David M. Eddy To a great extent, the quality and cost of health care are determined by the decisions made by physicians whose ultimate objective is to design and administer a treatment program to improve a patient's condition. Most of the decisions involve many factors, great uncertainty, and difficult value questions. This chapter examines one aspect of how these decisions are made, studying the use of probabilistic reasoning to analyze a particular prob- lem: whether to perform a biopsy on a woman who has a breast mass that might be malignant. Specifically, we shall study how physicians process information about the results of a mammogram, an X-ray test used to diagnose breast cancer. The evidence presented shows that physicians do not manage uncertainty very well, that many physicians make major eril'°rs in probabilistic reasoning, and that these errors threaten the quality of medical care. The problem A breast biopsy is not a trivial procedure. The most common type (around 80%) is the excisional biopsy, in which the suspicious mass is removed surgically for microscopic examination and histological diagnosis by a pathologist. Usually the patient is admitted to a hospital and given a full set of preoperative diagnostic tests. The biopsy is almost always done under general anesthesia (with a probability of approximately 2 out of 10,000 of an anesthetic death). A small (1- to 2-in.) incision is made, and tissue the size of a pecan to a plum is removed. In many cases (perhaps 1 in The preparation of this paper was supported by a grant from The Henry J. Kaiser Family Foundation.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

David M. Eddy
To a great extent, the quality and cost of health care are determined by thedecisions made by physicians whose ultimate objective is to design andadminister a treatment program to improve a patient's condition. Most ofthe decisions involve many factors, great uncertainty, and difficult valuequestions.
This chapter examines one aspect of how these decisions are made,studying the use of probabilistic reasoning to analyze a particular prob-lem: whether to perform a biopsy on a woman who has a breast mass thatmight be malignant. Specifically, we shall study how physicians processinformation about the results of a mammogram, an X-ray test used todiagnose breast cancer. The evidence presented shows that physicians donot manage uncertainty very well, that many physicians make majoreril'°rs in probabilistic reasoning, and that these errors threaten the qualityof medical care.
The problem
A breast biopsy is not a trivial procedure. The most common type (around80%) is the excisional biopsy, in which the suspicious mass is removedsurgically for microscopic examination and histological diagnosis by apathologist. Usually the patient is admitted to a hospital and given a fullset of preoperative diagnostic tests. The biopsy is almost always doneunder general anesthesia (with a probability of approximately 2 out of10,000 of an anesthetic death). A small (1- to 2-in.) incision is made, andtissue the size of a pecan to a plum is removed. In many cases (perhaps 1 in
The preparation of this paper was supported by a grant from The Henry J. Kaiser FamilyFoundation.
.pappe aJe s:>!1e~! a\j~ 'suo!~e~onb ~uanbasqns lIe pue S!\j~ uI
.UO!:j:>eue :j:>aIas ue:> ue!:>!sl..qd aq:j pue '.Ia:>ue:> seq 'swo:jdwl..s pue su~!s .IeIn:>!:j.Ied
.Iaq q:j!M ':jua!:jed aq:j :jeq:j a:>ueq:> aq:j ssasse ue:> ue!:>!sl..qd aq:j '(uO!saI
u~!uaq e I..sdo!q O:j :jou ~u!P!:>ap I..I.Iado.Id pue 'uo!saI :jueu~!Iew e ~U!SS!W
pue ~u!l..sdo!q :jou 'uo!saI :jueU~!IeW-UOu e Jo I..sdo!q I...xessa:>auun ue ~U!OP
'.Ia:>ue:> e ~u!sou~e!p I..I.Iado.Id '"~"a) sawo:>:jno aIq!ssod aq:j Jo san leA aq:t
Jo s:juawssasse q:j!M "ssew :jsea.Iq s,:jua!:jed 1? Jo sasne:> aIq!ssod aq:j azl..Ieueue!:>!sl..qd e dIaq O:j pasn aq ue:> uo!:jew.I°Ju! :>!:jS!I!qeqo.Id Jo adl..:j S!q.1
- ".Ia:>ue:> .I°J se naM se 'SUO!:j!puo:> :jsea.Iq .Iaq:jo uazop JIeq e pue
'ewne.I:j 's!so.I:>au :jeJ 'sewouapeo.Iqy .I°J aIqeI!eAe a.Ie suo!:jd!.I:>sap .IeI!w!s
(198-098.dd 'OL.6l'o:je~a}{ lap) tllews pue ald!:jlnw aJe s:Jsh aq:J 'ua:JJo aJOW .S:JSA:> qs!nlqa2Jel SMOqS /illuanba.tJu! aseas!p J!:JSAJ J!UOJq:> .pa~JeIUa :Jou /invnsn aJe sapouqdwAI AJen!>Ce aq.L .pa:J!w!lap naM pue Jaq:Joows /invnsn S! :J! :Jnq 'Jown:J e a'l!lstaal aseas!p J~:Jsh J~UOJqJ JO eaJe ue u~ :Jsh a~Jel V .p~ny Jeap u~etUOJ Aaqt J! ateu-!wnn~sueJt /iVIU pue tuentJny pue 'punOJ 'WJ9 aJe s:Jsh ald~tlnw .U!'IS ~U~ApaAO
aqt Ot uo~:Jex9 tnoqt!M pue uo!teJJewap dJeqs tnoqt!M asnJJ~p s! uo~sal aq.L 1last~aldd~u aqt u~ sa~ueqJ ou aJe aJaqt :Jnq 'saseJ aq:J JO %S'l /ilaIVIU!xo.tddv U! SJnJJO 'sno-Jas /invnsn 'a2JeqJs!p aldd!N .UOIUIUO:J aJe saJueqJnts~p lemtsuaw 2U~AUedwoJJe
pue 'po!Jad lemtSuawaJd aqt U! ApelnJ!tJed 'InJu!ed ualfo S! tI lSeaJq aJ!tuaaqt aAlOAU! AnemuaAa pue stJed Jaqto U! JnJJO /iVIU tnq :JueJpenb Ja:Jno Jaddnaqt U! /iluolUlUo:J IsolU tuasaJd S! tI .s:JseaJq news qt!M uaWOM snoJed U! SJnJJO
/invnsn tI lSeaJq aqt JO e~OU!JJeJ qt!M pasnJuOJ uatJo S! aseas!p J!:Jsh J!UOJq:>
"aseas!p :>!:jsl..:> :>!UO.Iq:> - aseas!pu~!uaq q:>ns auo saq!.I:>sap a~essed ~U!MOnOJ aq:j 'aIdwexa .I°d '.Ia:>ue:>
WO.IJ pa:je!:jua.IaJJ!p aq ue:> saseas!p :jueU~!IeW-Uou MOq aq!.I:>sap s'{ooq:jxa:t
Auew 'ue!:>!sl..qd aq:j dIaq 0.1 "q~noua q~!q S! uo!saI aIqe:jea.I:j Jaq:joue
.IO .Ia:>ue:> JO A-t!I!qeqo.Id aq:j J! I..sdo!q e w.IoJ.Iad pue ':jS!I aq:j uo saseas!p
aq:j JO q:>ea seq aqs :jeq:j a:>ueq:> aq:j a:jeW!:jsa ':jua!:jed aq:j U! S~U!puyaq:j q:j!M UO!:jeW.I°JU! S!q:j a.Iedwo:> 'aseas!p q:>ea q:j!M .In:>:>o swo:jdwl..s pue
su~!s SnO!.IeA q:>!qM q:j!M sa!:>uanbaJJ aq:j ssasse 'saseas!p aIq!ssod aq:j :jS!I
ue:> ue!:>!sl..qd e 'A-t!I!q!ssod S!q:j a:jeW!:jsa 0.1 ".Ia:>ue:> e S! ssew :jsea.Iq aq:j :jeq:t
A:j!I!q!ssod aq:j S! Asdo!q .I°J paau aq:j s:j:>aJJe :jeq:j .Io:j:>eJ :jue:j.Iodw! uy"pass!w aq I..ew uo!saI :jueU~!Iew ~u!:js!xa ue :jeq:j
U! aIqe!Ia.I ssaI aq O:j sue!:>!sl..qd I..uew I..q :jq~noq:j S!:j! '.IaAaMOH 'aA!suadxa
ssaI .IeJ S! pue 's:j:>aJJa Ienp!sa.I .Iaq:jo .IO .Ie:>s ou saAeaI 's!seq :jua!:jed:jno ue
uo auop aq ue:> S!q.1 "aIpaau e ~U!sn I..q anSS!:j u!e:jqo O:j sase:> awos U! .IaJa.Id
SUoa~.Ins awos 'I..sdo!q Ieuo!s!:>xa aq:j O:j aA!:jeU.Ia:jIe ue sy "e!saq:jsaue
Ie:>°I .Iapun pue s!seq :jua!:jed:jno ue uo auop aq ue:> a.Inpa:>o.Id S!q.L 'OO£,$
AIa:jew!xo.Idde S! a~.Ieq:> aq.L "s'{aaM Ie.IaAas .I°J :js!s.Iad ue:> :jeq:j a~eu!e.Ip
.IO UO!:j:>aJU! ue S! a.Iaq:j (ooz U! 1 sdeq.Iad) ase:> Ieuo!se:>:>o ue uI "~u!u!ewa.I
uo!:je:juapu! ue S! a.Iaq:j s.Iaq:jo U! ~aIqea:>!:jou I..Ia.Ieq S! anSS!:j Jo ssoI aq:j (z
10~.LNO:) aNY NOI.L YI~Y AO:)osz
251Probabilistic reasoning in clinical medicine
The case of mammography
Other diagnostic tests are available to help the physician estimate thechance that a particular woman's breast lesion is malignant. Perhaps themost important and commonly used is mammography. The value of thistest rests on the fact that the components of malignant cells absorb X raysdifferently from the components of non-malignant cells. By studying themammograms, a radiologist may be able to see certain signs that occurwith different frequencies in different lesions, and from this information ajudgment can be made about the nature of the lesion in question.Typically, mammograms are classified as positive or negative for cancer.Occasionally an expanded classification scheme is used, such as onecontaining the three classes: malignant, suspicious, and benign.
The test is not perfect, in that some malignant lesions are incorrectlyclassified as benign and some benign lesions are called malignant. Thus,one factor that is very important to the clinician is the accuracy of the test.
Probabilistic reasoning
Let us develop this notion more precisely. The purpose of a diagnostic testis to provide information to a clinician about the condition of a patient.The physician uses this information to revise the estimate of the patient'scondition and to select an action based on that new estimate. The actionmay be an order for further diagnostic tests, or if the physician issufficiently confident of the patient's condition, a therapeutic action maybe taken. The essential point is that the physician can have degrees ofcertainty about the patient's condition. The physician will gather evidenceto refine this certainty that the patient does or does not have cancer, andwhen that certainty becomes sufficiently strong (in the context of theseverity of the disease and the change in prognosis with treatment), actionwill be taken.
We can associate a probability, the physician's subjective probabilitythat the patient has cancer, with this degree of certainty. The impact onpatient care of a diagnostic test such as mammography, therefore, lies in itspower to change the physician's certainty or subjective probability that thepatient has cancer.
