Low-Dose Cardio–Respiratory Phase-Correlated Cone-Beam Micro-CT of Small Animals Stefan Sawall 1 , Frank Bergner 1 , Robert Lapp 2 , Markus Mronz 2 , Marek Karolczak 1 , Andreas Hess 3 , Marc Kachelrieß 1 1 Institute of Medical Physics, University of Erlangen–N¨ urnberg, Erlangen, Germany 2 CT Imaging GmbH, Erlangen, Germany 3 Institute of Experimental and Clinical Pharmacology and Toxicology,University of Erlangen–N¨ urnberg, Erlangen, Germany Send correspondence and reprint requests to: Stefan Sawall Institute of Medical Physics (IMP), University of Erlangen–N¨ urnberg Henkestraße 91, D–91052 Erlangen Tel.: +49–9131–8525535 Fax.: +49–9131–8522824 e–mail: [email protected]–erlangen.de

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Low-Dose Cardio–Respiratory Phase-CorrelatedCone-Beam Micro-CT of Small Animals
Stefan Sawall1, Frank Bergner1, Robert Lapp2, Markus Mronz2,Marek Karolczak 1, Andreas Hess3, Marc Kachelrieß1
1 Institute of Medical Physics, University of Erlangen–Nurnberg, Erlangen, Germany
2 CT Imaging GmbH, Erlangen, Germany
3 Institute of Experimental and Clinical Pharmacology and Toxicology,University of
Erlangen–Nurnberg, Erlangen, Germany
Send correspondence and reprint requests to:Stefan SawallInstitute of Medical Physics (IMP), University of Erlangen–NurnbergHenkestraße 91, D–91052 ErlangenTel.: +49–9131–8525535 Fax.: +49–9131–8522824e–mail: [email protected]–erlangen.de

Abstract
Purpose:
Micro–CT imaging of the animal heart typically requires a double gating procedure because scansduring a breath–hold are not possible due to the long scan times and the high respiratory rates.Simultaneous respiratory and cardiac gating (RC gating) can either be done prospectively or retro-spectively. True five–dimensional information can be either retrieved with retrospective gating orwith prospective gating if several prospective gates are acquired. In any case the amount of infor-mation available to reconstruct one volume for a given respiratory and cardiac phase is orders ofmagnitude lower than the total amount of information acquired. For example the reconstruction ofa volume from a 10% wide respiratory and a 20% wide cardiac window uses only 2% of the dataacquired. Achieving a similar image quality as a non–gated scan would therefore require to increasethe amount of data and thereby the dose to the animal by up to a factor of 50.Methods:
To achieve the goal of low–dose phase–correlated imaging we propose to use a highly efficient combina-tion of slightly modified existing algorithms. In particular we developed a variant of the McKinnon–Bates image reconstruction algorithm and combined it with bilateral filtering in up to five dimensionsto significantly reduce image noise without imparing spatial or temporal resolution.Results:
Our preliminary results indicate that the proposed low-dose phase-correlated (LDPC) reconstructionmethod typically reduces image noise by a factor of up to six (e.g. from 170 HU to 30 HU) while ourdose values lie in a range from 60 to 500 mGy. Compared to other publications that apply 250 mGyup to 1800 mGy for the same task ([1, 2, 3]), our LDPC approach therefore achieves a more thanten-fold dose usage improvement.Conclusions:
The LDPC reconstruction method improves phase-correlated imaging from highly undersampleddata. Artifacts caused by sparse angular sampling are removed and the image noise is decreasedwhile spatial and temporal resolution are preserved. Thus the administered dose per animal can bedecreased allowing for long term studies with reduced metabolic inference.

Figure 1: Illustration of the dual source concept and a picture of the scanner used for our study.Mouse 1 was scanned with a single source version while mouse 2 was scanned in the dual sourceversion.
1 Introduction
Double–gated in–vivo small animal cone–beam micro–CT scans provide five–dimensional informationabout the object: the three volume dimensions plus the temporal dimensions of the respiratory motionand the heart motion, respectively. Double gating is typically performed to separate respiratory fromcardiac motion when imaging the animal’s lung or heart.
When ignoring the fact that cardiac motion also induces motion in the lung itself imaging thelung can be done using respiratory gating only [4]. However, to image the heart of small animalsone cannot neglect the translations and deformations of the heart induced by the respiratory motion.Hence cardiac imaging requires double gating [1, 2, 3, 5, 6].
To obtain functional information of the heart or lung it may be important to cover the completemotion cycles and thereby to reconstruct four– or five–dimensional representations of the object.While this paper focuses on the five–dimensional reconstructions the low–dose phase–correlated imagereconstruction method we propose can also be applied to four–dimensional data.
It is our aim to improve the image quality achievable in low–dose single– or double–gated micro–CT scans of small specimen. On the one hand we want to reduce streak artifacts that result fromsparse angular sampling and on the other hand we want to reduce image noise resulting from thesmall amount of projections available in a given combination of respiratory and cardiac phase.
2 Method
2.1 Scan Mode
For our scans we chose a scan mode that acquires 7200 projections during 10 contiguous rotations.In case of unexpected incidences, such as object motion, we may use only the subset of data that isnot corrupted. In addition this scan mode allows us to study the dose reduction potential by doingreconstructions from only a subset of the data, e.g. by using only the first five rotations for imagereconstruction.
Data from an alternative scan mode that distributes the 7200 projections over a single rotationwere not available to us.
1
2.2 Intrinsic Gating
To correlate our reconstruction with the motion phases of the animal heart and lung we detectcorresponding synchronization information directly from the rawdata. This intrinsic gating tech-nique, which is also called wireless gating or kymogram–based gating, was first developed for clinicalcone–beam spiral CT scanners [7] and then adopted for the case of magnetic resonance imaging [8].Intrinsic gating in case of clinical CT is very difficult due to the fact that the scanner rotates up tothree times during one motion cycle and the motion detection needs to account for the varying viewangles using sophisticated mathematical models [7].
In our case of slowly rotating micro–CT scanners with a typical gantry rotation speed of about0.2 rad
s, or of flat detector CT scanners in general, a motion period is much shorter than the time
needed for a half or a full rotation. The respiratory cycle in a mouse for example takes 0.5 s onaverage (excluding mice with gasping caused by anesthesia) and the cardiac cycle takes 0.15 s onaverage (see table 1). Thus the extraction of the synchronization signal may neglect the gantryrotation and rather simple methods may be used to detect the periodic motion. Approaches thatevaluate the center of mass of certain ROIs within each two–dimensional projection image have beenquite successful to detect the respiratory and cardiac motion [6, 9, 10, 11]. We use a similar approachextended to two motion signals for our in–vivo mouse scans.
