Liver transplantation for acute liver failure in Europe: Outcomes over 20 years from the ELTR database Giacomo Germani 1,2, , Eleni Theocharidou 1, , Renè Adam 3, , Vincent Karam 3, , Julia Wendon 4, , John O’Grady 4, , Patrizia Burra 2, , Marco Senzolo 2, , Darius Mirza 5, , Denis Castaing 3, , Jurgen Klempnauer 6, , Stephen Pollard 7, , Andreas Paul 8, , Jacques Belghiti 9, , Emmanuel Tsochatzis 1, , Andrew K. Burroughs 1,⇑, 1 The Royal Free Sheila Sherlock Liver Centre, University Department of Surgery, Royal Free Hospital and UCL, London UK; 2 Gastroenterology, Department of Surgical and Gastroenterological Sciences, Padua University Hospital, Padua, Italy; 3 ELTR, Assistance Publique-Hôpitaux de Paris, Hôpital Paul Brousse, Centre Hepato-Biliaire, Universite ´Paris-Sud, Villejuif, France; 4 Liver Intensive Unit, Institute of Liver Studies, King’s College Hospital, London, UK; 5 The Queen Elizabeth Hospital, Birmingham, UK; 6 Medizinische Hochschule Hannover, Hannover, Germany; 7 St. Jame’s & Seacroft University Hospital, Leeds, UK; 8 C. U. K. GHs Essen, Essen, Germany; 9 Hôpital Beaujon, Clichy, France Background & Aims: Liver transplantation for acute liver failure (ALF) still has a high early mortality. We evaluated changes dur- ing 20 years, and identified risk factors for poor outcome. Methods: Donor, graft, and recipient variables from the European Liver Transplant Registry database (January 1988–June 2009), were analysed. Aetiologies and time periods were compared. Three and 12-month survival models were generated from sepa- rate training data sets, which were validated. A sub-analysis was performed for recipient older than 50 years. Results: Four thousand nine hundred and three patients were evaluated. One, 5- and 10-year patient, and graft survival rates were 74%, 68%, 63%, and 63%, 57%, 50%, respectively. Survival was better in 2004–2009 compared to previous quinquennia (p<0.001), despite donors >60 years increased from 1.8% to 21%. A higher incidence of suicide or non-adherence occurred in paracetamol-related ALF (p<0.001). Death or graft loss were independently associated with male recipients (adjusted OR 1.25), recipient >50 years (1.26), incompatible ABO matching (1.93), donors >60 years (1.21), and reduced size graft (1.54). For both 3- and 12-month models, incompatible ABO matching, non-viral aetiology, reduced size graft, and non-UW preservation fluid were associated with increased mortality/graft loss, whereas male recipients and age >50 years were associated only at 12 months. Both models had reasonable discriminative ability with good calibration at 3 months. Recipients >50 years, com- bined with donors >60 years resulted in 57% mortality/graft loss within the first year. Conclusions: Survival after liver transplantation has improved despite increases in donor/recipient age. Recipients >50 years paired with donors >60 years had a very high mortality/graft loss within the first year. Ó 2012 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved. Introduction Acute liver failure (ALF) accounted for 8% of indications for liver transplantation in Europe during 1988–2009 [1] and 7% in the USA during 1999–2008 [2]. The survival rates at 1 year have improved from 60% to 92% in large centres over the past 20 years [3–11], but are less than for cirrhosis [12]. The European Liver Transplant Registry (ELTR) holds data on 87,963 liver transplantations performed in 79,063 patients in 23 European countries over 43 years [13], and has been used to evalu- ate outcomes and evolution of liver transplantation in Europe [14]. The primary objective of this study was to use the ELTR data- base to evaluate outcomes after liver transplantation for ALF, comparing different aetiologies of ALF, and to evaluate these out- comes with respect to changes in recipient and donor characteris- tics, and in surgical techniques over the past 20 years. The secondary objective was to identify potential risk factors for death or graft loss after liver transplantation for ALF, so as to explore if these could be used to establish a particularly poor prognosis. Materials and methods The methods and details used to obtain the data have been described previously [15] (Supplementary material). The quality of ELTR data is controlled regularly by Journal of Hepatology 2012 vol. xxx j xxx–xxx Keywords: Liver transplantation; Acute liver failure; Europe. Received 14 November 2011; received in revised form 1 February 2012; accepted 8 March 2012 ⇑ Corresponding author. Address: The Royal Free Sheila Sherlock Liver Centre, Royal Free Hospital, Pond Street, NW3 2QG London, UK. Tel.: +44 02074726229; fax: +44 02074726226. E-mail address: [email protected] (A.K. Burroughs). For the European Liver and Intestine Transplant Association (ELITA) and on behalf of the European Liver Transplant Registry (ELTR) Liver Transplant Centres listed at www.eltr.org. Abbreviation: ALF, acute liver failure. Research Article Please cite this article in press as: Germani G et al. Liver transplantation for acute liver failure in Europe: Outcomes over 20 years from the ELTR data- base. J Hepatol (2012), http://dx.doi.org/10.1016/j.jhep.2012.03.017

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Research Article
Liver transplantation for acute liver failure in Europe: Outcomesover 20 years from the ELTR database
Giacomo Germani1,2,�, Eleni Theocharidou1,�, Renè Adam3,�, Vincent Karam3,�, Julia Wendon4,�,John O’Grady4,�, Patrizia Burra2,�, Marco Senzolo2,�, Darius Mirza5,�, Denis Castaing3,�,
Jurgen Klempnauer6,�, Stephen Pollard7,�, Andreas Paul8,�, Jacques Belghiti9,�,Emmanuel Tsochatzis1,�, Andrew K. Burroughs1,⇑,�
1The Royal Free Sheila Sherlock Liver Centre, University Department of Surgery, Royal Free Hospital and UCL, London UK; 2Gastroenterology,Department of Surgical and Gastroenterological Sciences, Padua University Hospital, Padua, Italy; 3ELTR, Assistance Publique-Hôpitaux de Paris,Hôpital Paul Brousse, Centre Hepato-Biliaire, UniversiteParis-Sud, Villejuif, France; 4Liver Intensive Unit, Institute of Liver Studies, King’s CollegeHospital, London, UK; 5The Queen Elizabeth Hospital, Birmingham, UK; 6Medizinische Hochschule Hannover, Hannover, Germany; 7St. Jame’s &
Seacroft University Hospital, Leeds, UK; 8C. U. K. GHs Essen, Essen, Germany; 9Hôpital Beaujon, Clichy, France
Background & Aims: Liver transplantation for acute liver failure with good calibration at 3 months. Recipients >50 years, com-
(ALF) still has a high early mortality. We evaluated changes dur-ing 20 years, and identified risk factors for poor outcome.Methods: Donor, graft, and recipient variables from the EuropeanLiver Transplant Registry database (January 1988–June 2009),were analysed. Aetiologies and time periods were compared.Three and 12-month survival models were generated from sepa-rate training data sets, which were validated. A sub-analysis wasperformed for recipient older than 50 years.Results: Four thousand nine hundred and three patients wereevaluated. One, 5- and 10-year patient, and graft survival rateswere 74%, 68%, 63%, and 63%, 57%, 50%, respectively. Survivalwas better in 2004–2009 compared to previous quinquennia(p <0.001), despite donors >60 years increased from 1.8% to21%. A higher incidence of suicide or non-adherence occurredin paracetamol-related ALF (p <0.001). Death or graft loss wereindependently associated with male recipients (adjusted OR1.25), recipient >50 years (1.26), incompatible ABO matching(1.93), donors >60 years (1.21), and reduced size graft (1.54).For both 3- and 12-month models, incompatible ABO matching,non-viral aetiology, reduced size graft, and non-UW preservationfluid were associated with increased mortality/graft loss, whereasmale recipients and age >50 years were associated only at12 months. Both models had reasonable discriminative abilityJournal of Hepatology 20
Keywords: Liver transplantation; Acute liver failure; Europe.Received 14 November 2011; received in revised form 1 February 2012; accepted 8March 2012⇑ Corresponding author. Address: The Royal Free Sheila Sherlock Liver Centre,Royal Free Hospital, Pond Street, NW3 2QG London, UK. Tel.: +44 02074726229;fax: +44 02074726226.E-mail address: [email protected] (A.K. Burroughs).
� For the European Liver and Intestine Transplant Association (ELITA) and onbehalf of the European Liver Transplant Registry (ELTR) Liver Transplant Centreslisted at www.eltr.org.Abbreviation: ALF, acute liver failure.
Please cite this article in press as: Germani G et al. Liver transplantation for acbase. J Hepatol (2012), http://dx.doi.org/10.1016/j.jhep.2012.03.017
bined with donors >60 years resulted in 57% mortality/graft losswithin the first year.Conclusions: Survival after liver transplantation has improveddespite increases in donor/recipient age. Recipients >50 yearspaired with donors >60 years had a very high mortality/graft losswithin the first year.� 2012 European Association for the Study of the Liver. Publishedby Elsevier B.V. All rights reserved.