The notion of a subjective probability or degree of certainty appears inmany different forms in the medical vernacular. For example, one authorwrites that "because the older age group has the greatest proportion ofmalignant lesions, there is heightened index of suspicion of cancer in themind of a clinician who faces an older patient" (Gold, 1969, p. 162).Another author states that the mammogram can reduce the number ofbreast biopsies "in many instances when the examining physician's ratherfirm opinion of benign disease is supported by a firm mammographic diagnosis
'ual\.!g~sn~ A:>eJn:>:>e aq~ q~!M ~JodaJ AeJ-X Ja!l!sod e pa:>npoJd seq ~S!~oIo!peJaq~ ~nq 'u8!uJq (%66) AIqeqoJd S! dwnI aq~ s'fU!q~ ue!:>!sAqd aq.L :Ja:>ue:> seq~ua!~ed S!q~ ~eq~ A:J!I!qeqoJd Mau aq~ JIaSJnOA JoJ ~u!~ew!~sa Aq walqoJds,ue!:>!sAqd aq~ Jo uo!~e!:>aJdde JnOA aseaJ:>u! ue:> noA ~u!od S!q~ ~Y
'(L.l'l' °d'9961 'J~pAUS) ,,~ua:> Jad L.S Jo A:>eJn:>:>e IIeJal\.o ue JoJ 'pasou~e!p AI~:>aJJO;);}JaM suo!saI u~!uaq SOl'l Jo ~ua:> Jad vo06 pue pasou~e!p AI~:>aJJo:> aJaMsuo!saI ~Ueu~!IeW S/,v Jo ~ua:> Jad 'l"6L. paMoqs s~InsaJ aq.L" a'f!I s~uawa~e~sAuew pug ue:> ue!:>!sAqdaq~ 'paJ!sap S! I!e~ap aJOW JI 0(S6 °d 'U61'uqO:),,~ua:>Jad SS o~ OS sa~eJal\.e ~seaJq aq~ Jo suo!saI ~ueu~!Iew ~u!sou~e!pAI~:>aJJo:> U! AqdeJgowwew Jo A:>eJn:>:>e aq.L" pue ~(16V 'd '£L.61 'o~eso}J
~ 'sewoq.L 'o~eso}J) "a~eJn:>:>e AIq~!q S! eWOU!:>Je:> Jo ~JodaJ [weJ~owwew]al\.!~!sod e [ssew ~seaJq e q~!M ~ua!~ed e] uI" ~(vl'l' 'd '9961'aJIoM) ,,~ua:>Jad06 AIa~eW!xoJdde S! AqdeJ~owwew Jo A:>eJn:>:>e aq.L" :~U!MOIIOJ aq~se q:>ns 's~uawa~e~s InJdIaq aIqeJawnuu! pug ue:> aJn~eJa~!I aq~. o~ SUJn~OqM ue!:>!sAqd Y °Ja:>ue:> seq ~ua!~ed aq~ ~eq~ A:J!I!qeqoJd aq~ Jo a~ew!~saMau s,ue!:>!sAqd aq~ uo puadap AISnO!l\.qo II!M ua'fe~ suo!~:>e aq~ pueuo!~ewJoJu! Mau S! S!q.L O~ueu~!Iew S! uo!saI aq~ uo!u!do S,~S!~oIo!peJ aq~u! ~eq~ ~JodaJ e al\.!a:>aJ pue weJ~owwew e JapJo ue!:>!sAqd aq~ ~aI MoN
'Ja:>ue:> seq ~ua!~ed S!q~ ~eq~ ~ual\.a aq~ o~ % 1 Jo A~!I!qeqoJdal\.!~:>a~qns e (AISnO!:>suo:>qns sdeqJad) u~!sse aJoJaJaq~ II!M ue!:>!sAqd aq~'uo!~ewJoJu! Jaq~o Aue ~u!'f:>el '001 Jo ~no 1 'Aes 'S! dnoJ~ S!q~ U! Ja:>ue;)Jo A:>uanbaJJ aq~ ~eq~ a:>ua!Jadxa S!q~ WOJJ SMOU'f ue!:>!sAqd aq~ asoddnspuy '~ua!~ed JeIn:>!~Jed S!q~ o~ JeI!w!s ale S~U!pug Ie:>!sAqd pue '£.Jo~S!qAI!weJ 'SW()~dWAS 'a~e se q:>ns s~:>adse ~ue~Jodw! lIe U! 'OqM uaWOMJo Jaqwnu e q~!M a:>ua!Jadxa peq seq ue!:>!sAqd aq~ asoddns °sMoII°.Jse "u~!uaq [001 Jo ~no 66] AIqeqoJd S! s'fU!q~ ue!:>!sAqd aq~ ~eq~" aseJqd aq~~aJdJa~u! ue:> no}.. '001 Jo ~no 66 aq A~!I!qeqoJd S!q~ ~al °u~!uaq AIqeqoJdS! s'fU!q~ ue!:>!sAqd aq~ ~eq~ ssew ~seaJq e q~!M ~ua!~ed e Jap!suo:> MoN
Iil{dvJ.80LULUVLU /0 li.JvJ.n.J.Jv Jl{l 8u!lJJ.dJ.J1U[
.u09:>e Jo as.Ino:> e ~:>aIasdIa\{ o~ wa\{~ Aq pasn a.Ie pue SUe!:>!sA\{d o~ Ie.In~eu a.Ie A~U!e~.Ia:> JO Saa.I~ap
}O SUO!~OU a\{~ ~e\{~ a:>Uap!Aa aIdwe S! a.Ia\{~ 'ssaIa\{~auoN .S!SAIeUe uo!s!:>appue ~!I!qeqo.Id aA!~:>a~qns JO s~da:>uo:> a\{~ \{~!M pa~u!enb:>e AneW.IO} a.Iesue!:>!sA\{d MaJ asne:>aq as!:>a.Id ~ou a.Ie s~uawa~e~s asa\{]. .\{t,I°J os pue '(Z6£.d 'U61 'ue~H) "s!sou811!p aa!l!sod a.lOUl e" '(8£1 .d 'L.961 'aJIoM) "Ii:Jul1u8
253Probabilistic reasoning in clinical medicine
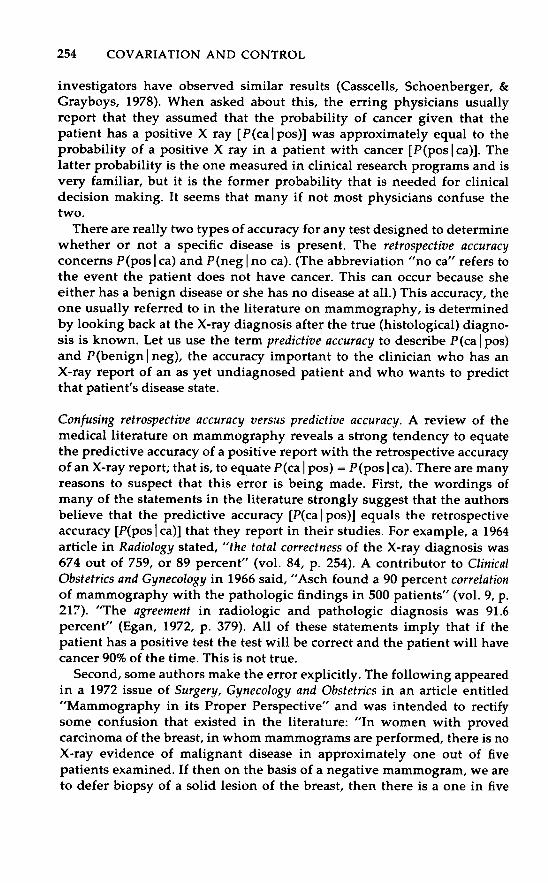
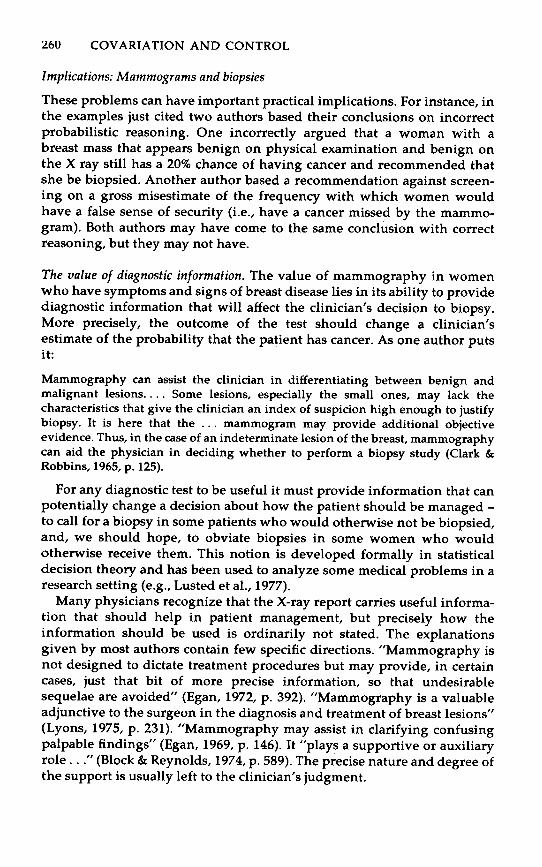
Table 1. Accuracy of mammography in diagnosing benign and malignant lesions
Results ofX ray
Malignant lesion(cancer)
Benign lesion(no cancer)
PositiveNegative
.792
.208.096.904
Source: The numbers are from Snyder (1966).
Bayes' formula can be applied to assess the probability. This formulatells us that
P(ca I pos) =
whereP(ca I pos) is the probability that the patient has cancer, given that
she has a positive X-ray report (the posterior probability)P(pos Ica) is the probability that, if the patient has cancer, the
radiologist will correctly diagnose it (the true-positive rate, orsensitivity)
P(ca) is the probability that the patient has cancer (prior probabili-
ty)P(benign) is the prior probability that the patient has benign
disease [P(benign) = 1 - P(ca)]P(pos I benign) is the probability that, if the patient has a benign
lesion, the radiologist will incorrectly diagnose it as cancer (thefalse-positive rate)
Table 1 summarizes the numbers given by Snyder. The entries in thecells are the appropriate probabilities (e.g., P(pos I ca) = .792).
Using 1% as the physician's estimate of the prior probability that themass is malignant and taking into account the new information providedby the test, we obtain
(0.792) (0.01)P(ca I pos) = (0.792) (0.01) + (0.096) (0.99) ~ .f
Thus, the physician should estimate that there is approximately an 8%chance that the patient has cancer.
