Long Term Administration of Endothelin Receptor Antagonist Improves Coronary Endothelial Function in Patients with Early Atherosclerosis Martin Reriani, MB ChB, Eugenia Raichlin, MD, Abhiram Prasad, MD, Verghese Mathew, MD, Geralyn M. Pumper, Rebecca E. Nelson, Ryan Lennon, MS, Charanjit Rihal, MD, Lilach O. Lerman, MD, PhD, and Amir Lerman, MD Abstract Background—Endothelin (ET-1) is one of the most potent vasoconstrictors, and plays a seminal role in the pathogenesis of atherosclerosis. The current study was designed to test the hypothesis that long term treatment with an endothelin-A (ET A ) receptor antagonist improves coronary endothelial function in patients with early coronary atherosclerosis. Methods and Results—Forty seven patients with multiple cardiovascular risk factors, nonobstructive coronary artery disease and coronary endothelial dysfunction were randomized in a double-blind manner to either the ET A receptor antagonist Atrasentan (10mg) or placebo for six months. Coronary endothelium-dependent vasodilation was examined by infusing acetylcholine (ACh10 −6 ml/L to 10 −4 mol/L) in the left anterior descending coronary artery (LAD). N G - monomethyl- L -arginine (L-NMMA) was administered to a sub group of patients. Endothelium independent coronary flow reserve (CFR) was examined using intracoronary adenosine and nitroglycerin. Baseline characteristics and incidence of adverse effects were similar between the two groups. There was a significant improvement in percent change of coronary blood flow (% Δ CBF) in response to ACh at six months from baseline in the Atrasentan group as compared to the placebo group (39.67 % (23.23, 68.21) vs.−2.22 % (−27.37, 15.28), P<0.001). No significant difference in the percent change of coronary artery diameter or change in coronary flow reserve (Δ CFR) was demonstrated. CBF, coronary artery diameter and the effect of L-NMMA were similar between the groups at baseline and at six months. Conclusion—This study demonstrates that six month treatment with Atrasentan improves coronary microvascular endothelial function and support the role of the endogenous endothelin system in the regulation of endothelial function in early atherosclerosis in humans. Keywords endothelin-1 (ET-1); Atrasentan; endothelium dependent coronary blood flow; endothelium independent coronary flow reserve; coronary artery diameter Correspondence: Amir Lerman, MD Division of Cardiovascular Diseases, Mayo Clinic Rochester, 200 First Street, SW, Rochester, MN 55905 Fax: (507)-255-2550; phone: (507)-255-4152 [email protected]. Clinical Trial Registration: Clinical trials.gov identifier NCT00271492 URL: www.clinicaltrials.gov Disclosures None This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain. NIH Public Access Author Manuscript Circulation. Author manuscript; available in PMC 2011 September 7. Published in final edited form as: Circulation. 2010 September 7; 122(10): 958–966. doi:10.1161/CIRCULATIONAHA.110.967406. NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Long Term Administration of Endothelin Receptor AntagonistImproves Coronary Endothelial Function in Patients with EarlyAtherosclerosis
Martin Reriani, MB ChB, Eugenia Raichlin, MD, Abhiram Prasad, MD, Verghese Mathew,MD, Geralyn M. Pumper, Rebecca E. Nelson, Ryan Lennon, MS, Charanjit Rihal, MD, LilachO. Lerman, MD, PhD, and Amir Lerman, MD
AbstractBackground—Endothelin (ET-1) is one of the most potent vasoconstrictors, and plays a seminalrole in the pathogenesis of atherosclerosis. The current study was designed to test the hypothesisthat long term treatment with an endothelin-A (ETA) receptor antagonist improves coronaryendothelial function in patients with early coronary atherosclerosis.
Methods and Results—Forty seven patients with multiple cardiovascular risk factors,nonobstructive coronary artery disease and coronary endothelial dysfunction were randomized in adouble-blind manner to either the ETA receptor antagonist Atrasentan (10mg) or placebo for sixmonths. Coronary endothelium-dependent vasodilation was examined by infusing acetylcholine(ACh10−6 ml/L to 10−4 mol/L) in the left anterior descending coronary artery (LAD). NG-monomethyl-L-arginine (L-NMMA) was administered to a sub group of patients. Endotheliumindependent coronary flow reserve (CFR) was examined using intracoronary adenosine andnitroglycerin.
Baseline characteristics and incidence of adverse effects were similar between the two groups.There was a significant improvement in percent change of coronary blood flow (% Δ CBF) inresponse to ACh at six months from baseline in the Atrasentan group as compared to the placebogroup (39.67 % (23.23, 68.21) vs.−2.22 % (−27.37, 15.28), P<0.001). No significant difference inthe percent change of coronary artery diameter or change in coronary flow reserve (Δ CFR) wasdemonstrated. CBF, coronary artery diameter and the effect of L-NMMA were similar betweenthe groups at baseline and at six months.
Conclusion—This study demonstrates that six month treatment with Atrasentan improvescoronary microvascular endothelial function and support the role of the endogenous endothelinsystem in the regulation of endothelial function in early atherosclerosis in humans.
Keywordsendothelin-1 (ET-1); Atrasentan; endothelium dependent coronary blood flow; endotheliumindependent coronary flow reserve; coronary artery diameter
Correspondence: Amir Lerman, MD Division of Cardiovascular Diseases, Mayo Clinic Rochester, 200 First Street, SW, Rochester,MN 55905 Fax: (507)-255-2550; phone: (507)-255-4152 [email protected] Trial Registration: Clinical trials.gov identifier NCT00271492 URL: www.clinicaltrials.govDisclosures NoneThis is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providingthis early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before itis published in its final citable form. Please note that during the production process errors may be discovered which could affect thecontent, and all legal disclaimers that apply to the journal pertain.
NIH Public AccessAuthor ManuscriptCirculation. Author manuscript; available in PMC 2011 September 7.
Published in final edited form as:Circulation. 2010 September 7; 122(10): 958–966. doi:10.1161/CIRCULATIONAHA.110.967406.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

IntroductionEndothelin -1 (ET-1) is a 21-amino acid peptide with both mitogenic and vasoconstrictingproperties.1 Circulating ET-1 is increased in patients with atherosclerosis2 and in thecoronary circulation of patients with early atherosclerosis and coronary endothelialdysfunction.3 ET-1 contributes to the complex regulation of vascular tone through two majorreceptors termed endothelin-A (ETA) and endothelin-B (ETB) receptors.4 ETA receptors arelocated on vascular smooth muscle and mediate vasoconstriction.5 ETB receptors are locatedon both endothelial cells, where they mediate dilatation by releasing nitric oxide, and onsmooth muscle cells, where they contribute to constriction.6
Acute blockade of ETA receptors results in coronary vasodilatation7, 8 and improvement inendothelial function.7, 9 We have previously reported that twelve week administration of anETA receptor antagonist in a porcine hypercholesterolemia model improved coronaryendothelial function.10 Atrasentan (Abbott Laboratory, ABT-627, A-147627; trace nameXinlay), an orally available, potent and highly selective antagonist of the ETA receptor11 hasbeen extensively tested in cancer therapy and its effects have been reported in several phaseIII trials of refractory malignanicies.12, 13 We have recently demonstrated the systemiceffects and the safety of long term administration of Atrasentan in humans.14 The effect oflong term therapy with an ETA receptor antagonist on the human coronary circulation isunknown. Thus, the current study was designed to extend our previous observations and totest the hypothesis that long term administration of an ETA receptor antagonist improvescoronary endothelial function in patients with early coronary atherosclerosis. Moreover, weevaluated the impact of therapy on coronary nitric oxide (NO) bioavailability.
