Long-term Outcomes in Patients with Retinal Vein Occlusion Treated with Ranibizumab The RETAIN Study Peter A. Campochiaro, MD, 1 Raafay Sophie, MD, 1 Joel Pearlman, MD, PhD, 2 David M. Brown, MD, 3 David S. Boyer, MD, 4 Jeffrey S. Heier, MD, 5 Dennis M. Marcus, MD, 6 Leonard Feiner, MD, PhD, 7 Arun Patel, MD, 2 for the RETAIN Study Group* Objective: To determine long-term outcomes of patients with ranibizumab-treated retinal vein occlusion (RVO). Design: Prospective follow-up of a subset of patients from 2 phase 3 trials. Participants: Thirty-four patients with branch RVO (BRVO) and 32 with central RVO (CRVO) who completed the Genentech-sponsored ranibizumab study RVO trials. Methods: Patients seen every month in year 1 and at least every 3 months in year 2 were treated with ranibizumab for intraretinal fluid. Patients requiring injections on consecutive visits were treated with ranibizumab plus scatter photocoagulation. Main Outcome Measures: Mean improvement in best-corrected visual acuity (BCVA) and percentage of patients with edema resolution. Results: With a mean follow-up of 49.0 months, 17 of 34 BRVO patients (50%) had edema resolution defined as no intraretinal fluid for 6 months or more after the last injection. The last injection was given within 2 years of treatment initiation in 76%. The mean number of injections required in unresolved patients in year 4 was 3.2. In patients with resolved edema mean improvement in BCVA was 25.9 letters versus 17.1 letters (P ¼ 0.09) in unresolved patients, and in both groups, approximately 80% had a final BCVA of 20/40 or better. With a mean follow-up of 49.7 months, 14 of 32 CRVO patients (44%) had edema resolution, with 71% receiving their last injection within 2 years of treatment initiation. The mean number of injections in unresolved patients in year 4 was 5.9. Compared with patients with unresolved CRVO, patients with resolved disease had greater improvement in BCVA (25.2 vs. 4.3 letters; P ¼ 0.002), and a greater percentage had a final BCVA of 20/40 or better (64.3% vs. 27.8%; P ¼ 0.04). Nine patients with BRVO and 9 with CRVO received scatter photocoagulation, and with mean follow-up of 9 months (BRVO) and 11 months (CRVO) after last laser, only 1 in each group had resolution of edema. Conclusions: Long-term outcomes in BRVO patients treated with ranibizumab were excellent, and although half still required occasional injections after 4 years, they maintained good visual potential. A substantial minority (44%) of patients with ranibizumab-treated CRVO had edema resolution and a good outcome within 4 years, but most (56%) still required frequent injections, had reduced visual potential, and have a guarded prognosis. Ophthalmology 2014;121:209-219 ª 2014 by the American Academy of Ophthalmology. *Group members listed online in the Appendix (http://aaojournal.org). Patients with central retinal vein occlusion (CRVO) have reduced vision, retinal hemorrhages, macular edema, and variable amounts of retinal nonperfusion (RNP). The presentation of patients with branch retinal vein occlusion (BRVO) is similar but less severe on average than that seen in patients with CRVO because venous return is compromised in approximately one quarter to one half of the retina, rather than the entire retina. Vascular endothelial growth factor (VEGF) plays an important role in the pathogenesis of macular edema in both CRVO and BRVO. Neutralization of VEGF by intraocular injections of ranibizumab (Lucentis; Genentech, Inc., South San Francisco, CA), a Fab fragment that specifically binds all isoforms of VEGF-A, reduces macular edema and improves vision. 1 The Ranibizumab for the Treatment of Macular Edema after Central Retinal Vein Occlusion Study: Evaluation of Efficacy and Safety (CRUISE) trial demonstrated that injection of 0.3 or 0.5 mg of ranibizumab every month for 6 months in patients with CRVO resulted in improvements in best-corrected visual acuity (BCVA) of 12.7 and 14.9 letters, respectively, compared with 0.8 letter in the sham group. 2 The Ranibizumab for the Treatment of Macular Edema 209 Ó 2014 by the American Academy of Ophthalmology ISSN 0161-6420/14/$ - see front matter Published by Elsevier Inc. http://dx.doi.org/10.1016/j.ophtha.2013.08.038

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Long-term Outcomes in Patients with RetinalVein Occlusion Treated with RanibizumabThe RETAIN Study
Peter A. Campochiaro, MD,1 Raafay Sophie, MD,1 Joel Pearlman, MD, PhD,2 David M. Brown, MD,3
David S. Boyer, MD,4 Jeffrey S. Heier, MD,5 Dennis M. Marcus, MD,6 Leonard Feiner, MD, PhD,7
Arun Patel, MD,2 for the RETAIN Study Group*
Objective: To determine long-term outcomes of patients with ranibizumab-treated retinal vein occlusion(RVO).
Design: Prospective follow-up of a subset of patients from 2 phase 3 trials.Participants: Thirty-four patients with branch RVO (BRVO) and 32 with central RVO (CRVO) who completed
the Genentech-sponsored ranibizumab study RVO trials.Methods: Patients seen every month in year 1 and at least every 3 months in year 2 were treated with
ranibizumab for intraretinal fluid. Patients requiring injections on consecutive visits were treated with ranibizumabplus scatter photocoagulation.
Main Outcome Measures: Mean improvement in best-corrected visual acuity (BCVA) and percentage ofpatients with edema resolution.
Results: With a mean follow-up of 49.0 months, 17 of 34 BRVO patients (50%) had edema resolution definedas no intraretinal fluid for 6 months or more after the last injection. The last injection was given within 2 years oftreatment initiation in 76%. The mean number of injections required in unresolved patients in year 4 was 3.2. Inpatients with resolved edema mean improvement in BCVA was 25.9 letters versus 17.1 letters (P ¼ 0.09) inunresolved patients, and in both groups, approximately 80% had a final BCVA of 20/40 or better. With a meanfollow-up of 49.7 months, 14 of 32 CRVO patients (44%) had edema resolution, with 71% receiving their lastinjection within 2 years of treatment initiation. The mean number of injections in unresolved patients in year 4 was5.9. Compared with patients with unresolved CRVO, patients with resolved disease had greater improvement inBCVA (25.2 vs. 4.3 letters; P ¼ 0.002), and a greater percentage had a final BCVA of 20/40 or better (64.3% vs.27.8%; P ¼ 0.04). Nine patients with BRVO and 9 with CRVO received scatter photocoagulation, and with meanfollow-up of 9 months (BRVO) and 11 months (CRVO) after last laser, only 1 in each group had resolution ofedema.
Conclusions: Long-term outcomes in BRVO patients treated with ranibizumab were excellent, and althoughhalf still required occasional injections after 4 years, they maintained good visual potential. A substantial minority(44%) of patients with ranibizumab-treated CRVO had edema resolution and a good outcome within 4 years, butmost (56%) still required frequent injections, had reduced visual potential, and have a guarded prognosis.Ophthalmology 2014;121:209-219 ª 2014 by the American Academy of Ophthalmology.
*Group members listed online in the Appendix (http://aaojournal.org).
Patients with central retinal vein occlusion (CRVO) havereduced vision, retinal hemorrhages, macular edema, andvariable amounts of retinal nonperfusion (RNP). Thepresentation of patients with branch retinal vein occlusion(BRVO) is similar but less severe on average than that seen inpatients with CRVO because venous return is compromisedin approximately one quarter to one half of the retina, ratherthan the entire retina. Vascular endothelial growth factor(VEGF) plays an important role in the pathogenesis ofmacular edema in both CRVO and BRVO. Neutralization ofVEGF by intraocular injections of ranibizumab (Lucentis;
� 2014 by the American Academy of OphthalmologyPublished by Elsevier Inc.