2.3 Image Reconstruction
Let f denote the object, X the x–ray transform operator, and p be the projection data, such thatp = Xf .
Our standard image reconstruction is the Feldkamp algorithm which we denote with X−1
Stdand
which results in the standard image fStd = X−1
Stdp [12]. The standard Feldkamp algorithm is not
phase–correlated and thus uses all acquired projections for reconstruction. We make use of it belowto define the McKinnon–Bates algorithm.
To perform respiratory and cardiac–correlated image reconstruction we use a phase–correlatedFeldkamp algorithm X
−1
PCthat filters and backprojects only those projections that lie in the desired
temporal window. The temporal window itself is defined by specifying the respiratory phase r andthe cardiac phase c, both are values between 0 and 1 and count relative to one motion period,and by specifying the widths ∆r and ∆c of these temporal windows. The respiratory and cardiacphase–correlated image is denoted as fPC = X
−1
PCp.
Since only few projections fall into the desired temporal window, streak artifacts may occur unlessa very large number of projections at very fine angular increments is acquired. The McKinnon–Bates(MKB) algorithm can be used to address this issue [13, 14]. It works as follows. First, a standardreconstruction is performed to obtain a prior image. This prior image is blurry in those regions wheremotion is present, and it is of high image quality elsewhere. Then, a forward projection of the priorimage is performed and subtracted from the measured rawdata. These subtracted data are then usedfor a phase–correlated reconstruction which is added to the prior image. Mathematically:
fMKB = fStd + X−1
PC(p− XfStd). (1)
To correctly compensate for the longitudinal truncation effects we rather perform
fMKB = X−1
StdXfStd + X
−1
PC(p− XfStd) (2)
= (X−1
Std− X
−1
PC)XfStd + X
−1
PCp (3)
= X−1
PCXfStd + X
−1
PCp. (4)
2

Figure 2: The MKB algorithm is implemented by using complementary weights. A 20% wide phaseweight is illustrated. Green weights would be applied to the measured data while red weights areapplied to the forward projected data. The blending method is a weighted sum of measured rawdataand forward projected data followed by standard reconstruction.
Figure 3: Three orthogonal slices of a mouse scanned with a dose of 175 mGy. The top row showsimages originating from a standard phase–correlated reconstruction. Row two shows the imagesobtained by the McKinnon-Bates algorithm. The LDPC reconstruction is presented in the bottomrow. (C=400 HU/W=1200 HU)
The new operator X−1
PCdenotes the complement of the phase–correlated reconstruction operator such
that the sum X−1
PC+ X
−1
PCis equal to the standard reconstruction X
−1
Std. Since our phase–correlated
reconstruction approach corresponds to nothing but a weighting of the projections prior to Feldkampreconstruction the MKB algorithm can be realized by adequate weighted blending of the forwardprojected prior image XfStd with the original rawdata p followed by another standard image recon-struction (figure 2).
Since the respiratory motion dominates the cardiac motion we extend the MKB approach to atwo step algorithm. In a first step we apply MKB only to respiratory gating and in the second stepwe use the respiratory–gated MKB image as a prior for the additional cardiac gating. This procedureensures the best possible prior for cardiac gating.
To reduce noise we apply edge preserving denoising bilateral filters [15] in up to five dimensions.To define the bilateral filter let us restrict to one dimension, for convenience. Bilateral filtering of a
3

function f(x) is then defined as
Bf(x) =
∫
dtD(x, t)R(x, t)f(t)∫
dtD(x, t)R(x, t)(5)
with B denoting the bilateral filtering operator and
D(x, t) = e−(x− t
σx
)2
(6)
R(x, t) = e−(f(x)− f(t)
σf
)2
(7)
being the domain and the range filter, respectively. The parameters σx and σf are the widths of theGaussian domain and range filters, respectively. Note that other shapes of range and domain filtersmay be used as well. In this study, however, we restricted ourselves to considering Gaussian–shapedfilters.
Since respiratory and cardiac gating yields five–dimensional volumes f(x, y, z, r, c), with r de-noting the respiratory and c denoting the cardiac phase, we can apply bilateral filtering in up tofive dimensions. The corresponding domain filter parameters are denoted as σx, σy, σz, σr and σc,respectively. We also apply the edge–preserving filtration to the first prior volume (in x, y, and z),and to the second prior volume (in x, y, z, and r) using the same filter parameters as for the finalfive–dimensional filtering.
Referring to equation (7) the parameter σf determines the edge–preserving or edge–smoothingcapabilities of the filter. To ensure that edges are preserved within the filter the parameter was setslightly above the noise values measure in the McKinnon-Bates reconstructions. The parameters σx,σy and σz where chosen as twice the spatial sampling ∆, in the case of our scan protocol as 160 µm,resulting in a full width at half maximum of the filter kernel of about about 380 µm. The quantitiesσc and σr where chosen as 2∆c and 2∆r respectively.
The final volume, obtained by bilateral filtering the MKB volume and the intermediate priorvolumes, is the low–dose phase–correlated volume
fLDPC = BfMKB (8)
which we want to compare against the conventional (and more simple) phase–correlated volume fPCin the following.
Figure 3 further presents the intermediate results of the LDPC algorithm compared to the stan-dard phase–correlated reconstruction (PC) as shown in the top row. Due to the sparse angularsampling the PC images suffer from a high noise level and severe streak artifacts are visible, espe-cially in the axial slice. The anatomical structures further seem distorted and their perceptibility isreduced as consequence of the artifacts. The application of the McKinnon-Bates algorithm (middlerow) has removed almost all of the streak artifacts and thus the image homogeneity is restored.However the image noise becomes more apparent and is the most limiting factor when interpretingthe images. The bottom row therefore shows the MKB images after the bilateral filter has beenapplied. The noise has been reduced while spatial resolution has been preserved, as will be shown inthe following sections.
