
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Luiz Henrique GebrimHospital Pérola Byington
UNIFESP
Os Trabalhos/Abstracts mais Relevantes emtratamento cirúrgico
Luiz Henrique Gebrim
Câncer de mama

1. Todos necessitam terapêutica?2. CDIS – Todos necessitam RT?3. Cir. conservadora ou radical em jovens ? 4. Adenectomia ou cir conservadora?5. Seguimento da mama oposta6. L sentinela + = linfadenectomia?7. Reconstrução imediata ou tardia?
Câncer precoce de mama

Mammograms don't save as many lives as women think screening for breast cancer with mammography.
Gøtzsche PC, Nielsen M.The Nordic Cochrane Centre, .Cochrane Database Syst Rev. 2011
• N= 600.000• Igual mortalidade 13 anos• Overtreatment CDIS (+30%)
• 10 em 2.000 (tratadas desnecessariamente)
• 200 falsos positivos

Effect of tamoxifen and radiotherapy in women with locally excised ductal carcinoma in situ: long-term results from the
UK/ANZ DCIS trialJack Cuzick,a* Ivana Sestak,a Sarah E Pinder,b et al, 2010
2. CDIS- Conclusões
•Multifocal•Diferentes formas Sem biomarcadores preditivos•RT (8 x 25%)Eficácia menor ( Tu<1cm, margem>1cm, >50 anos, G1,G2)
•HT ( - 29%)•R. Local = sobrevida
?

Indicações de Mastectomia nos EUA
2000 2002 2004 2006 2008 2010

First reported site of treatment failure for sentinel-node (SLN)-negative patients
STAGE I
RECURRENCE RATES IN YOUNG WOMEN WITH BREAST CANCER BY LOCOREGIONAL TREATMENT APPROACH
Beathe et al, Int J Radiat Onc Bio Phis, 2009

RECURRENCE RATES IN YOUNG WOMEN WITH BREAST CANCER BY LOCOREGIONAL TREATMENT APPROACH
Beathe et al, Int J Radiat Onc Bio Phis, 2009
STAGE II

3.Câncer precoce em jovensConclusões
• Risco de recidiva maior (20-30%)
• EI =Cir Conservadora +RT• EII =Mastectomia + RT • Sobrevida média 20 anos : 55%
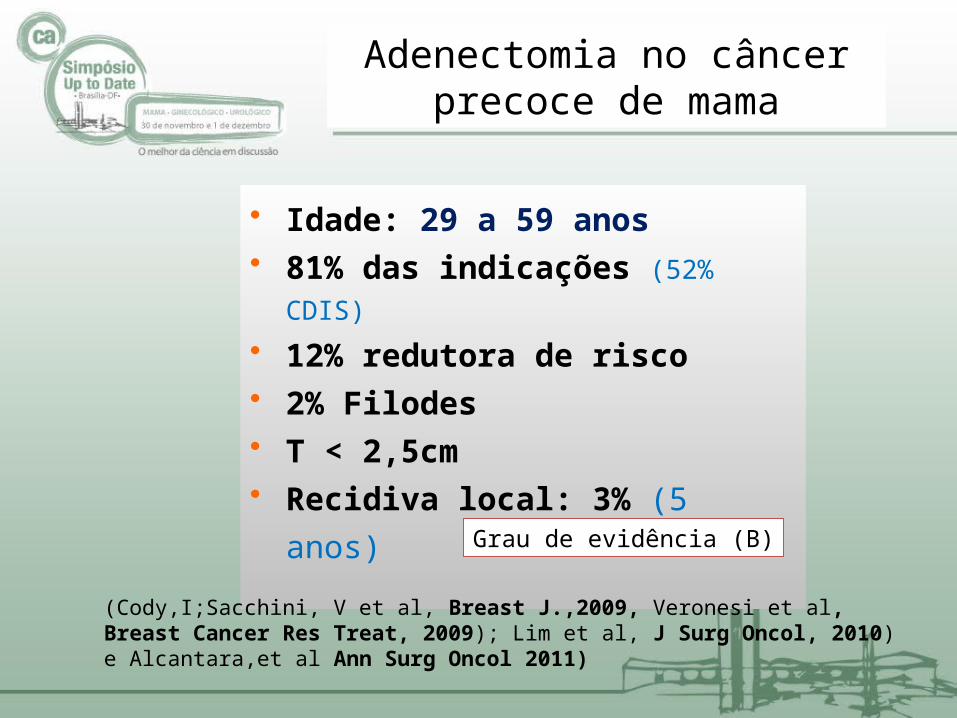
• Idade: 29 a 59 anos• 81% das indicações (52% CDIS)
• 12% redutora de risco• 2% Filodes• T < 2,5cm• Recidiva local: 3% (5 anos)
Grau de evidência (B)
(Cody,I;Sacchini, V et al, Breast J.,2009, Veronesi et al, Breast Cancer Res Treat, 2009); Lim et al, J Surg Oncol, 2010) e Alcantara,et al Ann Surg Oncol 2011)
Adenectomia no câncer precoce de mama
Controle local > C.conservadora RT menos indicada Procedimento único
(reconstrução e simetrização) Redução no risco (mama oposta,
jovens, BRCA +)
Vantagens da Adenectomia

