
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

8/4/2019 Lecture 1, Operative Dentistry (Script)
http://slidepdf.com/reader/full/lecture-1-operative-dentistry-script 1/12

8/4/2019 Lecture 1, Operative Dentistry (Script)
http://slidepdf.com/reader/full/lecture-1-operative-dentistry-script 2/12
Operative Dentistry Page 2
Operative Dentistry-
We start with a simple question: What is operative dentistry? Operative dentistry
is the art and science of the diagnosis, treatment and prognosis of teeth that do not
require full restoration or correction. Meaning that restorations inside the tooth (not
necessarily by carries), it could be a defect in the tooth unrelated to carries- also called
“Non-carious loss of tooth
structure” which could be as a
result of coronal defects of the
teeth, or defects caused by
carries. Operative dentistry
includes defects/restorations
inside the crown of the tooth=
Involved in INTRA-CORONAL
RESTORATIONS (any
restoration inside the tooth), any
restoration on the outside of the
tooth is called EXTRA-CORONAL RESTORATION.
Operative Dentistry also includes Prevention (we are also involved in preventing
the disease from occurring in the early stages) as well as preservation of the tooth
structure as well as interception of the disease (if you recall from cariology we can
interfere with the carious process and either slow it down or possible even reverse it at
a certain stage), and restoration (if it is too late to intercept and reverse the defect then
we must properly restore the tooth). So operative dentistry is basically based around:
Prevention, Intervention and restoration when required.

8/4/2019 Lecture 1, Operative Dentistry (Script)
http://slidepdf.com/reader/full/lecture-1-operative-dentistry-script 3/12
Operative Dentistry Page 3
Classifications of Dental Carries:
**Note: we previously took the following classifications in “CARIOLOGY” so the
doctor read the slides very quickly.
Classification according to initial state of the tooth:
Primary (initial) Caries: The process attacks the tooth surface for the first time,
regardless of progression or extent. This refers to a tooth that was not previously
carious but was attacked by carries for the first time.
Secondary (Recurrent) caries: The process attacks the tooth at the margin or
margins of an existing restoration, regardless of extension or progression. In
secondary carries a new carious lesion attacks a previously restored area of the
tooth or a nearby surrounding area.
Classification according to the situation of the tooth:
Acute Caries: Involves a large number of teeth in the mouth, and destruction of
tooth structure is usually quiet rapid.
Chronic Caries: Much lower progression of the lesion, and the average lesion
size is smaller than in acute caries.
Active caries: Describe lesion that progressively destroys more tooth structure.
Arrested caries: Occurs when the active degradative process is interrupted or
ceases, an example of arrested carries is if someone has a proximal region and

