Cutaneous leishmaniasis

Leismaniasis presentation.ppt modified
Nov 28, 2014
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Cutaneous leishmaniasis

INTRODUCTION
• DEFINITION,CLASSIFICATION• EPIDEMIOLOGY• ETIOLOGY• PATHOPHYSIOLOGY• CLINICAL MANIFESTATIONS• DX &DDX• TREATMENT• PROGNOSIS & PREVENTION

• It is a protozoal disease caused by a parasite called leshmania genus.
• It is an obligate intracellular parasite.• Which is transmitted to humans by a sand fly
bite.

EPIDEMIOLOGY
• Endemic in 88 countries of the old and new world(Africa,Asia,Europe,N.A& S.A, except Australia.
• 1.5-2million new cases seen every year (WHO estimates) • 40,000 – 80,000 deaths every year (esp. MCL,VL).• Race: no racial predilection• Sex: no sex predilection• Age: no specific age susceptibility is known.• The disease is seen in tropics,subtropics & highlands.

• Traditionally divided as Old World and New World leishmaniasis.
• Old World leishmaniasis: is caused by Leishmania species found in Africa, Asia, the Middle East, the Mediterranean, and India, and
• New World leishmaniasis: is caused by Leishmania species found in Central America and South America,

THE VECTORS
• Leishmania parasites are transmitted by sandflies of • the genus phlebotomus =in the old world and• the genus lutzomyia =in the new world.
• Sand flies are small in size mosquito like insects 1.5-4mm in size can pass through ordinary mesh screen and mosquito netting.
Only the females are blood sucking.

The parasite has two host life cycles.

Leishmania parasites• members of the order kinetoplastida family
trypanosomatidae• They are found in two morphologic forms= in mamalian with
in macrophages as round to oval non flagellated amastigotes &• in sandfly promastigotes elongated flagellated .
• Both forms of parasites have got a nucleus and DNA containing kinetoplast.

pathophysiology …• With in the macrophages the promastigotes
transform in to amastigotes (leishman-donovan bodies)→multiply by binary fission.
• When a macrophage become filled with amastigotes it disrupted →amastigotes reenter the extracellular space and taken up by other macrophages.

PATHOPHYSIOLOGY.• Parasites in the form of amastigotes from infected tissue or
blood are taken up from the mamalian host during feeding,• Then with in the mid gut of the sandfly the parasites under
go change to promastigotes form →multiply
• then they migrate to the pharynx and proboscis of the sandfly i.e. with in 8-2o days →they remain until they are injected in to a new host during a subsequent blood meal.
• Between 10-200 promastigotes enter the dermis during each feeding but most of them are destroyed by polymorphonuclear leukocytes,eosinophils & serum complement.
• Some of the promastigotes become attached to receptors of the dermal macrophages and are phagocytosed = in the macrophages the promastigotes resisting.




• Similar to Hansen disease, leishmaniasis is a disease in which the clinical diversity reflects a complex interplay between the virulence of the infecting species and the host's immune response.
• At one extreme, localized cutaneous disease demonstrates a strong immune response, with most cases resolving without intervention.
• This form of disease exhibits a helper T-cell subtype 1 (TH1) immune response, with cytokines that induce disease resolution.

Clinical manifestation
• Depending on the degree of the cell mediated host immune response &the type ,virulence of leishmania species the clinical classification are:
• Localized cutaneous leishmaniasis• Mucocutaneous leishmaniasis• Diffuse cutaneous lesihmaniasis• Visceral leishmaniasis


CUTANEOUS LEISHMANIASIS• OLD WORLD CL -L tropica &L. major ,L.infantum &
L.aethiopica.
• The disease begin as a small erythematus papule which may appear after the bite of the sand fly→the papules enlarges slowly in size (to 2 cm or more)
• Over a period of several weeks a lesion becomes crusted in the center.


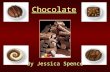
CL ON THE FACE.

CONTD…
• L.tropica


Moist (ulcerative)cutaneous leishmaniasis
• usually caused by L . major• characterized by multiple lesions,• short incubation period (1 to 3 weeks)• rapid and mild course • Spontanosly heals with in 6 months.• good response to therapy.


CL WITH S/C NODULES ALONG THE PROXIMAL LYMPHATICS.


New world CL
• found in Mexico,central America,texas& brazil.
• the lesions are similar to L.major• Lesions can develop on any part of the body
and• can involve the PINNA of the ears(chiclero
ulcer)
• L.brazilinesis can some time invade mucous mebrane.

Diffuse cutaneous leishmaniasis
• DCL in both old and new world caused by L.aethiopica& L.brazilinesis
• DCL is found in 20% of leishmania pts in Ethiopia and the Sudan .
• Clinically a single nodule spreads locally then by metastasis becomes wide spread with non ulcerating nodules over the face and trunk .
• It resembles lepromatous leprosy.

• DCL usually runs a protracted course but does not visceralize,
• responds to therapy poorly.• Parasites are abundant in skin smear and
biopsies.


