'Let me tell you what I really think about you' – evaluating nursing managers using anonymous staff feedback ILYA KAGAN MA, RN 1 , RONIT KIGLI-SHEMESH MA, RN 2 and NILLI TABAK PhD, RN, LLB 3 1 Head, Continuing Nursing Education Unit, Tel-Aviv University, Tel Aviv and Nursing Management Department, Assaf-HaRofeh Medical Center, Tzrifin, Israel, 2 Director of Nursing, Ness-Ziona Mental Health Center and Nursing Department, Tel-Aviv University, Tel Aviv and 3 Head, Nursing Department and Head, Ethics and Law Unit, School of Health Professions, Tel-Aviv University, Tel Aviv, Israel Introduction Nursing in Israel has undergone many organizational and managerial changes in recent years and its workings have come under intense scrutiny. Eliminating tenure in managerial positions has been proposed and increased efficiency and higher productivity has been demanded from nursing directors (Riba et al. 2004). The period- ical rotation of managerial posts and making senior managers’ retention of their job conditional on a com- prehensive achievements’ evaluation are other sugges- tions. Employee evaluation is considered a key manage- ment tool today (Martzki & Gureli 1990, Weizner 1998, McCarthy 2000, Harmati 2003, Kaspi & Ben-Dor 2003, Garman et al. 2004). In Israel, nurses’ performance evaluation generally takes the form of senior personnel evaluating junior employees – a ward nurse evaluated by her head nurse, or outpatient clinic head nurses evaluated by the district head nurse – and is performed periodically, at annual or semiannual intervals, or when the nurse enrols for special or ad- vanced training and the training facility requires evaluation for admittance. Despite the relatively well- developed procedures for the evaluation of junior employees, having line staff evaluate their managers and senior nurses has not achieved established status. We did not find any Israeli reports of subordinates evaluating senior nursing managers. We know that there have been local efforts to conduct dialogues in Correspondence Ilya Kagan 31/1 Tavor St PO Box 2217 Gan-Yavne 70800 Israel E-mail: [email protected] or [email protected] KAGAN I ., KIGLI-SHEMESH R. & TABAK N . (2006) Journal of Nursing Management 14, 356– 365 'Let me tell you what I really think about you' – evaluating nursing managers using anonymous staff feedback The evaluation of employees by their superiors is standard managerial practice but the value of the evaluation of superiors by their employees is much less recognized. This study describes a project where for 3 years (2000–02), in an Israeli mental health center, the Director of Nursing, clinical supervisors, ward head nurses and their deputies were evaluated by nurses and nursing aides. Feedback was gathered through anonymous questionnaires under conditions of confidentiality. Based on the findings, steps were taken to improve managers’ performance. Evaluators were also requested to evaluate the project’s contribution to themselves and the hospital in a second, open questionnaire. All parties, evaluators and evaluated, expressed satisfaction and recommended that the project continue on a regular basis. Nurses felt empowered and respected and that manager–subordinate relations were improved. Other results and recommendations are discussed. Keywords: anonymity, employee evaluation, nursing managers Accepted for publication: 21 April 2005 Journal of Nursing Management, 2006, 14, 356–365 356 ª 2006 Blackwell Publishing Ltd

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

'Let me tell you what I really think about you' – evaluating nursingmanagers using anonymous staff feedback
ILYA KAGAN MA , RN1, RONIT KIGLI-SHEMESH MA , RN
2 and NILLI TABAK P hD , RN , L L B3
1Head, Continuing Nursing Education Unit, Tel-Aviv University, Tel Aviv and Nursing Management Department,Assaf-HaRofeh Medical Center, Tzrifin, Israel, 2Director of Nursing, Ness-Ziona Mental Health Center and NursingDepartment, Tel-Aviv University, Tel Aviv and 3Head, Nursing Department and Head, Ethics and Law Unit, Schoolof Health Professions, Tel-Aviv University, Tel Aviv, Israel
Introduction
Nursing in Israel has undergone many organizational
and managerial changes in recent years and its workings
have come under intense scrutiny. Eliminating tenure in
managerial positions has been proposed and increased
efficiency and higher productivity has been demanded
from nursing directors (Riba et al. 2004). The period-
ical rotation of managerial posts and making senior
managers’ retention of their job conditional on a com-
prehensive achievements’ evaluation are other sugges-
tions.
Employee evaluation is considered a key manage-
ment tool today (Martzki & Gureli 1990, Weizner
1998, McCarthy 2000, Harmati 2003, Kaspi &
Ben-Dor 2003, Garman et al. 2004). In Israel, nurses’
performance evaluation generally takes the form of
senior personnel evaluating junior employees – a ward
nurse evaluated by her head nurse, or outpatient clinic
head nurses evaluated by the district head nurse – and
is performed periodically, at annual or semiannual
intervals, or when the nurse enrols for special or ad-
vanced training and the training facility requires
evaluation for admittance. Despite the relatively well-
developed procedures for the evaluation of junior
employees, having line staff evaluate their managers
and senior nurses has not achieved established status.
