Lithium Poisoning: Lithium Poisoning: when is hemodialysis when is hemodialysis indicated? indicated? Kent R. Olson, MD Kent R. Olson, MD Medical Director - SF Medical Director - SF Division Division California Poison Control California Poison Control

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Lithium Poisoning: when is Lithium Poisoning: when is hemodialysis indicated?hemodialysis indicated?
Kent R. Olson, MDKent R. Olson, MDMedical Director - SF DivisionMedical Director - SF Division
California Poison Control SystemCalifornia Poison Control System
CaseCase
• A 32 year old woman A 32 year old woman ingested 20 lithium carbonate 300 mg ingested 20 lithium carbonate 300 mg tablets in a suicide attempttablets in a suicide attempt
• She is drowsy and her speech is She is drowsy and her speech is slurredslurred
• Her serum Her serum Li = 6 mEq/LLi = 6 mEq/L
• Hemodialysis needed?Hemodialysis needed?
LithiumLithium
• Alkali metal (like Na, K)Alkali metal (like Na, K)
• Widely used for bipolar disorderWidely used for bipolar disorder
• Therapeutic rangeTherapeutic range 0.6-1.2 mEq/L 0.6-1.2 mEq/L
• Toxicity = mainly CNSToxicity = mainly CNS– Tremor, slurred speech, muscle twitchingTremor, slurred speech, muscle twitching– Confusion, delirium, seizures, comaConfusion, delirium, seizures, coma– Recovery may take weeksRecovery may take weeks
• Toxicity may occur as a result of Toxicity may occur as a result of acute acute overdose or overdose or chronic chronic useuse
PharmacokineticsPharmacokinetics
• Completely absorbed orallyCompletely absorbed orally– Volume of distribution approx 0.8 L/kgVolume of distribution approx 0.8 L/kg– Slow entry into CNSSlow entry into CNS– Initial serum levels do NOT reflect brain levelsInitial serum levels do NOT reflect brain levels
• Eliminated entirely by the kidneysEliminated entirely by the kidneys– Half-life 14-20 hoursHalf-life 14-20 hours– Prolonged in patients with renal insufficiencyProlonged in patients with renal insufficiency– Promoting saline excretion hastens Li removalPromoting saline excretion hastens Li removal
Li Case, continuedLi Case, continued
• Na = 140Na = 140
• K = 4.0K = 4.0
• Cl = 110Cl = 110
• HCO3 = 26HCO3 = 26
• BUN = 8 Cr = 1.0BUN = 8 Cr = 1.0
• Glucose = 98Glucose = 98
• EtOH = 0.16 gm% U Tox (+) benzo’sEtOH = 0.16 gm% U Tox (+) benzo’s
Enhanced drug elimination:Enhanced drug elimination:
• Who needs it?Who needs it?
• Will it work?Will it work?
• What’s the best technique?What’s the best technique?
Who needs it?Who needs it?
• Critically ill despite supportive careCritically ill despite supportive care– eg, phenobarbital OD w/ intractable shockeg, phenobarbital OD w/ intractable shock
• Known Known lethal dose or blood levellethal dose or blood level– eg, salicylate; methanol / ethylene glycoleg, salicylate; methanol / ethylene glycol
• Usual Usual route of elimination impairedroute of elimination impaired– eg, lithium OD in oliguric patienteg, lithium OD in oliguric patient
• Risk of prolonged comaRisk of prolonged coma– eg, phenobarbital OD w/ level of 250eg, phenobarbital OD w/ level of 250
Will it work?Will it work?
• Volume of distribution: Volume of distribution: – is the drug is the drug accessible?accessible?
– how big a volume to clear?how big a volume to clear?
• Clearance (CL):Clearance (CL):– does the method efficiently does the method efficiently
cleanse the blood?cleanse the blood?

