Magnetic Resonance Enteroclysis Nicholas C. Gourtsoyiannis and Nickolas Papanikolaou MR enteroclysis (MRE) is an emerging technique for the evaluation of small intestinal diseases. Administration of an iso-osmotic water solution through a nasojejunal catheter can guarantee adequate luminal distention, and in combination with ultrafast sequences, such as single shot TSE, true FISP, HASTE and 3D FLASH, results in excellent anatomic demonstration of the small intestine. MR fluoroscopy can be performed during MRE examination to monitor the filling process and might be useful in studying low-grade stenosis or motility related disorders. MRE is a very promising technique for the detection and characterization of involved small bowel segments in patients with Crohn’s disease while its diagnostic performance in disclosing lumen narrowing and extramural manifesta- tions and complications of the disease is outstanding. Initial experience shows that MRE is very efficient in the diagnosis of small bowel tumors and can be used in the evaluation of small bowel obstruction. Semin Ultrasound CT MRI 26:237-246 © 2005 Elsevier Inc. All rights reserved. E nteroclysis is widely recognized as a most reliable method for imaging evaluation of the small intestine. Adequate distention of the entire small bowel lumen by bar- ium contrast medium favors a detailed demonstration of anatomy and a more confident identification of morpholog- ical and functional abnormalities present. In long-term fol- low-up studies enteroclysis has been shown to be a highly accurate method with a sensitivity of 93.1% and a specificity of 96.9%. 1,2 The main limitation of enteroclysis remains its inability to demonstrate exoenteric pathology associated with small intestinal diseases. 3 The potential of magnetic resonance imaging (MRI) exam- ination of the small bowel has been explored in several re- ports. 3-14 The most important advantages of MRI can be sum- marized as the following: absence of radiation exposure, excellent soft tissue contrast that might improve tissue char- acterization, projectional and cross-sectional imaging capa- bilities in all three dimensions, which may be of importance when mapping small intestinal pathology, and multiple con- trast sources, which may favor a comprehensive morpholog- ical and functional evaluation of the small intestine. 15 Key technical issues for a successful MRI examination of the small intestine include hardware and software considerations, the type of intraluminal contrast agent, and the route of contrast administration. 16 Two major approaches concerning the lat- ter have been advocated, that is, per os administration and infusion through a nasojejunal catheter. A variety of intralu- minal contrast agents are in use with oral administration, including mannitol and sorbitol water solutions, 17 iron ox- ide, 7 or barium sulfate suspensions. 9 Fairly recently, ispa- ghula husk 18 or locust bean gum 19 have been added. These two substances are commonly used in the food industry as thickening agents and have the property of retaining large amounts of water up to 20 to 30 times their own volume. The feasibility of these agents has been proven so far only in normal subjects. Oral administration of intraluminal contrast agents is patient friendly, when compared to the infusion technique through duodenal intubation. However, it might prolong the examination time considerably, up to two hours. More importantly, luminal distention is not consistently ad- equate to guarantee a confident diagnosis, 3,4 and the accuracy of wall thickness measurements is rather questionable when optimal luminal distention is not provided. 3,4 MR enteroclysis, a combined functional and morphologi- cal imaging method, was only recently introduced in clinical practice with adequate image quality coupled by the benefits of volume challenge. 20 Results have so far shown that the functional information provided by MR enteroclysis equals that of conventional enteroclysis, whereas inherent advan- tages of the technique include detailed morphological evalu- ation of the bowel wall and the mesenteries. 3,20 This article provides an overview of the technical aspects of MR enteroclysis technique and reviews the clinical applica- tions of MR enteroclysis in small intestinal diseases. Department of Radiology, University Hospital of Iraklion, University of Crete Medical School, Iraklion Crete, Greece. Address reprint requests to Nicholas C. Gourtsoyiannis, MD, Department of Radiology, University Hospital of Iraklion, P.O. Box 1352, 711 10 Irak- lion Crete, Greece; Phone: (30 81) 392541-2; Fax: (30 81) 542-095; E-mail: [email protected] 237 0887-2171/05/$-see front matter © 2005 Elsevier Inc. All rights reserved. doi:10.1053/j.sult.2005.04.007

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
MN
EAiailaois
ipmeabwtitit
D
A
0d
agnetic Resonance Enteroclysisicholas C. Gourtsoyiannis and Nickolas Papanikolaou
MR enteroclysis (MRE) is an emerging technique for the evaluation of small intestinaldiseases. Administration of an iso-osmotic water solution through a nasojejunal cathetercan guarantee adequate luminal distention, and in combination with ultrafast sequences,such as single shot TSE, true FISP, HASTE and 3D FLASH, results in excellent anatomicdemonstration of the small intestine. MR fluoroscopy can be performed during MREexamination to monitor the filling process and might be useful in studying low-gradestenosis or motility related disorders. MRE is a very promising technique for the detectionand characterization of involved small bowel segments in patients with Crohn’s diseasewhile its diagnostic performance in disclosing lumen narrowing and extramural manifesta-tions and complications of the disease is outstanding. Initial experience shows that MRE isvery efficient in the diagnosis of small bowel tumors and can be used in the evaluation ofsmall bowel obstruction.Semin Ultrasound CT MRI 26:237-246 © 2005 Elsevier Inc. All rights reserved.
atimiigttafnatpMeoo
cpoftta
M
nteroclysis is widely recognized as a most reliablemethod for imaging evaluation of the small intestine.
dequate distention of the entire small bowel lumen by bar-um contrast medium favors a detailed demonstration ofnatomy and a more confident identification of morpholog-cal and functional abnormalities present. In long-term fol-ow-up studies enteroclysis has been shown to be a highlyccurate method with a sensitivity of 93.1% and a specificityf 96.9%.1,2 The main limitation of enteroclysis remains itsnability to demonstrate exoenteric pathology associated withmall intestinal diseases.3
The potential of magnetic resonance imaging (MRI) exam-nation of the small bowel has been explored in several re-orts.3-14 The most important advantages of MRI can be sum-arized as the following: absence of radiation exposure,
xcellent soft tissue contrast that might improve tissue char-cterization, projectional and cross-sectional imaging capa-ilities in all three dimensions, which may be of importancehen mapping small intestinal pathology, and multiple con-
rast sources, which may favor a comprehensive morpholog-cal and functional evaluation of the small intestine.15 Keyechnical issues for a successful MRI examination of the smallntestine include hardware and software considerations, theype of intraluminal contrast agent, and the route of contrast
epartment of Radiology, University Hospital of Iraklion, University ofCrete Medical School, Iraklion Crete, Greece.
ddress reprint requests to Nicholas C. Gourtsoyiannis, MD, Department ofRadiology, University Hospital of Iraklion, P.O. Box 1352, 711 10 Irak-lion Crete, Greece; Phone: (30 81) 392541-2; Fax: (30 81) 542-095;
tE-mail: [email protected]
887-2171/05/$-see front matter © 2005 Elsevier Inc. All rights reserved.oi:10.1053/j.sult.2005.04.007
dministration.16 Two major approaches concerning the lat-er have been advocated, that is, per os administration andnfusion through a nasojejunal catheter. A variety of intralu-
inal contrast agents are in use with oral administration,ncluding mannitol and sorbitol water solutions,17 iron ox-de,7 or barium sulfate suspensions.9 Fairly recently, ispa-hula husk18 or locust bean gum19 have been added. Thesewo substances are commonly used in the food industry ashickening agents and have the property of retaining largemounts of water up to 20 to 30 times their own volume. Theeasibility of these agents has been proven so far only inormal subjects. Oral administration of intraluminal contrastgents is patient friendly, when compared to the infusionechnique through duodenal intubation. However, it mightrolong the examination time considerably, up to two hours.ore importantly, luminal distention is not consistently ad-
quate to guarantee a confident diagnosis,3,4 and the accuracyf wall thickness measurements is rather questionable whenptimal luminal distention is not provided.3,4
MR enteroclysis, a combined functional and morphologi-al imaging method, was only recently introduced in clinicalractice with adequate image quality coupled by the benefitsf volume challenge.20 Results have so far shown that theunctional information provided by MR enteroclysis equalshat of conventional enteroclysis, whereas inherent advan-ages of the technique include detailed morphological evalu-tion of the bowel wall and the mesenteries.3,20
This article provides an overview of the technical aspects ofR enteroclysis technique and reviews the clinical applica-
ions of MR enteroclysis in small intestinal diseases.
