Loop-mediated isothermal amplification assay for rapid and sensitive diagnosis of tuberculosis Parveen Kumar a , Deepal Pandya b , Niti Singh c , Digambar Behera c,e , Praveen Aggarwal d , Sarman Singh a, * a Division of Clinical Microbiology and Molecular Medicine, All India Institute of Medical Sciences, New Delhi 110029, India b AmpliGene India Biotech Pvt. Ltd., Ahmedabad, Gujarat, India c National Institute of Tuberculosis and Respiratory Diseases, New Delhi, India d Department of Emergency Medicine, All India Institute of Medical Sciences, New Delhi, India Accepted 12 August 2014 Available online --- KEYWORDS LAMP; esat-6; Mycobacterium tuberculosis; Multiplex PCR Summary Objectives: Loop-mediated isothermal amplification (LAMP) is a newly developed molecular method that can be performed isothermally. We developed and evaluated a LAMP assay using novel primers to diagnose tuberculosis directly from clinical samples. Materials: Primers were designed to amplify the specific novel esat-6 gene target of Mycobac- terium tuberculosis (MTB). Quantitated DNA was used to determine analytical sensitivity and specificity was evaluated by testing 29 NTM and 37 other bacterial species. After standardiza- tion, its sensitivity and specificity were evaluated on samples from 118 TB suspected and 31 non-TB patients and compared it with smear, culture and mPCR methods. Results: LAMP was able to detect 5 fg DNA (one MTB) within 21 min and found to be 10 times more sensitive than mPCR and showed 100% specificity against NTM and other bacterial spe- cies. In clinical samples, LAMP showed highest MTB detection rate (52.5%) as compared to mPCR (44%) and culture (30.5%). On culture positive and mPCR positive samples, the sensitivity of LAMP was found to be 100% (95% CI 90.2e100) and 96.1% (95% CI 86.7e99.5) respectively with 93.5% (95% CI 78.5e99.2) of overall specificity. Conclusion: LAMP was found to be more sensitive than culture and mPCR for the detection of MTB. It showed specificity comparable to mPCR but was rapid and cost effective. ª 2014 The British Infection Association. Published by Elsevier Ltd. All rights reserved. * Corresponding author. Tel.: þ91 11 2658 8484; fax: þ91 11 2658 8663, þ91 11 2658 8641. E-mail addresses: [email protected], [email protected] (S. Singh). e Present address: Post-Graduate Institute of Medical Education and Research, Chandigarh, India. http://dx.doi.org/10.1016/j.jinf.2014.08.017 0163-4453/ª 2014 The British Infection Association. Published by Elsevier Ltd. All rights reserved. www.elsevierhealth.com/journals/jinf Journal of Infection (2014) xx,1e9 Please cite this article in press as: Kumar P, et al., Loop-mediated isothermal amplification assay for rapid and sensitive diagnosis of tuberculosis, J Infect (2014), http://dx.doi.org/10.1016/j.jinf.2014.08.017

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Journal of Infection (2014) xx, 1e9
www.elsevierhealth.com/journals/jinf
Loop-mediated isothermal amplificationassay for rapid and sensitive diagnosis oftuberculosis
Parveen Kumar a, Deepal Pandya b, Niti Singh c,Digambar Behera c,e, Praveen Aggarwal d, Sarman Singh a,*
aDivision of Clinical Microbiology and Molecular Medicine, All India Institute of Medical Sciences,New Delhi 110029, IndiabAmpliGene India Biotech Pvt. Ltd., Ahmedabad, Gujarat, IndiacNational Institute of Tuberculosis and Respiratory Diseases, New Delhi, IndiadDepartment of Emergency Medicine, All India Institute of Medical Sciences, New Delhi, India
Accepted 12 August 2014Available online - - -
KEYWORDSLAMP;esat-6;Mycobacteriumtuberculosis;Multiplex PCR
* Corresponding author. Tel.: þ91 1E-mail addresses: sarman_singh@ye Present address: Post-Graduate In
http://dx.doi.org/10.1016/j.jinf.20140163-4453/ª 2014 The British Infectio
Please cite this article in press as: Ktuberculosis, J Infect (2014), http://
Summary Objectives: Loop-mediated isothermal amplification (LAMP) is a newly developedmolecular method that can be performed isothermally. We developed and evaluated a LAMPassay using novel primers to diagnose tuberculosis directly from clinical samples.Materials: Primers were designed to amplify the specific novel esat-6 gene target of Mycobac-terium tuberculosis (MTB). Quantitated DNA was used to determine analytical sensitivity andspecificity was evaluated by testing 29 NTM and 37 other bacterial species. After standardiza-tion, its sensitivity and specificity were evaluated on samples from 118 TB suspected and 31non-TB patients and compared it with smear, culture and mPCR methods.Results: LAMP was able to detect 5 fg DNA (one MTB) within 21 min and found to be 10 timesmore sensitive than mPCR and showed 100% specificity against NTM and other bacterial spe-cies. In clinical samples, LAMP showed highest MTB detection rate (52.5%) as compared tomPCR (44%) and culture (30.5%). On culture positive and mPCR positive samples, the sensitivityof LAMP was found to be 100% (95% CI 90.2e100) and 96.1% (95% CI 86.7e99.5) respectivelywith 93.5% (95% CI 78.5e99.2) of overall specificity.Conclusion: LAMP was found to be more sensitive than culture and mPCR for the detection ofMTB. It showed specificity comparable to mPCR but was rapid and cost effective.ª 2014 The British Infection Association. Published by Elsevier Ltd. All rights reserved.
1 2658 8484; fax: þ91 11 2658 8663, þ91 11 2658 8641.ahoo.com, [email protected] (S. Singh).stitute of Medical Education and Research, Chandigarh, India.