-- - On77
Incorrect probabilistic reasonin~
Unfortunately, most physicians (approximately 95 out of 100 in an infor-mal sample taken by the author) misinterpret the statements about theaccuracy of the test and estimate P(ca I pos) to be about 75%. Other
aAg u! auo e s! aJa4:) ua4:) ':)seaJq a4:) Jo uo!sa{ P!{OS e Jo Asdo!q JaJap 0:)
aIe aM 'weJ~owwew aA!:)e~au e Jo s!seq a4:) uo ua4:) JI °pau!wexa s:)ua!:)ed
aAg Jo :)no auo A{a:)ew!xoJdde U! aseas!p :)ueu~!{ew Jo a:>uap!Aa AeJ-X
ou S! aJa4:) 'pawJoJJad aJe sweJ~owwew W04M U! ':)seaJq a4:) Jo ewou!:>J~:>
paAoJd 4:)!M uawoM uI" :am:)eJa:)!I a4:) U! pa:)s!xa :)e4:) uo!snJuo:> awos
AJ!:):>aJ 0:) papua:)u! seM pu~ "aA!:):>adsJad JadoJd s:)! U! A4deJ~owwew"
pa{:)!:)ua a{:>!:)Je ue U! S.J!,llc7lsqO puv 1i8ol°.Jc7uli.') '1i,lc78,lns Jo anss! U61 e U!paJeadde ~U!MOllOJ a4J. ° A{:)!:>!{dxa JoJJa a4:) a'{ew sJ04:)ne awos 'puo:>as
'am:) :)ou S! S!4J. °aw!:) a4:) Jo %06 Ja:>u~:>
aAe4 ll!M :)ua!:)ed a4:) pue :):>aJJo:> aq ll!M :)sa:J a4:) :)sa:) aA!:)!sod e se4 :)ua!:)~d
a4:J J! :)e4:) A{dw! s:)uawa:)e:)s asa4:) Jo llV '(6L.£ 'd 'U61 'ue~H) ,,:)ua:>Jad9°16 seM s!sou~e!p :>!~0{04:)ed pue :>!~o{o!peJ U! lUc7lUc7c7,l8v a4J." il.I'l
'd '6 'lOA) "s:)ua!:)ed OOS U! S~U!pug :>!~0{04:)ed a4:) 4:)!M A4de.I~owwew Jo
UO!lVlc7,l,lo.J :)ua:>Jad 06 e punoJ 4:>sV" 'P!es 9961 U! 1i8ol°.Jc7uli.') puv S.J!,llc7lsqO
Iv:J!U!!.J 0:) Jo:)nq!J:)uo:> V itSZ °d 't8 loA) ,,:)ua:>Jad 68 JO '6SL. Jo :)no tL.9
seM s!sou~e!p AeJ-X a4:) Jo SSc7UPc7,l,lO.J IV10l c7lll" 'pa:Je:)s 1i8o10!PVN U! a{:>!:)J~
J7961 ~ 'a{dwexa JOd °sa!pmS J!a4:) U! :)JodaJ Aa4:) :Je4:J [(e:> I sod)d] A:>eJn:>:>eaA!:):>adso.I:)aJ a4:) s{enba [(sod I e:»d] A:>em:>:>e aA!:):>!paJd a4:) :)e4:) aAa!{aq
SJ04:)ne a4:) :)~4:) :)sa~~ns A{~UOJ:)s am:)eJa:)!{ a4:) U! s:)uawa:Je:)s a4:) Jo AuewJO S~U!pJOM a4:J ':)SJ!d °apew ~u!aq S! JOJJa S!4:) :)e4:) :):>adsns 0:) suosea.IAuew aJe aJa4J. ie:> I sod)d = (sod I ~:»d a:)~nba O:J 'S! :)e4:) ~:)JodaJ AeJ-X ue Jo
AJem:>:>e aA.!:):>adsoJ:)aJ a4:) 4:)!M :)JodaJ aA!:)!sod e Jo A:>eJn:>:>e aA.!:):>!paJd a4:)
a:)enba 0:) A:>uapua:) ~UOJ:)s e S{eaAaJ A4de.I~owwew uo am:)eJa:)!{ {e:>!paw
a4:) Jo Ma!AaJ V 'li.Jv,ln.J.Jv c7a!p!pc7,ld SnS,lc7a li.Jv,ln.J.Jv c7a!pc7dso,llc7,l 8u!snJuo.:)
"a:Je:Js aseas!p s,:Jua!:Jed :Jeq:J:J:>!pa.ld O:J s:JueM. oqM. pue :Jua!:Jed pasouSe!pun :JaA se ue JO :J.loda.l Ae.l-Xue seq oqM. ue!:>!u!I:> aq:J O:J :Jue:J.lodw! A:>e.ln:>:>e aq:J '(Sau I uS!Uaq)d pue(sod I e:»d aq!.I:>sap O:J h:1vJ.n:1:1v Ja!p!pJJ.d w.la:J aq:J asn sn :Ja'l "UM.ou'{ S! S!S
-ouSe!p (Ie:>!SOI°:JS!q) an.l:J aq:J .la:J}e s!souSe!p Ae.l-X aq:J :Je '{:>eq SU!'{oOI Aqpau!w.la:Jap S! 'Aqde.lSowwew uo a.ln:Je.la:J!I aq:J U! O:J pa.l.laJa.l Anensn auoaq:J 'A:>e.ln:>:>e S!q.L ('ne :Je aseas!p ou seq aqs .10 aseas!p u~!uaq e seq .laq:J!a
aqs asne:>aq .In:>:>o ue:> S!q.L ".la:>ue:> aAeq :Jou saop :Jua!:Jed aq:J :JuaAa aq:}
O:J s.la}a.l "e:> ou" UO!:Je!Aa.lqqe aq.L) "(e:> ou I Sau)d pue (e:> I sod)d su.la:>uo:>!i:1vJ.n:1:1v Ja!I:1JdsoJ.IJJ. aq.L ":Juasa.ld S! aseas!p :>y!:>ads e :Jou .10 .laq:JaqM.
au!w.la:Jap O:J pauS!sap :Jsa:J Aue .l0} A:>e.ln:>:>e}o sadA:J OM.:J Anea.l a.le a.laq.L
"OM.:}aq:J asn}uo:> sue!:>!sAqd :Jsow :Jou }! Auew :Jeq:J swaas :JI "Su!'{ew uo!s!:>ap
Ie:>!U!I:> .l°J papaau S! :Jeq:J At!I!qeqo.ld .law.lo} aq:J S! :J! :Jnq '.le!I!we} A.xaAS! pue swe.lSo.ld q:>.leasa.l Ie:>!U!I:> U! pa.lnseaw auo aq:J S! At!I!qeqo.ld .la:J:JeI
aq.L "[(e:> I sod)d] .la:>ue:> q:J!M. :Jua!:Jed e U! Ae.l X aA!:J!sod e }O A:J!I!qeqo.ld
aq:J O:J Ienba Ala:JeW!xo.ldde geM. [(sod I e:»d] Ae.l X aA!:J!sod e seq :Jua!:Jedaq:J :Jeq:J UaA!S .la:>ue:> Jo A:J!I!qeqo.ld aq:J :Jeq:J pawnsse Aaq:J :Jeq:J :J.loda.l
Anensn sue!:>!sAqdSu!.I.la aq:J 'S!q:J :Jnoqe pa'{se uaqM "(8"61 'sAoqAe.l~l? '.laS.laquaoq:>s 'sna:>sse:) s:Jlnsa.l .leI!w!s paA.Iasqo aAeq s.lo:JeS!:JsaAU!
'IOM.LNO:) aNY NOI.L VIMV AO:)tS'l
Probabilistic reasoning in clinical medicine 255
chance that we are deferring biopsy of a malignant lesion" (vol. 134, p. 98).The author has incorrectly stated that P(neg I ca) = .2 implies P(ca I neg) =.2. His error becomes very serious when he concludes that "to defer biopsyof a clinically benign solid lesion of the breast that has been called benign onmammography is to take a step backward in the eradication of carcinomaof the breast in our female population." The chance that such a patient hascancer depends on the prior probability, but is less than 1 in 100. Hisanalysis is in error by more than a factor of 20.
Surgery, Gynecology and Obstetrics published in 1970 (vol. 131, pp. 93-98)the findings of another research group, who computed the "correlation ofradiographic diagnosis with pathologic diagnosis" as follows. They tookall the patients with histologically proven diagnoses and separated theminto three groups on the basis of the X-ray diagnosis - "benign," "carci-noma," and "suspected carcinoma." In the "X-ray benign" ("negative" inour terminology) group, the tally showed that 84% in fact had benignlesions. It was also noted that 87.5% of the "X-ray carcinoma" (or"positive") group had biopsy-proven malignant lesions. Thus, P(ca I pos) =87.5% and P(benign I neg) = 84%. But the authors mistook this predictive
accuracy for the retrospective accuracy. They stated that "A correctmammographic diagnosis was made in 84 percent of those with benign lesionsand in 87.5 percent of those with carcinoma." In fact, the true-positive rate[P(pos I ca)] in this study was actually 66% and the true-negative rate[P(neg I benign)] was 54%.
In a letter to the editor in the September 11, 1976, issue of the NationalObserver, a physician presented five "observations and facts" to support hisopinion that "routine [i.e., screening] mammography is not in the bestinterest of the population at large at any age." Here is the first set ofobservations.
(1) The accuracy of the examination of mammography is reported to be between 80percent and 90 percent, depending on such factors as the age of the patient,whether or not she has fibrocystic disease, the type of radiographic equipment, theexperience of the radiologist, and what our definition of "accurate" is. . . . Even ifwe conclude that accuracy is 85 percent generally (and I am sure that not everyradiologist in the nation can approach that figure in his own practice), then thatmeans that 15 percent of the women X-rayed will wind up with incorrect interpretations ofthe findings, or more likely, their mammograms will simply fail to demonstrate the disease.This means that 15 percent of the women will be given a false sense of security if they aretold~r X-rays are normal, if indeed they already have cancer. It is difficult to assessthe harm done to this group, for they would obviously be better off with noinformation rather than with incorrect information. Told that her mammogram isnormal and she need not come back for one more year, a woman with breast cancermay well ignore a lump in her breast which might otherwise send her to the doctor
immediately.
There are several errors in this author's reasoning. First, the "accuracy"of mammography cannot be expressed as a single number. Assume the
";[n:>:>o g pue y S~UaAa \{~oq ~e\{~ A:t!T!qeqO.ld ~U!o! a\{~ S! (g'Y)d z
1! \I~!M. aA1!aI II!M. wa\I~ }O gSt'g , A;)1!Jn;);)1! a\I~ }O a~1!W!~Sas!W S,Jo\I~n1!
a\I~ asn aM. }! PU1! 'pauaaJ;)S aJ1! uaWOM. ;)!~1!WO~dWAS1! 000'01 }! 'S! ~1!\Il.
(S66')(SSO) + (SOO")(sr') 68000' - (£00")(£1")
(e;) ou)d (e;) ou I ~au)cl + (e;)d (e;) I ~au)d(~au I e;)d
(\?;)d (\?;) I gau)d
'1!InWJoJ ,SaA1!g Aq MoNi~au 11!:»d a:J1!W!:Jsa O:J ~U!AJ:J aq O:J sJ1!add1! Joq:Jn1! aqj, ,,11!WJOU aJ1! SA1!J-XJ!aq:J Plo:J aJ1! Aaq:J J! A:J!Jn:>as JO asuas asI1!J 1! UaA!~ aq II!M UaWOM aq:J JO:Jua:>Jad ST" :J1!q:J U1!aw :JOU saop "a:J1!Jn~:>1!" %S8 :J1!q:J S! walqoJd Jaq:Jouy
"Ala'!!I SSiJ] saW!:J OOZ :Jnoq1! S! :JI "SZ6fT" = (sod'1!:> ou)d U1!q:J Ala'!!TaJOW IOU S! SlOOO" = (~au'1!:»d ,,"as1!as!p aq:J a:J1!J:Jsuowap o:J I!1!J ATdw!s
II!M SW1!J~OWW1!W J!aq:J 'ATa'!!I aJow" :J1!q:J U1!aw :Jou saop S!q:J 'JaAaMOH"sa:J1!:Js Joq:Jn1! aq:J S1! '%ST S! q:>!qM 'sJaqwnu OM:J asaq:J Jo wns aq:J S! [(sod'1!:>ou)d + (~aU'1!:»d '"a"!] uo!:J1!:JaJdJa:Ju! :J:>aJJo:>u! U1! Jo A:J!I!q1!qoJd 11!:Jo:J aqj,
SZ6fT" = (S66") (ST") "-< (1!:> ou)d (1!:> ou I sod)d = (sod'1!:> ou)d
'osYV
SL.OOO. = (SOO.) (SI(Sau'e:»a
'snl{l.