Genentech, Inc., South San Francisco, CA), a Fab fragmentthat specifically binds all isoforms of VEGF-A, reducesmacular edema and improves vision.1 The Ranibizumab forthe Treatment of Macular Edema after Central Retinal VeinOcclusion Study: Evaluation of Efficacy and Safety(CRUISE) trial demonstrated that injection of 0.3 or 0.5 mgof ranibizumab every month for 6 months in patients withCRVO resulted in improvements in best-corrected visualacuity (BCVA) of 12.7 and 14.9 letters, respectively,compared with 0.8 letter in the sham group.2 TheRanibizumab for the Treatment of Macular Edema
209ISSN 0161-6420/14/$ - see front matterhttp://dx.doi.org/10.1016/j.ophtha.2013.08.038

Ophthalmology Volume 121, Number 1, January 2014
following Branch Retinal Vein Occlusion: Evaluation ofEfficacy and Safety (BRAVO) study showed that after 6ranibizumab injections, the mean gain from baseline inBCVA was 16.6 and 18.3 letters in the 0.3-mg and 0.5-mgranibizumab groups, respectively, compared with 7.3 lettersin the sham group.3 After the initial 6 months, evaluationswere carried out every month, and if BCVA was 20/40 orworse or if central subfield thickness was 250 mm or more,patients in the ranibizumab groups received their assigneddose, and patients in the sham group received 0.5 mgranibizumab. At month 12 in the CRUISE trial, the meanimprovement from baseline BCVA was 13.9 letters in the 2ranibizumab groups and 7.3 letters in the sham/0.5-mggroup, and in the BRAVO trial, the mean improvementfrom baseline BCVA letter score was 16.4 and 18.3 letters inthe 0.3-mg and 0.5-mg ranibizumab groups, respectively, and12.1 letters in the sham/0.5-mg group.
After completion of the CRUISE or BRAVO trials,patients were offered enrollment in the retinal vein occlusion(RVO) cohort of An Open-Label, Multicenter ExtensionStudy to Evaluate the Safety and Tolerability of Ranibizu-mab in Subjects with Choroidal NeovascularizationSecondary to Age-Related Macular Degeneration orMacular Edema Secondary to Retinal Vein Occlusion WhoHave Completed a Genentech-Sponsored Ranibizumab(HORIZON) Study and were seen at least every 3 months(although they could be seen as frequently as every month atthe investigator’s discretion) and were treated with 0.5 mgof ranibizumab if their BCVA was 20/40 or worse or theircentral subfield thickness was 250 mm or more. Becausepatients entered HORIZON right after completing theCRUISE or BRAVO trials and exited within 1 month ofFood and Drug Administration approval of ranibizumab forRVO, the duration of follow-up varied considerably amongpatients. The data of patients who completed at least 1 yearof follow-up in HORIZON study were reported.4 In patientswith CRVO, the mean change in BCVA from the CRUISEstudy baseline was 9.4 letters, 14.9 letters, and 16.2 letters inthe sham/0.5-mg, 0.3-/0.5-mg, and 0.5-mg treatment groups,respectively, at HORIZON study baseline. After 1 year, themean change in BCVA letter score from the CRUISE studybaseline was 7.6 letters, 8.2 letters, and 12.0 letters,respectively, a statistically significant reduction in all 3groups. In patients with BRVO, the mean change fromBRAVO baseline was 13.2 letters, 16.8 letters, and 19.2letters in the sham/0.5-mg, 0.3-/0.5-mg, and 0.5-mg treat-ment groups, respectively, at HORIZON baseline. After 1year, the mean change from BRAVO baseline was 15.6,14.9, and 17.5 letters, respectively, which was not signifi-cantly different. These data indicate that initial visualbenefits seen after a year of aggressive ranibizumab treat-ment in patients with CRVO may decline during a secondyear in which there is reduced frequency of injectionsbecause of less frequent follow-up. Also, a substantialpercentage of patients with either CRVO or BRVO werestill requiring ranibizumab injections to control edema, andtheir long-term outcomes were uncertain. These resultssuggest many questions. Does allowing edema to recur andremain for a period of time before reinjecting and sup-pressing VEGF lead to gradual loss of vision in patients
210
with RVO? What is the percentage of patients with RVOtreated with ranibizumab who ultimately have completeresolution of edema and no longer require injections? Ifpatients are still requiring injections to control edema afterseveral years, can scatter or grid photocoagulation, or both,lead to resolution of edema and allow them to stop injec-tions? In this study, we sought to obtain additional long-term outcome data in patients with RVO treated with rani-bizumab to address these questions.
Methods
The Extended follow-up of patients with macular edema due tobRanch rETinal vein occlusion or centrAl retinal veIn occlusioNpreviously treated with intravitreal ranibizumab (RETAIN) study(ClinicalTrials.gov identifier: NCT01198327) was an investigator-initiated trial sponsored by the Macula Foundation (New York,NY) and Genentech, Inc., in which 7 of the highest enrollingHORIZON study sites presented each of their patients whocompleted HORIZON study with the option of participating. It wasan open-label, single-arm, multicenter extension trial that wasconducted in accordance with the Declaration of Helsinki, appli-cable US Food and Drug Administration regulations, and theHealth Insurance Portability and Accountability Act. The studyprotocol was approved by the respective institutional review boardsbefore study initiation, and all participating patients providedinformed consent. Patients with RVO were eligible for theRETAIN study if they completed the BRAVO or CRUISE trialsand had subsequent follow-up in HORIZON. The inclusion andexclusion criteria for BRAVO and CRUISE patients are summa-rized in Table 1 (available at http://aaojournal.org). The mean timefrom HORIZON study exit to entry in the RETAIN study was 92.7days, with a range of 68 to 150 days. Those who gave informedconsent were evaluated every month for 12 months and then atleast every 3 months (as frequently as every month if needed)for an additional 12 months, with measurement of BCVA usingthe Early Treatment Diabetic Retinopathy Study (ETDRS)protocol5; a complete eye examination; measurement of vitalsigns; review of medical history, including concurrentmedications and medical procedures; and optical coherencetomography using Stratus OCT III (Carl Zeiss Meditec, Inc.,Dublin, CA; software version 4.0 or higher). At each study visit,patients were eligible to receive an intravitreal injection of 0.5mg ranibizumab if there was any intraretinal fluid involving thefovea. If patients required an injection at 2 consecutive visits andBCVA was worse than 20/30, they were treated with scatterphotocoagulation to the far periphery and all areas of RNPoutside the macula combined with an intraocular injection of 0.5mg of ranibizumab (BRVO patients received treatment to thequadrants affected by the BRVO). If intraretinal fluid waspresent at 1 or 2 months after laser photocoagulation, the patientwas treated with injection of 0.5 mg of ranibizumab. Ifintraretinal fluid was present 3 months or longer after laserphotocoagulation and BCVA was worse than 20/30, scatterphotocoagulation was extended posteriorly, making sure to treatany areas of RNP combined with an injection of 0.5 mg ofranibizumab. If intraretinal fluid was present at 1 or 2 monthsafter laser photocoagulation, the patient was treated withinjection of 0.5 mg ranibizumab. If intraretinal fluid was presentat 3 months or more after laser photocoagulation and BCVA wasworse than 20/30, any remaining areas of retina judged to beischemic were treated with scatter photocoagulation and gridlaser therapy was given to any areas of leakage in the maculaoutside the foveal avascular zone. Fluorescein angiograms using

Campochiaro et al � Long-term Outcomes in RVO
an ultrawide angle camera (or 60� camera with sweeps if anultrawide-angle camera was not available) were performed atbaseline, at months 6, 12, 18, and 24, and before each treatmentwith laser photocoagulation.
Outcome assessments included the mean change in BCVA fromoriginal CRUISE or BRAVO study baseline measured in ETDRSletter score, the percentage of patients gaining or losing 15 lettersor more from baseline, the percentages of patients with Snellenequivalent BCVA of 20/40 or better or 20/200 or worse, the meanchange from baseline in central foveal thickness (CFT) by StratusOCT at each study visit, the percentage of patients with CFT of 250mm or less at each study visit, the percentage of patients who hadresolution of edema defined as no intraretinal or subretinal fluid inthe macula for at least 6 months after the last injection, and theincidence and severity of ocular and nonocular adverse events.
