Eruption Considerations Chapter 9, pp 184- 201; Chapter 27, pp 627-669; McDonald

Lecture 4 761 Pediataric Dentistry 2011.ppt
Jan 01, 2016
Pediataric Dentistry
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Eruption Considerations
Chapter 9, pp 184-201; Chapter 27, pp 627-669; McDonald
2
OverviewReview of spacingReview of space maintenance Local and systemic factors that influence eruption:
HabitsEctopic EruptionImpacted and Supernumerary teethAbnormal Labial FrenumAgenesis of TeethAnkylosed TeethEctodermal dysplasiaOther causes: Clefts, Cherubism, hypophosphatemia, acrodynia, Achondroplastic dwarfism,Cleidocranial dysplasia, Hypothyroidism, Hypopituitarism, Down, genetics,
post natal environment/nutrition, trauma, abcesses, early
losses, etc.

3
Review of spacing: Primary dentition
Interdental spacing-spacing between mesial of canines (across labial surfaces of anterior teeth)Accommodates larger permanent teeth
Primate space-between Mx canine and lateral Md canine and 1st molar
Closed primate space-no space availableSecondary incisor space-created by Md laterals forcing
primary Md canines laterally, which forces Mx canines laterally and widens the Mx intercanine arch length.Premature loss Md canines/caries/disking—borderline cases become extraction cases.
Leeway space—(Primary canines’+ Primary molars’ widths)- (Permanent canines’+Premolars’ widths) in each arch
Mx-3.4 mm/arch Md 0.9 mm/arch (large primaries)

4
Review of space maintenance
Band and Loop—unilateral/bilateralBilateral-appliance of choice mixed dentition
need 4 Md incisors/1st molars saves leeway spaceDistal shoe (contraindicated for poor oral hygiene,
blood dyscrasias, immunosuppressed, congenital heart defects, rheumatic fever history, diabetes, debilitation)—chronic inflammation with it--may want to regain space later, instead
RPD/fixed appliances—anterior collapse/space loss preventionreestablish anterior function/speech
5
Habit considerations
0-1 yo—clinging and oral habits
Compulsive habits—fixated
insecure/threatened
Damage from habits-duration
frequency
intensity
6
Thumbsucking
Incidence—47%
no residual effects if eliminated before mixed dentition
(6yo/school age)
Removable digital sucking appliance resembles a Hawley
If pt presents with thumbsucking habit, open bite/posterior X-bite refer for orthodontics (treatment may include Quad hexix)
7
Tongue Thrust/Infantile/Juvenile swallow
Infantile swallow—suckling associated with nursing, training cups
Usually adult swallow by age 6
The tongue can malpose teeth if the swallowing involves the tongue touching the Mx incisors
*Try muscle retraining first—practice placing tongue on incisive papilla and swallow
A tongue thrust appliance helps train the tongue to its proper position
8
Activity: Evaluate space maintenance/guidance/habit sample appliances brought to class

9
Ectopic eruptionAbnormal eruption positionIncidence: 3%, (boys more often)Common Sites:
Permanent Mx 1st molars Permanent Md laterals
Self corrects: 66% of molarsDX: evaluate radiographs closely TX for molars:
1. Monitor (usually lack of tuberosity development)2. Determine it is reversible (self-correcting)/irreversible between 7-8y3. If it is irreversible: orthodontic consult stating concerns/distally reposition it
McDonald 663 27-47

10
Ectopic eruption
Higher incidence-pts with Cleft lip and palate
Self correction rate-22% with a cleft
11
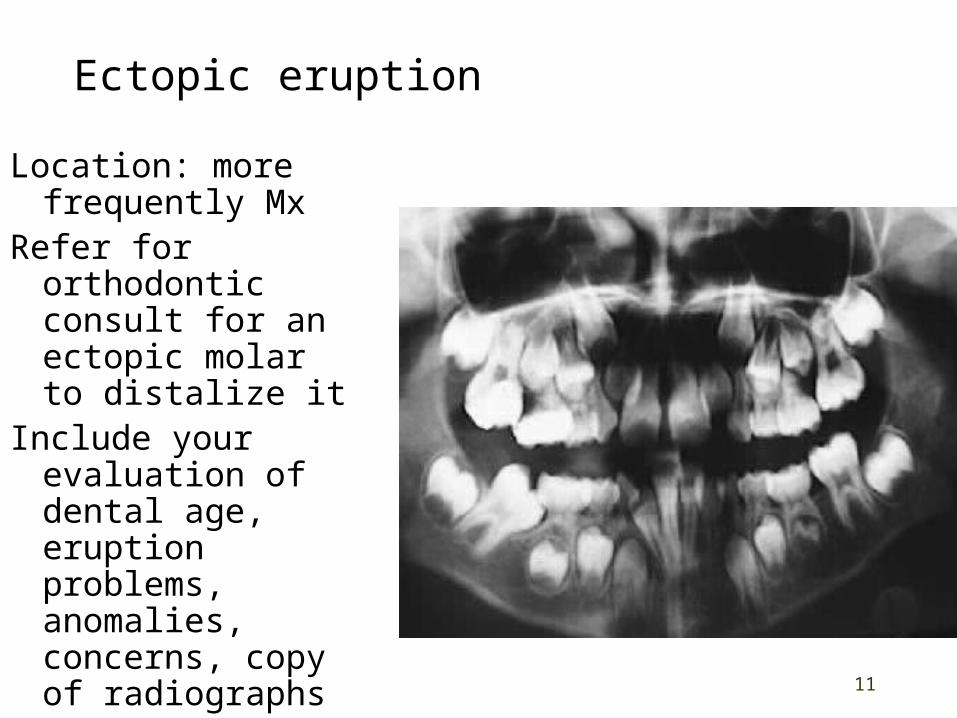
Ectopic eruption
Location: more frequently Mx
Refer for orthodontic consult for an ectopic molar to distalize it
Include your evaluation of dental age, eruption problems, anomalies, concerns, copy of radiographs

