1 London School of Hygiene and Tropical Medicine. MSc Project Report: Surgical management of upper limb nerve palsies in leprosy affected patients; literature review and project proposal. Candidate Number: 491839 Supervisor: Professor Diana Lockwood Submitted in part fulfillment of the requirements for the degree of MSc in: Tropical Medicine and International Health. Academic year: 2009-2010 Date of submission: 23 rd Aug 2010 Word count: 9062 Project length: Standard

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
London School of Hygiene and Tropical Medicine.
MSc Project Report:
Surgical management of upper limb nerve palsies in leprosy
affected patients; literature review and project proposal.
Candidate Number: 491839
Supervisor: Professor Diana Lockwood
Submitted in part fulfillment of the requirements for the
degree of MSc in:
Tropical Medicine and International Health.
Academic year: 2009-2010
Date of submission: 23rd
Aug 2010
Word count: 9062
Project length: Standard
2
Contents
1. …………………………………………………………………………………….Cover page.
2. ………………………………………………………………………………...Contents page.
3. ………………………………………………………………………………...Contents page.
4. ………………………………………………………………………………………..Abstract.
5. ……………………………...Introduction; Epidemiology and Disease Control Initiatives.
6. ……………………………………………..Pathophysiology and transmission of leprosy.
7. ……………………………………..Clinical manifestations and complications of leprosy.
8. ......................................................................................................Women and leprosy.
Diagnostics and Classification.
Ridley-Jopling Scheme.
WHO classification.
9. ……………………………………………………………………………Leprosy Treatment.
Drug Treatment for Leprosy.
Leprosy Prevention.
Disability.
10. ……………………………………………………….Measurement of disability in leprosy.
The leprosy affected hand impairment of normal function.
11. ………………………………………………………………………………………………..…
12. ……………………………………………………………………………….Leprosy surgery.
13. …………………………………………………………………………………………………..
14. ………………………………………………….Experience of leprosy surgery in the field.
Why do this review?
Aims and Objectives.
15. ………………………………………………………………………………………..Methods.
Types of studies.
Participants.
Interventions.
Outcomes measures.
Search methods.
Electronic searches.
16. ………………………………………………………………………………………….……….
17. ………………………………………………………………………………….Ongoing trials.
Unpublished data.
Language restrictions.
18. …………………………………………………………………Data collection and analysis.
Results.
3
Study descriptions (appendix 1).
Search results.
Included studies.
Excluded studies.
19. ………………………………………………………………………..….Intervention effects.
Which surgical options for stable upper limb paralysis have good outcomes?
In claw hand.
20. …………………………………………………………………………………………………..
21. ………………………………………………...……….…..For postoperative interventions.
22. ……………………………………………………………………………..For simian thumb.
23. …………………………………………………………………………………………………..
24. ……………………………………………………………………………..Quality of Studies.
25. …………………………………………………………………………………………………..
26. ………………………………………………………………………..Study Heterogeneity.
27. …….Most effective surgical intervention for the management of upper limb paralysis?
Interventions most effective at improving quality of life or stigma?
Adverse events/unwanted side effects of surgery?
28. …Is immediate physiotherapy better than immobilization in leprosy related paralysis?
29. ………………………………………………....……….Discussion and recommendations.
30. …………….. ………………………………………………………………. Future research.
31. ……………………………………..Appendix 1; detailed description of studies included.
32. …………………………………………………………………………………………………..
33. …………………………………………………………………………………………………..
34. …………………………………………………………………………………………………..
35. ……………………………………………………………...Appendix 2; research proposal.
36. …………………………………………………………………………..Acknowledgements.
37. …………………………………………………………………………………….References.
38. .……………………………………………………………………………………References.
39. …………………………………………………………………………………….References.
40-52.................................................................................................................CARE form.
4
Abstract
Background
Nerve damage affects 30% of leprosy patients. At present about 6-9% of individuals
newly presenting with leprosy have grade 2 disabilities and 3 million people worldwide are
disabled due to the affects of leprosy.
Objectives
To assess outcomes of surgery and post operative techniques to improve upper limb
nerve paralysis second to leprosy.
Search strategy
Data bases searched; Cochrane Central Register of Controlled Trials, Medline,
Embase, Global Health/Global Health Archives, Africa Wide NiPAD, CINAHL, LEYES (Latin
America and Caribbean) LILACS (South America) and online registers of ongoing trials.
Study selection
Leprosy affected patients with upper limb nerve paralysis that have been entered in
to studies looking at surgical or post operative intervention outcomes.
Data collection and analysis
Data was electronically or by hand retrieved and assessed for quality and content.
Main results
Eleven trials were included with a total of 1161 operations and 998 participants. All
trials were small, diverse and the quality was generally poor. Studies included had between
23 to 246 operations (20 and 216 participants) for leprosy related disabilities. Six studies
looked at correction of the claw hand, one randomized control trial looked at postoperative
intervention. Four studies looked at opponensplasty to correct the simian thumb. Studies
were from 1958 to 2008 spanning 60 years of surgical research.
Conclusions
Though there was some consensus among studies as to pre-operative function
predicting post operative function and the importance of physiotherapy the wide variability in
the type, design and techniques used prevented consensus being drawn on the best
surgical options for correction of the upper limb nerve palsy.
There is a severe lack of good quality research on the best practice for surgical
correction of upper limb nerve palsies in leprosy affected patients. New trials need to follow
modern standards for designing and reporting controlled trials.
5
Introduction
Epidemiology and Disease Control Initiatives.
Despite decades of intensive effort to control leprosy the disease remains an
important global issue. In 1985 it was estimated that there was approximately 12 million
people worldwide affected by leprosy. In 2006 the prevalence was registered as 224,717[1].
The remaining numbers are concentrated in a handful of countries clustered in limited
geographical sites and ethnic groups[2].
Early diagnosis efforts and the availability of free multi-drug therapy (MDT) through
the WHO have lead to a decrease in prevalence in most endemic countries. Some 11
million[1] people have been treated with MDT.
The 2009 WHO statistics show a continued decrease in prevalence. The lengthy
disease progression and because it occurs in the poorest most marginalized communities
makes epidemiological study difficult. Yearly incidence of new cases has not matched the
decline in prevalence; this may be due to better surveillance and detection or indicate
ongoing transmission.
In 1986 the elimination of leprosy by 2000 was first proposed. This was later modified
to “elimination as a public health problem” (less than 1 case per 10,000 population) and
adopted by the World Health Assembly in 1991[3]. This target has proved unattainable to
date. Leprosy cure with MDT however does not presuppose absence of disability.
Reactions, progressive silent neuronal damage and increasing disability can persist after
MDT completion.
The “Final Push” strategy launched by the WHO in 1999 ran from 2000 till 2005 and
was launched in recognition that elimination by 2000 could not be achieved. Focus shifted
toward intensified initiatives in countries where endemicity remains problematic[4]. “Global
strategy for further reducing leprosy burden and sustaining leprosy control activities”,
promoting an integrated approach, ran from 2006 to 2010. MDT remained the management
cornerstone but with added emphasis on community involvement[5]. There has been a
recent move to appreciate the chronicity of leprosy disability with stigma and social exclusion
adding further to patient burden. The proposed “New Enhanced Global Strategy for further
reducing the disease burden due to leprosy” will run from 2011 to 2015. This introduces the
global target of reducing new cases with grade 2 disabilities per 10,000 population by at
least 35% by 2015 compared to the 2010 baseline[6].
Areas where leprosy remains a problem and the WHO‟s target is still elusive include
India, Nepal, Angola, Brazil, Central African Republic, Democratic Republic of Congo,
6
Mozambique, Tanzania and Madagascar[1] India alone accounts for 64% of all Leprosy
cases worldwide[2].
Pathophysiology and Transmission
Leprosy is a disease caused by the intercellular Mycobacterium Leprae. The
mycobacterium has a predilection for macrophages and nerve Schwann cells and causes a
chronic granulomatous infection of nerves and skin[7]. Infectivity appears to be low and
many who become infected never manifest disease[8]. Proximity appears to be the most
important factor affecting risk of acquiring leprosy; a household contact runs 2-4 times the
risk of contracting leprosy cohabiting with someone who has tuberculoid disease and 8-10
times contacting lepromatous disease[9]. It is held that infection is due to nasal
secretions/respiratory transmission. Man is the only known reservoir although
Mycobacterium Leprae has been shown to be present in the nine-banded armadillo.
M. Leprae is difficult to study due to slow evolution of the disease, lack of animal
models and our inability to culture the organism. Clinical presentation is largely dictated by
the host‟s immune response. This separates those with Tuberculoid Leprosy: a strong
immune response to a small mycobacterial burden, from Lepromatous leprosy: patients with
minimal inflammatory response to a heavy mycobacterial load. Between these extremes are
three borderline levels; borderline tuberculoid, borderline and borderline lepromatous.
Intervals between infection and disease presentation are variable; on average10 years for
lepromatous leprosy and about four for tuberculoid[8].
The two extremes of disease are generally stable. Those suffering from borderline
disease are prone to reactions. Reactions can be Type 1 reversal reactions, which can affect
all types of borderline leprosy and post partum women, and is due to delayed
hypersensitivity to M. Leprae antigen in the nerves and skin[10]. Type 2 reactions,
(Erythema Nodosum Leprosum) affect those with lepromatous or borderline lepromatous
leprosy. These are due to T cell dysfunction with excess TNF production and immune
complex deposition within skin nerves and organs[10]. Neuritis can occur without reactions
and can be acute, chronic or silent with no symptoms until appearance of functional deficit.
Nerve involvement can leave patients with combinations of anesthesia and paralysis leading
to progressive disability and stigmatizing disfigurement.
7
Clinical manifestations and complications
Leprosy is a complex disease with a host of slow and fast evolving presentations. The
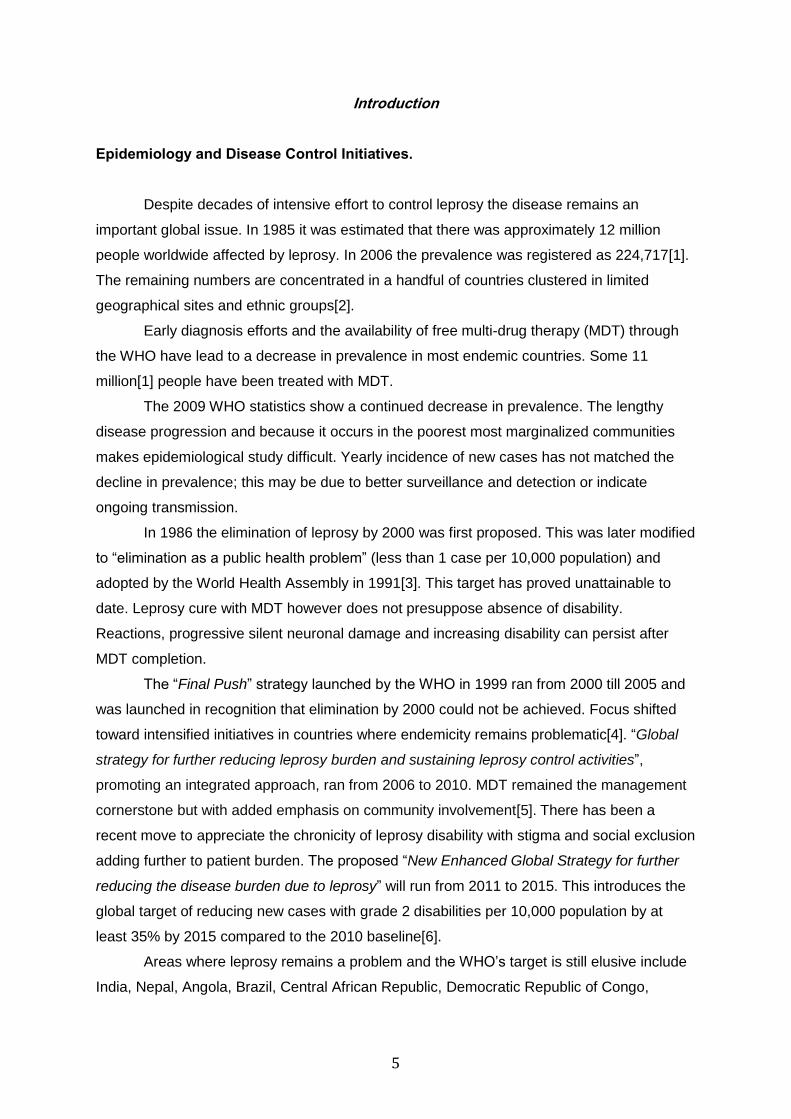
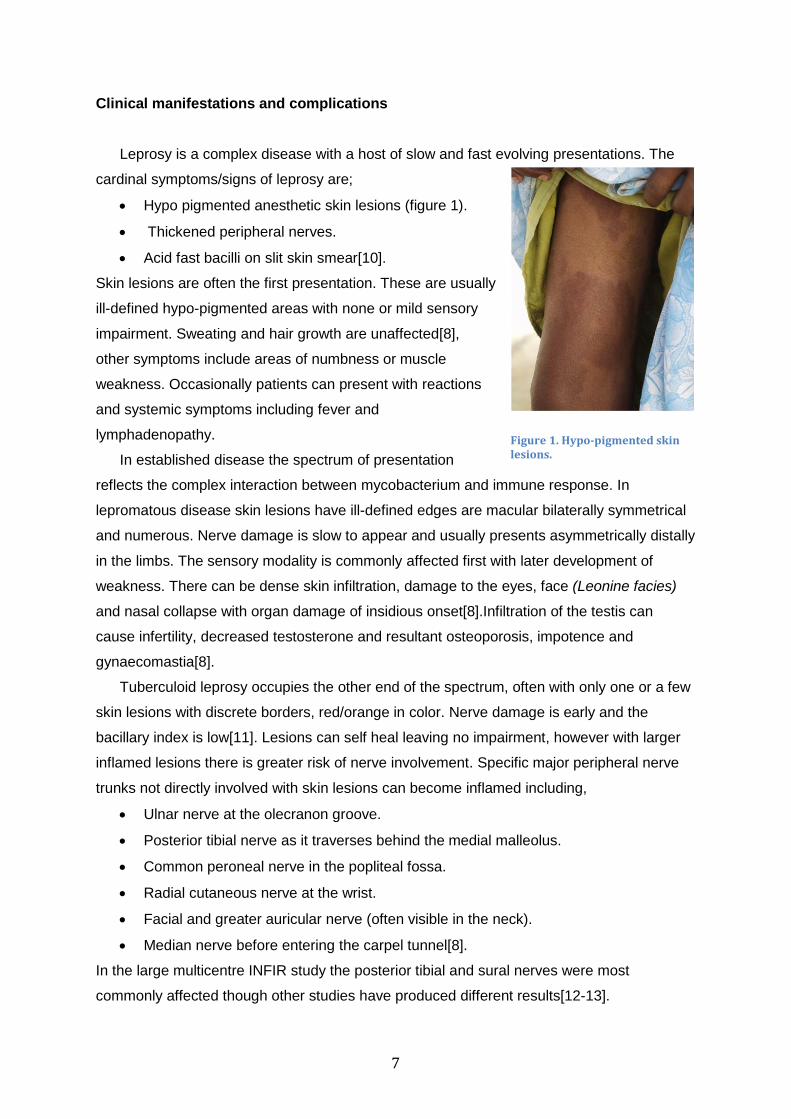
cardinal symptoms/signs of leprosy are;
Hypo pigmented anesthetic skin lesions (figure 1).
Thickened peripheral nerves.
Acid fast bacilli on slit skin smear[10].
Skin lesions are often the first presentation. These are usually
ill-defined hypo-pigmented areas with none or mild sensory
impairment. Sweating and hair growth are unaffected[8],
other symptoms include areas of numbness or muscle
weakness. Occasionally patients can present with reactions
and systemic symptoms including fever and
lymphadenopathy.
In established disease the spectrum of presentation
reflects the complex interaction between mycobacterium and immune response. In
lepromatous disease skin lesions have ill-defined edges are macular bilaterally symmetrical
and numerous. Nerve damage is slow to appear and usually presents asymmetrically distally
in the limbs. The sensory modality is commonly affected first with later development of
weakness. There can be dense skin infiltration, damage to the eyes, face (Leonine facies)
and nasal collapse with organ damage of insidious onset[8].Infiltration of the testis can
cause infertility, decreased testosterone and resultant osteoporosis, impotence and
gynaecomastia[8].
