Long-Lasting Evolution of Ptosis Control After Reduction Mammaplasty Using the Hammock Technique Jose´ M. Pe´rez-Macı´as, M.D. Pe´rez-Macı´as Plastic Surgery Clinic, Garcı´a Morato 39 1-b, 47006 Valladolid, Spain Abstract. Background: The hammock technique combines inferior pedicle mammaplasty with retropectoral and inferior sus- pensions to prevent displacement of breast tissue toward the inferior mammarian pole. This study aimed to assess the long-lasting internal suspension with the authorÕs mammary reduction technique. Methods: From 1987 to 2005, the hammock technique was performed for 623 breast reduction patients (1,201 breasts), including 318 women (636 breasts) who underwent the technique between 1994 and 2005. From the latter group, the author retrospectively reviewed the case histories of 281 patients who had come for long-term follow-up evaluation. All had significant ptosis associated with breast hypertro- phy. Preoperative and postoperative examinations included evaluation of postoperative bottoming out by monitoring of three measurements: the sternal notch-to-nipple length, the inferior areolar border-to-inframammary fold length, and the distance between the inframmary fold and the projection of the lowest breast contour on the chest wall. Results: The evaluation data on postoperative ptosis are derived from a control study at 30 months, 5 years, and 7 years or more for 281 women (562 breasts) of the 318 who underwent surgery using this technique over the 11-year period. Review after 2.5 to 7 years or more shows that inferior areolar border-inframammary fold distance in- creases no more than 10 mm. Conclusions: The hammock technique suspension achieves true permanent breast lifting through dermis strips from the inferior pedicle itself. This procedure also gives predictable results, a low morbidity rate, and good breast shape. Key words: Breast hypertrophy—Hammock technique— Ptosis control—Reduction mammaplasty Reduction mammaplasty methods have undergone multiple refinements in recent years. Mastopexy techniques are of great importance in maintaining breast uplift after reduction mammaplasty. The abundance of surgical options generated over the recent years attests to the lack of consensus for a single procedure to address all degrees of mammary ptosis [130]. Mammaplasty reduction has been performed according to the norms of the inferior and central dermoglandular pedicle techniques [6,3136] since 1982 [37]. The advantages of this technique are well known: nipple sensitivity conservation [33,3840], vascular security of the nippleareola complex (NAC) [4144], and lactiferous duct preservation [36,45]. However, this technique has a drawback: secondary breast sagging [4648]. To correct this problem, in 1987, we introduced internal suspension to support the inferior pedicle [15]. The hammock technique we present is an inferior pedicle procedure associated with retropectoral and inferior derm- opexies in breast reduction [49]. The name ‘‘hammock technique’’ was inspired in the 1970s by bladder suspension techniques [50]. This method has proved itself to be beneficial for patients with mammary ptosis and hypertrophy. It retains all the advantages provided by inferior pedicle proce- dures [51]. The average plastic surgery patient is far more educated about aesthetic procedures than in the past, and many request procedures that incorporate recent advances in breast surgery (shortened scars, postop- erative ptosis control). Mammaplasty suspension has already been established as a viable alternative in breast ptosis surgery, and scar-shortening procedures are now frequent in various breast techniques [14,17,20,21,23,5263]. Correspondence to Jose´ M. Pe´rez-Macı´as M.D. email: [email protected] Aesth. Plast. Surg. 31:266274, 2007 DOI: 10.1007/s00266-006-0188-3

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Long-Lasting Evolution of Ptosis Control After Reduction Mammaplasty
Using the Hammock Technique
Jose M. Perez-Macıas, M.D.
Perez-Macıas Plastic Surgery Clinic, Garcıa Morato 39 1-b, 47006 Valladolid, Spain
Abstract.
Background: The hammock technique combines inferiorpedicle mammaplasty with retropectoral and inferior sus-
pensions to prevent displacement of breast tissue towardthe inferior mammarian pole. This study aimed to assessthe long-lasting internal suspension with the author�smammary reduction technique.
Methods: From 1987 to 2005, the hammock technique wasperformed for 623 breast reduction patients (1,201 breasts),including 318 women (636 breasts) who underwent the
technique between 1994 and 2005. From the latter group,the author retrospectively reviewed the case histories of 281patients who had come for long-term follow-up evaluation.
All had significant ptosis associated with breast hypertro-phy. Preoperative and postoperative examinations includedevaluation of postoperative bottoming out by monitoringof three measurements: the sternal notch-to-nipple length,
the inferior areolar border-to-inframammary fold length,and the distance between the inframmary fold and theprojection of the lowest breast contour on the chest wall.
Results: The evaluation data on postoperative ptosis arederived from a control study at 30 months, 5 years, and 7years or more for 281 women (562 breasts) of the 318 who
underwent surgery using this technique over the 11-yearperiod. Review after 2.5 to 7 years or more shows thatinferior areolar border-inframammary fold distance in-
creases no more than 10 mm.Conclusions: The hammock technique suspension achievestrue permanent breast lifting through dermis strips from theinferior pedicle itself. This procedure also gives predictable
results, a low morbidity rate, and good breast shape.
Key words: Breast hypertrophy—Hammock technique—Ptosis control—Reduction mammaplasty
Reduction mammaplasty methods have undergonemultiple refinements in recent years. Mastopexytechniques are of great importance in maintainingbreast uplift after reduction mammaplasty. Theabundance of surgical options generated over therecent years attests to the lack of consensus for asingle procedure to address all degrees of mammaryptosis [1�30].
Mammaplasty reduction has been performedaccording to the norms of the inferior and centraldermoglandular pedicle techniques [6,31�36] since1982 [37]. The advantages of this technique are wellknown: nipple sensitivity conservation [33,38�40],vascular security of the nipple�areola complex(NAC) [41�44], and lactiferous duct preservation[36,45]. However, this technique has a drawback:secondary breast sagging [46�48]. To correct thisproblem, in 1987, we introduced internal suspensionto support the inferior pedicle [15]. The hammocktechnique we present is an inferior pedicle procedureassociated with retropectoral and inferior derm-opexies in breast reduction [49].
The name ‘‘hammock technique’’ was inspired inthe 1970s by bladder suspension techniques [50]. Thismethod has proved itself to be beneficial for patientswith mammary ptosis and hypertrophy. It retains allthe advantages provided by inferior pedicle proce-dures [51].
