Low Level Laser Therapy (LLLT) contra Light Emitting Diode Therapy (LEDT) - What is the difference? Lars Hode*, Jan Tuner P.OBOX 27137; 10252 Stockholm ABSTRACT The article aims to make a comparison, starting from a review of the available literature data, between the low level laser therapy (LLLT) and the light emitting diode therapy (LEDT) applied on human patients. The main conclusion is that too little research efforts have been devoted on the effects specific to LEDT. More than that, it is the authors opinion that every device claiming to heal has to prove the effectiveness in controlled studies. 1. INTRODUCTION All forms of light affects the living organism. it has been shown that white light in certain doses may influence seasonal depression conditions. Over 30 years ago, Endre mesters group in Budapest found that laser light can influence pain and wound healing. It is essential to clarify whether or not the biological effects obtained with laser therapy will appear only if the light source is a laser - that is, if the effects are laser specific. This is not just of theoretical interest. If one could just as well use a light bulb with a polarization filter and/or a colour filter -or light emitting diodes with a certain colour or with infrared light (such as in remote controls) - it would be considerably less expensive to manufacture therapeutic instruments. Many therapists think they are working with a laser, but in reality they have bought a Light Emitting Diode (LED) instrument and not a laser. But is then Light Emitting Diode Therapy (LEDT) as good as Low Level Laser Therapy (LLLT)? Does it really matter ifone or the other is used? Are there any comparing investigations? Yes, many comparisons have been made, also with different dose levels and different wavelengths. These comparisons show two things: 1. Till today, there is no study showing that LEDT is better than LLLT; and there is no study showing that LEDT is as good as LLLT. 2. LEDT seem to have biologic effects similar to the effects ofLLLT, though less pronounced. But if LEDT is less good than LLLT, why are LED instruments still produced? Our opinion is that they are produced only because they are cheaper and easier to power than lasers and not because they have been evaluated and compared with lasers and found to be better. Many producers of therapeutic instruments claim that treatment with LEDs is as effective as laser treatment. Then they make references to laser research in their marketing, obviously due to the lack of support from published LED effects. The question is not only a question of lasers or LED, it is rather a question if the reported effects are "laser specific" or not. There have been quite a number of studies conducted on laboratory an23456' 12, 13, 14, 17, 19,21,22,23,24,29 even blind studies — in which the effect oflaser light was compared with the effect of light from other sources, such as LED's. A significant effect was observed with lasers, which was not achieved with the other, less narrow-band light sources. Conclusion: Either all the investigators who conducted the research cheated, or the effects are specific to laser light. * Correspondence: P.O.BOX 27137; 10252 Stockhohn In Laser Florence '99: A Window on the Laser Medicine Worlc Longo, Hofstetter, Pascu, Waidelich, Editors, Proceedings of SPIE Vol. 4166 (2000) • 1605-7422/00/$1 5.00 90 Downloaded From: http://proceedings.spiedigitallibrary.org/ on 02/03/2014 Terms of Use: http://spiedl.org/terms

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Low Level Laser Therapy (LLLT) contra Light Emitting DiodeTherapy (LEDT) - What is the difference?
Lars Hode*, Jan Tuner
P.OBOX 27137; 10252 Stockholm
ABSTRACT
The article aims to make a comparison, starting from a review of the available literature data, between the low levellaser therapy (LLLT) and the light emitting diode therapy (LEDT) applied on human patients. The main conclusion isthat too little research efforts have been devoted on the effects specific to LEDT. More than that, it is the authorsopinion that every device claiming to heal has to prove the effectiveness in controlled studies.
1. INTRODUCTION
All forms of light affects the living organism. it has been shown that white light in certain doses may influenceseasonal depression conditions. Over 30 years ago, Endre mesters group in Budapest found that laser light caninfluence pain and wound healing. It is essential to clarify whether or not the biological effects obtained with lasertherapy will appear only if the light source is a laser - that is, if the effects are laser specific. This is not just oftheoretical interest. If one could just as well use a light bulb with a polarization filter and/or a colour filter -or lightemitting diodes with a certain colour or with infrared light (such as in remote controls) -it would be considerably lessexpensive to manufacture therapeutic instruments.
