REVIEW ARTICLE Liquid biopsy in ovarian cancer: the potential of circulating miRNAs and exosomes D193X X LYDIA GIANNOPOULOUD194X X , D195X X MARTHA ZAVRIDOUD196X X , D197X X SABINE KASIMIR-BAUERD198X X , and D199X X EVI S. LIANIDOUD200X X ATHENS, GREECE; and ESSEN, GERMANY Ovarian cancer still remains the most lethal female cancer, since in most cases it is diagnosed at an advanced stage. Usually after completion of primary treatment chemoD201X X resistance occurs, and recurrent disease is finally observed. Liquid biopsy, based on minimally invasive and serial blood tests, has the advantage of following tumor evolution in real time, offering novel insights on precision medicine. Circulat- ing tumor cells (CTCs), circulating tumor DNA (ctDNA), circulating cell-free micro- RNAs (cfmiRNAs) and circulating exosomes represent the major components of liquid biopsy analysis. Liquid biopsy has been already implemented in ovarian can- cer, and most studies so far are mainly focused on CTCs and ctDNA. This review is mainly focused on the clinical potential of circulating miRNAs and exosomes as a source of liquid biopsy biomarkers in ovarian cancer diagnosis, prognosis, and response to treatment. (Translational Research 2018; 000:1 15) Abbreviations: AUC = area under curve; cfDNA = cell-free DNA; cfmiRNAs = cell-free micro- RNAs; CNV = copy number variations; CTCs = circulating tumor cells; ctDNA = circulating tumor DNA; ddPCR = droplet digital PCR; EMT = epithelial-to-mesenchymal transition; EVs = extracel- lular vesicles; HGSC = high-grade serous ovarian cancer; LOH = loss of heterozygosity; NGS = next-generation sequencing; OS = overall survival; PARP = poly ADP-ribose polymerase; PFS = progression-free survival; ROC = receiver operating characteristic; snRNA = small nuclear RNA INTRODUCTION Ovarian cancer is the most lethal among gynecologi- cal malignancies and represents the fifth cause of can- cer-related mortality in women.D202X X 1 D203X X Epithelial ovarian cancer is the main type, characterized by remarkable histological and molecular heterogeneity. In the major- ity of new incidents, the disease is diagnosed at an advanced stage and regardless of the initial response to treatment, chemoD204X X resistance is observed.D205X X 2, D206X X 3 D207X X Primary epi- thelial ovarian cancer is treated with surgical removal of the tumor and a subsequent combination of platinum and taxane-based adjuvant chemotherapy.D208X X 4 D209X X The newest therapeutic approaches include Bevacizumab and the poly ADP-ribose polymerase (PARP) inhibitor Ola- parib; however, these targeted therapy agents are applied only in certain clinical situations.D210X X 5, D211X X 6 D212X X Metastasis in ovarian cancer is unique among all solid malignancies. It occurs via 2D213X X distinct routes: the transcoelomic passive dissemination of tumor cell spheroids in the peritoneal cavity through ascites and the hematogenous metastasis of ovarian cancer cells in systemic circulation followed by the preferred seeding From the Department of Chemistry, Analysis of Circulating Tumor Cells lab, Lab of Analytical Chemistry, University of Athens, Uni- versity Campus, Athens, Greece; Department of Gynecology and Obstetrics, University Hospital of Essen, University of Duisburg- Essen, Essen, Germany. Submitted for Publication July 31, 2018; received submitted October 8, 2018; accepted for publication October 8, 2018. Reprint requests: Evi S. Lianidou, Department of Chemistry, Analysis of Circulating Tumour Cells lab, Laboratory of Analyti- cal Chemistry, University of Athens, 15771, Athens, Greece. e-mail: [email protected]. 1931-5244/$ - see front matter Ó 2018 Elsevier Inc. All rights reserved. https://doi.org/10.1016/j.trsl.2018.10.003 1 ARTICLE IN PRESS

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ARTICLE IN PRESS
REVIEW ARTICLELiquid biopsy in ovarian cancer: the potentialof circulating miRNAs and exosomes
D193X XLYDIA GIANNOPOULOUD194X X, D195X XMARTHA ZAVRIDOUD196X X, D197X XSABINE KASIMIR-BAUERD198X X, and D199X XEVI S. LIANIDOUD200X X
ATHENS, GREECE; and ESSEN, GERMANY
From the Department of Chemistr
Cells lab, Lab of Analytical Chem
versity Campus, Athens, Greece;
Obstetrics, University Hospital of
Essen, Essen, Germany.
Submitted for Publication July 31,
8, 2018; accepted for publication O
Reprint requests: Evi S. Lianid
Analysis of Circulating Tumour C
cal Chemistry, University of A
e-mail: [email protected].
1931-5244/$ - see front matter
� 2018 Elsevier Inc. All rights rese
https://doi.org/10.1016/j.trsl.2018.1
Ovarian cancer still remains the most lethal female cancer, since in most cases it isdiagnosed at an advanced stage. Usually after completion of primary treatmentchemoD201X Xresistance occurs, and recurrent disease is finally observed. Liquid biopsy,based on minimally invasive and serial blood tests, has the advantage of followingtumor evolution in real time, offering novel insights on precision medicine. Circulat-ing tumor cells (CTCs), circulating tumor DNA (ctDNA), circulating cell-free micro-RNAs (cfmiRNAs) and circulating exosomes represent the major components ofliquid biopsy analysis. Liquid biopsy has been already implemented in ovarian can-cer, and most studies so far are mainly focused on CTCs and ctDNA. This review ismainly focused on the clinical potential of circulating miRNAs and exosomes as asource of liquid biopsy biomarkers in ovarian cancer diagnosis, prognosis, andresponse to treatment. (Translational Research 2018; 000:1�15)
Abbreviations: AUC=area under curve; cfDNA =cell-free DNA; cfmiRNAs = cell-free micro-RNAs; CNV =copy number variations; CTCs = circulating tumor cells; ctDNA=circulating tumorDNA; ddPCR= droplet digital PCR; EMT = epithelial-to-mesenchymal transition; EVs = extracel-lular vesicles; HGSC= high-grade serous ovarian cancer; LOH = loss of heterozygosity;NGS = next-generation sequencing; OS = overall survival; PARP = poly ADP-ribose polymerase;PFS = progression-free survival; ROC= receiver operating characteristic; snRNA= small nuclearRNA
INTRODUCTION
Ovarian cancer is the most lethal among gynecologi-
cal malignancies and represents the fifth cause of can-
cer-related mortality in women. D202X X1 D203X X Epithelial ovarian
y, Analysis of Circulating Tumor
istry, University of Athens, Uni-
Department of Gynecology and
Essen, University of Duisburg-
2018; received submitted October
ctober 8, 2018.
ou, Department of Chemistry,
ells lab, Laboratory of Analyti-
thens, 15771, Athens, Greece.
rved.
0.003
cancer is the main type, characterized by remarkable
histological and molecular heterogeneity. In the major-
ity of new incidents, the disease is diagnosed at an
advanced stage and regardless of the initial response to
treatment, chemo D204X Xresistance is observed. D205X X2, D206X X3 D207X XPrimary epi-
thelial ovarian cancer is treated with surgical removal
of the tumor and a subsequent combination of platinum
and taxane-based adjuvant chemotherapy. D208X X4 D209X XThe newest
therapeutic approaches include Bevacizumab and the
poly ADP-ribose polymerase (PARP) inhibitor Ola-
parib; however, these targeted therapy agents are
applied only in certain clinical situations. D210X X5, D211X X6D212X X
Metastasis in ovarian cancer is unique among all
solid malignancies. It occurs via 2 D213X Xdistinct routes: the
transcoelomic passive dissemination of tumor cell
spheroids in the peritoneal cavity through ascites and
the hematogenous metastasis of ovarian cancer cells in
systemic circulation followed by the preferred seeding
1

ARTICLE IN PRESSTranslational Research
2 Giannopoulou et al 2018
to the omentum. D214X X7, D215X X8D216X XThe final stage of both metastatic
routes is the colonization of cancer cells originating
from the ovary to distal organs, mainly the liver, the
spleen, and the lungs. D217X X9 D218X X
Liquid biopsy is a minimally invasive blood-based
approach that has the potential of providing informa-
tion on prognosis, response to therapeutic regimens
and recently even on early diagnosis and population
screening. D219X X10, D220X X11 D221X XThe detection and molecular characteri-
zation of circulating tumor cells (CTCs), the detection
of circulating tumor DNA (ctDNA), circulating cell-
free microRNAs (cfmiRNAs), and circulating extracel-
lular vesicles D222X Xlike exosomes, in the peripheral blood of
cancer patients, represent the main liquid biopsy
approaches (FigD223X X 1).11�14 It has also been recently
found that tumor-educated platelets can transfer
nucleic acids from the tumor, mainly RNA, to distant
organs. D224X X15 D225X XThe clinical significance of CTCs and ctDNA
in ovarian cancer has been intensively investigated in a
large number of research studies during the last 2 D226X Xdeca-
des and latest developments in this field have been
recently reviewed. D227X X16�21D228X X
Circulating miRNAs are a subclass of small nonD229X Xcoding
RNAs that have been detected in almost all body fluids.
Circulating miRNAs are involved in cell-to-cell commu-
nication and their main role is the up- or down-regulation
of the expression of their target genes. miRNAs biogene-
sis occurs first in the nucleus and then in the cytoplasm;
afterwards, they are released in the circulation as cell-
free miRNAs bound in specific RNA-binding proteins
(circulating cfmiRNAs) or encapsulated in exosomes
Fig. 1. Liquid biopsy in
(circulating exosomal miRNAs) along with proteins, lip-
ids, and nucleic acids.D230X X14,D231X X22,D232X X23D233X XExosomes are a subcategory
of extracellular vesiclesD234X X secreted by living cells in the
extracellular space or in blood circulation; in cancer
patients, exosomes are also secreted by tumor cells and it
is now believed that they play important roles in the met-
astatic process.D235X X24�26D236X XIn ovarian cancer, a large number of
studies suggest a possible role of exosomes in early diag-
nosis, prognosis, and response to treatment.D237X X26�28D238X X
In this review, we provide a brief description of the
most recent studies on CTCs and ctDNA in ovarian
cancer and a detailed overview of studies on circulating
cfmiRNAs and exosomes in ovarian cancer. We also
focus on the clinical significance of liquid biopsy in
ovarian cancer and attempt to clarify their role in early
diagnosis, prognosis, and response to treatment.