We did not find any Israeli reports of subordinates
evaluating senior nursing managers. We know that
there have been local efforts to conduct dialogues in
Correspondence
Ilya Kagan
31/1 Tavor St
PO Box 2217
Gan-Yavne 70800
Israel
E-mail: [email protected] or
KAGAN I., K IGL I - SHEMESH R. & TABAK N. (2006) Journal of Nursing Management 14, 356–
365
'Let me tell you what I really think about you' – evaluating nursing managersusing anonymous staff feedback
The evaluation of employees by their superiors is standard managerial practice butthe value of the evaluation of superiors by their employees is much less recognized.
This study describes a project where for 3 years (2000–02), in an Israeli mental
health center, the Director of Nursing, clinical supervisors, ward head nurses andtheir deputies were evaluated by nurses and nursing aides. Feedback was gathered
through anonymous questionnaires under conditions of confidentiality. Based on
the findings, steps were taken to improve managers’ performance. Evaluators werealso requested to evaluate the project’s contribution to themselves and the hospital
in a second, open questionnaire. All parties, evaluators and evaluated, expressed
satisfaction and recommended that the project continue on a regular basis. Nursesfelt empowered and respected and that manager–subordinate relations were
improved. Other results and recommendations are discussed.
Keywords: anonymity, employee evaluation, nursing managers
Accepted for publication: 21 April 2005
Journal of Nursing Management, 2006, 14, 356–365
356 ª 2006 Blackwell Publishing Ltd

which junior employees were encouraged to express
their opinions openly.
The aim of this project is to describe a 3-year project
where anonymous feedback supplied by subordinates
was tried (at the Abarbanel Mental Health Center, in
Bat Yam, Israel) as a method of evaluating the per-
formance of middle and senior nursing managers. And
we also examine what the Abarbanel Center’s nursing
staff, both evaluators and evaluated, had to say about
the benefits and disadvantages, the implications and
contributions of this type of evaluation as a manage-
ment tool.
Background
Employee evaluation today is considered an integral
part of business life. At least once a year both employers
and employees formally undergo an evaluation of
workplace performance. The declared purpose is to
identify the activities and components required for the
successful performance of specific organizational tasks.
It usually consists of two elements: a comprehensive
questionnaire and feedback supplied to the question-
naire items in discussion with a superior (Stockman
1996, Kaspi & Ben-Dor 2003). Two other principal
reasons are given for performing employee evaluation:
it increases motivation and thereby performance, and is
an important managerial tool for manpower decision-
making (salaries, promotions, dismissals, etc.). Some
experts contend, however, that employee evaluation is
gradually losing its impact (Longeneker 1999).
In Israel, the overall impression gained from the lit-
erature and from our experience is that employee eva-
luation is almost always conducted on the ‘top–down’
principal, reflecting the existing organizational hier-
archy. Junior employees are evaluated by their imme-
diate superiors; middle management is assessed by
senior management, and so on. In the nursing commu-
nity, worker assessment tends to lack focus and to lose
momentum almost entirely when it comes to senior
managers, such as directors of nursing and nursing
supervisors.
Evaluation from different angles
An alternative approach to evaluating performance,
especially where senior staff is involved, is to apply the
principal of ‘bottom–up’ evaluation. In other words,
employees appraise their managers. Both the ‘top–
down’ and ‘bottom–up’ approaches have merits and
each requires and serves a different management
approach. McCauley and Moxley (1996) claim that
performance evaluation by different status groups of
employees throws light on different features of per-
formance. Each group has its own viewpoint. The dis-
parity of reactions derives from a number of factors:
first, levels of interaction and contact will allow some
groups to appraise leadership aptitude more reliably
than others. Subordinates, for example, have a clearer
view of their manager’s efforts to develop and streng-
then his staff than his colleagues or superiors will have.
Secondly, the manager’s behaviour will differ towards
different groups. Her relationship to her subordinate
staff will not be the same as with his colleagues or
superiors. Evaluators’ expectations will also differ; the
managers’ staff will look for different qualities from
those expected by his superiors. Furnham (2002) has
examined the qualities looked for in a good employee
under three situations; evaluation by superiors, by peers
and by subordinates. A group of 149 subjects, of whom
half were top managers, a third middle management
and the rest juniors, were asked to define the ideal
manager, colleague and subordinate. Scores differed
significantly according to the expectations of the
responder.
Appreciating the disparities in perception of different
evaluator groups can thus both contribute to greater
self-awareness on the part of the evaluated and also be
used to design a more efficient evaluation process. The
evaluation of a nursing manager by junior nurses will
emphasize different characteristics and emphasize dif-
ferent features from an evaluation by her superiors, and
also promote trust and respect between them (Farrell
et al. 2002).
Bottom–up evaluation
Most of the research publications concerning manage-
ment evaluation come from industry or business. Most
are concerned with the variables that affect meeting
production quotas (Stathakopoulos 1998, Lockyer
2003) and derive from the assumption that evaluation
performance will improve the productivity of both
managers and staff. One exception is Porter (1997) who
evaluated management and leadership skills as viewed
by employees in an electronics factory. A group of 297
workers filled out a comprehensive evaluation ques-
tionnaire relating to output quotas, leadership qualities
and managerial performance. Based on the findings, a
programme was set up for improving the managers’
management and leadership skills.
