1 Nursing Care of a Family When a Child has a Respiratory Disorder General Nursing, 2010 Objectives ¬ Understand the anatomy and physiology of the paediatric respiratory tract. ¬ Identify the functions of the respiratory system. ¬ Describe the pathophysiology, clinical manifestations, treatment and nursing management of common respiratory conditions. E.g. asthma, upper respiratory infection, croup - laryngotracheobronchitis, pneumonia, bronchiolitis, respiratory distress and failure, and epiglottitis Anatomy and Physiology of the Respiratory System ¬ Upper respiratory tract - the nose, paranasal sinuses, pharynx, larynx, trachea and epiglottis ¬ Lower respiratory tract - the bronchi, bronchioles, alveoli (lungs) Development of the Respiratory system ¬ Infant (0 to 1 year) ¬ Respiratory rate (30 - 60 bpm average 40 bpm) ¬ Structure and function ¬ At birth, the lungs contain fluid; this is replaced by air as the infant begins respiration ¬ The respiratory tract is small and relatively delicate and it provides inadequate protection against infection. The close proximity of one structure to another eases the spread of infection. There is limited alveolar surface for gas exchange ¬ Ethmoidal and maxillary sinuses are present NOTE: ¬ At birth the chest wall is soft and pliable and the respiratory muscles underdeveloped resulting in poor expansion of the chest and decreased lung volumes at the end of exhalation In comparison with the adult, in the infant: ¬ The nasal passages are narrower. ¬ The trachea and chest wall are more compliant. ¬ The bronchi and bronchioles are shorter and narrower. ¬ The larynx is more funnel-shaped. ¬ The tongue is larger. ¬ There are significantly fewer alveoli. Anatomic differences ¬ Place the infant at higher risk for respiratory compromise. ¬ Furthermore, the lack of Ig A in the mucosal lining of the upper respiratory tract also contributes to the frequent infections that occur in infancy.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
Nursing Care of a FamilyWhen a Child has a
Respiratory Disorder
General Nursing, 2010
Objectives
¬ Understand the anatomy and physiology of thepaediatric respiratory tract.
¬ Identify the functions of the respiratorysystem.
¬ Describe the pathophysiology, clinicalmanifestations, treatment and nursingmanagement of common respiratoryconditions. E.g. asthma, upper respiratoryinfection, croup - laryngotracheobronchitis,pneumonia, bronchiolitis, respiratory distressand failure, and epiglottitis
Anatomy and Physiology of theRespiratory System
¬Upper respiratory tract - the nose,paranasal sinuses, pharynx, larynx,trachea and epiglottis
¬Lower respiratory tract - the bronchi,bronchioles, alveoli (lungs)
Development of the Respiratorysystem
¬ Infant (0 to 1 year)¬ Respiratory rate (30 - 60 bpm average 40 bpm)¬ Structure and function
¬ At birth, the lungs contain fluid; this is replaced by air as the infantbegins respiration
¬ The respiratory tract is small and relatively delicate and it providesinadequate protection against infection. The close proximity of onestructure to another eases the spread of infection. There is limitedalveolar surface for gas exchange
¬ Ethmoidal and maxillary sinuses are presentNOTE:¬ At birth the chest wall is soft and pliable and the
respiratory muscles underdeveloped resulting in poorexpansion of the chest and decreased lung volumes atthe end of exhalation
In comparison with the adult,in the infant:
¬ The nasal passages are narrower.¬ The trachea and chest wall are more
compliant.¬ The bronchi and bronchioles are
shorter and narrower.¬ The larynx is more funnel-shaped.¬ The tongue is larger.¬ There are significantly fewer alveoli.
Anatomic differences
¬ Place the infant at higher risk forrespiratory compromise.
¬ Furthermore, the lack of Ig A in themucosal lining of the upperrespiratory tract also contributes tothe frequent infections that occur ininfancy.

