nausea and vomiting uncontrollable with medication, and one at the request of the patient.
Agreement study
Five endoscopists (L.M-D., H.L-V., A.R., C.S., J.S.), who did not participate in the conceptualization of the endo- scopic pat terns, were asked to classify 20 endoscopic images (2 images per subgroup) on two occasions, with an interval of at least one day between observations. Before making any observation, the endoscopists were given a short explanation of the rationale for each group and sub- group classification. The reference classification was defined and proposed by the 2 endoscopists who initially identified the patterns, that is, those who performed the endoscopies and systematically reviewed the video tapes. All 5 of the endoscopist observers were blinded as to the classifications of the other observers, to the reference clas- sification, and, at the second observation, to the results of their first observation.
Histopathologic definitions
Biopsy specimens were taken in each area with a dif- ferent endoscopic pattern. The histopathologic interpreta- tion of these specimens was used as the reference stan- dard against which the accuracy of the endoscopic patterns was assessed. Lesions such as chronic gastritis, atrophy, and intest inal metaplas ia were considered nondysplastic but possibly associated with gastric cancer, according to the so-called Vienna classification described by Schlemper et al. 21 Chronic gastritis was defined as a chronic diffuse inflammatory infiltrate with lymphocytes
VOLUME 57, NO. 4, 2003 GASTROINTESTINAL ENDOSCOPY 499

M Dinis-Ribeiro, A da Costa-Pereira, C Lopes, et al. Magnification chromoendoscopy for intestinal metaplasia and gastric dysplasia
V K
Figure 2. Magnification chromoendoscopic Group II images (metaplastic mucosa; blue color change, regular pattern) sub- grouped by pit pattern: A, blue irregular marks (IIA); B, blue round and tubular pits (liB); C, blue villi (IIC); D, blue small pits (liD).
Figure 3. Magnification chromoendoscopic Group III images (dysplastic mucosa; no clear color change [heterogeneous], no clear pattern): A, loss of clear pattern with depression (IliA); B, loss of clear pattern or slight elevation (IIIB).
and plasmocytes, expanding the lamina propria and epithelium, with no atypical cellular nuclei. Atrophy was defined as the disappearance of the normal glands in a certain area of the stomach; with the so-called Sydney classification of Guarner et a1.,22 atrophy was further clas- sifted as mild or severe. Intestinal metaplasia was classi- fled as complete (type I) and incomplete (type II or III), based on special staining (for sulpho or syalomucins). 23 Gastric dysplasia, further classified as low-grade or high- grade, and invasive carcinoma werb considered according to the Vienna classification. 23 Two pathologists (C.L., M.G.) reviewed all slides independently.
Statistical analysis Cohen's kappa coefficient (1<) and proportion of agree-
ment (Pa) were calculated as measures of agreement between observers in the classification of endoscopic images. Strength of agreement was considered as follows: 0.01-0.2 slight, 0.21-0.4 fair, 0.41-0.6 moderate, 0.61-0.8 substantial, 0.81-1.0 almost perfect.24, 25 Sensitivity, speci- ficity, and predictive values were calculated. The classifi- cation (Group I, Group II [Subgroups IIA, IIB, IIC, IID], and Group III) made for each endoscopic image (n = 462) was compared against the histopathologic evaluation of each corresponding biopsy. A statistical software package was used for data collection and analysis (SPSS 9.0, SPSS, Inc., Chicago, Ill.).
RESULTS Definition of endoscopic patterns
Videotapes (n = 141) and single images (n = 462) of areas from which biopsy specimens were obtained were reviewed. Three groups and 10 subgroups of endoscopic findings were defined.
If the color of the mucosa did not change after application of methylene blue and a regular muco- sal pa t t e rn was defined, the a rea observed was allocated to Group I (nonmetaplastic, nondysplastic mucosa) (Fig. 1). If the mucosa stained blue and a regular pat tern was present, the observed area was assigned to Group II (metaplastic mucosa) (Fig.2). If no clear change in color (heterogeneous) and no clear mucosal pa t te rn were evident, the endo- scopic image was assigned to Group III (dysplastic mucosa) (Fig. 3).
