Local Delivery Plan 2016–2017 Driving Improvement in Health and Social Care

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Local Delivery Plan 2016–2017
Driving Improvement in Health and Social Care

© Healthcare Improvement Scotland 2016
First published July 2016
All images contained within this publication were sourced from the
NHSScotland Photo Library and are covered by © Crown copyright.
The contents of this document may be copied or reproduced for
use within NHSScotland and our partner organisations, or for
educational, personal or non-commercial research purposes only.
Commercial organisations must obtain written permission from
Healthcare Improvement Scotland before copying or reproducing
any part of this document.
www.healthcareimprovementscotland.org

3
Contents
Introduction 4
How we work – our principles 5
Our unique strategic advantages 6
Our seven strategic contributions to support the
transformation of health and social care in Scotland 7
Our Work Programme 2016–2017 8
Measurement and evaluation 26
Best use of resources 28
Appendix 1: 2020 Workforce Vision –
local implementation plan (2016–2017) 29

4
Introduction
This Local Delivery Plan 2016–2017 sets out our intent to support the
transformational change to public services that is taking place in Scotland. In
particular, our plan supports the Scottish Government’s ambition to build a safer,
healthier and fairer society and it sets out the contributions that we can make to
achieve the Scottish Government’s 2020 Vision for health and social care.
This is an ambitious plan which updates our Driving Improvement in Healthcare
Strategy (2014–2020) by positioning our role and our work across public services
and specifically within health and social care services in Scotland.
We have identified seven strategic contributions that demonstrate the role that
Healthcare Improvement Scotland (HIS) can play in supporting the significant
redesign of health and social care services in Scotland. We have incorporated key
principles from the National Clinical Strategy1, such as putting communities at the
centre of design and delivery of services that are evidence based, effective and
sustainable.
This plan also signals our move from measuring outputs to delivering outcomes.
We have mapped our work in the Local Delivery Plan to our seven contributions
and our evaluation framework, which is aligned with the nine national health
and wellbeing outcomes2, to ensure that all of our activity is linked to achieving
national outcomes and demonstrates progress.
1 Scottish Government. A National Clinical Strategy for Scotland. 2016. http://www.gov.scot/Resource/0049/00494144.pdf
2 Scottish Government. National Health and Wellbeing Framework. 2015. http://www.gov.scot/Resource/0047/00470219.pdf

5
How we work – our principles
We are uniquely placed as a national organisation to make a very substantial
and positive impact in supporting improvements in the quality of health care in
Scotland. As an integrated organisation, our blend of roles and functions offers a
highly effective, efficient and cohesive approach to supporting high quality care.
We will support the achievement of Scottish Government’s ambitions by adhering
to the following principles:
• Establishing the evidence for what will work best to integrate services and what high quality care would look like
• Supporting the redesign of services to achieve and sustain higher quality and increasingly integrated care
• Reviewing the current provision of services and supporting the commissioning and redesign of new services
• Working with citizens to ensure that their voice is heard in the design, and provision of health and social care.
• Ensuring that we have meaningful clinical and practitioner engagement and involvement across all of our work
• Working in Partnership with our stakeholders in NHS boards, Integration Authorities, Local Authorities and Government to drive improvement in health care across public services
• Assuring the quality of care that people are receiving and reporting our findings and recommendations without bias
• Ensuring that we can measure and demonstrate the impact of our work in support of the health and wellbeing outcomes and reducing inequalities
• Managing our resources efficiently and effectively and by achieving value for money

6
Our unique strategic advantages
There is a need for a strong and bold reshaping of care that places individuals
at the centre of the future model of service provision, but which also recognises
the need to tackle duplication, inappropriate variation and waste. It is about
preventing and tackling ill health and delivering a health and social care system
that consistently puts service users, carers and citizens first and supports self-
management wherever possible.
We have at least two unique strategic advantages:
1. We support both health and social care services to deliver higher quality care. We offer a strong and visible contribution to health and social care services in Scotland, in supporting their drive to be highly reliable organisations, providing consistently safe, effective and person-centred care.
2. The integrated and cohesive provision of a complementary range of functions which are aligned and mutually supportive.
These are substantial advantages, enabling us to provide a single gateway to a
range of strong, timely and effective mechanisms to support higher quality care,
for example:
• practical quality improvement support
• securing the voice of citizens in the design of services
• the latest good practice and evidence, or
• rigorous and independent external quality assurance
We will use our influence and our alliances with national organisations (United
Kingdom Improvement Alliance (UKIA), The Health Foundation and the Kings
Fund) and we will work alongside other improvement bodies to capitalise on
these strategic advantages, for example Advancing Quality Alliance (AQuA), Haelo
Innovation and Improvement Science Centre and Yorkshire and Humberside
Improvement Academy (YHIA).
7
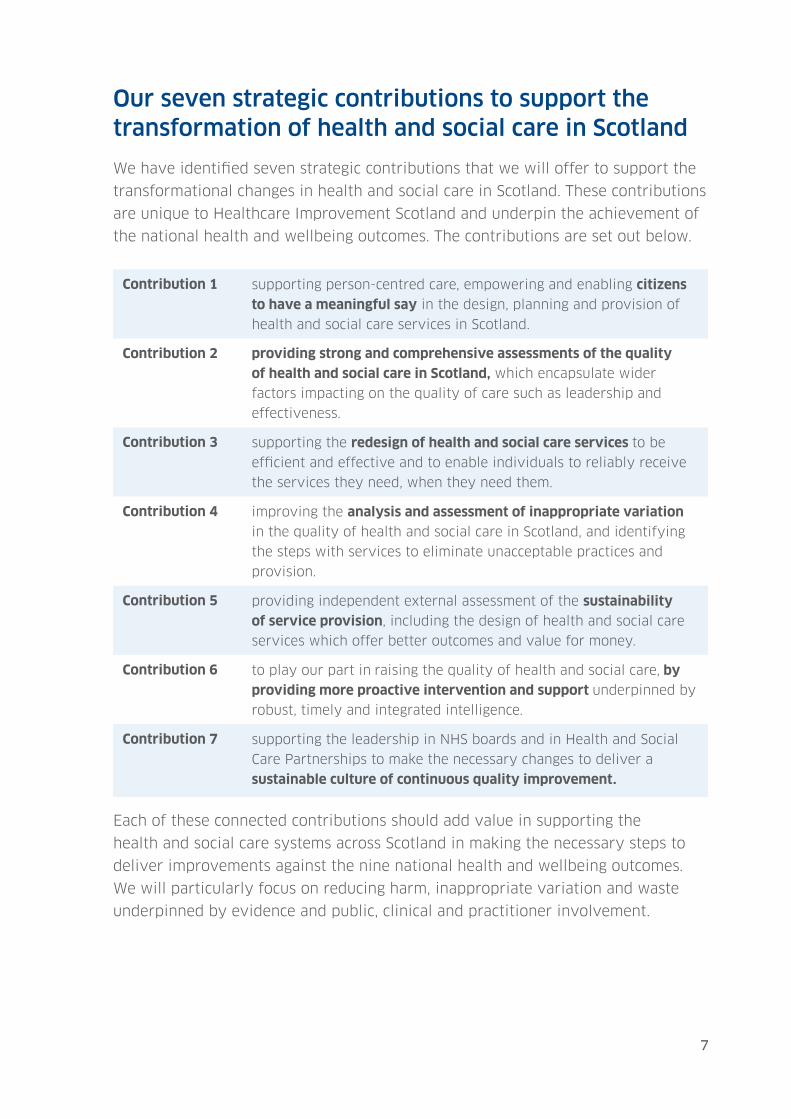
Our seven strategic contributions to support the transformation of health and social care in Scotland
We have identified seven strategic contributions that we will offer to support the
transformational changes in health and social care in Scotland. These contributions
are unique to Healthcare Improvement Scotland and underpin the achievement of
the national health and wellbeing outcomes. The contributions are set out below.
Contribution 1 supporting person-centred care, empowering and enabling citizens
to have a meaningful say in the design, planning and provision of
health and social care services in Scotland.
Contribution 2 providing strong and comprehensive assessments of the quality
of health and social care in Scotland, which encapsulate wider
factors impacting on the quality of care such as leadership and
effectiveness.
Contribution 3 supporting the redesign of health and social care services to be
efficient and effective and to enable individuals to reliably receive
the services they need, when they need them.
Contribution 4 improving the analysis and assessment of inappropriate variation
in the quality of health and social care in Scotland, and identifying
the steps with services to eliminate unacceptable practices and
provision.
Contribution 5 providing independent external assessment of the sustainability
of service provision, including the design of health and social care
services which offer better outcomes and value for money.
Contribution 6 to play our part in raising the quality of health and social care, by
providing more proactive intervention and support underpinned by
robust, timely and integrated intelligence.
Contribution 7 supporting the leadership in NHS boards and in Health and Social
Care Partnerships to make the necessary changes to deliver a
sustainable culture of continuous quality improvement.
Each of these connected contributions should add value in supporting the
health and social care systems across Scotland in making the necessary steps to
deliver improvements against the nine national health and wellbeing outcomes.
We will particularly focus on reducing harm, inappropriate variation and waste
underpinned by evidence and public, clinical and practitioner involvement.

