Dr. Michelle Haas Denver Metro Tuberculosis Program Denver Public Health Focus on TB Prevention Modesto, CA June 5, 2019 1 LTBI Basics Focus on TB Prevention June 5th, 2019 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES • I have no disclosures or conflicts of interest to report

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 1
LTBI Basics
Focus on TB PreventionJune 5th, 2019
Michelle Haas, M.D.
Associate Director
Denver Metro Tuberculosis Program
Denver Public Health
DISCLOSURES
• I have no disclosures or conflicts of interest to report
Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 2
Objectives
• List causes of indeterminate results for IGRAs
• Describe limitations of using IGRAs to diagnose LTBI in low risk populations
• Understand evidence supporting treatment of latent TB infection (LTBI)
• Understand advantages/disadvantages of current treatment options for LTBI
Patient with Preventable TB
• 28 year old woman, originally from Mexico, presented to her primary care provider 5 years ago essentially for well visit
• Went back to PCP 5 years later:• Cough for 2 months, wheezing noted on exam• Inhaler offered, PFTs scheduled
• Urgent care visit 3 days after that visit• Continued cough, CXR obtained…

Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 3
“atypical
pneumonia”:
azithromycin for 5
days
Patient with Preventable TB
• 5 months later: repeat PCP visit:
• continued cough, no relief with albuterol
• 8 lb. weight loss: BMI 18.6.
• QVAR and Claritin were added to her albuterol.
• Chest radiograph findings were noted→ referred to pulmonary, CT chest ordered.

Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 4
Patient with Preventable TB
• One month later: seen in the ED• continued chronic cough, tachycardic to 115. Was discharged
• Two days after ED visit in pulmonary clinic:• Working diagnosis of possible bronchiolitis, bronchoscopy planned but she
didn’t have the funds to cover to copay
Patient with Preventable TB
• 3 weeks after pulm visit, 7 months into her illness• Went to the ED with headache for 7 days, fever, nausea/vomiting
and body aches and sore throat
• DX→ strep throat • RX→ azithromycin
• Chest x-ray was noted to have “no acute findings.”
• Went back twice in one week: persistent headaches, nausea vomiting and now photophobia, visual disturbances
• DX→ tension headache
• RX → follow up with her primary care provider
Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 5
Patient with Preventable TB
• Two days later, 8 months into her illness: family took her to another hospital
• Somnolence, confusion• Continued nausea/vomiting
• 9/6: MRI/ brain: diffuse focal flair hyperintensity; diffuse leptomeningeal enhancement compatible with meningitis.
• LP: WBC 149, t prot 152, glucose 14• M. tuberculosis PCR positive
Patient with Preventable TB
• Bronchoalveolar lavage, smear positive for AFB and subsequently was identified to be Mycobacterium tuberculosis.
• Additional studies: –QuantiFERON positive–HIV negative
• Her hospital course was further notable for the development of seizures.
• Started on TB treatment with isoniazid, rifampin, pyrazinamide and ethambutol and steroids due to meningitis.
• Profoundly debilitated/confused and unable to care for herself at discharge

Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 6
A review of how to identify individuals at risk for TB infection

Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 7
Who should get tested?
• Use this tool to identify asymptomatic adults for latent TB infection (LTBI) testing.• Do not repeat testing unless there are new risk factors since the last test.• Do not treat for LTBI until active TB disease has been excluded
• No gold standard for diagnosing LTBI
• All tests assess T-cells for prior exposure to TB antigens
Slide courtesy of Dr. David Horne
Tests for identifying TB infection
Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 8
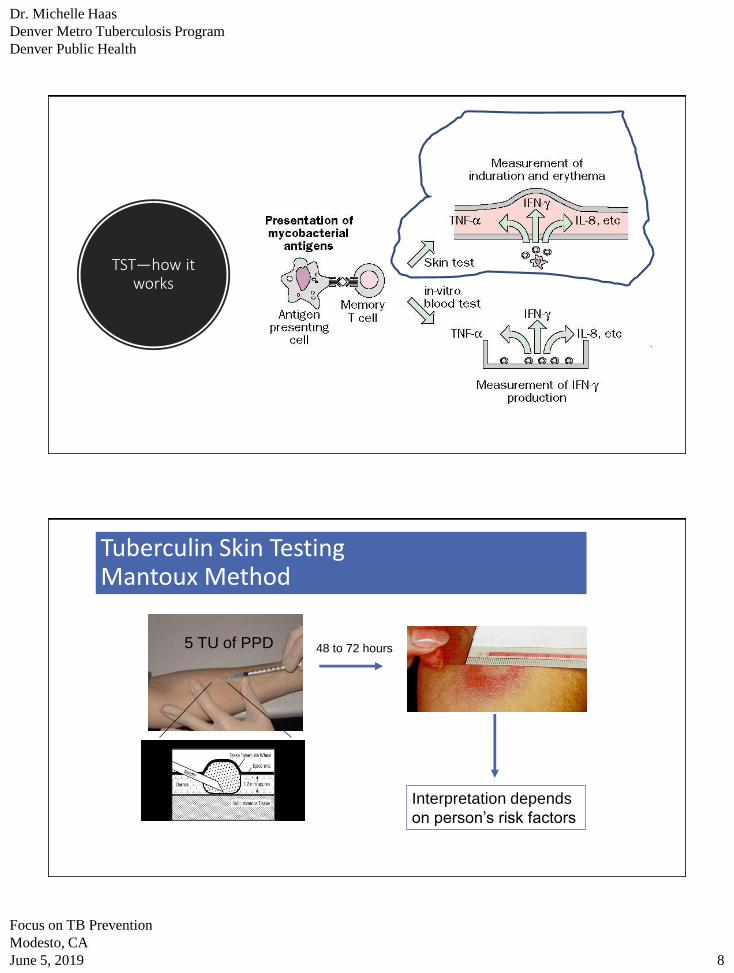
TST—how it works
Tuberculin Skin TestingMantoux Method
48 to 72 hours5 TU of PPD
Interpretation depends
on person’s risk factors
Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 9
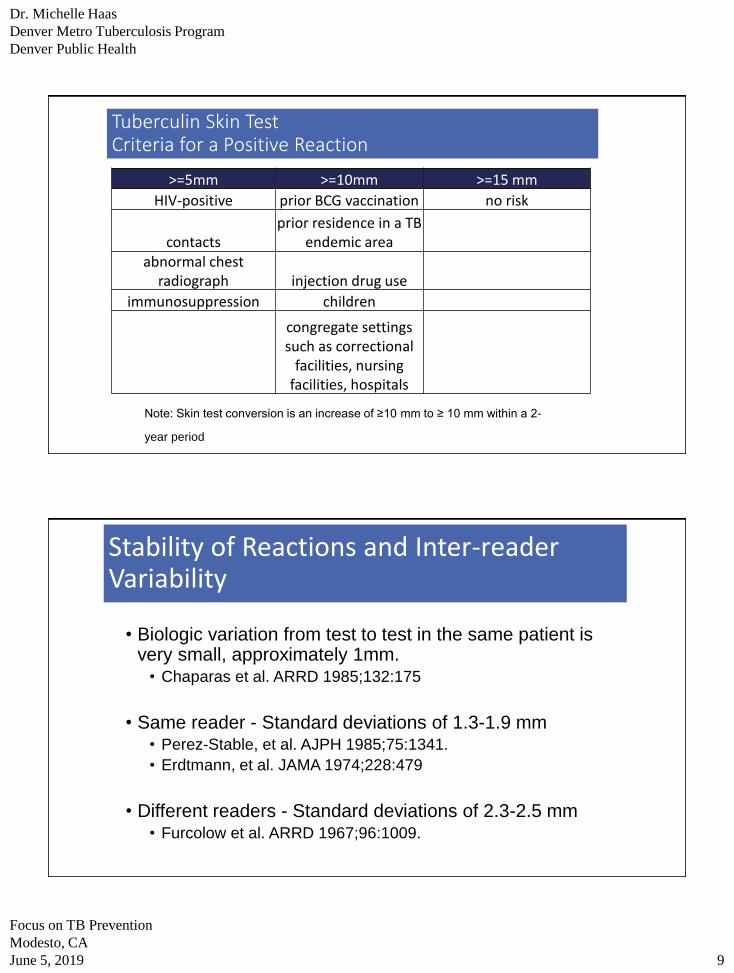
Tuberculin Skin TestCriteria for a Positive Reaction
Note: Skin test conversion is an increase of ≥10 mm to ≥ 10 mm within a 2-
year period
>=5mm >=10mm >=15 mm
HIV-positive prior BCG vaccination no risk
contactsprior residence in a TB
endemic areaabnormal chest
radiograph injection drug use
immunosuppression children
congregate settings such as correctional
facilities, nursing facilities, hospitals
Stability of Reactions and Inter-reader Variability
• Biologic variation from test to test in the same patient is very small, approximately 1mm.
• Chaparas et al. ARRD 1985;132:175
• Same reader - Standard deviations of 1.3-1.9 mm• Perez-Stable, et al. AJPH 1985;75:1341.
• Erdtmann, et al. JAMA 1974;228:479
• Different readers - Standard deviations of 2.3-2.5 mm• Furcolow et al. ARRD 1967;96:1009.
Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 10
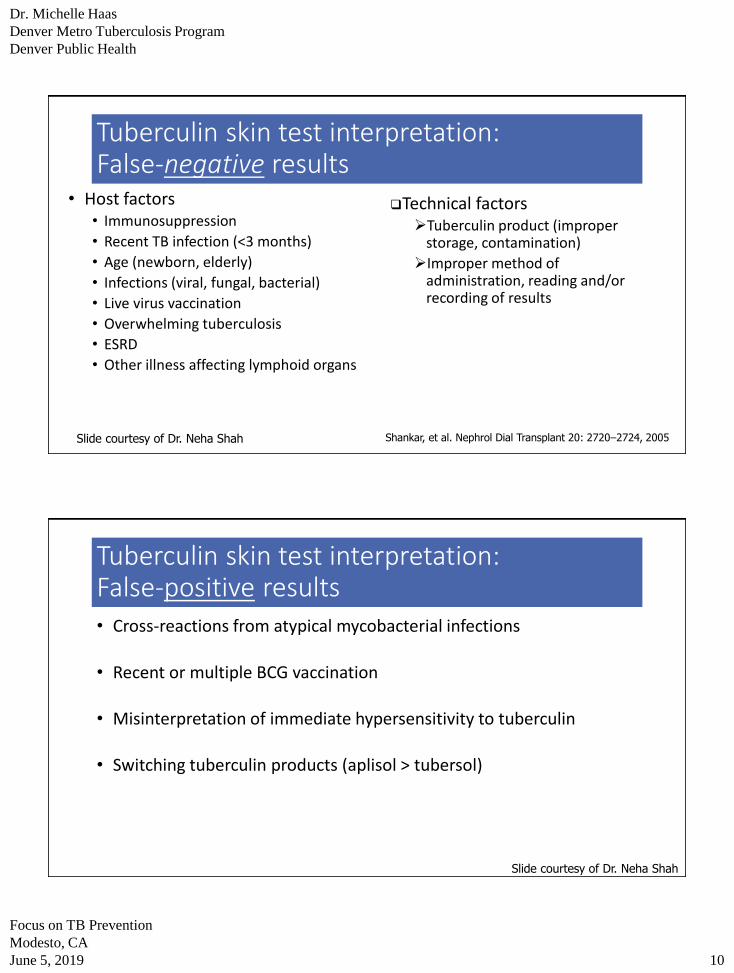
Tuberculin skin test interpretation: False-negative results
• Host factors • Immunosuppression
• Recent TB infection (<3 months)
• Age (newborn, elderly)
• Infections (viral, fungal, bacterial)
• Live virus vaccination
• Overwhelming tuberculosis
• ESRD
• Other illness affecting lymphoid organs
Shankar, et al. Nephrol Dial Transplant 20: 2720–2724, 2005
❑Technical factors ➢Tuberculin product (improper
storage, contamination)
➢Improper method of administration, reading and/or recording of results
Slide courtesy of Dr. Neha Shah
Tuberculin skin test interpretation: False-positive results • Cross-reactions from atypical mycobacterial infections
• Recent or multiple BCG vaccination