3 Measurements
We currently have several mouse data sets available for double gating that were measured in-house.Three of them shall be presented here. The first and second mouse was scanned with a dual source
4
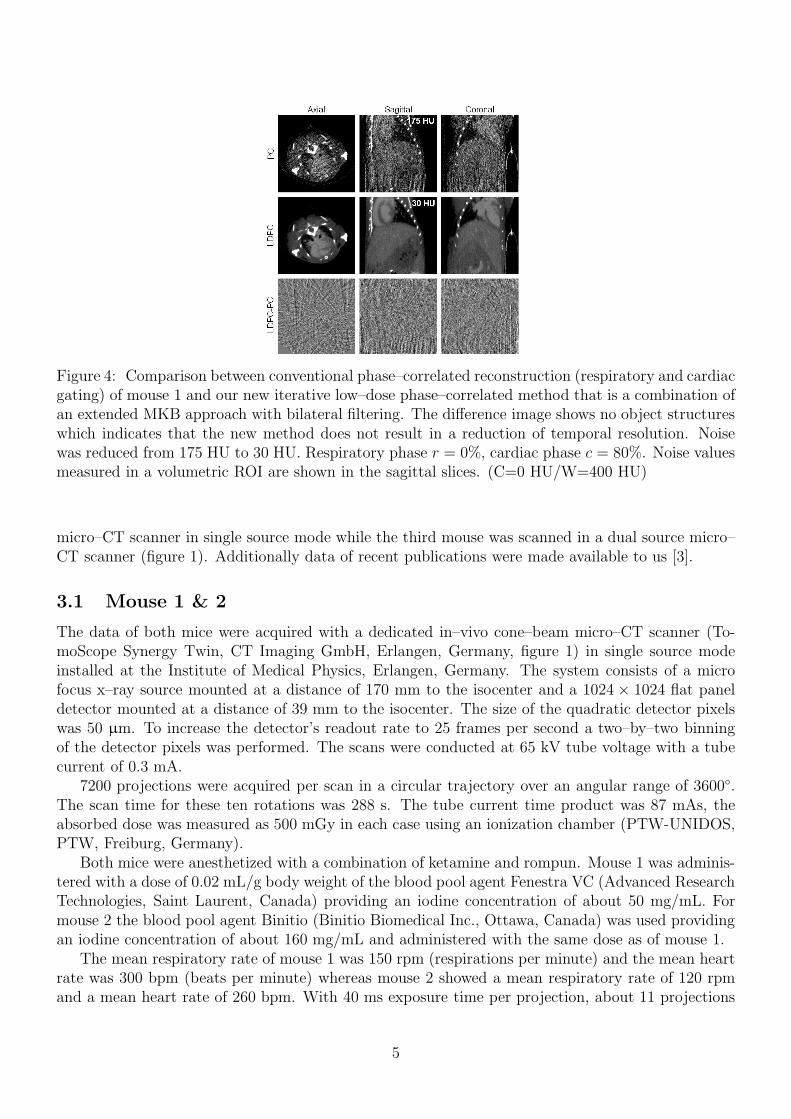
Figure 4: Comparison between conventional phase–correlated reconstruction (respiratory and cardiacgating) of mouse 1 and our new iterative low–dose phase–correlated method that is a combination ofan extended MKB approach with bilateral filtering. The difference image shows no object structureswhich indicates that the new method does not result in a reduction of temporal resolution. Noisewas reduced from 175 HU to 30 HU. Respiratory phase r = 0%, cardiac phase c = 80%. Noise valuesmeasured in a volumetric ROI are shown in the sagittal slices. (C=0 HU/W=400 HU)
micro–CT scanner in single source mode while the third mouse was scanned in a dual source micro–CT scanner (figure 1). Additionally data of recent publications were made available to us [3].
3.1 Mouse 1 & 2
The data of both mice were acquired with a dedicated in–vivo cone–beam micro–CT scanner (To-moScope Synergy Twin, CT Imaging GmbH, Erlangen, Germany, figure 1) in single source modeinstalled at the Institute of Medical Physics, Erlangen, Germany. The system consists of a microfocus x–ray source mounted at a distance of 170 mm to the isocenter and a 1024 × 1024 flat paneldetector mounted at a distance of 39 mm to the isocenter. The size of the quadratic detector pixelswas 50 µm. To increase the detector’s readout rate to 25 frames per second a two–by–two binningof the detector pixels was performed. The scans were conducted at 65 kV tube voltage with a tubecurrent of 0.3 mA.
7200 projections were acquired per scan in a circular trajectory over an angular range of 3600◦.The scan time for these ten rotations was 288 s. The tube current time product was 87 mAs, theabsorbed dose was measured as 500 mGy in each case using an ionization chamber (PTW-UNIDOS,PTW, Freiburg, Germany).
Both mice were anesthetized with a combination of ketamine and rompun. Mouse 1 was adminis-tered with a dose of 0.02 mL/g body weight of the blood pool agent Fenestra VC (Advanced ResearchTechnologies, Saint Laurent, Canada) providing an iodine concentration of about 50 mg/mL. Formouse 2 the blood pool agent Binitio (Binitio Biomedical Inc., Ottawa, Canada) was used providingan iodine concentration of about 160 mg/mL and administered with the same dose as of mouse 1.