Introduction
Acute liver failure (ALF) accounted for 8% of indications for livertransplantation in Europe during 1988–2009 [1] and 7% in theUSA during 1999–2008 [2]. The survival rates at 1 year haveimproved from 60% to 92% in large centres over the past 20 years[3–11], but are less than for cirrhosis [12].
The European Liver Transplant Registry (ELTR) holds data on87,963 liver transplantations performed in 79,063 patients in 23European countries over 43 years [13], and has been used to evalu-ate outcomes and evolution of liver transplantation in Europe [14].
The primary objective of this study was to use the ELTR data-base to evaluate outcomes after liver transplantation for ALF,comparing different aetiologies of ALF, and to evaluate these out-comes with respect to changes in recipient and donor characteris-tics, and in surgical techniques over the past 20 years. Thesecondary objective was to identify potential risk factors for deathor graft loss after liver transplantation for ALF, so as to explore ifthese could be used to establish a particularly poor prognosis.
Materials and methods
The methods and details used to obtain the data have been described previously[15] (Supplementary material). The quality of ELTR data is controlled regularly by
12 vol. xxx j xxx–xxx
ute liver failure in Europe: Outcomes over 20 years from the ELTR data-
Research Article
audit visits to the contributing centres [16]. The ELTR database does not includepre-transplant variables (i.e. renal support, ventilation, and prognostic scores)and alcoholic aetiology is not a grouping for ALF. We present analyses based ondata from first transplants performed in adults (aged 16 years or over) for ALFbetween January 1988 and June 2009.Procedures and statistical analysis
We used all ELTR variables whether continuous or categorical variables, related tothe donor, the recipient, the graft, and the liver transplant technique. The donorvariables were age, gender, type of donor (cadaveric, domino, living); recipientvariables were: age, gender, UNOS status, and donor/recipient blood groupmatching (identical, compatible, incompatible); graft variables were: type of graft(full size, split liver, reduced liver, partial liver from living donor); variablesrelated to liver transplant technique were: total ischemic time (minutes), typeof transplant (orthotopic, heterotopic, and non auxiliary, auxiliary), type of pres-ervation fluid, type of by-pass (extracorporeal, lateral clamping, none, other).
Patients were grouped according to the aetiology of ALF as follows: virus-related (HAV, HBV, HDV), paracetamol-related, other drug-related, other knowncauses (post-traumatic, post-operative, heat shock, toxic not drug-related, other),and unknown causes.
Patients were also classified according to different time periods (1988–1993,1994–1998, 1999–2003, and 2004–2009) to evaluate the evolution of recipient,donor, and surgical characteristics.
The causes of death or graft failure after first liver transplant for ALF wereevaluated: primary-non-function (PNF) or delayed function (PDF), intra-operativefailure, technical problems, infection, acute or chronic rejection (combined inthe analysis), renal disease, cardiovascular disease, pulmonary disease,
Table 1. Recipient, donor, surgical characteristics, and causes of death or graft loss
Aetiology of ALF Viral Paracetn = 1029 n = 536
Recipient gender, %MaleFemale
51.548.5
33.266.8
Recipient age (yr), mean ± SD 40.6 ± 13.1 34.2 ± 1Donor gender (%)
MaleFemale
55.344.7
52.747.3
Donor age (yr), mean ± SD 40.1 ± 16.1 43.6 ± 1Blood group matching (%)
IdenticalCompatibleIncompatible
73.419.27.3
66.731.61.7
Total ischemic time (min), mean ± SD 516.3 ± 191.1 552.9 ±Type of by-pass (%)
ExtracorporealLateral clampingNoneOthers
32.525.441.20.9
18.861.919.30
Type of donor (%)CadavericDominoLiving
98.50.21.3
10000
Graft type (%)Full sizeSplitReducedPartial for living
92.53.62.51.3
92.43.14.50
Type of transplant (%)Non-auxiliaryAuxiliary
982
96.13.9
Type of transplant (%)OrthotopicHeterotopic
99.40.6
98.91.1
n.s., not significant.
Please cite this article in press as: Germani G et al. Liver transplantation for acbase. J Hepatol (2012), http://dx.doi.org/10.1016/j.jhep.2012.03.017
2 Journal of Hepatology 201
cerebrovascular disease, gastrointestinal disease, multi-organ failure, recurrenceof primary liver disease, ‘‘de novo’’ tumours, lymphoproliferative disorders,‘‘social’’ problems (non-adherence to immunosuppressive medications, suicideor trauma). The causes of death or graft failure were compared across differentaetiologies and time periods.
Patient survival according to aetiology of ALF and to time period was evalu-ated using the life-table method and comparisons made by the log-rank test. Dis-crete variables are shown as percentages and continuous variables as meanvalues ± SD, as all had a normal distribution (Kolmogorov–Smirnov test).Chi-square test was used to compare discrete variables, Student’s t-test forcontinuous variables, and ANOVA analyses for comparisons of two groups ormore. Statistically significant differences were defined by a p-value 60.05.
The effect of recipient, donor, and surgical variables on patient and graftsurvival was evaluated by Cox analysis. Variables with statistically significantrisk-ratios at the univariate analysis (p value cut-off <0.05) were used for thesubsequent multivariate analysis.
Multivariate logistic regression was used to generate 3 and 12-month mortalityscores in a randomly chosen training set (�70% of transplants). We assessed modeldiscrimination and calibration on an independent validation dataset (�30% oftransplants) using methods already applied to the ELTR database and previouslypublished [14]. All the analyses were done with PASW statistics version 18.0.
Results
There were 6374 patients transplanted for ALF between January1988 and June 2009: 942 paediatric patients (<16 years) and
according to the aetiology of acute liver failure (ALF) in the ELTR database.
amol Other drugs Other known Unknown p valuen = 496 n = 744 n = 2098
37.562.5
41.758.3
34.865.2
<0.001
1.7 42.8 ± 14.8 42 ± 14.6 39.8 ± 13.5 <0.001
55.144.9
57.842.2
56.443.6
n.s.
6.1 42.6 ± 16.3 42.7 ± 16 39.9 ± 15.9 <0.001
72.622.84.5
77.918.53.6
69.523.66.9
<0.001
183.8 523.5 ± 198 481.3 ± 152.3 524.1 ± 195.8 <0.001
19.434.845.50.3
22.430.846.10.7
32.82343.90.2
<0.001
98.80.21
98.50.11.3
99.200.8
n.s.
91.434.41.2
94.52.71.41.4
9333.10.8
0.02
98.21.8
98.61.4
97.72.3
0.05
99.20.8
99.70.3
99.40.6
n.s.
ute liver failure in Europe: Outcomes over 20 years from the ELTR data-
2 vol. xxx j xxx–xxx
JOURNAL OF HEPATOLOGY
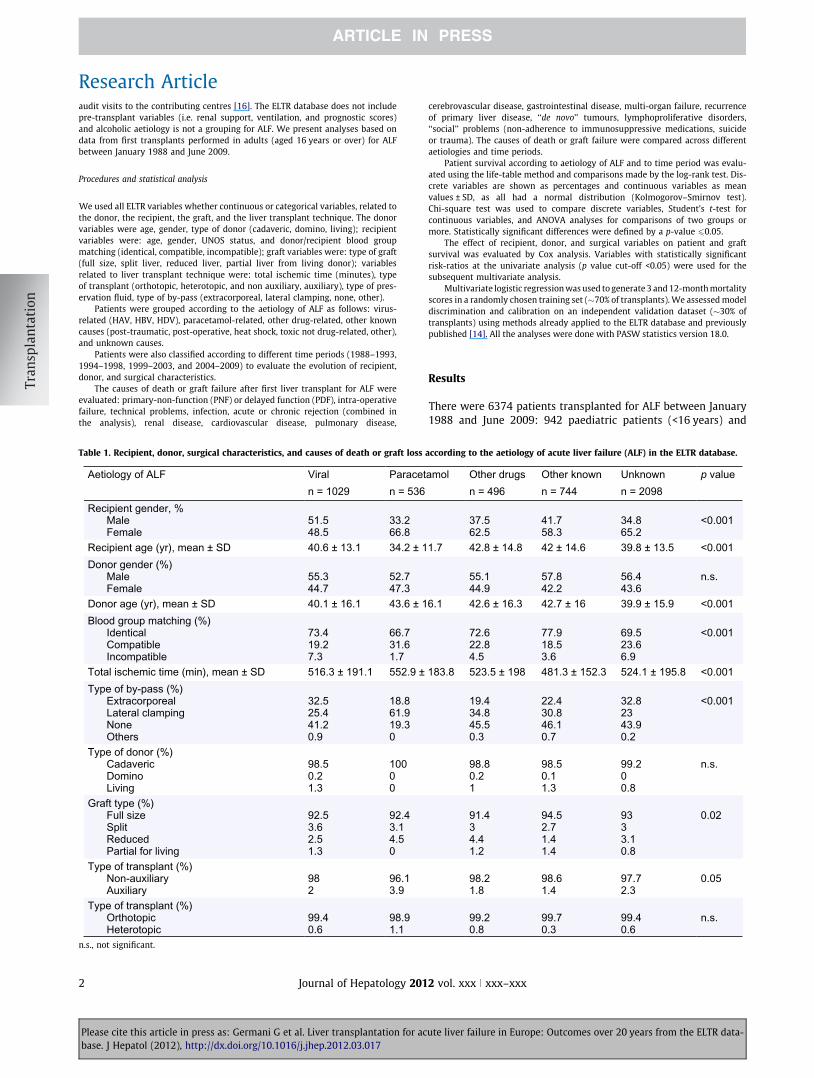
529 patients with a second underlying liver disease wereexcluded, leaving 4903 patients for the analysis.Donor variables
Male donors were 51.8% with a mean ± SD age of 41 ± 16 years(range: 2–88). Nearly 2/3 of liver transplants for ALF were per-formed using an identical donor/recipient ABO group match,whereas an incompatible ABO matching was used between 1.7%and 7.3% of cases across different aetiologies, being significantlyhigher in patients transplanted for virus-related ALF (7.3%) com-pared to other groups (paracetamol: 1.7%, p <0.001; other drugs:4.5%, p = 0.015; other known: 3.6%, p <0.001; unknown: 6.9%,p <0.001) (Table 1).