Volume of distribution (Vd)Volume of distribution (Vd)
• A calculated number - not realA calculated number - not real
= amt. of drug / plasma conc.= amt. of drug / plasma conc.= mg/kg / mg/L = L/kg= mg/kg / mg/L = L/kg
• Total body waterTotal body water = 0.7 L/kg or ~ = 0.7 L/kg or ~ 50 L50 L
• ECFECF = 0.25 L/kg or about = 0.25 L/kg or about 15 L15 L in adult in adult
• Blood or Blood or plasmaplasma = 0.07 L/kg or ~ = 0.07 L/kg or ~ 5 L5 L

Vd for some common drugsVd for some common drugs
Large Vd:Large Vd:
• camphorcamphor• antidepressantsantidepressants• digoxindigoxin• opioidsopioids• phencyclidinephencyclidine• phenothiazinesphenothiazines
Small Vd:Small Vd:
• alcoholsalcohols• lithiumlithium• phenobarbitalphenobarbital• phenytoinphenytoin• salicylatesalicylate• valproic acidvalproic acid
““But they reported the CLEARANCE But they reported the CLEARANCE was really good - - - 200 mL/min . . .”was really good - - - 200 mL/min . . .”
• But Cl is expressed in But Cl is expressed in mL/minmL/min . . . . . . NOT mg/min or gm/hr or tons/dayNOT mg/min or gm/hr or tons/day