Tuberculoid leprosy occupies the other end of the spectrum, often with only one or a few
skin lesions with discrete borders, red/orange in color. Nerve damage is early and the
bacillary index is low[11]. Lesions can self heal leaving no impairment, however with larger
inflamed lesions there is greater risk of nerve involvement. Specific major peripheral nerve
trunks not directly involved with skin lesions can become inflamed including,
Ulnar nerve at the olecranon groove.
Posterior tibial nerve as it traverses behind the medial malleolus.
Common peroneal nerve in the popliteal fossa.
Radial cutaneous nerve at the wrist.
Facial and greater auricular nerve (often visible in the neck).
Median nerve before entering the carpel tunnel[8].
In the large multicentre INFIR study the posterior tibial and sural nerves were most
commonly affected though other studies have produced different results[12-13].
Figure 1. Hypo-pigmented skin lesions.
8
Sensory nerve function is usually first affected however sensory motor and autonomic can
occur synchronously. Despite the range of complications that occur in leprosy it is thought
that many infections are subclinical, of those who do progress to clinical disease only 2%
progress to long term disability[14].
Women and Leprosy
Women are a minority when it comes to infection with leprosy.
Disability appears to occur just as commonly however. Studies tend to
find that women are less like to present for treatment leading to a
greater proportion of women being disabled long term[15]. This may be
due to increased difficulties for women in accessing health care for a
variety of reasons, including greater poverty and lower social standing.
One study looking at women with leprosy and the role of surgery found
admission and inpatient care for surgical correction of disability was
more distressing and a greater social upheaval for females than
men[16].
Diagnostics and Classification
Ridley-Jopling Classification
Leprosy diagnostics is a combination of clinical testing in combination with
identification of acid-fast bacilli on slit skin smears. This allows for the patient to be placed
on the Ridley Jopling[17] classification scale and guide management. Sensory nerve
dysfunction can be measured using monofilaments or simple sensory discrimination using a
ballpoint pen or cotton wool. Motor function can be assessed using voluntary muscle tests
and if available dynamometry. Nerve conduction studies are the often not available, gold
standard[18].
WHO Classification
In 1998 the WHO introduced [19] the simplified pauci and multibacillary criteria to
guide treatment. This field tool uses number of skin lesions to dictate classification with
paucibacillary being up to 5 lesions and multibacillary being 6 or more. Studies have shown
that the addition of further information such as nerve testing can add to sensitivity and
specificity of this simplified classification[19-20].
Figure 2 Nepali women affected by leprosy with severe disability.
9
Treatment
Drug Treatment
MDT is highly affective (relapse of less than 1%)[21] and
defends against resistance emergence. Paucibacillary disease is
treated with 6 months of Rifampicin and Dapsone. Multibacillary is
treated with Rifampicin Clofazimine and Dapsone for a year[10].
Acute nerve involvement in leprosy has been managed
medically and surgically. Reactions and neuritis are treated with
various regimes of steroids and steroid sparing alternatives[10]. A
meta-analysis looking at surgical decompression compared to steroid
treatment alone in acute nerve impairment does not support the use
of surgical management. This however was only based upon two
non-blinded randomized controlled trials of 88 people and the authors call for further studies
to be conducted[22]. The AMFES study found that 88% of those with a single acute
neuropathy treated with steroids made a full recovery[23-24]. The multicentre TRIPOD
randomized placebo controlled trial however has not shown a sustained reduction in
incidence of new reactions and nerve function impairment in using prophylactic steroids for
longer than a year to prevent new disability in MDT treated patients[25].
Prevention of Leprosy
Leprosy prevention would be the ideal to prevent related disability. There is
continuing efforts to prevent transmission through MDT. New research in to BCG given in
infancy and Rifampicin to household contacts show a combined protective effect of about
80%[26] and if this strategy could be deployed it might be the final step to control the
disease and prevent resulting disabilities.
Disability
Disabilities second to leprosy are due to interplay between leprosy type, reactions
occurring and interim between infection and treatment. Nerve involvement can affect eyes;
upper and lower limbs but early management can prevent damage occurring[27-28].
Management of individuals once damage has occurred is more difficult and there is a role for
surgery. The AMFES study in Ethiopia found that delay in presentation and age are the main
risk factors for impairment[29] and those with chronic and recurrent neuropathy have a
worse prognosis. Impairment at diagnosis was also associated with worse long term
Figure 3 Adult MDT combination drug packs.
10
disability[23] this is also supported by the BANDS study in Bangladesh[30]. The INFIR study
in India also identified that even subclinical nerve dysfunction along with increased serum
TNF were predictive of future nerve impairment[31].
To combat secondary damage occurring after nerve involvement self-care has been
promoted and has been demonstrated to be an effective means of preventing further tissue
damage, hence self-care education is being encouraged in primary care in leprosy affected
areas[32].
Measurements of Disability
Disability can be comprehensively measured by the WHO‟s International
Classification of Functioning Disability and Health (ICF) which assesses all aspects of
disability affecting quality of life[33]. This holistic but complex scoring system is appropriate
for any cause of disability but is not easily used in field settings. Specific for leprosy and
probably most widely used is the WHO disability grading for leprosy and consists of scoring
eyes hands and feet on left and right.
Alternative scoring systems for leprosy especially when looking at activity and
participation in low income countries include the SALSA score[34] and the WHODAS[35]
scoring system. There are also scoring systems that look specifically at disabilities in the
upper limb such as the DASH (Disabilities of the Arm, Shoulder and Hand) score[36].
The leprosy affected hand; impairment of normal function.
The function of the hand is based on grip and sensation. Leprosy produces severe
hand dysfunction through damage to the ulnar, median and radial nerves. Loss of ulnar and
median function paralyses the intrinsic muscles of the hand. This leads to loss of balance of
the digits, exacerbated by the uncontrolled pull of the long extrinsic muscles, flexor and
extensor.
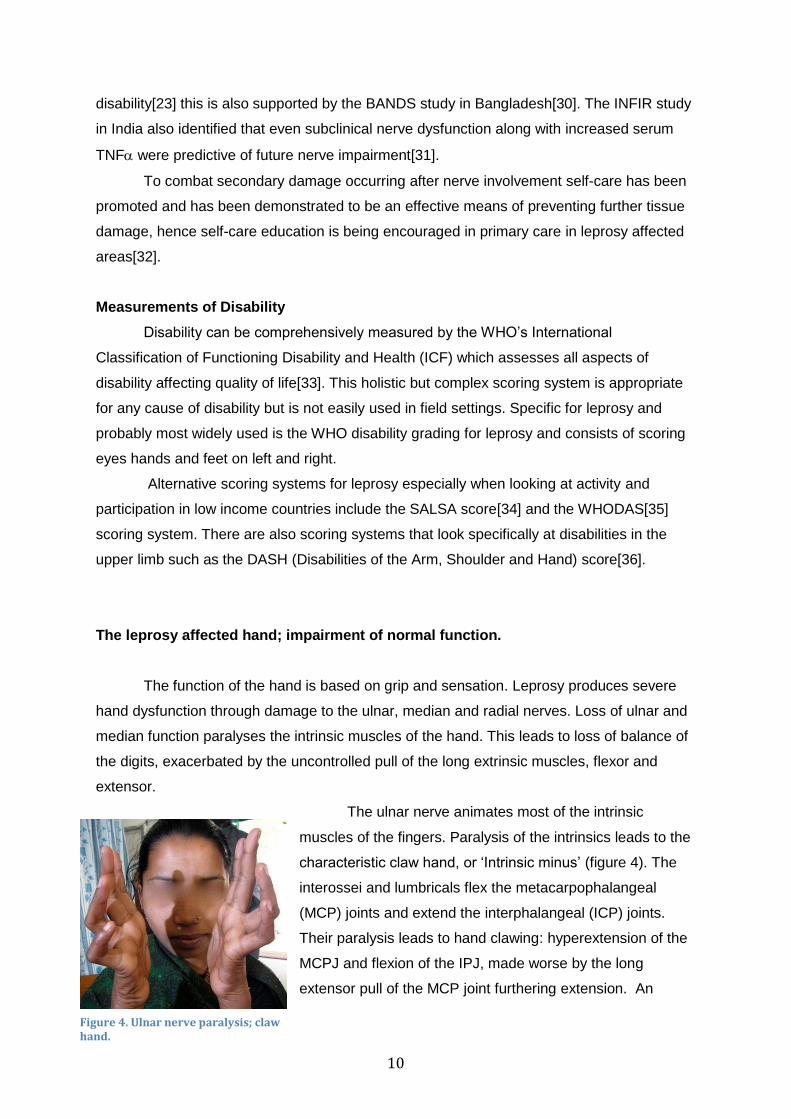
The ulnar nerve animates most of the intrinsic
muscles of the fingers. Paralysis of the intrinsics leads to the
characteristic claw hand, or „Intrinsic minus‟ (figure 4). The
interossei and lumbricals flex the metacarpophalangeal
(MCP) joints and extend the interphalangeal (ICP) joints.
Their paralysis leads to hand clawing: hyperextension of the
MCPJ and flexion of the IPJ, made worse by the long
extensor pull of the MCP joint furthering extension. An
Figure 4. Ulnar nerve paralysis; claw hand.
11
attempt to open the hand, to grasp an object is usually achieved by a synchronous extension
of the chain of digital joints. In the clawed hand there is acute hyperextension of the MCP,
while the IPJ‟s remain flexed and the patient‟s hand is unable to surround an object.
Synchronous flexion is also impaired. Normal closing of the hand allows for
maximum contact with an object and maximal grip. Functioning lumbricals ensure
simultaneous and synchronised flexion of the chain of digital joints. The clawed hand starts
from a position of severe flexion of the ICP joints and extension of the MCP joints with loss
of the controlling function of the lumbricals.
Adduction and abduction are also lost. The failure to spread the fingers wide, limits
the versatility of the hand, since the hand cannot conform to an uneven object wider than the
palm. Advantageous grip is lost and effective grip strength is further diminished.
The thumb occupies a unique role in the hand. The mechanism of loss outlined
above, also affects the thumb, with crucial loss of unique arcs of movement. Loss of
adduction in the thumb web space (adductor pollicis paralysis) weakens or abolishes key
grip[37], the grasp of an object between thumb tip and side of index finger. Opposition is a
composite movement made up of a sequential abduction, pronation and flexion, such that
the thumb comes to face the long digits centred on the middle finger. This opposition action
of the thumb is essential to the production of power grip to which the thumb contributes an
estimated 40%. Opposition also permits the grasping of a fine object between thumb, index
and middle fingers („Chuck‟ or „Three point‟ grip) and very precise manipulative function can
be achieved (e.g. holding a pen in writing).
Opposition is lost with paralysis of the median nerve, while pinch power will be
maintained if the ulnar nerve is not affected; in most cases median and ulnar palsy occur
together. For around 60 years tendon muscle unit transfer has been used to correct both
these deformities[38], often in the same procedure.
The adequate range of joints and powerful, synchronous function of muscles is
significantly handicapped by the loss of the other great modality in the hand: Sensation. Erik
Moberg, who pioneered sensory testing in the hand, wrote „The insensate hand is the blind
hand‟[39].
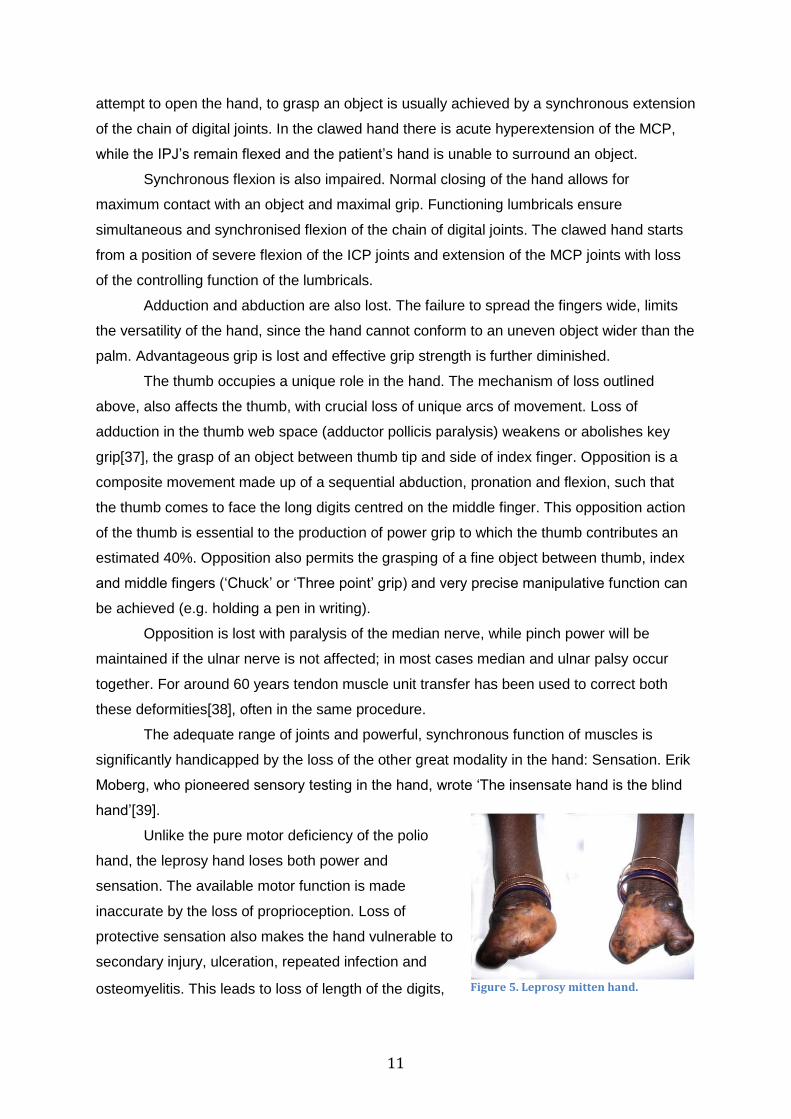
Unlike the pure motor deficiency of the polio
hand, the leprosy hand loses both power and
sensation. The available motor function is made
inaccurate by the loss of proprioception. Loss of
protective sensation also makes the hand vulnerable to
secondary injury, ulceration, repeated infection and
osteomyelitis. This leads to loss of length of the digits, Figure 5. Leprosy mitten hand.
12
secondary scarring and contractures. Progressively, the almost useless leprosy mitten hand
(figure 5) develops, leaving the patient severely disabled[40].
Leprosy Surgery
Surgery in leprosy has many roles. The surgeon can be involved in acute and
chronic nerve management, in the management of ulcers and in reconstructive and cosmetic
surgery. Surgery in the leprosy hand aims to make maximal use of the available resources
(muscle units). Active tendons are transferred to more essential functions; contractures are
released; joints are stabilised. The function overall is improved. All such surgery is directed
at the motor aspects of the disability.
No standard procedures are available for the restoration of sensation, other than
decompression of acute intraneural nerve abscesses aimed at halting progression of nerve
damage.
Principles of surgery in leprosy affected hands include:
1. Stiffness and limitation of passive range should be corrected first.
2. Instability must be corrected by procedures such as tenodeses, joint stabilisations
and selected fusion.
3. Dynamic instability, such as the claw hand, requires dynamic solutions.
4. Tendon transfer and stabilisation surgery should only be contemplated in the treated
patient with a stable motor pattern.
The improvement of function in the leprosy-affected hand with the use of tendon muscle
unit transfer is dependent on several factors. A functioning tendon muscle unit must be
available and in the case where multiple nerve palsies exist in a single limb these options
can be limited. The power ratio and the excursion of the transferred muscle must match the
function, which is being restored[37].
Correction of the claw hand is based on the principle that if the metacarpophalangeal
joints can be stabilised at 5-10 flexion then extensor digitorum communis can actively
extend the interphalangeal joints leading to finger opening[41]. Various muscle units can be
used.
The use of extensor carpi radialis longus (ECRL) in the extensor to flexor procedure was
introduced by Littler and popularised by Brand[38]. Palmaris longus (PL) transfer was
introduced by Lennox[38]. Flexor digitorum superficialis (FDS) transfer, using the one tendon
split into four tails, is amongst the commonest performed. These tendon slips can be
inserted into a choice of sites, including the extensor mechanism, the lumbrical tendon (as

13
popularised by Bunnell) or in a relatively static fashion, into the A1 pulley, the Zancolli lasso.