CIRCULATING TUMOR CELLS D239X X
In epithelial ovarian cancer, CTCs are involved in
the hematogenous metastatic routeD240X X17, D241X X29 D242X X Up to now,
many studies attempted to evaluate the clinical signifi-
cance of CTCs, especially their role as prognostic and/
or predictive biomarkers. D243X X19, D244X X20 D245X XA variety of technologies
have been used for CTCs enrichment and detection in
ovarian cancer; CTCs isolation and/or enrichment is
based mainly on immunomagnetic particles or is size-
based, while CTCs detection is based on immunocyto-
chemistry approaches (microscopic detection or the
FDA-cleared CellSearch D246X X system, Menarini, Silicon
Biosystems), reverse transcription polymerase chain
ovarian cancer.

ARTICLE IN PRESSTranslational ResearchVolume 00 Giannopoulou et al 3
reaction (RT-PCR) (AdnaTest, QIAGEN, Hilden, Ger-
many) and RT-qPCR. D247X X17, D248X X20 D249X X Novel technologies for
CTCs isolation and enrichment based on their physical
properties were also introduced by several research
groups, such as microfluidic devices for the isolation
and detection of CTCs in ovarian cancer patients. D250X X30, D251X X31 D252X X
The microfluidics-based ParsortixD253X X technology (Angle
plc) has been recently used for the D254X XCTC enrichment,
followed by RT-qPCR for CTC detection and molecu-
lar characterization. D255X X31 D256X X
A recent study attempted to investigate the incidence
of epithelial-to-mesenchymal transition (EMT)-like
CTCs in ovarian cancer patients, prior to surgery and
after platinum-based chemotherapy at the gene expres-
sion level. D257X X32 D258X XThe EMT-associated transcripts analyzed
were PIK3CA, AKT-2, and TWIST. Before surgery, the
presence of PI3K+EMT-like CTCs in combination
with epithelial CTCs was significantly associated with
worse overall survival (OS). In the International Feder-
ation of Gynecology and Obstetrics (FIGO) stage I-III
patients with residual tumor burden after surgery,
EMT-like CTCs were observed; furthermore, epithelial
CTCs significantly correlated with shorter progression-
free survival (PFS) and OS and the presence of PI3K+
CTCs was correlated with decreased OS. D259X X32 D260X X
In a recent study performed with a large group of
patients with ovarian cancer, which was conducted to
investigate whether the presence of CTCs could reveal
minimal residual disease, univariate, and multivariate
analysis indicated a worse OS in CTC positive patients
at the time of diagnosis. D261X X33 D262X X The alterations between
CTCs and the immune system were also investigated,
in a very recent study from the same group. D263X X34 D264X XThe pres-
ence of the immune activation marker neopterin and
the ratio of kynurenine to tryptophan were evaluated in
matched plasma samples from ovarian cancer patients,
where CTCs have already been detected. D265X X35 D266X XAt the time
of diagnosis and at follow-up, both, neopterin and
kynurenine to tryptophan levels were significantly
increased in PPIC positive CTCs when compared to
benign disease, suggesting that immune responses
occur not only in the primary tumor but also in the
circulation. D267X X34 D268X X
The potential of CTCs detection for the diagnosis of
ovarian cancer was evaluated in a recent study where a
size-based microfluidic device was used for CTCs isola-
tion, followed by their detection and identification
through immunofluorescent staining of CD45, HE4, and
the EMT markers EpCAM, pan-cytokeratins, and
vimentin. A group of women having an ovarian mass
participated in the study, and almost half of them were
diagnosed with ovarian cancer. More specifically, the
DAPI+/E&M+/CD45¡/HE4+CTC subpopulation was
significantly higher in ovarian cancer patients compared
to those with benign tumors. Furthermore, a better diag-
nostic sensitivity was estimated using receiver operating
characteristic (ROC) curves, when compared to the
most established tumor marker in ovarian cancer, serum
CA-125. The above CTC count was proposed as a bio-
marker for ovarian cancer early diagnosis in cases where
a pelvic mass was observed.D269X X36D270X XThe predictive value of
CTCs was also investigated in a very small group of
ovarian cancer patients (n = 13) that received standard
taxol and/or carboplatin chemotherapy; a statistically
significant association was observed between CTC lev-
els and disease progression.D271X X37D272X X
CIRCULATING TUMOR DNA D273X X
A number of studies on ctDNA in patients with ovar-
ian cancer attempted to evaluate its clinical value, in the
terms of early diagnosis, prognosis, and response to treat-
ment or even screening in the general population.D274X X16,D275X X38D276X XTo
this end, total ctDNA and/or circulating cell-free mito-
chondrial DNA quantification, or detection of different
genetic and epigenetic alterations, such as chromosomal
abnormalities and specific tumor loss of heterozygosityD277X X,
somatic and germline gene mutations and aberrant DNA
methylation, were correlated with diagnosis, prognosis,
and response to treatment.D278X X18D279X XIn a very recent study, short
ALU-115 repeat and long ALU-219 fragments were
amplified and used for the detection of plasma cell-free
DNA (cfDNA) concentrations and ALU-219/ALU-115
integrity index was measured in ovarian cancer patients.
Significantly higher ALU-219 fragment levels and integ-
rity index were observed in ovarian cancer when com-
pared to benign disease and healthy individuals,
suggesting a possible role of ctDNA analysis in early
diagnosis of ovarian cancer.D280X X39D281X X
Epigenetic alterations in ctDNA are also important
in ovarian cancer. It was recently shown that the meth-
ylation status of 3 D282X X genes (COL23A1, C2CD4D, and
WNT6), discovered using targeted ultra-high coverage
bisulfite sequencing, could discriminate successfully
the responders and non D283X Xresponders to platinum-based
neoadjuvant chemotherapy. D284X X40 D285X X We recently evaluated
for the first time ESR1 methylation status in plasma
ctDNA and paired primary tumors of patients with
high-grade serous ovarian cancer (HGSC), and found
an agreement between ESR1 methylation in primary
tumors and paired ctDNA. D286X X41 D287X X
Droplet digital PCR (ddPCR) was used for the eval-
uation of somatic TP53 mutations in plasma ctDNA
samples of patients with serous ovarian cancer. D288X X42, D289X X43 D290X X
TP53 mutations were investigated in serial ctDNA
samples of HGSC patients; the presence of TP53
mutant allele fractions in ctDNA, when compared to

ARTICLE IN PRESSTranslational Research
4 Giannopoulou et al 2018
serum CA-125, could indicate much earlier response to
chemotherapy. D291X X43D292X X
The importance of the reversion of BRCA1/2 muta-
tions in ctDNA as an indicator of response to platinum-
based and PARP inhibitor-based chemotherapy was
investigated. D293X X44, D294X X45 D295X XMore specifically, in ovarian cancer
patients with recurrent HGSC, the same BRCA1/2
reversions that were identified in paired tumor and
plasma ctDNA samples were present in the tumor.
Interestingly, resistance to platinum-based and PARP
inhibitor-based chemotherapy was observed in all
patients with BRCA1/2 reversions in ctDNA. D296X X44 D297X X The
BRCA1/2 reversion mutation status was also assessed
by using targeted massively parallel sequencing in
ctDNA samples of platinum resistant and/or refractory
ovarian cancer patients; putative BRCA1 or BRCA2
somatic reversion mutations or intragenic deletions
were detected in 21% of ovarian cancer ctDNA sam-
ples, and these results were further confirmed using
ddPCR. D298X X45 D299X X Germline and somatic BRCA1/2 mutations
were detected in plasma ctDNA of ovarian cancer
patients, by using next-generation sequencing (NGS)
technology. All germline BRCA1/2 mutations detected
in ctDNA were present in the primary tumor but
this concordance was not observed for somatic muta-
tions, indicating the incidence of intratumoral hetero-
geneity. D300X X46 D301X X
The clinical value of plasma ctDNA in treatment
monitoring was recently investigated in cases where
neoadjuvant chemotherapy is necessary. In this study,
NGS was performed in ctDNA samples before and
after neoadjuvant chemotherapy, using a specific panel
of 50 genes; before treatment, 59 genetic variants from
19 of these genes were identified but only 6 D302X X of them
were detected after neoadjuvant chemotherapy. D303X X47D304X X A
number of somatic mutations, polymorphisms, and
copy number variations D305X Xwere also detected in plasma
ctDNA samples of recurrent and drug-resistant recur-
rent ovarian cancer patients, using NGS. D306X X48 D307X X
The development of a novel massive parallel
sequencing approach named targeted error correction
sequencing, led to the identification of cancer-related
genomic changes in early stage malignancies, includ-
ing ovarian cancer. Somatic mutations of driver genes
were detected in 68% of ovarian cancer patients with
early stage disease and for all cancer types analyzed, a
high concordance between ctDNA and primary tumor
was observed. D308X X49 D309X X
The recently developed CancerSEEK blood test has
the potential to evaluate the levels of 8D310X Xproteins and the
presence of somatic mutations in 2D311X X001 genomic posi-
tions simultaneously.D312X X10D313X XWhen this test was evaluated in
1D314X X005 patients with already detected solid cancers,
including 54 patients with ovarian cancer, its sensitivity
varied in the different types of cancer tested, but the
higher diagnostic sensitivity was observed in ovarian
cancer (98%). The concordance between tissue and
ctDNA was also estimated, in cases where the primary
tumor was available, with the highest 100% concor-
dance being observed in ovarian cancer. This test could
also determine the location of the primary tumor based
on the obtained information from ctDNA and circulating
proteins. In ovarian cancer, 79% of the cases were pre-
dicted correctly as the most likely type and the percent-
age reached 92% when the second more likely type was
included.D315X X10D316X X
CIRCULATING CELL-FREE AND EXOSOMAL miRNAs
Many research studies aimed to elucidate the clinical
value of circulating cfmiRNAs and exosomal miRNAs
in serum and/or plasma of ovarian cancer patients. D317X X50�52D318X X
In a recent meta-analysis that was performed to estimate
the diagnostic significance of circulating cfmiRNAs in
ovarian cancer, the diagnostic value of circulating
cfmiRNAs was considered as moderate. However, only
ten research studies were included in the statistical ana-
lysis.D319X X53D320X XAdditionally, another nonD321X Xcoding RNA, circulat-
ing U2 small nuclear RNA (snRNA) was recently
proposed on having an important role in ovarian cancer
diagnosis.D322X X54D323X X
Most studies that investigated the clinical value of
circulating cfmiRNAs and exosomal miRNAs in ovar-
ian cancer are presented in detail below and are sum-
marized in Tables I and II. The assessment of clinical
significance resulting from these studies is also
reported (Table III). Only studies that included more
than 25 ovarian cancer patients were added in these
tables. As can be seen in Tables I�III, the results
obtained from the studies on circulating cfmiRNAs in
ovarian cancer were often controversial; a possible
explanation could be the different procedures used for
the isolation and characterization of these circulating
cfmiRNAs or the distinct reference miRNAs used for
the quantification of their expression levels.