Recipient variables
The aetiology of ALF was unknown in 43%, viral in 21%, paracet-amol overdose in 11%, other drugs-related in 10%, and due toother known causes in 15%.
Table 2. Change over time of liver transplantation for acute liver failure in the ELTR
Transplantation era 1988-1993 1n = 990 n
Recipient gender, %MaleFemale
36.363.7
36
Recipient age (yr), mean ± SD 37.6 ± 13 3Recipient age, %
≤3031-4041-5051-60>60
37.722.722.2143.3
32215
Donor gender, %MaleFemale
62.437.6
54
Donor age (yr), mean ± SD 32.7 ± 13.4 3Donor age, %
≤4041-60>60
70.227.91.8
448
Blood group matching, %IdenticalCompatibleIncompatible
6721.211.7
724
Total ischemic time (min), mean ± SD 518.4 ± 219.7 5Type of donor, %CadavericDominoLiving
99.900.1
900
Graft type, %Full sizeSplitReducedPartial for living
94.623.20.1
9350
Type of transplant, %Non-auxiliaryAuxiliary
99.20.8
94
n.s., not significant.⁄Data available until 31/06/2009.
Please cite this article in press as: Germani G et al. Liver transplantation for acbase. J Hepatol (2012), http://dx.doi.org/10.1016/j.jhep.2012.03.017
Journal of Hepatology 201
Female recipients were 61.2% with a mean ± SD age of40 ± 14 years (range: 16–75). The proportion of female recipientswas significantly higher in the paracetamol group (67%) com-pared to virus-related ALF (48.5%; p <0.001) and to ALF due toother known causes (58%; p = 0.002). Recipient age was signifi-cantly lower in the paracetamol group (34.2 ± 11.7 years) com-pared to other aetiologies (p <0.001 vs. all other groups) (Table 1).
Surgical characteristics
Whole cadaveric livers from brain stem dead donors were used in89.6%. The split liver technique was used between 2.7% and 3.6%,living donor liver transplantation between 0% and 1.3%, andauxiliary transplant between 1.4% and 3.9% across differentaetiologies. A reduced size graft was used more for paraceta-mol-related ALF (4.5%) compared to virus-related ALF (2.5%,p = 0.003) and to ALF due to other known causes (1.4%,p <0.001). No non-heart-beating donors were recorded in thiscohort. Mean ± SD total ischaemic time was 518.9 ± 188 min(Table 1).
database.
994-1998 1999-2003 2004-2009* p value = 1190 n = 1335 n = 1387
8.41.6
40.359.7
39.660.4
n.s.
8.9 ± 13.7 40.4 ± 13.8 41.7 ± 13.9 <0.001
3.42.21.17.5.8
29.222.92119.27.7
25.22422.5199.3
<0.001
7.32.7
54.845.2
51.448.6
<0.001
9.3 ± 15.2 42.4 ± 15.8 46.1 ± 16.4 <0.001
8.93.1
42.346.511.3
35.343.721
<0.001
0.74.4.9
74.222.83
73.122.34.5
<0.001
33.4 ± 193 522 ± 187.7 503.7 ± 162.7 0.001
9.7.1.2
98.70.11.2
98.10.11.8
<0.001
0.9.8
.2
93.63.31.91.2
933.12.11.8
<0.001
6 982
98.11.9
<0.001
ute liver failure in Europe: Outcomes over 20 years from the ELTR data-
2 vol. xxx j xxx–xxx 3
Research Article
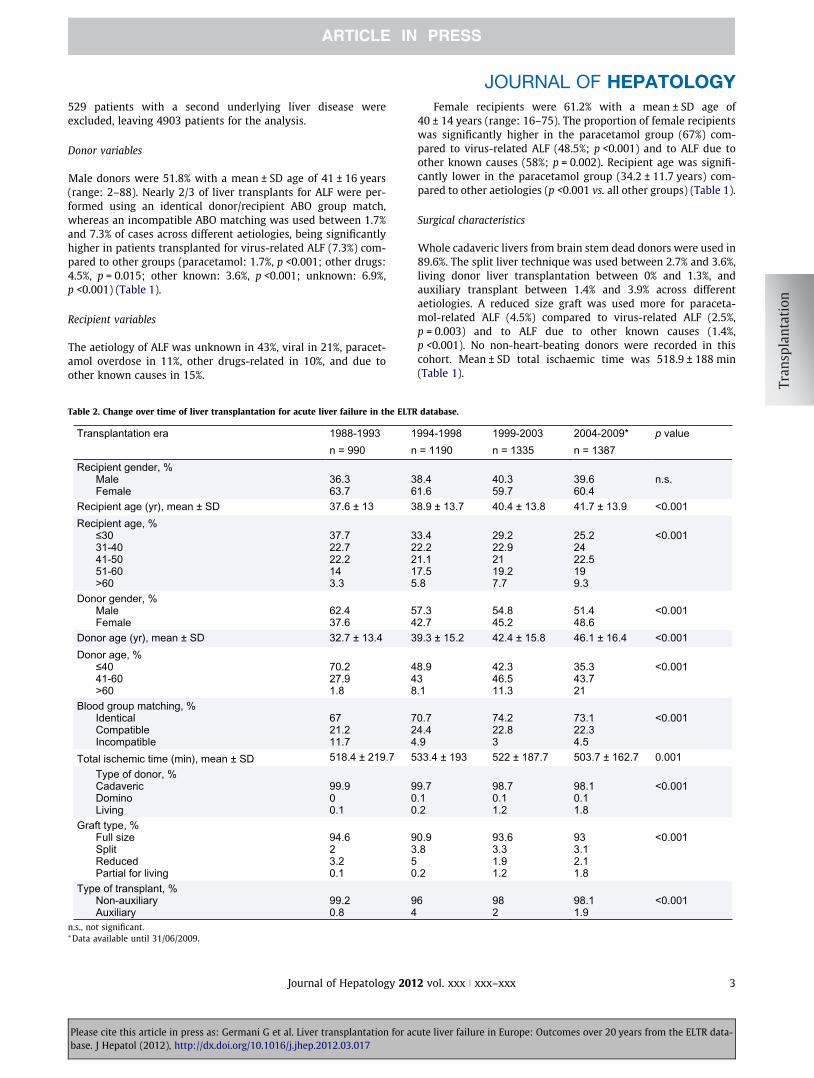
Evolution of liver transplantation for ALF over timeWe examined changes by comparing the latest period of trans-plantation (2004–2009) to the earliest (1988–1993) (Table 2).
Donor age significantly increased over this time from a meanof 33 ± 13 to 46 ± 16 (p <0.001). Over the study period, this repre-sents an increase in donor age of 2.5 years/year. Donors640 years of age have halved from 70% to 35% (p <0.001),whereas donors >60 years have increased more than ten timesfrom 1.8% to 21.1% (p <0.001) (Table 2).
