Lymphedema: Early Detection and Quantitative Assessment Harvey N. Mayrovitz PhD Professor of Physiology College of Medical Sciences Nova Southeastern University [email protected]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Lymphedema: Early Detection and
Quantitative Assessment
Harvey N. Mayrovitz PhD
Professor of Physiology
College of Medical Sciences
Nova Southeastern University

• Lymphedema Physiology
• Research into Early Detection
• ‘Evolving’ Research Projects
The Lymphatic System
and Lymphedema

Arterial Venous Lymphatic

Anchoring
Filaments
Lymphatic Capillary
INTERSTITIUM
Fluid & Protein enter
Lymph Capillaries
Endothelial Cell
Blood Capillary
Blood-Lymphatic Interaction

FiltrationResorption
~30 liters/day
Normal Fluid Balance
Blood Capillary
~27 liters/day
TISSUE AND CELLS

Lymphatic Capillary
Normal Fluid Balance
protein~3 liters/day
(10% of filtered) Back to
Venous
System
Start of the
Lymphatic
System
FiltrationResorption
~30 liters/day
Blood Capillary
~27 liters/day
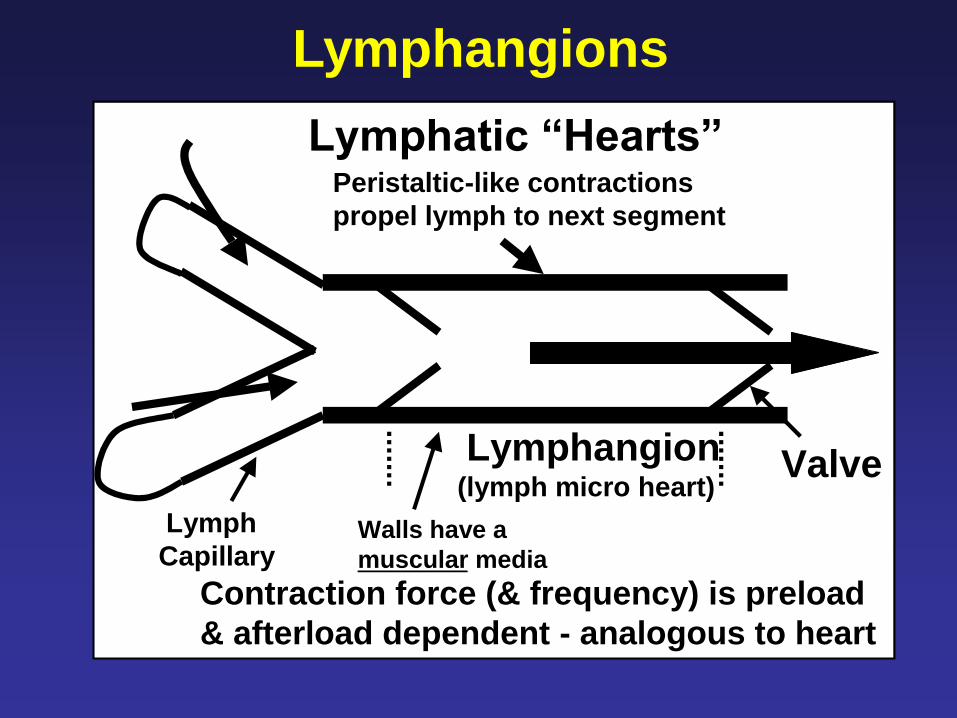
ValveLymphangion(lymph micro heart)
Lymph
CapillaryWalls have a
muscular media
Peristaltic-like contractions
propel lymph to next segment
Contraction force (& frequency) is preload
& afterload dependent - analogous to heart
Lymphatic “Hearts”
Lymphangions


Olszewski & Engeset, 1988
Effects of Muscular Contractions
on lymphatic Flow and pressureF
low
(ul)
Pre
ss
ure
(mm
Hg
)