• Total drug elimination depends on Total drug elimination depends on drug concentration:drug concentration:
mcg/mL x mL/min = mg/minmcg/mL x mL/min = mg/min
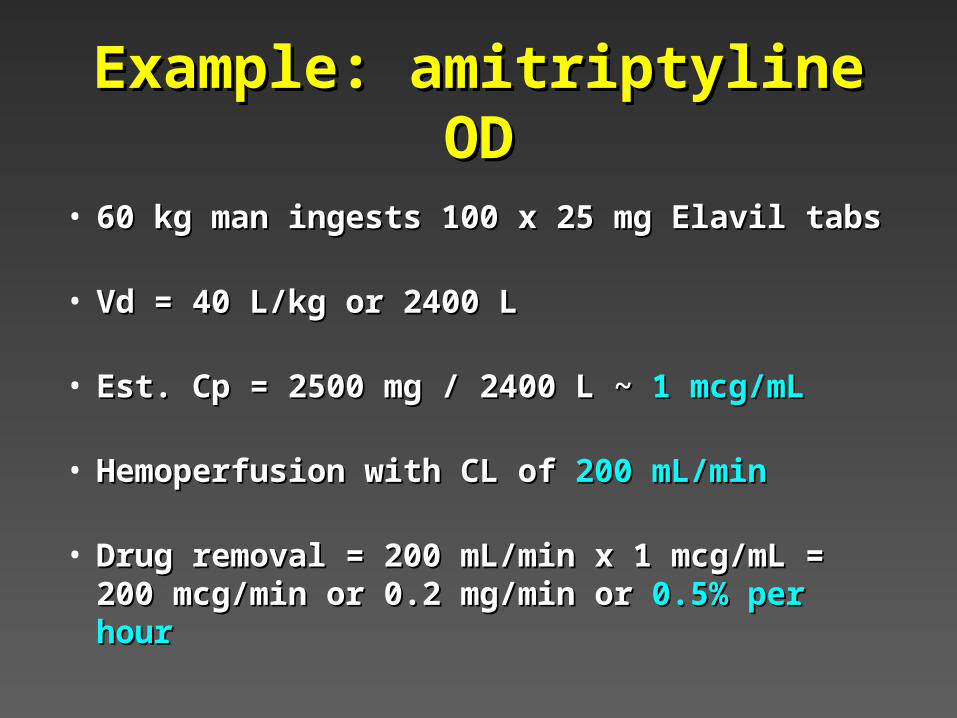
Example: amitriptyline ODExample: amitriptyline OD
• 60 kg man ingests 100 x 25 mg Elavil tabs60 kg man ingests 100 x 25 mg Elavil tabs
• Vd = 40 L/kg or 2400 LVd = 40 L/kg or 2400 L
• Est. Cp = 2500 mg / 2400 L ~ Est. Cp = 2500 mg / 2400 L ~ 1 mcg/mL1 mcg/mL
• Hemoperfusion with CL of Hemoperfusion with CL of 200 mL/min200 mL/min
• Drug removal = 200 mL/min x 1 mcg/mL = Drug removal = 200 mL/min x 1 mcg/mL = 200 mcg/min or 0.2 mg/min or 200 mcg/min or 0.2 mg/min or 0.5% per hour0.5% per hour
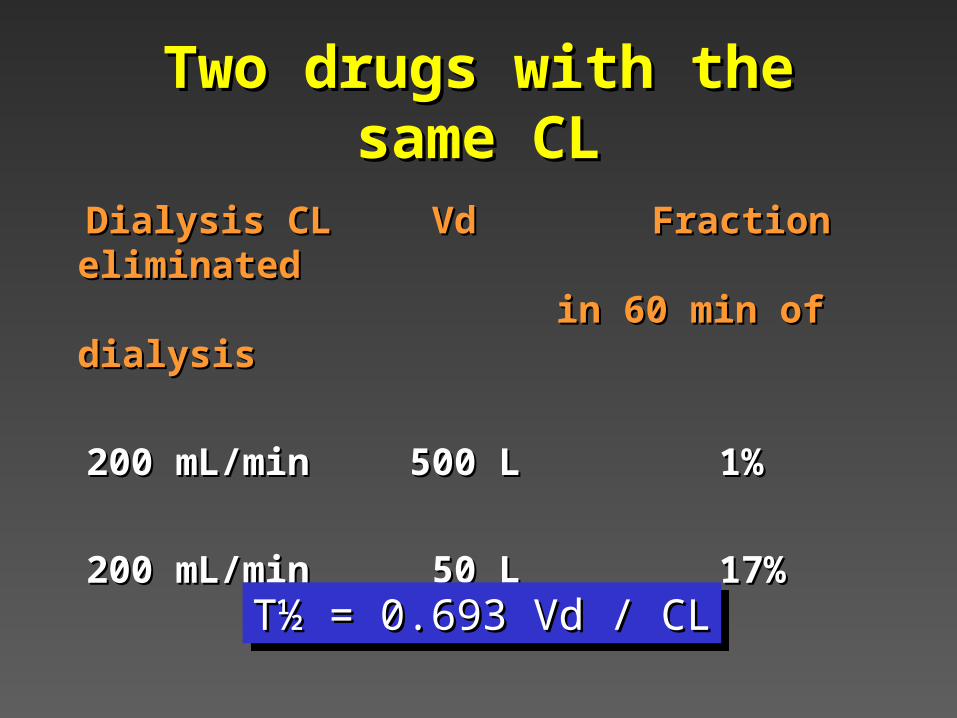
Two drugs with the same CLTwo drugs with the same CL
Dialysis CLDialysis CL Vd Vd Fraction eliminatedFraction eliminatedin 60 min of dialysisin 60 min of dialysis
200 mL/min200 mL/min 500 L 500 L 1% 1%
200 mL/min200 mL/min 50 L 50 L 17% 17%
T½ = 0.693 Vd / CLT½ = 0.693 Vd / CLT½ = 0.693 Vd / CLT½ = 0.693 Vd / CL
Which method?Which method?