CIRCULATING cfmiRNAs
Diagnosis. The first study that focused on circulating
cfmiRNAs in ovarian cancer was based on real-time PCR
quantification of specific miRNAs in serum samples
of ovarian cancer patients and healthy individuals;
miR-142-3p was used as a reference miRNA.D324X X55D325X XAccording
to this study, the expression of 8D326X XmiRNAs was signifi-
cantly differentiated in ovarian cancer patients when
compared to healthy controls, indicating a diagnostic
value; 5D327X X specific miRNAs were overD328X Xexpressed (miR-21,
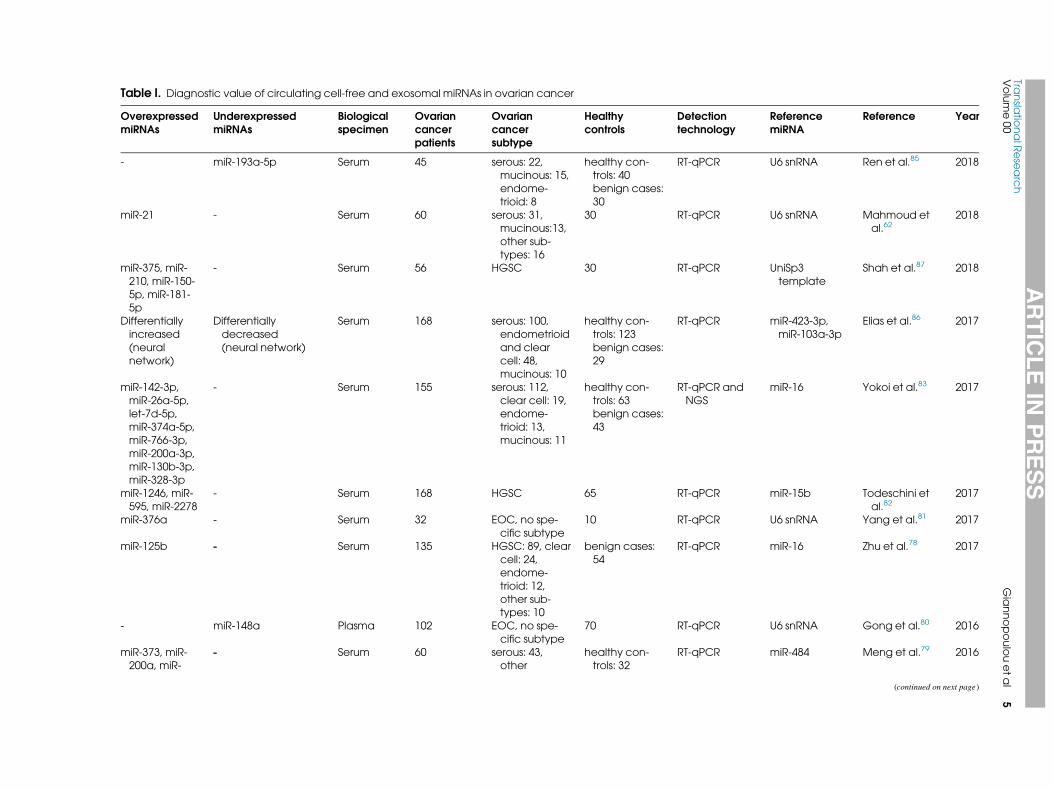
Table I. Diagnostic value of circulating cell-free and exosomal miRNAs in ovarian cancerD1X X
OverD2X XexpressedmiRNAs
UnderD3X XexpressedmiRNAs
Biologicalspecimen
OvarianD4X Xcancerpatients
OvarianD5X Xcancersubtype
Healthycontrols
Detectiontechnology
ReferencemiRNA
Reference Year
- miR-193a-5p Serum 45 serous: 22,mucinous: 15,endome-trioid: 8
healthy con-trols: 40benign cases:30
RT-qPCR U6 snRNA Ren et al. D6X X85D7X X 2018
miR-21 - Serum 60 serous: 31,mucinous:13,other sub-types: 16
30 RT-qPCR U6 snRNA Mahmoud etal. D8X X62D9X X
2018
miR-375, miR-210, miR-150-5p, miR-181-5p
- Serum 56 HGSC 30 RT-qPCR UniSp3template
Shah et al.D10X X87D11X X 2018
Differentiallyincreased(neuralnetwork)
Differentiallydecreased(neural network)
Serum 168 serous: 100,endometrioidand clearcell: 48,mucinous: 10
healthy con-trols: 123benign cases:29
RT-qPCR miR-423-3p,miR-103a-3p
Elias et al. D12X X86D13X X 2017
miR-142-3p,miR-26a-5p,let-7d-5p,miR-374a-5p,miR-766-3p,miR-200a-3p,miR-130b-3p,miR-328-3p
- Serum 155 serous: 112,clear cell: 19,endome-trioid: 13,mucinous: 11
healthy con-trols: 63benign cases:43
RT-qPCR andNGS
miR-16 Yokoi et al.D14X X83 D15X X 2017
miR-1246, miR-595, miR-2278
- Serum 168 HGSC 65 RT-qPCR miR-15b Todeschini etal. D16X X82D17X X
2017
miR-376a - Serum 32 EOC, no spe-cific subtype
10 RT-qPCR U6 snRNA Yang et al. D18X X81D19X X 2017
miR-125b - Serum 135 HGSC: 89, clearcell: 24,endome-trioid: 12,other sub-types: 10
benign cases:54
RT-qPCR miR-16 Zhu et al.D20X X78 D21X X 2017
- miR-148a Plasma 102 EOC, no spe-cific subtype
70 RT-qPCR U6 snRNA Gong et al. D22X X80D23X X 2016
miR-373, miR-200a, miR-
- Serum 60 serous: 43,other
healthy con-trols: 32
RT-qPCR miR-484 Meng et al.D24X X79 D25X X 2016
(continued on next page)
ARTICLE
INPRESS
Transla
tionalR
ese
arch
Volume00
Giannopoulouetal
5

Table I. (Continued)
OverD2X XexpressedmiRNAs
UnderD3X XexpressedmiRNAs
Biologicalspecimen
OvarianD4X Xcancerpatients
OvarianD5X Xcancersubtype
Healthycontrols
Detectiontechnology
ReferencemiRNA
Reference Year
200b, miR-200c
subtypes: 2,unknown: 15
benign cases:20
miR-125b - Serum 70 mucinous: 36,serous: 17,other sub-types: 17
70 RT-qPCR U6 snRNA Zuberi et al. D26X X77D27X X 2016
- miR-199a Serum 70 mucinous: 36,serous: 17,other sub-types: 17
70 RT-qPCR U6 snRNA Zuberi et al. D28X X76D29X X 2016
miR-373, miR-200a, miR-200b, miR-200c
- Serumexosomes
163 serous: 120,other sub-types: 15,unknown: 28
healthy con-trols: 32benign cases:20
RT-qPCR miR-484 Meng et al.D30X X94 D31X X 2016
miR-7, miR-429 miR-25, miR-93 Serum 180 EOC, no spe-cific subtype
66 RT-qPCR miR-484 Meng et al.D32X X75D33X X 2015
miR-200b - Plasma 51 EOC, no spe-cific subtype
healthy con-trols: 25benign cases:25
RT-qPCR miR-191 Kapetanakis etal. D34X X59D35X X
2015
miR-200a, miR-200b, miR-200c
- Serum 70 mucinous: 36,serous: 17,other sub-types: 17
70 RT-qPCR U6 snRNA Zuberi et al. D36X X58D37X X 2015
- miR-145 Serum 84 endometrioid:24, serous: 18,clear cell: 17,mucinous: 12,mixed: 13
healthy con-trols: 135benign cases:51
RT-qPCR U6 snRNA Liang et al. D38X X66D39X X 2015
miR-200c, miR-141
- Serum 74 serous: 16,endome-trioid: 15,clear cell: 14,mucinous: 12,undifferenti-ated: 17
50 RT-qPCR NR Gao et al.D40X X74 D41X X 2015
- let-7i-5p, miR-122,miR-152-5p, miR-25-3p
Serum 25 Serous benign cases:20
RT-qPCR has-miR-103a-3p, miR-27b-3p, miR-30b-
Langhe et al. D42X X71D43X X 2015
(continued on next page)
ARTICLE
INPRESS
Transla
tionalR
ese
arch
6Giannopoulouetal
2018

Table I. (Continued)
OverD2X XexpressedmiRNAs
UnderD3X XexpressedmiRNAs
Biologicalspecimen
OvarianD4X Xcancerpatients
OvarianD5X Xcancersubtype
Healthycontrols
Detectiontechnology
ReferencemiRNA
Reference Year
5p, miR-101-3p
miR-26a - Plasma 26 serous: 15,other sub-types: 11
19 RT-qPCR cel-miR-39 Shen et al.D44X X64D45X X 2014
miR-22, miR-93,miR-451
miR-106b Serum 31 EOC, no spe-cific subtype
healthy con-trols: 8 benigncases: 23
RT-qPCR andNGS
miR-16 Ji et al.D46X X73D47X X 2014
miR-625-3p,miR-720, miR-1274a
19 miRs including:miR-19b, miR-223,miR-16, miR-150,miR-20a, miR-126,miR-1290
Plasma 42 Serous healthy con-trols: 23benign cases:36
RT-qPCR Presurgicalsamples: miR-320, miR-720,miR- 1274b,U6 snRNA Allother sam-ples: 14miRNAs
Shapira et al.D48X X72 D49X X 2014
miR-205 let-7f Plasma 360 serous: 179,endome-trioid: 86,adenocarci-noma: 47,mucinous: 33,clear cell: 15
200 RT-qPCR NR Zheng et al.D50X X67D51X X 2013
miR-21 - Serum 94 serous: 68,other sub-types: 26
40 RT-qPCR U6 snRNA Xu et al. D52X X63D53X X 2013
miR-16, miR-21,miR-191, miR-4284
- Plasma 35 Endometriosis-associated(endome-trioid andclear cell)
healthy con-trols: 20 endo-metriosis: 33
RT-qPCR miR-132 Suryawanshi etal. D54X X68D55X X
2013
miR-92 - Serum 50 EOC, no spe-cific subtype
50 RT-qPCR cel-miR-54 Guo et al. D56X X61D57X X 2013
miR-221 - Serum 96 serous: 70,other sub-types: 26
35 RT-qPCR mmu-miR-295 Hong et al. D58X X60 D59X X 2012
miR-200a, miR-200b, miR-200c
- Serum 28 HGSC 28 RT-qPCR miR-103 Kan et al.D60X X57D61X X 2012
Serum 28 15 RT-qPCR miR-142-3p Resnick et al.D62X X55D63X X 2009
(continued on next page)
ARTICLE
INPRESS
Transla
tionalR
ese
arch
Volume00
Giannopoulouetal
7

Table
I.(C
ontinued)
OverD2XXexpressed
miRNAs
UnderD3XXexpressed
miRNAs
Biological
specim
en
Ovarian
D4XXcancer
patie
nts
Ovarian
D5XXcancer
subtype
Health
ycontrols
Detectio
ntechnology
Reference
miRNA
Reference
Year
miR-21,miR-92,
miR-93,m
iR-
126,m
iR-29a
miR-155,miR-127,
miR-99b
EOC,nosp
e-
cificsubtype
miR-21,miR-
141,m
iR-
200a,miR-
200c,miR-
200b,miR-
203,m
iR-205,
miR-214
-Se
rum
exo
somes
50
Serous
healthycon-
trols:10
benigncase
s:10
Microarrays
conta
ining
probes
NR
Tayloretal.D64XX93D65XX
2008
EOC:epithelia
lovaria
ncancer,NR:notreported
ARTICLE IN PRESSTranslational Research
8 Giannopoulou et al 2018
miR-92, miR-93, miR-126, and miR-29a) and 3D329X XunderD330X Xex-
pressed (miR-155, miR-127, and miR-99b).D331X X55D332X X When
peripheral blood samples from ovarian cancer patients
that relapsed were analyzed using specific microarrays,
the elevated expression of miR-30c-1 and the decreased
expression of 3D333X X circulating cfmiRNAs (miR-342-3p,
miR-181a, and miR-450b-5p) D334X Xwere reported.D335X X56D336X XIn another
study, miRNAs from the miR-200 family, namely miR-
200a, miR-200b, and miR-200c were found significantly
overD337X Xexpressed in serum samples of serous ovarian cancer
patients when compared to healthy donors, using miR-
103 as a reference miRNA. miR-182 levels were also
assessed, however, no significant increment was reported
for patients in contrast with the ovarian cancer cell lines
examined.D338X X57D339X X These miR-200 family members were also