The average plastic surgery patient is far moreeducated about aesthetic procedures than in the past,and many request procedures that incorporate recentadvances in breast surgery (shortened scars, postop-erative ptosis control). Mammaplasty suspension hasalready been established as a viable alternative inbreast ptosis surgery, and scar-shortening proceduresare now frequent in various breast techniques[14,17,20,21,23,52�63].Correspondence to Jose M. Perez-Macıas M.D. email:
Aesth. Plast. Surg. 31:266�274, 2007DOI: 10.1007/s00266-006-0188-3
The hammock technique has been refined over thepast 18 years [64], satisfying a combination of pa-tients� needs: long-term maintenance of postoperativeuplift and short inframammary scars. With our pro-cedure, internal suspension provides long-lastingstability while eliminating the inferior central scarsegment and keeping the lateral scar within the limitsof the anterior axillary line, yielding a smaller scar.
Patients and Methods
A total of 623 women (1,201 breasts) who had under-gone mammaplasty surgery over a 21-year period(1987�2005) received mammary reduction and mas-topexyby thehammock technique to correct ptosis andhypertrophy. In this retrospective study, the case his-tories of 318 women who underwent bilateral mam-maplasties (636 breasts) were reviewed with thistechnique between January 1994 and August 2005.The data for this subgroup were as follows. All the
patients had surgery under general anesthesia. Theaverage patient age was 35.85 years (range, 18�65years). The glandular tissue removed had a meanweight of 597.16 g (range, 220�1,450 g) per breast.The following measurements were obtained pre-
operatively and postoperatively with the patient instanding position for follow-up evaluations: the dis-tance from the inferior margin of the areola to theinframammary fold, the distance from the sternalnotch to the nipple, and the distance between theinframammary fold and the projection of the lowestbreast contour on the chest wall.The preoperative sternal notch�nipple distance
ranged from 27 to 39 cm, and the length from in-framammary fold to inferior areola border rangedfrom 11 to 20 cm. The breast ptosis degree variedfrom 5 to 13 cm, according to the projection of theinferior breast border on the chest wall.For the evaluation of prospective dermopexy con-
trol, the case histories of the 318 patients whounderwent surgery between 1994 and 2005 were ret-rospectively reviewed. Of these patients, 281 who hadreturned for follow-up evaluations until at least 30months (or more) after surgery were selected. Thedegree of postoperative ptosis and the quality ofbreast reshaping were the assessment criteria at eachpatient�s final follow-up evaluation. The percentageof complications was determined for the followingcase histories: complications of the hammock tech-nique for 318 women (636 breasts) who underwentsurgery between 1994 and 2005 and complications ofthe dermis suspension technique for the same group.
Surgical Technique
With the patient in standing position, the midclavic-ular line is marked downward through and past thenipple. The future top of the NAC, which is 19 to 22
cm from the suprasternal notch, depending on patientsize, is marked on this midclavicular vertical line at apoint determined by pushing the index finger upwardfrom the inframammary crease. This point also ismarked on the other breast. The horizontal distancebetween each new NAC top and the midsternal linesis verified, adjusting as necessary. This distanceshould never exceed 12 cm.
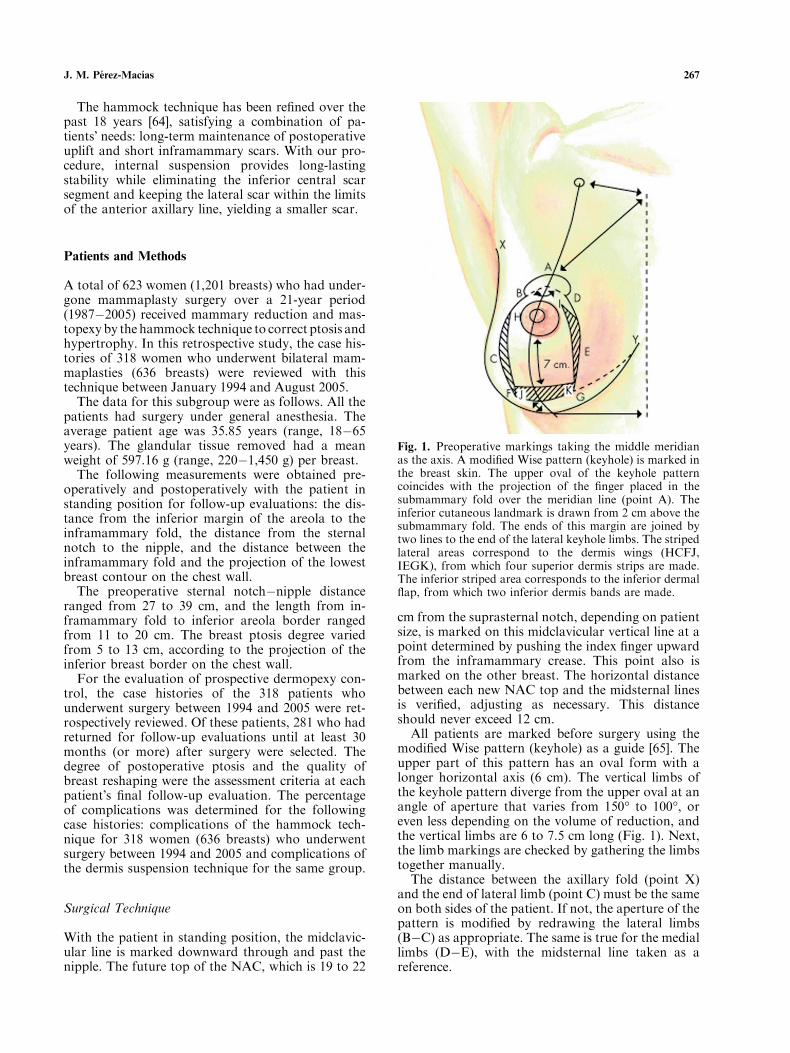
All patients are marked before surgery using themodified Wise pattern (keyhole) as a guide [65]. Theupper part of this pattern has an oval form with alonger horizontal axis (6 cm). The vertical limbs ofthe keyhole pattern diverge from the upper oval at anangle of aperture that varies from 150� to 100�, oreven less depending on the volume of reduction, andthe vertical limbs are 6 to 7.5 cm long (Fig. 1). Next,the limb markings are checked by gathering the limbstogether manually.
The distance between the axillary fold (point X)and the end of lateral limb (point C) must be the sameon both sides of the patient. If not, the aperture of thepattern is modified by redrawing the lateral limbs(B�C) as appropriate. The same is true for the mediallimbs (D�E), with the midsternal line taken as areference.
