1 Sitanala Community Survey (23 November – 15 December 2010) 1. Introduction The following is a report on a three-week survey conducted from 23 November to 15 December 2010 by JSPO Research & Development Director, Peter Carey, with the assistance of JSPO volunteer, Kerstin Fackler (OT from Austria) [Photo 1], and former Hansen’s disease (leprosy) patient, Mas Deden Sinuhaji [Photo 24], in Karangsari village (desa) – also known as Komplek Serbaguna (Multipurpose Complex) - situated between Sitanala Hansen’s disease Hospital in the Neglasari sub-district (kecamatan) of Tangerang municipality (pemkot) (Banten) and the Soekarno-Hatta International Airport at Cengkareng. The village extends over roughly four hectares of land owned by the Indonesian Ministry of Health (henceforth: MoH), some of which has been earmarked for the redevelopment of the planned integrated campus of Jakarta I and Jakarta II Polytechnics of Health Sciences. This raises the interesting possibility that the Karangsari community with its 100+ P&O patients, may one day become the principal local feeder community for the third-year training clinic of the Jakarta-I P&O Department. Permissions for our survey were obtained from each of the RT heads as we gradually progressed through the community, ending up in RT 05 on 6 December, where we met with the village head Pak RW), Pak Kisin, who chaired our public meeting on the night of Wednesday, 15 December 2010. At that meeting, three members of the JSPO faculty (Olle Hjelmström, Thou Sambath and Deby Eka Supadma) spoke to 57 of the 73 former Hansen’s disease patients whom we had interviewed during the course of the three-week survey. They introduced them to the process of how P&O patients will be treated at JSPO and appealed for model patients for the 3 rd Intake Trans-Tibial (TT) Module starting in late January 2011. The recent (2009) film on the young boy who received a TT Sitanala Community Survey – November-December 2010 Page 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
Sitanala Community Survey(23 November – 15 December 2010)
1. Introduction
The following is a report on a three-week survey conducted from23 November to 15 December 2010 by JSPO Research & DevelopmentDirector, Peter Carey, with the assistance of JSPO volunteer,Kerstin Fackler (OT from Austria) [Photo 1], and former Hansen’sdisease (leprosy) patient, Mas Deden Sinuhaji [Photo 24], inKarangsari village (desa) – also known as Komplek Serbaguna(Multipurpose Complex) - situated between Sitanala Hansen’sdisease Hospital in the Neglasari sub-district (kecamatan) ofTangerang municipality (pemkot) (Banten) and the Soekarno-HattaInternational Airport at Cengkareng. The village extends overroughly four hectares of land owned by the Indonesian Ministry ofHealth (henceforth: MoH), some of which has been earmarked forthe redevelopment of the planned integrated campus of Jakarta Iand Jakarta II Polytechnics of Health Sciences. This raises theinteresting possibility that the Karangsari community with its100+ P&O patients, may one day become the principal local feedercommunity for the third-year training clinic of the Jakarta-I P&ODepartment.
Permissions for our survey were obtained from each of the RTheads as we gradually progressed through the community, ending upin RT 05 on 6 December, where we met with the village head PakRW), Pak Kisin, who chaired our public meeting on the night ofWednesday, 15 December 2010. At that meeting, three members ofthe JSPO faculty (Olle Hjelmström, Thou Sambath and Deby EkaSupadma) spoke to 57 of the 73 former Hansen’s disease patientswhom we had interviewed during the course of the three-weeksurvey. They introduced them to the process of how P&O patientswill be treated at JSPO and appealed for model patients for the3rd Intake Trans-Tibial (TT) Module starting in late January2011. The recent (2009) film on the young boy who received a TT
Sitanala Community Survey – November-December 2010 Page 1
2
device at SLSPO in Ragama (Sri Lanka) was used by way ofintroduction. The assistance of both Kerstin Fackler and MasDeden were critical to the success of the present survey, thefirst bringing much appropriate information on the care of thehands and feet of former Hansen’s disease patients which shecould share with our interviewees, and the second making all therelevant introductions and contacts. Without Mas Deden’s localknowledge, skill and credibility as a former Hansen’s diseasepatient, recently and successfully treated at JSPO, theseinterviews could not have happened. I wish to acknowledge my debtto them both here.
Sitanala Community Survey – November-December 2010 Page 2
3
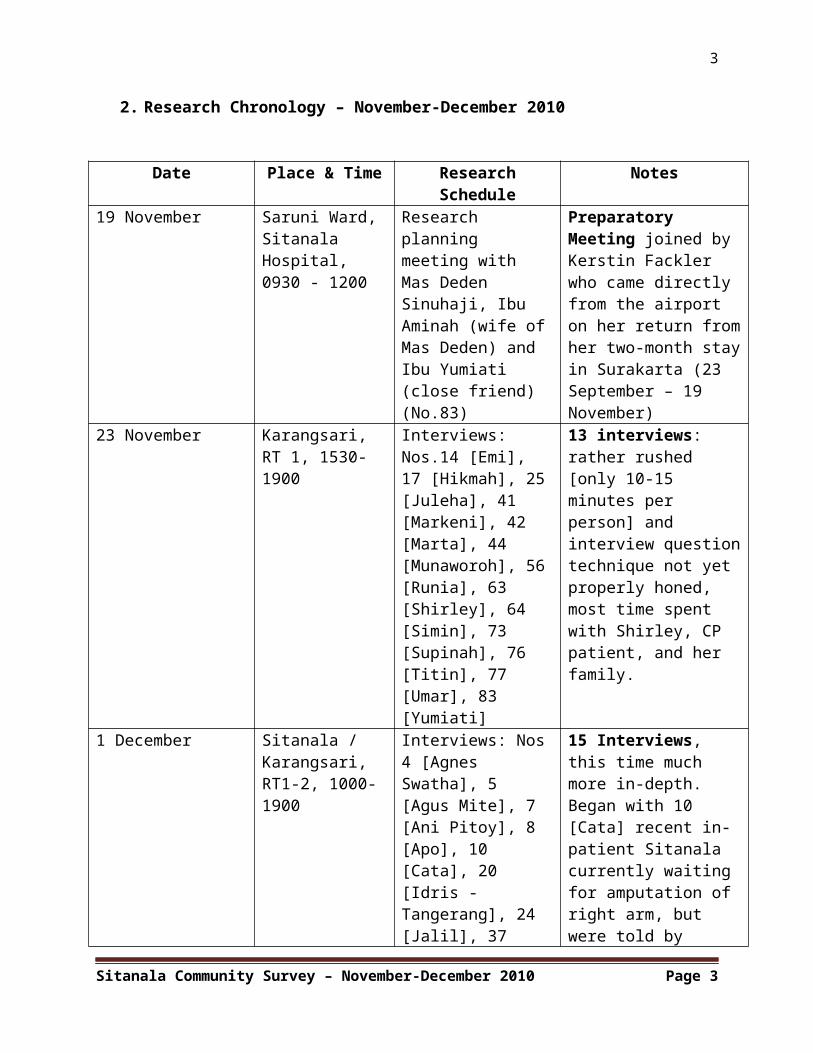
2. Research Chronology – November-December 2010
Date Place & Time ResearchSchedule
Notes
19 November Saruni Ward, Sitanala Hospital,0930 - 1200
Research planning meeting with Mas Deden Sinuhaji, Ibu Aminah (wife ofMas Deden) and Ibu Yumiati (close friend) (No.83)
Preparatory Meeting joined by Kerstin Fackler who came directly from the airport on her return fromher two-month stayin Surakarta (23 September – 19 November)
23 November Karangsari, RT 1, 1530-1900
Interviews: Nos.14 [Emi], 17 [Hikmah], 25[Juleha], 41 [Markeni], 42 [Marta], 44 [Munaworoh], 56[Runia], 63 [Shirley], 64 [Simin], 73 [Supinah], 76 [Titin], 77 [Umar], 83 [Yumiati]
13 interviews: rather rushed [only 10-15 minutes per person] and interview questiontechnique not yet properly honed, most time spent with Shirley, CP patient, and her family.
1 December Sitanala / Karangsari, RT1-2, 1000-1900
Interviews: Nos4 [Agnes Swatha], 5 [Agus Mite], 7 [Ani Pitoy], 8 [Apo], 10 [Cata], 20 [Idris - Tangerang], 24 [Jalil], 37
15 Interviews, this time much more in-depth. Began with 10 [Cata] recent in-patient Sitanala currently waiting for amputation of right arm, but were told by
Sitanala Community Survey – November-December 2010 Page 3
4
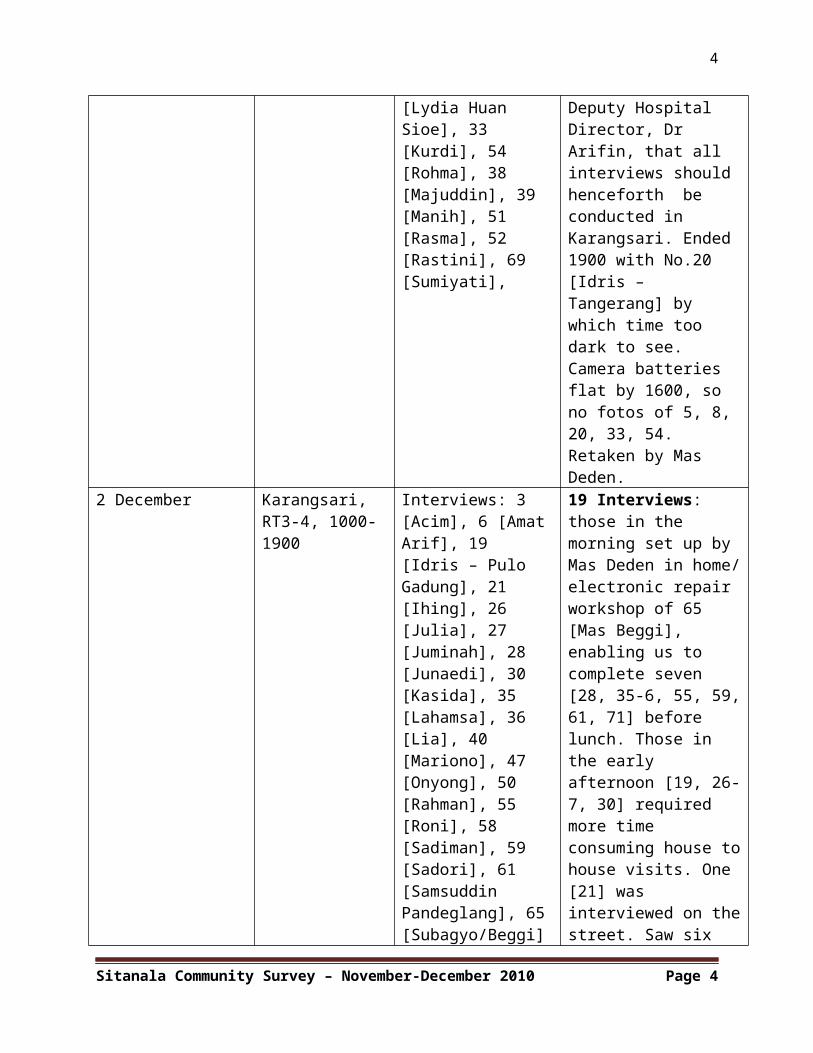
[Lydia Huan Sioe], 33 [Kurdi], 54 [Rohma], 38 [Majuddin], 39 [Manih], 51 [Rasma], 52 [Rastini], 69 [Sumiyati],
Deputy Hospital Director, Dr Arifin, that all interviews should henceforth be conducted in Karangsari. Ended 1900 with No.20 [Idris – Tangerang] by which time too dark to see. Camera batteries flat by 1600, so no fotos of 5, 8, 20, 33, 54. Retaken by Mas Deden.