found elevated using U6 snRNA as a reference in a dif-
ferent study.D340X X58D341X XMoreover, increased levels of circulating
miR-200b were reported in pre- and post-treatment ovar-
ian cancer patients.D342X X59D343X XIn this study, Kapetanakis et al. eval-
uated levels of the tumor marker CA-125 and circulating
miR-200b in a group of 51 ovarian cancer patients, how-
ever, no significant correlation was found. Circulating
miR-200b was not associated with the FIGO stage,
whereas CA-125 levels significantly correlated with the
FIGO stage; however, CA-125 levels were very low in 3D344X X
out of 4D345X X early staged cases of the group and circulating
miR-200b levels were above averageD346X X59D347X XFurthermore, cir-
culating miR-221D348X X60D349X XmiR-92,D350X X61D351X Xand miR-21D352X X62,D353X X63D354X Xwere signif-
icantly upD355X Xregulated in serum samples of ovarian cancer
patients when compared to healthy women. Conversely,
miR-26a was found upD356X Xregulated in plasma samples of
ovarian cancer patients compared to healthy controls, in a
different study.D357X X64D358X XDownD359X Xregulation of miR-145 was con-
firmed in another study in ovarian cancer tissues, cell
lines, and serum samples.D360X X65D361X XThe diagnostic value of circu-
lating miR-145 levels in sera from patients with ovarian
cancer was determined with the corresponding levels in
healthy subjects, with evaluation using ROC curves (area
under curve, AUC = 0.82).D362X X66D363X X
Circulating miR-205 and let-7f were significantly
over D364X Xexpressed and under D365X Xexpressed, respectively, in a
large number of ovarian cancer patients using a Taq-
Man low density array; the diagnostic value of the
combination of these 2 D366X Xcirculating cfmiRNAs was esti-
mated using a ROC curve (AUC = 0.831). When the
levels of circulating miR-205 and let-7f were combined
with CA-125 values, a better diagnostic sensitivity was
observed. D367X X67 D368X X In endometriosis-associated (endometrioid
and clear cell) ovarian and serous ovarian cancer a dis-
tinct expression of specific miRNAs was detected in
each type of ovarian cancer when compared to healthy
women; more specifically, endometriosis-associated
ovarian cancer was characterized by the over D369X Xexpres-
sion of miR-16, miR-21, and miR-191, whereas serous

Table II. Prognostic and predictive value of circulating cell-free and exosomal miRNAs in ovarian cancerD66X X
Over-expressedmiRNAs
Under-expressedmiRNAs
Biologicalspecimen
OvarianD67X Xcancerpatients
Ovarian D68X Xcancersubtype
Detectiontechnology
Reference miRNA Prognosticsignificance
Reference Year
miR-200b, miR-1274a, miR-141, miR-200c
- Plasma 207 serous: 137, clearcell: 27, mixed:21, other sub-types: 22
RT-qPCR miR-220, miR-19b,U6 snRNA, miR-320
Patients receiv-ing Bevacizu-mab: PFS(miR-200c,P = 0.006)
Halvorsen et al. D69X X92D70X X 2017
miR-125b - Serum 135 HGSC: 89, clearcell: 24, endo-metrioid: 12,other subtypes:10
RT-qPCR miR-16 PFS (P D71X X= 0.035) Zhu et al. D72X X78D73X X 2017
- miR-148a Plasma 102 EOC, no specificsubtype
RT-qPCR U6 snRNA OS (PD74X X= 0.002) Gong et al.D75X X80D76X X 2016
- miR-199a Serum 70 mucinous: 36,serous: 17, othersubtypes: 17
RT-qPCR U6 snRNA OS (P = 0.030) Zuberi et al.D77X X76D78X X 2016
miR-373, miR-200a, miR-200b, miR-200c
- Serumexosomes
163 serous: 120, othersubtypes: 15,unknown: 28
RT-qPCR miR-484 OS (miR-200bPD79X X= 0.007, miR-200cP = 0.017)
Meng et al. D80X X94D81X X 2016
miR-7, miR-429 miR-25, miR-93 Serum 180 EOC, no specificsubtype
RT-qPCR miR-484 OS (miR-429,PD82X X= 0.011)
Meng et al. D83X X75D84X X 2015
miR-200b - Plasma 51 EOC, no specificsubtype
RT-qPCR miR-191 PFS (P D85X X= 0.003) Kapetanakis et al. D86X X59D87X X 2015
- miR-145 Serum 84 endometrioid: 24,serous: 18, clearcell: 17, mucin-ous: 12, mixed:13
RT-qPCR U6 snRNA OS (PD88X X= 0.039) Liang et al.D89X X66D90X X 2015
miR-200c, miR-141
- Serum 74 serous: 16, endo-metrioid: 15,clear cell: 14,mucinous: 12,undifferentiated:17
RT-qPCR NR OS (miR-200c, P D91X X< 0.001)
Gao et al. D92X X74D93X X 2015
miR-625-3p,miR-720, miR-1274a
19 miRs including:miR-19b, miR-223, miR-16, miR-150, miR-20a,miR-126, miR-1290
Plasma 42 Serous RT-qPCR Presurgical sam-ples: miR-320,miR-720, miR-1274b, U6 snRNAAll other sam-ples: 14 miRNAs
OS (miR-1290,PD94X X= 0.004)
Shapira et al. D95X X72D96X X 2014
(continued on next page)
ARTICLE
INPRESS
Transla
tionalR
ese
arch
Volume00
Giannopoulouetal
9

Table
II.(Continued)
Over-
expressed
miRNAs
Under-expressed
miRNAs
Biological
specim
en
Ovarian
D67XXcancer
patie
nts
OvarianD68XXcancer
subtype
Detectio
ntechnology
ReferencemiRNA
Prognostic
significance
Reference
Year
miR-205
let-7f
Plasm
a360
serous:179,e
ndo-
metrioid:86,
adenocarci-
noma:47,
mucinous:33,
clearcell:15
RT-qPCR
NR
PFS
(let-7f,
PD97XX=0.006)
Zhengetal.D98XX67D99XX
2013
miR-21
-Se
rum
94
serous:68,other
subtypes:26
RT-qPCR
U6snRNA
OS(PD100XX=0.006)
Xuetal.D101XX63D102XX
2013
miR-221
-Se
rum
96
serous:70,other
subtypes:26
RT-qPCR
mmu-m
iR-295
OS(PD103XX=0.005)
Hongetal.D104XX60D105XX
2012
ARTICLE IN PRESSTranslational Research
10 Giannopoulou et al 2018
ovarian cancer by the over D370X Xexpression of miR-16,
miR-191, and miR-4284. The diagnostic value of these
combinations was evaluated using ROC curves. D371X X68 D372X XCir-
culating cfmiR-99a was found down D373X Xregulated both in
serum and primary tissue ovarian cancer samples,
using RT-qPCR and U6 snRNA as a reference. D374X X69 D375X XAyaz
et al. examined the expression of a large number of
plasma circulating cfmiRNAs in ovarian cancer
patients and reported an increase and a decrease on
the expression levels of 8 D376X X (miR-191-5p, miR-206,
miR-548a-3p, miR-320a, miR-574-3p, miR-590-5p,
miR-34c-5p, and miR-106b-5p) and 4 D377X X (miR-150-5p,
miR-645, miR-30a-5p, and miR-19a-3p) miRNAs,
respectively, when compared to healthy controls. D378X X70D379X X
In another study, circulating let-7i-5p, miR-122,
miR-152-5p, and miR-25-3p were significantly under-
D380X Xexpressed in ovarian cancer patients compared to
patients with benign serous cystadenomas. D381X X71 D382X XShapira et
al. investigated the expression of a large number of
plasma circulating cfmiRNAs and reported a decrease
in the expression levels of 19 circulating cfmiRNAs in
ovarian cancer patients when compared to healthy con-
trols and an increment in the expression levels of 3 D383X X
miRNAs (miR-625-3p, miR-720, and miR-1274a) in
patients’ plasma samples.D384X X72 D385X X Three miRNAs (miR-22,
miR-93, and miR-451) were significantly over D386X Xex-
pressed and one (miR-106b) was under D387X Xexpressed in
serum samples of ovarian cancer patients. D388X X73 D389X XAccording
to another study, circulating miR-200c and miR-141
were over D390X Xexpressed in ovarian cancer patients. D391X X74 D392X X
When TaqMan PCR miRNA assays and miR-484 as
a reference miRNA were used for the estimation of the
expression levels of specific circulating cfmiRNAs in a
larger cohort of ovarian cancer patients, 2 D393X X miRNAs
(miR-7 and miR-429) were found over D394X Xexpressed and 2 D395X X
(miR-25 and miR-93) under D396X Xexpressed. It is important
to mention that both over D397X Xexpressed miRNAs, miR-7,
and miR-429, are involved in the EMT process. D398X X75 D399X X