iSl?aJq al{:J }OJa:>Ul?:> a{ql?:J:>a:Jap-wl?J~OWWl?W :Jnq :>!:Jl?WO:JdWASl? Ul? JoqJl?l{ UaWOM ooo'r}O :Jno S Ul?l{:J JaMa} 'S! :Jl?l{l. 'SOO' Ul?l{:J Ssa{ S! :J! :Jl?l{:J U!l?:JJa:> A{ql?UOSl?aJ all?aM uo!:Jl?{ndod ~u!uaaJ:>s l? JO} :Jnq 'A{as!:>aJd (l?:»d MOU'{ :JOU op aM .aSl?:>
S!l{:J U! sr. s{l?nba aJo}aJal{:J PUl? (l?:> I sod)d }O :Juawa{dwo:> al{:J S! (l?:> I ~au)d
(l?:»d (l?:> I ~au)d = (~au'l?:»d
:Jl?l{:J MOU'{ aM AJoal{t A:J!{!ql?qOJd AJl?:Juawa{a wold ;(sod'l?:> ou)d
'Ja:>ul?:> aAl?l{ :Jou :Jnq UO!:Jl?u!wl?xa aA!:J!sod l? aAl?l{ Ul?:> al{s (q) JO ~(~aU'l?:»d
'UO!~!Wl?xa aA!:Jl?~aU l? PUl? Ja:>Ul?:> aAl?l{ Ul?:> :Jua!:Jl?d al{:J (l?) :In:>:>o Ul?:> UO!:J
-l?:JaJdJa:Ju! :J:>aJJo:>u! Ul? SAl?M OM:J all? aJal{l. .a:>ua:Juas puo:>as al{:J Jap!suo::)
.~U!UOSl?aJ al{:J U! sa!:>l?Jn:>:>l?U! {l?JaAaS pug aM '%SS ~u!sn uaAa 'pJ!l{l.. A{aA!:J:>adsaJ '%S6 PUl? %09 all? SWl?J~OJd ~u!uaaJ:>s
U! sa:Jl?J aA!:Jl?~au-anJ:J PUl? aA!:J!sod-anJ:J al{:J JO} sa:Jl?W!:Jsa a{ql?Uosl?aJ aJOW
.~u!ssaJppl? S! Jol{:Jnl? al{:J UO!:Jl?m!S al{:J S! l{:>!l{M 'UO!:Jl?U!Wl?xa ~u!uaaJ:>sl? U! :Jl{~nos ~u!aq SUo!sa{ al{:J Ul?l{:J pa:>Ul?Apl? aJOW Anl?JaUa~ all? suo!sal
l{:>ns 'SWO:JdWAS PUl? SU~!S UMOU'{ }O S!SOU~l?!P {l?!:JuaJaJ}!p l? a'{l?W O:J
pasn S! Al{dl?J~OWWl?W ual{M paAJasqo all? (%SS }o) sa:Jl?J asal{:J 'puo:>as
.%SS{l?nba l{:Joq sa:Jl?J aA!:Jl?~au-anJ:J PUl? aA!:J!sod-anJ:J al{:J :Jl?l{:J SUl?aw Jol{:Jnl?
10~lNO:) aNY NOll YI~Y AO:)9SZ

Probabilistic reasoning in clinical medicine 257
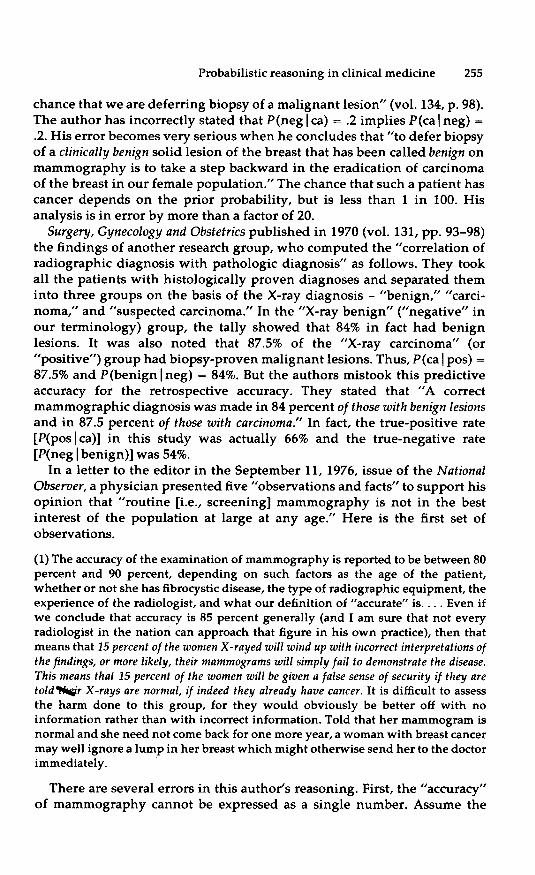
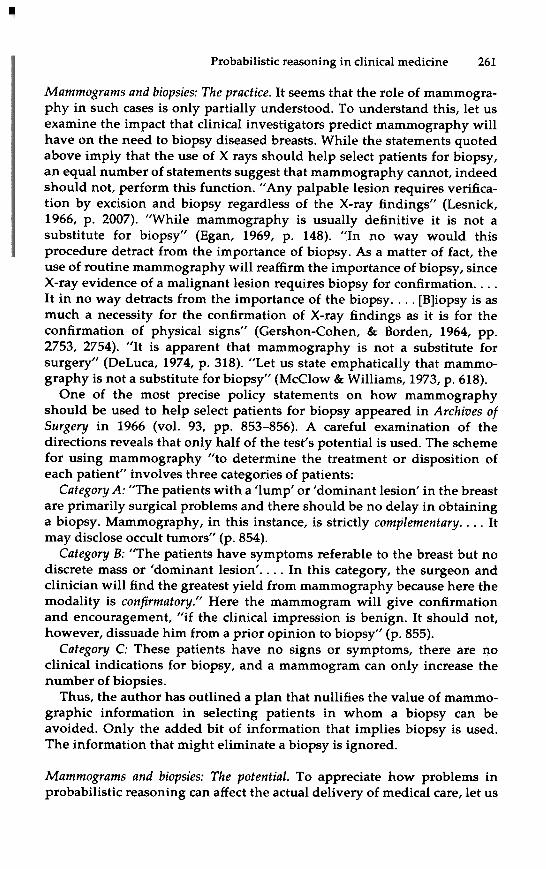
Table 2. Presence of cancer and results of X rays in 1000 women who have abnormalphysical examinations
Women withcancer
Women withno cancer Total
Women withpositive X rays
Women withnegative X rays
Total
74 110 184
810
920
816
1,000
6
80
Note: A true-positive rate of .92 (p(poslca) = 0.92) implies that of 80 women whohave cancer, 74 will have positive X rays and 6 will have negative X rays. Of all thewomen with positive X rays, 74/184 have cancer, or P(calpos) = 74/184 - 40%.Source: The numbers are from Wolfe (1964).
negative examination. The author thinks that about 1,269 of them willhave a false sense of security. In fact, only about 9 will. This number hasbeen overestimated by a factor of about 150.
Finally, adding the phrase, "if indeed they already have cancer" furtherconfuses the meaning of the sentence. The phrases "a false sense ofsecurity ," "if [given] they are told their X-rays are normal," and "if theyalready have cancer" translate symbolically into P(ca I neg,ca). This proba-bility is 1, not .15.
The importance of P(ca). In addition to confusing the two accuracies, manyauthors do n~eem to understand that, for a test of constant retrospectiveaccuracy, the meaning to the physician of the test results (the predictiveaccuracy) depends on the initial risk of cancer in the patient beingmammogrammed. Even if it is assumed that the true-positive and true-negative rates are constant for all studies, the proper interpretation of thetest results - the chance that a patient with a positive (or negative)mammogram has cancer - will depend on the prevalence of cancer in thepopulation from which the patient was selected, on the pretest probabilitythat a patient has cancer. This can be extremely important when onecompares the use of the test in a diagnostic clinic (where women havesigns and symptoms of breast disease) with its use in a screening clinic forasymptomatic women.
The importance of this is shown by an example. Suppose a clinician'spractice is to mammogram women who have an abnormal physicalexamination. The frequency of cancer in such women has been found inone study to be approximately 8% (Wolfe, 1964). In one series of mammo-grams in this population, a true-positive rate of 92% and a true-negativerate of 88% was obtained (Wolfe, 1964). Let the physician now face a
"(e:»d Jo a:>uetJodw! a\{t ateJtsuowap °t ATuO apew s! uondwnsse a\{J. "t:>atapat JapJe\{ pue Janews \{:>nw aq °t puat SJa:>ue:> a\{t asne:>aq UoneTndod :>neWOtdWAse ueU! tsat a\{t Su!sn S! auo Ua\{M JaMoT S! ateJ aAmsod-anlt a\{t 'aTdwexa JOd "saSue\{:> pau!wexaSu!aq UoneTndod a\{t se saSue\{:> "A:>eJn:>:>e" a\{t a:>u!s 'uondwnsse pooS e tau S! S!\{J. £
a\{:j U! sas1?as!p alq!ssod a\{:j Jo A:>uanba.IJ :>!S1?q a\{:j :jnoq1? UO!:j1?W.I°JU!asn U1?!:>!sA\{d 1? Plno\{s MO\{ 'SWO:jdWAS PU1? SU~!S s,:jua!:j1?d 1? a:j1?nl1?AaO:j ~U!A.r.:j Ua\{M - ~U!UOS1?a.I l1?:>!paw :jnoq1? uo!:jsanb .IOr1?W 1? saS!1?I S!\{j,
° .Ia:>U1?:>
S1?\{ W1?I~OWW1?W aA!:j!sod 1? \{:j!M U1?WOM 1? :j1?\{:j a:>U1?\{:> a\{:j U! J,JUJ.lJ1/!P
PloflilUJml 1? :jnoq1? aq U1?:> a.Ia\{:j 'pau!w1?xa ~u!aq S! O\{M uo ~u!puadap'sn\{j, O%Ot S1?M (sod 11?:»d 'SWO:jdWAS \{:j!M uaWOM paAl0AU! :j1?\{:j aldw1?xasno!Aa.Id a\{:j UI ,(£ alq1?j,) %O'Z :jnoq1? .IO '6t JO :jno 1 :jnoq1? S! «sod 11?:»d).Ia:>U1?:> S1?\{ tua!:j1?d a\{:j :j1?\{:j A:j!l!q1?qo.Id a\{:j ':j.Ioda.I A\{d1?I~oww1?WaA!:j!sod a\{:j UaA!~ °aA!:j!sod S! U1?WOM :>!:j1?WO:jdWAS1? S!\{:j U! W1?I~OWW1?Wa\{:j t1?\{:j s:j.Ioda.I :jS!~010!P1?I a\{:j A1?S 'aldw1?xa S!\{:j \{:j!M anU!:juo:> oj,
O%oaq(as1?as!p ou I sod)d :jal PU1? A\{d1?I~oww1?W O:j alq1?IOA1?J uo!:jdwnss1? U1?
a'I1?W OSl1? 111?\{S aM O%Ot :jnoq1? S! (u~!uaq)d PU1? %09 :jnoq1? S! (as1?as!p OU)d:j1?\{:j awnSS1? PU1? (S961) aJl~ Aq pa:juasa.Id 1?:j1?p a\{:j asn 111?\{S aM 'aldw1?xa
S!\{:j .I0,f .poo:jS.Iapun :jOU S! swalqo.Id asa\{:j JO S!SA11?U1? a\{:j U! a:>u1?:j.Iodw!.I!a\{t t1?\{:j t:>adsns O:j sn sp1?al :j! PU1? aA!:j:>n.I:jsu! S! S!\{j, 'a.Im1?Ia:j!l a\{:j U! An!