237
TMictiq(st(lMn
PAMcTia
gfS3ppdpcatqagdgcg
oomcoc
aatpell
Fwa
238 N.C. Gourtsoyiannis and N. Papanikolaou
echnical Requirementsotion sensitivity is a well-known prohibiting factor in MR
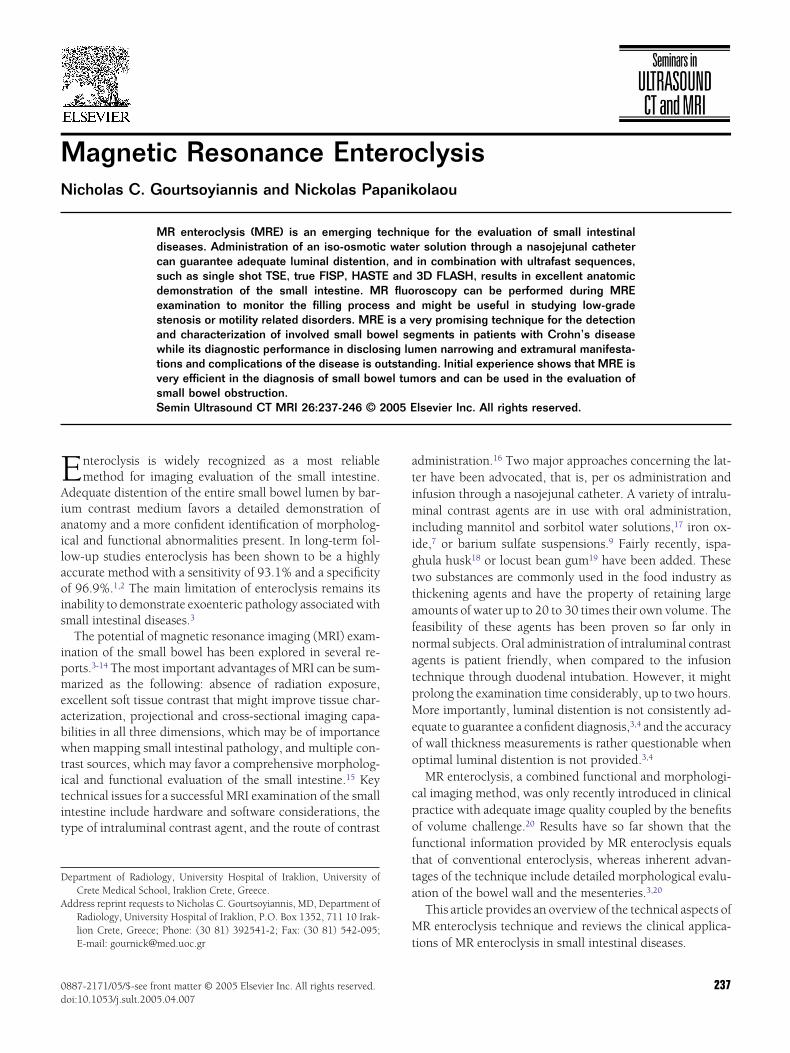
maging that may downgrade diagnostic information. Espe-ially MR imaging of the small intestine is largely susceptibleo respiratory and peristaltic motion problems. Initial smallntestinal applications, recruiting conventional pulse se-uences, were invariably suffering from motion artifacts3,4
Fig 1a). Improved performance of gradient systems led tohorter repetition and echo times in ultrafast pulse sequenceshat are of great importance in minimizing motion artifactsFig 1b). Recent introduction of novel techniques like paral-el imaging have increased further the spatial resolution of
R imaging, allowing detection of even subtle small intesti-al lesions.20
ulse Sequencesvariety of pulse sequences are currently used for intestinalRI applications. These can be classified, according to the
ontrast that they generate, either into (1) T1 weighted, (2)2 weighted, and (3) mixed contrast, or, in relation to their
maging speed capabilities, into (1) conventional, (2) fast,nd (3) ultrafast sequences.
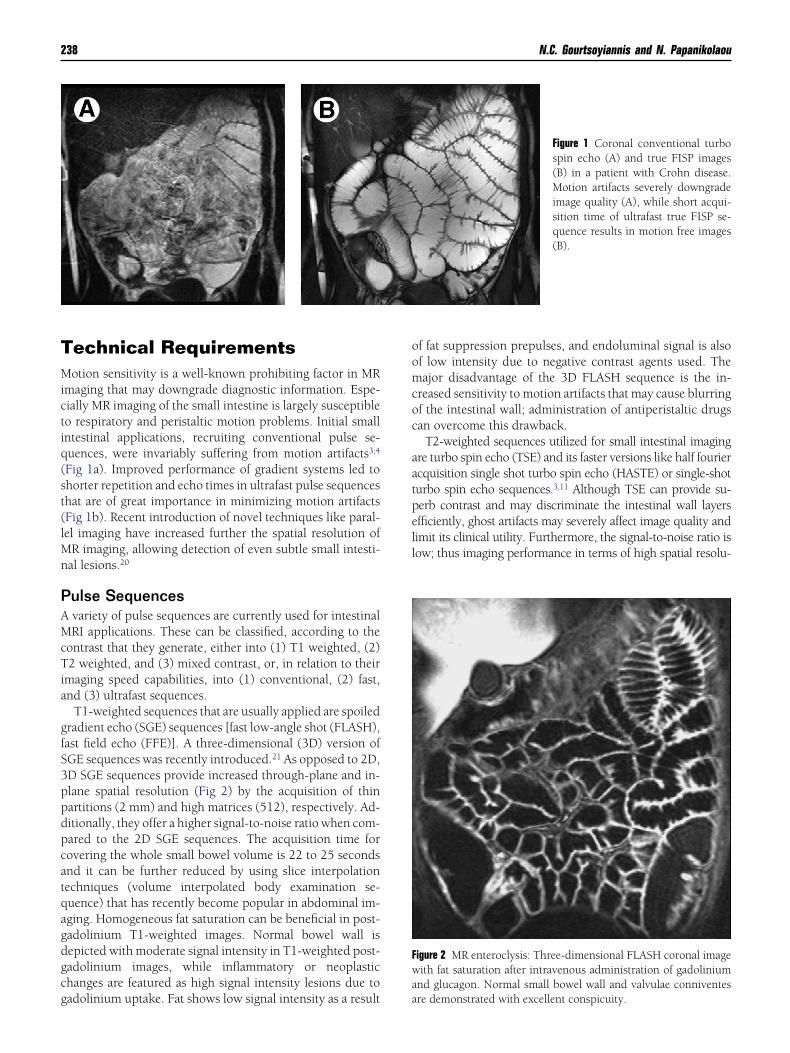
T1-weighted sequences that are usually applied are spoiledradient echo (SGE) sequences [fast low-angle shot (FLASH),ast field echo (FFE)]. A three-dimensional (3D) version ofGE sequences was recently introduced.21 As opposed to 2D,D SGE sequences provide increased through-plane and in-lane spatial resolution (Fig 2) by the acquisition of thinartitions (2 mm) and high matrices (512), respectively. Ad-itionally, they offer a higher signal-to-noise ratio when com-ared to the 2D SGE sequences. The acquisition time forovering the whole small bowel volume is 22 to 25 secondsnd it can be further reduced by using slice interpolationechniques (volume interpolated body examination se-uence) that has recently become popular in abdominal im-ging. Homogeneous fat saturation can be beneficial in post-adolinium T1-weighted images. Normal bowel wall isepicted with moderate signal intensity in T1-weighted post-adolinium images, while inflammatory or neoplastichanges are featured as high signal intensity lesions due to
adolinium uptake. Fat shows low signal intensity as a result af fat suppression prepulses, and endoluminal signal is alsof low intensity due to negative contrast agents used. Theajor disadvantage of the 3D FLASH sequence is the in-
reased sensitivity to motion artifacts that may cause blurringf the intestinal wall; administration of antiperistaltic drugsan overcome this drawback.