MethodsStudy Design
This study is a single center, double blind, randomized control trial, sponsored by theNational Institutes of Health. The study protocol was approved by the Mayo FoundationInstitutional Review Board.
Study PopulationSubjects were enrolled between July 2001 and December 2006 from those referred to thecardiac catheterization laboratory for evaluation of coronary artery disease, found to havenon-obstructive disease, and had comprehensive coronary physiology study including theassessment of endothelial function and non-endothelium-independent coronary flow reserve.Patients were included in this study if they had coronary microvascular endothelialdysfunction. According to our previous studies, we defined microvascular endothelialdysfunction as ≤ 50% increase in coronary blood flow (CBF) in response to the maximaldose of acetylcholine (ACh) compared with baseline CBF.15 Exclusion criteria for the studyhave been previously reported.15
Study ProtocolAt baseline, diagnostic coronary angiography and determination of endothelium-dependentand endothelium-independent flow reserve were performed as previously described.15 ADoppler guide wire (0.014-in diameter, FloWire, Volcano Incorporated) within a 2.2Fcoronary infusion catheter (Ultrafuse, SciMed Life System) was advanced and positioned inthe middle portion of the left anterior descending coronary artery (LAD). Intracoronarybolus injections of incremental doses (18 to 36 μg) of adenosine (Fujisawa), an endothelium-independent vasodilator (primarily of the microcirculation),16 were administered into theguiding catheter until maximal hyperemia was achieved.
Reriani et al. Page 2
Circulation. Author manuscript; available in PMC 2011 September 7.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Assessment of the endothelium-dependent coronary flow reserve was performed byselective infusion of ACh into the LAD. ACh (Iolab Pharmaceuticals) 10−6, 10−5, and 10−4
mol/L, was infused at 1 mL/min for 3 minutes.3, 15 Hemodynamic data (heart rate and meanarterial pressure), Doppler measurements, and coronary angiography were obtained aftereach infusion. Endothelium-independent epicardial vasodilation was assessed with anintracoronary bolus injection of nitroglycerin (200 μg, Abbott Laboratories).17
Assessment of Tonic Basal NO ReleaseIn a subset of patients whose consent was obtained prior to the baseline comprehensivecoronary physiology study (some patient were consented after their initial cardiaccatheterization and did not have this part of the study done), intracoronary NG-monomethyl-L-arginine (L-NMMA), a specific inhibitor of nitric oxide synthesis, wasinfused at a rate of 32 μmol/min for 5 minutes and then at 64 μmol/min for another 5minutes. Basal NO activity was evaluated by measuring the effect of L-NMMA on % Δcoronary artery diameter and % Δ CBF.
Quantitative Coronary AngiographyCoronary artery diameter (coronary artery diameter) was analyzed from digital images withuse of a modification of a previously described technique from this institution.15 The leftanterior descending coronary artery was divided into proximal, middle, and distal segments.For each segment, the measurements were performed in the region where the greatestchange had occurred during the acetylcholine infusion. An angiographically smooth segmentof the proximal, middle, and distal left anterior descending coronary arteries, free of anyoverlapping branch vessels, was identified in each patient and served as the referencediameter for calculation of diameter stenosis. End-diastolic cine frames that best showed thesegment were selected, and calibration of the video and cine images was done, identifyingthe diameter of the guide catheter. Quantitative measurements of the coronary arteries wereobtained using a computer-based image analysis system. Segment diameters weredetermined at baseline and after both acetylcholine and nitroglycerin administration. Theproximal segment was not exposed to Ach and thus served a control segment.
Assessment of Coronary Blood FlowDoppler flow velocity spectra were analyzed online to determine the time-averaged peakvelocity. Volumetric CBF was determined from the following relation: CBF=cross-sectionalarea × average peak velocity × 0.5.18 Endothelium-dependent coronary flow reserve wascalculated as % Δ CBF in response to ACh as previously described19. The endothelium-independent coronary flow reserve ratio was calculated by dividing the average peakvelocity after adenosine injection by the baseline average peak velocity.15 Coronary vascularresistance (CVR) was estimated as mean arterial blood pressure/CBF.20
Follow-UpThe patients were randomly assigned and treated in a double-blind fashion according to acomputer-generated code with either the ETA receptor antagonist Atrasentan at the dose of10 mg PO once a day or placebo for six months, in addition to standard medical therapy.Treatment assignments were concealed from participants and study staff except for thepharmacist technician. Study and placebo tablets (provided by Abbott Laboratory) weredistributed in bottles and were identical in appearance.
Six month follow-up coronary artery angiogram with coronary physiology study wasperformed by an independent investigator blinded to treatment allocation. The pre-specifiedprimary endpoint was the change at six months from baseline of % Δ CBF measured by
Reriani et al. Page 3
Circulation. Author manuscript; available in PMC 2011 September 7.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

intracoronary graded administration of ACh and % Δ CAD measured by quantitativecoronary angiography.
Statistical AnalysisPower calculation—Based on our previous studies21, and assuming a power of 80% andan alpha error=0.05, we calculated the magnitude difference that could be detected for the %Δ coronary artery diameter to ACh 10−4 as 3.9% and % Δ CBF to ACh 10−4 as 37.3% for asample size of 70 (35 in each group). With the above magnitude difference and given theobserved placebo mean from our previous studies of −25.9% for % Δ coronary arterydiameter to ACh 10−4 we would expect a significant result if the treatment mean is greaterthan −22.0%. Similarly given an observed placebo mean of 6.0% for % Δ CBF to ACh 10−4
from our previous studies we would expect a significant result if the treatment mean isgreater than 43.3%.
Data are displayed as means ± SD or count and percentage as appropriate. Variables withheavily skewed distribution are reported as medians with first and third quartiles inparenthesis. Analysis to compare different demographic and baseline clinical data betweenthe randomized groups was performed using the Student's t test for continuous data and thePearson's chi-squared test for categorical data. Baseline data for the CBF, CFR and coronaryartery diameter was compared using a rank sum test. Differences between the groups in theprimary end points were compared using Wilcoxon rank-sum test. Multiple linear regressionwas used to estimate the treatment effect adjusted for other covariates. All statistical testswere two-sided and a P<0.05 was considered to be statistically significant.