The mean respiratory rate of mouse 1 was 150 rpm (respirations per minute) and the mean heartrate was 300 bpm (beats per minute) whereas mouse 2 showed a mean respiratory rate of 120 rpmand a mean heart rate of 260 bpm. With 40 ms exposure time per projection, about 11 projections
5
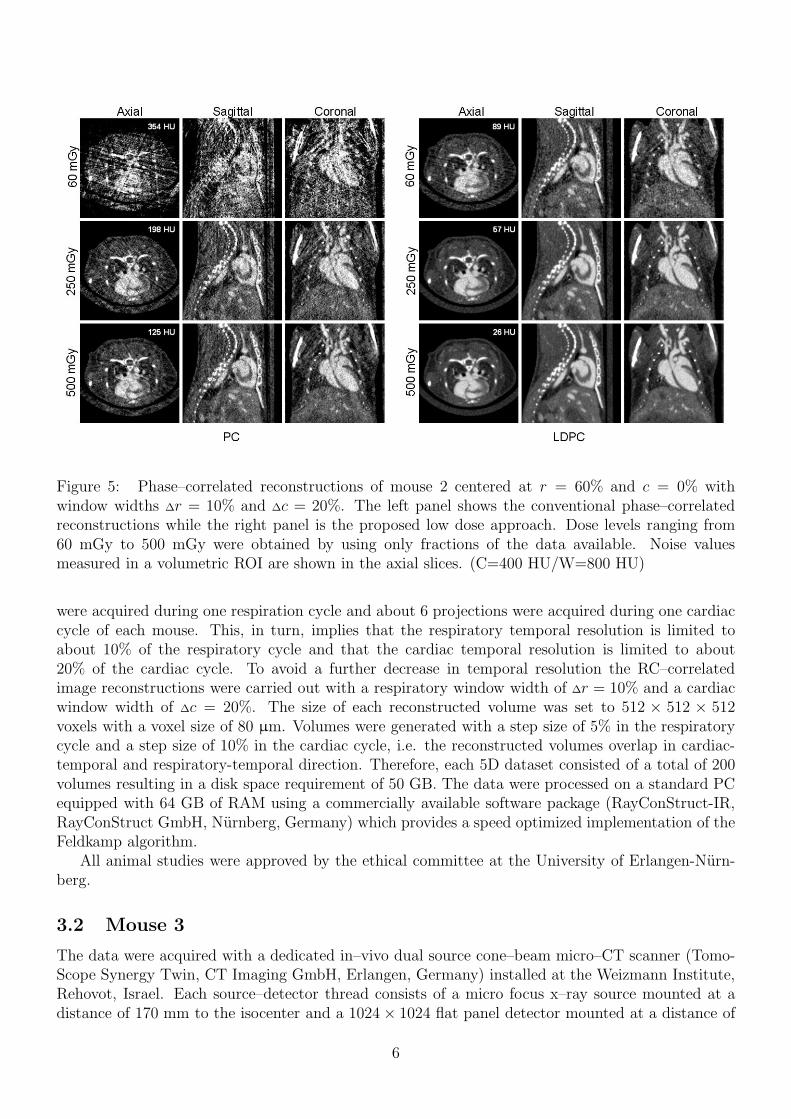
Figure 5: Phase–correlated reconstructions of mouse 2 centered at r = 60% and c = 0% withwindow widths ∆r = 10% and ∆c = 20%. The left panel shows the conventional phase–correlatedreconstructions while the right panel is the proposed low dose approach. Dose levels ranging from60 mGy to 500 mGy were obtained by using only fractions of the data available. Noise valuesmeasured in a volumetric ROI are shown in the axial slices. (C=400 HU/W=800 HU)
were acquired during one respiration cycle and about 6 projections were acquired during one cardiaccycle of each mouse. This, in turn, implies that the respiratory temporal resolution is limited toabout 10% of the respiratory cycle and that the cardiac temporal resolution is limited to about20% of the cardiac cycle. To avoid a further decrease in temporal resolution the RC–correlatedimage reconstructions were carried out with a respiratory window width of ∆r = 10% and a cardiacwindow width of ∆c = 20%. The size of each reconstructed volume was set to 512 × 512 × 512voxels with a voxel size of 80 µm. Volumes were generated with a step size of 5% in the respiratorycycle and a step size of 10% in the cardiac cycle, i.e. the reconstructed volumes overlap in cardiac-temporal and respiratory-temporal direction. Therefore, each 5D dataset consisted of a total of 200volumes resulting in a disk space requirement of 50 GB. The data were processed on a standard PCequipped with 64 GB of RAM using a commercially available software package (RayConStruct-IR,RayConStruct GmbH, Nurnberg, Germany) which provides a speed optimized implementation of theFeldkamp algorithm.
All animal studies were approved by the ethical committee at the University of Erlangen-Nurn-berg.
3.2 Mouse 3
The data were acquired with a dedicated in–vivo dual source cone–beam micro–CT scanner (Tomo-Scope Synergy Twin, CT Imaging GmbH, Erlangen, Germany) installed at the Weizmann Institute,Rehovot, Israel. Each source–detector thread consists of a micro focus x–ray source mounted at adistance of 170 mm to the isocenter and a 1024× 1024 flat panel detector mounted at a distance of
6
62 mm to the isocenter. Both detectors were laterally shifted to increase the field of measurementto a diameter of 60 mm while leaving an 18 mm inner field of measurement [16]. Both threads weremounted under an angle of approximately 90◦. Only the projections originating from source 1 wereused for reconstruction.
The size of the quadratic detector pixels was 50 µm. To increase the detector’s readout rate to25 frames per second a two–by–two binning of the detector pixels was performed. The scan wasconducted at 40 kV tube voltage with a tube current of 1.0 mA per tube. 7200 projections wereacquired in a circular scan over an angular range of 3600◦. The scan time for these ten rotationswas 288 s resulting in an overall tube current time product of 576 mAs and an absorbed dose of1077 mGy thus 500 mGy per source–detector system.
The mouse was anesthetized using a combination of ketamine and xylazine. The contrast agentused was Omnipaque Iohexol (GE Healthcare, Buckinghamshire, United Kingdom) containing 300mg/mL iodine and was administered at a dose of 0.02 mL/g body weight.
4 Results
4.1 Mouse 1 & 2
Although the contrast enhancement in the heart between blood and myocardium of mouse 1 is onlyabout 110 HU our reconstruction and postprocessing approach yields images of surprisingly highquality. Figure 4 compares the results of our new RC–gated approach (LDPC) with a conventionalRC–gated approach (PC) that simply feeds only those projections corresponding to the desiredmotion phases into a modified Feldkamp reconstruction algorithm. With our gating parametersof using a respiratory window of 10% width and a cardiac window of 20% width only 2% of theprojections fall into desired motion phases. Hence the conventional simple gating approach suffersfrom significantly increased image noise and from streak artifacts due to sparse view sampling. Withthe new and improved algorithm we can reduce image noise from 175 HU to 30 HU and we canremove all streak artifacts while maintaining the full temporal resolution (as far as one can tell fromthe difference images).
To further quantify that the proposed algorithm does not decrease spatial resolution figure 6compares several edge profiles measured within a sagittal slice of mouse 2 reconstructed with thestandard method and the new LDPC method. Thereby figure 6a shows the change in CT values froma costal arch to the sourrounding soft tissue. Figure 6b shows an edge between a contrast–enhancedstructure of the heart and the unenhanced soft tissue nearby. Additionally an edge between themouse bed to the adjacent air is shown in figure 6c. These profiles all indicate that there is no lossof edge information due to the new and improved algorithm compared to a reconstruction using thestandard PC algorithm.
It should be further noted that image noise was measured in difference images of adjacent slicesin z-direction obtained in a homogeneous region of interest (ROI) in the liver region. The same ROIwas used for all reconstructions and it is not necessarily intersecting those slices that are shown inthe images.
Regarding figure 7, which also shows the image quality obtained using a standard FDK recon-struction that is non–gated and where moving structures appear blurred, it is interesting to see thatRC–gating increases image noise by only 36% (corresponding to 8 HU) when our new reconstruc-tion approach is being used. This is quite remarkable because the gated images show a temporalresolution corresponding to using only 2% of the data available.