• Urinary pH manipulationUrinary pH manipulation
• Peritoneal dialysisPeritoneal dialysis
• HemodialysisHemodialysis
• HemoperfusionHemoperfusion
• Multiple dose activated charcoalMultiple dose activated charcoal
• Continuous hemofiltrationContinuous hemofiltration
Urinary pH manipulationUrinary pH manipulation
• Alkaline diuresisAlkaline diuresis– traps weak acids in alkaline urinetraps weak acids in alkaline urine– useful for salicylates, phenobarbital, useful for salicylates, phenobarbital,
chlorpropamidechlorpropamide– risk of fluid overloadrisk of fluid overload
• Acid diuresisAcid diuresis– traps weak basestraps weak bases– may enhance elimination of amphetaminesmay enhance elimination of amphetamines– TOO RISKY - may worsen myoglobinuric RFTOO RISKY - may worsen myoglobinuric RF
Peritoneal dialysisPeritoneal dialysis
• Theoretically useful if drug is:Theoretically useful if drug is:– water solublewater soluble– small (MW <500)small (MW <500)– not highly protein boundnot highly protein bound– not so bad you don’t mind waiting . . . TOO SLOWnot so bad you don’t mind waiting . . . TOO SLOW
• Rarely performed unless it’s the only Rarely performed unless it’s the only available methodavailable method

HemodialysisHemodialysis
• Can be arteriovenous or veno-Can be arteriovenous or veno-venous (double-lumen catheter)venous (double-lumen catheter)
• Requires anticoagulationRequires anticoagulation
• Best if drug is:Best if drug is:– water-solublewater-soluble– small (MW <500)small (MW <500)– not highly protein boundnot highly protein bound