8
Our Work Programme 2016–2017
Our work programme presented as the Local Delivery Plan for 2016–2017 is
strategically aligned with our seven strategic contributions and reflects our
medium term outcomes. It clearly sets out what will be delivered and the
objectives that have been set.
Contribution 1: Supporting person-centred care, and empowering and enabling
citizens to have a meaningful say in the design, planning and provision of health
and social care services in Scotland.
Title Aim Objectives Lead Director
Personal
Outcomes
Improving
personal outcomes
Take forward the Personal
Outcomes Partnership with Thistle
Foundation offering facilitated
development to staff working with
people to enhance focus on assets
and personal outcomes.
Director of
Improvement
Support and
ihub
Scottish Health
Council (SHC)
Volunteering
Supporting
volunteering in
Scotland
Provide national leadership
and guidance to ensure long
term vision and consistency
of approach and support for
volunteering across NHSScotland.
This support may extend in time
to integration authorities.
Director of
Scottish Health
Council
SHC Service
Change
Quality assurance
of service change
in Scotland
Provide advice and support to
NHS boards on involving patients
and communities in service
change processes, in line with
Scottish Government guidance.
Director of
Scottish Health
Council
SHC Public
Involvement
Unit
Promoting
greater public
involvement
Continue to ensure HIS meets its
equalities duties and the Duty
of User Focus and generally
demonstrate good practice in
involving users, carers and the
public in its activities.
Director of
Scottish Health
Council
SHC Community
Engagement
and
Improvement
Support
Strengthening
community
engagement
Provide tailored advice and
improvement support to 21 NHS
boards/special NHS boards. Work
to develop and support local peer
networks and build capacity for
communities to be involved in the
design and delivery of health and
care services.
Director of
Scottish Health
Council
9
Title Aim Objectives Lead Director
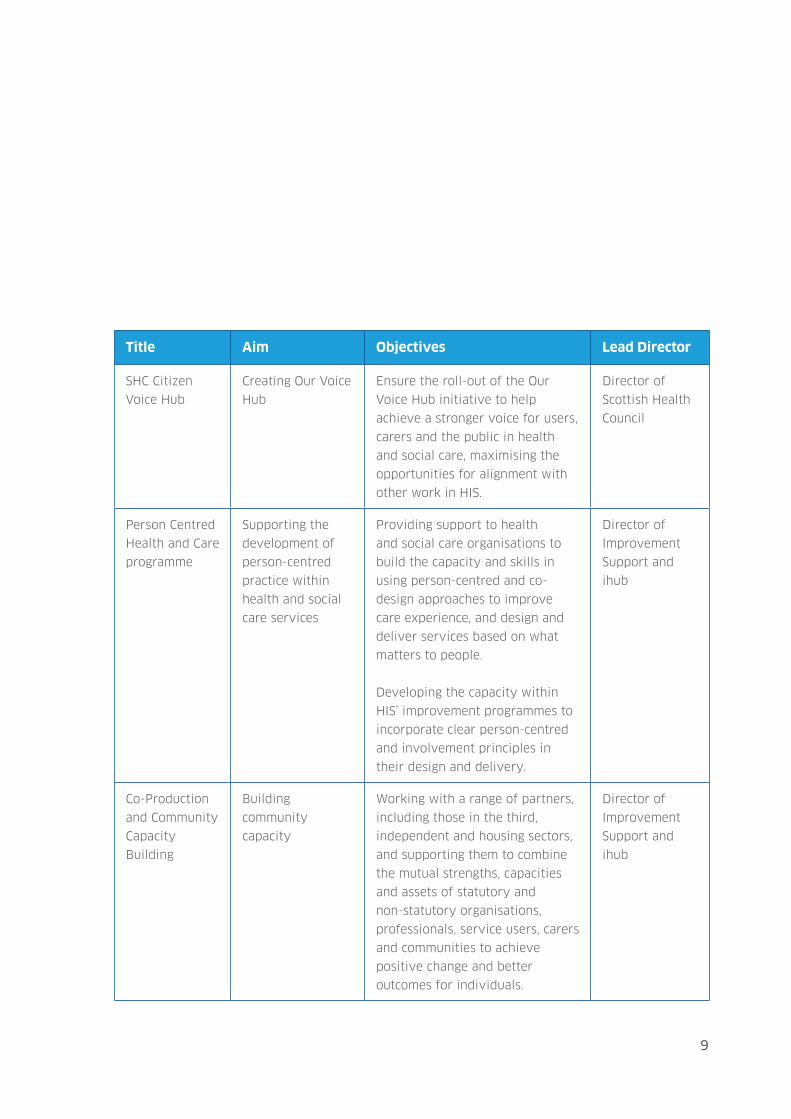
SHC Citizen
Voice Hub
Creating Our Voice
Hub
Ensure the roll-out of the Our
Voice Hub initiative to help
achieve a stronger voice for users,
carers and the public in health
and social care, maximising the
opportunities for alignment with
other work in HIS.
Director of
Scottish Health
Council
Person Centred
Health and Care
programme
Supporting the
development of
person-centred
practice within
health and social
care services
Providing support to health
and social care organisations to
build the capacity and skills in
using person-centred and co-
design approaches to improve
care experience, and design and
deliver services based on what
matters to people.
Developing the capacity within
HIS’ improvement programmes to
incorporate clear person-centred
and involvement principles in
their design and delivery.
Director of
Improvement
Support and
ihub
Co-Production
and Community
Capacity
Building
Building
community
capacity
Working with a range of partners,
including those in the third,
independent and housing sectors,
and supporting them to combine
the mutual strengths, capacities
and assets of statutory and
non-statutory organisations,
professionals, service users, carers
and communities to achieve
positive change and better
outcomes for individuals.
Director of
Improvement
Support and
ihub

10
Contribution 2: Providing strong and comprehensive assessments of the quality of
health and social care in Scotland, which encapsulate wider factors impacting on
the quality of care such as leadership and effectiveness.
Title Aim Objectives Lead Director
Strategic
Inspection of
Adult Services
External quality
assurance of
jointly delivered
adult services
Undertake joint inspections with
the Care Inspectorate.
Ensure delivery of robust,
affordable proposals for the
future design of joint adult
inspections in collaboration
with the Care Inspectorate and
informed by engagement with
external stakeholders.
Director
of Quality
Assurance
Scrutiny of
Prisoner
Healthcare
Quality assurance
of health care
provided to
prisoners
Provide clinical expertise to the
inspection programme of prisons
in Scotland.
Director
of Quality
Assurance
Inspection of
Services for
Older People in
Acute Hospitals
(OPAH)
Driving better care
for older people in
hospital
Continue to undertake inspections
of the care of older people in
acute hospitals and agree detailed
proposals for the extension of the
methodology to include non-acute
healthcare facilities, including
specialist dementia units.
Director
of Quality
Assurance
Joint Inspection
of Children’s
Services
Driving better care
for children
Led by the Care Inspectorate,
HIS works in partnership
with Education Scotland and
Her Majesty’s Inspectorate of
Constabulary Partners in the
multi-agency strategic inspections
of services for children. In
addition to being part of the
core team, ensure strong and
effective clinical assurance of the
inspection.
Director
of Quality
Assurance

