ORIGINAL ARTICLE Legg-Calvé-Perthes disease: multipositional power Doppler sonography of the proximal femoral vascularity Andrea S. Doria & Fabiano G. Cunha & Marcelo Modena & Rui Maciel & Laszlo J. Molnar & Carlos Luzo & Rahim Moineddin & Roberto Guarniero Received: 1 July 2007 / Revised: 19 November 2007 / Accepted: 5 December 2007 / Published online: 7 February 2008 # Springer-Verlag 2008 Abstract Background Selection of the most appropriate sonographic scanning approaches for evaluation of hips can improve the method efficacy and decrease the scanning time. Objective To determine the sonographic scanning planes that best assess the proximal femoral vascularity in asymptomatic and pathologic hips of children with Legg- Calvé-Perthes disease (LCPD) and evaluate the frequency (number of hips with evidence of perfusion) and intensity (number of color pixels per region) of color pixels representing superficial cartilaginous and deep transphyseal vascularity in different anatomic regions of pathologic and asymptomatic hips using multipositional power Doppler approaches. Materials and methods Seven scanning approaches (anterior- sagittal, anterior-transverse, coronal, adduction, perineal, 30° and 70° of abduction) were applied in 26 pathologic hips of 26 children with LCPD (age range 3–11 years) and in 25 contralateral asymptomatic hips. The color Doppler signals seen within the proximal femur were analyzed both qualitatively (overall/regional frequency) and quantitatively (intensity). Results The coronal ( P=0.009) and 30° abduction (P=0.047) approaches demonstrated a higher frequency of color pixels in pathologic than in asymptomatic hips. The anterior-sagittal, 30° abduction, adduction and anterior- transverse planes performed best of all approaches (P=0.02) to assess deep transphyseal perfusion. The physis demon- strated a greater intensity of color signals representing intraosseous vascularity than other regions in pathologic hips (P=0.027), as noted with the anterior-sagittal approach. There was a tendency (P=0.06) towards a greater intensity of pixels representing cartilaginous vascularity in patholog- ic hips’ physes with the coronal approach. Conclusion Specific sonographic scanning planes are rec- ommended for assessment of the proximal femoral vascu- larity of LCPD hips. The physis is the anatomic region that presents with the greatest intensity of color signals in pathologic hips. Keywords Legg-Calvé-Perthes disease . Power Doppler sonography . Hips . Children . Vascularity Introduction Although the normal vascular anatomy of the human growing femoral head has been extensively investigated in cadaveric studies by Trueta (46 specimens) [1], Lauritzen (6 specimens) [2], Ogden (20 specimens) [3] and Chung (150 specimens) [4], the literature on the vascularity of normal and pathologic hips assessed with noninvasive in vivo imaging techniques such as ultrasonography is scarce. Pediatr Radiol (2008) 38:392–402 DOI 10.1007/s00247-007-0726-4 A. S. Doria : L. J. Molnar Heart Institute, Diagnostic, Imaging, Hospital das Clinicas FMUSP, Sao Paulo, Brazil F. G. Cunha : M. Modena : R. Maciel : C. Luzo : R. Guarniero Department of Orthopedic Surgery, Hospital das Clinicas FMUSP, Sao Paulo, Brazil R. Moineddin Department of Public Health, University of Toronto, Toronto, Canada Permanent address: A. S. Doria (*) Department of Diagnostic Imaging, The Hospital for Sick Children, 555 University Ave, Toronto M5G1X8, Canada e-mail: [email protected]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ORIGINAL ARTICLE
Legg-Calvé-Perthes disease: multipositional power Dopplersonography of the proximal femoral vascularity
Andrea S. Doria & Fabiano G. Cunha &
Marcelo Modena & Rui Maciel & Laszlo J. Molnar &
Carlos Luzo & Rahim Moineddin & Roberto Guarniero
Received: 1 July 2007 /Revised: 19 November 2007 /Accepted: 5 December 2007 / Published online: 7 February 2008# Springer-Verlag 2008
AbstractBackground Selection of the most appropriate sonographicscanning approaches for evaluation of hips can improve themethod efficacy and decrease the scanning time.Objective To determine the sonographic scanning planesthat best assess the proximal femoral vascularity inasymptomatic and pathologic hips of children with Legg-Calvé-Perthes disease (LCPD) and evaluate the frequency(number of hips with evidence of perfusion) and intensity(number of color pixels per region) of color pixelsrepresenting superficial cartilaginous and deep transphysealvascularity in different anatomic regions of pathologic andasymptomatic hips using multipositional power Dopplerapproaches.Materials and methods Seven scanning approaches (anterior-sagittal, anterior-transverse, coronal, adduction, perineal, 30°and 70° of abduction) were applied in 26 pathologic hips of26 children with LCPD (age range 3–11 years) and in 25
contralateral asymptomatic hips. The color Doppler signalsseen within the proximal femur were analyzed bothqualitatively (overall/regional frequency) and quantitatively(intensity).Results The coronal (P=0.009) and 30° abduction(P=0.047) approaches demonstrated a higher frequency ofcolor pixels in pathologic than in asymptomatic hips. Theanterior-sagittal, 30° abduction, adduction and anterior-transverse planes performed best of all approaches (P=0.02)to assess deep transphyseal perfusion. The physis demon-strated a greater intensity of color signals representingintraosseous vascularity than other regions in pathologichips (P=0.027), as noted with the anterior-sagittal approach.There was a tendency (P=0.06) towards a greater intensityof pixels representing cartilaginous vascularity in patholog-ic hips’ physes with the coronal approach.Conclusion Specific sonographic scanning planes are rec-ommended for assessment of the proximal femoral vascu-larity of LCPD hips. The physis is the anatomic region thatpresents with the greatest intensity of color signals inpathologic hips.
Keywords Legg-Calvé-Perthes disease .
Power Doppler sonography . Hips . Children . Vascularity
Introduction
Although the normal vascular anatomy of the humangrowing femoral head has been extensively investigated incadaveric studies by Trueta (46 specimens) [1], Lauritzen (6specimens) [2], Ogden (20 specimens) [3] and Chung (150specimens) [4], the literature on the vascularity of normaland pathologic hips assessed with noninvasive in vivoimaging techniques such as ultrasonography is scarce.
