LYMPHOMA Dr Bruce Covell

LYMPHOMA Dr Bruce Covell. Each year in the UK about about 1500 people develop Hodgkin's disease, usually between 15-25 years of age. It can also develop.
Dec 22, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

LYMPHOMA
Dr Bruce Covell

Each year in the UK about about 1500 people develop Hodgkin's disease, usually between 15-25 years of age. It can also develop later in life in people over 60. In younger people the numbers of men to women are about the same but overall Hodgkin's affects more men.
Between 7000 and 7500 people develop non-Hodgkin's lymphoma each year. It is more common over the age of 60 and affects slightly more men than women.At present the cause of most lymphomas is unknown.


Thomas Hodgkin
English physcian and pathologist, born August 17, 1798, in Pentonville, St. James Parish, Middlesex; died April 5, 1866, Jaffa, Palestine [now Tel Aviv-Yafo, Israel].
members of "The Society of Friends"

The castle walls-first line of defence is the skin and the mucosa
The foot soldiers -macrophages Complement, and other immune cells send out chemical messengers to call for reinforcements.
The cavalry-neutrophils -small, short-lived immune cells ,swallow the invaders and kill them
The SAS-Antibodies recognise and stick to foreign material.B lymphocytes exist to produce antibodies. infection is over, most of the B cells die, but some live on as memory cells.
The generals-T lymphocytes major histocompatibility complex (MHC), Helper T cells Cytotoxic T cells recognise cells with foreign proteins attached to MHC on their surface and destroy them directly.
Defence against Infection

Disease states correlate with stages in normal B-cell development
Diseases: AML Pro-B-ALL Pre-B-ALL -B-CLL-DLBCL-FLL-BL-Mantle Cell lymphoma-Marginal Zone lymphoma-MALT-GALT-Hodgkins (?)
B-ALL -MGUS-Multiple Myeloma-Plasmacytoma
Lymphoid tumors that present as mature B-cellsmay have arisen as a result of the interplay between geneticlesions and normal processes that govern lymphoid tolerance,homeostasis and function

A minimalist view of a T cell response
1. EXPANSIONactivation and proliferation
3. CONTRACTION apoptosis and memory
2. EFFECTOR PHASEelimination of infection
T
T
T
T
TT T
TT
T
T
T
T
T
TT
Microbe
AUTOIMMUNITY CANCER
IMMUNO-DEFICIENCY


Cancer “stem-cells”?!

CLASSIFICATION
“Nowhere in pathology has a chaos of names clouded clear concepts as inthe subject of lymphoid tumors”
Willis R.A.: Pathology of tumors, Mosby 1948
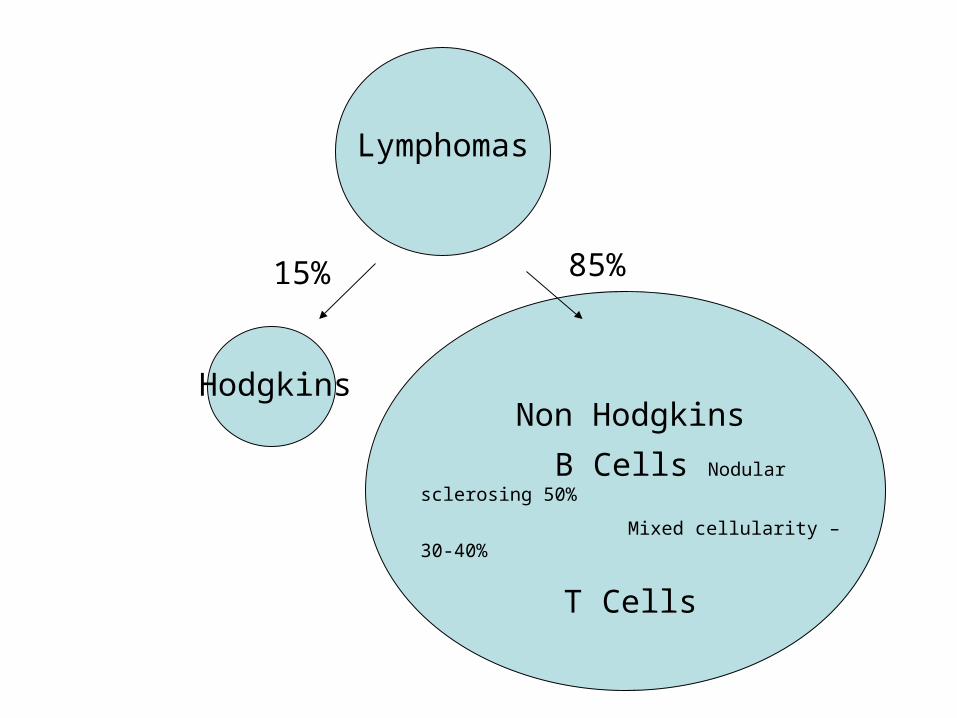
Lymphomas
HodgkinsNon Hodgkins
B Cells Nodular sclerosing 50%
Mixed cellularity –30-40%
T Cells
15% 85%