Many therapists think they are working with a laser, but in reality they have bought a Light Emitting Diode (LED)instrument and not a laser. But is then Light Emitting Diode Therapy (LEDT) as good as Low Level Laser Therapy(LLLT)? Does it really matter ifone or the other is used?
Are there any comparing investigations? Yes, many comparisons have been made, also with different dose levels anddifferent wavelengths. These comparisons show two things:
1. Till today, there is no study showing that LEDT is better than LLLT; and there is no study showing that LEDT isas good as LLLT.
2. LEDT seem to have biologic effects similar to the effects ofLLLT, though less pronounced.
But if LEDT is less good than LLLT, why are LED instruments still produced? Our opinion is that they areproduced only because they are cheaper and easier to power than lasers and not because they have been evaluated andcompared with lasers and found to be better. Many producers of therapeutic instruments claim that treatment withLEDs is as effective as laser treatment. Then they make references to laser research in their marketing, obviously dueto the lack of support from published LED effects.
The question is not only a question of lasers or LED, it is rather a question if the reported effects are "laser specific"or not. There have been quite a number of studies conducted on laboratory an23456' 12,13, 14, 17, 19,21,22,23,24,29
even blind studies — in which the effect oflaser light was compared with the effect of light from other sources, suchas LED's. A significant effect was observed with lasers, which was not achieved with the other, less narrow-bandlight sources.
Conclusion: Either all the investigators who conducted the research cheated, or the effects are specific to laser light.
*Correspondence: P.O.BOX 27137; 10252 Stockhohn
In Laser Florence '99: A Window on the Laser Medicine Worlc Longo, Hofstetter, Pascu, Waidelich,Editors, Proceedings of SPIE Vol. 4166 (2000) • 1605-7422/00/$1 5.0090
Downloaded From: http://proceedings.spiedigitallibrary.org/ on 02/03/2014 Terms of Use: http://spiedl.org/terms

The most important difference between LED's and lasers is the coherence. it has been said that the coherence is lostwhen laser light is scattered in tissue. In a little experiment we will show that the coherence oflaser light is not lost intissue due to scattering. Light is neither coherent nor incoherent but is more or less coherent (the light from a laser ismore coherent - longer coherence length -than light from LED's).
In the literature there is a good support for the hypothesis that at least some of the biostimulative effects in vivo arelaser specific. In fact, we have not yet found one single study indicating that non coherent light is as efficient ascoherent light. This does not mean non coherent light is not a useful therapy, only that it is less efficient and probablymost efficient on superficial structures.
We have found the following published comparisons between coherent and non coherent light (such as from LED):
Bihari2 treated three groups of patients with long-standing crural ulcers with HeNe, HeNe/GaAs and non-coherentunpolarized red light, respectively. Groups 1 and 2 demonstrated excellent healing, with group 2 slightly better thangroup 1, compared to group 3 with a low effective percentage.
Kubota3 found that 830 urn GaA1As laser increased flap survival area in a rat model. Laser treated flaps had betterperfusion, a greater number of larger blood vessels and significantly enhanced flow rate. There was no differencebetween control and LED 840 nm groups.
Berki4 used a HeNe laser to stimulate activation of cells in vitro. These effects (increased phagocytic activity,immunoglobulin secretion) were not seen when irradiating the cell cultures with normal monochromatic light of thesame wavelength and doses.
Mukliyarov5 used HeNe laser on zymosan arthritis in rats and found that the laser exerted an evident therapeuticeffect. Analysis ofthe cases where the rats were treated with ordinary red light revealed no essential differences fromthe control group.