Two circulating cfmiRNAs were investigated as
diagnostic biomarkers in ovarian cancer, using RT-
qPCR and U6 snRNA as a reference D400X X. D401X X76, D402X X77 D403X XThe levels of
miR-199a were significantly decreased in ovarian can-
cer patients when compared to healthy women. D404X X76 D405X X
Inversely, miR-125b was significantly over D406X Xexpressed
in ovarian cancer patients and its levels were signifi-
cantly correlated with FIGO stage, lymph node and dis-
tant metastasis. D407X X77 D408X X According to another study,
circulating cfmiR-125b was over D409X Xexpressed in serum
samples of ovarian cancer patients when compared to
benign controls. D410X X78 D411X X
Circulating cfmiRNAs were also investigated in a
large group of ovarian cancer patients, patients with
benign disease and healthy women. D412X X79 D413X XTaqMan miRNA
assays were used for the quantification of selected

Table III. Clinical significance of circulating cell-free and exosomal miRNAs in ovarian cancerD106X X
miRNAs Expression Clinical significance References
miR-21 OverD107X Xexpressed Diagnostic, Prognostic D108X X
55,D109X X
62,D110X X
63,D111X X
68,D112X X
93D113X X
miR-200a, miR-200b, miR-200c OverD114X Xexpressed Diagnostic, Prognostic D115X X
57-59,D116X X
74,D117X X
79,D118X X
83,D119X X
92-94D120X X
miR-141 OverD121X Xexpressed Diagnostic, Prognostic D122X X
74,D123X X
92,D124X X
93D125X X
miR-125b OverD126X Xexpressed Diagnostic, Prognostic D127X X
77,D128X X
78D129X X
miR-429 OverD130X Xexpressed Diagnostic, Prognostic D131X X
75D132X X
miR-221 Over-expressed Diagnostic, Prognostic D133X X
60D134X X
miR-26a OverD135X Xexpressed Diagnostic D136X X
64,D137X X
83D138X X
miR-205 OverD139X Xexpressed Diagnostic D140X X
67,D141X X
93D142X X
miR-210 OverD143X Xexpressed Diagnostic D144X X
87D145X X
miR-7 OverD146X Xexpressed Diagnostic D147X X
75D148X X
miR-373 OverD149X Xexpressed Diagnostic D150X X
79,D151X X
94D152X X
miR-375 OverD153X Xexpressed Diagnostic D154X X
87D155X X
miR-92 OverD156X Xexpressed Diagnostic D157X X
55,D158X X
61D159X X
miR-1246 OverD160X Xexpressed Diagnostic D161X X
82D162X X
miR-1274a OverD163X Xexpressed Diagnostic D164X X
72,D165X X
92D166X X
miR-93 OverD167X Xexpressed Diagnostic D168X X
55,D169X X
73D170X X
UnderD171X Xexpressed D172X X
75D173X X
let-7f UnderD174X Xexpressed Diagnostic, Prognostic D175X X
67D176X X
miR-145 UnderD177X Xexpressed Diagnostic, Prognostic D178X X
66D179X X
miR-199a UnderD180X Xexpressed Diagnostic, Prognostic D181X X
76D182X X
miR-25 UnderD183X Xexpressed Diagnostic, Predictive D184X X
71,D185X X
75D186X X
miR-148a UnderD187X Xexpressed Diagnostic, Prognostic D188X X
80D189X X
miR-1290 UnderD190X Xexpressed Prognostic D191X X
72D192X X
ARTICLE IN PRESSTranslational ResearchVolume 00 Giannopoulou et al 11
miRNAs and miR-484 was used as a reference. The
expression of 4 D414X XmiRNAs (miR-373, miR-200a, miR-
200b, and miR-200c) was significantly increased in
ovarian cancer patients when compared to healthy con-
trols; three of them (miR-200a, miR-200b, and miR-
200c) were also significantly increased in ovarian can-
cer patients compared to patients with benign disease.
Elevated levels of miR-373 were observed in advanced
stage patients exclusively, whilst these of miR-200a,
miR-200b, and miR-200c were observed in both, early
and advanced stage ovarian cancer. D415X X79 D416X XGong et al. inves-
tigated the expression levels of miR-148a in plasma
and observed a significant under D417X Xexpression in ovarian
cancer when compared to healthy controls. D418X X80 D419X XCirculat-
ing miR-376a was up D420X Xregulated in serum and primary
tumor ovarian cancer samples when compared to
healthy donors. D421X X81 D422X X
In a cohort of 168 HGSC patients, a significant
increase of the expression levels of 3 D423X XmiRNAs namely
miR-1246, miR-595, and miR-2278 in patients’ serum
samples when compared to healthy controls was
reported. According to ROC curves, miR-1246 was the
best diagnostic biomarker in HGSC ovarian cancer
(AUC = 0.89). D424X X82 D425X XYokoi et al. also recruited 155 ovarian
cancer patients and used a combination of 8 D426X Xcirculating
cfmiRNAs to establish a new diagnostic model for
early detection (Table I).D427X X83 D428X XIn 2 D429X Xvery recent studies, cir-
culating miR-1181 and miR-4314 were significantly
elevated in ovarian cancer samples when compared to
healthy donors D430X X84 D431X X and miR-193a-5p was significantly
decreased in serum samples.D432X X85 D433X X
Elias et al. developed a neural network of circulating
cfmiRNAs for ovarian cancer early detection by recruit-
ing 168 ovarian cancer patients of diverse histology and
healthy controls and identified a network of 14 differen-
tially expressed miRNAs. The proposed miRNA neural
network had 100% specificity and a significantly better
specificity and sensitivity compared to CA-125.D434X X86D435X X
When the diagnostic value of circulating cfmiRNAs
in combination with CA-125 in HGSC patients was
investigated using RT-qPCR, a significant over D436X Xexpres-
sion of 4 D437X XmiRNAs (miR-375, miR-210, miR-150-5p,
and miR-181-5p) in 2 D438X Xcohorts of HGSC patients com-
pared to healthy controls was reported; notably, a com-
bination of circulating miR-375 and CA-125 proved to
have a better diagnostic value, according to ROC
curves (AUC = 0.956). D439X X87 D440X X
A study on the role of circulating cfmiRNAs in clear
cell ovarian cancer and especially in disease recurrence
based on real-time PCR revealed that 4 D441X XmiRNAs were
found elevated in pre D442X Xoperative serum samples when
compared to post D443X Xoperative samples; interestingly,
miR-130a levels were increased in early recurrent dis-
ease, suggesting a possible role on the detection of can-
cer progression. D444X X88 D445X X Circulating cfmiR-135a-3p was
under D446X Xexpressed in serum samples of ovarian cancer
patients when compared to patients with benign disease
or healthy controls. D447X X89 D448X X

ARTICLE IN PRESSTranslational Research
12 Giannopoulou et al 2018
A very recent study, wherein the role of miR-590-3p
in the development epithelial ovarian cancer was inves-
tigated, revealed a possible involvement since over D449X Xex-
pression of miR-590-3p was observed in both, tissues
and plasma samples of ovarian cancer patients, com-
pared to patients with benign gynecological diseases. D450X X90D451X X
Prognosis. In a large number of studies, over- or
under D452X Xexpression of specific circulating cfmiRNAs was
significantly correlated with shorter OS and/or PFS,
indicating a possible prognostic value (Table II). More
specifically, over D453X Xexpression of circulating miR-21, D454X X63 D455X X
miR-221,D456X X60 D457X X miR-141 D458X X74 D459X X and miR-429, D460X X75 D461X X and under D462X Xex-
pression of miR-200c, D463X X74 D464X XmiR-1290 D465X X72 D466X XmiR-145, D467X X66 D468X XmiR-
199a D469X X76 D470X X and miR-148a, D471X X80 D472X Xwere correlated with shorter
OS. Additionally, increased levels of miR-200b D473X X59] and
miR-125b, D474X X78 D475X Xand decreased levels of let-7f D476X X67 D477X Xand miR-
135a-3p D478X X89 D479X X were significantly associated with shorter
PFS.