Pediatr Radiol (2008) 38:392–402DOI 10.1007/s00247-007-0726-4
A. S. Doria : L. J. MolnarHeart Institute, Diagnostic, Imaging,Hospital das Clinicas FMUSP,Sao Paulo, Brazil
F. G. Cunha :M. Modena : R. Maciel : C. Luzo : R. GuarnieroDepartment of Orthopedic Surgery, Hospital das Clinicas FMUSP,Sao Paulo, Brazil
R. MoineddinDepartment of Public Health, University of Toronto,Toronto, Canada
Permanent address:A. S. Doria (*)Department of Diagnostic Imaging,The Hospital for Sick Children,555 University Ave,Toronto M5G1X8, Canadae-mail: [email protected]

Previous studies have demonstrated the presence ofcartilaginous vascular canals that arise in the normalepiphysis and course towards the metaphysis traversingthe growing physis [5, 6]. These normal vascular canalsenhance after intravenous administration of gadolinium[7] and are well evaluated with MRI [7]. However, anMRI examination requires sedation in young children.Sonography arises as an appealing imaging modality forassessment of children’s joints because it does not involveradiation and does not require sedation. Previous authors[8–11] have reported the ability of power Dopplersonography to detect vascularity within cartilaginouscanals of normal neonatal proximal femoral chondroe-piphyses. Previous Doppler sonography studies [12–15]have investigated the normal and pathologic proximalfemoral vascularity in growing joints after the neonatalperiod. However, no previous investigation has beenconducted to evaluate the effect of different sonographicscanning approaches on the ability to depict proximalfemoral vascularity.
The major blood supply to the femoral head arises fromthe ascending cervical arteries (branches of the lateralcircumflex arteries) that run subsynovially along thefemoral neck. A secondary blood source is the medialcircumflex artery, which partially supplies the femoral headand neck [16]. Legg-Calvé-Perthes disease (LCPD) is anavascular necrosis of the proximal growing femoralepiphysis [17] that is likely caused by an interruption ofthe blood supply from the retinacular arteries, branches ofthe ascending cervical arteries, to the proximal femoralepiphysis, with associated decreased flow in the medialcircumflex artery [17]. Recognizing the scanningapproaches that best identify the healing-related neovascu-larity in pathologic hips that sustained prior local ischemiaand the normal vascularity in asymptomatic hips is crucialfor further sonographic investigation of the vascularity ofthe growing proximal femur. Although power Dopplersonography might not be able to depict the vascularityarising from the medial circumflex artery (posterior access)we hypothesized that it could identify the deep transphysealflow as a result of healing in pathologic hips of patientswith LCPD.
The purpose of our study was twofold: (1) to determinethe scanning planes that provided best qualitative andquantitative assessment of the proximal femoral vascularity(overall and regionally) in asymptomatic and pathologichips of children with LCPD using multipositional powerDoppler sonography; and (2) to evaluate the frequency(number of hips with evidence of perfusion) and intensity(number of color pixels per region) of cartilaginous anddeep transphyseal vascularity in different anatomic regionsof pathologic and asymptomatic hips using multipositionalapproaches.
Materials and methods
Patients
This study was approved by the Research Ethics Com-mittee of our institution and informed consent wasobtained from the parents of all patients. Children withLCPD who agreed to participate in the study and who hadnot undergone prior surgery of their hips were included inthe study. The diagnosis of LCPD was made based onclinical (limping hip with pain at mobilization) and radio-graphic findings. Of 26 patients included, 18 (69.2%) alsounderwent scintigraphy within a short time (range 0–11 days) from the power Doppler examination, whichensured that the observations on sonography representedreal changes related to the revascularization process of thedisease as noted by analysis of the images according tothe Conway’s patterns of neovascularization/revasculariza-tion of the femoral head in LCPD [18].
In 26 children with LCPD (18 boys, 8 girls; age 3.1–11.5 years, mean 7.1 years), 26 consecutive symptomatichips (11 left, 15 right) were evaluated. Of the 26 children,15 (54%) were younger than 7 years and 12 (46%) were7 years or older. Twenty five children had unilateral diseaseand one had bilateral disease. In the patient with bilateraldisease only the right hip, which had not undergone priorsurgery, was included in the study. The duration of symptom-atology ranged from 1month to 5.5 years (mean 12.8months).The 25 contralateral asymptomatic hips (14 left, 11 right)of the children included in the study were also assessed.
Definitions
Superficial cartilaginous vascularity is characterized bypower Doppler signals visualized externally to the corticalbone of the secondary ossification center of the proximalfemoral epiphysis. These signals represent vascular canalsthat course through the epiphyseal and superficial physealcartilage of the femoral head (Fig. 1).
Deep transphyseal perfusion is represented by powerDoppler signals visualized along the physis in the vicinityof the epiphyseal secondary ossification center and meta-physis (Fig. 1).
Sonographic image acquisition
Whenever possible, unenhanced power Doppler sonogramsof the hips were obtained in the supine position using sevenscanning approaches (Fig. 2): (1) anterior-sagittal (25asymptomatic hips, 26 pathologic hips), with the hips inneutral position (extension and slight external rotation), andthe transducer placed along the longitudinal axis of thefemoral shaft; (2) anterior-transverse (25 asymptomatic
Pediatr Radiol (2008) 38:392–402 393

hips, 26 pathologic hips), with the transducer placedperpendicular to the plane of the anterior-sagittal approach;(3) coronal (25 asymptomatic hips, 26 pathologic hips),with the transducer placed on the lateral side of the patient’ship angled at 90° in relation to the plane of the anterior-sagittal approach; (4) adduction (16 asymptomatic hips, 16pathologic hips), with the probe placed on the sameposition as for the sagittal-anterior approach but with thehip in slight internal rotation and the knee crossing over thecontralateral joint; (5) perineal (19 asymptomatic hips, 17pathologic hips), with the probe placed on the internalaspect of the thigh at the level of the femoral head,immediately lateral to the perineum area, with the hipabducted at 45° in relation to a sagittal line crossing thecentral aspect of the body; (6) hip at 30° abduction inrelation to the aforementioned imaginary line (22 asymp-tomatic hips, and 22 pathologic hips), with the probe placedon the same position as for the sagittal-anterior approach;(7) hip at 70° abduction (15 asymptomatic hips, 12pathologic hips) in relation to the imaginary line, with theprobe placed on the same position as for the sagittal-anterior approach. Standardized foam pads were used toabduct the patients’ thighs at preestablished angles for thesake of reproducibility of measurements. All efforts weremade to avoid causing any discomfort or pain to thepatients during the examinations. Specific scanningapproaches were not performed or immediately discontin-ued if they caused any discomfort or pain to the patient.
The sonographic examinations were performed with anHDI 5000 scanner (Advanced Technology Laboratories,Bothell, WA) by the same operator, who was unaware ofthe physiologic status of the hips (pathologic vs. asymp-tomatic), using a 10-MHz linear-array transducer. Imagingdepth was adjusted to the body habitus of each patient inorder to provide full view of the patient’s femoral head.Otherwise identical technical parameters (medium filter,pulse repetition frequency 700 Hz, and 79% color gainsettings) were used for all examinations. Doppler sono-graphic examination was limited to a maximum period of5 min per approach for each hip. Only vessels that could beidentified within the established time frame and for which apulsed Doppler waveform could be obtained were consid-ered for evaluation.