Haina6 compared the effects of HeNe-laser and incoherent light of the same wavelength. Experimental wounds werepunched out in the muscle fascia of249 Wistar rats. In the HeNe groups, the granulation tissue increased 13% at 0.5
J/cm2.and 22% at 1 .5 J/cm2. The increase in the incoherent group was less than 10%.
Rochkind'2 compared five different wavelengths, giving a single transcutaneous irradiation to injured peripheralnerves. HeNe prevented the drop in functional activity following crush injury. 830 nm laser was ineffective, 660 nmincoherent light was even less effective and 880 nm and 950 urn incoherent light was completely ineffective.
Laaks&7 studied to relationship between LLLT and opoids. In a double blind study 56 selected patients with chronicpain conditions were treated with 820 nm LLLT 25 mW, 670 nm LLLT 10 mW or 660 am LED 9.5 rnW. ACTH and
13 -endorphin levels were significantly elevated in the LLLT groups but not in the LED group.
Pöntinen19 compared the effect of laser light and light from a LED-source on head skin blood flow in 10 healthy
men, using laser doppler technology. Doses were from 0.1 to 1.36 JIcm2. Skin blood flow was measured before,immediately after and 30 minutes after each treatment at 4 sites on the scalp. The conclusion was that 670 urn laserinduced a temporary vasodilatation and increased blood flow when the dose given was in the range of 0.12 -0.36
J/cm2. The non-coherent visible monochromatic irradiation (LED: 635 nm) with doses between 0.68 and 1.36 J/cm2decreased blood flow at least for 30 minutes after irradiation.
Lederer2' found that "irradiation with coherent HeNe laser light effected leucocytes in migration inhibition assays.Incoherent light ofthe same wavelength and power density showed no influence."
Rosner2 evaluated the ability ofHeNe laser to delay the posttraumatic optical nerve degeneration in rats. The opticalnerve was crushed and irradiated through the eye. Interestingly enough, irradiation immediately before the injury wasas effective as irradiation beginning soon after it. Non coherent infrared light was ineffective or had adverse effect.However, the non coherent light had a wavelength of 904 nm, which makes comparisons difficult.
91
Downloaded From: http://proceedings.spiedigitallibrary.org/ on 02/03/2014 Terms of Use: http://spiedl.org/terms

NicoIa23 developed a technique of causing highly reproducible inflammatory lesions on the skin of rats. HeNe 1
J/cm2 produced an acceleration of the healing process. Incoherent light of the same wavelength and dose was lessfavourable.
Onac24 compared the effect of HeNe laser and monochromatic light at 61 8 nm. The intact skin of guinea pigs wasirradiated with different doses. They not only compared the two different light sources; they also compared them at
different doses (from 0.63 J/cm2 and up to 38.1 J/cm2) and came to the following conclusion: non coherent
monochromatic red light irradiation leads to tegument trophicity at 4.96 J/cm2 (but less than HeNe-laser); lowerdoses have no effect (but HeNe laser had) whereas higher ones causes focal epidermic hypertrophy. Thus, thetherapeutic window seems to be more narrow for monochromatic non coherent light.
NicoIa29 investigated the role of polarization and coherence of laser light on wound healing in rats. He had fourgroups of wounds:#1 was treated with coherent and polarized HeNe laser light (633 urn).#2 was treated with non polarized, coherent HeNe laser light (2=633 urn).#3 was tretated with polarized, low degree coherent light (2=633 nm).#4 was untreated and served as control.
After the fourth treatment, lesions #1 had healed completely; lesions #2 had not healed completely but showed moreadvanced healing process than lesions #3 . The lesions #4 showed a poor degree of cicatrization when compared tolesions #1, #2 and #3.