Factors Affecting Lymph Transport
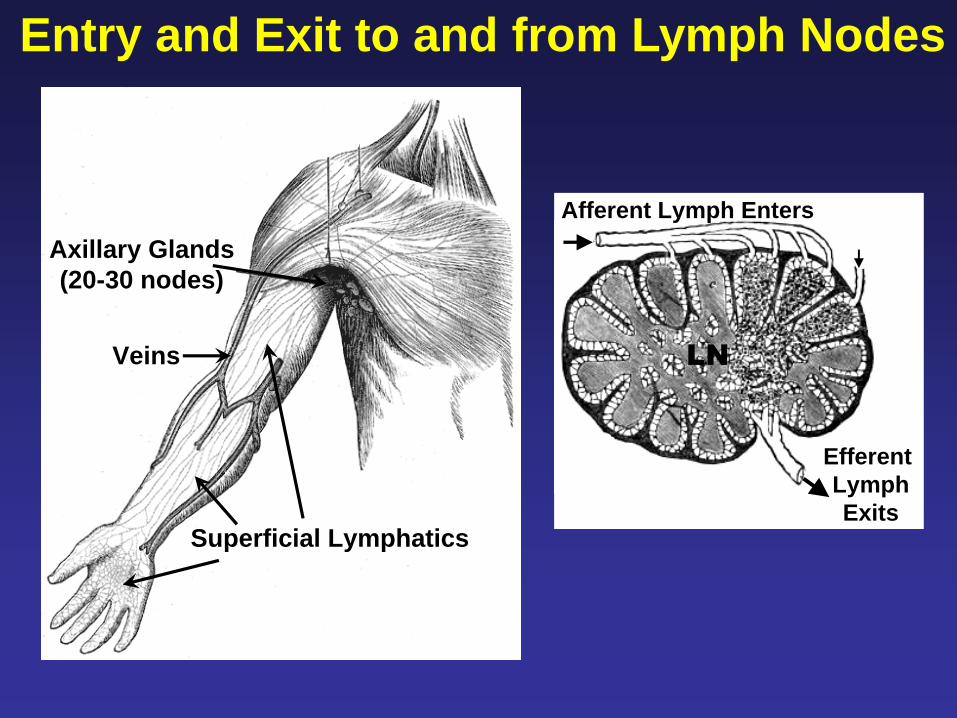
Axillary Glands
(20-30 nodes)
Superficial Lymphatics
Veins
Afferent Lymph Enters
Efferent
Lymph
Exits
LN
Entry and Exit to and from Lymph Nodes

LN
Vertical
Watershed
NORMAL
Transverse
Watershed
Veins
Lymphatic Drainage
Lymph flow and drainage
determined by normal
physiological processes
and lymphatic pathways

Overload = Edema
+ [Protein]
= Lymphedema
If Net Filtration Exceeds
Lymphatic Transport Capacity
Excess --> Lymphatics
Fluid +
Protein
capillary
Normal Lymphatic Function

LN
Vertical
Watershed
NORMAL
Transverse
Watershed
Veins LN
Vertical
Watershed
LYMPHEDEMA
Transverse
Watershed
Veins
Lymphatic Drainage
Lymph flow and drainage
determined by normal
physiological processes
and lymphatic pathways
Lymph flow through normal
pathways reduced or absent
due to nodal or lymph vessel
obstruction and dysfunction

Potential Outcome
System
Works
OK Here
System
Not OK
Here

General Principles of Care for
Persons At-Risk for Lymphedema

• Pre-surgical Assessment
• Periodic test via emerging
early detection methods
• Self recognition of symptoms
• Reduce Risk
• Detect Early
• Arrest & Reduce
• Maintain Gains
- Complications
Overall Goals

Surgery
RadiationSymptoms
Seek Therapy
Arrest & Reduce
Lym
ph
ed
em
a S
eve
rity
Fibrosis
Time
Develops
Late Treat
Worsens Without Treatment

Surgery
RadiationSymptoms
Seek Therapy
Arrest & Reduce
Lym
ph
ed
em
a S
eve
rity
Early Detection
“Sub-Clinical”
Fibrosis
Time
• Catch it Early
• More Treatable
• Less Complications
Develops
Late Treat
Early Treat
Pre-surgical
Assessment
Worsens Without Treatment

Quantitative Assessment Methods
• Limb Volumes
• Bioimpedance
• Local Tissue Fluid
• Tissue Properties
Early Detection and Treatment Effectiveness
Limbs
Any at Risk Location
(e.g. Trunk, Face and etc.)

Pre-Surgical
Baseline
Threshold Change Detection
Therapy
Initiation
Periodic Follow-ups
Measures and Criteria
•Limb Volumes and Metrics
•Limb Bioimpedance
•Local Tissue Water
Goal: Earlier Detection and Intervention
A Rationale and Sensible Approach
Dr. HN Mayrovitz
Goal: Early Detection – Timely Intervention

Pre-Surgical
Baseline
Threshold Change Detection
Therapy
Initiation
Not Often
Done
Periodic Follow-ups
Measures and Criteria
•Limb Volumes and Metrics
•Limb Bioimpedance
•Local Tissue Water
Can We Estimate Impact?
Goal: Earlier Detection and Intervention
Dr. HN Mayrovitz
Goal: Early Detection – Timely Intervention