Ten subgroups (4 in Groups I and II, 2 in Group III) were defined according to pit pattern. For Group
500 GASTROINTESTINAL ENDOSCOPY VOLUME 57. NO. 4, 2003

Magnification chromoendoscopy for intestinal metaplasia and gastric dysplasia M Dinis-Ribeiro, A da Costa-Pereira, C Lopes, et al.
Table 1. Intraobserver and interobserver agreement for magnification chromoendoscopic patterns in stomach and agreement with reference classification for first and second observations
vs. Reference vs. Reference Intraobserver Interobserver (1st observation) (2nd observation)
Pa ~ Pa K Pa ~ Pa
Groups I-III 0.91 0.86 0.84 0.74 0.84 0.75 0.88 0.80 All subtypes 0.70 0.67 0.51 0.45 0.58 0.55 0.63 0.55
Subtypes I A-D 0.72 0.78 0.48 0.46 0.63 0.55 0.72 0.62 Subtypes II A-D 0.72 0.48 0.55 0.41 0.54 0.42 0.67 0.52 Subtypes III A-B 0.66 0.63 0.33 0.12 0.33 0.11 0.50 0.36
K, Kappa; Pa, proportion of agreement.
Table 2. Magnification chromoendoscopic patterns in stomach vs. histopathologic evaluation of corresponding biopsy specimens
Histology N(%) Total
N or CG cIM iIM Dys N = 462
Endoscopic pat terns I A-D 124 (85) 3 (2) 18 (12) 1 (1) 146 II A-B 23 (24) 59 (62) 13 (14) 0 95 II C-D 10 (10) 24 (23) 69 (67) 0 103 III A-B 50 (42) 11 (9) 19 (16) 38 (33) 118
N or CG, Normal mucosa or chronic gastritis; cIM, complete intestinal metaplasia; iIM, incom- plete intestinal metaplasia; Dys, dysplasia or invasive cancer.
I, these were as follows: round-small (IA), round and tubular-small (IB), coarse-round (IC), and course- round pits with a s t raight pit (ID). For Group II, these were as follows: blue irregular marks (IIA), blue round and tubular pits (IIB), blue villi (IIC), and blue small pits (IID). For the images in Group III, the subgroups were as follows: loss of clear pat tern with depression (IIIA) or with slight elevation (IIIB).
Reproducibility of endoscopic patterns: intraob- server and interobserver variation
The classifications made by the 5 endoscopists (who did not perform the procedures) for the endo- scopic images (2 for each subgroup) were compared (Table 1).
Both for intraobserver evaluation (Pa = 0.91, ~: = 0.86) and for interobserver evaluation (Pa = 0.84, = 0.74), a substantial agreement was noted for clas- sification of the images by groups (I, II, or III).
As for the classification of the images into sub- groups, intraobserver agreement was still good (Pa range, 0.66 to 0.72; K = 0.48 to 0.78), but it was only moderate (Pa = 0.51, r = 0.45) for interobserver eval- uation. Interobserver agreement was moderate for images belonging to Subgroups IA through ID (Pa = 0.48; ~ = 0.46), and for Subgroups IIA through IID (Pa = 0.55; ,c = 0.41). For Subgroups IIIA and IIIB, inter- observer agreement could not be defined (~ = 0.1).
There were some subgroups in which the propor- tion of agreement wi th the reference endoscopic
classification was low (data not shown). When each subgroup was analyzed separately, Subgroups IB, IIB, IIC, and IIIB showed a proportion of agreement between observers ranging from 75% to 100%, that is, different observers agreed on the inclusion of the images in their respect ive subgroups. For images allocated to Subgroups IA and ID, 50% to 75% of the observers agreed with these classifications. For images in Subgroups IIA, IID, a n d IIIA, less than 50% of the observations coincided.
