Drugs 2008; 68 (13): 1787-1802 THERAPY IN PRACTICE 0012-6667/08/0013-1787/$53.45/0 © 2008 Adis Data Information BV. All rights reserved. Local Treatment of Vulvovaginal Candidosis General and Practical Considerations Jos´ e das Neves, 1,2,3 Eug´ enia Pinto, 1 Branca Teixeira, 3 Gustavo Dias, 3 Patroc´ inia Rocha, 3 Teresa Cunha, 3 B´ arbara Santos, 3 Maria H. Amaral 2 and Maria F. Bahia 2 1 Department of Microbiology, CEQUIMED, Faculty of Pharmacy, University of Porto, Porto, Portugal 2 Department of Pharmaceutical Technology, Faculty of Pharmacy, University of Porto, Porto, Portugal 3 Department of Pharmacy, Hospital Geral de Santo Ant ´ onio, Porto, Portugal Contents Abstract ................................................................................... 1787 1. Basic Concepts on Vulvovaginal Candidosis ............................................... 1788 1.1 Epidemiology ...................................................................... 1788 1.2 Classification ....................................................................... 1789 1.3 Pathogenesis ....................................................................... 1789 1.4 Clinical Findings and Diagnosis ....................................................... 1790 1.5 Risk Factors ......................................................................... 1791 2. Treatment of Vulvovaginal Candidosis: General Considerations ............................. 1792 2.1 Local versus Oral Therapy ........................................................... 1792 3. Local Treatment of Vulvovaginal Candidosis ............................................... 1793 3.1 General Considerations ............................................................. 1793 3.2 Antifungal Drugs for Local Treatment ................................................. 1795 3.3 Other Potential Local Therapeutic Options ............................................ 1795 4. Selection of Topical Antifungal Drug Formulations .......................................... 1796 4.1 General Considerations ............................................................. 1796 4.2 Conventional and Novel Antifungal Formulations ...................................... 1797 4.3 Potential and Investigational Antifungal Delivery Systems ............................... 1798 4.4 Safety Issues ........................................................................ 1798 5. Conclusions ............................................................................ 1799 Vulvovaginal candidosis is a common worldwide female medical problem, Abstract occurring mostly in women of childbearing age. Currently available options for the treatment of this condition include local and oral (systemic) therapy. Both alternatives have been considered equally effective in the treatment of uncompli- cated vulvovaginal candidosis, although oral regimens are often preferred by physicians and women. However, local treatment presents several advantageous and unique features that may favour this therapeutic approach. The availability of numerous antifungal drugs and products for topical administration makes the selection quite challenging as this task is mostly based on personal experience or

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Drugs 2008; 68 (13): 1787-1802THERAPY IN PRACTICE 0012-6667/08/0013-1787/$53.45/0
© 2008 Adis Data Information BV. All rights reserved.
Local Treatment ofVulvovaginal CandidosisGeneral and Practical Considerations
Jose das Neves,1,2,3 Eugenia Pinto,1 Branca Teixeira,3 Gustavo Dias,3 Patrocinia Rocha,3Teresa Cunha,3 Barbara Santos,3 Maria H. Amaral2 and Maria F. Bahia2
1 Department of Microbiology, CEQUIMED, Faculty of Pharmacy, University of Porto,Porto, Portugal
2 Department of Pharmaceutical Technology, Faculty of Pharmacy, University of Porto,Porto, Portugal
3 Department of Pharmacy, Hospital Geral de Santo Antonio, Porto, Portugal
ContentsAbstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17871. Basic Concepts on Vulvovaginal Candidosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1788
1.1 Epidemiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17881.2 Classification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17891.3 Pathogenesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17891.4 Clinical Findings and Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17901.5 Risk Factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1791
2. Treatment of Vulvovaginal Candidosis: General Considerations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17922.1 Local versus Oral Therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1792
3. Local Treatment of Vulvovaginal Candidosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17933.1 General Considerations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17933.2 Antifungal Drugs for Local Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17953.3 Other Potential Local Therapeutic Options . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1795
4. Selection of Topical Antifungal Drug Formulations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17964.1 General Considerations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17964.2 Conventional and Novel Antifungal Formulations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17974.3 Potential and Investigational Antifungal Delivery Systems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17984.4 Safety Issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1798
5. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1799
Vulvovaginal candidosis is a common worldwide female medical problem,Abstractoccurring mostly in women of childbearing age. Currently available options forthe treatment of this condition include local and oral (systemic) therapy. Bothalternatives have been considered equally effective in the treatment of uncompli-cated vulvovaginal candidosis, although oral regimens are often preferred byphysicians and women. However, local treatment presents several advantageousand unique features that may favour this therapeutic approach. The availability ofnumerous antifungal drugs and products for topical administration makes theselection quite challenging as this task is mostly based on personal experience or

1788 das Neves et al.
anecdotal data. Also, recent advances have been made in topical antifungalformulations and there is an increasing availability of over-the-counter products.Therefore, a review of both general and practical considerations related to thelocal treatment of vulvovaginal candidosis is timely.
In summary, azoles and short-term regimens are usually recommended for thelocal treatment of vulvovaginal candidosis, with nystatin and boric acid consid-ered as second-line alternatives. Unconventional approaches may also be regardedas suitable in patients refractory to usual treatments. In addition to the susceptibil-ity of implicated Candida spp. to the antifungal agents, this choice should takeinto consideration other important issues such as particular situations (e.g. preg-nancy, menopause, drug hypersensitivity), women’s preferences, and the availa-bility, particularities and cost of antifungal formulations.
Vulvovaginal candidosis is a mucocutaneous in- several over-the-counter (OTC) vaginal productsfection by yeasts of the genus Candida involving the and their wide use increases the responsibility ofvulva and vagina. It is a common worldwide prob- non-physician healthcare providers to adequatelylem, particularly in women of reproductive age.[1] respond to this situation. Therefore, it is important toVulvovaginal candidosis is also frequently referred review several general and practical considerationsto as vulvovaginal candidiasis, thrush and, rarely, related to the local treatment of vulvovaginal candi-moniliasis. However, recent standardization trends dosis in order to optimize its use in clinical practice.suggest that the nomenclature of fungal diseases
1. Basic Concepts oncaused by specific pathogens should include theVulvovaginal Candidosisgenus name followed by the suffix -osis. Although
not considered a severely debilitating condition, itsThe objective of this article is not to thoroughlyhigh prevalence and interference with daily activi-
review the subject of vulvovaginal candidosis be-ties and the well-being of women makes this diseasecause this has been recently addressed elsewhere byan important medical condition. Various highly ef-Sobel.[1] However, it is important to highlight sever-fective oral or local treatment regimens includingal important aspects related to the epidemiology,different drugs (mostly azole antifungals), regimens,classification, pathogenesis, clinical manifestations,durations of treatment and pharmaceutical dosagediagnosis and risk factors implicated in this infec-forms have been proposed and routinely used intion before discussing its local treatment. A briefclinical practice. Recent reports on the comparativeoverview is provided in the following sections.efficacy of local versus oral treatment of uncompli-
cated vulvovaginal candidosis found no significant1.1 Epidemiology
differences, or at least no conclusive differences,between either treatment modalities.[2,3] In addition, Vulvovaginal candidosis is one of the three mosttreatment guidelines issued worldwide do not favour common vaginal infections among women in theireither local or oral therapy. fertile years and accounts for 20–30% of all cases.[5]
Even if only equally effective as oral therapy, Epidemiological studies indicate that approximatelylocal treatment of vulvovaginal candidosis may pre- 75% of all women will have at least one episode ofsent several advantages when compared with oral vulvovaginal candidosis throughout their lifetime,therapy. However, physicians are not always aware while 40–50% will experience one or more subse-of the benefits and limitations of both treatment quent episodes. It is also noteworthy that the simplemodalities as they frequently prefer oral regimens presence of Candida spp. in the vulvovaginal areawhen prescribing.[4] Moreover, the availability of does not necessarily mean infection. Approximately
© 2008 Adis Data Information BV. All rights reserved. Drugs 2008; 68 (13)

Local Treatment of Vulvovaginal Candidosis 1789
10–20% of healthy women have vulvovaginal colo- and duration of symptoms (acute or chronic).[8] Un-nization by these yeasts without showing typical complicated vulvovaginal candidosis is character-symptoms of vulvovaginal candidosis; in some ized by sporadic episodes with light to mild symp-women (e.g. HIV-positive or pregnant women), this toms that are usually caused by C. albicans. Thisrate may be higher.[6,7] Vulvovaginal candidosis is situation corresponds to the majority of all vulvo-rarely associated with trichomoniasis or bacterial vaginal candidosis cases as they are sensitive tovaginosis, although mixed infections are possible.[8] almost all therapeutic regimens, including short-
course regimens. In contrast, complicated vulvo-The frequency with which several Candida spp.vaginal candidosis commonly refers to recurrent orare involved in vulvovaginal candidosis is relativelysevere cases that are usually caused by non-albicanswell known. C. albicans is the main species respon-Candida spp. Although recurrent vulvovaginalsible and accounts for 80–90% of all infections,candidosis corresponds to approximately 6–8% offollowed by C. glabrata, C. tropicalis and C. kruseiall cases in otherwise healthy women, this form ofwith 5–10%, 5% and 1%, respectively.[9-11] Uncom-the disease presents as more preoccupant and ismonly, other non-albicans Candida spp. may alsocharacterized by four or more confirmed episodesbe responsible. However, non-albicans Candidaper year.[8] Recurrence seems to be related to thespp. are more resistant to conventional antifungalincomplete eradication of Candida spp. after symp-therapies, making them important organisms in thetomatic relief because of either yeast virulence orprevalence of vulvovaginal candidosis. In fact,host factors (exacerbated immune response mayvulvovaginal candidosis caused by non-albicansplay an important role).[15,16] Nonetheless, other fac-Candida spp. has been increasing in recent years, ators may be implicated, namely the possibility offact that may be related to the widespread and inade-reinoculation from a persistent intestinal source.quate use of antifungal drugs, namely those avail-Vulvovaginal candidosis can also be classified asable as OTC products.[12,13] It is thought that inade-chronic when symptoms last for ≥6 months and isquate use of these drugs contributed to the elimina-usually associated with azole-resistant non-albicanstion of azole-sensitive C. albicans, allowing theCandida spp.[17] Lastly, this vaginal infection is notdevelopment of azole-resistant non-albicans Candi-considered a sexually transmitted disease (STD).da spp. However, a contradictory study thatHowever, vulvovaginal candidosis is usually con-analysed the prevalence of non-albicans Candidasidered in this group of infectious diseases, as it isstrains among women before and after the introduc-often diagnosed in women being evaluated for ation of OTC products seem to refute this claim.[14] ItSTD.has been estimated that only approximately 50% of
all cases of vulvovaginal candidosis caused by non-albicans Candida spp. respond to conventional oral 1.3 Pathogenesisor local therapy with azoles.
