Magnetocardiographic Pacemapping for Nonfluoroscopic Localization of Intracardiac Electrophysiology Catheters RICCARDO FENICI.* KATJA PESOLA,**,+ PETRI KORHONEN,t,* MARKKU MAKIJARVI.t,* JUKKA NENONEN,**,t LAURIE TOIVONEN.t,* PETER FENICI,* and TOIVO KATILA**,* From the *Clinical Physiology—Biomagnetism Research Center, Catholic University, Rome, Italy; **Laboratory of Biomedical Engineering, Helsinki University of Technology, Helsinki; tMedical Engineering Centre, BioMag Laboratory, University Central Hospital, Helsinki; and the ^Division of Cardiology, Helsinki University of Technology, Helsinki, Finland FENICI, R., ET AL.: Magnetocardiographic Pacemapping for Nonflouroscopic Localization of Intracar- diac Electrophysiology Catheters. The purpose of the study was to validate, in patients, the accuracy of magnetocardiography (MCG) for three-dimensional localization of an amagnetic catheter (AC) for multi- ple monophasic action potential (MAP) with a spatial resolution of 4 mm2. The AC was inserted in five patients after routine electrophysiological study. Four MAPs were simultaneously recorded to monitor the stability of endocardial contact of the AC during the MCG localization. MAP signals were band-pass fil- tered DC-500 Hz and digitized at 2 KHz. The position of the AC was also imaged by biplane fluoroscopy (XB), along with lead markers. MGG studies were performed with a multichannel SQUID system in the Helsinki BioMag shielded room. Current dipoles (5mm; 10mA), activated at the tip of the AC, were local- ized using the equivalent current dipole (ECD) model in patient-specific boundary element torso. The ac- curacy of the MCG localizations was evaluated by: (1) anatomic location of ECD in the MBI, (2) mismatch with XR. The AC was correctly localized in the right ventricle of all patients using MRI. The mean three- dimensional mismatch between XR and MCG localizations was 6 ± 2 mm (beat-to-beat analysis). The co- efficient of variation of three-dimensional localization of the AC was 1.37% and the coefficient of repro- ducibility was 2.6 mm. In patients, in the absence of arrhythmias, average local variation coefficients of right ventricular MAP duration at 50% and 90% of repolarization, were 7.4% and 3.1%, respectively. This study demonstrates that vtith adequate signal-to-noise ratio, MCC three-dimensional localizations are ac- curate and reproducible enough to provide nonfluoroscopy dependant multimodal imaging for high res- olution endocardial mapping of monophasic action potentials. (PACE 1998; 2l[Pt. U]:2492-2499) magnetocardiograpby, monopbasic action potential, amagnetic pacing catbeter, boundary element metbod, equivalent current dipole localization Introduction The identification of the mechanisms of focal arrhythmias and the localization of their suhstrate is sometimes difficult even with invasive electro- This work was supported by the EU HCM Large Scale Installa- tion in Biomagnetic Research (BIRCH) at Helsinki University of Technology, and by the Italian National Research Council (CNR). Address for reprints; Riccardo R. Fenici, M.D., Clinical Physi- ology—Biomagnetism Center, Catholic University of Rome, Largo A. Cemelli, 8, 00168, Rome, Italy. Fax: 39-6-3051343; e- mail; [email protected] physiological study. Therefore during the last years surface potential mapping^'^ and other non- invasive imaging techniques'"^ have been used, before and during electrophysiological study, to facilitate the localization of arrhythmogenic suh- strates and to improve the outcome of ablative in- terventions, while minimizing the use of fluo- roscopy. Magnetocardiographic mapping (MCG) is the most recent noninvasive method that provides quantitative three-dimensional localization and imaging of cardiac arrhythmias.^"^ A pacemap- ping method hased on MCG recordings was devel- 2492 Noveniber 1998, Part U PACE, Vol. 21

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Magnetocardiographic Pacemapping forNonfluoroscopic Localization of IntracardiacElectrophysiology Catheters
RICCARDO FENICI.* KATJA PESOLA,**,+ PETRI KORHONEN,t,*MARKKU MAKIJARVI.t,* JUKKA NENONEN,**,t LAURIE TOIVONEN.t,*PETER FENICI,* and TOIVO KATILA**,*
From the *Clinical Physiology—Biomagnetism Research Center, Catholic University, Rome, Italy;**Laboratory of Biomedical Engineering, Helsinki University of Technology, Helsinki; tMedical EngineeringCentre, BioMag Laboratory, University Central Hospital, Helsinki; and the ^Division of Cardiology,Helsinki University of Technology, Helsinki, Finland
FENICI, R., ET AL.: Magnetocardiographic Pacemapping for Nonflouroscopic Localization of Intracar-diac Electrophysiology Catheters. The purpose of the study was to validate, in patients, the accuracy ofmagnetocardiography (MCG) for three-dimensional localization of an amagnetic catheter (AC) for multi-ple monophasic action potential (MAP) with a spatial resolution of 4 mm2. The AC was inserted in fivepatients after routine electrophysiological study. Four MAPs were simultaneously recorded to monitor thestability of endocardial contact of the AC during the MCG localization. MAP signals were band-pass fil-tered DC-500 Hz and digitized at 2 KHz. The position of the AC was also imaged by biplane fluoroscopy(XB), along with lead markers. MGG studies were performed with a multichannel SQUID system in theHelsinki BioMag shielded room. Current dipoles (5mm; 10mA), activated at the tip of the AC, were local-ized using the equivalent current dipole (ECD) model in patient-specific boundary element torso. The ac-curacy of the MCG localizations was evaluated by: (1) anatomic location of ECD in the MBI, (2) mismatchwith XR. The AC was correctly localized in the right ventricle of all patients using MRI. The mean three-dimensional mismatch between XR and MCG localizations was 6 ± 2 mm (beat-to-beat analysis). The co-efficient of variation of three-dimensional localization of the AC was 1.37% and the coefficient of repro-ducibility was 2.6 mm. In patients, in the absence of arrhythmias, average local variation coefficients ofright ventricular MAP duration at 50% and 90% of repolarization, were 7.4% and 3.1%, respectively. Thisstudy demonstrates that vtith adequate signal-to-noise ratio, MCC three-dimensional localizations are ac-curate and reproducible enough to provide nonfluoroscopy dependant multimodal imaging for high res-olution endocardial mapping of monophasic action potentials. (PACE 1998; 2l[Pt. U]:2492-2499)
magnetocardiograpby, monopbasic action potential, amagnetic pacing catbeter, boundary elementmetbod, equivalent current dipole localization
Introduction
The identification of the mechanisms of focalarrhythmias and the localization of their suhstrateis sometimes difficult even with invasive electro-
This work was supported by the EU HCM Large Scale Installa-tion in Biomagnetic Research (BIRCH) at Helsinki University ofTechnology, and by the Italian National Research Council(CNR).