Changes in mean visual acuity and CFT were assessed using theWilcoxon signed-rank test. Differences in binary categorical vari-ables between patients with resolved and unresolved disease werecalculated using the Pearson chi-square or Fisher exact tests.Differences in continuous variables between patients with resolvedand unresolved disease were calculated using the independent-samples t test for parametric data and the ManneWhitney U testfor nonparametric data. All tests were run for a 2-tailed significancewith a type I error rate of 0.05.
Results
RETAIN Patients Are Representative of BRAVOand CRUISE Patients
Thirty-four patients with BRVO and 32 patients with CRVOwere enrolled. Table 2 shows a comparison between the RETAINtrial cohort, patients who were eligible for the RETAIN trial butdeclined to participate, and the entire BRAVO and CRUISE trialcohorts with regard to some baseline characteristics and outcomemeasures. In general, patients who entered the RETAIN studywere fairly representative of the entire population of BRAVOand CRUISE study patients with one difference: the 9 patientsin the BRVO sham group and the 9 patients in the CRVOsham group who were enrolled in the RETAIN study bychance had a better visual outcome on average during theBRAVO and CRUISE trials than the entire sham grouppopulations.
Patient Disposition
Of the patients enrolled in the RETAIN study, 26 of 34 withBRVO and 27 of 32 with CRVO completed 2 years of follow-up.Table 3 shows the disposition of the 8 BRVO and 5 CRVOpatients who left the study before the 2-year end point. Five ofthe 8 BRVO patients and 2 of the 5 CRVO patients showedresolution of macular edema with no injections for 9 months ormore and withdrew because they believed they did not needcontinued follow-up (in 2 instances, the patients failed to returnand could not be contacted). Six patients were considered to haveunresolved edema because they required an injection within 6months of withdrawal (3 BRVO patients and 1 CRVO patient) ordeath (2 CRVO patients). None of the 8 BRVO patients had a CFTof more than 250 mm at last visit, and the mean change in BCVAfrom the BRAVO study baseline to the last visit was þ31 letters.Two of the 5 CRVO patients had a CFT of more than 250 mm atthe last visit (254 and 377 mm), and the mean change in BCVAfrom the CRUISE study baseline to the last visit was þ18 letters.Thus, in general, patients did not leave the trial early because theywere doing poorly, but rather because they were no longer
receiving injections or the continued follow-up became tooburdensome.
Patients with Branch Retinal Vein OcclusionTreated with Ranibizumab Have an Excellent Long-term Outcome
Patients were evaluated at least every 3 months during HORIZON,every month during the first year of the RETAIN study, and at leastevery 3 months during the second year of the RETAIN study; ifintraretinal fluid was identified, an injection of 0.5 mg ranibizumabwas given. Figure 1A shows mean BCVA at the BRAVO trialbaseline and every 6 months thereafter through 48 months for allpatients enrolled in the RETAIN study. In the 28 patients forwhom data were available 4 years after the BRAVO studybaseline assessment, the mean ETDRS letter score was 74.1 (20/32), an improvement in BCVA of 20.1 letters from baseline,which is not statistically different from the improvement of 18.6letters at the 6-month primary end point of the BRAVO trial(P ¼ 0.6). At final visit with a mean follow-up of 50.2 months,61.8% of the 34 BRVO patients enrolled in the RETAIN trialshowed improvement in BCVA of 15 letters or more from theBRAVO trial baseline and 79.4% had a final BCVA of 20/40 orbetter. Three patients had reduction in BCVA consistingof �2, �4, and �41 letters compared with the BRAVO trialbaseline. The loss of 41 letters was the result of a superior hemi-retinal vein occlusion that occurred during the first year of theRETAIN trial in a patient with a prior inferior BRVO. Mean CFTchanged very little after year 2 (Fig 1B), and the mean number ofranibizumab injections per year was 2.6 in year 2, 2.1 in year 3, and2.0 in year 4 (Fig 1C).
An analysis including only the patients who completed theRETAIN trial had results similar to those of the full analysis. Themean follow-up duration at the end of the RETAIN study was 53.4months and the mean BCVA in ETDRS letters was 72.6 (20/32),an improvement of 16.4 letters from BRAVO baseline, which wasnot statistically different from the improvement of 18.5 lettersat the end of the BRAVO study for the same cohort of patients(P ¼ 0.9; Fig 2A, available at http://aaojournal.org). Mean CFTremained less than 200 mm throughout HORIZON and RETAINtrials (Fig 2B, available at http://aaojournal.org), and at the finalvisit, 88.5% of patients had a CFT of 250 mm or less. The meannumber of injections was 7.2 during the BRAVO study, 3.3during an average follow-up of 16.9 months in HORIZON, 2.4in the first year of the RETAIN trial, and 1.8 in the second year ofthe RETAIN trial, for a total of 14.8 during a mean of 53 months offollow-up (Fig 2C, available at http://aaojournal.org).
Resolution of Macular Edema in Patients withBranch Retinal Vein Occlusion
Resolution of macular edema was defined as an absence of intra-retinal fluid for at least 6 months after the last injection of ranibi-zumab. Five patients had no intraretinal fluid for a prolongedperiod (mean, 32 months) but a small amount of intraretinal fluidreappeared, requiring an injection within 6 months of the end of theRETAIN study, and therefore they had unresolved edema. Reso-lution of edema occurred in 5 of 8 BRVO patients who withdrewbefore the end of the RETAIN study (Table 2) and in 12 of 26patients who completed the RETAIN study, for a total 17 of 34patients (50%) who entered the RETAIN study. Figure 1Dshows the time of last injection plotted against the change inBCVA from BRAVO baseline to final study visit, excluding theone patient who had a second BRVO. There was a broad rangeof time over which resolution of edema occurred, as evidencedby time of last injection (mean, 17.6 months). Fifty-three percent
211
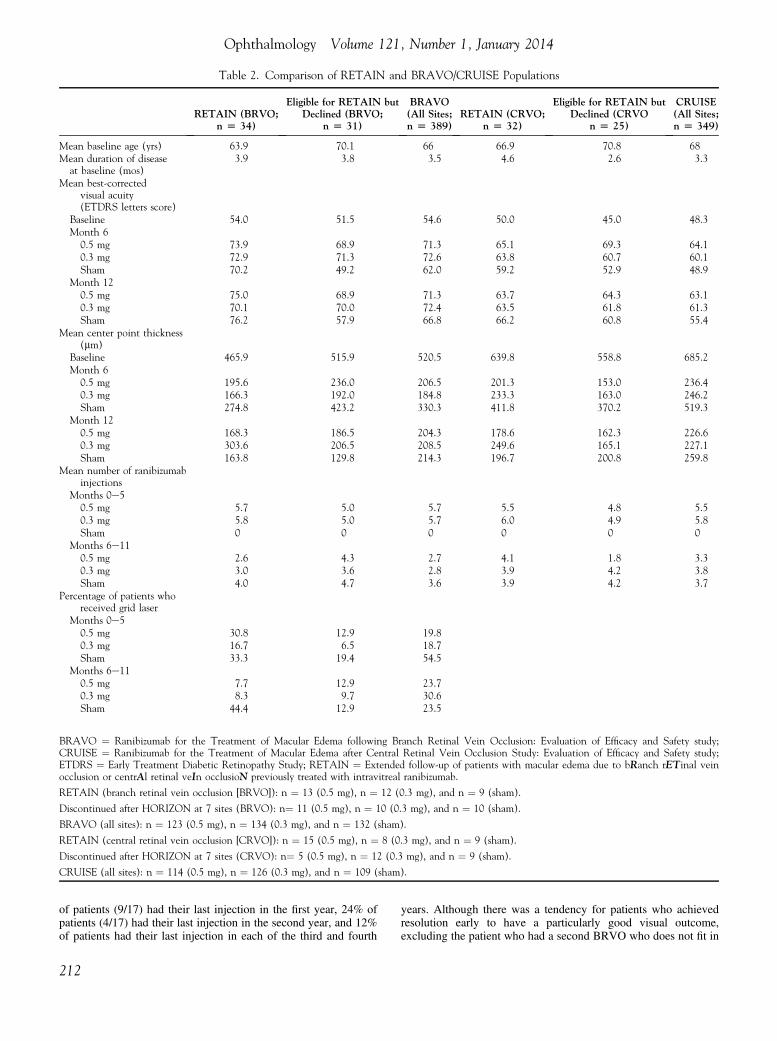
Table 2. Comparison of RETAIN and BRAVO/CRUISE Populations
RETAIN (BRVO;n [ 34)
Eligible for RETAIN butDeclined (BRVO;
n [ 31)
BRAVO(All Sites;n [ 389)
RETAIN (CRVO;n [ 32)
