Lebanese Medical Journal 2021 • Vol 69 (2) I JOURNAL MEDICAL LIBANAIS LEBANESE MEDICAL JOURNAL Publication du Comité Scientifique Ordre des Médecins du Liban Publication of the Scientific Committee Lebanese Order of Physicians Editorial “Paediatric orthopaedics” is not “adult orthopaedics” in children ! http://www.lebanesemedicaljournal.org/articles/69(2)/editorial.pdf I. B. GHANEM ........................................................................................................... 63 Practical guidelines to correct acetabular dysplasia in children and adolescents http://www.lebanesemedicaljournal.org/articles/69-2/pedsortho1.pdf N. KHOURI ................................................................................................................ 64 Recurrence of lower extremity rotational deformities after derotation osteotomy in ambulatory children with cerebral palsy http://www.lebanesemedicaljournal.org/articles/69-2/pedsortho2.pdf T. A. L. WREN, A. M. BROOM, S. A. RETHLEFSEN, R. M. KAY ............................ 70 Percutaneous metaphyseal juxta-physeal perforations A new potential approach to angular correction and limb lengthening An experimental pilot study http://www.lebanesemedicaljournal.org/articles/69-2/pedsortho3.pdf I. SALIBA, S. SKAFF, M. RIZKALLAH, D. GHANEM, A. SEBAALY. G. EL KHOURY, R. ELABIAD, I. GHANEM ..................................... 76 Management of the complex clubfoot http://www.lebanesemedicaljournal.org/articles/69-2/pedsortho4.pdf K. J. NOONAN .......................................................................................................... 82 Tarsal coalition Clinical and radiographic diagnosis and management http://www.lebanesemedicaljournal.org/articles/69-2/pedsortho5.pdf V. ROCCHI, S. MUBARAK ....................................................................................... 89 Challenges of pediatric reconstruction post limb sarcoma resection http://www.lebanesemedicaljournal.org/articles/69-2/pedsortho6.pdf A.S. NAJA, A. IBRAHIM, M. ISSA R. HAIDAR, S. SAGHIEH ......................................................................................... 95 Etiology of the so-called idiopathic scoliosis from birth to aging seen from a clinician side The biomechanical importance of the horizontal plane http://www.lebanesemedicaljournal.org/articles/69-2/pedsortho7.pdf J. DUBOUSSET ........................................................................................................ 107 Rédacteur en chef émérite Editor in chief emeritus Adel BERBARI Rédacteur en chef Editor in chief David ATALLAH Rédacteur en chef adjoint Associate editor Muhieddine SEOUD Directrice de la rédaction Managing editor Diala AL SAMARANI MOUSSA Secrétaire général General secretary George ARAJ Comité de rédaction Editorial board Amer Camille ABDALLAH Nizar BITAR Issam CHAARANI Michel DAHER Hadi FAKIH Nassim FARES Hadi HACHEM Zouheir El IMAD Karl JALLAD Roland KASSAB Joseph MAARRAWI Majed YAZBECK Coordinateur du site web Website coordinator Joseph MAARRAWI Consultant en statistiques Statistics advisor Bachir ATALLAH Secrétaire de rédaction Executive secretary Zeinab HAMMOUD FRONT COVER The painting was executed by Serwan Baran (Photo credit: Public domain) PAEDIATRIC ORTHOPAEDICS

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Lebanese Medical Journal 2021 • Vol 69 (2) I
JOURNAL MEDICAL LIBANAISLEBANESE MEDICAL JOURNAL
Publication du Comité ScientifiqueOrdre des Médecins du Liban
Publication of the Scientific CommitteeLebanese Order of Physicians
Editorial“Paediatric orthopaedics” is not “adult orthopaedics” in children !http://www.lebanesemedicaljournal.org/articles/69(2)/editorial.pdfI. B. GHANEM ........................................................................................................... 63
Practical guidelines to correct acetabular dysplasia in children and adolescentshttp://www.lebanesemedicaljournal.org/articles/69-2/pedsortho1.pdfN. KHOURI ................................................................................................................ 64
Recurrence of lower extremity rotational deformities after derotationosteotomy in ambulatory children with cerebral palsyhttp://www.lebanesemedicaljournal.org/articles/69-2/pedsortho2.pdfT. A. L. WREN, A. M. BROOM, S. A. RETHLEFSEN, R. M. KAY ............................ 70
Percutaneous metaphyseal juxta-physeal perforationsA new potential approach to angular correction and limb lengtheningAn experimental pilot studyhttp://www.lebanesemedicaljournal.org/articles/69-2/pedsortho3.pdfI. SALIBA, S. SKAFF, M. RIZKALLAH, D. GHANEM, A. SEBAALY. G. EL KHOURY, R. EL ABIAD, I. GHANEM ..................................... 76
Management of the complex clubfoothttp://www.lebanesemedicaljournal.org/articles/69-2/pedsortho4.pdfK. J. NOONAN .......................................................................................................... 82
Tarsal coalitionClinical and radiographic diagnosis and managementhttp://www.lebanesemedicaljournal.org/articles/69-2/pedsortho5.pdfV. ROCCHI, S. MUBARAK ....................................................................................... 89
Challenges of pediatric reconstruction post limb sarcoma resectionhttp://www.lebanesemedicaljournal.org/articles/69-2/pedsortho6.pdfA.S. NAJA, A. IBRAHIM, M. ISSAR. HAIDAR, S. SAGHIEH ......................................................................................... 95
Etiology of the so-called idiopathic scoliosis from birth to agingseen from a clinician sideThe biomechanical importance of the horizontal planehttp://www.lebanesemedicaljournal.org/articles/69-2/pedsortho7.pdfJ. DUBOUSSET ........................................................................................................ 107
Rédacteur en chef émériteEditor in chief emeritus
Adel BERBARI
Rédacteur en chefEditor in chief David ATALLAH
Rédacteur en chef adjointAssociate editor
Muhieddine SEOUD
Directrice de la rédactionManaging editor
Diala AL SAMARANI MOUSSA
Secrétaire généralGeneral secretary
George ARAJ
Comité de rédactionEditorial board
Amer Camille ABDALLAH
Nizar BITAR
Issam CHAARANI
Michel DAHER
Hadi FAKIH
Nassim FARES
Hadi HACHEM
Zouheir El IMAD
Karl JALLAD
Roland KASSAB
Joseph MAARRAWI
Majed YAZBECK
Coordinateur du site webWebsite coordinator
Joseph MAARRAWI
Consultant en statistiquesStatistics advisor
Bachir ATALLAH
Secrétaire de rédactionExecutive secretary
Zeinab HAMMOUD
FRONT COVER
The painting was executed by Serwan Baran (Photo credit: Public domain)
PPAAEEDDIIAATTRRIICC OORRTTHHOOPPAAEEDDIICCSS

II Lebanese Medical Journal 2021 • Vol 69 (2)
JML
JOURNAL MEDICAL
LIBANAIS
LMJ
LEBANESE
MEDICAL JOURNAL
Publication du
Comité Scientifique
Ordre des Médecins du Liban
Publication of
the Scientific Committee
Lebanese Order of Physicians
Adressertoute correspondance au
Rédacteur en ChefJournal Médical Libanais
Ordre des Médecins du LibanAutostrade Tawita
Furn el-Chebbak - BeyrouthLiban
Mailing address
Editor in ChiefLebanese Medical Journal
Lebanese Order of PhysiciansAutostrade Tawita
Furn el-Shebbak - BeirutLebanon
e-mail : [email protected]
www.lebanesemedicaljournal.org
Tel./Fax : +961 1 610710 ext 306
ProductionMichèle Valligny
Elie Ammar
A three-dimensional biomechanical analysis of the skeletonin adolescent idiopathic scoliosishttp://www.lebanesemedicaljournal.org/articles/69-2/pedsortho8.pdfM. KARAM, I. GHANEM, W. SKALLI, A. ASSI ..................................................... 109
Traitement des scolioses infantiles et juvéniles par corsets plâtrésÉtat des lieux, techniques et perspectives http://www.lebanesemedicaljournal.org/articles/69-2/pedsortho9.pdfF. MONGET, E. NECTOUX, D. FRON, F. CANAVESE ........................................... 126
Effectiveness of bracing alone in idiopathic scoliosis before6 years of agehttp://www.lebanesemedicaljournal.org/articles/69-2/pedsortho10.pdfI. BERNARDINI, R. COMPAGNON, F. ACCADBLED J. SALES de GAUZY .......................... .................................................................... 137
Complications in traditional growing rods used for early onset scoliosisA case series and a review of literaturehttp://www.lebanesemedicaljournal.org/articles/69-2/pedsortho11.pdfM. RIZKALLAH, D. GHANEM, A. ASSI, I. GHANEM ........................................... 141
ISSN 0023-9852Indexed by • Index Medicus • Embase (Excerpta Medica)
• Cab Abstracts and Global Health - CABI Publishing• Index Medicus (IMEMR)
Lebanese Medical Journal 2021 • Volume 69 (2) 63
When I was asked to guest-edit this special issue on paediatric orthopaedics, I thought it would bebest to introduce this topic through a specific approach of a lifetime experience.
Those of us who became orthopaedic surgeons, showed very early in medical school a particularinterest in functional anatomy, physiology, pathophysiology, as well as normal and abnormal boneand joint mechanics. Understanding the musculoskeletal system and its anomalies couldn’t be possiblewithout a three-dimensional (3D) approach of a part and/or the entire system. “Paediatric Ortho-paedics” adds to this 3D approach a fourth dimension related to growth, an element of utmost impor-tance while evaluating a musculoskeletal disorder and planning its treatment in a child.
When compared to adult orthopaedics, the management of musculoskeletal disorders in childreninvolves a wide range of disciplines such as genetics, embryopathology, biomechanics, orthopaedics,general paediatrics, oncology, obstetrics and gynaecology, metabolic and endocrine diseases, skeletaldysplasias, neurology, etc. Paediatric orthopaedic surgeons around the globe are trained to acquire amind-set compatible with this specificity.
The care of children with musculoskeletal disorders in Lebanon and the Middle East has evolvedduring the past decades, gaining more and more interest, leading to the development of the speciality toan international level. Despite the suboptimal political and socioeconomic situation in Lebanon, chil-dren with orthopaedic disorders continue to receive the best available management according tointernational standards, due to the devotion and passion of dedicated physicians, some of whom aresharing their experience in this issue of the journal. The increasing interest in basic and clinicalresearch in the field, mainly in university settings, along with scientific exchanges with internationalleading figures in this domain from Europe and the USA have led to this high level special editionof the Lebanese Medical Journal.
I can only salute, with a great honour and emotion, the extreme humbleness, kindness and friend-ship of the international authors from Europe and the USA who took of their busy schedules to contributeto the success of this issue, and I am deeply thankful to them on behalf of the Editor-in-Chief, theEditorial board and the Lebanese medical community.
The painting on the cover page is a scene of street cleaning and reconstruction of Beirut after thedramatic August 4, 2020 blast, executed by the famous Iraqi artist Serwan Baran, and was chosen forits similarity with bone reconstruction in disabled children by dedicated physicians from various disciplines.
Long live Lebanon and science in Lebanon.Long live the Lebanese Medical Journal !
Ismat B. GHANEM, MD*
* Professeur de Chirurgie Orthopédique. Chirurgien Orthopédique Pédiatrique, Hôpital Hôtel-Dieu de France,Université Saint-Joseph - Beyrouth. Liban. e-mail: [email protected]
PPAAEEDDIIAATTRRIICC OORRTTHHOOPPAAEEDDIICCSSEDITORIAL“Paediatric Orthopaedics” Is Not “Adult Orthopaedics” In Children !http://www.lebanesemedicaljournal.org/articles/69-2/editorial.pdf

Acetabular dysplasia is an increasingly complex disor-der. Rather than the traditionally understood isolated an-terolateral dysplasia, lateral, posterior, and global acetab-ular insufficiencies are recognized. Consequently, the op-erative procedure that is necessary to correct these pat-terns requires the ability to achieve tailored and multipla-nar corrections.
Reshaping osteotomies involves incomplete cuts inthe ilium (Fig. 1). Correction is achieved by hingingthrough the triradiate cartilage. Because the osteotomiesare incomplete, they are stable after graft placement. Theydo not change the orientation of the acetabular opening,but they do change the shape &volume of the acetabulum(Fig. 2). The Pemberton pelvic osteotomy primarily pro-vides anterior coverage, the Dega pelvic osteotomy cov-ers anterolaterally, & the San Diegoplasty covers laterally.
Redirectional acetabular osteotomies involve com-plete cuts in the pelvis and require internal fixation. Un-like reshaping osteotomies, these procedures do notchange the size or shape of the acetabulum but do reorient the position of the acetabulum in space and require con-
gruency of the joint. The classical example is the Salterinnominate osteotomy (Fig. 3), which involves a singlecomplete cut in the ilium. Coverage, predominantly an-terolateral, is obtained by rotation through the pubic sym-physis (Fig. 4). It provides less fragment mobility becausethe acetabulum is not completely freed. A dysplasticacetabulum with poor posterior coverage is a contrain-dication for a Salter osteotomy, as while it provides ex-cellent anterolateral coverage, it can further uncover thefemoral head posteriorly.
“Complete” redirectional osteotomies (Fig. 5), includ-ing the triple innominate osteotomy and the periacetab-ular osteotomy (PAO), completely free the acetabulumfrom the rest of the pelvis. First described by Lecoeur, thetriple innominate osteotomy (Fig. 6) involves completethree cuts in the ilium, ischium, and pubis. The triradiatecartilage is spared, and the procedure can therefore be per-formed in the skeletally immature. After its first descrip-tion, the procedure underwent several modifications withrespect to the osteomy site at the level of the pubis and theischium. Osteotomies can either be closer to the symphy-sis, as in Lecoeur and Sutherland procedure, or closer to the acetabulum, as recommended by Steel, Tonnis,Carlioz, Jawish (Fig. 7) and Rebello providing a greaterdegree of freedom.
64 Lebanese Medical Journal 2021 • Volume 69 (2)
PPAAEEDDIIAATTRRIICC OORRTTHHOOPPAAEEDDIICCSSPRACTICAL GUIDELINES TO CORRECT ACETABULAR DYSPLASIAIN CHILDREN AND ADOLESCENTS http://www.lebanesemedicaljournal.org/articles/69-2/pedsortho1.pdf
Néjib KHOURI*
Néjib Khouri. Practical guidelines to correct acetabular dysplasiain children and adolescents. J Med Liban 2021; 69 (2) :64-69.
*Pediatric orthopedic surgeon. Department of Pediatric Orthopedics, Necker Sick Children University Hospital, Paris 75743. Medical Director Gait Analysis Laboratory. Ellen Poidatz Foundation 77310 France. e-mail: [email protected]
Figure 1. Reshaping osteotomies

N. KHOURI – Achieving correction of acetabular dysplasia Lebanese Medical Journal 2021 • Vol 69 (2) 65
Figure 3. Salter innominate osteotomy
A. 4y adduction flexion contracture ofthe left hip with painful dislocation.
B. Posterior and superior dysplasia on3Dscan and operatively.
C. Location of the bone graft (blackarrow) to correct the acetabular de-ficiency during the surgical reduc-tion. On the follow-up 3Dscan thewhite arrow points to this electivereconstruction.
D. 8y right hip undergoes the same dis-location.
E. 13y last follow-up near maturity afterbilateral surgical reduction, acetabu-loplasty and femoral osteotomy.
Figure 2. Cerebral palsy gross motor function classification system (GMFCSV)
A B C
D E

66 Lebanese Medical Journal 2021 • Vol 69 (2) N. KHOURI – Achieving correction of acetabular dysplasia
Figure 4. Developmental dysplasia of the hip (DDH)A. 5 y. High superior dislocation. B. Three months after surgical reduction, femoral derotation shortening osteotomy &
innominate osteotomy. C. 16 y Last follow-up at maturity. The hip is supple and painless.
Figure 7Quadruple redirectional osteotomy.
Jawish, 2007. Figure 8. Bernese periacetabular osteotomy. Ganz, 1988.
Figure 6. A. 12y. Adduction deformity with painful dislocation. B. Immediate postop. AP radiograph after adductor release,femoral varus derotation shortening osteotomy and triple Lecoeur osteotomy. C. 19 y. Last followup at maturity.
The hip is supple and painless. Note the healing of the lateral acetabular roof.
Figure 5. Triple redirectional osteotomies. A wide spectrum.
A B C
A B C

The Ganz (Bernese) periacetabular osteotomy main-tains the integrity of the posterior column by performinga bone cut connecting the iliac osteotomy to the partialischial osteotomy (Figure 8). This osteotomy travelsthrough a very narrow column of bone in the young patient and cannot be performed in the skeletally imma-ture.
Salvage procedures are indicated when a congruentreduction of the hip cannot be obtained by other means.The hip is contained, and the weight-bearing surface isincreased without hyaline cartilage. These proceduresrely on metaplasia of the capsule to serve as the articularsurface. The two primary salvage procedures are theChiari osteotomy and the Shelf procedure.
N. KHOURI – Achieving correction of acetabular dysplasia Lebanese Medical Journal 2021 • Vol 69 (2) 67
Figure 9. Planning a reorientation after fixing momentarily the hip. Padovani, 1976.
Figure 10. Rotation of the acetabulum by the two levers maneuver

Traditionally there are two methods to rotate the ace-tabulum during a reorientation pelvic osteotomy : in theplane of the iliac wing (Salter) assuring an anterolateralcoverage or by fixing momentarily the hip (Padovani) ina position determined by the surgeon (Figure 9) accordingto the dysplasia to correct.
They can produce undesirable under- or hypercorrec-tions.
We propose a refined procedure to rotate the acetab-ulum without undesirable effect in the transverse plane.
Surgical procedure includes an elective spatial rotation ofthe acetabulum around two axes (Figure 10).
One antero-posterior (according to Y axis) correctingin the frontal plane the acetabular index, the other cranio-caudal (according to Z axis) correcting the anteversion-retroversion in the transverse plane thanks to two perpen-dicular pins inserted above the roof of the acetabulumand acting as levers.
Peroperative correction is appreciated by fluoroscopyand anticipated preoperatively (Figure 11) on the 3Dpelvis scan.
68 Lebanese Medical Journal 2021 • Vol 69 (2) N. KHOURI – Achieving correction of acetabular dysplasia
Figure 11. Planning a reorientation pelvic osteotomy pre- and peroperatively.
A. 13y Cerebral palsy. GMFCSIII. Adduction flexion contractturewith painful dislocation of the left hip.
B. Preoperative 3Dscan.C. Spatial correction according to Z and Y axes anticipated
preoperatively on the 3D pelvis scan.D. 16 y. Last follow-up after adductor release, surgical reduction,
femoral varus shortening, osteotomy and periacetabularosteotomy.
A B
C
D

SELECTED REFERENCES
_ Akiyama M, Nakashima Y, Oishi M et al. Risk factors foracetabular retroversion in developmental dysplasia of the hip : does the Pemberton osteotomy contribute? J Orthop Sci 2014 Jan ; 19 (1) : 90-6.
_ Kobayashi D, Satsuma S, Kinugasa M, Kuroda R,Kurosaka M. Does Salter innominate osteotomy predis-pose the patient to acetabular retroversion in adulthood ?Clin Orthop Relat Res. 2015 May ; 473 (5) : 1755-62.
_ Jawish R, Najdi H, Krayan A. Periacetabular quadrupleosteotomy of the pelvis in older children : computed to-mography scan analysis of acetabular retroversion andanterior overcoverage of the hip, preventing femoral ace-tabular impingement. J Pediatr Orthop B. 2018 May ; 27(3) : 257-63.
_ Tannast M, Fritsch S, Siebenrock KA, Steppacher SD.Which radiographic hip parameters do not have to becorrected for pelvic rotation and tilt? Clin Orthop RelatRes. 2015 Apr ; 473 (4) : 1255-66.
_ Wylie JD, Ross JA, Erickson JA, Anderson MB, Peters CL.Operative fluoroscopic correction is reliable and corre-lates with postoperative radiographic correction in peri-acetabular osteotomy. Clin Orthop Relat Res. 2017 Apr;475 (4) : 1100-6.
_ Zaltz I. How to properly correct and to assess acetabularposition : an evidence-based approach. J Pediatr Orthop.2013 Jul ; 33 (Suppl 1) : S21-8.
_ Ross JA, Peters CL. Operative fluoroscopic correction isreliable and correlates with postoperative radiographiccorrection in periacetabular osteotomy. Clin Orthop RelatRes. 2017 Apr ; 475 (4) : 1100-6.
N. KHOURI – Achieving correction of acetabular dysplasia Lebanese Medical Journal 2021 • Vol 69 (2) 69

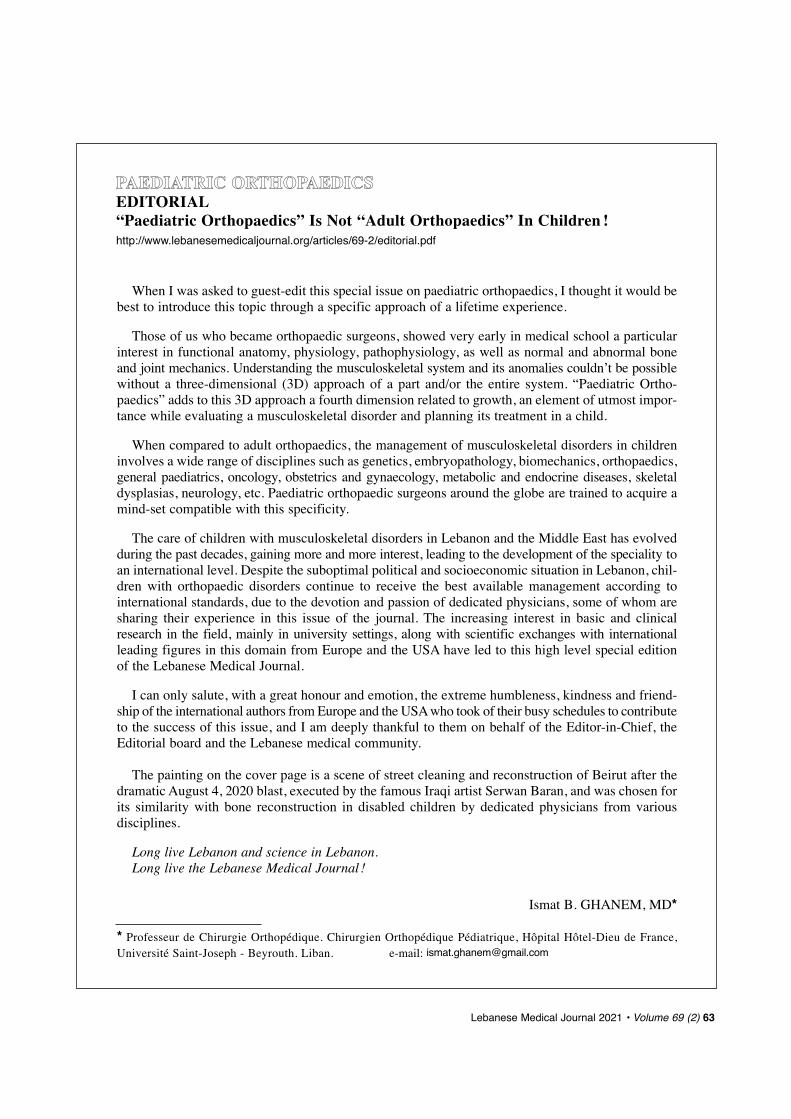
INTRODUCTION
Cerebral palsy (CP) is a non-progressive neurologicaldisorder that affects between 2.2 and 3.6 children per1000 live births [1]. Long bone torsional deformities ofthe legs are common in patients with CP and can affectthe femur and/or tibia. Lever arm dysfunction occurs dueto these transverse plane skeletal deformities, resultingin abnormal gait patterns, decreased metabolic efficien-cy [2] and decreased overall function. Although surgical
indications for femoral derotation osteotomy (FDRO)vary among centers [3], such osteotomies are often a com-ponent of single event multi-level surgery (SEMLS),which has become the standard of care in the surgical man-agement of patients with CP with the aim of improvingambulatory function [4-8]. Tibial derotation osteotomy(TDRO), when indicated, is also often recommended inchildren with CP and is effective in improving foot pro-gression during gait [9,10].
While the literature indicates that lasting correctioncan be achieved in many cases following FDRO in chil-dren with CP [11,12], recurrence of excess femoral rota-tion can also occur [11,12]. Age at surgery is one factorthat has been identified as a potential predictor of suchrecurrence in children with spastic diplegic CP [13,14].The causes of subsequent rotational deformity develop-ing after derotation of the femur and/or tibia remain un-certain. The purpose of this study was to examine poten-tial predictors of the development of femoral and/or tib-ial rotational deformity following primary derotation os-teotomy (DRO) in ambulatory children with CP.
METHODS
After receiving institutional review board approval, allambulatory patients with CP who underwent derotationosteotomy of the femur and/or tibia between January 1,1992 and November 5, 2018 at our institution were iden-tified. The procedures were usually performed as part ofmultilevel surgery aimed at improving gait. Only pa-tients with both pre- and postoperative gait analysis wereincluded. A chart review was performed to collect thefollowing measures hypothesized as possible preopera-tive factors affecting the development of subsequent ro-tational problems after the initial DRO : sex, age at sur-gery, body mass index (BMI), Gross Motor FunctionClassification System (GMFCS) level [15], distributionof CP (unilateral vs. bilateral), femoral anteversion, andtransmalleolar angle (TMA).
Gait analysis (including clinical examination of rangeof motion) was performed by one of three physical thera-pists, each with more than 20 years of experience in themotion analysis laboratory, using standard procedures.Femoral anteversion was measured using the trochan-teric prominence angle test [16]. Transmalleolar anglewas measured with the patient prone and the knee flexed
70 Lebanese Medical Journal 2021 • Volume 69 (2)
PPAAEEDDIIAATTRRIICC OORRTTHHOOPPAAEEDDIICCSSRECURRENCE OF LOWER EXTREMITY ROTATIONAL DEFORMITIES AFTERDEROTATION OSTEOTOMY IN AMBULATORY CHILDREN WITH CEREBRAL PALSYhttp://www.lebanesemedicaljournal.org/articles/69-2/pedsortho2.pdf
Tishya A. L. WREN1,2, Alexander M. BROOM2,3, Susan A. RETHLEFSEN1, Robert M. KAY1,2A
Wren TAL, Broom AM, Rethlefsen SA, Kay RM. Recurrenceof lower extremity rotational deformities after derotation os-teotomy in ambulatory children with cerebral palsy. J MedLiban 2021 ; 69 (2) : 70-75.
ABSTRACT • Objective : To determine predictors of recur-rent femoral and/or tibial rotational deformity following pri-mary derotation osteotomy in children with cerebral palsy(CP). Method: One hundred fifty-one patients with CP (GMFCSI-IV ; 61% male ; age 8.4, SD 2.4 years ; follow-up 3.8, SD2.5 years) underwent femoral and/or tibial derotation osteo-tomy with pre- and postoperative gait analysis. Rotationalproblems at final follow-up and potential predictive factorswere recorded retrospectively and analyzed using logisticregression. Results: New rotational problems developed in25% (58/234) of limbs, only in patients with bilateral invol-vement. New rotational problems were more common atGMFCS levels III/IV than levels I/II (OR 3.4, 95% CI 1.6 to 7.3,p = 0.002) and increased with more external transmalleolarangle (OR 1.04, 95% CI 1.01 to 1.07, p = 0.005). When newproblems occurred, the femur almost always ended up inter-nally rotated (34/36, 94%, p < 0.0001), and the tibia exter-nally rotated (28/34, 82%, p = 0.0002). Subsequent prob-lems occurred most commonly in limbs undergoing externalfemoral combined with internal tibial derotation (6/8, 75%).Conclusions: Though typically successful, subsequent femoral/tibial rotational abnormalities may develop after primary de-rotation osteotomy, particularly in less functional patientsand those with combined internal femoral rotation and externaltibial rotation. These patients may require additional surgery.
Keywords : femur ; tibia ; derotation osteotomy; gait ; cerebralpalsy.
‘1Children’s Orthopaedic Center, Children’s Hospital Los Angeles,Los Angeles, CA.
2Keck School of Medicine, University of Southern California,Los Angeles, CA.
3Oro Valley Hospital, Tucson, AZ.*Corresponding author: Susan A. Rethlefsen, PT, DPT.
e-mail: [email protected]

to 90° (positive values indicate external rotation of ankleaxis relative to knee axis). Computerized gait analysiswas performed for all subjects using an 8-10 camera 3-D motion capture system (Vicon 612 or Nexus 2,Vicon Motion Systems, Ltd., Oxford UK). Fifteen to 20retro-reflective markers were placed over specific bonylandmarks on the lower body following the Plug-in-Gaitimplementation of the conventional gait model [17].Subjects walked down a 15-meter walkway barefoot at aself-selected speed, using assistive devices as necessary.Kinematic data from at least three trials were averaged, andthe averaged data were included in the gait analysis report.
The primary outcome measure was occurrence of ro-tational deformity after the initial DRO, which was de-fined as positive if a subsequent derotation was eitherdone or recommended at a follow-up gait analysis test.The indications for primary and revision surgery fol-lowed the same criteria. At both time points, the indica-tions for FDRO and TDRO were lower extremity longbone rotational deformity with resultant lever arm dys-function causing impairment of gait and function. FDROwas indicated when excessive femoral anteversion wasmeasured statically (hip internal rotation at least 20-30°greater than external rotation) with kinematics duringgait showing dynamic internal hip rotation more thanone standard deviation (SD) above the mean of norma-tive data for the majority of the gait cycle. TDRO wasindicated when the measured TMA was abnormal (> 20°external or > 5° internal) and tibial torsion was deemedto be contributing significantly to the child’s in-toeing,out-toeing or lever arm dysfunction. Intraoperative goalsfor FDRO were adjusted based on the finding that, onaverage, patients at 1-year follow-up have 35-50% lesscorrection than was recorded at time of surgery [18-20].Thus, for a typical patient with 20° internal hip rotationduring gait, intraoperative femoral derotation would beapproximately 30-40° to normalize postoperative hip ro-tation. Tibial torsion was typically corrected to an intra-operative thigh-foot angle of 0-5° external, with the ex-pectation that full correction would be maintained at 1-year follow-up.
Intraoperatively, derotation wires were placed in thefemur and/or tibia undergoing surgery, and with the aidof a goniometer were used to confirm the amount of de-rotation and verify achievement of desired correction.Adequate correction was also verified intraoperativelyby checking that hip external rotation range of motionwas at least 20° greater than hip internal rotation follow-ing derotation and that thigh foot angle was 0-5° exter-nal. In cases where varus or valgus foot deformities werepresent, thigh-foot angle was rechecked intraoperativelyafter correction of the deformity, and TDRO was done ifthigh-foot angle remained abnormal.
Statistical analysisThe data were first examined descriptively, and it was ob-served that no new rotational problems appeared in unilater-ally involved patients. The primary analyses were thereforeperformed only on patients with bilateral involvement.
A one-sample test of proportions was used to evaluatewhether the new rotational problems that developed in eachbone were preferentially in one direction or the other (in-wards or outwards) compared with a hypothesis of equalproportions (0.5 in each direction). Logistic regression anal-ysis was then performed to examine the potential preopera-tive predictors of subsequent rotational deformity at any site(femur, tibia or both bones). First, each potential predictorwas examined separately including length of follow-up as acovariate to adjust for differing lengths of time over whichnew problems could develop. Multivariable logistic regres-sion was then performed including all factors that were sig-nificant in the individual analyses. Logistic regression analy-sis was also performed only in limbs that had undergoneFDRO to determine if the occurrence of subsequent rota-tional problems was related to the site of femoral osteotomy(proximal or distal). All statistical analysis was performed inSTATA (version 14.2, StataCorp LLC, College Station, TX)with a significance level of 0.05.
RESULTS
ParticipantsA total of 151 patients were identified, in whom 252 limbshad undergone 325 derotation osteotomies. Eighteen ofthe patients (12%) had unilateral involvement, and theremaining 133 patients (88%) had bilateral involvement(Table I). Length of follow-up ranged from 6.7 monthsto 11.2 years (mean 3.8, SD 2.5 years).
T. A. L. WREN et al. – Rotational deformity recurrence in CP Lebanese Medical Journal 2021 • Vol 69 (2) 71
TABLE I PARTICIPANT CHARACTERISTICS
Unilateral CP Bilateral CP(n = 18) (n = 133)
SexMale 14 (78%) 78 (59%)
Female 4 (22%) 55 (41%)
8.5 (2.7) 8.6 (2.5)
[5.0, 15.1] [4.4, 15.8]GMFCS
I 14 (78%) 19 (14%)
II 3 (17%) 43 (32%)
III 1 (6%) 60 (45%)
IV 0 11 (8%)
Length of follow-up (years)2.9 (2.1) 4.0 (2.6)
[0.9, 8.1] [0.6, 11.2]
Continuous variables are presented as mean (SD) [range]. Categorical variables are presented as n (%).

Among the 18 unilaterally involved patients, 2 hadundergone TDRO only, 9 had undergone FDRO on-ly, and 7 had undergone both TDRO and FDRO on theaffected side.
All derotations were in the external direction tocorrect excessive internal tibial torsion, anteversion,or intoeing. No subsequent rotational problems de-veloped in any of the unilaterally involved subjects.Therefore, only bilaterally involved patients were in-cluded in the primary analyses below.
Predictors of rotational problems following DRO inbilaterally involved patientsAmong the limbs from bilaterally involved patients, 60had undergone TDRO only, 108 had undergone FDROonly, and 66 had undergone both TDRO and FDRO(Figure 1). Overall, 58/234 limbs (25%) developed sub-sequent rotational problems. Of these, 24 problems in-volved the femur only (all ending up internal), 22 in-volved the tibia only (5 ending up internal, 17 external),and 12 involved both bones (1 with both bones internal,
72 Lebanese Medical Journal 2021 • Vol 69 (2) T. A. L. WREN et al. – Rotational deformity recurrence in CP
Figure 1. Flow chart of results for bilaterally involved patients stratified by type (femur and/or tibia) and direction (internal or external) of derotation osteotomy. The two bottommost rows of the chart show the number and percentage of recurrence within each subgroup.

