Chapter- 2- Review of Literature Page | 25 LITERATURE REVIEW A literature review is a body of text that aims to review the critical points of current knowledge including substantive findings as well as theoretical and methodological contributions to a particular topic. Literature reviews are secondary sources, and as such, do not report any new or original experimental work. Most often associated with academic-oriented literature, such as a thesis, a literature review usually precedes a research proposal and results section. Its ultimate goal is to bring the researcher up to date with current literature on a topic and forms the basis for another goal, such as future research that may be needed in the area. A well-structured literature review is characterized by a logical flow of ideas; current and relevant references with consistent, appropriate referencing style; proper use of terminology; and an unbiased and comprehensive view of the previous research on the topic. This study also followed number of national and International research, which are as follows: NATIONAL STATUS Mavalankar et al., (2009) 1 in their study ‘A preliminary estimate of immediate cost of chikungunya and dengue to Gujarat, India’, estimated cost of chikungunya and dengue by combining nine earlier studies on major cost factors such as costs of illness and control, and thus building a more comprehensive picture of the immediate cost of these Aedesmosquito-borne diseases to Gujarat. Dorret al.,(2008) 2 examined ‘Cost of illness: Evidence from a study in five resource-poor locations in India’ founds that health services are funded largely through out-of-pocket spending (OOPS). They carried out this study to collect data on the cost of an illness episode and parameters affecting cost in five locations in India. 1 Dileep V. Mavalankar, Tapasvi I. Puwar, DiptiGovil, Tina M. Murtola, S.S. Vasan (2009). A Preliminary Estimate of Immediate Cost of Chikungunya and Dengue to Gujarat, India. 2 David M. Dror, Olga van Putten-Rademaker& Ruth Koren,(2008). Cost of illness: Evidence from a study in five resource-poor locations in India” Indian J Med Res 127, pp 347-361

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Chapter- 2- Review of Literature
Page | 25
LITERATURE REVIEW
A literature review is a body of text that aims to review the critical points of current
knowledge including substantive findings as well as theoretical and methodological
contributions to a particular topic. Literature reviews are secondary sources, and as
such, do not report any new or original experimental work.
Most often associated with academic-oriented literature, such as a thesis, a literature
review usually precedes a research proposal and results section. Its ultimate goal is to
bring the researcher up to date with current literature on a topic and forms the basis for
another goal, such as future research that may be needed in the area.
A well-structured literature review is characterized by a logical flow of ideas; current and
relevant references with consistent, appropriate referencing style; proper use of
terminology; and an unbiased and comprehensive view of the previous research on the
topic. This study also followed number of national and International research, which are
as follows:
NATIONAL STATUS
Mavalankar et al., (2009)1in their study ‘A preliminary estimate of immediate cost of
chikungunya and dengue to Gujarat, India’, estimated cost of chikungunya and dengue
by combining nine earlier studies on major cost factors such as costs of illness and
control, and thus building a more comprehensive picture of the immediate cost of these
Aedesmosquito-borne diseases to Gujarat.
Dorret al.,(2008)2examined ‘Cost of illness: Evidence from a study in five resource-poor
locations in India’ founds that health services are funded largely through out-of-pocket
spending (OOPS). They carried out this study to collect data on the cost of an illness
episode and parameters affecting cost in five locations in India.
1Dileep V. Mavalankar, Tapasvi I. Puwar, DiptiGovil, Tina M. Murtola, S.S. Vasan (2009). A Preliminary Estimate of Immediate Cost of Chikungunya and Dengue to Gujarat, India. 2David M. Dror, Olga van Putten-Rademaker& Ruth Koren,(2008). Cost of illness: Evidence from a study in five resource-poor locations in India” Indian J Med Res 127, pp 347-361
Chapter- 2- Review of Literature
Page | 26
Dorr. et al., (2007)3 studied‘ Willingness to pay for health insurance among rural and
poor persons: Field evidence from seven micro health insurance units in India’ The
study provides evidence on Willingness to pay (WTP), gathered through a unidirectional
(descending) bidding game among 3024 households in seven locations where micro
health insurance units are in operation.
Usha Gupta (2006)4worked on the topic “Valuation of Urban Air Pollution: A Case
Study of Kanpur City in India’ . Theauthor estimated the monetary benefits to
individuals from health damages avoided as a result on reductions in air pollution in the
urban industrial city of Kanpur in India.
Gautam A. et al(2003)5 examined on “Impact of air pollution on Human Health in
Dehradoon City”. They studied on Air quality levels of Dehradoon city from four selected
sites and simultaneously collected the health effect data from the selected area and
calculate the effects of air pollution on human health
Shankar and Rao (June 2002)6 analyzed the “Impact of Air Quality on Human Health:
A case of Mumbai City, India,” and measured the levels of air pollution and estimated
the monetary benefits to individuals from health damages avoided as a result on
reductions in air pollution in the urban industrial city of Kanpur in India.
Srivastava and Kumar (2001)7have disclosed in their study “Economic valuation of
health impacts of air pollution in Mumbai” that air pollution leads to serious negative
impacts on health. An attempt has been made in this paper to establish dose-response
relationship of Ambient Air Quality Index and human health, based on time spent by an
individual in different microenvironments during one day. Economic valuation of
3David M. Dror, Ralf Radermacher& Ruth Koren (2008).Willingness to pay for health insurance among rural and poor persons: Field evidence from seven micro health insurance units in India 4Usha Gupta(2006),.him RaoAmbedkar College, University of Delhi. Valuation of Urban Air Pollution: A Case Study of Kanpur City in India. 5 A. Gautam, M. Mahajan& S. Garg (2003). Impact of air pollution on human health in Dehradoon city. 6P.Ravi Shankar, G.RamaRao. (2002).Impact of Air Quality on Human Health: A Case of Mumbai City, India, (Paper presented at the IUSSP Regional Conference on Southeast Asia’s Population in a Changing Asian Context, 10-13. 7Anjali Srivastava, RakeshKumar (2001). Economic valuation of health impacts of air pollution in Mumbai.inEnvironmental Monitoring and Assessment , 75:135-143.
Chapter- 2- Review of Literature
Page | 27
morbidity and mortality has been attempted through lost salary approach. The results
show that the avoidance cost is 29% of the total health damage cost.
Smith et.al. (2000)8in their paper “National burden of disease in India from indoor air
pollution” evaluated the existing epidemiological studies and applies the resulting risks
to more than three-quarters of Indian households dependent on such fuels. Allowance is
made for the existence of improved stoves with chimneys and other factors that may
lower exposures. Attributable risks are calculated in reference to the demographic
conditions and patterns of each disease in India.
Cropper, Simon, et al., (1997)9In their paper “The Health Benefits of Air Pollution
Control in Delhi.”Reported the result of relating levels of particulate matter to daily
deaths in Delhi, India, between 1991 and 1994. The focus is on Delhi because it is one
of the world’s most polluted cities. This study concludes, that the impact of particulate
matter on total non-trauma deaths in Delhi is smaller than effects found in the United
States. The impacts of air pollution on deaths by age group may be very different in
developing countries than in the United States, where peak effects occur among people
aged sixty-five and older. In Delhi, peak effects occur between the ages of fifteen and
forty-four, implying that a death associated with air pollution causes more life-years to
be lost.
INTERNATIONAL STATUS
SoyeonGuh, et al., (2008)10, in their study“ Comparison of cost-of-illness with
willingness-to-pay estimates to avoid shigellosis: evidence from China” have shown that
cost of illness (COI) measures are lower than the conceptually correct willingness-to-
pay (WTP) measure of the economic benefits of disease prevention. They compared 8Smith, K.R., Corvalan, C.F. and T. Kjellstrom, (1999).National burden of disease in India from indoor air pollution Factors, Epidemiology, 10, 573-584. 9Cropper, Simon, Alberini, Arora and Sharma (1997).The Health Benefits of Air Pollution Control in Delhi American Journal of Agricultural Economics, 79, 1625-1629. 10SoyeonGuh, Chen Xingbao, Christine Poulos, Zhang Qi, Cao Jianwen, Lorenz von Seidlein, Chen Jichao, XuanYi Wang, Xing Zhanchun, Andrew Nyamete, John Clemens and Dale Whittington (2008).Comparison of cost-of-illness with willingness-to-pay estimates to avoid shigellosis: evidence from China. Health Policy and Planning;23:pp 125–136
Chapter- 2- Review of Literature
Page | 28
COI with stated preference estimates of WTP associated with shigellosis in a rural area
of China.
George, et al., (2008)11 studied the “Costs of Illness Among Older Adults: An Analysis
of Six Major Health Conditions with Significant Environmental Risk Factors”had
estimated the cost burden associated with six major illnesses among Americans age 65
or older: chronic lung disease, ischemic heart disease, stroke, lung cancer, pneumonia,
and gastrointestinal illness. These illnesses were selected because of their relatively
high impact among older populations and because they include environmental
exposures as a significant risk factor. A prevalence-based cost-of-illness approach was
applied. Medical costs were estimated from Medicare claims data in 2000.
TanjimaPervinet. al., (2008)12carried out a research on the topic“Societal costs of air
pollution-related health hazards: A review of methods and results”.This paper aims to
provide a critical and systematic review of the societal costs of air pollution-related ill
health (CAP), to explore methodological issues that may be important when assessing
or comparing CAP across countries and to suggest ways in which future CAP studies
can be made more useful for policy analysis.
Spadaro and Rabl (2008)13in their paper“Estimating the uncertainty of damage costs of
pollution: A simple transparent method and typical results”lightingthat most (and in
many cases all) of the uncertainty calculation involves products and/or sums of products
and can be accomplished with an analytic solution which is simple and transparent.
They present their own assessment of the component uncertainties and calculate the
total uncertainty for the impacts and damage costs of the classical air pollutants; results
for a Monte Carlo calculation for the dispersion part werealso shown. The distribution of
11George van Houtven, Amanda A. Honeycutt, Boyd Gilman, Nancy T. Mccall, Wanda W. Throneburg, and Kathy E. Sykes (2008).Costs of illness among older adults: an analysis of six major health conditions with significant environmental risk factors. 12TanjimaPervin, Ulf-G Gerdtham and Carl H Lyttkens (2008) Societal costs of air pollution-related health hazards: A review of methods and results, http://www.resource-allocation.com/content/6/1/19 13Joseph V. Spadaro and Ari Rabl(2008). Estimating the uncertainty of damage costs of pollution: A simple transparent method and typical results in Environmental Impact Assessment ReviewVolume 28, Issues 2-3, pp 166-183
Chapter- 2- Review of Literature
Page | 29
the damage costs was approximately lognormal and can be characterized in terms of
geometric mean µg and geometric standard deviation σg, implying that the confidence
interval is multiplicative.
Marbek Resource Consultants and Colin Welburn (2007)14 have focused on
“Evaluation of Total Cost of Air Pollution Due to Transportation in Canada” have
focused on estimating the economic value of transport-caused air pollution, allocating
these costs by transport mode and province and estimating average unit pollutant costs.
The goal of the study was to provide reasonable and credible estimates of the total cost
of transport-caused air pollution in Canada in the year 2000.
Wen-Yi Chenet. al., (2007)15“The Willingness to Pay for the Health Care under
Taiwan’s National Health Insurance” have utilized the nested multinomial logit model to
estimate the willingness to pay (WTP) values for different National Health Insurance
(NHI) coverage plans in Taiwan. The WTP value for having care from clinics in a
hospital care only plan is NT$178 (US$6) per person/month. The WTP value for having
care from hospitals in a clinic care only plan is NT$1,342 (US$43) per person/month.
