American Journal of Transplantation 2008; 8: 2547–2557 Wiley Periodicals Inc. C 2008 The Authors Journal compilation C 2008 The American Society of Transplantation and the American Society of Transplant Surgeons doi: 10.1111/j.1600-6143.2008.02409.x Liver Transplantation for Hepatocellular Carcinoma: Results of Down-Staging in Patients Initially Outside the Milan Selection Criteria M. Ravaioli a , G. L. Grazi a, ∗ , F. Piscaglia b , F. Trevisani b , M. Cescon a , G. Ercolani a , M. Vivarelli a , R. Golfieri c , A. D’Errico Grigioni d , I. Panzini e , C. Morelli a , M. Bernardi b , L. Bolondi b and A. D. Pinna a a Department of Liver and Multi-organ Transplantation, b Department of Gastroenterology and Internal Medicine, c Department of Radiology and d Department of Onco-hematology, Pathology Division of the ‘F. Addarii’ Institute, Sant’ Orsola-Malpighi Hospital, University of Bologna, Bologna, Italy e Department of Research and Innovation, Hospital of Rimini, Rimini, Italy ∗ Corresponding author: Gian Luca Grazi, [email protected]; [email protected] Conventional criteria for liver transplantation for pa- tients with hepatocellular carcinoma are single HCC ≤ 5 cm or less than or equal to three HCCs ≤ 3 cm. We prospectively evaluated the possibility of slightly extending these criteria in a down-staging protocol, which included patients initially outside conventional criteria: single HCC 5–6 cm or two HCCs ≤ 5 cm or less than six HCCs ≤ 4 cm and sum diameter ≤ 12 cm, but within Milan criteria in the active tumors after the down-staging procedures. The outcome of patients down-staged was compared to that of Milan criteria after liver transplantation and since the first evalua- tion according to an intention-to-treat principle. From 2003 to 2006, 177 patients with HCC were considered for transplantation: the transplantation rate was com- parable between the Milan and down-staging groups: 88/129 cases (68%) versus 32/48 cases (67%), respec- tively. At a median follow-up of 2.5 years after trans- plantation, the 1 and 3 years’ disease-free survival rates were comparable: 80% and 71% in the Milan group ver- sus 78% and 71% in the down-staging. The actuarial intention-to-treat survival was 27/48 patients (56.3%) in the down-staging and 81/129 cases (62.8%) in the Milan group, p = n.s. The proposed down-staging crite- ria provide a comparable outcome to the conventional criteria. Key words: Allocation, hepatocellular carcinoma, liver transplantation, MELD score, patient survival, selec- tion criteria, tumor recurrence Received 12 March 2008, revised 30 June 2008 and accepted for publication 02 August 2008 Introduction Liver transplantation (LT) for hepatocellular carcinoma (HCC) preoperatively meeting the Milan criteria (MC) is an established effective treatment, with a tumor recurrence rate and 5-year patient survival close to 10% and 75%, respectively (1–3). Patients with HCC not meeting the MC are generally ex- cluded from LT (3,4), due to the poor results reported in the past in comparison to patients transplanted for cirrhosis, and are managed with alternative treatments which offer a lower survival than LT (5,6). Several authors believe these criteria, which include single nodule with a diameter ≤5 cm or multiple nodules up to three with a diameter ≤3 cm, could be slightly expanded without affecting the postoperative tumor recurrence rate and patient survival (7–18). However, there are no prospec- tive and comprehensive studies with new preoperative selection criteria, intention-to-treat analysis, including all tumor stages, and a median follow-up of more than 2 years. The extension of the selection criteria based on postopera- tive histological samples proposed in some studies should be carefully evaluated, due to the discrepancy between preoperative and postoperative tumor stages which may affect the analysis of patient outcome (1,19,20). Other debated issues are the type of priority on the wait- ing list for each tumor stage which HCC patients should receive and the management of these patients during the waiting time to avoid tumor progression or death due to liver failure (21–28). We performed a prospective study, applying a down- staging protocol for patients initially outside the conven- tional tumor criteria and meeting them after preoperative treatments (pre-Ts). The outcome of patients meeting the Milan criteria at the beginning and the outcome of patients included in the down-staging protocol were compared both after LT and after the first evaluation of the patients in an intention-to-treat analysis. 2547

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

American Journal of Transplantation 2008; 8: 2547–2557Wiley Periodicals Inc.
C© 2008 The AuthorsJournal compilation C© 2008 The American Society of
Transplantation and the American Society of Transplant Surgeons
doi: 10.1111/j.1600-6143.2008.02409.x
Liver Transplantation for Hepatocellular Carcinoma:Results of Down-Staging in Patients Initially Outsidethe Milan Selection Criteria
M. Ravaiolia, G. L. Grazia,∗, F. Piscagliab,
F. Trevisanib, M. Cescona, G. Ercolania,
M. Vivarellia, R. Golfieric, A. D’Errico Grigionid,
I. Panzinie, C. Morellia, M. Bernardib, L. Bolondib
and A. D. Pinnaa
aDepartment of Liver and Multi-organ Transplantation,bDepartment of Gastroenterology and Internal Medicine,cDepartment of Radiology and dDepartment ofOnco-hematology, Pathology Division of the ‘F. Addarii’Institute, Sant’ Orsola-Malpighi Hospital, University ofBologna, Bologna, ItalyeDepartment of Research and Innovation, Hospital ofRimini, Rimini, Italy∗Corresponding author: Gian Luca Grazi,[email protected]; [email protected]
Conventional criteria for liver transplantation for pa-tients with hepatocellular carcinoma are single HCC ≤5 cm or less than or equal to three HCCs ≤ 3 cm.We prospectively evaluated the possibility of slightlyextending these criteria in a down-staging protocol,which included patients initially outside conventionalcriteria: single HCC 5–6 cm or two HCCs ≤ 5 cm orless than six HCCs ≤ 4 cm and sum diameter ≤ 12 cm,but within Milan criteria in the active tumors after thedown-staging procedures. The outcome of patientsdown-staged was compared to that of Milan criteriaafter liver transplantation and since the first evalua-tion according to an intention-to-treat principle. From2003 to 2006, 177 patients with HCC were consideredfor transplantation: the transplantation rate was com-parable between the Milan and down-staging groups:88/129 cases (68%) versus 32/48 cases (67%), respec-tively. At a median follow-up of 2.5 years after trans-plantation, the 1 and 3 years’ disease-free survival rateswere comparable: 80% and 71% in the Milan group ver-sus 78% and 71% in the down-staging. The actuarialintention-to-treat survival was 27/48 patients (56.3%)in the down-staging and 81/129 cases (62.8%) in theMilan group, p = n.s. The proposed down-staging crite-ria provide a comparable outcome to the conventionalcriteria.
Key words: Allocation, hepatocellular carcinoma, livertransplantation, MELD score, patient survival, selec-tion criteria, tumor recurrence
Received 12 March 2008, revised 30 June 2008 andaccepted for publication 02 August 2008
Introduction
Liver transplantation (LT) for hepatocellular carcinoma(HCC) preoperatively meeting the Milan criteria (MC) is anestablished effective treatment, with a tumor recurrencerate and 5-year patient survival close to 10% and 75%,respectively (1–3).
Patients with HCC not meeting the MC are generally ex-cluded from LT (3,4), due to the poor results reported in thepast in comparison to patients transplanted for cirrhosis,and are managed with alternative treatments which offera lower survival than LT (5,6).
Several authors believe these criteria, which include singlenodule with a diameter ≤5 cm or multiple nodules up tothree with a diameter ≤3 cm, could be slightly expandedwithout affecting the postoperative tumor recurrence rateand patient survival (7–18). However, there are no prospec-tive and comprehensive studies with new preoperativeselection criteria, intention-to-treat analysis, including alltumor stages, and a median follow-up of more than2 years.
The extension of the selection criteria based on postopera-tive histological samples proposed in some studies shouldbe carefully evaluated, due to the discrepancy betweenpreoperative and postoperative tumor stages which mayaffect the analysis of patient outcome (1,19,20).
Other debated issues are the type of priority on the wait-ing list for each tumor stage which HCC patients shouldreceive and the management of these patients during thewaiting time to avoid tumor progression or death due toliver failure (21–28).