TABLE IVPREDICTION OF SUBSEQUENT ROTATIONAL PROBLEMS IN PATIENTS WITH BILATERAL INVOLVEMENT
USING MULTIVARIATE LOGISTIC REGRESSION (N = 223 LIMBS)
95% POdds Ratio Confidence z value
Interval
GMFCS HI/IV 3.4 [1.6, 7.3] 3.16 0.002
TMA (degrees) 1.04 [1.01, 1.07] 2.79 0.005
Length of follow-up (years) 1.4 [1.2, 1.6] 4.9 < 0.001
Constant 0.02 [0.007, 0.06] - 7.09 < 0.001
TMA was not measured in 11 limbs.
2 with both bones external, 9 with femur internal and ti-bia external). Rotational problems that developed in thefemur were more frequently in the inward direction(34/36, 94%, p < 0.0001), while problems that devel-oped in the tibia were more frequently in the outwarddirection (28/34, 82%, p = 0.0002).
The development of subsequent rotational problemswas related to GMFCS level and preoperative TMA(Tables II-IV). No relationship was observed with sex,age, BMI, or preoperative femoral anteversion. Rota-tional problems occurred in 35% (44/127) of limbs atGMFCS levels III and IV, compared with only 13%(14/107) of limbs at GMFCS levels I and II (Table II).The odds ratio for GMFCS III/IV compared withGMFCS I/II was 3.2 (95% CI: 1.5 to 6.5, p = 0.002) afteradjusting for length of follow-up in the logistic regres-sion model (Table III). The odds ratio for TMA perdegree in the external direction was 1.03 (95% CI : 1.01to 1.06, p = 0.02), again adjusting for length of follow-up (Table III). In multiple logistic regression, bothGMFCS level and TMA remained as significant predic-tors of subsequent rotational problems (Table IV).
Proximal FDROs were performed in 56 limbs, anddistal FDROs were performed in 113 limbs. The site of derotation was unavailable for 5 limbs. Rotationalproblems occurred in 16/56 limbs (29%) with proximalFDRO and 30/117 limbs (26%) with distal FDRO.Therefore, there was no influence of FDRO location onthe development of subsequent rotational problems (ORproximal 0.9, 95% CI 0.4 to 2.1, p = 0.82) adjusting forlength of follow-up in the logistic regression model.
T. A. L. WREN et al. – Rotational deformity recurrence in CP Lebanese Medical Journal 2021 • Vol 69 (2) 73
TABLE IIFREQUENCY OF SUBSEQUENT ROTATIONAL PROBLEMS BYGMFCS LEVEL IN PATIENTS WITH BILATERAL INVOLVEMENT
(N = 234 limbs)
Preoperative Functional N Subsequent RotationalStatus Problems, N (%)
GMFCS I 35 4 (11.4%)
GMFCS II 72 10 (13.9%)
GMFCS III 108 37 (34.3%)
GMFCS IV 19 7 (36.8%)
GMFCS indicates Gross Motor Function Classification System
TABLE IIIPREDICTION OF SUBSEQUENT ROTATIONAL PROBLEMS IN PATIENTS WITH BILATERAL INVOLVEMENT
USING LOGISTIC REGRESSION WITH A SINGLE PREDICTOR (N = 234 limbs)
95% POdds Ratio Confidence z value
Interval
Sex, female 1.3 [0.7, 2.5] 0.79 0.43
Age at surgery (years) 1.1 [0.9, 1.3] 1.08 0.28
BMI (kg/m2) 0.9 [0.8, 1.04] - 1.37 0.17
GMFCS III / IV 3.2 [1.5, 6.5] 3.12 0.002
Femoral anteversion (degrees) 1.01 [0.98, 1.04] 0.57 0.57
TMA (degrees)* 1.03 [1.01, 1.06] 2.37 0.02
Length of follow-up was included as a covariate in all analyses. * TMA was not measured in 11 limbs (N = 223)

DISCUSSION
The overall rate of long bone transverse plane deformi-ties requiring repeat surgery in children with bilateral CPinvolvement in the current study was 25%. This includ-ed recurrence of the same problem in the same bone,development of the opposite deformity in the same bone,and/or development of rotational deformity in the otherbone. We did not observe any rotational deformities fol-lowing derotational osteotomy in unilaterally involvedpatients, indicating that distribution of CP (unilateral vs.bilateral) is a significant predictor for successful surgicalcorrection.
In bilaterally involved patients, rotational problemsoccurred after both FDRO and TDRO, alone and in com-bination with each other. Most FDROs (169/174, 97%)were performed in the external direction to correct inter-nal hip rotation and in-toeing. Recurrence of internalfemoral rotation after external FDRO without or withoutconcomitant TDRO occurred in 27/174 limbs (15%),which is similar to rates of recurrence reported previous-ly [11, 21]. Dreher et al. documented recurrence of inter-nal hip rotation in 15% of 59 limbs that underwent ex-ternal FDRO in diplegic children with CP, defined as > 15o increase in internal hip rotation between one andnine year follow-up [11]. Õunpuu et al. reported a slight-ly lower rate of recurrence of 9% (2/27 limbs), an aver-age of 11 years after external FDRO in a combinedgroup of children with unilateral or bilateral CP [21]. Inall cases in which rotational deformity developed in thefemur following FDRO and/or TDRO, the femur endedup internally rotated. This is consistent with the previousfinding that hip internal rotation increases with age inambulatory children with CP [22]. Reverse deformitywas observed in the femur in only one limb in the cur-rent series and occurred after internal, rather than exter-nal, FDRO. Since proximal and distal FDRO resulted insimilar rates of subsequent rotational deformity, it doesnot appear that location of FDRO affects the risk of de-veloping rotational problems after this procedure.
The tibia was more variable with 20 (16%) internaland 106 (84%) external TDROs being performed. Out-comes were also more unpredictable for the tibia. AfterTDRO, the tibia sometimes re-rotated toward the originalmal-aligned position (recurrence), but often continuedfurther in the direction of surgical derotation (reversedeformity). When these subsequent rotational problemsoccurred, the tibia ended up externally rotated in 84% ofcases. This is consistent with other reports of long termoutcome of TDRO in children with CP which identify atrend toward progressive external rotation with time af-ter both internal and external TDRO [10, 23-25]. In allcases of “reverse deformity,” the final measure of tibial
torsion was greater than tibial torsion at the time of sur-gical correction, indicating that further remodeling oc-curred postoperatively. This was likely due to stressesplaced on the bone postoperatively, as previous serieshave shown that loss of reduction is rare [10, 23].
The highest rate of subsequent rotational problemswas seen in limbs with rotational malalignment that un-derwent external FDRO combined with internal TDRO(6/8, 75%). These limbs represent a small subset of thesample undergoing surgery on both bones (8/66 limbs,12%), but may be complex cases that are more difficultto treat successfully. Such patients and their parentsshould be cautioned that additional torsional deformitiesmay develop over time, and that repeat surgery may beneeded.
In addition to time since surgery, the only factors pre-dictive of development of subsequent rotational defor-mities were distribution of CP and GMFCS levels, withbilaterally involved patients functioning at GMFCS lev-els III and IV having higher odds of developing subse-quent problems. These findings suggest that factors as-sociated with lower functional levels, such as greaterweakness, limited weight bearing and mobility, or over-pull of spastic muscles may be related to the develop-ment of rotational deformity. Bone density is lower inpatients functioning at GMFCS levels III/IV versus I/II[26]. It is possible that bone remodeling is exaggeratedin these patients, even under conditions of limited load-ing, due to their poorer quality bone.
Younger age (< 10 years) at surgery has been previ-ously reported as predictive of recurrent femoral ante-version and internal rotation gait [13-14]. In the currentstudy, however, no such relationship was found. We alsopostulated that increased weight or body size would bepredictive of developing rotational deformity. Ultimate-ly, neither age at surgery nor BMI were predictive of thedevelopment of subsequent rotational problems. The av-erage age of patients in the current study was 8.5 months,ranging from 4.4 to 15.8 months.
Limitations of this study include the retrospective single-site design in which participants were treated pri-marily by one surgeon at one orthopedic center, possiblyimposing selection or treatment bias. Only patients withboth pre- and postoperative gait analyses were included.In many cases, postoperative tests were conducted toevaluate the need for additional intervention, which mayor may not have involved rotational problems. Since pa-tients without perceived problems often did not under-go postoperative gait analysis, the study sample may bebiased towards patients with poorer outcomes (thoughthe problems were not necessarily bony), possibly lead-ing to exaggerated estimates of the need for additionalsurgery. Finally, since derotation osteotomy (DRO) was
74 Lebanese Medical Journal 2021 • Vol 69 (2) T. A. L. WREN et al. – Rotational deformity recurrence in CP

defined at the beginning of multilevel surgery, variousconcomitant soft tissue or bony surgeries had been donefor most of the subjects and were not controlled for inthe current analysis.
In conclusion, the operative management of torsionaldeformity of the femur and tibia through DRO in chil-dren with CP is typically successful, but there is a risk ofsubsequent rotational abnormalities developing, particu-larly in patients with greater functional limitations andthose who have a combination of excess internal femo-ral rotation and excess external tibial rotation. Familiesshould be advised that revision surgery may be needed inthese patients. The fact that subsequent rotational defor-mities often develop not only in the bone that underwentDRO but in the other long bone highlights the complex-ity of transverse plane problems in children with CP andthe need for careful surgical planning and follow-up. Theresults of the current study can help inform clinicians,patients and families when making surgical decisions forambulatory patients with CP with rotational deformities.
REFERENCES
1. Ketelaar M, Gorter JW, Westers P, Hanna S, Verhoef M.Developmental trajectories of mobility and self-carecapabilities in young children with cerebral palsy. JPediatr. 2014 Apr; 164 (4): 769-74.
2. Waters RL, Mulroy S. The energy expenditure of normaland pathologic gait. Gait Posture. 1999; 9 (3): 207-31.
3. Schwartz MH, Rozumalski A, Novacheck TF. Femo-ral derotational osteotomy: surgical indications and out-comes in children with cerebral palsy. Gait Posture 2014Feb; 39 (2): 778-83.
4. Adolfsen SE, Ounpuu S, Bell KJ, DeLuca PA. Kinematicand kinetic outcomes after identical multilevel soft tissuesurgery in children with cerebral palsy. J Pediatr Orthop.2007; 27 (6): 658-67.
5. Karol LA. Surgical management of the lower extremityin ambulatory children with cerebral palsy. J Am AcadOrthop Surg. 2004; 12 (3): 196-203.
6. Gough M, Eve LC, Robinson RO, Shortland AP. Short-term outcome of multilevel surgical intervention in spas-tic diplegic cerebral palsy compared with the natural his-tory. Dev Med Child Neurol. 2004; 46 (2): 91-7.
7. Rodda JM, Graham HK, Nattrass GR, Galea MP, BakerR, Wolfe R. Correction of severe crouch gait in patientswith spastic diplegia with use of multilevel orthopaedicsurgery. J Bone Joint Surg Am. 2006; 88 (12): 2653-64.
8. Heimkes B, Martignoni K, Utzschneider S, Stotz S. Softtissue release of the spastic hip by psoas-rectus trans-fer and adductor tenotomy for long-term functional im-provement and prevention of hip dislocation. J PediatrOrthop B. 2011 Jul; 20 (4): 212-21.
9. Stefko RM, de Swart RJ, Dodgin DA et al. Kinematicand kinetic analysis of distal derotational osteotomy ofthe leg in children with cerebral palsy. J Pediatr Orthop.
1998; 18 (1): 81-7.10. Ryan DD, Rethlefsen SA, Skaggs DL, Kay RM. Results
of tibial rotational osteotomy without concomitant fibu-lar osteotomy in children with cerebral palsy. J PediatrOrthop. 2005; 25 (1): 84-8.
11. Dreher T, Wolf SI, Heitzmann D et al. Long-term out-come of femoral derotation osteotomy in children withspastic diplegia. Gait Posture. 2012; 36 (3): 467-70.
12. Ounpuu S, DeLuca P, Davis R, Romness M. Long-termeffects of femoral derotation osteotomies: an evaluationusing three-dimensional gait analysis. J Pediatr Orthop.2002; 22 (2): 139-45.
13. Kim H, Aiona M, Sussman M. Recurrence after femoralderotational osteotomy in cerebral palsy. J Pediatr Orthop.2005; 25 (6): 739-43.
14. Niklasch M, Wolf SI, Klotz MC et al. Factors associatedwith recurrence after femoral derotation osteotomy incerebral palsy. Gait Posture. 2015; 42 (4): 460-5.
15. Rosenbaum PL, Palisano RJ, Bartlett DJ, Galuppi BE,Russell DJ. Development of the Gross Motor FunctionClassification System for cerebral palsy. Dev Med ChildNeurol. 2008; 50 (4): 249-53.
16. Chung CY, Lee KM, Park MS, Lee SH, Choi IH, Cho TJ.Validity and reliability of measuring femoral anteversionand neck-shaft angle in patients with cerebral palsy. J BoneJoint Surg Am. 2010; 92 (5): 1195-205.
17. Davis RBI, Ounpuu S, Tyburski D, Gage JR. A gait anal-ysis data collection and reduction technique. HumanMovement Science. 1991; 10: 575-87.
18. Kay RM. Lower extremity surgery in children with cere-bral palsy. In: Tolo VTS, D.L., editor. Pediatrics (MasterTechniques in Orthopaedic Surgery). Philadelphia, PA:Lippincott Williams & Wilkins; 2008. p. 83-119.
19. Kay RM, Rethlefsen SA, Hale JM, Skaggs DL, Tolo VT.Comparison of proximal and distal rotational femoral os-teotomy in children with cerebral palsy. J Pediatr Orthop.2003; 23 (2): 150-4.
20. Pirpiris M, Trivett A, Baker R, Rodda J, Nattrass GR,Graham HK. Femoral derotation osteotomy in spasticdiplegia. Proximal or distal? J Bone Joint Surgery Br2003; 85 (2): 265-72.
21. Ounpuu S, Solomito M, Bell K, Pierz K. Long-term out-comes of external femoral derotation osteotomies in chil-dren with cerebral palsy. Gait Posture. 2017; 56: 82-8.
22. Wren TA, Rethlefsen S, Kay RM. Prevalence of specificgait abnormalities in children with cerebral palsy: influ-ence of cerebral palsy subtype, age, and previous sur-gery. J Pediatr Orthop. 2005; 25 (1): 79-83.
23. Dodgin DA, De Swart RJ, Stefko RM, Wenger DR, Ko JY.Distal tibial/fibular derotation osteotomy for correction oftibial torsion: review of technique and results in 63 cases.J Pediatr Orthop. 1998; 18 (1): 95-101.
24. Er MS, Bayhan IA, Rogers KJ et al. Long-term outcomeof external tibial derotation osteotomies in children withcerebral palsy. J Pediatr Orthop. 2017; 37 (7): 460-5.
25. Er MS, Abousamra O, Rogers et al. Long-term outcomeof internal tibial derotation osteotomies in children withcerebral palsy. J Pediatr Orthop. 2017; 37 (7): 454-9.
26. Wren TAL, Lee DC, Kay RM, Dorey FJ, Gilsanz V. Bonedensity and size in ambulatory children with cerebralpalsy. Dev Med Child Neurol. 2011; 53 (2): 137-41.
T. A. L. WREN et al. – Rotational deformity recurrence in CP Lebanese Medical Journal 2021 • Vol 69 (2) 75

INTRODUCTION
Bone modelling is the process by which bones changeshape or size in response to physiologic influences ormechanical forces [1]. Dysregulation of bone modellingin lower extremities due to genetic, environmental or bio-mechanical factors leads to angular varus-valgus defor-mities and leg length discrepancies [2-4]. These relative-ly common conditions may lead to gait disturbance, in-stability and pain, and predispose to early degenerativearticular changes later in adulthood if corrective surgeryis not performed [5- 6].
Since longitudinal growth occurs mostly around theknee, specifically around the distal femoral and proximaltibial physes, initial efforts to modulate lower limb growthconcentrated on this anatomical area [1]. Minimally inva-sive techniques aiming to reach permanent or reversiblehemiepiphysiodesis were developed including rigid sta-pling, percutaneous transphyseal screwing and tensionband plating among others [6-9]. These techniques fol-low the Hueter-Wolkman principle [10]. Also, limblengthening procedures has developed considerablysince the beginning of the 20th century [11-13]. Most ofthem rely on long bone distraction following osteotomythrough the shaft or the metaphysis [14-15]. Metaphy-seal osteotomies are associated with higher rates of con-solidation and faster bone healing [16-18], due to a greaterosteogenesis potential near the physis [16-18]. On theother hand, it has been shown that periosteal violationleads to appositional bone growth disturbance [19].
We postulated that percutaneous juxtaphyseal meta-physeal perforations could increase bone growth giventhe rich vascularisation of the metaphysis and its prox-imity to the physis, leading to bone shape and length mod-ification. This study was conducted to validate this hypo-thesis and to set grounds for future applications of thistechnique.
METHODS
This is an IRB approved experimental study on 18 NewZealand white growing rabbits aged between 8 and 9weeks performed according to ARRIVE Guidelines [20].Authors abided by the STROBE checklist for case con-trol studies [21] (Table I). Twenty-four weeks is the ageat which this species of rabbits ends its growth [10].
Rabbits careRabbits were sheltered in favorable conditions, accord-ing to animal testing guidelines and regulations [20, 22].Two rabbits were sheltered per cage without a raisedarea. Cages had a surface of 7100 cm2 with a height of60 cm. Temperature was kept stable around 18°C.
All rabbits were operated under general anaesthesiausing intramuscular injections of ketamine hydrochloride(50 mg/kg) and xylazine (5 mg/kg) [7]. Only ketaminehydrochloride intramuscular injections (50 mg/kg) wereused at each radiological control. A dose of 200 mg/kg ofparacetamol three times daily _ total dose not exceeding600 mg/kg/day _ was given to all rabbits in order to de-crease the painful stimuli during the first two postopera-tive weeks. The wellbeing of the rabbits was regularlyassessed twice a day by qualified lab technicians. Rab-bits that remained healthy at the end of the follow-upwere euthanized. Euthanasia was performed by an intra-venous overdosage of sodium phenobarbital at a dose of1 ml/4.5 kg.
Operating protocolThe proximal tibia was chosen as site of perforationsince it has an easy surgical access and a relatively flatgrowth plate compared to the undulated distal femoralgrowth plate [10]. The rabbits are placed supine, the sur-gery site is shaved and cleaned with Povidone-iodine(PVP-I) solution. Under fluoroscopy guidance, a 5 mm-incision is made facing the proximal tibial growth plate.A 1.6 mm-Kirshner wire is drilled through the lateralmetaphyseal cortex few millimeters below the physis(Figures 1, 2). A total of three to four adjacent unicorticalholes are made. The left tibia, kept intact, is used as reference.
76 Lebanese Medical Journal 2021 • Volume 69 (2)
PPAAEEDDIIAATTRRIICC OORRTTHHOOPPAAEEDDIICCSSPERCUTANEOUS METAPHYSEAL JUXTA-PHYSEAL PERFORATIONSA NEW POTENTIAL APPROACH TO ANGULAR CORRECTION AND LIMB LENGTHENING An Experimental Pilot Studyhttp://www.lebanesemedicaljournal.org/articles/69-2/pedsortho3.pdf
Ibrahim SALIBA1, Stephanie SKAFF1, Maroun RIZKALLAH1, Diane GHANEM3, Amer SEBAALY1,2
Georges EL KHOURY1, Rami EL ABIAD1,2, Ismat GHANEM1,2
Saliba I, Skaff S, Rizkallah M, Ghanem D, Sebaaly A,El Khoury G, El Abiad R. Ghanem I. Percutaneous metaphy-seal juxta-physeal perforations : a new potential approach toangular correction and limb lengthening. An experimentalpilot study. J Med Liban 2021 ; 69 (2) : 76-81.
From Beirut, Lebanon. 1Faculty of Medicine, Saint-Joseph University (USJ) 2Hôtel-Dieu de France University Hospital, USJ. 3Faculty ofMedicine, American University of Beirut. *Corresponding author: Rizkallah Maroun, MD e-mail: [email protected]

TABLE I STROBE STATEMENT _ CHECKLIST OF ITEMS THAT SHOULD BE INCLUDED IN REPORTS OF CASE-CONTROL STUDIES
Item No Recommendation
Title and abstract 1 (a) Indicate the study’s design with a commonly used term in the title or the abstract.(b) Provide in the abstract an informative and balanced summary of what was done and what was found.
IntroductionBackground/Rationale 2 Explain the scientific background and rationale for the investigation being reported.Objectives 3 State specific objectives, including any prespecified hypotheses.
MethodsStudy design 4 Present key elements of study design early in the paper.Setting 5 Describe the setting, locations and relevant dates, including periods of recruitment, exposure, follow-up,
and data collection.
Participants 6 (a) Give the eligibility criteria, and the sources and methods of case ascertainment and control selection. Give the rationale for the choice of cases and controls.
(b) For matched studies, give matching criteria and the number of controls per case.Variables 7 Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers.
Give diagnostic criteria, if applicable.Data sources/Measurement 8* For each variable of interest, give sources of data & details of methods of assessment (measurement).
Describe comparability of assessment methods if there is more than one group.Bias 9 Describe any efforts to address potential sources of bias.Study size 10 Explain how the study size was arrived at.Quantitative variables 11 Explain how quantitative variables were handled in the analyses. If applicable, describe which
groupings were chosen and why.
Statistical methods 12 (a) Describe all statistical methods, including those used to control for confounding.(b) Describe any methods used to examine subgroups and interactions.(c) Explain how missing data were addressed.(d) If applicable, explain how matching of cases and controls was addressed.(e) Describe any sensitivity analyses.
ResultsParticipants 13* (a) Report numbers of individuals at each stage of study _ e.g. numbers potentially eligible, examined
for eligibility, confirmed eligible, included in the study, completing follow-up, and analysed.(b) Give reasons for non-participation at each stage.(c) Consider use of a flow diagram.
Descriptive data 14* (a) Give characteristics of study participants (e.g. demographic, clinical, social) and information on exposures and potential confounders.
(b) Indicate number of participants with missing data for each variable of interest.
Outcome data 15* Report numbers in each exposure category, or summary measures of exposure.Main results 16 (a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates & their precision
(e.g. 95% confidence interval). Make clear which confounders were adjusted for and why theywere included).
(b) Report category boundaries when continuous variables were categorized.(c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period.
Other analyses 17 Report other analyses done _ e.g. analyses of subgroups and interactions, and sensitivity analyses.
DiscussionKey results 18 Summarise key results with reference to study objectives.Limitations 19 Discuss limitations of the study, taking into account sources of potential bias or imprecision.
Discuss both direction and magnitude of any potential bias.Interpretation 20 Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of
analyses, results from similar studies, and other relevant evidence.Generalisability 21 Discuss the generalisability (external validity) of the study results.
Other informationFunding 22 Give the source of funding and the role of the funders for the present study and, if applicable, for the
original study on which the present article is based.
*Give information separately for cases and controls.Note : An Explanation and Elaboration article discusses each checklist item, gives methodological background and published examples of transparent reporting.TheSTROBE checklist is best used in conjunction with this article (freely available on the Web sites of PLoS Medicine at http://www.plosmedicine.org/, Annals of InternalMedicine at http://www.annals.org/, and Epidemiology at http://www.epidem.com/). Information on the STROBE Initiative is available at http: //www.strobe-statement.org.

Radiographic measurements Anteroposterior (A/P) radiographs are performed for allrabbits at baseline and at postoperative weeks 8 and 16.Postoperative week 16 is equivalent to age 24-25 weeks,i.e. the age at which New Zealand white rabbits reachskeletal maturity. Radiographs are taken in strict supineposition at one meter SID _ source to image distance _
with care taken to keep both lower limbs symmetrical. A40 mm large metallic plate was used for calibration oflength measurements on X-rays (Figure 3).
Right and left tibial lengths are measured from themidpoint of the proximal tibial articular surface to themidpoint of the distal tibial articular surface (Figure 3).The difference between right and left tibial lengths (�L)is calculated. The ALDA angle _ articular line-diaphy-seal angle _ is measured between the lateral tibial pla-teau and the tibial anatomical axis (Figure 4) [10]. Thedifference between right and left tibial ALDA (�ALDA)is calculated. Varus is defined as a positive �ALDA
while valgus is defined as a negative �ALDA. Radiographic measurements were undertaken by two
independent radiologists using RadiAnt DICOM viewer(64-bit). Intra-observer reliability was assessed at oneweek interval for all measured variables. Inter-observerreliability for length and angles measurements was alsoassessed.
In case the measurement difference between the tworadiologists was less than 1 mm or 3 degrees for anygiven parameter, the first value was recorded. A thirdindependent radiologist was involved in case a largermeasurement difference existed between the two radiol-ogists for any given parameter.
Statistical analysisNormality is checked by using Shapiro-Wilk test. A paired2-tailed t-test is used to compare longitudinal and angulargrowth between the operated side (Right) and the controlside (Left). Significance is established with p < 0.05.
78 Lebanese Medical Journal 2021 • Vol 69 (2) I. SALIBA .et al. – Percutaneous juxta-physeal perforations & growth modulation
Figure 1 showing the pin introduced laterallyin the metaphysis of the right tibia.
Figure 2 showing the perforation carried outunder fluoroscopy guidance.
Figure 3 showing the measurement of the lengthsof the right and left tibias in each rabbit.
Figure 4 showing the measurement of the ALDA angleon the right and left tibias of each rabbit.

RESULTS
Four rabbits out of 18 died. Two of the rabbits died in theperioperative setting while the remaining two rabbitsdied during the first radiographic control, probably dueto complications from ketamine injection. Fourteen rab-bits survived till the last follow-up.
At baseline, the mean tibia longitudinal length was7.20 cm ± 2.27 at the operated side and 7.28 cm ± 2.14at the control side (p > 0.05). The same parameter meas-ured at week 8 was 9.17 cm ± 1.20 at the operated sidecompared to 8.90 cm ± 1.28 at the control side (p < 0.01)(Figure 5). The mean growth difference between rightand left tibias (�L) at postoperative week 8 was 2.63 mm(Figure 6). At week 16, the length of the operated sidewas 9.58 cm ± 1.03 versus 9.28 cm ± 1.16 for the con-trol side (p < 0.01) (Figure 5). The mean growth dif-ference between right and left tibias at 16 weeks reached(�L) = 2.95 mm (Figure 6).
Intra-observer length measurements reliability reached83%. Inter-observer reliability for same measurementswas 72%. A third radiologist was consulted for three dif-ferent measurements.
Concerning the angular deviation, at week 8, �ALDA R(operated side) was + 3.40° versus �ALDA L (control side)of - 0.04° (p = 0.038). At week 16, �ALDA R was + 4.36° versus �ALDA L of 0.80° (p = 0.038) (Figure 7).
Intra-observer angle measurements reliability reached86%. Inter-observer reliability for same measurementswas 75%.
DISCUSSION
This study confirms our hypothesis that metaphysealjuxta-physeal percutaneous perforations can modifybone growth. This is most probably due to the rich vas-cularisation of the metaphysis and its proximity to thephysis. Perforation would increase the physeal activitythrough hypervascularisation without risking a physealdamage [23]. This is also supported by the high osteo-genesis potential observed in the metaphysis [16-18,24].
Increased physeal activity after metaphyseal stimu-lation is one among other plausible theories explainingCozen’s phenomenon [25]. This phenomenon describesa valgus deformity of the tibia occurring after a patientsustains a non-displaced proximal tibial metaphysicalfracture [26]. The most accepted theory is an overgrowthphenomenon in which the proximal tibia fracture, throughincreased blood circulation and secondary local inflam-matory process, stimulates the physis to grow while anintact fibula acts as a tether, which produces valgus an-gulation [25-26].
I. SALIBA .et al. – Percutaneous juxta-physeal perforations & growth modulation Lebanese Medical Journal 2021 • Vol 69 (2) 79
Figure 5. Diagram showing the average longitudinalgrowth of the right tibia (blue) and left tibia (red)
at baseline, week 8 and week 16.
Figure 6. Diagram showing the average difference (�L)between length of the right (R) tibia & that of the left (L) tibia
at baseline, week 8 and week 16.
Figure 7. Diagram showing the mean angular deviation of theright tibia (blue) & left tibia (red) at baseline, week 8 & week 16.
Baseline Week 8 Week 16
Baseline Week 8 Week 16
Right Left

The current study shows that percutaneous juxtaphy-seal perforations in white New Zealand rabbits inducedangular deviation and to a lesser extent an increasedlength of the operated bone segment. Observed modifi-cations at week 8 of follow-up were sustained and evenaccentuated at week 16. Lateral metaphyseal perfora-tions lead to varus deformity. Although none of the rab-bits in this study underwent medial perforations, onewould suppose that they could induce valgus deformityof the proximal tibia.
Bone modulation procedures for angular correctionare widely performed using periphyseal stapling, tensionband plating or screwing [6-8]. When compared to thesetechniques the minimally invasive percutaneous meta-physeal periphyseal perforations proved to be effectiveand safe in the growing white New-Zealand rabbit.
Additional advantages of this new minimally invasivetechnique are numerous. It is simple, fast and easy to per-form. It does not require casting or any internal or externalfixation. Our assumption is that it could be used either forminimal to moderate (to be defined after a larger experi-ence on animals, and its use in humans) angular deformi-ties or limb shortening or for correction of residual defor-mities following the use of well-known techniques.
However, the amount of angular deviation followingthe procedure is still unpredictable and depends proba-bly on animal species or human ethnic background aswell as remaining growth, the bone type (long, short orflat), physeal characteristics in terms of anatomical pat-tern and growth activity, the distance between perfora-tions and the physis, along with other possible factors.Further application of this procedure may help establish-ing a mathematical formula linking the above cited para-meters, thereby giving an idea of the provisional amountof angular deviation to be ultimately produced. To a less-er extent, percutaneous juxtaphyseal perforations havealso led to an increased bone length. In this series, thelength of the operated tibia increased by 3.1% comparedto the control non-operated tibia. This is minimal thoughstatistically significant. We assume that if lengthening on-ly is contemplated, perforations should be undertakenboth medially and laterally at the metaphysis, in order toavoid undesired angular deviation. This study is prelimi-nary and should be refined to improve its accuracy. Infact, the authors are aware of this major limitation of thistreatment method in its current status, and conducted thispilot study to set the grounds for further investigations andadditional clinical applications.
Another limitation to this study is its small popula-tion. However, the results are consistent and show a sig-nificant and sustained trend towards inducing varus andbone lengthening over 8 and 16 weeks of follow-up. Thelack of a control group may also be considered as a limi-
tation. Since the included number of rabbits was limited,the contralateral tibia was chosen as control, which ledto the impossibility of blinding data collection. The pos-itive effect of such choice however is that it reduces thebias related to the possible difference in growth potentialbetween different rabbits (operated and controls). Onemore limitation of this study is the lack of postmortemCT-scan analysis of the tibia on the conserved cadavers.This would have reduced imprecision in measurements ;however, this was impossible due to strict laboratory reg-ulations for animal cadaver conservation in our institu-tion. The last limitation of this study is the lack of histo-logical evaluation of the physo-metaphyseal area due toa technical error in specimen preparation, discoveredfew weeks after termination of the study. However, sincewe observed obvious changes, we decided not to repeatthe experiment for histological purposes. Percutaneousmetaphyseal perforations around the knee have shown toproduce angular deviation and to a lesser extent limblengthening in New Zealand rabbits, probably through anincrease in physeal activity induced by hyper-vasculari-zation.
The procedure is simple, easy, effective, safe and maybe extended to children with moderate or residual defor-mities, provided unpredictable issues related to its useare solved. Unlike most of the studies that have dealtwith limb lengthening or angular correction procedures,this paper opens prospects for other experimental re-search assessing noninvasive techniques to modify bonegrowth ; it may also serve as a model for future studiesdealing with juxtaphyseal perforations in other parts ofthe skeleton, mainly around the hip.
Highlights_ Growth modulation became widely accepted for
correction of angular deformities._ This paper proposes a simple, easy, effective and
safe procedure that has shown to produce angulardeviation and to a lower extent limb lengthening inNew Zealand rabbits.
_ We believe that this simple cost sparing proceduremay be extended to children with moderate or re-sidual deformities after commonly performed pro-cedures provided that unpredictable issues relatedto its use are solved.
_ This paper opens prospects for other experimentalresearch assessing non-invasive techniques to mod-ify bone growth; and serves as a model for future stud-ies dealing with juxta-physeal perforations around thehip.
This research involving animals received an IRB ap-proval. Authors took care of the welfare of the animals.The rabbits were fed adequate dosage of analgesics (pa-
80 Lebanese Medical Journal 2021 • Vol 69 (2) I. SALIBA .et al. – Percutaneous juxta-physeal perforations & growth modulation

racetamol), weighted and monitored daily to make surethat they were growing according to the standard growthcharts. Rabbits were anesthetized using ketamine duringall manipulations. No rabbit exhibited signs of lethargyor suffering during the course of this study.
REFERENCES
1. Katsimbri P. The biology of normal bone remodelling.Eur J Cancer Care (Engl) 2017: 26 (6).https://doi.org/10.1111/ecc.12740
2. Schneider M, Buschbaum J, Joeris A et al. Biomechani-cal investigation of two long bone growth modulationtechniques by finite element simulations. J Orthop Res2018: 36:1398-1405.https://doi.org/10.1002/jor.23762
3. Sinha R, Weigl D, Mercado E et al. Eight-plate epiphysio-desis: are we creating an intra-articular deformity? BoneJoint J 2018; 100-B: 1112-1116.https://doi.org/10.1302/0301-620X.100B8.BJJ-2017-1206.R3
4. Mahapatra S, Hampannvar A, Sahoo M. Tension bandplating in growth modulation?: A review of current evi-dences. Acta Orthop Belg 2015; 81: 351-357.
5. Ruzbarsky JJ, Goodbody C, Dodwell E. Closing thegrowth plate: a review of indications and surgical options.Curr Opin Pediatr 2017; 29: 80-86.https://doi.org/10.1097/MOP.0000000000000438
6. Lykissas MG, Jain VV, Manickam V et al. Guided growthfor the treatment of limb length discrepancy: a compara-tive study of the three most commonly used surgicaltechniques. J Pediatr Orthop 2013; B 22: 311-317.https://doi.org/10.1097/BPB.0b013e32836132f0
7. Gaumétou E, Mallet C, Souchet P et al. Poor efficiencyof eight-plates in the treatment of lower limb discrepan-cy. J Pediatr Orthop 2016; 36: 715-719.https://doi.org/10.1097/BPO.0000000000000518
8. Friend L, Widmann RF. Advances in management oflimb length discrepancy and lower limb deformity. CurrOpin Pediatr 2008; 20: 46-51.https://doi.org/10.1097/MOP.0b013e3282f35eeb
9. Pesenti S, Iobst CA, Launay F. Evaluation of the exter-nal fixator TrueLok Hexapod System for tibial deformitycorrection in children. Orthop Traumatol Surg Res 2017;103: 761-764.https://doi.org/10.1016/j.otsr.2017.03.015
10. Ghanem I, El Hage S, Diab M et al. Radiofrequency ap-plication to the growth plate in the rabbit: a new poten-tial approach to epiphysiodesis. J Pediatr Orthop 2009;29: 629-635.https://doi.org/10.1097/BPO.0b013e3181b2bae7
11. Ilizarov GA. Clinical application of the tension-stress effect
for limb lengthening. Clin Orthop Relat Res 1990; 250: 8-26.12. Caton J. Allongement des membres chez l’adulte (adoles-
cents et jeunes adultes). In: Conférence d’enseignementde la SOFCOT (1995).
13. Latte Y. Application de la méthode d’Ilizarov en chirurgieorthopédique vétérinaire. Prat Med Chir Anim Comp1994; 29 (6): 545-570.
14. Gubin A, Borzunov D, Malkova T. Ilizarov method forbone lengthening and defect management review of con-temporary literature. Bull Hosp Jt Dis 2016; 74: 145-54.
15. Hvid I, Horn J, Huhnstock S, Steen H. The biology ofbone lengthening. J Child Orthop 2016; 10: 487-92.https://doi.org/10.1007/s11832-016-0780-2
16. Steen H, Fjeld TO. Lengthening osteotomy in the meta-physis and diaphysis. An experimental study in the ovinetibia. Clin Orthop Relat Res 1989; 247: 297-305.
17. Monticelli G, Spinelli R. Leg lengthening by closed me-taphyseal corticotomy. Ital J Orthop Traumatol 1983; 9:139-50.
18. Fischgrund J, Paley D, Suter C . Variables affecting timeto bone healing during limb lengthening. Clin OrthopRelat Res 1994; 301: 31-37.
19. Gkiatas I, Lykissas M, Kostas-Agnantis I et al. Factorsaffecting bone growth. Am J Orthop (Belle Mead NJ)2015; 44: 61-67.
20. Bosmans JWAM, Moossdorff M, Al-Taher M et al. Inter-national consensus statement regarding the use of animalmodels for research on anastomoses in the lower gas-trointestinal tract. Int J Colorectal Dis 2016; 31: 1021-30. https://doi.org/10.1007/s00384-016-2550-5
21. Vandenbroucke JP, von Elm E, Altman DG et al. Strength-ening the Reporting of Observational Studies in Epide-miology (STROBE): explanation and elaboration. PLoSMed 2007; 4 (10): e297.https://doi.org/10.1371/journal.pmed.0040297
22. Ferdowsian HR, Gluck JP. The ethical challenges of ani-mal research. Camb Q Healthc Ethics 2015; 24 (4): 391-406.https://doi.org/10.1017/S0963180115000067
23. Späth S-S, Andrade AC, Chau M, Nilsson O. Local regu-lation of growth plate cartilage. Endocr Dev 2011; 21:12-22.
24. Aldegheri R, Renzi-Brivio L, Agostini S. The callotasismethod of limb lengthening. Clin Orthop Relat Res1989; 241: 137-145.
25. Yang BW, Shore BJ, Rademacher E et al. Prevalence ofCozen’s phenomenon of the proximal tibia. J PediatrOrthop 2019; 39 (6): e417-e421.https://doi.org/10.1097/BPO.0000000000001354
26. Burton A, Hennrikus W. Cozen’s phenomenon revisited.J Pediatr Orthop B 2016; 25 (6): 551-555.https://doi.org/10.1097/BPB.0000000000000327
I. SALIBA .et al. – Percutaneous juxta-physeal perforations & growth modulation Lebanese Medical Journal 2021 • Vol 69 (2) 81

INTRODUCTION
The incidence of idiopathic clubfoot (Figure 1) variesamong different ethnic groups with an overall incidenceof approximately 1 per thousand live births. The ratio ofmale to female incidence is 3:1 and the deformity is bi-lateral in 40% of cases. A strong genetic component ispresent as the occurrence rate in families with affectedindividuals may be up to 10 times that seen in the nor-mal population. The clubfoot is one of the most common
congenital deformities and can be associated with neuro-muscular syndromes, chromosomal abnormalities,, and,in rare cases due to extrinsic causes, such as] constric-tion band syndrome. The goal of treatment for idiopath-ic clubfoot is to produce a flexible, plantar grade footthat is painless for the life of the individual and withoutthe need for orthotics.
Initial management of the clubfoot consists of non-operative treatment. Internationally, the Ponseti methodhas become the treatment of choice for the correction ofthe clubfoot deformity. The Ponseti method is successfulin avoiding the need for extensive surgical release ingreater than 90 percent of idiopathic clubfeet. Recentlythe “complex clubfoot” has been identified within theidiopathic clubfoot designation. These feet resist thestandard Ponseti manipulation and require a change instrategy. The purpose of this paper is to review the stand-ard Ponseti method and to focus on the detection and man-agement of the complex clubfoot.
ANATOMIC FEATURESOF THE IDIOPATHIC CLUBFOOT
At birth, the whole clubfoot appears to be severely supi-nated ; yet the forefoot is adducted and pronated relativeto the hindfoot, which is in varus and in equinus. It is help-ful to remember the four basic deformities of clubfeet bythe acronym C.A.V.E., cavus, adductus, varus and equi-
82 Lebanese Medical Journal 2021 • Volume 69 (2)
PPAAEEDDIIAATTRRIICC OORRTTHHOOPPAAEEDDIICCSSMANAGEMENT OF THE COMPLEX CLUBFOOThttp://www.lebanesemedicaljournal.org/articles/69-2/pedsortho4.pdf
Kenneth J. NOONAN*
ABSTRACT • Clubfoot is a congenital deformity which isseen once in 1000 live births ; most often considered idio-pathic, a certain number of patients may have an associat-ed diagnosis. Clubfeet are best managed by the Ponsetimethod of manipulation and casting, and initially correctsthe deformity in greater than 90 percent of idiopathic pa-tients. Yet a certain percentage of these feet resist the Pon-seti method and while undergoing the standard method de-velop characteristic features. Termed the “complex” club-foot, these feet are often red, swollen, painful and have fore-foot cavus with retraction of the great toe. When these occur,Ponseti recommended changing the strategy of correction.The purpose of this paper is to outline how we identify andmanage the complex clubfoot.
Keywords : computer clubfoot, Ponseti method, idiopathicclubfoot.
Noonan KJ. Management of the complex clubfoot. J MedLiban 2021 ; 69 (2) : 82-88.
*Chief of Pediatric Orthopaedics. University of Wisconsin. 6130 MFCB. 1685 Highland Avenue. Madison WI. 53705-2281.e-mail : [email protected]
Figure 1. This infant has typical feature of idiopathic clubfeet. Figure used with permission from the University of Wisconsin.

nus (Figure 2). The forefoot deformity is due to medialdisplacement of the navicular that articulates with themedial aspect of the head of the talus. The cuboid is alsoadducted in front of the calcaneus along with the meta-tarsals, which are further adducted on the midfoot. Thehindfoot deformity is due to malposition of the calca-neus in adduction and inversion under the talus. Al-though the entire foot is supinated, the forefoot prona-tion relative to the hind foot causes the cavus (high arch)deformity. The muscles and tendons of the gastrocso-leus, tibialis posterior and long toe flexors are short. Theposterior and medial ligaments of the ankle and tarsaljoints are thick and short.
Equinus deformity is due to the shortening of the ex-
trinsic tendons such as the gastrocsoleus, tibialis poste-rior and long toe flexors. The talus is plantar flexed inthe ankle plafond and the posterior ankle and subtalarcapsules are also tight. The physical assessment of actu-al hindfoot deformity can be deceptive when the foot isdorsiflexed due to midfoot breach resulting from hind-foot stiffness. In these cases the foot may appear to dor-siflex up to 10 degrees but the true equinus deformitycan be appreciated by palpating the heel fat pad whichfeels empty due to proximal retraction of the calcanealtuberosity. Radiographically, the tibial-calcaneal angle isincreased and a plantar flexed talus results in a rockerbottom deformity from the aforementioned midfoot breach(Figure 3).
K. J. NOONAN – Complex clubfoot management Lebanese Medical Journal 2021 • Vol 69 (2) 83
Figure 2. This figure represents the different components of the idiopathic clubfoot according to the CAVE acronym.Figure used with permission from the University of Wisconsin.
Figure 3. While the shape of this foot on the left would suggest that there is no equinus contracture, the lateral X-raydemonstrates that the calcaneus is high in the fat pad and there is midfoot breach.
Figure used with permission from the University of Wisconsin.