7
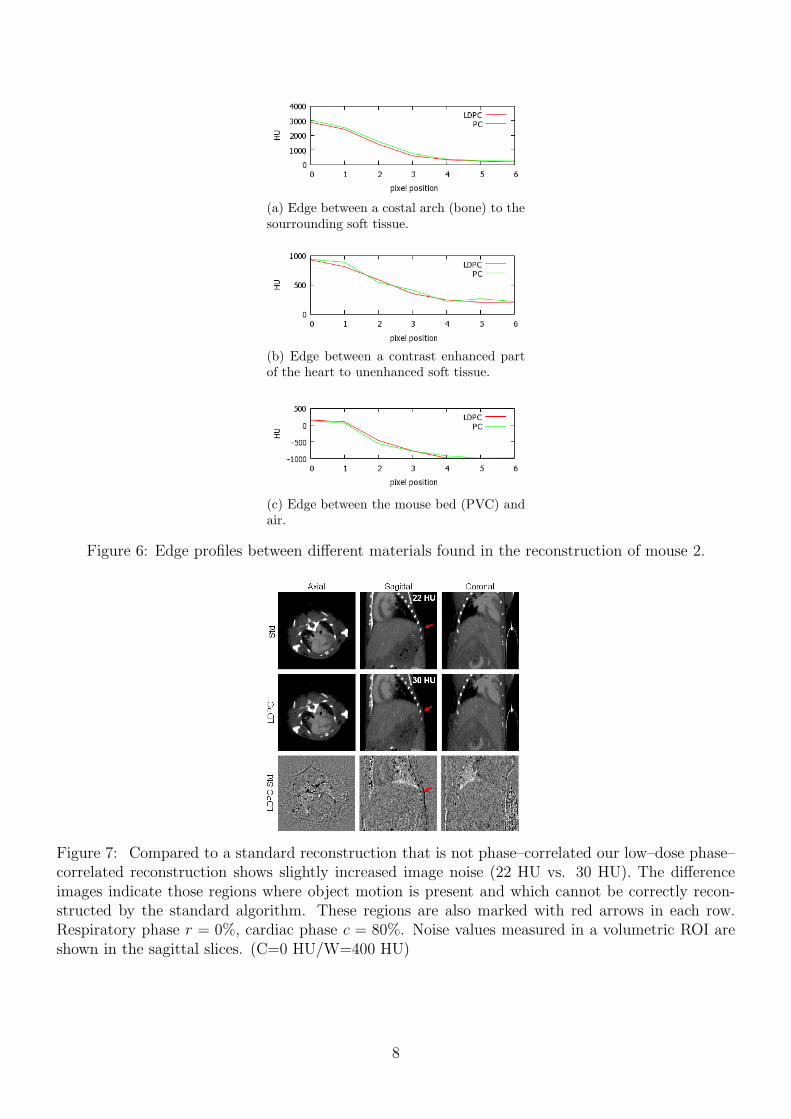
(a) Edge between a costal arch (bone) to thesourrounding soft tissue.
(b) Edge between a contrast enhanced partof the heart to unenhanced soft tissue.
(c) Edge between the mouse bed (PVC) andair.
Figure 6: Edge profiles between different materials found in the reconstruction of mouse 2.
Figure 7: Compared to a standard reconstruction that is not phase–correlated our low–dose phase–correlated reconstruction shows slightly increased image noise (22 HU vs. 30 HU). The differenceimages indicate those regions where object motion is present and which cannot be correctly recon-structed by the standard algorithm. These regions are also marked with red arrows in each row.Respiratory phase r = 0%, cardiac phase c = 80%. Noise values measured in a volumetric ROI areshown in the sagittal slices. (C=0 HU/W=400 HU)
8
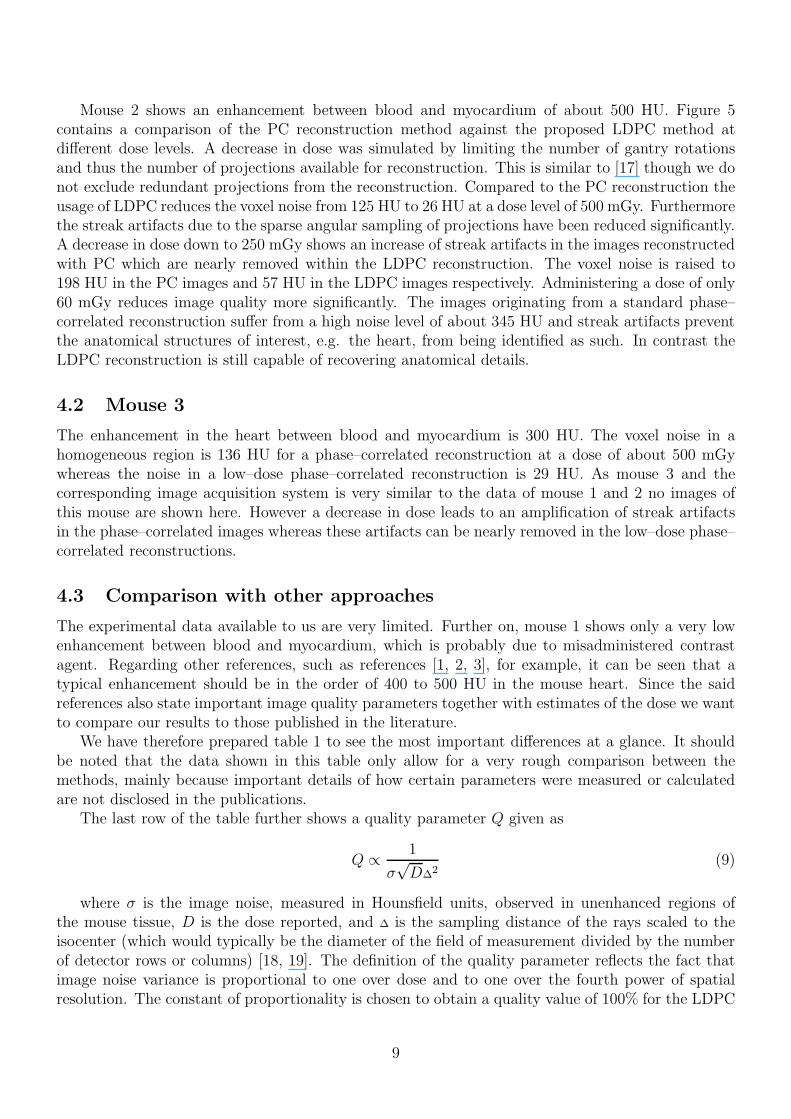
Mouse 2 shows an enhancement between blood and myocardium of about 500 HU. Figure 5contains a comparison of the PC reconstruction method against the proposed LDPC method atdifferent dose levels. A decrease in dose was simulated by limiting the number of gantry rotationsand thus the number of projections available for reconstruction. This is similar to [17] though we donot exclude redundant projections from the reconstruction. Compared to the PC reconstruction theusage of LDPC reduces the voxel noise from 125 HU to 26 HU at a dose level of 500 mGy. Furthermorethe streak artifacts due to the sparse angular sampling of projections have been reduced significantly.A decrease in dose down to 250 mGy shows an increase of streak artifacts in the images reconstructedwith PC which are nearly removed within the LDPC reconstruction. The voxel noise is raised to198 HU in the PC images and 57 HU in the LDPC images respectively. Administering a dose of only60 mGy reduces image quality more significantly. The images originating from a standard phase–correlated reconstruction suffer from a high noise level of about 345 HU and streak artifacts preventthe anatomical structures of interest, e.g. the heart, from being identified as such. In contrast theLDPC reconstruction is still capable of recovering anatomical details.