Fig. 1. Preoperative markings taking the middle meridianas the axis. A modified Wise pattern (keyhole) is marked inthe breast skin. The upper oval of the keyhole patterncoincides with the projection of the finger placed in thesubmammary fold over the meridian line (point A). Theinferior cutaneous landmark is drawn from 2 cm above thesubmammary fold. The ends of this margin are joined bytwo lines to the end of the lateral keyhole limbs. The stripedlateral areas correspond to the dermis wings (HCFJ,IEGK), from which four superior dermis strips are made.The inferior striped area corresponds to the inferior dermalflap, from which two inferior dermis bands are made.
J. M. Perez-Macıas 267
The new submammary fold is marked with thepatient supine. It is determined by pushing the breastupward, stretching the inferior pole skin 2 cm abovethe old submammary crease line. The horizontallength of the future submammary scar will be thesame as distance between this new line and the end ofthe lateral Wise pattern limb. The top, lateral, andmedial markings of the inferior areola�nipple pedicleare drawn within the limits of the keyhole pattern onthe lateral and medial margins of the inferior pedicle(HCFJ, IEGK). Triangular wings are drawn, fromwhich dermis strips will be fashioned for the retro-mastopexy (Fig. 1).The entire inferior pole, except for the NAC
(diameter, �4.5�5.0 cm), is deepithelialized, fol-lowing the cutaneous drawings. The lateral andmedial cutaneous fat breast flaps are dissectedtangentially up to the anterior musculo-aponeuroticwall. All dissection is performed with electrocau-tery. The thickness of the lateral, superior, andmedial flaps cannot be less than 2 or 3 cm.Redundant skin and breast tissue then are removedby circumferential resection in a horseshoe shape
between the inferior pedicle margins and the key-hole pattern skin markings. From two-thirds toone-half of the breast tissue making up the inferior
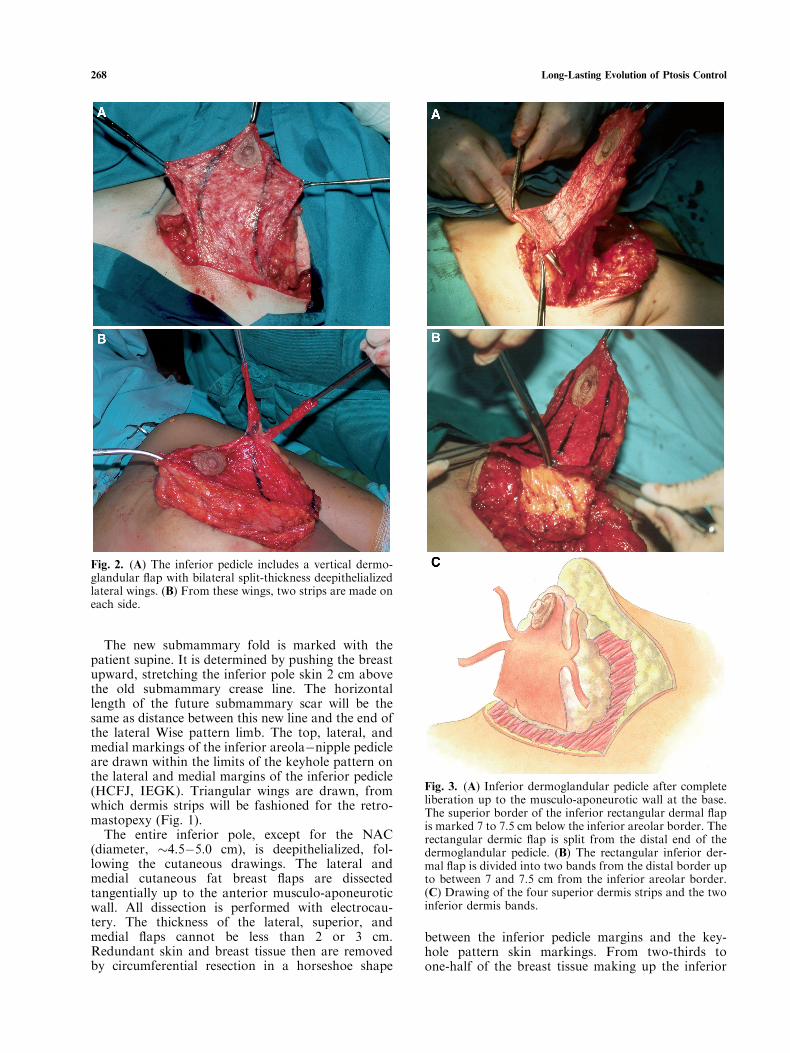
Fig. 2. (A) The inferior pedicle includes a vertical dermo-glandular flap with bilateral split-thickness deepithelializedlateral wings. (B) From these wings, two strips are made oneach side.
Fig. 3. (A) Inferior dermoglandular pedicle after completeliberation up to the musculo-aponeurotic wall at the base.The superior border of the inferior rectangular dermal flapis marked 7 to 7.5 cm below the inferior areolar border. Therectangular dermic flap is split from the distal end of thedermoglandular pedicle. (B) The rectangular inferior der-mal flap is divided into two bands from the distal border upto between 7 and 7.5 cm from the inferior areolar border.(C) Drawing of the four superior dermis strips and the twoinferior dermis bands.