11
Title Aim Objectives Lead Director
Healthcare
Environment
Inspectorate
(HEI)
Inspections
Promoting safer
and cleaner
hospitals
Undertake further HEI inspections
under the revised Healthcare
Associated Infection (HAI)
Standards, including theatres.
Manage and carry out wider
assessment of the progress in
the delivery of Lord Maclean’s
recommendations arising from the
Vale of Leven Inquiry.
Director
of Quality
Assurance
Medical
Revalidation
National
assessment of the
revalidation of
medical doctors
Undertake further national
assessment of the progress in
medical revalidation in Scotland.
Director
of Quality
Assurance
Management
of Controlled
Drugs
(Governance)
Ensuring Safe
Management of
Controlled Drugs
Maintain and publish the register
of controlled drugs accountable
officers in Scotland and provide
external quality assurance of the
governance arrangements in place
within each designated body
in Scotland to ensure the safe
management of controlled drugs.
Director
of Quality
Assurance
Regulation of
Independent
Healthcare
Driving better
bare and services
provided by the
independent
healthcare sector
Ensure effective and successful
extension of regulatory powers to
include independent clinics, with
all independent clinics registered
by 31 March 2017.
Continue programme of
inspections for independent
hospitals which includes hospices
and private psychiatric hospitals.
Director
of Quality
Assurance
Human
Tissue Bank
Accreditation
Ensuring a safe
network of Human
Tissue Banks
Undertake accreditation of the
regional tissue banks and external
quality assurance of the satellite
boards.
Director
of Quality
Assurance

12
Title Aim Objectives Lead Director
Assessment
of referral
from National
Confidential
Alert Line
(NCAL) and
concerns
passed to
HIS under
the Public
Information
Disclosure Act
(PIDA)
Assessment
of referral
from National
Confidential Alert
Line (NCAL) and
concerns passed
to HIS under the
Public Information
Disclosure Act
(PIDA)
Actively review and where
necessary take action in relation
to concerns about safety of
patient care.
Director
of Quality
Assurance
Thematic
Reviews of
Major Priorities
Comprehensive
assessments of the
quality of care in
Scotland
Establish the detailed operational
methodology and infrastructure to
implement comprehensive quality
of care reviews in Scotland,
ensuring that such reviews
are aligned to wider national
priorities, including the National
Clinical Strategy.
Director
of Quality
Assurance
Quality
Assurance of
Mental Health
Care Services in
Scotland
Driving
improvements in
mental health care
in Scotland
Within the context of quality of
care reviews, establish a robust
approach to the external quality
assurance of mental health
services in Scotland, working in
partnership with other agencies
such as the Mental Welfare
Commission.
Director
of Quality
Assurance
Review of
National
Screening
Programmes
Establish
consistent high
quality approach
to screening in
Scotland
Undertake scrutiny and assurance
activity of national screening
programmes against national
standards.
Director
of Quality
Assurance
13
Title Aim Objectives Lead Director
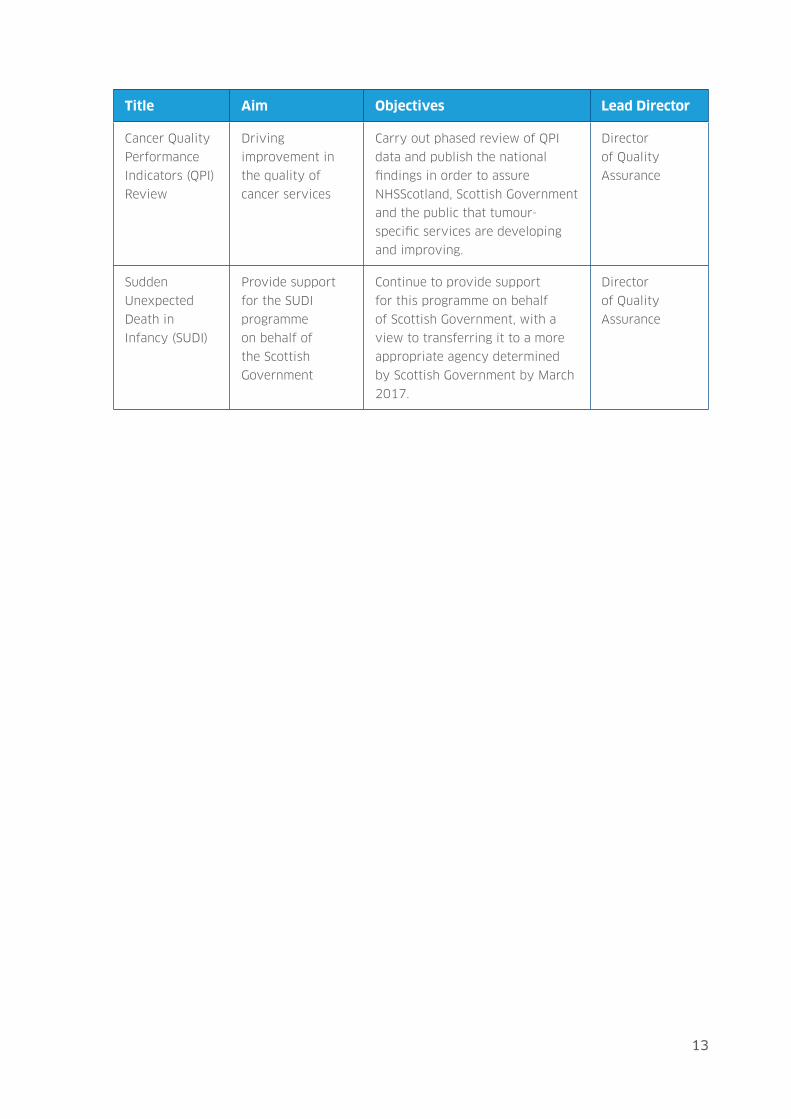
Cancer Quality
Performance
Indicators (QPI)
Review
Driving
improvement in
the quality of
cancer services
Carry out phased review of QPI
data and publish the national
findings in order to assure
NHSScotland, Scottish Government
and the public that tumour-
specific services are developing
and improving.
Director
of Quality
Assurance
Sudden
Unexpected
Death in
Infancy (SUDI)
Provide support
for the SUDI
programme
on behalf of
the Scottish
Government
Continue to provide support
for this programme on behalf
of Scottish Government, with a
view to transferring it to a more
appropriate agency determined
by Scottish Government by March
2017.
Director
of Quality
Assurance

14
Contribution 3: Supporting the redesign of health and social care services to be
efficient and effective and to enable individuals to reliably receive the services
they need, when they need them.
Title Aim Objectives Lead Director
Primary Care
Strategy
and Phase 1
Implementation
Driving
improvement
in the quality
of primary care
services
Complete strategy to inform
the capability and capacity
building needed to enhance the
pace and scale at which HIS
collaborates with and supports
healthcare organisations to drive
improvements in integrated
primary care services.
Executive
Clinical Director
National Review
of Out-of-
Hours Services
Quality & Safety
Programme
Driving
improvement to
deliver consistent,
high quality out-
of-hours services
HIS is scoping work aimed at
enabling NHS boards to become
self-sufficient in knowing how
their urgent care services are
performing against agreed
standards, what they need to
focus on improving, and have
the knowledge and skills to then
deliver and sustain the desired
improvements.
Executive
Clinical Director
Older People
in Acute Care
Improvement of
Care
Driving
improvement in
the quality of care
for older people
Build on work to date, which
supports improvement work
at a local level and promotes
local ownership, spread and
sustainability of change.
Critically, during 2016–2017 to
ensure an increasingly aligned
approach between scrutiny and
improvement.
Director of
Improvement
Support and
ihub