.08.017n Association. Published by Elsevier Ltd. All rights reserved.
umar P, et al., Loop-mediated isothermal amplification assay for rapid and sensitive diagnosis ofdx.doi.org/10.1016/j.jinf.2014.08.017

2 P. Kumar et al.
Introduction
Tuberculosis (TB) remains one of the leading infectiousdiseases, particularly in developing countries. India hasmore new TB cases annually than any other country. In2012, out of the 8.6 million global annual incidental casesof TB, 2.0e2.4 million were estimated to be from India.1
The biggest challenges in TB control remain early and accu-rate diagnosis. Though smear microscopy is the simplestand most rapid diagnostic procedure currently availablebut its sensitivity is very low and requires at least5 � 103 bacilli/ml in the clinical samples which is a very sol-emn issue specially in extra-pulmonary (EPTB) samples.2
The automated liquid culture based Mycobacteria GrowthIndicator Tube (MGIT) system has reduced this time, butstill it is not optimal.3
In last 6e7 years, the diagnosis of TB has undergone amajor breakthrough with the introduction of nucleic acidamplification (NAA) techniques. Using these methodsdirectly on clinical samples, results can be obtained within1e3 days with high sensitivity and specificity. Centers forDisease Control and Prevention (CDC)4 and AmericanThoracic Society (ATS)5 recommend well-standardizedNAA to be performed for rapid screening of patients withsigns and symptoms of pulmonary TB (PTB). Currently,several commercial NAA methods based on different princi-ples are available. These include, Roche’s COBAS AmplicorMTB test6,7 GenProbe’s Amplified M. tuberculosis Directtest (AMTD),6e8 BD’s ProbeTec-ET6,9 and Hain’s GenoTypeMycobacteria Direct assay (GTMD).10 Available real-timepolymerase chain reactions (RT-PCR) systems are, RocheCOBAS TaqMan MTB� test and the Cepheid Xpert MTB/RIFtest.11 These assays have been widely evaluated ondifferent clinical samples and strains. Most of the NAAshowed consistent specificity and good positive predictivevalues but modest and variable sensitivity, particularly insmear-negative and extra-pulmonary TB samples. Eventhough these NAAs are well established but requirementof sophisticated infrastructure, prices of commercial kitsand reagents are not affordable for most of the countrieswith high TB burden. To circumvent these limitations,many of these countries use poorly validated in-housePCR which show variability in their accuracy.12 Hence,there is a high demand of well validated, affordable com-mercial NAA for use in low-resource countries.
In year 2000, Notomi et al.13 developed a loop-mediatedisothermal amplification (LAMP) method for the detectionof viral pathogens. This nucleic acid amplification test isfound to be simple, rapid, highly efficient, specific andcost effective. LAMP assay has several advantages ascompared to the conventional PCR such as requires fewersteps, performed at a fixed temperature and the amplifiedproducts can be visualized from naked eye by adding thedye. LAMP assay has been developed for the detection ofa number of infectious agents, including Vibrio parahaemo-lyticus,14 Dengue virus,15 Trypanosoma brucei,16 Plasmo-dium parasitemia,17 Mycobacterium tuberculosis(MTB),18,19 M. bovis,20 M. avium21 and respiratory viruses22
as well as for nonhuman viruses.23 However, so far for MTBdetection in clinical samples only one commercial versionof this method has been developed. This commercial kit
Please cite this article in press as: Kumar P, et al., Loop-mediated istuberculosis, J Infect (2014), http://dx.doi.org/10.1016/j.jinf.2014.08
was recently evaluated by WHO/FIND. The WHO expertgroup analyzed this evaluation data and agreed that LAMPtechnology has potential as a rapid TB diagnostic tool butmade further recommendations to improve its perfor-mance.24 In the present study, we developed an improvisedversion of LAMP for the specific detection of MTB using thenovel gene target. The efficacy of the LAMP assay was as-sessed by comparing it with other standard TB diagnosticmethods.
Materials and methods
Study settings
The study was performed at the TB research laboratory,Division of Clinical Microbiology and Molecular Medicine, AllIndia Institute of Medical Sciences, New Delhi, which is anaccredited laboratory by the central TB division of theGovernment of India and certified by the STOP-TB for non-commercial rapid culture and drug susceptibility tests.25
The study was approved by the Institute Ethics Committee(Ref. No.IEC/NP-259/2010) and written informed consentwas obtained from all the participants.
LAMP primer designing
The primer designing is the most crucial step to develop asuccessful LAMP assay. LAMP primer sets were designedagainst MTB specific novel target east-6 gene by using theLAMP designer software version 1.10 (Optigene, UK). Thissoftware has special characteristics to design and shortlist superior five LAMP primer sets followed by checkingthe homology and specificity of primers by BLAST. A primerset was composed of outer primers F3 and B3, inner primersforward inner primer (FIP) and backward inner primer (BIP).Loop primers were forward loop primer (FLP) and backwardloop primer (BLP). FIP consists of F1c sequence comple-mentary to F1 and F2 sequence; BIP consists of B1csequence complementary to B1 and B2 sequence (Table 1).
Optimization of the LAMP reaction
LAMP reactions were performed in a volume of 25 mLconsisting of 20 pmol each of inner primers FIP and BIP,5 pmol each of outer primers F3 and B3, 10 pmol each ofloop primers FLP and BLP. The reaction mixture containedof 15 mL of isothermal master mix ISO 0001 (Optigene, UK)which included Geobacillus species DNA polymerase,thermo stable inorganic pyrophosphatase, optimized buffer(containing MgCl2, deoxynucleotide triphosphates anddouble-stranded DNA dye) and 5 mL of extracted DNA astemplate. The LAMP assay was optimized at 65 �C for35 min on a real-time fluorometer Genie II (Optigene,UK). The amplification reaction was terminated at 85 �Cfor 5 min. A melting curve was drawn after the amplifica-tion by measuring the fluorescence to detect the annealingtemperature. Further, the specificity of MTB LAMP wasexamined by performing the assay on 100 ng of genomicDNA isolated from 6 reference mycobacterial strains [MTBH37Rv (TMC-102), M. avium (NCTC-8551), M. intracellulare
othermal amplification assay for rapid and sensitive diagnosis of.017

Table 1 Nucleotide sequences of esat6-LAMP primers.
LAMP primers Nucleotide sequences Length (bp)
F3 CAAGCGCAATCCAGGG 16B3 GCTTCGCTGATCGTCC 16FIP(F1c þ F2) CGCTGCGAGCTTGGTCATGTCACGTCCATTCATTCC 36BIP(B1c þ B2) TAGCGGTTCGGAGGCGTACGTTGTTCAGCTCGGTAG 36Loop F CTGCTTCCCCTCGTCAAG 18Loop B AAATGGGACGCCACGG 16
LAMP assay for TB diangosis 3
(TMC1406), M. terrae (TMC-1450), M. smegmatis MC2155,M. bovis BCG], 37 laboratory maintained mycobacterialspecies and 37 non mycobacterial species as given inTable 2. In order to investigate the analytical sensitivity,LAMP assay was performed at different dilutions of DNA.For this, a known concentration of MTB H37Rv genomicDNA was 10-fold serially diluted in 1� TE buffer (pH 8.8)from 5 ng to 5 � 10�7 ng. The genome copy number ofeach dilution was calculated considering that a singlegenome of MTB is equivalent to approximately 5 fg ofDNA.18 After standardization the LAMP results could beread visually by a simply color change using SYBR green Idye (100�) (Invitrogen, USA).