Although not entirely understood, vaginalimmune and non-immune defences in healthy1.2 Classificationwomen are important in the pathophysiology ofvulvovaginal candidosis. As stated in section 1.2,Although not a potentially fatal pathology,vulvovaginal colonization by Candida spp. does notvulvovaginal candidosis is a common problem andnecessarily mean symptomatic infection.includes all women with positive cultures for Candi-
da spp., symptomatic or not.[1] Hence, this broad Indeed, several species are part of the normaldefinition means that vulvovaginal candidosis can vaginal flora but may become pathogens when thebe classified according to various criteria, namely vaginal environment undergoes change, such as inepisode frequency (sporadic or recurrent), severity the levels of lactobacilli (e.g. as a result of antibac-(complicated or uncomplicated), symptoms (asymp- terial therapy). These bacteria are capable of inhib-tomatic, mild to moderate, or severely symptomatic) iting the growth of a wide range of pathogens. In the
© 2008 Adis Data Information BV. All rights reserved. Drugs 2008; 68 (13)
1790 das Neves et al.
Mucus layer
Stratified squamousepithelium
Basement membrane
Lamina propria
Blastospores Hyphae
a b c
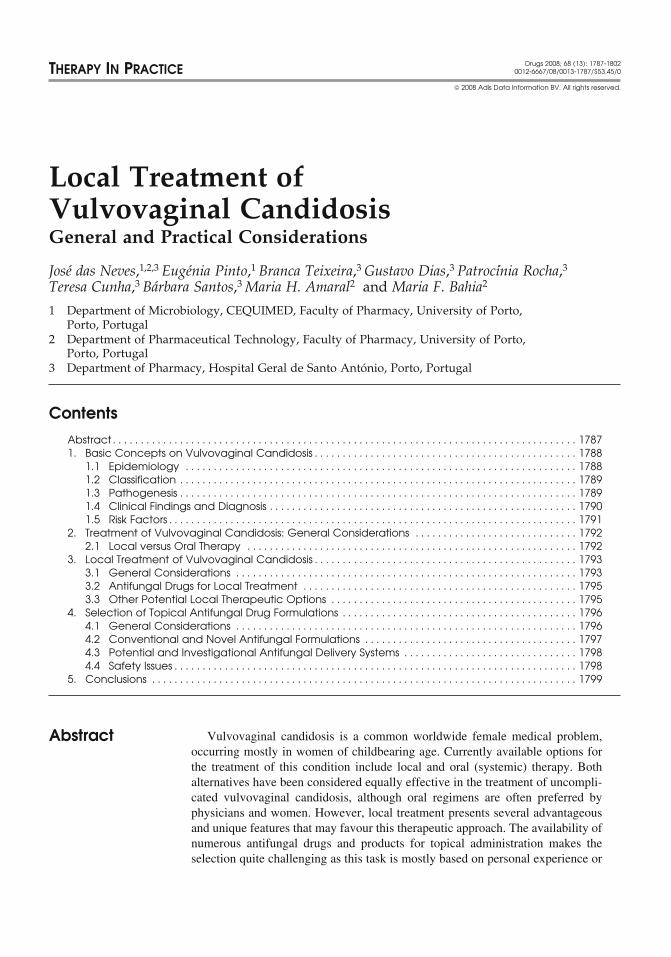
Fig. 1. Schematic drawing of the pathogenic mechanism of vaginal infection by Candida albicans. (a) Blastospores (budding yeast) are thedissemination and transmission form of C. albicans, and are associated with asymptomatic colonization of the vagina; (b) dimorphictransition to the filamentous form (hyphae) can be stimulated by various environmental conditions, resulting in increased adhesiveproperties to epithelial cells and production of lytic enzymes (mainly proteinases); (c) these enzymes facilitate epithelial invasion, resulting invaginal wall damage and inflammation, responsible for symptom occurrence.
case of vulvovaginal candidosis, lactobacilli may ure 1). This morphological conversion is dependenton multiple factors, namely vaginal pH, and humor-prevent the adhesion and/or germination of Candidaal and cellular immune status.[20] Factors that en-spp., thus providing a natural mechanism of defencehance or facilitate germination (e.g. estrogen ther-against symptomatic infection.[18] However, aapy, pregnancy) tend to precipitate symptomaticstraightforward relationship between colonizationvulvovaginal candidosis, whereas others that inhibitwith lactobacilli and the onset of vulvovaginalthis dimorphic change (e.g. bacterial flora) maycandidosis is unclear, as this pathology is also fre-prevent acute symptoms in women who are asymp-quently observed in women with normal levels oftomatic carriers. In addition, virulence of Candidalactobacilli.[19]
spp. is related to their capacity for adhesion toReproductive hormones (estrogens and proges-epithelial cells, which is a complex process that istogens) also play an important role in local immuni-not yet fully understood, and their increased proteo-ty as they are responsible for increased susceptibilitylytic activity.[21,22]
to infection with Candida spp. when their levels areelevated. These hormones decrease both humoral
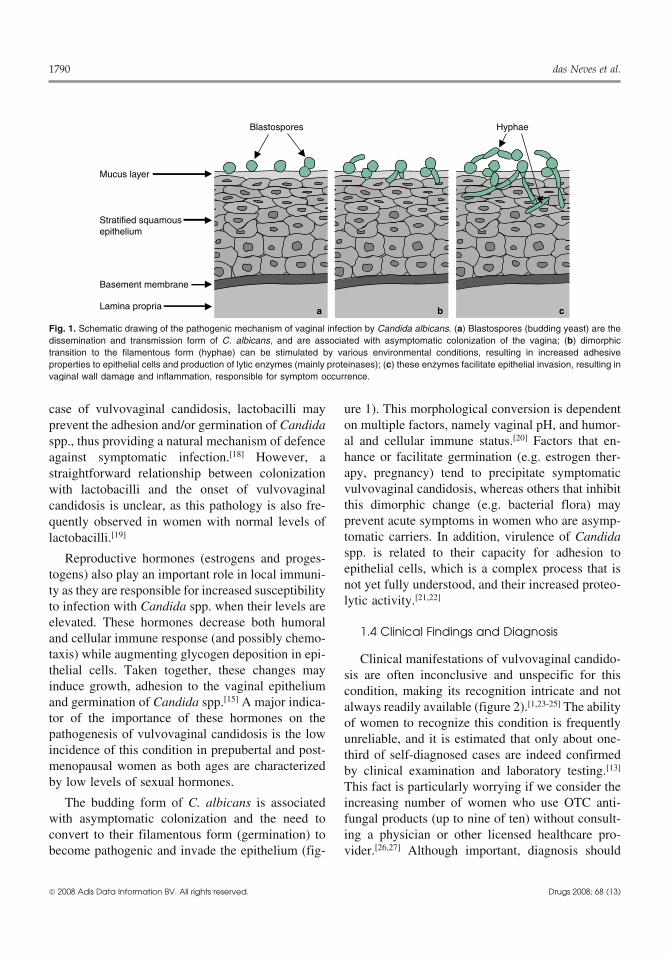
1.4 Clinical Findings and Diagnosisand cellular immune response (and possibly chemo-taxis) while augmenting glycogen deposition in epi- Clinical manifestations of vulvovaginal candido-thelial cells. Taken together, these changes may sis are often inconclusive and unspecific for thisinduce growth, adhesion to the vaginal epithelium condition, making its recognition intricate and notand germination of Candida spp.[15] A major indica- always readily available (figure 2).[1,23-25] The abilitytor of the importance of these hormones on the of women to recognize this condition is frequentlypathogenesis of vulvovaginal candidosis is the low unreliable, and it is estimated that only about one-incidence of this condition in prepubertal and post- third of self-diagnosed cases are indeed confirmedmenopausal women as both ages are characterized by clinical examination and laboratory testing.[13]
by low levels of sexual hormones. This fact is particularly worrying if we consider theThe budding form of C. albicans is associated increasing number of women who use OTC anti-
with asymptomatic colonization and the need to fungal products (up to nine of ten) without consult-convert to their filamentous form (germination) to ing a physician or other licensed healthcare pro-become pathogenic and invade the epithelium (fig- vider.[26,27] Although important, diagnosis should
© 2008 Adis Data Information BV. All rights reserved. Drugs 2008; 68 (13)
Local Treatment of Vulvovaginal Candidosis 1791
not be based solely on a patient’s clinical history, toms frequently emerge 1 week before menses anddisappear with the onset of menstruation. Vaginalpelvic examination and symptomatic assessment, asdischarge may be present or not, with variableonly microscopic observation (10% potassium hy-amounts and physicochemical properties (usuallydroxide) or mycological culture can accurately diag-without pronounced odour). Possible vulval symp-nose vulvovaginal candidosis.[28] The Whiff test andtoms also include erythema, oedema and swelling,pH determination are also useful tools, particularlyparticularly near the introitus.[1,8] The cervix is usu-in office-based practice.[29] Vaginal pH associatedally unaffected, while the vaginal mucosa presentswith vulvovaginal candidosis is similar to that ob-erythema and white plaques, this last feature beingserved in otherwise healthy women during theirtypical in women with vulvovaginal candidosisfertile years (approximately 3.5–4.5), which con-during pregnancy.[28]
trasts with increased values associated with bacterialvaginosis, trichomoniasis or mixed infections.[5] The
1.5 Risk Factorsmain symptom of vulvovaginal candidosis is pruri-tus, which can be accompanied by burning sensa- Several risk factors have been described fortion, pain, dysuria and dyspareunia. These symp- vulvovaginal candidosis,[30-41] even if most affected
Woman presenting vaginal symptoms
Pharmacist or other licensed healthcare providerPhysician1
Symptomassessmentand pelvic
examinationsuggest VVC?
Consider otherconditions
Wet mount microscopyreveals the presence
of yeast?
pH >5, excess WBC,trichomonads or
clue cells?
pH <5 and noexcess of WBC?
Initiate VVCtreatment
Considermixed
infectiontreatment
Considerother
conditions
Request laboratoryculture and consider
VVC treatment4
Proceed according tolaboratory information
Any of the following applies: Never diagnosed for VVC OR <16 or >60 years of age OR symptoms
suggesting other conditions OR pregnancy/breast feedingOR two or more VVC episodes in the last 6 mo OR
other predisposing condititions (e.g. diabetes mellitus)
Typical symptomsof VVC?
Symptomssuggesting
other condition?
Counseling
Refer to
Symptoms onset suggestsother than an acute episode?
Previous OTC treatment?
RecommendOTC treatment
Failure ofprevious OTC
treatment?