T2-weighted sequences utilized for small intestinal imagingre turbo spin echo (TSE) and its faster versions like half fouriercquisition single shot turbo spin echo (HASTE) or single-shoturbo spin echo sequences.3,11 Although TSE can provide su-erb contrast and may discriminate the intestinal wall layersfficiently, ghost artifacts may severely affect image quality andimit its clinical utility. Furthermore, the signal-to-noise ratio isow; thus imaging performance in terms of high spatial resolu-
Figure 1 Coronal conventional turbospin echo (A) and true FISP images(B) in a patient with Crohn disease.Motion artifacts severely downgradeimage quality (A), while short acqui-sition time of ultrafast true FISP se-quence results in motion free images(B).
igure 2 MR enteroclysis: Three-dimensional FLASH coronal imageith fat saturation after intravenous administration of gadolinium
nd glucagon. Normal small bowel wall and valvulae conniventes
re demonstrated with excellent conspicuity.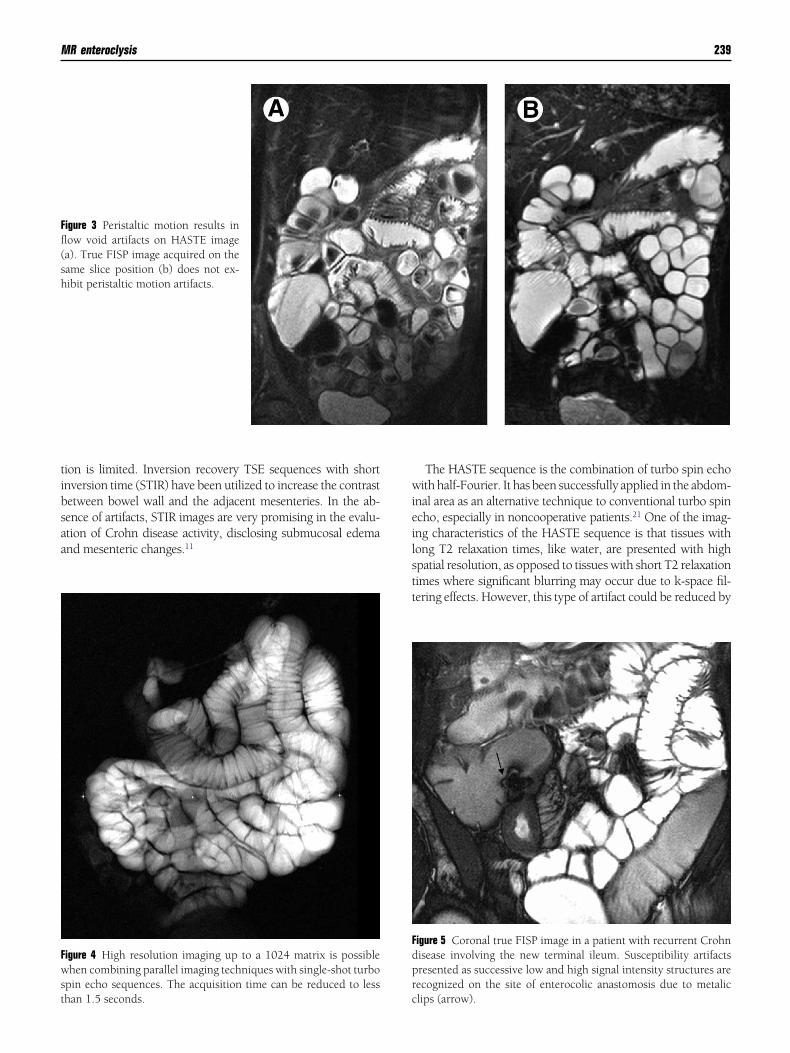
tibsaa
wieilstt
Ffl(sh
Fwst
Fdpr
MR enteroclysis 239
ion is limited. Inversion recovery TSE sequences with shortnversion time (STIR) have been utilized to increase the contrastetween bowel wall and the adjacent mesenteries. In the ab-ence of artifacts, STIR images are very promising in the evalu-tion of Crohn disease activity, disclosing submucosal edemand mesenteric changes.11
igure 3 Peristaltic motion results inow void artifacts on HASTE imagea). True FISP image acquired on theame slice position (b) does not ex-ibit peristaltic motion artifacts.
igure 4 High resolution imaging up to a 1024 matrix is possiblehen combining parallel imaging techniques with single-shot turbo
pin echo sequences. The acquisition time can be reduced to less
han 1.5 seconds. cThe HASTE sequence is the combination of turbo spin echoith half-Fourier. It has been successfully applied in the abdom-
nal area as an alternative technique to conventional turbo spincho, especially in noncooperative patients.21 One of the imag-ng characteristics of the HASTE sequence is that tissues withong T2 relaxation times, like water, are presented with highpatial resolution, as opposed to tissues with short T2 relaxationimes where significant blurring may occur due to k-space fil-ering effects. However, this type of artifact could be reduced by
igure 5 Coronal true FISP image in a patient with recurrent Crohnisease involving the new terminal ileum. Susceptibility artifactsresented as successive low and high signal intensity structures areecognized on the site of enterocolic anastomosis due to metalic
lips (arrow).
cssiottHlsdf
weitsaGi
ts(sqsfMtFqhtsd
TbDpwbt(
IVMa(atv
F
240 N.C. Gourtsoyiannis and N. Papanikolaou
ombining HASTE with parallel imaging techniques throughhortening of the echo spacing. HASTE belongs to the ultrafastequences providing subsecond imaging times and therefore it isnsensitive to respiratory motion. On the contrary, the absencef flow compensation capabilities renders this sequence sensi-ive to intraluminal flow-related artifacts due to peristaltic mo-ion20 (Fig 3). This problem may be overcome when acquiringASTE images following spasmolytic drug administration. The
ong echo train used in HASTE sequence renders it insensitive tousceptibility artifacts related to intraluminal air presence. Ad-itionally, it is not sensitive to chemical shift artifacts, allowingor accurate measurements of intestinal wall thickness.