15
Title Aim Objectives Lead Director
Mental Health
Access
Supporting swifter
access to mental
health care
The Mental Health Access
Improvement Support Team
(MHAIST) has been established
to support improved access
to both psychological therapy
interventions and Child and
Adolescent Mental Health
Services. The team will work
with NHS boards and Health
and Social Care Partnerships to
support a ‘deep dive’ diagnostic
to understand the barriers to
meeting the target of treatment
within 18 weeks of referral and
– on the basis of this – to then
agree an improvement plan to
enable reliable delivery of this
access target.
Director of
Improvement
Support and
ihub
Strategic
Commissioning
Supporting
good practice in
commissioning
services that offer
better outcomes
Support Health and Social Care
Partnerships to improve the
effectiveness of their strategic
commissioning arrangements and
practice. In doing so, enable them
to achieve a better alignment
of investment and delivered
outcomes whilst ensuring
that personalised services
and supports, a co-production
approach and more robust and
consistent decision-making
become more strongly embedded.
Director of
Improvement
Support and
ihub
Home, Place
and Housing
Portfolio
Supporting more
people to lead
independent and
healthier lives at
home
The Home, Place and Housing
Portfolio aims to make key
improvements to strategic
planning of housing and related
services to provide people with a
home environment that supports
greater independence and
improved health and wellbeing.
Director of
Improvement
Support and
ihub
16
Title Aim Objectives Lead Director
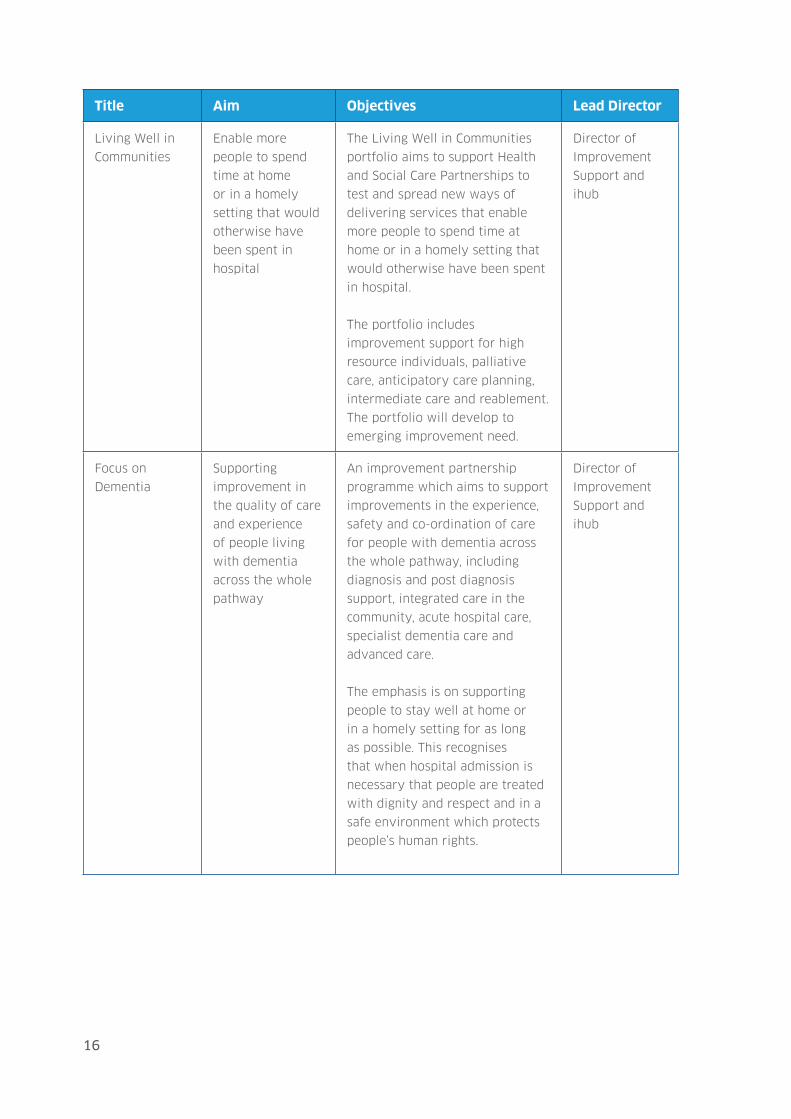
Living Well in
Communities
Enable more
people to spend
time at home
or in a homely
setting that would
otherwise have
been spent in
hospital
The Living Well in Communities
portfolio aims to support Health
and Social Care Partnerships to
test and spread new ways of
delivering services that enable
more people to spend time at
home or in a homely setting that
would otherwise have been spent
in hospital.
The portfolio includes
improvement support for high
resource individuals, palliative
care, anticipatory care planning,
intermediate care and reablement.
The portfolio will develop to
emerging improvement need.
Director of
Improvement
Support and
ihub
Focus on
Dementia
Supporting
improvement in
the quality of care
and experience
of people living
with dementia
across the whole
pathway
An improvement partnership
programme which aims to support
improvements in the experience,
safety and co-ordination of care
for people with dementia across
the whole pathway, including
diagnosis and post diagnosis
support, integrated care in the
community, acute hospital care,
specialist dementia care and
advanced care.
The emphasis is on supporting
people to stay well at home or
in a homely setting for as long
as possible. This recognises
that when hospital admission is
necessary that people are treated
with dignity and respect and in a
safe environment which protects
people’s human rights.
Director of
Improvement
Support and
ihub

17
Title Aim Objectives Lead Director
National Care
Standards
Development
of consistent
National Care
Standards
Deliver in collaboration with the
Care Inspectorate, a set of general
and specialist standards linked to
the principles signed off in March
2016.
Director of
Evidence
Scottish
Intercollegiate
Guidelines
Network (SIGN)
Guideline
Programme
Driving
improvements in
care by developing
SIGN clinical
guidelines
Continue to develop evidence-
based guidelines for healthcare
professionals, seeking appropriate
ways in which information can be
more rapidly disseminated.
Director of
Evidence
Standards
and Indicators
Programme
Driving
improvements in
care by developing
standards and
indicators
Further develop the programme of
standards, including pressure ulcer
standards and screening services
to underpin inspection processes
and indicators, in areas such as
palliative care and heart disease,
which are used to facilitate
ready comparison of services in
a nationally consistent manner
and generate data that provides a
baseline for improvement.
Director of
Evidence
RARE-
Bestpractices
Programme
Conclusion of the
European RARE-
Bestpractices
Programme
Continue with the RARE-
Bestpractices programme to
reduce inequality in care for
patients with rare diseases across
Europe.
Director of
Evidence

18
Contribution 4: Improving the analysis and assessment of inappropriate variation
in the quality of health and social care in Scotland, and identifying the steps with
services to eliminate unacceptable practices and provision.
Title Aim Objectives Lead Director
Death Certification
Review Service
Quality
assurance and
enhancing
the clinical
governance of the
death certification
process
Ensure the effective operation
of the Death Certification
Review Service and key
operational objectives are
consistently delivered.
Executive
Clinical
Director
Scottish Mortality
and Morbidity
Programme
(SMMP)
Maximising and
sharing learning
from the SMMP
Through the SMMP, ensure
an effective approach to
supporting the improved local
learning from deaths; improved
local action to reduce Hospital
Standard Morbidity Rates
(HSMR); thematic national data
for improvement; and improved
governance at local and national
level in relation to mortality
reviews.
Executive
Clinical
Director
Measurement and
Monitoring of
Safety Programme
Consolidate
learning
from testing
a conceptual
framework and
seek to support a
rounded approach
to safety
measurement
and monitoring
using leading
and predictive
measures
Spread and integrate the
framework for the measurement
and monitoring of safety across
Scotland. Work with UKIA
and partners across the UK
to further develop resources
and create a spread and
sustainability plan to support
others in their use of the
framework.
Executive
Clinical
Director
Scottish Patient
Safety Programme
(SPSP) Acute Adult
Driving
improvement in
safety for patients
in acute hospitals
Implement the new
arrangements arising from the
90-day process reviewing the
Acute Adult and Primary Care
safety programmes.
Director of
Improvement
Support and
ihub