Other muscles, such as Extensor carpi radialis brevis have been used.
Median nerve paralysis produces atrophy of the thenar muscles. The thumb is
habitually held flat in the plane of the palm (the „simian‟
thumb) and opposition is lost. Opponensplasty is
indicated, supplemented by an adductorplasty if ulnar
nerve paralysis has also caused loss of adductor pollicis
function. Opponensplasty aims to recreate abduction-
opposition of the thumb and stabilise the proximal phalanx
restoring three-finger pinch and a grip of adequate strength.
Bunnell was the first to clarify the requirements for a successful
opponensplasty: the tendon must pull subcutaneously in the direction of the pisiform bone
and should insert on the dorso-ulnar aspect of the base of the proximal phalanx of the
thumb. He preferred to use an available flexor superficialis with a pulley constructed at the
insertion of the flexor carpi ulnaris. Since that time almost every available tendon around the
wrist has been used, and most of the procedures require the construction of a pulley or the
use of an intervening tendon graft.
Surgical correction of radial nerve palsies is much less commonly indicated and
usually in combination with median and ulnar nerve paralysis. Triple nerve palsies occur in
less than 1% of those with nerve involvement due to leprosy[42-43] and have been omitted
from this review.
The use of surgery in the management of ulcer care, correction of nerve palsies in
the lower limb, eye care and aesthetic facial surgery have been documented in the literature
but good randomised controlled trials are lacking in these areas.
The timing of surgical corrections is also important. Surgery is not attempted on an
evolving picture, whether this is deteriorating or improving. Brandsma et al suggest that
functional recovery of ulnar or median nerve paralysis is unlikely after 6 months. This is the
watershed period beyond which tendon transfers should be considered on a stable clinical
picture[44].
This review does not consider non-surgical modalities, such as early steroid therapy.
A recent meta-analysis by Reinar et al[45] looked at ways to improve ulcer healing while
avoiding surgery, but includes the observation that much of the work in this field is poor and
of limited use to analysis.
Figure 6 Simian thumb
14
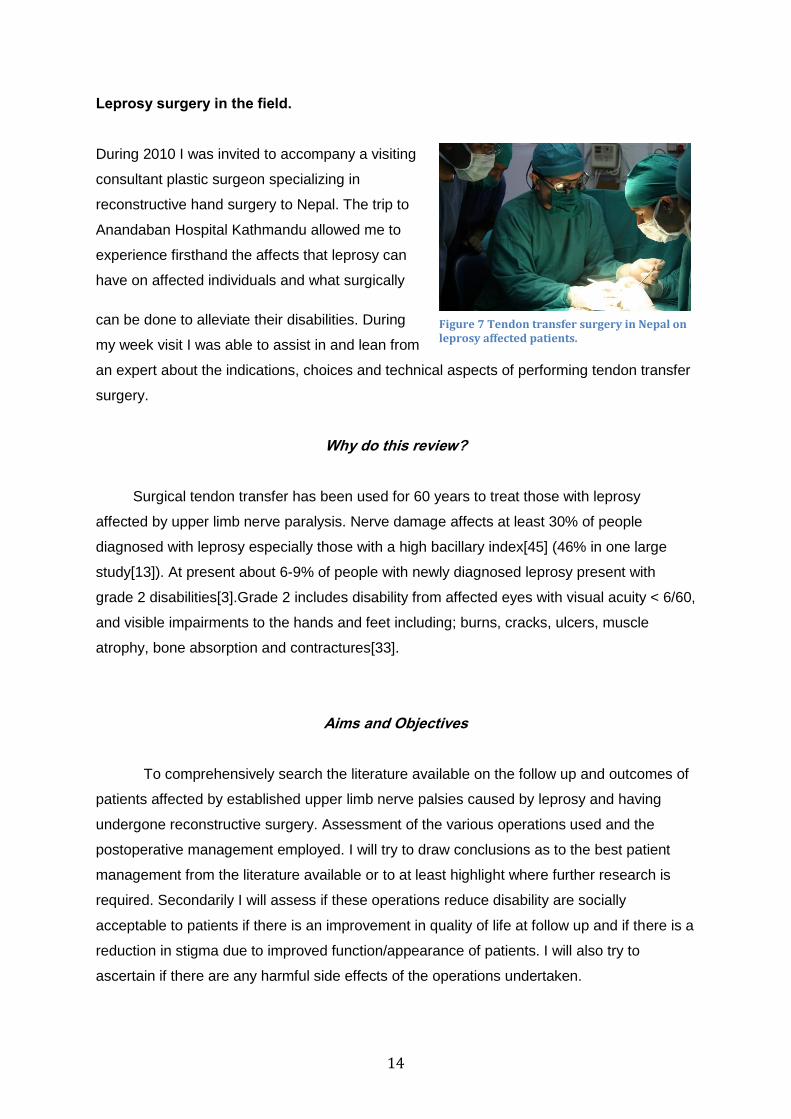
Leprosy surgery in the field.
During 2010 I was invited to accompany a visiting
consultant plastic surgeon specializing in
reconstructive hand surgery to Nepal. The trip to
Anandaban Hospital Kathmandu allowed me to
experience firsthand the affects that leprosy can
have on affected individuals and what surgically
can be done to alleviate their disabilities. During
my week visit I was able to assist in and lean from
an expert about the indications, choices and technical aspects of performing tendon transfer
surgery.
Why do this review?
Surgical tendon transfer has been used for 60 years to treat those with leprosy
affected by upper limb nerve paralysis. Nerve damage affects at least 30% of people
diagnosed with leprosy especially those with a high bacillary index[45] (46% in one large
study[13]). At present about 6-9% of people with newly diagnosed leprosy present with
grade 2 disabilities[3].Grade 2 includes disability from affected eyes with visual acuity < 6/60,
and visible impairments to the hands and feet including; burns, cracks, ulcers, muscle
atrophy, bone absorption and contractures[33].
Aims and Objectives
To comprehensively search the literature available on the follow up and outcomes of
patients affected by established upper limb nerve palsies caused by leprosy and having
undergone reconstructive surgery. Assessment of the various operations used and the
postoperative management employed. I will try to draw conclusions as to the best patient
management from the literature available or to at least highlight where further research is
required. Secondarily I will assess if these operations reduce disability are socially
acceptable to patients if there is an improvement in quality of life at follow up and if there is a
reduction in stigma due to improved function/appearance of patients. I will also try to
ascertain if there are any harmful side effects of the operations undertaken.
Figure 7 Tendon transfer surgery in Nepal on leprosy affected patients.
15
Methods; Criteria for considering studies for review
Types of studies
Randomized controlled trials are the ideal. Most likely only retrospective, follow up and
prospective trials are going to be available.
Participants
Anyone who has suffered from upper limb nerve paralysis due to leprosy having received
MDT and has been entered in to study looking at outcomes of surgery or postoperative
interventions.
Interventions
Types of surgery performed, postoperative interventions, complications of surgery.
Outcome measures
1. Improvement in hand mechanical outcomes post-operatively.
2. Improvement in disability (ability to do appropriate functional tasks post-
operatively).
3. Quality of life measures or other functional or psychological measures.
4. Adverse events/unwanted side effects of surgery.
5. Acceptability to patients of surgery/inpatient time.
6. Aesthetic improvement in hand(s).
7. Cost to patient including travel, time off work, and educational loss for those
school age.
8. Cost effectiveness of intervention(s).
Search methods for identifying studies.
Electronic Searches
Search of the Cochrane Central registrar of Controlled trials using;
#1 Leprosy: title abstract and keyword
#2 Hansen‟s: title abstract and keyword
#3 MeSH term Leprosy explode all trees
#4 (#1 OR #2 OR #3)
#5 Surgery: search all text
#6 Disability: search all text
#7 (#5 OR #6)
16
#8 (#4 AND #7)
Search results 19 (4 Cochrane reviews, 1 other review, 13 clinical trials, 1 economic
evaluation).
Search of Medline (OVID)
1) Leprosy- key word
2) Hansen* Disease- key word
3) Mycobacter* Leprae- key word
4) MeSH term Leprosy explode all trees
5) 1 OR 2 OR 3 OR 4
6) Surgical
7) Surgery
8) Operative
9) 6 OR 7 OR 8
10) Neuropath*
11) Nerve pals*
12) Nerve paralysis
13) Nerve damage*
14) 10 OR 11 OR 12 OR 13
15) 5 AND 9 AND 14
Search results 64
Search of Embase (OVID) same search used as for Medline.
Search results 143
Search of Global Health/Global Health Archives (OVID) same search as for Medline.
Search results 50
AfricaWideNiPAD
Search mode Boolean/Phrase
S1) Leprosy
S2) Hansen*
S3) (S1 OR S2)
S4) Surgery
S5) Hand*
S6) Upper limb*
S7) Arm*
17
S8) (S5 OR S6 OR S7)
S9) (S3 AND S4 AND S8)
Search results 23
Search of CINAHL
Same search as used for Africa Wide NiPAD
Search results 32
LEYES (Latin America & Caribbean)
Search term Leprosy AND Surgery
Search results 0
LILACS (South America)
Search term Leprosy AND Surgery
Search results 40
References from identified published data were used to trace further studies.
Ongoing trials
A search for ongoing trials was conducted (www.controlled-trials.com/mrct/,
www.who.int/trialsearch).
One study on the subject of disability management in leprosy patients that has recently been
completed is registered;
Clinic-Epidemiological Evaluation of Ulcers in Leprosy Patients and the Use of Low Level
Laser Therapy: a Randomized Clinical Trial. Clinical trials .gov identifier NCT00860717
No studies in to surgical management of disability in leprosy or further relevant studies have
been registered at this time.
Unpublished data
ELDIS
Search term “leprosy” produced 23 documents.
Language Only those studies in English where reviewed due to time restrictions.
18
Data collection and analysis
Study selection was based on any study that looked at surgical management or post
operative care of upper limb nerve palsies and either compared different techniques with
follow up, or looked at pre and post operative comparison for single surgical technique.
Included where follow up studies, prospective and retrospective studies.
Results
Detailed study descriptions. See Annex 1.
Search Results.
In total the search of the listed databases found 371 possibly relevant papers. 40
Papers were retrieved either electronically or by hand from libraries including London School
of Hygiene and Topical Medicine, The Royal College of Surgeons the British Medical
Association library and The British Library.
Included studies
11 trials were included, a total of 1161 operations conducted/reviewed and 998
participants. All trials were small and included between 20 and 216 participants (23 to 246
operations) for leprosy related disabilities. Six studies looked at correction of the claw hand,
one randomized control trial looked at postoperative intervention. Four studies looked at
opponensplasty to correct the simian thumb. Studies were from 1958 to 2008.
All of the studies had high risks of bias, due to non-random patient allocation lack of
blinding and poor documentation of losses to follow up. Only one study (the most recent) by
Rath et al made an attempt at randomization via sealed envelopes and at blinding of
assessors but was too small to draw definite answers from.
Excluded studies
Papers with very small numbers such as case studies were excluded. Papers without
English texts were excluded due to time constraints. Studies looking at the use of static
procedures (e.g. capsulorrhaphy[46]) were excluded. Papers that included studies on
sensory re-enablement were excluded, as this is not current practice. Research on surgery
in the lower limbs or face was excluded.
19
Intervention Effects.
Which surgical options for stable upper limb paralysis lead to good out comes?
Claw hand correction (ulnar paralysis)
Comparisons between operations for ulnar paralysis were difficult due to the various
ways in which outcomes where measured and also due to the wide variety of different
surgical techniques employed.
Correction of claw hand using Flexor Digitorum 4 Tailed procedure (FDS-4T) or
Zancolli’s Lasso procedure (ZLP) [37].
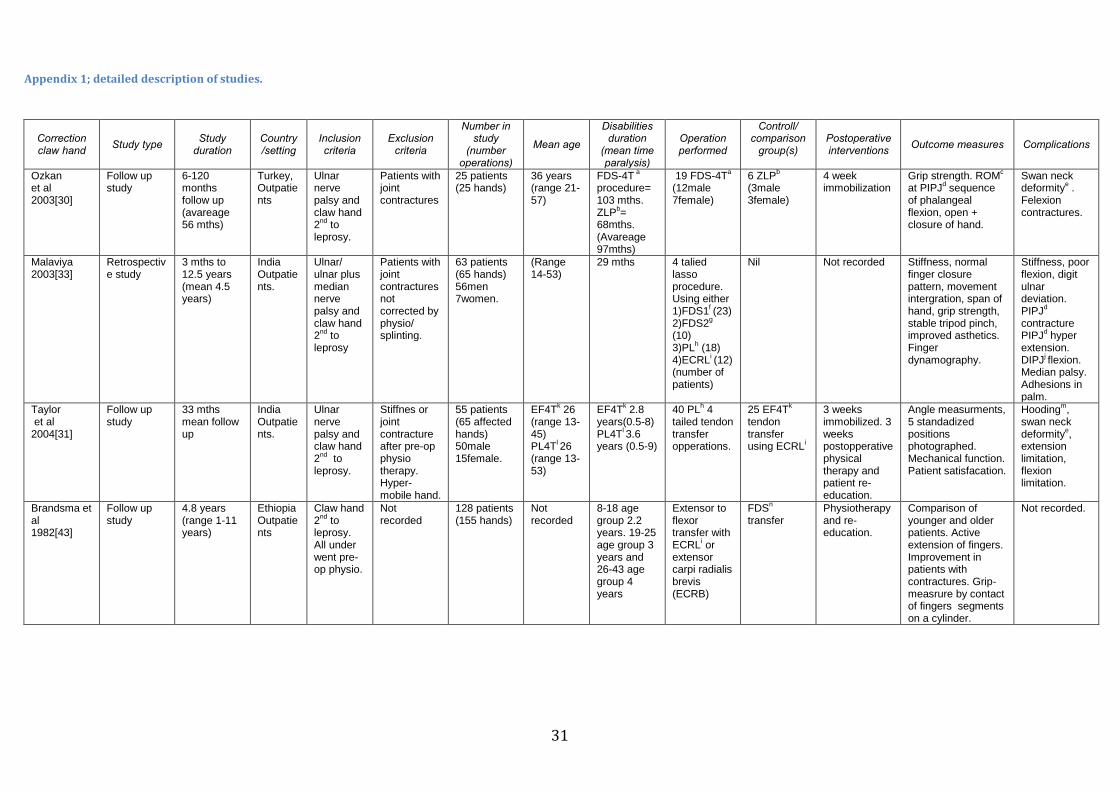
Ozkan et al‟s study in 2003 compared out comes in patients with ulnar nerve palsy
having undergone corrective surgery either with FDS-4T or ZLP procedure both use FDS but
attachment to the MCP joint varies. Conclusions drawn by the authors were that there was
no significant difference in grip strength in the two groups post operatively. Comparison with
pre-operative assessment showed a 20% increase in grip power of patients having
undergone ZLP and 1% in FDS-4T (P<0.05). The authors propose that this may show
evidence of a superior grip improvement with ZLP procedure. The authors also compare
hands that have undergone FDS-4T procedure with lesser or greater extensor lag
suggesting longer standing/more severe clawing of the hand. The conclusion drawn is that
those with lesser extent of extensor lag (<30) preoperatively benefit the most from
intervention (P<0.05). Final conclusions drawn are that while the FDS-4T procedure was
more effective at correcting claw hand deformity the ZLP procedure was more successful at
restoring grip strength [37]. This conclusion however this did not seem fully supported by the
research and appeared to be more based on the author‟s experience.
Comparison of effectiveness of different motor muscles in a lasso procedure for
correction of claw hand[41].
Malaviya in 2003 reported a retrospective study of 65 hand operations. All patients
underwent a modified lasso procedure but four different muscle tendon units were used.
Observations were that palmaris longus (PL) or extensor carpi radialis longus (ECRL)
resulted in good or excellent grades in most cases. The use of flexor digitorum superficialis
(FDS) from the index or middle finger produced poorer results. The authors also noted that
the working space of the hand (the ability of fingers to acquire postures needed for
manipulative activities) were best restored with PL or ECRL transfers the working space
being 50% less in those with FDS transfer. Problems with the use of PL are also highlighted
and the final conclusion is that the authors support the use of a lasso procedure with ECRL

20
at the tendon motor unit. The paper however doesn‟t assess presence of side affects when
using ECRL and the statement of preference is only partially supported by the findings.