2 December Karangsari, RT3-4, 1000-1900
Interviews: 3 [Acim], 6 [AmatArif], 19 [Idris – Pulo Gadung], 21 [Ihing], 26 [Julia], 27 [Juminah], 28 [Junaedi], 30 [Kasida], 35 [Lahamsa], 36 [Lia], 40 [Mariono], 47 [Onyong], 50 [Rahman], 55 [Roni], 58 [Sadiman], 59 [Sadori], 61 [Samsuddin Pandeglang], 65[Subagyo/Beggi]
19 Interviews: those in the morning set up by Mas Deden in home/electronic repair workshop of 65 [Mas Beggi], enabling us to complete seven [28, 35-6, 55, 59,61, 71] before lunch. Those in the early afternoon [19, 26-7, 30] required more time consuming house tohouse visits. One [21] was interviewed on thestreet. Saw six
Sitanala Community Survey – November-December 2010 Page 4
5
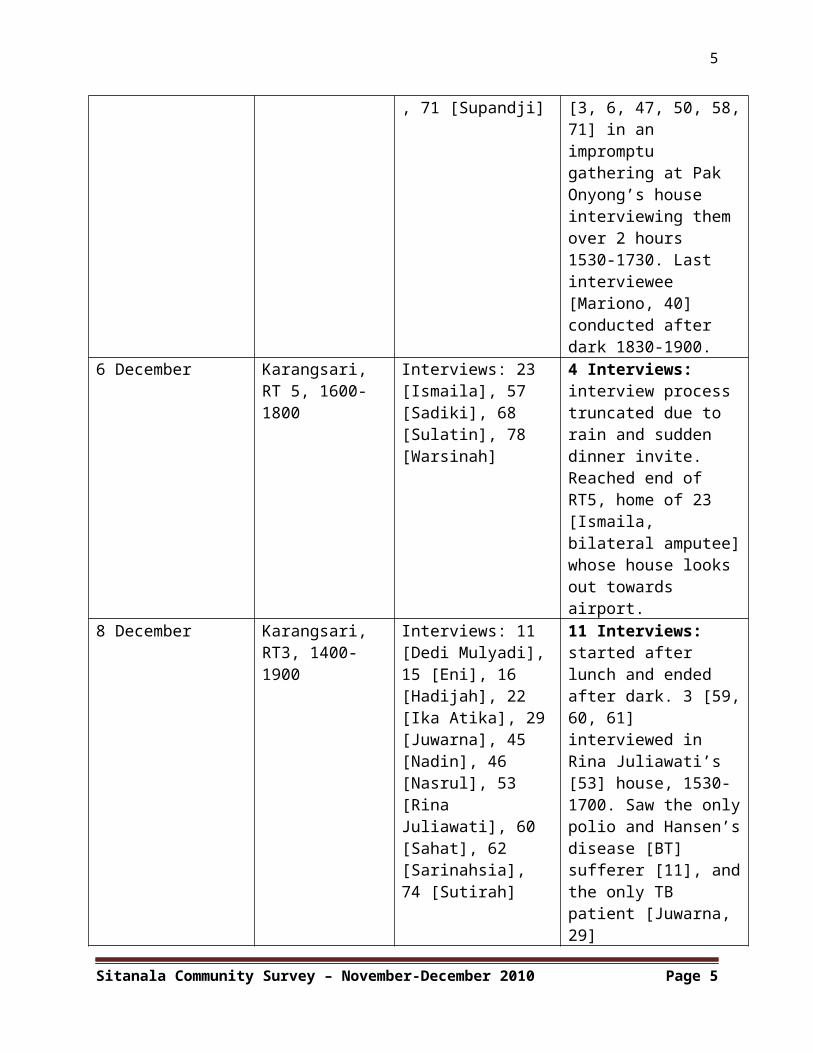
, 71 [Supandji] [3, 6, 47, 50, 58,71] in an impromptu gathering at Pak Onyong’s house interviewing them over 2 hours 1530-1730. Last interviewee [Mariono, 40] conducted after dark 1830-1900.
6 December Karangsari, RT 5, 1600-1800
Interviews: 23 [Ismaila], 57 [Sadiki], 68 [Sulatin], 78 [Warsinah]
4 Interviews: interview process truncated due to rain and sudden dinner invite. Reached end of RT5, home of 23 [Ismaila, bilateral amputee]whose house looks out towards airport.
8 December Karangsari, RT3, 1400-1900
Interviews: 11 [Dedi Mulyadi],15 [Eni], 16 [Hadijah], 22 [Ika Atika], 29[Juwarna], 45 [Nadin], 46 [Nasrul], 53 [Rina Juliawati], 60 [Sahat], 62 [Sarinahsia], 74 [Sutirah]
11 Interviews: started after lunch and ended after dark. 3 [59,60, 61] interviewed in Rina Juliawati’s [53] house, 1530-1700. Saw the onlypolio and Hansen’sdisease [BT] sufferer [11], andthe only TB patient [Juwarna, 29]
Sitanala Community Survey – November-December 2010 Page 5
6
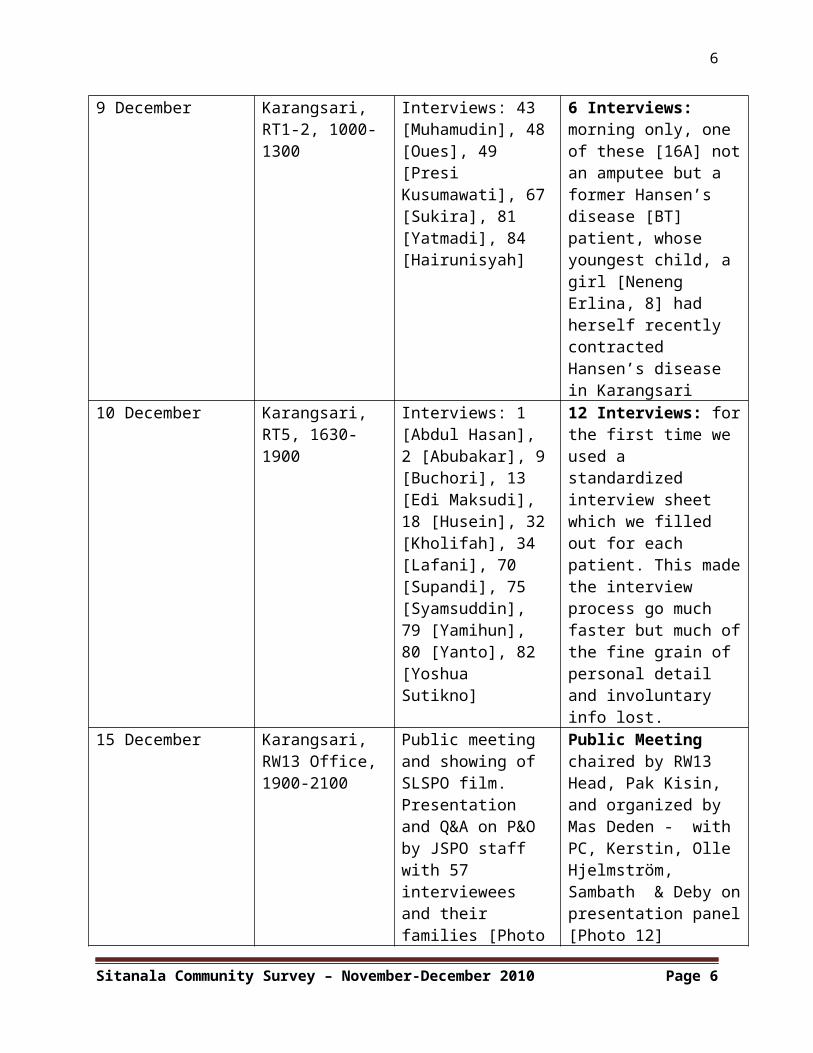
9 December Karangsari, RT1-2, 1000-1300
Interviews: 43 [Muhamudin], 48[Oues], 49 [Presi Kusumawati], 67[Sukira], 81 [Yatmadi], 84 [Hairunisyah]
6 Interviews: morning only, one of these [16A] notan amputee but a former Hansen’s disease [BT] patient, whose youngest child, a girl [Neneng Erlina, 8] had herself recently contracted Hansen’s disease in Karangsari
10 December Karangsari, RT5, 1630-1900
Interviews: 1 [Abdul Hasan], 2 [Abubakar], 9[Buchori], 13 [Edi Maksudi], 18 [Husein], 32[Kholifah], 34 [Lafani], 70 [Supandi], 75 [Syamsuddin], 79 [Yamihun], 80 [Yanto], 82 [Yoshua Sutikno]
12 Interviews: forthe first time we used a standardized interview sheet which we filled out for each patient. This madethe interview process go much faster but much ofthe fine grain of personal detail and involuntary info lost.
15 December Karangsari, RW13 Office, 1900-2100
Public meeting and showing of SLSPO film. Presentation and Q&A on P&O by JSPO staff with 57 interviewees and their families [Photo
Public Meeting chaired by RW13 Head, Pak Kisin, and organized by Mas Deden - with PC, Kerstin, Olle Hjelmström, Sambath & Deby onpresentation panel[Photo 12]
Sitanala Community Survey – November-December 2010 Page 6
7
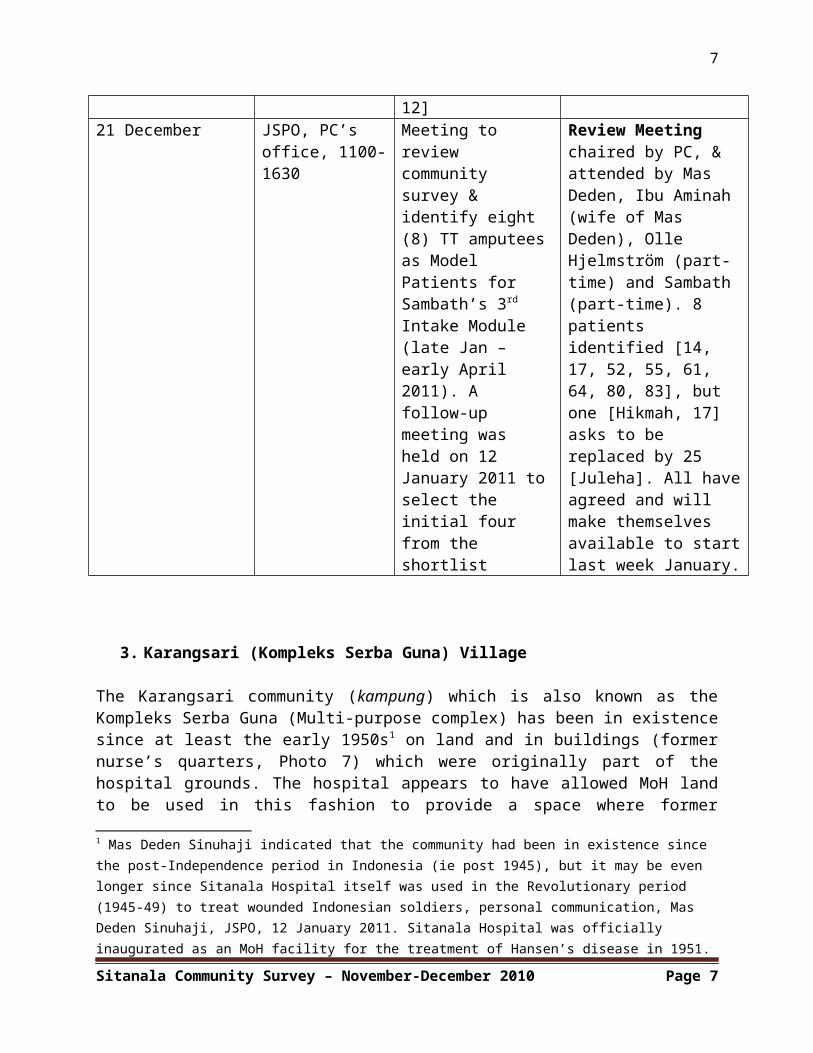
12]21 December JSPO, PC’s
office, 1100-1630
Meeting to review community survey & identify eight (8) TT amputeesas Model Patients for Sambath’s 3rd Intake Module (late Jan – early April 2011). A follow-up meeting was held on 12 January 2011 toselect the initial four from the shortlist
Review Meeting chaired by PC, & attended by Mas Deden, Ibu Aminah (wife of Mas Deden), Olle Hjelmström (part-time) and Sambath (part-time). 8 patients identified [14, 17, 52, 55, 61, 64, 80, 83], but one [Hikmah, 17] asks to be replaced by 25 [Juleha]. All haveagreed and will make themselves available to startlast week January.
3. Karangsari (Kompleks Serba Guna) Village
The Karangsari community (kampung) which is also known as theKompleks Serba Guna (Multi-purpose complex) has been in existencesince at least the early 1950s1 on land and in buildings (formernurse’s quarters, Photo 7) which were originally part of thehospital grounds. The hospital appears to have allowed MoH landto be used in this fashion to provide a space where former
1 Mas Deden Sinuhaji indicated that the community had been in existence since the post-Independence period in Indonesia (ie post 1945), but it may be even longer since Sitanala Hospital itself was used in the Revolutionary period (1945-49) to treat wounded Indonesian soldiers, personal communication, Mas Deden Sinuhaji, JSPO, 12 January 2011. Sitanala Hospital was officially inaugurated as an MoH facility for the treatment of Hansen’s disease in 1951.