The WTP value for the NHI with a universal coverage is NT$1,540 (US$49) per
person/month. The figure NT$1,540 (US$49) is equivalent to 8.77% of monthly
household income, much higher than the new premium rate of the new NHI tax (2.5%-
4% of monthly household income) proposed by the Taiwan’s government. Their result
suggests that Taiwan’s government may increase the new premium rate further in order
to make Taiwan’s NHI financially more sustainable.
Dave Sawyer et. al (2007)16 “Evaluation of Total Cost of Air Pollution Due to
Transportation in Canada” The Reduced Form Source-Receptor Tool, ReFSoRT,
developed by RWDI in collaboration with Environment Canada, was used to determine
14Dave Sawyer and Seton Stiebert (Marbek Resource Consultants),ColinWelburn(2007).Evaluation of Total Cost of Air Pollution Due to Transportation in Canada. 15Wen-Yi Chen a , Chunhuei Chi b , Yu-Hui Lin (2007) .The Willingness to Pay for the Health Care under Taiwan’s National Health Insurance2007 International Health Economics Association 6th World Congress in Copenhagen, Denmark. 16Dave Sawyer and Seton Stiebert (Marbek Resource Consultants),ColinWelburn(2007).Evaluation of Total Cost of Air Pollution Due to Transportation in Canada.

Chapter- 2- Review of Literature
Page | 30
changes in ambient air quality attributable to year 2000 transport emissions at the
census division level. A review of the year 2000 emission inventory indicates that the
transportation sector comprises a significant proportion of the total emissions for all the
relevant pollutants considered (SO2, NOX, PM2.5 and VOC). NOX transportation
emissions contributed the largest share of the overall emissions.
Alexander et. al.,(2004)17in his study“ Rich-Poor Differences in Health Care Financing”
have found that most community finance schemes have evolved in the context of
severe economic constraints, political instability, and lack of good governance. Usually
government taxation capacity is weak, formal mechanisms of social protection for
vulnerable populations absent, and government oversight of the informal health sector
lacking. In this context of extreme public sector failure, community involvement in
financing health care provides a critical, though insufficient, first step in the long march
toward improved health care access for the poor and social protection against the cost
of illness.
Wilson, (2004)18 worked on “A WTP Model Showing the Relationships Between Three
Approaches For Pollution Control”. In this study , a simple willingness to pay (WTP)
model that shows the theoretical relationships among three valuation approaches that
can be used to measure changes in health resulting from pollution has been developed.
The three valuation approaches considered are the contingent valuation (CV), cost of
illness (COI) and the defensive behavior approaches.
B. Schramm et al., (2003)19 in their study evaluated the “Cost of illness of moderate to-
severe atopic asthma and/or seasonal allergic rhinitis (SAR) in Germany” from the
perspective of third-party payers (TPP) and patients. Five-hundred patients (276
children/adolescents) with moderate-to-severe asthma and/ or SAR were included in
17Preker, Alexander, Carrin, Guy, Dror, David M., Jakab, Melitta, Hsiao, William and Arhin, Dyna, (2004). Rich-Poor Differences in Health Care Financing. Health Financing For Poor People: Resource Mobilization And Risk Sharing, Preker A.S., Carrin G., eds., pp. 3-51, World Bank. 18Clevo Wilson(2004). A WTP Model Showing the Relationships Between Three Approaches For Pollution. 19B. Schramm, B. Ehlken, A. Smala, K. Quednau, K. Berger, D. Nowak (2003) .Cost of illness of atopic asthma and seasonal allergic rhinitis in Germany: 1-yr retrospective study, ISSN 0903-1936
Chapter- 2- Review of Literature
Page | 31
this cross-sectional study. Information was collected using as pacific patient
questionnaire and the abstraction of patient records.
Anne Case et at.,(2002)20“Economic Status and Health in Childhood: The Origins of
the Gradien”.In the study the authors said that the well-known positive association
between health and income in adulthood has antecedents in childhood. Not only is
children's health positively related to household income, but the relationship between
household income and children's health becomes more pronounced as children age.
Part of the relationship can be explained by the arrival and impact of chronic conditions.
Children from lower income households with chronic conditions have worse health than
to those from higher-income households. The adverse health effects of lower income
accumulate over children's lives. Part of the intergenerational transmission of
socioeconomic status may work through the impact of parents' income on children's
health.
Caceres. et at.,(2001),21‘Indoor air pollution in a zone of extreme poverty of
metropolitan Santiago. The study represent an important risk factor for human health.
They have investigated the levels of carbon monoxide (CO), sulphur dioxide (SO2),
Respirable particulate matter(PM10), polycyclic aromatic hydrocarbons (PAHs) and
mutagen city in the PM5 fraction, as well as temperature and humidity, in the interior of
24 houses in La Pintana, Santiago. The survey showed that in children younger than 2
years, most respiratory diseases occur during winter (75%), the most frequent complaint
being bronchitis (62%) and obstructive bronchitis (50%). The higher pollutant
concentrations were observed during heating hours, in houses that used coal(mean
PM10 250 µg·m-3, CO 42 ppm, SO2 192 ppb) or firewood (mean PM10 489 µg·m-3,CO
57 ppm, SO2 295 ppb). PAHs were detected in all houses and they concluded that they
came from inside the house and not from outdoor infiltration.
20Case, Anne, Darren Lubotsky, and Christina Paxson. (2002). "Economic Status and Health in Childhood: The Origins of the Gradient ."American Economic Review, 92(5): 1308–1334. 21Caceres, D., M. Adonis, G. Retamal, P. Ancic, M. Valencia, X. Ramos, N. Olivares and L. Gil (2001).Indoor air pollution in a zone of extreme poverty of metropolitan Santiago. RevistaMedicaChilena 129:33-42.
Chapter- 2- Review of Literature
Page | 32
H. Sommer, et al.,(2000)22have come out with a study on “Economic evaluation of
health impacts due to road traffic-related air pollution (An impact assessment project of
Austria, France and Switzerland)”.In preparation for the Transport, Environment and
Health Session of the WHO Ministerial Conference on Environment and Health in
London (June 1999) a tri-lateral project was carried out by Austria, France and
Switzerland. The project assessed the health costs of road-traffic related air pollution in
the three countries using a common methodological framework.
Alberini and Krupnik (2000).23In their study“ Cost-of-Illness and Willingness-to-Pay
Estimates of the Benefits of Improved Air Quality: Evidence from Taiwan” have compare
cost-of-illness (COI) and willingness-to-pay (WTP) estimates of the damages from minor
respiratory symptoms associated with air pollution using data from a study in Taiwan in
1991-92. A contingent valuation survey is conducted to estimate WTP to avoid minor
respiratory illnesses. Health diaries are analyzed to predict the likelihood and cost of
seeking relief from symptoms and of missing work. As predicted by estimates, WTP is
exceeding on COI the latter by 1.61 to 2.26 times, depending on pollution levels. These
ratios are similar to those for the United States, despite the differences between the two
countries.
Thanh and Lefevre (2000)24carried out a research on the topic “Assessing Health
Impacts of Air Pollution from Electricity Generation: The Case of Thailand” and have
applied they apply the impact pathway approach (IPA) to estimate health impacts and
corresponding damage costs of sulfur dioxide (SO2) and emissions offline particulate
matter (PM10) from four power units using different fuels (lignite, oil, natural gas, and
coal) at four locations in Thailand. The results show that the damage cost related to
health effects of electricity generation in Thailand are relatively small, but not negligible,
ranging from 0.006 U.S. cent to 0.05 U.S. cent per kilowatt-hour (in 1995 dollars).
22H. Sommer, N. Künzli, R. Seethaler, O. Chanel, M. Herry, S. Masson, J-C. Vergnaud, P. Filliger, F. Horak JR., R. Kaiser, S. Medina. V. Puybonnieux-texier, P. Quénel, J. Schneider, M. Studnicka(2000).Economic Evaluation Of Health Impacts Due To Road Traffic-Related Air Pollution (An impact assessment project of Austria, France and Switzerland) 23Alberini, Anna and Alan Krupnick, (2000). .Cost-of-Illness and WTP Estimates of the Benefits of Improved Air Quality: Evidence from Taiwan.,Land Economics 76(1). 24Thanh, Bui Duy and Thierry Lefevre, (2000). .Assessing Health Impacts of Air Pollution from Electricity Generation: The Case of Thailand., Environmental Impact Assessment Review, 20, 137-158.
Chapter- 2- Review of Literature
Page | 33
Damage costs to the public health due to SO2 andPM10 emissions from electricity
generation not only depend on fuel and generating technology but also depend strongly
on power plant location. This implies that the assessment of adverse health impacts is
very important for technology choice and setting of new power plants.
Sean D. Sullivanet al.,(2000)25“The Economic Burden of COPD”. In this study they
found that COPD is one of the leading causes of morbidity and mortality worldwide and
imparts a substantial economic burden on individuals and society. Despite the intense
interest in COPD among clinicians and researchers, there is a paucity of data on health-
care utilization, costs, and social burden in this population. The total economic costs of
COPD morbidity and mortality in the United States were estimated at $23.9 billion in
1993. Direct treatments for COPD-related illness accounted for $14.7 billion, and the
remaining $9.2 billion were indirect morbidity and premature mortality estimated as lost
future earnings. Similar data from another US study suggest that 10% of persons with
COPD account for > 70% of all medical care costs.
Larson, Avaliani.et. al(1999)26“The Economics of Air Pollution Health Risks in Russia:
A case study of Volgograd” in the study a combined health risk assessment, cost-
effectiveness analysis, and benefit-cost analysis is undertaken for direct particulate
emissions from 29 stationary source polluters in the city of Volgograd, Russia. Annual
particulate-related mortality risks from these stationary sources are estimated to be
substantial, with an estimate in the range of 960- 2,667 additional deaths per year in this
city of one million. The majority of these risks are attributed to two major facilities in the
northern part of the city. For several emission reduction projects, the cost-per-life saved
was estimated to be quite low. The total net benefits to the city of implementing five of
the six identified projects, leading to roughly a 25% reduction in mortality risk, are
estimated to be at least $40 million in present value terms.
25Sean D. Sullivan,Scott D. Ramsey, Todd A. Lee. (2000)“The Economic Burden of COPD” in doi: 10.1378/chest.117.2_suppl.5S CHEST February 2000 vol. 117 no. 2 suppl 5S-9S 26Larson, Avaliani, Golub, Rosen, Shaposhnikov, Strukova, Vincent (1999) .The Economics of Air Pollution Health Risks in Russia: Acase study of Volgograd.,World Development, 10, 1803-1819.

Chapter- 2- Review of Literature
Page | 34
Clevo Wilson (1999)27“A WTP Model Showing The Relationships Between Three
Approaches For Pollution Control”. In this paper, a simple willingness to pay (WTP)
model that shows the theoretical relationships among three valuation approaches that
can be used to measure changes in health resulting from pollution is developed. The
three valuation approaches considered are the contingent valuation (CV), cost of illness
(COI) and the defensive behavior approaches. After showing the relationships between
the three valuation approaches, the model demonstrates that the CV approach exceeds
the COI and the defensive behavior approaches. The theoretical results are supported
by field survey data. The pollution referred to in this paper is direct exposure to
pesticides by farmers during handling and spraying on their farms.
McCubbin and Delucchi, (1999)28“The Health Costs of Motor-Vehicle-Related Air
Pollution”.Motor vehicles have significantly larger health costs than previously reported.
Particulates are the most damaging pollutant, while ozone and other pollutants have
smaller effects. Diesel vehicles cause more damages per mile than dogasoline vehicles,
because of greater particulate emissions. Very fine particles appear more dangerous
than larger particles, and combustion particles appear more dangerous than road dust.