1988-1993 1994-1998
Virus
1999-2003 2004-2009
Paracetamol
Other drugs
Other known
Unknown
59.5% 52.5%2.0%
9.3%
22.3%
6.9%
12.7%
8.2%
19.0%
8.2%
32.3% 33.0%
12.7%
10.8%
24.2%
20.1%
14.1%
11.8%
18.7%
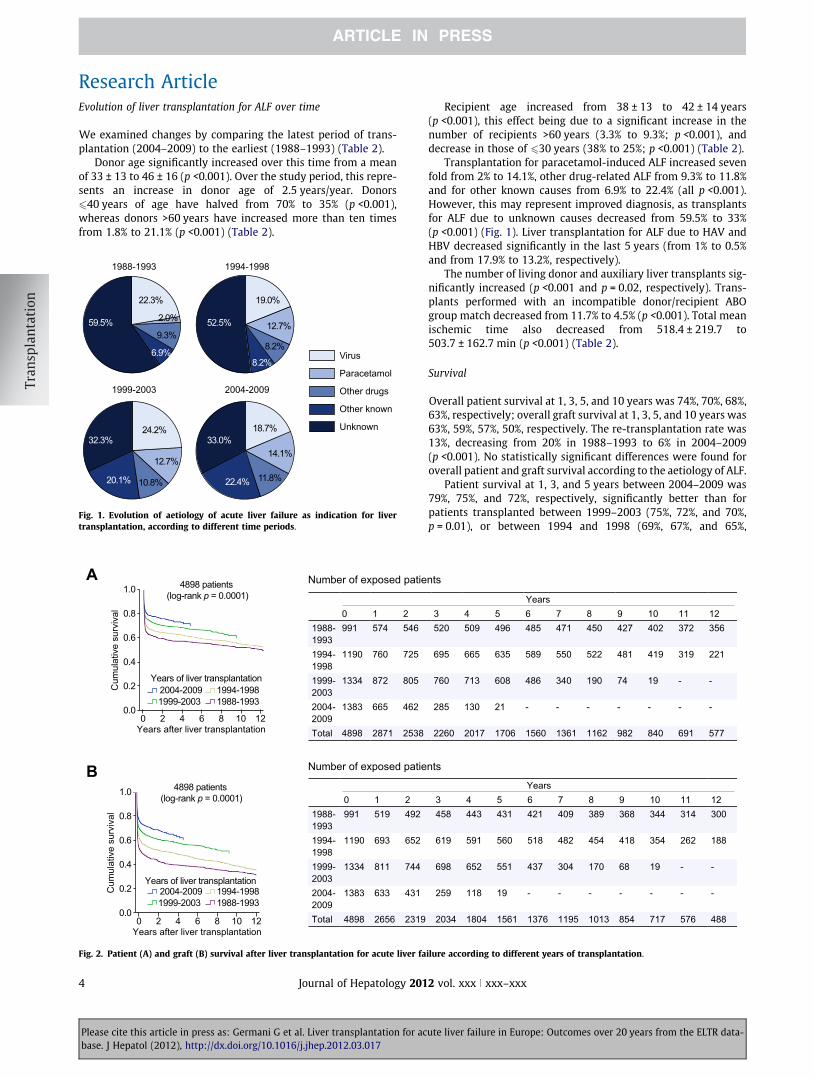
22.4%
Fig. 1. Evolution of aetiology of acute liver failure as indication for livertransplantation, according to different time periods.
Years after liver transplantation
Years of liver transplantation
A
Cum
ulat
ive
surv
ival
1.0
0.8
0.6
0.4
0.2
0.00 2 4 6 8 1210
4898 patients (log-rank p = 0.0001)
1988-19931994-1998
1999-20032004-2009
B4898 patients
(log-rank p = 0.0001)
Years of liver transplantation
Years after liver transplantation
Cum
ulat
ive
surv
ival
1.0
0.8
0.6
0.4
0.2
0.00 2 4 6 8 1210
Number of exposed patie
0 1 21988-1993
991 574 546
1994-1998
1190 760 725
1999-2003
1334 872 805
2004-2009
1383 665 462
Total 4898 2871 2538
0 1 21988-1993
991 519 492
1994-1998
1190 693 652
1999-2003
1334 811 744
2004-2009
1383 633 431
Total 4898 2656 2319
Number of exposed patie
1988-19931994-1998
1999-20032004-2009
Fig. 2. Patient (A) and graft (B) survival after liver transplantation for acute liver fa
Please cite this article in press as: Germani G et al. Liver transplantation for acbase. J Hepatol (2012), http://dx.doi.org/10.1016/j.jhep.2012.03.017
4 Journal of Hepatology 201
Recipient age increased from 38 ± 13 to 42 ± 14 years(p <0.001), this effect being due to a significant increase in thenumber of recipients >60 years (3.3% to 9.3%; p <0.001), anddecrease in those of 630 years (38% to 25%; p <0.001) (Table 2).
Transplantation for paracetamol-induced ALF increased sevenfold from 2% to 14.1%, other drug-related ALF from 9.3% to 11.8%and for other known causes from 6.9% to 22.4% (all p <0.001).However, this may represent improved diagnosis, as transplantsfor ALF due to unknown causes decreased from 59.5% to 33%(p <0.001) (Fig. 1). Liver transplantation for ALF due to HAV andHBV decreased significantly in the last 5 years (from 1% to 0.5%and from 17.9% to 13.2%, respectively).
The number of living donor and auxiliary liver transplants sig-nificantly increased (p <0.001 and p = 0.02, respectively). Trans-plants performed with an incompatible donor/recipient ABOgroup match decreased from 11.7% to 4.5% (p <0.001). Total meanischemic time also decreased from 518.4 ± 219.7 to503.7 ± 162.7 min (p <0.001) (Table 2).
Survival
Overall patient survival at 1, 3, 5, and 10 years was 74%, 70%, 68%,63%, respectively; overall graft survival at 1, 3, 5, and 10 years was63%, 59%, 57%, 50%, respectively. The re-transplantation rate was13%, decreasing from 20% in 1988–1993 to 6% in 2004–2009(p <0.001). No statistically significant differences were found foroverall patient and graft survival according to the aetiology of ALF.
Patient survival at 1, 3, and 5 years between 2004–2009 was79%, 75%, and 72%, respectively, significantly better than forpatients transplanted between 1999–2003 (75%, 72%, and 70%,p = 0.01), or between 1994 and 1998 (69%, 67%, and 65%,
nts
Years3 4 5 6 7 8 9 10 11 12520 509 496 485 471 450 427 402 372 356
695 665 635 589 550 522 481 419 319 221
760 713 608 486 340 190 74 19 - -
285 130 21 - - - - - - -
2260 2017 1706 1560 1361 1162 982 840 691 577
Years3 4 5 6 7 8 9 10 11 12458 443 431 421 409 389 368 344 314 300
619 591 560 518 482 454 418 354 262 188
698 652 551 437 304 170 68 19 - -
259 118 19 - - - - - - -
2034 1804 1561 1376 1195 1013 854 717 576 488
nts
ilure according to different years of transplantation.
ute liver failure in Europe: Outcomes over 20 years from the ELTR data-
2 vol. xxx j xxx–xxx
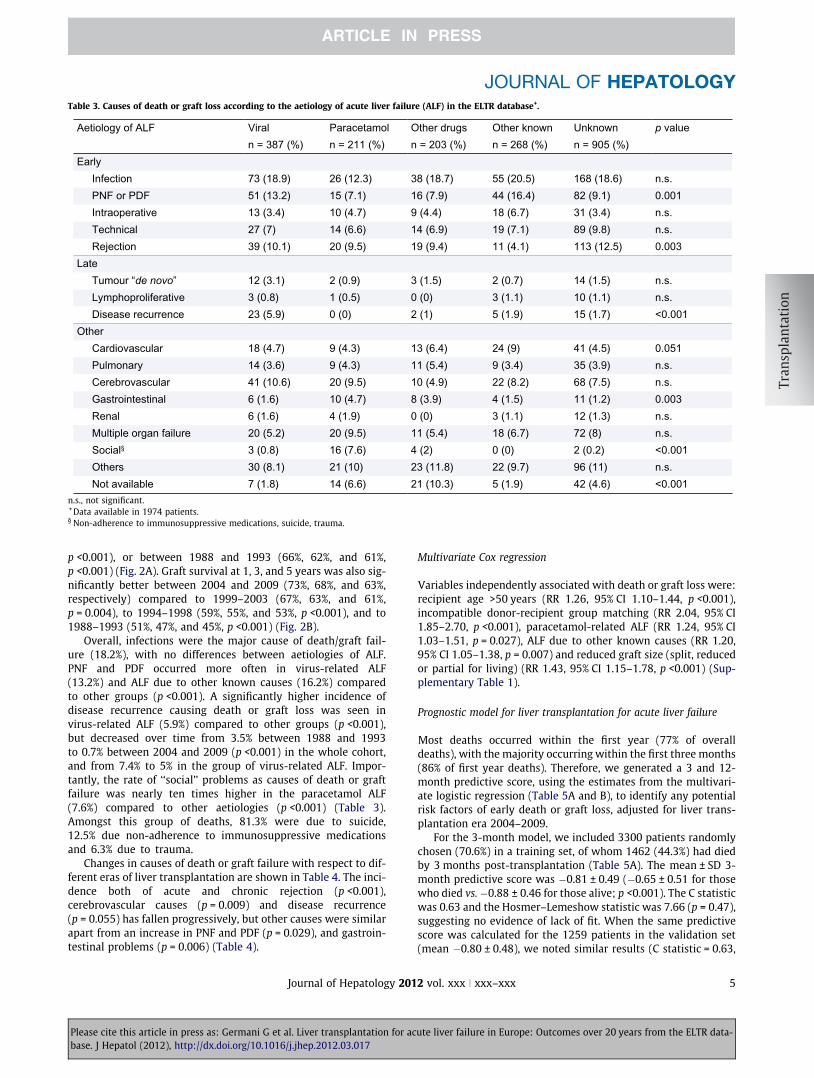
Table 3. Causes of death or graft loss according to the aetiology of acute liver failure (ALF) in the ELTR database+.
