LOCALIZATION OF CNS LESIONS RABIA SALEEM SAFDAR Postgraduate trainee Pediatrics Unit I 05/06/2022 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

05/03/20231
LOCALIZATION OF CNS LESIONS
RABIA SALEEM SAFDARPostgraduate trainee
Pediatrics Unit I

05/03/20232
APPROACH TO LOCALIZE THE LESION
History General physical examination Neurological examination

05/03/20233
HISTORY Biodata of Patient(name,age,sex,address) Chief complaint Quality of symptoms Mode of onset Course since onset Frequency of symptoms Severity of symptoms Precipitating factors if any Ameliorating factors like medications Pevious diagnostic evaluation

05/03/20234
HISTORY Prior medical history Natal perinatal and postnatal history Developmental milestones Immunization Trauma Surgery previously done Previously or present medications used Any bleeding disorder Previous history of any neurological problem Previous infection especially involving CNS

05/03/20235
HISTORY Family History Family tree Consanguinty Relatives having similar problems Age and state of health of living relatives Age and cuase of death of deceased relatives

05/03/20236
HISTORY Socioeconomic status
History of contact of TB
History of measels
History of travelling

05/03/20237
• Smell• Visual defect• Diplopia• Ptosis• Hearing disturbance• Vertigo, Lightheadedness• Swallowing difficulty• Speech disturbance• Sleep disturbance
• Involuntary movement• Weakness• Gait disturbance• Incoordination• Muscle atrophy• Tremor• Muscle Cramps• Bladder/bowel control• Weight change
• Pain• Numbness• Paresthesia/ aneasthesia• Headache• Seizure/syncope• Memory• Behavior/Mood change• Aphasia
SYSTEMIC INQUIRY RELEVANT TO CNS

05/03/20238
General physical examination
Involves review of systems Skin Eyes ear nose throat Respiratory Cardivascular Gastrointestinal Musculoskeletal Endocrinology Psychiatric

05/03/20239
NEUROLOGICAL EXAMINATION Higher mental functions Systemic review►Cranial Nerve examination
► Sensory system►Pyramidal System
► Extrapyramidal System ► Cerebellum ► Evaluation of Speech and Language

05/03/202310
HIGHER MENTAL FUNCTIONS Appearance and behavior Level of Consciousness Orientation with time and space Intelligence level Memory Thought process Primitive reflexes

05/03/202311
HIGHER MENTAL FUNCTION
Level of Consciousness Level of consciousness implies awareness of surroundings. Consciousness is dependent on the normal functioning of the
reticular activating system, which originates in the pons and projects to the cortex of bilateral hemispheres via the thalamus.
The reticular activating system activates the cortex when one awakens and inhibits the cortex when in sleep.
The hypothalamus is also important in maintaining level of alertness.

05/03/202312
HIGHER MENTAL FUNCTION
Level of Consciousness During brain herniation,compression of the reticular
activating system may produce profound coma
Metabolic abnormalities such as hyperglycemia or drugs may produce coma by impairing neuronal function diffusely within the brain.

05/03/202313
Evaluation of a comatose patient
Evaluation of a comatose patient requires examination of four steps
Pupils and Fundoscopy Ocular movements Motor response to pain Pattern of breathing

05/03/202314
Evaluation of a comatose patient
Pupil Examination
Normal pupils are 3 – 4mm in diameter & equally bilaterally reactive,constrict briskly & symmetricallyin response to light

05/03/202315
PUPIL LESIONSlightly smaller but reactive Early stage of thalmic damageFixed dilated(7mm) pupil ( non- reactive)
Oculomotor nerve lesion
Fixed midsized pupils(5mm) Mid brain lesionPinpoint pupils(1-1.5mm) Pontine lesion,opioid overdoseAsymmetrical pupils Normal in 20 % of population
but reactive..If one pupil is sluggish to react than the other think mid brain or oculomotor lesion