A popular tool for evaluating performance is ‘360-
degree-feedback’ – a comprehensive approach by which
a manager obtains multisource feedback from his
Staff feedback
ª 2006 Blackwell Publishing Ltd, Journal of Nursing Management, 14, 356–365 357

superiors, his colleagues, his subordinates, his instruc-
tors and even his clients. The evaluators are given
structured tools and requested to score the subject on
his performance. This can provide rigorous information
of high quality that can then be used for enrichment and
self-improvement (Luthans & Farner 2002, Lockyer
2003, Garman et al. 2004). It can also enable the
manager to evaluate his professional image, as it is
perceived by all around him in his working context and
so become more self-aware and successful. It is most
important to emphasize, however, that the reliability
and credibility of the feedback are governed by the
degree of anonymity of the responses. To protect indi-
vidual evaluators it is customary to present all ratings as
a summary score for each evaluator group (McCauley
& Moxley 1996, Olson 1996). There is a number of
reports on development of nursing managers’ evalua-
tion tools. Garman et al. (2004) developed and valid-
ated a 360-degree-feedback instrument for health care
administrators. In a further study, a data collection
instrument to assess the professional competence of
chief nursing executive by nursing personnel in organ-
ized delivery systems was developed and validated
(Farrell et al. 2002, Farrell 2004). Yet another Manager
Evaluation Tool was implemented by a director of
medical–surgical and transitional care (Olson 1996).
There is room to develop and research the subject of
manager evaluation in the health care system in Israel.
Our own managerial experience has been that in many
organizations the activity has not been implemented
systematically: evaluation by employees is made spor-
adically if at all. Some organizations attempt to obtain
feedback from employees through individual or group
dialogue. Such an initiative, although important, is
problematic as it is influenced by many factors. These
are principally the nervous tension associated with the
confrontation, the difficulty in openly expressing an
opinion from an inferior rank, and the evaluator’s
dependence on the rulings of the person who is
requesting the feedback. Even without the manager
intending it, the situation can sometimes become
threatening for the employee. Furthermore, one of the
most common mistakes made in appraising worker
performance and productivity by individual interview,
is interviewer bias, for the outcome largely depends on
the expectations and patterns of thought of the ques-
tioner himself (Furnham 2002).
McCauley and Moxley (1996), in discussing 360-
degree evaluation, define a number of guidelines that
should be adhered to when gathering feedback on
managers. The feedback itself should be genuinely
reflective of the scope and content of the evaluated
manager’s activities. The evaluation tool must be reli-
able and valid and designed to allow unproblematic
interpretation of the data. Significantly, the authors add
that feedback gathering in itself does not make a man-
ager more effective. This aim is achieved only after a
stepwise process of self-criticism and improvement that
the manager initiates after receiving the feedback and
with the strong support of the system employing him.
The very act of handing over the feedback to the eval-
uated manager and his superiors triggers sensitivities
that must be taken into account. The transfer often
leaves the evaluated very tense. Usually, they wish to
know who gave them such an assessment, and the weak
points needing correction will often be met with
defensive and emotional responses. To forestall this
tension and minimize the objections the following
points should be observed: (1) include the evaluated in
the decision to employ this evaluation procedure;
(2) define clearly the objectives of the evaluation;
(3) guarantee the confidentiality of the information
received; (4) allow the manager time to digest the
feedback received; (5) bring in an experienced instructor
to work one-on-one with the evaluated to clarify the
meaning of the feedback and reinforce the outstanding
weaknesses revealed. Another important consideration
is the timing of the evaluation relative to the subject’s
career. Suitable times are after the probationary period,
before a promotion, or when performance is in decline
due to burnout or stagnation (McCauley & Moxley
1996).
Anonymous evaluation
There is always the possibility of a manager retaliating
on his evaluators for their criticism. This problem can
usually be avoided by maintaining data confidentiality
and evaluator anonymity. However, it is difficult to
guarantee this with a small staff in a small organiza-
tion. Collins (2002) described a project conducted at
the Department of Environmental Health in Texas,
USA, in the framework of which managers were
evaluated by subordinates but not anonymously. The
results showed that the feedback was diplomatic rather
than critical and did not cross the barrier between
what might have been said and what the manager
would like to hear. Anonymous feedback is usually
proposed as overcoming the shortcomings of the face-
to-face method (Olson 1996, Farrell 2004). The col-
lection and interpretation bias could be related to the
anonymity of evaluation, i.e. evaluated workers can
overstate their negative feelings as to the manager
(Barnes 1997).
I. Kagan et al.
358 ª 2006 Blackwell Publishing Ltd, Journal of Nursing Management, 14, 356–365

Several Israeli organizations that are strictly hierar-
chical nonetheless insist on subordinates supplying
anonymous feedback on their superiors. In the Israeli
Defense Forces anonymous feedback plays a role in
some situations as a significant, even obligatory, step for
an officer to retain his position or continue training.
Another example is the evaluation of university lectur-
ers by their students, who fill out a comprehensive
anonymous questionnaire. In some academic institu-
tions this evaluation plays an important role in pro-
motions and sometimes can determine continuation of
employment. Zevulun (1993) describes the application
of a similar approach, under which 24 000 managers
over a period of 3 years were evaluated by subordinates
and also conducted simultaneously a process of self-
evaluation. There is a number of studies and reports
that recommends nurses supplying feedback on their
managers, maintaining anonymity to encourage a
higher level of compliance and quality of response
(Olson 1996, Willard 2000, Farrell et al. 2002, Farrell
2004). The possibility of applying the approach to
senior staff in the Israeli health services has been raised
from time to time in congresses but has yet to be
implemented.