-:>!ldxa passn:>s!p :jOU a.I1? (as1?as!p ou I sod)d PU1? '(as1?as!p OU)d '(u~!Uaq)d
[(as1?as!p ou)d(as1?as!p ou I sod)d +
(u~!Uaq)d(u~!Uaq I sod)d + (1?:»d(1?:>j sod)d]+ [(1?:»d(1?:> I sod)d] = (sod 11?:»d
'aS1?:> S!\{:j U! 'sn\{j, iS961 'aJl° M) 111? :j1? aS1?as!p ou p1?\{ uaWOM asa\{:jJo %09 :jnoq1? ApmS auo uI .sas1?as!p u~!uaq PU1? .Ia:>U1?:> aA1?\{ O\{M uaWOMU! :jsa:j a\{:j Jo A:>1?In:>:>1? aA!:j:>adso.I:ja.I a\{:j uo AluO 1?:j1?P sap!Ao.Id a.Im1?Iat!la\{j, E.%88 Jo (sUO!Sal u~!uaq Jo S!SOU~1?!P a\{:j .I°J) a:j1?I aA!:j1?~aU-an.I:j 1? PU1?%Z6 Jo a:j1?I aA!:j!sod-an.I:j 1? aA1?\{ U!~~1? W!\{ :jal s:jua!:j~d Jo Uo!:j~lndod S!\{:jU! 'S! :j1?\{:j - pa~ue\{:>un aq :jS!~olo!pe.I a\{:j Jo A:>e.In:>:>e aA!:j:>adso.I:ja.I a\{:j :jal
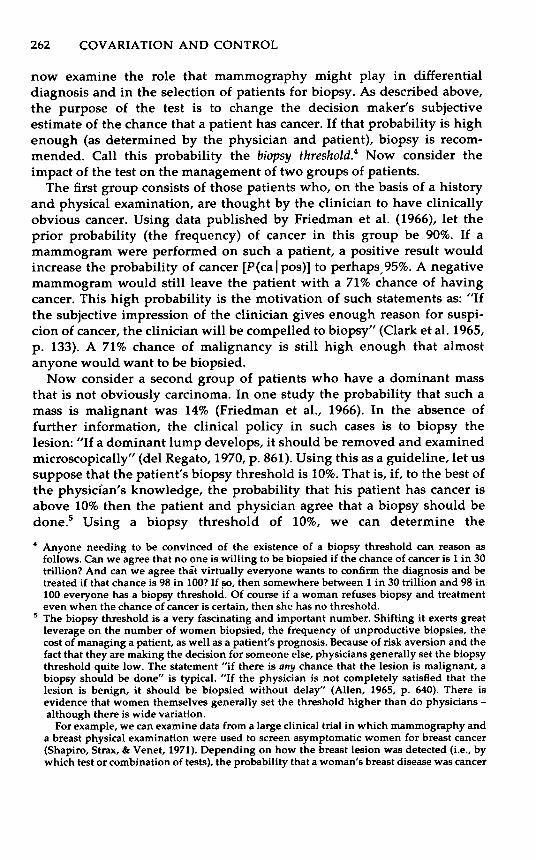
'aldwexa S!\{:j Jo sasod.Ind a\{:j .Io,f i£,961 ':jauaA:1? 'xe.I:jS 'o.I!de\{s "~'a) %01.:jnoqe S! uaWOM \{:>ns U! .Ia:>ue:> alqe:j:>a:jap-A\{de.I~owwew Jo a:>ualeAa.Ida\{j, .uo!:jeu!wexa le:>!sA\{d aA!:je~au e pue SWO:jdWAS ou se\{ O\{M uewoM..e U! .Ia:>ue:> .I°J uaa.I:>s O:j :jsa:j a\{:j s.Iap.Io ue!:>!u!l:> a\{:j asoddns 'MoN
.Z alqe.LU! UMO\{S S! a:j1?w!:jsa S!\{:j .I°J :>!~Ol a\{j, °%1 ue\{:j ssal An\{~!lS S! .Ia:>ue:>sel.{ 11!:js ':j.Ioda.I aA!:je~au e UaA!~ 'ueWOM S!l.{:j :jel.{:j A:I!l!qeqo.Id al.{j, l.Ia:>ue:>:jno paln.I aAel.{ :j.Ioda.I aA!:je~au e PlnoM o(Z alqej, aas) %Ot aq O:j pa:jeln:>le:>aq ue:> A:I!l!qeqo.Id :jel.{j, ..Ia:>ue:> sel.{ :jua!ted al.{:j :jel.{:j A:j!l!qeqo.Id Mau al.{:j uopaseq aq Plnol.{s Asdo!q e .Iap.Io O:j uo!s!:>ap S!H .:jS!~010!pe.I al.{:j WO.IJ :jlnsa.IaA!:j!sod e SaA!a:>a.I pue we.I~owwew e s.Iap.Io al.{ asoddns i%8 = (e:»d
:jal "a'!) UO!:jelndod aldwes S!l.{:j Jo aA!:je:juasa.Ida.I S! slaaJ al.{ Ol.{M :jua!:jed
10}Jl.NOJ aNY NOll. YI}JY 1\OJ8S"l

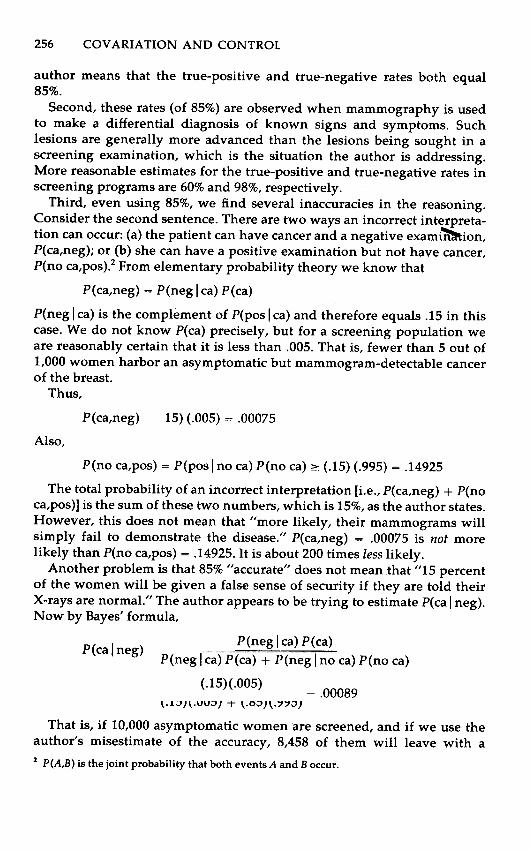
Probabilistic reasoning in clinical medicine 259
48 49
0
1
352
400
599
599
951
1,000
--
Women withpositive X rays
Women withnegative X rays
Total-
Note: A true-positive rate of 0.92 implies that the X ray will detect cancer in theone woman who has the disease. A true-negative rate of 0.88 for benign diseaseimplies that of 400 women with benign disease, 352 will have negative X rays,whereas in 48 the X ray will be {'ositive. Thus, 49 women will have positive X rays,but only one has cancer, or P(calpos) = 1/49 = 2%.
population at large? The profession appears to be confused about thisissue. On the one hand, physicians make statements that the relativecommonness of a disease should not affect the estimate of the probabilitythat a particular patient has the disease. This notion appears in severalmaxims, such as, "The patient is a case of one" and, "Statistics are for deadmen." In discussions of specific problems, the idea is sometimes expressedsubtly as in the statement, "The younger women obviously have a fewernumber of the malignancies which, however, should exert very littleinfluence on the individual case" (Wolfe, 1967, p. 138). It can also be statedexplicitly and presented as a rule to be obeyed. For example, the followingappeared in a textbook on clinical diagnosis: "When a patient consults hisphysician with an undiagnosed disease, neither he nor the doctor knowswhether it is rare until the diagnosis is finally made. Statistical methodscan only be applied to a population of thousands. The individual eitherhas a rare disease or doesn't have it; the relative incidence of two diseasesis completely irrelevant to the problem of making his diagnosis" (DeGo-win &1: DeGowin, 1969, p. 6).
On the other hand, these statements are often inconsistent with thebehavior of physicians who try, however imperfectly, to use this diagnos-tic information. Witness the following maxims that are passed on inmedical schools: "When you hear hoofbeats, think of horses not ofzebras," "Common things occur most commonly," "Follow Sutton's law:go where the money is," and so forth. It appears that many physicianssense the value of information on the prior probability of a disease but thatthe formal lessons of probability theory are not at all well understood.Without a formal theory, physicians tend to make the same kinds of errorsin probabilistic reasoning that have been observed in other contexts(Kahneman & Tversky, 1973,4; Lyon & Slovic, 1976).
tuaw~pn~ s,ue!:>!u!I:> al{t °t tJaI AIIensn S! tJoddns al{:JJO aaJ~ap pue aJmeu as!:>aJd al{j, i68S "d 'v£.6 1 'sPIouAa~ l? 'I:>oIg) ,," " " aIoJ
AJe!I!xne JO aA!tJoddns e sAeId" tI i9vl "d '6961 'ue~3) "S~U!puy aIqedIed~u!snJuo:> ~u!AJ!JeI:> U! ts!sse Aew Al{deJ~owwew" il£"l "d 'S£.61 'SUOA'I)"suo!saI tseaJq Jo tuawteaJt pue s!sou~e!p al{t U! uoa~Jns al{t °t aA!t:>un~peaIqenIeA e S! Al{deJ~owwew" "<"l6£ .d 'U6 1 'ue~3) "pap!OAe aJe aeIanbasaIqeJ!sapun tel{t os 'uo!tewJoJu! as!:>aJd aJOW Jo t!q tel{t tsn~ 'sase:>u!etJa:> U! 'ap!AoJd Aew tnq saJnpa:>oJd tuawteaJt atet:>!p °t pau~!sap tou
S! Al{deJ~owwew" "suo!t:>aJ!p :>y!:>ads MaJ u!etuo:> SJol{tne tSOw Aq UaA!Ssuo!teueIdxa al{j, .patets tOU AI!JeU!pJo S! pasn aq PInol{s uo!tewJoJu!al{t MOl{ AIas!:>aJd tnq 'tuawaSeuew tua!ted U! dIal{ PInol{s tel{t UO!t-ewJoJu! InJasn sa!JJe:> tJodaJ AeJ-X al{t tel{t az!u~o:>aJ sue!:>!sAl{d Auew
"(£.£.61 'le ta patsn'I '"S.a) Su!ttas l{:>JeasaJe U! swaIqoJd Ie:>!paw awos azAIeue °t pasn uaaq self pue AJoal{t uo!s!:>ap
Ie:>!ts!tets U! AIIewJoJ padoIaAap S! UO!tou S!l{j, .wal{t aA!a:>aJ as!M.Jal{toPInoM Ol{M uaWOM awos U! sa!sdo!q ate!Aqo °t 'adol{ PInol{s aM 'pue'pa!sdo!q aq tOU as!M.Jal{to PInoM Ol{M stua!ted awos U! Asdo!q e JoJ lIe:> °t- paSeuew aq PInol{s tua!ted al{t MOl{ tnoqe Uo!s!:>ap e a~uel{:> AIIe!tuatod
ue:> tel{t uo!tewJoJu! ap!AoJd tsnw t! InJasn aq °t tsat :>!tsou~e!p Aue JOd
"(S'l1 "d 'S961 'SU!qqo~~ 'IJeo) ApntS Asdo!q e WJoJJiJd °t JiJ\{tiJ\{M 2u!p!:>iJP U! ue!:>!sA\{d iJ\{t p!e ue:>A\{deJ20wwew 'tseiJJq iJ\{t JO UO!SiJY iJteU!WJiJtiJPU! ue JO iJse:> iJ\{t U! 'sn\{l. "a:>UiJp!A.aiJA.!t:>a!qo yeUo!t!ppe ap!A.oJd Aew weJ20wwew ".. iJ\{t te\{t iJJiJ\{ S! tI . Asdo!q
AJ!tSn! °t \{2nouiJ \{2!\{ uo!:>!dsns JO XiJPU! ue ue!:>!u!y:> iJ\{t iJA.!2 te\{t s:>!tS!JiJt:>eJe\{:>iJ\{t 'I:>ey Aew 'SiJUO news iJ\{t Ane!:>adsiJ 'SUO!SiJY iJWOS ."" .SUO!SiJY tueu2!yew
pue u2!uiJq UiJiJMtiJq 2u!te!tuiJJaJJ!p U! ue!:>!u!y:> iJ\{t tS!Sse ue:> A\{deJ20wwew
:t!stnd Joqtn~ auo sy . Ja:>u~:> s~q tua!t~d aqt t~qt At!I!q~qoJd aqt Jo at~w!tsaS,U~!:>!U!I:> ~ agu~q:> PInoqs tsat aqt Jo awo:>tno aqt I AIaS!:>aJd aJow. Asdo!q °t uo!s!:>ap S,U~!:>!U!I:> aqt t:>a.JJ~ II!M. t~qt UO!t~WJoJU! :>nsoug~!P
ap!AoJd °t A:t!I!q~ St! U! sa!I as~as!p ts~aJq Jo sug!S pu~ SWOtdwAS aA~q oqM.UaWOM. U! Aqd~Jgoww~w Jo anI~A aq.L 'UO!IVUlJOjU! J!lsou8v!p jo Jnlva JIfL
.aAeq :JOU AeW Aaq:J :Jnq '~U!UOSea.I
:J~aJJO~ q:J!M. uo!snl~uo~ awes aq:J O:J awo~ aAeq Aew SJoq:Jne q:Jog iweJ~-owwew aq:J Aq pass!w Ja~ue~ e aAeq I.a.!) A:J!Jn~as JO asuas asleJ e aAeq
PlnoM. uawoM. q~!qM. q:J!M. A~uanbaJJ aq:J Jo a:Jew!:Jsas!w SSOJ~ e uo ~U!