05/03/202316
Evaluation of a comatose patient
FundoscopyTo see Papilledema:disc margins are blurred,colour of disc
is pink and hyperemic,congested veins
Optic atrophy: optic disc becomes pale

05/03/202317
Evaluation of a comatose patient
Ocular MovementsCheck when cervical trauma has been ruled out
Pathway tested: Medial longitudinal fasciculusControl centers : FRONTAL EYE FIELD PARAMEDIAN PONTINE RETICULAR FORMATIONTests performed1. Doll`s eye maneuver(oculocephalic reflex)2. Caloric test(irrigation with cold water)

05/03/202318

05/03/202319
LESION SYMPTOMS
RIGHT ABDUCENT Right eye cannot look right
RIGHT PPRF(paramedian pontine reticular formation)
Neither eye can look right
LEFT MEDIAL LONGITUDIONAL FASCICULUS
Internuclear ophthalmoplegia left eye cannot look right,Right eye has nystagmus
LEFT FRONTAL EYE FIELD
Neither eye can look right but slow drift towards left

05/03/202320
A patient has the appearance shown in the diagram below on attempted gaze to the right. All other ocular movements are normal. Where is the lesion?
The abducens nerve innervates the lateral rectus muscle and mediates lateral gaze. The inability to abduct the right eye suggests a lesion in the right abducens nerve.

05/03/202321
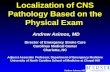
A patient has the appearance shown in the diagram below on attempted gaze to the left (A) or right (B). Convergence is normal. Where is the lesion?
BILATERAL MEDIAL LONGITUDIONAL FASCICULUS :The patient can abduct both eyes (lateral gaze is normal), but cannot adduct both eyes (medial gaze is impaired on voluntary eye movements). However, both oculomotor nuclei and nerves are intact since convergence is normal. Thus the lesion is in the medial longitudinal fasciculus (MLF), and information from the abducens nucleus is not reaching the oculomotor nucleus to mediate the medial component of voluntary conjugate gaze.

05/03/202322
Cold caloric testing andappropriate responses when the brainstem isintact (top) and when a pontine lesion is present(bottom) is demonstrated.
Cold water irrigation—nystagmus to opposite sideWarm water irrigation--- nystagmus to same sideCOWS----cold opposite,warm same

05/03/202323
Evaluation of a comatose patient
Motor response to pain
Look for lateralizing signs such as asymmetry of movement either spontaneously or to painful stimulation
Decorticate posturing is characterized by tonic flexion of the arms and extension of the legs and implies a lesion at the level of the midbrain
Decerebrate posturing is manifest as tonic adduction and extension of the arms and legs and suggests a lesion at the level of the pons.

05/03/202324
Decorticate posturing isillustrated on the left. Decerebrate posturingis on the right.

05/03/202325
Evaluation of a comatose patient
Respiratory patterns Cheyne-Stokes respiration:respiratory pattern of metabolic
disease.
Central neurogenic hyperventilation:manifest as rapid shallow breathing, indicates midbrain dysfunction.
Cluster or apneustic breathing:suggests pontine injury.
Ataxic, shallow breathing: results from medullary lesion.

05/03/202326
GLASGOW COMA SCALE(4-15Y)RESPONSE SCORE
EYE OPENING`Spontaneous 4To Speech 3To Painful Stimulus 2None 1
BEST MOTOR RESPONSEObeys Command 6 Localizes Pain 5Withdrawl 4Abnormal Flexion 3Extensor Repnse 2None 1
BEST VERBAL RESPONSEOriented 5Confused 4Inaappropriate words 3Incomprehensible words 2None 1

05/03/202327
GLASGOW COMA SCALE(<4y)RESPONSE SCORE
EYE OPENING`Spontaneous 4To Speech 3To Painful Stimulus 2None 1
BEST MOTOR RESPONSEObeys Command 6 Localizes Pain 5Withdrawl 4Abnormal Flexion 3Extensor Repnse 2None 1
BEST VERBAL RESPONSESmiles oriented to sounds,follows objects 5Crying interactcs 4
Consolable inappropriate 3 Inconsistently consolable Moaning 2
No response 1

05/03/202328
HIGHER MENTAL FUNCTIONS
Primitive reflexes
Primitive reflexes are automatic stereotypic movements directed from the brainstem and require no cortical involvement (thought).
Must be abated in order for proper neurological organization of the brain to develop.

