ORIGINAL CONTRIBUTION Leukocyte-Reduced Red Blood Cell Transfusions in Patients With Anemia and Human Immunodeficiency Virus Infection The Viral Activation Transfusion Study: A Randomized Controlled Trial Ann C. Collier, MD Leslie A. Kalish, ScD Michael P. Busch, MD, PhD Terry Gernsheimer, MD Susan F. Assmann, PhD Thomas A. Lane, MD David M. Asmuth, MD Michael M. Lederman, MD Edward L. Murphy, MD, MPH Princy Kumar, MD Meera Kelley, MD Timothy P. Flanigan, MD Deborah K. McMahon, MD Henry S. Sacks, MD, PhD Melanie S. Kennedy, MD Paul V. Holland, MD for the Viral Activation Transfusion Study Group A DVANCES IN ANTIRETROVIRAL treatment have markedly im- proved prognosis of persons infected with human immu- nodeficiency virus (HIV). 1-4 However, ac- quired immunodeficiency syndrome (AIDS) continues to occur since antiret- roviral therapy is not always tolerated, successful, or available and persons may be unaware of their infection until late clinical manifestations occur. One complication of advanced HIV in- fection is anemia, which may be caused by HIV, opportunistic diseases, and medications. 5-9 An estimated 21% to 58% of HIV patients are anemic, with increas- ing frequency in advanced HIV. 5-8,10 Anemia is associated with shorter sur- vival. 5-7,11 Management of anemia in- cludes stopping marrow-suppressive medications, use of erythropoietin, and Author Affiliations and other participating members of the Viral Activation Transfusion Study Group are listed at the end of this article. Corresponding Author and Reprints: Ann C. Collier, MD, Harborview Medical Center, 325 Ninth Ave, Box 359929, Seattle, WA 98104 (e-mail: acollier@u .washington.edu). Context Allogeneic blood transfusions have immunomodulatory effects and have been associated with activation of human immunodeficiency virus (HIV) and cyto- megalovirus (CMV) in vitro and of HIV in small pilot studies. Retrospective studies sug- gest that transfusions adversely affect the clinical course of HIV. Data in selected non– HIV-infected patients requiring blood transfusion have suggested clinical benefit with leukocyte-reduced red blood cells (RBCs). Objective To compare the effects of leukoreduced and unmodified RBC transfusions on survival, complications of acquired immunodeficiency syndrome, and relevant labo- ratory markers in HIV-infected patients. Design and Setting Double-blind randomized controlled trial conducted in 11 US academic medical centers from July 1995 through June 1999, with a median follow-up of 12 months (24 months in survivors). Patients A total of 531 persons infected with HIV and CMV, aged 14 years or older, who required transfusions for anemia; 259 received leukoreduced transfusions and 262 received unmodified transfusions (10 did not receive the planned transfusion). Main Outcome Measures Survival and change in plasma HIV RNA level 7 days af- ter transfusion, compared by type of transfusion. Results At entry, the groups were similar in demographic, clinical, and relevant labo- ratory characteristics. A total of 3864 RBC units were transfused. Two hundred eighty- nine deaths occurred (151 with leukoreduced transfusion; 138 with unmodified trans- fusion); median survival was 13.0 and 20.5 months, respectively (relative hazard [RH], 1.20; 95% confidence interval [CI], 0.95-1.51; log-rank P = .12). Analyses adjusted for prognostic factors suggested possible worse survival with leukoreduction (RH, 1.35; 95% CI, 1.06-1.72). There was no difference in time to new opportunistic event/death or fre- quency of transfusion reactions. No changes in plasma HIV RNA level were seen in either group at days 7, 14, 21, or 28, even in patients not taking antiretroviral drugs. There were no differences in trends between groups in CMV DNA, CD4 cell counts, activated (CD38% or human leukocyte antigen-DR) CD8 cell counts, or plasma cytokine levels. Conclusions We found no evidence of HIV, CMV, or cytokine activation following blood transfusion in patients with advanced HIV infection. Leukoreduction provided no clinical benefit in these patients. These data demonstrate the importance of conducting controlled studies of effects of leukoreduction in different patient populations, since smaller studies in other patient populations have suggested leukoreduction may be beneficial. JAMA. 2001;285:1592-1601 www.jama.com 1592 JAMA, March 28, 2001—Vol 285, No. 12 (Reprinted) ©2001 American Medical Association. All rights reserved. Downloaded From: http://jama.jamanetwork.com/ by a UCSF LIBRARY User on 05/27/2015

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ORIGINAL CONTRIBUTION
Leukocyte-Reduced Red Blood CellTransfusions in Patients With Anemia andHuman Immunodeficiency Virus InfectionThe Viral Activation Transfusion Study:A Randomized Controlled TrialAnn C. Collier, MDLeslie A. Kalish, ScDMichael P. Busch, MD, PhDTerry Gernsheimer, MDSusan F. Assmann, PhDThomas A. Lane, MDDavid M. Asmuth, MDMichael M. Lederman, MDEdward L. Murphy, MD, MPHPrincy Kumar, MDMeera Kelley, MDTimothy P. Flanigan, MDDeborah K. McMahon, MDHenry S. Sacks, MD, PhDMelanie S. Kennedy, MDPaul V. Holland, MDfor the Viral Activation TransfusionStudy Group
ADVANCES IN ANTIRETROVIRAL
treatment have markedly im-proved prognosis of personsinfected with human immu-
nodeficiency virus (HIV).1-4 However, ac-quired immunodeficiency syndrome(AIDS) continues to occur since antiret-roviral therapy is not always tolerated,successful, or available and persons maybe unaware of their infection until lateclinical manifestations occur.
One complication of advanced HIV in-fection is anemia, which may be causedby HIV, opportunistic diseases, andmedications.5-9 An estimated 21% to 58%of HIV patients are anemic, with increas-
ing frequency in advanced HIV.5-8,10
Anemia is associated with shorter sur-vival.5-7,11 Management of anemia in-cludes stopping marrow-suppressivemedications, use of erythropoietin, and
Author Affiliations and other participating membersof the Viral Activation Transfusion Study Group arelisted at the end of this article.Corresponding Author and Reprints: Ann C. Collier,MD, Harborview Medical Center, 325 Ninth Ave, Box359929, Seattle, WA 98104 (e-mail: [email protected]).
Context Allogeneic blood transfusions have immunomodulatory effects and havebeen associated with activation of human immunodeficiency virus (HIV) and cyto-megalovirus (CMV) in vitro and of HIV in small pilot studies. Retrospective studies sug-gest that transfusions adversely affect the clinical course of HIV. Data in selected non–HIV-infected patients requiring blood transfusion have suggested clinical benefit withleukocyte-reduced red blood cells (RBCs).
Objective To compare the effects of leukoreduced and unmodified RBC transfusionson survival, complications of acquired immunodeficiency syndrome, and relevant labo-ratory markers in HIV-infected patients.
Design and Setting Double-blind randomized controlled trial conducted in 11 USacademic medical centers from July 1995 through June 1999, with a median follow-upof 12 months (24 months in survivors).
Patients A total of 531 persons infected with HIV and CMV, aged 14 years or older,who required transfusions for anemia; 259 received leukoreduced transfusions and 262received unmodified transfusions (10 did not receive the planned transfusion).
Main Outcome Measures Survival and change in plasma HIV RNA level 7 days af-ter transfusion, compared by type of transfusion.
Results At entry, the groups were similar in demographic, clinical, and relevant labo-ratory characteristics. A total of 3864 RBC units were transfused. Two hundred eighty-nine deaths occurred (151 with leukoreduced transfusion; 138 with unmodified trans-fusion); median survival was 13.0 and 20.5 months, respectively (relative hazard [RH],1.20; 95% confidence interval [CI], 0.95-1.51; log-rank P=.12). Analyses adjusted forprognostic factors suggested possible worse survival with leukoreduction (RH, 1.35; 95%CI, 1.06-1.72). There was no difference in time to new opportunistic event/death or fre-quency of transfusion reactions. No changes in plasma HIV RNA level were seen in eithergroup at days 7, 14, 21, or 28, even in patients not taking antiretroviral drugs. There wereno differences in trends between groups in CMV DNA, CD4 cell counts, activated (CD38%or human leukocyte antigen-DR) CD8 cell counts, or plasma cytokine levels.
Conclusions We found no evidence of HIV, CMV, or cytokine activation followingblood transfusion in patients with advanced HIV infection. Leukoreduction provided noclinical benefit in these patients. These data demonstrate the importance of conductingcontrolled studies of effects of leukoreduction in different patient populations, since smallerstudies in other patient populations have suggested leukoreduction may be beneficial.JAMA. 2001;285:1592-1601 www.jama.com
1592 JAMA, March 28, 2001—Vol 285, No. 12 (Reprinted) ©2001 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a UCSF LIBRARY User on 05/27/2015

red blood cell (RBC) transfusion.8,12-14 Asurvey of transfusion practices in pa-tients with HIV infection showed thatone third of responding centers used leu-kocyte-reduced (hereafter called leuko-reduced) blood products routinely andnearly 30% used irradiated blood.14
Leukoreduced blood products are madeby passing the blood component (eg,RBCs, platelets) through a filter that trapsleukocytes. Retrospective studies havesuggested that RBC transfusion has anadverse effect on the course of HIV in-fection, may be associated with cyto-megalovirus (CMV) disease, and mayshorten survival.15,16
Immunomodulatory effects have beenassociated with transfusion of alloge-neic RBCs. Allogeneic RBC transfusionmay result in alloimmunization andmore frequent tumor recurrences.17-21
However, transfusion also may in-crease transplant survival, suppress in-flammatory disease, and prevent recur-rent abortion.22-27 Data are conflictingabout the impact of transfusion on post-operative infections.28-31 Removing leu-kocytes from RBC units may lessen theseeffects, suggesting they are mediated byantigenic stimulation from leukocytescontained in RBC units.32-38
For selected patients, use of leukore-duced blood components has beenshown in controlled studies to de-crease certain complications of transfu-sion, including febrile transfusion reac-tions and human leukocyte antigenalloimmunization.39 There are conflict-ing data about its potential benefits inother patient populations, and no pro-spective data on HIV-infected patients.Currently in the United States, discus-sion is ongoing about adopting a policyof universal leukoreduction.39-41
Allogeneic leukocytes, but not eryth-rocytes or platelets, have been shown toreactivate HIV in vitro.42 In addition, al-logeneic leukocytes may activate latentviruses, including CMV in vitro, as dotransfusions in animal models.43-45 Dataabout this topic were recently re-viewed.46 Pilot studies in HIV-infectedpersons showed modest increases in HIVp24 antigen and HIV RNA levels afterRBC transfusion.47,48 We hypothesized
that RBC transfusions containing leu-kocytes would result in immune and vi-ral activation, and adversely affect thecourse of HIV disease. The data from thisstudy are unique since this is one of thelargest randomized studies of leukore-duction, and the only large-scale pro-spective study of blood transfusions inHIV-infected persons.