One investigation that unexpectedly strengthen our hypothesis that most treatments of tissue are laser specific, ispublished by, Zhou30. The study concerns PDT (Photodynamic therapy) using three light sources: a) copper-vapourpumped-dye laser, b) HeNe laser, and c) non-coherent red light (filtered from a halogen lamp), when irradiating theliver in normal mice. The mice (each group containing 1 8 -20 mice) received haematoporphyrin derivative in a doseof 10 mg/kg intra-venous, 24 hours prior to light irradiation. The mice livers were directly irradiated with different
red light at a dose of 5, 10, 25, 50, or 100 J/cm2, respectively. Forty-eight hours later the mice were killed, and thedepth of liver necrosis was measured using a computer image-analysis system. No necrosis was found in the control
liver irradiated with 500 J/cm2 alone. The depth of photodynamic necrosis showed a light dose-dependent response.The mean depth of necrosis of all groups were compared statistically. The Cu-dye laser showed the best effect whilethe non-coherent light showed the poorest. There were significant differences between non-coherent light and laserirradiated groups, but not between Cu-dye and HeNe laser groups. The results indicate that among the examined lightsources, the Cu-dye laser is most suitable to photodynamic therapy (PDT) of tumours. However, the halogen lampwith a special filter device may still be occasionally used as a light source in PDT if needed.
In a wound healing study by Lowe1 mouse skin was irradiated with 20 Gy X-ray irradiation. 72 hours later a woundwas made on the dorsum and the area was treated with 890 nm monochromatic LED light three times weekly. There
was no effect on the wound healing using 0.18 J/cm2 or 0.54 J/cm2 but an inhibiting effect at 1.45 J/cm2.
2. HODE'S HAMBURGER
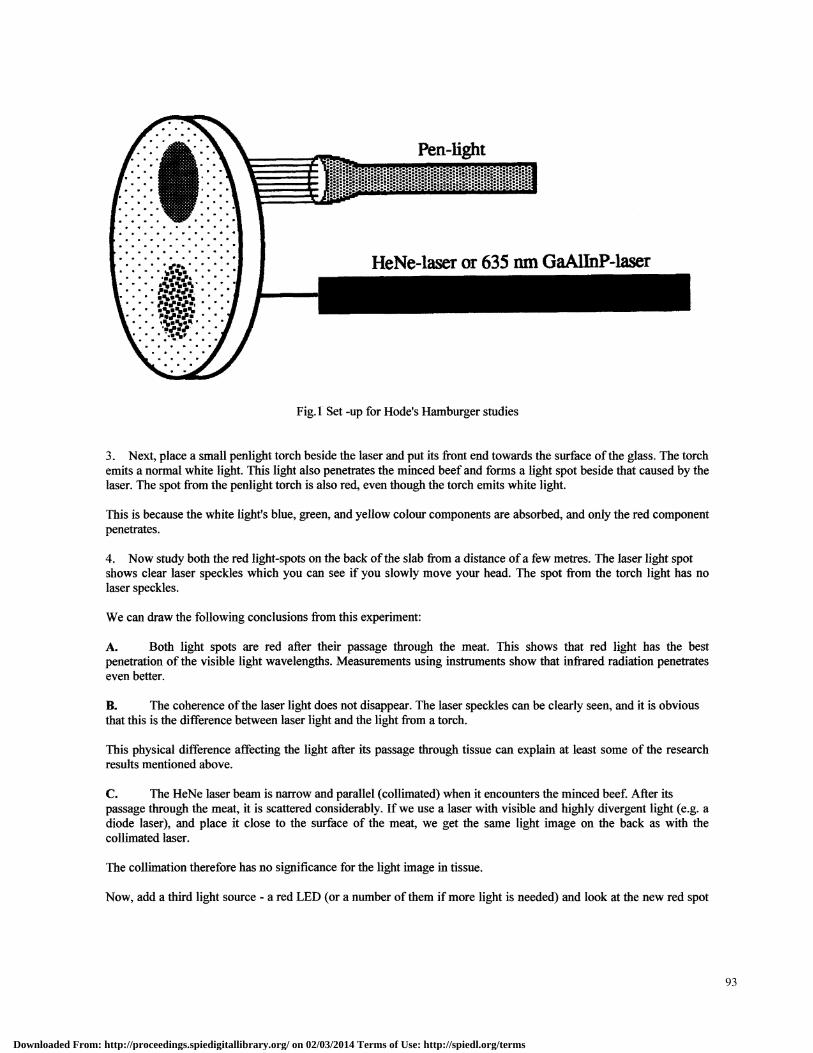
However, it is also possible to see that there is a clear difference between LED light and laser light after penetrationof tissue. This is due to the shorter coherence length of the LED light. It is well-known that the coherence lengthdecreases in the event of diffuse reflection, but it does not drop to zero. This was firmly established by means of anexperiment, Fig.l, first demonstrated by Lars Hode at The Ninth Congress of the International Society for LaserSurgery and Medicine in Los Angeles in 1991. Anyone with a HeNe laser can conduct this experiment:
1. Press together newly-minced fresh beef, e.g. raw hamburger meet between two glass plates so that you havea 5 - 10 mm thick minced beef plate.