-uaaJ~S :Jsu!e~e uo!:Jepuawwo~aJ e paseq Joq:Jne Jaq:Jouy .pa!sdo!q aq aqs
:Jeq:J papuawwo~aJ pue Ja~ue~ ~U!Aeq Jo a~ueq~ %O"l e seq l1!:Js AeJ X aq:Juo u~!uaq pue uo!:Jeu!wexa le~!sAqd uo u~!uaq sJeadde :Jeq:J ssew :JseaJq
e q:J!M. uewoM. e :Jeq:J pan~Je Ap~aJJO~u! auo .~u!uoseaJ ~!:JS!I!qeqoJd
:J~aJJO~U! uo suo!snl~uo~ J!aq:J paseq sJoq:Jne OM.:J pa:J!~ :Jsn~ saldwexa aq:J
U! 'a~ue:Jsu! J°:1 .suo!:Je~!ldw! le~!:J~eJd :Jue:JJodw! aAeq ue~ swalqoJd asaql.
siJ!sdo!q puv SlUVJ8olUlUVW :SUO!lVJ!1dlUI
'IO~.lNO:) aNY NOI.l YI~Y AO:)09Z
Probabilistic reasoning in clinical medicine 261
Mammograms and biopsies: The practice. It seems that the role of mammogra-phy in such cases is only partially understood. To understand this, let usexamine the impact that clinical investigators predict mammography willhave on the need to biopsy diseased breasts. While the statements quotedabove imply that the use of X rays should help select patients for biopsy,an equal number of statements suggest that mammography cannot, indeedshould not, perform this function. "Any palpable lesion requires verifica-tion by excision and biopsy regardless of the X-ray findings" (Lesnick,1966, p. 2007). "While mammography is usually definitive it is not asubstitute for biopsy" (Egan, 1969, p. 148). "In no way would thisprocedure detract from the importance of biopsy. As a matter of fact, theuse of routine mammography will reaffirm the importance of biopsy, sinceX-ray evidence of a malignant lesion requires biopsy for confirmation. . . .It in no way detracts from the importance of the biopsy. . . . [B]iopsy is asmuch a necessity for the confirmation of X-ray findings as it is for theconfirmation of physical signs" (Gershon-Cohen, & Borden, 1964, pp.2753, 2754). "It is apparent that mammography is not a substitute forsurgery" (DeLuca, 1974, p. 318). "Let us state emphatically that mammo-graphy is not a substitute for biopsy" (McClow & Williams, 1973, p. 618).
One of the most precise policy statements on how mammographyshould be used to help select patients for biopsy appeared in Archives ofSurgery in 1966 (vol. 93, pp. 853-856). A careful examination of thedirections reveals that only half of the test's potential is used. The schemefor using mammography "to determine the treatment or disposition ofeach patient" involves three categories of patients:
Category A: "The patients with a 'lump' or 'dominant lesion' in the breastare primarily surgical problems and there should be no delay in obtaininga biopsy. Mammography, in this instance, is strictly complementary. . . . Itmay disclose occult tumors" (p. 854).
Category B: "The patients have symptoms referable to the breast but nodiscrete mass or 'dominant lesion'. . . . In this category, the surgeon andclinician will find the greatest yield from mammography because here themodality is confirmatory." Here the mammogram will give confirmationand encouragement, "if the clinical impression is benign. It should not,however, dissuade him from a prior opinion to biopsy" (p. 855).
Category C: These patients have no signs or symptoms, there are noclinical indications for biopsy, and a mammogram can only increase thenumber of biopsies.
Thus, the author has outlined a plan that nullifies the value of mammo-graphic information in selecting patients in whom a biopsy can beavoided. Only the added bit of information that implies biopsy is used.The information that might eliminate a biopsy is ignored.
Mammograms and biopsies: The potential. To appreciate how problems inprobabilistic reasoning can affect the actual delivery of medical care, let us
Ja:Jue:J SeM aSeaS!p tSeaJq S,UeWOM e teqt .l.t!I!qeqoJd aqt '(stsat Jo uoHeu!qwo:J JO tsat q:J!qM.l.q "a"!) pat:Jatap seM uo!saI tseaJq aqt MOq UO 8u!puadaa '(U61 'tauaA 1? 'xeJtS 'oJ!deqs)Ja:Jue:J tseaJq JoJ uaWOM :JHeWotdw.l.se uaaJ:Js °t pasn aJaM uoHeu!wexa Ie:J!s.l.qd tseaJq epue.l.qdeJ80wwew q:J!qM U! Ie!.lt Ie:J!u!I:J a8JeI e WOJJ etep au!wexa ue:J aM 'aIdwexa JOd
'UOHe!.leA ap!M S! aJaqt q8noqtIe- sue!:J!s.l.qd op ueqt Jaq81q PloqsaJqt aqt tas .l.IIeJaua8 saAIaswaqt uaWOM teqt a:JuapIAasl aJaq.L '(Ot9 'd 'S961 'uany) ".l.eIap tnoqtlM palsdolq aq PInoqs tl 'u81uaq sl uo!saIaqt teqt paysHes .l.IataIdwo:J tOU sl uel:Jls.l.qd aqt JI" le:Jldi.t sl "auop aq PInoqs .l.sdOlqe 'tueu8new sl uolsaI aqt teqt a:Jueq:J null sl aJaqt J!" tuawatets aq.L 'MOI at!nb PIoqsaJqt.l.sdOlq aqt tas .l.neJaua8 suel:JlS.l.qd 'asIa auoawos JoJ uolsl:Jap aqt 8ul'iew aJe .l.aqt teqt t:JeJaqt pue UOlS,1aAe 'is!.l Jo asne:Jag 'S1Sou80Jd S,tuaHed e se naM se 'tUaHed e 8u18euew Jo tSO:Jaqt 'salsdolq aAH:JnpoJdun Jo .I.:JuanbaJJ aqt 'palsdolq uaWOM Jo Jaqwnu aqt uo a8eJaAaIteaJ8 St.Iaxa tl 8u!tJlqS 'Jaqwnu tuetJodWl pue 8uHeul:JseJ f.oIaA e SI PIoqsa.lqt .l.sdolq aq.L .
'PIoqsaJqt ou seq aqs uaqt 'uletJa:J S! Ja:Jue:J Jo a:Jueq:J aqt uaqM uaAatuawteaJt pue .l.sdolq sasnJaJ ueWOM e J! as,lnO:J JO 'PIoqsaJqt .l.sdo!q e seq auof.olaAa DOlUl 86 pue u°nI!.lt DE Ul1 uaaMtaq aJaqMawos uaqt 'os JUOOI Ul 86 SI a:Jueq:J teqt Jl pateaJtaqpue s1sou8elP aqt WJyuo:J °t StUeM auof.olaAa AnemJIA t!qt aaJ8e aM ue:J puy l,u°nI!.ltDE Ul1 SI Ja:Jue:J Jo a:Jueq:J aqt Jl palsdolq aq °t 8UnI!M SI auo ou teqt aaJ8e aM ue:) 'SMOnOJse UoseaJ ue:J PIoqsaJqt .l.sdOlq e JO a:Juatslxa aqt JO pa:JuIAuo:J aq °t 8u!paau auo.l.uy .
aq~ aU!W.Ia~ap ue:> aM '%01 Jo PIoqsa.Iq~ Asdo!q e ~U!Sfl s'auopaq PInoqs Asdo!q e ~eq~ aa.I~e ue!:>!sAqd pue ~ua!~ed aq~ uaq~ %01 aAoqeS! .Ia:>ue:> seq ~ua!~ed S!q ~eq~ ..\:J!I!qeqo.Id aq~ 'a~paIMou'{ s,ueJ:>!sAqd aq~Jo ~saq aq~ o~ 'J! 'S! ~eq.L '%01 S! PIoqsa.Iq~ Asdo!q s,~ua!~ed aq~ ~eq~ asoddnssn ~aI 'au!Iap!n~ e se S!q~ ~U!Sfl "(198 'd 'OI.6I'O~e~a}l lap) "AIIe:>!do:>so.I:>!Wpau!wexa pue paAOWa.I aq PInoqs ~! 'sdoIaAap dwnI ~ueu!wop e JI" :uo!saIaq~ Asdo!q o~ S! sase:> q:>ns U! A:>!Iod Ie:>!u!I:> aq~ 'uo!~ew.I°Ju! .Iaq~.InJJo a:>uasqe aq~ uI '(9961 ie ~a uewpa!.Id) %tI seM ~ueu~!Iew S! ssewe q:>ns ~eq~ ..\:J!I!qeqo.Id aq~ Apn~s auo uI 'ewou!:>.Ie:> AIsno!Aqo ~ou S! ~eq~ssew ~ueu!wop e aAeq OqM s~ua!~ed Jo dno.I~ puo:>as e .Iap!suo:> MoN
'pa!sdo!q aq o~ ~ueM PIn OM auoAue~sowIe ~eq~ q~noua q~!q II!~S S! A:>ueu~!IeW Jo a:>ueq:> %11. Y '(££1 'd'S96Ile ~a '{.IeD) "Asdo!q o~ paIIadwo:> aq II!M ue!:>!u!I:> aq~ '.Ia:>ue:> Jo UO!:>-!dsns .I°J uosea.I q~noua SaA!~ ue!:>!u!I:> aq~ Jo uo!ssa.Idw! aA!~:>a~qns aq~JI" :se s~uawa~e~s q:>ns Jo UO!~eA!~OW aq~ S! ..\:J!I!qeqo.Id q~!q S!q.L '.Ia:>ue:>~U!Aeq Jo a:>ueq:> %11. e q~!M ~ua!~ed aq~ aAeaI II!~S PInoM we.I~owwewaA!~e~aU Y '%S6 'sdeq.Iad o~ [(sod I e:»d] .Ia:>ue:> Jo A~!I!qeqo.Id aq~ asea.I:>U!PIn OM ~Insa.I aA!~!sod e '~ua!~ed e q:>ns uo paw.IoJ.Iad a.IaM we.I~owwewe JI '%06 aq dno.I~ S!q~ U! .Ia:>ue:> Jo (A:>uanba.IJ aq~) A~!I!qeqo.Id .Io!.Idaq~ ~aI '(9961) 'Ie ~a uewpa!.Id Aq paqs!Iqnd e~ep ~U!Sfl '.Ia:>ue:> SnO!AqoAIIe:>!U!I:> aAeq o~ ue!:>!u!I:> aq~ Aq ~q~noq~ a.Ie 'uo!~eu!wexa Ie:>!sAqd pueA.IO~S!q e Jo s!seq aq~ uo 'OqM s~ua!~ed asoq~ Jo S~S!suo:> dno.I~ ~S.Ig aq.L
's~ua!~ed Jo sdno.I~ o~ Jo ~uawa~euew aq~ uo ~sa~ aq~ Jo ~:>edw!