RESULTSCharacteristics of the patients
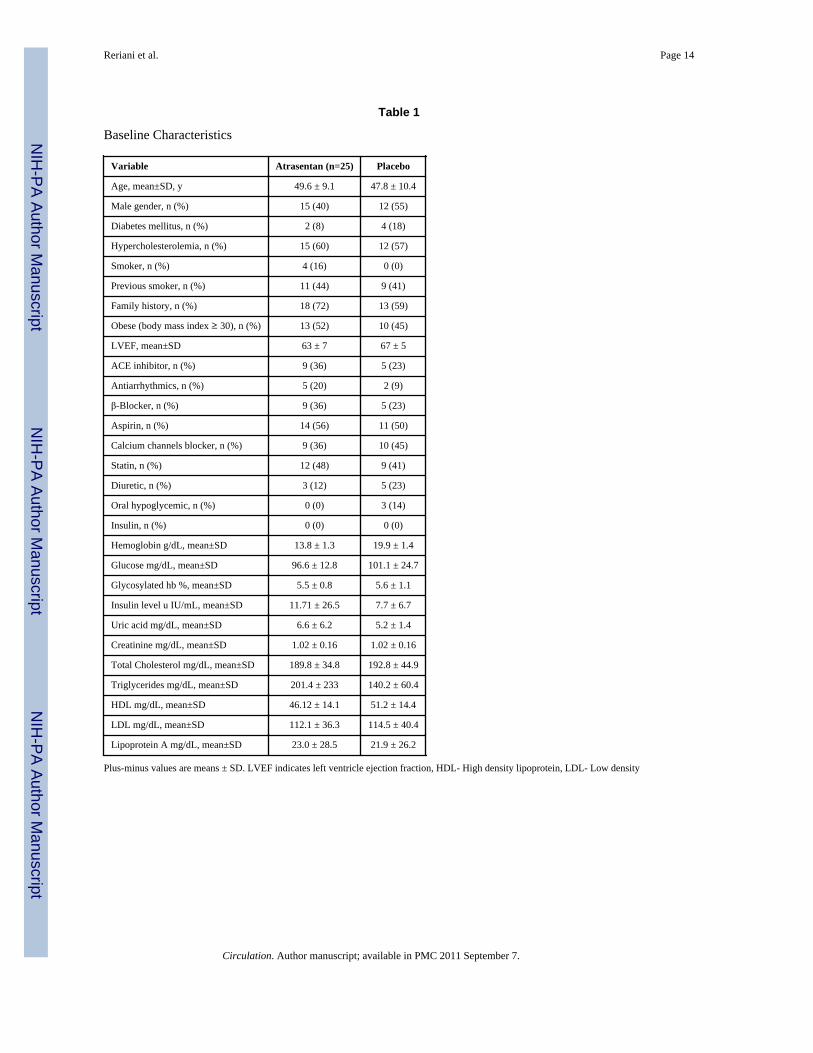
Of the seventy two patients randomized, forty seven had repeated coronary artery angiogramwith coronary physiology study at six months and were included in the final analysis (Figure1). The baseline characteristics of the 47 subjects were similar between the Atrasentan andthe placebo group (Table 1). Briefly the groups were well matched at baseline with regard toage, gender, race, coronary risk factors and medical treatment.
The baseline characteristics of the entire cohort have been reported previously14. Thepatients who had a follow-up coronary physiology study did not differ significantly fromthose who did not have a follow-up study. Patients who had a follow-up coronaryphysiology study however had a higher use of calcium channel blockers and diureticscompared at baseline compared to those who did not have a follow-up physiology study(Table 2).
Blood pressure and Heart rateThe baseline heart rate, systolic and diastolic blood pressures were similar between the twogroups. Long term administration of Atrasentan resulted in a reduction in diastolic bloodpressure from 74±3 to 59 ± 17 mmHg (P =0.02) and mean arterial pressure from 94±12 to86±12 mmHg (P=0.004) but reduction in systolic blood pressure from 120 ±36 to 113 ± 27mm Hg was not significant (P=0.96). Systolic, diastolic and mean arterial blood pressuresdid not change in the placebo group. There was no effect in heart rate (Table 3).
Effect of Atrasentan on Resting Coronary Vascular toneThere was no difference in the resting coronary artery diameter or CBF between the groupsat baseline and at six months (Table 3)
Reriani et al. Page 4
Circulation. Author manuscript; available in PMC 2011 September 7.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Effect of Atrasentan on Coronary Vascular resistanceLong term administration of Atrasentan decreased the CVR though it did not reach statisticalsignificance (P=0.08). CVR at six months was lower in the Atrasentan group compared toplacebo (P=0.04). The difference in CVR from baseline to 6 months between the Atrasentanand the placebo group was however not significant (P=0.5; Table 3).
Endothelium-Dependent and Independent Coronary Vascular Function Effect ofAtrasentan on the Epicardial circulation
Analysis of % Δ coronary artery diameter to ACh in the middle and distal segments of theLAD produced similar results and we reported only the results of the middle segment.Epicardial response to ACh did not improve after long term administration of Atrasentan(Figure 2). The percent change in coronary epicardial diameter in response to ACh at sixmonths was similar between the Atrasentan group and placebo (P=0.26; Table 3)
Effect of Atrasentan on Coronary microvascular endothelial functionLong term administration of Atrasentan resulted in significant improvement of coronarymicrovascular endothelial function (Figure 2). Compared to placebo, 6-month therapy withAtrasentan resulted in a significant improvement in % Δ CBF in response to ACh (P=0.003).There was also a significant difference in improvement in % Δ CBF between the Atrasentanand the placebo group at six months compared to baseline (P<0.001; Table 3). In adjustedanalysis using a linear regression model, Atrasentan compared to placebo significantlypredicted improvement in coronary microvascular endothelial function even after adjustingfor mean arterial pressure, glucose, triglycerides, lipoprotein A and uric acid (adjusteddifference in the mean % Δ CBF =.29.86 P<0.001).
Effect of Atrasentan on Coronary endothelium independent functionEndothelium independent CFR to Adenosine was lower with Atrasentan (P=0.01). CFR inthe placebo group also decreased though it did not reach statistical significance (P=0.06).Intracoronary administration of adenosine produced a lower CFR in the Atrasentan group atsix months compared to placebo (P=0.04). There was however no significant difference inthe change in CFR from baseline to 6 months between the Atrasentan and placebo group(P=0.64; Table 3)
Effect of Atrasentan in Response to Intracoronary NitroglycerinThere was no difference in the % Δ coronary artery diameter after administration ofintracoronary Nitroglycerin between the groups at baseline and at six months (Table 3).
Effect of L-NMMAA total of 30 patients (15 in each group) had L-NMMA administered at baseline and at sixmonths. Effect of L-NMMA on % Δ coronary artery diameter and % Δ CBF was similarbetween the Atrasentan and placebo group at baseline and after six months of treatment(Table 3) indicating similar blockade of tonic basal release of NO from the coronarycirculation in both the groups. The baseline characteristics of the patients who received theL-NMMA study were similar to the patients who did not suggesting that they may berepresentative of the whole cohort.
Effect of Atrasentan on renal function and metabolic characteristicsTriglyceride level (P=0.013), Lipoprotein-A (P=0.046), uric acid (P=0.006), fasting bloodglucose (P=0.026) and glycosylated hemoglobin (P=0.041) improved at six months in theAtrasentan-treated patients as compared with placebo-treated patients. Comparison of the
Reriani et al. Page 5
Circulation. Author manuscript; available in PMC 2011 September 7.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

difference at six months from baseline between the Atrasentan-treated patients and placebotreated patient was however significant only for fasting glucose (P=0.02). No significantdifference in changes at six months of the creatinine level (P=0.25) or estimated creatinineclearance (P=0.09) was demonstrated between the groups (Table 4).