268 Long-Lasting Evolution of Ptosis Control
pedicle remains joined directly to the musculo-aponeurotic wall. Most of the tissue is removedsupralaterally, with less removed medially. Theinferior pedicle ends up in the shape of a cone, withthe nipple at the apex. This pedicle includes avertical dermoglandular flap with bilateral split-thickness deepithelialized wings (Fig. 2A and C).From these wings, two strips are made on eachside, as shown (superior strips) (Fig. 2. B and C).Next, the inferior base of the pedicle is separated
by an incision through the dermis and breastparenchyma up to the musculo-aponeurotic wall topermit complete mobilization (Fig. 3A). The nextstep is to split a rectangular dermal flap from thedistal end of the inferior pedicle up to between 7and 7.5 cm from the inferior areola border(Fig. 3A). This then is divided in half into twodermis bands (inferior strips) (Fig. 3B and C),
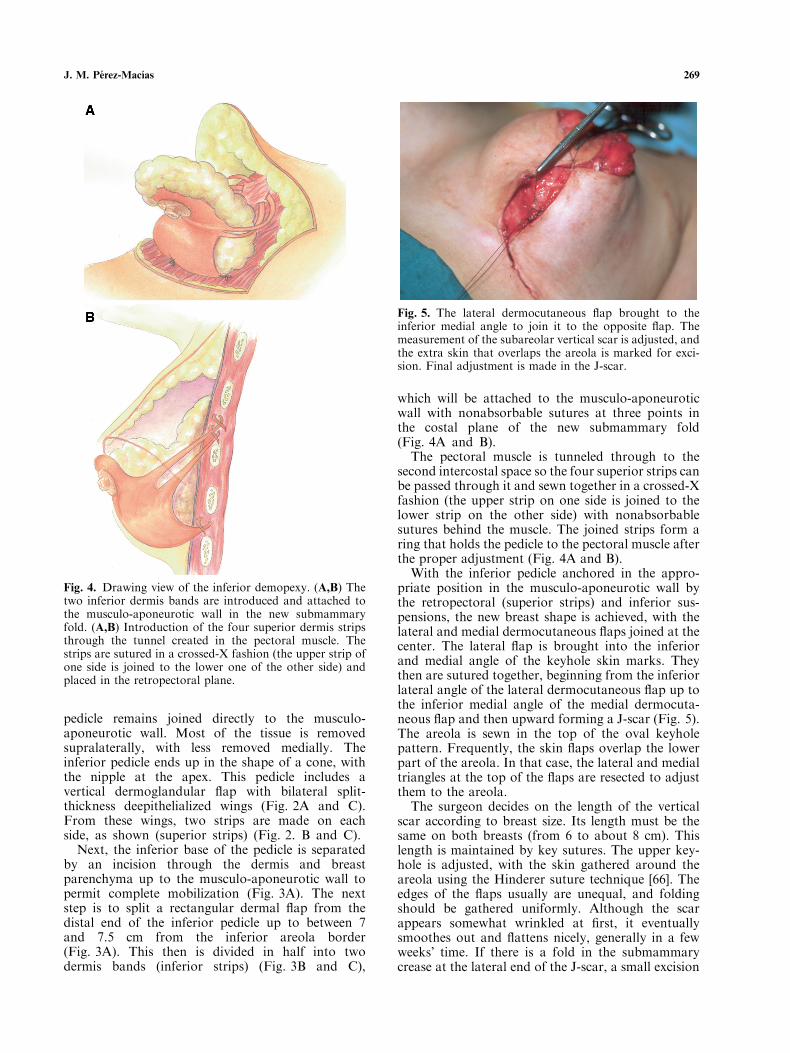
which will be attached to the musculo-aponeuroticwall with nonabsorbable sutures at three points inthe costal plane of the new submammary fold(Fig. 4A and B).
The pectoral muscle is tunneled through to thesecond intercostal space so the four superior strips canbe passed through it and sewn together in a crossed-Xfashion (the upper strip on one side is joined to thelower strip on the other side) with nonabsorbablesutures behind the muscle. The joined strips form aring that holds the pedicle to the pectoral muscle afterthe proper adjustment (Fig. 4A and B).
With the inferior pedicle anchored in the appro-priate position in the musculo-aponeurotic wall bythe retropectoral (superior strips) and inferior sus-pensions, the new breast shape is achieved, with thelateral and medial dermocutaneous flaps joined at thecenter. The lateral flap is brought into the inferiorand medial angle of the keyhole skin marks. Theythen are sutured together, beginning from the inferiorlateral angle of the lateral dermocutaneous flap up tothe inferior medial angle of the medial dermocuta-neous flap and then upward forming a J-scar (Fig. 5).The areola is sewn in the top of the oval keyholepattern. Frequently, the skin flaps overlap the lowerpart of the areola. In that case, the lateral and medialtriangles at the top of the flaps are resected to adjustthem to the areola.
The surgeon decides on the length of the verticalscar according to breast size. Its length must be thesame on both breasts (from 6 to about 8 cm). Thislength is maintained by key sutures. The upper key-hole is adjusted, with the skin gathered around theareola using the Hinderer suture technique [66]. Theedges of the flaps usually are unequal, and foldingshould be gathered uniformly. Although the scarappears somewhat wrinkled at first, it eventuallysmoothes out and flattens nicely, generally in a fewweeks� time. If there is a fold in the submammarycrease at the lateral end of the J-scar, a small excision
Fig. 4. Drawing view of the inferior demopexy. (A,B) Thetwo inferior dermis bands are introduced and attached tothe musculo-aponeurotic wall in the new submammaryfold. (A,B) Introduction of the four superior dermis stripsthrough the tunnel created in the pectoral muscle. Thestrips are sutured in a crossed-X fashion (the upper strip ofone side is joined to the lower one of the other side) andplaced in the retropectoral plane.
Fig. 5. The lateral dermocutaneous flap brought to theinferior medial angle to join it to the opposite flap. Themeasurement of the subareolar vertical scar is adjusted, andthe extra skin that overlaps the areola is marked for exci-sion. Final adjustment is made in the J-scar.
J. M. Perez-Macıas 269
or liposuction is required to remodel it. No drains areused, and hypoallergic tape plus adhesive elasticbandages are used as a dressing.
Results
Between 1994 and 2005, 281 of the 318 patients (562breasts) received follow-up evaluations for a mini-mum of 30 months. Of these, 85 received additionalrevisions 5 years postoperatively, and 42 came forfollow-up evaluations for 7 years or more.At the end of the operation, vertical the infra-
areolar�inframammary fold distance averaged 6.8cm (8 cm maximum). In the 30-month postopera-tive revision, this distance increased only minimally(7 mm maximum increase), with correct NACpositioning. Between the 30-month and the 5-yearfollow-up evaluations, the vertical distance barelyincreased, at most, 3 mm more than the 30-monthlength (10-mm maximum increase compared withthe initial postoperative distance). At this writing, 7years postoperatively, the vertical distance has notchanged.The sternal notch-to-nipple distance did not vary
significantly in either the short- or long-term revision
for any of the groups. The inframammary projectionof the lowest breast contour over the chest wall variedbetween 0 and 10 mm (average, 3.5 mm). The earlycomplications in this subgroup population (318 wo-men) included areolar epidermolysis (6 breasts,0.94%), which healed with topical treatment; partialareolar necrosis (4 breasts, 0.62%), which healedwithout secondary surgery; and suture dehiscence (12breasts, 0.88%), with five breasts (4 patients) requir-ing secondary surgery. Five patients experiencedhematoma postoperatively (0.78%), which did notneed to be drained. No cases of infection were ob-served.