2. Aim the light from a 5 - 10 mW HeNe- or InGaAlP-laser (red visible light) at the glass plates with theminced beef slab as shown in the Fig.l. You can see a red spot on the back of the minced beef where the light haspenetrated.
92
Downloaded From: http://proceedings.spiedigitallibrary.org/ on 02/03/2014 Terms of Use: http://spiedl.org/terms
*•
:::.• .'•
&
• •• &• •• •• • • •• •• • •• •• • • • • •• • • •R%' •
HeNe-laser or 635 nm GaAllnP4aser
I
Fig.1 Set -up for Hode's Hamburger studies
3. Next, place a small penlight torch beside the laser and put its front end towards the surface ofthe glass. The torchemits a normal white light. This light also penetrates the minced beef and forms a light spot beside that caused by thelaser. The spot from the penlight torch is also red, even though the torch emits white light.
This is because the white light's blue, green, and yellow colour components are absorbed, and only the red componentpenetrates.
4. Nowstudy both the red light-spots on the back ofthe slab from a distance ofa few metres. The laser light spotshows clear laser speckles which you can see if you slowly move your head. The spot from the torch light has nolaser speckles.
We can draw the following conclusions from this experiment:
A. Both light spots are red after their passage through the meat. This shows that red light has the bestpenetration of the visible light wavelengths. Measurements using instruments show that infrared radiation penetrateseven better.
B. The coherence ofthe laser light does not disappear. The laser speckles can be clearly seen, and it is obviousthat this is the difference between laser light and the light from a torch.
This physical difference affecting the light after its passage through tissue can explain at least some of the researchresults mentioned above.
C. The HeNe laser beam is narrow and parallel (collimated) when it encounters the minced beef. After itspassage through the meat, it is scattered considerably. If we use a laser with visible and highly divergent light (e.g. adiode laser), and place it close to the surface of the meat, we get the same light image on the back as with thecollimated laser.
The collimation therefore has no significance for the light image in tissue.
Now, add a third light source - a red LED (or a number of them if more light is needed) and look at the new red spot
93
Downloaded From: http://proceedings.spiedigitallibrary.org/ on 02/03/2014 Terms of Use: http://spiedl.org/terms

on the back side of the meet. No laser speckles can be seen!!
Fig.2 Enlarged real laser speckles. BriSht parts corresponds to areas (volumes) with higher intensity than average.Photo: Lars Hode
5. WHAT CHARACTERIZES THE LIGHT IN A LASER SPECKLE?
The phenomenon of speckles is a form of optical noise. It was observed long time before the laser arrived. Already in1877 reported Exner' about granulations in filtered mercury lamp light.
When the first lasers came, the speckles became not only much more noticed, but also a problem. Dennis Gabor, the"father of holography" published 1970 an article with the title: "Laser Speckle and Its Elimination" in which hedescribed different ways to get rid of speckles
Hode, Biedermann and Ek25' 27 investigated in 1972-1973 the possibility to use the inherent information in specklefields to observe surface deformation in real time.