Adverse EffectsThe incidence of reported adverse effects was similar between the treatment groups (Table5). The most common adverse effect with Atrasentan was nasal stuffiness, which occurred inthe first week after initiation and persisted during the study period. Headache occurred witha higher incidence in the patients receiving Atrasentan in the first month but was reported atthe same rate in the both groups on further follow-up. Edema (upper extremities and facial)occurred more frequently with the initiation of Atrasentan, but after 2 months of follow-upthere were no differences between the groups.
There were no changes in body weight in the patients treated with Atrasentan. There wereno changes in levels of sodium or albumin in the Atrasentan group. No patient developedproteinuria or hematuria during the study period.
A mild drop in hemoglobin concentration was observed within the first month of treatmentbut remained stable within the subsequent 5 months. In the Atrasentan group, the reductionsof mean hemoglobin at the end of the treatment were 1.18±1.17 g/dL as compared with0.63±0.90 g/dL in the placebo group (P=0.04). However, no patient required bloodtransfusion during the study period. No significant changes were observed in white bloodcount or platelet count in the Atrasentan-treated patients. There were no increases and noclinically significant changes in liver enzymes.
DiscussionThe present study demonstrates that long term ETA receptor antagonism improves coronarymicrovascular endothelial function in patients with early atherosclerosis and non obstructivecoronary artery disease. ET-1 mediated ETA receptor activation however did not have anysignificant effect on resting coronary vascular tone or epicardial endothelial function. Wehave also previously shown improvement of systemic hemodynamic and metabolic profilewith long term ETA receptor antagonism in humans14. The current study serves as a naturalextension of this study and supports a role for ET-1 in the regulation of coronary endothelialfunction in humans.
Effect of ETA Receptor Blockade on Coronary Vascular ToneThe present study did not show significant contribution of ET-1 mediated ETA receptoractivation to either the basal epicardial or microcirculatory coronary vasoconstrictor tone.Previous studies have demonstrated that acute blockade of ETA receptors resulted indilatation of coronary epicardial arterie.7, 8 The effects on the coronary microcirculation washowever much less pronounced9, with some studies showing no change in coronary bloodflow velocity after acute ETA receptor blockade.22 In one study, the vasodilation by ETAreceptor antagonism was greater in atherosclerotic coronary arteries compared to normalcoronary arteries22 reflecting the relative increase in vascular tissue and circulating ET-1concentrations in atherosclerotic plaques.2, 23, 24 Thus, the endogenous ET-1 pathway mayplay a more significant role in regulation of vascular tone in pathophysiological statesassociated with more advanced atherosclerotic plaques.2, 15 Therefore, the lack of the effectof ETA receptor antagonism on basal coronary vascular tone in the current study may berelated to the fact that the patient population did not have significant coronaryatherosclerosis.
Reriani et al. Page 6
Circulation. Author manuscript; available in PMC 2011 September 7.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Effects of ETA receptor Blockade on Microcirculatory Coronary Endothelial FunctionShort term ETA receptor antagonism causes improvement in the microcirculatory coronaryendothelial function.7, 9 One study showed an improvement in coronary microcirculationfunction in response to ACh infusion with the greatest impairment of endothelial functionderiving the greatest improvement after acute ETA blockade9. Recent studies have alsoshown that ETA receptor activation contributes to peripheral endothelial dysfunction25.Thus, our current study is in accord with these clinical observations and demonstrates for thefirst time the beneficial effects of long term administration of ETA receptor antagonist onmicrocirculation coronary endothelial function.
In the current study long term ETA antagonism did not affect epicardial vessel endothelium-dependent or independent function. Previous studies with acute ETA antagonism showedimprovement in epicardial coronary endothelial function only in those segments thatconstricted in response to ACh administration.9 Our study cohort included both coronaryvessels that constricted and those that dilated with ACH likely attenuating the vasodilatoryeffect of Atrasentan on the epicardial vessels.
Effect of ETA receptor blockade on Coronary endothelium independent functionLong term ETA receptor antagonism decreased endothelium independent CFR in response toadenosine. Coronary flow reserve is calculated as the ratio between hyperemic blood flowand resting coronary blood flow. The reduction in CFR to adenosine may thus reflect therelatively small increase in resting coronary blood flow (although not significant) or areduction in coronary vascular resistance to long term ETA receptor blockade.
Potential MechanismsLong term ETA receptor antagonism may improve coronary microvascular endothelialfunction through several potential mechanisms including direct effects on thevasoconstriction caused by ET-1 activity, decrease in oxidative stress and inflammation,improvement in metabolic characteristics, attenuation of atherosclerosis and augmentationof nitric oxide pathways.
Direct effect on Vasoconstriction activity of ET-1The sustained and potent vasoconstrictive response of ET-1 is mediated primarily throughactivation of ETA receptors24 which are the predominant receptors in vascular smoothmuscle cells. In this study and in previous studies of acute inhibition of ETA receptor inexperimental porcine hypercholesterolemia26 we did not show any attenuation in ACh-induced epicardial vasoconstriction. We previously reported the beneficial effects ofAtrasentan in lowering blood pressure observed in this study.14 Other clinical trials havealso shown similar beneficial effects of ETA receptor blockade on systemic blood pressure.27 The improvement in blood pressure observed in this study may have accounted for someof the improvement in the endothelial vasodilator function. However in the adjustedanalysis, the improvement in microvascular endothelial function occurred even afteradjusting for the hemodynamic and metabolic effects of Atrasentan. This suggests thatattenuation of the vasoconstricting effect is not the only mechanism of improvingendothelial function.
ET-1 and NOClassically endothelial dysfunction has been considered to be the result of a decrease in NObioavailability.3 Deficiency of the endothelium-derived NO is well documented in coronaryendothelial dysfunction28, 29 and in human atherosclerotic arteries.24 ET-1 can decrease NObioavailability by decreasing it production via inhibition of eNOS activity or by increasing it
Reriani et al. Page 7
Circulation. Author manuscript; available in PMC 2011 September 7.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

degradation via formation of oxygen radicals.30, 31 ET-1 also functionally offsets thevasodilator action of NO, and thereby participates in regulation of vascular tone.
Similar response to L-NMMA in the Atrasentan and placebo groups in this study impliesthat the effect on basal NO production by ETA receptor blockade is also not the mainmechanism in the improvement of microvascular endothelial function in patients with earlyatherosclerosis. Thus, the interaction between ET-1 and NO may involve the degradation ofNO. We have previously demonstrated the association between oxidative stress andendothelial dysfunction in animal models.29 32 Diet induced hypercholesterolemia in porcineexperimental models resulted in blunted endothelial function in the renal circulation29 aswell as in the coronary circulation32 and these were restored by antioxidant interventions.We have also recently shown that that coronary endothelial dysfunction in humans ischaracterized by local enhancement of oxidative stress.33 Both ETA and ETB receptors canincrease ROS production34, 35 which reacts with NO to produce peroxynitrite. ETA receptorblockade may lead to reduced production of ROS and decreased NO degradation leading toimprovement in NO dependent vasorelaxation.