Aetiology of ALF Viral Paracetamol Other drugs Other known Unknown p valuen = 387 (%) n = 211 (%) n = 203 (%) n = 268 (%) n = 905 (%)
EarlyInfection 73 (18.9) 26 (12.3) 38 (18.7) 55 (20.5) 168 (18.6) n.s.PNF or PDF 51 (13.2) 15 (7.1) 16 (7.9) 44 (16.4) 82 (9.1) 0.001Intraoperative 13 (3.4) 10 (4.7) 9 (4.4) 18 (6.7) 31 (3.4) n.s.Technical 27 (7) 14 (6.6) 14 (6.9) 19 (7.1) 89 (9.8) n.s.Rejection 39 (10.1) 20 (9.5) 19 (9.4) 11 (4.1) 113 (12.5) 0.003
LateTumour “de novo” 12 (3.1) 2 (0.9) 3 (1.5) 2 (0.7) 14 (1.5) n.s.Lymphoproliferative 3 (0.8) 1 (0.5) 0 (0) 3 (1.1) 10 (1.1) n.s.Disease recurrence 23 (5.9) 0 (0) 2 (1) 5 (1.9) 15 (1.7) <0.001
OtherCardiovascular 18 (4.7) 9 (4.3) 13 (6.4) 24 (9) 41 (4.5) 0.051Pulmonary 14 (3.6) 9 (4.3) 11 (5.4) 9 (3.4) 35 (3.9) n.s.Cerebrovascular 41 (10.6) 20 (9.5) 10 (4.9) 22 (8.2) 68 (7.5) n.s.Gastrointestinal 6 (1.6) 10 (4.7) 8 (3.9) 4 (1.5) 11 (1.2) 0.003Renal 6 (1.6) 4 (1.9) 0 (0) 3 (1.1) 12 (1.3) n.s.Multiple organ failure 20 (5.2) 20 (9.5) 11 (5.4) 18 (6.7) 72 (8) n.s.Social§ 3 (0.8) 16 (7.6) 4 (2) 0 (0) 2 (0.2) <0.001Others 30 (8.1) 21 (10) 23 (11.8) 22 (9.7) 96 (11) n.s.Not available 7 (1.8) 14 (6.6) 21 (10.3) 5 (1.9) 42 (4.6) <0.001
n.s., not significant.+ Data available in 1974 patients.§ Non-adherence to immunosuppressive medications, suicide, trauma.
JOURNAL OF HEPATOLOGY
p <0.001), or between 1988 and 1993 (66%, 62%, and 61%,p <0.001) (Fig. 2A). Graft survival at 1, 3, and 5 years was also sig-nificantly better between 2004 and 2009 (73%, 68%, and 63%,respectively) compared to 1999–2003 (67%, 63%, and 61%,p = 0.004), to 1994–1998 (59%, 55%, and 53%, p <0.001), and to1988–1993 (51%, 47%, and 45%, p <0.001) (Fig. 2B).
Overall, infections were the major cause of death/graft fail-ure (18.2%), with no differences between aetiologies of ALF.PNF and PDF occurred more often in virus-related ALF(13.2%) and ALF due to other known causes (16.2%) comparedto other groups (p <0.001). A significantly higher incidence ofdisease recurrence causing death or graft loss was seen invirus-related ALF (5.9%) compared to other groups (p <0.001),but decreased over time from 3.5% between 1988 and 1993to 0.7% between 2004 and 2009 (p <0.001) in the whole cohort,and from 7.4% to 5% in the group of virus-related ALF. Impor-tantly, the rate of ‘‘social’’ problems as causes of death or graftfailure was nearly ten times higher in the paracetamol ALF(7.6%) compared to other aetiologies (p <0.001) (Table 3).Amongst this group of deaths, 81.3% were due to suicide,12.5% due non-adherence to immunosuppressive medicationsand 6.3% due to trauma.
Changes in causes of death or graft failure with respect to dif-ferent eras of liver transplantation are shown in Table 4. The inci-dence both of acute and chronic rejection (p <0.001),cerebrovascular causes (p = 0.009) and disease recurrence(p = 0.055) has fallen progressively, but other causes were similarapart from an increase in PNF and PDF (p = 0.029), and gastroin-testinal problems (p = 0.006) (Table 4).
Please cite this article in press as: Germani G et al. Liver transplantation for acbase. J Hepatol (2012), http://dx.doi.org/10.1016/j.jhep.2012.03.017
Journal of Hepatology 201
Multivariate Cox regression
Variables independently associated with death or graft loss were:recipient age >50 years (RR 1.26, 95% CI 1.10–1.44, p <0.001),incompatible donor-recipient group matching (RR 2.04, 95% CI1.85–2.70, p <0.001), paracetamol-related ALF (RR 1.24, 95% CI1.03–1.51, p = 0.027), ALF due to other known causes (RR 1.20,95% CI 1.05–1.38, p = 0.007) and reduced graft size (split, reducedor partial for living) (RR 1.43, 95% CI 1.15–1.78, p <0.001) (Sup-plementary Table 1).
Prognostic model for liver transplantation for acute liver failure
Most deaths occurred within the first year (77% of overalldeaths), with the majority occurring within the first three months(86% of first year deaths). Therefore, we generated a 3 and 12-month predictive score, using the estimates from the multivari-ate logistic regression (Table 5A and B), to identify any potentialrisk factors of early death or graft loss, adjusted for liver trans-plantation era 2004–2009.
For the 3-month model, we included 3300 patients randomlychosen (70.6%) in a training set, of whom 1462 (44.3%) had diedby 3 months post-transplantation (Table 5A). The mean ± SD 3-month predictive score was �0.81 ± 0.49 (�0.65 ± 0.51 for thosewho died vs. �0.88 ± 0.46 for those alive; p <0.001). The C statisticwas 0.63 and the Hosmer–Lemeshow statistic was 7.66 (p = 0.47),suggesting no evidence of lack of fit. When the same predictivescore was calculated for the 1259 patients in the validation set(mean �0.80 ± 0.48), we noted similar results (C statistic = 0.63,
ute liver failure in Europe: Outcomes over 20 years from the ELTR data-
2 vol. xxx j xxx–xxx 5
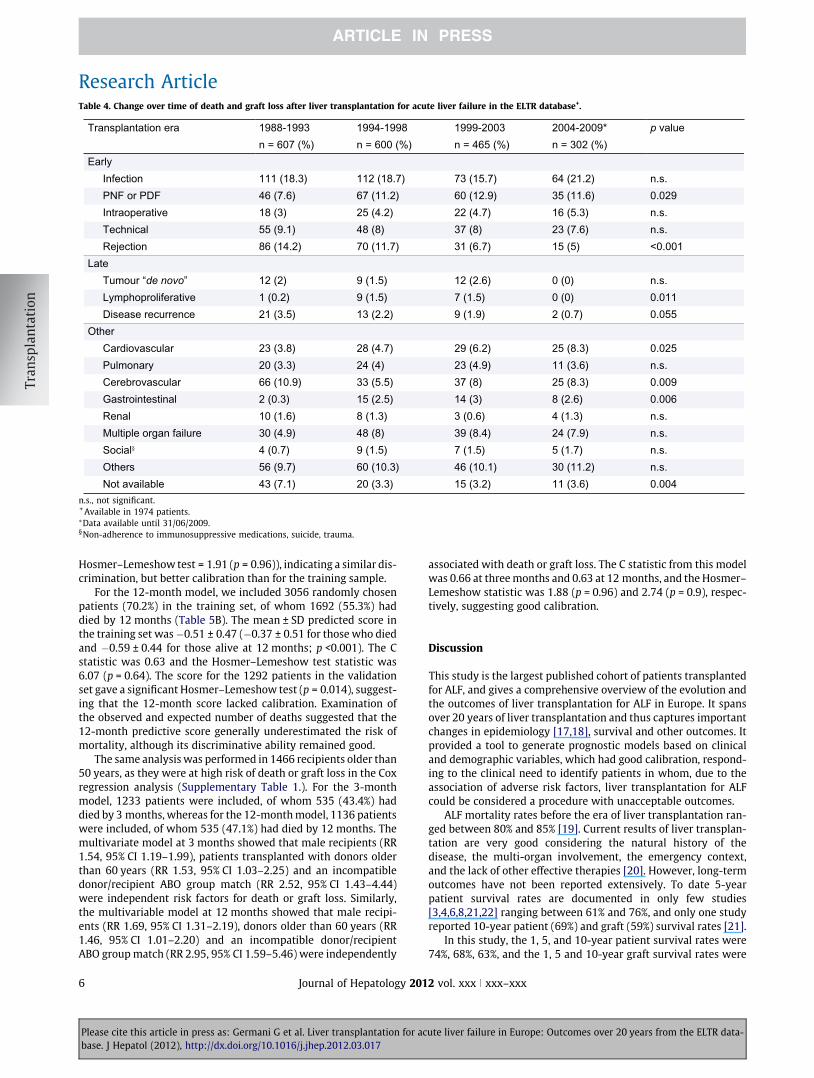
Table 4. Change over time of death and graft loss after liver transplantation for acute liver failure in the ELTR database+.
