RESEARCH FROM THE UNIVERSITY OF ALABAMA AT BIRMINGHAM Live Three-Dimensional Transthoracic Echocardiographic Assessment of Ventricular Noncompaction Kunal Bodiwala, M.D., Andrew P. Miller, M.D., Navin C. Nanda, M.D., Vinod Patel, M.D., Srinivas Vengala, M.D., Farhat Mehmood, M.D., Shailendra Upendram, M.D., and Ebenezer Frans, M.D. Division of Cardiovascular Diseases, University of Alabama at Birmingham, Birmingham, Alabama We present eight adult patients with noncompaction (four with isolated left ventricular noncompaction and four with combined left and right ventricular noncompaction) in whom live three-dimensional transthoracic echocardiography (3D TTE) demonstrated multiple, prominent myocardial trabecula- tions, deep intertrabecular recesses communicating with the ventricular cavity, and a typical honey- combing appearance. In the four patients with combined right and left ventricular noncompaction, very extensive trabeculations in the right ventricle were identified, much more than in normal or hypertrophied right ventricles. Five of the eight patients were not definitively identified to have non- compaction on two-dimensional (2D) TTE, but the diagnosis was made with 3D TTE. These cases demonstrate the potential usefulness of 3D TTE as a supplement to 2D TTE in the assessment of noncompaction. (ECHOCARDIOGRAPHY, Volume 22, August 2005) left ventricular noncompaction, right ventricular noncompaction, cardiomyopathy, live three- dimensional transthoracic echocardiography, heart failure Noncompaction of the ventricle is a rare disorder of endomyocardial morphogenesis characterized by echocardiographic findings consisting of multiple, prominent myocardial trabeculations and deep intertrabecular re- cesses communicating with the ventricular cavity. 1–4 The disease affects the left ventricle, with or without right ventricular involvement, and may result in both systolic and diastolic ventricular dysfunction with frequent progres- sion to clinical heart failure, and potential complications including arrhythmias and thromboembolic events. 5,6 Noncompaction was initially described in children; 7 however, recent Address for correspondence and reprint requests: Navin C. Nanda, M.D., University of Alabama at Birmingham, Heart Station SWB/S102, 619 19th Street South, Birmingham, AL 35249. Fax: 205-934-6747. E-mail: [email protected] studies have characterized this disease in adult populations, in whom this process may be underappreciated in prevalence. 6,8,9 Right ventricular involvement may be difficult to differentiate from normal anatomy but is characterized by both apical involvement and pathologically prominent trabeculations. 10 In this report, we describe eight cases of non- compaction (four of isolated left and four of combined left and right ventricular noncom- paction) with typical clinical and echocardio- graphic features of the disease, and findings are correlated with computed tomography (CT) or magnetic resonance imaging (MRI) in two pa- tients. Using live/real-time three-dimensional transthoracic echocardiography (3D TTE), we were able to make a definitive diagnosis of noncompaction with an en face view of the typical honeycombed-appearing myocardium; and in addition, we were able to clearly assess the segmental extent of involvement. Vol. 22, No. 7, 2005 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. 611

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

RESEARCH FROM THE UNIVERSITY OF ALABAMA ATBIRMINGHAM
Live Three-Dimensional TransthoracicEchocardiographic Assessment of VentricularNoncompactionKunal Bodiwala, M.D., Andrew P. Miller, M.D., Navin C. Nanda, M.D., Vinod Patel, M.D., SrinivasVengala, M.D., Farhat Mehmood, M.D., Shailendra Upendram, M.D., and Ebenezer Frans, M.D.
