Journal offiepafolog)~ 1999; 31: 60461 I Printed in Denrnurk All rights reserved Munksguurd Copenhu~rn Journal of Hepatology ISSN 0168-8278 Low virological response to intederon in children with chronic hepatitis C Pasqualina Pensati, Raffaele Iorio, Salvatore Botta, Concetta Tuccillo’, Sara Donetto, Pietro Vajro, Giuseppina Ciarlo and Angela Vegnente Department of Pediatriu, University of Naples “Federico II”, ‘Department of Internal Medicine “F: Mograssi”, Second University (?f Nuples, Italy Background/Aims: Children with chronic hepatitis C were recently found to have higher rates of sustained response to interferon compared to adults. The aim of this study was to verify the response to interferon using frequent viremia measurements. Methods: Sera from 25 children (13 males; mean age 7.9 years) with chronic hepatitis C, treated with re- combinant alpha-2b interferon for 12 months, were tested for liver function tests and viremia levels for a median of 27.5 months. Autoantibodies were evalu- ated during and after interferon. Results: Fifteen patients completed 12 months of in- terferon; treatment was stopped in 10 other patients. In 11 (44%) patients viremia was undetectable al- ready at the second administration of interferon; one of them remained viremia-free up to the end of fol- low-up and had persistently normal alanine-amino- transferase levels (complete sustained responder). A URRJZNTLY, C the only approved therapy for chronic hepatitis C is alpha-interferon ((x-INF) (l--3). Controlled studies in adults with chronic hepatitis C (CHC) have shown that a standard regimen of or-INF therapy induced normalization of alanine-aminotrans- ferase (ALT) serum levels during treatment in 35.-50% of the patients. Unfortunately, 50% to 80% of bio- chemical responders relapsed within 6 months of dis- continuation of therapy (4-9). With the advent of HCV genome tests, it became apparent that detectable HCV RNA in serum is a better indicator of response (10). However, HCV RNA has been found in 10-40%1 Received 9 Fehruqy; revised I9 April; accepted 26 April I999 Correspondence: Pasqualina Pensati, Dipartimento di Pe- diatria, UniversitB di Napoli “Federico II” Via Sergio Pansini n. 5 80131 Napoli, Italy. Tel: 39 81 746 3500. Fax: 39 81 545 1278. e-mail: [email protected] complete sustained response was observed only in one other patient, who normalized alanine amino- transferase and cleared viremia from the 3rd month of therapy. Three patients with persistent viremia normalized alanine-aminotransferase from the 3rd week of therapy up to the end of follow-up (biochem- ical sustained responders). Viremia was undetectable during treatment in four patients, who stopped inter- feron because of worsening in hypertransaminasemia. Three of these four patients were anti-liver-kidney microsomal type l-positive. Conclusions: In this study the response rate to inter- feron was very low and viremia and transaminase findings were often discordant. Key WV& Children; Chronic hepatitis; HCV viral load; Hepatitis C virus; Interferon alfa; Viral clear- ance. of adult patients with normal ALT serum levels after treatment with IFN (11,12). In recent studies, IFN was more effective in children than in adults in terms of ALT normalization and HCV RNA clearance (I 3-l 8). In most of these studies the virological response to IFN was evaluated on the basis of sporadic determinations of serum HCV RNA (13,15,16,18). However, a body of evidence suggests that HCV RNA level is not a constant, but varies spontaneously or as a consequence of endogenous fac- tors such as the magnitude of the immune response, medications such as corticosteroids and differences in serum sample preparation for HCV RNA determi- nation (18-23). Therefore, frequent quantitations of vi- remia during IFN therapy could provide a better measure of the response. Some pre-treatment characteristics in adults have been associated with a greater likelihood of response to a-INF; the most important are low basal levels of 604

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Journal offiepafolog)~ 1999; 31: 60461 I Printed in Denrnurk All rights reserved Munksguurd Copenhu~rn Journal of Hepatology
ISSN 0168-8278
Low virological response to intederon in children with chronic hepatitis C
Pasqualina Pensati, Raffaele Iorio, Salvatore Botta, Concetta Tuccillo’, Sara Donetto, Pietro Vajro,
Giuseppina Ciarlo and Angela Vegnente
Department of Pediatriu, University of Naples “Federico II”, ‘Department of Internal Medicine “F: Mograssi”, Second University (?f Nuples, Italy
Background/Aims: Children with chronic hepatitis C were recently found to have higher rates of sustained response to interferon compared to adults. The aim of this study was to verify the response to interferon using frequent viremia measurements. Methods: Sera from 25 children (13 males; mean age 7.9 years) with chronic hepatitis C, treated with re- combinant alpha-2b interferon for 12 months, were tested for liver function tests and viremia levels for a median of 27.5 months. Autoantibodies were evalu- ated during and after interferon. Results: Fifteen patients completed 12 months of in- terferon; treatment was stopped in 10 other patients. In 11 (44%) patients viremia was undetectable al- ready at the second administration of interferon; one of them remained viremia-free up to the end of fol- low-up and had persistently normal alanine-amino- transferase levels (complete sustained responder). A
URRJZNTLY, C the only approved therapy for chronic hepatitis C is alpha-interferon ((x-INF) (l--3).
Controlled studies in adults with chronic hepatitis C (CHC) have shown that a standard regimen of or-INF therapy induced normalization of alanine-aminotrans- ferase (ALT) serum levels during treatment in 35.-50% of the patients. Unfortunately, 50% to 80% of bio- chemical responders relapsed within 6 months of dis- continuation of therapy (4-9). With the advent of HCV genome tests, it became apparent that detectable HCV RNA in serum is a better indicator of response (10). However, HCV RNA has been found in 10-40%1
Received 9 Fehruqy; revised I9 April; accepted 26 April I999
Correspondence: Pasqualina Pensati, Dipartimento di Pe- diatria, UniversitB di Napoli “Federico II” Via Sergio Pansini n. 5 80131 Napoli, Italy. Tel: 39 81 746 3500. Fax: 39 81 545 1278. e-mail: [email protected]
complete sustained response was observed only in one other patient, who normalized alanine amino- transferase and cleared viremia from the 3rd month of therapy. Three patients with persistent viremia normalized alanine-aminotransferase from the 3rd week of therapy up to the end of follow-up (biochem- ical sustained responders). Viremia was undetectable during treatment in four patients, who stopped inter- feron because of worsening in hypertransaminasemia. Three of these four patients were anti-liver-kidney microsomal type l-positive. Conclusions: In this study the response rate to inter- feron was very low and viremia and transaminase findings were often discordant.