Recommend sameOTC treatment
Patientfeedback3Patient
feedback2
No
No
No
Yes
Yes
Yes NoYesNo
No
No
No
No
No
Yes
Yes
Yes
Yes
Individualsituationsmay justify
Yes
Yes
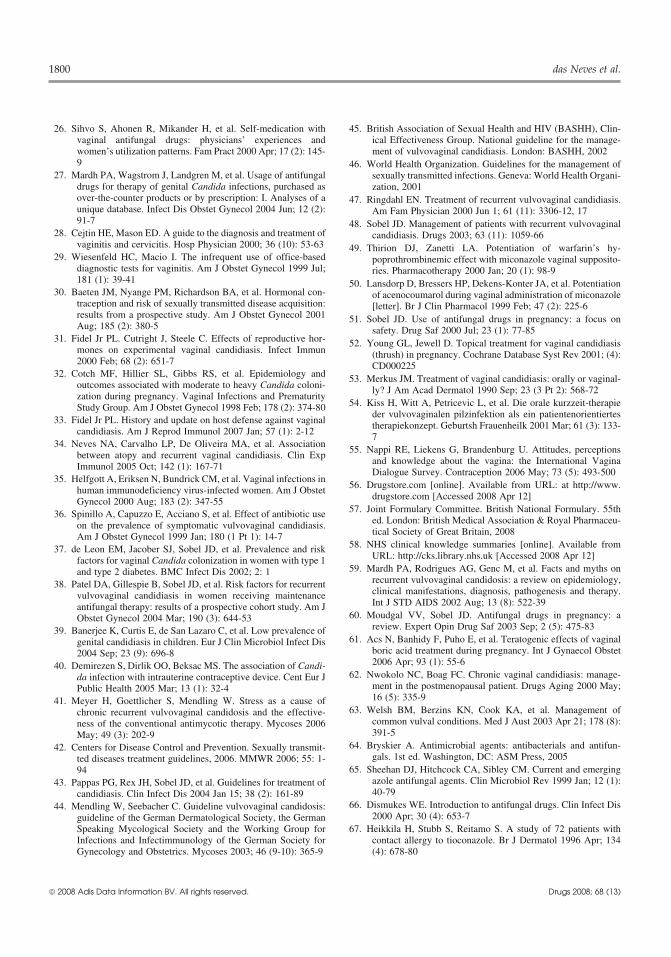
Fig. 2. Combined algorithm for office-based and over-the-counter (OTC) management of women presenting vaginal symptoms allegedlydue to vulvovaginal candidosis (VVC).[1,23-25] 1 Complicated cases may require reference to an experienced gynaecologist and/or infectiousdisease specialist. 2 In cases of treatment failure or short-term relapse consider possible drug-resistant or recurrent VVC, respectively. 3 Incases of treatment failure or relapse refer to physician. 4 Laboratory culture may also be required in other cases (e.g. chronic, recurrent orpresumably azole-resistant cases). WBC = white blood cells.
© 2008 Adis Data Information BV. All rights reserved. Drugs 2008; 68 (13)
1792 das Neves et al.
women may not present any of these. Table I pre- eral Candida spp. to antifungal drugs is document-sents a synopsis of the most important predisposing ed,[43] but individual isolates may not always fit thisfactors to vulvovaginal infection by Candida spp. pattern. Thus, laboratory susceptibility tests should
be performed whenever empirical therapy does not2. Treatment of Vulvovaginal produce a response.Candidosis: General Considerations
2.1 Local versus Oral TherapyGeneral guidelines for the management ofvulvovaginal candidosis have been issued by several
As mentioned in the introduction, efficacy ofgroups and organizations worldwide.[42-46] The
both oral and local therapy has been shown to bemain goal of vulvovaginal candidosis treatment
equivalent.[2,3] However, there are several other is-is to achieve rapid and complete relief of signs and
sues that may favour one therapeutic approach oversymptoms of vulvovaginal inflammation after
the other.48–72 hours, and mycological cure following
Local treatment presents several advantages.4–7 days.[43] Prevention of recurrence is also sought.Antifungal products administered in the vagina areMain therapeutic regimens include azoles (imidaz-usually designed to avoid extensive drug absorption,oles or triazoles), although others can be used. Thewith blood concentrations frequently being negligi-selection of individual drugs for vulvovaginalble. The incidence of adverse effects, particularlycandidosis therapy (oral or local) should be baseddue to prolonged systemic exposure to antifungals,upon their pharmacology and implicated Candidamay therefore be decreased with local therapy.[47,48]
spp. susceptibility. In general, the sensitivity of sev-Drug interactions frequently observed during oraladministration are uncommon when using topicalantifungals, with this fact being an important advan-tage over oral regimens. Nonetheless, their occur-rence should not be ignored since some reportsindicate that these interactions might also be observ-ed during local treatment, e.g. between topicalazoles and oral anticoagulants.[49,50] Oral azoles arecontraindicated or, at least, should be avoidedduring pregnancy and breast feeding because ofsafety issues to the fetus or baby, with local therapyusually being recommended.[51,52] For the same rea-sons, it is also prudent to choose local therapy whentreating women who are not using reliable birthcontrol methods or who are planning to becomepregnant.
Vaginal administration of antifungals also pre-sents some disadvantages. Women’s preferences donot favour local therapy. A review study in the early1990s found that approximately 50% of womenfavoured oral antifungal therapy, while only 5%preferred local therapy; the remaining women show-ed no preferences.[53] A study published in 2001corroborated these results; among 1348 women,58% preferred oral treatment, while 36% and 8%favoured vaginal suppositories and vaginal tablets,
Table I. Risk factors contributing for vulvovaginal candidosis occur-rence[30-41]
Hormonal Increased levels of endogenous estrogens (mainlyfactors during pregnancy)
Use of exogenous estrogens (oral contraceptives orhormonal replacement therapy)Increased levels of progesterone (?)
Immune Decreased cellular immunityfactors Immunosuppressed patients
High predisposition for atopia, allergic andhypersensitivity reactionsHIV infection (?)
Antibacterial Broad-spectrum antibacterials (systemic or local;use mostly during prolonged treatments)
Diabetes Particularly in patients with type 1 diabetes or inmellitus whom diabetes is not well controlled
Others ObesityDietary (?)Debilitating conditionsHeat, moisture and occlusive underwearIntrauterine contraceptive deviceContraceptive sponges or irritating vaginal products[e.g. containing nonoxynol-9] (?)Corticosteroids (?)Nappy or diaper dermatitis or sexual abuse inchildrenSexual activity [namely orogenital or high frequencyintercourse] (?)Stress factors
(?) = role in the occurrence of vulvovaginal candidosis remainscontroversial.
© 2008 Adis Data Information BV. All rights reserved. Drugs 2008; 68 (13)

Local Treatment of Vulvovaginal Candidosis 1793
respectively.[54] However, these results may be ment), with symptomatic and mycological cure be-changing towards local therapy as a result of the ing achieved in approximately 80–90% of patientsadvances in the formulation of vaginal products and who have completed the treatment. Prolonged ther-decrease of genitalia related taboos.[55] Antifungals apy (>7 days) is necessary for complicated or non-used for local treatment may cause local reactions, albicans Candida infections; after a symptomaticnamely burning or irritation. Although mild and cure, a maintenance regimen may be initiatedsomewhat occasional, these symptoms may cause and prolonged for 6 months (oral regimens) or inter-women to discontinue treatment or may even be mittently (local therapy).[42,43] Some experts recom-misinterpreted by healthcare providers as being mend clotrimazole 200 mg twice weekly, clo-caused by fungal persistence and lead to inadequate trimazole 500 mg once weekly, nystatincontinuation of local therapy. 100 000 units every other day or boric acid 600 mg
Another relevant aspect when comparing both every other day (then twice weekly) as examples oftreatment modalities is their cost. Affordability is, in local intermittent therapy.[59] Even if considered ef-fact, a critical issue related to treatment compliance fective, maintenance therapy does not guarantee aand should not be disregarded by clinicians. A rapid cure, with 30–50% or 50–70% of women experienc-analysis of US and UK markets reveals a wide range ing relapses in the following month or followingof prices among oral and local treatment options; 2 months after treatment cessation, respectively.[48]
this variability is observed between different drugs, This can be explained by the fungistatic action of thedosage regimens or even formulations (see table II drugs that are used and immunopathogenesis of thefor prices of local therapy regimens). A typical disease. In these patients with relapsing infections,example of an oral regimen is that of fluconazole subsequent maintenance therapy regimens may be(150 mg, single dose), which costs approximately considered. It is also important to further consider$US26 or £12.50 (2008 costings). Also, patients’ relevant factors related to the patient (e.g. identifica-healthcare plan financing and worldwide price vari- tion and control of risk factors, tolerability to theability may substantially influence treatment af- antifungal regimen), disease-causing Candida spp.fordability. Hence, general comparison between oral (particularly antifungal drug resistance), drug andand local regimen costs and specific recommenda- drug formulation (e.g. safety profile).tions on the subject are hard to perform. The golden
Special populations may have specific require-rule should always be ‘the best treatment at the bestments. In pregnant women, it is advisable to dupli-price’.cate the treatment period. In this particular group,miconazole, clotrimazole, butoconazole and ter-3. Local Treatment ofconazole are generally considered the most effectiveVulvovaginal Candidosisdrugs.[46] Alongside oral antifungals, several otherdrugs have been considered unsafe during preg-
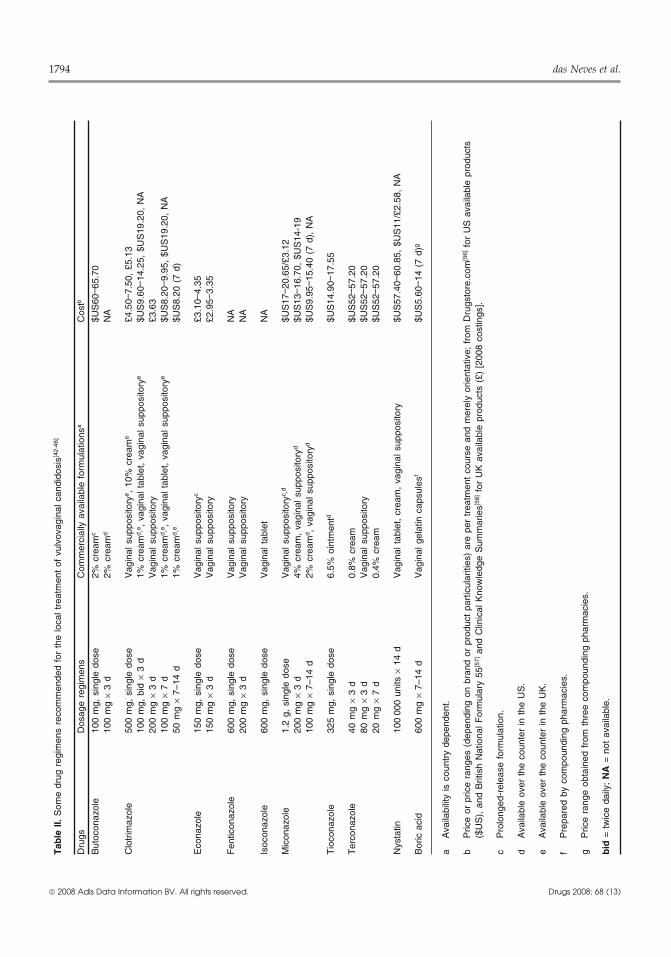
3.1 General Considerationsnancy (either locally or systemically), namely flu-cytosine and potassium iodide.[60] Boric acid useSeveral local drug regimens have been recom-also seems contraindicated in pregnant women.[61]mended and used in clinical practice (table II).[42-46]
HIV-positive women are usually treated forAzoles are recommended as first-line treatment un-vulvovaginal candidosis in the same way as HIV-less a confirmed or suspected azole-resistant Candi-negative women, although their vaginal coloniza-da strain is involved. Other situations may alsotion rates with Candida spp. are usually higher.[42]contraindicate azole therapy (e.g. hypersensitivity toPostmenopausal women should also be treated asthese agents) in which nystatin or boric acid shouldyounger fertile women, although several age-relatedbe used. Uncomplicated vulvovaginal candidosisaspects should be taken into consideration (e.g.usually responds quite rapidly to any empiricalhigher incidence of type 2 diabetes mellitus, highershort-course local regimen (up to 3 days of treat-
© 2008 Adis Data Information BV. All rights reserved. Drugs 2008; 68 (13)
1794 das Neves et al.