8/4/2019 Lecture 1, Operative Dentistry (Script)
http://slidepdf.com/reader/full/lecture-1-operative-dentistry-script 4/12
Operative Dentistry Page 4
an adjacent tooth was extracted exposure of the lesion to cleaning carious
lesion may arrest.
Classification according to Stage of
development of the lesion:
Incipient caries: The lesion is confined to enamel
and does not penetrate the DEJ. Also called White
Spot lesion when the Dentino-Enamel junction is
not reached (Lesion is confined to enamel = No undermining of enamel = no
cavity = remineralization of lesion is still possible).
Advanced caries:the other state of lesions in
teeth, when the lesion reaches or passes through
the DEJ and approaches the pulp. (if the lesion
reaches the DEJ then it is considered advanced).
Classification according to the Location of the Lesion:
Pit & fissure caries: originates in developmental irregularities, most often in the
occlusal surface of posterior teeth.
8/4/2019 Lecture 1, Operative Dentistry (Script)
http://slidepdf.com/reader/full/lecture-1-operative-dentistry-script 5/12
Operative Dentistry Page 5
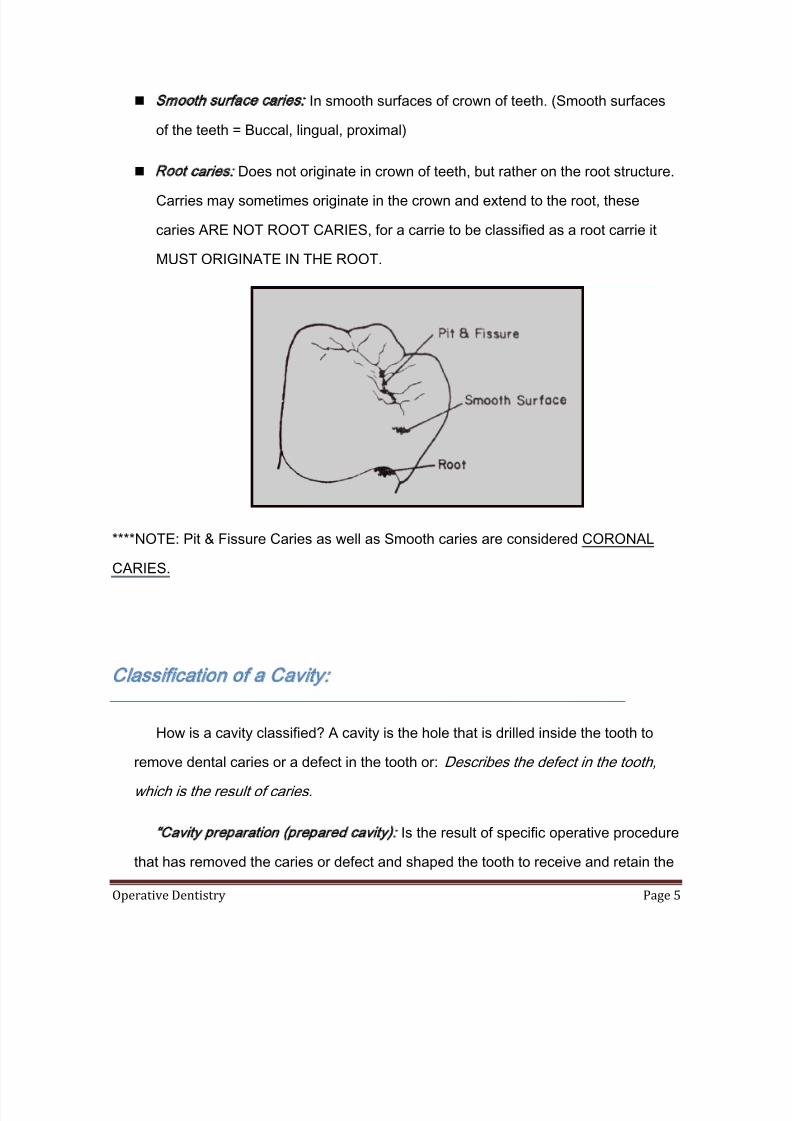
Smooth surface caries: In smooth surfaces of crown of teeth. (Smooth surfaces
of the teeth = Buccal, lingual, proximal)
Root caries: Does not originate in crown of teeth, but rather on the root structure.
Carries may sometimes originate in the crown and extend to the root, these
caries ARE NOT ROOT CARIES, for a carrie to be classified as a root carrie it
MUST ORIGINATE IN THE ROOT.
****NOTE: Pit & Fissure Caries as well as Smooth caries are considered CORONAL
CARIES.
Classification of a Cavity:
How is a cavity classified? A cavity is the hole that is drilled inside the tooth to
remove dental caries or a defect in the tooth or: Describes the defect in the tooth,
which is the result of caries.
“Cavity preparation (prepared cavity): Is the result of specific operative procedure
that has removed the caries or defect and shaped the tooth to receive and retain the

8/4/2019 Lecture 1, Operative Dentistry (Script)
http://slidepdf.com/reader/full/lecture-1-operative-dentistry-script 6/12
Operative Dentistry Page 6
restorative material.” Acavity is the hole in the tooth caused by the defect (usually
carries) and Cavity preparation the hole we prepare inside the tooth with certain
geometry to retain the restoration (such as mechanical retention by sloping the walls
of the cavity in amalgam fillings).
“Restorative material:is the material that is used to restore the cavity, i.e.
Amalgam.”
“Restoration: The cavity preparation plus the restorative material.”
There must be a common language/understanding between dentists to easily
relay information about a cavity to each other; this is called Blacks Classification of
Cavities, named after G.V. Black (The father of operative dentistry, who placed the
basic principles of operative dentistry). Black placed a classification of cavities to be a
common language between dentists, these cavities where divided into 6 categories
(Class I, Class II, Class III, Class IV, Class V, Class VI).

8/4/2019 Lecture 1, Operative Dentistry (Script)
http://slidepdf.com/reader/full/lecture-1-operative-dentistry-script 7/12
Operative Dentistry Page 7
Class I:class I originates in structural defects of the tooth such as pits and
fissures (usually on the occlusal surface of the tooth), preparation of a class I
cavity is called “class I preparation” and restoration of a class I cavity is also
called “class I restoration”. Any cavity found in the Lingual pit of Lateral Incisors is
also considered a class I cavity. (Class I does not define which surface the
structual defect is in, thus the lingual pit on the lingual surface of the tooth is
included).
Class II: Class II originates in the proximal (Mesial/Distal) surfaces of
MOLARS AND PRE-MOLARS. (in posterior teeth).