Attenuation of AtherosclerosisET-1 is increased in patients with atherosclerotic risk factors such hypertension diabetes andsmoking. It is also elevated locally in atherosclerotic plaques23, 24 and the circulation andvascular tissue levels correlate with severity of atherosclerotic lesions.2, 36 One of themechanisms by which long term ETA receptor antagonism improved coronarymicrocirculatory endothelial function may be by the reduction in risk factors that maycontribute to endothelial dysfunction. We have reported that long term treatment withAtrasentan resulted in a reduction of blood pressure, improvement in glucose and lipidmetabolism as well as improvement in renal function in a subset of patients not treated withACE inhibitors.14 Thus, the beneficial effect of the blockade of the endogenous ET-1pathway in the current study may be in part mediated by the reduction in blood pressure andimprovement in lipid and glucose metabolism. By modifying atherosclerotic risk factors andattenuating the atherosclerotic process it may be speculated that long term ETA receptorantagonists may attenuate the progression of atherosclerosis by reversing endothelialdysfunction.
LimitationsThere are several limitation to this study. First, a significant number of patients did not havea follow up coronary physiology study. Among these patients, some did not have a repeatangiogram and the rest had a repeat angiogram but developed coronary arteryvasoconstriction that precluded the endothelial function study. The baseline characteristicsof the patients who had a follow-up coronary physiology study however did not differsignificantly from those who did not. The rate of adverse effects were also similar betweenthe two groups. Even with these measures there still remains a risk of bias in the results.
Second, the number of subjects having repeat coronary physiology studies was lower thanexpected and this may have reduced the power to find significant differences in some of theendpoints.
Third, we did not perform an intent-to-treat analysis in our primary outcome as we did nothave follow-up coronary physiology study data on a significant number of patients. Fourth,the small sample size means that overfitting is a concern in the case of multiple regressionmodeling and may cause instability in model estimates. Overfitting is especially a concernwhen one is creating a prediction model with the intention of applying it to external datasets. In our case the model was not aimed at predicting future outcomes, but for controlling
Reriani et al. Page 8
Circulation. Author manuscript; available in PMC 2011 September 7.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

other factors in estimating the size of the Atrasentan effect. Still, overfitting could result ininstability of the effect estimate. We did not find this to be the case, however, as the adjustedAtrasentan estimate was nearly the same as the unadjusted estimate, and the standard errorwas not so large as to render the hypothesis test non-significant. Thus we are confident thatour conclusions with regards to Atrasentan are valid.
Fifth, the present study was not designed to explain the precise cellular mechanism of theeffects of long term administration of Atrasentan on coronary physiology. Due to lack ofstandardization in measurements of invasive endothelial function we are limited in ourability compare the observed effects with those from studies measuring more acute effects ofAtrasentan. The measured effects on coronary physiology may indeed reflect the acute effectfrom the last given dose(s). More studies are thus needed to elucidate the mechanisms oflong term ETA receptor antagonism in improving coronary microvascular endothelialfunction. Six we do not have data on the degree of atherosclerosis in the patients throughintra vascular ultrasound. We thus cannot correlate the improvement in endothelial functionobserved with the degree of atherosclerosis.
ConclusionThis study demonstrates that six month treatment with Atrasentan improves coronarymicrovascular endothelial function. It emphasizes the importance of ET-1 on thecardiovascular system and the potential of long term ETA receptor antagonism to improveendothelial dysfunction.
This study demonstrates for the first time that the endogenous ET-1 plays a role in long termcoronary microvascular endothelial function and in the pathogenesis and progression ofcoronary endothelial dysfunction a known prognostic factor for cardiovascular disease. Thecurrent study suggests a potential role for long term ETA receptor antagonists as atherapeutic option for patients with coronary endothelial dysfunction and non-obstructivecoronary artery disease.
Clinical Perspective
Endothelial dysfunction is considered critical in the initiation, progression andcomplications of coronary artery disease and is independently associated withcardiovascular (CV) events. It is a reversible process that represents the functionalexpression of an individual's overall CV risk factor burden and many therapies thatrestore endothelial function also lower CV events. Coronary endothelial function isregulated by the balance of endothelium derived vasodilator and vasoconstrictor factorssuch as ET-1. This study provides evidence that long term ETA receptor antagonistsimproves coronary microvascular endothelial function in humans and support a role forthe endogenous ET in the mechanism and potentially the treatment of coronaryendothelial function in humans.
AcknowledgmentsSources of Funding The study was supported by grants from the NIH: NIH K24 HL-69840, NIH R01 HL-63911,HL-77131, HL 92954, HL 085307, DK 73608, DK 77013 and Mayo Foundation.
References1. Mathew V, Hasdai D, Lerman A. The role of endothelin in coronary atherosclerosis. Mayo Clin
Proc. 1996; 7:769–777. [PubMed: 8691898]
Reriani et al. Page 9
Circulation. Author manuscript; available in PMC 2011 September 7.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

2. Lerman A, Edwards BS, Hallett JW, Heublein DM, Sandberg SM, Burnett JC Jr. Circulating andtissue endothelin immunoreactivity in advanced atherosclerosis. N Engl J Med. 1991; 325:997–1001. [PubMed: 1886637]
3. Lerman A, Holmes DR Jr. Bell MR, Garratt KN, Nishimura RA, Burnett JC Jr. Endothelin incoronary endothelial dysfunction and early atherosclerosis in humans. Circulation. 1995; 92:2426–2431. [PubMed: 7586341]
4. Winkles JA, Alberts GF, Brogi E, Libby P. Endothelin-1 and endothelin receptor mRNA expressionin normal and atherosclerotic human arteries. Biochem Biophys Res Commun. 1993; 191:1081–1088. [PubMed: 8466485]
5. Haynes WG, Strachan FE, Webb DJ. Endothelin ETA and ETB receptors cause vasoconstriction ofhuman resistance and capacitance vessels in vivo. Circulation. 1995; 92:357–363. [PubMed:7634449]
6. Verhaar MC, Strachan FE, Newby DE, Cruden NL, Koomans HA, Rabelink TJ, Webb DJ.Endothelin-A receptor antagonist-mediated vasodilatation is attenuated by inhibition of nitric oxidesynthesis and by endothelin-B receptor blockade. Circulation. 1998; 97:752–756. [PubMed:9498538]