Chen and Vine (1999)29“A Scoping Study on the Costs of Indoor Air Quality Illnesses:
Ann Insurance Loss Reduction Perspective”. This paper reports on the results of a
literature search of buildings-related, business and legal databases, and interviews with
insurance and risk management representatives aimed at finding information on the
direct costs to the insurance industry of poor building IAQ, as well as the costs of
litigation. The literature search turned up little specific cost information, but indicated
that there is strong awareness and growing concern over the silent crisis of IAQ and its
potential to cause large industry losses. The source of these losses includes both direct
27Clevo Wilson (1999) A WTP Model Showing The Relationships Between Three Approaches For Pollution Control published by Department of Economics, University of Queensland. 28McCubbin, Donald R., Mark A. Delucchi, (1999) .The Health Costs of Motor-Vehicle- Related Air Pollution., Journal of Transport Economics and Policy, 33(3), 253-286. 29Chen, Allen and Edward L. Vine, (1999).A Scoping Study on the Costs of Indoor Air Quality Illnesses: An Insurance Loss Reduction Perspective., Environmental Science and Policy, 2, 457-464.

Chapter- 2- Review of Literature
Page | 35
costs to insurers from paying health insurance and professional liability claims as well
as the cost of litigation.
Alberini and Krupnick (1998)30, have worked the study “Air Quality and Episodes of
Acute Respiratory Illness in Taiwan Cities: Evidence from Survey Data”. The paper
reports on a unique study that records daily health status for over nine hundred
residents of three urban areas in Taiwan and elicits their willingness to pay to avoid
episodes of illness. Incidence of illness is related to the ambient concentration levels of
particulate matter but the effects are much less pronounced than would be expected
from earlier U.S. studies. Willingness to pay to avoid illness is considerably higher than
that predicted by extrapolations of U.S. studies that rely on simple income adjustments.
Alberini, et al., (1997)31, in their study “Valuing Health Effects of Air Pollution in
Developing Countries: The Case of Taiwan”, conducted a contingent valuation survey in
Taiwan to elicit willingness to pay (WTP) to avoid a recurrence of the episode of acute
respiratory illness experienced by the respondent. They estimated a model in which
willingness to pay depends on the attributes of the illness (duration and number of
symptoms, and nature of the illness) and on respondent characteristics (such as income
and health history), and allow mitigating behavior to be endogenously determined with
willingness to pay.
30Alberini, Anna; Krupnick, Alan J. (1998).Air Quality and Episodes of Acute Respiratory Illness in Taiwan Cities: Evidence from Survey Data in Journal of Urban Economics (44). 31Alberini, Anna, Cropper, Maureen, Fu, Tsu-Tan, Krupnick, Alan, Liu, Jin-Tan, Shaw, Daigee, Harrington, Winston (1997)Valuing Health Effects of Air Pollution in Developing Countries: The Case of Taiwan”
Chapter- 2- Review of Literature
Page | 36
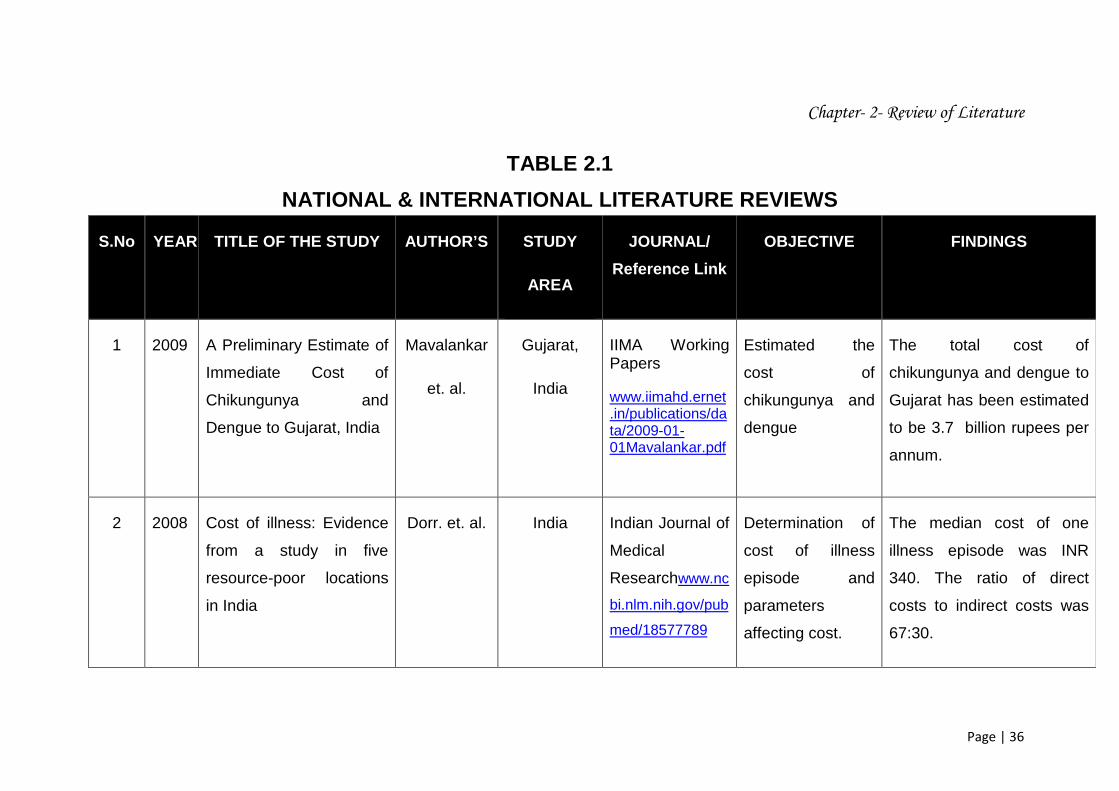
TABLE 2.1
NATIONAL & INTERNATIONAL LITERATURE REVIEWS
S.No YEAR TITLE OF THE STUDY AUTHOR’S STUDY
AREA
JOURNAL/
Reference Link
OBJECTIVE FINDINGS
1 2009 A Preliminary Estimate of
Immediate Cost of
Chikungunya and
Dengue to Gujarat, India
Mavalankar
et. al.
Gujarat,
India
IIMA Working Papers
www.iimahd.ernet.in/publications/data/2009-01-01Mavalankar.pdf
Estimated the
cost of
chikungunya and
dengue
The total cost of
chikungunya and dengue to
Gujarat has been estimated
to be 3.7 billion rupees per
annum.
2 2008 Cost of illness: Evidence
from a study in five
resource-poor locations
in India
Dorr. et. al. India Indian Journal of
Medical
Researchwww.nc
bi.nlm.nih.gov/pub
med/18577789
Determination of
cost of illness
episode and
parameters
affecting cost.
The median cost of one
illness episode was INR
340. The ratio of direct
costs to indirect costs was
67:30.
Chapter- 2- Review of Literature
Page | 37
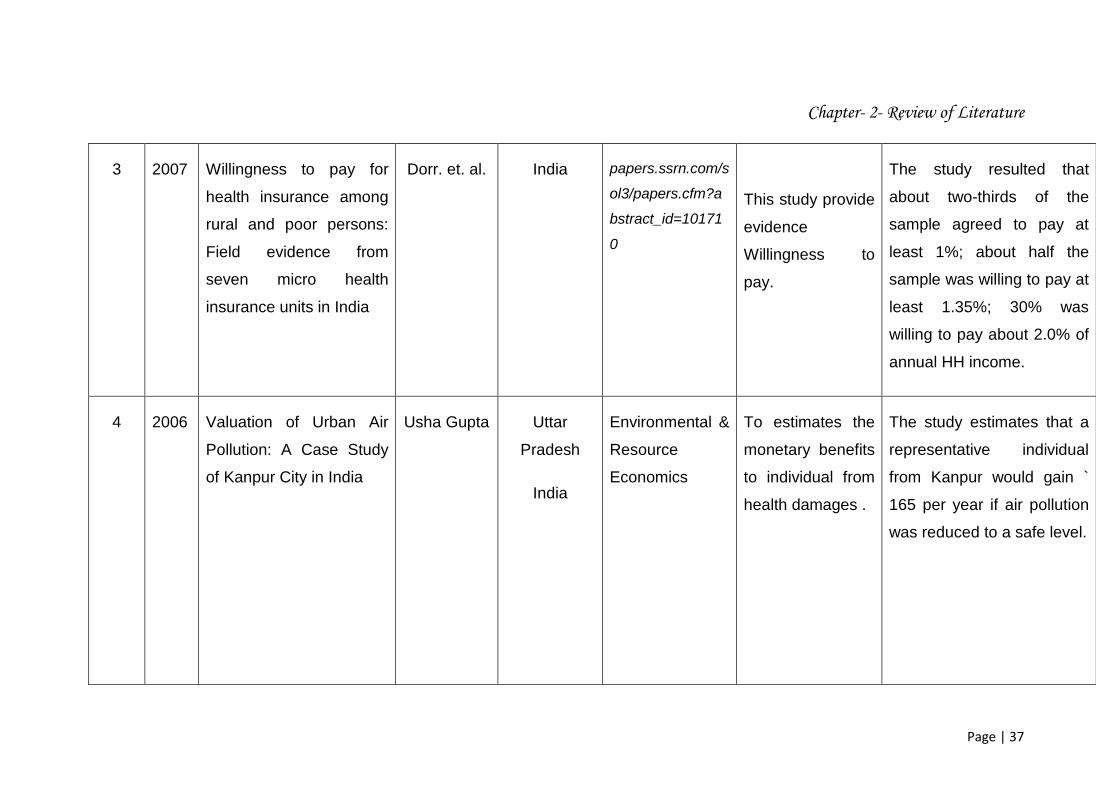
3 2007
Willingness to pay for
health insurance among
rural and poor persons:
Field evidence from
seven micro health
insurance units in India
Dorr. et. al. India papers.ssrn.com/s
ol3/papers.cfm?a
bstract_id=10171
0
This study provide
evidence
Willingness to
pay.
The study resulted that
about two-thirds of the
sample agreed to pay at
least 1%; about half the
sample was willing to pay at
least 1.35%; 30% was
willing to pay about 2.0% of
annual HH income.
4 2006 Valuation of Urban Air
Pollution: A Case Study
of Kanpur City in India
Usha Gupta Uttar
Pradesh
India
Environmental &
Resource
Economics
To estimates the
monetary benefits
to individual from
health damages .
The study estimates that a
representative individual
from Kanpur would gain `
165 per year if air pollution
was reduced to a safe level.