05/03/202329
HIGHER MENTAL FUNCTIONS
Causes of retained Primitive Reflexes Children born via cesarean section Trauma Toxicity exposure Anesthetics Early walkers Head injuries Excessive falls Chronic ear infections

05/03/202330

05/03/202331

05/03/202332
CRANIAL NERVES

05/03/202333
CRANIAL NERVES 12 pairs of cranial nerves
3 Types
SENSORY I , II, VIII MOTOR III, IV, VI, XI, XII MIXED V,VII,IX,X

05/03/202334
FUNCTIONS OF CRANIAL NERVESNO NAME FUNCTION
I OLFACTORY SmellII OPTIC SightIII OCULOMOTOR Eye movements except lateral rectus and
sup.obliqueIV TROCHLEAR Superior obliqueV TRIGEMINAL Mastication,facial sensationsVI ABDUCENT Lateral rectusVII FACIAL Fascial movements taste ant 2/3rd of tongueVIII VESTIBULOCOCHLEAR Hearing,balance
XI GLOSSOPHARYNGEAL Taste from post.1/3rd of tongue,caritid bodyand baroreceptors,parotid,pharyngeal muscles
X VAGUS Taste from epiglottic area,swalloing,palate elevation,abd viscera
XI ACESSORY Head turning,shuolder shruggingXII HYPOGLOSSAL Tongue movements

05/03/202335
NUCLEI OF CRANIAL NERVES
CRANIAL NERVE NUCLEI LOCATION
I and II Directly goes to cerebral cortex
III,IV midbrain
V,VI,VII and VIII pons
IX,X,XI,XII medulla

05/03/202336
You are testing the blink reflex on your patient. When you touch a piece of cotton to the right eye, both eyelids close in a blink. When you touch the left eye, neither eye closes. Which of the following cranial nerves is involved in a lesion?
Left trigeminal. The trigeminal nerve (CN 5) is the afferent arm of the blink reflex (corneal reflex) and the facial nerve (CN 7) is the efferent arm. If there is a lesion of left CN 5, sensation of touching the cornea will not be conveyed centrally, and neither eye will blink.

05/03/202337

05/03/202338
Reflexes Afferent Efferent
Corneal V (i) VII
Jaw jerk V (iii) sensory V (iii) motor
Gag IX IX , X
pupillary II III
CRANIAL NERVE REFLEXES

05/03/202339
Direct & consensual light reflexes – Pathway

05/03/202340
Direct & consensual light reflexes – Pathway

05/03/202341
CRANIAL NERVES
Cornea or Conjunctiva ↓ Ophthalmic branch of the TGN ↓ Main sensory ganglion of the TGN ↓Internuncial neurons connect with the motor nucleus of the facial nerve on Both
sides (Through the medial longitudinal fasciculus) ↓ Facial nerve ↓ Orbicularis oculi of both sides ↓ Closure of the eyelids
Corneal reflex : Light touching of the cornea or conjunctive results in blinking of the eye lids

05/03/202342
CRANIAL NERVES Accommodation reflex
When the eyes are directed from a distant object to a near object:
Medial recti contracts (Brings convergence) Lens thickens to increase the refractory power by
contracting ciliary muscles Pupils constrict to restrict light waves to the thickest
central part of the lens

05/03/202343
Accommodation reflex

05/03/202344
WHAT IS THE LESION?WHERE IS THE LESION?
Left sided facial palsy, LMN type lesion