We performed a prospective study, applying a down-staging protocol for patients initially outside the conven-tional tumor criteria and meeting them after preoperativetreatments (pre-Ts). The outcome of patients meeting theMilan criteria at the beginning and the outcome of patientsincluded in the down-staging protocol were compared bothafter LT and after the first evaluation of the patients in anintention-to-treat analysis.
2547

Ravaioli et al.
Patients and Methods
Study design and patient population
From January 2003 to January 2006, we prospectively evaluated 177 pa-tients considered for LT with a preoperative diagnosis of HCC. The diagnosisof HCC was made following the EASL and the AASLD guidelines (29,30).Nodules between 1 and 2 cm were considered HCCs when two radiologicaltechniques among ultrasonography (US), computed tomography (CT) andmagnetic resonance imaging (MRI) showed a typical hypervascular patternwith a washout in the venous phase. Nodules less than 2 cm with an equivo-cal imaging pattern were biopsied whenever possible and, if the biopsy wastechnically unfeasible, they were included in a US and CT scan surveillanceprogram (31).
The diagnosis of HCC was the only indication for LT in 15 cases (8.5%),while in the remaining cases it was associated with liver failure.
During the waiting time, pre-Ts were decided in each patient by a mul-tidisciplinary team according to the tumor stage, HCC location and liverfunction. Patients with a single nodule or two nodules located in the samesegment and preserved liver function were treated by liver resection (LR)and were listed for LT only if tumor recurrence within the MC or liverfailure occurred. Patients not suitable for LR were treated by transarterialchemo-embolization (TACE) and/or alcohol injection (PEI) or percutaneousradiofrequency ablation (RFA) aimed at achieving complete tumor necrosis(1,32,33).
Patients not meeting the MC were included on the waiting list after com-pleting the following down-staging protocol, drawn up by a multidisciplinaryteam at our hospital including surgeons, hepatologists, radiologists andpathologists, based on our previous experiences and studies (1,22,24–26,32–34).
Down-stage protocol
(1) The criteria approved by the committee were a single HCC ≤ 8 cm orbifocal HCCs ≤ 5 cm or multiple HCCs < 6 with a maximum diameter≤ 4 cm and a total tumor diameter ≤ 12 cm.
(2) All cases had to meet the MC after the down-staging procedures, con-sidering the still active tumors. The radiological response to the pre-Tswere evaluated in a blinded fashion by two different investigators and adisagreement of less than 0.5 cm was allowed during the measurementof nodules.
(3) TACE, LR, PEI or RFA were applied according to case-by-case discussionas described.
(4) After the pre-Ts, the nodules were considered active if contrast en-hancement of any extent was present at imaging techniques. Amongthe active nodules, the diameter of the whole lesion including thenecrotic portion was considered to establish the size to meet the MC.Only active nodules were considered to meet the selection criteria andthe new nodules appearing during the waiting time were put togetherwith the treated nodules. Indeed, the total number of nodules, eithertreated or not and either present at the beginning or developed subse-quently, should not exceed the number approved for the protocol.
(5) A minimum follow-up of 3 months of meeting the conventional criteriaafter the pre-Ts was considered necessary for patients to be includedon the waiting list. The alfa-feto protein level (AFP) had to remain <400ng/mL during the waiting time.
(6) Macrovascular or biliary invasion by the tumor were definitive exclusioncriteria. Portal thrombosis was not considered an exclusion criterion perse, but only if the contrast imaging technique and the ultrasound-guidedbiopsy were not able to definitively exclude a malignant nature of the
thrombus. Microvascular invasion or high tumor grade on the samplesafter LR were not considered a contraindication to LT. These criteriawere also applied for the other tumor stages.
When listed, patients with all tumor stages were followed with US, AFPdetermination and CT scan repeated at least every 3 months (1,34).
At the time of listing for LT, the HCC patients received priority according to acalculated score which was computed by adding a number of points basedon the tumor stage and the waiting time to the MELD (model for end-stageliver disease) score currently in use by UNOS (http://www.unos.org) (35,36).These points changed over the years, due to an ad interim analysis whichwas designed to maintain a comparable dropout rate between HCC andnon-HCC patients; further data on this policy are presented in two recentpublications (26,37).
The study was approved by the local institutional review committee.
Statistical analysis
Fisher’s exact test, Mann–Whitney test or Chi-square test were applied, asappropriate.
Waiting time on the list was calculated starting from the day of listing tothe day of dropout, LT or end of the follow-up on the list (January 2007)if the patient was still on the list at that date. In this way all patients hadat least 1 year of follow-up on the list if they were not transplanted orremoved from the list before this period. The causes of dropout weredeath, tumor progression exceeding the transplant criteria and too-sickcases (26).
The survival of patients after LT was calculated by the Kaplan–Meier methodstarting from the date of LT to the date of death or to the most recentfollow-up visit. The follow-up after LT started in January 2003 and ended inDecember 2007.
The chi-square test and logistic regression were used to assess the accu-racy of variables as predictors of tumor recurrence after LT.
The disease-free survival was computed by the Kaplan–Meier method start-ing from the date of LT to the date of the diagnosis of tumor recurrence ordeath.
The tumor-recurrence-free survival was computed by the Kaplan–Meiermethod starting from the date of LT to the date of the diagnosis of tu-mor recurrence; patients who died of causes other than tumor recurrencewere censored at the end of the follow-up.
The intention-to-treat survival of patients was calculated by the Kaplan–Meier method starting from the date of the patient evaluation for LT insideor outside the down-staging protocol to the date of death (during the waitingtime, after the exclusion from the list for tumor progression, after LT) or tothe most recent follow-up visit if the patient was alive.
None of the patients were lost during the follow-up.
Differences were compared by the log-rank test and variables were evalu-ated in the multivariate analysis using Cox’s proportional hazard model.
The cut-off of the AFP-level was established according to our previousexperience (1); its value at the time of LT and its delta measure (time of LT –time of listing) were related to tumor recurrence.
2548 American Journal of Transplantation 2008; 8: 2547–2557
Bologna HCC Criteria for Liver Transplantation
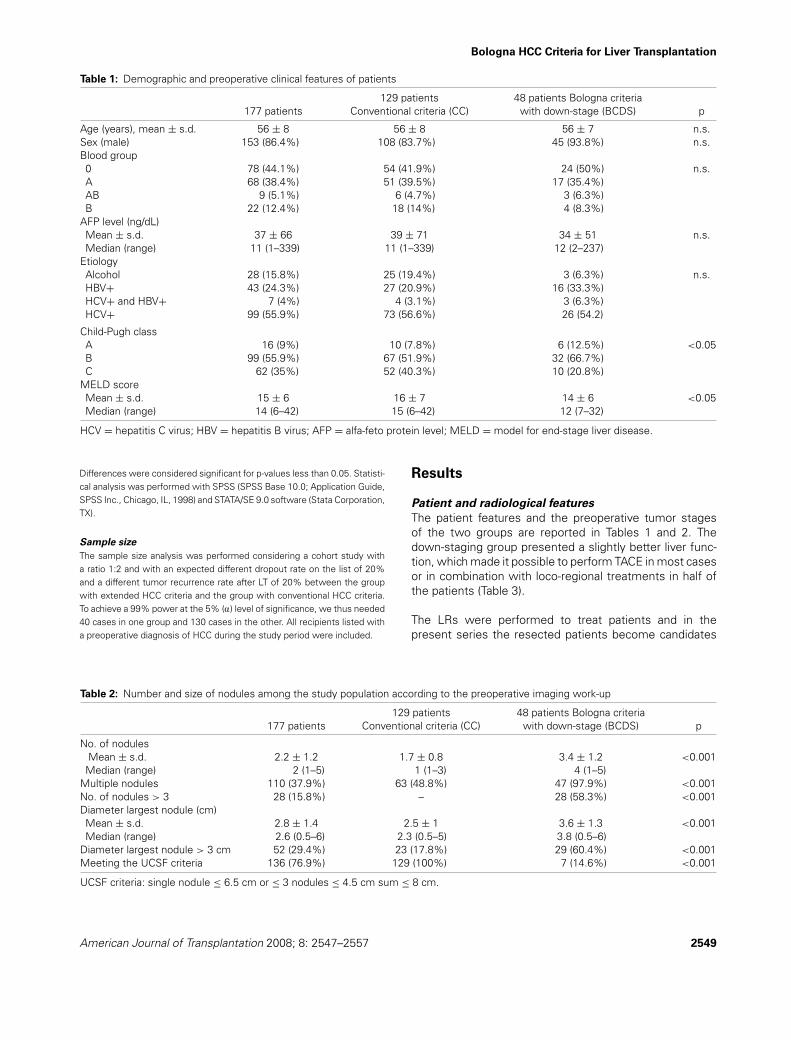
Table 1: Demographic and preoperative clinical features of patients
129 patients 48 patients Bologna criteria177 patients Conventional criteria (CC) with down-stage (BCDS) p
Age (years), mean ± s.d. 56 ± 8 56 ± 8 56 ± 7 n.s.Sex (male) 153 (86.4%) 108 (83.7%) 45 (93.8%) n.s.Blood group0 78 (44.1%) 54 (41.9%) 24 (50%) n.s.A 68 (38.4%) 51 (39.5%) 17 (35.4%)AB 9 (5.1%) 6 (4.7%) 3 (6.3%)B 22 (12.4%) 18 (14%) 4 (8.3%)
AFP level (ng/dL)Mean ± s.d. 37 ± 66 39 ± 71 34 ± 51 n.s.Median (range) 11 (1–339) 11 (1–339) 12 (2–237)
EtiologyAlcohol 28 (15.8%) 25 (19.4%) 3 (6.3%) n.s.HBV+ 43 (24.3%) 27 (20.9%) 16 (33.3%)HCV+ and HBV+ 7 (4%) 4 (3.1%) 3 (6.3%)HCV+ 99 (55.9%) 73 (56.6%) 26 (54.2)
Child-Pugh classA 16 (9%) 10 (7.8%) 6 (12.5%) <0.05B 99 (55.9%) 67 (51.9%) 32 (66.7%)C 62 (35%) 52 (40.3%) 10 (20.8%)
MELD scoreMean ± s.d. 15 ± 6 16 ± 7 14 ± 6 <0.05Median (range) 14 (6–42) 15 (6–42) 12 (7–32)
HCV = hepatitis C virus; HBV = hepatitis B virus; AFP = alfa-feto protein level; MELD = model for end-stage liver disease.