Division of Cardiovascular Diseases, University of Alabama at Birmingham, Birmingham,Alabama
We present eight adult patients with noncompaction (four with isolated left ventricular noncompactionand four with combined left and right ventricular noncompaction) in whom live three-dimensionaltransthoracic echocardiography (3D TTE) demonstrated multiple, prominent myocardial trabecula-tions, deep intertrabecular recesses communicating with the ventricular cavity, and a typical honey-combing appearance. In the four patients with combined right and left ventricular noncompaction,very extensive trabeculations in the right ventricle were identified, much more than in normal orhypertrophied right ventricles. Five of the eight patients were not definitively identified to have non-compaction on two-dimensional (2D) TTE, but the diagnosis was made with 3D TTE. These casesdemonstrate the potential usefulness of 3D TTE as a supplement to 2D TTE in the assessment ofnoncompaction. (ECHOCARDIOGRAPHY, Volume 22, August 2005)
left ventricular noncompaction, right ventricular noncompaction, cardiomyopathy, live three-dimensional transthoracic echocardiography, heart failure
Noncompaction of the ventricle is a raredisorder of endomyocardial morphogenesischaracterized by echocardiographic findingsconsisting of multiple, prominent myocardialtrabeculations and deep intertrabecular re-cesses communicating with the ventricularcavity.1–4 The disease affects the left ventricle,with or without right ventricular involvement,and may result in both systolic and diastolicventricular dysfunction with frequent progres-sion to clinical heart failure, and potentialcomplications including arrhythmias andthromboembolic events.5,6 Noncompaction wasinitially described in children;7 however, recent
Address for correspondence and reprint requests: Navin C.Nanda, M.D., University of Alabama at Birmingham, HeartStation SWB/S102, 619 19th Street South, Birmingham, AL35249. Fax: 205-934-6747. E-mail: [email protected]
studies have characterized this disease inadult populations, in whom this process may beunderappreciated in prevalence.6,8,9 Rightventricular involvement may be difficult todifferentiate from normal anatomy but ischaracterized by both apical involvement andpathologically prominent trabeculations.10 Inthis report, we describe eight cases of non-compaction (four of isolated left and four ofcombined left and right ventricular noncom-paction) with typical clinical and echocardio-graphic features of the disease, and findings arecorrelated with computed tomography (CT) ormagnetic resonance imaging (MRI) in two pa-tients. Using live/real-time three-dimensionaltransthoracic echocardiography (3D TTE), wewere able to make a definitive diagnosis ofnoncompaction with an en face view of thetypical honeycombed-appearing myocardium;and in addition, we were able to clearly assessthe segmental extent of involvement.
Vol. 22, No. 7, 2005 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. 611

BODIWALA, ET AL.
TABLE I
Clinical and Real-Time Two-Dimensional and Live Three-Dimensional Transthoracic Echocardiographic Features ofVentricular Noncompaction
Age (years)/ ClinicalCase No. Gender Presentation 2D TTE Live 3D TTE
1 31/Female Cardiac failure,hypertension
LVNC. All LV s involved except basalseptal s. N/C ratio 2.94, LVEF 20%and RVEF 25%. Medications:carvedilol, angiotensin II receptorblocker, warfarin, furosemide.Follow-up 2D TTE after 6 months:LVEF and RVEF improved to 45%and 55%, respectively
LVNC and RVNC. All LV and RV sinvolved except LV basal septal s.N/C ratio 3.92. Echo contrast studyshowed LV apical hypoperfusion.CT-scan showed LVNC
2 37/Male Cardiac failure,hypertension, HIVinfection
LVNC. All LV s involved except basalinferior and basal anterior s. N/Cratio 3.72. LVEF 15%, RVEF 15%.Medications: angiotensinconverting enzyme inhibitor,furosemide. No follow-up 2D TTE
LVNC. All LV s involved except basalinferior and basal anterior s. N/Cratio 4.65
3 53/Male Atypical precordialchest pain,hypertension,dyspnea onmoderate exertion
LVNC. All apical s involved. N/C ratio2.92. LVEF 50–55%, RVEF > 55%.Medications: labetalol, clonidine.No follow-up 2D TTE
LVNC. All apical and midposterolateral s involved. N/C ratio3.96