Transplantation era 1988-1993 1994-1998 1999-2003 2004-2009* p valuen = 607 (%) n = 600 (%) n = 465 (%) n = 302 (%)
EarlyInfection 111 (18.3) 112 (18.7) 73 (15.7) 64 (21.2) n.s.PNF or PDF 46 (7.6) 67 (11.2) 60 (12.9) 35 (11.6) 0.029Intraoperative 18 (3) 25 (4.2) 22 (4.7) 16 (5.3) n.s.Technical 55 (9.1) 48 (8) 37 (8) 23 (7.6) n.s.Rejection 86 (14.2) 70 (11.7) 31 (6.7) 15 (5) <0.001
LateTumour “de novo” 12 (2) 9 (1.5) 12 (2.6) 0 (0) n.s.Lymphoproliferative 1 (0.2) 9 (1.5) 7 (1.5) 0 (0) 0.011Disease recurrence 21 (3.5) 13 (2.2) 9 (1.9) 2 (0.7) 0.055
OtherCardiovascular 23 (3.8) 28 (4.7) 29 (6.2) 25 (8.3) 0.025Pulmonary 20 (3.3) 24 (4) 23 (4.9) 11 (3.6) n.s.Cerebrovascular 66 (10.9) 33 (5.5) 37 (8) 25 (8.3) 0.009Gastrointestinal 2 (0.3) 15 (2.5) 14 (3) 8 (2.6) 0.006Renal 10 (1.6) 8 (1.3) 3 (0.6) 4 (1.3) n.s.Multiple organ failure 30 (4.9) 48 (8) 39 (8.4) 24 (7.9) n.s.Social§ 4 (0.7) 9 (1.5) 7 (1.5) 5 (1.7) n.s.Others 56 (9.7) 60 (10.3) 46 (10.1) 30 (11.2) n.s.Not available 43 (7.1) 20 (3.3) 15 (3.2) 11 (3.6) 0.004
n.s., not significant.+ Available in 1974 patients.⁄Data available until 31/06/2009.§Non-adherence to immunosuppressive medications, suicide, trauma.
Research Article
Hosmer–Lemeshow test = 1.91 (p = 0.96)), indicating a similar dis-crimination, but better calibration than for the training sample.
For the 12-month model, we included 3056 randomly chosenpatients (70.2%) in the training set, of whom 1692 (55.3%) haddied by 12 months (Table 5B). The mean ± SD predicted score inthe training set was�0.51 ± 0.47 (�0.37 ± 0.51 for those who diedand �0.59 ± 0.44 for those alive at 12 months; p <0.001). The Cstatistic was 0.63 and the Hosmer–Lemeshow test statistic was6.07 (p = 0.64). The score for the 1292 patients in the validationset gave a significant Hosmer–Lemeshow test (p = 0.014), suggest-ing that the 12-month score lacked calibration. Examination ofthe observed and expected number of deaths suggested that the12-month predictive score generally underestimated the risk ofmortality, although its discriminative ability remained good.
The same analysis was performed in 1466 recipients older than50 years, as they were at high risk of death or graft loss in the Coxregression analysis (Supplementary Table 1.). For the 3-monthmodel, 1233 patients were included, of whom 535 (43.4%) haddied by 3 months, whereas for the 12-month model, 1136 patientswere included, of whom 535 (47.1%) had died by 12 months. Themultivariate model at 3 months showed that male recipients (RR1.54, 95% CI 1.19–1.99), patients transplanted with donors olderthan 60 years (RR 1.53, 95% CI 1.03–2.25) and an incompatibledonor/recipient ABO group match (RR 2.52, 95% CI 1.43–4.44)were independent risk factors for death or graft loss. Similarly,the multivariable model at 12 months showed that male recipi-ents (RR 1.69, 95% CI 1.31–2.19), donors older than 60 years (RR1.46, 95% CI 1.01–2.20) and an incompatible donor/recipientABO group match (RR 2.95, 95% CI 1.59–5.46) were independently
Please cite this article in press as: Germani G et al. Liver transplantation for acbase. J Hepatol (2012), http://dx.doi.org/10.1016/j.jhep.2012.03.017
6 Journal of Hepatology 201
associated with death or graft loss. The C statistic from this modelwas 0.66 at three months and 0.63 at 12 months, and the Hosmer–Lemeshow statistic was 1.88 (p = 0.96) and 2.74 (p = 0.9), respec-tively, suggesting good calibration.
Discussion
This study is the largest published cohort of patients transplantedfor ALF, and gives a comprehensive overview of the evolution andthe outcomes of liver transplantation for ALF in Europe. It spansover 20 years of liver transplantation and thus captures importantchanges in epidemiology [17,18], survival and other outcomes. Itprovided a tool to generate prognostic models based on clinicaland demographic variables, which had good calibration, respond-ing to the clinical need to identify patients in whom, due to theassociation of adverse risk factors, liver transplantation for ALFcould be considered a procedure with unacceptable outcomes.
ALF mortality rates before the era of liver transplantation ran-ged between 80% and 85% [19]. Current results of liver transplan-tation are very good considering the natural history of thedisease, the multi-organ involvement, the emergency context,and the lack of other effective therapies [20]. However, long-termoutcomes have not been reported extensively. To date 5-yearpatient survival rates are documented in only few studies[3,4,6,8,21,22] ranging between 61% and 76%, and only one studyreported 10-year patient (69%) and graft (59%) survival rates [21].
In this study, the 1, 5, and 10-year patient survival rates were74%, 68%, 63%, and the 1, 5 and 10-year graft survival rates were
ute liver failure in Europe: Outcomes over 20 years from the ELTR data-
2 vol. xxx j xxx–xxx
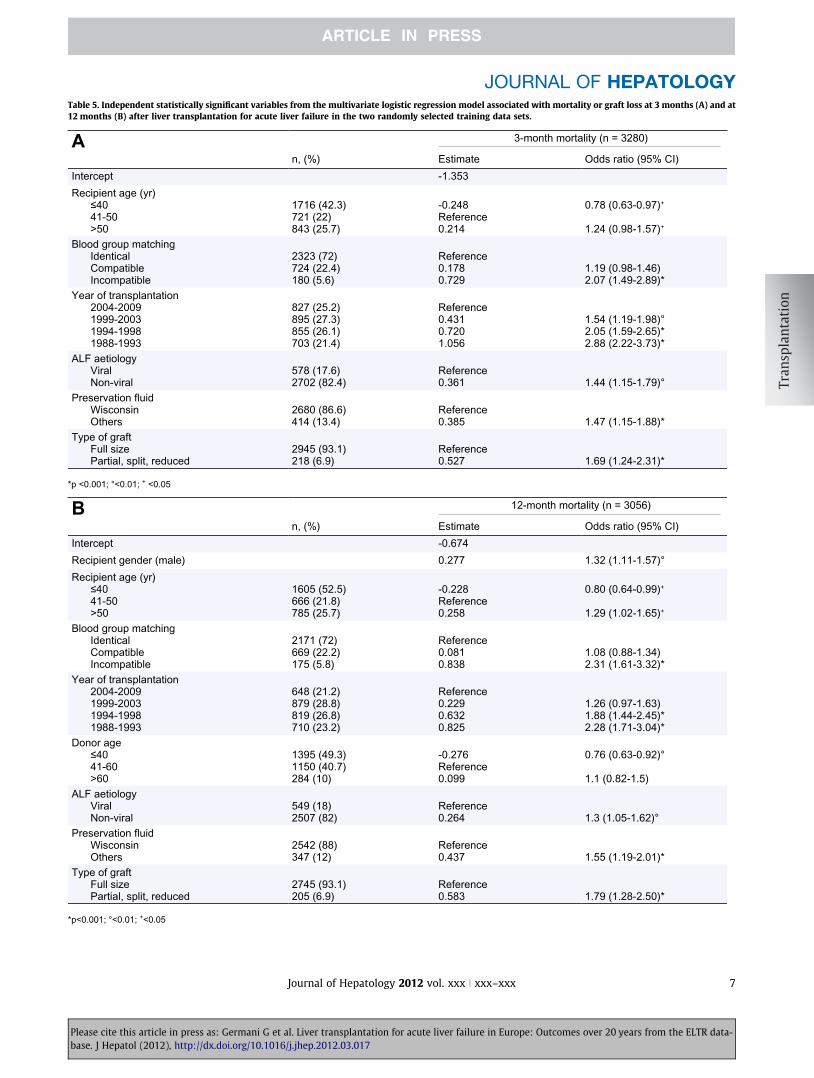
Table 5. Independent statistically significant variables from the multivariate logistic regression model associated with mortality or graft loss at 3 months (A) and at12 months (B) after liver transplantation for acute liver failure in the two randomly selected training data sets.