METHODSStudy Design and Treatment
The study was a randomized, double-blind, comparative study of leukore-duced vs unmodified RBCs.46 Theparticipants, investigators, study coor-dinators, and persons having any con-tact with the patients were blinded tostudy treatment assignments. Blood banktechnical staff who prepared the bloodproducts were aware of the treatment as-signments. All required procedures of theFood and Drug Administration andAmerican Association of Blood Bankswere followed during collection, test-ing, administration of blood compo-nents to the study enrollees, and leuko-reduction (ie, no more than 5×106/µL ofleukocytes per unit of blood).39 Leuko-reduction involves the use of a sterile,single-use filter that is inserted in the tub-ing between the RBCs and a secondarycollection bag. The blood is filtered us-ing gravity, and the filter removes leu-kocytes by mechanical trapping and ab-sorption. The RBC leukoreductionoccurred prior to storage and within 72hours of blood collection. At time oftransfusion, RBC units were to be nomore than 14 storage-days old. If enroll-ees required platelet transfusion, theyreceived leukoreduced platelets. Noscreening of blood products for CMV an-tibodies was performed prior to trans-fusion. If enrollees developed a newmedical condition that required irradi-ated blood products, they continued toreceive their blinded, assigned bloodcomponents, and irradiation was al-lowed. Gamma irradiation performedunder controlled procedures using regu-lated blood bank instruments results indamage to nucleic acids that precludesleukocytes, particularly lymphocytes,from proliferating and causing graft-vs-
host disease. It has no significant effecton the integrity of other blood ele-ments, including RBCs, platelets, andplasma proteins, nor does it have an im-pact on the infectivity of viruses or otherpathogens.
PatientsPatients had confirmed HIV infection,symptomatic anemia requiring RBCtransfusion as defined by their physi-cian, and were to receive nonemergentRBC transfusions within 72 hours of en-rollment. Enrollees were 14 years orolder, had documented CMV infection(by chart review or antibody testing), aKarnofsky performance score of 40 orhigher,49 and expected survival of morethan 1 month. Patients were ineligibleif they had a surgical reason for trans-fusion, a prior history of transfusion, re-nal failure requiring dialysis, thrombo-cytopenic purpura, used intravenousimmunoglobulin within 6 weeks of en-try, or had started new antiretroviraldrugs or systemic immunomodulators(eg, interleukin [IL]-2, interferons,granulocyte colony-stimulating factor)within 2 weeks of entry.
Study ProceduresThe study was approved by the institu-tional review boards at the 11 partici-pating institutions. Patients gave writ-ten informed consent. Treatmentallocation was made centrally by thestudy coordinating center, using strati-fied permuted blocks with dynamic bal-ancing within each center.50 Patientswere stratified by (1) CD4 cell count ofless than 50/µL at any time in the pastor 50/µL or greater, or if this informa-tion was unavailable, total lymphocytecount of less than 1000/µL or 1000/µLor greater,51 and (2) presence of CMVend organ disease. Patients receivedtransfusions as ordered by their physi-cian and underwent monitoring dur-ing transfusions per local policies.
Patients underwent standardizedevaluations. Occurrence of serious HIV-related complications, nonstudy trans-fusions, and type and dates of HIV-associated medications were assessed ateach visit. Use of antiretroviral therapy
VIRAL ACTIVATION TRANSFUSION STUDY
©2001 American Medical Association. All rights reserved. (Reprinted) JAMA, March 28, 2001—Vol 285, No. 12 1593
Downloaded From: http://jama.jamanetwork.com/ by a UCSF LIBRARY User on 05/27/2015

was classified as (1) potent ($3 antiret-roviral drugs with at least 1 proteaseinhibitor or 1 nonnucleoside reversetranscriptase inhibitor), (2) other anti-retroviral drugs, and (3) no antiretro-viral drugs. Patients had dilated eye ex-aminations by an ophthalmologist every6 months. At entry and every 3 months,patients had complete RBC and CD4 cellcounts and plasma HIV RNA and CMVDNA assays were performed.
Since itwashypothesizedthat immuneor viral activation might differ betweenfirst and later transfusions, we defined 2transfusion series for the purpose ofassessing possible short-term changes inlaboratory end points. The first seriesstarted at the patient’s first transfusionand included all subsequent RBC unitstransfused less than 7 days after a prior
unit. The second was defined only forpatients who had 1 or more transfu-sions starting at least 7 days after the endof the first series, and again included allsubsequent RBC units transfused lessthan 7 days after a prior unit. The HIVRNA and CMV DNA levels were mea-sured pretransfusion and at weeks 1, 2,3, and 4 after the start of each transfu-sionseries.Lymphocyteactivationmark-ers were measured pretransfusion and atweeks 1 and 4; cytokine levels were mea-sured pretransfusion and at week 1.Patients were evaluable for a transfu-sion series if they had a pretransfusionand at least 1 posttransfusion sampleavailable.
Laboratory testing was done cen-trally on batched specimens that wereseparatedwithin4hoursofcollectionand
stored at −70°C. The CMV antibodieswere assayed by enzyme immunoassay.After enrollment, blood from the base-lineblooddrawwas tested forCMVanti-bodies at the Viral Activation Transfu-sion Study (VATS) central laboratory.Each unit of donor blood was also testedretrospectively forCMVantibodies.Lym-phocyte subsets (CD3/CD4, CD3/CD8,and the proportion of CD8 cells express-ing activation markers CD38% andhumanleukocyteantigen-DR)weremea-sured by flow cytometry (FACScan, Bec-tonDickenson,SanJose,Calif).52,53 CD3/CD4 lymphocytes, often called CD4 Tcells, are a major target of HIV, and theirdepletion is used to measure progres-sionofHIVdisease.54 TheHIVRNAlevelwas measured using a reverse transcrip-tasepolymerasechainreactionassaywitha lower limitofquantificationof200cop-ies/mL (Amplicor Monitor assay, RocheMolecular Systems, Branchburg, NJ).55
The CMV DNA was initially assayedusingaqualitativepolymerasechainreac-tion assay, and if positive, a quantitativepolymerasechainreactionassaywassub-sequently applied (Roche MolecularSystems).56,57 The lower limitof thequan-titative assay was 400 copies/mL. Tumornecrosis factor, tumor necrosis factorreceptor, IL-6, and b2-microglobulinplasma levels were assayed by enzymeimmunoassays as detailed elsewhere.58
Qualitycontrolofresidual leukocytecon-tent of leukoreduced RBCs and plate-lets was previously described.53,59
End Points and Statistical MethodsPrimary end points were originally timetodeathor first seriousHIV-relatedcom-plicationandchange inplasmaHIVRNAlevel from baseline to week 1 after firsttransfusion series. Planned accrual was430, but 3 months into the study, addi-tionalresourceswereobtainedtoincreaseaccrual to 640 and change the primaryclinical end point to survival. The finaldesignassumed427deaths,andhad85%powerfordetectingarelativehazard(RH)of1.33for thesurvivalcomparison,usinga 2-sided test (a = .05). With improve-ment inthecourseofHIV, therewere289deaths, resulting in 85% power to detectan RH of 1.42 for survival.
Box. List of Predefined VATS Serious Clinical Event OutcomesRelated to HIV Infection*
Bacteremia†Catheter-relatedNoncatheter-related
Other serious bacterial/fungal infections (isolation from a normally sterile site)Cervical cancerCoccidioidomycosis (disseminated or extrapulmonary)Cryptococcosis (extrapulmonary)Cryptosporidiosis (.1 mo)Cytomegalovirus end organ diseaseHistoplasmosis (disseminated or extrapulmonary)Kaposi sarcoma (visceral)Mycobacterium avium complex (disseminated or extrapulmonary)Mycobacterium kansasii (disseminated or extrapulmonary)Mycobacterium tuberculosisNon-Hodgkin lymphoma (Burkitt, immunoblastic, or primary brain)Other mycobacterial species (disseminated or extrapulmonary)Pneumocystis carinii pneumoniaProgressive multifocal leukoencephalopathy‡Toxoplasmosis (brain)§*Adapted from the Centers for Disease Control and Prevention 1993 case definition for ac-
quired immunodeficiency syndrome.60 All diagnoses were definitive except for toxoplasmosis(see § footnote below).
†To be classified as a bacteremia, patients had to have systemic or focal symptoms or have2 or more cultures positive for the same organism. To be classified as a catheter-related bac-teremia, patients had no source of infection other than a catheter, and if they only had 1 posi-tive blood culture, they had to be treated with antimicrobial therapy and have had a favorableclinical response.
‡Required positive polymerase chain reaction for JC virus and compatible clinical syn-drome or diagnostic brain biopsy.
§Presumptive diagnosis was allowed if patients had compatible clinical findings, mass le-sions on brain imaging, and were toxoplasma antibody–positive or had a successful responseto therapy for toxoplasmosis.60
VIRAL ACTIVATION TRANSFUSION STUDY
1594 JAMA, March 28, 2001—Vol 285, No. 12 (Reprinted) ©2001 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a UCSF LIBRARY User on 05/27/2015
Secondary objectives included time todeath or first serious HIV-related com-plication, time to new or progressiveCMV end organ disease, plasma HIVRNA and CMV DNA levels, lympho-cyte subset markers, and change in cy-tokine and lymphocyte activation mark-ers. The HIV-related complications werepredefined and included specific AIDS-defining conditions and serious bacte-rial infections associated with mediansurvival times of less than 1 year or anacute mortality of more than 5% (BOX).60
Definitive diagnoses were required, ex-cept for toxoplasmosis, in which pa-tients were required to meet a standard-ized case definition.60 Progressive CMVretinitis required an ophthalmologist’sdiagnosis, as well as a change in therapy.Each clinical end point was confirmedto meet the study criteria.
Survival and other time-to-failureprobabilities were estimated by theKaplan-Meier method. Log-rank testsand proportional hazards models (withtime-varying covariates for factors de-termined after randomization) were usedto compare failure-time curves. The HIVRNA and CMV DNA levels and CD4 cellcounts were log transformed beforeanalyses. Changes in laboratory param-eters were calculated by comparisonwith pretransfusion values. Treat-ments were compared at selected timepoints using Wilcoxon rank-sum tests,and more globally using repeated mea-sures models adjusted for baseline value.Long-term trends in HIV RNA level andCD4 cell count were assessed with lin-ear random effects models. Discrete out-comes were analyzed with the Fisher ex-act test. All P values are 2-sided.
