Lumbar Rehabilitation

Lumbar Rehabilitation. Stability is the key to rehabilitation Once we have ‘normal’ mobility we need to stabilise within this new range This emphasises.
Dec 13, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Lumbar Rehabilitation

Lumbar Rehabilitation
• Stability is the key to rehabilitation• Once we have ‘normal’ mobility we need to
stabilise within this new range• This emphasises the need for manual therapy
techniques to restore mobility

Mobility Before Stability
• Bilateral Lumbar Paraspinals
• Bilateral Hip Flexors
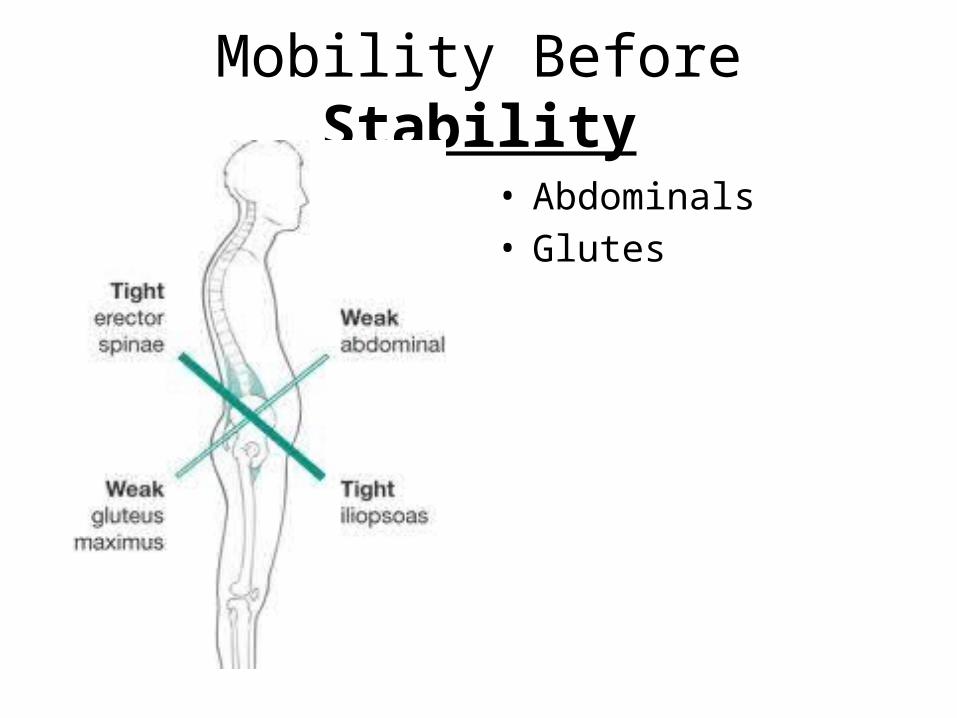
Mobility Before Stability
• Abdominals• Glutes
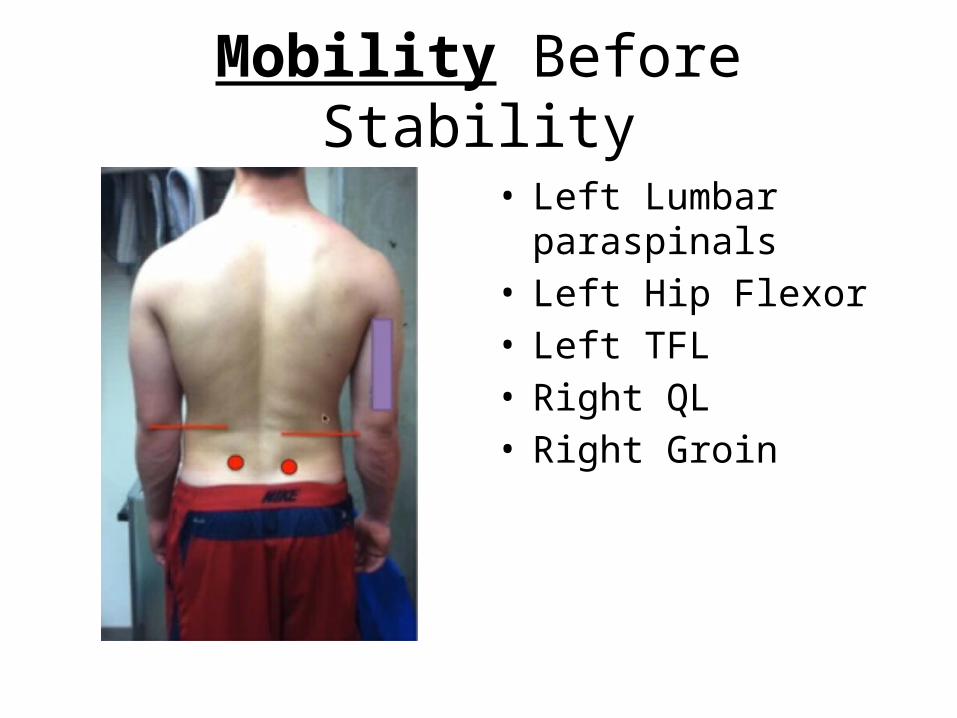
Mobility Before Stability
• Left Lumbar paraspinals• Left Hip Flexor• Left TFL• Right QL• Right Groin