Response to treatment. The role of circulating cfmiR-
NAs in predicting treatment response was first evalu-
ated in a phase II clinical trial (NCT00477386, www.
clinicaltrials.gov). D480X X91 D481X X Patients with recurrent and plati-
num-resistant ovarian cancer were treated with the
hypomethylating agent decitabine, followed by carbo-
platin. The expression levels of 78 circulating cfmiR-
NAs were measured before and after the first cycle of
treatment; the subgroups of responders and non D482X Xres-
ponders were characterized by a different profile of
miRNAs, as shown in Table II. Interestingly, when all
patients’ data were studied together, 3 D483X X circulating
cfmiRNAs namely miR-616, miR-532-3p, and miR-
148b-5p were significantly over D484X Xexpressed in respond-
ers, while under D485X Xexpression of miR-148b-5p was signif-
icantly correlated with worse PFS. D486X X91 D487X X
In another recent study, the addition of Bevacizumab
to standard chemotherapy was investigated in a large
group of ovarian cancer patients (n = 207); the
increased level of circulating miR-200c was associated
with worse PFS in the subgroup of patients who addi-
tionally received Bevacizumab. D488X X92 D489X X
CIRCULATING EXOSOMAL miRNAs
The first study on circulating exosomal miRNAs in
ovarian cancer was performed ten years ago. D490X X93 D491X XCircu-
lating exosomes were extracted from serum of patients
with serous ovarian cancer, patients with benign dis-
ease and healthy women, using an anti-EpCAM assay.
A large number of exosomal miRNAs was examined,
but only 8 D492X X (miR-21, miR-141, miR-200a, miR-200c,
miR-200b, miR-203, miR-205, and miR-214) were
found elevated both, in serum samples and paired pri-
mary tumors. These miRNAs were not detected in
healthy controls and patients with benign disease had a
significantly different profile compared to ovarian can-
cer patients, indicating a possible clinical value of
these circulating exosomal miRNAs in the early diag-
nosis of ovarian cancer.D493X X93 D494X X
In another study, circulating exosomal miRNAs
were also investigated in a large group of ovarian can-
cer patients, patients with benign disease and healthy
women. D495X X94D496X XSpecific miRNA TaqMan assays were used
for the quantification of selected miRNAs and miR-
484 was used as reference miRNA. Four miRNAs
namely miR-373, miR-200a, miR-200b, and miR-200c
had significantly over D497X Xexpressed in ovarian cancer
patients compared to healthy controls, with D498X X3 D499X Xof them
(miR-200a, miR-200b, and miR-200c) being signifi-
cantly increased in ovarian cancer patients compared
to patients with benign disease. The levels of exosomes
in total were also increased in ovarian cancer patients
compared to the other 2 D500X Xgroups. All these findings sug-
gest a diagnostic value of the above circulating exoso-
mal miRNAs. D501X X94 D502X X
Ying et al. studied the expression of miR-222-3p in
primary tumors and serum samples of patients with
epithelial ovarian cancer, as well as in ovarian cancer
cell lines and reported a significant up D503X Xregulation of cir-
culating exosomal miR-222-3p in serum samples when
compared to healthy controls. They also report an over-
D504X Xexpression of miR-222-3p in exosomes derived from
ovarian cancer cells and macrophages; their subsequent
experiments suggested a possible role of miR-222-3p
in the polarization of tumor-associated macrophages. D505X X95 D506X X
In another study, a number of circulating miRNAs was
evaluated in exosomes isolated from serum and in
paired tissue samples of ovarian cancer patients, using
RT-qPCR and U6 snRNA as reference; only circulat-
ing exosomal miR-101 was significantly under D507X Xex-
pressed in serum exosomes compared to healthy
controls. D508X X96 D509X X
So far, only one study suggested a prognostic value
of circulating exosomal miRNAs in ovarian cancer; the
elevated levels of both, miR-200b and miR-200c, were
significantly associated with worse OS. Interestingly,
the increased levels of miR-200b and miR-200c also
significantly correlated with CA-125 levels. D510X X94 D511X X
CONCLUSIONS
Despite the increasing number of research and clini-
cal studies, ovarian cancer still has very low survival
rates among all gynecological malignancies. D512X X1 D513X X This
could be attributed to the lack of effective tumor bio-
markers; especially to the absence of an FDA-cleared
biomarker for the early detection of this disease. CA-
125 and HE4 are FDA-approved predictive biomarkers
that are also used for the detection of recurrent disease

ARTICLE IN PRESSTranslational ResearchVolume 00 Giannopoulou et al 13
after the completion of first-line treatment. D514X X97 D515X X In addi-
tion to the CA-125 and HE4 tumor biomarkers, a num-
ber of supplementary algorithms are also developed;
the risk of ovarian malignancy algorithm D516X X is FDA-
approved and combines the levels of CA-125 and HE4
with menopausal status to generate a score that indi-
cates the likelihood of malignancy in adnexal mass
patients. D517X X98 D518X X However, none of these were appropriate
for early diagnosis of the disease and, most impor-
tantly, for population screening.
The clinical significance of CTCs and ctDNA has
been investigated in many types of cancer, D519X X99 D520X X including
ovarian cancer. However, no standard methods are
used for the isolation and detection in the bloodstream
and only a few studies recruited large cohorts of ovar-
ian cancer patients.
Circulating cfmiRNAs and circulating exosomes can
serve as tumor biomarkers with the potential of provid-
ing information on early diagnosis, prognosis, response
to therapy and development of chemo D521X Xresistance. In
ovarian cancer, a large number of studies revealed the
diagnostic and prognostic potential of circulating
cfmiRNAs and exosomes; additional studies that will
be focused on their role in predicting response to treat-
ment and chemo D522X Xresistance development would be of
great interest.
Liquid biopsy approaches are minimally invasive
and allow for easily tolerated serial measurements dur-
ing treatment. However, there is a lot to be done in
terms of pre D523X Xanalytical and post D524X Xanalytical conditions,
quality control, and validation of the assays used for
circulating cfmiRNAs and exosomes isolation, detec-
tion, and characterization, before their implementation
in clinical practice. In conclusion, circulating cfmiR-
NAs and exosomes constitute a main component of liq-
uid biopsy analysis, with the potential of contributing
to the development and establishment of personalized
medicine protocols in ovarian cancer patients.
ACKOWLEDGMENTS
All authors have read the journal’s policy on disclo-
sure of potential conflicts of interest and have declared
no conflicts of interest. All authors have read the jour-
nal’s authorship agreement and declare that the manu-
script has been reviewed and approved by all named
authors.
REFERENCES
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Can-
cer J Clin 2017;67:7–30.
2. Cancer Genome Atlas Research Network. Integrated genomic
analyses of ovarian carcinoma. Nature 2011;474:609–15.
3. Patch AM, Christie EL, Etemadmoghadam D, et al. Whole-
genome characterization of chemoresistant ovarian cancer.
Nature 2015;521:489–94.
4. Du Bois A, Pfisterer J. Future options for first-line therapy of
advanced ovarian cancer. Int J Gynecol Cancer 2005;15(Suppl
1):42–50.
5. Burger RA, Brady MF, Bookman MA, et al. Incorporation of
bevacizumab in the primary treatment of ovarian cancer. N Engl
J Med 2011;365:2473–83.
6. Ledermann J, Harter P, Gourley C, et al. Olaparib maintenance
therapy in patients with platinum-sensitive relapsed serous ovar-
ian cancer: a preplanned retrospective analysis of outcomes by
BRCA status in a randomised phase 2 trial. Lancet Oncol
2014;15:852–61.
7. Pradeep S, Kim SW, Wu SY, et al. Hematogenous metastasis of
ovarian cancer: rethinking mode of spread. Cancer Cell
2014;26:77–91.
8. Yeung TL, Leung CS, Yip KP, Au Yeung CL, Wong ST, Mok
SC. Cellular and molecular processes in ovarian cancer metasta-
sis. a review in the theme: cell and molecular processes in cancer
metastasis. Am J Physiol Cell Physiol 2015;309:444–56.
9. Prat J. Staging classification for cancer of the ovary, fallopian
tube, and peritoneum. Int J Gynaecol Obstet 2014;124:1–5.
10. Cohen JD, Li L, Wang Y, et al. Detection and localization of sur-
gically resectable cancers with a multi-analyte blood test. Sci-
ence 2018;359:926–30.
11. Lianidou E, Hoon D. Circulating Tumor Cells and circulating
Tumor DNA. In: Rifai Nader, Horvath Andea Rita,
Wittwer Carl, eds. Tietz Textbook of Clinical Chemistry and
Molecular Diagnostics, Sixth Edition, Elsevier, 2017:1111–44.