Key WV& Children; Chronic hepatitis; HCV viral load; Hepatitis C virus; Interferon alfa; Viral clear- ance.
of adult patients with normal ALT serum levels after treatment with IFN (11,12).
In recent studies, IFN was more effective in children than in adults in terms of ALT normalization and HCV RNA clearance (I 3-l 8). In most of these studies the virological response to IFN was evaluated on the basis of sporadic determinations of serum HCV RNA (13,15,16,18). However, a body of evidence suggests that HCV RNA level is not a constant, but varies spontaneously or as a consequence of endogenous fac- tors such as the magnitude of the immune response, medications such as corticosteroids and differences in serum sample preparation for HCV RNA determi- nation (18-23). Therefore, frequent quantitations of vi- remia during IFN therapy could provide a better measure of the response.
Some pre-treatment characteristics in adults have been associated with a greater likelihood of response to a-INF; the most important are low basal levels of
604

IFN treatment in children with chronic hepatitis C
serum HCV RNA, the absence of cirrhosis on the pre- treatment liver biopsy specimen, and the presence of a genotype other than lb (24-26).
To our knowledge, there is a lack of exhaustive data about basal viral load and its fluctuations during and after IFN treatment in children with CHC. We meas- ured HCV RNA levels, using frequent quantitations of viremia, in 25 children with CHC, treated with ol-IFN for 12 months. The aim of our study was to obtain a more accurate definition of end-of-treatment response and of sustained response (after 18 months of post- therapy follow-up). In addition, because IFN therapy is expensive, long-lasting and associated with several, and sometimes severe, side effects (27,28), we also attempted to identify parameters, particularly virolog- ic parameters such as HCV RNA levels and genotype, that could predict the response to IFN, in order to better select patients who could benefit from the treat- ment.
Materials and Methods Twenty-five consecutive patients (13 males; mean age 7.7 years; range 2.8-14.5 years) with CHC, attending the Liver Unit of the Depart- ment of Pediatrics of the University of Naples “Federico II”, were included in a prospective study lasting from November 1995 to June 1998. The patients’ basal characteristics are listed in Table 1.
TABLE 1
Basal characteristics of 25 patients with CHC
Male/Female/Median age 13/12/7.7 years (range 2.8-14.5)
Source of infection: No. pts (%) Blood transfusion 10 (40) Vertical transmission ll(44) Minor surgery 2 (8) Minor parenteral exposure 1 (4) Unknown 1 (4)
Median duration of HCV infection
Median ALT serum levels Median HCV RNA serum levels
3.4 years (range 0.5-l 1 .l)
89 U/l (range 62-200) 3.587X 10^6 Eq/ml (range 0.202-21.395)
Genotype: la lb 2a
3a 2a+lb 2a+2c
Histological features: Minimal chronic hepatitis Mild chronic hepatitis Moderate chronic hepatitis Severe chronic hepatitis
HCV positivity in parents:
Mother Mother and father None Unknown
no. pts (%)
6 (24) 13 (52)
3 (12) 1 (4) 1 (4) 1 (4)
no. pts (%)
4 (16) 15 (60)
6 (24) None (0) no. pts (%)
7 (28) 4 (16)
13 (52)
1 (4)
Diagnosis Chronic hepatitis C was diagnosed on the basis of elevated serum ALT levels (1.5 times above the normal range on at least two oc- casions) over 6 months, anti-HCV antibodies revealed by a third-gen- eration recombinant immunoblot assay (Ortho Diagnostic System, Raritan, NY, USA), serum HCV RNA and histological evidence of chronic hepatitis. Liver biopsy was performed in all patients within the 6 months before enrollment in the study, and liver histology was evaluated according to the criteria of Scheuer & Desmet et al. (29,30).
Causes of chronic liver disease other than HCV were excluded in all patients. None of the patients showed serological evidence of hepa- titis B virus (HBV), cytomegalovirus or human immunodeficiency vi- rus infection. Serum values of alpha-l antitrypsin were within the normal range. Autoimmune hepatitis was ruled out according to the criteria established by the International Autoimmune Hepatitis Group (31). Hemochromatosis was excluded on the basis of normal serum concentrations of iron, transferrin and ferritin. Ceruloplasmin serum concentration and urinary copper excretion were normal, thus ruling out Wilson’s disease. No patient had clinical and/or laboratory evidence of other more common inborn errors of metabolism associ- ated with hypertransaminasemia, such as galactosemia, hereditary fructose intolerance, glycogen storage disease, ornithine carbamyl transferase deficiency, tyrosinemia, mitochondrial cytopathies, Gaucher’s disease, and Niemann-Pick disease. No patient had evi- dence of drug- or toxin-induced liver injury.
Patients with cirrhosis or chronic systemic diseases were also ex- cluded. At the beginning of IFN treatment all the enrolled patients were asymptomatic and none had a history of acute liver injury, ma- lignancy, or prior use of IFN preparations.
IFN therapy Patients received recombinant a-2b IFN at the dosage of 5 million units (MU) per square meter of body surface, intramuscularly, three times a week for 12 months. According to previous studies (l&32,33), treat- ment was discontinued in case of severe side effects, including increases of ALT values to more than 6 times the upper reference limit, or because ALT levels did not decrease after 6 months of treatment. Interferon dis- continuation was not based on viremia because HCV RNA serum levels were determined at the end of the study in all patients.
Follow-up schedule Blood samples for serum HCV RNA and ALT determinations were collected at the following times: 2 weeks and 1 week before IFN ther- apy, weekly for the first 3 weeks of treatment, monthly until the 6th month of therapy, at the 9th and 12th month of therapy, and, there- after, at the lst, 3rd, 6th, 12th and 18th month of post-therapy follow- up. On the same occasions, clinical evaluation, hematological tests and the usual liver function tests were also performed. In all patients, serum HCV RNA determinations were performed at the end of fol- low-up. The baseline serum HCV RNA concentration for each pa- tient was calculated as the mean of the HCV RNA concentration determined at weeks -2 and - 1.