Mobility Before Stability
• Left Posterior Pelvic Tilt• Left adduction/ IR• Left Oblique• Right External Rotation

Stability
• What is it?– Functional Exercise?– Motor Control?– Isolated strengthening?

Static vs Dynamic Stability
• Static Stability– Osseous configuration– Capsules and Ligaments
• The knee is greater static stability than the shoulder
• Someone sitting in lumbar flexion relies on static stabilisers for stability, hence creep of tissues and therefore pain
• Dynamic Stability– Muscle function
• Dynamic Ligament Tension
• Force Couples• Joint Compression• Neuromuscular Control
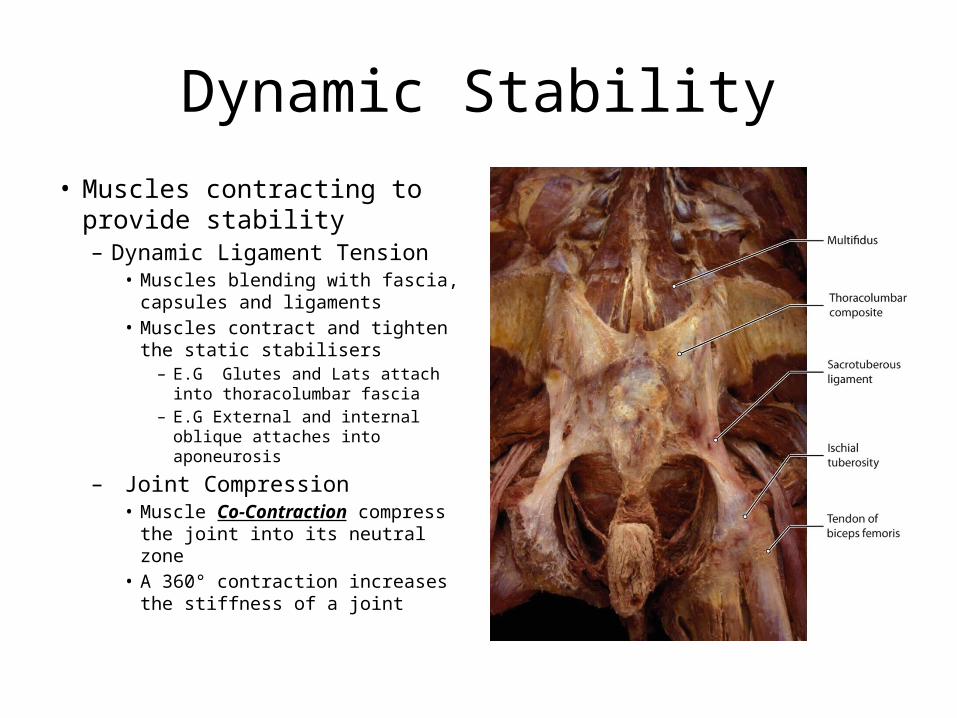
Dynamic Stability• Muscles contracting to provide
stability– Dynamic Ligament Tension
• Muscles blending with fascia, capsules and ligaments
• Muscles contract and tighten the static stabilisers– E.G Glutes and Lats attach into
thoracolumbar fascia– E.G External and internal
oblique attaches into aponeurosis
– Joint Compression• Muscle Co-Contraction compress
the joint into its neutral zone• A 360° contraction increases the
stiffness of a joint