Limb Volume or Girth AssessmentsMainly for Tracking and Documenting
CircumferenceIf unilateral then
lymphedema if
difference > X cm
Automated ManualMultiple Circumferences
Geometric Model
or Algorithm
If unilateral then lymphedema
if volume difference > Y ml
Limb Volumes
Limb Volumes and Circumference
www.limbvolumes.orgIf volume difference > Z %

Arm Lymphedema Metric CriteriaLE rate dependent on criteria used
Data from: Armer and Stewart Lymphat Res Biol. 2005;3(4):208-217.
0
20
40
60
80>=10% vol>=200 ml>=2 cm
Lym
ph
ed
em
a R
ate
(%
)
6 Months 12 Months
Differences • Between sides
• or vs. baseline

Bioimpedance Measurements
ImpediMed
(50 KHz)
Arm Electrical Impedance ~ Total Arm Tissue Water
Dr. HN Mayrovitz

0.8
1
1.2
1.4
1.6
Contol Ratios (N=60) 3SD = 0.102
Patients > 3SD of Controls and Confirmed LE
0
2
4
6
8
10
0 1 2 4 6 10
Re
sis
tan
ce
Ra
tio
Be
twe
en
Arm
s
LE confirmation (20/22)
Months after ‘positive’ test
3SD
Data from: Cornish BH et al. Lymphology. 2001;34(1):2-11.
Arm Lymphedema
N total = 102

Tissue Water via Dielectric Constant
MoistureMeter-D
• Low power 300 MHz
incident wave
• Reflected wave depends
on the tissue’s
dielectric constant
• Dielectric constant
depends on total tissue
water (free + bound)
• Pure water has a
dielectric constant of
about 78
• Calibrated for each
probe from 1 - 80
Penetration Depth (0.5 – 5 mm)
0.5 1.5 2.5 5.0 mmDr. HN Mayrovitz
Can measure at
almost any site!
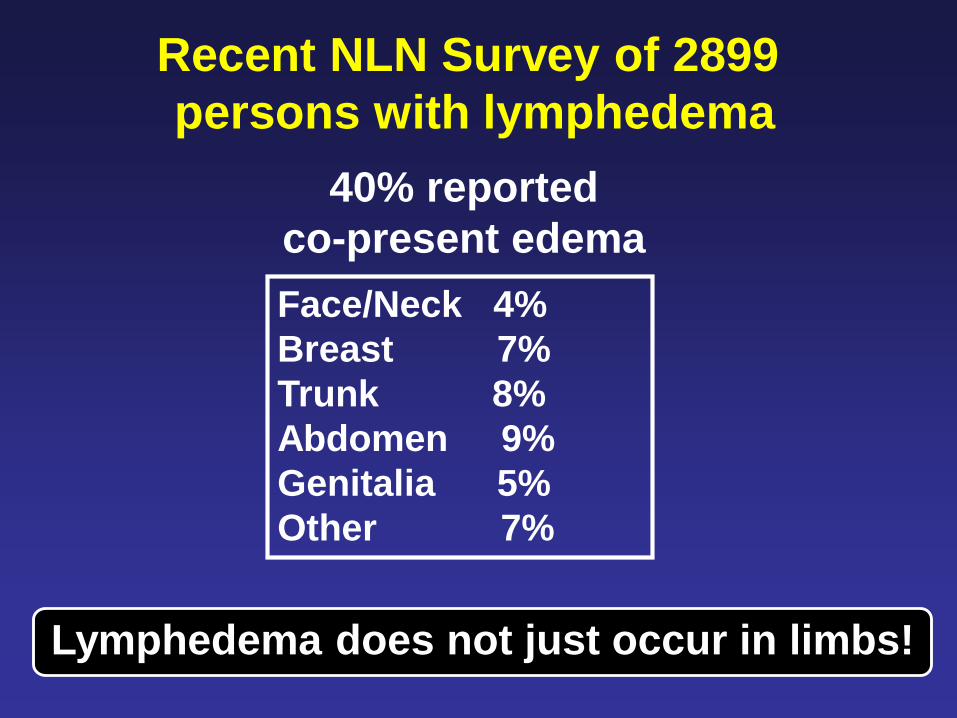
Recent NLN Survey of 2899
persons with lymphedema
40% reported
co-present edema
Face/Neck 4%
Breast 7%
Trunk 8%
Abdomen 9%
Genitalia 5%
Other 7%
Lymphedema does not just occur in limbs!