The three-dimensional structure of real speckles is manifest in a patient's tissue during irradiation with laser light. Itarises as a result of interference between different beams with a random direction, amplitude and phase. in laserspeckles which have a higher intensity than the surrounding environment, the light is linearly polarized, or partiallypolarizcd, because the higher intensity has come about as a result of constructive interference, which occurs only ifthe interfering waves have the same polarization.
In this way, islands of polarized light appear in the tissue, with an average size of a few tenths of a millimetre, that is,generally larger than the cells they surround. Interestingly enough, these islands occur regardless of whether theirradiating laser emits polarized or unpolarized light.
94
Downloaded From: http://proceedings.spiedigitallibrary.org/ on 02/03/2014 Terms of Use: http://spiedl.org/terms
Horvath15 has actually measured the light distribution in tissue when illuminated with coherent and incoherent light.He used a small detector and could verify that there is a three dimensional speckle structure ofthe light in the tissue ifilluminated by laser light but not when illuminated by incoherent light.
6. PORPIIYRINS AND POLARIZED LIGHT
If polarization is so important, can we not simply use polarized normal light or polarize the light from LED's? Theanswer is yes and no. If we illuminate cell cultures, the polarization remains unchanged through the thin layer ofcells. However, if we illuminate a highly scattering media, such as living tissue, the polarization is lost after apenetration of a millimetre or so. Therefore, if we polarize light from a pocket torch, and use it to irradiate skin, thepolarization will disappear before it encounters the deeper-lying tissues. However, we could use polarized normallight to treat open wounds and improve the healing'8 (if we filter off all wavelengths shorter than 600 nm as these arenegative to already stimulated cells), as the light would directly encounter the cells in the wound, where there is nooverlying skin to eliminate the polarization.
If we accept that laser light causes areas of polarized light in tissue (as earlier described), we might also ask thequestion: what is there in the body/tissue/cells that reacts to the light's polarization? Is there a polarization-sensitiveelement?
Yes, there is. It is known that matrix fixed chromophore molecules (e.g. the body's porhyrins) possess absorptiondipoles and both absorb and emit (e.g. through fluorescence) linearly polarized light of a determined polarity.Porphyrins are just one of the elements in the mitochondria's respirator chain, and are the molecules chieflyresponsible for the absorption of light. The polarization in the speckles created by laser light is significant here, andthis could explain why the studies mentioned above showed different results with lasers and incoherent light sources.
7. CELL CULTURES AND TISSUE HAVE DifFERENT OPTICAL PROPERTIES
In a number of studies in which the biologic effects of monochromatic light from various sources have beencompared, the following has been found:
1. In cell cultures laser light gives almost the same effect" as incoherent light (i.e. colour-filtered light from alight bulb or an LED ofthe same wavelength).
2. When tissue is irradiated, laser light gives stronger effect than incoherent light in all the studies so farconducted. In some of the studies, certain effects were also achieved with LEDs, but these were not as clear as withlaser light of the same wavelength and the same dose. It should be noted that in four of these studies adverse effectsfrom LED light was 922 24,30
3. if cell cultures are irradiated with polarized light, narrow band incoherent light gives go% of what polarizedlaser light ofthe same wavelength and dose would giv&°.
4. Even polarized broad-band light'8 has a clear effect on cell cultures and even some effect on open wounds andcertain skin problems, however, not as good as polarized laser light.
5. Under certain power density conditions non polarized broad-band light can, as well, have an influence on cells incultures'6'2°
Karu'1 has demonstrated stimulating biological effects in cell cultures from monochromatic incoherent light.