This study
The project at the Abarbanel Mental Health Center,
which we report on, was based on the concepts, pre-
sented above – that anonymous feedback on superiors
generates trustworthy and impartial evaluation at the
same time as it ensures maximum security for the
subordinate evaluators. The essence of the project was
that to the existing traditional annual top–down
evaluation of ward nurses by their head nurses it
added an anonymous evaluation in the opposite
direction. The idea behind the project arose when a
sharp change in hospital management and managerial
approach raised the need for reliable feedback on
existing senior and middle managerial staff. We also
added another feature, unique as far as we know – an
evaluation of the project itself: Should it continue?
What were its negative and positive aspects? How to
improve it?
The tools
To evaluate the management skills of senior nurses
(ward head nurses and their deputies) and nursing
managers (clinical supervisors) the Anonymous Feed-
back Instrument for Evaluating Managers (see Appen-
dix 1) was used. The tool, constructed by the project
planners on the basis of the published literature, focused
only on management skills and ignored clinical skills,
patient care, attitudes to patients, etc., for two reasons:
(1) to narrow the focus to what most interested the
evaluators and (2) to keep the content of the tool uni-
form for all evaluated: clinical supervisors do not care
directly for patients. The tool did not include demo-
graphic data on the responder in order to guarantee
anonymity. It consisted of 16 statements (reduced at the
data analysis stage to 14) regarding human relations,
communications, support for teamwork, problem sol-
ving, credibility and openness, competence and staff
development. An outside senior nursing manager and
two managers of psychiatric departments in our hospi-
tal tested the questionnaire’s face validity. Reliability
and internal consistency rated 0.73–0.91 on the Cron-
bach’s-a test. At the time of the project we did not find a
reliable and valid feedback survey for health care sys-
tems. Later, the appropriate tools were published
(Farrell et al. 2002, Garman et al. 2004).
The Project Evaluation Questionnaire (see Appen-
dix 2) was used to elicit the responders’ evaluation of
the evaluation project itself. It consisted of seven ques-
tions, three closed and four open-ended. We inserted
both open and closed questions in order to obtain as
wide and varied an outlook as possible and to allow free
expression. The closed questions were framed to furnish
direct answers on the evaluators’ overall satisfaction
with the project. The four open questions were designed
to allow a more detailed and wide-ranging appraisal on
the importance of the project, whether it should con-
tinue, its contribution, its strong and weak points, etc.
The replies to the open questions were grouped into
categories by area of content.
Project design and development
Initial response of senior and junior staff to the project
Abarbanel nurses were accustomed to be evaluated by
their immediate superiors once a year. Following a
change in the hospital’s management, in 2000 the
Director of Nursing and one of her five clinical nurse
supervisors proposed the idea of paralleling that top–
down evaluation with an evaluation in the other
direction. Only one other supervisor was supportive.
The objectors expressed themselves either through act-
ive refusal – they would not allow the project in the
wards they supervised – or by indirect, passive resist-
ance and simply ignoring the proposal. From its outset
the project aroused feelings of anxiety and worry,
which persisted even after the questionnaire had been
completed.
Staff feedback
ª 2006 Blackwell Publishing Ltd, Journal of Nursing Management, 14, 356–365 359

As for the junior staff, the evaluators, remarks and
questions were posed about the guarantee of complete
anonymity. Some were even inclined not to write their
answers, fearing their superiors might identify their
handwriting. From the emotional perspective, the nurses
had mixed feelings. At one extreme, they enthusiastic-
ally welcomed the chance to spell out what they had not
been able to say to their superiors, even anonymously,
for many years. At the other extreme, they feared
exposure for their lack of trust. Written evidence for this
emerges from the analysis of the open-ended questions in
the second tool (see Table 1). Ten nurses reported a
feeling of discomfort, embarrassment and anxiety when
writing their evaluation. As time progressed into the
second and third year of the project, the objections
raised became gradually fewer. Evaluation of senior staff
by their juniors came to be seen as inseparable from the
overall process of workforce evaluation. Junior nurses
asked when the evaluation of the seniors was to take
place and even requested that it take place prior to that
of the evaluation in the other direction.
Project design
2000
As noted, in 2000 only two of the five clinical super-
visors were in sympathy with the project and one
offered to participate in a pilot run. With the approval
of the hospital director and with the agreement of the
head nurses and their deputies of the three wards under
that supervisor’s supervision, the project was launched.
The nursing staff (including auxiliaries) of the three
wards supplied the anonymous feedback relating to the
clinical supervisor and to their own head and deputy
head nurse (i.e. all evaluators evaluated the supervisor
but the staff of each ward evaluated only their own two
head nurses, not the head nurses of other wards).
The Anonymous Evaluation Questionnaire was dis-
tributed and filled out at ward staff meetings, after all
senior nurses (head nurses, deputies and supervisors)
had left the room. The completed forms were put in
envelopes, sealed and gathered up by one of the par-
ticipants. Participants were then asked to fill out the
Project Evaluation Form, which was then collected
separately. All the forms were delivered together to an
outside analyst for analysis of the findings. His analysis
was delivered unopened to the Director of Nursing.