4 28/Female Cardiac failure LVNC versus septal mass. LVEF 15%,RVEF 15%. Medications: carvedilol,angiotensin converting enzymeinhibitor, furosemide. Follow-up 2DTTE after 7 months: LVEFimproved to 35%, RVEF unchanged
LVNC and RVNC. All LV and RV sinvolved except LV basal anteriorand RV basal septal s. N/C ratio10.34. MRI initially suggestedseptal mass consistent withmalignancy; on subsequent reviewno mass but LVNC
5 45/Male Cardiac failure,atypical chest pain,hypertension
? LV apical thrombus. LVEF 25–30%,RVEF 35%. Medications:hydralazine, clonidine. Follow-up2D TTE after 14 months: LVEF andRVEF improved to 55%
LVNC. All apical s and mid and basalseptal and posterolateral sinvolved. N/C ratio 3.40
6 41/Male Cardiac failure,hypertension, endstage renal disease
LVNC and RVNC not suspected.LVEF 15%, RVEF 15%.Medications: minoxidil, calciumchannel blocker. No follow-up 2DTTE
LVNC and RVNC. All LV and RV sinvolved except LV mid and basalanterior and basal inferior s andRV basal septal and basal inferiors. N/C ratio 4.98
7 52/Male Cardiac failure,probable angina,hypertension,previousmyocardialinfarction, diabetes
LVNC and RVNC not suspected.LVEF 15%, RVEF 30%.Medications: carvedilol, warfarin,amiodarone, furosemide,spironolactone, digoxin. Nofollow-up 2D TTE
LVNC and RVNC. All LV and RV sinvolved except RV basal s. N/Cratio 2.70
8 54/Male Hypertension,diabetes, acutemyelogenousleukemia, endstage renal disease
LVNC and RVNC not suspected.LVEF > 55%, RVEF > 55%.Medications: metoprolol,angiotensin converting enzymeinhibitor, furosemide. No follow-up2D TTE
LVNC. All LV s involved except basalseptal and basal inferior s. N/Cratio 3.75
CT = computed tomography; HIV = human immunodeficiency virus; LVEF = left ventricular ejection fraction; LVNC =left ventricular noncompaction; MRI = magnetic resonance imaging; N/C = noncompacted/compacted myocardium; RVEF= right ventricular ejection fraction; RVNC = right ventricular noncompaction; s = segment; 2D TTE = two-dimensionaltransthoracic echocardiography; 3D TTE = three-dimensional transthoracic echocardiography.
612 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. Vol. 22, No. 7, 2005

VENTRICULAR NONCOMPACTION
Embryology
In the early embryo, the heart is a loose in-terwoven mesh of muscle fibers that forms tra-beculae with deep intertrabecular recesses.11
During fetal ontogenesis, the developing my-ocardium gradually condenses, and largespaces within the trabecular meshwork flatten.These large intertrabecular spaces transforminto capillaries as the process of compaction oc-curs from epicardium to endocardium and frombase toward the apex of the heart, with trabecu-lar compaction being more complete in the leftventricular than in the right ventricular my-ocardium.
In the abnormal condition, the process of com-paction arrests at an early stage, leaving nu-merous, excessively prominent trabeculationsand deep intertrabecular recesses in a segmen-tal distribution usually from the apex.3,8 Theseproduce a typical honeycomb-like appearancewhen sectioned transversely. Thought to be acongenital disorder occurring by this mecha-nism, evidence supports the notion that non-compaction is present from birth.6,9 Interest-ingly, noncompaction can be associated withother congenital cardiac malformations, suchas anomalous origin of the left coronary arteryfrom pulmonary trunk and obstruction to rightor left ventricular outflow tracts.2,3,8,12
Diagnostic Criteria
The typical feature of noncompaction is atwo-layered myocardial wall structure, witha thin compacted myocardium on the epicar-dial side (epicardial layer) and thicker non-compacted myocardium on the endocardial side(endocardial layer).3 This results in a thick-ened ventricular wall with deep recesses filledwith blood from the ventricular cavity.3,5 Non-compaction can be described anatomically us-ing nine left ventricular segments.5,6 Not to beconfused with the diffuse hypertrophy createdby conditions such as hypertension and valvu-lar heart disease where prominent trabecula-tions (coursing from the free wall to the septum)may be noted, left ventricular noncompactionis typically apical, lateral, and inferior.5,6 Themajor echocardiographic criterion is a ratio ofnoncompacted-to-compacted (N/C) myocardiummeasured at a site of maximal thickness thatis ≥2.3 Of further use in conventional echocar-diography, color Doppler can differentiate deep