© 2008 Adis Data Information BV. All rights reserved. Drugs 2008; 68 (13)
Tab
le I
I. S
ome
drug
reg
imen
s re
com
men
ded
for
the
loca
l tre
atm
ent
of v
ulvo
vagi
nal c
andi
dosi
s[42-
46]
Dru
gsD
osag
e re
gim
ens
Com
mer
cial
ly a
vaila
ble
form
ulat
ions
aC
ostb
But
ocon
azol
e10
0 m
g, s
ingl
e do
se2%
cre
amc
$US
60– 6
5.70
100
mg
× 3
d2%
cre
amd
NA
Clo
trim
azol
e50
0 m
g, s
ingl
e do
seV
agin
al s
uppo
sito
rye ,
10%
cre
ame
£4.5
0–7.
50,
£5.1
310
0 m
g, b
id ×
3 d
1% c
ream
d ,e ,
vag
inal
tab
let,
vagi
nal s
uppo
sito
rye
$US
9.60
– 14.
25,
$US
19.2
0, N
A20
0 m
g ×
3 d
Vag
inal
sup
posi
tory
£3.6
310
0 m
g ×
7 d
1% c
ream
d ,e ,
vag
inal
tab
let,
vagi
nal s
uppo
sito
rye
$US
8.20
– 9.9
5, $
US
19.2
0, N
A50
mg
× 7–
14 d
1% c
ream
d ,e
$US
8.20
(7
d)
Eco
nazo
le15
0 m
g, s
ingl
e do
seV
agin
al s
uppo
sito
ryc
£3.1
0–4.
3515
0 m
g ×
3 d
Vag
inal
sup
posi
tory
£2.9
5–3.
35
Fen
ticon
azol
e60
0 m
g, s
ingl
e do
seV
agin
al s
uppo
sito
ryN
A20
0 m
g ×
3 d
Vag
inal
sup
posi
tory
NA
Isoc
onaz
ole
600
mg,
sin
gle
dose
Vag
inal
tab
let
NA
Mic
onaz
ole
1.2
g, s
ingl
e do
seV
agin
al s
uppo
sito
ryc ,
d$U
S17
– 20.
65/£
3.12
200
mg
× 3
d4%
cre
am,
vagi
nal s
uppo
sito
ryd
$US
13– 1
6.70
, $U
S14
-19
100
mg
× 7–
14 d
2% c
ream
d , v
agin
al s
uppo
sito
ryd
$US
9.95
– 15.
40 (
7 d)
, N
A
Tio
cona
zole
325
mg,
sin
gle
dose
6.5%
oin
tmen
td$U
S14
.90–
17.5
5
Ter
cona
zole
40 m
g ×
3 d
0.8%
cre
am$U
S52
– 57.
2080
mg
× 3
dV
agin
al s
uppo
sito
ry$U
S52
– 57.
2020
mg
× 7
d0.
4% c
ream
$US
52– 5
7.20
Nys
tatin
100
000
units
× 1
4 d
Vag
inal
tab
let,
crea
m,
vagi
nal s
uppo
sito
ry$U
S57
.40–
60.8
5, $
US
11/£
2.58
, N
A
Bor
ic a
cid
600
mg
× 7–
14 d
Vag
inal
gel
atin
cap
sule
sf$U
S5.
60– 1
4 (7
d)g
aA
vaila
bilit
y is
cou
ntry
dep
ende
nt.
bP
rice
or p
rice
rang
es (
depe
ndin
g on
bra
nd o
r pr
oduc
t pa
rtic
ular
ities
) ar
e pe
r tr
eatm
ent
cour
se a
nd m
erel
y or
ient
ativ
e; f
rom
Dru
gsto
re.c
om[5
6] f
or U
S a
vaila
ble
prod
ucts
($U
S),
and
Brit
ish
Nat
iona
l For
mul
ary
55[5
7] a
nd C
linic
al K
now
ledg
e S
umm
arie
s[58] f
or U
K a
vaila
ble
prod
ucts
(£)
[20
08 c
ostin
gs].
cP
rolo
nged
-rel
ease
for
mul
atio
n.
dA
vaila
ble
over
the
cou
nter
in t
he U
S.
eA
vaila
ble
over
the
cou
nter
in t
he U
K.
fP
repa
red
by c
ompo
undi
ng p
harm
acie
s.
gP
rice
rang
e ob
tain
ed f
rom
thr
ee c
ompo
undi
ng p
harm
acie
s.
bid
= t
wic
e da
ily;
NA
= n
ot a
vaila
ble.
Local Treatment of Vulvovaginal Candidosis 1795
drug usage and vaginal dryness).[62] The treatment ofmale sexual partners is usually not considered, ex-cept in women with recurrent vulvovaginalcandidosis or when partners present with genitalsymptoms.[42] In this situation, topical application ofnystatin or clotrimazole, lotion or cream, twice dailyfor 7 days may be useful.[46]
Alongside antifungal therapy, several other localtherapeutic approaches may be helpful, namely inthe relief of vulval dermatitis or intense pruritus.These measures may include the utilization of corti-costeroids (e.g. 1% hydrocortisone ointment) andapplying cold compresses on the affected areas.[63]
Corticosteroids should only be considered in severecases and used with caution as rebound effects maybe observed. Use of non-irritating moisturizers, im-plementation of adequate hygiene practices andavoidance of soap-containing cleansers are equallyimportant in the prevention and exacerbation ofthese symptoms.
3.2 Antifungal Drugs for Local Treatment
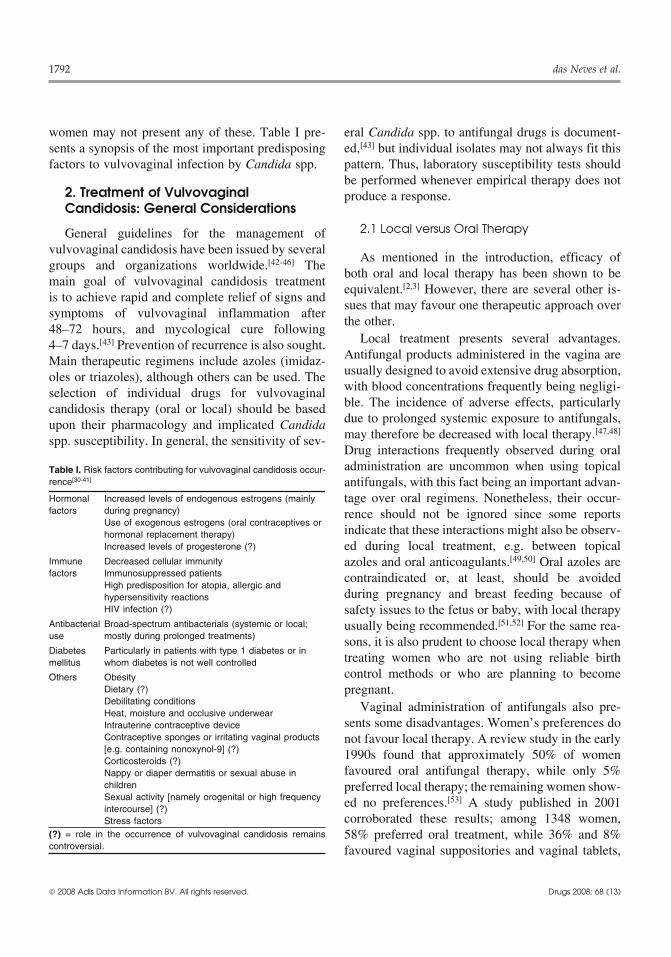
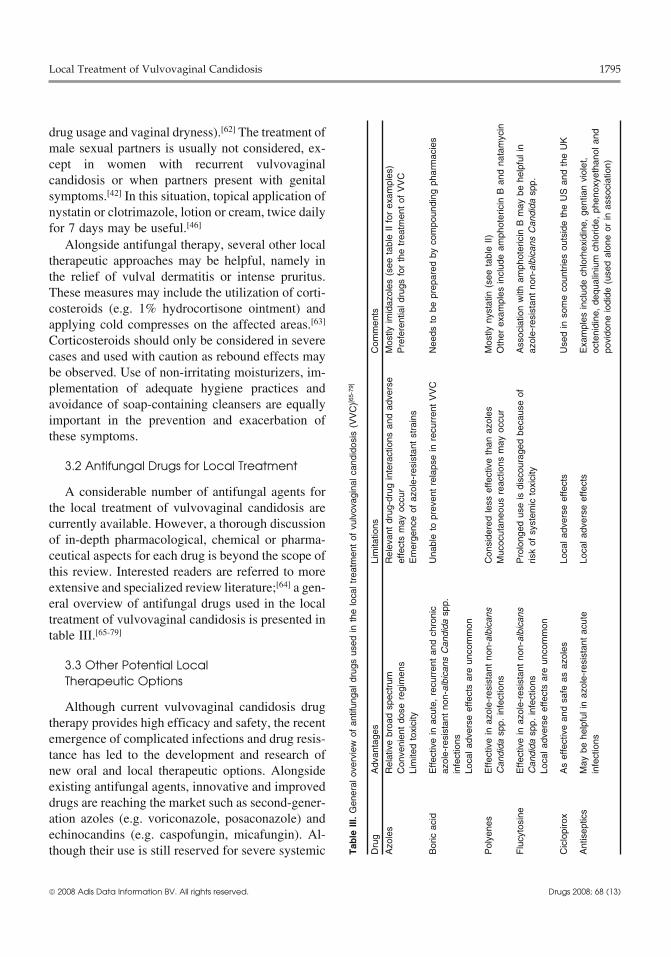
A considerable number of antifungal agents forthe local treatment of vulvovaginal candidosis arecurrently available. However, a thorough discussionof in-depth pharmacological, chemical or pharma-ceutical aspects for each drug is beyond the scope ofthis review. Interested readers are referred to moreextensive and specialized review literature;[64] a gen-eral overview of antifungal drugs used in the localtreatment of vulvovaginal candidosis is presented intable III.[65-79]
3.3 Other Potential LocalTherapeutic Options
Although current vulvovaginal candidosis drugtherapy provides high efficacy and safety, the recentemergence of complicated infections and drug resis-tance has led to the development and research ofnew oral and local therapeutic options. Alongsideexisting antifungal agents, innovative and improveddrugs are reaching the market such as second-gener-ation azoles (e.g. voriconazole, posaconazole) andechinocandins (e.g. caspofungin, micafungin). Al-though their use is still reserved for severe systemic
© 2008 Adis Data Information BV. All rights reserved. Drugs 2008; 68 (13)
Tab
le I
II. G
ener
al o
verv
iew
of
antif
unga
l dru
gs u
sed
in t
he lo
cal t
reat
men
t of
vul
vova
gina
l can
dido
sis
(VV
C)[6
5-79
]
Dru
gA
dvan
tage
sLi
mita
tions
Com
men
ts
Azo
les
Rel
ativ
e br
oad
spec
trum
Rel
evan
t dr
ug-d
rug
inte
ract
ions
and
adv
erse
Mos
tly im
idaz
oles
(se
e ta
ble
II fo
r ex
ampl
es)
Con
veni
ent
dose
reg
imen
sef
fect
s m
ay o
ccur
Pre
fere
ntia
l dru
gs f
or t
he t
reat
men
t of
VV
CLi
mite
d to
xici
tyE
mer
genc
e of
azo
le-r
esis
tant
str
ains
Bor
ic a
cid
Effe
ctiv
e in
acu
te,
recu
rren
t an
d ch
roni
cU
nabl
e to
pre
vent
rel
apse
in r
ecur
rent
VV
CN
eeds
to
be p
repa
red
by c
ompo
undi
ng p
harm
acie
saz
ole-
resi
stan
t no
n-al
bica
nsC
andi
da s
pp.