• Comprometimento do CAP• 0,9 - 3,0% (Morrow, 2005) Tu < 2cm Distantes do CAP Axila -• Congelação intra-operatória (Veronesi, 2009) A preservação não aumenta a recidiva local
Eis,EI, IIA.
Grau de evidência (B)
Higgins et al, J Natl Cancer. 2009; Lash et al, Lancet Oncol 2010; NCCN,( 2011)
Adenectomia no câncer precoce de mama

Local, regional, and systemic recurrence rates in patients undergoing skin-sparing mastectomy
compared with conventional mastectomy. Yi,M Hunt, KK Cancer 2011 (M D Anderson).
•N= 1.810 (E0-II)•Mastectomia = 1011 (idade média=60 anos)•Skin-sparing = 799 (48 anos)•Recidiva local =6,6% (ns)

Preoperative predictors of nipple-areola complex involvement for patients undergoing mastectomy for breast cancer. Billar JA et al. Ann Surg Oncol, 2011.
Clinicos :VPP= 61%•>3cm diâmetro•< 2cm distância
D.Imagem: VPP =38%• > 4 cm distância
Biomarcadores• G3•HER2

Adenectomia após reconstruçãocom implantes
(Gebrim e Sabino -2008)
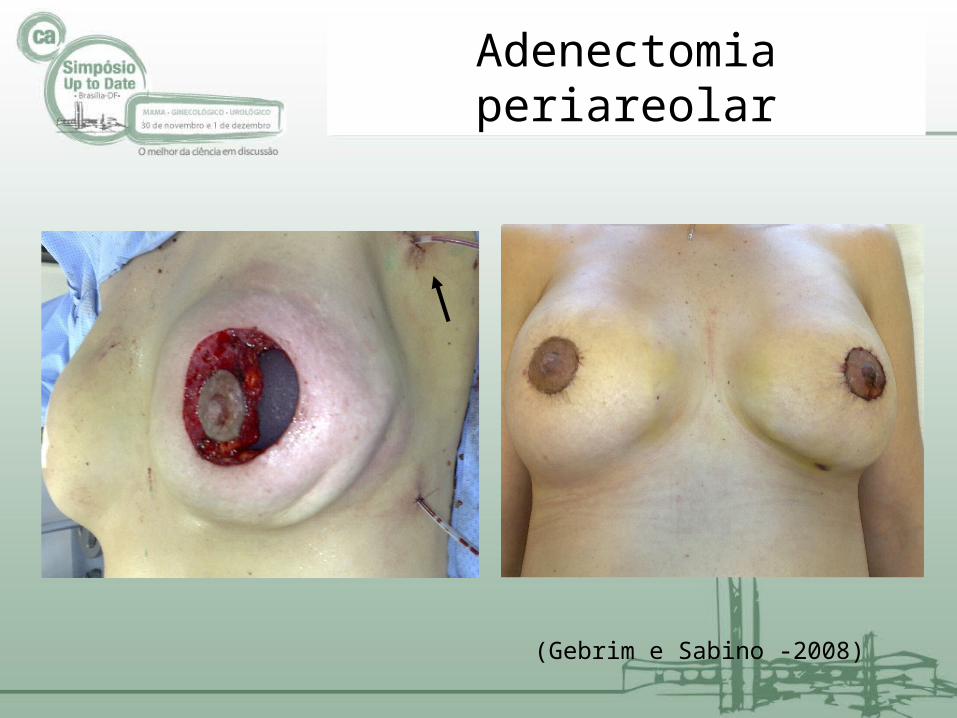
(Gebrim e Sabino -2008)
Adenectomia periareolar
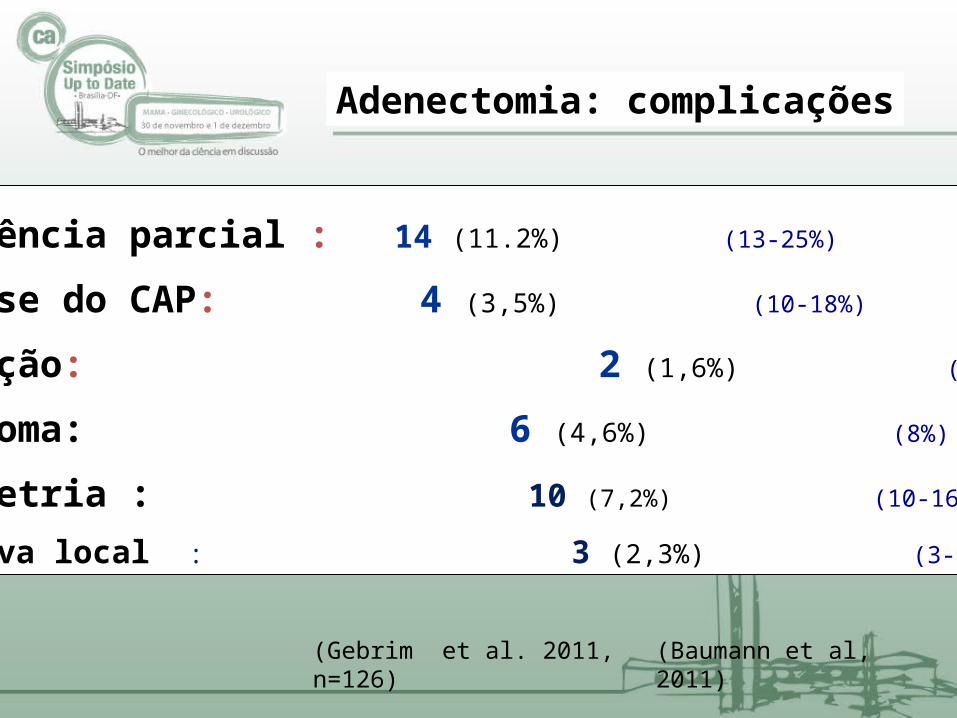
•Deiscência parcial : 14 (11.2%) (13-25%)
•Necrose do CAP: 4 (3,5%) (10-18%)
•Infecção: 2 (1,6%) (5-11%)
•Hematoma: 6 (4,6%) (8%)
•Assimetria : 10 (7,2%) (10-16%)
•Recidiva local : 3 (2,3%) (3-6%)
(Gebrim et al. 2011, n=126)
(Baumann et al, 2011)
Adenectomia: complicações