RESULTSPatients and Follow-up
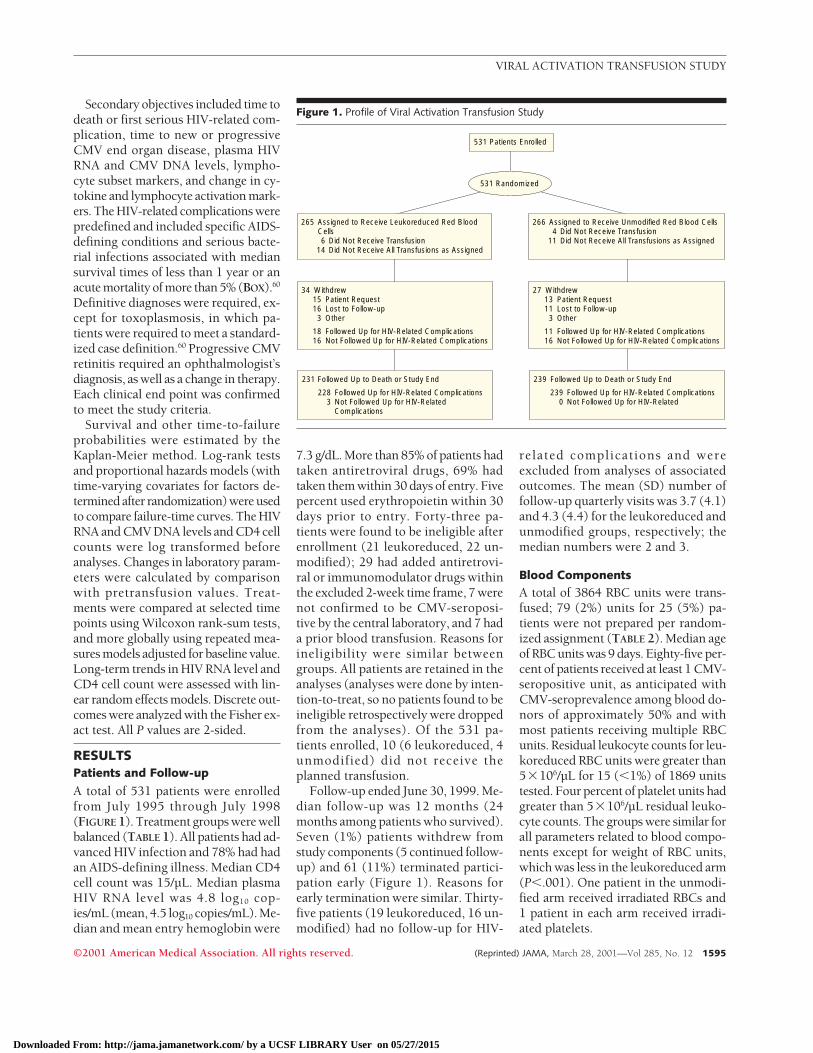
A total of 531 patients were enrolledfrom July 1995 through July 1998(FIGURE 1). Treatment groups were wellbalanced (TABLE 1). All patients had ad-vanced HIV infection and 78% had hadan AIDS-defining illness. Median CD4cell count was 15/µL. Median plasmaHIV RNA level was 4.8 log10 cop-ies/mL (mean, 4.5 log10 copies/mL). Me-dian and mean entry hemoglobin were
7.3 g/dL. More than 85% of patients hadtaken antiretroviral drugs, 69% hadtaken them within 30 days of entry. Fivepercent used erythropoietin within 30days prior to entry. Forty-three pa-tients were found to be ineligible afterenrollment (21 leukoreduced, 22 un-modified); 29 had added antiretrovi-ral or immunomodulator drugs withinthe excluded 2-week time frame, 7 werenot confirmed to be CMV-seroposi-tive by the central laboratory, and 7 hada prior blood transfusion. Reasons forineligibility were similar betweengroups. All patients are retained in theanalyses (analyses were done by inten-tion-to-treat, so no patients found to beineligible retrospectively were droppedfrom the analyses). Of the 531 pa-tients enrolled, 10 (6 leukoreduced, 4unmodified) did not receive theplanned transfusion.
Follow-up ended June 30, 1999. Me-dian follow-up was 12 months (24months among patients who survived).Seven (1%) patients withdrew fromstudy components (5 continued follow-up) and 61 (11%) terminated partici-pation early (Figure 1). Reasons forearly termination were similar. Thirty-five patients (19 leukoreduced, 16 un-modified) had no follow-up for HIV-
related complications and wereexcluded from analyses of associatedoutcomes. The mean (SD) number offollow-up quarterly visits was 3.7 (4.1)and 4.3 (4.4) for the leukoreduced andunmodified groups, respectively; themedian numbers were 2 and 3.
Blood ComponentsA total of 3864 RBC units were trans-fused; 79 (2%) units for 25 (5%) pa-tients were not prepared per random-ized assignment (TABLE 2). Median ageof RBC units was 9 days. Eighty-five per-cent of patients received at least 1 CMV-seropositive unit, as anticipated withCMV-seroprevalence among blood do-nors of approximately 50% and withmost patients receiving multiple RBCunits. Residual leukocyte counts for leu-koreduced RBC units were greater than53106/µL for 15 (,1%) of 1869 unitstested. Four percent of platelet units hadgreater than 53106/µL residual leuko-cyte counts. The groups were similar forall parameters related to blood compo-nents except for weight of RBC units,which was less in the leukoreduced arm(P,.001). One patient in the unmodi-fied arm received irradiated RBCs and1 patient in each arm received irradi-ated platelets.
Figure 1. Profile of Viral Activation Transfusion Study
531 Patients Enrolled
531 Randomized
265 Assigned to Receive Leukoreduced Red Blood Cells6 Did Not Receive Transfusion
14 Did Not Receive All Transfusions as Assigned
34 Withdrew15 Patient Request16 Lost to Follow-up3 Other
18 Followed Up for HIV-Related Complications16 Not Followed Up for HIV-Related Complications
231 Followed Up to Death or Study End
228 Followed Up for HIV-Related Complications3 Not Followed Up for HIV-Related
Complications
266 Assigned to Receive Unmodified Red Blood Cells4 Did Not Receive Transfusion
11 Did Not Receive All Transfusions as Assigned
27 Withdrew13 Patient Request11 Lost to Follow-up3 Other
11 Followed Up for HIV-Related Complications16 Not Followed Up for HIV-Related Complications
239 Followed Up to Death or Study End
239 Followed Up for HIV-Related Complications0 Not Followed Up for HIV-Related
VIRAL ACTIVATION TRANSFUSION STUDY
©2001 American Medical Association. All rights reserved. (Reprinted) JAMA, March 28, 2001—Vol 285, No. 12 1595
Downloaded From: http://jama.jamanetwork.com/ by a UCSF LIBRARY User on 05/27/2015
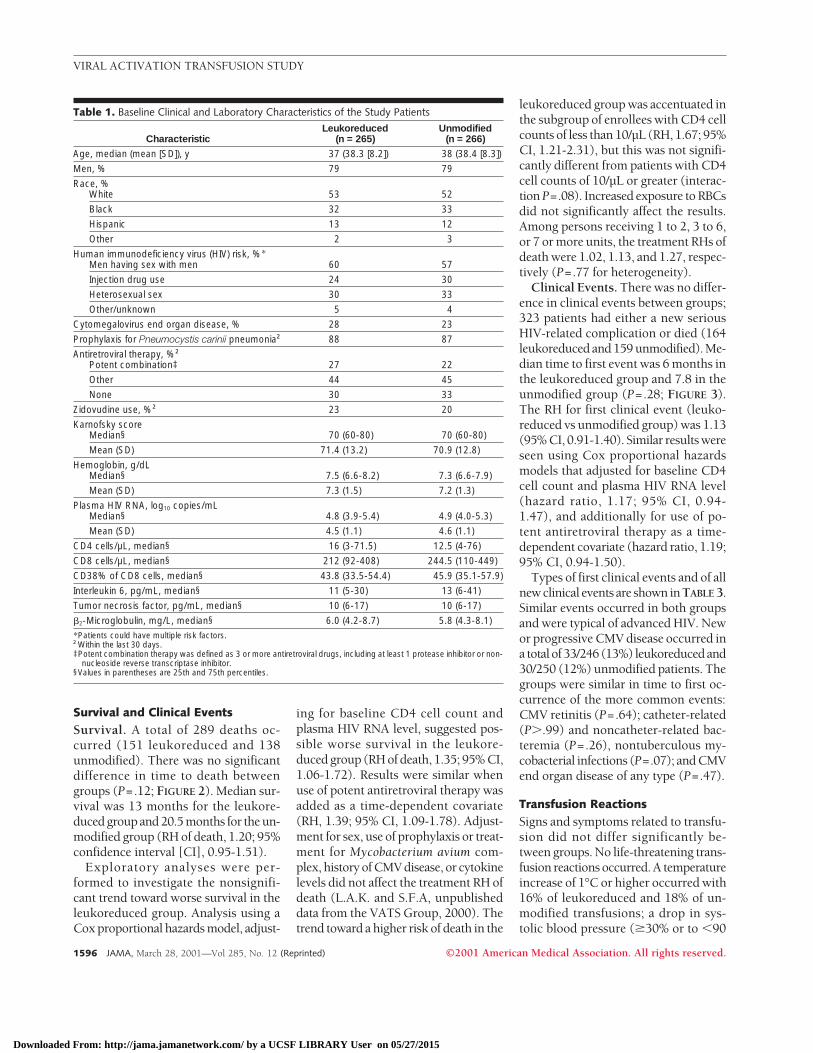
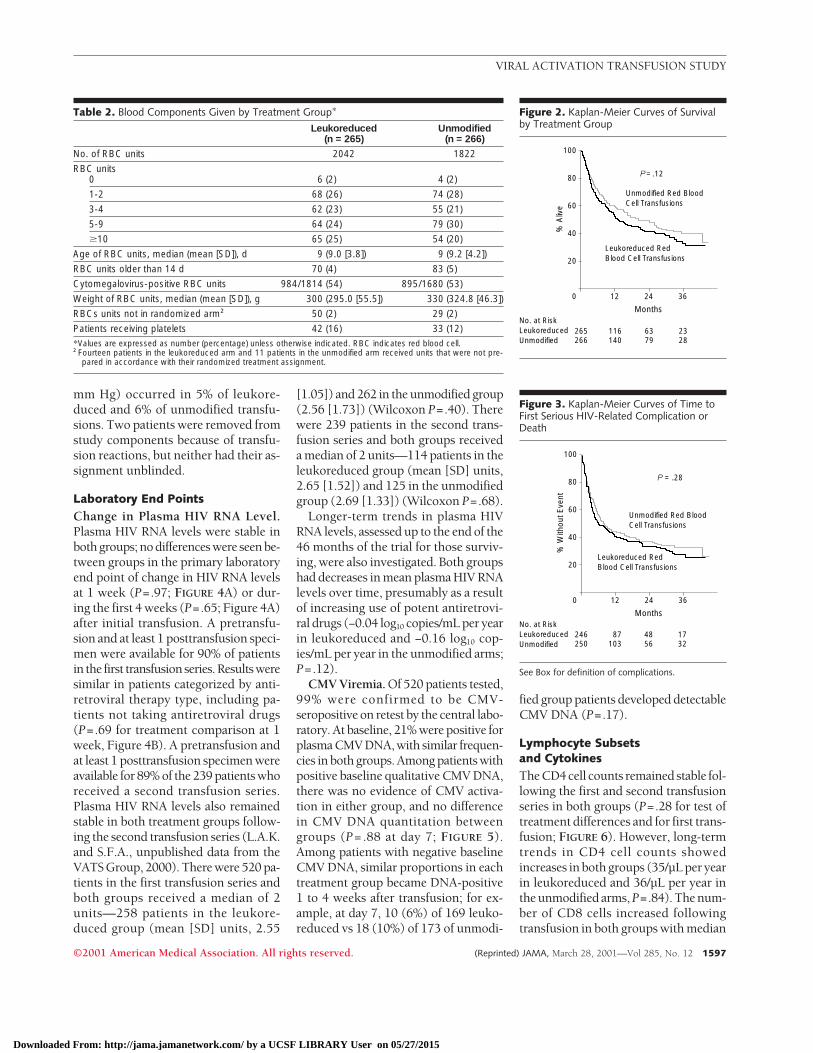
Survival and Clinical EventsSurvival. A total of 289 deaths oc-curred (151 leukoreduced and 138unmodified). There was no significantdifference in time to death betweengroups (P=.12; FIGURE 2). Median sur-vival was 13 months for the leukore-duced group and 20.5 months for the un-modified group (RH of death, 1.20; 95%confidence interval [CI], 0.95-1.51).