Use of LAMP assay on clinical samples
The optimized LAMP assay was performed on clinicalsamples to evaluate the feasibility of the test. For this,118 clinical samples (one each) from suspected TB patientssent from various hospitals within and around Delhi for TBdiagnosis were included. Of these 41 were pulmonarysamples (29 sputa, 7 BAL and 5 GA) and 77 extra pulmonarysamples (28 CSF, 11 pus, 15 pleural fluid, 2 ascitic fluid, 7lymph node aspirate, 5 urine, 3 abscess pus and 6 otherbody fluids). The clinical suspicion of TB was based onstandard clinico-radiological findings mentioned in the CDCand ATS guidelines,26,27 e.g. fever with or without cough;weight loss or night sweats lasting longer than 2 weeks;and/or cavitary lesions in the lung fields on radiological ex-amination; or suppurating or non-suppurating cold single ormated lymph nodes. In addition, a total of 31 samples frompatients having no past history of TB and having confirmeddiagnosis of Non-TB infectious or non-infectious diseaseswere included as disease controls. These included 11 sputafrom patients with chronic obstructive pulmonary diseases(COPD), 5 lymph node biopsies from patients of malignantlymphoma, 7 pus and 8 urine samples from patients withbacterial urinary tract infection. The methods of samplesprocessing, mycobacterial culturing, DNA extraction andmultiplex PCR (mPCR) were followed as described else-where.28,29 All study participants gave informed consent,as a standard routine TB diagnostic procedure of thelaboratory.
Statistical analysis
The results of LAMP assay were analyzed and comparedwith standard TB diagnostic methods. Data were main-tained on MS Excel 7.0 and statistically analyzed to
Please cite this article in press as: Kumar P, et al., Loop-mediated istuberculosis, J Infect (2014), http://dx.doi.org/10.1016/j.jinf.2014.08
calculate the sensitivity and specificity of the LAMP assay.Chi-squared test and Fisher’s exact test were also per-formed to analyze the results using Stata 11.1 software.The significance level for these analyzes was defined as a plevel of �0.05.
Results
Optimization of LAMP reaction time andtemperature
The LAMP reaction time, temperature, and primer con-centrations were optimized for the rapid detection of MTBwith the help of Genie II fluorometer. The Genie II displaysthe real time amplification signals and at the end of theassay it displays the time to positivity and annealing Tmfor each sample. During the standardization, the LAMPreaction was standardized at 65 �C isothermal tempera-ture and the amplification times were observed rangingfrom 10.8 to 24 min. The mean time to positivity for allpositive results was 17.2 � 6.19 min. Thus, the optimizedLAMP reaction was set to run for 35 min for testing allother samples.
Analytical sensitivity and specificity of LAMP assay
The optimized LAMP assay showed the lowest (5 fg) amountof MTB DNA was consistently detected within 21 min whichis equivalent to one copy of the MTB genome (Fig. 1A). Theresults showed that a reaction time of 35 min was sufficientto amplify one copy of genomic DNA. The mPCR was able todetect 5 � 10�5 ng of DNA which is a minimum of 10 copiesof purified MTB DNA (50 fg) (Fig. 1B). In conclusion, esat6-LAMP assay was 10 times more sensitive than conventionalmPCR. In addition, the LAMP results could be read visuallyby a change in the color/fluorescence after addition of5 mL of SYBR green (Fig. 2). In order to investigate the spec-ificity, the efficient amplification of DNA by esat6-LAMP wasobserved only in MTB strains within 35 min. In contrast, noDNA amplification was observed with the 29 NTM speciesand 37 other bacterial species, giving 100% specificity(Table 2).
LAMP assay on clinical samples
A total of 118 suspected TB patients, 75 (63.5%) men and 43(36.4%) women were enrolled in this study. Majority [80(67.7%)] of patients were more than 15 years of age (meanage of 38.1 � 16.95) and 38 (32.2%) patients aged less than
othermal amplification assay for rapid and sensitive diagnosis of.017

Figure 2 LAMP amplification results of positive and negative samples can be detected and differentiated with naked eyes (upperpanel A) as well as under ultraviolet light (middle panel B). LAMP results on 2% agarose gel electrophoresis (lower panel C). Panelsare showing LAMP positive results (3e10) and negative results (1e2).
Figure 1 Comparison of determination of analytical sensitivity of the LAMP (panel A) and mPCR (panel B). (A) Detection of sensi-tivity of LAMP assay by a real-time fluorometer Genie II. The results showed detection limit of esat6-LAMP was 5 � 10�6 ng (equal toone genome of MTB (5 fg)) (B) detection limit of mPCR was 5 � 10�5 ng (50 fg) of MTB DNA.