Adenectomia: complicações
•Indicação seletiva (I,II,BHGI)
•Jovens , mamas pequenas•Cirurgia oncoplástica•Preservação do CAP•Complicações: 5-22%•Recidiva: 3-6% (8 anos)
L H Gebrim
5-Adenectomia X Cir. conservadora Conclusoes
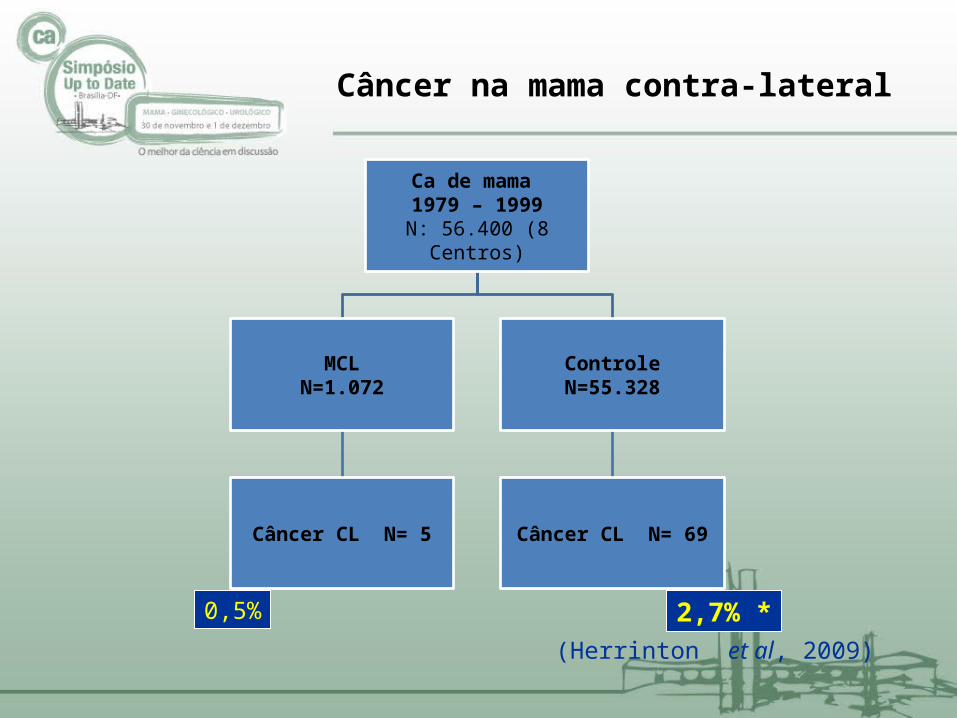
(Herrinton et al, 2009)
Ca de mama 1979 – 1999
N: 56.400 (8 Centros)
MCLN=1.072
Câncer CL N= 5
ControleN=55.328
Câncer CL N= 69
0,5% 2,7% *
Câncer na mama contra-lateral
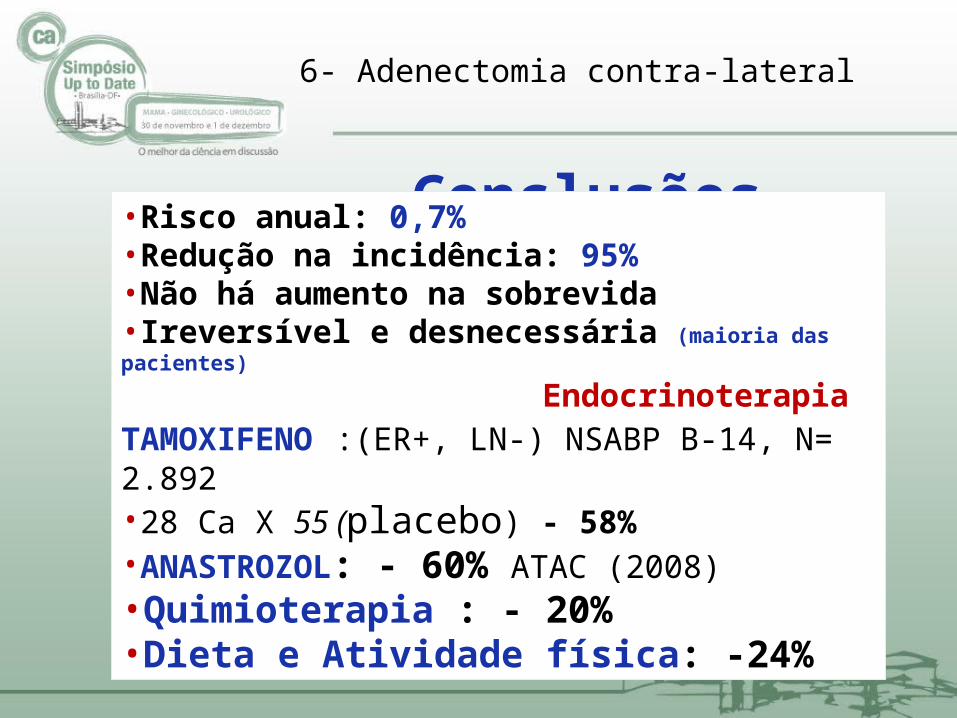
6- Adenectomia contra-lateral
Conclusões•Risco anual: 0,7%•Redução na incidência: 95%•Não há aumento na sobrevida•Ireversível e desnecessária (maioria das pacientes)
Endocrinoterapia TAMOXIFENO :(ER+, LN-) NSABP B-14, N= 2.892 •28 Ca X 55 (placebo) - 58% •ANASTROZOL: - 60% ATAC (2008)•Quimioterapia : - 20%•Dieta e Atividade física: -24%