The later complications included hypertrophy andwide scars (31 breasts, 4.8%) (secondary scar surgerywas offered to some patients, but few accepted),partial fat necrosis (4 breasts, 0.62%), and alterationsin sensitivity (24 breasts 3.77%).
Nine patients (2.8%) needed a small excision of aresidual dog ear at the end of the inferior lateral scar.Asymmetry was assessed in 13 cases (4%), In terms ofaesthetic form, the results were unsatisfactory for 14patients (4.4%). These negative results were related toobesity, severe hypertrophy, and severe ptosis. Whenthe patients were asked to evaluate aesthetic mor-phology and correct NAC positioning, 94% reported
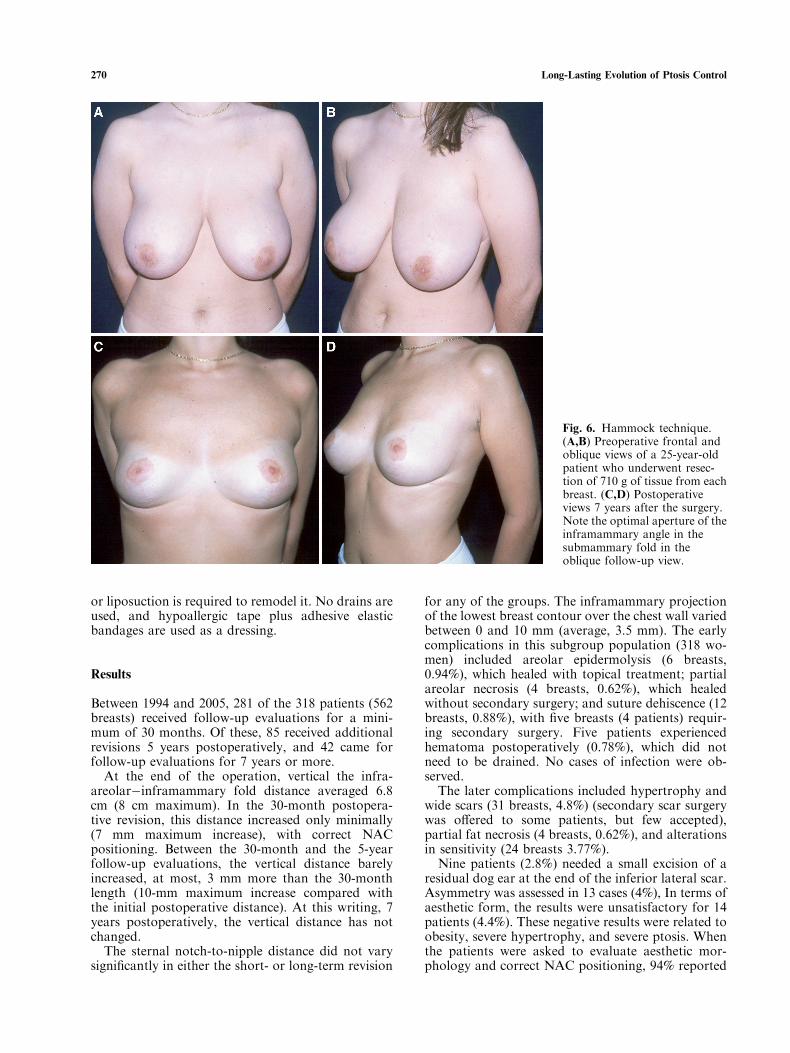
Fig. 6. Hammock technique.(A,B) Preoperative frontal andoblique views of a 25-year-oldpatient who underwent resec-tion of 710 g of tissue from eachbreast. (C,D) Postoperativeviews 7 years after the surgery.Note the optimal aperture of theinframammary angle in thesubmammary fold in theoblique follow-up view.
270 Long-Lasting Evolution of Ptosis Control
that they were highly pleased with the results (Figs. 6and 7).Complications related to dermis suspension mas-
topexies were experienced by 7 of the 318 patientswho underwent surgery between 1984 and 2005.These seven patients experienced failure of the infe-rior mastopexies (7 of 636 breasts, 1.1%) (Fig. 8).
Discussion
The main causes of unsatisfactory uplift results arethat the breast lacks true fixation to stabilize it in the
muscular plane. It also is covered by stretchable skinand dragged down by gravity. The concept of internalsuspension to support breast tissues, described in theearly years of mammaplasty techniques, allows onlyapproximation of breast tissues toward the musculo-aponeurotic wall. Simple sutures for suspension arenot sufficient [1,3,5�7], and the permanent fixationwith these techniques depends only on extensiveformation of fibrous tissue between the skin and thesurface of the breast gland [3,5]. With the standardinferior dermoglandular pedicle technique, recurrentptosis gradually develops with time because the lat-
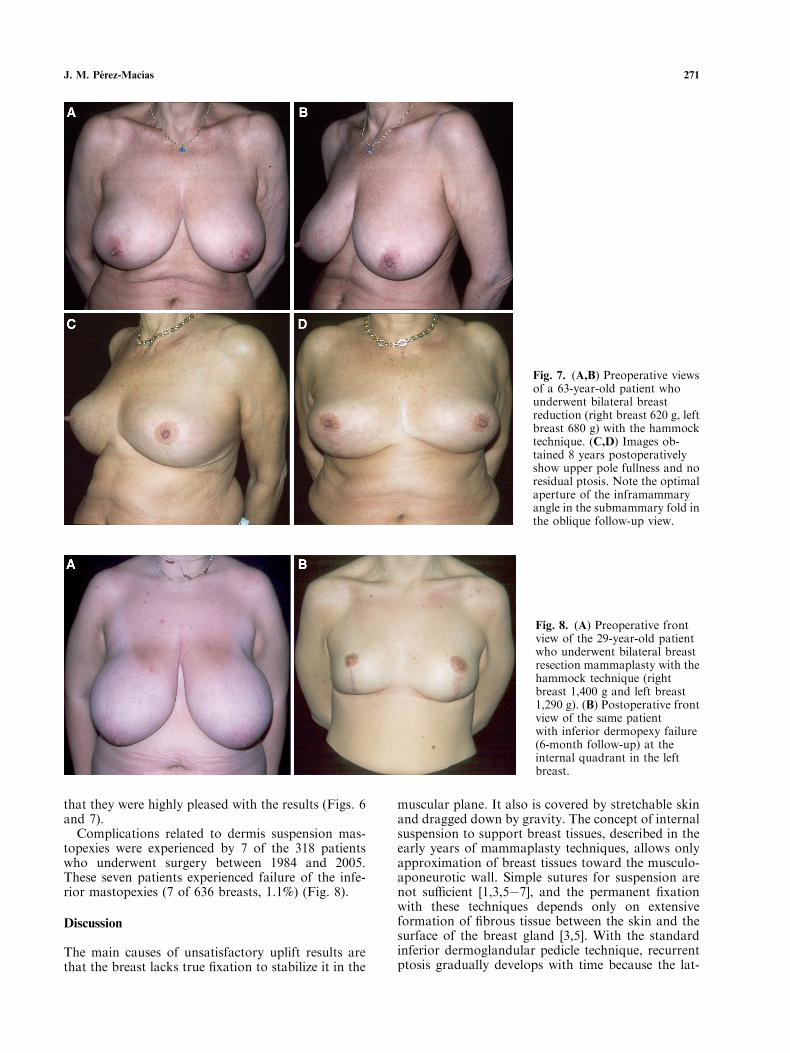
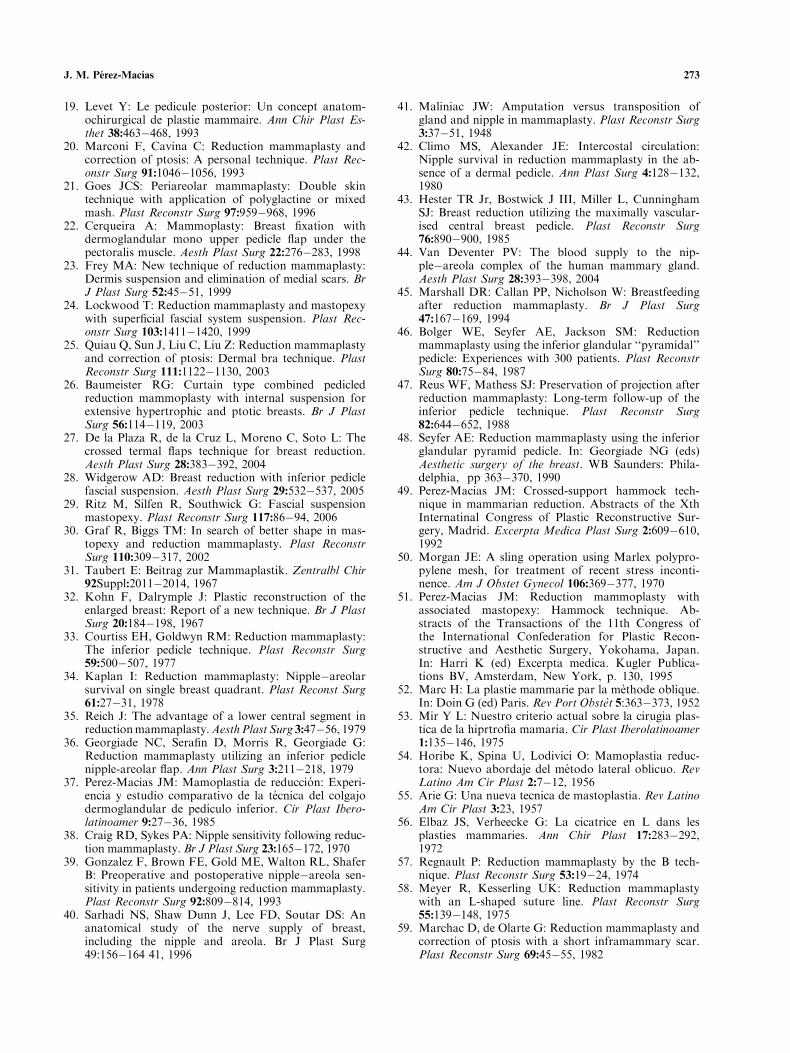
Fig. 7. (A,B) Preoperative viewsof a 63-year-old patient whounderwent bilateral breastreduction (right breast 620 g, leftbreast 680 g) with the hammocktechnique. (C,D) Images ob-tained 8 years postoperativelyshow upper pole fullness and noresidual ptosis. Note the optimalaperture of the inframammaryangle in the submammary fold inthe oblique follow-up view.