Address for reprints; Riccardo R. Fenici, M.D., Clinical Physi-ology—Biomagnetism Center, Catholic University of Rome,Largo A. Cemelli, 8, 00168, Rome, Italy. Fax: 39-6-3051343; e-mail; [email protected]
physiological study. Therefore during the lastyears surface potential mapping ' and other non-invasive imaging techniques'"^ have been used,before and during electrophysiological study, tofacilitate the localization of arrhythmogenic suh-strates and to improve the outcome of ablative in-terventions, while minimizing the use of fluo-roscopy.
Magnetocardiographic mapping (MCG) is themost recent noninvasive method that providesquantitative three-dimensional localization andimaging of cardiac arrhythmias.^"^ A pacemap-ping method hased on MCG recordings was devel-
2492 Noveniber 1998, Part U PACE, Vol. 21
NONFLUOROSCOPIC MCG LOCALIZATION OF ELECTRODE CATHETERS
oped at the Catholic University of Ronie.^°'^^ Inprevious studies MCG pacemapping was used tolocate the tip of the amagnetic pacing catheterand to fit the catheter position with the three-di-mensional MCG coordinates of the arrhythmo-genic target, with a reported localization accuracyranging between 5 and 25 mm.^^ This study wascarried out to: (1) quantify the three-dimensionalaccuracy of MCC to localize an intracardiacsource; (2) evaluate the accuracy of MCG to imagethe three-dimensional position of the tip of an am-agnetic catheter (AC) for electrophysiologicalstudy, without the use of fluoroscopy; (3) validatethe reliability of the new multipurpose AC forhigh resolution (HR) multiple monophasic actionpotential (MAP) recording; and (4) evaluate thefeasibility of the MCC method for multimodalthree-dimensional electroanatomical integrationof electrophysiological recordings carried out asclose as possihie to the arrhythmogenic substrate.
MethodsPatient Studies
Five patients, all investigated for supraven-tricular arrhythmias, volunteered for the MCG ad-ditional procedure after standard electrophysio-logical study. The research project was approvedhy the Ethical Committee of HUCH. After the di-agnostic electrophysiological study was com-pleted, the AC was inserted in the right ventricle.The position of the catheter tip was documentedin orthogonal fluoroscopic projections.
The AC
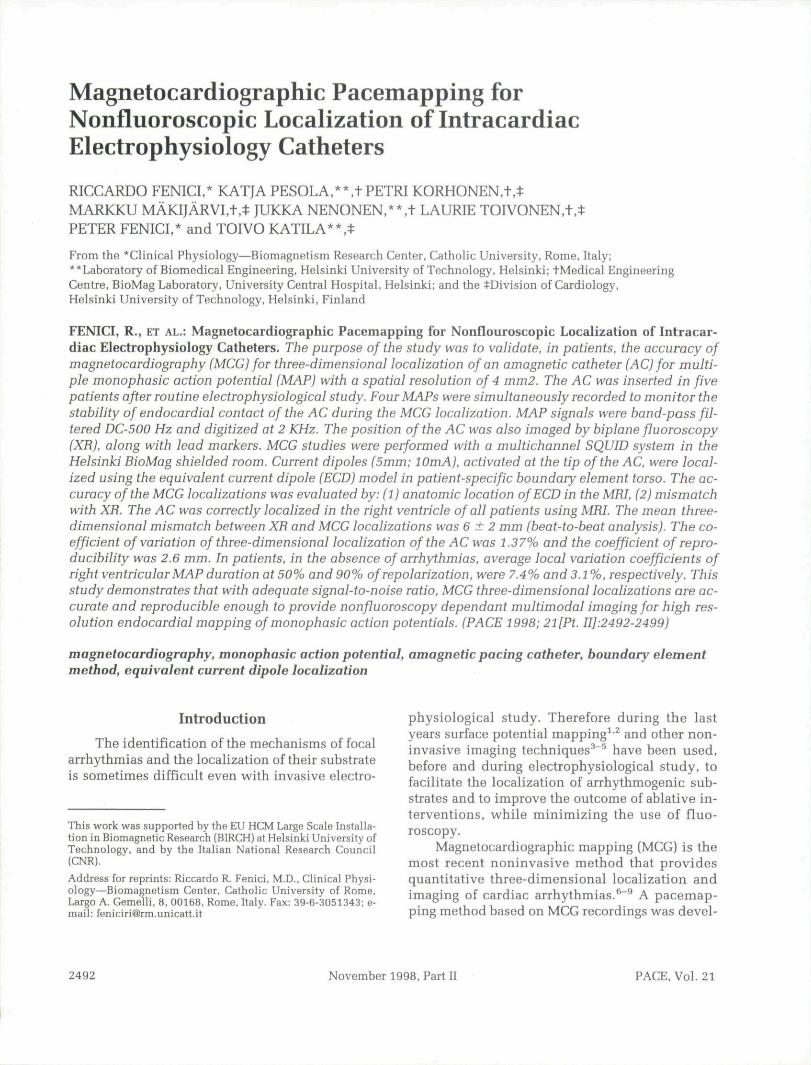
The multipurpose AC, for MCG-guided multi-ple simultaneous MAP recording is a patent of theItalian National Research.^^ The catheter's tip fea-tures several nonpolarizable amagnetic elec-trodes, arranged in such a way that current dipolesof different geometry and strength can be gener-ated in the patient's heart, without electromag-netic interfaces. This AC was used to test the ac-curacy of MCG localization of an intracardiacsource (by comparison with fluoroscopic imag-ing), and to record multiple simultaneous MAPs,with a spatial resolution of 4 mm^ (Fig. 1). The po-sition of the catheter's tip was automaticallymarked into the three-dimensional model of the
patient's heart, and in magnetic resonance imag-ing (MRI) slices (Figs. 2,3).