DCL ON FACE.

Mucocutaneous lesihmaniasis• MCL = is involvement of both skin & mucus memb of upper
resp tract→ by L.brazelinesis &L.aethiopica.• Mucosal lesions develop from CL in more than 75% of those
infected.• A small red papule develops at the site of a sandfly bite
gradually enlarges,ulcerates and the infections extends to the mucus of the mouth,nose,pharynx,to carrtillages of the upper resp tract(nose&the larynx)
• Oedema &inflam.changes occur →destruction of the cartilagenous structures(nasal septum,floor of the mouth →to marked disfigurement.
• BUT bony stuctures are spared.

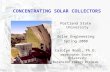
MCL WITH NASAL SEPTUM CARTILLAGE DESTRUCTION &DISFIGURMENT

MCL


MCL.





Visceral leishmaniasis• VL(KALAZAR)=Mainly affects the reticulo-endothelial systems
(spleen , BM,liver,lymphnodes)• L.DONOVANI,L.CHAGASI &L.INFANTUM• The disease present in china,india mid.east,east ,Africa
&S.America.
• It is one of the Common opprtunistic infection in HIV.• Patients will have splenomegally,pancytopenia,anaemia
fever,wasting& imbalance of serum protiens.

Visceral leishmniasis….
• Diagnosis =smears,cultures from BM biopsies,or spleen aspirates,serology tests are important.

POST KALAZAR DERMAL LEISHMANIASIS
• lesions usually appear with in a year after a course of therapy.
• Consists of macular,papular & nodular lesions on the face,trunk & extremities.
• PKDL has been reported to develop in 20% of Indian & in more than 50% of pts in the Sudan treated for VL.

PKDL

PKDL


WORKUP • Lab Studies:
• Cutaneous lesions– Skin scrapings are obtained from the base of an active ulcer or
biopsy of the edge of a suspicious lesion or ulcer. – Visualization of all 3 features (nucleus, cell membrane, and
kinetoplast) is required to make the Dx. microscopically.


• Cultures of tissue are regularly obtained to identify Leishmania species.
• PCR is now routinely used in experienced laboratories as a rapid diagnostic technique.

Serologic test
a direct agglutination test (DAT), and even a nitrocellulose dipstick test.
to date is an L chagasi recombinant amastigotes K39 (rK39)–based antigen test system that has been used with enzyme-linked immunosorbent assay (ELISA),
– The degree of conservation of the K39 gene is high among isolates of the L donovani family, including L chagasi and L infantum.
– Therefore, this test is useful for most recognized cases of visceral leishmania.
– Assays based on rK39 antigen are highly sensitive and specific and validated in several large studies worldwide.

ManagementTopical therapyTopical azoleCryotherapyLocal heat therapy(electrocautery)Topical parmomycine
• The mainstay of antileishmanial therapy has been pentavalent antimony (sodium stibogluconate or meglumine antimonate).
• Cutaneous disease: 20 mg/kg/d IV/IM for 20 D• Lesion borders: 1 mg/kg intralesional qwk.• Cure rates are 90-97%. These drugs are expensive and difficult to obtain.

Amphotericin B • Cure rates near 100%, except possibly in HIV infection. • Dose Amphotericin B (with deoxycholate): 1 mg/kg IV for 20 d

Ketoconazole • Azole antifungals have antileishmanial properties. • Not effective in visceral disease and should be used only as
second-line therapy in limited forms of cutaneous disease with known species sensitivity (eg, rapidly self-curing disease due to L mexicana but not L tropica).
• Gastric acid required for absorption. • Adult Dose 600 mg PO qd for 4 wk.

Pentamidine (Pentam-300, Pentacarinat, NebuPent) • - Inhibits growth of protozoa by blocking oxidative phosphorylation
and incorporation of nucleic acids into RNA and DNA, inhibiting protein and phospholipid synthesis.
• Cutaneous disease: 2 mg/kg IV (4 doses) • Resistance common in India; high relapse rates reported.

• Paromomycin (Aminosidine) -- Amebicidal and antibacterial aminoglycoside obtained from Streptomyces rimosus grain.
• Dose15 mg/kg/d IV for 20 d • Cytokines -- Interferon-gamma a TH1 cytokine, is used to enhance
host immunity to Leishmania parasites. • Interferon-gamma-1b (Actimmune) -- Recombinant DNA product.
Administered with sodium antimony gluconate (probably ineffective alone).
• Adult Dose 100 mg/m2/d IV for 28 d (with 20 mg/kg/d sodium antimony gluconate)

In addition to parenteral and oral medications , local therapies for some forms of cutaneous leishmaniasis:
• Cryotherapy; • Intralesional heat therapy with 40-42°C for 12 hours (One novel FDA-
approved device is called the Thermo Med device.); and
• Topical paromomycin preparations, typically 15% with 10% urea.

Mortality/Morbidity: • As many as 90% of localized cutaneous forms of leishmaniasis heal
spontaneously with scarring.
Related Documents