• Also good for correcting fluid & Also good for correcting fluid & electrolyte abnormalitieselectrolyte abnormalities
Hemodialysis, continued . . .Hemodialysis, continued . . .
• Newer machines have higher flow Newer machines have higher flow rates, better extraction ratiosrates, better extraction ratios
• Note: DON’T use the REDY system - Note: DON’T use the REDY system - these portable HD units have very these portable HD units have very limited volume dialysate which is limited volume dialysate which is recycled, and CL may be very poor recycled, and CL may be very poor
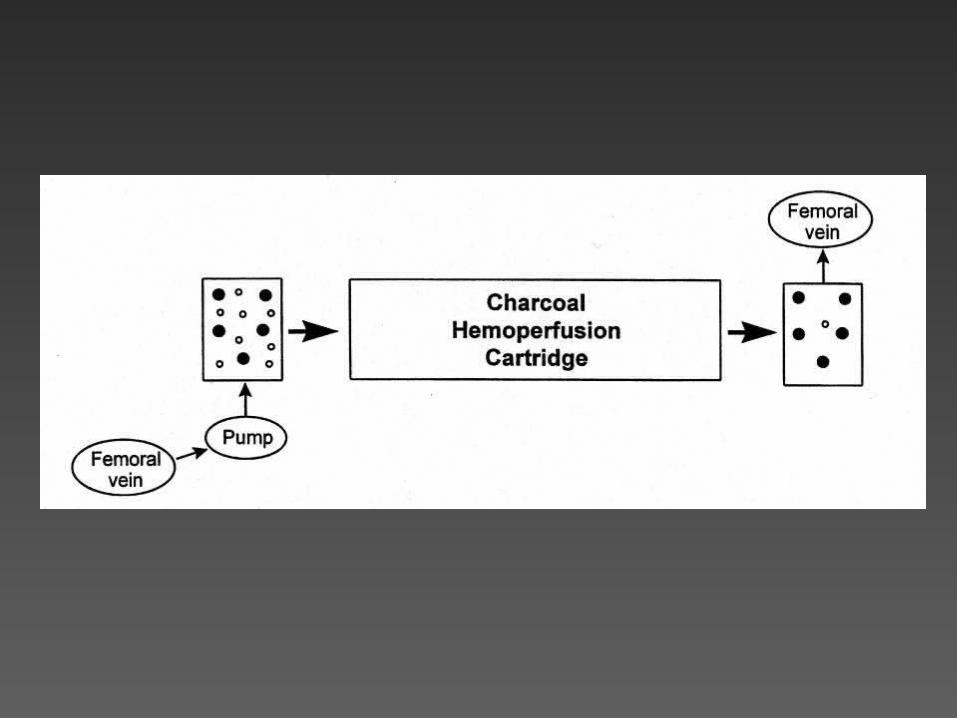
Charcoal hemoperfusionCharcoal hemoperfusion
• Uses same vascular access and Uses same vascular access and dialysis pumpsdialysis pumps
• Greater anticoagulation requiredGreater anticoagulation required
• Saturation of charcoal limits durationSaturation of charcoal limits duration
• But, it is But, it is not dependentnot dependent on on drug sizedrug size, , water solubilitywater solubility or or protein bindingprotein binding - - as long as drug binds to charcoal as long as drug binds to charcoal
• Can be used in series with dialysisCan be used in series with dialysis
Multiple dose oral charcoal - Multiple dose oral charcoal - “gut dialysis”“gut dialysis”
• Charcoal slurry along the entire Charcoal slurry along the entire intestinal tractintestinal tract
• Large surface area for adsorption of Large surface area for adsorption of drug diffusing across intestinal drug diffusing across intestinal epithelium from capillariesepithelium from capillaries