The agreement between observers and reference endoscopic classification was measured at a f irst and at a second observation. For the first classifica- tion into groups, the Pa was 0.84 with ~ = 0.75; for the second classification, agreement seemed to increase slightly (Pa = 0.88; ~ = 0.80). This was also noted when images were classified into subgroups: for those belonging to Group I (Subgroups IA through ID), Pa increased from 0.63 to 0.72; for images classified as belonging to Group II (Subgroups IIA through IID), Pa increased from 0.54 to 0.67; for the images of Group III, (Subgroups IIIA, IIIB), Pa with reference was 0.33 and 0.50 at first and second observations, respectively.
Chromoendoscopy and magnification endoscopy for diagnosis of gastric intestinal metaplasia and dysplasia
Biopsy specimens were obtained from all areas (n = 462) imaged. Histopathologic diagnoses in relation
VOLUME 57, NO. 4, 2003 GASTROINTESTINAL ENDOSCOPY 501

M Dinis-Ribeiro, A da Costa-Pereira, C Lopes, et al. Magnification chromoendoscopy for intestinal metaplasia and gastric dysplasia
Table 3. Magnification chromoendoscopy in the diagnosis of gastric intestinal metaplasia and dysplasia Sensitivity Specificity Positive PV Negative PV Validity
Histologic lesion % (95% CI) % (95% CI) % (95% CI) % (95% CI) % (95% CI)
Intestinal metaplasia 76.4 (72.4, 80.3) 86.6 (83.4, 89.8) 83.3 (79.9, 86.8) 80.7 (77.0, 84.4) 81.8 (68.4, 95.2) 165/316 213/236 165/198 213/264 378/462
Complete 60.8 (56.3, 65.4) 90.1 (87.4, 92.9) 62.1 (57.6, 66.6) 89.6 (86.8, 92.5) 83.9 (71.7, 96.2) 59/97 329/365 59/95 329/367 388/462
Incomplete 58.0 (53.4, 62.5) 90.0 (87.3, 92.9) 66.9 (62.6, 71.4) 86.1 (82.8, 89.3) 81.8 (68.6, 95.0) 69/119 309/343 69/113 309/359 378/462
Dysplasia 97.4 (96.0, 98.9) 81.1 (77.4, 84.7) 32.2 (27.8, 36.5) 99.7 (99.2, 100.0) 82.5 (74.0, 91.0) 38/39 343/413 38/118 343/344 381/462
PV, Predictive values.
to endoscopic pa t te rns are shown in Table 2. For 85% of the areas classified as Group I (n = 146), no mucosal lesion or gastr i t is was described histopathologically. For 83% of those in Group II (n = 198), intestinal metaplasia was found. Subgroups IIA and IIB were more often associated with com- plete intestinal metaplasia (62%), and IIC and IID with incomplete metaplasia (67%). For Group III (n = ll8)Amages, dysplasia was diagnosed histopatho- logically in 33%.
Results for the diagnosis of intestinal metaplasia and dysplasia are shown in Table 3. For the diagnosis of intestinal metaplasia, the classification had an accuracy of 82% (95% CI [68%, 95%]), sensitivity of 76% (95% CI [72%, 80%]), specificity of 87% (95% CI [83%, 89%]), positive predictive value of 83% (95% CI [80%, 87%]), and negative predictive value of 81% (95% CI [77%, 84%]). The overall accuracy for the diagnosis of complete and incomplete metaplasia was, respectively, 84% (95% CI [72%, 96%]) and 82% (95% CI [69%, 95%]). For the diagnosis of dysplasia, accura- cy was 83% (95% CI [74%, 91%]), sensitivity 97% (95% CI [96%, 99%]), specificity 81% (95% CI [77%, 84%]), positive predictive value 32% (95% CI [28%, 36%]), and negative predictive value was 99% (95% CI [99%,
�9 100%]). There was just one false negative: an area classified as belonging to Group I was found histopathologically to contain low-grade dysplasia.