Chapter- 2- Review of Literature
Page | 38
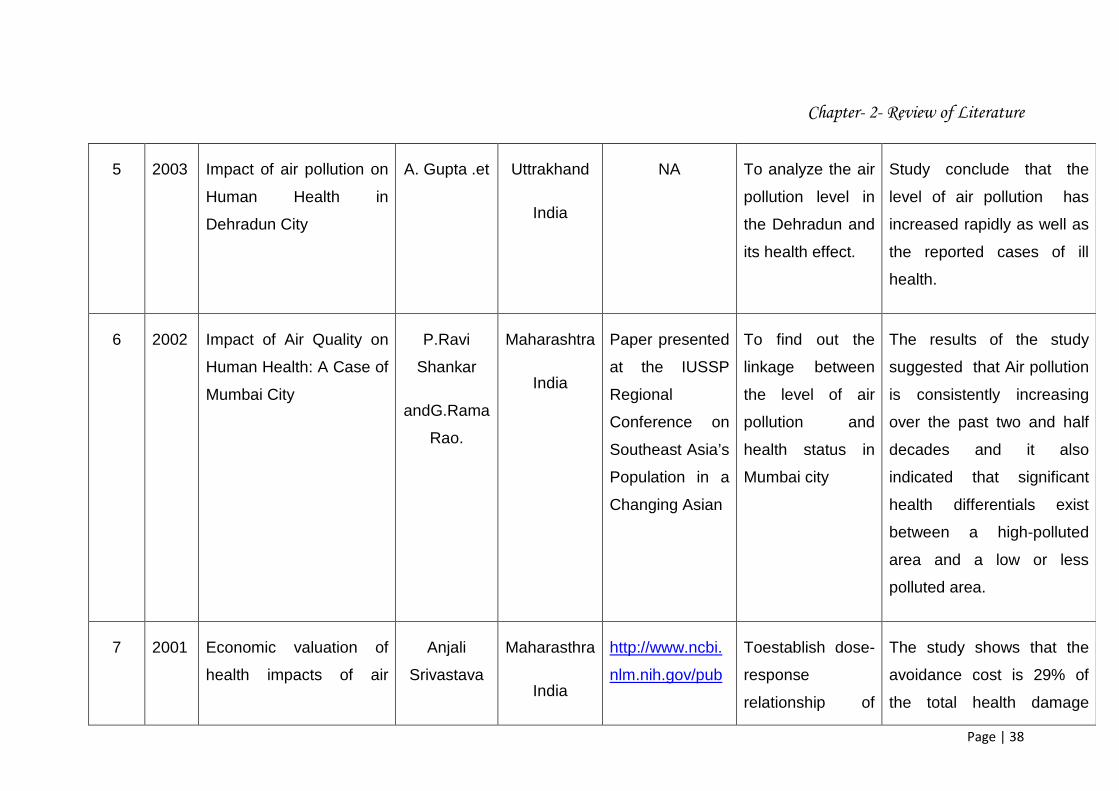
5 2003 Impact of air pollution on
Human Health in
Dehradun City
A. Gupta .et Uttrakhand
India
NA To analyze the air
pollution level in
the Dehradun and
its health effect.
Study conclude that the
level of air pollution has
increased rapidly as well as
the reported cases of ill
health.
6 2002 Impact of Air Quality on
Human Health: A Case of
Mumbai City
P.Ravi
Shankar
andG.Rama
Rao.
Maharashtra
India
Paper presented
at the IUSSP
Regional
Conference on
Southeast Asia’s
Population in a
Changing Asian
To find out the
linkage between
the level of air
pollution and
health status in
Mumbai city
The results of the study
suggested that Air pollution
is consistently increasing
over the past two and half
decades and it also
indicated that significant
health differentials exist
between a high-polluted
area and a low or less
polluted area.
7 2001 Economic valuation of
health impacts of air
Anjali
Srivastava
Maharasthra
India
http://www.ncbi.
nlm.nih.gov/pub
Toestablish dose-
response
relationship of
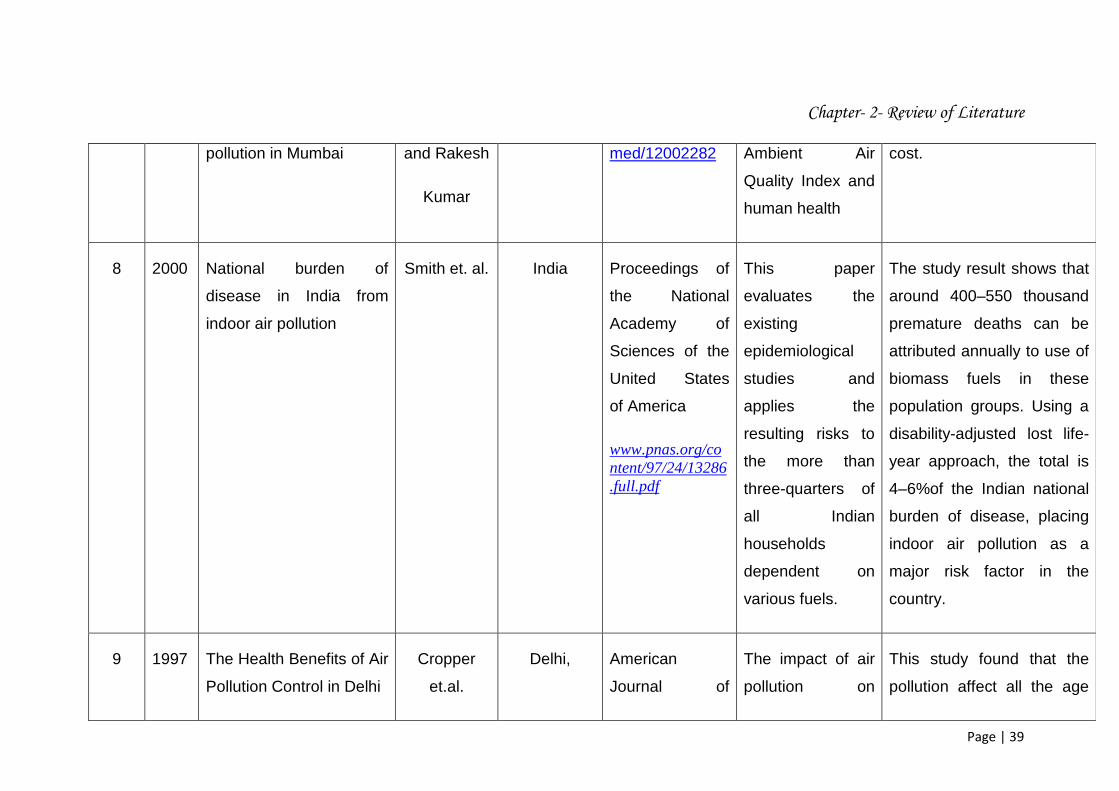
The study shows that the
avoidance cost is 29% of
the total health damage
Chapter- 2- Review of Literature
Page | 39
pollution in Mumbai and Rakesh
Kumar
med/12002282 Ambient Air
Quality Index and
human health
cost.
8 2000 National burden of
disease in India from
indoor air pollution
Smith et. al. India Proceedings of
the National
Academy of
Sciences of the
United States
of America
www.pnas.org/content/97/24/13286.full.pdf
This paper
evaluates the
existing
epidemiological
studies and
applies the
resulting risks to
the more than
three-quarters of
all Indian
households
dependent on
various fuels.
The study result shows that
around 400–550 thousand
premature deaths can be
attributed annually to use of
biomass fuels in these
population groups. Using a
disability-adjusted lost life-
year approach, the total is
4–6%of the Indian national
burden of disease, placing
indoor air pollution as a
major risk factor in the
country.
9 1997 The Health Benefits of Air
Pollution Control in Delhi
Cropper
et.al.
Delhi, American
Journal of
The impact of air
pollution on
This study found that the
pollution affect all the age
Chapter- 2- Review of Literature
Page | 40
India Agricultural
Economics
http://www.econ.
umd.edu/resear
ch/papers/137
deaths by
different age
group.
group except zero to four
and very old sixty five
above.
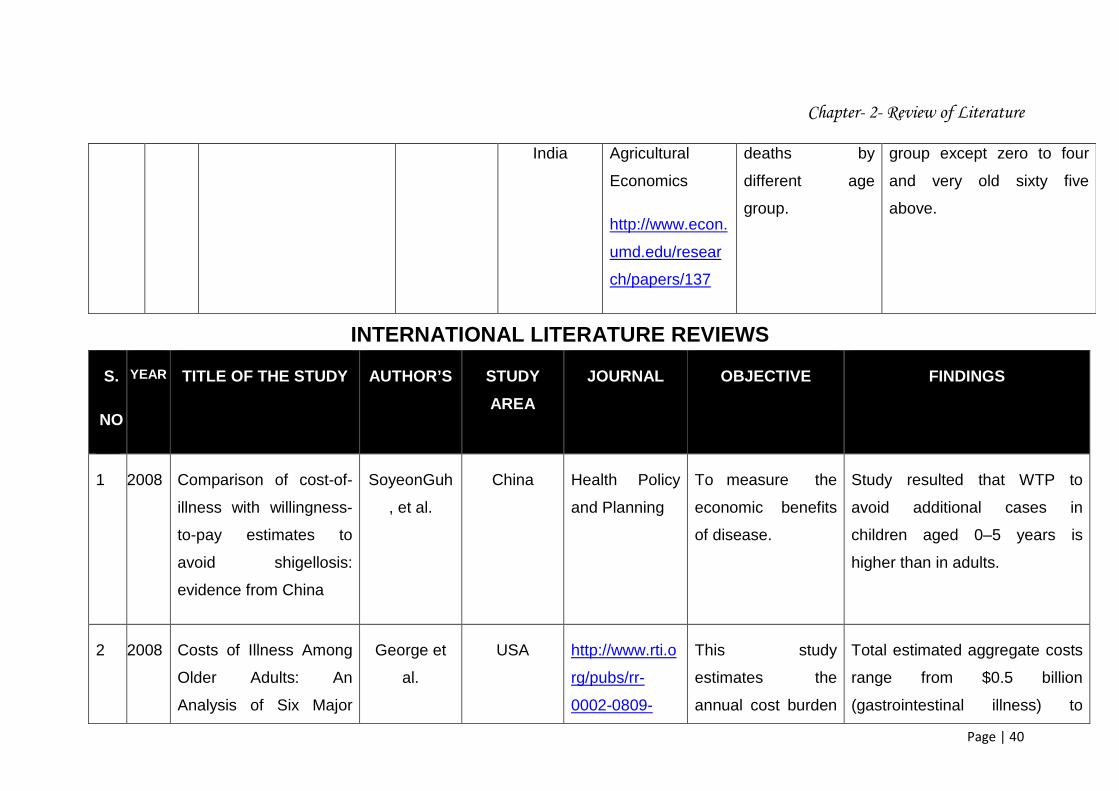
INTERNATIONAL LITERATURE REVIEWS
S.
NO
YEAR TITLE OF THE STUDY AUTHOR’S STUDY
AREA
JOURNAL OBJECTIVE FINDINGS
1 2008 Comparison of cost-of-
illness with willingness-
to-pay estimates to
avoid shigellosis:
evidence from China
SoyeonGuh
, et al.
China Health Policy
and Planning
To measure the
economic benefits
of disease.
Study resulted that WTP to
avoid additional cases in
children aged 0–5 years is
higher than in adults.
2 2008 Costs of Illness Among
Older Adults: An
Analysis of Six Major
George et
al.