MCG Mapping Systems
MCC studies were performed in the magneti-cally shielded room of the BioMag Laboratory ofHUCH, with a 67-channel instrumentation featur-ing seven coaxial (haseline 80 mm; aBz/az) and 60planar (baseline 16.2 mm, dBJdx and 5B2/ay) dc-SQUID (Superconducting QUantum InterferenceDevice) gradiometers, covering a surface with a di-ameter of 30 cm. The sensors are immersed in liq-uid helium inside a cylindrical dewar, supportedby a gantry system Before MCC recordings, thoraxcoordinates were defined by digitizing a set of ref-erence points, which were used to transfer MCGlocalization in MR images and for comparisonwith fluoroscopic images (XR) with the same co-ordinate system.
MCG Localization of the AC
Three-dimensional MCG localization of thetip of the catheter as calculated from stimuluspeaks generated by the 10 mA fed into thecatheter. The polarity of the magnetic field in-duced by the stimulus varied among the individ-ual patients, depending on the direction of the ar-tificial dipole (Fig. 4). In the computation, amoving equivalent current dipole in a realistic,homogeneous boundary element method (BEM),in which the torso model of the patient surface istessellated with plane triangles (Fig. 2). "* Theelectric potential is assumed to be linear in eachtriangle, and the discretized integral equations forthe electric potential and the magnetic field can bemanipulated into matrix equations that are fast tosolve.'^ The six parameters (position and mo-ment) of a current dipole were estimated withnonlinear least squares fitting.^^ All inverse com-putations were performed from raw MGG data;neither signal-averaging nor digital filtering wereapplied. The accuracy of the MGG localizationwas evaluated hy: (l) mismatch with XR and (2)anatomic location of EGD in MRI slices. The re-producihility of the measure was tested hy repeat-ing the same measurement five times and comput-ing the coefficient of variation and the coefficientof reproducibility.""
PACE, VoL 21 November 1998, Part 11 2493
FENICI, ET AL.
MRI
MRI was performed in a separate session. MRIdata were collected using a functional 1.5 tesla su-perconducting magnet device (Magnetom Vision,Siemens AG, Erlangen, Germany) at the Depart-ment of Radiology of HUCH. A set of 10-mm thicktransaxial slices were acquired from the waist tothe neck during early systole. In addition, 8-mm or10-mm slices were collected transaxially or in thedirection of the short axis of the heart to extract
the endo- and epicardial surfaces more accurately.Cross-shaped markers filled with MgCl-solutionwere applied in the marker positions defined dur-ing the MCG recordings to match the MRI andMCG coordinate frames.^^ In this study, the MRIdata were used for accurate representation of theindividual geometry of the thorax and the heart forboundary element computations. They also allowaccurate registration of MGG localization resultswith respect to the anatomy of the patient's heart[Figs. 2,3).'^
RAP SVT/RF AHLATION 3-26-gB U: 26:01 14:20:59: ?B3
^-^VF
3-Vl
A-VG
21-HAP 1
22-MAP 2
23-HAP 3
24-MAP 4lB-STIH 1
_A mna/a.