Eligible for RETAIN butDeclined (CRVO
n [ 25)
CRUISE(All Sites;n [ 349)
Mean baseline age (yrs) 63.9 70.1 66 66.9 70.8 68Mean duration of diseaseat baseline (mos)
3.9 3.8 3.5 4.6 2.6 3.3
Mean best-correctedvisual acuity(ETDRS letters score)
Baseline 54.0 51.5 54.6 50.0 45.0 48.3Month 6
0.5 mg 73.9 68.9 71.3 65.1 69.3 64.10.3 mg 72.9 71.3 72.6 63.8 60.7 60.1Sham 70.2 49.2 62.0 59.2 52.9 48.9
Month 120.5 mg 75.0 68.9 71.3 63.7 64.3 63.10.3 mg 70.1 70.0 72.4 63.5 61.8 61.3Sham 76.2 57.9 66.8 66.2 60.8 55.4
Mean center point thickness(mm)
Baseline 465.9 515.9 520.5 639.8 558.8 685.2Month 6
0.5 mg 195.6 236.0 206.5 201.3 153.0 236.40.3 mg 166.3 192.0 184.8 233.3 163.0 246.2Sham 274.8 423.2 330.3 411.8 370.2 519.3
Month 120.5 mg 168.3 186.5 204.3 178.6 162.3 226.60.3 mg 303.6 206.5 208.5 249.6 165.1 227.1Sham 163.8 129.8 214.3 196.7 200.8 259.8
Mean number of ranibizumabinjections
Months 0e50.5 mg 5.7 5.0 5.7 5.5 4.8 5.50.3 mg 5.8 5.0 5.7 6.0 4.9 5.8Sham 0 0 0 0 0 0
Months 6e110.5 mg 2.6 4.3 2.7 4.1 1.8 3.30.3 mg 3.0 3.6 2.8 3.9 4.2 3.8Sham 4.0 4.7 3.6 3.9 4.2 3.7
Percentage of patients whoreceived grid laser
Months 0e50.5 mg 30.8 12.9 19.80.3 mg 16.7 6.5 18.7Sham 33.3 19.4 54.5
Months 6e110.5 mg 7.7 12.9 23.70.3 mg 8.3 9.7 30.6Sham 44.4 12.9 23.5
BRAVO ¼ Ranibizumab for the Treatment of Macular Edema following Branch Retinal Vein Occlusion: Evaluation of Efficacy and Safety study;CRUISE ¼ Ranibizumab for the Treatment of Macular Edema after Central Retinal Vein Occlusion Study: Evaluation of Efficacy and Safety study;ETDRS ¼ Early Treatment Diabetic Retinopathy Study; RETAIN ¼ Extended follow-up of patients with macular edema due to bRanch rETinal veinocclusion or centrAl retinal veIn occlusioN previously treated with intravitreal ranibizumab.
RETAIN (branch retinal vein occlusion [BRVO]): n ¼ 13 (0.5 mg), n ¼ 12 (0.3 mg), and n ¼ 9 (sham).
Discontinued after HORIZON at 7 sites (BRVO): n¼ 11 (0.5 mg), n ¼ 10 (0.3 mg), and n ¼ 10 (sham).
BRAVO (all sites): n ¼ 123 (0.5 mg), n ¼ 134 (0.3 mg), and n ¼ 132 (sham).
RETAIN (central retinal vein occlusion [CRVO]): n ¼ 15 (0.5 mg), n ¼ 8 (0.3 mg), and n ¼ 9 (sham).
Discontinued after HORIZON at 7 sites (CRVO): n¼ 5 (0.5 mg), n ¼ 12 (0.3 mg), and n ¼ 9 (sham).
CRUISE (all sites): n ¼ 114 (0.5 mg), n ¼ 126 (0.3 mg), and n ¼ 109 (sham).
Ophthalmology Volume 121, Number 1, January 2014
of patients (9/17) had their last injection in the first year, 24% ofpatients (4/17) had their last injection in the second year, and 12%of patients had their last injection in each of the third and fourth
212
years. Although there was a tendency for patients who achievedresolution early to have a particularly good visual outcome,excluding the patient who had a second BRVO who does not fit in

Table 3. Summary of Patients Who Discontinued during the Trial
PatientIdentifier
Last Visit
Months SinceLast Injection Edema Status
Reason forDiscontinuationWeek
Best-Corrected VisualAcuity (Early
Treatment DiabeticRetinopathy Study Score)
Change inBest-CorrectedVisual Acuity(Letters)
Center PointThickness (mm)
B18 16 80 21 204 4 Unresolved Transportation difficultiesB34 24 79 51 148 10 Resolved Withdrew consentB03 32 90 51 231 27 Resolved Stable and intercurrent illnessB29 36 48 13 219 5 Unresolved Diagnosed with stomach cancerB06 40 93 29 217 19 Resolved Stable and moved awayB07 48 85 35 121 30 Resolved StableB19 72 73 8 114 39 Resolved Lost to follow-upB10 72 73 40 177 0 Unresolved Withdrew consentC16 12 72 3 199 2 Unresolved DiedC32 24 63 23 254 0 Unresolved DiedC03 36 86 19 145 9 Resolved Lost to follow-upC26 48 83 33 177 17 Resolved StableC13 72 73 14 377 0 Unresolved Transportation difficulties
Campochiaro et al � Long-term Outcomes in RVO
either category, the amount of improvement in BCVA at the lastvisit was not significantly greater for patients with resolved edemacompared with unresolved edema (25.9 vs. 17.1 letters; P ¼ 0.09).Also, although patients whose disease resolved achieved anexcellent mean BCVA earlier during follow-up, by 4 years, therewas no difference between the groups (final BCVA, 74.9 vs. 76.5letters; P ¼ 0.9; Fig 1E). The percentage of patients who had a finalBCVA of 20/40 or better was 82.4% for patients with resolveddisease and 81.3% for patients with unresolved disease. Asexpected, the unresolved group had a somewhat greater meanCFT at most time points (Fig 1F) and had a higher mean numberof ranibizumab injections over 4 years (18.9 vs. 9.9; P ¼ 0.002;Fig 1G).
The percentage of patients who enrolled in the RETAIN studywho received grid laser photocoagulation was 52.9% in patientswith resolved edema compared with 62.5% in patients with unre-solved edema, and they did not differ significantly in visualoutcome (Fig 3A, available at http://aaojournal.org). Patients whowere treated with grid laser photocoagulation did not havea greater reduction in mean CFT (Fig 3B, available at http://aaojournal.org) or required fewer injections of ranibizumab (Fig3C, available at http://aaojournal.org). Nine patients with BRVOrequired ranibizumab injections on consecutive visits andqualified for scatter photocoagulation. The mean follow-up afterthe last laser treatment was 9.3 months, and resolution of edemaoccurred in only 1 of the 9 patients during that time.
Patients with Central Retinal Vein OcclusionTreated with Ranibizumab Have a Good Long-termOutcome
In the 28 patients with CRVO for whom data were available 4years after the CRUISE study baseline, the mean ETDRS letterscore was 64.0 (20/50), an improvement of 14.0 letters from theCRUISE study baseline, which was not statistically different fromthe improvement of 13.1 letters at the end of the CRUISE study forthe same cohort of patients (P ¼ 0.3; Fig 4A). At the final visit,with a mean follow-up of 51.4 months, 53.1% of the 32 CRVOpatients enrolled in the RETAIN study gained 15 letters or more,and 43.8% had a final BCVA of 20/40 or better. Six patients hadreduced BCVA compared with the CRUISE study baseline, con-sisting of �33, �18, �11, �4, �3, and �3 letters. A detailed
analysis of these patients is described below. Central fovealthickness was 639.8 mm at the CRUISE study baseline, 201.4 mmat month 12, and 220.6 mm at month 48 (Fig 4B). The meannumber of ranibizumab injections per year was 4.5 in year 2, 3.6in year 3, and 3.3 in year 4 (Fig 4C).