Sitanala Community Survey – November-December 2010 Page 7
8
Hansen’s disease patients, who frequently experience prejudice orrejection in their home communities, can live in a supportive andinclusive environment. The village is divided into five RukunTetangga (RT) (Neighbourhood Associations, RT 01-05), each withroughly 760 people. The current (2011) population is 3,785, ofwhom 2,650 are former Hansen’s disease patients.2 These latterare particularly clustered in RT 01-03. The last two RT (04-05)have a higher percentage of non-former Hansen’s disease patients(known locally as ‘orang sehat’ – ‘healthy people’). Together theyform one Rukun Warga (RW) (Citizen’s association, formerly RukunKampung [RK] = hamlet association) – RW13 which is led by PakKisin, a local Jakartan (anak Betawi) born and bred who is nothimself a former Hansen’s disease sufferer. It has its ownschools (primary [SD] through to senior high [SMA]) run by aprivate Islamic association – the ar-Rahman Foundation. Inaddition to the local mosque, which was built by the first Vice-President of Indonesia, Muhammad Hatta (1902-80), subsequent tohis official inauguration of Sitanala Hospital in 1951, there isan Ecumenical Protestant Church (Maranata), which, together withthe Merpati Catholic Church just across the street from thehospital, provide subsidised lodging for Church members (AgnesSwatha [4] and Lydia Huan Sioe [37]) and employment(sewing/seamstressing) for others (Ibu Kholifah [32] and IbuWarsinah [78]). It also has a local P&O workshop – the Ali Sagaclinic (Photos 8-9) - run by a former artist who raises moneyfrom wealthy local donors like the Al-Azhar Islamic Foundationand the commercial TV station, Indosiar, to sponsor his products.Ali Saga works closely with staff at the Sitanala P&O workshop(Photos 10-11) in what is clearly a very profitable business: hisclinic is the only three-storey building in the village.Apparently there is money to be made out of P&O provision inKarangsari given that most patients have Medical Social Security(Jamskesmas) cards. This enables those making the devices toclaim back the material costs from the Government and then earn
2 Population statistics from the five RT heads obtained by Mas Deden Sinuhajiin May 2011. Some of these RT population statistics (RT 03-05) indicate whether inhabitants are former Hansen’s Disease patients (eks-penderita) or not (ie ‘orang sehat’ – ‘healthy people’), whereas those from RT 01-02 make no such distinctions.
Sitanala Community Survey – November-December 2010 Page 8
9
an additional fee from sponsorship. Finally, there is theproximity of the Sitanala Hospital itself which enables formerHansen’s disease patients to have access to free out-patient andin-patient services provided they have Jamskesmas cards andobtain a referral letter from the local Public Health clinic(Puskesmas) on the airport road.
The total population is now estimated to be 3,785 and contains anumber who are not former Hansen’s disease sufferers (the corepopulation of former Hansen’s disease sufferers is around 2,650),who are known locally as ‘orang sehat’ (‘healthy people’). Some ofthese are the children of former Hansen’s disease patients, ormembers of their extended family who have moved to the communityover the past decades, Many of the latter have settled there fromother parts of Indonesia to benefit from the village’s low livingcosts (rents in particular) and proximity to work opportunitiesin neighbouring Tangerang, which is a major manufacturing centrefor textiles, shoes, metal products and plastics: these lastinclude wheelchairs (PT Dharma Polymetal), as well as siliconesocket liners and orthotic shoe inlays (PT Silicone RubberSolutions, Bitung). Both the two trauma patients we interviewed –Pak Lahamsa [35] and Ibu Lia [36], who met in the Pondok Bambudetention centre for vagrants in East Jakarta – moved foreconomic and social reasons (low rents, opportunities to earnmoney on the street through begging and ease of obtaining aresidency permit [KTP] through local Karangsari ward [RT] heads).The same occurred with the family of the present author’s homehelp who recently transferred into the community from Majenang inWest Java after an elder female sibling married into the familyof a former Hansen’s disease sufferer. Besides extended family,there has also been a steady stream of able-bodied – non-formerHansen’s disease patients – who have sought to take advantage ofthe opportunities offered by Karangsari. As the fear and stigmaassociated with Hansen’s disease has diminished somewhat in thelocal population (although buses and other public transport(angkot) still tend to empty when disabled former Hansen’sdisease patients climb aboard3), these non-former Hansen’sdisease patients have sought to obtain local identity cards via3 Testimony of Pak Juwarna [29], Karangsari, 8 December 2010.
Sitanala Community Survey – November-December 2010 Page 9
10
the RT heads in what is clearly a lucrative process for the wardchiefs. One has the sense that relations between the formerHansen’s disease sufferers and the newcomers, who now constitutearound twenty percent of the total population, is somewhatproblematic: unless they are family of former patients, thenewcomers do not mix too well with the original residents.
4. Sitanala Hospital and Hansen’s disease in Indonesia
Sitanala Hansen’s disease Hospital was officially opened in 1951.It has Dutch colonial origins and is the latest in a long line ofHansen’s disease hospitals in the Indonesian capital dating backto 1666, when the original Leper Hospital was founded by theDutch East India Company (VOC) in Muara Angké (North Jakarta).4
It received its current name in the 1950s in memory of theAmbonese doctor and independence hero who pioneered Hansen’sdisease care in Indonesia, Dr Jacob Bernardus Sitanala (1889-1958). It is the second largest Hansen’s disease hospital in theworld. The largest is the Christian Medical College and Hospitalin Vellore, India, where the famous orthopedic surgeon Dr PaulBrand (1914-2003) pioneered his reconstructive hand surgery inthe 1950s. Sitanala covers a 24-hectare site and has a 550-bedcapacity with 11 wards (bangsal), although fewer than 15 Hansen’sdisease patients are now in residence and only 3 of the 11 wardsare in use by such patients (the others are now reserved for non-Hansen’s disease patients). This decline in patient numbers is inpart due to the prioritization of non-Hansen’s disease facilitiesat the Sitanala site, facilities which are more lucrative for thehospital. It is also a result of the MoH policy of localizingout-patient treatment through its post-1990 provision of freeanti-Hansen’s disease drugs (DDS [Dapsone], clofazimine[Lamprene], rifampicin) through its local public health centres(Puskesmas). Whereas in the days of the Netherlands Hansen’sdisease Mission (now Netherlands Hansen’s disease Relief) beforethe mid-1990s, there were eleven (11) Hansen’s disease wards –each with 50 beds – there are now only four (4), including thefemale Seruni Ward. One of these (Dahlia Ward used for post-4 Moved in 1681 to one of the islands (Purmerend) in the Bay of Jakarta.
Sitanala Community Survey – November-December 2010 Page 10
11
surgical cases) is empty and others have just two or threepatients.
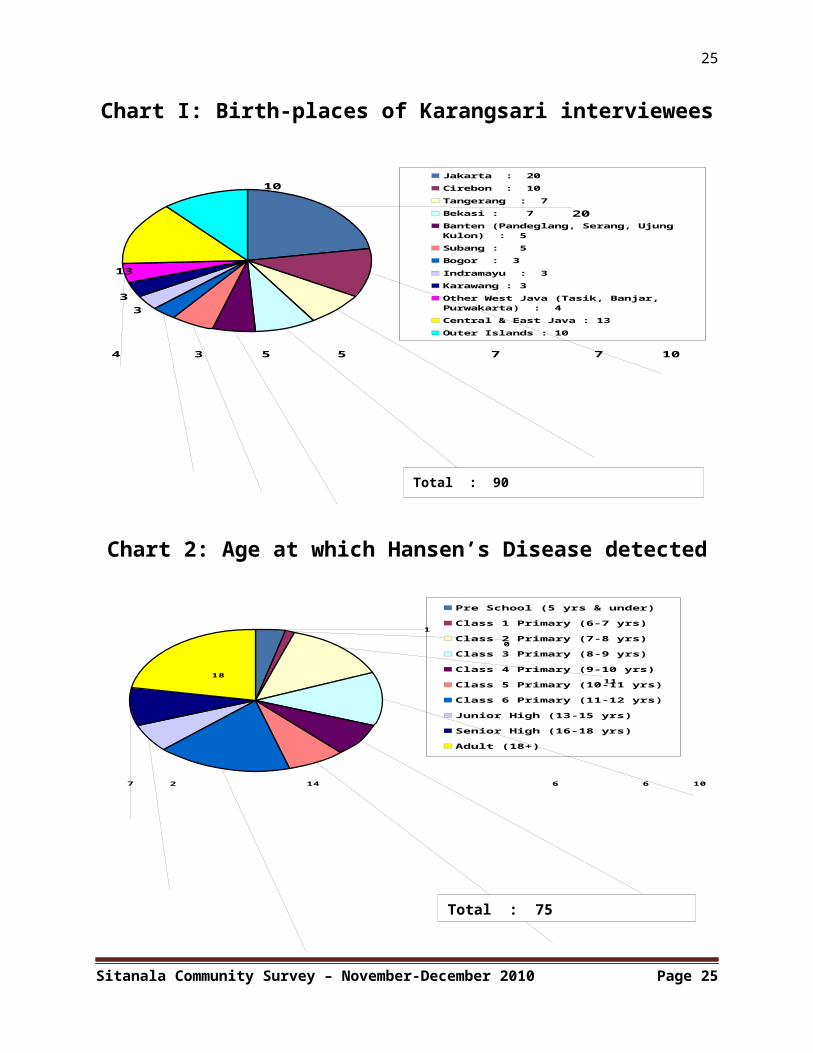
The funds available for the maintenance of the Hansen’s diseasesection of the hospital come from a variety of sources, theprincipal one being the central government budget or DIPA (DaftarInventaris Pajak Anggaran: Listed Inventory of Budgeted Taxes)and subventions from well-endowed local foundations like theMesjid Al-Ajar, which has regularly given in excess ofIDR100,000,000 per annum. Other types of support in kind comethrough the Tangerang Korean community, who operate many of thelocal shoe and garment factories, and Christian churches.Despite these subventions, funds are clearly not sufficient tomaintain the facility, parts of which are now abandoned orfalling into disrepair. One has a sense that the hospital hasseen better days. Many former patients interviewed in theKarangsari community commented that standards had declined sincethe Netherlands Hansen’s disease Mission (NLM – now NetherlandsHansen’s disease Relief) was asked to pull out in the mid-1990s.The IDR40,000,000 corruption case involving a former SitanalaHospital Director, who recently died in prison, has also had anegative effect. But the hospital has been - and still remains -the principle referral centre for Hansen’s disease patients fromall over Indonesia, a fact attested by the geographical range ofthe birth provinces of the former patients interviewed (Chart 1,Appendix I) just over ten percent of whom hailed from placesoutside Java: Manado (North Sulawesi, Sulut) 7], Makassar [5, 34]and Sengkang in South Sulawesi (Sulsel) [23], Ambon (Maluku)[47], Bagan Si-Api-Api (Riau) [4, 37], Samarinda (EastKalimantan) [75] and Pulau Bangka (East Sumatra) [8].
Amongst the 18 countries in the world where Hansen’s disease isstill endemic, Indonesia ranks in third place after India andBrazil. It has the highest proportion of Hansen’s diseasesufferers in Southeast Asia (Timor-Leste is in second place).5
Recent MoH statistics indicate that since 2000 there have beensome 17,000 to 18,000 new reported cases each year (a highproportion children), a figure which has remained stable over the5 Khanchit Limpakarnjanarat (WHO) quoted in Jakarta Post, 1 September 2010.
Sitanala Community Survey – November-December 2010 Page 11
12
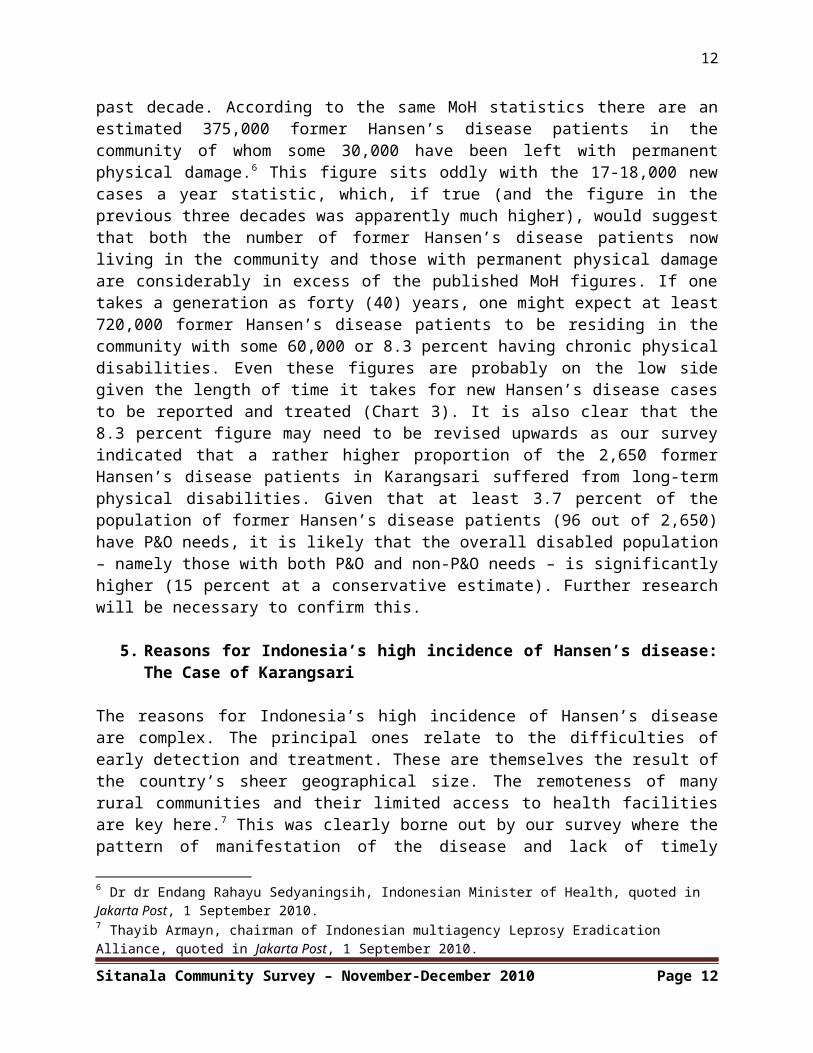
past decade. According to the same MoH statistics there are anestimated 375,000 former Hansen’s disease patients in thecommunity of whom some 30,000 have been left with permanentphysical damage.6 This figure sits oddly with the 17-18,000 newcases a year statistic, which, if true (and the figure in theprevious three decades was apparently much higher), would suggestthat both the number of former Hansen’s disease patients nowliving in the community and those with permanent physical damageare considerably in excess of the published MoH figures. If onetakes a generation as forty (40) years, one might expect at least720,000 former Hansen’s disease patients to be residing in thecommunity with some 60,000 or 8.3 percent having chronic physicaldisabilities. Even these figures are probably on the low sidegiven the length of time it takes for new Hansen’s disease casesto be reported and treated (Chart 3). It is also clear that the8.3 percent figure may need to be revised upwards as our surveyindicated that a rather higher proportion of the 2,650 formerHansen’s disease patients in Karangsari suffered from long-termphysical disabilities. Given that at least 3.7 percent of thepopulation of former Hansen’s disease patients (96 out of 2,650)have P&O needs, it is likely that the overall disabled population– namely those with both P&O and non-P&O needs – is significantlyhigher (15 percent at a conservative estimate). Further researchwill be necessary to confirm this.