Each of the evaluated heard the findings concerning him
or her individually, the evaluated supervisor from the
Director of Nursing and the head nurses and deputies
from the supervisor. In these one-on-one meetings the
findings were discussed in detail and guidance given by
the superior on what to improve and how. Each person
evaluated was given the feedback scores of each state-
ment in the form plus a summary score (the supervisor
received a summary score from each ward separately
and of all wards together; see Table 5).
In response to the findings, a training initiative
designed to improve and strengthen leadership and
administrative skills was introduced. A series of
Table 1Nine items from the clinical supervisor and head nurse evaluation form, showing the overall scores from one ward and their trend from 2000 to2001
Statement
Score 1–5 Score 1–100
Trend2000 2001 2000 2001
Works to improve the atmosphere among staff 4.41 3.87 88.2 77.4 DecreaseMaintains good personal relations 4.47 4.47 89.4 89.4 No changeIs open to others' opinions 4.18 4.27 83.6 85.4 No changePromotes projects at the health center 4.81 4.67 96.2 93.4 DecreaseTreats all staff equally 4.13 3.36 82.6 67.2 DecreaseIs a superior one can trust 3.87 3.93 77.4 78.6 No changePromotes professional training and advancement of staff 4.25 4.40 85 88 IncreaseWorks to promote the status of nursing staff at the center 4.25 4.0 85 80 DecreaseIs a pillar of support when needed 4.71 4.07 94.2 81.4 Decrease
Table 2Project evaluation, 2000–02
Year
Number ofProject EvaluationForms distributed
Number of evaluationforms returned
Responserate (%)
2000 46 28 612001 17* 13* 762002 22� 22 100Total 85 63 79
*The staffers who had returned a project evaluation in 2000 wereasked not to do so again in 2001, hence the low numbers.�Includes only head nurses and deputy head nurses. By contrast, in2000 and 2001 no head nurse or deputy head nurse filled out aProject Evaluation Form.
I. Kagan et al.
360 ª 2006 Blackwell Publishing Ltd, Journal of Nursing Management, 14, 356–365

interactive workshops led by outside instructors was
arranged for head and deputy head nurses, as well as
two workshops for supervisors.
The project evaluation
Table 2 shows the number of Project Evaluation Forms
distributed and returned for the 3 years of the project.
2001
The second run of the project followed the same
structure as the first, except that a second supervisor –
the only other that supported the project – agreed to be
evaluated. However, she stipulated that at this stage,
only one of the three wards she was responsible for
would evaluate her. The three wards polled in 2000
were repolled, so that in all four wards were polled. The
head nurses and deputies evaluated the previous year
could see if their scores had risen or fallen in the interim
(see Table 1). Again, in response to the scores the
Director of Nursing provided instruction and guidance
through ongoing personal supervision, which focused
on discussion of different conflict situations, interper-
sonal aspects of manager–employee relationship, and
enhancement of administration and leadership skills, to
the two clinical supervisors evaluated. In addition, all
senior nurse managers participated in a longitudinal
workshop, which was initiated by the Director of
Nursing and was supplied by external expertise in hu-
man resources management.
2002
The third stage of the project was planned to follow the
same structure as the first two with one important
addition. After the project’s second run, the ward head
nurses asked to give feedback on all senior nurse man-
agers that is the Director of Nursing and all her five
supervisors. The Director of Nursing agreed and in her
wake also the three stand-out supervisors. For two
reasons the body of evaluators was restricted to head
and deputy head nurses: (1) it was not felt practicable to
poll all the hospital’s nurses (the five supervisors were
responsible for all wards in the hospital) and (2) the
Director of Nursing and her team of supervisors worked
far more with head and deputy head nurses than with
rank and file nursing staff. This element of the evalua-
tion was carried out but before the head nurses them-
selves could be evaluated for a third year the hospital’s
new management ran into trouble with the staff over
other issues, the Director of Nursing quit the hospital,
and the evaluation project, planned to be a long-term
constituent of the hospital management regime, came to
a premature end.
Discussion
Perhaps the two outstanding findings of the evaluation
project are (1) the high response rates over the 3 years it
lasted – about 90% for the Personal Evaluation Ques-
tionnaire (Table 3) and almost 80% for the Project
Evaluation Questionnaire (Table 2) and (2) that 87% of
the responses to the second questionnaire supported and
justified the idea of juniors evaluating their seniors
(Table 4). About 61% of the responses to the second
questionnaire stated positively that junior–senior eval-
uation should continue at least once a year and all the
Table 3Evaluated and evaluators, 2000–02
Year Evaluated EvaluatorsResponse rate
(%)Number of
wards
2000 1 Nursing supervisor ? Nurses* 93 33 Ward head nurses ? Nursing aides*2 Deputy ward head nurses 43 Total responders6 Total managers evaluated 46 Total staff receiving
questionnaires2001 2 Nursing supervisors ? Nurses* 81 4�
4 Ward head nurses ? Nursing aides*3 Deputy ward head nurses 51 Total responders�
9 Total managers evaluated 63 Total staff receivingquestionnaires�
2002 1 Director of Nursing 21 Ward head nurses 100 All5 Nursing supervisors� 1 Deputy ward head nurse6 Total managersevaluated
22 Total staff receivingquestionnaires
*The distribution of responders between nurses and nursing aides is not known. There were on averagefour aides in each ward.�Includes the same wards and staffers as in 2000.�One supervisor was also training coordinator.