VTV
V V V
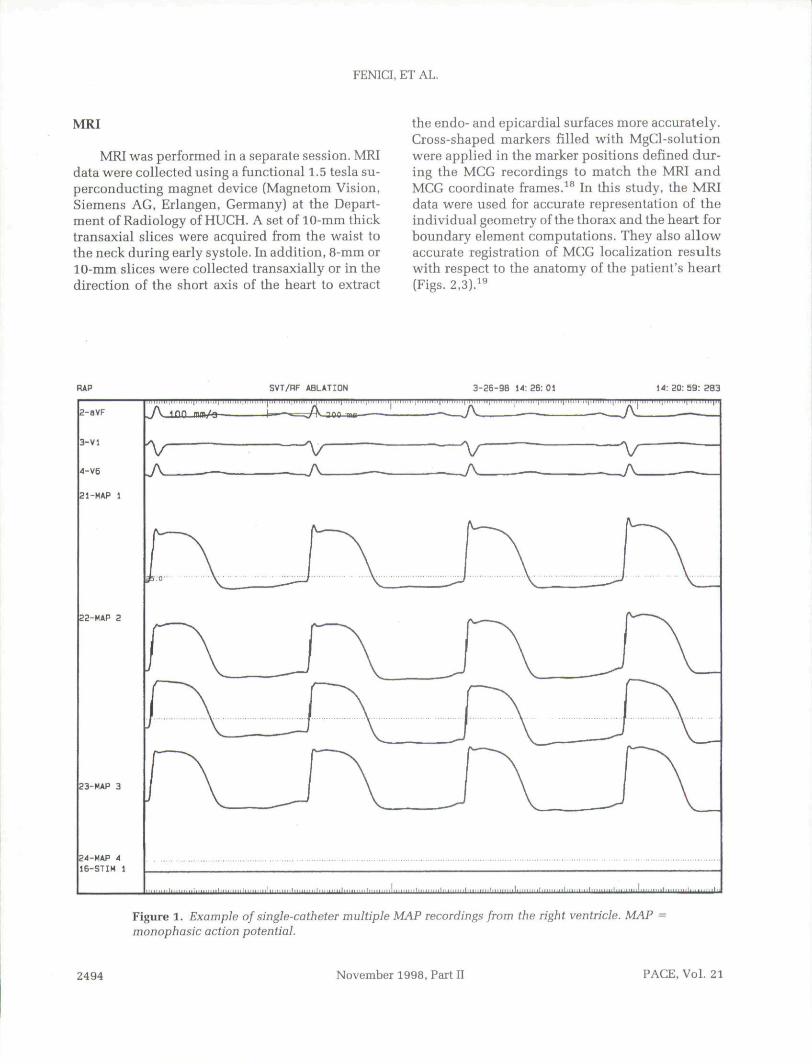
Figure 1. Example of single-catheter multiple MAP recordings from the right ventricle. MAP =monophasic action potential.
2494 November 1998, Part IT PACE, Vol. 21
NONFLUOROSCOPIC MCG LOCALIZATION OF ELECTRODE CATHETERS
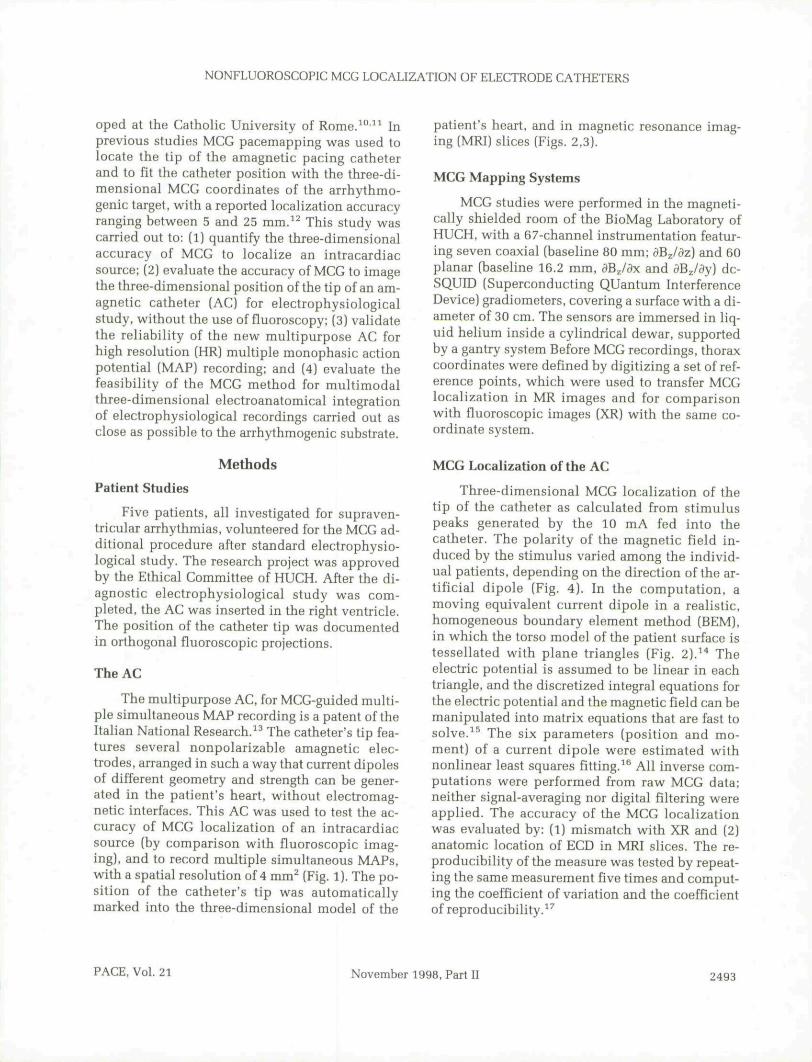
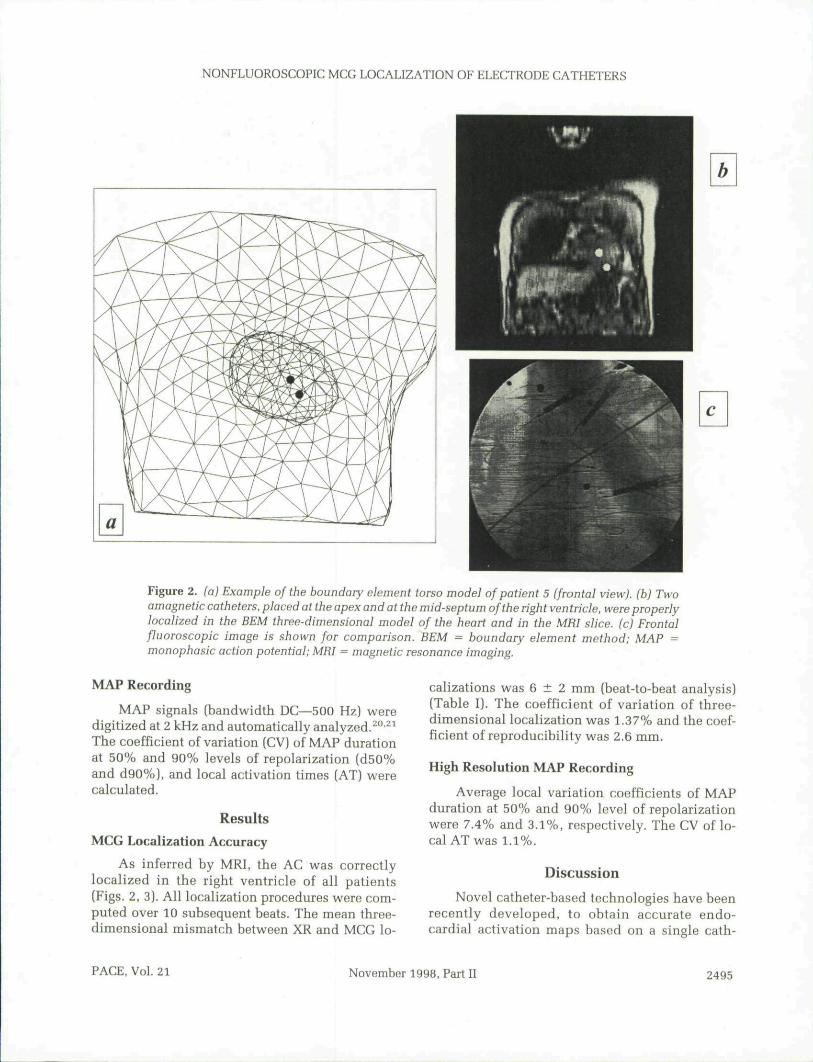
Figure 2. (a) Example of tbe boundary element torso mode! of patient 5 (frontal view), (b) Twoamagnetic catheters, placed at tbe apex and at tbe mid-septum of tbe rigbt ventricle, were properlylocalized in tbe BEM tbree-dimensional model of tbe beart and in tbe MRI slice, (c) Frontalfluoroscopic image is sbown for comparison. BEM = boundary element method; MAP =monopbasic action potential; MHl = magnetic resonance imaging.