infe
ctio
nsLo
cal a
dver
se e
ffect
s ar
e un
com
mon
Pol
yene
sE
ffect
ive
in a
zole
-res
ista
nt n
on-a
lbic
ans
Con
side
red
less
effe
ctiv
e th
an a
zole
sM
ostly
nys
tatin
(se
e ta
ble
II)C
andi
da s
pp.
infe
ctio
nsM
ucoc
utan
eous
rea
ctio
ns m
ay o
ccur
Oth
er e
xam
ples
incl
ude
amph
oter
icin
B a
nd n
atam
ycin
Flu
cyto
sine
Effe
ctiv
e in
azo
le-r
esis
tant
non
-alb
ican
sP
rolo
nged
use
is d
isco
urag
ed b
ecau
se o
fA
ssoc
iatio
n w
ith a
mph
oter
icin
B m
ay b
e he
lpfu
l in
Can
dida
spp
. in
fect
ions
risk
of s
yste
mic
tox
icity
azol
e-re
sist
ant
non-
albi
cans
Can
dida
spp
.Lo
cal a
dver
se e
ffect
s ar
e un
com
mon
Cic
lopi
rox
As
effe
ctiv
e an
d sa
fe a
s az
oles
Loca
l adv
erse
effe
cts
Use
d in
som
e co
untr
ies
outs
ide
the
US
and
the
UK
Ant
isep
tics
May
be
help
ful i
n az
ole-
resi
stan
t ac
ute
Loca
l adv
erse
effe
cts
Exa
mpl
es in
clud
e ch
lorh
exid
ine,
gen
tian
viol
et,
infe
ctio
nsoc
teni
dine
, de
qual
iniu
m c
hlor
ide,
phe
noxy
etha
nol a
ndpo
vido
ne io
dide
(us
ed a
lone
or
in a
ssoc
iatio
n)

1796 das Neves et al.
conditions, these drugs may find in the future a place tree oil)[88] demonstrated high antifungal activity invitro against Candida spp. commonly involved inin the therapy of complicated vulvovaginal candido-vulvovaginal candidosis. An interesting feature ofsis. The use of drugs with different mechanisms ofthese natural products is their similar activity againstaction may also be an interesting strategy. In vitroboth azole-sensitive and -resistant Candida spp.and animal data show synergistic effects between
commonly used azoles and other substances show-ing antifungal activity.[80] In addition, limited clin- 4. Selection of Topical Antifungalical case reports using flucytosine and amphotericin Drug FormulationsB seem to point in this direction.[75] However, fur-ther studies are required to test the possibility ofsynergistic drug use. 4.1 General Considerations
Probiotic local therapy with products containinglactobacilli has been proposed as an alternative op- As well as choosing an effective drug, an ade-tion for the prevention of vulvovaginal candidosis, quate antifungal product must be selected or evenparticularly for recurrent cases. A relatively com- sometimes compounded in order to fulfil a treatmentmon practice recommended by some gynaecologists regimen. This task should not be neglected as inade-
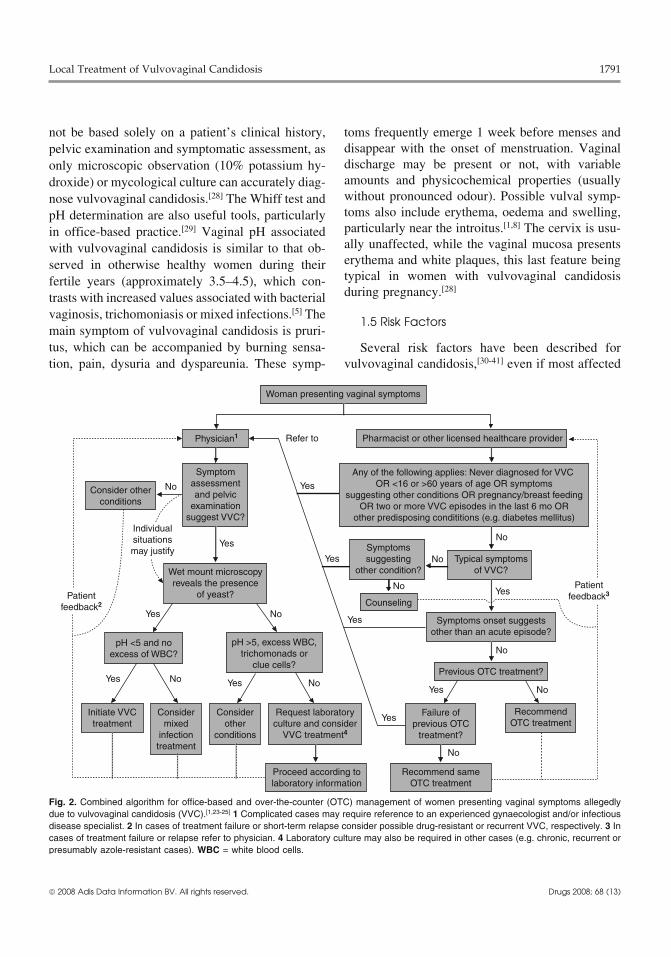
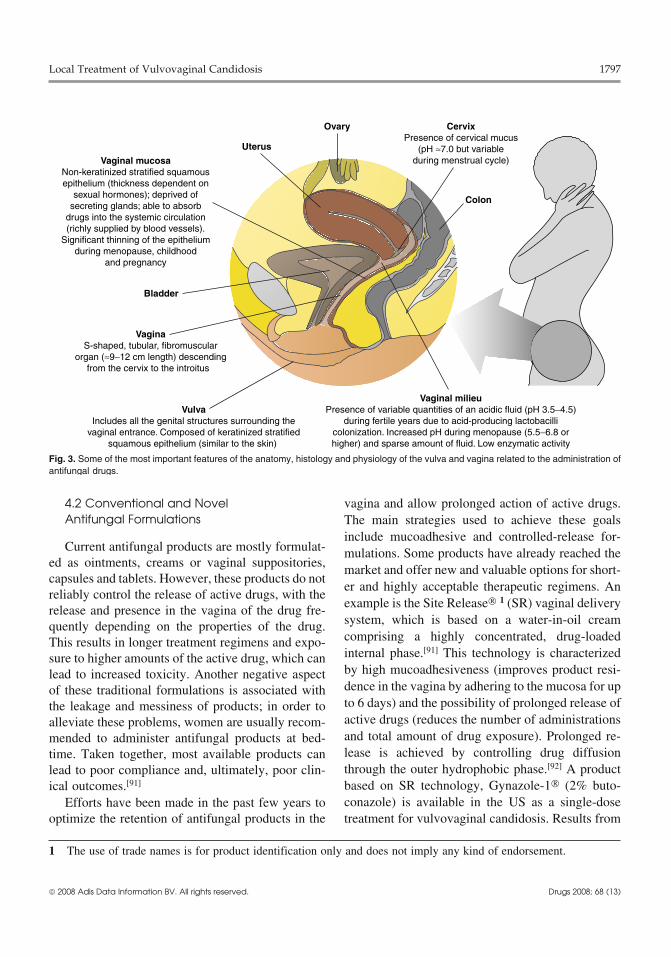
quate vaginal drug delivery systems may lead tohas been the administration of yogurt containingpoor clinical outcomes. Features related to the anat-lactobacilli into the vagina. Nevertheless, availableomy, histology and physiology of the vulva andclinical data fail to clearly demonstrate the benefi-vagina (figure 3) should be taken into account whencial outcome of this strategy.[81,82] Immunotherapy ischoosing a topical antifungal formulation for localalso being investigated, particularly in the field oftreatment of vulvovaginal candidosis.[89,90] Also, it isvaccine, antibody and cytokine development.[83,84]
occasionally necessary to compound antifungal for-The purpose of this strategy is to induce or regulatemulations in pharmacies when products are notthe local immune response against infection by Can-commercially available (e.g. boric acid capsules,dida spp., either by passive or active immunization.amphotericin B vaginal suppositories). WheneverFindings from a recent review of preclinical datapossible, these compounded formulations should beseems to support that the vaginal administration offully characterized and optimized for their biophar-diverse immunomodulatory compounds (e.g. anti-maceutical and pharmacotechnological features, as
bodies) can kill Candida spp. or inhibit its germina-vehicles are recognized to dramatically influence
tion and epithelial adhesion, thus reducing sympto-the release, in loco residence, and rate and extent of
matic infection; reduction of inflammatory humoral drug penetration into the mucosa. This last feature isand cellular response associated with vulvovaginal particularly important, as inadequate mucosal pene-candidosis also seems to be possible.[85] Although tration of antifungal drugs may lead to toxicity (withimmunotherapy is considered very promising, sev- excessive penetration) or poor cure rates (with pooreral important issues related to the correlation be- penetration). Although antifungal products are ad-tween disease, success and protection of this thera- ministered topically, their action is not merely on thepeutic approach still have to be resolved before mucosal surface or vaginal lumen; these agents needtranslation to clinical practice is possible. Natural to penetrate deep into the epithelium to reach inva-products have also shown antifungal activity in vitro sive Candida hyphae (figure 1) and exert a localagainst Candida spp., with their use being a poten- antifungal action there. Moreover, other importanttial option for the treatment of vulvovaginal candi- issues should not be disregarded such as women’sdosis in the future.[86] For example, Thymus spp. preferences, their ability to fully comply with theessential oil (thyme oil),[87] a commonly used food treatment (e.g. correct use of vaginal applicators)spice, and Melaleuca alternifolia essential oil (tea and treatment affordability.