12
Treatment of Ectopic eruption of a permanent first molar
Kesling spring (separator)
Prepare brass wire with double helix bend. Place active spring below contact of the primary 2nd molar and ectopic permanent molar.
TX time—3-4 weeks
McDonald 665 27-48

13
Treatment of Ectopic eruption of a permanent first molar with Kesling spring
Personal collection of Dr. Mike Bagby
14
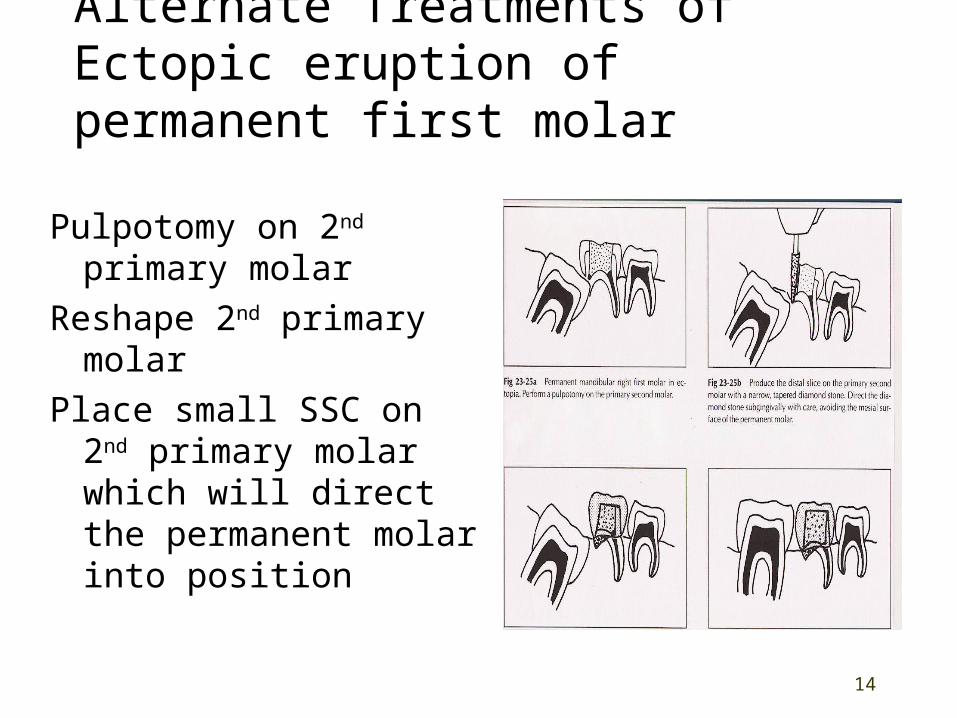
Alternate Treatments of Ectopic eruption of permanent first molar
Pulpotomy on 2nd primary molar
Reshape 2nd primary molar
Place small SSC on 2nd primary molar which will direct the permanent molar into position