ventricular recesses that invaginate the non-compacted myocardium.6
Case Studies
Eight cases of noncompaction of the left ven-tricle with or without right ventricular involve-ment were identified from all patients present-ing to the Echocardiography Laboratory overa 7-month period. All patients underwent two-dimensional (2D) TTE using a 3.5 MHz probeand a commercially available ultrasound sys-tem (Philips Sonos 7500, Andover, MA, USA)with capabilities for performing live 3D B-modeand color Doppler echocardiography.13 Aftercompletion of the standard 2D TTE in each pa-tient, 3D TTE images of the ventricles wereobtained using a 4 MHz 4× matrix probe. Ap-proximately 5–7 seconds of breath-holding wereneeded to collect one dataset. Data were storeddigitally and subsequently evaluated by a sin-gle echocardiographer to characterize noncom-pacted myocardium. The 3D pyramidal datasetwas cropped systematically to create an en faceview of the ventricular septum and apex, andevaluation was augmented with color Dopplerand/or intravenous echo contrast assessment.To define extent of noncompaction involvement,segmental evaluation of the left ventricles wasperformed, dividing it into basal, mid, and api-cal regions of the septal, inferior, posterolat-eral, and anterior walls. The right ventriclewas divided into apical, mid, and basal re-gions of the septal, diaphragmatic, and freewalls. Noncompacted-to-compacted ratios wereobtained from end-systolic measurements of thenoncompacted endocardial and the compactedepicardial layers in the maximally involved my-ocardium.6
Patient characteristics, 2D TTE and 3D TTEfindings, and correlation with other imagingmodalities are detailed in Table I. Of note, ahoneycombing appearance in the apical areawas visualized in all patients by 3D TTE. Im-ages revealed finger-like projections from theventricular wall with deep intertrabecular re-cesses between, when viewed en face. In five pa-tients, 2D TTE findings were not diagnostic ofnoncompaction, as one patient was felt to havea possible left ventricular mass (Case 4), an-other a left ventricular thrombus (Case 5), andthree patients were not suspected to have non-compaction (Cases 6–8).
In one case (Case 1), myocardial contrastechocardiography was performed. 2D TTE in
Vol. 22, No. 7, 2005 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. 613

BODIWALA, ET AL.
Figure 1. Continued. Figure 2. Continued.
614 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. Vol. 22, No. 7, 2005
VENTRICULAR NONCOMPACTION
Figure 2. Continued.
Figure 3. Continued. Figure 3. Continued.
Vol. 22, No. 7, 2005 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. 615

BODIWALA, ET AL.
Figure 3. Continued. Figure 3. Continued.
616 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. Vol. 22, No. 7, 2005

VENTRICULAR NONCOMPACTION
Figure 3. Continued.
Figure 4. Continued. Figure 4. Continued.
Vol. 22, No. 7, 2005 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. 617

BODIWALA, ET AL.
this case revealed extensive involvement of theentire posterolateral wall of the left ventricle(Fig. 1A). Using perflutren lipid microspheres(Definity, Bristol-Myers Squibb, North Biller-ica, MA, USA; 1.5 cc dissolved in 15 cc of nor-mal saline) injected intravenously slowly and ata steady rate, apical hypoperfusion of the non-compacted myocardium was visualized (Fig. 1Band 1C). Use of 3D TTE in this patient re-vealed pathologic noncompaction in both the
←−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−Figure 1. Two-dimensional transthoracic echocardiogra-phy in left ventricular noncompaction (Case 1). A. Arrowpoints to prominent trabeculations involving the whole ex-tent of left ventricular (LV) posterolateral wall consistentwith noncompaction. B. Myocardial perfusion study usingperflutren lipid microspheres demonstrated apical hypoper-fusion (arrowhead). C. Echo contrast time intensity curvesshow diminished rate of filling as well as peak filling in theLV apex as compared to the ventricular septum (VS). LA =left atrium; MV = mitral valve; RA = right atrium; RV =right ventricle.