Exploratory analyses were per-formed to investigate the nonsignifi-cant trend toward worse survival in theleukoreduced group. Analysis using aCox proportional hazards model, adjust-
ing for baseline CD4 cell count andplasma HIV RNA level, suggested pos-sible worse survival in the leukore-duced group (RH of death, 1.35; 95% CI,1.06-1.72). Results were similar whenuse of potent antiretroviral therapy wasadded as a time-dependent covariate(RH, 1.39; 95% CI, 1.09-1.78). Adjust-ment for sex, use of prophylaxis or treat-ment for Mycobacterium avium com-plex, history of CMV disease, or cytokinelevels did not affect the treatment RH ofdeath (L.A.K. and S.F.A, unpublisheddata from the VATS Group, 2000). Thetrend toward a higher risk of death in the
leukoreduced group was accentuated inthe subgroup of enrollees with CD4 cellcounts of less than 10/µL (RH, 1.67; 95%CI, 1.21-2.31), but this was not signifi-cantly different from patients with CD4cell counts of 10/µL or greater (interac-tion P=.08). Increased exposure to RBCsdid not significantly affect the results.Among persons receiving 1 to 2, 3 to 6,or 7 or more units, the treatment RHs ofdeath were 1.02, 1.13, and 1.27, respec-tively (P=.77 for heterogeneity).
Clinical Events. There was no differ-ence in clinical events between groups;323 patients had either a new seriousHIV-related complication or died (164leukoreduced and 159 unmodified). Me-dian time to first event was 6 months inthe leukoreduced group and 7.8 in theunmodified group (P=.28; FIGURE 3).The RH for first clinical event (leuko-reduced vs unmodified group) was 1.13(95% CI, 0.91-1.40). Similar results wereseen using Cox proportional hazardsmodels that adjusted for baseline CD4cell count and plasma HIV RNA level(hazard ratio, 1.17; 95% CI, 0.94-1.47), and additionally for use of po-tent antiretroviral therapy as a time-dependent covariate (hazard ratio, 1.19;95% CI, 0.94-1.50).
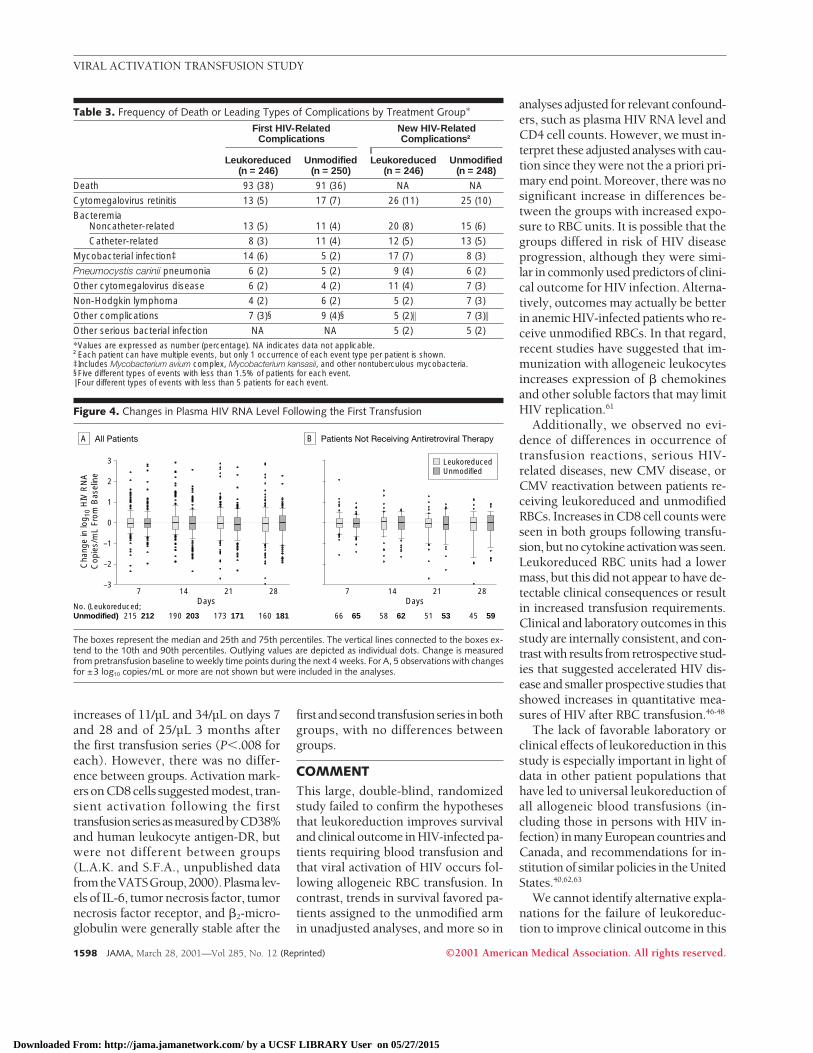
Types of first clinical events and of allnew clinical events are shown inTABLE 3.Similar events occurred in both groupsand were typical of advanced HIV. Newor progressive CMV disease occurred ina totalof33/246(13%) leukoreducedand30/250 (12%) unmodified patients. Thegroups were similar in time to first oc-currence of the more common events:CMV retinitis (P=.64); catheter-related(P..99) and noncatheter-related bac-teremia (P=.26), nontuberculous my-cobacterial infections (P=.07); and CMVend organ disease of any type (P=.47).
Transfusion ReactionsSigns and symptoms related to transfu-sion did not differ significantly be-tween groups. No life-threatening trans-fusion reactions occurred. A temperatureincrease of 1°C or higher occurred with16% of leukoreduced and 18% of un-modified transfusions; a drop in sys-tolic blood pressure ($30% or to ,90
Table 1. Baseline Clinical and Laboratory Characteristics of the Study Patients
CharacteristicLeukoreduced
(n = 265)Unmodified
(n = 266)
Age, median (mean [SD]), y 37 (38.3 [8.2]) 38 (38.4 [8.3])
Men, % 79 79
Race, %White 53 52
Black 32 33
Hispanic 13 12
Other 2 3
Human immunodeficiency virus (HIV) risk, %*Men having sex with men 60 57
Injection drug use 24 30
Heterosexual sex 30 33
Other/unknown 5 4
Cytomegalovirus end organ disease, % 28 23
Prophylaxis for Pneumocystis carinii pneumonia† 88 87
Antiretroviral therapy, %†Potent combination‡ 27 22
Other 44 45
None 30 33
Zidovudine use, %† 23 20
Karnofsky scoreMedian§ 70 (60-80) 70 (60-80)
Mean (SD) 71.4 (13.2) 70.9 (12.8)
Hemoglobin, g/dLMedian§ 7.5 (6.6-8.2) 7.3 (6.6-7.9)
Mean (SD) 7.3 (1.5) 7.2 (1.3)
Plasma HIV RNA, log10 copies/mLMedian§ 4.8 (3.9-5.4) 4.9 (4.0-5.3)
Mean (SD) 4.5 (1.1) 4.6 (1.1)
CD4 cells/µL, median§ 16 (3-71.5) 12.5 (4-76)
CD8 cells/µL, median§ 212 (92-408) 244.5 (110-449)
CD38% of CD8 cells, median§ 43.8 (33.5-54.4) 45.9 (35.1-57.9)
Interleukin 6, pg/mL, median§ 11 (5-30) 13 (6-41)
Tumor necrosis factor, pg/mL, median§ 10 (6-17) 10 (6-17)
b2-Microglobulin, mg/L, median§ 6.0 (4.2-8.7) 5.8 (4.3-8.1)
*Patients could have multiple risk factors.†Within the last 30 days.‡Potent combination therapy was defined as 3 or more antiretroviral drugs, including at least 1 protease inhibitor or non-
nucleoside reverse transcriptase inhibitor.§Values in parentheses are 25th and 75th percentiles.
VIRAL ACTIVATION TRANSFUSION STUDY
1596 JAMA, March 28, 2001—Vol 285, No. 12 (Reprinted) ©2001 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a UCSF LIBRARY User on 05/27/2015
mm Hg) occurred in 5% of leukore-duced and 6% of unmodified transfu-sions. Two patients were removed fromstudy components because of transfu-sion reactions, but neither had their as-signment unblinded.
Laboratory End PointsChange in Plasma HIV RNA Level.Plasma HIV RNA levels were stable inboth groups; no differences were seen be-tween groups in the primary laboratoryend point of change in HIV RNA levelsat 1 week (P=.97; FIGURE 4A) or dur-ing the first 4 weeks (P=.65; Figure 4A)after initial transfusion. A pretransfu-sion and at least 1 posttransfusion speci-men were available for 90% of patientsin the first transfusionseries.Resultsweresimilar in patients categorized by anti-retroviral therapy type, including pa-tients not taking antiretroviral drugs(P=.69 for treatment comparison at 1week, Figure 4B). A pretransfusion andat least 1 posttransfusion specimen wereavailable for 89% of the 239 patients whoreceived a second transfusion series.Plasma HIV RNA levels also remainedstable in both treatment groups follow-ing the second transfusion series (L.A.K.and S.F.A., unpublished data from theVATS Group, 2000). There were 520 pa-tients in the first transfusion series andboth groups received a median of 2units—258 patients in the leukore-duced group (mean [SD] units, 2.55
[1.05]) and 262 in the unmodified group(2.56 [1.73]) (Wilcoxon P=.40). Therewere 239 patients in the second trans-fusion series and both groups receiveda median of 2 units—114 patients in theleukoreduced group (mean [SD] units,2.65 [1.52]) and 125 in the unmodifiedgroup (2.69 [1.33]) (Wilcoxon P=.68).