DISCUSSION
The diagnosis of gastric mucosal intestinal meta- plasia and dysplasia, and the follow-up of patients with these lesions, depends upon randomly obtained endoscopic biopsy specimens. 26-35 However, because these lesions are probably multifocal and may be present in flat mucosa, diagnosis by conventional endoscopy is charac ter ized by unsa t i s fac tory intraobserver agreement and poor correlation with histopathologic findings. 13-2~ Sauerbruch et al. 12 found thickened mucosal folds,,erosions, and visible areae gastricae to be the endoscopic features with the highest agreement among different observers.
Laine et al. 11 also assessed agreement on endoscopic descriptions for the diagnosis of chronic gastritis. Only modera te ag reement was found: prominent areae gastricae in the body of the stomach (~ = 0.49), nodularity in the body (K = 0.65), and antral nodu- lari ty (K = 0.68). Thus far, no endoscopic pat terns that clearly define intestinal metaplasia or dyspla- sia in the stomach have been found.
Chromoendoscopy is a l ready a commonly used, valuable endoscopic procedure in different segments of the GI tract, whereas magnification endoscopy is still being developed, and its potential impact on endoscopic diagnosis has not been fully explored. Mucosal pat terns defined by magnification endos- copy in the colon have been found to be predictive of the histopathologic characteristics of polyps , 36 and the recognition of aber ran t crypts has led to new insights into colon carcinogenesis. 37 There are also some studies of magnification endoscopy and chro- moendoscopy in pat ients with Barre t t ' s esopha- gnS. 38-45 Magnification endoscopy has also been pro- posed as useful for the diagnosis of early stage, protruded forms of gastric cancer . 46-48
The aim of the present study was to describe the endoscopic appearance of the gastric mucosa using magnification chromoendoscopy. If these techniques can be shown to be reproducible and valid, they could be used to identify intestinal metaplasia and dysplasia. The gastric mucosa was examined in 141 patients, and biopsy specimens were obtained from 462 different areas based on differences in mucosal pat tern and color. Each area was classified into 1 of 3 groups based on mucosal pat tern and change in color in response to spraying with a 1% solution of methylene blue: Group I, regular mucosal pattern, no change in color; Group II, blue mucosal staining together with a clearly defined pattern; and Group III, heterogeneous blue s taining with no mucosal pattern. The 3 groups were fur ther divided into sub- groups, 10 in total, based on pit patterns. For Group I, there are 4 subgroups: round small pits (IA), round and tubular small pits (IB), coarse round pits
502 GASTROINTESTINAL ENDOSCOPY VOLUME 57. NO. 4. 2003

Magnification chromoendoscopy for intestinal metaplasia and gastric dysplasia M Dinis-Ribeiro, A da Costa-Pereira, C Lopes, et al.
(IC), and course round pits with a straight pit (ID). For Group II, there are 4 subgroups: blue irregular marks (IIA), blue round and tubular pits (IIB), blue villi (IIC), and blue small pits (IID). For Group II, there are 2 subgroups: a slight depression (IIIA) or a slight elevation (IIIB).
Five endoscopist observers a t tempted to classify 20 images (not seen previously) on 2 separate occa- sions. Although they were given an explanat ion prior to each classification procedure, they had no knowledge of the image classification (reference classification) conceived by the 2 endoscopists who obtained the images, nor of the classifications made by the other observers or their initial classification of the images at the second at tempt at classification. In t raobserver agreement was subs tan t ia l for the classification into groups and for most subgroups as well (Table 1). Furthermore, agreement with the ref- erence classification tended to increase with the sec- ond observation. Thus, the 5 observers seemed to be able to unders tand the concept for each category, to remember it, and to improve their classification of the images at a second attempt. Observers seemed to agree on the rationale and concept for the image classification, as high levels of interobserver agree- ment were also found concerning the dist inction between nonmetaplastic, nondysplastic, and meta- plastic or dysplast ic areas of gastric mucosal. However, for some subgroups, only a moderate level of agreement was found.