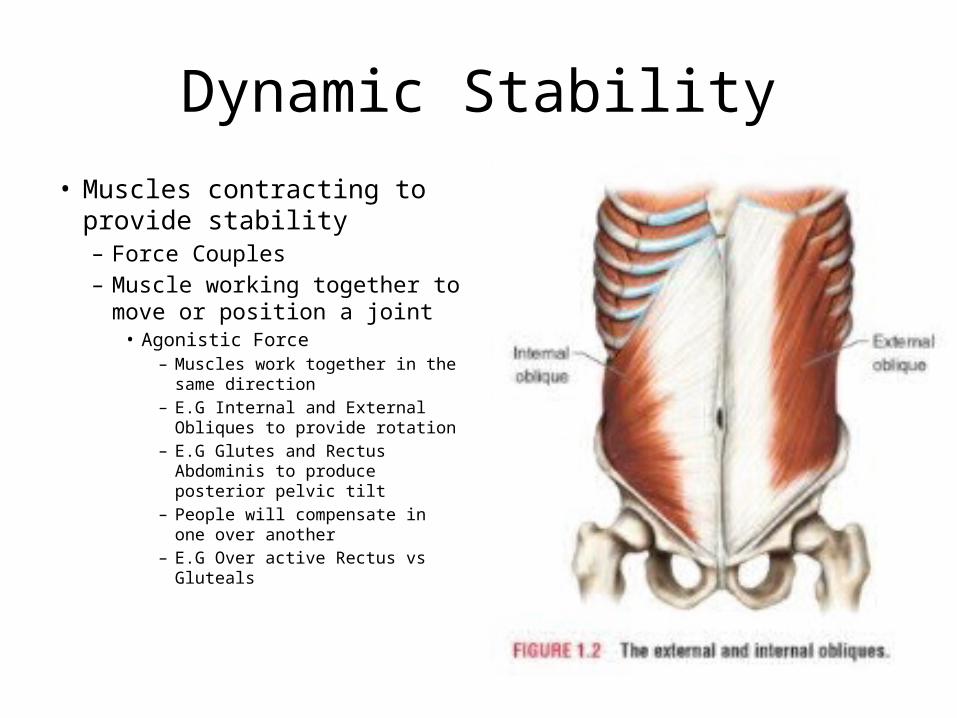
Dynamic Stability• Muscles contracting to provide
stability– Force Couples– Muscle working together to
move or position a joint• Agonistic Force
– Muscles work together in the same direction
– E.G Internal and External Obliques to provide rotation
– E.G Glutes and Rectus Abdominis to produce posterior pelvic tilt
– People will compensate in one over another
– E.G Over active Rectus vs Gluteals

Dynamic Stability
• Muscles contracting to provide stability– Force Couples
• Muscle working together to move or position a joint
• Antagonistic Force– Muscles work together in
opposite directions– E.G Rectus abdominis and
paraspinals– If one is over active joint
position will change– E.G Increase tone
paraspinals vs Rectus causes anterior pelvic tilt

Dynamic Stability
• Neuromuscular Control– Motor Response to a
Sensory Input• Proprioception
– Understanding where you body is in space
• Kinaesthesia– Understanding where
your body is MOVING in space

Dynamic Stability
• What can reduce Dynamic Stability– Muscle Weakness– Muscle Fatigue– Muscle Imbalances– Injury