Comparison of extensor to flexor operation or use of palmaris longus for correction
of claw hand[38].
Taylor et al conducted a follow up study in 2004 looking at differences in outcomes of
various operations to correct 65 claw hands. PL tendon transfer was conducted on 40
hands and extensor to flexor operation with ECRL was used on 25 hands. Each hand was
assessed prior to surgery and then post-operatively. The conclusions drawn were that there
was no statistically significant difference in the clinical outcomes of the two different
procedures neither in angle measurements (P>.05), technical grade (P=0.5) nor in patient
satisfaction (P>.05). However due to the supposed greater ease of patient re-education and
the lack of appreciable loss of function when removed from its original position the authors
recommend that where PL is available it should be first choice. This appears to contradict
Malaviya‟s study in 2003, it does seem to be more through with more statistical evidence
however again the study is small and how much solid evidence can be drawn form an
underpowered trial is questionable.
Claw Finger Correction: Result of Extensor-Flexor Many Tailed Operation[47].
Brandsma et al followed up 155 operations, 45% of the total operation list from an
Ethiopian hospital between 1967 and 1976. The authors initially highlight that there is some
improvement in function during pre-operative physiotherapy. They also demonstrate that in
their series younger patients tended to do better post-operatively excellent/good achieved in
58.5 % compared to 49% in the over 50‟s. They however feel that this is due to shorter
length of paralysis in the younger group rather than patient age. The study shows an
association between preoperative function and surgical outcome. Hands with flexion
deformities having poorer results than patients with less pre-op deformity (0º contracture
angle excellent/good outcome 47%, greater than 40º contracture angle 29% excellent/good
outcome). The size of this study makes it more convincing however there are some serious
flaws such as recall bias. Much of the conclusion also seems based on personal opinion
which while still valid is not completely supported by the research conducted.
Paralytic claw hand (1958) and Tendon Grafting (1961)[48-49].
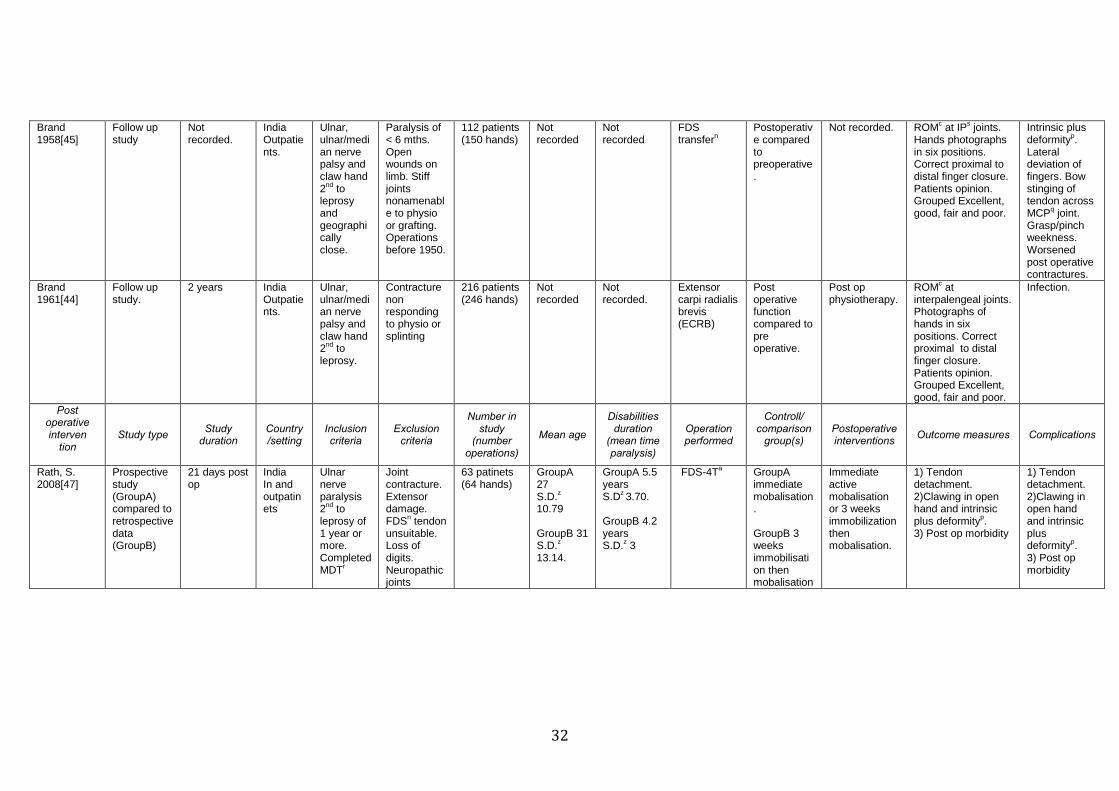
Brand conducted two studies one in 1958 and one in 1961. The first study followed-
up 150 operations (112 patients) having correction of claw hand by flexor digitorum
superficialis (FDS) procedure. They reported that the transfer gave good or excellent results
in 73% of fingers and commented that fingers that where stiff preoperatively produced
21
poorer results postoperatively. Analysis of fist closure postoperatively reported only 5% had
poor results and results for correct mechanism of finger closure (proximal to distal) only 2%
poor results. Overall the author cites that 75% of patients have restored hand opening and
over 90% correct hand closure. Brand then goes on to point out the complications of this
operation including the excessive force that the FDS can produce leading to new deformities
and also the weakness in the donor finger. From this he further suggests that FDS should
only be used in the stiff or contracted hand or that the tendon of a single FDS tendon should
be split to reduce excessive pull or other operations such as extensor to flexor transfer
should be considered. His second study in 1961 looked at outcomes of 246 hands having
had tendon graft using extensor carpi radialis brevis (ECRB) as the motor muscle. This
study concluded that this operation produce excellent results in 24% good/fair result in 71%
and poor results in only 2%. He reported that this was a better result than his previous study
using FDS but emphasized that this was not only due to the operative technique but to do
with case selection, which meant the operation was only performed on those with supple
non-contracted hands. Brands studies though large were conducted on two very different
patient populations and are not comparable. The conclusions drawn by the authors though
supported to some extent by their findings are not conducted against any control and so is
difficult to take the results as conclusive.
Postoperative intervention after claw deformity correction.
Only one study was identified that looked directly at postoperative interventions after
tendon transfer surgery in the leprosy hand. Many of the other studies (Taylor et al,
Brandsma et al, Brand) highlight the importance of postoperative physiotherapy in producing
good long-term results.
Randomized clinical trial comparing immediate active motion with immobilization
after tendon transfer for claw deformity[50].
Rath et al in 2009 published a study looking at immediate postoperative care. 50
claw hand deformities where randomized to two groups. For one group physiotherapy was
started days 2 postoperatively and in the other on day 22 after conventional immobilization.
Groups where compared on a number of outcomes (see appendix 1) and compared at
discharge and then at over one year. Four patients where lost to follow up. The author‟s
conclusions at the studies end were that there was no difference in outcomes except for pain
relief and restoration of hand function; these were achieved significantly earlier in the early
mobilization group. They state that morbidity was reduced by on average 22 days with early
active mobilization.
22
This study is a lot more like what is expected from current trials, with an attempt at
blinding and randomization. While the conclusions are supported by the results the main
problem with this study is that it is underpowered and further studies would need to be done
to support change in current practice.
Simian thumb correction (median median/ulnar nerve paralysis)
Four studies looked at correction of the simian thumb. It was impossible to compile
these studies due to the variety of operations conducted the varying technical operative
aspects and the different outcome measures.
Assessment of results of opponensplasty[51].
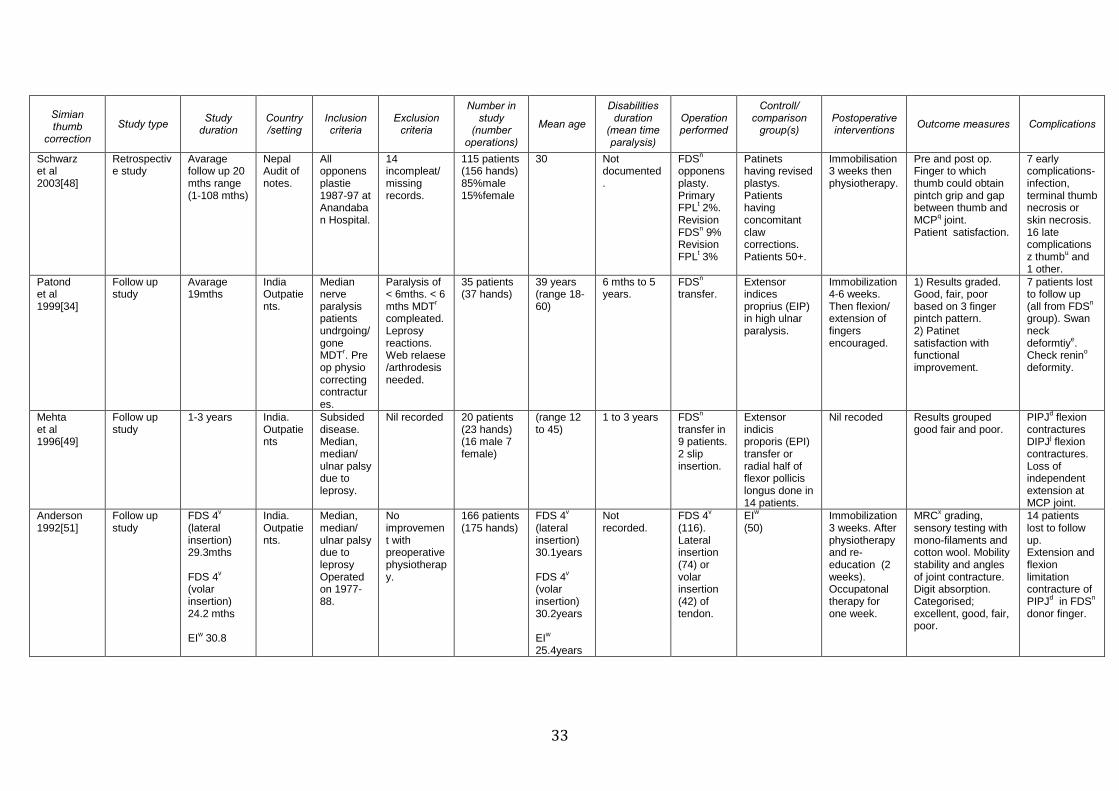
Schwarz reviewed 156 opponensplasties in 2003. The authors compared pre and
postoperative function. The majority were oppoensplasties using FDS (94%) the minority
were using flexor pollicis longus (FPL). Their findings were that there was an 89%
good/excellent result based on their scoring system (appendix1). They recorded that 94% of
patients who underwent subjective assessment reported good/fair satisfaction. The authors
highlighted that there was little correlation in patient‟s subjective opinion of outcome and
objective outcome measure. Subgroup analysis looked at whether older patients (50+) had
more difficulty in muscle reeducation but found no difference and suggest that surgery of this
kind is beneficial in older and younger patients. The observation that those undergoing
concomitant claw corrections had as good outcome as those having the opponensplasty
alone was also made. On average those having re-do operations had them at an average of
32 mouths (range 4-81 mouths) after the original operation. Complications where also
documented including early and late events (see appendix 1). The authors conclude that
subjective measurement of results by patients are important and should be included in
findings and that overall outcomes were good for the opponensplasty conducted with either
FDS or FPL.
This study was open to several types of bias and while it does include a relatively
good sized patient group most of the conclusions drawn are based on personal opinion and
experience making the applicability of the results to further studies minimal.
Results of thumb correction in leprosy using different techniques[52].
Study by Patond et al investigated outcomes of FDS or extensor indicis proprius
(EIP) for thumb reanimation. The use of FDS produced good results 87.5% of the time and
75% of the patients reported improvement in functional capabilities. EIP transfer was used in
seven hands due to high ulnar paralysis. 85.7 % had good results and 57% of patients
reported improvement in their functional capabilities. The authors recommend the use of
23
FDS as it provides greatest strength and as many leprosy affected individuals are in rural
settings in less developed countries a high proportion are farmers requiring powerful grip.
They also recommend the use of a window in the flexor retinaculum as the fulcrum as this
provides optimal direction of pull and isn‟t prone to stretching and tendon transfer laxity. The
use of EIP is only recommended where there is high ulnar nerve paralysis and the use of
FDS would lead to a functional deficit in the donor finger. Like other papers (Schwarz et al
and Brandsma et al) this study recommends that opponensplasty can be safely done
concurrently with claw hand correction however the paper produces little evidence to support
this conclusion. Like the other papers on opponensplasties there is no statistical back up to
support the recommendations and generally the size and quality of the trial does not make
for convincing conclusions to support recommendations.
Single tendon-two insertion versus two-tendon transfer for re-enablement of
ulnar/median paralyzed thumb in leprosy[53].
Methta et al‟s study in 1996 compares two different opponensplasties either extensor
indicis proporis (EIP) transfer plus radial half of flexor pollics longus (FPL) or flexor digitorum
superficialis (FDS) from the ring or middle finger. In hands where EIP and FPL were used (2
tendon transfer) overall satisfactory results were seen in 93%. Plus points for this choice of
operation were that all cases gained enough strength to reposition the thumb, there was no
requirement for a tendon graft to elongate the tendon and there was very little re-educating
of the patient required for good functional results.
In FDS transfer the overall satisfactory results where 66%. Complications for both
techniques listed in appendix 1. The author‟s highlight that incidence of postoperative
complications correlate with overlooked preoperative hand dysfunction for example stiffness
or contractures were present in 3 out of 4 thumbs having poor results. The authors conclude
that where two tendons were transferred (EPI and FPL) the outcome was better than FDS
transfer with two insertions extrapolating that this is due to the complex movement
opposition requires. They further state that in leprosy cases where combination nerve
palsies exist surgical outcomes are not as good as in single nerve paralysis however this
statement is not backed up by the evidence given and is based upon the authors findings in
practice not on a statistically significant finding from the study.
Opponensplasty by Extensor Indicis (EI) or FDS Tendon Transfer[54].
Anderson et al conducted a study comparing the results of opponensplasty using
either EI or FDS. EI group had 98% excellent and good results and the FDS group have
85% excellent and good, both having about 2% poor results. The conclusion drawn by the
authors were that the use of EI in thumb reanimation produced better results in supple
24
hands while the more powerful FDS tendon transfer was better in stiffer hands, however
again this conclusion seems to be based on personal opinion. The study does not actually
identify those with stiffer hands compared to those without undergoing the different
operations; hence it is difficult to ascertain the applicability of the studies to the wider leprosy
affected population.
Quality of studies included.
The quality of the studies reviewed where generally poor. Of the studies looking at
claw hand correction only three (Ozkan et al, Malaviya and Taylor et al) compared different
surgical techniques. Studies by Brandsma et al and by Brand compared pre and
postoperative function. All the papers had well defined clinical questions and all except one
(Brandsma et al) adequately described the surgical technique(s) employed. Where surgical
techniques where compared no patient randomization occurred.
In Ozkan et al‟s study there was no indication of how the patients were assigned to
their treatment group. The demographic of the patient groups did appear to be similar for
age sex and mean follow up time however there was a statistically significant difference in
the time at which the palsy had been present in the groups (P=0.03). This could significantly
add to study bias producing erroneous results.
Malaviya‟s study in 2003 also compared different techniques but again did not give
any indication of patient assignment resulting in possible selection bias. There was no
indication that group demographics where recorded and that chance could not have lead to
unacceptably large differences in the base line features. Taylor et al‟s study comparing two
different surgical techniques used retrospective data and didn‟t indicate the basis of surgical
group assignment.
Of the three follow up studies using pre and post operative out comes as
comparisons none of them made any comparison to patients undergoing conservative or
any other treatment so it‟s hard to draw conclusions as to what exactly lead to
improved/worsened outcomes. Only one paper by Brand in 1958 gave details as to case
selection for surgery and for follow up. Follow up was based on geography, likely to give
selection bias however there was an attempt to compensate for this by doing a smaller
thorough follow up in one area and compare demographics and outcomes with patients
selected by geography.