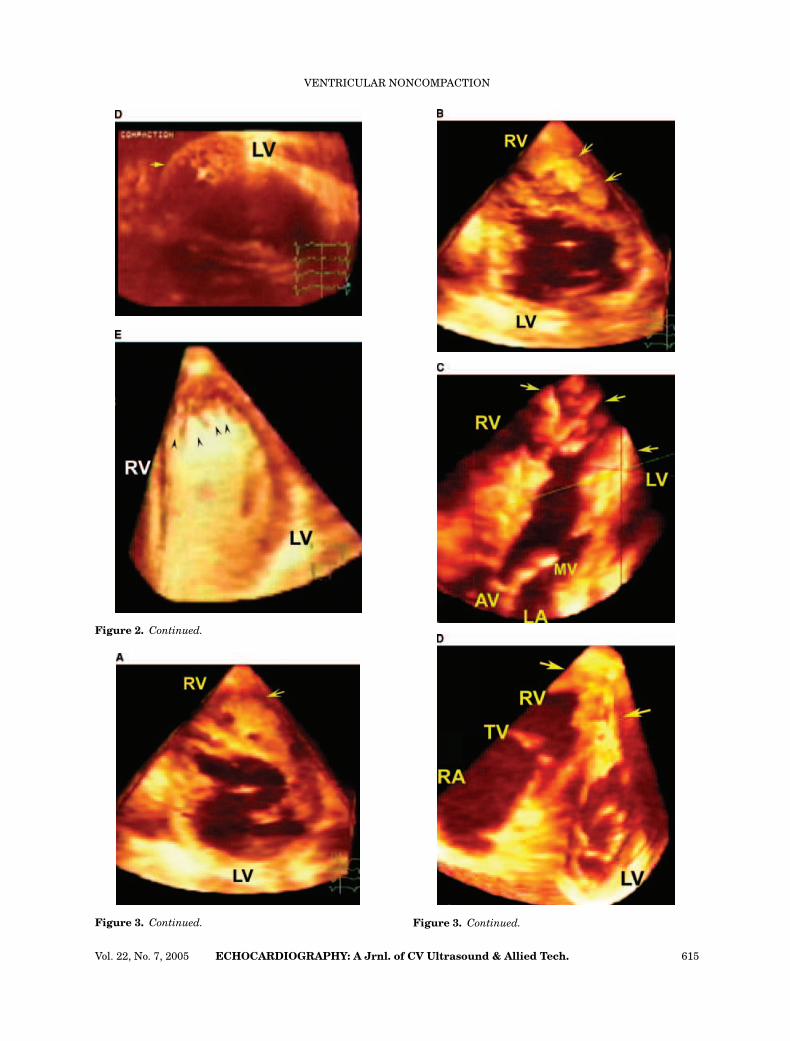
Figure 2. Live three-dimensional transthoracic echocar-diography in combined left and right ventricular noncom-paction (Case 1). A and B. Arrows point to prominent tra-beculations in both ventricles. C. Arrows show multipleprominent trabeculations in RV. D. Transverse cropping ofLV apical area shows a honeycomb-like appearance (arrow)typical of noncompaction. E. Echo contrast study using per-flutren lipid microspheres shows filling of intertrabecularrecesses with the contrast agent (arrowheads). AV = aorticvalve; other abbreviations as in Figure 1.
Figure 3. Live three-dimensional transthoracic echocar-diography in combined left and right ventricular noncom-paction in another patient (Case 4). A and B. Arrows pointto a cauliflower-like mass in RV mimicking a tumor. C-E.Arrows point to massive trabeculations in both LV and RVconsistent with noncompaction. F and G. Transverse (F)and anteroposterior (G) cropping of LV apical area showa honeycomb-like appearance (arrow) typical of noncom-paction. H. Arrowheads point to multiple trabeculations inRV. I and J. Arrow points to massive trabeculations in theventricular septal area. K. Arrows point to multiple trabec-ulations crossing the RV cavity transversely. TV = tricuspidvalve; AO = ascending aorta; RCA = right coronary artery;1 = anterior leaflet of tricuspid valve; 2 = septal leaflet oftricuspid valve. Other abbreviations as in previous figures.
Figure 4. Live three-dimensional transthoracic echocar-diography in dilated cardiomyopathy. A–C. Systematic andsequential anteroposterior cropping of RV demonstrates themoderator band (arrowhead) as well as other trabeculationsand papillary muscles (black arrow) in the RV. D and E.Further cropping shows paucity of trabeculations in the RVapex. There is no evidence of noncompaction. Yellow arrowin A, B, D, and E points to a false tendon in LV. Abbreviationsas in Figures 1–4.
right and the left ventricles, which was high-lighted with contrast injection (Fig. 2). The find-ings of noncompaction by 3D TTE correlatedwell with those of a thoracic CT scan in this pa-tient. Additionally, in follow up after treatmentwith carvedilol and other heart failure therapy,both right and left ventricular systolic functionimproved markedly.