7. Halcox JP, Nour KR, Zalos G, Quyyumi AA. Endogenous endothelin in human coronary vascularfunction: differential contribution of endothelin receptor types A and B. Hypertension. 2007;49:1134–1141. [PubMed: 17353514]
8. Kyriakides ZS, Kremastinos DT, Bofilis E, Tousoulis D, Antoniadis A, Webb DJ. Endogenousendothelin maintains coronary artery tone by endothelin type A receptor stimulation in patientsundergoing coronary arteriography. Heart. 2000; 84:176–182. [PubMed: 10908255]
9. Halcox JP, Nour KR, Zalos G, Quyyumi AA. Coronary vasodilation and improvement inendothelial dysfunction with endothelin ET(A) receptor blockade. Circ Res. 2001; 89:969–976.[PubMed: 11717152]
10. Best PJ, McKenna CJ, Hasdai D, Holmes DR Jr. Lerman A. Chronic endothelin receptorantagonism preserves coronary endothelial function in experimental hypercholesterolemia.Circulation. 1999; 99:1747–1752. [PubMed: 10190886]
11. Wessale JL, Adler AL, Novosad EI, Calzadilla SV, Dayton BD, Marsh KC, Winn M, Jae HS, vonGeldern TW, Opgenorth TJ, Wu-Wong JR. Pharmacology of endothelin receptor antagonistsABT-627, ABT-546, A-182086 and A-192621: ex vivo and in vivo studies. Clin Sci (Lond). 2002;103(Suppl 48):112S–117S. [PubMed: 12193067]
12. Nelson JB, Love W, Chin JL, Saad F, Schulman CC, Sleep DJ, Qian J, Steinberg J, Carducci M.Phase 3, randomized, controlled trial of Atrasentan in patients with nonmetastatic, hormone-refractory prostate cancer. Cancer. 2008; 113:2478–2487. [PubMed: 18785254]
13. Carducci MA, Saad F, Abrahamsson PA, Dearnaley DP, Schulman CC, North SA, Sleep DJ,Isaacson JD, Nelson JB. A phase 3 randomized controlled trial of the efficacy and safety ofAtrasentan in men with metastatic hormone-refractory prostate cancer. Cancer. 2007; 110:1959–1966. [PubMed: 17886253]
14. Raichlin E, Prasad A, Mathew V, Kent B, Holmes DR Jr. Pumper GM, Nelson RE, Lerman LO,Lerman A. Efficacy and safety of Atrasentan in patients with cardiovascular risk and earlyatherosclerosis. Hypertension. 2008; 52:522–528. [PubMed: 18695150]
15. Hasdai D, Gibbons RJ, Holmes DR Jr. Higano ST, Lerman A. Coronary endothelial dysfunction inhumans is associated with myocardial perfusion defects. Circulation. 1997; 96:3390–3395.[PubMed: 9396432]
16. Hori M, Kitakaze M. Adenosine, the heart, and coronary circulation. Hypertension. 1991; 18:565–574. [PubMed: 1937658]
17. Harrison DG, Bates JN. The nitrovasodilators. New ideas about old drugs. Circulation. 1993;87:1461–1467. [PubMed: 8491000]
18. Doucette JW, Corl PD, Payne HM, Flynn AE, Goto M, Nassi M, Segal J. Validation of a Dopplerguide wire for intravascular measurement of coronary artery flow velocity. Circulation. 1992;85:1899–1911. [PubMed: 1572046]
19. Ofili EO, Labovitz AJ, Kern MJ. Coronary flow velocity dynamics in normal and diseased arteries.Am J Cardiol. 1993; 71:3D–9D.
Reriani et al. Page 10
Circulation. Author manuscript; available in PMC 2011 September 7.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

20. Quyyumi AA, Dakak N, Andrews NP, Gilligan DM, Panza JA, Cannon RO 3rd. Contribution ofnitric oxide to metabolic coronary vasodilation in the human heart. Circulation. 1995; 92:320–326.[PubMed: 7634444]
21. Lerman A, Burnett JC Jr. Higano ST, McKinley LJ, Holmes DR Jr. Long-term L-argininesupplementation improves small-vessel coronary endothelial function in humans. Circulation.1998; 97:2123–2128. [PubMed: 9626172]
22. Kinlay S, Behrendt D, Wainstein M, Beltrame J, Fang JC, Creager MA, Selwyn AP, Ganz P. Roleof endothelin-1 in the active constriction of human atherosclerotic coronary arteries. Circulation.2001; 104:1114–1118. [PubMed: 11535565]
23. Lerman A, Webster MW, Chesebro JH, Edwards WD, Wei CM, Fuster V, Burnett JC Jr.Circulating and tissue endothelin immunoreactivity in hypercholesterolemic pigs. Circulation.1993; 88:2923–2928. [PubMed: 8252706]
24. Zeiher AM, Drexler H, Wollschlager H, Just H. Modulation of coronary vasomotor tone inhumans. Progressive endothelial dysfunction with different early stages of coronaryatherosclerosis. Circulation. 1991; 83:391–401. [PubMed: 1991363]
25. Cardillo C, Campia U, Kilcoyne CM, Bryant MB, Panza JA. Improved endothelium-dependentvasodilation after blockade of endothelin receptors in patients with essential hypertension.Circulation. 2002; 105:452–456. [PubMed: 11815427]
26. Hasdai D, Best PJ, Cannan CR, Mathew V, Schwartz RS, Holmes DR Jr. Lerman A. Acuteendothelin-receptor inhibition does not attenuate acetylcholine-induced coronary vasoconstrictionin experimental hypercholesterolemia. Arterioscler Thromb Vasc Biol. 1998; 18:108–113.[PubMed: 9445263]
27. Krum H, Viskoper RJ, Lacourciere Y, Budde M, Charlon V. The effect of an endothelin-receptorantagonist, bosentan, on blood pressure in patients with essential hypertension. BosentanHypertension Investigators. N Engl J Med. 1998; 338:784–790. [PubMed: 9504938]
28. Mathew V, Cannan CR, Miller VM, Barber DA, Hasdai D, Schwartz RS, Holmes DR Jr. LermanA. Enhanced endothelin-mediated coronary vasoconstriction and attenuated basal nitric oxideactivity in experimental hypercholesterolemia. Circulation. 1997; 96:1930–1936. [PubMed:9323083]
29. Chade AR, Krier JD, Rodriguez-Porcel M, Breen JF, McKusick MA, Lerman A, Lerman LO.Comparison of acute and chronic antioxidant interventions in experimental renovascular disease.Am J Physiol Renal Physiol. 2004; 286:F1079–1086. [PubMed: 14722019]
30. Iglarz M, Clozel M. Mechanisms of ET-1-induced endothelial dysfunction. J CardiovascPharmacol. 2007; 50:621–628. [PubMed: 18091577]
31. Landmesser U, Harrison DG. Oxidant stress as a marker for cardiovascular events: Ox marks thespot. Circulation. 2001; 104:2638–2640. [PubMed: 11723010]
32. Rodriguez-Porcel M, Lerman LO, Holmes DR Jr. Richardson D, Napoli C, Lerman A. Chronicantioxidant supplementation attenuates nuclear factor-kappa B activation and preserves endothelialfunction in hypercholesterolemic pigs. Cardiovasc Res. 2002; 53:1010–1018. [PubMed:11922911]
33. Lavi S, Yang EH, Prasad A, Mathew V, Barsness GW, Rihal CS, Lerman LO, Lerman A. Theinteraction between coronary endothelial dysfunction, local oxidative stress, and endogenous nitricoxide in humans. Hypertension. 2008; 51:127–133. [PubMed: 18086957]
34. Duerrschmidt N, Wippich N, Goettsch W, Broemme HJ, Morawietz H. Endothelin-1 inducesNAD(P)H oxidase in human endothelial cells. Biochem Biophys Res Commun. 2000; 269:713–717. [PubMed: 10720482]
35. Loomis ED, Sullivan JC, Osmond DA, Pollock DM, Pollock JS. Endothelin mediates superoxideproduction and vasoconstriction through activation of NADPH oxidase and uncoupled nitric-oxidesynthase in the rat aorta. J Pharmacol Exp Ther. 2005; 315:1058–1064. [PubMed: 16144972]
36. Rossi GP, Colonna S, Pavan E, Albertin G, Della Rocca F, Gerosa G, Casarotto D, Sartore S,Pauletto P, Pessina AC. Endothelin-1 and its mRNA in the wall layers of human arteries ex vivo.Circulation. 1999; 99:1147–1155. [PubMed: 10069781]
Reriani et al. Page 11
Circulation. Author manuscript; available in PMC 2011 September 7.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 1.Flow chart of random assignment to treatment, completion of the trial, and reasons for notcompleting it.