19
Title Aim Objectives Lead Director
SPSP Venous
Thromboembolism
(VTE)
Reduction of
incidence of VTE
Undertake a ‘deep dive’ with
one NHS board to understand
the factors mitigating against
reducing unwarranted variation
in the management of VTE, test
solutions and identify learning
for spread across Scotland.
Director of
Improvement
Support and
ihub
SPSP Mental
Health
Reduce harm for
patients with
mental illness
Support NHS boards to improve
outcomes for people with
mental illness through a focus
on reducing harm, including
restraint and seclusion,
improving medicine safety risk
assessment and safety planning
at key transition points.
Director of
Improvement
Support and
ihub
SPSP Primary Care Driving
improvements in
the quality and
safety of primary
care
Implement the new
arrangements arising from the
90-day process reviewing the
Acute Adult and Primary Care
safety programmes.=
Director of
Improvement
Support and
ihub
SPSP Pressure
Ulcers
Support for a
reduction in
incidence and
prevalence of
pressure ulcers
The programme will work
in collaboration with NHS
boards, Health and Social Care
Partnerships, Scottish Care and
care homes across Scotland to
reduce the incidence of pressure
ulcers for residents in care
homes.
Director of
Improvement
Support and
ihub
SPSP Maternity
and Children
Driving
improvement
in the safety
of care offered
to mothers and
children
Implement SPSP Maternity and
Children programme to improve
outcomes by providing a safe,
high quality care experience for
all women, babies and children,
in these settings in Scotland.
Director of
Improvement
Support and
ihub

20
Title Aim Objectives Lead Director
SPSP Healthcare
Associated
Infections (HAI)
Support reduction
in HAI
Provide overall co-ordination of
all HAI-related activities within
HIS to ensure an integrated
and planned approach. Provide
improvement advice and
support to the NHS boards on
HAI issues.
Director of
Improvement
Support and
ihub
SPSP Pharmacy in
Primary Care
Driving
improvement in
safer prescribing
and dispensing in
primary care
Continue to improve reliability
of a number of processes,
including the prescribing,
monitoring and dispensing of
high risk medicines, medicines
reconciliation at discharge from
acute hospital, and developing a
safety culture.
Director of
Improvement
Support and
ihub
SPSP Medicines Reducing harm
from medicines
SPSP Medicines aims to reduce
harm from medicines through
supporting the medicines
streams within each of the SPSP
improvement programmes,
with a focus on medicines
reconciliation and high risk
medicines.
Director of
Improvement
Support and
ihub
Sharing
Intelligence for
Health & Care
Maximise the
sharing of
intelligence to
identify areas for
improvement
Build on the work of the Sharing
Intelligence Group to provide
a proactive and supportive
environment for collaboration;
regular opportunities to build
stronger working relationships
and understanding of roles;
a shared view of risks to
quality through our collective
intelligence; an early warning
mechanism of risks; and co-
ordinated action to drive
improvement.
Director
of Quality
Assurance
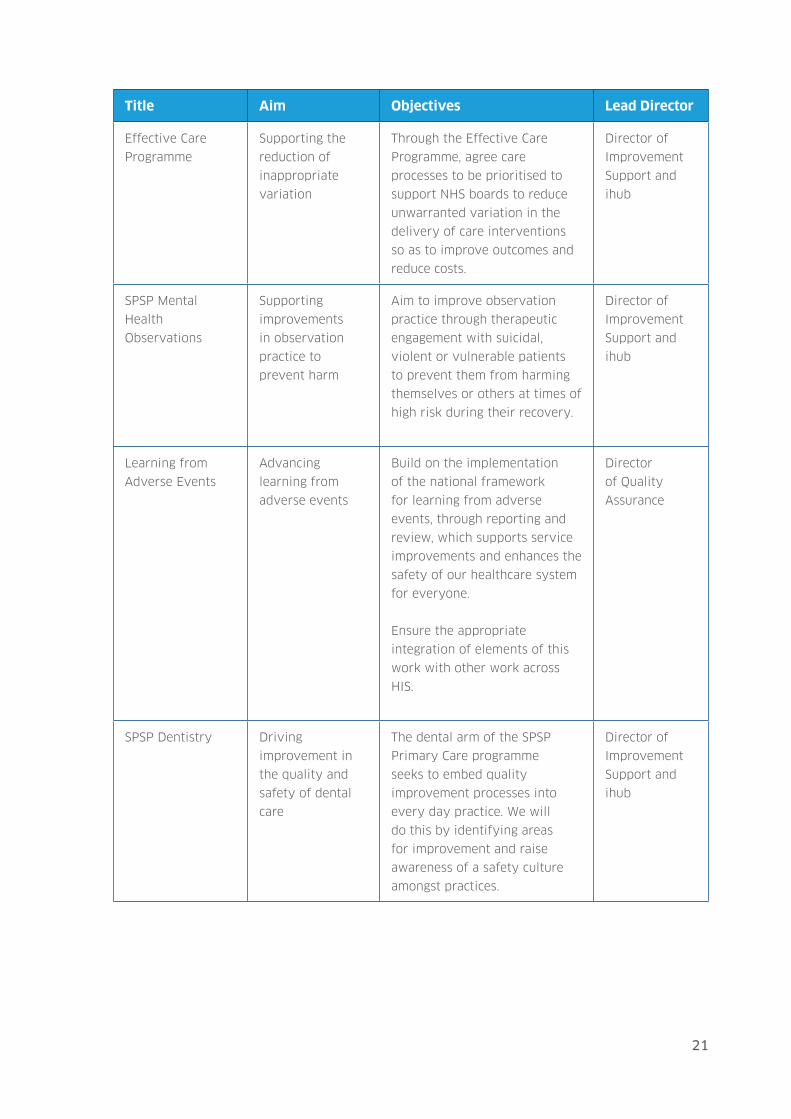
21
Title Aim Objectives Lead Director
Effective Care
Programme
Supporting the
reduction of
inappropriate
variation
Through the Effective Care
Programme, agree care
processes to be prioritised to
support NHS boards to reduce
unwarranted variation in the
delivery of care interventions
so as to improve outcomes and
reduce costs.
Director of
Improvement
Support and
ihub
SPSP Mental
Health
Observations
Supporting
improvements
in observation
practice to
prevent harm
Aim to improve observation
practice through therapeutic
engagement with suicidal,
violent or vulnerable patients
to prevent them from harming
themselves or others at times of
high risk during their recovery.
Director of
Improvement
Support and
ihub
Learning from
Adverse Events
Advancing
learning from
adverse events
Build on the implementation
of the national framework
for learning from adverse
events, through reporting and
review, which supports service
improvements and enhances the
safety of our healthcare system
for everyone.
Ensure the appropriate
integration of elements of this
work with other work across
HIS.
Director
of Quality
Assurance
SPSP Dentistry Driving
improvement in
the quality and
safety of dental
care
The dental arm of the SPSP
Primary Care programme
seeks to embed quality
improvement processes into
every day practice. We will
do this by identifying areas
for improvement and raise
awareness of a safety culture
amongst practices.
Director of
Improvement
Support and
ihub