05/03/202345

05/03/202346
SENSORY SYSTEMLOCALIZATION OF LESIONS OF

05/03/202347
Sensory system Sensory modalities Superficial sensation light touch pain temperature sensibility Deep sensation joint and vibratory sensibility pain from deep muscle and ligamentous structures

05/03/202348
Sensory system Neuroanatomical pathways Spinothalmic tract
Lateral spinothalamic tract(pain, temp) Anterior spinothalamic tract(touch ,pressure)
Dorsal column tract(position,vibration)

05/03/202349
Spinal tracts anatomy and function
Tract 1st order neuron
Synapse 1 2nd order neuron Synapse 2 3rd order neuron
Dorsal column
Sensory nerve ending―cell body in dorsal root ganglion―ascend ipsi -lateral in spinal cord
Ipsilateral nucleus cuneatus n gracilis
Decussate in medulla―ascend contralaterally in medial leminiscus
VPL of thalmus
Sensory cortex

05/03/202350
Spinal tracts anatomy and function
Tract 1st order neuron
Synapse 1 2nd order neuron
Synapse 2
3rd order neuron
AnterolateralSpinothalmictract
Sensory nerve ending―cell body in dorsal root ganglion—enters spinal cord
Ipsilateral grey matter of spinal cord
Decussate and ascend contralaterally
VPLOf thalmus
Sensory cortex

05/03/202351

05/03/202352
Localization of Sensory lesion
Peripheral nerve lesion Isolated nerve palsy(Mononeuropathy) Mononeuritis multiplex Sensory peripheral neuropathy(polyneuropathy) Root lesion Spinal cord Brainstem Thalamus Cortex

05/03/202353
Localization of Sensory lesion
Isolated nerve palsy(Mononeuropathy)
Sensory loss is in the distribution of that nerve invoved.
Example Ulnar nerve lesion(sensory loss is over the medial
one and a half fingers both anteriorly and posteriorly)

05/03/202354
Sensory distribution of the ulnar nerve .

05/03/202355
Localization of Sensory lesion
Mononeuritis multiplex
Combinations of peripheral nerve lesions occur, usually caused by nerve infarcts
secondary to vasculitis or diabetic vasculopathy.

05/03/202356
Localization of Sensory lesion
Sensory peripheral neuropathy Disease affecting peripheral nerves may affect the
Schwann cell myelin sheath (demyelinating neuropathy) or the nerve axons (axonal neuropathy).
Peripheral neuropathy characteristically symmetrical and greater distally than proximally(gloove and stocking pattern).

05/03/202357
Localization of Sensory lesion
Sensory peripheral neuropathy
In any peripheral nerve or root lesion the sensory or motor arc of the deep tendon reflex can be interrupted leading to diminished or absent deep tendon reflexes.
Distal reflexes (ankle) are diminished more than proximal reflexes (biceps).

05/03/202358
Localization of Sensory lesion
Root lesion(Rediculopathy)The location of common root paresthesias are C-5 shoulder region; C-6 thumb; C7 middle finger; C-8 5th finger; L-4 knee L-5great toe S-1 medial sole of the foot

05/03/202359
SYMPTOMS OF NERVE ROOT LESION

05/03/202360

05/03/202361
Localization of Sensory lesion
Spinal cord Ascending and descending pathways are interrupted
sensation is usually diminished distal to the lesion Localizing signs would be Localized root pain Sensory loss below the level of the lesion, An absent root reflex at the level of the lesion Increased reflexes below this level.