5. Reasons for Indonesia’s high incidence of Hansen’s disease:The Case of Karangsari
The reasons for Indonesia’s high incidence of Hansen’s diseaseare complex. The principal ones relate to the difficulties ofearly detection and treatment. These are themselves the result ofthe country’s sheer geographical size. The remoteness of manyrural communities and their limited access to health facilitiesare key here.7 This was clearly borne out by our survey where thepattern of manifestation of the disease and lack of timely
6 Dr dr Endang Rahayu Sedyaningsih, Indonesian Minister of Health, quoted in Jakarta Post, 1 September 2010.7 Thayib Armayn, chairman of Indonesian multiagency Leprosy Eradication Alliance, quoted in Jakarta Post, 1 September 2010.
Sitanala Community Survey – November-December 2010 Page 12
13
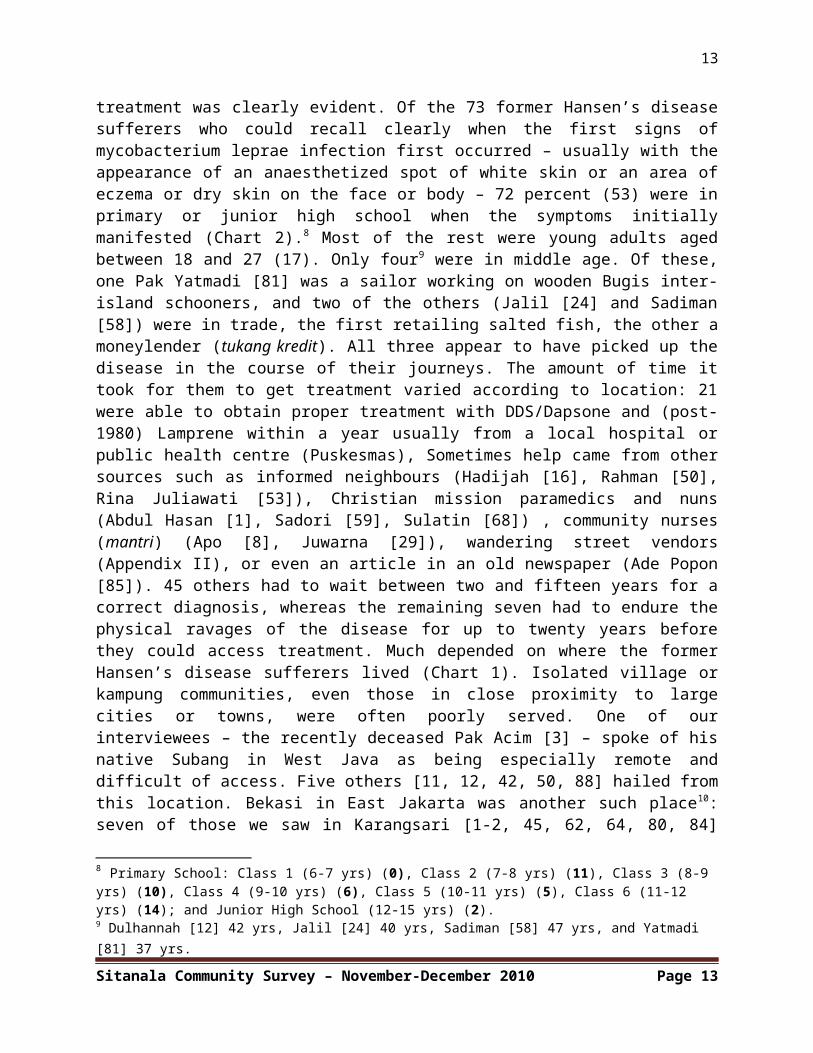
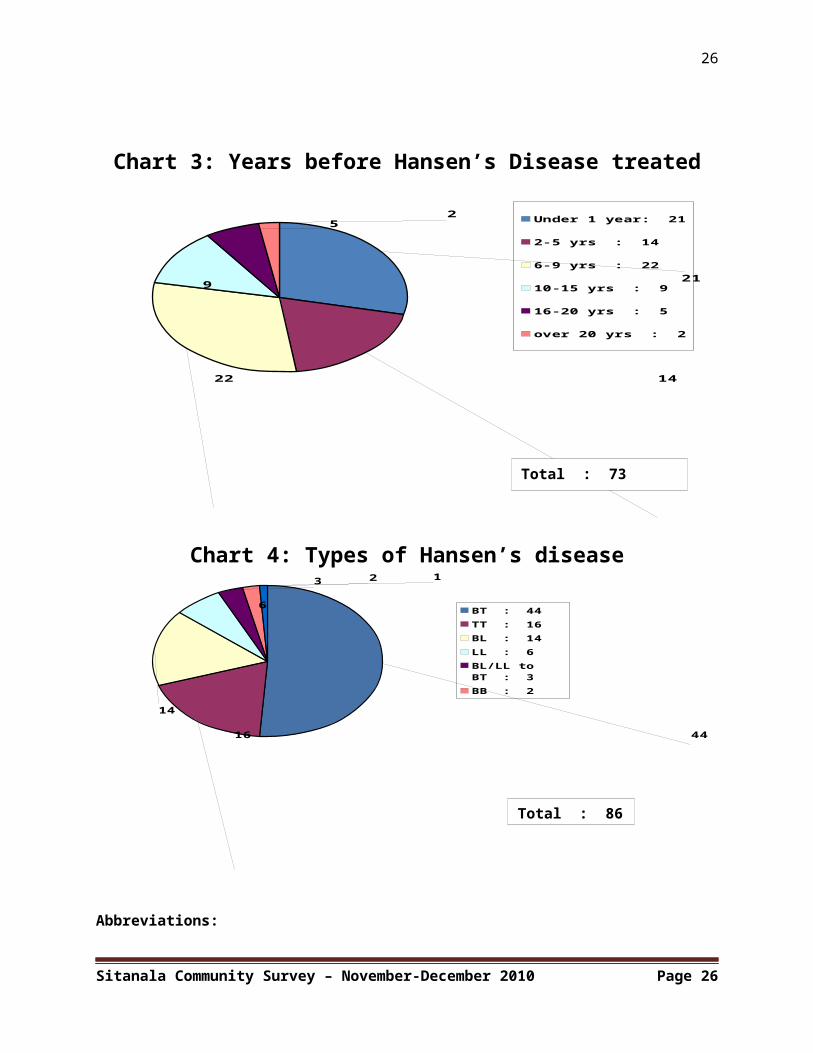
treatment was clearly evident. Of the 73 former Hansen’s diseasesufferers who could recall clearly when the first signs ofmycobacterium leprae infection first occurred – usually with theappearance of an anaesthetized spot of white skin or an area ofeczema or dry skin on the face or body – 72 percent (53) were inprimary or junior high school when the symptoms initiallymanifested (Chart 2).8 Most of the rest were young adults agedbetween 18 and 27 (17). Only four9 were in middle age. Of these,one Pak Yatmadi [81] was a sailor working on wooden Bugis inter-island schooners, and two of the others (Jalil [24] and Sadiman[58]) were in trade, the first retailing salted fish, the other amoneylender (tukang kredit). All three appear to have picked up thedisease in the course of their journeys. The amount of time ittook for them to get treatment varied according to location: 21were able to obtain proper treatment with DDS/Dapsone and (post-1980) Lamprene within a year usually from a local hospital orpublic health centre (Puskesmas), Sometimes help came from othersources such as informed neighbours (Hadijah [16], Rahman [50],Rina Juliawati [53]), Christian mission paramedics and nuns(Abdul Hasan [1], Sadori [59], Sulatin [68]) , community nurses(mantri) (Apo [8], Juwarna [29]), wandering street vendors(Appendix II), or even an article in an old newspaper (Ade Popon[85]). 45 others had to wait between two and fifteen years for acorrect diagnosis, whereas the remaining seven had to endure thephysical ravages of the disease for up to twenty years beforethey could access treatment. Much depended on where the formerHansen’s disease sufferers lived (Chart 1). Isolated village orkampung communities, even those in close proximity to largecities or towns, were often poorly served. One of ourinterviewees – the recently deceased Pak Acim [3] – spoke of hisnative Subang in West Java as being especially remote anddifficult of access. Five others [11, 12, 42, 50, 88] hailed fromthis location. Bekasi in East Jakarta was another such place10:seven of those we saw in Karangsari [1-2, 45, 62, 64, 80, 84]
8 Primary School: Class 1 (6-7 yrs) (0), Class 2 (7-8 yrs) (11), Class 3 (8-9 yrs) (10), Class 4 (9-10 yrs) (6), Class 5 (10-11 yrs) (5), Class 6 (11-12 yrs) (14); and Junior High School (12-15 yrs) (2).9 Dulhannah [12] 42 yrs, Jalil [24] 40 yrs, Sadiman [58] 47 yrs, and Yatmadi [81] 37 yrs.
Sitanala Community Survey – November-December 2010 Page 13
14
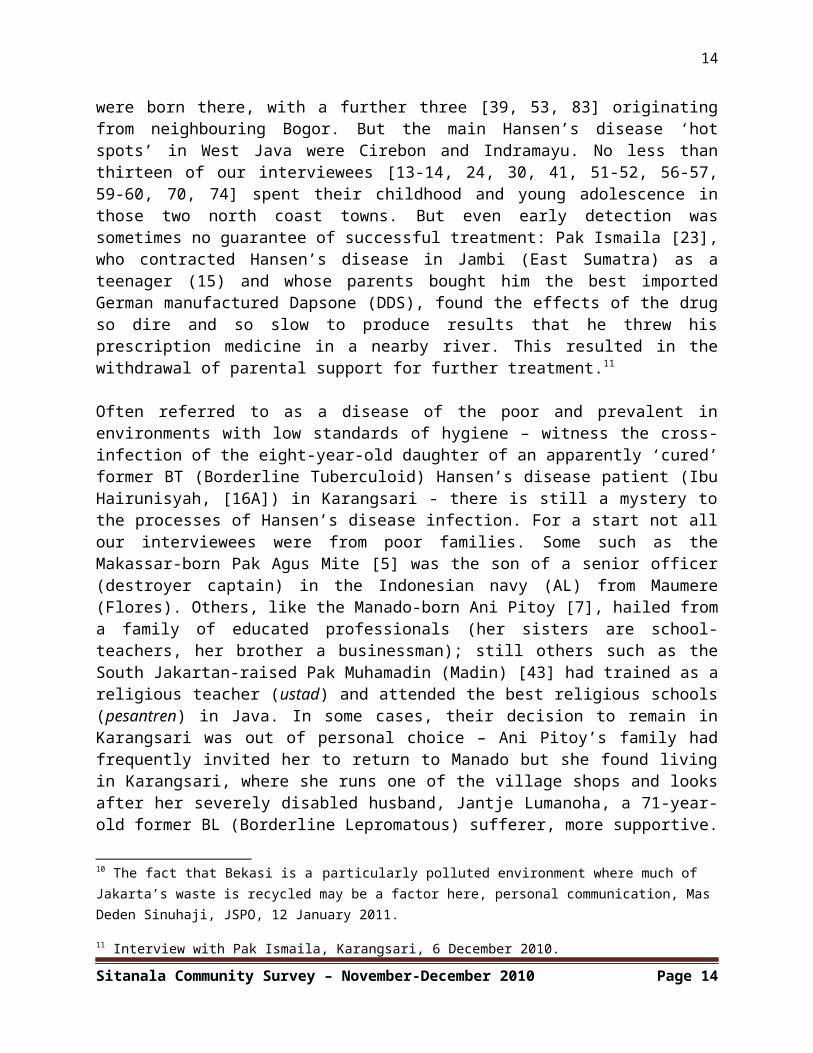
were born there, with a further three [39, 53, 83] originatingfrom neighbouring Bogor. But the main Hansen’s disease ‘hotspots’ in West Java were Cirebon and Indramayu. No less thanthirteen of our interviewees [13-14, 24, 30, 41, 51-52, 56-57,59-60, 70, 74] spent their childhood and young adolescence inthose two north coast towns. But even early detection wassometimes no guarantee of successful treatment: Pak Ismaila [23],who contracted Hansen’s disease in Jambi (East Sumatra) as ateenager (15) and whose parents bought him the best importedGerman manufactured Dapsone (DDS), found the effects of the drugso dire and so slow to produce results that he threw hisprescription medicine in a nearby river. This resulted in thewithdrawal of parental support for further treatment.11
Often referred to as a disease of the poor and prevalent inenvironments with low standards of hygiene – witness the cross-infection of the eight-year-old daughter of an apparently ‘cured’former BT (Borderline Tuberculoid) Hansen’s disease patient (IbuHairunisyah, [16A]) in Karangsari - there is still a mystery tothe processes of Hansen’s disease infection. For a start not allour interviewees were from poor families. Some such as theMakassar-born Pak Agus Mite [5] was the son of a senior officer(destroyer captain) in the Indonesian navy (AL) from Maumere(Flores). Others, like the Manado-born Ani Pitoy [7], hailed froma family of educated professionals (her sisters are school-teachers, her brother a businessman); still others such as theSouth Jakartan-raised Pak Muhamadin (Madin) [43] had trained as areligious teacher (ustad) and attended the best religious schools(pesantren) in Java. In some cases, their decision to remain inKarangsari was out of personal choice – Ani Pitoy’s family hadfrequently invited her to return to Manado but she found livingin Karangsari, where she runs one of the village shops and looksafter her severely disabled husband, Jantje Lumanoha, a 71-year-old former BL (Borderline Lepromatous) sufferer, more supportive.