Differences were considered significant for p-values less than 0.05. Statisti-cal analysis was performed with SPSS (SPSS Base 10.0; Application Guide,SPSS Inc., Chicago, IL, 1998) and STATA/SE 9.0 software (Stata Corporation,TX).
Sample size
The sample size analysis was performed considering a cohort study witha ratio 1:2 and with an expected different dropout rate on the list of 20%and a different tumor recurrence rate after LT of 20% between the groupwith extended HCC criteria and the group with conventional HCC criteria.To achieve a 99% power at the 5% (a) level of significance, we thus needed40 cases in one group and 130 cases in the other. All recipients listed witha preoperative diagnosis of HCC during the study period were included.
Table 2: Number and size of nodules among the study population according to the preoperative imaging work-up
129 patients 48 patients Bologna criteria177 patients Conventional criteria (CC) with down-stage (BCDS) p
No. of nodulesMean ± s.d. 2.2 ± 1.2 1.7 ± 0.8 3.4 ± 1.2 <0.001
Median (range) 2 (1–5) 1 (1–3) 4 (1–5)Multiple nodules 110 (37.9%) 63 (48.8%) 47 (97.9%) <0.001No. of nodules > 3 28 (15.8%) – 28 (58.3%) <0.001Diameter largest nodule (cm)Mean ± s.d. 2.8 ± 1.4 2.5 ± 1 3.6 ± 1.3 <0.001Median (range) 2.6 (0.5–6) 2.3 (0.5–5) 3.8 (0.5–6)
Diameter largest nodule > 3 cm 52 (29.4%) 23 (17.8%) 29 (60.4%) <0.001Meeting the UCSF criteria 136 (76.9%) 129 (100%) 7 (14.6%) <0.001
UCSF criteria: single nodule ≤ 6.5 cm or ≤ 3 nodules ≤ 4.5 cm sum ≤ 8 cm.
Results
Patient and radiological features
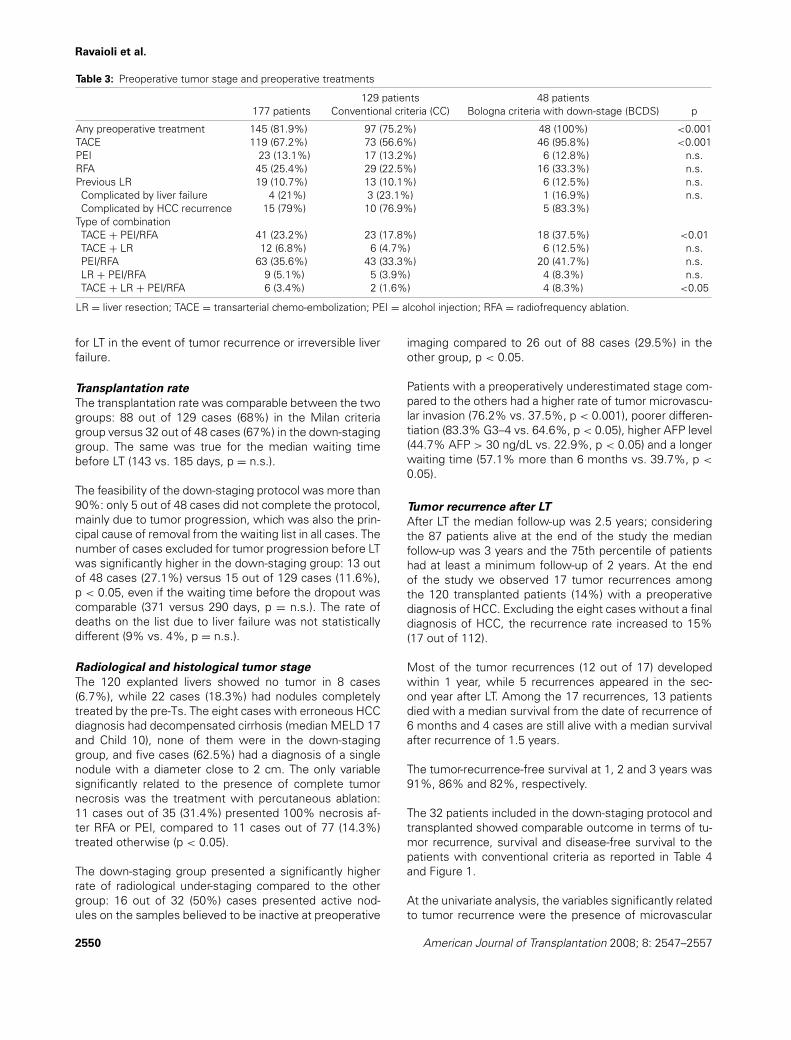
The patient features and the preoperative tumor stagesof the two groups are reported in Tables 1 and 2. Thedown-staging group presented a slightly better liver func-tion, which made it possible to perform TACE in most casesor in combination with loco-regional treatments in half ofthe patients (Table 3).
The LRs were performed to treat patients and in thepresent series the resected patients become candidates
American Journal of Transplantation 2008; 8: 2547–2557 2549
Ravaioli et al.
Table 3: Preoperative tumor stage and preoperative treatments
129 patients 48 patients177 patients Conventional criteria (CC) Bologna criteria with down-stage (BCDS) p
Any preoperative treatment 145 (81.9%) 97 (75.2%) 48 (100%) <0.001TACE 119 (67.2%) 73 (56.6%) 46 (95.8%) <0.001PEI 23 (13.1%) 17 (13.2%) 6 (12.8%) n.s.RFA 45 (25.4%) 29 (22.5%) 16 (33.3%) n.s.Previous LR 19 (10.7%) 13 (10.1%) 6 (12.5%) n.s.Complicated by liver failure 4 (21%) 3 (23.1%) 1 (16.9%) n.s.Complicated by HCC recurrence 15 (79%) 10 (76.9%) 5 (83.3%)
Type of combinationTACE + PEI/RFA 41 (23.2%) 23 (17.8%) 18 (37.5%) <0.01TACE + LR 12 (6.8%) 6 (4.7%) 6 (12.5%) n.s.PEI/RFA 63 (35.6%) 43 (33.3%) 20 (41.7%) n.s.LR + PEI/RFA 9 (5.1%) 5 (3.9%) 4 (8.3%) n.s.TACE + LR + PEI/RFA 6 (3.4%) 2 (1.6%) 4 (8.3%) <0.05
LR = liver resection; TACE = transarterial chemo-embolization; PEI = alcohol injection; RFA = radiofrequency ablation.
for LT in the event of tumor recurrence or irreversible liverfailure.