22
Contribution 5: providing independent external assessment of the sustainability
of service provision, including the design of health and social care services which
offer better outcomes and value for money.
Title Aim Objectives Lead Director
Scottish Health
Technologies
Group (SHTG)
Appraisal and
provision of
evidence on new
non-medicines
technologies
Provide advice on the evidence
about the clinical and cost
effectiveness of existing
and new non-medicine
technologies likely to have
significant implications for
patient care in Scotland.
Implement key actions from the
Non-Medicines Technologies
Strategic Plan (2016–2018),
including the commissioned
work on landing zones for
advice within NHSScotland.
Director of
Evidence
Scottish Medicines
Consortium (SMC)
- Implementation
of New Medicines
Review
Recommendations
Support the
introduction of
recommendations
arising from the
review of access
to new medicines
Consider and implement
recommendations arising
from the ‘Montgomery review’
relating to the policy change for
new medicines.
Director of
Evidence
SMC Core Business Appraisal of new
drug therapies
to deliver safe,
clinically effective
and cost effective
medicines
Deliver robust SMC decisions
and continue to refine the
process.
Director of
Evidence
Scottish
Antimicrobial
Prescribing Group
(SAPG)
Ensuring safe and
evidence-based
provision of
antibiotics
Support the work of SAPG
in containing the spread of
Antimicrobial Resistance (AMR)
in Scotland and reducing
patient harm by maintaining
the national antimicrobial
stewardship agenda from HAI.
Director of
Evidence
23
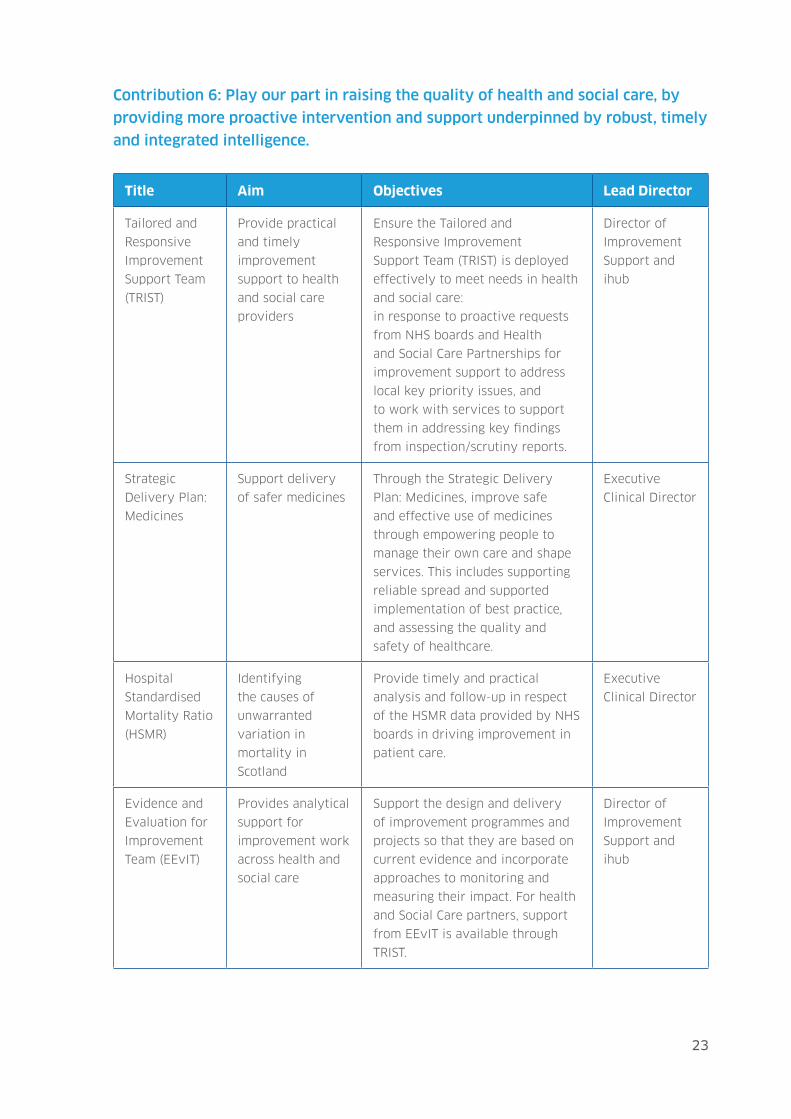
Contribution 6: Play our part in raising the quality of health and social care, by
providing more proactive intervention and support underpinned by robust, timely
and integrated intelligence.
Title Aim Objectives Lead Director
Tailored and
Responsive
Improvement
Support Team
(TRIST)
Provide practical
and timely
improvement
support to health
and social care
providers
Ensure the Tailored and
Responsive Improvement
Support Team (TRIST) is deployed
effectively to meet needs in health
and social care:
in response to proactive requests
from NHS boards and Health
and Social Care Partnerships for
improvement support to address
local key priority issues, and
to work with services to support
them in addressing key findings
from inspection/scrutiny reports.
Director of
Improvement
Support and
ihub
Strategic
Delivery Plan:
Medicines
Support delivery
of safer medicines
Through the Strategic Delivery
Plan: Medicines, improve safe
and effective use of medicines
through empowering people to
manage their own care and shape
services. This includes supporting
reliable spread and supported
implementation of best practice,
and assessing the quality and
safety of healthcare.
Executive
Clinical Director
Hospital
Standardised
Mortality Ratio
(HSMR)
Identifying
the causes of
unwarranted
variation in
mortality in
Scotland
Provide timely and practical
analysis and follow-up in respect
of the HSMR data provided by NHS
boards in driving improvement in
patient care.
Executive
Clinical Director
Evidence and
Evaluation for
Improvement
Team (EEvIT)
Provides analytical
support for
improvement work
across health and
social care
Support the design and delivery
of improvement programmes and
projects so that they are based on
current evidence and incorporate
approaches to monitoring and
measuring their impact. For health
and Social Care partners, support
from EEvIT is available through
TRIST.
Director of
Improvement
Support and
ihub

24
Title Aim Objectives Lead Director
Improvement
Fund
Provide grant
awards to support
improvement for
Health and Social
Care Partnerships
Provide grant awards to applicants
with a strong proposal to either
test a change idea locally or
spread improvement nationally.
The aim of the fund is to invest in
and expand innovative practices
that demonstrate impact on the
national health and wellbeing
outcomes.
Director of
Improvement
Support and
ihub
Contribution 7: supporting the leadership in NHS boards and in Health and Social
Care Partnerships to make the necessary changes to deliver a sustainable culture
of continuous quality improvement.
Title Aim Objectives Lead Director
Implementation
and
Improvement
Support of
Area and Drug
Therapeutic
Committees
(ADTCs)
Support ADTC to
implement best
practice
Following the Scottish Government
response to the Health and Sport
Committee inquiry into access
to new medicines in 2013,
continue to provide effective
support to the application of the
recommendations as they pertain
to ADTCs.
Executive
Clinical Director
Hospital
Electronic
Prescribing
and Medicines
Administration
(HEPMA) Phase
2
Support delivery
of cost effective
and safe
prescribing
Support a collaborative approach
to implementation of HEPMA
across NHS boards ensuring
lessons learned, minimisation of
risk, and securing overall benefits
of safer prescribing.
Executive
Clinical Director
Quality
Improvement
(QI) Skills
Development
Developing QI
capacity within
Board members
across Scotland
Develop the skills of staff working
across health and social care
services to support the work of
QI through funding 56 places a
year on the Scottish Improvement
Leaders course provided by NHS
Education for Scotland.
Director of
Improvement
Support and
ihub

25
Title Aim Objectives Lead Director
Networks and
Knowledge
Exchange
Making effective
use of networks to
share learning
Develop and implement a
network strategy to support the
Improvement Hub and partners to
connect and share learning.
Director of
Improvement
Support and
ihub
QI for Board
Members
Developing QI
capability of
Board members
within Scotland
To create opportunities for
Board members to increase their
understanding of QI so that they
can lead and govern organisations
to continuously improve and
contribute to the nine national
health and wellbeing outcomes.
Director of
Improvement
Support and
ihub
Independent
Care Sector
Programme
Maximise the
contribution of
the independent
care sector to
improvements
in health and
wellbeing
Take forward the Independent
Care Sector Programme which
is designed to support the
development of this sector
as a full partner in delivering
improvements in health and
wellbeing at both strategic and
local levels.
Director of
Improvement
Support and
ihub

26
Measurement and evaluation
We have created a logic model which incorporates our seven strategic
contributions and has aligned them to the nine national health and wellbeing
outcomes. We are developing effective evaluation processes to better evidence the
outcomes, benefits and impact of our work. This includes developing indicators to
enable us to measure progress toward achieving our outcomes and a prioritisation
process to ensure strategic fit and that we are making best use of resources.
This work is developmental and, during the course of 2016–2017, we will
be testing and refining the model to ensure that it meets our needs and can
demonstrate impact.
We will also develop our performance management arrangements to improve
reporting of the progress that we are making with our work and any changes we
might need to make. This will include measuring and reporting of our work in
a matrix way to suit the most appropriate circumstances as clearly as possible,
for example by outcome, theme or programme. We believe that by incorporating
this flexibility of approach to reporting we will be able to identify the cross-
organisational value that is added to our work.