Single-shot TSE (SSTSE) sequence provides heavily T2-eighted images in projectional mode. In the case of MR
nteroclysis it has been proved helpful for monitoring thenfusion process and assessing the degree of luminal disten-ion13,16; it can also provide functional information related tomall bowel motility.3 With the advent of gradient systemsnd parallel imaging techniques such as SENSE andRAPPA, acquisition of high resolution SSTSE projectional
mages become feasible (Fig 4).Hybrid ultrafast pulse sequences, which provide a mixed
ype of contrast, are balanced steady-state free precessionequences, such as true fast imaging with steady precessionFISP), balanced fast field echo, and fast imaging employingteady state acquisition. Important features of such se-uences include high intrinsic signal-to-noise ratio, superbpatial resolution, and insensitivity to motion-related arti-acts.4,22,23 True FISP sequence was recently introduced for
R examination of the small bowel using duodenal intuba-ion.4 Water solutions exhibit high signal intensity on trueISP images due to their high T2/T1 ratio. True FISP se-uence is excellent in demonstrating the mesenteries, due toigh contrast resolution between the bright peritoneal fat andhe dark vessels and lymph nodes.4 As opposed to HASTEequences, true FISP is insensitive to intraluminal flow voids,
ue to its balanced and symmetric gradient design (Fig 3). prue FISP sequence is sensitive to susceptibility (Fig 5) andlack boundary artifacts that may downgrade image quality.emonstration of normal bowel wall and intestinal folds thatresent intermediate signal intensity, as well as detection ofall thickening, are not usually affected by the presence oflack boundary artifacts. Alternatively, the combination ofrue FISP sequences with spectral fat saturation prepulses24
Fig 6) can overcome misinterpretation of such findings.
ntraluminal Contrast Agentsarious contrast agents have been proposed for small bowelRI applications.4,25-36 The most important characteristics of
n intraluminal contrast agent suitable for gastrointestinalGI) applications may be summarized as follows: uniformnd homogeneous lumen opacification, high contrast resolu-ion between the lumen and bowel wall, no significant ad-erse effects, and low cost. In addition, minimal mucosal
Figure 6 Coronal true FISP spot viewof the terminal ileum in a patient withCrohn disease. (A) Black boundaryartifact (arrows) is recognized as ablack thin line along the borders ofthe thickened bowel wall and themesenteric fat. (B) The same sequenceapplied with fat saturation prepulses.Note that the black boundary artifacthas been eliminated.
igure 7 Axial true FISP image showing fissure ulcers (arrows) in a
atient with active Crohn disease.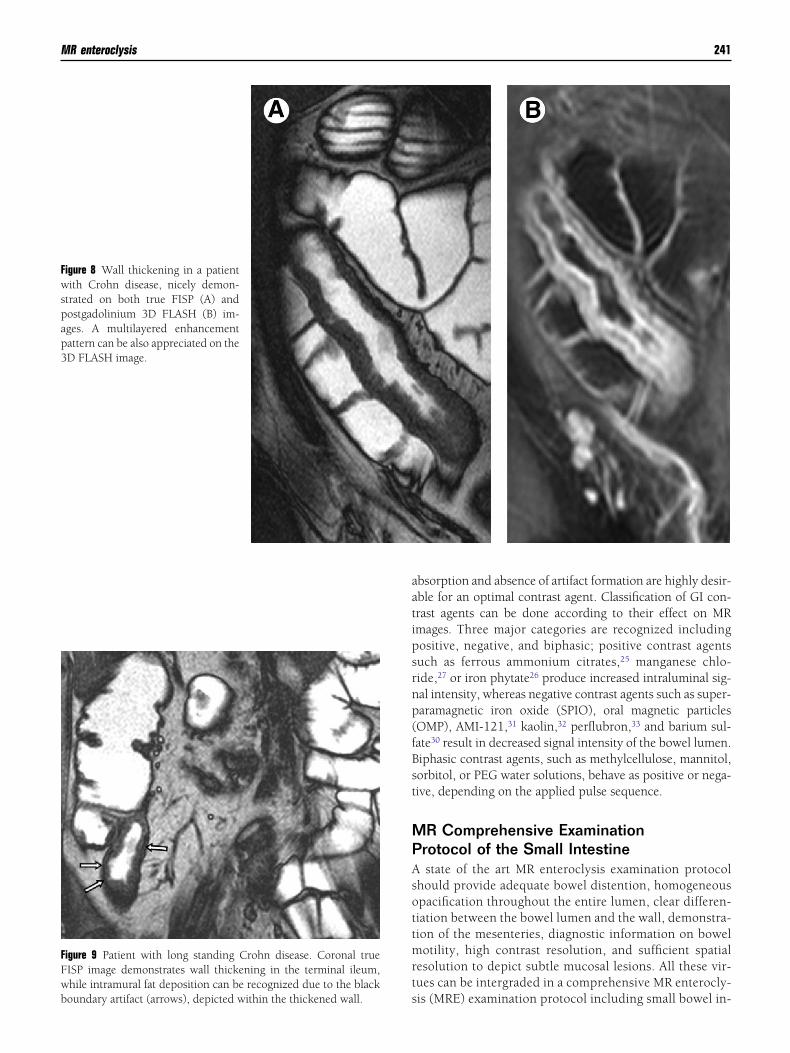
aatipsrnp(fBst
MPAsottmrts
Fwspap3
FFwboundary artifact (arrows), depicted within the thickened wall.
MR enteroclysis 241
bsorption and absence of artifact formation are highly desir-ble for an optimal contrast agent. Classification of GI con-rast agents can be done according to their effect on MRmages. Three major categories are recognized includingositive, negative, and biphasic; positive contrast agentsuch as ferrous ammonium citrates,25 manganese chlo-ide,27 or iron phytate26 produce increased intraluminal sig-al intensity, whereas negative contrast agents such as super-aramagnetic iron oxide (SPIO), oral magnetic particlesOMP), AMI-121,31 kaolin,32 perflubron,33 and barium sul-ate30 result in decreased signal intensity of the bowel lumen.iphasic contrast agents, such as methylcellulose, mannitol,orbitol, or PEG water solutions, behave as positive or nega-ive, depending on the applied pulse sequence.