Sonographic imaging analysis
Qualitative assessment Two radiologists (A.S.D. and L.J.M.) graded the presence or absence of color pixel signalswithin the proximal femur (binary response) with regard to:
1. Overall assessment of color Doppler signal in theproximal femur
2. Region of the proximal femur: epiphysis, physis ormetaphysis (Fig. 1)
3. Type of vascularity: superficial cartilaginous or deepphyseal (Fig. 1)
Fig. 1 Anatomy of the arterial blood supply to the proximal femur inrelation to the secondary ossification center of the proximal epiphysis,physis and metaphysis. a Cross section of the proximal femur at thelevel of the joint capsule: a superficial cartilaginous vascularity(visualized on color Doppler sonography); b anterior ascending cervicalartery; c lateral circumflex artery; d posterior ascending cervical artery;e medial circumflex artery; f epiphysis; g physis (where deeptransphyseal perfusion can be identified in pathologic hips); h meta-physis (Drawing modified with permission from reference 15). bSuperficial cartilaginous vascularity extending externally to the cortical
bone at the level of the metaphysis and physis of the proximal femur.Normal vascularity arising from the intracapsular subsynovial arterialring in the femoral head of a cadaveric specimen of a 9-month-old girl.The anterior half of the specimen, perfused with barium sulfate andshown in the coronal plan, demonstrates the intracapsular subsynovialring (white arrows) with branches of the anterior ascending cervicalarteries (B) crossing through the periphery of the cartilaginousepiphysis and other sets of blood vessels supplying different areas ofthe ossification center (black arrows, A). E epiphysis; P physis; Mmetaphysis (reprinted with permission from reference 4)
394 Pediatr Radiol (2008) 38:392–402

Fig. 2 a, c, e, g, i, k, m Photographs obtained during sonographicscanning in children in the supine position using the anterior-sagittal(a), anterior-transverse (c), lateral-sagittal (e), adduction (g), perineal(i), 30° of abduction (k), and 70° of abduction (m) approaches. b, d, f,h, j, l, n Power Doppler signals in the pathologic hip of an 8-year-oldboy using the anterior-sagittal (b), anterior-transverse (d), [coronal](f), adduction (h), perineal (j), 30° of abduction (l), and 70° ofabduction (n) scanning approaches. h, l, n Color pixels represent
vessels located within the fragmented femoral head (arrows) ofaffected hips. d, f Power Doppler signals visualized externally to thebone contour within the ossifying cartilage of the femoral head andalong the external contour of the proximal femoral metaphysis areshown using the anterior-transverse (d) and coronal (f) approaches(arrows). f, n Note cartilaginous vascular canals seen with the coronalplane (f arrowheads) and a flash artefact from the femoral artery(asterisk) with the 70° abduction approach (n)
Pediatr Radiol (2008) 38:392–402 395
Power Doppler signals could be identified either within asingle region or within multiple regions of the proximalfemur. The readers reviewed the images on both digitalformat and on videotapes. They were blinded to the clinicalhistory of the patients; however, the pathologic status of thehips could be assumed in some patients based on thecharacteristic imaging features of LCPD on gray-scale USimaging. The two readers reached consensus as to thepresence or absence of color pixels in specific anatomicregions for discordant cases (3/26, 11.5%, overall analysis).
Quantitative assessment The overall and regional quantita-tive assessment of the superficial cartilaginous and deeptransphyseal proximal femoral vascularity was performedby counting the number of color pixels spread through thethree regions of the proximal femur. The images obtainedwere printed as hard copies and digitalized by an HR5-PROcolor scanner (Kye Systems, Taipei, Taiwan) using 200 dpi,with 100% image size. The region-of-interest (ROI) of thesonographic image measured 7.5×9.5 cm (width×height)and was saved in a JPG image file format. The images weretransferred to a PC and analyzed using Photoshop 5.0(Adobe Systems, Mountain View, CA). On completion ofthe image analysis, the data were matched to each patient’sclinical information and the sonographic scanning approachused.
Statistical analysis
The number of hips with evidence of perfusion (frequency)presenting with color pixels that represented superficialcartilaginous or deep transphyseal perfusion was determinedaccording to different sonographic scanning approaches,pathologic or asymptomatic status of the hip joint, andanatomic region of the hip using Fisher’s exact test. Thenumbers of color pixels per region (intensity) identifiedin different anatomic regions of pathologic and asymp-tomatic hips were compared using two-tailed Student’st-tests, 95% confidence intervals or one-factor analysis ofvariance, as appropriate. To assess the ability to detectpixels of the sonographic scanning approaches frequencieswere grouped using the Duncan test. P values less than0.05 were considered significant.