However, she has also shown that cell cultures which are first irradiated with laser light, and have consequentlyexhibited biological effects, and then are irradiated with broadband (that is, non-monochromatic and incoherent)light, subsequently have their laser-produced biological effects reduced to almost nothing9. This indicates that thereare more mechanisms at work here than simply the excitation of polarization-sensitive chromophores.
It is important to understand the purely optical difference between irradiating tissue, which spreads light verydiffusely, and a thin transparent cell layer in culture. If a thin layer of cells in culture is irradiated with polarized light,
95
Downloaded From: http://proceedings.spiedigitallibrary.org/ on 02/03/2014 Terms of Use: http://spiedl.org/terms

the polarization is maintained right through the whole layer. This means that the cells are entirely surrounded bypolarized light.
Mester has shown that leucocytes in culture are affected by both polarized laser light and polarized incoherent light,but not by unpolarized incoherent light'0.
6 CONCLUSION
It is a fact that a lot ofLED instruments are used in therapy. Still, it is more or less unknown which wavelengths anddoses are optimal. Simply, too little research is done on the effects of LEDT. It would be valuable to find out whichparameters are good for what condition.
Our opinion is that every device claiming to heal has to prove its own effectiveness in controlled studies. That is thebest tool we have after all. Just to say that "it is as good as ..."jnot good enough.
REFERENCES
I. J. Tuner and L. Hode, Low Level Laser Therapy, Clinical Practice and Scientjflc Background, ISBN 91 -630-7616 - 0, Prima Books Ltd, Spjutvtgen I 1, 77232 Grängesberg, Sweden, 1999
2. I. Bihari and A. Mester, "The biostimulative effect of low level laser therapy of long-standing crural ulcerusing Helium Neon laser, Helium Neon plus infrared lasers and noncoherent light: Preliminary report of arandomized double blind comparative study", Laser Therapy 1(2), p. 97, 1989.
3. J. Kubota and T. Ohshiro, "The effects ofdiode laser low reactive-level laser therapy (LLLT) on flapsurvival in a rat model", Laser Therapy 1(3), p. 127, 1989.
4. T. Berki Ct al, "Biological Effect ofLow-power Helium-Neon (HeNe) Laser Irradiation", Lasers in MedicalScience 3, p. 35, 1988.
5. P. Muldiyarov et a!, "Effect ofMonochromatic Helium-Neon Laser Red Light on the Morphology ofZymosan Arthritis in Rats, Biull Eksp Biol Med 1 p. 55, 1983.
6. D. Haina et a!, "Animal Experiments on Light-Induced Wouñdhealing", Biophysica Berlin 35(3), pp. 227-230, 1973
7. R. Cherry, "Measurement of Protein Rotational Diffusion in Membranes by Flash Photolysis", Methods inEnzymology 54, p. 47, 1978.
8. R. Lubart, Y. Woliman, H. Friedman, S. Rochkind and I. Laulicht, "Effects ofvisible and near-infrared laserson cell cultures" I Photochem. Photobiol. B 12, pp. 305-310, 1992.
9. 1. Karu, "Photobiological Fundamentals of Low Power Laser Therapy", iEEE Journal of QuantumElectronic,. 23(10), p. 1703, 1987.
10 E. Mester et al, "Auswirkungen direkter Laserbestrahiung auf menschliche Lymphozyten", Arch DermatolRes, 5:p. 31, 1978.
I I T. Karu et a!, "Biostimulation ofHeLa-cells by low-Intensity Visible Light", Nuovo Cimento ID (6), p. 828,1982.
12 5. Rochkind et al, "A single Transcutaneous Light Irradiation to Injured Peripheral Nerve: ComparativeStudy with Five Different Wavelengths", Lasers in MedicalScience, 4, p. 259, 1989.
13 J. Kana, G. Hutschenreiter, D. Haina and W. Waidelich, "Effect of low-power density laser radiation onhealing ofopen skin wounds in rats", Arch surg. 116, p. 293, 1981.
14 C. Shiroto et al, "Effects of diode laser radiation in vitro on activity of human neutrofils", Laser TherapyI(3),p. 135, 1989.