Fig. 8. (A) Preoperative frontview of the 29-year-old patientwho underwent bilateral breastresection mammaplasty with thehammock technique (rightbreast 1,400 g and left breast1,290 g). (B) Postoperative frontview of the same patientwith inferior dermopexy failure(6-month follow-up) at theinternal quadrant in the leftbreast.
J. M. Perez-Macıas 271

eral and medial skin flaps cannot support the weightof the inferior pedicle [46�48].However, mastopexies using the hammock tech-
nique correct the tendency of the breast to sag. Forthis reason, it also prevents postoperative NAC up-ward migration, confirmed by the follow-up sternalnotch-to nipple distance measurement.With the hammock technique, the suspension
achieves true permanent lifting of the mammary tis-sues through deepithelialized dermis strips from thebreast itself [15,49,51].The deepithelialized dermisstrips are part of the inferior pedicle, which they forminto a unit. They stabilize the mobile inferior tissuewhen the fixations are established [63,64]. It isimportant to emphasize that the step of disconnectingthe base of the inferior pedicle from the lower infra-mammary tissues is what makes it possible to lift andplace the breast tissues correctly.The hammock technique differs from others in
various aspects. The breast suspension is associatedwith an inferior dermoglandular pedicle, whereasother techniques use dermis strips with superiordermoglandular pedicles [9�14,16,20] or syntheticmaterials with a periareolar approach [17,21]. Someauthors introduce lateral dermis suspension from theinferior dermoglandular pedicle in an attempt toprevent breast ptosis, without consistent success [19].Others use free dermis strips [4,5,9], fascia lata [2,8], orother synthetic materials, transfixing the mammarygland and pectoral muscle [13]. A previous publica-tion emphasized the function of the superficial fascialsystem in breast tissues, showing how its use improvesbreast suspension [24]. Hanrahan and others [4,12]earlier recommended lifting the breast using its ‘‘truesuspensory ligaments’’ given that these ligaments havelost their suspensory function when ptosis occurs.Recently, some authors published a description of
a mastopexy procedure that provides similar inferiordermis fixation [23,26,28]. However, the originalhammock technique [49] suspends the inferiordermoglandular pedicle superiorly and inferiorly, andboth contribute to lifting of the breast when the stripsare tightened. The complications of this technique aresimilar to those of other procedures [67,68].With respect to residual submammary scars, ours
are similar to those for the lateral or L techniques[14,23,56�58,61,62]. However, skin reshaping is dif-ferent, reducing scar length considerably, with thetissues wrinkled and sutured.