© 2008 Adis Data Information BV. All rights reserved. Drugs 2008; 68 (13)
Local Treatment of Vulvovaginal Candidosis 1797
Colon
VulvaIncludes all the genital structures surrounding the
vaginal entrance. Composed of keratinized stratifiedsquamous epithelium (similar to the skin)
VaginaS-shaped, tubular, fibromuscular
organ (≈9−12 cm length) descendingfrom the cervix to the introitus
Vaginal mucosaNon-keratinized stratified squamousepithelium (thickness dependent on
sexual hormones); deprived ofsecreting glands; able to absorb
drugs into the systemic circulation(richly supplied by blood vessels).
Significant thinning of the epitheliumduring menopause, childhood
and pregnancy
Ovary CervixPresence of cervical mucus
(pH ≈7.0 but variableduring menstrual cycle)
Uterus
Bladder
Vaginal milieuPresence of variable quantities of an acidic fluid (pH 3.5−4.5)
during fertile years due to acid-producing lactobacillicolonization. Increased pH during menopause (5.5−6.8 orhigher) and sparse amount of fluid. Low enzymatic activity
Fig. 3. Some of the most important features of the anatomy, histology and physiology of the vulva and vagina related to the administration ofantifungal drugs.
4.2 Conventional and Novel vagina and allow prolonged action of active drugs.Antifungal Formulations The main strategies used to achieve these goals
include mucoadhesive and controlled-release for-Current antifungal products are mostly formulat- mulations. Some products have already reached the
ed as ointments, creams or vaginal suppositories, market and offer new and valuable options for short-capsules and tablets. However, these products do not
er and highly acceptable therapeutic regimens. Anreliably control the release of active drugs, with the
example is the Site Release® 1 (SR) vaginal deliveryrelease and presence in the vagina of the drug fre-system, which is based on a water-in-oil creamquently depending on the properties of the drug.comprising a highly concentrated, drug-loadedThis results in longer treatment regimens and expo-internal phase.[91] This technology is characterizedsure to higher amounts of the active drug, which canby high mucoadhesiveness (improves product resi-lead to increased toxicity. Another negative aspectdence in the vagina by adhering to the mucosa for upof these traditional formulations is associated withto 6 days) and the possibility of prolonged release ofthe leakage and messiness of products; in order toactive drugs (reduces the number of administrationsalleviate these problems, women are usually recom-and total amount of drug exposure). Prolonged re-mended to administer antifungal products at bed-lease is achieved by controlling drug diffusiontime. Taken together, most available products canthrough the outer hydrophobic phase.[92] A productlead to poor compliance and, ultimately, poor clin-based on SR technology, Gynazole-1® (2% buto-ical outcomes.[91]
conazole) is available in the US as a single-doseEfforts have been made in the past few years tooptimize the retention of antifungal products in the treatment for vulvovaginal candidosis. Results from
1 The use of trade names is for product identification only and does not imply any kind of endorsement.
© 2008 Adis Data Information BV. All rights reserved. Drugs 2008; 68 (13)

1798 das Neves et al.
clinical trials demonstrated that treatment with SR prolonged drug release is valuable (e.g. maintenancecream is as safe and effective as 7-day treatment therapy for recurrent vulvovaginal candidosis). Oth-with conventional 2% miconazole cream or oral er interesting drug delivery approaches have alsofluconazole, with the advantage of allowing faster been proposed. Chang et al.[99] and Bilensoy etrelief of symptoms.[93,94] Clinical data also suggest al.[100] designed thermosensitive formulations thatthat SR technology may be used for the vaginal are able to release clotrimazole in a controlled fash-administration of other antifungal agents (e.g. flu- ion. Besides allowing longer administration inter-trimazole).[95] Another currently commercially vals than conventional products, the fact that theseavailable prolonged-release product in the US is formulations are liquids at room temperature andMonistat-1® (1.2 g miconazole); in the UK it is mucoadhesive semisolid gels at body temperaturecommercialized as Gyno-Daktarin® 1200 mg vagi- facilitates their administration while guaranteeingnal capsule. This ovule-shaped insert is comprised good retention in the vagina.of miconazole suspended in an ointment base (min- Nanocarriers, such as liposomes,[101] prolipo-eral oil, white petrolatum and lecithin), which is somes[102] or niosomes,[103] may also play a futurecovered by a soft gelatin hydrogel layer that controls role in the treatment of vulvovaginal candidosis.drug release. Single-dose Monistat-1® was shown to These spherical vesicles have been shown to effec-be as effective as 7-day treatment with conventional tively deliver antifungals (e.g. clotrimazole) deeply2% miconazole cream and achieved symptom relief into the vaginal epithelium and provide prolongedfaster.[96] Moreover, it demonstrated the convenient drug release without being submitted to the naturalfeature of equal efficacy either with daytime or vaginal cleansing mechanism responsible for leak-bedtime use.[97] The same product is available in age of conventional products.combination with a 2% miconazole cream to beapplied in the vulva for symptomatic relief (Monis-
4.4 Safety Issuestat-1® Combination Pack). Similar single-dose, pro-longed-release vaginal products are also availableworldwide that contain econazole 150 mg (Ecosta- Safety concerns with antifungal products are nottin-1® E.R. and Gyno-Pevaryl® LP) or sertacon- exclusively related to the toxic effects of activeazole 300 mg (Monazol®), and have been shown to drugs. Excipients commonly present in antifungalbe effective and well tolerated in vulvovaginal products administered in the vulvovaginal area maycandidosis.[98] be responsible for adverse effects, particularly local
ones. For example, local irritation or allergic reac-tion has been attributed to propylene glycol,[104]4.3 Potential and Investigational Antifungalpolysorbates[105] and benzyl alcohol.[106] Thus, it isDelivery Systemsimportant to assess the patient’s hypersensitivity
Recent investigations in drug delivery have history to the ingredients of antifungal formulations.opened the way for some new and interesting ap- Conversely, some excipients (acidic polymers orproaches for the vaginal administration of antifun- moisturizers) may contribute to the re-establishmentgals. Key objectives remain the same: to improve in of a healthy vaginal milieu.[107,108] Women shouldloco residence and achieve prolonged drug release. also be informed that the use of vaginal antifungalThe development of user-acceptable products is also products may damage condoms or other vaginaldesirable. For example, drugs for Candida infec- contraceptive devices (e.g. diaphragms); when ap-tions may benefit from innovative drug dose forms, plicable, a 3-day break is usually recommendedsuch as mucoadhesive gels, foams or vaginal before using condoms or contraceptive devices. Inrings.[89] These dosage forms, which are already all cases, information about individual productscommercially available for the management of other should be checked before prescribing and/or dis-conditions, may be particularly advantageous when pensing.