• Useful if drug likes AC, small Vd, low Useful if drug likes AC, small Vd, low protein bindingprotein binding
• Clinical benefit unprovenClinical benefit unproven
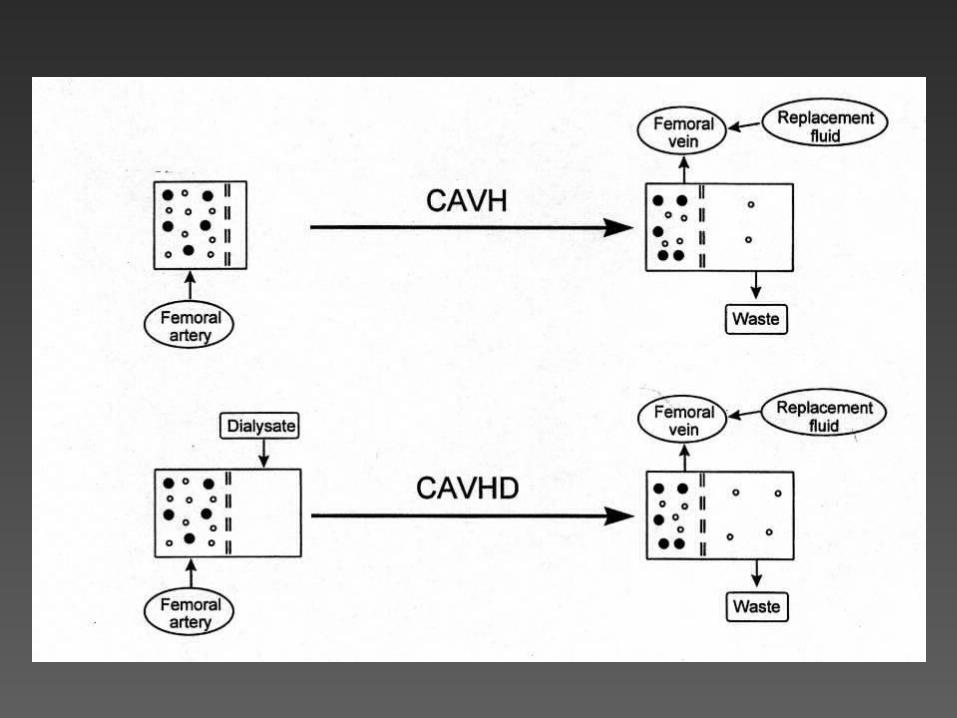
Continuous hemofiltrationContinuous hemofiltration
• Plasma moves across Plasma moves across semipermeable membrane under semipermeable membrane under hydrostatic pressurehydrostatic pressure
• No dialysateNo dialysate
• Solutes follow the plasma water - Solutes follow the plasma water - size up to MW ~ 10,000-40,000size up to MW ~ 10,000-40,000
• CL lower than HD or HP, but it can be CL lower than HD or HP, but it can be performed 24 hrs/dayperformed 24 hrs/day
Salicylate poisoningSalicylate poisoning
• Indications for dialysis:Indications for dialysis:– severe metabolic acidosissevere metabolic acidosis– serum level > 100 mg/dL (acute OD)serum level > 100 mg/dL (acute OD)– level > 60 mg/dL (elderly, chronic OD)level > 60 mg/dL (elderly, chronic OD)
• Note:Note:– alkalinize serum and urinealkalinize serum and urine– dialysis preferred: can correct electrolyte and fluid dialysis preferred: can correct electrolyte and fluid
abnormalitiesabnormalities
Methanol, Ethylene GlycolMethanol, Ethylene Glycol
• Indications for dialysis:Indications for dialysis:– elevated level > 50 mg/dLelevated level > 50 mg/dL– severe acidosissevere acidosis– increased osmolal gap > 10-15 mmol/Lincreased osmolal gap > 10-15 mmol/L
• Notes:Notes:– HD only - not adsorbed to ACHD only - not adsorbed to AC– give blocking drug (EtOH, 4-MP) - Note: need to give blocking drug (EtOH, 4-MP) - Note: need to
increase dosing during dialysisincrease dosing during dialysis