12. Alix-Panabieres C, Pantel K. Clinical applications of circulating
tumor cells and circulating tumor DNA as liquid biopsy. Cancer
Discov 2016;6:479–91.
13. Panagiotara A, Markou A, Lianidou ES, Patrinos GP, Katsila T.
Exosomes: a cancer theranostics road map. Public Health Geno-
mics 2017;20:116–25.
14. Schwarzenbach H, Nishida N, Calin GA, Pantel K. Clinical rele-
vance of circulating cell-free microRNAs in cancer. Nat Rev
Clin Oncol 2014;11:145–56.
15. Mader S, Pantel K. Liquid biopsy: current status and future per-
spectives. Oncol Res Treat 2017;40:404–8.
16. Cheng X, Zhang L, Chen Y, Qing C. Circulating cell-free DNA
and circulating tumor cells, the “liquid biopsies” in ovarian can-
cer. J Ovarian Res 2017;10:75.
17. Gasparri ML, Savone D, Besharat RA, et al. Circulating tumor
cells as trigger to hematogenous spreads and potential bio-
markers to predict the prognosis in ovarian cancer. Tumour Biol
2016;37:71–5.
18. Giannopoulou L, Kasimir-Bauer S, Lianidou ES. Liquid biopsy
in ovarian cancer: recent advances on circulating tumor cells and
circulating tumor DNA. Clin Chem Lab Med 2018;56:186–97.
19. Romero-Laorden N, Olmos D, Fehm T, Garcia-Donas J, Diaz-
Padilla I. Circulating and disseminated tumor cells in ovarian
cancer: a systematic review. Gynecol Oncol 2014;133:632–9.
20. Van Berckelaer C, Brouwers AJ, Peeters DJ, Tjalma W, Trinh
XB, van Dam PA. Current and future role of circulating tumor
cells in patients with epithelial ovarian cancer. Eur J Surg Oncol
2016;42:1772–9.
21. Zhou Q, Li W, Leng B, et al. Circulating Cell Free DNA as the
Diagnostic Marker for Ovarian Cancer: A Systematic Review
and Meta-Analysis. PLoS One 2016;11:e0155495.
22. Anfossi S, Babayan A, Pantel K, Calin GA. Clinical utility of cir-
culating non-coding RNAs - an update. Nat Rev Clin Oncol
2018;15:541–63.
ARTICLE IN PRESSTranslational Research
14 Giannopoulou et al 2018
23. Fabbri M. MicroRNAs and miRceptors: a new mechanism of
action for intercellular communication. Philos Trans R Soc Lond
B Biol Sci 2018;373:1737.
24. Kalluri R. The biology and function of exosomes in cancer. J
Clin Invest 2016;126:1208–15.
25. Keup C, Mach P, Aktas B, et al. RNA Profiles of Circulating
Tumor Cells and Extracellular Vesicles for Therapy Stratifica-
tion of Metastatic Breast Cancer Patients. Clin Chem
2018;64:1054–62.
26. Li X, Wang X. The emerging roles and therapeutic potential of
exosomes in epithelial ovarian cancer. Mol Cancer 2017;16:92.
27. Dorayappan KDP, Wallbillich JJ, Cohn DE, Selvendiran K. The
biological significance and clinical applications of exosomes in
ovarian cancer. Gynecol Oncol 2016;142:199–205.
28. Nawaz M, Fatima F, Nazarenko I, et al. Extracellular vesicles in
ovarian cancer: applications to tumor biology, immunotherapy
and biomarker discovery. Expert Rev Proteomics 2016;13:395–
409.
29. Kolostova K, Matkowski R, Jedryka M, et al. The added value of
circulating tumor cells examination in ovarian cancer staging.
Am J Cancer Res 2015;5:3363–75.
30. Lee M, Kim EJ, Cho Y, et al. Predictive value of circulating
tumor cells (CTCs) captured by microfluidic device in patients
with epithelial ovarian cancer. Gynecol Oncol 2017;145:361–5.
31. Obermayr E, Maritschnegg E, Agreiter C, et al. Efficient leuko-
cyte depletion by a novel microfluidic platform enables the
molecular detection and characterization of circulating tumor
cells. Oncotarget 2017;9:812–23.
32. Chebouti I, Kasimir-Bauer S, Buderath P, et al. EMT-like circu-
lating tumor cells in ovarian cancer patients are enriched by plat-
inum-based chemotherapy. Oncotarget 2017;8:48820–31.
33. Obermayr E, Bednarz-Knoll N, Orsetti B, et al. Circulating
tumor cells: potential markers of minimal residual disease in
ovarian cancer? A study of the OVCAD consortium. Oncotarget
2017;8:106415–28.
34. Gostner JM, Obermayr E, Braicu IE, et al. Immunobiochemical
pathways of neopterin formation and tryptophan breakdown via
indoleamine 2,3-dioxygenase correlate with circulating tumor
cells in ovarian cancer patients- A study of the OVCAD consor-
tium. Gynecol Oncol 2018;149:371–80.
35. Obermayr E, Castillo-Tong DC, Pils D, et al. Molecular charac-
terization of circulating tumor cells in patients with ovarian can-
cer improves their prognostic significance � a study of the
OVCAD consortium. Gynecol Oncol 2013;128:15–21.
36. Guo YX, Neoh KH, Chang XH, et al. Diagnostic value of HE4+
circulating tumor cells in patients with suspicious ovarian can-
cer. Oncotarget 2018;9:7522–33.
37. Pearl ML, Dong H, Tulley S, et al. Treatment monitoring of
patients with epithelial ovarian cancer using invasive circulating
tumor cells (iCTCs). Gynecol Oncol 2015;137:229–38.
38. Merker JD, Oxnard GR, Compton C, et al. Circulating tumor
DNA analysis in patients with cancer: American Society of Clin-
ical Oncology and College of American Pathologists joint
review. J Clin Oncol 2018;36:1631–41.
39. Zhang R, Pu W, Zhang S, et al. Clinical value of ALU concentra-
tion and integrity index for the early diagnosis of ovarian cancer:
a retrospective cohort trial. PLoS One 2018;13:e0191756.
40. Widschwendter M, Zikan M, Wahl B, et al. The potential of cir-
culating tumor DNA methylation analysis for the early detection
and management of ovarian cancer. Genome Med 2017;9:116.
41. Giannopoulou L, Mastoraki S, Buderath P, et al. ESR1 methyla-
tion in primary tumors and paired circulating tumor DNA of
patients with high-grade serous ovarian cancer. Gynecol Oncol
2018;150:355–60.
42. Park YR, KimYM, Lee SW, et al. Optimization to detect TP53muta-
tions in circulating cell-free tumor DNA from patients with serous
epithelial ovarian cancer. Obstet Gynecol Sci 2018;61:328–36.
43. Parkinson CA, Gale D, Piskorz AM, et al. Exploratory analysis of
TP53 mutations in circulating tumour DNA as biomarkers of treat-
ment response for patients with relapsed high-grade serous ovarian
carcinoma: a retrospective study. PLoSMed 2016;13:e1002198.
44. Christie EL, Fereday S, Doig K, Pattnaik S, Dawson SJ, Bowtell
DDL. Reversion of BRCA1/2 Germline Mutations Detected in
Circulating Tumor DNA From Patients With High-Grade Serous
Ovarian Cancer. J Clin Oncol 2017;35:1274–80.
45. Weigelt B, Comino-Mendez I, de Bruijn I, et al. Diverse BRCA1 and
BRCA2 reversion mutations in circulating cell-free DNA of therapy-
resistant breast or ovarian cancer. Clin Cancer Res 2017;23:6708–20.
46. Ratajska M, Koczkowska M, Zuk M, et al. Detection of BRCA1/2
mutations in circulating tumor DNA from patients with ovarian
cancer. Oncotarget 2017;8:101325–32.
47. Arend RC, Londono AI, Montgomery AM, et al. Molecular
Response to Neoadjuvant Chemotherapy in High-Grade Serous
Ovarian Carcinoma. Mol Cancer Res 2018;16:813–24.
48. Du ZH, Bi FF, Wang L, Yang Q. Next-generation sequencing unrav-
els extensive genetic alteration in recurrent ovarian cancer and unique
genetic changes in drug-resistant recurrent ovarian cancer. Mol Genet
Genomic Med 2018;6:638–47, May 24 [Epub ahead of print] .
49. Phallen J, Sausen M, Adleff V, et al. Direct detection of early-
stage cancers using circulating tumor DNA. Sci Transl Med
2017;9:1–12, pii: eaan2415.
50. Nakamura K, Sawada K, Yoshimura A, Kinose Y, Nakatsuka E,
Kimura T. Clinical relevance of circulating cell-free microRNAs
in ovarian cancer. Mol Cancer 2016;15:48.
51. Zheng H, Liu JY, Song FJ, Chen KX. Advances in circulating
microRNAs as diagnostic and prognostic markers for ovarian
cancer. Cancer Biol Med 2013;10:123.
52. Zhou Q, Zuo MZ, He Z, Li HR, Li W. Identification of circulat-
ing microRNAs as diagnostic biomarkers for ovarian cancer: a
pooled analysis of individual studies. Int J Biol Markers 2018:
1–10, Apr 1:1724600818766500.
53. Wang H, Wang T, Shi W, Liu Y, Chen L, Li Z. Comprehensive
analysis on diagnostic value of circulating miRNAs for patients
with ovarian cancer. Oncotarget 2017;8:66620–8.
54. Kuhlmann JD, Baraniskin A, Hahn SA, et al. Circulating U2 small
nuclear RNA fragments as a novel diagnostic tool for patients with
epithelial ovarian cancer. Clin Chem 2014;60:206–13.
55. Resnick KE, Alder H, Hagan JP, Richardson DL, Croce CM,
Cohn DE. The detection of differentially expressed microRNAs
from the serum of ovarian cancer patients using a novel real-
time PCR platform. Gynecol Oncol 2009;112:55–9.