05/03/202362
Localization of Sensory lesion
Common cord syndromes are: Brown-Séquard syndrome Central cord syndrome (cervical) Complete cord transection

05/03/202363

05/03/202364
CorticospinalTract(motor)
Dorsal Column(Joint Positionsense lighttouch)
Pyramidal TractWeaknes
Absent Position& Vibrationsense
Absent pain& temperature
Brown-Séquard syndrome • ipsilateral plegia below the lesion• ipsilateral proprioception and light touch loss below the lesion• contralateral pain and temperature loss below the lesion

05/03/202365
Central cord syndrome (cervical)• shawl distribution pain and temperature loss• sparing of light touch and proprioception• lower motor neuron weakness of the affected cord levels (anterior horn cell involvement)
Shawl distribution pain &temperature loss if anterior horncells involved get flaccidweakness of involvedlevels.
Lesion involved crossing pain andtemperature fibers in theanterior commisure

05/03/202366
Complete cord transection. • loss of all modalities below the level of the lesion

05/03/202367
Neurological examination revealed: ---paralysis and increased DTRs of left leg ---loss of vibration and proprioception of left leg ---loss of pain and temperature sensation in the right leg Where is the lesion?
This is an example of the Brown-Sequard syndrome (hemisection of the spinal cord). Tracts involved in a lesion of the left spinal cord involve (1) the left corticospinal tract, which will synapse with lower motor neurons in the left limbs; (2) the left dorsal column containing primary sensory neurons for vibration and proprioception from the left limbs; and (3) the left spinothalamic tract containing secondary sensory neurons for pain and temperature sensation coming from the right limbs (the pain/temperature neurons cross at the level of entry in the anterior commissure after synapsing in the dorsal horn).

05/03/202368
Localization of Sensory lesion
BrainstemBrainstem lesions at the level of the medulla has: Ipsilateral loss of pain and temperature of the face Contralateral loss on the body. Light touch and proprioceptive loss is contralateral Above this level all sensory modality findings are
contralateral to the side of the lesion because all pathways have crossed.

05/03/202369
Localization of Sensory lesion
Thalamus
Thalamic lesions produce contralateral loss of all sensory modalities in the face,extremities and trunk.
Stimulation may be perceived as uncomfortable and painful(dysesthesia).

05/03/202370
Localization of Sensory lesion
Cortical lesions
Lesions of the cerebral cortex cause diminution of all sensory modalities on the contra lateral side of the body.
In addition, higher integrative sensory functions are impaired causing defects in stereo gnosis, two-point discrimination etc

05/03/202371
Lesion FINDINGS
Peripheral nerve All sensory modalities are affected.The borders are sharply demarcated.There may be hyperesthesia, discomfort and pain
Root All sensory modalities are affected.Sensory loss is vague but in a dermatomal distribution.Pain is present and may radiate in the dermatome distribution.
Spinal cord There is sensory dissociation.A unilateral lesion produces ipsilateral loss of light touch and proprioception and contralateral loss of pain and temperature
SUMMARYCharacteristics of sensory system lesions

05/03/202372
Lesion FindingsMedulla There is sensory dissociation.
Pain and temperature are lost on the ipsilateral side of the face and contralateral side of the body.Light touch and proprioception are lost on the contralateral side of the body.
Upper brainstem There is sensory dissociation.All sensory modalities are now crossed and on the same side.Unilateral lesions cause contralateral loss of sensory modalities
Thalamus Sensory dissociation is no longer present.Ipsilateral lesions produce contralateral loss of all modalities.
Cerebral cortex Sensory dissociation is absent.Ipsilateral lesions produce contralateral loss of all modalities.Discriminative sensory functions are lost.

05/03/202373
PYRAMIDAL TRACT(MOTOR SYSTEM)
LOCALIZATION OF LESIONS OF

05/03/202374
Pyramidal SystemTract 1st order
neuronSynapse 1 2nd order
neuronSynapse 2 D
ESCENDINGTRACT
Lateral Corticospinal tract
UMN:Cell body in motor cortex descend s ipsilaterally through internal capsule until decussate at pyramid and descends contralaterally
Cell body of anterior horn of spinal cord
LMNleaves Spinal cord
Neuro-muscular junction

05/03/202375

05/03/202376
Pyramidal System Inspection and observation Muscle tone Muscle power Tendon reflexes Co-ordination Gait