Because both CHC and IFN treatment may be associated with autoimmunity, cryoglobulinemia and thyroid diseases (3438), all pa- tients were tested, before enrollment, every 3 months during therapy and every 6 months after therapy, for antinuclear (ANA), anti-smooth muscle (SMA), anti-liver-kidney microsomal type 1 (LKM-1) and anti-gastric parietal cell (GPC) autoantibodies, cryoglobulins, total
thyroxine (T4), free thyroxine (fT4), total tri-iodothyronine (T3), free tri-iodothyronine (ff3), and thyroid stimulating hormone (TSH).
Approval Each patient’s parent gave written informed consent to the study. The study was approved by our Hospital Ethics Committee. The Declar- ation of Helsinki on experimentation in humans was observed in all aspects of this study.
Virological studies Blood samples for serum HCV RNA determination were centrifuged within 2 h of collection and immediately separated. Serum samples
605
P. Pensati et al.
TABLE 2
Type of response to IFN therapy at the end of treatment and during post-therapy follow-up in 25 children with CHC
End of IFN therapy 1st month post-therapy follow-up 6th month post-therapy follow-up 12th month post-therapy follow-up 18th month post-therapy follow-up
Complete Virological Biochemical No response response response response
3 (12%) 0 4* (16%) 18 (56%) 3# (12%) 0 2 (8%) 20 (80%) 2 (8%) 0 3 ( 12%) 20 (80%) 2 (8%) 0 3 ( 12%) 20 (80%) 2 (8%) 0 3 (12%) 20 (80%)
Values are given as number of patients with different type of response * 2 of these patients became nonresponders. # 1 of these patients became a biochemical responder.
were stored in aliquots at -80” C until the analysis was performed. The HCV RNA titer was measured with the most recent version of the branched-chain DNA (bDNA) assay (Quantiplex HCV-RNA 2.0 Assay, Chiron Corporation Emeryville, CA, USA). This version is more sensitive than version 1.0, having a sensitivity limit of approxi- mately 200 000 equivalent genomes/ml. In addition, it is less depend- ent on HCV genetic variability and provides a more accurate quant- itation of genotypes 2 and 3 (39).
In patients with serum HCV RNA levels below the bDNA 2.0 as- say detection threshold, a commercially available reverse trancriptase polymerase chain reaction (RTPCR) method (Amplicor, Roche Mol- ecular Diagnostic System, Branchburg. NJ, USA) was used to detect serum HCV RNA. This method has a sensitivity limit of about 100 copies/ml. Genotypes were determined by reverse hybridization with a probe hybridization assay (InnoLiPA HCV Innogenetics, Ghent, Belgium) that has been shown to accurately identify HCV genotypes 1 through 6, according to the classification proposed by Simmonds et al. (40).
Criteria for response
The criteria for response are according to Lindsay (7). Complete end- of-treatment response was defined as normalization of serum ALT and undetectable serum HCV RNA by RTPCR during and up to the
25
20
15
# .$ 10 a
“0
E5
0
I
end of treatment. Complete sustained response was defined as the persistence of this response until the end of the post-therapy follow- up. The occurrence, during treatment, of undetectable HCV RNA by RT-PCR or serum ALT normalization, persisting until the end of therapy, was considered to be a virologicul and a biochemical end-of’ treatment response, respectively. The same conditions persisting until the end of post-therapy follow-up were considered to be a virological and a biochemical sustnined response, respectively. The term relupsc
was used to describe an increase of ALT serum levels or the appear- ance of HCV RNA after a biochemical or virological end-of-treat- ment response.
IFN side ejJect.7 All patients and their parents were invited to record on a diary-card the side effects that occurred during IFN therapy; cards were col- lected at each consultation. Evaluation and management of IFN-re- lated adverse reactions were as previously reported (28).
Statistical analysis
Results were expressed as median and range unless indicated other- wise. The Mann-Whitney U and Fisher exact tests were used for stat- istical analysis. In all cases, a p-value co.05 indicated statistical sig- nificance.
2 3 8 12 4 5 6 9 12 1 3 6 12
I i Weeks of IFN therapy ’ Months of post-therapy
follow-up No. of patients tested at each control: 25 25 25 25 25 23 20 20 15 15 25 25 25 25
18
-I
25
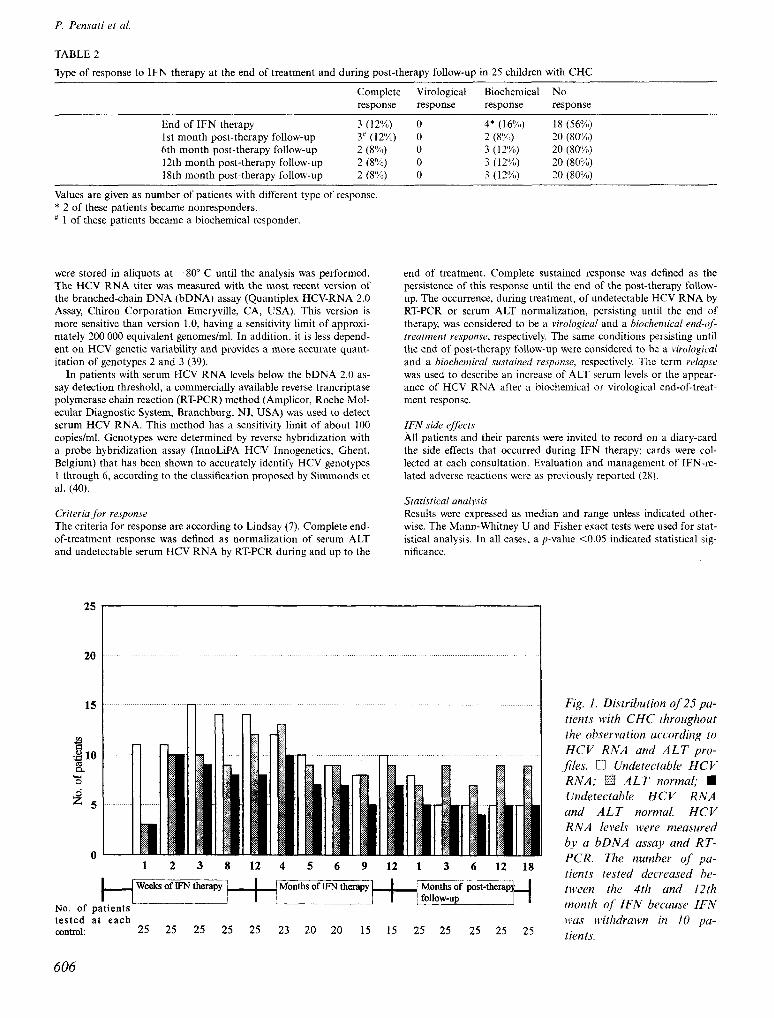
Fig. 1. Distribution of 25 pa- tients with CHC throughout the observation uccording to HCV RNA und ALT pro- Jiles. q Undetectuble HCV RNA; q ALT normal; n Undetectable HCV RNA and ALT normal. HCV RNA levels were measured by a bDNA assay and RT- PCR. The number of’ pu- tients tested decreased be- tween the 4th and 12th month of IFN becuuse IFN wus cc?thdrawn in IO pu- tients.