Only Ozkan et al attempted any sort of statistical analysis beyond simple comparison
of percentages using analysis of variance (ANOVA) for comparison of quantitative variables
and the qui squared test for comparison of categorical variables. None of the studies
attempted to blind the assessors and often it was a member of the surgical team that
25
assessed the outcome creating problems of reporter bias. Only one study by Taylor
indicated that a physiotherapist “not attached to the surgical team” did the postoperative
assessment.
Malaviya reported two patients lost to follow up. Brands study in 1958 requested
review of 184 patients with a response of 112 patients, reasons such as poverty, inability to
read and write and change of address quoted as affecting follow up. Brandsma was only
able to follow up 45% of the patients operated on. None of the other studies documented
losses to follow up which would affect validity of results.
Most of the studies mentioned postoperative intervention. The standard for this was
between 2 and 4 weeks of immobilization in the majority of cases followed up by
physiotherapy, and in one study occupational therapy (Anderson 1992). The one study
found directly looking at postoperative intervention was a small randomized controlled trial
comparing immediate activity with immobilization after claw hand repair. The study used
mixing of opaque envelopes containing allocation details in a box for randomization. This
method is poor and prone to error but made an attempt at reduction in selection bias. Follow
up was conducted by therapists not involved in earlier care and blinded to postoperative
technique used hence controlling of reporting bias. Demographic details of the two groups
where analyzed attempting to identify if chance could have affected results; this did not
appear to be a problem.
Studies identified looking at opponensplasty again where very variable and often
poor. Three of the four studies compared different operative techniques (Patond et al, Mehta
et al and Anderson et al) but none of these were randomized controlled trials. The study by
Patond et al was small and analyzed results of thumb correction in 37 operations. 7 patients
were lost to follow up. The paper gave clear inclusion criteria but the allocation of surgical
technique was based upon type of paralysis so the results are not comparable between
grups. Like all the studies looking at opponensplasty there was good documentation of the
operation(s) performed. The use of arbitrary divisions in to good fair and poor (and
sometimes excellent as well) was commonly used (Brandsma et al, Mehta et al, Brand and
Anderson) but these all had different contributing objective and subjective measurements so
were non-comparable. These arbitrary divisions are also open to interpretation and error in
use and therefore give results difficult to apply to other patient groups.
A much larger study done by Schwarz assessed 156 opponensplasties. This was a
retrospective study and used patient notes to look at operative outcomes. Retrospective
studies are inherently flawed, as they can only be as good as the documentation they are
based on and are open to the bias of those that write and those that review the notes. 14
notes were also missing or incomplete adding to the bias of the study. Some operations
26
used within the analysis where also re-do‟s (156 operations on 137 hands) giving a false
impression of outcome.
The study by Anderson et al though larger and conducted on patients at follow up
had flaws. There was no blinding of the allocation process and no indication in the study as
to how patients were allocated to operations. Base line differences were recorded in the
subgroups and in one group there was a discrepancy of 5 years in average participant age
that could have adverse affect on results. No indication of assessor blinding is given leaving
another source of bias. The patient‟s opinion was not sort in this trial (and many others) and
as patient satisfaction is an important predictor for good surgical outcome this is another
area lacking. This study also included a small numbers of patients who did not have leprosy
(trauma, polio, burns and congenital causes) this could affect the studies applicability to
leprosy.
Overall study quality was poor. Study power is often insufficient and there is little
attempt to correct for selection or assessor bias or for chance. The studies are all open to
type 1 and type 2 errors and many contain personal views as conclusions. Mostly, apart
from very basic percentage comparisons, statistical analysis was not used and due to the
varying ways and stratification techniques done for outcome measures compilation of data to
increase power couldn‟t be achieved.
Study Heterogeneity.
Studies included where very heterogenous. Eight studies were done in India two in
Ethiopia, one in Nepal and one in Turkey. Age groups, the length of time that paralysis had
been present and presence of secondary problems were widely variable. The type of leprosy
was only occasionally documented (Patond et al, Sundararaj et al) different classification
systems were used, having implications for results. Pre and postoperative care also varied
some undergoing intensive preoperative physiotherapy (Patond et al, Brandsma et al) or
surgery for contractures. Some had no preoperative care and some studies excluded those
with contractures altogether (Rath Ozkan et al and McEvitt et al). The experience and skill of
the surgeons also plays a role in affecting outcomes. Only one study by Malaviya provided
the information that all operations where done by the same surgeon. Outcome measures
were variable some very simple and some sophisticated using photographs and
dynamography (Malaviya) again affected comparison between the different studies.
27
According to present literature what is the most effective surgical interventions for
management of stable upper-limb paralysis?
All studies reported on mechanical function (such as finger angles and fist formation)
and reported overall improvement post-operatively. In those papers where two operations
where compared with one another Ozkan et al, Malaviya and Taylor for claw hand
correction, Patond, Mehta and Anderson for opponensplasty and Rath et al for post
operative care. The large differences in choice of operation/intervention, technical aspects of
the operations, the operative skill of the surgeon, differences in patients involved, length of
time to follow up and outcome measures make comprehensive comparisons and assimilated
conclusions impossible.
Interventions most affective at improving quality of life or stigma?
None of the papers looked directly at or measured improvement in quality of life or
related stigma. Measurement of functional skills such as ability to manage appropriate
activities of daily living was attempted by Brand using graded cylinders simulating use of
tools. This had to be abandoned due to patients learning to improve scores by dampening
their hands and increasing grip by friction, all the other studies used mechanical
measurements. Patond et al and Taylor et al did ask the patient if there had been an
improvement in their daily functioning but this was not quantified by an examination, no other
assessment of daily activity was attempted.
Acceptability to patients of surgery/inpatient time was not assessed in any of the
papers. None of the studies assessed the cost effectiveness of surgical intervention(s). The
cost to the patient including travel, time off work, and educational loss for those school age,
was also not evaluated in any paper. Rath et el mentions that early active mobilization may
save expense but does not go on to quantify this. Similarly Patond et al comments that one
stage correction of fingers and thumb in combined nerve paralysis may lead to earlier return
to work but this is not further explored.
Any adverse events/unwanted side effects of surgery?
A variety of adverse events were documented in the papers chosen for this review.
All of the papers except one by Brandsma et al gave specific complications related to the
operative technique used. Several of the papers noted that deformities could occur in the
FDS donor finger for claw or simian thumb correction. These included distal inter-phalangeal
(DIP) and proximal inter-phalangeal (PIP) flexion contractures (Check rein deformity) (Ozkan
et al, Malaviya, Anderson, Mehta et al, Patond) this is a well known complication and
Brandsma et al in 1992 wrote a paper on long term follow up and occurrence of adverse
28
events in the FDS donor finger[55]. Patond also reported this deformity in fingers using
extensor indicies (EI) transfer though Anderson reported no such complications with EI use.
Infection was an early complication mentioned in a few studies that lead to
significantly poorer results (Brand 61, Oberlin, Schwarz et al). Swan neck deformity (hyper
extended PIP joint and a flexed DIP joint) occurred in Ozkan et al‟s study using FDS but also
in Taylor‟s study using Palmaris longus the reason proposed being excessive tension at the
transfer. A complication quoted for the use of ECRL was ulnar deviation (Malaviya) and
Taylor comments that his study should have included testing for this along with wrist
extension power to look for defects second to ECRL‟s transfer. Other complications inherent
to most hand surgery such as stiffness, skin necrosis or suture breakdown are sporadically
mentioned[56].
Median nerve damage second to surgery occurred in one study (Malaviya, et al)
though rare the implications for iatrogenic nerve damage lead Brandsma et al in 1985 to look
at if there is an increase in median nerve damage after tendon transfer. His findings where
that there is no association[56]. Further studies looking at adverse events have been written
and suggestions on how to avoid complications are in much of the literature[57-59].
Is immediate physiotherapy better than immobilization after surgery in leprosy related
paralysis?
Many of the studies highlighted the importance of postoperative training and
physiotherapy of the patient (Taylor et al, Mehta et al and Brand). Preoperative function was
noted by several authors to be an important predictor of postoperative outcome (Ozkan et al,
Mehta et al Brandsma et al and Brand).
The one trial by Rath et al suggests that immediate mobilization is preferable to the
conventional postoperative immobilization in plaster. This study is based on only 50 patients
however and will need further larger studies before it can be accepted in to current practice.
29
Discussion and Recommendations
Leprosy can lead to disability in two ways. Primary
disability comes from the direct sensory and motor dysfunction
leading to the paralyzed and insensate hand. This can lead to
secondary disabilities from joint contractures and tissue loss;
second to trauma infection and inappropriate limb use[37].
Once primary disability has developed early and affective
educational and surgical management of affected hands can
prevent development of irreversible secondary deformities and
disabilities.
Of all deformities in leprosy 80% require minor surgery
and the rest major surgery[60]. Tendon transfer is the only option available in cases of
deformities like simian thumb, claw hand, and wrist drop[61]. At present we can only correct
the motor component and that only to an extent. Sensory loss and its dangers continue and
care in the management of the anesthetic part via patient education and tools is essential to
maintain integrity of any restored digits[52]. Early attempts have been made to surgically
correct sensation in the hand recognizing that this could not only prevent disability but also
decrease development of secondary disabilities. None of the pioneering techniques have so
far made the transfer in to common use [62-64].
The studies that I have discussed looking at surgical options for the leprosy affected
hand have helped shape current practice. These have increased the knowledge base on
outcomes for these patients. In some of the studies where there was comparison of different
techniques this provided reference for those faced with choosing the best operative
procedure. These studies have helped guide surgeons, disseminate information on new and
evolving practices and highlight postoperative complications and pitfalls. However the
evidence base for current surgical practice in these patients is weak. This is due to a number
of problems with research that has been conducted on leprosy surgery.
The studies looked at in this paper are often small not controlled or blinded and use a
host of pre post and inter-operative techniques making assimilated conclusions difficult. The
different inclusion and exclusion criteria for the trials and the great variability in the outcome
measures used make over reaching conclusions impossible. The lack of assessment and
documentation of how “every day” function is improved, or not postoperatively means that
relevance to the patient‟s daily living is not easily elucidated. There is also almost no
documentation of affects on stigma or other aspect of the patent‟s lives such as relief of
financial or relationship burdens. These are areas that the WHO is keen to highlight in the
Figure 8. Tool used to improve hand function.
30
more holistic initiatives of long-term disability management in leprosy and that future surgical
trials may need to attempt to assess more adequately.
The areas that the studies mostly do seem to agree on are that preoperative function
is an important predictor of surgical result. That physiotherapy appears to be an important
factor in producing good outcomes and that the different operations used can produce
multiple different complications but that overall function is improved.
Future Research
The lack of consistency and great variability in outcomes and techniques in surgical options
for upper limb paralysis in leprosy would suggest that further rigorous and controlled trials
which conform to current standards for design and reporting are greatly desirable to guide
best evidence based practice for care of leprosy patients with disabilities. The structure,
requirements and pitfalls for a trial are discussed in appendix 2.
31
Correction claw hand
Study type Study
duration Country /setting
Inclusion criteria
Exclusion criteria
Number in study
(number operations)
Mean age
Disabilities duration
(mean time paralysis)
Operation performed
Controll/ comparison
group(s)
Postoperative interventions
Outcome measures Complications
Ozkan et al 2003[30]
Follow up study
6-120 months follow up (avareage 56 mths)
Turkey, Outpatients
Ulnar nerve palsy and claw hand 2
nd to
leprosy.
Patients with joint contractures
25 patients (25 hands)
36 years (range 21-57)
FDS-4T a
procedure= 103 mths. ZLP
b=
68mths. (Avareage 97mths)
19 FDS-4Ta
(12male 7female)
6 ZLPb
(3male 3female)
4 week immobilization
Grip strength. ROMc
at PIPJd sequence
of phalangeal flexion, open + closure of hand.
Swan neck deformity
e .
Felexion contractures.
Malaviya 2003[33]
Retrospective study
3 mths to 12.5 years (mean 4.5 years)
India Outpatients.
Ulnar/ ulnar plus median nerve palsy and claw hand 2
nd to
leprosy
Patients with joint contractures not corrected by physio/ splinting.
63 patients (65 hands) 56men 7women.
(Range 14-53)
29 mths 4 talied lasso procedure. Using either 1)FDS1
f (23)
2)FDS2g
(10) 3)PL
h (18)
4)ECRLi (12)
(number of patients)
Nil Not recorded Stiffness, normal finger closure pattern, movement intergration, span of hand, grip strength, stable tripod pinch, improved asthetics. Finger dynamography.
Stiffness, poor flexion, digit ulnar deviation. PIPJ
d
contracture PIPJ
d hyper
extension. DIPJ
j flexion.
Median palsy. Adhesions in palm.
Taylor et al 2004[31]
Follow up study
33 mths mean follow up
India Outpatients.
Ulnar nerve palsy and claw hand 2
nd to
leprosy.
Stiffnes or joint contracture after pre-op physio therapy. Hyper-mobile hand.
55 patients (65 affected hands) 50male 15female.
EF4Tk 26
(range 13-45) PL4T
l 26
(range 13-53)
EF4Tk 2.8
years(0.5-8) PL4T
l 3.6
years (0.5-9)
40 PLh 4
tailed tendon transfer opperations.
25 EF4Tk
tendon transfer using ECRL
i
3 weeks immobilized. 3 weeks postopperative physical therapy and patient re-education.
Angle measurments, 5 standadized positions photographed. Mechanical function. Patient satisfacation.
Hoodingm,
swan neck deformity
e,
extension limitation, flexion limitation.
Brandsma et al 1982[43]
Follow up study
4.8 years (range 1-11 years)
Ethiopia Outpatients
Claw hand 2
nd to
leprosy. All under went pre-op physio.
Not recorded
128 patients (155 hands)
Not recorded
8-18 age group 2.2 years. 19-25 age group 3 years and 26-43 age group 4 years
Extensor to flexor transfer with ECRL
i or
extensor carpi radialis brevis (ECRB)
FDSn
transfer Physiotherapy and re-education.
Comparison of younger and older patients. Active extension of fingers. Improvement in patients with contractures. Grip- measrure by contact of fingers segments on a cylinder.
Not recorded.
Appendix 1; detailed description of studies.
32
Brand 1958[45]
Follow up study
Not recorded.
India Outpatients.
Ulnar, ulnar/median nerve palsy and claw hand 2
nd to
leprosy and geographically close.
Paralysis of < 6 mths. Open wounds on limb. Stiff joints nonamenable to physio or grafting. Operations before 1950.
112 patients (150 hands)
Not recorded
Not recorded
FDS transfer
n
Postoperative compared to preoperative.
Not recorded. ROMc at IP
s joints.
Hands photographs in six positions. Correct proximal to distal finger closure. Patients opinion. Grouped Excellent, good, fair and poor.
Intrinsic plus deformity
p.
Lateral deviation of fingers. Bow stinging of tendon across MCP
q joint.
Grasp/pinch weekness. Worsened post operative contractures.
Brand 1961[44]
Follow up study.
2 years India Outpatients.
Ulnar, ulnar/median nerve palsy and claw hand 2
nd to
leprosy.
Contracture non responding to physio or splinting
216 patients (246 hands)
Not recorded
Not recorded.
Extensor carpi radialis brevis (ECRB)
Post operative function compared to pre operative.
Post op physiotherapy.
ROMc at
interpalengeal joints. Photographs of hands in six positions. Correct proximal to distal finger closure. Patients opinion. Grouped Excellent, good, fair and poor.
Infection.
Post operative interven
tion
Study type Study
duration Country /setting
Inclusion criteria
Exclusion criteria
Number in study
(number operations)
Mean age
Disabilities duration
(mean time paralysis)
Operation performed
Controll/ comparison
group(s)
Postoperative interventions
Outcome measures Complications
Rath, S. 2008[47]
Prospective study (GroupA) compared to retrospective data (GroupB)
21 days post op
India In and outpatinets
Ulnar nerve paralysis 2
nd to
leprosy of 1 year or more. Completed MDT
r
Joint contracture. Extensor damage. FDS
n tendon
unsuitable. Loss of digits. Neuropathic joints
63 patinets (64 hands)
GroupA 27 S.D.
z
10.79 GroupB 31 S.D.
z
13.14.
GroupA 5.5 years S.D
z 3.70.