A 3-month mortality (n = 3280)
n, (%) Estimate Odds ratio (95% CI)Intercept -1.353Recipient age (yr)
≤4041-50>50
1716 (42.3)721 (22)843 (25.7)
-0.248Reference0.214
0.78 (0.63-0.97)+
1.24 (0.98-1.57)+
Blood group matchingIdenticalCompatibleIncompatible
2323 (72)724 (22.4)180 (5.6)
Reference0.1780.729
1.19 (0.98-1.46)2.07 (1.49-2.89)*
Year of transplantation2004-20091999-20031994-1998 1988-1993
827 (25.2)895 (27.3)855 (26.1)703 (21.4)
Reference0.4310.7201.056
1.54 (1.19-1.98)°2.05 (1.59-2.65)*2.88 (2.22-3.73)*
ALF aetiologyViralNon-viral
578 (17.6)2702 (82.4)
Reference0.361 1.44 (1.15-1.79)°
Preservation fluidWisconsinOthers
2680 (86.6)414 (13.4)
Reference0.385 1.47 (1.15-1.88)*
Type of graftFull sizePartial, split, reduced
2945 (93.1)218 (6.9)
Reference0.527 1.69 (1.24-2.31)*
*p <0.001; °<0.01; + <0.05
B 12-month mortality (n = 3056)
n, (%) Estimate Odds ratio (95% CI)Intercept -0.674Recipient gender (male) 0.277 1.32 (1.11-1.57)°Recipient age (yr)
≤4041-50>50
1605 (52.5)666 (21.8)785 (25.7)
-0.228Reference0.258
0.80 (0.64-0.99)+
1.29 (1.02-1.65)+
Blood group matchingIdenticalCompatibleIncompatible
2171 (72)669 (22.2)175 (5.8)
Reference0.0810.838
1.08 (0.88-1.34)2.31 (1.61-3.32)*
Year of transplantation2004-20091999-20031994-1998 1988-1993
648 (21.2)879 (28.8)819 (26.8)710 (23.2)
Reference0.2290.6320.825
1.26 (0.97-1.63)1.88 (1.44-2.45)*2.28 (1.71-3.04)*
Donor age≤4041-60 >60
1395 (49.3)1150 (40.7)284 (10)
-0.276Reference0.099
0.76 (0.63-0.92)°
1.1 (0.82-1.5)ALF aetiology
ViralNon-viral
549 (18)2507 (82)
Reference0.264 1.3 (1.05-1.62)°
Preservation fluidWisconsinOthers
2542 (88)347 (12)
Reference0.437 1.55 (1.19-2.01)*
Type of graftFull sizePartial, split, reduced
2745 (93.1)205 (6.9)
Reference0.583 1.79 (1.28-2.50)*
*p<0.001; °<0.01; +<0.05
JOURNAL OF HEPATOLOGY
Please cite this article in press as: Germani G et al. Liver transplantation for acute liver failure in Europe: Outcomes over 20 years from the ELTR data-base. J Hepatol (2012), http://dx.doi.org/10.1016/j.jhep.2012.03.017
Journal of Hepatology 2012 vol. xxx j xxx–xxx 7

Donor age>60 years
Malerecipient
Donor age>60 years
Malerecipient
IncompatibleABO match
Donor age>60 years
IncompatibleABO match
Malerecipient
IncompatibleABO match
Donor age>60 years
Malerecipient
IncompatibleABO match
Donor age>60 years
Malerecipient
Donor age>60 years
Malerecipient
IncompatibleABO match
Donor age>60 years
IncompatibleABO match
Malerecipient
IncompatibleABO match
Donor age>60 years
Malerecipient
IncompatibleABO match
32%A
33%
43%
44%
55%
55%
65%
44%B
47%
57%
61%
70%
73%
80%
Hosmer and Lemeshow test = 1.88 (0.96)Area under the ROC = 0.66
Hosmer and Lemeshow test = 2.74 (0.90)Area under the ROC = 0.63
Fig. 3. Risk of 3-month (A) and 12-month (B) mortality or graft loss inpatients older than 50 years transplanted for ALF according to the presence ofindependently associated risk factors.
Research Article
63%, 57%, 50%. In the United States, between 1997 and 2004, the1-year and 5-year patient and graft survival rates were 82%, 70%and 76%, 61%, respectively [2]. Based on the same time-interval inthe ELTR database, the five-year patient and graft survival rateswere similar at 69% and 60%, whereas the 1-year survival rateswere lower at 74% and 66%, respectively. All patients had a min-imum of 1 year follow-up and thus time periods are comparable,without bias of varying follow-up times. The differences in sur-vival occur in this first year, and then survival curves remain par-allel. This suggests that improvements are related to pre-, peri-and immediately post-operative care.The ELTR data showed a constant and progressive improve-ment in the survival rate over time, with only small changes inaetiology: HAV- and HBV-related ALF decreased over time andALF due to paracetamol increased. These improved outcomesare not only important ‘‘per se’’, but is crucial to understand thatthis occurred despite a dramatic increase in the donor age, withdonors older than 60 years being nearly ten times more numerousbetween 2004 and 2009 than between 1988 and 1993. These find-ings reflect the worldwide increase of age of donors [23], which isan established adverse factor for both elective and emergencyliver transplantation [14]. Thus, the increased prevalence of thisadverse factor has been compensated by a substantial improve-ment in the pre-, peri- and post-operative patient managementof ALF with liver transplantation. Thus, it is unlikely there is a sin-gle or most important factor responsible for the improved survivalafter liver transplantation for ALF in the most recent 5 years. ALFpatients have always been considered super-urgent and are notunder the MELD system, thus the allocation system has not chan-ged. Selection also probably has not changed, as it is unlikely thatsicker patients were not selected, but this cannot be verified fromthe ELTR database. The introduction of new immunosuppressantsmay have contributed to improved survival. This is suggested by asignificant reduction in rejection incidence as a cause of death orgraft loss (from 14.2% in 1988–1993 to 5% in 2004–2009). How-ever, in addition, improved anaesthesia and intensive care willhave contributed, as it has been shown following liver transplan-tation for cirrhosis, where progressive improvements in survivalhave been documented in Europe [14].
Despite the significant improvement in patient and graft sur-vival over time, a high early mortality rate still persists aftertransplantation for ALF, especially within the first year. Therefore,we decided to identify potential risk factors for poor prognosis inthe early post-transplant period and to generate 3- and 12-monthprognostic models with the aim to stratify patients according tothe risk of death or graft loss. The 3-month model was well cali-brated, but the 12-month model showed a tendency to underes-timate mortality rates. The most likely explanation for the lack ofcalibration in the 12-month model is that other factors such asrecurrent disease and renal function post-operatively becomeimportant and peri-operative variables lose their importance.Moreover, the lack of information regarding the clinical statusof the recipient before liver transplantation such as ventilationstatus, renal function, presence/absence of cerebral oedema,which are not recorded by the ELTR, could weaken the predictivevalue of the model and is a limitation of the models.