606
IFN treatment in children with chronic hepatitis C
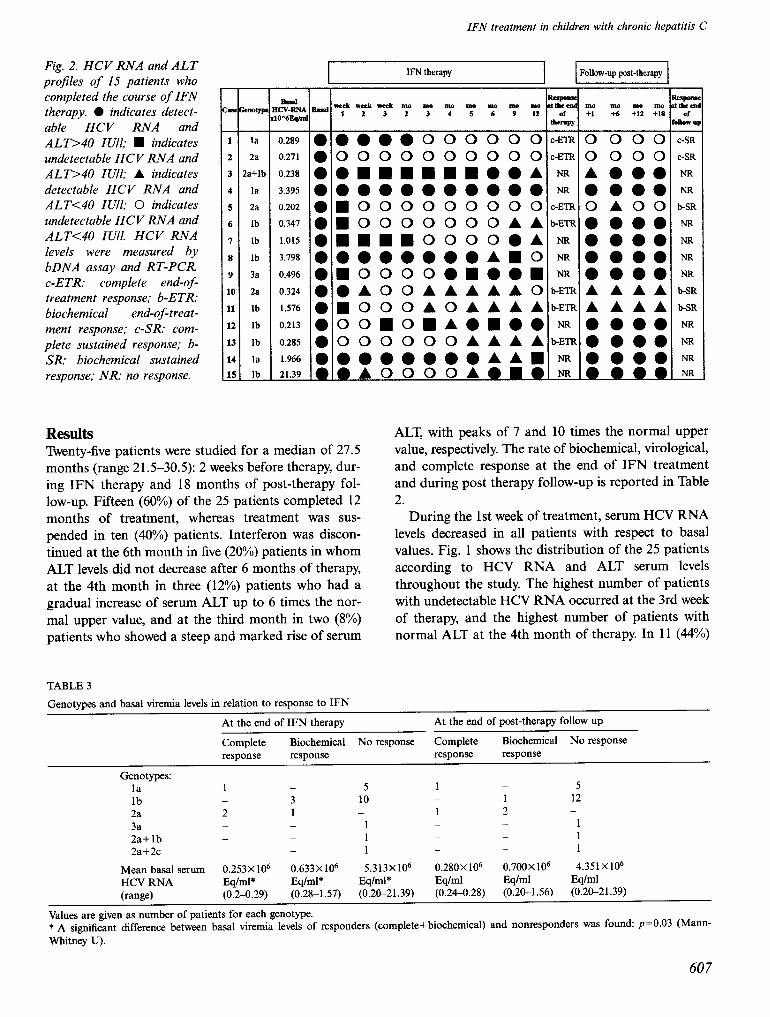
Fig. 2. HCV RNA and ALT projiles of 15 patients who completed the course of IFN therapy. l indicates detect- able HCV RNA and ALT>40 IUll; W indicates undetectable HCV RNA and ALT>IO IUll; A indicates detectable HCV RNA and ALT<IO Ml; 0 indicates undetectable HCV RNA and ALT<40 IUll. HCV RNA levels were measured by bDNA assay and RT-PCR. c-ETR: complete end-of- treatment response; b-ETR:
biochemical end-of-treat- ment response; c-SR: com- plete sustained response; b- SR biochemical sustained
response,. NR: no response.
1
2
3
4
5
6
I
8
9
10
11
12
13
14
15 -
- la
2a
!a+lb
la
2a
lb
lb
lb
3a
2a
lb
lb
lb
la
lb -
0.289
0.271
0.238
3.395
0.202
0.347
1.015
3.798
0.496
0.324
1.576
0.213
0.285
1.966
21.39
IFN therapy
*ul we& We& 4 1110 Dy) In0 IIY) 1110 In0 Ino 1 2 3 1 3 * s 6 9 IS
l aaoaoooooo
~0000000000
•o~m~~~~.aA
l oooooooooo
~~000000000
l woooooooAr
l mu~~oooo.A
l OOOOOOOA~~
l ~ooooomoem
l eAOOAAAAA0 l UOOOAOAAAA l oomomremee l OOOOOOAAAA
Results Twenty-five patients were studied for a median of 27.5 months (range 21.5-30.5): 2 weeks before therapy, dur- ing IFN therapy and 18 months of post-therapy fol- low-up. Fifteen (60%) of the 25 patients completed 12 months of treatment, whereas treatment was sus- pended in ten (40%) patients. Interferon was discon- tinued at the 6th month in five (20%) patients in whom ALT levels did not decrease after 6 months of therapy, at the 4th month in three (12%) patients who had a gradual increase of serum ALT up to 6 times the nor- mal upper value, and at the third month in two (8%) patients who showed a steep and marked rise of serum
?2? of
hmPY
z-i C-ETR
NTt
NR
c-ETl?
bETR
NR
NR
NR
b-ETA
b-ETA
NR
b-ETF
NR
NR
0ucWup post-therapy
In0 no Ino mo +1 +6 +n +18
0 000
0000
A0.e
l eee
OAOO l eee l eee l eeo l eee AAAA AAAA l eee l eee l eeo
zzi of
laov-q
C-SR
c-SR
NR
NR
b-SR
NR
NR
NR
NR
b-SR
b-SR
NR
NR
NR
NR
ALT, with peaks of 7 and 10 times the normal upper value, respectively. The rate of biochemical, virological, and complete response at the end of IFN treatment and during post therapy follow-up is reported in Table 2.