GroupB 4.2 years S.D.
z 3
FDS-4Ta GroupA
immediate mobalisation. GroupB 3 weeks immobilisation then mobalisation
Immediate active mobalisation or 3 weeks immobilization then mobalisation.
1) Tendon detachment. 2)Clawing in open hand and intrinsic plus deformity
p.
3) Post op morbidity
1) Tendon detachment. 2)Clawing in open hand and intrinsic plus deformity
p.
3) Post op morbidity
33
Simian thumb
correction
Study type Study
duration Country /setting
Inclusion criteria
Exclusion criteria
Number in study
(number operations)
Mean age
Disabilities duration
(mean time paralysis)
Operation performed
Controll/ comparison
group(s)
Postoperative interventions
Outcome measures Complications
Schwarz et al 2003[48]
Retrospective study
Avarage follow up 20 mths range (1-108 mths)
Nepal Audit of notes.
All opponensplastie 1987-97 at Anandaban Hospital.
14 incompleat/ missing records.
115 patients (156 hands) 85%male 15%female
30 Not documented.
FDSn
opponensplasty. Primary FPL
t 2%.
Revision FDS
n 9%
Revision FPL
t 3%
Patinets having revised plastys. Patients having concomitant claw corrections. Patients 50+.
Immobilisation 3 weeks then physiotherapy.
Pre and post op. Finger to which thumb could obtain pintch grip and gap between thumb and MCP
q joint.
Patient satisfaction.
7 early complications- infection, terminal thumb necrosis or skin necrosis. 16 late complications z thumb
u and
1 other.
Patond et al 1999[34]
Follow up study
Avarage 19mths
India Outpatients.
Median nerve paralysis patients undrgoing/gone MDT
r. Pre
op physio correcting contractures.
Paralysis of < 6mths. < 6 mths MDT
r
compleated. Leprosy reactions. Web relaese /arthrodesis needed.
35 patients (37 hands)
39 years (range 18-60)
6 mths to 5 years.
FDSn
transfer. Extensor indices proprius (EIP) in high ulnar paralysis.
Immobilization 4-6 weeks. Then flexion/ extension of fingers encouraged.
1) Results graded. Good, fair, poor based on 3 finger pintch pattern. 2) Patinet satisfaction with functional improvement.
7 patients lost to follow up (all from FDS
n
group). Swan neck deformtiy
e.
Check renino
deformity.
Mehta et al 1996[49]
Follow up study
1-3 years India. Outpatients
Subsided disease. Median, median/ ulnar palsy due to leprosy.
Nil recorded 20 patients (23 hands) (16 male 7 female)
(range 12 to 45)
1 to 3 years FDSn
transfer in 9 patients. 2 slip insertion.
Extensor indicis proporis (EPI) transfer or radial half of flexor pollicis longus done in 14 patients.
Nil recoded Results grouped good fair and poor.
PIPJd flexion
contractures DIPJ
j flexion
contractures. Loss of independent extension at MCP joint.
Anderson 1992[51]
Follow up study
FDS 4v
(lateral insertion) 29.3mths FDS 4
v
(volar insertion) 24.2 mths EI
w 30.8
India. Outpatients.
Median, median/ ulnar palsy due to leprosy Operated on 1977-88.
No improvement with preoperative physiotherapy.
166 patients (175 hands)
FDS 4v
(lateral insertion) 30.1years FDS 4
v
(volar insertion) 30.2years EI
w
25.4years
Not recorded.
FDS 4v
(116). Lateral insertion (74) or volar insertion (42) of tendon.
EIw
(50) Immobilization 3 weeks. After physiotherapy and re-education (2 weeks). Occupatonal therapy for one week.
MRCx grading,
sensory testing with mono-filaments and cotton wool. Mobility stability and angles of joint contracture. Digit absorption. Categorised; excellent, good, fair, poor.
14 patients lost to follow up. Extension and flexion limitation contracture of PIPJ
d in FDS
n
donor finger.
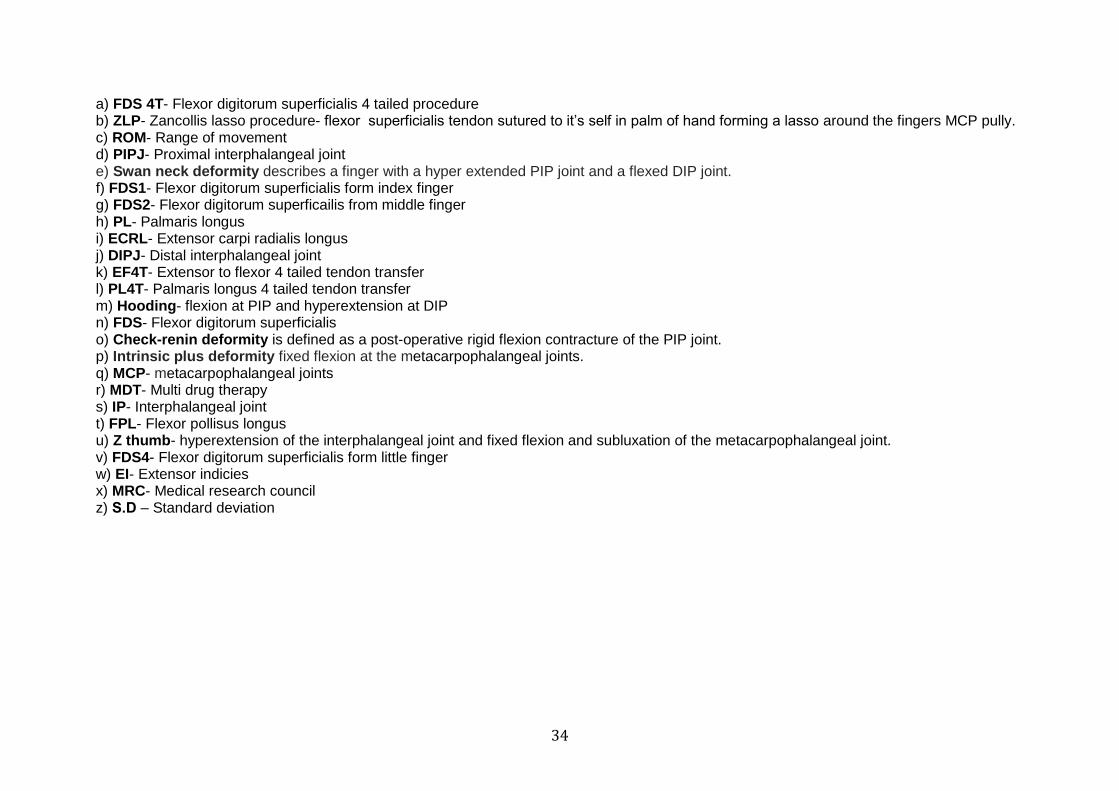
34
a) FDS 4T- Flexor digitorum superficialis 4 tailed procedure b) ZLP- Zancollis lasso procedure- flexor superficialis tendon sutured to it‟s self in palm of hand forming a lasso around the fingers MCP pully. c) ROM- Range of movement d) PIPJ- Proximal interphalangeal joint e) Swan neck deformity describes a finger with a hyper extended PIP joint and a flexed DIP joint. f) FDS1- Flexor digitorum superficialis form index finger g) FDS2- Flexor digitorum superficailis from middle finger h) PL- Palmaris longus i) ECRL- Extensor carpi radialis longus j) DIPJ- Distal interphalangeal joint k) EF4T- Extensor to flexor 4 tailed tendon transfer l) PL4T- Palmaris longus 4 tailed tendon transfer m) Hooding- flexion at PIP and hyperextension at DIP n) FDS- Flexor digitorum superficialis o) Check-renin deformity is defined as a post-operative rigid flexion contracture of the PIP joint. p) Intrinsic plus deformity fixed flexion at the metacarpophalangeal joints. q) MCP- metacarpophalangeal joints r) MDT- Multi drug therapy s) IP- Interphalangeal joint t) FPL- Flexor pollisus longus u) Z thumb- hyperextension of the interphalangeal joint and fixed flexion and subluxation of the metacarpophalangeal joint. v) FDS4- Flexor digitorum superficialis form little finger w) EI- Extensor indicies x) MRC- Medical research council z) S.D – Standard deviation
35 of 52
Appendix 2; Research project.
Areas requiring further trials include;
1) Best operative management of the claw hand in the stiff and supple hand.
2) Best operative management of correction of the simian thumb.
3) Best operative management of those with combined ulnar and median nerve
paralysis.
4) Best postoperative management of patients undergoing surgery on the leprosy
affected hand.
Randomized double blind placebo controlled trials are the ideal though these are
inherently difficult to achieve in surgical management. Randomization of treatment arm
allocation should be achieved using computer generated random numbers, which assign a
participant to a group eliminating selection bias. Blinding of both patient and of physician is
preferred but this is only possible up to a point with the surgeon required to perform the
operation. Assessors of outcome however should be blinded and be independent of the
surgical team so as to not have a vested interest. The use of placebo in surgery can be
achieved using “sham operations” but this is often un-ethical and difficult to perform. All
studies must be ethically approved and advantageous to participants.
Studies need to be adequately powered allowing for statistically significant results to be
obtained. For a disease such as leprosy with relatively few surgical procedures carried out in
each centre a multi center study would be appropriate including individuals from many
countries and treatment in many health care facilities by many different surgeons. Inclusion
and exclusion criteria need to be well specified and adhered to through all the different
centers. Once a hypothesis has been stated data needs to be appropriately statistically
analyzed and the hypothesis proved or refuted. Data should be analyzed with patient‟s
intention to treat.
Write up of studies should conform to the CONSORT statement (Consolidated Standards of
Reporting Trials) which encompasses various initiatives developed by the CONSORT Group
to alleviate the problems arising from inadequate reporting of randomized controlled
trials[65]. Adequately produced randomized controlled trials allows for future meta-analysis
such as those registered with the Cochrane database.
36 of 52
Acknowledgements
I would like to thank Donald Sammut for his generous help. James Mackie for his support,
Lilli Cooper for her encouragement and Natasha Hezalgrave for the cups of tea.
References.
1. WHO. Leprosy today. 2010 [cited 2010 22 June 2010]; Available from: http://www.who.int/lep/en/.
2. Britton, W.J. and D.N.J. Lockwood, Leprosy. Lancet, 2004. 363(9416): p. 1209-19. 3. Lockwood, D.N., Leprosy elimination-a virtual phenomenon or a reality? BMJ,
2002. 324(7352): p. 1516-8. 4. Sharma, R., Complete elimination of leprosy still elusive. BMJ, 2001. 322(7282): p.
318e-. 5. World Health Organization Regional Office for South-East Asia New, D., Global
strategy for further reducing the leprosy burden and sustaining leprosy control activities 2006-2010. Operational guidelines. Leprosy Review, 2006. 77(3): p. IX.
6. WHO, Enhanced Global Strategy for Further Reducing the Disease Burden Due to Leprosy
Operational Guidelines (Updated) (2011-2015). 2009, WHO Regional Office of South East Asia. 7. Wilder-Smith, E.P. and W.H. Van Brakel, Nerve damage in leprosy and its
management. Nat Clin Pract Neurol, 2008. 4(12): p. 656-63. 8. Bryceson, A.P., R. E., Leprosy. 3rd ed. Medicine in the Tropics. 1990, Edinburgh
London Melbourne and New York: Churchill Livingstone. 9. Hastings, R.C., Leprosy. 2nd ed. Medicine in the tropics series. 1994, Edinburgh
New York Churchill Livingstone. 10. Gill, G.B., N., Lecture notes Tropical Medicine. 2009, Wiley Blackwell. p. 171-184. 11. Parry, E.G., R. Mabey, D. Gill, G., Principles of Medicine in Africa. 3rd ed. 2004,
Cambridge: Cambridge University Press. 12. Van Brakel, W.H., et al., The INFIR Cohort Study: Assessment of sensory and motor
neuropathy in leprosy at baseline. Leprosy Review, 2005. 76(4): p. 277-295. 13. Van Brakel, W.H., et al., The INFIR Cohort Study: Investigating prediction, detection
and pathogenesis of neuropathy and reactions in leprosy. Methods and baseline results of a cohort of multibacillary leprosy patients in North India. Leprosy Review, 2005. 76(1): p. 14-34.
14. Murthy, P.K., Clinical manifestations, diagnosis and classification of leprosy. Journal of the Indian Medical Association, 2004. 102(12): p. 678-9.
15. Goulart, I.M. and L.R. Goulart, Leprosy: diagnostic and control challenges for a worldwide disease. Arch Dermatol Res, 2008. 300(6): p. 269-90.
16. Sarkar, K., Corrective surgery for deformities in women leprosy patients. Indian Journal of Leprosy, 2004. 76(3): p. 233-5.
17. Ridley, D.S. and W.H. Jopling, Classification of leprosy according to immunity. A five-group system. International Journal of Leprosy & Other Mycobacterial Diseases, 1966. 34(3): p. 255-73.
18. Khambati, F.A., et al., Sensitivity and specificity of nerve palpation, monofilament testing and voluntary muscle testing in detecting peripheral nerve abnormality,
37 of 52
using nerve conduction studies as gold standard; A study in 357 patients. Leprosy Review, 2009. 80(1): p. 34-50.
19. Mehndiratta, R.C., et al., Does nerve examination improve diagnostic efficacy of the WHO classification of leprosy? Indian Journal of Dermatology, Venereology & Leprology, 2008. 74(4): p. 327-30.
20. Banerjee, S., et al., Development and application of a new efficient and sensitive multiplex polymerase chain reaction (PCR) in diagnosis of leprosy. Journal of the Indian Medical Association, 2008. 106(7): p. 436-40.
21. WHO, WHO Expert Committee on Leprosy. World Health Organ Tech Rep Ser, 1998. 874: p. 1-43.
22. Van Veen, N.H.J., et al., Decompressive surgery for treating nerve damage in leprosy. A Cochrane review. Leprosy Review, 2009. 80(1): p. 3-12.
23. Saunderson, P., The epidemiology of reactions and nerve damage. Leprosy Review, 2000. 71(SUPPL): p. S106-S110.
24. Saunderson, P., et al., The pattern of leprosy-related neuropathy in the AMFES patients in Ethiopia: Definitions, incidence, risk factors and outcome. Leprosy Review, 2000. 71(3): p. 285-308.
25. Smith, W.C.S., et al., Steroid prophylaxis for prevention of nerve function impairment in leprosy: Randomised placebo controlled trial (TRIPOD 1). British Medical Journal, 7454. 328(7454): p. 1459-1462.
26. Schuring, R.P., et al., Protective effect of the combination BCG vaccination and rifampicin prophylaxis in leprosy prevention. Vaccine, 1999. 27(50): p. 7125-8.
27. Srinivasan, H., Nerve damage, surgery and rehabilitation in leprosy. Tropical Medicine and Parasitology, 1990. 41(3): p. 347-349.
28. Srinivasan, H., Algorithms as guides for the prevention of permanent nerve damage in leprosy patients. Indian Journal of Leprosy, 2004. 76(4): p. 321-324.
29. Meima, A., et al., Factors associated with impairments in new leprosy patients: The AMFES cohort. Leprosy Review, 1999. 70(2): p. 189-203.
30. Van Veen, N.H.J., A. Meima, and J.H. Richardus, The relationship between detection delay and impairment in leprosy control: A comparison of patient cohorts from Bangladesh and Ethiopia. Leprosy Review, 2006. 77(4): p. 356-365.
31. Smith, W.C.S., et al., Predicting neuropathy and reactions in leprosy at diagnosis and before incident events - Results from the INFIR cohort study. PLoS Neglected Tropical Diseases, 2009. 3(8).
32. Smith, W.C.S., Review of current research in the prevention of nerve damage in leprosy. Leprosy Review, 2000. 71(SUPPL): p. S138-S145.
33. Brakel, D.W.H.v. Current practices in disability grading and monitoring. 2009 [cited 2010 7th July]; Lacture notes]. Available from: http://www.ilep.org.uk/fileadmin/uploads/Documents/WHO_TAG_Meetings/Informal_Consultations_G2D_and_Chemoprophylaxis/Current_Practices_in_G2D_Assessment_and_Monitoring.pdf.