MAP Recording
MAP signals (bandwidth DC—500 Hz) weredigitized at 2 kHz and automatically analyzed.^°-^^The coefficient of variation (CV) of MAP durationat 50% and 90% levels of repolarization (d50%and d90%), and local activation times (AT) werecalculated.
Results
MCG Localization Accuracy
As inferred by MRI, the AC was correctlylocalized in the right ventricle of all patients(Figs. 2, 3). All localization procedures were com-puted over 10 subsequent beats. The mean three-dimensional mismatch between XR and MCG lo-
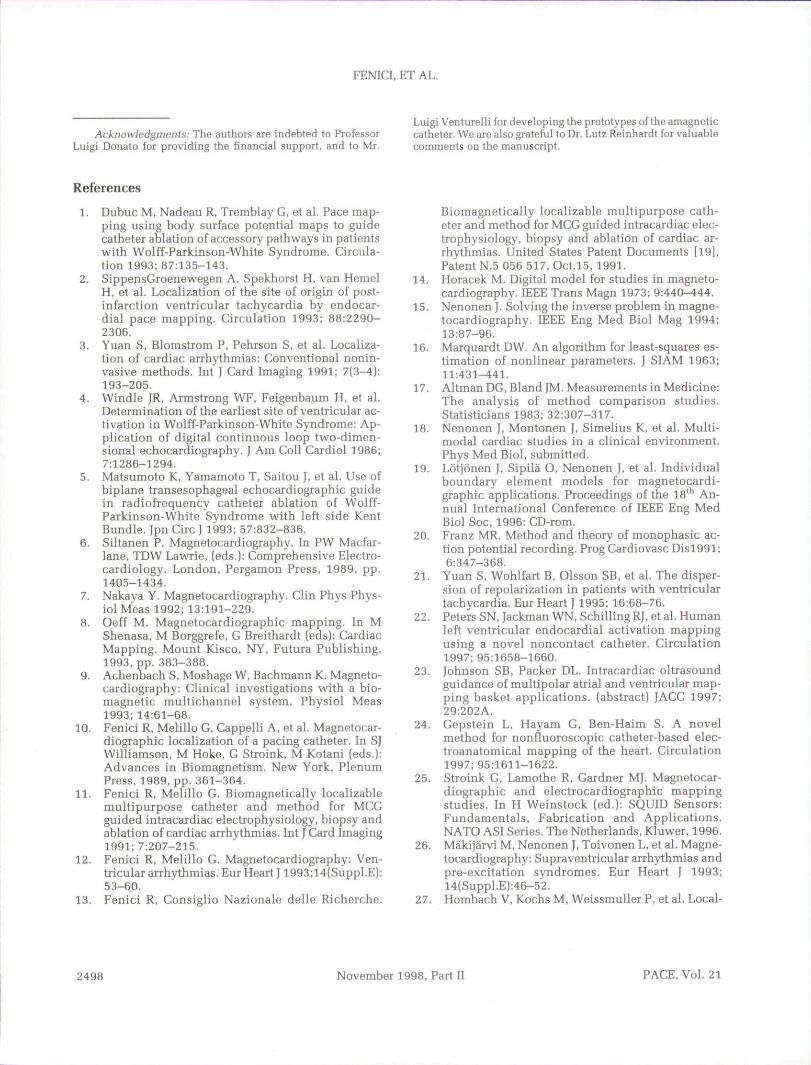
calizations was 6 ± 2 mm (beat-to-beat analysis)(Table I). The coefficient of variation of three-dimensional localization was 1.37% and the coef-ficient of reproducibility was 2.6 mm.