Dynamic Stability
• What do we need to do to train Dynamic Stability• A complete rehabilitation programme includes the
following– Motor Control
• Teach the body/muscles to move/contract in the order/way they are supposed to
• E.g delayed firing diaphragm, trans abs, multifidus
– Isolated Strengthening– Endurance– Neuromuscular Control
• Exercises are progressed to become more challenging
What’s Wrong with Current Core Programmes
• Sit Ups, Crunches, Russian Twists etc– Based upon the ‘ACTION’ of a muscle– Not based upon its true role– Sit up creates 320 Kg force through
lumbar spine– Twisting the lumbar spine- Discs don’t
like rotational shearing forces
• Abdominal Hollowing– Notoriously difficult to teach– Diane Lee reports she uses Ultrasound
for 30 mins until a correct contraction occurs
– Isolating Trans abs does not provide 360° stability• Isolated strengthening, if needed, Yes,
but must transfer into 360° contraction (Bracing)
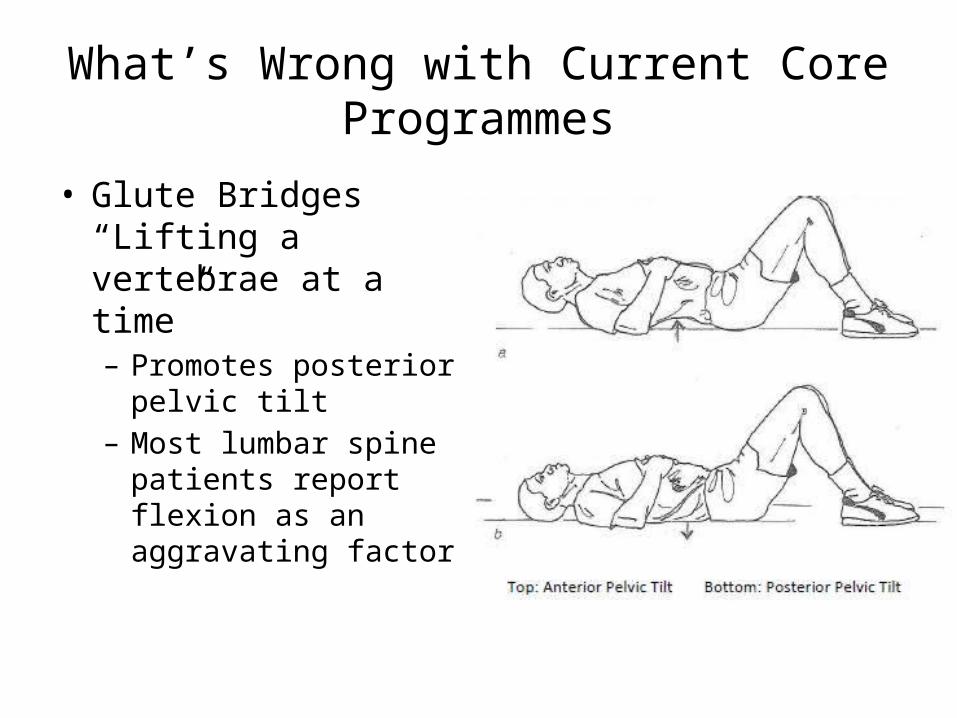
What’s Wrong with Current Core Programmes
• Glute Bridges “Lifting a vertebrae at a time”– Promotes posterior
pelvic tilt– Most lumbar spine
patients report flexion as an aggravating factor

Lumbar Spine Pain
• Delayed onset transversus abdominis• Decreased and delayed multifidus• Delayed diaphragm• Fatigue back extensors• Lumbar spine buckles in a certain plane at
without 360° muscular co contraction