Longer-term trends in plasma HIVRNA levels, assessed up to the end of the46 months of the trial for those surviv-ing, were also investigated. Both groupshad decreases in mean plasma HIV RNAlevels over time, presumably as a resultof increasing use of potent antiretrovi-ral drugs (−0.04 log10 copies/mL per yearin leukoreduced and −0.16 log10 cop-ies/mL per year in the unmodified arms;P=.12).
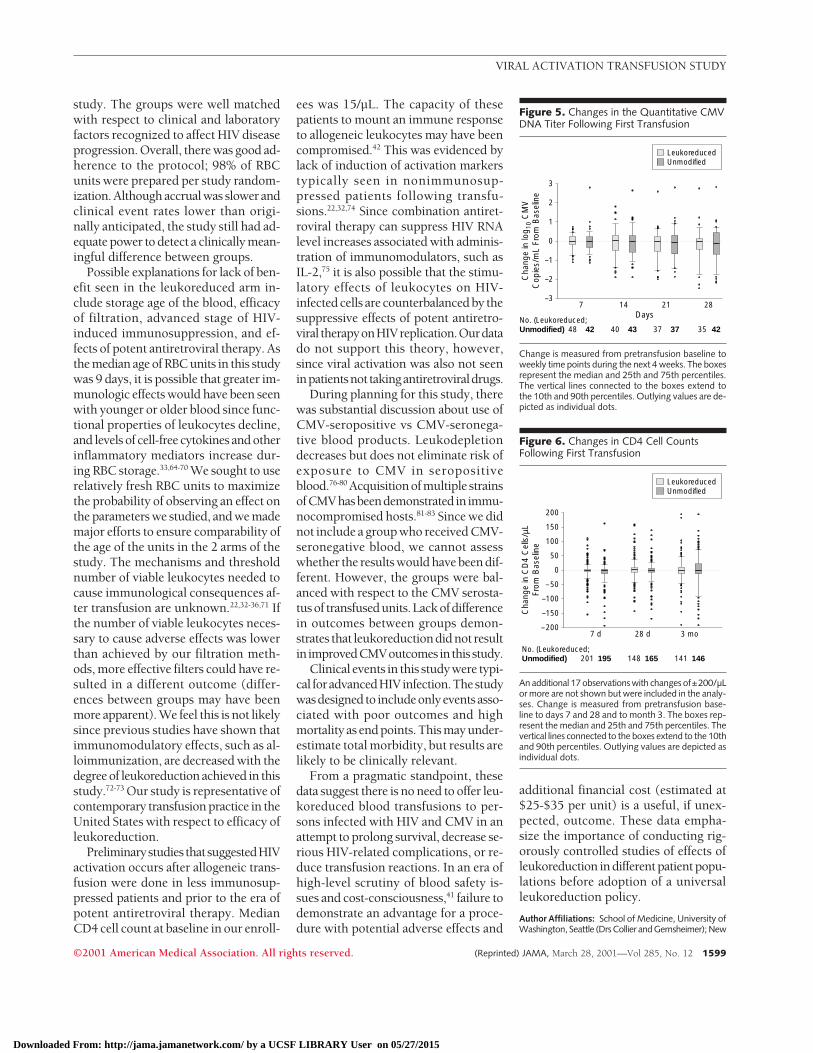
CMV Viremia. Of 520 patients tested,99% were confirmed to be CMV-seropositive on retest by the central labo-ratory. At baseline, 21% were positive forplasma CMV DNA, with similar frequen-cies in both groups. Among patients withpositive baseline qualitative CMV DNA,there was no evidence of CMV activa-tion in either group, and no differencein CMV DNA quantitation betweengroups (P= .88 at day 7; FIGURE 5).Among patients with negative baselineCMV DNA, similar proportions in eachtreatment group became DNA-positive1 to 4 weeks after transfusion; for ex-ample, at day 7, 10 (6%) of 169 leuko-reduced vs 18 (10%) of 173 of unmodi-
fied group patients developed detectableCMV DNA (P=.17).
Lymphocyte Subsetsand CytokinesThe CD4 cell counts remained stable fol-lowing the first and second transfusionseries in both groups (P=.28 for test oftreatment differences and for first trans-fusion; FIGURE 6). However, long-termtrends in CD4 cell counts showedincreases in both groups (35/µL per yearin leukoreduced and 36/µL per year inthe unmodified arms, P=.84). The num-ber of CD8 cells increased followingtransfusion in both groups with median
Figure 2. Kaplan-Meier Curves of Survivalby Treatment Group
100
80
60
40
20
0 12 3624
Months
% A
live
No. at RiskLeukoreducedUnmodified
Unmodified Red Blood Cell Transfusions
Leukoreduced Red Blood Cell Transfusions
P = .12
265266
116140
6379
2328
Figure 3. Kaplan-Meier Curves of Time toFirst Serious HIV-Related Complication orDeath
100
80
60
40
20
0 12 3624
Months
% W
ithou
t Eve
nt
No. at RiskLeukoreducedUnmodified
Unmodified Red Blood Cell Transfusions
Leukoreduced Red Blood Cell Transfusions
P = .28
246250
87103
4856
1732
See Box for definition of complications.
Table 2. Blood Components Given by Treatment Group*
Leukoreduced(n = 265)
Unmodified(n = 266)
No. of RBC units 2042 1822
RBC units0 6 (2) 4 (2)
1-2 68 (26) 74 (28)
3-4 62 (23) 55 (21)
5-9 64 (24) 79 (30)
$10 65 (25) 54 (20)
Age of RBC units, median (mean [SD]), d 9 (9.0 [3.8]) 9 (9.2 [4.2])
RBC units older than 14 d 70 (4) 83 (5)
Cytomegalovirus-positive RBC units 984/1814 (54) 895/1680 (53)
Weight of RBC units, median (mean [SD]), g 300 (295.0 [55.5]) 330 (324.8 [46.3])
RBCs units not in randomized arm† 50 (2) 29 (2)
Patients receiving platelets 42 (16) 33 (12)
*Values are expressed as number (percentage) unless otherwise indicated. RBC indicates red blood cell.†Fourteen patients in the leukoreduced arm and 11 patients in the unmodified arm received units that were not pre-
pared in accordance with their randomized treatment assignment.
VIRAL ACTIVATION TRANSFUSION STUDY
©2001 American Medical Association. All rights reserved. (Reprinted) JAMA, March 28, 2001—Vol 285, No. 12 1597
Downloaded From: http://jama.jamanetwork.com/ by a UCSF LIBRARY User on 05/27/2015
increases of 11/µL and 34/µL on days 7and 28 and of 25/µL 3 months afterthe first transfusion series (P,.008 foreach). However, there was no differ-ence between groups. Activation mark-ers on CD8 cells suggested modest, tran-sient activation following the firsttransfusionseriesasmeasuredbyCD38%and human leukocyte antigen-DR, butwere not different between groups(L.A.K. and S.F.A., unpublished datafromtheVATSGroup,2000).Plasmalev-els of IL-6, tumor necrosis factor, tumornecrosis factor receptor, and b2-micro-globulin were generally stable after the
firstandsecondtransfusionseries inbothgroups, with no differences betweengroups.
COMMENTThis large, double-blind, randomizedstudy failed to confirm the hypothesesthat leukoreduction improves survivaland clinical outcome in HIV-infected pa-tients requiring blood transfusion andthat viral activation of HIV occurs fol-lowing allogeneic RBC transfusion. Incontrast, trends in survival favored pa-tients assigned to the unmodified armin unadjusted analyses, and more so in
analyses adjusted for relevant confound-ers, such as plasma HIV RNA level andCD4 cell counts. However, we must in-terpret these adjusted analyses with cau-tion since they were not the a priori pri-mary end point. Moreover, there was nosignificant increase in differences be-tween the groups with increased expo-sure to RBC units. It is possible that thegroups differed in risk of HIV diseaseprogression, although they were simi-lar in commonly used predictors of clini-cal outcome for HIV infection. Alterna-tively, outcomes may actually be betterin anemic HIV-infected patients who re-ceive unmodified RBCs. In that regard,recent studies have suggested that im-munization with allogeneic leukocytesincreases expression of b chemokinesand other soluble factors that may limitHIV replication.61
Additionally, we observed no evi-dence of differences in occurrence oftransfusion reactions, serious HIV-related diseases, new CMV disease, orCMV reactivation between patients re-ceiving leukoreduced and unmodifiedRBCs. Increases in CD8 cell counts wereseen in both groups following transfu-sion, but no cytokine activation was seen.Leukoreduced RBC units had a lowermass, but this did not appear to have de-tectable clinical consequences or resultin increased transfusion requirements.Clinical and laboratory outcomes in thisstudy are internally consistent, and con-trast with results from retrospective stud-ies that suggested accelerated HIV dis-ease and smaller prospective studies thatshowed increases in quantitative mea-sures of HIV after RBC transfusion.46-48
The lack of favorable laboratory orclinical effects of leukoreduction in thisstudy is especially important in light ofdata in other patient populations thathave led to universal leukoreduction ofall allogeneic blood transfusions (in-cluding those in persons with HIV in-fection) in many European countries andCanada, and recommendations for in-stitution of similar policies in the UnitedStates.40,62,63
We cannot identify alternative expla-nations for the failure of leukoreduc-tion to improve clinical outcome in this
Figure 4. Changes in Plasma HIV RNA Level Following the First Transfusion
3
2
1
0
–1
–2
–3
No. (Leukoreduced;Unmodified)
Cha
nge
in lo
g 10
HIV
RN
AC
opie
s/m
L Fr
om B
asel
ine
A
Days
All Patients B Patients Not Receiving Antiretroviral Therapy
LeukoreducedUnmodified
28
181160
21
173 171
14
190 203
7
212215
Days7
66 65
21
5351
28
45 59
14
58 62
The boxes represent the median and 25th and 75th percentiles. The vertical lines connected to the boxes ex-tend to the 10th and 90th percentiles. Outlying values are depicted as individual dots. Change is measuredfrom pretransfusion baseline to weekly time points during the next 4 weeks. For A, 5 observations with changesfor ±3 log10 copies/mL or more are not shown but were included in the analyses.