27
Fina
ncia
l re
sour
ce
Flex
ible
, en
gage
d an
d ap
prop
riate
ly
skill
ed
wor
kfor
ce th
at is
su
stai
nabl
e,
capa
ble,
fully
in
tegr
ated
and
su
ppor
ted
by
effe
ctiv
e le
ader
ship
Eff
icie
nt a
nd
effe
ctiv
e H
R,
Fina
nce,
IT a
nd
Com
mun
icat
ions
Inpu
ts
Act
iviti
es
R
each
O
utco
mes
1.Pe
ople
are
abl
e to
look
afte
r and
impr
ove
thei
row
n he
alth
and
wel
lbei
ng a
nd li
ve in
goo
dhe
alth
for l
onge
r
2.Pe
ople
, inc
ludi
ng th
ose
with
disa
bilit
ies o
r lon
gte
rm c
ondi
tions
, or w
ho a
re fr
ail, a
re a
ble
toliv
e, as
far a
s rea
sona
bly
prac
ticab
le,
inde
pend
ently
and
at h
ome
or in
a h
omel
yse
tting
in th
eir c
omm
unity
3.Pe
ople
who
use
hea
lth a
nd so
cial
care
serv
ices
have
pos
itive
exp
erie
nces
of t
hose
serv
ices
and
have
thei
r dig
nity
resp
ecte
d
4.H
ealth
and
soci
al ca
re se
rvic
es a
re c
entre
d on
help
ing
to m
ainta
in o
r im
prov
e th
e qu
ality
of
life
of p
eopl
e w
ho u
se th
ose
serv
ices
5.H
ealth
and
soci
al ca
re se
rvic
es c
ontri
bute
tore
duci
ng h
ealth
ineq
ualit
ies
6.Pe
ople
who
pro
vide
unp
aid c
are
are
supp
orte
dto
look
afte
r the
ir ow
n he
alth
and
wel
lbei
ng,
incl
udin
g re
duce
any
neg
ativ
e im
pact
of t
heir
carin
g ro
le o
n th
eir o
wn
healt
h an
d w
ellb
eing
7.Pe
ople
usin
g he
alth
and
soci
al ca
re se
rvic
es a
resa
fe fr
om h
arm
8.Pe
ople
who
wor
k in
hea
lth a
nd so
cial
care
serv
ices
feel
eng
aged
with
the
wor
k th
ey d
o an
dar
e su
ppor
ted
to c
ontin
uous
ly im
prov
e th
ein
form
atio
n, su
ppor
t, ca
re a
nd tr
eatm
ent t
hey
prov
ide
9.Re
sour
ces a
re u
sed
effe
ctiv
ely
and
effic
ient
ly in
the
prov
ision
of h
ealth
and
soci
al se
rvic
es
Pers
on-c
entre
d H
ealth
and
Car
e Pr
ogra
mm
e
Inap
prop
riate
var
iatio
n in
ca
re is
redu
ced
[4]
Impr
ovem
ent i
n he
alth
and
soci
al ca
re p
rovi
sion
is su
ppor
ted
by in
telli
genc
e led
pr
oact
ive
inte
rven
tion
[6]
Citi
zens
hav
e a
mea
ning
ful
say
in th
e de
sign,
plan
ning
an
d pr
ovisi
on a
nd d
eliv
ery
of h
ealth
and
soci
al ca
re
serv
ices
[1]
Hea
lth a
nd so
cial
care
se
rvic
es a
re su
stain
able
and
pr
ovid
e in
divi
dual
care
that
is
appr
opria
te a
nd ti
mel
y [3
]
Citi
zens
, boa
rds,
Scot
tish
Gov
ernm
ent a
nd c
are
prov
ider
s are
ass
ured
abo
ut
the
quali
ty o
f ser
vice
s [2]
Citi
zens
, boa
rds,
SG a
nd
care
pro
vide
rs a
re a
ssur
ed
abou
t the
sust
ainab
ility
of
serv
ices
[5]
Sust
ainab
le q
ualit
y im
prov
emen
t is d
eliv
ered
by
supp
ortin
g ch
ange
thro
ugh
effe
ctiv
e le
ader
ship
[7]
Com
mun
ity e
ngag
emen
t and
supp
ort
Can
cer/
scre
enin
g pr
ogra
mm
e Q
A
NH
S bo
ards
, in
tegr
ated
join
t bo
ards
, hea
lth a
nd
soci
al ca
re
partn
ersh
ips,
third
se
ctor
and
in
depe
nden
t sec
tor
Inde
pend
ent c
are
prov
ider
s
Our
staf
f
Publ
ic, p
atie
nts,
care
rs a
nd
com
mun
ities
Staf
f in
healt
h an
d so
cial
care
Scot
tish
Parli
amen
t an
d Sc
ottis
h G
over
nmen
t
Eff
ectiv
e C
are
Prog
ram
me
SPSP
QI C
apac
ity a
nd C
apab
ility
bui
ldin
g
Shar
ing
Inte
llige
nce
Qua
lity
of c
are
revi
ews
Insp
ectio
n pr
ogra
mm
es
TRIS
T
Our
Voi
ce
Pers
onal
outc
omes
Tech
nolo
gies
pro
gram
me
Prof
essio
nal r
evali
datio
n
IHC
regu
latio
n
Prim
ary
care
/OO
H
Priso
ner h
ealth
care
OPA
C
Adv
erse
eve
nts
Stan
dard
s
SAPG
EE
vIT
Logi
c m
od
el

28
Best use of resources
This Local Delivery Plan has been prepared as part of our integrated planning
process. This ensures that we work within our resources – people and finances –
and deliver a high quality work programme. We effectively manage our resources
through good governance processes and prioritisation of our work.
This plan incorporates an outline of our implementation plan for Delivering
Everyone Matters: 2020 Workforce Vision in Appendix 1.

29
Appendix 1: 2020 Workforce Vision – local implementation plan (2016–2017)
Our 2020 Workforce Vision local implementation plan (2016–2017) provides a
range of actions that support the achievement of our outcomes, and contribute to
the ongoing development of our organisation. The actions are outlined below:
Healthy organisational culture: we are developing promotional materials to
support employee understanding of their contribution to the workforce vision.
We are improving our measurement of staff engagement through full roll-out of
iMatter, and the use of pulse surveys. A co-ordinated approach to team briefing
across the organisation will be developed, and our monthly staff huddles are being
continuously improved following employee feedback. We are undertaking work
to gain a deeper understanding of the causes of unplanned absence in order to
inform the ways we can more effectively support our employees.
Sustainable workforce: we established a Change Management Board in 2015–
2016 that has oversight of all organisational change across HIS, including changes
in structure and service delivery. The Board considers how change impacts our
workforce, and how change in one area of our organisation can affect other areas
while ensuring appropriate action is taken to manage this. During 2016–2017,
the main focus of the Change Management Board will be to ensure oversight of
changes relating to our Improvement Support and Quality Assurance offerings,
as well as the development of Our Voice within the Scottish Health Council. This
activity will benefit from our learning around organisational changes implemented
in the past 12 months.
Capable workforce: we will be providing health inequalities awareness sessions
for all employees during 2016–2017 as well as exploring options for balancing
measures on inequalities as part of our Improvement Hub performance framework.
Employees will be supported to understand the benefits and challenges of using
social media for business purposes. Employee awareness raising of the critical role
of carers will be part of the internal communications that support the launch of
Our Voice. Also, there will be awareness activities planned and delivered detailing
how strategic inspections have a focus on the Partnerships Carers Strategy, Carers
Assessments and Outcomes for Carers.