4.2 Mouse 3
The enhancement in the heart between blood and myocardium is 300 HU. The voxel noise in ahomogeneous region is 136 HU for a phase–correlated reconstruction at a dose of about 500 mGywhereas the noise in a low–dose phase–correlated reconstruction is 29 HU. As mouse 3 and thecorresponding image acquisition system is very similar to the data of mouse 1 and 2 no images ofthis mouse are shown here. However a decrease in dose leads to an amplification of streak artifactsin the phase–correlated images whereas these artifacts can be nearly removed in the low–dose phase–correlated reconstructions.
4.3 Comparison with other approaches
The experimental data available to us are very limited. Further on, mouse 1 shows only a very lowenhancement between blood and myocardium, which is probably due to misadministered contrastagent. Regarding other references, such as references [1, 2, 3], for example, it can be seen that atypical enhancement should be in the order of 400 to 500 HU in the mouse heart. Since the saidreferences also state important image quality parameters together with estimates of the dose we wantto compare our results to those published in the literature.
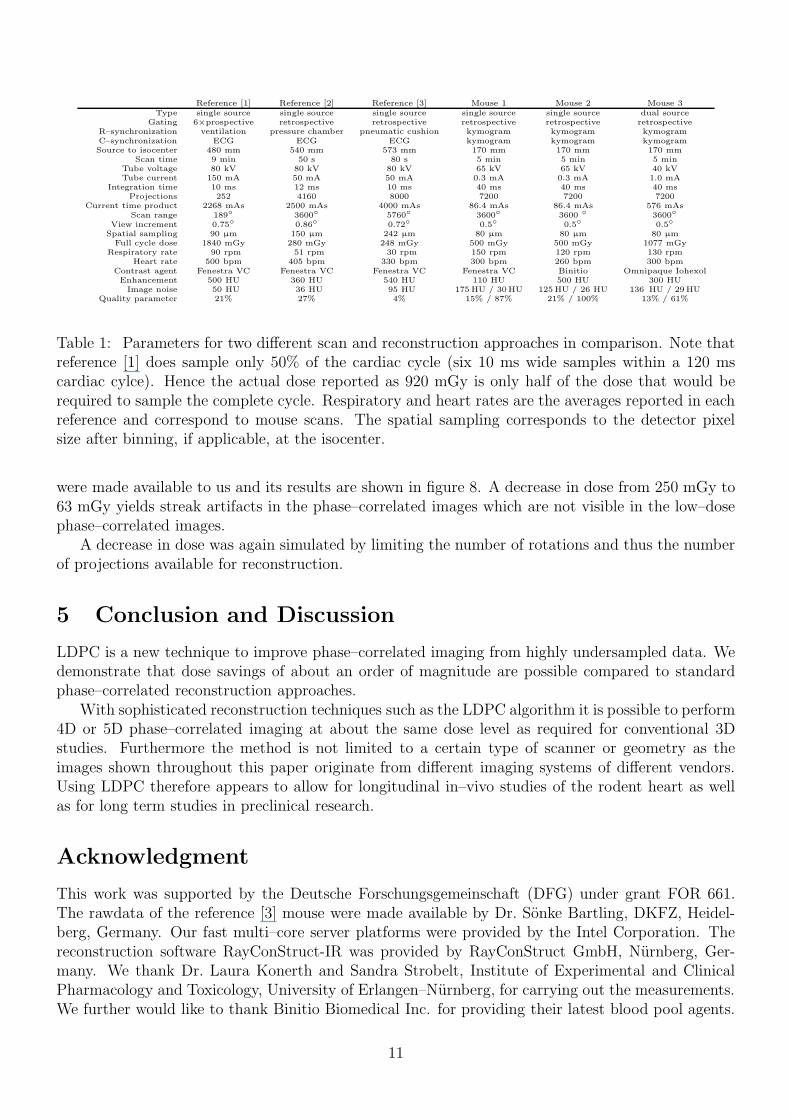
We have therefore prepared table 1 to see the most important differences at a glance. It shouldbe noted that the data shown in this table only allow for a very rough comparison between themethods, mainly because important details of how certain parameters were measured or calculatedare not disclosed in the publications.