Results
Superficial cartilaginous vascularity of proximal femur
Overall assessment of frequency of color pixels
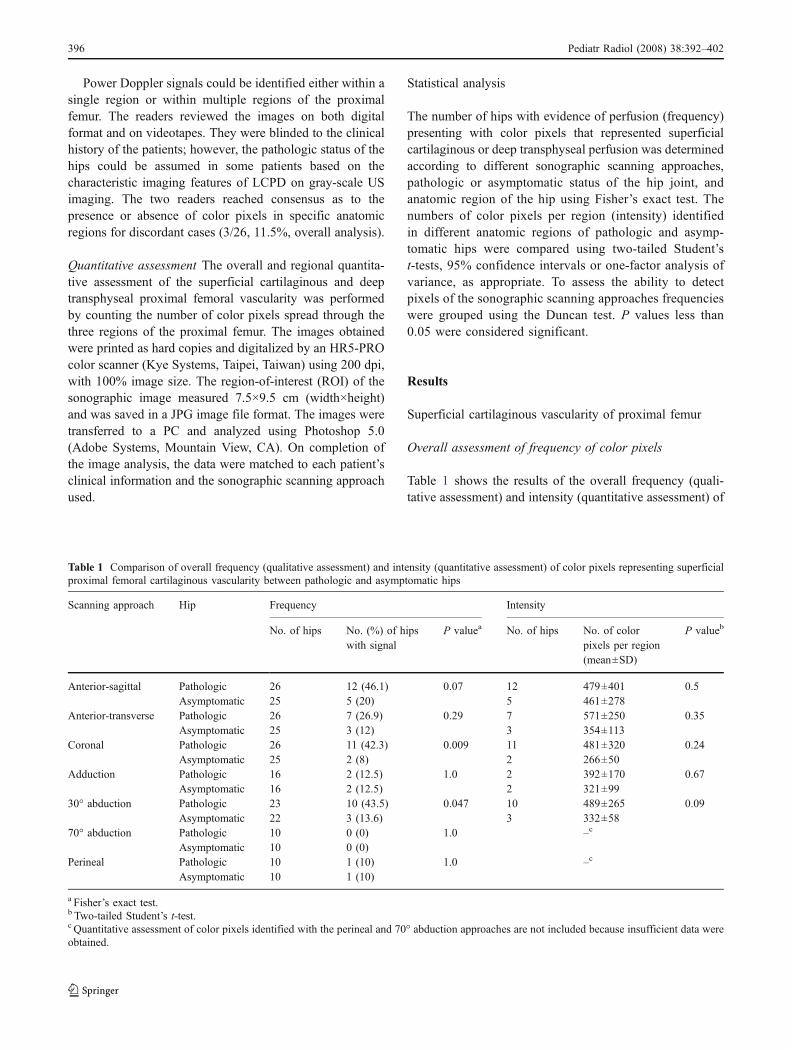
Table 1 shows the results of the overall frequency (quali-tative assessment) and intensity (quantitative assessment) of
Table 1 Comparison of overall frequency (qualitative assessment) and intensity (quantitative assessment) of color pixels representing superficialproximal femoral cartilaginous vascularity between pathologic and asymptomatic hips
Scanning approach Hip Frequency Intensity
No. of hips No. (%) of hipswith signal
P valuea No. of hips No. of colorpixels per region(mean±SD)
P valueb
Anterior-sagittal Pathologic 26 12 (46.1) 0.07 12 479±401 0.5Asymptomatic 25 5 (20) 5 461±278
Anterior-transverse Pathologic 26 7 (26.9) 0.29 7 571±250 0.35Asymptomatic 25 3 (12) 3 354±113
Coronal Pathologic 26 11 (42.3) 0.009 11 481±320 0.24Asymptomatic 25 2 (8) 2 266±50
Adduction Pathologic 16 2 (12.5) 1.0 2 392±170 0.67Asymptomatic 16 2 (12.5) 2 321±99
30° abduction Pathologic 23 10 (43.5) 0.047 10 489±265 0.09Asymptomatic 22 3 (13.6) 3 332±58
70° abduction Pathologic 10 0 (0) 1.0 –c
Asymptomatic 10 0 (0)Perineal Pathologic 10 1 (10) 1.0 –c
Asymptomatic 10 1 (10)
a Fisher’s exact test.b Two-tailed Student’s t-test.c Quantitative assessment of color pixels identified with the perineal and 70° abduction approaches are not included because insufficient data wereobtained.
396 Pediatr Radiol (2008) 38:392–402
color pixels representing the superficial proximal femoralcartilaginous vascularity in pathologic and asymptomatichips. Both the coronal and 30° abduction approachesdemonstrated a greater frequency of color pixels in patho-logic hips as compared with asymptomatic hips (P=0.009coronal approach; P=0.047 30° abduction approach) with atendency towards the anterior-sagittal approach also show-ing a difference in the frequency of color pixels betweenpathologic and asymptomatic hips (P=0.07). The 30°abduction approach demonstrated superficial proximalfemoral cartilaginous vascularity in 10 of 23 pathologichips (43.5%), the coronal approach in 11 of 26 pathologichips (42.3%) and the anterior-sagittal approach in 12 of 26pathologic hips (46.1%). No significant differences in theintensity of color pixels were found between pathologic andasymptomatic hips with any of the approaches (Table 1).
With regard to the frequency of detection of proximalfemoral vascularity according to patient age group, nodifferences in the frequency of color pixels identified in theproximal femora of children younger than 7 years or 7 yearsor older were noted with any of the sonographic scanningapproaches. Although not reaching statistical significance,superficial cartilaginous vascularity pixels tended to bedepicted more frequently in children less than 7 years ofage than in older children with the coronal approach inpathologic hips (P=0.08) and with the adduction approachin asymptomatic hips (P=0.07).
Regional assessment of intensity of color pixels
No definite color signals were identified within the epiphysealcartilage of asymptomatic hips. The anterior-sagittal approach
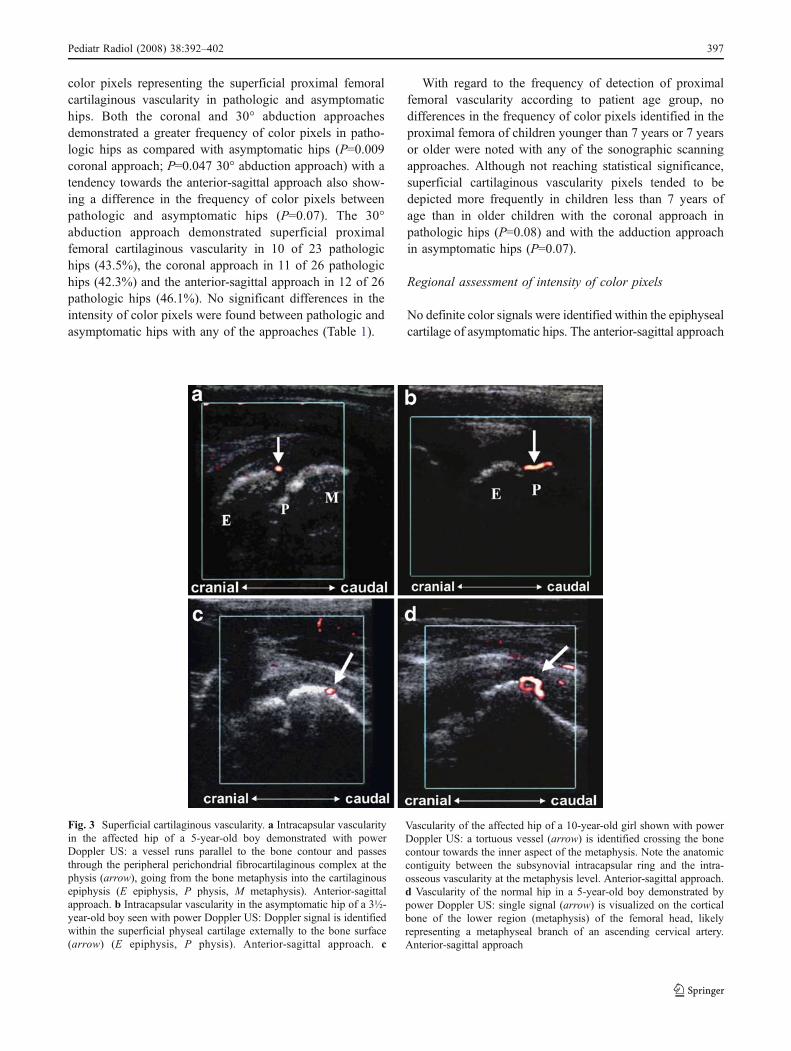
