Long Island Radiological Society Interesting Case Panel March 11, 2014

Long Island Radiological Society Interesting Case Panel March 11, 2014.
Dec 26, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Long Island Radiological SocietyInteresting Case Panel
March 11, 2014

Case 1
30yo obese female, restrained driver rollover MVC. Positive “seat-belt sign.” Tenderness over multiple areas
of the abdomen.
Presented by Brian Goodman, MD PGY-3Presented by Brian Goodman, MD PGY-3


STOP. Proceed to Diagnosis.

Rare, associated with high-impact blunt trauma (eg, high-velocity motor vehicle accidents), which produces increased intra-abdominal pressure sufficient to disrupt the abdominal wall musculature.
Seat belt use increases the risk for traumatic hernias.
The most common locations are areas of relative anatomic weakness, such as the lower abdomen and the lumbar region.
Easily overlooked at physical examination performed at initial presentation.
Traumatic Abdominal Wall Hernia

Traumatic Abdominal Wall Hernia
Incarceration and strangulation of hernia contents is common, and up to 60% of cases are associated with additional intra-abdominal injuries.
For these reasons, traumatic abdominal wall hernias usually require emergent laparotomy (not in our case).
Multi–detector row CT permits reliable diagnosis and assessment of traumatic hernias, including characterization of hernia contents, visualization of disrupted abdominal muscle layers, and identification of associated intra-abdominal injuries.

References
RSNA Radiographics. November-Decemeber 2005, Volume 25, Issue 6.“Abdominal Wall Hernias: Imaging Features, Complications, and Diagnostic Pitfalls at Multi-Detector Row CT.” Aguirre D, Santosa A, Casola G, Sirlin C
Hernia. Aug 2011; 15(4): 443-445 :”Acute Traumatic Abdominal Wall Hernia.” Hartog D, Tuinebreijer WE, Oprell PP, Patka P

Case 2
28yo female with generalized weakness. No PMHx.
Submitted by HyukJun Yoon, MD PGY 2



STOP. Proceed to Diagnosis.
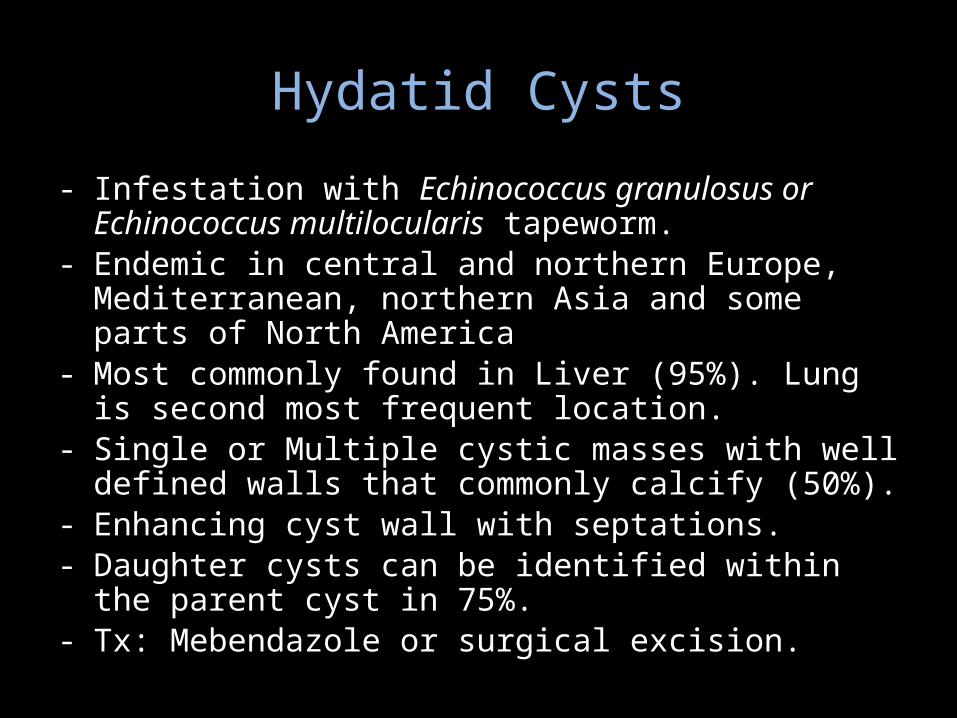
Hydatid Cysts
- Infestation with Echinococcus granulosus or Echinococcus multilocularis tapeworm.
- Endemic in central and northern Europe, Mediterranean, northern Asia and some parts of North America
- Most commonly found in Liver (95%). Lung is second most frequent location.
- Single or Multiple cystic masses with well defined walls that commonly calcify (50%).
- Enhancing cyst wall with septations.- Daughter cysts can be identified within the parent cyst in 75%.- Tx: Mebendazole or surgical excision.