34. The SALSA Collaboative Study Group. Ebenso, J.F., P. Melchior, H. Wexler, R. Shumin, C. Piefer, A. Premkumar, R. Benbow, C. Nicholls, P. Velema, J. Saunderson, P. Lehman, L. SALSA Beta Testing Package. 2004 Web page [cited 2010 9th July]; Available from: http://www.ilep.org.uk/fileadmin/uploads/Documents/Infolep_Documents/Salsa/Beta_Testing_Package_V1.0_S.pdf.
35. WHO’s Classification, T.a.S.T.C. and w.t.f.o.t.W.N.J.P.o.A.a.C.o. Disability. WORLD HEALTH ORGANIZATION
38 of 52
DISABILITY ASSESSMENT SCHEDULE 2.0. [Web site] 2009; Available from: http://www.unescap.org/stat/disability/census-ws/WHODAS-English.pdf.
36. (AAOS), D.b.t.I.f.W.H.a.t.A.A.o.O.S. DASH "Disabilities of the Arm, Shoulder and Hand." Outcome measure. 2009 [cited 2010 9th July]; Available from: http://www.dash.iwh.on.ca/.
37. Ozkan, T., et al., Surgical reconstruction of irreversible ulnar nerve paralysis in leprosy. Leprosy Review, 2003. 74(1): p. 53-62.
38. Taylor, N.L., et al., The correction of ulnar claw fingers: a follow-up study comparing the extensor-to-flexor with the palmaris longus 4-tailed tendon transfer in patients with leprosy. Journal of Hand Surgery - American Volume, 2004. 29(4): p. 595-604.
39. Moberg, E.G., S., Emergency Surgery of the Hand. 1967, Edinburgh and London: E & S Livingstone Ltd.
40. Roy, C., N.C. Nath, and S.R. Saha, Reconstructive surgery in upper limbs in leprosy. Journal of the Indian Medical Association, 2004. 102(12): p. 702-3.
41. Malaviya, G.N., Comparative evaluation of effectiveness of different motor muscles in modified lasso procedure for correction of finger clawing. Journal of Hand Surgery - British Volume, 2003. 28(6): p. 597-601.
42. Sundararaj, G.D. and K. Mani, Surgical reconstruction of the hand with triple nerve palsy. Journal of Bone and Joint Surgery Series B, 1984. 66(2): p. 260-264.
43. McEvitt, E. and R. Schwarz, Tendon transfer for triple nerve paralysis of the hand in leprosy. Leprosy Review, 2002. 73(4): p. 319-25.
44. Brandsma, J.W. and T. Lijftogt, Timing of tendon-transfer surgery. Leprosy Review, 1983. 54(2): p. 109-114.
45. Reinar Liv, M., et al., Interventions for skin changes caused by nerve damage in leprosy. Cochrane Database of Systematic Reviews: Reviews, 2008(3).
46. Palande, D., Correction of paralytic claw finger in leproy by capsulorrhaphy and pully advancement. Journal of Bone and Joint Surgery Series A, 1976. 58A(1): p. 59-66.
47. Brandsma, W., Claw finger correction; Results of extensor flexor many tailed opperation. The Hand, 1982. 14(3): p. 307-312.
48. Brand, P.W., Tendon Grafting. The Journal of Bone and Joint Surgery, 1961. 43B(3): p. 444-453.
49. Brand, W., P., Paralytic claw hand. The Jounal of Bone and Joint Surgery, 1958. 40B(4): p. 618-632.
50. Rath, S., et al., A randomized clinical trial comparing immediate active motion with immobilization after tendon transfer for claw deformity. The Journal of hand surgery, 2009. 34(3): p. 488-94, 494.el-5.
51. Schwarz, R.J. and M. Macdonald, Assessment of results of opponensplasty. Journal of Hand Surgery - British Volume, 2003. 28(6): p. 593-6.
52. Patond, K.R., B.D. Betal, and V. Gautam, Results of thumb correction in leprosy using different techniques. Indian Journal of Leprosy, 1999. 71(2): p. 155-66.
53. Mehta, R., et al., Single tendon-two insertion versus two tendon transfers for reablement of ulnar-median palsied thumb in leprosy. Acta leprologica, 1996. 10(2): p. 105-109.
54. Anderson, G.A., V. Lee, and G.D. Sundararaj, Opponensplasty by extensor indicis and flexor digitorum superficialis tendon transfer. Journal of Hand Surgery - British Volume, 1992. 17(6): p. 611-4.
39 of 52
55. Brandsma, J.W. and M.W. Ottenhoff-De Jonge, Flexor digitorum superficialis tendon transfer for intrinsic replacement. Long-term results and the effect on donor fingers. Journal of Hand Surgery - British Volume, 1992. 17(6): p. 625-8.
56. Brandsma, J.W. and P.W. Brand, Median nerve function after tendon transfer for ulnar paralysis. Journal of Hand Surgery - British Volume, 1985. 10(1): p. 30-2.
57. Malaviya, G.N., Unfavourable results after surgical correction of claw fingers in leprosy. Indian Journal of Leprosy, 1997. 69(1): p. 43-52.
58. Malaviya, G.N., Some more about unfavourable results after corrective surgery as seen in leprosy. Indian Journal of Leprosy, 2002. 74(3): p. 243-257.
59. Malaviya, G.N., Median nerve palsy following claw finger correction in leprosy: Effect of M. Leprae or a consequence of surgery. Indian Journal of Leprosy, 2002. 74(3): p. 217-220.
60. Virmond, M. and H. Da Rosa Pereira, Surgical correction of deformities and disabilities in leprosy patients. Indian Journal of Leprosy, 2000. 72(3): p. 401-412.
61. Agrawal, A., et al., Leprosy, nerves, and surgery. Infectious Diseases in Clinical Practice, 2008. 16(6): p. 345-348.
62. Ganopol, J., M. Antola, and M.C. Ortiz, Neuropathy in leprosy: Results of surgical treatment. International Journal of Leprosy, 1979. 47(2 Sup).
63. Pereira, J.H., et al., Nerve repair by denatured muscle autografts promotes sustained sensory recovery in leprosy. Journal of Bone and Joint Surgery Series B, 2008. 90(2): p. 220-224.
64. Ozkan, T., K. Ozer, and A. Gulgonen, Restoration of sensibility in irreparable ulnar and median nerve lesions with use of sensory nerve transfer: long-term follow-up of 20 cases. Journal of Hand Surgery - American Volume, 2001. 26(1): p. 44-51.
65. CONSORT, G. The CONSORT statement. 2010 [cited 2010 17/8/10]; Web page]. Available from: http://www.consort-statement.org/consort-statement/overview0/.
40 of 52
London School of Hygiene & Tropical Medicine (University of London)
Combined Academic, Risk assessment and Ethics (CARE) approval form for MSc Project Reports
*This form must be completed electronically. For detailed guidance, please refer to the
Project Handbook for your course.
SECTION 1 – STUDENT AND COURSE INFORMATION
MSc DETAILS AND DEADLINES (deadlines to be communicated by Course Director)
Academic Year 2009-10
MSc course (and stream, where applicable) TMIH
Deadline for Supervisor approval Friday 28th May 2010
Deadline for Course Director approval Friday 28th May 2010
Deadline for submission to Ethics Committee Friday 30 April 2010
Target for approved form to be passed to TSO Friday 28th May 2010
STUDENT, SUPERVISOR AND TUTOR DETAILS (to be completed by student)
Full name of student
Student email address
Year of study (part-time students
only)
First Year Second Year
Supervisor name
Professor Dianna Lockwood
Supervisor email address [email protected]
Supervisor status (at time of this
version of the form being completed)
Confirmed Provisional Still to be
identified
Name of personal tutor (where
Supervisor is still to be identified)
SECTION 2 – APPROVAL AND SUBMISSION STATUS
*Students please note: It is a requirement of your LSHTM degree that you obtain all
required approvals before beginning your project work. To comply with legal requirements,
your Supervisor and Course Director must specifically give Risk Assessment approval. Ethical
approval must also be obtained if required (answers in Section 5 will help determine if so).
STUDENT DECLARATION (to be completed for all projects)
I agree to conduct my project on the basis set out in this form, and to
consult staff (initially, my Supervisor) if making any subsequent changes –
especially any that would affect the information given with respect to
ethics approval.
I agree to comply with the relevant safety requirements, and will submit a
separate request for LSHTM travel insurance where relevant.
*Where seeking ethical approval for a study involving human subjects, please also attach
41 of 52
copies of any information sheets, consent forms, and other relevant documents.
Date of declaration 30/04/10
*Further note: when submitting your final project report at the end of the summer, you
should also include a copy of your approved CARE form (which will be seen by the project
markers); but to preserve anonymity, the page above – with your name – should be omitted.
42 of 52
STAFF APPROVAL
*Staff please note: Sections 3 and 4 of the form should be completed by the student before
you are asked to sign. If you tick ‘no’ to any of the ‘Yes/No’ questions below, or disagree with
any of the statements given, or have any other concerns, then you should not give approval –
instead, please contact the student immediately to inform them of your concerns and discuss
changes which they may need to make before you may be willing to give approval.
*Supervisors and Course Directors should also be aware that in the exceptional case of a
request to undertake a project in a country or region to which the Foreign & Commonwealth
Office advise against travel, the student would need to fill out a separate form which will then
need further School-level approval by the Safety Manager and Secretary & Registrar.
SUPERVISOR’S APPROVAL (required for all projects – this approval should be given first)
I agree that Section 3 of this form is a reasonable summary of the
proposed project.
Yes No
I agree that responses in Section 4 of this form address the main
risks connected with a project of this nature.
Yes No
Name of Supervisor (if not yet identified, personal
tutor or Course Director should approve)
Professor Dianna Lockwood
Date of approval 4/5/10
COURSE DIRECTOR’S APPROVAL (required for all projects – should follow Supervisor approval)
I agree that the academic content of the proposed project, set out at
Section 3 of this form, is suitable for this MSc.
Yes No
I agree that responses in Section 4 of this form address the main
risks connected with a project of this nature.
Yes No
Name of Course Director (or nominee) Robin Bailey
Date of approval 5/5/10
DEPARTMENTAL SAFETY SUPERVISOR’S APPROVAL (only required if project involves working
with pathogenic organisms, human blood or radiochemicals – should follow Supervisor approval)
I agree that the proposed project, as set out in this form and
particularly Section 4, may proceed.
Yes No
Name of Departmental Safety Supervisor (or
nominee)
Michael Smith
Date of approval 4/5/10
ETHICAL APPROVAL (required for all projects involving human subjects or human data, except for
public domain data that cannot enable the identification of living people – NB that Supervisor approval must have been received before the application is submitted to the Ethics Committee)
Date application received 4/6/10
Ethics Committee application number assigned 009/438
On behalf of the Ethics Committee, I approve the project
proposal set out on this form.
Yes No
Name of Ethics Committee scrutineer Paula Elliott
Date of approval 4/6/10
43 of 52
SECTION 3 – APPLICATION FOR ACADEMIC APPROVAL
*All students should complete all sub-sections (3.1, 3.2 and 3.3); if particular questions
are not applicable to you then please write ‘N/A’.
3.1 PROJECT OUTLINE (should not normally exceed 750 words total)
Proposed project title: (should not normally exceed 20 words)
To undertake a literature search looking at long term follow up and out comes of Leprosy
affected patients who have undergone reconstructive hand surgery for nerve paralysis in
the upper limb. Combined with this I will undertake an audit of hand surgery occurring in
Leprosy affected patients in Anandaban Hospital Nepal. From this work I will put
together a project proposal for a follow up study of reconstructive plastic surgery in
patients with Leprosy in Nepal and their long term out comes.
Proposed project type:
*See course-specific section of Project Handbook for details of project types permitted
for each MSc. Be aware that restrictions may apply for individual courses.
A paper describing a piece of research work carried out by the student during the course including a comprehensive and original review of the literature on the relevant subject and culminating in a proposal for a longer term project.
Proposed project length:
*For almost all students, this will be ‘Standard’. Long and extended projects are only
available for certain ITD courses; they have a different schedule and allow a slightly
greater word count.
Standard Long Extended
Background: (about 200 words)
*Indicate why this topic is of interest or relevance.
*If the project involves work with a specific organisation please give details.
*Please give any other details specifically relevant for consideration by the Ethics
Committee, e.g. related to purpose.
I intend to conduct a systematic review of the current literature on long term outcomes
of Leprosy patients having undergone reconstructive hand surgery for upper limb nerve
palsies. Through this I will high light the need for further research to be conducted in
this area. I will combine with this an audit of the presentation; operations performed and
follow up of patients having undergone reconstructive hand surgery second to Leprosy at
Anandaban Hospital Nepal over a five-year period. This will generate new data on
surgical practice and need with in this region. I will then put forward a proposal for a
larger long term follow up study on outcomes of patients who have undergone
reconstructive hand surgery in Nepal. This will add to the data set on functional status
and resulting disability experienced by these patients in the years post operatively.
Hypothesis: (about 30 words, where applicable)
Overall aim of project: (about 30 words)
To identify the operable upper limb nerve palsies that are presenting to a Leprosy
hospital in Nepal and are undergoing surgery, and to review the literature on out comes
and follow up of post operative reconstructive hand surgery patients with Leprosy. From
this work I intend to propose a longer term follow up study to look at function and
disability in post surgical Leprosy patients in Nepal.
Specific objectives of project: (about 70 words)
To investigate the current literature on the functional out comes disability and follow up
44 of 52
of leprosy affected patients who have undergo reconstructive surgery in the hand to
correct upper limb nerve palsies. Using patient notes I will then conduct an audit on the
current presentation and operations performed for hand palsies second to Leprosy at a
Leprosy Hospital in Nepal in an attempt to identify the type of operations being
performed and the surgical need in this resource poor setting.
I then intend on proposing a long term follow up study of patients in Nepal who undergo
surgery and their functional out comes and disability at 5 years. My intention is to
provide evidence as to where the allocation of scarce plastic surgical resources may be
best directed in Nepal’s Leprosy care facilities.
Proposed methods: (about 200 words)
*Please summarise methods, and include any relevant details for consideration by
the Ethics Committee such as numbers of participants and procedures to be
performed.
The systematic literature review shall be conducted at the LSHTM and from my home
(London). I will use the library and on line data resources to comprehensively cover all
published and other resources (such as gray literature) to the best of my ability ensuring
an encompassing over view of the subject.
The audit on presentation and operation performed on patients with upper limb nerve
palsies second to Leprosy will be conducted at Anandaban Leprosy Hospital Nepal. All
data collected will be anonymised and collected on a secure encrypted data spread
sheet. Any demographic or data that could identify a patient will be remove from the
data set. I will ensure that I have received ethics approval from the LSHTM and from the
Nepal ethics committee before any data collection occurs. The number of patient notes
used will vary dependent on the number of operations performed over the last five years
but I estimate of about 250 notes will be used. I will endeavour to ensure that my
activates are as a minimal a disruption to the notes department at Anandaban hospital
as possible. The writing up and further project proposal aspect of my summer project
will occur back in the UK. When proposing my further research I will take in to
consideration the constrains sensitivities and ethics that are appropriate for conducting
research in Nepal. I aim to propose a project that will be of scientific value not only to
Anandaban Hospital but to all those providing surgical care to Leprosy patients in
resource poor settings.
References: (max 150 words)
*List any key references which will shape the project, including for methods to be used.
It should not normally be necessary to quote more than 5 references.
The role of surgery in leprosy rehabilitation - a general overview.
Antia N.H. International Journal of Leprosy. 47(2 Sup.)(pp X 316), 1979.
Incidence of acute nerve function impairment and reactions in Leprosy: a
prospective cohort analysis after 5 years of follow up. Richards J. H,
Nicholls P. G, Croft R. P, Withington S. G, Smith W. C. S. International Journal of
Epidemiology 2004;33:337-343.
Reconstructive surgery in upper limbs in Leprosy. Roy C, Nath N. C, Saha S.
R. Journal of the Indian Medical Association. 102(12):702-3, 2004 Dec.
Leprosy Britton J. W, Lockwood D. N. J. The Lancet 2004;363:1209-19.
Leprosy. A disease of the Schwann cell. Leprosy In India. 54(4)(pp 599-604),
1982. Date of Publication: 1982.
Prior work: (only where relevant; max 100 words)
*Indicate any previous work you have done related to this project topic, including
student work, professional work, or publications.
I have spent a week assisting a visiting consultant plastic surgeon at Anandaban Hospital
Nepal. I am familiar with the staff and hospital setting there all though I have not
conducted any research at this site before.