USA http://www.rti.o
rg/pubs/rr-
0002-0809-
This study
estimates the
annual cost burden
Total estimated aggregate costs
range from $0.5 billion
(gastrointestinal illness) to
Chapter- 2- Review of Literature
Page | 41
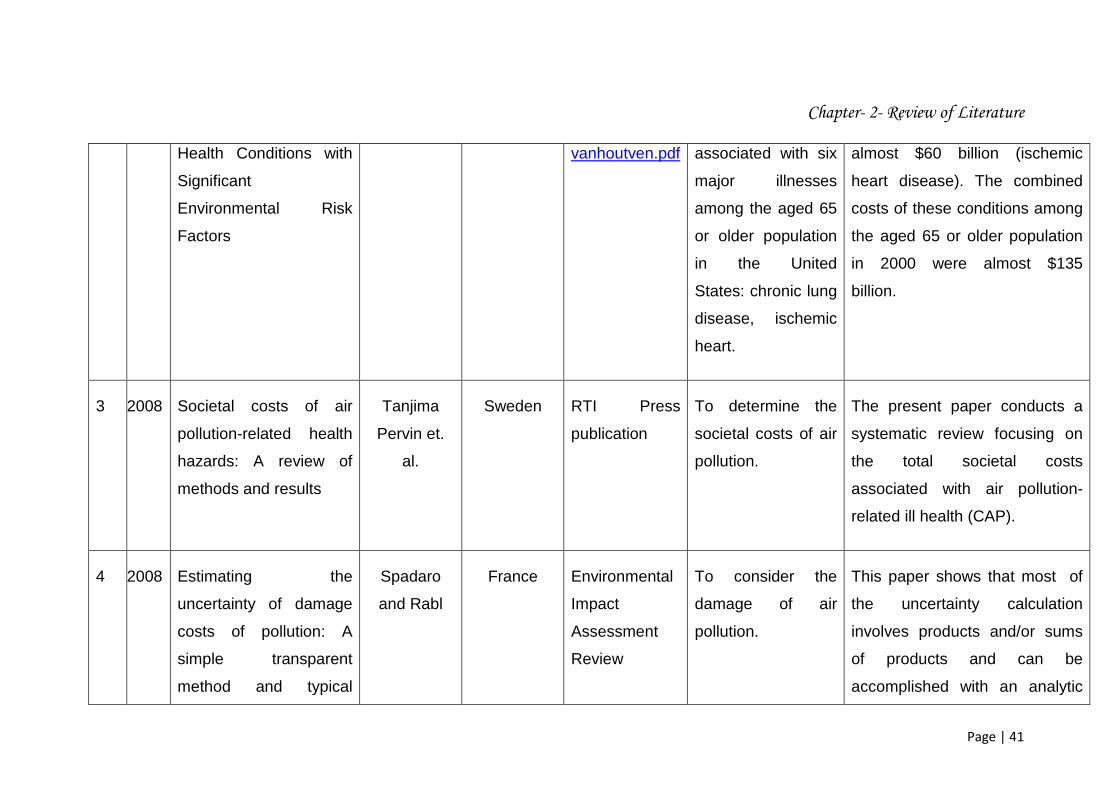
Health Conditions with
Significant
Environmental Risk
Factors
vanhoutven.pdf associated with six
major illnesses
among the aged 65
or older population
in the United
States: chronic lung
disease, ischemic
heart.
almost $60 billion (ischemic
heart disease). The combined
costs of these conditions among
the aged 65 or older population
in 2000 were almost $135
billion.
3 2008 Societal costs of air
pollution-related health
hazards: A review of
methods and results
Tanjima
Pervin et.
al.
Sweden RTI Press
publication
To determine the
societal costs of air
pollution.
The present paper conducts a
systematic review focusing on
the total societal costs
associated with air pollution-
related ill health (CAP).
4 2008 Estimating the
uncertainty of damage
costs of pollution: A
simple transparent
method and typical
Spadaro
and Rabl
France Environmental
Impact
Assessment
Review
To consider the
damage of air
pollution.
This paper shows that most of
the uncertainty calculation
involves products and/or sums
of products and can be
accomplished with an analytic

Chapter- 2- Review of Literature
Page | 42
results solution which is simple and
transparent.
5 2007 Evaluation of Total Cost
of Air Pollution Due to
Transportation in
Canada
Dave
Sawyer et.
al.
Canada Government of
Canada
Publications
To measures the
economic value of
transport-caused air
pollution.
This study provides credible
estimates of the total costs of
transport-caused air pollution in
Canada in the year 2000.
6 2007 The Willingness to Pay
for the Health Care
under Taiwan’s National
Health Insurance.
Wen-Yi
Chen et. al.
Taiwan International
Health
Economics
Association
Estimate the
willingness to pay
(WTP) values for
different National
Health Insurance
coverage plans in
Taiwan.
In the study it was found that
WTP value for having care from
clinics in a hospital care only
plan is NT$178 (US$6) per
person/month.
7 2004 Rich-Poor Differences in
Health Care Financing
Alexander
et. al.
USA WHO To estimate the
health care facilities
among the different
countries.
In the study it was found that in
most of the community finance
schemes have evolved in the
context of severe economic
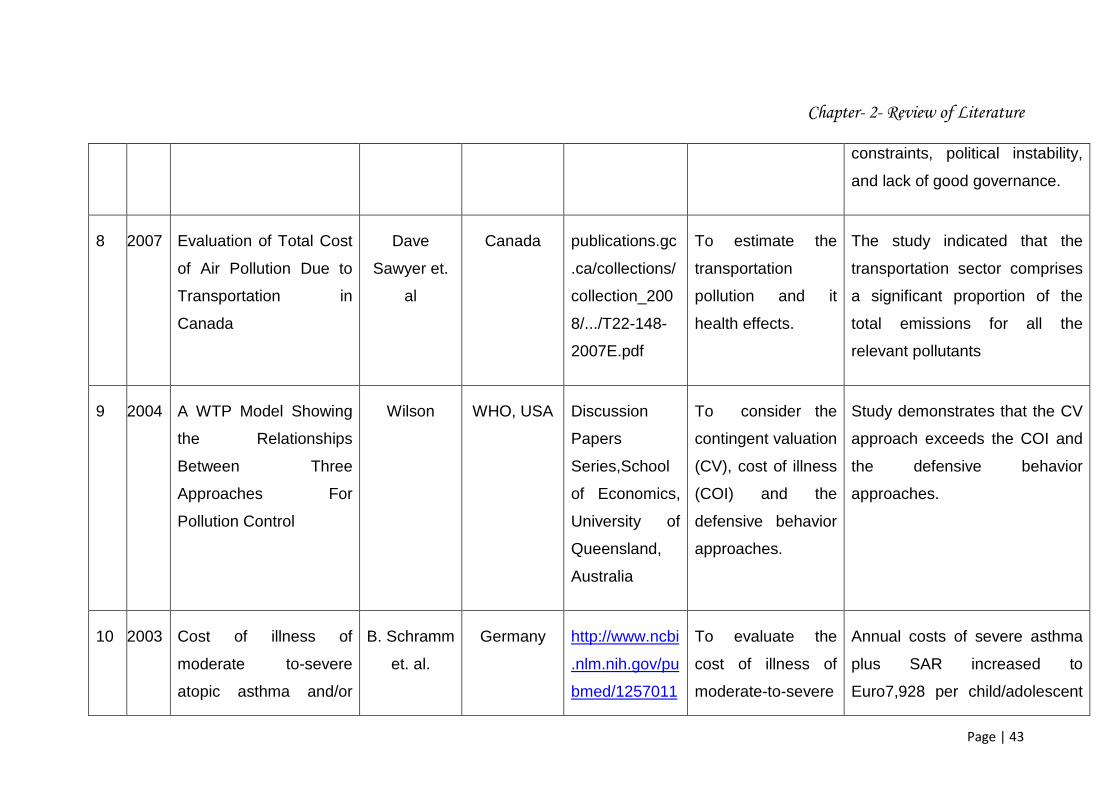
Chapter- 2- Review of Literature
Page | 43
constraints, political instability,
and lack of good governance.
8 2007 Evaluation of Total Cost
of Air Pollution Due to
Transportation in
Canada
Dave
Sawyer et.
al
Canada publications.gc
.ca/collections/
collection_200
8/.../T22-148-
2007E.pdf
To estimate the
transportation
pollution and it
health effects.
The study indicated that the
transportation sector comprises
a significant proportion of the
total emissions for all the
relevant pollutants
9 2004 A WTP Model Showing
the Relationships
Between Three
Approaches For
Pollution Control
Wilson WHO, USA Discussion
Papers
Series,School
of Economics,
University of
Queensland,
Australia
To consider the
contingent valuation
(CV), cost of illness
(COI) and the
defensive behavior
approaches.
Study demonstrates that the CV
approach exceeds the COI and
the defensive behavior
approaches.
10 2003 Cost of illness of
moderate to-severe
atopic asthma and/or
B. Schramm
et. al.
Germany http://www.ncbi
.nlm.nih.gov/pu
bmed/1257011
To evaluate the
cost of illness of
moderate-to-severe
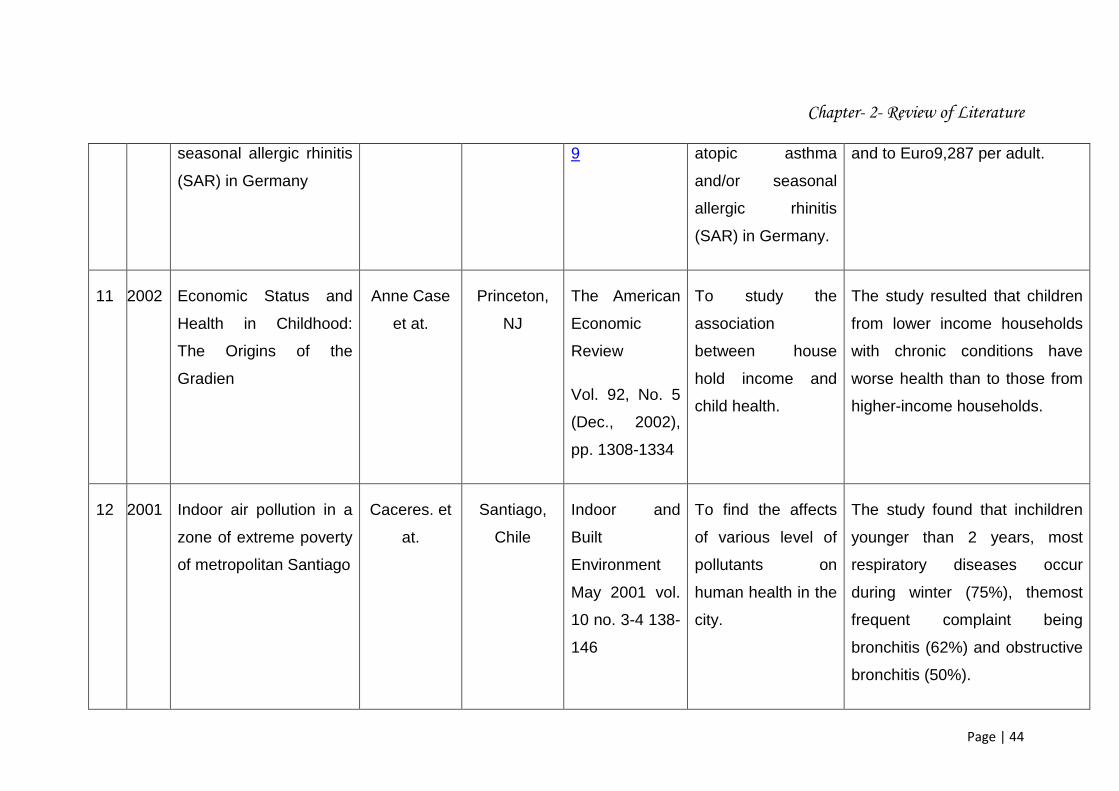
Annual costs of severe asthma
plus SAR increased to
Euro7,928 per child/adolescent
Chapter- 2- Review of Literature
Page | 44
seasonal allergic rhinitis
(SAR) in Germany
9 atopic asthma
and/or seasonal
allergic rhinitis
(SAR) in Germany.
and to Euro9,287 per adult.
11 2002 Economic Status and
Health in Childhood:
The Origins of the
Gradien
Anne Case
et at.
Princeton,
NJ
The American
Economic
Review
Vol. 92, No. 5
(Dec., 2002),
pp. 1308-1334
To study the
association
between house
hold income and
child health.
The study resulted that children
from lower income households
with chronic conditions have
worse health than to those from
higher-income households.
12 2001 Indoor air pollution in a
zone of extreme poverty
of metropolitan Santiago
Caceres. et
at.
Santiago,
Chile
Indoor and
Built
Environment
May 2001 vol.
10 no. 3-4 138-
146
To find the affects
of various level of
pollutants on
human health in the
city.