The endoscopic subgroups seemed to be valid for the diagnosis of lesions associated with gastric can- cer, at least for the exclusion of more advanced lesions such as incomplete metaplasia or dysplasia. High negative predictive values and reasonable sen- sitivity, specificity, and validity were found based on actual histopathologic diagnoses. The positive pre- dictive value for dysplasia was low. Further studies are needed to improve reproducibility and address further questions such as the clinical applicability and acceptance magnification chromoendoscopy.
The definition of Groups II and III should be revised. Additionally, the descript ion of the sub- groups can be optimized.
For Group II, Subgroups IIA and IIB, and Sub- groups IIC and IID could be combined. Complete intestinal metaplasia was the main histopathologic lesion associated with images classified as IIA or IIB, and incomplete intestinal metaplasia was the change found in biopsy specimens from areas of mucosa clas- sified endoscopically as IIC and IID. Low levels of agreement were found for Subgroups IIA and IID. If the observers had been asked to classify the endo- scopic images such that Subgroups IIA and IIB were combined, as well as IIC and IID, intraobserver and
interobserver agreement would improve from slight to moderate (from Pa = 0.48 to 0.71 for IIA and IIB combined; and Pa = 0.41 to 0.62 for subgroups IIC and IID considered together). Also, the subdivision of Group III into Subgroups IIIA and IIIB should be abandoned, as there was no interobserver agreement with regard to this distinction, both represent the same histopathologic changes, and the observers had difficulty distinguishing them.
In conclusion, the diagnosis of gastric lesions associated with gastric cancer, metaplasia as well as dysplasia, by magnification chromoendoscopy with methylene blue seems to be valid and reproducible. These results suggest that, after a learning curve (to be defined), this procedure could be applied to the follow-up of pat ients with gastric intestinal meta- plasia and dysplasia.4,9, 26-33
REFERENCES
1. Black RJ, Bray F, Ferlay J, Parkin DM. Cancer incidence and mortality in the European Union: cancer registry data and estimates of national incidence for 1990. Eur J Cancer 1997;33:1075-107.
2. Levi F, La Vecchia C, Lucchini F, Negri E. Cancer mortality in Europe, 1990-92. Eur J Cancer Prev 1995;4:389-417.
3. Hundahl SA, Menck HR. Mansour EG, Winchester DP. The national cancer data base report on gastric carcinoma. Cancer 1997;80:2333-41.
4. Carneiro F, Machado JC, David L, Reis C, Nogueira AMMF, Sobrinho-SimSes M. Current thoughts on the histopathogen- esis of gastric cancer. Eur J Cancer Prev 2001;10:101-2.
5. Correa P. Human gastric carcinogenesis: a multistep and multifactorial process. First American Cancer Society award lecture on cancer epidemiology and prevention. Cancer Res 1992;52:6735-40.
6. Sipponen P, Hyv~irinen H, Sepp~il~i K, Blaser MJ. Review arti- cle: pathogenesis of the transformation from gastritis to malignancy. Aliment Pharmacol Ther 1998;12:61-71.
7. Conchillo JM, Houben G, de Bruine A, Stockbrugger RW. Is type III intestinal metaplasia an obligatory precancerous lesion in intestinal-type gastric carcinoma? Eur J Cancer Prev 2001;10:307-12.
8. Reis C, David L, Correa P, Carneiro F, BolSs C, Garcia E, et al. Intestinal metaplasia of human stomach displays distinct patterns of mucin (MUC1, MUC2, MUC5AC, and MUC6) expression. Cancer Res 1999;59:1003-7.
9. Rugge M, Farinati F, Baffa R, Sonego F, Di Mario F, Leandro G, et al. Gastric epithelial dysplasia in the natural history of gastric cancer: a multicenter prospective follow-up study. Gastroenterology 1994;107:1288-96.
10. Rugge M, Leandro G, Farinati F, Di Mario F, Sonego F, Cassaro M, et al. Gastric epithelial dysplasia. How clinico- pathologic background relates to management. Cancer 1995;76:376-82.
11. Laine L, Cohen H, Sloane R, Marin-Sorensen M, Weinstein WM. Interobserver agreement and predictive value of endo- scopic findings for H pylori and gastritis in normal volun- teers. Gastrointest Endosc 1995;42:420-3.