Transplantation rate
The transplantation rate was comparable between the twogroups: 88 out of 129 cases (68%) in the Milan criteriagroup versus 32 out of 48 cases (67%) in the down-staginggroup. The same was true for the median waiting timebefore LT (143 vs. 185 days, p = n.s.).
The feasibility of the down-staging protocol was more than90%: only 5 out of 48 cases did not complete the protocol,mainly due to tumor progression, which was also the prin-cipal cause of removal from the waiting list in all cases. Thenumber of cases excluded for tumor progression before LTwas significantly higher in the down-staging group: 13 outof 48 cases (27.1%) versus 15 out of 129 cases (11.6%),p < 0.05, even if the waiting time before the dropout wascomparable (371 versus 290 days, p = n.s.). The rate ofdeaths on the list due to liver failure was not statisticallydifferent (9% vs. 4%, p = n.s.).
Radiological and histological tumor stage
The 120 explanted livers showed no tumor in 8 cases(6.7%), while 22 cases (18.3%) had nodules completelytreated by the pre-Ts. The eight cases with erroneous HCCdiagnosis had decompensated cirrhosis (median MELD 17and Child 10), none of them were in the down-staginggroup, and five cases (62.5%) had a diagnosis of a singlenodule with a diameter close to 2 cm. The only variablesignificantly related to the presence of complete tumornecrosis was the treatment with percutaneous ablation:11 cases out of 35 (31.4%) presented 100% necrosis af-ter RFA or PEI, compared to 11 cases out of 77 (14.3%)treated otherwise (p < 0.05).
The down-staging group presented a significantly higherrate of radiological under-staging compared to the othergroup: 16 out of 32 (50%) cases presented active nod-ules on the samples believed to be inactive at preoperative
imaging compared to 26 out of 88 cases (29.5%) in theother group, p < 0.05.
Patients with a preoperatively underestimated stage com-pared to the others had a higher rate of tumor microvascu-lar invasion (76.2% vs. 37.5%, p < 0.001), poorer differen-tiation (83.3% G3–4 vs. 64.6%, p < 0.05), higher AFP level(44.7% AFP > 30 ng/dL vs. 22.9%, p < 0.05) and a longerwaiting time (57.1% more than 6 months vs. 39.7%, p <
0.05).
Tumor recurrence after LT
After LT the median follow-up was 2.5 years; consideringthe 87 patients alive at the end of the study the medianfollow-up was 3 years and the 75th percentile of patientshad at least a minimum follow-up of 2 years. At the endof the study we observed 17 tumor recurrences amongthe 120 transplanted patients (14%) with a preoperativediagnosis of HCC. Excluding the eight cases without a finaldiagnosis of HCC, the recurrence rate increased to 15%(17 out of 112).
Most of the tumor recurrences (12 out of 17) developedwithin 1 year, while 5 recurrences appeared in the sec-ond year after LT. Among the 17 recurrences, 13 patientsdied with a median survival from the date of recurrence of6 months and 4 cases are still alive with a median survivalafter recurrence of 1.5 years.
The tumor-recurrence-free survival at 1, 2 and 3 years was91%, 86% and 82%, respectively.
The 32 patients included in the down-staging protocol andtransplanted showed comparable outcome in terms of tu-mor recurrence, survival and disease-free survival to thepatients with conventional criteria as reported in Table 4and Figure 1.
At the univariate analysis, the variables significantly relatedto tumor recurrence were the presence of microvascular
2550 American Journal of Transplantation 2008; 8: 2547–2557
Bologna HCC Criteria for Liver Transplantation
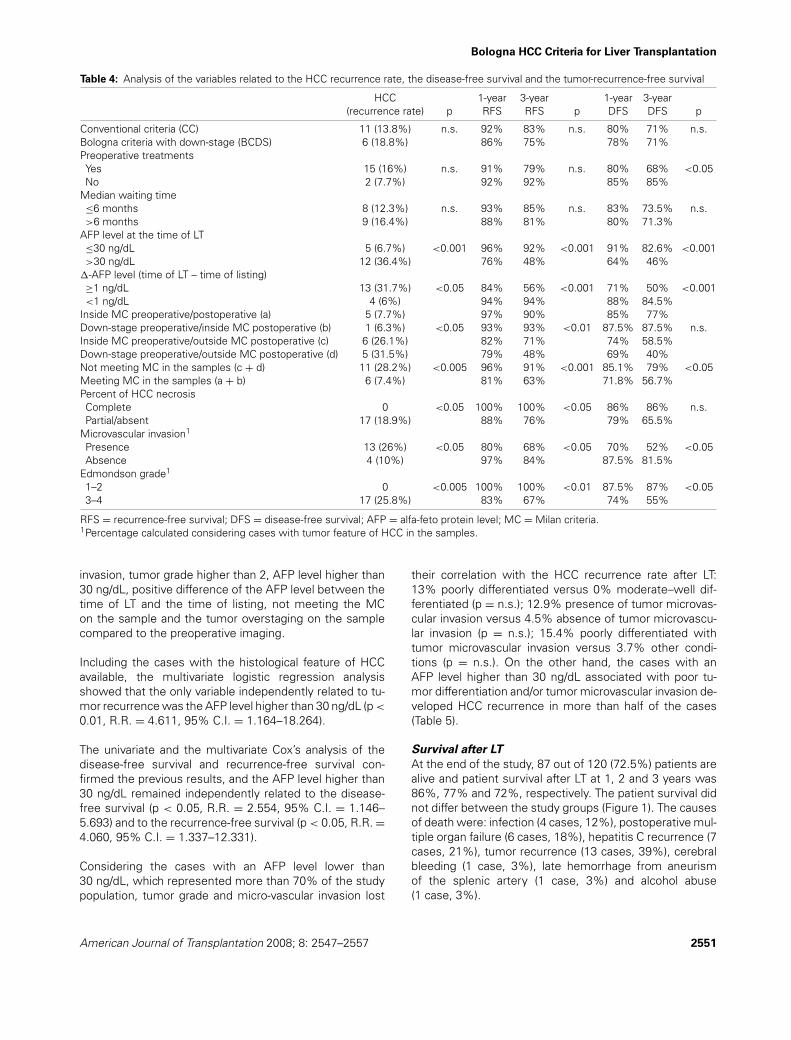
Table 4: Analysis of the variables related to the HCC recurrence rate, the disease-free survival and the tumor-recurrence-free survival
HCC 1-year 3-year 1-year 3-year(recurrence rate) p RFS RFS p DFS DFS p
Conventional criteria (CC) 11 (13.8%) n.s. 92% 83% n.s. 80% 71% n.s.Bologna criteria with down-stage (BCDS) 6 (18.8%) 86% 75% 78% 71%Preoperative treatmentsYes 15 (16%) n.s. 91% 79% n.s. 80% 68% <0.05No 2 (7.7%) 92% 92% 85% 85%
Median waiting time≤6 months 8 (12.3%) n.s. 93% 85% n.s. 83% 73.5% n.s.>6 months 9 (16.4%) 88% 81% 80% 71.3%
AFP level at the time of LT≤30 ng/dL 5 (6.7%) <0.001 96% 92% <0.001 91% 82.6% <0.001>30 ng/dL 12 (36.4%) 76% 48% 64% 46%
�-AFP level (time of LT – time of listing)≥1 ng/dL 13 (31.7%) <0.05 84% 56% <0.001 71% 50% <0.001<1 ng/dL 4 (6%) 94% 94% 88% 84.5%
Inside MC preoperative/postoperative (a) 5 (7.7%) 97% 90% 85% 77%Down-stage preoperative/inside MC postoperative (b) 1 (6.3%) <0.05 93% 93% <0.01 87.5% 87.5% n.s.Inside MC preoperative/outside MC postoperative (c) 6 (26.1%) 82% 71% 74% 58.5%Down-stage preoperative/outside MC postoperative (d) 5 (31.5%) 79% 48% 69% 40%Not meeting MC in the samples (c + d) 11 (28.2%) <0.005 96% 91% <0.001 85.1% 79% <0.05Meeting MC in the samples (a + b) 6 (7.4%) 81% 63% 71.8% 56.7%Percent of HCC necrosisComplete 0 <0.05 100% 100% <0.05 86% 86% n.s.Partial/absent 17 (18.9%) 88% 76% 79% 65.5%
Microvascular invasion1
Presence 13 (26%) <0.05 80% 68% <0.05 70% 52% <0.05Absence 4 (10%) 97% 84% 87.5% 81.5%
Edmondson grade1
1–2 0 <0.005 100% 100% <0.01 87.5% 87% <0.053–4 17 (25.8%) 83% 67% 74% 55%
RFS = recurrence-free survival; DFS = disease-free survival; AFP = alfa-feto protein level; MC = Milan criteria.1Percentage calculated considering cases with tumor feature of HCC in the samples.
invasion, tumor grade higher than 2, AFP level higher than30 ng/dL, positive difference of the AFP level between thetime of LT and the time of listing, not meeting the MCon the sample and the tumor overstaging on the samplecompared to the preoperative imaging.