Fig. 3 Superficial cartilaginous vascularity. a Intracapsular vascularityin the affected hip of a 5-year-old boy demonstrated with powerDoppler US: a vessel runs parallel to the bone contour and passesthrough the peripheral perichondrial fibrocartilaginous complex at thephysis (arrow), going from the bone metaphysis into the cartilaginousepiphysis (E epiphysis, P physis, M metaphysis). Anterior-sagittalapproach. b Intracapsular vascularity in the asymptomatic hip of a 3½-year-old boy seen with power Doppler US: Doppler signal is identifiedwithin the superficial physeal cartilage externally to the bone surface(arrow) (E epiphysis, P physis). Anterior-sagittal approach. c
Vascularity of the affected hip of a 10-year-old girl shown with powerDoppler US: a tortuous vessel (arrow) is identified crossing the bonecontour towards the inner aspect of the metaphysis. Note the anatomiccontiguity between the subsynovial intracapsular ring and the intra-osseous vascularity at the metaphysis level. Anterior-sagittal approach.d Vascularity of the normal hip in a 5-year-old boy demonstrated bypower Doppler US: single signal (arrow) is visualized on the corticalbone of the lower region (metaphysis) of the femoral head, likelyrepresenting a metaphyseal branch of an ascending cervical artery.Anterior-sagittal approach
Pediatr Radiol (2008) 38:392–402 397
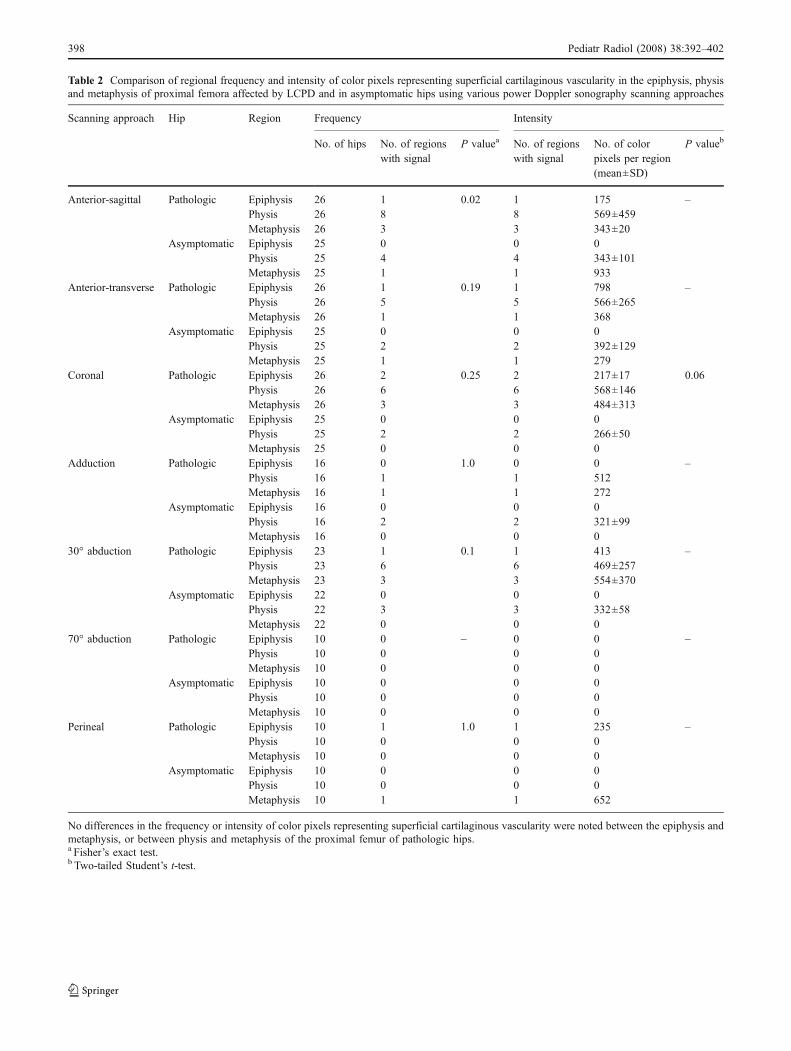
Table 2 Comparison of regional frequency and intensity of color pixels representing superficial cartilaginous vascularity in the epiphysis, physisand metaphysis of proximal femora affected by LCPD and in asymptomatic hips using various power Doppler sonography scanning approaches
Scanning approach Hip Region Frequency Intensity
No. of hips No. of regionswith signal
P valuea No. of regionswith signal
No. of colorpixels per region(mean±SD)
P valueb
Anterior-sagittal Pathologic Epiphysis 26 1 0.02 1 175 –Physis 26 8 8 569±459Metaphysis 26 3 3 343±20
Asymptomatic Epiphysis 25 0 0 0Physis 25 4 4 343±101Metaphysis 25 1 1 933
Anterior-transverse Pathologic Epiphysis 26 1 0.19 1 798 –Physis 26 5 5 566±265Metaphysis 26 1 1 368
Asymptomatic Epiphysis 25 0 0 0Physis 25 2 2 392±129Metaphysis 25 1 1 279
Coronal Pathologic Epiphysis 26 2 0.25 2 217±17 0.06Physis 26 6 6 568±146Metaphysis 26 3 3 484±313
Asymptomatic Epiphysis 25 0 0 0Physis 25 2 2 266±50Metaphysis 25 0 0 0
Adduction Pathologic Epiphysis 16 0 1.0 0 0 –Physis 16 1 1 512Metaphysis 16 1 1 272
Asymptomatic Epiphysis 16 0 0 0Physis 16 2 2 321±99Metaphysis 16 0 0 0
30° abduction Pathologic Epiphysis 23 1 0.1 1 413 –Physis 23 6 6 469±257Metaphysis 23 3 3 554±370
Asymptomatic Epiphysis 22 0 0 0Physis 22 3 3 332±58Metaphysis 22 0 0 0
70° abduction Pathologic Epiphysis 10 0 – 0 0 –Physis 10 0 0 0Metaphysis 10 0 0 0
Asymptomatic Epiphysis 10 0 0 0Physis 10 0 0 0Metaphysis 10 0 0 0
Perineal Pathologic Epiphysis 10 1 1.0 1 235 –Physis 10 0 0 0Metaphysis 10 0 0 0
Asymptomatic Epiphysis 10 0 0 0Physis 10 0 0 0Metaphysis 10 1 1 652
No differences in the frequency or intensity of color pixels representing superficial cartilaginous vascularity were noted between the epiphysis andmetaphysis, or between physis and metaphysis of the proximal femur of pathologic hips.a Fisher’s exact test.b Two-tailed Student’s t-test.