HODGKINS LYMHOMA % Of Lymphomas
Age of Incidence Prognosis Comment
With appropriate treatment, more than 80% of people with stage I or II Hodgkin's survive for at least 10 years. With widespread disease, the treatment is more intense and the 5-year survival rate is about 60%.1.
Classical •
Nodular sclerosing - 50% commonest of all types of Hodgkin's lymphoma.
Commonest in women in their 20’s and 30’s.
less favourable prognosis than the lymphocyte predominant
usually picked up at an early stage from enlarged lymph nodes in the neck.
Mixed cellularity - . 30 – 40%- Commonest in older people.
•Lymphocyte depleted
rare worst prognosis
Lymphocyte-rich –
rare
2. Nodular lymphocyte predominance
1% most favourable prognosis
'popcorn' cells.

B Cell lymphoma % Of Lymphomas Age of Incidence Prognosis Comment
Diffuse large B-cell lymphoma (DLBCL):
31% mid-60s. 40% to 50% are cured fast growing 2 kinds Genetics One serious
Follicular lymphoma 22% 60. rare in very young 5-year survival rate60% to 70%.
slow growingcan (transform) into a fast growing diffuse B-cell lymphoma.
Chronic lymphocytic leukemia (CLL)/small lymphocytic lymphoma (SLL):
7% live well over 10 years not considered curable are slow growing can transform into a more aggressive type of lymphoma
Mantle cell lymphoma: 6% Men most often affected. average age 63
very serious. 20% of patients survive at least 5 years.
Extranodal marginal zone B-cell lymphomas - mucosa-associated lymphoid tissue (MALT) lymphomas
8% average age about 60 slow growing lymphoma often curable in its early stages.
stomach Helicobacter pylori.
Nodal marginal zone B-cell lymphoma:
2% slow growing cured if diagnosed in early stages.
cells are small.
Splenic marginal zone B-cell lymphoma
rare often elderly and male slow growing,
Primary mediastinal B-cell lymphoma
2% two thirds women. 30s. About half of patients can be cured. fast growing
mediastinum closely related to Hodgkin disease
Burkitt lymphoma:
2% 90% of patients are
male, and the average age is about 30
half of patients are cured by aggressive chemotherapy.
medium size fast growing African jaws d US, abdomen,
Lymphoplasmocytic lymphoma (Waldenstrom macroglobulinemia
1% not curable, most live longer than 5 years.
slow growing Thick blood Symptoms
Hairy cell leukemia:
rare Patients are older in
general.slow growing, some patients never need treatment
Primary central nervous system (CNS) lymphoma:
rare patients with AIDS poor. 30% 5 years. called primary brain lymphoma

% Of Lymphomas Age of Incidence Prognosis Comment
Precursor T-lymphoblastic lymphoma/leukaemia:
2% (75%) men, average age 25
No bone marrow cure quite good. involve bone marrow, 20% cured.
lymphoma or leukaemia. fast growing,
Peripheral T-cell lymphomas:, 7% There are several kinds of peripheral T-cell lymphomas
Cutaneous T-cell lymphoma (mycosis fungoides, Sezary syndrome):
1% 50s or 60s survival at 5 years ranges 58% slow-growing lymphomas 5% faster growing ones
Skin Sezary syndrome spread all over the body OR mushroom-like (so first named mycosis fungoides
Angioimmunoblastic T-cell lymphoma:
Extranodal natural killer/T-cell lymphoma, nasal type
Enteropathy type T-cell lymphoma
outlook is poor Coeliac disease
Subcutaneous panniculitis-like T-cell lymphoma
cannot be cured
Anaplastic large T/null-cell lymphoma
2% cured.
Unspecified:
T Cell Lymphoma