In another case (Case 4), 2D TTE and car-diac MRI findings were most consistent witha septal mass (tumor) extending into the leftand right ventricles. However, when 3D TTEwas performed, the diagnosis of combined rightand left ventricular noncompaction was madewith involvement sparing only the basal an-terior wall of the left ventricle and basal sep-tal wall of the right ventricle (Fig. 3). This pa-tient also demonstrated a dramatic response tocarvedilol and other optimal heart failure ther-apy with an increase in left ventricular systolicfunction in follow-up.
For comparison, a patient with dilated car-diomyopathy with extensive trabeculations in adilated and hypertrophied right ventricle is pre-sented (Fig. 4). Notably, 3D TTE reveals sparingof the right ventricular apex and lack of trulynoncompacted tissue, while there is hypertro-phy of normal structures (moderator band andtrabecular muscle), in this patient. In contrast,all the cases demonstrated here with right ven-tricular noncompaction (Cases 1, 4, 6, 7) showmarked involvement of the right ventricularapex.
Discussion
These cases demonstrate both 2D and 3DTTE assessment of noncompaction of the leftand right ventricles, and the potential useful-ness of live 3D TTE as a supplement to 2D TTEin evaluation of this disorder. The major find-ings of this manuscript are that 3D TTE addsincremental value in delineating segmental in-volvement of noncompaction and in differenti-ating noncompaction from other conditions. Thecharacteristic 3D TTE findings presented hereincrease the confidence level in, and often make,the definitive diagnosis.
Doppler and echocardiographic criteria for di-agnosis of ventricular noncompaction are as fol-lows:
1.A N/C tissue ratio ≥2,2.The presence of numerous excessively promi-nent trabeculations and deep intertrabecularrecesses producing a typical honeycomb-like ap-pearance when viewed en face, and
618 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. Vol. 22, No. 7, 2005

VENTRICULAR NONCOMPACTION
3.Intertrabecular recesses perfused from theventricular cavity as visualized on colorDoppler or echo contrast imaging.
The differential diagnosis of noncompactioninvolves several other clinical entities includ-ing left or right ventricular hypertrophy, api-cal hypertrophic cardiomyopathy, right or leftventricular dysplasia, endocardial fibroelasto-sis, and intracardiac masses such as thrombusand tumors. Differentiation from these entitiesis enhanced by full characterization of segmen-tal involvement (especially of the right ven-tricular apex) and by correct measurement ofthe N/C ratio (best performed in cross-sectionalviews obtained perpendicular to the heart’saxis). 3D TTE offers an advantage in both ofthese imaging aspects. Additionally, noncom-paction, with its honeycombing appearance, isanatomically differentiated from other condi-tions such as right ventricular dysplasia that ischaracterized by severe dilatation and saccularaneurysms of the right ventricle.14
Use of contrast echocardiography, such as inCase 1 of this report, has been previously de-scribed in noncompaction.15,16 For characteri-zation of apical trabeculations, contrast admin-istration increases confidence in border defini-tion and, hence, the diagnosis of noncompactionby both 2D and 3D TTE. In addition, myocar-dial contrast echocardiography demonstrateshypoperfusion in some of the involved segmentsof the noncompacted ventricle as in Case 1 ofour series and in a previous report.16 Thoughtto be due to impaired microvascular functionin the noncompacted ventricle, this finding hasbeen validated by other myocardial perfusionimaging modalities.9,17–19
In this report, 3D TTE offers additional clin-ically important information. The ability toquantify the depth of penetration of the in-tertrabecular recesses in addition to localizingthe exact dimensions and severity of noncom-paction provides prognostic value. Since exten-sive left ventricular involvement is associatedwith a poorer prognosis and can, by itself, elicitreferral for transplantation or prophylactic de-fibrillator implantation,6 full characterizationof noncompaction with 3D TTE should be of clin-ical value. Additionally, 3D TTE may offer a bet-ter modality for following patient response totherapy, including use of beta-blocking agentssuch as carvedilol that have been associatedwith improvements in ventricular function asdemonstrated by others20 and in two patientsof our series.
In summary, the emerging technology of 3DTTE may offer a more definitive diagnostic toolin the assessment, recognition, and manage-ment of this clinical syndrome.