Including the cases with the histological feature of HCCavailable, the multivariate logistic regression analysisshowed that the only variable independently related to tu-mor recurrence was the AFP level higher than 30 ng/dL (p <
0.01, R.R. = 4.611, 95% C.I. = 1.164–18.264).
The univariate and the multivariate Cox’s analysis of thedisease-free survival and recurrence-free survival con-firmed the previous results, and the AFP level higher than30 ng/dL remained independently related to the disease-free survival (p < 0.05, R.R. = 2.554, 95% C.I. = 1.146–5.693) and to the recurrence-free survival (p < 0.05, R.R. =4.060, 95% C.I. = 1.337–12.331).
Considering the cases with an AFP level lower than30 ng/dL, which represented more than 70% of the studypopulation, tumor grade and micro-vascular invasion lost
their correlation with the HCC recurrence rate after LT:13% poorly differentiated versus 0% moderate–well dif-ferentiated (p = n.s.); 12.9% presence of tumor microvas-cular invasion versus 4.5% absence of tumor microvascu-lar invasion (p = n.s.); 15.4% poorly differentiated withtumor microvascular invasion versus 3.7% other condi-tions (p = n.s.). On the other hand, the cases with anAFP level higher than 30 ng/dL associated with poor tu-mor differentiation and/or tumor microvascular invasion de-veloped HCC recurrence in more than half of the cases(Table 5).
Survival after LT
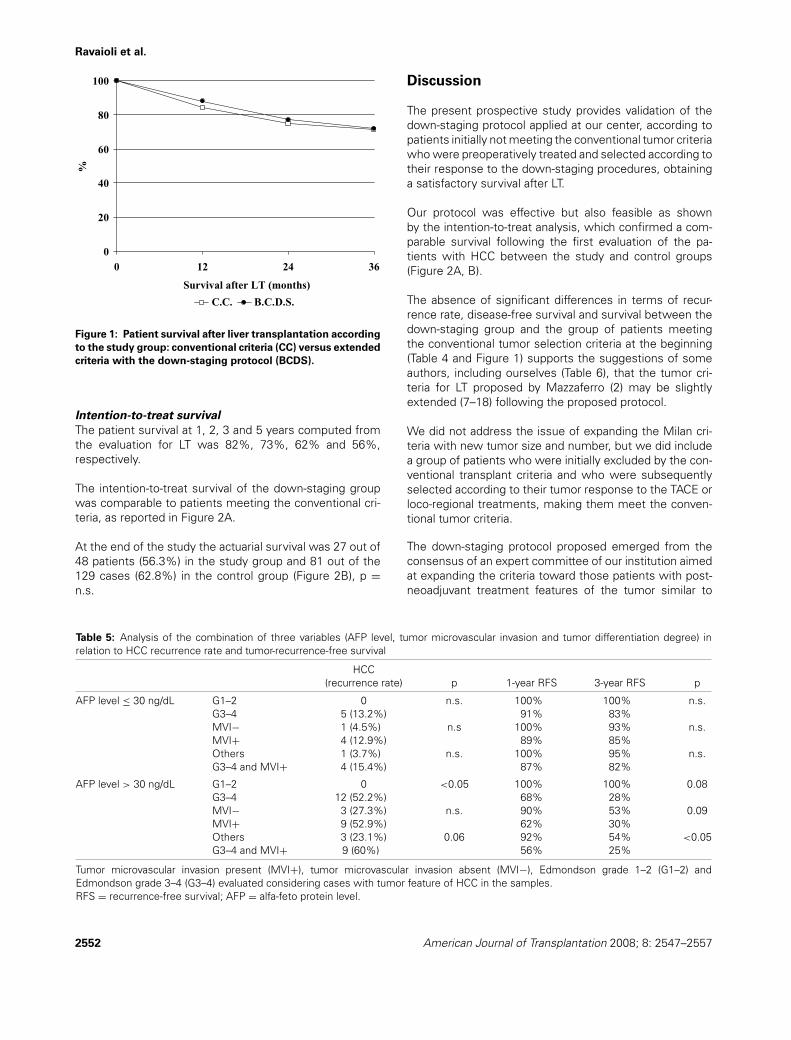
At the end of the study, 87 out of 120 (72.5%) patients arealive and patient survival after LT at 1, 2 and 3 years was86%, 77% and 72%, respectively. The patient survival didnot differ between the study groups (Figure 1). The causesof death were: infection (4 cases, 12%), postoperative mul-tiple organ failure (6 cases, 18%), hepatitis C recurrence (7cases, 21%), tumor recurrence (13 cases, 39%), cerebralbleeding (1 case, 3%), late hemorrhage from aneurismof the splenic artery (1 case, 3%) and alcohol abuse(1 case, 3%).
American Journal of Transplantation 2008; 8: 2547–2557 2551
Ravaioli et al.
0
20
40
60
80
100
0 12 24 36
Survival after LT (months)
%
C.C. B.C.D.S.
Figure 1: Patient survival after liver transplantation according
to the study group: conventional criteria (CC) versus extended
criteria with the down-staging protocol (BCDS).
Intention-to-treat survival
The patient survival at 1, 2, 3 and 5 years computed fromthe evaluation for LT was 82%, 73%, 62% and 56%,respectively.
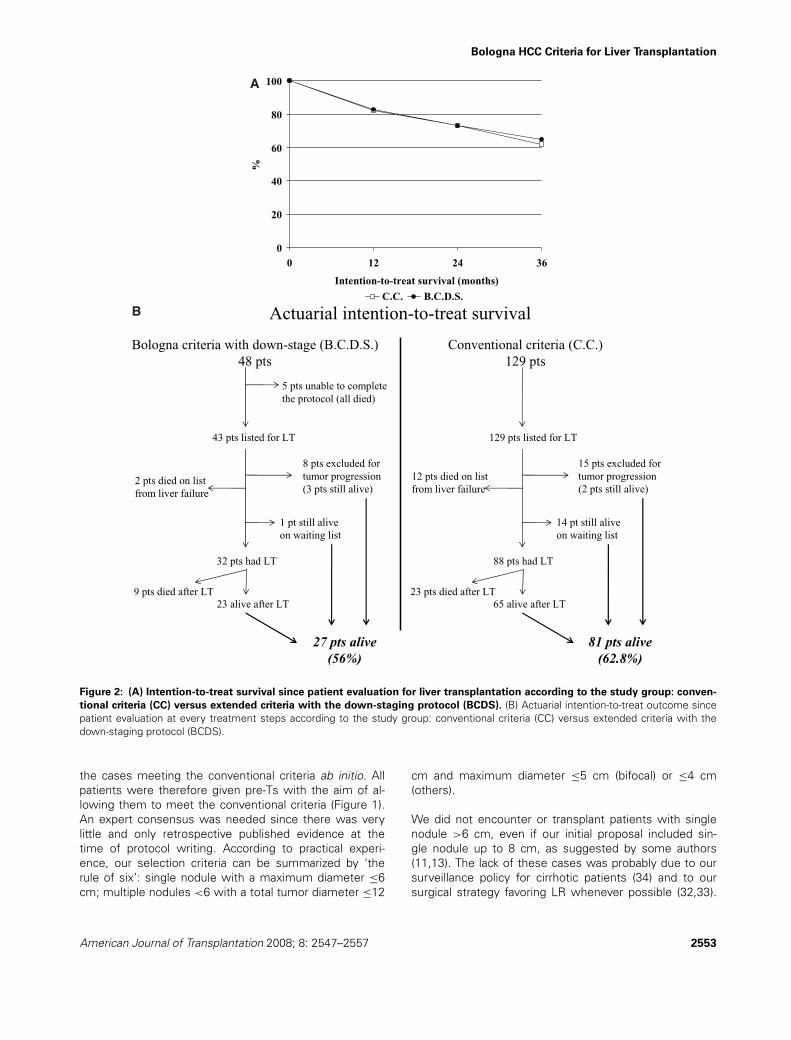
The intention-to-treat survival of the down-staging groupwas comparable to patients meeting the conventional cri-teria, as reported in Figure 2A.