The study found that inchildren
younger than 2 years, most
respiratory diseases occur
during winter (75%), themost
frequent complaint being
bronchitis (62%) and obstructive
bronchitis (50%).
Chapter- 2- Review of Literature
Page | 45
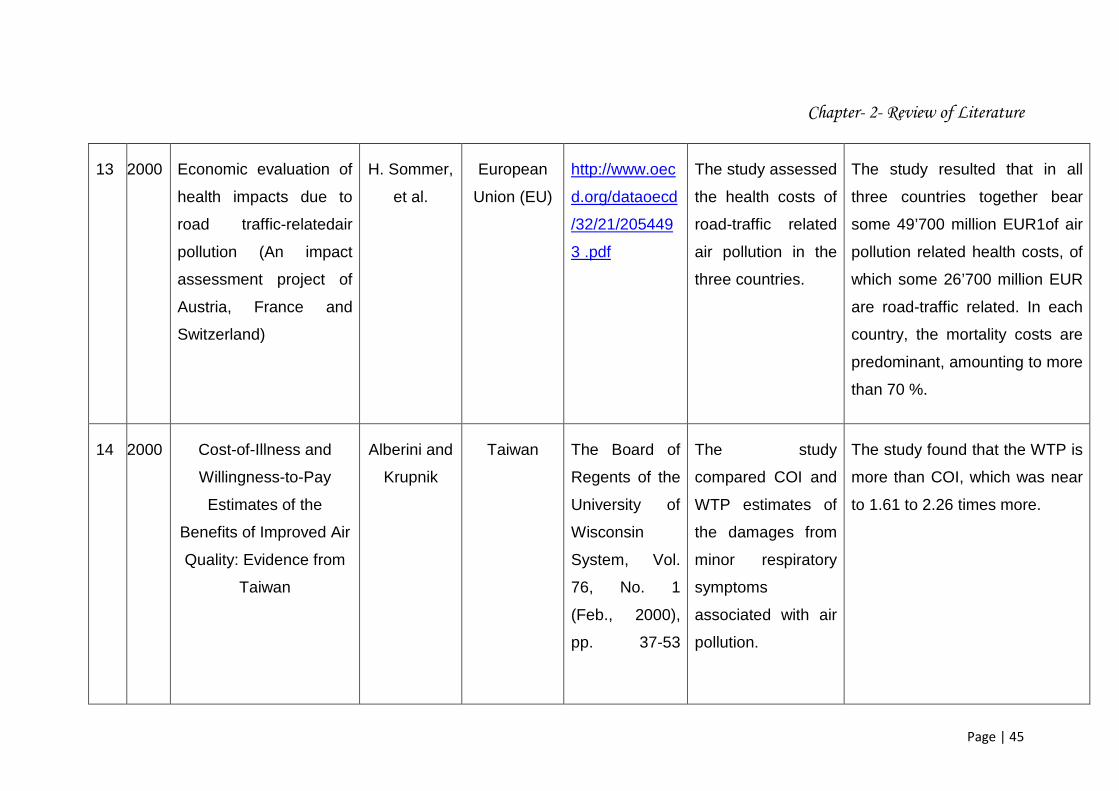
13 2000 Economic evaluation of
health impacts due to
road traffic-relatedair
pollution (An impact
assessment project of
Austria, France and
Switzerland)
H. Sommer,
et al.
European
Union (EU)
http://www.oec
d.org/dataoecd
/32/21/205449
3 .pdf
The study assessed
the health costs of
road-traffic related
air pollution in the
three countries.
The study resulted that in all
three countries together bear
some 49’700 million EUR1of air
pollution related health costs, of
which some 26’700 million EUR
are road-traffic related. In each
country, the mortality costs are
predominant, amounting to more
than 70 %.
14 2000 Cost-of-Illness and
Willingness-to-Pay
Estimates of the
Benefits of Improved Air
Quality: Evidence from
Taiwan
Alberini and
Krupnik
Taiwan The Board of
Regents of the
University of
Wisconsin
System, Vol.
76, No. 1
(Feb., 2000),
pp. 37-53
The study
compared COI and
WTP estimates of
the damages from
minor respiratory
symptoms
associated with air
pollution.
The study found that the WTP is
more than COI, which was near
to 1.61 to 2.26 times more.

Chapter- 2- Review of Literature
Page | 46
15 2000 Assessing Health
Impacts of Air Pollution
from Electricity
Generation: The Case of
Thailand
Thanh and
Lefevre
Thailand Environmental
Impact
Assessment
Review.
Volume 20,
Issue 2, April
2000, Pages
137–158
To estimate health
impacts and
corresponding
damage costs of
various air
pollutants from four
power units using
different fuels at
four locations in
Thailand.
The study results shows that the
damage cost related to health
effects of electricity generation
in Thailand are relatively small,
but not negligible, ranging from
0.006 U.S. cent to 0.05 U.S.
cent per kilowatt-hour.
16 2000 The Economic Burden
of COPD
Sean D.
Sullivan et
al
Washington
, Seattle,
WA
CHEST
February 2000
vol. 117 no. 2
supply 5S-9S
To study the
impact of COPD on
individuals and
society.
The study estimated that the
direct treatments for COPD-
related illness accounted for
$14.7 billion, and the remaining
$9.2 billion were indirect
morbidity and premature
mortality estimated as lost future
earnings.
Chapter- 2- Review of Literature
Page | 47
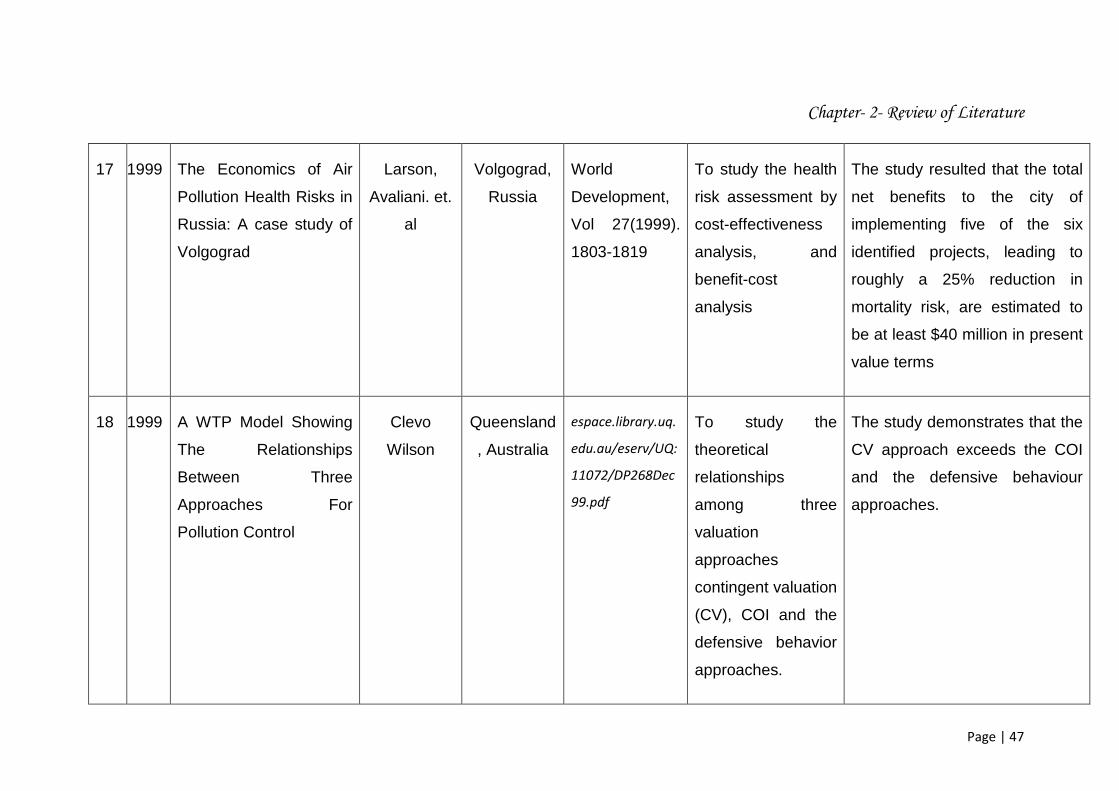
17 1999 The Economics of Air
Pollution Health Risks in
Russia: A case study of
Volgograd
Larson,
Avaliani. et.
al
Volgograd,
Russia
World
Development,
Vol 27(1999).
1803-1819
To study the health
risk assessment by
cost-effectiveness
analysis, and
benefit-cost
analysis
The study resulted that the total
net benefits to the city of
implementing five of the six
identified projects, leading to
roughly a 25% reduction in
mortality risk, are estimated to
be at least $40 million in present
value terms
18 1999 A WTP Model Showing
The Relationships
Between Three
Approaches For
Pollution Control
Clevo
Wilson
Queensland
, Australia
espace.library.uq.
edu.au/eserv/UQ:
11072/DP268Dec
99.pdf
To study the
theoretical
relationships
among three
valuation
approaches
contingent valuation
(CV), COI and the
defensive behavior
approaches.
The study demonstrates that the
CV approach exceeds the COI
and the defensive behaviour
approaches.
Chapter- 2- Review of Literature
Page | 48
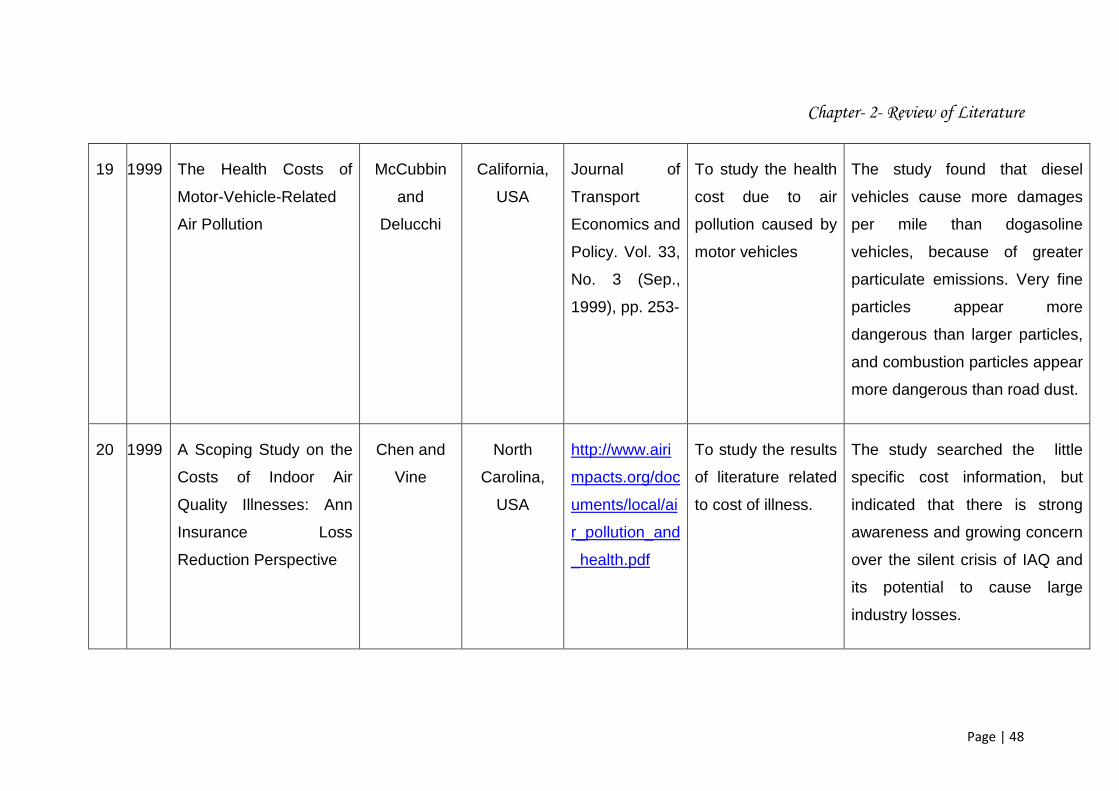
19 1999 The Health Costs of
Motor-Vehicle-Related
Air Pollution
McCubbin
and
Delucchi
California,
USA
Journal of
Transport
Economics and
Policy. Vol. 33,
No. 3 (Sep.,
1999), pp. 253-
To study the health
cost due to air
pollution caused by
motor vehicles
The study found that diesel
vehicles cause more damages
per mile than dogasoline
vehicles, because of greater
particulate emissions. Very fine
particles appear more
dangerous than larger particles,
and combustion particles appear
more dangerous than road dust.