Table 3. Frequency of Death or Leading Types of Complications by Treatment Group*
First HIV-RelatedComplications
New HIV-RelatedComplications†
Leukoreduced(n = 246)
Unmodified(n = 250)
Leukoreduced(n = 246)
Unmodified(n = 248)
Death 93 (38) 91 (36) NA NA
Cytomegalovirus retinitis 13 (5) 17 (7) 26 (11) 25 (10)
BacteremiaNoncatheter-related 13 (5) 11 (4) 20 (8) 15 (6)
Catheter-related 8 (3) 11 (4) 12 (5) 13 (5)
Mycobacterial infection‡ 14 (6) 5 (2) 17 (7) 8 (3)
Pneumocystis carinii pneumonia 6 (2) 5 (2) 9 (4) 6 (2)
Other cytomegalovirus disease 6 (2) 4 (2) 11 (4) 7 (3)
Non-Hodgkin lymphoma 4 (2) 6 (2) 5 (2) 7 (3)
Other complications 7 (3)§ 9 (4)§ 5 (2)\ 7 (3)\
Other serious bacterial infection NA NA 5 (2) 5 (2)
*Values are expressed as number (percentage). NA indicates data not applicable.†Each patient can have multiple events, but only 1 occurrence of each event type per patient is shown.‡Includes Mycobacterium avium complex, Mycobacterium kansasii, and other nontuberculous mycobacteria.§Five different types of events with less than 1.5% of patients for each event.\Four different types of events with less than 5 patients for each event.
VIRAL ACTIVATION TRANSFUSION STUDY
1598 JAMA, March 28, 2001—Vol 285, No. 12 (Reprinted) ©2001 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a UCSF LIBRARY User on 05/27/2015
study. The groups were well matchedwith respect to clinical and laboratoryfactors recognized to affect HIV diseaseprogression. Overall, there was good ad-herence to the protocol; 98% of RBCunits were prepared per study random-ization. Although accrual was slower andclinical event rates lower than origi-nally anticipated, the study still had ad-equate power to detect a clinically mean-ingful difference between groups.
Possible explanations for lack of ben-efit seen in the leukoreduced arm in-clude storage age of the blood, efficacyof filtration, advanced stage of HIV-induced immunosuppression, and ef-fects of potent antiretroviral therapy. Asthe median age of RBC units in this studywas 9 days, it is possible that greater im-munologic effects would have been seenwith younger or older blood since func-tional properties of leukocytes decline,and levels of cell-free cytokines and otherinflammatory mediators increase dur-ing RBC storage.33,64-70 We sought to userelatively fresh RBC units to maximizethe probability of observing an effect onthe parameters we studied, and we mademajor efforts to ensure comparability ofthe age of the units in the 2 arms of thestudy. The mechanisms and thresholdnumber of viable leukocytes needed tocause immunological consequences af-ter transfusion are unknown.22,32-36,71 Ifthe number of viable leukocytes neces-sary to cause adverse effects was lowerthan achieved by our filtration meth-ods, more effective filters could have re-sulted in a different outcome (differ-ences between groups may have beenmore apparent). We feel this is not likelysince previous studies have shown thatimmunomodulatory effects, such as al-loimmunization, are decreased with thedegree of leukoreduction achieved in thisstudy.72-73 Our study is representative ofcontemporary transfusion practice in theUnited States with respect to efficacy ofleukoreduction.
Preliminarystudies thatsuggestedHIVactivation occurs after allogeneic trans-fusion were done in less immunosup-pressed patients and prior to the era ofpotent antiretroviral therapy. MedianCD4 cell count at baseline in our enroll-
ees was 15/µL. The capacity of thesepatients to mount an immune responseto allogeneic leukocytes may have beencompromised.42 This was evidenced bylack of induction of activation markerstypically seen in nonimmunosup-pressed patients following transfu-sions.22,32,74 Since combination antiret-roviral therapy can suppress HIV RNAlevel increases associated with adminis-tration of immunomodulators, such asIL-2,75 it is also possible that the stimu-latory effects of leukocytes on HIV-infected cells are counterbalanced by thesuppressive effects of potent antiretro-viral therapyonHIVreplication.Ourdatado not support this theory, however,since viral activation was also not seeninpatientsnot takingantiretroviraldrugs.
During planning for this study, therewas substantial discussion about use ofCMV-seropositive vs CMV-seronega-tive blood products. Leukodepletiondecreases but does not eliminate risk ofexposure to CMV in seropositiveblood.76-80 Acquisitionofmultiple strainsofCMVhasbeendemonstrated in immu-nocompromised hosts.81-83 Since we didnot include a group who received CMV-seronegative blood, we cannot assesswhether the results would have been dif-ferent. However, the groups were bal-anced with respect to the CMV serosta-tusof transfusedunits.Lackofdifferencein outcomes between groups demon-strates that leukoreductiondidnot resultinimprovedCMVoutcomesinthisstudy.
Clinical events in this studywere typi-cal foradvancedHIVinfection.Thestudywasdesignedto includeonlyeventsasso-ciated with poor outcomes and highmortality as end points. This may under-estimate total morbidity, but results arelikely to be clinically relevant.
From a pragmatic standpoint, thesedata suggest there is no need to offer leu-koreduced blood transfusions to per-sons infected with HIV and CMV in anattempt to prolong survival, decrease se-rious HIV-related complications, or re-duce transfusion reactions. In an era ofhigh-level scrutiny of blood safety is-sues and cost-consciousness,41 failure todemonstrate an advantage for a proce-dure with potential adverse effects and
additional financial cost (estimated at$25-$35 per unit) is a useful, if unex-pected, outcome. These data empha-size the importance of conducting rig-orously controlled studies of effects ofleukoreduction in different patient popu-lations before adoption of a universalleukoreduction policy.
Author Affiliations: School of Medicine, University ofWashington, Seattle (Drs Collier and Gernsheimer); New
Figure 5. Changes in the Quantitative CMVDNA Titer Following First Transfusion
3
2
1
0
–1
–2
–3
No. (Leukoreduced;Unmodified)
Cha
nge
in lo
g 10
CM
VC
opie
s/m
L Fr
om B
asel
ine
Days
LeukoreducedUnmodified
7
48 42
28
35 42
21
37 37
14
40 43
Change is measured from pretransfusion baseline toweekly time points during the next 4 weeks. The boxesrepresent the median and 25th and 75th percentiles.The vertical lines connected to the boxes extend tothe 10th and 90th percentiles. Outlying values are de-picted as individual dots.
Figure 6. Changes in CD4 Cell CountsFollowing First Transfusion
200
150
50
100
0
–50
–100
–150
–200
No. (Leukoreduced;Unmodified)
Cha
nge
in C
D4
Cel
ls/µ
LFr
om B
asel
ine
LeukoreducedUnmodified
3 mo
146141
28 d
165148
7 d
201 195
An additional 17 observations with changes of±200/µLor more are not shown but were included in the analy-ses. Change is measured from pretransfusion base-line to days 7 and 28 and to month 3. The boxes rep-resent the median and 25th and 75th percentiles. Thevertical lines connected to the boxes extend to the 10thand 90th percentiles. Outlying values are depicted asindividual dots.
VIRAL ACTIVATION TRANSFUSION STUDY
©2001 American Medical Association. All rights reserved. (Reprinted) JAMA, March 28, 2001—Vol 285, No. 12 1599
Downloaded From: http://jama.jamanetwork.com/ by a UCSF LIBRARY User on 05/27/2015
England Research Institutes, Watertown, Mass (Drs Ka-lish and Assmann); Blood Centers of the Pacific, SanFrancisco, Calif (Dr Busch); School of Medicine, Uni-versity of California, San Francisco (Drs Busch and Mur-phy); Puget Sound Blood Center, Seattle, Wash (DrGernsheimer); School of Medicine, University of Cali-fornia, San Diego (Dr Lane); School of Medicine, Uni-versity of Texas, Galveston (Dr Asmuth); School of Medi-cine, Case Western Reserve University, Cleveland, Ohio(Dr Lederman); School of Medicine, Georgetown Uni-versity, Washington, DC (Dr Kumar); School of Medi-cine, University of North Carolina, Chapel Hill (Dr Kel-ley); School of Medicine, Brown University, Providence,RI (Dr Flanigan); School of Medicine, University of Pitts-burgh, Pittsburgh, Pa (Dr McMahon); School of Medi-cine, Mount Sinai, New York, NY (Dr Sacks); Ohio StateUniversity Medical Center, Columbus (Dr Kennedy); andSacramento Medical Foundation Blood Centers, Sac-ramento, Calif (Dr Holland).Author Contributions: Study concept and design: Col-lier, Kalish, Busch, Gernsheimer, Lane, Asmuth, Le-derman, Murphy, Kumar, Flanigan, McMahon, Sacks,Kennedy, Holland.Acquisition of data: Collier, Busch, Gernsheimer, Lane,Asmuth, Lederman, Murphy, Kumar, Kelley, Flani-gan, McMahon, Sacks.Analysis and interpretation of data: Collier, Kalish, Busch,Gernsheimer, Assmann, Lane, Lederman, Murphy, Kel-ley, Sacks.Drafting of the manuscript: Collier, Kalish, Busch, Gern-sheimer, Lane, Lederman.Critical revision of the manuscript for important intel-lectual content: Collier, Kalish, Busch, Gernsheimer,Assmann, Lane, Asmuth, Lederman, Murphy, Kumar,Kelley, Flanigan, McMahon, Sacks, Kennedy, Hol-land.Statistical expertise: Kalish, Assmann.Obtained funding: Collier, Kalish, Busch, Gernshei-mer, Lane, Asmuth, Lederman, Flanigan, Sacks.Administrative, technical, or material support: Col-lier, Kalish, Busch, Gernsheimer, Lane, Lederman, Ku-mar, Flanigan, Holland.Study supervision: Collier, Kalish, Busch, Gernshei-mer, Lane, Asmuth, Lederman, Murphy, Kelley, Sacks,Kennedy.Financial Disclosures: Dr Collier received research fund-ing from, was a consultant for, or prepared material forAbbott, Agouron, AnorMed, Gilead Sciences, GlaxoSmithKline, Hoffman La Roche, JAMA HIV/AIDS In-formation Center (Web site), Medscape (Web site),Merck, Pharmacia-Upjohn, The Body (Web site), Vi-rologic, and the National Institute of Allergy and In-fectious Diseases. Drs Kalish and Assmann received re-search funding from Baxter Healthcare Corp andAmerican Red Cross. Dr Kalish also received fundingfrom National Institute of Allergy and Infectious Dis-eases, National Institute of Child Health and HumanDevelopment, and National Institute on Drug Abuse.Dr Busch received research funding or honoraria from,or consulted for or advised for the Centers for DiseaseControl and Prevention, National Institute of Allergy andInfectious Diseases, National Heart, Lung, and BloodInstitute, State of California, Acrometrix, Chiron Corp,Gambro BCT (Cobe), Gen-Probe, Haemonetics, andRoche Molecular Systems Inc; and was vice presidentfor research, Blood Centers of the Pacific and Blood Sys-tems Inc; and was involved with development of as-says for Chiron and Roche. [Reagents used for the mainVATS study except for the CMV DNA assays were pur-chased by the study (see below). Dr Busch’s fundingby Chiron and Roche and collaboration with these com-panies has to do with development of blood donorscreening and microchimerism assays.] Dr Lane re-ceived research funding or reagents from or consultedfor American Red Cross, Amgen, Baxter, and Immu-nex. Dr Asmuth received funding from National Insti-tute of Allergy and Infectious Diseases and had stockin Abbott Laboratories. Dr Lederman received re-
search funding, speaker honoraria, assay kits, or re-agents from, or consulted for Abbott, Agouron, Anor-Med, Bristol-Myers Squibb, Chiron, Dupont, GlaxoSmithKline, Immunex, Merck, Roche, Schering Plough,Triangle, and National Institute of Allergy and Infec-tious Diseases. Dr Murphy received research supportfrom National Heart, Lung, and Blood Institute and Na-tional Institute on Drug Abuse. Dr Kumar received re-search support from National Institute of Allergy andInfectious Diseases. Dr Flanigan is a consultant to Bristol-Myers Squibb and Glaxo SmithKline and received re-search support from National Institute of Allergy andInfectious Diseases, National Institute on Drug Abuse,and National Heart, Lung, and Blood Institute. Dr Mc-Mahon received research funding from Chiron Corp,Merck and Co Inc, and National Institute of Allergy andInfectious Diseases, and honoraria from DuPont Pharmaand Glaxo SmithKline. Dr Sacks received research fund-ing or honoraria from Bristol-Myers Squibb, Agouron,Dupont Merck, Parexel, Upjohn, and National Insti-tute of Allergy and Infectious Diseases. Dr Kennedy re-ceived research support from the National Cancer In-stitute. Dr Holland received research funding fromAbbott, Ortho, Roche, and the Centers for Disease Con-trol and Prevention.Funding/Support: Reagents for detection and quan-titation of CMV DNA by polymerase chain reaction werecontributed by Roche Molecular Systems (Alameda,Calif). Supported by National Heart, Lung, and BloodInstitute contract RR00046. The following contracts arealso from the National Heart, Lung, and Blood Insti-tute and the numbers are listed by site. Case WesternReserve University, Cleveland, Ohio (N01-HB-57115); Georgetown University, Washington, DC (N01-HB-57116); Miriam Hospital/Brown University, Provi-dence, RI (N01-HB-57117); Mount Sinai MedicalCenter, New York, NY (N01-HB-57118); Ohio StateUniversity, Columbus (N01-HB-57119); University ofCalifornia, San Diego (N01-HB-57120); University ofCalifornia, San Francisco (N01-HB-57121); Universityof North Carolina, Chapel Hill (N01-HB-57122); Uni-versity of Pittsburgh, Pittsburgh Pa (N01-HB-57123);University of Texas Medical Branch, Galveston (N01-HB-57124); University of Washington/Puget SoundBlood Center, Seattle (N01-HB-57125); Blood Cen-ters of the Pacific and University of California/Mt ZionMedical Center, San Francisco (N01-HB-57126); andNew England Research Institutes, Watertown, Mass,and Beth Israel Deaconess Medical Center, HarvardMedical School, Boston, Mass (N01-HB-57127).Viral Activation Transfusion Study Group: Clinical Sites:Case Western Reserve University: Roslyn Yomtovian,MD, Michael Chance, RN, Donna Hendrix, RN; George-town University: S. Gerald Sandler, MD, Karyn Hawk-ins, RN; Miriam Hospital/Brown University: Joseph D.Sweeney, MD, Maria Mileno, MD, Melissa Di Spigno,RN, Michelle Dupuis, MT (SSB); Mt. Sinai Medical Cen-ter: Kala Mohandas, MD, Frances R. Wallach, MD, LettyMintz, ANP; Ohio State University: Michael F. Para, MD,Jane Russell, RN, David Krugh, MT; University of Cali-fornia (San Diego): W. Christopher Mathews, MD,Peggy Mollen-Rabwin, RN; University of California (SanFrancisco): Steven G. Deeks, MD, Maurene Viele, MD,Chaolun Han, MD, Joanne Moore, MT (ASCP) SBB; Uni-versity of North Carolina, Chapel Hill: Charles van derHorst, MD, Mark E. Brecher, MD, Linh Ngo, FNP; Uni-versity of Pittsburgh: John W. Mellors, MD, Darrell J.Triulzi, MD, Sharon Riddler, MD; University of TexasMedical Branch: Richard B. Pollard, MD, Janice Curry,PA-C, Gerald Shulman, MD; University of Washington/Puget Sound Blood Center: Dee Townsend-McCall, RN,Jill Corson, RN; Central Laboratory: Blood Centers ofthe Pacific: Tzong-Hae Lee, MD, PhD, W. LawrenceDrew, MD, PhD, Megan Laycock; Coordinating Cen-ter: New England Research Institutes: Jane D. Carring-ton, RN, BS, Margot S. Kruskall, MD, Ruth Eisenbud,BA; Sponsoring Agency: National Heart, Lung, and BloodInstitute: George J. Nemo, PhD (project officer), Paul
R. McCurdy, MD, Dean Follmann, PhD; Data SafetyMonitoring Board: Jeffrey McCullough, MD (chair), Vic-tor DeGruttola, ScD, Peter Frame, MD, Janice G. Mc-Farland, MD, Ronald T. Mitsuyasu, MD, Elizabeth J.Read, MD, Dorothy E. Vawter, PhD.Acknowledgment: We thank Linda Page, BA, for as-sistance with manuscript preparation, the patients fortheir participation, and the nurses and transfusion ser-vice personnel at each medical center for their assis-tance.
REFERENCES
1. Hammer SM, Squires KE, Hughes MD, et al. A con-trolled trial of two nucleoside analogues plus indina-vir in persons with human immunodeficiency virus in-fection and CD4 cell counts of 200 per cubic millimeteror less. N Engl J Med. 1997;337:725-733.2. Palella FJ Jr, Delaney KM, Moorman AC, et al. De-clining morbidity and mortality among patients with ad-vanced human immunodeficiency virus infection. N EnglJ Med. 1998;338:853-860.3. Egger M, Hirschel B, Francioli P, et al. Impact of newantiretroviral combination therapies in HIV-infected pa-tients in Switzerland. BMJ. 1997;315:1194-1199.4. Moore RD, Chaisson RE. Natural history of HIV in-fection in the era of combination antiretroviral therapy.AIDS. 1999;13:1933-1942.5. Sullivan PS, Hanson DL, Chu SY, et al. Epidemiol-ogy of anemia in human immunodeficiency virus (HIV)-infected persons. Blood. 1998;91:301-308.6. Mocroft A, Kirk O, Barton SE, et al. Anaemia is anindependent predictive marker for clinical prognosis inHIV-infected patients from across Europe. AIDS. 1999;13:943-950.7. Moore RD, Keruly JC, Chaisson RE. Anemia and sur-vival in HIV infection. J Acquir Immune Defic Syndr.1998;19:29-33.8. Coyle TE. Hematologic complications of human im-munodeficiency virus infection and the acquired im-munodeficiency syndrome. Med Clin North Am. 1997;81:449-470.9. Kreuzer KA, Rockstroh JK. Pathogenesis and patho-physiology of anemia in HIV infection. Ann Hematol.1997;75:179-187.10. Patton LL. Hematologic abnormalities among HIV-infected patients. Oral Surg Oral Med Oral Pathol OralRadiol Endod. 1999;88:561-567.11. Moore RD. Human immunodeficiency virus in-fection, anemia, and survival. Clin Infect Dis. 1999;29:44-49.12. Henry DH, Beall GN, Benson CA, et al. Recombi-nant human erythropoietin in the treatment of ane-mia associated with human immunodeficiency virus(HIV) infection and zidovudine therapy. Ann Intern Med.1992;117:739-748.13. Phair JP, Abels RI, McNeill MV, Sullivan DJ. Re-combinant human erythropoietin treatment. Arch In-tern Med. 1993;153:2669-2675.14. Popovsky MA, Benson K, Glassman AB, et al. Trans-fusion practices in human immunodeficiency virus-infected patients. Transfusion. 1995;35:612-616.15. Sloand E, Kumar P, Klein HG, et al. Transfusionof blood components to persons infected with hu-man immunodeficiency virus type 1. Transfusion. 1994;34:48-53.16. Vamvakas E, Kaplan HS. Early transfusion and lengthof survival in acquired immune deficiency syndrome.Transfusion. 1993;33:111-118.17. Blumberg N, Peck K, Ross K, Avila E. Immune re-sponse to chronic RBC transfusion. Vox Sang. 1983;44:212-217.18. Brantley SG, Ramsey G. Red cell alloimmuniza-tion in multitransfused HLA-typed patients. Transfu-sion. 1988;28:463-466.19. Vamvakas EC. Transfusion-associated cancer re-currence and postoperative infection. Transfusion. 1996;36:175-186.