At the end of the study the actuarial survival was 27 out of48 patients (56.3%) in the study group and 81 out of the129 cases (62.8%) in the control group (Figure 2B), p =n.s.
Table 5: Analysis of the combination of three variables (AFP level, tumor microvascular invasion and tumor differentiation degree) inrelation to HCC recurrence rate and tumor-recurrence-free survival
HCC(recurrence rate) p 1-year RFS 3-year RFS p
AFP level ≤ 30 ng/dL G1–2 0 n.s. 100% 100% n.s.G3–4 5 (13.2%) 91% 83%MVI− 1 (4.5%) n.s 100% 93% n.s.MVI+ 4 (12.9%) 89% 85%Others 1 (3.7%) n.s. 100% 95% n.s.G3–4 and MVI+ 4 (15.4%) 87% 82%
AFP level > 30 ng/dL G1–2 0 <0.05 100% 100% 0.08G3–4 12 (52.2%) 68% 28%MVI− 3 (27.3%) n.s. 90% 53% 0.09MVI+ 9 (52.9%) 62% 30%Others 3 (23.1%) 0.06 92% 54% <0.05G3–4 and MVI+ 9 (60%) 56% 25%
Tumor microvascular invasion present (MVI+), tumor microvascular invasion absent (MVI−), Edmondson grade 1–2 (G1–2) andEdmondson grade 3–4 (G3–4) evaluated considering cases with tumor feature of HCC in the samples.RFS = recurrence-free survival; AFP = alfa-feto protein level.
Discussion
The present prospective study provides validation of thedown-staging protocol applied at our center, according topatients initially not meeting the conventional tumor criteriawho were preoperatively treated and selected according totheir response to the down-staging procedures, obtaininga satisfactory survival after LT.
Our protocol was effective but also feasible as shownby the intention-to-treat analysis, which confirmed a com-parable survival following the first evaluation of the pa-tients with HCC between the study and control groups(Figure 2A, B).
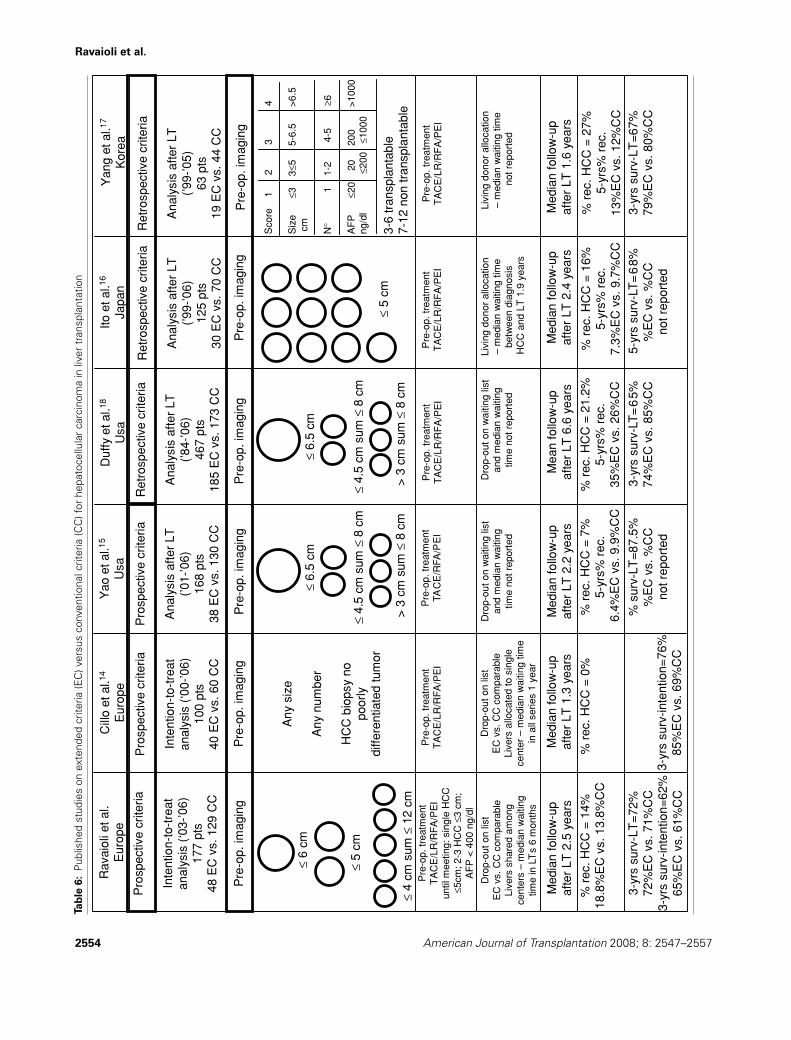
The absence of significant differences in terms of recur-rence rate, disease-free survival and survival between thedown-staging group and the group of patients meetingthe conventional tumor selection criteria at the beginning(Table 4 and Figure 1) supports the suggestions of someauthors, including ourselves (Table 6), that the tumor cri-teria for LT proposed by Mazzaferro (2) may be slightlyextended (7–18) following the proposed protocol.
We did not address the issue of expanding the Milan cri-teria with new tumor size and number, but we did includea group of patients who were initially excluded by the con-ventional transplant criteria and who were subsequentlyselected according to their tumor response to the TACE orloco-regional treatments, making them meet the conven-tional tumor criteria.
The down-staging protocol proposed emerged from theconsensus of an expert committee of our institution aimedat expanding the criteria toward those patients with post-neoadjuvant treatment features of the tumor similar to
2552 American Journal of Transplantation 2008; 8: 2547–2557
Bologna HCC Criteria for Liver Transplantation
0
20
40
60
80
100
0 12 24 36
Intention-to-treat survival (months)
%
C.C. B.C.D.S.
A
Actuarial intention-to-treat survival
Bologna criteria with down-stage (B.C.D.S.)48 pts
Conventional criteria (C.C.)129 pts
5 pts unable to complete the protocol (all died)
43 pts listed for LT
8 pts excluded for tumor progression(3 pts still alive)
2 pts died on list from liver failure
1 pt still alive on waiting list
32 pts had LT
23 alive after LT9 pts died after LT
27 pts alive(56%)
129 pts listed for LT
15 pts excluded for tumor progression(2 pts still alive)
12 pts died on list from liver failure
14 pt still alive on waiting list
88 pts had LT
65 alive after LT23 pts died after LT
81 pts alive(62.8%)
B
Figure 2: (A) Intention-to-treat survival since patient evaluation for liver transplantation according to the study group: conven-
tional criteria (CC) versus extended criteria with the down-staging protocol (BCDS). (B) Actuarial intention-to-treat outcome sincepatient evaluation at every treatment steps according to the study group: conventional criteria (CC) versus extended criteria with thedown-staging protocol (BCDS).
the cases meeting the conventional criteria ab initio. Allpatients were therefore given pre-Ts with the aim of al-lowing them to meet the conventional criteria (Figure 1).An expert consensus was needed since there was verylittle and only retrospective published evidence at thetime of protocol writing. According to practical experi-ence, our selection criteria can be summarized by ‘therule of six’: single nodule with a maximum diameter ≤6cm; multiple nodules <6 with a total tumor diameter ≤12
cm and maximum diameter ≤5 cm (bifocal) or ≤4 cm(others).
We did not encounter or transplant patients with singlenodule >6 cm, even if our initial proposal included sin-gle nodule up to 8 cm, as suggested by some authors(11,13). The lack of these cases was probably due to oursurveillance policy for cirrhotic patients (34) and to oursurgical strategy favoring LR whenever possible (32,33).