References
1. Engberding R, Bender F: Echocardiographic detec-tion of persistent myocardial sinusoids. Z Kardiol1984;73:786–788.
2. Jenni R, Goebel N, Tartini R, et al: Persisting my-ocardial sinusoids of both ventricles as an isolatedanomaly: Echocardiographic, angiographic and patho-logic anatomical findings. Cardiovasc Intervent Radiol1986;9:127–131.
3. Chin TK, Perloff JK, Williams RG, et al: Isolated non-compaction of left ventricular myocardium. A study ofeight cases. Circulation 1990;82:507–513.
4. Weiford BC, Subbarao VD, Mulhern KM: Noncom-paction of the ventricular myocardium. Circulation2004;109:2965–2971.
5. Jenni R, Oechslin E, Schneider J, et al: Echocardio-graphic and pathoanatomical characteristics of iso-lated left ventricular noncompaction: A step towardsclassification as a distinct cardiomyopathy. Heart2001;86:666–671.
6. Oechslin EN, Jost CHA, Rojas JR, et al: Long-term follow-up of 34 adults with isolated left ven-tricular noncompaction: A distinct cardiomyopathywith poor prognosis. J Am Coll Cardiol 2000;36:493–500.
7. Grant RT: An unusual anomaly of the coronary vesselsin the malformed heart of a child. Heart 1926;93:841–842.
8. Ritter M, Oechslin E, Sutsch G, et al: Isolated noncom-paction of the myocardium in adults. Mayo Clin Proc1997;72:26–31.
9. Ichida F, Hamamichi Y, Miyawaki T, et al: Clinicalfeatures of isolated noncompaction of the ventricularmyocardium: Long-term clinical course, hemodynamicproperties, and genetic background. J Am Coll Cardiol1999;34:233–240.
10. Cavusoglu Y, Ata N, Timuralp B, et al: Noncompactionof the ventricular myocardium: Report of two caseswith bicuspid aortic valve demonstrating poor progno-sis and with prominent right ventricular involvement.Echocardiography 2003;20:379–383.
11. Sedmera D, Pexieder T, Vuillemin M, et al: Devel-opmental patterning of the myocardium. Anat Rec2000;258:319–337.
12. Agmon Y, Connolly HM, Olson LJ, et al: Noncom-paction of the ventricular myocardium. J Am SocEchocardiogr 1999;12:859–863.
13. Mehmood F, Vengala S, Nanda NC, et al: Usefulnessof live three-dimensional transthoracic echocardiogra-phy in the characterization of atrial septal defects inadults. Echocardiography 2004;21:707–713.
14. Yoerger DM, Marcus F, Sherrill D, et al: Echocardio-graphic findings in patients meeting task force cri-teria for arrhythmogenic right ventricular dysplasia:New insights from the multidisciplinary study of rightventricular dysplasia. J Am Coll Cardiol 2005;45:860–865.
15. Koo BK, Choi D, Ha JW, et al: Isolated noncompactionof the ventricular myocardium: Contrast echocardio-graphic findings and review of the literature. Echocar-diography 2002;19:153–156.
Vol. 22, No. 7, 2005 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. 619

BODIWALA, ET AL.
16. Borges AC, Kivelitz D, Baumann: Isolated left ventric-ular noncompaction: Cardiomyopathy with homoge-neous transmural and heterogeneous segmental per-fusion. Heart 2003;89:e21.
17. Soler R, Rodriquez E, Monserrat L, et al: MRI of suben-docardial perfusion deficits in isolated left ventricularnoncompaction. J Comput Assist Tomogr 2002;26:373–375.
18. Junga G, Kneifel S, von Smekal A, et al: Myocardialischemia in children with isolated ventricular noncom-paction. Eur Heart J 1999;20:910–916.
19. Jenni R, Wyss CA, Oechslin, et al: Isolated ventricularnoncompaction is associated with coronary microcir-
culatory dysfunction. J Am Coll Cardiol 2002;39:450–454.
20. Toyono M, Kondo C, Nakajima Y, et al: Effects ofcarvedilol on left ventricular function, mass, andscintigraphic findings in isolated left ventricular non-compaction. Heart 2001;86:e4.
Supplementary Material
The following supplementary material isavailable for this article online:
Movie Clips: Figures 2 and 3.
620 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. Vol. 22, No. 7, 2005
Related Documents