VIRAL ACTIVATION TRANSFUSION STUDY
1600 JAMA, March 28, 2001—Vol 285, No. 12 (Reprinted) ©2001 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a UCSF LIBRARY User on 05/27/2015
20. Blajchman MA, Bardossy L, Carmen R, et al. Allo-geneic blood transfusion-induced enhancement of tu-mor growth. Blood. 1993;81:1880-1882.21. George CD, Morello PJ. Immunologic effects ofblood transfusion upon renal transplantation, tumor op-erations, and bacterial infections. Am J Surg. 1986;152:329-337.22. Bordin JO, Heddle NM, Blajchman MA. Biologiceffects of leukocytes present in transfused cellular bloodproducts. Blood. 1994;84:1703-1721.23. Opelz G, Sengar DP, Mickey MR, Terasaki PI. Ef-fect of blood transfusions on subsequent kidney trans-plants. Transplant Proc. 1973;5:253-259.24. Opelz G, Vanrenterghem Y, Kirste G, et al. Pro-spective evaluation of pretransplant blood transfu-sions in cadaver kidney recipients. Transplantation. 1997;63:964-967.25. Williams JG, Hughes LE. Effect of perioperativeblood transfusion on recurrence of Crohn’s disease. Lan-cet. 1989;2:1524.26. Peters WR, Fry RD, Fleshman JW, Kodner IJ. Mul-tiple blood transfusions reduce the recurrence rate ofCrohn’s disease.Dis Colon Rectum.1989;32:749-753.27. Gatenby PA, Cameron K, Simes RJ, et al. Treat-ment of recurrent spontaneous abortion by immuni-zation with paternal lymphocytes. Am J Reprod Im-munol. 1993;29:88-94.28. Jensen LS, Kissmeyer-Nielsen P, Wolff B, Qvist N.Randomised comparison of leukocyte-depleted versusbuffy-coat-poor blood transfusion and complications af-ter colorectal surgery. Lancet. 1996;348:841-845.29. Houbiers JG, van de Velde CJ, van de WateringLM, et al. Transfusion of red cells is associated with in-creased incidence of bacterial infection after colorectalsurgery. Transfusion. 1997;37:126-134.30. Koval KJ, Rosenberg AD, Zuckerman JD, et al. Doesblood transfusion increase the risk of infection after hipfracture? J Orthop Trauma. 1997;11:260-265.31. Vamvakas EC. Multicenter randomized con-trolled trials in transfusion medicine. Transfus Med Rev.2000;14:137-150.32. Bordin JO, Chiba AK, Carvalho KI, et al. The ef-fect of unmodified or prestorage white cell-reduced al-logeneic red cell transfusions on the immune respon-siveness in orthopedic surgery patients. Transfusion.1999;39:718-723.33. Mincheff MS, Meryman HT, Kapoor V, et al. Bloodtransfusion and immunomodulation. Vox Sang. 1993;65:18-24.34. Dzik WH. Mononuclear cell microchimerism andthe immunomodulatory effect of transfusion. Trans-fusion. 1994;34:1007-1012.35. Klein HG. Immunomodulation caused by bloodtransfusion. In: Peltz LD, Swisher SN, Kleinman S, et al,eds. Clinical Practice of Transfusion Medicine, Edition3. New York, NY: Churchill Livingstone Inc; 1996:59-69.36. Hillyer CD, Lankford KV, Roback JD, et al. Trans-fusion of the HIV-seropositive patients. Transfus MedRev. 1999;13:1-17.37. Vamvakas EC. Meta-analysis of randomized con-trolled trials of the efficacy of white cell reduction inpreventing HLA-alloimmunization and refractoriness torandom-donor platelet transfusions. Transfus Med Rev.1998;12:258-270.38. Blajchman MA. Transfusion-associated immuno-modulation and universal white cell reduction. Trans-fusion. 1999;39:665-670.39. Dzik S, Aubuchon J, Jeffries L, et al. Leukocyte re-duction of blood components. Transfus Med Rev. 2000;14:34-52.40. American Association of Blood Banks. BPAC rec-ommends universal leukoreduction. AABB News Briefs.1998;20:16.41. AuBuchon JP, Birkmeyer JD, Busch MP. Safety ofthe blood supply in the United States. Ann Intern Med.1997;127:904-909.42. Busch MP, Lee T-H, Heitman J. Allogeneic leu-
kocytes but not therapeutic blood elements induce re-activation and dissemination of latent human immu-nodeficiency virus type 1 infection. Blood. 1992;80:2128-2135.43. Soderberg-Naucler C, Fish KN, Nelson JA. Reac-tivation of latent human cytomegalovirus by alloge-neic stimulation of blood cells from healthy donors. Cell.1997;91:119-126.44. Olding LB, Jensen FC, Oldstone MB. Pathogen-esis of cytomegalovirus infection, I. J Exp Med. 1975;141:561-572.45. Cheung K-S, Lang DJ. Transmission and activa-tion of cytomegalovirus with blood transfusion.J Infect Dis. 1977;135:841-845.46. Busch MP, Collier A, Gernsheimer JD, et al. TheViral Activation Transfusion Study (VATS). Transfu-sion. 1996;36:854-859.47. Mudido PM, Georges D, Dorazio D, et al. Humanimmunodeficiency virus type 1 activation after bloodtransfusion. Transfusion. 1996;36:860-865.48. Groopman JE. Impact of transfusion on viral loadin human immunodeficiency virus infection. Semin He-matol. 1997;34(suppl 2):27-33.49. Karnofsky DA. Problems and pitfalls in the evalu-ationofanticancerdrugs.Cancer.1965;18:1517-1528.50. Zelen M. The randomization and stratification ofpatients to clinical trials. J Chronic Dis. 1974;27:365-375.51. Blatt SP, Lucey CR, Butzin CA, et al. Total lympho-cyte count as a predictor of absolute CD4+ count andCD4+ percentage in HIV-infected persons. JAMA. 1993;269:622-626.52. Fiebig EW, Johnson DK, Hirschkorn DF, et al. Lym-phocyte subset analysis on frozen whole blood. Cy-tometry. 1997;29:340-350.53. Lee TH, Sakahara NS, Fiebig EW, et al. Quantita-tion of white cell subpopulations by polymerase chainreaction using frozen whole-blood samples. Transfu-sion. 1998;38:262-270.54. Report of the NIH Panel to Define Principles ofTherapy of HIV Infection. Ann Intern Med. 1998;128:1057-1078.55. Mulder J, McKinney N, Christopherson C, et al.Rapid and simple PCR assay for quantitation of hu-man immunodeficiency virus type 1 RNA in plasma.J Clin Microbiol. 1994;32:292-300.56. Long CM, Drew L, Miner R, et al. Detection of cy-tomegalovirus in plasma and cerebrospinal fluid speci-mens from human immunodeficiency virus-infected pa-tients by the AMPLICOR CMV test. J Clin Microbiol.1998;36:2434-2438.57. Pellegrin I, Garrigue I, Binquet C, et al. Evaluationof new quantitative assays for diagnosis and monitor-ing of cytomegalovirus disease in human immunode-ficiency virus-positive patients. J Clin Microbiol. 1999;37:3124-3132.58. Lederman MM, Kalish LA, Asmuth D, et al. ‘Mod-eling’ relationships among HIV-1 replication, immuneactivation and CD4+ T-cell losses using adjusted cor-relative analyses. AIDS. 2000;14:951-958.59. Lee TH, Stromberg RR, Heitman J, et al. Quan-titation of residual white cells in filtered blood com-ponents by polymerase chain reaction amplificationof HLA DQ-A DNA. Transfusion. 1994;34:986-994.60. Centers for Disease Control and Prevention. 1993revised classification system for HIV infection and ex-panded surveillance case definition for AIDS among ado-lescents and adults. MMWR Morb Mortal Wkly Rep.1992;417(RR-17):1-20.61. Wang Y, Tao L, Mitchel l E, et al. Al lo-immunization elicits CD8+ T cell-derived chemokines,HIV suppressor factors and resistance to HIV infectionin women. Nat Med. 1999;5:1004-1009.62. British Committee for Standards in Haematology,Blood Transfusion Task Force. Guidelines on the clini-cal use of leucocyte-depleted blood components. Trans-fus Med. 1998;8:59-71.63. DanishSocietyofClinical Immunology.Danish rec-
ommendations for thetransfusionof leukocyte-depletedblood components. Vox Sang. 1996;70:185-186.64. Schechter GP, Soehnlen F, McFarland W. Lym-phocyte response to blood transfusion in man. N EnglJ Med. 1972;287:1169-1173.65. Fiebig E, Hirschkorn DF, Maino VC, et al. Assess-ment of donor T-cell function in cellular blood com-ponents by the CD69 induction assay. Transfusion.2000;40:761-770.66. HyllnerM,Arnestad JP,Bengtson JP, et al.Comple-mentactivationduringstorageofwholeblood, redcells,plasma,andbuffycoat.Transfusion.1997;37:264-268.67. Kristiansson M, Soop M, Saraste L, Sundqvist KG.Cytokines in stored RBC concentrates. Acta Anaesthe-siol Scand. 1996;40:496-501.68. Weisbach V, Wanke C, Zingsem J, et al. Cytokinegeneration in whole blood, leukocyte-depleted and tem-porarily warmed RBC concentrates. Vox Sang. 1999;76:100-106.69. Frabetti F, Musiani D, Marini M, et al. White cellapoptosis in packed red cells. Transfusion. 1998;38:1082-1089.70. Chin-Yee I, Keeney M, Krueger L, et al. Superna-tant from stored red cells activates neutrophils. Trans-fus Med Rev. 1998;8:49-56.71. Prince HE, Arens L. Effect of storage on lympho-cyte surface markers in whole blood units. Transplan-tation. 1986;41:235-238.72. Trial to Reduce Alloimmunization to Platelets StudyGroup. Leukocyte reduction and ultraviolet B irradia-tion of platelets to prevent alloimmunization and re-fractoriness to platelet transfusions. N Engl J Med. 1997;337:1861-1869.73. Jensen LS. Benefits of leukocyte-reduced bloodtransfusion in surgical patients. Curr Opin Hematol.1998;5:376-380.74. Kirkley SA, Cowles J, Pellegrini VD, et al. Blood trans-fusion and total joint replacement surgery.Transfus Med.1998;8:195-204.75. Kovacs JA, Vogel S, Albert JM, et al. Controlled trialof interleukin-2 infusions in patients infected with thehuman immunodeficiency virus. N Engl J Med. 1996;335:1350-1356.76. deGraan-Hentzen YC, Gratama JW, Mudde GC,et al. Prevention of primary cytomegalovirus infectionin patients with hematologic malignancies by inten-sive white cell depletion of blood products. Transfu-sion. 1989;29:757-760.77. Gilbert GL, Hayes K, Hudson IL, James J, for theNeonatal Cytomegalovirus Infection Study Group. Pre-vention of transfusion-acquired cytomegalovirus in-fection in infants by blood filtration to remove leuco-cytes. Lancet. 1989;1:1228-1231.78. Bowden RA, Slichter SJ, Sayers M, et al. A com-parison of filtered leukocyte-reduced and cytomega-lovirus (CMV) seronegative blood products for the pre-vention of transfusion-associated CMV infection aftermarrow transplant. Blood. 1995;86:3598-3603.79. Hillyer CD, Emmens RK, Zago-Novaretti M, Berk-man EM. Methods for the reduction of transfusion-transmitted cytomegalovirus infection. Transfusion.1994;34:929-934.80. Larsson S, Soderberg-Naucler C, Wang FZ, Mol-ler E. Cytomegalovirus DNA can be detected in periph-eral blood mononuclear cells from all seropositive andmost seronegative healthy blood donors over time.Transfusion. 1998;38:271-278.81. Spector SA, Hirata KK, Newman TR. Identifica-tion of multiple cytomegalovirus strains in homo-sexual men with acquired immunodeficiency syn-drome. J Infect Dis. 1984;150:953-956.82. Eizuru Y, Minamishima Y, Hirose M, et al. Isolationof multiple cytomegalovirus strains from a patient withadult T cell leukemia. Intervirology. 1990;31:355-358.83. Baldanti F, Sarasini A, Furione M, et al. Coinfec-tion of the immunocompromised but not the immu-nocompetent host by multiple human cytomegalovi-rus strains. Arch Virol. 1998;143:1701-1709.
VIRAL ACTIVATION TRANSFUSION STUDY
©2001 American Medical Association. All rights reserved. (Reprinted) JAMA, March 28, 2001—Vol 285, No. 12 1601
Downloaded From: http://jama.jamanetwork.com/ by a UCSF LIBRARY User on 05/27/2015
Related Documents