15
Ectopic eruption of permanent lateralsProblem: ectopic permanent Mx/Md
lateral can cause premature primary canine loss (7y)
Serious problem: ectopic permanent Mn lateral can cause premature primary canine and 1st primary molar loss with transposition of permanent lateral/canine
DX: Obtain/review appropriate radiographs
TX: Unilateral condition, no midline shift: space maintenance Unilateral condition, midline shift, crowding, loss of 1 primary canine: orthodontic consult extract contralateral canine passive lingual arch McDonald 666 27-50
16
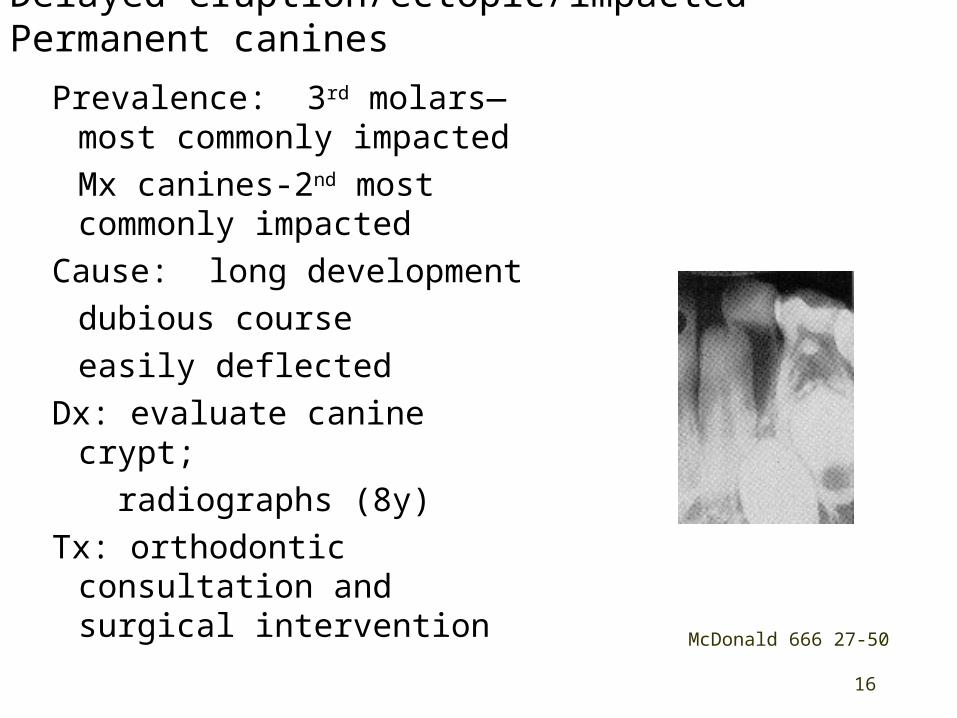
Delayed eruption/ectopic/impacted Permanent canines
Prevalence: 3rd molars—most commonly impactedMx canines-2nd most commonly impacted
Cause: long developmentdubious courseeasily deflected
Dx: evaluate canine crypt; radiographs (8y)
Tx: orthodontic consultation and surgical intervention
McDonald 666 27-50
17
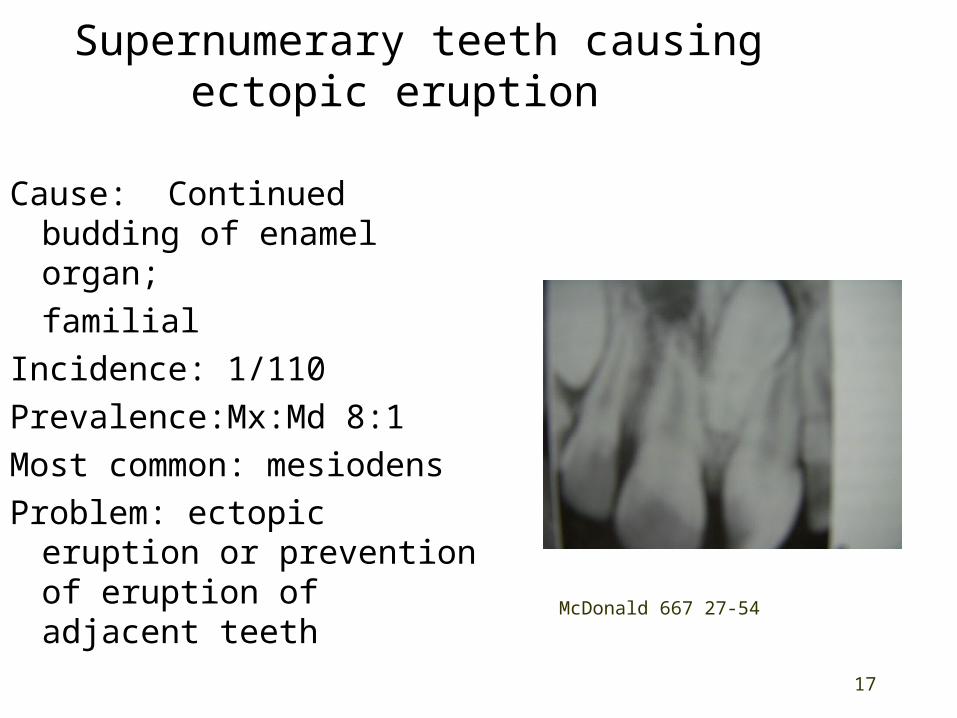
Supernumerary teeth causing ectopic eruption