20 1999 A Scoping Study on the
Costs of Indoor Air
Quality Illnesses: Ann
Insurance Loss
Reduction Perspective
Chen and
Vine
North
Carolina,
USA
http://www.airi
mpacts.org/doc
uments/local/ai
r_pollution_and
_health.pdf
To study the results
of literature related
to cost of illness.
The study searched the little
specific cost information, but
indicated that there is strong
awareness and growing concern
over the silent crisis of IAQ and
its potential to cause large
industry losses.

Chapter- 2- Review of Literature
Page | 49
21 1998 Air Quality and Episodes
of Acute Respiratory
Illness in Taiwan Cities:
Evidence from Survey
Data
Alberini and
Krupnick
Washington
, DC, USA
Journal of
Urban
Economics,
Vol. 44, Issue
1, July 1998,
Pages 68–92
To study the health
status and
willingness to pay
to avoid episodes of
illness.
The study found that the
Willingness to pay to avoid
illness is considerably higher
than episodes of illness.
22 1997 Valuing Health Effects of
Air Pollution in
Developing Countries:
The Case of Taiwan
Alberini, et
al.,
Taiwan Journal of
Environmental
Economics and
Management.
Vol. 37(1997)
pp.107-126
To study the CV
and WTP value.
This study investigated the
value of reducing illness in
Taiwan and related
methodological issues.
Chapter- 2- Review of Literature
Page | 50
The studies taken into consideration for the related area of the research have further
been classified on the basis of the study for which they were primarily under taken.
These objective have been broadly classified into four categories:
1. Studies considering air pollution and its effects.
2. Studies based to estimate cost of illness.
3. Studies related to determine willingness to pay for health care.
4. Studies considering cost of illness and willingness to pay.
These studies have been presented in the following tables 2.2, 2.3, 2.4, and 2.5
respectively.
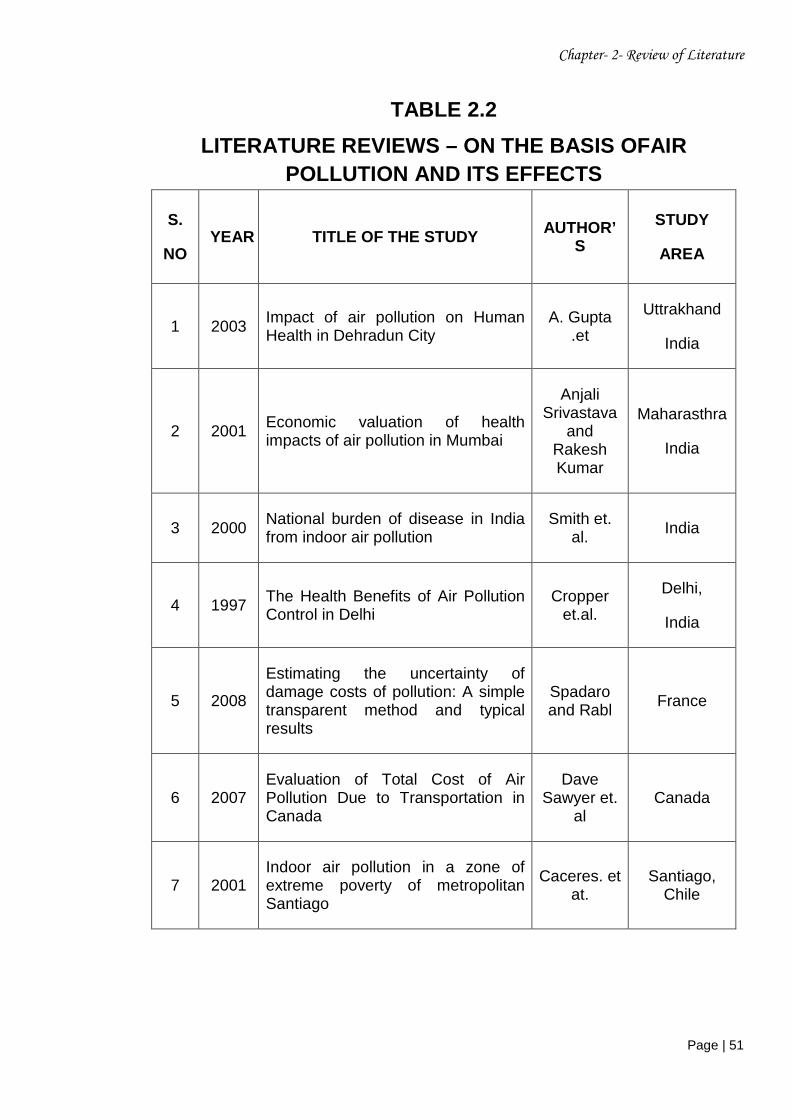
The table 2.2 shows that in the past few years there has been a great awareness
among the researchers to analyses the impact of air pollution on human health. The
table shows that various authors have around the taken up the above aspect in the
study as thrust area of research.
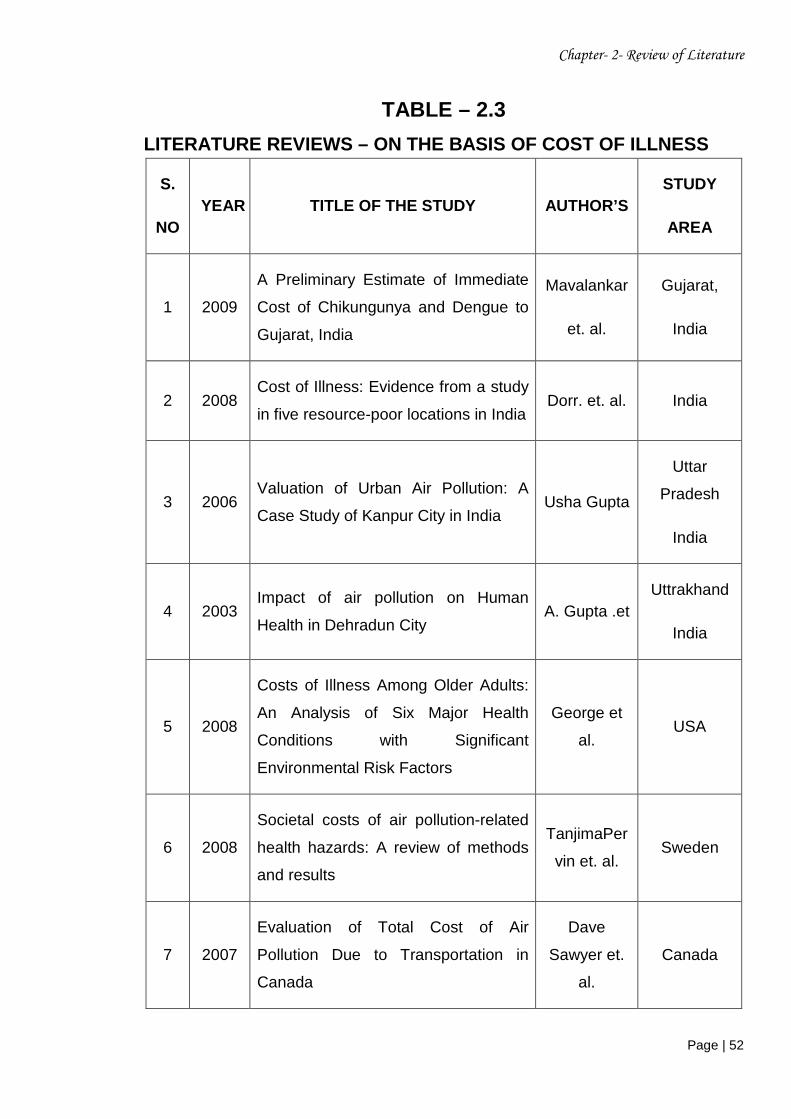
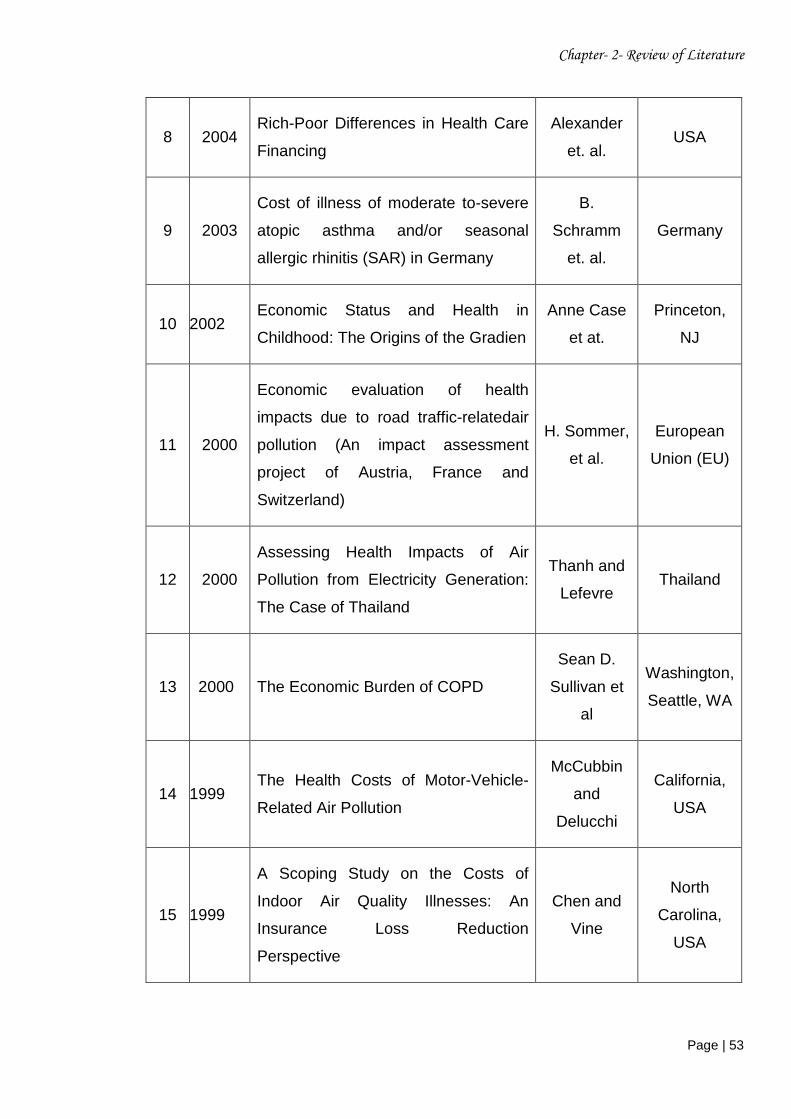
The table 2.3 shows that large number of study has been based on determination of
cost of illness due to air pollution and other factors. A large number of study has
been carried in abroad India and few studies has been carried out in India
particularly for the cities like Kanpur, Dehradun and the state of Gujarat. No such
study was carried out in Agra, which is one of the major tourist place of India and
highly polluted.