05/03/202377
Pyramidal SystemInspection and observation Size and bulk of muscle Any obvious wasting Visible fasciculations Position of the limb General body posture Scar marks or lacerations Ulceration Swelling Hip: Internaly rotated in anterior dislocation of hip Externaly rotation-posterior dislocation of hip

05/03/202378
Pyramidal System Muscle tone The resistance of a muscle against the passive
movement of the jointAssessed by Observing the position of the extremities at rest By pulpating the musle belly Determining the resistance against passive stretch

05/03/202379
Pyramidal System Hypertonia Spasticity: consists of an increase in tone that affects different
muscle groups to different extent. Rigidity: consists of increased resistance to passive movement
that is independent of direction of movement i-e it effects the flexors as well as extensors equally.
Hypotonia : defined as reduced resistance to the passive movement-the distal portion of the limb is easily waved when limb is shaken to and fro.
Paratonia: it seems to be rigidity when the examiner moves the limb rapidly but normal tone when the limb is moved slowly.

05/03/202380
Pyramidal System
Muscle power Checked in individual muscles and compared on both sides so that
the minor degree of weakness can be recognizedGrading of muscle power according to MEDICAL RESEARCH COUNCIL
Grade Muscle power
5 Normal power
4 Active movement against resistance and gravity
3 Active movement against gravity not resistance
2 Active movement possible only with gravity eliminated
1 Flicker or trace of movements
0 No movement

05/03/202381
Pyramidal System Tendon Reflexes Superfial reflexes Planter reflex Abdominal reflex Anal reflex Cremasteric reflex Deep tendon reflexes Knee jerk Ankle jerk Biceps jerk Supinator jerk Triceps jerk

05/03/202382
SUPERFICIAL REFLEXES
REFLEX HOW EXCITED
CLINICAL RESULT
LEVEL OF CORD
PLANTAR REFLEX Scrathing laterally on sole of foot
Flexion of big toe(downward movement)
L5 ,S1
SCAPULAR REFLEX Scrathing skin in intrascapular region
Contraction of scapular muscles
C 5 to T 1
ABDOMINAL REFLEX
Scrathing on abdominal wall below costal margin and in iliac fossa
Contraction of abdominal muscles
T 7 to T 12
ANAL REFLEX Scratching near anus Contraction of anal sphincter
S3, S4
CREMESTERIC REFLEX
Stoking skin at upper and inner thigh
Upward movement of testes
L1,L2

05/03/202383
Deep tendon reflexesREFLEX SEGMENTAL
INNERVATIONNERVE
KNEE REFLEX L3,L4 Femoral
BICEPS JERK C 5,C 6 Musculocutaneous
BRACHIORADIALIS JERK
C 5, C6 Radial
TRICEPS JERK C 7,C8 Radial
ANKLE JERK S 1,S 2 Tibial
JAW JERK Pons Mandibular branch of trigeminal nerve

05/03/202384
Grading of tendon reflexes
0 ABSENT1 PRESENT (as normal ankle jerk)
2 BRISK
3 VERY BRISK
4 CLONUS

05/03/202385
Pyramidal System
Coordination
Finger nose test
Heel Knee test

05/03/202386

05/03/202387
GAIT Gait Disturbances in Pyramidal Tract Lesions
HEMIPLEGIC GAIT:Patient does not lift his leg off the ground so that toes remain in contact with ground.Leg swings forward and outward in a circular fashion(ONLY ONE LEG INVOVED)
SPASTIC GAIT (Scissor Like Gait) Patient don’t lift his feet from the ground UMN paraplegia

05/03/202388
Comparison and Contrast b/w UML and LMN lesion
SIGN UMN lesion LMN lesion
Weakness Present Present
Atrophy Absent Present
Fasciculations Absent Present
Reflexes Brisk Dimished
Tone Increase Decrease
Babinski Upgoing Downgoing
Spastic paralysis Present Absent
UMN lesions may ipsilateral or contralateral while LMN lesions are usually ipsilateral.