10 The fact that Bekasi is a particularly polluted environment where much of Jakarta’s waste is recycled may be a factor here, personal communication, Mas Deden Sinuhaji, JSPO, 12 January 2011.
11 Interview with Pak Ismaila, Karangsari, 6 December 2010.
Sitanala Community Survey – November-December 2010 Page 14
15
In the two other cases, it seems that their families havedisowned them thus giving them little choice but to remain inKarangsari. The fact that the majority of the former Hansen’sdisease sufferers we interviewed indicated that they were theonly members of their immediate family and local community whohad contracted the disease, meant that they were oftenstigmatized and isolated. Unlike TB, polio or the now globallyeradicated smallpox, there seem to be no clearly defined vectorsfor the spread of M. leprae. Much seems to depend on the geneticmake-up, resistance to infection and other physical propensitiesof those exposed to the Hansen’s disease mycobacterium. Mostpeople have such high resistance that they cannot get Hansen’sdisease no matter how closely they are in contact with infectiouscases of the disease.12
6. Types of Hansen’s disease
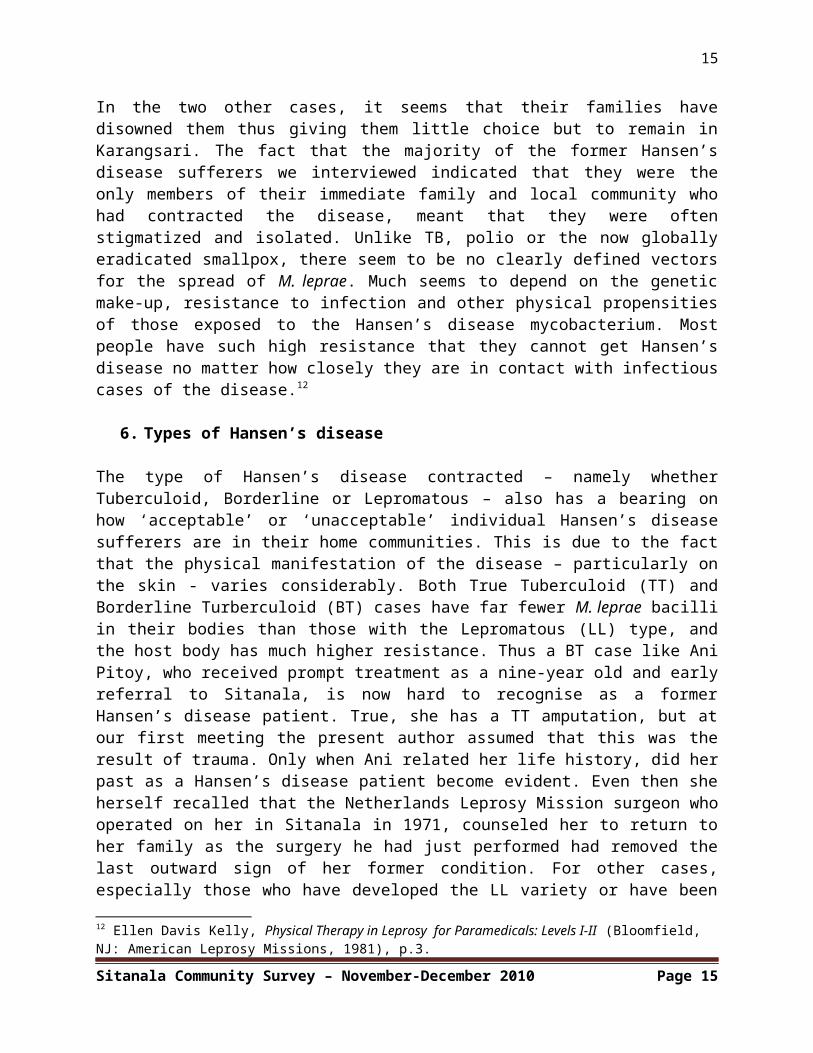
The type of Hansen’s disease contracted – namely whetherTuberculoid, Borderline or Lepromatous – also has a bearing onhow ‘acceptable’ or ‘unacceptable’ individual Hansen’s diseasesufferers are in their home communities. This is due to the factthat the physical manifestation of the disease – particularly onthe skin - varies considerably. Both True Tuberculoid (TT) andBorderline Turberculoid (BT) cases have far fewer M. leprae bacilliin their bodies than those with the Lepromatous (LL) type, andthe host body has much higher resistance. Thus a BT case like AniPitoy, who received prompt treatment as a nine-year old and earlyreferral to Sitanala, is now hard to recognise as a formerHansen’s disease patient. True, she has a TT amputation, but atour first meeting the present author assumed that this was theresult of trauma. Only when Ani related her life history, did herpast as a Hansen’s disease patient become evident. Even then sheherself recalled that the Netherlands Leprosy Mission surgeon whooperated on her in Sitanala in 1971, counseled her to return toher family as the surgery he had just performed had removed thelast outward sign of her former condition. For other cases,especially those who have developed the LL variety or have been
12 Ellen Davis Kelly, Physical Therapy in Leprosy for Paramedicals: Levels I-II (Bloomfield, NJ: American Leprosy Missions, 1981), p.3.
Sitanala Community Survey – November-December 2010 Page 15
16
treated late as TT or BT patients, the physical damage from M.leprae infected nerve trunks is irreversible. Cata [10], the 27-year-old from Karawang, who had waited several years beforetreatment, had severe infiltration of M. leprae on the skin of hisright hand resulting in ‘banana fingers’ (swollen fingerstapering at the fingertips) and loss of sensation (anaesthesia)in his entire right arm resulting in the need for immediateamputation. In a BL case like that of Pak Amat Arif [6]infiltration of the eye-balls had caused a constant watering andweakness in the eyelid muscles (lagopthalmous), preventing himfrom closing his right eye completely and necessitating constantvoluntary blinking. So complete was the anaesthesia in hisremaining left leg that rats had recently eaten off part of hislittle toe [Photo 26]. Another former BL patient Pak Sahat [60],had to lie down frequently so debilitating was the impact of hisprevious M. lepromatosis infection and the demands of earning hisliving on the street.
Over two-thirds of those former Hansen’s disease patients we sawin Karangsari had the BT (50 percent) or TT (20 percent) type(Chart 4). The majority of the rest were BL (15 percent). Only in8 percent of cases was the full-blown Lepromatous (LL) typeconfirmed. The number of true Borderline (BB) cases was evensmaller (2.5 percent). Finally, there were a handful of instances(5 percent) where Borderline Lepromatous or Lepromatous Leprosy(LL) had morphed into Borderline Tuberculoid due to the strengthof the host’s immune system [Ibu Oues, 48; Pak Sadori, 59 and IbuSulatin, 68]. In only one case did the reverse occur withBorderline Tuberculoid becoming full-blow Lepromatous Leprosy(LL) [Amat Arif, 6]. In the case of Ibu Oues [48], a twenty-eight-year old former long distance runner and high school sportsenthusiast from Karawang, it was suggested that her strongphysique had helped her to build up such resistance to heroriginally contracted LL type that it eventually turned intoBL.13 At the end of our survey, we asked our co-researcher, MasDeden, himself a former BT type sufferer, to reflect on what hesaw as the difference between the Tuberculoid and Lepromatoustypes. His reply was that with the first one had to live with a13 Personal communication Mas Deden Sinhuhaji, Karangsari, 9 December 2010.
Sitanala Community Survey – November-December 2010 Page 16
17
damaged ‘body’, but with the latter one also had to contend witha damaged ‘soul’.14
7. The Physical impact of Hansen’s disease I: Employment anddisability
Even with the presence of a supportive community, the physicalenvironment of Karangsari is tough. Opportunities for employmentare few, and there is no social security system in Indonesia. Themajority of those we interviewed earned their keep as beggars onthe streets around the hospital: the nearby sluice gate – PintuAir – and its adjacent traffic lights (lampu merah) beingfavourite spots. Those few in employment tend to work as streetcleaners for Tangerang municipality (pemkot), a physicallydemanding and low paid job, requiring the sweeping of a kilometerof road a day with no days off for a monthly salary of justIDR700,000 (USD75). Such situations have a significant impact onM. leprae damaged hands and feet. This is especially the case forthose who experience significant loss of feeling (anaesthesia).Poorly designed prosthetic and orthotic devices compound theproblem. Lack of biomechanical knowledge in socket design takesan immediate toll on amputees who earn their living on the streeteither as beggars or as sweepers. Pak Nadin [45], the thirty-fiveyear old pemkot (municipal) cleaning service employee, who haslimited feeling in his right stump, has abrasion sores behind hisknee and on his tibia and condulus lateralis, as well asextensive swelling on his hands. Even his still healthy left foothas problems and he now has only passive dorsi-flexion with it.An open wound (plantar ulcer) on the sole of his left toerequires him to steep his foot in warm salt water every night toprevent further deterioration. He would like to find lessphysically challenging employment, but the lack of jobs open toformer Hansen’s disease patients (there is still discriminationin the work force) means that he has no alternative but tocontinue his daily work as a municipal sweeper. His TT device,his second sponsored by the Indosiar commercial TV station sincehis amputation in Sitanala in 2000, was made for him in what he
14 His words in Indonesian were ‘rusak raga’ (broken body) and ‘rusak jiwa’ (broken soul/spirit), personal communication, Mas Deden Sinuhaji, 12 January 2011.
Sitanala Community Survey – November-December 2010 Page 17
18
describes as a ‘Menteng’ clinic, presumably a local P&O workshopin Central Jakarta which may well have taken a cast but then didnot have the biomechanical capacity to ensure proper weightdistribution in the socket. Even with multiple layers of stumpsocks and elasticated bandage, he has not been able to avoidsevere abrasion sores.
It is clear that long before most of the current Karangsariresidents arrived at Sitanala, the physical problems, which wouldlater necessitate amputation surgery, were already evident. Thelong-term physical impact of M. leprae infection, particularly inthe BT and TT types, tends to take a predictable course. This isparticularly the case for those living in rural areas wheremanual labour is the norm. Dr Brand once observed that if he hadone gift to give his patients it would be the gift of pain.15
Loss of the ability to feel pain in the extremities of the bodyis the main cause of physical disability in Hansen’s disease. Thedisease affects the nervous system and over time leads to loss offeeling (anaesthesia). This in turn triggers tissue damage whichescalates when its victims ignore, or more likely, are unable toperceive, early warnings of pain. The development of plantarulcers on the feet was the main cause of amputation amongst theformer Hansen’s disease patients we saw in Karangsari. Hailingfrom backgrounds where heavy manual work is the one source ofpaid employment, even patients whose Hansen’s disease conditionhad been detected early – and in some cases treated in a timelyfashion – still have to contend with long-term physicaldisability. Pak Ismaila [23], the fifteen-year-old who dumped hisGerman imported Dapsone in the river, ended up working in acoconut plantation for eight years in his late teens and earlytwenties with predictable effects for his hands and feet. It wasthe same for Pak Mariono [40], who began manual labour in apineapple plantation on leaving school as a thirteen-year-old –the same year his Dapsone treatment started. By his earlyforties, he was a TT amputee. Even those who were able to secureless rigorous physical employment could not escape the problems15 Al Schmidt (Spokane), ‘Life Saver Hero: Dr Paul Brand’, downloaded on http://myhero.com/go/hero.asp?hero=P_Brand_whitworth_US_2009, on 4 January 2011.