• Misinterpretation of immediate hypersensitivity to tuberculin
• Switching tuberculin products (aplisol > tubersol)
Slide courtesy of Dr. Neha Shah
Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 11
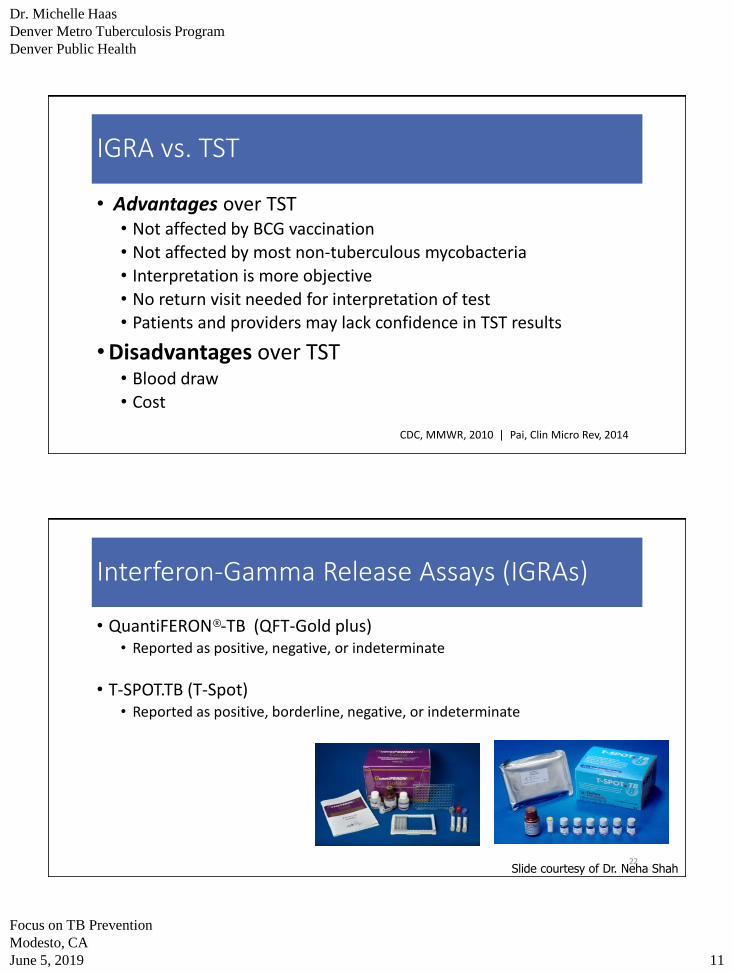
IGRA vs. TST
• Advantages over TST• Not affected by BCG vaccination
• Not affected by most non-tuberculous mycobacteria
• Interpretation is more objective
• No return visit needed for interpretation of test• Patients and providers may lack confidence in TST results
• Disadvantages over TST• Blood draw
• Cost
CDC, MMWR, 2010 | Pai, Clin Micro Rev, 2014
Interferon-Gamma Release Assays (IGRAs)
• QuantiFERON®-TB (QFT-Gold plus)• Reported as positive, negative, or indeterminate
• T-SPOT.TB (T-Spot)• Reported as positive, borderline, negative, or indeterminate
22Slide courtesy of Dr. Neha Shah
Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 12
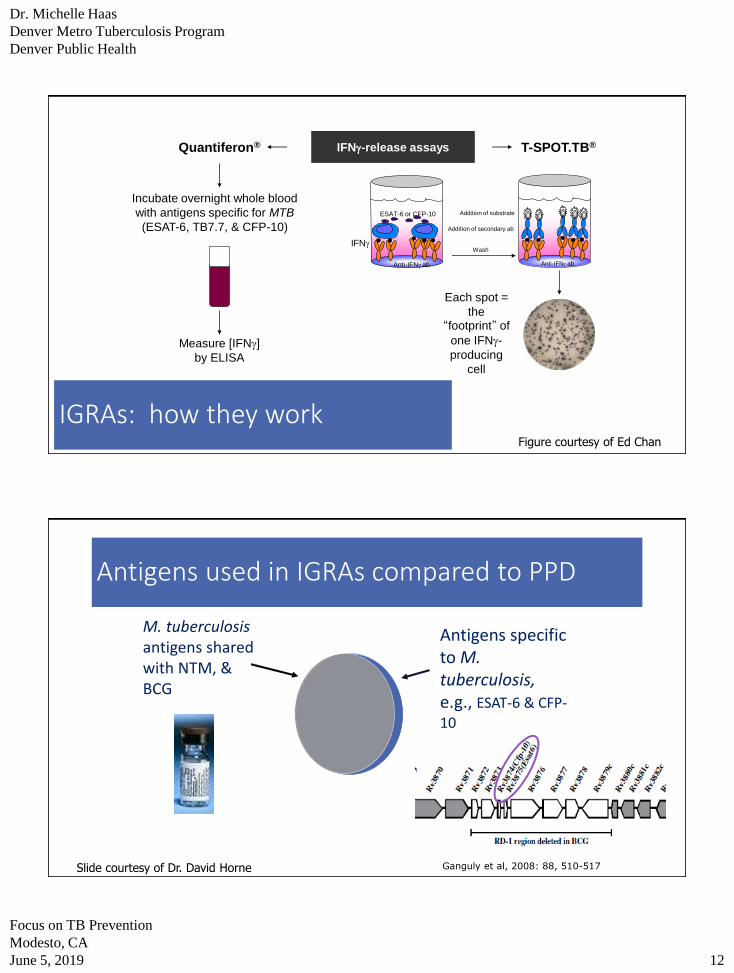
IFNg-release assays T-SPOT.TB®
Measure [IFNg]
by ELISA
Quantiferon®
Incubate overnight whole blood
with antigens specific for MTB
(ESAT-6, TB7.7, & CFP-10)
Anti-IFNg ab
IFNg
ESAT-6 or CFP-10
Wash
Anti-IFNg ab
Addition of secondary ab
Addition of substrate
Each spot =
the “footprint” of
one IFNg-
producing
cell
IGRAs: how they workFigure courtesy of Ed Chan
Antigens used in IGRAs compared to PPD
Antigens specific to M. tuberculosis, e.g., ESAT-6 & CFP-10
M. tuberculosisantigens shared with NTM, & BCG
Ganguly et al, 2008: 88, 510-517Slide courtesy of Dr. David Horne
Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 13
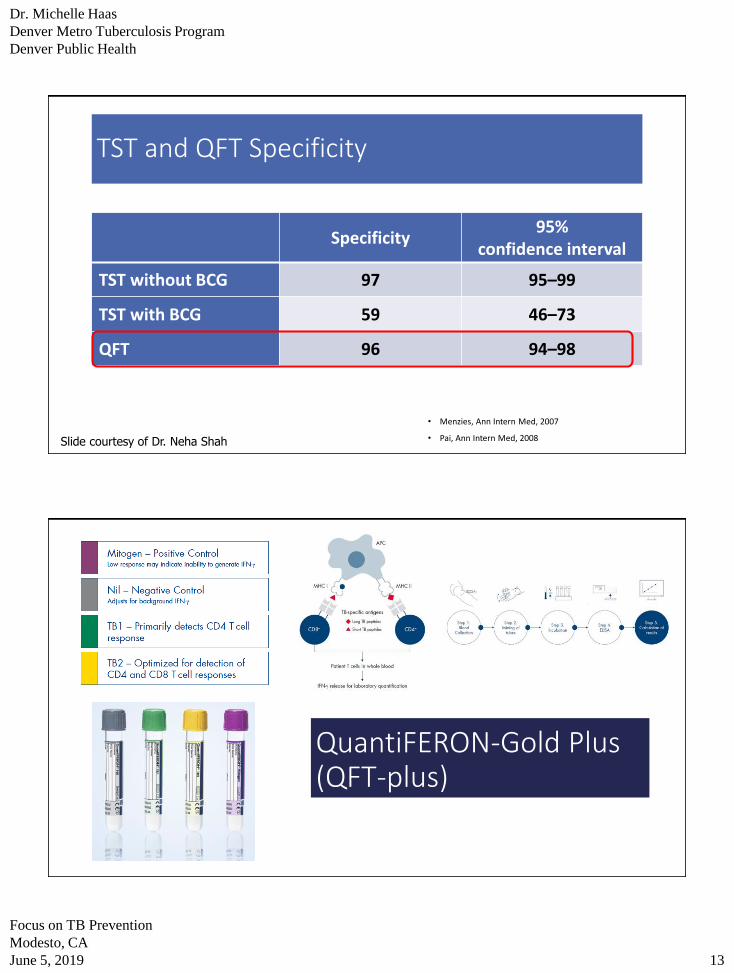
TST and QFT Specificity
Specificity95%
confidence interval
TST without BCG 97 95–99
TST with BCG 59 46–73
QFT 96 94–98
• Menzies, Ann Intern Med, 2007
• Pai, Ann Intern Med, 2008Slide courtesy of Dr. Neha Shah
QuantiFERON-Gold Plus (QFT-plus)
Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 14
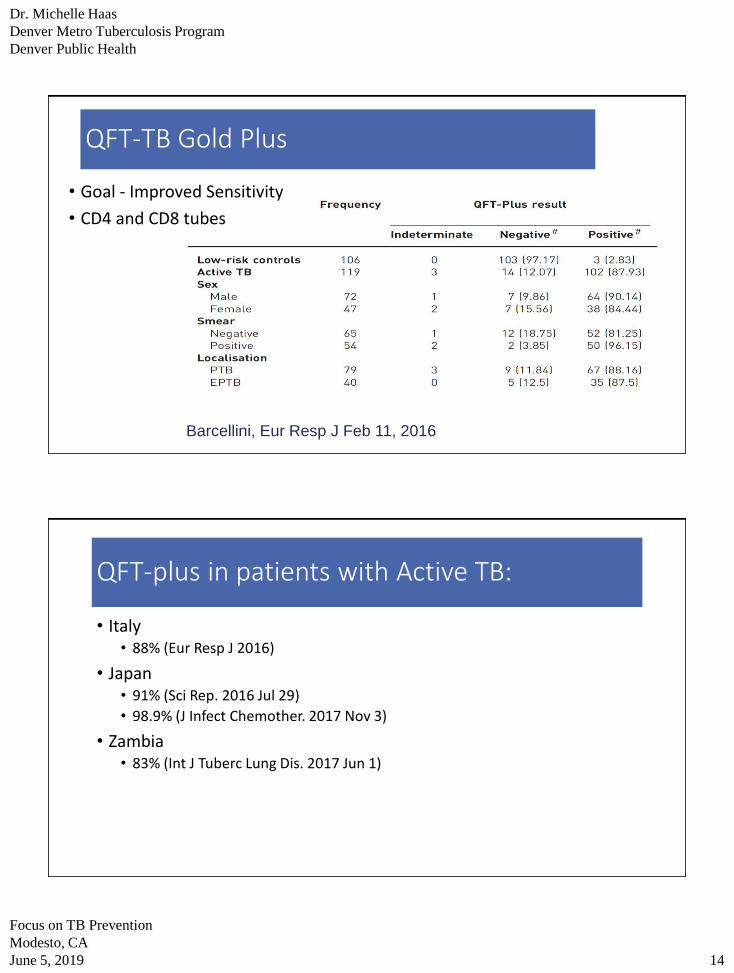
QFT-TB Gold Plus
Barcellini, Eur Resp J Feb 11, 2016
• Goal - Improved Sensitivity
• CD4 and CD8 tubes
QFT-plus in patients with Active TB:
• Italy • 88% (Eur Resp J 2016)
• Japan• 91% (Sci Rep. 2016 Jul 29)
• 98.9% (J Infect Chemother. 2017 Nov 3)
• Zambia • 83% (Int J Tuberc Lung Dis. 2017 Jun 1)
Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 15
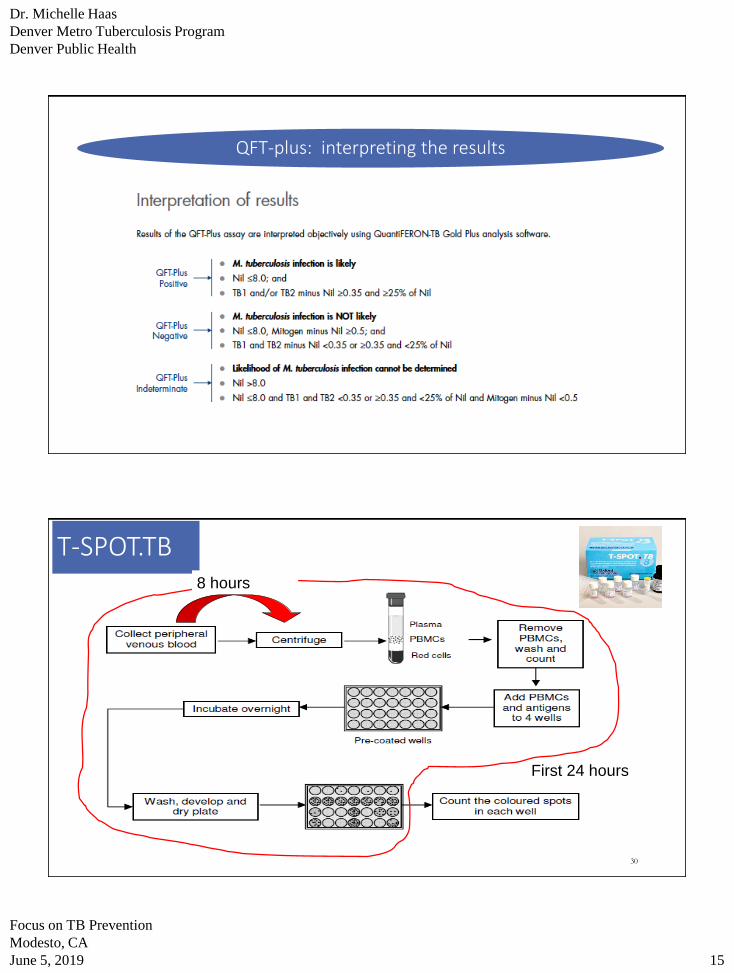
QFT-plus: interpreting the results
30
T-SPOT.TB
First 24 hours
8 hours

Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 16
T-SPOT Interpretation
Positive Negative Borderline Indeterminate
T Spot TB ≥ 8 spots* ≤ 4 spots* 5-7 spots*
Controls fail:• High Nil• Poor Mitogen
response
* (TB Ag - Nil) and assumes appropriate control responses
IGRAs –Basic similarities
• Single blood draw
• Incubate blood cells with antigens from the region of difference 1 (RD1)
• not contained in BCG but present in M.bovis
• Antigens present in M. marinum, kansasii, szulgai, and flavescens
• Results available in 1 day

Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 17
Indeterminate/borderline results
• Cannot determine whether someone has TB infection
• Low lymphocyte count
• Low lymphocyte activation potential
• Specimen collection errors
• Repeat test with valid result (pos/neg) in 68% (Banach IJTLD 2011)• Repeating the test is often the next step
Sources of variability and indeterminate results
Pai, Clin Micro Rev, 2014
• IFN-γ may vary by +0.24 IU/ml
when result between 0.25-0.80
(Metcalfe AJRCCM 2013)
• S. Africa study of serial QFTs –
“converters” who had levels <
0.7 IU/ml had same TB risk as
those with levels <0.2
IU/ml(Nemes AJRCCM 2017)
Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 18
Why do we repeat tests for TB infection?
• You don’t like the first test result so you repeat it to get the one you like
• Positive result in low risk individual (healthcare worker who is required to undergo testing)
• High risk individual who has a negative result• Repeating in person with HIV whose CD4 has risen above 200
• 8 week testing in the context of a contact investigation
Clinical Scenario #1
• 20-year-old man with prior residence in India:
• Required to undergo TB testing for college
• 11 mm TST, normal CXR
“It’s due to my BCG”• QFT positive (TB-nil = 1.15)
• TB antigen 2.08 IU, nil 0.93 IU, and mitogen > 10 IU. TB antigen- nil = 1.15 IU which was above the cutoff of > 0.35 IU that defines a positive test.
“It’s boosting from the TST. I would like to be tested again.”
What would you do next?

Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 19
Interpretation and Management
• 1- interpret QFT as positive and offer treatment for LTBI, decline his request for further testing
• 2- Attempt to explain that “boosting” from BCG still means that he was infected with TB at some point in his life, that no additional testing is needed and offer latent treatment
• 3- he lived for a long time in a TB endemic area so agree to will repeat the QFT anyway because of course it will be positive
Clinical Scenario #1
• 20-year-old man with prior residence in India:
• Required to undergo TB testing for college
• 11 mm TST, normal CXR
“It’s due to my BCG”• QFT positive (TB-nil = 1.15)
• TB antigen 2.08 IU, nil 0.93 IU, and mitogen > 10 IU. TB antigen- nil = 1.15 IU which was above the cutoff of > 0.35 IU that defines a positive test.
“It’s boosting from the TST. I would like to be tested again.”
A second QFT a few weeks later was negative (TB-nil was 0.34 IU). He believed this was the ”true” results and declined further testing
Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 20
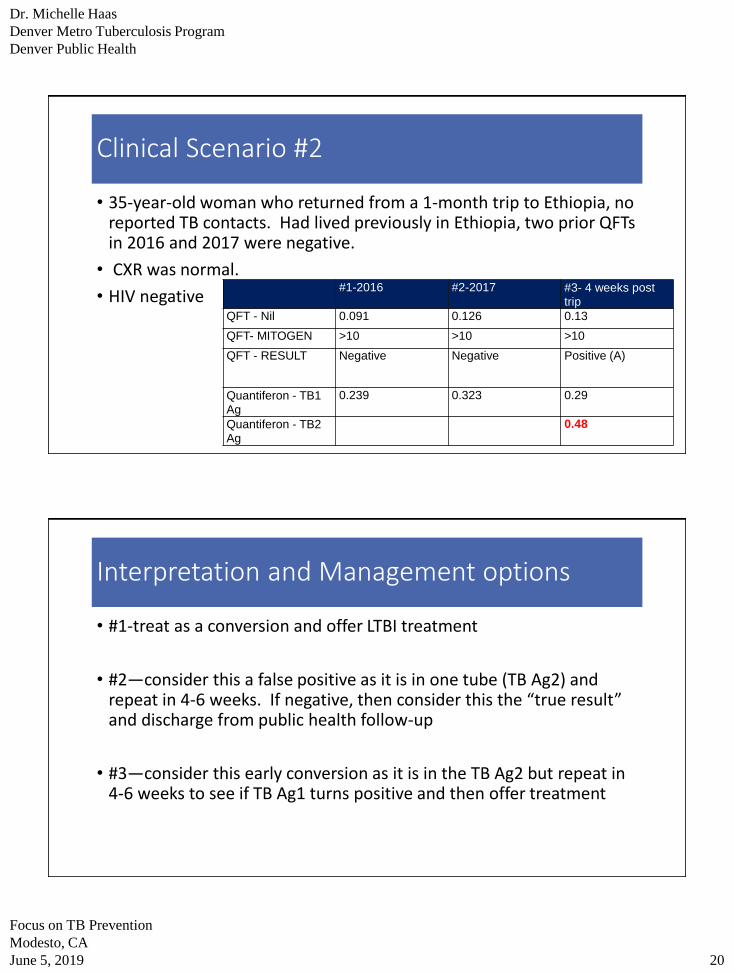
Clinical Scenario #2
• 35-year-old woman who returned from a 1-month trip to Ethiopia, no reported TB contacts. Had lived previously in Ethiopia, two prior QFTs in 2016 and 2017 were negative.
• CXR was normal.
• HIV negative#1-2016 #2-2017 #3- 4 weeks post
trip
QFT - Nil 0.091 0.126 0.13
QFT- MITOGEN >10 >10 >10
QFT - RESULT Negative Negative Positive (A)
Quantiferon - TB1
Ag
0.239 0.323 0.29
Quantiferon - TB2
Ag
0.48
Interpretation and Management options
• #1-treat as a conversion and offer LTBI treatment
• #2—consider this a false positive as it is in one tube (TB Ag2) and repeat in 4-6 weeks. If negative, then consider this the “true result” and discharge from public health follow-up
• #3—consider this early conversion as it is in the TB Ag2 but repeat in 4-6 weeks to see if TB Ag1 turns positive and then offer treatment
Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 21
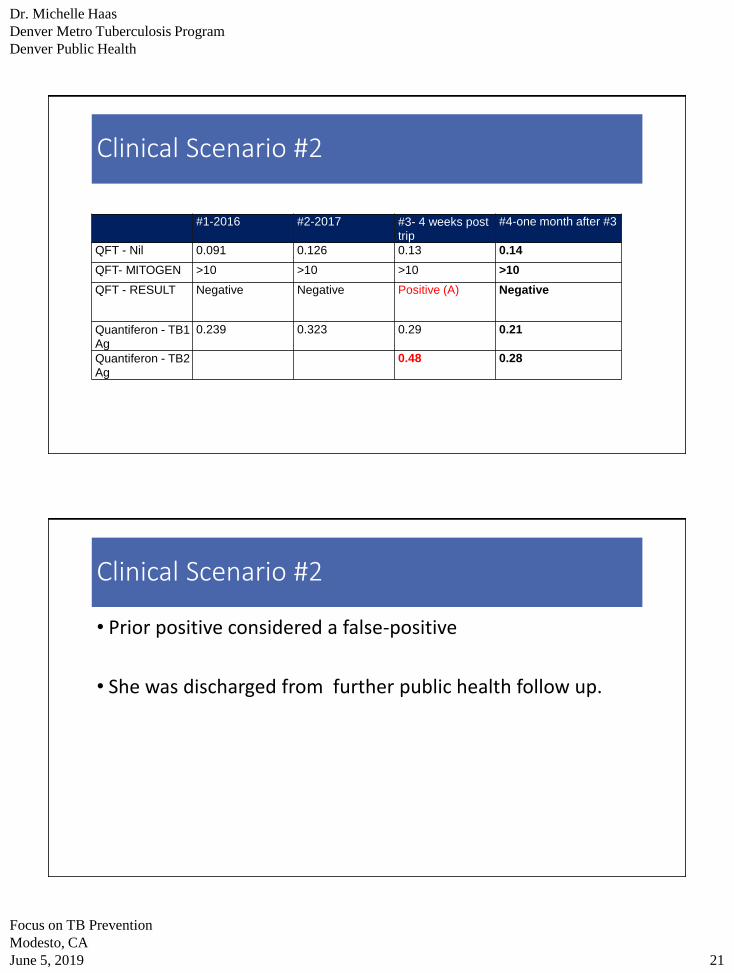
Clinical Scenario #2
#1-2016 #2-2017 #3- 4 weeks post
trip
#4-one month after #3
QFT - Nil 0.091 0.126 0.13 0.14
QFT- MITOGEN >10 >10 >10 >10
QFT - RESULT Negative Negative Positive (A) Negative
Quantiferon - TB1
Ag
0.239 0.323 0.29 0.21
Quantiferon - TB2
Ag
0.48 0.28
Clinical Scenario #2
• Prior positive considered a false-positive
• She was discharged from further public health follow up.

Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 22
• IGRA responses may change over time
• 2400 U.S. HCW, serial TST, QFT, T-SPOT (Dorman AJRCCM 2014)
• Conversions occurred: TST 0.9% QFT 6.1% T-SPOT 8.3%
IGRA Screening & Low LTBI Risk
Diagnosing Latent TB Infection
• TSTs and IGRAs cannot distinguish between latent TB infection and active TB disease
• Always evaluate for underlying active TB
• IGRAs and TSTs can be falsely negative in up to 25% of individuals with active TB
Positive TST or IGRA
Latent TB infectionActive TBdisease
? ?
Slide courtesy of Dr. Neha Shah

Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 23
Can IGRAs be use to monitor a response to treatment?
Clifford Tuberculosis 2015
• 15 studies that evaluated LTBI responses
• No consistent pattern using reversions or quantitative IFN-gamma levels
Slide courtesy of Dr. David Horne
Pros and Cons
IGRA
• in vitro
• Specific Mtb antigens
• 1 patient visit
• phlebotomy
• stimulate within hours
• results possible in 1 day
• complex laboratory test
• Much that is not understood
TST
• in vivo
• PPD
• 2 patient visits
• intracutaneous injection
• injected = done
• results in 2–3 days
• point-of-care test
• data storage—varies

Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 24
TB infection screening risk: examples of different work flows• Medical assistant asks about TB risk during rooming of the patient
• Orders IGRA or TST if at risk
• Health maintenance sections in electronic health record• Maintained by clinic nurses
• Taking a travel history only• Registration? (similar to Ebola?)• Medical assistant• Clinic nurse• Provider driven
• Assessing birth country at the time of registration
Perform TST/IGRAReason for test: ICD-10 Z91.89 “At high risk for tuberculosis infection”
Yes
No
Perform symptom screen if you determine they are at risk for TB infection: new/progressive cough for 2-3 weeks, night sweats, unexplained weight loss, subjective feverAre symptoms present?
Example Work-flow for TB infection diagnosis and treatment
Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 25
Diagnostic testing for active M. tuberculosis
Chest radiography
(AFB) sputum smear
30-50% may be AFB smear negative
AFB sputum culture—gold standard, limit of detection 10 organisms/mL sputum
Nucleic acid amplification test (NAAT) to detect M. tuberculosis in sputum samples Molecular beacon assays (”Xpert”)
Line probe assays “Hain)
MTB probe: amplified mycobacterium direct test
Your patient has no symptoms of active TB—what next?

Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 26
Perform chest radiograph and consider repeat symptom screen and/or review of systems. Are either abnormal?
IGRA/TST positive?
Evaluation for active TB and/or refer to public health
Yes
NoNo further intervention
Yes
Offer LTBI therapy if risk of developing active TB is >3%-5* by the age of 80 or greater than 0.1% annually: (http://www.tstin3d.com/)
No
Perform TST/IGRAReason for test: ICD-10 Z91.89 “At high risk for tuberculosis infection”

Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 27
Perform chest radiograph and consider repeating symptom screen. Are either abnormal?
If risk factors present, perform symptom screen. Symptom screen positive?
Evaluate for active TB/refer to public health
Yes
No
No further intervention
Yes
Offer LTBI therapy if risk of developing active TB is >3% by the age of 80 or >0.1% annually: (http://www.tstin3d.com/)Options:1) Rifampin 10mg/kg max dose 600mg daily x 4 months. Review drug
interactions.2) Isoniazid/rifapentine once weekly for 12 doses. Review drug interactions.3) INH 5mg/kg max dose 300mg daily with 25mg B6 x 9 months.
No
Example Work-flow for TB infection diagnosis and treatment
Perform QFT. QFT positive? No
LTBI Treatment: Key considerations
Efficacy• Ability to prevent
disease among individuals adhering to medication
Effectiveness (adherence)• Ability to prevent
disease when used in public health practice
Drug interactions & adverse events
Monitoring requirements,
cost, availability
Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 28
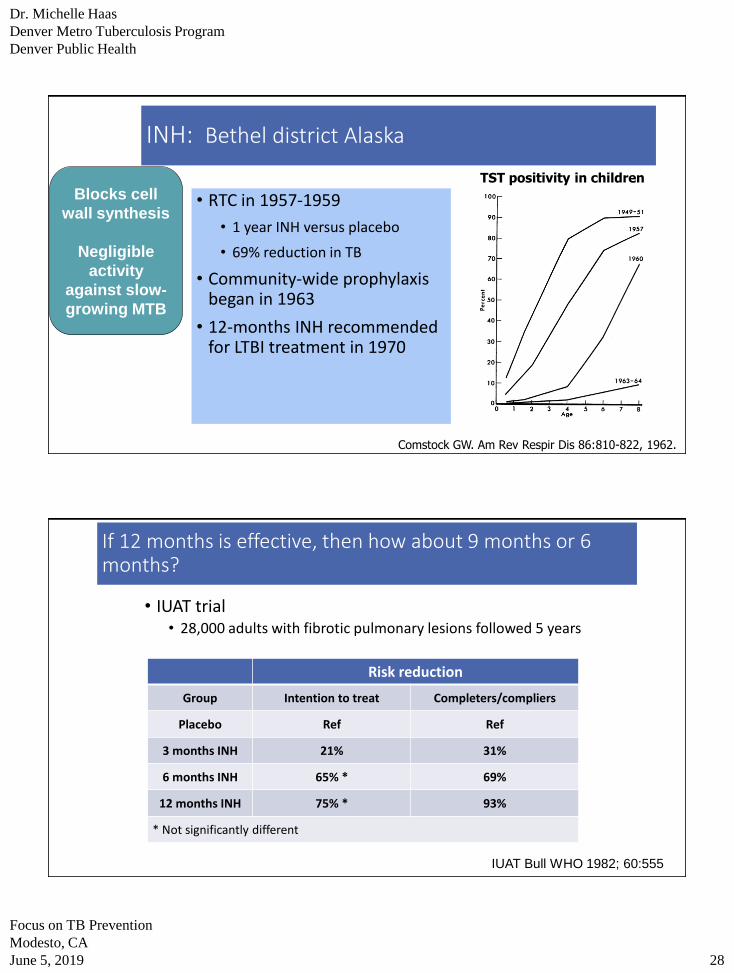
INH: Bethel district Alaska
• RTC in 1957-1959
• 1 year INH versus placebo
• 69% reduction in TB
• Community-wide prophylaxis began in 1963
• 12-months INH recommended for LTBI treatment in 1970
Comstock GW. Am Rev Respir Dis 86:810-822, 1962.
TST positivity in children
Blocks cell
wall synthesis
Negligible
activity
against slow-
growing MTB
IUAT Bull WHO 1982; 60:555
If 12 months is effective, then how about 9 months or 6 months?
• IUAT trial • 28,000 adults with fibrotic pulmonary lesions followed 5 years
Risk reduction
Group Intention to treat Completers/compliers
Placebo Ref Ref
3 months INH 21% 31%
6 months INH 65% * 69%
12 months INH 75% * 93%
* Not significantly different

Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 29
0 6 12 18 24
Months of Treatment
Cases
per 100
5
4
3
2
1
0
Observed values
Calculated curve
Calculated values
Comstock Int J Tuberc Lung Dis. 1999 3; 10:847
• Lower TB rates among
those who took 0-9
months
• No significant increase
among those who took >9
months
If 12 months is effective, then how about 9 months or 6 months?
Isoniazid: monitoring
• Check baseline labs if:
▪ HIV-positive
▪ History of liver disease
▪ Regular alcohol use
▪ Age >35
▪ Pregnant or post-partum (within 3 months)
▪ H/o injection drug use
▪ On hepatotoxic medications
• Labs during follow-up only if baseline labs elevated
or symptomatic
• Monthly follow-up recommended
Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 30
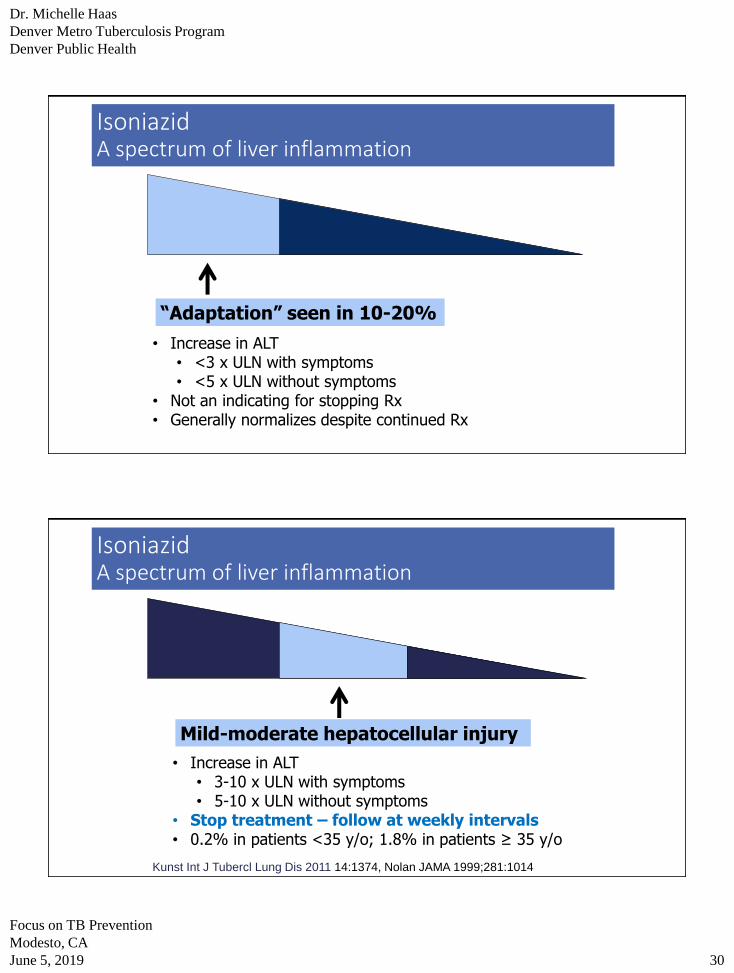
IsoniazidA spectrum of liver inflammation
“Adaptation” seen in 10-20%
• Increase in ALT • <3 x ULN with symptoms• <5 x ULN without symptoms
• Not an indicating for stopping Rx• Generally normalizes despite continued Rx
Mild-moderate hepatocellular injury
• Increase in ALT • 3-10 x ULN with symptoms• 5-10 x ULN without symptoms
• Stop treatment – follow at weekly intervals• 0.2% in patients <35 y/o; 1.8% in patients ≥ 35 y/o
Kunst Int J Tubercl Lung Dis 2011 14:1374, Nolan JAMA 1999;281:1014
IsoniazidA spectrum of liver inflammation
Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 31
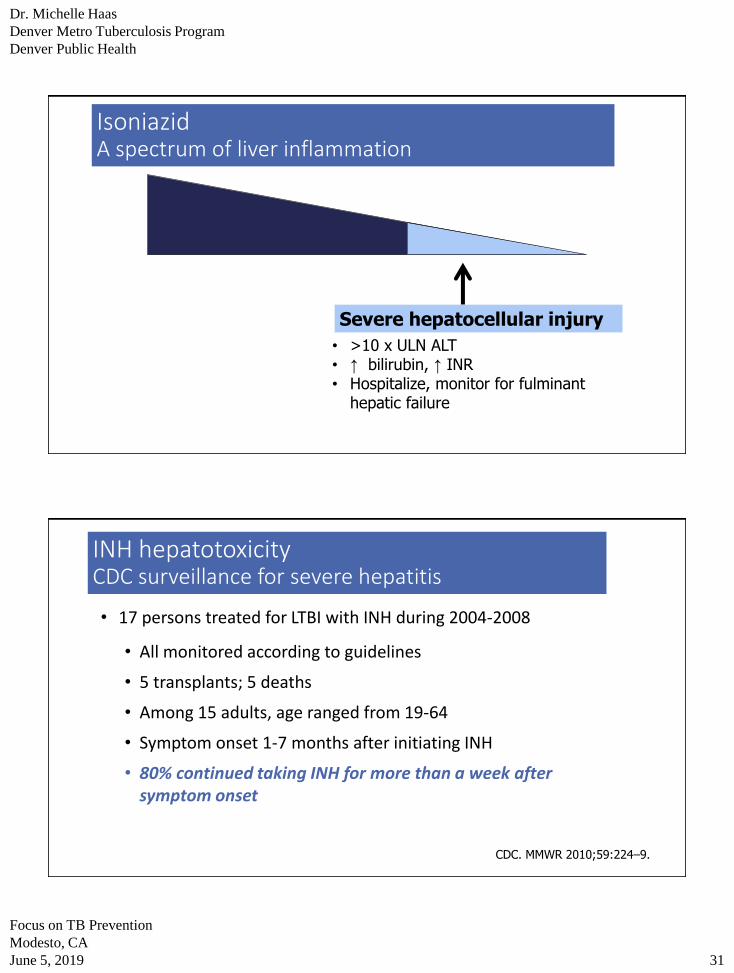
Severe hepatocellular injury
• >10 x ULN ALT • ↑ bilirubin, ↑ INR• Hospitalize, monitor for fulminant
hepatic failure
IsoniazidA spectrum of liver inflammation
INH hepatotoxicityCDC surveillance for severe hepatitis
• 17 persons treated for LTBI with INH during 2004-2008
• All monitored according to guidelines
• 5 transplants; 5 deaths
• Among 15 adults, age ranged from 19-64
• Symptom onset 1-7 months after initiating INH
• 80% continued taking INH for more than a week after symptom onset
CDC. MMWR 2010;59:224–9.

Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 32
INH ADVERSE EVENTS
• Neurologic - interference in vitamin B6 absorption
• Higher risk in DM, renal insufficiency, alcoholism, malnutrition, HIV, pregnancy, seizure disorder
• GI• Hepatotoxicity
• Nausea/vomiting
• Skin rash
• Drug interactions—always check!
Offer B6 at 25-50mg daily to individuals at higher risk for peripheral neuropathy
Self-administered rifampinEfficacy for LTBI
• 679 patients with silicosis & LTBI in Hong Kong
• Randomized to:
• Placebo - 27% developed TB within 5 years!
• 6 months INH
• 3 months INH/RIF
• 3 months RIF
Hong Kong Chest Service Am Rev Resp Dis 1992;145:36
Inhibits RNA synthesis
Potent activity against slow-
growing MTB
4 months10mg/kg = 600mg daily unless underweight

Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 33
Self-administered rifampinEfficacy for LTBI
H = isoniazidR = rifampinPl = placebo
Hong Kong Chest Service Am Rev Resp Dis 1992;145:36
63% protection relative to
placebo
Self-administered rifampin: better adherence than INH
Rifampin:
78% completion
INH:
60% completion
Menzies D, Ann Intern Med 2008; 149:689
847 adults with LTBI in Canada, Brazil & Saudi Arabia
Randomized to:
4 months RIF (n=420)
9 months INH (n=424)
Rifampin INH
Any adverse
event3.8% 5.7%
Grade 3-4
Hepatotoxicity0.7% 3.8%

Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 34
Menzies D et al. N Engl J Med 2018;379:440-453
Self-administered Rifampin
• Adverse effects
• Dyspepsia
• Orange discoloration to body fluids
• Rash
• Thrombocytopenia• Rare: neutropenia,
hemolytic anemia, thrombocytopenia
• Drug interactions
• Hormonal anti-contraceptives
• Coumadin
• Thyroid hormone
• Anti-seizure agents
• Antihypertensives
• Antipsychotics
• Plus many more
Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 35
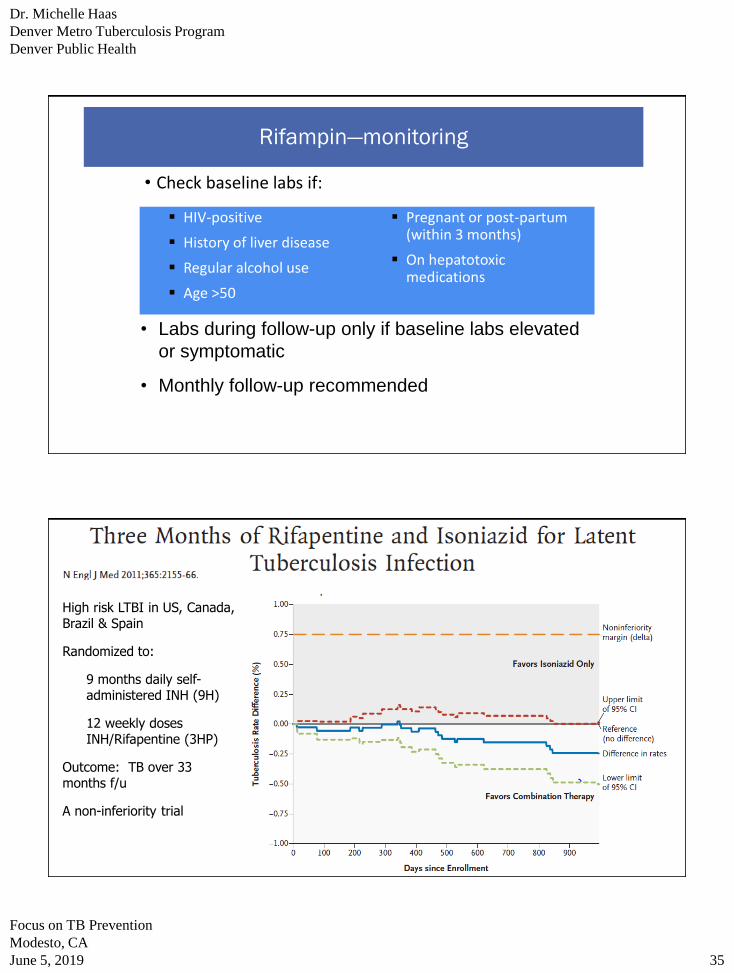
Rifampin—monitoring
• Check baseline labs if:
▪ HIV-positive
▪ History of liver disease
▪ Regular alcohol use
▪ Age >50
▪ Pregnant or post-partum (within 3 months)
▪ On hepatotoxic medications
• Labs during follow-up only if baseline labs elevated
or symptomatic
• Monthly follow-up recommended
High risk LTBI in US, Canada, Brazil & Spain
Randomized to:
9 months daily self-administered INH (9H)
12 weekly doses INH/Rifapentine (3HP)
Outcome: TB over 33 months f/u
A non-inferiority trial

Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 36
Isoniazid with rifapentine
• Adverse effects
• Dyspepsia
• Nausea/vomiting
• Fatigue
• Flu-like illness• Headaches
• Hepatotoxicity
• rash
• Drug interactions—some overlap with rifampin
• Hormonal anti-contraceptives
• Coumadin
• Antihypertensives
• antiretrovirals
Isoniazid and Rifapentine both once weekly for 12 doses
• Isoniazid: 15 mg/kg, rounded up to the nearest 50 or 100 mg; 900 mg maximum
• Rifapentine
• 10 to 14 kg: 300 mg
• 14.1 to 25 kg: 450 mg • 25.1 to 32 kg: 600 mg
• 32.1 to 49.9 kg: 750 mg
• >50 kg: 900 mg maximum
• Obtain LFTs:
• if aged >35
• has underlying liver disease
• pregnant/or within 3 months post-partum, o
• Regular EtOH consumption or taking other hepatotoxic agents

Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 37
Self-administered INH/Rifapentine: iAdhere study
• DOT
• SAT
• eSAT (with weekly text reminders)
Adherence trial with three arms:
USA (75%), Spain, Hong Kong, South Africa
Outcome: completion
Measured by self-report, pill count, MEMS
15% non-inferiority margin
Belknap R, et al. Ann Intern Med. 2017;167:689-697.
iAdhere results
• Overall• Non-inferiority not established for
SAT or eSAT
• In US • iAdhere supports use of
INH/rifapentine via SAT
DOT SATDifference from DOT
eSATDifference from DOT
ALL 86.9% 74.4% 12.4 (6.6, 18.2) 75.4% 11.8 (5.9, 17.6)
USA 85.0% 78.3% 6.8 (0.1, 13.4) 76.0% 9.5 (2.6, 16.4)

Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 38
Summary Efficacy & Completion
Regimen Efficacy Mean completion
9 months INH 90-92% 53-63%
6 months INH 41-76% 49-79%
4 months RifampinEquivalent to 9
months of INH72-79%
3 months INH -
Rifapentine
Equivalent to 9
months of INH 78%
Adapted from Landry Int J Tubercl Lung Dis 2008; 12:1352;
Menzies D, Ann Intern Med 2008; 149:689
Belknap R, et al. Ann Intern Med. 2017; 167:6
Summary
• Neither an IGRA or TST can distinguish between latent TB infection and active TB
• A negative test does not exclude active TB
• Test people at risk for infection • 1⁰ people born or lived in a high-burden country• Prioritize those with risk for exposure AND progression (HIV,
DM, ESRD etc.) on a programmatic level or clinic level to allow for scaling up of TB testing

Dr. Michelle Haas
Denver Metro Tuberculosis Program
Denver Public Health
Focus on TB Prevention
Modesto, CA
June 5, 2019 39
Summary
• Treatment for LTBI should be discussed with all patients • Recommend only for those with significant risk of
progression that outweighs the risk of adverse effects• Most experts would recommend LTBI treatment if lifetime
risk is greater than 3-5%
Patient -follow up
• Completed 12 months of treatment
• Was able to make a complete recovery!
Related Documents


![3 printable LTBI TX Keh - currytbcenter.ucsf.edunid]/3... · Sharma SK, et al. Rifamycins(rifampicin, rifabutinand rifapentine) compared to isoniazid for preventing tuberculosis in](https://static.cupdf.com/doc/110x72/5dd14202d6be591ccb64fa8d/3-printable-ltbi-tx-keh-nid3-sharma-sk-et-al-rifamycinsrifampicin-rifabutinand.jpg)