4 P. Kumar et al.
Please cite this article in press as: Kumar P, et al., Loop-mediated isothermal amplification assay for rapid and sensitive diagnosis oftuberculosis, J Infect (2014), http://dx.doi.org/10.1016/j.jinf.2014.08.017
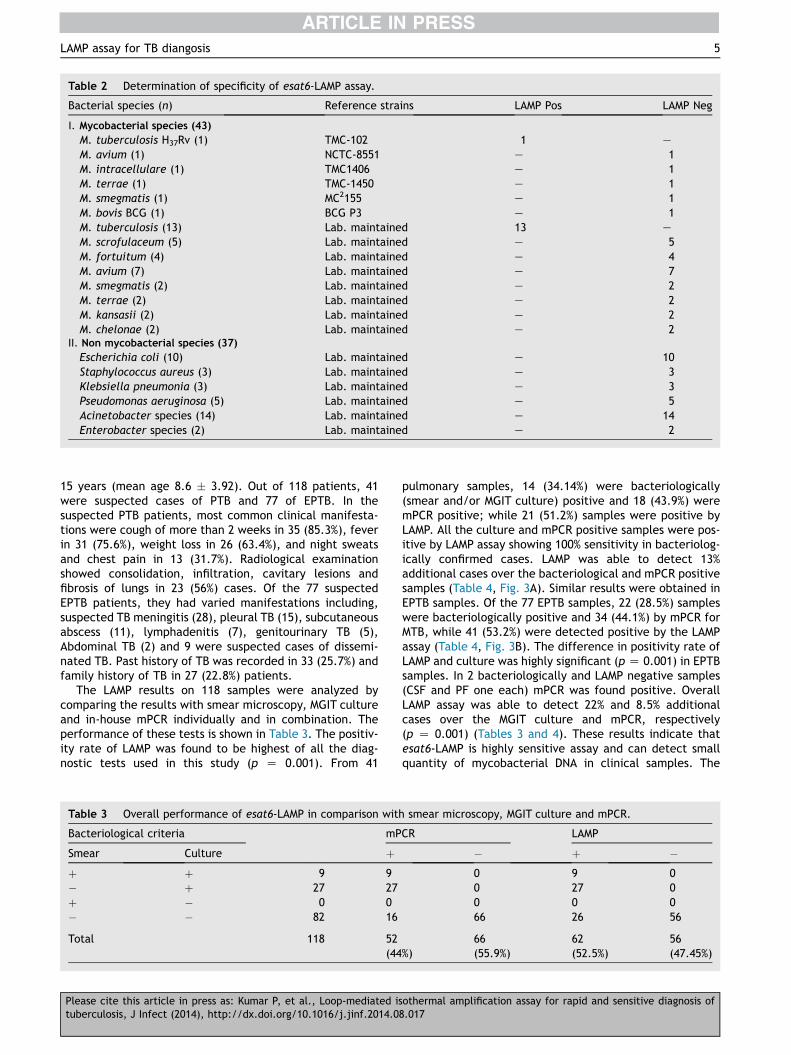
Table 2 Determination of specificity of esat6-LAMP assay.
Bacterial species (n) Reference strains LAMP Pos LAMP Neg
I. Mycobacterial species (43)
M. tuberculosis H37Rv (1) TMC-102 1 e
M. avium (1) NCTC-8551 e 1M. intracellulare (1) TMC1406 e 1M. terrae (1) TMC-1450 e 1M. smegmatis (1) MC2155 e 1M. bovis BCG (1) BCG P3 e 1M. tuberculosis (13) Lab. maintained 13 e
M. scrofulaceum (5) Lab. maintained e 5M. fortuitum (4) Lab. maintained e 4M. avium (7) Lab. maintained e 7M. smegmatis (2) Lab. maintained e 2M. terrae (2) Lab. maintained e 2M. kansasii (2) Lab. maintained e 2M. chelonae (2) Lab. maintained e 2
II. Non mycobacterial species (37)
Escherichia coli (10) Lab. maintained e 10Staphylococcus aureus (3) Lab. maintained e 3Klebsiella pneumonia (3) Lab. maintained e 3Pseudomonas aeruginosa (5) Lab. maintained e 5Acinetobacter species (14) Lab. maintained e 14Enterobacter species (2) Lab. maintained e 2
LAMP assay for TB diangosis 5
15 years (mean age 8.6 � 3.92). Out of 118 patients, 41were suspected cases of PTB and 77 of EPTB. In thesuspected PTB patients, most common clinical manifesta-tions were cough of more than 2 weeks in 35 (85.3%), feverin 31 (75.6%), weight loss in 26 (63.4%), and night sweatsand chest pain in 13 (31.7%). Radiological examinationshowed consolidation, infiltration, cavitary lesions andfibrosis of lungs in 23 (56%) cases. Of the 77 suspectedEPTB patients, they had varied manifestations including,suspected TB meningitis (28), pleural TB (15), subcutaneousabscess (11), lymphadenitis (7), genitourinary TB (5),Abdominal TB (2) and 9 were suspected cases of dissemi-nated TB. Past history of TB was recorded in 33 (25.7%) andfamily history of TB in 27 (22.8%) patients.
The LAMP results on 118 samples were analyzed bycomparing the results with smear microscopy, MGIT cultureand in-house mPCR individually and in combination. Theperformance of these tests is shown in Table 3. The positiv-ity rate of LAMP was found to be highest of all the diag-nostic tests used in this study (p Z 0.001). From 41
Table 3 Overall performance of esat6-LAMP in comparison with
Bacteriological criteria mP
Smear Culture þþ þ 9 9� þ 27 27þ � 0 0� � 82 16
Total 118 52(44
Please cite this article in press as: Kumar P, et al., Loop-mediated istuberculosis, J Infect (2014), http://dx.doi.org/10.1016/j.jinf.2014.08
pulmonary samples, 14 (34.14%) were bacteriologically(smear and/or MGIT culture) positive and 18 (43.9%) weremPCR positive; while 21 (51.2%) samples were positive byLAMP. All the culture and mPCR positive samples were pos-itive by LAMP assay showing 100% sensitivity in bacteriolog-ically confirmed cases. LAMP was able to detect 13%additional cases over the bacteriological and mPCR positivesamples (Table 4, Fig. 3A). Similar results were obtained inEPTB samples. Of the 77 EPTB samples, 22 (28.5%) sampleswere bacteriologically positive and 34 (44.1%) by mPCR forMTB, while 41 (53.2%) were detected positive by the LAMPassay (Table 4, Fig. 3B). The difference in positivity rate ofLAMP and culture was highly significant (p Z 0.001) in EPTBsamples. In 2 bacteriologically and LAMP negative samples(CSF and PF one each) mPCR was found positive. OverallLAMP assay was able to detect 22% and 8.5% additionalcases over the MGIT culture and mPCR, respectively(p Z 0.001) (Tables 3 and 4). These results indicate thatesat6-LAMP is highly sensitive assay and can detect smallquantity of mycobacterial DNA in clinical samples. The
smear microscopy, MGIT culture and mPCR.