R Comprehensive Examinationrotocol of the Small Intestinestate of the art MR enteroclysis examination protocol
hould provide adequate bowel distention, homogeneouspacification throughout the entire lumen, clear differen-iation between the bowel lumen and the wall, demonstra-ion of the mesenteries, diagnostic information on bowelotility, high contrast resolution, and sufficient spatial
esolution to depict subtle mucosal lesions. All these vir-ues can be intergraded in a comprehensive MR enterocly-
igure 8 Wall thickening in a patientith Crohn disease, nicely demon-
trated on both true FISP (A) andostgadolinium 3D FLASH (B) im-ges. A multilayered enhancementattern can be also appreciated on theD FLASH image.
igure 9 Patient with long standing Crohn disease. Coronal trueISP image demonstrates wall thickening in the terminal ileum,hile intramural fat deposition can be recognized due to the black
is (MRE) examination protocol including small bowel in-
tiwMTsw
ufdHtcFdm
CCTeon
Fmfgn
FP
242 N.C. Gourtsoyiannis and N. Papanikolaou
ubation, administration of a biphasic contrast agent, thats, an iso-osmotic water solution (PEG), heavily T2-eighted single-shot turbo spin echo (SSTSE) images forR fluoroscopy and for monitoring the infusion process,2-weighted imaging employing HASTE and true FISPequences with and without fat saturation in combinationith parallel imaging, and dynamic T1-weighted imaging
igure 11 Patient with active Crohn disease. Terminal ileum involve-ent is demonstrated on a coronal postgadolinium 3D FLASH,
eaturing increased gadolinium uptake (dashed arrow). Moderateadolinium enhancement of accompanying mesenteric lymph
odes (arrows) are also shown. ssing a postgadolinium 3D and 2D FLASH sequence withat suppression.20,37 This protocol can provide anatomicemonstration of the normal intestinal wall (true FISP,ASTE, 3D FLASH), identification of wall thickening or
umorous lesions (true FISP, HASTE, 3D FLASH), lesionharacterization or evaluation of disease activity (3D, 2DLASH, true FISP), assessment of exoenteric/mesentericisease extension (true FISP, 3D, 2D FLASH), and infor-ation concerning intestinal motility (SSTSE).20
linical Applicationsrohn Disease
he most common clinical indication for MR enteroclysisxamination is Crohn disease. The most attractive featuref MR enteroclysis over conventional enteroclysis exami-ations is its capacity to provide with intra- and extralu-
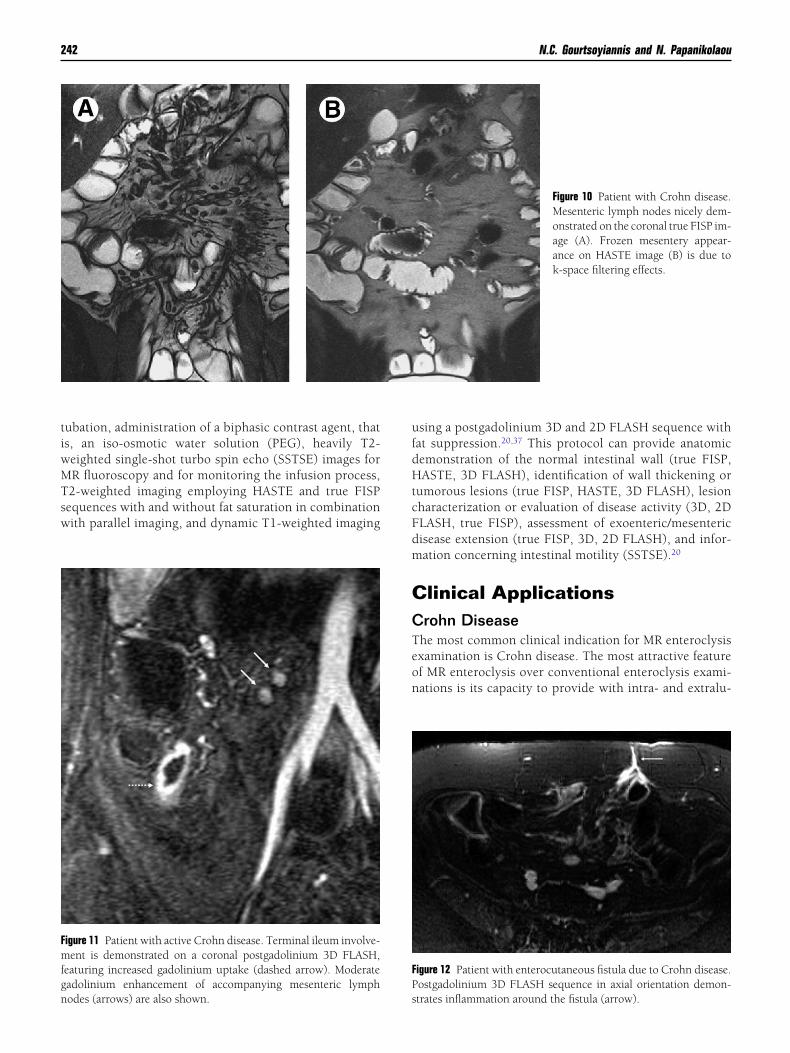
Figure 10 Patient with Crohn disease.Mesenteric lymph nodes nicely dem-onstrated on the coronal true FISP im-age (A). Frozen mesentery appear-ance on HASTE image (B) is due tok-space filtering effects.
igure 12 Patient with enterocutaneous fistula due to Crohn disease.ostgadolinium 3D FLASH sequence in axial orientation demon-
trates inflammation around the fistula (arrow).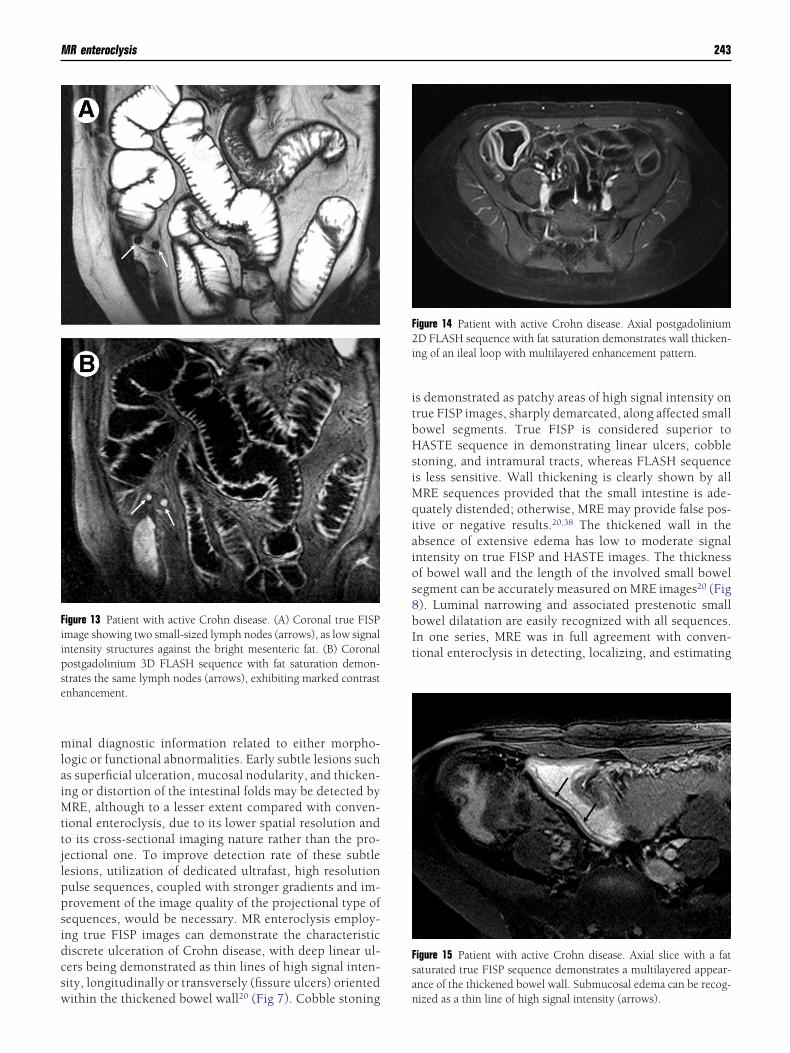
mlaiMttjlppsidcsw
itbHsiMqiaios8bIt
Fiipse
F2i
Fsa
MR enteroclysis 243
inal diagnostic information related to either morpho-ogic or functional abnormalities. Early subtle lesions suchs superficial ulceration, mucosal nodularity, and thicken-ng or distortion of the intestinal folds may be detected by
RE, although to a lesser extent compared with conven-ional enteroclysis, due to its lower spatial resolution ando its cross-sectional imaging nature rather than the pro-ectional one. To improve detection rate of these subtleesions, utilization of dedicated ultrafast, high resolutionulse sequences, coupled with stronger gradients and im-rovement of the image quality of the projectional type ofequences, would be necessary. MR enteroclysis employ-ng true FISP images can demonstrate the characteristiciscrete ulceration of Crohn disease, with deep linear ul-ers being demonstrated as thin lines of high signal inten-ity, longitudinally or transversely (fissure ulcers) oriented
igure 13 Patient with active Crohn disease. (A) Coronal true FISPmage showing two small-sized lymph nodes (arrows), as low signalntensity structures against the bright mesenteric fat. (B) Coronalostgadolinium 3D FLASH sequence with fat saturation demon-trates the same lymph nodes (arrows), exhibiting marked contrastnhancement.