Recent Survey of 50
Lymphedema Therapists
3
4
5 YES
NO
Avera
ge I
mp
ort
an
ce Use or recommend IPC?
N=28
N=22
Multi-
Chamber
Wound
Treat
Trunk
Treat
Calibrated
Pressure
Work
and
Release
Fibrosis
Treat
* *
* p<0.01
Therapist IPC Important Features

Pre-Surgical
Baseline
Threshold Change Detection
Therapy
Initiation
Periodic Follow-ups
Measures and Criteria
•Limb Volumes and Metrics
•Limb Bioimpedance
•Local Tissue Water
Goal: Earlier Detection and Intervention
A Rationale and Sensible Approach
Dr. HN Mayrovitz
N=50
Ongoing Research Study
Women Diagnosed with Breast Cancer

TDC Measurement Sites
Lateral Thorax Axilla
Forearm Biceps
2.5 mm Probe
Dr. HN Mayrovitz

24.9±3.1 24.7±3.3
21.7±3.0 21.9±2.7
34.5±7.6 35.3±7.9
25.5±4.6 25.4±4.8
Arm Volumes (ml)
2249±701 2271±702
Z=305±39Z=305±39
Cancer vs. Healthy SidesNo difference between sides
Cancer
SideHealthy
Side
•TDC
•BIOZ
•VOLUME
Dr. HN Mayrovitz
N = 50
Pre-surgery Assessments
Insignificant Side-to-Side Differentials

Number of Patients Evaluated
50
32
22
1512
74
0
10
20
30
40
50
60
1 2 3 4 5 6 7
Visit Number
Nu
mb
er
of
Pa
tie
nts
Getting close but insufficient follow-ups for conclusions

Some Newly Initiated
Research Studies

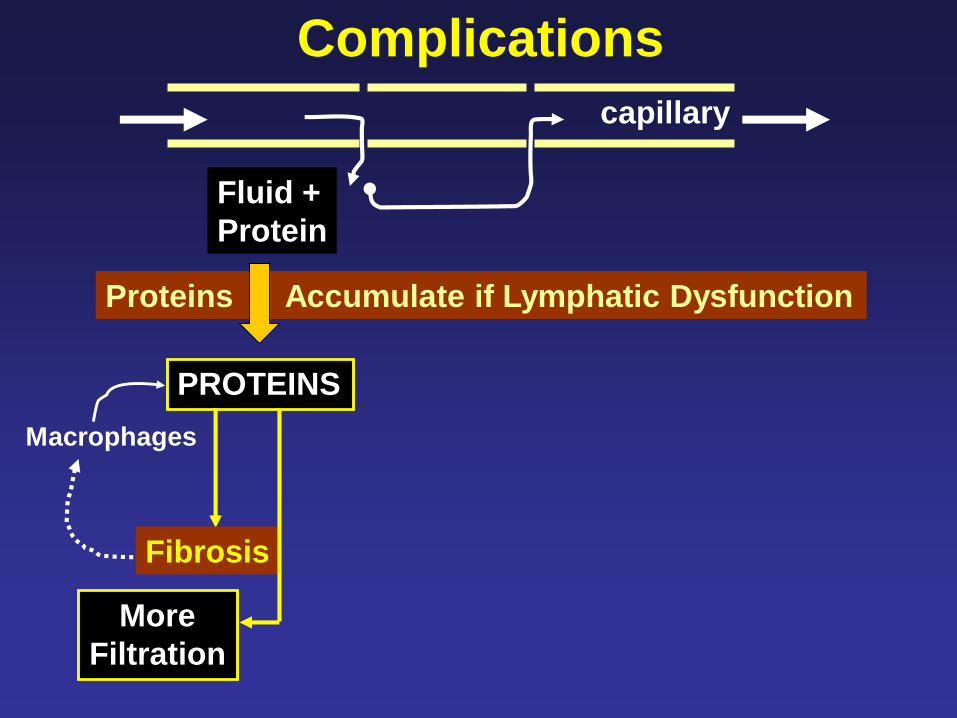
Fluid +
Protein
PROTEINS
Proteins Accumulate if Lymphatic Dysfunction
Macrophages
Stimulus for Chronic Inflammation
Vasodilation
• Increased filtration
• Tissue warmingBacterial
Growth
Bacterial/Fungal Infections
Fibrosis
More
Filtration
capillary
ComplicationsMeasure and Characterize Lymphedema Related Fibrosis

Force
Indentation
Principle: Indentation Force ~ Tissue ‘Hardness’
Fibrosis and Tissue Property Changes