CR LAMP
� þ �0 9 00 27 00 0 066 26 56
%)66(55.9%)
62(52.5%)
56(47.45%)
othermal amplification assay for rapid and sensitive diagnosis of.017
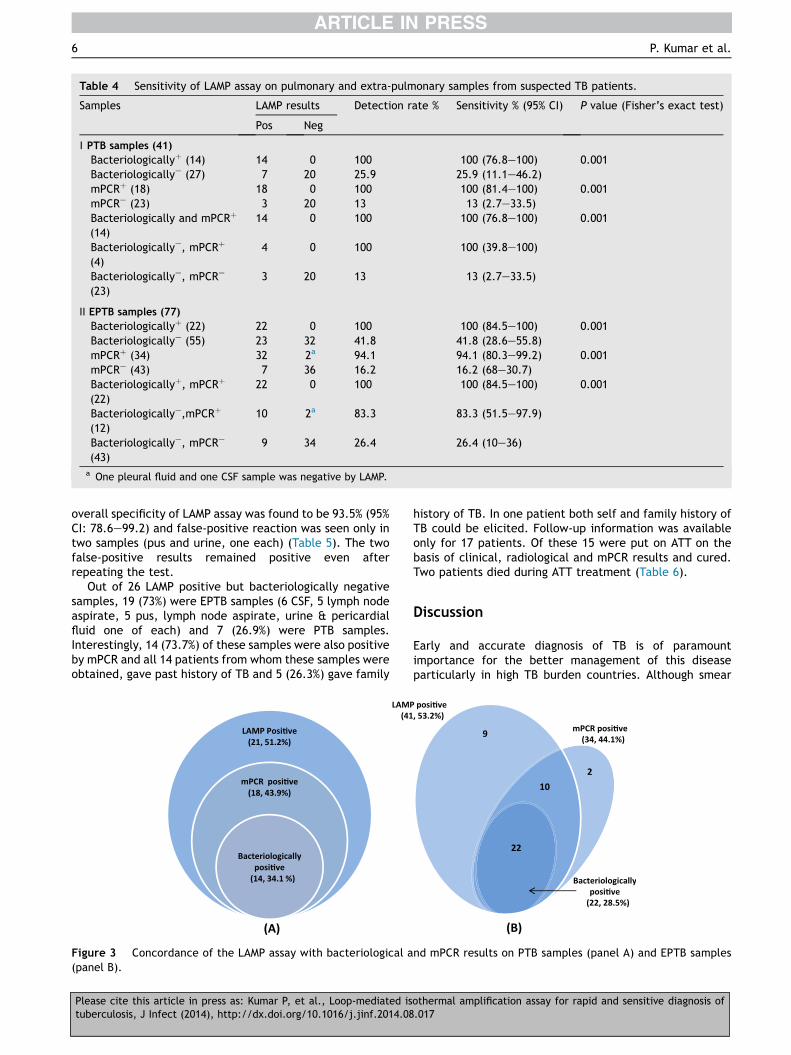
Table 4 Sensitivity of LAMP assay on pulmonary and extra-pulmonary samples from suspected TB patients.
Samples LAMP results Detection rate % Sensitivity % (95% CI) P value (Fisher’s exact test)
Pos Neg
I PTB samples (41)
Bacteriologicallyþ (14) 14 0 100 100 (76.8e100) 0.001Bacteriologicallye (27) 7 20 25.9 25.9 (11.1e46.2)mPCRþ (18) 18 0 100 100 (81.4e100) 0.001mPCRe (23) 3 20 13 13 (2.7e33.5)Bacteriologically and mPCRþ
(14)14 0 100 100 (76.8e100) 0.001
Bacteriologicallye, mPCRþ
(4)4 0 100 100 (39.8e100)
Bacteriologicallye, mPCRe
(23)3 20 13 13 (2.7e33.5)
II EPTB samples (77)
Bacteriologicallyþ (22) 22 0 100 100 (84.5e100) 0.001Bacteriologicallye (55) 23 32 41.8 41.8 (28.6e55.8)mPCRþ (34) 32 2a 94.1 94.1 (80.3e99.2) 0.001mPCRe (43) 7 36 16.2 16.2 (68e30.7)Bacteriologicallyþ, mPCRþ
(22)22 0 100 100 (84.5e100) 0.001
Bacteriologicallye,mPCRþ
(12)10 2a 83.3 83.3 (51.5e97.9)
Bacteriologicallye, mPCRe
(43)9 34 26.4 26.4 (10e36)
a One pleural fluid and one CSF sample was negative by LAMP.
6 P. Kumar et al.
overall specificity of LAMP assay was found to be 93.5% (95%CI: 78.6e99.2) and false-positive reaction was seen only intwo samples (pus and urine, one each) (Table 5). The twofalse-positive results remained positive even afterrepeating the test.
Out of 26 LAMP positive but bacteriologically negativesamples, 19 (73%) were EPTB samples (6 CSF, 5 lymph nodeaspirate, 5 pus, lymph node aspirate, urine & pericardialfluid one of each) and 7 (26.9%) were PTB samples.Interestingly, 14 (73.7%) of these samples were also positiveby mPCR and all 14 patients from whom these samples wereobtained, gave past history of TB and 5 (26.3%) gave family
Figure 3 Concordance of the LAMP assay with bacteriological a(panel B).
Please cite this article in press as: Kumar P, et al., Loop-mediated istuberculosis, J Infect (2014), http://dx.doi.org/10.1016/j.jinf.2014.08
history of TB. In one patient both self and family history ofTB could be elicited. Follow-up information was availableonly for 17 patients. Of these 15 were put on ATT on thebasis of clinical, radiological and mPCR results and cured.Two patients died during ATT treatment (Table 6).