During the 1st week of treatment, serum HCV RNA levels decreased in all patients with respect to basal values. Fig. 1 shows the distribution of the 25 patients according to HCV RNA and ALT serum levels throughout the study. The highest number of patients with undetectable HCV RNA occurred at the 3rd week of therapy, and the highest number of patients with normal ALT at the 4th month of therapy. In 11 (44%)
TABLE 3
Genotypes and basal viremia levels in relation to response to IFN
At the end of IFN therapy At the end of post-therapy follow up
Complete Biochemical No response Complete Biochemical No response response response response response
Genotypes: la 1 5 1 _ _ 5 lb - 3 10 _ 1 12 2a 2 1 _ 1 2 3a _ - _ - 1 1 2a+lb _ _ 1 _ _ 1 2a+2c _ _ _ _ 1 1
Mean basal serum 0.253x lo6 0.633x lo6 5.313X106 0.280X lo6 0.700x 106 4.351x106 HCV RNA Eq/ml* Eq/ml* Eq/ml* Eqlml Eqlml Eq/ml
(range) (0.2-0.29) (0.28-1.57) (0.2c21.39) (0.24-0.28) (0.20-1.56) (0.2c21.39)
Values are given as number of patients for each genotype. * A si@icant difference between basal viremia levels of responders (complete+biochemical) and nonresponders was found: ~~0.03 (Mann- Whitney U).
607
P. Pensati et al.
1000 HCV-RNA xl C% Eq/d
L /
la lb 2a 3a 2a+zc Ib+2a
Genotype
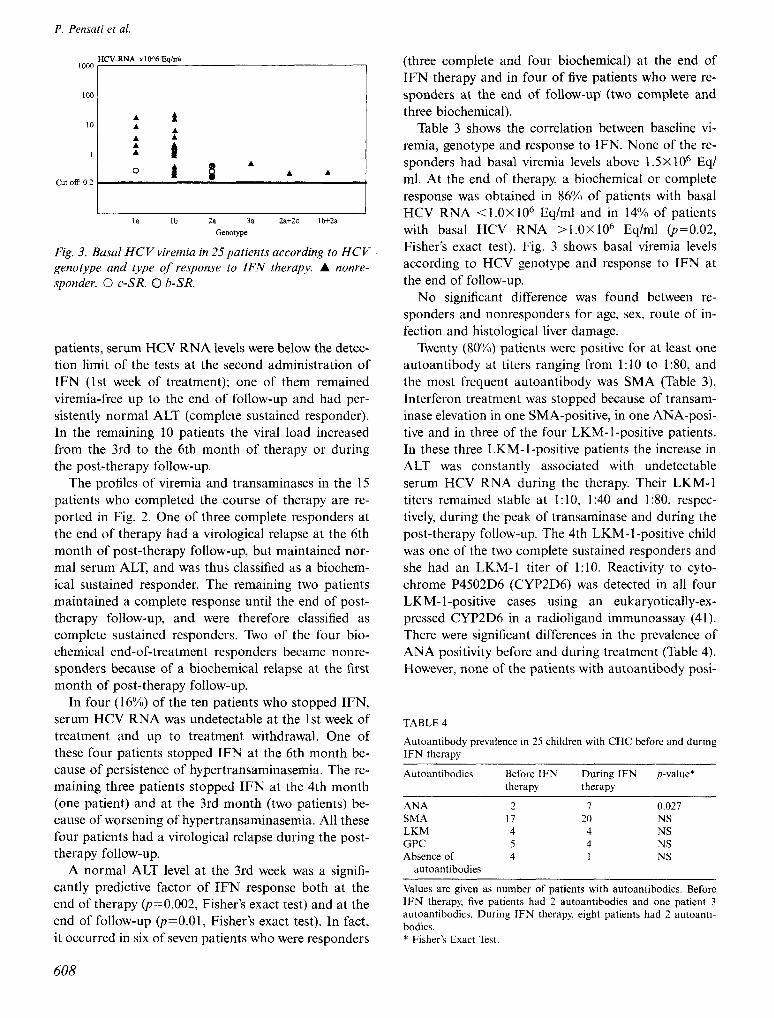
Fig. 3. Basal HCV viremia in 25 patients according to HCV genotype and type of response to IFN therupy. A nonre- sponder. 0 c-SR. 0 h-SR.
patients, serum HCV RNA levels were below the detec- tion limit of the tests at the second administration of IFN (1st week of treatment); one of them remained viremia-free up to the end of follow-up and had per- sistently normal ALT (complete sustained responder). In the remaining 10 patients the viral load increased from the 3rd to the 6th month of therapy or during the post-therapy follow-up.
The profiles of viremia and transaminases in the 15 patients who completed the course of therapy are re- ported in Fig. 2. One of three complete responders at the end of therapy had a virological relapse at the 6th month of post-therapy follow-up, but maintained nor- mal serum ALT, and was thus classified as a biochem- ical sustained responder. The remaining two patients maintained a complete response until the end of post- therapy follow-up, and were therefore classified as complete sustained responders. Two of the four bio- chemical end-of-treatment responders became nonre- sponders because of a biochemical relapse at the first month of post-therapy follow-up.
In four (16%) of the ten patients who stopped IFN, serum HCV RNA was undetectable at the 1st week of treatment and up to treatment withdrawal. One of these four patients stopped IFN at the 6th month be- cause of persistence of hypertransaminasemia. The re- maining three patients stopped IFN at the 4th month (one patient) and at the 3rd month (two patients) be- cause of worsening of hypertransaminasemia. All these four patients had a virological relapse during the post- therapy follow-up.
A normal ALT level at the 3rd week was a signifi- cantly predictive factor of IFN response both at the end of therapy (p=O.O02, Fisher’s exact test) and at the end of follow-up Cp=O.Ol, Fisher’s exact test). In fact, it occurred in six of seven patients who were responders
(three complete and four biochemical) at the end of IFN therapy and in four of five patients who were re- sponders at the end of follow-up (two complete and three biochemical).
Table 3 shows the correlation between baseline vi- remia, genotype and response to IFN. None of the re- sponders had basal viremia levels above 1.5X lo6 Eq/ ml. At the end of therapy, a biochemical or complete response was obtained in 86% of patients with basal HCV RNA < 1.0X 10” Eq/ml and in 14% of patients with basal HCV RNA >l.OX lo6 Eq/ml @=0.02, Fisher’s exact test). Fig. 3 shows basal viremia levels according to HCV genotype and response to IFN at the end of follow-up.