STANDARD PONSETI METHOD OF MANIPULATION
In general, the ability to obtain full correction via thisapproach is enhanced when treatment is instituted with-in the first month of life. In these instances the need forposterior medial and lateral release is avoided in greaterthan 90 percent of cases. The successful treatment of theclubfoot with the Ponseti method is dependent on an ap-preciation of pathoanatomy and an understanding thatcorrection of deformity should proceed in an orderly fash-ion. The acronym C.A.V.E. is helpful as it not only de-scribes the clinical position of the clubfoot but also out-lines the general order of deformity correction via the Pon-seti method (cavus, adductus, varus and finally equinus).
The protocol consists of stretching and manipulation ofthe foot and application of holding casts until the next ses-sion 5 to 7 days later. To stretch the ligaments and gradu-ally correct the deformity, the foot is manipulated for 1 to3 minutes. The correction is maintained for 5 to 7 dayswith a plaster cast extending from the toes to the upperthird of the thigh with the knee at 90 degrees of flexion.Five or six cast changes are sufficient to correct mostclubfeet. Casting is usually timed to coincide with routinefeedings ; after manipulation, the baby is fed a bottle thattends to relax the infant allowing easier cast application.
The first goal is correction of the cavus deformity byforefoot supination relative to the hindfoot. This manip-ulation seems counterintuitive, as it tends to exaggeratethe appearance of overall foot inversion. Elevation of thefirst metatarsal and supination of the forefoot is in con-tradistinction to other methods of manipulation that pro-pose correction of the cavus by pronation of the firstmetatarsal. At the first session the forefoot is simultane-ously supinated and abducted. The cavus is almost al-ways corrected with the first cast.
At successive manipulation and casting sessions, met-atarsus adductus and hind foot varus are simultaneouslycorrected by abducting the foot while counter pressure isapplied laterally. With this technique, the calcaneus, thenavicular and cuboid are gradually displaced laterally.Forefoot abduction should be performed with the foot inslight supination. As such, correction of the cavus defor-mity is preserved but also co-linearity of the metatarsalsis maintained, thereby producing an efficient lever armfor abduction. It is also important to avoid forceful dor-siflexion prior to correction of hindfoot varus as a rock-er bottom deformity could develop. Finally, care is takento locate the fulcrum for counter pressure on the lateralhead of the talus. Correction of hindfoot varus and cal-caneal inversion would be hindered if counter pressurewere applied to the lateral column of the foot. In gener-al, three to four weekly manipulation and casting ses-sions are usually required to loosen the medial ligamen-
tous structures of the tarsus and partially mold the joints.After each cast, the foot supination is gradually decreas-ed to correct the inversion of the tarsal bones while thefoot is further abducted under the talus.
The equinus is the last deformity that is corrected andshould be attempted when the hindfoot is in neutral toslight valgus and the foot is abducted 70 degrees relativeto the leg. Equinus may be completely corrected throughfurther progressive stretching and casting. However, to fa-cilitate more rapid correction, a subcutaneous heel cordtenotomy is done in 95% of patients. Tenotomy may beperformed in a surgical suite with a thin cataract knife orin the clinic under sterile technique after application ofEMLA cream.
RECOGNIZING THE COMPLEX CLUBFOOT
Recently the “complex clubfoot” has been identified with-in the idiopathic clubfoot designation. Most practitionershave great difficulty in predicting which feet (which ini-tially look like a standard clubfoot) will develop a com-plex pattern with the Ponseti method. This foot is usual-ly a shorter foot with a first ray that is proximally re-cessed from the later four toes. In addition, a deep plan-tar crease extends from the medial arch to the lateral bor-der of the foot. These feet tend to be fatter with a highercavus than normally seen and are much more difficult totreat as a result of the intrinsic stiffness (Figure 4).
In the author’s experience it can be hard to predict whichfeet will develop the complex clubfoot pattern. We agreewith Dragoni et al. (2018) that the complex clubfoot maybe a result of iatrogenic errors in the use of the Ponsetimethod; thus it makes sense that it would be challenging topredict the occurrence based upon the appearance of thefoot. Yet a characteristic pattern of problems usually ensuein these feet that are undergoing treatment. In the typicalPonseti method, the foot is manipulated (as describedabove) and many infants find this to be uncomfortable andwill cry during the manipulation. The well trained practi-tioner will recognize that it’s important to cast the foot in aposition slightly less than what it was stretched to and thatdoes not distract the baby from nursing.
Children who have a complex clubfoot pattern tend tocry throughout the entire process from cast removal tocast application. Often it appears to be an angry anxiouscry that is difficult to console. The foot is red, swollenand highly sensitive even when touched lightly. We likenthis to an active case of reflex sympathetic dystrophywith indurated skin and swelling. Other features includea history of casts falling off or toes drawing back in thecast, the retracted foot not only prevents correction butcan lead to midfoot breach and increase in cast sores onthe heel. It is very hard to compare the results of treat-
84 Lebanese Medical Journal 2021 • Vol 69 (2) K. J. NOONAN – Complex clubfoot management

ment in the complex clubfoot as the differentiation ofeach foot is largely qualitative. Even though classifica-tion systems exist to try to classify these feet, the authorremains that these are challenging to reproduce acrossinstitutions. We use the term complex clubfoot for thosepatients with severe deformity that resist the standardmethod and appear to be on the verge of requiring a pos-terior medial release.
PONSETI’S APPROACH TO COMPLEX CLUBFOOT
About 15 years ago just prior to his death, Ponseti de-scribed a different manipulation strategy for the complexclubfoot. Ponseti et al. (2006), suggested a treatment
strategy change as soon as the practitioner suspects amorphogenesis into the pattern. He advocated to stop thetreatment for a few weeks and that parents begin lightmassage to desensitize the foot. Once the swelling abatesand the child’s foot can be touched without discomfort,the method can be restarted with emphasis on goingslowly. Repeat forefoot abduction is started with a goalof 10 to 20 degrees external rotation. Once this obtainedthe practitioner then works on progressive dorsiflexionof the foot with pressure on the midfoot (Figure 5). Hy-perflexion of the knee to 120 degrees can prevent thecast from loosening or falling off. In many cases thechild may need to have earlier tenotomy and then havecontinued stretching and casting afterwards.
K. J. NOONAN – Complex clubfoot management Lebanese Medical Journal 2021 • Vol 69 (2) 85
Figure 4. Classic appearance of complex clubfoot with retracted great toe (circled on the right) &a prominent plantar crease (circled on the left). Figure used with permission from the University of Wisconsin.
Figure 5. The modified Ponseti method for complex clubfoot involves working on stretching with pressure in the sole of the foot.Figure used with permission from the University of Wisconsin.

MANAGEMENT OF THE COMPLEX CLUBFOOT
Once the complex club foot pattern has been appreciat-ed, the treating provider must have a detailed discussionwith the family regarding the current situation and dif-ferent options for further treatment. It is essential that theteam stop the current treatment regimen, and give the in-fant time to recover.
We explain to the family that the child’s foot is verysensitive and that we will resume treatment when symp-toms and appearance improve. Returning to the previousanalogy, we tend to treat these feet as if they are in anactive phase of reflex sympathetic dystrophy, or causal-gia. This includes foot massage, desensitization, and oc-casional use of acetaminophen to decrease the symptomsof pain and irritation. It may take 3 to 4 weeks of absti-nence from casting and with appropriate massage for theinflammation and the sensitivity of the foot to abate.
Each instance of complex clubfoot is different and avariety of strategies is considered; it is reasonable to con-sider asking another practitioner to resume manipulationand casting. Sometimes a slight subtle difference in footpressure, technique and approach can be more successfulin another provider hands.
Authors preferred methodIn our experience, one of the greatest obstacles to correctthe complex club foot includes overcoming severe equi-nus contracture which compounds the forefoot cavusthat Ponseti identified. It is challenging to treat these feetbecause the hindfoot equinus makes it more likely thatthe clubfoot cast can slide off and the attempts to dorsi-flex the foot can lead to midfoot breach, pain and irrita-tion ; all of which can lead back to an irritated and in-flamed foot.
As Ponseti described, the main goal at this stage ofthe complex clubfoot is not obtaining 70 degrees of ab-duction that is required prior to tenotomy in the uncom-plicated clubfoot. This can lead to iatrogenic metatarsusabductus. In the more challenging complex clubfoot, af-ter the initial inflammation and symptoms have resolved ,we begin the treatment with manipulation and casting thefoot to about 15 to 20° of forefoot abduction. This is usu-ally obtained in one to two casting sessions and then wework on gentle stretching of the heel cord as Ponseti de-scribed with pressure in the midfoot to prevent a rocker-bottom deformity. Use of benzoin and hyperflexion ofthe cast can help prevent it from falling off. We continuethis strategy until it becomes apparent we are not gain-ing anymore improvement or if the child is starting toredevelop pain and swelling.
Previous practitioners [Alvarez et al. (2009), Alvarez(2018) and Cummings (2009)] have injected botulinum
toxin (BTX-a) into the calf as method to correct equinusin lieu of heel cord tenotomy for the idiopathic clubfoot.While we do not use this for the uncomplicated foot, yetwe have found it useful in the complex clubfoot. Ourstrategy is based on the understanding that an early teno-tomy may be needed in order to “gain control of thefoot” but that further stretching will be needed after-ward. Simultaneous injection of BTX-a will make subse-quent stretching easier in the face of a temporarily para-lyzed gastrocsoleus complex.
We like to perform this procedure in the operatingroom, while both injection and tenotomy have been in-dividually performed in the outpatient clinic. The combi-nation of these with the need for a well-fitting cast is bestperformed in the most controlled environment possible.Under general anesthesia we inject five units per kilo-gram of BTX-a into the gastrocsoleus complex of eachaffected leg. Once this is performed, we then perform aheel cord tenotomy in the standard fashion. A well mold-ed fiberglass cast is applied with the foot maximally dor-siflexed. In these patients we prefer to use fiberglass ma-terial which is stronger and lighter and would allow us toperform cast wedging in the clinic in one week.
The following week the infant is seen back in the clin-ic where a posterior cut in the back of the cast is made inorder to gain progressive dorsiflexion without the needfor painful cast removal so soon after surgery (Figure 6).A cast spacer is inserted and keeps the wedge open thusapplying more stretch to the achilles. Typically we areable to increase the dorsiflexion with wedging the cast 2-3 times in weekly increments. The cast is maintainedfor one month at which time it is removed and repeatmanipulation and casting is reinstituted if needed. Thesuccessive sessions of manipulation and casting aremuch easier in the face of the temporarily weakened gas-trocsoleus. Once the child has gained 15 degrees of dor-siflexion conversion to and abduction orthosis or a nighttime stretching, AFO is started.
Clinical resultsAt the University Wisconsin, we have eight childrenwith 12 complex clubfeet that underwent the abovetreatment (Figure 7). We have a greater than two-yearfollow-up in five of these children with seven complexclubfeet. All of these patients underwent the protocol ofcombination botulinum toxin injection and heel cord te-notomy with additional stretching and casting one monthafter the index procedure. Five of these feet have had nofurther treatment at an average of five years follow-up(Figure 8). One foot required a repeat percutaneousAchilles lengthening and anterior tibialis tendon transferat age 5. One foot required posterior-medial release at 13months of age.
86 Lebanese Medical Journal 2021 • Vol 69 (2) K. J. NOONAN – Complex clubfoot management

K. J. NOONAN – Complex clubfoot management Lebanese Medical Journal 2021 • Vol 69 (2) 87
Figure 6. Cast wedging one week after tenotomy and BTX-a injection allows one to gain some stretch without removing the cast.Figure used with permission from the University of Wisconsin.
Figure 7. AC has history of complex clubfoot pattern that underwent BTX-a injection and heel cord tenotomy of both feet followed by serial casting. Figure used with permission from the University of Wisconsin.
Figure 8. Five years later AC has had an excellent clinical result. Figure used with permission from the University of Wisconsin.

CONCLUSION
In summary, the complex club foot is an uncommon re-sult of the Ponseti method utilized in idiopathic clubfeet.It is important for the practitioner to recognize whenthey are developing this pattern and to change treatmentstrategies in order to effectuate a good outcome. Thecomplex club foot presents with a pattern similar toreflex sympathetic dystrophy with a painful, irritated redand swollen foot that resists treatment. We follow theprinciples of Ponseti who advocated stopping the treat-ment until symptoms abate and then to work on gentleheel cord stretching. We have modified his method byinclusion of early heel cord tenotomy and BTX-a injec-tion which helps facilitate further stretching after theheel cord has healed. Our numbers are small but ourresults appear to be slightly better than that presented inthe literature using the modified Ponseti method. In com-parison to Matar et al. (2016), they had 11 children with17 complex clubfeet that underwent the modified Ponsetimethod for the complex clubfoot. In this paper, 53 percentof feet had relapse requiring further treatment. Theseresults are similar to Dragoni et al. (2018) that had recur-rence in 55 percent. It is difficult to compare our resultsto these papers as the definition of complex clubfoot isqualitative and subjective. In our minds the complexclubfoot is that foot that is extremely difficult to treatand whereby we consider the possibility of posterior-medial release to be a reasonable next step. Our resultsare similar to Duman et al. (2020) who published theirresults in 32 complex clubfeet that underwent the modi-fied Ponseti method with 78% excellent and 22% goodresults. In our series of complex clubfeet we have not hadany long-term weakness or effect of the use of BTX-a.
Our method appears to be a safe and effective adjunct toPonseti’s method for the management of this problem.
REFERENCES
_ Alvarez CM, Wright JG, Chhina H, Howren A, Law P. Bot-ulinum toxin type A versus placebo for idiopathic clubfoot:A two-center, double-blind, randomized controlled trial. J Bone Joint Surg Am. 2018 Sep 19; 100 (18): 1589-96.doi: 10.2106/JBJS.17.01652. PMID: 30234623.
_ Alvarez CM, De Vera MA, Chhina H, Williams L,Durlacher K, Kaga S. The use of botulinum type A toxinin the treatment of idiopathic clubfoot: 5-year follow-up.J Pediatr Orthop. 2009 Sep; 29 (6): 570-5.doi: 10.1097/BPO.0b013e3181b2b3d4. PMID:19700985.
_ Cummings RJ. The effectiveness of botulinum A toxin as an adjunct to the treatment of clubfeet by the Ponsetimethod: a randomized, double-blind, placebo controlledstudy. J Pediatr Orthop. 2009 Sep; 29 (6): 564-9.doi: 10.1097/BPO.0b013e3181b2f21d. PMID: 19700-984.
_ Duman S, Camurcu Y, Cobden A, Ucpunar H, Karahan N,Bursali A. Clinical outcomes of iatrogenic complex club-foot treated with modified Ponseti method. Int Orthop.2020 Sep; 44 (9): 1833-1840.doi: 10.1007/s00264-020-04529-6. Epub 2020 May 6. PMID: 32377781.
_ Dragoni M, Gabrielli A, Farsetti P, Bellini D, Maglione P,Ippolito E. Complex iatrogenic clubfoot: is it a real enti-ty? J Pediatr Orthop B. 2018 Sep; 27 (5): 428-434.doi: 10.1097/BPB.0000000000000510. PMID: 29578 933.
_ Matar HE, Beirne P, Bruce CE, Garg NK. Treatment ofcomplex idiopathic clubfoot using the modified Ponsetimethod: up to 11 years follow-up. J Pediatr Orthop B. 2017Mar; 26 (2): 137-142.doi: 10.1097/BPB.0000000000000321. PMID: 271049-2.
_ Ponseti IV, Zhivkov M, Davis N, Sinclair M, Dobbs MB,Morcuende JA. Treatment of the complex idiopathic club-foot. Clin Orthop Relat Res. 2006 Oct; 451: 171-6.doi: 10.1097/01.blo.0000224062.39990.48. PMID: 1678 8-408.
88 Lebanese Medical Journal 2021 • Vol 69 (2) K. J. NOONAN – Complex clubfoot management
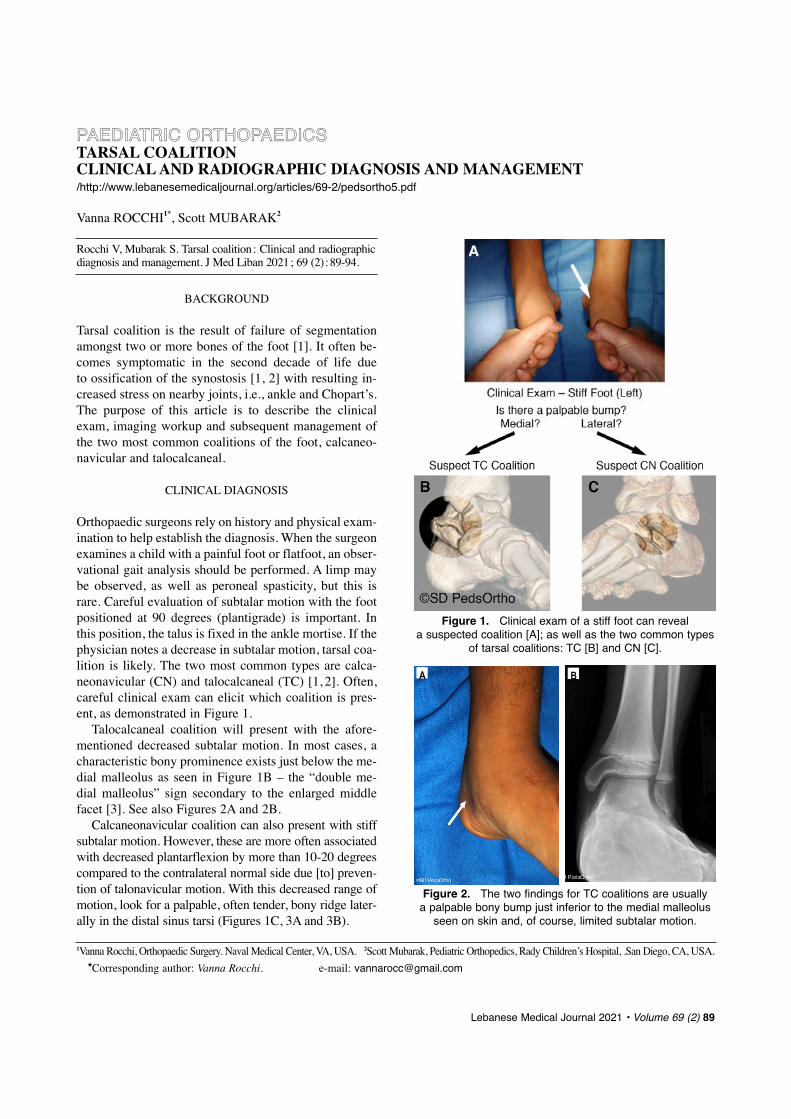
BACKGROUND
Tarsal coalition is the result of failure of segmentationamongst two or more bones of the foot [1]. It often be-comes symptomatic in the second decade of life due to ossification of the synostosis [1, 2] with resulting in-creased stress on nearby joints, i.e., ankle and Chopart’s.The purpose of this article is to describe the clinicalexam, imaging workup and subsequent management ofthe two most common coalitions of the foot, calcaneo-navicular and talocalcaneal.
CLINICAL DIAGNOSIS
Orthopaedic surgeons rely on history and physical exam-ination to help establish the diagnosis. When the surgeonexamines a child with a painful foot or flatfoot, an obser-vational gait analysis should be performed. A limp maybe observed, as well as peroneal spasticity, but this israre. Careful evaluation of subtalar motion with the footpositioned at 90 degrees (plantigrade) is important. Inthis position, the talus is fixed in the ankle mortise. If thephysician notes a decrease in subtalar motion, tarsal coa-lition is likely. The two most common types are calca-neonavicular (CN) and talocalcaneal (TC) [1, 2]. Often,careful clinical exam can elicit which coalition is pres-ent, as demonstrated in Figure 1.
Talocalcaneal coalition will present with the afore-mentioned decreased subtalar motion. In most cases, acharacteristic bony prominence exists just below the me-dial malleolus as seen in Figure 1B _ the “double me-dial malleolus” sign secondary to the enlarged middlefacet [3]. See also Figures 2A and 2B.
Calcaneonavicular coalition can also present with stiffsubtalar motion. However, these are more often associatedwith decreased plantarflexion by more than 10-20 degreescompared to the contralateral normal side due [to] preven-tion of talonavicular motion. With this decreased range ofmotion, look for a palpable, often tender, bony ridge later-ally in the distal sinus tarsi (Figures 1C, 3A and 3B).
Lebanese Medical Journal 2021 • Volume 69 (2) 89
PPAAEEDDIIAATTRRIICC OORRTTHHOOPPAAEEDDIICCSS TARSAL COALITIONCLINICAL AND RADIOGRAPHIC DIAGNOSIS AND MANAGEMENT/http://www.lebanesemedicaljournal.org/articles/69-2/pedsortho5.pdf
Vanna ROCCHI1*, Scott MUBARAK2
Rocchi V, Mubarak S. Tarsal coalition : Clinical and radiographicdiagnosis and management. J Med Liban 2021; 69 (2) :89-94.
Figure 1. Clinical exam of a stiff foot can reveal a suspected coalition [A]; as well as the two common types
of tarsal coalitions: TC [B] and CN [C].
Figure 2. The two findings for TC coalitions are usually a palpable bony bump just inferior to the medial malleolus
seen on skin and, of course, limited subtalar motion.
A B
1Vanna Rocchi, Orthopaedic Surgery. Naval Medical Center, VA, USA. 2Scott Mubarak, Pediatric Orthopedics, Rady Children’s Hospital, .San Diego, CA, USA.
*Corresponding author: Vanna Rocchi. e-mail: [email protected]

RADIOGRAPHIC DIAGNOSIS
Once we have established a clinical suspicion for a tarsalcoalition, appropriate imaging can be obtained. Tarsal co-alitions may be difficult to appreciate on standard imag-ing. Bilateral weight bearing (standing) AP and lateralradiographs are needed for comparison (Figure 4).
Standing lateral radiographs may demonstrate a C-sign,
which is a fairly reliable indicator of talocalcaneal coali-tion (Figure 4D). This is seen when there is a confluenceof the subchondral bone of the talar dome with the pos-terior and inferior edge of the enlarged middle facet co-alition and the sustentaculum tali. This was studied indetail by Moraleda and colleagues [4]. A complete C-sign is present in 41% of TCCs and 77% will have anincomplete C-sign. However, an incomplete C-sign is
90 Lebanese Medical Journal 2021 • Vol 69 (2) V. ROCCHI, S. MUBARAK – Tarsal coalition
Figure 3. Three findings for a CN coalition are : limited subtalar motion, a palpable bony ridge in the distal sinus tarsi (absent in 3, present in 3), and decreased plantarflexion up to 20 degrees due to lack of motion across Chopart’s joint.
Figure 4. Radiographic pathway for suspected TC coalition [A] and CN coalition [B]. Coalition-specific films include the Harris calcaneal view [C] which will show an enlarged sustentaculum tali on the involved
side and middle facet joints that are out of plane or absent. Often a C-sign is present on the standing lateral [D].The internal oblique film is ideal for the CN coalition, which may show an osseous or fibro-osseous connection [E].
A B

also common in flexible flatfeet on standing lateral radi-ographs (44%) [2]. If TC coalition is suspected, then theHarris heel radiographic view is useful (Figure 4C). Innormal feet, the posterior and middle subtalar joints ap-pear parallel, whereas in feet with TC coalition the mid-
dle facet is often angled, with subsequent loss of paral-lelism. Our research has shown that an additional find-ing on this view is an abnormally enlarged sustentacu-lum tali and sometimes complete bridging of the talocal-caneal joint, seen with an osseous coalition [3].
V. ROCCHI, S. MUBARAK – Tarsal coalition Lebanese Medical Journal 2021 • Vol 69 (2) 91
Figure 5. CN coalition resection is accomplished utilizing an oblique incision centered over the coalition [A].An example coalition is seen in the 3D CT reconstruction [B], with freer elevators on either side protecting the talar head
and the cuboid [C]. An osteotome is used to resect the bar [D - line drawing, E - live] and a kerrison rongeur may be usedto remove all remaining connections [F]. Intraoperative fluoroscopy shows resection [G]. An intraoperative CT scan
is obtained to confirm complete resection [H]. Finally, a fat graft (abdominal or buttock) is interposed in the resulting defect [I].
A B C
D E F
G H I

When CN coalition is suspected, an internal obliqueview is needed (Figure 4E). This will show fibro-carti-laginous and/or osseous bridging of the anterior calca-neal process and lateral aspect of the navicular bone.
Continuing along this diagnostic pathway, after appro-priate plain radiographs, we advise CT scan with 3D re-constructed images to assist with surgical planning. Thisallows assessment of the shape, defines the size and typeof coalition and confirms that there are not multiple coali-tions in the foot [5, 6]. The 5 types of TC coalitions andtheir prevalence are detailed by Rozansky et al. [6].
TREATMENT
We rarely treat a tarsal coalition with immobilization ina brace or cast. The underlying issue is a pathologic coa-
lition of two tarsal bones, which fundamentally changesfoot mechanics. Surgical excision may prevent futurepathology, such as ankle sprains, fractures of the ankle orfoot, and ankle arthritis, by restoring more normal footand ankle kinematics. In nearly all cases we recommendsurgical excision once the diagnosis is made [7].
Surgical steps for calcaneonavicular resection are detailed in Figure 5. CN coalition is excised using anoblique skin incision centered over the coalition. The ex-tensor digitorum brevis (EDB) muscle is identified andfreed at its proximal insertion to expose the coalition.Freer elevators are inserted to protect the talar head andcuboid while a small osteotome is used to resect the coali-tion. Kerrison rongeurs should be used to remove any re-maining deeper bony connections. A fat graft (abdomen orbuttock) is then inserted into the defect prior to closure.
92 Lebanese Medical Journal 2021 • Vol 69 (2) V. ROCCHI, S. MUBARAK – Tarsal coalition
Figure 6. Surgical steps of TC coalition resection.The incision is centered over the prominent coalition inferior to the medial malleolus [A - line drawing, B - on skin].
The posterior tibialis (blue tendon - line drawings) and flexor digitorum tendons (green tendon - line drawings) are retractedto expose periosteum overlying the medial coalition [C]. The periosteum is incised [D]. The fibrocartilaginous physis
is identified, based on preoperative CT scan [E]. Removal is completed with osteotomes, rongeur and high-speed burrs until normal-appearing cartilage is visualized [F]. If a posterior TCC exists, care must be taken to also identify and protect
the flexor hallucis longus tendon and neurovascular bundle [G]. Intraoperative CT and assessment of hindfoot motion are performed [H]. Fat grafting is used for adequate interposition [I).

V. ROCCHI, S. MUBARAK – Tarsal coalition Lebanese Medical Journal 2021 • Vol 69 (2) 93
Figure 7. Clinical and radiographic pathway for diagnosis and classification of tarsal coalitions.

Fat interposition grafting is preferred over an EDB in-terposition graft given the depth of the coalition (25 mm)and inadequate size of EDB (17 mm), as verified on CTand cadaver studies [8, 9]. The procedure is detailed inFigure 6. After closure, the patient is placed into a castfor two weeks, after which therapy is initiated. CN coali-tion excision is a successful operation in 90%, restoringfunction, motion and relieving pain.
Talocalcaneal coalition excision, as demonstrated inFigure 6, is performed using an incision centered overthe prominent coalition inferior to the medial malleolus.The posterior tibialis and flexor digitorum tendons areretracted to expose periosteum overlying the medialcoalition. If a posterior TCC exists, care must be taken toalso identify and protect the flexor hallucis longus ten-don and neurovascular bundle (Figure 6G). Based onpreoperative templating, the appropriate plane of resec-tion is identified, often compared to a fibrocartilaginous“physis”, and then removal is completed using osteo-tomes, rongeurs, and high-speed burrs until normal ap-pearing cartilage of the posterior facet is visualized.Again, fat grafting is used for adequate interposition. In-traoperative assessment of hindfoot motion as well asintraop CT scanning after the resection of the coalitionhas been shown to alter surgical decision-making, whichresults in an improved ability to obtain a complete resec-tion [5, 10]. Postoperative management is similar to thatof CN coalition excision. We expect near 90% relief ofsymptoms even in these more difficult coalitions.
In the setting of concomitant severe planovalgus,triple C (3C) osteotomies, including calcaneal, cuboidand cuneiform osteotomies should be considered, but notuntil 6-12 months after first obtaining motion [11].
SUMMARY
Careful clinical exam of a patient with a painful or stifffoot or a patient with recurrent sprains or ankle/foot frac-tures will lead to increased tarsal coalition recognition.The three findings for a CN coalition are : limited subta-
lar motion, a palpable bony ridge in the distal sinus tar-si, and decreased plantarflexion due to lack of motionacross Chopart’s joint. There are two main findings seenin a TC coalition : limited subtalar motion and a palpablebony bump just inferior to the medial malleolus.
With this knowledge, the surgeon can now order thebest radiographs and CT scans to elucidate the diagnosis(Figure 7). Once the coalitions are characterized, exci-sion of the tarsal coalition can provide effective sympto-matic relief and prevent future injury and arthritis.
REFERENCES
1. Docquier PL, Maldaque P, Bouchard M. Tarsal coalitionin paediatric patients. Orthop Traumatol Surg Res 2019,105 (1S): S123-S131.
2. Mosca VS. Subtalar coalition in pediatrics. Foot AnkleClin 2015, 20 (2): 265-81.
3. Rocchi V, Huang MT, Bomar JD, Mubarak S..The “DoubleMedial Malleolus” : A new physical finding in talocalca-neal coalition. J Pediatr Orthop 2018 Apr, 38 (4) : 239-243..
4. Moraleda L, Gantsoudes GD, Mubarak SJ. C sign: ta-localcaneal coalition or flatfoot deformity? J PediatrOrthop 2014, 34 (8): 814-19.
5. Kemppainen J et al. The use of a portable CT scanner forthe intraoperative assessment of talocalcaneal coalitionresections. J Pediatr Orthop 2014, 34 (5): 559-64.
6. Rozansky A et al. A radiologic classification of talocal-caneal coalitions based on 3D reconstruction. J ChildOrthop 2010, 4 (2): 129-35.
7. Li S, Myerson MS. Excision of a middle facet tarsal co-alition. JBJS Essent Surg Tech 2020, 10 (1): e0114.1-14.
8. Mubarak SJ et al. Calcaneonavicular coalition: treatmentby excision and fat graft. J Pediatr Orthop 2009, 29 (5):418-26.
9. Upasani VV, Chambers RC, Mubarak SJ. Analysis of cal-caneonavicular coalitions using multi-planar three-dimen-sional computed tomography. J Child Orthop 2008, 2 (4):301-7.
10. Gantsoudes GD, Roocroft JH, Mubarak SJ. Treatment oftalocalcaneal coalitions. J Pediatr Orthop 2012, 32 (3):301-7.
11. Rathjen KE, Mubarak SJ. Calcaneal-cuboid-cuneiformosteotomy for the correction of valgus foot deformities inchildren. J Pediatr Orthop 1998, 18 (6): 775-82.
94 Lebanese Medical Journal 2021 • Vol 69 (2) V. ROCCHI, S. MUBARAK – Tarsal coalition

INTRODUCTION
Primary malignant bone tumors account for approximate-ly 6% of all pediatric neoplasms in patients younger than20 years-old [1]. The two predominant primary bonetumors in the pediatric population are osteosarcoma andEwing’s sarcoma. They account for 64% and 34% re-spectively of newly diagnosed cases. In the late seven-ties of the last century, surgeons started to explore limbsparing resection techniques as a viable option for localcontrol. The use of chemotherapy in neoadjuvant pro-tocols improved markedly the success of these limb sal-vage surgeries.
That being said, a shift from extremity amputationthat used to be the standard care toward limb sparingwide resection occurs in today’s practice [2]. With theadvancement of imaging modalities allowing a robustlocalization of tumor extent and evolution of surgicaltechniques, excision of the cancerous lesions while pre-serving lower extremity function became more attainable[3]. However, the reconstruction of the limb remainschallenging and needs specialized surgical expertise.
Endoprosthetic reconstruction has been widely usedto substitute bone and joint loss. They encompass expan-dable and non-expandable prosthesis. The former un-derwent technological advancement whereby expansionmechanism shifted from surgery requiring procedure tominimally invasive bedside technique. Nevertheless,many potential problems are still unsolved including butnot limited to the extent of possible expansion, the ex-pansion mechanism breakage, the longevity of the pros-thesis in addition to well-known prosthesis associatedsurgical complications like infection, wound complica-tions, etc.
The main objective of biological reconstruction islong lasting durability. Free vascularized fibula graftsare the most used biologic constructs. Despite excellent
reported outcome, many obstacles remain that orthope-dic oncology surgeon has to face in his/her daily prac-tice. They include but are not limited to soft tissue in-tegrity, size of the defect, age of the pediatric patient,potential of growth, functional demands and psycholog-ical expectations of the child and caregivers. Perfectingall the above raised many facets in reconstructive sur-gery rendering it extremely exacting, giving birth to sev-eral hurdles which include mainly longevity of the re-construction and limb length discrepancy that will beextensively tackled in this review.
We will point out the surgical and functional chal-lenges that orthopedic oncologists face when dealingwith reconstruction of post malignant tumor resection inthe upper and lower extremity of a pediatric patient. Wewill shed the light on some of the modifiable and non-modifiable factors that may influence surgeon decisionto adopt strategies that will optimize patient functionaloutcomes without affecting cancer-related survival.
CHALLENGES IN PEDIATRIC ONCOLOGICRECONSTRUCTION
The main two challenges that are characteristic for pedi-atric limb salvage procedures are how to achieve a longlasting reconstruction and decrease the anticipated leglength discrepancy.
Long lasting reconstructionThe increasing survival of oncological patients with pri-mary bone tumors has called for an enhancement in thereconstruction methods offered for these patients [4].Many advancements have been seen over the past fewyears in tribology and fixation method of prosthetic de-vices in adults to accommodate for this increased sur-vival rate [5].
Endoprosthesis has many potential advantages includ-ing early weight bearing mobilization, good emotionalacceptance and high functional scores [6]. Different mod-ular tumor prosthesis types exist in the market. The lon-gevity of these implants can be satisfactory in adults(survival rate 58% at 8 years) but not in children [7].
The expandable prostheses were popularized as anappealing solution to accommodate for the loss of thegrowth plate of the involved bone. However, they failedto provide a long lasting solution. The 10-year failure-
Lebanese Medical Journal 2021 • Volume 69 (2) 95
PPAAEEDDIIAATTRRIICC OORRTTHHOOPPAAEEDDIICCSSCHALLENGES OF PEDIATRIC RECONSTRUCTION POST LIMB SARCOMA RESECTIONhttp://www.lebanesemedicaljournal.org/articles/69-2/pedsortho6.pdf
Ahmad Salaheddine NAJA1, Amir IBRAHIM2, Mohamad ISSA1, Rachid HAIDAR1, Said SAGHIEH1*
Naja AS, Ibrahim A, Issa M, Haidar R, Saghieh S. Challengesof pediatric reconstruction post limb sarcoma resection. J MedLiban 2021 ; 69 (2) : 95-106.
1Orthopaedic Surgery Department, American University of Bei-rut Medical Center (AUBMC), Beirut, Lebanon.
2Plastic Surgery Department, AUBMC.*Corresponding author: Said Saghieh, MD.
e-mail: [email protected]
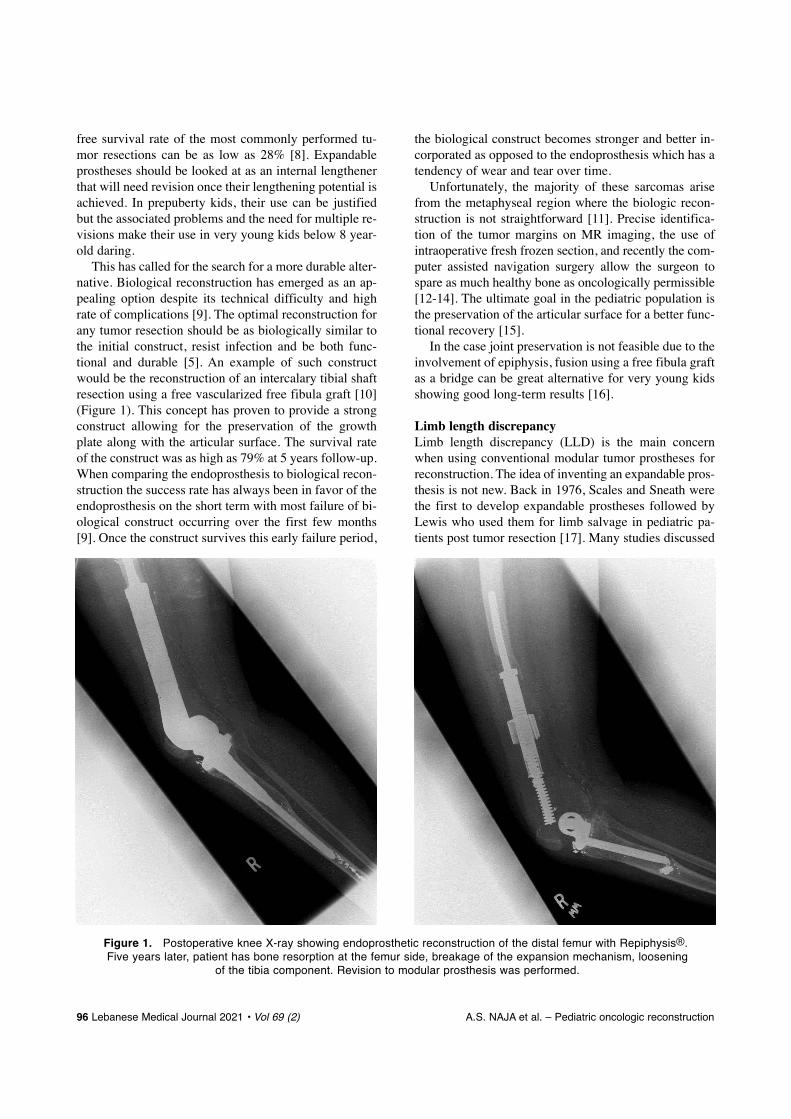
free survival rate of the most commonly performed tu-mor resections can be as low as 28% [8]. Expandableprostheses should be looked at as an internal lengthenerthat will need revision once their lengthening potential isachieved. In prepuberty kids, their use can be justifiedbut the associated problems and the need for multiple re-visions make their use in very young kids below 8 year-old daring.
This has called for the search for a more durable alter-native. Biological reconstruction has emerged as an ap-pealing option despite its technical difficulty and highrate of complications [9]. The optimal reconstruction forany tumor resection should be as biologically similar tothe initial construct, resist infection and be both func-tional and durable [5]. An example of such constructwould be the reconstruction of an intercalary tibial shaftresection using a free vascularized free fibula graft [10](Figure 1). This concept has proven to provide a strongconstruct allowing for the preservation of the growthplate along with the articular surface. The survival rateof the construct was as high as 79% at 5 years follow-up.When comparing the endoprosthesis to biological recon-struction the success rate has always been in favor of theendoprosthesis on the short term with most failure of bi-ological construct occurring over the first few months[9]. Once the construct survives this early failure period,
the biological construct becomes stronger and better in-corporated as opposed to the endoprosthesis which has atendency of wear and tear over time.
Unfortunately, the majority of these sarcomas arisefrom the metaphyseal region where the biologic recon-struction is not straightforward [11]. Precise identifica-tion of the tumor margins on MR imaging, the use ofintraoperative fresh frozen section, and recently the com-puter assisted navigation surgery allow the surgeon tospare as much healthy bone as oncologically permissible[12-14]. The ultimate goal in the pediatric population isthe preservation of the articular surface for a better func-tional recovery [15].
In the case joint preservation is not feasible due to theinvolvement of epiphysis, fusion using a free fibula graftas a bridge can be great alternative for very young kidsshowing good long-term results [16].
Limb length discrepancyLimb length discrepancy (LLD) is the main concernwhen using conventional modular tumor prostheses forreconstruction. The idea of inventing an expandable pros-thesis is not new. Back in 1976, Scales and Sneath werethe first to develop expandable prostheses followed byLewis who used them for limb salvage in pediatric pa-tients post tumor resection [17]. Many studies discussed
96 Lebanese Medical Journal 2021 • Vol 69 (2) A.S. NAJA et al. – Pediatric oncologic reconstruction
Figure 1. Postoperative knee X-ray showing endoprosthetic reconstruction of the distal femur with Repiphysis®.Five years later, patient has bone resorption at the femur side, breakage of the expansion mechanism, loosening
of the tibia component. Revision to modular prosthesis was performed.