© 2008 Adis Data Information BV. All rights reserved. Drugs 2008; 68 (13)

Local Treatment of Vulvovaginal Candidosis 1799
4. McCaig LF, McNeill MM. Trends in prescribing for5. Conclusionsvulvovaginal candidiasis in the United States. Pharmacoepi-demiol Drug Saf 2005 Feb; 14 (2): 113-20
In addition to equivalent efficacy, local treatment 5. Sobel JD. Vaginitis. N Engl J Med 1997 Dec 25; 337 (26): 1896-903of vulvovaginal candidosis presents several advan-
6. Ferrer J. Vaginal candidosis: epidemiological and etiologicaltageous features when compared with oral therapy.factors. Int J Gynaecol Obstet 2000 Dec; 71 Suppl. 1: 21-7
These include a low rate of adverse events (partic- 7. Mitchell H. Vaginal discharge: causes, diagnosis, and treatment.BMJ 2004 May 29; 328 (7451): 1306-8ularly systemic ones), safe utilization during preg-
8. Sobel JD, Faro S, Force RW, et al. Vulvovaginal candidiasis:nancy and breast feeding, and the availability ofepidemiologic, diagnostic, and therapeutic considerations. Am
several efficacious agents against azole-resistant J Obstet Gynecol 1998 Feb; 178 (2): 203-119. Richardson MD, Warnock DW. Fungal infection: diagnosis andCandida spp. However, the wide variety of anti-
management. 3rd ed. Malden (MA): Blackwell Publishing,fungal drugs, regimens and products that is currently 2003available for the local treatment of vulvovaginal 10. Singh S, Sobel JD, Bhargava P, et al. Vaginitis due to Candida
krusei: epidemiology, clinical aspects, and therapy. Clin Infectcandidosis requires an adequate choice of therapeu-Dis 2002 Nov 1; 35 (9): 1066-70
tic approach that is based on a systematic assess- 11. Spinillo A, Capuzzo E, Egbe TO, et al. Torulopsis glabratavaginitis. Obstet Gynecol 1995 Jun; 85 (6): 993-8ment of diverse aspects related to the women, and
12. Martens MG, Hoffman P, El-Zaatari M. Fungal species changesCandida spp. responsible for episode. Azoles andin the female genital tract. J Low Genit Tract Dis 2004 Jan; 8
short-course regimens are used as first-line treat- (1): 21-413. Ferris DG, Nyirjesy P, Sobel JD, et al. Over-the-counter anti-ment, with nystatin and boric acid usually consid-
fungal drug misuse associated with patient-diagnosed vulvo-ered as alternative agents. However, particular situa-vaginal candidiasis. Obstet Gynecol 2002 Mar; 99 (3): 419-25
tions may benefit from other drugs and regimens 14. Walker PP, Reynolds MT, Ashbee HR, et al. Vaginal yeasts inthe era of “over the counter” antifungals. Sex Transm Infectwhen previous therapy has failed. Choosing a con-2000 Dec; 76 (6): 437-8venient antifungal drug formulation should not be 15. Fidel Jr PL, Sobel JD. Immunopathogenesis of recurrent
neglected as they can facilitate or complicate the vulvovaginal candidiasis. Clin Microbiol Rev 1996 Jul; 9 (3):335-48clinical outcome; recent advances in vaginal drug
16. Giraldo P, Neuer A, Korneeva IL, et al. Vaginal heat shockdelivery have brought interesting and convenient protein expression in symptom-free women with a history of
recurrent vulvovaginitis. Am J Obstet Gynecol 1999 Mar; 180options for the local treatment of vulvovaginal(3 Pt 1): 524-9candidosis. Additionally, non-physician healthcare
17. Nyirjesy P. Chronic vulvovaginal candidiasis. Am Fam Physi-providers must be made aware of the main features cian 2001 Feb 15; 63 (4): 697-702
18. Strus M, Kucharska A, Kukla G, et al. The in vitro activity ofof vulvovaginal candidosis in order to correctlyvaginal Lactobacillus with probiotic properties against Candi-counsel women about OTC antifungal products, or da. Infect Dis Obstet Gynecol 2005 Jun; 13 (2): 69-75
effectively identify those patients who require a 19. Sobel JD, Chaim W. Vaginal microbiology of women withacute recurrent vulvovaginal candidiasis. J Clin Microbiolphysician’s attention.1996 Oct; 34 (10): 2497-9
20. Fidel Jr PL. Immunity in vaginal candidiasis. Curr Opin InfectAcknowledgements Dis 2005 Apr; 18 (2): 107-11
21. Sundstrom P. Adhesion in Candida spp. Cell Microbiol 2002No sources of funding were used to assist in the prepara- Aug; 4 (8): 461-9
tion of this review. The authors have no conflicts of interest 22. Schaller M, Bein M, Korting HC, et al. The secreted aspartylproteinases Sap1 and Sap2 cause tissue damage in an in vitrothat are directly relevant to the content of this review.model of vaginal candidiasis based on reconstituted humanvaginal epithelium. Infect Immun 2003 Jun; 71 (6): 3227-34
References 23. Watson MC, Bond CM. Evidence-based guidelines for non-prescription treatment of vulvovaginal candidiasis (VVC).1. Sobel JD. Vulvovaginal candidosis. Lancet 2007 Jun 9; 369Pharm World Sci 2003 Aug; 25 (4): 129-34(9577): 1961-71
24. Eckert LO, Hawes SE, Stevens CE, et al. Vulvovaginal candi-2. Watson MC, Grimshaw JM, Bond CM, et al. Oral versus intra-diasis: clinical manifestations, risk factors, management al-vaginal imidazole and triazole anti-fungal agents for the treat-gorithm. Obstet Gynecol 1998 Nov; 92 (5): 757-65ment of uncomplicated vulvovaginal candidiasis (thrush): a
systematic review. BJOG 2002 Jan; 109 (1): 85-95 25. Ryan CA, Courtois BN, Hawes SE, et al. Risk assessment,3. Nurbhai M, Grimshaw J, Watson M, et al. Oral versus intra- symptoms, and signs as predictors of vulvovaginal and cervi-
vaginal imidazole and triazole anti-fungal treatment of uncom- cal infections in an urban US STD clinic: implications for useplicated vulvovaginal candidiasis (thrush). Cochrane Database of STD algorithms. Sex Transm Infect 1998 Jun; 74 Suppl. 1:Syst Rev 2007; (4): CD002845 59-76
© 2008 Adis Data Information BV. All rights reserved. Drugs 2008; 68 (13)
1800 das Neves et al.
26. Sihvo S, Ahonen R, Mikander H, et al. Self-medication with 45. British Association of Sexual Health and HIV (BASHH), Clin-vaginal antifungal drugs: physicians’ experiences and ical Effectiveness Group. National guideline for the manage-women’s utilization patterns. Fam Pract 2000 Apr; 17 (2): 145- ment of vulvovaginal candidiasis. London: BASHH, 20029 46. World Health Organization. Guidelines for the management of
27. Mardh PA, Wagstrom J, Landgren M, et al. Usage of antifungal sexually transmitted infections. Geneva: World Health Organi-drugs for therapy of genital Candida infections, purchased as zation, 2001over-the-counter products or by prescription: I. Analyses of a 47. Ringdahl EN. Treatment of recurrent vulvovaginal candidiasis.unique database. Infect Dis Obstet Gynecol 2004 Jun; 12 (2): Am Fam Physician 2000 Jun 1; 61 (11): 3306-12, 1791-7 48. Sobel JD. Management of patients with recurrent vulvovaginal
28. Cejtin HE, Mason ED. A guide to the diagnosis and treatment of candidiasis. Drugs 2003; 63 (11): 1059-66vaginitis and cervicitis. Hosp Physician 2000; 36 (10): 53-63 49. Thirion DJ, Zanetti LA. Potentiation of warfarin’s hy-
29. Wiesenfeld HC, Macio I. The infrequent use of office-based poprothrombinemic effect with miconazole vaginal supposito-diagnostic tests for vaginitis. Am J Obstet Gynecol 1999 Jul; ries. Pharmacotherapy 2000 Jan; 20 (1): 98-9181 (1): 39-41 50. Lansdorp D, Bressers HP, Dekens-Konter JA, et al. Potentiation
30. Baeten JM, Nyange PM, Richardson BA, et al. Hormonal con- of acenocoumarol during vaginal administration of miconazoletraception and risk of sexually transmitted disease acquisition: [letter]. Br J Clin Pharmacol 1999 Feb; 47 (2): 225-6results from a prospective study. Am J Obstet Gynecol 2001 51. Sobel JD. Use of antifungal drugs in pregnancy: a focus onAug; 185 (2): 380-5 safety. Drug Saf 2000 Jul; 23 (1): 77-85
31. Fidel Jr PL. Cutright J, Steele C. Effects of reproductive hor- 52. Young GL, Jewell D. Topical treatment for vaginal candidiasismones on experimental vaginal candidiasis. Infect Immun (thrush) in pregnancy. Cochrane Database Syst Rev 2001; (4):2000 Feb; 68 (2): 651-7 CD000225
32. Cotch MF, Hillier SL, Gibbs RS, et al. Epidemiology and 53. Merkus JM. Treatment of vaginal candidiasis: orally or vaginal-outcomes associated with moderate to heavy Candida coloni- ly? J Am Acad Dermatol 1990 Sep; 23 (3 Pt 2): 568-72zation during pregnancy. Vaginal Infections and Prematurity
54. Kiss H, Witt A, Petricevic L, et al. Die orale kurzzeit-therapieStudy Group. Am J Obstet Gynecol 1998 Feb; 178 (2): 374-80der vulvovaginalen pilzinfektion als ein patientenorientiertes
33. Fidel Jr PL. History and update on host defense against vaginal therapiekonzept. Geburtsh Frauenheilk 2001 Mar; 61 (3): 133-candidiasis. Am J Reprod Immunol 2007 Jan; 57 (1): 2-12 7
34. Neves NA, Carvalho LP, De Oliveira MA, et al. Association55. Nappi RE, Liekens G, Brandenburg U. Attitudes, perceptions
between atopy and recurrent vaginal candidiasis. Clin Expand knowledge about the vagina: the International Vagina
Immunol 2005 Oct; 142 (1): 167-71Dialogue Survey. Contraception 2006 May; 73 (5): 493-500
35. Helfgott A, Eriksen N, Bundrick CM, et al. Vaginal infections in56. Drugstore.com [online]. Available from URL: at http://www.human immunodeficiency virus-infected women. Am J Obstet
drugstore.com [Accessed 2008 Apr 12]Gynecol 2000 Aug; 183 (2): 347-5557. Joint Formulary Committee. British National Formulary. 55th36. Spinillo A, Capuzzo E, Acciano S, et al. Effect of antibiotic use
ed. London: British Medical Association & Royal Pharmaceu-on the prevalence of symptomatic vulvovaginal candidiasis.tical Society of Great Britain, 2008Am J Obstet Gynecol 1999 Jan; 180 (1 Pt 1): 14-7
58. NHS clinical knowledge summaries [online]. Available from37. de Leon EM, Jacober SJ, Sobel JD, et al. Prevalence and riskURL: http://cks.library.nhs.uk [Accessed 2008 Apr 12]factors for vaginal Candida colonization in women with type 1
59. Mardh PA, Rodrigues AG, Genc M, et al. Facts and myths onand type 2 diabetes. BMC Infect Dis 2002; 2: 1recurrent vulvovaginal candidosis: a review on epidemiology,38. Patel DA, Gillespie B, Sobel JD, et al. Risk factors for recurrentclinical manifestations, diagnosis, pathogenesis and therapy.vulvovaginal candidiasis in women receiving maintenanceInt J STD AIDS 2002 Aug; 13 (8): 522-39antifungal therapy: results of a prospective cohort study. Am J