No significant difference was found between re- sponders and nonresponders for age, sex, route of in- fection and histological liver damage.
Twenty (80%) patients were positive for at least one autoantibody at titers ranging from 1: 10 to 1:80, and the most frequent autoantibody was SMA (Table 3). Interferon treatment was stopped because of transam- inase elevation in one SMA-positive, in one ANA-posi- tive and in three of the four LKM-l-positive patients. In these three LKM-l-positive patients the increase in ALT was constantly associated with undetectable serum HCV RNA during the therapy Their LKM-1 titers remained stable at 1: 10, 1:40 and 1:80, respec- tively, during the peak of transaminase and during the post-therapy follow-up. The 4th LKM-l-positive child was one of the two complete sustained responders and she had an LKM-1 titer of 1:lO. Reactivity to cyto- chrome P4502D6 (CYP2D6) was detected in all four LKM-l-positive cases using an eukaryotically-ex- pressed CYP2D6 in a radioligand immunoassay (41). There were significant differences in the prevalence of ANA positivity before and during treatment (Table 4). However, none of the patients with autoantibody posi-
TABLE 4
Autoantibody prevalence in 25 children with CHC before and during IFN therapy
Autoantibodies Before IFN During IFN therapy therapy
p-value*
ANA SMA LKM GPC Absence of
autoantibodies
2 7 0.027 17 20 NS 4 4 NS 5 4 NS 4 1 NS
Values are given as number of patients with autoantibodies. Before IFN therapy, five patients had 2 autoantibodies and one patient 3 autoantibodies. During IFN therapy, eight patients had 2 autoanti- bodies. * Fisher’s Exact Test.
608
IFN treatment in children with chronic hepatitis C
tivity fulfilled the score criteria for a diagnosis of “de- finite” or “probable” autoimmune hepatitis (31).
A transitory influenza-like syndrome, characterized by fever, chills, myalgia and arthralgia, occurred in all patients soon after starting treatment. The most fre- quent side effects were anorexia, abdominal pain, headache, myalgia, vomiting, and irritability All pa- tients experienced at least one adverse reaction to IFN treatment; 80% had more than 5 side effects. In two children, who experienced a severe reaction (febrile seizure and relapsing episodes of epistaxis, respec- tively), IFN had been stopped at the 4th month of therapy, also because of increases in ALT serum levels up to 6 times the normal upper value. In seven children (28%) the neutrophil count fell below lOOO/mmc and promptly increased when IFN was temporarily discon- tinued. There was no evidence of cryoglobulinemia and thyroid disorders in any patient.
Discussion This study has brought to light new aspects of the effi- cacy of IFN therapy in children with CHC. Only 8% of treated children of our study had a complete sustained response at the 18th month of post-therapy follow-up versus 3340% recently reported in other pediatric studies (17,18). This discrepancy is probably attribu- table to two factors: the virological response in other studies was evaluated on the basis of sporadic determi- nations of HCV RNA serum levels; and the very strict response criteria used in our study. If we had con- sidered HCV RNA serum levels only at the end of treatment and at the end of post-therapy follow-up, the rate of complete response would have been 20% and 12%, respectively. Our data are consistent with a recent international randomized controlled trial, in which 1071 adults with CHC were treated with different types of IFN (42). In the latter study the rate of sustained response (at the 12th month of post-therapy follow-up) was 6.7% in patients treated with IFN-a-2b.
Our data also show that a biochemical response does not correspond to a virological response. In fact, at the end of therapy, only three of seven patients, and at the end of post-therapy follow-up, only two of five patients with persistent ALT normalization had cleared HCV RNA. Consequently, persistent ALT nor- malization is not invariably associated with a virolo- gical response. Moreover, in four patients in whom IFN was withdrawn because of persistence or worsen- ing of hypertransaminasemia, HCV RNA was un- detectable throughout the treatment period.
In our study, a biochemical response was more fre- quent than a virological response: 8% of patients had a complete sustained response and 20% had long-term
ALT normalization. A weaker histological activity, a lower fibrosis score and a slower progression rate of fibrosis have been found in HCV-infected adults with normal ALT after IFN therapy than in HCV patients with elevated ALT (43). Thus, although the desirable end-point of IFN treatment is HCV RNA clearance, a long-lasting biochemical response is an alternative, practically feasible goal. Although the main aim of this study was the evaluation of viremia during IFN ther- apy, the assessment of histological changes could be interesting. On the other hand, since a follow-up bi- opsy in the present study was scheduled 2 years after the completion of IFN therapy, histological findings are not available.
In five children, IFN therapy was associated with a worsening of hypertransaminasemia. The marked elev- ation of serum aminotransferase levels, observed in these children during the treatment, could be related to the rapid elimination of infected hepatocytes by IFN- induced activation of the cytolytic response (44). Three of these children, who were LKM-l-positive, had per- sistently undetectable HCV RNA throughout the treat- ment period. It is noteworthy that the coexistence of persistently undetectable HCV RNA and ALT worsen- ing occurred only in LKM-l-positive patients. This seems to point to a peculiar immunological response to viral components in LKM-l-positive patients during IFN therapy. The role of molecular mimicry between the HCV genome and the molecular target of LKM-1 autoantibodies could be investigated in order to ex- plain this peculiar immunological response. A molecu- lar mimicry between viral antigens and host proteins has been invoked as trigger of autoimmune diseases (45). As for viral hepatitis, it has been reported that HBV shares epitopes with the molecular target of ANA and SMA (46).
According to previous observations, the low titer of autoantibodies, typically associated with autoimmune liver disease, was a common finding in children with CHC and did not seem to be due to IFN treatment (47). With the exception of ANA, autoantibody fre- quency did not change significantly during treatment. Although in our study the LKM-1 autoantibody was frequently associated with a significant biochemical de- terioration (observed in three of four LKM-l-positive patients) during IFN treatment, the presence of LKM- 1 autoantibodies does not seem to affect the response to IFN, because one of the only two complete sus- tained responders was LKM-l-positive.