Staff feedback
ª 2006 Blackwell Publishing Ltd, Journal of Nursing Management, 14, 356–365 361
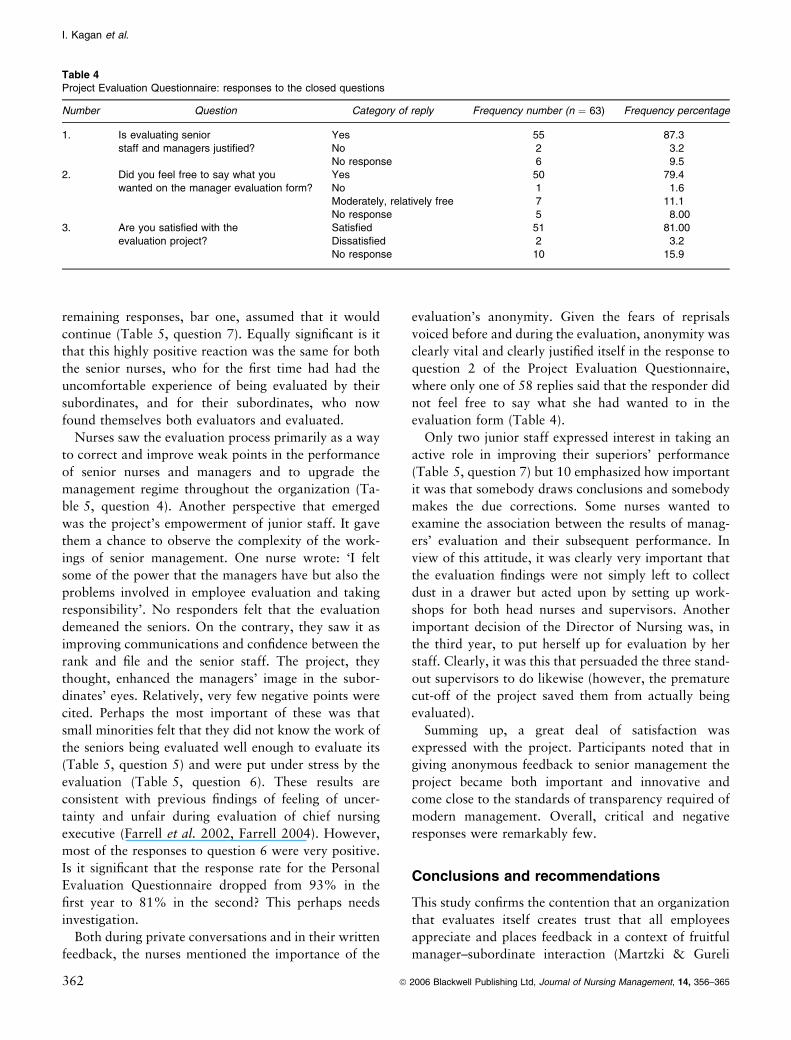
remaining responses, bar one, assumed that it would
continue (Table 5, question 7). Equally significant is it
that this highly positive reaction was the same for both
the senior nurses, who for the first time had had the
uncomfortable experience of being evaluated by their
subordinates, and for their subordinates, who now
found themselves both evaluators and evaluated.
Nurses saw the evaluation process primarily as a way
to correct and improve weak points in the performance
of senior nurses and managers and to upgrade the
management regime throughout the organization (Ta-
ble 5, question 4). Another perspective that emerged
was the project’s empowerment of junior staff. It gave
them a chance to observe the complexity of the work-
ings of senior management. One nurse wrote: ‘I felt
some of the power that the managers have but also the
problems involved in employee evaluation and taking
responsibility’. No responders felt that the evaluation
demeaned the seniors. On the contrary, they saw it as
improving communications and confidence between the
rank and file and the senior staff. The project, they
thought, enhanced the managers’ image in the subor-
dinates’ eyes. Relatively, very few negative points were
cited. Perhaps the most important of these was that
small minorities felt that they did not know the work of
the seniors being evaluated well enough to evaluate its
(Table 5, question 5) and were put under stress by the
evaluation (Table 5, question 6). These results are
consistent with previous findings of feeling of uncer-
tainty and unfair during evaluation of chief nursing
executive (Farrell et al. 2002, Farrell 2004). However,
most of the responses to question 6 were very positive.
Is it significant that the response rate for the Personal
Evaluation Questionnaire dropped from 93% in the
first year to 81% in the second? This perhaps needs
investigation.
Both during private conversations and in their written
feedback, the nurses mentioned the importance of the
evaluation’s anonymity. Given the fears of reprisals
voiced before and during the evaluation, anonymity was
clearly vital and clearly justified itself in the response to
question 2 of the Project Evaluation Questionnaire,
where only one of 58 replies said that the responder did
not feel free to say what she had wanted to in the
evaluation form (Table 4).
Only two junior staff expressed interest in taking an
active role in improving their superiors’ performance
(Table 5, question 7) but 10 emphasized how important
it was that somebody draws conclusions and somebody
makes the due corrections. Some nurses wanted to
examine the association between the results of manag-
ers’ evaluation and their subsequent performance. In
view of this attitude, it was clearly very important that
the evaluation findings were not simply left to collect
dust in a drawer but acted upon by setting up work-
shops for both head nurses and supervisors. Another
important decision of the Director of Nursing was, in
the third year, to put herself up for evaluation by her
staff. Clearly, it was this that persuaded the three stand-
out supervisors to do likewise (however, the premature
cut-off of the project saved them from actually being
evaluated).