The last row of the table further shows a quality parameter Q given as
Q ∝1
σ√D∆
2(9)
where σ is the image noise, measured in Hounsfield units, observed in unenhanced regions ofthe mouse tissue, D is the dose reported, and ∆ is the sampling distance of the rays scaled to theisocenter (which would typically be the diameter of the field of measurement divided by the numberof detector rows or columns) [18, 19]. The definition of the quality parameter reflects the fact thatimage noise variance is proportional to one over dose and to one over the fourth power of spatialresolution. The constant of proportionality is chosen to obtain a quality value of 100% for the LDPC
9
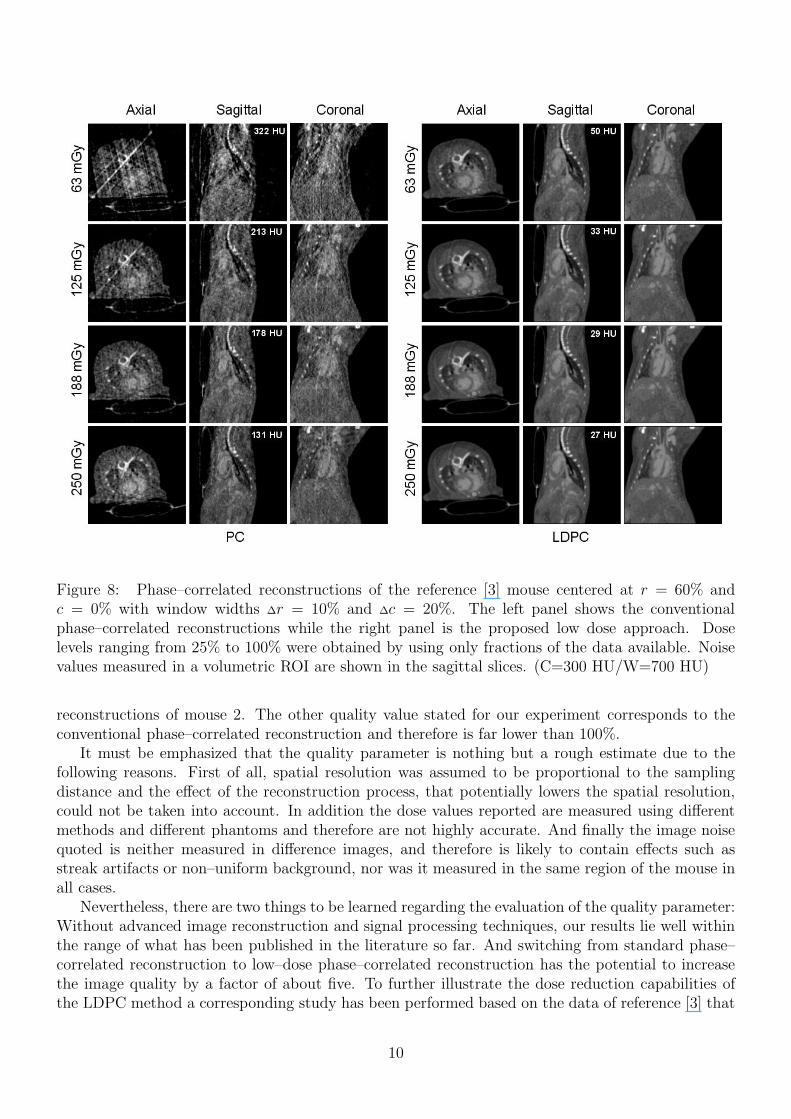
Figure 8: Phase–correlated reconstructions of the reference [3] mouse centered at r = 60% andc = 0% with window widths ∆r = 10% and ∆c = 20%. The left panel shows the conventionalphase–correlated reconstructions while the right panel is the proposed low dose approach. Doselevels ranging from 25% to 100% were obtained by using only fractions of the data available. Noisevalues measured in a volumetric ROI are shown in the sagittal slices. (C=300 HU/W=700 HU)
reconstructions of mouse 2. The other quality value stated for our experiment corresponds to theconventional phase–correlated reconstruction and therefore is far lower than 100%.
It must be emphasized that the quality parameter is nothing but a rough estimate due to thefollowing reasons. First of all, spatial resolution was assumed to be proportional to the samplingdistance and the effect of the reconstruction process, that potentially lowers the spatial resolution,could not be taken into account. In addition the dose values reported are measured using differentmethods and different phantoms and therefore are not highly accurate. And finally the image noisequoted is neither measured in difference images, and therefore is likely to contain effects such asstreak artifacts or non–uniform background, nor was it measured in the same region of the mouse inall cases.
Nevertheless, there are two things to be learned regarding the evaluation of the quality parameter:Without advanced image reconstruction and signal processing techniques, our results lie well withinthe range of what has been published in the literature so far. And switching from standard phase–correlated reconstruction to low–dose phase–correlated reconstruction has the potential to increasethe image quality by a factor of about five. To further illustrate the dose reduction capabilities ofthe LDPC method a corresponding study has been performed based on the data of reference [3] that
10
Reference [1] Reference [2] Reference [3] Mouse 1 Mouse 2 Mouse 3Type single source single source single source single source single source dual source
Gating 6×prospective retrospective retrospective retrospective retrospective retrospectiveR–synchronization ventilation pressure chamber pneumatic cushion kymogram kymogram kymogramC–synchronization ECG ECG ECG kymogram kymogram kymogramSource to isocenter 480 mm 540 mm 573 mm 170 mm 170 mm 170 mm
Scan time 9 min 50 s 80 s 5 min 5 min 5 minTube voltage 80 kV 80 kV 80 kV 65 kV 65 kV 40 kVTube current 150 mA 50 mA 50 mA 0.3 mA 0.3 mA 1.0 mA
Integration time 10 ms 12 ms 10 ms 40 ms 40 ms 40 msProjections 252 4160 8000 7200 7200 7200
Current time product 2268 mAs 2500 mAs 4000 mAs 86.4 mAs 86.4 mAs 576 mAsScan range 189◦ 3600◦ 5760◦ 3600◦ 3600 ◦ 3600◦
View increment 0.75◦ 0.86◦ 0.72◦ 0.5◦ 0.5◦ 0.5◦
Spatial sampling 90 µm 150 µm 242 µm 80 µm 80 µm 80 µmFull cycle dose 1840 mGy 280 mGy 248 mGy 500 mGy 500 mGy 1077 mGy
Respiratory rate 90 rpm 51 rpm 30 rpm 150 rpm 120 rpm 130 rpmHeart rate 500 bpm 405 bpm 330 bpm 300 bpm 260 bpm 300 bpm
Contrast agent Fenestra VC Fenestra VC Fenestra VC Fenestra VC Binitio Omnipaque IohexolEnhancement 500 HU 360 HU 540 HU 110 HU 500 HU 300 HUImage noise 50 HU 36 HU 95 HU 175 HU / 30HU 125HU / 26 HU 136 HU / 29HU
Quality parameter 21% 27% 4% 15% / 87% 21% / 100% 13% / 61%
Table 1: Parameters for two different scan and reconstruction approaches in comparison. Note thatreference [1] does sample only 50% of the cardiac cycle (six 10 ms wide samples within a 120 mscardiac cylce). Hence the actual dose reported as 920 mGy is only half of the dose that would berequired to sample the complete cycle. Respiratory and heart rates are the averages reported in eachreference and correspond to mouse scans. The spatial sampling corresponds to the detector pixelsize after binning, if applicable, at the isocenter.
were made available to us and its results are shown in figure 8. A decrease in dose from 250 mGy to63 mGy yields streak artifacts in the phase–correlated images which are not visible in the low–dosephase–correlated images.
A decrease in dose was again simulated by limiting the number of rotations and thus the numberof projections available for reconstruction.
5 Conclusion and Discussion
LDPC is a new technique to improve phase–correlated imaging from highly undersampled data. Wedemonstrate that dose savings of about an order of magnitude are possible compared to standardphase–correlated reconstruction approaches.