Recipients above 50 years were at risk for increased mortality,confirming data from 236 patients in a single centre [3], and from1457 patients (UNOS database, 1988–2003) [22], and it can beprobably explained by an age-related reduction in physiologicalreserve [3]. Therefore, a sub-analysis was performed in recipients
Please cite this article in press as: Germani G et al. Liver transplantation for acbase. J Hepatol (2012), http://dx.doi.org/10.1016/j.jhep.2012.03.017
8 Journal of Hepatology 201
>50 years, based on the 3 and 12-month prognostic models. Con-sidering mortality or graft loss rate of more than 50% at12 months as an unacceptable outcome, there are several combi-nations of three risk factors, when liver transplantation for ALFcould be considered futile, especially when all risk factors arepresent (35% and 20% of death or graft loss at 3 and 12 months,respectively) (Fig. 3). Thus, an ABO incompatible graft remainsan important adverse factor for patient and graft survival con-firming previous studies [24], but in contrast to two others[25,26]. The database does not include data on therapies usedto prevent consequences of ABO incompatible mismatch.Recently, a more selective approach, based on antigen-specificimmunoadsorption with immunoadsorbent columns with orwithout rituximab, has been proposed in order to reduce the highrisk of sepsis occurring with previous regimens [27]. In addition,in the whole cohort, a reduced size graft (split liver, reduced, orpartial for living) compared to a full size graft, increased
ute liver failure in Europe: Outcomes over 20 years from the ELTR data-
2 vol. xxx j xxx–xxx

JOURNAL OF HEPATOLOGY
mortality or graft loss by 1.5 times. In order to reduce the mortal-ity risk in this specific sub-group of recipients >50 years, donors>60 years should be avoided, as well as use of reduced size grafts.ABO incompatible matching could be also circumvented [28].The results of our models may help clinicians to decide whenan outcome might be unacceptable as another recipient may ben-efit far more from use of a particular donor liver. However, thedecisions must always be focused on the individual patient, andthe model predictions should not be used as guidelines. Althoughin an emergency situation, it may be difficult not to choose to useparticular donors, the centre, and the national transplant com-munity need to review the use of older donors for certain recip-ients with ALF, as the outcomes may not justify the choices taken.
Lastly, we showed that in Europe there has been a significantand constant increase in liver transplantation for paracetamol-related ALF. Among these patients, nearly 8% died or lost the graftfor ‘‘social’’ complications, with suicide and non-adherence toimmunosuppressive medications accounting for nearly 94% ofthese deaths, 57% of which occur within the first year after trans-plant (and 40% within the first three months). Therefore, in theearly post-transplant phase, more psychological/psychiatric, andsocial support should be offered to patients transplanted for par-acetamol overdose, to lessen graft loss and death.
In conclusion, despite a progressive and constant improve-ment in the survival rate after liver transplantation for ALF, a highmortality and graft loss rate still persist, especially within thefirst year post-transplant. Data shown in our analysis strengthensthe importance of a re-evaluation of the selection of olderpatients with ALF as potential recipients for liver transplantation.This is particularly so, as outcomes with older donors >60 years(currently 21% of all donors) result in poor survival. Therefore,a strategy to improve outcomes could be firstly to identifypatients, estimated to have an unacceptable high risk of deathor graft loss within one year of liver transplantation based onutilitarian principles, and secondly to avoid in these patients,and particularly in those older than 50 years (especially if males),use of grafts from donors >60 years, ABO incompatible matching(without novel technological solutions) and a reduced size graft.
Conflict of interest
The authors who have taken part in this study declared that theydo not have anything to disclose regarding funding or conflict ofinterest with respect to this manuscript.
Supplementary data
Supplementary data associated with this article can be found, in theonline version, at http://dx.doi.org/10.1016/j.jhep. 2012.03.017.
References
[1] Available from <http://www.eltr.org>.[2] 2009 Annual Report of the US Organ Procurement Transplant Network and
Scientific Registry of Transplant Recipients: transplant data 1999–2008,<http://optn.transplant.hrsa.gov/ar2009>.
[3] Bernal W, Cross TJ, Auzinger G, Sizer E, Heneghan MA, Bowles M, et al.Outcome after wait-listing for emergency liver transplantation in acute liverfailure: a single centre experience. J Hepatol 2009;50:306–313.
Please cite this article in press as: Germani G et al. Liver transplantation for acbase. J Hepatol (2012), http://dx.doi.org/10.1016/j.jhep.2012.03.017
Journal of Hepatology 201
[4] Bismuth H, Samuel D, Castaing D, Adam R, Saliba F, Johann M, et al.Orthotopic liver transplantation in fulminant and subfulminant hepatitis.The Paul Brousse experience. Ann Surg 1995;222:109–119.
[5] O’Grady JG, Alexander GJ, Thick M, Potter D, Calne RY, Williams R. Outcomeof orthotopic liver transplantation in the aetiological and clinical variants ofacute liver failure. Q J Med 1988;68:817–824.
[6] Wigg AJ, Gunson BK, Mutimer DJ. Outcomes following liver transplantationfor seronegative acute liver failure: experience during a 12-year period withmore than 100 patients. Liver Transpl 2005;11:27–34.
[7] Ascher NL, Lake JR, Emond JC, Roberts JP. Liver transplantation for fulminanthepatic failure. Arch Surg 1993;128:677–682.
[8] Farmer DG, Anselmo DM, Ghobrial RM, Yersiz H, McDiarmid SV, Cao C, et al.Liver transplantation for fulminant hepatic failure: experience with more than200 patients over a 17-year period. Ann Surg 2003;237:666–675, [discussion675–666].
[9] Bjoro K, Ericzon BG, Kirkegaard P, Hockerstedt K, Soderdahl G, Olausson M,et al. Highly urgent liver transplantation: possible impact of donor–recipientABO matching on the outcome after transplantation. Transplantation2003;75:347–353.
[10] Emond JC, Aran PP, Whitington PF, Broelsch CE, Baker AL. Liver transplan-tation in the management of fulminant hepatic failure. Gastroenterology1989;96:1583–1588.
[11] Lee WM. Acute liver failure in the United States. Semin Liver Dis2003;23:217–226.
[12] Bernal W, Auzinger G, Dhawan A, Wendon J. Acute liver failure. Lancet2010;376:190–201.
[13] Adam R, McMaster P, O’Grady JG, Castaing D, Klempnauer JL, Jamieson N,et al. Evolution of liver transplantation in Europe: report of the EuropeanLiver Transplant Registry. Liver Transpl 2003;9:1231–1243.
[14] Burroughs AK, Sabin CA, Rolles K, Delvart V, Karam V, Buckels J, et al. 3-month and 12-month mortality after first liver transplant in adults inEurope: predictive models for outcome. Lancet 2006;367:225–232.
[15] Adam R, Cailliez V, Majno P, Karam V, McMaster P, Caine RY, et al.Normalised intrinsic mortality risk in liver transplantation: European LiverTransplant Registry study. Lancet 2000;356:621–627.
[16] Karam V, Gunson B, Roggen F, Grande L, Wannoff W, Janssen M, et al. Qualitycontrol of the European Liver Transplant Registry: results of audit visits tothe contributing centers. Transplantation 2003;75:2167–2173.
[17] Escorsell A, Mas A, de la Mata M. Acute liver failure in Spain: analysis of 267cases. Liver Transpl 2007;13:1389–1395.
[18] Ichai P, Samuel D. Epidemiology of liver failure. Clin Res Hepatol Gastro-enterol 2011;35:610–617.
[19] Bernuau J, Rueff B, Benhamou JP. Fulminant and subfulminant liver failure:definitions and causes. Semin Liver Dis 1986;6:97–106.
[20] O’Grady JG. Postoperative issues and outcome for acute liver failure. LiverTranspl 2008;14 (Suppl 2):S97–101.
[21] Chan G, Taqi A, Marotta P, Levstik M, McAlister V, Wall W, et al. Long-termoutcomes of emergency liver transplantation for acute liver failure. LiverTranspl 2009;15:1696–1702.
[22] Barshes NR, Lee TC, Balkrishnan R, Karpen SJ, Carter BA, Goss JA. Riskstratification of adult patients undergoing orthotopic liver transplantationfor fulminant hepatic failure. Transplantation 2006;81:195–201.
[23] Merion RM. Current status and future of liver transplantation. Semin LiverDis 2010;30:411–421.
[24] Bismuth H, Samuel D, Castaing D, Williams R, Pereira SP. Liver transplan-tation in Europe for patients with acute liver failure. Semin Liver Dis1996;16:415–425.
[25] Farges O, Kalil AN, Samuel D, Saliba F, Arulnaden JL, Debat P, et al. The use ofABO-incompatible grafts in liver transplantation: a life-saving procedure inhighly selected patients. Transplantation 1995;59:1124–1133.
[26] Toso C, Al-Qahtani M, Alsaif FA, Bigam DL, Meeberg GA, James Shapiro AM,et al. ABO-incompatible liver transplantation for critically ill adult patients.Transpl Int 2007;20:675–681.
[27] Saliba F, Ichai P, Azoulay D, Habbouchi H, Antonini T, Sebagh M, et al.Successful long-term outcome of ABO-incompatible liver transplantationusing antigen-specific immunoadsorption columns. Ther Apher Dial2010;14:116–123.
[28] Tanabe M, Kawachi S, Obara H, Shinoda M, Hibi T, Kitagawa Y, et al. Currentprogress in ABO-incompatible liver transplantation. Eur J Clin Invest2010;40:943–949.
ute liver failure in Europe: Outcomes over 20 years from the ELTR data-
2 vol. xxx j xxx–xxx 9
Related Documents