Summing up, a great deal of satisfaction was
expressed with the project. Participants noted that in
giving anonymous feedback to senior management the
project became both important and innovative and
come close to the standards of transparency required of
modern management. Overall, critical and negative
responses were remarkably few.
Conclusions and recommendations
This study confirms the contention that an organization
that evaluates itself creates trust that all employees
appreciate and places feedback in a context of fruitful
manager–subordinate interaction (Martzki & Gureli
Table 4Project Evaluation Questionnaire: responses to the closed questions
Number Question Category of reply Frequency number (n ¼ 63) Frequency percentage
1. Is evaluating seniorstaff and managers justified?
Yes 55 87.3No 2 3.2No response 6 9.5
2. Did you feel free to say what youwanted on the manager evaluation form?
Yes 50 79.4No 1 1.6Moderately, relatively free 7 11.1No response 5 8.00
3. Are you satisfied with theevaluation project?
Satisfied 51 81.00Dissatisfied 2 3.2No response 10 15.9
I. Kagan et al.
362 ª 2006 Blackwell Publishing Ltd, Journal of Nursing Management, 14, 356–365

1990, Weizner 1998, Edwards 2001, Collins 2002,
Garman et al. 2004). Subordinate staff needs a feed-
back opportunity because they know that they have the
ability to think, to disagree and to substantiate their
opinions, even ones that the boss does not agree with
(McCarthy 2000). Obtaining feedback from subordin-
ates is a first step to showing willingness to introduce
changes into the managerial culture and organizational
values (Edwards 2001).
The anonymous evaluation of managers is an effect-
ive tool by which real feedback is gathered on ‘things,
which are not talked about’. It is the nearest thing to
objectivity that can be obtained today in the area of
senior health care staff performance. For low-rank
employees it is an almost unique opportunity to convey
a message to their manager without fear of exposure or
reprisals on their chances of promotion or of keeping
their jobs. Moreover, supplying anonymous feedback
increases trust in the organization and its managers.
Periodic anonymous feedback can also be useful in
assessing how new senior staff are adapting to their new
positions.
In view of this study’s findings it is worth considering
using anonymous feedback by employees for the routine
evaluation of nursing managers’ performance. It is also
desirable to extend it to other staff sectors, such as
doctors, administrators and maintenance staff. But
before it can become fully established all tools need to
Table 5Project Evaluation Questionnaire: responses to the open questions
Number Question ItemsFrequencynumber
Totalresponses %
4. What are the project'spositive points?
Will enable senior staff to improve their performance 38 113 33.6Guarantees anonymity and immunity to responders 10 8.9Allows genuine and objective evaluation 18 15.9Makes staffers' opinions important and empowers them 11 9.7Indicates a positive change in management regime 11 9.7Informs managers how subordinates see them 13 11.5Improves relations and ties betweenseniors and subordinates
11 9.7
There are no positive points 1 0.9Did not respond 18
5. What are the project'snegative points?
There are no negative points 17 50 34.0Causes staff feelings of uneasiness,embarrassment, stress
9 18.0
There is no guarantee that lessons will be learntand conclusions drawn
3 6.0
Subjective; not objective 3 6.0The questionnaire is not comprehensive 3 6.0The questionnaire is not anonymous enough 2 4.0Evaluators are not familiar enough with the workof some of the seniors evaluated
12 24.0
Lets disgruntled employees `get even' 1 2.0Did not respond 19
6. What were your feelings as youfilled out the form?
Good, at ease, satisfaction, free 27 50 54.0Feelings of partnership, belonging, equality,that I meant something
10 20.0
Uncertain, embarrassed, uneasy 10 20.0Confidence, in control, power 3 6.0Did not respond 16 32.0
7. Recommendations forproject's continuation
It should continue at annual/biannual rate 38 62 61.3Would like to be partner in work to improve performance 2 3.2Improve and expand the evaluation form 3 4.8Draw conclusions and take correctivemeasures accordingly
10 16.1
The project should not continue 1 1.6Present the findings for open group discussion 2 3.2Replicate for all staffers and sectors 5 8.1Consider doing an open evaluation 1 1.6Did not respond 12
*These four open questions evoked a wide variety of responses, which were categorized by content. Some respondents preferred to give severalanswers to a question; at times these related to different areas of content. In some cases the responses were partial and only parts of the openquestions were addressed. As a result the number of responses does not necessarily match the number of responders.
Staff feedback
ª 2006 Blackwell Publishing Ltd, Journal of Nursing Management, 14, 356–365 363

be systematically validated and the entire process
empirically examined. It is possible that the 360-degree-
feedback survey developed by Garman et al. (2004) can
be useful in Israeli health care services.
References
Barnes P. (1997) Making appraisal work in the new millennium.
Management Services 41, 14–16.
Collins B. (2002) Meeting employee expectations: exploring
change through employee feedback. Journal of Environmental
Health 7, 30–33.
Edwards J.D. (2001) Examining employees from all angles: the
360-degree evaluation. Interview with Shirley Arney. Behavi-
oral Health Management July–August, 60–61.
Farrell M. (2004) Evaluating the chief nurse executive. JONA 34,
458–462.