Hodgkin's Lymphoma VS Non-Hodgkin's Lymphomas
Age Average age is 27.7 with two age peaks, the major one between 15 and 24 with a lesser peak after age 55.
Average age is about 67.
Chance of getting in all people over an entire lifetime
Men 0.23%Women 0.20%
Men 2.12%Women 1.79%
Occurrence About 15% of all lymphomas About 85% of all lymphomas
Location The disease occurs most often in lymph nodes above the collar bone. In Hodgkin's it is also more likely to appear in the chest cavity between the lungs (the mediastinum), particularly in younger patients.
Only about 15% to 20% of cases are found in areas below the diaphragm.
Disease occurs outside the nodes in about 4% of cases.
In NHL it is more likely to appear in the nodes in the abdomen (called the mesenteric nodes).
The disease occurs in the chest cavity in less than 40% of patients. (An exception, lymphoblastic lymphoma, which is seen most often in young people, is likely to first appear in the chest.)
Disease occurs outside the nodes in about 23% of patients. Slow-growing lymphomas are common in the liver and bone marrow.
Affected Lymph Cells B-Lymphocytescharacterized by the Reed-Sternberg Cell
B-Lymphocytes, T-Lymphocytes or Natural Killer (NK) Cells depending on the subtype
Symptoms More likely than NHL (40%) to have systemic ("B") symptoms (such as fever and night sweats) at the time of diagnosis.
Less likely than HL to have systemic ("B") symptoms (27%) at the time of diagnosis.
Progression Less likely than NHL to be diagnosed in stage IV (10%). Hodgkin's disease usually progresses in an orderly way from one lymph node region to the next. This process may be slow, particularly in younger people, or very aggressive. The disease typically spreads downward from the initial site. If it spreads below the diaphragm, it usually reaches the spleen first; the disease then may spread to the liver and bone marrow. If the disease starts in the nodes in the middle of the chest, it may spread outward to the chest wall and areas around the heart and lungs.
More likely than HD to be diagnosed in stage IV (36%) but this will vary by NHL subtype. The Non-Hodgkin's lymphomas are less predictable in their course than Hodgkin's and they are more apt to spread.

Lymphoma Symptoms (Hodgkin's Disease = HL, or a form of Non-Hodgkin's Lymphoma = NHL):
•Lymph node swelling, often in the upper body area but it can be in almost any node or related organ. The node is usually NOT painful as opposed to infected lymph nodes which are common and can be painful (HL, NHL) •A lack of energy, general fatigue. (HL, NHL) •Weight loss - usually at least 10% over a short time (HL, NHL) •Fevers which can come and go. This can be accompanied by chills or a feeling of temperature swings (HL, NHL) •Night sweats - unexplained sweating at night, often drenching (more often HL than NHL) •Itching - itching without an apparent cause or rash, sometimes deep in the skin rather than on the surface, sometimes on different parts of the body (more often HL than NHL)
Less Often:•Some people have lower back pain that is unexplained (may be caused by expanding lymph nodes pressing on nerves). (HL, NHL) •Lymph nodes are possibly painful after alcohol consumption. (HL)
What now?A good percentage of diagnoses are made during routine tests, x-rays, or even while pregnant. This is how difficult it is to diagnose lymphoma based on external symptoms alone
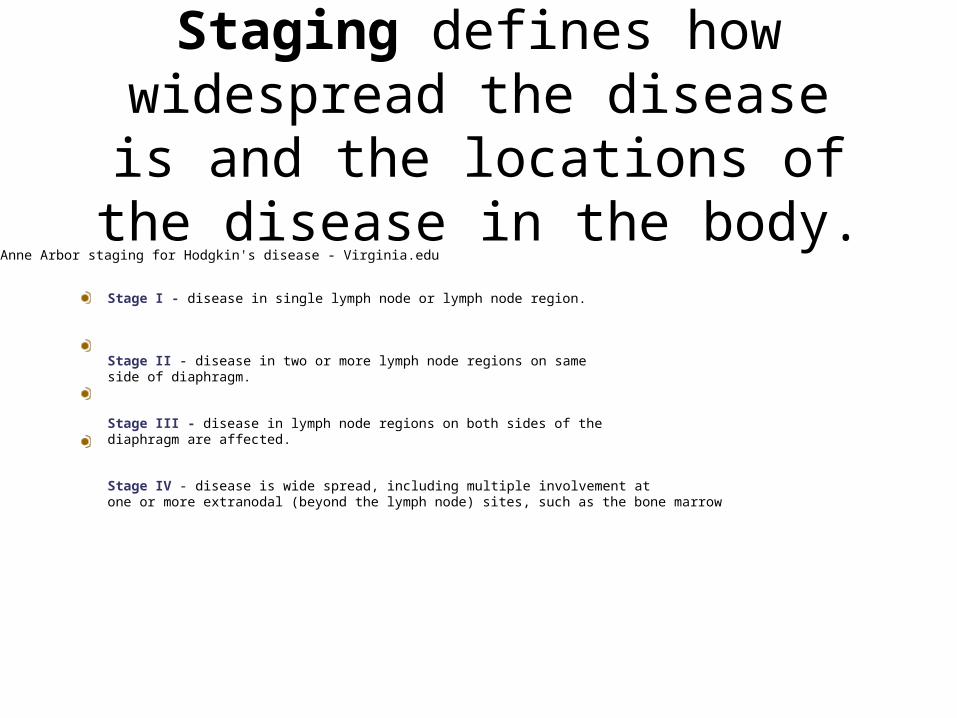
Staging defines how widespread the disease is and the locations of the
disease in the body. Anne Arbor staging for Hodgkin's disease - Virginia.edu
Stage I - disease in single lymph node or lymph node region.
Stage II - disease in two or more lymph node regions on same side of diaphragm.
Stage III - disease in lymph node regions on both sides of the diaphragm are affected.
Stage IV - disease is wide spread, including multiple involvement at one or more extranodal (beyond the lymph node) sites, such as the bone marrow