First reported site of treatment failure for sentinel-node (SLN)-negative patients
Sentinel noderesection +
axillary disection
Sentinel noderesection
Location of failure
No. % No. %
Local recurrence
54 2.7 49 2.4
Regional node recurrence
8 0.4 14 0.7
Distant metastasis
55 2.8 64 3.2
Opposite breast
56 2.8 44 2.2
Second non-breast cancer
89 4.5 109 5.4
Dead, no evidence of disease
53 2.7 56 2.8
Total First Events
315 15.9 336 16.7
Alive, event free
1660 84.1 1675 83.3
Patients followed
1975 100.0 2011 100.0
Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negative patients with breast cancer: overall survival findings from the NSABP B-32 randomized phase 3 trial Krag DN, Anderson SJ, Julian TB et al, Lancet Oncol, 2010.

Axillary dissection vs no axillary dissection in women with invasive
breast cancer and sentinel node metastasis: a randomized clinical trial. Giuliano AE, Morrow, M - JAMA, 2011.
G1= 445 Linfadenectomia axilar (17 linfonodos)G2= 446 L. sentinela (02 linfonodos) Igual prognóstico e controle loco-regional (5 anos)
Sentinel lynph node biopsy in early breast cancer. The experience of the European Institute of Oncology of Milan. Toesca A, Luini A, Veronesi P - Breast Care 2011;6(3):208-14.
•Cirurgia prévia (sentinela ou plástica)•Gestação•Qt primária•CDIS (> 3cm)•Axila clinicamente negativa

Survival of the ALND X SLND alone
Axillary Dissection vs No Axillary Dissection in Women With Invasive Breast Cancer and Sentinel Node Metastasis. JAMA, Feb 9, 2011 vol 305-n6

ACOZOG Z0011• Não houve diferença entre os grupos
Recidiva local1
Reidiva regional1
Sobrevida global2
• Linfadenectomia axilar não é necessária para pacientes T1 e T2 N0 com BLS+
1 Giuliano AE, McCall L, Beitsch P et al. (2010) Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: the American College of Surgeons Oncology Group Z0011 randomized trial. Ann Surg 252:426–32;
2 Axillary Dissection vs No Axillary Dissection in Women With Invasive Breast Cancer and Sentinel Node Metastasis. JAMA, Feb 9, 2011 vol 305-n6

6. Sentinel lymph node micrometastasis in breast cancer: An update
Salhab M, Patani N, Mobkel K, Surgical Oncol, 2011.
Conclusoes:• Linfadenectomia axilar pode ser evitada• Não sentinelas em geral são negativos• Prognóstico desfavorável• Falta de padronização na interpretação
histopatológica (escassez de material,cortes insuficientes, estudos não randomizados e tempo de seguimento)
Menor (custo e impacto emocional)
Igual (Prognóstico)
Maior (complicações :20% e insatisfação, 81% implantes)
Retardo no tratamento oncológico (15%) 19% Imediatas (EUA, Canada)
(Alderman & Wilkins, Plast Reconstr Surg, 2011, Gurunluoglu, et al Ann Plast Surg, 2011)
7. Reconstrução imediata x tardia Conclusoes