Discussion
Early and accurate diagnosis of TB is of paramountimportance for the better management of this diseaseparticularly in high TB burden countries. Although smear
nd mPCR results on PTB samples (panel A) and EPTB samples
othermal amplification assay for rapid and sensitive diagnosis of.017
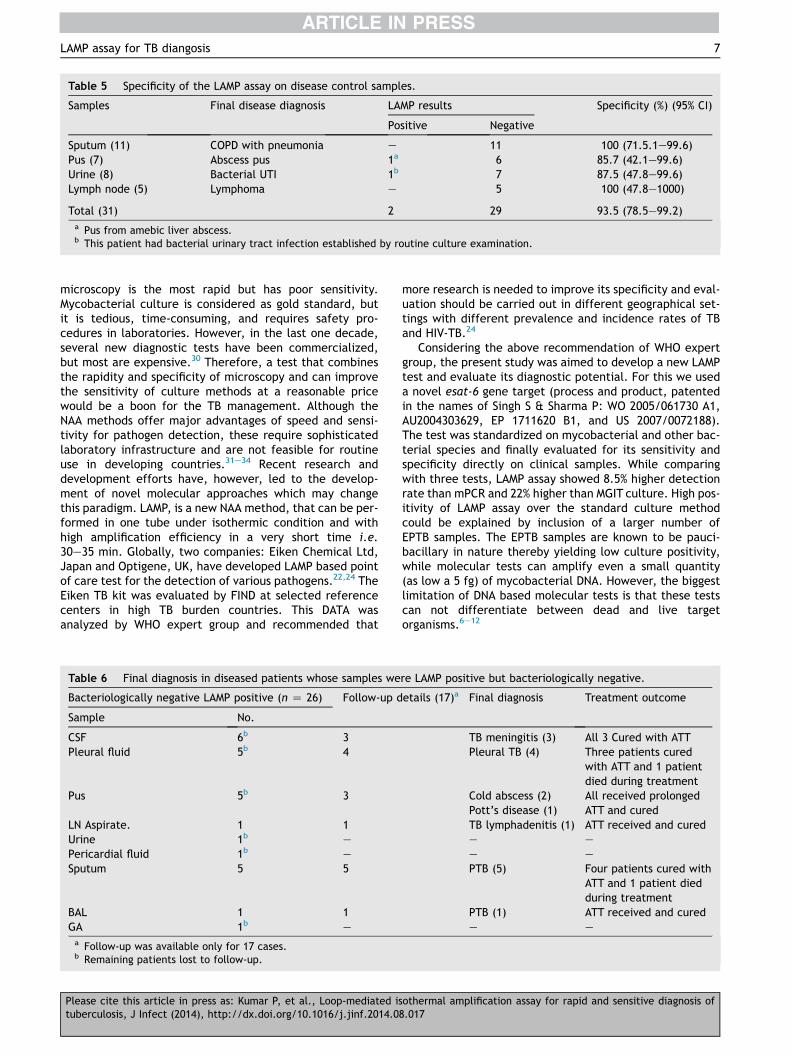
Table 5 Specificity of the LAMP assay on disease control samples.
Samples Final disease diagnosis LAMP results Specificity (%) (95% CI)
Positive Negative
Sputum (11) COPD with pneumonia e 11 100 (71.5.1e99.6)Pus (7) Abscess pus 1a 6 85.7 (42.1e99.6)Urine (8) Bacterial UTI 1b 7 87.5 (47.8e99.6)Lymph node (5) Lymphoma e 5 100 (47.8e1000)
Total (31) 2 29 93.5 (78.5e99.2)a Pus from amebic liver abscess.b This patient had bacterial urinary tract infection established by routine culture examination.
LAMP assay for TB diangosis 7
microscopy is the most rapid but has poor sensitivity.Mycobacterial culture is considered as gold standard, butit is tedious, time-consuming, and requires safety pro-cedures in laboratories. However, in the last one decade,several new diagnostic tests have been commercialized,but most are expensive.30 Therefore, a test that combinesthe rapidity and specificity of microscopy and can improvethe sensitivity of culture methods at a reasonable pricewould be a boon for the TB management. Although theNAA methods offer major advantages of speed and sensi-tivity for pathogen detection, these require sophisticatedlaboratory infrastructure and are not feasible for routineuse in developing countries.31e34 Recent research anddevelopment efforts have, however, led to the develop-ment of novel molecular approaches which may changethis paradigm. LAMP, is a new NAA method, that can be per-formed in one tube under isothermic condition and withhigh amplification efficiency in a very short time i.e.30e35 min. Globally, two companies: Eiken Chemical Ltd,Japan and Optigene, UK, have developed LAMP based pointof care test for the detection of various pathogens.22,24 TheEiken TB kit was evaluated by FIND at selected referencecenters in high TB burden countries. This DATA wasanalyzed by WHO expert group and recommended that
Table 6 Final diagnosis in diseased patients whose samples we
Bacteriologically negative LAMP positive (n Z 26) Follow-up d
Sample No.
CSF 6b 3Pleural fluid 5b 4
Pus 5b 3
LN Aspirate. 1 1Urine 1b e
Pericardial fluid 1b e
Sputum 5 5
BAL 1 1GA 1b e
a Follow-up was available only for 17 cases.b Remaining patients lost to follow-up.
Please cite this article in press as: Kumar P, et al., Loop-mediated istuberculosis, J Infect (2014), http://dx.doi.org/10.1016/j.jinf.2014.08
more research is needed to improve its specificity and eval-uation should be carried out in different geographical set-tings with different prevalence and incidence rates of TBand HIV-TB.24
Considering the above recommendation of WHO expertgroup, the present study was aimed to develop a new LAMPtest and evaluate its diagnostic potential. For this we useda novel esat-6 gene target (process and product, patentedin the names of Singh S & Sharma P: WO 2005/061730 A1,AU2004303629, EP 1711620 B1, and US 2007/0072188).The test was standardized on mycobacterial and other bac-terial species and finally evaluated for its sensitivity andspecificity directly on clinical samples. While comparingwith three tests, LAMP assay showed 8.5% higher detectionrate than mPCR and 22% higher than MGIT culture. High pos-itivity of LAMP assay over the standard culture methodcould be explained by inclusion of a larger number ofEPTB samples. The EPTB samples are known to be pauci-bacillary in nature thereby yielding low culture positivity,while molecular tests can amplify even a small quantity(as low a 5 fg) of mycobacterial DNA. However, the biggestlimitation of DNA based molecular tests is that these testscan not differentiate between dead and live targetorganisms.6e12
re LAMP positive but bacteriologically negative.
etails (17)a Final diagnosis Treatment outcome
TB meningitis (3) All 3 Cured with ATTPleural TB (4) Three patients cured
with ATT and 1 patientdied during treatment
Cold abscess (2)Pott’s disease (1)
All received prolongedATT and cured
TB lymphadenitis (1) ATT received and curede e
e e
PTB (5) Four patients cured withATT and 1 patient diedduring treatment
PTB (1) ATT received and curede e
othermal amplification assay for rapid and sensitive diagnosis of.017