Conclusions
With the hammock technique, inferior pedicle mam-maplasty is combined with retropectoral (superiorlevel) and inferior (inferior level) suspension by adermis strip from this inferior breast pedicle in asingle procedure. This allows bottoming out of thebreast to be prevented effectively. Our technique re-lies on reshaping and anchoring of internal tissues to
obtain improved breast contours. In addition, itmaintains superior pole fullness because it elevatesthe entire inferior breast pedicle after liberating it atthe base, with the pedicle maintained by the dermisstrip mastopexies.
The hammock technique is a versatile procedurethat can readily be adapted to a wide spectrum ofbreast volume reduction and mastopexy require-ments. This reduction mammaplasty technique withan inferior pedicle and hammock suspension main-tains the anatomic and functional unity of the breastand prevents recurrence of ptosis with limited scar-ring. It is easily reproducible and offers very satisfy-ing, long-lasting results.
References
1. Girard C: Uber Mastoptose und Mastopexie. Langen-becks Arch Klin Chir 92:829�842, 1910
2. Gobell R: Uber Autoplastiche freie Fascien and Apo-neurosentransplantation nach Martin Kirchner. ArchKlin Chir 146:478�480, 1927
3. Bames HO: Reduction of massive breast hypertrophy.Plast Reconstruct Surg 3:560�569, 1948
4. Hanrahan EM: Mammaplasty: One-stage transpositionoperation. Plast Reconstr Surg 6:110�118, 1950
5. Maliniac JW: Evaluation of principal mammaplasticprocedures. Plast Reconstr Surg 4:359�373, 1949
6. Aufricut A: Mammaplasty for pendulous breasts:Empiric and geometric planning. Plast Reconstr Surg4:13�29, 1949
7. Erczy M: New method of mammaplasty by doublewedge-shaped excision and submuscular suspension ofthe gland. Plast Reconstr Surg 16:374�386, 1955
8. Lewis GK: A method of mastopexy with fascia latatransplants. J Int Coll Surg 26:346�353, 1956
9. Da Silva G: Mastopexy with dermal ribbon for sup-porting the breast and keeping it in shape. Plast Rec-ontr Surg 34:403�405, 1964
10. Hinderer UT: Plastia mamaria modelante de dermop-exia superficial y retromamaria. Rev Esp Cir Plast5:52�58, 1972
11. Garcia Padron J: Mammareduktionsplastik (Abstract):Transacta der III Tagung der Vereinigung der Deuts-chen, Plastischen, Chirurgen, pp. 85, 1972
12. Figallo E: Surgical treatment of mammary ptosis with-out hypertrophy. Plast Reconstr Surg 60:189�196, 1977
13. Johnson GW: Central core reduction mammaplastiesand and Marlex suspension of breast tissue. Aesth PlastSurg 5:77�84, 1981
14. De Longis E: Mammaplasty with an L-shaped limitedscar and dermopexy.Aesth Plast Surg 10:171�175, 1986
15. Perez-Macias JM: Reduction mammaplasty: Thehammock technique. Abstracts of the Xth Interna-tional ISAPS Congress, Zurich, pp. 144, 1989
16. Svedman P: Correction of breast ptosis utilizing a ‘‘foldover’’ deepithelialized lower thoracic fasciocutaneousflap. Aesth Plast Surg 15:43�47, 1991
17. Bustos RA: Periareolar mammaplasty with siliconesupporting lamina. Plast Reconstr Surg 89:646�657,1992
18. Rodrigo Cucalon MA: Mamoplastia tecnica ‘‘de lapelota.’’. Cir Plast Iberolatinoamer 18:147�165, 1992
272 Long-Lasting Evolution of Ptosis Control
19. Levet Y: Le pedicule posterior: Un concept anatom-ochirurgical de plastie mammaire. Ann Chir Plast Es-thet 38:463�468, 1993
20. Marconi F, Cavina C: Reduction mammaplasty andcorrection of ptosis: A personal technique. Plast Rec-onstr Surg 91:1046�1056, 1993
21. Goes JCS: Periareolar mammaplasty: Double skintechnique with application of polyglactine or mixedmash. Plast Reconstr Surg 97:959�968, 1996
22. Cerqueira A: Mammoplasty: Breast fixation withdermoglandular mono upper pedicle flap under thepectoralis muscle. Aesth Plast Surg 22:276�283, 1998
23. Frey MA: New technique of reduction mammaplasty:Dermis suspension and elimination of medial scars. BrJ Plast Surg 52:45�51, 1999
24. Lockwood T: Reduction mammaplasty and mastopexywith superficial fascial system suspension. Plast Rec-onstr Surg 103:1411�1420, 1999
25. Quiau Q, Sun J, Liu C, Liu Z: Reduction mammaplastyand correction of ptosis: Dermal bra technique. PlastReconstr Surg 111:1122�1130, 2003
26. Baumeister RG: Curtain type combined pedicledreduction mammoplasty with internal suspension forextensive hypertrophic and ptotic breasts. Br J PlastSurg 56:114�119, 2003
27. De la Plaza R, de la Cruz L, Moreno C, Soto L: Thecrossed termal flaps technique for breast reduction.Aesth Plast Surg 28:383�392, 2004
28. Widgerow AD: Breast reduction with inferior pediclefascial suspension. Aesth Plast Surg 29:532�537, 2005
29. Ritz M, Silfen R, Southwick G: Fascial suspensionmastopexy. Plast Reconstr Surg 117:86�94, 2006
30. Graf R, Biggs TM: In search of better shape in mas-topexy and reduction mammaplasty. Plast ReconstrSurg 110:309�317, 2002
31. Taubert E: Beitrag zur Mammaplastik. Zentralbl Chir92Suppl:2011�2014, 1967
32. Kohn F, Dalrymple J: Plastic reconstruction of theenlarged breast: Report of a new technique. Br J PlastSurg 20:184�198, 1967
33. Courtiss EH, Goldwyn RM: Reduction mammaplasty:The inferior pedicle technique. Plast Reconstr Surg59:500�507, 1977