aq~ .Iap!suo:> MoN t'Pl°l{sa.ll{l /isdo!q aq~ A~!I!qeqo.Id S!q~ lIe:) 'papuaw-wo:>a.I S! Asdo!q '(~ua!~ed pue ue!:>!sAqd aq~ Aq pau!w.Ia~ap se) q~nouaq~!q S! A~!I!qeqo.Id ~eq~ JI '.Ia:>ue:> seq ~ua!~ed e ~eq~ a:>ueq:> aq~ Jo a~ew!~saaA!~:>a~qns s,.Ia'{ew uo!s!:>ap aq~ a~ue\{:> o~ S! ~sa~ aq~ Jo asod.Ind aq~'aAoqe paq!.I:>sap sy . Asdo!q .I°J s~ua!~ed Jo uo!~:>aIas aq~ U! pue s!sou~e!p
Ie!~ua.IaJJ!p U! AeId ~q~!W Aqde.I~owwew ~eq~ aI°.I aq~ au!wexa MOU
'IOMlNOJ aNY NOll YIMY AOJZ9Z
Probabilistic reasoning in clinical medicine 263
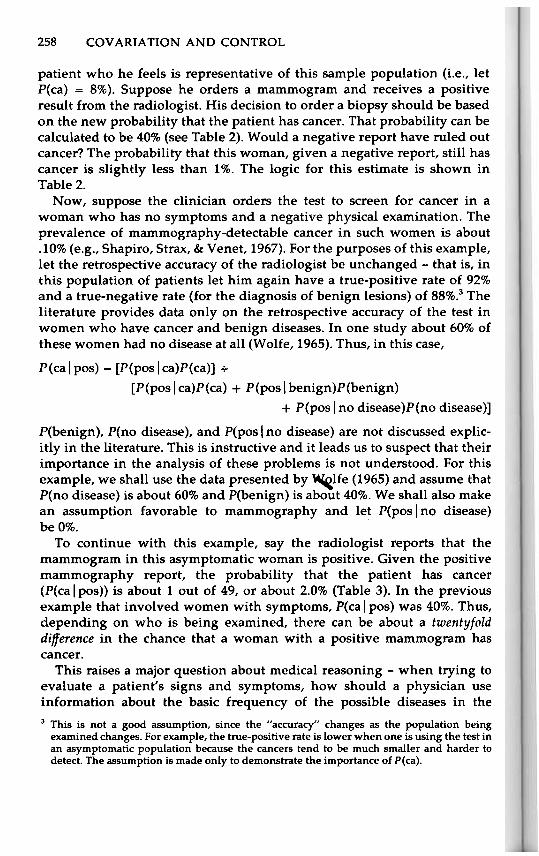
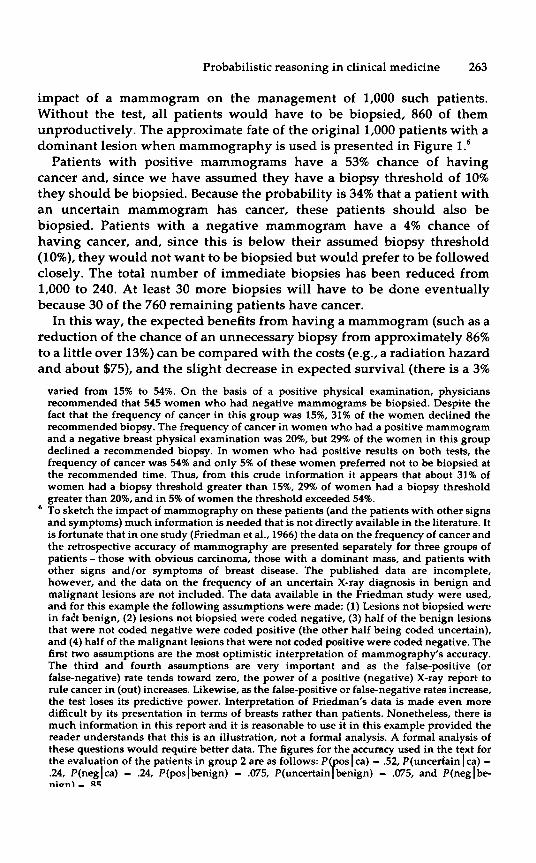
impact of a mammogram on the management of 1,000 such patients.Without the test, all patients would have to be biopsied, 860 of themunproductively. The approximate fate of the original 1,000 patients with adominant lesion when mammography is used is presented in Figure 1.6
Patients with positive mammograms have a 53% chance of havingcancer and, since we have assumed they have a biopsy threshold of 10%they should be biopsied. Because the probability is 34% that a patient withan uncertain mammogram has cancer, these patients should also bebiopsied. Patients with a negative mammogram have a 4% chance ofhaving cancer, and, since this is below their assumed biopsy threshold(10%), they would not want to be biopsied but would prefer to be followedclosely. The total number of immediate biopsies has been reduced from1,000 to 240. At least 30 more biopsies will have to be done eventuallybecause 30 of the 760 remaining patients have cancer.
In this way, the expected benefits from having a mammogram (such as areduction of the chance of an unnecessary biopsy from approximately 86%to a little over 13%) can be compared with the costs (e.g., a radiation hazardand about $75), and the slight decrease in expected survival (there is a 3%
varied from 15% to 54%. On the basis of a positive physical examination, physiciansrecommended that 545 women who had negative mammograms be biopsied. Despite thefact that the frequency of cancer in this group was 15%,31% of the women declined therecommended biopsy. The frequency of cancer in women who had a positive mammogramand a negative breast physical examination was 20%, but 29% of the women in this groupdeclined a recommended biopsy. In women who had positive results on both tests, thefrequency of cancer was 54% and only 5% of these women preferred not to be biopsied atthe recommended time. Thus, from this crude information it appears that about 31% ofwomen had a biopsy threshold greater than 15%, 29% of women had a biopsy thresholdgreater than 20%, and in 5% of women the threshold exceeded 54%.
. To sketch the impact of mammography on these patients (and the patients with other signs
and symptoms) much information is needed that is not directly available in the literature. Itis fortunate that in one study (Friedman et al., 1966) the data on the frequency of cancer andthe retrospective accuracy of mammography are presented separately for three groups ofpatients - those with obvious carcinoma, those with a dominant mass, and patients withother signs and/or symptoms of breast disease. The published data are incomplete,however, and the data on the frequency of an uncertain X-ray diagnosis in benign andmalignant lesions are not included. The data available in the Friedman study were used,and for this example the following assumptions were made: (1) Lesions not biopsied werein fact benign, (2) lesions not biopsied were coded negative, (3) half of the benign lesionsthat were not coded negative were coded positive (the other half being coded uncertain),and (4) half of the malignant lesions that were not coded positive were coded negative. Thefirst two assumptions are the most optimistic interpretation of mammography's accuracy.The third and fourth assumptions are very important and as the false-positive (orfalse-negative) rate tends toward zero, the power of a positive (negative) X-ray report torule cancer in (out) increases. Likewise, as the false-positive or false-negative rates increase,the test loses its predictive power. Interpretation of Friedman's data is made even moredifficult by its presentation in terms of breasts rather than patients. Nonetheless, there ismuch information in this report and it is reasonable to use it in this example provided thereader understands that this is an illustration, not a formal analysis. A formal analysis ofthese questions would require better data. The figures for the accuracy used in the text forthe evaluation of the patients in group 2 are as follows: P(pos I ca) ~ .52, P(uncertain I ca) -.24, P(neglca) - .24, P(poslbenign) - .075, P(uncertainlbenign) - .075, and P(neglbe-rugn\ - R~

UO pal!nbal SeM ASdO!q 'ssew ~ueu!wop e 4~!M s~ua!~ed a4~ Jo Apn~S a4:JuI i6SS 'd 'SOl lOA '1'1.61 'liJ.iJ'SJ.ns /0 siJa!l{:JJ.V WO1J) "Asdo!q sal!nbal 's:>!:J-S!la~:>ele4:> UMO S~! Jo s!seq a4~ uo '~e4~ aynpou ~sealq ayqedyed [Ane:>!SA4d"a'!] Ane:>!U!Y:> a4~ Jo ~uawageuew a4~ o~ ay~~!y sppe A4delgowwew" '1
:s~uawa~e~s A:>!yod gU!MOnOJ a4~ a~enyeAa sn sdya4 ogle ~I 'suo!say
SnO!leA Jo s!souge!p ye!~Uala.J.J!p a4~ U! A4delgowwew Jo ssauynJasny~!~ua~od a4~ leay:> a'lew sdya4 S!SAyeue Jo ad~ S!4.L 'piJl!S!aiJJ. iJ:J!l:JI1J.d iJl{L
'spunOJg Ja\{~o uo pa9!tsn~aq o~ aAe\{ pynOM. ase:> s!\{~ U! A\{deJgommem Jo asfl 'AsdO!q °t uo!s!:>apa\{~ o~ pa~nq!J~uo:> aAe\{ taU pynoM. uo!~emJoJu! S!\{~ ~nq uo!~emJoJu!amos ue!:>!u!y:> a\{~ UaA!g aAe\{ Aem meJgommem a\{l. o(pyo\{saJ\{~ S!\{~paa:>xa pynoM. Ja:>ue:> Jo a:>ue\{:> %17 e) Asdo!q a\{t JoJ paau a\{t pateu!m!yaaAe\{ tOu pynoM. ~JodaJ meJgommem aA!~egau e ua\{~ - Asdo!q e tueJJeM. o~tua!:>9Jns seM. Ja:>ue:> gU!Ae\{ JO a:>ue\{:> 001 U! 1 e ~e\{~ ~yaJ ~ua!~ed a\{~ J! 'S!~em - % 1 ~e pyo\{saJ\{~ a\{~ ~as Fe\{ ~ua!~ed S!\{ pue ue!:>!sA\{d a\{~ JI °passaJ~S
aq pyno\{s aydmexa S!\{~ U! pyo\{saJ\{~ Asdo!q a\{~ JO a:>ue~Jodm! a\{l.0(688 'd '9961 '"Ie ~a uempa!Jd) "s8u!puy J!l{dv.l80UlUlVUl jo SSJIP.lv8J.l 'Asdo!q
e aAe\{ pyno\{s [dnoJg S!\{t U!] stua!ted TIe ~e\{~ S! aJa\{ snsuasuo:> ye:>!gJnsa\{~" S!SAyeue Jo adAJ, S!\{~ Jo a:>uasqe a\{~ uI 0 Asdo!q e paJeds aq pynoM.smeJgommem aA!~egau Fe\{ O\{M. dnoJg S!\{~ U! s~ua!~ed Auem 'pasn aJaM.I..xoa\{~ AJ,!y!qeqoJd aydm!s amos pue pyo\{saJ\{~ Asdo!q e Jo UO!~OU a\{~ JI '(osJO \{~uom e pauod~sod aq TI!M. uo!say ~ueug!yem e JO s!souge!p te\{~ a:>ue\{:>
°suo!sal tueu!wop \{t!M. uawoM. U! Ja:>ue:> Jo At!I!qeqOJd °1 a.Ing!d
OCl.