High Resolution MAP Recording
Average local variation coefficients of MAPduration at 50% and 90% level of repolarizationwere 7.4% and 3.1%, respectively. The CV of lo-cal AT was 1.1%.
Discussion
Novel catheter-based technologies have beenrecently developed, to obtain accurate endo-cardial activation maps based on a single cath-
PACE. Vol. 21 November 1998, Part II 2495
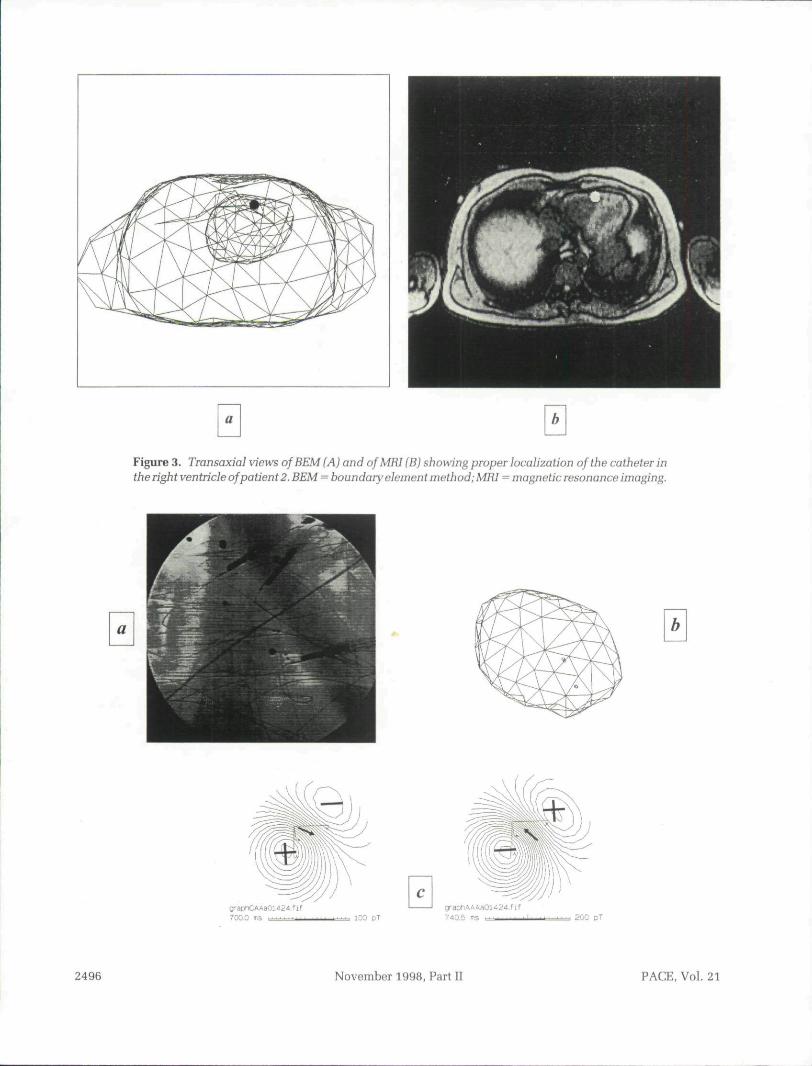
Figure 3. Transaxial views of BEM (A) and of MRI (B) sbowing proper localization of the catbeter intbe rigbt ventricle of patient 2. BEM = boundary element metbod; MRI = magnetic resonance imaging.
a
2uG pT
2496 November 1998, Part II PACE. Vol. 21
NONFLUOROSCOPIC MCG LOCALIZATION OF ELECTRODE CATHETERS
Table I.
Three-dimensional Localization Errorof the Amagnetic Catheter
Patient n.
12
34
5
Mean (mm)
SD (mm)
Mismatch between MCG
X
3,0- 0,7
1,62,8
2,2
1.8
1,3
and Fluoroscopy
y
7,0
1,9
6,16,7
5,7
5,5
1,9
z
1,00,7
0,4- 1,0
- 2,0
- 0,2
1,1
3D
7,72,1
6.37,4
6,4
6,0
2,0
MCG = magnetocardiographic mapping; SD - standard devia-tion
22.23 Qj g Q them provides nonfluoroscopicthree-dimensional navigation for electroanatomi-cal reconstruction of sequentially acquired con-tact catheter data with minimal use of fluo-roscopy.^'' The interest for such new methods isobvious, as they should provide better localiza-tion accuracy of arrhythmogenic areas, with lessinvasion and lower exposure to radiation for boththe patient and the operator, during interven-tional electrophysiological study. However theuse of these methods is confined to invasive elec-trophysiological study. In fact, none of them canbe used for preoperative noninvasive localizationofthe arrhythmogenic target and combine such "apriori" knowledge with the navigation of thecatheters during electrophysiological study. MCG
has such potential, reported in several studies,which demonstrated its clinical usefulness for lo-calizing sites of arrhythmias.^^"^^ In addition, ourpresent work has quantified the MCG accuracy forlocalization of intracardiac dipolar sources. In-deed MCG is adequate for noninvasive localiza-tion of the site of origin of focal arrhythmias andfunctional imaging of arrhythmogenic targets onthree-dimensional images of the patient heart(model and/or MRI slices). Its precision and re-producihility is on the order of a few millimeters.Furthermore it has been shown that the AC usedfor this study is very reliable for multiple simul-taneous MAP recordings with a well-defined andhigh spatial resolution (4 mm^). This device de-signed for MCG pacemapping can be imagedthree-dimensionally into a patient's MRI slicesand/or in a three-dimensional BEM model of theheart. Such images can be rotated by the operatorin real time and represent a new user-friendly in-terface for electroanatomical investigation of thesite of origin of focal arrhythmias, with minimalexposure to radiation. Multiple MAP recordingsfrom the arrhythmogenic area can pinpoint local-ized arrhythmogenic mechanisms.^^'^"'^^ The lim-itation of the method is, at the moment, the lackof a multichannel mapping system offering thesame sensitivity outside of a high performanceshielded room, necessary to achieve an optimalsignal-to-noise ratio, which is a critical require-ment for MGG accuracy. In fact, in our unshieldedEP laboratory the localization uncertainty hadbeen almost four times higher.^^ This implies thatfurther investments are needed to construct amore compact multichannel MGG instrumenta-tion, reliable in unshielded EP laboratories.^^Technological progress is fast and such a tacticalchoice could dramatically drop the instrumenta-tion costs and favor a wider clinical applicationof MGG.