398 Pediatr Radiol (2008) 38:392–402
was able to demonstrate a difference in the frequency ofvisualization of color pixels representing superficial cartilag-inous vascularity in the physis compared with the epiphysis inpathologic hips (P=0.02; Fig. 3; Table 2). Although notreaching statistical significance, there was a tendencytowards the coronal approach showing a greater intensityof color pixels representing superficial cartilaginous vascu-larity at the level of the physis (mean number of pixels 568±146) compared to the epiphysis (mean number of pixels 217±17) in pathologic hips (P=0.06; Table 2). No differences werenoted in the mean number of pixels identified within themetaphysis and physis of pathologic hips, or within the meta-physis and epiphysis of pathologic hips with any of thesonographic scanning approaches (Fig. 3; Table 2).
Deep transphyseal vascularity of proximal femur
Overall assessment of frequency of color pixels
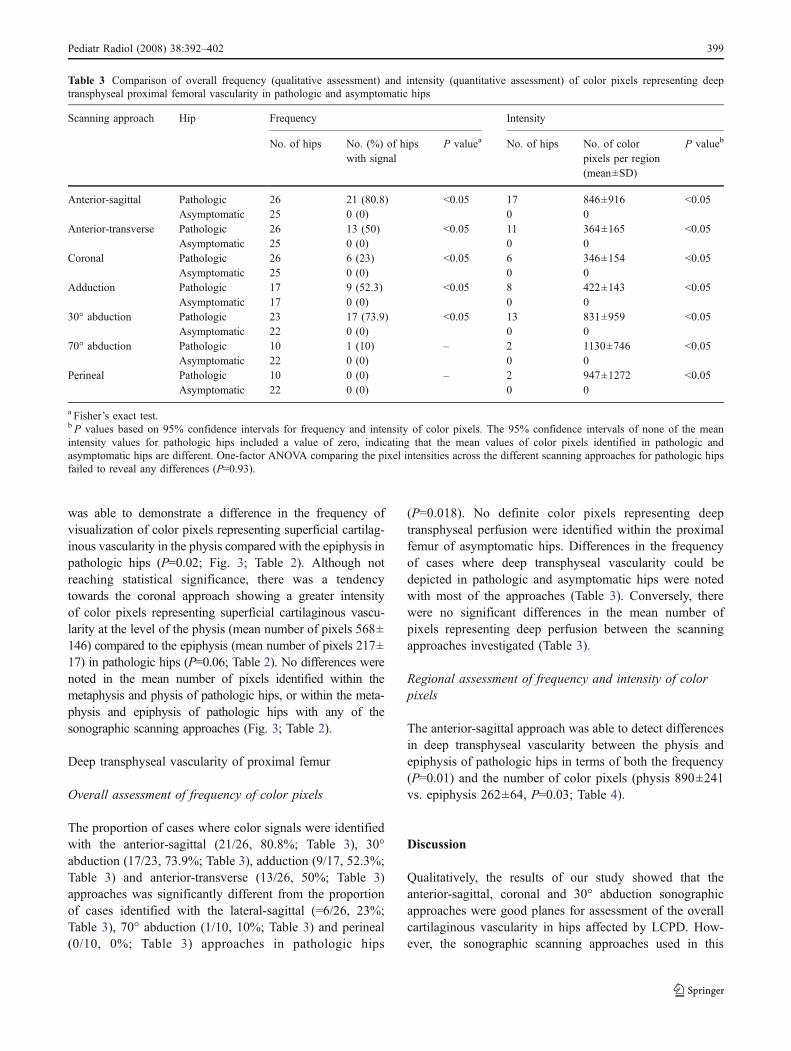
The proportion of cases where color signals were identifiedwith the anterior-sagittal (21/26, 80.8%; Table 3), 30°abduction (17/23, 73.9%; Table 3), adduction (9/17, 52.3%;Table 3) and anterior-transverse (13/26, 50%; Table 3)approaches was significantly different from the proportionof cases identified with the lateral-sagittal (=6/26, 23%;Table 3), 70° abduction (1/10, 10%; Table 3) and perineal(0/10, 0%; Table 3) approaches in pathologic hips
(P=0.018). No definite color pixels representing deeptransphyseal perfusion were identified within the proximalfemur of asymptomatic hips. Differences in the frequencyof cases where deep transphyseal vascularity could bedepicted in pathologic and asymptomatic hips were notedwith most of the approaches (Table 3). Conversely, therewere no significant differences in the mean number ofpixels representing deep perfusion between the scanningapproaches investigated (Table 3).
Regional assessment of frequency and intensity of colorpixels
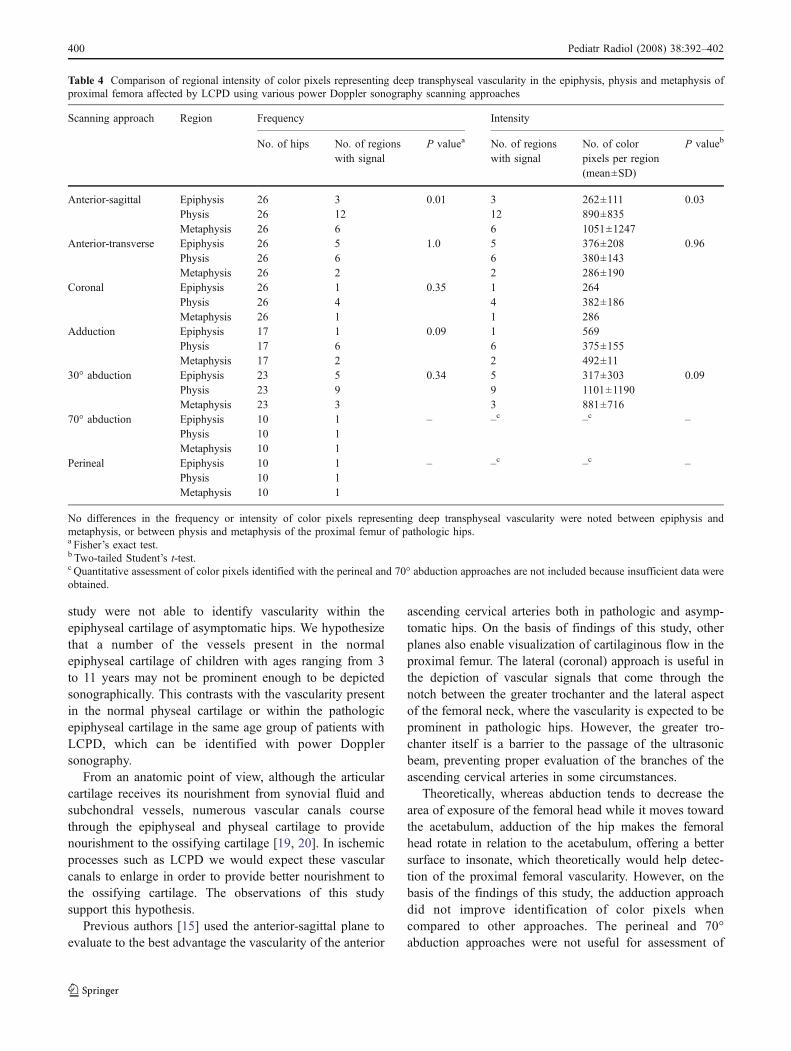
The anterior-sagittal approach was able to detect differencesin deep transphyseal vascularity between the physis andepiphysis of pathologic hips in terms of both the frequency(P=0.01) and the number of color pixels (physis 890±241vs. epiphysis 262±64, P=0.03; Table 4).