Extranodal notations
Extranodal means 'beyond nodal' - sites are identified by the following notation:

ANN ARBOR notations Ann Arbor staging further classifies patients with lymphoma into A or
B categories:A = without symptoms
B = with symptoms including unexplained weight loss (10% in 6 months prior to diagnosis, unexplained fever, and drenching night
sweats. Disease Staging may also be accompanied by local involvement of
an extranodal organ or site.Example involving spleen and Ann Arbor notation: Stage IIIS A

Treatment
Lymphomas are usually treated by a combination of chemotherapy, radiation, surgery, and/or bone
marrow transplants. The cure rate varies greatly depending on the type of lymphoma and the progression of
the disease.

Regimen Drugs
CHOP Cyclophosphamide, Doxorubicin, Vincristine, Prednisone
BACOP Bleomycin, Doxorubicin, Cyclophosphamide, Vincristine. Prednisone
M-BACOD Methotrexate, Leucovorin, Bleomycin, Cyclophosphamide, Vincristine, Dexamethasone
ProMACE/MOPP
Prednisone, Methotrexate, Leucovin, Doxorubicin, Cyclophosphamide, Etoposide
MACOP-B Methotrexate, Leucovorin, Doxorubicin, Cyclophosphamide, Vincristine, Bleomycin, Prednisone, Trimethoprim-sulfamethoxazole
Current up-front treatment regimens for aggressive lymphomas
(Used at various doses, with, or without radiation)

Additional experimental therapies for B-cell lymphomas:
-CD20-specific antibodies (Rituximab, Bexxarr, Zevalin):target a tetraspanin on the surface of all B-cells and ablatesthe entire B-cell compartment for over 6 months. Mechanismof action is unknown. Rarely used as up-front therapy.
-Clonotypic antibodies to individual lymphomas: pioneeredby Ron Levy and his colleagues at Stanford. Current successrate is 1 patient in 15 years.

Evidence for a possible role of outside agent in lymphomagenesis:
-pristane-induced plasmacytomas in mice and rats (Andreson and Potter, 1969)
-Retroviral infection of mice elicits T-cell lymphomas only in those strains that couldmount an immune response to the virus (McGrath and Weissman, 1979, Lee andIhle, 1981)
-Infection with Helicobacter pylori correlates well with MALT lymphoma - antibiotictreatment leads to remission in these patients (Casella et al, 2001).
-Long-term untreated chronic GVHD after transplantation (Gleichmannand Gleichmann, 1971)
-Large B-cell lymphomas (DLBCL, FLL, BL) have been shown to express Igmolecules on their surface, which bear the scars of affinity maturation; anantigen-driven process (Klein et al, 1995, Chapman et al, 1995, Kuppers et al, 1997)
-The gene expression profiles of DLBCL cells resemble those of B-cells thathave mounted a response to antigen (Alizadeh et al, 2000).
These findings prompt the hypothesis that an antigenic stimulus may cooperatewith other tumorigenic influences in the genesis of lymphoid tumors

Autoimmunity and lymphoid neoplasia may represent differentparts of a single disease-spectrum:
-Patients who suffer from several autoimmune syndromes are50-200 fold more likely to develop B-cell lymphomas(Sjörgen’s syndrome, autoimmune thyroditis, autoimmune hemolyticanemia, systemic lupus erythematosus, rheumatoid arthritis)
-Patients who develop the HTLV-1 associated tropical spastic parapesisare also highly prone to develop T-cell lymphomas.
-Patients with NHL have been found to have high titers ofautoantibodies in their sera, and accompanying symptoms, suchas autoimmune hemolytic anemia.
-EBV infection correlates with some autoimmune diseases,such as Hashimoto’s thyroditis.
Key differences: clonality of expanded population, disease grade, site ofanatomical presentation, FACS pattern, histopathology
Related Documents