Cause: Continued budding of enamel organ;familial
Incidence: 1/110Prevalence:Mx:Md 8:1Most common: mesiodensProblem: ectopic eruption
or prevention of eruption of adjacent teeth McDonald 667 27-54
18
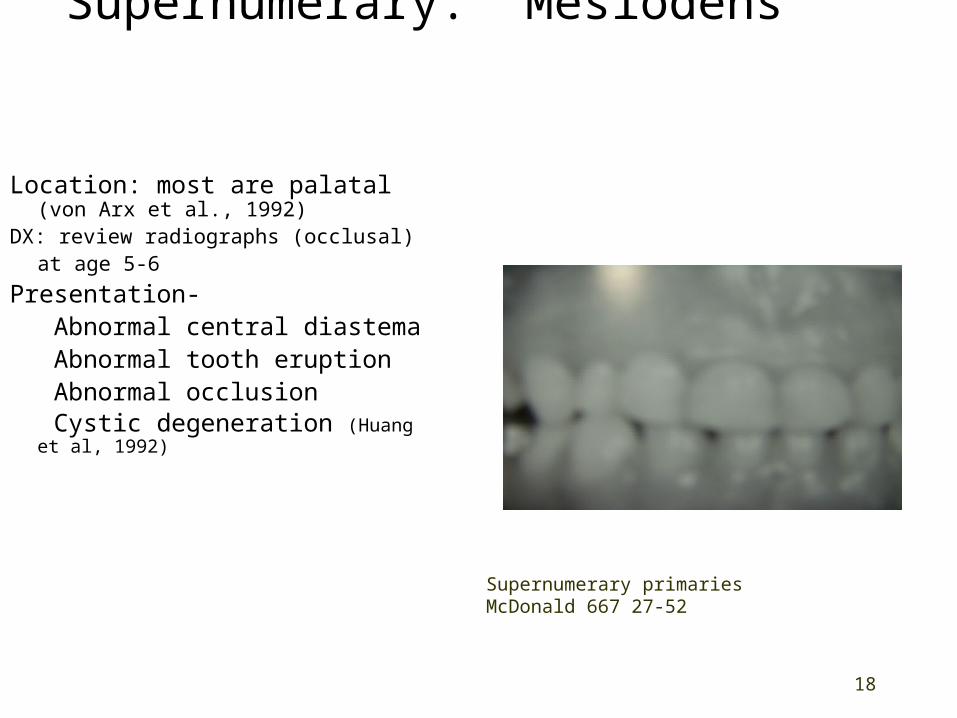
Supernumerary: Mesiodens
Location: most are palatal (von Arx et al., 1992)
DX: review radiographs (occlusal)at age 5-6
Presentation- Abnormal central diastema Abnormal tooth eruption Abnormal occlusion Cystic degeneration (Huang et al,
1992)
Supernumerary primaries
McDonald 667 27-52
19
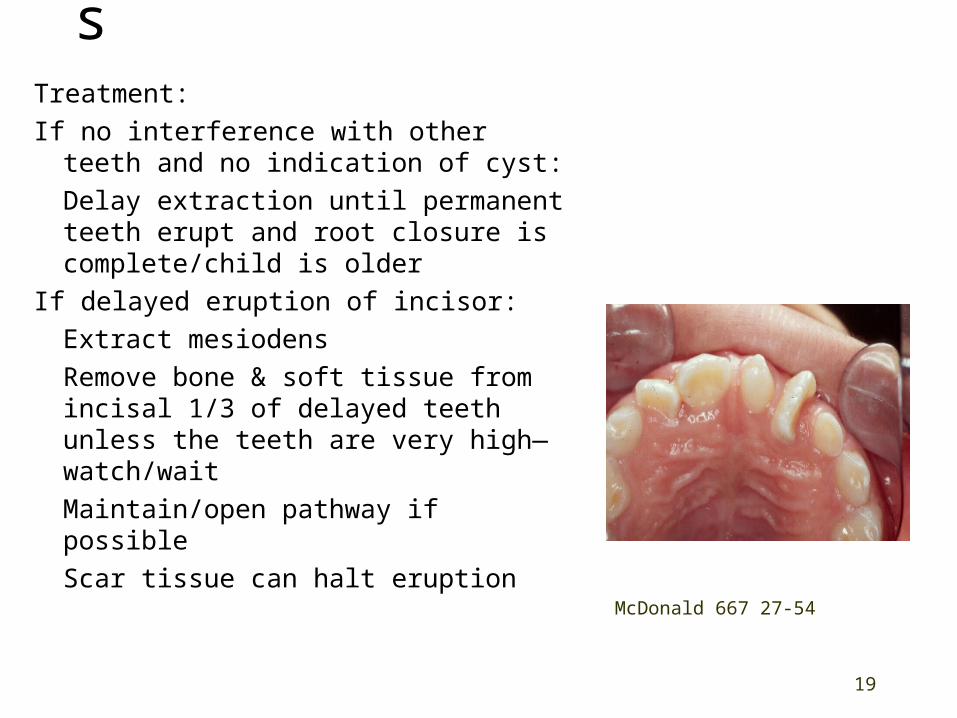
Supernumerary:MesiodensTreatment:
If no interference with other teeth and no indication of cyst:
Delay extraction until permanent teeth erupt and root closure is complete/child is older
If delayed eruption of incisor:
Extract mesiodens
Remove bone & soft tissue from incisal 1/3 of delayed teeth unless the teeth are very high—watch/wait
Maintain/open pathway if possible
Scar tissue can halt eruption McDonald 667 27-54