American Journal of Transplantation 2008; 8: 2547–2557 2553
Ravaioli et al.
Tab
le6:
Publ
ishe
dst
udie
son
exte
nded
crite
ria(E
C)v
ersu
sco
nven
tiona
lcrit
eria
(CC
)for
hepa
toce
llula
rca
rcin
oma
inliv
ertr
ansp
lant
atio
n
2554 American Journal of Transplantation 2008; 8: 2547–2557

Bologna HCC Criteria for Liver Transplantation
Furthermore, such large tumors often present satellite nod-ules, or macrovascular or biliary invasion by the tumor (38),which were exclusion criteria.
Concerning multiple nodules, we moved from the previouslimit of 3 nodules to <6 nodules and we increased theprevious maximum diameter from 3 to 5 cm in the case ofbifocal lesions.
Our choice was based on the assumption that multiplesmall nodules may have a lower risk of recurrence after LTthan a single large nodule, the tumor size being strongly re-lated to the probability of tumor vascular invasion (1,39,40).Following these principles, our study population was verydifferent from the cases included in the UCSF criteria (15)where cases with more than 3 nodules were excluded. Asreported in Table 2, less than 15% of patients in our studygroup met the UCSF criteria.
Besides size and number of nodules, the other importantselection criterion was the response to the TACE and loco-regional treatments: 10% of cases were not able to com-plete the protocol and close to 30% of patients were ex-cluded during the waiting time. In this way, as suggestedby some authors (40), we clinically selected the HCCs witha more favorable biology.
Our allocation policy obviously played an important role, butthis issue has been discussed in other studies (26,37) andthe comparable transplantation rate between the study andcontrol groups avoided any bias on the intention-to-treatanalysis.
The last relevant issue to be pointed out concerning ourresults was the mismatch between the preoperative andpostoperative tumor stages. The inaccuracy of preopera-tive radiological imaging was a key variable in predicting un-favorable outcome: cases with an underestimated tumorstage had more aggressive tumor features and a higher re-currence rate (close to 30%). This stresses the importanceof preoperative staging and treatments to further improvethe results after LT.
The previous reported rate of radiological under-staging be-tween 20% and 30% (2,15) is in accordance with our dataon the control group, while the down-staging group pre-sented a higher rate.
This high rate of radiological under-staging was probablysecondary to the low sensitivity of the CT scan after TACEwith lipiodol in detecting active HCC nodules (41,42). Whenour study was planned in 2002, we decided to follow pa-tients during the waiting time on the list and after pre-Tswith US, AFP determination and CT scan at least every 3months according to our previous experience (1,34) andaccording to the low availability of MRI exams in our hos-pital. CT scan failed several times to distinguish histolog-
ically active HCCs in the presence of lipiodol from previ-ous TACE and this limit was amplified in the down-staginggroup, where many pre-Ts were applied. We therefore be-lieve that the use of contrast-enhanced US and MRI shouldbe significantly extended to evaluate the effectiveness ofTACE and loco-regional treatments (43,44) for patients likeour study group, who were outside the conventional tu-mor selection and who were candidates for LT accordingto their response to pre-Ts.
Another important strategy for the follow-up of the recip-ients on the list may be the evaluation of the AFP level.As previously reported by our group and others (1,17),the AFP level at the time of LT and evaluated dynami-cally during the waiting time (Table 5) was extremely ef-fective in predicting HCC recurrence. Its evaluation shouldprobably be stressed at the time of registration on thelist and during the waiting time, in particular for thosecases at the top of the list with high priority for LT. Forthose cases with AFP levels higher than 30 ng/dL, the tu-mor follow-up should be stricter and more accurate: mea-surement of AFP level every month associated with are-evaluation by alternative imaging techniques. The AFPlevel could thus help to reduce the cases with a histo-logical overstaging on the samples and its role as a se-lection criteria should probably be planned for prospectivestudies.
On the other hand, the cases with an AFP level lower thanthis cut-off (close to 70% of the series) had a favorableprognosis even in the presence of poor differentiation ofthe tumor or in the presence of tumor microvascular inva-sion, and these two histological features lost their statisti-cal correlation with HCC recurrence (Table 5). We there-fore believe that the poor tumor differentiation degree,which was present in more than half of our cases, shouldnot be an absolute contraindication to LT as proposedby some authors (14), at least in cases with normal AFPlevels.
The presence of high AFP levels and unfavorable histolog-ical features (high tumor grade and tumor microvacular in-vasion) was associated with HCC recurrence after LT closeto 50% and we therefore believe that patients with theseknown features (all of them available only after LR) shouldnot be considered for LT.
The principal limitation of this study was its nonrandomizednature (LT vs. other treatments); however, the outcome af-ter LT and the intention-to-treat survival of the study groupwas comparable to the patients meeting the conventionalcriteria and the series reported by Mazzaferro (2), whichhas guided clinical practice during these last 10 years.
We believe these data make any randomized protocol un-ethical and we considered the present study design clini-cally probative, based on an intention-to-treat principle, on
American Journal of Transplantation 2008; 8: 2547–2557 2555

Ravaioli et al.
preoperative tumor stage assessment and reaching a me-dian follow-up of more than 2 years.
In conclusion, the present prospective study advocates anew patient selection based on slightly extended preoper-ative staging and on the clinical response to pre-Ts, whichwere validated to be effective and safe by the compara-ble outcome according to both intention-to-treat analysisand survival after LT. According to the proposed protocol,among the 48 patients believed to be beyond any curativetherapeutic strategy such as LT, the intention-to-treat sur-vival at 3 years was close to 60%; this result opens newprospectives for HCC patients respecting these criteria.
Acknowledgments
The author thank the colleagues of the University of Bologna, who gavetheir support to the management of patients: Augusto Lauro, M.D.; Mas-simo Del Gaudio, M.D.; Giovanni Varotti, M.D.; Gaetano Vetrone, M.D.;Alessandro Cucchetti, M.D.; Giuliano La Barba, M.D.; Matteo Zanello, M.D.;Alessandro Dazzi, M.D.; Francesco Tuci, M.D.; Chiara Zanfi, M.D.; ClaudiaSama, M.D.; Sonia Berardi, M.D.; Piero Andreone, M.D.; Maurizio Biselli,M.D.; Paolo Caraceni, M.D.; Giorgio Ballardini, M.D.; Marco Lenzi, M.D.;Maria Rosa Tame, M.D.; Giuseppe Mazzella, M.D.; Fabio Tumietto, M.D.;Paolo Costigliola, M.D.; Marco Zoli, M.D.; Gian Paolo Bianchi, M.D.; AlbertaCappelli, M.D.; Emanuela Giampalma, M.D.; Walter Franco Grigioni, M.D.;Michelangelo Fiorentino, M.D.; Barbara Corti, M.D.
Conflict of Interest Statement
Statistical analysis was performed by I.P.
References
1. Ravaioli M, Ercolani G, Cescon M et al. Liver transplantation forhepatocellular carcinoma: Further considerations on selection cri-teria. Liver Transpl 2004; 10: 1195–1202.
2. Mazzaferro V, Regalia E, Doci R et al. Liver transplantation forthe treatment of small hepatocellular carcinomas in patients withcirrhosis. N Engl J Med 1996; 334: 693–699.
3. Llovet JM, Schwartz M, Fuster J, Bruix J. Expanded criteriafor hepatocellular carcinoma through down-staging prior to livertransplantation: Not yet there. Semin Liver Dis 2006; 26: 248–253.
4. Sauer P, Kraus TW, Schemmer P et al. Liver transplantation forhepatocellular carcinoma: Is there evidence for expanding the se-lection criteria? Transplantation 2005; 80: S105–S108.
5. Ringe B, Wittekind C, Bechstein WO, Bunzendahl H, PichlmayrR. The role of liver transplantation in hepatobiliary malignancy. Aretrospective analysis of 95 patients with particular regard to tumorstage and recurrence. Ann Surg 1989; 209: 88–98.
6. Pichlmayr R, Weimann A, Ringe B. Indications for liver transplan-tation in hepatobiliary malignancy. Hepatology 1994; 20: 33S–40S.
7. Yao FY. Expanded criteria for hepatocellular carcinoma: Down-staging with a view to liver transplantation—yes. Semin Liver Dis2006; 26: 239–247.