Lithium case, cont . . .Lithium case, cont . . .
• The Poison Control Center was The Poison Control Center was consulted about hemodialysisconsulted about hemodialysis
• The toxicologist advised:The toxicologist advised:
• IV saline at a rate of 150 cc/hrIV saline at a rate of 150 cc/hr
• Recheck serum Li in 4 hoursRecheck serum Li in 4 hours

Li case, cont . . .Li case, cont . . .
• After 4 hrs, the Li was After 4 hrs, the Li was 2.2 mEq/L2.2 mEq/L
• A 3A 3rdrd level 4 hrs later was level 4 hrs later was 1.11.1
• The patient gradually recovered from The patient gradually recovered from her alcohol and benzodiazepine her alcohol and benzodiazepine intoxicationintoxication
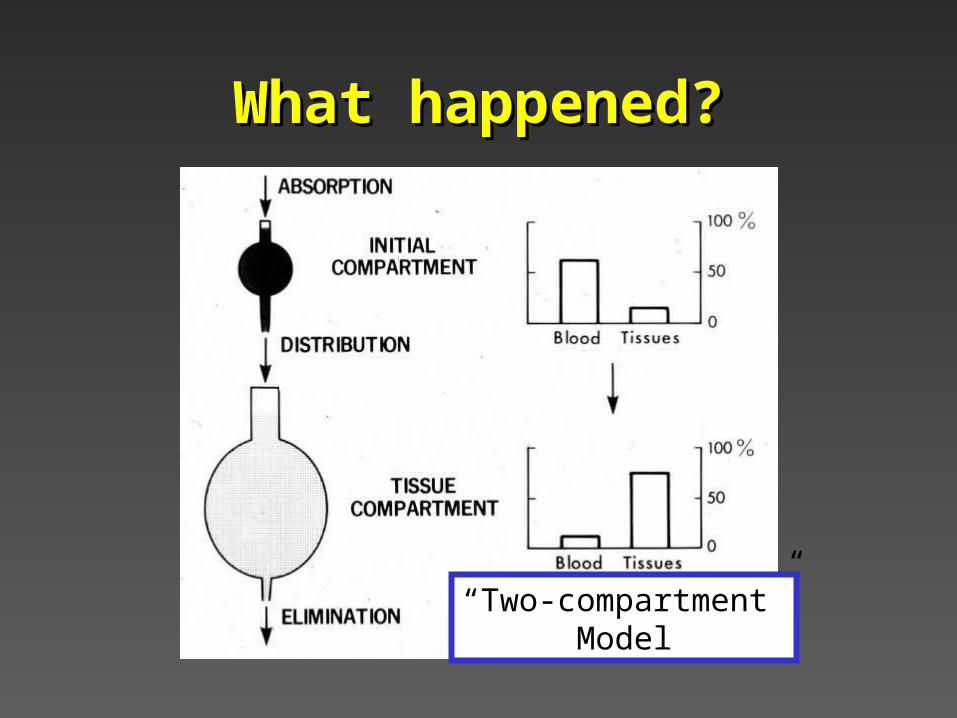
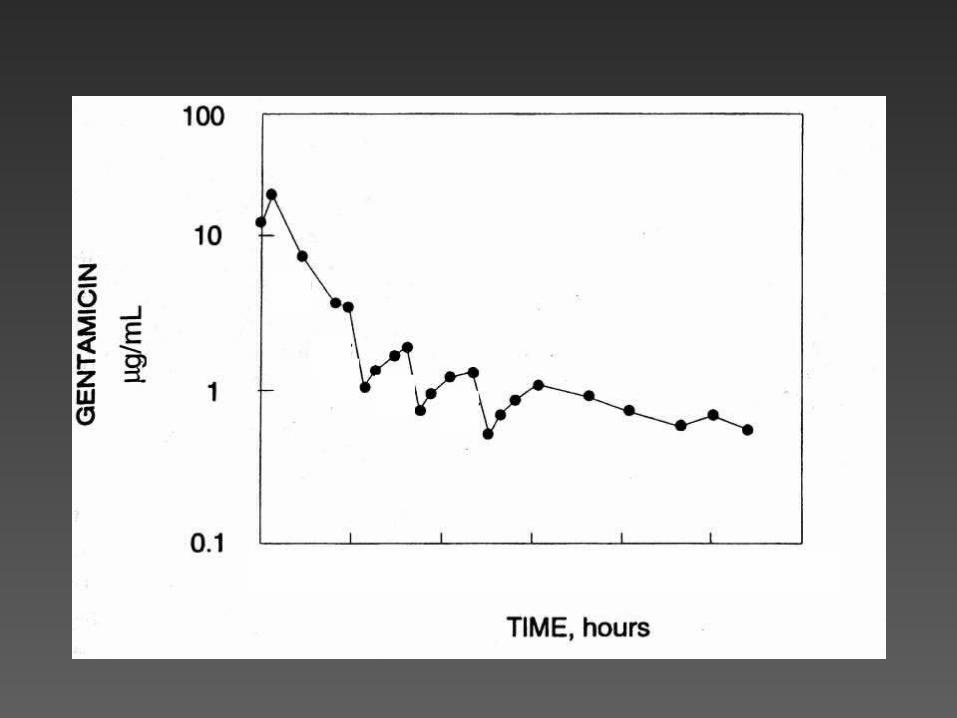
What happened?What happened?
“Two-compartment”Model
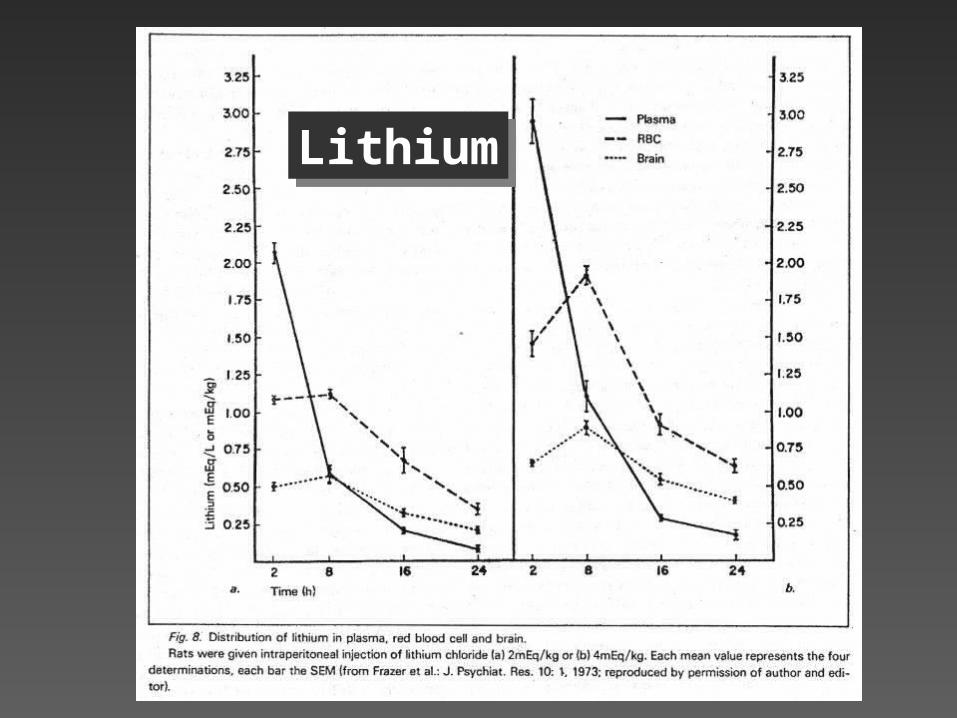
LithiumLithium
Another Lithium CaseAnother Lithium Case
• A 42 year old man brought from a A 42 year old man brought from a board and care with mumbling, board and care with mumbling, tremor, has a seizure in the EDtremor, has a seizure in the ED
• Chronic Li use, no other medsChronic Li use, no other meds
• BUN = 44 Cr = 2.6 Na = 148BUN = 44 Cr = 2.6 Na = 148
• Li = 3.8 mEq/LLi = 3.8 mEq/L
• Repeat Li 4 hours later =Repeat Li 4 hours later = 3.6 mEq/L 3.6 mEq/L
Acute vs Chronic LiAcute vs Chronic Li
• Acute:Acute:– High level, drops rapidlyHigh level, drops rapidly– Absent symptomsAbsent symptoms
• Chronic:Chronic:– Often associated w/ renal insufficiency, DIOften associated w/ renal insufficiency, DI– Occurs graduallyOccurs gradually– Symptoms more severe, even with lower Symptoms more severe, even with lower