56. Hausler SF, Keller A, Chandran PA, et al. Whole blood-derived
miRNA profiles as potential new tools for ovarian cancer screen-
ing. Br J Cancer 2010;103:693–700.
57. Kan CW, Hahn MA, Gard GB, et al. Elevated levels of circulat-
ing microRNA-200 family members correlate with serous epi-
thelial ovarian cancer. BMC Cancer 2012;12:627.
58. Zuberi M, Mir R, Das J, et al. Expression of serum miR-200a,
miR-200b, and miR-200c as candidate biomarkers in epithelial
ovarian cancer and their association with clinicopathological fea-
tures. Clin Transl Oncol 2015;17:779–87.
59. Kapetanakis NI, Uzan C, Jimenez-Pailhes AS, et al. Plasma miR-
200b in ovarian carcinoma patients: distinct pattern of pre/post-treat-
ment variation compared to CA-125 and potential for prediction of
progression-free survival. Oncotarget 2015;6:36815–24.
60. Hong F, Li Y, Xu Y, Zhu L. Prognostic significance of serum
microRNA-221 expression in human epithelial ovarian cancer. J
Int Med Res 2013;41:64–71.

ARTICLE IN PRESSTranslational ResearchVolume 00 Giannopoulou et al 15
61. Guo F, Tian J, Lin Y, Jin Y, Wang L, Cui M. Serum microRNA-
92 expression in patients with ovarian epithelial carcinoma. J Int
Med Res 2013;41:1456–61.
62. Mahmoud EH, Fawzy A, RA AE. Serum MicroRNA-21 nega-
tively relates to expression of programmed cell death-4 in
patients with epithelial ovarian cancer. Asian Pac J Cancer Prev
2018;19:33–8.
63. Xu YZ, Xi QH, Ge WL, Zhang XQ. Identification of serum
microRNA-21 as a biomarker for early detection and prognosis
in human epithelial ovarian cancer. Asian Pac J Cancer Prev
2013;14:1057–60.
64. Shen W, Song M, Liu J, et al. MiR-26a promotes ovarian cancer
proliferation and tumorigenesis. PLoS One 2014;9:e86871.
65. Wu H, Xiao Z, Wang K, Liu W, Hao Q. MiR-145 is downregu-
lated in human ovarian cancer and modulates cell growth and
invasion by targeting p70S6K1 and MUC1. Biochem Biophys
Res Commun 2013;441:693–700.
66. Liang H, Jiang Z, Xie G, Lu Y. Serum microRNA-145 as a novel
biomarker in human ovarian cancer. Tumour Biol
2015;36:5305–13.
67. Zheng H, Zhang L, Zhao Y, et al. Plasma miRNAs as diagnostic
and prognostic biomarkers for ovarian cancer. PLoS One
2013;8:e77853.
68. Suryawanshi S, Vlad AM, Lin HM, et al. Plasma microRNAs as
novel biomarkers for endometriosis and endometriosis-associ-
ated ovarian cancer. Clin Cancer Res 2013;19:1213–24.
69. Jiang H, Qu L, Wang Y, Cong J, Wang W, Yang X. miR-99a
promotes proliferation targeting FGFR3 in human epithelial
ovarian cancer cells. Biomed Pharmacother 2014;68:163–9.
70. Ayaz L, Cayan F, Balci S, et al. Circulating microRNA expression
profiles in ovarian cancer. J Obstet Gynaecol 2014;34:620–4.
71. Langhe R, Norris L, Saadeh FA, et al. A novel serum microRNA
panel to discriminate benign from malignant ovarian disease.
Cancer Lett 2015;356:628–36.
72. Shapira I, Oswald M, Lovecchio J, et al. Circulating biomarkers
for detection of ovarian cancer and predicting cancer outcomes.
Br J Cancer 2014;110:976–83.
73. Ji T, Zheng ZG, Wang FM, et al. Differential microRNA expres-
sion by Solexa sequencing in the sera of ovarian cancer patients.
Asian Pac J Cancer Prev 2014;15:1739–43.
74. Gao YC, Wu J. MicroRNA-200c and microRNA-141 as poten-
tial diagnostic and prognostic biomarkers for ovarian cancer.
Tumour Biol 2015;36:4843–50.
75. Meng X, Joosse SA, Muller V, et al. Diagnostic and prognostic
potential of serum miR-7, miR-16, miR-25, miR-93, miR-182,
miR-376a and miR-429 in ovarian cancer patients. Br J Cancer
2015;113:1358–66.
76. Zuberi M, Khan I, Gandhi G, Ray PC, Saxena A. The conglomera-
tion of diagnostic, prognostic and therapeutic potential of serummiR-
199a and its association with clinicopathological features in epithelial
ovarian cancer. Tumour Biol 2016;37:11259–66.
77. Zuberi M, Khan I, Mir R, Gandhi G, Ray PC, Saxena A. Utility
of serum miR-125b as a diagnostic and prognostic indicator and
its alliance with a panel of tumor suppressor genes in epithelial
ovarian cancer. PLoS One 2016;11:e0153902.
78. Zhu T, Gao W, Chen X, et al. A pilot study of circulating micro-
RNA-125b as a diagnostic and prognostic biomarker for epithe-
lial ovarian cancer. Int J Gynecol Cancer 2017;27:3–10.
79. Meng X, Muller V, Milde-Langosch K, Trillsch F, Pantel K,
Schwarzenbach H. Circulating cell-free miR-373, miR-200a,
miR-200b and miR-200c in patients with epithelial ovarian can-
cer. Adv Exp Med Biol 2016;924:3–8.
80. Gong L, Wang C, Gao Y, Wang J. Decreased expression of
microRNA-148a predicts poor prognosis in ovarian cancer and
associates with tumor growth and metastasis. Biomed Pharmac-
other 2016;83:58–63.
81. Yang L, Wei QM, Zhang XW, Sheng Q, Yan XT. MiR-376a pro-
motion of proliferation and metastases in ovarian cancer: poten-
tial role as a biomarker. Life Sci 2017;173:62–7.
82. Todeschini P, Salviato E, Paracchini L, et al. Circulating miRNA
landscape identifies miR-1246 as promising diagnostic bio-
marker in high-grade serous ovarian carcinoma: a validation
across two independent cohorts. Cancer Lett 2016;388:320–7.
83. Yokoi A, Yoshioka Y, Hirakawa A, et al. A combination of cir-
culating miRNAs for the early detection of ovarian cancer.
Oncotarget 2017;8:89811–23.
84. Ruan L, Xie Y, Liu F, Chen X. Serum miR-1181 and miR-4314
associated with ovarian cancer: MiRNA microarray data analysis
for a pilot study. Eur J Obstet Gynecol Reprod Biol
2018;222:31–8.
85. ren x, zhang h, cong h, et al. Diagnostic model of serum miR-
193a-5p, HE4 and CA125 improves the diagnostic efficacy of
epithelium ovarian cancer. Pathol Oncol Res 2018;24:739–44.
86. Elias KM, Fendler W, Stawiski K, et al. Diagnostic potential for
a serum miRNA neural network for detection of ovarian cancer.
Elife 2017;6:pii: e28932.
87. Shah JS, Gard GB, Yang J, et al. Combining serum microRNA
and CA-125 as prognostic indicators of preoperative surgical
outcome in women with high-grade serous ovarian cancer. Gyne-
col Oncol 2018;148:181–8.
88. Chao A, Lai CH, Chen HC, et al. SerummicroRNAs in clear cell car-
cinoma of the ovary. Taiwan J Obstet Gynecol 2014;53:536–41.
89. Fukagawa S, Miyata K, Yotsumoto F, et al. MicroRNA-135a-3p
as a promising biomarker and nucleic acid therapeutic agent for
ovarian cancer. Cancer Sci 2017;108:886–96.
90. Salem M, O’Brien JA, Bernaudo S, et al. miRNA-590-3p pro-
motes ovarian cancer growth and metastasis via a novel FOXA2-
versican pathway. Cancer Res 2018;78:4175–90.
91. Benson EA, Skaar TC, Liu Y, Nephew KP, Matei D. Carboplatin
with decitabine therapy, in recurrent platinum resistant ovarian
cancer, alters circulating mirnas concentrations: a pilot study.
PLoS One 2015;10:e0141279.
92. Halvorsen AR, Kristensen G, Embleton A, et al. Evaluation of
prognostic and predictive significance of circulating micrornas
in ovarian cancer patients. Dis Markers 2017;2017:3098542.
93. Taylor DD, Gercel-Taylor C. MicroRNA signatures of tumor-
derived exosomes as diagnostic biomarkers of ovarian cancer.
Gynecol Oncol 2008;110:13–21.
94. Meng X, Muller V, Milde-Langosch K, Trillsch F, Pantel K,
Schwarzenbach H. Diagnostic and prognostic relevance of circu-
lating exosomal miR-373, miR-200a, miR-200b and miR-200c
in patients with epithelial ovarian cancer. Oncotarget
2016;7:16923–35.
95. Ying X, Wu Q, Wu X, et al. Epithelial ovarian cancer-secreted
exosomal miR-222-3p induces polarization of tumor-associated
macrophages. Oncotarget 2016;7:43076–87.
96. Xu Y, Xu L, Zheng J, Geng L, Zhao S. MiR-101 inhibits ovarian
carcinogenesis by repressing the expression of brain-derived
neurotrophic factor. FEBS Open Bio 2017;7:1258–66.
97. Bottoni P, Scatena R. The role of CA 125 as tumor marker: bio-
chemical and clinical aspects. Adv Exp Med Biol
2015;867:229–44.
98. Leung F, Diamandis EP, Kulasingam V. Ovarian cancer bio-
markers: current state and future implications from high-
throughput technologies. Adv Clin Chem 2014;66:25–77.
99. Ignatiadis M, Lee M, Jeffrey SS. Circulating tumor cells and cir-
culating tumor DNA: challenges and opportunities on the path to
clinical utility. Clin Cancer Res 2015;21:4786–800.
Related Documents