8 P. Kumar et al.
Although culturing is gold standard test for diagnosis ofTB but it can yield false-negative results when samplecontains dormant bacilli, less than 102 bacilli/ml, or non-culturable bacilli (because of over decontamination processand under treatment). However, in the analysis of results,reference standard test is the comparator for the test un-der evaluation, especially for sensitivity evaluation. The se-lection and the quality of the reference standard testdirectly affect the measurement of test performance.35 Inour study, the analytical sensitivity of our LAMP assay washigher than conventional mPCR. Aryan et al.18 also reportedthat LAMP is more sensitive than conventional PCR in pauci-bacillary sputum samples. However, other authors haveobserved that LAMP assay had broadly similar sensitivityand specificity in pulmonary samples as of PCR and cultureresults.19,36e38
The limitation of our study was small sample size. Astudy with larger sample size using the case controlapproach would be desirable. A prospective study toevaluate the utility of LAMP test in the disease prognosisand treatment success also need to be carried out. Thespecificity may be a concern in ultrasensitive test methodssuch as LAMP. But this can be improved by using theflouremeter Genie II real time system. This system providesa closed tube approach that minimizes the number of liquidhandling steps, and reduces possibility of cross contamina-tion significantly18
In conclusion, the LAMP assay could be highly useful toolfor diagnosing pauci-bacillary cases of tuberculosis such asEPTB cases. The test is highly sensitive, cost effective, andrapid with a turnaround time of less than 6 h. The patientcan be diagnosed on the same day and need not to comeagain to the laboratory.
Conflict of interest
The corresponding author holds the process and productpatent on using esta-6 primer sequences for the moleculardiagnosis of Mycobacterium tuberculosis in the names ofSingh S & Sharma P: WO 2005/061730 A1, AU2004303629,EP 1711620 B1, and US 2007/0072188. Another author(Deepal Pandya) works for AmpliGene India Biotech Pvt.Ltd., Ahmedabad, Gujarat, India, who markets fluorometerGenei-II in India.
Acknowledgments
We wish to thank Ms. Syed Beenish Rufai, Deepika Anandand Mr. Vinod Kumar for their technical help. Financialsupport from the Department of Biotechnology, Govern-ment of India (vide grant no BT/PR-15206/Med/29/281/2011) to SS is acknowledged. A senior research fellowshipto PK from Department of Biotechnology, Government of In-dia is also acknowledged.
References
1. World Health Organization. Global tuberculosis report. 2013.WHO/HTM/TB/2013.11. Geneva, Switzerland. Retrievedfrom: http://apps.who.int/iris/bitstream/10665/91355/1/9789241564656_eng.pdf.
Please cite this article in press as: Kumar P, et al., Loop-mediated istuberculosis, J Infect (2014), http://dx.doi.org/10.1016/j.jinf.2014.08
2. Gopinath K, Kumar S, Sankar MM, Singh S. Novel method forclearing red blood cell debris from BacT/ALERT blood culturemedium for improved microscopic and anti-mycobacterial drugsusceptibility test results. J Clin Lab Anal 2007;21(4):220e6.
3. Lu PL, Yang YC, Huang SC, Jenh YS, Lin YC, Huang HH, et al.Evaluation of the Bactec MGIT 960 system in combinationwith the MGIT TBc identification test for detection of Mycobac-terium tuberculosis complex in respiratory specimens. J ClinMicrobiol 2011;49(6):2290e2.
4. Centers for Disease Control and Prevention (CDC). Updatedguidelines for the use of nucleic acid amplification tests inthe diagnosis of tuberculosis. MMWR Morb Mortal Wkly Rep2009;58(01):7e10.
5. American Thoracic Society Documents (ATS), AmericanThoracic Society/Centers for Disease Control and Preventio-n/Infectious Diseases Society of America. Controlling tubercu-losis in the United States. Am J Respir Crit Care Med 2005;172:1169e227.
6. Ling DI, Flores LL, Pai M. Commercial nucleic-acid amplifica-tion tests for diagnosis of pulmonary tuberculosis in respiratoryspecimens: meta-analysis and meta-regression. PLoS One 2008;3(2):e1536.
7. Goessens WHF, de Man P, Koeleman GM, Luijendijk A, teWitt R, Endtz HP, et al. Comparison of the COBAS AMPLICORMTB and BDProbeTec ET assays for detection of Mycobacteriumtuberculosis in respiratory specimens. J Clin Microbiol 2005;43(6):2563e6.
8. Coll P, Garrig�o M, Moreno C, Martı N. Routine use of gen-probeamplified Mycobacterium Tuberculosis Direct (MTD) test fordetection of Mycobacterium tuberculosis with smear-positiveand smear-negative specimens. Int J Tuberc Lung Dis 2003;7(9):886e91.
9. Miragliotta G, Antonetti R, Di Taranto A, Mosca A, Del Prete R.Direct detection of Mycobacterium tuberculosis complex inpulmonary and extrapulmonary samples by BD ProbeTec ET sys-tem. New Microbiol 2005;28(1):67e73.
10. de Luna FF, Ruiz P, Gutierrez J, Casal M. Evaluation of the Ge-noType Mycobacteria Direct assay for detection of Mycobacte-rium tuberculosis complex and four atypical mycobacterialspecies in clinical samples. J Clin Microbiol 2006;44(8):3025e7.
11. Antonenka A, Hofmann-Thiel S, Turaev L, Esenalieva A,Abdulloeva A, Sahalchyk E, et al. Comparison of Xpert MTB/RIFwith ProbeTec ET DTB and COBAS TaqMan MTB for direct detec-tion of M. tuberculosis complex in respiratory specimens. BMCInfect Dis 2013;13:280.
12. Flores LL, Pai M, Colford JM, Riley LW. In-house nucleic acidamplification tests for the detection of Mycobacterium tuber-culosis in sputum specimens: meta-analysis and meta-regres-sion. BMC Microbiol 2005;5:55.
13. Notomi T, Okayama H, Masubuchi H, Yonekawa T, Watanabe K,Amino N, et al. Loop mediated isothermal amplification ofDNA. Nucleic Acids Res 2000;28(12):e63.
14. Wataru Y, Ishibashi M, Kawahara R, Inoue K. Development of aloop-mediated isothermal amplification assay for sensitive andrapid detection of Vibrio parahaemolyticus. BMC Microbiol2008;8:163.
15. Parida M, Horioke K, Ishida H, Dash PK, Saxena P, Jana AM,et al. Rapid detection and differentiation of dengue virus sero-types by a real-time reverse transcription-loop-mediatedisothermal amplification assay. J Clin Microbiol 2005;43(6):2895e903.
16. Njiru ZK, Mikosza ASJ, Armstrong T, Enyaru JC, Ndung’u JM,Thompson ARC. Loop-mediated isothermal amplification(LAMP) method for rapid detection of Trypanosoma brucei rho-desiense. PLoS Negl Trop Dis 2008;2:e147.