Discussion
Qualitatively, the results of our study showed that theanterior-sagittal, coronal and 30° abduction sonographicapproaches were good planes for assessment of the overallcartilaginous vascularity in hips affected by LCPD. How-ever, the sonographic scanning approaches used in this
Table 3 Comparison of overall frequency (qualitative assessment) and intensity (quantitative assessment) of color pixels representing deeptransphyseal proximal femoral vascularity in pathologic and asymptomatic hips
Scanning approach Hip Frequency Intensity
No. of hips No. (%) of hipswith signal
P valuea No. of hips No. of colorpixels per region(mean±SD)
P valueb
Anterior-sagittal Pathologic 26 21 (80.8) <0.05 17 846±916 <0.05Asymptomatic 25 0 (0) 0 0
Anterior-transverse Pathologic 26 13 (50) <0.05 11 364±165 <0.05Asymptomatic 25 0 (0) 0 0
Coronal Pathologic 26 6 (23) <0.05 6 346±154 <0.05Asymptomatic 25 0 (0) 0 0
Adduction Pathologic 17 9 (52.3) <0.05 8 422±143 <0.05Asymptomatic 17 0 (0) 0 0
30° abduction Pathologic 23 17 (73.9) <0.05 13 831±959 <0.05Asymptomatic 22 0 (0) 0 0
70° abduction Pathologic 10 1 (10) – 2 1130±746 <0.05Asymptomatic 22 0 (0) 0 0
Perineal Pathologic 10 0 (0) – 2 947±1272 <0.05Asymptomatic 22 0 (0) 0 0
a Fisher’s exact test.bP values based on 95% confidence intervals for frequency and intensity of color pixels. The 95% confidence intervals of none of the meanintensity values for pathologic hips included a value of zero, indicating that the mean values of color pixels identified in pathologic andasymptomatic hips are different. One-factor ANOVA comparing the pixel intensities across the different scanning approaches for pathologic hipsfailed to reveal any differences (P=0.93).
Pediatr Radiol (2008) 38:392–402 399
study were not able to identify vascularity within theepiphyseal cartilage of asymptomatic hips. We hypothesizethat a number of the vessels present in the normalepiphyseal cartilage of children with ages ranging from 3to 11 years may not be prominent enough to be depictedsonographically. This contrasts with the vascularity presentin the normal physeal cartilage or within the pathologicepiphyseal cartilage in the same age group of patients withLCPD, which can be identified with power Dopplersonography.
From an anatomic point of view, although the articularcartilage receives its nourishment from synovial fluid andsubchondral vessels, numerous vascular canals coursethrough the epiphyseal and physeal cartilage to providenourishment to the ossifying cartilage [19, 20]. In ischemicprocesses such as LCPD we would expect these vascularcanals to enlarge in order to provide better nourishment tothe ossifying cartilage. The observations of this studysupport this hypothesis.
Previous authors [15] used the anterior-sagittal plane toevaluate to the best advantage the vascularity of the anterior
ascending cervical arteries both in pathologic and asymp-tomatic hips. On the basis of findings of this study, otherplanes also enable visualization of cartilaginous flow in theproximal femur. The lateral (coronal) approach is useful inthe depiction of vascular signals that come through thenotch between the greater trochanter and the lateral aspectof the femoral neck, where the vascularity is expected to beprominent in pathologic hips. However, the greater tro-chanter itself is a barrier to the passage of the ultrasonicbeam, preventing proper evaluation of the branches of theascending cervical arteries in some circumstances.
Theoretically, whereas abduction tends to decrease thearea of exposure of the femoral head while it moves towardthe acetabulum, adduction of the hip makes the femoralhead rotate in relation to the acetabulum, offering a bettersurface to insonate, which theoretically would help detec-tion of the proximal femoral vascularity. However, on thebasis of the findings of this study, the adduction approachdid not improve identification of color pixels whencompared to other approaches. The perineal and 70°abduction approaches were not useful for assessment of
Table 4 Comparison of regional intensity of color pixels representing deep transphyseal vascularity in the epiphysis, physis and metaphysis ofproximal femora affected by LCPD using various power Doppler sonography scanning approaches
Scanning approach Region Frequency Intensity
No. of hips No. of regionswith signal
P valuea No. of regionswith signal
No. of colorpixels per region(mean±SD)
P valueb
Anterior-sagittal Epiphysis 26 3 0.01 3 262±111 0.03Physis 26 12 12 890±835Metaphysis 26 6 6 1051±1247
Anterior-transverse Epiphysis 26 5 1.0 5 376±208 0.96Physis 26 6 6 380±143Metaphysis 26 2 2 286±190
Coronal Epiphysis 26 1 0.35 1 264Physis 26 4 4 382±186Metaphysis 26 1 1 286
Adduction Epiphysis 17 1 0.09 1 569Physis 17 6 6 375±155Metaphysis 17 2 2 492±11
30° abduction Epiphysis 23 5 0.34 5 317±303 0.09Physis 23 9 9 1101±1190Metaphysis 23 3 3 881±716
70° abduction Epiphysis 10 1 – –c –c –Physis 10 1Metaphysis 10 1
Perineal Epiphysis 10 1 – –c –c –Physis 10 1Metaphysis 10 1
No differences in the frequency or intensity of color pixels representing deep transphyseal vascularity were noted between epiphysis andmetaphysis, or between physis and metaphysis of the proximal femur of pathologic hips.a Fisher’s exact test.b Two-tailed Student’s t-test.c Quantitative assessment of color pixels identified with the perineal and 70° abduction approaches are not included because insufficient data wereobtained.
400 Pediatr Radiol (2008) 38:392–402

deep transphyseal vascularity. Nevertheless, the ischemiceffect of hyperabduction of the femoral chondroepiphysis,which has been previously reported [8, 19, 21, 22] in thecontext of hip dysplasia, is not something that clinicians areconcerned about during therapy of LCPD. With the perinealapproach many soft-tissue planes interpose between theprobe and the femoral head, which limits the use of thisapproach for Doppler sonographic assessment of thevascularity of the hip. The 70° abduction approach impedesvisualization of the proximal femoral vascularity and resultsin greater exposure of the femoral artery, which can produceartefacts that hinder proper evaluation of vascularity.