34. Kaplan I: Reduction mammaplasty: Nipple�areolarsurvival on single breast quadrant. Plast Reconst Surg61:27�31, 1978
35. Reich J: The advantage of a lower central segment inreductionmammaplasty.AesthPlast Surg 3:47�56, 1979
36. Georgiade NC, Serafin D, Morris R, Georgiade G:Reduction mammaplasty utilizing an inferior pediclenipple-areolar flap. Ann Plast Surg 3:211�218, 1979
37. Perez-Macias JM: Mamoplastia de reduccion: Experi-encia y estudio comparativo de la tecnica del colgajodermoglandular de pedıculo inferior. Cir Plast Ibero-latinoamer 9:27�36, 1985
38. Craig RD, Sykes PA: Nipple sensitivity following reduc-tion mammaplasty. Br J Plast Surg 23:165�172, 1970
39. Gonzalez F, Brown FE, Gold ME, Walton RL, ShaferB: Preoperative and postoperative nipple�areola sen-sitivity in patients undergoing reduction mammaplasty.Plast Reconstr Surg 92:809�814, 1993
40. Sarhadi NS, Shaw Dunn J, Lee FD, Soutar DS: Ananatomical study of the nerve supply of breast,including the nipple and areola. Br J Plast Surg49:156�164 41, 1996
41. Maliniac JW: Amputation versus transposition ofgland and nipple in mammaplasty. Plast Reconstr Surg3:37�51, 1948
42. Climo MS, Alexander JE: Intercostal circulation:Nipple survival in reduction mammaplasty in the ab-sence of a dermal pedicle. Ann Plast Surg 4:128�132,1980
43. Hester TR Jr, Bostwick J III, Miller L, CunninghamSJ: Breast reduction utilizing the maximally vascular-ised central breast pedicle. Plast Reconstr Surg76:890�900, 1985
44. Van Deventer PV: The blood supply to the nip-ple�areola complex of the human mammary gland.Aesth Plast Surg 28:393�398, 2004
45. Marshall DR: Callan PP, Nicholson W: Breastfeedingafter reduction mammaplasty. Br J Plast Surg47:167�169, 1994
46. Bolger WE, Seyfer AE, Jackson SM: Reductionmammaplasty using the inferior glandular ‘‘pyramidal’’pedicle: Experiences with 300 patients. Plast ReconstrSurg 80:75�84, 1987
47. Reus WF, Mathess SJ: Preservation of projection afterreduction mammaplasty: Long-term follow-up of theinferior pedicle technique. Plast Reconstr Surg82:644�652, 1988
48. Seyfer AE: Reduction mammaplasty using the inferiorglandular pyramid pedicle. In: Georgiade NG (eds)Aesthetic surgery of the breast. WB Saunders: Phila-delphia, pp 363�370, 1990
49. Perez-Macias JM: Crossed-support hammock tech-nique in mammarian reduction. Abstracts of the XthInternatinal Congress of Plastic Reconstructive Sur-gery, Madrid. Excerpta Medica Plast Surg 2:609�610,1992
50. Morgan JE: A sling operation using Marlex polypro-pylene mesh, for treatment of recent stress inconti-nence. Am J Obstet Gynecol 106:369�377, 1970
51. Perez-Macias JM: Reduction mammoplasty withassociated mastopexy: Hammock technique. Ab-stracts of the Transactions of the 11th Congress ofthe International Confederation for Plastic Recon-structive and Aesthetic Surgery, Yokohama, Japan.In: Harri K (ed) Excerpta medica. Kugler Publica-tions BV, Amsterdam, New York, p. 130, 1995
52. Marc H: La plastie mammarie par la methode oblique.In: Doin G (ed) Paris. Rev Port Obstet 5:363�373, 1952
53. Mir Y L: Nuestro criterio actual sobre la cirugia plas-tica de la hiprtrofia mamaria. Cir Plast Iberolatinoamer1:135�146, 1975
54. Horibe K, Spina U, Lodivici O: Mamoplastia reduc-tora: Nuevo abordaje del metodo lateral oblicuo. RevLatino Am Cir Plast 2:7�12, 1956
55. Arie G: Una nueva tecnica de mastoplastia. Rev LatinoAm Cir Plast 3:23, 1957
56. Elbaz JS, Verheecke G: La cicatrice en L dans lesplasties mammaries. Ann Chir Plast 17:283�292,1972
57. Regnault P: Reduction mammaplasty by the B tech-nique. Plast Reconstr Surg 53:19�24, 1974
58. Meyer R, Kesserling UK: Reduction mammaplastywith an L-shaped suture line. Plast Reconstr Surg55:139�148, 1975
59. Marchac D, de Olarte G: Reduction mammaplasty andcorrection of ptosis with a short inframammary scar.Plast Reconstr Surg 69:45�55, 1982
J. M. Perez-Macıas 273
60. Lassus C: An ‘‘all-season’’ mammoplasty. Aesth PlastSurg 10:9�15, 1986
61. Chiari AC Jr: The L short-scar mammaplasty: A newapproach. Plast Reconstr Surg 90:233�246, 1992
62. Rodriguez-Camps S: Mamaplastia de reduccion en‘‘L’’: Un nuevo camino. Cir Plast Iberolatinoamer25:45�55, 1999
63. Perez-Macias JM: Dermis suspension in mammoplasty.Br J Plast Surg 52:421, 1999
64. Perez-Macias JM: Personal mastopexy technique forbreast stabilisation:Update.Br JPlast Surg 57:178, 2004
65. Moufarrage R: Dermoglandular pedicle mammoplastyIn: Georgiade NG (ed) Aesthetic surgery of the breastWB Saunders, Philadelphia, pp 371�386, 1990
66. Hinderer UT: Circumareolar dermo-glandular plica-tion: A new concept for correction of breast ptosis.Aesth Plast Surg 25:404�420, 2001
67. Mandrekas AD, Zambacos GJ, Anastasopoulos, et al.Reduction mammaplasty with the inferior pedicletechnique: Early and late complications in 371 patients.Br J Plast Surg 49:442�446, 1996
68. OGrady KF, Thoma A, Dan Cin A: A comparisonof complication rates in large and small inferior pedi-cle reduction mammaplasty. Plast Reconstr Surg115:736�742, 2005
274 Long-Lasting Evolution of Ptosis Control
Related Documents