The Core
• More of a Tent than a corset
• Includes the diaphragm and pelvic floor
• Includes the obliques, rectus abdominis
• Includes Quadratus Lumborum – If this muscle doesn’t
work you CANNOT walk
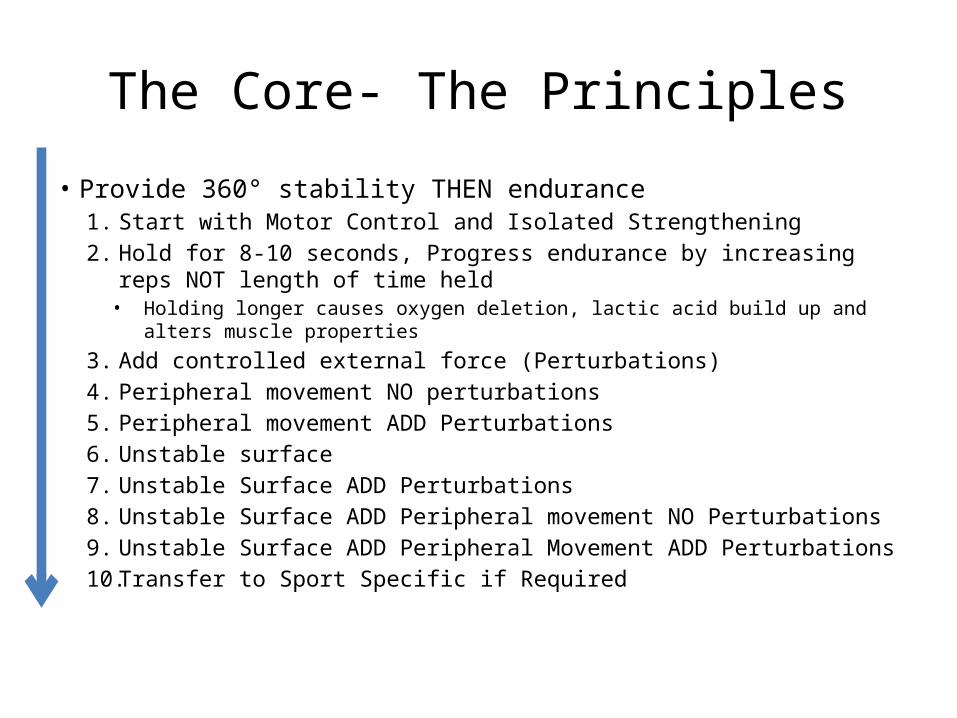
The Core- The Principles• Provide 360° stability THEN endurance
1. Start with Motor Control and Isolated Strengthening2. Hold for 8-10 seconds, Progress endurance by increasing reps NOT
length of time held• Holding longer causes oxygen deletion, lactic acid build up and alters muscle
properties
3. Add controlled external force (Perturbations) 4. Peripheral movement NO perturbations5. Peripheral movement ADD Perturbations6. Unstable surface7. Unstable Surface ADD Perturbations8. Unstable Surface ADD Peripheral movement NO Perturbations9. Unstable Surface ADD Peripheral Movement ADD Perturbations10. Transfer to Sport Specific if Required

Isolated Core
• Focus On– Anterior Core (Anti
Extension)– Posterior Core (Anti
Flexion)– Lateral Core (Anti Side
Flexion)– Anti Rotational Core
(Anti Rotation)

Before Isolated Strengthening
• Every exercise starts with the same– Neutral Lumbopelvic
position (Pain Free)– Diaphragmatic Breathing– Bracing
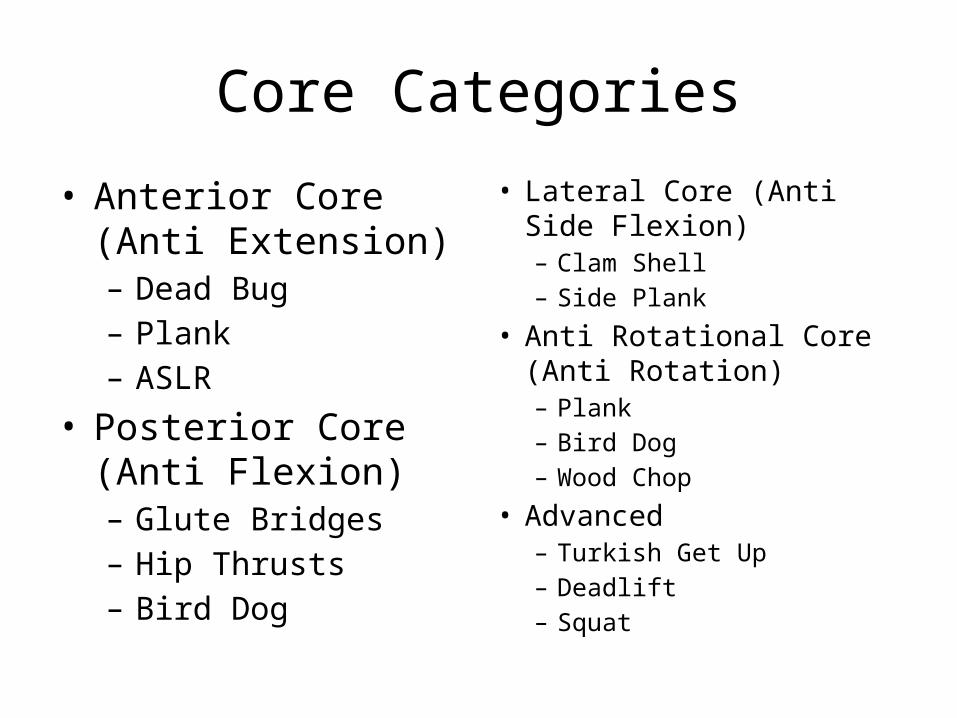
Core Categories
• Anterior Core (Anti Extension)– Dead Bug– Plank– ASLR
• Posterior Core (Anti Flexion)– Glute Bridges– Hip Thrusts– Bird Dog
• Lateral Core (Anti Side Flexion)– Clam Shell– Side Plank
• Anti Rotational Core (Anti Rotation)– Plank– Bird Dog– Wood Chop
• Advanced– Turkish Get Up– Deadlift– Squat