100
200
300
400
500 pre-MLD
pst-MLD
Fo
rce
(g
)
Calf Thigh
Single MLD Treatment
P<0.001 P<0.01~
N=22 N=6
Lower Extremity
Lymphedema
Tissue
‘softening’
Some Initial Applications and Outcomes

Evaluate Efficacy of Low Level Laser Therapy (LLLT)
Single Laser Treatment Fibrosis Hardness Tissue Water
Initial Results are Encouraging – Conclusions Premature

Develop a Reference Framework for Facial Edema
FL
CL
ML
Ophthalmic
Maxillary
Mandibular
Different
Innervation
Territories

Cross section of upper arms, autopsy samples.
Hypertrophied adipose tissue of the lymphedematous left arm.
Dr. C-H Håkansson, Dept of Oncology,
Lund University Hospital

Liposuction in Chronic Lymphedema

Courtesy H. Brorson M.D.
15 years
later



HUMAN MOUSE

TREATMENT

PHASE I
• Manual Lymphatic Drainage
• Compression Bandaging
• Decongestive Exercise
• Skin Care
• Reduce Risk
• Detect Early
• Arrest & Reduce
• Maintain Gains
- Complications
Overall Goals

• Manual Lymph Drainage (MLD)
• Compression Bandaging
• Exercise and Skin Care
• ± Intermittent Pneumatic
Compression (IPC)
Phase I - Intensive
Complete Decongestive
Physiotherapy (CDP)

MLD Compressive
Bandage
Decongestive
Exercise
Phase I - Intensive
Complete Decongestive
Physiotherapy (CDP)

LN
Vertical
Watershed
NORMAL
Transverse
Watershed
Veins
Lymphatic Drainage
Lymph flow and drainage
determined by normal
physiological processes
and lymphatic pathways

LN
Vertical
Watershed
NORMAL
Transverse
Watershed
Veins LN
Vertical
Watershed
LYMPHEDEMA
Transverse
Watershed
Veins
Lymphatic Drainage
Lymph flow and drainage
determined by normal
physiological processes
and lymphatic pathways
Lymph flow through normal
pathways reduced or absent
due to nodal or lymph vessel
obstruction and dysfunction
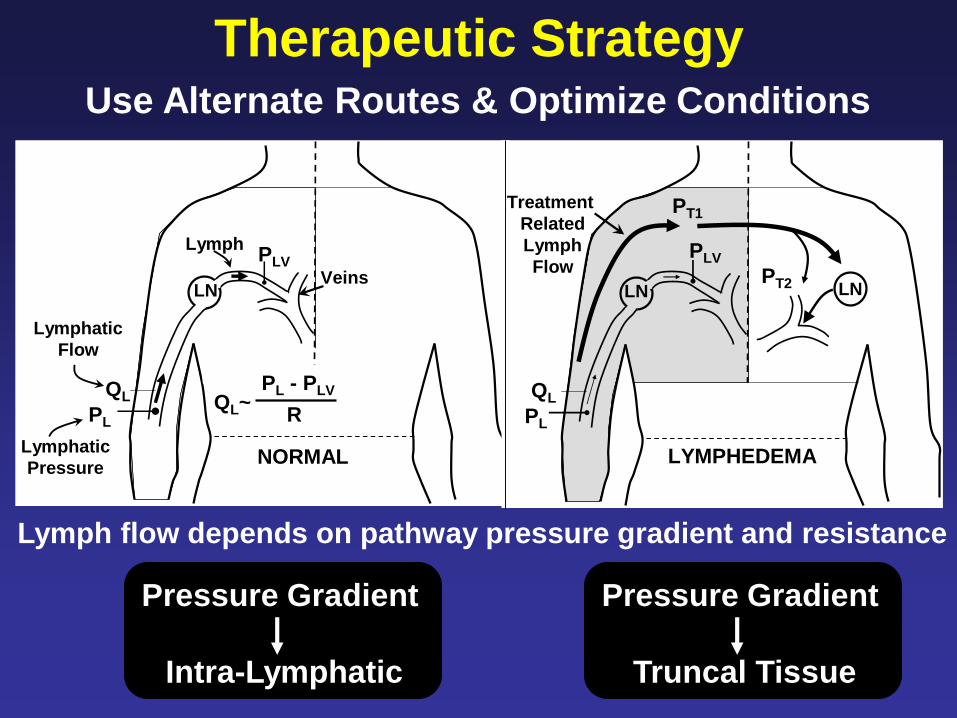
PL
PLV
QL
Lymphatic
Pressure
Lymphatic
Flow
LNVeins
Lymph
QL~PL - PLV
R
NORMAL
PL
PLV
QL
LYMPHEDEMA
LN LN
Treatment
Related
Lymph
Flow
PT1
PT2
Therapeutic StrategyUse Alternate Routes & Optimize Conditions
Lymph flow depends on pathway pressure gradient and resistance
Pressure Gradient
Intra-Lymphatic
Pressure Gradient
Truncal Tissue