Tendências da terapêutica do câncer precoce de mamaTake home message
1-Biomarcadores preditivos de resposta 2-Terapêutica de curta duração (QT ou HT)3- Linfonodo sentinela (prognóstico)4-Cirurgia oncoplástica individualizada (idade, biomarcadores)

Câncer de mama no Brasil e em São Paulo (n=1.023) em 2011
0
10
20
30
40
50
60
E 0 E I E II E III E IV
BrasilCRSM
Cir. conservadora após neoadjuvânciaIndicações
Volume/ tumorResposta total ou parcial• Tumores T2 e T3 únicosDiagnóstico por Imagem• Microcalcificações agrupadas < 3cm• Mensuração pela MMG e US• Lesões monofocaisHistopatológicos• Margens livres• Localizados• L. sentinela é controverso
(NCCN, EUSOMA, 2010)
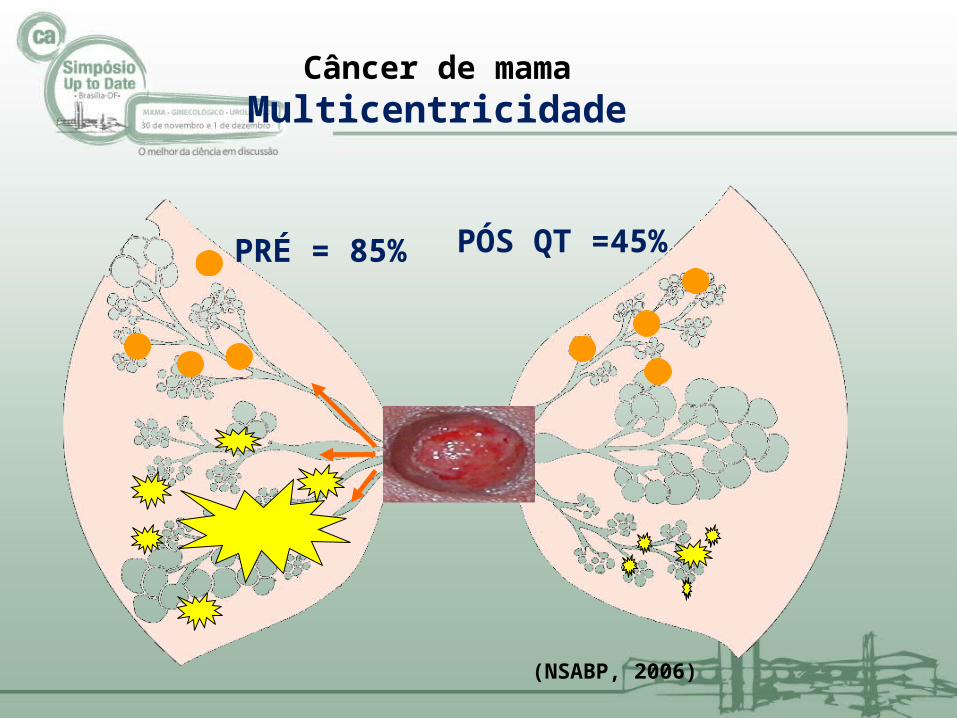
Câncer de mamaMulticentricidade
PRÉ = 85% PÓS QT =45%
(NSABP, 2006)
CANCER DE MAMAQUIMIOTERAPIA PRIMÁRIA
• N= 3.173• IIB (17%),IIIA (36%) e IIIB (41%)• AC (3 ciclos)• RP 75% (21% completa)• Cir.conservadora= 23% (<5cm)• Sobrevida média 27 meses• Recidiva local 4-35% (Cons.) e 4-7% (Radical)
(Cochrane, NSABP, 2010 )