the promising benefits of expandable prosthesis and itsusefulness to a certain extent in compensating for the leg length discrepancy caused by the epiphysis resectionwhen compared to the contralateral leg [18,19]. The ma-jor limitation of these prostheses was the necessity toundergo open surgical intervention each time length ex-pansion was needed. This led to major complicationslike infections, postop stiffness and neurovascular injury[19, 20]. It wasn’t until late 90s where noninvasive ex-pandable prostheses came into the market with a mainobjective of providing expansion without open surgeries. Many designs were manufactured with different expan-
sion mechanisms [21]. They include (but are not limited to) Repiphysis®
(Microport Orthopedics, Arlington, Tennessee USA, orig-inally manufactured as the Phenix prosthesis, PhenixMedical, Paris, France) (Figure 5), MUTARS (implant-cast GmbH, Buxtehude Germany) and the Juvenile Tu-mour System (Stanmore Implants, Elstree, UK) [22]. Nev-ertheless many complications arose from the use of en-doprosthesis in general and expandable prosthesis spe-cifically. These include but not limited to loosening ofthe prosthesis, fractures, infections and failure of expan-sion mechanism [23].
Through our 7 years of experience with the Repiphysissystem we analyzed the outcomes and complications as-sociated with this design in limb salvage of skeletallyimmature patients. Although we decreased the rate ofsurgical procedures to attain the required leg length, westill encountered a high complication rate : 6 mechanicaldysfunctions mainly due to failure of the extension mech-anism, 2 tibia fractures, and 3 infections which necessi-tated 7 revision operations [18]. Most of the patients re-quired revision with another modular prosthesis mainlyfor the defective extension mechanism. Another studypublished in 2015 by Staals et al. summarized the out-comes of Repiphysis and found out an extremely highcomplication rate mainly because of mechanical failurewith low Musculoskeletal Tumor Society/MSTS scoreand even stopped from using this design in their practice.Our 20 years of follow-up showed a high complicationrate exceding 85% using this prosthesis and thus a fulldisclosure of the short- and long-term complicationsprofile is needed as well as alternative therapeutic op-tions. (Masrouha et al., in press JPO 2021). Dukan et al.reported lower complication rate with the use of JuvenileTumour System/JTS, Stanmore System, but none of thepatients was younger than 6 years old and follow-up wasnot long enough due to a more recent insertion of theprosthesis which might underestimate the rate of compli-cations and revision rate [24]. Rate of complication waslower than the older designs with less risk of mechani-cal failure. But none of the patients was younger than
6 years old and follow-up was not long enough due to amore recent insertion of the prosthesis which mightunderestimate the rate of complications and revision rate[24]. An important observation worth shedding the lighton, is the limited expansion potential of the prosthesisthat is directly proportional to the length of the body ofthe prosthesis (i.e. equal to the resected bone).
Expandable prostheses are of use mainly in patientswho are above 11-12 years in whom the predicted limblength discrepancy, according to the Anderson and greengrowth chart, can be offset by the prostheses expansionmechanism [18,21,25]. (Figure 1). These prostheses canbe coupled to epiphysiodesis of the contralateral limb toinclude younger patients or in case of underestimation ofthe longitudinal growth potential [22, 26]. However, inpatients who are less than 9 years, the predicted discrep-ancy is usually beyond the capacity of the expansionmechanism which prompts the need of a second expand-able prosthesis and revision to a modular design later on[27]. All of the above constitute an undesirable impact of using expandable prosthesis on these very young pa-tients.
Hence, a long-lasting method with ability for longitu-dinal growth is needed for limb salvaging and approxi-mation of limb length discrepancy in very young pa-tients, biological reconstruction surfaced in literature andgained popularity as a salvage technique in the pediatricspopulation post limb sarcoma resection. Pioneered byHahn, back in 1884, free fibular bone graft has been in-corporated as a biological breakthrough for reconstruc-tion of bone defects [28]. During the last decades, theadvancement of microsurgery enabled the incorporationof a free vascularized fibular graft (FVFG) with arterialand venous anastomosis at the recipient site [29]. Union,hypertrophy and growth are the three most importantcornerstones when dealing with an adequately harvestedviable free fibula graft reconstruction.
The distinctive characteristic of FVGF is the ability toact like a normal viable bone with its remodeling capa-bility, and its plasticity for longitudinal growth if its epi-physis was assimilated with the graft [30, 31]. Very lim-ited are the studies with large sample size tackling thepotential growth of vascularized epiphyseal transfer ; thelargest was done by Innocenti et al. [32] showing that theannual growth trend ranged between 0.7 and 1.35 cm.Nevertheless, precocious closure of the growth plate wasseen in 30% of patients. That was mainly attributed tothe scarce blood supply or to iatrogenic injury duringfixation.
Lengthening by distraction osteogenesis can be usedin patients after biologic reconstruction that violated thegrowth plate, infected prosthesis that had to be removed(combined to a fusion) or infected structural bone graft.
A.S. NAJA et al. – Pediatric oncologic reconstruction Lebanese Medical Journal 2021 • Vol 69 (2) 97

Many of these patients may need one or two lengtheningprocedures depending on the age at the time of resection[33].
According to the involved anatomical sites on MRI,Kumta et al. [34] classified the location and extension ofosteosarcoma in bone into five subtypes as follows :Type 1, the tumor is located > 2 cm from the epiphysealcartilage ; type II, the tumor is located within ≤ 2 cm ofthe epiphyseal cartilage ; type III, the tumor extends to orbeyond the epiphyseal cartilage, but > 1 cm of epiphy-seal tissue is retained ; type IV, the tumor breaches thephyses and extends to the subchondral region but doesnot breach the articular surface ; and type V, the tumorbreaches the articular surface and involves the adjacentjoint [34].
The use of these microvascular free fibula transferwill follow 4 schemes ;
1 _ Intercalary resection (Kumta type 1) : That is thebest scenario where the growth plate remains open.No LLD is anticipated.
2 _ Metaphyseal Resection (Kumta type 2) : The growthplate is saved but the fixation used to fix the grafthas to extend across it. The side plate and the epi-physeal screws will play the role of temporary epi-physiodesis. They should be removed as soon asthe fibula graft heals to allow the longitudinalgrowth to resume.
3 _ Epiphyseal Resection (Kumta type 3) : The growthplate is resected. There will be a leg length discre-pancy that can be addressed by distraction osteo-genesis once the fibula graft incorporates and hy-pertrophies.
4 _ Transarticular Resection (Kumta type 4,5) : Ar-throdesis is performed with the free fibula. Thisoption should be limited to patients who have acontraindication or can’t afford prosthetic replace-ment because of the loss of joint. However, it maybe an option for very young kids with extension ofthe tumor to the knee joint for instance.
BONE SPECIFIC CHALLENGES
Long bone shaftIntercalary reconstruction consists of resecting diaphy-seal portion of a long bone and replacing it with eitherallograft, autograft (most commonly free-fibula), seg-mental endoprosthesis or bone transport using distrac-tion osteogenesis [30, 35-38]. Intercalary reconstructionusing segmental endoprosthesis is far less common com-pared to allo/autografts [39-40]. The main advantages ofsegmental endoprosthesis is the early weight bearing,quick rehabilitation and return to near baseline function.They are mostly used for patients with limited life ex-
pectancy or when there is urgency for immediate fixa-tion by cementation without healing time [41]. How-ever, the substantial amount of complications associatedwith segmental endoprosthesis made them one of theleast frequently used reconstruction options in interca-lary resection. They include, but are not limited to asep-tic loosening, infection, mechanical wear and low sur-vival especially in younger patients [35,37,42]. The sur-vival of segmental endoprosthesis is a major concern. Asa matter of fact, their 10 years survival range between68% and 80% and complications arising from implantfailure can reach up to 30% [37, 39, 43]. Distraction os-teogenesis is an excellent technique for bone regenera-tion in segmental bone loss of less than 6 cm. Its use inacute oncologic reconstruction is limited by the size ofdefect and the use of postoperative chemotherapy thatmay increase the risk of pin site infection [44]. Allo-grafts gained popularity rapidly, however with long-termfollow-up, many serious complications arose like infec-tion, fracture and disease transmission, putting it loweston the list for intercalary reconstruction. This is whenautograft came into use with the vascularized fibulargraft as the most frequently used in intercalary replace-ment [45].
The main superiority of free-fibula compared to allo-graft is its inherent ability to resemble biology of normalbone healing decreasing the rate of infection, non-unionand fracture that is seen more commonly with allografts.In addition, the vascularized properties of the fibula al-lows its incorporation into the host without having opti-mal soft tissue conditions. Also, segmental resection ofthe fibula while preserving the proximal and the distalend does not jeopardize the integrity of the ankle andknee stability [45]. Free fibula graft can be used as a solebone replacement or as a double barrel depending on thelocation of the tumor excision ; it can be combined withan allograft whenever additional support is needed and[it] can be used as an onlay graft through longitudinal os-teotomy for partial cortical defect [41, 46]. As a generalrule, the humerus, radius and the ulna can be construct-ed without the need for allograft reinforcement. Howev-er, for the lower extremity, where weight bearing stressis significant, intercalary fibula graft needs to be supple-mented with an additional allograft where the fibula getsincorporated in the canal of the allograft as illustrated bythe Capanna technique [47]. Recently, we reported ourresults in single barel isolated free fibula transfer for re-construction of long bone post sarcoma resection [48].Out of 7 patients, 6 patients were able to resume theirregular daily activities with full range of motion of theproximal joint. Bony union at both ends of the fibula withevident hypertrophy on imaging was seen in 5 out these6 patients (71.4%). Full weight bearing was achieved in
98 Lebanese Medical Journal 2021 • Vol 69 (2) A.S. NAJA et al. – Pediatric oncologic reconstruction

83.3% of the cases at an average of 14 months follow-up.The only case where no fibula hypertrophy was docu-mented, the mode of fixation was with a locking plate.This can be explained by the rigid nature of fixationwhere the plate shields the graft from stress provoked byweight bearing and hindering hypertrophy from occur-ring (Figure 2). No case on non-union was reported, butthe sample size was small.
Proximal humerus It is one of the most preferred sites for free microvascu-lar fibula graft reconstruction. Due to its vascularizedproperties the fibula graft is an autologous bone withoutrisk of resorption (Figure 1). It can get thickened resem-bling the properties of the recipient site [49]. However,this reconstruction is not without any challenges specif-ically pertaining to the unique properties of the shoulderjoint and its mobility. When embarking on such recon-struction, the surgeon has to address the following con-cerns :
1 _ Shoulder joint reconstruction.2 _ Shoulder joint motion restoration.3 _ Incorporation of the graft : union and hypertrophy.4 _ Prevention of graft fracture.5 _ Longitudinal growth and prevention of LLD.
Shoulder reconstruction : The most primitive functionof any graft reconstruction would be creating a spacer al-lowing for the preservation of the proximal edge of thearm and prevention of dead space. Free vascularized fib-ula graft when coupled with the fibula head would pro-vide a strong construct resembling the initial humeralhead and with long term durability resisting resorption[10, 50] (Figure 3A). Harvesting the fibula head withdouble pedicle anastomosis allows for possible longitu-dinal growth when positioned in a favorable positionwith the glenoid [51]. This vascularized growth platecould help prevent a detrimental limb length discrepan-cy in very young children which we will be discussingfurther later in this section. In contrast to what is seen inforearm reconstruction where the free fibula reshapes toaccommodate the radiocarpal articulation, the discrepan-cy in the size of femoral head and that of the resectedproximal humerus is usually significant enough to pre-vent the proper stability needed [52]. The major concernin this case is the possible proximal migration leadingto subacromial displacement [52]. Many different tech-niques have been proposed to stabilize the “new shoul-der” ; one of the first methods postulated was the use ofthe long tendon of the biceps brachii through an obliquehole in the fibular head and anchored at the superior as-pect of the glenoid [53]. The use of mesh or Gortex graftsutured to the glenoid on one side and around the graft
on the other side is another possible method to prevent thesuperior displacement of the fibular head [54]. K-wiresfixation can stabilize the joint temporary as well to allowtime for the new soft tissue envelope to heal. We haveintroduced a technique where the flexible nail fixing thefibula distally will go proximally as well into the glenoidfor around 3 cm serving as a fulcrum around which thefibula can swing (Figure 3B). The use of the biceps fe-moris tendon or palmaris longus muscles as a stringattached to the acromion is yet another anchoring tech-nique described for the fibula head reconstruction [55].In selected patients, preserving the osteochondral part ofthe head when oncologically feasible or using extracor-poreally-irradiated osteochondral autograft will allowfixation of the fibula and thus salvaging the articular sur-face however high incidence of AVN and articular sur-face changes has been postulated [56] (Figure 3C).
Restoration of shoulder joint mobility and function isa challenging process given the high mobility of thisjoint and the loss of the soft tissue envelope during re-section. In the majority of proximal humerus reconstruc-tions the soft tissue component of the free fibula is su-tured to the remnant of the rotator cuff remaining afterresection [57]. In order to achieve a more reliable func-tional restoration, concomitant or delayed rotator cuff re-construction should be entertained. Multiple tendon trans-fer procedures have been described to restore the functionof lost rotator cuff muscles. Latissimus dorsi transfer toachieve active abduction and external rotation is a wide-ly used technique to accommodate for deficient infraspi-natus and teres minor muscles [58]. The restoration of
A.S. NAJA et al. – Pediatric oncologic reconstruction Lebanese Medical Journal 2021 • Vol 69 (2) 99
Figure 2. Postoperative AP leg X-ray of vascularized freefibula reconstruction of tibia shaft post sarcoma resection.Fixation was done using a long medial proximal tibia plate
and flexible intramedullary nail.

this function depends on the presence of functional sub-scapularis muscle. Pagnotta et al. describe long-termfunctional active external reduction with loss of abduc-tion in series of 203 children undergoing latissimus dorsitransfer for obstetric palsy [59]. Pectoralis major muscleis another possible tendon transfer to restore active inter-nal rotation when the subscapularis muscle is deficient..A recent study by Ernstbrunner et al. has revealed ap-pealing long-term results with this reconstruction tech-nique [60]. The pectoralis major transfer can also beused to restore the anterosuperior rotator cuff accommo-dating for supraspinatus as well [61]. Elhassan et al.described the use of yet another muscle, the trapeziusmuscle, for reconstruction of a lacking external rotation[62].
Incorporation of the graft into the recipient humerussite is of utmost importance to achieve the necessarylong-term functional outcome [57]. Union at the incor-poration site depends widely on the vascularity and typeof fixation used. Most studies in the literature describethe telescoping of the distal segment of fibula few cen-timeters into the reamed distal humeral shaft with fixa-tion using screws or locking plates [57-58, 63]. We have
found that flexible intra medullary nails/IMN are thebest type of fixation. They allow for a solid constructdistally and when well anchored proximally, they cancreate some compression effect on the interface improv-ing healing potential. The addition of K-wires can pro-vide more stability to the construct when needed. Theunion is achieved in most cases of free fibula transferpertaining to the good vascularity provided by the pedi-cled graft [58, 63]. As with union, hypertrophy is alsodependent on the degree of vascularity which in fewcases is better achieved with a bipedicled graft or usinganterior tibial vessel-based pedicle [58,64]. In studies byZelenski et al. and Stevenson et al., the hypertrophy in-dex graft increase ranged from 62% - 65% when usingthe vascularized fibula graft [57, 63].
Fracture is the most common complication seen withvascularized free fibula reconstruction in proximal hu-merus post tumor excision where most fractures occurduring the first year following surgery [65]. The mainreason is the mismatch between the diameter of the fibu-la compared to the humerus followed by high functionaldemand in the pediatric population and low compliance[63]. One possible solution for this complication is theadjuvant use of a larger allograft [35]. This technique
100 Lebanese Medical Journal 2021 • Vol 69 (2) A.S. NAJA et al. – Pediatric oncologic reconstruction
Figure 3. Postoperative AP X-ray of the left humerus of vascularized free fibula fixation to the glenoid using flexible nailsand K-wires post proximal humerus sarcoma resection. A: Bipedicled graft with hypertrophy of the fibula and preservation
of the head. B: Flexible nail tip anchored into the glenoid. C: Salvage of osteoarticular humeral head.
A B C
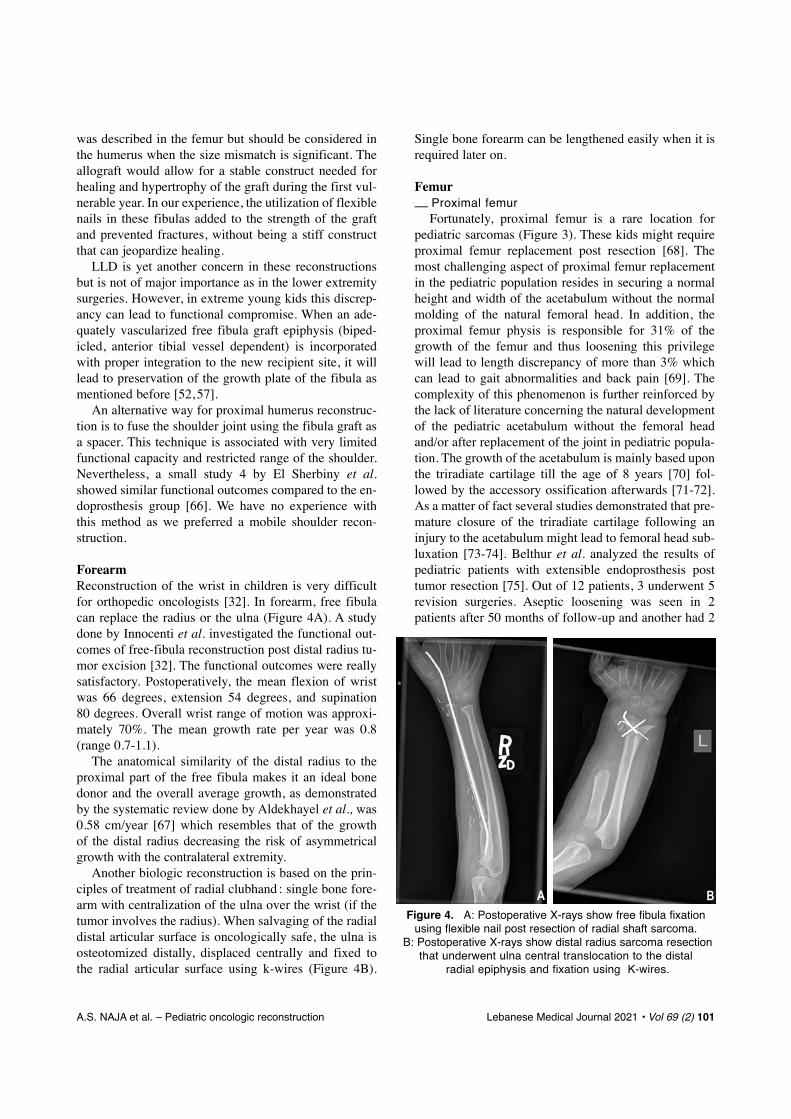
was described in the femur but should be considered inthe humerus when the size mismatch is significant. Theallograft would allow for a stable construct needed forhealing and hypertrophy of the graft during the first vul-nerable year. In our experience, the utilization of flexiblenails in these fibulas added to the strength of the graftand prevented fractures, without being a stiff constructthat can jeopardize healing.
LLD is yet another concern in these reconstructionsbut is not of major importance as in the lower extremitysurgeries. However, in extreme young kids this discrep-ancy can lead to functional compromise. When an ade-quately vascularized free fibula graft epiphysis (biped-icled, anterior tibial vessel dependent) is incorporatedwith proper integration to the new recipient site, it willlead to preservation of the growth plate of the fibula asmentioned before [52, 57].
An alternative way for proximal humerus reconstruc-tion is to fuse the shoulder joint using the fibula graft asa spacer. This technique is associated with very limitedfunctional capacity and restricted range of the shoulder.Nevertheless, a small study 4 by El Sherbiny et al.showed similar functional outcomes compared to the en-doprosthesis group [66]. We have no experience withthis method as we preferred a mobile shoulder recon-struction.
ForearmReconstruction of the wrist in children is very difficultfor orthopedic oncologists [32]. In forearm, free fibulacan replace the radius or the ulna (Figure 4A). A studydone by Innocenti et al. investigated the functional out-comes of free-fibula reconstruction post distal radius tu-mor excision [32]. The functional outcomes were reallysatisfactory. Postoperatively, the mean flexion of wristwas 66 degrees, extension 54 degrees, and supination 80 degrees. Overall wrist range of motion was approxi-mately 70%. The mean growth rate per year was 0.8(range 0.7-1.1).
The anatomical similarity of the distal radius to theproximal part of the free fibula makes it an ideal bonedonor and the overall average growth, as demonstratedby the systematic review done by Aldekhayel et al., was0.58 cm/year [67] which resembles that of the growth of the distal radius decreasing the risk of asymmetricalgrowth with the contralateral extremity.
Another biologic reconstruction is based on the prin-ciples of treatment of radial clubhand : single bone fore-arm with centralization of the ulna over the wrist (if thetumor involves the radius). When salvaging of the radialdistal articular surface is oncologically safe, the ulna isosteotomized distally, displaced centrally and fixed tothe radial articular surface using k-wires (Figure 4B).
Single bone forearm can be lengthened easily when it isrequired later on.
Femur__ Proximal femur
Fortunately, proximal femur is a rare location forpediatric sarcomas (Figure 3). These kids might requireproximal femur replacement post resection [68]. Themost challenging aspect of proximal femur replacementin the pediatric population resides in securing a normalheight and width of the acetabulum without the normalmolding of the natural femoral head. In addition, theproximal femur physis is responsible for 31% of thegrowth of the femur and thus loosening this privilegewill lead to length discrepancy of more than 3% whichcan lead to gait abnormalities and back pain [69]. Thecomplexity of this phenomenon is further reinforced bythe lack of literature concerning the natural developmentof the pediatric acetabulum without the femoral headand/or after replacement of the joint in pediatric popula-tion. The growth of the acetabulum is mainly based uponthe triradiate cartilage till the age of 8 years [70] fol-lowed by the accessory ossification afterwards [71-72].As a matter of fact several studies demonstrated that pre-mature closure of the triradiate cartilage following aninjury to the acetabulum might lead to femoral head sub-luxation [73-74]. Belthur et al. analyzed the results ofpediatric patients with extensible endoprosthesis posttumor resection [75]. Out of 12 patients, 3 underwent 5revision surgeries. Aseptic loosening was seen in 2patients after 50 months of follow-up and another had 2
A.S. NAJA et al. – Pediatric oncologic reconstruction Lebanese Medical Journal 2021 • Vol 69 (2) 101
Figure 4. A: Postoperative X-rays show free fibula fixationusing flexible nail post resection of radial shaft sarcoma.
B: Postoperative X-rays show distal radius sarcoma resectionthat underwent ulna central translocation to the distal
radial epiphysis and fixation using K-wires.
A B

revision surgeries because of infection at 16 months fol-low-up. Most common complications were hip disloca-tion and infection. One patient had distal femur growtharrest secondary to cement induced thermal injury dur-ing femoral fixation. Kampen et al. analyzed post-opera-tive outcomes of tumor resection in children with ce-mented proximal femur replacement ; 15 out of 27 pa-tients survived [68]. Among 7 patients who had their oper-ation before 11 years old, only 2 patients survived till age23 years without complications (loosening of the acetab-ulum and infection). And among patients above 11 yearsold, 1 patient needed revision and 2 others presented dislo-cations that were treated by closed reduction and bracing.
For unipolar prosthesis the results were not reassur-ing. Most of the patients had complications and for veryyoung patients (2 years old), both required shelf proce-dures. As for the lengthening, although expandible mini-mally invasive prostheses have been used in very youngskeletally immature patients ; however, close monitoringwith frequent lengthening visits are needed with a sub-stantial risk of increasing joint instability which makes itan unfavorable option for this subset of patients [68]. Adistal contralateral femur epiphysiodesis can be useful todecrease the amount of anticipated leg length discrepan-cy. The overall survival of all proximal femur replace-ments was about 74% at 5 years and 47% at 10 years [76].
Despite the enthusiasm for prosthetic replacement,biologic treatment may be used particularly in young agegroups or when resection can be done at the intertro-chanteric ridge or distal to it (Figure 5). Preservation ofgreater trochanter will assure better function of the ab-
ductors and thus better gait. However, reconstruction isa much more complicated surgery and needs expertise. Acase report published in Lancet described biological re-construction of hip using vascularized free fibula in a 4years old patient with Ewing sarcoma of the pelvis [51].The surgeon used ipsilateral proximal fibula to recon-struct the femoral metaphysis and a massive femoral al-lograft to hold the new hip. Then reaming of the femoralmedullary canal was done and the fibula was fixated in-side and fractured to maintain the shape of the femoralneck angle and to allow periosteal continuity. Anotherstudy done by Germain et al. where fibula graft includ-ing the proximal joint cartilage and the growth plate andfibular graft with massive allograft was used for recon-struction post sarcoma resection [49]. They included pa-tients with proximal femur reconstruction. The resultswere promising with only benign complication(s) and nopostoperative death. Peterson et al. illustrated two cases,4 and 6 years old, who underwent vascularized free-fibu-la reconstruction of the proximal femur post sarcoma resection. One patient died and had hip disarticulationwhich was attributed to suboptimal resection of the tu-mor and the other had decent results with acceptablefunctional outcomes [77].
Failure to union will lead to graft fracture, hardwarefailure or coxa vara. Bone grafting is recommended atthe end of the chemotherapy if there is no radiographicbone union. Although scare, the available literature inproximal femur replacement is guiding the authors to-ward shifting their practice to biological reconstructionusing free-fibula in view of promising functional out-comes, possible lengthening of the graft and potential ofhypertrophic remodeling with the use of supporting allo-graft. This holds true especially for very young patientswhere endoprosthetic replacement is hard to be achievedor to last.
Rotationplasty remains a useful surgical technique forreconstruction of these tumors ; however, it is very diffi-cult to obtain consent both from patients and families forthe procedure [78].
__ Distal femur and proximal tibiaThese are the most common sites for sarcoma. Most of
these tumors reside in the metaphyseal area. Prostheticreplacement with expandable and non-expandable pros-thesis (in patients near skeletal maturity) is the standardof care. The reconstruction is more difficult in proximaltibia where the extensor apparatus needs to be reattachedto the fibula graft with a tendon autograft. Medial gastroc-nemius rotational flap is the most commonly used. Dif-ferent variations in the original technique were described[79-81]. Patella superior migration and extension gap
102 Lebanese Medical Journal 2021 • Vol 69 (2) A.S. NAJA et al. – Pediatric oncologic reconstruction
Figure 5. Postoperative X-ray of the left thigh showingvascularized free-fibula reconstruction with allograft
reinforcement post proximal femur sarcoma resection.Fixation was done using a long LCP plate and K-wires.

remain the main complications [79, 82-83]. Short andlongterm complications of prosthetic replacement havebeen discussed earlier.
__ Biologic reconstruction can be attempted in thefollowing situations :
1_ Resection can be performed without sacrificing the growth plate. The tumor as identified on pre-and post-chemotherapy MRI does not extend to thegrowth plate. Fixation of the graft with a side platehalts the growth temporary. Epiphyseal screws orplate removal after union can allow growth to resume.
2 _ Resection is planned through the growth plate. Theidea is to salvage the articular cartilage in veryyoung kids and allow for long lasting reconstruc-tion with a normal joint. Nevertheless, these pa-tients will require lengthening of their fibula or thenative bone later on.
3 _ Transarticular or extraarticular resection when tu-mor invades the epiphysis or the joint. Arthrodesiswith a fibula graft may be an alternative for pros-thetic replacement as discussed earlier. Lengthen-ing on either or both sides of the joint will ensureequal leg length
There are few more topics for discussion in these biolog-ic reconstructions :
1 _ Use of concomitant structural allograft to increasethe strength of the fibula and prevents fracture [84].The surgeon has to balance between higher risk ofinfection and increase cost with the risk of graftfracture. In very young patients, where most ofthese reconstructions are performed, the use of flex-ible nail seems to strengthen the graft and preventsfracture without the need for any structural allo-graft.
2 _ Graft fixation : flexible nails may not be enough forgraft fixation in lower extremity. Anatomical platesusually are not adequate in preadolescent kids be-cause of screws size. Alternatively, distal tibia plate(2.7/3.5) can be used. The main drawback is pos-sible axial deviation that may result if the surgeondoes not pay enough attention to the planning andplate application.
3 _ Soft tissue coverage remains as important as inprosthetic reconstruction. It is rarely needed on thefemoral side but remains highly recommended onthe tibia side. Medial gastrocnemius flap offers theadvantage of soft tissue coverage along the exten-sor apparatus reconstruction. They are the gold stand-ard for soft tissue reconstruction around the knee.The blood supply is based on medial sural arterywhich should be preserved during tumor resection.Another solution will be to harvest the free fibula
with a soft tissue and skin paddle to be able to pro-vide good coverage of the area to prevent skin break-down. This is useful in tumor extending to the shaftwith prior open biopsy scar.
Donor site morbidityThe free fibula donor harvesting procedure has its owndonor site morbidity. Some of these complications arerelated to the harvesting procedure itself while othersvary according to site of the segment removed. Local-ized complications like wound healing issues, infectionsor bleeding are potential obstacles that might be encoun-tered at the donor site. These are related to the harvest-ing procedure, the use of skin grafts for closure in somecases, the chemotherapy/radiotherapy administration, andgeneral status of the patient. They can be as high as 53%[85]. Pain is present in the majority of patients but it ismild to moderate and disappears in 88% of the subjectswithin three months [85]. Functional complications suchas balancing/walking problems and sensation abnormal-ities may be faced as well after free fibula harvesting[86].
Site specific complications are usually related to theinvolvement of the ends of the fibula, whether the fibu-la head is removed and/or the size of the distal stump ofthe fibula left at the ankle. Valgus ankle deformity oc-curs mainly when either no transfixion of the residualfibular stump with the distal tibia occurs or when it is toosmall for fixation (Figure 6). In skeletally immature pa-tients the residual stump should be 6 to 10 cm long withfixation using cortical screws for prevention of valgus
A.S. NAJA et al. – Pediatric oncologic reconstruction Lebanese Medical Journal 2021 • Vol 69 (2) 103
Figure 6. Valgus deformity in a 9 year-old girl 2 yearsafter free fibula harvesting despite the relatively long
remaining distal fibula stump.

deformity [46]. In our recent series, valgus deformityand ankle instability could be prevented [48].
Another debilitating complication is the developmentof flexion contractures related to the displacement of theinterosseous membrane during harvesting and damage tothe extensors of the foot. Hammer and claw toes and def-icits in dorsal extension of the hallux can occur in 27%of patients [86]. This complication can be prevented byextension of the osteotomy to approximately 2/3 of theentire fibula and/or by early stretching exercises to pre-vent flexion contracture from occurring. Peroneal nervepalsy occurs approximately in half of the patients whounderwent fibula harvesting and mainly in those wherethe fibula head is involved [32]. Fortunately, most ofthem are related to nerve stretching during the procedureleading to a transient neuropraxia.
CONCLUSION
This review shed the light on the major challenges ortho-pedic oncologist might face in pediatric post limb sarco-ma resection and reconstruction. We also highlighted thedifferent reconstruction modalities in the most commonlocations in the appendicular skeleton while highlightingthe hurdles that might be encountered with the possiblepreventive methods.
REFERENCES
1. Ries LAG. Cancer incidence and survival among childrenand adolescents: United States SEER program, 1975-1995: National Cancer Institute, 1999.
2. Nagarajan R, Neglia JP, Clohisy DR, Robison LL. Limbsalvage and amputation in survivors of pediatric lower-extremity bone tumors: what are the long-term implica-tions? J Clin Oncol 2002; 20 (22): 4493-501.
3. Nesbit M, Perez CA, Tefft M et al. Multimodal therapyfor the management of primary, nonmetastatic Ewing’ssarcoma of bone: an Intergroup Study. Natl Cancer InstMonogr 1981; 56: 255-62.
4. Lichtenberg FR. The impact of pharmaceutical innova-tion on premature mortality, hospital separations, and can-cer survival in Australia. Economic Record. 2017; 93(302): 353-78.
5. Guzik G. Results of the treatment of bone metastases withmodular prosthetic replacement _ analysis of 67 patients.J Orthop Surg Res 2016; 11 (1): 1-9.
6. Kawai A, Muschler GF, Lane JM, Otis JC, Healey JH.Prosthetic knee replacement after resection of a malig-nant tumor of the distal part of the femur. Medium tolong-term results. JBJS. 1998; 80 (5): 636-47.
7. Pala E, Trovarelli G, Calabrò T, Angelini A, Abati CN,Ruggieri P. Survival of modern knee tumor megaprosthe-ses: failures, functional results, and a comparative statis-tical analysis. Clinical Orthopaedics and Related Re-search®. 2015; 473 (3): 891-9.
8. Tsuda Y, Tsoi K, Stevenson JD, Fujiwara T, Tillman R,Abudu A. Extendable endoprostheses in skeletally imma-
ture patients: a study of 124 children surviving more than10 years after resection of bone sarcomas. JBJS. 2020;102 (2): 151-62.
9. Futani H, Minamizaki T, Nishimoto Y, Abe S, Yabe H,Ueda T. Long-term follow-up after limb salvage in skele-tally immature children with a primary malignant tumor ofthe distal end of the femur. JBJS. 2006; 88 (3): 595-603.
10. Abed Y, Beltrami G, Campanacci D, Innocenti M,Scoccianti G, Capanna R. Biological reconstruction afterresection of bone tumours around the knee: long-termfollow-up. J Bone Joint Surg Br. 2009; 91 (10): 1366-72.
11. Heare T, Hensley MA, Dell’Orfano S. Bone tumors: os-teosarcoma and Ewing’s sarcoma. Curr Opin Pediatr.2009; 21 (3): 365-72.
12. Wong K, Kumta S, Chiu K, Antonio G, Unwin P, Leung K.Precision tumour resection and reconstruction using image-guided computer navigation. J Bone Joint Surgery Br2007; 89 (7): 943-7.
13. Fisher JE, Burger PC, Perlman EJ et al. The frozen sec-tion yesterday and today: pediatric solid tumors - crucialissues. Pediatr. Dev. Pathol. 2001; 4 (3): 252-66.
14. Young P, Bell S, Mahendra A. The evolving role of com-puter-assisted navigation in musculoskeletal oncology.Bone Joint J. 2015; 97 (2): 258-64.
15. Takeuchi A, Yamamoto N, Hayashi K et al. Joint-preser-vation surgery for pediatric osteosarcoma of the kneejoint. Cancer Metastasis Rev. 2019; 38 (4): 709-22.
16. Wada T, Usui M, Nagoya S, Isu K, Yamawaki S, Ishii S.Resection arthrodesis of the knee with a vascularised fib-ular graft: medium-to long-term results. J Bone JointSurgery Br. 2000; 82 (4): 489-93.
17. Lewis MM. The use of an expandable and adjustableprosthesis in the treatment of childhood malignant bonetumors of the extremity. Cancer. 1986; 57 (3): 499-502.
18. Saghieh S, Abboud MR, Muwakkit SA, Saab R, Rao B,Haidar R. Seven-year experience of using Repiphysis®
expandable prosthesis in children with bone tumors.Pediatr Blood Cancer. 2010; 55 (3): 457-63.
19. Ward WG, Yang R-S, Eckardt JJ. Endoprosthetic bonereconstruction following malignant tumor resection inskeletally immature patients. Orthop Clin North Am. 1996;27 (3): 493-502.
20. Schindler OS, Cannon SR, Briggs TW, Blunn GW. Stan-more custom-made extendible distal femoral replace-ments: clinical experience in children with primary ma-lignant bone tumours. J Bone Joint Surg Br. 1997; 79 (6):927-37.
21. Neel MD, Wilkins RM, Rao BN, Kelly CM. Early multi-center experience with a noninvasive expandable pros-thesis. Clinical Orthopaedics & Related Research 2003;415: 72-81.
22. Dominkus M, Krepler P, Schwameis E, Windhager R,Kotz R. Growth prediction in extendable tumor prosthe-ses in children. Clinical Orthopaedics & Related Re-search® (1976-2007). 2001; 390: 212-20.
23. Nystrom LM, Morcuende JA. Expanding endoprosthesisfor pediatric musculoskeletal malignancy: current con-cepts and results. Iowa Orthop J 2010; 30: 141-9.
24. Dukan R, Mascard E, Langlais T et al. Long-term out-comes of non-invasive expandable endoprostheses forprimary malignant tumors around the knee in skeletally-immature patients. Arch Orthop and Trauma Surg. 2021Jan 8: 1-10.
25. Wilkins RM, Soubeiran A. The Phenix expandable pros-
104 Lebanese Medical Journal 2021 • Vol 69 (2) A.S. NAJA et al. – Pediatric oncologic reconstruction
thesis: early American experience. Clin Orthop RelatRes (1976-2007). 2001 Jan (382): 51-8.
26. Arteau A, Lewis VO, Moon BS, Satcher RL, Bird JE,Lin PP. Tibial growth disturbance following distal femoralresection and expandable endoprosthetic reconstruction. J Bone Joint Surg Am. 2015; 97 (22): e72.
27. Yoshida S, Yokoyama R, Sakamoto A. Treatment of pel-vic defect and infection with endoprosthesis exposure bytopical negative pressure and irrigation with myocuta-neous flap. Microsurgery. 2011; 31 (8): 655-8.
28. Ozger H, Bulbul M, Eralp L. Complications of limb sal-vage surgery in childhood tumors and recommended so-lutions. Strategies Trauma Limb Reconst. 2010; 5 (1):11-15.
29. Taylor GI, Miller GD, Ham FJ. The free vascularizedbone graft. A clinical extension of microvascular tech-niques. Plast Reconstr Surg. 1975; 55 (5): 533-44.
30. Muscolo DL, Ayerza MA, Aponte-Tinao LA, Ranalletta M.Partial epiphyseal preservation and intercalary allograft re-construction in high-grade metaphyseal osteosarcoma ofthe knee. JBJS. 2004; 86 (12): 2686-93.
31. Goldberg V, Shaffer J, Field G, Davy D. Biology of vas-cularized bone grafts. Orthop Clin North Am. 1987; 18(2): 197-205.
32. Innocenti M, Delcroix L, Manfrini M, Ceruso M, Capanna R.Vascularized proximal fibular epiphyseal transfer for dis-tal radial reconstruction. J Bone Joint Surg Am. 2004; 86(7): 1504-11.
33. Lesensky J, Prince DE. Distraction osteogenesis recon-struction of large segmental bone defects after primarytumor resection: pitfalls and benefits. Eur J Ortho SurgTraumatol. 2017; 27 (6): 715-27.
34. Kumta SM, Chow TC, Griffith J, Li CK, Kew J, LeungPC. Classifying the location of osteosarcoma with refer-ence to the epiphyseal plate helps determine the optimalskeletal resection in limb salvage procedures. ArchOrthop Trauma Surg. 1999; 119 (5-6): 327-31.
35. Rabitsch K, Maurer-Ertl W, Pirker-Frühauf U, Wibmer C,Leithner A. Intercalary reconstructions with vascularisedfibula and allograft after tumour resection in the lowerlimb. Sarcoma. 2013 (12): 160295.
36. Yang Y-s, Zhang G-m, Xu Z-h, Wang J-w. Homeochro-nous usage of structural bone allografts with vascular-ized fibular autografts for biological repair of massivebone defects in the lower extremities after bone tumorexcision. J Reconstr Microsurg. 2010; 26 (02): 109-15.
37. Hanna S, Sewell M, Aston W et al. Femoral diaphysealendoprosthetic reconstruction after segmental resectionof primary bone tumours. J Bone Joint Surg Br. 2010; 92(6): 867-74.
38. Said GZ, El-Sherif EK. Resection-shortening-distractionfor malignant bone tumours. A report of two cases. J BoneJoint Surg Br. 1995; 77 (2): 185-8.
39. Ahlmann E, Menendez L. Intercalary endoprostheticreconstruction for diaphyseal bone tumours. J Bone JointSurg Br. 2006; 88 (11): 1487-91.
40. Rosen ED, Hsu CH, Wang X et al. C/EBPalpha inducesadipogenesis through PPARgamma: a unified pathway.Genes Dev. 2002; 16 (1): 22-6.
41. Fuchs B, Ossendorf C, Leerapun T, Sim FH. Intercalarysegmental reconstruction after bone tumor resection. EurJ Surg Oncol. (EJSO). 2008; 34 (12): 1271-6.
42. Ruggieri P, Mavrogenis AF, Bianchi G, Sakellariou VI,Mercuri M, Papagelopoulos PJ. Outcome of the intrame-
dullary diaphyseal segmental defect fixation system forbone tumors. J Surg Oncol. 2011; 104 (1): 83-90.
43. Aldlyami E, Abudu A, Grimer R, Carter S, Tillman R.Endoprosthetic replacement of diaphyseal bone defects.Long-term results. Int Orthop. 2005; 29 (1): 25-9.
44. Yang Z, Jin L, Tao H, Yang D. Reconstruction of largetibial bone defects following osteosarcoma resectionusing bone transport distraction: A report of two cases.Oncol Lett. 2016; 12 (2): 1445-7.
45. Gur E, Kollender Y, Meller I, Amir A, Zaretski A, Bickels J.The use of free vascularized fibular grafts for reconstruc-tion of segmental bone defects. Operative techniques inorthopaedic surgical oncology. Lippincott Williams &Wilkins, Philadelphia. 2012.
46. Beris AE, Lykissas MG, Korompilias AV et al. Vascular-ized fibula transfer for lower limb reconstruction. Micro-surgery. 2011; 31 (3): 205-11.
47. Capanna R, Campanacci DA, Belot N et al. A new recon-structive technique for intercalary defects of long bones:the association of massive allograft with vascularizedfibular autograft. Long-term results and comparison withalternative techniques. Orthop Clin North Am. 2007; 38(1): 51-60.
48. Karami RA, Ghieh FM, Saghieh SS, Ibrahim AE. Theuse of the fibula flap in post oncologic reconstruction oflong bone in pediatric patients: A retrospective cohortstudy. Journal of Plastic, Reconstructive & Aesthetic Sur-gery (JPRAS), 2021.
49. Germain MA, Mascard E, Dubousset J, Nguefack M.Free vascularized fibula and reconstruction of long bonesin the child _ our evolution. Microsurgery: Official Jour-nal of the International Microsurgical Society and the Eu-ropean Federation of Societies for Microsurgery. 2007; 27 (5): 415-19.
50. Ou Q, Wu P, Zhou Z, Pan D, Tang JY. Complication ofosteo reconstruction by utilizing free vascularized fibularbone graft. BMC Surgery. 2020; 20 (1): 1-11.
51. Manfrini M, Innocenti M, Ceruso M, Mercuri M. Origi-nal biological reconstruction of the hip in a 4-year-oldgirl. The Lancet. 2003; 361 (9352): 140-2.
52. Innocenti M, Delcroix L, Romano GF, Capanna R. Vas-cularized epiphyseal transplant. Orthop Clin North Am.2007; 38 (1): 95-101.
53. Tang CH. Reconstruction of the bones and joints of theupper extremity by vascularized free fibular graft: reportof 46 cases. J Reconstr Microsurg. 1992; 8 (4): 285-92.
54. Marulanda GA, Henderson E, Cheong D, Letson GD.Proximal and total humerus reconstruction with the useof an aortograft mesh. Clin Orthop Rel Res. 2010; 468(11): 2896-903.
55. Wada T, Usui M, Isu K, Yamawaki S, Ishii S. Recon-struction and limb salvage after resection for malignantbone tumour of the proximal humerus: a sling procedureusing a free vascularised fibular graft. J Bone Joint SurgBr. 1999; 81 (5): 808-13.
56. Muramatsu K, Fukano R, Ihara K, Iwanaga R, Taguchi T.Reconstruction of the proximal humerus by combineduse of extracorporeally-irradiated osteochondral graft andfree vascularized fibula following resection of Ewing sar-coma. J Plast Reconstruc Aesthet Surge. 2010; 63 (12):2177-80.
57. Stevenson J, Doxey R, Abudu A et al. Vascularized fibu-lar epiphyseal transfer for proximal humeral reconstruc-tion in children with a primary sarcoma of bone. Bone
A.S. NAJA et al. – Pediatric oncologic reconstruction Lebanese Medical Journal 2021 • Vol 69 (2) 105