2
Development of the respiratorysystem
¬Toddler/Preschooler (1 to 6 years)¬Respiratory rate (20 to 30 bpm)¬Structure and function
¬Lung volume increases and susceptibility toinfection decreases
¬After age 2 years the right bronchus isshorter, wider and more vertical
Development of the respiratorysystem
¬School-age child (6 to 12 years)¬Respiratory rate (15 to 20 bpm)¬Structure and function
¬Respiratory system achieves adult maturity. Therespiratory rate slows as the amount of airexchanged increases with each breath. Lungcapacity becomes proportionate to body size
¬Frontal and sphenoidal sinuses develop betweenages 6 and 8 years.
Development of the respiratorysystem
¬Adolescent (12 to 21 years)¬Respiratory rate¬Structure and function
¬Inadequate oxygenation occurs as therespiratory system grows slowly in proportionto the rest of the body. Males have greatervital capacity due to greater chest size, andtheir lung capacity matures later than femaleswho reach adult capacity at age 17 or 18.
Remember
¬ Size of the infant’s trachea and lowerairway are approximately 1/3 to 1/2 ofthe an adult’s airway.
¬ The infant and young child’s nose,nasopharynx and pharynx are smaller andmore vulnerable to obstruction. Infantsare obligate nose breathers.
¬ Infants have limited alveolar space for gasexchange (20 million alveoli). By 3 - 8years children’s lungs contain more than300 million alveoli (same as adult)
Functions of respiratorysystem
¬ The major functions to deliver O2 to arterial blood andremove CO2 from venous blood (gas exchange).
¬ Normal gas exchange depends on:¬ Ventilation¬ Diffusion¬ Perfusion
¬ Control of gas exchange involves:¬ The neural system¬ Chemical processes
¬ Differences in respiratory response¬ Poor tolerance of nasal congestion¬ Increased susceptibility to ear infection¬ Increased severity of respiratory symptoms¬ A total body response to respiratory tract infection
Nursing Process:Respiratory Disorder
¬Assessment¬Nursing diagnosis¬Outcome identification and
planning¬Implementation¬Outcome evaluation

3
Assessing Respiratory Illness
¬Physical assessment¬Cough¬Rate and depth of respirations¬Retractions¬Restlessness¬Cyanosis
Assessing Respiratory Illness
¬Physical assessment¬Clubbing of the fingers¬Adventitious sounds¬Chest diameter
Assessing Respiratory Illness
¬Laboratory tests¬Blood gas analysis¬Pulse oximetry

4
Assessing Respiratory Illness
¬Laboratory tests¬Nasopharyngeal culture¬Respiratory syncytial virus nasal
washings¬Sputum analysis
Assessing Respiratory Illness
¬Diagnostic procedures¬Chest x-ray¬Pulmonary function studies
Health promotion and riskmanagement
¬Hand washing¬Proper disposal of tissues¬Covering mouth while coughing¬ Immunizations (e.g. HIB)

5
Therapeutic Techniques
¬Expectorant therapy¬Liquefying agents¬Humidification¬Vaporizers¬Nebulizers
¬Coughing¬Chest physiotherapy
Therapeutic Techniques
¬Therapy to improve oxygenation¬Oxygen administration¬Pharmacologic therapy¬Metered-dose inhalers
¬Incentive spirometry¬Breathing techniques
Therapeutic Techniques
¬Therapy to improve oxygenation¬Tracheostomy¬Emergency intubation¬Suctioning technique
Therapeutic Techniques
¬Therapy to improve oxygenation¬Endotracheal intubation¬Assisted ventilation
¬Lung transplantation
Upper Respiratory TractDisorders
¬Acute nasopharyngitis¬Assessment¬Therapeutic management