In patients with CRVO who completed the RETAIN study, themean BCVA in ETDRS letter score was 61.3 (20/63), animprovement of 12.6 letters from the CRUISE study baseline,which was not statistically different from the improvement of 13.6letters at the end of the CRUISE study for the same cohort ofpatients (P ¼ 0.5; Fig 5A, available at http://aaojournal.org).Central foveal thickness was reduced markedly between baselineand the end of the CRUISE trial and fluctuated thereafterdepending on the frequency of follow-up (Fig 5B, available athttp://aaojournal.org). The mean number of injections was 7.9during the CRUISE trial, 4.7 during an average of 18.2 monthsof follow-up in HORIZON, 4.1 in the first year of the RETAINstudy, and 2.5 in the second year of the RETAIN study, for a meanof 19.2 during 54 months of follow-up (Fig 5C, available at http://aaojournal.org).
Resolution of Macular Edema in Patients withCentral Retinal Vein Occlusion
Resolution of edema occurred in 2 of 5 patients who withdrewbefore completing the RETAIN study (Table 2) and in 12 of 27patients who completed the RETAIN study, for a total of 14 of32 patients (43.8%). Figure 4D shows the distribution of lastinjections over time (mean time in resolved patients, 17.8months). Fifty-seven percent (8/14) had their last injection inthe first year, 14% (2/14) had their last injection in the secondyear, 21% (3/14) had their last injection in the third year, and7% (1/14) had their last injection in the fourth year. Unlike thesituation in patients with BRVO, patients with CRVO who hadresolution of edema had a superior outcome compared withthose who did not; the mean change in BCVA at the last visit,the percentage of patients who gained 15 letters or more, andthe percentage of patients who had a final vision of 20/40 orbetter was 25.2 letters, 78.6%, and 64.3%, respectively,for those with resolved disease versus 4.3 letters (P ¼ 0.002),33.3% (P ¼ 0.02), and 27.8% (P ¼ 0.04) for those with unre-solved disease. At the 4-year visit, the mean BCVA was 73.2
213
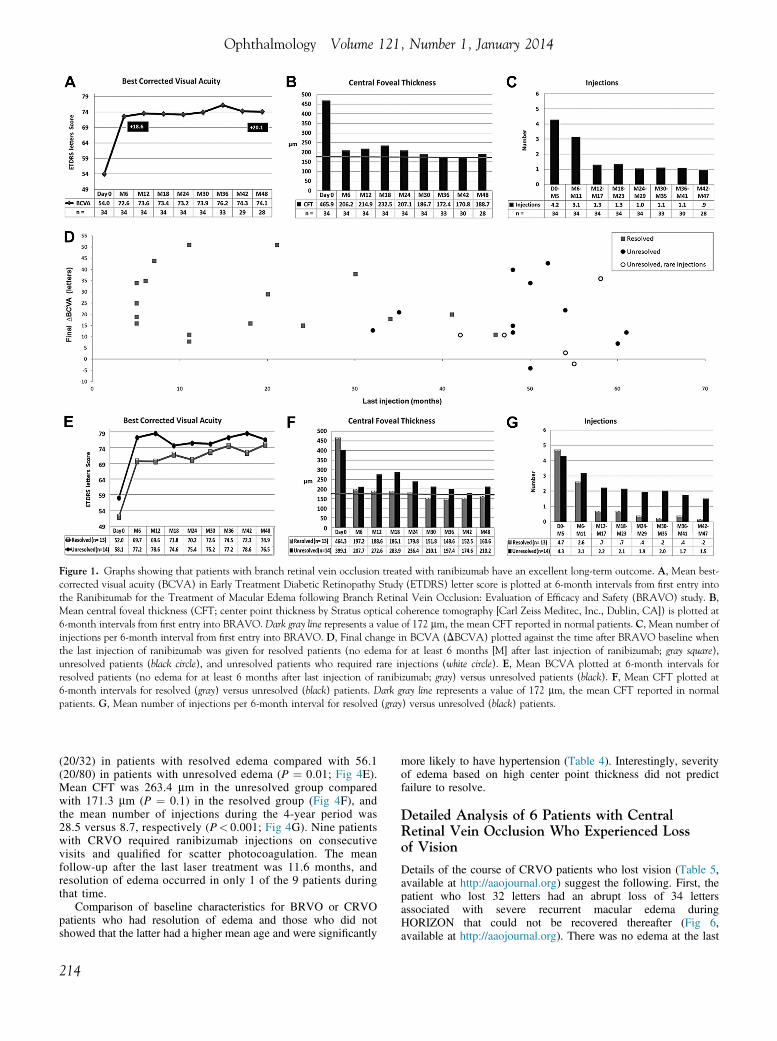
Figure 1. Graphs showing that patients with branch retinal vein occlusion treated with ranibizumab have an excellent long-term outcome. A, Mean best-corrected visual acuity (BCVA) in Early Treatment Diabetic Retinopathy Study (ETDRS) letter score is plotted at 6-month intervals from first entry intothe Ranibizumab for the Treatment of Macular Edema following Branch Retinal Vein Occlusion: Evaluation of Efficacy and Safety (BRAVO) study. B,Mean central foveal thickness (CFT; center point thickness by Stratus optical coherence tomography [Carl Zeiss Meditec, Inc., Dublin, CA]) is plotted at6-month intervals from first entry into BRAVO. Dark gray line represents a value of 172 mm, the mean CFT reported in normal patients. C, Mean number ofinjections per 6-month interval from first entry into BRAVO. D, Final change in BCVA (DBCVA) plotted against the time after BRAVO baseline whenthe last injection of ranibizumab was given for resolved patients (no edema for at least 6 months [M] after last injection of ranibizumab; gray square),unresolved patients (black circle), and unresolved patients who required rare injections (white circle). E, Mean BCVA plotted at 6-month intervals forresolved patients (no edema for at least 6 months after last injection of ranibizumab; gray) versus unresolved patients (black). F, Mean CFT plotted at6-month intervals for resolved (gray) versus unresolved (black) patients. Dark gray line represents a value of 172 mm, the mean CFT reported in normalpatients. G, Mean number of injections per 6-month interval for resolved (gray) versus unresolved (black) patients.
Ophthalmology Volume 121, Number 1, January 2014
(20/32) in patients with resolved edema compared with 56.1(20/80) in patients with unresolved edema (P ¼ 0.01; Fig 4E).Mean CFT was 263.4 mm in the unresolved group comparedwith 171.3 mm (P ¼ 0.1) in the resolved group (Fig 4F), andthe mean number of injections during the 4-year period was28.5 versus 8.7, respectively (P< 0.001; Fig 4G). Nine patientswith CRVO required ranibizumab injections on consecutivevisits and qualified for scatter photocoagulation. The meanfollow-up after the last laser treatment was 11.6 months, andresolution of edema occurred in only 1 of the 9 patients duringthat time.
Comparison of baseline characteristics for BRVO or CRVOpatients who had resolution of edema and those who did notshowed that the latter had a higher mean age and were significantly
214
more likely to have hypertension (Table 4). Interestingly, severityof edema based on high center point thickness did not predictfailure to resolve.