Joint J. 2018; 100-B (4): 535-41.58. Erdmann D, Garcia RM, Blueschke G, Brigman BE,
Levin LS. Vascularized fibula-based physis transfer forpediatric proximal humerus reconstruction. Plast ReconstrSurg. 2013; 132 (2): 281e-7e.
59. Pagnotta A, Haerle M, Gilbert A. Long-term results onabduction and external rotation of the shoulder after la-tissimus dorsi transfer for sequelae of obstetric palsy.Clin Orthop Relat Res. 2004; 426: 199-205.
60. Ernstbrunner L, Wieser K, Catanzaro S et al. Long-termoutcomes of pectoralis major transfer for the treatment ofirreparable subscapularis tears: results after a mean fol-low-up of 20 years. JBJS. 2019; 101 (23): 2091-100.
61. Moroder P, Schulz E, Mitterer M, Plachel F, Resch H,Lederer S. Long-term outcome after pectoralis majortransfer for irreparable anterosuperior rotator cuff tears.JBJS. 2017; 99 (3): 239-45.
62. Elhassan B. Lower trapezius transfer for shoulder exter-nal rotation in patients with paralytic shoulder. J HandSurg Am. 2014; 39 (3): 556-62.
63. Zelenski N, Brigman BE, Levin LS, Erdmann D, Eward WC.The vascularized fibular graft in the pediatric upper ex-tremity: a durable, biological solution to large oncologicdefects. Sarcoma. 2013; 2013: 321201.
64. Ad-El DD, Paizer A, Pidhortz C. Bipedicled vascularizedfibula flap for proximal humerus defect in a child. PlastReconstr Surg. 2001; 107 (1): 155-7.
65. Gebert C, Hillmann A, Schwappach A et al. Free vascu-larized fibular grafting for reconstruction after tumor re-section in the upper extremity. J Surg Oncol. 2006; 94(2): 114-27.
66. El-Sherbiny M. Reconstruction of the proximal humerusafter wide resection of tumors: comparison of three re-constructive options. J Egypt Natl Can Inst. 2008; 20 (4):369-78.
67. Aldekhayel S, Govshievich A, Neel OF, Luc M. Vascu-larized proximal fibula epiphyseal transfer for distal ra-dius reconstruction in children: a systematic review.Microsurgery. 2016; 36 (8): 705-11.
68. Van Kampen M, Grimer RJ, Carter SR, Tillman RM,Abudu A. Replacement of the hip in children with a tu-mor in the proximal part of the femur. JBJS. 2008; 90 (4):785-95.
69. Song KM, Halliday SE, Little DG. The effect of limb-length discrepancy on gait. JBJS. 1997; 79 (11): 1690-8.
70. Ponseti IV. Growth and development of the acetabulumin the normal child. Anatomical, histological, and roent-genographic studies. J Bone Joint Surg Am. 1978; 60 (5):575-85.
71. Harris NH. Acetabular growth potential in congenital dis-location of the hip and some factors upon which it maydepend. Clin Orthop Relat Res. 1976 (119): 99-106.
72. Weinstein SL. Congenital hip dislocation. Long-rangeproblems, residual signs, and symptoms after successful
treatment. Clin Orthop Relat Res. 1992 (281): 69-74.73. Bucholz R, Ezaki M, Ogden J. Injury to the acetabular
triradiate physeal cartilage. J Bone Joint Surg Am.. 1982;64 (4): 600-9.
74. Hallel T, Salvati EA. Premature closure of the triradiatecartilage. A case report and animal experiment. ClinOrthop Relat Res. 1977 (124): 278-81.
75. Belthur MV, Grimer RJ, Suneja R, Carter SR, Tillman RM.Extensible endoprostheses for bone tumors of the proxi-mal femur in children. J Pediatr Orthop. 2003; 23 (2):230-5.
76. Ramseier LE, Sukthankar A, Exner GU. Minimal inva-sive epiphysiodesis using a modified “Canale” _ tech-nique for correction of angular deformities and limb leglength discrepancies. J Child Orthop 2009; 3 (1): 33-7.
77. Petersen MM, Hovgaard D, Elberg JJ, Rechnitzer C,Daugaard S, Muhic A. Vascularized fibula grafts for re-construction of bone defects after resection of bone sar-comas. Sarcoma. 2010; 2010: 524721.
78. Sakkers R, van Wijk I. Amputation and rotationplasty inchildren with limb deficiencies: current concepts. J ChildOrthop 2016; 10 (6): 619-26.
79. Madi NS, Masrouha KZ, Haidar RK, Saghieh SS. Use ofhamstring autograft to reconstruct the patellar tendon after endoprosthetic replacement of the proximal tibiafor bone sarcomas. J Pediatr Orthop B. 2020; 29 (5):510-13.
80. Browne JA, Hanssen AD. Reconstruction of patellar ten-don disruption after total knee arthroplasty: results of anew technique utilizing synthetic mesh. JBJS. 2011; 93(12): 1137-43.
81. Ichikawa J, Matsumoto S, Shimoji T, Ae K, Tanizawa T,Gokita T. A new technique using mesh for extensor re-construction after proximal tibial resection. Knee 2015;22 (6): 659-63.
82. Jentzsch T, Erschbamer M, Seeli F, Fuchs B. Extensorfunction after medial gastrocnemius flap reconstructionof the proximal tibia. Clin Orthop Relat Res. 2013; 471(7): 2333-9.
83. Grimer R, Carter S, Tillman R et al. Endoprosthetic re-placement of the proximal tibia. J Bone Joint Surg Br.1999; 81 (3): 488-94.
84. Zekry KM, Yamamoto N, Hayashi K et al. Reconstructionof intercalary bone defect after resection of malignant bonetumor. J Orthop Surg. 2019; 27 (1): 2309499019832970.
85. Sieg P, Taner C, Hakim SG, Jacobsen HC. Long-termevaluation of donor site morbidity after free fibula trans-fer. Br J Oral Maxillofac Surg. 2010; 48 (4): 267-70.
85. Hakim SG, Tehrany AS, Wendlandt R, Jacobsen HC,Trenkle T, Sieg P. The impact of harvest length and de-tachment of the interosseous membrane on donor-sitemorbidity following free fibula flap surgery _ A biome-chanical experimental study. J Cranio-Maxillofac Surg.2018; 46 (11): 1939-42.
106 Lebanese Medical Journal 2021 • Vol 69 (2) A.S. NAJA et al. – Pediatric oncologic reconstruction

INTRODUCTION
One of the specificity of the human nature is the erect pos-ture standing or sitting. Most of the studies about the etiol-ogy of the so-called idiopathic scoliosis, after excludingknown evident reasons, congenital malformations, para-lytic, dystrophic, metabolic as for bone as for soft tissues,are searching about multiple pathways such as genetic,metabolic, neuro-sensory, biomechanics. They start fromprevious studies dividing this deformity according to theage of the patient at onset, young, adolescent, adult, orlook about difference in the localization of the deformity,thoracic, thoraco-lumbar or lumbar, They look about thevarious aspects of genetic, neuromuscular, metabolic, hor-monal, even biomechanical specificities. Regarding thislast point, most of the time they are focusing on the infor-mation given by the frontal and sagittal projections of theX-rays and even after a so-called 3D computer reconstruc-tion, don’t look in reality on the horizontal plane projec-tion and especially on the horizontal plane of the bodygiven for example by the view from the top. The addictionof the medical community to these frontal and sagittalprojections is so strong that all classifications, even themost modern ones, have difficulties to think about scolio-sis as an architect would do, especially using always thetop view of the building they are planning to build.
The aim of this paper is to demonstrate that no matterthe age of the patient, the localization and the type, thespeed of progression of the deformity, the search about acommon factor available for every patient any time, mustbe found.
This common factor I identified is that the startingpoint is, biomechanically, always a disorder within thehorizontal plane, with a similar and constant reaction tothe gravity. The resulting spinal deformity is in reality thecompensation of the rotatory inducing factor. This con-cept would unify the various aspects of this deformityand perhaps increase the fields of research.
CLINICAL OBSERVATIONS BY THE AUTHOR
_ Idiopathic scoliosis like doesn’t exist spontaneously in quadrupedal animals, erect posture is necessary.
_ I have never seen cases of idiopathic scoliosis in pa- tients with congenital blindness.
_ Movements are permanent in standing or sitting erectposture, even at rest sometimes minimal, but constantlooking for the best balance with the minimal of mus-cle consumption within the cone of economy of thechain of balance with the major compensatory role of the pelvic vertebra.
_ The search for a horizontal gaze is constant for anyspinal deformity at rest or during motion.
_ A horizontal adaptation in rotation of the successive joints from feet to head is observed during walking in the human, (the most evident is the pelvic step from Ducroquet’s brothers, and its subsequent shoul-der adaptation).
_ Clinical observation of a scoliotic patient at rest in a standing or sitting position, seen from the top whencompared to normal or purely kyphotic patient, demon-strate always a horizontal torsion of the shoulder axis,of the pelvis axis, and more or less of the thoracic, tho-racolumbar or lumbar areas.
ANATOMICAL OBSERVATIONS BY THE AUTHOR
_ Analysis of cadaveric spine of subjects with signifi- cant idiopathic scoliosis looking globally kyphoticdemonstrates that deformity I described as “paradox- ical kyphosis” was in reality theaspect given by thehyper apical torsion, where the apical vertebrae pro-jected at same level on AP and sagittal, is truely locat-ed in lordosis one to the nextone. This was beautiful-ly demonstrated by the anatomical accurate measure-ment of the vertebrae of a scoliotic specimen byRené Perdriole.
_ Analysis of cadaveric spine moderate so-called lordo tho-racic scoliosis, where it was easy to show that at the
Lebanese Medical Journal 2021 • Volume 69 (2) 107
PPAAEEDDIIAATTRRIICC OORRTTHHOOPPAAEEDDIICCSSETIOLOGY OF THE SO-CALLED IDIOPATHIC SCOLIOSIS FROM BIRTH TO AGINGSEEN FROM A CLINICIAN SIDEThe Biomechanical Importance of the Horizontal Planehttp://www.lebanesemedicaljournal.org/articles/69-2/pedsortho7.pdfJean DUBOUSSET*
Dubousset J. Etiology of the so-called idiopathic scoliosisfrom birth to aging seen from a clinician side. The biomedicalimportance of the horizontal plane. J Med Liban 2021 ; 69 (2) :107-108.
* Académie nationale de médecine, 16 rue Bonaparte, 75006Paris, France.
e-mail: [email protected]

upper part of the thoracic curve the vertebra just above was horizontally oriented in a reverse directionof the one below : it was the definition of the junction-al zone, again perfectly defined by René Perdriolle un-der the name of “specific rotation” as soon as 1979.
_ Lewis Sayre experimental model with rigid frame,spine skeleton, elastic horizontal bands, flexible brassrod slipped inside the spinal canal, where vertical pres-sure on the rod creates scoliosis and on the contrarytraction decreases it.
_ Similarly, the biomechanical model developed at EN-SAM where an axial intervertebral rotation is neces-sary to simulate scoliosis, by vertical pressure on thetop of the model to simulate growth.
COMBINED CLINICAL, RADIOLOGICAL &3D COMPUTER RECONSTRUCTION OBSERVATIONS
_ Analysis of the evolution of the infantile idiopathicscoliosis where we prove that the prognostic of the evo-lution (progression/regression) was under the aspectof the spine on the horizontal plane projection.
_ Evidently the Crankshaft phenomenon is a typical ob-servation of such inducing horizontal factor.
_ Paralytic pelvic obliquity is better assessed by 3Dbuttocks pressure than with spine Cobb angles.
_ Progression of AIS studied from the top projection isthe same typical horizontal increasing deformity espe-cially compared to the progression of a Scheuermannkyphosis where horizontal axial deformity does not existbetween 2 successive vertebrae. It is why I call these scolioses occurring during the growing time of the chil-dren : “ascending” scolioses, where the twisting of thespine is simultaneous to the growth in height of the pa-tient creating this 3D deformity with always the hori-zontal plane importance well demonstrated on the viewfrom the top.
_ Starting point and progression of de novo adult sco-liosis or purely degenerative scoliosis in the adult,
where induction starts with a failure of the rotatory sta-bility of the disc in this horizontal plane realizing adiscogenic cascade giving the same aspect seen fromthe top. It is why I call these scolioses “descending”because associated with a collapse of the spine and anevident loss in height of the patient.
_ The horizontal plane plays an important role in the
rotational dislocation of the spine, able to occur atany level and any age, where the intermediate verte-bra between two curves in lordosis is particularly un-stable because the discs above and below are rotated in the axial plane in an opposite direction. It is a typical junctional mechanism evolving always in a kyphosisprojection.
_ EOS imaging system was designed especially to ad-dress this 3D horizontal plane vision from the top (orthe bottom) of the entire body properly within the erect posture. Unfortunately the marketing business devel-oped mainly its 2D applications thanks to the radiationdose reduction and forgot the real 3D and especially thehorizontal plane studies despite the fact that it was in- cluded inside the software. Very few studies appeareddesigned from this view from the top, so great was theaddiction to the AP and sagittal projections coming from the time of the discovery of the X-rays.
_ Nevertheless, Tamas Illes vectors appeared properlyto address this problem and it is true that this simpli-fied horizontal vision of the entire spine allows in a glance to estimate, and more, to measure any spinaldeformity.
_ Kazuhiro Hazegawa improved this measurement for apractical use in clinics every day thanks to the hori-zontal 3D & volumetric projection including head,spine, pelvis, lower limbs and feet representation,much more reliable than the angular approximations coming from the sagittal alignment of the odontoid orlocation of the sella turcica.
CONCLUSION
First, the Spine community is very addicted, nowadays,toward the sagittal plane, getting no ways where to go toprogress. They must consider the major importance of thehorizontal plane in the erect posture and the induction ofthe deformity at any age and work to predict, to correct itor better prevent it with cast braces or even localized sur-gery done before a too large deformity.
Second, as the erect posture is necessary in the patho-geny of idiopathic scoliosis, all research factors neces-sary to achieve this function must be included in the ge-netic, neurosensory, metabolic, biomechanical researchfields.
Despite my personal intuition drive toward a probablepreponderance of the neurological and neurosensoryfields, in relation with balance, each one of the four mainsections must be opened as widely as possible to any lab-oratory in the world for proposal, looking on such goals.
108 Lebanese Medical Journal 2021 • Vol 69 (2) J. DUBOUSSET – Etiology of the so-called idiopathic scoliosis

INTRODUCTION
Adolescent idiopathic scoliosis (AIS) is a three-dimen-sional complex deformity of the spine. It is the mostcommon form of scoliosis. It reaches around 0.2 to 0.6%of the general population.
The main cause of this pathology is still unknown,hence its name “idiopathic” (Konieczny, Senyurt, &Krauspe, 2013).
While being a deformity that alters the alignment ofthe spine especially in the frontal plane, scoliosis alsoaffects the sagittal plane by modifying the curvatures ofthe back leading to its flattening in the majority of cases(Mac-Thiong, Labelle, Charlebois, Huot, & de Guise,2003). In addition, Professor Dubousset has long en-
couraged the scientific community to place additionalimportance on the scoliotic deformity in the horizontalplane which induces vertebral rotations (Jean Dubousset,2011), hence the importance of diagnosing the scolioticdeformity in the three planes.
Routine radiographic procedures that allow 3D recon-struction of the spine (such as CT-scan) are often associ-ated with a high rate of radiation. Likewise, these radio-graphs are taken in the supine position, which can maskthe spinal deformity. Hence the interest of low-dose bi-planar X-ray radiograph performed in a standing posi-tion.
The scoliotic spinal deformity can be stable or pro-gressive and occurs in one or more segments of the spine(thoracic, thoracolumbar and lumbar curvatures) whileaffecting other skeletal levels. Despite the three-dimen-sional aspect of spinal deformity, the treatment decisionfor subjects with AIS depends on several factors, in par-ticular the frontal Cobb angle, which is commonly usedas an indicator of the severity of the deformity. The diag-nosis and/or treatment decision may be biased if basedsolely on the frontal Cobb angle because it is a projec-tion of a true 3D deformity in a 2D frontal plane. Cotreland Dubousset showed the importance of the 3D evalu-ation of the scoliotic deformity, mainly in the sagittaland horizontal planes, as being an important indicator onthe planning of the treatment (J. Dubousset & Cotrel,1991). In addition, the horizontal plane has been shownto be essential in predicting the progression of spinal de-formity (Courvoisier, Drevelle, Dubousset, & Skalli,2013) as well as defining the severity index to differen-tiate between progressive and non-progressive scolioticdeformity (Skalli et al., 2017). Hence the interest of athree-dimensional evaluation of spinal deformity in dif-ferent types of curvatures.
The three-dimensional alteration of the spine directlyinfluences the rib cage through the costo-vertebral jointswhich leads to a morphological deformity of the ribcage. In addition, the progression of both spinal and ribcage deformities are associated with mechanical dys-functions of the chest wall and diaphragm, thus leadingto disturbances of respiratory function (Bouloussa et al.,
Lebanese Medical Journal 2021 • Volume 69 (2) 109
PPAAEEDDIIAATTRRIICC OORRTTHHOOPPAAEEDDIICCSSA THREE-DIMENSIONAL BIOMECHANICAL ANALYSIS OF THE SKELETONIN ADOLESCENT IDIOPATHIC SCOLIOSIShttp://www.lebanesemedicaljournal.org/articles/69-2/pedsortho8.pdf
Mohamad KARAM1, Ismat GHANEM1, Wafa SKALLI2, Ayman ASSI1,2
ABSTRACT • The objective of this review was to conduct athree-dimensional biomechanical analysis of the skeleton insubjects with adolescent idiopathic scoliosis (AIS).
Over 200 subjects with AIS and 64 controls underwent lowdose biplanar X-rays in the free-standing position with 3Dreconstructions of the skeleton.
Results have shown that the scoliotic deformity is corre-lated in the three planes, especially in thoracic curvatures.However, these correlations could not fully explain the defor-mities in a single plane. In addition, we have found that pa-tients with severe morphological deformities of the rib cagecan be classified depending on : high gibbosity, high volu-metric spine penetration index (VSPI) or both. Gibbosity wascorrelated to the frontal and horizontal deformities, whileVSPI was correlated to the sagittal deformity. Moreover, thelowered side of the pelvis exhibited a decreased acetabularabduction and an increased external hip coverage angle.Both sides of the hip showed decreased anterior coverageas well as increased acetabular anteversion. These changeswere determined by the pelvic tilt.
This three-dimensional approach allows to better under-stand the morphological deformities of the skeleton and helpsin better decision-making in the treatment of AIS.
Keywords :adolescent idiopathic scoliosis ; spine ; rib cage ;hip ; lower limbs ; three-dimensional analysis.
Karam M, Ghanem I, Skalli W, Assi A. A three-dimensionalbiomechanical analysis of the skeleton in adolescent idiopathicscoliosis. J Med Liban 2021 ; 69 (2) : 109-125.
1 Faculty of Médecine, Saint-Joseph University, Beirut, Lebanon. 2 Institut de Biomécanique Humaine Georges Charpak, Arts et Métiers ParisTech, Paris, France.
*Corresponding author: Ayman Assi, PhD e-mail: [email protected]

2019 ; Dreimann et al., 2014 ; Johnston et al., 2011 ;Yaszay, Bastrom, Bartley, Parent & Newton, 2017).Hence it would be interesting to evaluate the rib cagedeformities and their relationship to the spinal ones.
In addition, 3D deformity of the spine in adolescentidiopathic scoliosis causes alterations in the orientationof the pelvis (Jean Dubousset, 1990 ; Pasha et al., 2014).The pelvis is an integral part of the spine, so any alter-ation could change its orientation in the frontal and sagit-tal planes and its rotation in the horizontal plane. It hasbeen shown that some alterations are encountered at thehip and lower limbs, hence the interest of the analysis ofthe alterations that can occur at these levels and their re-lationship to the spinal deformity.
The objective of this review was therefore to conducta three-dimensional approach of the entire skeleton insubjects with AIS.
METHODS
This is a review study based on IRB approved (CEHDF742) cross-sectional descriptive studies of non-operatedsubjects with AIS who had previously consulted for radi-ographic follow-up. Non-scoliotic control subjects for-merly recruited for previous studies were also included.Written and informed consent was obtained from all sub-jects and their legal guardians.
In the case of subjects with AIS, inclusion criteriawere age 10 to 18 years, and frontal Cobb angle ≥ 10° ;exclusion criteria were congenital or neurological scoli-osis, infantile and juvenile scoliosis, structural leg lengthdiscrepancy ≥ 1 cm.
In the case of controls, inclusion criteria were age 10to 18 years, and no known underlying musculoskeletalor neurological disorders; the exclusion criterion was afrontal Cobb angle ≥ 10°.
Demographic data (age, weight, height and sex) werecollected for all subjects.
Data acquisitionAll subjects underwent full-body low-dose biplanar X-rays (EOS Imaging®, Paris, France). Subjects were placedin the free-standing position (Chaibi et al., 2012 ; Faro,Marks, Pawelek, & Newton, 2004). 3D reconstructionsof their spine, rib cage, pelvis and lower limbs were per-formed by trained operators using SterEOS® (EOS®
Imaging, Paris, France ; version 1.8.99.20R) and a dedi-cated software (Arts et Métiers ParisTech, Paris, France).
The collected spino-pelvic parameters were: pelvic in-cidence (PI in°), pelvic tilt (PT in°), sacral slope (SS in°),L1S1 lordosis (LL in °), T10L2 thoracolumbar junctionangle (negative values indicate kyphosis) (°), T4T12 (in °) and T1T12 kyphosis (TK in °), frontal Cobb (in °),
apical vertebral rotation (AVR in °) and vertebral axialrotations (°).
The radiological parameters used to calculate the se-verity index were extracted (Skalli et al., 2017) : inter-vertebral axial rotation at the upper and lower junction(UIAR and LIAR respectively in °) ; torsion index (TI in °), calculated as the mean of the two sums of the inter-vertebral axial rotations within the scoliotic segment,from lower to upper junction ; hypokyphosis/lordosis in-dex (HI in °), calculated as the difference between localkyphosis/lordosis, at the apical level, of the scoliotic sub-ject, and the mean value at the equivalent level of a non-scoliotic control group (Skalli et al., 2017). A negativevalue could mean either hypokyphosis (thoracic seg-ment) or hypolordosis (lumbar segment). The aforemen-tioned parameters were presented in Figure 1.
The collected 3D rib cage parameters (Figure 2) werethickness (mm) as the maximum antero-posterior distancebetween the most posterior point of the rib cage and itsprojection on the sternal vertical axis ; width (mm) as themaximum frontal width of the rib cage ; volume (cm3) asthe integration of different layered surfaces extracted from rib cage reconstructions (Pietton, Bouloussa, Vergari,Skalli, & Vialle, 2020) ; gibbosity (°) as the angle betweenthe horizontal axis and the axis passing through the mostposterior prominent points on both sides of the rib cage(Aubert et al., 2016) ; local gibbosity (°) at each vertebrallevel from T1 to T10 ; volumetric spinal penetration in-dex (VSPI) (%) as the ratio of the spinal volume pene-trating the chest to the rib cage volume (Jean Dubousset,Wicart, Pomero, Barois, & Estournet, 2003). The validi-ty and reliability of these parameters have already beenevaluated in previous studies (Aubert et al., 2016 ; Cour-voisier, Ilharreborde et al., 2013 ; Pietton et al., 2020).
The collected 3D acetabular parameters included : ace-tabular tilt (°) (Lazennec et al., 2004), acetabular ante-version (°), acetabular abduction (°) (Anda, Svenningsen,Grontvedt, & Benum, 1990), center edge angle (CEA in °)(Tönnis & Heinecke, 1999), anterior and posterior sectorangles (°) (Anda, Svenningsen, Dale & Benum, 1986),sacro-acetabular angle (SA in °) (Lazennec et al., 2004).Acetabular anteversion and abduction were calculatedmorphologically, i.e. in the Lewinnek plane (M), and po-sitionally (P), i.e. in the horizontal or vertical planes.
The collected 3D lower limb parameters were : fem-oral torsion (°), hip-knee shaft angle (HKS in °), kneeflexion-extension (°), neck-shaft angle (NSA in °), tibialtorsion (°), valgus/varus of the knee (hip knee angle :HKA in °) and the tibial mechanical angle (°) (AymanAssi et al., 2012). The ratio of the femur length over thetibial length (Rampal et al., 2018), as well as the anatom-ical (sum of the femur and tibia lengths in cm) and func-tional lengths (distance between the center of the fem-
110 Lebanese Medical Journal 2021 • Volume 69 (2) M. KARAM et al. – 3D biomechanics in adolescent idiopathic scoliosis

oral head to the center of the ankle in cm) of the fulllower limbs were also calculated and normalized toheight. The validity and reliability of the aforementionedparameters have already been studied (Ayman Assi et al.,2013 ; Ghostine et al., 2017). In addition, lateral pelvicobliquity (LPA in mm) (distance between iliac crests cal-
culated in the frontal plane) and the pelvic axial rotation(PAR in °) (in the horizontal plane) were calculated.
The global postural parameters were also collected :sagittal vertical axis (SVA : as the distance in mm fromthe C7 plumbline to the posterior corner of the sacrum),CAM-HA plumbline (as the distance in mm from the
M. KARAM et al. – 3D biomechanics in adolescent idiopathic scoliosis Lebanese Medical Journal 2021 • Vol 69 (2) 111
Figure 2. Rib cage parametersa) Volumetric spine penetration index. b) Rib cage volume. c) Thickness and width. d) Gibbosity.
Figure 1. Spino-pelvic and severity index parametersa) 1. T1T12 kyphosis. 2. T4T12 kyphosis. 3. L1S1 lumbar lordosis. 4. Sacral slope. 5. Pelvic incidence. 6. Pelvic tilt.
b) Hypokyphosis/lordosis index. c) Frontal Cobb angle.d) 1. Upper intervertebral axial rotation. 2. Apical vertebral rotation. 3. Lower intervertebral axial rotation. 4. Torsion index.

plumbline passing by the center of auditory meatus tothe center of the hip axis), T1 and T9 tilt (°), C7CSL (thedistance in mm from the center of C7 plumbline to thecenter of the sacral plate in the frontal plane). These pa-rameters were presented in Figure 3.
Subject classificationThe current study was divided into three parts. The 1st
section of this study investigated the spine deformity atthe level of the scoliotic segment (A. Assi et al., 2018).The 2nd section evaluated the 3D rib cage deformity (A. Assi, Karam, Skalli, & Vergari, 2021). The 3rd sec-tion assessed the 3D hip and lower limbs deformity insubjects with AIS (Karam et al., 2020).
• In the 1st section, subjects were grouped by majorcurve type (Lenke et al., 2001) : thoracic (T, apex be-tween T2 and T11), thoracolumbar (TL, apex at T12 orL1) and lumbar (L, apex between L2 and L4).
• In the 2nd section, subjects with AIS were groupedaccording to gibbosity and VSPI. Subjects with normalor slightly elevated gibbosity and VSPI, but lower thanthe 95th percentile of the control values, were grouped asmild rib cage deformity (group I). The remaining sub-jects who presented a high gibbosity and/or VSPI, greaterthan the 95th percentile of control values, were grouped assevere rib cage deformity (group II) and further dividedinto 3 subgroups : only high gibbosity (group IIa), only
high VSPI (group IIb), and both high gibbosity and VSPI(group IIc).
• In the 3rd section, the two limbs were included foreach subject with AIS and grouped according to thepelvic obliquity in the frontal plane (obtained from the3D reconstruction) into elevated side (ES) and loweredside (LS). Subjects were grouped according to the distri-bution of the acetabular parameters. CEA, NSA and ace-tabular anteversion were compared between groups ac-cording to specific ranges used in clinical classifications(CEA for risk of overcoverage or dysplasia ; NSA andacetabular anteversion for risk of femoro-acetabular im-pingement) (Stem, O’Connor, Kransdorf, Crook, & StemES, O’Connor MI, Kransdorf MJ, 2006 ; Tannast, Hanke,Zheng, Steppacher & Siebenrock, 2015; Tönnis &Heinecke, 1999). When no clinical classifications werefound in the literature, the control group was dividedinto three classes defined as : low, if inferior to mean-1sd(17% of subjects) ; intermediate, if it falls betweenmean-1sd and mean + 1sd (66% of subjects) ; high, ifsuperior to mean + 1sd (17% of subjects). The distribu-tion of the AIS sides was then evaluated based on theseclassifications.
StatisticsDemographic characteristics were compared betweengroups.
112 Lebanese Medical Journal 2021 • Volume 69 (2) M. KARAM et al. – 3D biomechanics in adolescent idiopathic scoliosis
Figure 3. Acetabular, lower limbs and postural parametersa ) 1. Acetabular tilt. 2. Acetabular anteversion. 3. Acetabular abduction. 4. Center edge angle. 5. Anterior sector angle.
6. Posterior sector angle. 7. Femoral torsion. 8. Tibial torsion. 9. Femoral mechanical angle. 10. Tibial mechanical angle. b ) 1. C7CSL. 2. T1 tilt. 3. T9 tilt. 4. SVA. 5. CAM-HA.
a b

• In the 1st section : the spino-pelvic and severity in-dex parameters were compared between types of curva-ture. In order to investigate the relationship between theaxial plane and both the frontal and sagittal planes, amultiple linear regression was computed while consider-ing the type of major curvature (ANCOVA model).
• In the 2nd section, differences in rib cage, spino-pelvic and scoliosis parameters were investigated be-tween controls and the different groups of rib cage de-formities. Relationships between the rib cage deformi-ty (gibbosity and VSPI) in group II and the 3D spinal deformity (frontal plane: Cobb angle, sagittal plane :T1T12, and horizontal plane : TI) were investigatedusing a Pearson’s correlation test. The relationship be-tween the vertebral axial rotation and the local gibbosityat the level of the apical vertebra and its adjacent unitsproximally and distally was also evaluated.
• In the 3rd section, acetabular, lower limb and 3Dlength parameters were first compared between eachside of AIS (ES or LS). For the control group, the leftand right sides were averaged after confirmation of nostatistical differences between both sides. Then each sideof the AIS was compared to controls. Differences be-tween groups were also investigated by studying the dis-tribution of the parameters. In order to investigate therelationship between the 3D acetabular and lower limbsparameters and spino-pelvic parameters, a univariateanalysis using Pearson’s correlation test was applied.Then, in order to explore the most significant determi-nants of the acetabular and lower limb 3D parametersamong demographics and spino-pelvic parameters, amultivariate analysis using stepwise multiple linear re-gression was computed.
The level of significance was set at 0.05 and correct-ed in case of multiple comparisons. Statistics were per-formed using Xlstat® (version 2019.1.2, Addinsoft3®,Paris, France).
RESULTS
DemographicsThese studies included between 200 to 274 subjects withAIS and 64 to 84 controls. Demographic characteristicsfor both groups were : age = 14 ± 2 years (mean ± SD),weight = 53 ± 11 kg and height = 1.6 ± 0.1 m. Demo-graphic parameters did not differ between groups (allp > 0.05). 83% of subjects with AIS and 72% of controlswere females. Mean frontal Cobb angle in subjects withAIS was 43 ± 23° [10-128°].
The 3D scoliotic segmentIn brief, frontal Cobb was significantly higher in subjectswith T and TL curves compared to L curves (47 ± 20° and
40 ± 13° vs. 31 ± 11°, respectively). TI, UIAR and LIARwere significantly higher in subjects with T curves whencompared to both TL and L curves (TI : 16 ± 8° vs. 9 ± 5°and 6 ± 4° ; UIAR : 8 ± 4° vs. 6 ± 3° and 4 ± 2° ; LIAR :9 ± 5° vs. 7 ± 4° and 6 ± 3°, respectively). When control-ling for frontal Cobb, the HI did not differ between typesof curvature. However, the TI, UIAR and LIAR werestill significantly higher in T curves compared to TL andL curves (all p < 0.05). Regarding postural parameters,subjects with major lumbar curves presented a higher T9tilt compared to major thoracic curves (11 ± 4 mm vs. 9 ± 4 mm, p = 0.02). C7CSL was found to be higher insubjects with TL curves compared to both T and L(13 ± 9 mm vs. 10 ± 8 mm and 9 ± 8 mm, p = 0.03). SeeTable I for detailed results.
Correlations between frontal Cobb and HI were sig-nificant for the T curves (r = _ 0.51, p < 0.001), but notfor the TL and L curves (p = 0.08 and p = 0.6, respective-ly). Correlations between HI and TI were significant forT curves (r = _ 0.37, p < 0.001), but not for TL and Lcurves (p = 0.07, p = 0.74, respectively). Correlationsbetween TI and frontal Cobb were significant for the 3types of curvature (T : r = 0.76, p < 0.001 ; TL : r = 0.57,p < 0.001 ; L : r = 0.52, p = 0.005). Correlations betweenthe 3 planes are plotted in Figure 4.
The multiple linear regressions showed a relationshipbetween the torsion index and frontal Cobb, the HI andthe type of major curvature (adjusted : R2 = 0.6).
Rib cage deformityThe control group allowed for the definition of thethreshold of high gibbosity (> 9°) and VSPI (> 6.3%)according to the 95th percentile. As for the novel rib cagedeformity classification, 44% (n = 88) of AIS had bothnormal or subnormal gibbosity and VSPI and were clas-sified as group I with mild rib cage deformity ; 24% (n = 48) of AIS had high gibbosity and were classified asgroup IIa ; 24% (n = 48) of AIS had high VSPI and wereclassified as group IIb ; the remaining 8% (n = 16) of AIShad both high gibbosity and VSPI and were classified asgroup IIc. In total, 56% (n = 112) of subjects with AISwere classified as group II with severe rib cage deformity.
Subjects in group II had smaller rib cage volumes com-pared to group I and controls (p = 0.008) and higher gib-bosity and VSPI (p < 0.001). Subjects in group IIb showeddecreased thickness and higher VSPI compared to groupsI, IIa & controls (thickness : 135 mm vs. 144 mm vs. 148mm and 144 mm respectively, p = 0.002; VSPI: 7% vs. 5%vs. 5% and 4% respectively, p < 0.001). Rib cage volumewas significantly lower in group IIb compared to group I(4731cm3 vs. 5257cm3, p = 0.01). Additionally, gibbositywas significantly higher in group IIa compared to groupsI, IIb & controls (15° vs. 5° vs. 6° and 4° respectively).
M. KARAM et al. – 3D biomechanics in adolescent idiopathic scoliosis Lebanese Medical Journal 2021 • Vol 69 (2) 113