05/03/202389
Upper Motor Neuron lesion
Cardinal features Weakness or paralysis Spasticity Brisk reflexes Upgoing plantars Loss of superficial abdominal reflexes

05/03/202390
UMN lesionSites Motor cortex Internal capsule Brain stem Spinal cord

05/03/202391
UMN lesion
Lesion of motor cortex results in monoplegia
Specific menifestations are present according to the lobes involved

05/03/202392

05/03/202393

05/03/202394

05/03/202395
LOBES IMPORTANT REGIONS
DEFICIT AFTER LESION
FRONTAL LOBE Primary motor cortex
Contralateral spastic paresis(area of homonculus affected),premotor:apraxia
Frontal eye field Eye deviation to ipsilateral side
Broca`s area Expressive aphasia
Prefrontal cortex Frontal lobe syndrome:poor judement,difficulty in concentrating,inappropriate social behaviour
PARIETAL LOBE Primary somatosensory
Contralateral hemihypesthesia
Superior parietal lobule
Contralateral asteriognosis,apraxia
Inferior parietal lobule
Contralateral hemianopia, rt n lft confusion (dominant)alexia,dyscalculia,unilateral neglect(non- dominant)

05/03/202396
LOBES IMPORTANT REGION DEFICIT AFTER LESION
TEMPORAL Primary auditory cortex Deafness :bilateral damage
Wernick s area Receptive aphasia
Hippocampus Bilateral lesion leads to poor short term and long term memory
Olfactory bulb Ipsilateral anosmia
Mayer loop Contralateral upper quadrantanopia
OOCIPITAL Primary visual cortex Cortical blindness with macular sparing

05/03/202397
UMN lesionInternal capsule lesion
Produces dense hemiplegia and facial nerve palsy of opposite side(uncrossed hemiplagia)

05/03/202398
UMN lesion

05/03/202399
UMN lesionCharacteristics of internal capsule lesion:
1- Hemi-plegia i.e. paralysis of the muscles present in the opposite side of the body due to damage of pyramidal and extra- pyramidal tracts fibers.
2- Hemi-anesthesia i.e. loss of all sensations from the opposite side of the body due to damage of sensory radiation.

05/03/2023100
UMN lesion
3- Hemi-anopia i.e. loss of vision in the opposite halves of visual fields of both eyes. So, lesion in the right internal capsule leads to loss of vision in the left halves of visual fields of both eyes. It is due to damage of optic radiation.
4- Decrease hearing; it is due to damage of auditory radiation. No deafness because each ear is bilaterally represented in the cerebral cortex.

05/03/2023101
UMN lesion Brain stem lesion produces crossed hemiplegia i-e
cranial nerve is affected on one side and the hemiplegia of the opposite side
If 3rd nerve is involved. Lesion is in mid-brain If 6th and 7th nerve is involved,lesion is in pons. If 9th and 10th nerves are involved, lesion is in medulla

05/03/2023102
UMN lesion Spinal cord
Whenever there is a lesion of spinal cord ,there will be UMN signs below the level of lesion
Upper limb involved ---- above C 5 Absent abdominal reflexes----- above T 8 Specific sensory level is always present

05/03/2023103
Lower Motor Neuron lesion
Cardinal features
Weakness or paralysis Wasting of individual muscles Hypotonia Diminished tendon jerks Downgoing plantars Fasciculations

05/03/2023104
LMN LESION Sites
Nuclei of cranial nerves Anterior horn cells Nerve roots Nerves(crania and peripheral)

05/03/2023105
LMN LESION Cranial nerves: Produces paralysis of muscles supplied
by the cranial nerves and LMN type of lesion of cranial nerve
Anterior horn cell : paraparesis or quadriparisis
Root: muscle supplied by root is paralysed
Single peripheral nerve :muscle supplied by that nerve is paralysed

05/03/2023106
THANK YOU
Related Documents