15 Z. Donko, "Possible ab-initio explanation of laser "biostimulation" effects", Laser Applications in Medicineand Surgery, Proc 3rd World Congr -mtSoc Low Power Laser Appln in Medicine 57, Ed. G. Galletti et al,Monduzzi Editore S.p.A., Bologna, 1992.
16 R. Lubart, H. Friedmann, I. Peled and N. Grossman, "Light effect on fibroblast proliferation", Laser Therapy5, p. 55, 1993.
17 E. L. Laakso et al, "Plasma ACTH and l -endorphin levels in response to low level laser therapy (LLLT) formyofascial trigger points", Laser Therapy 6, pp. 133-142, 1994.
18 M. Feny et al, "Theoretical and experimental basis of biostimulation by laser irradiation", Optics and LaserTechnology 4, p. 209, 1984.
19 P. Pöntinen P et a!, "Comparative effects of exposure to different light sources (He-Ne laser, InGaAl diode
96
Downloaded From: http://proceedings.spiedigitallibrary.org/ on 02/03/2014 Terms of Use: http://spiedl.org/terms

laser, a specific type of noricoherent LED) on skin blood flow for the head", Acupunct Electrother Res 21(2), pp.105-118, 1996.
20 R. Lubart et a!, "A light source for phototherapy", Laser Therapy 1, p. 1 5, 1991.21 . H. Lederer et al, "Influence oflight on human immunocompetent cells in vitro", Proc. Laser Opto-Elektronik,
Munich, 1981.22. M. Rosner et al, "Dose and temporal parameters in delaying injured optic nerve degeneration by low-energy
laser irradiation", Lasers Surg Med 13 (6), pp. 61 1-617, 1993.23. J. H. Nicola et a!, "The role of coherence in wound heating stimulation by non-thermal laser radiation",
Surgical andMedicalLasers 2-3(2), p. 70, 1989.24. I. Onac et a!, "Histological study regarding the effects of HeNe (632.8 mu) laser biostimulation upon the
tegument of Cavia Cobaia as compared with that ofmonochromatic red light (618 inn,) ",Proc. 2nd C'ongressWorldAssnfor Laser Therapy, Kansas City, p. 52-53, 1998.
25. L. Hode and K. Biedermann, "Observation of surface deformation in real time using laser speckles", ProcConference in Physics, Lund, Sweden, June 12-14,1972.
26. S.I. Ragnarsson, Vision Research 12, p. 41 1, 1972.27. L. Hode, "Elektronisk bildbehandling fZSr speckelinterferometri i reel! tid", Proj 1006, Institutet für Optisk
Forskning, Kung!. Tekniska Hogskolan, (in Swedish), 197328. J. M. Burch, Interferometty with Scattered Light. Optical Instruments and Techniques, J. Home, Dickson ed.
(Reading Conf. 1969). One! Press, New Castle upon Tyne, p. 213, 1970.29. J.H. Nicola, E. M. D. Nicola, M. Simoes and J. R. Paschoal, Role ofpolarization and Coherence of Laser
Light on Wound Healing. Laser Tissue Interaction V, S.L. Jacques ed., Proc SPIE 2134A, pp. 448-450, 1994.30 Thou Chuannong, Song, Xuyan, Deng Jinsheng, Liang Junlin, Thang Hua, Huang Wenjia, Liu Tao and Ha
Xian-Wen, "Photodynamic effect of copper-vapor pumped-dye laser, HeNe laser, and noncoherent red lightto the liver in normal mice", International Conference on Photodynamic Therapy and Laser Medicine, Jim-Heng Li ed, Proc. SPIE 1616, p. 239-245, 1993.
97
Downloaded From: http://proceedings.spiedigitallibrary.org/ on 02/03/2014 Terms of Use: http://spiedl.org/terms
Related Documents