114 Lebanese Medical Journal 2021 • Volume 69 (2) M. KARAM et al. – 3D biomechanics in adolescent idiopathic scoliosis
N.B
. Sig
nifi
cant
p-v
alue
s in
bol
d.TAB
LEI
MEA
N C
OM
PAR
ISO
NS
OF
3D P
ELVI
C, S
PIN
O-P
ELVI
C, S
CO
LIO
SIS
AND
PO
STU
RAL
PAR
AMET
ERS
BETW
EEN
THO
RAC
IC (T
), TH
OR
ACO
LUM
BAR
(TL
) AN
D L
UM
BAR
(L) C
UR
VES
OF
SUBJ
ECTS
WIT
H A
IS

Subjects in group IIc had higher gibbosity than group IIband higher VSPI than group IIa.
When analyzing subgroups in subjects with severe ribcage deformity (group II), subjects in group IIb withhigh VSPI showed lower kyphosis when compared togroups I, IIa and controls (i.e. T1T12: 21° vs. 36° vs. 33°and 42° respectively, p < 0.001). Subjects in group IIchad a similar sagittal profile to groups IIa and IIb, and amore severe scoliotic deformity in the frontal and hori-zontal planes. Detailed results were presented in Table II.
VSPI was negatively correlated to T1T12 (r = _ 0.47,p < 0.001) in all subjects in group II (Figure 5a). Gibbosi-ty was positively correlated to the frontal Cobb angle (r = 0.54, p < 0.001) & TI (r = 0.41, p < 0.001) in groupsIIa & IIc, but not in group IIb (Figures 5b & 5c).
In subjects in group IIa, vertebral axial rotation andlocal gibbosity increased simultaneously from the prox-imal adjacent units until reaching the apex (Figure 6) ;while the vertebral axial rotation started to decreasewhen descending distally, the local gibbosity continuedto increase. In subjects in group IIb, the vertebral axialrotation had a similar pattern to that in group IIa, butlocal gibbosity remained constant.
Lower limb alterationsDetailed comparisons of acetabular and lower limbparameters between the ES, LS in AIS and controls werepresented in Table III. Acetabular abduction (M & P) wassignificantly higher in the ES group (59.2 ± 6°, 56.6 ± 4°,respectively) when compared to both LS (55.6 ± 6°, 53.9 ± 4°, respectively) and controls (57.5 ± 4°, 55.5 ± 4°,respectively). CEA and acetabular anteversion (M and P)were significantly higher in the LS (32 ± 6°, 20.5 ± 6°,15.9 ± 5°, respectively) group when compared to both
ES (28.7 ± 5°, 19.8 ± 5°, 15.5 ± 4.5°, respectively) andcontrols (29.8 ± 5°, 19.1 ± 4°, 14.8 ± 4°, respectively).The anterior sector angle was significantly lower in bothES (59.1 ± 6°) and LS (59.2 ± 6.5°) groups when com-pared to controls (61 ± 4°). Femoral torsion, NSA, tibialtorsion and valgus/varus did not differ between groups.Both normalized anatomical and functional lengths weresignificantly higher in the ES (0.475±0.02, 0.478±0.02,respectively) while compared to both LS in AIS (0.474±0.02, 0.477 ± 0.02, respectively) and controls (0.471 ±0.01, 0.474 ± 0.01, respectively).
When the CEA was evaluated based on the clinicalranges published by Tannast (Tannast et al., 2015), theES group tended towards dysplasia and the LS groupwas significantly shifted towards overcoverage (Figure7a). Acetabular anteversion and NSA were similar tonormal ranges when assessing the risk of femoro-acetab-ular impingement based on the clinical classificationspublished in the literature (Stem et al., 2006 ; Tönnis &Heinecke, 1999). When the distribution of the ES and LSgroups were compared to controls for both the morpho-logical and positional acetabular abduction, the LS grouptended towards the low class and the ES to the high classof controls (Figure 7b). For the anterior sector angle, bothES and LS groups tended towards the low class of con-trols (Figure 7c). For the acetabular anteversion, both ESand LS groups tended towards the high class of controls(Figure 7d).
CEA was significantly correlated to : age (r = _ 0.20,p = 0.05), T1 tilt (r = _ 0.25, p = 0.01) and PT (r = _ 0.25,p = 0.01). Positional acetabular abduction was signifi-cantly correlated to : T1 tilt (r = 0.23, p = 0.02), T9 tilt (r = 0.25, p = 0.01), SS (r = _ 0.20, p = 0.04) and PT(r = 0.32, p = 0.001) (Figure 5).
M. KARAM et al. – 3D biomechanics in adolescent idiopathic scoliosis Lebanese Medical Journal 2021 • Vol 69 (2) 115
Figure 4. Correlations between scoliotic deformity parameters in the 3 planes in different types of major scoliotic curvatures(T : Thoracic TL: Thoracolumbar L: Lumbar)
a. Axial (torsion index) vs. frontal plane (frontal Cobb angle). b. Sagittal (hypokyphosis index) vs. frontal plane (frontal Cobb angle). c. Sagittal (hypokyphosis index) vs. axial plane (torsion index).

TAB
LEII
ME
AN
CO
MPA
RIS
ON
S O
F S
PIN
O-P
ELV
IC, S
CO
LIO
SIS
AN
D R
IB C
AG
E P
AR
AM
ETE
RS
BE
TWE
EN
CO
NTR
OLS
AN
D
SU
BG
RO
UP
S O
F S
UB
JEC
TS W
ITH
AIS
CLA
SS
IFIE
D A
CC
OR
DIN
G T
O T
HE
SE
VE
RIT
YO
F TH
E R
IB C
AG
E D
EFO
RM
ITY
Tabl
e IIa
116 Lebanese Medical Journal 2021 • Volume 69 (2) M. KARAM et al. – 3D biomechanics in adolescent idiopathic scoliosis
* B
old
: si
gn
ifica
nt
p-va
lue
.

Positional acetabular anteversion was significantlycorrelated to CAM-HA plumb line (r = _ 0.36, p < 0.01),T1 tilt (r = 0.30, p = 0.002), PI (r = 0.41, p < 0.001) andPT (r = 0.45, p < 0.001) (Figure 8). The multivariateanalysis showed that CEA was determined (adjusted R2 = 0.08) by PT (ß = _ 0.08 ; p = 0.003).
Positional acetabular abduction was determined (ad-justed R2 = 0.19) by PT (ß = 0.32 ;p < 0.001) and lateralpelvic obliquity (ß = 0.07 ; p = 0.03). Positional aceta-bular anteversion was determined (adjusted R2 = 0.32) by frontal Cobb angle (ß = 0.18 ; p < 0.001), T1T12 ky-phosis (ß= 0.07 ; p = 0.04) and PT (ß= 0.51, p < 0.001).
DISCUSSION
It is known that subjects with AIS present an alteredskeletal deformity at the level of the scoliotic segment,rib cage, hips and lower limbs. This review aimed todescribe these deformities and to investigate their deter-minants.
At the level of the scoliotic segment, subjects withmajor T curves presented with more severe frontal, sagit-tal and axial deformities compared to TL and L curvesand showed moderate to strong correlations between thedeformities in the three planes.
At the level of the rib cage, four groups of rib cagedeformity patterns were identified in subjects with AIS :group I with mild rib cage deformity ; group II withsevere rib cage deformity, further stratified into groupIIa with high gibbosity, group IIb with high volumetricspinal penetration index, and group IIc with both highgibbosity and VSPI.
At the level of hip and lower limbs, subjects with AIShad a more abducted acetabulum at the lowered side,more anteverted acetabulum and a lack of anterior cov-erage of both acetabula. These alterations were stronglyrelated to pelvic tilt.
The 3D scoliotic segmentT1T12 kyphosis was lower in T curves in accordancewith previous studies (Newton, Osborn, Bastrom, Doan,& Reighard, 2019).
Subjects with major T curves presented high TI,UIAR and LIAR when compared to TL and L curves.This finding indicates that subjects with major T curvesrepresent the major deformity in the axial plane through-out the scoliotic segment when compared to TL and L curves.
A previous study including only mild scoliosis (Cobb< 25°) showed that subjects with major T curves pre-sented the same Cobb angle, with the same UIAR andLIAR compared to major TL and L curves but higher TI(Courvoisier, Drevelle, et al., 2013).
M. KARAM et al. – 3D biomechanics in adolescent idiopathic scoliosis Lebanese Medical Journal 2021 • Vol 69 (2) 117
Tabl
e IIb

118 Lebanese Medical Journal 2021 • Volume 69 (2) M. KARAM et al. – 3D biomechanics in adolescent idiopathic scoliosis
TAB
LEA
UIII
BETW
EEN
-GR
OU
PC
OM
PAR
ISO
NS
OF
3D A
CET
ABU
LAR
AN
D L
OW
ER L
IMBS
PAR
AMET
ERS
IN C
ON
TRO
LS, E
LEVA
TED
SID
E (E
S) &
LOW
ERED
SID
E (L
S) O
F SU
BJEC
TS W
ITH
AD
OLE
SCEN
TID
IOPA
THIC
SC
OLI
OSI
S.

M. KARAM et al. – 3D biomechanics in adolescent idiopathic scoliosis Lebanese Medical Journal 2021 • Vol 69 (2) 119
Figure 5. Correlation between rib cage deformity and spino-pelvic parameters in Group II
Figure 6. Local gibbosity and vertebral axial rotation at vertebral levels of the scoliotic segment.AV indicates apical vertebra.

120 Lebanese Medical Journal 2021 • Volume 69 (2) M. KARAM et al. – 3D biomechanics in adolescent idiopathic scoliosis
Figure 7. Distribution of (a) center edge angle according to the criteria’s as defined by Tannast et al. 2005.
In addition to the distribution of (b) acetabular abduction angle, (c) anterior sector angle,
(d) acetabular anteversion according to the normative classes
(low, intermediate and high) as defined by the control group. *p value < 0.05.
Figure 8. Correlations between center edge angle, acetabular abduction, acetabular anteversion and pelvic tilt

The current study, having included subjects withmore severe scoliosis (Cobb ≥ 20°), showed that majorT curves presented higher Cobb, TI, UIAR and LIARwhen compared to TL and L curves. It might be possiblethat AIS patients with major lumbar curves presentedwith minimal axial and sagittal deformity because oftheir low Cobb angle.
The hypokyphosis/lordosis index was found to be com-parable between the three major and minor types of cur-vature. This shows that the location of the scoliotic de-formity creates the same amount of sagittal deformity(loss of lordosis/kyphosis), independently of the type ofcurvature.
Several studies attempted to evaluate the relationshipbetween the three planes of the scoliotic deformity (Huet al., 2016 ; Morrison, Chan, Hill, Parent, & Lou, 2015 ;Ni et al., 2010 ; Pizones, Zúñiga, Sánchez-Mariscal &Izquierdo, 2016), but were limited by the use of 2D fron-tal and lateral radiographs with a less accurate evaluationof the axial plane. A recent study, using bi-planar X-rayswith subsequent 3D reconstructions, found significantcorrelations between the three planes while consideringonly subjects with major thoracic scoliosis (Sullivan,Reighard, Osborn, Parvaresh & Newton, 2017). The cur-
rent study, including all three types of major and minorcurves, showed that only subjects with T scoliosis pre-sented significant correlations between the three planes,with TL and L groups only presenting correlations be-tween the frontal and axial planes. This could be due tothe fact that the thoracolumbar and lumbar segments ofthe spine behave differently than the thoracic segment,due to the absence of the rib cage, and to the higher mo-bility of the thoracolumbar and lumbar segments.
The present study showed that 60% of the axial defor-mity was determined by the frontal deformity in AIS.Thus, 40% of the axial deformity remained uneluci-dated, highlighting the importance of evaluating the tor-sional deformity in addition to the frontal deformitywhen assessing the severity of scoliosis in patients withAIS. The same reasoning applies to the sagittal deformi-ty which highlights the importance of assessing all threeplanes in AIS.
Additionally, the axial deformity was highly correlat-ed to both the frontal and sagittal deformities in majorcurves, and to the type of curvature. Since 40% of theaxial deformity remained unexplained, this may suggestthat any surgery correcting both frontal and sagittalplanes might not automatically fully correct the axial
M. KARAM et al. – 3D biomechanics in adolescent idiopathic scoliosis Lebanese Medical Journal 2021 • Vol 69 (2) 121
Figure 9. Examples of AIS subjects with high gibbosity (group IIa) and high VSPI (group IIb)
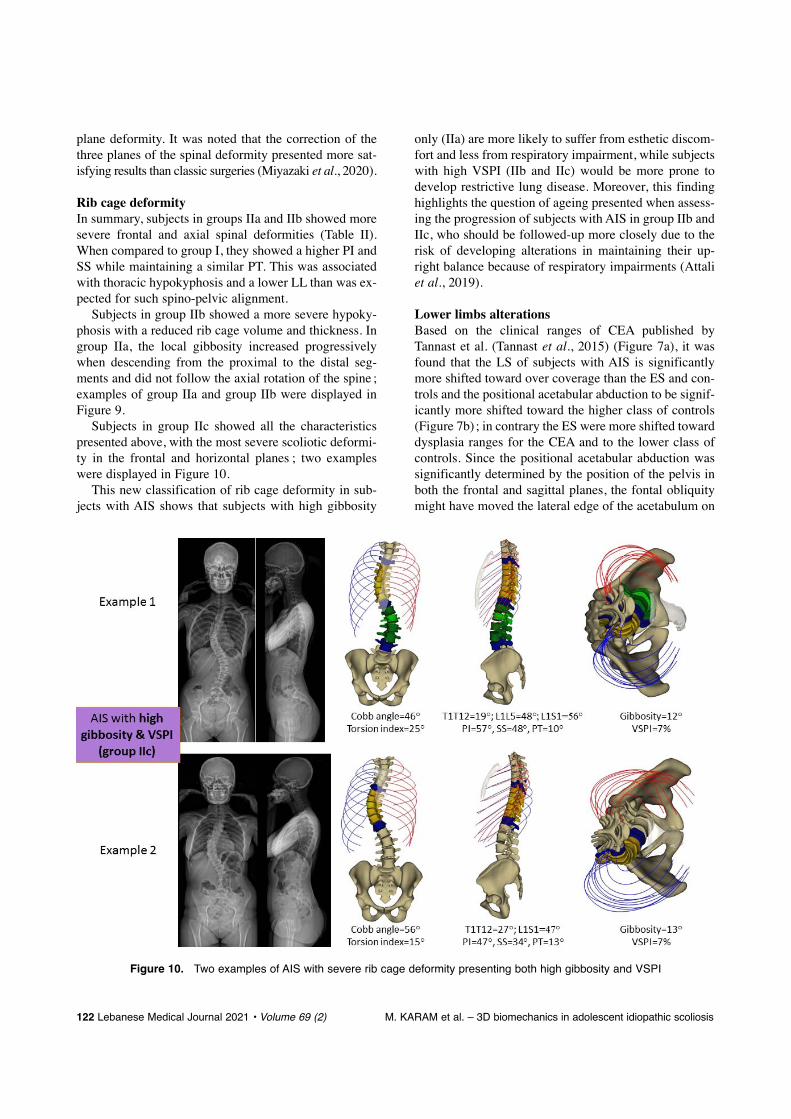
plane deformity. It was noted that the correction of thethree planes of the spinal deformity presented more sat-isfying results than classic surgeries (Miyazaki et al., 2020).
Rib cage deformityIn summary, subjects in groups IIa and IIb showed moresevere frontal and axial spinal deformities (Table II).When compared to group I, they showed a higher PI andSS while maintaining a similar PT. This was associatedwith thoracic hypokyphosis and a lower LL than was ex-pected for such spino-pelvic alignment.
Subjects in group IIb showed a more severe hypoky-phosis with a reduced rib cage volume and thickness. Ingroup IIa, the local gibbosity increased progressivelywhen descending from the proximal to the distal seg-ments and did not follow the axial rotation of the spine ;examples of group IIa and group IIb were displayed inFigure 9.
Subjects in group IIc showed all the characteristicspresented above, with the most severe scoliotic deformi-ty in the frontal and horizontal planes ; two exampleswere displayed in Figure 10.
This new classification of rib cage deformity in sub-jects with AIS shows that subjects with high gibbosity
only (IIa) are more likely to suffer from esthetic discom-fort and less from respiratory impairment, while subjectswith high VSPI (IIb and IIc) would be more prone todevelop restrictive lung disease. Moreover, this findinghighlights the question of ageing presented when assess-ing the progression of subjects with AIS in group IIb andIIc, who should be followed-up more closely due to therisk of developing alterations in maintaining their up-right balance because of respiratory impairments (Attaliet al., 2019).
Lower limbs alterations Based on the clinical ranges of CEA published byTannast et al. (Tannast et al., 2015) (Figure 7a), it wasfound that the LS of subjects with AIS is significantlymore shifted toward over coverage than the ES and con-trols and the positional acetabular abduction to be signif-icantly more shifted toward the higher class of controls(Figure 7b) ; in contrary the ES were more shifted towarddysplasia ranges for the CEA and to the lower class ofcontrols. Since the positional acetabular abduction wassignificantly determined by the position of the pelvis inboth the frontal and sagittal planes, the fontal obliquitymight have moved the lateral edge of the acetabulum on
122 Lebanese Medical Journal 2021 • Volume 69 (2) M. KARAM et al. – 3D biomechanics in adolescent idiopathic scoliosis
Figure 10. Two examples of AIS with severe rib cage deformity presenting both high gibbosity and VSPI

the LS externally, which might lead to a lower acetab-ular abduction, and consequently to a higher externalcoverage of the femoral head. The opposite effect takesplace on the ES, showing more subjects having undercoverage compared to controls.
When analyzing the anterior sector angle, the ES andLS hips were shifted toward the low class in controls(Figure 7c), thus indicating a high prevalence of de-creased anterior femoral head coverage in subjects withAIS in both hips (ES and LS). Moreover, positionalacetabular anteversion in both sides of AIS pelvis wassignificantly shifted toward the high class of controls(Figure 7d). This increase in acetabular anteversion wasalso present morphologically. Both the increase of ace-tabular anteversion and the decrease of the anterior sec-tor angle show that subjects with AIS have a more ex-posed femoral head anteriorly on both the ES and LSthat could predispose them to hip dysplasia.
Moreover, acetabular anteversion and acetabular ab-duction were both positionally and morphologically sig-nificantly different between groups (Table III), thismight show that subjects with AIS have already morpho-logical alterations of the acetabula in addition to the po-sitional impact of the spinal deformity on the acetabula.
The alterations of the CEA, acetabular abduction andanteversion were found to be correlated (Figure 8) andmostly determined by PT (ß = 0.08, ß = 0.32 and ß = 0.51respectively) showing that the alteration of the positionof the pelvis in the sagittal plane have a major impact onthe acetabular coverage over the femoral head as shownin a previous study (Henebry & Gaskill, 2013).
Surgical spinal realignment of subjects with adult spi-nal deformity showed that improving the sagittal align-ment by increasing the lumbar lordosis had consequent-ly decreased the pelvic tilt and acetabular anteversion(Buckland et al., 2015). In this study, the acetabular an-teversion, abduction and CEA were correlated and deter-mined by the pelvic tilt ; this might highlight the impor-tance of the continuous monitoring of the sagittal align-ment of subjects with AIS since they might be at risk ofdeveloping acetabular alteration in case they did not reachthe proper sagittal alignment.
In conclusion, this three-dimensional approach ofsubjects with AIS highlighted the importance of not rely-ing solely on the deformity in the frontal plane but toassess and follow the scoliotic deformity in the threeplanes :
1) At the level of the horizontal plane : the deformitycannot be explained by the frontal and sagittal ones andshould be considered when assessing the scoliotic spine. Inaddition, we have shown that the progression of the hori-zontal deformity may worsen the gibbosity in the rib cage.
2) At the level of the sagittal plane : a reduction in tho-racic kyphosis may lead to an increase in the VSPI andconsequently induce an alteration of the respiratoryfunctions, hence the interest of modifying the therapeu-tic ap-proach in subjects with a high VSPI. Likewise, anincrease in the pelvic tilt risks creating dysplasia on thehigh side and excess coverage of the hip on the loweredside.
REFERENCES
Anda S, Svenningsen S, Dale LG & Benum P. (1986). The ace-tab-ular sector angle of the adult hip determined by computedtomography. Acta Radiologica Diagnosis, 27 (4), 443-447.
Anda S, Svenningsen S, Grontvedt T & Benum P. (1990).Pelvic inclination and spatial orientation of the acetabu-lum. A radiographic, computed tomographic and clinicalinvestigation. Acta Radiologica (Stockholm, Sweden,1987), 31 (4), 389-394.
Assi A, Chaibi Y, Presedo A, Dubousset J, Ghanem I & Skalli W.(2013). Three-dimensional reconstructions for asympto-matic and cerebral palsy children’s lower limbs using abiplanar X-ray system: A feasibility study. Eur J Radiol.82 (12), 2359-64.https://doi.org/10.1016/j.ejrad.2013.07.006
Assi A, Karam M, Skalli W & Vergari C. (2021). PRIMARYRESEARCH. A novel classification of 3D rib cage defor-mity in subjects with adolescent idiopathic scoliosis, 0 (0), 1-11.
Assi A, Karam M, Skalli W, Vergari C, Bakouny Z, Otayek J,… Ghanme I. (2018). The 3D deformity in adolescentidiopathic scoliosis depends on the type of curvature.
Assi A, Presedo A, Baudoin A, Mitton D, Ghanem I & Skalli W.(2012). Specific 3D reconstruction for children lowerlimbs using a low dose biplanar X-ray system. Reprodu-cibility of clinical parameters for cerebral palsy patients.Computer Methods in Biomechanics and BiomedicalEngineering 10 (Suppl. 1).https://doi.org/10.1080/10255840701479065
Attali V, Clavel L, Rouch P, Rivals I, Rémy-Néris S, Skalli W,… Similowski T. (2019). Compensation of respiratory-related postural perturbation is achieved by maintenanceof head-to-pelvis alignment in healthy humans. Frontiersin Physiology 10 (APR), 1-10.https://doi.org/10.3389/fphys.2019.00441
Aubert B, Vergari C, Ilharreborde B, Courvoisier A, Skalli W,Ilharreborde B, … Courvoisier A. (2016). 3D reconstruc-tion of rib cage geometry from biplanar radiographsusing a statistical parametric model approach. ComputerMethods in Biomechanics and Biomedical Engineering:Imaging & Visualization 4 (5), 281-295.https://doi.org/10.1080/21681163.2014.913990
Bouloussa H, Pietton R, Vergari C, Haen TX, Skalli W &Vialle R. (2019). Biplanar stereoradiography predictspulmonary function tests in adolescent idiopathic sco-liosis: a cross-sectional study. European Spine Journal 9 (123456789), 1962-1969.https://doi.org/10.1007/s00586-019-05940-3
Buckland AJ, Vigdorchik J, Schwab FJ, Errico TJ, Lafage R,Ames C, … Lafage V. (2015). Acetabular anteversionchanges due to spinal deformity correction: Bridging the
M. KARAM et al. – 3D biomechanics in adolescent idiopathic scoliosis Lebanese Medical Journal 2021 • Vol 69 (2) 123

gap between hip and spine surgeons. The Journal of Boneand Joint Surgery. American Volume 97 (23), 1913-20.https://doi.org/10.2106/JBJS.O.00276
Chaibi Y, Cresson T, Aubert B, Hausselle J, Neyret P, Hauger O,… Skalli W. (2012). Fast 3D reconstruction of the lowerlimb using a parametric model and statistical inferencesand clinical measurements calculation from biplanar X-rays. Computer Methods in Biomechanics and Biomedi-cal Engineering 15 (5), 457-466.https://doi.org/10.1080/10255842.2010.540758
Courvoisier A, Drevelle X, Dubousset J & Skalli W. (2013).Transverse plane 3D analysis of mild scoliosis. EuropeanSpine Journal 22 (11), 2427-2432.https://doi.org/10.1007/s00586-013-2862-x
Courvoisier A, Ilharreborde B, Constantinou B, Aubert B,Vialle R & Skalli W. (2013). Evaluation of a three-di-mensional reconstruction method of the rib cage of mildscoliotic patients. Spine Deformity 1 (5), 321-327.https://doi.org/10.1016/j.jspd.2013.07.007
Dreimann M, Hoffmann M, Kossow K, Hitzl W, Meier O &Koller H. (2014). Scoliosis and chest cage deformitymeasures predicting impairments in pulmonary function:A cross-sectional study of 492 patients with scoliosis toimprove the early identification of patients at risk. Spine39 (24), 2024-2033.https://doi.org/10.1097/BRS.0000000000000601
Dubousset J. (1990). [CD instrumentation in pelvic tilt]. DerOrthopade 19 (5), 300-308.
Dubousset J. (2011). Reflections of an orthopaedic surgeon onpatient care and research into the condition of scoliosis.Journal of Pediatric Orthopaedics 31 (1 Suppl.), 1-8. https://doi.org/10.1097/BPO.0b013e3181f73beb
Dubousset J & Cotrel Y. (1991). Application technique of Cotrel-Dubousset instrumentation for scoliosis deformities. Clini-cal Orthopaedics and Related Research (264), 103-10.http://www.ncbi.nlm.nih.gov/pubmed/1997225
Dubousset J, Wicart P, Pomero V, Barois A & Estournet B.(2003). Spinal penetration index: New three-dimension-al quantified reference for lordoscoliosis and other spinaldeformities. Journal of Orthopaedic Science 8 (1), 41-49.https://doi.org/10.1007/s007760300007
Faro FD, Marks MC, Pawelek J & Newton PO. (2004). Evalu-ation of a functional position for lateral radiograph ac-quisition in adolescent idiopathic scoliosis. Spine 29 (20),2284-2289.https://doi.org/00007632-200410150-00017
Ghostine B, Sauret C, Assi A, Bakouny Z, Khalil N, Skalli W& Ghanem I. (2017). Influence of patient axial malposi-tioning on the trueness and precision of pelvic parame-ters obtained from 3D reconstructions based on biplanarradiographs. European Radiology 27 (3), 1295-1302.https://doi.org/10.1007/s00330-016-4452-x
Henebry A & Gaskill T. (2013). The effect of pelvic tilt on radi-ographic markers of acetabular coverage. American Jour-nal of Sports Medicine 41 (11), 2599-2603.https://doi.org/10.1177/0363546513500632
Hu P, Yu M, Liu X, Zhu B, Liu X & Liu Z. (2016). Analysis ofthe relationship between coronal and sagittal deformities inadolescent idiopathic scoliosis. European Spine Journal 25 (2), 409-416. https://doi.org/10.1007/s00586-015-3986-y
Johnston CE, Stephens Richards B, Sucato DJ, Bridwell KH,Lenke LG & Erickson M. (2011). Correlation of pre-
operative deformity magnitude and pulmonary functiontests in adolescent idiopathic scoliosis. Spine 36 (14),1096-1102.https://doi.org/10.1097/BRS.0b013e3181f8c931
Karam M, Bizdikian AJ, Khalil N, Bakouny Z, Obeid I,Ghanimeh J, … Assi, A. (2020). Alterations of 3D acetab-ular and lower limb parameters in adolescent idiopathicscoliosis. European Spine Journal 29 (8), 2010-2017.https://doi.org/10.1007/s00586-020-06397-5
Konieczny MR, Senyurt H & Krauspe R. (2013). Epidemiolo-gy of adolescent idiopathic scoliosis. Journal of Children’sOrthopaedics 7 (1), 3-9.https://doi.org/10.1007/s11832-012-0457-4
Lazennec JY, Charlot N, Gorin M, Roger B, Arafati N, Bissery A& Saillant G. (2004). Hip-spine relationship: A radio-ana-tomical study for optimization in acetabular cup position-ing. Surgical and Radiologic Anatomy 26 (2), 136-144. https://doi.org/10.1007/s00276-003-0195-x
Lenke LG, Betz RR, Harms J, Bridwell KH, Clements DH,Lowe TG & Blanke KM. (2001). Adolescent idiopathicscoliosis: a new classification to determine extent of spi-nal arthrodesis. The Journal of Bone and Joint Surgery.American Volume 83-A (8), 1169-81.https://doi.org/10.1097/00007632-200101010-00009
Mac-Thiong JM, Labelle H, Charlebois M, Huot MP & de Guise JA. (2003). Sagittal plane analysis of the spineand pelvis in adolescent idiopathic scoliosis according tothe coronal curve type. Spine 28 (13), 1404-9.https://doi.org/10.1097/01.BRS.0000067118.60199.D1
Miyazaki M, Ishihara T, Abe T, Kanezaki S, Notani N, Kataoka M& Tsumura H. (2020). Analysis of reciprocal changes inupper cervical profiles after posterior spinal fusion withthe simultaneous double rod rotation technique for ado-lescent idiopathic scoliosis. Orthopaedics and Trauma-tology: Surgery and Research 106 (7), 1275-1279.https://doi.org/10.1016/j.otsr.2020.03.017
Morrison DG, Chan A, Hill D, Parent EC & Lou EHM. (2015).Correlation between Cobb angle, spinous process angle(SPA) and apical vertebrae rotation (AVR) on postero-anterior radiographs in adolescent idiopathic scoliosis(AIS). European Spine Journal 24 (2), 306-312.https://doi.org/10.1007/s00586-014-3684-1
Newton PO, Osborn EJ, Bastrom TP, Doan JD & Reighard FG.(2019). The 3D sagittal profile of thoracic versus lumbarmajor curves in adolescent idiopathic scoliosis. SpineDeformity 7 (1), 60-65.https://doi.org/10.1016/J.JSPD.2018.05.003
Ni H, Zhu X, He S, Yang C, Wang C, Zhao Y, … Li M. (2010).An increased kyphosis of the thoracolumbar junction iscorrelated to more axial vertebral rotation in thoracolum-bar/lumbar adolescent idiopathic scoliosis. Spine (PhilaPa 1976) 35 (23), E1334-E1338.https://doi.org/10.1097/BRS.0b013e3181e5370b
Pasha S, Aubin CE, Sangole AP, Labelle H, Parent S & Mac-Thiong JM. (2014). Three-dimensional spinopelvic rela-tive alignment in adolescent idiopathic scoliosis. Spine39 (7), 564-70https://doi.org/10.1097/BRS.0000000000000193
Pietton R, Bouloussa H, Vergari C, Skalli W & Vialle R.(2020). Rib cage measurement reproducibility using bipla-nar stereoradiographic 3D reconstructions in adolescentidiopathic scoliosis. Journal of Pediatric Orthopaedics 40 (1), 36-41.
124 Lebanese Medical Journal 2021 • Volume 69 (2) M. KARAM et al. – 3D biomechanics in adolescent idiopathic scoliosis

https://doi.org/10.1097/BPO.0000000000001095Pizones J, Zúñiga L, Sánchez-Mariscal F & Izquierdo E.
(2016). Relationship between the different torsion-relatedthoracic deformity parameters of adolescent idiopathicscoliosis. European Journal of Orthopaedic Surgery andTraumatology. https://doi.org/10.1007/s00590-016-1762-2
Rampal V, Rohan PY, Assi A, Ghanem I, Rosello O, Simon AL… Wicart P. (2018). Lower-limb lengths and angles inchildren older than six years: Reliability and referencevalues by EOS® stereoradiography. Orthopaedics &Traumatology: Surgery & Research 104 (3), 389-395.https://doi.org/10.1016/j.otsr.2017.10.007
Skalli W, Vergari C, Ebermeyer E, Courtois I, Drevelle X,Kohler R … Dubousset, J. (2017). Early detection of pro-gressive adolescent idiopathic scoliosis: A severity in-dex. Spine 42 (11), 823-830.https://doi.org/10.1097/BRS.0000000000001961
Stem ESE., O’Connor MIM, Kransdorf MJM, Crook J & StemES, O’Connor MI, Kransdorf MJ, C. J. (2006). Computedtomography analysis of acetabular anteversion andabduction. Skeletal Radiology 35 (6), 385-389.
https://doi.org/10.1007/s00256-006-0086-4Sullivan TB, Reighard FG, Osborn EJ, Parvaresh KC & Newton
PO (2017). Thoracic idiopathic scoliosis severity is high-ly correlated with 3D measures of thoracic kyphosis. TheJournal of Bone and Joint Surgery. American Volume 99(11), e54.https://doi.org/10.2106/JBJS.16.01324
Tannast M, Hanke MS, Zheng G, Steppacher SD & SiebenrockKA (2015). What are the radiographic reference valuesfor acetabular under- and overcoverage? Clinical Ortho-paedics and Related Research.https://doi.org/10.1007/s11999-014-4038-3
Tönnis D & Heinecke A. (1999). Acetabular and femoral an-teversion: relationship with osteoarthritis of the hip. TheJournal of Bone and Joint Surgery. American 81 (12),1747-1770.https://doi.org/10.2106/JBJS.L.00710
Yaszay B, Bastrom TP, Bartley CE, Parent S & Newton PO.(2017). The effects of the three-dimensional deformity ofadolescent idiopathic scoliosis on pulmonary function.European Spine Journal 26 (6), 1658-1664.https://doi.org/10.1007/s00586-016-4694-y
M. KARAM et al. – 3D biomechanics in adolescent idiopathic scoliosis Lebanese Medical Journal 2021 • Vol 69 (2) 125