With sophisticated reconstruction techniques such as the LDPC algorithm it is possible to perform4D or 5D phase–correlated imaging at about the same dose level as required for conventional 3Dstudies. Furthermore the method is not limited to a certain type of scanner or geometry as theimages shown throughout this paper originate from different imaging systems of different vendors.Using LDPC therefore appears to allow for longitudinal in–vivo studies of the rodent heart as wellas for long term studies in preclinical research.
Acknowledgment
This work was supported by the Deutsche Forschungsgemeinschaft (DFG) under grant FOR 661.The rawdata of the reference [3] mouse were made available by Dr. Sonke Bartling, DKFZ, Heidel-berg, Germany. Our fast multi–core server platforms were provided by the Intel Corporation. Thereconstruction software RayConStruct-IR was provided by RayConStruct GmbH, Nurnberg, Ger-many. We thank Dr. Laura Konerth and Sandra Strobelt, Institute of Experimental and ClinicalPharmacology and Toxicology, University of Erlangen–Nurnberg, for carrying out the measurements.We further would like to thank Binitio Biomedical Inc. for providing their latest blood pool agents.
11
References
[1] C.T. Badea, B. Fubara, L.W. Hedlund, and G.A. Johnson. 4D micro–CT of the mouse heart.Molecular Imaging, 4(2):110–116, April/June 2005.
[2] Maria Drangova, Nancy L. Ford, Sarah A. Detombe, Andrew R. Wheatley, and David W.Holdsworth. Fast retrospectively gated quantitative four–dimensional (4D) cardiac micro com-puted tomography imaging of free–breathing mice. Investigative Radiology, 42(2):85–94, Febru-ary 2007.
[3] Soenke H. Bartling, Wolfram Stiller, Michael Grasruck, Bernhard Schmidt, Peter Peschke,Wolfhard Semmler, and Fabian Kiessling. Retrospective motion gating in small animal CTof mice and rats. Investigative Radiology, 42(10):704–714, oct 2007.
[4] Nancy L. Ford, Hristo N. Nikolov, Chris J.D. Norley, Michael M. Thornton, Paula J. Foster,Maria Drangova, and David W. Holdsworth. Prospective respiratory–gated micro–CT of freebreathing rodents. Med. Phys., 32(9):2888–2898, September 2005.
[5] C.T. Badea, L.W. Hedlund, and G.A. Johnson. Micro–CT with respiratory and cardiac gating.Med. Phys., 31(12):3324–3329, December 2004.
[6] Julien Dinkel, Soenke H. Bartling, Jan Kuntz, Michael Grasruck, Annette Kopp-Schneider,Masayoshi Iwasaki, Stefanie Dimmeler, Rajiv Gupta, Wolfhard Semmler, Hans-Ulrich Kauc-zor, and Fabian Kiessling. Intrinsic gating for small–animal computed tomography: A robustECG–less paradigm for deriving cardiac phase information and functional imaging. Circulation:Cardiovascular Imaging, 1(3):235–243, 2008.
[7] Marc Kachelrieß, Dirk-Alexander Sennst, Wolfgang Maxlmoser, and Willi A. Kalender. Kymo-gram detection and kymogram–correlated image reconstruction from subsecond spiral computedtomography scans of the heart. Med. Phys., 29(7):1489–1503, July 2002.
[8] Andrew C. Larson, Richard D. White, Gerhard Laub, Elliot R. McVeigh, Debiao Li, and Or-lando P. Simonetti. Self–gated cardiac cine MRI. Magnetic Resonance in Medicine, 51:93–102,2004.
[9] Lambert Zijp, Jan-Jakob Sonke, and Marcel van Herk. Extraction of the respiratory signalfrom sequential thorax cone–beam x–ray images. Proc. of the 14th ICCR, Seoul, Korea, pages507–509, 2004.
[10] Jan-Jakob Sonke, Lambert Zijp, Peter Remeijer, and Marcel van Herk. Respiratory correlatedcone beam CT. Med. Phys., 32(4):1176–1186, April 2005.
[11] Soenke H. Bartling, Julien Dinkel, Wolfram Stiller, Michael Grasruck, Ijad Madisch, Hans-UlrichKauczor, Wolfhard Semmler, Rajiv Gupta, and Fabian Kiessling. Intrinsic respiratory gating insmall–animal CT. European Radiology, 18(7):1375–1384, July 2008.
[12] L.A. Feldkamp, L.C. Davis, and J.W. Kress. Practical cone–beam algorithm. Journal of the
Optical Society of America, 1(6):612–619, June 1984.
[13] Graeme C. McKinnon and R.H.T. Bates. Towards imaging the beating heart usefully with aconventional CT scanner. IEEE Transactions on Biomedical Engineering, BME-28(2):123–127,February 1981.
12
[14] Kathryn L. Garden and Richard A. Robb. 3-D reconstruction of the heart from few projections:A practical implementation of the McKinnon–Bates algorithm. IEEE Transactions on Medical
Imaging, MI-5(4):233–239, December 1986.
[15] C. Tomasi and R. Manduchi. Bilateral filtering for gray and color images. Proc. 6th Int. Conf.
Computer Vision, pages 839–846, 1998.
[16] Clemens Maaß, Michael Knaup, Robert Lapp, Marek Karolczak, Willi A. Kalender, and MarcKachelrieß. A new weighting function to achieve high temporal resolution in circular cone–beamCT with shifted detectors. Med. Phys., 35(12):5898–5909, December 2008.
[17] Nancy L. Ford, Andrew R. Wheatley, David W. Holdsworth, and Maria Drangova. Optimizationof a retrospective technique for respiratory–gated high speed micro–ct of free–breathing rodents.Physics in Medicine and Biology, 52(19):5749–5769, October 2007.
[18] Willi A. Kalender. Computed Tomography. Wiley & Sons, 2005. ISBN 3–89578–216–5, 2ndEdition.
[19] Marc Kachelrieß, Katia Sourbelle, and Willi A. Kalender. Extended parallel backprojec-tion (epbp) for spiral and circular cardiac cone–beam CT with up to 256 slices. Radiology,229(P):427–428, November 2003.
[20] Marc Kachelrieß, Oliver Watzke, and Willi A. Kalender. Generalized multi–dimensional adaptivefiltering (MAF) for conventional and spiral single–slice, multi–slice and cone–beam CT. Med.
Phys., 28(4):475–490, April 2001.
[21] Anja Borsdorf, Steffen Kappler, Rainer Raupach, Frederic Noo, and Joachim Hornegger. Localorientation–dependent noise propagation for anisotropic denoising of CT–images. IEEE Medical
Imaging Conference Record, pages M02–2, 2472–2475, October 2009.
13
Related Documents