• Type 1: Simple cyst without internal architecture.• Type 2a : Peripherally located round daughter cysts.• Type 2b: Large, irregular coutour daughter cysts
occupying the mother cyst.• Type 2c: Oval shaped masses with scattered
calcifications and some daughter cysts.• Type 3: Calcified cyst.• Type 4: Complicated cyst.
Hydatid Cysts
References
• William E. Brant and Clyde A. Helms ,2012,Fundamentals of Diagnostic Radiology, Lippincott Williams & Wilkins, Philadelphia, PA, p. 709
• Jourdan JL, Morris DL. Hydatid liver disease. In: Holzheimer RG, Mannick JA, editors. Surgical Treatment: Evidence-Based and Problem-Oriented. Munich: Zuckschwerdt; 2001.
• Pedrosa I, Saíz A, Arrazola J et-al. Hydatid disease: radiologic and pathologic features and complications. Radiographics. 20 (3): 795-817.

Case 3
34yo female with syncopal episode. No PMHx.
Submitted by Jonathan Holstad, MD PGY 3
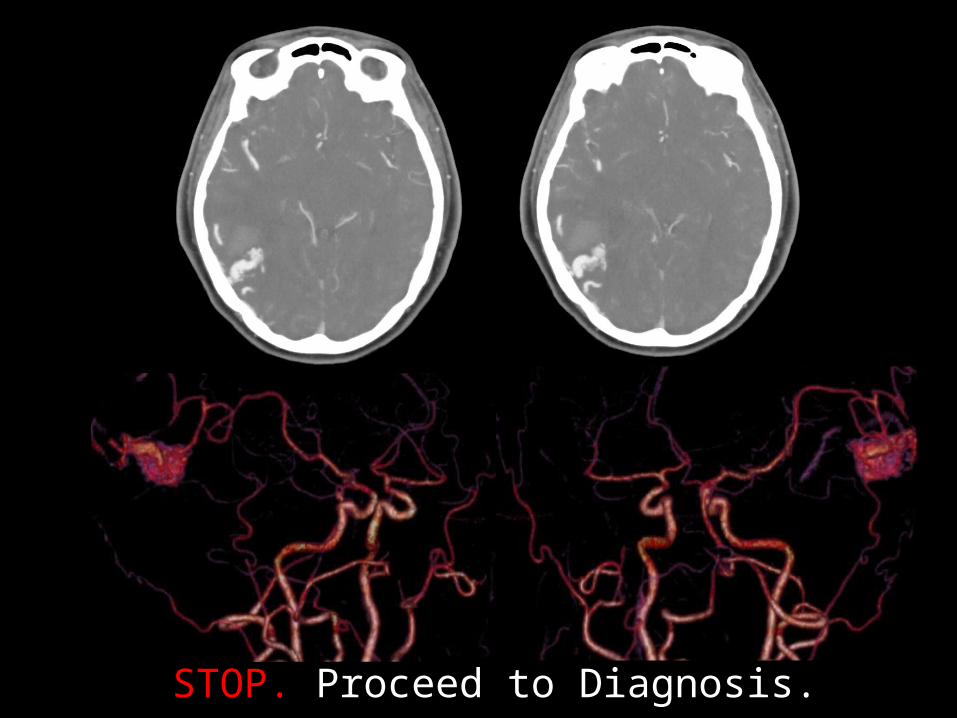
STOP. Proceed to Diagnosis.

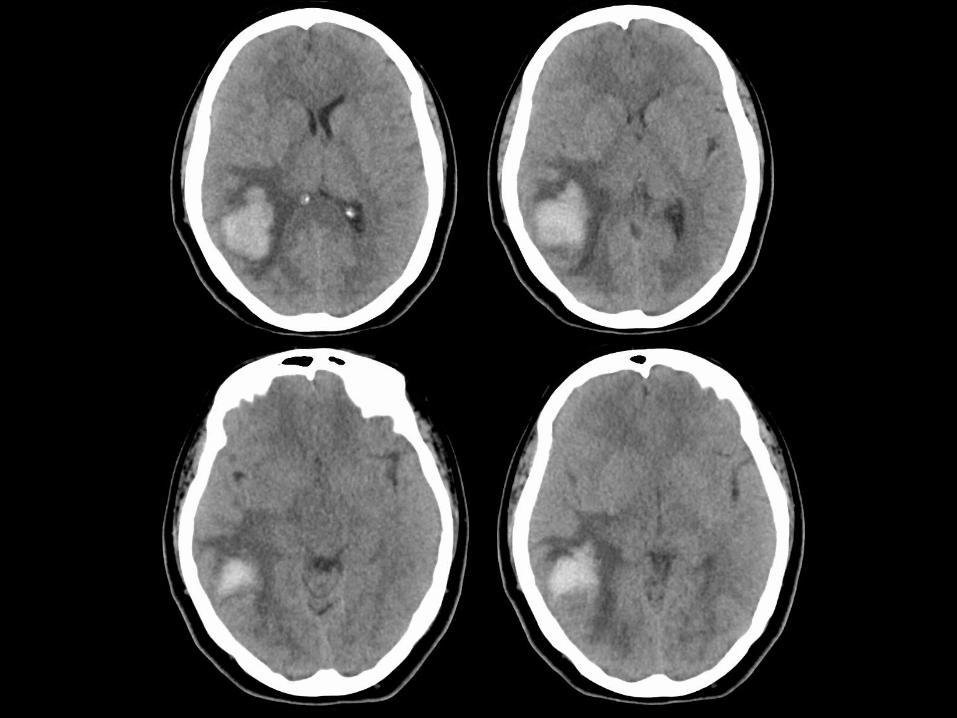
Arterovenous MalformationMost common type of brain vascular malformation.
98% Sporadic: Hox D3/B3 malfunction->dysregulated angiogenesis
Abnormal tangle of enlarged feeding artieries and central tightly packed nidus directly communicating with veins, no intervening brain parenchyma or capillary network.
Typically young adult with non-traumatic hemorrhage/headache, seizures, or focal neurological deficit.
Approximately 1/3 have a dual supply with dura/pia.
2-4% risk of hemorrhage per year, 2x-3x if previous hemorrhage