20From Creighton University
Multiple mesiodens in a 3yo at 4yo no tx Surgery
indicated

21
Multiple wisdom teeth

22
Anterior Diastema
Postpone until complete eruption of canines unless:
1. laterals are erupting lingually and do not have space to be moved labially; 2. heavy labial frenum—close the space, then do surgery;
3. Other valid reason

23
Abnormal labial frenum
Labial frenum: 2 layers of epithelium with a loose vascular connective tissue and muscle fibers from the orbicularis oris
Origin: midline on inner lip (wide)Insertion: midline in outer layer
periosteum and CT of internal MX suture and alveolar process to: above the crest of the ridge, or
at ridge, or through centrals to palatine
papilla McDonald 142 7-49

24
Abnormal labial frenumWNL (within normal limits): midline
diastema in pre-school children. Diastema usually closes when canines erupt.
Diagnostic test in mid-late mixed dentition:Press on frenum then identify location of alveolar attachment—a blanching of the palatine papilla indicates abnormality.
Other concerns:Interference with speechInterference with eatingDifficulty brushing
McDonald 142 7-49
25
Abnormal labial frenumFrenectomy: Orthodontic consult Evaluate esthetics/function Possible laser surgery Traditional surgery: Do not disturb mesial of free marginal tissue of incisors. Remove wedge section of tissue between incisors to nasal palatine papilla (transeptal fibers). Lateral incisions on either side of frenum to bone. con’t
26
Abnormal labial frenumFrenectomy con’t:
Excise the tissue.
Recontour labial and/or palatal gingival papilla if there is excessive tissue
Do not remove mesial free gingiva
Suture inside the lip to approximate free tissue margins
27
Agenesis of Teeth-failure of teeth to form
Anodontia – all teeth fail to developHypodontia–1 or more teeth fail to
formOlder term: Oligodontia – oligo-few; few teeth presentInaccurate older terms: Congenitally absent-permanent teeth are not expected at birth Partial anodontia-anodontia is complete absence; how does one have a partial complete absence?
Absence of teeth may be: Nonsyndromic/syndromic
One syndrome is Ectodermal Dysplasias
28
Anodontia
Autosomal recessive
No permanent dentition
The primary dentition is usually not affected
Treatment :
Overlay denture
McDonald 130 7-37