In this study, patients considered responders both at the end of therapy and at the end of follow-up, as re- ported in Table 2, usually normalized ALT and cleared HCV-RNA within the first 3 weeks of treatment; only
609
P. Pensati et al.
one patient, a complete sustained responder, had a late ALT normalization and undetectable HCV RNA, at the third month of therapy. While early ALT normal- ization is predictive of a biochemical response, early undetectable HCV RNA (occurring at the second ad- ministration of IFN in 44% of patients) is a frequent phenomenon also in nonresponders.
A low baseline HCV RNA serum level was a predic- tive factor of response to IFN, similar to findings in adults (21-23). In fact, there was a significant differ- ence in basal HCV RNA serum levels between patients who were responders at the end of treatment and non- responders: none of the responders had basal viremia levels above I .5X IO6 Eq/ml and patients with viremia below 1 X106 Eq/ml had a significantly higher prob- ability of response.
We are unable to comment on the role of genotype because the frequency of genotypes other than lb is very low in our patients. No complete sustained re- sponder and only one biochemical responder had genotype 1 b. The poor response in patients with geno- type 1 b does not seem to be related to basal viremia levels. In fact, patients with genotype 1 b and low basal viremia did not have a favorable response to INF (Fig.
3). In summary, only a very low proportion of children
affected by CHC and treated with (x-INF for 12 months have long-term viral suppression associated with biochemical quiescence. Low baseline viral load is an essential factor for IFN response. Because long- term ALT normalization tends to be associated with a better histological prognosis and because it was ob- tained in 20% of treated children, IFN therapy could be recommended in children with low basal viremia. In LKM-l-positive children, who in this study invariably had a virological response frequently associated with a worsening of hypertransaminasemia, IFN could be administered at a lower dosage, at least during the first months of therapy, to limit the detrimental effect of IFN on transaminases. Since it has been reported that in adult patients with CHC, therapy with IFN and ri- bavirin is more effective than IFN alone in inducing virologic and histologic improvement (48), this combi- nation therapy should be considered in the future also in children with CHC.
References 1. Hoofnagle JH, Di Bisceglie AM. The treatment of chronic viral
hepatitis. N Engl J Med 1997; 336: 347-56. 2. Davis GL, Balart LA, Schiff ER, Lindsay K, Bodenheimer HC,
Perrillo RP, et al. Treatment of chronic hepatitis C with recom- binant interferon-alpha: a multicenter randomized controlled trial. N Engl J Med 1989; 321: 1501-6.
3. Di Bisceglie AM. Interferon therapy for chronic viral hepatitis [editorial] N Engl J Med 1994; 330: 137-8.
4. Fried MW. Hoofnagle JH. Therapy of hepatitis C. Semin Liver Dis 1995; 15: 82-91.
5. Carithers RL, Emerson SS. Therapy of hepatitis C: meta-analysis of interferonalpha2b trials. Hepatology 1997; 26: 83S-8s.
6. Farrell GC. Therapy of hepatitis C: interferon-alphaN trials.
Hepatology 1997; 26: 96S-100s. 7. Lindsay KL. Therapy of hepatitis C: overview. Hepatology 1997;
26: ?lS-7s. 8. Keeffe EB, Hollinger FB. Therapy of hepatitis C: consensus in-
terferon trials. Consensus Interferon study group. Hepatology 1997; 26: lOlS7S.
9. Lee WN. Therapy of hepatitis C: interferon alfa-2a trials. Hep- atology 1996; 26: 89S95S.
10. Shindo M, Di Bisceglie AM, Hoofnagle JH. Long-term follow up of patients with chronic hepatitis C treated with alpha-interferon. Hepatology 1992; 15: 1013-~6.
I 1. Saracco G, Rosina F, Abate ML, Chiandussi L, Gallo \! Cerutti E, et al. Long-term follow up of patients waith chronic hepatitis C treated with different doses of interferonalpha2b. Hepatology 1993; 18: 1300.5.
12. Castillo 1, Bartolome J, Navas S, Gonzales S, Herrero M, Car- reno V. Virological and biochemical long-term follow up of pa-
tients with chronic hepatitis C treated with interferon. Hep- atology 1994; 19: 1342-6.
13. Bortolotti F Giacchino R, Vajro P, Barbera C, Crivellaro C, Al- berti A, et al. Recombinant interferon-alpha therapy in children with chronic hepatitis C. Hepatology 1995; 22: 1623-6.
14. Fujisawa T, Inui A, Ohkawa T, Komatsu H, Miyakawa Y, Onoue M. Response to interferon therapy in children with chronic hepa- titis C. J Pediatr 1995; 127: 660-3.
15. Iorio R, Pensati P, Porzio S, Fariello 1, Guida S, Vegnente A. Lymphoblastoid alpha-interferon therapy in chronic hepatitis C. Arch Dis Child 1996; 74: 15226.
16. Matsuoka S, Mori K. Nakano 0, Yuasa Y, Taguchi Y. Hayabuchi Y, et al. Efficacy of interferon in treating children with chronic hepatitis C. Eur J Pediatr 1997; 156: 7048.
17. Jonas M, Ott MJ, Nelson SP Badizadegan K, Perez-Atayde AR. Interferon-alpha treatment of chronic hepatitis C virus infection in children, Pediatr Infect Dis J 1998: 17: 241-6.
18. Sawada A. Tajiri H. Kozaiwa K, Guo W Tada K. Etani Y, et al. Favorable response to lymphoblastoid interferon-alpha in children with chronic hepatitis C. J Hepatol 1998; 28: 1848.
19. Collins ML, Zayati C, Detmer JJ, Daly B, Kolberg JA, Cha T-A, et al. Preparation and characterization of RNA standards for use
in quantitative branched DNA hybridization assays. Anal Bio- them 1995; 226: 120-9.
20. Davis GL, Lau JYN, Urdea MS, Neuwald P Wilber JC, Lindsay K, et al. Quantitative detection of hepatitis C virus RNA by a
solid phase signal amplification method: definition of optimal conditions for specimen collection and clinical application in in- terferon-treated patients. Hepatology 1994; 19: 133741.
21. Alter HJ, Sanchez-Pescador R, Urdea MS, Wilber JC, Lagier RJ, Di Bisceglie AM, et al. Evaluation of branched DNA signal am- plification for the detection of hepatitis C virus RNA, J Viral Hepatitis 1995; 2: 121.-32.
22. Nelson DR. Marousis CG, Davis GL, Lau JYN. Defining the role of intrahepatic HCV-specific cytotoxic T-lymphocytes in chronic hepatitis C [abstract]. Hepatology 1995; 22: 287A.