9£."0~~
O£
s~ua!~Ed OOO'I
VI::
10~.LNO::> aNY NOI.L YI~Y AO::>t9Z
265Probabilistic reasoning in clinical medicine
clinical grounds alone. The use of mammography split the group intosubgroups with frequencies of cancer ranging from 53% to 4%. Biopsymight be avoided in the latter group and the number of biopsies might bereduced 73% (from 1,000 per 1,000 to 270 per 1,000).
2. "For clinical purposes mammography must provide accuracy atapproximately the 100 percent level before it alone can direct manage-ment" (from Archives of Surgery, 1974, vol. 108, p. 589). In a population likethe second group discussed above, it might be quite rational to letmammography select patients for biopsy. Recall that the true-positive rateused in that example was 52% and that a more accurate test would be evenmore valuable.
3. "Mammography is not a substitute for biopsy" (from Oncology, 1969,vol. 23, p. 148). The purpose of both mammography and biopsy is toprovide information about the state of the patient. Some patients, in theabsence of mammography, require biopsy. In some of these patients anegative mammogram would obviate the biopsy, and in these cases themammogram would replace the biopsy.
4. "Every decision to biopsy should be preceded by a mammogram"(from Oncology, 1969, vol. 23, p. 146). Consider clinically obvious carci-noma. The probability of cancer will be above almost anyone's biopsythreshold no matter what the outcome of the mammogram. The primaryjustification for this policy in such a case must lie in the chance that theclinically obvious is benign (otherwise the patient would have to have amastectomy [breast removal] anyway) and that there is a hidden, non-palpable, malignant lesion. The probability of this compound event is theproduct of the probabilities of the two events, which is extremely small(on the order of lout of 5,000).
5. "To defer biopsy of a clinically benign lesion of the breast which hasbeen called benign on mammography is to take a step backward in theeradication of carcinoma of the breast" (from Surgery, Gynecology andObstetrics, 1972, vol. 134, p. 98). Let "clinically benign" be represented by aP(ca) of ~%. After a negative mammogram, the probability that such apatient has cancer is approximately 1%. Out of 100 biopsies, 99 would beunproductive. Is the deferral of biopsy here a step backward or forward?The other point is that if the policy were followed, all lesions from"clinically benign" through clinically obvious carcinoma would require abiopsy no matter what the outcome of the test was. This seems tocontradict the author's statement that "when used in its proper perspec-tive, mammography is an excellent adjunct to the physician in themanagement of carcinoma of the breast" (from Surgery, Gynecology andObstetrics, 1972, vol. 134, p. 98).
6. "Mammography must never be used instead of biopsy when dealingwith a 'dominant lesion' of the breast and should never change the basicsurgical approach in breast diseases, i.e., a 'lump is a lump' and must be

ual(t 'awo;)tno weJ~owwew al(t Aq paAOWUn aq pue UO!S!;)ap ASdO!q Jo!Jde °t aJal(pe SAeMle Plnol(s ue!;)!sAl(d al(t puel( Jal(to al(t uo jl .uo!t;)unj tel(twJoJJad tsat al(t tal °t tl(~no aM ual(t ' Asdo!q 1? S1? l(;)ns aJnpa;)oJd ;)!tewneJt
pue aA!SUatXa aJow e stua!ted awos ~u!Jeds AqaJal(t 'aseas!p tseaJq
tueu~!leW WOJJ u~!uaq l(s!n~u!ts!P SU1?!;)!sAl(d dIal( °t S! Al(deJ~owwewJo asodJnd al(t J! tel(t ,!se °t alqeuoseaJ waas plnOM t! 'AJewwns UI
,;alqe11aJ ~ua;)Jad S6 aq PlnoM s1sou~e1P al{~ f..es S;)1~S1~e~s al{~ 'weJ~owwewal{~ WOJJ SaJn~;)1d XOJax al{~ l{~1M SaaJ~e ~1 J1 pue 'aA1~e~aU JO aA1~1Sod Jal{~1a s,~el{tJI 'weJ~owJal{~ e aAel{ O~ ~uaw~u10dde ue palnpal{;)s aAJ ~SJ9 'oS' . . 'aw1~ al{~ Jo
~ua;)Jad S8 ~noqe ~l{~1J s,~1 sf..es JO~;)OP Jno puy 'ssan~ I 'UO o~ o~ ~u1l{~aWOs s,~I"
",a;)eld ~SJ9 al{~ U1 ua'{e~ f..eJ-X al{~ ~a~ f..l{M 05",,'~no awo;) o~ aAe4
111M dwnl aq~ S1 ~lnsaJ al{~ JaAa~el{M 'ual{.L 'weJ~wweWOJax e Op o~ s~ueM aH"
",f..es JO~;)OP al{~ P1P ~el{M"'pueqsnl{ Jal{ l{~1M walqoJd al{~ pasSn;)s1P ual{~ ueWOM al{.L
,,'ado;)sOJ;)1We JapUn ~1 ~e '{OOI pue ~no ~U1l{~ al{~ ~n;) o~ S1 U!e~Ja;) aq O~ f..eM f..luO al{~- ~UeU~11eW ~,US1 dwnl al{~ sueaw l{;)1l{M - aA!~e~aU S! ~U!peaJ al{~ J1 UaAa" 'paUJeM
all ,,'MOU'{ noA 'aq ue;) aJn~;)!d f..ue se a~eJn;);)e se ~noqe f..lqeqOJd" 'pa~~nJl{s aH
",a~eJn;);)e ~! sl",,'s~seaJq al{~ JO saJn~;)!d
- sweJ~owwew a'{ew o~ f..eM Mau e s,~1 'weJ~owweWOJax e ~a~ o~ nof.. a,{11 p,l"
"ue!:>!sAqd.laq q~!M uo!~e~lnsuo:> e paq!.I:>sap pue ~sea.lq .laq u! ssew e pa.laAO:>S!p~snr peq .la~.loda.l UeWOM Y "(91.61 '.lauqsn)l) 3P!UOJZf.J o:>s!:>ue.ld ues aq~ U!pa.leadde ~eq~ £..Io~s 8U!MOnOJ aq~ a~e!:>a.ldde o~ uo!~!sod e U! MOU a.le aM
,,"~sea.lq aq~ ueq~ s!sou8e!p Jo spoq~aw .la~~aq Aq pap!OAeaq Plno:> q:>!qM pa~e~!ssa:>au S! £..Ia8.1ns q:>nw os q:>!qM U! sea.le Mala.le a.laq~" '~! s~nd nasw!q ~uawa~e~s aAoqe aq~ Jo .loq~ne aq~ se 'asne:>aqaweqs e S! S!q.L "A:>!10d S!q~ Aq pap!OAeaq n!M Asdo!q a18u!s e ~oN "(Z811"d '6961 'speoq}I) "Aqde.l80wwew q~!M paq:>ea.l sasou8e!p aA!~!sod-asleJJo .laqwnu u!e~.la:> e ueq~ sno!.las a.low q:>nw S! pue neJ o~ pua~ neaM q:>!qM O~U! de.I~ le:>!80loq:>Asd e S! S!q.L "A:J!A!~!sod uo Ala.l A1UO Plnoqsauo uaqM 'we.l80wwew aq~ JO A~!A!~e8au aq~ uo a:>ue!la.l O~ nasw!qpa~~!wwo:> seq A1SnO!:>suo:>un auo ,'Ae.l-X ue ~a8 s,~al- S!q~ ~noqe a.lnsa~!nb ~ou we I, '~ua!~ed e O~ shes aq J! A1.Ieln:>!~.led pue 'nasw!q o~ Shes auose uoos sy "we.l80wwew e .lap.lo uaq~ 'uo!~eu!wexa le:>!sAqd .10 £..Ia8.1ns.l°J Uo!~e:>!pu! ou S! a.laq~ a.lns a.le noA JI "~! op uaq~ 'Asdo!q e op PlnoMnoA JI "alqel!eAe ~ou a.laM Ae.l-X J! Asdo!q e op ~ou PlnoM .10 PlnoM noA
.laq~aqM ap!:>ap o~ ~sea.lq aq~ 8u!~edled pue 8u!u!wexa .la~Je le!~uassa S! ~I"sase:> lnJ~qnop U! [Aqde.l80wwew] uo 8u!Ala.l U! sawo:> A:>eneJ aq.L" "I.
"~uawa~e~s S!q~ q~!M aa.l8es!p PlnoM %S.laAO sploqsa.lq~ Asdo!q pue suo!sal ~ueu!wop q~!M s~ua!~ed itS8 "d '£6 "lOA'9961 'IiJ3SJns /0 S312!ZfJJV WO.lJ) "uo!~e.l!dse .10 UO!S!:>U! Aq .laq~!a pa!sdo!q
'10}l.LNOJ aNY NOI.L VI}lV AOJ007

267Probabilistic reasoning in clinical medicine
we ought not to claim that the purpose of the test is to help distinguishbenign from malignant disease, since that distinction will be made defini-tively from a biopsy. Finally, if the purpose of the test is to search forhidden and clinically unsuspected cancer in a different area of the breast(away from a palpable mass that needs biopsy anyway), we ought torecognize explicity that the chances of such an event are extremely smalland that the use of the test amounts to screening.
My purpose is not to argue for a specific mammography or biopsypolicy - to do so would require better data and a better assessment ofpatient values. It is to suggest that we have not developed a formal way ofreasoning probabilistically about this type of problem, that clinical judg-ment may be faulty, and that current clinical policies may be inconsistentor incorrect.
Discussion
These examples have been presented to illustrate the complexity ofmedical decision-making and to demonstrate how some physiciansmanage one aspect of this complexity - the manipulation of probabilities.The case we have studied is a relatively simple one, the use of a singlediagnostic test to sort lesions into two groups, benign and malignant. Thedata base for this problem is relatively good. The accuracy and diagnosticvalue of the test has been studied and analyzed in many institutions formany years. As one investigator put it, "1 know of no medical procedurethat has been more tested and retested than mammography" (Egan, 1971,p. 1555).
The probabilistic tools discussed in this chapter have been available forcenturies. In the last two decades they have been applied increasingly tomedical problems (e.g., Lusted, 1968), and the use of systematic methodsfor managing uncertainty has been growing in medical school curricula,journal articles, and postgraduate education programs. At present, howev-er, the application of these techniques has been sporadic and has not yetfiltered down to affect the thinking of most practitioners. As illustrated inthis case study, medical problems are complex, and the power of formalprobabilistic reasoning provides great opportunities for improving thequality and effectiveness of medical care.
Related Documents