12. Sauerbruch T, Schreiber MA, Schiissler P, Permanetter W. Endoscopy in the diagnosis of gastritis. Diagnostic value of endoscopic criteria in relation to histological diagnosis. Endoscopy 1984;16:101-4.
VOLUME 57, NO. 4, 2003 GASTROINTESTINAL ENDOSCOPY 503

M Dinis-Ribeiro, A da Costa-Pereira, C Lopes, et al. Magnification chromoendoscopy for intestinal metaplasia and gastric dysplasia
13. Atkins L, Benedict EB. Correlation, of gross gastroscopic find- ings with gastroscopic biopsy in gastritis. N Engl J Med 1956; 254:641-4.
14. Belair PA, Metz DC, Faigel DO, Furth EE. Receiver operator characteristic analysis of endoscopy as a test for gastritis. Dig Dis Sci 1997;42:2227-33.
15. Carpenter HA, Talley NJ. Gastroscopy is incomplete without biopsy: clinical relevance of distinguishing gastropathy from gastritis. Gastroenterology 1995;108:917-24.
16. Heinkel K. Correlation of gastroscopy, gastric photography and biopsy in diagnosis. Gastrointest Endosc 1969;16:81-5.
17. Khakoo SI, Lobo A1, Shepherd NA, Metz DC. Histologic assessment of the Sydney classification of endoscopic gastri- tis. Gut 1994;36:1172-5.
18. Maratka Z. Endoscopic diagnosis of gastritis: pros and cons. J Clin Gastroenterol 1995;20:92-3.
19. Stathopoulos G, Goldberg RD, Blackstone MO. Endoscopic diagnosis of intestinal metaplasia. Gastrointest Endosc 1990; 36:544-5.
20. Meshkinpour H, Orlando RA, Arguello JF, DeMicco MP. Significance of endoscopically visible blood vessels as an index of atrophic gastritis. Am J Gastroenterol 1979;71:376-9.
21. Schlemper RJ, Riddell RH, Kato Y, Borchard F, Cooper HS, Dawsey SM, et al. The Vienna classification of gastrointesti- nal epithelial neoplasia. Gut 2000;47:251-5.
22. Guarder J, Herrera-Goepfert R, Mohar A, Sanchez L, Halperin D, Ley C, et al. Interobserver variability in applica- tion of the revised Sydney classification of gastritis. Hum Pathol 1999;30:1431-4.
23. Filipe MI, Barbatis C, Sandey A, Metz DC. Expression of intestinal mucin antigens in the gastric epithelium and its relationship with malignancy. Hum Pathol 1998; 19:19-26.
24. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986;I:307-10.
25. Chien PF, Khan KS. Evaluation of a clinical test. II: assess- ment of validity. BJOG 2001; 108:568-72.
26. Fertitta AM, Comin U, Terruzzi V, Minoli G, Zambelli A, Camatelli G, et al. Clinical significance of gastric dysplasia: a multicenter follow-up study. Endoscopy 1993;25:265-8.
27. You WC, Li JY, B10t WY, Chang YS, Jin ML, Gail MH, et al. Evolution of precancerous lesions in a rural Chinese popula- tion at high risk of gastric cancer. Int J Cancer 1999;83:615-9.
28. Sipponen P, Kekki M, Haapakoski J, Ihmaki T, Siurala M. Gastric cancer risk in chronic atrophic gastritis: statistical calculations of cross-sectional data. Int J Cancer 1985;35: 173-7.
29. Di Gregorio C, Morandi P, Fante R, De Caetani C. Gastric dys- plasia. A follow-up study. Am J Gastroenterol 1993;88:1714-9.
30. Bearzi I, Brancorsini D, Santinelli A, Rezai B, Mannello B, Ranaldi R. Gastric dyspiasia: a ten-year follow-up study. Path Res Pract 1994;190:61-8.