17. Hopkins H, Gonz�alez IJ, Jolley SD, Angutoko P, Ategeka J,Asiimwe C, et al. Highly sensitive detection of Malaria
othermal amplification assay for rapid and sensitive diagnosis of.017
LAMP assay for TB diangosis 9
parasitemia in a malaria-endemic setting: performance of anew loop-mediated isothermal amplification kit in a remoteclinic in Uganda. J Infect Dis 2013;208(4):645e52.
18. Aryan E, Makvandia M, Farajzadeha A, Huygenb K, Bifanib P,Mousavic SL, et al. A novel and more sensitive loop-mediatedisothermal amplification assay targeting IS6110 for detectionof Mycobacterium tuberculosis complex. Microbiol Res 2010;165(3):211e20.
19. George G, Mony P, Kenneth J. Comparison of the efficacies ofloop-mediated isothermal amplification, fluorescence smearmicroscopy and culture for the diagnosis of tuberculosis.PLoS One 2011;6(6):1007.
20. Zhu RY, Zhang KX, Zhao MQ, Liu YH, Xu YY, Ju CM, et al. Use ofvisual loop-mediated isotheral amplification of rimM sequencefor rapid detection of Mycobacterium tuberculosis and Myco-bacterium bovis. J Microbiol Methods 2009;78(3):339e43.
21. Iwamoto T, Sonobe T, Hayashi K. Loop-mediated isothermalamplification for direct detection of Mycobacterium tubercu-losis complex, M. avium, and M. ntracellulare in sputum sam-ples. J Clin Microbiol 2003;41(6):2616e22.
22. Mahony J, Chong S, Bulir D, Ruyter A, Mwawasi K, Waltho D.Development of a sensitive loop-mediated isothermal amplifi-cation assay that provides specimen-to-result diagnosis of res-piratory syncytial virus infection in 30 minutes. J Clin Microbiol2013;51(8):2696e701.
23. Peng J, Shi M, Xia Z, Huang J, Fan Z. Detection of cucumbermosaic virus isolates from banana by one-step reverse tran-scription loop-mediated isothermal amplification. Arch Virol2012;157(11):2213e7.
24. World Health Organization. The use of a commercial loop-mediated isothermal amplification assay (TB-LAMP) for thedetection of tuberculosis. 2013. WHO/HTM/TB/2013.05.Geneva, Retrieved from: http://apps.who.int/iris/bitstream/10665/83142/1/WHO_HTM_TB_2013.05_eng.pdf.
25. Singh S, Kumar P, Sharma S, Mumbowa F, Martin A, Durier N.Rapid identification and drug susceptibility testing of Mycobac-terium tuberculosis: standard operating procedure for non-commercial assays: part 1: microscopic observation drug sus-ceptibility assay v2.4.12. J Lab Physicians 2012;4:120e6.
26. American Thoracic Society (ATS). Diagnostic standards andclassification of tuberculosis in adults and children. This offi-cial statement of the American Thoracic Society and the Cen-ters for Disease Control and Prevention was adopted by the ATSBoard of Directors, July 1999. This statement was endorsed bythe Council of the Infectious Disease Society of America. Am JRespir Crit Care Med 1999;161:1376e95.
Please cite this article in press as: Kumar P, et al., Loop-mediated istuberculosis, J Infect (2014), http://dx.doi.org/10.1016/j.jinf.2014.08
27. Reves R, Reichman LB, Simone PM, Starke JR, Vernon AA.American Thoracic Society/Centers for Disease Control andPrevention/Infectious Diseases Society of America: treatmentof tuberculosis. Am J Respir Crit Care Med 2003;167:603e62.
28. Kumar P, Benny P, Jain M, Singh S. Comparison of an in-housemultiplex PCR with two commercial immuno-chromatographictests for rapid identification and differentiation of MTB fromNTM isolates. Int J Mycobacteriol 2014;3(1):50e6.
29. Gopinath K, Singh S. Multiplex PCR assay for simultaneousdetection and differentiation of Mycobacterium tuberculosis,Mycobacterium avium complexes and other mycobacterial spe-cies directly from clinical specimens. J Appl Microbiol 2009;107(2):1364e72.
30. Verma S, Dhole TN, Kumar M, Kashyap S. A novel approach forimproving sensitivity of AFB microscopy using ReaSLR method.J Clin Microbiol 2013;51(11):3597e601.
31. Dora JM, Geib G, Chakr R, Paris Fd, Mombach AB, Lutz L, et al.Polymerase chain reaction as a useful and simple tool for rapiddiagnosis of tuberculous meningitis in a Brazilian tertiary carehospital. Braz J Infect Dis 2008;12(3):245e7.
32. Lorino G, Lilli D, Rivanera D, Guarino P, Angeletti S,Gherardi G, et al. Polymerase chain reaction, with sequencing,as a diagnostic tool in culture-negative bacterial meningitis.Clin Microbiol Infect 1999;5(2):92e6.
33. Pai M, Flores LL, Pai N, Hubbard A, Riley LW, Colford JM. Diag-nostic accuracy of nucleic acid amplification tests for tubercu-lous meningitis: a systematic review and meta-analysis. LancetInfect Dis 2003;3(10):633e43.
34. Pal RB, Desai MM. Polymerase chain reaction for the rapid diag-nosis of tuberculous meningitis. J Indian Med 2007;105(1):21e4.
35. Peeling RW, Smith PG, Bossuyt PMM. A guide for diagnosticevaluations. Nat Rev Microbiol 2010:S2e6.
36. Tomita N, Mori Y, Kanda H, Notomi T. Loop-mediatedisothermal amplification (LAMP) of gene sequences and simplevisual detection of products. Nat Protoc 2008;3(5):877e82.
37. Leila K, Shahhosseiny MH, Razavi MR, Parivar K, Moslemi E,Werngren J. Evaluation of loop mediated isothermal amplifica-tion for diagnosis of Mycobacterium tuberculosis complex inclinical samples. Afr J Biotechnol 2011;10:5096e101.
38. Greco S, Rulli M, Girardi E, Piersimoni C, Saltini C. Diagnosticaccuracy of in-house PCR for pulmonary tuberculosis insmear-positive patients: metaanalysis and metaregression. JClin Microbiol 2009;47(3):569e76.
othermal amplification assay for rapid and sensitive diagnosis of.017
Related Documents