60. Moudgal VV, Sobel JD. Antifungal drugs in pregnancy: aObstet Gynecol 2004 Mar; 190 (3): 644-53review. Expert Opin Drug Saf 2003 Sep; 2 (5): 475-8339. Banerjee K, Curtis E, de San Lazaro C, et al. Low prevalence of
61. Acs N, Banhidy F, Puho E, et al. Teratogenic effects of vaginalgenital candidiasis in children. Eur J Clin Microbiol Infect Disboric acid treatment during pregnancy. Int J Gynaecol Obstet2004 Sep; 23 (9): 696-82006 Apr; 93 (1): 55-640. Demirezen S, Dirlik OO, Beksac MS. The association of Candi-
62. Nwokolo NC, Boag FC. Chronic vaginal candidiasis: manage-da infection with intrauterine contraceptive device. Cent Eur Jment in the postmenopausal patient. Drugs Aging 2000 May;Public Health 2005 Mar; 13 (1): 32-416 (5): 335-941. Meyer H, Goettlicher S, Mendling W. Stress as a cause of
63. Welsh BM, Berzins KN, Cook KA, et al. Management ofchronic recurrent vulvovaginal candidosis and the effective-common vulval conditions. Med J Aust 2003 Apr 21; 178 (8):ness of the conventional antimycotic therapy. Mycoses 2006391-5May; 49 (3): 202-9
64. Bryskier A. Antimicrobial agents: antibacterials and antifun-42. Centers for Disease Control and Prevention. Sexually transmit-gals. 1st ed. Washington, DC: ASM Press, 2005ted diseases treatment guidelines, 2006. MMWR 2006; 55: 1-
65. Sheehan DJ, Hitchcock CA, Sibley CM. Current and emerging94azole antifungal agents. Clin Microbiol Rev 1999 Jan; 12 (1):43. Pappas PG, Rex JH, Sobel JD, et al. Guidelines for treatment of40-79candidiasis. Clin Infect Dis 2004 Jan 15; 38 (2): 161-89
66. Dismukes WE. Introduction to antifungal drugs. Clin Infect Dis44. Mendling W, Seebacher C. Guideline vulvovaginal candidosis:2000 Apr; 30 (4): 653-7guideline of the German Dermatological Society, the German
Speaking Mycological Society and the Working Group for 67. Heikkila H, Stubb S, Reitamo S. A study of 72 patients withInfections and Infectimmunology of the German Society for contact allergy to tioconazole. Br J Dermatol 1996 Apr; 134Gynecology and Obstetrics. Mycoses 2003; 46 (9-10): 365-9 (4): 678-80
© 2008 Adis Data Information BV. All rights reserved. Drugs 2008; 68 (13)
Local Treatment of Vulvovaginal Candidosis 1801
68. Sanglard D, Odds FC. Resistance of Candida species to anti- 87. Pina-Vaz C, Goncalves Rodrigues A, Pinto E, et al. Antifungalfungal agents: molecular mechanisms and clinical conse- activity of Thymus oils and their major compounds. J Eurquences. Lancet Infect Dis 2002 Feb; 2 (2): 73-85 Acad Dermatol Venereol 2004 Jan; 18 (1): 73-8
69. Phillips AJ. Treatment of non-albicans Candida vaginitis with 88. Hammer KA, Carson CF, Riley TV. Antifungal activity of theamphotericin B vaginal suppositories. Am J Obstet Gynecol components of Melaleuca alternifolia (tea tree) oil. J Appl2005 Jun; 192 (6): 2009-12 Microbiol 2003; 95 (4): 853-60
70. Dan M. Severe vulvovaginitis associated with intravaginal nys- 89. das Neves J, Amaral MH, Bahia MF. Vaginal drug delivery. In:tatin therapy. Am J Obstet Gynecol 2001 Jul; 185 (1): 254-5 Gad SC, editor. Pharmaceutical manufacturing handbook: pro-
71. Sobel JD, Chaim W, Nagappan V, et al. Treatment of vaginitis duction and processes. 1st ed. Hoboken (NJ): Wiley, 2008:caused by Candida glabrata: use of topical boric acid and 809-78flucytosine. Am J Obstet Gynecol 2003 Nov; 189 (5): 1297- 90. das Neves J, Santos B, Teixeira B, et al. Vaginal drug adminis-300 tration in the hospital setting. Am J Health Syst Pharm 2008;
72. Ray D, Goswami R, Banerjee U, et al. Prevalence of Candida 65 (3): 254-9glabrata and its response to boric acid vaginal suppositories in 91. Merabet J, Thompson D, Saul Levinson R. Advancing vaginalcomparison with oral fluconazole in patients with diabetes and drug delivery. Expert Opin Drug Deliv 2005 Jul; 2 (4): 769-77vulvovaginal candidiasis. Diabetes Care 2007 Feb; 30 (2): 92. Henzl MR. Properties of sustained-release single-dose formula-312-7 tions for vulvovaginal candidiasis: the example of butocona-
73. Sobel JD, Chaim W. Treatment of Torulopsis glabrata vagini- zole vaginal emulsion as a drug-sparing formulation. Am Jtis: retrospective review of boric acid therapy. Clin Infect Dis Drug Deliv 2005; 3 (4): 227-371997 Apr; 24 (4): 649-52
93. Brown D, Henzl MR, Kaufman RH. Butoconazole nitrate 2%74. Horowitz BJ. Topical flucytosine therapy for chronic recurrent for vulvovaginal candidiasis: new, single-dose vaginal cream
Candida tropicalis infections. J Reprod Med 1986 Sep; 31 (9): formulation vs. seven-day treatment with miconazole nitrate.821-4 Gynazole 1 Study Group. J Reprod Med 1999 Nov; 44 (11):
75. White DJ, Habib AR, Vanthuyne A, et al. Combined topical 933-8flucytosine and amphotericin B for refractory vaginal Candida
94. Seidman LS, Skokos CK. An evaluation of butoconazole nitrateglabrata infections. Sex Transm Infect 2001 Jun; 77 (3): 212-32% site release vaginal cream (Gynazole-1) compared to fluco-
76. Garcia Figueroa RG, Sauceda L, Ramirez Palacios D, et al. nazole 150 mg tablets (Diflucan) in the time to relief ofEficacia y seguridad de ciclopirox olamina en crema vaginal al symptoms in patients with vulvovaginal candidiasis. Infect Dis1% contra terconazol en crema vaginal al 0.8% en el Obstet Gynecol 2005 Dec; 13 (4): 197-206tratamiento de candidiasis genital. Ginecol Obstet Mex 2000
95. del Palacio A, Sanz F, Sanchez-Alor G, et al. Double-blindApr; 68: 154-9randomized dose-finding study in acute vulvovaginal77. Friese K, Neumann G, Siebert J. Topical antiseptics as ancandidosis: comparison of flutrimazole site-release cream (1, 2alternative in the treatment of acute vulvovaginal candidosis.and 4%) with placebo site-release vaginal cream. MycosesArch Gynecol Obstet 2003 Aug; 268 (3): 194-72000 Oct; 43 (9-10): 355-65
78. Molteni B, D’Antuono A, Bandini P, et al. Efficacy and tolera-96. Upmalis DH, Cone FL, Lamia CA, et al. Single-dosebility of a new chlorhexidine-based vaginal gel in vaginal
miconazole nitrate vaginal ovule in the treatment ofinfections. Curr Med Res Opin 2004 Jun; 20 (6): 849-53vulvovaginal candidiasis: two single-blind, controlled studies
79. Petersen EE, Weissenbacher ER, Hengst P, et al. Local treat-versus miconazole nitrate 100 mg cream for 7 days. J Womens
ment of vaginal infections of varying etiology with dequalini-Health Gend Based Med 2000 May; 9 (4): 421-9
um chloride or povidone iodine: a randomised, double-blind,97. Barnhart K. Safety and efficacy of bedtime versus daytimeactive-controlled, multicentric clinical study. Arzneimittelfor-
administration of the miconazole nitrate 1200 mg vaginalschung 2002; 52 (9): 706-15ovule insert to treat vulvovaginal candidiasis. Curr Med Res80. Stevens DA, Calderon L, Martinez M, et al. Zeamatin, clo-Opin 2005 Jan; 21 (1): 127-34trimazole and nikkomycin Z in therapy of a Candida vaginitis
98. Dellenbach P, Thomas JL, Guerin V, et al. Topical treatment ofmodel. J Antimicrob Chemother 2002 Sep; 50 (3): 361-4vaginal candidosis with sertaconazole and econazole sus-81. Pirotta M, Gunn J, Chondros P, et al. Effect of Lactobacillus intained-release suppositories. Int J Gynaecol Obstet 2000 Dec;preventing post-antibiotic vulvovaginal candidiasis: a random-71 Suppl. 1: 47-52ised controlled trial. BMJ 2004 Sep 4; 329 (7465): 548
99. Chang JY, Oh YK, Kong HS, et al. Prolonged antifungal effects82. Falagas ME, Betsi GI, Athanasiou S. Probiotics for preventionof clotrimazole-containing mucoadhesive thermosensitive gelsof recurrent vulvovaginal candidiasis: a review. J Antimicrobon vaginitis. J Control Release 2002 Jul 18; 82 (1): 39-50Chemother 2006 Aug; 58 (2): 266-72
100. Bilensoy E, Rouf MA, Vural I, et al. Mucoadhesive, thermosen-83. Wozniak KL, Palmer G, Kutner R, et al. Immunotherapeuticsitive, prolonged-release vaginal gel for clotrimazole:beta-approaches to enhance protective immunity against Candidacyclodextrin complex. AAPS PharmSciTech 2006; 7 (2): E38vaginitis. Med Mycol 2005 Nov; 43 (7): 589-601
101. Pavelic Z, Skalko-Basnet N, Jalsenjak I. Characterisation and in84. Magliani W, Conti S, Cassone A, et al. New immunotherapeuticvitro evaluation of bioadhesive liposome gels for local therapystrategies to control vaginal candidiasis. Trends Mol Med 2002of vaginitis. Int J Pharm 2005 Sep 14; 301 (1-2): 140-8Mar; 8 (3): 121-6
102. Ning MY, Guo YZ, Pan HZ, et al. Preparation and evaluation of85. Cassone A, De Bernardis F, Santoni G. Anticandidal immunityproliposomes containing clotrimazole. Chem Pharm Bull 2005and vaginitis: novel opportunities for immune intervention.Jun; 53 (6): 620-4Infect Immun 2007 Oct; 75 (10): 4675-86
86. Hammer KA, Carson CF, Riley TV. Antimicrobial activity of 103. Ning M, Guo Y, Pan H, et al. Preparation, in vitro and in vivoessential oils and other plant extracts. J Appl Microbiol 1999 evaluation of liposomal/niosomal gel delivery systems forJun; 86 (6): 985-90 clotrimazole. Drug Dev Ind Pharm 2005 May; 31 (4-5): 375-83
© 2008 Adis Data Information BV. All rights reserved. Drugs 2008; 68 (13)

1802 das Neves et al.
104. Motoyoshi K, Nozawa S, Yoshimura M, et al. The safety of 108. Caswell M, Kane M. Comparison of the moisturization efficacypropylene glycol and other humectants. Cosmet Toilet 1984; of two vaginal moisturizers: pectin versus polycarbophil tech-99 (10): 83-91 nologies. J Cosmet Sci 2002 Mar-Apr; 53 (2): 81-7
105. Shelley WB, Talanin N, Shelley ED. Polysorbate 80 hypersensi-tivity [letter]. Lancet 1995 May 20; 345 (8960): 1312-3
106. Sestini S, Mori M, Francalanci S. Allergic contact dermatitis Correspondence: Dr Jose das Neves, Department of Pharma-from benzyl alcohol in multiple medicaments. Contact Derma- ceutical Technology, Faculty of Pharmacy, University oftitis 2004 May; 50 (5): 316-7
Porto, Rua Anibal Cunha, 164, 4050-047, Porto, Portugal.107. das Neves J, Bahia MF. Gels as vaginal drug delivery systems.E-mail: [email protected] J Pharm 2006 Aug 2; 318 (1-2): 1-14
© 2008 Adis Data Information BV. All rights reserved. Drugs 2008; 68 (13)
Related Documents