29
Hypodontia Most common: 3rd molarsMost common in children:
Md 2nd premolars Mx lateral incisors Mx 2nd premolars
Most common primary:Mx lateral
Several genes may be involvedPAX9 gene produces DNA
binding protein that controls other genes in tooth development and was mutated in one family with hypodontia
30
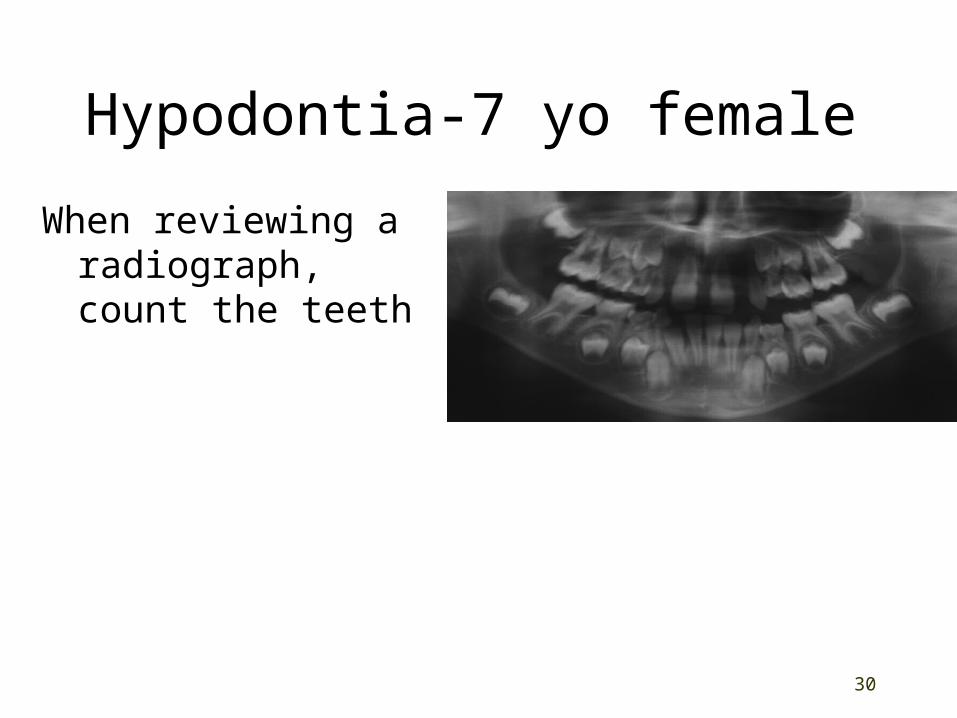
Hypodontia-7 yo female
When reviewing a radiograph, count the teeth
31
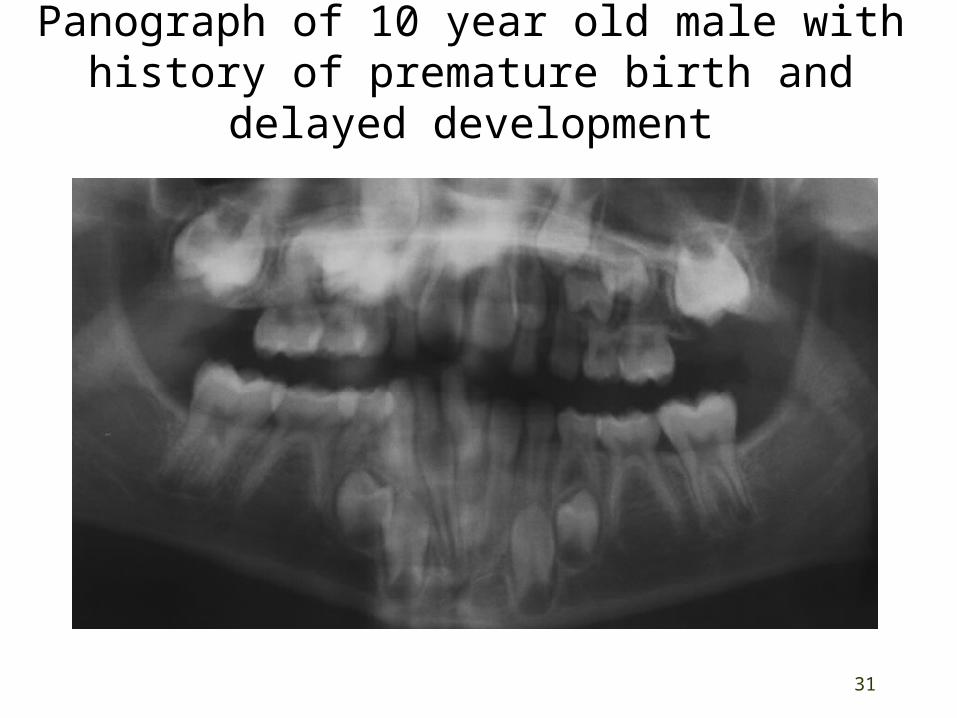
Panograph of 10 year old male with history of premature birth and delayed
development
32
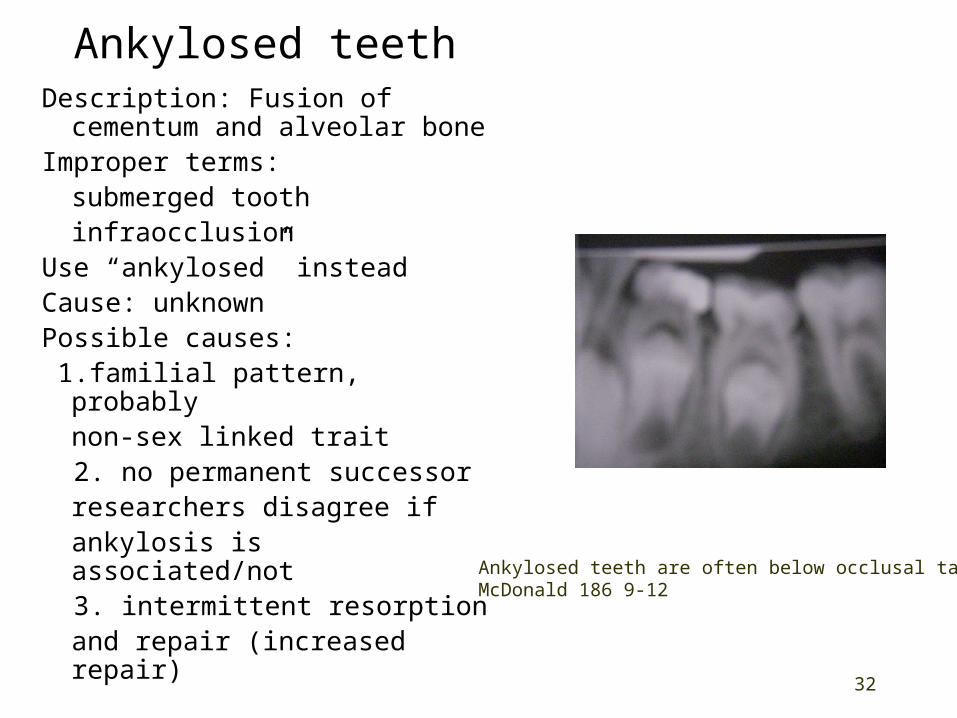
Ankylosed teethDescription: Fusion of
cementum and alveolar boneImproper terms:
submerged toothinfraocclusion
Use “ankylosed” insteadCause: unknownPossible causes: 1.familial pattern, probably
non-sex linked trait 2. no permanent successor
researchers disagree if ankylosis is associated/not
3. intermittent resorption and repair (increased repair)
Ankylosed teeth are often below occlusal tableMcDonald 186 9-12
33
Ankylosed teethOther possible causes
Inadequate Arch spacePre-eruptive proximity of permanent molarsEctopic eruption of permanent molarsCaries
Occurrence: usually after root resorption beginsor after trauma (anterior teeth)
Highest Incidence- Md primary molars Diagnosing:
Tooth appears depressedTapping - solid sound (normal teeth have a cushioned sound)Tooth not mobilePDL on radiograph is discontinuous
McDonald 186 9-12