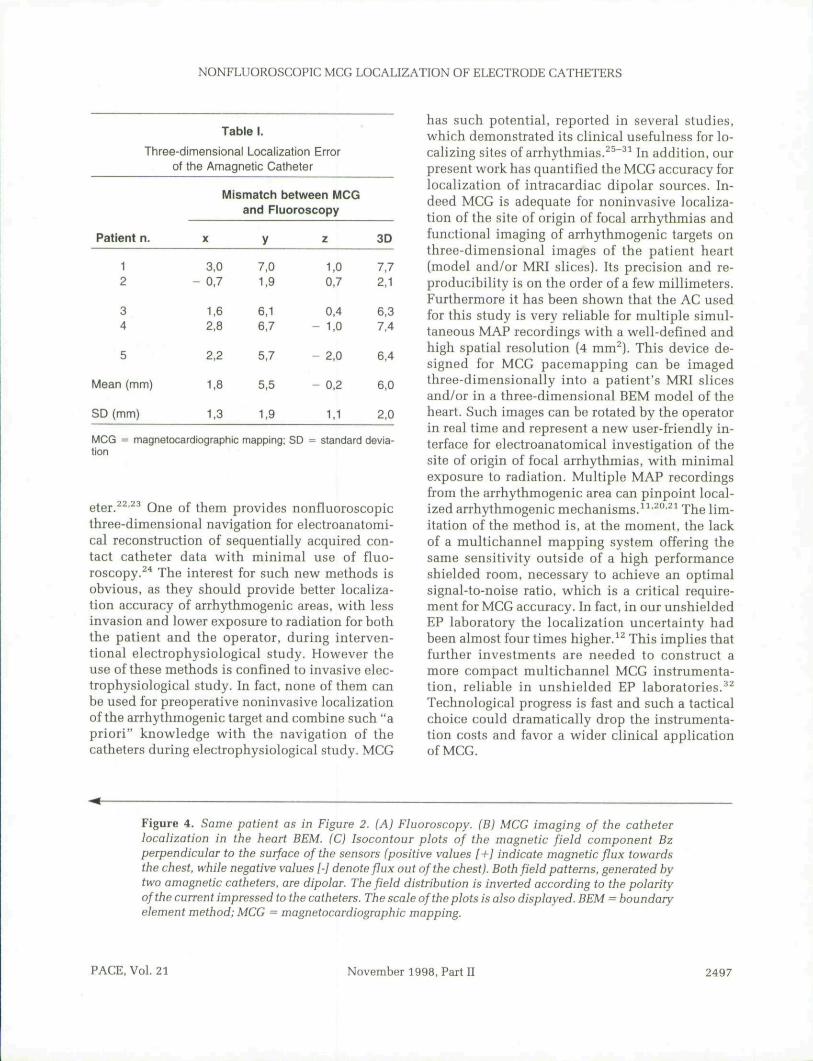
Figure 4. Same patient as in Figure 2. {A) Fluoroscopy. (B) MCG imaging of the catheterhcalizotion in the heart BEM. (C) Isocontour plots of the magnetic field component Bzperpendicular to tbe surface ofthe sensors (positive values [+} indicate magnetic flux towardsthe chest, while negative values [-] denote flux out of the chest). Both field patterns, generated by-two amagnetic catheters, are dipolar. The field distribution is inverted according to the polarityofthe current impressed to the catheters. The scale of the plots is also displayed. BEM = boundaryelement method; MCG = magnetocardiographic mapping.
PACE. Vol. 21 November 1998. Part II 2497
FENICI.ETAL.
Acknowledgments: The authors are indebted to ProfessorLuigi Donato for providing the financial support, and to Mr.
Luigi VentureMi for developing the prototypes of the amagneticcatheter. We are also grateful to Dr. Lutz Reinhardt for valuablecomments nn the manuscript.
References
1. Dubuc M, Nadeau R, Tremblay G, et al. Pace map-ping using body surface potential maps to guidecatheter ablation of accessory pathways in patientswith Wolff-Parkinson-White Syndrome. Circula-tion 1993; 87:135-143.
2. SippensGroenewegen A, Spekhorst H, van HemelH, et al. Localization of the site of origin of post-infarction ventricular tachycardia by endocar-dial pace mapping. Circulation 1993; 88:2290-2306.
3. Yuan S, Blomstrom P, Pehrson S, et al. Localiza-tion of cardiac arrhythmias: Conventional nonin-vasive methods. Int J Card Imaging 1991; 7(3—4):193-205.
4. Windlc JR, Armstrong WF, Feigenbaum H, et al.Determination of the earliest site of ventricular ac-tivation in Wolff-Parkinson-White Syndrome: Ap-plication of digital continuous loop two-dimen-sional echocardiography. J Am Coll Cardiol 1986;7:1286-1294.
5. Matsumoto K, Yamamoto T, Saitou J, et al. Use ofbiplane transesophageal echocardiographic guidein radiofrequency catheter ablation of Wolff-Parkinson-White Syndrome with left side KentBundle. Jpn Circ J 1993; 57:832-836.
