LOCALIZED FIBROUS TUMOR OF PLEURA GENERAL THRACIC SURGERY CHAPTER 64

LOCALIZED FIBROUS TUMOR OF PLEURA GENERAL THRACIC SURGERY CHAPTER 64.
Dec 15, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

LOCALIZED FIBROUS TUMOR OF PLEURA
GENERAL THRACIC SURGERY
CHAPTER 64

Localized fibrous tumor
• Previous name— Localized mesothelioma of pleura, benign or malignant.
• Scharifker and Kaneko— Cell origin of these tumor is noncommitted mesenchymal cell present in the areolar tissue subjacent to the mesothelial lining of the pleura, not from mesothelial cell of pleura.
• Malignant variety— Localized malignant fibrous tumor of the pleura.
Benign localized fibrous tumor of the pleura
• From visceral pleura. • On a stalk, project into pleural space. • May inward growth into lung parenchyma. • Occasionally within fissure. • May from mediastinal, diaphragm, costal
portion of parietal pleura— Often malignant. • Solitary, ovoid round.
Benign localized fibrous tumor of the pleura
• Histology— Fibroblastlike cell and connective tissue.
• Lack keratin reactivity and positive CD34 antigen– Differentiates fibrous tumor from mesothelioma.
• Table 64-1.

Benign localized fibrous tumor of the pleura– Clinical feature
• Equal frequency in both sex.
• Common in 5th to 8th decades.
• Half asymptomatic,
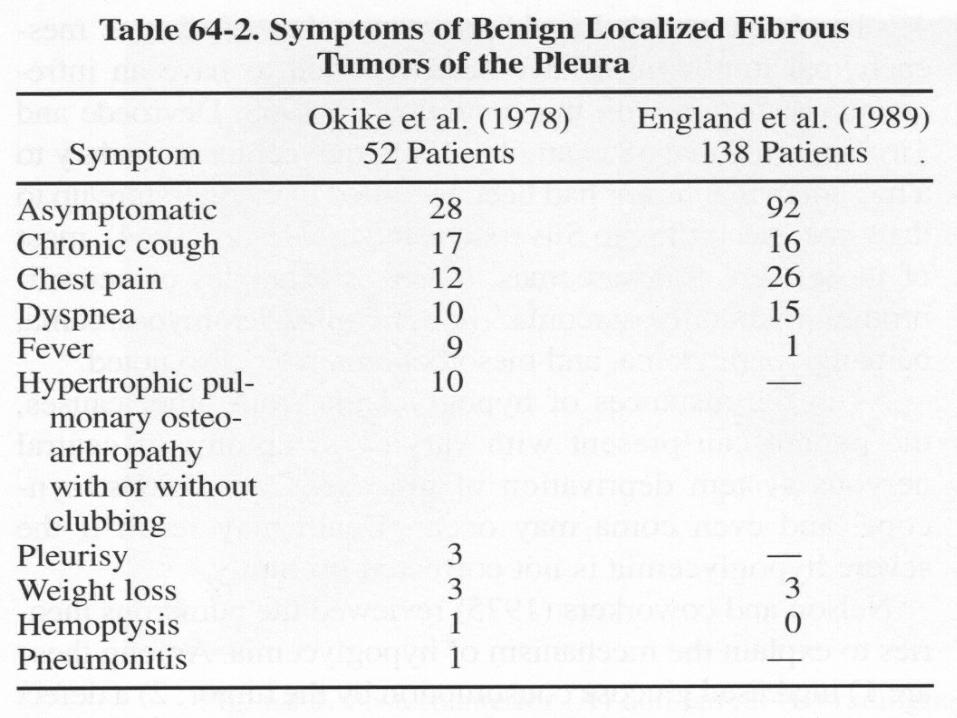
• Chronic cough, chest pain, dyspnea. Table 64-2.
• Chest pain – Most lesion arise from parietal pleura.

Benign localized fibrous tumor of the pleura– Clinical feature
• Hypertrophic pulmonary osteoarthropathy (20%)– Stiffness of the joint, edema of ankle, arthralgia, pain of long bone (especially the tibia).
• Gynecomastia. • Clubbing finger. • Hypoglycemia (3-4%)– Tumor production insulin
like growth factors or somatomedins. • Galactorrhea.
Benign localized fibrous tumor of the pleura
• Radiographic features—
Circumscribed mass of varying size.
Located in the lung periphery.
Margin sharply defined.
Movable with change position.

Benign localized fibrous tumor of the pleura
• Diagnosis—
Fine needle aspiration.
Biopsy.
Benign localized fibrous tumor of the pleura – Treatment
• Surgical resection.
• Lesion within parenchyma– Lung resection.
• Tumor within fissure – Bilobectomy.
• Tumor located in mediastinum, diaphragm, parietal pleura – Should be excised widely – Because of associated malignancy.
Benign localized fibrous tumor of the pleura
• Prognosis— Cured by adequate excision.
• Recurrence – 2%.

Malignant localized fibrous tumor of the pleura
• Incidence—12%. • Gross feature – Table 64-3. • Clinical features— 3/4 have symptoms:
Chest pain, cough, dyspnea, fever, osteoarthropathy (rarely), hypoglycemia (11%).
• Radiographic features— Tumor more large, pleural effusion (32%), rib erosion.


Malignant localized fibrous tumor of the pleura
• Diagnosis—Most until the histologic examination. • Treatmen—Wide local excision, pulmonary and
pleural excision, from parietal pleura should be resected with chest wall, post-operative radiotherapy and chemotherapy.
• Prognosis—45% long term survival, chest wall invasion or pleural effuison are poor prognostic feature.
• Recurrence– Less than 5 years.
Related Documents


![Solitary Fibrous Tumor of the Pleura: Histology, CT Scan Images … · 2019. 1. 6. · Solitary fibrous tumor of the pleura is a rare neoplasm. In Literature up to 800 cases [1-3]](https://static.cupdf.com/doc/110x72/6081a8834487a75fc349fbe2/solitary-fibrous-tumor-of-the-pleura-histology-ct-scan-images-2019-1-6-solitary.jpg)