Reriani et al. Page 12
Circulation. Author manuscript; available in PMC 2011 September 7.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 2.Difference in the mean percent change in Coronary Blood Flow and Coronary ArteryDiameter in response to acetylcholine at six months from baseline for Atrasentan andplacebo groups
Reriani et al. Page 13
Circulation. Author manuscript; available in PMC 2011 September 7.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Reriani et al. Page 14
Table 1
Baseline Characteristics
Variable Atrasentan (n=25) Placebo
Age, mean±SD, y 49.6 ± 9.1 47.8 ± 10.4
Male gender, n (%) 15 (40) 12 (55)
Diabetes mellitus, n (%) 2 (8) 4 (18)
Hypercholesterolemia, n (%) 15 (60) 12 (57)
Smoker, n (%) 4 (16) 0 (0)
Previous smoker, n (%) 11 (44) 9 (41)
Family history, n (%) 18 (72) 13 (59)
Obese (body mass index ≥ 30), n (%) 13 (52) 10 (45)
LVEF, mean±SD 63 ± 7 67 ± 5
ACE inhibitor, n (%) 9 (36) 5 (23)
Antiarrhythmics, n (%) 5 (20) 2 (9)
β-Blocker, n (%) 9 (36) 5 (23)
Aspirin, n (%) 14 (56) 11 (50)
Calcium channels blocker, n (%) 9 (36) 10 (45)
Statin, n (%) 12 (48) 9 (41)
Diuretic, n (%) 3 (12) 5 (23)
Oral hypoglycemic, n (%) 0 (0) 3 (14)
Insulin, n (%) 0 (0) 0 (0)
Hemoglobin g/dL, mean±SD 13.8 ± 1.3 19.9 ± 1.4
Glucose mg/dL, mean±SD 96.6 ± 12.8 101.1 ± 24.7
Glycosylated hb %, mean±SD 5.5 ± 0.8 5.6 ± 1.1
Insulin level u IU/mL, mean±SD 11.71 ± 26.5 7.7 ± 6.7
Uric acid mg/dL, mean±SD 6.6 ± 6.2 5.2 ± 1.4
Creatinine mg/dL, mean±SD 1.02 ± 0.16 1.02 ± 0.16
Total Cholesterol mg/dL, mean±SD 189.8 ± 34.8 192.8 ± 44.9
Triglycerides mg/dL, mean±SD 201.4 ± 233 140.2 ± 60.4
HDL mg/dL, mean±SD 46.12 ± 14.1 51.2 ± 14.4
LDL mg/dL, mean±SD 112.1 ± 36.3 114.5 ± 40.4
Lipoprotein A mg/dL, mean±SD 23.0 ± 28.5 21.9 ± 26.2
Plus-minus values are means ± SD. LVEF indicates left ventricle ejection fraction, HDL- High density lipoprotein, LDL- Low density
Circulation. Author manuscript; available in PMC 2011 September 7.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Reriani et al. Page 15
Table 2
Baseline Characteristics of Completers vs. Non completers
Characteristics Completers (n=47) Non Completers (n=25) P
Age, mean±SD, y 48.7 ± 9.6 48.8 ± 11.6 0.98
Male gender, n (%) 20 (43) 10 (48) 0.69
Diabetes mellitus, n (%) 6 (13) 2 (9) 0.7
Hypercholesterolemia, n (%) 27 (57) 16 (76) 0.3
Smoker, n (%) 4 (9) 4 (19) 0.21
Previous smoker, n (%) 20 (42) 10 (47) 0.7
Family history, n (%) 31 (66) 15 (71) 0.69
Obese (body mass index ≥30), n (%) 23 (49) 6 (29) 0.12
LVEF, mean±SD 66 + 6 56 -
ACE inhibitor, n (%) 14 (30) 8 (38) 0.5
Antiarrhythmics, n (%) 7 (15) 3 (14) 0.95
β-Blocker, n (%) 15 (32) 5 (24) 0.5
Aspirin, n (%) 25 (53) 16 (76) 0.07
Calcium channels blocker, n (%) 19 (40) 17 (81) 0.002
Statin, n (%) 21 (45) 14 (67) 0.09
Diuretic, n (%) 8 (17) 0 (0) 0.04
Oral hypoglycemic, n (%) 3 (6) 1 (5) 0.79
Insulin, n (%) 0 (0) 1 (5) 0.8
LVEF indicates left ventricle ejection fraction
Circulation. Author manuscript; available in PMC 2011 September 7.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Reriani et al. Page 16
Table 3
Baseline and Follow-Up of outcome measures.