Autor• Hortobaggi (1998)
• Yeh (2001)• Bauerfeind (2003)• Veronesi (2010)• CRSM (2011)
Rec. local (5 anos)
......... 8 %
......... 9 %
......... 12 %
......... 4 %
......... 7,8%
Cirurgia conservadora e recidiva local após QT neoadjuvante (EIII)

Early stage breast cancer: is exclusive radiotherapy an option for early breast cancers with complete clinical response after neoadjuvant chemotherapy?Daveau et al-Cancer Radiother, 2011.
N= 1477N= 165 (R Completa)G1 = 100 (Cir. Conservadora + RT) Rec Local =17%G2= 65 (Radioterapia) Rec local 31%Sobrevida= 71% (ns)

Terapêutica neoadjuvante(Hospital Pérola Byington- 2010)
N= 228 (22 HT)Cirurgias conservadoras = 55 (24%)Recidiva local = 7,8% (50 meses)Perda no seguimento : 32%

Cirurgia conservadora após neoadjuvância
•Impact of neoadjuvant chemotherapy on breast reconstruction (Greenberg et al, 2011) Imediatas(44 x 23%), complicações (30 x 31%)
•Can we predict local recurrence after neoadjuvant chemotherapy? (Cabrecos et al, 2010) 7 a 11%, pT3, HER-2, ER/PR, multifocalidade
•Is Radiotherapy an option for early breast cancers with complete response after neoadjuvant chemotherapy? (Daveau, et al, 2010),
Sobrevida e ILD iguais, 31 x 17% (R.Local)
Cirurgia conservadora após neoadjuvânciaTake home message
•Indicação seletiva (20 a 30%)
•Igual sobrevida•Indicar após término da Qt•Recidiva maior (< 40 anos, margens +,mamas densas, Her2 +,triplo -, diâmetro)•RT e oncoplástica seletivas•L. Sentinela ainda controverso
(NCCN, EUSOMA, 2011)
Câncer avançado de mamaQual o melhor momento da pesquisa do linfonodo
sentinela ?
Melhor acurácia no início
Custo maior Retardo no tratamento Morbidade
(Zhang et al, 2012)

Câncer avançado de mama Estadiamento loco-regional
• Linfonodo sentinela• Ultra-som com biópsia• PET/CT

• Citologia = 38% • Histopatologia = 13%• Imunoistoquímica = 2%
(Diest et al.1999)
LINFONODO SENTINELAFalso negativo no exame intra-operatório

LINFONODO SENTINELALimitações
Micrometástase, necrose gordurosa, fibrose, sinushistiocitose

Linfonodo sentinela após quimioterapia neoadjuvante
• N=343 (retrospectiva)• Taxa de detecção: 80,8%• Falso negativo:19,5%• Menor acurácia (axila +)• Variações técnicas• Não recomendada
(Petcha et al, 2011)

Avaliação linfonodal pré-operatória com ultra-som e punção biópsia
• N=382 (retrospectiva)• Sem adenomegalia clínica• 129 metastáticos• 121 achados US suspeitos (50 a 71% de
especificidade)• US + PAAF (96% de especificidade)
• Excluiu resposta completa • 62/382 dispensariam a
linfadenectomia
(Park et al, 2011)
Pesquisa de metástase linfonodal com PET/ CT
• N = 311• Escala (2 a 3)• Sensitividade 82%• Especificidade: 92%• VPP=98%• VPN=53%• 10% metástases ocultas (M. interna e
claviculares)
(Koolen, et al- Breast Cancer Research and Treat, 2012)

Considerar a pesquisa do LS em tumores únicos e mensuráveis (nódulos).
O US com biópsia (PAAF) é útil nos casos de dúvida clínica e nas pacientes com morbidades
O método com radioisótopos possui maior acurácia para identificação (95%)
O patologista deve ser experiente A remoção dos para-sentinelas evita re-
operação sem morbidade adicional.
Linfadenectomia no câncer avançadoTake home message
Related Documents