Sitanala Community Survey – November-December 2010 Page 18
19
of loss of feeling: Pak Subagyo (Mas Beggi) [65], who grew up inthe shadow of the prestigious Marriott Hotel in downtown Jakarta,received treatment as an out-patient in one of the Indonesiancapital’s best hospitals – RSUP Tjipto Mangunkusumo – and secureda job in a nearby photographic studio – was a partial footamputee by the age of eighteen: the chemicals (potassium bromide)he had to handle every day had exacerbated a wound (plantarulcer) on the sole of his right foot leading to amputation.
Nor was this a situation confined to men: both Ibu PresiKusumawati [49] and Ibu Sukira [67], who started work at thirteenand eighteen respectively on leaving school, the latter in afactory bagging sugar and rice in the Cimone area of Tanggerang,experienced physical problems as young adults: in Ibu Presi’scase she had wounds ‘all over her body’ in her late teens and aplantar ulcer in her right foot which necessitated a TTamputation when she was just 22. Ibu Sukira, who had begun tolose feeling in her lower legs in her early twenties, got a nailin the heel of her left foot while working at the Cimone factory,and now has an inverted foot, a direct result of having to walkon the ball of her foot during the past fifteen years.
8. The Physical Impact of Hansen’s disease II: P&O Provision
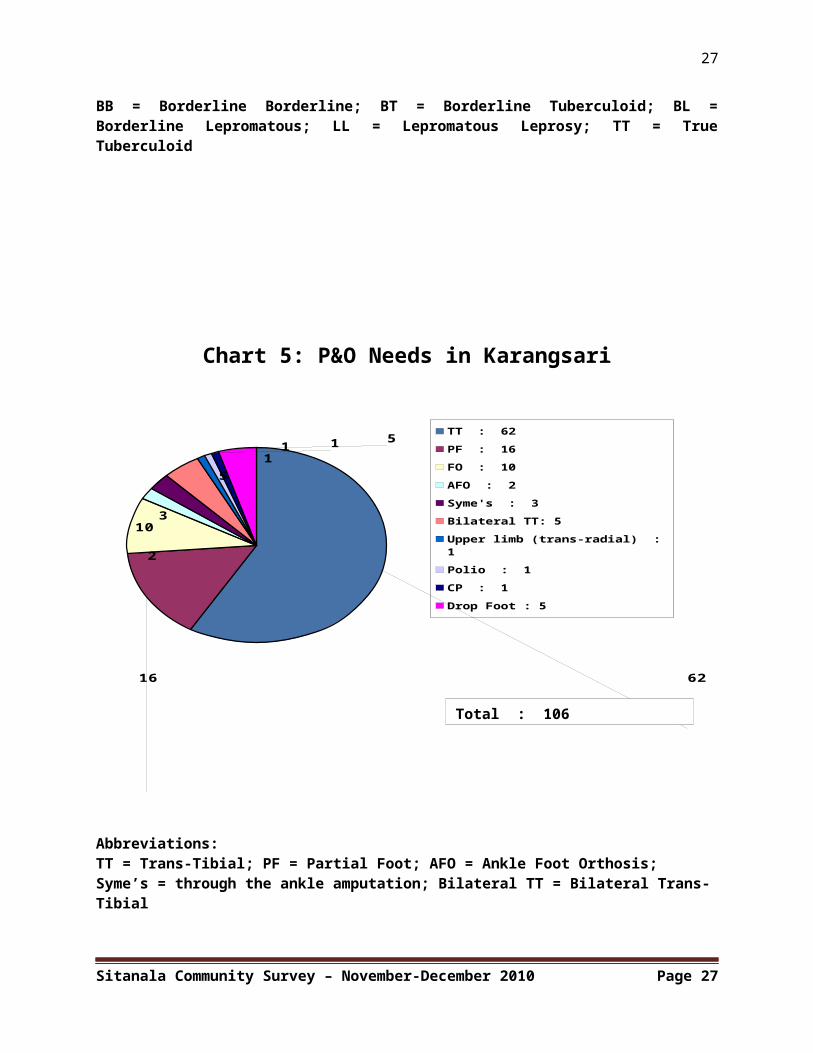
While many of the former Hansen’s disease patients we saw inKarangsari had prostheses, these were almost all Trans-Tibial(TT) (Chart 5). None of the 16 partial foot (PF) patients – apartfrom Mas Deden who had been recently treated at JSPO – had AFO(Ankle Foot Orthosis) devices. It was the same with the twoSyme’s patients and the ten who required foot orthoses.Furthermore, as we have just seen, in nearly all cases where TTdevices had been fabricated (Section 7 above), there wereproblems with their use: either the prostheses were too old, orthere were problems with the biomechanics of the socket design,alignment and fit.
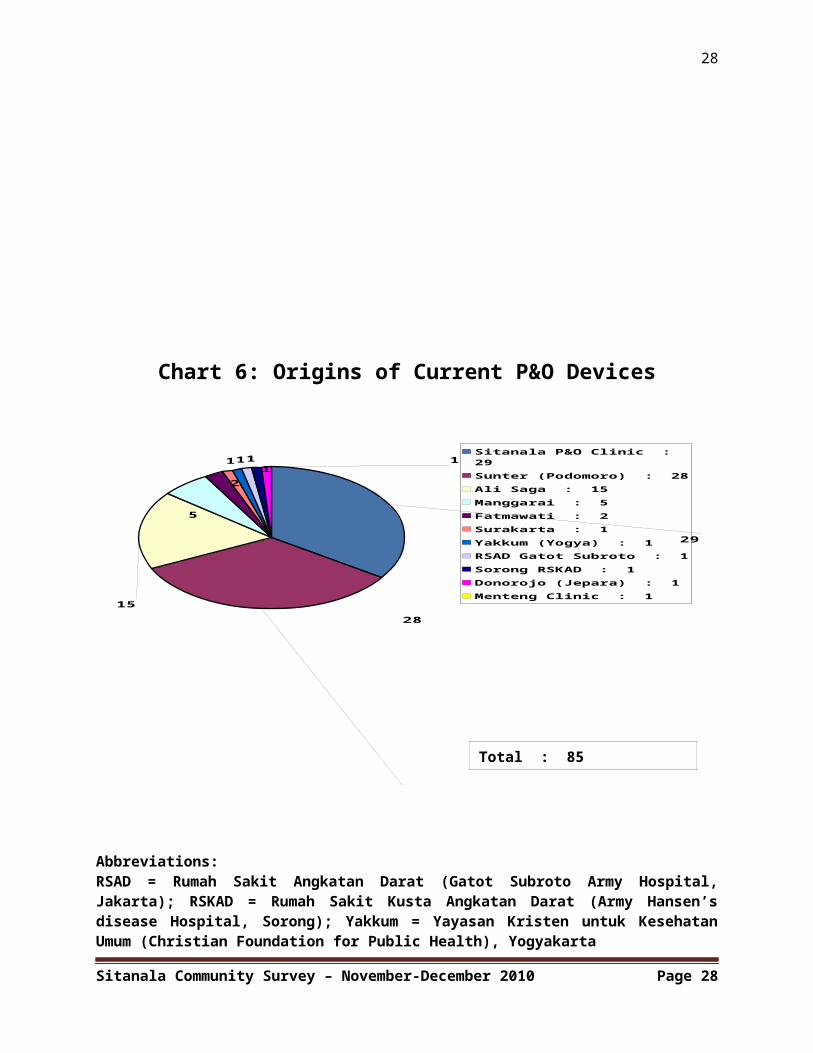
The three main places for TT prosthetic fabrication were theJaipur-originated Sunter limb centre in North Jakarta, theSurakarta P&O-staffed clinic at Sitanala Hospital, and the Ali
Sitanala Community Survey – November-December 2010 Page 19
20
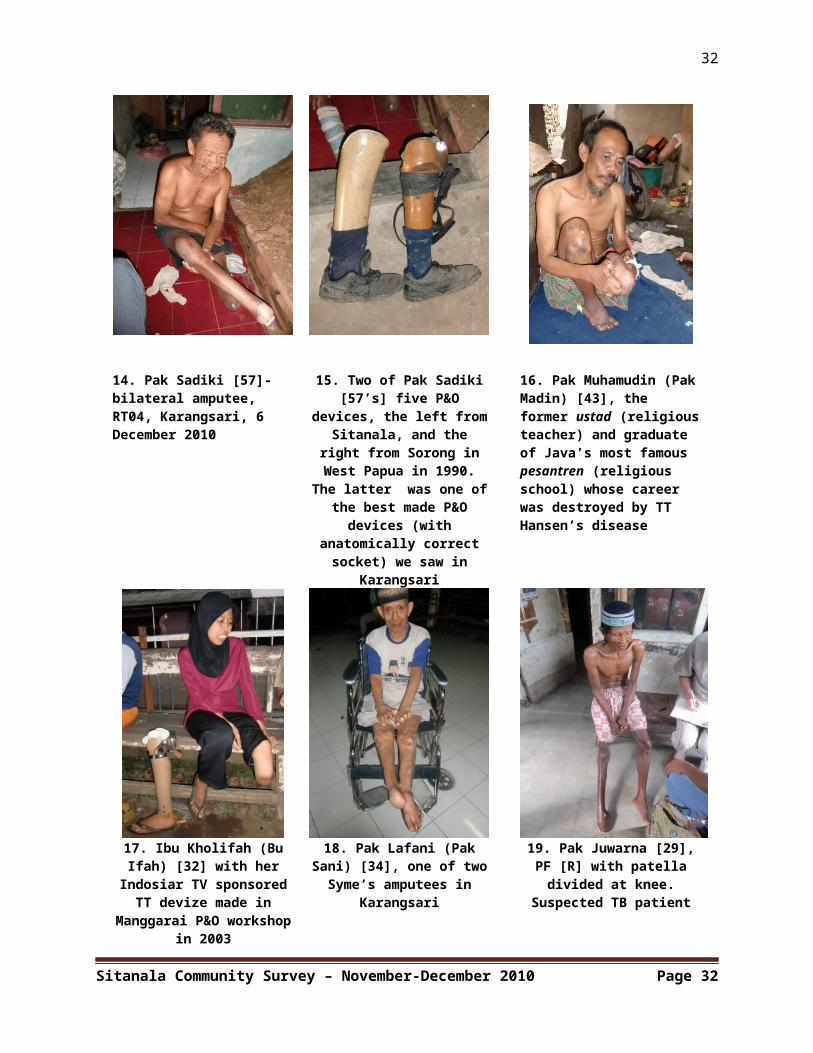
Saga workshop in Karangsari set up by a local artist. There werealso a handful of prostheses dating from the 1980s and 1990swhich were made elsewhere (Chart 6). These include prosthesesmade in the P&O workshop at Fatmawati, the Gatot Subroto ArmyHospital and a now defunct P&O clinic in Manggarai (Jalan Tambak,South Jakarta), previously supported by a section of the Indianexpat community in Jakarta who hailed from a different area fromthose – mainly Sindhi - involved with the Sunter workshop (seebelow).16 Ironically, perhaps the best designed and most durableTT prosthetic device we saw was made at the other end ofIndonesia, nearly 3,000 kilometers away in Sorong (Biak district,West Papua) by Hansen’s disease patients at the local IndonesianArmy Hansen’s disease Hospital (RSKAD) (Photo 15). Although nolonger usable, Pak Sadiki, the bilateral TT amputee for whom itwas originally made, is still cannibalizing its superiormaterials to keep his more recent and inferior quality Sunter andAli Saga prostheses in commission.17
Of the three main centres of prosthetic fabrication, Sunter(Yayasan Peduli Tuna Daksa, Sunter Jaya, North Jakarta) wouldseem to be the most competent. Established in 2007 by the smallbut wealthy Indian Sindhi business community in Jakarta at thebehest of their spiritual mentor, Dada J.P. Vaswani (born 1923),the centre has brought in technicians from Jaipur to trainIndonesian counterparts in fibre plastic (laminate) and resintechnologies. Unlike Sitanala, it is able to manufacture Trans-Femoral (TF) (above-knee) prostheses as well as upper limbprosthetics. Since 2007, it has produced 3,800 artificial limbsfor persons with disabilities throughout Indonesia and these aredistributed free of charge with donations and sponsorship moneybeing raised from a variety of different sources, includingIndosiar TV, PT Semen Padang (for devices distributed in theaftermath of the 30 September 2009 West Sumatra earthquake) andthe local PT Agung Podomoro Property Developers. The techniciansworking in Sunter boast that they can turn out a TT device every
16 Interview with Mas Deden Sinhuhaji, JSPO, 8 February 2011.17 Interview with Pak Sadiki, Karangsari, 6 December 2010.
Sitanala Community Survey – November-December 2010 Page 20
21
two hours.18 Their output is certainly impressive, but theirprostheses suffer from the lack of any possible alignmentadjustment at the socket once the device has been made. Theweight of the Jaipur rubber foot also makes their TT limb veryheavy, the foot itself being poorly engineered with a badly madewooden keel structure which gives it reduced durability.