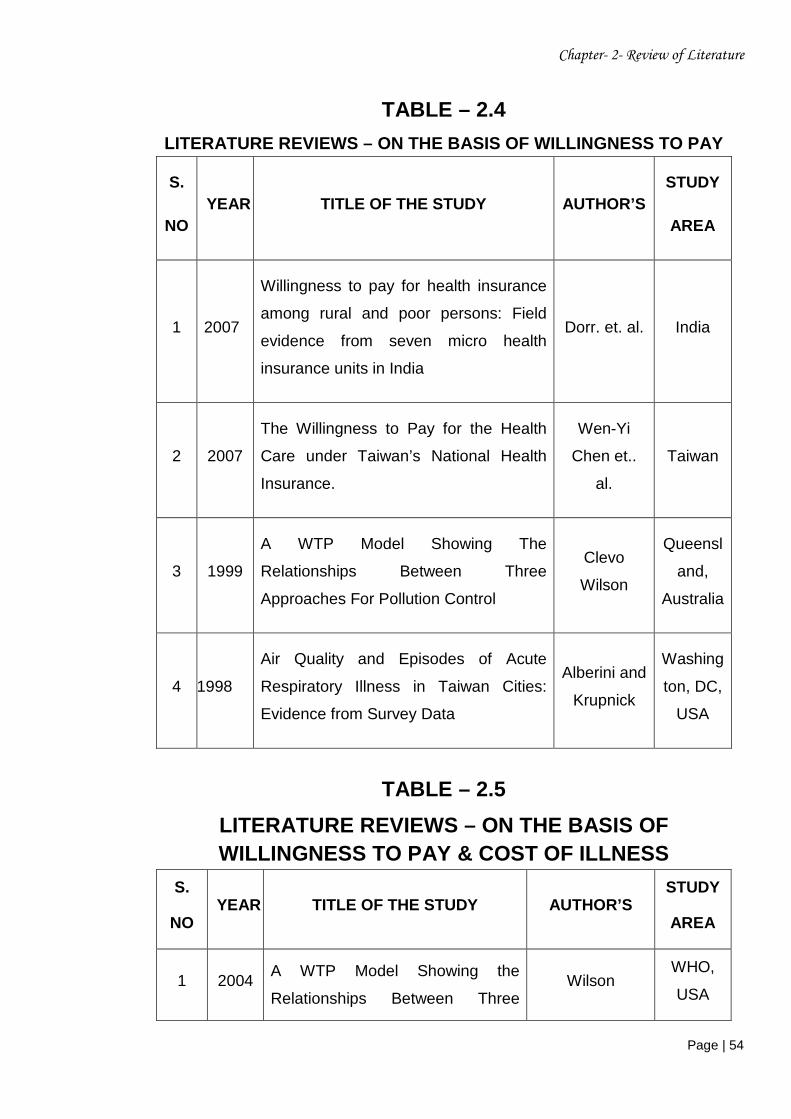
The table 2.4shows, only four studies has been carried out specially on willingness
to pay model. Out of the four studies only a single study has been carried out in
India.
The table 2.5 shows that there were only five studies which have considered both
cost of illness and willingness to pay approach. Out of these five studies none of the
study considering both the aspect have ever been carried out in India.
Chapter- 2- Review of Literature
Page | 51
TABLE 2.2
LITERATURE REVIEWS – ON THE BASIS OFAIR POLLUTION AND ITS EFFECTS
S.
NO YEAR TITLE OF THE STUDY AUTHOR’
S
STUDY
AREA
1 2003 Impact of air pollution on Human Health in Dehradun City
A. Gupta .et
Uttrakhand
India
2 2001 Economic valuation of health impacts of air pollution in Mumbai
Anjali Srivastava
and Rakesh Kumar
Maharasthra
India
3 2000 National burden of disease in India from indoor air pollution
Smith et. al. India
4 1997 The Health Benefits of Air Pollution Control in Delhi
Cropper et.al.
Delhi,
India
5 2008
Estimating the uncertainty of damage costs of pollution: A simple transparent method and typical results
Spadaro and Rabl
France
6 2007 Evaluation of Total Cost of Air Pollution Due to Transportation in Canada
Dave Sawyer et.
al Canada
7 2001 Indoor air pollution in a zone of extreme poverty of metropolitan Santiago
Caceres. et at.
Santiago, Chile
Chapter- 2- Review of Literature
Page | 52
TABLE – 2.3
LITERATURE REVIEWS – ON THE BASIS OF COST OF ILLNESS
S.
NO YEAR TITLE OF THE STUDY AUTHOR’S
STUDY
AREA
1 2009
A Preliminary Estimate of Immediate
Cost of Chikungunya and Dengue to
Gujarat, India
Mavalankar
et. al.
Gujarat,
India
2 2008 Cost of Illness: Evidence from a study
in five resource-poor locations in India Dorr. et. al. India
3 2006 Valuation of Urban Air Pollution: A
Case Study of Kanpur City in India Usha Gupta
Uttar
Pradesh
India
4 2003 Impact of air pollution on Human
Health in Dehradun City A. Gupta .et
Uttrakhand
India
5 2008
Costs of Illness Among Older Adults:
An Analysis of Six Major Health
Conditions with Significant
Environmental Risk Factors
George et
al. USA
6 2008
Societal costs of air pollution-related
health hazards: A review of methods
and results
TanjimaPer
vin et. al. Sweden
7 2007
Evaluation of Total Cost of Air
Pollution Due to Transportation in
Canada
Dave
Sawyer et.
al.
Canada
Chapter- 2- Review of Literature
Page | 53
8 2004 Rich-Poor Differences in Health Care
Financing
Alexander
et. al. USA
9 2003
Cost of illness of moderate to-severe
atopic asthma and/or seasonal
allergic rhinitis (SAR) in Germany
B.
Schramm
et. al.
Germany
10 2002 Economic Status and Health in
Childhood: The Origins of the Gradien
Anne Case
et at.
Princeton,
NJ
11 2000
Economic evaluation of health
impacts due to road traffic-relatedair
pollution (An impact assessment
project of Austria, France and
Switzerland)
H. Sommer,
et al.
European
Union (EU)
12 2000
Assessing Health Impacts of Air
Pollution from Electricity Generation:
The Case of Thailand
Thanh and
Lefevre Thailand
13 2000 The Economic Burden of COPD
Sean D.
Sullivan et
al
Washington,
Seattle, WA
14 1999 The Health Costs of Motor-Vehicle-
Related Air Pollution
McCubbin
and
Delucchi
California,
USA
15 1999
A Scoping Study on the Costs of
Indoor Air Quality Illnesses: An
Insurance Loss Reduction
Perspective
Chen and
Vine
North
Carolina,
USA
Chapter- 2- Review of Literature
Page | 54
TABLE – 2.4
LITERATURE REVIEWS – ON THE BASIS OF WILLINGNESS TO PAY
S.
NO YEAR TITLE OF THE STUDY AUTHOR’S
STUDY
AREA
1 2007
Willingness to pay for health insurance
among rural and poor persons: Field
evidence from seven micro health
insurance units in India
Dorr. et. al. India
2 2007
The Willingness to Pay for the Health
Care under Taiwan’s National Health
Insurance.
Wen-Yi
Chen et..
al.
Taiwan
3 1999
A WTP Model Showing The
Relationships Between Three
Approaches For Pollution Control
Clevo
Wilson
Queensl
and,
Australia
4 1998
Air Quality and Episodes of Acute
Respiratory Illness in Taiwan Cities:
Evidence from Survey Data
Alberini and
Krupnick
Washing
ton, DC,
USA
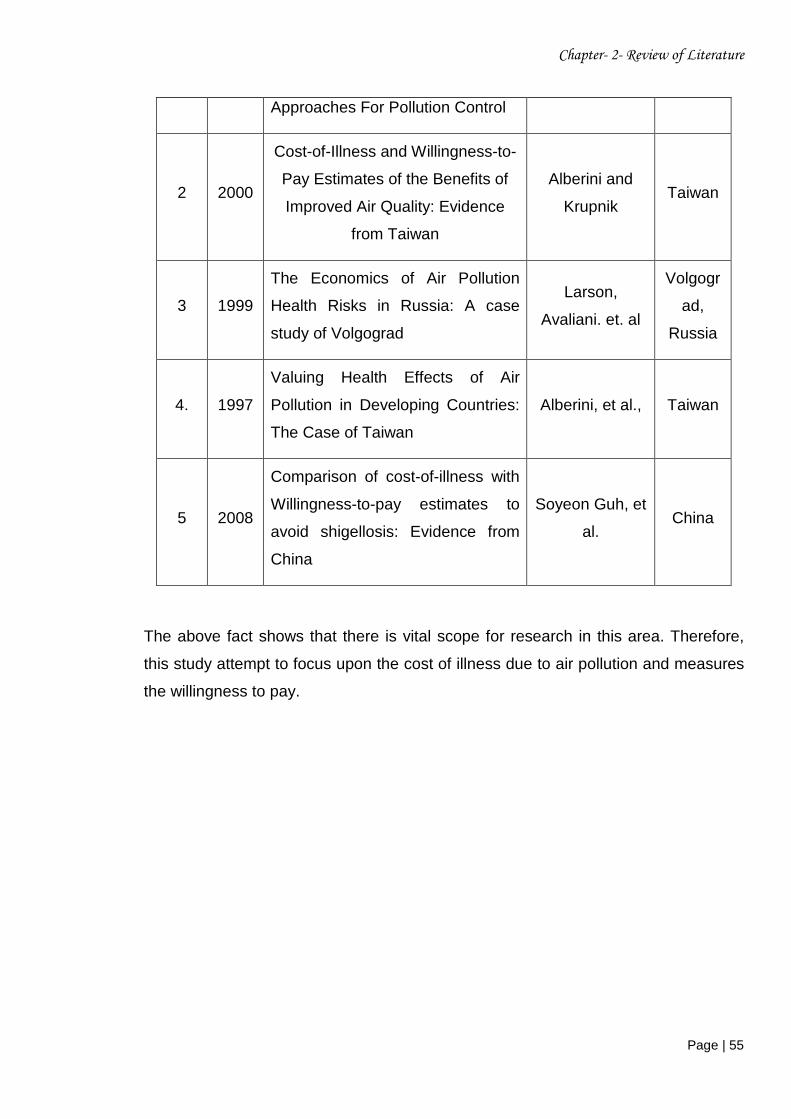
TABLE – 2.5
LITERATURE REVIEWS – ON THE BASIS OF WILLINGNESS TO PAY & COST OF ILLNESS
S.
NO YEAR TITLE OF THE STUDY AUTHOR’S
STUDY
AREA
1 2004 A WTP Model Showing the
Relationships Between Three Wilson
WHO,
USA
Chapter- 2- Review of Literature
Page | 55
Approaches For Pollution Control
2 2000
Cost-of-Illness and Willingness-to-
Pay Estimates of the Benefits of
Improved Air Quality: Evidence
from Taiwan
Alberini and
Krupnik Taiwan
3 1999
The Economics of Air Pollution
Health Risks in Russia: A case
study of Volgograd
Larson,
Avaliani. et. al
Volgogr
ad,
Russia
4. 1997
Valuing Health Effects of Air
Pollution in Developing Countries:
The Case of Taiwan
Alberini, et al., Taiwan
5 2008
Comparison of cost-of-illness with
Willingness-to-pay estimates to
avoid shigellosis: Evidence from
China
Soyeon Guh, et
al. China
The above fact shows that there is vital scope for research in this area. Therefore,
this study attempt to focus upon the cost of illness due to air pollution and measures
the willingness to pay.
Related Documents