45 of 52
3.2 FEASIBILITY (about 100 words total – but can write more or write less if
appropriate)
What could cause this project to fail, i.e. prevent you from achieving your
objectives?
*Please indicate any aspects of your proposed approach which could potentially
experience difficulties, e.g. delays with permissions, data collection or storage problems,
lack of sufficient comparable information, etc. You may also wish to mention any wider
matters which could affect your project, e.g. civil unrest, natural disasters, transport
availability.
Difficulties in gaining ethical consent.
Political difficulties in Nepal preventing travel to the country.
Aeronautical restrictions (such as volcanic ash) preventing travel.
Difficulties in travel with in the country due to strikes, road conditions, weather
(monsoon season) etc.
Difficulties in identifying adequate patient notes for audit purposes.
Language difficulties and problems with translation.
What alternative plans do you have in case you encounter any of the potential
problems you have identified?
If difficulties that are insurmountable are met then a more extensive and broad
systematic literature search on surgery in Leprosy affected patients will be conducted.
3.3 INTELLECTUAL PROPERTY, COPYRIGHT AND OTHER PERMISSIONS
*Please also see Section 5.2 regarding any specific data rights limitations arising from
local ethical or research governance requirements
If you expect to use existing data, how will you obtain it and what permissions
will be required?
N/A
Having considered whether intellectual property rights (IPR) or copyright
issues may affect your project, will any specific agreements be required?
*Please tick all boxes that apply, and attach copies of any forms/agreements (even if in
draft).
No specific IPR, Copyright or permissions issues should apply to this project (student
retains Copyright and related IPR by default, in line with LSHTM registration
declaration)
IPR to be retained by LSHTM (specific LSHTM form to be completed)
Copyright to be transferred to LSHTM (specific LSHTM form to be completed)
IPR, Copyright or other agreements/permissions required with external
parties/organisations
Please give any further relevant details about IPR, copyright or other
permissions.
SECTION 4 – APPLICATION FOR RISK ASSESSMENT APPROVAL
*All students should answer all questions in sub-section 4.1; this will make clear which
of the following sub-sections you need to complete.
Ensuring safety during project work is the responsibility of each individual
46 of 52
student, and not of LSHTM or LSHTM staff. *Please see the Project Handbook for
further guidance.
4.1 TYPE OF RISK (to be completed by all students)
Where will the project be carried out? (please tick all that apply)
*Note that work away from LSHTM or outside the UK means any form of work for your
project, not just primary data collection. Some courses may have specific restrictions on
this.
All work will take place either at LSHTM, in libraries in the UK, or at my
personal residence in the UK. [If so, you do not need to complete either section 4.2
or section 4.3]
Some work will take place in the UK that is away from LSHTM sites in
London, is non-Library-based, and is not at my personal residence. [If so, section
4.2 on ‘Work away from LSHTM’ must be completed]
Some work will take place at my personal residence outside the UK [If so,
section 4.3 on ‘Work outside the UK’ must be completed]
Some work will take place outside the UK that is not at my personal
residence [If so, both sections 4.2 and 4.3 on ‘Work away from LSHTM’ and ‘Work
outside the UK’ must be completed]
Will the project involve working with or handling any of the following
materials?
Pathogenic organisms Yes No
Human blood Yes No
Radiochemicals Yes No
[If ‘Yes’ to any of the above, Sections 4.4 and 4.5 must be completed]
Are any other potentially hazardous activities likely to be carried out during the
project?
Yes No
[If ‘Yes’, Section 4.5 must be completed]
Do any special requirements (e.g. disability-related issues) or other concerns
need to be taken into account for either you as a student, study participants or
colleagues?
Yes No
[If ‘Yes’, Section 4.6 must be completed]
4.2 WORK AWAY FROM LSHTM (to be completed if any work will be done away from
LSHTM, other than at your home or at libraries elsewhere in the UK)
Will the project be based in an established hospital, college,
research institute, NGO headquarters, field station or other
institutional site? If ‘Yes’, please give the name and location of the
site(s); describe approximately what proportions of your project will be
spent there; and state name and role of person who has confirmed
willingness to support you at each site (indicating extent of
correspondence, especially what they have confirmed in writing).
Yes
No
Anandaban Leprosy Hospital, PO Box 151, Kathmandu, Nepal. Between 2-4 weeks will
be spent at the hospital and it will be the primary site for data collection. Dr Indra Napit/
Deanna Hagge have been contacted via email and I have met in person on a previous
visit to Nepal.
Will you have an ‘external supervisor’, co-supervisor or other Yes
47 of 52
main advisor, or be working with any specific organisation(s),
during your work away from LSHTM? If ‘Yes’, please indicate the
name, role, contact details, and level of support that any such external
advisors are expected to provide, and give details about any
organisations you will be working with.
No
Advisory and support role; Mr D Sammut (Consultant Plastic Surgeon specialist in Hand
surgery) The Hand Clinic Oakley Green Windsor SL4 4LHb England. Tel: 01753832109. [email protected]
Will the project involve personal visits, interviews or interactions
with people in their homes, workplaces, community settings or
similar? If ‘Yes’, please give details, including approximately what
proportion of your project this will involve.
Yes
No
Will the project involve lone/isolated work or significant travel? If
‘Yes’, please give details, including approximately what proportion of your
project this will involve, and state how you can be contacted while
working or travelling.
Yes
No
International flight London to Nepal. Accompanied travel to Anandaban Hospital (aprox 1
hr car ride). Can be reached by email and by phone during this time.
What arrangements are proposed for contact with your main supervisor while
you are away from LSHTM? Indicate expected ease and frequency of contact, and
communication methods to be used.
Email and phone which can be achieved with relative ease.
Please tick to
confirm:
I have read the LSHTM Code of Practice on off-site
work.
4.3 WORK OUTSIDE THE UK (to be completed if any work will be done outside the UK)
What form of project work will be undertaken outside the UK? (please tick all that
apply)
Work at my family home or personal residence only
Work at an established hospital, college, research institute, NGO
headquarters, field station or other institutional site
Work away from my personal residence or an established site
*Note that for either the second or third options, you should also have completed
Section 4.2.
Name the country/countries and region(s) in which work will be undertaken:
Country or countries: Nepal Region(s) : Kathmandu Valley
Do the Foreign & Commonwealth Office’s (FCO) Travel Advice
Notices (www.fco.gov.uk/en/travelling-and-living-overseas/travel-
advice-by-country/) advise against travel to the regions(s), country
or countries involved?
*Note that if ‘Yes’, the School will not normally permit such travel for project work. In exceptional circumstances only, requests may be considered by the Safety Committee and require approval by the Safety Manager and Secretary & Registrar.
Yes
No
Please tick to confirm: I understand that LSHTM travel insurance is
required for any international travel as part of my
project.
48 of 52
*Travel insurance can be applied for using a separate form.
4.4 WORK WITH HAZARDOUS SUBSTANCES (to be completed if the project involves
any work with pathogenic organisms, human blood or radiochemicals – NB that this will
require approval by the Departmental Safety Supervisor)
Name the organism or organisms to be used:
N/A
Identify all potential routes of infection:
N/A
Name the radiochemical or radiochemicals to be used:
N/A
List laboratories where work with pathogens or radioisotopes will be carried
out:
N/A
List disinfectants to be used, and describe arrangements for disposal of used
material:
N/A
Will or might Health Surveillance be required for you or any staff
working with you? If ‘Yes’, please give details.
Yes
No
N/A
4.5 PRECAUTIONS AGAINST HAZARDS (to be completed if any potentially hazardous
activities are likely to be carried out during the project. Refer to Project Handbook and
School safety documentation for further information. Departmental Safety Supervisor’s
approval should be obtained where felt appropriate by project Supervisor.)
Indicate any procedures, activities or aspects of the proposed project which
may entail hazards (including work with hazardous substances as per Section
4.4, or anything else relevant). Please set distinct hazards out separately, in a
numbered list.
N/A
Indicate the precautions you will take to prevent or mitigate such potential
hazards. Please number these to refer to the specific hazards identified in the preceding
question.
N/A
4.6 SPECIAL REQUIREMENTS (to be completed if the project involves any special
requirements, e.g. disability-related issues, or other concerns that need to be taken into
account for either you as a student, study participants or colleagues)
What special requirements or concerns need to be taken into account?
N/A
Do these need to be considered in planning arrangements?
If ‘Yes’, please give details.
Yes
No
N/A
Do these impact on supervision arrangements? Yes
No
49 of 52
If ‘Yes’, please give details.
N/A
Does the project location need to be considered in relation to
these?
If ‘Yes’, please give details.
Yes
No
N/A
Do arrangements for access to specialist medical treatment need
to be considered?
If ‘Yes’, please give details.
Yes
No
N/A
SECTION 5 – APPLICATION FOR ETHICS APPROVAL
*All students should answer all questions in sub-sections 5.1 and 5.2. Answers to
5.1 will make clear whether approval by the LSHTM Ethics Committee is necessary, and
which later sub-sections you may need to complete. Section 5.2 covers any external
approvals required.
5.1 SCOPE OF STUDY (to be completed by all students)
*Before completing this part of the form, please read the Ethics Approval Policy &
Procedure plus guidance notes at http://intra.lshtm.ac.uk/reference/ethicsstuds.html .
This describes what to do next if formal LSHTM ethics approval is required. NB that
supervisor approval must be obtained before an application is submitted to the Ethics
Committee.
Which of the following applies to your project? (please tick one option only)
*Note – the term ‘human data’ includes any documentary data, datasets or biological
samples.
Project does not involve any human subjects or any human data. [If so, formal
LSHTM ethics approval is not required and you do not need to complete Sections 5.3 or
5.4]
Project involves human data, but all this human data is fully in the public
domain. [If so, formal LSHTM ethics approval is not required and you do not need to
complete Sections 5.3 or 5.4]
*Public domain human data must be: available to any member of the public without
special permission; to which access is not restricted in any way; and which does not
enable the identification of living people, either directly or by linking to other data.
Project involves some non-public-domain human data, all of which was
previously collected in another study or studies. [If so, formal LSHTM ethics
approval is required and Section 5.3 must be completed]
Project involves some additional collection of data, further to an ongoing or
previously completed study or studies. [If so, formal LSHTM ethics approval is
required and Section 5.4 must be completed]
Project is a completely new study which will involve human subjects or
human data. [If so, formal LSHTM ethics approval is required and Section 5.4 must be
completed]
5.2 LOCAL ETHICAL APPROVAL OR RESEARCH GOVERNANCE APPROVAL (to be
completed by all students)
* As well as approval from the LSHTM Ethics Committee, projects may require specific
50 of 52
approval from other involved or responsible bodies. For example, in the UK you may
need specific authorisation to work in an NHS facility, or to work with vulnerable groups
such as patients or children. Outside the UK a wide range of requirements may apply
e.g. from local or national Ethics Committees, government departments etc. Students
must investigate all potential local approval required for your project work.
Failure to check or gain any necessary external approval may invalidate LSHTM
approval.
Is local approval required for the work being done (whether this
approval is still to be obtained, or has already been granted)?
*This should include any forms of ethical approval, research governance
approval or other specific permissions that may apply.
Yes
No
If ‘Yes’, give details of local approval to be obtained (this must be in place
before commencing fieldwork) or which has already been granted.
*Please name all bodies whose approval is required, or indicate where work is expected
to take place using permissions already granted for a ‘parent’ project. Where approval
has already been granted, quote approval reference numbers and if possible give web
links to documents.
If ‘No’, explain why formal local approval is not required, and describe any less
formal permissions, invitations or support you are being given for this work.
*If you will be working away from LSHTM with human subjects or human data, but
cannot identify a local Ethics Committee or believe that no formal approval is required,
then please give details and explain what you have done to check this. In such cases, if
you do not have formal approval you should always demonstrate appropriate local
support, such as correspondence with local government officials or an involved Non-
Governmental Organisation.
Nepal research council ethics approval.
For data to be used or collected in the project, will any specific
data rights permissions be required or usage limitations apply?
Yes
No
5.3 PROJECTS USING ONLY PREVIOUSLY-COLLECTED HUMAN DATA (to be
completed if project involves non-public-domain human data, datasets or biological
samples previously collected in another study or studies; if collecting any new data,
complete Section 5.4 instead)
*Further guidance is given at http://intra.lshtm.ac.uk/reference/ethicsstuds.html
Summary of purpose and methods of the original study or studies: (max 100
words)
N/A
Give details of all approvals under which the original study or studies took
place:
*Please quote names of Ethics Committees and approval reference numbers (required if
previous approval was from LSHTM); if possible give web link to original study
application.
N/A
Proposed study: Ensure that the project outline given in Section 3.1 states the
purpose, methods and procedures of the new work to be done in your project,
and describes how this builds on the previous study or studies (for which
participants will already have been recruited, data or samples collected, and
procedures performed). Do not reproduce here.
51 of 52
Will your analyses be for purposes not covered by the original
application detailed above? If ‘Yes’, indicate how you will obtain (i)
permission to use the data from the principal investigator responsible for
each original study; and (ii) retrospective consent, where appropriate,
from the participants in each original study.
Yes
No
N/A
Does the project involve analysis of documentary information
and/or data already collected from or about human subjects? If
‘Yes’, specify analyses briefly.
Yes
No
N/A
Does the project involve laboratory analysis of human biological
samples already collected, or new or additional analysis of stored
samples? If ‘Yes’, specify the laboratory analyses or tests to be
performed.
Yes
No
N/A
Specify how confidentiality will be maintained. When small numbers are
involved, indicate how possible identification of individuals will be avoided.
N/A
5.4 PROJECTS COLLECTING ANY NEW HUMAN DATA (to be completed if project
involves collection of human data, datasets or human biological samples – either as a
completely new study, or collecting additional data further to an ongoing or previously
completed study)
*Further guidance is given at http://intra.lshtm.ac.uk/reference/ethicsstuds.html
Proposed study: Ensure that the project outline given in Section 3.1 contains
sufficient detail (inc. purpose, methods, procedures for both new data collection
and any work building on previous studies), so as to allow the Ethics Committee
to make an informed decision without reference to other documents. Do not
reproduce here.
Is your project a randomised trial? Yes
No
Will any human biological samples be collected? If ‘Yes’, specify
details.
Yes
No
Will any human biological material be stored at LSHTM for more
than 24 hours? If ‘Yes’, specify which samples and how they will be
stored.
*Further guidance is given at
http://intra.lshtm.ac.uk/safety/Safety%20manual-3-HTA.pdf
Yes
No
Specify the number - with scientific justification for sample size – age, gender,
source and method of recruiting subjects for the study.
Audit of approximately 250 patients medical notes (last 5 years of operations notes) to
form an anonymised data set for analysis.
State the location and likely duration of new or additional human data
collection, and the extent to which this will be carried out by you alone, or in
collaboration with others, or by others.
52 of 52
Location of data collection is Anandaban Hospital Nepal. Data collection will take
approximately 2-4 weeks conducted by me alone with assistance from the records
department at the hospital.
State the potential distress, discomfort or hazards, and their likelihood, to
which research subjects may be exposed (these may include physical,
biological and/or psychological hazards). What precautions are being taken to
control and modify these hazards?
Medical notes will be used and data anonymised to ensure that no distress could occur to
patients whose notes are used in the study.
Specify how confidentiality will be maintained. When small numbers are
involved, indicate how possible identification of individuals will be avoided.
The numbers I am planning to collect will help maintain confidentiality I will also only be
collecting minimal demographics such as age gender type of leprosy, presence and type of
nerve palsy, and operation conducted. The data will be stored in a secure encrypted data
base and any specifics that may identify a patient will be omitted from the audit to ensure
confidentiality.
State the manner in which consent will be obtained from subjects and supply
copies of the information sheet and consent form.
Written consent is normally required. Where not possible, explain why and confirm
that a record of those giving verbal consent will be kept.
Where appropriate, please state if and how the information and consent form will be
translated into local language(s).
Consent from patients not required as collecting data for audit purpose.
As well as collecting new data, will your project also make use of
any human data or biological samples collected in a previous study
or studies? If ‘Yes’, summarise the purpose and methods of the original
study or studies – for which participants will already have been recruited,
data or samples collected, and procedures performed. (max 100 words)
Yes
No
Related Documents