ithin the thickened bowel wall20 ( Fig 7). Cobble stoning n
s demonstrated as patchy areas of high signal intensity onrue FISP images, sharply demarcated, along affected smallowel segments. True FISP is considered superior toASTE sequence in demonstrating linear ulcers, cobble
toning, and intramural tracts, whereas FLASH sequences less sensitive. Wall thickening is clearly shown by all
RE sequences provided that the small intestine is ade-uately distended; otherwise, MRE may provide false pos-
tive or negative results.20,38 The thickened wall in thebsence of extensive edema has low to moderate signalntensity on true FISP and HASTE images. The thicknessf bowel wall and the length of the involved small bowelegment can be accurately measured on MRE images20 ( Fig ). Luminal narrowing and associated prestenotic smallowel dilatation are easily recognized with all sequences.n one series, MRE was in full agreement with conven-ional enteroclysis in detecting, localizing, and estimating
igure 14 Patient with active Crohn disease. Axial postgadoliniumD FLASH sequence with fat saturation demonstrates wall thicken-
ng of an ileal loop with multilayered enhancement pattern.
igure 15 Patient with active Crohn disease. Axial slice with a fataturated true FISP sequence demonstrates a multilayered appear-nce of the thickened bowel wall. Submucosal edema can be recog-
ized as a thin line of high signal intensity (arrows).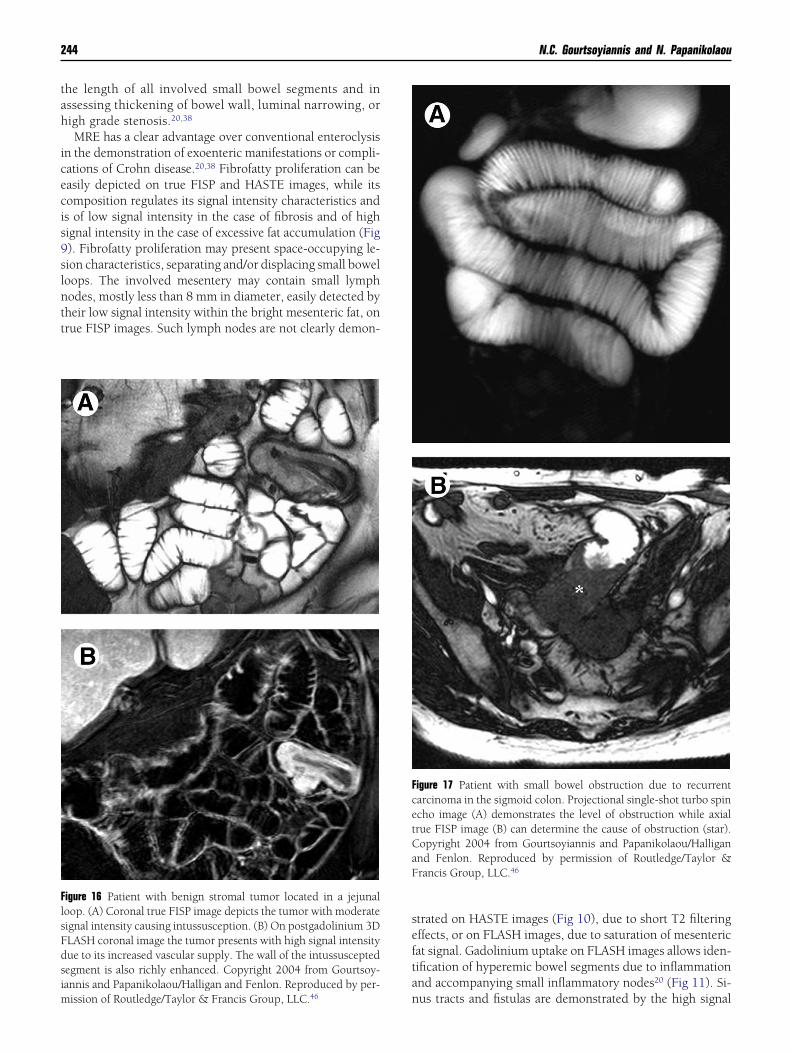
tah
icecis9slntt
sefta
FlsFdsim
FcetCaF
244 N.C. Gourtsoyiannis and N. Papanikolaou
he length of all involved small bowel segments and inssessing thickening of bowel wall, luminal narrowing, origh grade stenosis.20,38
MRE has a clear advantage over conventional enteroclysisn the demonstration of exoenteric manifestations or compli-ations of Crohn disease.20,38 Fibrofatty proliferation can beasily depicted on true FISP and HASTE images, while itsomposition regulates its signal intensity characteristics ands of low signal intensity in the case of fibrosis and of highignal intensity in the case of excessive fat accumulation (Fig). Fibrofatty proliferation may present space-occupying le-ion characteristics, separating and/or displacing small boweloops. The involved mesentery may contain small lymphodes, mostly less than 8 mm in diameter, easily detected byheir low signal intensity within the bright mesenteric fat, onrue FISP images. Such lymph nodes are not clearly demon-
igure 16 Patient with benign stromal tumor located in a jejunaloop. (A) Coronal true FISP image depicts the tumor with moderateignal intensity causing intussusception. (B) On postgadolinium 3DLASH coronal image the tumor presents with high signal intensityue to its increased vascular supply. The wall of the intussusceptedegment is also richly enhanced. Copyright 2004 from Gourtsoy-annis and Papanikolaou/Halligan and Fenlon. Reproduced by per-
nission of Routledge/Taylor & Francis Group, LLC.46
trated on HASTE images (Fig 10), due to short T2 filteringffects, or on FLASH images, due to saturation of mesentericat signal. Gadolinium uptake on FLASH images allows iden-ification of hyperemic bowel segments due to inflammationnd accompanying small inflammatory nodes20 (Fig 11). Si-
igure 17 Patient with small bowel obstruction due to recurrentarcinoma in the sigmoid colon. Projectional single-shot turbo spincho image (A) demonstrates the level of obstruction while axialrue FISP image (B) can determine the cause of obstruction (star).opyright 2004 from Gourtsoyiannis and Papanikolaou/Halligannd Fenlon. Reproduced by permission of Routledge/Taylor &rancis Group, LLC.46
us tracts and fistulas are demonstrated by the high signal

iacice
ecuocsdsoescaissrmhsans
eaisvbFes(
NMwhmis(icMttas
ncpcs
twhnaF
SMtStow
qgTcsii
CMstmAtTcbspiadtaittd
R
MR enteroclysis 245
ntensity of their fluid content on true FISP and HASTE im-ges. Accompanying inflammation (Fig 12) around a fistulaan be easily depicted on postgadolinium SGE T1-weightedmages due to increased contrast uptake. Abscess formationan be recognized by fluid content and wall post contrastnhancement.