31. Correa P, Haenszel W, Cuello C, Zavala D, Fontham E, Zarama G, et al. Gastric precancerous process in a high risk popula- tion: cohort follow-up. Cancer Research 1990;50:4737-40.
32. Riddell RH. Premalignant and early malignant lesions in the
gastrointestinal tract: definitions, terminology and problems. Am J Gastroenterol 1996;91:864-72.
33. Kokkola A, Haapiainen R, Laxen F, Puolakkainen P, Kivilaakso E, Virtamo J, et al. Risk of gastric carcinoma in patients with mucosal dysplasia associated with atrophic gas- tritis: a follow up study. J Clin Pathol 1996;49:979-84.
34. Pickover LM. Gastric biopsies: a matter of routine? Gastro- enterology 1995;109:664-5.
35. Talley NJ, Faigel DO. Gastric biopsies: a matter of routine [letter]? Gastroenterology 1995;109:665.
36. Kudo S, Tamura S, Nakajima T, Yamano H, Kusaka H, Watanabe H. Diagnosis of colorectal tumors lesions by mag- nifying endoscopy. Gastrointest Endosc 1996;44:8-14.
37. Takayama T, Katsuki S, Takahashi Y, Ohi M, Nojiri S, Sakamaki S, et al. Aberrant crypt foci of the colon as precur- sors of adenoma and cancer. N Engl J Med 1998;339:1277-84.
38. Shrestha S, Xiao SY, Reeves AL, Waxman I. Can high resolu- tion and high magnification endoscopy (HRHME) accurately predict the presence of specialized intestinal metaplasia in patients with Barrett's esophagus and serve as a surrogate optical biopsy [abstract]? Endoscopy 2001;53:121.
39. Stevens PD, Lightdale CJ, Green PHR, Siegel LM, Garcia- Carrasquillo RJ, Rotterdam H. Combined magnification endoscopy with chromoendoscopy for the evaluation of Barrett's esophagus. Gastrointest Endosc 1994:40:747-9.
40. Sharma P, Weston AP. Magnification chromoendoscopy for the detection of intestinal metaplasia and dysplasia in Barrett's esophagus [abstract]. Gastrointest Endosc 2001;53:AB62.
41. Jung M, Kiesslich R. Chromoendoscopy and intravital stain- ing techniques. Baillieres Best Pract Res Clin Gastroenterol 1999;13:11-9.
42. Canto MIF, Setrakian S, Willis J, Chak A, Petras R, Powe NR, et al. Methylene blue-directed biopsies improve detection of intestinal metaplasia and dysplasia in Barrett's esophagus. Gastrointest Endosc 2000;51:560-8.
43. Canto MIF, Setrakian S, Willis J, Chak A, Petras R, Sivak MV Jr. Methylene blue staining of dysplastic and non-dysplastic Barrett's esophagus: an in vivo and ex vivo study. Endoscopy 2001;33:391-400.
44. Bouma BE, Tearney GJ, Compton CC, Nishioka NS. High-res- olution imaging of the human esophagus and stomach in vivo using optical coherence tomography. Gastrointest Endosc 2000;51:467-73.
45. TSth E, SjSlund K, Fork FT, LindstrSm C. Chronic atrophic fundic gastritis diagnosed by a modified Congo Red test. Endoscopy 1995;27:654-8.
46. Guelrud M, Herrera I, Essenfeld H, Castro J. Usefulness of enhanced magnification endoscopy in Barrett's esophagus [abstract]. Am J Gastroenterol 2000;95:M144.
47. Tajiri H, Doi T, Endo H, Nishina T, Terao T, Hirasaki S, et al. The application of magnifying endoscopy to gastric cancer diagnosis: a prospective study [abstract]. Endoscopy 2001;53:123.
48. Yamaguchi Y, Takahashi H, Ukawa K, Shoji T, Fujita R. Usefulness of magnifying endoscopy and new techniques for diagnosis of protruded early gastric cancer [abstract]. Endos- copy 2001;53:123.
504 GASTROINTESTINAL ENDOSCOPY VOLUME 57, NO. 4, 2003
Related Documents