LNVeins
3
4
5
Clear
normal
adjacent
trunk areas
LN
122Clear
affected
trunk areas
LNInguinal
Nodes
Prepare
abdominal
region
MLD and New IPC Approach
First sequentially treat
lymph receiving
regions (15) to
optimize gradient and
minimize resistance
for subsequent limb
drainage procedures
Mayrovitz et al. (2009) Home Health Care Management & Practice (in press)

LNVeins
3
4
5
Clear
normal
adjacent
trunk areas
LN
122Clear
affected
trunk areas
LNInguinal
Nodes
Prepare
abdominal
region
First sequentially treat
lymph receiving
regions (15) to
optimize gradient and
minimize resistance
for subsequent limb
drainage procedures
Then progressive treatment of limb and trunk
with suitable manual or pump pressures
starting at the most peripheral region (5 1)
MLD and New IPC Approach

Adjunctive IPC Therapy
Basic Limited Adjustability – Non-Programmable
Advanced Calibrated – Sequential - Programmable
ROLE
Phase I Component of in-clinic therapy
Phase II Component of at-home maintenance therapy
• With Truncal Clearance Capability
• No Truncal Clearance Capability
TYPES

IPC Parameters
Calibrated
Pressure setting (manual or programmed)
corresponds to pressure delivered to skin
Sequential
During drainage phase, compression progresses
distal proximal consistent with physiological concepts
Programmable
Software control to permit customization of compression
parameters to account for variable patient conditions
e.g. painful, ulcerated or fibrotic areas

Differences Among Therapy Parameters
Newer IPC Approach• Initial ‘preparation phase’
• ‘Work & Release’
‘Older generation’ IPC
• Limb drainage
• ‘Squeeze & Hold’
Flexitouch® Lympha Press®
Adjunctive IPC Therapy

0
10
20
30
40
50
60
70
0 10 20 30 40 50
G1
G2
G3
G4
G5
Flexitouch® SystemP
ressu
re (
mm
Hg
)Pressure Timing and Pattern
0
10
20
30
40
50
60
70
0 10 20 30 40 50
G1
G2
G3
G4
G5
Seconds
Lympha Press® System
Drainage
‘Work &
Release’
Mayrovitz HN
Physical Therapy
2007;87:1379-1388
‘Squeeze
& Hold”

0
400
800
1200
1600
Lymphapress®
Flexitouch® Preparation Phase
Flexitouch® Drainage PhaseP
res
su
re-T
ime
(m
mH
g x
se
c)
Pressure-Time Integral
G1 G2 G3 G4 G5
****
****
**
†
† † † †
Mayrovitz HN
Physical Therapy
2007;87:1379-1388
Concerns of too high a pressure have been raised in the literature
regarding ‘older generation’ IPC1 and poor pressure calibration2
“Compression pumps should be used only under the supervision of a trained health care professional
because high external pressure can damage the lymphatic vessels near the skin surface.”
http://www.cancer.gov/cancertopics
1Eliska & Eliskova Lymphology 1995;28:21-30 2Segers et al. Phys Ther 2002;82:1000-1008