6. Siltanen P. Magnetocardiography. In PW Macfar-lane, TDW LawTie, [eds.]: Comprehensive Electro-cardiology. London, Pergamon Press, 1989, pp.1405-1434.
7. Nakaya Y. Magnetocardiography. Clin Phys Phys-iol Meas 1992; 13:191-229.
8. Oeff M. Magnetocardiographic mapping. In MShenasa. M Borggrefe, G Breithardt (eds): CardiacMapping, Mount Kisco. NY. Futura Publishing,1993. pp. 383-388.
9. Achenbach S, Moshage W, Bachmann K. Magneto-cardiography: Clinical investigations with a bio-magnetic multichannel system. Physiol Meas1993; 14:61-68.
10. Fenici R. Melillo C, Cappelli A, et al. Magnetocar-diographic localization of a pacing catheter. In SJWilliamson, M Hoke, C Stroink, M Kotani (eds.):Advances in Biomagnetism. New York, PlenumPress. 1989, pp. 361-364.
11. Fenici R, Melillo C. Biomagnetically localizablemultipurpose catheter and method for MCCguided intracaidiac electrophysiology, biopsy andablation of cardiac arrhythmias. Int J Card Imaging1991; 7:207-215.
12. Fenici R, Melillo C. Magnetocardiography: Ven-tricular arrhythmias. Eur Heart 11993;14(Suppl.E):53-60.
13. Fenici R, Consiglio Nazionale delle Richerche.
Biomagnetically localizable multipurpose cath-eter and method for MCG guided intracardiac elec-trophysiology, biopsy and ablation of cardiac ar-rhythmias. United States Patent Documents [19],Patent N.5 056 517, Oct.l5, 1991.
14. Horacek M. Digital model for studies in magneto-cardiography. IEEE Trans Magn 1973; 9:440^44.
15. Nenonen J. Solving the inverse problem in magne-tocardiography. IEEE Eng Med Bid Mag 1994;13:87-96.
16. Marquardt DW. An algorithm for least-squares es-timation of nonlinear parameters. J SIAM 1963;11:431-441.
17. Altman DG, Bland IM. Measurements in Medicine:The analysis of method comparison studies.Statisticians 1983; 32:307-317.
18. Nenonen J, Montonen J, Simelius K, et al. Multi-modal cardiac studies in a clinical environment.Phys Med Biol, submitted.
19. Lotjonen J, Sipila O, Nenonen J, et al. Individualboundary element models for magnetocardi-graphic applications. Proceedings of the 18' An-nual International Conference of IEEE Eng MedBiol Soc, 1996: CD-rom.
20. Franz MR. Method and theory of monophasic ac-tion potential recording. Prog Cardiovasc Disl991;6:347-368.
21. Yuan S, Wohlfart B, Olsson SB, et al. The disper-sion of repolarization in patients with ventriculartachycardia. Eur Heart J 1995; 16:68-76.
22. Peters SN, Jackman WN, Schilling Rl, et al. Humanleft ventricular endocardial activation mappingusing a novel noncontact catheter. Circulation1997; 95:1658-1660,
23. Johnson SB, Packer DL. Intracardiac oltrasoundguidance of multipolar atrial and ventricular map-ping basket applications, (abstract) JACC 1997;29:202A.
24. Cepstein L, Hayam C. Ben-Haim S. A novelmethod for nonfluoroscopic catheter-based elec-troanatomical mapping of the heart. Circulation1997; 95:1611-1622.
25. Stroink C, Lamothe R, Gardner MJ. Magnetocar-diographic and electrocardiographic mappingstudies. In H Weinstock (ed.): SQUID Sensors:Fundamentals, Fabrication and Applications.NATO ASI Series. The Netherlands, Kluwer, 1996.
26. Makijarvi M, Nenonen J, Toivonen L, et al. Magne-tocardiography: Supraventricular arrhythmias andpre-excitation syndromes. Eur Heart J 1993;14(Suppl.E):46-52.
27. Hombach V, Kochs M, WeissmuUer P, et al. Local-
2498 November 1998, Part II PACE, Vol. 21
NONFLUOROSCOPIC MCG LOCALIZATION OF ELECTRODE CATHETERS
ization of ectopic ventricular depolarization by is-pect-radionuclide ventriculography and by mag-netocardiography. Int J Card Imaging 1991; 7(3-4):225-235.
28. Oeff M, Burghoff M. Magnetocardiographic local-ization of the origin of ventricular ectopic beats.PACE 1994; 17:517-522.
29. Moshage W, Achenbach S. Gahl K, et al. Evalua-tion of the non-invasive localization accuracy ofcardiac arrhythmias attainable by multichannelmagnetocardiography (MCG). Int ) Card Imaging1996; 12:47-59.
30. Fenici R, Covino M, Cellerino C, et al. Magneto-
cardio-graphically guided catheter ablation. J In-terven Cardiol 1995; 8(Suppl):825-836.
31. Nenonen J, Makijarvi M, Toivonen L, et al. Non-in-vasive magnetocardiographic localization of ven-tricular pre-excitation in the Wolff-Parkinson-White syndrome using a realistic torso model. EurHeart J1993; 14:168-174.
32. Fenici R, Fenici P, van Bosheide J. Amagneticcatheter for biomagnetically guided endocardialmapping and ablation of cardiac arrhythmias. InH Reichl, A Heuberger, {eds.): Micro System Tech-nologies. Berlin, VDE-Verlag GmbH, 1996, pp.711-716.
PACE, Vol. 21 November 1998, Part II 2499

Related Documents