Detailed Analysis of 6 Patients with CentralRetinal Vein Occlusion Who Experienced Lossof Vision
Details of the course of CRVO patients who lost vision (Table 5,available at http://aaojournal.org) suggest the following. First, thepatient who lost 32 letters had an abrupt loss of 34 lettersassociated with severe recurrent macular edema duringHORIZON that could not be recovered thereafter (Fig 6,available at http://aaojournal.org). There was no edema at the last
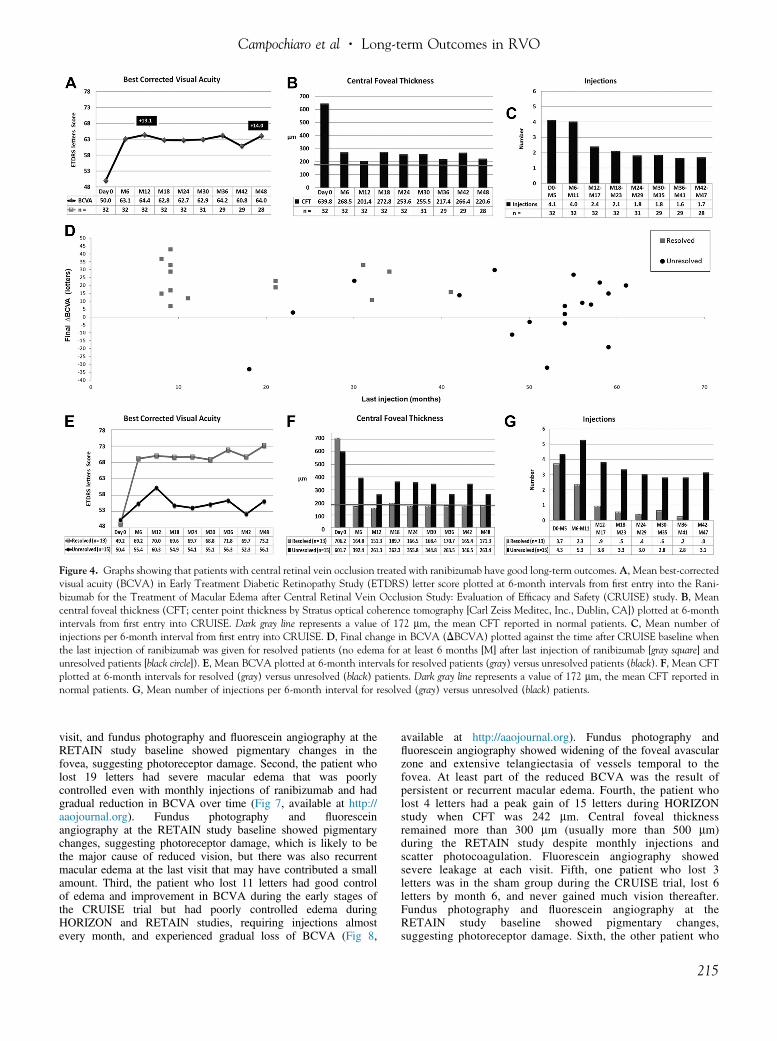
Figure 4. Graphs showing that patients with central retinal vein occlusion treated with ranibizumab have good long-term outcomes. A, Mean best-correctedvisual acuity (BCVA) in Early Treatment Diabetic Retinopathy Study (ETDRS) letter score plotted at 6-month intervals from first entry into the Rani-bizumab for the Treatment of Macular Edema after Central Retinal Vein Occlusion Study: Evaluation of Efficacy and Safety (CRUISE) study. B, Meancentral foveal thickness (CFT; center point thickness by Stratus optical coherence tomography [Carl Zeiss Meditec, Inc., Dublin, CA]) plotted at 6-monthintervals from first entry into CRUISE. Dark gray line represents a value of 172 mm, the mean CFT reported in normal patients. C, Mean number ofinjections per 6-month interval from first entry into CRUISE. D, Final change in BCVA (DBCVA) plotted against the time after CRUISE baseline whenthe last injection of ranibizumab was given for resolved patients (no edema for at least 6 months [M] after last injection of ranibizumab [gray square] andunresolved patients [black circle]). E, Mean BCVA plotted at 6-month intervals for resolved patients (gray) versus unresolved patients (black). F, Mean CFTplotted at 6-month intervals for resolved (gray) versus unresolved (black) patients. Dark gray line represents a value of 172 mm, the mean CFT reported innormal patients. G, Mean number of injections per 6-month interval for resolved (gray) versus unresolved (black) patients.
Campochiaro et al � Long-term Outcomes in RVO
visit, and fundus photography and fluorescein angiography at theRETAIN study baseline showed pigmentary changes in thefovea, suggesting photoreceptor damage. Second, the patient wholost 19 letters had severe macular edema that was poorlycontrolled even with monthly injections of ranibizumab and hadgradual reduction in BCVA over time (Fig 7, available at http://aaojournal.org). Fundus photography and fluoresceinangiography at the RETAIN study baseline showed pigmentarychanges, suggesting photoreceptor damage, which is likely to bethe major cause of reduced vision, but there was also recurrentmacular edema at the last visit that may have contributed a smallamount. Third, the patient who lost 11 letters had good controlof edema and improvement in BCVA during the early stages ofthe CRUISE trial but had poorly controlled edema duringHORIZON and RETAIN studies, requiring injections almostevery month, and experienced gradual loss of BCVA (Fig 8,
available at http://aaojournal.org). Fundus photography andfluorescein angiography showed widening of the foveal avascularzone and extensive telangiectasia of vessels temporal to thefovea. At least part of the reduced BCVA was the result ofpersistent or recurrent macular edema. Fourth, the patient wholost 4 letters had a peak gain of 15 letters during HORIZONstudy when CFT was 242 mm. Central foveal thicknessremained more than 300 mm (usually more than 500 mm)during the RETAIN study despite monthly injections andscatter photocoagulation. Fluorescein angiography showedsevere leakage at each visit. Fifth, one patient who lost 3letters was in the sham group during the CRUISE trial, lost 6letters by month 6, and never gained much vision thereafter.Fundus photography and fluorescein angiography at theRETAIN study baseline showed pigmentary changes,suggesting photoreceptor damage. Sixth, the other patient who
215

Table 4. Comparison of Baseline Characteristics in Patients with Resolved versus Unresolved Edema
Resolved Unresolved P Value
No. 31 34Mean age (SD), yrs 62.4 (11.6) 67.8 (9.6) 0.04Mean duration of disease (SD), mos 4.1 (4.3) 4.5 (4.5) 0.6Mean initial BCVA (SD), ETDRS letters score 49.5 (13.7) 53.9 (14.8) 0.2Mean initial CPT (SD), mm 616.6 (238.4) 497.9 (218.8) 0.04Hypertensive, n (%) 18 (58.1) 30 (88.2) 0.006Female sex, n (%) 10 (32.3) 17 (50.0) 0.1White race, n (%) 25 (80.6) 28 (84.8) 0.7Diabetic, n (%) 4 (12.9) 7 (20.6) 0.40.3- or 0.5-mg Ranibizumab group, n (%) 23 (74.2) 25 (73.5) 0.9
Boldface values indicate resolved patients had no macular edema for at least 6 months after their last injection of ranibizumab. Unresolved patients were stillrequiring injections of ranibizumab for macular edema within 6 months of last follow up.BCVA ¼ best-corrected visual acuity; CPT ¼ center point thickness; ETDRS ¼ Early Treatment Diabetic Retinopathy Study; SD ¼ standard deviation.
Ophthalmology Volume 121, Number 1, January 2014
lost 3 letters demonstrated an epiretinal membrane that wasbelieved to be contributing to reduced vision.
Safety
Tables 6 and 7 show all of the severe adverse events that occurredduring the RETAIN study. There were 4 ocular severe adverseevents, and none were attributable to ranibizumab. Two patientshad events probably related to vitreous traction: a vitreoushemorrhage in the absence of identifiable neovascularization thatresolved spontaneously and a retinal tear occurring many monthsafter the last injection of ranibizumab. One patient experienceda severe reaction to povodone iodine. The most serious event wasa superior hemiretinal vein occlusion in a patient who had resolvededema from an inferior BRVO with no injections of ranibizumabfor 27 months before the second RVO that resulted in severe lossof vision from macular ischemia.
Thirteen patients experienced severe systemic adverse events,and in 12 patients, the events were related to pre-existing disease,with no evidence suggesting a role for ranibizumab. One patientdied unexpectedly of an unknown cause within 2 months ofa ranibizumab injection; there is no evidence implicating ranibi-zumab, but it is not possible to rule out a role without moreinformation. The patient’s family did not respond to queries despitenumerous requests.