Farrell M., George V., Brukwitzki G. & Burke L. (2002) Trust
through feedback to the chief nurse executive: preliminary re-
sults of a pilot study to evaluate performance competence (on
the scene). Nursing Administration Quarterly 26, 26–34.
Furnham A. (2002) Rating a manager, a colleague and a subor-
dinate. Journal of Managerial Psychology 17, 655–671.
Garman A.N., Tyler J.L. & Darnall J.S. (2004) Development and
validation of 360-degree-feedback instrument for healthcare
administrators. Journal of Healthcare Management 49, 307–
322.
Harmati H. (2003) Employer Evaluation. Available at: http://
www.iew3.technion.ac.il (in Hebrew) accessed on 6 June 2004.
Kaspi A. & Ben-Dor B. (2003) Cranet Survey, Israel 2001–2002.
Available at: http://www.biu.ac.il/SOC/sb/cranet/2002execu-
tive_report_heb.html, accessed on 09.02.2005 (in Hebrew).
Lockyer J. (2003) Multisource feedback in the assessment of
physician competencies. The Journal of Continuing Education
in Health Professions 23, 4–12.
Longeneker C.O. (1999) Creating effective performance evalua-
tions. Industrial Management October–November, 18–23.
Luthans K.W. & Farner S. (2002) Expatriate development: the
use of 360-degree feedback. Journal of Management Develop-
ment 21, 780–793.
Martzki J. & Gureli S. (1990) Giving feedback: the key to suc-
cessful management. Mashabei Enosh 28, 32–34 (in Hebrew).
McCarthy J. (2000) How to conduct productive performance
evaluations. Journal of Property Management September–
October, 23–25.
McCauley C.D. & Moxley R.S. (1996) Developmental 360: how
feedback can make managers more effective. Career Develop-
ment International 1/3, 15–19.
Olson H. (1996) A progressive management tool. Medical-Sur-
gical Nursing 5, 201–203.
Porter G. (1997) Employees’ perception on management: a case
for leadership training. International Journal of Training and
Development 1, 271–286.
Riba S., Greenberger C. & Reches H. (2004) State involvement in
professional nursing development in Israel promotive or
restrictive. OJIN: Online Journal of Issues in Nursing. Avail-
able at: http://www.nursingworld.org/ojin/topic12/tpc12_11.
htm, accessed on 02.09.2004.
Stathakopoulos V. (1998) Enhancing the performance of mar-
keting managers. Aligning strategy, structure and evaluating
systems. European Journal of Marketing 32, 536–558.
Stockman N. (1996) Employee evaluation. Hamif’al 418, 6–8 (in
Hebrew).
Weizner A. (1998) An approach to evaluating army officers and
their rewards. Ma’arachot 360, 16–20 (in Hebrew).
Willard J. (2000) When releasing a temp nurse give the agency
good feedback. Nursing Management 31 19. Available at:
http://www.nursingmanagement.com
Zevulun A. (1993) Manager development on the basis of feedback
from their employees. Mashabei Enosh 64, 6–8 (in Hebrew).
I. Kagan et al.
364 ª 2006 Blackwell Publishing Ltd, Journal of Nursing Management, 14, 356–365

Appendix 1 Anonymous Evaluation Questionnaire for hospital managers and senior nurses
Please use this form to give your feedback on the performance of _______. Before you are 16 statements characterizing the work ofthese senior staff; please circle the number that reflects your level of agreement with the statement, on the following scale.
Definitely correct Largely correct Moderately correct Not very correct Not at all correct
5 4 3 2 1
Number Statement Feedback scale
1 Works to improve the atmosphere among staff 1 2 3 4 52 Promotes professional training and advancement of staff 1 2 3 4 53 When I have a problem in the ward I feel comfortable asking her for help 1 2 3 4 54 Every time I turn to her for help I get a positive response 1 2 3 4 55 Maintains good personal relations 1 2 3 4 56 Is open to others' opinions 1 2 3 4 57 Works to promote projects at the health center 1 2 3 4 58 Treats all staff equally 1 2 3 4 59 Sets staff a personal example 1 2 3 4 510 Is a superior one can trust 1 2 3 4 511 Works to promote the status of nursing staff at the center 1 2 3 4 512 Cultivates a new generation of psychiatric nursing staff 1 2 3 4 513 Demonstrates real professionalism 1 2 3 4 514 Backs up the ward head nurse's decisions 1 2 3 4 515 Is a pillar of support when needed 1 2 3 4 516 She performs satisfactorily in her present position 1 2 3 4 5
Note: During the process of data analysis the 16 statements were reduced to 14.
Appendix 2 Questionnaire on the evaluation project itself
Thank you for your feedback on senior nursing staff. We now request that in this form you express your opinion about the evaluation project itself.Your opinion will help decide whether it continues and in what format.
1. Is evaluating senior staff and managers justified?(1) Yes (2) No, Specify
2. Did you feel free to say what you wanted on the manager evaluation form?(1) Yes (2) No, Specify
3. Are you satisfied with the evaluation project?(1) Yes (2) No, Specify
4. What are the project's positive points?5. What are the project's negative points?6. What were your feelings as you filled out the form?7. What are your recommendations for the project's continuation?
Staff feedback
ª 2006 Blackwell Publishing Ltd, Journal of Nursing Management, 14, 356–365 365
Related Documents