30
Workforce to deliver integrated services: we will support development of quality
improvement capacity across health and social care by funding over 50 places on
the Scottish Improvement Leaders programme. We will work with other national
organisations including the Scottish Government, NHS Education for Scotland
and the Scottish Social Services Council to identify workforce implications across
Scotland attached to improvement and service redesign work, and develop
appropriate interventions that are solutions-focused. Our provision of practical
improvement support will be delivered through a mixture of planned programmes
and responsive support. In equipping our employees to support this work, we
will ensure awareness and understanding of the pressures health and social care
partnerships face, and address skills and experience gaps at individual and team
levels.
Effective leadership and management: our focus for 2016–2017 will be on
strengthening change leadership capacity and capability. This will be facilitated
through topic specific leadership discussion groups on adaptive leaderships,
complexity and emergence, and how these relate to cross-organisation and cross-
sector working. Promoting NHSScotland and HIS organisational values will be
supported by the development of values-based recruitment processes and the
establishment of values-oriented objectives built into leaders’ and managers’
2016–2017 work objectives. Performance management and iMatter training will
be provided to all managers to support open and honest discussions with our
employees. This should support them to maximise their contribution and agree
action plans to secure improvement. We will progress succession planning and
talent management discussion with the Executive Team to reach agreement on
a consistent approach. We will continue to provide support for facilitated team
building and development, targeted towards teams directly affected by change.
This includes ensuring understanding and awareness of the HIS approach to
organisational change management, and supporting managers to implement this
effectively, and be responsive to the need to continuously improve the way we
work.
Over the course of 2016–2017, we anticipate recruitment challenges with the
following staffing groups:
• Health Economists
• Improvement Advisors
• Inspectors, and
• Medical Reviewers.

31
All of the above staff groups are either specialist or highly specialist and are
critical to the success of our Local Delivery Plan. In the case of Health Economists,
there is a significant shortage of supply within Scotland. Moreover, the private
sector is continually able to attract the limited numbers of suitably qualified and
experienced individuals who are available with higher salaries than we currently
can offer via the Agenda for Change framework. To mitigate this, we have trialled
traineeships in order to attract newly qualified individuals, with dedicated
coaching and mentorship available to ‘fast track’ the acquisition of skills and
experience. This has had mixed success, and we intend to refocus on other ways to
mitigate the situation during 2016–2017.
Given our expanded remit in terms of facilitating improvement across health
and social care from 1 April 2016, there will be a significant requirement for
appropriately skilled and experienced Improvement Advisors drawn from both
health and social care backgrounds. We have a good track record in supporting
NHS boards with expertise and personnel to deliver improvement interventions.
There continues to be a national shortage of qualified and experienced
Improvement Advisors, and this represents a risk for us in the delivery of our
programmes in the short to medium term. The new integrated improvement
resource will be investing in Improvement Advisor and Associate Improvement
Advisor posts, with a strong focus on succession planning and retention to ensure
as much stability as possible is built into the structure. We are also creating
alternative ways of staffing national improvement programmes so as not to
simply take key individuals away from local delivery organisations. This includes
the development of our Improvement Associate framework, the use of joint
appointments where individuals work part-time nationally and part-time locally,
and the development of a grant making arm. Parallel to work on infrastructures,
skills mapping and skill gap analysis will be carried out to inform the workforce
development priorities. The Quality Improvement Framework along with the new
QI Development Diagnostic tool will be used as part of this process.
We have worked collaboratively with a range of stakeholders in the development
of our new Quality of Care reviews, which we believe will have a positive impact
on quality assurance across the service, and become an effective lead-in for
quality improvement. We are also building capacity in independent healthcare
inspection during 2016–2017. Both these important developments require skilled
and experienced Inspectors to support our operational capability. A barrier to
our ability to attract suitable talent from the social care sector is our terms and
conditions of service through the Agenda for Change framework. We will work to
find a solution to this barrier during 2016–2017 so that certainty can be brought
to recruitment processes, and the best possible terms and conditions can be
offered to prospective entrants.

32
The nature of the Death Certification Review Service requires Medical Reviewers
who are highly experienced medical professionals, drawn from the General
Practitioner and Consultant communities. This has required HIS to appoint
individuals on to differing terms and conditions that reflect their backgrounds, but
the same salary scale in order to avoid question marks over equal pay. A solution
to the terms and conditions situation is needed to bring clarity to our employment
offering, and we will fully participate in any discussions relating to the creation of
new contracts led by Scottish Government colleagues in 2016–2017.
Our employee age profile remains broadly consistent with previous years.
Compared to other NHS employers, HIS has proportionately less staff under
the age of 25. The main cause of this is the skills and experience required
for the majority of our posts. We recognise the important contribution that
under 25s can provide and that our current position is neither sustainable nor
desirable. During 2016–2017, we will develop a range of initiatives to encourage
youth employment, with the chief focus on Modern Apprenticeships within
administrative services.
During 2015–2016, there was a slight increase in sickness absence rates, but these
remain below the established 4% expectation. There continues to be work required
with people managers on improving the capture of unplanned absence causes.
However, there has been an increase in the numbers of employees indicating
anxiety, depression and stress, and this will be explored in detail in early 2016–
2017. One aspect of this exploration will be determining if there is any linkage
between increased absence levels and our approach to vacancy management.
A challenging budgetary environment in 2015–2016 required HIS, through the
established Change Management Board and process, to assiduously manage
vacancies and deliver headcount reductions. For 2016–2017, a vacancy factor of
7.7% has been agreed in order to accrue financial savings that will contribute to
a balanced budget. This will be closely monitored to ensure achievement of our
budgetary goals, and our people are supported in terms of manageable workloads
and performance expectations.

Levels of anticipated workforce growth during 2016–2017, particularly within the
Improvement Hub and the Directorate of Quality Assurance, require us to urgently
consider the application of agile working approaches for colleagues based within
our two main offices – Gyle Square (Edinburgh) and Delta House (Glasgow). The
ready availability of additional workstation space is particularly challenging in
Delta House. A subgroup of the Change Management Board has been considering
the situation and is coming forward with recommendations. These include
switching the majority of available workstations to ‘hot desk’ status, and ensuring
that all employees are provided with information communication technology that
facilitates cross-site and home-working whenever appropriate.
To be able to deliver on our work programme and achieve changes in the way we
work, we need a flexible workforce that is able to be responsive to changes in
the work plan due to changing context and to urgent unplanned work demands.
The Change Management Board is working to support the workforce to build
approaches to work more flexibly across the organisation so that we can respond
more efficiently to fluctuations in workload and optimise use of existing workforce
capacity and capability. This will require traditional team and directorate
structures to support an increased level of cross-organisational working. Members
of the Change Management Board have sought examples of flexible workforce
approaches from Audit Scotland and from Scott-Moncrieff and have presented
these models to Partnership Forum and Corporate Management Team as a way
of stimulating thinking about a model that would work for HIS. In addition we are
building case studies of pieces of work being carried out across the organisation
that are testing out ways of working more flexibly. We will build on these during
2016–2017 and use them to engage staff in taking forward changes in ways of
working.
33

Edinburgh Office
Gyle Square
1 South Gyle Crescent
Edinburgh
EH12 9EB
0131 623 4300
Glasgow Office
Delta House
50 West Nile Street
Glasgow
G1 2NP
0141 225 6999
www.healthcareimprovementscotland.org
You can read and download this document from our website.
We are happy to consider requests for other languages or
formats. Please contact our Equality and Diversity Advisor on
0141 225 6999 or email [email protected]
The Healthcare Environment Inspectorate, Improvement Hub, Scottish
Health Council, Scottish Health Technologies Group, Scottish Intercollegiate
Guidelines Network (SIGN) and Scottish Medicines Consortium are part of
Healthcare Improvement Scotland.
Related Documents