23. Wright TL, Donegan E, Hsu HH, Ferrell L, Lake JR, Kim M, et al. Recurrent and acquired hepatitis C viral infection in liver transplant recipients. Gastroenterology 1992; 103: 3 17722.
24. Davis GL. Prediction of response to interferon treatment of chronic hepatitis C. J Hepatol 1994; 21: l-3.
25. Martinot-Peignoux M, Marcellin P Pouteau M, Castelnau C. Boyer N, Poliquin M, et al. Pretreatment serum hepatitis C virus RNA levels and hepatitis C virus genotype are the main and inde- pendent prognostic factors of sustained response to interferon alfa therapy in chronic hepatitis C. Hepatology 1995; 22: 105s 6.
26. Conjeevaram HS, Everhart JE, Hoofnagle JH. Predictors of a
610

IFN treatment in children with chronic hepatitis C
sustained beneficial response to interferon alfa therapy in chronic hepatitis C. Hepatology 1995; 22: 1326-9.
27. Vial T, Descotes J. Clinical toxicity of the interferons. Drug Safety 1994; 10: 115-50.
28. Iorio R, Pensati P, Botta S, Moschella S, Impagliazzo N, Vajro P,
et al. Side effects of alpha-interferon therapy and impact on health-related quality of life in children with chronic viral hepa- titis. Pediatr Infect Dis J 1997; 16: 98490.
29. Scheuer PJ, Ashrafzadeh P Sherlock S, Brown D, Dusheiko GM. The pathology of hepatitis C. Hepatology 1992; 15: 567-7 1.
30. Desmet VJ, Gerber M. Classification of chronic hepatitis: diag- nosis, grading and staging. Hepatology 1994; 19: 1513-20.
31. Johnson PJ, McFarlane IG. Meeting report: International Auto- immune Hepatitis Group. Hepatology 1993; 18: 998-1050.
32. Davis GL, Balart LA, Schiff ER, Linsay K, Bodenheimer HC,
Perrillo RP, et al. Treatment of chronic hepatitis C with recom- binant interferon alfa: a multicentre randomized controlled trial. N Engl J Med 1989; 321: 1501-6.
33. Davis GL. Prediction of response to interferon treatment of chronic hepatitis C. J Hepatol 1994; 20: l-3.
34. Vergani D, Mieli-Vergani G. Type II autoimmune hepatitis: the
conundrum of cytochrome P450IID6. Clin Exp Immunol 1993; 92: 367-8.
35. Misiani R, Bellavita P Fenili D, Vicari 0, Marchesi D, Sironi PL, et al. Interferon alfa-2a therapy in cryoglobulinemia associated with hepatitis C virus. N Engl J Med 1994; 330: 751-6.
36. Lunel F, Musset L, Cacoub I’, Frangeul L, Cresta P, Perrin M, et al. Cryoglobulinemia in chronic liver diseases: role of hepatitis C virus and liver damage. Gastroenterology 1994; 106: 1291-300.
37. Lisker-Mehnan M, Di Bisceglie AM, Usala SJ, Weintraub B, Murray LM, Hoofnagle JH. Development of thyroid disease dur- ing therapy of chronic viral hepatitis with interferon alfa. Gastro- enterology 1992; 102: 215560.
38. Tran A, Quaranta JF, Benzaken S, Thiers V, Chau HT, Hastier P,
et al. High prevalence of thyroid autoantibodies in a prospective series of patients with chronic hepatitis C before interferon ther- apy. Hepatology 1993; 18: 253-7.
39. Detmer J, Lagier R, Flynn J, Zayati C, Kolberg J, Collins M, et al. Accurate quantification of HCV-RNA from all HCV geno-
types using branched DNA (b-DNA) technology. J Clin Micro- biol 1996; 34: 901-7.
40. Simmonds E McOmish F, Yap PL, Chan SW, Lin CK, Dusheiko G, et al. Sequence variability in the 5’ non-coding region of hepa- titis C virus: identification of a new virus type and restrictions on sequence diversity. J Gen Virol 1993; 74: 661-8.
41. Ma Y, Gregorio G, Gaken J, Muratori L, Bianchi FB, Mieli- Vergani G, et al. Establishment of a novel radioligand assay using eukaryotically expressed cytochrome P4502D6 for the measure- ment of liver kidney microsomal type 1 antibody in patients with autoimmune hepatitis and hepatitis C virus infection. J Hepatol 1997; 26: 1396402.
42. Farrell GC, Bacon BR, Goldin RD. Lymphoblastoid interferon alfa-nl improves the long-term response to a 6-month course of treatment in chronic hepatitis C compared with recombinant in- terferon alfa-2b: results of an international randomized con- trolled trial. Clinical Advisory Group for the Hepatitis C Com- parative Study. Hepatology 1998; 27: 1121-7.
43. Mathurin P Moussalli J, Cadranel JF, Thibault V, Charlotte F, Dumouchel P, et al. Slow progression rate of fibrosis in HCV patients with persistently normal ALT activity. Hepatology 1998; 27: 868-72.
44. Baron S, Tyring SK, Fleischmann WR Jr, Coppenhaver DH, Nie- se1 DW, Klimpel GR, et al. The interferons. Mechanisms of ac- tion and clinical applications. JAMA 1991; 266: 1375-83.
45. Oldstone MBA. Molecular mimicry and autoimmune disease. Cell 1987; 50: 819-20.
46. Gregorio GV, Choudhuri K, Mieli-Vergani G, Vergani D. Mim- icry between HBV-DNA polymerase and antigenic targets of nu- clear and smooth-muscle antibodies in chronic hepatitis B virus
infection [abstract]. Hepatology 1996; 24: 28A. 47. Gregorio GV, Pensati P Iorio R, Vegnente A, Mieli-Vergani G,
Vergani D. Autoantibody prevalence in children with liver disease due to chronic hepatitis C virus (HCV) infection. Clin Exp Im- munol 1998; 112: 471-6.
48. McHutchison JG, Gordon SC, Schiff ER, Schiffman ML, Lee WM, Rustgi VK, et al. Interferon alfa-2b alone or in combi- nation with ribavirin as initial treatment for chronic hepatitis C.
N Engl J Med 1998; 339: 1485-92.
611
Related Documents