Discussion
The CRUISE and BRAVO studies demonstrated that anintraocular injection of ranibizumab every month for 6months resulted in marked improvement in edema andvisual acuity and that the benefits were maintained for
Table 6. Ocular Severe Adverse Events
Vitreous hemorrhage, resolved spontaneouslyPatient with an inferior branch retinal vein occlusion had resolution ofedema, but a superior branch vein occlusion developed 27 months afterlast ranibizumab injection; had severe ischemia, and neovascularglaucoma developed
Retinal tear in a patient with branch retinal vein occlusion who did notreceive any treatment during the trial
Severe reaction to povodone iodine
216
another 6 months when patients were evaluated monthly andgiven injections only if there was persistent or recurrentedema.2,3,6,7 Similar results have been obtained in patientswith CRVO treated with aflibercept,8,9 and thus it is clearthat suppression of VEGF provides excellent short-termoutcomes in patients with RVO. It was hoped that ifedema could be controlled for a year or so, collaterals woulddevelop and eliminate the underlying problem and theneed for continued injections. However, HORIZONdemonstrated that many patients with BRVO or CRVOcontinued to require injections of ranibizumab 2 years afterinitiation of treatment and that less frequent follow-upduring year 2 resulted in worsening of edema and reducedvision in many patients with CRVO.4 In this study, weprovided additional follow-up for a cohort of BRVO andCRVO patients who completed HORIZON. With a meanfollow-up of 50.2 months, 50% of BRVO patients hadresolution of edema, defined as no intraretinal fluid withoutinjection of ranibizumab for at least 6 months. Thesepatients had an excellent visual outcome, with a final visionof 20/40 or better in approximately 80%. The other 50% stillrequired an average of 3 injections of ranibizumab duringtheir last year of follow-up, but 80% of them had a finalvision of 20/40 or better. Thus, the problem was solved witha good outcome in half the BRVO patients, and although theultimate outcome is still uncertain in the other half, most ofthem have maintained good visual potential and requireinfrequent injections to control recurrent edema.
In patients with CRVO, with a mean follow-up of 51.4months, 44% had resolution of edema and an excellentvisual outcome, with 78% gaining 15 letters or more anda final visual acuity of 20/40 or better in 64%. However, theother 56% still required 6 injections of ranibizumab onaverage during their last year of follow-up, only 33% gained15 letters or more, and 28% had a final vision of 20/40 orbetter. Thus, slightly less than half of CRVO patientsexperienced resolution of the disease with a good outcome,and slightly more than half lost a substantial amount ofvisual potential and still have an uncertain future.
These results should be a reasonable estimate of long-term results for patients with RVO who fit the eligibility

Table 7. Systemic Severe Adverse Events
Description of EventTime Since LastInjection (mos) Outcome
Death resulting from pre-existing idiopathic pulmonary fibrosis 1.5 DeathDeath of unknown cause 2 DeathECG for elective knee surgery showed inverted T waves, patientasymptomatic, admitted for workup
0.1 Coronary artery bypass surgery, recovered
Mild chest discomfort for 6 mos, coronary angiography showed 2obstructions
1.25 Elective placement of 2 stents without complications,recovered
Tachycardia and went to the emergency department 2 Cardioverter defibrillator implanted, recoveredSyncope with fall because of arrhythmia 1 Pacemaker implanted, recoveredChronic atrial fibrillation, CVA; treated with tissue plasminogen activator;bladder cancer identified during hospitalization
28 Pacemaker implanted, administered anticoagulants,underwent surgery for bladder cancer; recovered
Head injury resulting from fall 1 Received staples for scalp laceration, recoveredUrinary tract infection leading to septic shock 5 Hospitalized, recoveredHospitalized for pneumonia 5 RecoveredHospitalized for pneumonia ×2 17, 49 RecoveredHospitalized for elective back surgery 16 RecoveredHospitalized for elective surgery ×2: rotator cuff, interphalangeal joint 4, 20 Recovered
CVA ¼ cerebrovascular accident; ECG ¼ electrocardiogram.
Campochiaro et al � Long-term Outcomes in RVO
criteria for the BRAVO or CRUISE trials, are treatedaccording to those protocols, and then have frequent follow-up and optical coherence tomographyeguided treatmentthereafter. They do not necessarily apply to patients with anafferent pupil defect or BCVA worse than 20/400 in theinvolved eye. One difference between our cohort and theentire cohorts of the BRAVO and CRUISE trials is that thesham patients in our cohort fared somewhat better during theBRAVO or CRUISE trials than the entire sham cohorts. It ispossible that the better early outcome in these subgroups ofsham patients led to better long-term outcomes. Our BRVOcohort contained 26% of patients originally assigned tosham, and in our CRVO cohort, 28% had a sham assign-ment and neither showed a significant difference in long-term outcome compared with corresponding patientsoriginally assigned to 0.3 or 0.5 mg ranibizumab. However,we cannot rule out the possibility that the outcomes reportedhere are slightly better than what would have been seen ifthe entire BRAVO and CRUISE populations had been fol-lowed up for 4 years.
Despite the excellent 4-year outcomes in most patients inthis study, there were some who lost vision. Detailedexamination of the course of patients who lost vision in thecurrent study and in a previous study10 suggests that itoccurs as a result of damage to photoreceptors fromischemia, recurrent edema, or both. Some patientsexperience ischemic damage to the fovea at the time of orsoon after the occlusion, and therefore visual potential islimited from the outset of treatment. Other patients havegood visual potential initially but lose that potential overtime from progressive ischemic damage to the fovea,photoreceptor damage from the edema, or both. It seemsthat photoreceptor damage is more likely when edema issevere and prolonged, repeated, or both, but it also seemsthat some individuals may be more susceptible than otherswho maintain good vision despite repeated bouts ofedema. This raises an important question for future
investigations. Monthly injections of ranibizumab preventprogression of RNP and ischemic damage11 and in mostpatients prevent large swings in retinal thickening andintraretinal fluid. Could more aggressive treatment at theonset of RVO or sustained delivery approaches aimed atpreventing progression of RNP and repeated episodes ofedema prevent visual loss in susceptible patients? Anotherunanswered question is why has edema resolutionoccurred in approximately half the patients, whereas theother half continue to experience bouts of recurrent edema4 years after initiation of treatment? Patients whose edemafailed to resolve had a higher mean age compared withthose whose edema resolved, and thus older age at onsetof occlusion is one factor. Another possible factor ishypertension: compared with patients with resolution ofedema, a significantly higher percentage of those in whomedema failed to resolve had hypertension. This is animportant area of investigation for future studies. Perhapsthe unresolved group had more retinal ischemia, resultingin higher levels of VEGF that was more difficult toneutralize by injections of ranibizumab, particularly duringperiods of less frequent follow-up and hence less frequentinjections. The worsening of RNP and ischemia by highlevels of VEGF may cause a positive feedback loop thatpromotes chronicity.
In patients with RVOwith chronic or recurrent edemawhostill require frequent injections several years after institutingtherapy, it is prudent to consider whether other alternatives oradditions should be considered. The first step is to definechronic in this context. Because roughly 75% of patients withBRVO or CRVO who experienced resolution of edema hadtheir last injection of ranibizumab within the first 2 years oftreatment, it is reasonable to consider adjunctive or alternativetreatments if relatively frequent injections are needed 2 yearsafter instituting treatment. One adjunctive treatment that isreasonable to consider is scatter photocoagulation, because ifproduction ofVEGFby ischemic peripheral retina is the cause
217

Ophthalmology Volume 121, Number 1, January 2014
of chronicity, one would expect scatter photocoagulation tothe peripheral retina to promote resolution of edema. In ourstudy, patients were not assigned randomly to receive scatterphotocoagulation, so we cannot say for certain whether itprovides benefit, but we can say that the protocol that we usedis not amagic bullet that rapidly promotes edema resolution inpatients with RVO who still require ranibizumab injectionsafter several years of treatment. One caveat is that in ourprotocol, laser photocoagulation was directed primarily toareas of RNP and to the far periphery, where it is difficult toassess perfusion status. However, although RNP is a markerfor retinal ischemia, it is not an ideal marker because hypo-perfused retina may be ischemic but still appear perfused onfluorescein angiography. Only 2 of 9 patients with CRVOreceived complete scatter photocoagulation outside thetemporal arcade vessels, and 1 of 9 patients with BRVOreceived complete scatter photocoagulation to the affectedhemisphere of the retina. It is possible that more completescatter photocoagulation would have a different effect thanwhat we observed. It is also possible that in a substantialpercentage of patients, RVO results in changes to the retinalvasculature that are not easily remedied or reversed. Fluo-rescein angiograms in patients with recurrent edema oftenshow telangiectatic vessels in the macula that leak. Suchabnormal vessels may be particularly sensitive to the leakage-promoting effects of VEGF, so that even small patches ofischemic retina in the posterior pole are sufficient to causerecurrent bouts of edema. In this situation, scatter photoco-agulation to peripheral retina may have little effect. Beforepassing final judgment on the effect of scatter photocoagu-lation, it is necessary to determine its effect when assignedrandomly to patients followed up in a prospective manner.