Additional information regarding MRI evaluation of dis-ase activity has been presented.8,10-14 In a recent study,39
ertain MR imaging findings, including the presence of deeplcers, wall thickness of more than 7 mm, and marked gad-linium enhancement of mesenteric lymph nodes were wellorrelated with the clinical activity index (CDAI) and it isuggested that such findings may serve as indicators of Crohnisease activity. Identification of deep ulcers was the mostensitive MRI criterion for disease activity, since more thanne deep ulcer was invariably present in active Crohn dis-ase.39 Previous studies of disease activity have not reporteduch a relationship or even disclosure of deep ulcers that areonsidered characteristic of Crohn disease and are tradition-lly recognized on conventional enteroclysis. However, MRmaging protocols in these studies have not included eitherpecific techniques for bowel distention or high contrast andpatial resolution pulse sequences like true FISP or FLASH,espectively.11,40,41 Mesenteric lymph nodes exhibitingarked enhancement after gadolinium administration wereighly suggestive of active Crohn disease (Fig 13). A fewmall nonenhancing mesenteric lymph nodes were occasion-lly seen close to nonactive bowel segments, whereas markedodal enhancement was found to accompany only involvedegments with active inflammation.39
One of the earliest imaging signs that correlated with dis-ase activity was the degree of contrast enhancement by usingbolus injection and acquisition of T1-weighted dynamic
mages preferably with fat saturation.11,40 Wall thickening,ignificant enhancement of the mucosa compared to nearbyessels, and relatively hypointense submucosal edema haveeen reported as common findings on postgadoliniumLASH images in active Crohn disease11 (Fig 14). Active dis-ase in small bowel segments may also be manifested by highignal intensity of intestinal wall on T2-weighted images11
Fig 15).
eoplastic Bowel DiseaseRE incorporates the advantages of cross-sectional MRIith those of conventional enteroclysis, which has provenighly sensitive in the detection of small bowel (SB) tu-ors. On true FISP images the high signal intensity of
ntraluminal fluid and mesenteric fat allows the demon-tration of tumors exhibiting intermediate signal intensity Fig 16). Small bowel neoplasms are mildly hypointense tosointense in comparison with the intestinal wall on pre-ontrast non-fat suppressed T1-weighted gradient echoR images and present various enhancement patterns af-
er gadolinium administration.42 High contrast betweenhe tumor and surrounding high signal intensity fat en-bles MRI to demonstrate the local extension of the le-
ions.42,43Small bowel gastrointestinal stromal tumors (GIST), ade-ocarcinoma, carcinoid tumor, and lymphoma present post-ontrast enhancement that is better appreciated on fat sup-ressed T1-weighted FLASH images. Strong enhancementan be seen with carcinoid tumors and benign and malignanttromal tumors.
Lipomatous tumors and tumor hemorrhage can be de-ected on nonenhanced, non-fat suppressed FLASH images,hich should be acquired in addition to the MRE compre-ensive imaging protocol. Small bowel loop distortion oreoplastic invasion is depicted by all MRE sequences, whilessociated lymphadenopathy is well demonstrated on trueISP and FLASH images.
mall Bowel ObstructionRE can provide anatomic and functional information iden-
ical to that provided by conventional enteroclysis in cases ofB obstruction.3 In addition, extraluminal causes may be bet-er shown by using MRE, and malignant and benign types ofbstruction are better defined on gadolinium-enhanced T1-eighted images.44
MR fluoroscopy, utilizing dynamic projectional SSTSE se-uences (Fig 17), is extremely helpful in diagnosing lowrade stenosis and in determining the level of obstruction.rue FISP and post-gadolinium-enhanced 3D FLASH imagesan disclose the level and the cause of obstruction. In a recenttudy of 27 patients with postsurgical adhesions, cine MRmaging using the true FISP technique resulted in a sensitiv-ty of 87.5% and a specificity of 92.5%.45
onclusionsR imaging has a potential to change the way we evaluate
mall intestinal pathology, due to its superb soft tissue con-rast and the functional information it can provide, its directultiplanar capabilities, and the lack of radiation exposure.dequate bowel distention, homogeneous lumen opacifica-
ion, fast sequences with breath-hold acquisition times, both1- and T2-weighted imaging, and contrast enhancement areornerstones for an optimal MRI examination of the smallowel. A comprehensive MR enteroclysis imaging protocolhould comprise SSTSE, true FISP, HASTE, and fat sup-ressed 3D FLASH sequences. SSTSE is utilized for monitor-
ng the infusion process and MR fluoroscopy, while true FISPnd HASTE are mainly used for anatomic delineation andetection of abnormalities present. 3D FLASH sequences af-er intravenous gadolinium injection may aid in tissue char-cterization. Inflammatory or neoplastic diseases, includingntestinal wall abnormalities, exoenteric disease manifesta-ions and complications, disease activity, and to a lesser ex-ent, mucosal abnormalities, can be appreciated with confi-ence on MRE.