Arterovenous Malformation
Treatment involves embolization, microneurosurgical resection, and stereotactic radiosurgery.
Spetzler-Martin scale estimates surgical risk (1-5)small <3cm – 1ptmedium 3-6cm – 2 ptslarge >6cm – 3ptsInvolves “eloquent” brain? – 1ptDeep draining vein? - 1pt

References
William E. Brant and Clyde A. Helms, 2012, Fundamentals of Diagnostic Radiology, Lippincott Williams & Wilkins, Philadelphia, PA, p. 102.
Santos ML et al: Angioarchitechture and clinical presentation of brain arteriorvenous malformations. Arg Neuropsiquiatr. 67(2A):316-21, 2009.

Case 4
62yo male, fell on ice.
Submitted by Asim Maher, MD PGY2


STOP. Proceed to Diagnosis.

Ossification of the Posterior Longitudinal Ligament (OPLL)
• Begins in the cervical spine (75%) but may extend into the thoracic spine (15%) or lumbar spine (10%).
• Most common location C4-C6.
• 95% of ossification is located in C spine.
• Associated with DISH.

Ossification of the Posterior Longitudinal Ligament (OPLL)
• Cause is unclear, Oriental races especially Japanese, men, obesity, poor calcium absorption, ankylosing spondylitis and diabetics have an increase incidence.
• Most people are asymptomatic, However it can cause spinal stenosis and compression of the anterior part of the cord.
• Treatment is NSAIDs. If conservative treatment is unsuccessful, spine surgery may be recommended to relieve pressure on the spinal cord.

• Stages of spinal cord damage by OPLL• stage 0 - normal or mild compression of
anterior horn without neuronal loss. • stage 1 - mild compression of ant. horn with
partial neuronal loss. • stage 2 - marked deformity of anterior horn;
severe neuronal loss. • stage 3 - severe spinal cord damage
Ossification of the Posterior Longitudinal Ligament (OPLL)
References• http://www.emoryhealthcare.org/spine/medical-conditions/ossification-p
osterior-longitudinal-ligament.html
• http://www.orthobullets.com/spine/2046/ossification-posterior-longitudinal-ligament
• http://radiopaedia.org/articles/ossification-of-the-posterior-longitudinal-ligament

Case 5
40yo female with hemoptysis.
Submitted by HyukJun Yoon MD PGY2


STOP. Proceed to Diagnosis.

Aspergilloma(Fungus Ball)
• Mass-like fungus balls, which are collections of fungal hypahe, mucus, and cellular debris including inflammatory cells in preexisting structural lung disease (i.e. bulla or cavitary lesions)
• Usually solitary and located in the upper lungs,similar to post primary pulmonary TB: posterior segments of the upper lobes or superior segments of the lower lobes.
• Typically infection with Aspergillus fumigatus.• Commonly occurs in immunocompetent patients.

• Rounded, ovoid soft tissue density well formed focal intracavitary mass outlined by air (Monod sign), mobile with altered position of the patient.
• May calcify, adjacent pleural thickening common
• Tx: Antifugal (Amphotericin) agent administration into the cavitary lesion.
• Surgical resection for repeated hemoptysis
Aspergilloma(Fungus Ball)

References
• William E. Brant and Clyde A. Helms, 2012, Fundamentals of Diagnostic Radiology, Lippincott Williams & Wilkins, Philadelphia, PA, p. 445-446
• Franquet T, Müller NL, Giménez A et-al. Spectrum of pulmonary aspergillosis: histologic, clinical, and radiologic findings. Radiographics. 21 (4): 825-37.
Related Documents