8/4/2019 Lecture 1, Operative Dentistry (Script)
http://slidepdf.com/reader/full/lecture-1-operative-dentistry-script 8/12
Operative Dentistry Page 8
Class III: Class III cavities originate in the proximal surfaces (Mesial/Distal) of
Anterior teeth (Central, Lateral & canines), BUT DOES NOT INVOLVE the loss
or removal of the incisal angle/edge.
1 Class III cavities do NOT include the incisal edge of the tooth
Class IV:When a cavity involves the proximal surface of an anterior tooth alongwith the incisal edge of the tooth this is considered a Class IV (4) cavity.

8/4/2019 Lecture 1, Operative Dentistry (Script)
http://slidepdf.com/reader/full/lecture-1-operative-dentistry-script 9/12
Operative Dentistry Page 9
Class IV:Class V cavities are found in the gingival/cervical (lower 1/3 rd) of any
tooth on the facial or lingual side (anterior/posterior), with the exclusion of Class I
pit/fissure caries.
**Note: the Buccal pit of the lower first molar is considered CLASS I , as well
as the palatal pit of the upper first molar- because these are NOT located in
the gingival third of the tooth.
Class VI: is a VERY RARE CASE, found located on the incisal edges of
canines and incisors, as well as the cusp tips of canines and posterior teeth.
.
.

8/4/2019 Lecture 1, Operative Dentistry (Script)
http://slidepdf.com/reader/full/lecture-1-operative-dentistry-script 10/12
Operative Dentistry Page 10
Classification by Complexity of Cavity:
This type of classification depends on the number of tooth surfaces involved, and
it is not as commonly used as Blacks classification but you should still know it:
Simple: Involves only a single tooth surface (regardless of which surface it is).
Compound: Involves any two tooth surfaces (must be connected, otherwise its
considered two simple cavities not one complex cavity).
Complex: Involves three or more tooth surfaces.
Classification by Surfaces:
Prepared cavities or restorations take the name of the respective surfaces, for
example a cavity on the occlusal surface is called “O”, a cavity on two surfaces such as
the occlusal and Mesial surfaces is called “MO” (mesio-occlusal), involving three
services such as Mesial, Occlusal, and distal is called “MOD” (Mesio-Occlusal-Distal).

8/4/2019 Lecture 1, Operative Dentistry (Script)
http://slidepdf.com/reader/full/lecture-1-operative-dentistry-script 11/12
Operative Dentistry Page 11
Components of Prepared Cavity:We also have names for the components of the prepared cavity including walls
floors and angles. The wall of the prepared cavity is the inclosing side of the prepared
cavity that takes the name of the adjacent surface of the tooth (Mesial wall/Distal wall),
the wall facing the distal side is the distal wall; the one on the mesial side is the mesial
wall… etc.
In class I cavities the surface facing the Pulp is called the PULPAL
FLOOR, in all other cavity classes the part facing the pulp is called
the AXIAL SURFACE.
Class II cavities are composed of an occlusal part and a proximal part, similar to
a step on a stairs, therefore it has both Pulpal and Axial internal walls. (you will
understand this better once we take it in the lab).
“Line angle: The line, or angle formed
when two walls of a prepared cavity
meet. It is named by combining the

8/4/2019 Lecture 1, Operative Dentistry (Script)
http://slidepdf.com/reader/full/lecture-1-operative-dentistry-script 12/12
Operative Dentistry Page 12
names of intersecting walls, i.e. Linguopulpal line angle.” We have two
neighboring walls in the cavity for example the mesial wall and the pulpal floor,
the line that joins these walls together is called the Mesio-Pulpal line angle, in a
class two cavity it is possible to have a PulpoAxial line angle at the intersection
between the occlusal part of the cavity and the proximal part.
Point angle: when three walls meet they
will join in a POINT not a line, this point
angle will be named according to the
three walls forming it
(Linguoaxiogingival forming between
Axial-lingual-gingival walls).
Cavosurface angle: is a very important
angle in tooth restoration it is “The line
or angle formed by the junction of a
cavity wall with the unprepared surface
of the tooth”, or the angle formed
between the wall of the prepared cavity
and the unprepared tooth surface, this
angle will decide which restoration must be used on the cavity (in amalgam the
cavosurface angle must be 90 degrees).
Done by: Ali Al-Qudsi
Related Documents