levels (eg, 2 - 2.5 and above)levels (eg, 2 - 2.5 and above)
Lithium and dialysisLithium and dialysis
• Indications for dialysis:Indications for dialysis:
– serum level serum level > 6?> 6? 8?8? 10?10? (acute OD) (acute OD)
– level > 4 ? (chronic)level > 4 ? (chronic)
– level 2.5-4 with severe Sx?level 2.5-4 with severe Sx?
Lithium and dialysisLithium and dialysis
• Usual renal CL 25-35 mL/minUsual renal CL 25-35 mL/min
• Hemodialysis adds 100-150 mL/minHemodialysis adds 100-150 mL/min– But only for 3-4 hours at a timeBut only for 3-4 hours at a time– Rebound between dialysis sessionsRebound between dialysis sessions– NotNot very good at removing very good at removing intracellular Liintracellular Li
CVVH (a.k.a. CRRT)CVVH (a.k.a. CRRT)
• CVVH adds 20-35 mL/minCVVH adds 20-35 mL/min– But can be provided continuouslyBut can be provided continuously– Volume cleared ~ 50L/dayVolume cleared ~ 50L/day
vs 36 L/day w/ 4 hours of HDvs 36 L/day w/ 4 hours of HD– No rebound No rebound
Lithium: summaryLithium: summary
• 2-compartment model2-compartment model– Early levels misleadingly highEarly levels misleadingly high– By the way --- don’t use a green-top tube!By the way --- don’t use a green-top tube!
• Acute vs chronic intoxicationAcute vs chronic intoxication
• Dialysis is not rapidly effectiveDialysis is not rapidly effective– Li is slow to leave intracellular compartmentLi is slow to leave intracellular compartment
• IV fluids often the best betIV fluids often the best bet
Related Documents