3
4
5 YES
NO
Ave
rag
e I
mp
ort
an
ce Use or recommend IPC?
Therapist IPC Important Features
N=28
N=22
Multi-
Chamber
Wound
Treat
Trunk
Treat
Calibrated
Pressure
Work
and
Release
Fibrosis
Treat
* *
* p<0.01
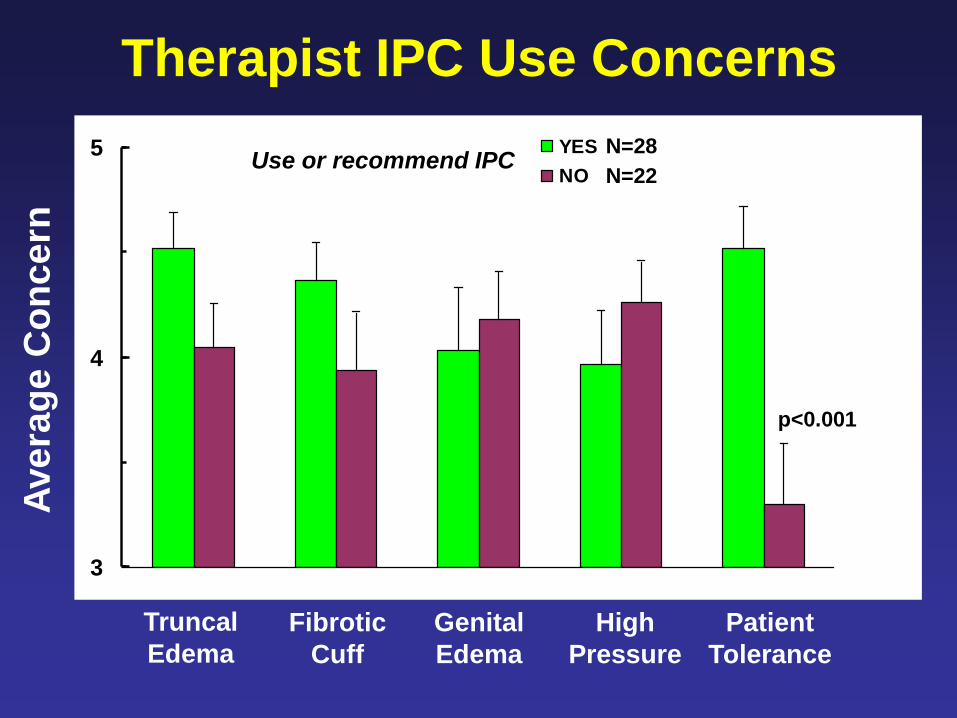
3
4
5 YES
NO
Ave
rag
e C
on
ce
rn
Use or recommend IPCN=28
N=22
p<0.001
Truncal
Edema
Fibrotic
Cuff
Genital
Edema
High
Pressure
Patient
Tolerance
Therapist IPC Use Concerns


• Reduce Risk
• Detect Early
• Arrest & Reduce
• Maintain Gains
- Complications
PHASE II
• Self MLD
• Compression Garment
• Self Bandaging
Overall Goals

Potential Risks of Ineffective
Home Self Maintenance
• Loss/Reversal of Phase I Achievements
• Interim Development of Complications
e.g. Fibrosis, Inflammation, Cellulitis, Pain
• Therapeutic Interventions for Complications
and new rounds of Phase I therapy requiring
additional patient time, suffering and costs

After Vignes et al.
Breast Cancer Res Treat
(2007) 101:285–290
Lym
ph
ed
em
a V
olu
me
(m
l)
Start Phase I 6 months 12 months
Phase II
N=537 newly
diagnosed pts
End
2 wks – 10 Tx
N= 426 356
Breast Cancer Treatment-Related Lymphedema
Self MLD
Elastic Sleeve
LS Bandage
Compared to end of Phase I
Increased > 10% 51%
“Stable” ± 10% 20%
Decrease >-10% 29%

Compliance – Risk of Increase
Vignes et al. Breast Cancer Res Treat (2007) 101:285–290
No added risk?

• Low Stretch Bandaging
• Compression Garment
Phase II Outcomes: Compliance
Fairly Conclusive
MLD - Inconclusive
1. Phase I MLD Major initial reductions
2. Self reported use/non-use as an index may
or may not be valid
3. Impact of MLD on stable and decrease?
4. No measure or knowledge that proper
self-MLD technique was used!

IF Phase I outcome is very effective and
IF patients are ~100% compliant with respect to
garment use, bandages and exercises
THEN Self MLD may not add much to outcome
BUT --- the above is at best only sometimes true
SO ---- Assistance in MLD compliance is needed
Personal View
• ROM and Functional impairments
• Aging population of cancer survivors
• Physical demands of effective MLD
• Difficulty of properly done self-MLD
• ~35% of patients report doing self-MLD1
1Ridner et al. Oncol Nurs Forum 2008;35:671-680.

10
12
14
16
18 Flexitouch
Self-MLD
% E
xc
es
s V
olu
me
~Pre-Treat Post-Treat
Data from: Wilburn et al. BMC Cancer 2006, 6:84
Short-Term Home MaintenanceMLD Assistance via Advanced IPC
BCRL N=10
2 wks tx with
each modality
P<0.001 NS
*

Phase II Outcomes: Compliance
IPC Usage
1. Lynnworth, M. NLN Newsletter 1997;(10)
2. Ridner et al. Oncol Nurs Forum 2008;35:671-680
Users Abandoning Pump Use by 6-7 Months
0
5
10
15
20
25
30
35
40 Older GenerationPumps - 1
Advanced Pump(Flexitouch) - 2
37.7%
4.0 %

• Pre-surgical Assessment
• Periodic test via emerging
early detection methods
• Self recognition of symptoms
• Reduce Risk
• Detect Early
• Arrest & Reduce
• Maintain Gains
- Complications
Overall Goals

Quantitative Assessment Methods
• Limb Volumes
• Bioimpedance
• Local Tissue Fluid
• Tissue Properties
Early Detection & Treatment Effectiveness
Limbs
Any at Risk Location
(e.g. Trunk, Face and etc.)