INTRODUCTION
Les scolioses infantiles (SI) et juvéniles (SJ) sont despathologies incontournables et délicates à prendre encharge en orthopédie pédiatrique. Le traitement doit êtreprécoce, et doit idéalement permettre de contrôler la pro-gression de la déformation tout en respectant la crois-sance de la colonne vertébrale et le développement de lacage thoracique.
Les SI et les SJ diffèrent de la scoliose idiopathiquede l’adolescent car l’âge d’apparition est plus précoce(SI : < 5 ans ; SJ : < 10 ans), le risque d’aggravation estplus important et la fréquence d’anomalies médullairesassociées est plus élevée [1]. Les modifications induitespar une scoliose à début précoce sur la colonne verté-brale et la cage thoracique d’un organisme en croissancepeuvent être dramatiques et, dans certains cas graves,entraîner la mort du patient.
Une colonne vertébrale qui ne grandit pas normale-ment affecte le potentiel de croissance de toute la cagethoracique, entraîne une réduction de la taille assise, untronc sous-développé, déformé et disproportionné, uneincapacité à assurer une respiration normale, un faiblepoids et des dysfonctionnements cardiaques. La pré-sence simultanée de ces signes caractérise le syndromed’insuffisance thoracique (SIT) [2].
Le traitement idéal des SI et des SJ n'a pas encore étéidentifié. Une arthrodèse précoce de la colonne verté-brale n’est pas une solution satisfaisante même si ellecorrige, au moins en partie et dans l’immédiat, la défor-mation scoliotique. En effet, une arthrodèse vertébraleprécoce n’est pas en mesure de corriger les anomaliesmorphologiques de la cage thoracique, de permettre ledéveloppement normal du parenchyme pulmonaire et depréserver la fonction cardiaque [3].
La technique de moulage d’un corset plâtré par élon-gation, dérotation et flexion (EDF) a été décrite pour lapremière fois par les chirurgiens français Yves Cotrel etGeorges Morel en 1963 [4]. Il s’agit d’un corset thoraco-lombaire sur mesure qui agit comme une force positivecapable de corriger la déformation scoliotique dans lestrois plans de l’espace, de guider la croissance de la co-lonne vertébrale, de contrôler, au moins en partie, l’évo-
126 Journal Médical Libanais 2021 • Volume 69 (2)
PPAAEEDDIIAATTRRIICC OORRTTHHOOPPAAEEDDIICCSSTRAITEMENT DES SCOLIOSES INFANTILES ET JUVÉNILES PAR CORSETS PLÂTRÉSÉTAT DES LIEUX, TECHNIQUES ET PERSPECTIVEShttp://www.lebanesemedicaljournal.org/articles/69-2/pedsortho9pdf
Faustine MONGET1, Eric NECTOUX1-2, Damien FRON1, Federico CANAVESE1-2
RÉSUMÉ • Introduction : Les scolioses infantiles et juvénilesreprésentent, parmi les déformations rachidiennes, un défi pourles chirurgiens orthopédistes pédiatriques. Si le traitement parcorsets plâtrés est actuellement considéré comme la méthodede référence dans les scolioses infantiles (SI) idiopathiques, sonefficacité dans les scolioses juvéniles (SJ) et congénitales (SC)est beaucoup plus discutée, et moins étudiée. Le but de cet ar-ticle est de faire l’état des lieux via une revue de la littérature desrésultats du traitement par corsets plâtrés chez les patients avecune SI, SJ ou SC en abordant les complications décrites au seinde ces études. Méthodes: Nous avons effectué la rechercheau sein des bases de données PUBMED Medline et EMBASEallant de Janvier 1955 à Janvier 2021, avec les termes de re-cherche suivants : • congenital scoliosis/scoliose congénitale •early onset scoliosis/scoliose à début précoce • serial casting/corsets successifs • EDF casting/corset EDF • Risser frame/cadre de Risser • Cotrel frame/cadre de Cotrel • et children/enfants ; les limites suivantes ont été utilisées : • langue an-glaise • langue française et • tous les enfants de 0 à 10 ans.Les résultats de chaque article ont été compilés au sein d’untableau comparatif détaillant pour chacun, la date de publication,les auteurs, le type de scoliose étudié (SI et SJ, idiopathique ousyndromique, et SC), l’âge moyen des patients au début dutraitement, le taux de correction (angle de Cobb) et le délai entrela fin du traitement et l’éventuelle prise en charge chirurgicale.Les complications retrouvées dans ces études ont égalementété répertoriées, comptabilisées et classées. Résultats: Un to-tal de 32 articles a été analysé. La réalisation de corsets plâtréssuccessifs est une alternative efficace à la chirurgie chez lespatients atteints de scoliose à début précoce. Sa réalisation est systématiquement associée à une diminution de l’angle deCobb moyen chez les patients atteints de SI idiopathique ou non.Son efficacité dans les SJ et SC est plus discutée mais elle per-met de retarder la prise en charge chirurgicale au prix de peu de complications, majoritairement réversibles et peu sévères.Conclusion: Aucune étude au sein de ce travail ne fait état decontre-indication ou de complications sévères impliquées par laréalisation de corsets plâtrés dans les scolioses à début précoce.Le traitement par corsets plâtrés successifs permet de retarder letraitement chirurgical dont le taux de complications est plus élevé.En règle générale, l’efficacité du traitement par corset est d’autantplus importante que l’enfant est jeune (< 2 ans), que le traitementest mis en place tôt et sur de faibles courbures initiales.
Mots-clés: scoliose infantile; scoliose juvénile; scoliose à débutprécoce; corset EDF; corsets successifs
Monget F, Nectoux E, Fron D, Canavese F. Traitement des sco-lioses infantiles et juvéniles par corsets plâtrés : état des lieux,techniques et perspectives. J Med Liban 2021; 69 (2) :126-136.
1 Service de chirurgie orthopédique pédiatrique, Hôpital Jeanne de Flandre, Avenue Eugène Avinée. 59037 Lille, France.2 Université de Lille, Faculté de Médecine Henri Warembourg, F-59045 Lille Cedex, France
*Auteur correspondant : Pr. Federico Canavese e-mail: [email protected]
lution de la déformation et d’accompagner le développe-ment de l’enfant pour lui permettre de mieux tolérerd’autres formes de traitement.
Plusieurs techniques de réalisation de corsets plâtrésont été décrites et sont aujourd’hui disponibles [5].Certaines techniques impliquent l’utilisation de cadresspéciaux (cadre de Cotrel, cadre de Risser ou cadre deMehta) permettant de soutenir la tête, la nuque et lesmembres inférieurs de l’enfant, tout en laissant le torselibre. D’autres techniques ne nécessitent pas l’utilisationd’un cadre spécifique, et sont donc potentiellement plusaccessibles à toutes les équipes.
Cette revue de la littérature vise à effectuer un état deslieux du traitement par corsets plâtrés des SI et SJ idio-pathiques et syndromiques, et des SC en détaillant lesrésultats et les complications induites par ce type de trai-tement en fonction de l’étiologie de la déformation sco-liotique, idiopathique, syndromique ou congénitale.
MATÉRIEL ET MÉTHODE
Nous avons effectué notre recherche au sein des basesde données PUBMED Medline et EMBASE en couvrantla période allant du mois de janvier 1955 au mois de jan-vier 2021, avec les termes de recherche suivants : • con-genital scoliosis/scoliose congénitale • early onset sco-liosis/scoliose à début précoce • serial casting/corsetssuccessifs • EDF casting/corset EDF • Risser frame/cadre de Risser • Cotrel frame/cadre de Cotrel et • children/enfants.
Les résultats de chaque article ont ensuite été com-pilés au sein d’un tableau comparatif détaillant pour cha-cun d’entre eux, la date de publication, les auteurs, letype de scoliose étudié (SI et SJ idiopathique ou syn-dromique, et SC), l’âge moyen des patients à la mise enplace du traitement, le taux de correction (angle de Cobb)et le délai entre la fin du traitement par corsets plâtrés etl’éventuelle prise en charge chirurgicale. Les complica-tions retrouvées dans ces études ont également été réper-toriées, comptabilisées et classées (Tableaux I-III).
Un total de 32 articles a été analysé par deux auteursde l’article (FM et FC).
TECHNIQUES
Corset plâtré avec cadre EDFEDF signifie élongation, dérotation et flexion. Il s’agit
d’une méthode de réduction orthopédique de la scoliosegrâce à l’utilisation d’un cadre spécifique (cadre de Co-trel) qui permet de tracter la patient (correction axiale),de déroter la déformation (correction dans le plan trans-versal), d’appliquer un plâtre thoraco-lombo-sacré et decorriger ultérieurement la déformation scoliotique par
une compression latérale (correction dans le plan frontal).Entre 1975 et 2000 Min H. Mehta a modifié la tech-
nique EDF développée par Yves Cotrel et Georges Morelet a introduit le concept de corsets plâtrés successifs(serial casting). Avec le protocole de Min H. Metha(Mehta Growth Guidance Casting Protocol), les plâtresEDF sont changés toutes les 8 à 12 semaines sous anes-thésie générale [6].
Le patient est soutenu par deux barres métalliques ho-rizontales (l’une sous les épaules et l’autre soutenant lebassin). Une traction axiale entre le menton et l’occiputet les crêtes iliaques est exercée de façon progressive.Dans le même temps, une bande entourant le patient ducôté convexe de la courbe scoliotique est mise en tensionpermettant de déroter la déformation.
Dans le cas d’une double courbe, une deuxième bandepeut être appliquée dans le sens et le côté opposé, au ni-veau de cette deuxième convexité.
Ensuite, les deux barres de support sont enlevées et leplâtre est appliqué à partir des crêtes iliaques en direc-tion disto-proximale. Alors que le plâtre est encore mal-léable, une pression latérale d’une main est appliquée ducôté de la convexité et une contre-pression est appliquéedu côté de la concavité et maintenue jusqu’à ce que le plâtre durcisse. Le plâtre est ensuite renforcé parquelques couches de résine et une fenêtre thoraco-abdominale est ouverte de manière à obtenir une décom-pression de l’abdomen antérieur (estomac et intestins) etune meilleure expansion de la cage thoracique (Figure 1).
Corset plâtré sans cadre EDFEn 2002, Richard Schwend [7] et l’équipe médicale
du projet Perfect World ont proposé l’utilisation d’unebarre en métal de 40 x 2.5 cm qui permet de maintenirl’enfant entre deux supports, et d’avoir accès à la cagethoracique dans sa totalité. La barre est suffisammentfine pour pouvoir être glissée sous le jersey et suffisam-ment rigide pour pouvoir soutenir les enfants jusqu’à en-viron 30 kg de poids. Un lubrifiant était parfois appliquésur la barre afin qu’elle puisse être retirée facilement unefois le plâtre terminé.
Les deux extrémités de la barre métallique peuventêtre placées entre deux supports posés sur la table d’opé-ration ; en alternative, une extrémité de la barre peut êtreposée sur la table d’opération (perpendiculaire à celle-ci)et l’autre extrémité sur un support de la même hauteur.Indépendamment de la configuration choisie, la tête estcontrôlée par les mains de l’anesthésiste et posée sur latable d’opération ou sur le support, la colonne repose sur la barre et un membre du personnel tient les deuxmembres inférieurs et exerce une traction axiale. La poi-trine et l’abdomen de l’enfant sont protégés par un t-shirtde jersey et par de l’ouate.
F. MONGET et al. – Corsets plâtrés et scoliose Journal Médical Libanais 2021 • Volume 69 (2) 127

Le plâtre est ensuite appliqué. La traction axiale estexercée par l’aide qui tracte les membres inférieurs del’enfant tandis que les manoeuvres de dérotation et decorrection sur le plan frontal sont effectuées par le chi-rurgien.
Cette technique permet la prise en charge des SI et desSJ en respectant les principes correctifs d’élongation, dedérotation et de flexion sans besoin d’utiliser un cadrespécifique (Figure 2).
RÉSULTATS
Trente-deux articles, publiés entre janvier 1955 et jan-vier 2021 ont été répertoriés et analysés ; 29 articles surles 32 (90%) ont été publiés après l’étude de Min H.Mehta de 2005 [6]. Au total 27 articles sur 32 étaientanalysables (84,4%) car cinq articles ne donnaient pas dechiffres utilisables pour notre revue de la littérature.
Les patients analysés par ces articles sont souvent hé-
térogènes ; en effet, 24 articles sur 27 analysent des pa-tients avec SI idiopathiques et non idiopathiques, 3 ar-ticles (37 patients) étudient des patients avec SJ idiopa-thiques (2 études et 29 patients) et non idiopathiques (1 étude et 8 patients) et 5 études concernent les patientsavec SC (77 patients) ; les SI idiopathiques sont de loinles plus étudiées (1043 sur 1157 patients).
Scoliose infantile idiopathiqueLa SI est généralement thoracique gauche et plus fré-
quente chez les garçons. En règle générale elle est diag-nostiquée avant l’âge de 3 ans.
Mehta a décrit la différence de l’angle costo-vertébral(rib-vertebral angle difference ou RVAD) et a rapportéqu’un RVAD > 20° et le chevauchement de la côte con-vexe sur le corps vertébral au niveau de l’apex de ladéformation sont des indicateurs fiables d’un risque de progression élevé de la scoliose [8]. Dans une autreétude, Mehta a aussi présenté les données radio-cliniques
128 Journal Médical Libanais 2021 • Volume 69 (2) F. MONGET et al. – Corsets plâtrés et scoliose
Figure 1. Réalisation d’un corset plâtré EDF sur cadre de CotrelA. Patient en traction sur cadre. B. Bandes de plâtre appliquées. C. Mise en place des pressions correctrices.
D. Fenêtrage après avoir appliqué de la résine.
A B
C D

de 136 enfants avec SI traitées par corset plâtré EDFselon la technique de Cotrel et Morel [4, 6]. Trente-sixenfants de la cohorte (26,5%) présentaient une SI nonidiopathique. Parmi les 136 patients, 94 ont montré unerésolution complète de la déformation scoliotique (69,1%)suite à un traitement précoce par corsets plâtrés ; les meil-leurs résultats ont été observés lorsque le corset plâtréétait effectué avant l’âge de 2 ans. Cependant, il est im-possible de vérifier si la guérison a été spontanée ou in-duite par le traitement.
En 2020, Alassaf et al. dans leur méta-analyse de 10études sur le traitement des SI traitées par corsets plâtrésont rapporté une amélioration moyenne de l’angle de Cobbde 25° [9] ; néanmoins, les données analysées étaient trèshétérogènes, comme souligné auparavant par Mehta [6].Alassaf et al. ont montré que l’amélioration était d’au-tant plus importante que le traitement était mis en placetôt et sur de faibles courbures initiales [9].
Nous avons identifié 19 études analysant les angles de
Cobb pré- et post-traitement par corsets plâtrés chez desenfants avec SI idiopathique, et [nous] avons retrouvéune amélioration moyenne de l’angle de Cobb de 29°,corroborant les résultats d’Alassaf et al. [9].
Toutes les études réalisées sur le sujet considèrent laréalisation de corsets plâtrés comme un traitement effi-cace et avec un faible taux de complications chez les en-fants avec une SI idiopathique. Le traitement est d’au-tant plus efficace qu’il est réalisé sur des patient jeunes (< 2 ans), avec des courbures de moindre sévérité (30°-45°) et sans pathologies associées [6, 10-28].
Scoliose infantile non idiopathique La SI non idiopathique est diagnostiquée avant l’âge
de 3 ans et survient sur une pathologie sous-jacente d’ori-gine syndromique, génétique, osseuse, neurologique cen-trale ou périphérique. Ces situations sont beaucoup plusrares que les précédentes rendant la réalisation d’étudesde puissance suffisante difficile.
F. MONGET et al. – Corsets plâtrés et scoliose Journal Médical Libanais 2021 • Volume 69 (2) 129
Figure 2. Réalisation d’un corset plâtré sans cadre spécifique [7]A. Patient installé (posé sur la barre soutenue par deux supports). B) Traction distale.
C. Correction. D. Fenêtrage après avoir appliqué de la résine.
A B
C D

Parmi les 13 études analysant des patients avec SI non idiopathiques, les angles de Cobb pré- et post-trai-tement étaient disponibles dans 8 études [10, 16-19, 23,25, 29] et l’amélioration moyenne retrouvée était de 10°.Ces résultats sont issus d’études très hétérogènes et uneinterprétation significative des résultats est difficile à ob-tenir.
Scoliose juvénileLes SJ sont découvertes entre l’âge de 5 et 10 ans
(Figure 3). Parmi les scolioses à début précoce, la SJ estla forme la moins étudiée; en particulier, la SJ idiopa-thique n’est abordée que dans deux études pour un totalde 37 patients. Au sein des deux études, l’améliorationmoyenne de l’angle de Cobb avant et après traitementétait d’environ 5° [5, 30].
Les séries de corsets plâtrés ont moins de succès chezles enfants avec SJ avec un taux d’arthrodèse vertébraleentre 27% et 100% après traitement conservateur. Laplupart des études ont également montré une perte decorrection entre la pose du premier corset plâtré et la findu traitement.
Plus récemment, Van Hessem et al. ont revu rétro-spectivement 3 patients avec SJ traités par corsets plâtrés
avec un suivi moyen de 4,6 ans [30]. Dans cette petitesérie, l’angle de Cobb a été corrigé en moyenne de 12°(de 25° à 37°) et aucune chirurgie d’arthrodèse n’a étéréalisée pendant le suivi. Van Hessem et al. ont concluque le traitement par corsets plâtrés pourrait éviter laprogression de la déformation scoliotique et réduire lerecours à la chirurgie chez les patients avec SJ [30].
Canavese et al. ont étudié 44 enfants avec SJ idiopa-thique et non idiopathique traités par corsets plâtrés réa-lisés sur cadre EDF [31]. Les auteurs ont rapporté que lecorset plâtré réalisé sous anesthésie générale associé àdes curares (18 enfants) permettait une meilleure correc-tion initiale de la déformation par rapport aux patientschez qui le corset plâtré était réalisé sous anesthésie gé-nérale (12 patients) ou éveillés (14 patients) [31].
Les SJ non idiopathiques sont quant à elles étudiéesdans un unique article rétrospectif portant sur 8 patients.Canavese et al. ont rapporté une amélioration moyennede l’angle de Cobb d’environ 5° entre les radiographiesprétraitement et le dernier suivi (2 ans) [31].
Scoliose congénitaleLes SC sont étudiées dans cinq articles pour un total
de 77 patients avec une amélioration moyenne de l’angle
130 Journal Médical Libanais 2021 • Volume 69 (2) F. MONGET et al. – Corsets plâtrés et scoliose
Figure 3. Radiographies avant et après la pose du premier corset plâtré chez un patient de 9 ans avec SJ idiopathique (A); bonne correction sous corset plâtré (B).
A B

de Cobb de 7°. L’efficacité thérapeutique des corsets plâ-trés chez les enfants avec SC n’est pas prouvée, et lesavantages potentiels du corset plâtré ont été mis en évi-dence à court terme uniquement.
Cao et al. ont comparé les résultats du traitement parcorsets plâtrés entre SC (8 patients) et scolioses non con-génitales (15 patients) [13] ; ils ont trouvé que même sil’angle de Cobb avait diminué chez tous les patients, letaux de correction était significativement plus élevé chezles patients avec une scoliose non congénitale (50%) quechez les patients avec SC (20%).
Demirkiran et al. dans une étude sur 11 patientsavec SC traités par corsets plâtrés ont retrouvé unediminution de l’angle de Cobb de 15° dans le planfrontal et de 16° dans le plan sagittal [32]. L’âgemoyen à la mise en place du premier corset plâtréétait de 40 mois avec un nombre de plâtre moyen de6.2. Dans cette étude, aucun des patients pris encharge n’a nécessité de chirurgie ni n’a développé decomplications. Demirkiran et al. ont conclu que lecorset plâtré est une stratégie sûre et efficace pourretarder la chirurgie (26 mois en moyenne) chez lesenfants avec SC. Même si l’efficacité thérapeutiqueest limitée chez les patients avec SC, le corset plâtréreste une option précieuse pour retarder la chirurgie[13,32] (Tableaux I-II) (Figure 4).
ComplicationsLes complications entraînées par la mise en place
d’un corset plâtré sont rares mais certaines d’entre ellespeuvent être potentiellement graves.
Quinze articles (365 patients) sur 36 (42.6%) ont rap-porté des complications (85 cas ; 23%) au cours du traite-ment par corsets plâtrés. La plupart des complications ré-pertoriées sont “mineures” et réversibles sans séquelle ;néanmoins des complications majeures ont aussi été dé-crites, généralement chez des patients présentant de mul-tiples comorbidités [23]. La grande majorité des compli-cations est représentée par les troubles cutanés réversibles(51 cas; 60%) généralement entraînés par le frottement duplâtre sur la peau ; elles vont de la simple irritation cuta-née à l’ulcère et retardent parfois la prise en charge, enparticulier si le corset plâtré doit être changé (Figure 5).
Le deuxième type de complication la plus fréquenteest le trouble respiratoire peu sévère et réversible (12cas; 14,2%) suivi par les troubles gastro-intestinaux etles nausées (5 cas ; 5,9%).
Dans les SI idiopathiques les complications sont men-tionnées dans 14 études sur 23 pour un total de 59 pa-tients sur 293 (14 études ; 20% de complications). Dansles SI non idiopathiques, elles sont mentionnées dansseulement 3 études sur 13 soit 20 patients sur 77 (26%de complications).
F. MONGET et al. – Corsets plâtrés et scoliose Journal Médical Libanais 2021 • Volume 69 (2) 131
Figure 4. Radiographie (A) et scanner thoracique (B) préopératoires et radiographie après la pose du premier corset plâtré (C)chez un patient de 14 mois avec SC; la correction de la courbe scoliotique est moindre.
A B C
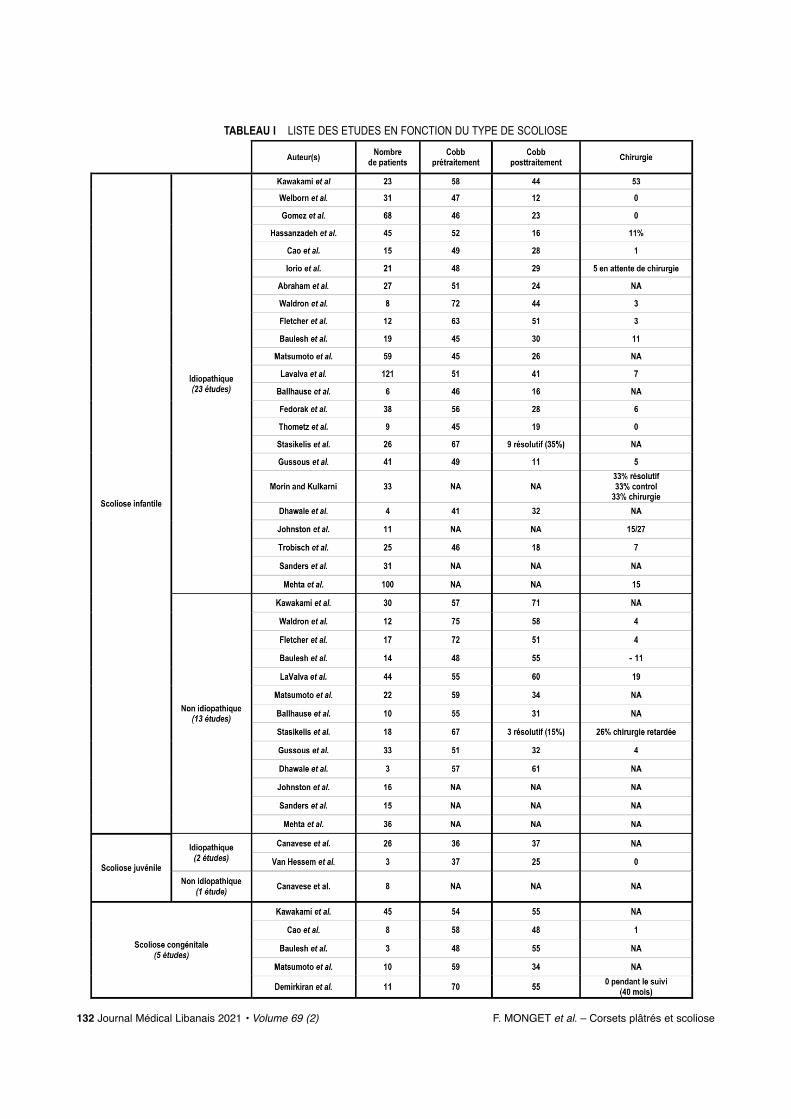
TABLEAU I LISTE DES ETUDES EN FONCTION DU TYPE DE SCOLIOSE
132 Journal Médical Libanais 2021 • Volume 69 (2) F. MONGET et al. – Corsets plâtrés et scoliose

Dans les SJ une seule complication a été mentionnéedans une étude de 7 patients (14% de taux de complica-tion).
Dans les SC, 2 études sur 5 mentionnent 5 complica-tions pour 53 patients (10% de complications).
Les autres complications sont quasi anecdotiquesmais l’on mentionne tout de même l’étude de Gussous etal. qui rapporte trois cas de complications rares maisnotables dont une fracture d’humérus survenue lors de lapose du plâtre, une thrombose de la veine sous-clavièresur compression et un cas de décès lors d’une exacerba-tion de crise d’asthme sévère chez un enfant avec d’autrescomorbidités [23]. La thrombose de la veine sous-clavièrepar compression après application du corset plâtré avaitpour la première fois été décrite par Badlani et al. en2013 [33]. Le Tableau III détaille l’ensemble des com-plications retrouvées.
DISCUSSION
Les scolioses à début précoce représentent un défipour le chirurgien orthopédiste pédiatrique car il doitcontrôler la déformation scoliotique sans perturber lacroissance de la colonne vertébrale et de la cage thora-cique et sans altérer la fonction pulmonaire et cardiaque.Ce travail est une revue de la littérature qui vise à établirl’état des lieux du traitement par corsets plâtrés des en-fants avec scoliose à début précoce et inclut les SI idio-pathiques et non idiopathiques, les SJ et les SC.
La majorité des études disponibles concerne les SIidiopathiques et les auteurs de ces travaux considèrent lecorset plâtré comme le traitement de choix car il permetde contrôler la progression de la déformation lorsqu’ilest débuté tôt, si l’enfant est très jeune (< 2 ans) et si ladéformation est idiopathique. Al Alassaf et al. ont con-
F. MONGET et al. – Corsets plâtrés et scoliose Journal Médical Libanais 2021 • Volume 69 (2) 133
Figure 5. ComplicationLésion de grattage sévère après ablation du premier corset plâtré
(enfant avec SI idiopathique de 17 mois)
TABLEAU II RÉCAPITULATIF DES ÉTUDES ET COMPLICATIONS
TABLEAU IIICOMPLICATIONS RETROUVÉES DANS LES ÉTUDES LES MENTIONNANT
Type de complications Nombre de complications(15 études & 365 patients)
Irritations et ulcérations cutanées 51
Troubles respiratoires peu sévères 12
Troubles gastro-intestinaux et nausées 5
Intolérance ou non compliance au traitement 3
Plâtre trop serré 9
Exacerbation épilepsie 1
Thrombose de la veine sous-clavière 1
Fracture induite par le plâtre 1
Complication liée à l’anesthésie 1(arrêt cardiaque, non fatal)
Décès (crise d’asthme) 1
85 (23%)
Nombre de patients
Cobb Cobb prétraitement posttraitement
Nombre de complications Taux de complication
Scoliose infantile
773Idiopathique
65°(23 études)
36°(sur 19 études) (sur 19 études)
59 sur 293 patients 20%
(14 études)
Non 270idiopathique
59°(13 études)
51°(sur 10 études) (sur 10 études) 26%
Scoliose
20 sur 77 patients (3 études)
juvénile
33Idiopathique (2 études) 36.5° 31°
(sur 2 études) (sur 2 études) 1 sur 7 patients 14%(1 étude)
Non 8idiopathique
NA(1 étude) NA NA NA
77 55°Scoliose congénitale (5 études)
48°(sur 5 études) (sur 5 études) 10%5 sur 53 patients
(2 études)

firmé que l’amélioration de l’angle de Cobb chez lesenfants avec SI idiopathique était d’autant plus impor-tante que le traitement était mis en place tôt, et sur defaibles courbures initiales ; ils ont également mis en évi-dence que l’effet diminue avec l’âge [9].
Toutes les études incluses au sein de notre revue de lalittérature ont démontré une amélioration significativede l’angle de Cobb exclusivement chez les enfants avecune SI idiopathique.
Les SI non idiopathiques ne font pas l’objet d’étudesspécifiques et sont généralement étudiées au sein d’é-tudes incluant surtout des SI idiopathiques.
Ballhause et al. dans une étude rétrospective de 16 pa-tients (6 SI idiopathiques et 10 non idiopathiques) ontretrouvé une diminution de l’angle de Cobb de 44% chezles patients avec SI non idiopathiques contre 65% chezles patients avec SI idiopathique. Par contre, le traite-ment permettait de diminuer le recours à la chirurgiechez tous les patients [19].
Gussous et al. dans une étude rétrospective réaliséesur 19 patients avec SI idiopathique et 9 patients avec SInon idiopathique traités par corsets plâtrés, ont rapportéune correction moyenne de l’angle de Cobb en fin detraitement d’environ 5° chez les enfants avec SI nonidiopathique contre 20° chez les enfants avec SI idio-pathique [23].
Plus récemment, Lavalva et al. dans leur étude rétro-spective de 44 SI non idiopathiques (26 syndromiques et18 neuromusculaires) ont retrouvé une amélioration mo-dérée de l’angle de Cobb (amélioration > 10°) chez 30%des patients [29] ; néanmoins, la courbe scoliotique s’estaggravée, malgré le traitement, chez 55% des patients,dont 43% ont nécessité une prise en charge chirurgicalependant le suivi (3 ans). La durée entre la mise en placedu premier corset plâtré et la chirurgie était en moyennede 34,5 mois [29]. Les auteurs concluent en une effica-cité moindre du corset plâtré sur l’amélioration de lacourbure scoliotique chez les patients avec SI non idio-pathique mais affirment également que le traitement per-met, au prix de peu de complications, de retarder effica-cement le recours à la chirurgie [29].
Johnston et al. ont comparé les enfants avec SI traitéspar corsets plâtrés avec ceux qui ont bénéficié d’un mon-tage de croissance [26]. Dans leur étude comparative (27patients) ils ont retrouvé certes une meilleure correctiondans le groupe ayant bénéficié d’une chirurgie, mais letaux de complications était 10 fois plus élevé que chezles enfants traités par corset. Ils ont souligné l’impor-tance de retarder la chirurgie le plus possible, et de con-sidérer le traitement par corset comme la stratégie per-mettant d’atteindre cet objectif, avec une balance béné-fice-risque positive [26].
L’efficacité des corsets plâtrés dans les SJ, par contre,
est peu étudiée et le taux d’arthrodèse vertébrale varieentre 27% et 100% après traitement conservateur [10,13, 18, 26, 31]. En plus, la plupart des études ont égale-ment montré une perte de correction entre la pose du pre-mier corset plâtré et la fin du traitement.
Van Hessem et al. ont revu rétrospectivement une pe-tite série de patients avec SJ traités par corsets plâtrésavec un suivi moyen de 4,6 ans. Van Hessem et al. ontconclu que le traitement par corsets plâtrés pourrait ré-duire le recours à la chirurgie chez les patients avec SJcar aucune chirurgie d’arthrodèse vertébrale n’a été réa-lisée pendant le suivi [30].
Canavese et al. ont étudié 44 enfants avec SJ traitéspar corsets plâtrés réalisés sur cadre EDF et ont montréque l’association entre curare et anesthésie générale per-mettait une meilleure correction de la déformation sco-liotique par rapport à l’anesthésie générale seule ou à laréalisation du corset chez des patients éveillés [31]. Surle long terme, par contre, les deux modalités de réalisa-tion du corset aboutissent aux mêmes résultats, avec uneperte de l’effet ‘positif’ du curare permettant une meil-leure correction initiale (résultats préliminaires non en-core publiés).
Par contre, l’efficacité du corset plâtré chez les en-fants avec SC n’est étudiée qu’à court terme et les ar-ticles publiés concordent sur le fait que même si le tauxde correction est réduit, le corset plâtré permet de retar-der la prise en charge chirurgicale [10,13,18, 32].
Globalement, les études qui se focalisent sur le traite-ment par corset des scolioses à début précoce sont trèshétérogènes et impliquent généralement un nombre li-mité de patients ; de plus, la plupart des études analysentl’angle de Cobb pré- et post traitement, sans véritable-ment différencier les sous-types de scoliose. En particu-lier nous avons constaté une perte de correction entre laradiographie post-corset plâtré peropératoire, avec pa-tient allongé, et la radiographie de suivi avec corset plâ-tré réalisée avec le patient débout (résultats préliminairesnon encore publiés).
En conséquence, la correction angulaire est variable.Elle est plus importante et durable chez les enfants lesplus jeunes qui ont pu bénéficier du traitement lorsque la déformation ne dépassait pas les 45° [11,12,14]. Lescomplications ne sont pas mentionnées dans toutes lesétudes mais elles sont globalement peu fréquentes et ré-versibles.
Cette révision de la littérature présente plusieurs li-mites car il s’agit d’un travail descriptif dépendant de laqualité du recueil réalisé et de l’accès aux sources citées.Les études incluses sont trop hétérogènes pour permettreune analyse statistique significative. Le faible nombred’études disponibles notamment concernant les SJ et SCne permet pas d’obtenir une puissance suffisante pour in-
134 Journal Médical Libanais 2021 • Volume 69 (2) F. MONGET et al. – Corsets plâtrés et scoliose

terpréter strictement les résultats. De plus, les donnéesconcernant l’amélioration de l’angle de Cobb sont hété-rogènes et parfois non présentes dans le texte. Les com-plications répertoriées sont probablement sous-estiméeset dépendent du choix des auteurs de les mentionner ounon au sein des études.
Néanmoins, même si l’efficacité des corsets plâtrésest moindre dans les déformations scoliotiques non idio-pathiques, ils permettent de retarder le recours à la chi-rurgie avec peu de complications, très souvent mineureset transitoires. Les quelques rares cas de complicationsmajeures sont survenus dans des contextes de comorbi-dités importantes. Par ailleurs, le taux de complicationslors du traitement conservateur est dix fois moins impor-tant que dans le traitement chirurgical par montage decroissance ou arthrodèse.
CONCLUSION
La SI et la SJ représentent un défi pour les chirurgiensorthopédistes pédiatriques car ils doivent respecter lacroissance de la colonne vertébrale et de la cage thora-cique tout en essayant de contrôler la déformation sco-liotique et la fonction cardio-respiratoire.
La majorité des études sur le sujet concernent les SIidiopathiques et les auteurs considèrent le traitement parcorsets plâtrés successifs comme le traitement de choix.Plusieurs techniques de réalisation du corset sont pos-sibles et certaines d’entre elles ne nécessitent pas de ma-tériel spécifique comme les cadres de Cotrel, de Risserou de Mehta.
Même si l’efficacité du traitement par corsets plâtrésest moindre dans les déformations non idiopathiques etchez les enfants avec SJ par rapport aux SI idiopa-thiques, il permet néanmoins de retarder le recours à lachirurgie au prix de peu de complications, généralementtransitoires et moins fréquentes que celles rapportéeschez les patients opérés avec un montage de croissanceou avec une arthrodèse définitive.
REFERENCES
1. LeFever D, Menger RP. Infantile & Juvenile Scoliosis. Stat-Pearls, Treasure Island (FL): StatPearls Publishing;2020.
2. Ramírez N, Devaris A, Arroyo S et al. [Thoracic insuffi-ciency syndrome]. Acta Ortop Mex 2020; 34: 254-60.
3. Karol LA. Early definitive spinal fusion in young children:what we have learned. Clin Orthop 2011; 469: 1323-9.
4. Cotrel Y, Morel G, Rey JC. [Idiopathic scoliosis]. ActaOrthop Belg 1965; 31: 795-810.
5. Canavese F, Rousset M, Mansour M, Samba A, Dimeglio A.Serial elongation derotation flexion (EDF) casting for pa-tients with infantile and juvenile scoliosis. Minerva Pediatr2016; 68: 56-65.
6. Mehta MH. Growth as a corrective force in the early
treatment of progressive infantile scoliosis. J Bone JointSurg Br 2005; 87: 1237-47.
7. Schwend RM. Spica & spine casting with inexpenivemetal bar n.d.:2.ht tps: / /g lobalhe lp .org/publ icat ions/books/he lp_tipsspicaspinacasting.pdf.
8. Mehta MH. The rib-vertebra angle in the early diagno-sis between resolving and progressive infantile scoliosis. J Bone Joint Surg Br 1972; 54: 230-43.
9. Alassaf N, Tabard-Fougère A, Dayer R. Casting in infan-tile idiopathic scoliosis as a temporising measure: A sys-tematic review and meta-analysis. SAGE Open Med 2020;8: 2050312120925339.
10. Kawakami N, Koumoto I, Dogaki Y et al. Clinical impactof corrective cast treatment for early onset scoliosis: Is ita worthwhile treatment option to suppress scoliosis pro-gression before surgical intervention? J Pediatr Orthop2018; 38: e556-61.
11. Welborn MC, D’Astous J, Bratton S, Heflin J. Infantileidiopathic scoliosis: Factors affecting EDF casting suc-cess. Spine Deform 2018; 6: 614-20.
12. Gomez JA, Grzywna A, Miller PE et al. Initial cast cor-rection as a predictor of treatment outcome success forinfantile idiopathic scoliosis. J Pediatr Orthop 2017; 37:e625-30.
13. Cao J, Zhang X-J, Sun N et al. The therapeutic character-istics of serial casting on congenital scoliosis: a compari-son with non-congenital cases from a single-center expe-rience. J Orthop Surg 2017; 12: 56.
14. Iorio J, Orlando G, Diefenbach C et al. Serial casting forinfantile idiopathic scoliosis: Radiographic outcomes andfactors associated with response to treatment. J PediatrOrthop 2017; 37: 311-6.
15. Abraham R, Sponseller PD. Focused molding usingadhesive pads in Mehta casting for early-onset scoliosis.Spine Deform 2014; 2: 454-9.
16. Waldron SR, Poe-Kochert C, Son-Hing JP, Thompson GH.Early onset scoliosis: the value of serial risser casts. JPediatr Orthop 2013; 33: 775-80.
17. Fletcher ND, McClung A, Rathjen KE, Denning JR,Browne R, Johnston CE. Serial casting as a delay tacticin the treatment of moderate-to-severe early-onset sco-liosis. J Pediatr Orthop 2012; 32: 664-71. https://doi.org/10.1097/BPO.0b013e31824bdb55.
18. Baulesh DM, Huh J, Judkins T, Garg S, Miller NH,Erickson MA. The role of serial casting in early-onsetscoliosis (EOS). J Pediatr Orthop 2012; 32: 658-63.https://doi.org/10.1097/BPO.0b013e318269c438.
19. Ballhause TM, Moritz M, Hättich A, Stücker R, MladenovK. Serial casting in early onset scoliosis: syndromic scolio-sis is no contraindication. BMC Musculoskelet Disord2019; 20: 554.https://doi.org/10.1186/s12891-019-2938-9.
20. Fedorak GT, D’Astous JL, Nielson AN, MacWilliams BA,Heflin JA. Minimum 5-year follow-up of mehta casting totreat idiopathic early-onset scoliosis. J Bone Joint SurgAm 2019; 101: 1530-8.https://doi.org/10.2106/JBJS.18.01268.
21. Thometz J, Liu X-C. Serial CAD/CAM bracing: An alter-native to serial casting for early onset scoliosis. J PediatrOrthop 2019; 39: e185-9.https://doi.org/10.1097/BPO.0000000000001287.
22. Stasikelis PJ, Carpenter AM. Results of casting in severe
F. MONGET et al. – Corsets plâtrés et scoliose Journal Médical Libanais 2021 • Volume 69 (2) 135

curves in infantile scoliosis. J Pediatr Orthop 2018; 38:e186-9. https://doi.org/10.1097/BPO.0000000000001140.
23. Gussous YM, Tarima S, Zhao S et al. Serial derotationalcasting in idiopathic and non-idiopathic progressive early-unset scoliosis. Spine Deform 2015; 3: 233-8.https://doi.org/10.1016/j.jspd.2014.10.001.
24. Morin C, Kulkarni S. ED plaster-of-Paris jacket for in-fantile scoliosis. Eur Spine J 2014; 23 Suppl 4: S412-418.https://doi.org/10.1007/s00586-014-3336-5.
25. Dhawale AA, Shah SA, Reichard S et al. Casting for in-fantile scoliosis: the pitfall of increased peak inspiratorypressure. J Pediatr Orthop 2013; 33: 63-7.https://doi.org/10.1097/BPO.0b013e318264936f.
26. Johnston CE, McClung AM, Thompson GH, Poe-Kochert C, Sanders JO. Growing Spine Study Group.Comparison of growing rod instrumentation versus seri-al cast treatment for early-onset scoliosis. Spine Deform2013; 1: 339-42.https://doi.org/10.1016/j.jspd.2013.05.006.
27. Trobisch PD, Samdani A, O’Neil C, Betz R, Cahill P.[Non-operative treatment for severe forms of infantileidiopathic scoliosis]. Z Orthopadie Unfallchirurgie 2012;150: 52-5. https://doi.org/10.1055/s-0031-1280330.
28. Sanders JO, D’Astous J, Fitzgerald M, Khoury JG,
Kishan S, Sturm PF. Derotational casting for progressiveinfantile scoliosis. J Pediatr Orthop 2009; 29: 581-7.https://doi.org/10.1097/BPO.0b013e3181b2f8df.
29. LaValva S, Adams A, MacAlpine E et al. Serial casting in neuromuscular and syndromic early-onset scoliosis(EOS) can delay surgery over 2 years. J Pediatr Orthop2020; 40: e772-9.https://doi.org/10.1097/BPO.0000000000001568.
30. van Hessem L, Schimmel JJP, Graat HCA, de Kleuver M.Effective nonoperative treatment in juvenile idiopathicscoliosis. J Pediatr Orthop Part B 2014; 23: 454-60.https://doi.org/10.1097/BPB.0000000000000077.
31. Canavese F, Botnari A, Dimeglio A et al. Serial elonga-tion, derotation and flexion (EDF) casting under gener-al anesthesia and neuromuscular blocking drugs im-prove outcome in patients with juvenile scoliosis: pre-liminary results. Eur Spine J 2016; 25: 487-94.https://doi.org/10.1007/s00586-015-4100-1.
32. Demirkiran HG, Bekmez S, Celilov R, Ayvaz M, Dede O,Yazici M. Serial derotational casting in congenital scoliosisas a time-buying strategy. J Pediatr Orthop 2015; 35: 43-9.https://doi.org/10.1097/BPO.0000000000000229.
33. Badlani N, Korenblit A, Hammerberg K. Subclavian veinthrombosis after application of body cast. J PediatrOrthop 2013; 33: e1-3.https://doi.org/10.1097/BPO.0b013e31827363e7.
136 Journal Médical Libanais 2021 • Volume 69 (2) F. MONGET et al. – Corsets plâtrés et scoliose

INTRODUCTION
Idiopathic scoliosis before the age of 6 years old are rare,their prevalence is estimated at less than 1% of all scol-iosis [1]. Their prognosis depends on the scalability ofthe curve. Mehta [2] identified on X-ray two risk factorsof progression or spontaneous resolution of the curve :the initial Cobb angle and the initial rib vertebral angledifference (RVAD) angle.
The usual orthopedic treatment is based on EDF-type (elongation, derotation, flexion) plasters casts [3].They are made on a Cotrel frame [4]. They are re-newed every 6 weeks in order to obtain a gradual cor-rection of the deformation. Then treatment is followedby a brace.
We propose to treat in first intention with a Cheneau-Toulouse-Munster (CTM) brace which has direct sup-ports on the gibbosity areas and large opening to mobi-lize the entire trunk (Figure 1). This avoids the risks ofa bad development of the chest. This treatment hasseveral advantages. It does not require hospitalizationnor general anesthesia and its tolerance is good duringdaily life.
The purpose of this study is to evaluate the effective-ness of the CTM brace for the treatment of idiopathicscoliosis before the age of 6 years. It is a preliminarystudy whose results will have to be evaluated at the endof growth.
MATERIAL AND METHOD
We retrospectively analyzed data from all patientstreated with CTM brace for idiopathic scoliosis diag-nosed before the age of 6 years between 1999 and2015 in our department. The minimum follow-up was18 months.
Non idiopathic scoliosis were excluded. No patientshad been treated before the CTM brace was placed. Thebrace was worn 22 hours per day initially for at least 6months and then reduced to 12 hours a day in case of sat-isfactory correction. The wearing time of the brace, theCobb angle at each consultation and the initial Mehtaangle (RVAD) were noted.
Lebanese Medical Journal 2021 • Vol 69 (2) 137
PPAAEEDDIIAATTRRIICC OORRTTHHOOPPAAEEDDIICCSS EFFECTIVENESS OF BRACING ALONE IN IDIOPATHIC SCOLIOSISBEFORE 6 YEARS OF AGEhttp://www.lebanesemedicaljournal.org/articles/69-2/pedsortho10.pdf
Isabelle BERNARDINI1, Roxane COMPAGNON1, Frank ACCADBLED1, Jérôme SALES de GAUZY1*
ABSTRACT • Introduction : Scoliosis before 6 years ofage are usually managed with serial casting to reduce thecurve then thoraco-lumbar orthosis to maintain the reduc-tion. Our strategy was to use only bracing, without prelim-inary serial casting. The goal of this study was to analysethe results of this strategy. Material and method : We re-trospectively reviewed the data of all children who hadbeen treated for idiopathic scoliosis diagnosed before the age of 6 years with CTM brace, between 1999 and2015 at a single institution. The minimal follow-up was 18months. Secondary scoliosis were excluded. Daily bracetime was 22 hours, decreased to 12 h in case of satisfac-tory correction without progression. Bracing was interrupt-ed when the spine was balanced and the curve showed noprogression at 6-month interval. Bracing time, Cobb angleand rib vertebra angle difference (RVAD) were recorded.Results : Forty-six patients were included (27 girls and 19boys). Mean age at diagnosis was 35 months (9-71).Cobb angle at onset of treatment was 35° (13-70) andRVAD was 20.5° (0-60). Forty patients had a satisfactoryresult. Mean age at diagnosis was 35 months (9-71),RVAD was 18° (0-55). Cobb angle at the onset of treat-ment was 32° (13-60) and 27° (0-60) at latest follow-up.Mean full time bracing was 25.2 months (4-42) and halftime 18.5 months (0-72). Mean follow-up after bracing was47 months (0-145). In six patients scoliosis progresseddespite bracing. Five were managed with serial castingand one with a Milwaukee brace. Discussion : Non oper-ative management is well accepted since excellent re-sults have been reported for curves below 60°. Plastercast requires specific frame and often general anesthesia.It can be a burden for the patient and his family. Bracetreatment alone stands as an alternative in case of satis-factory curve correction. Brace treatment alone has beenreported as less effective, resulting in progression of thecurve in up to 52% of patients. However, recent studiesshowed that casting and/or bracing is effective for themanagement of juvenile scoliosis. The results with bracingalone were similar to results of serial casting from the lit-erature. Conclusion : Bracing alone is an interesting alternative to serial casting for idiopathic scoliosis. It pro-vides in most of cases satisfactory correction which allowsstopping the treatment before skeletal maturity. In case offailure serial casting can be performed.
Keywords : early onset scoliosis ; bracing ; infantile scoliosis ;orthopaedic treatment.
1Service d’orthopédie pédiatrique. Hôpital des Enfants CHU de Toulouse. Avenue de Grande-Bretagne. 31026 Toulouse cedex France.*Corresponding author: Jérôme Sales de Gauzy, MD. e-mail: [email protected]
Bernardini I, Compagnon R, Accadbled F, Sales de Gauzy J.Effectiveness of bracing alone in idiopathic scoliosis before 6 years of age. J Med Liban 2021 ; 69 (2) : 137-140.