Sitanala comes in second place. It has half a dozen staff, themajority of whom are Surakarta Poltekkes graduates from the onemid-1980s graduating class and the more recent post-2003 P&Ocourse. Although the devices are distributed free to those withJamskesmas (Medical Social Security) cards, the Sitanala P&Oworkshop’s production range and capacity is limited: the currentfacility is poorly equipped with many machines now out ofcommission. Their products also suffer from many of the problemsinherent in the Solo Poltekkes training curriculum: fit, design,alignment and biomechanics all leave much to be desired. WhenKarangsari residents complain that they have problems with thesocket fit and alignment of the new TT prostheses made atSitanala, the usual response from workshop staff is that suchproblems are ‘normal’ and that the TT amputees will ‘get used’ tousing them provided they walk far enough. This is usually arecipe for abrasion sores. For active amputees holding down jobsas municipal cleaners the long-term effects of poorly designedprosthetic devices soon become obvious.
Finally, there is Ali Saga’s private P&O clinic, which worksclosely with staff from the Sitanala P&O workshop and uses thesame laminate and resin technologies. His devices look good asbefits an artist and sculptor, but they are not viable except forthose few in Karangsari who do not have to move far to theirplace of work – namely those handful of women who run their ownstores or who work as seamstresses in the local churches. UnlikeSitanala, Ali Saga does, however, produce upper limb prosthesesand in the view of the senior JSPO lecturer who visited on thenight of 15 December these have potential if only from the18 Personal communication, Sébastien Dubois, P&O Student Montmorency Collège, Quebec, Canada, 26 January 2011. Mr Dubois visited the Sunter Workshop on 25 January 2011.
Sitanala Community Survey – November-December 2010 Page 21
22
cosmetic point of view. A proper assessment by professionallytrained P&O personnel is necessary before any firm conclusionscan be drawn regarding the potential or lack of it of all threeof these Jakarta-based P&O providers. One suspects that onceproperly trained International Society of Prosthetics & Orthotics(ISPO) qualified Category-2 P&Os begin to make an impact on theprovision of P&O devices in Jakarta that some of the existingproviders need to upgrade their production techniques or face asharp decline in the number of their clients.
9. Conclusions
The current survey on the P&O needs of Karangsari residents is awork in progress. For a start, there are still fifteen formerHansen’s disease patients [85-99], including the only femalebilateral TT amputee (Ibu Gemi [86]), who have yet to beinterviewed. Two others – Pak Acim [3] and Ibu Supinah [73] –have died (April 2011) since we interviewed them. Still others,who are part-time residents of Karangsari – like Pak Edi Maksudi[13] - may come forward in the future to be registered. But themain outlines are clear: in this specific community of formerHansen’s disease patients and their children, numbering at least2,650 people, 3.7 percent have P&O needs. Only about 60 percentof their P&O needs are currently being addressed and then onlyfor TT amputees. The principal providers are the two local(Sitanala and Ali Saga) and one North Jakarta-based (Sunter) P&Oworkshops, but their devices fall far short of what is requiredto ensure long-term pain-free mobility for their users.Furthermore, most of these devices are still in commission longafter they should have been replaced: some residents (Pak Simin[64], Ibu Suharti [66], and Ibu Yumiati [83]) are using deviceswhich are over a decade old. Others like Pak Sadiki [57] arecannibalising them because their quality is better than anythingthey have subsequently been able to acquire.
Apart from TT prosthetics, the range of P&O services on offerfrom these three workshops is limited. Sunter (Yayasan TunaDaksa) would seem to be the most competent, but even they do notprovide the type of orthotic devices required by the 16 Partial
Sitanala Community Survey – November-December 2010 Page 22
23
Foot and two AFO (Chart 5) clients in Karangsari. One of theseAFO clients was our research assistant, Mas Deden (Appendix II).A Partial Foot amputee, he admitted that he was seriouslycontemplating a further below-knee amputation of his right leg sothat he could at least get a serviceable prosthetic device whichwould enable him to walk again. His current AFO device made byone of the JSPO lecturers (Photo 24) has transformed his life. Hecan now walk without pain, carry sacks of rice on his shoulders,tend his market garden and raise tropical fish for sale tosuppliers in downtown Jakarta. Indeed, so radical has the changebeen for him that he has also just decided to get married (7November 2010) to his long-time partner, Ibu Aminah, whom he metin 2007-8 as a Sitanala in-patient when he was having his partialfoot operation. It is remarkable what USD30 worth ofpolypropylene, Velcro and orthotic shoe can do if shaped by aproperly-trained P&O. There are many such stories waiting tohappen – and they will if JSPO graduates deliver what they havebeen trained for.
_________
Sitanala Community Survey – November-December 2010 Page 23
24
Pie-Charts
1. Birth places of Karangsari interviewees
2. Age at which Hansen’s disease first detected
3. Years before Hansen’s disease treated
4. Types of Hansen’s disease5. P&O needs in Karangsari6. Origins of P&O devices
Sitanala Community Survey – November-December 2010 Page 24
25
Chart I: Birth-places of Karangsari interviewees
20
1077553
33
4
13