eferences1. Dixon PM, Roulston ME, Nolan DJ: The small bowel enema: A 10-year
review. Clin Radiol 4:46-48, 1993
2. Barloon TJ, Lu CC, Honda H, et al: Does a normal small-bowel entero-
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
246 N.C. Gourtsoyiannis and N. Papanikolaou
clysis exclude small-bowel disease? A long-term follow-up of consecu-tive normal studies. Abdom Imaging 19:113-115, 1994
3. Umschaden HW, Szolar D, Gasser J, et al: Small-bowel disease: Com-parison of MR enteroclysis images with conventional enteroclysis andsurgical findings. Radiology 215:717-725, 2000
4. Gourtsoyiannis N, Papanikolaou N, Grammatikakis J, et al: MR imag-ing of the small bowel using a true-FISP sequence after enteroclysiswith water solution. Invest Radiol 35:707-711, 2000
5. Lomas DJ, Graves MJ: Small bowel MRI using water as a contrast me-dium. Br J Radiol 72:994-997, 1999
6. Aschoff A, Zeitler H, Merkle EM, et al: MR enteroclysis for nuclear spintomographic diagnosis of inflammatory bowel diseases with contrastenhancement. Fortschr Röntgenstr 167:387-391, 1997
7. Holzknecht N, Helmberger T, von Ritter C, et al: MRI of the smallintestine with rapid MRI sequences in Crohn disease after enteroclysiswith oral iron particles. Radiologe 38:29-36, 1998
8. Rieber A, Wruk D, Nüssle K, et al: MRI of the abdomen in combinationwith enteroclysis in Crohn disease with oral and intravenous Gd-DTPA.Radiologe 38:23-28, 1998
9. Low RN, Francis IR: MR imaging of gastrointestinal tract with IV gad-olinium and diluted barium oral contrast media compared with unen-hanced MR imaging and CT. Am J Roentgenol 169:1051-1059, 1997
0. Schunk K, Metzmann U, Kersjes W, et al: Serial observation in Crohndisease: Can hydro-MRI replace follow-through examinations? FortschrRöntgenstr 166:389-396, 1997
1. Maccioni F, Viscido A, Broglia L, et al: Evaluation of Crohn diseaseactivity with magnetic resonance imaging. Abdom Imaging 25:219-228, 2000
2. Minowa O, Ozaki Y, Kyogoku S, et al: MR imaging of the small bowelusing water as a contrast agent in a preliminary study with healthyvolunteers. Am J Roentgenol 173:581-582, 1999
3. Prassopoulos P, Papanikolaou N, Grammatikakis J, et al: MR entero-clysis imaging of Crohn disease. Radiographics 21:S161-S172, 2001
4. Lee JK, Marcos HB, Semelka RC: MR imaging of the small bowel usingthe HASTE sequence. AJR Am J Roentgenol. 170:1457-1463, 1998
5. Papanikolaou N, Prassopoulos P, Grammatikakis I, et al: Technicalchallenges and clinical applications of magnetic resonance enteroclysis.Top Magn Reson Imaging 13:397-408, 2002
6. Gourtsoyiannis N, Papanikolaou N, Grammatikakis J, et al: MR entero-clysis: Technical considerations and clinical applications. Eur Radiol12:2651-2658, 2002
7. Ajaj W, Goehde SC, Schneemann H, et al: Oral contrast agents for smallbowel MRI: Comparison of different additives to optimize bowel dis-tension. Eur Radiol 14:458-64, 2004
8. Patak MA, Froehlich JM, von Weymarn C, et al: Non-invasive disten-sion of the small bowel for magnetic-resonance imaging. Lancet 22;358:987-988, 2001
9. Lauenstein TC, Schneemann H, Vogt FM, et al: Optimization of oralcontrast agents for MR imaging of the small bowel. Radiology 228:279-283, 2003
0. Gourtsoyiannis N, Papanikolaou N, Rieber A, et al: Evaluation of thesmall intestine by MR imaging, in Gourtsoyiannis N, ed: RadiologicalImaging of the Small Intestine. Berlin, Heidelberg, New York, Springer,2002:157-170
1. Gourtsoyiannis N, Papanikolaou N, Grammatikakis J, et al: MR entero-clysis protocol optimization: Comparison between 3d FLASH with fatsaturation after intravenous gadolinium injection and true FISP se-quences. Eur Radiol 11:908-913, 2001
2. Semelka RC, Kelekis NL, Thomasson D, et al: HASTE MR imaging:Description of technique and preliminary results in the abdomen. JMagn Reson Imaging 6:698-699, 1996
3. Haacke M, Tkach J: Fast MR imaging: Techniques and clinical applica-tions. AJR Am J Roentgenol 155:951-964, 1990
4. Oppelt A, Graumann R, Barfuss H, et al: A new fast MRI sequence.
Electromed 3:15-18, 19865. Scheffler K, Heid O, Hennig J: Magnetization preparation during thesteady state: Fat-saturated 3D TrueFISP. Magn Reson Med 45:1075-1080, 2001
6. Kivelitz D, Gehl HB, Heuck A, et al: Ferric ammonium citrate as apositive bowel contrast agent for MR imaging of the upper abdomen:Safety and diagnostic efficacy. Acta Radiol 40:429-435, 1999
7. Hahn PF: Advances in contrast enhanced MR imaging: Gastrointestinalcontrast agents. AJR Am J Roentgenol 156:252-254, 1991
8. Small WC, DeSimone-Macchi D, Parker JR, et al: A multisite phase IIIstudy of the safety and efficacy of a new manganese chloride-basedgastrointestinal contrast agent for MRI of the abdomen and pelvis. JMagn Resin Imaging 10:15-24, 1999
9. Mirowitz SA, Susman N: Use of a nutritional support formula as agastrointestinal contrast agent for MRI. J Comput Assist Tomogr 16:908-915, 1992
0. A. Karantanas N, Papanikolaou J, Kalef-Ezra, et al: Blueberry juice usedper os in upper abdominal MR imaging: Composition and initial clin-ical data. Eur Radiol 10:909-913, 2000
1. Rubin DL, Muller HH, Young SW: Formulation of radiographicallydetectable gastrointestinal contrast agents for magnetic resonance im-aging: Effects of barium sulfate additive on MR contrast agent effective-ness. Magn Reson Med 23:154-165, 1992
2. Faber SC, Stehling MK, Holzknecht N, et al: Pathologic conditions inthe small bowel: Findings at fat-suppressed gadolinium-enhanced MRimaging with an optimized suspension of oral magnetic particles. Ra-diology 205:278-282, 1997
3. Mitchell DG, Vinitski S, Mohamed FB, et al: Comparison of Kaopectatewith barium for negative and positive enteric contrast at MR imaging.Radiology 181:475-480, 1991
4. Mattrey RF, Trambert MA, Brown JJ, et al: Perflubron as an oral contrastagent for MR imaging: Results of a phase III clinical trial. Radiology191:841-848, 1994.
5. Weinreb JC, Maravilla KR, Redman HC, et al: Improved MR imaging ofthe upper abdomen with glucagons and gas. J Comput Assist Tomogr8:835-838, 1984
6. Reiber A, Aschoff A, Nussle K, et al: MRI in the diagnosis of small boweldisease: Use of positive and negative oral contrast media in combina-tion with enteroclysis. Eur Radiol 10:1377-1382, 2000
7. Papanikolaou N, Prassopoulos P, Grammatikakis J, et al: Optimizationof a contrast medium suitable for conventional enteroclysis, MR entero-clysis, and virtual MR enteroscopy. Abdom Imaging 27:517-522, 2002
8. Prassopoulos P, Papanikolaou N, Grammatikakis J, et al: MR entero-clysis imaging findings in Crohn disease. Radiographics 21;Spec No:S161-S172, 2001
9. Gourtsoyiannis N, Papanikolaou N, Grammatikakis J, et al: Assessmentof Crohn disease activity in the small bowel with MR and conventionalenteroclysis: Preliminary results. Eur Radiol. 14:1017-1024, 2004
0. Schunk K, Kern A, Oberholzer K, et al: Hydro-MRI in Crohn’s disease:Appraisal of disease activity. Invest Radiol 35:431-437, 2000
1. Koh DM, Miao Y, Chinn RJ, et al: MR imaging evaluation of the activityof Crohn’s disease. AJR Am J Roentgenol 177:1325-1332, 2001
2. Semelka RC, John G, Kelekis N, et al: Small bowel neoplastic disease:Demonstration by MRI. J Magn Reson Imaging 6:855-860, 1996
3. Low RN, Chen SC, Barone R: Distinguishing benign from malignantbowel obstruction in patients with malignancy: Findings at MR imag-ing. Radiology 228:157-165, 2003
4. Ha HK, Lee EH, Lim CH, et al: Application of MRI for small intestinaldiseases. J Magn Reson Imaging 8:375-383, 1998
5. Lienemann A, Sprenger D, Steitz HO, et al: Detection and mapping ofintraabdominal adhesions by using functional cine MR imaging: Pre-liminary results. Radiology 217:421-425, 2000
6. Gourtsoyiannis N, Papanikolaou N: Evaluation of the small intestine byMR imaging, in Halligan S, Fenlon HM, (eds). New techniques ingastrointestinal imaging. Basel Marcel, Dekker New York, 2004, pp
115-132.
Related Documents