RESULTS
Forty-six patients were included (27 girls and 19 boys).Mean age at diagnosis was 35 months (9-71).
Cobb angle at onset of treatment was 35° (13-70) and theRVAD angle (Mehta angle) was 20.5 degrees (0-60 degrees)
The evolution of the curve with the brace shows adecrease in the Cobb angle. At the last follow-up theaverage Cobb angle was 25.8 degrees (0-60).
Forty patients had a satisfactory result (Figures 2 & 3).For these cases, mean age at diagnosis was 35 months(9-71), RVAD was 18° (0-55). Cobb angle at the onset oftreatment was 32° (13-60) and 27° (0-60) at latest fol-low-up. Mean full time bracing was 25.2 months (4-42)and half time 18.5 months (0-72). Mean follow-up after
bracing was 47 months (0-145). Six patients had a curve progression despite the brac-
ing and were treated by a pop cast (Figure 3).In univariate analysis, over the entire cohort, there is
a statistically significant correlation between the Cobbangle at the beginning of treatment and the Cobb angleat the last follow-up.
In univariate analysis, over the entire cohort, there is al-so a statistically significant correlation between the initialRVAD angle and the Cobb angle at the last follow-up.
DISCUSSION
Our study shows the effectiveness of CTM brace treat-ment for early onset idiopathic scoliosis. It allows, in
138 Lebanese Medical Journal 2021 • Vol 69 (2) I. BERNARDINI et al. – Bracing alone in idiopathic scoliosis before 6 years of age
Figure 1. CTM brace. X-rays without and with brace.
Figure 2. A & B : Infantile scoliosis treated with CTM brace. C : Two years old X-ray at diagnosis. D : X-ray at 5 years old. good reduction, brace is stopped. E : X-ray at 15 years old.
A B C D
A B C D E

some cases, a total correction of the deformity and in alot of other cases a diminution of the curve. If correctionis not sufficient, definitive arthrodesis surgery can beperformed at the end of growth [5]. Our results are con-sistent with the literature, which found good results withplaster casts and bracing [5, 6, 7, 8, 9].
The effectiveness of the treatment by series of plastercasts had already been demonstrated [4, 5, 10]. We re-serve this treatment for severe deformations or in case offailure of the CTM brace.
EDF pop cast requires a Cotrel frame and a trainedteam. In a North American survey only 66% of profes-
I. BERNARDINI et al. – Bracing alone in idiopathic scoliosis before 6 years of age Lebanese Medical Journal 2021 • Vol 69 (2) 139
Figure 3. Infantile scoliosis A. Three years old. B. Three years old with brace. C. Result at 5 years old.
Figure 4. A. Curve progression despite the bracing. B & C. Treatment with a pop cast.
A B C
A B C

sionals had access to a Cotrel frame [11]. The choice oforthotic treatment may then be a reasonable alternative,especially for deformations of small amplitudes.
For some authors, brace treatment alone is less ef-fective. In the series of Smith et al. 53% of patientstreated with brace alone had a progression of deformi-ty [12]. Nevertheless, in patients who responded tobrace treatment, the overall correction of curvaturewas very satisfactory and close to treatment with plas-ter cast.
Plaster casting needs general anesthesia. Cumulativeexposure to general anesthesia has been quantified byseveral authors [1, 13]. Exposure to anesthetic productsespecially in small children can lead to learning disor-ders and cognitive difficulties [8, 13].
Finally, hospitalizations, discomfort and recovery timeafter general anesthesia, repeated consultations or nu-merous surgical complications are no cause of very im-portant constraints for the patient and his family. Theycan lead to over-added psychosocial difficulties.
There are limitations to our study. Follow-up isshort. This is a retrospective study with missing dataduring follow-up decreasing the power of this evalua-tion. Similarly, no sufficient information was availableon the study of the sagittal plan. Given the low inci-dence of this pathology, the number of patients includ-ed was small.
Finally, we had no concomitant data on the assess-ment of chest and lung growth or respiratory function.
CONCLUSION
CTM brace only treatment is an interesting alternativeto the usual plaster series treatment for scoliosis diag-nosed before the age of 6. It allows in most of the casesa satisfactory correction while avoiding the constraintsand risks associated with repeated surgical proceduresand general anesthesia. As with all treatments availableto date, efficacy is highest for young patients with an ini-tial low Cobb angle and a low initial RVAD angle. If this
treatment fails, more traditional treatment per series ofplaster casts can be carried out.
REFERENCES
1. Van Hessem L, Schimmel JJP, Graat HCA, de Kleuver M.Effective nonoperative treatment in juvenile idiopathicscoliosis. J Pediatr Orthop Part B. 2014; 23 (5): 454-460.
2. Mehta MH. The rib-vertebra angle in the early diagnosisbetween resolving and progressive infantile scoliosis. J Bone Joint Surg Br. 1972; 54 (2): 230-243.
3. Cunin V. Early-onset scoliosis: current treatment. OrthopTraumatol Surg Res OTSR. 2015; 101(Suppl 1): S109-118.
4. Cotrel Y, Morel G. The elongation-derotation-flexiontechnic in the correction of scoliosis. Rev Chir OrthopReparatrice Appar Mot. 1964; 50: 59-75.
5. D’Astous JL, Sanders JO. Casting and traction treatmentmethods for scoliosis. Orthop Clin North Am. 2007; 38(4): 477-484.
6. Dede O, Sturm PF. A brief history and review of moderncasting techniques in early onset scoliosis. J Child Orthop.2016; 10 (5): 405-411.
7. Mehta MH. The conservative management of juvenile idio-pathic scoliosis. Acta Orthop Belg. 1992; 58 Suppl 1: 91-97.
8. Sanders JO, D’Astous J, Fitzgerald M, Khoury JG,Kishan S, Sturm PF. Derotational casting for progressiveinfantile scoliosis. J Pediatr Orthop. 2009; 29 (6): 581-587.
9. Stasikelis PJ, Carpenter AM. Results of casting in severecurves in infantile scoliosis. J Pediatr Orthop. 2018; 38(4): e186-e189.
10. Mehta MH. Growth as a corrective force in the earlytreatment of progressive infantile scoliosis. J Bone JointSurg Br. 2005; 87 (9): 1237-1247.
11. Fletcher ND, Larson AN, Richards BS, Johnston CE.Current treatment preferences for early onset scoliosis: asurvey of POSNA members. J Pediatr Orthop. 2011; 31(3): 326-330.
12. Smith JR, Samdani AF, Pahys J et al. The role of bracing,casting, and vertical expandable prosthetic titanium ribfor the treatment of infantile idiopathic scoliosis: a sin-gle-institution experience with 31 consecutive patients.Clinical article. J Neurosurg Spine. 2009; 11 (1): 3-8.
13. Goldstein MJ, Kabirian N, Pawelek JB et al. Quanti-fying anesthesia exposure in growing rod treatment forearly onset scoliosis. J Pediatr Orthop. 2017; 37 (8):e563-e566.
140 Lebanese Medical Journal 2021 • Vol 69 (2) I. BERNARDINI et al. – Bracing alone in idiopathic scoliosis before 6 years of age

INTRODUCTION
Early onset scoliosis (EOS) refers to a three dimension-al spine deformity with a coronal plane curvature ex-ceeding 10 degrees, present before the age of 10 [1, 2].EOS comprises a myriad of etiologies and is thereforecategorized into five subtypes: idiopathic, congenital, tho-racogenic, neuromuscular and syndromic [1, 2].
The treatment of EOS remains challenging with manyparadigm shifts through the past years [3]. Patients withEOS may sometimes be underweight with poor soft tis-sues ; their vertebrae are often osteopenic ; and curves areoccasionally severe, stiff, and kyphotic [3-5]. Left un-treated, patients with EOS are at high risk of progressionwith remaining growth, leading to severe thoracic insuf-ficiency and early demise [6, 7]. This is a life threaten-ing condition and the rule of thumb in the treatment ofEOS is to optimize pulmonary function by allowing thegrowth of a well-developed chest while minimizingspine deformity [2, 5, 6]. Thus, growth-friendly methodsof deformity control are indicated in EOS treatment asthey allow surgeons to achieve a crucial maximal T1-T12 length, therefore optimizing lung function [1, 4, 7].
Despite the shift to early surgical intervention andinstrumentation for EOS patients in the beginning of thethird millennium, registered complications in these frailpatients with comorbidities have swung the pendulumback to initial conservative approach [6]. Non operativetreatment including bracing, casting and halo-gravitytraction should be considered first [4, 8, 9]. This “buy-time” strategy led to satisfactory results by slowing pro-gression and delaying surgery until frailty in these pa-tients is adequately addressed [1, 4, 9].
Once surgery is indicated, growth friendly techniquesare favored for the reasons shown above [10, 11]. Theseare categorized into three types : distraction based (con-ventional growing rods, magnetically controlled grow-ing rods and vertical expandable prosthesis titanium ribs/VEPTR), compression based (vertebral body stapling ortethering), and growth-guided based (Shilla system, mo-dern Luque trolley) [3-5, 10, 11].
Traditional growing rods (TGR), which were first in-troduced by Harrington in 1962, are the most commonly
Lebanese Medical Journal 2021 • Vol 69 (2) 141
PPAAEEDDIIAATTRRIICC OORRTTHHOOPPAAEEDDIICCSS COMPLICATIONS IN TRADITIONAL GROWING RODS USED FOR EARLY ONSET SCOLIOSISA Case Series and a Review of Literaturehttp://www.lebanesemedicaljournal.org/articles/69-2/pedsortho11.pdf
Maroun RIZKALLAH1, Diane GHANEM2, Ayman ASSI3, Ismat GHANEM1
ABSTRACT • Introduction: Early-onset scoliosis (EOS) is de-fined as > 10° spine curvature in children with onset before 10years of age. It may severely impact lung development and sig-nificantly reduce life expectancy. When surgery is indicated, itshould allow growth while maintaining an acceptable deformitycorrection. Traditional growing rods (TGR) is the surgical goldstandard treatment of EOS. Aim: To review the cases of EOSoperated at our institution with TGR, and analyze the outcomesand complications. Findings will be compared to similar seriesafter a thorough review of literature. Material and Methods :Patients with EOS operated at our institution between January2007 and July 2019 were included. Charts and X-rays werereviewed to assess demographic data, etiology of EOS, age andweight at surgery, type of construct, magnitude of main coronalcurve, sagittal profile, incidence and types of complications, andmortality. Results : Thirty-seven patients were included. Meanfollow-up was 45 months. Mean age at surgery was 6.5 years (3to 10 years). Mean coronal main curve angle went from 82° pre-operatively to 45° at last follow-up (p = 0.01). Mean T1-S1 lengthwent from 26.7 preoperatively to 33.3 cm at the last follow-up (p = 0.03). Mean weight went from 32 kg to 45 kg at the last fol-low-up (p = 0.03). Fifteen patients (40.54%) had a severe thora-columbar kyphosis. Twenty patients (54.05%) had an initial dual rods construct. Sixteen complications were recorded in 13patients (35%) with 13 mechanical failures of the construct. Sub-group analysis showed that in patients with severe kyphosis,53.33% had complications, compared to 22.72% in the remain-ing patients (p = 0.01). In patients with dual rod constructs, 15%had complications, compared to 58.82% of those with single rod constructs (p = 0.02). Mean preoperative main curve Cobbangle in patients with complications averaged 84°, compared to72° in patients without any complication (p = 0.04). Mean preop-erative weight of the 13 patients with complications was 26.3 kgcompared to 34.5 kg in the remaining patients (p = 0.03).Discussion : Despite allowing growth and maintaining accept-able curve correction, a high rate of complications following TGRis reported in our series as was as in all similar series in literature.The increased severity of spine deformity, the thoracolumbarkyphosis, the low preoperative weight and the single rod con-structs increase significantly the complication rate in our studygroup. Surgical intervention when main curve reaches 60°, usingall pedicle screws constructs with dual-rods, with close follow-upespecially in patients with thoraco-lumbar kyphosis, and preoper-ative nutritional optimization would help lower complications.
Keywords: early onset scoliosis; growing rods; complica-tions; thoracolumbar kyphosis; dual rod construct
Rizkallah M, Ghanem D, Assi A, Ghanem I. Complications in tra-ditional growing rods used for early onset scoliosis: A case seriesand a review of literature. J Med Liban 2021; 69 (2) :141-146.
1 Saint Joseph University, Faculty of Medicine & Department of Orthopedic Surgery, Hôtel-Dieu de France Hospital, Beirut, Lebanon. 2 Faculty of Medicine, American University of Beirut. 3Laboratory of Biomechanics & Medical Imaging, Faculty of Medicine, Saint-Joseph University, Beirut. Corresponding author: Maroun Rizallah, MD e-mail: [email protected]

applied technique and considered the gold standard forEOS surgical treatment [12, 13]. Proximal and distal in-strumentation and fusion maintain the deformity correc-tion that is achieved with distraction and repetitive length-ening procedures [3,13-14]. Indications for TGR includeprogression under bracing or casting treatment in pa-tients without rib anomalies and a physiologically seg-mented spine, curvature of more than 60 degrees and ageyounger than 10 years old. Despite being the gold stan-dard for EOS, this technique is associated with a highrate of complications, exceeding 50% in some series [1,4, 13].
In this study, we review the results of EOS cases oper-ated at our institution using the TGR, focusing on re-corded complications and their possible risk factors.These results will be compared to findings from similarseries, through a thorough literature review.
MATERIAL AND METHODS
This is a retrospective monocentric study performed af-ter the Institutional Review Board (IRB) approval. Allpatients with confirmed EOS operated at our institutionbetween January 2007 and July 2019 with a minimal fol-low-up of 12 months were included. Patients operatedbefore the age of 3 years and those operated after the ageof 10 years were excluded. Patients who failed to com-plete 12 months of follow-up were also excluded. Chartsof the patients were reviewed to assess their demographicdata, the etiology of EOS, age at surgery, incidence andtypes of complications, and mortality. Preoperative andlast-follow-up A/P and lateral full spine X-rays werereviewed and main curve coronal Cobb angle and T1-S1length were recorded. Severe thoraco-lumbar kyphosiswas defined as T10-L2 kyphosis > 25°. Surgical distrac-
tion was scheduled at 6 months interval. All patients hada hybrid pedicle screw/proximal hooks constructs, withchrome-cobalt 4 mm rods. They were operated by thesame surgeon.
Paired t-test was used to compare quantitative vari-ables preoperatively and postoperatively in the same pa-tients. Differences in quantitative variables were testedusing a Wilcoxon rank test. Differences in qualitativevariables were tested using Fisher’s exact test. Thesetests were used due to the small number of patients insubgroup analysis (< 30). Multiple logistic regressionwas not used due to limited number of events.
All analyses were performed using the R softwareversion 3.6.1 (R Foundation for Statistical Computing,Vienna, Austria).
RESULTS
Thirty-seven patients with EOS were included in thisstudy, with a mean follow-up of 45 months (12 to 150months). There were 20 males and 17 females. Mean ageat surgery was 6.5 years (3 years–10 years). Mean coro-nal main curve angle went from 82° (55° – 100°) preop-eratively to 45° (35° – 70°) at last follow-up (Figure 1) (p = 0.01).
Mean T1-S1 length went from 26.7 cm (22 cm–32.1 cm)preoperatively to 33.3 cm (27 cm – 40.3 cm) at the last fol-low-up, with a mean increase of 6.6 cm (p = 0.03). Meanweight went from 32 kg (20 kg – 52 kg) to 45 kg (29 kg– 70 kg) at the last follow-up (p = 0.03) (Table I).
Fifteen patients (40.54%) had a severe thoracolum-bar junction kyphosis. There were 12 patients (32.4%)with congenital EOS, 17 (45.95%) with neurologic EOS,4 (10.81%) with myopathies, and 4 (10.81%) patientshad idiopathic EOS. Twenty patients (54.05%) had an
142 Lebanese Medical Journal 2021 • Vol 69 (2) M. RIZKALLAH et al. – Complications in [traditional] growing rods used for EOS
Figure 1. Figure showing anteroposterior full spine X-rays of the same patient at different follow-ups. A. Preoperative traction X-ray. B-E. X-rays during follow-up after iterative rods distraction.
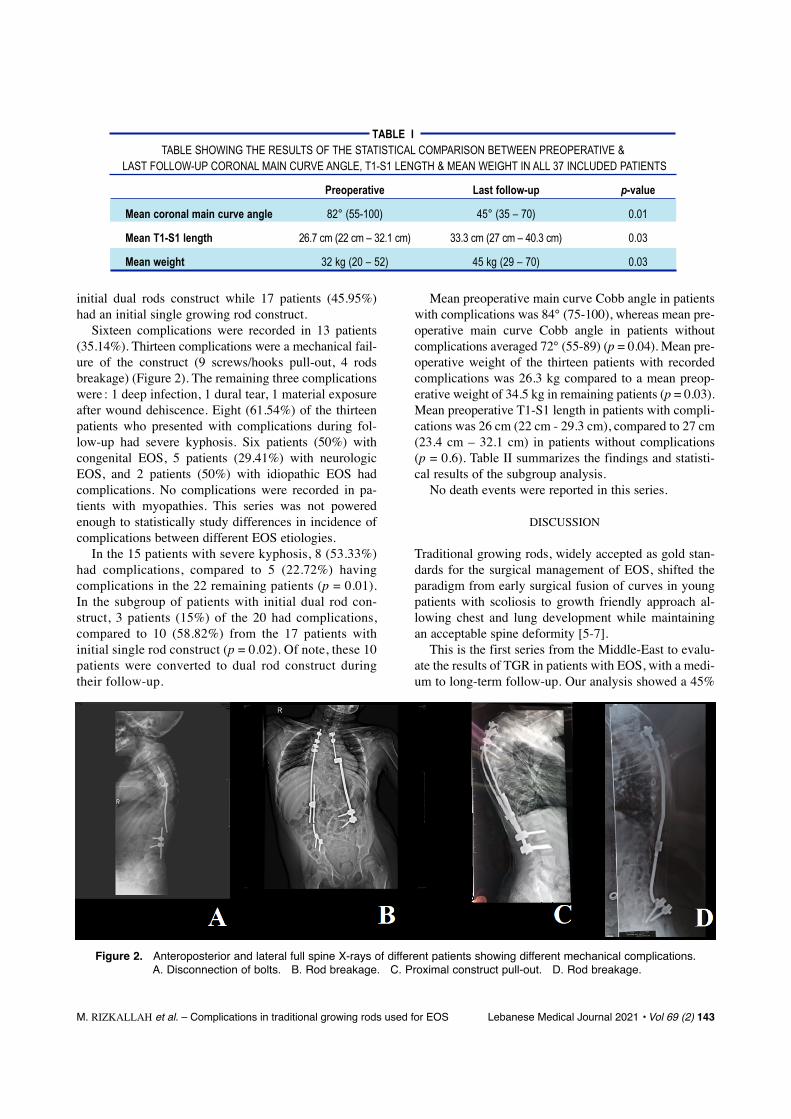
initial dual rods construct while 17 patients (45.95%)had an initial single growing rod construct.
Sixteen complications were recorded in 13 patients(35.14%). Thirteen complications were a mechanical fail-ure of the construct (9 screws/hooks pull-out, 4 rodsbreakage) (Figure 2). The remaining three complicationswere : 1 deep infection, 1 dural tear, 1 material exposureafter wound dehiscence. Eight (61.54%) of the thirteenpatients who presented with complications during fol-low-up had severe kyphosis. Six patients (50%) withcongenital EOS, 5 patients (29.41%) with neurologicEOS, and 2 patients (50%) with idiopathic EOS hadcomplications. No complications were recorded in pa-tients with myopathies. This series was not poweredenough to statistically study differences in incidence ofcomplications between different EOS etiologies.
In the 15 patients with severe kyphosis, 8 (53.33%)had complications, compared to 5 (22.72%) havingcomplications in the 22 remaining patients (p = 0.01).In the subgroup of patients with initial dual rod con-struct, 3 patients (15%) of the 20 had complications,compared to 10 (58.82%) from the 17 patients withinitial single rod construct (p = 0.02). Of note, these 10patients were converted to dual rod construct duringtheir follow-up.
Mean preoperative main curve Cobb angle in patientswith complications was 84° (75-100), whereas mean pre-operative main curve Cobb angle in patients withoutcomplications averaged 72° (55-89) (p = 0.04). Mean pre-operative weight of the thirteen patients with recordedcomplications was 26.3 kg compared to a mean preop-erative weight of 34.5 kg in remaining patients (p = 0.03).Mean preoperative T1-S1 length in patients with compli-cations was 26 cm (22 cm - 29.3 cm), compared to 27 cm(23.4 cm – 32.1 cm) in patients without complications (p = 0.6). Table II summarizes the findings and statisti-cal results of the subgroup analysis.
No death events were reported in this series.
DISCUSSION
Traditional growing rods, widely accepted as gold stan-dards for the surgical management of EOS, shifted theparadigm from early surgical fusion of curves in youngpatients with scoliosis to growth friendly approach al-lowing chest and lung development while maintainingan acceptable spine deformity [5-7].
This is the first series from the Middle-East to evalu-ate the results of TGR in patients with EOS, with a medi-um to long-term follow-up. Our analysis showed a 45%
M. RIZKALLAH et al. – Complications in traditional growing rods used for EOS Lebanese Medical Journal 2021 • Vol 69 (2) 143
Figure 2. Anteroposterior and lateral full spine X-rays of different patients showing different mechanical complications.A. Disconnection of bolts. B. Rod breakage. C. Proximal construct pull-out. D. Rod breakage.
TABLE ITABLE SHOWING THE RESULTS OF THE STATISTICAL COMPARISON BETWEEN PREOPERATIVE &
LAST FOLLOW-UP CORONAL MAIN CURVE ANGLE, T1-S1 LENGTH & MEAN WEIGHT IN ALL 37 INCLUDED PATIENTS
Preoperative Last follow-up p-value
Mean coronal main curve angle 82° (55-100) 45° (35 – 70) 0.01
Mean T1-S1 length 26.7 cm (22 cm – 32.1 cm) 33.3 cm (27 cm – 40.3 cm) 0.03
Mean weight 32 kg (20 – 52) 45 kg (29 – 70) 0.03

main coronal curve correction at last follow-up in ourpatients. A 6.6 cm mean T1-S1 length increase equiva-lent to 1.75 cm of growth per year of follow-up was rec-orded. These results confirm the success of TGR in themanagement of EOS and are comparable to those shownby main series published in the literature. Akbarnia et al.had a 56% improvement of deformity with 1.3 cm/yearof T1-S1 growth [13]. In another series, the growingspine study group reached a 67% deformity correctionat last follow-up together with 1.6 cm/year of T1-S1growth [15]. Wang et al. from Beijing, China, had near50% main curve correction with 1.49 cm/year of T1-S1growth [16]. Zarei et al. in their recent study, reported a32% correction rate of the main curve deformity [17].Finally, Upasani et al., El Sebai et al. and Bess et al. hadrespectively 43%, 29% and 37% of main curve correc-tion [18-20]. Therefore, the findings from our series to-gether with the available data in the literature confirmthe efficacy of TGR in the treatment of EOS, as both settargets are reached, allowing growth while maintainingan acceptable spine deformity.
However, one of the major drawbacks of TGR in EOSis the high incidence of complications, mainly related tothe mechanical failure of the construct. Our series reportsa 35% complication rate. This rate varied considerablyin similar published series ranging from 17% in the se-ries published by Zarei et al. to 79% of patients havingat least one complication in the series published byUpasani et al. [16-20]. Despite this wide range of varia-tion in complications rate, 5 of the 7 similar series avail-able in the literature showed a complication rate > 40%,with main issues being related to failure of construct [16,20]. We believe that this wide variability of reportedcomplication rates is due to the heterogeneity of the se-ries. Patients included in these series had different curvemagnitudes, EOS etiologies, age at surgery, comorbidi-ties and mainly, different types of constructs (all screws,hybrid with screws and hooks, single rod, dual rods, dif-ferent types of connecting bolts) [13, 15-16, 19-20].
Table III summarizes our findings and those from 7similar series in the literature, showing the number of in-cluded patients, the severity of the original deformity,
144 Lebanese Medical Journal 2021 • Vol 69 (2) M. RIZKALLAH et al. – Complications in [traditional] growing rods used for EOS
TABLE IIITABLE SUMMARIZING FINDINGS FROM OUR SERIES AND THOSE FROM 7 SIMILAR SERIES IN THE LITERATURE,
SHOWING THE NUMBER OF INCLUDED PATIENTS, THE SEVERITY OF THE ORIGINAL DEFORMITY, THE DEGREE OF CORRECTION, THE TYPE OF CONSTRUCT AND THE RATE OF COMPLICATIONS
Authors Year Patients Mean Mean correction Construct ComplicationCobb angle of curve rate
Our series 2021 37 82 45% Mixed 35%
Zarei et al. [17] 2021 42 42.9 32% Dual rod 17%
Wang et al. [16] 2012 30 72.3 50% Dual rod 23.3%
Akbarnia et al. [13] 2005 23 82 56% Dual rod 48%
GSSG [15] 2008 13 81 67% Dual rod 60%
Upasani et al. [18] 2016 110 75.5 43% Mixed 79%
Elsebai et al. [19] 2011 19 66 29% Mixed 42%
Bess et al. [20] 2010 140 75 37% Mixed 58%
TABLE IITABLE SUMMARIZING THE STATISTICAL RESULTS OF THE SUBGROUP ANALYSIS
Patients with complications Patient without complications p-value
Kyphosis 53.33% 22.72% 0.01
Dual rod construct 15% 85% < 0.01
Single rod construct 58.82% 41.18% 0.04
Mean preoperative curve Cobb angle 84? (75-100) 78? (55-89) 0.037
Mean preoperative weight 26.3 kg 34.5 kg 0.03
Mean preoperative T1-S1 length 26 cm 27 cm 0.6
Dual rod construct Single rod constructComplication rate 15% 58.82% 0.02

the degree of correction, the type of construct and therate of complications.
Subgroup analysis in our series showed the severityof spine deformity, the thoracolumbar kyphosis, the pre-operative weight and the single rod constructs to affectsignificantly the complication rate. Magnitude of spinedeformity, thoracolumbar kyphosis and single rod con-structs are previously known risk factors of complica-tions after TGR in EOS patients [21-22]. More severecurves at presentation are usually stiffer, with retractedsoft tissues. This increases significantly the mechanicalstress on the construct that is subject to repetitive micro-motion of the non-fused spine. Severely altered sagittalprofile, with mainly thoracolumbar kyphosis, increasespull-out stress on the proximal and distal anchors of theconstruct, leading to increased risk of rod breakage,screws/hooks pull-out and bolts disconnections [21-22].Double rod constructs were shown to significantly de-crease mechanical complications, to yield better correc-tions, yet minimally increasing complications related tosoft tissue coverage [22-23]. Risk factors for rods frac-tures include prior rod fracture, single rods, stainlesssteel rods, small diameter rods (< 4 mm), short connec-tors and patient ambulation [22-23]. Lengthening inter-val were not statistically associated to mechanical com-plications. Myung et al. reported fewer implant-relatedcomplications in all pedicle-screw constructs comparedto hooks [24]. Of note, patients included in our serie hada severe EOS (preoperative mean Cobb angle 82°), a sig-nificantly altered sagittal balance with near 41% of pa-tients having severe thoracolumbar kyphosis, and wereoperated using single and double rods constructs. Thismakes our study group at high risk of developing com-plications following TGR for EOS. The recorded 35% islower than the expected rate when comparing for similarseries in the medical literature (Table III).
One previously unexplored risk factor for postopera-tive complications is preoperative weight. It was shownin our series that lower preoperative weight is signifi-cantly associated with increased complication risk. Lowpreoperative weight indicates mainly a suboptimal nutri-tional profile of patient with subsequent implications onsubcutaneous and muscular tissue quality, together withreduced vertebral mineral density. We believe that thisleads to lower purchase of screws, higher mechanicalstress on the construct, and increased muscle and subcu-taneous tissue ischemia. Therefore, we recommend a sys-tematic preoperative nutritionist consult for these frailpatients with subsequent nutritional optimization. Thisshould reduce mechanical complications and those relat-ed to surgical site infection and delayed wound healing.
This study has several limitations. First, being retro-spective, it risks selection bias and incomplete data col-
lection due to recall bias. However, all eligible patientswith EOS operated and followed-up in our center wereincluded, and all data was collected from charts, whereinformation was entered prospectively with the follow-up. Another limitation is the low number of included pa-tients. However, the size of our study group is compara-ble to that of similar series in the literature. This is prob-ably due to the low incidence of EOS and to the mono-centric design of the study. Including more centers couldhave led to more included cases, but also to divergentpractices, organization and management. This would havealso increased bias related to data collections.
TGR remains the gold standard for EOS when surgi-cal treatment is indicated. Despite fulfilling the aim ofallowing residual growth while maintaining an accept-able spine deformity correction, a considerable rate ofcomplications is recorded in series of EOS patients treat-ed with TGR. These complications are mainly mechani-cal in nature and are due to continuous loading and mi-cromotion on a construct distracting an unfused spine invery young patients with small vertebrae, low bone min-eral density, and frail skin and muscle tissues. We be-lieve that surgical intervention when main curve reaches60 of magnitude, using all-screws-constructs with dual-rods, especially in patients with thoraco-lumbar kypho-sis, and nutritionally optimizing EOS patients preopera-tively would help lower the increased rate of complica-tions that reached > 50% in some series.
REFERENCES
1. Yang S, Andras LM, Redding GJ, Skaggs DL. Early-onset scoliosis: A review of history, current treatment,and future directions. Pediatrics 2016; 137 (1): e20150709.
2. Karol LA. The Natural History of Early-onset Scoliosis. J Pediatr Orthop 2019; 39 (6), Suppl 1: S38-S43.
3. Senkoylu A, Riise RB, Acaroglu E, Helenius I. Diverseapproaches to scoliosis in young children. EFORT OpenRev. 2020; 5 (10): 753-762.
4. Zhang YB, Zhang JG. Treatment of early-onset scoliosis:techniques, indications, and complications. Chin. Med. J.(Engl) 2020; 133 (3): 351-357.
5. Hardesty CK et al. Early-onset coliosis: Updated treat-ment techniques and results. Spine Deform. 2018; 6 (4):467-472.
6. Hasler CC. Early-onset scoliosis: Contemporary decision-making and treatment options. J Pediatr Orthop 2018; 38(Suppl1): S13–S20.
7. Bekmez S, Dede O, Yazici M. Advances in growing rodstreatment for early onset scoliosis. Curr Opin PediatrFeb 2017; 29 (1): 87-93.
8. Deng Z, Gong L, Zhang Q, Hao L, Ding Y, Niu X. Out-come of osteofibrous dysplasia-like versus classic ada-mantinoma of long bones: a single-institution experi-ence. J Orthop Surg Res Jul 2020; 15 (1): 268.
9. Mahajan R, Kishan S, Mallepally AR, Shafer C, Marathe N,Chhabra HS. Evolution of casting techniques in early-onset
M. RIZKALLAH et al. – Complications in traditional growing rods used for EOS Lebanese Medical Journal 2021 • Vol 69 (2) 145

and congenital scoliosis. J Clin Orthop Trauma 2020; 11(5): 810-815.
10. Wessell NM, Martus JE, Halanski MA, SnydeB, Truong W.What’s new in pediatric spine growth modulation andimplant technology for early-onset scoliosis ? J PediatrOrthop Jan 2018; 38 (1): e3-e13.
11. Odent T et al. Fusionless surgery in early-onset scoliosis.Orthop Traumatol Surg Res Oct 2015; 101 (6) Suppl:S281-S288.
12. Helenius IJ. Standard and magnetically controlled grow-ing rods for the treatment of early onset scoliosis. AnnTransl Med Jan 2020; 8 (2): 26,
13. Akbarnia BA, Marks DS, Boachie-Adjei O, Thompson AG,Asher MA. Dual growing rod technique for the treatmentof progressive early-onset scoliosis: a multicenter study.Spine (Phila. Pa. 1976) Sep. 2005, 30 (17) Suppl: S46-S57.
14. Dede O, Demirkiran G, Yazici M. 2014 Update on the‘growing spine surgery’ for young children with scolio-sis. Curr Opin Pediatr Feb. 2014, 26 (1): 57-63.
15. Akbarnia BA et al. Dual growing rod technique followedfor three to eleven years until final fusion: the effect offrequency of lengthening. Spine (Phila. Pa. 1976) Apr2008, 33 (9): 984-990.
16. S. Wang et al. Dual growing rods technique for congeni-tal scoliosis: more than 2 years outcomes: preliminary re-sults of a single center. Spine (Phila. Pa. 1976) 37 (26):E1639-44, Dec 15th 2012.
17. M. Zarei et al. Complications of dual growing rod with all-pedicle screw instrumentation in the treatment of early-onset scoliosis. J Orthop Surg Res Feb. 2021; 16 (1): 112.
18. Upasani VV et al. Age at initiation and deformity magni-tude influence complication rates of surgical treatmentwith traditional growing rods in early-onset acoliosis.Spine Deform 2016; 4 (5): 344-350.
19. Elsebai HB et al. Safety and efficacy of growing rod tech-nique for pediatric congenital spinal deformities. J PediatrOrthop 2020; 31 (1): 1-5.
20. Bess S et al. Complications of growing-rod treatment forearly-onset scoliosis: analysis of one hundred and forty pa-tients. J Bone Joint Surg Am Nov 2010; 92 (15): 2533-43.
21. Akbarnia BA, Emans JB. Complications of growth-spar-ing surgery in early onset scoliosis. Spine (Phila. Pa. 1976)Dec. 2010; 35 (25): 2193-204.
22. Yang JS et al. Growing rod fractures: risk factors andopportunities for prevention. Spine (Phila. Pa. 1976) Sep.2011; 36 (20): 1639-44.
23. Xu GJ, Fu X, Tian P, Ma, JX & X.-L. Ma XL. Compari-son of single and dual growing rods in the treatment ofearly onset scoliosis: a meta-analysis. J Orthop Surg ResJul. 2016; 11 (1): 80.
24. Myung KS, Skaggs DL, Johnston CE, Akbarnia BA &Growing Spine Study Group. The use of pedicle screwsin children 10 years of age and younger with growingrods. Spine Deform Nov. 2014; 2 (6): 471-474.
146 Lebanese Medical Journal 2021 • Vol 69 (2) M. RIZKALLAH et al. – Complications in [traditional] growing rods used for EOS
Related Documents