10Jakarta : 20Cirebon : 10Tangerang : 7Bekasi : 7Banten (Pandeglang, Serang, Ujung Kulon) : 5Subang : 5Bogor : 3Indramayu : 3Karawang : 3Other West Java (Tasik, Banjar, Purwakarta) : 4Central & East Java : 13Outer Islands : 10
Chart 2: Age at which Hansen’s Disease detected
1
0
11
10661427
18
Pre School (5 yrs & under)
Class 1 Primary (6-7 yrs)
Class 2 Primary (7-8 yrs)
Class 3 Primary (8-9 yrs)
Class 4 Primary (9-10 yrs)
Class 5 Primary (10-11 yrs)
Class 6 Primary (11-12 yrs)
Junior High (13-15 yrs)
Senior High (16-18 yrs)
Adult (18+)
Sitanala Community Survey – November-December 2010 Page 25
Total : 90
Total : 75
26
Chart 3: Years before Hansen’s Disease treated
21
1422
9
52 Under 1 year: 21
2-5 yrs : 14
6-9 yrs : 22
10-15 yrs : 9
16-20 yrs : 5
over 20 yrs : 2
Chart 4: Types of Hansen’s disease
4416
14
6
3 2 1
BT : 44TT : 16BL : 14LL : 6BL/LL to BT : 3BB : 2
Abbreviations:
Sitanala Community Survey – November-December 2010 Page 26
Total : 73
Total : 86
27
BB = Borderline Borderline; BT = Borderline Tuberculoid; BL =Borderline Lepromatous; LL = Lepromatous Leprosy; TT = TrueTuberculoid
Chart 5: P&O Needs in Karangsari
6216
10
2
3
511 1 5 TT : 62
PF : 16FO : 10AFO : 2Syme's : 3Bilateral TT: 5Upper limb (trans-radial) : 1Polio : 1CP : 1Drop Foot : 5
Abbreviations:TT = Trans-Tibial; PF = Partial Foot; AFO = Ankle Foot Orthosis; Syme’s = through the ankle amputation; Bilateral TT = Bilateral Trans-Tibial
Sitanala Community Survey – November-December 2010 Page 27
Total : 106
28
Chart 6: Origins of Current P&O Devices
29
2815
5
21
111 1Sitanala P&O Clinic : 29Sunter (Podomoro) : 28Ali Saga : 15Manggarai : 5Fatmawati : 2Surakarta : 1Yakkum (Yogya) : 1RSAD Gatot Subroto : 1Sorong RSKAD : 1Donorojo (Jepara) : 1Menteng Clinic : 1
Abbreviations: RSAD = Rumah Sakit Angkatan Darat (Gatot Subroto Army Hospital,Jakarta); RSKAD = Rumah Sakit Kusta Angkatan Darat (Army Hansen’sdisease Hospital, Sorong); Yakkum = Yayasan Kristen untuk KesehatanUmum (Christian Foundation for Public Health), Yogyakarta
Sitanala Community Survey – November-December 2010 Page 28
Total : 85
29
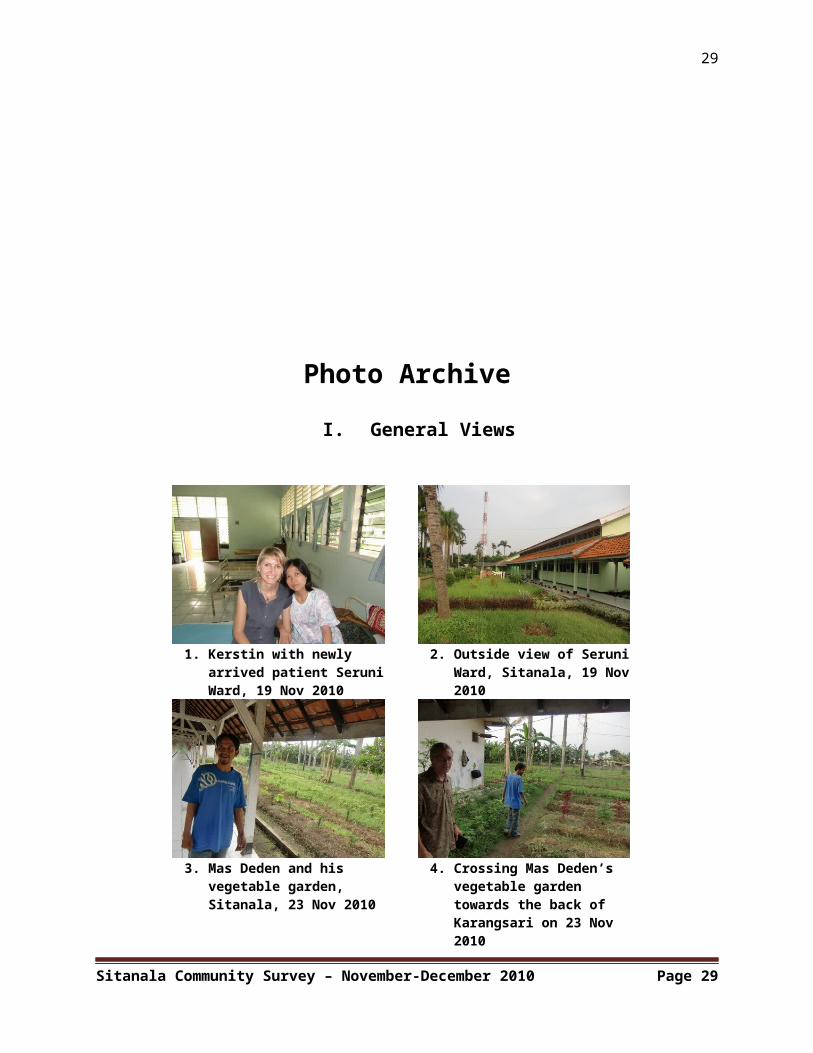
Photo ArchiveI. General Views
1. Kerstin with newly arrived patient SeruniWard, 19 Nov 2010
2. Outside view of Seruni Ward, Sitanala, 19 Nov 2010
3. Mas Deden and his vegetable garden, Sitanala, 23 Nov 2010
4. Crossing Mas Deden’s vegetable garden towards the back of Karangsari on 23 Nov 2010
Sitanala Community Survey – November-December 2010 Page 29
30
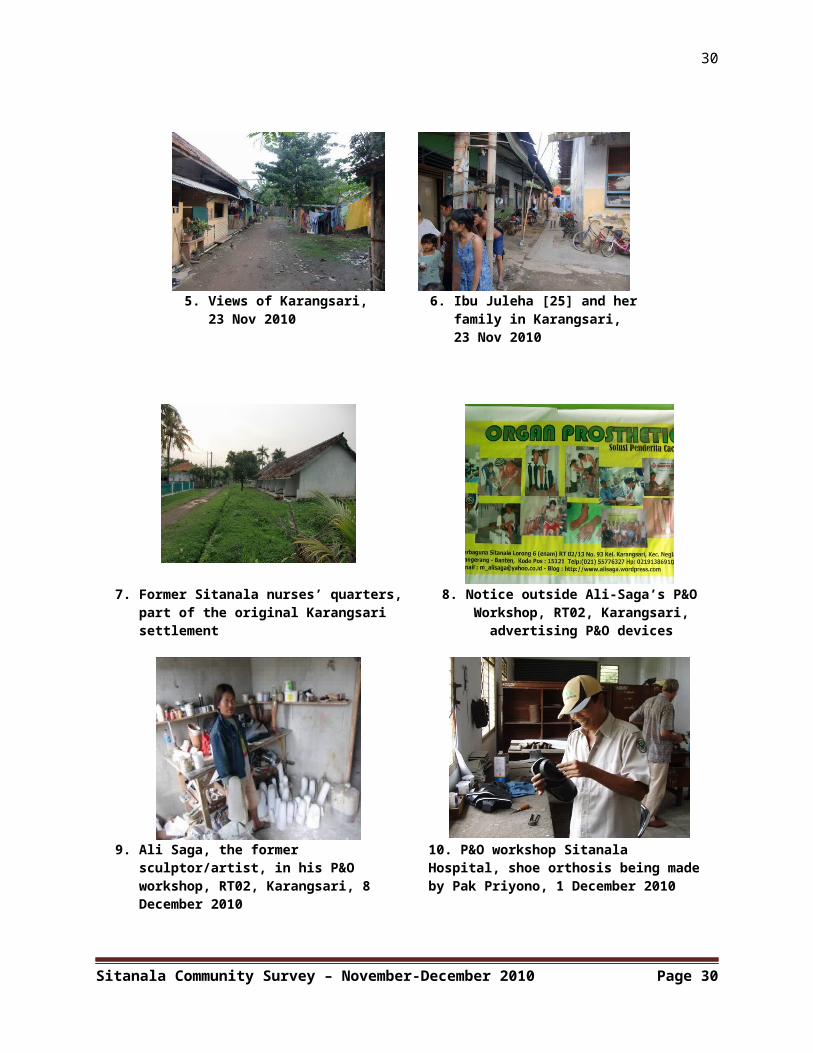
5. Views of Karangsari, 23 Nov 2010
6. Ibu Juleha [25] and herfamily in Karangsari, 23 Nov 2010
7. Former Sitanala nurses’ quarters, part of the original Karangsari settlement
8. Notice outside Ali-Saga’s P&OWorkshop, RT02, Karangsari,advertising P&O devices
9. Ali Saga, the former sculptor/artist, in his P&O workshop, RT02, Karangsari, 8 December 2010
10. P&O workshop Sitanala Hospital, shoe orthosis being madeby Pak Priyono, 1 December 2010
Sitanala Community Survey – November-December 2010 Page 30
31
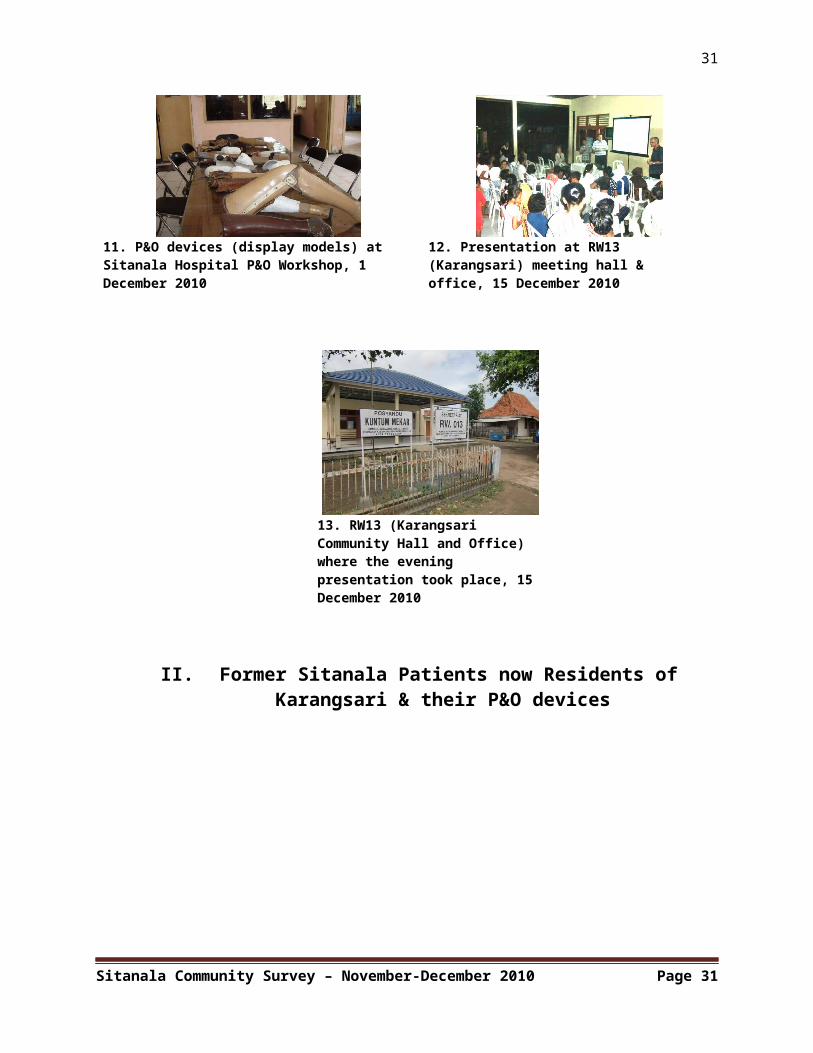
11. P&O devices (display models) at Sitanala Hospital P&O Workshop, 1 December 2010
12. Presentation at RW13 (Karangsari) meeting hall & office, 15 December 2010
13. RW13 (Karangsari Community Hall and Office) where the evening presentation took place, 15 December 2010
II. Former Sitanala Patients now Residents ofKarangsari & their P&O devices
Sitanala Community Survey – November-December 2010 Page 31
32
14. Pak Sadiki [57]- bilateral amputee, RT04, Karangsari, 6 December 2010
15. Two of Pak Sadiki[57’s] five P&O
devices, the left fromSitanala, and the
right from Sorong inWest Papua in 1990.
The latter was one ofthe best made P&Odevices (with
anatomically correctsocket) we saw in
Karangsari
16. Pak Muhamudin (PakMadin) [43], the former ustad (religiousteacher) and graduate of Java’s most famous pesantren (religious school) whose career was destroyed by TT Hansen’s disease
17. Ibu Kholifah (BuIfah) [32] with herIndosiar TV sponsoredTT devize made in
Manggarai P&O workshopin 2003
18. Pak Lafani (PakSani) [34], one of twoSyme’s amputees in
Karangsari
19. Pak Juwarna [29],PF [R] with patelladivided at knee.
Suspected TB patient
Sitanala Community Survey – November-December 2010 Page 32
33
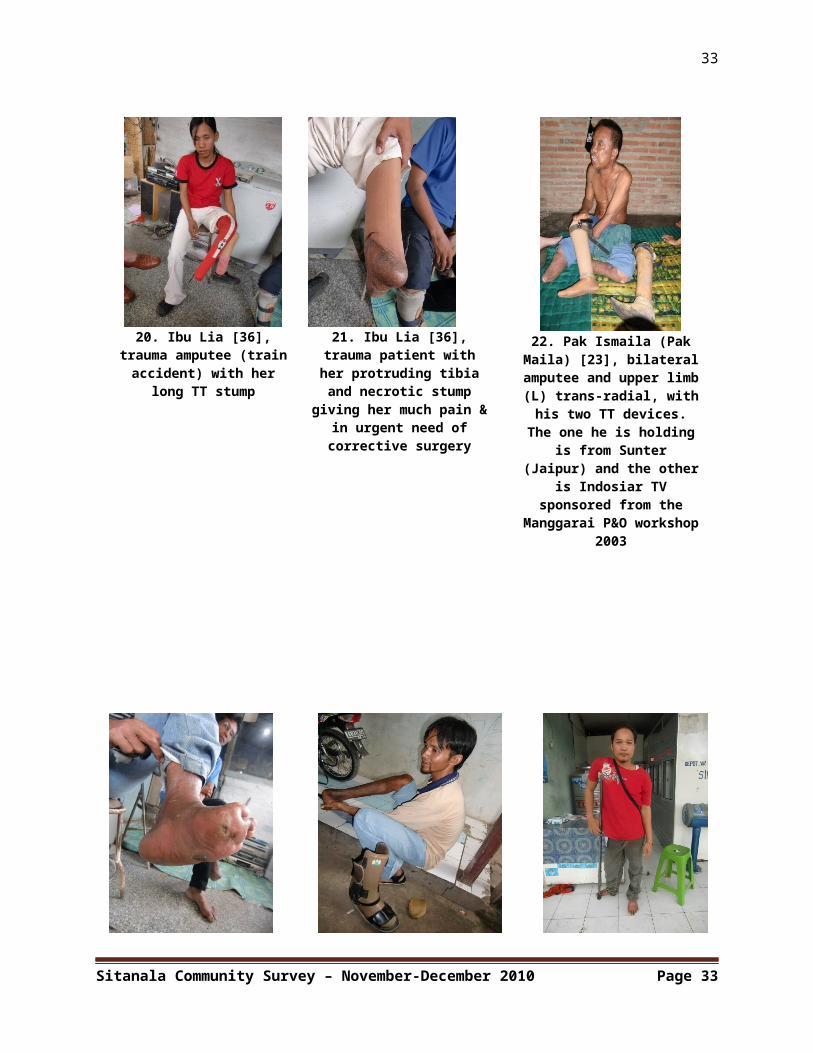
20. Ibu Lia [36],trauma amputee (trainaccident) with her
long TT stump
21. Ibu Lia [36],trauma patient withher protruding tibiaand necrotic stump
giving her much pain &in urgent need ofcorrective surgery
22. Pak Ismaila (PakMaila) [23], bilateralamputee and upper limb(L) trans-radial, withhis two TT devices.The one he is holding
is from Sunter(Jaipur) and the other
is Indosiar TVsponsored from the
Manggarai P&O workshop2003
Sitanala Community Survey – November-December 2010 Page 33
34
Sitanala Community Survey – November-December 2010 Page 34
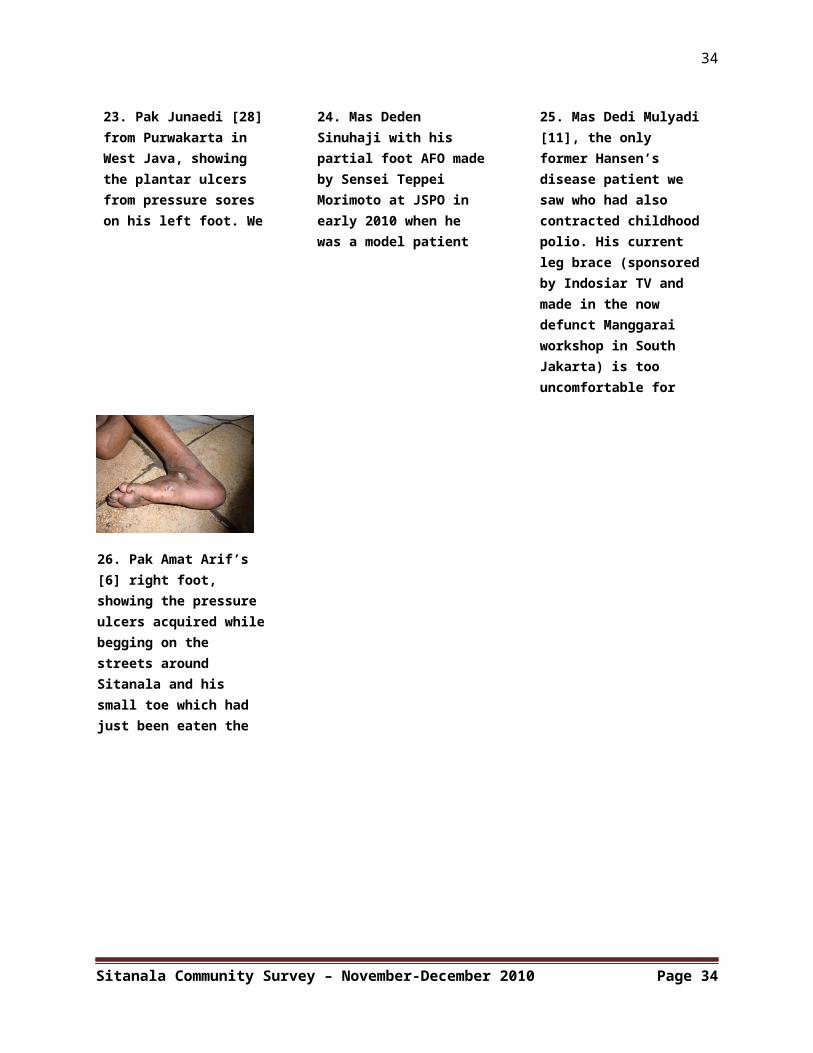
24. Mas Deden Sinuhaji with his partial foot AFO madeby Sensei Teppei Morimoto at JSPO in early 2010 when he was a model patient and which has
25. Mas Dedi Mulyadi[11], the only former Hansen’s disease patient we saw who had also contracted childhoodpolio. His current leg brace (sponsoredby Indosiar TV and made in the now defunct Manggarai workshop in South Jakarta) is too uncomfortable for
23. Pak Junaedi [28] from Purwakarta in West Java, showing the plantar ulcers from pressure sores on his left foot. We saw much worse than
26. Pak Amat Arif’s [6] right foot, showing the pressure ulcers acquired whilebegging on the streets around Sitanala and his small toe which had just been eaten the previous night by
Related Documents