6
Upper Respiratory TractDisorders
¬Pharyngitis¬Viral pharyngitis¬Streptococcal pharyngitis¬Assessment¬Therapeutic management
¬Tonsillitis¬Assessment¬Therapeutic management
¬Tonsillectomy
Upper Respiratory TractDisorders
¬Epistaxis¬Sinusitis¬Laryngitis¬Congenital
laryngomalacia/tracheomalacia
Upper Respiratory TractDisorders
¬Croup (laryngotracheobronchitis)¬Assessment¬Therapeutic management
¬Epiglottitis¬Assessment¬Therapeutic management
Upper Respiratory TractDisorders
¬Aspiration¬Bronchial obstruction¬Assessment¬Therapeutic management
Lower Respiratory TractDisorders
¬Influenza¬Bronchitis¬Bronchiolitis¬Respiratory syncytial virus
bronchiolitis
7
Lower Respiratory TractDisorders
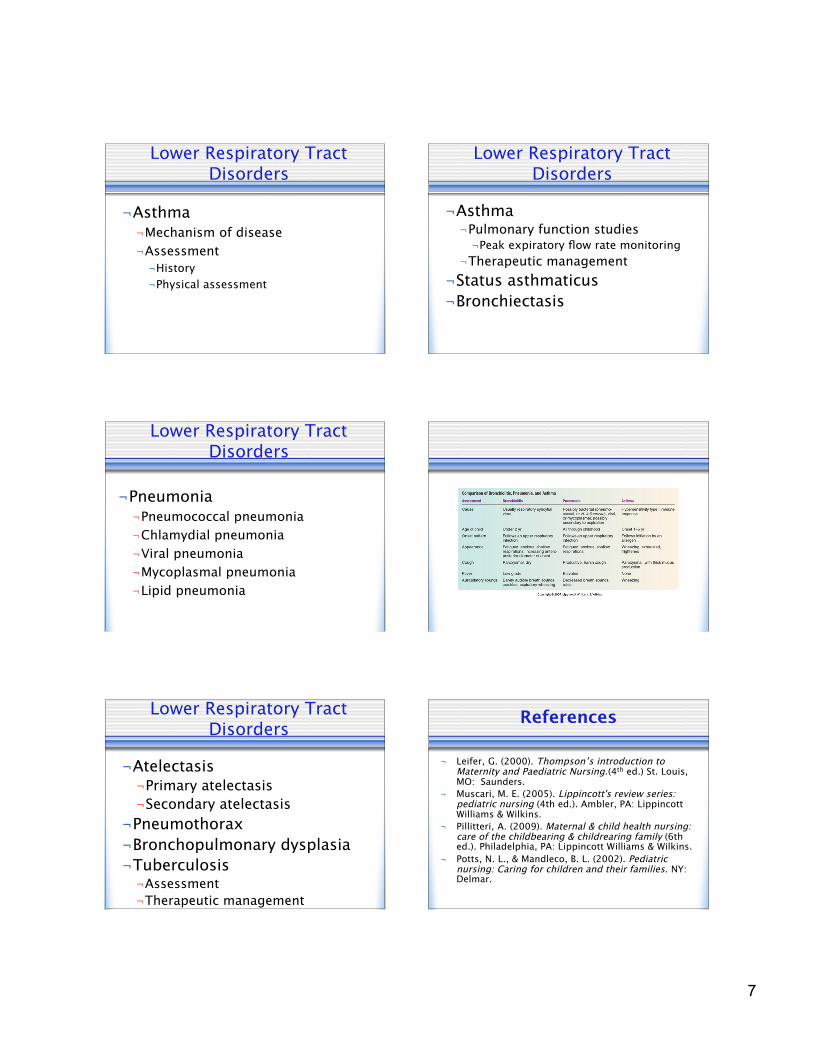
¬Asthma¬Mechanism of disease¬Assessment¬History¬Physical assessment
Lower Respiratory TractDisorders
¬Asthma¬Pulmonary function studies¬Peak expiratory flow rate monitoring
¬Therapeutic management¬Status asthmaticus¬Bronchiectasis
Lower Respiratory TractDisorders
¬Pneumonia¬Pneumococcal pneumonia¬Chlamydial pneumonia¬Viral pneumonia¬Mycoplasmal pneumonia¬Lipid pneumonia
Lower Respiratory TractDisorders
¬Atelectasis¬Primary atelectasis¬Secondary atelectasis
¬Pneumothorax¬Bronchopulmonary dysplasia¬Tuberculosis¬Assessment¬Therapeutic management
References
¬ Leifer, G. (2000). Thompson’s introduction toMaternity and Paediatric Nursing.(4th ed.) St. Louis,MO: Saunders.
¬ Muscari, M. E. (2005). Lippincott's review series:pediatric nursing (4th ed.). Ambler, PA: LippincottWilliams & Wilkins.
¬ Pillitteri, A. (2009). Maternal & child health nursing:care of the childbearing & childrearing family (6thed.). Philadelphia, PA: Lippincott Williams & Wilkins.
¬ Potts, N. L., & Mandleco, B. L. (2002). Pediatricnursing: Caring for children and their families. NY:Delmar.
Related Documents




![Respiratory disorders(student)[1]](https://static.cupdf.com/doc/110x72/55655061d8b42a77078b48de/respiratory-disordersstudent1.jpg)