8. Malago M, Sotiropoulos GC, Nadalin S et al. Living donor livertransplantation for hepatocellular carcinoma: A single-center pre-liminary report. Liver Transpl 2006; 12: 934–940.
9. Takada Y, Ueda M, Ito T et al. Living donor liver transplantation asa second-line therapeutic strategy for patients with hepatocellularcarcinoma. Liver Transpl 2006; 12: 912–919.
10. Todo S, Furukawa H. Japanese Study Group on Organ Transplan-tation. Living donor liver transplantation for adult patients withhepatocellular carcinoma: Experience in Japan. Ann Surg 2004;240: 451–459.
11. Yao FY, Ferrell L, Bass NM, Bacchetti P, Ascher NL, Roberts JP.Liver transplantation for hepatocellular carcinoma: Comparison ofthe proposed UCSF criteria with the Milan criteria and the Pitts-burgh modified TNM criteria. Liver Transpl 2002; 8: 765–774.
12. Broelsch CE, Frilling A, Malago M. Should we expand the criteria forliver transplantation for hepatocellular carcinoma—Yes, of course!J Hepatol 2005; 43: 569–573.
13. Yao FY, Hirose R, LaBerge JM et al. A prospective study on down-staging of hepatocellular carcinoma prior to liver transplantation.Liver Transpl 2005; 11: 1505–1514.
14. Cillo U, Vitale A, Grigoletto F et al. Intention-to-treat analysis ofliver transplantation in selected, aggressively treated HCC patientsexceeding the Milan criteria. Am J Transplant 2007; 7: 972–981.
15. Yao FY, Xiao L, Bass NM, Kerlan R, Ascher NL, Roberts JP.Liver transplantation for hepatocellular carcinoma: Validation ofthe UCSF-expanded criteria based on preoperative imaging. AmJ Transplant 2007; 7: 2587–2596.
16. Ito T, Takada Y, Ueda M et al. Expansion of selection criteria forpatients with hepatocellular carcinoma in living donor liver trans-plantation. Liver Transpl 2007; 13: 1637–1644.
17. Yang SH, Suh KS, Lee HW et al. A revised scoring system utilizingserum alphafetoprotein levels to expand candidates for living donortransplantation in hepatocellular carcinoma. Surgery 2007; 141:598–609.
18. Duffy JP, Vardanian A, Benjamin E et al. Liver transplantation cri-teria for hepatocellular carcinoma should be expanded: A 22-yearexperience with 467 patients at UCLA. Ann Surg 2007; 246: 502–509.
19. Shah SA, Tan JC, McGilvray ID et al. Accuracy of staging as apredictor for recurrence after liver transplantation for hepatocellularcarcinoma. Transplantation 2006; 81: 1633–1639.
20. Sotiropoulos GC, Malago M, Molmenti E et al. Liver transplantationfor hepatocellular carcinoma in cirrhosis: Is clinical tumor classifi-cation before transplantation realistic? Transplantation 2005; 79:483–487.
21. Graziadei IW, Sandmueller H, Waldenberger P et al. Chemoem-bolization followed by liver transplantation for hepatocellular car-cinoma impedes tumor progression while on the waiting listand leads to excellent outcome. Liver Transpl 2003; 9: 557–563.
22. Ravaioli M, Grazi GL, Ercolani G et al. Partial necrosis on hepato-cellular carcinoma nodules facilitates tumor recurrence after livertransplantation. Transplantation 2004; 78: 1780–1786.
23. Hayashi PH, Ludkowski M, Forman LM et al. Hepatic arterychemoembolization for hepatocellular carcinoma in patientslisted for liver transplantation. Am J Transplant 2004; 4: 782–787.
24. Ravaioli M, Grazi GL, Ercolani G et al. Liver allocation for hepato-cellular carcinoma: A European Center policy in the pre-MELD era.Transplantation 2006; 81: 525–530.
25. Trevisani F, De Notariis S, Rossi C, Bernardi M. Randomized controltrials on chemoembolization for hepatocellular carcinoma: Is thereroom for new studies? J Clin Gastroenterol 2001; 32: 383–389.
26. Ravaioli M, Grazi GL, Ballardini G et al. Liver transplantation withthe Meld system: A prospective study from a single Europeancenter. Am J Transplant 2006; 6: 1572–1577.
2556 American Journal of Transplantation 2008; 8: 2547–2557

Bologna HCC Criteria for Liver Transplantation
27. Wiesner RH, Freeman RB, Mulligan DC. Liver transplantation forhepatocellular cancer: The impact of the MELD allocation policy.Gastroenterology 2004; 127: S261–S267.
28. Yao FY, Bass NM, Nikolai B et al. Liver transplantation for hepato-cellular carcinoma: Analysis of survival according to the intention-to-treat principle and dropout from the waiting list. Liver Transpl2002; 8: 873–883.
29. Bruix J, Sherman M, Llovet J et al. Clinical management of hep-atocellular carcinoma. Conclusion of the Barcellona-2000 EASLconference. J Hepatol 2001; 35: 4210–4230.
30. Bruix J, Sherman M. Practice Guidelines Committee, AmericanAssociation for the Study of Liver Diseases. Management of hep-atocellular carcinoma. Hepatology 2005; 42: 1208–1236.
31. Stigliano R, Burroughs AK. Should we biopsy each liver mass sus-picious for HCC before liver transplantation? No, please don’t. JHepatol 2005; 43: 563–568.
32. Grazi GL, Cescon M, Ravaioli M et al. Liver resection for hepa-tocellular carcinoma in cirrhotics and noncirrhotics. Evaluation ofclinicopathologic features and comparison of risk factors for long-term survival and tumour recurrence in a single centre. AlimentPharmacol Ther 2003; 17: 119–129.
33. Ercolani G, Grazi GL, Ravaioli M et al. Liver resection for hepatocel-lular carcinoma on cirrhosis: Univariate and multivariate analysis ofrisk factors for intrahepatic recurrence. Ann Surg 2003; 237: 536–543.
34. Bolondi L, Sofia S, Siringo S et al. Surveillance programme of cir-rhotic patients for early diagnosis and treatment of hepatocellularcarcinoma: A cost effectiveness analysis. Gut 2001; 48: 251–259.
35. Kamath PS, Wiesner RH, Malinchoc M et al. A model to predictsurvival in patients with end-stage liver disease. Hepatology 2001;33: 464–470.
36. Bambha K, Kim WR, Kremers WK et al. Predicting survivalamong patients listed for liver transplantation: An assessmentof serial MELD measurements. Am J Transplant 2004; 4: 1798–1804.
37. Piscaglia F, Camaggi V, Ravaioli M et al. A new priority policy forpatients with hepatocellular carcinoma awaiting liver transplanta-tion within the model for end-stage liver disease system. LiverTranspl 2007; 13: 857–866.
38. Pawlik TM, Delman KA, Vauthey JN et al. Tumor size predictsvascular invasion and histologic grade: Implications for selectionof surgical treatment for hepatocellular carcinoma. Liver Transpl2005; 11: 1086–1092.
39. Shetty K, Timmins K, Brensinger C et al. Liver transplantation forhepatocellular carcinoma validation of present selection criteria inpredicting outcome. Liver Transpl 2004; 10: 911–918.
40. Otto G, Herber S, Heise M et al. Response to transarterialchemoembolization as a biological selection criterion for liver trans-plantation in hepatocellular carcinoma. Liver Transpl 2006; 12:1260–1267.
41. Guan YS, Sun L, Zhou XP, Li X, Zheng XH. Hepatocellular carci-noma treated with interventional procedures: CT and MRI follow-up. World J Gastroenterol 2004; 10: 3543–3548.
42. Chung YH. A strategy for early detection of recurrent hepatocel-lular carcinoma following initial remission by transcatheter arterialchemoembolization. Intervirology 2005; 48: 46–51.
43. Vossen JA, Buijs M, Kamel IR. Assessment of tumor responseon MR imaging after locoregional therapy. Tech Vasc Interv Radiol2006; 9: 125–132.
44. Taouli B, Krinsky GA. Diagnostic imaging of hepatocellular carci-noma in patients with cirrhosis before liver transplantation. LiverTranspl 2006; 12: S1–S7.
American Journal of Transplantation 2008; 8: 2547–2557 2557
Related Documents