Variable Atrasentan Placebo P
Systolic Blood Pressure n=25 n=22
Baseline, mean (SD) 120 ± 36 124 ± 18 0.2
6 months, mean (SD) 113 ± 27 126 ± 14 0.07
Difference, median (IQR) −5 (−29,5) 3.5 (−19.75,19) 0.27
Diastolic Blood Pressure n=25 n=22
Baseline, mean (SD) 74 ± 3 76 ± 8 0.58
6 months, mean (SD) 59 ± 17 75 ± 11.5 0.002
Difference, median (IQR) −15 (−22,−2) 2.5 (−16.5,9.5) 0.062
Mean Arterial Pressure n=25 n=22
Baseline, mean (SD) 94 ± 12 97 ± 18 0.43
6 months, mean (SD) 86 ± 12 96 ± 12 0.004
Difference, median (IQR) −11 (−17,−1) −1 (−8.5,5) 0.024
Heart Rate n=25 n=22
Baseline, mean (SD) 68 ± 9 73 ± 14 0.1
6 months, mean (SD) 71 ± 8 75 ± 11 0.1
Difference, median (IQR) 4 (−5,10) 2.5 (−2,9.25) 0.97
Coronary Blood Flow, ml/min n=25 n=22
Baseline, median (IQR) 48.67 (30.57, 73.89) 44.15 (30.55, 69.91) 0.65
6 months, median (IQR) 59.51 (46.13, 89.63) 51.08 (43.03, 68.06) 0.24
Difference, median (IQR) 15.26 (−7.08, 39.50) 5.56 (−23.50, 19.0) 0.25
Coronary Artery Diameter, mm n=25 n=22
Baseline, median (IQR) 2.1 (1.95, 2.68) 2.2 (1.76, 2.5) 0.45
6 months, median (IQR) 2.39 (2.03, 2.6) 2.3 (2, 2.9) 0.85
Difference, median (IQR) 0.2 (−0.5, 0.55) 0.005 (−0.37, 0.53) 0.62
Coronary vascular resistance mmHg ml-1 n=25 n=22
Baseline, median (IQR) 1.83 (1.36, 3.23) 2.11 (1.49, 3.27) 0.5
6 months, median (IQR) 1.47 (1.06, 1.88) 1.60 (1.45, 2.21) 0.04
Difference, median (IQR) −0.55 (−1.32, −0.15) −0.31 (1.23, 0.58) 0.5
% Change in coronary blood flow (Ach) n=25 n=22
Baseline, median (IQR) −11.32 (−46.06, 13) 4.81 (−44.22, 37.70) 0.25
6 months, median (IQR) 38.21 (2.76, 62.47) -6.35 (-30.36, 11.53) 0.003
Difference, median (IQR) 39.67 (23.24, 68.22) −2.2 (−27.37, 15.28) 0.0001
% Change coronary artery diameter (Ach) n=25 n=22
Baseline, median (IQR) −33.33 (−41.94, −16.30) −21.36 (−31.64, −13.45) 0.07
6 months, median (IQR) −34.78 (−48.33,−3.77) −16.67 (−33.39, −6.51) 0.26
Circulation. Author manuscript; available in PMC 2011 September 7.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Reriani et al. Page 17
Variable Atrasentan Placebo P
Difference, median (IQR) 1.07 (−10.40, 20.56) 8.05 (−17.5, 19.24) 0.6
% Change coronary flow reserve (Adenosine) n=25 n=22
Baseline, median (IQR) 2.9 (2.55, 3.2) 3.0 (2.68, 3.82) 0.51
6 months, median (IQR) 2.6 (2.2, 2.85) 2.8 (2.4, 3.42) 0.04
Difference, median (IQR) −0.3 (−0.55, 0) −0.25 (−0.63, 0.1) 0.65
% Change coronary artery diameter (Ntg) n=25 n=22
Baseline, median (IQR) 10 (0.75 17.52) 11.56 (2.78, 22.14) 0.59
6 months, median (IQR) 11.43 (6.57, 30.29) 16.33 (6.55, 23.62) 0.76
Difference, median (IQR) 3.33 (−8.0, 20.58) 9.16 (−7.81, 14.92) 0.99
% Change coronary blood flow to 64mcg L-NMMA n=15 n=15
Baseline, median (IQR) −23.47 (−44.20, −18.42) −17.14 (−41.56, −2) 0.31
6 months, median (IQR) −20.74 (−34.69, −0.91) −31.14 (−43.91, −23.05) 0.17
Difference, median (IQR) −1.28 (−12.83, 28.52) −11.53 (−33.87, 14.58) 0.09
% Change coronary artery diameterto 64mcg L-NMMA n=15 n=15
Baseline, median (IQR) −13.16 (−22.73, −9.68) −4.57 (−10.82, 0) 0.03
6 months, median (IQR) −13.79 (−17.39, 0) −13.33 (−17.22, −5.36) 0.98
Difference, median (IQR) 3.52 (−8.93, 15.71) −2.43 (−19.19, 9.04) 0.19
Circulation. Author manuscript; available in PMC 2011 September 7.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Reriani et al. Page 18
Table 4
Baseline and follow-up metabolic characteristics
Variable Atrasentan (n=31) Placebo (n=34) P
Creatinine, mg/dl
Baseline, mean (SD) 1 ± 0.15 1.02 ± 0.14 0.56
6 months, mean (SD) 0.90 ± 0.12 0.96 ± 0.15 0.25
Difference, mean (SD) −0.1 ± 0.13 0.06 ± 0.14 0.254
Creatinine clearance ml/min
Baseline, mean (SD) 58 ± 16 58 ± 17 0.83
6 months, mean (SD) 62 ± 14 60 ± 15 0.09
Difference, mean (SD) 4 ± 15 2 ± 16 0.6
Uric acid, mg/dl
Baseline, mean (SD) 4.9 ± 1.16 4.9 ± 1.14 0.95
6 months, mean (SD) 4.8±1.6 5.1±1.3 0.048
Difference, mean (SD) −0.1 ± 1.43 0.2 ± 1.23 0.08
Glucose, mg/dl
Baseline, mean (SD) 96.1 ± 18.3 96.0 ± 23.0 0.99
6 months, mean (SD) 93.0 ± 14.6 104.5 ± 32.0 0.026
Difference, mean (SD) 3.1 ± 5.3 8.5 ± 28.6 0.02
Glycosylated hb, %
Baseline, mean (SD) 5.5 ± 0.7 5.4 ± 0.9 0.71
6 months, mean (SD) 5.4 ± 0.8 5.5 ± 0.7 0.041
Difference, mean (SD) 0.1 ± 0.75 0.1 ± 0.81 0.3
Triglycerides, mg/dl
Baseline, mean (SD) 181.7 ± 202.5 127.9 ± 56.0 0.14
6 months, mean (SD) 126.0 ± 137.2 133.4 ± 75.2 0.013
Difference, mean (SD) −55.7 ± 179 5.5 ± 67.7 0.07
Lipoprotein A, mg/dl
Baseline, mean (SD) 25.5 ± 26.9 25.0 ± 28.9 0.82
6 months, mean (SD) 18.4 ± 20.5 27.9 ± 42.9 0.046
Difference, mean (SD) −7.1 ± 1.45 2.9 ± 1.75 0.2
Weight, kg
Baseline, mean (SD) 86.9 ± 21.3 88.6 ± 16.1 0.71
6 months, mean (SD) 87.6 ± 20.9 87.0 ± 27.7 0.6
Difference, mean (SD) 0.7 ± 21.1 −1.6 ± 1.75 0.68
Data show the ANOVA test with treatment group as the factor and baseline values as the covariate
Data are mean (SD)
Circulation. Author manuscript; available in PMC 2011 September 7.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Reriani et al. Page 19
Table 5
Symptoms and Adverse Effects
Variable Atrasentan Placebo P
Adverse effects, n 32 27 0.067
Headache, n 25 20 0.18
Nasal Stuffiness, n 30 19 <0.001
Edema
Lower extremities, n 24 20 0.3
Upper extremities, n 19 11 0.034
Facial, n 18 5 <0.001
Shortness of breath, n 27 23 0.25
Fatigue, n 27 27 0.78
Vertigo, n 19 22 0.54
Lightheadedness, n 24 22 0.46
Flushing, n 19 14 0.17
Insominia, n 19 16 0.37
Withdraw, n 4 2 0.65
Time to withdraw, range, d 56±55 67±66 0.74
Hospitalizations
Hospitalizations, n 19 21 0.62
Reason for hospitalizations
Chest pain, n 17 21 0.13
Atrial fibrilation, n 2 0
Circulation. Author manuscript; available in PMC 2011 September 7.
Related Documents