34
Ankylosed tooth with permanent successor
Treatment:
Watchful waiting for normal exfoliation or
Extraction and placement of any needed space maintainers

35
Ankylosed tooth with no permanent successorIf there is adequate crown exposure
and sufficient root length, no successor and ankylosis occurs late:Keep as a functional unit
Restore proximal and occlusal contacts
Restore with SSC, composite resin, crown, gold casting crown, etc.
Assess perio periodically on adjacent teeth
If ankylosed tooth is extracted:Orthodontic referral/therapy or
Prepare for prosthodontics with space maintainance
36
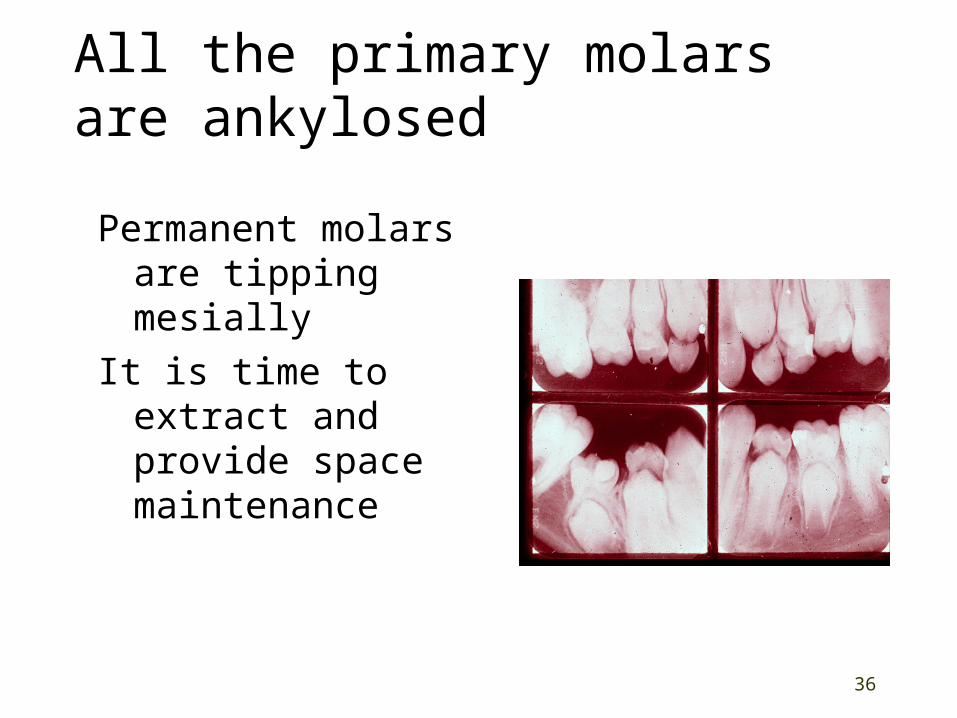
All the primary molars are ankylosed
Permanent molars are tipping mesially
It is time to extract and provide space maintenance

37
Ankylosed permanent teeth
The incomplete eruption of a permanent molar may be related to a small area of root ankylosis
TX:
Remove soft tissue and bone covering the occlusal of the tooth for a path for eruption
If unsuccessful:
Surgical consult to luxate and break the ankylosis
A delay in treatment may result in permanent ankylosis