Anterior Core (Anti Extension) - Dead Bug

Anterior Core (Anti Extension) - Plank

Anterior Core (Anti Extension) - ASLR

Posterior Core (Anti Flexion and Anti Extension) - Glute bridges

Posterior Core (Anti Flexion and Anti Extension) - Hip Thrusts

Posterior Core (Anti Flexion) - Bird Dog
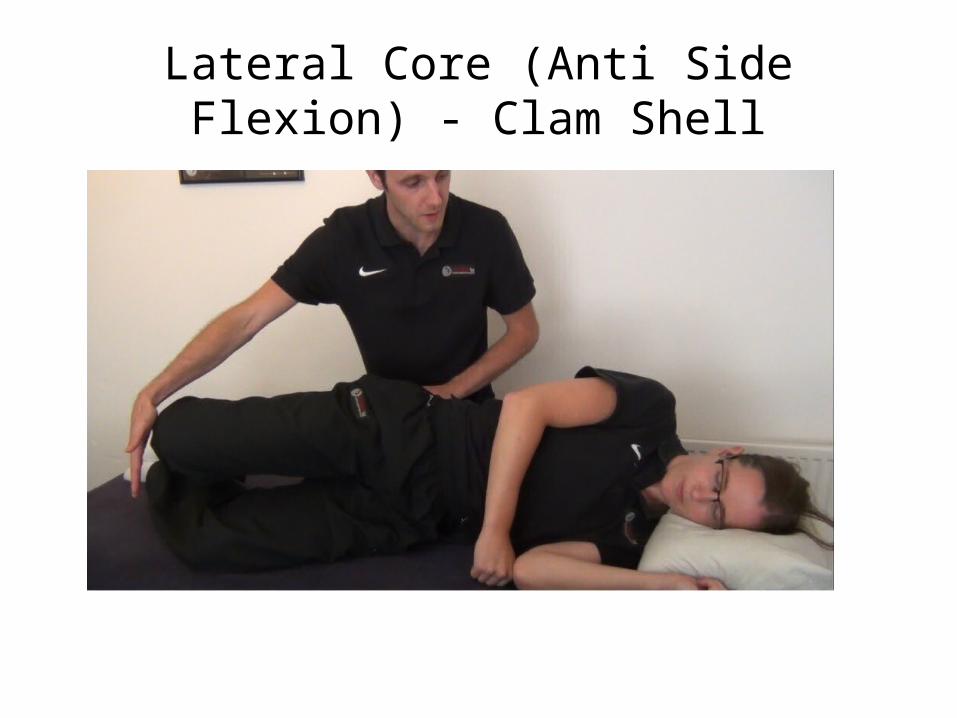
Lateral Core (Anti Side Flexion) - Clam Shell

Anti Rotational Core - Wood Chop

Advanced - Deadlift

Advanced - Turkish Get Up

Misc - 90/90 Hip Lift with Balloon
Related Documents