20
30
40
50 pre-MLD
pst-MLD
Calf Thigh
TD
C V
alu
eSingle MLD Treatment
Lower Extremity Lymphedema
P<0.001 P<0.05
N=20 N=6
Mayrovitz et al. Lymphology 2008;41:87-92

25.7±3.1 25.2±3.6
22.4±2.9 22.3±2.9
34.7±8.3 33.4±9.0
24.9±5.2 24.3±4.5
Cancer Side Healthy Side
Arm Volumes (ml)
2160±564 2164±509
Bioz306±34
Bioz307±34
Breast Cancer Pre-Surgical N=30
Insignificant Side-to-Side Differentials at Baseline
TDCTDC
Mayrovitz et al. Clinical Physiology and Functional Imaging 2008;28:337-342

Force
Indentation
Fibrosis & Tissue Property ChangesPrinciple: Indentation Force ~ Tissue ‘Hardness’

0
50
100
150
200
250
300
350
1 2 3 4 5
Pre-FT
Pst-FT
Single Flexitouch® ApplicationF
orc
e (
g)
Indentation Depth (mm)
N = 12
P<0.001
Tissue
‘Softening’
30 minute below
knee application

100
200
300
400
500 pre-MLD
pst-MLD
Fo
rce (
g)
Calf Thigh
Single MLD Treatment
P<0.001 P<0.01~
N=22 N=6
Lower Extremity
Lymphedema
Tissue
‘softening’

Summary
• Risk Reduction Catch it early Treat it intensively Maintain Gains
• Historically and Generally Accepted Approaches CDP ± IPC
• Phase I: MLD + SS Compression Bandage + Exercise + Skin Care
• Phase II: Self MLD + Elastic Garment + Bandage + Exercise + Skin Care
• Phase II compliance is a factor in maintaining gains
IPC use if programmable and if it provides truncal clearance prior
to limb pumping may increase compliance and improve outcomes
• Early detection with biophysical measures should be actively pursued
• Pre-surgical assessments can likely aid in the early detection process


Arterial
system
Venous
System
Blood
Capillaries
Lymphatic
Capillaries
Lymphatic
Vessels
Lymph
Nodes
Ly
mp
ha
tic
Sy
ste
m
Heart
Arteries
Pulmonary
Circulation
Sy
ste
mic
Cir
cu
lati
on
RALA
LVRV
Arterioles

Fluid +
Protein
PROTEINS
Proteins Accumulate if Lymphatic Dysfunction
More
Filtration
capillary
Complications
Lymphatic vessel/node
•Trauma
•Removal
•Radiation
•Blockage
•Overload
•Genetic - Primary
Fluid +
Protein
PROTEINS
Proteins Accumulate if Lymphatic Dysfunction
Macrophages
Fibrosis
More
Filtration
capillary
Complications

Fluid +
Protein
PROTEINS
Proteins Accumulate if Lymphatic Dysfunction
Macrophages
Stimulus for Chronic Inflammation
Vasodilation
• Increased filtration
• Tissue warmingBacterial
Growth
Bacterial/Fungal Infections
Fibrosis
More
Filtration
capillary
Complications

• Reduce Risk
• Detect Early
• Arrest & Reduce
• Maintain Gains
- Complications
Overall Goals

• Patient do’s & don’ts soon
after they become at risk
• Patient precaution compliance
• Reduce Risk
• Detect Early
• Arrest & Reduce
• Maintain Gains
- Complications
Overall Goals
• Multiple Web Sites with Good Info
• Not all precautions validated
• Some may be ‘over-kill’
• Informed and educated patient
• Common Sense Approach

0.6
1.0
1.4
1.8
2.2
Patient ArmsAffected/Control
1.64 ± 0.30
N=18
Premenopausal Postmenopausal1.04 ± 0.04 1.04 ± 0.04
N=15 N=15
Die
lec
tric
Co
ns
tan
t (R
ati
o)
Control Arms (Max/Min)
No overlap between
Patients vs. Controls
Potential Diagnostic Utility
Mayrovitz HN (2007) Lymphology 2007;40:87-94
Related Documents