38
Ectodermal Dysplasias-100 typesPresentation: Ectodermally derived
structures are altered:Anodontia or hypodontia of primary/permanent teethRetained primary teethHair-hypotrichosis absent/lanugo (fine) Sweat glands-hypohydrosis deficient
uncomfortable in warm weatherXerostomiaFissuring at corners of mouthSkeletal structures—normal with normal jaw development
Types:1. XLHED-X-linked recessive hypohidrotic
ectodermal dysplasia also called anhidrotic ectodermal dysplasia and Christ-Siemens-Touraine syndrome
2. Autosomal recessive ectodermal dysplasia
McDonald 133 7-39
39
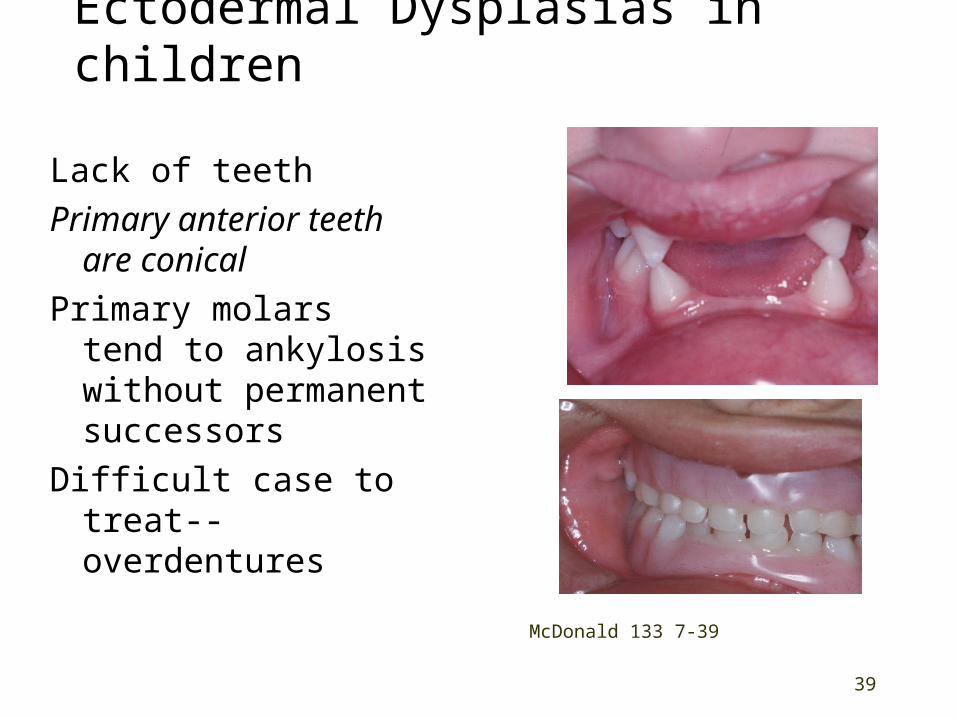
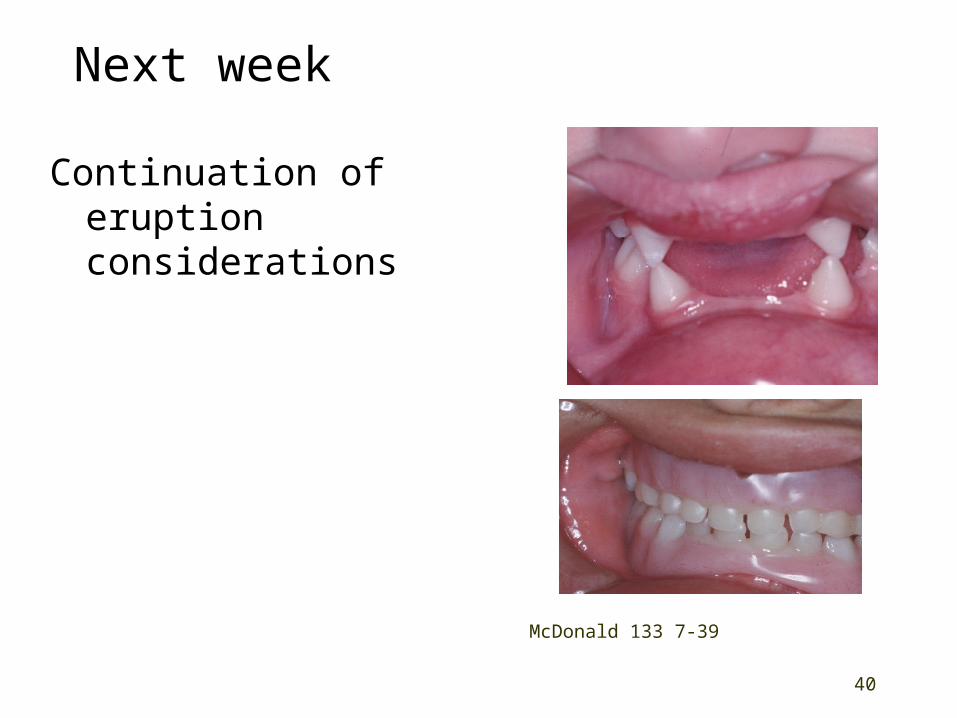
Ectodermal Dysplasias in children
Lack of teethPrimary anterior
teeth are conicalPrimary molars tend
to ankylosis without permanent successors
Difficult case to treat--overdentures McDonald 133 7-39
40
Next week
Continuation of eruption considerations
McDonald 133 7-39

41
Objectives
Define primate, leeway, secondary and closed spaces; agenesis, anodontia, hypodontia, oligodontia, and ankylosis.
List when the distal shoe is not indicated.
State when an RPD may be indicated to replace D, E, F, or G.
Identify sites with frequent ectopic/missing teeth.
Describe the consequences of ectopically positioned teeth
Describe the dx/tx for:Ectopic/impacted teethSuperrnumerariesAnkylosed teethAnterior diastemaAbnormal labial frenum
Explain why these terms are inaccurate“congenitally absent permanent teeth”“partial anodontia”“submerged teeth”“infra-occlusion”
Describe ectodermal dysplasia.
Related Documents