Previous studies [20] have shown that the cartilaginouscanals concentrate in the vicinity of the physeal region. Theanterior-sagittal approach was able to demonstrate a greaterintensity of color pixels representing deep transphysealperfusion within the physis of affected hips. There was also atendency towards color pixels representing superficial carti-laginous vessels being more prominent in the physeal regionof affected hips, as noted with the coronal approach. Theseresults confirm the findingsof a previousMRI investigation [7].
The major limitation of this study was its observationaldesign, which lacked a reference standard measure thatcould confirm the accuracy of the data. We used thepresence of Doppler tracing for a given color pixelrepresenting vascularity as a marker of real blood flowrather than motion artefacts. Although branches of thelateral femoral circumflex artery, including the anteriorascending cervical arteries, comprise the anterior portion ofthe intracapsular arterial ring of the hip, branches of themedial femoral circumflex artery comprise the posteriorportion of the intracapsular arterial ring [3]. The lattervessels penetrate the proximal femur posteriorly andtherefore are more difficult to visualize using anteriorsonographic approaches [8]. However, given the lack ofdirect comparison between color Doppler pixels and acorresponding reference standard method we were unableto differentiate color pixels related to branches of the lateralor medial femoral circumflex arteries. Also, we shouldconsider that multiple tests of hypotheses were performedin the statistical analysis of this study, which could have ledto the significant associations and trends seen. A muchlarger sample size would have been required to testhypotheses for seven different scanning approaches if wehad planned to control for the problem of multiple testingusing a post-hoc test such as the Bonferroni correction test.In this case, a P value of at least 0.007 would have beenrequired for a test to be considered statistically significant.
Power Doppler hip sonography is an imaging techniquethat holds potential value for follow-up of patients withLCPD and evaluation of the extent of injuries to the
cartilage in musculoskeletal trauma as further informationin the field accumulates. Overall results of our study showthat the superficial cartilaginous vascularity and intraoss-eous/deep transphyseal vascularity of pathologic hips canbe more effectively evaluated using specific sonographicscanning approaches, notably the 30° abduction plane. Thissonographic plane is effective for assessment of bothsuperficial cartilaginous vascularity and intraosseous/deeptransphyseal vascularity. The physis was the anatomicregion of the proximal femur that presented with greaterintensity of color signals representing deep transphysealvascularity in pathologic hips, as noted with the anterior-sagittal approach. The intensity of pixels was greater inaffected hips compared with asymptomatic hips. Werecommend the use of specific sonographic scanning planesto assess the proximal femoral vascularity of LCPD hips.Selection of appropriate scanning approaches for evaluationof hips can improve the efficacy of the method anddecrease the scanning time.
Acknowledgement We would like to thank Dr. Robert B. Salter forhis valuable suggestions and comments and Luke Itani for thegraphical design for Fig. 1a.
References
1. Trueta J (1957) The normal vascular anatomy of the humanfemoral head during growth. J Bone Joint Surg Br 39B:358–394
2. Lauritzen J (1974) The arterial supply to the femoral head inchildren. Acta Orthop Scand 45:724–736
3. Ogden JA (1974) Changing patterns of proximal femoralvascularity. J Bone Joint Surg Am 56A:941–950
4. Chung SMK (1976) The arterial supply of the developingproximal end of the human femur. J Bone Joint Surg Am58A:961–970
5. Wilsman N, Van Sickle D (1970) The relationship of cartilagecanals to the initial osteogenesis of secondary centers ofossification. Anat Rec 168:381–392
6. Wilsman N, Van Sickle D (1972) Cartilage canals, theirmorphology and distribution. Anat Rec 173:79–94
7. Barnewolt CE, Shapiro F, Jaramillo D (1997) Normal gadolini-um-enhanced MR images of the developing appendicularskeleton: part I. Cartilaginous epiphysis and physis. AJR 169:183–189
8. Bearcroft PW, Berman LH, Robinson AHN et al (1996)Vascularity of the neonatal femoral head: in vivo demonstrationwith power Doppler US. Radiology 200:209–211
9. Keller MS (1996) Sonographic detection of femoral headvascularity in neonates. Radiology 200:28–29
10. Amodio J, Rivera R, Prinkney L et al (2006) The relationshipbetween alpha angle and resistive index of the femoral epiphysisin the normal and abnormal infant hip. Pediatr Radiol 36:841–844
Pediatr Radiol (2008) 38:392–402 401

11. Schwartz DS, Keller MS, Fields JM et al (1998) Arterialwaveforms in the femoral heads of healthy neonates. AJR170:465–466
12. Doria AS, Guarniero R, Molnar LJ et al (2000) Three-dimensional(3D) contrast-enhanced power Doppler imaging in Legg-Calvé-Perthes disease. Pediatr Radiol 30:871–874
13. Doria AS, Guarniero R, Cunha FG et al (2002) Contrast-enhanced power Doppler sonography: assessment of revascular-ization flow in Legg-Calvé-Perthes disease. Ultrasound Med Biol28:171–182
14. Graif M, Schweitzer ME, Nazarian L et al (1998) Color Dopplerhemodynamic evaluation of flow to normal hip. J Ultrasound Med17:275–280
15. Robben SG, Lequin MH, Diepstraten AFM et al (2000) Dopplersonography of the anterior ascending cervical arteries of the hip.AJR 174:1629–1634
16. Jaramillo D, Shapiro F (1998) Growth cartilage – normalappearance, variants and abnormalities. MRI Clin North Am6:455–471
17. Gruber H, Lachman RS, Rimoin D (1990) Quantitative histologyof cartilage vascular canals in the human rib: findings in normalneonates and children, and in achondrogenesis II-hypochondro-genesis. J Anat 173:69–75
18. Conway JJ (1993) A scintigraphic classification of Legg-Calvé-Perthes disease. Semin Nucl Med 23:274–295
19. Salter RB (1999) Textbook of disorders and injuries of themusculoskeletal system, 3rd edn. Williams & Wilkins, Baltimore,pp 339–350
20. Lutfi AM (1970) Mode of growth, fate and functions of cartilagecanals. J Anat 106:135–145
21. Jaramillo D, Villegas-Medina OL, Doty DK et al (1996)Gadolinium-enhanced MR imaging demonstrates abduction-caused hip ischemia and its reversal in piglets. AJR 166:879–887
22. Salter RB, Kostuik J, Dallas S (1969) Avascular necrosis of thefemoral head as a complication of treatment for congenitaldislocation of the hip in young children: a clinical andexperimental investigation. Can J Surg 12:44–61
402 Pediatr Radiol (2008) 38:392–402
Related Documents