In conclusion, treatment with ranibizumab as needed tocontrol macular edema provides excellent long-term resultsin patients with BRVO. With a mean follow-up of 50.2months, 80% of BRVO patients had BCVA of better than20/40, regardless of whether there was complete resolutionof edema. One half showed resolution of edema, and theother half continued to require an average of 3 injections peryear. Although there is room for improvement, these arevery encouraging results. In patients with CRVO, the long-term outlook is more guarded. Slightly less than half hadresolution of edema with a mean follow-up of 51.4 months,and approximately two thirds of that group had BCVA of20/40 or better; however, slightly more than half stillrequired an average of 6 injections during year 4 to controledema, and only 25% of those patients had BCVA of 20/40or better. Furthermore, the frequent bouts of recurrent edema
218
in these patients are a risk for further loss of vision in thefuture. Thus, although we have made considerable progressin the treatment of patients with CRVO, new treatmentparadigms are needed.
References
1. Campochiaro PA, Hafiz G, Shah SM, et al. Ranibizumabfor macular edema due to retinal vein occlusions: implica-tion of VEGF as a critical stimulator. Mol Ther 2008;16:791–9.
2. Brown DM, Campochiaro PA, Singh RP, et al; CRUISEInvestigators. Ranibizumab for macular edema followingcentral retinal vein occlusion: six-month primary end point ofa phase III study. Ophthalmology 2010;117:1124–33.
3. Campochiaro PA, Heier JS, Feiner L, et al; BRAVO Investi-gators. Ranibizumab for macular edema following branchretinal vein occlusion: six-month primary endpoint results ofa phase III study. Ophthalmology 2010;117:1102–12.
4. Heier JS, Campochiaro PA, Yau L, et al. Ranibizumab formacular edema due to retinal vein occlusions: long-termfollow-up in the HORIZON trial. Ophthalmology 2012;119:802–9.
5. Early Treatment Diabetic Retinopathy Study Research Group.Photocoagulation for diabetic macular edema: Early TreatmentDiabetic Retinopathy Study report number 1. Arch Oph-thalmol 1985;103:1796–806.
6. Campochiaro PA, Brown DM, Awh CC, et al. Sustainedbenefits from ranibizumab for macular edema followingcentral retinal vein occlusion: twelve-month outcomes ofa phase III study. Ophthalmology 2011;118:2041–9.
7. Brown DM, Campochiaro PA, Bhisitkul RB, et al. Sustainedbenefits from ranibizumab for macular edema followingbranch retinal vein occlusion: 12-month outcomes of a phaseIII study. Ophthalmology 2011;118:1594–602.
8. Brown DM, Heier JS, Clark WL, et al. Intravitreal afliberceptinjection for macular edema secondary to central retinal veinocclusion: 1-year results from the phase 3 COPERNICUSStudy. Am J Ophthalmol 2013;155:429–37.
9. Holz FG, Roider J, Ogura Y, et al. VEGF Trap-Eye formacular oedema secondary to central retinal vein occlusion:6-month results of the phase III GALILEO study. Br J Oph-thalmol 2013;97:278–84.
10. Sophie R, Hafiz G, Scott A, et al. Progression of retinal non-perfusion in patients with retinal vein occlusion. Am J Oph-thalmol. In press.
11. Campochiaro PA, Bhistikul RB, Shapiro H, Rubio RG.Vascular endothelial growth factor promotes progressiveretinal nonperfusion in patients with retinal vein occlusion.Ophthalmology 2013;120:795–802.
Footnotes and Financial Disclosures
Originally received: May 31, 2013.Final revision: August 21, 2013.Accepted: August 27, 2013.Available online: October 8, 2013. Manuscript no. 2013-884.1 The Wilmer Eye Institute, Johns Hopkins University, Baltimore,Maryland.2 Retina Consultants, Sacramento, California.3 Retina Consultants of Houston, Methodist Hospital, Houston, Texas.
4 Retina-Vitreous Associates Medical Group, Beverly Hills, California.5 Ophthalmic Consultant of Boston, Boston, Massachusetts.6 Southeast Retina Center, Augusta, Georgia.7 Retina Associates of New Jersey, Teaneck, New Jersey.
*Members of the RETAIN Study Group are listed in the Appendix (http://aaojournal.org).
Campochiaro et al � Long-term Outcomes in RVO
Financial Disclosure(s):The author(s) have made the following disclosure(s): Peter A. Campochiaro- Consultant - Genentech, Regeneron, Aerpio, Kala, Applied GeneticTechnologies Corporation, Allergan; Data and Safety MonitoringCommittee - Advanced Cell Technology; Financial support - Genentech,Regeneron, Genzyme, Allergan, Oxford BioMedica, Molecular Partners,Aerpio; Advisory board (for which Johns Hopkins receives compensation) -Genentech, Inc., Regeneron, Aerpio
Joel Pearlman - Consultant - Genentech, Inc.; Financial support - Regen-eron, Alcon, Alimera Sciences, Pfizer, Ophthotech
David Brown - Consultant - Genentech/Roche, Regeneron/Bayer, Allergan,Alcon, ThromboGenics, Heidelberg Engineering, Optos, Zeiss, QLT;Financial support - Genentech, Regeneron, Allergan, Alcon, Thrombo-Genics, Acucela, GSK, Pfizer, Novartis, Xcovery Vision, Genzyme
David Boyer - Consultant - Allergan, Alcon, Bausch and Lomb, Allegro,Genentech, GSK, Merck, Bayer, Regeneron, Abbvie; Financial support -Alcon, Regeneron, Genentech, Ohr, Allergan, Juvenile Diabetes Associa-tion, GlaxoSmithKline; Data and Safety Monitoring Committee - AdvancedCell Technology
Jeffrey S. Heier - Consultant - Acucela, Aerpio, Allergan, Bausch & Lomb,Bayer, Dutch Ophthalmic, Endo Optiks, Forsight, Genzyme, HeidelbergEngineering, Kanghong, Notal Vision, Ohr Pharmaceutical, Ophthotech,QLT, Regeneron, Roche, Sequenom, ThromboGenics, Vertex, Xcovery;
Financial support - Aerpio, Alcon, Alimera, Allergan, Fovea, Genentech,Inc., Genzyme, GlaxoSmithKline, Neovista, Notal Vision, Novartis, Oph-thotech, Paloma, RegeneronDennis Marcus - Consultant - Genentech, Inc.,Regeneron, ThromboGenics; Financial support - Allergan, Genentech, Inc.,Pfizer, Regeneron, ThromboGenics, Quark, Lpath; Speakers’ bureau -Genentech, Inc., Regeneron; Advisory board - Genentech, Inc., Regeneron,ThromboGenics
Leonard Feiner - Speakers’ bureau - Roche, Regeneron
Arun Patel - Financial support - ThromboGenics
Supported by a grant from The Macula Foundation, New York, New York;and Genentech, Inc., South San Francisco, California. The Macula Foun-dation and Genentech had no role in the design or conduct of this research.
Correspondence:Peter A. Campochiaro, MD, The Wilmer Eye Institute, Johns HopkinsUniversity School of Medicine, 600 North Wolfe Street, Maumenee 719,Baltimore, MD 21287e9277. E-mail: [email protected].
219
Related Documents